
Naturalistic social cognition: Methodology, assessment, and validation
Social structure, social cognition, and physicalactivity: A test of four models
Gaston Godin1*, Paschal Sheeran2, Mark Conner3,Ariane Belanger-Gravel4, Maria Cecılia B. J. Gallani5 andBertrand Nolin61Canada Research Chair on Behaviour and Health, Faculty of Nursing,Laval University, Quebec, Canada
2Department of Psychology, The University of Sheffield, UK3Institute of Psychological Sciences, University of Leeds, UK4Research Group on Behaviour and Health, Faculty of Nursing,Laval University, Quebec, Canada
5Department of Nursing, Faculty of Medical Sciences, State University of Campinas,Sao Paulo, Brazil
6Institut National de Sante Publique du Quebec, Canada
Objective. This study investigated the combined influence of social structural factors(e.g. income) and cognitions in predicting changes in physical activity. Four models weretested: (a) direct effects (social structural factors influence behaviour controlling forcognitions), (b) mediation (cognitions mediate social structural influence), (c) moderation(social structural factors moderate cognition–behaviour relations), and (d) mediatedmoderation (cognitions mediate the moderating effects of social structural position).
Design. Baseline and 3-month follow-up surveys.
Methods. A random sample of 1,483 adults completed self-report measures ofphysical activity at baseline and 3-month follow-up. Measures of age, gender, education,income, material and social deprivation, intention, perceived behavioural control (PBC),and intention stability also were taken.
Results. Apart from age, social structural factors exhibited very small or marginaleffects on behaviour change, and only education moderated the intention–behaviourrelation. In contrast, the magnitude of direct effects of the social cognition variables wascomparatively large and intention stability mediated the moderating effect of education.
Conclusions. Stable intentions and PBC are the key predictors of changes in physicalactivity. Consequently, our findings would suggest the value of focusing on cognitionsrather than social structural variableswhenmodelling the determinants of physical activity.
* Correspondence should be addressed to Professor Gaston Godin, Canada Research Chair on Behaviour and Health, Faculty ofnursing, Laval University, Paul-Comtois Building, 4108-A, Quebec, Canada G1K 7P4 (e-mail: [email protected]).
TheBritishPsychologicalSociety
79
British Journal of Health Psychology (2010), 15, 79–95
q 2010 The British Psychological Society
www.bpsjournals.co.uk
DOI:10.1348/135910709X429901
A key starting point for the development of social cognition models of health behaviour
such as the health belief model (Rosenstock, 1966) and the theory of planned behaviour
(Ajzen, 1991)was the observation that although social structural factors (e.g. age, gender,
and socio-economic status) are reliably associated with health actions, it is usually
difficult, and sometimes impossible, to modify these factors. Thus, in order to generate
interventions that will change behaviour, researchers began to identify modifiable
individual characteristics that (a) were strongly associated with behaviour and (b)reflected differences in socialization that accrue fromoccupying different positions in the
social structure. Health cognitions (beliefs about health behaviours that are shared by
some individuals but not by others) were identified as these characteristics. Accumulated
evidence indicates that health cognitions have strong associations with behaviour
(for reviews, see, Abraham, Sheeran, & Johnston, 1998; Conner & Norman, 2005; de
Ridder & deWit, 2006), and that interventions which change health cognitions engender
changes in subsequent behaviour (Bandura, 2000; Webb & Sheeran, 2006). However,
little research has examined the assumptionmade by health behaviour models that socialstructural factors no longer influence behaviour once relevant health cognitions have
been taken into account. The present research provides an overdue test of this mediation
assumption, and examines four models that delineate how social structural factors and
health cognitions combine to influence physical activity.
Social structural factors and physical activitySocial structural position refers to individuals’ standing in the social hierarchy and is
measured by factors such as age, gender, income, and indices of deprivation. Socialstructural factors should influence levels of physical activity because these variables
capture the roles, status, and expectations associated with the membership of particular
social categories as well as the resources and opportunities that accrue from such
membership (Stryker, 1980, 1983). Evidence that social structural factors are associated
with physical activity comes from reviews by Sallis and Owen (1999) and updated in
2002 (Trost, Owen, Bauman, Sallis, & Brown, 2002; see also Humpel, Owen, & Leslie,
2002). Findings showed that age has a ‘repeatedly documented negative relationship
with physical activity’ (i.e. the 1999 and 2002 reviews both found consistent negativeassociations), whereas gender, education, and income/socio-economic status each have
a repeatedly documented significant relationship with physical activity (Trost et al.,
2002). These reviews indicate that young people, men, the better educated, and those
belonging to higher social classes are more likely to be physically active compared with
their counterparts. Analyses of neighbourhood-level indices of deprivation offer the
same conclusion about the positive relationship between socio-economic status and
physical activity (Cubbin et al., 2006; Sundquist, Malmstrom, & Johansson, 1999).
Although accumulated research thus indicates that social structural factors showconsistent associations with levels of physical activity, it is notable that the evidence to
date is almost entirely cross-sectional (Trost et al., 2002). Longitudinal studies that
control for past behaviour are needed in order to demonstrate that social structural
factors are associated with changes in physical activity.
Social cognition models and physical activityPerhaps, the most widely used and best validated social cognition model of health
behaviour is the theory of planned behaviour (TPB). According to the TPB, the most
80 Gaston Godin et al.
immediate and important predictor of behaviour is the person’s decision or intention to
engage in it (e.g. ‘I intend to engage in regular physical activity in the next year’).
Intentions should be translated into behaviour provided (a) people possess the requisite
abilities, resources, and opportunities to initiate action (i.e. have ‘actual control’ over
the behaviour) and (b) intentions do not change (i.e. remain stable) during the interim
between intention formation and execution of the behaviour. To take account of theextent of volitional control over action, the TPB includes the concept of perceived
behavioural control (PBC; e.g. ‘For me to engage in regular physical activity would be
easy/difficult’) as an additional direct predictor of behaviour alongside intentions.
Several meta-analyses attest to the predictive validity of intentions and PBC in predicting
physical activity (Downs & Hausenblas, 2005; Godin & Kok, 1996; Hagger,
Chatzisarantis, & Biddle, 2002). To capture the role of changes in intention, researchers
typically measure the temporal stability of intention (e.g. using absolute differences
between intention scores taken at two time-points; Conner, Sheeran, Norman, &Armitage, 2000). Findings support the idea that stable intentions better predict
behaviour when compared with unstable intentions (Conner & Godin, 2007; Conner
et al., 2000; Sheeran & Abraham, 2003; Sheeran, Orbell, & Trafimow, 1999).
