Restoring expression of miR-16: a novel approach to therapy for malignant pleural mesothelioma
8
12. Benson AB, 3rd, Guillem JG, Minsky BD. Have the changes in treatment of rectal cancer made a significant difference to our patients? Oncology 2011; 25: 1323–1329. 13. Clark JW, Niedzwiecki D, Hollis D et al. Phase II trial of 5-fluororuacil (5-FU), leucovorin (LV), oxaliplatin (Ox), and trastuzumab (T) for patients with metastatic colorectal cancer (CRC) refractory to initial therapy. ASCO Annual Meeting Proc 2003; 22: A-3584. 14. Conradi LC, Styczen H, Sprenger T et al. Frequency of HER-2 positivity in rectal cancer and prognosis. Am J Surg Pathol 2013; 37: 522–531. 15. Al-Kuraya K, Novotny H, Bavi P et al. HER2, TOP2A, CCND1, EGFR and C-MYC oncogene amplification in colorectal cancer. J Clin Pathol 2007; 60: 768–772. 16. Vance GH, Barry TS, Bloom KJ et al. Genetic heterogeneity in HER2 testing in breast cancer: anel summary and guidelines. Arch Pathol Lab Med 2009; 133: 611–612. 17. Yoon HH, Shi Q, Sukov WR et al. Adverse prognostic impact of intratumor heterogeneous HER2 gene amplification in patients with esophageal adenocarcinoma. J Clin Oncol 2012; 30: 3932–3938. 18. Owens MA, Horten BC, Da Silva MM et al. HER2 Amplification ratios by fluorescence in situ hybridization and correlation with immunoistochemistry in a cohort of 6556 breast cancer tissues. Clin Breast Cancer 2004; 5: 63–69. 19. Ross JS, Fletcher JA, Linette GP et al. The Her-2/neu gene and protein in breast cancer 2003: biomarker and target of therapy. Oncologist 2003; 8: 307–325. 20. Spitzner M, Emons G, Kramer F et al. A gene expression signature for chemoradiosensitivity of colorectal cancer cells. Int J Radiat Oncol Biol Phys 2010; 78: 1184–1192. 21. Yonesaka K, Zejnullahu K, Okamoto I et al. Activation of ERBB2 signaling causes resistance to the EGFR-directed therapeutic antibody cetuximab. Sci Transl Med 2011; 3: 99ra86. 22. Bertotti A, Migliardi G, Galimi F et al. A molecularly annotated platform of patient- derived xenografts (‘xenopatients’) identifies HER2 as an effective therapeutic target in cetuximab-resistant colorectal cancer. Cancer Discov 2011; 1: 508–523. Annals of Oncology 24: 3128–3135, 2013 doi:10.1093/annonc/mdt412 Published online 22 October 2013 Restoring expression of miR-16: a novel approach to therapy for malignant pleural mesothelioma G. Reid 1 * , M. E. Pel 1,2 , M. B. Kirschner 1 , Y. Y. Cheng 1 , N. Mugridge 3 , J. Weiss 3 , M. Williams 1 , C. Wright 1 , J. J. B. Edelman 4 , M. P. Vallely 4 , B. C. McCaughan 4 , S. Klebe 5 , H. Brahmbhatt 3 , J. A. MacDiarmid 3 & N. van Zandwijk 1 1 Asbestos Diseases Research Institute, University of Sydney, Sydney, Australia; 2 Department of Pulmonology, Academic Medical Centre, Amsterdam, The Netherlands; 3 EnGeneIC Ltd, Sydney; 4 Cardiothoracic Surgical Unit, Royal Prince Alfred Hospital, Sydney, Australia; 5 Department of Pathology, Flinders University, Adelaide, Australia Received 29 May 2013; revised 30 August 2013; accepted 30 August 2013 Background: Malignant pleural mesothelioma (MPM) is recalcitrant to treatment and new approaches to therapy are needed. Reduced expression of miR-15/16 in a range of cancer types has suggested a tumour suppressor function for these microRNAs, and re-expression has been shown to inhibit tumour cell proliferation. The miR-15/16 status in MPM is largely unknown. Materials and methods: MicroRNA expression was analysed by TaqMan-based RT-qPCR in MPM tumour specimens and cell lines. MicroRNA expression was restored in vitro using microRNA mimics, and effects on proliferation, drug sensitivity and target gene expression were assessed. Xenograft-bearing mice were treated with miR-16 mimic