Stored red blood cells: A changing universe waiting for its map(s)
12
Review Stored red blood cells: A changing universe waiting for its map(s) Niels Lion a,b, ⁎ , David Crettaz a , Olivier Rubin a , Jean-Daniel Tissot a a Service Régional Vaudois de Transfusion Sanguine, Lausanne, Switzerland b Laboratoire d'Electrochimie Physique et Analytique (LEPA), Ecole Polytechnique Fédérale de Lausanne (EPFL), Switzerland ARTICLE INFO ABSTRACT Article history: Received 29 June 2009 Accepted 4 November 2009 The availability of stored red blood cells (RBCs) for transfusion remains an important aspect of the treatment of polytrauma, acute anemia or major bleedings. RBCs are prepared by blood banks from whole blood donations and stored in the cold in additive solutions for typically six weeks. These far from physiological storage conditions result in the so-called red cell storage lesion that is of importance both to blood bankers and to clinical practitioners. Here we review the current state of knowledge about the red cell storage lesion from a proteomic perspective. In particular, we describe the current models accounting for RBC aging and response to lethal stresses, review the published proteomic studies carried out to uncover the molecular basis of the RBC storage lesion, and conclude by suggesting a few possible proteomic studies that would provide further knowledge of the molecular alterations carried by RBCs stored in the cold for six weeks. © 2009 Published by Elsevier B.V. Keywords: Red blood cell RBC Erythrocyte Senescence Blood banking Eryptosis Band 3 clustering Blood storage lesion RBC microvesicle Contents 1. Introduction .......................................................... 375 2. Facts about the red cell storage lesion ............................................ 375 3. Known senescence pathways ................................................ 377 3.1. The eryptosis model ................................................. 377 3.2. The Band 3 clustering model ............................................. 378 4. Relevance to the red cell storage lesion ........................................... 380 5. Proteomic insights into red cell storage lesion ........................................ 380 6. Conclusion ........................................................... 381 References ............................................................. 382 JOURNAL OF PROTEOMICS 73 (2010) 374 – 385 ⁎ Corresponding author. Service Régional Vaudois de Transfusion Sanguine, route de la Corniche 2, CH1066 Epalinges, Switzerland. Fax: +41 21 314 65 78. E-mail address: [email protected] (N. Lion). 1874-3919/$ – see front matter © 2009 Published by Elsevier B.V. doi:10.1016/j.jprot.2009.11.001 available at www.sciencedirect.com www.elsevier.com/locate/jprot
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Stored red blood cells: A changing universe waiting for its map(s)

J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r . com/ loca te / j p ro t
Review
Stored red blood cells: A changing universe waitingfor its map(s)
Niels Liona,b,⁎, David Crettaza, Olivier Rubina, Jean-Daniel Tissota
aService Régional Vaudois de Transfusion Sanguine, Lausanne, SwitzerlandbLaboratoire d'Electrochimie Physique et Analytique (LEPA), Ecole Polytechnique Fédérale de Lausanne (EPFL), Switzerland
A R T I C L E I N F O
⁎ Corresponding author. Service Régional VaFax: +41 21 314 65 78.
E-mail address: niels.lion@mavietonsang.
1874-3919/$ – see front matter © 2009 Publisdoi:10.1016/j.jprot.2009.11.001
A B S T R A C T
Article history:Received 29 June 2009Accepted 4 November 2009
The availability of stored red blood cells (RBCs) for transfusion remains an important aspectof the treatment of polytrauma, acute anemia or major bleedings. RBCs are prepared byblood banks from whole blood donations and stored in the cold in additive solutions fortypically six weeks. These far from physiological storage conditions result in the so-calledred cell storage lesion that is of importance both to blood bankers and to clinicalpractitioners. Here we review the current state of knowledge about the red cell storagelesion from a proteomic perspective. In particular, we describe the current modelsaccounting for RBC aging and response to lethal stresses, review the published proteomicstudies carried out to uncover themolecular basis of the RBC storage lesion, and conclude bysuggesting a few possible proteomic studies that would provide further knowledge of themolecular alterations carried by RBCs stored in the cold for six weeks.
© 2009 Published by Elsevier B.V.
Keywords:Red blood cellRBCErythrocyteSenescenceBlood bankingEryptosisBand 3 clusteringBlood storage lesionRBC microvesicle
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3752. Facts about the red cell storage lesion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3753. Known senescence pathways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 377
3.1. The eryptosis model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3773.2. The Band 3 clustering model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
4. Relevance to the red cell storage lesion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3805. Proteomic insights into red cell storage lesion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3806. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 382
udois de Transfusion Sanguine, route de la Corniche 2, CH1066 Epalinges, Switzerland.
ch (N. Lion).
hed by Elsevier B.V.

375J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
1. Introduction
Red blood cell (RBC) transfusion is a life-saving procedurewhose primary objective is to sustain tissue and organoxygenation in case of massive haemorrhage, or acuteanemia, often associated with hypovolemia. In Switzerlandalone (6.5 million inhabitants), approximately 300,000 eryth-rocyte concentrates (ECs) are delivered each year to patients.ECs are obtained from whole blood donation, and as in manyother countries, blood donation is a voluntary act without anypayback. On one hand, blood supply thus highly depends onthe ability of blood banks to recruit donors. In Switzerland, it isestimated that 2–3% of the population give blood (source:Swiss Red Cross).
After blood collection in anticoagulants (typically CPD,citrate-phosphate-dextrose), ECs are prepared by plasmaremoval and leucocyte depletion, and RBCs are stored inadditive solutions, most often slightly hypertonic SAGM(sodium–adenine–glucose–mannitol, 376 mOsm/L) or isotonicPAGGSM (phosphate–adenine–glucose-guanosin–saline–man-nitol, 285 mOsm/L) at 4 °C. The storage duration is legallydefined as the time after which 70–75% of transfused RBCssurvive in the recipient's blood flow 24 h after transfusion.This storage duration depends on the additive solution used;for example it is most often 42 days for SAGM and 50 days forPAGGSM. This limited storage duration has implications forblood bankers, because it is our experience that at least inurban areas, seasonal near-shortage situations can occasionn-ally occur when donors are in holidays, typically in mid-summer and during the Christmas break. Prolonged storageduration would thus smooth these seasonal effects.
More importantly, these far from physiologic storageconditions result in alterations in stored RBCs; no one canexpect that RBCs stored in vitro for 42 days at 4 °C in additivesolutions be as functional as fresh RBCs just punctured from adonor. Storing RBCs for transfusion thus consists in minimiz-ing deleterious alterations. Following others, Bennett-Guer-rero et al. have identified severemacroscopic changes in bloodbags during storage, such as increases in potassium, lactate,and Hb oxygen saturation, as well as concomitant decrease inpH, 2,3-diphosphoglycerate (2,3-DPG), and RBC deformability;some of these alterations occur within the first hours ofstorage, such as the pH drop, lactate and potassium increases,whereas others occur over a few days [1–3]. Not surprisingly,these macroscopic changes are accompanied by a number ofcellular and molecular changes that alter the integrity ofstored RBCs (see below). These phenomena, collectivelyknown as the red cell storage lesion, are of importance notonly for blood bankers, but also to clinical practitioners: thereis indeed accumulating evidence that the storage durationdoes make a difference in the biomedical value of a blood bag.A recent example of this has been provided by Koch et al., whoclearly demonstrated that patients having received transfu-sion in the course of cardiac surgery had different recoveriesdepending on the age of the blood bags they received [4]. It is afact that this study has been criticized in its design andstatistical analysis, and it is a general consensus that there isno sound body of clinical evidence of the detrimental effect oftransfusion of older red blood cells [5]. However, this kind of
study raises questions from clinical practitioners to bloodbankers about the quality of the products delivered topatients. What makes a biomedical difference between anolder unit of red blood (stored for 42 days) and a fresher one isstill a matter of debate; basically, the age of blood bags maycontribute to decreased biomedical efficiency through threeaspects: decreased oxygenation capacity, release of damagingconstituents (such as free Hb that can act as a circulatingsource of reactive oxygen species, ROS, or chemokines), orhampered circulation capacity (through adhesion to theendothelial surface and then proinflammatory properties,for example) [6]. Another possible consequence of the RBCstorage lesion is the generation of allo- or autoantibodiesagainst erythrocyte antigens by the transfusion recipient.Immunization occurs in approximately 10% of transfusedpatients by a yet unknown mechanism; but the patient'sinflamation status clearly plays a role in the immunization.This phenomenon parallels the fact that asmuch as 25–30% oftransfused RBCs are rapidly cleared from the recipient's bloodflow; despite active research in the last decades, no evidentparameter discriminates these 25–30% RBCs in the blood bagsthat are bound to be rapidly cleared, which tends to indicatethat more subtle clearance mechanisms are at work such asthe ones that participate in the physiological control of RBClifespan.
