
Self-Care Dependent-Care Nursing The Official Journal of the ...
30
& Self-Care Dependent-Care Nursing The Official Journal of the International Orem Society Volume 13, No. 1, December 2005 Contents Editorial 3 Parting shot Michael J. Morgan 3 Foreword by Guest Editor Violeta A. Berbiglia Original manuscripts 4 A Self-Care Deficit Nursing Theory practice model for advanced practice psychiatric/mental health nursing Victoria T. Grando 9 Development and examination of psychometric properties of Self-Care instruments to measure nutrition practices for English and Spanish-speaking adolescents Jean Moore, Lisa Pawloski, Heibatollah Baghi, Karen Whitt, Claudia Rodriguez, Laura Lumbi, and Adel Bashatah 17 Teaching practically practical nursing science Anna J. Biggs 22 Development and application of the Community Care Deficit Nursing Model (CCDNM) in two populations Serey Shum, Rebecca McGonigal, Barbara Biehler Teaching Strategy Column 26 Show me how Violeta A. Berbiglia IOS News 27 From the president Barbara Banfield 28 In memory of Margarethe Lorensen 29 Concept Formalization in Nursing reprint offer 30 New IOS Web Presentation
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Self-Care Dependent-Care Nursing The Official Journal of the ...
&Self-CareDependent-CareNursing The Official Journal of the International Orem Society
Volume 13, No. 1, December 2005
ContentsEditorial
3 Parting shotMichael J. Morgan
3 Foreword by Guest EditorVioleta A. Berbiglia
Original manuscripts4 A Self-Care Deficit Nursing Theory practice model for
advanced practice psychiatric/mental health nursingVictoria T. Grando
9 Development and examination of psychometric properties of Self-Care instruments to measure nutrition practices for English and Spanish-speakingadolescentsJean Moore, Lisa Pawloski, Heibatollah Baghi, Karen Whitt,Claudia Rodriguez, Laura Lumbi, and Adel Bashatah
17 Teaching practically practical nursing scienceAnna J. Biggs
22 Development and application of the Community CareDeficit Nursing Model (CCDNM) in two populationsSerey Shum, Rebecca McGonigal, Barbara Biehler
Teaching Strategy Column26 Show me how
Violeta A. Berbiglia
IOS News27 From the president
Barbara Banfield28 In memory of Margarethe Lorensen29 Concept Formalization in Nursing reprint offer30 New IOS Web Presentation
Author guidelinesSelf-care, Dependent-care, & Nursing is the
official journal of the International Orem Societyfor Nursing Science and Scholarship. The editorwelcomes manuscripts that address the missionof the Journal.
MANUSCRIPT PREPARATION
Use Standard English. The cover page mustinclude the author’s full name, title, mailingaddress, telephone number, and eMail address.So that we may use masked peer review, noidentifying information is to be found onsubsequent pages. Include a brief abstract(purpose, methods, results, discussion) followedby MeSH key words to facilitate indexing.
The use of metric and International Units isencouraged. Titles should be descriptive but short.Full-length articles should not exceed 15 double-spaced pages. Use of the Publication Manual ofthe American Psychological Association (5th ed.) isstrongly encouraged but not mandatory. Whenrequired by national legal or ethical regulations,research-based manuscripts should contain astatement regarding protection of human subjects.
M i s s i o n :To disseminate information related to thedevelopment of nursing science and itsarticulation with the science of self-care.
V i s i o n :To be the venue of choice for interdisciplinaryscholarship regarding self-care.
V a l u e s :
We value scholarly debate, the exchange ofideas, knowledge utilization, and developmentof health policy that supports self- anddependent-care.
REVIEW PROCESS
Manuscripts are reviewed anonymously. Oneauthor must be clearly identified as the lead, orcontact, author who must have eMail access. Thelead author will be notified by eMail of the editor'sdecision regarding publication.
INTELLECTUAL PROPERTY
Authors submit manuscripts for considerationsolely by SCDCN. Accepted manuscripts becomethe property of SCDCN, which retains exclusiverights to articles, their reproduction, and sale. It isthe intention of the editor to facilitate the flow ofinformation and ideas. Authors are responsible forchecking the accuracy of the final draft.
SUBMISSION
Manuscripts are to be submitted in MS Wordformat as an eMail attachment to the editor, KarenCox, RN, PhD [email protected] will be immediately acknowledged.It is assumed that a manuscript is sent forconsideration solely by SCDCN until the editorsends a decision to the lead author.
2

