
Resting-state functional connectivity abnormalities in limbic and salience networks in social...
10
Resting-state functional connectivity abnormalities in limbic and salience networks in social anxiety disorder without comorbidity J. Nienke Pannekoek a,b,n , Ilya M. Veer b,c,d , Marie-Jos e van Tol e,h , Steven J.A. van der Werff a,b , Liliana R. Demenescu f , Andr e Aleman e , Dick J. Veltman g , Frans G. Zitman a , Serge A.R.B. Rombouts b,c,d , Nic J.A. van der Wee a,b a Department of Psychiatry, Leiden University Medical Center, Leiden, The Netherlands b Leiden Institute for Brain and Cognition (LIBC), Leiden University, The Netherlands c Department of Radiology, Leiden University Medical Center, Leiden, The Netherlands d Institute of Psychology, Leiden University, Leiden, The Netherlands e BCN NeuroImaging Center, University of Groningen, The Netherlands f Department of Psychiatry, Psychotherapy and Psychosomatics, RWTH Aachen, Germany g Department of Psychiatry, VU Medical Center, Amsterdam, The Netherlands h Clinical Affective Neuroimaging Laboratory, Center for Behavioral Brain Sciences, Leibniz Institute for Neurobiology, Magdeburg, Germany Received 13 December 2011; received in revised form 16 March 2012; accepted 27 April 2012 KEYWORDS Resting-state functional connectivity; Social anxiety disorder; Amygdala; Anterior cingulate cortex; Salience network; Default mode network Abstract The neurobiology of social anxiety disorder (SAD) is not yet fully understood. Structural and functional neuroimaging studies in SAD have identified abnormalities in various brain areas, particularly the amygdala and elements of the salience network. This study is the first to examine resting-state functional brain connectivity in a drug-naive sample of SAD patients without psychiatric comorbidity and healthy controls, using seed regions of interest in bilateral amygdala, in bilateral dorsal anterior cingulate cortex for the salience network, and in bilateral posterior cingulate cortex for the default mode network. Twelve drug-naive SAD patients and pair-wise matched healthy controls, all drawn from the Netherlands Study of Depression and Anxiety sample, underwent resting-state fMRI. Group differences were assessed with voxel-wise gray matter density as nuisance regressor. All results were cluster corrected for multiple comparisons (Z42.3, po.05). Relative to control subjects, drug-naive SAD patients demon- strated increased negative right amygdala connectivity with the left middle temporal gyrus, left supramarginal gyrus and left lateral occipital cortex. In the salience network patients showed increased positive bilateral dorsal anterior cingulate connectivity with the left www.elsevier.com/locate/euroneuro 0924-977X/$ - see front matter & 2012 Elsevier B.V. and ECNP. All rights reserved. http://dx.doi.org/10.1016/j.euroneuro.2012.04.018 n Corresponding author at: Department of Psychiatry, B1-P, University Medical Center, PO Box 9600, 2300RC Leiden, The Netherlands. Tel.: +31 71 5261173; fax: +31 71 5248156. E-mail address: [email protected] (J.N. Pannekoek). European Neuropsychopharmacology (2013) 23, 186–195
-
Upload
rwth-aachen -
Category
Documents
-
view
4 -
download
0
Transcript of Resting-state functional connectivity abnormalities in limbic and salience networks in social...

Resting-state functional connectivity abnormalities
in limbic and salience networks in social anxiety
disorder without comorbidity
J. Nienke Pannekoeka,b,n, Ilya M. Veerb,c,d, Marie-Jos !e van Tole,h,Steven J.A. van der Werffa,b, Liliana R. Demenescuf, Andr !e Alemane,Dick J. Veltmang, Frans G. Zitmana, Serge A.R.B. Romboutsb,c,d,Nic J.A. van der Weea,b
aDepartment of Psychiatry, Leiden University Medical Center, Leiden, The NetherlandsbLeiden Institute for Brain and Cognition (LIBC), Leiden University, The NetherlandscDepartment of Radiology, Leiden University Medical Center, Leiden, The NetherlandsdInstitute of Psychology, Leiden University, Leiden, The NetherlandseBCN NeuroImaging Center, University of Groningen, The NetherlandsfDepartment of Psychiatry, Psychotherapy and Psychosomatics, RWTH Aachen, GermanygDepartment of Psychiatry, VU Medical Center, Amsterdam, The NetherlandshClinical Affective Neuroimaging Laboratory, Center for Behavioral Brain Sciences, Leibniz Institute for Neurobiology,
Magdeburg, Germany
Received 13 December 2011; received in revised form 16 March 2012; accepted 27 April 2012
KEYWORDSResting-statefunctionalconnectivity;Social anxietydisorder;Amygdala;Anterior cingulatecortex;Salience network;Default mode network
Abstract
