sir salimullah medical college journal
77
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of sir salimullah medical college journal
SIR SALIMULLAH MEDICAL COLLEGE JOURNAL
VOL. 28, NO. 2, JULY 2020
An Official Journal
of
Sir Salimullah Medical College Teachers’ Association
EDITORIAL BOARD
Address of Correspondence
Dr. Sudip Das Gupta, Editor-in-chief, Sir Sanimullah Medical College Journal
Department of Urology, Sir Salimullah Medical College Mitford Hospital, Dhaka-1100
E-mail: [email protected]
Date of Publication: March 2021
Chairman
Professor Dr. Md. Nurul Hooda Lanin
Principal of SSMC
Editor-in-Chief
Dr. Sudip Das Gupta
Joint Editors
Professor Dr. Zahed Ali
Professor Dr. Ahmed Hossain
Dr. Sunirmal Roy
Professor Dr. Gobinda Chandra Saha
Professsor Dr. Muna Shalima Jahan
Assistant Editors
Dr. Afshan Zareen
Dr. Ranajit Sen Chowdhury
Dr. Amiruzzaman
Dr. Mohammad Moshiur Rahman Khokon
Members
Professor Dr. Dewan Golam Md. Akaiduzzaman
Professor Dr. Chandra Shekhar Majumder
Professor Dr. Md. Abu Jafar
Professor Dr. Shikha Paul
Dr. Irin Parvin Alam
Dr. Tarek Mahbub Khan
Dr. Nasrin Rosy
Dr. Pallab Kanti Saha
Dr. Showkat Hossain Romol

The Sir Salimullah Medical College Journal a biannual (January &
July) Journal published by the Editorial Board on behalf of Sir
Salimullah Medical College Teachers’ Association. Each issue
includes editorial, original articles, review articles and case reports
of exceptional merit on any discipline of medical science.
Submission of manuscripts
Papers are accepted for publication with an understanding that
they are submitted solely to the Sir Salimullah Medical College
Journal. Statements and opinions expressed in the papers,
communications, and letter herein are those of author(s) and not
necessarily those of editor or publisher. Three hard / printed copies
in A4 size paper should be sent to the Editor. In addition an
electronic/digital version of the article should also be submitted.
Preparation of Manuscripts
Manuscripts should be typed on one side of good quality paper, with
margins of at least 25mm and using double space throughout. Each
component of the manuscript should begin on a new page in the
sequence of title page, abstract, text, references, tables, and legend
for illustrations. The title page should include the title of the paper,
name of the author(s), name of the department(s) to which the work
should be attributed. The text should be presented in the form of
Introduction, Materials and Methods, Results, and Discussion.
The authors should sign a covering letter mentioning that final
manuscript has been seen and approved by all authors. The letter
should mention the name of the person (with address and telephone
number) responsible for negotiation concerning the manuscript.
Abstracts
Provide on a separate page an abstract of not more than 250 words.
They should briefly describe the problem being addressed in the
study, how the study was performed, the salient results, and what
the authors conclude from the results.
Table
Each table should be typed in on separate sheet. Table should have
brief title for each, should be numbered consecutively using Roman
numbers and be cited in the in consecutive order internal horizontal
and vertical rules should not be used.
Results should be presented in logical sequence in the text, tables or
illustration. Do not repeat in the text all data in the tables or
illustrations; emphasize or summarize only important observations.
Drug names
Generic names should generally be used. When proprietary brands
are used in research, include the brand name in parentheses in the
Methods section.
Illustrations
Figure should be professionally designed symbols, lettering and
numbering should be clear and large. The back of each figure should
include the sequence number and the proper orientation (e.g., "top").
Photographs and photomicrographs should be supplied as glossy
black and white prints unmounted. Legend for each illustration
should be submitted in separate sheets. All photographs, graphs,
and diagrams should be referred to as figures numbered consecutively
in the text.
Instruction to Contributors
President
Dr. Sudip Das Gupta
Vice President
Dr. Shahnaz Begum
General Secretary
Dr. Md. Abdus Satter Sarkar
Treasurer
Dr. Md. Moshiur Rahman Khokon
Joint Secretary
Dr. Amiruzzaman
Organizing Secretary
Dr. Abul Fazal Md. Helal Uddin
Press and Publication Secretary
Dr. Sunirmal Roy
Scientific Secretary
Professor Dr. Muna Shalima Jahan
Office Secretary
Dr. Pallab Kanti Saha
Cultural & Entertainment
Secretary
Dr. Runa Akhter Dola
Social Welfare Secretary
Dr. Ashim Chakraborty
International Secretary
Dr. Md. Harun-Ar-Rashid
Members
Professor Mahmuda Begum
Professor Dr. ABM Bayezid Hossain
Professor Md. Abdul Kader Akanda
Professor Harunur Rashid Khan Shilpi
Professor Salma Yesmin Choudhury
Professor Chandra Shekhar Majumder
Professor Md. Abu Jafar
Professor Ahmed Hossain
Professor Gobinda Chandra Saha
Professor Md. Sirajul IslamDr. Md. Aminul IslamDr. Nasrin Rosy
Sir Salimullah MedicalCollege Teachers’ Association
EXECUTIVE COMMITTEE
Published byDr. Sunirmal RoyPublication SecretaryOn behalf of Sir Salimullah MedicalCollege Teachers’ Association.Mobile: 01771084056

Discussion
Emphasize the new and important aspects of the study
and the conclusion that follow from them. The detail
data or other material given in the Introduction or the
Results section should not be repeated. The
implications of the findings and their limitations,
including implication for future research should be
included in the Discussion section. The observations
should be compared and related to other relevant
studies. New hypothesis is appreciated, however they
should be clearly labeled as such. Recommendations
may be included only when appropriate.
References
References should be numbered consecutively in the order
in which they are first mentioned in the text. Identify
references in the text, tables and legend by Roman numerals
in parenthesis. Use the styles of the example below, which
are based on the formats used by the US National Library
of Medicine (NLM) in the Index Medicus.
Avoid using abstracts as references. References to paper
accepted but not yet published should be designated as
"in press" or "forthcoming"; authors should obtain written
permission to cite such papers as well as verification that
they have been accepted for publication. Information from
manuscripts submitted but not accepted should be cited
as "unpublished observations" with written permission
from the source. Avoid using a "personal communication"
unless it provides essential information not available from
a public source. For scientific articles, authors should
obtain written permission and confirmation of accuracy
from the source of a personal communication.
The references must be verified by the author(s) against
the original documents.
1. Articles in Journal
a. List all six authors when six or less;
Vega KJ, Pina I, Krevsky B. Heart transplantation
is associated with an increased risk for
pancreatobiliary disease. Ann Intern Med 1996;
124 : 980-3.
b. When seven or more, list the first three and
then add et al; Parkin DM, Clayton D, Black
RJ et al. Childhood leukemia in Europe after
Chernobyl 5-year follow-up. BR J Cancer 1996;73 : 1006-12.
c. No author given
Cancer in South Africa (editorial). S Afr Med J
1994; 84 : 15.
d. Organization as author
The Cardiac Society of Australia and New
Zealand. Clinical exercise stress training. Safety
and performance guideline. Med J Aust 1996;
164 : 282-4.
2. Books and Others Manuscripts
a. Personal author
Laurence DR, Bennett PN, Brown MJ. Clinical
Pharmacology Eighth ed. New York : Churchill
Livingstone; 1997.
b. Editor(s), (s) as author
Katzung BG, editor,. Basic & Clinical
Pharmacology. 6th ed. Connecticut : Appleton
& Lange; 1995.
c. Organization as author and publisher
World Health Organization, Ethical criteria for
Medical Drug Promotion: World Health
Organization; 1988.
d. Chapter in a book
Philips SJ, Whisnant JP. Hypertension and
stroke. In : Laragh JH, Brenner BM, editors.
Hypertension: pathophysiology, diagnosis, and
management. 2nd ed. New York : Raven Press;
1995; p. 465-78.
e. Dissertation
Kaplan SJ. Post-hospital home health care :
the elderly's access and utilization
(dissertation). St. Louis (MO) : Washington
Univ; 1995.
3. Other published material
a. Newspaper article
Lee G. Hospitalizations tied to ozone pollution
: study estimates 50,000 admissions annually.
The Washington Post 1996; June 21; Sect. A : 3
(col. 5).
b. Dictionary and similar references
Student's medical dictionary. 26th ed.
Baltimore : Williams & Wilkins; 1995.
Apraxia; p. 119-20.
4. Unpublished material
a. In press
Leshner Al. Molecular mechanisms of cocaine
addition. N Engl J med In Press 1997.
5. Electronic Material
a. Journal articles in electronic format
Morse SS. Factors in the emergence of
infectious diseases. Emerg Infect Dis I Serial
online I 1995 Jan-Mar I cited 1996 June 5 I;
1(1) : 24 screens I.
Available from : URL : http: //www.cdc.gog/
ncidod/ EID/eid.htm
Permissions
A written statement must accompany materials taken
from other sources from both author and publisher giving
permission to the Journal for reproduction. Obtain
permision in writing from at least one author of papers
still in press unpublished data, and personal
communications.
Review and Action
All submitted manuscripts will be reviewed by the
Editorial Board and reviewer. Rejected manuscripts will
not be returned. Ethical aspects will be considered in
the assessment of the paper.

Editorial
Sir Salimullah Med Coll J 2020; 28: 49-50
The world is passing a challenging period due tothe coronavirus disease (COVID-19) pandemic,which has disordered the whole world. The rapidlyrising incidence and death rates of cases of COVID-19 continue to be recorded worldwide. Accordingto WHO’s situation report dated December 12 2020,the total confirmed cases of COVID-19 are71,290,820, with a total death estimate of 1,598,666globally. About 49,637,225 people have alreadyrecovered from this virus worldwide.1 Precau-tionary measures for preventing transmissionwere notable, including maintaining socialdistancing, personal hygiene, and face-protectionwith masks. There are currently some approvedvaccines for use for protecting this virus, but still,most of the privileges will be available to developedcountries.2
Scientists have been researching cures for thisdisease extensively. They also proposedmedications, like Azithromycin, Hydroxy-chloroquine, Favipiravir, Remdesivir, Dexameth-asone, and a few others that have been used byhealthcare professionals against the COVID-19disease.3,4 Some of these therapies have provento be successful in the treatment process of COVID-19, but substantial clinical benefits are not yet wellestablished. Because of these challenges, theadoption of traditional interventions has re-emerged as viable options in regulating thisdisease. Nevertheless the subject of concern hasrecently been convalescent plasma therapy (CPT).Evidence supported that this CPT as a treatmentoption among different virus infected patientsduring the last few years.5 CPT method involvesusing plasmapheresis in survivors with previousinfections caused by that specific pathogens ofinterest, who have later developed antibodiesagainst that causative agent.5,6
“Convalescent Plasma Therapy in COVID-19 Disease”
In recent times, reports claim that the use of CPTas a measure in shortening COVID-19 has beenvital, particularly in low-and middle-incomecountries, as people struggle to afford ventilatorsor abide by restriction policies over the long-term.7
It’s also beneficial for the developed countries. Anexcellent An example was reported from the USfrom a conceptual perspective, which detailed theuse of CPT in COVID-19 management around thestarting of July 2020.8 Meanwhile, the findingsshowed a positive difference in better oxygenation,sequential organ failure assessment (SOFA) scores,and ultimately reduced need for ventilator use.Two main disadvantages to this study were that itwas not a well-designed randomized study, andother drugs were combined with CPT.8,9 Incontinuance to its advantageous nature, researchclaims that antibodies from convalescent plasmacontribute to restrictions of viral replications,whereas when administered to patients withhemorrhagic fevers such as Ebola, other plasmaelements were helpful in replenishing coagulationfactors.10
Patients who recovered from COVID-19 wereregarded as a valuable donor source of CPT, Inparticular, those COVID-19 patients recovered witha high neutralizing antibody titer at or above 1:640dilution. It is necessary to remember that bloodsafety and reliability must not be sacrificed forpractical therapeutic methods due to the sensitivityand idiosyncrasy attached to this matter. It isessential to note that blood safety and reliabilitymust not be sacrificed for practical therapeuticmethods due to the sensitivity and idiosyncrasyattached to this matter.11 Neutralizing antibodylevels varied, with geometric mean titer 1:333(range< 1:10–1:2,560). The highest levels ofneutralizing antibodies were found in donorshospitalized with laboratory-confirmed SARS-CoV-

2 infection, those who were older, and those whodonated <60 days from diagnosis. A study indicatesthat commercial ELISA (e.g., SARS-CoV-2 infectedcell lysate ELISA assay and Euroimmun ELISA)can perform effectively as a substitute for predictingneutralizing antibody titers and represent astreamlined and rapid way to guide convalescentplasma donor selection.12
Few studies were performed to evaluate the safetyand related risks of CPT in patients with COVID-19 . (8,13) Only a few reported cases have shownany serious adverse effects of CPT as a therapeuticmeasure for the COVID-19 disease. The focusshould be on susceptible groups such as pediatricpatients, gravid women, aged individuals, andpatients with co-morbidities. The most commonadverse events from convalescent plasmadonations are transfusion-related events. Theseincludes chills, fever, anaphylactic reactions,TRALI, TACO, hemolysis, and transfusion-transmitted diseases.14,15 The grave risksassociated with convalescent plasma transfusioninclude allergic reactions, harm to the lungs, andbreathing difficulty.16 Studies suggested pre-donation tests should include ABO and Rhesusgrouping and screening for HCV, HIV, HBV,Syphilis, and other locally spread diseases. Donor-recipient screening remains crucial for ensuringbetter clinical outcome. COVID-19 patients showedbetter recovery from the disease without severeadverse reactions. However, some patients facednegligeable side effects.17
Despite the limitations surrounding CPT, it maybe inferred that CPT is beneficial for COVID-19persons even among vulnerable age groups. Morestudies are required at the various phases of theillness and prevention to demonstrate safety andefficacy of convalescent plasma therapy amongCOVID-19 patients.18 As a scientific and clinicalcommunity, we must unlock the specific factorsregarding CP effectiveness to standardize thetreatment of COVID-19 disease in order to combatthe pandemic.
Dr. Daanish Arefin Biswas
Associate Professor and Head, Department ofTransfusion Medicine, Sir Salimullah MedicalCollege, Dhaka. e-mail: [email protected]
References:1. World Health Organization. WHO coronavirus disease
(COVID-19) dashboard. October 16, 2020. Available from:https://covid19.who.int/. Accessed December 12, 2020.
2. https:/ /www.thefinancialexpress.com.bd/views/equitable-access-to-covid-19-vaccines-massive-challenge-in-a-polarised-world-1605539804. AccessedDecember 12, 2020.
3. Horby P, Lim WS, Emberson JR, et al.; RECOVERYCollaborative Group. Dexamethasone in hospitalizedpatients with Covid-19 - preliminary report. N Engl JMed. 2020:NEJMoa2021436.
4. Wong HK, Lee CK. The pivotal role of convalescentplasma in managing emerging infectious diseases. VoxSang. 2020;115(7):545–547.
5. Marano G, Vaglio S, Pupella S, et al. Convalescentplasma: new evidence for an old therapeutic tool? BloodTransfus. 2016;14(2):152–157.
6. Mair-Jenkins J, Saavedra-Campos M, Baillie JK, et al.;Convalescent Plasma Study Group. The effectivenessof convalescent plasma and hyperimmune immuno-globulin for the treatment of severe acute respiratoryinfections of viral etiology: a systematic review andexploratory meta-analysis. J Infect Dis. 2015;211(1):80-90.
7. Syal K. COVID-19: herd immunity and convalescent plasmatransfer therapy. J Med Virol. 2020;92(9):1380–1382.
8. Duan K, Liu B, Li C, et al. Effectiveness of convalescentplasma therapy in severe COVID-19 patients. Proc NatlAcad Sci USA. 2020;117(17):9490–9496.
9. Shen C, Wang Z, Zhao F, et al. Treatment of 5 CriticallyIll Patients With COVID-19 With Convalescent Plasma.JAMA. 2020;323(16):1582–1589.
10. Zhang L, Pang R, Xue X, et al. Anti-SARS-CoV-2 virusantibody levels in convalescent plasma of six donorswho have recovered from COVID-19. Aging (AlbanyNY). 2020;12(8):6536–6542.
11. Rojas M, Rodríguez Y, Monsalve DM, et al. Convalescentplasma in Covid-19: possible mechanisms of action.Autoimmun Rev. 2020;19(7):102554.
12. Harvala Heli , Mehew Jennifer , Robb Matthew L. et al.Convalescent plasma treatment for SARSCoV-2infection: analysis of the first 436 donors in England,April 22 to May 12 2020. Euro Surveill. 2020;25(28).
13. Bloch EM, Shoham S, Casadevall A, et al. Deploymentof convalescent plasma for the prevention andTreatment of COVID-19. J Clin Invest. 2020;130(6):2757-2765.
14. Luke TC, Kilbane EM, Jackson JL, Hoffman SL. Meta-analysis: convalescent blood products for Spanishinfluenza pneumonia: a future H5N1 treatment? AnnIntern Med. 2006;145(8):599–609.
15. MacLennan S, Barbara JA. Risks and side effects oftherapy with plasma and plasma fractions. Best PractRes Clin Haematol. 2006;19(1):169–189.
16. Frazier SK, Higgins J, Bugajski A, Jones AR, BrownMR. Adverse reactions to transfusion of blood productsand best practices for prevention. Crit Care Nurs ClinNorth Am. 2017;29(3):271–290.
17. Zhang B, Liu S, Tan T, et al. treatment with convalescentplasma for critically Ill patients with severe acuterespiratory syndrome coronavirus 2 infection. Chest.2020;158(1):e9–e13.
18. Roback JD, Guarner J. Convalescent Plasma to TreatCOVID-19: Possibilities and Challenges. JAMA.2020;323(16):1561–1562.
50 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Effect of Carbon Dioxide Insufflation on Hepatic
Function Following Laparoscopic SurgeryGobinda Chandra Saha1, Md. Hasib-Al-Mamun2, Debashis Dey3, Md. Ziaur Rahman4,
Ahmed Manjurul Islam5
Abstract:
Background: Laparoscopic surgeries have revolutionized the field of surgery. However,
many studies have disclosed a variety of changes in postoperative liver function tests
(LFTs) which is difficult to explain. It was also noted that, following laparoscopic surgery,
serum level of certain hepatic enzymes raised markedly in most patients who had shown
normal LFTs preoperatively. Carbon dioxide insufflation during laparoscopic surgery
potentially influences hepatic microcirculatory perfusion.
Objective: The purpose of this study was to investigate the effect of carbon dioxide
insufflation during laparoscopic surgery on hepatic function.
Methods: A quasi-experimental study was conducted in Sir Salimullah Medical College
Mitford Hospital, Dhaka, from November 2018 to April 2019. Blood samples were collected
from 66 patients undergoing various laparoscopic procedures preoperatively once and
postoperatively on day-1 and day-7. They were tested for hepatic dysfunction by comparing
the level of serum bilirubin, ALT, SGPT and ALP. The duration of carbon dioxide
insufflation was also measured. These parameters were assessed using paired t test.
Results: The level of serum bilirubin, ALT/SGPT and ALP increased significantly during
the first 24 hours postoperatively. By the 7th day post operation, the level of bilirubin,
ALT/SGPT and ALP returned to near pre-operative values.
Conclusion: Transient change in the parameters of the liver biomarkers during laparoscopic
surgeries by CO2 pneumoperitoneum had no apparent clinical implication in patients with
normal hepatic function. However, caution should be maintained in patients with poor
liver function or preexisting liver disease.
Original Article
1 Professor, Department of Surgery, Sir Salimullah Medical College, Dhaka2 Registrar, Department of Burn and Plastic Surgery, Sir Salimullah Medical College Mitford Hospital, Dhaka3 Assistant Professor, Department of Surgery, Sir Salimullah Medical College, Dhaka4 Assistant Registrar, Department of Surgery, Sir Salimullah Medical College Mitford Hospital, Dhaka5 Officer on special duty, Directorate General of Health Services, Dhaka, On deputation, Department of Surgery,
Bangabandhu Sheikh Mujib Medical University, DhakaAddress of Correspondence: Gobinda Chandra Saha; Professor, Department of Surgery, Sir Salimullah Medical CollegeMitford Hospital, Dhaka; Phone: +8801819134530. E-mail: [email protected]
Key words:
Laparoscopy, Laparoscopicsurgery, Hepatic enzyme,Carbon dioxide insufflation,Pneumoperitoneum
Article information
Received: 01.04.2020Accepted: 01.06.2020
Cite this article:
Saha GC, Mamun MHA,Dey D, Rahman MZ, IslamAM. Effect of CarbonDioxide Insufflation onHepatic Function FollowingLaparoscopic Surgery. SirSalimullah Med Coll J 2020;28(2): 51-57
Sir Salimullah Med Coll J 2020; 28: 51-57
Introduction:
Laparoscopy is the mainstay of modern-day surgicalintervention. Most common laparoscopic procedureis laparoscopic cholecystectomy (LC). LC is nowfirmly established as gold standard therapy forsymptomatic gallstone disease.1 Besides LC someother commonly performed laparoscopicprocedures are laparoscopic appendicectomy,
repair of ventral hernias, inguinal hernioplasty,ovarian cystectomy, hysterectomy, diagnosticlaparoscopy etc. The ideal insufflating gas isinexpensive, chemically stable, highly soluble,rapidly eliminated, non-combustible and withminimal physiological effects. Carbon dioxide isthe closest to such a gas. Oxygen and air are notused because they can cause combustion especially

52 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
with bipolar diathermy and laser. Helium andargon are relatively insoluble but can result inserious complications should intravascular gasembolization occur. Nitrous oxide has been foundto be advantageous for some procedures, howeverits main drawbacks are related to the fact that itcan cause expansion of gas filled spaces includingair embolus.
Many studies have disclosed a variety of changeswhich is difficult to explain in postoperative liverfunction tests (LFTs) in patients undergoinglaparoscopic surgery2,3. It was also noted that,following laparoscopic surgery, serum level ofcertain liver enzymes raised markedly in mostpatients who had shown normal LFTspreoperatively4,5,6. Many researchers believe that,the procedure involving increased intraabdominalpressure maintained by continuous carbon dioxide(CO2) insufflation during laparoscopic surgerypotentially influences hepatic microcirculatoryperfusion7,8,9. CO2 insufflation into the peritonealcavity to the pressure of 12-14 mmHg, which isconsidered standard10,11. It is still higher than thenormal intraabdominal pressure(<10mmHg) andnormal portal venous pressure of 7-10 mmHg.Increment of intraabdominal pressure duringlaparoscopic surgery is related to reduction ofportal venous flow and compromise intraabdominalflow resulting in reduced splanchniccirculation12,13,14. The pressure of createdpneumoperitoneum and its duration has shown toinfluence the degree of hepatic ischaemia and causean elevation in liver enzymes7,15,16.
The aim of this study is to observe if there is anyeffect on hepatic function evidenced by alterationsin the serum level of hepatic biomarkers likebilirubin, ALT, ALP due to increased intra-abdominal pressure by CO2 insufflation duringlaparoscopic surgery performed under standardpressure of 12-14 mmHg.
Materials and methods:
This quasi-experimental study was conducted inSir Salimullah Medical College Mitford Hospital,Dhaka after obtaining ethical clearance fromEthical Review Board of the same institution fromNovember, 2018 to April, 2019. Data was collectedfrom total 66 consenting patients who meet theinclusion criteria. Inclusion criteria includespatients aged between 18 – 60 years, both male
and female gender, patients undergoing electivelaparoscopic surgery, preoperative serum level ofhepatic enzymes within normal range, normalbiliary channel by ultrasonography, patientsclassified under American Society ofAnaesthesiologists (ASA) grade-1 and grade-2.Preoperative and postoperative changes in meanvalues ± standard deviation (SD) of serum HCO3
-
and hepatic biomarkers (S. bilirubin, ALT/SGPT,ALP) was expressed. The levels of biomarkers weremeasured preoperatively once (24-48 hours beforesurgery) and then postoperatively on Day-1(24hours after surgery) and Day- 7. Data waspresented in tables, pie chart, bar chart and graphsfor the purpose of this study. All data were expressedas mean ± standard deviation. The data wasanalyzed for finding the significance of the effectof laparoscopy on hepatic function by using thestudents paired t test. The P value less than 0.005was considered to be statistically significant.
Results:
The youngest patients age was 21 years and oldest60 years. The average age of the patients was 38years (± 12.3). Female patients were more thanmale patients. Highest number of patientsunderwent Laparoscopic Cholecystectomy;amongst them 38 were female and 12 were male.Amongst the surgeries undertaken, 76% wereLaparoscopic Cholecystectomy. The procedurewhich the least number (4%) of patients underwentis Laparoscopic Inguinal Hernioplasty (Figure 1).
Figure 2, 3, 4 and 5 below shows bar charts of themean values obtained from laboratoryinvestigations done preoperatively, on the firstpostoperative day and on the seventh postoperativeday for Serum bilirubin, SGPT, Serum ALP andSerum HCO3
-. The values raised on the firstpostoperative day compared to preoperative resultsand returned to near normal on the seventhpostoperative day.
The difference of mean between preoperative andpostoperative values of the laboratoryinvestigations in relation to duration of operationare described in tables I, II, III, IV. For S. bilirubin,for the surgical procedures that took less than anhour to complete, the mean increase in S. bilirubinlevels on the first postoperative day compared topreoperative day was statistically significant witha P value of 0.0000 (<0.05). The mean difference of

mean values of S. bilirubin levels of firstpostoperative day and seventh postoperative daywas 0.13 mg/L (± 0.15). This decrease wasstatistically significant. Similarly, for the surgicalprocedures that took more than an hour tocomplete, the mean increase in S. bilirubin levelson the first postoperative day compared topreoperative day and the decrease in S. bilirubinlevels on the seventh postoperative day comparedto first postoperative day was statisticallysignificant as well. (Table I).
For the surgical procedures that took less than anhour to complete, the mean increase in SGPT/ALTlevels on the first postoperative day compared topreoperative day was 9.9 IU/L (SD ± 10.6). Thisincrease was statistically significant with a P valueof 0.0000 (<0.05). The mean difference of meanvalues of SGPT/ALT levels of first postoperativeday and seventh postoperative day was 4.6 IU/L (±8.2) and this decrease was statistically significant(P value=0.0014). For the surgical procedures thattook more than an hour to complete, similarobservation was noted (Table II).
For S. ALP, for the surgical procedures that tookless than an hour to complete, the mean increasein S. ALP levels on the first postoperative day
compared to preoperative day was statisticallysignificant with a P value of 0.0001 (<0.05). Themean difference of mean values of S. ALP levelsof first postoperative day and seventh postoperativeday was 28.8 IU/L (± 0.15) and this decrease wasstatistically significant as well. For the surgicalprocedures that took more than an hour tocomplete, similar observation was noted (Table III).
For the surgical procedures that took less than anhour to complete, the mean increase in S. HCO3
-
levels on the first postoperative day compared topreoperative day was 91.1 mmol/L with standarddeviation of 1.2 and this increase was statisticallysignificant with a P value of 0.0000 (<0.05). Themean difference of mean values of S. HCO3
- levelsof first postoperative day and seventh postoperativeday was 0.7 mmol/L (±0. 8) and this decrease wasstatistically significant (P value=0.0000). Similarly,for the surgical procedures that took more thanan hour to complete, the mean increase in S.HCO3
- levels on the first postoperative daycompared to preoperative day and the meandecrease of S. HCO3
- levels on the seventhpostoperative day compared to the firstpostoperative day were statistically significant.This is an indirect evidence of CO2 absorptionfollowing pneumoperitoneum by CO2 insufflation(Table IV).
Table I. Difference of mean between preoperative and postoperative values of Serum Bilirubin in
relation to duration of operation
Difference of mean in S. Bilirubin Duration of Operationlevels (mg/dL) <= 1 hour >1 hour
Mean SD P value* Mean SD P value*
Preoperative vs 1st Postoperative Day 0.21 0.21 0.0000 0.20 0.24 0.0000Preoperative vs 7th Postoperative Day 0.07 0.15 0.0033 0.06 0.22 0.05631st Postoperative Day vs 7th Postoperative Day 0.13 0.22 0.0008 0.13 0.23 0.0010
* P value obtained by paired student’s t-test
Table II: Difference of mean between preoperative and postoperative values of SGPT/ALT in relation
to duration of operation
Difference of mean in SGPT Duration of Operation levels (IU/L) <= 1 hour >1 hour
Mean SD P value* Mean SD P value*
Preoperative vs 1st Postoperative Day 9.9 10.6 0.0000 13.8 12.0 0.0000Preoperative vs 7th Postoperative Day 5.3 7.2 0.0001 7.6 13.7 0.00161st Postoperative Day vs 7th Postoperative Day 4.6 8.2 0.0014 6.2 14.0 0.0076* P value obtained by paired student’s t-test
Effect of Carbon Dioxide Insufflation on Hepatic Function Gobinda Chandra Saha et al 53
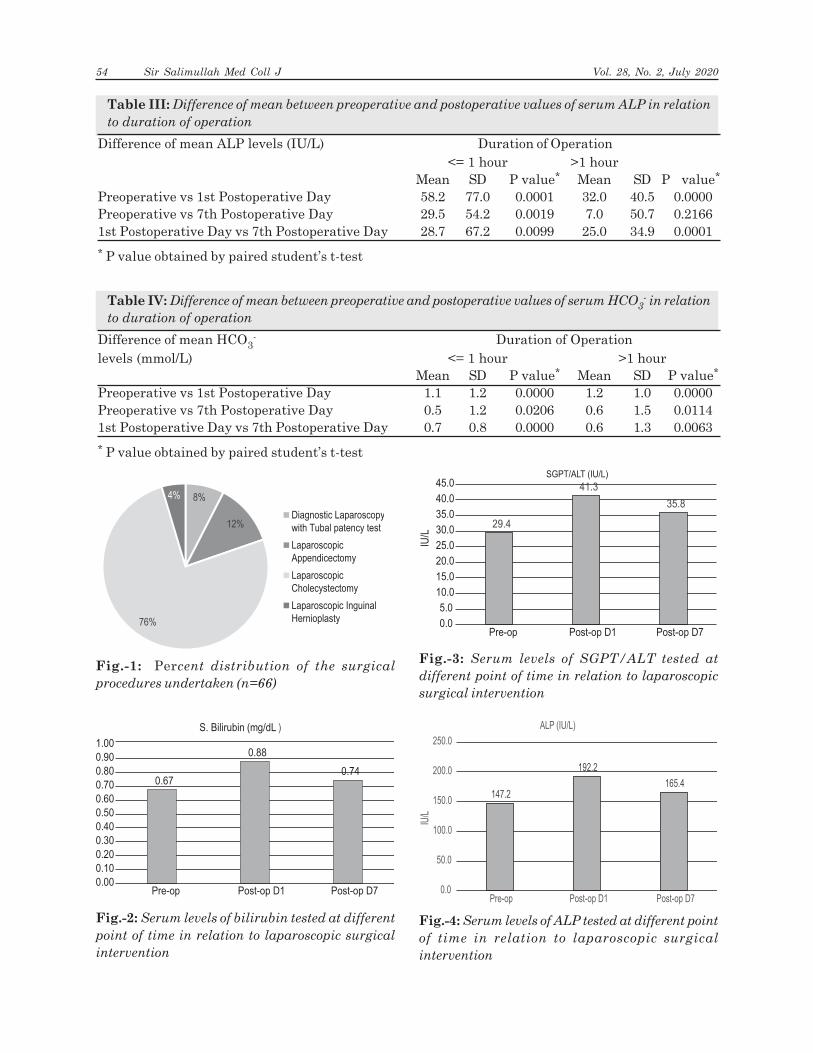
Table III: Difference of mean between preoperative and postoperative values of serum ALP in relation
to duration of operation
Difference of mean ALP levels (IU/L) Duration of Operation<= 1 hour >1 hour
Mean SD P value* Mean SD P value*
Preoperative vs 1st Postoperative Day 58.2 77.0 0.0001 32.0 40.5 0.0000Preoperative vs 7th Postoperative Day 29.5 54.2 0.0019 7.0 50.7 0.21661st Postoperative Day vs 7th Postoperative Day 28.7 67.2 0.0099 25.0 34.9 0.0001
* P value obtained by paired student’s t-test
Table IV: Difference of mean between preoperative and postoperative values of serum HCO3- in relation
to duration of operation
Difference of mean HCO3- Duration of Operation
levels (mmol/L) <= 1 hour >1 hourMean SD P value* Mean SD P value*
Preoperative vs 1st Postoperative Day 1.1 1.2 0.0000 1.2 1.0 0.0000Preoperative vs 7th Postoperative Day 0.5 1.2 0.0206 0.6 1.5 0.01141st Postoperative Day vs 7th Postoperative Day 0.7 0.8 0.0000 0.6 1.3 0.0063
* P value obtained by paired student’s t-test
Fig.-1: Percent distribution of the surgical
procedures undertaken (n=66)
8%
12%
76%
4%
Diagnostic Laparoscopy
with Tubal patency test
Laparoscopic
Appendicectomy
Laparoscopic
Cholecystectomy
Laparoscopic Inguinal
Hernioplasty
0.67
0.88
0.74
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Pre-op Post-op D1 Post-op D7
S. Bilirubin (mg/dL )
Fig.-2: Serum levels of bilirubin tested at different
point of time in relation to laparoscopic surgical
intervention
29.4
41.3
35.8
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
Pre-op Post-op D1 Post-op D7
IU/L
SGPT/ALT (IU/L)
Fig.-3: Serum levels of SGPT/ALT tested at
different point of time in relation to laparoscopic
surgical intervention
147.2
192.2
165.4
0.0
50.0
100.0
150.0
200.0
250.0
Pre-op Post-op D1 Post-op D7
IU/L
ALP (IU/L)
Fig.-4: Serum levels of ALP tested at different point
of time in relation to laparoscopic surgical
intervention
54 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Discussion:
In this study, assessment of presence of clinicalsignificance of unexplained disturbances in liverenzymes following laparoscopic surgeries wasobserved to evaluate the potential deleterious effectof laparoscopic surgeries on hepatic functionthrough the following parameters: S. bilirubin,SGPT/ALT, S. ALP. Pneumoperitoneum by CO2insufflation might be one of the reasons behindthis changes. About 66 patients constituted thestudy population. 49 were female patients and 17were male. All the patients were between 21 to 60years of age. The average age of the patients was38 years (±12.3).
We observed, in all patients the levels of serumbilirubin, serum ALT/SGPT and serum ALP waschecked preoperatively once and post operativelyon day 1 and day 7. The mean level of S. bilirubinpreoperatively was 0.67 ± 0.17 mg/dL.Postoperatively on day 1 and day 7 the levels were0.87 ± 0.24mg/dL and 0.74 ± 0.16mg/dLrespectively. Other studies like Marakis et al.found similar increase in S. bilirubin in their studywhere preoperative value was 0.64±0.24 mg/dlwhich showed significant rise to 0.95±0.58 mg/dl24 hours after laparoscopic surgery.17 In this study,the preoperative mean value was 0.67 ± 0.17 mg/dL which also showed significant rise to 0.87 ± 0.24mg/dL 24 hour after surgery. The mean values ofSGPT levels preoperatively, on the firstpostoperative day and on the seventh postoperativeday were 29.4±10.05 IU/L, 41.3±14.23 IU/L and35.8±10.53 IU/L respectively. Tan et al. showedsimilar statistically significant (p<0.05) increase in
postoperative liver transaminases compared topreoperative values2. Sakorafas et al. ( 21.6±13.4IU/L to 82.8±19.1 IU/L);15 Guven et al. (21.55±8.92IU/L to 60.30±32.17 IU/L);18 and Marakis et al.(31.88±74.77 IU/L to 61.62±54.87 IU/L)17 alsoshowed resembling increase in postoperative SGPTlevel from preoperative values similar to this study(29.4±10.05 IU/L to 41.3±14.23 IU/L). Studies byGuven et al18. Omari et al.19; Marakis et al.17
showed no significant alterations in serum ALPlevel which is different than this study where meanpreoperative value of ALP was 147.2±56.49 IU/Land on first postoperative day was 192.2±67.15 IU/L . However, this finding was similar to that ofTauro et al3. where there is significant rise inpostoperative value of ALP in comparison topreoperative value.
The transient postoperative increases in the serumbiomarkers of liver were seen in the studypopulation irrespective of the type of laparoscopicsurgery they underwent. However, if the changesare found to be permanent then breach of integrityof biliary tree should be suspected and furtherinvestigations are warranted.
With the increase in duration of laparoscopicsurgery, the changes in parameters of liverfunction was supposed to be more pronounced. But,in this study, although the changes of laparoscopicsurgeries having more than 60 minutes are foundto be statistically significant but not morepronounced than laparoscopic surgeries having lessthan 60 minutes duration. So, this finding is notconsistent with other published articles like Morinoet al.20 The probable reason behind thisinconsistency may be the lesser number of samplesize having longer duration of laparoscopic surgeryand shorter study and follow up period.
Increase in HCO3- level is an indirect evidence ofCO2 absorption following pneumoperitoneum byCO2 insufflation. This changes in HCO3- level asan indirect evidence of CO2 absorption is consistentwith the finding of Hakeem et al.21 In all thepatients where there was a transient rise in theenzyme levels, the values returned to nearpreoperative concentrations within one week aftersurgery. None of the patients presented withclinical hepatic dysfunction after the surgeryaccording to follow up observations and feedbackfrom the patients. As the standard intraabdominal
Fig.-5: Serum levels of HCO3- tested at different
point of time in relation to laparoscopic surgical
intervention
24.5 25.6 24.9
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
Pre-op Post-op D1 Post-op D7
mm
ol/L
HCO3-(mmol/L)
Effect of Carbon Dioxide Insufflation on Hepatic Function Gobinda Chandra Saha et al 55