packaged in minicells targeted with epidermal growth factor receptor (EGFR)-specific antibodies. Results: Expression of the miR-15 family was consistently downregulated in MPM tumour specimens and cell lines. A decrease of 4- to 22-fold was found when tumour specimens were compared with normal pleura. When MPM cell lines were compared with the normal mesothelial cell line MeT-5A, the downregulation of miR-15/16 was 2- to 10-fold. Using synthetic mimics to restore miR-15/16 expression led to growth inhibition in MPM cell lines but not in MeT-5A cells. Growth inhibition caused by miR-16 correlated with downregulation of target genes including Bcl-2 and CCND1, and miR-16 re-expression sensitised MPM cells to pemetrexed and gemcitabine. In xenograft-bearing nude mice, intravenous administration of miR-16 mimics packaged in minicells led to consistent and dose-dependent inhibition of MPM tumour growth. Conclusions: The miR-15/16 family is downregulated and has tumour suppressor function in MPM. Restoring miR-16 expression represents a novel therapeutic approach for MPM. Key words: mesothelioma, miR-16, microRNA, minicells *Correspondence to: Dr Glen Reid, Asbestos Diseases Research Institute, University of Sydney, PO box 3628, Rhodes, NSW 2138, Australia. Tel: +61-2-9767-9800; Fax: +61-2-9767-9860; E-mail: [email protected] original articles Annals of Oncology © The Author 2013. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected]. at University of Sydney on March 27, 2014 http://annonc.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Restoring expression of miR-16: a novel approach to therapy for malignant pleural mesothelioma

12. Benson AB, 3rd, Guillem JG, Minsky BD. Have the changes in treatment of rectalcancer made a significant difference to our patients? Oncology 2011; 25:1323–1329.
13. Clark JW, Niedzwiecki D, Hollis D et al. Phase II trial of 5-fluororuacil (5-FU),leucovorin (LV), oxaliplatin (Ox), and trastuzumab (T) for patients with metastaticcolorectal cancer (CRC) refractory to initial therapy. ASCO Annual Meeting Proc2003; 22: A-3584.
14. Conradi LC, Styczen H, Sprenger T et al. Frequency of HER-2 positivity in rectalcancer and prognosis. Am J Surg Pathol 2013; 37: 522–531.
15. Al-Kuraya K, Novotny H, Bavi P et al. HER2, TOP2A, CCND1, EGFR and C-MYConcogene amplification in colorectal cancer. J Clin Pathol 2007; 60: 768–772.
16. Vance GH, Barry TS, Bloom KJ et al. Genetic heterogeneity in HER2 testing in breastcancer: anel summary and guidelines. Arch Pathol Lab Med 2009; 133: 611–612.
17. Yoon HH, Shi Q, Sukov WR et al. Adverse prognostic impact of intratumorheterogeneous HER2 gene amplification in patients with esophagealadenocarcinoma. J Clin Oncol 2012; 30: 3932–3938.
18. Owens MA, Horten BC, Da Silva MM et al. HER2 Amplification ratios byfluorescence in situ hybridization and correlation with immunoistochemistry ina cohort of 6556 breast cancer tissues. Clin Breast Cancer 2004; 5:63–69.
19. Ross JS, Fletcher JA, Linette GP et al. The Her-2/neu gene and protein in breastcancer 2003: biomarker and target of therapy. Oncologist 2003; 8: 307–325.
20. Spitzner M, Emons G, Kramer F et al. A gene expression signature forchemoradiosensitivity of colorectal cancer cells. Int J Radiat Oncol Biol Phys 2010;78: 1184–1192.
21. Yonesaka K, Zejnullahu K, Okamoto I et al. Activation of ERBB2 signaling causesresistance to the EGFR-directed therapeutic antibody cetuximab. Sci Transl Med2011; 3: 99ra86.
22. Bertotti A, Migliardi G, Galimi F et al. A molecularly annotated platform of patient-derived xenografts (‘xenopatients’) identifies HER2 as an effective therapeutictarget in cetuximab-resistant colorectal cancer. Cancer Discov 2011; 1:508–523.