The gist of this review is to describe the state of knowledgein the red cell storage lesion from a proteomic perspective.Recent reviews have been published that are more focused ontransfusionmedicine [7,8]. We will first outline the alterationsor senescence pathways known from in vivo and in vitrophysiological and toxicological studies ; in the second part ofthis review, we will review in detail the proteomic approachesto the red cell storage lesion, and propose a few complemen-tary studies that would provide insight into molecularmechanisms at work during blood storage.
2. Facts about the red cell storage lesion
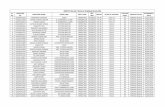
As mentioned above, stored RBCs undergo a number ofalterations during storage in blood banking conditions. Themost striking one is the change of shape undergone by afraction of RBCs, from the normal smooth discoid shape to anechinocyte shape or spheroid shape with specula, as shown inFig. 1 [9]. These shape changes are first reversible bytransfusion, but become irreversible at the end of the storageperiod [2].
A more subtle effect of storage on RBCs that has a directimpact on their function is the loss of S-nitrosothiol-haemo-globin (SNO-Hb): in the circulation, vasodilatation is controlledby NO. When the local oxygen tension is low, erythrocytesproduce NO that induces local vasodilatation and allow theRBC flow to match the oxygen demand. The pioneeringobservation that SNO-Hb was elevated in the arterial flowand decreased in the venous flow [10] led to the stronghypothesis that SNO-Hb was involved in the generation of NOby the erythrocytes. Whereas this hypothesis is now ques-tioned by mutational analysis [11,12], there is still a largeconsensus than SNO-Hb plays an important role in thegeneration of NO by erythrocytes. At the same time there is

Fig. 1 – Evolution of a fraction of stored RBCs during storage. Evolution froma smooth discoid shape (top left) to echinocytes (top right)and spheroid shape with specula (bottom). Reproduced from [9] with permission.
376 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
definitive evidence that SNO-Hb disappears from stored bloodjust a few days after collection [1,13], and that this decline inSNO-Hb correlates with a loss of vasodilatory activity of storedRBCs.
More classical are the observed fluxes of sodium andpotassium: at the storage temperature of 4 °C, the Na+/K+
pump is inactive, resulting in an influx of sodium into theerythrocytes and a massive loss of K+ in the storage medium[1], which makes massive transfusion risky for newborns orinfants, for whom cell washing or removal of the storagemedium is necessary [14]. After transfusion, the recovery ofnormal sodium concentration inside the cell typically takes24 h, whereas normalisation of potassium concentration cantake up to four days [15].
Another key feature of the RBC storage is the almostdisappearance of 2,3-diphosphoglycerate over one week ofstorage [1]; 2,3-DPG is a glycolytic intermediate that binds tohaemoglobin to modulate its affinity for oxygen. Higher 2,3-DPG concentration allosterically favours O2 release fromhaemoglobin, whereas lower 2,3-DPG concentration increasesthe affinity of haemoglobin for oxygen. The disappearance of2,3-DPG from RBCs thus impedes the ability of haemoglobin todeliver oxygen. Cho et al. recently demonstrated that a yetunknown 2,3-DPG phosphatase that is still fully active at 4 °C,
might be responsible for the rapid clearance of 2,3-DPG inbanked erythrocytes [16]. 2,3-DPG recovery after transfusiontypically occurs at the following rate: 25–30% after 1 h, 50%after 24 h and 100% after three days [17,18].
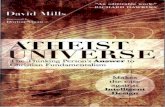
Another important feature of RBC storage in blood bankingconditions is the shedding of microvesicles. Microvesicles arephospholipid-rich vesicles of less than 0.5 μm that are emittedby RBCs (as by many other cell types in vivo). Thoughmicrovesicle emission seems to be a controlled process, theirfunctions are still unknown; they might be a way for viablecells to get rid of deleterious compounds (see below) thatwould otherwise trigger definitive cell lesions or target thecells to the clearance system [19]. Fig. 2 shows the increase inthe concentration of microvesicles in blood bags that has beenobserved in our laboratory [20], as well as by others [21].
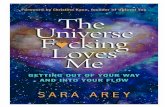
Kriebardis et al. studied the localisation of Band 3, acarbonate/chloride exchanger and the most abundant proteinof the RBCmembrane; they found that upon storage, the Band3 cytosolic part appears in the whole cytosol, demonstrating acleavage of the N-terminus of the protein and loss oflocalisation, as shown in Fig. 3. Concomitantly, the sameauthors evidenced the accumulation of IgGs at the cell surface,as well as a reorganisation of lipid raft proteins such asstomatin and flotillins [22]. The same authors, following

Fig. 2 – Increase in the concentration of microvesicles duringstorage of RBCs in SAGM(sodium–adenine–glucose–mannitol) at 4 °C. Values aremean±standard deviation over 7 samples. Reproduced withpermission from [20].
377J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
classical studies [23], demonstrated an accumulation ofoxidatively damaged membrane proteins throughout storage[24], aswell as an accumulation and clustering of haemoglobindimers at the internal side of the plasma membrane [25].
Membrane reorganisation is accompanied in some cases byphosphatidylserine (PS) exposure to the outer leaflet of theplasma membrane. Normally PS is sequestered to the innerleaflet of theplasmamembraneby a complex systemcomposedof flippase, floppase and scamblase. There is no clear consensusif a fraction of stored erythrocytes exhibits this PS exposure:some authors observed PS exposure [26], typically by flowcytometric analysis of Annexin binding, whereas others did not[27]. In most cases, PS exposure was observed after inducingspecific stresses in vitro that are hypothesised to mimic RBCsenescence, but the relevance of these observations to sponta-neousRBC alterations during storage remains questionable [28].
Lastly, Sparrow et al. studied the binding of RBCs to variouslectins throughout storage, and found that various lectinsbound differently to RBCs depending on the storage duration:whereas the binding of lectins specific for (α-2,3)-linked sialicacids showed no difference in the course of storage, thebinding of lectins to N-acetylglucosamine and (α-2,6)-linkedsialic acids showed marked difference between the beginningof storage (day 1) and the end of storage (day 42) [29]. The studywas further complicated by the difference in lectin bindingaccording to the age of erythrocytes at collection: whereas
Fig. 3 – Localisation of the N-terminal, cytosolic part of Band 3 thrstorage. Right: erythrocyte stored for 30 days in blood banking co
young and old erythrocytes had the same lectin bindingbehaviour for N-acetylglucosamine and (α-2,6)-linked sialicacids throughout storage, a marked difference was found withregards to (α-2,3)-linked sialic acids. Put together with otherstudies [30], these results point out the probable remodellingof surface carbohydrates during storage.
In summary, stored RBCs undergo a wide range ofalterations, from shape, metabolic status, surface carbohy-drate exposure, membrane organisation, microvesicle shed-ding… This inventory “à la Prévert” points out the difficulty inorganising this heterogeneous data into a coherent model ofRBC alteration during blood banking. The following section ofthe present paper aims at describing the models that havebeen proposed to account for RBC alterations.
3. Known senescence pathways
RBC is totally devoid of protein synthesis capability; all itsphysiology thus depends on proteins and enzymes present atthe end of its maturation from reticulocytes. This fixedmolecular machinery is responsible for the main function ofRBCs (i.e. oxygen delivery), for cell survival (maintenance ofosmotic homeostasis, membrane integrity, energy productionfrom glycolysis...), and response to external stresses (such asosmotic shock, exposure to toxics, or oxidative stress, seebelow). Given the static nature of the RBC proteome andenzymatic repertoire, it is not surprising that it undergoesprogressive loss of function during its lifespan of 120±4 daysin the circulation (such as increased cytoskeleton rigidity,decreased glycolysis rates...). Two major pathways or senes-cence models have been proposed to describe RBCs alterationand response to stresses in vivo, namely the eryptosis model,and the Band 3 clustering model.
3.1. The eryptosis model
The term “eryptosis” has been introduced a few years ago byFlorian Lang to describe a set of mechanisms at work in RBCsin response to various stresses, that closely resemblesclassical apoptosis pathways. Common to all studies is alarge influx of ionic calcium as a very initial event in RBCinjury [31–38]. Reasons for this calcium intake are largelyunknown, but altered activity of non-specific (NS) cationchannels is often mentioned as a possible cause. As shownin [39], one documented activation of non-specific cationchannels can occur through prostaglandin E2 stimulation, thatcan be synthesized by the phospholipase A2/cyclooxygenase
oughout storage. Left: control erythrocyte at the beginning ofnditions. Reproduced from [22] with permission.

