scrutiny board (adults and health) - Meetings, agendas, and ...
184
Please note: Certain or all items on this agenda may be recorded Principal Scrutiny Adviser: Steven Courtney Tel: (0113) 37 88666 Produced on Recycled Paper A SCRUTINY BOARD (ADULTS AND HEALTH) Meeting to be held in Civic Hall, Leeds, LS1 1UR on Tuesday, 18th July, 2017 at 1.30 pm (A pre-meeting will take place for ALL Members of the Board at 1.00 p.m.) MEMBERSHIP Councillors C Anderson Adel and Wharfedale; J Chapman Weetwood; B Flynn Adel and Wharfedale; H Hayden (Chair) Temple Newsam; A Hussain Gipton and Harehills; J Jarosz Pudsey; G Latty Guiseley and Rawdon; C Macniven Roundhay; J Pryor Headingley; D Ragan Burmantofts and Richmond Hill; P Truswell Middleton Park; S Varley Morley South; Co-opted Member (Non-voting) Dr J Beal - Healthwatch Leeds Public Document Pack
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of scrutiny board (adults and health) - Meetings, agendas, and ...

Please note: Certain or all items on this agenda may be recorded
Principal Scrutiny Adviser:Steven CourtneyTel: (0113) 37 88666
Produced on Recycled Paper
A
SCRUTINY BOARD (ADULTS AND HEALTH)
Meeting to be held in Civic Hall, Leeds, LS1 1UR onTuesday, 18th July, 2017 at 1.30 pm
(A pre-meeting will take place for ALL Members of the Board at 1.00 p.m.)
MEMBERSHIP
Councillors
C Anderson Adel and Wharfedale;J Chapman Weetwood;
B Flynn Adel and Wharfedale;H Hayden (Chair) Temple Newsam;
A Hussain Gipton and Harehills;J Jarosz Pudsey;G Latty Guiseley and Rawdon;
C Macniven Roundhay;J Pryor Headingley;
D Ragan Burmantofts and Richmond Hill;P Truswell Middleton Park;
S Varley Morley South;
Co-opted Member (Non-voting)
Dr J Beal - Healthwatch Leeds
Public Document Pack

B
A G E N D A
ItemNo
Ward/Equal Opportunities
Item NotOpen
PageNo
1 APPEALS AGAINST REFUSAL OF INSPECTION OF DOCUMENTS
To consider any appeals in accordance with Procedure Rule 25* of the Access to Information Procedure Rules (in the event of an Appeal the press and public will be excluded).
(* In accordance with Procedure Rule 25, notice of an appeal must be received in writing by the Head of Governance Services at least 24 hours before the meeting).
2 EXEMPT INFORMATION - POSSIBLE EXCLUSION OF THE PRESS AND PUBLIC
1. To highlight reports or appendices which officers have identified as containing exempt information, and where officers consider that the public interest in maintaining the exemption outweighs the public interest in disclosing the information, for the reasons outlined in the report.
2. To consider whether or not to accept the officers recommendation in respect of the above information.
3. If so, to formally pass the following
resolution:-
RESOLVED – That the press and public be excluded from the meeting during consideration of the following parts of the agenda designated as containing exempt information on the grounds that it is likely, in view of the nature of the business to be transacted or the nature of the proceedings, that if members of the press and public were present there would be disclosure to them of exempt information, as follows:
No exempt items have been identified.

C
3 LATE ITEMS
To identify items which have been admitted to the agenda by the Chair for consideration.
(The special circumstances shall be specified in the minutes.)
4 DECLARATION OF DISCLOSABLE PECUNIARY INTERESTS
To disclose or draw attention to any disclosable pecuniary interests for the purposes of Section 31 of the Localism Act 2011 and paragraphs 13-16 of the Members’ Code of Conduct.
5 APOLOGIES FOR ABSENCE AND NOTIFICATION OF SUBSTITUTES
To receive any apologies for absence and notification of substitutes.
6 MINUTES - 27 JUNE 2017
To approve as a correct record the minutes of the meeting held on 27 June 2017.
1 - 6
7 HEALTH AND WELLBEING BOARD - DRAFT MINUTES FROM 20 JUNE 2017
To receive for information purposes the draft minutes of the Health and Wellbeing Board meeting held on 20 June 2017.
7 - 12
8 EXECUTIVE BOARD - DRAFT MINUTES FROM 21 JUNE 2017
To receive for information purposes the draft minutes of the Executive Board meeting held on 21 June 2017.
13 - 28
D
9 CHAIR'S UPDATE
To receive an update from the Chair on relevant scrutiny activity since the previous Board meeting that is not specifically included elsewhere on the agenda.
29 - 30
10 UPDATE ON EARLY INTERVENTIONS AND REDUCING HEALTH INEQUALITIES BREAKTHROUGH PROJECT
To receive and consider a report from the Director of Public Health that provides an update on progress of the Early Interventions and Reducing Health Inequalities Breakthrough Project against the three identified priorities, with a particular focus on inequalities.
31 - 52
11 QUALITY OF CARE SERVICES IN LEEDS
To receive and consider a report from the Head of Governance and Scrutiny Support introducing a range of information relevant to the Scrutiny Board’s continued focus on the quality of care services in Leeds.
53 - 110
12 HEALTHWATCH LEEDS ANNUAL REPORT (2016/17) AND FUTURE WORK PROGRAMME
To receive and consider a report from the Head of Governance and Scrutiny Support introducing HealthWatch Leeds’ Annual Report for 2016/17 and its future work programme for 2017/18.
111 - 150

E
13 CLOSURE OF THE BLOOD DONOR CENTRE IN SEACROFT - RESPONSES TO SCRUTINY BOARD STATEMENT
To receive and consider a report from the Head of Governance and Scrutiny Support that introduces responses to the previous Scrutiny Board’s statement following NHS Blood and Transplant’s decision to close the blood donor centre in Seacroft, Leeds.
151 - 174
14 WORK SCHEDULE
To consider the Scrutiny Board’s draft work schedule for the 2017/18 municipal year.
175 - 178
15 DATE AND TIME OF NEXT MEETING
Tuesday, 5 September 2017 at 1:30pm (pre-meeting for all Scrutiny Board members at 1:00pm).
THIRD PARTY RECORDING
Recording of this meeting is allowed to enable those not present to see or hear the proceedings either as they take place (or later) and to enable the reporting of those proceedings. A copy of the recording protocol is available from the contacts on the front of this agenda.
Use of Recordings by Third Parties – code of practice
a) Any published recording should be accompanied by a statement of when and where the recording was made, the context of the discussion that took place, and a clear identification of the main speakers and their role or title.
b) Those making recordings must not edit the recording in a way that could lead to misinterpretation or misrepresentation of the proceedings or comments made by attendees. In particular there should be no internal editing of published extracts; recordings may start at any point and end at any point but the material between those points must be complete.

This page is intentionally left blank

Draft minutes to be approved at the meeting to be held on Tuesday, 18th July, 2017
SCRUTINY BOARD (ADULTS AND HEALTH)
TUESDAY, 27TH JUNE, 2017
PRESENT:
Councillor H Hayden in the Chair
Councillors C Anderson, J Chapman, B Flynn, M Harland, A Hussain, J Jarosz, G Latty, J Pryor, D Ragan, P Truswell and S Varley
Co-opted Members: Dr J Beal (Healthwatch Leeds)
1 Late Items
The following late information was submitted to the Board:
Agenda item 10 – Proposed Changes to Prescribing Guidance across Leeds – Confirmation from NHS England on national work going forward
Agenda item 12 – Draft outline work schedule. The above information was not available at the time of agenda despatch, but was subsequently made available on the Council’s website.
2 Declaration of Disclosable Pecuniary Interests
There were no disclosable pecuniary interests declared to the meeting, however the following matters were brought to the attention of the Scrutiny Board for information:
- Councillor P Truswell advised that a family member was likely to be affected by proposed prescribing changes.
- Councillor J Chapman advised that a family member had accessed residential care services.
The above Board Members remained present for the duration of the meeting.
3 Apologies for Absence and Notification of Substitutes
An apology for absence was submitted by Councillor C Macniven. Notification had been received that Councillor M Harland was to substitute for Councillor C Macniven.
4 Minutes - 25 April 2017
RESOLVED – That the minutes of the Scrutiny Board (Adult Social Services, Public Health, NHS) meeting held on 25 April 2017 be approved as a correct record.
Page 1
Agenda Item 6

Draft minutes to be approved at the meeting to be held on Tuesday, 18th July, 2017
5 Co-opted Members
The Head of Governance and Scrutiny Support submitted a report which sought the Board’s formal consideration for the appointment of co-opted members. The Board was informed that they could appoint the following:
Up to five non-voting co-opted members for a term of office that does not go beyond the next Annual Meeting of the Council; and/or
Up to two non-voting co-opted members for a term of office that relates to the duration of a particular and specific scrutiny inquiry.
RESOLVED –
(a) That Dr John Beal representing HealthWatch Leeds be appointed as a non-voting co-opted Member of the Board for the 2017/18 municipal year.
(b) That the Board considers the appointment of co-opted members on an ad-hoc basis for any inquiries where it was deemed appropriate.
6 Scrutiny Board Terms of Reference
The Head of Governance and Scrutiny Support submitted a report which presented terms of reference for the Adults and Health Scrutiny Board for Members’ information. RESOLVED – That the Board’s terms of reference be noted.
7 Sources of Work
The Head of Governance and Scrutiny Support submitted a report which provided information and guidance on potential sources of work and areas of priority within the Board’s terms of reference. The following information was appended to the report:
- Vision for Scrutiny in Leeds - Best Council Plan 2017/18: Tackling poverty and reducing inequalities - Leeds Health and Wellbeing Strategy (2016-2021) - NHS Leeds West CCG Integrated Quality and Performance Report
(May 2017) - Financial Performance – Outturn Financial year ended 31 March 2017
– Report to Executive Board dated 21 June 2017 - Financial Health Monitoring 2017/18 – Month 2 (May 2017) – Report to
Executive Board dated 21 June 2017. The following were in attendance:
Page 2

Draft minutes to be approved at the meeting to be held on Tuesday, 18th July, 2017
- Councillor Rebecca Charlwood (Executive Member for Health,
Wellbeing and Adults) - Shona McFarlane (Chief Officer (Access and Care Delivery)) – Adult
Social Care, Leeds City Council. A number of work areas were put forward for consideration within the overall work schedule, including:
Partnership working, including development of Leeds’ health and care plan and associated cost implications.
Quality of care affecting all service users, especially focused on social care providers judged as ‘requiring improvement’.
The types of support offered as part of the transforming care agenda – i.e. around the repatriation of patients subject to long-term hospital placements.
A potential review of care arrangements for offenders in prison.
GP provision across the city.
Support available to working age adults.
Transition from hospital to home (hospital discharge), developing links with housing (specifically in relation to adaptations) and work across localities.
The development of digital technology to support patient care needs.
The role of public health, particularly in relation to health inequalities.
Mental health provision with a particular focus on transition from children to adults.
NHS performance and workforce issues.
Progress of the ‘One Voice’ project
The role of third sector in the delivery of health and social care services, including but not restricted to the neighbourhood networks, and associated funding arrangements.
Maintaining an overview of proposed service changes. As part of the discussions, the Board acknowledged there would be limitations on the work schedule due to the resources directly available to support the Board’s work. It was also acknowledged that the Scrutiny Board would need to prioritise the focus of its work schedule. RESOLVED –
(a) That the above issues be used to inform the further development of the Board’s draft work schedule for the 2017/18 municipal year.
(b) That authority be given to the Chair of the Scrutiny Board (Adults and Health), in conjunction with officers, to draw up inquiry terms of reference for subsequent approval by the Scrutiny Board, where required.
(Councillor G Hussain left them meeting at 2.00pm during the consideration of this item.)
Page 3

Draft minutes to be approved at the meeting to be held on Tuesday, 18th July, 2017
8 Proposed changes to prescribing guidance across Leeds - formal consultation
The Head of Governance and Scrutiny Support submitted a report which introduced some proposed changes to prescribing guidance across Leeds, as part of the formal public consultation. The following information was appended to the report:
- Proposed Prescribing Changes: Formal Consultation – Report to Scrutiny Board (Adult Social Services, Public Health, NHS) on 25 April 2017.
The following were in attendance:
- Sue Robins, Director of Commissioning and Strategy, NHS Leeds CCGs Partnership
- Heather Edmonds, Head of Medicines Optimisation, NHS Leeds CCGs Partnership.
The key areas of discussion were:
Concern about the potential issue of creating a postcode prescribing arrangement. The Board discussed the need for clear national guidance to ensure consistency of approach – as previously identified during discussions in April 2017.
Concern about the potential impact of the proposals on patients and subsequently health inequalities across the City.
An update that consultation on the proposals was due to end in July. It was suggested that an update be provided to the Board 6 months after implementation.
Confirmation that the proposals were anticipated to save approximately £1m, although the total amount was dependent on clinical needs.
A request that the Board be provided with an update on changes to prescribing guidance implemented in North Yorkshire.
RESOLVED –
(a) That the contents of the report and appendices be noted. (b) That the Principal Scrutiny Adviser draft a statement to the CCG to
highlight the Board’s concerns about the proposed changes. (c) That the Board be provided with an update on changes to prescribing
guidance implemented in North Yorkshire. (d) That the CCG be requested to provide an update to the Board 6
months after implementation.
9 Chair's Update
The Chair provided a verbal update on recent scrutiny activity that had not been specifically included elsewhere on the agenda.
Page 4

Draft minutes to be approved at the meeting to be held on Tuesday, 18th July, 2017
The key updates included:
A visit to Donisthorpe Hall on 7 June 2017 (Honorary Life President, Geoff Caplan) and subsequent facilitation of discussions between the provider and the Executive Board member;
York Road Surgery and the planned dispersal of the patient list – with the surgery due to close 30 September 2017;
Cottingley Surgery (retirement of Dr Pai) – due to retire on 30 June 2017, Dr Pai had written to all patients on 22 June 2017 advising of his retirement and temporary arrangements in place, as follows: o Leeds Clinical Commissioning Groups Partnership had
commissioned Windsor House Group Practice in Morley to take on the current registered patient list for the next 12 months, to ensure continuity of care for the registered patients;
o Over the next few weeks, the CCG would be sending out a survey to patients to help understand patients’ preferences for accessing and receiving GP care in the future.
Care Quality Commission (CQC) – Hospital Mental Health directorate report update; o Waterloo Manor – Targeted inspection in March 2017 (covering
Safe and Well-led domains) and judged as ‘Requires Improvement’ for both domains and overall. CQC to monitor breaches of regulation through ongoing engagement with the service, including monthly meetings to review their action plan response;
o St Anne’s Community Services – Alcohol Services – inspected in April 2017 against the regulatory breaches and recommended actions from the previous comprehensive inspection (March 2016).
Closure of Blood Donor Centre in Seacroft – responses received from NHS Blood and Transplant (NHSBT) and the Independent Reconfiguration Panel (IRP). No response yet from the Department of Health, but had until 30 June 2017. Details of the responses to be considered at July’s Scrutiny Board meeting;
Joint Health Overview and Scrutiny Committee (Yorkshire and Humber) meeting on 5 July 2017 to formally consider NHS England’s proposals for the future provision of Congenital Heart Disease Services for children and adults. The outcome to be reported to the Scrutiny Board at its next meeting.
RESOLVED – That the Chair’s update be noted.
10 Work Schedule
The Head of Governance and Scrutiny Support submitted a report which invited Members to consider the Board’s work schedule for the 2017/18 municipal year. RESOLVED – That the draft work schedule be amended to take account of the sources of work discussion at the meeting (minute 7 refers).
Page 5

Draft minutes to be approved at the meeting to be held on Tuesday, 18th July, 2017
11 Date and Time of Next Meeting
Tuesday, 18 July 2017 at 1.30pm (pre-meeting for all Board Members at 1.00pm) (The meeting concluded at 3.05pm)
Page 6

Draft minutes to be approved at the meeting to be held on Thursday, 28th September, 2017
HEALTH AND WELLBEING BOARD
TUESDAY, 20TH JUNE, 2017
PRESENT: Councillor R Charlwood in the Chair
Councillors D Coupar, B Flynn, S Golton, and L Mulherin
Representatives of Clinical Commissioning GroupsNigel Gray NHS Leeds North CCG
Directors of Leeds City CouncilDr Ian Cameron – Director of Public HealthSteve Hume – LCC Adults and Health Sue Rumbold – LCC Children and Families
Representative of NHS (England)Louise Auger - NHS England
Third Sector RepresentativeKerry Jackson – St Gemma’s Hospice
Representative of Local Health Watch OrganisationLesley Sterling-Baxter – Healthwatch Leeds Tanya Matilainen – Healthwatch Leeds
Representatives of NHS providersSara Munro - Leeds and York Partnership NHS Foundation TrustDean Royles - Leeds Teaching Hospitals NHS Trust Thea Stein - Leeds Community Healthcare NHS Trust
1 Welcome and introductions The Chair welcomed all present and brief introductions were made.
Additionally, Councillor Charlwood noted that Dr Alistair Walling had been appointed to represent NHS Leeds South and East Clinical Commissioning Group by Annual Council on 25th May 2017.
2 Appeals against refusal of inspection of documents There were no appeals against the refusal of inspection of documents.
3 Exempt Information - Possible Exclusion of the Press and Public The agenda contained no exempt information.
4 Late Items No late of business were added to the agenda.
5 Declarations of Disclosable Pecuniary Interests No declarations of disclosable pecuniary interests were made.
Page 7
Agenda Item 7
Draft minutes to be approved at the meeting to be held on Thursday, 28th September, 2017
6 Apologies for Absence Apologies for absence were received from Councillor G Latty, Gordon Sinclair, Phil Corrigan, Julian Hartley, Cath Roff, Steve Walker, Moira Dumma and Julian Hartley. The Board welcomed Councillor Flynn, Dean Royles, Steve Hume, Sue Rumbold and Louise Auger as substitutes to the meeting.
7 Open Forum No matters were raised by members of the public under the Open Forum.
8 Minutes RESOLVED – The minutes of the previous meeting held 20th April 2017 were agreed as a correct record.
9 Leeds Health and Care Plan: Progressing a conversation with citizens The Board considered an overview of the emerging Leeds Health and Care Plan – Leeds’ description of what it envisaged health and care will look like in the future and how it will contribute to the delivery of the vision and objectives of the Leeds Health and Wellbeing Strategy 2016-21.
Paul Bollom, Interim Executive Lead for the Leeds Health and Care Plan, presented the report seeking support from the Board for the draft narrative of the Plan to be published in order to develop a citywide conversation with citizens. Stuart Barnes, NHS Leeds North CCG was also in attendance.
The draft narrative set the Leeds Plan in context with the West Yorkshire Sustainability and Transformation Plan. To achieve the maximum chance of engaging the public and delivering change; the Plan was user friendly and accessible reflecting the core value of working with the population. Discussion would be held alongside the wider future discussion on provision of public services – ‘changing Leeds’ discussions.
A copy of the draft ‘Leeds Health and Care Plan’ narrative document was attached as Appendix A along with a copy of the ‘Changing Leeds’ document at Appendix B
During discussions the following matters were raised: Acknowledged and welcomed the opportunity for the Community
Committees to have had early discussions on the Leeds Plan during the Spring 2017. A request for an update to the community committees was noted
The need to realise the value of the collective Leeds Pound and emphasise this within the health economy and beyond; acknowledging that service users may be buyers as well as consumers who could form co-operatives or social enterprises. This was also an opportunity to engage businesses in the ambitions of the Leeds Health and Care Plan; to interact with inclusive growth alongside Leeds Growth Strategy and with the Leeds Academic Health Partnership
Page 8

Draft minutes to be approved at the meeting to be held on Thursday, 28th September, 2017
A request for the draft Plan to include a foreword emphasising the role of feedback in shaping a live document that will evolve. Associated to this, a review of the language and phrasing to ensure a plain English approach and to avoid inadvertently suggesting that areas of change have already been decided. The narrative to also clarify who will make decisions in the future
The Plan to include case studies Acknowledged the need to broaden the scope of the Plan in order to “if
we do this, then this how good our health and care services could be” and to provide more detail on what provision may look like in the future
Noted the request for the Plan to provide more focus on some of the options from the Joint Health and Wellbeing Strategy
References to taking self-responsibility for health should also include urgent care/out of hospital health
References to the role of the Leeds Health and Wellbeing Board and the Joint Health and Wellbeing Strategy to be strengthened and appear earlier in the Plan
Assurance was sought that the Plan would be co-produced as part of the ongoing conversation
A focus on Leeds figures rather than national Requested that a follow up paper with more detail, including the
extended primary care model, be brought back in September.
In conclusion, the Chair noted that the Board was supportive of the draft Plan being released for consultation, subject to the amendments suggested being made. Additionally, she expressed her support for the ‘plan on a page’ approach but noted that a decision needed to be made on whether to have a generic approach or provide specific information within the Plan i.e. detail had been provided on some health issues but not others such as Primary Care. In response, it was agreed that the SRO’s, the Interim Executive Lead for the Leeds Plan, a representative of Healthwatch and the Health Partnership Team would review the draft Plan narrative, including the ‘plain English’ request and report back to the Board in September 2017. RESOLVED
a) To note the contents of the report and the comments made during discussions;
b) That having considered the draft narrative for the ‘Leeds Plan’, the feedback provided on whether it provides appropriate information to progress our conversation with citizens about the future of health and care in Leeds be noted.
c) To note the intention for the SRO’s, the Interim Executive Lead, a representative of Healthwatch for the Leeds Plan and the Health Partnership Team to review the draft Plan narrative, including the ‘plain English’ request; and would report back to the Board in September 2017.
Page 9

Draft minutes to be approved at the meeting to be held on Thursday, 28th September, 2017
d) To approve plans to progress a conversation with the public, based around the content of the summary report, and delivered in conjunction with the ‘Changing Leeds’ discussion.
10 Leeds Health and Care Quarterly Financial Reporting The Board considered the report of the Leeds Health and Care Partnership Executive Group (PEG) which provided an overview of the financial positions of the health and care organisations in Leeds, brought together as one single citywide quarterly financial report.
The report provided a financial ‘health check’ to clarify where the current and expected financial pressures were in the local health and care system. This gave the Board an opportunity to direct action to support an appropriate and effective response as part of the Boards role in having strategic oversight of both the financial sustainability of the Leeds health and care system; and of the executive function carried out by the Leeds Health and Care Partnership Executive Group.
Bryan Machin, Chair of the Citywide Directors of Finance Group, presented the report. He highlighted key headlines from the report including:
- The Leeds health & care system ended 2016/17 in a more favourable position than that predicted at quarter 3.
- The plans for health and care services within Leeds City Council and for the Leeds CCGs demonstrated the delivery of a breakeven position across the future 4-year planning period. However, this was reliant on the assumed delivery of significant levels of recurrent savings and the CCGs being able to access some of their previously accumulated surpluses.
- The aggregate 4-year plans of the three NHS Trusts would not achieve breakeven across the whole period without receipt of additional national funding, better management of demand, and delivery of significant levels of savings.
- The significant financial risk associated with the plans of all partners and that further citywide action is required to mitigate the risks in single organisation plans.
A question was raised over whether budget sharing to further the ‘one approach’ to health and care would be supported by the Directors of Finance. It was noted that although this approach may be viewed favourably, consideration would have to be given to the evidence required to support this approach. Members recognised that statutory and regulatory responsibilities may impact on collaboration but felt that this approach should be explored.
Further discussions noted the continuing austerity measures and the challenge of finding money upfront to invest in collaborative working. Concern was expressed that CCGs may not be able to draw down any previously accumulated surplus funds, as suggested in the report, due to Treasury restrictions and national funding pressures. An approach to PEG was suggested in the first instance to consider the opportunities for collaboration and budget sharing.
Page 10

Draft minutes to be approved at the meeting to be held on Thursday, 28th September, 2017
RESOLVED – a) Having reviewed the Leeds health & care quarterly financial report, the
Board noted its contents and the comments made during discussions;b) To note the extent of the financial challenge over the next year and
until 2021 and the need to further develop a shared system-wide response and assurance that this challenge will be met;
c) As part of the Boards’ role to provide clear guidance to the Leeds Health and Care Partnership Executive Group on the possible actions required to achieve financial sustainability, the Board asked that PEGi) Convene a workshop to consider and identify the opportunities
for collaboration and budget sharingii) Undertake a piece of work to gather and understand savings
and Return on Investment.
11 Being the Best City For Health Requires the Best Workforce Tony Cooke, Chief Officer Health Partnerships Team, presented a report summarising the city’s challenges relating to workforce and three potential and developing solutions. The Board was asked to consider it’s’ role in progressing, steering and directing future work to address the challenges, in the short term these were identified as:
- The impact of nursing bursaries (25% drop in applications) - The impact of Brexit (96%fall in people coming to the UK to work)- The number of health and care practitioners due to retire within the
next 5 years (600,000)
The challenges ahead had highlighted the need to systematically “Grow your own workforce” with a focus on the establishment of a Health and Care Academy for Leeds, promotion of the living wage and supporting disabled people into employment. Health & Care Academy – The Health and Social Care Academy would support a better targeting of employment opportunities in the city’s more deprived areas. In answer to a query the Board received assurance that the Health Academy would focus on business as well as clinical skills, recognising the role of small and medium businesses in the health and care sector.Work Related Long Term Illness - 32,000 people in Leeds received Employment & Support Allowance (ESA) - financial support for those who were unable to work through disability or illness. Of these, it was suggested that a large number had work related anxiety or musculoskeletal issues; and with the right support available to employers, that skilled and/or experienced workforce could be retained.
Dave Roberts, LCC Financial Inclusion Manager, provided the Board with information on the ‘Living Wage’, in particular:
- The influence the public sector had on the private sector - 60% of children living in poverty are from working households- The proven link between poverty and ill-health
Discussion followed on the proposal for public services to collaborate and develop a strategy to encourage momentum within the private sector for the Living Wage, noting a seminar had been proposed by the Integrated
Page 11

Draft minutes to be approved at the meeting to be held on Thursday, 28th September, 2017
Commissioning Executive (ICE) as an initial focus for the strategy. Comments included:
- Quality Care work – Paying appropriate wages will encourage staff retention, boost health and care outcomes and alleviate child poverty
- One approach to training - 57,000 people in Leeds work in the health and care sector and were largely trained within the organisation they work for. ‘One approach’ to training would encourage rotation throughout the health and care sector settings and break down barriers between the health and care settings in the public/private sector.
- The opportunities for joined up learning and training, recognising that there were issues across the public and private sectors which required the same training – such as moving/handling technique
- Awareness that many working in the health and care sector do so whilst they gain non-health and care related qualifications and/or language skills. Once complete, they often move out of the health and care sector
- The impact of the Apprenticeship Levy and whether this could be invested in health and care apprenticeships
RESOLVED - a) That, having considered the role of the Health and Wellbeing Board in
overcoming challenges relating to workforce; the comments made during discussions be used to provide direction for progress towards the priorities of the Leeds Health and Wellbeing Strategy 2016-21.
b) To support the engagement of members in discussions about the Living Wage and attend the Low Pay Seminar when arranged.
c) To oversee/raise the profile of the Supporting Disabled People into Employment Project to ensure it remains consistent with the city’s health and wellbeing priorities and participate in a ‘health, wellbeing and employment workshop’ in October 2017.
d) To continue to note and support the development of Leeds Health and Social Care Academy and to receive regular updates on progress.
e) To note that the City Workforce Work stream should be used to understand and plan responses to these challenges and keep the Board up to date with progress.
12 For information: Better Care Fund Quarterly Reports Steve Hume, Chief Officer, Resources & Strategy (LCC Adults & Health) presented a report for information on the completed Better Care Fund (BCF) reporting templates for quarters 2, 3 and 4 for 2016-17. The report noted that a requirement of the BCF is that completed reporting templates are submitted quarterly to NHS England to provide assurance that the conditions of the BCF are being met. RESOLVED – That the completed BCF reporting templates for quarters 2, 3 and 4 for 2016-17 be noted for information.
13 Date and Time of Next Meeting RESOLVED – To note the date and time of the next formal Board meeting as Thursday 28th September 2017 at 10.00am (with a pre-meeting for Board members at 9.30am).
Page 12

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
EXECUTIVE BOARD
WEDNESDAY, 21ST JUNE, 2017
PRESENT: Councillor J Blake in the Chair
Councillors S Golton, R Charlwood, D Coupar, R Lewis, J Lewis, L Mulherin, M Rafique, L Yeadon and B Anderson
Apologies Councillor
1 Substitute Member Under the provisions of Executive and Decision Making Procedure Rule 3.1.6, Councillor B Anderson was invited to attend the meeting on behalf of Councillor A Carter, who had submitted his apologies for absence from the meeting.
2 Exempt Information - Possible Exclusion of the Press and Public RESOLVED – That, in accordance with Regulation 4 of The Local Authorities(Executive Arrangements) (Meetings and Access to Information) (England) Regulations 2012, the public be excluded from the meeting during consideration of the following parts of the agenda designated as exempt on the grounds that it is likely, in view of the nature of the business to be transacted or the nature of the proceedings, that if members of the public were present there would be disclosure to them of exempt information so designated as follows:-
(a) Appendix 6 to the report entitled, ‘East Leeds Orbital Road: Land Assembly and Financing’, referred to in Minute No. 19 is designated as exempt from publication in accordance with paragraph 10.4(3) of Schedule 12A(3) of the Local Government Act 1972 on the grounds that it contains information relating to the financial or business affairs of particular people, and of the Council. It is therefore considered that the release of such information would, or would be likely to prejudice the Council’s commercial interests in relation to potential transactions.
3 Declaration of Disclosable Pecuniary Interests There were no declarations of Disclosable Pecuniary Interests made at the meeting.
4 Minutes RESOLVED – That the minutes of the previous meeting held on 19th April 2017 be approved as a correct record.
5 Chair's Opening Comments The Chair welcomed all in attendance to the meeting and reflected upon the number of significant events which had occurred since the previous Board meeting on 19th April 2017, including the General Election.
Public Document Pack
Page 13
Agenda Item 8

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
Specifically however, the Chair made reference to the atrocities which had occurred in London and Manchester in recent weeks, and also to the fire which had recently occurred at Grenfell Tower, London. On behalf of the Board, the Chair extended the Council’s sympathies to all of those who had lost their lives and to all of those who had been affected by those terrible events.
With regard to the fire at Grenfell Tower, the Chair invited the Director of Resources and Housing to provide an update and also reassurance, as to the actions which the Council was taking in light of the Grenfell Tower fire.
The Board noted that checks had been undertaken on the cladding systems used in Leeds, with reassurance being provided that none of the systems used had been comparable to those at Grenfell Tower. It was also noted that as a precautionary measure, further testing would take place on the materials used in the city’s high rise buildings. Reassurance was also provided on the ‘compartmentation’ system used in Leeds which had been established in order to contain fires within high rise buildings. Members also received an update on the installation of sprinkler systems which had occurred in a number of blocks in the city to date, and it was noted that this programme had prioritised those blocks which had been reserved for older residents. In light of the Grenfell Tower fire, emphasis was also placed upon the wish to continue to promote the importance of sprinkler systems in high rise buildings as a key fire safety measure on a national level.
Finally, the importance of the communication and engagement work with tenants was highlighted, and that this programme of engagement would continue.
Members welcomed the update and the reassurance provided, thanked the Executive Member for Communities for the lead which she had taken on such issues, and requested that Members be kept informed of developments in this area, as and when they occurred.
ENVIRONMENT AND SUSTAINABILITY
6 Waste Depot Development The Director of Communities and Environment submitted a report outlining the current depot provision across the Council and the current operational and financial risks associated with this. The report also outlined the work that had been undertaken to develop options in order to mitigate such risks, including the costs, issues and benefits associated with these options, and which sought approval for capital funding in order to deliver a new depot for the use of Waste Management and other Council services.
In response to a Members’ enquiries, the Board received assurances on the proposed development, specifically in respect of the service’s efficiency levels and its impact upon carbon output levels. In addition, with regard to the issue
Page 14

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
of continuity of service, it was acknowledged that a robust continuity plan would be established as part of this development.
Responding to an enquiry, assurances were provided in terms of keeping Elected Members informed of developments as they occurred in this area.
RESOLVED – (a) That the contents of the submitted report, be noted;
(b) That the injection of £4.01m of unsupported borrowing into the capital programme, in order to fund the development of a new operational depot on Newmarket Approach, be authorised;
(c) That authorisation be given to begin the process to tender for the construction of a new operational depot, on the land off Newmarket Approach behind the Refuse and Energy Recovery Facility (RERF), subject to necessary consultation and Planning permission;
(d) That it be noted that the Chief Officer, Waste Management, will be responsible for the implementation of such matters.
CHILDREN AND FAMILIES
7 Outcome of consultation to change the age range of Hovingham Primary School from 3-11years to 2-11years. The Director of Children and Families submitted a report regarding the outcome of consultation on a proposal to change the age range of Hovingham Primary School from 3-11 years to 2-11 years, and which sought approval to publish a statutory notice in respect of this proposal.
RESOLVED – (a) That the publication of a Statutory Notice to lower the age limit of
Hovingham Primary School from 3 to 2, changing the school’s age range from 3-11 years to 2-11 years, be approved, which would enable the school to deliver free early education entitlement for eligible 2 year olds;
(b) That it be noted that the responsible officer for the implementation of such matters is the Head of Learning Systems.
8 Learning Places Programme - Capital Programme Update Further to Minute No. 127, 14th December 2016, the Director of Children and Families, the Director of Resources and Housing and the Director of City Development submitted a joint report presenting an update on the 3 year strategy for providing sufficient school places in the city, on the progress of the projects currently forming part of the Learning Places Programme, outlining the revised programme of governance arrangements and which sought relevant approvals in order to progress the programme.
The Board acknowledged the complexities of the challenges being tackled by the Programme, and in response to an enquiry, Members highlighted the
Page 15

