
Subjective and Objective Measures of Parent-Child Relationship Dysfunction, Child Separation...
16
Psychiatry 73(2) Summer 2010 130 Subjective and Objective Measures of Parent-Child Relationship Dysfunction, Child Separation Distress, and Joint Attention Daniel S. Schechter, Erica Willheim, Claudia Hinojosa, Kimberly Scholfield-Kleinman, J. Blake Turner, Jaime McCaw, Charles H. Zeanah, Jr., and Michael M. Myers The literature suggests an adverse impact of maternal stress related to interper- sonal violence on parent-child interaction. The current study investigated associa- tions between a mother's self-reported parent-child relationship dysfunction and what she does in response to her child's cues. It also examined whether mater- nal perception of parent-child dysfunctional interaction and child behavior when stressed by separation, along with maternal behavior in response to child distress, predicted impaired joint attention (JA) during play. Participant mothers (n - 74) and their children ages 12-48 months were recruited from community pediatrics clinics and completed two videotaped visits. After correlations, multiple linear regression was applied to find the best model fit that would predict outcomes of interest. We found that both maternal subjective report of self-reported parent- child relationship dysfunction and observed child separation distress together predicted atypical maternal behavior. Self-reported parent-child relationship dysfunction, observed atypical maternal behavior, and child separation distress combined significantly predicted less time spent in joint attention during play. Maternal posttraumatic stress predicted less maternal availability after separation stress. Clinicians should thus carefully assess and listen to parents' communica- tion of disturbances in their relationship with their young child. Left untreated, parent-child relationship dysfunction may well lead to impairment in learning and social-emotional development. Daniel S. Schechter, M.D., is Chief of the Consult-Liaison Unit and Parent-Infant Research, Department of Child &c Adolescent Psychiatry, University of Geneva Hospitals and Faculty of Medicine, Geneva, Switzerland. He is also Ad- junct Assistant Professor of Psychiatry (Division of Developmental Neuroscience & Behavior), Columbia University College of Physicians & Surgeons, in New York City. Erica Willheim, Ph.D. is Director of the Family Peace Program/ Columbia SafeStart, and Instructor, the Parent-Infant Program, Department of Psychiatry, New York-Presbyterian Hospital and the Columbia University College of Physicians & Surgeons, in New York Gity. Claudia Hinojosa, M.S., is Research Technician, Department of Psychiatry (Division of Developmental Neuroscience Se Behavior), Columbia University Gollege of Physicians &C Surgeons, in New York. Kimberly Scholfield-Kleinman, M.S.W., is Instructor in the Parent-Infant Program, Golumbia University Genter for Psychoanalytic Training & Research, New York. /. Blake Turner, Ph.D., is Assistant Professor of Glinical Psychiatry (Division of Ghild &c Adolescent Psychiatry), Golumbia University Gollege of Physicians &C Surgeons and the Mailman School of Public Health, New York. Jaime McCaw, B.A., is Research Goordinator, Department of Psychiatry (Division of Developmental Neuroscience 6c Be- havior), Golumbia University Gollege of Physicians &C Surgeons, New York. Charles H. Zeanah, Jr., M.D., is Sellars- Polchow Professor, Department of Psychiatry and Neurology, Tulane University School of Medicine, New Orleans, Louisiana. Michael M. Myers, Ph.D., is Professor of Glinical Psychiatry and Ghief of the Division of Developmental Neuroscience and Behavior, Golumbia University Gollege of Physicians & Surgeons, New York. Address correspondence to Daniel S. Schechter, Ghef de l'Unité de Liaison et de la Recherche Parents-Bébé, Service de Psychiatrie de l'Enfant e de l'Adolescent (SPEA), Hôpitaux Universitaires de Genève, 51 Boulevard de la Gluse, 2ème Etage, GH-1205 Genève, Switzerland. E-mail: [email protected].
Transcript of Subjective and Objective Measures of Parent-Child Relationship Dysfunction, Child Separation...
Psychiatry 73(2) Summer 2010 130
Subjective and Objective Measures ofParent-Child Relationship Dysfunction, Child
Separation Distress, and Joint AttentionDaniel S. Schechter, Erica Willheim, Claudia Hinojosa,
Kimberly Scholfield-Kleinman, J. Blake Turner, Jaime McCaw,Charles H. Zeanah, Jr., and Michael M. Myers
The literature suggests an adverse impact of maternal stress related to interper-sonal violence on parent-child interaction. The current study investigated associa-tions between a mother's self-reported parent-child relationship dysfunction andwhat she does in response to her child's cues. It also examined whether mater-nal perception of parent-child dysfunctional interaction and child behavior whenstressed by separation, along with maternal behavior in response to child distress,predicted impaired joint attention (JA) during play. Participant mothers (n - 74)and their children ages 12-48 months were recruited from community pediatricsclinics and completed two videotaped visits. After correlations, multiple linearregression was applied to find the best model fit that would predict outcomes ofinterest. We found that both maternal subjective report of self-reported parent-child relationship dysfunction and observed child separation distress togetherpredicted atypical maternal behavior. Self-reported parent-child relationshipdysfunction, observed atypical maternal behavior, and child separation distresscombined significantly predicted less time spent in joint attention during play.Maternal posttraumatic stress predicted less maternal availability after separationstress. Clinicians should thus carefully assess and listen to parents' communica-tion of disturbances in their relationship with their young child. Left untreated,parent-child relationship dysfunction may well lead to impairment in learningand social-emotional development.
Daniel S. Schechter, M.D., is Chief of the Consult-Liaison Unit and Parent-Infant Research, Department of Child &cAdolescent Psychiatry, University of Geneva Hospitals and Faculty of Medicine, Geneva, Switzerland. He is also Ad-junct Assistant Professor of Psychiatry (Division of Developmental Neuroscience & Behavior), Columbia UniversityCollege of Physicians & Surgeons, in New York City. Erica Willheim, Ph.D. is Director of the Family Peace Program/Columbia SafeStart, and Instructor, the Parent-Infant Program, Department of Psychiatry, New York-PresbyterianHospital and the Columbia University College of Physicians & Surgeons, in New York Gity. Claudia Hinojosa, M.S.,is Research Technician, Department of Psychiatry (Division of Developmental Neuroscience Se Behavior), ColumbiaUniversity Gollege of Physicians &C Surgeons, in New York. Kimberly Scholfield-Kleinman, M.S.W., is Instructorin the Parent-Infant Program, Golumbia University Genter for Psychoanalytic Training & Research, New York./ . Blake Turner, Ph.D., is Assistant Professor of Glinical Psychiatry (Division of Ghild &c Adolescent Psychiatry),Golumbia University Gollege of Physicians &C Surgeons and the Mailman School of Public Health, New York. JaimeMcCaw, B.A., is Research Goordinator, Department of Psychiatry (Division of Developmental Neuroscience 6c Be-havior), Golumbia University Gollege of Physicians &C Surgeons, New York. Charles H. Zeanah, Jr., M.D., is Sellars-Polchow Professor, Department of Psychiatry and Neurology, Tulane University School of Medicine, New Orleans,Louisiana. Michael M. Myers, Ph.D., is Professor of Glinical Psychiatry and Ghief of the Division of DevelopmentalNeuroscience and Behavior, Golumbia University Gollege of Physicians & Surgeons, New York.Address correspondence to Daniel S. Schechter, Ghef de l'Unité de Liaison et de la Recherche Parents-Bébé, Servicede Psychiatrie de l'Enfant e de l'Adolescent (SPEA), Hôpitaux Universitaires de Genève, 51 Boulevard de la Gluse,2ème Etage, GH-1205 Genève, Switzerland. E-mail: [email protected].
