
Serum HBs Ag and anti HBs in Brazilian families of index cases with Hepatitis
29
1 1 Title Serum HBsAg and anti-HBs in Brazilian families of index cases with Hepatitis B Virus Chronic Liver Disease: Comparison of Oriental and Occidental origin. Flair J Carrilho *1 , Suzane K Ono-Nita 1 , Rita A Cardoso 1 , Luís EP Fonseca 1 , José EM Medeiros-Filho 1 , Eduardo LR Cancado 1 , João RR Pinho 1 , Venâncio AF Alves 2 , Luiz CC Gayotto 2 , Luiz C Da Silva 1 Address: 1 Hepatology Branch, Department of Gastroenterology and 2 Department of Pathology, University of São Paulo School of Medicine, São Paulo, Brazil E-mail: Flair J Carrilho * - [email protected] ; Suzane K Ono-Nita - [email protected]; Rita A Cardoso - [email protected] ; Luís EP Fonseca - [email protected]; José EM Medeiros-Filho – [email protected] ; Eduardo LR Cancado – [email protected] ; João RR Pinho – [email protected]; Venâncio AF Alves - [email protected]; Luiz CC Gayotto - [email protected]; Luiz C Da Silva - [email protected] * Corresponding author
Transcript of Serum HBs Ag and anti HBs in Brazilian families of index cases with Hepatitis
11
Title
Serum HBsAg and anti-HBs in Brazilian families of index cases with Hepatitis
B Virus Chronic Liver Disease: Comparison of Oriental and Occidental origin.
Flair J Carrilho*1, Suzane K Ono-Nita1, Rita A Cardoso1, Luís EP Fonseca1, José
EM Medeiros-Filho1, Eduardo LR Cancado1, João RR Pinho1, Venâncio AF Alves2,
Luiz CC Gayotto2, Luiz C Da Silva1
Address: 1Hepatology Branch, Department of Gastroenterology and 2Department
of Pathology, University of São Paulo School of Medicine, São Paulo, Brazil
E-mail:
Flair J Carrilho* - [email protected];
Suzane K Ono-Nita - [email protected];
Rita A Cardoso - [email protected];
Luís EP Fonseca - [email protected];
José EM Medeiros-Filho – [email protected];
Eduardo LR Cancado – [email protected];
João RR Pinho – [email protected];
Venâncio AF Alves - [email protected];
Luiz CC Gayotto - [email protected];
Luiz C Da Silva - [email protected]
* Corresponding author
22
Background
Several sero-epidemiological studies in the general and blood-donor populations
have identified asymptomatic carriers of the viral surface antigen of hepatitis B
(HBsAg). Upon investigation, a significant proportion of those individuals turned out
to have some liver injury, from minor alterations to chronic active hepatitis, liver
cirrhosis and hepatocellular carcinoma [1].
Hepatitis B Virus (HBV) chronic infection in humans is frequent in certain
regions of the world, where the prevalence of HBV carriers in the general
population is high [2 - 5].
In Brazil, studies on the HBsAg prevalence were carried out in the general
population, but mainly in volunteer candidates for blood donation [1]. The observed
prevalence was 0.3% in the South of the country [6] and 11.3% in the Amazon
region [7]. For the state of São Paulo, about 1.0 % was found in the capital and
from 0.3 to 1.3% in the interior [1, 8].
The prevalence of asymptomatic carriers varies among countries, being
considered as low- (0.2- 0.5%), median- (2.0 – 7.0%) and high-prevalent (8.0 –
20.0%) areas [9, 10]. As discussed below, this prevalence also varies within
countries, from region to region, depending on different factors, such as
socioeconomic conditions, drug addiction, alcoholism, professional blood donation,
homosexualism and high familial incidence [1, 2, 11 - 20].
The familial occurrence of the HBV infection is well established for some ethnic
groups. Initially, OHBAYASHI et al. reported three Japanese families, in which 36
of the 54 members were HBsAg positive. Among these, there were healthy carriers
as well as individuals with liver cirrhosis and hepatocellular carcinoma [21].
Similar observations were reported for the American [2, 22 - 27], European [28 -
32] and Asian continents [21, 26, 33 - 36].
However, there are only few comparisons among populations of different ethnic
backgrounds living in the same country [26, 37, 38].
Among us, research on familial HBV carriers began in 1971 at the “Hospital das
Clínicas” (Discipline of Clinical Gastroenterology, University of São Paulo – School
of Medicine). Even so the preliminary data have not been published and until 1984,
33
when our group started this work, there was not a publication on this issue from
Brazil.
In view of the need of knowing the familial HBV occurrence in our environment
and comparing it among different ethnic groups, the aim of this study was to
prospectively determine the presence of HBV markers in the relatives of patients
with chronic liver disorders related to HBV of Japanese and occidental ethnicity.
Material and Methods
Patients
Nineteen patients of Japanese background and 26 of occidental origin were
attended at the Hepatology Branch, Discipline of Clinical Gastroenterology,
University of São Paulo School of Medicine. These patients were considered the
index cases and their relatives were prospectively studied as two groups regarding
their familial relation: (i) genetic-related group – consanguineous (parents,
brothers, sisters, sons, daughters, grandparents, aunts, uncles, cousins, nieces
and nephews) and (ii) non-genetic-related group - non-consanguineous (husband,
wife, brothers-in-law, sisters-in-law, and others that could directly or indirectly be in
contact with the family). Altogether, 165 relatives from Japanese background and
186 from occidental origin were enrolled.
Inclusion criteria
Index cases were HBsAg seropositive with a chronic liver disease, including
chronic hepatitis, liver cirrhosis and hepatocellular carcinoma, diagnosed by liver
biopsy. Parents of the index cases belonged to the same ethnicity.
Methods
Seroimmunologic markers for present (HBsAg) and past (anti-HBs) HBV
infection were searched for in the relatives of the index cases.
Identification
For each index case and respective relatives, the parameters age, sex,
ethnic origin and degree of familial relation were evaluated.
HBsAg and anti-HBs determination
44
The presence of the antigen HBsAg and the antibody anti-HBs in serum was
determined by the enzyme-immunoassays AUSZYME II and AUSAB EIA,
respectively, provided by ABBOTT LABORATORIES (U.S.A).
Statistical analysis
The mean age of index cases in both ethnic groups (Japanese and
Occidental) were compared using t-test [39]. Categorical variables were compared
by chi-square or Fisher’s exact test.
The influence of the ethnic origin (Japanese and Occidental) and degree of
familial relation (genetic- and non-genetic-related) on the serum immunologic
markers were evaluated by linear model methods as typified by the Grizzle,
Starmer, Koch [40, 41] approach.
Four sub-populations determined by the variables ethnic group and familial
degree were considered (Japanese genetic-related, Japanese non-genetic-related,
Occidental genetic-related and Occidental non-genetic-related). The results of the
HBV serum markers were considered the response variable (HBsAg, anti-HBs and
negative).
The calculations were made using the SAS System, following the CATMOD
procedure [42].
Results
Index cases
Nineteen patients from oriental (Japanese) and 26 from occidental origin
were the index cases, for whom the gender (11 males / 8 females and 21 males / 5
females, respectively; p = 0.0945) and the mean age did not differ significantly
[39.8 + 11.3 (19 – 63) and 34.5 + 17.3 (7 – 61) years old, respectively (p > 0.05)].