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
need for the Council to continue to work in a cohesive cross-party manner in order to effectively address such challenges.
Also, the Board received further information on the actions which were being taken with the aim of ensuring that the planning process in this area operated as smoothly as possible, and discussed the process by which proposals were brought forward as part of the Learning Places Programme.
Members also considered the Community Infrastructure Levy (CIL), and how such monies could potentially be utilised to help address those issues being tackled by the Learning Places Programme, and it was noted that a report regarding CIL was scheduled to be submitted to the July meeting of the Board.
In conclusion, it was undertaken that should any specific Board Members require it, a briefing on such matters could be provided to them. RESOLVED –
(a) That the ‘authority to spend’ on the Learning Places Programme for the three schemes, as detailed in the submitted report, at a total value of £19.3m, be approved;
(b) That approval be given for the balance of the programme capital risk fund to be reset from £6.13m to £10.771m, in order to facilitate effective risk management at programme level, with approval also being given on the ‘authority to spend’ on the increase of £4.641m;
(c) That approval be given to the revision of the programme governance arrangements, which are proposed to maintain an appropriate level of check and challenge, which include:-
the delegation of the approval of design and cost reports for the schemes which form part of the programme, approved by Executive Board, to the Director of Children & Families, and that these approvals shall be subject to the agreement of the Director of City Development and the Director of Resources & Housing, in consultation with the appropriate Executive Member, and that these reports will be open to scrutiny by Members; and
the delegation of the management and use of the basic need risk capital fund to the Director of Children & Families, and that these decisions shall be subject to the agreement of the Director of City Development and the Director of Resources & Housing, in consultation with the appropriate Executive Member, and that decisions on these matters will be open to scrutiny by Members.
(d) That the following be noted:-
Page 16

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
(i) The good progress made on this challenging programme of work, which is currently valued at £128.651m.
(ii) That the following benefits have been delivered from the Projects commissioned via the programme from 2014 onwards. These have been called off through either the YORbuild arrangements and/or in conjunction with the Leeds Local Education Partnership (LLEP). The programme has in total supported 72 new and existing apprentices and 102 people into employment. These figures relate to employees of both main contractors and their supply chains. These schemes have also recycled or reused 99% of the waste generated during the construction process with only 1% going to landfill.
(iii) The projected funding deficit which currently stands at £71.20m based on Education Funding Agency rates, and that with this in mind, Executive Board support be given to the arrangement of a meeting between the Executive Member for Children’s & Families and the Education Funding Agency.
(iv) That in the current reporting period there has been one request to access the programme capital risk fund for Bramley Primary School totalling £0.57m, which was approved in accordance with the Executive Board governance arrangements.
(v) That any savings made on applications on the programme capital risk fund are returned to the risk fund in order to support continued management of programme risks.
COMMUNITIES
9 Illegal Money Lending Team Progress Report Further to Minute No. 23, 15th July 2015, the Director of Communities and Environment submitted a report which provided an update on the activities of the national Illegal Money Lending Team (IMLT) within Leeds, together with an updated action plan.
Members welcomed the submitted report, paid tribute to the vital work being undertaken in this area, and highlighted the need to ensure that such good work was communicated as effectively as possible.
RESOLVED – That the contents of the submitted report together with the Illegal Money Lending Team Action Plan, as set out within Appendix 1, be noted, and that the Director of Communities and Environment be requested to monitor the progress of the Illegal Money Lending Team against the plan, and prepare a further report in 12 months’ time on the activities of the IMLT within Leeds.
ECONOMY AND CULTURE
10 Graduate retention and mobility and its impact on the Leeds economy
Page 17

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
The Director of City Development submitted a report which presented the main findings from recent and current research in respect of graduate mobility to and from Leeds, and which outlined Leeds’ response as a city.
Responding to a Members’ enquiries, the Board received further detail on the actions being taken to engage with graduates in order to identify and understand the issues that were important to them in making a city an attractive place to live and work.
RESOLVED – (a) That the need for more graduates in Leeds to cope with an increasing
demand for skilled jobs in the city, be noted;
(b) That the Chief Officer (Economy and Regeneration) be authorised to roll out a programme of initiatives, as outlined in section 3.18 of the submitted report, in order to attract more graduates to the city and to increase retention of graduates from the city’s Universities.
EMPLOYMENT, SKILLS AND OPPORTUNITY
11 Delivering Social Value through Employment and Skills Obligations The Director of City Development submitted a report which provided a summary of the employment and skills obligations which had been delivered through the Council’s procurement and planning activity from September 2012 to March 2017. The report also highlighted the learning which had taken place from the implementation of the employment and skills obligations and the review work which had been undertaken by the ‘More Jobs, Better Jobs’ Partnership. Additionally, the report recommended a revised approach towards the targeting of opportunities for priority groups.
Members welcomed the contents of the submitted report, specifically the proposal to revise the existing approach in order to target priority groups. Responding to an enquiry, the Board received further information on how associated data was collected and monitored, with it also being highlighted that a key aspect of the new approach was to make it as streamlined as possible for participating businesses.
RESOLVED – (a) That the success of the approach achieved to date in delivering social
value via the application of employment and skills planning obligations and through contracts, be noted;
(b) That the proposed revised approach towards targeting the priority groups, as set out within paragraph 3.6.2 of the submitted report be agreed, which will aim to ensure that this approach continues to deliver Council policy objectives for inclusive growth;
(c) That it be noted that the officer responsible for the further development of the revised approach and its implementation is the Head of Employment Access and Growth.
Page 18

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
RESOURCES AND STRATEGY
12 Treasury Management Outturn Report 2016/17 The Chief Officer (Financial Services) submitted a report which provided a final update on Treasury Management Strategy and operations for 2016/17.
RESOLVED – That the Treasury Management outturn position for 2016/17 be noted, together with the fact that treasury activity has remained within the treasury management strategy and policy framework.
13 Financial Performance - Outturn Financial year ended 31st March 2017 The Chief Officer (Financial Services) submitted a report presenting the Council’s financial outturn position for 2016/17 for both revenue and capital, and which also included details in respect of the Housing Revenue Account and spending on schools. The report also highlighted the position regarding other key financial health indicators including Council Tax and Business Rates collection statistics, sundry income, reserves and the prompt payment of creditors.
Members discussed the Council’s final outturn position at the close of the 2016/17 financial year, considered the individual outturn position of several directorates, and discussed the proposed use of surpluses, as detailed within the submitted report.
RESOLVED – (a) That the outturn position for 2016/17 be noted, and that approval be
given to the creation of earmarked reserves, as detailed in paragraphs 3.5 and 5.5 of the submitted report, and that authority to release such reserves be delegated to the Chief Officer (Financial Services).
(b) That it be noted that the Chief Officer (Financial Services) will be responsible for the implementation of such actions, following the conclusion of the ‘call in’ period.
14 Financial Health Monitoring 2017/18 - Month 2 (May 2017) The Chief Officer (Financial Services) submitted a report presenting the Council’s projected financial health position for 2017/18, as at month 2. The report reviewed the position of the budget and highlighted any potential key risks and variations after the first two months of the financial year.
The Board highlighted the importance of the transparent approach which was being taken towards the presentation of budgetary information, and discussed how the presentation of such information could help to identify where specific budgetary pressures existed.
RESOLVED – (a) That the projected financial position of the authority, as detailed within
the submitted report, be noted;
Page 19

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
(b) That the injection of £14.702m of additional Better Care funding into the Adults and Health 2017/18 revenue budget, be approved, with the proposals in respect of the use of the grant being submitted to a forthcoming Leeds Health and Wellbeing Board, and subsequently reported to a future Executive Board. With it also being noted that the Director of Adults and Health has the responsibility for the implementation of the decision;
(c) That the injection of £1.636m of Flexible Homelessness Grant into the Resources and Housing 2017/18 revenue budget, be approved, with it being noted that the Director of Resources and Housing is responsible for implementing decisions as to the use of the grant.
15 Implementation of business rates relief measures announced at Spring Budget 2017, including the design of a local discount scheme The Chief Officer (Financial Services) submitted a report which sought approval to implement the proposed locally administered West Yorkshire discretionary discount scheme, which had been designed in liaison with the other West Yorkshire authorities. In addition, the report also sought approval to implement two national rate relief schemes, which had been introduced by Government.
RESOLVED – (a) That the proposed locally administered West Yorkshire business rate
discount scheme, which is intended to provide targeted support to businesses affected by the 2017 business rates revaluation, be approved;
(b) That approval be given to the use of any remaining government funds in order to support large businesses, to be considered on a case by case basis;
(c) That formal approval be given to the implementation of the two national business rate relief schemes, as announced by Government, namely: support for small businesses losing Small Business Rate Relief and a £1,000 business rate discount for public houses with a rateable value of up to £100,000;
(d) That following approval of the local and national schemes (as detailed in the resolutions above), the intention to implement the three schemes at the earliest opportunity be noted, together with the fact that reliefs awarded will be backdated to 1st April 2017;
(e) That it be noted that implementation of the local and national schemes will be undertaken by the Business Rates Manager.
16 Leeds Cycling Starts Here (CSH) Strategy The Director of City Development submitted a report which provided an update on the progress made with regard to the promotion of cycling in the
Page 20

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
city, and which presented for the Board’s endorsement the Leeds ‘Cycling Starts Here’ Strategy.
In acknowledging the progress which had been made in recent years in Leeds with regard to cycling, Members discussed the role of the proposed strategy and how it would be used as a starting point to make further progress in this area. The Board acknowledged the multifaceted nature of cycling and how this would need to be reflected by the strategy, and discussed the role to be played by Scrutiny in the Strategy’s development.
RESOLVED – (a) That the contribution of partners and stakeholders towards the
production of the Leeds ‘Cycling Starts Here’ Strategy, be noted;
(b) That the findings of the consultation process, as detailed within the submitted report, be noted;
(c) That the Leeds ‘Cycling Starts Here’ Strategy be endorsed;
(d) That the progress made on the Strategy and related matters be reported to Scrutiny Board annually;
(e) That future updates on the ‘Cycling Starts Here’ Strategy be presented to Executive Board, as necessary;
(f) That it be noted that the Chief Officers for Highways & Transportation and Culture & Sport will be responsible for the implementation of such matters.
REGENERATION, TRANSPORT AND PLANNING
17 Leeds Public Transport Investment Programme The Director of City Development submitted a report which sought ‘authority to spend’ a total of up to £15.31m from the £173.5m funding which the Department for Transport had agreed in April 2017 for the Leeds Public Transport Investment Programme. Additionally, the report detailed the next steps for the delivery of the Programme.
Responding to a Member’s enquiry, the Board received further information regarding when the proposed programme of works would need to be delivered by, together with further detail on the proposed new rail stations, and the current position with regard to Network Rail funding. The Board also noted that discussions were ongoing with bus companies, with Members highlighting the need for all residents of Leeds to benefit from improvements to bus transport, and not just those users of specific bus companies.
Responding to Members’ comments regarding investment in different modes of transport, it was highlighted that the public transport network needed to become as seamless as possible, in order to ensure that the public benefit was maximised from the investment being made.
Page 21

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
The Board discussed the cross-party working group, noted the comments made during the discussion, and reaffirmed the importance of cross-party working in this area.
Regarding the Council debate on public transport which had been scheduled for 17th May 2017, but had been subsequently cancelled following the Prime Minister’s announcement to hold a General Election, it was highlighted that a comprehensive discussion on such matters was still a priority, and that further work and discussion on the scheduling of this would be undertaken.
RESOLVED – (a) That the Government approval of £173.5m funding towards public
transport improvements in Leeds, together with the content of the related correspondence, as detailed at Appendix 1 to the submitted report, be noted;
(b) That approval be given to inject the Department for Transport grant of up to £173.5m towards public transport improvements in Leeds, as set out within the contents of the approval letter (as appended to the submitted report), subject to the finalisation of a grant agreement with West Yorkshire Combined Authority (WYCA) in accordance with their assurance framework and those elements of the programme to be delivered directly by WYCA;
(c) That expenditure of up to £15.31m from the £173.5m Government funding be approved in order to progress the Leeds Public Transport Improvement Programme, subject to finalising those elements to be directly delivered by WYCA;
(d) That it be noted that officers will return to Executive Board in due course in order to seek approval to carry out detail design and construction on schemes as they are developed;
(e) That negotiations with bus operators, developers and partners continue in order to leverage significant additional financial investments to support the Leeds Public Transport Investment Programme;
(f) That the necessary authority be provided in order to enter into a Grant Agreement with the West Yorkshire Combined Authority for the expenditure of monies;
(g) That it be noted that the Chief Officer (Highways and Transportation) is responsible for the delivery of the programme.
18 Design and Cost Report - Claypit Lane/ Woodhouse Lane Junction and Public Realm lmprovements The Director of City Development submitted a report which sought approval to carry out a major junction improvement at the Claypit Lane/Woodhouse Lane
Page 22

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
junction, and sought approval for the necessary ‘Authority to Spend’, in order to facilitate such improvements.
RESOLVED – (a) That ‘authority to spend’ £2.526m from existing Capital Scheme Nos.
32214 and 16256 for the proposed highway and public realm improvement works at the junction of Clay Pit Lane and Woodhouse Lane, as detailed within the submitted report, be approved;
(b) That the actions required to implement the decision, together with the proposed timescale to progress the project, as detailed in paragraph 3.1 and 3.2 of the submitted report, be noted;
(c) That it be noted that the Chief Officer (Highways and Transportation) will be responsible for the implementation of such matters.
19 East Leeds Orbital Road - Land Assembly and Financing Further to Minute No. 149, 8th February 2017, the Director of City Development submitted a report which sought approval for the Council to make a Compulsory Purchase Order and related Side Roads Order in order to assemble the land necessary for the construction and adoption of the East Leeds Orbital Road (ELOR). The report also sought agreement to a financing package for the ELOR scheme, and presented an update on the work undertaken on this project to date.
In considering the report, further to the Wards highlighted within the submitted report, it was highlighted that Alwoodley Ward would also be affected by the initiative, specifically the advanced junctions work.
Responding to a Member’s enquiry, it was confirmed that although there was no provision for a bus lane on the East Leeds Orbital Road itself, there were a number of public transport improvements proposed to be undertaken as part of the overall East Leeds Extension programme.
Following consideration of Appendix 6 to the submitted report designated as exempt from publication under the provisions of Access to information Procedure Rule 10.4(3), which was considered in private at the conclusion of the meeting, it was
RESOLVED – (a) That the Director of City Development be authorised to make the Leeds
City Council (East Leeds Orbital Road) Compulsory Purchase Order 2017 ("the CPO") under sections 239, 240, 246, 249, 250 and 260 of the Highways Act 1980, the Acquisition of Land Act 1981 and all other enabling powers, as per the details set out in paragraphs 3.5 – 3.8 of the submitted report, and the plan at Appendix 3 (subject to any final amendments the Director of City Development considers necessary);
(b) That the Director of City Development be authorised to make the Leeds City Council (A6120 (East Leeds Orbital Road Classified Road) Side
Page 23

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
Roads and Other Works) Order 2017 ("the SRO") under sections 14 and 125 of the Highways Act 1980 and all other enabling powers, as per the details set out in paragraphs 3.5 – 3.8 of the submitted report and the plan at Appendix 4, (subject to any final amendments the Director of City Development considers necessary);
(c) That the Director of City Development be authorised to take all necessary steps to proceed with, and secure confirmation of the CPO and SRO, including the service of all requisite notices on affected parties in connection with the making, confirmation and implementation of the CPO and SRO and making of agreements and undertakings with landowners and other affected parties necessary in order to secure removal of any objections made to the CPO and SRO (where such agreements and undertakings are appropriate), and subject to the confirmation of the CPO, the making of one or more general vesting declarations under the Compulsory Purchase (Vesting Declarations) Act 1981 or the service of Notice to Treat and Notice of Entry under the Compulsory Purchase Act 1965, and if necessary presenting the Council’s case at any public inquiry or other proceedings;
(d) That approval be given to the provisional financing package for the East Leeds Orbital Road, as set out within section 4.4 of the submitted report, and as detailed within exempt Appendix 6, and that approval be delegated to the Director of City Development: to enter into a funding agreement with the West Yorkshire Combined Authority for an initial grant from the West Yorkshire Transport Fund of £11.81m and to draw down the full amount of an £82.95m grant allocation; and also for the approval of a provisional borrowing requirement of £43.68m;
(e) That approval be given for the Council to underwrite all land assembly costs and compensation costs arising from the making and implementation of the CPO and SRO in the event that these exceed the available WYTF grant available, and on the basis that such costs will be fully recoverable through roof tax payments, as set out in section 4 of the submitted report;
(f) That approval be given for the scheme to be injected into the Council’s Capital Programme, and subject to confirmation of the WYTF Grant, that ‘Authority to Spend’ be delegated to the Director of City Development, in consultation with the Chief Officer (Financial Services), to procure and let the construction contract or contracts for the East Leeds Transport Package;
(g) That in the event that the Council will need to acquire additional land or interests in order to ensure that ELOR is delivered, the Director of City Development, in consultation with the Chief Officer (Financial Services) and Executive Member for Regeneration, Transport and Planning be authorised to inject relevant schemes to the capital programme and be provided with the necessary delegated authority to agree ‘authority to
Page 24

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
spend’ for such schemes, with it also being noted that such additional costs will be recovered through the East Leeds Extension roof tax;
(h) That approval be given for the estimated cost of land assembly for interests that include land outside the direct route of ELOR (as set out in exempt Appendix 6 to the submitted report), to be injected into the Capital Programme, and that the Director of City Development be authorised to agree appropriate terms and acquire such land or interests in land that may be necessary in order to enable the delivery of the ELOR scheme;
(i) That it be agreed that the information as contained within Appendix 6 to the submitted report be treated as exempt from publication under the provisions of Access to Information Procedure Rule 10.4(3), and that the recommendations, as detailed within the exempt Appendix 6 (considered in private at the conclusion of the meeting), be approved.
20 City Centre Vehicle Access Management Scheme The Director of City Development submitted a report which sought authority to progress the detailed design and implementation of an automated vehicle access system to manage and control vehicular access within the pedestrianised core of Leeds city centre, together with an injection of £1,400,000 into the 2017/18 Capital Programme necessary to develop the scheme. In addition, the report also sought authority to progress the more detailed investigation and option appraisal for four measures at four other locations in the city centre where access by vehicles is prohibited or restricted.
RESOLVED – (a) That the injection and expenditure of £1,400,000 into the 2017/18
Capital Budget be approved.
(b) That the detailed design and implementation of an automated vehicle access system to control vehicle access within the central pedestrianised core of Leeds city centre, be authorised.
(c) That the detailed evaluation of a manually operated access control system at four other key locations within the city centre, as identified in section 3.4.6 of the submitted report, where vehicle access is restricted, be authorised.
(d) That approval be given for the invitation of tenders, and that subject to the tender sums being within the tendered budget, agreement be given to approve and authorise the award of the Contract to undertake the construction of the scheme;
(e) That the Director of City Development be instructed to expedite the implementation of all reasonable measures in the most timely manner as possible, and that the necessary authority be delegated to the Director of City Development in order to approve, consult and
Page 25

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
implement such measures as should be identified at the four key locations identified in section 3.4.6 of the submitted report;
(f) That it be noted that the Chief Officer (Highways & Transportation) will be responsible for the implementation of such matters.
21 Approval for the Construction of a Flood Alleviation Scheme at Westfield, Allerton Bywater The Director of City Development submitted a report regarding the flooding issues which existed within the Westfield area in Allerton Bywater, with the report also seeking approval to implement the Westfield Flood Alleviation Scheme, and to give authority to incur expenditure on the proposed works.
In considering the submitted report, assurances were provided that the proposed scheme would not create negative impact in other areas, either upstream or downstream of this site.
RESOLVED – (a) That the implementation of Westfield Flood Alleviation scheme at
Westfield , as shown within Appendix A to the submitted report (on drawing FRM/253271/001 rev B), be approved;
(b) That authority be given to incur expenditure of £472,000 on the Westfield Flood Alleviation scheme, funded by Leeds City Council Capital resources (£177,000) and Environment Agency grant (£295,000);
(c) That it be noted that the Chief Officer (Highways & Transportation) will be responsible for the delivery of the scheme.
22 Street Lighting Energy Saving Programme The Director of City Development submitted a report which presented an update on the progress made with regard to street lighting energy saving, which explored options for further energy saving measures, and which sought approval to undertake public consultation on further energy saving measures.
In considering the submitted report, a Board Member highlighted his objection to the Street Lighting Energy Saving Programme, and in acknowledging the comments made, Members discussed the effect of the programme to date and the proposal to undertake public consultation regarding options for further energy saving measures.
With regard to the public consultation exercise which was proposed, it was suggested that a view from West Yorkshire Police and/or Safer Leeds regarding the street lighting energy saving programme could potentially be incorporated into such consultation.
RESOLVED – (a) That the progress of the selective part-night street lighting contribution
towards energy savings, be noted;
Page 26

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
(b) That the proposal to undertake public consultation in order to explore options for further energy saving measures, be approved;
(c) That it be noted that the Chief Officer (Highways and Transportation) will be responsible for the implementation of such matters.
(Under the provisions of Council Procedure Rule 16.5, Councillor Golton required it to be recorded that he abstained from voting on the decisions referred to within this minute)
HEALTH, WELLBEING AND ADULTS
23 Leeds Commitment to Carers The Director of Adults and Health submitted a report which presented the ‘Leeds Commitment to Carers’, and which invited Leeds City Council tosign up to the commitment, requesting that each directorate undertook to complete its own commitment and action plan.
Further to the introduction provided by the Executive Member for ‘Health, Wellbeing and Adults’, Val Hewison, Chief Executive of the ‘Carers Leeds’ organisation was in attendance and provided the Board with an update and further information on the crucial role played by the many carers throughout the city, the range of support which needed to be provided to carers and the partnership and multi-agency approach which needed to be taken in order to do this.
Members welcomed the information provided, confirmed the Board’s support for the Council to sign up to the ‘Leeds Commitment to Carers’, and requested that a further report be submitted to a future Board meeting which detailed the actions being taken by each directorate in response to the ‘Commitment’.
RESOLVED – (a) That each directorate of Leeds City Council be requested to consider
their contribution towards making Leeds the best city for carers, and for each directorate to complete a ‘Leeds Commitment to Carers’ action plan.
(b) That approval be given for Leeds City Council as an organisation to sign up to the ‘Leeds Commitment to Carers’.
(c) That a further report be submitted to a future meeting of the Board which details the actions being taken by each directorate in response to the Council signing up to the ‘Leeds Commitment to Carers’.
24 Adult Social Care Use of Resources Peer Challenge September 2016 The Director of Adults and Health submitted a report which presented the results from the recent Local Government Association (LGA) peer challenge of the Adult Social Care directorate’s use of resources. In addition, the report outlined the actions being taken in response to the review.
Page 27

Draft minutes to be approved at the meeting to be held on Monday, 17th July, 2017
Members welcomed the contents of the submitted report, with specific reference being made to the actions that the directorate was taking in response to the key messages arising from the review.
RESOLVED – That the contents of the submitted report be noted.
DATE OF PUBLICATION: FRIDAY, 23RD JUNE 2017
LAST DATE FOR CALL INOF ELIGIBLE DECISIONS: 5.00 P.M., FRIDAY, 30TH JUNE 2017
Page 28

Report of Head of Governance and Scrutiny Support
Report to Scrutiny Board (Adult and Health)
Date: 18 July 2017
Subject: Chairs Update – July 2017
Are specific electoral Wards affected? Yes No
If relevant, name(s) of Ward(s):
Are there implications for equality and diversity and cohesion and integration?
Yes No
Is the decision eligible for Call-In? Yes No
Does the report contain confidential or exempt information? Yes No
If relevant, Access to Information Procedure Rule number:
Appendix number:
1 Purpose of this report
1.1 The purpose of this report is to provide an opportunity to formally outline some of the areas of work and activity of the Chair of the Scrutiny Board since the previous Scrutiny Board meeting on June 2017.
2 Main issues
2.1 Invariably, scrutiny activity can often occur outside of the formal monthly Scrutiny Board meetings. Such activity may involve a variety of activities and can require specific actions of the Chair of the Scrutiny Board.
2.2 The purpose of this report is, therefore, to provide an opportunity to formally update the Scrutiny Board on the Chair’s activity and actions, including any specific outcomes, since the previous Scrutiny Board meeting on June 2017. It also provides an opportunity for members of the Scrutiny Board to identify and agree any further scrutiny activity that may be necessary.
2.3 The Chair and Principal Scrutiny Adviser will provide a verbal update on other activity at the meeting, as required.
3. Recommendations
3.1 Members are asked to:a) Note the content of this report and the verbal update provided at the meeting. b) Identify any specific matters that may require further scrutiny input/ activity.
Report author: Steven CourtneyTel: (0113) 37 88666
Page 29
Agenda Item 9

4. Background papers1
4.1 None used
1 The background documents listed in this section are available to download from the Council’s website, unless they contain confidential or exempt information. The list of background documents does not include published works.
Page 30

Report author: Anna Frearson / Tim Taylor
Tel: 07712 214816 / 07891 278231
Report of Director of Public Health
Report to Scrutiny Board (Adults and Health)
Date: 18 July 2017
Subject: Update on Early Interventions and Reducing Health Inequalities Breakthrough Project
Are specific electoral wards affected? Yes No
If yes, name(s) of ward(s):
The Locality Community Health Development and Improvement Service service operates in: Armley, Alwoodley, Beeston and Holbeck, Bramley and Stanningley, Burmantofts and Richmond Hill, Chapel Allerton, City and Hunslet, Cross Gates and Whinmoor, Farnley and Wortley, Gipton and Harehills, Hyde Park and Woodhouse, Killingbeck and Seacroft, Kirkstall, Middleton Park, Moortown, Pudsey, Roundhay, Temple Newsam and Weetwood wards.
The Inner South Physical Activity work is planned for Beeston and Holbeck, City and Hunslet and Middleton Park.
The Inner East Physical Activity work is planned for Burmantofts and Richmond Hill, Gipton and Harehills, Crossgates and Whinmoor, Killingbeck and Seacroft, Temple Newsam and Chapeltown.
Are there implications for equality and diversity and cohesion and integration? Yes No
Is the decision eligible for call-in? Yes No
Does the report contain confidential or exempt information? Yes No
If relevant, access to information procedure rule number:
Appendix number:
Summary of main issues
1. The report provides an update on progress by the Early Interventions and Reducing Health Inequalities Breakthrough Project against the three priorities below with a particular focus on inequalities: i. To commission an Integrated Healthy Living Service (IHLS) and Locality
Community Health Development and Improvement Service (CHID).
Page 31
Agenda Item 10

2 of 22
ii. To ensure strategic alignment with healthy living services commissioned by partners
iii. To inspire communities and partners to work differently to reduce health inequalities – physical activity selected as the focus.
2. The Integrated Healthy Living Service is currently being mobilised and will be operational in October 2017. The Community Health Development and Improvement service commenced on 1st April 2017.
3. A series of proposed work programme priorities are outlined around physical activity.
Recommendations
The Scrutiny Board (Adults & Health) is asked:
1. To note the overall progress against the three priorities of the Early Interventions and Reducing Health Inequalities Breakthrough Project.
2. To note the early positive indications of the impact of effective outreach and engagement with hard to reach groups by the CHID - Better Together Service providers.
3. To comment and advise on the proposed priorities around physical activity.
Page 32

1. Purpose of this report
1.1 This report provides an update on the progress of the Early Interventions and Reducing Health Inequalities Breakthrough Project with a particular focus on the impact across the project upon reducing inequalities.
2. Background information
2.1 There are around 2,200 deaths of people under the age of 75 years each year. Of these, around 1,520 can be considered avoidable. The largest contributions to premature death are lifestyles/behaviour (40%), followed by genetic pre-disposition (30%), social circumstances (15%), health care (10%) and environmental exposure (5%). Early deaths are disproportionally experienced by people living in the most deprived areas of Leeds. Figure 1 shows age standardised rates per 100,000 of all age all cause mortality for under 75 years. 2011-15 for deprived Leeds are 573 compared to the Leeds rate of 362. The ward with the lowest rate is Harewood (216) compared to Burmantofts and Richmond Hill (661) - the ward with the highest. There is a 10 year difference in life expectancy (see figure 2) between communities with Harewood having the longest life expectancy at 86 years compared to Burmantofts and Richmond Hill at 75.5 years.
2.2 Evidence suggests that where ill health is related to lifestyle behaviour, it is significantly worse in deprived areas. Appendix A contains key health statistics for people living in the most deprived areas of Leeds compared to more affluent areas.
2.3 Smoking is still the single biggest preventable cause of early death. Good progress has been made on reducing smoking. In 2014, 30% of adults in Leeds smoked. The latest figures (2016) show this has reduced to 17.8% - a reduction of just under 59,000 smokers. This still leaves around 125,000 current smokers – who are not evenly distributed across the city. Figure 3 shows age standardised smoking rates per 100,000 by ward for adults in Leeds using GP recorded figures from January 2017 audit data. The rate for deprived Leeds is 30,581 compared to 19,557 for Leeds. The ward with the lowest prevalence is Harewood (10,029) and the ward with highest prevalence is Burmantofts and Richmond Hill (30,574).
2.4 Figure 4 shows age standardised rates per 100,000 of GP recorded obesity (Body Mass Index over 30) in adults from January 2017 audit data. The rate for deprived Leeds is 28,571 compared to 23,637 for Leeds. The lowest rate is in Headingley (16,362) and the highest is in Middleton Park (30,943).
2.5 Though there is strong national evidence relating to physical inactivity and the positive impact of being active on health outcomes, local data around physical activity is poor. Improving information in this area is one of the proposed priorities of the Breakthrough Project (see report section 3.4). Figure 5 shows participation in sport and active recreation 3 x 30 minutes per week by MSOA in Leeds 2011/12. The map illustrates that adults in affluent communities are more active than adults living in deprived Leeds.
2.6 Figure 6 shows age standardised rates per 100,000 of GP recorded diabetes from January 2017 audit data. The rate of diabetes in deprived Leeds is 8,592 compared to the Leeds rate of 6,055. The lowest rate is in Harewood (3,493) and the highest is in Gipton and Harehills (10,998).
Page 33

2.7 Figure 7 shows age standardised rates per 100,000 of GP recorded Coronary Heart Disease (CHID) from January 2017 audit data. The rate of CHID in deprived Leeds is 4,904 compared to the Leeds rate of 3,947. The lowest rate is in Harewood (3,070) and the highest is in Middleton Park (5,026).
2.8 Figure 8 shows age standardised rates per 100,000 of GP recorded Chronic Obstructive Pulmonary Disease (COPD) from January 2017 audit data. The rate of COPD in deprived Leeds is 4,846 compared to the Leeds rate of 2,573. The lowest rate is in Adel and Wharfedale (1,003) and the highest is in Middleton Park (5,286).
2.9 The Early Interventions and Reducing Health Inequalities Breakthrough Project is aligned to the Health and Wellbeing Strategy outcome that “Leeds will be a healthy and caring city for all ages, where people who are the poorest will improve their health the fastest”. The breakthrough project also supports the priorities in the Leeds Health and Care Plan and the West Yorkshire and Harrogate Sustainability and Transformation Plan (STP)”. The Breakthrough Project has three priorities:
To commission an Integrated Healthy Living Service (IHLS) and Locality Community Health Development & Improvement Service (CHID) for Leeds.
To ensure strategic alignment with healthy living services commissioned by partners.
To inspire communities and partners to work differently to reduce health inequalities.
2.10 The Executive Board report in March 2016 set out the approach to the three priorities and received permission to proceed with the re-commissioning of the Integrated Healthy Living Service (ILHS) and Locality Community Health Development and Improvement Service (CHID). An update was then provided to Executive Board in March 2017 via the Health Breakthrough Project Annual Report. This Health Scrutiny report provides a further update on the progress against the three priorities with a particular focus on the impact across the project upon reducing inequalities.
Main issues
3.1 Integrated Healthy Living Service (IHLS) - “One You Leeds”
Following the procurement process, the contract to deliver the IHLS service known as “One You Leeds” was awarded to Reed Momenta Ltd. Mobilisation of the service began on 1st April 2017 and will be fully operational on 1st October 2017. One You Leeds will provide support to adults to achieve lifestyle behaviour change, particularly focusing on smoking cessation, weight management, cooking skills, healthy eating and physical activity. This will be done in conjunction with other services across the city including CHID and social prescribing.
3.2 People will have a single point of access to healthy lifestyle support for the new service, which will improve both professional referral and self-referral pathways. They will be offered a range of options including support to self-help, targeted face to face healthy living interventions in a range of community venues and one-to-one personal support to those of highest need to develop the confidence and motivation to change. The service will also: deliver targeted outreach activities and campaigns,
Page 34

provide training to the wider public health workforce and support people to access wider opportunities in the community to maintain behaviour change on leaving the service.
3.3 While the service will provide universal support, in order to improve outcomes for those who experience the poorest quality health, face to face support and outreach work will be targeted at the most deprived areas of Leeds. Within “deprived Leeds” the following target groups will be prioritised:
o People with, or at risk of developing, long term health conditions (serious mental illness, chronic obstructive pulmonary disease, cardio vascular disease, diabetes)
o Pregnant women and their familieso People with mild to moderate mental health problemso People with mild to moderate learning disabilitieso People from black or minority ethnic communities o New and emerging migrant communities
3.4 One You Leeds will prioritise the geographical location of services to ensure good access for people living in deprived parts of the city, however, the service will continue to provide a universal provision and anyone living in Leeds will be able to access the service regardless of their postcode. Clinic locations will be positioned where possible with adequate parking, opportunities to access by cycling or walking and good links to public transport. The service will also offer comprehensive digital opportunities with follow up for people who would prefer to self-help. Further information on specific buildings from where services will be delivered, will be provided once these have been identified and confirmed.
3.5 A Communications Plan has been developed as part of the mobilisation process to continue to keep stakeholders informed about the new service. A briefing paper and Frequently Asked Questions document has just been produced and the process of sharing this with stakeholders and partners including Elected Members, Clinical Commissioning Groups, GP Practices, Leeds Teaching Hospital Trust and Sport Leeds Board Members has begun.
4 Locality Community Health Development and Improvement Service (CHID) – Better Together
4.1 Better Together is the name for the new locality community health development service, which started in April 2017. Following a service review and procurement, contracts were awarded to third sector providers in the following areas of Leeds:
East North East Leeds – Feel Good Factor (consortia lead), Shantona, Space2, Touchstone, Zest
South and East Leeds – Health for All (consortia lead), Asha, Hamara West North West Leeds – Barca
The three new contracts replace the 14 previous separate locality contracts.
Page 35

