Study of impact of antitubercular therapy on quality of life
7
66 3 AND 4 ORIGINAL ARTICLES Fine needle aspiration cytology of swellings of head and neck region Gunvanti B. Rathod, Pragnesh Parmar ............ ............ 49 Evaluation of awareness about pharmacovigilance and adverse drug reaction monitoring in resident doctors of a tertiary care teaching hospital Sonali A. Pimpalkhute, K. M. Jaiswal, S. D. Sontakke, C. S. Bajait, A. Gaikwad ............ ............ 55 Variations of the gallbladder in sudanese subjects with literature review A. E. Abdalla, T. O. Ali, Assad Ali Rezigalla, M. I. Abdalla, M. Z. H. Mohamed ............ ............ 62 Fatal aluminum phosphide poisoning in Tehran-Iran from 2007 to 2010 Kambiz Soltaninejad, Lewis S. Nelson, Seyed Ali Bahreini, Shahin Shadnia ............ ............ 66 Study of impact of antitubercular therapy on quality of life Abhishek Balgude, Smita Sontakke ............ ............ 71 Acute myocardial infarction in a 28 year man with familial hypercholesterolemia Ahmed Al Montasir, Mainul Hasan Sadik ............ ............ 78 A case report of evans syndrome R. V. Dosi, A. P. Ambaliya, R. D. Patell, R. S. Patil, P. J. Shah ............ ............ 82 Gastric antral vascular ectasia with aortic stenosis: Heydes syndrome R. V. Dosi, A. P. Ambaliya, R. D. Patell, N. N. Sonune ............ ............ 86 Anesthetic management of a patient with bicuspid aortic valve and hashimoto's thyroiditis posted for abdominal hysterectomy Renuka Holyachi, Basavaraj Patil, Shivanand L. Karigar ............ ............ 90 Never underestimate simple splenic cyst Khalid Rasheed, Ajaz Ahmed Telwani, Shoukat Ali Zarger, Muhammed Yasin Mujoo ............ ............ 94 CASE REPORTS MARCH AND APRIL 2012 VOLUME NUMBER
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Study of impact of antitubercular therapy on quality of life

66
3 AND 4
ORIGINAL ARTICLES
Fine needle aspiration cytology of swellings of head and neck regionGunvanti B. Rathod, Pragnesh Parmar ............ ............ 49
Evaluation of awareness about pharmacovigilance and adverse drug reaction monitoring in resident doctors of a tertiary care teaching hospitalSonali A. Pimpalkhute, K. M. Jaiswal, S. D. Sontakke, C. S. Bajait, A. Gaikwad ............ ............ 55
Variations of the gallbladder in sudanese subjects with literature reviewA. E. Abdalla, T. O. Ali, Assad Ali Rezigalla, M. I. Abdalla, M. Z. H. Mohamed ............ ............ 62
Fatal aluminum phosphide poisoning in Tehran-Iran from 2007 to 2010Kambiz Soltaninejad, Lewis S. Nelson, Seyed Ali Bahreini, Shahin Shadnia ............ ............ 66
Study of impact of antitubercular therapy on quality of lifeAbhishek Balgude, Smita Sontakke ............ ............ 71
Acute myocardial infarction in a 28 year man with familial hypercholesterolemiaAhmed Al Montasir, Mainul Hasan Sadik ............ ............ 78
A case report of evans syndromeR. V. Dosi, A. P. Ambaliya, R. D. Patell, R. S. Patil, P. J. Shah ............ ............ 82
Gastric antral vascular ectasia with aortic stenosis: Heydes syndromeR. V. Dosi, A. P. Ambaliya, R. D. Patell, N. N. Sonune ............ ............ 86
Anesthetic management of a patient with bicuspid aortic valve and hashimoto's thyroiditis posted for abdominal hysterectomyRenuka Holyachi, Basavaraj Patil, Shivanand L. Karigar ............ ............ 90
Never underestimate simple splenic cystKhalid Rasheed, Ajaz Ahmed Telwani, Shoukat Ali Zarger, Muhammed Yasin Mujoo ............ ............ 94
CASE REPORTS
MARCH AND APRIL 2012
VOLUME
NUMBER

49
Indian Journal of Medical Sciences, Vol. 66, No. 3 and 4, March and April 2012
FINE NEEDLE ASPIRATION CYTOLOGY OF SWELLINGS OF HEAD AND NECK REGION
GUNVANTI B. RATHOD, PRAGNESH PARMAR1
ABSTRACT
Head and neck mass lesions are frequently found in clinical practice. A spectrum of pathological lesions ranging from simple benign lesion to highly malignant manifestation is observed. OBJECTIVES: To make clinicopathological correlation of head and neck lesions and to assess the frequency of incidences of different sites, age groups, sex, and distribution among inflammation and neoplastic lesion. MATERIALS AND METHODS: A retrospective study was conducted from January 2011 to April 2012. Fine‑needle aspiration diagnosis was correlated with details of relevant clinical findings and investigations. Patients aged between 1 and 70 years were included in the study. A total of 200 patients with the swellings of head and neck underwent fine‑needle aspiration cytology (FNAC). RESULTS: Out of 200 fine‑needle aspiration procedures, 52% were of thyroid, 28.50% were of lymph node, 11% from salivary gland, and 4% from soft tissue and miscellaneous swellings. There were 4.5% cases in which diagnosis was not possible. In inflammatory swelling (33%), tuberculous lymph node (42.12%) involvement is common than all other sites with male preponderance (55%). CONCLUSION: FNAC is a simple, quick, inexpensive, and minimally invasive technique to diagnose different types of head and neck swellings. It could differentiate the infective process from neoplastic one and avoids unnecessary surgeries. Thus, FNAC can be recommended as a first line of investigation in the diagnosis of head and neck swellings.