Familial HBV Markers
HBsAg and anti-HBs
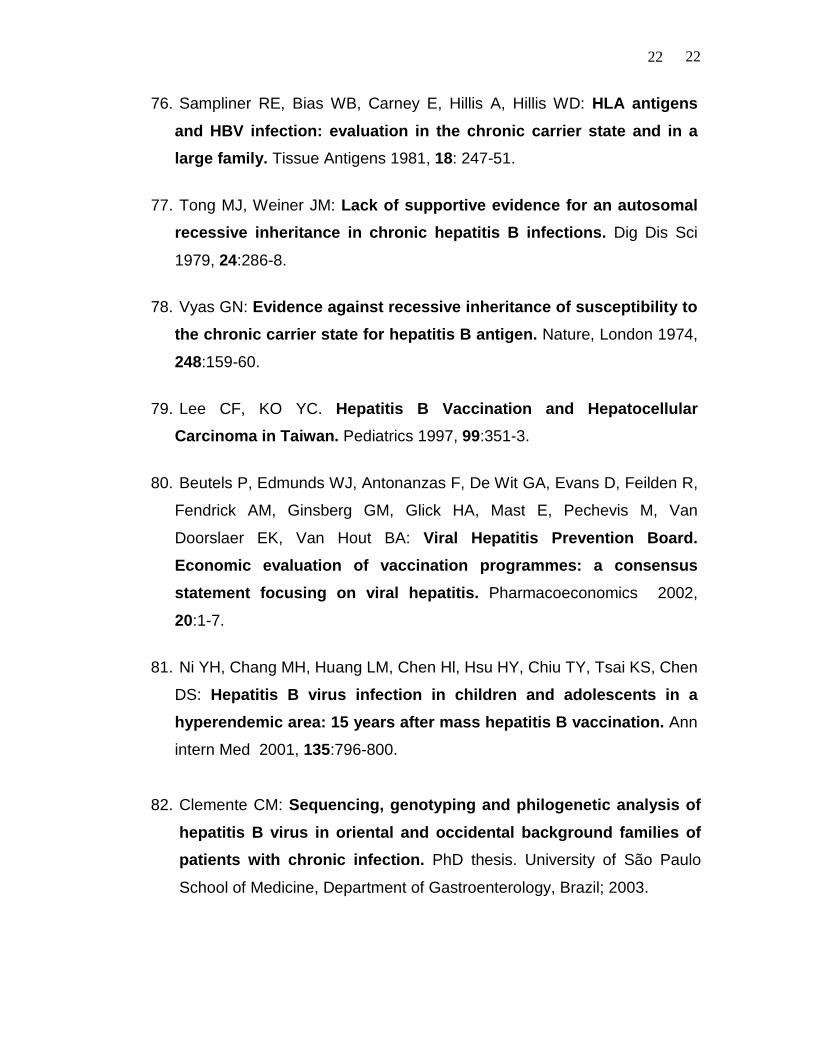
Altogether the frequency of both HBsAg and anti-HBs was 135/165 (81.8%)
for the Japanese relatives and 68/186 (36.5%) for those of occidental origin (p <
0.0001). Significant differences were also observed between the brothers and
55
sisters (p <0.0001), sons and daughters (p < 0.0001) and other relatives (p <
0.0007) of both groups (oriental and occidental) as shown in Table 1. Among the
parents of the index cases, in turn, there was just a trend to a significant difference
(p = 0.0578). Such a small number of cases was further compensated with the
inclusion of other parents belonging to the same familial hub.
HBsAg
A significant difference (p = 0.0001) was found between the frequency of the
HBsAg obtained for the Japanese relatives, 79/165 (47.9%), and for the occidental
ones, 10/186 (10.7%). Concerning the degree of familial relation, there was a
significant difference for the mothers (p = 0.0045), brothers and sisters (p <
0.0001) and sons and daughters (p < 0.0001) between the two groups.
Anti-HBs
The anti-HBs frequency found for the oriental relatives was 56/165 (33.9%),
which was not significantly different (p = 0.1209) from that of the occidental group,
48/186 (25.8%). Regarding the degree of familial relation, a significant difference
was observed only for the parents (0.0170) and other familial relatives (p =
0.0388).
Frequency of Familial Aggregation Rate per Ethnic Group
The familial aggregation frequency, given by the number of families having
at least one HBsAg or anti-HBs positive member (except the index case) per total
of studied families, was 94.7% and 88.5% for the Japanese and occidental groups,
respectively (p = 0.4319; Table 2).
HBV Markers in Progeny to HBsAg Positive Mothers
The progeny to 16 mothers of Japanese- and seven of occidental-
background was studied (Table 3); of the 67 from the former group, 56 (83.6%)
presented HBsAg and five (7.5%) anti-HBs, whereas of the 20 members from the
latter group, eight (40%) were HBsAg and four (20.8%) anti-HBs positive (p =
0.0004).
HBV Markers in Progeny to HBsAg Positive Fathers
Ten fathers of Japanese and 20 of occidental origin were enrolled in the
study (Table 4). Of the 30 members of the Japanese progeny, seven (23.3%) were
66
HBsAg and seven (23.3%) anti-HBs positive. For the 69 occidental descendents,
the markers were found in eight (11.6%) and six (8.7%) members, respectively (p =
0.0255).
HBV Markers in Progeny to Fathers or Mothers (HBsAg) of Japanese
origin
Nine HBsAg-positive fathers and 15 HBsAg-positive mothers having a 26-
and 63-member progeny, respectively, were enrolled in this investigation. HBsAg
was detected in three (11.6%) and anti-HBs in seven (26.9%) members of the first
group. While for the second group, 52 (82.6%) were found to be HBsAg and five
(7.9%) anti-HBs positive (difference significance: p < 0.0001). One family was
excluded from the results presented, for both father and mother were HBsAg
positive.
HBV Markers in Progeny to Fathers or Mothers (HBsAg) of Occidental
origin
Eighteen HBsAg-positive fathers gathering a progeny of 64 members and
five mothers having 15 children were studied. HBsAg was detected in seven
(10.9%) and anti-HBs in six (9.4%) of the 64 descendents of the first group; while
for the 15 of the second group, HBsAg was found in seven (46.6%) and anti-HBs in
four (26.7%) individuals (p = 0.0002). Two families were excluded from the results
presented, for both father and mother were HBsAg positive.
Frequency of HBV Markers in Progeny to Fathers or Mothers (HBsAg)
from Japanese and Occidental origins
The progenies enclosing 90 and 78 individuals from 27 fathers and 20
mothers (HBsAg-positives), respectively, were investigated. Among the first group,
HBsAg was detected in 10 (11.1%) and anti-HBs in 13 (14.4%) members; whereas
out of the second group, the frequency found for these markers was 75.7% (59/78)
and 11.5% (9/78), respectively (p = 0.0001).
Frequency of HBV Markers per Ethnic Group and Degree of Familial
Relation
The frequency of the HBV markers according to the ethnic origin (Japanese
and occidental) and the degree of familial relation (genetic- and non-genetic

77
related) were compared and presented in Table 5; the variance analysis has
shown significant difference (p = 0.0001) in both comparisons.
Since the interaction between ethnic group and familial relation was not
significant, the model was adjusted taking into consideration only the main effects.
Finally, the analysis for categorical data has shown that the observed and
expected probabilities were perfectly concordant (Table 6).
Discussion
Families make up an excellent model to look for qualitative and quantitative
features concerning host response to certain etiologic agents and transmission
mechanisms through people exposed to a variety of environmental characteristics
[43]. Familial studies have been proven important to the knowledge of viral
hepatitis B that shows little clinical symptoms but a clear trend to chronicity [25, 44,
45].
The mechanisms of hepatitis B transmission are not fully understood, but
they seem to have various aspects [22, 25, 26, 28, 46, 47]; the genetic component,
in particular, is still debated [48 - 50].
Despite all those unclear features, there are few studies worldwide in large
scale, including geographic areas of low- and high- incidence of HBV infection.
Numerous reports of families with multiple cases of acute and chronic hepatitis B
[25, 27, 51 - 56] have confirmed the possibility of familial aggregation. However,
they are of little value for estimating the frequency of these events in the population
and for the understanding of certain aspects of HBV familial aggregation [29, 57].