Combining social structural and social cognition factors: Four modelsTPB is construed as a sufficient model of health behaviour in the sense that (stable)
intentions and PBC are considered the only variables that directly determine behaviour
(Ajzen, 1991). A strict interpretation of this theory is that other variables (e.g. attitudes,
norms, personality characteristics, and social structural factors) have no direct effect on
behaviour (i.e. these variables do not influence behaviour after intentions and PBC have
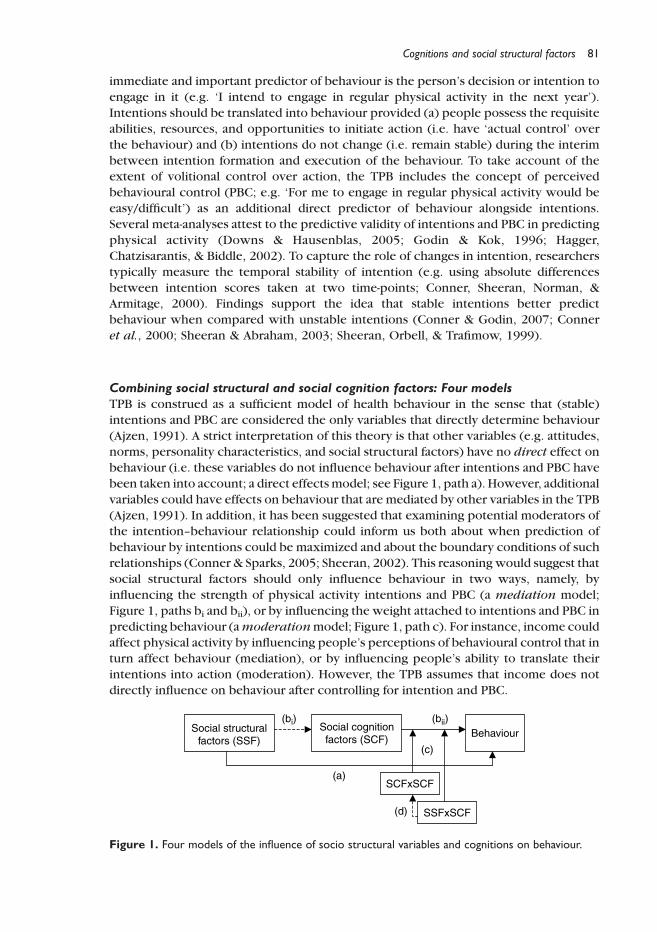
been taken into account; a direct effectsmodel; see Figure 1, path a). However, additional
variables could have effects on behaviour that are mediated by other variables in the TPB
(Ajzen, 1991). In addition, it has been suggested that examining potential moderators ofthe intention–behaviour relationship could inform us both about when prediction of
behaviour by intentions could be maximized and about the boundary conditions of such
relationships (Conner & Sparks, 2005; Sheeran, 2002). This reasoningwould suggest that
social structural factors should only influence behaviour in two ways, namely, by
influencing the strength of physical activity intentions and PBC (a mediation model;
Figure 1, paths bi and bii), or by influencing the weight attached to intentions and PBC in
predicting behaviour (amoderationmodel; Figure 1, path c). For instance, income could
affect physical activity by influencing people’s perceptions of behavioural control that inturn affect behaviour (mediation), or by influencing people’s ability to translate their
intentions into action (moderation). However, the TPB assumes that income does not
directly influence on behaviour after controlling for intention and PBC.
Figure 1. Four models of the influence of socio structural variables and cognitions on behaviour.
Cognitions and social structural factors 81

A fourth possibility for the impact of social structural variables on physical activity is a
mediated moderation model (Figure 1, path d; e.g. Muller, Judd, & Yzerbyt, 2005).
Sheeran and Abraham (2003) illustrated the nature of this model. Findings showed that
temporal stability of intention, anticipated regret, and self-schemas each had significant
interactions with intentions in predicting exercise behaviour (i.e. participants who had
more stable intentions, those who anticipated regret if they did not exercise, andparticipants whowere schematic for exercise weremore likely to translate their exercise
intentions into behaviour compared with their counterparts). However, findings also
showed that the intention £ intention stability interaction term mediated the impact of
other moderators of the intention–behaviour relation (i.e. the other interactions were no
longer significant when the intention £ intention stability interaction term was taken
into account). In the present context, the mediated moderation of social structural
factors would be observed if findings showed that interactions between intentions and
social structural factors (e.g. intention £ education) were mediated by social cognitionvariables. Previous research would suggest intention stability as the key mediator of any
moderation effects of social structural variables, although we also tested the effects of
intentions and PBC here (Sheeran & Abraham, 2003).
These four models of influence – direct, mediation, moderation, and mediated
moderation – reflect differences in the importance that different theorists attach to
social structural factors versus health cognitions as determinants of behaviour. Theorists
with a social structuralist orientation consider income and similar factors as key
determinants of physical activity. Evidence that social structural factors have substantialdirect effects on physical activity or moderate the impact of intentions or PBC on
behaviour would be consistent with this theoretical perspective. Theorists who hold a
social cognition orientation, on the other hand, see beliefs as having the greatest
influence on behaviour (Conner & Norman, 2005). Thus, findings showing that
social/health cognitions have substantial effects, mediating the impact of social
structural variables, or mediating any moderating effects of these variables would
support the social cognition perspective. The aim of the present research was to
provide evidence that permits evaluation of the tenets of the social structuralist versussocial cognition perspective. In particular, we provide the first combined test of four
models that describe how key social structural factors (age, gender, education, income,
material deprivation, and social deprivation) and key social cognition variables
(intentions, PBC) together influence physical activity using a longitudinal design and
that also takes account of past behaviour.
Method
Sample and data collectionAt Time 1, a sample of 2,153 individuals, aged 15 years or older, was randomly selected
from a pool of 24,127 respondents to a national health survey. This survey used a
stratified design to obtain a representative sample of the Province of Quebec, Canada
(Daveluy, Pica, Audet, Courtemanche, & Lapointe, 2000). In this survey, all participants
had completed a questionnaire that measured their health habits and behaviours,including physical activity. Three months later (Time 2), 75.4% of these 2,153
individuals were successfully contacted by telephone to report their physical activity
(Nolin, Prud’homme, Godin, & Hamel, 2002). For the purposes of the present study,
pregnant women, and respondents younger than 18 years and older than 80 years were
82 Gaston Godin et al.

excluded. Consequently, 1,483 respondents were included in the present analyses. This
study was approved by the ethics committee of Sante Quebec and was carried out in
accordance with universal ethical principles.
Social cognition measuresBefore answering the questionnaire, physical activity was defined to participants as any
physical activities practised in leisure time. Intention was measured by askingparticipants, ‘Do you intend to participate regularly in physical activities for 20–30min
per session within the next year?’ Responses were on a five-point scale (definitely
no–definitely yes). The test–retest reliability of this measure is high (r ¼ .65–.77) and its
validity is well established (Godin, Valois, Shephard, & Desharnais, 1987; Valois, Godin,
& Bertrand, 1992). PBC was measured by the item, ‘For me, practising regular physical
activity for 20–30min per session in my leisure time during the next year would
be : : : difficult–easy (five-point scale). The test–retest reliability of the PBC measure is
also high (r ¼ .66; Godin, Valois, & Lepage, 1993) and its validity has been demonstratedpreviously (Gagne & Godin, 2007). Based on previous research, temporal stability of
intention was measured by the absolute difference in intention scores between Time 1
and Time 2 (Conner et al., 2000).