pressure of 12-14mmHg used in this study washigher than the normal portal blood pressure of 7-10mmHg, the surgery might therefore reduce theportal blood flow and cause alteration in liverfunction.8,22
During laparoscopic procedure, the suddenalteration of intraabdominal pressure could causefluctuation of portal blood flow. This fluctuationand “re-irrigation of organs” and blood flow maygive rise to “ischaemia and re-irrigation” damageof tissues and organs, especially the Kupffer andendothelial cells of hepatic sinusoids.23 This canalso cause free radical generation.24 It was alsofound in this study that with the increased durationof CO2 pneumoperitoneum, the elevation in liverenzymes are increased which is consistent withthe findings of Schilling et al.25 So, if the patients’pre-operative liver function is very poor,laparoscopic surgery might not be the optimalchoice for treating certain abdominal diseases.Studies done by Giraudo et al. suggest that recentadvances in laparoscopic surgery like gaslesslaparoscopy can avoid causing alterations in hepaticfunction. [26] So, this could be tried as an alternativeto routine laparoscopic surgeries using carbondioxide insufflation, in patients with poor liverfunction.
Conclusion:
All types of laparoscopic procedures can causetransient elevation of hepatic biomarkers for whichthe major causative factor seems to be thepneumoperitoneum by carbon dioxide insufflation.Though this change caused no apparent clinicalimplications in patients with normal hepaticfunction but laparoscopic surgery may not be thebest choice for patients with poor hepatic function.Besides carbon dioxide insufflation, other factorsmay also contribute to the liver function alterationssuch as surgical manipulation, use of electro-surgical devices, general anaesthesia and so on.
References:1. Cuschieri A, Hanna G. Essential surgical practice: higher
surgical training in general surgery.5th ed .CRC Press;2015 Jan 20.p671-756
2. Tan M, Xu FF, Peng JS, Li DM, Chen LH, Lv BJ, ZhaoZX, Huang C, Zheng CX. Changes in the level of serumliver enzymes after laparoscopic surgery. World Journalof Gastroenterology: WJG. 2003 Feb 15;9(2):364
3. Tauro LF, Sheethal CM, Aithala PS, Shetty SR, D’souzaCS, Rao BS. Evaluation of Effects of Laparoscopic
Surgery on Hepatic Function. J Clin Diagn Res.2008;2:1155
4. Eryýlmaz HB, Memiþ D, Sezer A, Inal MT. The effectsof different insufflation pressures on liver functionsassessed with LiMON on patients undergoinglaparoscopic cholecystectomy. The Scientific WorldJournal. 2012;2012
5. Sharma A, Dahiya D, Kaman L, Saini V, Behera A.Effect of various pneumoperitoneum pressures onfemoral vein hemodynamics during laparoscopiccholecystectomy. Updates in surgery. 2016 Jun1;68(2):163-9.
6. Krishnegowda U, kumar Gupta A, Sharma R, GuptaN, Durga CK. A comparative study between low andnormal pressure pneumoperitoneum in laparoscopiccholecystectomy with special reference to shoulder tippain. Hellenic Journal of Surgery. 2016 Jan 1;88(1):13-7
7. Hasukiæ Š. Postoperative changes in liver function tests:randomized comparison of low-and high-pressurelaparoscopic cholecystectomy. Surgical Endoscopy andOther Interventional Techniques. 2005 Nov1;19(11):1451-5
8. Schmandra TC, Kim ZG, Gutt CN. Effect of insufflationgas and intraabdominal pressure on portal venous flowduring pneumoperitoneum in the rat. Surgicalendoscopy. 2001Apr 1;15(4):405-8.
9. Saber AA, Laraja RD, Nalbandian HI, Pablos-MendezA, Hanna K. Changes in liver function tests afterlaparoscopic cholecystectomy: not so rare, not alwaysominous. The American surgeon. 2000 Jul 1;66(7):699.
10. Joris J, Cigarini I, Legrand M, Jacquet N, De Groote D,Franchimont P, Lamy M. Metabolic and respiratorychanges after cholecystectomy performed vialaparotomy or laparoscopy. BJA: British Journal ofAnaesthesia. 1992 Oct 1;69(4):341-5.
11. Berggren U, Gordh T, Grama D, Haglund U, Rastad J,Arvidsson D. Laparoscopic versus opencholecystectomy: hospitalization, sick leave, analgesiaand trauma responses. British journal of surgery. 1994Sep;81(9):1362-5.
12. Jakimowicz J, Stultiens G, Smulders F. Laparoscopicinsufflation of the abdomen reduces portal venous flow.Surgical endoscopy. 1998 Feb 1;12(2):129-32.
13. Schäfer M, Krähenbühl L. Effect of laparoscopy on intra-abdominal blood flow. Surgery. 2001 Apr 1;129(4):385-9.
14. Odeberg S, Ljungqvist O, Sollevi A. Pneumoperitoneumfor laparoscopic cholecystectomy is not associated withcompromised splanchnic circulation. European Journalof Surgery. 1998 Oct;164(11):843-8.
15. Sakorafas G, Anagnostopoulos G, Stafyla V, Koletis T,Kotsifopoulos N, Tsiakos S, Kassaras G. Elevation ofserum liver enzymes after laparoscopic cholecys-tectomy. NZ Med J. 2005 Feb 25;118(1210): U1317.
56 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

16. Hasukic S, Kosuta D, Muminhodzic K. Comparison ofpostoperative hepatic function between laparoscopic andopen cholecystectomy. Medical Principles and Practice.2005;14(3):147-50
17. Marakis G, Pavlidis T, Ballas K, Rafailidis S, Psarras K,Symeonidis N, Triantafyllou A, Sakantamis A.Alterations in liver function tests following laparoscopiccholecystectomy. The Internet J Surg. 2006;8:245-7
18. Guven HE, Oral S. Liver enzyme alterations afterlaparoscopic cholecystectomy. Journal of Gastro-intestinal and Liver Diseases. 2007 Dec 1;16(4):391
19. Omari A, Bani-Hani KE. Effect of carbon dioxidepneumoperitoneum on liver function followinglaparoscopic cholecystectomy. Journal of Laparo-endoscopic & Advanced Surgical Techniques. 2007 Aug1;17(4):419-24
20. Morino M, Giraudo G, Festa V. Alterations in hepaticfunction during laparoscopic surgery. Surgicalendoscopy. 1998 Jul 1;12(7):968-72.
21. Hakeem A, Iqbal A, Dawood M, Saleem b, hameed A.Effects of CO2 pneumoperitonium on arterial partialpressure of carbon dioxide ph, end tidal carbn dioxide
and bicarbonate in patients during laparoscopiccholecystectomy. Journal of Evolution of Medical andDental-JEMDS. 2016 May 12;5(38):2299-302.
22. Bendet N, Morozov V, Lavi R, Panski M, Halevy A,Scapa E. Does laparoscopic cholecystectomy influenceperi-sinusoidal cell activity?. Hepato-gastroenterology.1999; 46(27):1603-6.
23. Volz J, Köster S, Spacek Z, Paweletz N. Characteristicalterations of the peritoneum after carbon dioxidepneumoperitoneum. Surgical endoscopy. 1999 Jun1;13(6):611-4.
24. Sare M, Yilmaz I, Hamamci D, Birincioglu M, ÖzmenM, Yesilada Ö. The effect of carbon dioxide pneumo-peritoneum on free radicals. Surgical endoscopy. 2000Jul 1;14(7):649-52.
25. Schilling MK, Redaelli C, Krähenbühl L, Signer C,Büchler MW. Splanchnic microcirculatory changesduring CO2 laparoscopy. Journal of the AmericanCollege of Surgeons. 1997 Apr;184(4):378-82.
26. Giraudo G, Contul RB, Caccetta M, Morino M. Gaslesslaparoscopy could avoid alterations in hepatic function.Surgical endoscopy. 2001 Jul 1;15(7):741-6.
Effect of Carbon Dioxide Insufflation on Hepatic Function Gobinda Chandra Saha et al 57

Comparison of Outcome of Ureteric Catheter andDJ Stent after URS ICPL for Lower Ureteric StonesAshraf Rahman1, Sudip Das Gupta2, Mazaharul Islam3, Md. Mahmudur Rahman5, Md. Naved
Yousuf4, Md. Rumman Asif1, Sayef Ullah Sujan1, Md. Sanaullah1, Dhanarjaj Dey1
Abstract
Background. Ureterorenoscopy (URS) is commonly practiced procedure in urology for
the management of lower ureteric stones. Most urologists advocate placement of routine
DJ stent for 4 to 6 weeks after ureteroscopic lithotripsy especially to reduce the incidence of
postoperative ureteral oedema and ureteral stricture development, and possibly to assist in
the passage of small stone fragments. However, the use of ureteral stents is not without its
attendant complications. Two days indwelling of ureteric catheter following URS for
lower ureteric stone might be a good alternative to the use of DJ stent for conventional 4 to
6 weeks. Temporary ureteral catheters, in contrast to DJ stent ones, do not expose patients
to higher risks of migration, infection, breakage, encrustation, and stone formation.
Objective. To compare the outcome of ureteric catheter and D-J stent after URS ICPL of lower
ureteric stones by the means of Visual Analogue Scale score of flank pain, Analgesic requirement
and willingness to Re-surgery, Irritative features, Urine and stent/ureteric catheter tip culture,
Organisms isolated from urine, DJ stent and ureteric catheter tip culture
Materials and method. Study population included 90. Among them, 02 dropped out from
the study. Finally, Group A (Ureteric catheter) was included 43 and Group B (DJ stent)
included 45 patients. A Quasi-experimental study done between July 2017 to July 2019 in
the Department of Urology, Sir Salimullah Medical College and Mitford Hospital, Dhaka,
Bangladesh. Patients were enrolled and reviewed by Visual Analogue Scale score of flank
pain, Analgesic requirement and willingness to Re-surgery, Irritative features, Urine and
stent/ureteric catheter tip culture, Organisms isolated from urine, DJ stent and ureteric
catheter tip culture. Institutional ethical committee clearance was taken before
commencement of the study.
Results. Flank pain was assessed by VAS score. Mean VAS score was significantly higher in
Group-B on Postoperative Day 1, 2.49 (±1.94) versus 3.78 (±1.84) (p= 0.55) ; on day 7 and 14,
0.52 versus 2.90 and 0.17 versus 2.40 (p<0.05). 74.41% and 28.89% patients in Group-A and
Group-B responded affirmatively when asked “Whether you would opt for the same procedure
again as treatment if you develop ureteral stones in the future?” (p< 0.05). Irritative features
at 2 weeks postoperatively was 2.53 and 10.82 in Group-A and Group-B respectively (p< 0.05).
the rate of growth of organism in urine did not differ significantly between two groups (p>
0.05). But colonization of bacteria in DJ stent was significantly higher than ureteric catheter
colonization (p<0.05). Pseudomonas and E.coli were most common pathogens.
Conclusion. Short duration (2 days) ureteric catheter placement after URS can reduce
postoperative loin pain, irritative voiding symptoms, increased patient compliance, urinary
bacterial growth and ureteric catheter colonization in comparison to conventional placement
of DJ stent for 3 weeks following URS ICPL of lower ureteric stone. Hence, it can be inferred
that placement of open-ended catheter was better tolerated by patients compared with an
indwelling DJ stent.
Original Article
1. Resident, Department of Urology, Sir Salimullah Medical College, Dhaka2. Associate Professor and Head, Department of Urology, Sir Salimullah Medical College, Dhaka3. EMO, Sir Salimullah Medical College Mitford Hospital, Dhaka4. IMO, Department of Urology, Sir Salimullah Medical College Mitford Hospital, Dhaka5. Registrar, Department of Urology, Sir Salimullah Medical College Mitford Hospital, DhakaAddress of Correspondence: Dr. Ashraf Rahman, Resident, Department of Urology, Sir Salimullah Medical College, Dhaka
Key words:
Lower Ureteric stone,Ureterorenoscopy, ICPL,Ureteric catheter, DJ stent
Article information
Received: 15.03.2020Accepted: 12.05.2020
Cite this article:
Rahman A, Gupta SD,Islam M, Rahman MM,Yousuf MN, Asif MR.Comparison of Outcome ofUreteric Catheter and DJStent after URS ICPL ofLower Ureteric Stones. SirSalimullah Med Coll J 2020;28: 58-62
Sir Salimullah Med Coll J 2020; 28: 58-62

Introduction
Among treatment options for ureteric stones,ureteroscopy is the favoured approach for mid anddistal ureteral stones1. With the development ofsmaller calibre semi-rigid and flexibleureteroscopes and the introduction of differenttypes of improved lithotrites, Ureterorenoscopyhas evolved into a safer and more efficaciousmodality for treatment of stones in all locations inthe ureter with increasing experience worldwide.
Ureteral stents have been conventionally placedto reduce the colicky pain and ureteral edemafollowing ureteroscopic removal of stones, toprevent or reduce the occurrence of ureteralstricture2. However,recognized complications havebeen associated with the use of stents with reportsin the literature of a 10% to 85% incidence of stentrelated symptoms and morbidity3.
On the contrary of the growing consensusregarding stentless URS, a recent trend of shortduration ureteral drainage by ureteric catheter isalso developing now a days. Placing a ureteralcatheter for the first 24-48 hours seemed toeliminate the possibility of early ureteral oedema,secondary hydronephrosis and flank pain.
This study was intended to assess the efficacy andsafety of a 2-day indwelling period of an open endedureteral catheter following URS for lower ureteralstones compared with the conventional long-termindwelling of a DJ stent.
Materials & Methods
The study was conducted in patients admitted inthe Urology ward with a diagnosis of lower uretericstone during the period from January 2018 to June2019 in Sir Salimullah Medical College Hospitaland different private hospitals in Dhaka City.
Ninety patients of single lower ureteric stones of6mm to 10 mm sizes were selected for the study.Patients with Multiple or impacted ureteric stonesor Concomitant renal stone or Patients having historyof previous ureteroscopy or failed treatment of thesame stone or having ureteral stent preoperativelyor Patient who suffered significant ureteral mucosalinjury during the surgery or Patients having impairedrenal function were excluded.Eligible patients wereallocated into two groups, Group-A and Group-B bypurposive sampling. The locations and sizes of theureteral stones were assessed by preoperative plainx-ray KUB and ultrasound scanning with IVU or CTUrogram. Stones located below the inferior border
of the sacroiliac joint were considered as distalureteric stone.
The Ethical Committee of Sir Salimullah MedicalCollege Mitford Hospital approved the study..Allpatients gave written informed consent beforeparticipation. With all preoperative preparation &precaution surgery was done by using a 9.5-Fr.semi-rigid ureteroscope (Karl Storz, Germany).Ureteral stones were fragmented by using anintracorporeal pneumatic lithotripter (ICPL) bySwiss Lithoclast. A basket (3Fr) was used forcomplete stone extraction if necessary. In all casesof fragmentation the site of impaction wasinspected for ureteral injury and perforation.Procedures were considered successful if thecalculus removed in its entirety or no fragment ispresent on radiographic follow-up.
Study Design
After successful procedure, patients were selectedin every alternate sequence. Odd numbers forureteric catheter insertion and designated asGroup-A. Even numbers for DJ stent insertion anddesignated as Group-B. First case was selected bylottery method. Open-ended polyurethane ureteralcatheter 6Fr (Devon)was used in Group-A and keptfor 2 days following surgery. The ureteric catheterwas exposed ex vivo and was fixed by using adhesiveband along with a urethral Foley catheter.On theother hand, a 6 Fr. double-J stent (Devon) wasplaced for 3 weeks postoperatively in Group-B.
The outcomes measured were Flank pain,Irritativevoiding symptoms: frequency, urgency andnocturia,Analgesic use,Willingness of re-surgery,Post-operative urine culture andsensitivity,DJ stent and catheter tip culture andsensitivity.
Statistical Analysis
All the collected data were compiled. The resultswere presented in tables, figures and diagrams.Quantitative data were expressed as mean andstandard deviation and compared by Student “t” test.Qualitative data were expressed as frequency andpercentage, compared by Chi square test. FurtherStatistical analyses of the results were obtained byusing Microsoft Xcel, 2010 (Microsoft Corporation,Washington, U.S.) and web based computersoftware – Graph Pad Software, 2019 (Graph PadSoftware, Inc, USA). A probability value (p) of lessthan 0.05 was considered to indicate statisticalsignificance. The summarized findings were thenpresented in the form of tables and graphs.
Comparison of Outcome of Ureteric Catheter and DJ Stent after URS ICPL Ashraf Rahman et al 59

2.49
0.52
0.17
3.78
2.9
2.4
0
0.5
1
1.5
2
2.5
3
3.5
4
Day 1 Day 7 DAY 14
Vis
ua
l A
na
log
ue
Sca
le s
co
re
Projected time
Group-A
Group-B
Line chart showing Visual Analogue Scale score of flankpain (vertical axis) over time (horizontal axis).Group A: Ureteric catheterGroup B: DJ stent
Fig-1: Visual Analogue Scale (VAS) score of flank
pain
Results
A total of 90 patient with distal ureteric stone wereselected according to definite selection criteria forthe study. They were equally allocated into Group-A and Group-B by purposive sampling technique.An open ended ureteric catheter and aconventional DJ stent were placed following URSICPL in each patients of Group-A and Group-Brespectively. Then the patients were followed upat post operative day one, seven & fourteen andcompared between two groups. Two patient fromgroup A were dropped out during follow upperiod.The different parameter of rest of thepatients have been sown in tabulated form andstatistical analysis has been done in both group tosee any significant difference.p value was set at0.05& p<0.05 was considered as significant. therewas no significant difference regarding Age, Sex,Stone size, Stone laterality of the patients of Group-A and Group-B(p>0.05)(table 1)
Table-I : General characteristics of the study
subjects (n=88)
General Group-A Group-Bcharacteristics (n=43) (n=45)
Age (year) 46.27 ± 11.15 49.76 ± 13.42 0.1891
Sex 26:17 31:15 0.5452
(Male: Female)
Stone size (mm) 8.92 ± 1.20 8.41 ± 1.28 0.511
Stone laterality 23:20 21:24 0.5222
(Right: Left)
Figures in the parentheses indicate corresponding percentageFigures in the parentheses indicate corresponding percentageFigures in the parentheses indicate corresponding percentage.Age & Stone Size were expressed as (Mean+/-SD) Datawere analyzed by using Student’s t-test1and chi square test2.Group A: Ureteric catheterGroup B: DJ stent
On postoperative day 1, the mean VAS scores forflank pain in Group-A and Group-B was notsignificantly different (p= 0.55). At postoperativeday 7 and 14 however, the mean VAS scores forflank pain showing statistically significantdifference (p<0.01).
On postoperative day 7, the irritative voidingsymptoms (frequency, urgency, and nocturia) werefound significantly higher in Group-B (p<0.05).
Table-II: Irritative voiding symptoms onpostoperative day 7 (n=88)
Irritative voiding Group-A Group-B P valuesymptoms (n=43) (n=45)
Frequency 2.02 ± 0.63 5.34 ± 0.68 <0.001s
Urgency 0.51 ± 0.47 4.21 ± 1.09 <0.001s
Nocturia 0.00 1.27 ± 0.85 <0.001s
S=significant Data were expressed as (Mean ± SD) Datawere analyzed by using Student’s t-test.Group A: Ureteric catheterGroup B: DJ stent
Additional dose of analgesic requirement neededmore frequently in Group-B, but the differencebetween Group-A and Group-B was not statisticallysignificant (p>0.05). On the other hand, thewillingness to re-surgery was significantly higherin Group-A (p<0.001)
Table-III: Frequency of analgesic use andwillingness to re-surgery (n=88)
Group-A Group-B(n=43) (n=45)
Use of analgesic 06 (13.95%) 11(24.44%) 0.329ns
Willingness of 32 (74.41%) 13(28.89%) <0.001s
re-surgery
s=significant, ns=not significant Data were analyzed by usingChi square test.Group A: Ureteric catheterGroup B: DJ stent
60 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

the rate of growth of organism in urine did notdiffer significantly between two groups (p>0.05).
Table-IV: Distribution of the patients by urine
culture
Urine culture Group-A Group-B P value
(n=43) (n=45)
Growth 15(34.88%) 09 (16.00%) 0.117ns
No growth 28 (65.12%) 36 (84.00%)
ns=not significant Data were analyzed by Chai square test.Group A: Ureteric catheterGroup B: DJ stent
Discussion
In the present study, On postoperative day 1, themean VAS scores for flank pain in Group-A andGroup-B was not significantly different but atpostoperative day 7 and 14 result was significant.Irritative voiding symptoms at 1 weekpostoperatively was significantly higher in Group-B. Similar finding was seen by Moon et al2 andChauhan et al.4 The pathophysiology of thesesymptoms has not been completely elucidated, butit is most commonly believed that adverse stentsymptoms are induced by bladder mucosalirritation due to contact by the distal curl of thestent, smooth muscle spasm, and reflux of urineresulting in flank pain.
Djaladat et al5 reported that when ureteroscopywas performed without catheterization, flank painand renal colic could result from early ureteraloedema implying that some postoperative drainageis better than no drainage at all. This formed thepremise of using the open-ended ureteral catheterin immediate postoperative period in our seriesand the significantly lower VAS scores suggest thattheir placement can be as effective as stents withminimal irritative symptoms.
There was no significant difference in analgesicrequirement in the two groups in our study; 6 and11 patients in group-A and B respectively requiredadditional dose of analgesic on postoperative days1 and 2. No patient needed analgesics beyond thesecond postoperative day which is comparable tothe series by Moon et al2 and Nabi et al.6
In present study, the rate of growth of organismin urine did not differ significantly between twogroups (p>0.05). But colonization of bacteria in DJ
stent was significantly higher than uretericcatheter colonization (p<0.05). Pseudomonas andE.coli were most common pathogens. Almostsimilar result was elucidated by Kehinde et al7.Patients with indwelling ureteral stents and asterile urine culture may benefit from prophylacticantibiotic treatment prior to endourologicprocedures.
Apart from the adverse stent related symptoms,removal of indwelling stent constitutes anadditional procedure, which not only is physicalbut also a financial burden to the patient especiallyin a developing country like ours. Although we didnot measure the mean VAS score for stent removalunder local anaesthesia in our series, we found itvery distressful in most of the patients. Kim et al8
& Moon et al.2 reported similar.
In our study, 74.41% and 28.89% patients inGroup-A and Group-B responded affirmativelywhen asked Whether they would opt for the sameprocedure again as treatment if they developureteral stones in the future (p<0.05).
Hence, it can be inferred that placement of open-ended catheter (removed on day 2) was bettertolerated by patients compared with an indwellingstent–only procedure.
Conclusion
In URS ICPL of lower ureteric stone, shortduration (2 days) ureteric catheter placement canreduce postoperative loin pain, irritative voidingsymptoms, increased patient compliance, urinarybacterial growth and ureteric catheter colonizationin comparison to conventional placement of DJstent for 3 weeks.
References1. Auge, B.K., Sarvis, J.A., L’Esperance, J.O. and
Preminger, G.M., 2007. Practice patterns of ureteralstenting after routine ureteroscopic stone surgery: asurvey of practicing urologists. Journal of
endourology, 21(11), pp.1287-1292.
2. Moon, K.T., Cho, H.J., Cho, J.M., Kang, J.Y., Yoo, T.K.,Moon, H.S. and Lee, S.W., 2011. Comparison of anindwelling period following ureteroscopic removal ofstones between Double-J stents and open-endedcatheters: a Prospective, pilot, randomized, multicenterstudy. Korean journal of urology, 52(10), pp.698-702.
3. Netto, N.R., Ikonomidis, J. and Zillo, C., 2001. Routineureteral stenting after ureteroscopy for ureterallithiasis: is it really necessary?. The Journal of
urology, 166(4), pp.1252-1254.
Comparison of Outcome of Ureteric Catheter and DJ Stent after URS ICPL Ashraf Rahman et al 61

4. Chauhan, V.S., Bansal, R. and Ahuja, M., 2015.Comparison of efficacy and tolerance of short-durationopen-ended ureteral catheter drainage and tamsulosinadministration to indwelling double J stents followingureteroscopic removal of stones. Hong Kong Med
J, 21(2), pp.124-30.
5. Djaladat, H., Tajik, P., Payandemehr, P. and Alehashemi,S., 2007. Ureteral catheterization in uncomplicatedureterolithotripsy: a randomized, controlled trial.European urology, 52(3), pp.836-841.
6. Nabi, G., Cook, J., N’dow, J. and McClinton, S., 2007.Outcomes of stenting after uncomplicated ureteroscopy:
systematic review and meta-analysis. bmj, 334(7593),p.572
7. Kehinde, E.O., Rotimi, V.O., Al-Hunayan, A., Abdul-
Halim, H., Boland, F. and Al-Awadi, K.A., 2004.
Bacteriology of urinary tract infection associated with
indwelling J ureteral stents. Journal of endourology,
18(9), pp.891-896.
8. Kim, K.S., Kim, J.S. and Park, S.W., 2006. Study on the
effects and safety of propofol anesthesia during
cystoscopy. Korean Journal of Urology, 47(11), pp.1230-
1235.
62 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Pattern of Visual Outcome after Nd: YAG Laser
Capsulotomy in Patients with Posterior Capsular
Opacity after Cataract Surgery of 30 CasesAsif-Ur-Rahman1, Lt. Col. Zakir Hossain2, Eram Mustafiz3
Abstract
Objective: To evaluate the visual acuity before and after Nd:YAG (Yutrium, Aluminium
and Garnet) laser capsulotomy.
Method: A Prospective study was conducted with the total of 30 patients of both sexes
with posterior capsular opacity and free from other ocular diseases and aged between 40
to 85 years in eye department of Uttara Adhunik Medical College Hospital and Combined
Military Hospital (CMH) of Dhaka Cantonment respectively, from July 2013 to July
2018.
Results: Five patients (16.66%) had pre- Nd:YAG laser visual acuity 6/12, 2 patients
(6.66%) had visual acuity of 6/18, 4 patients(13.33%) had visual acuity 6/24, 1 patient
(3.33%) had visual acuity 6/36, 7 patients(23.33%) had visual acuity of 6/60, 4 patients
(13.33%) had visual acuity of 3/60, 5 patients (16.66%) had visual acuity of CF 5ft, and 2
patients (6.66%) had visual acuity of CF 4ft. After 7 days, 23 patients (76.66%) had visual
acuity of 6/12 or better; p-value is 0.002 which is significant. After 30 days, 27 patients
(90.0 %) had visual acuity 6/12 or better; p- value is 0.001.
Conclusion: Nd:YAG laser capsulotomy in posterior capsule opacification can significantly
improve vision to a greater extent. This improvement can be further augmented with
refractive correction.
Original Article
Key words:
Nd:YAG laser capsulotomy
Article information
Received: 30.07.2020Accepted: 01.09.2020
Cite this article:
Rahman AU, Lt. Col.Hossain Z, Mustafiz E.Pattern of Visual Outcomeafter Nd: YAG LaserCapsulotomy in Patientswith Posterior CapsularOpacity after CataractSurgery of 30 Cases. SirSalimullah Med Coll J 2020;28(2): 63-66
Sir Salimullah Med Coll J 2020; 28(1): 63-66
1. Associate Professor, Department of Ophthalmology, Uttara Adhunik Medical College and Hospital, Uttara, Dhaka.2. Eye Specialist, Combined Military Hospital (CMH), Dhaka Cantonment.3. Associate Professor, Department of Biochemistry, Uttara Adhunik Medical College and Hospital, Uttara, Dhaka.Address of Correspondence: Dr. Asif-Ur-Rahman, Associate Professor, Department of Ophthalmology, Uttara AdhunikMedical College and Hospital, Uttara, Dhaka-1230.
Introduction:
Cataract is the leading cause of blindness globally,which is 42% of all global blindness. Worldwide,314 million people are visually impaired, out ofwhich 45 million of them are blind. About 87% ofthe visually impaired population live in theimpoverished developing country.1
In Bangladesh, National Survey on Blindnessrevealed that cataract is the highest and accountedfor the 82% of all blindness.2
For successful cataract surgery, a fully equippedoperation theatre with an operating microscope,
micro- surgical instruments and vitrectomyequipment are required. Either ‘Small incision’ or‘phaco-technique’ preferred. Lens implantation inthe bag is more preferred than sulcus implantation.
The final visual outcome will depend on thepatients’ age, presence or absence of systemicdiseases namely, diabetes mellitus andhypertension. Post operative visual acuity of 6/12or better is achieved in 96% of patients under theage of 60, reducing to 75% to 85%, if aged above 80years, provided no other ocular pathology ispresent.3

Posterior capsular opacification (PCO) is the mostcommon late complication of uneventfulextracapsular cataract extraction (ECCE).4,5 Within5 years, 28% of eyes develop PCO6, although nearly100% opacification occurs in case of children.7
Posterior capsule opacification (PCO) varies fromElschnig pearls to fibrous membrane formation.Before Nd:YAG laser came into being, thiscondition was treated by performing posteriorcapsulotomy with a 27 gauge needle either as aprimary or secondary procedure. In the last twodecades, Nd:YAG laser has gained popularity as anon- invasive method for treating PCO (posteriorcapsule opacification). Aim of treatment is to createan opening in the posterior capsule. Commonindications for the YAG laser capsulotomy includediminished visual acuity, diplopia, glare andinadequate fundus visualization.
Laser is an acronym for light amplification bystimulated emission of radiation. Laser is coherent(all photons have same wavelength) and collimated(all light waves are parallel).8 The NeodymiumYttrium Argon Garnet (Nd:YAG) laser is a solidtype of laser, causes tissue disruption by ionizationmode of action. It has 1064 nm wavelength withinfrared radiation. It is a powerful continuous waveand usually Q switched when used to treat theeye. It is used to disrupt the posterior capsulefollowing cataract surgery, iridotomy in narrowangle glaucoma and to cut vitreous band.9
It provides 4 spot aiming beam system. The 4spots then merged to form a single spot. The sizeof the capsulotomy depends on the indications.Most capsulotomies were done for the visualreasons and the size of the capsulotomy was inthe range of 3 to 4 mm respectively. Largeropening was required for panretinal photocoagulation (PRP) in diabetic retinopathy.10
Materials and methods:
A prospective study was done. In the Eye OPD ofUttara Adhunik Medical College Hospital andCombined Military Hospital (CMH) of DhakaCantonement from July 2013 to July 2018.
Patients with posterior capsular opacification ofeither sex, aged between 40- 85 years and all whomet the inclusion criteria were included in thestudy. Those who gave their consent were selectedin the study.
A prospective intervention study was done in theeye department of Uttara Adhunik Medical CollegeHospital and Combined Military Hospital (CMH)
of Dhaka Cantonment respectively, on 30 patientsand they were all treated with Nd:YAG lasercapsulotomy during period of 5 years from July2013 to July 2018 respectively, of either sex andaged between 40 to 85 years. Diagnosis of posteriorcapsule opacification was made from the symptomspresented by the patients and signs found duringexamination by an ophthalmologist.
Symptoms of reduction of vision, glare or anycomplaints that seemed the cataract had returnedand sign of loss of posterior capsule transparencydetected by ophthalmoscope and confirmed by slit-lamp biomicroscope under dilated pupil was takenas diagnostic. An arbitrary classification was madedepending on the thickness of the posterior capsuleopacification as mild, moderate and severely dense,basing on the visual- acuity, slit- lamp examinationand funduscopy.
The study excluded the patients with cornealopacity, history of glaucoma, posterior segmentdisease like, vitreous opacity, macular diseases,optic nerve diseases or any retinopathy causingfunctional impairment of vision.
A proformed data was prepared basing on theparticulars of the patients, pre-laser and post- laserassessment of the patients. The pre-laserophthalmic evaluation includes a history andcomplete ocular examinations.
Topical surface anaesthsia (0.4% Oxybuprocaine) wasused in each patient before laser therapy.Tropicamide 1% eye drop was used to dilate the pupilat a dose of 3 times at 10 minutes interval prior tothe laser therapy. Following the laser therapy, anti-glaucoma drop i.e. Timolol maleate (1 drop 2 times aday for 7 days) and steroid eye drop (1 drop 4 times aday for 7 days) were used in the post-laser eye.
A slit-lamp laser delivery was performed afterhelium-neon aiming beam was brought into focus.The pulse energy threshold was 0.9- 3.0 mJ/ pulsewith mode locked system depending on thethickness of the posterior capsule. Initially lowesteffective energy output was used. Higher energylevel was used in case of dense fibrosis of theposterior capsule. Capsulotomy was done by aseries of punctures either in a cruciate or circularpattern, with the punctures aimed at the visualaxis. An opening of about 2.5 mm to 3.0 mm wascreated to improve the vision. Pre and post laservisual acuity and IOP of the respective eye wasrecorded. Pre laser visual acuity was recorded justbefore the laser was given. Post laser visual acuitywas taken at least one week after the capsulotomy.
64 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Results:
Table-I. Pre and post laser visual acuity (after 7 days)
Visual Acuity Pre- laser number Post- laser number Total (pre and post p-(VA) of patients of patients laser) number value
(post laser 7th day) of patients
6/6 - 1 (3.33%) 1 (1.66%)
6/9 - 2 (6.66%) 2 (3.33%)
6/12 5 (16.66%) 20 (66.66%) 25 (41.66%)
6/18 2 (6.66%) 4 (13.33%) 6 (10%)
6/24 4 (13.33%) - 4 (6.66%)
6/36 1 (3.33%) 1 (3.33%) 2 (3.33%) 0.002
6/60 7 (23.33%) 2 (6.66%) 9 (15%)
3/60 4 (13.33%) - 4 (6.66%)
CF (8ft) 5 (16.66%) - 5 (8.33%)
CF (4ft) 2 (6.66%) - 2 (3.33%)
CF (2ft) - - -
CF (1/2ft) - - -
Total 30 (100%) 30 (100%) 60 (100%)
Table- II. Pre and post laser visual acuity (after 30 days)
Visual Acuity Pre laser number Post laser number Total (pre and post p-(VA) of patients of patients laser) number value
(post laser 30 days) of patients
6/6 - 1 (3.33%) 1 (1.66%)
6/9 - 2 (6.66%) 2 (3.33%)
6/12 5 (16.66%) 24 (80%) 29 (48.33%)
6/18 2 (6.66%) 2 (6.66%) 4 (6.66%)
6/24 4 (13.33%) 1 (3.33%) 5 (8.33%)
6/36 1 (3.33%) - 1 (1.66%) 0.001
6/60 7 (23.33%) - 7 (11.66%)
3/60 4 (13.33%) - 4 (6.66%)
CF (8 ft) 5 (16.66%) - 5 (8.33%)
CF (4 ft) 2 (6.66%) - 2 (3.33%)
CF (2 ft) - - -
CF (1/2 ft) - - -
Total 30 (100%) 30 (100%) 60 (100%)
Discussion:
The study was conducted in the eye department ofUttara Adhunik Medical College Hospital andCombined Military Hospital (CMH) of DhakaCantonment, respectively.
The main aim was to evaluate the visual acuity ofthe concerned eye following Nd: YAG lasercapsulotomy. The evaluation was done both forthe distant and near vision. It was evident in thestudy that substantial number of patients had
Pattern of Visual Outcome after Nd: YAG Laser Capsulotomy in Patients Asif-Ur-Rahman et al 65