Parting shotsI do not know how well the title of my final
editorial will be perceived by the non-NorthAmerican readership, so I will translate: a partingshot is a statement, often acerbic and over theshoulder, as a person leaves a situation (or triesto get the last word in during an argument). WhileI am not engaged in an argument with anyone inparticular, I do have a parting shot and hope itstimulates discussion, not ends it.
It has been 5 years since Kathie McLaughlinRenpenning turned the IOS Newsletter over to mewith the sage/rueful advice, “You can’t publishwhat you don’t receive.” I wish I could say thatSelf-care scholarship has flourished in those 5years, but I would be hard pressed to find theevidence. Biennial Congresses notwithstanding,our scholarship is not being presented to thediscipline of nursing. One barrier is the dearth ofscholarship; another is ongoing intradisciplinaryhostility to nursing theory. I believe it is up to theIOS to fund the development of scholarship, asfew others will do it. I implore readers to becomepart of the process. We have few researchersfunded at significant levels to produce the type ofscholarship necessary to improve, extend,expand, and even refute some of the theorizedrelationships among the various aspects of Self-care Deficit Nursing Theory. What can we doabout that?
We can continue to volunteer to be reviewersfor grant applications. We can pressure suchdeep-pocket funding sources (National Institutefor Nursing Research) to fund theory-basedinvestigations. We can pressure our colleaguesby asking, “What is the contribution of ourdiscipline in that effort?” I am still dismayed thatNINR continues to fund proposals with the phrase“self-care” yet give cursory mention of SCDNT.The traditional big grant winners continue tosupply the reviewers who continue to fund non-nursing research—all under the umbrella ofnursing! NINR continues to fund “nurses whoresearch” rather than nurses doing “nursingresearch.” The same thing goes for Sigma ThetaTau, International. I have given up bothering toread their journal for nursing research, yet itclaims to be the journal of nursing research. (Seewhat I mean about a parting shot?) To paraphrasewhat I have asked before, “Who is the keeper ofthe disciplinary flame?”
EBSCO has received all the back issues ofthis Journal, and the articles therein should beavailable via EBSCO products in the very nearfuture. Our scholarship can now be accessed bypeople whose library subscribes to EBSCO,
which is nearly every university library in NorthAmerica and dozens across the globe. Self-care,Dependent-care & Nursing continues to be an on-ramp to the information highway. Please join mein wishing the new editor, Karen Cox, RN, PhD asshe gets behind the wheel. Give her the fuel(manuscripts) as she heads the journal into thefuture. (Please forgive the metaphors, but I do livein Detroit, Michigan, “the Motor City.”
Best wishes,Michael J. Morgan,
Editor
About this issueDr. Violeta Berbiglia volunteered to be Guest
Editor for an SCDCN devoted to education. Shesolicited and edited all of the articles contained inthis issue. Her enthusiasm for SCDNT anddedication to excellence in nursing educationshines through.
FOREWORD FROM THE GUEST EDITORIt has been a pleasure to serve as your guest
editor for this issue. This special issue on SCDNT-based education includes 3 contributors from theUSA and 1 from Canada. All are known for theircontributions to the IOS and their excellence innursing education. Also, they are interested inyour response to their conceptualizations and increating a dialog with you. I have included aTeaching Strategy Column that I hope willcontinue in future issues. Enjoy your reading andplan to attend my Educators' Meeting inJohannesburg.
Violeta A. Berbiglia, RN, EdD
3
AbstractBecause advanced practice nurses often use treatmentstrategies in common with other healthcare providers,controversy continues concerning their role within the healthcare delivery system. This is particularly true forpsychiatric/mental health nurse practitioners whose practiceoverlaps with that of psychiatrists, psycholinguists, socialworkers, and counselors. To address this issue, a practicemodel based Orem’s Self-Care Deficit Nursing Theory wasdeveloped as part of a family psychiatric/mental health nursepractitioner master’s specialty program. The practice modelfocuses on minimizing the self-care deficits of patients withmental health issues by improving their self-care agency,meeting their therapeutic self-care demands, and establishingtherapeutic self-care systems. This paper provides a valuableand timely contribution to the literature on the advancement ofnursing discipline-specific knowledge and practice activities bypresenting a practice model grounded in a nursing conceptualmodel: Orem’s S-CDNT. Key words: Self-care, Orem,Psychiatric/Mental Health Nursing; Advanced PracticeNursing; practice models
Nursing leaders continue to wrestle with theparameters that define the scope of advancednursing practice. A review of nursing literaturereveals the ongoing dialogue regarding whethernurse practitioners are engaged in advancednursing or delegated medicine (Cody, 2003;Fawcett, Newman, & McAllister, 2004; Geden &Taylor, 1997; Geden, 2001; Grando, 1998;Watson, 1995). These leaders hold that the role ofadvanced practice nurses needs to bedifferentiated from the role of other health careprofessionals by clearly delineating nursing’sproper object that is the unique focus of nursing.Indeed, Fawcett (2003) argues that nursing’sfuture rests in the advancement of nursingdiscipline-specific knowledge and practiceactivities grounded in nursing conceptual modelsthat provide nursing’s distinct perspective onphenomena of interest to the profession: humanbeings, environment, health, and nursing.Although an important issue for all advancedpractice nurses, it is especially so for advancedpractice psychiatric/mental health nurses whohave recently experienced a major shift in theirpractice environment. The purpose of this paper
is twofold. First, it traces the historical backgroundof nurses’ concern for their patients’ ability to carefor themselves. And, second, it describes apractice model based on Orem’s S-CDNT thatwas developed to educate family psychiatric/mental health nurse practitioners.
Psychiatric/Mental Health Nursing in TransitionPrior to the decline of inpatient psychiatric
services brought about by managed care, the roleof psychiatric nurses was unique: managing theround-the-clock therapeutic milieu of psychiatricunits. This included, among other things,engaging patients in therapeutic communication,assisting patients in learning new behaviors andidentifying feelings, teaching patients to deal withstress, improving patients’ social skills, managingmedications, helping patients develop andmanage their self-care systems, runningpsychoeducational groups, and performingpsychotherapy. Their role was clearly definedwhether they based their care on nursingconceptual models or not.
Today, however, many advancedpsychiatric/mental health nurses work in primarycare as psychiatric/mental health nursepractitioners. In these settings, their practiceoverlaps that of other mental health professionals.For example, psychiatric/mental health nursepractitioners and psychiatrists share prescriptiveauthority while psychiatric/mental health nursepractitioners, psychiatrists, psychologists, socialworkers, and counselors use psychotherapy astheir primary treatment strategy. Moreover, thetheoretical frameworks that are the basis forpsychotherapy are derived from other disciplines.These factors underscore the critical need forpsychiatric/mental health nurse practitioners tobase their practice on conceptual models ofnursing if they are to have a distinct role. I believethat Orem’s Self-Care Deficit Nursing Theory (S-CDNT) provides a nursing framework for today’sadvanced practice psychiatric/mental healthnurses. However, there is a void in the recent
4
A Self-Care Deficit Nursing Theory practice modelfor advanced practice psychiatric/mental healthnursing
Victoria T. Grando
literature on the topic of advanced practicepsychiatric/mental health nursing and the use ofS-CDNT as a guiding framework. This paper fillsthis void by providing a valuable and timelycontribution to the literature on the advancementof nursing discipline-specific knowledge andpractice activities by presenting a practice modelgrounded in a nursing conceptual model: Orem’sS-CDNT.
Historical Background Since the inception of modern nursing in the
mid-nineteenth century, nurses have assistedtheir patients’ achieve health by providing nursingcare that promotes both the body’s healingprocess and the patients’ ability to care for theirhealth related needs. Florence Nightingalearticulated these views in, Notes on Nursing:What it is and What it is not (1859, 1946). In thislandmark book, she delineates the nature ofnursing while making the following three points.
First, the role of nursing is distinct from therole of medicine. Nightingale believed that the aimof both physicians and nurses was to enhance thebody’s ability to heal itself. Physicians achievedthis by intervening surgically and prescribingmedications. Nurses achieved this by preventingcomplications of poor sanitation, inadequatenutrition, prolonged confinements to sick beds,and unnecessary emotional stress as well ascarefully observing the patient’s condition.
Second, she held that patients and theirenvironment were the focus of nurses rather thanphysician’s orders. This view was clearly stated inNotes on Nursing by the following:
It (nursing) has been limited to signifylittle more than the administration ofmedicines and the application ofpoultices. It ought to signify the properuse of fresh air, light, warmth,cleanliness, quiet, and the properselection and administration of diet—allat the least expense of vital power of thepatient. (Nightingale, p. 6)
Lastly, Nightingale believed that nurses’ rolewas not only to care for the sick, but to teach theproper methods of caring to those who care forthe health of others. The fact that Notes onNursing was not a manual of nursing, but a guidefor women on how to care for their family’s healthneeds shows her commitment to this belief.
Nursing strategies advocated by Nightingalewere highly effective. The phenomenal success ofNightingale’s nurses in reducing the mortality ratein military hospitals during the Crimean war andthe rapid growth of American hospitals after the
introduction of trained nurses (Ashley, 1976;Grando, 1994) provides evidence of theeffectiveness of these nursing interventions.
The writings of another influential nursingleader, Virginia Henderson, echo Nightingale’sviews on nursing. Henderson believed that thefocus of nursing was to help patients achievehealth by assisting them to perform health relatedactivities and gain independence. Furthermore,she believed that nurses should focus on dailyactivities such as breathing normally, eatingadequately, getting sufficient rest and sleep,avoiding dangers, communicating with others,and learning how to achieve normal development.In her book, The Nature of Nursing (1966), sheprovides the following definition of nursing:
The unique function of the nurse is toassist the individual, sick or well, in theperformance of those activities contributingto health or its recovery (or to a peacefuldeath) that he would perform unaided if hehad the necessary strength, will orknowledge, And to do this in such a way asto help him gain independence as rapidlyas possible. (p. 15)
Orem’s (2001) beliefs about nursing aresimilar to those of Nightingale and Henderson, butshe advanced their views by placing greateremphasis on achieving health by focusing onpatients’ ability to care for themselves. Accordingto Orem, nursing’s proper object is self-care. Thefollowing excerpt from her book, Nursing:Concepts for Practice (2001), illustrates herviews:
Nursing has as its special concern man’sneed for self-care action and theprovision and maintenance of it on acontinuous basis in order to sustain lifeand health, recover from disease andinjury, and cope with their effects. Thecondition that validates the existence of arequirement for nursing in an adult is theabsence of the ability to maintain forhimself continuously that amount andquality of self-care which is therapeutic insustaining life and health, in recoveringfrom disease or injury or in coping withtheir effects. (p. 22)
Orem’s S-CDNT and Advanced PracticePsychiatric/Mental Health Nursing
It is evident from the writings of theseinfluential nursing leaders that promoting healthand the ability to care for self are nurses’ uniquecontributions to health care. Inspired by thistradition, I developed a practice model: Treating
5
Self-Care Deficits Related to Mental HealthFunctioning. It is based on Orem’s S-CDNT and isthe foundation of a new family psychiatric/mentalhealth nurse practitioner master’s specialtyprogram. The following assumptions guided thedevelopment of the practice model: (a) nurseshave an important role in the process of healing,(b) psychiatric/mental health nurse practitionersplay a distinct role in mental health, (c) self-care isthe proper object of psychiatric/mental healthnursing, and (d) Orem’s S-CDNT (Orem, 1979,2001) is an excellent model on which to base thepractice of psychiatric/mental health nursepractitioners.
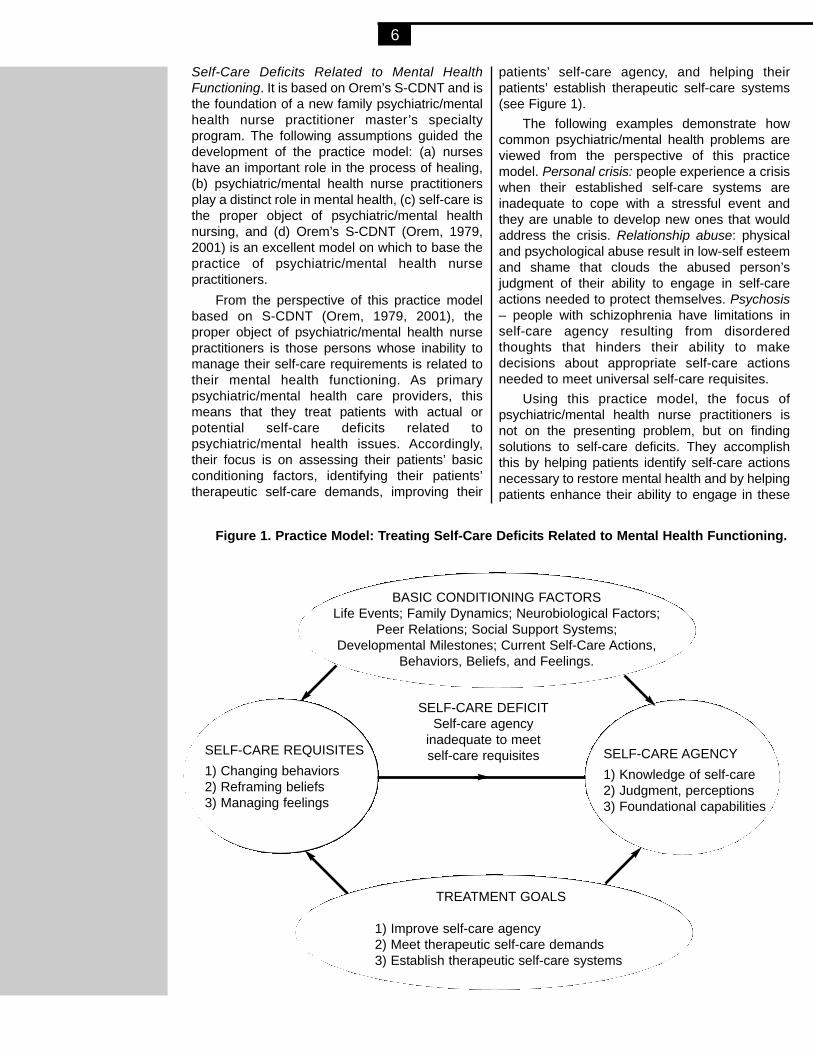
From the perspective of this practice modelbased on S-CDNT (Orem, 1979, 2001), theproper object of psychiatric/mental health nursepractitioners is those persons whose inability tomanage their self-care requirements is related totheir mental health functioning. As primarypsychiatric/mental health care providers, thismeans that they treat patients with actual orpotential self-care deficits related topsychiatric/mental health issues. Accordingly,their focus is on assessing their patients’ basicconditioning factors, identifying their patients’therapeutic self-care demands, improving their
patients’ self-care agency, and helping theirpatients’ establish therapeutic self-care systems(see Figure 1).
The following examples demonstrate howcommon psychiatric/mental health problems areviewed from the perspective of this practicemodel. Personal crisis: people experience a crisiswhen their established self-care systems areinadequate to cope with a stressful event andthey are unable to develop new ones that wouldaddress the crisis. Relationship abuse: physicaland psychological abuse result in low-self esteemand shame that clouds the abused person’sjudgment of their ability to engage in self-careactions needed to protect themselves. Psychosis– people with schizophrenia have limitations inself-care agency resulting from disorderedthoughts that hinders their ability to makedecisions about appropriate self-care actionsneeded to meet universal self-care requisites.
Using this practice model, the focus ofpsychiatric/mental health nurse practitioners isnot on the presenting problem, but on findingsolutions to self-care deficits. They accomplishthis by helping patients identify self-care actionsnecessary to restore mental health and by helpingpatients enhance their ability to engage in these
6
BASIC CONDITIONING FACTORSLife Events; Family Dynamics; Neurobiological Factors;
Peer Relations; Social Support Systems;Developmental Milestones; Current Self-Care Actions,
Behaviors, Beliefs, and Feelings.
TREATMENT GOALS
1) Improve self-care agency 2) Meet therapeutic self-care demands3) Establish therapeutic self-care systems
SELF-CARE REQUISITES1) Changing behaviors2) Reframing beliefs3) Managing feelings
SELF-CARE AGENCY1) Knowledge of self-care2) Judgment, perceptions3) Foundational capabilities
SELF-CARE DEFICITSelf-care agency
inadequate to meet self-care requisites
Figure 1. Practice Model: Treating Self-Care Deficits Related to Mental Health Functioning.
therapeutic self-care actions. The goals oftreatment include the following: (a) enhancingself-care agency by strengthening capabilitiesand minimizing limitations, (b) determining self-care actions necessary to change behaviors,reframing beliefs, and managing feelings; and (c)establishing therapeutic self-care systems.
Achieving these goals is often difficultbecause patients frequently have longestablished dysfunctional self-care patterns.However, engaging patients in treatment planningfacilitates the achievement of their goals. The firststep in this process is a comprehensivepsychiatric/mental health history and assessmentthat focuses on strengths as well as limitations. Itbegins by evaluating the patient’s BasicConditioning Factors that influence the currentsituation such as family dynamics;neurobiological factors; peer relations; socialsupport systems; developmental milestones;current behaviors, beliefs, and feelings; and onwhat routine self-care actions are working andthose that are not. Next it focuses on determiningthe patient’s Therapeutic Self-Care Requisites(Universal, Developmental, and Health Deviation)and the self-care actions necessary to meet theserequisites. And lastly, it involves determining theadequacy of the patient’s Self-Care Agency byassessing the following: (a) the patient’sknowledge about self-care (empirical,experiential, or technical), (b) the patient’s abilityto make sound judgments and decisions aboutself-care, and (c) the status of the patient’sfoundational capabilities (such as learning ability,priority systems, attention, perception, and self-understanding), which are necessary to engage indeliberate action.
After assessing the pertinent patientinformation, psychiatric/mental health nursepractitioners work with their patients to resolve thecurrent situation. Treatment goals are directed atsolutions and not dissecting the perceivedproblem. From a S-CDNT perspective (Orem,1979, 2001), the solution is achieved bydetermining therapeutic self-care demands,establishing therapeutic self-care action system,and enhancing self-care agency.
The following two case examplesdemonstrate how the practice model can beapplied to persons having difficulty meeting thetherapeutic self-care demands. A young adultcomes to see the psychiatric/mental health nursepractitioner because she has been cautioned thather continued tardiness at work will result in herlosing her job. She states that she has always hadtrouble getting up in the morning, but recently sheis unable get to up on time because she is tired in
the mornings. Moreover, she feels “down” andhas lost enjoyment in being at work. The problemstarted a few months after her best friend waskilled in a car accident. The assessment revealsthat the patient’s recent loss has lead todepression, which has exacerbating her chronicproblem of getting up in the morning. The focus oftreatment is to meet her therapeutic self-caredemand, which is to get to work on time. Thetreatment goals include treating the depressionthat interferes with her ability to perform self-care,helping her identify what actions she is currentlyperforming that help her get-up, guiding heridentifying new actions needed to get her get-up,and assisting her develop a system of self-careactions that will effectively get her to work on time.Treatment strategies might include anti-depressants, teaching the patient cognitivereframing skills, and exploring actions thateffectively wake get her up.
A middle aged man has come in to be seenbecause he is afraid that he has an “alcoholproblem”. The assessment reveals that his intakeof alcohol has been steadily increasing over thepast year and that he is not eating a sufficientquantity of protein because of his high alcoholconsumption. The focus of treatment would be tomeet the patient’s self-care demands: to reducehis alcohol intake and to eat a balanced diet. Thetreatment plan would address the addictivebehaviors, his eating patterns, and theconnections between the two. Treatmentstrategies would include joining a treatment groupfocused on reducing his alcohol dependency,identifying the positive aspects of his current diet,and guiding him to develop a balanced eatingplan.
The Practice Model for Treating Self-careDeficits Related to Mental Health Functioningprovides a treatment orientation that differentiatespsychiatric/mental health nurse practitioners’ carefrom that of other mental health professionals byfocusing on patients’ self-care requisites,identifying patients’ therapeutic self-caredemands, improving patients’ self-care agency,and assisting patients develop self-care systems.A self-care orientation is especially appropriate formental health patients because it focuses on theirability to solve their mental health problems.Moreover, helping patients achieve health bymanaging their own care needs is a longstandingnursing challenge.
Victoria T. Grando, PhD, APRN, BC, is Associate Professor,University of Arkansas for Medical Sciences College ofNursing, Little Rock, AR. Contact Dr. Grando at:[email protected]
7
References
Ashley, J. A. (1976). Hospitals, paternalism, and the role of thenurse. New York: Teachers College Press.
Cody, W. K. (2003). Scholarly dialogue. Nursing theory as aguide to practice. Nursing Science Quarterly, 16(3), 225.
Fawcett, J. (2003). Guest editorial: On bed baths andconceptual models of nursing. Journal of AdvancedNursing, 44(3), 229.
Fawcett, J., Newman, D. M., & McAllister, M. (2004).Advanced practice nursing and conceptual models ofnursing. Nursing Science Quarterly, 17(2), 135-138.
Geden, E., & Taylor, S. (1997). How is nursing expressed bynurse practitioners in the primary health care setting.International Orem Society Newsletter, 5(2), 9.
Geden, E. A. (2001). Self-care deficit nursing theory and thenurse practitioner’s practice in primary care settings.Nursing Science Quarterly, 14(1), 29-33.
Grando, V. T. (1994). Nurses’ struggle for economic equity:1945 to 1965. Dissertation Abstracts International,55(09B), 3815.: (University Microfilms International No.9504017).
Grando, V. T. (1998). Articulating nursing for advance practicenursing. In T. J. Sullivan (Ed.), Collaboration: A healthcare imperative (pp. 499-514). New York: McGraw Hill.
Henderson, V. (1966). The nature of nursing: A definition andits implications for practice, research, and education.New York: The Macmillan Company.
Nightingale, F. (1859, 1946). Notes on nursing: What it is andwhat it is not. Philadelphia: J. B. Lippincott Co.
Orem, D. E. (1979). Concept Formalization in Nursing Processand Product. Boston: Little, Brown and Company.
Orem, D. E. (2001). Nursing concepts of practice (6th ed.). StLouis: Mosby.
Watson, J. (1995). Advanced nursing practice. And what mightbe. N & HC
Perspectives on Community, 16(2), 78-83.
8