Key words: Fine‑needle aspiration cytology, head and neck swellings, thyroid lesions
ORIGINAL ARTICLE
Departments of Pathology and 1Forensic Medicine, Mahatma Gandhi Medical College and Research Institute, Pondicherry, India
Address for correspondence: Dr. Gunvanti B. Rathod, Department of Pathology, Mahatma Gandhi Medical College and Research Institute, Pondicherry ‑ 607 402, India. E‑mail: [email protected]
INTRODUCTION
In 1930, two doctors from a New York hospital, Martin and Colley, and a technical developer, Ellis, conducted aspirations from several organs and carried out cytological studies
on them.[1‑4] Fine‑needle aspiration cytology (FNAC) is a simple, quick, and cost‑effective method to sample superficial masses found in the head and neck.[5] FNAC is also widely used in the head and neck regions, such as in the
Access this article onlineQuick Response Code: Website:
www.indianjmedsci.org
DOI:10.4103/0019-5359.110896PMID:
*****************************
Azhar
Rectangle

50 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 66, No. 3 and 4, March and April 2012
thyroid, lymph nodes, major salivary glands, and other neoplasias.[2,4,6‑8] In the head and neck regions, FNAC is of great value because of the multiplicity of accessible organs and heterogeneous pathologies encountered. An early differentiation of benign from malignant pathology greatly influences the planned treatment.[9]
MATERIALS AND METHODS
In this study, FNAC was performed in 200 patients presented with lesions in the head and neck regions. All the patients of study were from the otorhinolaryngology, pediatric, and surgery departments. All patients were asked about history related to neck swelling and relevant questions to the etiological cause along with present, past, and family history of tuberculosis and history of sexual exposure for syphilis and AIDS. Patients were explained about the procedure and its advantages and their oral consent was taken. The area to be aspirated was cleaned with spirit and a 23‑gauge needle with syringe and trocar was inserted at convenient angles to the lesions and multiple hits were made within the lesion, with sufficient negative pressure; the needle was removed and the pressure was applied to the area of aspiration to avoid bleeding or hematoma formation. The technique was performed in the outpatient department with minimal trauma to the patient without any risk of complication. The aspirated material was smeared on minimum two clean glass slides and later, they were either wet‑dried or air‑dried as per the staining procedure adopted. Smears were stained by Giemsa and Pap stain and special stains were carried out as and when required.
RESULTS
The study included 200 cases ranged from 1 to 70 years of age in which 59% were male and 41% were female. Maximum incidences observed in the age group of 21‑30 years and out of 200 cases, 174 were below 50 years of age. Among the diagnostic outcome, higher incidence of lesion was in the neck region than in the head region.
Incidence of thyroid lesions was highest in 104 cases (52%) than other lesions in head and neck regions. Overall, incidence of thyroid lesions was proportionately more in females (84.61%). Totally, 57 cases (28.50%) were of lymph node involvement among which male preponderance was noted in 32 cases (56.14%). Out of 22 cases of salivary gland lesions, incidence of pleomorphic adenoma (36.36%) was highest. Incidence of keratinous cyst was highest followed by lipoma among soft tissue and miscellaneous lesions in our study as shown in Table 1.