achieved better visual acuity for distant vision after7 days of capsulotomy. That improvement was evengreater after 30 days of capsulotomy with orwithout refraction. From Table-I, it is revealed thatpre- capsulotomy visual acuity was 6/12 in 5patients (16.66%), 6/18 in 2 patients (6.66%), 6/24in 4 patients (13.33%), 6/36 in 1 patient (3.33%), 6/60 in 7 patients (23.33%), 3/60 in 4 patients(13.33%), CF (8ft) in 5 patients (16.66%), CF (4ft)in 2 patients (6.66%) respectively. From Table-I, itis revealed that after 7 days of posteriorcapsulotomy, visual acuity improved to 6/6 in 1patient (3.33%), 6/9 in 2 patients (6.66%), 6/12 in20 patients (66.66%), 6/18 in 4patients (13.33%), 6/36 in 1 patient (3.33%), 6/60 in 2 patients (6.66%)respectively. From Table-II, it is revealed that after30 days, visual acuity improved to 6/6 in 1 patient(3.33%), 6/9 in 2 patients (6.66%), 6/12 in 24 patients(80%), 6/18 in 2 patients (6.66%), 6/24 in 1 patient(3.33%) respectively.
A question still remains to be answered why visualacuity did not improve to 6/6 or 6/9 in the majorityof the cases. This is because of the pre existingocular diseases including ARMD (Age RelatedMacular Degeneration), CMO (Cystoid MacularOedema), glaucoma, ischaemic optic neuropathyand amblyopia12 that were undiagnosed beforelaser capsulotomy.
The findings of my study co-related with thefindings of the study conducted by Uddin M G etal13. In the said Uddin M G et al study, beforecapsulotomy visual acuity was 6/9 in 11(7.8%)patients, 6/12 in 12(8.57%) patients, 6/18 in 25(17.85%) patients, 6/24 in 26(18.57%) patients, 6/36 in 35 (25.05%) patients and 6/60 or less in31(22.14%) patients respectively. Uddin M G et alstudy revealed that after capsulotomy the visualacuity was 6/6 in 26 (18.57%) patients, 6/9 in24(17.14%) patients, 6/12 in 32 (22.85%) patients,6/18 in 31 ( 22.14%) patients, 6/24 in 12 (8.57%1)patients, 6/36 or less in 15 (10.71%) patientsrespectively.
Our study has similar findings conducted byHossain MM et al. In their study, among 100patients 36 of them achieved (36%) visual acuity of6/6, 48 patients (48%) achieved visual acuity of 6/9, 9 patients (9%) achieved visual acuity of 6/12, 2patients (2%) achieved visual acuity of 6/18 andanother 2 patients (2%) had visual acuity 6/60 after
laser capsulotomy. These patients had visual acuity6/12 in 15 (15%) patients, 6/18 in 23 (23%) patients,6/24 in 31 (31%) patients, 6/36 in 17 (17%) patients,6/60 in 11 (11%) patients, less than 6/60 in 3 (3%)patients before laser capsulotomy.
My study has similar findings conducted byHossain AM et al. In Hossain et al study, beforelaser capsulotomy, patients had visual acuity of >6/12 in 6.9%, 6/12 -6/24 in 28.6%, 6/24 -6/36 in 48.4%,6/36 -6/60 in 13.6% and <6/60 in 2.5% respectively.In the said study, after laser capsulotomy, patientshad visual acuity >6/12 in 85.9%, 6/12 - 6/24 in8.10%, 6/24 - 6/36 in 1.70%, 6/36 -6/60 in 2.5%, andless than 6/60 in 1.8% respectively.
Conclusion:
The study results revealed that Nd:YAG lasercapsulotomy in posterior capsular opacification cansubstantially improve the visual outcome. Thisimprovement can be further augmented byrefractive corrections one month following thelaser capsulotomy. Although, the results wereinterpreted with short time follow up, long timefollow up is required to evaluate the ultimateoutcome.
References1. Thyletors B, Negrel AD, Global Data on Blindness of
WHO, 73, 115-21.
2. Klein B, Klein R, Linton K, Prevalence of Age- RelatedLens Opacities in a Population. The Beaver Dam EyeStudy, Ophthalmology, 1992, 99; 546 -552.
3. Laske MC, Sperduto RD, The Epidemiology of SenileCataract; Am. J. Epidemiology 1983; 118: 152 -165.
4. Stark WJ, Holladay JT et al. The FDA report onintraocular lenses. Ophthalmology 1983; 311- 317.
5. Desai P. The National Cataract Surgery Survey II:Clinical Outcomes. 1993; 7; 489- 494.
6. Apple DJ, Solomon KD et al. Posterior CapsuleOpacification. Survey of Ophthalmology 1992. 37: 73-116.
7. Constable IJ, Lim ASM. Laser: Its Clinical Use in EyeDiseases. Second edition, Singapore, P.G. Publishing;1990: 147- 148.
8. Nishi O. Posterior Capsule Opacification, Part- 1,Experimental Investigation J. 1999, 75; 107- 112.
9. Schaumbug DA, Dana MR et al. A Systemic Overviewof the Incidence of Posterior Capsular Opacification,Ophthalmology 1998; 105, 1213-1221.
10. F.S.Roger, J.C.Robert et al. Complications of CataractSurgery, Albert & Jacobiec, 2nd edition; 2000: vol- 2.W.B. Saunders Company. 1577- 1579.
66 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
Serum Vitamin D and Severe Preeclampsia: A
Case Control StudyShahina Akhter1, M Anwar Hussain2, Begum Nasrin3, Shamim Ara Begum4, MM Karim5
Abstract
Introduction: Preeclampsia is a pregnancy-specific syndrome characterized by new-onset
hypertension and proteinuria, occurring usually after 20 weeks gestation. It causes
significant mortality & morbidity both mother & foetus. Even though, widespread researches
are now being carried out but, regretfully the main causes for this disorder (preeclampsia)
have not been specifically determined so far. So, most of the preeclampsia cases remain
unrecognized until severe complications occur. Early recognition of preeclampsia is of
great importance for maternal and fetal outcome.
Objective: To assess the association of serum vitamin D level with severe preeclampsia.
Method: The present case-control study was conducted in the department of Obstetrics
and Gynecology of BSMMU, Dhaka, Bangladesh, from January, 2015 to December, 2015 to
explore the association between serum vitamin D level and severe preeclampsia. The study
included 30 severe preeclamptic women as cases and 30 normotensive pregnant women as
controls through purposive sampling. Proteinuria was measured by dip-stick method and
serum 25(OH)D level was measured by chemiluminescence Method in Nutritional
Biochemistry Lab. in ICDDRB. Result was expressed as, mean ± SD. Mann-Whitney U test,
Chi-square test, Pearson’s correlation-coefficient (r) test & Spearmen’s rho correlation-
coefficient test were used as and where necessary. Collected data were analyzed by using
window based software devised with statistical packages for social sciences. A p-value
smaller than 0.05 was considered to indicate a significant difference.
Result: In this study, comparison of mean serum 25(OH)D level between severe preeclamptic
and normotensive pregnant subject showed that serum 25(OH)D level was significantly
lower in subjects with severe preeclampsia in comparison to normotensive pregnant control.
The mean serum 25(OH)D level in cases and controls was 17.53±9.93 nmol/L and
31.09±19.07 nmol/L respectively. So, mean serum 25(OH)D level was 43.62% lower in
severe preeclamptic women than normotensive pregnant control. Using the cut off point of
25 nmol/L, it was observed that serum 25(OH)D deficiency was significantly associated
with cases than that of their control counterpart (76.7% vs 43.3%, p< .01). The risk of
developing severe preeclampsia is 4.3 times higher in pregnant women with serum 25(OH)D
level<25 nmol/L than those of pregnant women with serum 25(OH)D level e” 25 nmol/L
in this study. There was positive relationship between serum vitamin D level and gravidity
but correlation-coefficient was not statistically significant. Also serum 25(OH)D had
negative correlation with systolic and diastolic blood pressure and coefficients were both
statistically significant.
Conclusion: This study shows a potential association between low levels of vitamin D
and severe preeclampsia. However, the study does not prove that low levels of vitamin D
cause preeclampsia. So, further study is needed to understand the impact of vitamin D
deficiency on risk of preeclampsia. If these results are confirmed, vitamin D supplementation
in early pregnancy could be an effective and safe means of preventing preeclampsia.
Original Article
Key words:
Vitamin D, Preeclampsia.
Article information
Received: 01.06.2020Accepted: 02.07.2020
Cite this article:
Akhter S, Hussain MA,Nasrin B, Begum SA,Karim MM. Serum VitaminD and SeverePreeclampsia: A CaseControl Study. SirSalimullah Med Coll J 2020;28: 67-72
Sir Salimullah Med Coll J 2020; 28: 67-72
1. Assistant Professor, Department of Obstetrics and Gynaecology, Sir Salimullah Medical College, Dhaka.2. Professor, Ex-Chairman, Department of Obstetrics and Gynaecology, Bangabandhu Sheikh Mujib Medical University, Dhaka.3. Professor, Department of Obstetrics and Gynaecology, Bangabandhu Sheikh Mujib Medical University, Dhaka.4. Assistant Professor, Department of Obstetrics and Gynaecology, Cox’sbazar Medical College, Cox’sbazar.5. Colonel, Department of Clinical Haematology and Bone Marrow Transplantation, Combined Military Hospital, Dhaka.Address of correspondence: Dr. Shahina Akhter, Assistant Professor, Department of Obstetrics and Gynaecology, SirSalimullah Medical College, Dhaka. Mobile: 01911542337, E-mail:shahina123456akhter@ gmail.com

Introduction
Preeclampsia is a serious, pregnancy-specific multisystemic disorder that affects up to 8% of pregnantwomen. It is diagnosed by new-onset hypertensionand proteinuria after 20 weeks of gestation1,2. Itis a leading cause of maternal and perinatalmortality and morbidity in the world3. Despitedecades of research, the pathogenesis ofpreeclampsia is still not understood fully. Earlyrecognition of the syndrome still presents achallenge to clinicians as there is no specificdiagnostic test and treatment is based onmanagement of symptoms and prevention ofcomplications rather than specific therapy4.
It has been suggested that preeclampsia resultsfrom a breakdown of tolerance to the developingfetus after maternal immune maladaptation.Several of the proposed immunomodulatoryproperties of the hormonal vitamin D system couldpotentially have beneficial effects for successfulimplantation and maintenance of pregnancy1. Astudy done by the University of Pittsburgh Schoolsof the Health Sciences found that vitamin Ddeficiency early in pregnancy is associated with afive-fold increased risk of preeclampsia5. Theproposed pathogenesis is that vitamin D deficiencyimpairs the normal Th1 to Th2 cytokine balance,with higher Th1 cytokine expression impairingimmunological tolerance of embryo implantation6.Evidence proposes that ensuring adequate vitaminD status / intake may help in the prevention andmanagement of preeclampsia1.
Pregnancy provides an immunological challenge,as the fetus is essentially an allogenic tissue graftcarrying paternally derived antigens. Despite this,under normal circumstances, maternal immunedefense allows for implantation, and the motheris able to carry the fetus to full-term. It is believedthat domination by the T helper type 2 (Th2)cytokine response is one of the critical stepsrequired for the maintenance of normalpregnancy.1,25(OH)2D has an important role inpromoting the shift to a Th2-dominated immuneresponse pattern during pregnancy1,7.
Recent reports suggest that preeclampsia isassociated with a Th1 predominant profile and maybe considered as a failure of the tolerance systemallowing the second physiological trophoblasticinvasion. A significant positive correlation was
observed between mean blood pressure andconcentrations of Th1-type cytokines (IL-2, IFN-ã, TNF-á). These results strongly suggest thatthere is a Th1/Th2 imbalance in preeclampticpatients with predominant Th1-type immunity. Th1predominant immunity is closely related toinflammation, endothelial dysfunction and poorplacentation. The syndrome of preeclampsia haspreviously been ascribed to generalized maternalendothelial dysfunction, poor placentation andexcessive maternal inflammatory response8.
Preeclampsia is taken into account as one of thefrequent diseases during pregnancy that could leadto serious outcomes including death. Hence,identification of causative agent for thisphenomenon and establishing pathophysiologyseems quite vital that might help in takingpreventive measures. Under the above perspectivethe present study has been undertaken toinvestigate serum vitamin D status in womenaffected by preeclampsia and to explore theassociation of serum vitamin D level withpreeclamptic women who attended the departmentof Obstetrics and Gynaecology of BSMMU Hospital.
Materials and Methods
This case control study was conducted fromJanuary, 2015 to December, 2015 in Departmentof Obstetrics and Gynaecology, BSMMU Hospital,Dhaka, Bangladesh. The study included 30 severepreeclamptic women as cases and 30 normotensivepregnant women as controls. Method of samplingwas purposive. Calculated sample size was 68 ineach group but due to financial constraint only 60study subjects (cases-30 and controls-30) wereenrolled. After taking informed written consentsamples were collected on the basis of inclusionand exclusion criteria. A predesigned data collectionsheet was used to collect data. Proteinuria wasmeasured by dip-stick method and serum 25(OH)Dlevel was measured by chemiluminescence Methodin Nutritional Biochemistry Lab. in ICDDR, B.Result was expressed as, mean ± SD. Mann-Whitney U test, Chi-square test, Pearson’scorrelation-coefficient (r) test & Spearmen’s rhocorrelation-coefficient test were used as and wherenecessary. Collected data were analyzed by usingwindow based software devised with statisticalpackages for social sciences. A p-value smaller than0.05 was considered to indicate a significantdifference.
68 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
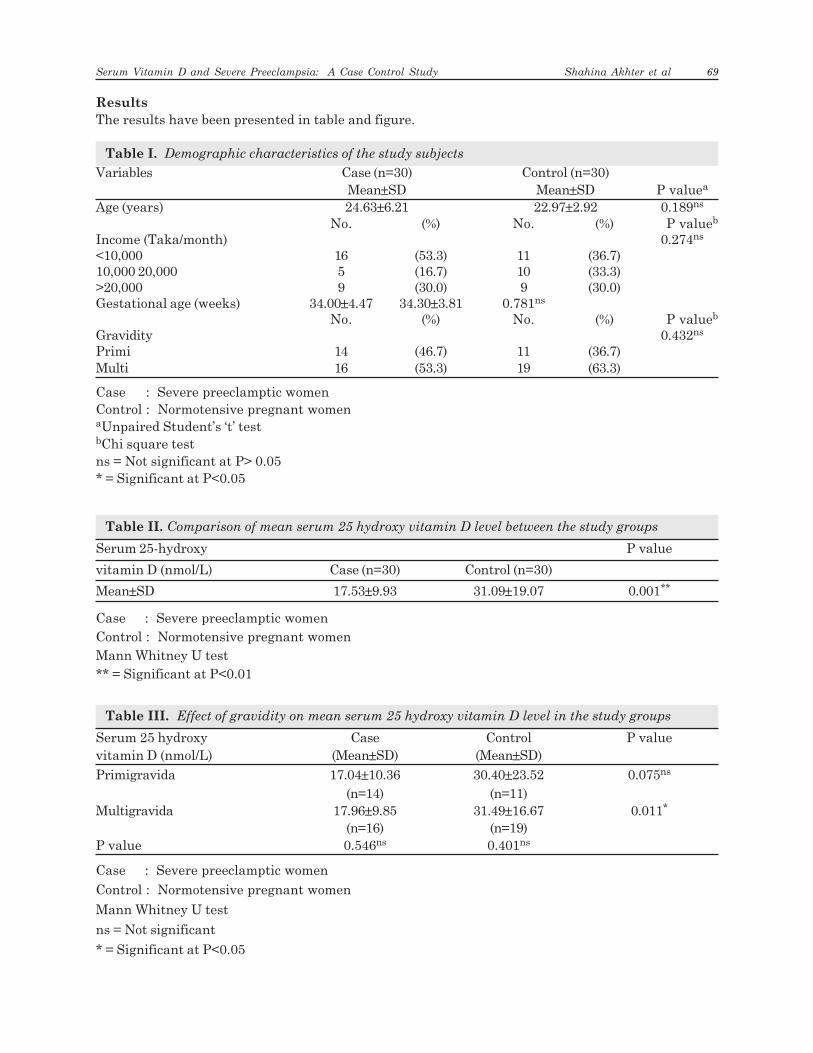
Results
The results have been presented in table and figure.
Table I. Demographic characteristics of the study subjects
Variables Case (n=30) Control (n=30)Mean±SD Mean±SD P valuea
Age (years) 24.63±6.21 22.97±2.92 0.189ns
No. (%) No. (%) P valueb
Income (Taka/month) 0.274ns
<10,000 16 (53.3) 11 (36.7)10,000 20,000 5 (16.7) 10 (33.3)>20,000 9 (30.0) 9 (30.0)Gestational age (weeks) 34.00±4.47 34.30±3.81 0.781ns
No. (%) No. (%) P valueb
Gravidity 0.432ns
Primi 14 (46.7) 11 (36.7)Multi 16 (53.3) 19 (63.3)
Case : Severe preeclamptic womenControl : Normotensive pregnant womenaUnpaired Student’s ‘t’ testbChi square testns = Not significant at P> 0.05* = Significant at P<0.05
Table II. Comparison of mean serum 25 hydroxy vitamin D level between the study groups
Serum 25-hydroxy P value
vitamin D (nmol/L) Case (n=30) Control (n=30)
Mean±SD 17.53±9.93 31.09±19.07 0.001**
Case : Severe preeclamptic womenControl : Normotensive pregnant womenMann Whitney U test** = Significant at P<0.01
Table III. Effect of gravidity on mean serum 25 hydroxy vitamin D level in the study groups
Serum 25 hydroxy Case Control P valuevitamin D (nmol/L) (Mean±SD) (Mean±SD)
Primigravida 17.04±10.36 30.40±23.52 0.075ns
(n=14) (n=11)Multigravida 17.96±9.85 31.49±16.67 0.011*
(n=16) (n=19)P value 0.546ns 0.401ns
Case : Severe preeclamptic women
Control : Normotensive pregnant women
Mann Whitney U test
ns = Not significant
* = Significant at P<0.05
Serum Vitamin D and Severe Preeclampsia: A Case Control Study Shahina Akhter et al 69
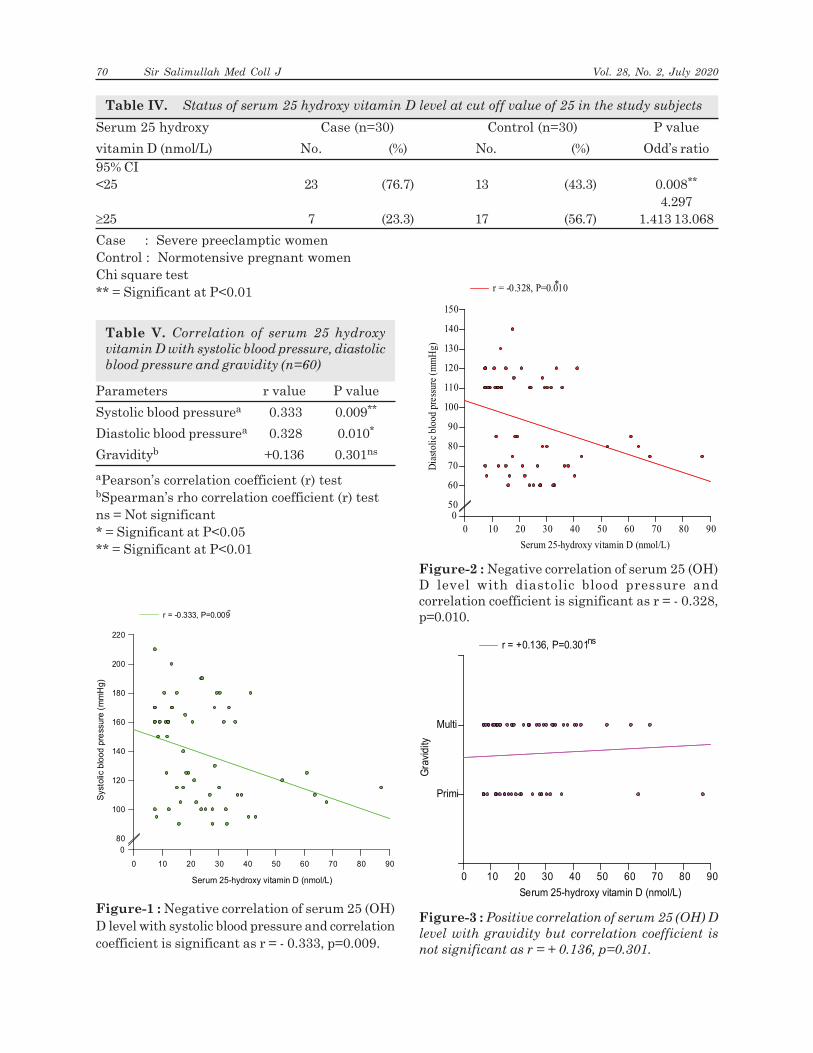
Table IV. Status of serum 25 hydroxy vitamin D level at cut off value of 25 in the study subjects
Serum 25 hydroxy Case (n=30) Control (n=30) P value
vitamin D (nmol/L) No. (%) No. (%) Odd’s ratio95% CI<25 23 (76.7) 13 (43.3) 0.008**
4.297³25 7 (23.3) 17 (56.7) 1.413 13.068
Case : Severe preeclamptic womenControl : Normotensive pregnant womenChi square test** = Significant at P<0.01
Table V. Correlation of serum 25 hydroxy
vitamin D with systolic blood pressure, diastolic
blood pressure and gravidity (n=60)
Parameters r value P value
Systolic blood pressurea 0.333 0.009**
Diastolic blood pressurea 0.328 0.010*
Gravidityb +0.136 0.301ns
aPearson’s correlation coefficient (r) testbSpearman’s rho correlation coefficient (r) testns = Not significant* = Significant at P<0.05** = Significant at P<0.01
Figure-1 : Negative correlation of serum 25 (OH)D level with systolic blood pressure and correlationcoefficient is significant as r = - 0.333, p=0.009.
Serum 25-hydroxy vitamin D (nmol/L)
0 10 20 30 40 50 60 70 80 90
Syst
olic
blo
od
pre
ssu
re (
mm
Hg
)
0
80
100
120
140
160
180
200
220
r = -0.333, P=0.009**
Serum 25-hydroxy vitamin D (nmol/L)
0 10 20 30 40 50 60 70 80 90
Dia
stol
ic b
lood
pre
ssur
e (m
mH
g)
050
60
70
80
90
100
110
120
130
140
150
r = -0.328, P=0.010*
Figure-2 : Negative correlation of serum 25 (OH)D level with diastolic blood pressure andcorrelation coefficient is significant as r = - 0.328,p=0.010.
Figure-3 : Positive correlation of serum 25 (OH) D
level with gravidity but correlation coefficient is
not significant as r = + 0.136, p=0.301.
Serum 25-hydroxy vitamin D (nmol/L)
0 10 20 30 40 50 60 70 80 90
Gra
vid
ity
Primi
Multi
r = +0.136, P=0.301ns
70 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Discussion
This study was carried out with an objective toevaluate the association between serum 25(OH)Dlevel and severe preeclampsia. A total of 60pregnant women with severe preeclampsia as case(30) and normotensive control (30) were includedin the study. Controls were selected matching formaternal age, gestational age, gravidity and familyincome with cases as these were the potentialconfounding factors might affect the outcomevariable, serum 25(OH)D level.
Preeclampsia occurs with increased frequencyamong young, nulliparous women. However, thefrequency distribution is bimodal, with a secondpeak occurring in multiparous women > 35 yearsof age9. Relative risk of developing preeclampsiais 2.91, CI:1.28-6.61 in case of nulliparouswomen10. So, nulliparous women may have lower25(OH)D level than multiparous women. There isno report regarding the relationship betweengravidity and vitamin D level. The present studydid not show significant difference in serum25(OH)D level between primigravida andmultigravida. There was positive relationshipbetween serum vitamin D level and gravidity butcorrelation coefficient was not statisticallysignificant. We had a smaller sample, thereforelimited power to detect an interaction between25(OH)D concentrations and gravidity.
In pregnancies with preeclampsia, the reportedmean maternal serum or plasma levels of either25(OH)D3 or total 25(OH)D are 15-57% lower thanin normal pregnancies.11,2,12,13 In this study serum25(OH)D level is 43.62% lower in severepreeclampsia than in normotensive pregnantcontrol. Comparison of mean serum 25(OH)D levelbetween severe preeclamptic and normotensivepregnant subjects showed that serum 25(OH)Dlevel was significantly lower in subjects with severepreeclampsia in comparison to control. The meanserum 25(OH)D level in cases and controls was17.53±9.93 nmol/L and 31.09 ± 19.07 nmol/Lrespectively. Another study reported that meanserum 25(OH)D level was 24.86 ng/ml in controlsand 23.96 ng/ml in preeclampsia and this differencewas statistically significant.14 Several other studiesfound significantly decreased levels of plasma25(OH)D in severe preeclamptic women thannormotensive control.13,15 However, one studyfound that preeclamptic and normotensive
pregnant women had equivalent levels of25(OH)D.16
Maternal vitamin D deficiency has been proposedas a risk factor for preeclampsia14. Recent datasuggest that abnormal cell-mediated immunityactivation by fetal allograft may contribute to thedevelopment of preeclampsia.7 The immune-modulatory properties of 1,25(OH)2D may play akey role in maintaining immunological tolerancein pregnancy and ensuring adequate vitamin Dstatus may help in the prevention of preeclampsia1.In this study, using the cut off point of 25nmol/L,it was observed that serum 25(OH)D deficiency(<25 nmol/L) was significantly associated withcases than that of their control counterpart (76.7%vs 43.3%, p<.01).
The risk of developing an event in the case groupcompared to the control group was estimated byodds ratio which had shown that the risk ofdeveloping severe preeclampsia was 4.3 timeshigher in pregnant women with serum 25(OH)Dlevel < 25 nmol/L than those pregnant women withserum 25(OH)D level e”25 nmol/L in this study.Here p - value is < .01 which is statisticallysignificant.
Vitamin D deficiency has also been implicated inthe development of hypertension in several clinicaland epidemiological studies.14 A recent reviewarticle demonstrates that eight out of tenobservational studies and 3 randomized controlledtrials strongly support an inverse relation betweenvitamin D and blood pressure.17 Vitamin D is apotent endocrine suppressor of renin biosynthesisto regulate the renin-angiotensin system.18
Notably, vascular structure and function includingvascular compliance, elasticity and intima mediathickness are more favourable among womensupplemented with vitamin D.19 Consistent withthe most previous studies, the present studyshowed that serum 25(OH)D had negativecorrelation with systolic and diastolic bloodpressure and coefficients were both statisticallysignificant.
Ambiguity in results obtained in different studies,methodological limitation in the studies necessitatemore comprehensive research to be performed toanswer the relevant questions. Since, preeclampsiais considered as one of the crucial events duringpregnancy that could lead to appalling
Serum Vitamin D and Severe Preeclampsia: A Case Control Study Shahina Akhter et al 71

circumstances. Therefore, exploration for findingthe cause of this phenomenon can create valuableprogress in prevention and cure of diseased women.
Conclusion
This work will enrich our knowledge regardingcorrelation between this proposed marker (serumvitamin D) and severe preeclampsia specially whenBangladesh is concerned that might help in takingpreventive measures.
References:1. HyppÖnen, E. Vitamin D for the prevention of
preeclampsia ? A hypothesis. Nutr Rev 2005; 63 : 225 –232.
2. Bodnar LM, Catov JM, Simhan HN, Holick MF, PowersRW and Roberts JM. Maternal Vitamin D DeficiencyIncreases the Risk of Preeclampsia. J Clin EndocrinolMetab 2007a; 92 (9) : 3517 – 3522.
3. Islam SN, Ahsan T, Khatun S, Khan MNI and AhsanM. Serum Vitamin E, C and A Status in Pre-eclampsiaand Eclampsia Patients, and Their correlation withBlood Pressure : A Study in Dhaka, Bangladesh. Mal JNutr 2004; 10(2): 207 - 214.
4. Mushambi MC, Halligan AW & Williamson K. Recentdevelopments in the pathophysiology and managementof preeclampsia. Br. J. Anaesth 1996; 76 :133– 148.
5. Bodnar LM, Catov JM and Roberts JM. Racial/ethnicdifferences in the monthly variation of preeclampsiaincidence. Am J Obstet Gynecol 2007b; 196:324.e1-324.e5.
6. Yakoob MY. Vitamin D deficiency during pregnancyand the risk of preeclampsia. J Pak Med Assoc 2011;61(7): 827-28.
7. Darmochwal – Kolarz D, Leszczynska – Gorzelak B,Rolinski J & Oleszczuk J.T helper 1 – type and T helper2 – type cytokine imbalance in pregnant women withpreeclampsia. European Journal of Obstetrics andGynecology and Reproductive Biology 1999; Volume86, Issue 2 : pages 165 – 170.
8. Saito S. and Sakai M. Th 1/ Th 2 balance in preeclampsia.Journal of Reproductive Immunology 2003; 59: 161 –173.
9. DeCherney HA, Nathan L, GooDwin MT, Laufer N.Current diagnosis and treatment, Obstetrics andGynaecology.11th ed. New York: McGraw-HillCompanies: 2013; 454-464
10. Edmonds KD. Dewhurts’s text book of Obstetrics &Gynaecology. 8th Ed. Oxford: Blackwell Publishing. 2012;104-109
11. August P, Marcaccio B, Gertner JM, Druzin ML, ResnickLM, Laragh JH. Abnormal 1,25-dihydroxyvitamin Dmetabolism in preeclampsia. Am J Obstet Gynecol 1992;166(4): 1295-9.
12. Halhali A, Tovar AR, Torres N, Bourges H, GarabedianM, Larrea F. Preeclampsia Is Associated with LowCirculating Levels of Insulin-Like Growth Factor I and1,25 Dihydroxyvitamin D in Maternal and UmbilicalCord Compartments. The journal of ClinicalEndocrinology and Metabolism 2000; Vol 85, No.5: 1828-1830.
13. Robinson CJ, Alanis MC, Wagner CL, Hollis BW,Johnson DD. Plasma 25-hydroxyvitamin D levels inearly-onset severe preeclampsia. Am J Obstet Gynecol2010; 203 (4): 366. e1-6.
14. Ullah MI, Koch CA, Tamanna S, Rouf S, ShamsuddinL. Vitamin D Deficiency and the Risk of Preeclampsiaand Eclampsia in Bangladesh. Horm Metabl Res 2013;45:682-687.
15. Kolusari A, Kurdoglu M, Yildizhan R, Adali E, Edirne T,Cebi A et.al. Catalase Activity, Serum Trace Elementand Heavy Metal Concentrations and vitamin A, D andE levels in preeclampsia. Journal of Internationalmedical Research 2008; 36:1335-1341.
16. Seely EW, Wood RJ, Brown EM, Graves SW. Lowerserum ionized calcium and abnormal calciotropichormone levels in preeclampsia. J Clin EndocrinolMetab 1992; 1436 – 40.
17. Feneis JF, Arora RR. Role of vitamin D in blood pressurehomeostasis. AM J Ther 2005; 17:221-229
18. Li YC, Qiao G, Uskokovic M, Xiang W, Zheng W, KongJ. Vitamin D : a negative endocrine vitamin regulatorof renin angiotensin system and blood pressure. JSteriod Bioche Mol Biol 2004; 89:387-392
19. Braam LA, Hoeks AP, Brouns F, Hamulyak K,Gerichhausen MJ, Vermeer C. Beneficial effects ofvitamins D and K on the elastic properties of the vesselwall in postmenopausal women: a follow-uo study.Thromb Haemost 2004; 91: 373-380.
72 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
Status of Erythrocyte Glutathione Level in
Diabetes MellitusRobiul Islam1, Zafar Khaled2, Nuzhat Chowdhury3, Moshiur Rahaman4,Shahidul Islam Nurre5,
Chandra Shekhar Majumdar 6
Abstract:
Objectives: The purpose of this study was to compare the level of erythrocyte glutathione
in adult onset diabetes mellitus patients with and without retinopathy.
Method and procedure: This was a prospective type of case-control study which was
conducted in the department of Ophthalmology, BSMMU in collaboration with the
department of Pharmacology, BSMMU, Dhaka from September, 2013 to January 2016. A
total number of 60 patients who had adult onset diabetes mellitus fulfilling inclusion and
exclusion criteria were enrolled in this study and they were divided into two groups as
group A and group B. Group A comprised 30 patients who had only diabetes mellitus
without retinopathy and group B comprised another 30 patients who had diabetes mellitus
with retinopathy.To maintain confidentiality, each of the study subjects was given an ID
number. All the research data was coded and stored in a locked cabinet. A well informed,
voluntarily signed written consent was taken in an understandable local language from
the study subjects. No experimental drug or placebo was used for this study. Diagnosis of
diabetic retinopathy was done by fundus oculi examination with direct and indirect
ophthalmoscope, colour fundus photograph (CFP) of both eyes. Then 3 ml blood was
collected by venous puncture in an EDTA containing test tube.
After collecting blood, erythrocyte reduced glutathione level was measured by Ellman’s
method (Ellman, 1959) and compared between two groups.
Results: In this study, the patients were matched in relation to age and sex. It was observed
that majority (40.0%) patients were belonged to age 41-50 years in group A and 10 (33.3%)
in group B. The mean age was found 55.8 ± 8.8 years in group A and 58.3 ± 9.4 years in
group B. More than half (53.3%) patients were female in group A and 12 (40.0%) in group
B. The mean duration of diabetes was found 7.6 ± 5.4 years in group A and 11.6 ± 6.9 years
in group B. The mean duration of diabetes was statistically significant (p<0.05) between
two groups. The mean glutathione level was found 9.8 ± 2.3 mg/ml in group A and 4.7 ± 1.0
mg/ml in group B. The difference was statistically significant (p<0.05) between two groups.
Conclusion: Diabetic patients have lower glutathione level with or without retinopathy.
Original Article
Key words:
Diabetic retinopathy,Glutathione(GSH),OxidisedGlutathione(GSSG),Antioxidants
Article information
Received: 01.05.2020Accepted: 01.08.2020
Cite this article:
Islam R, Khaled Z,Chowdhury N, RahamanM, Nurre MI, MajumdarCS. Status of ErythrocyteGlutathione Level inDiabetes Mellitus. SirSalimullah Med Coll J 2020;28: 73-77
Sir Salimullah Med Coll J 2020; 28: 73-77
1. Assistant Professor, Department of Ophthalmology, Sir Salimullah Medical College, Dhaka2. Professor, Department of Ophthalmology, BSMMU3. Associate professor, Department of Ophthalmology, BSMMU4. Registrar, Department of Ophthalmology, Sir Salimullah Medical College, Dhaka5. Assistant Register,Department of Ophthalmology, Sir Salimullah Medical College, Dhaka6. Professor, Department of Ophthalmology, Sir Salimullah Medical College, Dhaka
Address of Correspondence: Dr. Robiul Islam, Assistant Professor, Department of Ophthalmology, Sir Salimullah MedicalCollege Mitford Hospital, Dhaka
Introduction:
Free radicals cause cell injury by lipid peroxidationof membrane, oxidative modification of proteinsand DNA breakdown1. In order to compensate theeffects of free radicals, there are defense
mechanisms in the organism called antioxidants.These antioxidants may be classified as enzymesor small non-enzymatic protein moleculesaccording to their structure.2 The enzymes thatact as free radical scavenging system are catalase,