Measures of social structural factorsLevel of education (the number of school years completed), family income (the total
income of members of the household), gender, and age were assessed in the Time 1
questionnaire. Two objective measures of participants’ living conditions were also
taken, namely, material deprivation and social deprivation. These indices are derivedfrom the most basic geographical unit in Canada, i.e. the enumeration area (EA) which is
formed, on average, by 750 people and can be determined using postal codes. These
indices have been validated for the Province of Quebec (Pampalon & Raymond, 2000).
According to Townsend (1987), indices of deprivation measure social inequalities in
health. Material deprivation involves deprivation of the goods and conveniences that are
part of modern life and is based on a composite score of three indicators: the proportion
of individuals living in the EAwho have no high school diploma, the rate of employment,
and the average income of the EA. This index thus reflects variations in education,employment, and income at neighbourhood level. Social deprivation is closely related to
the concept of social capital and is also based on a composite score of three indicators:
the proportion of individuals in the EA who are separated, divorced or widowed, the
proportion of single-parent families in the EA, and the proportion of individuals in the
EA living alone. Both deprivation scores are computed by ranking EAs from least to most
deprived and dividing the distribution into quintiles (quintile 1 represents the least
deprived residential areas whereas quintile 5 represents the most deprived areas).
Measures of past and future behaviourTo assess past behaviour, respondents were asked how often they had participated in
one or more physical activities for 20–30min per session during free time in the last 3
months (seven-point scale; never – four times or more per week). The reliability and
validity of this measure of physical activity is well established (Gionet & Godin, 1989;
Godin, Jobin, & Bouillon, 1986; Godin & Shephard, 1986).
Cognitions and social structural factors 83
To ensure that shared method variance did not overestimate the strength of past
behaviour–future behaviour relations (see Ajzen, 1991, for discussion of this problem;
see Conner, Warren, Close, & Sparks, 1999, for an empirical demonstration), we used a
different measure of behaviour at Time 2 compared to Time 1. Physical activity at follow-
up was assessed by an adaptation of a questionnaire developed by Taylor et al. (1978)
and further validated by Jacobs, Ainsworth, Hartman, and Leon (1993). In brief, theparticipants first indicated if they practiced (participated in) one or more of 30 physical
activities (type) during their leisure time (yes or no) over the last 3 months. If yes,
information on frequency, duration, and intensity (three levels: low, moderate, and high)
was obtained and used to compute a total energy expenditure score (kcal/kg/week).
Based on these four dimensions of physical activity, an algorithm was created to classify
as active only the respondents who met public health recommendations for physical
activity (Kesaniemi et al., 2001). Thus, respondents could be classified in one of the
following four levels of physical activity: inactive (1), somewhat active (2), moderatelyactive (3), and active (4).
Results
Sample characteristicsAt baseline, 26.0% of the respondents reported being physically active at least three times a
week during their leisure time in the previous 3months. Intentions (M ¼ 4.08, SD ¼ 1.09)
and PBC (M ¼ 3.55, SD ¼ 1.06) were both positive. A majority of the respondents had
completed a high school level of education (65.5%), reported a family incomeabove 30,000
Canadian dollars (53.1%), and were women (59.4%). Themean age of the samplewas 44.5
years (SD ¼ 17.0). For the indices of deprivation, a near equal distribution was observed
per quintile for both material and social deprivation. At three-month follow-up, thepercentage of participants who were sedentary, somewhat active, moderately active, and
very active during their leisure time were 28, 16, 15, and 41%, respectively.
Direct and mediated effects of social structural factorsWe first examined whether social structural factors have direct effects on physical
activity or whether cognitions mediate social structural influences using procedures
recommended by Baron and Kenny (1986) and Preacher and Hayes (2008). Statistical
software used for all analyses was SAS version 9.1 (SAS Institute Inc., Cary, NC, USA).
The mediated moderation was tested by a SAS macro developed by Preacher and Hayesfor multiple mediator models available at http://www.comm.ohio-state.edu/ahayes/
SPSS%20programs/indirect.htm.
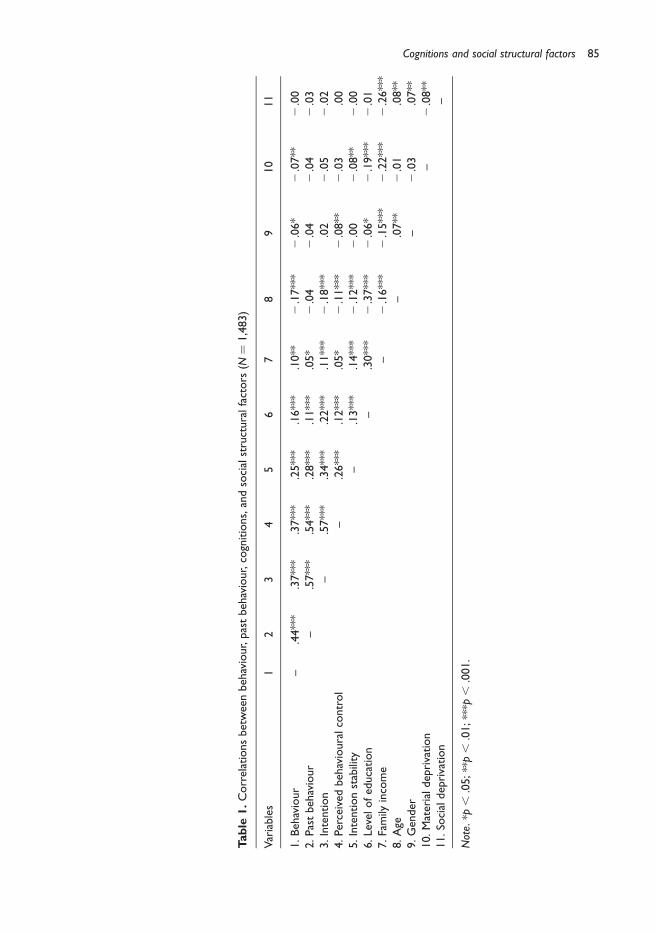
To this end, zero-order correlations were computed between the study variables
and future behaviour (see Table 1). Significant associations were observed for all of the
variables except social deprivation. Past behaviour and the cognitions (intention, PBC,
intention stability) showed the strongest relationships with behaviour. Physical activity
was more likely among participants who had engaged in physical activity in the past,
had a stronger activity intention, had higher PBC, had more stable intentions, hadgreater education and income, were younger, were men, and experienced lower
material deprivation. Because social deprivation was not related to physical activity,
this factor was not considered further. Correlations among the predictors were of small
to medium magnitude and did not engender concerns about multicollinearity
(Tabachnick & Fidell, 2001).
