Capturing Christ's Tears: in Medieval and Early Modern France

Shocked into Tears 1
Shocked into Tears:
Depression and Posttraumatic Stress Disorder in a
Sample of Syrian Refugees
Amanda Aoun, Lea Debal, and Amanda Raidy
Notre Dame University

Shocked into Tears 2
Abstract
This study examined the levels of depression and posttraumaticstress disorder in Syrian refugees in Lebanon using the BeckDepression Inventory (21 items) and the PTSD Checklist (17items). 94 acceptable participant responses were considered inthe study. All participants were above the age of 18. High levelsand an existing correlation between the two disorders wereexpected as well as greater scores and correlations for womencompared to men. Moderate levels of depression were found whilehigh degrees of PTSD were recorded. Males scored higher thanfemales in both scales but females had a higher correlationbetween the disorders. The study suggests that: refugees areprone to develop both posttraumatic stress disorder anddepression; a positive correlation exists between the disorders;male refugees develop higher degrees of PTSD and depression thanfemales and females have a greater possibility of developing oneof the disorders when the other is present.

Shocked into Tears 3
Shocked into Tears: Depression and Posttraumatic Stress Disorderin a
Sample of Syrian Refugees
“You do not need papers to tell you how depressed we are,
you can see it on our faces” said a refugee woman cradling her
infant boy (13/12/2013).
“I’m sorry, it upsets me too much to think of these
questions” said various refugee men and women across the field
(23/12/2013).
Depression is a common and significant mood disorder which
impairs daily functioning in various ways. As with most
psychiatric illnesses, depressed people rarely seek treatment. In
the cases of patients who pursue treatment, the combination of
medication and psychotherapy is usually effective (World Health
Organization, n.d.). Depression is characterized via various
symptoms. According to the text revised fourth edition of the
Diagnostic and Statistical Manual (DSM-IV-TR), the symptoms of
depression are: “depressed mood most of the day, diminished
interest or pleasure in all or most activities, significant
unintentional weight loss or gain, insomnia or sleeping too much,
agitation or psychomotor retardation noticed by others, fatigue

Shocked into Tears 4
or loss of energy, feelings of worthlessness or excessive guilt
and diminished ability to think or concentrate, or
indecisiveness” (American Psychiatric Association, 2000).
A person develops Posttraumatic Stress Disorder (PTSD) after
surviving a traumatic incident which may have involved physical
harm. The disorder was brought to light due to its context in
war-related events. However, it was then also found in people who
suffered from other terrifying events such as rape or accidents
(National Institute of Mental Health, n.d.). It is indicated by
symptoms such as repetitive intrusive thoughts and memories of a
traumatic event, nightmares, avoidance of situations or people
related to the event, and emotional numbing (American Psychiatric
Association, 2000). Similarly to depression, both
psychopharmacology and psychotherapy are combined in the
treatment of patients with post-traumatic stress disorder (The
National for PTSD).
According to the United Nations, a person who was obligated
to leave their country due to the presence of maltreatment, war,
or violence is coined a refugee (UN refugees, 2013).
Specifically, refugees of Syrian nationality found shelter in

Shocked into Tears 5
Turkey, Jordan, Iraq, Egypt and Lebanon mainly. The Lebanese
government estimates that there are around one million Syrian
refugees in Lebanon. According to the UNHCR, over 857 thousand
refugees have been recorded to this date while almost 56 thousand
await registration. In 2013 alone, over 700 thousand refugees
were registered in Lebanon (UNHCR, 2013).
The results found across various studies were all
complementary in the sense of concept. Refugees are expected to
have an elevated level of depression (Cummings, Sull, Davis &
Worley, 2011). Studies done on PTSD and depression in refugee
children showed a significant correlation between them
(Heptinstall, Sethna & Taylor, 2004). In South Lebanon, the
prevalence of PTSD in Lebanese ranged from 17.6 % to 33.3% across
six villages, while the prevalence of depression varied from 9.2%
to 19.7% (Farhood & Dimassi, 2011). According to the Psychosocial
Assessment of Displaced Syrians in Lebanon, the most cited impaired
tasks were self-neglect, less productivity, isolation, fatigue,
inability to communicate, and self alienation ranging from 25% to
60% of the sample. The most mental health related problems
recorded are anxiety, depressed feelings, lethargy, eating