superoxide dismutase and glutathione peroxidase.1
Superoxide dismutase removes superoxide anion(O2
-) by converting it to hydrogen peroxide whichis then removed by glutathione peroxidase orcatalase.3 Among the non-enzymatic smallmolecules antioxidants, these are glutathione,melatonin, carotenoids, retinoid and vitamins Cand E 2. Under normal circumstances, free radicalsare rapidly eliminated by antioxidants such asreduced glutathione, vitamin C, and vitamin E.
Glutathione (GSH) is a major antioxidant in thebody synthesized predominantly in hepatocytesfrom the amino acids cysteine, glutamate, andglycine 4,5 . The synthesis of GSH from glutamate,cysteine, and glycine is catalyzed sequentially bytwo cytosolic enzymes, gama-glutamylcysteinesynthetase (GCS) and GSH synthetase. Thispathway occurs in virtually all cell types, with theliver being the major producer and exporter of GSH6 .In healthy tissue, more than 99% of the totalglutathione pool is in the reduced form (GSH) andless than 1% exists in the oxidized (disulfide) form(GSSG) 4. Most of the cellular glutathione (85-90%)is present in the cytosol, with the remainder inmany organelles (including the mitochondria,nuclear matrix, and peroxisomes).6 About 99.5%of blood glutathione is contained in red blood cells.It is the central member of complex antioxidantsystem protecting the cell from oxidative stress.4
It also acts as a cofactor for many enzymes suchas glutathione peroxidase, which catalyzesdetoxification of intracellular peroxides.7 Reducedglutathione can again be regenerated from oxidizedglutathione (GSSG) by the enzyme glutathionereductase (GSR) with NADPH. In diabetes, thelevels of reduced glutathione intracellularantioxidant are decreased in the retina and theenzymes responsible for its metabolism arecompromised.8
There are many ways by which hyperglycemia mayincrease the generation of free radicals.
In diabetic patient, there is an elevated level ofoxidative stress due to deficiency of reducedglutathione, which occurs because of the decreasedsynthesis caused by limited availability of theprecursor amino acids cysteine and glycine.5 Inaddition, reduced glutathione deficiency may resultfrom depletion of NADPH in polyol pathway.8
Protein damage due to the protein glycosylation
may be a mechanism that lowers the activities ofprimary antioxidant enzyme. In addition, GSHdeficiency may result from depletion of NADH inpolyol pathway. The retina has high content ofpolyunsaturated fatty acids and has the highestoxygen uptake and glucose oxidation relative toany other tissue. This phenomenon renders retinamore susceptible to oxidative stress. It has beensuggested that the correlation betweenhyperglycemia, changes in the redox homeostasis,and oxidative stress are the key events in thepathogenesis of diabetic retinopathy.8 In diabeticretinopathy, aldose reductase is activated andsorbitol levels are elevated in retina, and activationof protein kinase C increases vascularpermeability, alterations in blood flow andneovascularization.9 A hallmark of early diabeticretinopathy is the change in the structure andcellular composition of the microvasculature.10
Pericytes are essential cellular components in theregulation of retinal capillary perfusion and damageto these cells in diabetes leads to altered retinalhemodynamics, including abnormal autoregulationof retinal blood flow. Loss of retinal pericytes alsorepresents another early feature of diabeticretinopathy and correlates with microaneurysmformation.11 Another common feature of diabeticretinopathy is the thickening of the capillarybasement membrane and increased deposition ofextracellular matrix components. This feature maycontribute to the development of abnormal retinalhemodynamics including abnormal autoregulationof retinal blood flow.12 There is evidence thatretinal leukostasis may play an important role inthe pathogenesis of diabetic retinopathy.Leukocytes possess large cell volume, highcytoplasmic rigidity, a natural tendency to adhereto the vascular endothelium, and a capacity togenerate toxic superoxide radicals and proteolyticenzymes. In diabetes, there is increased retinalleukostasis which affects retinal endothelialfunction, retinal perfusion, angiogenesis andvascular permeability.13 In diabetes, chronicexposure of retinal cells to high concentrations ofglucose caused decreased synthesis of glutathione,reducing the size of the glutathione pool.4 Thisstudy is carried out to compare the level oferythrocyte reduced glutathione level in adultonset diabetes mellitus patients withoutretinopathy and those having adult onset diabetesmellitus with retinopathy.
74 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Methods and procedure:
A Case-control study was done in the departmentof Ophthalmology, in collaboration with thedepartment of Pharmacology, BSMMU fromSeptember 2013 to January 2016. Patientsattended in the department of Ophthalmology,BSMMU who have adult onset diabetes Mellituswere the study population. Purposive samplingtechnique was applied and total 60 patients, whofulfilled the inclusion and exclusion criteria, wereselected in two divided groups. Group A contained30 patients who had adult onset diabetes mellituswithout retinopathy and Group B containedanother 30 patients who had adult onset diabetesmellitus with retinopathy. Written informedconsent was taken before enrollment. Clinicalevaluation including history, physical examination,relevant ocular examinations, were done in theophthalmology department. With all asepticprecautions, 3 ml blood (8 hours fasting) wascollected by venous puncture in an EDTAcontaining test tube. After collecting blood, itwas centrifuged at room temperature at 3500 rpmfor 10 minutes. The plasma and buffy coat wasseparated from the top. The packed Red blood cellswere washed thrice with five volumes of cold 0.9%
saline by centrifugation at 3500 rpm for 10minutes. The packed cells were suspended in fivevolumes of deionized distilled water at 4p C for 24hours to lyse RBCs. Then it was centrifuged at4000 rpm for 10 min to collect RBCs lysate. Allsamples were stored temporarily at -20p C in thepharmacology department, BSMMU. Then reducedglutathione was estimated weekly from thehemolysate by the spectrophotometer (UV-1800,Shimadzu spectrophotometer) at 412 nmwavelength using Ellman’s method (Ellman 1959)14.Statistical analysis of the results was done byusing computer based software, SPSS 16.0 (SPSSInc, Chicago, IL, USA).A probability ‘P’ value of0.05 or less was considered as significant.
Results and Observations:
It was observed that majority (40.0 %) patientswere belonged to age 41-50 years in group A and10 (33.3 %) in group B. The mean age was found55.8 ± 8.8 years in group A and 58.3 ± 9.4 years ingroup B. More than half (53.3%) patients werefemale in group A and 12 (40.0 %) in group B. Themean duration of diabetes was found 7.63 ± 5.4years in group A and 11.6 ± 6.9 years in group B.The mean duration of diabetes was statisticallysignificant (p<0.05) between two groups.
Table I: Particulars of the study patients (n=60)
Particular of the Group-A(n=30) Group-B (n=30) P valuepatients n % n %Age (in years) 41 - 50 12 40.0 10 33.3
51 - 60 9 30.0 7 23.361 - 70 8 26.7 11 36.771 - 80 1 3.3 1 3.3
>80 0 0.0 1 3.3Mean ± SD 55.8 ± 8.8 58.3 ± 9.4 a 0.294ns
Range (min, max) 42 , 73 46, 81Sex
Male 14 46.7 18 60.0 b0.301ns
Female 16 53.3 12 40.0Duration of diabetes(years)
£10 21 70.0 18 60.011-20 9 30.0 9 30.0>20 0 0.0 3 10.0
Mean ± SD 7.6 ± 5.4 11.6 ± 6.9 a0.017s
Range (min, max) 42 , 73 46 , 81
s= significant, ns= not significantaP value reached from unpaired t-testbP value reached from chi square test
Status of Erythrocyte Glutathione Level in Diabetes Mellitus Robiul Islam et al 75

It was observed that majority (50.0%) patients wereglutathione level <4.0 mg/ml in group A and 15(50.0%) in group B. The mean glutathione levelwas found 9.8 ± 2.3 mg/ml in group A and 4.7 ± 1.0mg/ml in group B. The difference was statisticallysignificant (p<0.05) between two groups.
Table II: Distribution of the study patients by
glutathione level (n=60)
Glutathione Group-A Group-B P(mg/ml) (n=30) (n=30) value
n % n %<4.0 15 50.0 15 50.04.0-10.0 (Normal) 4 13.3 10 33.3>10.0 11 36.7 5 16.7Mean ± SEM 9.8± 2.3 4.7± 1.0 0.049s
Range (min, max) 0, 41.78 0, 17.5
s= significantP value reached from unpaired t-test
Discussion:
One of the major complications of diabetes mellitusis diabetic retinopathy and it is the leading causeof blindness worldwide.5 The prevalence of diabeticretinopathy is 11.1% in Bangladesh.15 Accordingto the World Health Organization, approximately5 million individuals have diabetic retinopathy,which accounts for about 5% of world blindness.9
Reduced Glutathione is an important endogenousantioxidant and lower level level in the erythrocyteindicates that there is impairment of antioxidantdefense system.16
The present study was aimed to assess the extentof oxidative stress and the antioxidant statusagainst reactive oxygen species (ROS) in patientsof diabetes mellitus.It is now well established bymany studies that progression of diabeticretinopathy is positively correlated with durationof diabetes mellitus. It has significant associationwith duration of diabetes.17,18 Our present studyalso shows similar findings. The mean duration ofdiabetes was found higher in group B than in groupA. The mean duration of diabetes was statisticallysignificant (p<0.05) between two groups. The meanglutathione level was found higher (9.8 ± 2.3 mg/ml) in group A and lower (4.7 ± 1.0 mg/ml) in groupB. The difference was statistically significant(p<0.05) between two groups. The similar findingsalso observed by many other studies. Kalkan etal. 2013 found significant difference with respectto mean glutathione values between the diabeticretinopathy determined subjects and diabeticretinopathy was not determined. Jain et al. 2000showed that erythrocytes of diabetic patients havea lower level of glutathione compared with non-diabetic subject and it is a risk factor for thedevelopment of pathological states such asretinopathy. Atamer et al. 1998 showed thatglutathione activity has decreased in both diabeticgroups.19 They also showed that the level ofenzymes that act as free radical scavenging systemwere also significantly decreased in the group ofretinopathy in comparison to without retinopathy.Hartnett et al. 2000 determined increase in themarkers of oxidative stress and decrease in theantioxidant enzyme levels in subjects with diabeticretinopathy.20 Sree Kumar found significancedecrease in the concentration of reducedglutathione was observed in diabetic cases with orwithout retinopathy in comparison to normalcontrols.
Conclusion:
It may be concluded that there is oxidative stressand decrease antioxidant defense system in adultonset type 2 diabetic patients and it is moremarked in those who have developed diabeticretinopathy. Oxidative stress is reflected by thelower level of erythrocyte reduced glutathione.
Reactive oxygen species can be eliminated by anumber of enzymatic and non-enzymaticantioxidant mechanisms. Non-enzymatic
70.0
30.0
0.0
60.0
30.0
10.0
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
≤10 11-20 >20
Perc
en
tage
Duration of diabetes (years)
Group-A
Group-B
Fig.1: Bar diagram shows duration of diabetes of
the study patients
76 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

antioxidants include vitamins A, C and E;glutathione; á-lipoic acid; carotenoids; traceelements like copper, zinc and selenium; coenzymeQ10 (CoQ10); and cofactors like folic acid, uric acid,albumin, and vitamins B1, B2, B6 and B12.Glutathione (GSH) acts as a direct scavenger aswell as a co-substrate for Glutathione peroxidase.Further study is needed with a larger sample sizeto get more conclusive result. As the antioxidantdefense system is found reduced in this study,every diabetic patient should be managedprophylactically with antioxidant drugs to preventthe complications like retinopathy.
References1. Kumar V, Abbas AK, & Fausto N , Robbins and cotran
pathologic basis of disease, 7th edn, Elsevier Saunders,Philadelphia, Pennsylvania 2004, pp.16-18.
2. Gurler, B, Vural, H, Yilmaz, N, Oguz, H, Satici, A &Aksoy, N , ‘The role of oxidative stress in diabeticretinopathy’, Eye2000, vol. 14, no. 5, pp. 730-35.
3. Evans, P and Halliwell, B , ‘Micronutrients: oxidant/antioxidant status’, British Journal of Nutrition 2001,vol.85, Suppl. 2, pp.67-74.
4. Livingstone C, & Davis J , ‘Targeting therapeuticsagainst glutathione depletion in diabetes and itscomplications’ The British Journal of Diabetes andVascular Disease, 2007, vol. 7, p. 258.
5. Sekhar, RV, Mckay, SV, Patel, SG, Guthikonda, AP,Reddy, VT, Balasubramanam, A & Jahoor, F ,‘Glutathione Synthesis Is Diminished in Patients WithUncontrolled Diabetes and Restored by DietarySupplementation With Cysteine and Glycine’, DiabetesCare 2011,vol. 34, no.1, pp.162–67.
6. Wu G, Fang YZ, Yang S, Lupton JR & TurnerND,‘Glutathione Metabolism and Its Implications forHealth’, The Journal of nutrition 2004, vol. 134, no. 3,pp. 489-92.
7. Jain, SK, Mcvie, R & Smith, T ,‘Vitamin ESupplementation Restores Glutathione andMalondialdehyde to Normal Concentrations inErythrocytes of Type 1 Diabetic Children’, Diabetes Care2000, vol. 23, no. 9, pp. 1389–94.
8. Deore, AB, Sapakal, VD, & Naikwade, NS 2011, ‘Roleof oxidative stress in the pathogenesis of diabetes andits comlpicatications’, Pharmacologyonline 2011, vol. 2,pp. 603-21.
9. Santos, JM, Mohammad, G, Zhong, Q & Kowluru, RA ,‘Diabetic Retinopathy, Superoxide Damage andAntioxidants’, Curr Pharm Biotechnol 2011, vol. 12, no.3,pp.352-61.
10. Kubawara T, Cogan DG , ‘Retinal vascular patterns,VI: mural cells of the retinal capillaries’, ArchOphthalmology1962, Vol. 69, pp. 492-502.
11. Paget C, Lecomte M, Ruggiero D, Wiernperger N &Lagarde M, ‘Modification of enzymatic antioxidants inretinal microvascular cells by glucose or advancedglycation end products’, Free Radic Biol Med1998, Vol.25, pp. 121-29.
12. Williamson JR & Kilo C, ‘Extracellular matrix changesin diabetes mellitus’.In Scorpelli DG, Mogahi DG editors.Comparative pathobiology of Major Age –RelatedDiseases, New York: 1984 ,Liss, pp.269-88.
13. Miyamoto K & Ogura Y, ‘Pathogenetic potential ofleukocytes in diabetic retinopathy’1999, vol. 14, pp. 233-39.
14. Ellman GL 1959, ‘Tissue sulfhydryl groups’, Archives ofbiochemistry and biophysics, Vol.82, pp.70-77.
15. Rahman AHJ. A H editors , Diabetic retinopathy and itsmanagement, first edition, Diabetic association ofBangladeshi 1998, vol.32, pp.3-15.
16. Kalkan, IH & Suher, M , ‘The relationship between thelevel of glutathione, impairment of glucose metabolismand complications of diabetes mellitus’, Pak J Med Sci2013, vol. 29, no. 4, pp. 938-42.
17. Subhan, SS , Rahman, AHS, Sayeed, A, Hasin, F,Karim, R & Ali, L , ‘The Role of Duration of Diabetes inthe Development of Diabetic Retinopathy in YoungDiabetic Patients in Bangladesh’, Journal of BangladeshCollege of Physicians and Surgeons 2009, vol. 27, no. 3,pp. 133-38.
18. Benarous R, Sasongko MB, Qureshi S, Fenwick E,Dirani M,Wong TY, & Lamoureux EL , ‘Differentialassociation of serum lipids with diabetic retinopathyand diabetic macular oedema’, Investigativeophthalmology and visual science 2011, vol.52 (10),pp.7464-7469.
19. Atamer Y, Kocyigit Y, Atamer A, Mete N, Canoruc N,Toprak G , ‘Alterations of Erythrocyte and Plasma LipidPeroxides as well as Antioxidant Mechanism in Patientswith Type II Diabetes Mellitus (NIDDM)’,Tr. J. OfMedical Sciences 1998, vol.28, pp.143-148.
20. Hartnett ME, Stratton RD, Browne RW, Rosner BA,Lanham RJ, Armstrong D, ‘Serum Markers of OxidativeStress and Severity of Diabetic Retinopathy’, DiabetesCare, Vol. 23, No.2, pp.234-240.
Status of Erythrocyte Glutathione Level in Diabetes Mellitus Robiul Islam et al 77

Abstract
Background: Now a days typhoid fever is very common disease affecting both adult and
children. It transmits through faeco oral route. Common symptoms are fever, headache
and gastrointestinal symptoms. It requires long time treatment with appropriate antibiotics.
Many drugs are available for treatment among them injectable ceftriaxone is the most
potent drug. Exact defervasence period with injection ceftriaxone is not known definitely.
Objectives: To evaluate defervacence period of typhoid fever in children treating with
injection ceftriaxone.
Method: It was a cross sectional study. The study was conducted in the Department of
Paediatrics, Dr. M R Khan Shishu Hospital and ICH, Mirpur-2, Dhaka over a period of 1
year from July 2018 to June 2019. All hospitalized children with clinical diagnosis of
typhoid fever admitted in the above mention place were the study population. A total of 50
hospitalized children with laboratory diagnosis of typhoid fever(confirmed by blood culture)
admitted in the above mention place were selected as the study subjects.
Results: In our study, most of the study subjects were more than 5 years of age and mean
age was 8.4 ± 2.8year (the range of 2-15 years). Females were dominating the sex distribution
which are 19(63%) and most of the study subjects were in middle class status which are
16(53.3%) in the socio-economic distribution. Fever were the common symptoms of all
study participants and continues 5-6 days in most of the participants 19(63.3%); headache
were another most common symptoms in 7(23.3) of the study subjects. Signs were
Hepatomegaly, Splenomegaly and Coated tongue in 53.3 %, 43.3% and 93.3% cases
respectively. The mean temperature before treatment was 102.1 ± 2°F. Sixty percent of the
patients had defervescence between 3 – 5 days after treatment with injection ceftriaxone
and 40% between 6 – 9 days. The mean period of defervescence was 5.3 ± 1.5 days and all
children recovered completely after treatment.
Conclusion: Majority of case had fever clearance time less than 6 days.
Original Article
Key words:
Injection ceftriaxone,Typhoid fever, Treatment,Culture positive case.
Article information
Received: 01.09.2020Accepted: 01.11.2020
Cite this article:
Iman K, Haque F, Rahat F,Kahanam M, Zinnatunnassa.An Evaluation of Defer-vescance Period of CulturePositive Typhoid Fever inChildren Treated withInjection Ceftriaxone. SirSalimullah Med Coll J 2020;28: 78-82
Sir Salimullah Med Coll J 2020; 28: 78-82
An Evaluation of Defervescance Period of Culture
Positive Typhoid Fever in Children Treated with
Injection CeftriaxoneKazi Iman1, Fazlul Haque2, Farhana Rahat3, Morsheda Kahanam4, Zinnatunnassa5
1. Registrar, Dr. M R Khan Shishu Hospital and ICH, Mirpur, Dhaka.2. Professor, Dr. M R Khan Shishu Hospital and ICH, Mirpur, Dhaka.3. Assistant Professor, Dr. M R Khan Shishu Hospital and ICH, Mirpur, Dhaka.4. Assistant Professor, Dr. M R Khan Shishu Hospital and ICH, Mirpur, Dhaka.5. Medical Officer, Dr. M R Khan Shishu Hospital and ICH, Mirpur, Dhaka.Address of Correspondence: Dr. Kazi Iman, Registrar, DR. M R Khan Shishu Hospital and ICH, Mirpur, Dhaka, email:[email protected], 01711317493.
Introduction
Enteric fever is a common infectious disease whichencompass two similar clinical illnesses, causedby different serotypes of the bacterium Salmonellaenterica.1 Typhoid fever is generally more
common, but recent reports suggest that therelative frequency of paratyphoid fever may beincreasing and more severe2-8.World wide in theyear 2000, there were an estimated 21.6 millioncases of typhoid fever, death occurred 210000,

paratyphoid fever were reported in 5.1 millioncases.9- 10 The symptoms of typhoid fever can varyamong children of different ages and are usuallynon-specific.11 Common symptoms of enteric feverincludes fever, body ache, headache, gastro-intestinal symptoms like nausea, vomiting,abdominal pain, diarrhea, constipation and loss ofappetite.12-13 Severe disease occurs in 10 to15% ofchildren with complications. Complications areintestinal perforation, intestinal bleeding, shock,pancreatitis, pneumonia, myocarditis, meningitisor psychosis; may occur usually after the illnesshas lasted more than 14 days 11. The bacteria maybe sheded in the faeces during the acute illness,during convalescence and occasionally forprolonged periods when the patient is labeled a‘chronic carrier’.14 Infection occurs whencontaminated foods or water are ingested. Theorganisms then penetrate the intestinal lining,multiply in lymphoid tissues and are released intothe blood stream through which they spreadthroughout the body to various organs; mostcommonly the liver, spleen, bone marrow and gallbladder.15 Ceftriaxone is a drug of third-generationcephalosporin. In common with most of the otherthird generation agents, it has an aminothiazolylsubstitution at the R1 position of the â-lactam ring.Since the mid-1980s when ceftriaxone was firstintroduced, the drug has been used extensivelybecause of its improved stability against âlactamases, efficacy in a broad range of infectionsand its pharmacokinetic and tolerability profile.16
Pharmacokinetic properties of ceftriaxone, suchas sustained tissue drug levels over 24 hours aftera single injection; good penetration of the antibioticinto cells; significant biliary excretion as activeunchanged compound and high potency against S.typhi, should make it possible to significantlyshorten the treatment duration of typhoid fever.Although the efficacy of ceftriaxone in enteric feveris well documented, the precise duration ofceftriaxone therapy in children with enteric feveris not established and varies from 3 to 14 days.17
This has been well discussed by Tatli et al.18 in aprospective randomized study, ceftriaxone used fortreatment of 72 children who had bacteriologicallyconfirmed enteric fever. Ceftriaxone was given ata dose of 75 mg/kg per day (maximally 2 g/day)intravenously, in two doses until defervescenceand continued 5 days after that time. Meandefervescence time was in 5.4 days in the
ceftriaxone group. Clinical cure withoutcomplications was achieved in all patients and nopatient relapsed. They suggested that a flexible-duration of ceftriaxone therapy given untildefervescence time, followed by an additional 5 daysof therapy is a reasonable treatment in childrenwith enteric fever.19 Other study has shownceftriaxone was the commonly prescribed antibioticand duration of treatment ranged from 10 to 14days. Nalidixic acid-resistant S typhi was seen in56%. The mean duration of hospitalisation was 6.94days. In light of these findings, ceftriaxone showeda safe and effective alternative therapy to first linetherapies for the treatment of enteric fever inchildren. In addition, ceftriaxone shortens durationof fever substantially, thus reducing the hospitalstay.20 In our country, so far, no study has beencarried out to find out the defervescence time aswell as total duration of treatment in enteric feverwith ceftriaxone.
Typhoid fever is a global health problem; risk ishighest among children living in poverty in thedeveloping world like Bangladesh where water andsanitation services are inadequate and continuesto be a major health problem despite the use ofantibiotics and the development of newerantibacterial drugs. The highest incidence has beenreported in children between 5 and 10 years ofages. For improved treatments of enteric fever andmultidrug resistant S. typhi in particular, attentionhas been focused on ceftriaxone because of itsexcellent efficacy. This highly active drug reducesthe duration of treatment from the traditional 14days that is necessary for first line antibiotics.There is still lacking of fever clearance time ofthis disease treatment with injection ceftriaxone.
The aim of our study is to evaluate fever clearancetime in children with typhoid fever treating withinjection ceftriaxone.
Materials and methods
It was a cross sectional study. The study wasconducted in the Department of Paediatrics, DR.
M R Khan Shishu Hospital and ICH, Mirpur-2,Dhaka over a period of 1year from July218 to June2019. All hospitalized children with clinicaldiagnosis of typhoid fever admitted in the abovemention place were the study population. Thisstudy was done over 1 year. Fifty(50) children aged2 to 15 years with culture positive typhoid feverwere included in the study. Suspected typhoid feverbut culture negative cases were excluded from the
An Evaluation of Defervescance Period of Culture Positive Typhoid Fever in Children Kazi Iman et al 79

study. For all suspected cases of typhoid fever afteradmission in hospital, detailed history was takenand clinical examination was done. Theninvestigations were sent like CBC, blood culture,urine R/E. On the basis of clinical suspicion ofenteric fever empirical treatment was started withI/V injection ceftriaxone from the first day ofhospitalization. Dose of drug was 75 mg/kg/daymax. 2g. Only the culture positive cases weretreated over a period of 10 to 14 days. Six hourlytemperature chart was strictly maintained and thepoint fever clearance time was recorded.
Results:
The findings of the study derived from data analysisare presented below
Table-1: Distribution of patients by age, sex and
Socio-economic class (n = 50)
Age Frequency Percentage
£5 years 10 206 – 8 years 26 52>8 years 16 32Mean Age (8.4 ± 2.8)Range (2 – 12) yearsSexMale 20 40Female 30 60Socio-economic statusPoor 22 44Middle Class 18 36Upper Class 10 20
Table-II: Clinical presentation of the study
population (n = 50)
Sign and symptoms Frequency Percentage
Fever 50 100Duration of fever5 – 6 days 29 587 – 8 days 21 42Loose stool 15 30Anorexia 35 70Headache 16 32Abdominal pain 22 44Diarrhoea 22 44Vomiting 12 24Coated tongue 38 76Hepatomegaly 25 50Splenomegaly 12 24
Table-III: Distribution of patients by duration
of treatment and period of defervascence (n = 50)
Outcome Frequency% Mean±SD
Duration of treatment
7 – 10 days 13(26) 10.1±1.4
10 – 14 days 37(74)
Day of defervescence
3 – 5 days 18(36) 5.3±1.5
6 – 9 days 12(24)
Recovery 50(100)
Discussion
Typhoid fever still remains a serious problem indeveloping countries, with an estimated 12.5-16.6million cases and 600 000 deaths each year. Itcontinues to be a major cause of morbidity andmortality in tropical countries, especially childrenare affected more.21- 22 However, in some regionsof the world, proper sanitation has successfullydiminished the infections with S. typhi. Typhoidfever in children in the first 2 years of life exhibitssome differences in the clinical course incomparison to adults.23 The results of our studyconform with those of other studies which usedceftriaxone in cases of enteric fever i.e., thisantibiotic achieved highly satisfactory clinical andbacteriologic responses.24-25 In our study, 20% ofpatients were 5 years or less than 5 years, 52%between 6 – 8 years and 32% more than 8 years.Previous studies have also shown that about 22%to 30% of enteric fever cases in children upto 15yrs of age are of less than 5 yrs of age.26, 5 Anotherstudy in Northern India also showed that themajority of cases occurred in children among 5 to12 years, 22.8% of cases were in children up to 5years of age and 6% to 21 % were in less than 2years of age.27 Almost similar study done by Sinhaet al.28 showed 24% children were aged less than5 years. In our study, among 50 culture positiveenteric fever cases 40% were male and 60% werefemale. This finding was closely similar withDeshmukh et al. 29 who reported 31% male and69% female. Another study done by Butler et al. 30
also showed that infection rate is higher in female,perhaps reflecting greater exposure of female tocontaminated food and water outside the home.
Typhoid fever may be particularly difficult todiagnose in infants, as Secmeer et al. in 1995 have
80 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

reported, 10 patients in their study having mildillness characterized by non-specific symptoms likefever and cough. In our study fever was the mostcommonest presentation in all of the patients. Theother symptoms were headache (32%), loose stools(30%), anorexia (70%) and abdominal pain ( 44%)of patients. Hepatomegaly was detected (50%),splenomegaly (24%) and coated tongue (76% )ofpatients. These findings were almost similar tothose of a previous study by Threlfall et al. 31, whichshowed fever in 95% of patients, headache in22.7%, loose stool in 9%, anorexia in 5.1% andabdominal pain in 3.9%. In another retrospectiveanalysis of 52 cases of enteric fever in a tertiarycare hospital in Dhaka city conducted byMutanabbi et al. observed that hepatomegaly andsplenomegaly were the major physical findings intheir study. Few other studies have also foundthese to be inconsistent features of enteric fever.Rafiq et al. in32 noted that fever, vomiting,abdominal pain, loss of appetite; diarrhea and coughwere the predominant symptoms. Hepatomegalywas detected in 9 (9%), splenomegaly in 13 (13%)patients. Yaramis et al.33 reported in their studyhepatomegaly was higher than splenomegaly (71%vs.52%). Long et al.34 reported in their serieshepatomegaly was almost twice as frequent assplenomegaly. Threlfall et al 31 also reported in alarge series of children with enteric fever, 32%had elevated liver enzymes, while only 9% hadhepatomegaly with or without splenomegaly. Inanother study Cooke et al.35 found 17%encephalopathy, 73% hepatitis, 4% pneumonia, 4%gastrointestinal bleeding; but we did not find suchfeatures.
The present cross sectional study revealed theeffectiveness of injection ceftriaxone in term offever clearance and effective treatment in childrenwith typhoid fever.
All 50 enrolled cases responded to ceftriaxonetherapy with no treatment failure. Majority of casehad fever clearance time for less than 7 days. Thesame was stated in other study conducted byMadhulika et al.36 Several studies done in Indiaand other part of world also showed considerablevariation in fever clearance time for ceftriaxonefor typhoid fever in children. The mean feverclearance time with ceftriaxone observed in ourstudy was 5.3 days as against 6.1 days in
literature.11 In another study by Kumar et al. fromDelhi in year 2007, 93 blood culture proven typhoidcases in children were randomized to ofloxacintreatment group and ceftriaxone group. Meandefervescence time with ceftriaxone and ofloxacinwas 4.25 and 4.96 days respectively. A retrospectiveanalysis of 135 typhoid cases was conducted inKuwait in 2007 by Dimitrov et al. total 108 childrenwere treated with Ceftriaxone and meandefervescence time was 6.3 days. A retrospectivechart review of all cases of culture proven entericfever was carried out at a tertiary care privatehospital in Mumbai over the period January 2003to September 2005 by Jog et al.37; total 72 childrenwere treated with ceftriaxone and meandefervescence time of 4.2 days was noted. The meandefervescence time in our study is similar to thefinding in various previously done studies. In year1992, Gulati S et al. randomized fifteen culturesproven typhoid cases in three groups (ceftriaxone,cefotaxim, and ciprofloxacin) and noticed meanfever clearance time 5.1 days in ceftriaxone group.In another trial Tatil et al. in year 2003 Ceftriaxonewas given in 72 bacteriological confirmed typhoidfever children resulted in mean fever clearancetime of 5.4 days.
Conclusion:
In the conclusion, we can say that injectionceftriaxone is an effective drug for treatingchildren with typhoid fever. Majority of case hadfever clearance time less than 7 days. Our studywas conducted in a single centre with small samplesize. We are recommending multi-centre studywith large sample size for a better outcome.
References1. Kidenya V, Ferson MJ. Typhoid and paratyphoid fever
in south-eastern Sydney, 1992-1997. Communicablediseases intelligence. 2000 Aug; 24(8): 233-5.
2. Chandel DS, Chaudhry R, Dhawan B, Pandey A, DeyAB. Drug-resistant Salmonella enterica serotypeparatyphi A in India. Emerging infectious diseases. 2000Jul;6(4):420.
3. Ahmad K. Experts call for surveillance of drugresistanttyphoid at a global level. The Lancet. 2002;359(9306):592.
4. Butt T, Ahmad RN, Salman M, Kazmi SY. Changingtrends in drug resistance among typhoid salmonellaein Rawalpindi, Pakistan.
5. Ochiai RL, Acosta CJ, Danovaro-Holliday M,Baiqing D,Bhattacharya SK, Agtini MD, Bhutta ZA, Canh DG, AliM, Shin S, Wain J. A study of typhoid fever in five Asian
An Evaluation of Defervescance Period of Culture Positive Typhoid Fever in Children Kazi Iman et al 81

countries: disease burden and implications for controls.Bulletin of the world health organization. 2008;86:260-8.
6. Jesudason MV. Paratyphoid fever in Vellore, SouthIndia. Tropical doctor. 2005 Jul;35(3):191.
7. Woods CW, Murdoch DR, Zimmerman MD, Glover WA,Basnyat B, Wolf L, Belbase RH, Reller LB. Emergenceof Salmonella enterica serotype Paratyphi A as a majorcause of enteric fever in Kathmandu, Nepal.Transactions of the Royal Society of Tropical Medicineand Hygiene. 2006 Nov 1;100(11):1063-7.
8. Maskey AP, Basnyat B, Thwaites GE, Campbell JI,Farrar JJ, Zimmerman MD. Emerging trends in entericfever in Nepal: 9124 cases confirmed by blood culture1993–2003. Transactions of the Royal Society of TropicalMedicine and Hygiene. 2008 Jan 1;102(1):91-5.
9. Ochiai RL, Wang X, Von Seidlein L, Yang J,Bhutta ZA,Bhattacharya SK, Agtini M, Deen JL, Wain J, Kim DR,Ali M. Salmonella paratyphi A rates, Asia. Emerginginfectious diseases. 2005 Nov;11(11):1764.
10. Crump JA, Luby SP, Mintz ED. The global burden oftyphoid fever. Bulletin of the World HealthOrganization. 2004;82:346-53.
11. Parry CM, Hien TT &Dougan G, ‘Typhoid fever’, N Engl
J Med. 2002; 347(22) pp.1770-82.
12. Lee TP, Hoffman SL. Typhoid fever. In: StricklandGT(eds). Hunter’s Tropical medicine and emerginginfectious diseases. 8th Edition. Philadelphia. London:
Saunders. 2000.
13. Richens J. Typhoid fever. In: Armstrong D, CohenJ(eds). Infectious diseases. 1st Edition. London: Mosby.
2000.
14. Bhan MK, Bahl R, Bhatnagar S. Typhoid andparatyphoid fever. The Lancet. 2005 Aug 27;366(9487):749-62.
15. Braunwald E, Fauci AS, Kasper DL, Hauser SL, LongoDL, Jameson JL. Harrison’s principles of internalmedicine. McGraw Hill; 2001.
16. Fluit AC, Jones ME, Schmitz FJ, Acar J, Gupta R,Verhoef J. Antimicrobial susceptibility and frequencyof occurrence of clinical blood isolates in Europe fromthe SENTRY antimicrobial surveillance program, 1997and 1998. Clinical Infectious Diseases. 2000 Mar1;30(3):454-60.
17. Kalra SP, Naithani N, Mehta SR, Swamy AJ. Currenttrends in the management of typhoid fever. MedicalJournal, Armed Forces India. 2003 Apr;59(2):130
18. Tatli MM, Aktas G, Kosecik M, Yilmaz A. Treatment oftyphoid fever in children with a flexible-duration ofceftriaxone, compared with 14-day treatment withchloramphenicol. International journal of antimicrobialagents. 2003 Apr 1;21(4):350-3.
19. Ismail A. New advances in the diagnosis of typhoid anddetection of typhoid carriers. The Malaysian journal ofmedical sciences: MJMS. 2000 Jul;7(2):3.
20. Lalitha J, Vasanthi T, Malathi S, Ganesh R, Aparna V,Lakshmi M. Clinical profile and outcome of typhoid feverin children from a tertiary care hospital. 2008.
21. Scragg J, Rubidge CA, Wallace HL. Typhoid fever inAfrican and Indian children in Durban. Archives ofdisease in childhood. 1969 Feb;44(233):18.
22. Pang T, Bhutta ZA, Finlay BB, Altwegg M. Typhoidfever and other salmonellosis: a continuing challenge.Trends in microbiology. 1995 Jul 1;3(7):253-4.
23. Hornick R, Greisman SE, Woodward TE, DuPont HL,Dawkins AT, Snyder MJ. Typhoid fever: pathogenesisand immunologic control. New England journal ofmedicine. 1970 Sep 24;283(13):686-91.
24. Islam A, Butler T, Nath SK, Alam NH, Stoeckel K,Houser HB, Smith AL. Randomized treatment ofpatients with typhoid fever by using ceftriaxone orchloramphenicol. Journal of Infectious Diseases. 1988Oct 1;158(4):742-7.
25. Lasserre R, Sangalang RP, Santiago L. Three-daytreatment of typhoid fever with two different doses ofceftriaxone, compared to 14-day therapy withchloramphenicol: a randomized trial. Journal ofAntimicrobial Chemotherapy. 1991 Nov 1;28(5):765-72.
26. Rowe B, Ward LR, Threlfall EJ. MultidrugresistantSalmonella typhi: a worldwide epidemic. ClinicalInfectious Diseases. 1997 Jan 1;24(Supplement_1):S106-9.
27. Kanungo S, Dutta S, Sur D. Epidemiology of typhoidand paratyphoid fever in India. The Journal of Infectionin Developing Countries. 2008 Dec 1;2(06):454-60.
28. Sinha A, Sazawal S, Kumar R, Sood S, Reddaiah VP,Singh B, Rao M, Naficy A, Clemens JD, Bhan MK.Typhoid fever in children aged less than 5 years. TheLancet. 1999 Aug28;354(9180):734-7.
29. Deshmukh CT, Nadkarni UB, Karande SC. An analysisof children with typhoid fever admitted in 1991. Journalof postgraduate medicine. 1994 Oct 1;40(4):204.
30. Butler T, Islam A, Kabir I, Jones PK. Patterns ofmorbidity and mortality in typhoid fever dependent onage and gender: review of 552 hopitalized patients withdiarrhea. Reviews of infectious diseases. 1990Jan;13(1):85-90.
31. Threlfall EJ, Day M, De Pinna E, Lewis H, Lawrence J.Drug-resistant enteric fever in the UK. The Lancet.2006 May 13;367(9522):1576.
32. Rafiq H, Rashid Z, Samina N. Typhoid Fever–Continues. As a Major Threat in Children. Biomedica.2009 Jul;25:1-2.
33. Yaramis A, Yildirim I, Katar S, Ozbek MN, Yalcin I, TasMA, Hosoglu S. Clinical and laboratory presentation oftyphoid fever. International Pediatrics. 2001;16(4):227-31.
34. Long SS, Pickering LK, Prober CG. Principles andpractice of pediatric infectious diseases. Shock. 2003Jul 1;20(1):98.
35. Cooke FJ, Day M, Wain J, Ward LR, Threlfall EJ. Casesof typhoid fever imported into England, Scotland andWales (2000–2003). Transactions of the Royal Societyof Tropical Medicine and Hygiene. 2007 Apr 1;101(4):398-404.
36. Madhulika U, Harish BN, Parija SC. Current pattern inantimicrobial susceptibility of Salmonella Typhi isolatesin Pondicherry. Indian Journal of Medical Research.2004 Aug 1;120(2):111.
37. Jog S, Soman R, Singhal T, Rodrigues C, Mehta A,Dastur FD. Enteric fever in Mumbai–clinical profile,sensitivity patterns and response to antimicrobials. JAPI.2008 Apr;56:237-40.
82 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
Study on COVID-19 Positive Pregnant Woman
and Pregnancy OutcomeAmitun Nessa1, Khondoker Roksana Momtaj2, Sanzida Parvin3, Sumona Parvin4, Umma Salma5,
Mohammad Abdus Sattar Sarker6, Mohammad Selim Shahi7, Nahida Zafrin8
Abstract
Background: COVID-19 may pose a threat to pregnant women, who are often predisposed
to viral respiratory infections due to physiological changes such as diaphragm elevation,
increased oxygen consumption, edema of respiratory tract mucosa, and altered cellular
immunity.
Objective: This study is to describe the clinical manifestations, maternal and fetal outcome
of pregnant women with COVID-19.
Methods: This was a prospective observational study of 33 pregnant women who were
admitted into the Department of Obstetrics & Gynaecology, Corona Dedicated Mughda
Medical College Hospital, Dhaka during March’2020 to August’2020.Throat swabs were
collected from all these patients and were sent to the laboratory of the tests of SARS-CoV-
2 using the standard kit. Data were collected using pre-designed data collection sheet and
data were analysis using SPSS for windows version 20.
Results: This study shows the average age was 29.42 years. Maximum (33.3%) were affected
by self then hospital (18.2%), husband (12.1%), unknown (9.1%). The common clinical
presentations were fever (30.3%) then headache (18.2%), less fetal movement (18.2%),
respiratory distress severe (9.1%), cough (9.1%) and pain lower abdomen (9.1%). Majority
had no any pregnancy complication and only 18.2% had complication due to cause of GDM
(9.1%) and PIH (9.1%). Majority (72.7%) was LUCS and 27.3% were spontaneous expulsion
of product. Majority (93.9%) was live birth and only 6.1% were neonatal death due to cause
of still birth (3%) and impending eclampsia (3%). Fetal complications were prematurity
(16.7%), IUGR (3%) and respiratory distress syndrome (3%). Only 3% need admission in
neonatal unit and 3% need admission in neonatal ICU. All babies were covid-19 negative
following delivery within 72 hours of birth.
Conclusions: This study suggested that most pregnant women do not have severe illness
and that transmission of infection to infants of infected mothers can occur but is uncommon.
Covid-19 with pregnant women admitted with infection needs urgent investigation and
explanation.
Original Article
Key words:
COVID-19, PregnantWomen Outcome
Article information
Received: 01.08.2020Accepted: 30.10.2020
Cite this article:
Nessa A, Momtaj KR,Parvin S, Parvin S, SalmaU, Sarker MAS, Shahi MS,Zafrin Z. Study on COVID-19 Positive PregnantWoman and PregnancyOutcome. Sir SalimullahMed Coll J 2020; 28: 83-87
Sir Salimullah Med Coll J 2020; 28: 83-87
1. Resident Surgeon (Gynae &Obs), Mugdha Medical College Hospital, Dhaka2. Assistant Professor, Dept. of Gyane & Obstetrics, Mugdha Medical College, Dhaka3. Lecturer, Dept. of Anatomy, Sir Salimullah Medical College, Dhaka4. Lecturer, Dept of Pathology, Sir Salimullah Medical College, Dhaka5. Associate Professor, Dept. of Medicine,Dhaka National Medical College,Dhaka.6. Associate Professor, Dept.of Medicine, Sir Salimullah Medical College, Dhaka.7. Associate Professor, Neuromedicine.National Institute of Neuroscience, Dhaka.8. Assistant Professor, Dept. of MedicineSylhet MAG Osmani Medical College, Sylhet.Address to correspondence: Dr. Amitun Nessa, MS (Gyane & Obs), Resident Surgeon (Gynae), Mugdha Medical CollegeHospital, Dhaka, e-mail:[email protected], Mobile-01741065245
Introduction
Novel Coronavirus 2019 (COVID-19) has beendefined as a pandemic infecting millions ofindividuals with a significantly high mortality andmorbidity rate.1 The World Health Organization
declared a global pandemic of coronavirus disease2019 (covid-19) caused by severe acute respiratorysyndrome coronavirus 2 (SARS-CoV-2) in March2020.2 As the number of confirmed cases increases,evidence on the transmission, incidence, and effect