84 Gaston Godin et al.
Table
1.Correlationsbetweenbehaviour,pastbehaviour,cognitions,andsocialstructuralfactors
(N¼
1,483)
Variables
12
34
56
78
910
11
1.Behaviour
–.44***
.37***
.37***
.25***
.16***
.10**
2.17***
2.06*
2.07**
2.00
2.Pastbehaviour
–.57***
.54***
.28***
.11***
.05*
2.04
2.04
2.04
2.03
3.Intention
–.57***
.34***
.22***
.11***
2.18***
.02
2.05
2.02
4.Perceivedbehaviouralcontrol
–.26***
.12***
.05*
2.11***
2.08**
2.03
.00
5.Intentionstability
–.13***
.14***
2.12***
2.00
2.08**
2.00
6.Levelofeducation
–.30***
2.37***
2.06*
2.19***
2.01
7.Family
income
–2.16***
2.15***
2.22***
2.26***
8.Age
–.07**
2.01
.08**
9.Gender
–2.03
.07**
10.Materialdeprivation
–2.08**
11.So
cialdeprivation
–
Note.*p
,.05;**p,
.01;***p
,.001.
Cognitions and social structural factors 85
Hierarchical multiple regression analyses were conducted to provide formal tests of
the direct and indirect (mediated) effects of social structural factors on physical activity.
Past behaviour entered the equation on the first step because we were interested in
behaviour change. Cognitions (intention, PBC, and intention stability) were entered on
the second step. Each of the social structural variables that showed significant bivariate
correlations with physical activity (education, income, age, gender, and materialdeprivation) were then entered one at a time in successive three steps (Baron & Kenny,
1986). We were interested in whether social structural factors retained a significant
effect on physical activity after controlling for the cognitive variables and in the size of
this effect (i.e. evidence of direct unmediated effects). Also of interest was whether the
effect of each social structural factor was significantly mediated by the cognitive
variables (evidence of indirect mediated effects). This mediation analysis was tested in
one multiple mediators model by means of bootstrapping procedures developed by
Preacher and Hayes (2008) to estimate a total mediated effect and to compute a 95%confidence interval for this effect (i.e. a significance test for mediation similar to a Sobel
test). This procedure allowed us to examine also the 95% confidence interval for each
individual mediator comprised in the global model to determine which cognitions were
important in mediating particular effects (see the upper panel of Table 2).
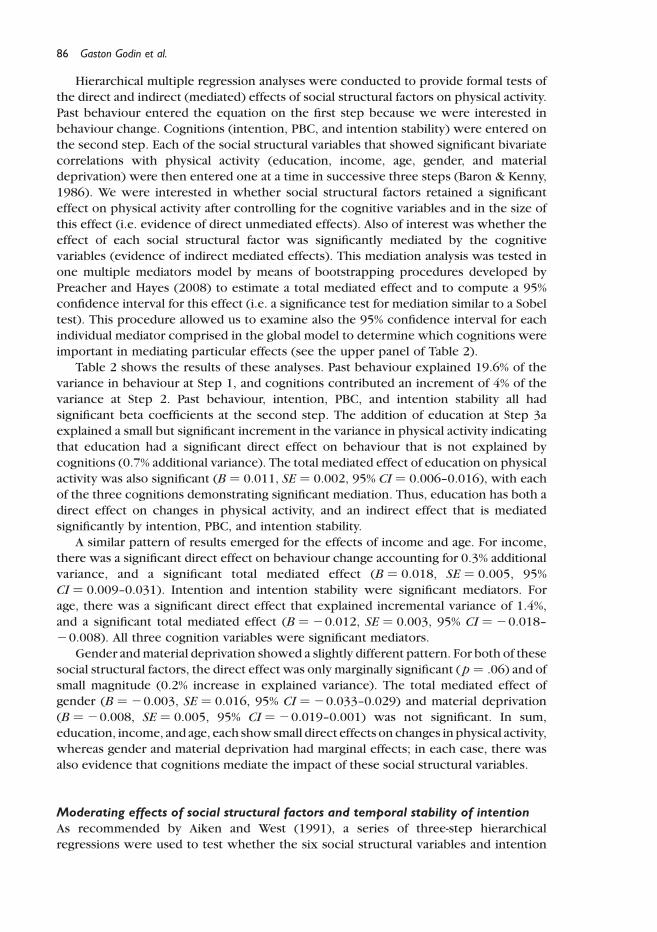
Table 2 shows the results of these analyses. Past behaviour explained 19.6% of the
variance in behaviour at Step 1, and cognitions contributed an increment of 4% of the
variance at Step 2. Past behaviour, intention, PBC, and intention stability all had
significant beta coefficients at the second step. The addition of education at Step 3aexplained a small but significant increment in the variance in physical activity indicating
that education had a significant direct effect on behaviour that is not explained by
cognitions (0.7% additional variance). The total mediated effect of education on physical
activity was also significant (B ¼ 0.011, SE ¼ 0.002, 95% CI ¼ 0.006–0.016), with each
of the three cognitions demonstrating significant mediation. Thus, education has both a
direct effect on changes in physical activity, and an indirect effect that is mediated
significantly by intention, PBC, and intention stability.
A similar pattern of results emerged for the effects of income and age. For income,there was a significant direct effect on behaviour change accounting for 0.3% additional
variance, and a significant total mediated effect (B ¼ 0.018, SE ¼ 0.005, 95%
CI ¼ 0.009–0.031). Intention and intention stability were significant mediators. For
age, there was a significant direct effect that explained incremental variance of 1.4%,
and a significant total mediated effect (B ¼ 20.012, SE ¼ 0.003, 95% CI ¼ 20.018–
20.008). All three cognition variables were significant mediators.
Gender andmaterial deprivation showed a slightly different pattern. For both of these
social structural factors, the direct effect was only marginally significant (p ¼ .06) and ofsmall magnitude (0.2% increase in explained variance). The total mediated effect of
gender (B ¼ 20.003, SE ¼ 0.016, 95% CI ¼ 20.033–0.029) and material deprivation
(B ¼ 20.008, SE ¼ 0.005, 95% CI ¼ 20.019–0.001) was not significant. In sum,
education, income, and age, each showsmall direct effects on changes in physical activity,
whereas gender and material deprivation had marginal effects; in each case, there was
also evidence that cognitions mediate the impact of these social structural variables.