378 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
(COX) system in response, for example, to an osmotic shock.Synthesis of PGE2 has been reported to be induced by exposureto high osmolarity [39]; in this case, PGE2 may activate NScation channels whether intracellularly, or after secretionthrough the multidrug resistant protein 4. The same stimulusresults in the synthesis of the platelet-activating factor (PAF)that can activate sphingomyelinase, thus producing ceramideand disrupting the RBC membrane organisation [40], and alsosensitize Gardos channels to Ca2+ activation.
Elevation of intracellular Ca2+ concentration leads to directactivation of the Gardos channels and thus to loss of K+, Cl−
and water, activation of scramblase, which perturbs thenormal asymmetry of RBC membrane and leads to phospha-tidylserine externalization [41,42]. Intracellularly, Ca2+ influxalso activates calpains [43,44], a family of cysteine proteasesthat is physiologically inhibited by the binding of calpastatin.Upon calpastatin release and calciumbinding, calpains bind tothe inner side of the membranes, where they degradecytoskeletal proteins, such as proteins 2.1 and 4.1 andspectrin. Calcium increase also directly activates transgluta-minase 2 (TG2), which crosslinks proteins of the cytoskeleton[45,46]. The combined action of calpain degradation and TG2 ismost probably responsible for the loss of cytoskeletonplasticity and cellular deformability. Of importance is alsothe role of calcium in the disruption of the interaction betweenBand 3, a major membrane protein and anion exchanger, withprotein tyrosine phosphatase 1B (PTP1B); in physiologicalconditions, PTP1B binds to the cytoplasmic domain of Band 3and maintains the phosphorylation status of two tyrosines[47–49]. When the interaction is disrupted by calcium, SRCkinase syk and kinases lyn remain unchallenged and thephosphorylation status of the cytoplasmic domain of Band 3 ismodified. The role of these tyrosine phosphorylations is notfully understood, but as the cytoplasmic domain of Band 3plays multiple roles in the anchorage with the cytoskeleton(through interaction with protein 4.2 and spectrin), binding ofglycolytic enzymes, and binding of haemoglobin, it is highlyprobable that modification of the phosphorylation status ofthe cytoplasmic domain of Band 3 serves as a signaling event(see below) [50–55].
The eryptosismodel accountswell for toxicological studies,where RBC degradation occurs following exposure to inorganicions such as gold, cadmium [56], selenium [57], tin [58]..., orvarious drugs such as zidovudine [59], cyclosporine , azathi-oprine, PPARγ agonists, cisplatin [60]... It also correlates wellwith observed RBC response to osmotic stress [61] and energydepletion [62] (Fig. 4).
However, if the eryptosismodel explains the loss of cellulardeformability, possible glycolysis alteration through modifiedinteractions with the cytosolic domain of Band 3, it does notaccount for the remarkable control of the RBC lifespan in theblood flow, and its relevance to aging or storage-associatedsenescence still has to be established.
3.2. The Band 3 clustering model
In circulation, human RBCs have a lifespan of 120±4 days. It isvery unlikely that such a precise control results from aprogressive, linear accumulation of lesions, resulting in RBCdeath and haemolysis, but muchmore probable that it results
from a specific, controlled, non linear mechanism inducingRBC clearance from the blood flow. Several versions of thesamemodel have been proposed through the years by Kay [63–66], Low [65,67,68] and Lutz [69–71]. Basically, they all relate tothe observation that in aged erythrocytes, Band 3 formsclusters that are recognised by naturally occurring antibodies[72,73]. The mechanism of cluster formation is not fullyunderstood, but is largely attributed to oxidative lesions,hemichrome formation and polymerisation with the cytosolicdomain of Band 3.
The RBC is constantly exposed to a flux of O2 [74,75]; uponoxygen binding, one electron is transferred from iron to thebound oxygen to form a ferric-superoxide anion complex. Theshared electron is normally returned to the iron upon oxygenrelease, however a fraction of dissociation events results incapture of the electron by oxygen, thus forming a superoxideO2•− and leaving iron in the ferric state, i.e. met-Hb. This
haemoglobin autooxidation transforms around 2% of Hb intomet-Hb per day. This met-Hb containing a Fe(III) ion isnormally recycled back to functional Hb by the met-Hbreductase system, a NAD/NADH dependent system, but canalso accumulate at the inner side of the RBCmembrane, whereit further generates reactive oxygen species (ROS) through theFenton and Haber–Weiss reactions. This local ROS productioncan be highly deleterious for proteins, resulting in proteincleavage, cross-linking and side-chain modifications, as wellas for the membrane itself, through lipid peroxidation. Thisprocess can be clearly identified by the presence of hemi-chromes in RBC ghosts, i.e. by haemoglobin-derived productstightly linked to the inner side of the RBC membrane [76–81].
The met-Hb reductase system is complemented by asophisticated antioxidant system, either enzymatic or meta-bolic. The main enzymes responsible for antioxidant defenceare catalase, which converts H2O2 resulting from the sponta-neous or catalysed dismutation of O2
•− into oxygen and water;catalase is recycled during the catalytic cycle and is thusindependent of any cofactor, but can be inactivated byreaction with excess O2
•−. Superoxide dismutase (SOD) catal-yses the dismutation of O2
•− into H2O2 and oxygen; SOD is alsoself-recycled during the catalytic process. Peroxyredoxinscatalyse the reduction of H2O2, ROOH and peroxynitrite;there are two classes of peroxyredoxins: 1-Cys peroxiredoxinsthat are recycled by sulfiredoxins in a NAD(P)/NAD(P)H andATP dependent manner, and 2-Cys peroxiredoxins that areself-recycled during the catalytic process in a NAD(P)/NAD(P)Hdependent manner. Peroxiredoxins can be irreversibly inacti-vated by excess of ROS. Lastly glutathione peroxidase catal-yses the reduction of H2O2 into water, and is recycled by theglutathione reductase system in a NADPH dependent manner.
Non-enzymatic antioxidant defences are mainly constitut-ed by glutathione (GSH), which reacts with ROS to form GSSGand is thus a redox “sacrificial” buffer for all cells. GSSG isrecycled back to GSH by the glutathione reductase system in aNADPH dependent manner. In physiological conditions, theGSH/GSSG balance is in high favour of GSH, thus providingefficient buffering. In altered conditions, the GSH/GSSG ratiodiminishes and indicates that oxidative stress has overcomeantioxidant defences. Another important component of thenon-enzymatic antioxidant system is ascorbate (vitamin C)that reduces various free radicals such as OH•, RO•, ROO•;

Fig. 4 – Known pathways leading to eryptosis.
Fig. 5 – Scheme of the Band 3/Rh macromolecular complex.The Band 3 tetramer functions as anHCO3−/Cl- exchanger, Rhfamily proteins as CO2 and O2 channels; CO2 is converted intoHCO3− by carbonic anhydrase (CAII). Reproduced withpermission from [149].
379J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
ascorbate is recycled by various enzymatic systems in a GSH orNADPH dependent manner.
As described in the previous paragraph, RBCs are underconstant oxidative stress due to the high flux of oxygen, andautooxidation processes. The main, directly visible feature ofthe oxidatively altered RBC is the accumulation of oxidized,denatured haemoglobin at the inner side of the RBC mem-branes. These haemoglobin-derived compounds are thoughtto be crosslinked haemoglobin fragments, reversibly or non-reversibly linked to cytoskeleton proteins such as spectrin. Assuch, the formation of these hemichromes is directly respon-sible for alterations of cytoskeleton plasticity and increasedRBC rigidity [76–81].
Hemichromes are also thought to promote the formation ofBand 3 clusters [78,79,81]. The cytoplasmic domain of Band 3 isamajor organisation centre for RBCs and an anchorage site fora number of membrane-associated proteins such as protein4.1, 4.2, glycolytic enzymes such as glyceraldehyde 3-phos-phate dehydrogenase, phosphofructokinase, aldolase, as wellas hemichromes, haemoglobin and protein tyrosine phospha-tase (PTP1B) and protein tyrosine kinase (p72syk). Damagingproperties of hemichromes result in the formation of poly-mers that promote clustering of Band 3 in the membrane. Inphysiological conditions, Band 3 appears to be present in theRBC membrane as tetramers complexed with Rh proteins, asshown in Fig. 5.