Taking into consideration some informations from outside Brazil [2, 11, 28,
37, 51, 58] and preliminary data [1] from our environment about relatives of HBV-
positive patients with liver disease, two populations of distinct ethnic origins were
studied — the relatives of index cases from Japanese and Occidental origins. The
choice was based on the fact that the immigrants of these two ethnic groups
comprise a great proportion of the population of the State of São Paulo. In fact,
São Paulo accounts for the largest Japanese-descendent population after Japan.
88
One of the main objectives of the present work was to investigate whether
our data are similar to the reported in the literature.
Concerning the inclusion criteria, it is worth mentioning the work from other
authors. BRUGUERA et al. [59] have studied 100 relatives of 29 patients with
HBV-related liver disease admitted at the Hospital of the University of Barcelona.
HBsAg was detected in 12 members of the families and, of these, eight were
asymptomatic HBV carriers, one had cirrhosis and three progressed to acute
hepatitis. There was no report of parenteral exposure within the familial contacts.
The HBsAg frequency (12.0%) in the families was considerably higher than the
prevalence of the antigen in patients (0.3%) without liver disease and in volunteer
blood donors (0.4%).
The same group from Barcelona [57] has published a study about familial
contacts to index cases with acute hepatitis, chronic hepatitis and healthy HBV
carriers, establishing the occurrence of HBsAg and anti-HBs in comparison to
volunteer blood donors. The prevalence of these markers was significantly higher
among the 178 relatives (39.2%) with domestic contact to the 54 HBsAg carriers
than in the control group of 834 blood donors (12.1%; p < 0,001). They came to the
conclusion that the risk of acquiring HBV infection for the relatives of patients with
some HBV-related liver disease (acute = 33.0%; chronic = 46.3%) was higher than
for those individuals with no familial case of liver disorders (13.4%; p < 0.01).
Similar data were reported by others [2, 23, 25, 29, 30, 32, 35, 38].
Due to the relevance of those results and the ease to study patients with
chronic liver diseases as compared to the acute forms, the families of the chronic
cases were given priority in this study. Unpublished data have shown us that the
existence of a member with a chronic form of liver disease greatly motivates the
family to join up the study.
Searching for HBsAg and anti-HBs has been generally adopted to detect
present or past HBV infection [62]. The anti-HBc is also another marker for HBV
infection that is largely used [26, 60].
In relation to age and gender, the index cases of Japanese and occidental
origin were not significantly different.
99
This work has shown that the general occurrence of the HBsAg and anti-
HBs markers, that expresses HBV contact, was 81.8% for the Japanese and
36.5% for the occidental families (Table 1). This difference is significant and our
data are comparable to those of OHBAYASHI et al. [21] in Japan (79.9%) and of
TONG et al. [26] in members of families of Chinese people living in the United
States in comparison to members living in the Orient. Our findings are also similar
to reports from various European (26.0% - 71.1%) [29, 57, 61] and American
authors (32.0% - 46.0%) [23, 26] in relation to the occidental people.
Concerning the degree of familial relation, the HBsAg has been found in
90.0% of the mothers, 79.6% of the brothers and sisters and 37.9% of the
progenies of oriental origin and, for the occidental equivalents, in 30.7%, 8.5% and
3.3%, respectively. These differences are significant and suggest, specially for the
Japanese subjects, that vertical or peri-natal transmission from mothers are the
most important way of acquiring HBV infection, as it will be seen later. These
results also corroborate with the literature [23, 25, 33, 35, 37, 46, 57].
The presence of anti-HBs, that indicates in the majority of the cases a host
immune response to the HBV and past infection [62], occurred in 33.9% of the
members of the Japanese families and in 25.8% of those of occidental origin. This
difference was not significant, and the literature reported occurrence for this
antibody in 2.2% to 50.0% of the oriental [21, 25, 26, 37, 46] and in 16.0% to
57.4% of the occidental subjects [22, 26, 37, 57].
Regarding the degree of familial relation, the anti-HBs occurred in 100% of
the fathers and in 78.6% of the partners of oriental origin. For those of occidental
origin, the occurrence was 40.0% and 70.0%, respectively; the difference was
significant between the groups of oriental and occidental fathers.
It is worth emphasizing that there is no similar concomitant study with these
two ethnic groups in the literature.
In general, 41 (91.1%) of the 45 families presented familial aggregation,
characterized by the existence of members (except the index case) with signs of
present (HBsAg positive) or past (anti-HBs positive) infection. Such aggregation
occurred in 94.7% and 88.5% of the Japanese and occidental families, respectively
1010
(p = 0.4319; Table 2). These values are higher than those observed by
BRUGUERA et al. (68.5%) in Spain [57], by COLTORTI et al. (77.7%) in Italy [29]
and by SZMUNESS et al. (8.4% - 21.0%) in the United States [38]. This
discrepancy may be viewed, at least in part, as a consequence of the various
behaviors of the families in different situations: chronic or acute liver disorders or
HBsAg healthy carriers [2, 38, 57, 63].
The analysis of the HBsAg and anti-HBs markers in progenies to mothers or
fathers positive for the antigen was carried out taking into consideration all the
familial possibilities; for instance, children from a genetic-related relative of the
index case were also included to increase the sampling for the statistical analysis.
The analysis of the HBV markers and degree of familial relation revealed
that the HBsAg was more frequent within those genetic-related individuals,
whereas among the non-genetic related ones, the anti-HBs was more prevalent
(Table 5).
The Japanese subjects showed an alarming high frequency of HBsAg
among the genetic-related relatives, being the parents, brothers, sisters, children
(47.9%, Table 1), or also other genetic-related members of the family (60.3%,
Table 1). These frequencies are higher than the ones found for any other risk
group ever investigated [64].
Altogether, the results presented here show that: 1. There is a high
frequency of intra-familial HBV spreading, especially in those of Japanese origin; 2.
Applying certain statistical methodology [40 - 42] allows the prediction of the
frequency of the HBV markers per ethnic group and per degree of familial relation;
in fact, the observed values are in agreement with the expected ones (Table 6).
This is a valuable contribution of practical use and, as far as we know, there is no
similar report in the literature; 3. Among the families from both ethnic groups, the
infected mothers are the most likely to spread the HBV. This fact strongly suggests
that vertical transmission is an important way of getting the infection. On the other
hand, the non-genetic related relatives presented a higher trend for developing
anti-HBs upon contact with HBsAg-positive carriers. The reason for such
1111
phenomenon is because the contact with HBV is in the adult phase, when the
possibility to eliminate the virus is more frequent.
The present results have shown fundamental differences in the HBsAg
occurrence between families of Japanese and occidental origin, and similar facts
were observed by others [26, 37, 46, 68]. It is worth noting, however, the lack of
publications on related studies, including different ethnic groups from a single
country. Altogether, these studies have shown that the spreading and persistence
of the HBV are more efficient within the Asian people than other ethnic groups [4,
26, 66 - 69]. To explain such phenomenon, hypotheses have been raised
concerning environmental, nutritional and genetic factors, yet they remain
unproved [29, 51, 70 - 78].
The HBsAg carriers should be clinically investigated, monitored by
laboratorial tests and, if appropriate, to undergo biopsy [6].
The practice of these prophylactic measures including active immunization
has significantly decreased the incidence of HBV infection in both occidental and
oriental countries [79 - 81].
The search for other HBV markers (anti-HBc, HBeAg, anti-HBe, HBsAg
subtypes and HBV genotyping) in the relatives of patients are under investigation
in our group [82].