4.2 The Better Together service providers link with other local partners to improve health and reduce health inequalities by targeting and focusing on the 10% most deprived neighbourhoods in the city.
4.3 The new service focuses primarily on issues that lead to poor health such as poverty, unemployment, relationships and housing issues and use a community development approach to work with individuals, groups and communities to identify local needs and work with them to find appropriate support and interventions that can help them improve their situation. It is part of the wide range of activity across the city helping people look after their own health, helping us look after each other and making the most of the strengths and assets we all have as individuals and communities.
4.4 The service complements the Leeds Integrated Healthy Living Service (IHLS) service. The ‘Better Together’ Service focuses primarily on addressing the wider determinants of health, whereas the LIHLS focuses primarily on promoting and improving healthy lifestyle services. The two services will work very closely together.
4.5 The first set of quarterly monitoring information is due in mid-July. We have worked closely with providers during mobilisation and the first quarter of activity. There are encouraging early signs of effective outreach and engagement for hard to reach residents and communities.
5.0 Strategic Alignment with Healthy Living Services
5.1 To ensure that the newly commissioned services meet the needs of the Leeds population, a health needs assessment and extensive consultation exercises were conducted, capturing the views of service users, current providers, primary care staff and commissioners. These findings informed the development of a model describing how an integrated healthy living service for Leeds could be commissioned within the broader system of assets in the city which support healthy lifestyles (see appendix B). The system aims to align citywide support around healthy lifestyles, with stronger interfaces between services commissioned by Leeds City Council, primary care services and third sector organisations. The model shown in appendix A illustrates how the IHLS and CHID services will interface and interact within the broader context of the health system in Leeds.
5.2 We have engaged with colleagues across Leeds City Council and partners in the city to align services with this model and ensure pathways are in place to connect up people and services. We have ensured the Leeds Integrated Healthy Living System has been incorporated into the development of the new Leeds Health & Care Plan and intend to use this to influence and align with the new service models for primary care and community services that are now being developed as part of this plan. In addition, we wish to use the model to influence the investment decisions that will be made by the Leeds Clinical Commissioning Partnership later in the year - for example on social prescribing.
6.0 Inspiring communities and partners to work differently to reduce health inequalities - Physical Activity
Page 36

6.1 A city wide Outcomes Based Accountability (OBA) event was held to launch the Health Breakthrough Project in September 2015 and led by Cllr Mulherin. This was attended by 135 partners and overwhelmingly, the key issue that emerged was the need to increase physical activity amongst groups who experience particularly poor health outcomes. As a result the third priority of the breakthough work was then focused on what more we can do as a city to work with people in ways that increase their movement, improve their wellbeing and ultimately reduce health inequalities.
6.2 A second OBA session was held in July 2016 and led by Cllr Charlwood, Cllr Coupar and Cllr J. Lewis to focus specifically on issues relating to physical activity in the city. The feedback from the attendees at these events, public and service user consultation and a report produced by the Sport and Active Lifestyles Service led to the emergence of the following themes around physical activity:
The need for a whole system buy in - influencing decision makers and
commissioners Promote the benefits of physical activity - as the norm and part of everyday
life Environment - engage partners to ensure the physical activity agenda is
addressed and prioritised in the developing built infrastructure Improve the measurement of physical activity in the city Take a Community approach with a focus on assets
6.3 In response, a Physical Activity Steering Group has been set up to drive forward these recommendations. The group is jointly chaired by Public Health and Active Lifestyles and is comprised of representatives from Public Health, Sport and Active lifestyles, Parks and Countryside, Transport, Planning and Regeneration, Culture, PPPU and the Health and Wellbeing Service (Healthy Schools). This cross-directorate approach to an issue lies at the heart of the Council’s aim for Breakthrough projects. External partners will be included in the group reports to the Sport Leeds Board which provides a useful external strategic reference group.
The Physical Activity Steering Group has developed a draft work programme based around the following priorities described below.
6.4 Support the delivery of a whole systems approach to physical activity – with a focus on the inner east and inner south of the city
6.4.1 Given the strong link between inactivity and deprivation an expression of interest was submitted to Sport England based on taking one (large) deprived part of the city where it is believed that significant impacts can be made in terms of a holistic approach to addressing inactivity. Unfortunately the bid was unsuccessful but there are still plans to continue to drive this work forward given the momentum gained from across the Council and partners and the potential long term benefits that could accrue. . The proposed areas for this work are in the Inner East:
Burmantofts and Richmond Hill Gipton and Harehills Crossgates and Whinmoor Killingbeck and Seacroft Temple Newsam Chapeltown
Page 37

6.4.2 The areas outlined provide an appropriate level of scale to work within and have high levels of deprivation. Other important factors include:
The housing growth and highways infrastructure planned for inner and outer east Leeds.
A number of high profile regeneration plans in the inner east area of the city (Neighbourhood Framework plans e.g. Killingbeck and Seacroft /East Leeds extension/Halton Moor). These local frameworks identify opportunities for housing development on both Council and third party land, improvements to open space and green connectivity, improvements to public transport including walking and cycling to help local people access training and job opportunities in the local area.
A move to more focused locality working within the Council and with key wider stakeholders. This is at estate level with potential for focus on physical inactivity, social cohesion and employability. Two of the six priority areas are within the defined catchment - Lincoln Green and Torres in Burmantofts and Spencer Place, Bankside Street and St Shepherd’s Lane plus Clifton / Newalls in Harehills / Chapeltown.
A focus on locality profiling to better inform and prioritise interventions, alongside the integration and alignment of service provision.
Two large city parks of national significance serving the catchment (Roundhay and Temple Newsam) with green corridors enabling connectivity.
Integrated facility developments e.g. potential major development of existing Fearnville site into a large “activity park” concept including a mix of wellbeing centre / park life / open space / playing pitches / walking / commercial outdoor development / colocation with Adult Social care and other services e.g. Health / partnerships with British cycling and British Triathlon. There are also ongoing discussions with Children’s Services about a possible new high school. A report will also be brought forward that will identify the preferred site for a new Wellbeing centre in the inner east of the city.
6.4.3 In parallel to this work officers have also been looking at potentially developing a similar approach in the inner south of the city focussing on the wards of Beeston and Holbeck, City and Hunslet and Middleton Park) . The approach would aim to support the council’s locality based approach to future service delivery in the six most deprived communities in the city (chosen from the 17 LSOAs in the bottom 1%) where services will focus their resources with the aim of reducing health inequalities. Two of these areas - Crosby Street, Recreations, Bartons in Holbeck & Stratford Street and Beverleys in Beeston Hill - sit within the project scope. Following recent discussions with the Communities Team there is a possibility of extending the project scope into the New Wortley area.
In addition, the project will complement the Locality Community Health Development and Improvement Service (CHID) with its focus on the 10% most deprived areas of the city/and be part of a wider integrated healthy living system. Area based contracts will be a key part of a whole systems approach to physical activity in a place.
Page 38

There has been initial consultation with key partners, community leaders and organisations and although the full scoping work is still to be undertaken, gaps within a “systems approach” are emerging and include;
Research / insight including data and intelligence access and share Community development and wider partner engagement Workforce development Digital technology, solutions, access and use
.Given the local delivery pilot bid was unsuccessful officers are now in discussion with Sport England about developing an investment plan for both the inner east and the inner south areas. There is potentially a minimum sum of £500k on offer to move this wider work forward with the aim of working with partners over the next 3 months in to develop a wider investment plan to then discuss with Sport England later this year in October.
6.5 Coordination of communications, key messages & marketing campaigns in relation to physical activity
There is a priority to create key physical activity messages for the city working with Sport Leeds and partners. Key campaigns will be utilised and built upon including Active 10, This Girl Can/ Leeds Girls Can and Change for Life. The aim will be to make physical activity messages consistent and visible and connect them to other related campaigns around for example air quality and active travel. A “virtual hub” is also proposed to pull together information on physical activity opportunities. The creation of which will be scoped and tested in the Inner South.
6.6 Influencing Role
There is a priority to ensure that physical activity is on the agenda of internal and external partners and contributes to service design, and commissioning decisions. The plan will focus on the following aspects:
One Council Approach Strong leadership in the city for physical activity Effective governance of physical activity Engaging city wide partners
6.7 Support the design, planning and development of the physical infrastructure that will support and enable communities to become more active based around:
Housing Active travel Public realm Parks / green space
There is a proposal to develop key principles of design for health and wellbeing - including a strong focus on physical activity. The plan is to update design guidance that can be referred to by developers and communities. The intention is to engage with community groups who understand their local areas and the potential for
Page 39

improving the public realm / placemaking and creating winter/wet weather uses for parks.
6.8 Managing Outdoor Spaces for Recreational Use - how do we use and manage our “green and blue” Infrastructure?
The following priorities have been proposed:
Targeting and prioritising blue and green space projects Connecting green/blue spaces across Leeds - providing opportunities for active
travel along green/blue corridors Connect up with the cycling and walking Implementation plan Community Infrastructure Levy (CIL) to investigate green infrastructure (GI)
opportunities Parks and Countryside’s management of parks and trees (Parks and
Greenspace Strategy) Work with the West Yorkshire Combined Authority (WYCA) who are signed up
to ‘Green Streets’ (cycling/pedestrian friendly)
7 Corporate considerations
7.1 Consultation and engagement
7.1.2 In order to shape the direction of the breakthrough project, the project team brought together information from a range of consultation and insight. Consultation was undertaken with the following groups:
The public Existing service users Service providers Potential co-commissioners Public health colleagues Wider stakeholders
Significant consultation was undertaken during the Healthy Living and Community Health Development service reviews and service specifications were developed to ensure that needs were accurately identified and taken into account. Wider stakeholders had an opportunity to input into the service delivery approach. Consultation with stakeholders included service users and potential services users, current and potential providers, strategic city partners, health professionals, senior LCC officers and Elected Members including Locality Health and Wellbeing Champions.
7.2 Equality and diversity / cohesion and integration
7.2.1 The new IHLS and CHID Services are focused on providing services to individuals, and communities living in the most deprived areas of the city. Specific geographic areas have been identified through the service review process and are detailed in the service specification.
Page 40

7.2.2 Equality, Diversity Cohesion and Integration Impact Assessments were undertaken and were subsequently reviewed at key stages of the procurement projects for the IHLS and CHID services.
7.2.3 The physical activity priorities include a focus on working with deprived communities in the inner east and south of the city.
7.3 Council policies and Best Council plan
7.3.1 This collaborative breakthrough project supports the ambition for Leeds to be the Best City in the UK by 2030. It also contributes to the Best Council Plan, Joint Health and Wellbeing Strategy Leeds Health and Care Plan and West Yorkshire and Harrogate Sustainability and Transformation Partnership Plan.
7.4 Resources and value for money
7.4.1 The breakthrough projects by definition are intended to make best use of existing resources by working innovatively as a team for Leeds. The breakthrough project is taking a citizen and asset based approach, working with partners to deliver projects.
7.4.2 Work to reduce unhealthy lifestyles is highly cost effective. The National Institute for Health and Care Excellence (NICE) have assessed the economic and health benefits of lifestyle services and conclude that most activities aimed at improving the public's health are extremely good value for money and generally offer more health benefits than the alternatives tested. Such activities include: stop smoking services, healthy eating initiatives, physical activity programmes and alcohol interventions. Some activities can be 'cost saving', that is, in the long run they reduce costs by more than the total spent on them.
7.4.3 The procurement processes were designed to drive improvements in service quality and value for money. The new services will operate on a reduced budget compared to the previous service provision and have been made more efficient for example for the IHLS by merging a number of individual contracts into one contract and for the LCHID/I services by having three providers to achieve reduced management costs.
7.5 Legal implications, access to information, and call-in
7.5.1 The recommissioning of the IHLS and CHID services were conducted in accordance with the Council’s contract procedure rules and procurement law. The decision maker’s authority falls under Part 3 Section 3E (09) of the Council Constitution, Officer Delegation Scheme (Executive Functions) – Director of Public Health. This decision is the implementation of a Key Decision from Executive Board of 9th March 2016 – minute number 147. There are no further specific legal implications associated with the issues identified in this report. The report is subject to call in.
7.6 Risk management
7.6.1 The scope of this programme of work is substantial particularly as the involvement of external partners across the city who have a role to play in supporting healthy living is key to its success. The issues tackled are complex and there is a need to be mindful of health inequalities and the impact upon more vulnerable people living
Page 41

in the city. A key challenge for this project is creating a strong joint narrative to promote the aims of this breakthrough project positively both within the council and to external partners and the general public in a climate of cuts to services. Risks associated with the re-commissioning of the Integrated Healthy Living Service have been and will continue to be identified, reviewed and managed through the mobilisation period. The identification of new and increasing risks has taken place an on-going basis and will continue to through the management of both the IHLS and CHID contracts.
8 Conclusions
8.1 The Early Interventions and Reducing Health Inequalities Breakthrough project is making progress against its three priorities and has the potential to make a positive contribution to the ambitions of improving health and reducing inequalities in the city as set out in the Leeds Health & Wellbeing Strategy. The new IHLS – One You Leeds service is currently being mobilised and will be operational in October 2017. One You Leeds will provide support to adults to achieve lifestyle behaviour change, particularly focusing on smoking cessation, weight management, cooking skills, healthy eating and drinking and physical activity. Whilst the One You service will provide universal support, in order to improve outcomes for those who experience the poorest quality health, face to face support and outreach work will be targeted at the most deprived areas of Leeds.
8.2 The CHID – Better Together service successfully launched in April and the first quarter of monitoring will be available at the end of July. The new service will focus primarily on issues that lead to poor health, such as poverty, unemployment, relationships and housing issues and use a community development approach to work with individuals, groups and communities to identify local needs and work with them to find appropriate support and interventions.
8.3 Following two OBA events physical activity was identified as a priority focus for the Breakthrough Project and a cross Council Steering Group has been established to drive forward the work. A series of priorities have been proposed for the physical activity work programme including locality pilots in Inner East and South Leeds the latter funded by Sport England. Other priorities include co-ordination of communications, better planning and design to encourage physical activity and managing outdoor spaces for recreational use.
9 Recommendations
The Scrutiny Board (Adults & Health) is asked:9.1 To note the overall progress against the three priorities of the Early Interventions
and reducing Health Inequalities Breakthrough Project.9.2 To note the early positive indications of the impact of effective outreach and
engagement with hard to reach groups by the CHID - Better Together Service providers.
9.3 To comment and advise on the proposed priorities around physical activity.
Page 42

Appendix A: Maps showing inequalities between deprived and non- deprived Leeds
Figure 1:
Page 43

Figure 2:
Page 44

Figure 3:
Page 45

Figure 4:
Page 46

Figure 5:
Page 47

Figure 6:
Page 48
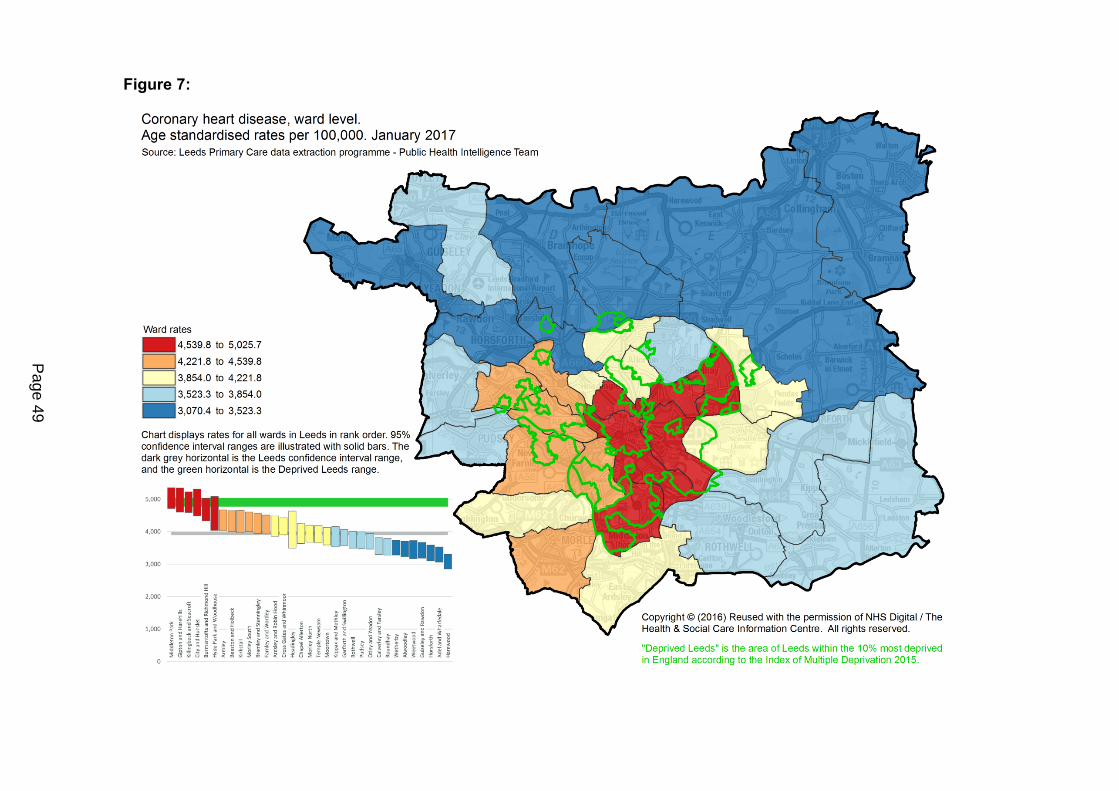
Figure 7:
Page 49
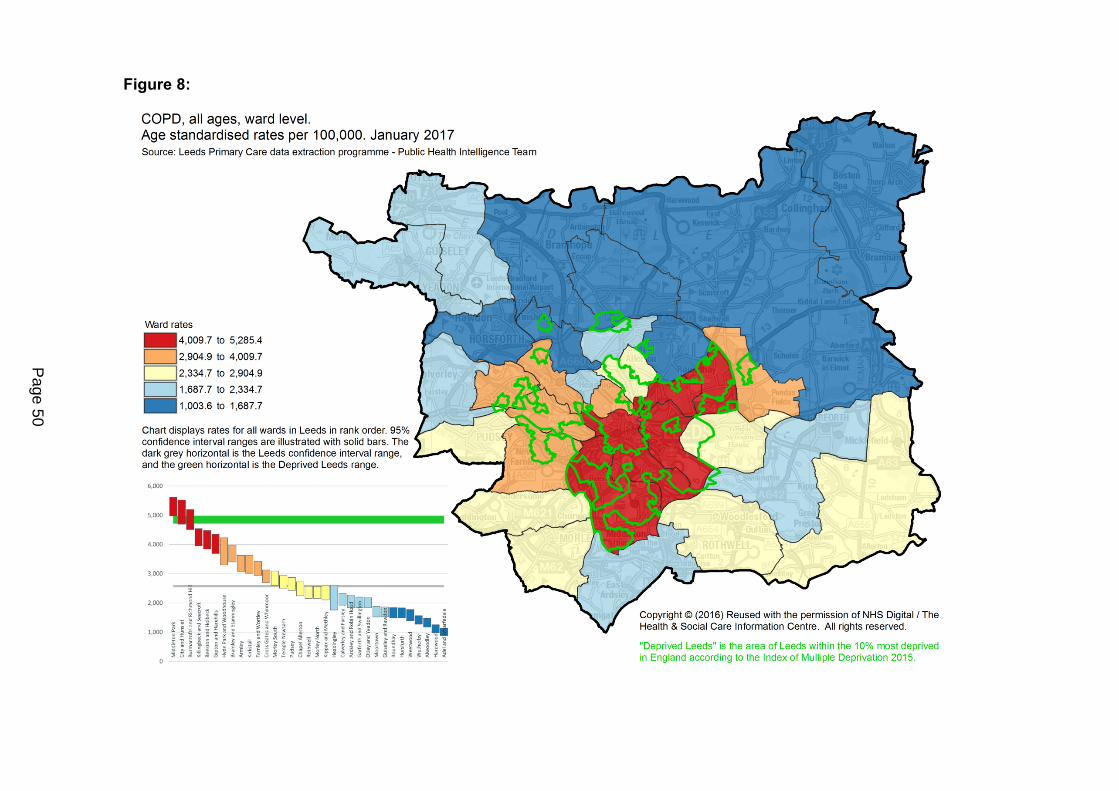
Figure 8:
Page 50
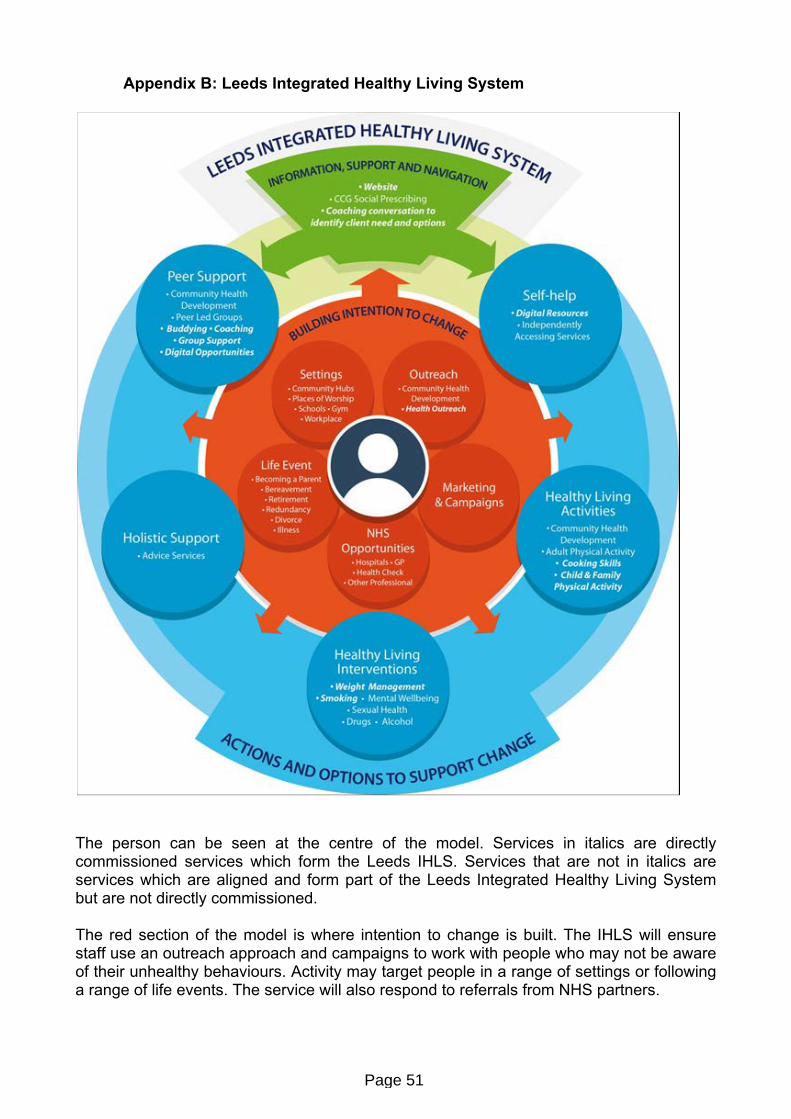
Appendix B: Leeds Integrated Healthy Living System
The person can be seen at the centre of the model. Services in italics are directly commissioned services which form the Leeds IHLS. Services that are not in italics are services which are aligned and form part of the Leeds Integrated Healthy Living System but are not directly commissioned.
The red section of the model is where intention to change is built. The IHLS will ensure staff use an outreach approach and campaigns to work with people who may not be aware of their unhealthy behaviours. Activity may target people in a range of settings or following a range of life events. The service will also respond to referrals from NHS partners.
Page 51

The green section of the model provides information, support and navigation to a service user. Service users could have a coaching conversation with a navigator to access the right support, or independently access the One You website which may provide enough information and support to make a behaviour change themselves.
The blue section of the model describes the range of services to choose from to facilitate and support change. These include self-help, accessing healthy living activities in the community, accessing a more traditional healthy living intervention, receiving holistic support to work to remove barriers to behaviour change or a peer support approach. People wishing to make a behaviour change can enter and exit the system at any single point - there is no set pathway.
Drawing on service reviews, the Community Health Development outcomes are increased social capital, increased community and individual resilience and reduced health inequalities with a focus on the wider determinants of health. The IHLS outcomes are increased confidence to change, increased level of motivation, increased physical activity, healthier weight, healthier nutrition, reduced problematic alcohol use, improved emotional health and reduced smoking.
Page 52

Report of the Head of Governance and Scrutiny Support
Report to Scrutiny Board (Adults and Health)
Date: 18 July 2017
Subject: Quality of Care Services in Leeds
Are specific electoral Wards affected? Yes No
If relevant, name(s) of Ward(s):
Are there implications for equality and diversity and cohesion and integration?
Yes No
Is the decision eligible for Call-In? Yes No
Does the report contain confidential or exempt information? Yes No
If relevant, Access to Information Procedure Rule number:
Appendix number:
1 Purpose of this report
1.1 The purpose of this report is to introduce a range of information relevant to the Scrutiny Board’s continued consideration of matters associated with the quality of care services across Leeds.
2 Background
2.1 During the municipal year 2015/16, the previous Scrutiny Board established a process to routinely consider published Care Quality Commission (CQC) inspection outcomes and reports for all health and care providers in Leeds. Since that time, the process has developed and been refined, resulting in quarterly reports being presented to the Scrutiny Board (due to commence in September 2017).
2.2 The previous Scrutiny Board also received details of the ‘One City Care Home Quality and Sustainability’ project aimed at ensuring that ‘citizens of Leeds receive high quality care in independent sector care home settings and that our contracts incentivise care homes to provide this high quality care’.
3 Summary of main issues
One City: Care Home Quality and Sustainability’ project3.1 As part of the overall project, a conference and project launch event was held in April
2017, which included the input of the Executive Member (Health, wellbeing and Adults) and the former Chair of the Scrutiny Board.
Report author: Steven CourtneyTel: (0113) 378 8666
Page 53
Agenda Item 11

3.2 Appended to the report, for consideration by the Scrutiny Board, is a briefing note which summarises progress since the launch across the following work areas:
One city approach to quality – development and implementation of a ‘one city care home quality improvement action plan’.
One city approach to market development – development of a ‘Joint Market Position Statement’ that sets out a shared vision for the sector that will support providers in developing future services.
Re-Commissioning of the Adult Social Care Residential and Nursing Care Services (Framework Arrangement) Contract – a review of the current contract and monitoring arrangements will inform an options appraisal to determine a service delivery model and procurement process, in readiness for replacing the existing contract with a new one from December 2017.
3.3 It should also be noted that as the details presented in Appendix 1 are a statement of fact, CQC representatives are not routinely invited to attend the Scrutiny Board. Should members of the Scrutiny Board have any specific matters they wish to raise directly with the CQC, these will have to be dealt with outside of the meeting and/or at a future Scrutiny Board.
3.4 Appropriate officers will attend the Scrutiny Board meeting to present the briefing note and address any questions from members of the Board.
The state of adult social care services 2014 to 2017
3.5 Also appended to this report is the recent Care Quality Commission (CQC) report on the state of adult social care services (2014 to 2017). This provides a summary report setting out the CQCs overall findings following two and a half years of inspections using a new methodology and ratings system to assess the quality of care and establish whether adult social care services are safe, effective, caring, responsive and well-led.
3.6 It should be noted the attached report provides a national overview and is not presented to provide a Leeds specific assessment or summary. Rather it is presented to help the Scrutiny Board in its future work during the course of the municipal year.
3.7 It should be noted that CQC representatives have not been specifically invited to attend the Scrutiny Board on this occasion.
Quality of Care Services in Leeds
3.8 It should be noted that further consideration of information and progress in relation to the ‘Quality of Care Services in Leeds’ theme are presented in the Board’s developing work schedule, and is likely to include matters such as:
Quarterly updates on published CQC inspection reports/ outcomes (commencing September 2017);
Leeds Quality Account (September / October 2017)
Page 54

Leeds Better Lives Strategy – update reports on the overall strategy; progress of Phase 4; and implementation updates for Phases 2 and 3 (Timing to be confirmed)
Re-Commissioning of the Adult Social Care Residential and Nursing Care Services Contract – overview of progress and outcomes (Timing to be confirmed)
4. Recommendations
4.1 That the Scrutiny Board considers the details presented in this report and its appendices; and determines any further scrutiny activity and/or actions, as appropriate.
5. Background papers1
None used.
1 The background documents listed in this section are available to download from the Council’s website, unless they contain confidential or exempt information. The list of background documents does not include published works.
Page 55

This page is intentionally left blank

1
Purpose
To provide Scrutiny Board members with a progress update since the previous brief to Scrutiny Board in March 2017, and following the projects launch event on the 7th April 2017.
Background Information
Under The Care Act 2014, the Council has legal obligations and the Director of Adults and Health has specific statutory duties to facilitate and shape a diverse and sustainable older people’s care home market.
There are significant concerns around the quality and sustainability of the current older people’s care home market, with the following issues all putting pressure on the sector;
An ageing population with increased complexity of need, co-morbidities, and dementia needs.
The financial sustainability of the market and the need to co-produce a “true cost of care” for Leeds, and to negotiate an appropriate fee that is proportionate to the expectations of quality service delivery and to the financial situation facing the local authority.
Quality of care services rated at 48% Good by the Care Quality Commission (CQC), in comparison with a national average of 65.5%. Scrutiny Board and the Executive Member for Health, Wellbeing and Adults’ aspiration1 is that this should be at least 80% for Leeds.
Significant workforce pressures affecting the ability to recruit and foster a skilled and sustainable workforce. Such pressures include; including salary expectations, access to training and suitable career pathways, job requirements and levels of accountability in comparison to other job options (e.g. Leeds strong retail sector), and potential implications of the Brexit decision.
Varying degrees of integration/duplication with existing initiatives and schemes to support quality of care in older people’s care homes, and a reported lack of open, honest and trusted relationships.
As such, Adult Social Care (ASC) and NHS Partners will deliver the One City Care Home Quality & Sustainability project, through partnership working with Commissioners, Care Home Providers and Older People’s Residents/Residents Representatives.
The overarching aim of the One City Care Home Quality & Sustainability project is: To ensure that citizens of Leeds receive high quality care in independent sector care home settings and that our contracts incentivise care homes to provide this high quality care. There are three parallel strands of work:
Strand 1: One city approach to quality - Development and implementation of a ‘one city care home quality improvement action plan’.
Strand 2: One city approach to market development – Development of a ‘Joint Market Position Statement’ that sets out a shared vision for the sector that will support providers in developing future services.
Strand 3: Re-Commissioning of the ASC Residential and Nursing Care Services (Framework Arrangement) Contract – A review of the current contract and monitoring arrangements will inform an options appraisal to determine a service delivery model and procurement process, in readiness for replacing the existing contract with a new one from December 2017.
1 Scrutiny Board Meeting Minutes, November 2016.
One City Care Home Quality & Sustainability Project UpdateBrief for Scrutiny Board (Adult Social Services, Public Health, NHS), June 2017
Page 57