of SARS-CoV-2 infection in mothers and their babiesremains limited. Pregnant women are not thoughtto be more susceptible to the infection than thegeneral population.3,4 However, changes to theimmune system mean that pregnant women maybe more vulnerable to severe infection.5 Evidencefrom other similar viral illnesses, such as influenzaA/H1N1,6-9 severe acute respiratory syndrome,10
and Middle East respiratory syndrome,11 suggestthat pregnant women are at greater risk of severematernal and neonatal morbidity and mortality.Some evidence suggests that the risk of criticalillness may be greatest in the later stages ofpregnancy.12
Most reported cases occurred in the third trimester,and around half of women gave birth during theacute infection episode. Most women weredelivered by caesarean section, predominantly formaternal indication, although at least three studiesreported cases of fetal distress.12
Most women developed mild or moderatesymptoms including cough, fever, andbreathlessness, and only a small number developedsevere disease.12 Evidence suggests that severecovid-19 in pregnancy is associated with iatrogenicpreterm delivery (75%), predominantly formaternal indication and in the third trimester.12
Most neonates born to mothers with confirmedSARS-CoV-2 infection were asymptomatic anddischarged home well. A small number of neonateshad symptoms, with a minority needing admissionto neonatal specialist care12 .The purpose of thisstudy was to describe the clinical manifestationsof pregnant women with COVID-19.
Material and methods
This was a prospective observational study carriedout in the Department of Obstetrics &Gynaecology, Corona Dedicated Mugda MedicalCollege Hospital, Dhaka who were admittedpregnant women with covid-19. Sample size was33 and study period was March’ 2020 to August’2020. This study followed the clinical diagnosiscriteria for COVID-19 pneumonia. Throat swabswere collected from all these patients and sent tothe laboratory of the tests of SARS-CoV-2 usingthe standard kit. Diagnosis criteria of COVID-19infection includes 1) typical chest CT imaging ofpatchy shadowing and ground-glass opacity, and2) positive in reverse transcription polymerasechain reaction (RT-PCR) tests for SARS-CoV-2.
Results
Maximum (36.4%) were 26-30 years followed by24.2% were 31-35 years, 21.2% were 21-25 years,15.2% were 36-40 years and only 3% were d•20years. The average age was 29.42 years. Maximum(33.3%) were affected by self then hospital (18.2%),husband (12.1%), unknown (9.1%). Other depictedin tables. The common clinical presentations werefever (30.3%) then headache (18.2%), less fetalmovement (18.2%), respiratory distress severe(9.1%), cough (9.1%) and pain lower abdomen(9.1%). Majority had no pregnancy complicationand only 18.2% had complication due to cause ofGDM (9.1%) and PIH (9.1%). Majorities (72.7%)were LUCS and 27.3% were spontaneous expulsionof product. Majority (75.8%) had no maternalcomplication and 24.2% had complication due tocause of respiratory distress (15.2%), scar infection(6.1%) and PPH (3%). Only 6.1% were death.Majorities (93.9%) were live birth and only 6.1%were neonatal death due to cause of still birth (3%)and impending eclampsia (3%). Fetal complicationswere prematurity (16.7%), IUGR (3%) andrespiratory distress syndrome (3%). Majorities(57.6%) were 2.5 kg and 42.4% were d•2.5 kg. Only3% need admission in neonatal unit and 3% needadmission in neonatal ICU. In results all babieswere Covid-19 negative.
Table I. Demographic characteristics of the
study subjects (n=33)
Age in years Frequency Percentage (%)
£20 years 1 3.0
21-25 years 7 21.2
26-30 years 12 36.4
31-35 years 8 24.2
36-40 years 5 15.2
Mean±SD 29.42±5.33
Educational status
Illiterate 2 6.1
Primary 5 15.2
Secondary 7 21.2
Higher secondary 11 33.3
Graduate 8 24.2
Occupational status
House wife 26 78.8
Service 3 9.1
Others 4 12.1
84 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
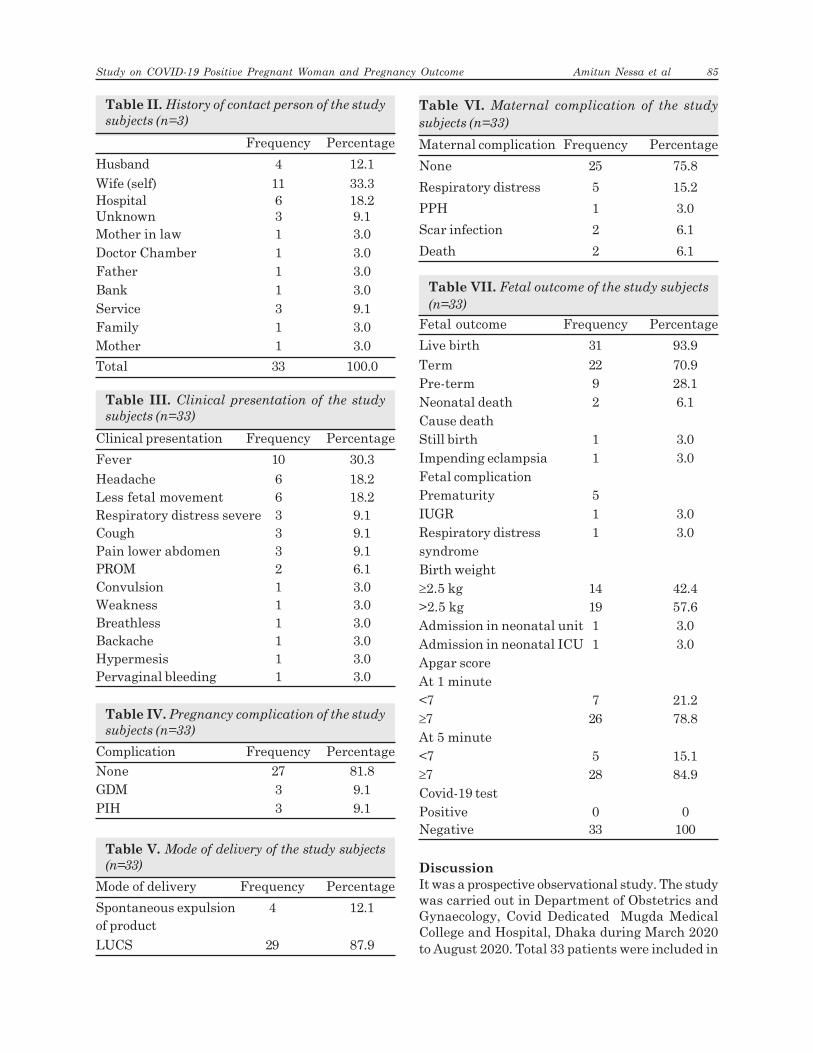
Table II. History of contact person of the study
subjects (n=3)
Frequency Percentage
Husband 4 12.1
Wife (self) 11 33.3Hospital 6 18.2Unknown 3 9.1Mother in law 1 3.0Doctor Chamber 1 3.0Father 1 3.0Bank 1 3.0Service 3 9.1Family 1 3.0Mother 1 3.0
Total 33 100.0
Table III. Clinical presentation of the study
subjects (n=33)
Clinical presentation Frequency Percentage
Fever 10 30.3
Headache 6 18.2Less fetal movement 6 18.2Respiratory distress severe 3 9.1Cough 3 9.1Pain lower abdomen 3 9.1PROM 2 6.1Convulsion 1 3.0Weakness 1 3.0Breathless 1 3.0Backache 1 3.0Hypermesis 1 3.0Pervaginal bleeding 1 3.0
Table IV. Pregnancy complication of the study
subjects (n=33)
Complication Frequency Percentage
None 27 81.8GDM 3 9.1PIH 3 9.1
Table V. Mode of delivery of the study subjects
(n=33)
Mode of delivery Frequency Percentage
Spontaneous expulsion 4 12.1of product
LUCS 29 87.9
Table VI. Maternal complication of the study
subjects (n=33)
Maternal complication Frequency Percentage
None 25 75.8
Respiratory distress 5 15.2
PPH 1 3.0
Scar infection 2 6.1
Death 2 6.1
Table VII. Fetal outcome of the study subjects
(n=33)
Fetal outcome Frequency Percentage
Live birth 31 93.9
Term 22 70.9Pre-term 9 28.1Neonatal death 2 6.1Cause deathStill birth 1 3.0Impending eclampsia 1 3.0Fetal complicationPrematurity 5IUGR 1 3.0Respiratory distress 1 3.0syndromeBirth weight³2.5 kg 14 42.4>2.5 kg 19 57.6Admission in neonatal unit 1 3.0Admission in neonatal ICU 1 3.0Apgar scoreAt 1 minute<7 7 21.2³7 26 78.8At 5 minute<7 5 15.1³7 28 84.9Covid-19 testPositive 0 0Negative 33 100
Discussion
It was a prospective observational study. The studywas carried out in Department of Obstetrics andGynaecology, Covid Dedicated Mugda MedicalCollege and Hospital, Dhaka during March 2020to August 2020. Total 33 patients were included in
Study on COVID-19 Positive Pregnant Woman and Pregnancy Outcome Amitun Nessa et al 85

this study. All pregnant women who confirmed withcovid-19 were enrolled for the study. This studywas done to describe the clinical manifestationspregnant women with COVID-19. The presentstudy findings were discussed and compared withpreviously published relevant studies. To our bestknowledge, this is the study to describe the clinicalmanifestations and maternal and fetal outcome ofpregnant women with COVID-19.
This study shows maximum (36.4%) were 26-30years followed by 24.2% were 31-35 years, 21.2%were 21-25 years, 15.2% were 36-40 years and only3% were d™20 years. The average age was 29.42years. Therefore, the findings of the study are inwell agreement with the findings of the otherresearch works.14 The found the average age was29.40±3.65 years. Another study Capobianco et al.reported 30.3±1.5 years.15
This study shows the common clinicalpresentation were fever (30.3%) then headache(18.2%), less fetal movement (18.2%), respiratorydistress severe (9.1%), cough (9.1%) and pain lowerabdomen (9.1%). This findings consistent withKnight et al.12 Wu et al.14 and Zhu et al.16 Anotherstudy Capobianco et al.15 found patients mainlycomplained of fever and cough proportions were76.0 % and 38.0 respectively.15 Similar study Liuet al.17 found the most common onset symptomsof COVID-19 pneumonia in pregnant women werefever (13/15 patients) and cough (9/15 patients).
In this study found majority had no pregnancycomplication and only 18.2% had complication dueto cause of GDM (9.1%) and PIH (9.1%). Therefore,the findings of the study are in well agreementwith the findings of the other researchworks.9,10,14,17
In present study shows majority (87.9%) werecaesarean delivery and 12.1% were spontaneousexpulsion of product. This findings consistent withCapobianco et al.15 study they found 88% caesareansection and 12% were vaginal delivery. Liu et al.17
they found 90.9% were LUCS and 9.1 were vaginaldelivery. Similar study Wu et al.14 they found93.1% were caesarean delivery and 6.9% werevaginal delivery. All study found majority werecaesarean delivery.
Regarding maternal complication majority (75.8%)had no maternal complication and 24.2% had
complication due to cause of respiratory distress(15.2%), scar infection (6.1%) and PPH (3%). Only6.1% were death. Therefore, the findings of thestudy are in well agreement with the findings ofthe other research works.1,6,11,14
Majority (93.9%) were live birth and only 6.1% wereneonatal death due to cause of still birth (3%) andimpending eclampsia (3%). Fetal complication wasprematurity (16.7%), IUGR (3%) and respiratorydistress syndrome (3%). Majority (57.6%) were 2.5kg and 42.4% were d”2.5 kg. Only 3% needadmission in neonatal unit and 3% need admissionin neonatal ICU. All babies were negative in Covid-19 test within 72 hours after delivery. All studiesfound prematurity were more common in fetalcomplication.
Conclusion
This study shows the common clinical presentationwere fever then headache, less fetal movement,respiratory distress, severe cough and pain lowerabdomen in pregnant mother with covid-19pandemic. Majority were delivered by caesareansection. Fetal complication were prematurity,IUGR and respiratory distress syndrome. All babieswere negative covid-19 pandemic. This studysuggested that systematic screening of anysuspected covid-19 infection during pregnancy andextend intensive follow-up for confirmed mothersand their fetuses.
References1. Douedi S, Albayati A, Alfraji N, Mazahir U, Costanzo E.
Successful Maternal and Fetal Outcomes in COVID-19Pregnant Women: An Institutional Approach. Am J CaseRep. 2020;21:e925513.
2. World Health Organization. Rolling updates oncoronavirus disease (covid-19). 2020. https://www.who.int/emergencies/diseases/novelcoronavirus-2019/events-as-they-happen.
3. Royal College of Obstetricians and Gynaecologists andThe Royal College of Midwives. Coronavirus (covid-19)infection in pregnancy: information for healthcareprofessionals. Royal College of Obstetricians andGynaecologists, 2020.
4. Chen Y, Li Z, Zhang YY, Zhao WH, Yu ZY. Maternalhealth care management during the outbreak ofcoronavirus disease 2019. J Med Virol 2020.
5. Favre G, Pomar L, Musso D, Baud D. 2019-nCoVepidemic: what about pregnancies?Lancet 2020;395:e40.
6. ANZIC Influenza Investigators and AustralasianMaternity Outcomes Surveillance System. Criticalillness due to 2009 A/H1N1 influenza in pregnant and
86 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

postpartum women: population based cohort study. BMJ2010;340:c1279.
7. Jamieson DJ, Honein MA, Rasmussen SA, et al, NovelInfluenza A (H1N1) Pregnancy Working Group. H1N12009 influenza virus infection during pregnancy in theUSA. Lancet 2009;374:451-8.
8. Louie JK, Acosta M, Jamieson DJ, Honein MA,California Pandemic (H1N1) Working Group. Severe2009 H1N1 influenza in pregnant and postpartumwomen in California. N Engl J Med 2010;362:27-35.
9. Siston AM, Rasmussen SA, Honein MA, et al, PandemicH1N1 Influenza in Pregnancy Working Group.Pandemic 2009 influenza A(H1N1) virus illness amongpregnant women in the United States. JAMA2010;303:1517-25.
10. Wong SF, Chow KM, Leung TN, et al. Pregnancy andperinatal outcomes of women with severe acuterespiratory syndrome. Am J Obstet Gynecol2004;191:292-7.
11. Mullins E, Evans D, Viner RM, O’Brien P, Morris E.Coronavirus in pregnancy and delivery: rapid review.Ultrasound Obstet Gynecol 2020;55:586-92.
12. Knight M, Bunch K, Vousden N, Morris E, Simpson N,Gale C. Characteristics and outcomes of pregnantwomen admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohortstudy. BMJ 2020;369:m2107
13. Zeng L, Xia S, Yuan W. Neonatal early-onset infectionwith SARS-CoV-2 in 33 neonates born to mothers withcovid-19 in Wuhan, China. JAMA Pediatr 2020.
14. Wu Y-T, Liu J, Xu J-J, Chen Y-F, Yang W, Chen Y.Neonatal outcome in 29 pregnant women with COVID-19: A retrospective study in Wuhan, China. PLoS Med2020;17(7):e1003195
15. Capobianco G, Saderi , Aliberti S, Mondoni M, Piana A,Dessole F, Dessole M, Cherchi PL, Dessole S, Sotgiu G.COVID-19 in pregnant women: A systematic reviewand meta-analysis. Eur J Obstet Gynecol Reprod Biol.2020:S0301-2115(20)30446-2.
16. Zhu H, Wang L, Fang C, Peng S, Zhang L, Chang G.
Clinical analysis of 10 neonates born to mothers with2019-nCoV pneumonia. Transl Pediatr 2020;9(1):51-60
17. Liu D, Li L, Wu X, Zheng D, Wang J, Yang L, Zheng C.Pregnancy and Perinatal Outcomes of Women WithCoronavirus Disease (COVID-19) Pneumonia:APreliminary Analysis. AJR 2020; 215:127–132.
Study on COVID-19 Positive Pregnant Woman and Pregnancy Outcome Amitun Nessa et al 87
Enterocutaneous Fistula after Bowel Surgery-
Study of 100 CasesProdip Kumar Mandal1, Ishtiaq Alam2, Md. Kamrul Ahsan3, Debashis Dey4
Abstract
Background: The commonest cause of entercutaneous fistula is surgical intervention.
Injury to bowel during adhesionlysis, devascularisation of gut wall and anastomotic
leakage are responsible for the majority of enterocutaneous fistula.
Objective: To evaluate the management pattern of enterocuteneous fistula.
Methods: It was a prospective study conducted in Department of Surgery, Dhaka Medical
College Hospital and Casualty Block, DMCH and Sir Salimullah Medical College Mitford
Hospital. Total 100 cases were included in this study during the period January 2015 to
June 2016. In this study gastrojejunostomy operations are not included.
Results : In the present study out of 100 respondents 24% had diabetic, 20% had typhoid
fever, 10% had tuberculosis, 4% had crohn’s disease and 15% had malignancy.
Enterocutaneous fistula developed maximum in emergency operations (82%) and less in
elective operation (18%). Spontaneous closure of fistula after taking conservative measure
in 10 cases, early surgical intervention taking in 4 patients & delayed surgical intervention
were necessitated in 2 cases.
Conclusion: As consequences of enterocutaneous fistula are still life threatening in our
country, so maximum awareness is needed to prevent it.
Original Article
Key words:
Enterocutaneous, fistula,bowel surgery,management, complication.
Article information
Received: 01.09.2020Accepted: 30.10.2020
Cite this article:
Mandal PK, Alam I, AhsanMK, Dey D. Enterocuta-neous Fistula after BowelSurgery- Study of 100Cases. Sir Salimullah MedColl J 2020; 28: 88-92
Sir Salimullah Med Coll J 2020; 28: 88-92
1. Assistant Professor, Department of Surgery, SSMC, Dhaka2. Assistant Professor, Department of Surgery, SSMC, Dhaka3. Medical Officer, Department of Surgery, SSMC Mitford Hospital, Dhaka4. Assistant Professor, Department of Surgery, SSMC, DhakaAddress of correspondence: Dr. Prodip Kumar Mandal, Assistant Professor, Department of Surgery, Sir SalimullahMedical College Mitford Hospital, Dhaka, Mobile-+8801922755644, E-mail:drprodip2008@ gmai.com
Causes of enterocutaneous fistula includeinadequate surgical technique, diverticulities,biliary tract obstruction and malignant disease. Ina review of 79 patients with 116 fistulas Kuvsshinoffet al. found 82% to be postoperative, 6.3% due toCrohn’s disease, 3.8% due to neoplasm andinfection each, 2.5% iatrogenic and 1.3% due toradiation.3
The management of enterocutancous fistula ischallenging, with significant associated morbidityand mortality. Management of enterocutancousfistula should initially concentrate on correction
Introduction
Enterocutaneous fistulas present a challenge tomedical and nursing staff. If not adequatelymanaged, a patient with a high-output fistula candevelop fluid and electrolyte imbalance andmetabolic acidosis in a relatively short period oftime. Fistulas typically develop in a surgical incisionor dehisced wound; the patient faces a 35.0% risk ofdying. Spontaneous closure occurs in approximately57.0% of all enteric fistulas within 8 weeks as alongas adequate nutrition and perenteral or oral fluidand electrolyte balance are maintained and thepatient remains on bowel rest.1,2

of fluid and electrolyte imbalances, drainage ofcollections, treatment of sepsis and control offistula output. The routine use of somatostatininfusion and somatostatin analogues remaincontroversial; although there are data suggestingreduced time to fistula closure, there is littleevidence of increased probability of spontaneousclosure. Malnutrition is common and adequatenutritional provision is essential, enteral wherepossible, although supplemental nutrition is oftenrequired for high-output small bowel fistulas. Therole of immunonutrition is unknown. Surgicalrepair should be attempted when spontaneousfistula closure does not occur, but it should bedelayed for at least 3 months.4
Surgery is usually not an immediate priority exceptto deal with complications. When surgicalintervention is required to deal with the fistula:resection and anastomosis or bypass procedure arethe preferred surgical options. Simple suture of thefistula is not recommended. Although many fistulaewill close with such conservative strategies,persistent fistulae require definitive surgicalintervention. This generally involved a majorlaparotomy and should be delayed to allow resolutionof intra-abdominal inflammatory adhesions forpatients in the early postoperative phase.5
Materials and Methods
It was a prospective study carried out in theDepartment of Surgery, Dhaka Medical CollegeHospital and Sir Salimullah Medical CollegeMitford Hospital, Dhaka. From January 2015 toJune 2016. Patients having bowel surgery afteradmission in the Department of Surgery, DhakaMedical College Hospital and Casualty Block,DMCH and Sir Salimullah Medical College MitfordHospital, Dhaka was taken as study population.Total 100 samples were included in this study. Ina pre-designed case record from detail history,physical examination, necessary laboratory andradiological investigations were recorded and thedetails of the operative findings andhistopathological report were noted. Collected datawere edited after data were analyzed usingcomputer based programme statistical package forsocial science (SPSS) for windows version 20.Patients admitted in general surgery wardrequiring bowel surgery and casualty wardrequiring emergency exploratory laparotomy &small and large gut surgery were included.Exclusion criteria were (i) Patient who refused tobe included in the study (ii) unconscious patients,
(iii), patients with multiple pathology (iv) patientstreated by non surgical methods.
Fig.-1: Entercutaneous fistula followed by
laparotomy
Results
Table I. Demographic characteristics of the
respondents by age (n=100)
Characteristics No of patients Percentage
Age group in years
<20 16 1621-30 38 3831-40 22 2241-50 18 18>50 6 6Mean±SD 31.88±10.30SexMale 86 86Female 14 14
Table II. Distribution of the respondents by
current medical history
Medical history No of patients Percentage
Diabetic 24 24
H/O typhoid fever 20 20H/O tuberculosis 10 10H/O crohn’s disease 4 4H/O malignancy 16 16
Table III. Types of surgery
Type of operation No of patients Percentage
Emergency 82 82
Routine 18 18
Enterocutaneous Fistula after Bowel Surgery- Study of 100 Cases Prodip Kumar Mandal et al 89

Table IV. Surgical complication associated with fistula formation (n=16)
Type of complications No. of patients PercentageLeakage or dehiscence of anastomosis 13 81.25Leakage or dehiscence of perforation 3 18.75Surgical injuriesLysis of adhesion 3 18.75Extensive mobilization 2 12.5Technical errorsTight/strangulating suture 8 50.00Rigid drain 0 00Narrow outlet of anastomosis etc. 3 18.75Accidental diathermy use 2 12.5
Table V. Routine and emergency operations
complicated by enterocutaneous fistula (n=16)
Emergency operation No. of patients PercentageJejunum and ileumResection and anastomosis 10 62.5Rt hemicolectomy 3 18.75ColonResection and anastomosis 1 6.25Hemicolectomy 0 00Routine operationLeft hemicolectomy 2 12.50Resection and anastomosis 0 00
Table VI. Complication of enterocutaneous fistula
(n=16)
Complication No. of patients PercentageSpecificFluid and electrolyte 10 62.5imbalanceMalnourishment 8 50.0InfectionWound infection 16 100.00Generalized peritonitis 5 31.25Septicaemia 3 18.75Skin excoriation 12 75.0Bowel obstruction 0 00Non specificPneumonia 5 31.25ARDS 3 18.75Jaundice 0 00Deep vein thrombosis 0 00Pulmonary embolism 0 00Bedsore 3 18.75Urinary tract infection 5 31.25Acute renal failure 4 25.0
Table VII. Method of management (n=16).
Methods No. of patients Percentage
Early surgical intervention 4 25.0
Conservative treatment 10 62.5
Early conservative and 2 12.5
delayed surgical intervention
Discussion
In the present study out of 100 respondent 56%were under 31 years age, 20% were between 31-40, 18% were between 41-50 and 6% were above50 years. Out of 100 respondent 86% were maleand 14% were female. Male and female ratio was6.14:1. Wainstein et al.6 in a study of ninety-onepatients, where 73 (69.2%) were men whose meanage was 48 years. Lynch et al.7 reviewed recordsof patients who had ECF surgery. In their studyamong 205 patients, 89 males, 43%; median age,51 years; range, 16-86 years. Memon and Siddiqui,8
in a descriptive study of forty patients withpostoperative fistula showed 25 males and 15females with 50% of the patients being in age groupof 21-30 years. The results of the present studynearly similar with them.
Out of 100 respondents 24% had diabetic, 20% hadH/O typhoid fever, 10% had H/O tuberculosis, 4%had H/O crohn’s disease and 15% had H/Omalignancy.
All respondents were presented with surgicalwound. Majority were developed skin excoriation(75%) due to fistula effluent. Here 87.5% patientswith single external fistula opening and 12.5patients with multiple openings. Content of fistula
90 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

were serious in 18.75 patients and liquid in 75patients of enterocutaenous fistula.
In (10%) respondents the initial pathology wereintestinal TB followed by thyphoid ulcer (20.0%),malignancy (15%), blunt Trauma (10%),penetrating Trauma (6. %). Eni et al.9 in a study of54 patients with ECF showed eighteen cases (33%)following appendicectomy, 12(22%) followinglaparotomy for intestinal obstruction, 10(18.5%)following laparotomy for abdominal malignancies,7(13%) followed laparotomy for penetratingabdominal injuries, 3(5.5%) followed laparotomyfor perforated typhoid enteritis, 2 (3.7%) cases weredue to spontaneous rupture of strangulated andneglected inguinal hernia, 1(1.9%) case followedchest tube insertion for pleural effusion in a PTBpatient and 1(1.9%) case followed a native healer’sincision on a lumber hernia. Martinez et al.10 in astudy of 174 patients found the most frequent siteof origin of fistula was the small bowel (90 patients:48 jejunal, and 42 ileal), followed in frequency bythe colon (50 patients). Postoperativeenterocutaneous fistula closure was achieved in151 patients (86%), being spontaneous in 65 (37%)and surgical in 86 (49%).
Out of 16 respondents 6 (37.5%) were high outputand 10(62.5%) were low output fistula, maximumrespondents (87.5%) were presented with singlefistula and 12.5% respondents presented withmultiple fistulas. Eni et al. retrospectively reviewed54 patients with ECF. Fourty one (76%) were highoutput type, while 13 (24%) were low output type.D’Harcour et al.11 evaluated retrospectively theresults of percutaneous catheter management ofenterocutaneous fistulas. One hundred eleven ofthese patients (76%) had developed fistulas aftersurgery were included. Ninety-three of 147patients (63%) had high-output fistulas, and 54 (37%) had low-output fistulas.
Draus et aI.12 studied the etiology, treatment, andoutcome of enterocutaneous fistulas in 106 patientsto evaluate the current practice and the impact ofnewer therapy Of the 106 patients in the study. 31had a high output fistula, 44 had a low outputfistula, and, in 31 patients, the fistula output waslow but there was no record of volume.
All respondents were presented after an initialoperation. Most of them under gone resection andanastomosis (62.5%) followed by hemicolectomy
(18.75%). Eni et al.9 in a study showed that themain cause of ECF in their environment ispostoperative (94.4%) with post appendicectomycases alone accounting for 33%. Majority of theirpatients (66.7%) were managed conservatively.Hollington et al.13 retrospectively reviewed 277consecutive patients of enterocutaneous fistulatreated over an 11-year period. In their study themost of the fistulas occurred secondary toabdominal surgery, and a high proportion (52.7 percent) occurred in association with inflammatorybowel disease.
Among the respondents of the present study properantibiotic after culture and sensitivity of the woundswab was needed for all respondents to controlsepsis. Enteral feeding was given to the allrespondents. Operative Procedures were done in37.5% of the respondents. Lynch et al.7 reviewedrecords of patients who had ECF surgery. In theirstudy management strategy involved earlydrainage of sepsis and nutritional support prior toelective ECF repair, with selective defunctioningproximal stoma formation.
In the present study fistula after takingconservative measure in 10 cases, early surgicalintervention taking in 4 patients & delayed surgicalintervention were necessitated in 2 cases. Lynchet al.7 reviewed records of patients who had ECFsurgery. In their study total of 203 patients haddefinitive ECF repair. Forty-four had over sewingor wedge resection of the fistula, and 159 hadresection and reanastornosis of the involved smallbowel segment or ileocolic anastomosis.
In the present study three modalities ofmanagement have been followed, namely earlysurgical intervention, conservative approach, earlyconservative and delayed surgical treatment. Fourof the patient (25%) in this study have undergoneearly operative approach to the fistula.
Rest of 10 cases have been treated by conservativemeasure. The conservative method which isappreciated all over the world for its success hasnot produced expected result in this study and twocases expired due this modality treatment.Patients with low output fistulae have beenmanaged by an initial period of perenteral nutritionuntil formation of the fistulous tract and thereaftermanaged mainly by oral feeding with intermittentintravenous supplementation to electrolyte
Enterocutaneous Fistula after Bowel Surgery- Study of 100 Cases Prodip Kumar Mandal et al 91

imbalance and to improve nutritional status of thepatients.
Conclusions
The present study shows a treatment guidelinefor patients with enterocutaneous fistula.Knowledge of the pathophysiology and risk factorsfor the development of enterocutaneous fistulasmay optimize the ability to avoid their creation inthe first place. The aetiologies, classification,clinical features, investigations, complications,different methods of management with theirsuccess rates and incidence of enterocutaneousfistula after different type of routine & emergencyoperations etc. have been studied. Once thiscatastrophic complication occurs, the bestoutcomes result from a rational, well-definedmanagement protocol. Early diagnosis of the fistulaand resuscitation of the patient, the control ofsepsis, and the provision of nutritional support maylimit the morbidity and mortality associated withthis complication. After adequate stabilization, anattempt at nonoperative management may allowfor spontaneous closure of the fistula, thus avoidingthe risks of a major reoperative procedure. Carefulplanning and meticulous dissection, reanastomosis,and reconstruction of the abdominal wall maximizethe patient’s chances of successful resolution.
References:1. Pellegrini CA, Gordon RL. Abdominal abscesses and
gastrointestinal fistulas. In: Sleisinger MH, Forham JS(editors). Gastrointestinal Disease. Philadelphia, WBSaunders 1993; 76(5) : 1019-33.
2. Lloyed D A.J, Gabe SM, Windsor AC J. Nutrition andmanagement of enterocutaneous fistula. BritishJournal of surgery 2006; 93(9):1045-1055.
3. Kuvshinoff BW, Brodish RJ, MeFadden DW, FischerJE. Scrum transferrin as prognostic indicator ofspontancous closure and mortality in gastrointestinalcutancous fistulas. Ann Surg 1993;217:615-623.
4. Memon AS, Siddiqui FG. Causes and management ofpost-operative enterocutaneous fistula. J Cel Phy SurgPak 2004; 14: 25-28.
5. Howard RA, Cart R, Way LW, Englebert DJ.Management of external gastrointestinal fistulas. AnnSurg 2006:188.
6. Fallouji MAR. Abdominal Trauma, Post graduatesurgery, the candidates guide, 2nd edition, ButterworthHeinemann, 1992:334-337.
7. Lynch RP, Olde Damink SWM, Winkens B, Soeters PBand van Gemert WG. Treatment Strategies in 135Consecutive Patients with Enterocutaneous Fistulas.World JSurg 2008;32(3):445—453.
8. Memon AS and Siddiqui FG. Causes and managementof postoperative enterocutaneous fistula. J CollPhysicians Surg Pak 2004;14(1):25-8.
9. Eni FR, Bradley J. Andrew. Transplantation. In RusselR.C.G, Williams NS and Buistrode CJK, Editor. “Baileyand loves Short Practice of Surgery”. 24th edition. Arnoldpublisher. 2004:183-206.
10. Martinez SL, Shires GT, Spencer FC, Husses WC.Endocrine and metabolic Response to injury. In:Principles of Surgery. 6th ed. New York, McGraw-HillboiL company, 2009:33-39.
11. D’Harcour JIB, Boverie 11-I and Dondelinger RF.Percutaneous management of enterocutaneousfistulas. American Journal of Roentgenology2007;167:33-38.
12. Draus MP, Hoyt DB, Engelhardt S, Hansbrough JF.The injured patient, In: Cuschieri A, Steele RJ, MoosaAR, editors. Essential Surgical Practice, Basic SurgicalTraining, 4th edition, Arnold, 2001:83-124.
13. Hollignton P, Mawdsley J, I am W, Gabe SM, Forbes A,Windsor AJ. An 11-year experience of enterocutaneousfistula. Br J Surg 2004; 91(12) : 1646-1641.
92 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Effect of Atorvastatin Alone and Combined Effect of
Atorvastatin and Allicin in Dyslipidaemic PatientsMaher Banu1*, Iram Shahriar2, Zahidul Hasan3, AFM Muntasir Reza4, Sanjana Sharmin Shashi5,
Abdus Sattar Sarker6
Abstract
Background: Dyslipidaemia contributes significantly to the prevalence and severity of
atherosclerosis and coronary artery diseases.
Objective: To compare the effect of Atorvastatin alone and combination of Atorvastatin
and Allicin in dyslipidemic patients.
Method: This interventional study was carried out in the department of Pharmacology,
Sir Salimullah Medical College Mitford Hospital (SSMCMH), Dhaka from January 2016
to December 2016. Total numbers of sixty four dyslipidemic subjects of both sexes, age 20
to 70 years, were included. The study subjects were divided into two groups, each comprising
of 32 subjects. Group A was supplemented with Atorvastatin only of dose 10mg/day and
the subjects in the group were designated as, A1- On the 1st day of study and A2, After
12weeks of the study and group B was given Atorvastatin of dose 10mg and Allicin (garlic
capsule) of dose 10 mg/day The subject of this group was categorized as B1- before
supplementation of allicin, taking only atorvastatin (on day 1). B2- After 12th week’s
supplementation of allicin and atorvastatin. Systolic blood pressure, diastolic blood
pressure, body mass index (BMI) and fasting serum lipid profile of each group were
measured before and after treatment with an interval of 12 weeks. Serum lipid profile (TC,
TAG, LDL-C, HDL-C) of all subjects were estimated by enzymatic method. Statistical
analysis was done by using paired and unpaired sample t-test.
Result: In this study, mean serum TC of subjects were 260.07±27.55 and 259.02±31.25,
serum TAG were 238.05±84.44 and 237.72±101.58,serum LDL-C were 151.83±23.60 and
149.06±28.95, serum HDL-C were 37.18±6.20 and 40.87±6.49 group A1 and B1 respectively.
After 12 weeks of different interventions, serum TC were 207.41±36.45 and 187.60±23.41mg/
dl, serum TAG were 218.72±69.49 and 195.59±84.60 mg/dl, serum LDL-C were 113.53±27.39
and 96.91±18.88 mg/dl, serum HDL-C were 39.72±4.46 and 45.59±6.21 mg/dl in group A2
and B2 respectively. From the results it is evident that both the interventions worked well
to reduce (p<0.001) the lipid profile parameters after 12 weeks of intervention. When
compared the differences between group A2 and B2 all the parameter changes were
significantly (p<0.001) better in group B2. Moreover in this study BMI levels of the subjects
were 25.85±1.26 and 26.50±1.38 kg/m2 in between group A1 and B1 respectively. After 12
weeks of different interventions, BMI levels were 25.23±0.91 and 24.78±0.87 kg/m2 in
group A2 and B2 respectively. From this result it is evident that BMI lowering effect was
significantly (P <0.001) well in combination treatment with Atorvastatin and Allicin than
12 weeks treated Atorvastatin only. Group B2 has reduced BMI in comparison to group A2.
Conclusion: Allicin has a significant role in reducing dyslipidaemia and overweight.
Original Article
Key words:
Atorvastatin, Allicin,dyslipidaemia, BMI.
Article information
Received: 01.10.2020Accepted: 01.12.2020
Cite this article:
Banu M, Shahriar I, HasanZ, Reza AFMM, Shashi SS,Sarker AS. Effect of Atorvas-tatin Alone and CombinedEffect of Atorvastatin andAllicin in DyslipidaemicPatients. Sir Salimullah MedColl J 2020; 28: 93-99
Sir Salimullah Med Coll J 2020; 28: 93-99
1. Assistant Professor, Department of Pharmacology, Dr. Sirajul Islam Medical College, Dhaka.2. Professor and Head, Department of Pharmacology,Sir Salimullah Medical College, Dhaka.3. Assistant Professor, Department of Medicine, Sir Salimullah Medical College, Dhaka.4. Assistant Registar, Department of Urology, Dhaka Medical College and Hospital, Dhaka.5. Assistant Professor, Department of Surgery, US Bangla Medical College, Narayngonj.6. Associate Professor, Department of Medicine, Sir Salimullah Medical College, Dhaka.*Correspondence: Dr. Maher Banu, E-mail: banumaher [email protected]