Annals of Oncology 24: 3128–3135, 2013doi:10.1093/annonc/mdt412
Published online 22 October 2013
Restoring expression of miR-16: a novel approachto therapy for malignant pleural mesotheliomaG. Reid1*, M. E. Pel1,2, M. B. Kirschner1, Y. Y. Cheng1, N. Mugridge3, J. Weiss3, M. Williams1,C. Wright1, J. J. B. Edelman4, M. P. Vallely4, B. C. McCaughan4, S. Klebe5, H. Brahmbhatt3,J. A. MacDiarmid3 & N. van Zandwijk11Asbestos Diseases Research Institute, University of Sydney, Sydney, Australia; 2Department of Pulmonology, Academic Medical Centre, Amsterdam, The Netherlands;3EnGeneIC Ltd, Sydney; 4Cardiothoracic Surgical Unit, Royal Prince Alfred Hospital, Sydney, Australia; 5Department of Pathology, Flinders University, Adelaide, Australia
Received 29 May 2013; revised 30 August 2013; accepted 30 August 2013
Background:Malignant pleural mesothelioma (MPM) is recalcitrant to treatment and new approaches to therapy areneeded. Reduced expression of miR-15/16 in a range of cancer types has suggested a tumour suppressor function forthese microRNAs, and re-expression has been shown to inhibit tumour cell proliferation. The miR-15/16 status in MPM islargely unknown.Materials and methods:MicroRNA expression was analysed by TaqMan-based RT-qPCR in MPM tumourspecimens and cell lines. MicroRNA expression was restored in vitro using microRNA mimics, and effects on proliferation,drug sensitivity and target gene expression were assessed. Xenograft-bearing mice were treated with miR-16 mimicpackaged in minicells targeted with epidermal growth factor receptor (EGFR)-specific antibodies.Results: Expression of the miR-15 family was consistently downregulated in MPM tumour specimens and cell lines. Adecrease of 4- to 22-fold was found when tumour specimens were compared with normal pleura. When MPM cell lineswere compared with the normal mesothelial cell line MeT-5A, the downregulation of miR-15/16 was 2- to 10-fold. Usingsynthetic mimics to restore miR-15/16 expression led to growth inhibition in MPM cell lines but not in MeT-5A cells.Growth inhibition caused by miR-16 correlated with downregulation of target genes including Bcl-2 and CCND1, andmiR-16 re-expression sensitised MPM cells to pemetrexed and gemcitabine. In xenograft-bearing nude mice, intravenousadministration of miR-16 mimics packaged in minicells led to consistent and dose-dependent inhibition of MPM tumourgrowth.Conclusions: The miR-15/16 family is downregulated and has tumour suppressor function in MPM. Restoring miR-16expression represents a novel therapeutic approach for MPM.Key words:mesothelioma, miR-16, microRNA, minicells
*Correspondence to: Dr Glen Reid, Asbestos Diseases Research Institute, University ofSydney, PO box 3628, Rhodes, NSW 2138, Australia. Tel: +61-2-9767-9800;Fax: +61-2-9767-9860; E-mail: [email protected]
original articles Annals of Oncology
© The Author 2013. Published by Oxford University Press on behalf of the European Society for Medical Oncology.All rights reserved. For permissions, please email: [email protected].
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

introductionMalignant pleural mesothelioma (MPM), caused by inhalationof asbestos fibres, is an aggressive tumour originating in thelining of the thoracic cavities. The prognosis for MPM patientsis poor, with median survival around 12 months, and therapy ismainly palliative [1]. Selected patients presenting with early-stage disease may receive a combination of chemotherapy,surgery and radiotherapy. However, despite intensive combinedmodality therapy, the disease will recur in almost all cases. In2004, the pemetrexed with cisplatin doublet was identified as themost effective chemotherapy combination [2], but there has beenalmost no progress since. Unlike the situation in non-small-celllung cancer where driver mutations have been identified, trials oftargeted therapies in MPM were not successful [3], and newtreatment approaches are urgently required.In common with other cancers, the microRNA expression in
MPM displays characteristic alterations [4–9]. However, none ofthese changes were present in a large proportion of tumours orcell lines, limiting their clinical utility. In a previous study, wenoted a significant downregulation of miR-16 expression intumour samples from patients who underwent extrapleuralpneumonectomy [10]. Here, we report that compared withnormal mesothelium or mesothelial cell lines, a consistentdownregulation of the miR-15/16 family was observed in allMPM tumours and cell lines investigated. Restoring expressionof miR-16 resulted in inhibition of cell growth in vitro, andusing epidermal growth factor receptor (EGFR)-targetedminicells to deliver miR-16 mimics to MPM xenograftedtumours in vivo caused profound inhibition of tumour growth.Together, these results suggest that miR-16 replacementrepresents a novel approach to therapy for MPM patients.
materials andmethods
clinical samplesThe 60 tumour samples used in this study were formalin-fixed paraffin-
embedded (FFPE) specimens from patients undergoing extrapleuralpneumonectomy, and are part of a series described previously [11].Formalin-fixed normal pleural tissues were collected from 23 patientsundergoing cardiac or aortic surgery at Royal Prince Alfred Hospital(RPAH), Sydney. Awritten, informed consent was obtained from all patientsand the study was approved by the Human Research Ethics Committees atRPAH and Concord Repatriation General Hospital, Sydney (supplementaryTable S1, available at Annals of Oncology online).