2
Progress Update
Strand 1 and 2:The 7th April One City Quality event was opened by Cllr Rebecca Charlwood, and saw presentations from speakers across the sector including Scrutiny Board Chair Cllr Peter Gruen, followed by workshops and a panel Q&A. These provided opportunity to better understand the current market position in relation to care quality, and to discuss on what good looks like and how we can work together to get there, with a focus on practical solutions. Headline themes from the event workshops and panel Q&A have been shared. Attendees were also given an open invitation to be involved as the work develops and to further comment, either from those in attendance or who due to other commitments were unable to attend on the day.
Two of the key findings from the event were; The need for targeted, specialist, strength-based support to care homes, the need for an integrated approach,
and that this could take the form of a supportive/mentoring team with a specific focus on driving quality improvements and supporting care homes to deliver high quality care.
A skilled, sustainable network of registered care home managers is crucial to ensuring that care homes are well-led and deliver high quality care.
A recurrent £300K investment, initially over 3 years, has been identified out of the additional 1% precept that Councils have been given permission to levy. This will be used to establish a Care Quality Team and to support workforce development in the sector, for example, a Leadership Academy/Support Programme for registered managers. There is potential for further funding investment from Leeds CCGs.
The remit and focus of a Care Quality Team and Leadership Academy are being developed. They will be informed by the One City event findings and other engagement activities that have taken place including the stakeholder questionnaire review of the existing A&H Residential and Nursing Care Services Framework Contract, a workshop with NHS partners to gather their initial requirements for a Care Quality Team, and discussions with other local authorities. To date, conversations have taken place with Barnet, Leicestershire and Durham who have such teams already established, and a discussion with My Home Life2 about their work delivering leadership support, integrated care, and community engagement transformation packages.
These engagement activities are also being used to inform the requirements for the quality improvement action plan and market position statement. As an example, feedback from the event reiterated the advice from the project’s Strategic Advisory Group, to streamline existing care home meeting forums and governance routes. This will reduce duplication, provide integration and clarity in focus and decision making, and to ensure that care home owners and directors are effectively engaged, as well as registered managers. It will also encourage engagement with many care home providers who struggle to find capacity to attend the various existing arrangements. A meeting between A&H, NHS and care home owner/director representatives has been arranged for the 29th June to discuss the strategic direction for the sector, and a proposed model for future forum meetings and governance is being developed.
Strand 3: Independent consultants Mazars have completed the Cost of Care review. The findings of the review are being considered by A&H in relation to the financial implications for the Council, and initial fee rate proposals are due to be discussed at the project’s Strategic Advisory Group on the 13th July. Work continues to develop the Market Analysis report and to review existing contract documentation such as the quality framework standards and equipment schedule. This is informed by learning from the various engagement activities and from workshops with a care home reference group.
2 My Home Life is a charitable organisation whose vision is “a world where care homes are great places to live, die, visit and work; where care homes are: supported to deliver to their potential, valued and trusted by those who work with them, cherished by their local communities”. Leeds City Council are registered members of the My Home Life/Kings Fund Network.
Page 58

CQC-377-072017
How to contact us Call us on 03000 616161Email us at [email protected] Look at our website www.cqc.org.uk Write to us at Care Quality CommissionCitygateGallowgateNewcastle upon TyneNE1 4PA
Follow us on Twitter @CareQualityComm
Please contact us if you would like this report in another language or format.
The state of adult social care services2014 to 2017 Findings from CQC’s initial programme of comprehensive inspections in adult social care
Page 59

Our purpose
The Care Quality Commission is the independent regulator of health and adult social care in England. We make sure that health and social care services provide people with safe, effective, compassionate, high-quality care and we encourage care services to improve.
Our role
• We register health and adult social care providers.
• We monitor and inspect services to see whether they are safe, effective, caring, responsive and well-led, and we publish what we find, including quality ratings.
• We use our legal powers to take action where we identify poor care.
• We speak independently, publishing regional and national views of the major quality issues in health and social care, and encouraging improvement by highlighting good practice.
Our values
Excellence – being a high-performing organisation
Caring – treating everyone with dignity and respect
Integrity – doing the right thing
Teamwork – learning from each other to be the best we can
Page 60

Contents
Foreword from the Chief Inspector ............................................................ 2
1. Introduction ............................................................................................. 4
2. What have we found in our inspections? ............................................... 8
3. What can the sector learn from our inspections? ................................ 24
4. What do we do about poor care? .......................................................... 33
5. Have adult social care services improved? ........................................... 39
6. What is next for the regulation of adult social care services? ............. 47
Acknowledgements ................................................................................... 49
References ................................................................................................. 49
Page 61

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 2
Foreword from the Chief Inspector
In my first month in post in October 2013, I wrote:
“To make sure that our regulatory approach is truly personalised I want us to consider for every service we look at – is this good enough for my Mum (or any other member of my family)? If it is, that is fantastic. If it’s not then we need to do something about it.”
The ‘Mum Test’ has guided our work ever since. I wanted CQC’s regulation and indeed, the commissioning and provision of adult social care, to be truly personalised and firmly focused on the people receiving it. After extensive co-production, engagement and testing, CQC formally rolled out its new inspection framework for adult social care in October 2014, when, for the first time, we rated services as outstanding, good, requires improvement or inadequate. By February 2017, we had inspected all adult social care services registered with us in October 2014 – many more than once. That’s more than 33,000 inspections of around 24,000 different locations, including care homes, care in people’s own homes, Shared Lives schemes and supported living services.
What have we found? Are adult social care services meeting the Mum Test? When we choose care for ourselves or our loved ones, can we be confident that it is safe, effective, caring, responsive to our needs and well-led? The wealth of information gathered from our inspections means that the picture of adult social care – its successes, its failures and the challenges ahead – is clearer. I can say that most of the adult social care sector is meeting the Mum Test, providing safe and high-quality care that we would be happy for anyone we love, or ourselves, to receive. Over three-quarters (77%) of adult social care services are good – this should be and is celebrated. These are services with leaders who inspire a positive culture focused on providing person-centred care – treating people as people and not just as recipients of care. These leaders motivate, develop and value their staff who work tirelessly and skilfully to support people to live their lives to the full, with dignity and respect. The lives of people using adult social care can be transformed or their final days remembered for the care and compassion they and their families and carers experienced.
However, quality across England is undeniably variable. We have completed our initial comprehensive inspection programme with only 2% of services being rated as outstanding. While we make no apology for setting the bar high, this is considerably lower than we originally expected. It is clear that it is more difficult to achieve this highest standard of quality.
And there is too much poor care: 2% of services are currently rated as inadequate, and 19% of services are rated as requires improvement and are struggling to improve. Through our inspections, we have seen examples of unacceptable care, occasionally resulting in actual harm to people using services.
Page 62

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 3
This is awful for people receiving this care, as well as their families and carers. But it also undermines the public’s confidence in the sector as a whole – a sector that we are becoming increasingly reliant on as our population ages and people’s needs at all ages become more complex.
Quality regulation is playing its part to ensure people receive the safe, high-quality and compassionate care they have every right to expect. We can see that many providers are responding to our concerns and rising to the challenge. Eighty-one per cent of services rated as inadequate improved their overall rating following re-inspection, which is testament to the commitment of staff to deal with problems and achieve better care. In particular, we have found that having a committed and consistent registered manager can have a big influence on the quality of care that people receive – for example, by making sure staff have training to understand the needs of people in their care.
However, too many services are not improving or seem incapable of improving. Thirty-eight per cent retain their rating of requires improvement following re-inspection, despite knowing from our inspections what needs to change and 5% of these services had deteriorated. Not all services that were originally rated as good maintain quality. Where we have re-inspected them, usually prompted by concerns, over a quarter (26%) have received a lower rating.
In our report The state of health care and adult social care in England last October, we gave a stark warning that adult social care in England was ‘approaching a tipping point’. This was driven by a growing and ageing population, more people with increasingly complex conditions and in a challenging economic climate a greater demand on services but more problems for people in accessing care, and further issues across the health and care sector. The risk of adult social care approaching that tipping point is still real. We will explore what effect this is having on people using services and the wider health and care landscape in our next report in the autumn.
CQC will keep its relentless focus on quality by sharing successes, identifying failings, taking action to ensure areas in need of improvement are tackled, and at all times, by being transparent and acting in the public’s best interests. To achieve this, our regulation of adult social care will become even more targeted, risk-based and intelligence-driven over the next few years.
I hope people using adult social care services, their families and carers will find this report helpful and that providers, commissioners and funders, improvement bodies and the government will use our information to place quality firmly at the heart of the continuing debate about the future of adult social care. There are stories to inspire, lessons to learn and warning signals to heed. With everyone at CQC, I remain committed to shining a spotlight on quality, encouraging and recognising improvement and holding providers to account. But we cannot do it alone. Everyone must play their part in transforming adult social care and making sure that all services pass the Mum Test so that people using services, their families and carers can be confident that quality matters and will be delivered.
Andrea Sutcliffe Chief Inspector of Adult Social Care
Page 63
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 4
1. Introduction
In 2013, CQC set out its plans to radically transform the regulation of adult social care services. A year later, we began our new programme of comprehensive inspections, with ratings to make it easy for people to understand the quality of care and to help them choose care; a focus on identifying, highlighting and celebrating good practice; and a determination to drive improvement and hold providers to account for poor care. Understanding the experiences of people who use adult social care services is key. They are often in very vulnerable circumstances and their care can affect every part of their lives. Social care supports older people coping with several health conditions; some are living with dementia while others may be isolated and lonely. But adult social care is not just a service for older people; meeting the needs of people with mental health issues, younger people with a disability and people with a learning disability is also very significant. People using adult social care services have different needs, aspirations and circumstances. This incredible diversity in the adult social care sector means that personalisation is critical so that people can identify their individual needs; be empowered to take control; and make informed choices about the way they live their lives. Good services recognise this by delivering truly person-centred care. We have now completed this initial programme of comprehensive inspections and ratings – some 33,000 in all across two and a half years. This report sets out what we found: are our adult social care services safe, effective, caring, responsive and well-led?
1.1 How we work
We register providers that apply to CQC when they are able to satisfy us that they meet the requirements. We make intelligent use of data, evidence and information, including information shared with us by staff and people using services, their families and carers to decide when, where and what to inspect. Our inspectors use their professional judgement, supported by objective measures and evidence, to assess services against our five key questions. Supported by people who have experience of using care services (Experts by Experience) in the majority of inspections, our inspectors use feedback from people who use services, their carers and families to inform their judgements. We always ask the following five questions of services.
• Are they safe?
• Are they effective?
Page 64

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 5
• Are they caring?
• Are they responsive to people’s needs?
• Are they well-led? We rate services to highlight where care is outstanding, good, requires improvement or inadequate. We rate services at two levels:
1. We rate each one of the five questions.
2. We aggregate these separate ratings to give an overall rating for the location. This approach to comprehensive inspections was launched on 1 October 2014. It was developed through testing and consultation with the public, people who use services, providers and organisations with an interest in our work. We are continuing to refine our approach and in June 2017 published a new, consolidated assessment framework, which will be adopted from November 2017. Our enforcement policy sets out what action we take to require services to improve and, where necessary, the action we take to make sure those responsible for poor care are held accountable for it.
1.2 Background to the sector
Adult social care can make a real difference to people’s lives. It is the largest sector that CQC regulates, with a large number and range of providers, a strong private and voluntary sector, and wide differences in the size and types of services and care provided. The sector covers:
• accommodation and personal care provided in residential care homes, nursing homes and specialist colleges (around 16,000 locations, with the capacity to provide care for around 460,000 people)
• personal care provided in the community for more than half a million people, of which the majority is care provided in people’s homes through domiciliary care services (around 8,500 services), as well as extra care housing, Shared Lives schemes and supported living services.a
Adult social care is estimated to contribute £20 billion to the economy1 and employ around 1.4 million people – 5.3% of the total workforce in England2. It can help individuals and the families of people who need care and support to carry on working. Adult social care services are facing a number of challenges. These include:
a We will be publishing a separate report later this year that looks at quality in hospice services. From 2017/18 hospices services be assessed under the healthcare assessment framework. They will therefore become part of the responsibility of the Chief Inspector of Hospitals. Hospice services are included in the data for ‘all’ adult social care services in this report.
Page 65

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 6
• An ageing population with increasing needs. o The number of people aged 85 or over in England is set to more than double over
the next two decades.3 o More than a third of people aged over 85 have difficulties undertaking five or more
tasks of daily living without assistance, and are therefore most likely to need health and care services.4
• Difficulties in recruiting and retaining staff to care for people. o In 2015/16 the overall staff vacancy rate across the whole of the care sector was
6.8% (up from 4.5% in 2012/13), rising to 11.4% for home care staff. Turnover rates have risen from 22.7% to 27.3% a year over the same three-year period.5
o Potential changes to immigration policy resulting from the vote to leave the European Union could have serious consequences for the social care workforce. Around one in 20 (6%) of England’s growing social care workforce are non-British European Economic Area nationals – around 84,000 people.6
• Rising costs of adult social care. o In 2015/16, the gross expenditure of all councils with adult social services
responsibilities was £16.97 billion. Although this is 18% higher in absolute terms than in 2005/06, after accounting for inflation it is 1.5% lower than in that year.7
o Findings from the most recent Association of Directors of Adult Social Services budget survey have estimated that the National Living Wage will cost councils around £151 million plus at least £227.5 million in implementation and associated costs in 2017/18. This will affect both direct council costs and increased provider fees.8
• Concerns about funding to meet these costs and a reliance on those who pay for their own care. o Age UK estimates that an additional £4.8 billion a year is needed to ensure that
every older person who currently has one or more unmet needs has access to social care, rising to £5.75 billion by 2020/21.9
o Some providers, particularly in domiciliary care, have withdrawn from local authority contracts where they felt there was too little funding to enable them to be responsive to people’s needs.
o Despite additional funding that has been made available for adult social care, only 7% of directors of adult social services are fully confident that savings targets will be met in 2019/20.10
o The public have expressed concerns over the higher charges self-funders tend to pay, compared with state-funded residents. A sample of care home groups operating in 12 English counties in 2015 found self-funders pay over 40% more on a like-for-like basis.11
In this challenging context, CQC’s role as the quality regulator is ever more important. We have to make sure that we do not compromise on the quality of care and ensure that people using services, their families and carers are at the heart of everything we do.
Page 66

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 7
1.3 This report
This report looks at what we found about the quality of care across the whole range of adult social care services that we regulate. Our report is based on more than 33,000 inspections of around 24,000 different locations published up to May 2017. It is one of a series of reports across the sectors that CQC regulates, which aim to give an in-depth review of services based on our initial programme of comprehensive inspections. We illustrate the quantitative findings from our ratings datab with qualitative information and examples from a sample of inspection reports. We recognise there is fragility in the adult social care sector influenced by funding and resource pressures. But as the quality regulator, our focus in this report is on the quality of adult social care services and the impact that this has on people who use services.
b Although we completed our initial programme of comprehensive inspections in January 2017, we have used data extracted on 5 May to allow time for inspection reports and ratings to be published.
Page 67

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 8
2. What have we found in our inspections?
Key points
• At the end of our initial comprehensive inspection programme, almost four out of five adult social care services in England were rated as good or outstanding overall. Nearly a fifth of services were rated as requires improvement. We are particularly concerned about the 343 locations (2%) that were still rated as inadequate.
• We have observed differences in performance from region to region, with the East of England showing almost 10% more locations rated as good or outstanding than the North West.
• Of the five key questions that we asked all services, safe and well-led have the poorest ratings, with around a quarter requires improvement and inadequate.
• Caring was the best rated key question – 92% good and 3% outstanding.
• Community social care services (such as supported living and Shared Lives) were rated the best overall. Nursing homes remain the biggest concern.
• Generally, smaller services that are designed to care for fewer people were rated better than larger services.
• The public values the information in our inspection reports.
2.1 Introduction
Since October 2014, when CQC completely overhauled and transformed our regulatory approach for adult social care services in England, people have been using our inspection reports and ratings as an important source of information to support their choice of care services. This was reflected in CQC’s 2016 public inspection report survey that showed 90% of people who were looking at residential adult social care reports said they found them useful. CQC’s judgements published in inspection reports are informed by a range of detailed information that we gather from providers, partners, commissioners and, importantly, people’s own experiences of care and the views of their families and carers. Our inspection teams are trained and equipped to support a consistent and robust approach to making these judgements by asking five key questions – is this service safe, caring, effective, responsive to people’s needs and well-led – so that we are really getting under the skin of care services in a more consistent, detailed and thorough way than ever before.
Page 68

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 9
Our approach not only supports people to make informed decisions about care, but the detail of CQC’s inspection reports also highlights shortcomings in the quality of care for providers and commissioners to respond to and act on. If providers do not respond well enough and fail to give people who use their services the standards they have a right to expect, we will take action to enforce improvement.
2.2 Overall ratings – all England
A service’s overall rating is very visible. All services are required to show it on their websites and in their services. Where services are good or outstanding, many providers have been keen to promote this further – on banners, on literature and through local media. We welcome this; it’s right that providers should be proud of their good and outstanding services, and of the staff who help to achieve this. By the end of our initial comprehensive programme of more than 33,000 inspections, almost four-fifths of adult social care services in England were rated as good (77%) or outstanding (2%) overall. Nearly a fifth of services were rated as requires improvement. This proportion is too high. As part of our next phase of inspections we will target these services to make sure that providers do not view this overall rating of requires improvement as acceptable and, alongside commissioners, they work hard to improve care. We are particularly concerned about the 343 locations (2%) that are currently rated as inadequate (figure 1). We estimate that these services may collectively have the capacity to care for almost 20,000 people. Since poor care can have such a shocking impact on people’s day-to-day lives, it has to be everyone’s responsibility to make sure that people’s care is safe, compassionate and of high quality. CQC will work with providers and commissioners to ensure the necessary changes to improve care are made.
Figure 1: Adult social care overall ratings
Source: CQC ratings data, 5 May 2017. Numbers above bars show total active locations rated
Page 69

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 10
2.3 Overall ratings – regional breakdown
Completion of our initial comprehensive inspection programme has provided the public with a full picture of performance for their area. As well as detailed inspection reports for each adult social care service – searchable by postcode – there is a map on our website that enables people to see and compare the ratings of services in their area. Region-by-region analysis shows that there was a difference between the region with the best ratings (East of England, where 82% of locations were rated as good and 1% as outstanding), compared with Yorkshire and the Humber (74% and 1%) and the North West (72% and 2%) (figure 2).
Figure 2: Overall adult social care ratings by region
Source: CQC ratings data, 5 May 2017. Figures in bars are % of rated locations. Numbers in brackets show total active locations rated
Figure 3 maps this regional performance across the local authorities in England. The lighter areas on the map show where, on average, we found the highest rated adult social care services – note the clusters in the midlands. And the darker areas show where the lowest rated services were – note the clusters in areas of the North West and West Yorkshire and some of the London boroughs in the North and East. This map, as well as the other maps and charts in this report, can be viewed in a separate document on our website.
Page 70

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 11
Figure 3: Adult social care ratings by local authority area
Source: CQC ratings data, 5 May 2017. Quintiles are based on local authority ratings scores, based on all key question ratings for each adult social care location
Figure 3 shows average ratings across all adult social care services, but we can look at the three main types of care in more detail. Figure 4 maps nursing home, residential home and domiciliary care performance across local authorities. Compared with all services, the cluster of high performance in the midlands is even more notable in residential homes, and for nursing homes high average ratings are particularly grouped in the far South West. Parts of the North West and West Yorkshire stand out as areas of poorer care, although this is more marked among residential and nursing homes than in domiciliary care. However, it is worth noting the cluster of poorer domiciliary care services in Greater London; 14 London boroughs feature in the lowest fifth of average ratings for domiciliary care, compared with eight boroughs for residential homes and seven boroughs for nursing homes.
Highest performing
Lowest performing
All adult social care services
Page 71

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 12
Beyond the clusters of patterns in performance, the maps below show many examples of variations in types of service within the same local authority. For example, Northumberland is in the highest performing 20-40% of nursing home provision, whereas it is among the lowest performing authorities in its residential home and domiciliary care provision. At the other end of the country, the London Borough of Bromley shows a similar pattern of performance.
We continue to observe these geographical differences in quality, and while the differences on average between the poorest fifth and best fifth of areas is not enormous, we are seeing that there are parts of the country where good quality adult social care may be harder to access. We will continue to analyse this data in discussion with partner organisations to see if we can explain the variation we observe.
Figure 4: Nursing home, residential home and domiciliary care ratings by local authority area
Nursing homes
Highest performing
Lowest performing
Page 72

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 13
Residential homes
Highest performing
Lowest performing
Page 73

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 14
Source: CQC ratings data, 5 May 2017. Quintiles are based on local authority area ratings scores, based on all key question ratings for each adult social care location
2.4 Ratings by key question
As well as the overall rating, we give all adult social care services a rating for each of the five questions we ask of all care services. These allow us to look into greater detail at the issues that matter to people: are services safe, effective, caring, responsive to people’s needs and well-led? Figure 5 shows how all adult social care services were rated against the five key questions.
Domiciliary care
Highest performing
Lowest performing
Page 74

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 15
Figure 5: Adult social care ratings by key question
Source: CQC ratings data, 5 May 2017. Figures in bars are percentages
Safe When we ask whether a service is safe, we find out if people are protected from abuse and avoidable harm.
SAFE IN AN INSPECTION REPORT ‘One member of care staff told us, “We try to build a trusting relationship so if people had any problems or concerns they would come to us and tell us.” One person told us, “If anyone hurt me I would talk to the staff about it.”’
However, of the five key questions that we asked all services, safe had the poorest ratings, with 23% rated as requires improvement and 2% as inadequate.
Low ratings are concerning and indicate poor quality that can have a real impact on people using services. For example, poor safety can mean systems and processes that are not adequate for managing medicines or determining staffing levels. This can result in people not getting their prescribed medicines to help keep them well. In domiciliary care agencies, for example, staff that do not have enough time on home visits to have meaningful discussions with people about their needs and preferences will not be able to give them good person-centred care. Effective When we ask whether a service is effective, we find out if people’s care, treatment and support achieves good outcomes, promotes a good quality of life and is based on the best available evidence.
EFFECTIVE IN AN INSPECTION REPORT ‘Care workers were proactive in identifying if people's needs changed. For example one person told us, "I usually make all my medical appointments, but one day the carer noticed something wrong with my ankle and called in the district nurse for me."’
Page 75

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 16
More than four out of five services were able to show that their care was effective and that people’s care, treatment and support enables them to have a good quality of life. This has been achieved, for example, by involving people in training, to help staff understand the needs of those in their care. Eighty-one per cent of services were rated as good and 1% as outstanding for the key question ‘are services effective?’. Caring When we say that a service is caring, we find out if staff involve and treat people with compassion, kindness, dignity and respect.
CARING IN AN INSPECTION REPORT ‘People who used the service and their relatives confirmed they were treated with dignity and respect by carers who empathised with them. One person said, "I'm very slow on my feet now and they know that – they never rush me." Another person told us how their carer, "always helps me do as much as I can – they're very tactful". In a questionnaire returned to CQC one relative stated, "The carers and managers have provided an excellent service underpinned by total respect and dignity.”’
In the majority of cases, our inspectors have seen and heard that staff involve people in their care and treat them with compassion, kindness, dignity and respect. When people may not be able to fully describe this themselves – for example, people with a learning disability and those living with dementia and other conditions that may affect their ability to communicate – our inspectors have used our Short Observational Framework for Inspection, which helps us to analyse how well staff interact with and support the people they are caring for. People using services were often very keen to tell us of the close relationships built up over time with staff who know their likes and dislikes. These factors led to ‘caring’ being the most highly rated of all the questions we ask services. More than nine out of 10 services were rated as good (92%) or outstanding (3%) for caring. Responsive When we ask whether a service is responsive, we find out if services are organised so that they meet people’s needs.
RESPONSIVE IN AN INSPECTION REPORT ‘All staff went out of their way to maintain family lives and relationships. Relatives’ comments included, "I'm always made to feel welcome anytime", "I bring the grandchildren in to visit, we sometimes go in the garden or just spend time in their room, there is plenty of space".’
Our reports show that in high-performing responsive services everyone has equal access to care, regardless of their particular characteristics. Eighty-five per cent of services were rated as good or outstanding for responsiveness, while 14% were rated requires improvement. One per cent of services were rated as inadequate for responsiveness.
Page 76

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 17
Well-led When we ask whether a service is well-led, we find out if the leadership, management and governance of the organisation assures the delivery of high-quality, person-centred care, supports learning and innovation, and promotes an open and fair culture.
WELL-LED IN AN INSPECTION REPORT ‘The registered manager and provider had developed an open and inclusive culture by meeting and working with people’s relatives, staff and external health and social care professionals. A comment from a relative read, “The kindness, patience and care shown to my relative is wonderful. The team is led by a truly marvellous manager whose standards are the highest possible.”’
Like the safe key question, our assessment of whether services are well-led shows relatively poor performance, with 22% of services rated as requires improvement and 2% as inadequate. Our data shows that if a service is rated as good or outstanding in well-led, it is more likely to be rated as good or outstanding overall, compared with any other key question. Services that are rated as requires improvement or inadequate in their well-led rating can indicate that staff are not being adequately supported or that people who use services, their families and carers are not being taken seriously if they raise a concern.
2.5 Types of services
People who use services, their families and carers can use these different types of adult social care service, depending on their needs. By looking at the registration data that we collect we can see how provision has changed over the last seven years as different providers enter and leave the market. By following the historical patterns, we get an idea of how services are responding to needs of local populations, and how they are balancing this with financial and resource pressures. Figure 6 shows a pattern of decreasing numbers of residential homes and increasing numbers of domiciliary care agencies of various sizes. It also shows a long-term trend of increasing numbers of nursing home beds and decreasing numbers of residential home beds. However, we flagged in The state of health care and adult social care in England last year that the increase in nursing home beds came to a halt around March 2015. Since then, the provision of nursing home beds has declined and there are nearly 4,000 fewer nursing home beds open than there were at the peak in March 2015. This decline in nursing home beds may have abated; the latest data shows a small rise in bed numbers. As demand increases it will be important for CQC nationally and commissioners locally to monitor the availability of services and understand the reasons for changes.
Page 77
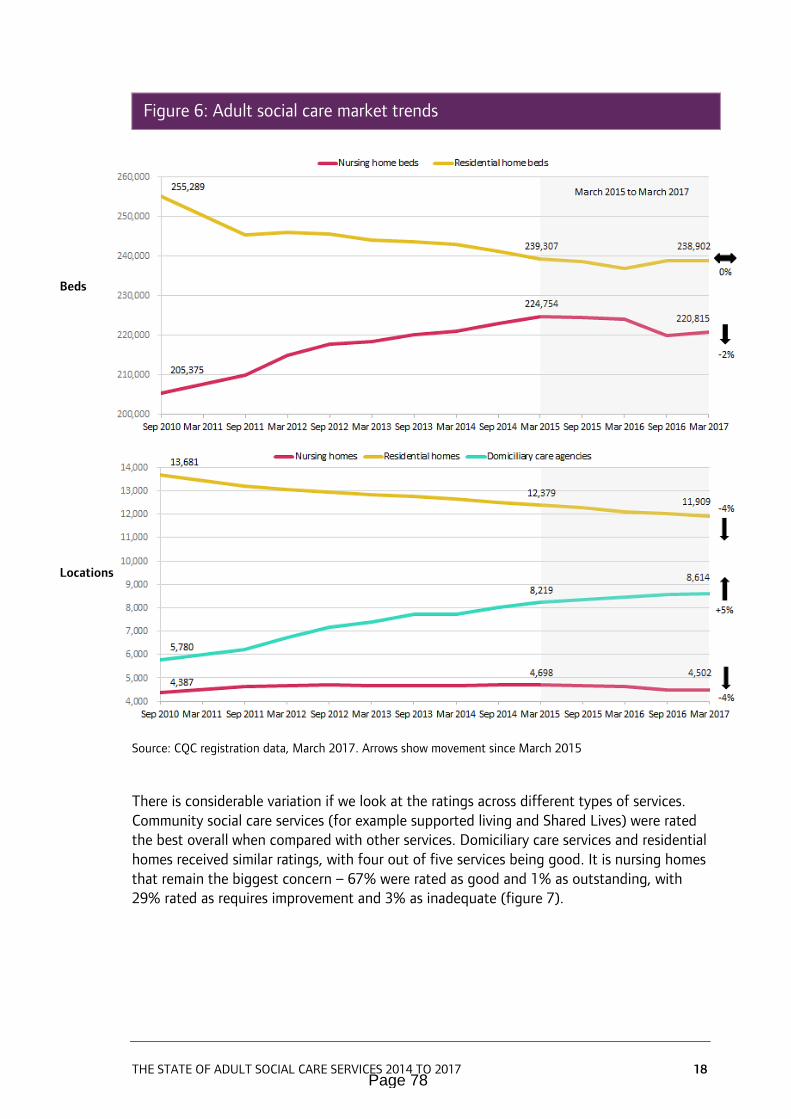
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 18
Figure 6: Adult social care market trends
Source: CQC registration data, March 2017. Arrows show movement since March 2015
There is considerable variation if we look at the ratings across different types of services. Community social care services (for example supported living and Shared Lives) were rated the best overall when compared with other services. Domiciliary care services and residential homes received similar ratings, with four out of five services being good. It is nursing homes that remain the biggest concern – 67% were rated as good and 1% as outstanding, with 29% rated as requires improvement and 3% as inadequate (figure 7).
Beds
Locations
Page 78
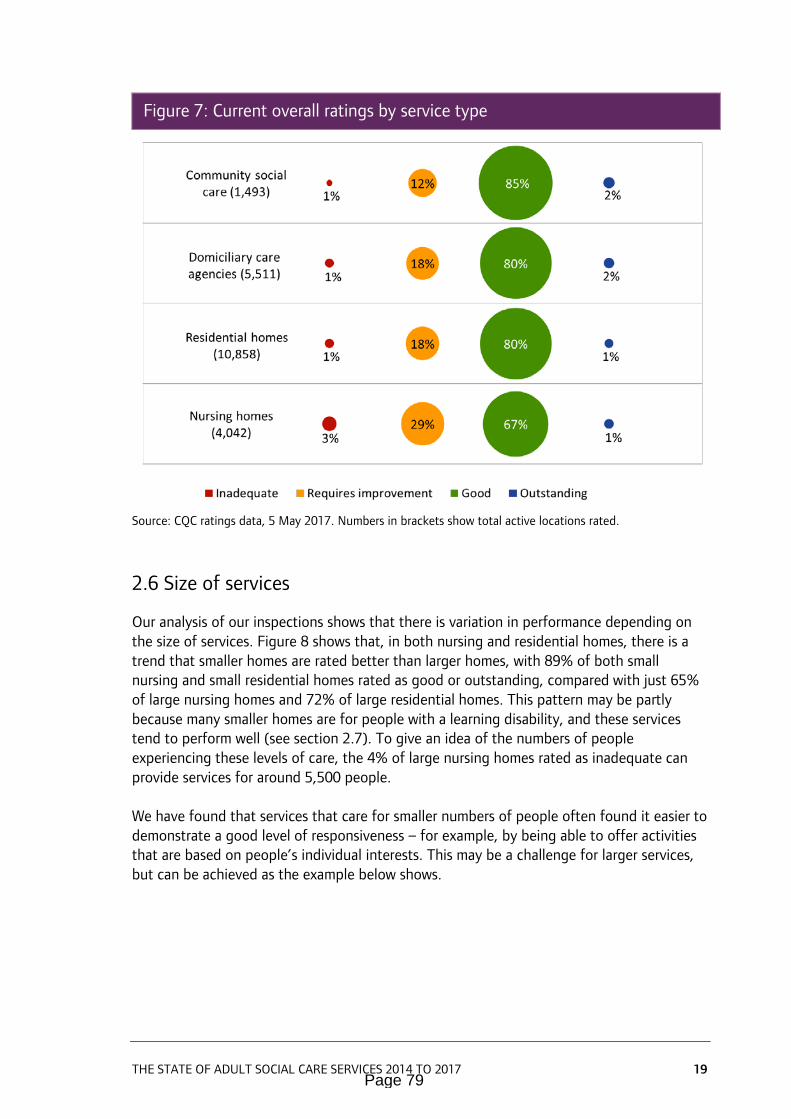
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 19
Figure 7: Current overall ratings by service type
Source: CQC ratings data, 5 May 2017. Numbers in brackets show total active locations rated.
2.6 Size of services
Our analysis of our inspections shows that there is variation in performance depending on the size of services. Figure 8 shows that, in both nursing and residential homes, there is a trend that smaller homes are rated better than larger homes, with 89% of both small nursing and small residential homes rated as good or outstanding, compared with just 65% of large nursing homes and 72% of large residential homes. This pattern may be partly because many smaller homes are for people with a learning disability, and these services tend to perform well (see section 2.7). To give an idea of the numbers of people experiencing these levels of care, the 4% of large nursing homes rated as inadequate can provide services for around 5,500 people. We have found that services that care for smaller numbers of people often found it easier to demonstrate a good level of responsiveness – for example, by being able to offer activities that are based on people’s individual interests. This may be a challenge for larger services, but can be achieved as the example below shows.
Page 79