Moderating effects of social structural factors and temporal stability of intentionAs recommended by Aiken and West (1991), a series of three-step hierarchical
regressions were used to test whether the six social structural variables and intention
86 Gaston Godin et al.
Table
2.Hierarchicalregressionofphysicalactivity
onpredictors:Testsofdirecteffectsandmediationofsocialstructuralfactors
bycognitions
Step/variable
entered
Model1
Model
2Model3a
Model
3b
Model3c
Model3d
Model
3e
Regressionanalyses
1–
Pastbehaviour
.44***
.29***
.29***
.29***
.30***
.29***
.29***
2–
Intention
.10**
.08*
.09**
.07*
.10**
.10*
Perceivedbehaviouralcontrol
.13***
.13***
.13***
.13***
.13***
.13***
Intentionstability
.10***
.09**
.09**
.09**
.10***
.09***
3a–Levelofeducation
.08**
3b–Family
income
.05*
3c–Age
2.12***
3d–Gender
2.04†
3e–Materialdeprivation
2.04†
R2
.196
.236
.242
.238
.249
.237
.237
DR2
–.040
.007
.003
.014
.002
.002
DF
–25.66***
13.10**
5.57*
27.27***
3.66*
3.63*
Mediationanalyses
BCa95%CI
Total
(.006;.016)
(.009;.031)
(2.017;2
.007)
(2.032;.029)
(2.020;.001)
Intention
(.001;.008)
(.002;.013)
(2.009;2
.001)
(.002;.031)
(2.008;.001)
Perceivedbehaviouralcontrol
(.001;.006)
(2.002;.009)
(2.007;2
.002)
(2.037;2
.003)
(2.007;.004)
Intentionstability
(.001;.007)
(.004;.018)
(2.007;2
.001)
(2.010;.017)
(2.012;2
.001)
Note.
†p¼
.06;*p
,.05;**p,
.01;***p
,.001.BCa95%CI;biascorrectedandaccelerated95%confidence
intervals.
Cognitions and social structural factors 87

stability moderate intention–behaviour and PBC–behaviour relations. Behaviour was
regressed on the respective cognition at Step 1, the social structural variable factor was
entered on the second step, and the social structural variable factor £ intention
interaction term entered the equation on the third step. Out of the 12 tests of
moderation by social structural variables, only one interaction term was significant: the
level of education moderated the impact of intentions on behaviour (b ¼ 0.06,p , .05).1 Simple slopes were computed at low (M 2 1SD) and high (M þ 1SD) levels of
the moderator, and showed that intentions better predicted physical activity among
more educated (B ¼ 0.490, SE ¼ 0.043, p , .001) as compared with less educated
participants (B ¼ 0.352, SE ¼ 0.035, p , .001).
As expected, the intention £ intention stability interaction term proved significant
after intention and intention stability had entered the regression equation (b ¼ 0.19,
p , .001). Simple slope analyses confirmed that more stable intentions better predicted
behaviour (B ¼ 0.603, SE ¼ 0.042, p , .001) compared with less stable intentions(B ¼ 0.257, SE ¼ 0.033, p , .001).
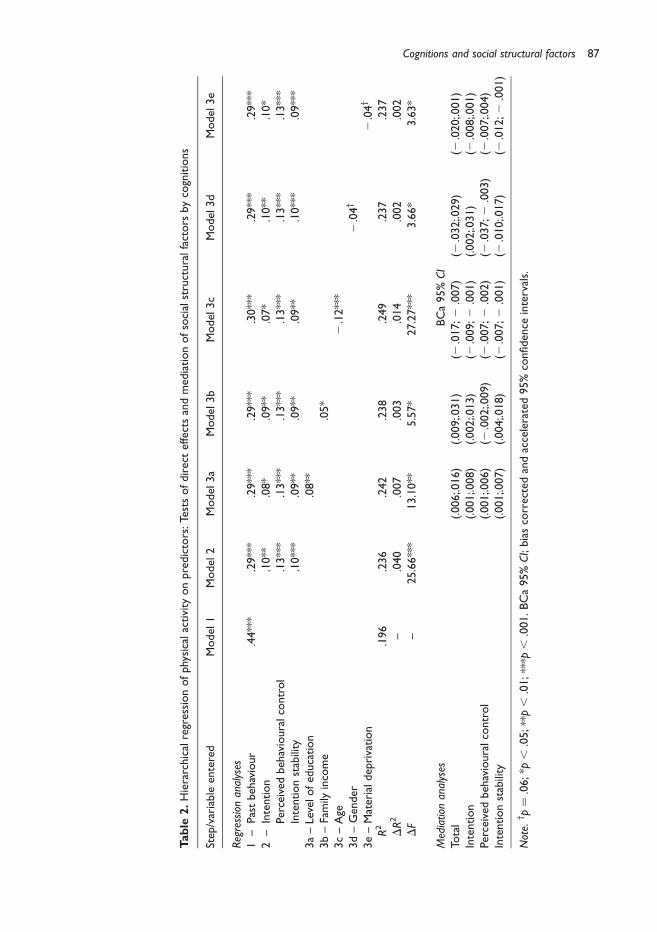
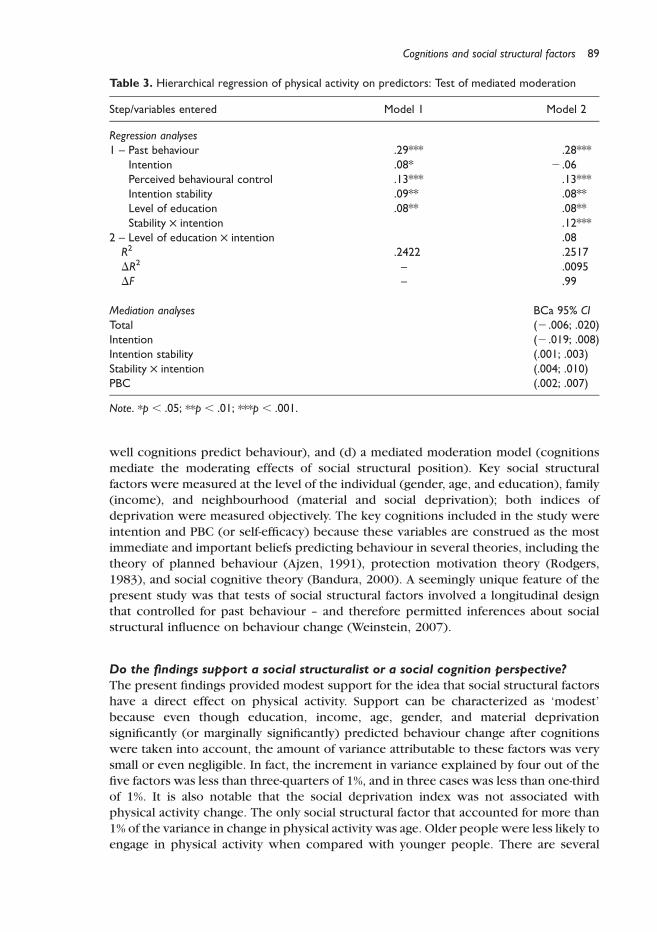
Mediation of moderating effects of social structural variablesA two-step hierarchical regression analysis was used to test whether intention stability
or the other cognitions mediate the observed moderation of the intention–behaviour
relation by education. Behaviour was regressed on past behaviour, cognitions,education, and the intention £ intention stability interaction term on the first step. On
the second step, the intention £ education interaction term was added to the equation.