Schechter et al. 131
Parent-child relationship disturbancesduring the formative development of affectregulation, within the first years of life, havesignificant public health implications (Sk-ovgaard et al., 2007). Disturbances in theparent-child relationship in early childhoodare known risk-factors for later psychologi-cal maladjustment (Dutra et al., 2009). Con-tinuing refinements in the identification ofunderlying causal factors and the directionalrelationships embedded in impaired early in-teraction patterns support the developmentof more effective, better individually matchedclinical assessment and treatment (Schechter& Willheim, 2009).
Multiple studies have identified fac-tors that can adversely impact interactionsbetween a parent and their very young child,for example, poverty and immigration (Ger-shoff. Aber, Raver, & Lennon, 2007), paren-tal psychopathology such as major depres-sion (Dietz, Jennings, Kelley, & Marshal,2009), and intergenerational disturbances inattachment patterns (Fraiberg, Adelson, &Shapiro, 1975). Of particular interest to thepresent authors has been the contribution ofviolence exposure and its sequelae to parent-child relational disturbances (Levendoskyet al., 2006). Specifically, the authors havebeen concerned with the impact of maternalstress related to interpersonal violence onpatterns of parent-child interaction, the de-velopment of intersubjective understanding,and broader social cognition. Interpersonalviolence in this paper, as in previous papersby the present authors, encompasses physicaland/or sexual abuse and/or assault, as well asdomestic violence exposure and/or victimiza-tion throughout the lifespan (Schechter et al.,2008).
Recently, at least two studies haveraised the question of whether there is some-thing particularly salient about exposureto child distress for mothers with a historyof interpersonal violence (Cohen, Hien, &cBatchelder, 2008; Schechter et al., 2008).These two studies have found that follow-ing laboratory-induced mother-child separa-tions, mothers with violence-related PTSD
are more avoidant, withdrawing, and laissez-faire in their caregiving than controls (Cohenet al., 2008; Schechter et al., 2008). Cohenand colleagues study, involved 176 mothersdivided into four groups: substance usingwith PTSD, depressed with PTSD, comorbid(depressed, substance abusing) with PTSD,and healthy controls. This study suggestedthat cumulative violent trauma and associat-ed comorbidity (i.e., PTSD, depression, andsubstance abuse together) contributed mostto insensitive caregiving behavior.
The Schechter study, by contrast, fo-cused specifically on 41 maternal violence-exposed mothers within a non-controlled,clinical sample, who had varying degrees ofPTSD. The severity of maternal PTSD wasfound to be associated with negative and dis-torted mental representations of their youngchildren and their relationship with theirchildren. Those representations, in turn,were significantly predictive of problematicor "atypical" maternal behavior with theirchild, that is behavior that tends to disorga-nize and stress the child rather than organizeand soothe the child (Schechter et al., 2008).While comorbid depression alone did notsignificantly alter the findings with respect tothe Schechter and colleagues a priori hypoth-eses, additional comorbidity was not consid-ered in further detail in that study.
The question of the psychologicalmechanisms by which cumulative violent ex-periences and associated comorbid psycho-pathology affect parenting behavior thereforeremains unanswered. An important clinicalobservation noted in the Schechter study wasthat 59% of mothers within the clinical sam-ple studied remarked that their young childwas among the top three Stressors in theirlife (Schechter et al., 2008). Thus subjectiveparenting stress within a population of vio-lence-exposed mothers, and how this stresstranslates into parent-child interactions andintersubjective states, is salient.
In order to explore this question ofpsychological mechanisms more fully, thepresent study examines the interplay of fourprinciple variables among a population of vi-
132 Parent-Child Dysfunction
olence-exposed mothers; maternal perceptionof the parent-child relationship, child distressupon separation, caregiving behavior, andjoint attention. The study further examinesthe association of maternal violence-relatedPTSD to these four principle variables.
As noted above, negative or distortedmaternal representations of her child andtheir relationship have been found to be pre-dictive of maternal behavior that tends todisorganize and stress the child. In the pres-ent study, the Parent-Child DysfunctionalInteraction (PCDI) subscale of the ParentingStress Index (PSI) (Abindin, 1995) was em-ployed to tap maternal perception of overalldysfunction within the relationship —ratherthan specific representations —in relationto the other study variables. Scores on thisself-report measure have been found to be re-lated to both parental psychopathology andpsychosocial risk (Whiteside-Mansell et al.,2006).
We also wished to explore the impactof child expression of negative emotion dur-ing helpless states, such as during separationfrom the mother in the laboratory, on mater-nal perception and behavior. Despite exten-sive study within the attachment literature ofchild behavior upon reunion with the mother,there has been less emphasis on the behaviorof the child during separation or its effect onthe parent. One study has demonstrated thatreunion behaviors were often at least partial-ly mediated by the intensity of children's sep-aration distress (Kochanska & Coy, 2002).We wondered if a mother's impression thather child poses a stress for her, and thus is thecause of the dysfunctional parent-child rela-tionship, might be determined by the degreeof expressed child separation distress. In aneffort to quantify this variable, the authorsdeveloped a scale to code child behavioralexpression of stress during separation (seeMethods).
"Atypical maternal behavior" (i.e.,non-contingent, disruptive and disrupted,social communication) has been studied inmothers during reunion episodes follow-ing the stress of separation episodes, and is
predictive of disorganized attachment in tod-dlerhood (Lyons-Ruth, Bronfman, and Par-sons, 1999). It has further been found to bepredictive of subsequent disturbances in psy-chosocial functioning during adolescence, in-cluding dissociative symptoms (Dutra et al.,2009). Given the significance of this factor,we wished to explore the question of whichvariables might impact —or derive from—caregiving behavior, that is, what is the re-lationship between caregiving behavior andmaternal perception of the relationship and/or child distress?
Joint attention is the capacity to at-tend to external objects or events "jointly"(i.e., together) and internal states and feel-ings intersubjectively. The maintenance ofjoint attention may well relate to the capac-ity to maintain attention to feeling states andthoughts that are crucial in the formation ofsuccessful social relationships (Schechter etal., 2008). Difficulty in maintaining joint at-tention to external reality has been describedas a marker for other adverse consequencesin childhood: disruptive behavior (Sheinko-pf, Mundy, Claassen, &c Willoughby, 2004),disturbances in language development(Watt, Wetherby, & Shumway, 2006) anddisturbances in learning and social cogni-tion (Tomasello & Carpenter, 2007; Moll etal., 2007; Vaughan van Hecke et al., 2007).These same three consequences have beenprospectively linked to the subsequent de-velopment of violence, trauma, and relatedpsychopathology in adulthood (Simonoff etal., 2004).
The capacity to "be together" requiresa level of comfort and openness to othersand one's surroundings that is not compat-ible with a fear-induced state of hypervigi-lance, survival planning, and physiologicalself-regulation of arousal in the face of threat(Purges, 2007). If anticipated or actual childstates of helplessness, distress, and aggres-sion are experienced as "threatening" by ahighly stressed or traumatized mother, wewould anticipate that she might become lessemotionally available to her child during orafter such states, experience the relationship
Schechter et al. 133
as more dysfunctional, and that as a result,joint attention would be more difficult to at-tain.