Although the researchers had been conducting nutritioneducation classes and collecting qualitative dietary informationsuch as 24-hour dietary recall and usual meal content on girlsin Nicaragua for several years, determining dietary changeand, therefore, program effectiveness, from such informationwas very difficult. First, it was not possible to identify specificnutrition behavior, particularly intellectual behavior, from suchinformation. Further, when changes in the diet occurred, it wasunclear whether it was due to a girl’s or her mother’s influence.To resolve these issues, the researchers decided to develop aquantitative, self-report approach to measure behavior changefor both girls and mothers asking for typical self-care activitiesbefore and after the nutrition education classes. The followingpaper relates the process of development of theseinstruments.
V. Berbiglia, Guest Editor
AbstractThere is a need for health professionals to develop nutritioneducation programs that inspire good self-care nutritionpractices among adolescents and their caregivers, as well asinstruments to measure the effectiveness of these programs.The purpose of this study was to develop and assess thevalidity and reliability of two self-care instruments to measurenutrition practices in English and Spanish-speakingadolescents and their parents. One instrument, theAdolescent Nutrition Self-Care Questionnaire (ANSCQ), wasdesigned to measure adolescents’ nutrition self-care practicesand the second, the Parent Nutrition Dependent-CareQuestionnaire (PNDCQ), was created to measure parents’nutrition dependent-care behavior for their children. Thequestionnaires were developed and tested first in English andthen translated into Spanish, back-translated, and tested.Orem’s self-care deficit nursing theory was used as thetheoretical framework for this study. Specifically, Orem’s(2001) estimative, transitional, and production self-careoperations were used as the structure for instrumentdevelopment. The researchers developed and tested theinstruments using methodology suggested by Evers and byNunnally and Bernstein. The researchers examined thepsychometric properties of the instruments including contentvalidity, item analysis, and reliability. In general, the expertsagreed that the items were clear, represented the nutritioncontent, and were unbiased. The Adolescent Nutrition Self-Care Questionnaire (ANSCQ) and the Parent NutritionDependent-Care Questionnaire (PNDCQ) can be valuableinstruments for various investigations, such as describingnutrition practices, comparing adolescents and parents’behavior, comparing practices in English- and Spanish-speaking populations, examining adolescents’ and parents’self-care operations, and determining the effectiveness of anutrition intervention.
Key words: nutrition, measurement instruments, self-care,dependent-care, adolescents, Spanish, self-care operations
The development of healthy nutritionalbehaviors in childhood and adolescencecontributes to lifelong health and well-being.Eating a healthy diet reduces the risk forcardiovascular disease, some cancers, diabetes,and other diseases (U.S. Department of Healthand Human Services, 1998). Worldwide, manychildren and adolescents do not meet healthguidelines for adequate nutrition. For example,research from Latin America has shown that whilemany countries within this region of the world areimproving economically, a transition has occurredin which fewer children suffer from lack of food,but many are now at risk of overconsumption ofhigh fat, high calorie, carbohydrate rich foods.Further, their consumption of nutrient dense fruitsand vegetables has decreased (Pena andBacallao, 2000). A survey of eating trends in theUnited States reported that fewer than 15% offamilies with children eat the recommended 5 ormore servings of fruit and vegetables per day(Produce for Better Health Foundation, 2003). Inthe United States, the nutritional problems ofadolescents and children are due mainly to poorfood choices such that children are consuminghigh calorie and low nutrient dense foods. Formany United States’ families convenienceoutranks price or nutrition in the importance ofselecting food (Guthrie, Lin, & Frazao, 2002). Indeveloping countries malnutrition amongadolescents and children is a major public healthproblem and the World Health Organization hascalled for the development of nutrition programsto lower the incidence of malnutrition in thesecountries (de Onis, Frongillo, & Blossner, 2000).
Parents and guardians play a critical role inestablishing healthy eating behaviors in theirchildren. Parents and caregivers are traditionallythe gatekeepers of a child’s food supply and serveas role models for food consumption. Positiveparental modeling and involvement significantlyinfluence healthy eating behaviors in children andadolescents (Norton, 2003).
There is a need for health professionals to
9
Development and examination of psychometricproperties of Self-Care instruments to measurenutrition practices for English and Spanish-speaking adolescents
Jean Burley Moore, Lisa Pawloski, Heibatollah Baghi, Karen Whitt,Claudia Rodriguez, Laura Lumbi and Adel Bashatah

develop nutrition education programs that inspiregood self-care nutrition practices amongadolescents and their parents, as well asinstruments to measure the effectiveness of theseprograms. The intent of this study was to developand examine the psychometric properties of twoself-care instruments to measure nutritionpractices in English- and Spanish-speakingadolescents and their parents.
Theoretical FrameworkOrem’s self-care deficit nursing theory (2001;
Orem Study Group, 2004) was used as thetheoretical framework for this study. Specifically,Orem’s (2001) estimative, transitional, andproduction self-care operations were used as thestructure for instrument development. Dennis(1997) defines an operation as “an intellectual orpsychomotor action directed toward a goal” (p.21).So operations are practices, activities, orbehaviors enacted to perform self-care for oneselfor dependent-care for one’s dependent.Estimative operations are defined as activities thatinvolve gathering information, acquiringknowledge, and identifying alternatives (Orem,2001; Dennis, 1997). Transitional operations arebehaviors such as considering various options,making decisions, and planning what action needsto be taken (Orem, 2001; Dennis, 1997).Production operations involve taking action,identifying resources, and evaluating the results ofthe action to meet the need for self-care ordependent-care (Orem, 2001; Dennis, 1997).Dennis (1997) describes estimative andtransitional operations as primarily cognitiveactivities and production as primarily psychomotor.
Orem’s discussion of operations is instructivewhen examining self-care practices. Self-carepractices related to the universal self-care
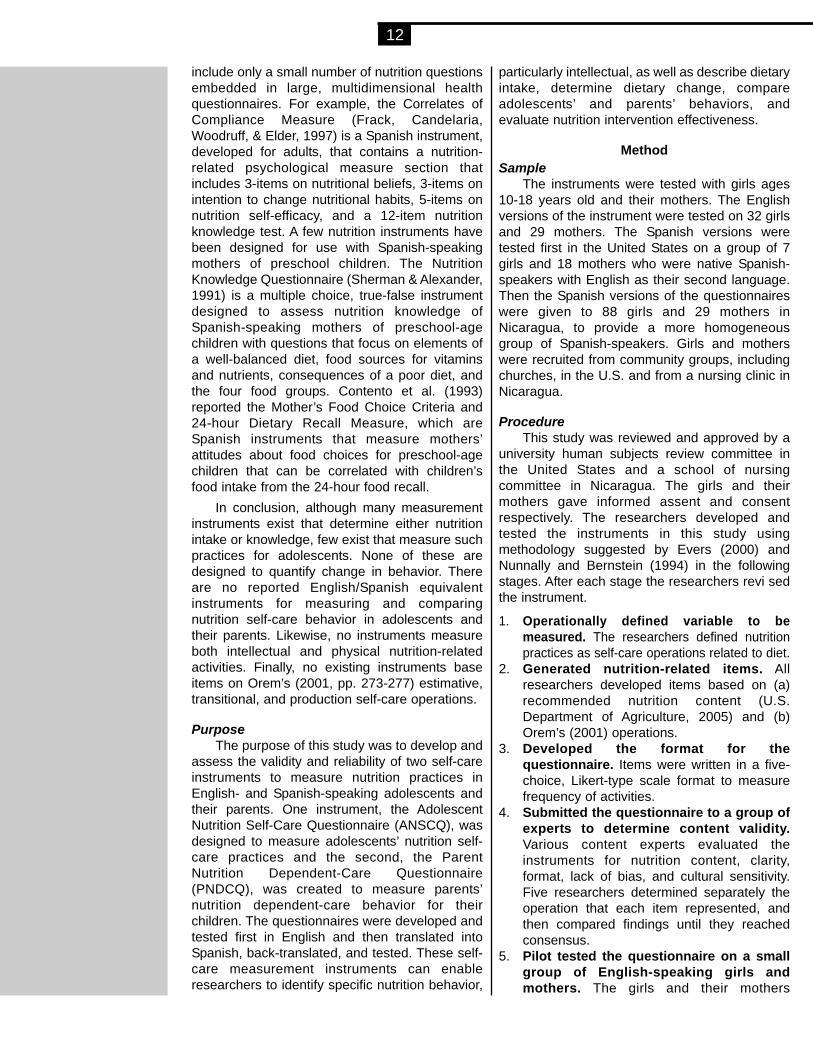
requisite “maintenance of a sufficient intake offood”, for example, involve more than just eatingactivities, according to Orem. Acquiringinformation about foods containing specificnutrients, identifying alternative healthier food,making food-buying decisions, and planninghealthy meals can be among the importantcognitive antecedent activities for meeting thisrequisite. Since the researchers’ goal in this studywas to design instruments to measure bothcognitive and psychomotor nutrition-relatedbehaviors of adolescents and parents, they usedOrem’s operations as a framework for writingitems. Examples of items appear in Table 1. Theyreasoned that measurement of nutrition-relatedoperations, both cognitive and psychosocial, isnecessary to determine current behaviors, designeffective education interventions, or measureoutcomes.
Literature ReviewSince formal publication of Orem’s Self-Care
Deficit Nursing Theory in 1971, a number ofinstruments have been developed to measure theconcepts and aspects of self-care (Dodd, 2004).Most of the self-care instruments that have beendeveloped to date are for use in adults. Severalself-care instruments have been developed foruse with children, adolescents, and theirdependent caregivers. The Denyes Self-CareAgency Instrument (1981) is a 35-item Likertscale instrument that measures the ability ofadolescents to manage self-care. Deynes (1988)also developed a 17-item self-responseinstrument to measure general self-care actionsin adolescents. The Dependent Care AgentQuestionnaire (DCAQ) was developed to studymother’s performances of self-care activities forchildren (Moore & Gaffney, 1989). The Child and
10
Examples of Operation from Instrument ItemAdolescents Parents
I encourage my daughter to:Estimative:• Identify Alternatives
I suggest healthy foods for myfamily to buy
suggest healthy foods for thefamily to buy
Transitional:• Make Decisions• Choose Among
Alternatives• Plan
I eat a variety of food eat a variety of food
I choose to drink soda instead ofwater
choose to drink soda instead ofwater
I plan my meals so that they arehealthy
plan her meals so that they arehealthy
Productive:• Take Action• Evaluate Action
I eat breakfast every day eat breakfast every day
I think about whether my diethas enough protein
think about whether her diet hasenough protein
Table 1 Operations identified in Self-Care nutrition questionnaires