RNA isolation, reverse transcription and real-timeqPCRTotal RNA from cell lines (see supplementary Information, available atAnnals of Oncology online, for details) was isolated using TRIzol reagent(Life Technologies) according to the manufacturer’s instructions. RNAisolation from FFPE sections was carried out after laser-capturemicrodissection (LCM) as described [10]. Measurement of microRNAexpression was carried out using microRNA-specific TaqMan assays, withexpression of target gene mRNA analysed by standard RT and SYBR Green-based real-time qPCR (see supplementary Information, available at Annalsof Oncology online, for details).
MicroRNAmimics and transfectionSynthetic microRNA mimics (supplementary Table S2, available at Annalsof Oncology online) were purchased from Shanghai GenePharma. Followingreverse transfection (and where indicated, additional treatment withchemotherapeutic drugs), effects on proliferation, colony formation, cell
cycle and apoptosis were analysed by standard assays (see supplementaryInformation, available at Annals of Oncology online, for detailed methods).
xenograft studiesThe effect on tumour growth of EGFR-targeted minicells loaded with miR-16 was evaluated in a subcutaneous human xenograft model of MPM innude mice, in experiments approved by the EnGeneIC Animal EthicsCommittee. See supplementary Information, available at Annals of Oncologyonline, for detailed methods.
results
the miR-15 family is downregulated in MPMIn a previous report, we observed a downregulation of miR-16in a small series of MPM tumour specimens [10]. Here, wecompared miR-16 expression in a larger sample set consisting of60 archival FFPE blocks, and 23 normal pleural tissue samples.This revealed that miR-16 expression was 22-fold lower intumours than normal tissue (Figure 1A). Similarly, the levels ofthe co-expressed miR-15a and miR-15b were also reduced intumours, by 4- and 10-fold, respectively (Figure 1A). Theexpression of miR-195, the remaining member of the miR-15family, was 11-fold lower in tumours (Figure 1A). We thenprofiled expression of 760 microRNAs in the mesothelial cellline MeT-5A and four MPM cell lines (supplementaryFigure S3, available at Annals of Oncology online). This revealedthat expression of the miR-15 family members was lower inMPM cell lines. These data were confirmed by RT-qPCR,showing a two- to fivefold decrease for each microRNA(Figure 1B) across six MPM cell lines.A comparison of MeT-5A cells and MPM cell lines revealed a
relationship between downregulation of the miR-15 familymicroRNAs (all of which contain the AGCAGC seed) andhigher expression of a number of their predicted target mRNAs(Figure 1C). This relationship was confirmed experimentally bythe observed decrease in the mRNA expression of a number ofpredicted targets of this microRNA following transfection withmiR-16 mimic (Figure 1D). In addition, the protein expressionof the well-characterised targets of miR-16- Bcl-2 and CCND1 –was decreased following transfection with miR-16 mimic(Figure 1E).