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 20
Figure 8: Current overall ratings by size and type of care home
Source: CQC ratings data, 5 May 2017. Figures in brackets are numbers of locations rated. Small = 1-10 beds, Medium = 11-49, Large = 50+
EXAMPLE OF PERSON-CENTRED CARE IN A LARGE SERVICE
Deerhurst Care Home is a care home with nursing care for up to 66 predominantly older people in Bristol.
A relative said:
• “As my mother’s needs have changed the staff have changed the way they look after her. Nothing seems to faze them and they always keep us informed [about] what is happening.”
Deerhurst has a ‘homemaker’ role, which staff take it in turns to fill. They are an extra dedicated member of staff to support and reassure people, and also to monitor what people are eating or drinking.
The service went the extra mile in caring for people when it arranged for a specially adapted
Page 80

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 21
double bed to be provided for one of its residents. This was because the resident had always shared a double bed and missed the cuddles with their loved one. The person was able to spend time with their loved one, watching television, lying on the bed until falling asleep in each other’s arms. The relative then returned to the family home knowing their loved one was settled for the night.
Read the whole report at www.cqc.org.uk
When looking at domiciliary care services, our data shows that locations providing care to a smaller number of people were also performing better than larger services. Our ratings data shows that 85% of small services (for one to 50 people) were rated as good or outstanding, whereas only 73% of larger services (for 101 to 250) achieved the same results (figure 9).
Figure 9: Current overall ratings by size of domiciliary care service
Source: CQC ratings data, 5 May 2017. Figures in brackets are numbers of locations rated
Page 81
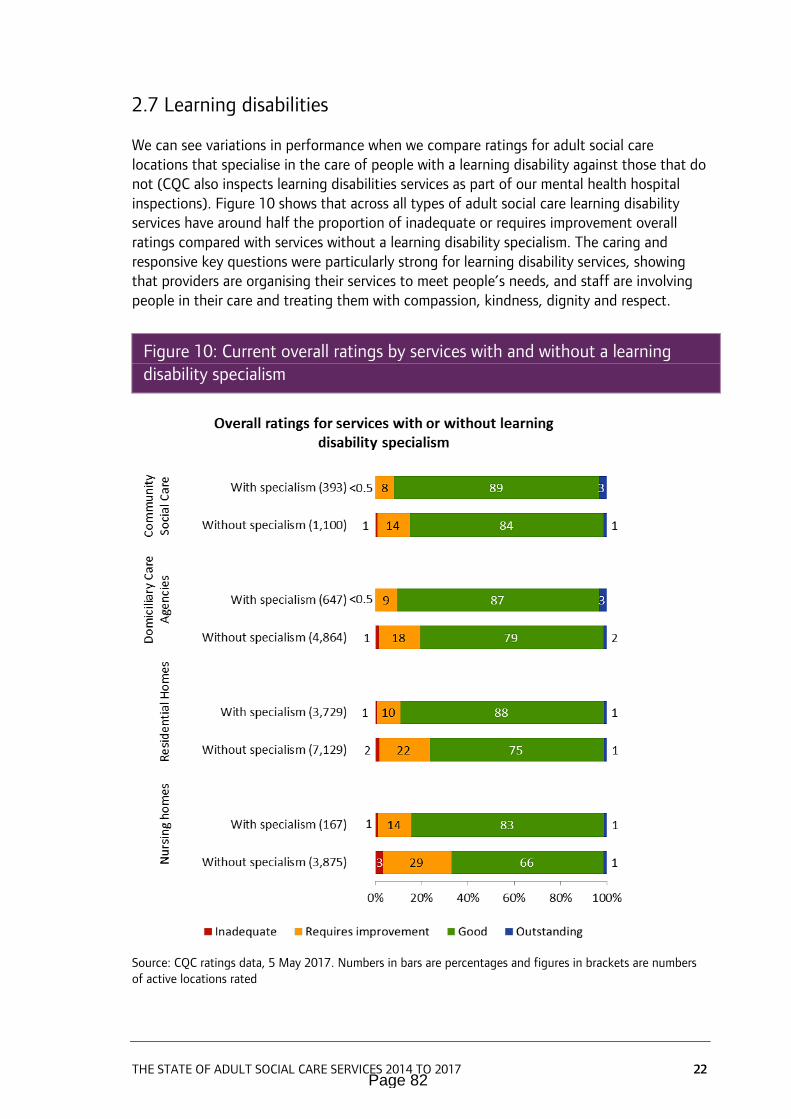
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 22
2.7 Learning disabilities
We can see variations in performance when we compare ratings for adult social care locations that specialise in the care of people with a learning disability against those that do not (CQC also inspects learning disabilities services as part of our mental health hospital inspections). Figure 10 shows that across all types of adult social care learning disability services have around half the proportion of inadequate or requires improvement overall ratings compared with services without a learning disability specialism. The caring and responsive key questions were particularly strong for learning disability services, showing that providers are organising their services to meet people’s needs, and staff are involving people in their care and treating them with compassion, kindness, dignity and respect.
Figure 10: Current overall ratings by services with and without a learning disability specialism
Source: CQC ratings data, 5 May 2017. Numbers in bars are percentages and figures in brackets are numbers of active locations rated
Page 82
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 23
EXAMPLE OF A CARING SERVICE FOR PEOPLE WITH A LEARNING DISABILITY
Mill Green provides accommodation and personal care for people who may have physical disabilities or long-term conditions, acquired brain injury and cognitive or learning disabilities.
One person said:
• "Staff here are great, but they have a lot to do. I do a bit of washing and drying up. It feels more homely if I help."
The provider's emphasis on person-centred care was understood by all staff. Staff saw beyond people's medical conditions, and encouraged and supported them to 'be themselves'. One person, who was not able to walk independently, had spent their morning happily painting the garden shelter with staff, while sitting in their wheelchair. People and relatives told us they had noticed a difference in the way people used the garden since a care coordinator had taken ownership of the 'garden project'. People also enjoyed an outdoor exercise class to music because all the staff, including the manager, housekeeper and senior manager joined in, which made them feel less self-conscious.
People were supported to maintain their independence with eating and drinking. Sometimes people chose to eat out and sometimes people chose to buy their own meals to re-heat at home, which promoted their independence.
Staff were committed to personalising the way they communicate with people. For example, one person with limited speech and mobility liked staff to walk in front of them, so they could hold their shoulders while they walked round the home.
Read the whole report at www.cqc.org.uk
Page 83

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 24
3. What can the sector learn from our inspections?
Key points
• All providers can learn from high-quality care services and should know what to do to avoid poor care.
• Strong leaders had a pivotal role in high-performing services. This was seen at registered manager and provider level, where strong vision and values were communicated to all staff, encouraging a culture of openness and transparency.
• Positive and supportive cultures are characterised by staff who were well-trained, caring, skilled, dedicated, enthusiastic and focused on positive outcomes for people.
• A key theme that shone through in terms of high-quality services and improvement was a clear focus on person-centred care. In these services, staff really get to know people as people, understanding their interests, likes and dislikes.
In this section, we focus on the main features of high-quality care that we have seen during our initial comprehensive programme of inspections, illustrated with examples from our inspections of high-performing providers. All providers can learn from each other – especially those that are rated as inadequate or requires improvement. Good and outstanding providers can also learn from the best practice and, as can be seen in the next section, quality in even the highest rated services can decline, so a focus on continuous improvement is vital to maintain quality care for people.
3.1 Characteristics that have led to high-quality care
Good leaders, both at registered manager and provider level, have a big influence on the quality of adult social care that people receive. They have an important role in shaping a positive culture in a service – including creating a supportive environment for staff, listening to their concerns, and communicating well with them, other professionals, and people who use services and their families and carers. They also genuinely appreciate diversity and seek ways to meet equality, diversity and human rights.
Leaders in the highest performing services also inspire a culture where people are at the centre – treating people as people, as opposed to just recipients of care. Staff sought to build relationships with people to find out what works for them. We found that good leadership, based around person-centred care inspired a positive culture (figure 11).
Page 84
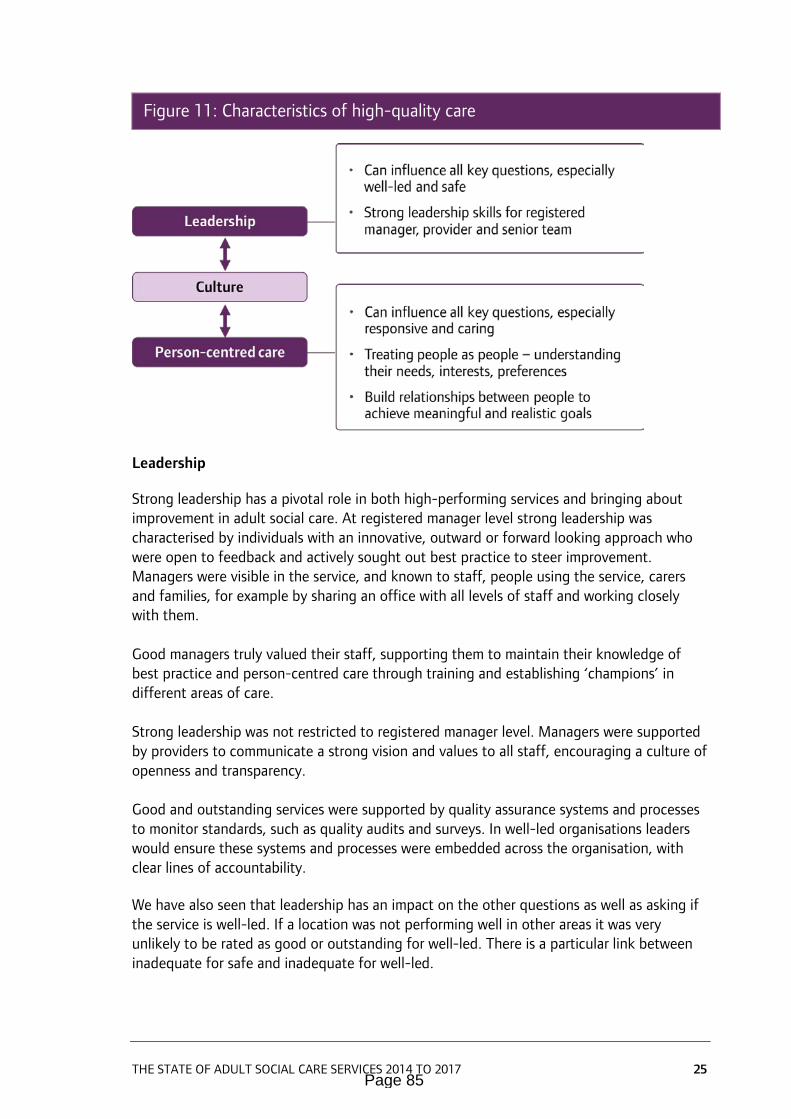
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 25
Figure 11: Characteristics of high-quality care
Leadership
Strong leadership has a pivotal role in both high-performing services and bringing about improvement in adult social care. At registered manager level strong leadership was characterised by individuals with an innovative, outward or forward looking approach who were open to feedback and actively sought out best practice to steer improvement. Managers were visible in the service, and known to staff, people using the service, carers and families, for example by sharing an office with all levels of staff and working closely with them. Good managers truly valued their staff, supporting them to maintain their knowledge of best practice and person-centred care through training and establishing ‘champions’ in different areas of care. Strong leadership was not restricted to registered manager level. Managers were supported by providers to communicate a strong vision and values to all staff, encouraging a culture of openness and transparency. Good and outstanding services were supported by quality assurance systems and processes to monitor standards, such as quality audits and surveys. In well-led organisations leaders would ensure these systems and processes were embedded across the organisation, with clear lines of accountability. We have also seen that leadership has an impact on the other questions as well as asking if the service is well-led. If a location was not performing well in other areas it was very unlikely to be rated as good or outstanding for well-led. There is a particular link between inadequate for safe and inadequate for well-led.
Page 85

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 26
Innovation was identified as a characteristic of outstanding services, with good leaders described as being ‘innovative’ or ‘creative’, especially when adopting really person-centred practice and solutions to individual care needs, instead of simply seeing the risks or barriers.
EXAMPLE OF VALUING STAFF AND INDIVIDUALISED CARE IN A HIGH-PERFORMING SERVICE
Care By Us is a large organisation that offers personal care and other related services in East, West and North Hertfordshire, Essex and North London. They provide a wide range of care services in people’s own homes. They serve around 1,600 people, employing about 500-600 staff.
People who used the service said:
• “Staff do very well at lifting my mood if I’m feeling a bit bad. They are very caring.”
• “They [staff] are so gentle when they get me out of bed, they don’t rush me or seem keen to go. I feel like they’re looking after me ever so well. Fantastic service!”
Beyond the necessary mandatory training, such as safeguarding and food hygiene, a lot more core training was given to staff – especially in their first weeks. For example, staff attended cookery lessons where they learnt basic cookery skills and how to promote healthy eating for the people they were supporting.
Training was supported by appointing Champions across the organisation – for example, for dementia, falls prevention, nutrition and medication. The Champions actively trained and coached staff. One staff member said, “We are learning a lot about safe handling of medicines and what best practice means. If we are unsure we have our Champions, they know how to guide us.”
The provider had a very personalised approach to care planning that sought to enable people to live as long as possible in their own home. They sat down with each person and looked at what good care looked like for them. There was a team who went out to talk to people who were not happy with the initial assessment of their care – for example the number or timing of the calls. This team of managers met with people and laid out all the options, talked about these and adapted the plan of care. Staff adapted to the people, not people to the staff. One person told us, “Care by Us came and discussed it [care needs], they did suggest three times a day but we have chosen to have mornings and evenings." One relative told us, "Yes, it was the senior management who came to discuss the care plan and care needs. I was there; it was very professional and very understanding of my [relative’s] needs."
Care By Us have their own IT department, which developed technology for their own use. They were using telecare equipment, for example a GPS watch for people who cannot find their way home, so that the service could locate them and pick them up.
Read the whole report at www.cqc.org.uk
Page 86

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 27
Culture
Positive culture was something that characterised good performance and improvement, and the links to the leadership finding outlined above are clear. Both staff, people who use services and inspectors commented on particularly positive and supportive cultures characterised by staff who were well-trained, caring, skilled, dedicated, enthusiastic and focused on positive outcomes for people. The cultures of the services were also highlighted as being open and transparent, with a culture of improvement based on good practice and feedback. A review of CQC inspection reports carried out by Skills for Care highlighted the importance of creating and maintaining an inclusive culture. It also identified a link between organisational vision and values and quality. It found that in the majority of CQC inspection reports reviewed from services rated as requires improvement or inadequate, there was little or no evidence of the organisation’s vision or values. By comparison, it was rare to find an inspection rated as good or outstanding that did not include some positive evidence of how vision and values have helped the service to achieve high standards of care.12 Practical examples of how a positive culture was created included:
• Staff not wearing uniforms in recognition that they were in people’s home and viewing themselves as ‘guests’.
• Involving people who use services in training.
• Staff designated as ‘champions’ in particular areas.
Person-centred care
The third key theme that shone through in terms of high-quality services and improvement was a clear focus on person-centred care. Good leadership that generates a positive and inclusive culture leads to genuinely person-centred care. These vital characteristics can have a real impact on the lives of people using services, their families and carers. In high-quality services, staff really get to know people as people, understanding their interests, likes and dislikes. This supports relationships where staff and people who use services work together to set and achieve meaningful and realistic goals. The way these services engaged with and supported carers and family members also showed an inclusive approach to care. Good person-centred care was achieved through people using services and their carers and families being fully involved in all areas of their care, such as writing care plans. Our report, Better care in my hands, used analysis from a literature review and from CQC inspections of outstanding services, and evidence from our national thematic reviews to identify a common set of achievements that have helped services to ensure people are involved in their care (box A).
Page 87

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 28
BOX A: The importance of involving people in adult social care to achieve person-centred care
1. I am involved in discussions about my care, treatment and daily life as I want to be How is this achieved? By involving people in all aspects of care is a priority for the organisation and managers take a leadership role, encouraging staff to involve people
Inspection report example “We saw that people’s preferences and views were reflected, such as the name they preferred to be called and personal care preferences such as, ‘I like to have a shower every day.’ We spoke with this person and they confirmed that they had a daily shower.” 2. My wishes and preferences are respected How is this achieved? There are management systems in place to monitor how people’s wishes and preferences are being acted on
Inspection report example “The main emphasis was that people were at home; they dressed in their preferred clothes and continued to undertake their individual hobbies. We observed people were able to do what they wished, making their own decisions helped and supported by staff. A member of staff we spoke with told us, ‘The residents are not pushed to have a certain routine; we go with the flow so people live the life they choose.’” 3. My family and loved ones help me plan my care and support How is this achieved? Services coordinate how they involve people and their families in their care
Inspection report example “I am always consulted about everything. The manager and staff keep me informed and we always have a six monthly review meeting when we discuss every aspect of my mother’s care. I find communication to be excellent.” (Relative of a care home resident) 4. Staff in different services work with me to adapt my plans as my needs change How is this achieved? Key staff work together across services to coordinate people’s involvement in their care
Inspection report example “A hospital passport was completed for each person. If a person needed to go into hospital other professionals would be made aware of people's preferences regarding their care, support needs and their current treatments that were best for them.” 5. I am offered appropriate information, support and advocacy about key decisions
for my care and treatment How is this achieved? Tailored and timely accessible information is used to support discussions and the involvement of people and their families
Page 88

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 29
Inspection report example “We observed a member of staff sitting next to a person who had no verbal communication. The staff member was holding the person’s hand and pointing out the various picture meal options available for lunch.” 6. I am involved in daily life choices in care settings How is this achieved? Services are organised to provide continuity of staff working with people using services over time
Inspection report example “Care staff worked with Mr J and his wife to understand his life story and find out what would make him happier. Mr J had been a firefighter and relished the responsibility of keeping people safe. Care staff supported Mr J to check the environment for safety and standards and also involved him in practical daily tasks.” 7. My capacity to be involved is taken into account – wherever I receive care How is this achieved? There is flexible advocacy provision as people use different services (when people lack capacity to make a decision or need support to represent their interests)
Inspection report example “One 17 year old had a continuing healthcare assessment which was very person-centred. His support needs were clearly outlined and recorded in simple language and using his own words. It had a strong focus on his likes, dislikes and wishes. His father told us, ‘The team have worked creatively to expand and enrich his social and practical skills. As a result his ability to join in and socialise with his siblings and peers has grown significantly.’” Adapted from: CQC: Better care in my hands: A review of how people are involved in their care, May 2016
Tailoring activities to individuals’ likes and interests was an important way of achieving person-centred care. This often involved using the arts to find creative ways of enhancing people’s quality of life. For example, there is building evidence13 that music and singing interventions work to improve the wellbeing of adults living with diagnosed conditions or dementia:
• Targeted, culturally relevant music and singing interventions can enhance mental wellbeing and decrease depression in older people with chronic conditions in residential and community settings.
• Participation in individual personalised music listening sessions can reduce anxiety and/or depression in nursing home residents with dementia and that listening to music may enhance overall wellbeing for adults with dementia.
• Participation in extended (12 months) community singing programmes can improve quality of life and social and emotional wellbeing in adults living with chronic conditions.
Page 89
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 30
Practical examples of how person-centred care was achieved included:
• Staff actively supporting links with the wider community and involving volunteers in day-to-day activities.
• Arranging the environment so it provided positive living, learning and social experiences. For example placing objects around the home that were meaningful to people and that they could interact with. One home used iPads to engage with and create a stimulating and fulfilling environment for people living with a learning disability and dementia. This meant that one person, who had no verbal communication, was able to build up a picture/video diary and could tell their family what they had been doing during their visits.
EXAMPLE OF PERSON-CENTRED CARE IN A HIGH-PERFORMING SERVICE Mary & Joseph House is a care home in Manchester, providing accommodation and personal care to adult men with enduring mental health needs.
A person who used the service said:
• “The staff here know what they are doing. They have supported me so well, I was close to death when I first arrived, now I am strong and feel great.”
Mary and Joseph House are careful about people having realistic aims and objectives. They want to make sure that, if people are moving out, they have their finances sorted out correctly. There was an example of a person who was due to move out back into his own family home. The service was supporting him over a number of months, to visit his home regularly, to try and build up links with the community, to find new volunteering opportunities, and to know that he can still come back to Mary and Joseph House informally for a cup of tea or have a meal.
Arts and creativity were an integral part of the service provided at Mary and Joseph House:
• The service had a choir and an instrumental band which had been organised by the staff and people.
• A therapeutic gardener and art teacher were employed. The gardening team have worked with the art group to achieve Gold Awards in various Royal Horticultural Society competitions.
We saw one example of a person living with dementia who started a project five years ago to make a ceramic picture of what the home did. He took pictures to show where he was up to with the project. The home continually supported him to finish the project. It was a massive achievement for him. Read the whole report at www.cqc.org.uk
Page 90

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 31
3.2 Focus on Shared Lives
CQC regulates, inspects and rates Shared Lives services, which match adults who have care needs with approved carers. Shared Lives carers accept people into their own homes and provide care, support and mentorship to people.
The Shared Lives model of care is geared towards achieving positive outcomes for people who use the service. The placement of people in a family home with carefully selected and screened carers helps create a supportive family environment, which helps to ensure person-centred care that is focused on independence and positive risk taking. Shared Lives represent a small proportion of the services we regulate. Between October 2014 and May 2017, we inspected and rated 98 Shared Lives services. According to Shared Lives Plus, this form of care is less expensive than other forms of care, while achieving good outcomes for people. Half of the 12,000 people using Shared Lives are living with their Shared Lives carer as part of a supportive household; half visit their Shared Lives carer for day support or short breaks. Shared Lives is also used as a stepping stone for someone to find their own home.14 CQC ratings data shows that they perform very well; over 90% are rated as good or outstanding and there are currently no locations rated as inadequate (figure 12). The key questions of caring and responsive are rated particularly highly compared with all adult social care services (for example, there are no locations rated as requires improvement or inadequate for the caring key question). This reflects the personalised approach of Shared Lives services that can bring positive results for people using them (see the example below).
Figure 12: Shared Lives overall ratings
Source: CQC ratings data, 5 May 2017. Numbers above bars show total active locations rated
Page 91

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 32
The characteristics that have led to high ratings and remarkable support to people using services as shown in the case study below are:
• Strong leadership features again, with managers who maintained strong relationships with other local health and local authority services, who were forward looking and focused on solutions to maintain placements.
• Positivity of staff reflects strong leadership and careful recruitment. Staff were dedicated, enthusiastic and motivated by achieving positive outcomes for people using the service.
• Carers were carefully selected, screened and assessed, ensuring that people were highly suited to the role and able to demonstrate the necessary skills and qualities required. This was followed by a robust process for matching a person with a carer, which took into account a wide range of aspects to ensure that the needs of the person were catered for.
• People who use services, carers and staff were all well supported through effective communications, the availability of training, and monitoring processes to proactively identify areas for support.
• An open and transparent culture was present, which meant that issues could be highlighted and addressed.
EXAMPLE OF A HIGH-PERFORMING SHARED LIVES SERVICE
The Shared Lives Service in Lancashire provides long-term placements, short breaks, respite care, day care and emergency care for adults with a range of needs, within carers' own homes. It is the largest Shared Lives provider in England.
A person who used the service said:
• “Shared Lives are amazing. This is my home and I am made to feel part of the family. Staff are really nice and friendly."
One carer said:
• “We wanted to see what [the person’s] potential could be. They have gone from doing almost nothing to being outgoing and making decisions for themselves, including where they want to go and who they want to see. It's been amazing to see the transformation.”
Person-centred model • One person we spoke with showed us photographs of themselves when they had moved
into their Shared Lives home a few years ago to show us they had lost a significant amount of weight. They were proud of this achievement and it was obvious they had been given a lot of support from their carer and support officer to eat well and lead a healthy and active life.
Read the whole report at www.cqc.org.uk
Page 92

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 33
4. What do we do about poor care?
Key points
• When we find poor care, we take action to make sure providers and managers tackle their problems and put things right for the benefit of people using services, their families and carers.
• Adult social care providers say that our enforcement regime encourages services to make sure they meet fundamental standards.
• Poor quality can have a real impact on people using services, particularly in the areas of staffing and medicines management.
• The areas of the regulations that we have taken the most enforcement actions relate to a lack of good governance, and issues with safe care and treatment, staffing and person-centred care.
CQC understands there are financial pressures facing the adult social care sector, but this does not mean that we will compromise on our purpose of ensuring people receive care that is safe, effective, compassionate and high-quality. Our inspections show that services of all types and in all circumstances can provide high-quality care for people. Where there is poor care, we will encourage improvement but if we need to take action that stops unsafe care and protects people from abuse and avoidable harm, then we will do that. If, during our inspections, we identify aspects of care that need to improve, we ask the provider to evidence how they are going to make sure people receive the care and support that meets the standards they have a right to expect. We go back to inspect to find out whether they have kept to their commitments and if these have had the required effect. If they have not, we will use the enforcement powers we have available to take appropriate action. Our focus is always on the people using services – they have a right to receive safe, compassionate and effective care. When this does not happen we will take action on their behalf. Our most recent annual provider survey, due to be published in the autumn, showed that providers think that our enforcement regime encourages services to meet fundamental standards that people have a right to expect whenever they receive care. Of the three main care sectors that we regulate, adult social care had the highest results in this area – with 74% agreeing that the prospect of enforcement action is an effective deterrent to encourage services to make sure they meet fundamental standards.
Page 93

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 34
4.1 Characteristics that have led to poor-quality care
Of the five key questions that we asked all services, safe had the poorest ratings, with 23% rated as requires improvement and 2% as inadequate. Poor quality can have a real impact on people using services, particularly in the areas of staffing and medicines management. Staffing
Staffing levels were a key factor in providers rated as inadequate or requires improvement for safety. Our inspectors look at safe staffing levels in terms of whether people’s needs were being responded to in a timely manner. They do this by talking to people using services and their families and visiting professionals, observing whether people’s needs are met and they are safe, checking systems for assessing staffing levels, and talking to a range of staff to hear their views on the staffing at the service. In care homes, for example, inadequate staffing levels led to alarm calls not being responded to promptly, which meant that people did not get the support they needed when they needed it. The layout of a home and peak times affected the number and deployment of staff. This could have an impact on whether people’s needs were responded to promptly, whether medication was given, whether staff were able to spend time in communal areas, and (considering people with challenging needs) ultimately that people were safe. Rotas had shown care staff being deployed to assist in the kitchen for example, during lunch time, when staff were required to safely assist people to the dining room. The impact of inadequate staffing on care provided for people receiving help from a domiciliary care agency was that they would receive rushed one-to-one assistance instead of the two-to-one support required, and this could be provided by a different carer every day. Even where appropriate numbers of staff were in place, if they did not have the necessary skills this could have an impact on safety. During one inspection of a service that was rated as inadequate, we found that the manager did not know what skills their agency workers had, and we found that they did not have the skills needed to support the people with complex needs. Staff training was also a factor on safety, particularly in areas such as infection control, risk assessments, safeguarding and medicines. We also found shortfalls in staff understanding of the training, with no evaluation of staff competency after the training or practical supervision.
Medicines management
Medicines management was a key factor associated with unsafe care. Specific issues included:
• Medicines not being administered properly
Page 94
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 35
• Staff lacking knowledge of medicines and their side effects
• Issues with record keeping, including timeliness
• A lack of medicines audits
• Medicines being out of date and not being stored correctly.
In some cases poor medicines management were described as having extremely serious consequences, with failure to check that a member of staff was able to administer medicines on an ongoing basis leading to actual harm to people using services. Conversely, staff that have an understanding of the medicines they were administering were able to talk to people about any possible side effects.
The next section discusses what we do when we find poor-quality care, with examples of some of the poor care described above, and what providers have done to make improvements.
Information and resources to support improvement can be found on Care Improvement Works, which is a free online tool developed by Skills for Care, the Social Care Institute for Excellence and the National Institute for Health and Care Excellence.
4.2 Using our civil enforcement powers
Where we identify poor care, or where registered providers and managers do not meet the standards required in the regulations, we have a wide set of enforcement powers that allow us to protect the public and hold those responsible to account.
The actions we take depend on how serious the problems we have identified are and how they affect the people who use the service. Actions range from giving providers notices setting out what improvements they must make and by when, to placing them in ‘special measures’, which gives them a clear timetable within which they must improve the quality of care they provide. If providers do not improve we will take further action (for example, cancelling their registration). The example on page 38 shows the work that is done to ensure continuity of care for people when a registration is cancelled.
Figure 13 shows the number of breaches in each area of the regulations that contributed to inadequate ratings. The enforcement actions we took ranged in severity from warning notices through to cancellation of registration. The most common breaches relate to the issues we have highlighted in this report. In these services there was a lack of good governance, and issues with safe care and treatment, staffing and person-centred care. This may mean that providers and leaders were failing to check the quality of their care, seek the views of people using the service, administer medicines safely, and make sure that staffing levels are adequate to provide care in a person-centred way. A similar pattern emerges for enforcement actions against locations rated as requires improvement, although with fewer civil actions and cancellations.
Page 95

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 36
Figure 13: Enforcement actions against locations rated as inadequate
Source: CQC ratings and enforcement data, 5 May 2017. The numbers relate to regulations breached, not total numbers of locations (which will be fewer as a number of locations breach more than one regulation)
4.3 Using our criminal enforcement powers
Since 1 April 2015, enforcement responsibility for health and safety incidents in the health and social care sector transferred from the Health and Safety Executive and local authorities to CQC. We have subsequently prosecuted five providers using these powers (figure 14). While all prosecutions so far have related to a breach in safe care and treatment requirements, the cases have covered a wide range of safety issues, including medication errors, uncovered radiators and use of bed rails. Recurring themes, which have been highlighted in legal analysis,15 included:
• Issues with documentation: for example, errors regarding medication dosages and strengths and timings not being accurately recorded.
• Risk assessments: for example, one care home was found to have no proper system for assessing the risks to the health and safety of people using services (including failing to prevent a blind resident repeatedly falling in her room and a resident repeatedly choking).
Page 96
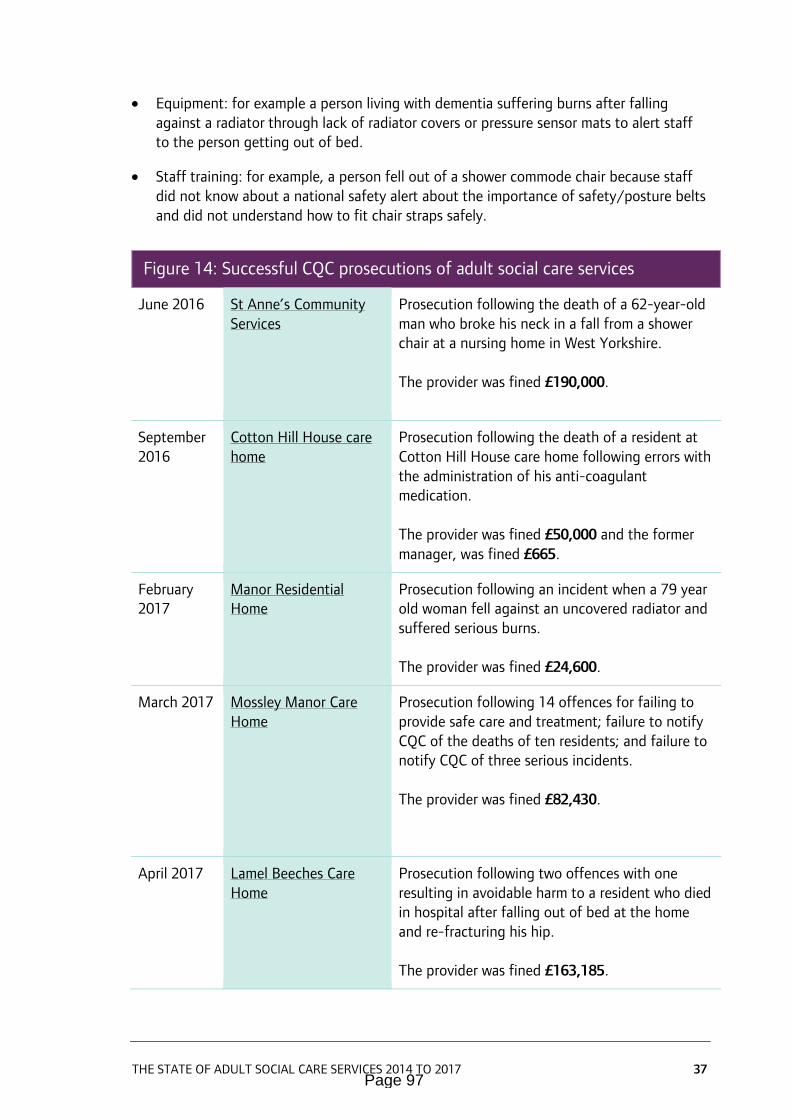
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 37
• Equipment: for example a person living with dementia suffering burns after falling against a radiator through lack of radiator covers or pressure sensor mats to alert staff to the person getting out of bed.
• Staff training: for example, a person fell out of a shower commode chair because staff did not know about a national safety alert about the importance of safety/posture belts and did not understand how to fit chair straps safely.
Figure 14: Successful CQC prosecutions of adult social care services
June 2016 St Anne’s Community Services
Prosecution following the death of a 62-year-old man who broke his neck in a fall from a shower chair at a nursing home in West Yorkshire. The provider was fined £190,000.
September 2016
Cotton Hill House care home
Prosecution following the death of a resident at Cotton Hill House care home following errors with the administration of his anti-coagulant medication. The provider was fined £50,000 and the former manager, was fined £665.
February 2017
Manor Residential Home
Prosecution following an incident when a 79 year old woman fell against an uncovered radiator and suffered serious burns. The provider was fined £24,600.
March 2017 Mossley Manor Care Home
Prosecution following 14 offences for failing to provide safe care and treatment; failure to notify CQC of the deaths of ten residents; and failure to notify CQC of three serious incidents. The provider was fined £82,430.
April 2017 Lamel Beeches Care Home
Prosecution following two offences with one resulting in avoidable harm to a resident who died in hospital after falling out of bed at the home and re-fracturing his hip. The provider was fined £163,185.
Page 97