Though the role of macromolecular assembly is poorlyunderstood in the function of Band 3 and Rh proteins, it seemsthat the association is relatively loose and dynamic inphysiological conditions. When hemichromes accumulateand crosslink Band 3 cytoplasmic domains, Band 3 multimers
appear to cluster within the membrane. The role of Band 3clusters in RBC senescence and clearance from the blood flowhas been successively described by the groups of Kay, Low andLutz [63–71]. The most comprehensive models put forwardsthat Band 3 clustering is recognised by naturally occurring

380 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
autoantibodies (Nabs). These IgGs seem to have a low affinityto physiological Band 3 multimers, but more than 3 orders ofmagnitudemore affinity to clustered Band 3, probably becauseof structural modifications in the extracellular domains ofBand 3 induced by clustering. In Lutz' model, these lowaffinity, low abundance Nabs are not able to induce anyopsonisation alone, and concomitant C3b complement depo-sition is necessary to obtain efficient opsonisation [82–85]. Ithas been shown that 1% oligomerised Band 3 was sufficient toelicit deposition of autologous anti-Band 3 IgGs (Nabs), andsubsequent complement activation through the alternativepathway.
Oxidative stress is also hypothesised to play another role inRBC senescence: several authors postulate that oxidativestress can directly activate pro-apoptotic proteolytic machin-eries such as caspases. It has been indeed proven thaterythroid progenitor cells are equipped with a functionalcaspases cascade that actually plays a role in erythroiddifferentiation termination. In mature red blood cells, someauthors, though able to detect caspases 3 and 8 for example,failed to measure any caspase activity in aging erythrocyte,even under classical apoptotic stimulations [22,86–89]. Con-versely, others were able to detect caspase activity: forexample, Ficarra et al. proved that active caspase 3 processedthe cytoplasmic domain of Band 3, resulting in both alteredanion transport and membrane modifications [90].
In summary, according to Lutz' model of RBC senescence,the formation of hemichromes at the RBC membrane inducesBand 3 clustering and aggregation; these Band 3 clusters arerecognised by low abundance autoantibodies that have abinding site for C3b and thus activate the alternative pathwayof the complement. Final senescent RBC clearance is thenassured by efficient phagocytosis. Whether other apoptoticmechanisms, such as caspase activation and Band 3 degrada-tion at the cytoplasmic domain, can be induced by oxidativestress in mature erythrocytes is still a matter of debate.
4. Relevance to the red cell storage lesion
The eryptosismodel describes RBC response to various stresses(osmotic shock, exposure to toxics...) and leads to intracellularcalcium increase, phosphatidylserine exposure on the outerside of the RBC membrane, microvesiculation, and internalproteinprocessing. Inparticular phosphatidylserine exposure isthought tomediateRBCclearancebymacrophages.Ontheotherhand, the Band3model accounts for physiological RBCaging (asit was demonstrated mainly on the 1% of older cells as isolatedby density centrifugation), and explains “normal”RBC clearancefrom the blood flow by phagocytosis.
Which of these two main pathways (if any) occur duringRBC storage in blood banking conditions is still a matter ofdebate. For example, some authors have found increased levelof intracellular calcium, phosphatidylserine exposing cellsand microvesicles in older blood bags [28,91,92], whereasothers did not. In our hands, the number of microvesiclespresent in blood bags increases constantly during storage,whereas the number of phosphatidylserine exposing cellsremains low (data not shown) [20].
On the other hand, there is accumulating evidence thathallmarks of the Band 3 clusteringmodel are present in storedRBCs. For example, Kriebardis et al. demonstrated accumula-tion of denatured haemoglobin on the cytoskeleton, modifi-cation of Band 3 localisation, and IgG deposition [22,25]. Thesame group measured extensive membrane protein carbon-ylation, a hallmark of protein oxidative lesions [24].
Focusing on oxidative stress, d'Amici et al. were able toshow that during the 14 first days of storage, the two-dimensional electrophoresis maps of RBCs were relativelystable; after 14 days, a lot of protein processing appearsthrough the increase in the number of spots on the 2D maps.Furthermore, this increase in spot numbers was almost absentin RBC bags stored under helium (i.e. in the absence ofoxygen), indicating that oxidative stress plays a role in themodifications occurring after 14 days of storage [93]. Remark-ably, this 14 day storage duration, after which protein proces-sing is visible on 2D maps, corresponds to the duration thatmakes a difference in the patient's recovery after transfusion,as statistically determined by Koch et al. [4].
From a metabolic point of view, this 14 days storageduration is the time necessary for 2,3-DPG concentration tofall down to almost zero, for the pH to fall down rapidly from6.8 to 6.5, for pO2 to start increasing rapidly from approxi-mately 50 mm Hg to 250 mm Hg (at day 42), and for lactate tostart increasing from 5mM to 20 mM (day 42) [1]. Though nodefinitivemodel has been described to explain for this 14 daystime lag and subsequent molecular processes at work in RBCstorage lesion, the above described lines of evidence altogeth-er start to build a picture of RBC evolution during storage:during 14 days, RBCs maintain more or less their metabolism(2,3-DPG is still present at millimolar levels), and no spectac-ular change is detectable. After 14 days of storage, themetabolic rates fall down, presumably because of energydepletion; as glycolysis diminishes, some important antioxi-dant factors, such as GSH, NADP and NADPH are no morerecycled to their reduced form, and ROS are no morechallenged by antioxidant defences, resulting in oxidativelesions, such as hemichrome formation, Band 3 clustering,possibly caspase activation, protein carbonylation... thataccumulate during the rest of the storage period (up to42 days).
5. Proteomic insights into red cell storage lesion
In the recent years, proteomics has entered the field ofhaematology and transfusion science massively [94–104].Proteomics has been applied to the establishment of referenceproteomes of RBCs [105–110], as well as the investigation ofseveral diseases [111]. More recently, proteomic approacheshave been applied to the investigation of the RBC storagelesion: for example, Anniss et al. compared by two-dimen-sional difference gel electrophoresis (2D-DIGE) the superna-tant of blood bags prepared with or without leukoreduction;not surprisingly, both types of blood bags contained highamounts of plasma proteins (10 mg/mL, identified mainly asalbumin, haptoglobin, apolipoprotein, and transferrin), butauthors were also able to identify haemolysis products that

381J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
appeared in the supernatant in the course of storage (such ashaemoglobin, thioredoxin, and carbonic anhydrase). In thenon-leukodepleted blood bags, authors found platelet proteinssuch as CTAP-III that upon proteolytic processing has thepotential to prime neutrophils. Of interest is the fact that innon-leukodepleted blood bags, the number of protein spotsobserved on 2D gels increased from blood sampling to day 14,presumably due to the release of platelet proteins, whereasafterward the number of protein spots diminished, whichauthors attributed to proteolytic degradation of releasedplatelet proteins. The presence of platelets in RBC concen-trates can readily occur in routine, depending on the processused to isolate RBCs. This 14 day threshold in spot number iswell in line with the clinical observation that blood bagsfresher than 14 days of storage have a better biomedical valuecompared to blood bags stored for more than 14 days [4].Proteins accumulating in leukocyte-reduced blood bags wereidentified as carbonic anhydrase I and thioredoxin peroxidaseB. But as leukocyte reduction prior to storage has become astandard in blood banks, these results are of questionablerelevance to the currently observed red cell storage lesion.
As described above, d'Amici et al. attributed the increasedspot number throughout storage mainly to oxidative damage[112], which is consistent with the independent observationthat anaerobic storage of RBCs may lessen the blood storagelesion [113–118].
Recently, Bosman et al. analysed the proteome of RBCmembranes and microvesicles by semi-quantitative onedimensional gel electrophoresis (1D-GE) followed by nano-LC-MS/MS in the course of storage [119]. More specifically,authors analysed RBC ghosts, microvesicles of mean diameterof 180 nm isolated by centrifugation of the RBC supernatant at40,000 g and nanovesicles of mean diameter 80 nm furtherisolated by centrifugation at 100,000 g. Authors confirmedalready observed data such as the accumulation of haemo-globin in the RBC membrane fractions as well as immuno-globulin deposition in the course of storage. Of importance arealso the losses of cytoskeleton and membrane proteins suchas spectrin, ankyrin, CD47 and Band 3, especially in the secondhalf of storage (day 21 to day 42), as well as the disappearancefrom the membrane fraction of metabolic enzymes, signaltransduction proteins, and small G proteins. In parallel,immunoglobulins and complement proteins were found toaccumulate in nanovesicles, and Band 3 in microvesicles.More specifically, Band 3 was identified in a large part in themicrovesicles from 1D-GE bands that do not correspond to themolecular weight of the intact Band 3 protein, indicating thatBand 3 has been processed sometime during its export intomicrovesicles.
In our hands, the microvesicles shed by RBCs duringstorage appeared to display proteomic profile markedlydifferent from their parent cells, especially in terms ofprocessed proteins. For example, the 1D-GE bandcorresponding to an average molecular weight of 25–35 kDacontains a lot of haemoglobin subunits (intact MW of 15–15 kDa), Band 3 and Rhesus (respectively of 102 and 45 kDa)[20].