Table 3 shows that all of the predictors had significant beta coefficients in the first
equation. Including the interaction between education and intention in the regression
equation did not improve the fit of the model, and the interaction term was not
significant (b ¼ 0.08, ns). Preacher and Hayes’ (2008) bootstrapping procedures
indicated that although the total mediated effect was not significant (B ¼ 0.008,
SE ¼ 0.007, 95% CI ¼ 20.006–0.021), three cognitions – PBC, intention stability, andthe interaction between intention and intention stability – significantly mediated the
moderating effect of education. In sum, social structural variables generally did
not moderate intention–behaviour or PBC–behaviour relations, and the one significant
moderating effect (intention £ education) appeared to be mediated by cognitive
factors, and in particular by the intention £ intention stability interaction term.
Discussion
The present study examined a key – but apparently little tested – assumption made by
social cognition models of health behaviour that structural factors such as gender, age,
and socio-economic status affect health behaviours entirely through their influence on
behaviour-relevant beliefs among an adult population. To provide a comprehensive test
of this assumption, four models of social structural and social cognition influence were
assessed: (a) a direct effects model (social structural factors influence behaviour over
and above the effects of cognitions), (b) a mediation model (cognitions mediate socialstructural influence), (c) a moderation model (social structural factors influence how
1 A table describing the moderated regression analyses for each social structural variable is available from the first author.
88 Gaston Godin et al.
well cognitions predict behaviour), and (d) a mediated moderation model (cognitions
mediate the moderating effects of social structural position). Key social structural
factors were measured at the level of the individual (gender, age, and education), family(income), and neighbourhood (material and social deprivation); both indices of
deprivation were measured objectively. The key cognitions included in the study were
intention and PBC (or self-efficacy) because these variables are construed as the most
immediate and important beliefs predicting behaviour in several theories, including the
theory of planned behaviour (Ajzen, 1991), protection motivation theory (Rodgers,
1983), and social cognitive theory (Bandura, 2000). A seemingly unique feature of the
present study was that tests of social structural factors involved a longitudinal design
that controlled for past behaviour – and therefore permitted inferences about socialstructural influence on behaviour change (Weinstein, 2007).
Do the findings support a social structuralist or a social cognition perspective?The present findings provided modest support for the idea that social structural factors
have a direct effect on physical activity. Support can be characterized as ‘modest’
because even though education, income, age, gender, and material deprivation
significantly (or marginally significantly) predicted behaviour change after cognitions
were taken into account, the amount of variance attributable to these factors was very
small or even negligible. In fact, the increment in variance explained by four out of the
five factors was less than three-quarters of 1%, and in three cases was less than one-thirdof 1%. It is also notable that the social deprivation index was not associated with
physical activity change. The only social structural factor that accounted for more than
1% of the variance in change in physical activity was age. Older people were less likely to
engage in physical activity when compared with younger people. There are several
Table 3. Hierarchical regression of physical activity on predictors: Test of mediated moderation
Step/variables entered Model 1 Model 2
Regression analyses1 – Past behaviour .29*** .28***
Intention .08* 2 .06Perceived behavioural control .13*** .13***Intention stability .09** .08**Level of education .08** .08**Stability £ intention .12***
2 – Level of education £ intention .08R2 .2422 .2517DR2 – .0095DF – .99
Mediation analyses BCa 95% CITotal (2 .006; .020)Intention (2 .019; .008)Intention stability (.001; .003)Stability £ intention (.004; .010)PBC (.002; .007)
Note. *p , .05; **p , .01; ***p , .001.
Cognitions and social structural factors 89
plausible mechanisms for such direct effects of age including biomedical factors (e.g.
illness rates, increased infirmity) and social expectations (reduced activity is associated
with the elderly stereotype; see Bargh, Chen, & Burrows, 1996).
The present findings were also consistent with partial mediation – the idea that
social structural factors influenced physical activity in part because of their influence on
cognitions. The finding that all five social structural variables that had significantassociations with behaviour also (a) had significant associations with at least one of the
cognition variables and (b) were significantly mediated by the cognition variables speak
to this interpretation (Baron & Kenny, 1986).
Even though it seems intuitively plausible that social structural factors would
influence people’s capacity to translate their intentions and PBC into action, the present
study found little support for this moderation model. Age, gender, income, and material
deprivation did not moderate cognition–behaviour relations. The only significant
finding from 12 moderator analyses was that greater education was associated withimproved consistency between intentions and subsequent physical activity. However,
temporal stability of intention did significantly moderate intention–behaviour relations –
and also mediated the effect of the education £ intention interaction on physical
activity. That is, greater education was associated with improved intention–behaviour
consistency because greater education was associated with more stable intentions.
These findings do not support the idea that social structural position is an important
determinant of how well cognitions guide physical activity; however, the present
findings contribute to evidence indicating that temporal stability of intention is a keyindicator of ‘strong’ intentions – more stable intentions better predicted behaviour
(Conner et al., 2000; Sheeran et al., 1999), and mediated the effects of other moderating
variables here (Sheeran & Abraham, 2003).
Overall, the present findings better support the social cognition perspective than the
social structural perspective. Apart from age, social structural variables offer little
additional predictive power after considering intentions and PBC when modelling the
determinants of physical activity. Indeed, the magnitude of the direct effects of social
structural factors was very small (DR2 ¼ .002–.014), and intentions and perceivedcontrol together explained 2.85–20.0 times more variance compared with each
social structural factor. Thus, the present findings suggest that the assumption made by
social cognitions models that social structural factors no longer influence behaviour
once relevant health cognitions have been taken into account is, strictly speaking,
accurate. The small/marginal effect sizes obtained for social structural factors here is
consistent with the social cognition view that behaviour-relevant beliefs capture the
most important influences on change in physical activity.
Possible objectionsTwo possible objections to the present analyses should be considered. First, it might be
argued that controlling for past behaviour is not legitimate, or that this type of analysis
served to obscure the influence of social structural factors. Weinstein (2007) pointed
out that controlling for past behaviour is a conservative strategy and may underestimate
other influences on behaviour, whereas failing to control for past behaviour is also likelyto be misleading, and overestimate how influential are the focal predictor variables. To
limit the attenuation associated with integrating past behaviour, we used two different
measures to assess physical activity levels at baseline and follow-up. Doing so ensures
that the strong association between past and future behaviour is not due to shared
90 Gaston Godin et al.
method variance (Conner et al., 1999). On the other hand, the use of two different
measures could lead to an underestimation of the effect of past behaviour as a result of
the measurement of two different aspects of a given behaviour. Given that health
psychologists are not usually in a position to intervene before participants have had the
opportunity to engage in physical activity, and thus, almost inevitably, are concerned
with behaviour change, we believe that controlling for past behaviour is the preferable(albeit conservative) analytic strategy. It is also the case that controlling for past
behaviour in the present analyses did not obscure the effects of social structural factors
or privilege the role of cognitions. For instance, a hierarchical regression of behaviour at
Time 2 on intention and PBC at Step 1, followed by age at Step 2 (the best social
structural predictor in the original analyses), indicated that age explained less – not
more – variance when past behaviour was not controlled (1.4% vs. 1.0%).