Out of 104 cases of thyroid lesions, 70 cases (67.30%) were having benign neoplastic lesions. Totally, 21 cases (20.19%) were having inflammatory lesions, which include Hashimoto’s thyroiditis [Figures 1 and 2], de Quervain’s thyroiditis, and chronic lymphocytic thyroiditis. One case of medullary carcinoma, one case of anaplastic carcinoma, and 11 cases of papillary carcinoma [Figures 3 and 4] were noted in our study as malignant thyroid lesions as shown in Table 2.
Out of 57 cases of lymph node lesions, 24 cases (42.11%) were having tuberculous inflammation. Out of 14 malignant cases (24.55%), metastatic lesions were the

51FINE‑NEEDLE ASPIRATION CYTOLOGY OF SWELLINGS OF HEAD AND NECK
Indian Journal of Medical Sciences, Vol. 66, No. 3 and 4, March and April 2012
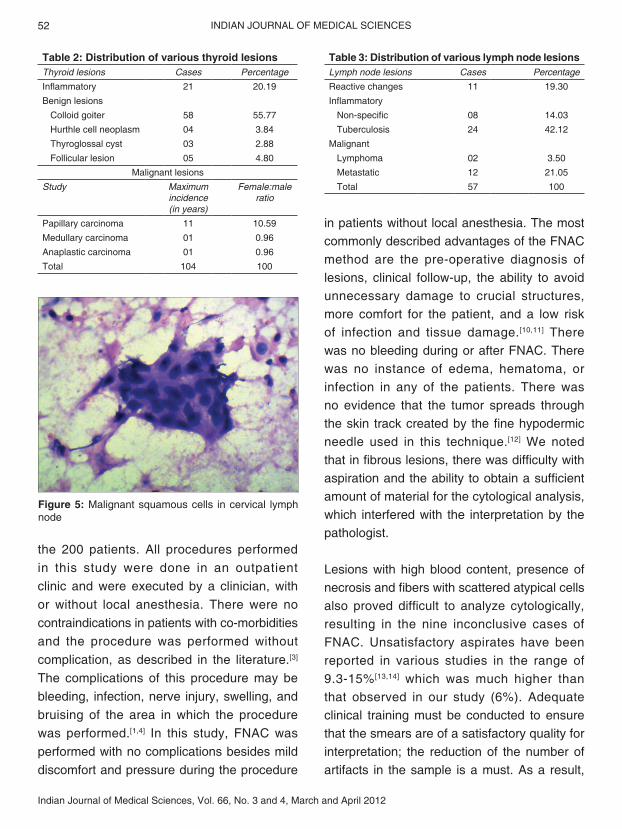
highest which include metastatic squamous cell carcinoma [Figure 5] and metastatic adenocarcinoma as shown in Table 3.
DISCUSSION
In this study, FNAC was performed in swellings of the head and neck regions of
Table 1: Case distribution of head and neck lesionsOrgan involved Total cases Inflammation Neoplastic lesions
Non‑specific Tuberculosis Benign MalignantThyroid 104 21 ‑ 70 13Lymph node 57 08 24 11 14Salivary gland 22 09 ‑ 10 03Soft tissue and miscellaneous 08 02 ‑ 06 ‑Inconclusive 09 ‑ ‑ ‑ ‑Total 200 66 ‑ 104 30
Figure 1: Hashimoto’s thyroiditis: Pronounced lymphocytic infiltration with hurthle change of the follicular epithelium. (Pap stain, ×10)
Figure 4: Papillary carcinoma: Intra nuclear inclusions (H and E, ×40)Figure 3: Papillary carcinoma: The nuclei are enlarged
and variable in size with intra nuclear inclusions and grooving (Pap stain, ×40)
Figure 2: Hashimoto’s thyroiditis: Groups of hurthle cells with inflammatory cells (May grunwald giemsa stain, ×40)
52 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 66, No. 3 and 4, March and April 2012
the 200 patients. All procedures performed in this study were done in an outpatient clinic and were executed by a clinician, with or without local anesthesia. There were no contraindications in patients with co‑morbidities and the procedure was performed without complication, as described in the literature.[3] The complications of this procedure may be bleeding, infection, nerve injury, swelling, and bruising of the area in which the procedure was performed.[1,4] In this study, FNAC was performed with no complications besides mild discomfort and pressure during the procedure
in patients without local anesthesia. The most commonly described advantages of the FNAC method are the pre‑operative diagnosis of lesions, clinical follow‑up, the ability to avoid unnecessary damage to crucial structures, more comfort for the patient, and a low risk of infection and tissue damage.[10,11] There was no bleeding during or after FNAC. There was no instance of edema, hematoma, or infection in any of the patients. There was no evidence that the tumor spreads through the skin track created by the fine hypodermic needle used in this technique.[12] We noted that in fibrous lesions, there was difficulty with aspiration and the ability to obtain a sufficient amount of material for the cytological analysis, which interfered with the interpretation by the pathologist.