The current study was thus designedto test the following specific hypotheses:
l(a).There will be a positive associa-tion between the severity of currentmaternal posttraumatic stressdisorder (PTSD) and each of thefollowing three variables: maternalperception of dysfunctional parent-child interaction, child distressduring separation, and atypicalmaternal behavior.l(b). There will be a negative as-sociation between maternal PTSDseverity and the amount of timemothers and their children engagein joint attention prior to separa-tion.2(a). There will be a positive asso-ciation between maternal percep-tion of parent-child dysfunctionalinteraction and the degree of atypi-cal maternal behavior.2(b). There will be a positive asso-ciation between greater child stressduring separation and maternalperception of parent-child dysfunc-tional interaction, as well as with agreater degree of atypical maternalbehavior.2(c). There will be a statisticallypredictive interaction between amother's perception of parent-childdysfunctional interaction and thedegree of child distress during sep-aration, with these two variablestogether predicting a significantlygreater degree of atypical maternalbehavior.3. There will be a negative associa-tion between the amount of timemothers and their children engagein joint attention (prior to separa-tion) and each of the followingthree variables: maternal percep-tion of dysfunctional parent-child
interaction, child distress duringseparation, and atypical maternalbehavior.
METHODS
Participants
Permission to conduct this study wasobtained from the institutional review boardof the Columbia University Department ofPsychiatry. Participant mothers and theirchildren were recruited from hospital-affili-ated community general and specialty pedi-atrics clinics. All participants were reachedthrough IRB-approved flyers posted on bul-letin boards and distributed among staff inthe clinics and main medical center buildings.Flyers targeted mothers with children age 1to 4 years and in the follow-up phone call,research staff stated to the parent that thestudy was designed to look at how stress inparents' lives affected their relationship withtheir young children. Participants were com-pensated with $50 and toys and/or books fortheir child.
Participants were included in this studyif they were between the ages of 18 and 48,were the child's biological mother, had livedwith the child for the majority of the child'slife, and if they suffered no major physical ormental disability that would preclude themfrom participating in the study-tasks, whichincluded play, mobility, and fundamental lit-eracy (i.e., equivalent to a 5* grade level) inEnglish or Spanish. All measures and inter-views were available in English and Span-ish, depending on the mother's preference,and all research staff-members were fluent inEnglish and Spanish. Potential participantswere excluded if they reported or were as-sessed as manifesting psychotic symptoms orevidence of a chronic psychotic illness, cur-rent moderate to severe substance abuse ordependence, or acute suicidality requiringimmediate attention.
134 Parent-Child Dysfunction
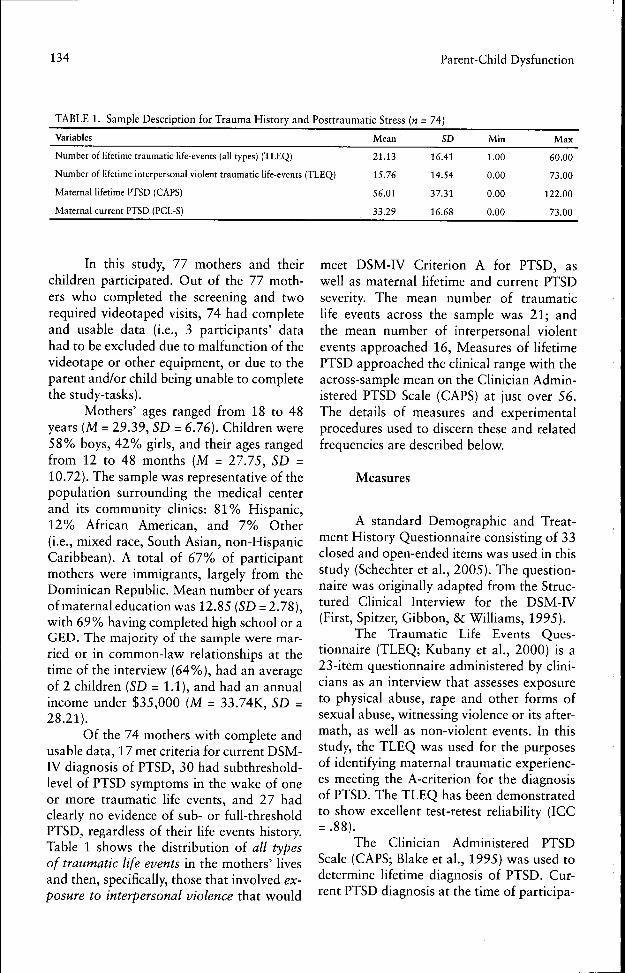
TABLE 1. Sample Description for Trauma History and Posttraumatic Stress (« = 74)
Variables Mean SD Min Max
Number of lifetime traumatic life-events (all types) (TLEQ)
Number of lifetime interpersonal violent traumatic life-events (TLEQ)
Maternal lifetime PTSD (CAPS)
Maternal current PTSD (PCL-S)
21.13
15.76
56.01
33.29
16.41
14.54
37.31
16.68
1.00
0.00
0.00
0.00
60.00
73.00
122.00
73.00
In this study, 77 mothers and theirchildren participated. Out of the 77 moth-ers who completed the screening and tworequired videotaped visits, 74 had completeand usable data (i.e., 3 participants' datahad to be excluded due to malfunction of thevideotape or other equipment, or due to theparent and/or child being unable to completethe study-tasks).
Mothers' ages ranged from 18 to 48years (M = 29.39, SD = 6.76). Children were58% boys, 42% girls, and their ages rangedfrom 12 to 48 months (M = 27.75, SD =10.72). The sample was representative of thepopulation surrounding the medical centerand its community chnics: 81% Hispanic,12% African American, and 7% Other(i.e., mixed race. South Asian, non-HispanicCaribbean). A total of 67% of participantmothers were immigrants, largely from theDominican Republic. Mean number of yearsof maternal education was 12.85 {SD = 2.78),with 69% having completed high school or aGED. The majority of the sample were mar-ried or in common-law relationships at thetime of the interview (64%), had an averageof 2 children (SD = 1.1), and had an annualincome under $35,000 (M = 33.74K, SD =28.21).
Of the 74 mothers with complete andusable data, 17 met criteria for current DSM-IV diagnosis of PTSD, 30 had subthreshold-level of PTSD symptoms in the wake of oneor more traumatic life events, and 27 hadclearly no evidence of sub- or full-thresholdPTSD, regardless of their life events history.Table 1 shows the distribution of all typesof traumatic life events in the mothers' livesand then, specifically, those that involved ex-posure to interpersonal violence that would
meet DSM-IV Criterion A for PTSD, aswell as maternal lifetime and current PTSDseverity. The mean number of traumaticlife events across the sample was 21; andthe mean number of interpersonal violentevents approached 16, Measures of lifetimePTSD approached the clinical range with theacross-sample mean on the Clinician Admin-istered PTSD Scale (CAPS) at just over 56.The details of measures and experimentalprocedures used to discern these and relatedfrequencies are described below.
Measures
A standard Demographic and Treat-ment History Questionnaire consisting of 33closed and open-ended items was used in thisstudy (Schechter et al., 2005). The question-naire was originally adapted from the Struc-tured Clinical Interview for the DSM-FV(First, Spitzer, Gibbon, & Williams, 1995).
The Traumatic Life Events Ques-tionnaire (TLEQ; Kubany et al., 2000) is a23-item questionnaire administered by clini-cians as an interview that assesses exposureto physical abuse, rape and other forms ofsexual abuse, witnessing violence or its after-math, as well as non-violent events. In thisstudy, the TLEQ was used for the purposesof identifying maternal traumatic experienc-es meeting the A-criterion for the diagnosisof PTSD. The TLEQ has been demonstratedto show excellent test-retest reliability (ICC= .88).