Conclusions
(i) The frequency of familial aggregation – given by the presence of one of the HBV
markers (HBsAg or anti-HBs) in serum in one or more relatives of patients with a
HBV-related liver disease – was equally elevated in groups from oriental and
occidental origin; (ii) The general occurrence of the HBsAg and anti-HBs was
significantly higher in families of Japanese origin; (iii) The HBsAg occurrence was
significantly higher in relatives of patients from Japanese background with close
genetic relation (mothers, daughters, sons, brothers and sisters); (iv) Concerning
the anti-HBs, there was no significant difference between relatives of oriental and
occidental origin. This marker was more frequently found in the fathers, sexual
partners and in the group of other relatives; (v) The children to HBsAg-positive
1212
mothers from Japanese origin presented higher frequency of HBV infection than
those from occidental mothers; the same fact was observed for the children to
Japanese fathers; (vi) Comparing mothers and fathers from Japanese origin,
transmission from the former group to their children was significantly higher; (vii)
Among the closely related individuals, the HBsAg was the more frequent marker,
whereas within the more distantly related subjects, the anti-HBs was the
predominant one; (viii) These facts strongly suggest the occurrence of vertical
transmission among the closely genetic related relatives; and, (ix) The high intra-
familial dissemination of the HBV calls for prophylatic measures. (x) Some
statistical methods allow the prediction of the frequency of the HBV markers per
ethnic group and per familial degree relation, with a close agreement with the
observed values. This is a valuable contribution of practical use and, as far as we
know, there is no similar report in the literature.
List of abbreviations
HBV, Hepatitis B Virus
HBsAg, Hepatitis B surface antigen
Anti-HBs, Hepatitis B surface antibody
Anti-HBc, Hepatitis B core antibody
HBeAg, Hepatitis B e antigen
Anti-HBe, Hepatitis B e antibody
HBV DNA, Hepatitis B Virus deoxyribonucleic acid
Competing interests
None declared.
Authors’ contributions
FJC conceived, designed, carried out the entire study in addition to the
standardization of the protocol and preparation of the manuscript. SKON, LEPF,
JEMMF and ELRC assisted in data collection. JRRP participated of the
1313
determination of HBV markers. RAC participated ofthe design of the study and
performed the statistical analysis. VAFA, LCCG and LCDS all participated of the
design and preparation of the manuscript. All authors read and approved the final
manuscript.
Acknowledgments
This study was in part supported by research grants from the FINEP –
Financiadora de Estudos e Projetos and Alves de Queiróz Family Fund for
Research. Authors thank Dr. Gabriela Ribeiro-dos-Santos for critically reviewing
the manuscript.
References
1. Carrilho FJ, Corrêa MCJM: Magnitude of hepatitis B and C in Latin
America. In Therapies for Viral Hepatitis. Edited by Schinazi RF,
Sommadossi JP, Thomas HC. London: International Medical Press;
1998:25-34.
2. Barrett DH, Burks JM, McMahon B, Elliott S, Berquist KR, Bender TR,
Maynard JE: Epidemiology of hepatitis B in two Alaskan
communities. Amer J Epidem 1977, 105:118-22.
3. Beasley RP, Hwang LY, Lin CC, Leu ML, Stevens CE, Szmuness W,
Chen KP: Incidence of hepatitis B virus infections in pre-school
children in Taiwan. J infect Dis 1982, 146:198-204.
4. Hann HW, Kim CY, London WT, Whiteford P, Blumberg BS: Hepatitis B
virus and primary hepatocellular carcinoma: family studies in Korea.
Int J Cancer 1982, 30:47- 51.
1414
5. Kashiwagi S, Hayashi J, Ikematsu H, Nomura H, Kusaba T, Shingu T,
Hayashida K, Kaji M: An epidemiologic study of hepatitis B virus in
Okinawa and Kyushu, Japan. Amer J Epidem 1983, 118:787-94.
6. Carrilho FJ, Baldy JLS, Takata PK, Adum S, Zeitune JMR: Prevalence
and study of asymptomatic carriers of hepatitis B surface antigen
(HBsAg, in blood donors in Londrina, South of Brazil. Gastroent
Endosc Digest, S. Paulo 1984, 3:13- 20.
7. Gayotto LCC, Quarentei AA, Cabral GL: Soro epidemiologia das
hepatites A e B nas regiões dos rios Biá e Alto Juruá, Amazônia
Ocidental. Gastroent Endosc Digest, S Paulo 1984, 3:106-12.
8. Foccacia R, Conceição OJG, Sette Jr H et al: Estimated prevalence of
viral hepatitis on the general population of the municipality of São
Paulo, measured by serological markers through samples collected
from a stratified, randomized and residence-based population
survey. Braz J Infect Dis 1998, 2:268-83.
9. Zuckerman AJ: Controversies in immunization against hepatitis B.
Hepatology 1985, 5:1227-30.
10.The EASL Jury: EASL International Consensus Conference on
Hepatitis B. J Hepatol 2003, 38:533-40.
11.Berris, B, Wrobel DM, Sinclair JC, Feinman SV: Hepatitis B antigen in
families of blood donors. Ann Intern Med 1973, 79:690-93.
12.Coleman JC, Waugh M, Dayton R: Hepatitis B antigen and antibody in
a male homosexual population. Brit J vener Dis 1977, 53:132-34.
13.Drachler DH: Hashish and the transmission of hepatitis. N Engl J Med
1975, 293:667.
1515
14.Ellis WR, Coleman JC, Fluker JL, Keeling PWN, Banatvala JE, Murray-
Lyon IM, Evans BA, Bull J, Simmons PD, Willcox JR, Thompson RPH:
Liver disease among homosexual males. Lancet 1979, 1:903-5.
15.Hadziyannis SJ, Merikas GE: Australia antigen in a family. Lancet
1970, 1:1057-8.
16.Lim KS, Wong VT, Fulford KWM, Catterall RD, Briggs M, Dane DS: Role
of sexual and non-sexual practices in the Transmission of hepatitis
B. Brit. J vener Dis 1977, 53:190-2.
17.Mazzur S, Blumberg BS, Friedlaender JS: Silent maternal transmission
of Australia Antigen. Nature, London 1974, 247:41- 3.
18.Steinberg SC, Alter HJ, Leventhal BG: The risk of hepatitis
transmission to family contacts of leukemia patients. J Pediat 1975,
87:753-6.
19.Szmuness W, Much MI, Prince AM, Hoofnagle JH, Cherubin CE, Harley
EJ, Blockj GH: On the role of sexual behavior in the spread of
hepatitis B infection. Ann intern Med 1975, 289:489-95.
20.Van Etta LL, Peterson LR, Gerding DN: Asymptomatic hepatitis B
carriers in a family. N Engl J Med 1981, 305:1093-4.
21.Ohbayashi A, Okochi K, Mayumi M: Familial clustering of
asymptomatic carriers of Australia antigen and patients with chronic
liver disease or primary liver cancer. Gastroenterology 1972, 62:618-
625.
22.Bernier RH, Sampliner R, Gerety R, Tabor E, Hamilton F, Nathanson N:
Hepatitis B infection in households of chronic carriers of hepatitis B
surface antigen. Amer J Epidem 1982, 116:199-211.
1616
23.Sampliner RE, Loevinger BL, Tabor E, Gerety RJ: Intrafamilial cluster of
hepatitis B virus infection: study of a large family in the United
States. Amer J Epidem 1981, 113:50- 4.
24.Szmuness W, Prince AM, Hirsch RL, Brotman B: Familial clustering of
hepatitis B infection. N Engl J Med 1973, 289:1162-6.
25.Tong MJ, Thursby MW, Lin JH, Welssman JY, McPeakj CM: Studies on
the maternal-infant transmission of the hepatitis B virus and HBV
infection within families. Prog med Virol 1981, 27:137-47.