restoring expression of miR-15 or miR-16 inhibitsMPM cell growth and miR-16 sensitises toantimetabolitesThe microRNAs of the miR-15/16 family share extensivesequence identity with identical seed sequences, and there isoverlap in their predicted mRNA targets. Transfecting with asynthetic mimic of miR-16, miR-15a or miR-15b led to growthinhibition in MPM cell lines but not in normal MeT-5A cells(Figure 2A). Growth inhibition was most effective followingtransfection with miR-16 mimic, and we focused on thismicroRNA in subsequent experiments. The effects of miR-16
Annals of Oncology original articles
Volume 24 | No. 12 | December 2013 doi:10.1093/annonc/mdt412 |
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

levels were dose-dependent and evident following transfectionwith 1 nM mimic (supplementary Figure S4, available at Annalsof Oncology online). Transfection with miR-16 also reduced theability of MPM cells to form colonies when plated at lowdensity, but did not affect normal cells (Figure 2B). Furtherinvestigation revealed that restoring miR-16 in MSTO-211Hcells resulted in a G0/G1 accumulation (Figure 2C), and a morestriking induction of apoptosis evidenced by DNA
fragmentation (Figure 2D) and increased annexin V staining(Figure 2E).To determine whether microRNA expression was related to
drug resistance, we combined mimics with thechemotherapeutic drugs frequently used for the treatment ofMPM. Transfection of MSTO-211H or MM05 cells with miR-16 mimic increased sensitivity of the cells to treatment withgemcitabine as well as pemetrexed, and these effects were
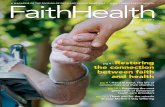
Figure 1. Expression of miR-15 family miRs in MPM tumours and cell lines. (A) The expression of miR-15 family members was measured in MPM tumourspecimens and normal pleura controls. The expression of each microRNAwas normalized to RNU6B and data are presented as values relative to the average ofthe normal pleura controls (*P < 0.0.5, **P < 0.01). (B) Downregulation of miR-15 family members was confirmed in MPM cell lines via real-time qPCR. Levelswere normalized to RNU6B, expressed as negative fold change relative to MeT-5A and are the average of 3 biological replicates (for P values, seesupplementary Table S2, available at Annals of Oncology online). (C) Basal mRNA expression of predicted target genes of miR-16 was evaluated in MeT-5Aand 6 MPM cell lines, and indicates a trend towards increased expression of miR-5A. (D) H28 and MSTO-2011H cells were transfected with miR-16 mimic(5 nM) and the mRNA expression of predicted target genes assessed by real-time qPCR. Expression levels are normalized to 18S and relative to control mimic-treated cells. Line represents twofold downregulation. (E) levels of BCL2 and CCND1 protein were assessed by Western blot with beta-actin used as control.
original articles Annals of Oncology
| Reid et al. Volume 24 | No. 12 | December 2013
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

Figure 2. Transfection with microRNA mimics inhibits MPM cell proliferation. (A) Cells were transfected with miR-15b, miR-16 or control mimics at a finalconcentration of 5 nM. Growth was measured at 48, 72, 96 and 120 h after transfection (*P < 0.05, **P < 0.01), (B) Colony-forming ability was measured in cellstransfected with 0.2 or 1 nM miR-16 mimic in MSTO-211H and MeT-5A cells. Data are representative of three experiments giving equivalent results.(C) MSTO-211H cells were transfected with 5 nM control or miR-16 mimic, and cell cycle distribution was analysed 72 h later. For each population, 10 000events were counted and the proportion of the cells in each phase of the cell cycle is shown. The data are representative of three experiments giving similarresults. MSTO-H211 cells were transfected with miR-16 or control mimic (1 or 5 nM) and apoptosis analysed by DNA fragmentation at 72 and 96 h (D) orannexin V/PI staining at 96 h (E). Genomic DNA revealed fragmentation with band sizes indicating typical apoptotic DNA fragmentation, and PI stainingincreased with miR-16 mimic concentration.
Annals of Oncology original articles
Volume 24 | No. 12 | December 2013 doi:10.1093/annonc/mdt412 |
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

dependent on mimic dose (Figure 3). At a concentration of5 nM, miR-16 increased the sensitivity of cells to gemcitabineand pemetrexed by three and sevenfold, respectively, but did notaffect sensitivity of MeT-5A cells to either drug (Figure 3). Incontrast, restoring levels of miR-16 restoration did not affectcisplatin sensitivity of MPM cells (supplementary Figure S5,available at Annals of Oncology online).
systemic delivery of a miR-16 mimic inhibits MPMtumour growth in vivoThe strong growth inhibitory response to restoration of miR-16expression in MPM cell lines observed in vitro suggested that a
similar approach might have a potential clinical application. Toexplore this, we administered miR-16-containing minicells tonude mice bearing MSTO-211H-derived xenografts viaintravenous injection. Minicells are formed through asymmetricbacterial cell division and have been shown to deliver drugs andsiRNAs to tumour xenografts, via a combination of passiveaccumulation at sites of leaky vasculature and specific targetingusing antibodies to tumour surface antigens [12, 13]. We usedan EGFR-specific antibody for targeting, and to increase thestability of the miR-16 mimic the sequence included four20O-methyl-modified nucleotides at each end of the passengerstrand (supplementary Figure S6, available at Annals ofOncology online).