Shocked into Tears 6
problems, and sleeping problems across 33% to 70% of the sample
(International Medical Corps, 2011).
Due to the little or no research done on Syrian Refugees in
Lebanon and in other countries of the region, our current study
aims at examining the levels of PTSD and depression in Syrian
Refugees found in Lebanon.
Hypothesis 1: Refugees will show high levels of depression and Post-
traumatic stress disorder.
Hypothesis 2: Depression will correlate positively with PTSD.
Hypothesis 3: Females will have higher levels of depression and PTSD
than males.
Hypothesis 4: Females will have a higher correlation between
depression and PTSD than males.
Methods
The scales were distributed to a total of 130 Syrian
refugees waiting for registration at the UNHCR branch found in
Jnah. A total of 94 acceptable questionnaires were completed. All
participants were above the age of 18 and varied in gender with a
ratio of 9:11 males to females. Some of the chosen participants

Shocked into Tears 7
were illiterate and were read to. The questionnaire required
approximately 10 minutes to complete. It involved an informed
consent form, two scales testing the levels of depression and
PTSD, and inquiry about the participants’ age and gender.
The chosen scale to test depression was the Beck Depression
Inventory (BDI). The used version was a previously translated and
validated scale. A former study done to test the validation of
the Arabic BDI showed internal consistency and stability
affirming its reliability. The scale results were also compared
to the diagnoses of Arab clinicians which confirmed the high
degree of validity of the chosen BDI (West, 1985). The BDI
consists of 21 items covering the various symptoms of depression.
Each item provided the participant with four options specific to
the item. The options were presented in increasing order of
intensity and numbered 1 through 4.The sum of the BDI answers are
put into a range of normal, slight depression, moderate
depression, and severe depression according to ranges of 0 to 11,
12 to 19, 20 to 27, and 28 to 63 respectively.
As for the scale chosen to test PTSD, the PTSD Checklist
(PCL) was used. The PCL’s reliability was tested in a previous

Shocked into Tears 8
study proving high internal consistency (International Society
for Traumatic Stress Studies, 1993). The PCL is formed of 17
items testing the symptoms of PTSD. A Likert scale was used
ranging from 1 to 5 (1 being “Not at all” and 5 being
“Extremely”). The scoring of the PCL is also based on the sum of
the chosen numbers and is split into four categories. People
having little or no symptoms of PTSD scored between 17 and 27.
Participants who scored either 28 or 29 have some PTSD symptoms.
Scores between 30 and 44 imply moderate to moderately high
severity of PTSD symptoms and scores between 45 and 85 represent
a high severity of symptoms.
Participants were given consent forms which they read
carefully and agreed to. Each consent form contained an
identification number. The consent form thoroughly explained the
purpose, content and confidentiality of the study. It also
included the freedom to refuse or withdraw, the possible
disadvantages of taking part in the study and the use of the
filled information. It provided the participants with the
required contact information in the case of further inquiries.
The participants kept a copy of the consent form which was

Shocked into Tears 9
presented in Arabic. The form was both translated and back-
translated from an English version prior to distribution by the
authors of this article. Since no deception was used throughout
the study, debriefing was not necessary. The two scales were
counterbalanced in order to test if the chronology of the scales
would affect the answers of the participants. They were coined as
Version A, PCL before BDI, and Version B, BDI before PCL. In
contrast to the BDI scale that was already translated, the PCL
scale was retrieved in English, translated and back-translated by
the authors of this article. The freedom to withdraw was highly
emphasized when approaching the participants. In case any
difficulties came up when filling the scales, participants were
explained to. However, if participants faced emotional
disturbances, they were informed that they had the freedom to
skip the item or the entire scale or even withdraw from the
entire study.
The answers of each participant were then entered
into the IBM Statistical Package for the Social Sciences (SPSS)
version 21 along with the gender and age.