26.Tong MJ, Weiner JM, Ashcavai MW, Redeker AG, Comparini S, Vyas
GN: A comparative study of hepatitis B viral markers in the family
member of Asian and Non-Asian patients with hepatitis B surface
antigen-positive hepatocellular carcinoma and with chronic hepatitis
B infection. J infect Dis 1979, 140:506-12.
27.Velasco M, Giaconi J, Cruz-Coke R, Fuente C, Ruiz A: Distribuición
familiar del antígeno Australiano en poblacion chilena. Rev méd
Chile 1973, 101:758-62.
28.Bosch J, Bruguera M, Rodés J: Familial spread of type-B hepatitis.
Lancet 1973, 2 :457.
29.Coltorti M, Del Vecchio-Blanco C, Caporaso N, SuozzoR, Servillo F:
Familial clustering of HBV infection and chronic liver disease. Front
gastroint Res 1984, 8:169-79.
30.Eliakin M, Ligumski M, Sandler Sg, Zlotnick A: Familal clustering and
immune response in family contacts of patients with HBsAg-positive
liver cirrhosis. Dig Dis Sci 1978, 23:407-12.
1717
31.Hellawell JM, Woolf IL, Jones DM, Dymock IW: Epidemiological
observations on the families of hepatitis B antigen carriers and
hepatitis B antibody-positive individuals. Gut 1975, 16: 402.
32.Hess G, Born M, Dormeyer H, Zoller B, Arnold W, Knolle J: Hepatitis B
virus markers among family contacts of asymptomatic HBsAg
carriers. Scand J Gastroent 1979, 14:373-8.
33.Anderson KE, Stevens CE, Tsuci JJ, Lee WC, Sun SC, Beasley RP:
Hepatitis B antigen in infants born to mothers with chronic hepatitis
antigenemia in Taiwan. Amer J Dis Child 1975, 129:1389-92.
34.Beasley RP, Hwang LY, Stevens CE, Lin CC, Hsieh FJ, Wang KY, Sunj
TS, Szmuness W: Efficacy of hepatitis B immune globulin for
prevention of perinatal transmission of the hepatitis B virus carrier
state: Final report of a randomized double-blind placebo-controlled
trial. Hepatology 1983, 3:135-41.
35.Grossman RA, Benenson MW, Scott RM, Snitbhan R, Top Jr FH,
Pantuwatana S: An epidemiologic study of hepatitis B Virus in
Bangkok, Thailand. Amer J Epidem 1975, 101:144-59.
36.Scobie B, Woodfield DG, Fong R: Familial hepatocellular carcinoma
and hepatitis B antigenemia in a New Zealand chinese family. Aust N
Z J Med 1983, 13:236-9.
37.Asami K, Tsuchiya M: Comparative study of incidence of HBV
infection in Japanese descendents and native bolivians in Santa
Cruz, Bolivia. Acta gastroent Bolivia 1983, 3 :5-8.
38.Szmuness W, Harley EJ, Prince AM: Intrafamilial spread of
asymptomatic hepatitis B. Amer J med Sci 1975, 270:293-304.
1818
39.Snedecor GW, Cochran WG: The comparison of two samples. In
Statistical methods. 7th edition. Edited by Snedecor GW, Cochran WG.
Ames: The Iowa State University Press; 1980:83-102.
40.Grizzle JE, Starmer CF, Koch GG: Analysis of categorical data by
linear models. Biometrics 1969, 25:489-504.
41.Koch GG, Imrey PB, Singer JM, Atkinson SS, Stokes JME: Lecture notes
for analyses of categorical data Post graduate Course in the Department
of Biostatistics. Chapel Hill: University of North Carolina Press; 1984.
42.SAS Institute Inc: SAS User´s Guide: Statistics. 5nd edition. Cary: SAS
Institute; 1985.
43.Frost WH: The familial aggregation of infectious disease. In Papers of
Wade Hampton Frost, MD: a contribution to epidemiological method.
Edited by Maxcy KF. New York: Commonwealth Fund; 1993:120-269.
44.Lo KJ, Tong MJ, Chien MC, Tsai YT, Liaw YF, Yang KC, Chian H, Liu
HC, Lee SD: The natural course of hepatitis B surface antigen-
positive chronic active hepatitis in Taiwan. J infect Dis 1982, 146:205-
10.
45.Sung J.L, Chen DS: Maternal transmission of hepatitis B surface
antigen in patients with hepatocellular carcinoma in Taiwan. Scand J
Gastroenterol 1980, 15:321-4.
46. Kashiwagi S, Hayashi J, Ikematsu H, Nomura H, Kajiyama W, Shingu T,
Hayashida K, Kaji M: Transmission of hepatitis B virus among
siblings. Amer J Epidem 1984, 120:617-25.
47. Marinier E, Barroi V, Larouze B, London WT, Cofer A, Diakhate L,
Blumberg BS: Lack of perinatal transmission of hepatitis B virus
infection in Senegal, West. Africa. J Pediat 1985, 106:843-9.
1919
48. Lok AS, Heathcote EJ, Hoofnagle JH: Management of Hepatitis B:
2000 – Summary of a Workshop. Gastroenterology 2001, 120:1828-53.
49. Conjeevaram HS, Lok AS. Management of chronic hepatitis B. J
Hepatol 2003, 38:S90-S103.
50. Liaw YF, Leung N, Guan R, Lau GKK, Merican I: Asian-Pacific
consensus statement on the management of chronic hepatitis B: An
update. J Gastroenterol Hepatol 2003, 18:239-45.
51. Boss LP, Bender TR, Schreeder MT, Lanier AP, Hardison HH, Maynard
JE: Hepatitis B testing in the families and villages of five young
Eskimos with primary hepatocellular carcinoma. Amer J Epidem
1981, 114:95- 101.
52. Bruguera M, Bosch J, Rodés J: Family outbreak of hepatitis B. N Engl
J Med 1973, 289:1144.
53. Koff RS, Slavin MM, Connelly LJD, Rosen DR: Contagiousness of
acute hepatitis B. Secondary attack rates in household contacts.
Gastroenterology 1977, 72:297-300.
54. Mitch WE, Wands JR, Maddrey WC: Hepatitis B transmission in a
family. J Amer med Assoc 1974, 227:1043-4.
55. Reeves WC, Peters CJ, Moon TE, Purcell RH: Familial clustering of
hepatitis B surface antigen among Panamanian indians. J infect Dis
1975, 131:61- 70.
56. Tong MJ, Coj RL: Hepatitis B virus markers in Asian families. Ann
intern Med 1985, 103:307-8.
2020
57. Bruguera M, Caballeria J, Acero D, Bosch J, Rodés J: Transmission
intrafamiliar del virus de la hepatitis B. Gastroent Hepatol 1980, 3:13-
8.
58. Beasley RP, Trepo C, Stevens CE, Szmuness W: The e antigen and
vertical transmission of hepatitis B surface antigen. Amer J Epidem
1977, 105:94- 8.
59. Bruguera M, Bosch J, Rodés J, Pedreira J: Familial clustering of
hepatitis B antigen: A study in relatives of patients with liver
diseases and hepatitis B antigenaemia. Brit Med J 1974, 3:495-97.
60. Papaevangelou G, Karaboyia-Karafyllidis P, Kyriakidou A: Prevalence
and epidemiologic significance of to hepatitis B core antigen in
Greece. Amer J Epidem , 1977, 106: 502-6.
61. Hadziyannis SJ: Nonparenteral transmission of viral hepatitis in
Greece. Amer J med Sci 1975, 270:313-8.
62. Holland PV: Hepatitis B surface antigen and antibody. In Hepatitis B.
Edited by Gerety RJ. Orlando: Academic Press; 1985:5-25.