A second potential objection to the present analyses might be that the effect size for
social cognition variables was smaller than expected (intentions and PBC explained 3%of the additional variance in behaviour change), and seem to be out of line with
published meta-analytic findings. In fact, intentions and PBC explained 17% of the
variance in behaviour when past behaviour was not controlled for – these values are
only slightly lower than those reported for application of the TPB for health-related
behaviours (e.g. Armitage & Conner, 2001; Godin & Kok, 1996) including physical
activity (Downs & Hausenblas, 2005; Hagger et al., 2002). We also reanalysed data from
the Ouellette and Wood’s (1998) meta-analysis of the influence of intentions on future
behaviour (controlling for past behaviour) to further test the representativeness of thepresent findings. Ouellette and Wood’s (1998) data pertained to behaviours that likely
come under the control of habits (i.e. behaviours that are frequently performed in stable
contexts, as is the case for physical activities). These analyses showed that intentions
and PBC together explained 5% of the variance in behaviour when past behaviour was
taken into account.2 Thus, findings from the present study are not out of line with the
results of previous meta-analytic reviews. Rather, the findings are consistent with
evidence indicating that intentions and PBC have a small-to-medium, but important,
impact on behaviour change (Webb & Sheeran, 2006).
Limitations of the present study and directions for future researchLimitations of the present research should be acknowledged. First, although the
sample used in the present study was representative of the population from whichit was drawn, further empirical work is needed to determine whether the present
findings generalize to other samples and populations. Second, the present research
used single-item measures of intention and PBC to reduce participant burden and
optimize response rates. These measures used here proved reliable and valid in
previous research (Gagne & Godin, 2007; Godin et al., 1987, 1993; Valois et al.,
1992); however, it would have been desirable to test reliability in the present study
(e.g. using multiple items). Finally, the measures of past and future behaviour, as
well as measures of key social structural variables (e.g. income) relied on self-report.Corroboration of the present findings using more objective indices for both sets of
variables would be desirable.
2 A table describing the regression analyses based on correlations presented in Table 2 of Ouellette and Wood’s (1998)meta-analysis can be obtained from the first author.
Cognitions and social structural factors 91

The present research also leaves open several important questions to which future
research might profitably be directed. For instance, the present findings indicate that
social structural factors influence physical activity in part by influencing behaviour-
relevant beliefs. However, it is not yet clear what are the processes by which social
structural position influences cognitions. For instance, are cultural and social networks
or lack of amenities and opportunity responsible for the findings showing that incomeengenders weaker intentions to be physically active, or that material deprivation and
lack of education serve to undermine intention stability. The present study also did not
examine features of the physical environment (e.g. access to footpaths and green
spaces, distance to sports grounds and gymnasia, calibres of recreational facilities; see
Spence & Lee, 2003; for a review), and thus the (potentially complex) interplay between
social structure, social cognition, and environmental features in determining rates of
physical activity remains to be investigated in future studies.
Finally, the present study included only two explicit cognition measures (intentionand PBC), and thus overlooked the possibility that other cognition variables (such as
attitudes and norms), or implicit measures of cognitions, might be important. For
instance, evidence indicates that images of the type of person who exercises predict
exercise behaviour over and above the effects of past behaviour, intention, and PBC
(Rivis & Sheeran, 2003), and a recent meta-analysis showed that implicit measures
capture a significant increment in the variance explained in behaviour after controlling
for explicit measures (Poehlmann, Uhlmann, Greenwald, & Banaji, 2007). Thus,
although the present study possesses limitations and leaves important questionsunanswered, it suggests several useful directions for further research.
In conclusion, this study made an important first step in delineating different routes
by which social structural and social cognition factors combine to influence physical
activity. The use of a large, representative sample, and a longitudinal design that also
controlled for past behaviour provided a stricter test of four models of influence (direct
effects, mediated, moderation, and mediated moderation) than has been afforded
heretofore. Findings indicated that the magnitude of the direct influence of social
structural factors was small both in absolute terms and compared with influence bycognitions; moreover, social structural factors did not moderate cognition–behaviour
consistency. Thus, the present findings are more consistent than not with the
assumption that social structural factors have little influence on behaviour once
cognitions have been taken into account, and support the idea that cognitions are the
key predictors of behaviour change.
References
Abraham, C., Sheeran, P., & Johnston, M. (1998). From health beliefs to self-regulation: Theoretical
advances in the psychology of action control. Psychology and Health, 13, 569–591.
Aiken, L., &West, S. (1991).Multiple regression: Testing and interpreting interactions. Thousand
Oaks, CA: Sage.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision
Processes, 50, 179–211.
Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: A meta-analytic
review. British Journal of Social Psychology, 40, 471–479.
Bandura, A. (2000). Health promotion from the perspective of social cognitive theory.
In P. Norman, C. Abraham, & M. Conner (Eds.), Understanding and changing health
behaviour: From health beliefs to self-regulation (pp. 239–299). Amsterdam: Harwood
Academic.
92 Gaston Godin et al.
Bargh, J. A., Chen, M., & Burrows, L. (1996). Automaticity of social behavior: Direct effects of trait
construct and stereotype-activation on action. Journal of Personality and Social Psychology,
71, 230–244.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social
psychological research: Conceptual, strategic, and statistical considerations. Journal of
Personality and Social Psychology, 51, 1173–1182.
Conner, M., & Godin, G. (2007). Temporal stability of behavioural intention as a moderator of
intention–health behaviour relationships. Psychology and Health, 22, 875–897.
Conner, M., & Norman, P. (2005). Predicting health behaviour (2nd ed.). Beckshire: Open
University Press.
Conner, M., Sheeran, P., Norman, P., & Armitage, C. J. (2000). Temporal stability as a moderator of
relationships in the theory of planned behaviour. British Journal of Social Psychology, 39,
469–493.
Conner, M., & Sparks, P. (2005). Theory of planned behaviour and health behaviour. In M. Conner
& P. Norman (Eds.), Predicting health behaviour: Research and practice with social
cognition models (Vol. 2nd, pp. 170–222). Maidenhead: Open University Press.
Conner, M., Warren, R., Close, S., & Sparks, P. (1999). Alcohol consumption and the theory of
planned behavior: An examination of the cognitive mediation of past behavior. Journal of
Applied Social Psychology, 29(8), 1676–1704.
Cubbin, C., Sundquist, K., Ahlen, H., Johansson, S. E., Winkleby, M. A., & Sundquist, J. (2006).
Neighborhood deprivation and cardiovascular disease risk factors: Protective and harmful
effects. Scandinavian Journal of Public Health, 34, 228–237.
Daveluy, C., Pica, L., Audet, N., Courtemanche, R., & Lapointe, F. (2000). Enquete sociale et de
sante 1998. Quebec: Institut de la statistique du Quebec.
de Ridder, D., & de Wit, J. (2006). Self-regulation in health behavior. Chichester: Wiley.