The Clinician Administered PTSDScale (CAPS; Blake et al., 1995) was used todetermine hfetime diagnosis of PTSD. Cur-rent PTSD diagnosis at the time of participa-
Schechtet et al. 135
tion in the research protocol was determinedby clinician interview using the CAPS andby the subject's self-report about her presentsymptoms using the Posttraumatic SymptomChecklist—Short Version (PCL-S; Weathers&c Ford, 1996). Additionally, to measure co-morbid depressive symptoms, we used theBeck Depression Inventory II (BDI-II; Beck,Steer, & Brown, 1996). The CAPS, PCL-S,and BDI-II are all standard assessment psy-chiatric measures and have excellent validityand reliability (Beck et al., 1996; Carlson,1997 pp. 221 & 232; Schechter &c Willheim,2009).
The Parent-Child Dysfunctional In-teraction (PCDI) subscale of the ParentingStress Index—Short Form (PSI-SF; Abidin,1995) contains 12 items (ICC = .83 respec-tively for each subscale of the PSI). This sub-scale measures a parent's perceptions aboutthe emotional quality of his or her relation-ship with their child, in light of his or herexpectations about the parent-child relation-ship. Parents are asked how much they agreeor disagree with statements such as: "Mosttimes I feel that my child does not like meand does not want to be close to me" or"Sometimes my child does things that botherme just to be mean." This subscale has beenassociated with parent reports of psychologi-cal symptoms as well as psychosocial riskfactors (Whiteside et ah, 2006). This particu-lar subscale independently has good inter-nal reliability with a Cronbach's alphaof.82.
A review of the attachment literatureyielded many studies utilizing multiple cod-ing schemes to quantify and clarify childbehaviors during play and during reunionepisodes, but not during separation. Sincemothers often wait just outside the door ofthe playroom during the separation, and cannot only imagine but hear the cries of theirchildren during these stressful minutes-typ-ically three minutes as in the Strange Situa-tion (Ainsworth 6c Wittig, 1969) and in theprocedure used here-we felt that the impactof child separation distress on mothers' per-
ception and behavior deserved greater atten-tion. We therefore consulted with ethologistswho had created a measure pertaining onlyto rat pup vocalizations during separation(Brunelli & Hofer, 2007) and created a be-havioral observation measure applicable tohuman child subjects.
The resulting measure is the Separa-tion Distress Scale (SDS; Schechter & Mc-Caw, 2005) in which videos of child distressduring separation are rated on a 5-point scaleby two independent raters naive to child ormaternal history (rating 0 = no observabledistress, 1 = marking separation with nega-tive expression but no crying or agitation, 2= calling for mother with negative expressionbut no crying or agitation, 3 = crying withno physical agitation, 4 = crying and physicalagitation). The consistency of the responseof the child to separation across two separa-tions was robust (Cronbach's alpha = .82).Inter-rater reliability was achieved on therating of the degree of child distress indepen-dently by two trained college-graduate raterswho watched the videotapes, one of whomwas blind as to the children's or mother's his-tory. Interrater reliability was excellent (ICC= 0.95, p<.001). In this paper, we operation-ally refer to severity of child scores on thisscale in terms of Child Separation Distress(CSD).
The Atypical Maternal Behavior In-strument (AMBI or "Ambiance"; Lyons-Ruth et al., 1999) is an observational mea-sure of caregiving behavior designed for usein videotaped laboratory protocols that in-clude sequences of separation and reunion.The measure yields an overall rating for ex-tent of atypical maternal behavior with thechild (also described in the literature as ma-ternal disrupted communication) on a scaleof 1 (no disrupted communication) to 7 (ex-treme and persistent disrupted communica-tion). This overall score is rated by codingvideotaped behavior across five dimensions:affective communication errors, withdrawal,disoriented behavior, hostility/intrusiveness,and role-confusion. The AMBI has provento be a strongly predictive measure of inse-
136 Parent-Child Dysfunction
cure, disorganized-type attachment acrossa variety of settings, with diverse samplesand across a range of ages from infancy tosix years (Madigan et al., 2007). For a simi-lar study of inner-city mothers, the level ofdisrupted communication was found to behighly reliable among raters (ICC = 0.93)(Madigan et al., 2007).
In this study, two history-naive codersused the AMBI coding scheme to rate the vid-eotapes of the interaction sequence knownas the Modified Crowell Procedure (Zeanahet al., 2000. See Procedures.). The coders,who were bilingual in Spanish and Enghsh,watched all 25 minutes of videotape multipletimes. Both were trained to reliability by Dr.Lyons-Ruth and her team, achieving excel-lent interrater reliability (ICC = 0.91).
The Coordinated Joint Attention Scales(Adamson, Baker, & Deckner, 2004) mea-sure the time that parents and children areengaged in coordinated joint attention, whenthey are "actively involved with the same ob-ject or event, and the child [was] actively andrepeatedly acknowledging the mother's par-ticipation [and the mother, hers]" (Adamsonet al., 2004, p. 1176). For the present study,two naive raters used this coding scheme tomeasure the number of seconds during the8-minute free-play portion of the protocolduring which child and mother were engagedin coordinated joint attention. Raters viewedand reviewed the videotapes in order to iden-tify clear beginnings and ends of coordinatedjoint attention engagement, identifying (a)time of onset and offset, and then countingthe duration in seconds of each of these in-teractions from onset to offset, and (b) whichdyadic partner initiated and ended the boutof attention. Raters also coded the amountof time each dyadic partner spent trying toengage the other partner without success.This specific item is coded by counting thenumber of seconds that one dyadic partnergestures and/or looks at the other partnerto initiate joint attention but receives no re-sponse.
The Joint Attention Scales coding wasapplied at two points during the mother-
child interaction procedure: 1) It was appliedto free, unstructured play with mother for 8minutes at the start of the protocol; and 2) Itwas again applied to free, unstructured playwith mother following the stress of separa-tion-reunion (4 minutes). This was done tosee if the stress of separation-reunion wouldimpact upon maternal availability to readchild cues in a direction proportional to themother's degree of posttraumatic stress symp-tom severity. Inter-rater reliability on the tim-ings (ICC = .87) and on initiation attempts(ICC = .76) both pre- and post-separationwere good. These values are consistent withthe previous use of this measure in which themeasure's authors achieved reliability usingstatistical analyses that corrected for chanceagreement that was between .70 and .80, in-dicating good to excellent interrater observa-tional reliability (Adamson et al., 2004).
PROCEDURES
The protocol consisted of two 2-hourvideotaped visits that followed informedconsent and screening in person.
During the initial videotaped visit,mothers were administered a clinical andtreatment history interview regarding theirchild and their relationship with their child.Mothers were then asked about stressfulevents during their own lives via the clini-cian's administration of the TLEQ. After re-viewing the violent events that had been ratedas "traumatic" by the mother, the clinicianasked the mother to describe, if there weremultiple events rated, the top three "mosttraumatic events" in further detail (i.e., interms of impact close to the time of the eventin the past if the event was not recent, andin terms of impact within the month priorto the current interview). The evaluation ofPTSD using the CAPS and PCL-S was thenbased on the mother's responses. The Parent-Child Dysfunctional Interaction (PCDI) sub-scale of the PSI-SF (Abidin, 1995) was alsoadministered during this first visit to evaluate

Schechter et al. 137
TABLE 2. Sample Description for Key Variables (n = 74)
Variables
Parent-child dysfunctional interaction
Child separation distress (0-4)
Atypical maternal hehavior
Time spent in joint attention (out of 8 minutes)
Mean
51.49
2.21
4.13
5.41 minutes
SD
7.18
1.38
1.51
1.57 minutes
Min
25.00
0.00
0.00
0.97 minutes
Max
60.00
4.00
7.00
6.95 minutes
mother's perception of dysfunction in the re-lationship with her child.