Figure 3. Restoring miR-16 increases sensitivity of MPM cells to gemcitabine and pemetrexed. MSTO-211H (A, B), MM05 (C, D) and Met-5A cells (E, F)were transfected with miR-16 mimic (at the indicated concentrations as labelled in (F)) and 24 h later exposed to pemetrexed (A, C, E) or gemcitabine (B, D, F)for 72 h. Compared with control mimic, transfection with miR-16 mimic increased toxicity of both pemetrexed and gemcitabine in MPM cells but not controlMeT-5A cells. Data are mean ± SD of triplicate measurements, and are representative of three independent experiments giving similar results.
original articles Annals of Oncology
| Reid et al. Volume 24 | No. 12 | December 2013
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

Dosing mice with 1 × 109 minicells containing miR-16 mimic(∼0.3 µg [12]) one, two or four times per week for 3 weeksresulted in a significant and dose-dependent inhibition oftumour growth compared with controls (Figure 4A). Increasingthe dose to 2 × 109 minicells four times per week led to evengreater inhibition of tumour growth (Figure 4B). In tumoursfrom mice receiving the higher dose of miR-16-containingminicells, there was a consistent grade 3 or 4 lymphocyteinfiltration observed (compared with grades 1–2 in controlmice), and a twofold reduction in the number of mitosesobserved (supplementary Table S7, available at Annals ofOncology online), but otherwise, no non-specific effects wereobserved (supplementary Figure S8, available at Annals ofOncology online). The results from DNA fragmentation assays
revealed an increase in DNA fragmentation in sections frommiR-16-treated mice compared with controls (Figure 4C).
discussion
MPM is remarkably resistant to therapy and so far, theevaluation of targeted agents and experimental (immuno)therapy approaches in clinical trials has not provided newtreatment opportunities [3]. The marked heterogeneity of MPMtumours and global upregulation of multiple genes involved inmetabolism, proliferation and avoidance of apoptosis mayexplain the lack of success observed with single-target agents inthe clinic. In light of this heterogeneity, targeting aberrant
Figure 4. Delivery of miR-16 mimic leads to inhibition of tumour growth in vivo. (A) MSTO-211H xenograft-bearing mice received 1 × 109 minicells perdose, 1×, 2× or 4× per week (the arrows indicate days on which mice were treated in each group, as indicated on the y-axis). In the right panel, tumour-bearingmice received 2 × 109 minicells per dose on the days indicated by the arrows. *P < 0.05, **P < 0.01. (B) Excised tumours from mice treated with saline, controlduplex or miR-16 mimic. Images are representative of the entire treatment group, which was processed immediately. (C) DNA fragmentation assay was carriedout on sections taken from tumours in each group. Nuclei are stained with DAPI, DNA fragmentation with TdT.
Annals of Oncology original articles
Volume 24 | No. 12 | December 2013 doi:10.1093/annonc/mdt412 |
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

microRNA expression to reassert control over entire geneexpression networks provides an attractive means tosimultaneously control multiple genes within the same and/orrelated pathways. Several studies have investigated the effects ofrestoring the expression of downregulated microRNAs in MPM.The expression of miR-29c-5p was decreased twofold in MPMcell lines compared with mesothelial cells, and re-expression ledto inhibition of growth and invasion [9]. Increasing expressionof miR-31, co-deleted with the CDKN2A locus in 32% oftumours, had similar effects [7]. A downregulation in miR-34band miR-34c expression was observed in 50% of tumoursanalysed, and cells stably transfected with a miR-34b/cconstruct exhibited reduced colony formation, migration andinvasion [14]. An adenoviral-based miR-34b/c vector reducedMPM cell viability. None of these studies, however, investigatedthe effects of microRNA replacement strategies on the growth ofnormal mesothelial cells, nor did they demonstrate the effects ofmicroRNA changes in tumours in vivo. Here, we report thatdownregulation in expression of the miR-15 family in MPMseems to be more frequent than changes in other microRNAs,and is a more common event than the most frequent single-genetic events such as deletion of the CDKN2A locus. Theseobservations, together with those reported previously, suggestthat targeting microRNA expression may have applicability inthe treatment of MPM patients presenting with an epithelioidor biphasic subtype.The consistent downregulation of the miR-15 family that we