Adolescent Self-Care Practice Questionnaire(CASCPQ) (Moore, 1995) determines children’sand adolescents’ performance as self-careagents. Adapted versions of the CASCPQ andDCAQ were created for use with children withcancer and their parents, respectively (Moore &Mosher, 1997).
A search for nutrition self-care instrumentsbased on Orem’s theory in the CINAHL databaseidentified only two studies that used nutrition self-care instruments. One study used an instrumentto measure self-care/dependent care nutritionknowledge and practices of dependent olderadults and their caregivers (Biggs & Freed, 2000).Another study used an instrument to measurenutrition self-care behavior of myocardialinfarction patients (Aish & Isenberg, 1996). Nostudies were identified that used instrumentsbased on Orem’s Self-Care Theory to measureadolescent nutrition self-care behaviors orparents’ nutrition dependent-care behavior fortheir children.
Regarding the performance of Orem’s self-care operations, only one study has beenreported. Moore and Beckwitt (in press) examinedchildren’s and parents’ performance of operationsin a qualitative study, finding that both childrenand parents reported performing operations in allthree categories.
A variety of methods have been used tomeasure nutrition behavior in children andadolescents. In some studies, the measurementof nutrition behavior in adolescents has beenincorporated into multidimensional instrumentsthat measure many variables, such as healthperceptions, safety, lifestyle practices, and dentalhealth with only a few questions related tonutrition behavior (Graham & Uphold, 1992;McCaleb & Cull, 2004). The Youth Risk BehaviorSurvey is an example of a multidimensionalinstrument that includes a brief section on dietarybehaviors (Centers for Disease Control, 2000).Neumark-Sztainer, Story, Hannan, & Croll (2002)noted that instruments used in large,comprehensive, population-based studies ofadolescent health include very few questionsassessing eating behaviors and these questionshave been limited in scope and not adequatelytested for reliability and validity. The majority ofinstruments used to measure child andadolescent nutrition behavior in studies publishedwithin the past ten years have examined foodconsumption only, such as food frequencyquestionnaires, 24-hour food recalls, or 3-dayfood diaries (Birnbaum, et al, 2002; Frenn, 2003;Hawks, Merrill, & Madanat, 2004; Lytle, Siefert,Greenstein, & McGovern, 2000; Middleman,
Vasquez, & Durant, 1998; National Institutes ofHealth, 2002; Neumark, et al., 2004; Prochaska &Sallis, 2004; Rhiderknecht & Smith, 2004; Siega-Riz, Carson, & Popkin, 1998; Stanton, Fries, &Danish, 2003).
Contento, Randell, & Basch, (2002) reviewedinstruments used in 265 nutrition educationstudies conducted between 1980 and 1999 in sixpopulation groups: preschool children, schoolaged children, adults, pregnant women, olderadults, and professionals. This review noted thatthere were a wide variety of instruments andmethods used to evaluate nutrition educationeffectiveness. Measures evaluating nutritionknowledge and skills were used to evaluatenutrition education effectiveness in 85% of thestudies of school-aged children. Instrumentsmeasuring nutrition attitudes, diet self-efficacy,and intentions to change nutrition behavior werealso used to evaluate nutrition educationeffectiveness in studies of school-aged children.With regard to measuring behavioral outcomes ofnutrition education in school-aged children,Contento et al. (2002) reports that directobservation of actual consumption of school lunchand snacking practices has been used, as wellas, 24 hour dietary recall, 3-day food records, andfood selection inventories.
The outcome of choice in measuring theeffectiveness of nutrition education programs ischange in dietary behavior (Contento et al, 2002).There is no standard definition of nutritionbehavior in dietary studies, however, andmeasurement of behaviors can range from actualintake of specific nutrients to actual food relatedbehaviors. Contento et al. (2002) suggests thatfood related behaviors and eating patterns aremore likely to be correlated with health, ratherthan specific nutrients or foods and thus,instruments that measure food-related behaviorsand eating patterns are a more effectiveevaluation of nutrition education. Contento et al.(2002) identified 10 studies that used instrumentsto measure food-related behaviors and eatingpatterns in adults, but no studies were mentionedthat used food-related behavior or eating patterninstruments in school-aged children.
In general, there is a scarcity of Spanishlanguage instruments available for research withHispanic populations (Carlson, 2000). A search ofthe Health and Psychosocial Instrumentsdatabase from 1985 to 2005 revealed no Spanishinstruments that measure nutrition self-carebehaviors in adolescents and their parents andvery few Spanish instruments that measurenutrition-related variables. Most nutrition-relatedSpanish instruments are designed for adults and
11
include only a small number of nutrition questionsembedded in large, multidimensional healthquestionnaires. For example, the Correlates ofCompliance Measure (Frack, Candelaria,Woodruff, & Elder, 1997) is a Spanish instrument,developed for adults, that contains a nutrition-related psychological measure section thatincludes 3-items on nutritional beliefs, 3-items onintention to change nutritional habits, 5-items onnutrition self-efficacy, and a 12-item nutritionknowledge test. A few nutrition instruments havebeen designed for use with Spanish-speakingmothers of preschool children. The NutritionKnowledge Questionnaire (Sherman & Alexander,1991) is a multiple choice, true-false instrumentdesigned to assess nutrition knowledge ofSpanish-speaking mothers of preschool-agechildren with questions that focus on elements ofa well-balanced diet, food sources for vitaminsand nutrients, consequences of a poor diet, andthe four food groups. Contento et al. (1993)reported the Mother’s Food Choice Criteria and24-hour Dietary Recall Measure, which areSpanish instruments that measure mothers’attitudes about food choices for preschool-agechildren that can be correlated with children’sfood intake from the 24-hour food recall.
In conclusion, although many measurementinstruments exist that determine either nutritionintake or knowledge, few exist that measure suchpractices for adolescents. None of these aredesigned to quantify change in behavior. Thereare no reported English/Spanish equivalentinstruments for measuring and comparingnutrition self-care behavior in adolescents andtheir parents. Likewise, no instruments measureboth intellectual and physical nutrition-relatedactivities. Finally, no existing instruments baseitems on Orem’s (2001, pp. 273-277) estimative,transitional, and production self-care operations.
PurposeThe purpose of this study was to develop and
assess the validity and reliability of two self-careinstruments to measure nutrition practices inEnglish- and Spanish-speaking adolescents andtheir parents. One instrument, the AdolescentNutrition Self-Care Questionnaire (ANSCQ), wasdesigned to measure adolescents’ nutrition self-care practices and the second, the ParentNutrition Dependent-Care Questionnaire(PNDCQ), was created to measure parents’nutrition dependent-care behavior for theirchildren. The questionnaires were developed andtested first in English and then translated intoSpanish, back-translated, and tested. These self-care measurement instruments can enableresearchers to identify specific nutrition behavior,
particularly intellectual, as well as describe dietaryintake, determine dietary change, compareadolescents’ and parents’ behaviors, andevaluate nutrition intervention effectiveness.
MethodSample
The instruments were tested with girls ages10-18 years old and their mothers. The Englishversions of the instrument were tested on 32 girlsand 29 mothers. The Spanish versions weretested first in the United States on a group of 7girls and 18 mothers who were native Spanish-speakers with English as their second language.Then the Spanish versions of the questionnaireswere given to 88 girls and 29 mothers inNicaragua, to provide a more homogeneousgroup of Spanish-speakers. Girls and motherswere recruited from community groups, includingchurches, in the U.S. and from a nursing clinic inNicaragua.
ProcedureThis study was reviewed and approved by a
university human subjects review committee inthe United States and a school of nursingcommittee in Nicaragua. The girls and theirmothers gave informed assent and consentrespectively. The researchers developed andtested the instruments in this study usingmethodology suggested by Evers (2000) andNunnally and Bernstein (1994) in the followingstages. After each stage the researchers revi sedthe instrument.
1. Operationally defined variable to bemeasured. The researchers defined nutritionpractices as self-care operations related to diet.
2. Generated nutrition-related items. Allresearchers developed items based on (a)recommended nutrition content (U.S.Department of Agriculture, 2005) and (b)Orem’s (2001) operations.
3. Developed the format for thequestionnaire. Items were written in a five-choice, Likert-type scale format to measurefrequency of activities.
4. Submitted the questionnaire to a group ofexperts to determine content validity.Various content experts evaluated theinstruments for nutrition content, clarity,format, lack of bias, and cultural sensitivity.Five researchers determined separately theoperation that each item represented, andthen compared findings until they reachedconsensus.
5. Pilot tested the questionnaire on a smallgroup of English-speaking girls andmothers. The girls and their mothers
12

evaluated the instruments for directions,clarity, format, and time for administration.
6. Translated the questionnaire into Spanish.Guidelines for translation, as discussed byCarlson (2000), were followed. These includeselection of an expert translator, back-translation, pretesting in a field test, and pilottesting.
7. Pretested the questionnaire on a smallgroup of Spanish-speaking girls andmothers. Spanish-speaking girls andmothers in the U. S. suggested manyrevisions in the Spanish translation.
8. Consulted a nursing faculty member inNicaragua to translate the items intoNicaraguan Spanish. The Nicaraguanresearcher and another native Spanish-speaker suggested changes in the Spanishtranslation based on the language and cultureof Nicaragua.
9. Pilot tested the questionnaire with girlsand their mothers in Nicaragua. TheSpanish versions of the questionnaires wereused with girls and mothers in Nicaragua.
10. Conducted item analysis on thequestionnaire. Item analyses werecalculated on both English and Spanishversions for girls and mothers.
11. Calculated reliability. Reliabilities werecalculated for both English and Spanishversions for girls and mothers.
12. Performed an additional check forevidence of validity. Participants were askedwhether they could answer the before andafter questions accurately.
InstrumentsThe Adolescent Nutrition Self-Care
Questionnaire (ANSCQ), designed by theresearchers, is a 37-item questionnaire tomeasure nutrition self-care practices based onOrem’s operations (2001). The questionnairemeasures frequency of behavior in a 5-choiceLikert-type scale format with choices of never,rarely, sometimes, most of the time, and alwayswith higher scores indicating better nutritionpractices. Eleven of the items are reversed.
The Parent Nutrition Dependent-CareQuestionnaire (PNDCQ) was developed by theresearchers to measure nutrition dependent-careoperations that parents perform for their daughters.It is a 37-item instrument that measures frequencyof behavior in a 5-choice Likert-type scale formatwith the same choices ranging from never toalways. All items are prefaced with the statement,“I encourage my daughter to…” Its itemscorrespond with the same topics in the same orderas the girl’s questionnaire. For example, item # 6
on the girl’s questionnaire is, “I suggest healthyfoods for my family to buy.” Item #6 on the parents’questionnaire is, with the preface, “Suggesthealthy foods for the family to buy.” The same 11items are reversed. See Table 1 for additionalexamples of items.
The questionnaires are designed to measurebefore and after behaviors on the same form atthe same time. For other research they could bedivided into tools that measure behaviors at onetime only.
Content validityContent validity is defined in the Standards for
Education and Psychological Testing (AmericanEducational Research Association, 1999) as alogical analysis of the adequacy with which thetest content represents the content domain. Theresearchers developed the items based on the U.S. Department of Agriculture guidelines (2005)and Orem’s (2001) operations. To provide furthercontent validity evidence, the questionnaires werereviewed by a panel of 11 experts including apediatric nurse researcher, a nutritionalanthropologist, a psychometrician, a nurseanthropologist, a nutritionist, two native Spanishspeakers, and four nursing doctoral students. Ofthese experts, four had been conducting anutrition intervention study in Nicaragua for fouryears, one was a native of Nicaragua and a facultymember at a school of nursing in Nicaragua, twohad been involved in various nursing projects inNicaragua, and one was conducting dissertationresearch on pediatric nutrition.
The experts made several suggestions forchanges in substance, wording, and format for thequestionnaires that were implemented. Oneexpert questioned whether participants couldremember previous dietary behavior and theresearchers investigated that issue during the pilotstudy. As a check for memory of before and afterbehavior, the researchers asked both English andSpanish-speaking groups if they could accuratelyanswer the questions. Participants reported thatthey could do so successfully. In general, theexperts agreed that the items were clear,represented the nutrition content, and wereunbiased. When the researchers assigned eachitem to an operational category, they reachedconsensus that items represented the threeoperational categories as shown in Table 1.
FindingsThe researchers examined the psychometric
properties of the instruments including contentvalidity, item analysis, and reliability. The contentvalidity was established using Orem’s (2001)operations, U.S. Department of Agriculture
13

guidelines (2005), and content expert evaluation.The results indicated that there was acorrespondence between the questionnaire itemsand the intended content domain.
Researchers conducted item analysis on theitems, examined the item-total correlations, foundthem to be acceptable, and estimated the internalconsistency reliability of the instruments. Theinternal consistency method of estimatingreliability focuses on the shared content of theitems or whether the items are homogeneous. Inthis study, estimates of internal consistency weredetermined using coefficient alpha. Methods forestimating reliability differ with respect to thesources of error being addressed. The presentstudy used coefficient alpha because itaddresses errors due to sampling of content ordomain, that is the degree to which the items arerepresentative of the content being measured(Pedhazur & Schmelkin, 1991). The coefficientsalpha were estimated and reported for theEnglish and Spanish versions of the before andafter data for both instruments. Although theminimum recommended standard for coefficientalpha varies among psychometricians, Nunnallyand Bernstein (1994) recommend a threshold of.70. The reliability coefficients for the instrumentsin this study are shown in Table 2. Thecoefficients alpha are above the threshold for allversions, except for the English version of theparents’ posttest at .67. If one specific item in thatversion were dropped, the coefficient alphawould be.72.
Table 2 Reliability Coefficients for the NutritionBehavior Questionnaires
Girls: Nutrition Self-Care BehaviorQuestionnaire
Coefficient CoefficientAlpha Alpha
Mothers: Nutrition Dependent-CareBehavior Questionnaire
Coefficient CoefficientAlpha Alpha
DiscussionBoth the Adolescent Nutrition Self-Care
Questionnaire and the Parent Nutrition Dependent-Care Questionnaire are instruments that werecreated to measure nutrition behaviors in English-or Spanish-speaking populations. Validity andreliability have been examined and established forthese instruments. For construct validity, factoranalysis will be conducted in the future on theinstruments when sample sizes in each group aresufficient.
Orem’s (2001) theory was useful in developingitems to measure both cognitive and psychomotoractivities. At present the majority of items measureoperations in the “take action” category, rather thanbeing evenly distributed among variousoperations. More items should be added to theinstruments reflecting the operations “acquiringknowledge”, “making decisions”, and “planningactions.” When compared to other nutritionmeasurement instruments in the literature, theseinstruments target areas previously unaddressed:matching adolescents and their parents,English/Spanish equivalent forms, comparison ofbefore and after behaviors, and inclusion of bothcognitive and psychomotor behaviors. So far theseinstruments have been tested only on girls andmothers and only in the United States andNicaragua. Nicaraguan Spanish may be somewhatdifferent than Spanish spoken in other countries.
The Adolescent Nutrition Self-CareQuestionnaire (ANSCQ) and the Parent NutritionDependent-Care Questionnaire (PNDCQ) can bevaluable instruments for various future researchinvestigations, such as describing nutritionpractices, comparing adolescents and parents’behavior, comparing practices in English- andSpanish-speaking populations, examiningadolescents and parents’ self-care operations,and determining the effectiveness of a nutritionintervention.
We will be pleased to share the questionnaireswith other researchers. We would appreciatethose researchers sharing their results with us sothat we can perform further analysis on thequestionnaires in the future.
Jean Burley Moore, RN, PhD, is Associate Professor, Collegeof Nursing, Lisa Pawloski, PhD, Heibatollah Baghi, PhD, KarenWhitt, MSN, Doctoral Candidate, Claudia Rodriguez, BS andAdel Bashatah, MS, Doctoral candidate, all with George MasonUniversity, Fairfax, Virginia. Laura Lumbi, MSN, is withUniversidad Politecnica de Nicaragua, Managua, Nicaragua.Contact Dr. Moore: Email: [email protected].
References
Aish, A. E., & Isenberg, M. (1996). Effects of Orem-basednursing intervention on nutritional self-care of myocardialinfarction patients. International Journal of Nursing
14
Before
After
English Version Spanish Version.8258 .9096
.8132 .9053
Before
After
English Version Spanish Version.7500 .8156
.6694 .9419