63. Pastore G, Dentico P, Angarano G, Lapedota E, Schiraldi O: Infectivity
markers in HBsAg chronic carriers and intrafamilial spread of
hepatitis B virus infection. Hepato-Gastroenterol 1981, 28:20- 2.
64. Carrilho FJ, Nita SKO, Da Silva LC, Cardoso RA, Fonseca LEP, Alves
VAF, Gayotto LCC: Behavior of HBV markers in Brazilian families of
occidental and oriental origin of patients with chronic HBV infection
[abstract]. Hepatology 1996, 24(4, Pt 2):493A.
65. Arakawa, K, Tsuda F, Takahashi K, Ise I, Naito S, Kosugi E, Miyakawa
Y, Mayumi M: Maternofetal Transmission of IgG-bound hepatitis B e
antigen. Pediat Res 1982, 16:247-50.
2121
66. Stevens CE, Beasley RP, Tsui J, Lee WC: Vertical transmission of
hepatitis B antigen in Taiwan. N Engl J Med 1975, 292:771-4.
67. Pongpipat D, Suvatte V, Assateerawatts A: Vertical transmission of the
hepatitis B surface antigen in Thailand. Southeast Asian J trop Med
publ Hlth 1980, 11:582-7.
68. Derso A, Boxall EH, Tarlow M J, Flewett TH: Transmission of HBsAg
from mother to infant in four ethnic groups. Brit med J 1978, 1:949-52.
69. Skinhoj P, Aldershvile J, Kjersem M, Black F: Hepatitis B infection in
Vietnamese families. J med Vir 1983, 11:125-9.
70. Chang MH, Hsu HJC, Lee CY, Chen DS, Lee CH, Lin KS: Fraternal
hepatocellular carcinoma in young children in two families. Cancer
1984, 53:1807-10.
71. Follett EAC, McMichael S, Goel KM, Thomson R: Hepatitis B in the
school environment. Brit med J 1978, 1:1279-80.
72. Helske, T, Nevanlinna HR: Familial accumulation of carriers of Au
antigen. J med Genet, 1973, 10:270-2.
73. Jeannet M, Farquet JJ: HLA antigens in asymptomatic chronic HBAg
carriers. Lancet 1974, 2:1383-4.
74. Kashiwagi S, Naito S, Kaneoka H, Miyanaga O, Jimi S, Yamaguchi M,
Kaji M: A family study of HBsAg carrier and major histocompatibility
antigens. Fukuoka Acta med 1978, 69:156-61.
75. Nasrallah SM, Nassar VH, Shammaa MH: Genetic and immunological
aspects of familial chronic active hepatitis (type B). Gastroenterology
1978, 69: 302-306.
2222
76. Sampliner RE, Bias WB, Carney E, Hillis A, Hillis WD: HLA antigens
and HBV infection: evaluation in the chronic carrier state and in a
large family. Tissue Antigens 1981, 18: 247-51.
77. Tong MJ, Weiner JM: Lack of supportive evidence for an autosomal
recessive inheritance in chronic hepatitis B infections. Dig Dis Sci