During the second visit, approximatelyone to two weeks later, mothers and childrenwere videotaped for 30 minutes while en-gaged in the Modified Crowell Procedure: a)playing together as they would at home usinga range of toys provided (8 minutes); b) sepa-rating (3 minutes) and reuniting (3 minutes);c) cleaning up the play area (2 minutes); d)engaging in a challenging structured activity,such as building a tower (toddlers) or doinga puzzle (preschoolers) (4 minutes); e) sepa-rating (3 minutes) and reuniting (3 minutes)for a second time; and f) exploring novel toyswith mother and clinician (4 minutes).
The AMBI, Child Separation DistressScale, and Joint Attention Scales are all mea-sures that were coded from this interactionprocedure based on repeated viewings of thevideotapes. That being said, each of thesemeasures focused on different segments ofthe interaction procedure so as to minimizeoverlap. The Child Separation Distress Scalefocused on the child's behavior during thesecond and more stressful of the two sepa-rations. The AMBI concentrated on overallmaternal caregiving behavior (i.e., coderswatched all 30 minutes at least once) but thenfocused particularly on the two reunions.Maternal behavior in response to child cuesduring the reunion is weighted heavily in thiscoding system.
The Joint Attention Scales focused onthe 8-minute period of free play prior to thefirst separation-reunion and the two periodsof two minutes each following both separa-tion-reunions (total of 4 minutes). The cod-ing of mother-child behavior during the free-
play was used to test the a priori hypothesisdescribed above. We therefore coded the in-teraction for the maximal time possible (i.e.,8 minutes). The post-separation coding wasused for exploratory analysis only. For theselatter analyses, we were restricted to the 4minutes allowed by the protocol.
Data Analysis
Pearson correlations were conductedto determine confounders and to confirmimportant relationships among key variablesbased on our a priori hypotheses. A series ofmultiple linear regression models containingsignificantly associated variables were thenestimated in order to find the best modelfit that would predict outcomes of interest.Models were subsequently adjusted in orderto test interaction effects between variablesand according to our hypotheses. All report-ed results are two-tailed.
RESULTS
To provide a sample-wide context forthe key variables pertaining to the hypoth-eses, we present the frequencies of thesevariables across the 74 subjects in Table 2.Good variability is noted across these fourkey measures: Parent-child dysfunctional in-teraction (PCDI) as subjectively reported bymother. Child separation distress (CSD) asobserved and coded by naive raters. Atypicalmaternal behavior on the AMBI as observedand coded by naive raters, and Time spent inJoint Attention (JA) during play as observed
138 Parent-Child Dysfunction
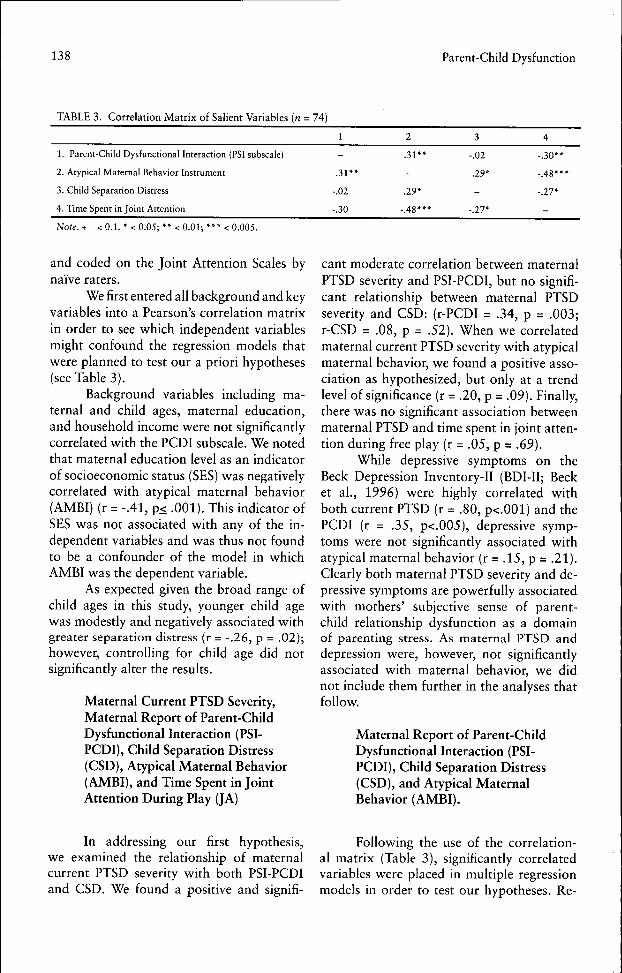
TABLE 3. Correlation Matrix of Salient Variables (« = 74)
I. Parent-Child Dysfunctional Interaction (PSI subscale)
2. Atypical Maternal Behavior Instrument
3. Child Separation Distress
4. Time Spent in Joint Attention
1
-
.31**
-.02
-.30
2
.31**
-
.29*
-.48***
3
-.02
.29*
-
-.27*
4
-.30**
-.48***
-.27*
-
Note. + < 0.1. * < 0.05; ** < 0.01; *** < 0.005.
and coded on the Joint Attention Scales bynaive raters.
We first entered all background and keyvariables into a Pearson's correlation matrixin order to see which independent variablesmight confound the regression models thatwere planned to test our a priori hypotheses(see Table 3).
Background variables including ma-ternal and child ages, maternal education,and household income were not significantlycorrelated with the PCDI subscale. We notedthat maternal education level as an indicatorof socioeconomic status (SES) was negativelycorrelated with atypical maternal behavior(AMBI) (r = -.41, p< .001). This indicator ofSES was not associated with any of the in-dependent variables and was thus not foundto be a confounder of the model in whichAMBI was the dependent variable.
As expected given the broad range ofchild ages in this study, younger child agewas modestly and negatively associated withgreater separation distress (r = -.26, p = .02);however, controlling for child age did notsignificantly alter the results.
Maternal Current PTSD Severity,Maternal Report of Parent-ChildDysfunctional Interaction (PSI-PCDI), Child Separation Distress(CSD), Atypical Maternal Behavior(AMBI), and Time Spent in JointAttention During Play (JA)
cant moderate correlation between maternalPTSD severity and PSI-PCDI, but no signifi-cant relationship between maternal PTSDseverity and CSD: (r-PCDI = .34, p = .003;r-CSD = .08, p = .52). When we correlatedmaternal current PTSD severity with atypicalmaternal behavior, we found a positive asso-ciation as hypothesized, but only at a trendlevel of significance (r = .20, p = .09). Finally,there was no significant association betweenmaternal PTSD and time spent in joint atten-tion during free play (r = .05, p = .69).
While depressive symptoms on theBeck Depression Inventory-II (BDI-II; Becket al., 1996) were highly correlated withboth current PTSD (r = .80, p<.001) and thePCDI (r = .35, p<.005), depressive symp-toms were not significantly associated withatypical maternal behavior (r = .15, p = .21).Clearly both maternal PTSD severity and de-pressive symptoms are powerfully associatedwith mothers' subjective sense of parent-child relationship dysfunction as a domainof parenting stress. As maternal PTSD anddepression were, however, not significantlyassociated with maternal behavior, we didnot include them further in the analyses thatfollow.
Maternal Report of Parent-ChildDysfunctional Interaction (PSI-PCDI), Child Separation Distress(CSD), and Atypical MaternalBehavior (AMBI).