Downs, D. S., & Hausenblas, H. A. (2005). The theories of reasoned action and planned
behavior applied to exercise: A meta-analytic update. Journal of Physical Activity and
Health, 2, 76–97.
Gagne, C., & Godin, G. (2007). Does the easy–difficult item measure attitude or perceived
behavioural control? British Journal of Health Psychology, 12, 543–557.
Gionet, N. J., & Godin, G. (1989). Self-reported exercise behavior of employees: A validity study.
Journal of Occupational Medicine, 31, 969–973.
Godin, G., Jobin, J., & Bouillon, J. (1986). Assessment of leisure time exercise behavior by self-
report: A concurrent validity study. Canadian Journal of Public Health, 77, 359–362.
Godin, G., & Kok, G. (1996). The theory of planned behavior: A review of its applications to health-
related behaviors. American Journal of Health Promotion, 11, 87–98.
Godin, G., & Shephard, R. J. (1986). A simple method to assess exercise behavior in the
community. Canadian Journal of Applied Sport Sciences, 10, 141–146.
Godin, G., Valois, P., & Lepage, L. (1993). The pattern of influence of perceived behavioral control
upon exercising behavior: An application of ajzen’s theory of planned behavior. Journal of
Behavioral Medicine, 16, 81–102.
Godin, G., Valois, P., Shephard, R. J., & Desharnais, R. (1987). Prediction of leisure-time exercise
behavior: A path analysis (LISREL V) model. Journal of Behavioral Medicine, 10, 145–158.
Hagger, M. S., Chatzisarantis, N. L. D., & Biddle, S. J. H. (2002). A meta-analytic review of the
theories of reasoned action and planned behavior in physical activity: Predictive validity and
the contribution of additional variables. Journal of Sport and Exercise Psychology, 24, 3–32.
Humpel, N., Owen, N., & Leslie, E. (2002). Environmental factors associated with adults’
participation in physical activity: A review. American Journal of Preventive Medicine, 22,
188–199.
Jacobs, D. R., Jr, Ainsworth, B. E., Hartman, T. J., & Leon, A. S. (1993). A simultaneous evaluation of
10 commonly used physical activity questionnaires. Medicine and Science in Sports and
Exercise, 25, 81–91.
Cognitions and social structural factors 93
Kesaniemi, Y. K., Danforth, E., Jr, Jensen, M. D., Kopelman, P. G., Lefebvre, P., & Reeder, B. A.
(2001). Dose-response issues concerning physical activity and health: An evidence-based
symposium. Medicine and Science in Sports and Exercise, 33, S351–S358.
Muller, D., Judd, C., & Yzerbyt, V. (2005). When moderation is mediated and mediation is
moderated. Journal of Personality and Social Psychology, 89, 852–863.
Nolin, B., Prud’homme, D., Godin, G., & Hamel, D. (2002). Enquete quebecoise sur l’activite
physique et la sante 1998. Quebec: Institut de la satistique du Quebec, Institut National de
sante publique du Quebec et Kino-Quebec.
Ouellette, J. A., &Wood, W. (1998). Habit and intention in everyday life: The multiple processes by
which past behavior predicts future behavior. Psychological Bulletin, 124, 54–74.
Pampalon, R., & Raymond, G. (2000). A deprivation index for health and welfare planning in
Quebec. Chronic Diseases in Canada, 21, 104–113.
Poehlmann, T. A., Uhlmann, E. L., Greenwald, A. G., & Banaji, M. R. (2007). Understanding and
using the implicit association test: III. Meta-analysis of predictive validity. Unpublished
manuscript. Yale University.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and
comparing indirect effects in multiple mediator models. Behavior Research Methods, 40,
879–891.
Rivis, A., & Sheeran, P. (2003). Social influences and the theory of planned bahaviour: Evidence for
a direct relationship between prototypes and young people’s exercise behaviour. Psychology
and Health, 18, 567–583.
Rodgers, R. (1983). Cognitive and physiological processes in fear appeals and attitude change:
A revised theory of protection motivation. In J. Cacioppo & R. Petty (Eds.), Social
psychophysiology: A source book. New York: Guilford Press.
Rosenstock, I. M. (1966). Why people use health services. The Milbank Memorial Fund
Quarterly, 44, 94–124.
Sallis, J. F., & Owen, N. (1999). Physical activity and behavioral medicine. Thousand Oaks, CA:
Sage.
Sheeran, P. (2002). Intention–behavior relations: A conceptual and empirical review. European
Review of Social Psychology, 12, 1–36.
Sheeran, P., & Abraham, C. (2003). Mediator of moderators: Temporal stability of intention and the
intention–behavior relation. Personality and Social Psychology Bulletin, 29, 205–215.
Sheeran, P., Orbell, S., & Trafimow, D. (1999). Does the temporal stability of behavioral intentions
moderate intention–behavior and past behavior–future behavior relations? Personality and
Social Psychology Bulletin, 25, 724–730.
Spence, J., & Lee, R. (2003). Toward a comprehensive model of physical activity. Psychology of
Sport and Exercise, 4, 7–24.
Stryker, S. (1980). Symbolic interactionism: A social structural version. Menlo Park, CA: The
Benjamin/Cummings Publishing Company.
Stryker, S. (1983). Social psychology from the standpoint of a structural symbolic interactionist:
Towards an inter-disciplinary social psychology. Advances in Experimental Social
Psychology, 16, 181–218.
Sundquist, J., Malmstrom, M., & Johansson, S. E. (1999). Cardiovascular risk factors and the
neighbourhood environment: A multilevel analysis. International Journal of Epidemiology,
28, 841–845.
Tabachnick, B. G., & Fidell, L. S. (2001). Using multivariate statistics (4th ed.). Needham Heights,
MA: Allyn and Bacon.
Taylor, H. L., Jacobs, D. R., Schucker, B., Knudsen, J., Leon, A. S., & DeBaker, G. (1978).
A questionnaire for the assessment of leisure-time physical activity. Journal of Chronic
Disease, 31, 741–755.
Townsend, P. (1987). Deprivation. Journal of Social Policy, 16, 125–146.
94 Gaston Godin et al.
Trost, S. G., Owen, N., Bauman, A. E., Sallis, J. F., & Brown, W. (2002). Correlates of adults’
participation in physical activity: Review and update. Medicine and Science in Sports and
Exercise, 34, 1996–2001.
Valois, P., Godin, G., & Bertrand, R. (1992). The reliability of constructs derived from attitude-
behavior theories: An application of generalizability theory in the health sector. Quality and
Quantity, 26, 291–305.
Webb, T. L., & Sheeran, P. (2006). Does changing behavioral intentions engender behavior
changes? A meta-analysis of the experimental evidence. Psychological Bulletin, 132, 249–268.
Weinstein, N. D. (2007). Misleading tests of health behavior theories. Annals of Behavioral
Medicine, 33, 1–10.
Received 31 October 2008; revised version received 18 February 2009
Cognitions and social structural factors 95
Copyright © 2022 FDOKUMEN




