have observed in MPM patient samples and cell lines mirrorsthe changes seen in these microRNAs in other solid tumours—most notably in cancers of the prostate [15], lung [16] ovary[17] and colon [18]. Consistent with the other tumour types,multiple transcripts dysregulated in MPM are predicted to betargets of the miR-15 family. We observed a number of thesepotential targets to be expressed at higher levels in MPM celllines compared with MeT-5A cells (concordant withdownregulation of microRNA expression), and alsodemonstrated a number to be downregulated upon ectopicexpression of miR-16. Together with the similar levels of growthinhibition we observed following re-expression of miR-16, miR-15a or miR-15b in MPM cells (but not normal mesothelialcells), this suggests that they are likely to be controllingproliferation through their effects on the cell cycle andapoptosis-related genes. The regulation of a related set of cellcycle- and apoptosis-related genes by the miR-34 family, andthe frequent methylation-induced silencing of miR-34b/c inMPM tumours [14], further underline the importance of thesepathways in MPM.As is the case for other tumours, microRNAs are likely to
contribute to the drug sensitivities of MPM cells. In the case ofmiR-15b and miR-16, both have been linked to the multidrugresistance of gastric cancer cells to vincristine, etoposide andAdriamycin [19]. Following miR-16 re-expression in MPMcells, we observed sensitisation to gemcitabine and pemetrexed.While there appears to be no obvious overlap between targets ofthese drugs (RRM1 and TYMS) and the predicted gene targetsof miR-16, it is noteworthy that the chemopreventive agentcurcumin sensitises pancreatic cancer cells to gemcitabine.Curcumin has been shown to downregulate Bcl-2 and cyclinsthrough inhibition of NF-kB in pancreatic cancer [20], and to
stimulate expression of miR-15a/16-1 leading todownregulation of WT1 and growth inhibition in CLL cell linesand tumour cells [21]. Regardless of the mechanism, the abilityof miR-16 to sensitise cells to antimetabolite drugs used to treatMPM patients has potential clinical implications.The application of microRNA replacement as a therapeutic
option for MPM patients is dependent on the ability toeffectively deliver synthetic microRNA mimics in vivo. Inpreviously reported pre-clinical studies, inhibition of tumourgrowth following the restoration of miR-16 expression in vivohas been reported in a prostate cancer model using lentivirus[15] or atelocollagen [22], and in multiple myeloma usingneutral lipid emulsion [23]. In our study, we made use of thetumour targeting afforded by EGFR-coated minicells [12] todeliver synthetic miR-16 mimic to established MPM xenograftsderived from MSTO-211H cells, which in common with mostMPM tumours, express EGFR [24]. Our results confirm thetumour inhibitory effects of miR-16 re-expression and,importantly, we show that tumour growth can be effectivelyinhibited with systemic administration of doses of <1 µg miR-16mimic. This compares very favourably with the 50 µg miR-16mimic [22, 23] or 20 µg miR-34a mimic [25] required to achievegrowth inhibition in previous studies.In conclusion, we have demonstrated a consistent
downregulation of multiple members of the miR-15/16 familyacross MPM cell lines and tumour samples. Restoring miR-16in vitro resulted in growth inhibitory and drug sensitising effectsin MPM cell lines, but not normal mesothelial cells.Furthermore, our demonstration that miR-16 mimics can beeffectively delivered using EGFR-targeted minicells resulting intumour regression in vivo, together with the safety profile ofminicells and their current assessment in a phase I clinical trial,suggests that this approach may bear fruit in the clinic.
fundingThis work was supported by the Cancer Institute NSW(11/TPG/3-06 to NvZ and GR), the Asbestos Research Fund (grantto GR), and the Dust Diseases Board of NSW (2009/1 to GR).
disclosureNM, JW, HB and JM are employees of, and NM, HB and JMhold stock in, EnGeneIC Ltd. All other authors have declaredno conflicts of interest.
references1. Tsao AS, Wistuba I, Roth JA et al. Malignant pleural mesothelioma. J Clin Oncol
2009; 27: 2081–2090.2. Vogelzang NJ, Rusthoven JJ, Symanowski J et al. Phase III study of pemetrexed in
combination with cisplatin versus cisplatin alone in patients with malignant pleuralmesothelioma. J Clin Oncol 2003; 21: 2636–2644.
3. Kelly RJ, Sharon E, Hassan R. Chemotherapy and targeted therapies forunresectable malignant mesothelioma. Lung Cancer 2011; 73: 256–263.
4. Balatti V, Maniero S, Ferracin M et al. MicroRNAs Dysregulation in HumanMalignant Pleural Mesothelioma. J Thorac Oncol 2011; 6: 844–851.
5. Busacca S, Germano S, De Cecco L et al. MicroRNA signature of malignantmesothelioma with potential diagnostic and prognostic implications. Am J RespirCell Mol Biol 2010; 42: 312–319.
original articles Annals of Oncology
| Reid et al. Volume 24 | No. 12 | December 2013
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

6. Guled M, Lahti L, Lindholm PM et al. CDKN2A, NF2, and JUN are dysregulatedamong other genes by miRNAs in malignant mesothelioma -A miRNA microarrayanalysis. Genes Chromosomes Cancer 2009; 48: 615–623.