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 38
To illustrate the terrible cases of neglect and abuse that are behind these prosecutions, the following example gives the detail of the Mossley Manor Care Home case.
EXAMPLE OF A CQC PROSECUTION
As a result of concerns from the family of a prospective resident, we inspected Mossley Manor Care Home during May and June 2015 and were appalled at what we found. Some residents were unkempt and smelled strongly of urine or body odour, having not received a bath or shower in the previous three weeks. Bedrooms were not being cleaned regularly and some contained mouldy and congealed tea and coffee cups. Carpets were dirty and dusty. Communal toilets did not contain soap, hand towels or bins. When there was no hot water staff had to boil pans of water in the kitchen to wash residents.
The care home had also failed to control risks of serious injury. There was no proper system in place for assessing the risks to the health and safety of individual people. One woman who was blind and had a history of falls was found injured on the floor of her room on three occasions but the provider failed to take action to stop it happening again. A 77-year-old man who was at risk of choking was twice taken to hospital – but there was conflicting advice for staff on how they should support him to eat and drink safely.
Initially we gave the owners 24 hours to submit an action plan to make urgent improvements. On visiting again a few days later to check if this was being implemented there were still serious concerns. CQC applied to Liverpool Magistrates to urgently cancel the provider’s registration and close Mossley Manor. We worked closely with Liverpool City Council at the time so that people living at the home could find alternative accommodation.
The registered providers were fined £60,000 for failing to provide safe care and treatment and £20,800 for the 13 offences of failing to notify CQC. They were also ordered to pay the prosecution costs of £1,510 and a £120 victim surcharge.
Taking criminal action and prosecuting providers is a detailed process that involves the care and comprehensive collection of evidence. We test each case on whether there is sufficient evidence to secure a prosecution and, if so, is it in the public interest to prosecute. We currently have two prosecution cases that have been listed for a magistrates’ court hearing, and six cases that are likely to be listed for a magistrates’ court first hearing by March 2018.
Page 98

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 39
5. Have adult social care services improved?
Key points
• Adult social care providers say that our inspections encourage improvement.
• More than four-fifths (81%) of locations that were initially rated as inadequate have improved their rating after a CQC inspection.
• Only 56% of locations that initially required improvement have improved their rating after a CQC inspection.
• Committed managers, who are supported by the provider, can drive improvement in a previously failing service.
The previous section of this report describes how we use our enforcement powers when we find poor care. It is our expectation that providers should take responsibility for the quality of the care they provide. We expect them to use our findings and reports as an opportunity to tackle their problems and put things right for the benefit of people using services, their families and carers, so that we should not have to resort to the more severe actions in our enforcement policy. Our most recent annual provider survey showed that providers think that our inspections encourage improvement. Of the three main sectors that we regulate, adult social care had the highest results in this area – with 80% agreeing that inspections help them to identify areas of improvement. This section focuses on how services have responded to our initial programme of comprehensive inspections in terms of improvement.
5.1 Inadequate services that improve their quality
Throughout our initial programme of comprehensive inspections in adult social care we have seen improvements across all types of services. This improvement is most evident in services that originally had the poorest quality, and were rated as inadequate. These services may not be keeping people safe – there may be widespread and significant shortfalls in the care, support and outcomes people experience; staff may not treat people with respect, and may sometimes be unkind and lack compassion; people may not be involved in the development of their care; and these things may stem from a lack of good leadership. Whatever factors have contributed to poor care, it is important that providers take action to protect people, improve their service and deliver on the legal obligations they accept when registering with CQC.
Page 99

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 40
Figure 15 shows what has happened to the 916 services where we gave a first rating of inadequate. Almost one-third (295 locations) are no longer active; many of these will be locations that were deregistered by their providers before we could take further action – half of them became inactive before we were able to re-inspect them. Nearly a quarter of the 295 locations (24%) remained inadequate on re-inspection before they became inactive. A small number of locations are now inactive because CQC cancelled their registration – see page 35. Of the 68% of services (621 locations) that were initially rated as inadequate and continued to provide services, over three-quarters improved (482 services). We continue to monitor the progress of the remaining 22% to make sure that people are protected and will take further action as necessary.
Figure 15: What has happened to services first rated as inadequate?
Source: CQC ratings data, 5 May 2017
Figure 16 shows a simpler picture of performance for those services that were first rated as inadequate and only includes those that have been re-inspected. It is encouraging to see that many providers are responding to our concerns. Eighty-one per cent improved their inadequate overall rating following re-inspection; 50% to requires improvement and 30% moved two ratings to good. We will continue to focus on those services that continue to be rated as inadequate (19%).
Page 100

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 41
Figure 16: Re-inspection of services rated as inadequate – all providers
Source: CQC ratings data, 5 May 2017. Percentages do not add up to 100% due to rounding.
EXAMPLE OF IMPROVEMENT THROUGH LISTENING TO CQC AND PEOPLE WHO USE SERVICES
In November and December 2015, a domiciliary care service was inspected and rated as inadequate overall.
Six months on, in June 2016, the service was re-inspected and ‘significant improvements’ were found. The service was rated good overall and good in all the areas we assessed. Seventeen people were receiving support from the service at this time.
The first inspection identified a range of issues and risks across the five areas we look at, relating to recruitment, medicines management, staff training and supervision, poor assessments of people’s needs and records management. Some people using the service and their relatives also highlighted issues about the delivery and continuity of care.
In preparation for the second inspection, the service had carried out another quality survey, which received positive feedback. When we talked to people using the service and their
Page 101

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 42
relatives, they confirmed they were now involved in care planning and staff were described as very caring and friendly and found to be proactive in supporting people and their relatives.
Both the registered provider and registered manager remained in post throughout the process, but a fundamental change to the service led to the improvements.
When we look at the overall ratings of corporate providers (a provider with 20 or more locations), they are very similar to the ratings of all providers. For example, 80% of corporate-owned locations were rated good or outstanding overall, compared with 79% of other locations. Corporate providers, however, have been better at improving since a first rating of inadequate; of the locations originally rated as inadequate, only 15% of locations owned by corporate providers remained inadequate at their last rating, compared with 22% of non-corporate locations (figure 17). This might suggest that corporate providers are more equipped to step in to support any of their locations that are performing poorly and we are aware of larger corporate providers establishing quality turn-around teams to address problems at individual locations. It is important to ensure that the immediate action taken to address problems is sustained once the turn-around team has left. There is also a key role for local commissioners to consider what support they may be able to provide to smaller providers to help them improve.
Page 102

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 43
Figure 17: Re-inspection of services rated as inadequate – corporate locations and non-corporate locations
Source: CQC ratings data, 5 May 2017
Impact of registered manager on improvement
It is clear from section 3 of this report that good leaders have a big influence on the quality of care that people receive. This applies not only to high-quality services, though, but also to services that have improved between inspections. A committed registered manager, who is supported by the provider, can drive improvement in a previously failing service:
• The presence and capability of the registered manager was key to improvement. One of the examples in this section shows that improvement can be achieved by a consistent manager who is supported to bring about fundamental change. In the other example, improvement was brought about through recruiting a new registered manager who was quickly able to address staff issues by providing training that helped them understand the needs of the people in their care.
• Similarly, acceptance and ownership of the issues raised by CQC by the registered manager and provider was highlighted as important.
• The improvement driven by the registered manager involved moving to a more person-centred approach and culture, for example by involving people more in their care.
Page 103

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 44
EXAMPLE OF IMPROVEMENT THROUGH A CHANGE IN MANAGER
The first inspection of a 58-bed residential care home, providing care to older adults with a range of support and care needs, in December 2015 revealed that the manager in place was not knowledgeable, approachable or responsive. Staff were process driven and did not support people in caring way that protected their dignity and privacy. The combination of these two aspects led to the service being rated as inadequate.
After this first inspection, the acting manager left their post and a new manager was appointed. At the second inspection the manager, with support from the owner, had been able to achieve a great deal of improvement in a short period of time. This included:
• Staff teams were mixed up so that “problematic cliques” could be broken up and staff could be exposed to best practice at other parts of the service.
• Person-centred caring training for staff. This included dignity challenges that aimed to give staff a better understanding of how it feels to be cared for, for example being fed by another person while wearing a blindfold. At the second inspection, staff also commented on how important the training had been for their role.
• More frequent staff meetings and weekly memos to improve communications between staff and the manager.
The overall rating of requires improvement reflected the work that the manager had been able to achieve, but still showed there was more to do.
At the third inspection the inspector saw improvements in the areas identified at the previous inspection and no new issues were identified and was able to rate the home as good.
5.2 Services that fail to improve their quality
Although it is very encouraging to see so much attention given to inadequate services that has enabled them to improve, we have not seen the same rate of improvement in services that have been rated as requires improvement. We are clear that providers and commissioners must work to improve services rated as requires improvement to good and outstanding as well.
Of the 3,951 locations originally rated as requires improvement that were re-inspected, 56% (2,211 locations) had improved to a rating of good (figure 18). Of these, 6% (126) first deteriorated to a rating of inadequate, before improving to a rating of good.
However, in 38% of cases, there had been no change, and in 5% of cases, quality had deteriorated, resulting in a rating of inadequate. This means locations that require improvement have improved at a much lower rate than inadequate locations.
Page 104

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 45
Figure 18: Re-inspection of services rated as requires improvement
Source: CQC ratings data, 5 May 2017.
5.3 Services where good quality deteriorates
It is important that even good services maintain their focus on quality. Having completed our initial programme of comprehensive inspections, we are now looking at the movement in quality, not only of services rated as inadequate or requires improvement (which we check more frequently), but also those that at first inspection we rated as good. Although these are smaller in number, and the re-inspections are likely to have been prompted by concerns from staff, people using services and their families, or notifications from the provider itself, analysis is beginning to show that even those services that have provided the highest quality can deteriorate.
Of the 1,830 originally good locations that we have re-inspected (some planned as part of our timetable for return inspections but mainly prompted by concerns), only 1% had improved to outstanding. In 73% of cases, there had been no change, but in 26% of cases, quality had deteriorated, resulting in a rating of requires improvement (22%) or inadequate (4%). Even people who use the services of outstanding services can experience a decline in their care – of the eight services originally rated as outstanding that we have re-inspected, half of these have deteriorated by two ratings to requires improvement (figure 19).
Page 105

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 46
Figure 19: Re-inspection of services rated as good or outstanding
Source: CQC ratings data, 5 May 2017
This early information shows that the sector continues to be fragile. Providers cannot afford to be complacent and need to monitor the quality of their services constantly, particularly when there are changes, for example the departure of the registered manager, to maintain a culture of person-centred care supported by well-trained, confident staff.
These findings from our inspections of services originally rated as good mean that we are not as confident as we need to be that services can always sustain their good practice. As we move into a more responsive and targeted phase of our inspections we will keep this under close review. We need to continue to improve the way we listen to and respond to the vital information that alerts us to poor performance, even among those services that have formerly been the best.
Page 106

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 47
6. What is next for the regulation of adult social care services?
6.1 Improving how we work
In A Fresh Start for the Regulation and Inspection of Adult Social Care in 2013 we set out how we would change the way we do things – developing our regulatory approach, including ratings, and supporting our staff to deliver a programme of inspections that would build confidence among people who use services, their families and carers; providers; and commissioners.
We have now completed this initial programme of inspections, and we are able to take what we have learned to strengthen our assessments of adult social care services to make sure we continue to find out whether services are safe, effective, caring, responsive and well-led.
In line with our strategy for 2016 to 2021, our regulation of adult social care will also be more targeted, responsive and collaborative so that more people get high-quality care. A new, consolidated assessment framework for all of adult social care was published in June 2017 that reduced duplication between the key lines of enquiry and made more explicit the characteristics of inadequate, requires improvement, good and outstanding services. The consultation also launched in June 2017 seeks your views on the proposed further changes to help us realise our strategy, improve what we do, and to help us adapt to a changing adult social care market.
6.2 Improving services
This report has shown that high-quality services exist in adult social care, and all providers can use the examples here and on our website to strive for excellence. This is positive and to be celebrated but the variability in services means that too many people are experiencing care that we would not want for anyone we love. The difficulties some providers experience in making improvements and the deterioration we have seen in services originally rated as good or outstanding, point to a fragility in the sector that needs to be addressed. We want more and more services to improve so that people’s experiences of care continue to rise. CQC has been working as part of a collaborative group with sector leaders and people using services, their families and carers to create a shared commitment to high-quality, person-centred adult social care – Quality matters. This initiative aims to make a difference in care services by working across the sector with people who use these services, carers and families. One of Quality matters central messages is that quality is the responsibility of everyone involved in adult social care. Ensuring people are at the heart of everything we do will help all of us who work in adult social care make a difference for people using services, their
Page 107

THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 48
families and carers. This is what CQC will continue to focus on by setting clear expectations; monitoring services, inspecting and rating them; celebrating good care and sharing good practice; ensuring providers know what action they need to take to improve; and taking action if they do not. The conclusion of our initial programme of comprehensive inspections shows that there is much for the adult social care sector to be proud of but there is still much more for us all to do to ensure the public can have confidence that every service meets the Mum Test.
Page 108
THE STATE OF ADULT SOCIAL CARE SERVICES 2014 TO 2017 49
Acknowledgements
CQC would like to thank the stakeholders in the adult social care sector who have helped us develop this report. We particularly appreciate the support given by the Editorial Panel, which included Ruth Iveson, Jennifer Pearl and Julie Thorpe. They represented the Experts by Experience who have been an important element in our initial programme of comprehensive inspections.
We are grateful to the providers, managers, staff and people who use services that have provided the feedback and practice in our examples in this report that illustrate the very good work that is seen across England in adult social care.
And we would like to thank the CQC inspection staff who have worked hard to complete the initial programme of comprehensive inspections. They have provided a wealth of information, not only for this report, but for individuals looking to choose care and to providers to bring about improvement.
References
1 IFG, GHK and Skills for Care, The economic value of the adult social care sector in England, 2013 2 Skills for Care, The state of the adult social care sector and workforce in England, 2016 3 Office for National Statistics 2015, 2014-based National Population Projections 4 Marmot M and others, English Longitudinal Study of Ageing: Waves 0-7, 1998-2015, 25th Edition, UK Data Service. SN: 5050 5 Skills for Care, The state of the adult social care sector and workforce in England, 2016 6 Independent Age, Brexit and the future of migrants in the social care workforce, 2016 7 NHS Digital, Personal Social Services: Expenditure and Unit Costs, England – 2015-16, 2016 8 ADASS, ADASS Budget Survey 2017, 2017 9 Age UK, Briefing: Health and Care of Older People in England 2017, February 2017 10 ADASS, ADASS Budget Survey 2017, 2017 11 Competition and Markets Authority, Care homes market study: Update paper, June 2017 12 Skills for Care, Good and outstanding care guide, April 2017 13 What Works Centre for Wellbeing, Music, singing and wellbeing in adults with diagnosed conditions or dementia, December 2016 14 Shared Lives Plus, State of Shared Lives in England, 2017 15 http://www.lexology.com/library/detail.aspx?g=d28ebead-0399-40da-9639-5add9d95bda2&l=7UZ7ZPK
Page 109

CQC-377-072017
How to contact us Call us on 03000 616161Email us at [email protected] Look at our website www.cqc.org.uk Write to us at Care Quality CommissionCitygateGallowgateNewcastle upon TyneNE1 4PA
Follow us on Twitter @CareQualityComm
Please contact us if you would like this report in another language or format.
The state of adult social care services2014 to 2017 Findings from CQC’s initial programme of comprehensive inspections in adult social care
Page 110

Report of Head of Governance and Scrutiny Support
Report to Scrutiny Board (Adults and Health)
Date: 18 July 2017
Subject: Healthwatch Leeds Annual Report (2016/17) and Future Work Programme
Are specific electoral Wards affected? Yes No
If relevant, name(s) of Ward(s):
Are there implications for equality and diversity and cohesion and integration?
Yes No
Is the decision eligible for Call-In? Yes No
Does the report contain confidential or exempt information? Yes No
If relevant, Access to Information Procedure Rule number:
Appendix number:
1 Purpose of this report
1.1 The purpose of this report is to present Healthwatch Leeds’ (HWL) Annual Work Report (2016/17) and its future work programme.
2 Main issues
2.1 Healthwatch was established to be an effective, independent consumer champion for health and social care. Healthwatch England is an umbrella organisation that provides a leadership and support role for the local Healthwatch network.
2.2 Given the respective roles of the Scrutiny Board and Healthwatch bodies, there is the potential for overlap and duplication in respective priority areas. In order to avoid or minimise duplication, the Scrutiny Board and Healthwatch Leeds (as the local Healthwatch body) have developed a productive relationship, which has included the appointment of a non-voting co-opted member onto the membership of the Scrutiny Board since 2014/15. The re-appointment of Healthwatch Leeds’ co-Chair was recently confirmed for the duration of the 2017/18 municipal year.
2.3 To help ensure a good understanding and awareness of previous work undertaken by Healthwatch Leeds, the Annual Report for 2016/17 is appended to this report. Likewise, to help avoid or minimise areas of duplication, Healthwatch Leeds future work programme is also appended to this report.
2.4 In formulating this report, HealthWatch Leeds has confirmed the future work programme is likely to translate into:
Report author: Steven CourtneyTel: (0113) 37 88666
Page 111
Agenda Item 12

Work around people with complex (mainly physical) conditions sharing their experience (filming);
A review of an aspect of health visiting (To be confirmed); An aspect of the equipment service (probably short term aids and their
return); Learning Disabled services in the NHS; Engagement with adult men about their health and care experience
(discussions taking place with HMP Leeds); and, Completion of the rolling program of visiting all out-patient clinics provided by
LTHT (total of 19; currently around 50% completed)
2.5 It should be noted that HWL’s second home care survey has recently been completed, in addition to work on the integrated occupational therapy (OT) service.
2.6 It should also be noted there is a degree of flexibility in HWL’s future work programme – to allow for additional, unplanned work items coming forward. This approach is also reflective of the Scrutiny Board’s approach to its own work schedule.
2.7 HWL’s co-Chair and non-voting co-opted member on the Scrutiny Board will be in attendance to assist the Scrutiny Board in its consideration of the details presented.
3. Recommendations
3.1 Members of the Scrutiny Board are asked to consider the details presented in this report and appendices and agree any specific matters that may require further scrutiny action, input or activity.
4. Background papers1
4.1 None used
1 The background documents listed in this section are available to download from the Council’s website, unless they contain confidential or exempt information. The list of background documents does not include published works.
Page 112

Annual Report 2016/17
Healthwatch Leeds is here to help local people get the best out of local health and care services by bringing their voice to those who plan and deliver services in Leeds.
Page 113

2 Healthwatch Leeds
Contents
Contents ...................................................................................................... 2
Message from our Chairs ................................................................................... 3
Snapshot of our work ..................................................................................... 4-7
Youthwatch Leeds ........................................................................................8-11
Volunteering ............................................................................................ 12-13
Information and signposting .............................................................................. 14
Socially Speaking ........................................................................................... 15
Working across the city ............................................................................... 16-17
Enter & View ............................................................................................ 18-19
Working together .......................................................................................... 20
Progress update ............................................................................................ 21
Outpatient work........................................................................................ 22-23
A message from Tanya, our CEO ..................................................................... 24-25
Governance & Board ....................................................................................... 26
The Team .................................................................................................... 27
Glossary ..................................................................................................... 28
Finance ...................................................................................................... 29
We are Moving/Contact us................................................................................ 30
Year at a glance ............................................................................................ 31
Page 114

3Healthwatch Leeds
2016-17 has been a year of new approaches to ongoing challenges, against a background of fast paced changes to local health and social care. Healthwatch Leeds began to work as a new Community Interest Company. The new company meant a new board and provided us with the opportunity to test out a new approach to the role of Chair.
We chose to make the role a job share, and we definitely feel this has been a resounding success. There are many demands on the time of a Healthwatch Chair, and having two people in the role has resulted in (almost!) twice the time and energy available.
It has also meant a much wider range of skills to call on as we have very different backgrounds. John brings a clinical and public health specialist perspective in dentistry and Lesley brings a health policy and patient and public engagement perspective. It means we are able to manage potential conflicts of interest, and are consequently able to have the Healthwatch Chair attend both the
Health and Wellbeing Board and the Local Authority Scrutiny Committee.
Our new board has changed its approach to meetings. The beginning of the year needed a real focus on governance to ensure our Community Interest Company has a sound foundation. Then we concentrated on hearing about the real issues faced by some of the poorest groups in Leeds. We have had presentations from those working with travellers and people with a learning disability. These were extremely helpful in energising and grounding our work.
A new communication strategy and strategic plan has been created, to guide everyone’s efforts over the next 3-5 years, when a complete change in the health and social care landscape of Leeds is being planned. Our work will continue to be about making sure the people of Leeds are able to have their voices listened to in the planning and delivery of local NHS and care and support services.
Lesley Sterling-Baxter & Dr John Beal
Message from our Chairs
Page 115

4 Healthwatch Leeds
Sexual Health Clinics ReviewThis project was part of a citywide review of sexual health services in Leeds, following significant changes to the service. We took on the role of reviewing services at the five sexual health clinics in the city.
Over the course of three weeks in September 2016 we carried out 18 visits to clinics and spoke with 220 people about their experience of making an appointment, waiting times and the care and support they received.
We found:• There were high levels of
satisfaction with the service and their website.
• Waiting times were identified as a key concern. There was a lack of clear communication and information in relation to expected waiting times.
• Privacy was highlighted as a concern for many.
We met with the service providers and commissioners to discuss our recommendations and an action plan has been produced and shared with us.
“Working alongside Healthwatch to review the Leeds Sexual Health Clinics has been a really positive and worthwhile experience. The final report is excellent and clearly written. Staff at Leeds Sexual Health have welcomed the report findings and are currently developing strategies to address the highlighted areas for improvement, to ensure that all clients receive the best possible experience when visiting a clinic.”Kerry Swift Health Improvement Specialist (Sexual Health) Leeds City Council
Snapshot of our workIt has been a very busy year for us, here’s just a taste of some of the projects we’ve been doing.
Page 116

5Healthwatch Leeds
Home Care Services ReviewAt the beginning of 2016 we carried out telephone interviews with 60 people receiving Home Care services in Leeds. The feedback we received highlighted some issues and concerns about which we made some recommendations. The full report is available on our website at: http://bit.ly/2nupeb8
Leeds City Council shared the report with the new Home Care providers who commenced delivery of a new contract on 1st June 2016. A key feature of the new contract is a set of standards that all providers must be able to demonstrate that they comply with. The standards address the key messages and recommendations made within our report.
In February 2017 we repeated the telephone surveys and spoke to over 130 people receiving home care to see if things had changed or improved for people since we carried out the original survey. The full report is available on our website.
Patient Transport Service (PTS) Between December 2015 and January 2016, five Healthwatch organisations in West Yorkshire carried out a survey with 545 patients and carers at 14 hospital sites across the region. We asked about their experience of pre-booked patient transport return journeys from hospital.
We found:• The vast majority of journeys
involved patients waiting less than 90 minutes - the agreed target waiting time.
• However, most of the patients told us whilst they didn’t mind waiting, they wanted updates about their transport.
• A number of patients felt unable to access food or drink or use the toilet whilst they were waiting as they were afraid of missing their transport.
We received initial action plans from the various hospital Trusts and Yorkshire Ambulance Service and are working with them to make improvements based on our recommendations.
Leeds Teaching Hospitals Trust has initially committed to reviewing how volunteers can offer further support to PTS patients in the waiting rooms and will be putting new signage in the Chancellor Wing, at St James Hospital.
Page 117

6 Healthwatch Leeds
Aspire We worked with local learning disability organisation Aspire to find out how clients and carers would like to get involved in improving their service.
It was great to speak to so many clients and carers who shared their views with us about things like keyworkers, activities and giving feedback about Aspire.
Our easier read report and recommendations were presented at Aspire’s Board meeting and we received an action plan which highlighted some of the things they are doing to improve their service, such as; • A commitment to help improve the
emerging relationship between keyworker and client.
• Developing an easy-read leaflet explaining how people can get involved and how their feedback is used to improve the service.
• Reviewing their comment, compliment and complaint process to ensure there is a consistent approach for all.
Patient Participation GroupsWe worked with Leeds North Clinical Commissioning Group (CCG) on a project around Patient Participation Groups (PPG) in GP practices.Based on conversations with patients, members of PPG groups and co-ordinators across 8 practices in north Leeds, we produced a report which illustrates what people think are the key factors for a well-functioning PPG.
Whilst some PPG’s work really well and offer patients a fantastic opportunity to work with their Practice to improve services, there are others that do not function so well. Our report sets out to highlight why this might be, and what can be done to make PPG’s more effective. The Leeds CCGs said: “The report, which has been shared with all the Leeds CCGs, made a series of recommendations and we are pleased to say that most of these are already being actioned. You can view the report and all the tools and resources available to Leeds PPGs here: https://www.leedswestccg.nhs.uk/get-involved/how/patient-participation-group/ The Leeds CCGs Communications and Engagement Team will continue to support their primary care teams in their work with local practices to develop and deliver effective and meaningful PPGs. We will use the Healthwatch Leeds report to identify gaps in our practices’ PPGs and work with them to champion the voice of the wider public”.
Page 118

7Healthwatch Leeds
Healthwatch FilmsAt Healthwatch, we are always looking for new ways to provide information or get a message across.
We’ve got several short films on our website that have been shared across the city. Some are about volunteering with us, some are thoughts on the future of health and care, and we also have a very powerful video from someone sharing their experience of mental health crisis in Leeds. All well worth a watch.
Future Me 2026Imagine if you could see into the future. That’s what we tried to do when we held our Future Me 2026 event. We brought members of the public, health professionals and the third sector together to look at our vision of health and social care in ten years time. Information and support, partnership working between services and making the best use of technology were some of the main themes that came out on the day. The summary report from the day was shared and promoted across Leeds with planners, commissioners and providers of health and care.
Page 119

8 Healthwatch Leeds
YouthWatch Leeds
Future in Mind: Leeds reportDuring autumn 2016, Healthwatch Leeds worked with Common Room*, to gather experiences about children and young people’s mental health and wellbeing service provision across Leeds. We did this using a combination of surveys and workshops.
We wanted to go back to talk to young people, their parents and carers and professionals to find out what, if anything had changed for them in terms of their experience of mental health and wellbeing services.
The report was shared with the Future in Mind: Leeds Strategic Board along with providers and commissioners of all the services featured in the report.
They all have provided us with an action plan responding to each of our recommendations. We will follow up any progress against these in April 2018.
Key findings Key RecommendationsThere is an overall trend toward Improvements to waiting times, particularly within specialist CAMHS. 54 (81%) young people said that they had waited 12 weeks or less.
Commissioners should consider ways they can work with providers to ensure that communication and support offered during the wait is consistent across services.
Young people and families were generally not aware of the MindMate** website.
Explore ways in which the MindMate website can be more widely publicised, and include more detailed, useful information.
There is a lack of awareness amongst young people and parents of MindMate Single Point of Access (SPA)
Raise awareness and accessibility of MindMate SPA amongst parents and young people.
The introduction of MindMate SPA has been welcomed by professionals but there is room for improvement in terms of communication with referrers and parents.
Continue to evaluate MindMate SPA. Identify how referral pathways and communication with referrers and parents could be improved.
Family and friends were a vital source of support for children and young people who were waiting to access or using services.
Ensure services build in ways (where appropriate) to support parents to help their children.
*promotes the views and expertise of people with lived experience across disability, health and mental health**MindMate is a Leeds-based website for young people, their families and the professionals who support them
It has been a very productive and exciting year for YouthWatch Leeds. Making videos, taking part in Takeover challenges and follow up work to our 2015 Child and young people’s mental health services report.
Page 120

9Healthwatch Leeds
Young facilitators deliver ‘Rights in the NHS’ session to other young peopleIn November 2016, we trained 10 YouthWatch volunteers as young facilitators. Since then, they have gone on to work with Healthwatch Leeds to co-produce a session on young people’s rights in the NHS. The session uses the brilliant ‘Get your rights’ resources produced by the Council for Disabled Children to introduce young people to what their rights are under the NHS constitution. It helps them to think about when they’ve received good or bad care and tells them what they can do if they think their rights haven’t been met.
The young facilitators have delivered the session to a variety of youth groups including Young Dads Collective North, HYPE group at The Market Place (a young people’s emotional wellbeing service) and the young adult carers group at Carers Leeds. We have
also delivered a session to a year 6 class at Stanningley Primary School. 38 (83%) out of 46 children and young people who took part in the session said that they would be more likely to take action if they thought their rights hadn’t been met:
“I would definitely act and encourage other people to do so as well. There are lots of organisations that I could go to to ”
“no matter how old or who you are everyone has rights”
“I have a right to correct doctors if they disrespect my rights”
“Everyone has a right and you can speak up and complain at any age”
“I have learnt what NHS means”
“I have learnt that doctors have to communicate to everyone.”
Our Healthwatch Team (from left to right): Name; Name; Name
Page 121

YouthWatch volunteers who helped facilitate the sessions also learnt a lot…
“What once started off as a meeting looking into our Rights within the NHS to now being able to deliver the message to other young adults and children is mindblowing!! It just shows a small idea – with the added spark of passion can take you a real long long way” (YouthWatch volunteer, age 18)
We are currently making links with more PSHE* leads in local schools, with the hope of rolling out the session to more
primary and secondary schools in the coming year.
*Personal & Social Health Education
Page 122

11Healthwatch Leeds
Takeover of the Health and Wellbeing BoardAs part of the Children’s Commissioner’s Takeover Challenge this year, YouthWatch Leeds volunteers took over, not one but TWO Board meetings – our own Healthwatch Leeds Board and the Leeds Health and Wellbeing Board.
Since chairing a small part of the Healthwatch Leeds Board meeting last year as part of Takeover, YouthWatch Leeds volunteer Chloe has gone on to become deputy chair of the Board. This year Chloe went solo for Takeover and chaired the whole Board meeting.
“Even with years of experience, taking the position of Chair feels daunting. Chloe’s careful preparation, and determination to get things right was obvious, but so was her passion and enthusiasm for what we do. Young people bring so much energy, it’s like a shot in the arm. I made a mental note that we need to have more takeovers, more routinely. We would all benefit!”
Lesley, Healthwatch Leeds Chair
YouthWatch volunteers Sam and Eleni were involved in the Takeover Challenge of a Health and Wellbeing Board workshop to show some of the excellent work that young people
have been doing to get their voices heard.
Eleni talked like a pro to all the Chief Executives and Councillors on the Board, whilst Sam helped to run a workshop to raise awareness about the Doctors Talk to Me video she had been involved in.
At the end of the workshop, all board members filled in a ‘lightbulb moment’ about how they as a board want to keep ensuring children and young people’s voices are heard.We hope that this is the beginning of an ongoing conversation to keep young people’s voices on the agenda.
Eleni - YouthWatch Volunteer
Page 123