Studies, 33(3), 259-270.American Educational Research Association, American
Psychological Association & National Council onMeasurement in Education. (1999). Standards foreducational and psychological testing, Washington, DC:Author.
Biggs, A. J., & Freed, P. E. (2000). Nutrition and older adults:What do family caregivers know and do? Journal ofGerontological Nursing, 26(8), 6-14.
Birnbaum, A. S., Lytle, L. A., Story, M., Perry, C. L., & Murray,D. M. (2002). Are differences in exposure to amulticomponent school-based intervention associatedwith varying dietary outcomes in adolescents? HealthEducation & Behavior, 29(4), 427-443.
Carlson, E. D. (2000). A case study in translation methodologyusing the Health-Promotion Lifestyle Profile II. PublicHealth Nursing, 17(1), 61-70.
Centers for Disease Control and Prevention. (2000). Youth riskbehavior surveillance- United States, 1999. MMWRMorbidity and Mortality Weekly Report, 49, 1-89.
Contento, I. R., Basch, C., Shea, S., Gutin, B., Zybert, P.,Michela, J. L., et al. (1993). Relationship of mothers’ foodchoice criteria to food intake of preschool children;Identification of family subgroups. Health EducationQuarterly, 20, 243-259.
Contento, I. R., Randell, J. S., & Basch, C. (2002). Review andanalysis of evaluation measures used in nutritioneducation intervention research. Journal of NutritionEducation and Behavior, 34(1), 2-25.
de Onis, M., Frongillo, E. A., & Blossner, M. (2000). Ismalnutrition declining? An analysis of changes in levelsof child malnutrition since 1980. Bulletin of the WorldHealth Organization, 78(10), 1222-1233.
Dennis, C. M. (1997). Self-care deficit theory of nursing. St.Louis: Mosby.
Denyes, M. J. (1981). Development of an instrument tomeasure self-care agency in adolescents.University ofMichigan, Dissertation Abstracts International, 41(5),1715B.
Denyes, M. J. (1988). Orem’s model used for healthpromotion: Directions for research. Advances in NursingScience, 11, 13-21.
Dodd, M. J. (2004). Measuring Self-Care Activities. In M.Frank-Stromborg & S. J. Olsen (Eds.), Instruments forClinical Health-Care Research (3rd ed.). London: Jonesand Bartlett.
Evers, G. (2000, February). Measurement of self-care in clinicalpractice. Paper presented at the 6th International Self-CareDeficit Nursing Theory conference, Bangkok, Thailand.
Frack, S. A., Candelaria, J., Woodruff, S. I., & Elder, J. P.(1997). Correlates of compliance with measurementprotocols in a Latino nutrition-intervention study.American Journal of Preventive Medicine, 13, 131-136.
Frenn, M. (2003). Peer leaders and adolescents participatingin a multicomponent school based nutrition interventionhad dietary improvements. Evidence-Based Nursing,6(2), 44.
Graham, M. V., & Uphold, C. R. (1992). Health perceptionsand behaviors of school-age boys and girls. Journal ofCommunity Health Nursing, 9(2), 77-86.
Guthrie, J. F., Lin, B. H., & Frazao, E. (2002). Role of foodprepared away from home in the American diet 1977-78versus 1994-96. Journal of Nutrition Education andBehavior, 34, 140-150.
Hawks S. Merrill RM. Madanat HN. The Intuitive Eating Scale(IES) (2004). American Journal of Health Education,35(2): 90-9.
Lytle, L. A., Seifert, S., Greenstein, J., & McGovern, P. (2000).How do children’s eating patterns and food choiceschange over time? American Journal of HealthPromotion, 14(4), 222-228.
McCaleb, A., & Cull, V. V. (2000). Sociocultural influences andself-care practices of middle adolescents. Journal ofPediatric Nursing, 15(1), 30-35.
Middleman, A. B., Vazquez, I., & Durant, R. H. (1998). Eatingpatterns, physical activity, and attempts to change weightamong adolescents. Journal of Adolescent Health, 22(1),37-42.
Moore, J. B. (1995). Measuring the self-care practice ofchildren and adolescents: Instrument development.Journal of Maternal Child Nursing, 23(3), 101-108.
Moore, J. B. (in press). Self-care operations and nursinginterventions for children with cancer and their parents.Nursing Science Quarterly.
Moore, J. B., & Gaffney, K. F. (1989). Development of aninstrument to measure mothers’ performance of self-careactivities for children. Advances in Nursing Science,12(1), 76-83.
Moore, J. B., & Mosher, R. (1997). Adjustment responses ofchildren and their mothers to cancer: Self-care andanxiety. Oncology Nursing Forum, 24, 519-525.
National Institutes of Health, Applied Research Program,National Cancer Institute, (2002). Diet HistoryQuestionnaire, Version 1.0.
Neumark-Sztainer, D., Story, M., Hannan, P. J., & Croll, J.(2002). Overweight status and eating patterns amongadolescents: Where do youths stand in comparison withthe Healthy People 2010 objectives? American Journal ofPublic Health, 92(5), 844-851.
Norton, D. E. (2003). Eating and exercise behaviors inpreadolescents: Parental influence? UnpublishedDissertation, University of California, San Francisco.
Nunnally, J., & Bernstein, I. (1994). Psychometric Theory. NewYork: McGraw Hill.
Orem, D.E. (2001). Nursing: Concepts of practice (6th ed.). St.Louis: Mosby.
Orem Study Group (2004). Working papers. Cloppenburg,Germany: Institute fur Pflegediagnosik & Praxisforschung.
Pedhazur, E. J., & Schmelkin, L. P. (1991). Measurement,design, and analysis. Hillsdale, NJ: Lawrence Erlbaum.
Pena, M. and Bacallao, J. (2000) eds. Obesity and Poverty: Anew public health challenge. Washington DC: PanAmerican Health Organization.
Prochaska, J. J., & Sallis, J. F. (2004). A randomized controlledtrial of single versus multiple health behavior change:Promoting physical activity and nutrition amongadolescents. Health Psychology, 23(3), 314-318.
Produce for Better Health Foundation. (2003). State of theplate: Study on America’s consumption of fruits andvegetables. Wilmington, DE: Produce for Better HealthFoundation.
Rinderknecht, K., & Smith, C. (2004). Social cognitive theoryin an after-school nutrition intervention for urban NativeAmerican youth. Journal of Nutrition Education andBehavior, 36(6), 298-304.
Sherman, J. B., & Alexander, M. A. (1991). Nutrition KnowledgeQuestionnaire. Public Health Nursing, 8, 53-58.
Siega-Riz, A. M., Carson, T., & Popkin, B. (1998). Threesquares or mostly snacks—what do teens really eat?: Asociodemographic study of meal patterns. Journal ofAdolescent Health, 22(1), 29-36.
Stanton, C. A., Fries, E. A., & Danish, S. J. (2003). Racial andgender differences in the diets of rural youth and their
15
mothers. American Journal of Health Behavior, 27(4),336-347.
U. S. Department of Health and Human Services. (1998). TheSurgeon General’s Report on Nutrition and Health.Washington, DC: U. S. Department of Health and HumanServices.
U. S. Department of Health and Human Services. (2000).Healthy People 2010. Retrieved July 14, 2005, fromhttp://www.healthypeople.gov
U.S. Department of Agriculture (2005). MyPyramid.gov: Newsand Media. Retrieved July 19, 2005, fromhttp://www.mypyramid.gov/global_nav/media.html
16

We are fortunate to have one of our experienced educatorsrelate to us her Self-Care Deficit Nursing Theory (SCDNT)-based curriculum experiences. Part I features the initialhermeneutic journey and teaching nursing using Orem’sSCDNT in a baccalaureate degree completion program. PartII will follow in our next issue on Education. The focus of PartII will be on teaching nursing assessment and fundamentalskills and clinical courses for traditional baccalaureate nursingstudents, including application of SCDNT in a theoreticalnursing assessment and nursing care plan forms used by theprogram and graduate nursing theory, again emphasizingapplication and use of Orem’s SCDNT.
V. Berbiglia, Guest Editor
BackgroundHaving taught nursing in two associate degree
programs in Southwestern and Western UnitedStates, I began preparations for entering a doctorof philosophy (PhD) in a nursing program. Ibelieved I needed further education as theprogram where I was teaching developed a two-plus-two baccalaureate nursing program. This wasat a time when physical assessment wasbecoming a nursing buzzword; and I wanted tounderstand better what a nursing assessment was.
Doctoral StudiesEarly in my doctoral studies, the director of
the doctoral program invited newly admittedstudents to her home to meet a visiting nursephilosopher and theorist, Martha Rogers. I,admittedly, did not know much about any nursingtheory or nursing theorist, so decided I had betterread a book that had come to my office as a deskcopy for review and possible course adoption.The book (Nursing Theories Conference Group,1980) was a synopsis of several nursing theories,including Martha Rogers’ Science of Unitary Man(before the change to Human Being) andDorothea Orem’s Self-Care Deficit NursingTheory, among others. While this first encounterwith Orem’s theory was in a secondary source, itwas the beginning of my hermeneutic journey.
I am a scribbler in books, making marginalnotes and underlining or highlighting passages ofthe text that stand out to me. A few years later,
when I was working on my dissertation onmetaphors of nursing in Orem’s work, I needed togo back to this first source on Orem, and, to mysurprise, found many marginal notes andunderlining and a picture of my infant daughter asa bookmark in the chapter on Orem’s theory.There were fewer marks in the chapter on Rogers’theory, which I had thought I should read beforemeeting Martha Rogers! I was surprised becauseI had no real recollection of having read andmarked up the chapter on Orem’s theory! Inhermeneutics, this is spoken of as being graspedby the theory rather than grasping it (Bleicher,1980; Ricoeur 1975, 1976, and 1981).
During the PhD Program there was, ofcourse, the required course on theoryconstruction, development, analysis andevaluation. I read, studied and used a variety ofarticles and books on analyzing and evaluatingtheory (Ellis, 1968; Duffey & Mulhenkamp, 1974;Stevens, 1979; Fawcett, 1978; Fawcett, 1980;Meleis, 1985; Chinn & Jacobs, 1983). Finally, Ifocused my attention on Orem’s SCDNT, feelingdrawn to the philosophy and theory. Still there wasdissatisfaction with knowing what the Self-CareDeficit Nursing Theory says using theaforementioned traditional methods of theoryanalysis and evaluation which put questions(sometimes more than 60 questions!) to thetheory, looking for the hidden meaning of thetheory. I began searching for understanding themeaning of the theory using hermeneuticinterpretation method (Ricoeur, 1975). This led toidentifying the metaphors of nursing in Orem’swork: Nursing as a Practice Discipline; Nursing asDeliberate Action; Nursing as a Helping, HumanHealth Service and Science; and Nursing asCare—Self-Care of Another Self (Biggs, 1999).Metaphors carry the meaning of a text or theoryand are projected upfront and not hidden in thetext or the mind of the author. The identification ofthese metaphors of nursing and the nexus ofmetaphors connected with them and with theconcepts of the General Theory of Nursing
17
Teaching Practically Practical Nursing Science,Part I
Anna J. Biggs