In addressing our first hypothesis,we examined the relationship of maternalcurrent PTSD severity with both PSI-PCDIand CSD. We found a positive and signifi-
Following the use of the correlation-al matrix (Table 3), significantly correlatedvariables were placed in multiple regressionmodels in order to test our hypotheses. Re-
Schechter et al. 139
TABLE 4a. Predictors of Atypical Maternal Behavior (AMBIANCE) (n = 74) Unadjusted model
Unadjusted model R-square F (df 2,72) ß
0.16 5.96*
CSD
PSI-PCID
.25*
.30*
TABLE 4b. Model Above Adjusted for the CSD X PSI-PCDI Interaction
Adjusted model R-square f(df3,71)
0.16 3.50*
CSD
PSI-PCDI
CSD X PSI-PCID
0.28
.35+
0.07
Note, p < + 0.10, * 0.05, **0.01, ***0.001
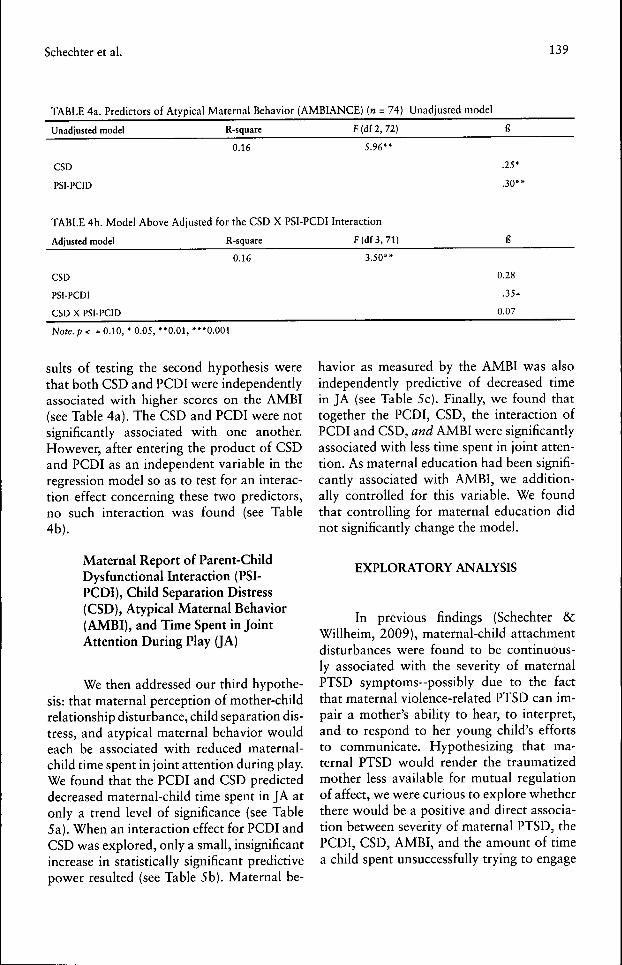
suits of testing the second hypothesis werethat both CSD and PCDI were independentlyassociated with higher scores on the AMBI(see Table 4a). The CSD and PCDI were notsignificantly associated with one another.However, after entering the product of CSDand PCDI as an independent variable in theregression model so as to test for an interac-tion effect concerning these two predictors,no such interaction was found (see Table4b).
Maternal Report of Parent-ChildDysfunctional Interaction (PSI-PCDI), Child Separation Distress(CSD), Atypical Maternal Behavior(AMBI), and Time Spent in JointAttention During Play (JA)
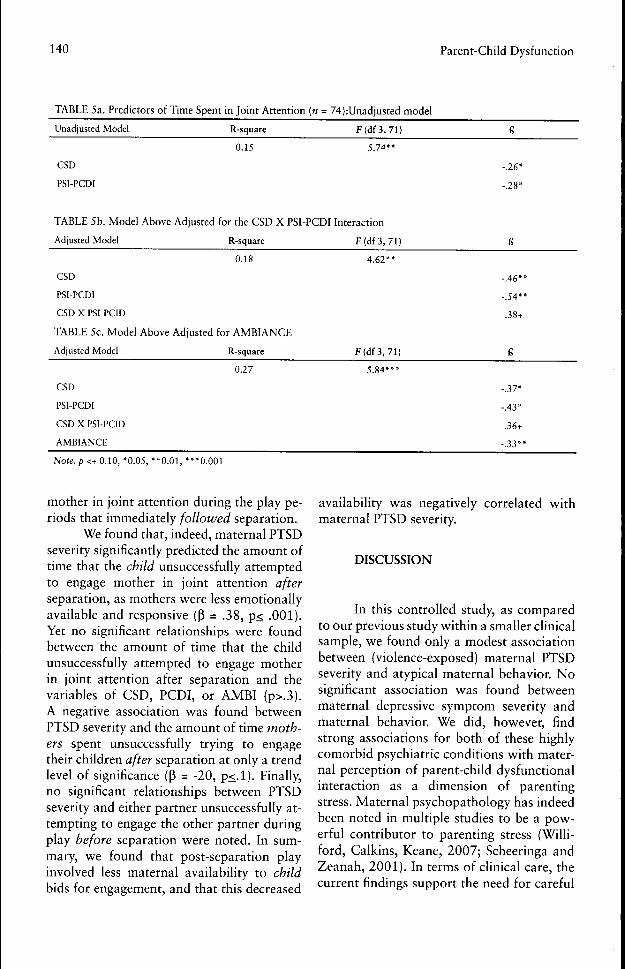
We then addressed our third hypothe-sis: that maternal perception of mother-childrelationship disturbance, child separation dis-tress, and atypical maternal behavior wouldeach be associated with reduced maternal-child time spent in joint attention during play.We found that the PCDI and CSD predicteddecreased maternal-child time spent in JA atonly a trend level of significance (see Table5a). When an interaction effect for PCDI andCSD was explored, only a small, insignificantincrease in statistically significant predictivepower resulted (see Table 5b). Maternal be-
havior as measured by the AMBI was alsoindependently predictive of decreased timein JA (see Table 5c). Finally, we found thattogether the PCDI, CSD, the interaction ofPCDI and CSD, and AMBI were significantlyassociated with less time spent in joint atten-tion. As maternal education had been signifi-cantly associated with AMBI, we addition-ally controlled for this variable. We foundthat controlling for maternal education didnot significantly change the model.
EXPLORATORY ANALYSIS
In previous findings (Schechter &cWillheim, 2009), maternal-child attachmentdisturbances were found to be continuous-ly associated with the severity of maternalPTSD symptoms-possibly due to the factthat maternal violence-related PTSD can im-pair a mother's ability to hear, to interpret,and to respond to her young child's effortsto communicate. Hypothesizing that ma-ternal PTSD would render the traumatizedmother less available for mutual regulationof affect, we were curious to explore whetherthere would be a positive and direct associa-tion between severity of maternal PTSD, thePCDI, CSD, AMBI, and the amount of timea child spent unsuccessfully trying to engage
140 Parent-Child Dysfunction
TABLE 5a. Predictors of Time Spent in Joint Attention (n = 74):Unadjusted model
Unadjusted Model R-square f (df3, 71)
0.15 5.74*
CSD
PSI-PCDI
-.26*
-.28*
TABLE 5b. Model Above Adjusted for tbe CSD X PSI-PCDI Interaction
Adjusted Model R-square F(df3,71)
CSD
PSI-PCDI
CSD X PSI-PCID
TABLE 5c. Model
Adjusted Model
CSD
PSI-PCDI
CSD X PSI-PCID
AMBIANCE
0.18
Above Adjusted for AMBIANCE
R-square
0.27
4.62**
f (df3, 71)
5.84***
-.46**
-.54**
.38+
ß
-.37*
-.43*
.36+
-.33**
Note, p <+ 0.10, *0.05, **0.01, ***0.001
mother in joint attention during the play pe-riods that immediately followed separation.