Shocked into Tears 10
The data was then checked for normality via the formation of
histograms and tests of skewness and kurtosis. Finally, data
analysis was done to retrieve frequencies (mean, median mode,
range, minimum, maximum) and to test correlations and t-testing
following the standardization of the results.
Results
Before the initiation of analysis the data was checked for
accuracy of entry and missing values. Missing values on both
scales exceeded 5% of the cutoff and they were replaced using
expectation maximization. All scores were standardized across the
items of both scales. Univariate Outlier Analysis using z-scores
found no outliers on both scales. All scores were therefore
retained. Normality of the data for all continuous variables was
checked and confirmed through the standardized kurtosis
statistics, standardized skew statistics (z skew) and histograms.
There was no significant difference between the two
counterbalanced versions. This implies that the order of the
scales does not affect the scores. Reliability of the scales was

Shocked into Tears 11
tested. Cronbach’s alpha was calculated to be 0.81 which confirms
that the study is reliable.
In respect to the first hypothesis, participants were
expected to show high levels of both PTSD and depression based on
our scales. The sum of each participant’s responses was
calculated per scale. A descriptive analysis of the sums was done
to calculate the mean, median, mode, standard deviation, minimum
and maximum of the results. Results are shown in Table 1. The
mean, median, and mode of the participants were all between 20
and 27 which is the range of moderate depression (Mean=25.15,
Median=24.00, Mode=25.00). As for the PCL, the mean and median of
the scores were between 45 and 85 which is the range of high
severity of PTSD symptoms (Mean=50.37, Median=51.00). However,
the mode of the scores was between 30 and 44 which is the range
of moderate to moderately high severity of PTSD symptoms
(Mode=41.00). The results show that both the average and the
majority of the participants in the study are moderately
depressed which is lesser in degree than expected in the
hypothesis. Additionally, the results prove that the average of
the participants’ scores shows a high level of PTSD severity

Shocked into Tears 12
which confirms our hypothesis. On the other hand, the outcome of
the statistical analysis shows that the majority of the
participants had moderate to high severity of PTSD symptoms which
is subordinate to the expected level.
As for the second hypothesis, a positive correlation between
PTSD and depression was expected. A Pearson Correlation of the
scores was calculated. Results are shown in table 2. Since there
exists a correlation of 0.38, which is considered to be a weak
correlation but nevertheless a positive one, the hypothesis was
confirmed (p>0.01). Additionally, the correlation between age and
depression was calculated. Results showed a negative weak
correlation (r= -0.233, p>0.05). This means that as age
increased, the scores of our participants on the BDI decreased.
Similarly, the correlation between age and PTSD was also
calculated. Results showed an almost null correlation (r= -
0.087). This showed that there is no notable relationship between
age and PTSD scores.
The third hypothesis expected higher results on the BDI and
PCL for females compared to males. The means of both PTSD and