Introduction
Cardiovascular disease is the primary cause ofmortality and morbidity worldwide. Numerousfactors, such as age, family history, high cholesteroland hypertension, lifestyle and diet rich insaturated fats play an important role in thedevelopment of dyslipidaemia, which contributesignificantly in the prevalence and severity ofatherosclerosis and coronary artery diseases suchas angina, myocardial infarction.1 Dyslipidaemiais a metabolic disorder characterized by alterationin serum lipid and lipoprotein profile due toincreased concentration of Total cholesterol (TC),Low density lipoprotein (LDL-C) and Triglycerides(TAG) with concomitant decrease in theconcentration of High Density Lipoprotein (HDL-C) in the blood circulation.2 Dyslipidaemia isusually associated with hepatic fat accumulationand elevated plasma lipids which is the predictorof coronary artery disease.3 Epidemiological studieshave shown that there is a positive correlationbetween the incidence of coronary heart diseaseand the blood cholesterol level. An interventionalstudy showed that reduction of total cholesterolby 11.5% reduced cardiovascular disease eventsby 33%.4,5 Dislipidemia is the presence of elevatedabnormal levels of lipid and or lipoproteins in theblood. Lipid and lipoprotein abnormalities areextremely common in the general population, andare regarded as a highly risk factor forcardiovascular disease. Cholesterol is one of themost clinically relevant lipid substances inatherosclerosis.6,7
According to American Heart Association Report,cardiovascular disease is a major cause of deathand constituted about 35.2% of death rate in 2012,55% of population have cholesterol levels greaterthan (200mg/dl) and are at increased risk for thedevelopment of coronary artery diseases.8
Cardiovascular disease is also the leading cause ofdeath in Asian countries. The general consensusis that the main treatment of dyslipidaemia islifestyle modification, like exercise, weightreduction, dietary reduction of saturated fat andcholesterol. Pharmacological agents such lipidlowering drugs used for treating high-risk personsinclude 3-hydroxy-3methylglutaryl coenzyme Areductase inhibitors (statins), bile acid sequestrans,fibrates, and nicotinates.9 The National CholesterolEducation Program in 1993, considered diet
modification as a foundation of the primarytreatment proposing a dietary reduction ofsaturated fat and cholesterol consumed by riskypatients.10 Lipid lowering agents, statins are themost used drugs in the world for the wide evidenceof safety, cost effectiveness, potency in decreasingcoronary artery disease and stroke risk in bothprimary and secondary hyperlipidaemia.11,12
Allicin, a sulfur-containing active compound ofgarlic and it is widely used around the world witha history of human use of over 7000 years forculinary and medicinal purpose.13 As and activecompound allicin exhibits hypocholesterolemiceffects,14 antithrombotic, anticoagulant,hypotensive, antioxidant effects,15 anti-carcinogenic effect, hypoglycemic activities.16
Recently, different formulations of Allicin arewidely used for the prevention of cardiovasculardiseases, dyslipidaemia, hypertension.17 Moreover,a number of interventional studies have shownthat Allicin( active component of garlic) exertssignificiant role on reducing plasma lipids, speciallyplasma cholesterol and LDL cholesterol level inhumans.18 It also inhibit LDL oxidation and possessbeneficial effects for the prevention ofcardiovascular diseases. It was known as aneffective material in decreasing blood pressure alsocan inhibit LDL oxidation.19,20 There has been anincreasing recognition that certain naturalsubstances of plant origin have the potential toreduce the detrimental effect of cardiovascular riskfactors.21 The use of natural substance has becomemore widespread over the past few years drivenundoubtedly by the belief that natural substancesmay have fewer side effects and easily availableand cheap with good efficacy.22
This study is carried out to see the effect of Allicinin reducing serum lipid profile and also to observethe effect on lipid profile in combination withAtorvastatin (10mg), Allicin capsule (10mg) oncedaily could act as an additive therapy in decreaseof lipid profile and can reduce the adverse effectsproduced by Atorvastatin alone.
Materials and Methods
The objective of this study was to assess theadditive effect of Allicin along with Arorvastatinon dyslipidemic patients. This interventional studywas conducted in the department of Pharmacology,Sir Salimullah Medical College Mitford Hospital
94 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

(SSMCMH), Dhaka during the period of Januaryto December 2016. A total number of 64 subjectswere selected by purposive sampling procedure anddivided into two groups each group comprised to32 subjects. Protocol was approved by InstitutionalEthical committee (IEC) of SSMCMH and informedwritten consent was taken from the patients.Subjects meeting the inclusion & exclusion criteriaand willing to participate in the study wererecruited from the outpatient department ofCardiology, SSMCMH. All informations werecollected and a structured questionnaire was filledup for each patient. Data were collected by usingdata collection sheet and laboratory investigationswere done in Microbiology department of SirSalimullah Medical College. Serum lipid profile(Total cholesterol, TG, LDL, HDL) of all patientswere measured in morning after overnight fasting(12hrs) and considered as control. Patients wereinstructed to take the medications for 12 weeks atbed time. After treatment for 12 weeks, 10ml ofvenous blood was taken from each patient for lipidprofile assessment, centrifuged at 2500 revolutionsper minute to obtain serum, which was stored forenzymatic colorimetric method. Systolic & diastolicblood pressures were measured by auscultatorymethod and height and weight were also measuredfor BMI calculation before and after 12 weeks ofboth interventions (A2 and B 2 respectively).
Data analysis:
Collected data were checked, edited and processed,then expressed as mean ± SD. Statistical analysiswas done by using Statistical Package of SocialScience (SPSS), for Windows version 21. Pairedand unpaired sample‘t’ test were used as tests ofsignificance and ‘p’ value <0.05 was considered assignificant.
Results
Table 1, shows that out of total 64 dyslipidaemicpatients, majority in both groups A and B,18(56.25%) and 20(62.5%) respectively, werebetween 41-50 years age group and were malepredominance. Differences of BMI of both groups(A and B) were non-significant beforeinterventions. Most of the patients of both groups(n=64) were from higher socio-economic group.
Table I. Gender, age, BMI and Socio-economic
conditions in different groups (n=64)
Parameters Group A Group B P value
Male 18 (56.25%) 20 (62.5%)
Female 14 (43.75%) 12 (37.5%)
Age (years) 34-60 28-65 0.62ns
(mean±SD) 44.63±5.92 45.63±9.55
BMI (kg/m2) 25.16-29.41 25.16-31.25 0.06ns
(mean±SD) 25.85±1.26 26.50±1.38
Socio-economic condition
Low 07 (21.88%) 08 (25%)
Middle 09(28.12%) 10 (31.25%)
High 16(50%) 14 (43.75%)
ns: non significant
Table II and table III shows that systolic and diastolicblood pressure were statistically non significant ingroups both before and after treatment.
Table II. Blood pressure in different groups
before treatment (n= 64).
Blood pressure Group A1 Group B1 P value(n=32) (n=32)
Before treatmentSystolic Blood 125.31±7.29 124.53±6.01 0.64ns
Pressure (mmHg) (110-140) (110-140)Diastolic Blood 79.69±4.39 79.38±5.20 0.80ns
Pressure (mmHg) (70-85) (70-85)
Table III. Blood pressure in different groups
after treatment (n=64):
Group A2 Group B2 P value(n=32) (n=32)
Systolic Blood 120±4.02 119.38±4.54 0.64ns
Pressure (mmHg) (110-130) (110-130)Diastolic Blood 77.81±3.07 77.19±4.00 0.56ns
Pressure (mmHg) (65-85) (70-80)
Group A1: Before treatment with Atorvastatin alone(Day 1)Group A2: After 12 weeks of treatment withAtorvastatin aloneGroup B1: Before supplementation of Allicin (Day1),patient taking atorvastatain only.Group B2: After 12 weeks of supplementation withAtorvastatin and Allicinns: non-significant
Effect of Atorvastatin Alone and Combined Effect of Atorvastatin and Allicin Maher Banu et al 95

In Table IV shows that, the mean serum TC, TAG,LDL-C and HDL-C levels were almost similar andthe difference were not statistically significantbetween group A1 and group B1. In group A showedlipid profile parameters were significantly (<0.001)improved in patients after 12 weeks of treatmentwith Atorvastatin alone (A2) compared to groupA1 before Atorvastatin supplementation. In groupB, lipid profile parameters were also significantly(<0.001) improved in patients after 12 weeks ofsupplementation with Allicin and Atorvastatin (B2)
compared to before supplementation of Allicin, ingroup B1 .
Table V reveals that, after 12 weeks of treatmentwith Atorvastatin alone in group A2 compared to12 weeks of treatment with Allicin and Atorvastatinin group B2, serum lipid profile parameters werehighly significant (<0.001) and individualparameters were also significant which showedthat all parameters reduced more in group B2 thanin group A2 .
Table IV. Lipid profile before and after treatment in different groups
Serum lipid Group A1 Group A2 P value Group B1 Group B2 P valueprofile (n=32) (n=32) (n=32) (n=32)
(mg/dl) Mean±SD Mean±SD Mean±SD Mean±SD
Serum TC 260.07±27.55 207.41±36.45 < 0.001*** 259.02±31.25 187.60±23.41 <0.001***
(210-321) (108-292) (192-320) (140-234)
Serum TAG 238.05±84.44 218.72±69.49 < 0.001*** 237.72±101.58 195.59±84.60 <0.001***
(120-497) (148-362) (102-498) (80-387)
Serum LDL-C 151.83±23.60 113.53±27.39 < 0.001*** 149.06±28.95 96.91±18.88 <0.001***
(121-196) (82-155) (85-195) (60-150)
Serum HDL-C 37.18±6.20 39.72±4.46 < 0.001*** 40.87±6.49 45.59±6.21 <0.001***
(28-55) (31-52) (29-51) (32-58)
Group A1: Before treatment with Atorvastatin alone (Day 1)Group A2: After 12 weeks of treatment with Atorvastatin aloneGroup B1: Before supplementation of Garlic (Day 1)Group B2: After 12 weeks of supplementation with Atorvastatin and Garlic*: significant
Table V. Comparison of lipid profile between the groups after 12 weeks of different treatment (N=64)
Serum lipid profile Group A2 (n=32) Group B2 (n=32) P value
(mg/dl) Mean±SD Mean±SD
Serum TC 207.41±36.45 187.60±23.41 0.02**
(108-292) (140-234)
Serum TAG 218.72±69.49 195.59±84.60 0.04**
(148-362) (80-387)
Serum LDL-C 113.53±27.39 96.91±18.88 0.02**
(82-155) (60-150)
Serum HDL-C 39.72±4.46 45.59±6.21 <0.001***
(31-52) (32-58)
*: significant
96 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Table VI shows that there were a significant(<0.001) reduction of BMI level after 12 weeks ofsupplementation with Allicin and Atorvastatin ingroup B2 compared to group B1, beforesupplementation of Allicin. It was also evident thatBMI reduced significantly in group B2 comparedto group A2, where the readings were taken frompatients who were treated for 12 weeks withAtorvastatin only.
Table VII. Adverse effects in both groups after
12 weeks of treatment
Adverse effects Atorvastatin Allicin and
n=32(%) Atorvastatinn=32(%)
Muscle pain 5 (15.62) 2 (6.25)Leg cramps 11 (34.38) 2 (6.25)Myalgia 8 (25) 1 (3.12)Nausea 0(0) 3 (9.38)Diarrhea 1 (3.12) 2 (6.25)Hypersensitivity 0(0) 0(0)Cold symptom 3 (9.38) 0(0)(runny nose, sneezing,coughing)Heart burn 1 (3.12) 4 (12.5)
No complaints 3 (9.38) 18 (56.25)
N 32(100) 32(100)
Table VII shows that combination of Allicin andAtorvastatin reduced the adverse effects producedby Atorvastatin alone. Allicin reduced leg crampsfrom 11(34.38%) to 2(6.25%) and myalgia from8(25%) to 1(3.12%). Most of the patients 18(56.25%)did not give any complaints with this combinationtherapy.
Discussion
Dyslipidaemia significantly produces varioushazards, so effective management is frequentlyintended for such patients. In clinical managementof dyslipidaemia, Atorvastatin and other statingroups are mainly indicated for dyslipidaemiachiefly involving raised cholesterol level.Atorvastatin successfully reduce blood LDL-Cthough, Atorvastatin alone is ineffective for optimalLDL-C level as recommended via the currentguiding principle National Cholesterol EducationProgram (NCEP ATP III).23 Moreover, anti-lipidaemic medications are not free of adverseeffects. Atorvastatin treatment elevated the risksof liver enzymes, myalgia, and elevated liverenzymes and some have been associated withpotential carcinogenicity.21 Herbal treatment canbe a safe and cost effective way to combatdyslipidaemia. An increasing interest in herbalmedicine of plant origin has led to a search for
Table VI. BMI in different groups before and after treatment (N=64)
Group A1 (n=32) Group B1 (n=32) P value
Mean±SD Mean±SD
BMI (kg/m2) 25.85±1.26 26.50±1.38 0.06ns
(25.16-29.41) (25.16-31.25)
Group A1 (n=32) Group A2 (n=32)Mean±SD Mean±SD
BMI (kg/m2) 25.85±1.26 25.23±0.91 0.56 ns
(25.10-29.41) (23.53-27.10)
Group B1 (n=32) Group B2 (n=32)Mean±SD Mean±SD
BMI (kg/m2) 26.50±1.38 24.78±0.87 < 0.001***
(25.15-31.25) (23.43-27.73)
Group A2 (n=32) Group B2 (n=32)Mean±SD Mean±SD
BMI (kg/m2) 25.23±0.91 24.78±0.87 0.04**
(23.53-27.10) (23.43-27.73)ns: non-significant*: significant
Effect of Atorvastatin Alone and Combined Effect of Atorvastatin and Allicin Maher Banu et al 97

effective natural therapies that have significanteffects on blood lipid parameters.24
Male and female subjects of the present study ingroup A were 56.25% and 43.75%, while in groupB were 62.50 % and 37.50% respectively. Highestnumber of subjects belongs to male category. Theage of participants ranged between 20-70 years inboth groups, where 41-50 years group constitutedthe highest number. This may be due to increasedlipid catabolism after 40years in men, though pre-menopausal and menopause tends to abolish thisdifference.
The prevalence of higher socio-economic group(50% and 43.75%) was high in this study, due toeconomic liberalization with widespread presenceof transitional food outlets, availability of packagedfood with low cost and better affordability and alsolack of awareness regarding dyslipidaemia. Thesefindings were similar with the work of Misra Aand Shrivastava U.25 Systolic blood pressure anddiastolic blood pressure were almost similar andshowed no significant difference (p>0.05) in bothgroups before and after 12 weeks of differenttreatment as analogous to the findings of Shah Set al.22
Lipid profile level
In this study, the mean serum TC, TAG, LDL-Cand HDL-C levels were almost similar and thedifference were not statistically significant betweengroup A1 and group B1. Serum TC, TAG, LDL-C,VLDL-C and HDL-C level were improvedsignificantly (p<0.001) in subjects who took 12weeks of treatment with Atorvastatin alone. It alsoimproved significantly (p<0.001) in subjects whotook supplementation of Atorvastatin and Allicinfor 12 weeks compared to before supplementationof Allicin (Day 1).
Moreover, serum total TC, TAG, LDL-C, VLDL-Cdecreased and HDL-C level were increasedsignificantly (p<0.001) after 12 weekssupplementation of Atorvastatin and Allicincompared to that of 12 weeks treatment withAtorvastatin. These findings were similar with thework of some researchers.26,27
n this study, Allicin capsule (garlic) was given at10mg daily for 12 weeks in patients withdyslipidaemia taking Atorvastatin. This finding issimilar with that of other investigators.14,22,28 It
could be due to presence of flavonoids and sulphurcontaining compounds within it.22
Body mass index (BMI)
In this study, BMI level was decreased nonsignificantly (p>0.001) after 12 weeks treated ofAtorvastatin in comparison to that of Atorvastatintreated (Day 1). Again, BMI level was decreasedsignificantly (p<0.001) after 12 weekssupplementation of Atorvastatin and Allicincompared to that of before supplementation ofGarlic (Day 1). Moreover, BMI level was decreasedsignificantly (p<0.05) after 12 weekssupplementation of Atorvastatin and Allicincompared to that after12 weeks treated ofAtorvastatin .This finding is similar with someother researchers.17,18,29
The study also revealed that combination of Allicinand Atorvastatin reduced the adverse effectsproduced by Atorvastatin alone. Allicin reduced legcramps from 11(34.38%) to 2(6.25%), arthalgia from8(25%) to 1(3.12%) and 18(56.25%) patients did notgive any complaints about this combinationtherapy. This was due to the presence of biologicallymost active compounds allicin, flavonoids and S-allyl cysteine present in Garlic.22,29,30
Conclusion
From this study it can be concluded that, Allicin(Allium sativum) has got significant effect onimprovement of lipid profile by lowering serumlevel of total cholesterol (TC), triglyceride (TG),low density lipoprotein Cholesterol (LDL-C), verylow density lipoprotein Cholesterol (VLDL-C) andincreasing serum high density lipoproteincholesterol (HDL-C). In addition, Allicin alsosignificantly decreases body mass index (BMI).Therefore, dyslipidaemic patients may besuggested to take certain amount of Allicin dailyto reduce bad cholesterol (TC, TAG, LDL-C, VLDL-C) including BMI and to increase good cholesterolHDL-C.
References1. Gosain Anderson KM, Odrell PM, Wilson PW, Kannel
WB. Cardiovascular disease risk profiles. Am heart J.
2010; 121: 293-298.
2. Ochani K, Mello D. Cholesterol in the prediction ofatherosclerotic disease. New perspectives based on theFramingham study. Ann Intern Med. 2009.
3. Helal T, Kashimoto N, Kasuga S, Hassan HT. Ajoene(natural Garlic compound): a new anti-lipidemic agent
98 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

for dyslipidemia therapy. Leuk Res. 2011; 28(7); 667-671.
4. Nakamura HT, Verschu WM, Jacobs DR, BloembergBP, Kromhut D, Menotti A, Aravains C. Serum totalcholesterol and long term coronary heart disease indifferent cultures. Twenty five year follow up of the
seven countries study JAMA 2007.
5. Hamed PK, De B Backer G, Graham I, Poole WP, WoodD. Prevention of coronary heart disease in clinicalpractice. Recommendations of the task force of theEuropean society of cardiology. European
atherosclerosis society, European society of hypertension
society. 2010.
6. Durrington L, Zhang Thomas AS, Varughese P, SawJT, Lim YH. Potential drug-herb interaction with drugs,complementary therapeutics in clinical practice 2003.
7. Zhang A, Othman I, Gulzar U, Ali A. Role of herbalextracts in the prevention of oxidative stress andmodulation of atherogenic risk factors in experimentallyinduced DM. Diabetes Metab 2011;
8. Rosamond SJ. A tale of two trials; the west of Scotlandcoronary prevention study and Texas coronaryAtherosclerosis prevention study. Atheroselerosis. 2008.
9. Summary of the second report of the NationalCholesterol Education Program-NCEP.Expert Panel onDetection, Evolution and Treatment of High BloodCholesterol in Adults (Adult Treatment Panel II) JAMA
1993; 269:3015-3023.
10. Khanabadi M, Anderson KM, Odell PM, Kennel W B.Cardiovascular disease risk profiles. Am heart J 2006;121:293-298.
11. Mason M, Liao J K, Laufs U. Effects of statins. Annu
Rev Pharmacol Toxicol 2009; 45:89-118.
12. Mcelduff C, Newman G, Palmer H S, Danesh FR. Safetyof Atorvastatin derived from analysis of 44 completedtrials in 9416 patients. Am J Cardiol 2006.
13. Ensminger AH. Foods and Nutrition Encyclopedia.CRP
Press. 1994;1:750.
14. Khalid S. Al-Numair. Hypocholesteromic andAntioxident effects of Garlic (Allium sativum L). Extractin Rats Fed High Cholesterol diet. Pakistan journal of
Nutrition.2009; 8(2):161-166
15. Vilela M, Vega GL, Mishra A, Weyer C. The mood ofaction of allicin: Trapping of radiclals and interactionwith thiol containing proteins. Biocheim Biophys Acta
2010; 1379: 233-244.
16. Zavaragh F. Influence of Garlic and sumac power onperformance, carcass and blood biochemical of Japanesequails. Annals of Biological Research 2011; 2(6): 542-545.
17. Steiner M, Liu W. Garlic extracts a modular ofcardiovascular risk factors: A dose finding study on the
effect of Garlic on platelet functions. Journal of
nutrition 2001; 131(3): 980-984.
18. Yeh Y, Lin R, Yeh S, Evens S. Garlic reduce plasmacholesterol in hypercholesterolemic men maintaininghabitual diet in food factors for cancer prevention.Springer 1997: 226-230.
19. Heiner L, Rahbani K M, Evens L. Evaluation of theeffects of Garlic oil preparation on serum lipoproteinsand cholesterol metabolism. JAMA 1998; 279:1900-1904.
20. Elkayam A, Mirelman E, Peleg M, Wilchek T, Miron A,Rabinkov M, Henman O. The effect of allicin on weightin fructose induced hyperinsulinemic, hyperlipidemic,hypertensive rats. Am J Hypertens 2003; 16:1053-1056.
21. Stevenson CM, Pittler H. Garlic for treatinghypercholesterolemia. Ann Intern Med 2000; 133: 420-429.
22. Shah S, Gaurang F, Shah B. Comparative study withlasuna and Atorvastatin in obese and hyperlipidemiccases. Scholars research Library ISSN 0975-5071
(DerpharmaLetttre)2012; 4(3):1013-1021.
23. National Cholesterol Education Program (NCEP) Expertpanel on Direction, Evaluation and Treatment of HighCholesterol in Adults (Adult Treatment Panel III).ThirdReport of the National Cholesterol Education Program(NCEP) Expert panel on Detection, Evaluation andTreatment of High Blood cholesterol in Adults (AdultTreatment Panel III) final report. Circulation 2002;106:3143-3421.
24. El-Moselhy MA, El-Sheikh AA, Evans V. Protectivemechanisms of Atorvastatin against doxorubicin inducedhepato-renal toxicity. Biomed Pharmacother 2014;
68(1):101-110.
25. Misra A, Shrivastava U. Obesity and Dyslipidemia inSouth Asians. Nutrients 2013; 5:2708-2733.
26. Ashraf R, Amir K, Shaik AR, Ahmed T. Effects of Garlicon dyslipidemia in patients with type 2 diabetics mellitus.J Ayub Med Cell Abbottabad 2005;3: 17.
27. McMahon F, Vargas R, Jain A. Can Garlic reduce levelsof serum lipids? A controlled clinical study. Am J. Med
2013; 94: 632-635.
28. Satitvipawce P, Rawdaree P, Indrabhakti S,RatanaSuwan T, Getn-Gern P, Viwatwongka C. Noeffect of Garlic extract supplement on serum lipids levelsin hypercholesterolemic subjects. Journal of Medicine
Association 2003; 86(8):750-757.
29. Zuhair MH, Luma TA, Qutuba GH. Effect of Atorvastatinand Garlic on lipid profile in hyperlipidemic patients.University of Diyalia 2012;
30. Mahmoodi M, Islami MR, Karam GRA. Study of theeffect of raw Garlic consumption on the level if lipidsand other blood biochemical factors in hyperlipidemicindividuals. Pakistan journal of pharmaceutical
sciences.2006; 19(4): 295-298.
Effect of Atorvastatin Alone and Combined Effect of Atorvastatin and Allicin Maher Banu et al 99

Role of Computed Tomography Scan in the
Evaluation of Urinary Bladder Mass with
Histopathological ComparisonNusrat Jahan1, Mohammad Rued Hossain2, Partha Pratim Saha3, Kamrun Nahar4, Mohammad
Sazzad Hossain5, Asifa Sattar6, Lovely Yasmin7
Abstract
Background: Bladder cancer is the 7th most common cancer seen worldwide, with a
higher incidence in the USA and Europe compared with Asian countries. Though the
incidence of bladder cancer in Bangladesh is not known.
Objectives: To diagnose the urinary bladder mass on the basis of Computed Tomography
findings. To compare CT scan findings with that of histopathological findings of urinary
bladder mass. To calculate the sensitivity, specificity, positive predictive value, negative
predictive value and accuracy of CT scan in the diagnosis of urinary bladder mass.
Methods: A cross-sectional study was carried out in the department of Radiology and
Imaging of Sir Salimullah Medical College and Mitford Hospital, Dhaka enrolling 60
patients who were referred to department of Radiology and Imaging of Sir Salimullah
Medical College and Mitford Hospital as clinically suspected cases of urinary bladder
mass for contrast CT scan of whole abdomen, during the period of July 2015 to June
2017. After taking informed consent, data were collected in a structured questionnaire by
taking history, the finding and interpretation of the CT scan and histopathological
reports. Histopathological diagnosis was considered as gold standard of diagnostic
criteria.
Result: Considering histopatholgical diagnosis as gold standard test, Sensitivity,
Specificity, Positive Predictive Value, Negative Predictive Value and Accuracy of CT scan
in diagnosis of urinary bladder mass were 96.08%, 88.88%, 98%, 80% and 95% respectively.
Conclusion: Considering the validity parameters it can be concluded that CT scan is a
useful modality for detection of urinary bladder mass.
Original Article
Key words:
Urinary bladder mass, CTscan
Article information
Received: 01.08.2020Accepted: 01.09.2020
Cite this article:
Jahan N, Hossain MR,Saha PP, Nahar K, HossainMS, Sattar A, Yasmin L.Role of ComputedTomography Scan in theEvaluation of UrinaryBladder Mass withHistopathologicalComparison. Sir SalimullahMed Coll J 2020; 28: 100-5
Sir Salimullah Med Coll J 2020; 28: 100-107
1. Radiologist, Department of Radiology and Imaging, SSMC & MH, Dhaka.2. Professor, Department of Radiology and Imaging, SSMC, Dhaka.3. Assistant Professor, Department of Radiology and Imaging, SSMC, Dhaka.4. Radiologist, 250 Bed District Hospital, Feni.5. Assistant Professor, Department of Radiology and Imaging, SSMC, Dhaka.6. Associate Professor, Department of Radiology and Imaging, SSMC, Dhaka.7. Assistant Professor, Department of Radiology and Imaging, NITOR, Dhaka.Address of Correspondence: Dr. Nusrat Jahan, Radiologist, Department of Radiology and Imaging, SSMC & MH, Dhaka.Mobile: 01711317475, e-mail: [email protected]
Introduction
The human bladder is a retroperitoneal muscularorgan which acts as temporary reservoir of urine,after urine is filtered by the kidneys. Pathologiccondition of the bladder can manifest as a focalbladder mass or diffuse wall thickening. Focal
masses may be neoplastic or may developsecondary to congenital, inflammatory, idiopathicor infectious sources. Diffuse bladder wallthickening can develop secondary to non neoplasticconditions including infection with bacteria oradenovirus, schistosomiasis, tuberculosis,