Put together all these results tend to plead for the Band 3clustering model: it indeed seems that oxidative stress plays alarge role in the global alteration of stored RBCs, as demon-
strated by several authors [24,25,93,120]. Oxidative stressmight thus result in accumulation of haemichromes on thered cell membrane, providing a local source of furtheroxidizing species that alter the cytoskeleton microenviron-ment. The direct link between oxidative stress and Band 3clustering and processing remains to be firmly established[121,122], but as pointed by Bosman et al., perturbation of thecytoskeleton microenvironment (binding of glycolyticenzymes, membrane proteins/cytokeleton proteins interac-tions...) could well alter the tight balance between thecytoskeleton pressure and the membrane bending stress,thus resulting in microvesiculation [119]. Another alternativeis that deposition of immunoglobulins on the red cell surfacemight well trigger microvesiculation itself. In these twohypotheses, microvesiculation serves as a defence mecha-nism to help cells to get rid of deleterious or alteredmembranedomains. Cells unable to microvesiculate or that carry toimportant oxidative lesions would then be targeted toclearance through the Band 3 clustering model.
6. Conclusion
Whereas the known molecular data about the red blood cellstorage lesion start to build a consistent picture of whathappens to stored red blood cells, many issues remainunresolved. For example, the eryptosis model points out therole of calpains for the degradation of cytoskeleton proteinsfollowing a calcium uptake, whereas other authors were ableto detect caspase activity in stored RBCs following oxidativestress injury [22,86–90]. However, this issue remains unsettled,and the recent development of proteomic methodologies todetect and map proteolytic activities promises to prove usefulin elucidating the processes at work during RBC senescence[123–132].
Another central point is the role of Band 3 in the function ofthe RBC: as shown in Fig. 5, Band 3 is part of a macromolecularmembrane complex that comprise Rhesus proteins, whoseprobable function is to serve as channels, glycophorins A andB and CD47. On the internal part of the cell, the cytoplasmicdomain of Band 3 provides anchoring sites for carbonicanhydrase that converts carbon dioxide to carbonate [133],deoxy-haemoglobin, and glycolytic enzymes. The deoxy-Hbbinding site is very close to the binding sites of ankyrin,protein 4.1, and glycolytic enzymes, which strongly suggestthat the oxygenation state of the RBC (i.e. the intracellularconcentration of deoxy-Hb) can modulate both the cytoskel-eton properties and the metabolic activity of the cell [55,134–136]. As mentioned above, Band 3 is under tight phosphory-lation control [137], and there is large evidence that thesephosphorylation events control both the interaction of Band 3with glycolytic enzymes as well as are implied in the volumeregulation of the cell [138]. Several studies have highlightedthe interplay between oxidative stress and the phosphoryla-tion status of Band 3 [139–148], which might provide a linkbetween oxidative stress and Band 3 clustering. However, tothe best of our knowledge, no large-scale interaction study hasbeen conducted to identify themolecular interactors of Band 3in various conditions relating to blood banking. If coupledwith

382 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
phosphoproteomic analysis of RBC membrane proteins, such astudy would provide valuable information about the functionalrole of Band 3 modifications in RBC senescence as well as inexplaining the molecular aspects of the RBC storage lesion.
R E F E R E N C E S
[1] Bennett-Guerrero E, Veldman TH, Doctor A, TelenMJ, Ortel TL,ReidTS, etal. Evolutionofadversechanges instoredRBCs. ProcNatl Acad Sci USA 2007;104:17063–8.
[2] Hess JR, Greenwalt TG. Storage of red blood cells: newapproaches. Transfus Med Rev 2002;16:283–95.
[3] Meryman HT, Hornblower MLS, Syring RL. Prolonged storageof red-cells at 4-degrees-C. Transfusion 1986;26:500–5.
[4] Koch CG, Li L, Sessler DI, Figueroa P, Hoeltge GA,Mihaljevic T,et al. Duration of red-cell storage and complications aftercardiac surgery. N Engl J Med 2008;358:1229–39.
[5] Hess JR. Blood storage, personnal communication, Viterbo, Italy.[6] Anniss AM, Sparrow RL. Variable adhesion of different red
blood cell products to activated vascular endothelium underflow conditions. Am J Hematol 2007;82:439–45.
[7] Bosman GJCGM, Werre JM, Willekens FLA. Novotn√Ω VMJ.Erythrocyte ageing in vivo and in vitro: structural aspects andimplications for transfusion. Transfus Med 2008;18:335–47.
[8] van deWatering LMG, Brand A. Effects of storage of red cells.Transfusion Medicine and Hemotherapy 2008;35:359–67.
[9] Holme S. Current issues related to the quality of stored RBCs.Transf Apheres Sci 2005;33:55–61.
[10] Jia L, Bonaventura C, Bonaventura J, Stamler JS.S-nitrosohaemoglobin: a dynamic activity of blood involvedin vascular control. Nature 1996;380:221–6.
[11] De RosaMC, Alinovi CC, Galtieri A, Scatena R, Giardina B. Theplasma membrane of erythrocytes plays a fundamental rolein the transport of oxygen, carbon dioxide and nitric oxideand in the maintenance of the reduced state of the hemeiron. Gene 2007;398:162–71.
[12] Isbell TS, Sun CW, Wu LC, Teng XJ, Vitturi DA, Branch BG, et al.SNO-hemoglobin is not essential for red blood cell-dependenthypoxic vasodilation. Nat Med 2008;14:773–7.
[13] Reynolds JD, Ahearn GS, Angelo M, Zhang J, Cobb F, StamlerJS. S-nitrosohemoglobin deficiency: a mechanism for loss ofphysiological activity in banked blood. Proc Natl Acad SciUSA 2007;104:17058–62.
[14] Klein HG, Spahn DR, Carson JL. TransfusionMedicine 1— redblood cell transfusion in clinical practice. Lancet2007;370:415–26.
[15] Hogman CF, Meryman HT. Storage parameters affecting redblood cell survival and function after transfusion. TransfusMed Rev 1999;13:275–96.
[16] Cho J, King JS, Qian X, Harwood AJ, Shears SB.Dephosphorylation of 2, 3-bisphosphoglycerate by MIPPexpands the regulatory capacity of the Rapoport-Lueberingglycolytic shunt. Proc Natl Acad Sci USA 2008;105:5998–6003.
[17] Beutler E, Wood L. In vivo regeneration of red cell 2,3diphosphoglyceric acid (DPG) after transfusion of storedblood. J Lab Clin Med 1969;74:300.
[18] Valeri CR, Collins FB. Physiologic effect of transfusingpreserved red cells with low 2,3-diphosphoglycerate andhigh affinity for oxygen. Vox Sang 1971;20:397.
[19] Willekens FLA, Werre JM, Groenen-Dopp YAM,Roerdinkholder-Stoelwinder B, De Pauw B, Bosman GJCGM.Erythrocyte vesiculation: a self-protective mechanism? Br JHaematol 2008;141:549–56.
[20] Rubin O, Crettaz D, Canellini G, Tissot JD, Lion N.Microparticles in stored red blood cells: an approach usingflow cytometry and proteomic tools. Vox Sang2008;95:289–97.
[21] Greenwalt TJ. The how and why of exocytic vesicles.Transfusion 2006;46:143–52.
[22] Kriebardis AG, Antonelou MH, Stamoulis KE,Economou-Petersen E, Margaritis LH, Papassideri IS.Storage-dependent remodeling of the red blood cellmembrane is associated with increased immunoglobulin Gbinding, lipid raft rearrangement, and caspase activation.Transfusion 2007;47:1212–20.
[23] Wolfe LC, Byrne AM, Lux SE. Molecular defect in themembrane skeleton of blood-bank storedred-cells — abnormal spectrin protein 4.1-actincomplex-formation. J Clin Invest 1986;78:1681–6.
[24] Kriebardis AG, Antonelou MH, Stamoulis KE,Economou-Petersen E, Margaritis LH, Papassideri IS.Membrane protein carbonylation in non-leukodepletedCPDA-preserved red blood cells. Blood Cells Mol Dis2006;36:279–82.
[25] Kriebardis AG, Antonelou MH, Stamoulis KE,Economou-Petersen E, Margaritis LH, Papassideri IS.Progressive oxidation of cytoskeletal proteins andaccumulation of denatured hemoglobin in stored red cells. JCell Mol Med 2007;11:148–55.
[26] Stewart A, Urbaniak S, Turner M, Bessos H. The applicationof a new quantitative assay for the monitoring ofintegrin-associated protein CD47 on red blood cells duringstorage and comparison with the expression of CD47 andphosphatidylserine with flow cytometry. Transfusion2005;45:1496–503.