(SCDNT) (Orem, 1985; Orem, 2001) provided thedeeper understanding of the world of nursing thatI was seeking so that I could better express tostudents what a nursing assessment would be.
Teaching in a SCDNT- Based CurriculumAfter completing my doctorate, I began
teaching in a baccalaureate completion program(RN to BSN) in a mid-western United Statespublic university in a major metropolitan area,where Orem’s theory was the conceptualframework for the curriculum. I was delighted tobe assigned to teach an introductory course onthe dimensions of professional nursing where Iwould be introducing undergraduate nursingstudents (formerly diploma and associate degreeregistered nurses) to Dorothea Orem’s theory. Irecall one semester where, as usual, I had askedstudents why they became a nurse and jottedtheir responses of wanting to help people on theblackboard. I then used that notion of helpingpeople to begin talking about Dorothea Orem’stheory and the metaphors of nursing that hadhelped me better understand nursing. Onestudent had her arms crossed and took no notesduring the entire introduction to the course,assignments, and requirements. When I movedon into talking about helping as one of themetaphors of nursing in SCDNT and how wewould use a practice model (see Figure 1) toexamine the dimensions of professional nursing, Inoticed this student writing notes as rapidly aspossible. She came up during a break and askedfor some additional references and I thought,“you’ve been caught as I was!” In fact, she laterserved as a research assistant on some of myresearch to test the Biggs’ Elderly Self-CareAssessment Tool (BESCAT) (Biggs, 1990).
One of the activities in this course was tocritically analyze the kardexes and nursing careplans in use in students’ current employmentsituations. Students were challenged to see ifthere could be connections made to Orem’sSCDNT. I was impressed with their efforts. Someexamples of their applications of SCDNTincluded:
• Connecting orders for pulse oximetryreadings and oxygen administration to“maintaining an adequate intake of air”
• Changing the wording regarding parenteral(IV) fluid administration to “maintaining anadequate intake of water”
• Altering standardized nursing care plans forfall prevention to address “prevention ofhazards”
Students were able to reconceptualizekardexes and nursing care plans in terms of
universal self-care requisites. This new foundability may not seem tremendous or impressive tothose who have been using Orem’s theory, but,for nurses prepared at a technical level, returningfor their baccalaureate degree, this is an eyeopening or gestalt experience. Most weredelighted to have a better appreciation for all thethings they did to care for patients. They felt thatthe nursing care they gave, using Orem’s theory,was actually moving them from a technical level ofnursing to a more professional level.
Students working in pediatrics and obstetricsalso used maturational and situationaldevelopmental self-care requisites, respectively,in developing appropriate nursing care plans,along with universal self-care requisites. Therewas a diabetes nurse educator in one of theclasses who exclaimed, regarding the healthdeviation self-care requisites, “Now, I have amore comprehensive way of looking at andteaching diabetes self-care management. WithOrem’s theory to help my patients understandtheir pathological condition, be aware of andattend to the effects of their diabetes and carry outthe prescribed therapy and regulate theirfunctioning, modify their self-concept byaccepting themselves as having a pathologiccondition and needing specific forms of healthcare, all the while learning to live with theircondition in a life-style that promotes theircontinued personal development! This is just whatI have needed for a long time!”
Dorothea Orem (1985) noted that nurses oftenstart at the level of universal and developmentalself-care requisites and basic conditioning factors.However, she concluded that there is a need forcloser examination of the health deviation self-carerequisites and a thorough description anddiscussion of “nursing cases” concerning thehealth deviation self-care requisites and the powercomponents of self-care agency. For thesebeginning professional nurses, I believed theirstrides toward a more comprehensive nursingapproach to be note-worthy.
When we examined currently used nursinghistory forms, students were distressed to see howmuch of the nursing history was really a repetitionof the medical history and physical examination.That led to discussions of the proper object ofnursing and the domain of nursing (Orem,1980,1985, 1995, 2001) as well as how the initialnursing history forms could be more relevant tonursing care. As we moved into examining thebasic conditioning factors (BCF’s) (see Figure 1) toindividualize the universal, developmental andhealth deviation self-care requisites, most of theseregistered nurses began seeing the need for
18

19
Figure1. Practice Model of Orem's Self-Care Deficit Nursing Theory
Self-Care Requisites are individualized by theBASIC CONDITIONING FACTORS
Resulting in the determination of theTHERAPEUTIC SELF-CARE DEMAND
which is compared with
SELF-CARE AGENCYAssessed by analyzing the ten power components toevaluate development, operability and adequacy for
meeting self-care demandsand demonstrates or identifies the
SELF-CARE DEFICIT
which determines the
NURSING SYSTEMWholly compensatory, Partly Compensatory, Supportive-Educative
Implemented by the METHODS OF ASSISTINGActing for/doing for Another, Guiding Another, Supporting Another,
Providing an Environment for the development of Self-Care Agency,Teaching Another
Reassess TSCD, Evaluate Outcomes , and Replan/Redesignthe NURSING SYSTEM
The Universal, Developmental, and Health-Deviation Self-Care Requisites (SCR's) are individualized by the BasicConditioning Factors (BCF's) to determine the person's (patient's) Therapeutic Self-Care Demand (TSCD), thetotal care needed at this point in time. When we compare the Self-Care Agency (SCA, ability to care for self) orthe Dependent-Care Agency (DCA, one's ability to care for one's dependents) with the TSCD, we find whether ornot the person has a Self-Care Deficit (SCD, inability to care for one's self) or a Dependent-Care Deficit (DCD,inability to care for one's dependents) because of the situation of personal health. A Self-Care Deficit (orDependent-Care Deficit) is what legitimizes the need for nursing. If there is an SCD or DCD due to the person'sor dependent's health state, then a Nursing System is needed and designed. The Nursing System is prescribedas Wholly Compensatory, Partly Compensatory, or Supportive-Educative. The designed Nursing System isimplemented by means of the five Methods of Assisting, and is further specified by the nursing actions to be takenwithin the general method of assisting. The designed Nursing System is evaluated in terms of the development ofregained ability to exercise and regulate Self-Care Agency (or Dependent-Care Agency). Reassessment,replanning or redesigning results from this evaluation in the management of nursing care.
UNIVERSALSELF-CAREREQUISITES
DEVELOPMENTALSELF-CAREREQUISITES
HEALTHDEVIATION SELF-CARE REQUISITES
If TSCD < or = SCA, then noSCD, and no NursingSystem is needed
TSCD - SCA = SCDor
TSCD > SCA = SCD

altering their employer’s nursing history forms toaddress more of the items in the BCF’s becausethat was truly the information nurses needed toprovide nursing care.
Discussions of which nursing system wasapplicable in certain nursing situations werelikewise very stimulating. Students posedquestions such as:
• When is a patient in need of a whollycompensatory nursing system?
• What if there were family members who couldmake decisions for needed care andparticipate in care?
• If patients could do nothing for themselves,such as in an intensive care unit of sedated-ventilated patients, were the patients in awholly compensatory nursing system?
• How did family involvement in decision-making and care fit with definitions ofdependent care agency?
• How did nursing agency link with self-careagency and/or dependent-care agency?
Students who were in home health careagencies or who were patient educators inhospital settings were very interested in theconcepts of “multi-person units” of families andpopulations of patients. They recognized that theultimate basic unit of care was the individual, the“Another Self” (Orem, 1980, 1985, 1995, 2001),who needed self-care; but, because of thesituation of personal health, was unable toprovide care for self.
Students were also able to classify nursinginterventions from the standardized care plansused in their employment situations with thecategories of the methods of assisting. They foundthat much of the focus at that time was onteaching patients, with much less attention toacting for/doing for another, guiding another,supporting another, and providing an environmentin which patients could develop their self-careagency. Seeing that nursing was so much morethan only teaching helped many of them to workon expanding the care plans that were in use andto join practice committees at their employinginstitutions to try to make some of these changes.I believe this change in attitude of technical nursesin a baccalaureate completion program, as theyexamined the focus, nature and structure ofnursing in preparation for becoming professionalnurses, is an example of what Orem discussed ina recent article on Nursing Practice Science:
Nurses who have or are achievingprofessional status have responsibility forthe development of nursing science.Becoming and being professional
requires understanding of the focus, thenature, the structure, the content, and thedomain of nursing science in relationshipto the focus of and the realities that definethe domain of nursing practice (Orem,2004, p. 4).
These positive reflections should not beconstrued to mean that there were never groansor murmuring and complaining about “having tostudy Orem.” There was plenty of that, too.Students who did not want to have to read, studyand think/reflect about their nursing practice werevocal in their preference for continuing theiratheoretical nursing practice. They preferred theirreflexive knee-jerk responses to situations like anempty IV or a patient’s request for painmedication, or a critical situation such as internalbleeding or wound dehiscence and evisceration.My intent was to foster a reflective (deliberate)nursing practice where:
• The IV might have been ready before thecurrent bag was empty (to maintain anadequate intake of water).
• The patient’s pain might be anticipated andmedications offered to manage pain before itbecame severe (promoting normalcy).
• Internal bleeding might have been thought ofas a possibility and assessments madebefore it became a critical situation(maintaining an adequate intake of air asoxygen at the cellular level and the impact ofbleeding and shock on air and oxygenation).
• A fragile wound might be managed by nursingcare to prevent or at least find the earliestsigns before there was evisceration(prevention of hazards).
Students who did not want to have tochallenge their supervisors and colleagues to ahigher level of practice were also among thosewho didn’t want to use a theory that might causethem to have to rock the boat. It is probablyapparent which group of nurses would bepreferred for caring for family members of thoseascribing to the use of Orem’s Self-Care DeficitNursing Theory! The challenge to faculty was totry to find the message that would hook the moreresistant students or to acknowledge that notevery student would be able to move into thatlevel of professional thinking and practice.
Change from Teaching in a SCDNT-BasedCurriculum to a Self-Care Systems Model-Based Curriculum
Sadly, at a curriculum workday in this college,a part-time clinical instructor, who rarely attendedfaculty committees or workdays, asked why wehad to keep using Orem’s theory because she
20
had not read it and did not plan to and thought weought to just drop it. I was nearly speechless andspent the lunch time writing about what usingOrem’s theory did in terms of helping to structureand organize the curriculum and nursing practice,using an analogy of lemonade made from powder,or frozen concentrate with lemonade made fromfresh lemons. However, I was one lone voice; andthe vote was to change to an undefined (and un-definable without using Orem’s SCDNT!) “self-care systems model”. The courses weresubsequently changed and re-titled, so there wasno longer a course entitled “Designing NursingSystems for Families and Groups”, nor a courseon “Teaching and Supporting Individuals andGroups” and so forth. The entire curriculum lost itsstructure, cohesiveness and organization andbecame a listing of required courses for obtaininga bachelor’s degree in nursing.
Because Orem’s SCDNT pervaded mynursing practice or my own structure andorganization as an educator, I was able tocontinue teaching in this program. My teachingassignment was changed to teaching a course oncomputers in nursing, where students used wordprocessing to write essays about “self-carenursing systems” after reading a description ofwholly compensatory, partly compensatory andsupportive-educative nursing systems. Studentsdevised databases to collect information on basicconditioning factors. They created spreadsheetswith narrative and numerical data on maintainingan adequate intake of oxygen and hemodynamicmonitoring data; or maintaining an adequateintake of water and food with IV fluid and totalparenteral nutrition (TPN) ingredients or oral foodintake. When students would ask where I got theideas for their assignments, I would smile andthen give them the reference to the current editionof Orem’s work. Some would respond with “Wow,that is really interesting that all this could comefrom a nursing theory!” So, even a computercourse could be used to fulfill my need to continueto use Orem’s theory in teaching and practice.
When a nursing educator is committed to atheory-based nursing practice using SCDNT,teaching nursing students to know and perhapseven understand and appreciate Orem’s SCDNT,will be natural, even in the face of curricular andteaching assignment changes. The second article(Part II) will continue the discussion of usingOrem’s SCDNT in a traditional baccalaureateprogram in a variety of courses: nursingassessment, fundamental skills, clinical practice,and graduate nursing.
Anna J. Biggs, RN, PhD, is Assistant Professor at St. LouisUniversity, St. Louis, MO. Contact Dr. Biggs at:[email protected]
References
Biggs, A.J. (1990). Family caregiver versus nursingassessments of elderly self-care abilities. Journal ofGerontological Nursing, 16(8), 11-16, 36-37.
Biggs, A.J. (1999, April). The language of Self-Care DeficitTheory. International Orem Society Newsletter, 7(1), 3-7.
Bleicher, J. (1980). Contemporary hermeneutics:Hermeneutics as method, philosophy, and critique.London: Routledge and Kegan Paul.
Chinn, P. L., & Jacobs, M. K. (1983). Theory and nursing: Asystematic approach. St. Louis: Mosby
Duffey, M., & Muhlenkamp, A. F. (1974). A framework fortheory analysis. Nursing Outlook, 22(9), 570-574.
Ellis, R. (1968). Characteristics of significant theories. NursingResearch, 17, 217-222.
Fawcett, J. (1978). The relationship between theory andresearch: A double helix. Advances in Nursing Science,1(1), 49-62.
Fawcett, J. (1980, Nov-Dec). A framework for analysis andevaluation of conceptual models of nursing. NurseEducator, 5(6), 10-14.
Meleis, A. (1985). Theoretical nursing: Development andprogress. Philadelphia: J. B. Lippincott Company.
The Nursing Theories Conference Group. (1980). Nursingtheories: The base for professional nursing practice.Englewood Cliffs, N. J.: Prentice-Hall.
Orem, D. E. (1980). Nursing: Concepts of practice. (Secondedition). New York: McGraw-Hill.
Orem, D. E. (1985). Nursing: Concepts of practice. (Thirdedition). New York: McGraw-Hill.
Orem, D. E. (1991). Nursing: Concepts of practice. (Fourthedition). St. Louis: Mosby.
Orem, D. E. (1995). Nursing: Concepts of practice. (Fifthedition). St. Louis: Mosby.
Orem, D. E. (2001). Nursing: Concepts of practice. (Sixthedition). St. Louis: Mosby.
Orem, D. E. (2004). Reflections on nursing practice science:The nature, the structure and the foundation of nursingsciences. Self-Care, Dependent-Care and Nursing,12(3), 4 – 11.
Ricoeur, P. (1975). The rule of metaphor: Multidisciplinarystudies of the creation of meaning in language. Toronto:University of Toronto Press.
Ricoeur, P. (1976). Interpretation theory: Discourse and thesurplus of meaning. Fort Worth, TX: The Texas ChristianUniversity Press.
Ricoeur, P. (1981). Hermeneutics and the human sciences.Cambridge, MA: Cambridge University Press.
Stevens, B. (1979). Nursing theory. Boston: Little Brown andCoimpany.
21