inflammatory conditions such as cystitis andexposure to chemotherapy (particularly withcyclophosphamide) or irradiation and mimicmalignancy1.
Bladder cancer is the 7th most common cancer seenworldwide, with a higher incidence in the USA andEurope compared with Asian countries2. It is the4th most common cancer in male and the 10th mostcommon cancer in female. Though the incidenceof bladder cancer in Bangladesh is not known itwas estimated that 70,530 new cases werediagnosed and 14,680 deaths were caused bybladder cancer in the United States in 20103.
Bladder cancer rates are nearly four times higherin men than in women. Although bladder cancercan be detected at any age, more than 70% of newcases are diagnosed in patients who are 65 yearsof age or older. In addition, up to 70% of patientstreated for bladder cancer will experience arecurrence after treatment4.
The most common etiologic factors of bladdercancer are cigarette smoking and occupationalexposure to chemical carcinogen such as anilinedyes5. Although it is rare, there is a geneticpredisposition to the development of urothelialtumor in some families6.
Patient symptoms are all nonspecific. The mostcommon presenting symptom is painlesshaematuria (80% cases)2 although microscopichaematuria may be detected at urinalysis. Patientsmay also experience voiding symptoms such asincreased frequency, dysuria, and pelvic pain andpressure7.
Bladder cancer is a heterogeneous disease with70% of patients presenting with superficial tumorswhich tends to recur but are generally not lifethreatening, and 30% presenting as muscleinvasive disease associated with a high risk ofdeath from distant metastasis8. 95% of bladderneoplasms arise from the epithelium; the mostcommon subtype is urothelial carcinoma, whichaccounts for 90% of cases. Squamous cell carcinomaaccounts for 2%–15%, with rates varying widelyaccording to geographic location. Adenocarcinoma(primary bladder, urachal, or metastatic)represents less than 2%. Other rarer subtypes such
as small cell carcinoma account for fewer than 1%of the case7.
Several imaging modalities have been used in theevaluation of bladder mass. Historically,intravenous urography (IVU) has been the primarymethod of imaging in these patients. Currently,the examinations that are commonly used toevaluate patients with bladder mass include IVU,ultrasonography (US), computed tomography (CT),MRI and cystoscopy9.
MDCT allows the entire urinary tract to be imagedduring a single breath hold with thin collimation.As a result, thin section images obtained in anyplane provides higher spatial resolution than CTimages in the past9. It has an accuracy of 97% forcancer detection for all bladder cancers and 85%for bladder cancer shorter than 1 cm maximaldiameter10. It has a sensitivity and specificity ofover 90% for the diagnosis of bladder cancer inpatients with haematuria11.
The most commonly used CT protocol comprisesthree phases: pre contrast scan which revealswall calcification that may be sometimesassociated with transitional cell carcinoma orsquamous cell carcinoma12. The nephrographicphase, which is acquired following a delay of 90 -100 seconds after administration of 120 ml ofintravenous iodinated contrast, to evaluate therenal parenchyma. This is followed by thepyelographic phase taken 5 to 10 minutesfollowing contrast administration, to evaluatethe urothelium from the pelvicaliceal system tothe bladder13. Both the intraluminal andextraluminal component of the bladder cancershow intravenous contrast enhancement. Withcontrast enhance spiral CT, the enhancingbladder wall is contrasted against unopacifiedurine to outline the intra vesical extent of thetumor14.
A CT scan of the abdomen and pelvis may alsoprovide some clinical information regarding thepelvic and retroperitoneal lymph node. In lymphnode staging CT has 100% specificity15.
Methods
This cross-sectional study was carried out in thedepartment of Radiology and Imaging of SirSalimullah Medical College and Mitford Hospital,Dhaka, during the period of July 2015 to June
Role of Computed Tomography Scan in the Evaluation of Urinary Bladder Mass Nusrat Jahan et al 101
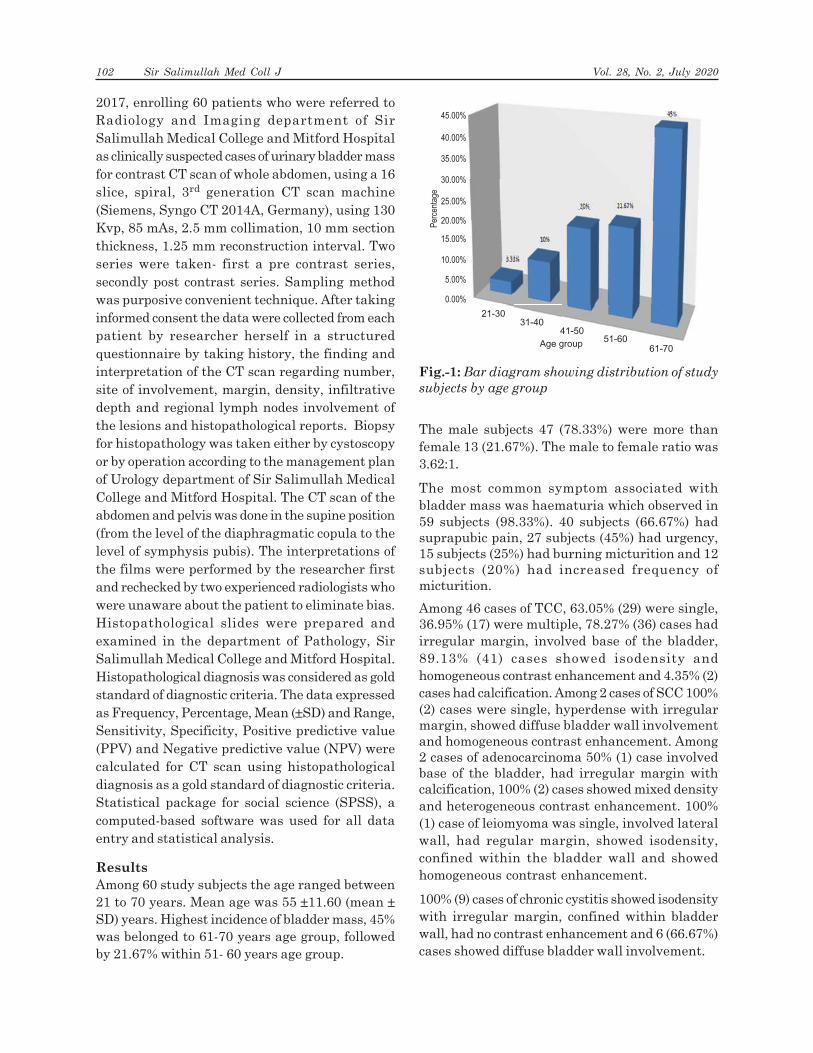
2017, enrolling 60 patients who were referred toRadiology and Imaging department of SirSalimullah Medical College and Mitford Hospitalas clinically suspected cases of urinary bladder massfor contrast CT scan of whole abdomen, using a 16slice, spiral, 3rd generation CT scan machine(Siemens, Syngo CT 2014A, Germany), using 130Kvp, 85 mAs, 2.5 mm collimation, 10 mm sectionthickness, 1.25 mm reconstruction interval. Twoseries were taken- first a pre contrast series,secondly post contrast series. Sampling methodwas purposive convenient technique. After takinginformed consent the data were collected from eachpatient by researcher herself in a structuredquestionnaire by taking history, the finding andinterpretation of the CT scan regarding number,site of involvement, margin, density, infiltrativedepth and regional lymph nodes involvement ofthe lesions and histopathological reports. Biopsyfor histopathology was taken either by cystoscopyor by operation according to the management planof Urology department of Sir Salimullah MedicalCollege and Mitford Hospital. The CT scan of theabdomen and pelvis was done in the supine position(from the level of the diaphragmatic copula to thelevel of symphysis pubis). The interpretations ofthe films were performed by the researcher firstand rechecked by two experienced radiologists whowere unaware about the patient to eliminate bias.Histopathological slides were prepared andexamined in the department of Pathology, SirSalimullah Medical College and Mitford Hospital.Histopathological diagnosis was considered as goldstandard of diagnostic criteria. The data expressedas Frequency, Percentage, Mean (±SD) and Range,Sensitivity, Specificity, Positive predictive value(PPV) and Negative predictive value (NPV) werecalculated for CT scan using histopathologicaldiagnosis as a gold standard of diagnostic criteria.Statistical package for social science (SPSS), acomputed-based software was used for all dataentry and statistical analysis.
Results
Among 60 study subjects the age ranged between21 to 70 years. Mean age was 55 ±11.60 (mean ±SD) years. Highest incidence of bladder mass, 45%was belonged to 61-70 years age group, followedby 21.67% within 51- 60 years age group.
The male subjects 47 (78.33%) were more thanfemale 13 (21.67%). The male to female ratio was3.62:1.
The most common symptom associated withbladder mass was haematuria which observed in59 subjects (98.33%). 40 subjects (66.67%) hadsuprapubic pain, 27 subjects (45%) had urgency,15 subjects (25%) had burning micturition and 12subjects (20%) had increased frequency ofmicturition.
Among 46 cases of TCC, 63.05% (29) were single,36.95% (17) were multiple, 78.27% (36) cases hadirregular margin, involved base of the bladder,89.13% (41) cases showed isodensity andhomogeneous contrast enhancement and 4.35% (2)cases had calcification. Among 2 cases of SCC 100%(2) cases were single, hyperdense with irregularmargin, showed diffuse bladder wall involvementand homogeneous contrast enhancement. Among2 cases of adenocarcinoma 50% (1) case involvedbase of the bladder, had irregular margin withcalcification, 100% (2) cases showed mixed densityand heterogeneous contrast enhancement. 100%(1) case of leiomyoma was single, involved lateralwall, had regular margin, showed isodensity,confined within the bladder wall and showedhomogeneous contrast enhancement.
100% (9) cases of chronic cystitis showed isodensitywith irregular margin, confined within bladderwall, had no contrast enhancement and 6 (66.67%)cases showed diffuse bladder wall involvement.
Fig.-1: Bar diagram showing distribution of study
subjects by age group
21-30
3.33%
10%
20%
45.00%
Per
cent
age
40.00%
35.00%
30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%
21.67%
45%
31-4041-50
51-6061-70
Age group
3.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33.33%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%3%
10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%10%
20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20% 21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.21.67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%67%
45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%45%
102 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020
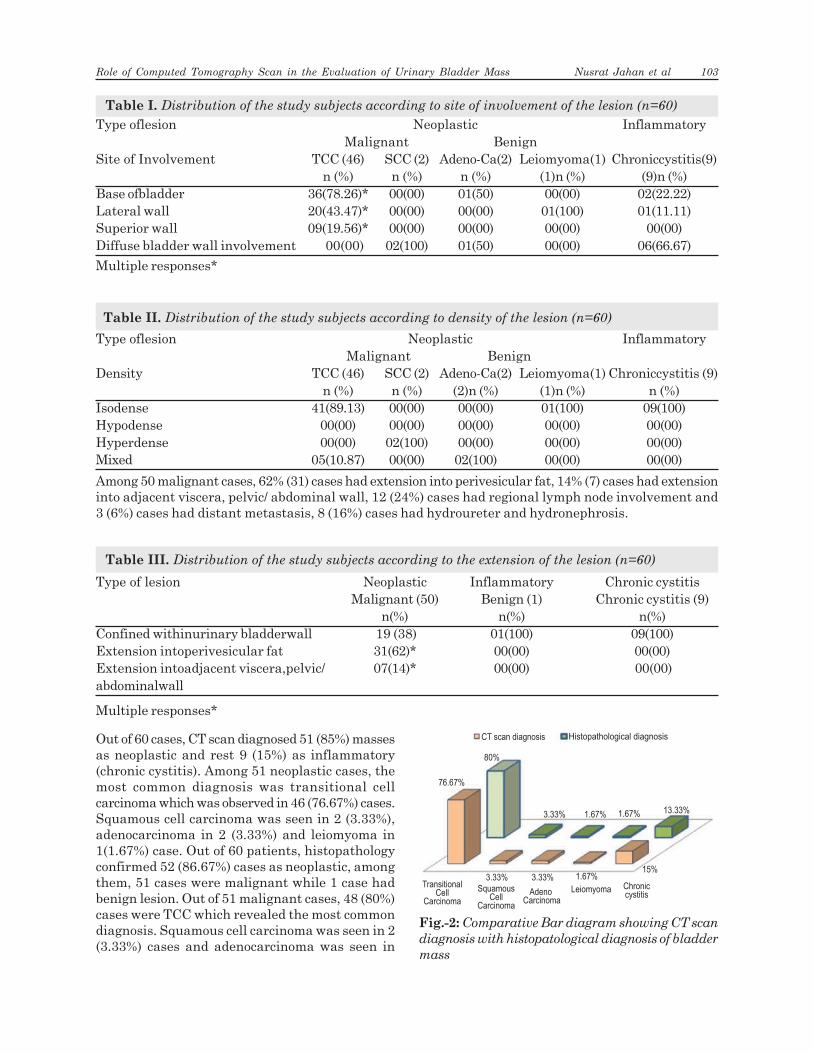
Table I. Distribution of the study subjects according to site of involvement of the lesion (n=60)
Type oflesion Neoplastic Inflammatory Malignant Benign
Site of Involvement TCC (46) SCC (2) Adeno-Ca(2) Leiomyoma(1) Chroniccystitis(9)n (%) n (%) n (%) (1)n (%) (9)n (%)
Base ofbladder 36(78.26)* 00(00) 01(50) 00(00) 02(22.22)Lateral wall 20(43.47)* 00(00) 00(00) 01(100) 01(11.11)Superior wall 09(19.56)* 00(00) 00(00) 00(00) 00(00)Diffuse bladder wall involvement 00(00) 02(100) 01(50) 00(00) 06(66.67)
Multiple responses*
Table II. Distribution of the study subjects according to density of the lesion (n=60)
Type oflesion Neoplastic Inflammatory Malignant Benign
Density TCC (46) SCC (2) Adeno-Ca(2) Leiomyoma(1) Chroniccystitis (9)n (%) n (%) (2)n (%) (1)n (%) n (%)
Isodense 41(89.13) 00(00) 00(00) 01(100) 09(100)Hypodense 00(00) 00(00) 00(00) 00(00) 00(00)Hyperdense 00(00) 02(100) 00(00) 00(00) 00(00)Mixed 05(10.87) 00(00) 02(100) 00(00) 00(00)
Among 50 malignant cases, 62% (31) cases had extension into perivesicular fat, 14% (7) cases had extensioninto adjacent viscera, pelvic/ abdominal wall, 12 (24%) cases had regional lymph node involvement and3 (6%) cases had distant metastasis, 8 (16%) cases had hydroureter and hydronephrosis.
Table III. Distribution of the study subjects according to the extension of the lesion (n=60)
Type of lesion Neoplastic Inflammatory Chronic cystitisMalignant (50) Benign (1) Chronic cystitis (9)
n(%) n(%) n(%)Confined withinurinary bladderwall 19 (38) 01(100) 09(100)Extension intoperivesicular fat 31(62)* 00(00) 00(00)Extension intoadjacent viscera,pelvic/ 07(14)* 00(00) 00(00)abdominalwall
Multiple responses*
Out of 60 cases, CT scan diagnosed 51 (85%) massesas neoplastic and rest 9 (15%) as inflammatory(chronic cystitis). Among 51 neoplastic cases, themost common diagnosis was transitional cellcarcinoma which was observed in 46 (76.67%) cases.Squamous cell carcinoma was seen in 2 (3.33%),adenocarcinoma in 2 (3.33%) and leiomyoma in1(1.67%) case. Out of 60 patients, histopathologyconfirmed 52 (86.67%) cases as neoplastic, amongthem, 51 cases were malignant while 1 case hadbenign lesion. Out of 51 malignant cases, 48 (80%)cases were TCC which revealed the most commondiagnosis. Squamous cell carcinoma was seen in 2(3.33%) cases and adenocarcinoma was seen in
CT scan diagnosis
80%
76.67%
3.33% 1.67% 1.67% 13.33%
15%1.67%3.33%3.33%
TransitionalCell
Carcinoma
SquamousCell
Carcinoma
Adeno Carcinoma
Leiomyoma Chroniccystitis
Histopathological diagnosis
Fig.-2: Comparative Bar diagram showing CT scan
diagnosis with histopatological diagnosis of bladder
mass
Role of Computed Tomography Scan in the Evaluation of Urinary Bladder Mass Nusrat Jahan et al 103

1(1.67%). 1 (1.67%) benign lesion was diagnosed asleiomyoma. Rest 8(13.33%) cases had chroniccystitis. Perivesical fat plane invasion was foundin 27 cases.
Table- IV shows, out of the 60 study subjects, 51cases were histopathologically confirmed asmalignant mass. Among the confirmed subjects,49 (True positive) cases were diagnosed asmalignant mass in CT scan accurately, while in 2(False negative) subjects, CT scan failed to clearly
diagnose malignant mass. One subject was falsepositively considered as malignant bladder mass.8 (True negative) subjects had inflammatory/benign lesion as diagnosed by both CT scan andHistopathological examination.
Considering histopathological diagnosis as goldstandard test Sensitivity, Specificity, PositivePredictive Value, Negative Predictive Value andAccuracy of CT scan in diagnosis of urinary bladdermass were 96.08%, 88.88%, 98%, 80% and 95%respectively.
Table IV. Evaluation of CT scan diagnosis on the basis of Histopathology as a gold standard test fordiagnosis of urinary bladder mass
CT scan diagnosis Histopathological diagnosis Total(+) ve for malignancy (-) ve for malignancy
(+) ve for malignancy 49 (TP) 01 (FP) 50
(-) ve for malignancy 02 (FN) 08 (TN) 10
Total 51 09 60
Table V. Sensitivity, Specificity, Positive
Predictive Value, Negative Predictive Value and
Accuracy of CT scan for diagnosis of urinary
bladder mass considering Histopathology as
gold standard test
Test Statistics Value (%)
Sensitivity 96.08
Specificity 88.88Positive Predictive Value 98.00NegativePredictive Value 80.00Accuracy 95.00
Discussion
The goal of cancer screening is to detect cancer atan early stage when it is treatable and curable.The standard imaging work-up for suspectedurothelial tumor has shifted from excretoryurography to cross-sectional non invasivemodalities such as ultrasonography (US), CT, andmagnetic resonance (MR) imaging. Althoughcystoscopy and histopathology remain the
Fig.3: Axial non enhanced CT scan of urinary
bladder showing- Transitional Cell Carcinoma
involving base and left lateral bladder wall
Fig.-4: Axial contrast enhanced (late phase) CT scan
of urinary bladder showing- Transitional Cell
Carcinoma involving base and left lateral bladder wall
104 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

reference standard for bladder cancer detection,both are invasive procedure and are uncomfortablein some patients. To observe the interior of thebladder wall, perivesical tissues, the neighbouringstructures and distant metastasis ComputedTomography is the preferred modality.
Current study was an endeavor to evaluate therole of CT scan in the evaluation of differenturinary bladder mass lesions with description ofCT scan findings of different masses and to findout Sensitivity, Specificity, Positive PredictiveValue, Negative Predictive Value and Accuracy ofCT scan. It was carried out in Radiology andImaging department, Sir Salimullah MedicalCollege and Mitford Hospital, Dhaka, among 60patients of clinically suspected urinary bladdermass lesion. All of them underwent CT scan fortheir current pathology and subsequentlyhistopathology was performed. Histopathologyreport was used as a foundation for confirming theactual diagnosis of patients and was used as a goldstandard for comparing the procedure. Thefindings of the study are discussed on the basis ofrelated previous studies concerning the objectiveof the study.
The age group mostly affected was 61-70 years andfollowed by 51-60 years which was agreed withVikram, Sandler and Ng (2009)4 who found thatprevalence of bladder lesion increased withincreases of age. About 66.67% was found above51 years age group and uncommon in thoseyounger than 40 years. Lynch and Cohen (1995)16
found cancers of the urinary bladder were morecommon in 51-80 years and rare in patientsyounger than age 40. There were 47 (78.33%) malesand 13 (21.67%) females. The male to female ratiowas 3.62:1. In previous study, Vikram, Sandler andNg (2009)4 reported that urinary bladder neoplasmwas four times greater in men than in women.
The most common symptom was haematuria whichobserved in 59 study subjects (98.33%). Previousstudy done by Panchal and Khandige (2015)2
showed that 80% of patients with bladder cancerpresent with haematuria.
In current study, among 46 cases of TCC, 29(63.05%) were single, 17 (36.95%) were multiple,
78.27% (36) cases had irregular margin, involvedbase of the bladder, 89.13% (41) cases showedisodensity and homogeneous contrastenhancement and 4.35% (2) cases had calcification.Among 2 cases of SCC 100% (2) cases were single,hyperdense with irregular margin, showed diffusebladder wall involvement and homogeneouscontrast enhancement. Among 2 cases ofadenocarcinoma 50% (1) case involved base of thebladder, had irregular margin with calcification,100% (2) cases showed mixed density andheterogeneous contrast enhancement. 100% (1)case of leiomyoma was single, involved lateral wall,had regular margin, showed isodensity, confinedwithin the bladder wall and showed homogeneouscontrast enhancement. These results werecomparable with Wong-You-Cheong et al. (2006)7
who found 60% TCC were single, 30-40% weremultiple, 80% involved in bladder base. Most ofthe TCC were iso-hypodense, had papillary andnodular margin and showed early homogeneouscontrast enhancement. Approximately 5% of casesshowed tumoral calcification. Most of the SCCdiffusely involved lateral wall and trigon of thebladder, had irregular margin, hyperdense andshowed homogeneous contrast enhancement. Mostof the adenocarcinoma had irregular margin withmixed density and showed heterogeneous contrastenhancement. Most of the leiomyoma had regularmargin, isodense, and showed homogeneouscontrast enhancement.
Shu-Yu Wu et al. (2016) observed that most of thecystitis cases were non-enhancing isodense lesionswith irregular margin. Comparable results wererevealed in present study where it was seen that100% (9) cases of chronic cystitis showed isodensitywith irregular margin, had no contrastenhancement.
Out of 50 cases of malignant mass, 38% (19) caseswere superficial and remaining 62% (31) cases hadextension beyond the bladder wall. Kirkali, Chanand Manoharan (2005)17 reported that 70% caseswere superficial and remaining 30% has invadedthe muscle. This disparity may be due to delayeddiagnosis. CT scan demonstrates perivesicalinvasion in 31 cases and histopathology confirmed
Role of Computed Tomography Scan in the Evaluation of Urinary Bladder Mass Nusrat Jahan et al 105

27 (87.09%) cases. Kim et al. (2004)10 foundperivesical invasion in 18 cases and histopathologyconfirmed 16 (88.88%) cases.
In this study, among 50 malignant cases, 24% (12)cases showed regional lymph node involvementand 3 (6%) cases had distant metastasis. Vikram,Sandler and Ng (2009)4 reported the incidence ofnodal metastasis was less than 30% and Arumugamet al. (2011)18 found 5.5% distant metastasis onCT.
Among 60 cases, 51 (85%) masses were neoplasticand rest 9 (15%) were inflammatory as diagnosedby CT scan. Among 51 neoplastic masses, 50 weremalignant arises from epithelium and 1 was benignlesion. Out of 50 malignant cases, 46 (76.67%)cases were TCC, 2 (3.33%) cases wereadenocarcinoma and 2 (3.33%) cases were SCC.Wong-You-Cheong et al. (2006)7 reported that 95%of bladder neoplasms arise from the epithelium;the most common subtype is urothelial carcinoma.Squamous cell carcinoma accounts for 2%–15%.Adenocarcinoma represents less than 2%.
Considering histopatholgical diagnosis as goldstandard test, Sensitivity, Specificity, PositivePredictive Value, Negative Predictive Value andAccuracy of CT scan in diagnosis of malignantbladder mass were 96.08%, 88.88%, 98%, 80% and95% respectively. These results were in agreementwith Turney et al. (2006)19 who found Sensitivityof Computed Tomography was 93%, with 98%Positive Predictive Value and Kim et al. (2004)10
observed that CT scan was highly Sensitive (92%)and Accurate (97%) method for detecting bladdercancer.
Conclusion
The present study is conducted to assess thediagnostic usefulness of computed tomography inthe evaluation of urinary bladder mass. Studyrevealed high sensitivity, specificity and accuracyof the CT scan in the diagnosis of urinary bladdermass. From the present study findings, it could beconcluded that CT scan is a useful diagnostic toolfor diagnosis of urinary bladder mass.
References1. Wong-You–Cheong, Jade, J., Paula, J., Woodward,
Maria, A., Manning, Charles, J. and DaviS, J.R. (2006)
Inflammatory And Nonneoplastic Bladder Masses:
Radiologic-Pathologic Correlation. Radiographics. 26,
pp. 1847–1868.
2. Panchal, J. and Khandige, S. (2015) A Gamut Of
Histopathological Lesion Of Cancer Of Urinary Bladder-
A Study Of 43 Cases. International Journal of
Biomedical and Advance Research. 6(03), pp. 212- 219.
3. Jemal, A., Siegel, R., Xu, J. and Ward, E. (2010) Cancer
Statistics. A Cancer Journal for Clinicians. 60, pp. 277–
300
4. Vikram, R., Sandler, C.M. and Ng, C.S. (2009) Imaging
And Staging Of Transitional Cell Carcinoma: Part 1,
Lower Urinary Tract. American Journal Of
Roentgenology. 192, pp. 1481–1487
5. Murta-Nascimento, C., Schmitz-Drager, B.J. and
Zeegers, M.P. (2007) Epidemiology Of Urinary Bladder
Cancer: From Tumor Development To Patients Death.
World Journal Of Urology. 25(3), pp. 285-295.
6. Aben, K.K., Witjes, J.A., Schoenberg, M.P., Hulsbergen-
Van-De-Kaa, C., Verbeek, A.L. and Kiemency, L.A.
(2002) Familial aggregation of urothelial cell carcinoma.
International Journal of Cancer. 98(2), pp. 274-278.
7. Wong-You–Cheong, Jade, J., Paula, J., Woodward,
Maria, A., Manning, Isabell, A. and Sesterhenn (2006)
Neoplasms Of The Urinary Bladder: Radiologic-
Pathologic Correlation. Radiographics. 26, pp. 553–580.
8. Kaufman, D.S., Shipley, W.U. And Feldman, A.S. (2009)
Bladder Cancer. Lancet. 374(9685), pp.239-249.
9. Joffe, S.A., Servaes, S., Okon, S. and Horowitz, M. (2003)
Multidetector Row CT Urography in the Evaluation of
Hematuria. Radiographics. 23, pp. 1441–1456.
10. Kim, J.K., Park, S.Y., Ahn, H.J., Kim, C.S. and Cho,
K.S. (2004) Bladder Cancer: Analysis Of Multi-Detector
Row Helical CT Enhancement Pattern And Accuracy
In Tumor Detection And Perivesical Staging. Radiology.
231(3), pp. 725-731.
11. Caterino, M., Giunta, S., Finocchi,V., Giglio, L.,
Mainiero,G., Carpanese, L. and Crecco, M. (2001)
Primary Cancer Of The Urinary Bladder: CT Evaluation
Of The T parameter With Different Techniques.
Abdominal Imaging. 26, pp. 433–438.
12. Caoili, E.M., Cohan, R.H., Inampudi, P., Ellis, J.H., Shah,
R.B., Faerber, G.J. and Montie, J.E. (2005) MDCT
Urography Of Upper Tract Urothelial Neoplasms.
American Journal of Roentgenology. 184, pp. 1873–
1881.
106 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

13. Maher, M.M., Kalra, M.K., Rizzo, S., Mueller, P.R. and
Saini, S. (2004) Multidetector CT Urography In Imaging
Of The Urinary Tract In Patients With Hematuria.
Korean Journal of Radiology. 5, pp. 1-10.
14. Su, H.S. And Harisinghani, M.G. (2009) Male Pelvis. In:
JR. Haaga, VS. Dogra, M. Forsting, R.C. Gilkeson, H.K.
HA, M. Sundaram, eds. CT and MRI Of The Whole
Body. 5th ed. Philadelphia: Mosby Elsevier. pp. 2043-
2064.
15. Lodde, M., Lacombe, L., Friede, J., Morin, F., Saourine,
A. and Fradet, Y. (2010) Evaluation of Fluorodeo-
xyglucose Positron-Emission Tomography with
Computed Tomography for Staging of Urothelial
Carcinoma. British Journal of Urology International.
106, pp. 658– 663.
16. Lynch, C.F. and Cohen, M.B. (1995) Urinary System.
Cancer. 75, p. 316.
17. Kirkali, Z., Chan, T. and Manoharan, M. (2005) Bladder
Cancer: Epidemiology, Staging And Grading, And
Diagnosis. Urology. 66(1), pp. 4-34.
18. Arumugam, R., Heminder, S., Rachael, F., Kevin, M.A.
and Michael, B.J.G. (2011) Role Of Whole-Body Staging
Computed Tomographic Scans For Detecting Distant
Metastases In Patients With Bladder Cancer. Journal
Of Computed Assisted Tomography. 35(3), pp. 402-405.
19. Turney, B.W., Willatt, J.M., Nixon, D., Crew, J.P. and
Cowan, N.C. (2006) Computed Tomography Urography
For Diagnosing Bladder Cancer. British journal of
urology international. 98(2), pp. 345-348.
Role of Computed Tomography Scan in the Evaluation of Urinary Bladder Mass Nusrat Jahan et al 107

Massive Transfusion in Clinical PracticeDaanish Arefin Biswas1, Md. Wasim2, Md. Rafiqul Haque3, Hasiba Akhter Bhuiyan4
Abstract:
Massive transfusion (MT) is important part of management of massive hemorrage to
maintain adequate circulation and haemostasis. For optimal management of massively
bleeding patients, regardless of causes effective preparation and communication between
transfusion medicine department, other laboratory services and clinical teams are
essential. A well-defined MT protocol (MTP) is a valuable tool to delineate how blood
products are ordered, prepared and delivered. It also dictate algorithms to be used as
transfusion guidelines and specify duties and facilitate communication between involved
personnel in different clinical settings. This review will define MT and review expert
guidelines available for MTPs, provide guidance for the use of therapeutic hemostatic
products, discuss the relevance investigations and selection of appropriate blood product
with ratios during an MTP both in trauma and non-trauma settings.
Review Article
Key words:
Massive transfusion,protocols, managements,blood product ratios
Article information
Received: 01.11.2020Accepted: 01.12.2020
Cite this article:
Biswas DA, Wasim M, HaqueMR, Bhuiyan HA. MassiveTransfusion in ClinicalPractice. Sir Salimullah MedColl J 2020; 28: 108-109
Sir Salimullah Med Coll J 2020; 28: 108-117
1. Associate Professor and Head, Department of Transfusion Medicine, Sir Salimullah Medical College, Dhaka.2. Assistant Professor, Department of Transfusion Medicine, Sir Salimullah Medical College, Dhaka.3. Associate Professor, Department of Transfusion Medicine, Ibn Sina Medical College, Dhaka,4. Medical Officer, Department of Transfusion Medicine, Sir Salimullah Medical College, Dhaka.Correspondence: Dr. Daanish Arefin Biswas, Associate Professor and Head, Department of Transfusion Medicine, SirSalimullah Medical College, Dhaka. Mobile: +8801715005808. E-mail: [email protected]
Introduction:
Massive haemorrhage requires massivetransfusion (MT) to maintain adequate circulationand haemostasis. Most deaths due to blood lossoccur within the first 6 hours1 For optimalmanagement of massively bleeding patients,regardless of aetiology (trauma, obstetrical,surgical), effective preparation and communicationbetween transfusion and other laboratory servicesand clinical teams are essential. A well-defined MTprotocol is a valuable tool to delineate how bloodproducts are ordered, prepared, and delivered;determine laboratory algorithms to use astransfusion guidelines; and outline duties andfacilitate communication between involvedpersonnel. This review will define MT and reviewexpert guidelines available for MTPs, provideguidance for the use of therapeutic hemostaticproducts, discuss the relevance of point-of-care(POC) coagulation testing and blood product ratios
during an MTP both in trauma and non-traumasetting.
Definition of MT
MT refers to the transfusion of large volume ofblood products over a short period of time to apatient who has severe or un-controlledhaemorrhage. In adults, several definitions of MTexist based on the volume of the blood productstransfused and also the time frames over whichthese transfusions occurred.2-4
The four most common definitions of MT in adultpatients are:
1. Transfusion of ³10 red blood cell (RBC) units,which approximates the total blood volume (TBV)of an average adult patient, within 24 hours.
2. Transfusion of >4 RBC units in 1 h withanticipation of continued need for blood productsupport.

3. Replacement of >50% of the TBV by bloodproducts within 3 h.
4. Transfusion support to more than 150 ml/minute of blood loss.
Epidemiology of MT
Trauma related mortality is the fourth leadingcause of death in the USA and according to theCenters for Disease Control and Prevention,unintentional injury accounted for more than120000 deaths in 2010.5 About 40% of traumarelated mortality is due to uncontrolled bleeding.It has been estimated that among the injuredpatients admitted to trauma centres, up to 10% ofmilitary and up to 5% of civilian patients requireMT.6,7 In general, injury severity and transfusionrequirement are associated with mortality. Most(99%) of the patients receiving <10 RBC unitswithin the first 24 h survived, whereas only 60%of patients who received >10 RBC units within thefirst 24 h survived.8 Obstetrical haemorrhage isanother common cause of MT.9 Other causes ofMT include gastrointestinal haemorrhage andmajor surgeries, such as cardiac, spinal, and liversurgery and liver and multivisceral trans-plantation.
Pathophysiological changes as a result of massivehaemorrhage & transfusionThe majority of the current concepts regardingthe haemostasis and pathophysiological changesthat occur during massive haemorrhage and theresultant MT are derived from animal and adulttrauma patient studies.10-13 The haemostaticdefects in massive haemorrhage are dynamic andhave multifactorial pathogenesis that relate toearly trauma induced coagulopathy (ETIC, alsotermed acute coagulopathy of trauma), transfusionof blood products, and infusion of crystalloids.14
Trauma induced tissue damage results in therelease of tissue factor and subsequent activationof the coagulation cascade. Hypoperfusion that thatoccurs after massive blood loss causes increasedexpression of thrombomodulin in turn binding tothrombin & activating protein C. Activated proteinC inhibits cofactors V & Viii and in excess alsodepletes plasminogen activator inhibitor 1,reducing tissue plasminogen activator inhibition& accelerating the formation of plasmin &fibrinolysis. Similar pathophysiological changes
can occur during major surgery with massive bloodloss.10
Coagulopathy may also develop during massivetransfusion, as a result of haemodilution fromvolume replacement and can be exacerbated byhypothermia & acidosis. The storage temperatureof blood products of blood products at 1-6oC cancontribute to hypothermia in patients requiringmassive transfusion. For each 1oC decrease intemperature, coagulation factor activity decreasesby 10%. Below 34o C, clotting time prolongsplatelets pool within the spleen and there isimpaired adherence and aggregation. Significanthypocalcaemia (ionized calcium <0.6 mmol/L)induced by citrate binding to circulating serumcalcium and acidosis (PH<7.3) reduces theactivation of coagulation on platelet cell surfaceson platelet cell surfaces and disrupts haemo-stasis.15
Historically, ETIC was attributed to crystalloid andRBC transfusion without administration ofplatelets, plasma, or both. However, subsequentstudies in both adult and paediatric trauma patientsdemonstrated that ETIC was present in 24%, andup to 56% in severely injured patients, usuallywithin 30 min of injury, even before receiving RBCand fluid resuscitation.11,16-19, The presence ofETIC correlates with poor clinical outcomesindependent of the severity of injury.11,16-19 Inbrief, tissue injury from trauma or surgery releasestissue factor, locally and subsequentlysystematically, which activates coagulationpathways. This initiation results in massiveconsumptive coagulopathy leading to a DIC likesyndrome, which is most commonly seen inpatients with severe head injury or extensivemuscle damage.20,21
The administration of RBC units without additionalclotting factors or platelets during MT results infurther impairment of haemostasis from bothhaemodilution (dilutional coagulopathy andthrombocytopenia) and metabolic derangement(acidosis and hypocalcaemia from citrate in storagesolution, and hypothermia from refrigera-tion).15,22,23 All of these ‘exogenous’ factorscontribute to the vicious cycle of progressivecoagulopathy due to the ‘lethal triad’ of refractorycoagulopathy, progressive hypothermia, andpersistent metabolic acidosis.
Massive Transfusion in Clinical Practice Daanish Arefin Biswas et al 109

When to initiate MTP
Initiation of MTP was formerly under cliniciansconsideration. This intuition appears to have onlya 50% predictive value in identification of patientswho will need MTP.24 Recently, clinicians developedmassive resuscitation scoring systems toaccurately identify patients who will ultimatelyrequire large volume blood product resuscitationupon arrival to the emergency department. Earlyrecognition & prompt initiation of MTP,immediately in the emergency room rather thanlater in the operating room, improves both short-term and long-term survival.25 Implementationof MTP guidelines both decrease mortality and theoverall amount of blood use in 24 h, due to betterproximal resuscitation.26.
The German originated trauma associated severehemorrhage score (TASH) was the first massivetransfusion scoring system. It has 7 variablesinvolving history (gender), physical findings (FAST,long-bone or pelvic fractures), vital signs (heartrate, blood pressure),and laboratory values (basedeficit, hemoglobin).27
The Assessment of Blood Consumption score wasdesigned to be applicable on immediate arrival tothe emergency room without additional laboratorytesting or need for additional calculations. Itassigns one point to: Penetrating mechanism,heart rate > 90 bpm, positive FAST, or SBP < 90mmHg. An Assessment of Blood Consumptionscore of greater than 2 was determined to be theappropriate trigger for MTP, with a sensitivity andspecificity of 75% and 86%, respectively.28
Cessation of MTP may more reliant on clinicianconsideration given the potentially rapidly changingcurrent of the patients’ clinical condition in theshort hours after admission. Following surgicalcontrol of bleeding, the restoration ofhemodynamics, correction of acidosis andcoagulopathy, and signs of sufficient end organperfusion (mental status, urine output) all may beused as surrogates for adequate resuscitation.Despite aforementioned calculations for initiationand cessation of MTP, providers will often initiateMTP on the early evidence or concern forsignificant hemorrhage. It is our suggestion to placeinstitutional protocols depending on availablefacilities will save more lives. A National guidelineis necessary.
Current MT guidelines
Guidelines are designed to provide evidence based,well balanced information regarding the benefitsand limitations of therapeutic interventions. Twomajor guidelines are available for MT: theEuropean guidelines by the Task Force forAdvanced Bleeding Care in Trauma (updated in2013) and the Trauma Quality ImprovementProgram (TQIP) recommendations from theAmerican College of Surgeons.29 The Task Forcehas included a new section discussing theimplementation and adherence to evidence based,protocolled clinical practices relating to bloodtransfusion in bleeding trauma patients. Notably,a significant portion of these guidelines is dedicatedto a discussion of the utility of rapid and pertinentlaboratory tests, evaluation of clinically significanthemorrhage, and administration of appropriateblood products for resuscitation in a timelymanner. Similarly, the 2011 update on the clinicalpractice guidelines for blood conservation from theSociety of Thoracic Surgeons and the Society ofCardiovascular Anesthesiologists also advocatesthe judicious use of blood products, factorconcentrates, hemostatic agents, and blood salvageto minimize blood loss. In addition, the AmericanCollege of Surgeons has established the TQIP toprovide recommendations for the care provided totrauma patients. It also provides guidelines forMTPs, which emphasize tight collaboration amongblood banks, emergency departments,anesthesiologists, and trauma services. TQIPrecommends that an MTP needs to define protocoltriggers for activation or deactivation, an algorithmfor preparation and delivery of blood products,including continued support in the non-emergencydepartment (ED) setting. The guidelines advocatethe establishment of transfusion targets,recommend the use of pharmacologic hemostaticagents, and suggest ongoing evaluation ofcumulative MTP performance. A recent survey byTQIP evaluated over 180 registered trauma centerson their current MTP practices.
Massive transfusion protocols
One way to coordinate the care for patientsrequiring MT is to develop an institutional MTPto facilitate communication between differentservices (trauma, nursing, transfusion medicine,and other laboratories), avoid delay in clinical care,laboratory testing and blood product transfusion,
110 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

and nursing care. MTPs have demonstratedimproved patients survival and reduced rates oforgan failure and post-trauma complications.(30)The development, implementation, andcontinuous improvement of an MTP requireongoing collaboration between different clinicalservices.
When developing an MTP, determining qualityindicators will enable clear parameters to trackand trend, such as the time for productspreparation and issue, product wastage, laboratoryturnaround time, laboratory values, andindications for MTP in order to continuouslyimprove the MTP. An MTP should have thefollowing components:
1. When and who should initiate MTP.
2. Notification of the transfusion service andlaboratory regarding start and stop of MTP.
3. Laboratory testing algorithm [prothrombintime (PT), activated partial thromboplastin time(aPTT), fibrinogen level, blood gas, andcomplete blood count], and thrombo-elastography if available.
4. Blood product preparation and delivery (i.e. pre-determined transfusion packages).
5. Other patient care needs (such as bloodwarmers, nursing care).
MTPs can include preparation and administrationof blood products based on laboratory test results,predetermined transfusion packages orintegration of both.31 Although the number andtiming of blood component delivery, laboratorytesting algorithms, and other aspects of the MTPsvaries between institutions, most current MTPsuse predetermined transfusion packages.31 MTPsvary in their pre-determined transfusionpackages, but all include platelet and plasma unitswith RBC units.32-37 Furthermore, patients withobstetrical haemorrhage should also be monitoredclosely for fibrinogen level, because it has beenshown that women with fibrinogen level >400 mg/dl did not develop postpartum haemorrhage.Similarly, data from neurology and cardiacsurgery showed that there is increased bleedingtendency if the fibrinogen level is ,150 – 200 mg /
dl.38,39 Moreover, a retrospective review from aUS Army hospital demonstrated that increasingthe ratio of fibrinogen : RBC is associated withimproved survival to hospital discharge bydecreasing death from bleeding.40 Thus,monitoring fibrinogen level and/or earlytransfusion of fibrinogen concentrate orcryoprecipitate could be potentially beneficial.
The military uses fresh whole blood whenapheresis platelet products are not available. Inthe recent military experiences in Iraq andAfghanistan, whole blood transfusion comparedwith RBC, plasma, and apheresis platelet usereduced pulmonary and tissue oedema, whichdecreased the ventilation time and also allowedclosure of the abdomen with minimal delay.41
Furthermore, retrospective analysis suggestedthat patients who received both fresh whole bloodand component therapy had better clinicaloutcomes compared with those who received onlycomponent therapy.42 However, concern fortransfusion transmitted infections and transfusionassociated graft v host disease remains.43,44
Selection of blood products
Red blood cells
To minimize blood product wastage, most bloodbanks aim to transfuse the oldest units first.recently.45 Wang et al suggested that transfusingolder blood is significantly associated with anincreased mortality risk. The age of transfusedRBCs increased significantly when the patient wasswitched to type-specific RBCs.46
Immune-mediated hemolysis is another clinicalconcern during the MTP. Due to the emergentneed for blood products, routine pre transfusiontesting is bypassed and uncrossmatched Group ORhD negative RBCs are often given. This removalof safety assurances received from the antibodyscreen and product cross-matching leavesalloimmunized patients at increased risk for acuteor delayed hemolysis.47
In addition, residual plasma within Group O RBCunits can accumulate when large quantities ofGroup O RBC units are transfused. This maytheoretically lead to hemolysis due to ABOincompatibility.48,49
Massive Transfusion in Clinical Practice Daanish Arefin Biswas et al 111