Shocked into Tears 13
depression were calculated based on gender. The results are shown
in table 3. Variance t tests on depression levels found for
females and males were insignificant (Mean males = 1.20; Mean
females = 1.17). Differences on means on the PTSD levels
indicated a significant difference between means of males and
females (Mean males = 3.16; Mean females = 2.93). The results
show that male and female Syrian refugees received similar scores
on the BDI indicating similar levels of depression. To the
contrary, the results show that males scored significantly higher
than females on the PCL suggesting a higher level of PTSD in
males. This shows that this hypothesis is incorrect.
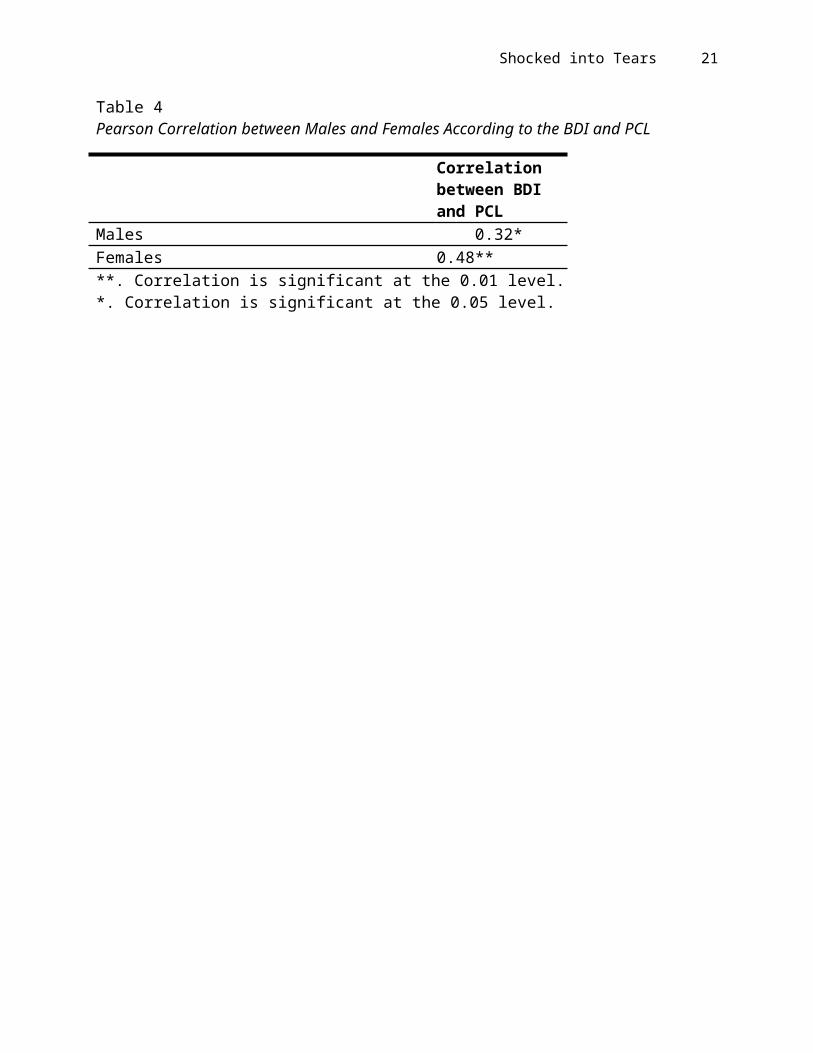
The expectation that females will have a higher correlation
between PTSD and depression than males forms the fourth
hypothesis. A Pearson Correlation was calculated. The results are
shown in Table 4. Males showed a correlation of 0.32 (p>0.05)
while females showed a correlation of 0.48 (p>0.01). The results
show that females who have one of depression or PTSD are more
likely to have the other as well than males which confirms the
hypothesis.

Shocked into Tears 14
The sum of each participant’s scores on each scale were
calculated and put into the suitable range. 5.3% of participants
were recorded to have normal results on the BDI. 23.4% had a
slight score of depression while 31.9% had a moderate degree.
Finally, 39.4% of the participants were classified as having a
severe degree of depression. As for the PCL, 1.1% of participants
had little to no severity and 1.1% had some PTSD symptoms. 34%
were recorded to have a moderate to moderately high level of PTSD
symptoms while a total of 63.8% of participants were scored as
having a high severity of PTSD symptoms.
Discussion
The purpose of the study was to assess the levels of PTSD
and depression in a sample of Syrian refugees. Four predictions
were made prior to the study: high levels of PTSD and depression,
a positive correlation between PTSD and depression, greater
scores for females than males, and a greater correlation between
PTSD and depression for females than males.
The findings of this study are consistent with the results
of Cummings, Sull, Davis and Worley (2011) where the majority of

Shocked into Tears 15
the refugees are considered to be depressed. The results of PTSD
are also similar to those recorded in a study conducted with
Bosnian refugees (Vojvoda, Weine, McGlashan, Becker & Southwick,
2008). However, the results are more amplified than those found
in a study done on Lebanese citizens also testing for PTSD and
depression (Farhood & Dimassi, 2011). In the study of Farhood and
Dimassi, results showed that there is a minor prevalence of PTSD
and depression in participants of the area. The findings of this
study, on the other hand, recorded that the majority of
participants were depressed and had sufficient symptoms of PTSD.
The results showed that the average and the majority of the
participants in the study are moderately depressed. The average
of the participants’ scores also shows a high level of PTSD
severity. However, the majority of the participants had moderate
to high severity of PTSD symptoms. This may be caused by the
difficulties the refugees underwent in both the physical and
psychological damages caused by war and fleeing their country.
Statistical analysis of the results showed a positive correlation
between PTSD and depression. A significant comorbidity between
PTSD and depression has been previously established (Campbell et