We found that, indeed, maternal PTSDseverity significantly predicted the amount oftime that the child unsuccessfully attemptedto engage mother in joint attention afterseparation, as mothers were less emotionallyavailable and responsive (ß = .38, p< .001).Yet no significant relationships were foundbetween the amount of time that the childunsuccessfully attempted to engage motherin joint attention after separation and thevariables of CSD, PCDI, or AMBI (p>.3).A negative association was found betweenPTSD severity and the amount of time moth-ers spent unsuccessfully trying to engagetheir children after separation at only a trendlevel of significance (ß - -20, p<.l). Finally,no significant relationships between PTSDseverity and either partner unsuccessfully at-tempting to engage the other partner duringplay before separation were noted. In sum-mary, we found that post-separation playinvolved less maternal availability to childbids for engagement, and that this decreased
availability was negatively correlated withmaternal PTSD severity.
DISCUSSION
In this controlled study, as comparedto our previous study within a smaller clinicalsample, we found only a modest associationbetween (violence-exposed) maternal PTSDseverity and atypical maternal behavior. Nosignificant association was found betweenmaternal depressive symptom severity andmaternal behavior. We did, however, findstrong associations for both of these highlycomorbid psychiatric conditions with mater-nal perception of parent-child dysfunctionalinteraction as a dimension of parentingstress. Maternal psychopathology has indeedbeen noted in multiple studies to be a pow-erful contributor to parenting stress (Willi-ford. Calkins, Keane, 2007; Scheeringa andZeanah, 2001). In terms of clinical care, thecurrent findings support the need for careful
Schechter et al. 141
evaluation and treatment of parental psycho-pathology.
While violent trauma-related PTSDwas significantly correlated with mothers'perception of dysfunctional interaction,there were no further direct significant re-lationships between maternal PTSD and themain variables of interest in this paper. Theone exception, found in post-hoc explor-atory analysis, was a significant associationbetween current maternal PTSD symptomseverity and greater time spent by the childunsuccessfully attempting to engage themother in joint attention during the periodof play following separation and reunion.
This finding suggests to us that ma-ternal PTSD as one extreme contributor toparental stress does indeed limit maternalavailability for joint attention in the wake ofthe acute Stressor of separation. This is con-sistent with our previous work suggestingthat the child's expression of negative emo-tion during helpless states such as separationimpacts maternal perception and behavior(Schechter et al., 2006). Indeed, we wonderwhether the interpersonal Stressor of separa-tion might even have promoted dissociativestates of mind in traumatized mothers who,prior to the separation Stressor, were able toengage in joint attention. While this area re-quires further study, we conclude that ma-ternal violence-related PTSD does have cer-tain specific consequences with respect to theparent-child relationship that are potentiallyquite important to clinical intervention. YetPTSD is but one sequela of interpersonal vio-lence that can adversely augment parentingstress and affect the parent-child relationship(Cohen et al., 2008).
Consistent with our a priori hypoth-eses, we found that there are indeed impor-tant independent effects between maternalperception of parent-child dysfunctional in-teraction as a dimension of parenting stressand atypical maternal behavior. Additional-ly, there were important independent effectsbetween the observed child level of distressduring separation and atypical maternal be-havior, although there was no statistically
significant interaction effect for dysfunction-al interaction plus child distress with atypicalmaternal behavior. This means that child dis-tress and dysfunctional interaction did notsynergistically magnify each other's effectson maternal behavior, but rather exertedtheir effects independently of one another.
In contrast to our initial hypotheses,we found that mothers' reports of dysfunc-tional interaction with their children werenot associated with the degree of their child'sseparation distress. This suggests that actualchild distress is not infiuencing maternal per-ception of dysfunction as much as her preex-isting mental representation of her child (andher child's distress) and her relationship withher child.
As predicted, all three variables-ma-ternal perception of parent-child dysfunc-tional interaction, child separation distress,and atypical maternal behavior, both in-dependently and in interaction-were sig-nificantly associated with the total amountof time mothers and their children spent injoint attention during play {prior to separa-tion). This latter set of findings supports butdoes not conclusively prove that the capacityto share in joint attention is mediated by allthree of these variables. We therefore sug-gest that in the absence of an acute Stressor,mothers' subjective view of their relationshipwith their child, their child's actual level ofdistress, and mothers' objectively observ-able behavior all contribute to the supportor impairment of mother and child's capac-ity to share in both joint attention to objects/events in their environment (i.e., learning)and intersubjective states of mind (i.e., socialcognition). These findings echo previouslypublished clinical studies among violence-exposed, traumatized and depressed caregiv-ers, and otherwise disadvantaged and adopt-ing families (Fraiberg, Adelson, & Shapiro,1975; Goldsmith & Rogoff, 1997; van Lon-den et al., 2007).
One limitation, due to the cross-sec-tional design of the present study, is the pos-sibility of an alternate interpretation of thefindings. It could be argued that both atypi-
142 Parent-Child Dysfunction
cal maternal behavior and decreased timespent in joint attention are poor caregivingoutcomes related to maternal negative anddistorted experience of her relationship withher young child. Also, the fact that the sam-ple was largely of Caribbean Hispanic ori-gin, including many immigrants, may meanthat the present findings may not be general-izable to a more diverse population. A finallimitation may be the use of the SeparationDistress Scale (Schechter & McCaw, 2005)to measure Child Separation Distress. Whiledemonstrating high interrater reliability, themeasure has yet to be validated in furtherstudies.
Finally, it was interesting to note thata greater number of years of maternal edu-cation was significantly associated with lessatypical maternal behavior. Does this meanthat one could decrease disturbances in care-giving behavior via education? Or that great-er intelligence and/or resources may help amother interpret and respond to her child'scommunication? Alternatively, could this as-sociation be a marker of resilience to psycho-pathology? Since this study lacked a prospec-tive design and larger sample, such questionsawait further investigation
REFERENCES
Abidin, R.R. (1995). Parenting Stress Index(3rd ed.). Odessa, FL: Psychological Assess-ment Resources.
Adamson, L.B., Bakerman, R., & Deckner, D.F.(2004). The development of symbol-infusedjoint engagement. Child Development, 75(4),1171-1187.
Ainsworth, M.D. & Witing, B.A. (1969). At-tachment and exploratory behavior of one-year-olds in a strange situation. In B.M. Foss(Ed.), Determination of Infant Behavior, (vol.4, pp. 113-136). London: Methuen
Beck, A.T., Steer, R.A., 8c Brown, C.K. (1996).Manual for Beck Depression Inventory -II. SanAntonio, TX: Psychological Corporation.
Blake, D.D., Weathers, FW, Nagy, L.M., Ka-loupek, D.C., Cusman, F.D., Charney, D.S.,& Keane, T.M. (1995). The development of aclinician-administered PTSD scale. Journal ofTrauma Stress, 8(1), 75-90.
Brunelli, S.A., & Hofer, M.A. (2007). Selectivebreeding for infant rat separation-induced ul-trasonic vocalizations: Developmental precur-sors of passive and active coping styles. Behav-ior and Brain Research, 182(2), 193-207.
Carlson, E.B. (1997). Trauma Assessments: AClinician's Guide. New York: The CuilfordPress, Inc.
Cohen, L.R., Hien, D.A., & Batchelder, S.(2008). The impact of cumulative maternaltrauma and diagnosis on parenting behavior.Child Maltreatment, 13(1), 27-38.
Dietz, L.J., Jennings, K.D., Kelley, S.A., &Marshal, M. (2009). Maternal depression, pa-ternal psychopathology, and toddlers' behav-ioral problems. Journal of Clinical Child andAdolescent Psychology, 38(1), 48-61.