Lesions with high blood content, presence of necrosis and fibers with scattered atypical cells also proved difficult to analyze cytologically, resulting in the nine inconclusive cases of FNAC. Unsatisfactory aspirates have been reported in various studies in the range of 9.3‑15%[13,14] which was much higher than that observed in our study (6%). Adequate clinical training must be conducted to ensure that the smears are of a satisfactory quality for interpretation; the reduction of the number of artifacts in the sample is a must. As a result,
Table 2: Distribution of various thyroid lesionsThyroid lesions Cases PercentageInflammatory 21 20.19Benign lesions
Colloid goiter 58 55.77Hurthle cell neoplasm 04 3.84Thyroglossal cyst 03 2.88Follicular lesion 05 4.80
Malignant lesionsStudy Maximum
incidence (in years)
Female:male ratio
Papillary carcinoma 11 10.59Medullary carcinoma 01 0.96Anaplastic carcinoma 01 0.96Total 104 100
Table 3: Distribution of various lymph node lesionsLymph node lesions Cases PercentageReactive changes 11 19.30Inflammatory
Non‑specific 08 14.03Tuberculosis 24 42.12
MalignantLymphoma 02 3.50Metastatic 12 21.05Total 57 100
Figure 5: Malignant squamous cells in cervical lymph node

53FINE‑NEEDLE ASPIRATION CYTOLOGY OF SWELLINGS OF HEAD AND NECK
Indian Journal of Medical Sciences, Vol. 66, No. 3 and 4, March and April 2012
the experience of the pathologist for interpreting these patterns in the cell smears should be considered. The presence of a pathologist at the time of sample collection, as well as during the staining for the rapid interpretation, may help the clinician at the time of aspiration. This can, therefore, help to minimize the rate of inconclusive cases.
Out of 200 FNAC procedures, 52% cases are of thyroid lesion with female preponderance (84.61%). Maximum incidence of thyroid les ions was found in the age group of 20‑30 years while in Charry’s study,[15] maximum incidence was between 20 and 40 years. In Charry’s study[15] and in this study, female: male ratio was 4:1, whereas in Pranesh Prasad’s study,[16] it was 5:1 as shown in Table 4. Female preponderance in various thyroid lesions was comparatively well observed in this study. Highest incidence of benign thyroid lesions diagnosed in our study was colloid goiter (55.77%) and malignant lesions were papillary carcinoma.
Tuberculous lymphadenitis was found to be the most common pathology of lymph node lesions in our study accounting for 42.12% of cases followed by metastatic carcinoma found in 21.05% of cases and reactive/non‑specific lymphadenitis constituting 19.30% of cases. El Hag, et al.[17] carried out a similar study in Saudi Arabia over a period of 5 years which included 225 patients which showed reactive/
non‑specific lymphadenitis to be the commonest cause of neck masses accounting for 33% of cases. Tuberculous lymphadenitis was found to be the next most common pathology constituting 21% of cases followed by malignant swellings found in 13% of cases. Pleomorphic adenoma is the commonest tumor of salivary gland. In this study, out of 22 cases of salivary gland lesions, 9 cases were of pleomorphic adenoma.
Commonest malignancy in the salivary gland tumor was mucoepidermoid carcinoma which was compared with Michael Cohen’s study[18] as shown in Table 5. All cases of FNAC were subsequently confirmed either by follow‑up for a minimum of 12 months or by surgical biopsy wherever needed. Overall, the procedure was simple and rapid obviating the need of surgical intervention.
CONCLUSION
Nowadays, with increasing cost of medical facilities, any technique which speeds up the process of diagnosis, limits the physical and psychological trauma to the patient, and saves the expenditure of hospitalization, will be of tremendous value. It may also help the surgeon to select, guide, and modify surgical planning in patients requiring surgery. Our study found that FNAC is a simple, quick, inexpensive, and minimally invasive technique to diagnose different types of head and neck swellings. It could differentiate the infective process from neoplastic one and avoids unnecessary Table 4: Study of relationship of thyroid lesions
with age and sexStudy Maximum
incidence (in years)Female:male
ratioCharry[15] 20‑40 4:1Pranesh Prasad[16] 30‑50 5:1This study 20‑30 4:1
Table 5: Comparison study of mucoepidermoid carcinomaStudy PercentageMichael, Cohen[18] 35This study 13.63

54 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 66, No. 3 and 4, March and April 2012
surgeries. Thus, FNAC can be recommended as a first line of investigation in the diagnosis of head and neck swellings.
ACKNOWLEDGMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals, and books from where the literature for this article has been reviewed and discussed.
REFERENCES
1. Costas A, Castro P, Martín‑Granizo R, Monje F, Marrón C, Amigo A. Fine needle aspiration biopsy (FNAB) for lesions of the salivary glands. Br J Oral Maxillofac Surg 2000;38:539‑42.
2. Amedee RG, Dhurandhar NR. Fine‑needle aspiration biopsy. Laryngoscope 2001;111:1551‑7.
3. Fulciniti F, Califano L, Zupi A, Vetrani A. Accuracy of fine needle aspiration biopsy in head and neck tumors. J Oral Maxillofac Surg 1997;55:1094‑7.
4. Kline TS. Handbook of Fine Needle Aspiration Biopsy Cytology. 2nd ed. New York: Churchill Livingstone; 1988. p. 492.
5. Orell SR, Sterrett GF, Walters NI, Whitaker D. Manual and Atlas of FNAC, 2nd ed. New York: Churchill Livingstone; 1995. p. 250.
6. Florentine BD, Staymates B, Rabadi M, Barstis J, Black A; Cancer Committee of the Henry Mayo Newhall Memorial Hospital. The reliability of fine‑needle aspiration biopsy as the initial diagnostic procedure for palpable masses: A 4‑year experience of 730 patients from a community hospital‑based outpatient aspiration biopsy clinic. Cancer 2006;107:406‑16.
7. Batra M, Wadhwa N, Mishra K. Cytologic diagnosis in benign odontogenic tumor with abundant calcification: A case report. Acta Cytol 2009;53:460‑2.
8. C a r r i l l o J F , R a m í r e z R , F l o r e s L , Ramirez‑Ortega MC, Arrecillas MD, Ibarra M, et al. Diagnostic accuracy of fine needle aspiration biopsy in preoperative diagnosis of patients with parotid gland masses. J Surg Oncol 2009;100:133‑8.
9. Watkinson JC, Wilson JA, Gaze M, Stell PM, Maran AGD. Stell and Maran’s Head and Neck Surgery. 4th ed. Oxford: Butterworth Heinemann; 2000. p. 20‑1.
10. Saleh HA, Clayman L, Masri H. Fine needle aspiration biopsy of intraoral and oropharyngeal mass lesions. Cytojournal 2008;5:4.
11. Shah SB, Singer MI, Liberman E, Ljung BM. Transmucosal fine‑needle aspiration diagnosis of intraoral and intrapharyngeal lesions. Laryngoscope 1999;109:1232‑7.
12. Russel RC, William NS, Bulstrode CJ. Bailey and Love's Short Practice of Surgery. 24th ed. London: Arnold; 2004. p. 950.
13. Smallman LA, Young JA, Oates J, Proops DW, Johnson AP. Fine needle aspiration cytology in the management ENT of patients. J Laryngol Otol 1988;102:909‑13.
14. Sismanis A, Strong MS, Merriam J. Fine needle aspiration biopsy diagnosis of neck masses. Otolaryngol Clin North Am 1980;13:421‑9.
15. Charry AK. Role of FNAB in thyroid swelling. Indian J Surg 1980;346‑8.
16. Pranesh Prasad. Comparative study of FNAC and histopathology in diagnosis of thyroid swellings. Indian J Surg 1992;54:287‑91.
17. el Hag IA, Chiedozi LC, al Reyees FA, Kollur SM. Fine needle aspiration cytology of head and neck masses. Seven years’ experience in a secondary care hospital. Acta Cytol 2003;47:387‑92.
18. Cohen MB, Fisher PE, Holly EA, Ljung BM, Löwhagen T, Bottles K. Fine needle aspiration biopsy diagnosis of mucoepidermoid carcinoma. Statistical analysis. Acta Cytol 1990;34:43‑9.
How to cite this article: Rathod GB, Parmar P. Fine needle aspiration cytology of swellings of head and neck region. Indian J Med Sci 2012;66:49‑54.Source of Support: Nil. Conflict of Interest: None declared.