[27] Mitrofan-Oprea L, Palii C, Tissier JP, Héron A, Verpoort T,BehagueM, Smagghe E, Schooneman F, Huart JJ, Goudaliez F,Montreuil J, Bratosin D. Novel criteria for assessing red bloodcell viability in blood banks. Nouveaux critères d'évaluationde la viabilité des hématies destinées à la transfusion 2007;14: 393–401.
[28] Bosman GJCGM,Willekens FLA, Werre JM. Erythrocyte aging:a more than superficial resemblance to apoptosis? CellPhysiol Biochem 2005;16:1–8.
[29] Sparrow RL, Veale MF, Healey G, Payne KA. Red blood cell(RBC) age at collection and storage influences RBCmembrane-associated carbohydrates and lectin binding.Transfusion 2007;47:966–8.
[30] Bratosin D, Mazurier J, Debray H, Lecocq M, Boilly B,Alonso C, et al. Flow cytofluorimetric analysis of young andsenescent human erythrocytes probed with lectins.Evidence that sialic acids control their life span. Glycoconj J1995;12:258–67.
[31] Lang F, Lang KS, Wieder T, Myssina S, Birka C, Lang PA, et al.Cation channels, cell volume and the death of anerythrocyte. Pflugers Arch 2003;447:121–5.
[32] Lang F, Birka C,Myssina S, Lang KS, Lang PA, Tanneur V, et al.Erythrocyte ion channels in regulation of apoptosis. Adv ExpMed Biol 2005;559:211–7.
[33] Lang KS, Lang PA, Bauer C, Duranton C, Wieder T, Huber SM,et al. Mechanisms of suicidal erythrocyte death. Cell PhysiolBiochem 2005;15:195–202.
[34] Wieder T, Lang PA, Lang KS, Kempe DS, Niemoeller OM,Duranton C, et al. Studying mechanisms of eryptosis.Cytotechnology 2005;49:117–32.
[35] Lang F, Lang KS, Lang PA, Huber SM, Wieder T. Mechanismsand significance of eryptosis. Antioxid Redox Signal2006;8:1183–92.
[36] Lang F, Huber SM, Szabo I, Gulbins E. Plasma membrane ionchannels in suicidal cell death. Arch Biochem Biophys2007;462:189–94.
[37] F√∂ller M, Huber SM, Lang F. Erythrocyte programmed celldeath. IUBMB life 2008;60:661–8.
[38] Lang F, Gulbins E, Lerche H, Huber SM, Kempe DS, Foller M.Eryptosis, a window to systemic disease. Cell PhysiolBiochem 2008;22:373–80.

383J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
[39] Lang PA, Kempe DS, Myssina S, Tanneur V, Birka C, Laufer S,et al. PGE2 in the regulation of programmed erythrocytedeath. Cell Death Differ 2005;12:415–28.
[40] LangKS,MyssinaS,BrandV,SanduC, LangPA,BerchtoldS, et al.Involvement of ceramide inhyperosmotic shock-induceddeathof erythrocytes. Cell Death Differ 2004;11:231–43.
[41] Nicolay J, Bentzen PJ, Ghashghaeinia M, Wieder T, Lang F.Stimulation of erythrocyte cell membrane scrambling byamiodarone. Cell Physiol Biochem 2007;20:1043–50.
[42] Sopjani M, Foeller M, Lang F. Gold stimulates Ca2+ entry intoand subsequent suicidal death of erythrocytes. Toxicology2008;244:271–9.
[43] Foeller M, Huber SM, Lang F. Erythrocyte programmed celldeath. Iubmb Life 2008;60:661–8.
[44] Lang F, Gulbins E, Lerche H, Huber SM, Kempe DS, Foeller M.Eryptosis, a window to systemic disease. Cellular Physiologyand Biochemistry 2008;22:373–80.
[45] Zaidi A, Saleemuddin M. Ca2+-induced alterations in theactivity of membrane (Ca2+–Mg2+)-atpase of human and raterythrocytes. Indian Journal of Biochemistry & Biophysics1993;30:98–102.
[46] Redding GS, Record DM, Raess BU. Calcium-stressederythrocyte-membrane structure and function for assessingglipizide effects on transglutaminase activation. Proc SocExp Biol Med 1991;196:76–82.
[47] Low PS, Allen DP, Zioncheck TF. Tyrosine phosphorylation ofband 3 inhibits peripheral protein binding. J Biol Chem1987;262:4592–6.
[48] Yannoukakos D, Meyer HE, Vasseur C, Driancourt C,Wajcman H, Bursaux E. Three regions of erythrocyte band 3protein are phosphorylated on tyrosines: characterization ofthe phosphorylation sites by solid phase sequencingcombined with capillary electrophoresis.Biochimica et Biophysica Acta — Biomembranes1991;1066:70–6.
[49] Yannoukakos D, Vasseur C, Piau JP, Wajcman H, Bursaux E.Phosphorylation sites in human erythrocyte band 3 protein.Biochimica et Biophysica Acta - Biomembranes1991;1061:253–66.
[50] Willardson BM, Thevenin BJM, Harrison ML, Kuster WM,Benson MD, Low PS. Localization of the ankyrin-binding siteon erythrocyte membrane protein, band 3. J Biol Chem1989;264:15893–9.
[51] Thevenin BJM, Low PS. Kinetics and regulation of theankyrin-band 3 interaction of the human red blood cellmembrane. J Biol Chem 1990;265:16166–72.
[52] Harrison ML, Rathinavelu P, Arese P, Geahlen RL, Low PS.Role of band 3 tyrosine phosphorylation in the regulationof erythrocyte glycolysis. J Biol Chem 1991;266:4106–11.
[53] Low PS, Willardson BM, Mohandas N, Rossi M, Shohet S.Contribution of the band 3-ankyrin interaction toerythrocyte membrane mechanical stability. Blood1991;77:1581–6.
[54] Low PS, Rathinavelu P, Harrison ML. Regulation of glycolysisvia reversible enzyme binding to the membrane protein,band 3. J Biol Chem 1993;268:14627–31.
[55] Weber RE, Voelter W, Fago A, Echner H, Campanella E, LowPS. Modulation of red cell glycolysis: interactions betweenvertebrate hemoglobins and cytoplasmic domains of band 3red cell membrane proteins. Am J Physiol Regul Integr CompPhysiol 2004;287:R454–64.
[56] Sopjani M, Foller M, Dreischer P, Lang F. Stimulation oferyptosis by cadmium ions. Cellular Physiology andBiochemistry 2008;22:245–52.
[57] Sopjani M, Foller M, Gulbins E, Lang F. Suicidal death oferythrocytes due to selenium-compounds. CellularPhysiology and Biochemistry 2008;22:387–94.
[58] Tan TN, Foller M, Lang F. Tin triggers suicidal death oferythrocytes. J Appl Toxicol 2009;29:79–83.
[59] Kucherenko Y, Geiger C, Shumilina E, FoÃàller M, Lang F.Inhibition of cation channels and suicidal death of humanerythrocytes by zidovudine. Toxicology 2008;253:62–9.
[60] Mahmud H, Foller M, Lang F. Suicidal erythrocyte deathtriggered by cisplatin. Toxicology 2008;249:40–4.
[61] Lang F, Lang KS, Lang PA, Huber SM, Wieder T. Osmoticshock-induced suicidal death of erythrocytes.Acta Physiologica 2006;187:191–8.
[62] Klarl BA, Lang PA, Kempe DS, Niemoeller OM, Akel A,Sobiesiak M, et al. Protein kinase C mediates erythrocyte“programmed cell death” following glucose depletion.American Journal of Physiology — Cell Physiology 2006;290:C244–53.
[63] Kay MMB, Goodman SR, Sorensen K. Senescent cell antigenis immunologically related to band 3. Proc Natl Acad Sci USA1983;80:1631–5.
[64] Kay MMB. Localization of senescent cell antigen on band 3.Proc Natl Acad Sci USA 1984;81:5753–7.
[65] Kay MMB, Flowers N, Goodman J, Bosman G. Alteration inmembrane protein band 3 associated with acceleratederythrocyte aging. Proc Natl Acad Sci USA 1989;86:5834–8.
[66] Kay MMB, Wyant T, Goodman J. Autoantibodies to band 3during aging and disease in aging interventions. Ann N YAcad Sci 1994;719:419–47.
[67] Low PS, Westfall MA, Allen DP, Appell KC. Characterizationof the reversible conformational equilibrium of thecytoplasmic domain of erythrocyte membrane band 3.J Biol Chem 1984;259:13070–6.