Dutra, L., Bureau, J.F., Holmes, B., Lyubchik,A., & Lyons-Ruth, K. (2009). Quality of ear-ly care and childhood trauma: A prospectivestudy of developmental pathways to dissocia-tion. Journal of Nervous and Mental Disease,197(6), 383-390.
First, M.B., Spitzer, R.L., Gibbon, M., & Wil-liams, J.B. (1995). Structured Clinical Inter-view for DSM-IY Axis I Disorders. Washing-ton, DC: American Psychiatric Press.
Fraiberg, S., Adelson, E., & Shapiro, V. (1975).Chosts in the nursery: A psychoanalytic ap-proach to impaired infant-mother relationships.Journal of the American Academy of Child &Adolescent Psychiatry, 14(3), 387-421.
Cershoff, E.T., Aber, J.L., Raver, C.C, & Len-non, M.C. (2007). Income is not enough: In-corporating material hardship into models ofincome associations with parenting and child
Schechter et al. 143
development. Child Development, 78(1),70-95.
Goldsmith, D.F., & Rogoff, B. (1997). Moth-ers' and toddlers' coordinated joint focus ofattention: Varations with maternal dysphoricsymptoms. Developmental Psychology, 33(1),113-119.
Kochanska, G., & Coy, K.C. (2002). Childemotionality and maternal responsiveness aspredictors of reunion behaviors in the strangesituation: Links mediated and unmediated byseparation distress. Child Development, 73(1),228-240.
Kubany, E.S., Haynes, S.N., Leisen, M.B., Ow-ens, J.A., Kaplan, A.S., Watson, S.B., & Burns,K. (2000). Development and preliminary vali-dation of a brief broad-spectrum measure oftrauma exposure: The Traumatic Life EventsQuestionnaire. Psychological Assessment, 12,210-224.
Levendosky, A.A., Leahy, K.L., Bogat, G.A.,Davidson, W.S., & von Eye, A. (2006). Domes-tic violence, maternal parenting, maternal men-tal health, and infant externalizing behavior.Journal of Family Psychology, 20(4), 544-552.
Lyons-Ruth, K., Bronfman, E., & Parsons, E.(1999). Maternal frightened, frightening, oratypical behavior and disorganized infant at-tachment patterns. Monographs of the Societyfor Research on Child Development, 64(3),67-96.
Madigan, S., Moran, G., Schuengel, C , Peder-son, D.R., & Otten, R. (2007). Unresolved ma-ternal attachment representations, disruptedmaternal behavior and disorganized attachmentin infancy: Links to toddler behavior problems.Journal of Child Psychology and Psychiatry,48(10), 1042-1050.
Moll, H., Carpenter, M., & Tomasello, M.(2007). Fourteen-month-olds know what oth-ers experience only in joint engagement. Devel-opmental Science, 10(6), 826-835.
Porges, S.W. (2007). The polyvagal perspective.Biological Psychology, 74(2), 116-143.
Schechter, D.S. & McCaw, J. (2005). The Sepa-ration Distress Scale (SDS). Unpublished mea-sure, Columbia University, New York, NY
Schechter, D.S., Coates, S.W., Kaminer, T.,Coots, T., Zeanah, C.H., Davies, M., Schon-feld, I.S., Marshall, R.D., Liebowitz, M.R.,Trabka, K.A., McCaw, J.E., & Myers, M.M.(2008). Distorted maternal mental representa-tions and atypical behavior in a clinical sampleof violence-exposed mothers and their tod-dlers. Journal of Trauma and Dissociation,9(2),123-147.
Schechter, D.S., Coots, T., Zeanah, C.H., Da-vies, M.S., Coates, S.W., Trabka, K.A., Mar-shall, R.D., Liebowitz, M.R., & Myers, M.M.(2005). Mental representations of the child inan inner-city clinical sample: Violence-relatedposttraumatic stress and reflective functioning.Attachment and Human Development, 7(3),713-731.
Schechter, D.S., & Willheim, E. (2009). Dis-turbances of attachment and parental psycho-pathology in early childhood. Child and Ado-lescent Psychiatric Clinics of North America,18(3), 665-687.
Scheeringa, M.S., &c Zeanah, C.H. (2001). Arelational perspective on PTSD in early child-hood. Journal of Traumatic Stress, 14(4),799-815.
Scheeringa, M.S., Zeanah, C.H., Myers, L., &Putnam, F.W. (2003). New findings on alterna-tive criteria for PTSD in preschool children.Journal of the American Academy of Child andAdolescent Psychiatry, 42(5), 561-570.
Sheinkopf, S.J., Mundy, P., Claussen, A.H., &Willoughby, J. (2004). Infant joint attentionskill and preschool behavioral outcomes in at-risk children. Development and Psychopathol-ogy, 16(2), 273-291.
Simonoff, E., Elander, J., Holmshaw, J., Pick-les, A., Murray, R., & Rutter, M. (2004). Pre-dictors of antisocial personality: Continuitiesfrom childhood to adult life. British Journal ofPsychiatry, 184, 118-127.
144 Parent-Child Dysfunction
Skovgaard, A.M., Houmann, T., Christiansen,E., Landorph, S., Joergensen, T., et al. (2007).The prevalence of mental health problems inchildren 11/2 years of age: The CopenhagenChild Cohort 2000. Journal of Child Psychol-ogy and Psychiatry, 48(1), 62-70.
Tomasello, M., & Carpenter, M. (2007).Shared intentionality. Developmental Science,10(1), 121-125.
van Londen, W.M., Juffer, E, &C van IJzen-doorn, M.H. (2007). Attachment, cognitive,and motor development in adopted children:Short-term outcomes after international adop-tion. Journal of Pédiatrie Psychology, 32(10),1249-1258.
Vaughan van Hecke, A., Mundy, P.C., Acra,C.E, Block, J.J., Delgado, C.E., Parlade, M.V.,Meyer, J.A., Neal, A.R., & Pomares, Y.B.(2007). Infant joint attention, temperament,and social competence in preschool children.Child Development, 78(1), 53-69.
Watt, N., Wetherby, A., & Shumway, S. (2006).Prelinguistic predictors of language outcome at3 years of age. Journal of Speech, Language,and Hearing Research, 49(6), 1224-1237.
Weathers, EW., & Ford, J. (1996). Psychomet-ric properties of the PTSD Checklist (PCL-C,PCL-S, PCL-M, PCL-PR). In B.H. Stamm (Ed.),Measurement of Stress, Trauma, and Adapta-tion (pp. 250-252). Lutherville, MD: SidranFoundation & Press.
Whiteside-Mansell, L., Ayoub, C , McKelvey,L., Ealdowski, R. A., Hart, R. A., & Shears,J. (2006). Parenting stress of low-income par-ents of toddlers and preschoolers: Psychomet-ric properties of a short form of the parentingstress index. Parenting: Science and Practice, 7,27-56.
Williford, A.P., Calkins, S.D. & Keane, S.P.(2007). Predicting change in parenting stressacross early childhood: Childhood and mater-nal factors. Journal of Abnormal Child Psy-chology, 35(2), pp 257-263
Zeanah, C.H., Larrieu, J.A., Heller, S.S., &Valliere, J. (2000). Infant-parent relationshipassessment. In C.H. Zeanah (Ed.), Handbookof Infant Mental Health (pp. 222-235). NewYork: Guilford Press.
Copyright of Psychiatry: Interpersonal & Biological Processes is the property of Guilford Publications Inc. and
its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.




