12 Healthwatch Leeds
Our volunteers have contributed 3,041 hours this year. That’s a fantastic amount of help and a huge increase of 415 hours from last year! A big, big thank you to everyone that’s volunteered for us, from those that have volunteered just the once to those that continue to do so on a regular basis. Your input is invaluable! Over the year we have provided quality training and development opportunities for our volunteers. This includes, Healthwatch Induction (27 volunteers), Safeguarding Adults (16 volunteers) and Young Facilitators training (10 volunteers), Enter & View (9 volunteers), Equality & Diversity (9 volunteers). In total 82 people have attended our training this year.
100% of people completing the Induction training rate it as either good or excellent!
“Following the induction I have a greater understanding of Healthwatch as well as health and social care services in Leeds.”
Volunteers
“The volunteers
are so motivated and well supported
and the work they do on behalf of HWL is outstanding.”Carol McGrathPrincipal Commissioning OfficerAdult Social Care
Page 124
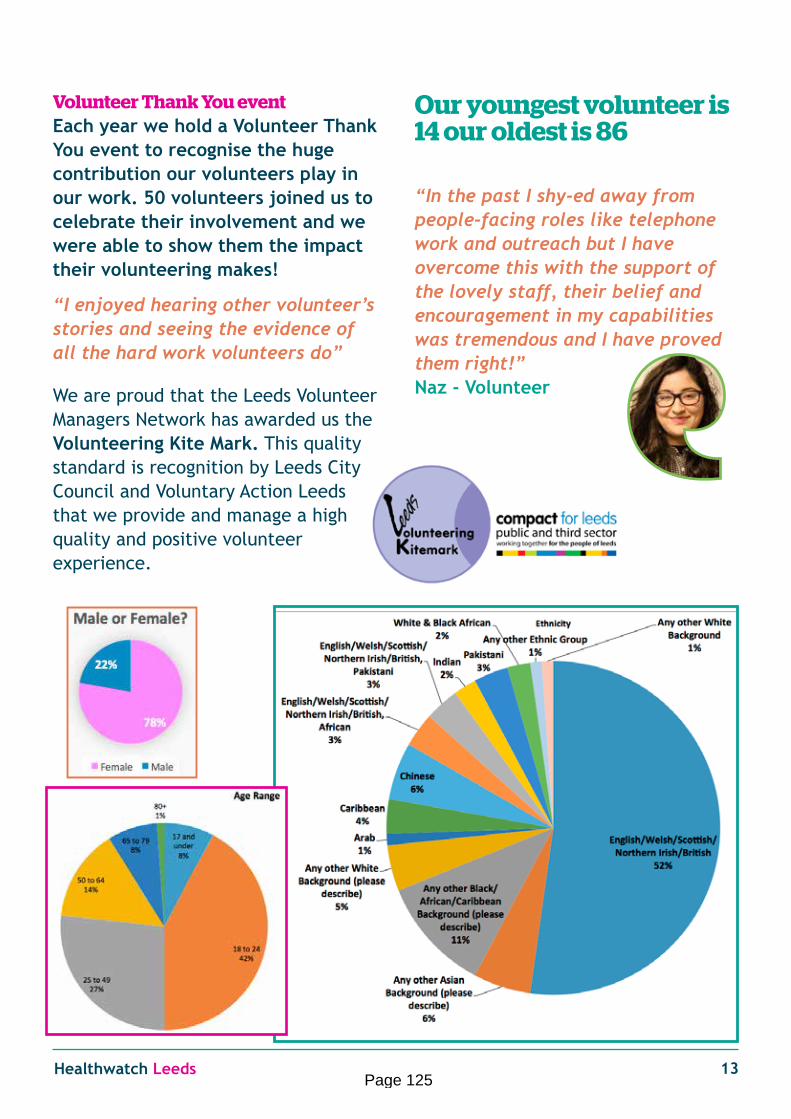
13Healthwatch Leeds
Volunteer Thank You event Each year we hold a Volunteer Thank You event to recognise the huge contribution our volunteers play in our work. 50 volunteers joined us to celebrate their involvement and we were able to show them the impact their volunteering makes!
“I enjoyed hearing other volunteer’s stories and seeing the evidence of all the hard work volunteers do”
We are proud that the Leeds Volunteer Managers Network has awarded us the Volunteering Kite Mark. This quality standard is recognition by Leeds City Council and Voluntary Action Leeds that we provide and manage a high quality and positive volunteer experience.
Our youngest volunteer is 14 our oldest is 86
“In the past I shy-ed away from people-facing roles like telephone work and outreach but I have overcome this with the support of the lovely staff, their belief and encouragement in my capabilities was tremendous and I have proved them right!” Naz - Volunteer
Page 125

14 Healthwatch Leeds
Healthwatch Leeds provides an Information, Advice and Signposting service. We know that the health and care system can be complicated and hard to navigate, so we do our best to help people who often don’t know where to start looking, or have been through the system and have nowhere else to go.
This year we have received 277 direct enquiries (110 more than last year). Our staff regularly attend training and updates about changes in healthcare to ensure that we are giving the public the best possible service.
“I emailed with a dental pricing query and received a reply very quickly, telling me what to do should my problem not be resolved with the dentist. Very happy with your service.”
“Thanks for your help, you’ve been the only person that has listened and given me clear information on what I can do next”
“This is the second time I’ve called Healthwatch and both times they have been very helpful. They advised me on where to go to resolve a dental issue. I heard about Healthwatch following their outreach visit to a community centre I attend, I got their number from one of the mugs they left”.
“Thank you so much for your help, I’ve been trying to contact people all day and this is the closest I have come to finding a solution”.
Since November 2016 we have had 67 separate requests for information from the Care Quality Commission (CQC). We have been able to provide information on 16 occasions. Some of these have influenced areas of CQC inspection.
Information and Signposting
Page 126
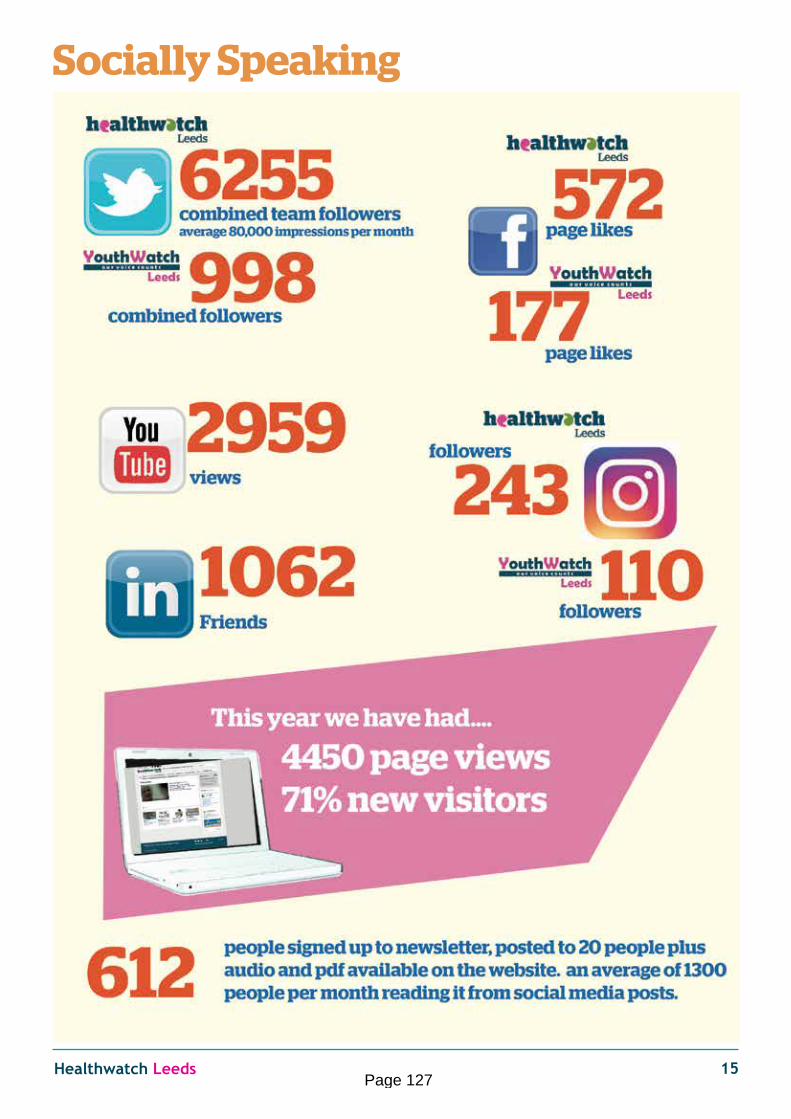
15Healthwatch Leeds
Socially Speaking
Page 127
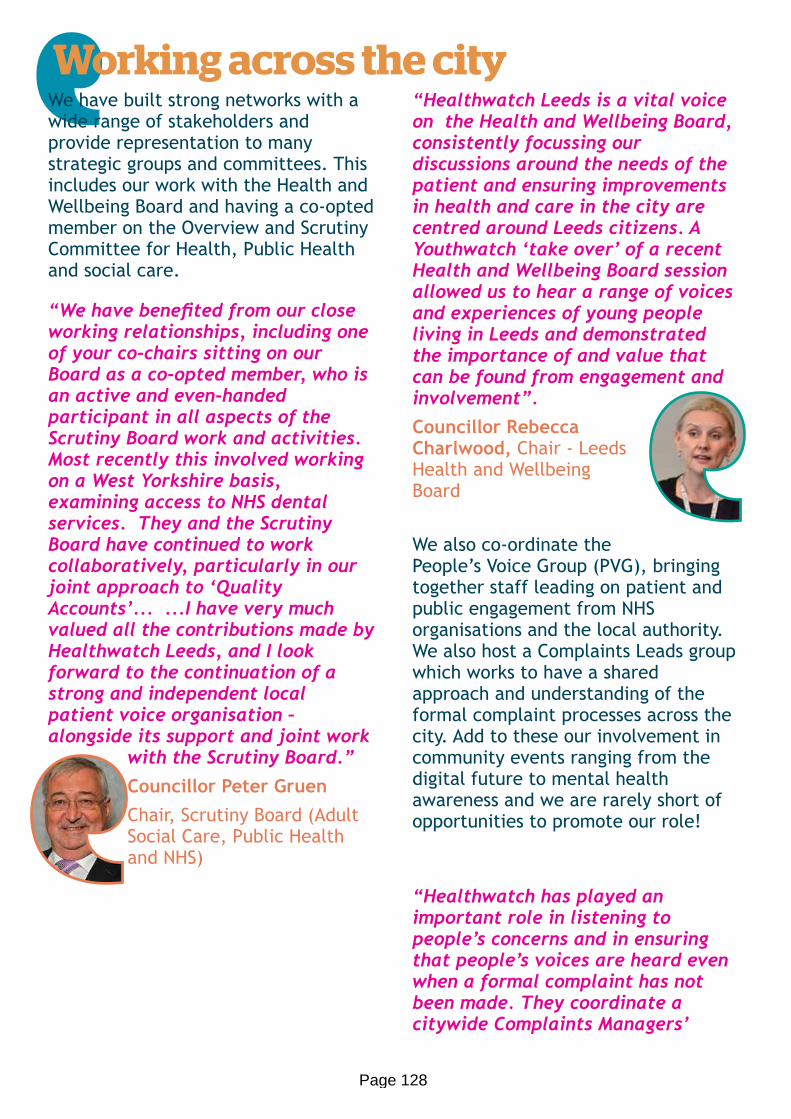
We have built strong networks with a wide range of stakeholders and provide representation to many strategic groups and committees. This includes our work with the Health and Wellbeing Board and having a co-opted member on the Overview and Scrutiny Committee for Health, Public Health and social care.
“We have benefited from our close working relationships, including one of your co-chairs sitting on our Board as a co-opted member, who is an active and even-handed participant in all aspects of the Scrutiny Board work and activities. Most recently this involved working on a West Yorkshire basis, examining access to NHS dental services. They and the Scrutiny Board have continued to work collaboratively, particularly in our joint approach to ‘Quality Accounts’... ...I have very much valued all the contributions made by Healthwatch Leeds, and I look forward to the continuation of a strong and independent local patient voice organisation – alongside its support and joint work
with the Scrutiny Board.” Councillor Peter GruenChair, Scrutiny Board (Adult Social Care, Public Health and NHS)
“Healthwatch Leeds is a vital voice on the Health and Wellbeing Board, consistently focussing our discussions around the needs of the patient and ensuring improvements in health and care in the city are centred around Leeds citizens. A Youthwatch ‘take over’ of a recent Health and Wellbeing Board session allowed us to hear a range of voices and experiences of young people living in Leeds and demonstrated the importance of and value that can be found from engagement and involvement”.Councillor Rebecca Charlwood, Chair - Leeds Health and Wellbeing Board
We also co-ordinate the People’s Voice Group (PVG), bringing together staff leading on patient and public engagement from NHS organisations and the local authority. We also host a Complaints Leads group which works to have a shared approach and understanding of the formal complaint processes across the city. Add to these our involvement in community events ranging from the digital future to mental health awareness and we are rarely short of opportunities to promote our role!
“Healthwatch has played an important role in listening to people’s concerns and in ensuring that people’s voices are heard even when a formal complaint has not been made. They coordinate a citywide Complaints Managers’
Working across the city
Page 128

17Healthwatch Leeds
Group with representation from Social Care, the NHS and the local independent advocacy organisation, Advonet.
By working closely with Social Care, the NHS and Advonet, people’s experience of the complaints process across the city has been improved by everyone. Some of the joint initiatives have included:• Working to a “no wrong door”
approach for people wishing to access the complaints procedure
• Having a shared consent approach, reducing duplication in cross-organisational complaints and speeding up the process
• Providing the same core information to promote all feed back
• providing training to staff within integrated teams”
Judith Kasolo, Head of Complaints, Adult Social Care, Leeds City Council
“The PVG has been a great way to share good practice with my colleagues across the city. It has helped us to work in partnership to develop an engagement hub which offers training and peer support to patients and staff in Leeds”
Chris Bridle - Engagement Lead CCG
“The PVG helped us to think creatively about how working together could maximise impact and has shown that there are gains to be made by crossing organisational boundaries and finding opportunities for partnering. It also provides space for reflection and exploring the art of the possible, with a focus on practical solutions and action in practice”Krystina Kozlowska, Head of Patient Experience, Leeds Teaching Hospitals NHS Trust
“Having a PVG in Leeds has helped me build relationships with colleagues with different perspectives, learn from their experiences and knowledge. It feels good to be part of a collective effort to strengthen our organisations’ commitment to people’s voices and experiences shaping services.”
Matthew Lund Senior Policy and Performance Officer, Intelligence and Policy Service, Leeds City Council
Page 129

This year we have continued using our specially trained volunteers to carry out enter and view visits, to look at how health and care services are provided, and talk to service users, their families and carers.
The visits can be part of a programme of themed visits to a particular service or a single visit where we have been made aware of issues or concerns.
We have carried out two single visits to care homes where we were made aware of some concerns. We have also undertaken five enter and view visits to the acute gynaecology service at Leeds Teaching Hospitals NHS Trust, as part of our programme of themed visits. All the visit reports and action plans are available on our website.
Spring Gardens Care Home
We visited Spring Gardens Care Home following a report published by the CQC, rating the home as requiring improvement in four out of five areas. We were also made aware of a number of concerns from different sources about the home.
During the visit residents and relatives expressed satisfaction with the care that they received. However, the visit team identified many areas for improvement including activities, the internal environment and the outside building and areas.
Following our visit we were pleased to note that several improvements were made, specifically around activities for residents and décor of the Home. We received an update from Leeds City Council highlighting the changes made as a result of our visit.
Enter & View
Page 130

19Healthwatch Leeds
Knowle Manor Care Home
Having visited Knowle Manor in 2014, and received generally very positive feedback, we decided to revisit the home following some concerns raised, specifically around activities for residents.
During the visit we found there were high levels of satisfaction with the care and support received, and we had no concerns about the care given. Residents were complimentary about the availability and choice of food on offer. Residents told us there were a lack of activities available. We were also told that activities advertised didn’t always take place.
Following the visit we made a number of recommendations relating to activities and how these are advertised. There were also recommendations relating to signage and communication with residents.
We are pleased to report that all the recommendations were taken on board by the home who provided us with an action plan clearly outlining what steps have been taken to address the concerns raised.
Women’s Services
Healthwatch Leeds carried out five visits to acute gynaecology services. These were part of our planned programme of enter and view visits and also as a response to some issues that had been highlighted through our enquiries and engagement work.
There was positive feedback about the care and support received from the staff and the visit team were impressed with the overall environment of the department. People felt that they were treated with dignity and respect and there were good levels of satisfaction with the information and communication from staff.
The key concerns expressed related to cancellation of procedures and the short notice given to patients. Some concerns were also raised about the lack of availability of hot food for patients who had stayed more than a few days on the ward. The full report and recommendations are available on our website.
Page 131

This year we have worked in partnership with other local Healthwatch organisations as well as local organisations in Leeds.
Community Dentistry We led on some work with local Healthwatch in West Yorkshire to bring peoples experience of Community Dentistry to influence the NHS England Public Health Dental Team’s review of the service. Our report shows that out of the 334 people we spoke with who used the service during July, 73% thought that the dental staff understood their complex needs. Others thought access and appointment times could be improved. The review of the service is currently on hold.
Orthodontics Joining forces with local Healthwatch organisations in Yorkshire & Humber we spoke to 117 people about orthodontic services, to feed into the NHS England (NHSE) orthodontic service review. A very high percentage of people were happy with the treatment they received. Our report contributed to the evidence in a paper that went to NHSE Directors with a procurement update.
Hear, See and TreatThere are plans in place to improve urgent and emergency care across West Yorkshire. This plan is called ‘Hear, See and Treat’. Alongside West Yorkshire and Harrogate Healthwatch organisations we engaged with 2,585 people to find out what they thought about the plans and proposals. A shared report formed part of the
business case for change that Yorkshire Ambulance Service (YAS) put to the Clinical Commissioning Groups (CCG) in Yorkshire.
We produced a Leeds summary report that was shared with the Leeds Teaching Hospitals NHS Trust, YAS, CCG’s and the Urgent Care Board.
Children and Young Peoples Involvement in Health and CareWe worked with Health Together at Leeds Becket University and the Leeds City Council Voice, Influence and Change team to find out how children and young people are involved in health and care services in Leeds. We were able to highlight good practice and things that don’t work so well. We shared this with the Health and Well-Being Board.
Working Together
Page 132

21Healthwatch Leeds
Quality Accounts As in previous years we have hosted sessions that bring together providers, our volunteers and representatives of the Overview and Scrutiny Committees to look at and hear about local Quality Accounts. Every NHS provider organisation is required to publish Quality Accounts and invite their local Healthwatch to comment.
These sessions promote good practice amongst providers. We will be commenting after the final session in May 2017.
Access to Health and Care for the Deaf and Hard of Hearing CommunityBack in 2014 we did some work with health and care providers to try and improve access to services for people who are Deaf and Hard of Hearing. Our report was positively received and we continue to get feedback on what is being done to hopefully improve experiences for people in Leeds.
This year we received an update from Leeds Teaching Hospitals Trust which highlighted changes to the booking system, text messaging, training and interpreting. We shared this with Leeds DEAForum.
HIV and Dentistry In 2014 we carried out some work to look at the experience of people with HIV when going to the dentist. The report we produced highlighted a number of concerns that we shared with the Yorkshire and the Humber Dental Public Health Team amongst others. Influencing change can often take a long time. This year they produced a factsheet on HIV and blood borne viruses was produced and we helped run a short consultation on this. The factsheet was updated following the feedback received.
There are plans for the factsheet to be published and distributed to all Yorkshire & Humber Dental Teams, undergraduate Dental and Hygiene and therapy students and Foundation Dentists. If published it will be available as a national resource.
Progress Update
Page 133

We are working in partnership with Leeds Teaching Hospitals NHS Trust (LTHT) to look at people’s outpatient experience, with a view to making improvements where possible.
The focus for the outpatient project is to look at the quality of information and communication patients receive before and during their appointment, waiting time concerns and access.
We have been gathering views at different outpatient departments across the Trust. We visited 6 departments and plan to visit a further 10 in the coming year. During the visits we spoke to 562 patients.
Each outpatient department we visited received a brief report of the findings and any suggestions for improvement. The Trust is continuously responding to our reports and recommendations and working to improve patient experience.
Eye Clinic (Pilot) Chancellor Wing, St James Hospital
This was chosen as the pilot as it is one of the busiest clinics. We visited during May 2016 and spoke with 148 patients.
Findings: 93% of patients received clear information to prepare them for their appointment. However, some patients found that signage and font style used in letters they received was hard to read.
Action: The Trust is looking into costing up replacement signage to be fit for purpose for the Ophthalmogy patients. This work is also a part of their service review and patient flow.
Area’s 7&8 Chancellor Wing St James Hospital
In November 2016 we visited outpatient areas 7 and 8. In total we spoke with 42 patients.
Findings: 50% of patients used self-check-in however, some patients found that the machines instructed them to go to waiting area 9 instead of 7&8.
Actions: This is being looked at as part of the work with InTouch (self-check-in provider). On-going maintenance of systems if changes are made seems to be the issue.
Endocrinology Outpatients (Chancellor Wing) at St James Hospital
We visited the Endocrinology outpatients in December 2016. In total we spoke to 86 patients.
Findings: Patients felt a poster titled ‘speak to a sister or Matron’ was friendly and welcoming. Patients also commented about the hospital being too warm but
Outpatient work
Page 134

23Healthwatch Leeds
appreciated the availability of drinks in the waiting area.
We are currently awaiting response
Gynaecology Outpatients Chancellor Wing St James Hospital
We spoke to 78 patients at the Gynaecology Outpatients.
Findings: some patients attending an appointment said they had their original appointment rescheduled by the hospital but received another appointment within a reasonable time. Some patients waited longer than others and were not informed of any delays. Two people said “staff only inform you of a delay when you ask them”.
We are currently awaiting response
Outpatient 1 Lincoln Wing St James Hospital
We visited Lincoln Wing Outpatient 1 in January 2017 and spoke to 108 patients.
Findings: Generally patients were happy with the clinic. One patient felt the service was “one of the best in the world”. Care and treatment was also praised, with long term patients talking about how the service has improved over the years.
We are currently awaiting response
Main Outpatients at Seacroft Hospital
In February 2017 we visited the Main Outpatients department. We spoke to 87 patients.
Findings: Patients were impressed with the cleanliness of the waiting areas (and of the hospital in general).The majority of patients did not wait over their allotted appointment time. For those who did, the wait was no longer than 30 minutes but most patients were seen within 15 minutes.
Many patients commented that the tea bar was closed in the afternoon and they did not have access to any refreshments during their wait.
Action: The tea bar opening times will be discussed with Facilities and the ‘Friends of Seacroft volunteers’ to look at options.
Next steps
There will be an overall report once all visits are completed and we will do follow up visits to see what has improved or changed.
Page 135

It was our fourth Birthday this year and as a part of a review by our commissioners we did some work to record our progress since April 2013. We found strong evidence of our development, giving us a good platform to plan our work for the coming year.
Some of the developments we made may not sound too exciting, policies, frameworks and decision making tools. However what these things give us is a strong base to evidence where local people are heard, have an impact and influence change.
We continue to promote local people’s voices and work to increase our reach.
We have learned to value and develop our connections and networks. Our shared reach is much wider than any of us would achieve on our own. We work with our fellow Healthwatch, with
community groups and with commissioners and providers.
We are fortunate in being asked to join many groups, sit on a range of Boards and strategic groups and to attend many events and meetings. The big challenge for us is capacity.
We manage a lot but are grateful for the review of our local commissioning arrangements to a Leeds “One Voice” way of working that has significantly reduced the number of formal meetings to attend.
We are seeing significant system change and challenge in health and care.
A message from Tanya, our CEO
Page 136

25Healthwatch Leeds
There is no need to have any “secret knowledge” to know that the resources are stretched. We live longer, have increasing care needs and the technology marches on, providing solutions and enabling people to live longer, healthier lives.
Most local people understand that the system struggles, they tell us about how busy the staff they see are, how much pressure there is on services and how difficult it can be at times to see the right person at the right time.
Our challenge, on behalf of Leeds citizens, is how people access, receive and experience care:
• How have you worked with the local people and communities from the beginning. What did you learn and change from what you heard?
• How are you making it easy for people to find out what has changed and how it affects them.
• Have you made clear where people can go if there is a problem with the services they receive?
There is a lot of good practise about what good looks like. We are not looking to re-invent any of that. But our job is to keep challenging, on behalf of the people of Leeds.
Tanya Matilainen CEO
Page 137

26 Healthwatch Leeds
Governance & Board
The Healthwatch Leeds Board is made up of ten volunteers and two staff members. The Board is responsible for the strategic leadership and development of Healthwatch Leeds. There are two sub-committees of the Board: the Quality and Resource Sub-Committee looks at finance resources and quality assurance, and the Peoples Sub-Committee covers staff and volunteers.
The Healthwatch Leeds Board (Left to Right) Moneer Sharif, Chloe Rankin (Deputy Chair), Linn Phipps (Deputy Chair), Dr John Beal (Chair), Tanya Matilainen (CEO), Joanna Barszcak, Stuart Morrison, Sally Morgan, Karen McMahon, Niccola Swan, Lesley Sterling-Baxter (Chair), Richard Taylor
You can find out more about our Board by visiting our website at www.healthwatchleeds.co.uk
Page 138

27Healthwatch Leeds
The Team
The Healthwatch Leeds Team (Left to Right)
Dex Hannon - Communications Manager, Tatum Yip - Community Project Worker, Tanya Matilainen - CEO, Parveen Ayub - Community Project Worker, Stuart Morrison - Team Leader, Tay Babbage - Senior Administrator, Sharanjit Boughan - Community Project Worker, Craig McKenna - Volunteer Coordinator, Harriet Wright - Community Project Worker. You can find out more about our Staff by visiting our website at www.healthwatchleeds.co.uk
Page 139

28 Healthwatch Leeds
GlossaryHealth & Well-Being Board (HWBB): The HWBB is in place to oversee improvements in health and care for people in Leeds. It makes strategic decisions about health and care services. The Board includes: Local Councillors, representatives from children and adult social care, Clinical Commissioning Groups, Public Health, voluntary organisations and Healthwatch Leeds.
Scrutiny Board (Adult Social Services, Public Health and NHS): This Board reviews and scrutinises (examines in detail) the performance of local NHS, Adult Social Care and Public Health. It also scrutinises decisions made by the main decision making body of the Council (Executive Board) relating to Adult Social Care.
Clinical Commissioning Groups (CCGs): These are groups of medical professionals who make decisions about what is needed and what to buy, according to what people in their area need.
Commissioning: Planning, paying for and monitoring services. Choosing what to buy, who to buy from and checking you got a good deal.
Care Quality Commission (CQC): The regulator for all health and social care services in England. It checks that services meet the government’s standards and rules about care.
CAMHS (Child and adolescent mental health services): CAMHS is used as a term for all services that work with children and young people who have difficulties with their emotional or behavioural wellbeing.
Page 140

29Healthwatch Leeds
Income £
Funding received from local authority to deliver local Healthwatch statutory activities 374,400
Additional Income 25,000
Total income 399,400
Expenditure £
Operational costs 52,458
Staffing costs 294,069
Office costs 48,879
Total expenditure 395,406
The small surplus will be invested in our work 2017-18
Finance
Page 141

30 Healthwatch Leeds
Contact usHealthwatch Leeds Community Interest CompanyThe Old Fire Station, Gipton Approach, Gipton, Leeds. LS9 6NLTelephone: 0113 898 0035Text: 07551 122289Email: [email protected] number: 9542077
We will be making this annual report publicly available on 30 June 2017 by publishing it on our website and sharing it with Healthwatch England, CQC, NHS England, Clinical Commissioning Groups, Overview and Scrutiny Committees, and our local authority.
We confirm that we are using the Healthwatch Trademark (which covers the logo and Healthwatch brand) when undertaking work on our statutory activities as covered by the licence agreement.
If you require this report in an alternative format please contact us at the address above.
© Copyright Healthwatch Leeds 2017
As of August 2017, we are planning to have moved into a newly renovated, multi-purpose community centre. Our new office is at the Old Fire Station, Gipton. The fire station originally opened in 1937 and was West Yorkshire’s oldest operational fire station when it closed at the end of 2015. We are pleased to be part of a centre that can become the heart of the local community.
We will be sharing the building with several other voluntary organisations and charities who will be delivering a range of services. There will also be a community café and spaces available for the local community to hire. Part of the cost of the renovation is being met by Jimbo’s Fund, which was established by the late Leeds philanthropist Jimi Heselden.
For more information on the centre, please visit:
www.theoldfirestationgipton.org.uk
Page 142

31Healthwatch Leeds
This year we reached out & connected to 13,000 local people on social media.
We have 55 active volunteers
We have published over 20 reports
We’ve spoken to 1,137 people at Health & Care premises
We’ve visited 36 Health & Social Care premises in Leeds
We’ve engaged with over 4,000 people at events & outreach sessions & project work
The Year at a glance
Page 143

www.healthwatchleeds.co.uk t: 0113 898 0035 e:[email protected] tw: @HWLeeds fb: facebook.com/HealthwatchLeedsInstagram: Healthwatchleeds
Healthwatch LeedsThe Old Fire Station, Gipton Approach,Gipton,Leeds. LS9 6NL
Page 144

Page 1 of 6 Community Interest Company number: 9542077
HWL Workplan 2017-18
No. Our priorities – what we want to do
Outcome - what we want to happen
Activities – how we will do the work Measures & Evidence – how do we know and measure what we have
done
1. We will engage and connect with a range of communities and individuals, identifying themes and priorities and raise awareness of these with commissioners and providers.
Local people will feel more able to share their views and experiences, and have a say about any changes to services.
Our plans, projects and evaluations will be co-produced with volunteers and others who want to take part in our work.
A diverse range of people including those that are seldom heard will feel that their voices can be heard.
We will promote opportunities to have a say through our contacts, networks, website and social media.
We will work with commissioners to identify opportunities to engage.
We ask for feedback and plans from all commissioners and providers and local stakeholders.We undertake a planning session with our Board.We will undertake an annual 360 stakeholder survey which will ask for people’s views and opinions about key issues and priorities.
We will encourage volunteers to get involved in planning and evaluation of all projects.
We collect information We review and identify themes and key issues to feedback to commissioners and providers.
We will maintain and develop our links to a wide range of groups and communities community events and outreach work
Project scopes and plans will show how local voices have influenced our work and volunteers have been involved.
Reports to Board and commissioners summarizing community engagement activity.
Updated and accessible website.
Volunteer activity records and feedback will show how volunteers have been involved in planning and evaluation of projects.
Our monitoring data will show engagement with seldom heard groups
Page 145

Page 2 of 6 Community Interest Company number: 9542077
We will invest additional resource to engage with seldom heard groups.
2. We will provide information and signposting to people about choices in their health and care, and options for sharing their voice and experience
Local people will be better informed about their choices and options in relation to health and care.
We will continue to raise our profile to ensure we are visible and accessible to local people.
We will continue to provide an information, advice and signposting phone line for the public.
We will raise awareness of our information and signposting serviceWe will respond promptly to any requests for information or advice, and ensure that what we provide is current and accurate. Where specialist sources of information exist we will guide people towards them.
We will develop our knowledge and maintain and update our advice & signposting handbook for staff..
We will co-ordinate a complaints leads group city wide to promote joint work, review themes, support good practice and enable early identification of concerns.
We will maintain a partnership approach for those needing advice or advocacy, connecting people directly if they agree to share their information.
We will review our information, identify key issues or trends and share at least
Database monitoring of information, advice and signposting activity. This includes source, number and nature of enquiries.
We will collect and report feedback annually and quarterlyShared feedback and joint work with other local advocacy organisations.
Page 146

Page 3 of 6 Community Interest Company number: 9542077
quarterly with commissioners and providers.
3. We will deliver a Healthwatch that makes a difference to the people of Leeds
People who come into contact with Healthwatch will feel that it is a helpful and useful service.
Health and social care services will improve the way they work as a result of our work.
We will work with providers and commissioners of services to try and ensure that there are actions to any recommendations that we make. We will follow up any actions and impact for all projects.
We will focus on impact and outcomes in our widely circulated annual report.
We will seek feedback from all stakeholders annually as part of our 360 review. We will adapt and develop our service in response to feedback and the diverse and changing communities of Leeds.
We will maintain our role in providing an independent assurance within health and social care, and publish our findings.
We aim to identify opportunities where local voices can have an impact and influence the outcome.
Actions and impact of specific projects will be monitored. Quarterly reporting to Board and commissioners.We collect feedback on our work from organisations and individuals through the “Treasure Chest”. We will monitor progress of all work and projects against our annual and strategic plans-.
Page 147

Page 4 of 6 Community Interest Company number: 9542077
4. We will work together to help ensure the best outcomes for people.
Stakeholders in the city will recognize Healthwatch Leeds as a valuable partner, which adds value.
We will develop and maintain our networks both locally and nationally to guide the direction and strengthen the impact of our work.
We will work collaboratively to maximise our capacity, explore opportunities for joint work and influence new and emerging models of health and social care.
We will provide HW representation to a wide range of strategic Boards and Committees.
We will meet Board level Chairs and Directors regularly to maintain links and updates.
We will work with local commissioners and providers to check that the voices of local people have been listened to in the planning and delivery of their services. We will challenge to promote good engagement.
We will continue to develop meaningful feedback mechanisms and a joint approach to our role among our representatives
Representation levels on strategic boards and partnerships in the city.
We will track how local people’s voices have influenced reviews and commissioning.
Feedback from stakeholders about our work including via our annual 360 review.
Page 148

Page 5 of 6 Community Interest Company number: 9542077
We will take part and promote good practice in regional and national networks eg. West Yorkshire, regional and national Healthwatch networks
We will comment and sign-post to good practice even where we cannot support the actual engagement
We will co-ordinate the Leeds wide People’s Voice group to support best practice and information sharing.
5. We will support and develop our staff and volunteers
Staff and volunteers will feel they are well supported and have opportunities for development.
We will recruit a sufficient and representative mix of staff and volunteers to help reflect the many communities of Leeds, and work to remove any barriers to involvement.
We will offer a wide range of volunteer opportunities and roles.
We will ask all volunteers about any support needs and all regular volounteers will be allocated a named worker.
All volounteers will have an induction and further training opportunities according to their role.
Staff will have bimonthly 1:1 meetings
Feedback from volunteers and staff, including via our annual 360 review.
Tracking number of volunteers, individual volunteer activity and time given.
Number of training sessions and inductions run and attendance levels. Feedback from training evaluations.
Tracking of volunteer destinations following their time volunteering with us.
Range of volunteer roles on offer.
Page 149

Page 6 of 6 Community Interest Company number: 9542077
and annual appraisals where any support and development issues will be addressed.
We will recognise and celebrate the contribution our volunteers make, both on an ongoing basis and through our annual volunteer thank you event.
We will use inclusive processes in both volunteer and staff recruitment.
We will seek feedback from volunteers regularly about how we work. There will be opportunities for co-production of events and projects.
Page 150