Plasma
During massive hemorrhage, significant bloodvolume loss could lead to uncompensatedcoagulopathy. Until recently, universal Group ABplasma has been the standard product used duringMT when the patient’s blood group is initiallyunknown.
The selection of the plasma product is determinedby product availability and the coagulation factorcontent. Thawing large amounts of frozen plasmaduring an MTP presents a formidable logisticalchallenge to deliver the plasma products within5–10 minutes of the request. Fresh frozen plasmabe prepared within 6 hours of collection. Whenthawed it can be used with up to five more days ofshelf life mortality.50 Liquid plasma (LP) is plasmarecovered within 5 days of expiration from a WBproduct (never frozen); therefore, it has a shelflife of 26 days from the day of collection.
Platelet
After collection from blood donors, platelets aretypically stored between 20oC and 24oC withconstant agitation for up to 5 days. In vitro andanimal model-based studies have shown thatrefrigerated platelets have a shortened half-life incirculation.51,52 While refrigeration (1oC–6oC) isassociated with decreased platelet viability and postinfusion increments, cold platelets have beenshown to more readily aggregate in vitro and tohave a better metabolic profile.53,54 Duringemergency resuscitation, it is more importantachieving rapid hemostasis rather than a durableincrease in platelet count. Therefore, refrigeratedplatelets dedicated for emergency transfusion.
Whole blood
The direct use of WB for bleeding trauma patientsin a civilian setting has gained increasing attention.A platelet-sparing leukoreduction filter to be used.A single institution RCT evaluated the 24-hourtransfusion volume in trauma patients receivingeither WB or blood component therapy. While WBtransfusion did not significantly reduce thetransfusion volume in all patients, a portion of thetrauma patients transfused with WB did receivesignificantly less blood volume.55
Blood product ratios
Many early studies fresh frozen plasma (FFP) toblood and platelet ratios were affected by survivalor selection biases and mixed populations (56–58)With the findings of the Pragmatic RandomizedOptimal Platelet and Plasma Ratios (PROPPR)study group published in 2015, many hospitals havedecided on a 1:1:1 ratio of products (59) ThePROPPR group prospectively randomized patientsat 12 centers to receive 1:1:1 or 1:2:1. No increasein transfusion-related complications was noted inthe 1:1:1 group. A fibrinogen level lower than <100 mg/dL substantially increases in hospitalmortality.60
Hemostatic therapy /alternative medicationsincluded in MTP/ adjuncts to massive transfusion
TXA is a lysine analog which inhibits fibrinolysis.The antifibrinolytic effect is attributed to itscompetitive inhibition of the lysine binding site onplasminogen, resulting in the molecules stabilityand prevents further degradation of the existingclot61,62 In 2010 the Clinical Randomization of anAntifibrinolytic in Significant Hemorrhage(CRASH)-2 study reported an improvement in allcause mortality and mortality attributed tohemorrhage with the use of TXA within 3 h fromtime of injury which was a 20000 patient RTC inwhich the effects of TXA on mortality andtransfusion requirements in adult patients whowere traumatically injured and in hemorrhagicshock63. Regarding thromboembolic events, therewas an observed increase in pulmonary embolusand deep venous thrombosis in the MATTERsstudy.64,65
The use of supplemental fibrinogen, RecombinantFactor VII (rFVIIa), and prothrombin complex(PCC) as adjuncts have also been explored. Severalnonrandomized trials have evaluated the usefibrinogen in the trauma patient.69-68 In each ofthese studies there was a reduced requirementfor blood product transfusion and associatedreduced potential for multi-organ failure.
Prothrombin complex concentrate (PCC) has beenused to treat congenital coagulation disorders andfor warfarin reversal in patients with activebleeding or undergoing urgent procedures. To date,
112 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

there has not been any prospective randomizedcontrolled trial to evaluate the efficacy and safetyof PCC in massively bleeding patients. In addition,PCC might be associated with thromboembolic riskas shown in animal studies.69-70 Hence, it isrecommended that PCC usage should becontinually evaluated & risks & benefits of usingPCC as an adjunctive therapy in MTP should bediscussed.
Laboratory monitoring during MTP
MTP requires adequate laboratory support tooxygen-carrying capacity, haemostasis, andmetabolic status in order to address and correctabnormalities. In addition, laboratory results canbe used retrospectively to assess the need forMTP adjustment. A metabolic panel should beused to monitor metabolic abnormalities duringMT, such as hyperkalaemia and hypocalcaemia.Arterial blood gases measurement is helpful inmonitoring oxygenation. Monitoring haemostasisis challenging because there is no validatedcoagulation assay that can detect thecoagulopathies in massively bleeding patients.Conventional coagulation assays, such as PT,aPTT, and fibrinogen levels, are likely notavailable in realtime fashion. In addition, thesetests do not detect some haemostaticabnormalities, such as platelet dysfunction,hyperfibrinolysis, and factor XIII deficiency. Theyalso do not quantify the relative contribution ofprocoagulant and anticoagulant factors.71,72
.These do not predict the future need for MTPand have limited utility to direct ongoing bloodcomponent therapy in real time because of slowturnaround times.73
Recently, it has been suggested that point of carehaemostasis assays, such as thromboelastography(TEG) and rotational thromboelastometry(ROTEM), might be better at assessingcoagulopathy in patients requiring MT,74 Whichoffer clinicians a graphic representation of thecoagulation process. In addition, the parametersobtained from TEG/ ROTEM could provide aquantitative measure of individual components ofthe haemostatic process. Hence, guide bloodcomponent therapies in a more timely manner.74
There are several advantages of using TEG/ROTEM.10
1. Turn around time for these assays is shortercompared with conventional assays (15–30min);75
2. These assays can detect hyperfibrinolysis, animportant component of haemostaticabnormalities in patients with MT that cannotbe detected by PT and aPTT assays.74
3. Unlike the PT and aPTT that can only testsecondary haemostasis, whole blood assaysassess all phases of coagulation, such as thecontribution of platelets to primary haemostasisand factor XIII to cross-linking the fibrin clot.
4. TEG/ROTEM can be performed at the patient’strue temperature, which makes it moresensitive for detection of coagulopathy due tohypothermia.76
Equipment during a massive transfusion
Administration of large volumes of blood productsrequires adequate vascular access. Duringpaediatric trauma where massive haemorrhage issuspected, if no access is established in two attemptsthen, intraosseous access is appropriate. Bloodneed to be warmed and the rate of transfusion willindicate which method of warming will be mostsuitable. Warming via insulating iv tubing can beeffective or utilizing an in line warmer close tothe infusion site.
Blood salvage can be used in case of surgery.Fixed volume bowls are used or more recentlycontinuous disc or centrifugal processing allowingsmaller volumes of blood to be processed faster.77
Cell savers have an additional use as they can washPRBC before transfusion in cases where significantblood loss is expected.
Complications of MTP -
Besides the risk of transfusion reactions that occurwith single unit transfusions, patients with MTare at risk of other adverse events due to largetransfusion volumes. The patient should bemonitored closely for these complications becausethey might contribute further to coagulopathy.Paediatric patients, patients with pre-existingcardiac, hepatic, and renal disease, or older patientsare more at risk for having these complications.(Table 1).
Massive Transfusion in Clinical Practice Daanish Arefin Biswas et al 113

Table 1: Probable adverse events or reactions following massive transfusion.
Adverse events Potential treatments& prevention
Transfusion reaction
Allergic Can vary from simple urticaria to anaphylaxis. Steroid& antihistamine might be given.
Hemolytic transfusion reaction Might be reduced by transfusing group O RBC & AB(acute & delayed) plasma as emergency blood products
Febrile non hemolytic transfusion reaction Diagnosis of exclusion & symptomatic managementof fever
Immunological reactions
Transfusion related acute lung injury( TRALI) Can be reduced by transfusing male only plasmaTransfusion related immunomodulation (TRIM) Might be responsible for increased risk of bacterial
infection
Transfusion associated graft versus host disease Irradiation of cellular blood products in patients at(TA-GVHD) risk (such as neonate and immunosupreesed patients)
to prevent TA- GVHDPost transfusion purpura (PTP) Treated with IVIG infusion steroid or plasma
exchangeMetabolic complication
Hypocalcemia Due to citrate overload Monitor ionized calcium level and correct if from rapid transfusion necessary.
Hypomagnesaemia Because of large volume of magnesium poor fluidand citrate overload. Monitor ionized magnesiumlevel and correct if necessary.
Hypokalaemia Because of reentry into transfused RBC, release ofstress hormones or metabolic alkalosis. Monitorpotassium level & correct if necessary.
Metabolic alkalosis Because of citrate overload. Monitor acid base status.
Metabolic acidosis Because of hypoperfusion, liver dysfunction andcitrate overload. Monitor acid base status.
Hypothermia Because of infusion of cold fluid and blood products,opening of body cavities, decrease heat productionand impaired thermal control. Blood warmer shouldbe used.
Other adverse events
Haemostatic defects Result from complex mechanism.
Infection Can result from blood products or other resuscitationprocedures.
Transfusion associated circulatory Should be differentiated from TRALI. Infants andoverload (TACO) patients with preexisting cardiac disease are at
increased risk. Oxygen and diuretics can be used.
Air embolism A rare fatal complication. Instructions and orprotocols on how to use rapid infuser must befollowed.
114 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Conclusion
The finer points of massive transfusion, such asratios of blood products, adjuncts, and transfusiontriggers and endpoints will continue to be studiedand debated in the literature for years to come.However, it cannot be argued that a massivetransfusion protocol saves lives. A defined, hospital-specific MTP allows trained providers to recognizepatients at risk of high-volume blood loss early,initiation of massive transfusion quickly and hasspecific end points to limit over-transfusion. Werecommend that all centers that take care ofcritically ill patients of all varieties should evaluatethe literature and develop their own MT protocol.
Referenes:1. Callcut RA, Cotton BA, Muskat P, Fox EE, Wade CE,
Holcomb JB, et al. Defining when to initiate massivetransfusion: a validation study of individual massivetransfusion triggers in PROMMTT patients. J TraumaAcute Care Surg. 2013;74:59–65, 67–68.
2. Raymer JM, Flynn LM, Martin RF. Massive transfusionof blood in the surgical patient. Surg Clin North Am.2012;92:221 – 34.
3. Levy JH. Massive transfusion coagulopathy. SeminHematol. 2006;43:59 – 63.
4. Malone DL, Hess F JR, A. Massive transfusion practicesaround the globe and a suggestion for a common massivetransfusion protocol. J Trauma. 2006;60:91 – 6.
5. Deaths and Mortality Centers for Disease Control andPrevention [Internet]. 2010. Available from: http://www.cdc.gov/nchs/fastats/deaths
6. Sauaia A, Moore FA, Moore EE. Epidemiology of traumadeaths: a reassessment. J Trauma. 1995;38:185 – 93.
7. Holcomb JB, Jenkins D, Rhee P. Damage controlresuscitation: directly addressing the early coagulopathyof trauma. J Trauma. 2007;62:307 – 10.
8. Como JJ, Dutton RP, Scalea TM, Edelman BB, Hess J.Blood trans-fusion rates in the care of acute trauma.Transfusion. 2004;44:809 – 13.
9. Friedman AJ. Obstetric hemorrhage. J CardiothoracVasc Anesth. 2013;27:44 – 8.
10. Diab YA, Wong EC, Luban NL. Massive transfusion inchildren and neonates. Br J Haematol. 2013;161:15 –26.
11. Brohi K, Singh J, Heron M, Coats T. Acute traumaticcoagulopathy. J Trauma. 2003;54:1127 – 30.
12. Chesebro BB, Rahn P, Carles M. Increase in activatedprotein C mediates acute traumatic coagulopathy inmice. Shock. 2009;32:659 – 65.
13. Gruen RL, Brohi K, Schreiber M. Haemorrhage controlin se-verely injured patients.
14. Reiss RF. Hemostatic defects in massive transfusion:rapid diagnosis and management. Am J Crit Care.2000;9:158 – 65 66 – 7.
15. Lier H, Krep H, Schroeder S, Stuber F. Preconditionsof hemostasis in trauma: a review The influence ofacidosis, hypocalcemia, anemia, and hypothermia onfunctional hemostasis in trauma. J Trauma. 2008;65:951– 60.
16. Floccard B, Rugeri L, Faure A. Early coagulopathy intrauma patients: an on scene and hospital admissionstudy. Injury. 2012;43:26 – 32.
17. Hendrickson JE, Shaz BH, Pereira G. Coagulopathy isprevalent and associated with adverse outcomes intransfused pediatric trauma patients. J Pediatr.2012;160:204 – 9 3.
18. MacLeod JB, Lynn M, McKenney MG, Cohn SM, EarlyMM. J Trauma. 2003;55:39–44.
19. Patregnani JT, Borgman MA, Maegele M, Wade CE,Blackbourne LH, Spinella PC. Coagulopathy and shockon admission is associated with mortality for childrenwith traumatic injuries at combat support hospitals.Pediatr Crit Care Med. 2012;13:273 – 7.
20. Lustenberger T, Talving P, Kobayashi L. Earlycoagulopathy after isolated severe traumatic braininjury: relationship with hypoperfusion challenged. JTrauma. 2010;69:1410 – 4.
21. Talving P, Lustenberger T, Lam L. Coagulopathy afterisolated severe traumatic brain injury in children. JTrauma. 2011;71:1205 – 10.
22. Watts DD, Trask A, Soeken K, Perdue P, Dols S.Kaufmann C Hypo-thermic coagulopathy in trauma:effect of varying levels of hypo-thermia on enzymespeed, platelet function, and fibrinolytic activity. JTrauma. 1998;44:846 – 54.
23. Martini WZ, Holcomb JB. Acidosis and coagulopathy:the differen-tial effects on fibrinogen synthesis andbreakdown in pigs. Ann Surg. 2007;246:831 – 5.
24. Pommerening MJ, Goodman MD, Holcomb JB, WadeCE, Fox EE, Del Junco DJ, et al. Clinical gestalt and theprediction of massive transfusion after trauma. Injury.2015;46:807 –813.
25. Cotton BA, Dossett LA, Au BK, Nunez TC, RobertsonAM, Young PP. Room for (performance) improvement:provider-related factors associated with poor outcomesin massive transfusion. J Trauma. 2009;67:1004–1012.
26. Cotton BA, Gunter OL, Isbell J, Au BK, Robertson AM,Morris JA, et al. Damage control hematology: the impactof a trauma exsanguination protocol on survival andblood product utilization. J Trauma. 2008;64:1177–11821182–1183.
27. Yücel N, Lefering R, Maegele M, Vorweg M, Tjardes T,Ruchholtz S, et al. Trauma Associated SevereHemorrhage (TASH)-Score: probability of masstransfusion as surrogate for life threateninghemorrhage after multiple trauma. J Trauma. 2006;60:1228–1236 1236–1337.
Massive Transfusion in Clinical Practice Daanish Arefin Biswas et al 115

28. Nunez TC, Voskresensky D IV, LA S, R D, WD C, B.A.Early prediction of massive transfusion in trauma:simple as ABC (assessment of blood consumption)? JTrauma. 2009;66:346–352.
29. Spahn DR, Bouillon B, Cerny V. Management ofbleeding and coagulopathy following major trauma: anupdated European guideline. Crit Care. 2013;17(2):76.
30. Cotton BA, Au BK, Nunez TC, Gunter OL, RobertsonAM, Young PP. Predefined massive transfusionprotocols are associated with a reduction in organ failureand postinjury complications. J Trauma. 2009Jan;66(1):41–8; discussion 48-49.
31. Shaz BH, Dente CJ, Harris RS, MacLeod JB, HillyerCD. Transfusion management of trauma patients.Anesth Analg. 2009 Jun;108(6):1760–8.
32. Cotton BA, Guy JS, JA M Jr, Abumrad NN. The cellular,metabol-ic, and systemic consequences of aggressivefluid resuscitation strategies. Shock. 2006;26:115 – 21.
33. Cushing M, Shaz BH. Blood transfusion in traumapatients: unre.
34. Dente CJ, Shaz BH, Nicholas JM. Improvements inearly mortality and coagulopathy are sustained betterin patients with blunt trauma after institution of amassive transfusion protocol in a civilian level I traumacenter. J Trauma. 2009;66:1616 – 24.
35. Nunez TC, Young PP, Holcomb JB, Cotton BA. Creation,implemen-tation, and maturation of a massivetransfusion protocol for the exsanguinating traumapatient. J Trauma. 2010;68:1498 – 505.
36. O’Keeffe T, Refaai M, Tchorz K, Forestner JE, SarodeR. A massive transfusion protocol to decrease bloodcomponent use and costs. Arch Surg. 2008;143:686 – 9090 – 1.
37. Riskin DJ, Tsai TC, Riskin L. Massive transfusionprotocols: the role of aggressive resuscitation versusproduct ratio in mortality reduction. J Am Coll Surg.2009;209:198 – 205.
38. Gerlach R, Tolle F, Raabe A, Zimmermann M,Siegemund A, Seifert V. Increased risk forpostoperative hemorrhage after intra-cranial surgeryin patients with decreased factor XIII activity:implications of a prospective study. Stroke. 2002;33:1618– 23.
39. Blome M, Isgro F, Kiessling AH. Relationship betweenfactor XIII activity, fibrinogen, haemostasis screeningtests and post operative bleeding in cardiopulmonarybypass surgery. Thromb Haemost. 2005;93:1101 – 7.
40. Stinger HK, Spinella PC, Perkins JG. The ratio offibrinogen to red cells transfused affects survival incasualties receiving massive transfusions at an armycombat support hospital. J Trauma. 2008;64:79 – 85 85.
41. Spinella PC, Perkins JG, Grathwohl KW. Fresh wholeblood transfusions in coalition military, foreign national,and enemy combatant patients during Operation IraqiFreedom at a U.S. combat support hospital. World JSurg. 2008;32:2 – 6.
42. Spinella PC, Perkins JG, Grathwohl KW, Beekley AC,Holcomb JB. Warm fresh whole blood is independentlyassociated with improved survival for patients withcombat-related traumatic in-juries. J Trauma. 66:69 – 76.
43. Chandler MH, Roberts M, Sawyer M, Myers G. The USmilitary experi-ence with fresh whole blood during theconflicts in Iraq and Af-ghanistan. Semin CardiothoracVasc Anesth. 2012;16:153 – 9.
44. Gilstad C, Roschewski M, Wells J. Fatal transfusion-associated graft-versus-host disease with concomitantimmune hemolysis in a group A combat trauma patientresuscitated with group O fresh whole blood.Transfusion 2012. 52:930 – 5.
45. Zimring JC. Fresh versus old blood: are there differencesand do they matter? Hematology Am Soc Hematol EducProgram. 2013;651–655.
46. McDaniel LM, Triulzi DJ, Cramer J. Massive transfusionprotocol activation does not result in preferential use ofolder red blood cells. J Blood Transfus. 2014;328967.
47. Dutton RP, Shih D, Edelman BB, Hess J, Scalea TM.Safety of uncross-matched type-O red cells forresuscitation from hemorrhagic shock. J Trauma.2005;59(6):1445–1449.
48. McManigal S, Sims KL. Intravascular hemolysissecondary to ABO incompatible platelet products. Anunderrecognized transfusion reaction. Am J Clin Pathol.1999;111(2):202–206.
49. Fung MK, Downes KA, Shulman IA. Transfusion ofplatelets containing ABO-incompatible plasma: asurvey of 3156 North American laboratories. ArchPathol Lab Med. 2007;131(6):909–916.
50. Radwan ZA, Bai Y, Matijevic N. An emergencydepartment thawed plasma protocol for severely injuredpatients. JAMA Surg. 2013;148(2):170–175.
51. Murphy S, Gardner FH. Effect of storage temperatureon maintenance of platelet viability. N Engl J Med.1969;280(20):1094–1098.
52. Jansen AJ, Josefsson EC, Rumjantseva V. Desialylationaccelerates platelet clearance after refrigerationandinitiates GPIbalpha metalloproteinase-mediatedcleavage in mice. Blood. 2012;119(5):1263–1273.
53. Enhanced shear-induced platelet aggregation due tolow-temperature storage. Transfusion. 2013;53(7):1520–1530.
54. Reddoch KM, Pidcoke HF, Montgomery RK. Hemostaticfunction of apheresis platelets stored at 4 degrees Cand 22 degrees C. Shock. 2014;41 Suppl 1:54–61.
55. Cotton BA, Podbielski J, Camp E. A randomizedcontrolled pilot trial of modified whole blood versuscomponent therapy in severely injured patientsrequiring large volume transfusions. Ann Surg.2013;258(4):527–532 532–523.
56. Bhangu A, Nepogodiev D, Doughty H, Bowley DM.Meta-analysis of plasma to red blood cell ratios and
116 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

mortality in massive blood transfusions for trauma.Injury. 2013;44:1693–1699.
57. Godier A, Samama CM, Susen S. Plasma/platelets/redblood cell ratio in the management of the bleedingtraumatized patient: does it matter? Curr Opin.Anaesthesiol. 2012;25:242–247.
58. Hallet J, Lauzier F, Mailloux O, Trottier V, ArchambaultP, Zarychanski R, et al. The use of higher platelet. RBCtransfusion ratio in the acute phase of traumaresuscitation: a systematic review. 2013;41:2800–2811.
59. Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE,Podbielski JM, et al. Transfusion of plasma, platelets,and red blood cells in a 1: 1: 1 vs a 1: 1: 2 ratio andmortality in patients with severe trauma: the PROPPRrandomized clinical trial. JAMA. 2015;313.
60. Inaba K, Karamanos E, Lustenberger T, Schöchl H,Shulman I, Nelson J, et al. Impact of fibrinogen levelson outcomes after acute injury in patients requiring amassive transfusion. J Am Coll Surg. 2013;216:290–297.
61. Bailey AM, Baker SN, Weant KA. Tranexamic acid fortrauma-related hemorrhage. Adv Emerg Nurs J.2014;36:123–131 132–133.
62. Okamoto S, Hijikata-Okunomiya A, Wanaka K, OkadaY, Okamoto U. Enzyme-controlling medicines:introduction. Semin Thromb Hemost. 1997;23:493–501.
63. Roberts I, Shakur H, Coats T, Hunt B, Balogun E,Barnetson L, et al. The CRASH-2 trial: a randomisedcontrolled trial and economic evaluation of the effectsof tranexamic acid on death, vascular occlusive eventsand transfusion requirement in bleeding traumapatients. Health Technol Assess. 2013;17:1–79.
64. Morrison JJ, Dubose JJ, Rasmussen TE, MidwinterMJ. Military Application of Tranexamic Acid in TraumaEmergency Resuscitation (MATTERs) Study. ArchSurg. 2012;147:113–119.
65. Eckert MJ, Wertin TM, Tyner SD, Nelson DW, IzenbergS, Martin MJ. Tranexamic acid administration topediatric trauma patients in a combat setting: thepediatric trauma and tranexamic acid study (PED-TRAX. J Trauma Acute Care Surg. 2014;77.
66. Schöchl H, Solomon C, Traintinger S, Nienaber U,Tacacs-Tolnai A, Windhofer C, et al. Thrombo-elastometric (ROTEM) findings in patients suffering
from isolated severe traumatic brain injury. JNeurotrauma. 2011;28:2033–2041.
67. Schöchl H, Nienaber U, Maegele M, Hochleitner G,Primavesi F, Steitz B, et al. Transfusion in trauma:thromboelastometry-guided coagulation factorconcentrate-based therapy versus standard fresh frozenplasma-based therapy. Crit Care. 2011;15:83.
68. Aubron C, Reade MC, Fraser JF, Cooper DJ. Efficacyand safety of fibrinogen concentrate in trauma patients–a systematic review. J Crit Care. 2014;29:471 11–47117.
69. Mitterlechner T, Innerhofer P, Streif W. Prothrombincomplex concentrate and recombinant prothrombinalone or in combination with recombinant factor X andFVIIa in dilutional coa-gulopathy: a porcine model. JThromb Haemost. 2011;9:729–37.
70. Grottke O, Braunschweig T, Spronk HM. Increasingconcentra-tions of prothrombin complex concentrateinduce disseminated intravascular coagulation in a pigmodel of coagulopathy with blunt liver injury. Blood.2011;118:1943 – 51.
71. Tripodi A, Chantarangkul V, Mannucci PM. Acquiredcoagulation disorders: revisited using global coagulation/anticoagulation testing. Br J Haematol. 2009;147:77 –82.
72. Mann KG, Butenas S, Brummel K. The dynamics ofthrombin formation. Arterioscler Thromb Vasc Biol.2003;23:17 – 25.
73. Dzik WH. Predicting hemorrhage using preoperativecoagulation screening assays. Curr Hematol Rep.2004;3:324 – 30.
74. Davenport R, Khan S. Management of major traumahaemor-rhage: treatment priorities and controversies.Br J Haematol. 2011;155:537 – 48.
75. Bolliger D, Seeberger MD, Tanaka KA. Principles andpractice of thromboelastography in clinical coagulationmanagement and transfusion practice. Transfus MedRev. 2012;26:1 – 13.
76. Kettner SC, Kozek SA, Groetzner JP. Effects ofhypothermia on thrombelastography in patientsundergoing cardiopulmonary bypass. Br J Anaesth.1998;80:313 – 7.
77. Smith C, K. Principles of fluid and blood warming intrauma. Int Trauma care (ITACCS. 2008;19:71–9.
Massive Transfusion in Clinical Practice Daanish Arefin Biswas et al 117

Endogenous Endophthalmitis Associated with
Liver Abscess: A Case ReportMowsumi Chowdhury1, Sohel Ahmed2, Chandra Shekhar Majumder3, Robiul Islam4
Abstract
Endogenous endophthalmitis associated with a liver abscess is a rare combination of
diseases.We treated such a 34-year-old female diabetic patient admitted in the medicine
ward with abdominal pain, high fever and debilitating health condition. The diagnosis of
the liver abscess was established by clinical evaluation aided by ultrasonography of the
abdomen. She was treated by broad-spectrum antibiotics, insulin and aspiration of pus
under ultrasonography guidance. After 48 hours she was referred to the department of
ophthalmology with pain, redness, blurring of vision in her right eye. Clinical examination
revealed anterior uveitis with hypopyon, vitreous haze and absent red fundal glow, B-scan
ultrasosnography and vitreous sampling showed feature of endophthalmitis. Patient was
treated with intravitreal antibiotics and topical medications but final visual outcome was
poor.
Case Report
Key words:
Endogenous Endophthalmitis,Liver Abscess
Article information
Received: 01.11.2020Accepted: 30.12.2020
Cite this article:
Chowdhury M, Ahmed S,Majumder CS, Islam R.Endogenous Endophtha-lmitis Associated with LiverAbscess: A Case Report. SirSalimullah Med Coll J 2020;28: 118-112
Sir Salimullah Med Coll J 2020; 28: 118-120
1. MS Resident, Phase-B, Department of Ophthalmology, Sir Salimullah Medical College, Dhaka2. MS Resident, Phase-B, Department of Ophthalmology, Sir Salimullah Medical College, Dhaka3. Professor and Head, Department of Ophthalmology, Sir Salimullah Medical College, Dhaka4. Assistant Professor, Department of Ophthalmology, Sir Salimullah Medical College, DhakaAddress of correspondence: Dr. Mowsumi Chowdhury. MS Resident, Phase-B, Department of Ophthalmology, SirSalimullah Medical College, DhakaE-mail: [email protected]
Introduction
Endogenous endophthalmitis is an intraocularinfection, occurs due to haematogenous spread oforganism from a systemic source of infection. Itmay result in severe loss of vision with devastatingocular complications. It is common in patients withcomorbid conditions like diabetes mellitus,immunocompromised state, extensive gastro-intestinal surgery, endoscopy, and dentalprocedures. The extraocular infection sources arehepatobiliary infection including pyogenic liverabscess, urinary tract infection, peumonia, lungabscess, indwelling catheter and dialysis vascularaccess. In South-East Asia, the liver abscess is thecommonest extraocular infection source, andKlebsiella pneumoniae is the commonest
organism.1 However, Endogenous KlebsiellaEndophthalmitis is associated with a poor visualoutcome.2 We treated such a diabetic patientwhere, despite all measures, she lost right eyevision. As it is a rare but exciting case, we wish topublish it with useful clinical information.
Case report
A 34-year-old female patient was referred to thedepartment of Ophthalmology with the complaintsof pain, redness and blurring of vision in the righteye for two days. Initially, she was admitted tomedicine ward with complaints of fever with chillsand rigor, abdominal pain and vomiting and severeweakness. It was diagnosed as a case of liverabscess by clinical evaluation and ultrasonogram

(USG) of the abdomen (Figure-1). She was diabeticbut normotensive. Accordingly, she was treatedthere with intravenous Ceftriaxone andMetronidazole in an adequate dose. Ultraso-nography guidance aspiration of pus from theabscess was done and sent for C/S and cytology.The C/S showed growth of Klebsiella. However,cytology was negative for malignant cells.
We took history and performed a thorough clinicalexamination and found mildly anaemic andmalnourished. The body temperature was 1000F,pulse 100 beats/minute and BP: 110/70 mm of Hg.On ocular examination, visual acuity in the righteye was hand movement, pupillary light reactionwas sluggish. Slit-lamp examination revealed ciliaryinjection, multiple keratic precipitates in cornea,cells (2+), moderate flare and hypopyon of about 2mm in height (Figure-2). The red fundal glow wasabsent, and fundus could not be visualized. Lefteye examination showed normal findings withvisual acuity 6/6.
We performed B-scan ultrasonography of the righteye revealed vitreous opacity with posteriorvitreous detachment (Figure-3). The vitreoussample was sent for Gram staining and culturesensitivity. The staining showed Gram-negativebacilli 3+ and fungal element and culture yieldedgrowth of Klebsiella species. Our diagnosis was acase of Endogenous Endophthalmitis of the righteye. We performed counselling repeatedly aboutthe disease, the consequences, including her righteye vision and the treatment options.
Accordingly, we treated her with intravitrealinjection Ceftazidime 2 mg/0.1 ml and Vancomycin2 mg/0.1 ml. We also applied topical moxifloxacin,corticosteroid and anticholinergic and followed hernext 24 hours. However, her eye condition did notimprove, and we used a second dose of intravitrealantibiotic, Ceftazidime 2 mg/0.1 ml andVancomycin 2 mg/0.1 ml. Despite this treatment,there was no improvement after the next 24 hoursand patient was suggested for pars planavitrectomy. But the patient denied it. Follow up
Fig.-1
Fig.-2
Fig.-3
Endogenous Endophthalmitis Associated with Liver Abscess Mowsumi Chowdhury et al 119

after one week showed that her right eye visionwas reduced to no perception of light. However,the general condition improved, fever subsided.We omitted intravenous infusion of antibiotics andprescribed oral Cefixime 200 mg twice daily forone week. Subsequently, she lost our follow up.
Discussion
Endogenous endophthalmitisis is an uncommonocular condition having devastating ocularcomplications. A most common cause in East Asiais Klebsiella associated pyogenic liver abscess2.The significant risk factor for developingendogenous endophthalmitis is an immuno-compromised state such as diabetes mellitus,malignancy, SLE, HIV infection. The criteria fordiagnosis of endogenous endophthalmitis includedin a study are: 1) posterior and/ or anterior ocularinflammation for which no aetiology other thaninfection is identified 2) positive micro-organismsare obtained from vitreous humor, blood or otherextraocular sites 3) primary extraocular source isidentified 4) no prior ocular surgery or trauma inthe affected eye2.
In our case, the clinical findings, B scanultrasonography, vitreous tap for Gram stainingand culture, liver abscess on USG, microbiologyof aspirated pus from liver abscess confirmed thediagnosis. Plain X-ray chest, routine examinationof urine, liver function tests were done to rule outother source of systemic infection. EndogenousKlebsiella Endophthalmitis is associated with gravevisual outcome even with aggressive treatment.Klebsiella Pneumonia is a highly virulent organismand causes rapid, irreversible photoreceptordamage as early as 48 hours after infection2.Yanget al found early diagnosis and prompt treatmentwithin 48 hours may salvage vision in somepatients2. Therefore, prompt treatment withempirical antibiotic should be started and it canbe modified according to C/S findings3,4. However,eye symptoms may be ignored while managingcrucial systemic condition that attributed delayeddiagnosis and poor outcome5 and our case is aunique example of it. The patient was referred tous 48 hours after onset of visual symptoms as shewas initially admitted and treated in medicine unitfor liver abscess. We treated the patient withintravitreal injection of Ceftazidime 2 mg/0.1 mland Vancomycin 2 mg/0.1ml twice within 48 hoursaccording to the protocol of treatment. However,
her eye condition did not improve. We advised thepatient for pars plana vitrectomy, but the patientdenied. In a study, Lim WS in 2020 noticeda littlebetter outcome with intravitreal Ceftriaxone andWang Y in a study supported initial pars planavitrectomy with intravitreal antibiotic and foundvisual outcome CF or better in 31% patients butin others overall visual outcome was poor4,5.
Conclusion
Patients of endogenous endophthalmitis associatedwith a liver abscess may present with abdominalpain, high fever and debilitating general conditionand get admission in medicine unit. In such apatient, the early symptoms of endogenousendophthalmitis may be missed or ignoredmanaging the general critical condition. Therefore,diagnosis is late, and despite all measures, theresults are disappointing with a loss of vision.Therefore, early diagnosis and treatment ofendogenous endophthalmitis in a liver abscesspatient is very important satisfactory visualoutcome.
Conflict of interest: None
Acknowledgement
We are grateful to the Department of Medicinefor referring a rare and interesting case. We arealso thankful to the patient for her consent to usethe images, pictures and treatment material inthe article’s publication.
References1. CiprianDanielescu, Nicoleta Anton, Horia Tudor Stanca,
MihneaMunteanu, “Endogenous Endophthalmitis: AReview of Case Series Published between 2011 and2020”, Journal of Ophthalmology 2020; vol. 2020, ArticleID 8869590, 13 pages.
2. Yang SC, Tsai HY, Sung CS, Lin HK, Lee FL, Hsu WM.Endogenous Klebsiellaendophthalmitis associated withpyogenic liver abscess. Americal Academy ofOphthalmology. 2007; 114(5): 876-880.
3. Brinbaum F, Gupta G. Endogenous Endophthalmitis:Diagnosis and Treatment. American academy ofOphthalmology. Ophthalmic Pearl. Eye Net Magazine.June 2016. Available from URL:https://www.aao.org/eyenet/article/endogenous-endophthalmitis-diagnosis-treatment.
4. Lim WS, Sung Y, Kwon HJ, Song WK. Case Report:Endogenous Endophthalmitis associated with liverabscess successfully treated with vitrectomy andintravitreal empirical antibiotic injections. Hndawi CaseReports in Ophthalmic Medicine2020; vol 2020, ArticleID 8165216: 4 pages.
5. Wang, Y., Wang, X. & Di, Y. Surgery combined withantibiotics for the treatment of endogenousendophthalmitis caused by liver abscess. BMC InfectiousDiseases. 2020; 20: 661.
120 Sir Salimullah Med Coll J Vol. 28, No. 2, July 2020

Obituary News
Sir Salimullah Med Coll J 2020; 28: 121
Dr. ASM Hasanuzzaman Sahin
Associate ProfessorDepartment of Paediatric Surgery, SSMCDied on 10th January 2021 at the age of 52 yearsHe was suffering from Pleural mesothelioma
Dr. Farhana Ahmed Jewel
Assistant ProfessorDepartment of Obstretrics and Gynaecology, SSMCJoint Secrary, SSMC Teachers AssociationDied on 5th November 2020She was suffering from ovarian cancerMay almighty bless the departed soulsOur heartiest commiseration to the deceased’s family.Our prayers are with them during this difficult moment of their life.