[68] Christian JA, Rebar AH, Boon GD, Low PS. Senescence ofcanine biotinylated erythrocytes: increased autologousimmunoglobulin binding occurs on erythrocytes aged invivo for 104 to 110 days. Blood 1993;82:3469–73.
[69] Lutz HU, Stringaro-Wipf G. Senescent red cell-bound IgG isattached to band 3 protein. Biomedica Biochimica Acta1983;42:S117–21.
[70] Lutz HU, Flepp R, Stringaro-Wipf G. Naturally occurringautoantibodies to exoplasmic and cryptic regions of band 3protein, the major integral membrane protein of human redblood cells. J Immunol 1984;133:2610–8.
[71] Hornig R, Lutz HU. Band 3 protein clustering on humanerythrocytes promotes binding of naturally occurringanti-band 3 and anti-spectrin antibodies. Exp Gerontol2000;35:1025–44.
[72] Arese P, Turrini F, Schwarzer E. Band 3/complement-mediated recognition and removal of normally senescentand pathological human erythrocytes. Cell Physiol Biochem2005;16:133–46.
[73] Pantaleo A, Giribaldi G, Mannu F, Arese P, Turrini F. Naturallyoccurring anti-band 3 antibodies and red blood cell removalunder physiological and pathological conditions.Autoimmunity Reviews 2008;7:457–62.
[74] Minetti M, Malorni W. Redox control of red blood cellbiology: the red blood cell as a target and source ofprooxidant species. Antioxid Redox Signal 2006;8:1165–9.
[75] CÃßimen MYB. Free radical metabolism in humanerythrocytes. Clin Chim Acta 2008;390:1–11.
[76] Rachmilewitz EA. Formation of hemichromes fromoxidized hemoglobin subunits. Ann N Y Acad Sci1969;165:171–84.
[77] Rachmilewitz EA, Thorell B. Hemichromes in single inclusion bodies in red cells of beta thalassemia. Blood1972;39:794–800.
[78] Waugh SM, Low PS. Hemichrome binding to band 3:nucleation of Heinz bodies on the erythrocyte membrane.Biochemistry 1985;24:34–9.
[79] Waugh SM, Walder JA, Low PS. Partial characterization ofthe copolymerization reaction of erythrocyte membraneband 3 with hemichromes. Biochemistry 1987;26:1777–83.
[80] Kannan R, Labotka R, Low PS. J Biol Chem 1988;263:13766–73.

384 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
[81] Mannu F, Arese P, Cappellini MD, Fiorelli G, Cappadoro M,Giribaldi G, et al. Role of hemichrome binding to erythrocytemembrane in the generation of band-3 alterations inŒ≤-thalassemia intermedia erythrocytes. Blood1995;86:2014–20.
[82] Lutz HU, Stammler P, Fasler S. How naturally occurringanti-band 3 antibodies stimulate C3b deposition tosenescent and oxidatively stressed red blood cells. BiomedBiochim Acta 1990;49:S224–9.
[83] Lutz HU, Stammler P, Kock D, Taylor RP. Opsonic potential ofC3b-anti-band 3 complexes when generated on senescentand oxidatively stressed red cells or in fluid phase. Adv ExpMed Biol 1991;307:367–76.
[84] Lutz HU, Nater M, Stammler P. Naturally occurring anti-band3 antibodies have a unique affinity for C3. Immunology1993;80:191–6.
[85] Jelezarova E, Lutz HU. IgG naturally occurring antibodiesstabilize and promote the generation of the alternativecomplement pathway C3 convertase. Mol Immunol2005;42:1393–403.
[86] Berg CP, Engels IH, Rothbart A, Lauber K, RenzA, Schlosser SF,et al. Human mature red blood cells express caspase-3 andcaspase-8, but are devoid of mitochondrial regulators ofapoptosis. Cell Death Differ 2001;8:1197–206.
[87] Mandal D, Moitra PK, Saha S, Basu J. Caspase 3 regulatesphosphatidylserine externalization and phagocytosis ofoxidatively stressed erythrocytes. FEBS Lett 2002;513:184–8.
[88] Mandal D, Baudin-Creuza V, Bhattacharyya A, Pathak S,Delaunay J, Kundu M, et al. Caspase 3-mediated proteolysisof the N-terminal cytoplasmic domain of the humanerythroid anion exchanger 1 (Band 3). J Biol Chem2003;278:52551–8.
[89] Mandal D, Mazumder A, Das P, Kundu M, Basu J.Fas-, caspase 8-, and caspase 3-dependent signalingregulates the activity of the aminophospholipid translocaseand phosphatidylserine externalization in human erythro-cytes. J Biol Chem 2005;280:39460–7.
[90] Ficarra S, Tellone E, Giardina B, Scatena R, Russo A, Misiti F,et al. Derangement of erythrocytic AE1 in beta-thalassemiaby caspase 3: pathogenic mechanisms and implications inred blood cell senescence. J Membr Biol 2009;228:43–9.
[91] Bosman GJCGM, Lasonder E, Luten M,Roerdinkholder-Stoelwinder B. Novotn√Ω VMJ, Bos H, DeGrip WJ. The proteome of red cell membranes and vesiclesduring storage in blood bank conditions. Transfusion2008;48:827–35.
[92] Salzer U, Zhu R, Luten M, Isobe H, Pastushenko V, Perkmann T,et al. Vesicles generatedduring storageof red cells are rich in thelipid raft marker stomatin. Transfusion 2008;48:451–62.
[93] D'Amici GM, Rinalducci S, Zolla L. Proteomic analysis of RBCmembrane protein degradation during blood storage.Journal of Proteome Research 2007;6:3242–55.
[94] Cristea IM, Gaskell SJ, Whetton AD. Proteomics techniquesand their application to hematology. Blood 2004;103:3624–34.
[95] Kaiser T, Kamal H, Rank A, Kolb HJ, Holler E, Ganser A, et al.Proteomics applied to the clinical follow-up of patients afterallogeneic hematopoietic stem cell transplantation. Blood2004;104:340–9.
[96] Rees-Unwin KS, Morgan GJ, Davies FE. Proteomics and thehaematologist. Clin Lab Haematol 2004;26:77–86.
[97] Seshi B. Proteomics knocks on hematology's door. Blood2004;103:3607-3607.
[98] Caron M, Joubert-Caron R. Proteomics in hematologicmalignancies. Expert Review of Proteomics 2005;2:567–76.
[99] Thadikkaran L, Siegenthaler MA, Crettaz D, Queloz PA,Schneider P, Tissot JD. Recent advances in blood-relatedproteomics. Proteomics 2005;5:3019–34.
[100] Unwin RD, Whetton AD. How will haematologists useproteomics? Blood Rev 2007;21:315–26.
[101] Liumbruno G, D'Amici GM, Grazzini G, Zolla L. Transfusionmedicine in the era of proteomics. Journal of Proteomics2008;71:34–45.
[102] Zolla L. Proteomics and transfusion medicine. BloodTransfusion 2008;6:67–9.
[103] Lion N, Tissot JD. Application of proteomics to hematology:the revolution is starting. Expert Review of Proteomics2008;5:375–9.
[104] Zolla L, Liumbruno GM, D'Amici GM, Grazzini G. Adverseeffects related to storage lesions: Proteomic profiles of redblood cells during storage. Blood Transfusion 2009; 7.
[105] Olivieri E, Herbert B, Righetti PG. The effect of proteaseinhibitors on the two-dimensional electrophoresis patternof red blood cell membranes. Electrophoresis 2001;22:560–5.
[106] BruschiM, Seppi C, Arena S, Musante L, Santucci L, Balduini C,et al. Proteomic analysis of erythrocyte membranes by softimmobiline gels combined with differential protein extrac-tion. Journal of Proteome Research 2005;4:1304–9.
[107] Pasini EM, KirkegaardM, Mortensen P, Lutz HU, Thomas AW,Mann M. In-depth analysis of the membrane and cytosolicproteome of red blood cells. Blood 2006;108:791–801.
[108] Roux-Dalvai F, de Peredo AG, SimoC, Guerrier L, Bouyssiee D,Zanella A, et al. Extensive analysis of the cytoplasmicproteome of human erythrocytes using the peptide ligandlibrary technology and advanced mass spectrometry.Molecular & Cellular Proteomics 2008;7:2254–69.
[109] Simo C, Bachi A, Cattaneo A, Guerrier L, Fortis F, Boschetti E,et al. Performance of combinatorial peptide libraries incapturing the low-abundance proteome of red blood cells. 1.Behavior of mono- to hexapeptides. Anal Chem2008;80:3547–56.
[110] Bachi A, Sim C, Restuccia U, Guerrier L, Fortis F, Boschetti E,et al. Performance of combinatorial peptide libraries incapturing the low-abundance proteome of red blood cells. 2.Behavior of resins containing individual amino acids. AnalChem 2008;80:3557–65.