Shocked into Tears 16
al., 2007). Additionally, males scored higher than females on
both scales but females showed a greater correlation between PTSD
and depression than males. Males may have scored higher because
they may have been more exposed to the direct traumas of war than
females since few or no women are involved in direct battle.
Also, women are more prone than men to develop depression so
perhaps developing PTSD eases the development of depression and
thus explains the higher correlation (Noble, 2005).
There were various limitations to the study. One main
difficulty faced throughout the study was that a variety of
participants was emotionally unable to complete both scales and
decided to skip one of them. This caused the elimination of about
20 questionnaires. Also, since some of the participants were
illiterate and read to, their answers might have been compromised
by the idea of declaring their personal responses. Some of the
refugees became very emotionally touched and terminated the study
without completion or completed the study while crying however
their freedom to withdraw was repeated to them. In addition, the
participants were awaiting registration and might have been
preoccupied with the many forms they had to fill and the children

Shocked into Tears 17
they had to care for while waiting. As for the questionnaire
itself, two main weaknesses existed. The first weakness was that
the used version of the BDI was not the most recent one. The
second limitation was the inability to find a proper Arabic
translation for an item of the PCL (item #12) which might have
been misrepresented in the scale.
In conclusion, the study provided a valid understanding
about the levels of PTSD and depression in male and female Syrian
refugees. It showed that significant degrees of both disorders
were present in the sample and had a positive correlation
relationship. This study and future studies contributed to the
understanding of refugees as a whole and their psychological
difficulties. The International Medical Corps has taken
consideration of the assistance this issue requires. “While
social and outreach workers have been deployed in the North by
other agencies, there is a need for capacity building of non-
specialized staff, including community workers, volunteers, and
NGO staff to provide basic emotional and practical support to
individuals and families crossing the border” (International
Medical Corps, 2011).

Shocked into Tears 18

Shocked into Tears 19
Table 1Scale Descriptives (1)
Sum of Beck Depression Inventory Scores
Sum of PTSD Checklist Scores
Mean 25.15 50.37Median 24.00 51.00Mode 25.00a 41.00a
Standard Deviation 9.68 12.34Minimum 1.00 1.00Maximum 4.00 4.00a. Multiple modes exist. The smallest value is shown.
Table 2Pearson Correlation between the BDI and the PCL
Mean of Beck Depression Inventory
Mean of PTSD Checklist
Age
Mean of Beck Depression Inventory Correlation
1.00
Mean of PTSD Checklist Correlation
0.384** 1.00
Age Correlation -0.233* -0.087 1.00**. Correlation is significant at the 0.01 level.*. Correlation is significant at the 0.05 level.
Table 3Scale Descriptives (2)
Mean of Beck Depression Inventory Scores
Mean of PTSDChecklist

Shocked into Tears 20
Males 1.21 3.16Females 1.17 2.93
Shocked into Tears 21
Table 4Pearson Correlation between Males and Females According to the BDI and PCL
Correlation between BDI and PCL
Males 0.32*Females 0.48****. Correlation is significant at the 0.01 level.*. Correlation is significant at the 0.05 level.

Shocked into Tears 22
References
American Psychiatric Association. (2000). Diagnostic and Statistical Manual.
Campbell D. et al. (2008). Posttraumatic Stress Disorder Symptomsin Bosnian Refugees 3 1/2 Years After Resettlement.
Cummings S,. Sull L., Davis C., Worle N. (2011). Correlates of Depression among Older Kurdish Refugees.
Farhood L., Dimassi H. (2011). Prevalence and Predictors for Post-traumatic Stress Disorder, Depression and General Health in a Population from Six Villages in South Lebanon.
Heptinstall E., Sethna V., Taylor, E. (2004). PTSD and Depressionin Refugee Children.
International Medical Corps. (2011). Psychosocial Assessment of Displaced Syrians.
International Society for Traumatic Stress Studies. (1993). Posttraumatic Stress Disorder Checklist.
National Institute of Mental Health. (n.d.). Post-traumatic Stress Disorder.
Noble R. (2005). Depression in Women.
UN Refugees. (2013). What Is a Refugee?
UNHCR. (2013). Syria Regional Refugee Response.
Vojvoda D., Weine SM., McGlashan T., Becker DF., Southwick SM. (2008) Posttraumatic Stress Disorder Symptoms in Bosnian Refugees3 ½ Years After Resettlement.
West J. (1985). An Arabic Validation of a Depression Inventory.
World Health Organization. (n.d.). Depression.
Copyright © 2022 FDOKUMEN