1979, 24:286-8.
78. Vyas GN: Evidence against recessive inheritance of susceptibility to
the chronic carrier state for hepatitis B antigen. Nature, London 1974,
248:159-60.
79. Lee CF, KO YC. Hepatitis B Vaccination and Hepatocellular
Carcinoma in Taiwan. Pediatrics 1997, 99:351-3.
80. Beutels P, Edmunds WJ, Antonanzas F, De Wit GA, Evans D, Feilden R,
Fendrick AM, Ginsberg GM, Glick HA, Mast E, Pechevis M, Van
Doorslaer EK, Van Hout BA: Viral Hepatitis Prevention Board.
Economic evaluation of vaccination programmes: a consensus
statement focusing on viral hepatitis. Pharmacoeconomics 2002,
20:1-7.
81. Ni YH, Chang MH, Huang LM, Chen Hl, Hsu HY, Chiu TY, Tsai KS, Chen
DS: Hepatitis B virus infection in children and adolescents in a
hyperendemic area: 15 years after mass hepatitis B vaccination. Ann
intern Med 2001, 135:796-800.
82. Clemente CM: Sequencing, genotyping and philogenetic analysis of
hepatitis B virus in oriental and occidental background families of
patients with chronic infection. PhD thesis. University of São Paulo
School of Medicine, Department of Gastroenterology, Brazil; 2003.
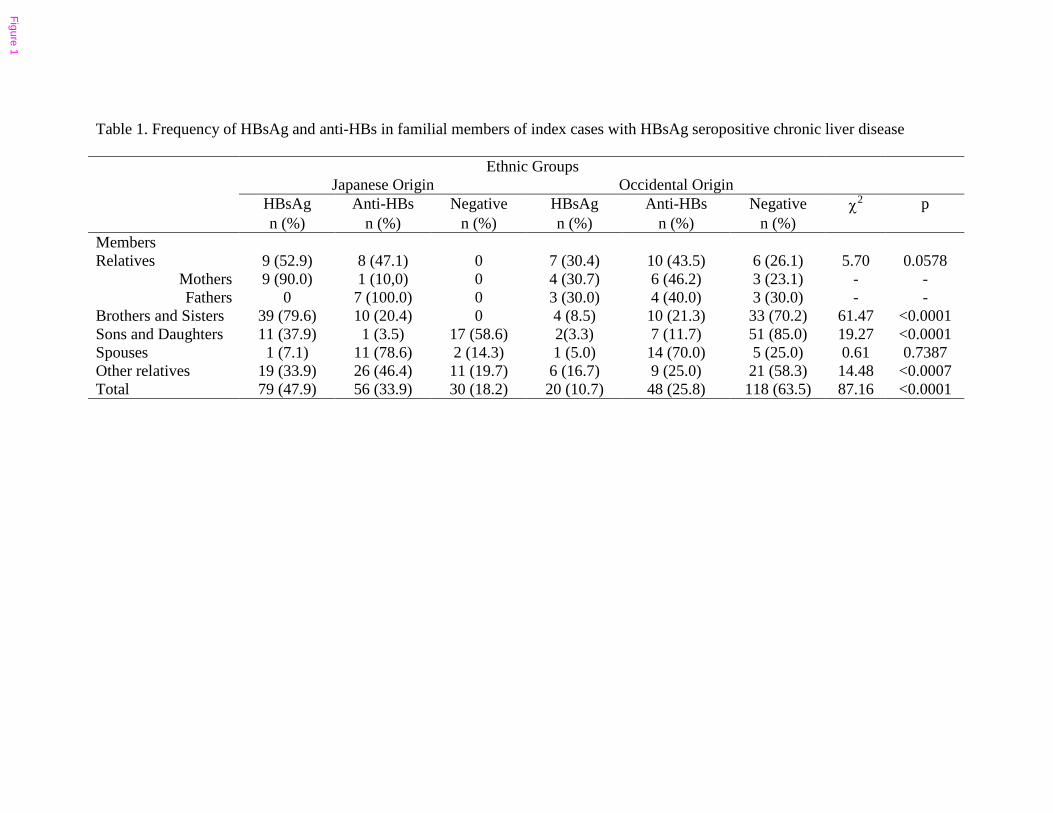
Table 1. Frequency of HBsAg and anti-HBs in familial members of index cases with HBsAg seropositive chronic liver disease
Ethnic GroupsJapanese Origin Occidental Origin
HBsAg Anti-HBs Negative HBsAg Anti-HBs Negative χ2 pn (%) n (%) n (%) n (%) n (%) n (%)
MembersRelatives 9 (52.9) 8 (47.1) 0 7 (30.4) 10 (43.5) 6 (26.1) 5.70 0.0578
Mothers 9 (90.0) 1 (10,0) 0 4 (30.7) 6 (46.2) 3 (23.1) - -Fathers 0 7 (100.0) 0 3 (30.0) 4 (40.0) 3 (30.0) - -
Brothers and Sisters 39 (79.6) 10 (20.4) 0 4 (8.5) 10 (21.3) 33 (70.2) 61.47 <0.0001Sons and Daughters 11 (37.9) 1 (3.5) 17 (58.6) 2(3.3) 7 (11.7) 51 (85.0) 19.27 <0.0001Spouses 1 (7.1) 11 (78.6) 2 (14.3) 1 (5.0) 14 (70.0) 5 (25.0) 0.61 0.7387Other relatives 19 (33.9) 26 (46.4) 11 (19.7) 6 (16.7) 9 (25.0) 21 (58.3) 14.48 <0.0007Total 79 (47.9) 56 (33.9) 30 (18.2) 20 (10.7) 48 (25.8) 118 (63.5) 87.16 <0.0001
Figure 1
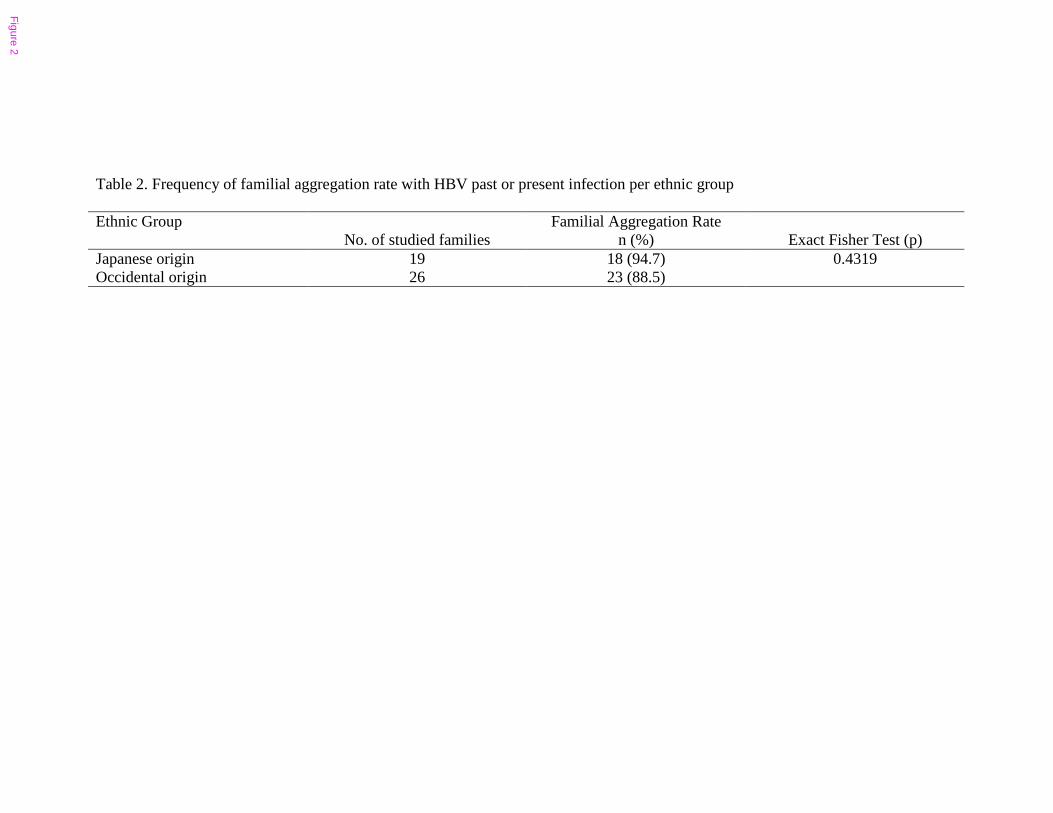
Table 2. Frequency of familial aggregation rate with HBV past or present infection per ethnic group
Ethnic Group Familial Aggregation RateNo. of studied families n (%) Exact Fisher Test (p)
Japanese origin 19 18 (94.7) 0.4319Occidental origin 26 23 (88.5)
Figure 2