AbstractThe purposes of this paper are to describe the CommunityCare Deficit Nursing Model (CCDNM) and two caseapplications using the CCDNM in the education of graduatestudents. The students were able to apply the model to benefitthe communities studied. Students derived a holisticunderstanding of the communities and the actual CommunityDeficits from the perspective of the community members.
Key terms: Theory, CCDNM, Orem, Community, Public Health,Teaching, Graduate Education
Orem’s Self-Care Deficit Nursing Theory (S-CDNT) has been applied extensively to individuals.Fewer applications have been accomplished incommunity care when a population is themultiperson unit of care. The Community CareDeficit Model (CCDM) and Diagnosis ofCommunity Care Deficit Instrument (DCCDI) weredeveloped by faculty and graduate students atWest Texas A& M University (WTAMU). Orem’s(2001) Self-Care Deficit Nursing Theory (S-CDNT)is the foundation for all graduate nursing courses,as well as the practice theory for faculty andstudents at WTAMU. The development of thisframework and its utilization were integral parts ofthe teaching methodology used in a master’s levelcommunity health nursing course.
ProcessStudents began the community health course
with a review of the community health nursingliterature. Notably lacking was a full extension ofS-CDNT to the population as the multiperson unitof care and the recognition that, as a unity of care,the population must meet unit health demands.Therefore, the foundational work of Taylor andRenpenning (cited in Orem, 2001; Taylor andMcLaughlin, 1991) were used as a launchingpoint from which to begin the process of derivinga theory of population care from S-CDNT. Theprinciples and process of theory derivationdescribed by Walker and Avant (1995) werehelpful in the process of developing this model.Through examining analogous relationships,theory derivation stimulates the invention of new
constructs and explanations related to aphenomenon in one field in order to obtainconcepts and explanations in another field. Theprocess was modified to use S-CDNT to derivenew constructs that would be helpful in extendingthe theory to describe a community or populationas the unit of service. The results were thedevelopment of a conceptual model ofCommunity Care Deficit Nursing extension of S-CDNT and a community diagnosis instrumentbased on the model.
A Community Care Deficit Instrument wasdeveloped based on the Community Care DeficitModel. Both the model and the instrument werecompared to community health nursing theoriesand community assessment models in terms ofphilosophical underpinnings, assumptions,concepts and propositions. Specifically, Helvie’sEnergy Theory of Communities (1991) andAnderson and McFarlane’s Community as Partner(2004) were chosen to confirm the accuracy andcomprehensiveness of the new model andinstrument in relation to current communitydiagnosis, population health management andcommunity health nursing practice.
The term community is used to indicate themultiperson unit of service. In this modelcommunity, as the unit of service, is different fromcommunity as a setting for providing care to anindividual, exemplified by a community primarycare clinic, or a community based home healthagency. It is also different from community as aconditioning factor for the individual. As the unit ofservice, the community is the care agent and hasconditioning factors that are unique and affect theunit’s agency and demands.
Community is the type of multiperson unitdescribed by Taylor and Renpenning (cited inOrem 2001) as a group of persons impersonallyrelated who come together for shared purposes,and shared problem resolution. It fits the categoryof a type 2 multiperson care system in thatmembers are of a “structured, enduring social
22
Development and application of the Community CareDeficit Nursing Model (CCDNM) in two populations
Serey Shum, Rebecca McGonigal and Barbara Biehler
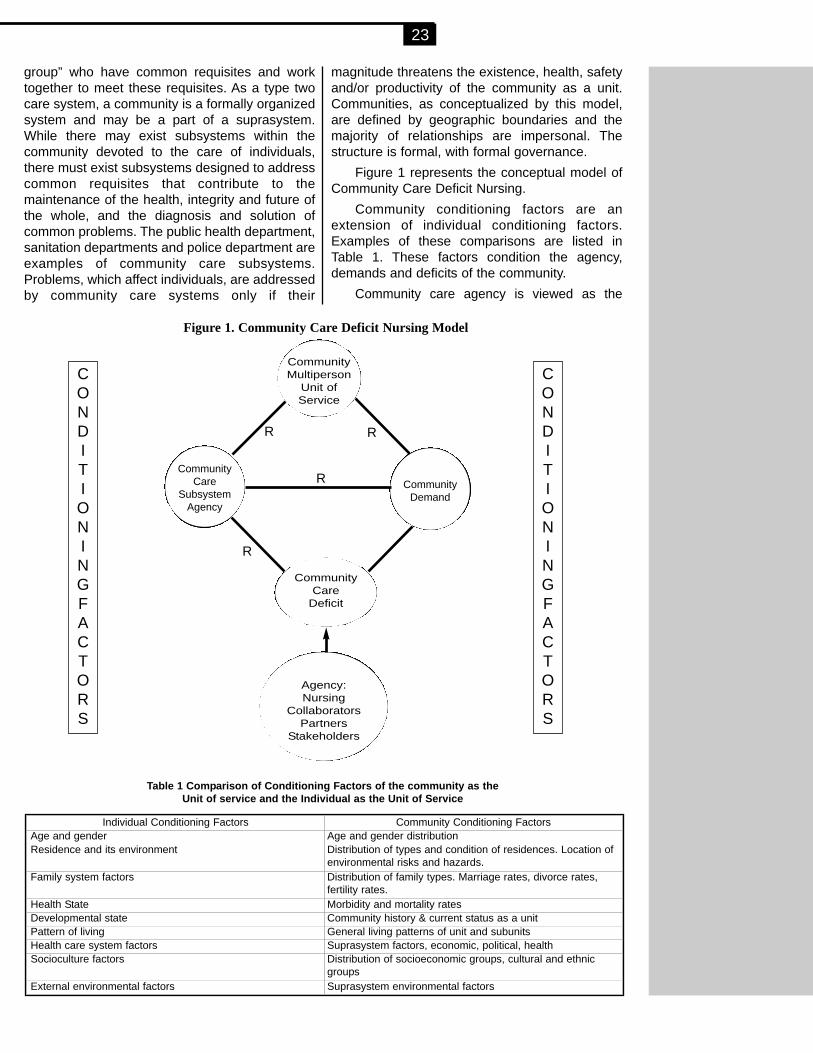
group” who have common requisites and worktogether to meet these requisites. As a type twocare system, a community is a formally organizedsystem and may be a part of a suprasystem.While there may exist subsystems within thecommunity devoted to the care of individuals,there must exist subsystems designed to addresscommon requisites that contribute to themaintenance of the health, integrity and future ofthe whole, and the diagnosis and solution ofcommon problems. The public health department,sanitation departments and police department areexamples of community care subsystems.Problems, which affect individuals, are addressedby community care systems only if their
magnitude threatens the existence, health, safetyand/or productivity of the community as a unit.Communities, as conceptualized by this model,are defined by geographic boundaries and themajority of relationships are impersonal. Thestructure is formal, with formal governance.
Figure 1 represents the conceptual model ofCommunity Care Deficit Nursing.
Community conditioning factors are anextension of individual conditioning factors.Examples of these comparisons are listed inTable 1. These factors condition the agency,demands and deficits of the community.
Community care agency is viewed as the
23
CONDITIONINGFACTORS
CONDITIONINGFACTORS
CommunityMultiperson
Unit ofService
CommunityCare
Deficit
Agency:Nursing
CollaboratorsPartners
Stakeholders
CommunityCare
SubsystemAgency
CommunityDemand
R
RR
R
Figure 1. Community Care Deficit Nursing Model
Individual Conditioning Factors Community Conditioning FactorsAge and gender Age and gender distribution Residence and its environment Distribution of types and condition of residences. Location of
environmental risks and hazards.Family system factors Distribution of family types. Marriage rates, divorce rates,
fertility rates. Health State Morbidity and mortality ratesDevelopmental state Community history & current status as a unitPattern of living General living patterns of unit and subunitsHealth care system factors Suprasystem factors, economic, political, healthSocioculture factors Distribution of socioeconomic groups, cultural and ethnic
groupsExternal environmental factors Suprasystem environmental factors
Table 1 Comparison of Conditioning Factors of the community as the Unit of service and the Individual as the Unit of Service
ability of the community system and subsystems toevaluate and perform the functions needed tomaintain the health, integrity and growth of thecommunity. The power for community care lieswithin its governmental subsystems such asdepartments of health, sanitation, recreation, andpublic safety. Such power can also be exercised byless formal subsystems such as volunteer groups,non-profit agencies, religious groups, politicalgroups and influential citizens and citizen groups.
The individual has self-care requisites. Anextension of this construct is to think of thecommunity as a multiperson unit which has unitcare requisites. For example, individual universalself-care requisites include air, water and food. Acommunity requires a safe water source, pollutionfree air and adequate corporate food supplies.Other examples of community requisites arecontrol and regulation of communicable disease,control of safety hazards, reduction ofpreventable morbidity and premature death.These requisites place demands on thecommunity and its subsystems; demands, whichmust be met to maintain a functional, integratedunit. The methods and strategies to meetcommunity care requisites are population basedwith restoration of population health as the goalrather than individual care based with recovery ofthe individual as the goal.
When community care demands exceedcommunity care agency, a deficit occurs. Thisdeficit may be diagnosed through the routinemonitoring of requisites and demands bycommunity care subsystems or by a formalprocess of community assessment and diagnosisor a combination of the two methods. Thediagnosis of a deficit concurrently diagnoses adeficit in community care agency. For example, anincrease in sexually transmitted disease ratesamong adolescents is a community care deficitindicating also an agency deficit for thosesubsystems charged with the management andcontrol of sexually transmitted diseases. Whensuch a deficit exists there is a need for intervention.
Population based community care is of such acomplex nature that nursing care agency mayrequire partners, e.g., other disciplines both withinand outside the community as well as individualmembers of the community, to address the deficit.The outcome of such intervention may result inadjustments or augmentation of existingcommunity care subsystems or the planning andimplementation of new population-basedcommunity care interventions. These interventionsare population-based programs with the goal ofrestoring community care.
Nursing agency may be required in the
diagnosis of community deficits as well as theplanning, implementation and evaluation ofcommunity care interventions. To the extent thatthe community care deficit falls within the scope ofnursing practice, nursing agency may be all that isrequired to address the community care deficit.More commonly nursing partners with care agentsto address the community deficits.
The Diagnosis of Community Care DeficitInstrument based on this model was developed toguide the student in defining the communityaccording to geographic and system boundaries.The suprasystem(s) are identified, as well as theformal subsystems, which exist to maintain thehealth, functioning and integrity of the community.
Community conditioning factors aredescribed as well as community requisites anddemands. From these data, an analysis is madeas to whether or not requisites and demands aremet or not met. From those that are not met, aformal diagnosis is derived. Following this,students can use the program planning process todefine agency requirements for addressing thecommunity care deficit. Nursing agencyrequirements are specified as well as the agencyrequirements of partners of nursing from otherdisciplines and care systems.
Community Care Deficit Nursing Model(CCDNM) Application
To describe the teaching of the CCDNM in amaster’s program, we will first describe thecourse, then course procedures and experiencesusing the model in two clinical settings. Thecourse is a required core course in the master’sprogram and is designed to teach public healthmaterial according to various accreditationcriteria. It is a didactic/clinical course that buildson undergraduate community health concepts.
Course Requirements include texts andpublic health resources, two papers, participationin classroom discourse, community assessmentdone in small clinical groups, and a formalpresentation to their respective communities.Required materials have included Orem,epidemiology reference, public health resources,and Healthy People 2010. The first or secondweek of the semester students divide themselvesinto small groups for the clinical components. Thesmall group determines the general populationthey want to work with.
The focus of the first of the two papers isglobal analysis of a population using the CCDNM.The second paper focuses on refinement of theCommunity Care Deficit. Resources for the firstpaper are more generic public health than thesecond in which students refer to information
24