7. Ivanov SV, Goparaju CM, Lopez P et al. Pro-tumorigenic effects of miR-31 loss inmesothelioma. J Biol Chem 2010; 285: 22809–22817.
8. Kubo T, Toyooka S, Tsukuda K et al. Epigenetic silencing of microRNA-34b/c playsan important role in the pathogenesis of malignant pleural mesothelioma. ClinCancer Res 2011; 17: 4965–4974.
9. Pass HI, Goparaju C, Ivanov S et al. hsa-miR-29c* is linked to the prognosis ofmalignant pleural mesothelioma. Cancer Res 2010; 70: 1916–1924.
10. Kirschner MB, Cheng YY, Badrian B et al. Increased circulating miR-625-3p: apotential biomarker for patients with malignant pleural mesothelioma. J ThoracOncol 2012; 7: 1184–1191.
11. Kao SC, Lee K, Armstrong NJ et al. Validation of tissue microarray technology inmalignant pleural mesothelioma. Pathology 2011; 43: 128–132.
12. MacDiarmid JA, Amaro-Mugridge NB, Madrid-Weiss J et al. Sequential treatmentof drug-resistant tumors with targeted minicells containing siRNA or a cytotoxicdrug. Nat Biotechnol 2009; 27: 643–651.
13. MacDiarmid JA, Mugridge NB, Weiss JC et al. Bacterially derived 400 nm particlesfor encapsulation and cancer cell targeting of chemotherapeutics. Cancer Cell2007; 11: 431–445.
14. Tanaka N, Toyooka S, Soh J et al. Frequent methylation and oncogenic role ofmicroRNA-34b/c in small-cell lung cancer. Lung Cancer 2012; 76: 32–38.
15. Bonci D, Coppola V, Musumeci M et al. The miR-15a-miR-16-1 cluster controlsprostate cancer by targeting multiple oncogenic activities. Nat Med 2008; 14:1271–1277.
16. Bandi N, Zbinden S, Gugger M et al. miR-15a and miR-16 are implicated incell cycle regulation in a Rb-dependent manner and are frequently deleted or
down-regulated in non-small cell lung cancer. Cancer Res 2009; 69:5553–5559.
17. Bhattacharya R, Nicoloso M, Arvizo R et al. MiR-15a and MiR-16 control Bmi-1expression in ovarian cancer. Cancer Res 2009; 69: 9090–9095.
18. Wang X, Wang J, Ma H et al. Downregulation of miR-195 correlates with lymphnode metastasis and poor prognosis in colorectal cancer. Med Oncol 2012; 29:919–927.
19. Xia L, Zhang D, Du R et al. miR-15b and miR-16 modulate multidrug resistanceby targeting BCL2 in human gastric cancer cells. Int J Cancer 2008; 123:372–379.
20. Kunnumakkara AB, Guha S, Krishnan S et al. Curcumin potentiates antitumor activityof gemcitabine in an orthotopic model of pancreatic cancer through suppression ofproliferation, angiogenesis, and inhibition of nuclear factor-kappaB-regulated geneproducts. Cancer Res 2007; 67: 3853–3861.
21. Gao SM, Yang JJ, Chen CQ et al. Pure curcumin decreases the expression of WT1by upregulation of miR-15a and miR-16-1 in leukemic cells. J Exp Clin CancerRes 2012; 31: 27.
22. Takeshita F, Patrawala L, Osaki M et al. Systemic delivery of synthetic microRNA-16 inhibits the growth of metastatic prostate tumors via downregulation of multiplecell-cycle genes. Mol Ther 2010; 18: 181–187.
23. Sun CY, She XM, Qin Y et al. miR-15a and miR-16 affect the angiogenesis ofmultiple myeloma by targeting VEGF. Carcinogenesis 2013; 34: 426–435.
24. Kurai J, Chikumi H, Hashimoto K et al. Therapeutic antitumor efficacy of anti-epidermal growth factor receptor antibody, cetuximab, against malignant pleuralmesothelioma. Int J Oncol 2012; 41: 1610–1618.
25. Trang P, Wiggins JF, Daige CL et al. Systemic delivery of tumor suppressormicroRNA mimics using a neutral lipid emulsion inhibits lung tumors in mice. MolTher 2011; 19: 1116–1122.
Annals of Oncology original articles
Volume 24 | No. 12 | December 2013 doi:10.1093/annonc/mdt412 |
at University of Sydney on M
arch 27, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from