Table 3. Frequency of HBV markers in progeny to HBsAg positive mothers
Ethnic Group HBsAg (+) Mothers Total Children HBsAg Anti-HBs HBV negative markers
n n n (%) n (%) n (%)Japanese origin 16 67 56 (83.6) 5 (7.5) 6 (9.5)Occidental origin 7 20 8 (40.0) 4 (20.0) 8 (40.0)χ2 = 15.54 p = 0.0004
Figure 3
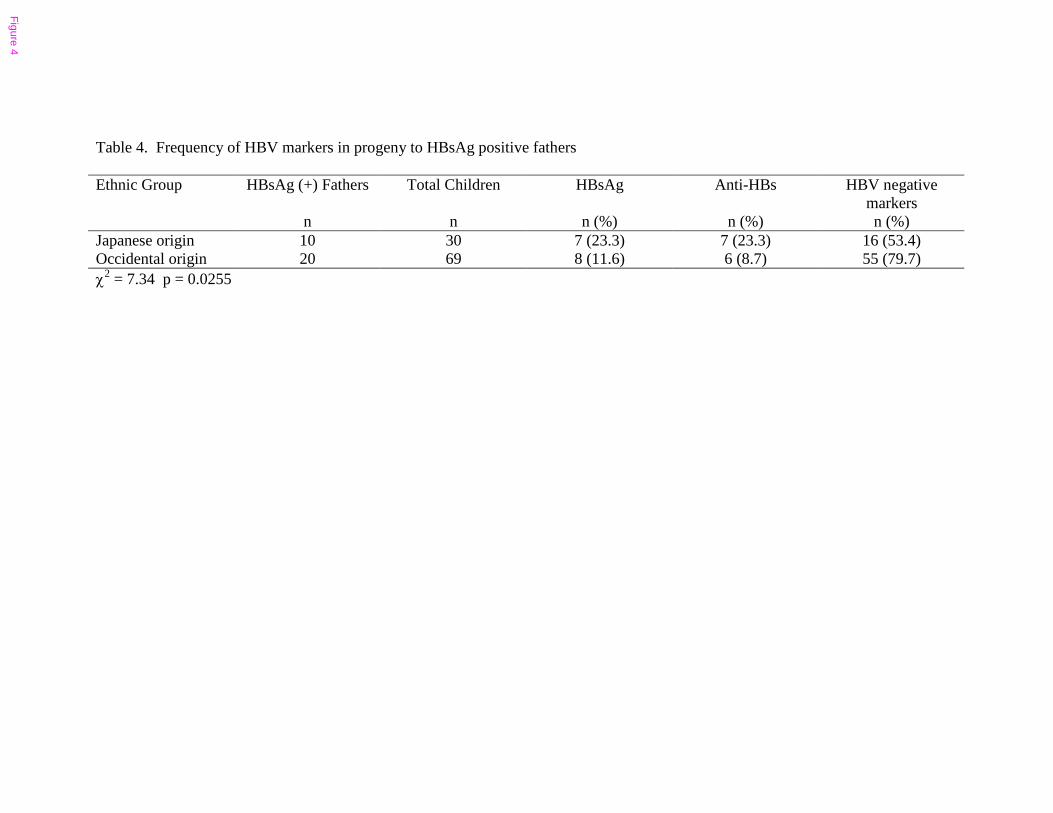
Table 4. Frequency of HBV markers in progeny to HBsAg positive fathers
Ethnic Group HBsAg (+) Fathers Total Children HBsAg Anti-HBs HBV negative markers
n n n (%) n (%) n (%)Japanese origin 10 30 7 (23.3) 7 (23.3) 16 (53.4)Occidental origin 20 69 8 (11.6) 6 (8.7) 55 (79.7)χ2 = 7.34 p = 0.0255
Figure 4
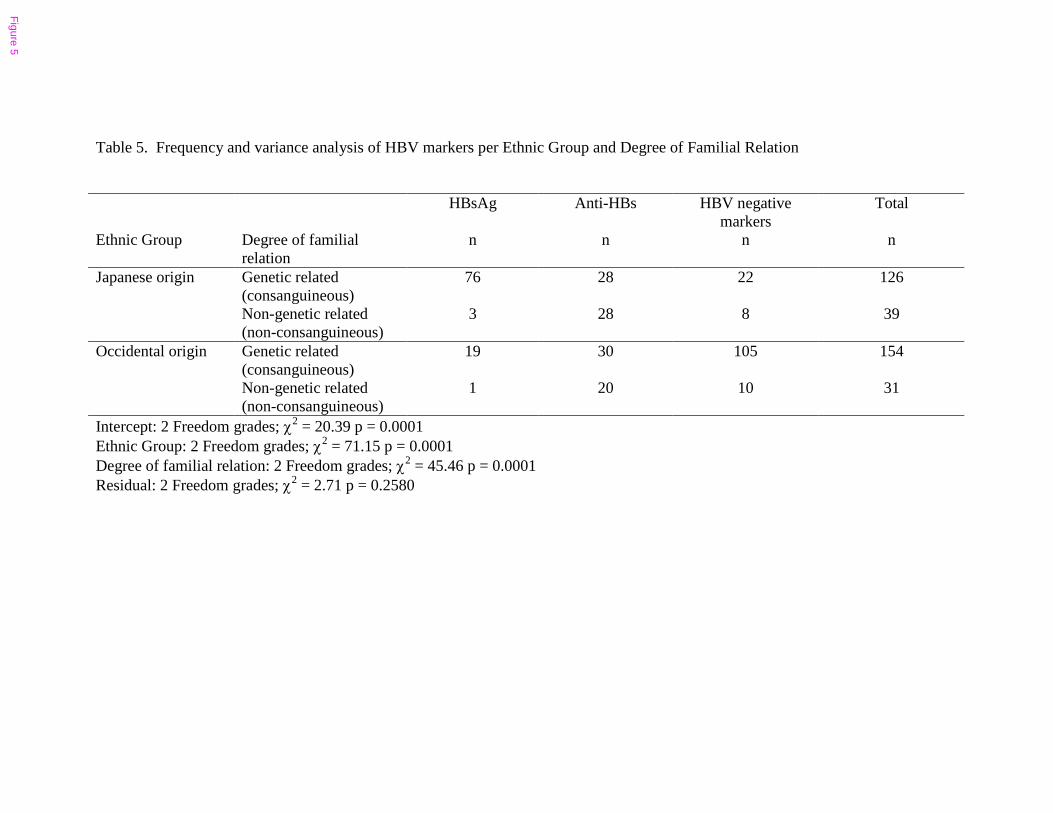
Table 5. Frequency and variance analysis of HBV markers per Ethnic Group and Degree of Familial Relation
HBsAg Anti-HBs HBV negative markers
Total
Ethnic Group Degree of familial relation
n n n n
Genetic related (consanguineous)
76 28 22 126Japanese origin
Non-genetic related (non-consanguineous)
3 28 8 39
Genetic related (consanguineous)
19 30 105 154Occidental origin
Non-genetic related (non-consanguineous)
1 20 10 31
Intercept: 2 Freedom grades; χ2 = 20.39 p = 0.0001Ethnic Group: 2 Freedom grades; χ2 = 71.15 p = 0.0001Degree of familial relation: 2 Freedom grades; χ2 = 45.46 p = 0.0001Residual: 2 Freedom grades; χ2 = 2.71 p = 0.2580
Figure 5
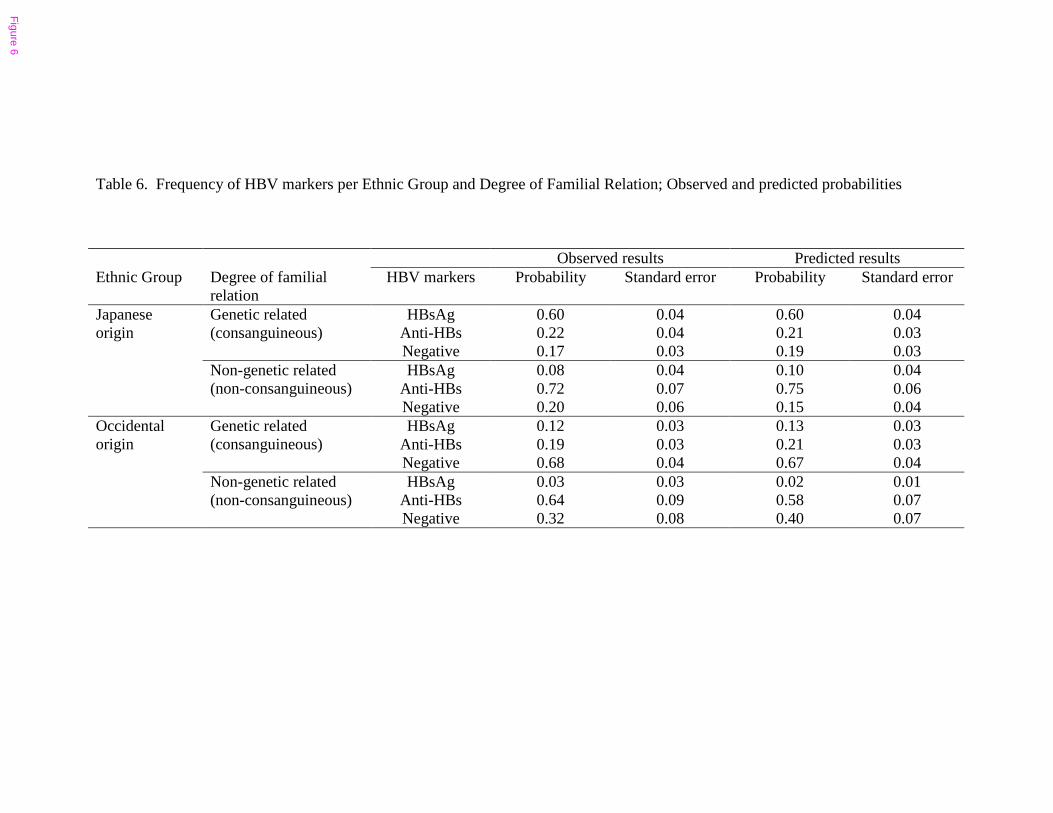
Table 6. Frequency of HBV markers per Ethnic Group and Degree of Familial Relation; Observed and predicted probabilities
Observed results Predicted resultsEthnic Group Degree of familial
relationHBV markers Probability Standard error Probability Standard error
HBsAg 0.60 0.04 0.60 0.04Anti-HBs 0.22 0.04 0.21 0.03
Genetic related (consanguineous)
Negative 0.17 0.03 0.19 0.03HBsAg 0.08 0.04 0.10 0.04
Anti-HBs 0.72 0.07 0.75 0.06
Japanese origin
Non-genetic related (non-consanguineous)
Negative 0.20 0.06 0.15 0.04HBsAg 0.12 0.03 0.13 0.03
Anti-HBs 0.19 0.03 0.21 0.03Genetic related (consanguineous)
Negative 0.68 0.04 0.67 0.04HBsAg 0.03 0.03 0.02 0.01
Anti-HBs 0.64 0.09 0.58 0.07
Occidental origin
Non-genetic related (non-consanguineous)
Negative 0.32 0.08 0.40 0.07
Figure 6
Additional files provided with this submission:
Additional file 1: Tables160703.doc : 73KBhttp://www.biomedcentral.com/imedia/2073115740193534/sup1.doc




