about the specific community deficit. Requiredclassroom participation continues throughout thesemester. Discourse focus moves from generalpublic health information to a later specific clinicalapplication focus. During the semester studentswill have reviewed S-CDNT in general, theCCDNM, public health concepts andepidemiology. Once students have begun to workwith and study their selected populations theybring these data for class discussion.
These classroom discussions become theheart of learning public health concepts within themodel. Each student brings information about aparticular Community Care Requisite thinkingher/his studied requisite is of major importance.Then, through faculty-student debate studentscome to recognize that all requisites are importantto a community, but that Community Agency is thedetermining factor in identifying the CommunityDeficit. Because this is an academic experience,student must also consider what is doable within asemester’s time and within the realm of publichealth nursing. These discussions focus on adialectic that involves concepts such as population,setting, multiperson units, and communities. Taylorand Renpenning’s work provides the basis forthese discussions (cited in Orem, 2001).
For example, students recently studied twosouthwest communities: one an air force baseand another, a low-income community served bya nurse practitioner clinic. With discussion ofcommunity care requisites, the community caredemands and community agencies, studentsdiscovered that the Community Care Deficit wasdifferent than their initial impressions.
Discussions related to the air force basebegan with students’ thinking that the closing ofthe base hospital forcing patients to usecommunity resources could be the problem.Students also reviewed one year’ retrospectiverecord of emergency room use and interviewedwith base parents. These data demonstrated alack of primary care resources for pediatricpatients. Using the model and focusing theirliterature review based on the refinement of data,students then looked at available resources forparenting, anticipatory guidance and emergencycare for pediatric families, thus addressing thisspecific Community Care Deficit.
In the case of the low-income clinicpopulation, students began with a concern for theageing population. What the model led them towas that their specific population’s deficit relatedto grandparents raising grandchildren. Thisanalysis led them to seeking specific resourcesfor aging grandparents with low incomes raisingtheir grandchildren.
Up to this point the clinical component hasincluded: l) data gathering from public documents;2) survey of the selected communities withanalysis and discussion at each point using theCCDNM; and 3) interviewing the multi-person unitswithin their selected communities. The final clinicalexperience is the student feedback presentationsto the selected communities. This is the high pointof the semester. Students use radio spots andflyers to invite the community to the forums. Theyinvite community members they have justsurveyed and interviewed as well as thecommunity stakeholders, and any professionalsthey can prevail upon to share their expertise tohelp with problem solving. In some cases studentshad family members that are CPA and attorneyswho participated in the forum. Also invited aremembers of the class, faculty and other students.
Each small group selects a time of the daymost appropriate to its population and preparespresentation media for the event. Information isshared and discussion follows. The dialogueshave resulted in eye opening experiences for theclients, the stakeholders and professionals. Therewere often resources available that were notbeing accessed because of lack of information.Some stakeholders expressed an interest incontinuing the dialogue. Both graduate studentsand community members learned that nursingagency has an important role in the health of acommunity. Teaching public health conceptswithin the CCDNM enables graduate students tosee that nursing can make a positive difference tothe health of a community.
Serey Shum PhD, RN, CNS is with West Texas A&M University,Division of Nursing, Canyon, TX. Rebecca McGonigal PhD RN, iswith Brenau University Dept. of Nursing, Gainesville, GA; and :Barbara Biehler, EdD RN PNP lives in Amarillo, TX. Contact Dr.Shum at [email protected]
References
Anderson, E.T. & McFarlane, J.M. (2004) Community aspartner. Philadephia: Lippincott, Williams and Wilkins.
Helvie, C.O. (Ed). (1998). Community health nursing theoryand practice. Thousand Oaks: Sage Publications.
Orem, D.E. (2001). Nursing concepts of practice. St. Louis:Mosby Publishing.
Taylor, S.G. & McLaughlin, K (1991). Orem’s general theory ofnursing and community nursing. Nursing ScienceQuarterly 4:153-169.
Walker, L.O. & Avant, K.C. (1995). Strategies for theoryconstruction in nursing. Norwalk: Appleton and Lange.
U.S. Department of health and Human Services, HealthyPeople 2010: What are the leading indicators? Retrieved4/16/05 fromhttp://healthypeople.gov/document/html/objective/14-29.htm
25
SCDNT – Tell Me About It
Game Design: Violeta A. Berbiglia
The Game
Purpose: To accomplish formative andsummative evaluation on concept attainment ofthe SCDNT concepts.
Game Content: The questions come directlyfrom classroom content (lecture, discussion,handouts, etc.). Only content that students havebeen exposed to in class is used for questions.Categories of questions are: history, concepts,rationales, trivia, and student-generated questions.The teacher develops all of the questions (exceptthe student-generated questions) prior to classtime.
Rules of the Game
1. Create 2 or more groups (not over 4 to 6 pergroup).
2. Each group selects a leader.3. Only the group leader can answer questions.4. Groups sit together at a distance from other
groups. All course materials must be putaway.
5. Select 1 individual to assist the teacher inrecognizing group leaders when they stand.
6. Explain the rules and scoring to the groups.7. Request each group to develop and answer
2 to 3 questions, write them on separatesheets of paper, and give them to theteacher.
Rules for Play
1. The teacher chooses the 1st category for aquestion.
2. The teacher announces the category.3. The teacher asks a question from that
category.4. Groups confer within the group and agree on
an answer.5. The group leader stands, is recognized and
provides the answer.6. If several leaders stand, they are recognized
in the order of standing. If the 1st standinganswers incorrectly, the next standing isrecognized, etc.
7. The group answering the question correctlyselects the next category and anotherquestion is asked by the teacher.
Scoring
1. The scoreboard is posted on a blackboard,poster, flip chart, etc. Also, the categories areposted separate from the scoreboard. Whencorrect answers are given, groups receive aletter (letters are given sequentially under theSCDNT Dorothea E. Orem.) If the answer isincomplete, the group will be given a part of aletter. The following scoreboard shows that all3 groups have answered questions. If groupsare tied at the end of the game, ask acomplex question to break the tie. Uponcompletion of the game, the group with themost correct answers receives a prize.
S C D N T D o r o t h e a E. O r e m
Group 1 S N
Group 2 C D
Group 3 T D
Suggestions for a Fun Game Process:
1. Just after explaining the rules, ask the groupsif they have any “handicaps” (for example: nomales in group, no females in the group, 1less group member than in other groups, toomany younger (or older members), etc. If agroup determines they have a handicap,award the group a letter on the scoreboard.
2. Request the groups to use their own words toparaphrase content – not memorized words.This gives them increased ownership of thetheory.
3. Include humor.4. Refrain from criticizing individuals/groups.5. Don’t play the game too long. The interest
will lag and fun decreases.
Violeta A. Berbiglia, RN, EdD lives in Helotes, TX. Contact Dr.Berbiglia: [email protected]
26
Teaching Strategy Column

IOS News
From the presidentDear Members of IOS,
What a year it has been. The devastation andsuffering resulting from so many natural disastershave been overwhelming. Yet, in all the tragedyand sadness, there is evidence of the tremendouscapability of human beings to persevere and tostrive to do good.
The IOS web site has been moved. The newaddress is www.scdnt.com. There is still morework to be done on the web site. If you have anyexpertise with web site development, pleaseconsider volunteering to help with this ongoingwork. If interested, send me an e-mail. A bigThank You to Gerd Bekel for his work on gettingthe new web site going.
At the end of this year, Michael Morgan will bestepping down as Editor of the journal. During histime as editor, Dr. Morgan has contributed a greatdeal, including moving the format of the journalfrom print to electronic format. Thank You Dr.Morgan for all the work you have done.
Karen Cox has been appointed by the Boardof Directors of IOS to serve as Editor for theremainder of the term, ending Dec. 2006. Pleasesee Dr. Cox’s announcement in this journalregarding the submission deadlines for next year.
The term for office for the Board of Directorswas changed from 4 years to 2 years in therevised bylaws. Beginning in 2006, elections willbe held yearly. The positions to be filled willalternate from year to year so that there is somecontinuity on the board. Think about running foran office or for chairperson of one of thecommittees (see below).
The 9th World Congress of SCDNT isscheduled for July 20-22 in Johannesburg, SouthAfrica. I encourage you all to attend. Check outthe web site at www.worldcongress-scdnt.com forspecific details regarding the conference. Also,think about submitting an abstract for theconference. Information regarding the call forabstracts can be found on the web site.
I am asking each member to take a fewminutes to look at the mission statement of theIOS as well as the mission statement of thejournal. The accomplishment of the IOS missionis dependent on the contributions of individualmembers. As you think about your New Year’sresolutions, please make a commitment to dosomething that helps the IOS move towardaccomplishment of its mission. There are anumber of ways you can contribute; submit anarticle for publication in the journal, submit an
abstract for the 9th World Congress, volunteer toserve on a committee, volunteer to help withfurther development of the web site, and/orconsider running for an office or for chairperson ofa committee.
May you all have a meaningful holidayseason and a Happy New Year.
Barbara Banfield, PresidentFor your information:The composition of the Board of Directors is:
• Founding Members• President-Banfield-term expires 12/2007• VP-Beth Geden-term expires 12/2006• Secretary-Connie Dennis-term expires
12/2007• Treasurer-Connie Brooks-term expires
12/2006• At Large Members-Violeta Berbiglia-term
expires 12/2006Kathie Renpenning-term expires 12/2007Marcel Sailer-term expires 12/2007
• Nominating Committee-Barbara Biehler-termexpires 12/2006Sheila Jesek-Hale-term expires 12/2006Monika Lovgren-term expires 12/2006Jacqueline Fawcett-term expires 12/2007Jane Ransom-term expires 12/2007
• Program Chair-Gerd Bekel-term expires12/2006
• Public Affairs Chair-Andrea Hintze-termexpires 12/2006
• Public Relations Chair-Andrea Hintze-termexpires 12/2006
• Publication Chair-Michael Morgan-steppingdown 12/2005-replacement is Karen Cox-term expires 12/2006
• Scholarly Endeavor Chair-MargaretheLorensen-term expires 12/2006
Mission Statement:The mission of the International Orem Society
is to advance nursing science and scholarshipthrough the use of Dorothea E.
Orem's nursing conceptualizations in nursingeducation, practice, and research.
27
Memorial to Dr. MargaretheLorensen, Institute of Nursing
Science, Oslo University,Norway
Professor Margarethe Lorensen1942-2005
Professor Margarethe Lorensen died October30th 2005, at the age of 63, in her home inDenmark with her two sons beside her.
Dr. Lorensen’s colleague, Dr. MonikaLovgren, expresses the loss she feels andprovides a translation of the informationconcerning Margarethe’s life:
Doctor Lorensen began her nursing career in1964 as registered nurse at SonderjyskeSygeplejeskole (Nursing College); and in 1969,she continued her nursing education atDenmark’s School of Nursing, Aarhus University.
Margarethe’s early interest was nursingresearch. She was awarded a scholarship forstudies in USA. There, she received a MastersDegree of Arts in Education (Northern ArizonaUniversity, 1972) and a Masters Degree inNursing (University of Colorado, 1973).Margarethe was the first Danish nurse tocomplete a PhD (Arizona State University, 1976).When she returned to Denmark, she worked asResearch Consultant on the Danish NursingCouncil (1978). She established the DanishCouncil’s Nursing Research. Margarethe servedas supervisor for 25 years and as the publisher ofthe journal for Nursing Research for 21 years.
In 1983, Margarethe was appointed ViceDirector for the Deaconess Foundation(Copenhagen). In 1986, she became the Director. She developed a Somatic Hospital into aGeriatric Center. This was the first time inDenmark that a PhD prepared nurse wasappointed a supervisor. She used Orem’s Self-Care Deficit Nursing Theory in her practice in thecare of the elderly.
Dr. Lorensen was the first nurse to receive aresearch award in health and nursing care fromthe Danish Medical Research Council. The awardmade it possible for her to conduct her project,“Elderly and Self-Care”.
From 1987 until her death, Margarethe was aProfessor in Nursing Science at Oslo University.She worked very hard to define an autonomousand independent nursing science, nursingresearch and nursing practice.
The International Orem Society for Nursing
Science and Scholarship celebrates the life ofMargarethe and pays tribute to her contributionsto the IOS and to the nursing profession.Dorothea Orem recalls the early contributions ofMargarethe and comments: “Her researchconcerned women and their recovery undercertain conditions. She was very active in that shehad the research instruments she developed overtime to study women who were hospitalized or inrehabilitation. She was an interesting woman.Walene and I enjoyed our time with her inWashington. Walene called her ‘the statute ofliberty’.”
Vi Berbiglia also recalls Margarethe’s statureand strong leadership qualities. She served onIOS committees and fostered the use of theSCDNT in many parts of the world. The IOS andthe faculty of the Institute of Nursing Science,Oslo University feel a great loss. Margarethecontinued to meet with her university colleauesuntil a few days before her death. We all share agreat appreciation for Dr. Margarethe Lorensen’scontributions and express our sympathy to herfamily.
Memorial prepared by: Drs. Monika Lovgren, Dorothea Orem,and Violeta Berbiglia
28

Concept Formalization inNursing reprint offerReprint of Concept Formalization in Nursing isnow availble
The IOS has supported the reprint of the 2ndedition of Concept Formalization in Nursing:Process and Product. The book was one of themost selling nursing theory books in 1979.
The second edition of CONCEPTFORMALIZATION IN NURSING: PROCESS ANDPRODUCT reflects the progress made till 1979.This volume refines previous conclusions andmoves on to descriptions of the individual orgroup dynamics associated with formulation,expression, and acceptance of nursing’sconceptual structure. Orem’s general theory ofnursing is used to provide the conceptualframework for research and the structuring ofnursing knowledge. Research carried out byConference members Melba Anger Malatesta,Louise Hartnett Rauckhorst, and the late JoanBackscheider is also presented.
Throughout the text, drawings, tables, charts,and graphs are used to illustrate key points. Thebook is divided into two parts.
Part I focuses on nursing as a practicediscipline, explains the position of the professionin the world of human affairs, and analyzes 14concepts of nursing. Part II delves into theNursing Development Conference Group’s workon the structure of nursing knowledge and appliesinsights into the conclusions of the first edition.Two chapters explore the implications of the self-care agency. Throughout the text, the skillfulintegration of a substantial amount of newmaterial serves to provide a complete update ofthe initial concerns.
For more information visit www.scdnt.com-/pub/pub.html or for any order information contactGerd Bekel ([email protected]).
29

• The new IOS Webpage is available to thepublic.
• You will find new information related to S-CDNT and IOS.
• Please bookmark our domain and give noticeto your colleagues, students and friends.
• You’ll find the webpage at www.scdnt.com• Please Feel free to send us commends and
information you’d like to be presented.• We would like to develop two more sections
on SCDNT Research and on Internationalaffairs.
• If you or your students would like to report onyour current research work, please contactGerd Bekel ([email protected]).
30
New IOS Web Presentation




