Report of Head of Governance and Scrutiny Support
Report to Scrutiny Board (Adults and Health)
Date: 18 July 2017
Subject: Closure of the Blood Donor Centre in Seacroft – responses to Scrutiny Board statement
Are specific electoral Wards affected? Yes No
If relevant, name(s) of Ward(s):
Are there implications for equality and diversity and cohesion and integration?
Yes No
Is the decision eligible for Call-In? Yes No
Does the report contain confidential or exempt information? Yes No
If relevant, Access to Information Procedure Rule number:
Appendix number:
1 Purpose of this report
1.1 The purpose of this report is to present the responses to the former Scrutiny Board’s statement in relation to NHS Blood and Transplant’s decision to close the Blood Donor Centre in Seacroft.
2 Main issues
2.1 The Scrutiny Board (Adult Social Services, Public Health, NHS) first became aware of NHS Blood and Transplant’s proposed closure of the Blood Donor Centre in Seacroft in December 2016. Various exchanges of correspondence between the Chair of the Scrutiny Board (on behalf of the Scrutiny Board) and NHS Blood and Transplant followed.
2.2 Following consideration of the all information made available, in April 2017 (subject to final drafting amendments) the Scrutiny Board agreed a statement in response to NHS Blood and Transplant’s closure decision. The agreed statement, published in May 2017, is attached to this report for information.
2.3 In line with the Scrutiny Board’s agreed statement, responses were sought from the identified organisations in May 2017, with a deadline of 30 June 2017. The responses received are appended to this report, as follows:
NHS Blood and Transplant – dated 6 June 2017 The Independent Reconfiguration Panel (IRP) – dated 21 June 2017 Department of Health (NHS Blood and Transplant triennial review team) – no
response received (as at 10 July 2017).
Report author: Steven CourtneyTel: (0113) 37 88666
Page 151
Agenda Item 13

3. Recommendations
3.1 Members of the Scrutiny Board are asked to consider the attached responses and identify and agree any specific matters that may require further scrutiny action, input or activity.
4. Background papers1
4.1 None used
1 The background documents listed in this section are available to download from the Council’s website, unless they contain confidential or exempt information. The list of background documents does not include published works.
Page 152

Scrutiny Board Statement
Closure of Blood Donor Centre in Seacroft, Leeds Scrutiny Board (Adult Social Services, Public Health, NHS) May 2017
Page 153

Page 154

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 1
Introduction
1. As a Scrutiny Board we (the Scrutiny Board (Adult Social Services, Public Health, NHS) discharge Leeds City Council’s health scrutiny function. In this we would specifically highlight the following functions:
• To review and scrutinise any matter
relating to the planning, provision and operation of the health service in its area and to make reports and recommendations on any such matter it has reviewed or scrutinised;
• To comment on, make recommendations about, or report to the Secretary of State in writing about such proposals as are referred to the authority by a relevant NHS body or a relevant health service provider.
2. In December 2016, we first became
aware of the proposed closure for the Blood Donor Centre in Seacroft. Press coverage reported proposals to close the blood donor centre in Seacroft on 27 January 2017.
3. At our Board meeting on 20 December 2016 we raised concerns about the apparent lack of consultation regarding the proposals and ensured further details were being sought from the provider of the service/facility, NHS Blood and Transplant (NHSBT).
4. Accordingly, a letter was sent to
NHSBT by the Chair on 22 December 2016, detailing our concerns and requesting further details about the reported closure, alongside any service user/public consultation and engagement that may have taken place.
5. We received a response from NHSBT on 13 January 2017 and considered all the additional information provided at our Board meeting on 24 January 2017. At that Board meeting we:
• Noted the intended closure of the
Blood Donor Centre in Seacroft had been brought forward from the end of February 2017 to 27 January 2017- due to the centre running at a reduced capacity.
• Noted evidence of attempts by NHS Blood and Transplant (NHSBT) to inform/engage with the local scrutiny process, however out of date contact details had been used and there were no details around how NHSBT may have tried to verify the information.
• Highlighted our concerns around the lack of any formal public consultation regarding the proposed closure.
• Highlighted further concerns regarding the general lack of awareness of the proposal across Leeds ‘Health and Social Care economy (including service commissioners and providers alike).
• Considered the proposed closure as a substantial variation that merited a much more robust approach to engagement and consultation.
6. Subsequently, we considered whether
or not to refer the closure to the Secretary of State for Health.
Page 155

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 2
Introduction
7. After much deliberation, and taking a
somewhat pragmatic approach given the timings and reported current state of the service, we agreed not to make a formal referral to the Secretary of State for Health on this occasion.
8. However, we agreed the Chair should write to NHSBT and other key stakeholders setting out our concerns and seeking assurances that lessons would be learned.
9. We also agreed to request a further
report from NHSBT to consider the impact of the closure on service users and the levels of blood donation across Leeds.
10. In addition, we requested this report be
provided for September 2017, which will also require appropriate NHSBT staff to attend the Scrutiny Board meeting to present the report and address any of our questions and/or concerns at that time.
Page 156

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 3
Comments and Observations
11. The following comments and observations should be considered alongside the timeline of key events and dates, attached at Appendix 1.
12. We recognise NHSBT is a Special Health Authority for England and Wales that supplies critical biological products and related clinical services to the NHS within a highly regulated environment.
13. We also recognise this is a national service and that NHSBT holds a special relationship with the Department of Health and is accountable directly to that department.
14. Nonetheless, we are disappointed by NHSBT’s decision to close a Blood Donor Centre in Leeds without any involvement, engagement or consultation with the local body charged with maintaining oversight of health services across the City.
15. While we recognise that NHSBT
deliver a national service, we are also concerned by NHSBT’s apparent lack of awareness or disregard for its duties and responsibilities to proactively involve, engage and consult with local Health Overview and Scrutiny Committees.
16. We believe that NHSBT is “a
responsible person”, as defined by ‘The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013’, and is therefore subject to the same requirements and has the same responsibilities as any other body within that definition.
17. As such, NHSBT has responsibility to help support local authorities to discharge their health scrutiny functions. In this instance, we believe NHSBT has failed to adequately discharge this responsibility.
18. We would view the closure of the
NHSBT Blood Donor Centre as a ‘substantial variation’ of service, as we would of any proposed closure of a local health care facility. As such, we believe the proposals should have been subject to a process of formal public consultation, alongside full engagement with the Scrutiny Board.
19. As a minimum, and in line with the
2013 regulations, we would have expected NHSBT to:
• Formally consult with us (the Scrutiny Board);
• Provide details of the intended date of decision;
• Be explicit about the date when any response to the proposals should be provided;
• Inform us of any changes to its decision-making timetable.
• Formally publish details of this decision-making timetable.
20. Furthermore, from the ongoing
exchange of correspondence, we remain unconvinced that NHSBT acknowledge its specific responsibilities around public consultation and engagement with the health scrutiny process. Rather, NHSBT appear to suggest that its relationship with the Department of Health absolves it of these fundamental duties and responsibilities.
Page 157

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 4
Comments and Observations
21. Although we recognise there is some evidence of NHSBT attempting to engage with the local scrutiny process, it has ultimately been proven ineffective for the following reasons:
• The use of out of date contact details with no details of how NHSBT may have tried to verify the information. Councillor Coupar ceased to be the Chair of the Scrutiny Board in May 2015.
• The use of a residential address for correspondence rather than the formal business address for Leeds City Council.
• Failure to provide the authority with the proposed date by which NHSBT intended to make a decision as to whether to proceed with the proposal; and the date by which NHSBT required the authority to provide any comments.
• Failure to inform the authority of any change to the dates provided; and,
• Failure to publish those dates, including any change in those dates.
22. From our perspective, we believe
NHSBT has failed to comply with the regulations associated with service reconfiguration.
23. We understand that the regulations should also be considered alongside the ‘four tests of service change’ which the government mandate requires NHS England to test proposed service changes against.
24. We have discussed NHSBT’s role as a Special Health Authorities with the Independent Reconfiguration Panel (IRP). The IRP has made clear that NHSBT should be required to consider its proposed service changes against the following ‘four tests’:
1) Strong public and patient engagement
2) Clear, clinical evidence base 3) Support for proposals from
commissioners 4) Consistency with current and
prospective need for patient choice
25. As we have not been proactively notified and/or engaged in the development of NHSBT’s plans, it is difficult to fully assess the extent to which NHSBT has taken into account all the key considerations.
26. Nonetheless, based on the information which has been provided to us, our assessment against each of the four tests is set out below.
Strong public and patient engagement
27. By its own admission, NHSBT failed
to undertake any formal public consultation regarding the proposed closure of the Blood Donor Centre in Seacroft.
28. While existing and known service
users may have been informed of the closure this should not be mistaken for formal consultation.
Page 158

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 5
Comments and Observations
29. The approach did not seek the views of service users on the ‘proposals’: Rather it provided information on the consequences of a decision already taken to close the centre.
30. This failed to provide the opportunity
for existing service users to adequately input into the decision-making process.
31. It also failed to provide the opportunity for prospective or future service users to have a voice in the decision-making process and future design of the service..
32. Furthermore, there was also a complete lack of awareness of NHSBT’s proposals across the local health and social care economy. This failed to provide any opportunity for other matters or prospective changes across the local landscape to be adequately identified and/or considered as part of the decision-making process.
33. We can perhaps conclude that NHSBT failed to meet the government’s first test or standard for service reconfiguration.
Clear, clinical evidence base
34. Despite NHSBT providing some
clinical evidence base and information in support of the decision to close the site in Seacroft, in our view, NHSBT has not provided sufficient information in relation to the following:
• Evidence of support for the service model from senior clinicians whose services will be affected by the reconfiguration.
• Evidence of engagement with clinical commissioners on the outcome of internal and independent external reviews of the clinical evidence base.
• Evidence of plans for the future.
35. Therefore we believe NHSBT has failed to deliver a clear, clinical evidence base for its proposed reconfiguration.
Support for proposals from commissioners
36. As mentioned elsewhere, we have not been provided with any evidence to suggest NHSBT has worked collaboratively to inform its decision-making process. Our enquiries suggest there was a lack of awareness across the various statutory bodies that make up Leeds local health and social care economy.
37. As a result, we believe NHSBT failed to provide any real opportunity for other matters or prospective changes across the local health and social care economy to be adequately identified and/or considered as part of the decision-making process.
Consistency with current and prospective need for patient choice
38. We have already established that
NHSBT did not carry out any public/service user consultation regarding the proposed closure of the donor centre. However, we are aware that affected donors were informed of the proposal to close the centre with invitations to attend alternative sessions in the area.
Page 159

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 6
Comments and Observations
39. We acknowledge there is another donor centre located in the city centre of Leeds and that NHSBT run mobile sessions in community venues across the Leeds area; therefore donors still have the opportunity to donate locally.
40. However, we believe the failure to
properly engage and consult on the proposed closure has resulted in there being a lack of any local intelligence regarding future demand and patient choice or preferences.
41. In addition, we are equally concerned
that the Department of Health Triennial Review of NHS Blood and Transplant did little to enhance or reinforce NHSBT’s duties and responsibilities in relation to service reconfiguration when recommending that, ‘…NHSBT’s blood collection modernisation strategy be accelerated, but monitored through a phased plan, with key decision points reflecting analysis of the impact on donor behaviours’
42. While recognising the need to
consider donor behaviour, in our view, there was a missed opportunity to reinforce NHSBT’s responsibilities to engage with local health overview and scrutiny committees, other local health and social care bodies and local service users, when considering specific actions and any proposed changes to the local service offer.
Page 160

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 7
Summary and Conclusions
43. Following local media coverage of the proposed closure for the Blood Donor Centre in Seacroft; we first raised concerns about the lack of NHSBT’s engagement and consultation at our Board meeting on 20 December 2016.
44. We invited NHSBT to attend a
meeting with us to discuss the proposals and we also asked NHSBT to delay the proposed closure to allow more time to consider and review the proposals.
45. NHSBT did not attend a meeting with
us and advised the proposed closure would occur earlier than originally planned due to prevailing circumstances – particularly in terms of staffing.
46. Nonetheless, we believe NHSBT has:
• Failed to comply with the letter and the spirit of current legislation and regulations governing service reconfiguration within the NHS; and,
• Failed to adequately address the majority (if not all) of the government’s tests for service reconfiguration.
47. The interests of patients, service
users and the general public are paramount. As such, we are most concerned by the lack of any formal public engagement or consultation regarding the proposed closure of the Blood Donor Centre in Seacroft.
48. Failure to observe statutory duties
regarding service reconfiguration permits us to refer the closure decision to the Secretary of State for
Health. Our original decision was not to take this formal course of action, but to stress the importance for NHSBT to consider its actions and provide assurances that lessons have been learned for future reference.
49. We also agreed to request a further report from NHSBT by September 2017, to consider the impact of the closure on service users and levels of blood donation across Leeds.
50. However, given the latest response
from NHSBT (Mike Stredder, Director of Blood Donation) on 10 March 2017, we have significant concerns regarding NHSBT’s understanding of its duties and responsibilities and how regulations and guidance apply to it as a Special Health Authority.
51. As such, we will formally submit this
statement and seek responses to its findings from:
• NHS Blood and Transplant • The Department of Health • The independent
Reconfiguration Panel.
52. We trust this statement and the views expressed will serve to enhance future decision-making processes, and we would like to thank all those that have contributed to the production of this statement.
Cllr Peter Gruen, Chair Scrutiny Board (Adult Social Services, Public Health, NHS)
May 2017
Page 161

Page 162

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 9
Appendix 1: Timeline
Date Summary of event
DECEMBER 2016
20 December
Scrutiny Board (Adult Social Services, Public Health, NHS) first became aware of the proposed closure for the Blood Donor Centre in Seacroft.
o Scrutiny Board Meeting - Concerns were raised about the apparent lack of consultation regarding the proposals and ensured further details were being sought from the provider of the service/facility, NHS Blood and Transplant (NHSBT).
22 December Letter to NHSBT – detailing the concerns and requests for further details of NHSBT’s decision and any service user/public consultation and engagement that informed the decision.
JANUARY 2017
13 January
o NHSBT response – letter highlights details of the decision & engagement/consultations: - Due to two blood donor centres in Leeds that collect both
platelets and whole blood (NHSBT centre at Bridle Path and City Centre of Leeds) in close proximity led to reviewing donor centre provision.
- Decision by Department of Health Advisory Committee on the Safety of Blood Tissues and Organs (SaBTO) to collect fewer platelets by apheresis procedure and ongoing decline in hospital demand for blood.
- Leeds Headrow site best placed to serve Leeds (bigger blood donor base, higher footfall, better placed to attract BME donors).
- Closure of Leeds Bridle Path Donor Centre will not affect NHSBT’s ability to collect and supply blood/blood products to meet demand of hospitals
- NHSBT wrote to Cllr Coupar (May 2016) regarding long term options of centres in Leeds and Sheffield. Further letter (September 2016) informing the decision to close the Leeds Bridle Path Blood Donor Centre.
- Collective consultation with staff side representatives for those impacted by the proposed change
- Decision to go ahead with closure of the Bridle Path Donor Centre taken on 4 November 2016.
- Individual consultation with affected staff.
Page 163

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 10
Appendix 1: Timeline
Date Summary of event
17 January
o Email from Principal Scrutiny Adviser on behalf of the Chair – requesting a range of information: - Electronic copies of letters sent to Cllr Coupar, confirmation of
capacity in which Cllr Coupar was contacted, information used to confirm Cllr Coupar as the appropriate contact, confirmation on how the letters were originally sent and attempts made to confirm receipt.
- Details of any local stakeholders involved in discussions around the proposed closure and/or those informed once a closure decision had been made.
- Details of any local ward councillors involved in discussion about the proposed closure (including any feedback received).
- Details of any public/service user engagement and involvement, including feedback. (To share any communications/engagement plan developed as part of the process around the proposed closure).
- Date on which the decision to close the blood donor centre was agreed and to confirm the decision-making body, details of any minutes and paperwork from the meeting.
- Confirmation on who owns the blood donor centre in Seacroft and any future plans for the facility
- Details to confirm current arrangements for blood donations across Leeds (times and locations), and the changes once the proposed closure is implemented (how are blood donors and wider public being informed of these).
20 January
o Letter to NHSBT, requesting for the proposed closure of the Leeds Bridle Pathway Donor Centre (scheduled 27 January 2017) to be deferred for the foreseeable future, in order to allow sufficient time for the Scrutiny Board to fully consider all the available information.
Page 164

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 11
Appendix 1: Timeline
Date Summary of event
23 January
o NHSBT response - Following the queries raised via email on 17 January 2017 the following further information was provided: - Electronic copies of the two letters sent to Cllr Coupar in May
2017 and September 2016 were included. - Information regarding the process for contacting Cllr Coupar was
limited due to the member of staff who contacted Cllr Coupar being on maternity leave. The standard procedure for NHSBT is to check the council website for details of relevant committee members to contact.
- In terms of discussions with other local stakeholders around the proposed closure, NHSBT wrote to the following MPs: Rachel Reeves MP, Fabian Hamilton MP, Greg Mulholland MP, Hilary Benn MP and Richard Burgon MP. The letters provided the same information that was included in the letters to Cllr Coupar.
- NHSBT did not contact any ward Councillors in relation to the proposed closure.
- NHSBT did not carry out any public/service user engagement consultations about the proposed closure. NHSBT wrote to affected donors in September 2016 to inform them they were considering a proposal to close the donor centre and wrote to them again in December 2016 to confirm this closure, inviting them to alternative sessions in the area.
- The decision to close the blood donor centre was formally communicated to staff on 4 November 2016 after the collective staff consultations came to an end on 28 October 2016. Documents of the minutes for consultation meetings and the final decision were also provided.
- Confirmation that the NHSBT Leeds Bridle Path site, which included the donor centre, is owned by NHSBT.
- There are currently two blood donor centres in Leeds that collect platelets and whole blood. One is located at the NHSBT centre at Bridle Path, while the other donor centre is located in the city centre of Leeds at a leased property.
- NHSBT currently runs 488 mobile sessions per year in community venues across the Leeds area, of these around 50 sessions are within 6 miles of the current Bridle Path site. Following the closure of the donor centre at Bridle Path, all donors wishing to donate locally will still have the opportunity to do so.
Page 165

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 12
Appendix 1: Timeline
Date Summary of event
Also, following the request the defer the closure of the donor centre as set out in the letter sent by the Chair on 20 January 2017: NHSBT stated they are unable to do so due to already running the centre at reduced capacity (3 rather than 6 donation beds) and reduced opening hours due to some staff leaving early ahead of the closure, going on sick leave, agreeing with mutual consent to terminate employment early. As a result the closure was brought forward from the end of February to 27 January, donors informed of the closure date and staff redeployment/redundancy dates have been agreed. Therefore it would not be operationally viable to continue opening the centre beyond this point.
24 January
o Scrutiny Board Meeting - Details of the exchange in correspondence between the Chair of the Scrutiny Board and NHSBT were shared with the Board. The Scrutiny Board considered the additional information and: - Noted the intended closure in Seacroft being brought forward
from the end of February 2017 to 27 January 2017- due to the centre running at reduced capacity.
- Noted Evidence of attempts by NHSBT to inform/engage with the local scrutiny process, however out of date contact details had been used and there were no details around how NHSBT may have tried to verify the information.
- Raised concerns around lack of any formal public consultation regarding the proposed closure.
- Raised further concerns regarding the general lack of awareness of the proposals across Leeds’ Health and Social Care economy (including both service commissioners and providers).
- Considered whether or not to register the closure to the Secretary of State for Health.
After some deliberation, the Scrutiny Board agreed not to make a formal referral to the Secretary of State for Health but agreed that the Chair should write to NHSBT and other key stakeholders setting out the concerns of the Scrutiny Board regarding the process followed by NHSBT and seeking assurances that lessons would be learned. The Scrutiny Board agreed to request a further report from NHSBT to consider the impact of the closure on service users and the levels of blood donation across Leeds.
Page 166

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 13
Appendix 1: Timeline
Date Summary of event
FEBRUARY 2017
17 February
o Letter to NHSBT following the Scrutiny Board meeting held on Tuesday 24 January 2017, in which the proposed closure of the Leeds Bridle Path Donor Centre was considered. An extract of the draft minutes were enclosed to summarise the discussion and outcome. The letter highlighted the main issues considered by the Scrutiny Board which centred on the lack of any:
- Formal public consultation regarding the proposed closure; and, - Effective engagement with the Scrutiny Board.
The letter includes the Boards intention to contact NHSBT again with fuller details of the Scrutiny Boards concerns and observations. Also included is the final resolution of the Scrutiny Board; that in September 2017, NHSBT provide a further report on the impact of the closure.
22 February
o Letter sent to Mr Mike Stredder (Director of Blood Donation, NHSBT), following the comments attributed to him in the Yorkshire Evening Post (17 Feb 2017).
The letter requests Mr Stredder to explain his views regarding NHSBT not having any obligation to consult with the public on the proposal to close the Leeds Bridle Path Donor Centre. The Scrutiny Boards views on the matter are made clear as well as the intention to contact NHSBT again with fuller details of the Boards concerns and observations.
MARCH 2017
10 March
o Response from Mike Stredder received - highlighting the following in regards to public consultation:
- NHSBT did not carry out any public consultation but donors were informed of the proposal and decision to close.
- Unlike other local health service providers, NHSBT does not have a mandatory requirement to provide a specific number of donation sessions in a given area and responsibility is to collect enough blood to meet hospital demand.
- The closure of the site does not prevent donors from donating in the Leeds area.
As an Arm’s Length Body (ALB), NHSBT is accountable directly to the Department of Health and ensures both DH Sponsors and the Secretary of State for Health is kept updated on planned changes.
Page 167

Closure of the Blood Donor Centre in Seacroft Published May 2017 Page | 14
Page 168

Page 169

Scrutiny Board (Adult Social Services, Public Health, NHS)
Closure of the Blood Donor Centre in Seacroft
May 2017
Report author: Steven Courtney
Page 170

Councillor Peter Gruen Chair, Scrutiny Board (Adult Services, Public Health, NHS) 3rd Floor (East) Civic Hall Leeds LS1 1UR By email 06 June 2017 Dear Councillor Gruen, Re: Closure of the Leeds Bridle Path Donor Centre in Seacroft I respond to your letter of 3 May, regarding feedback from the Leeds Health Scrutiny Board about NHSBT’s decision to close the blood donation centre at our Leeds Bridle Path site. I have considered carefully the points you have made. NHSBT’s responsibility is to collect enough blood nationally to care for patients across England. We do not provide a local health service. In 2016/17 NHSBT collected just over 1.6 million donations from around 900,000 donors across England. Once collected each donation is processed and tested before being issued to hospitals throughout England in line with patient need. The amount of blood hospitals need is lower than it was due to improvements in clinical practice. We need to react to this by proposing some changes to collections. As a publicly funded organisation, we have a duty to collect blood as efficiently and effectively as possible. Every saving we make is money that is released back to hospitals to invest in frontline patient care. I would again like to stress that the closure of the Leeds Bridle Path Donor Centre will not affect NHSBT’s ability to collect and supply enough blood and blood products to meet the demand of hospitals in Leeds or anywhere else in England. In addition, every donor that wants to give blood will still have the opportunity to do so. Point 16 of the Scrutiny Board statement you have sent us states that “We believe that NHSBT is “a responsible person”, as defined by „The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013‟, and is therefore subject to the same requirements and has the same responsibilities as any other body within that definition.”
The 2013 Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) regulations says “a responsible person means a relevant NHS body or a health service provider” and clarifies that this definition is based on section 244(3) of the NHS Act 2006 as amended by the section 190(1) and (4) of the Health and Social Care Act 2012. The definitions in both Acts also have clauses that clearly state that “relevant NHS body” in relation to overview and scrutiny committees means an NHS body, other than a Special Health Authority, which is prescribed for those purposes in relation to the authority.
Head Office
Oak House
Reeds Crescent
Watford
Hertfordshire
WD24 4QN
Tel: 01923 366800
www.nhsbt.nhs.uk
Page 171

NHSBT is a Special Health Authority. We remain committed to ensuring that we are as open as possible when communicating changes to our blood collection programme. We are not bound, however, to the same duties and responsibilities in relation to engagement and consultation with local Health Scrutiny Committees that local health providers are by legislation. I hope that the information provided here has been helpful in addressing the queries raised. Please do not hesitate to contact me if you have any further queries. Yours sincerely
Mike Stredder Director of Blood Donation
Page 172

IRP
Independent Reconfiguration PanelTel: 020 7389 8045/6 E Mail: [email protected]
Website: https://www.gov.uk/government/organisations/independent-reconfiguration-panel
6th Floor157-197 Buckingham Palace Road
LondonSW1W 9SP
Cllr Peter GruenChair, Scrutiny BoardLeeds City Council3rd Floor Civic HallLeeds LS1 1UR
21 June 2017Dear Cllr Gruen
Closure of the Leeds Bridle Path Blood Donor Centre in Seacroft
Thank you for your letter of 3 May 2017 regarding the above requesting a response by 30 June 2017 to the Scrutiny Board Statement that accompanied your letter.
The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013 define “a responsible person” as “a relevant NHS body or a relevant health service provider”. Examination of the primary legislation underpinning the Regulations confirms that the meaning of “relevant NHS body” and “relevant health service provider” is contained in section 244(3) of the National Health Service Act 2006 as amended by section 190(1) and (4) of the Health and Social Care Act 2012. Subsection (4) states:
(4) For subsection (3) substitute—“(3) For the purposes of subsections (2) and (2ZA)—
“relevant NHS body”, in relation to an authority to which this section applies, means an NHS body, other than a Special Health Authority, which is prescribed for those purposes in relation to the authority; “relevant health service provider”, in relation to an authority to which this section applies, means a body or person which— (a) provides services in pursuance of arrangements made—
(i) by the Board or a clinical commissioning group under section 3, 3A, 3B or 4 or Schedule 1,
(ii) by a local authority for the purpose of the exercise of its functions under or by virtue of section 2B or 6C(1) or Schedule 1, or
(iii) by the Board, a clinical commissioning group or a local authority by virtue of section 7A, and
(b) is prescribed, or is of a description prescribed, for those purposes in relation to the authority.”
You may wish to seek advice from your own legal department but the IRP takes this section to mean that special health authorities are exempt from the requirements for health scrutiny by local authorities that apply to other NHS bodies.
The introduction of the Secretary of State’s four tests for service change (reconfiguration) was announced by the then Secretary of State for Health, Andrew Lansley, in May 2010. The tests, that apply to proposals for changes to NHS clinical services, are “designed to build confidence within the service, with patients and communities”. Guidance on the application of the tests was issued to all NHS chief executives on 29 July 2010. While it is not known by the IRP whether the guidance was intended to cover special health authorities
Page 173

IRP
Independent Reconfiguration PanelTel: 020 7389 8045/6 E Mail: [email protected]
Website: https://www.gov.uk/government/organisations/independent-reconfiguration-panel
(unlike the scrutiny legislation, it does not appear specifically to exclude them), it seems reasonable to the Panel that any proposal to implement a clinical service change should be subject to evaluation against the four tests, including the strength of public and patient engagement.
The NHS, and indeed, the government is committed to the principle of public and patient involvement in NHS service development. Much guidance has been issued to the NHS in this respect. The IRP agrees with the broad thrust of your Statement that there are lessons to be learnt for the future and hopes that, moving forward, the parties involved in this matter can work together in a spirit of co-operation, openness and transparency.
Yours sincerely
Martin HoughtonSecretary to IRP
Page 174

Report of Head of Governance and Scrutiny Support
Report to Scrutiny Board (Adults and Health)
Date: 18 July 2017
Subject: Work Schedule
Are specific electoral Wards affected? Yes No
If relevant, name(s) of Ward(s):
Are there implications for equality and diversity and cohesion and integration?
Yes No
Is the decision eligible for Call-In? Yes No
Does the report contain confidential or exempt information? Yes No
If relevant, Access to Information Procedure Rule number:
Appendix number:
1 Purpose of this report
1.1 The purpose of this report is to consider the Scrutiny Board’s work schedule for the forthcoming municipal year.
2 Main issues
2.1 During discussions at the Board previous meeting on 27 June 2017, the Scrutiny Board discussed a range of matters for possible inclusion within the overall work schedule for 2017/18. The areas discussed included the following matters:
Partnership working, including development of Leeds’ health and care plan and associated cost implications.
Quality of care affecting all service users, especially focused on social care providers judged as ‘requiring improvement’.
The types of support offered as part of the transforming care agenda – i.e. around the repatriation of patients subject to long-term hospital placements.
A potential review of care arrangements for offenders in prison. GP provision across the city. Support available to working age adults. Transition from hospital to home (hospital discharge), developing links with
housing (specifically in relation to adaptations) and work across localities. The development of digital technology to support patient care needs. The role of public health, particularly in relation to health inequalities. Mental health provision with a particular focus on transition from children to
adults. NHS performance and workforce issues.
Report author: Steven CourtneyTel: 0113 378 8666
Page 175
Agenda Item 14

Progress of the ‘One Voice’ project The role of third sector in the delivery of health and social care services,
including but not restricted to the neighbourhood networks, and associated funding arrangements.
Maintaining an overview of proposed service changes.
2.2 The Board previously acknowledged that, due to the resources directly available to support the Board’s work, there would be limitations on the work schedule; and that the Scrutiny Board would need to prioritise its main areas of focus for 2017/18.
2.3 The following areas are proposed as particular priorities for the remained of the municipal year 2017/18. These areas are proposed following further consideration of the matters previously identified and discussed by the Scrutiny Board; and subsequent discussions with the Chair of the Scrutiny Board.
Quality of Care Services in Leeds2.4 The proposal is to maintain the Board’s focus on service quality, with a particular
emphasis on social care provision. As reflected elsewhere on the agenda, this would include:
Quarterly updates on published CQC inspection reports/ outcomes (commencing September 2017);
Leeds Quality Account (September / October 2017) Leeds Better Lives Strategy – update reports on the overall strategy; progress of
Phase 4; and implementation updates for Phases 2 and 3 (Timing to be confirmed) Re-Commissioning of the Adult Social Care Residential and Nursing Care
Services Contract – overview of progress and outcomes (Timing to be confirmed)2.5 Within the overall theme of quality, the Board may also wish to consider issues
associated with hospital discharges and any associated quality issues. The Board had previously identified ‘hospital discharges’ as an area for specific consideration.
Health and Care Needs of Offenders2.6 Based on the initial discussions in June 2017, understanding the Council’s care
obligations in relation to offenders and the associated implications would be a key aim. It would also consider the current commissioning and delivery arrangements of offender health services, particularly focusing on HMP Leeds.
2.7 Other key considerations could include focusing on the specific health issues identified in the recent Annual Report of the Independent Monitoring Board (published 21 June 2017). This is likely to include some consideration of the provision of mental health service.
2.8 Subject to further discussions with Healthwatch Leeds, there may be an opportunity to undertake some joint work and/or consider the outcome of Healthwatch Leeds’ proposal to consider men’s experience of health and care services.
Leeds Health and Care Plan2.9 Maintaining an overview on the development of Leeds Health and Care Plan,
including any specific service change proposals that result. There would also be a
Page 176

balance between the activity happening locally and any proposals being developed on a wider, West Yorkshire and Harrogate footprint.
2.10 A key consideration would be undertaking complementary work to that being undertaken through the West Yorkshire Joint Health Overview and Scrutiny Committee arrangements in place.
Current provision of GP services and the future vision2.11 A specific aspect of this area would be to consider the current delivery of Primary
Care (GP) services across the City, with a specific focus around the South East of the City in order to understand the current challenges and how these will be addressed in the short-term.
2.12 Another aspect of this work would be to consider system integration proposals and the vision for services in the future, including the involvement and engagement of patients and the public; and the potential role and implications for the Third Sector.
Health Service Developments Working Group2.13 In previous years, the Scrutiny Board has formed a working group to help discharge
its health scrutiny function in relation to proposed NHS services changes and/or developments. As highlighted at the meeting in June 2017, this is an important aspect of the Scrutiny Board’s remit and is not reflected in the remit of any other Scrutiny Board.
2.14 However, the Board have also identified other areas of work / activity that it may be possible to integrate into the work group arrangements. This could include:
Quarterly NHS provider updates. NHS key performance reports. Adults and Health 2017/18 budget performance reports. 2018/19 budget proposals
2.15 The aim of this approach would be for the Working Group to meet in September, December and March to consider some or all of the matters identified above, in addition to any specific NHS service change / development proposals at that time. It should be noted that due to nature of any service change proposals, it may be necessary to meet outside the proposed 3 meeting schedule.
Summary2.16 A revised work schedule is being drafted to reflect the Board’s previous discussions
and the proposals set out above. This will be provided in advance of the meeting.
3. Recommendations
3.1 Members are asked to consider and agree/ amend the proposals identified in this report, specifically in relation to:
The overall work schedule as the basis for the Board’s work for the remainder of 2017/18.
The specific matters set out in paragraphs 2.4 – 2.15 above.
Page 177

4. Background papers1
4.1 None used
1 The background documents listed in this section are available to download from the Council’s website, unless they contain confidential or exempt information. The list of background documents does not include published works.
Page 178