[111] Kakhniashvili DG, Griko NB, Bulla LA, Goodman SR. Theproteomics of sickle cell disease: profiling of erythrocytemembrane proteins by 2D-DIGE and tandem massspectrometry. Exp Biol Med 2005;230:787–92.
[112] D'Amici GM, Rinalducci S, Zolla L. Proteomic analysis of RBCmembrane protein degradation during blood storage. JProteome Res 2007;6:3242–55.
[113] Yoshida T, Lee J, McDonoughW, Friedman K, Bitensky M.Anaerobic refrigerated-storage of red blood cells for 9weeks: in vivo and in vitro characteristics. Transfusion 1997;37:S414-S414.
[114] Dumont LJ, Yoshida T, AuBuchon JP. Anaerobic storage ofred blood cells in a novel additive solution improves in vivorecovery. Transfusion 2009;49:458–64.
[115] Yoshida T, AuBuchon JP, Dumont LJ, Gorham JD, Gifford SC,Foster KY, et al. The effects of additive solution pH andmetabolic rejuvenation on anaerobic storage of red cells.Transfusion 2008;48:2096–105.
[116] Yoshida T, AuBuchon JP, Tryzelaar L, Foster KY, BitenskyMW.Extended storage of red blood cells under anaerobic condi-tions. Vox Sang 2007;92:22–31.
[117] Hess JR. Storage of red blood cells under anaerobicconditions. Vox Sang 2007;93:183-183.
[118] Yoshida T, AuBuchon JP. Storage of red blood cells underanaerobic conditions: reply. Vox Sang 2007;93:184-184.
[119] Bosman G, Lasonder E, Luten M,Roerdinkholder-Stoelwinder B, Novotny VMJ, Bos H, et al.The proteome of red cell membranes and vesicles duringstorage in blood bank conditions. Transfusion2008;48:827–35.
[120] Kriebardis AG, Antonelou MH, Stamoulis KE,Economou-Petersen E, Margaritis LH, Papassideri IS.RBC-derived vesicles during storage: ultrastructure, protein

385J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 3 7 4 – 3 8 5
composition, oxidation, and signaling components.Transfusion 2008;48:1943–53.
[121] Galtieri A, Tellone E, Romano L, Misiti F, Bellocco E, Ficarra S,et al. Band-3 protein function in human erythrocytes: effectof oxygenation-deoxygenation. Bba-Biomembranes2002;1564:214–8.
[122] Teti D, Crupi M, BusaM, Valenti A, Loddo S,MondelloM, et al.Chemical and pathological oxidative influences on band 3protein anion-exchanger. Cell Physiol Biochem2005;16:77–86.
[123] Lopez-Otin C, Overall CM. Protease degradomics: a newchallenge for proteomics. Nat Rev, Mol Cell Biol2002;3:509–19.
[124] Thiede B, Treumann A, Kretschmer A, Sohlke J, Rudel T.Shotgun proteome analysis of protein cleavage in apoptoticcells. Proteomics 2005;5:2123–30.
[125] LiuMC, Akle V, ZhengW, Dave JR, Tortella FC, Hayes RL, et al.Comparing calpain- and caspase-3-mediated degradationpatterns in traumatic brain injury by differential proteomeanalysis. Biochem J 2006;394:715–25.
[126] Mahrus S, Trinidad J, Burlingame A, Wells JA. Degradomics:the proteolysis of cell death. Molecular & Cellular Proteomics2007; 6: 5.2.
[127] Doucet A, Butler GS, Rodriguez D, Prudova A, Overall CM.Metadegradomics toward in vivo quantitative degradomicsof proteolytic post-translational modifications of the cancerproteome. Molecular & Cellular Proteomics 2008;7:1925–51.
[128] Doucet A, Overall CM. Protease proteomics: revealingprotease in vivo functions using systems biologyapproaches. Mol Aspects Med 2008;29:339–58.
[129] LamkanfiM, Kanneganti TD, VanDammeP, VandenBergheT,Vanoverberghe I, Vandekerckhove J, et al. Targeted peptide-centric proteomics reveals caspase-7 as a substrate of thecaspase-1 inflammasomes. Molecular & Cellular Proteomics2008;7:2350–63.
[130] Schilling O, Overall CM. Proteome-derived,database-searchable peptide libraries for identifyingprotease cleavage sites. Nat Biotechnol 2008;26:685–94.
[131] Van Damme P, Vandelkerckhove J, Gevaert K.Disentanglement of protease substrate repertoires. BiolChem 2008;389:371–81.
[132] Van Damme P, Maurer-Stroh S, Plasman K, Van Durme J,Colaert N, Timmerman E, et al. Analysis of proteinprocessing by N-terminal proteomics reveals novelspecies-specific substrate determinants of granzyme Borthologs. Molecular & Cellular Proteomics 2009;8:258–72.
[133] Vince JW, Reithmeier RAF. Identification of the carbonicanhydrase II binding site in the Cl-/HCO3-anion exchangerAE1. Biochemistry 2000;39:5527–33.
[134] Chu H, Breite A, Ciraolo P, Franco RS, Low PS.Characterization of the deoxyhemoglobin binding site onhuman erythrocyte band 3: implications for O-2 regulationof erythrocyte properties. Blood 2008;111:932–8.
[135] Campanella ME, Chu H, Low PS. Assembly and regulation ofa glycolytic enzyme complex on the human erythrocytemembrane. Proc Natl Acad Sci USA 2005;102:2402–7.
[136] CampanellaME, ChuH,WanderseeNJ, Peters LL,MohandasN,Gilligan DM, et al. Characterization of glycolytic enzymeinteractions with murine erythrocyte membranes inwild-type and membrane protein knockout mice. Blood2008;112:3900–6.
[137] Brunati AM, Bordin L, Clari G, James P, QuadroniM, Baritono E,et al. Sequential phosphorylation of protein band 3 by Syk andLyn tyrosine kinases in intact human erythrocytes: identifi-cation of primary and secondary phosphorylation sites. Blood2000;96:1550–7.
[138] Minetti G, Piccinini G, Balduini C, Seppi C, Brovelli A.Tyrosine phosphorylation of band 3 protein inCa2+/A23187-treated human erythrocytes. Biochem J1996;320:445–50.
[139] Mallozzi C, Di Stasi AMM,Minetti M. Peroxynitritemodulatestyrosine-dependent signal transduction pathway of humanerythrocyte band 3. FASEB J 1997;11:1281–90.
[140] Mallozzi C, Di Stasi AMM, Minetti M. Activation of srctyrosine kinases by peroxynitrite. FEBS Lett 1999;456:201–6.
[141] Mallozzi C, Di Stasi MAM, Minetti M.Peroxynitrite-dependent activation of src tyrosine kinaseslyn and hck in erythrocytes is under mechanisticallydifferent pathways of redox control. Free Radic Biol Med2001;30:1108–17.
[142] Minetti M, Mallozzi C, Di Stasi AMM. Peroxynitrite activateskinases of the src family and upregulates tyrosinephosphorylation signaling. Free Radic Biol Med2002;33:744–54.
[143] Ciana A, Minetti G, Balduini C. Phosphotyrosinephosphatases acting on band 3 in human erythrocytes ofdifferent age: PTP1B processing during cell ageing.Bioelectrochemistry 2004;62:169–73.
[144] Minetti G, Ciana A, Balduini C. Differential sorting of tyrosinekinases and phosphotyrosine phosphatases acting on band3 during vesiculation of human erythrocytes. Biochem J2004;377:489–97.
[145] Matarrese P, Straface E, Pietraforte D, Gambardella L, Vona R,Maccaglia A, et al. Peroxynitrite induces senescence andapoptosis of red blood cells through the activation ofaspartyl and cysteinyl proteases. FASEB J 2005;19:416–8.
[146] Serafini M, Mallozzi C, Di Stasi AMM, Minetti M.Peroxynitrite-dependent upregulation of Src kinases in redblood cells: strategies to study the activation mechanisms.Methods Enzymol 2005;396:215–29.
[147] PietraforteD,Matarrese P, Straface E,Gambardella L,MetereA,Scorza G, et al. Two different pathways are involved inperoxynitrite-induced senescence and apoptosis of humanerythrocytes. Free Radic Biol Med 2007;42:202–14.
[148] Metere A, Iorio E, Pietraforte D, Podo F, Minetti M.Peroxynitrite signaling in human erythrocytes: Synergisticrole of hemoglobin oxidation and band 3 tyrosinephosphorylation. Archives of Biochemistry and Biophysics2008.
[149] Daniels G. Functions of red cell surface proteins. Vox Sang2007;93:331–40.