The neurobiology of social anxiety disorder (SAD) is not yet fully understood. Structural andfunctional neuroimaging studies in SAD have identified abnormalities in various brain areas,particularly the amygdala and elements of the salience network. This study is the first toexamine resting-state functional brain connectivity in a drug-naive sample of SAD patientswithout psychiatric comorbidity and healthy controls, using seed regions of interest in bilateralamygdala, in bilateral dorsal anterior cingulate cortex for the salience network, and in bilateralposterior cingulate cortex for the default mode network. Twelve drug-naive SAD patients andpair-wise matched healthy controls, all drawn from the Netherlands Study of Depression andAnxiety sample, underwent resting-state fMRI. Group differences were assessed with voxel-wisegray matter density as nuisance regressor. All results were cluster corrected for multiplecomparisons (Z42.3, po.05). Relative to control subjects, drug-naive SAD patients demon-strated increased negative right amygdala connectivity with the left middle temporal gyrus,left supramarginal gyrus and left lateral occipital cortex. In the salience network patientsshowed increased positive bilateral dorsal anterior cingulate connectivity with the left
www.elsevier.com/locate/euroneuro
0924-977X/$ - see front matter & 2012 Elsevier B.V. and ECNP. All rights reserved.http://dx.doi.org/10.1016/j.euroneuro.2012.04.018
nCorresponding author at: Department of Psychiatry, B1-P, University Medical Center, PO Box 9600, 2300RC Leiden, The Netherlands.Tel.: +31 71 5261173; fax: +31 71 5248156.
E-mail address: [email protected] (J.N. Pannekoek).
European Neuropsychopharmacology (2013) 23, 186–195

precuneus and left lateral occipital cortex. Default mode network connectivity was notdifferent between groups. These data demonstrate that drug-naive SAD patients withoutcomorbidity show differences in functional connectivity of the amygdala, and of areas involvedin self-awareness, some of which have not been implicated in SAD before.& 2012 Elsevier B.V. and ECNP. All rights reserved.
1. Introduction
Social anxiety disorder (SAD) is characterized by persistentfear of social or performance situations in which judgmentor scrutiny by others and embarrassment can occur. Socialsituations are preferably avoided or otherwise experiencedwith extreme anxiety and discomfort (American PsychiatricAssociation, 1994; Furmark, 2002). The number of neuroi-maging studies investigating SAD is rather modest, but thesehave provided some insight in the brain circuitry involved inthis disorder. Structural neuroimaging studies have beenscarce, and have used different approaches, reportinginconsistent results with some studies showing no abnorm-alities and others decreases in volume of the amygdala,right posterior right temporal gyrus and (para)hippocampus(Irle et al., 2010; Liao et al., 2011; Potts et al., 1994). Thenumber of functional studies is much greater, with most ofthese studies focusing on the processing of emotional facesor using symptom provocation designs (Blair et al., 2008a;Blair et al., 2008b; Blair et al., 2011; Damsa et al., 2009;Etkin and Wager, 2007; Freitas-Ferrari et al., 2010; Gentiliet al., 2009; Shin and Liberzon, 2010). A recent systematicreview on neuroimaging studies in SAD by Freitas-Ferrariet al. (2010), mainly focusing on functional connectivity,found the amygdala and its connections in the emotionaland fear circuitry to play a key role in SAD (Freitas-Ferrariet al., 2010). However, other areas such as the insula (Shahet al., 2009), anterior cingulate cortex (Amir et al., 2005;Blair et al., 2011) and ventromedial prefrontal cortex havealso been reported to be involved in SAD (Damsa et al.,2009; Etkin and Wager, 2007; Freitas-Ferrari et al., 2010).
1.1. Resting-state fMRI
Resting-state fMRI (RS-fMRI) enables the monitoring of brainactivity and connectivity in the absence of externallycontrolled tasks or stimuli (Fox and Raichle, 2007). Consis-tently reported RS networks of functionally interconnectedbrain regions include the default mode network (DMN)(precuneus/posterior cingulate cortex, medial prefrontalcortex, and lateral parietal cortex) (Raichle et al., 2001),and the salience network (Biswal et al., 2010; Seeley et al.,2007). The salience network is important in assessing therelevance of internal and external stimuli in order to guidebehavior (Seeley et al., 2007). Its principal areas are thebilateral anterior insula and bilateral dorsal anterior cingu-late cortex, two areas frequently reported to be involved inSAD (Freitas-Ferrari et al., 2010). So far, five RS-fMRIconnectivity studies in SAD have been published, four ofwhich were conducted by the same research group withinoverlapping cohorts of SAD patients (Ding et al., 2011; Hahnet al., 2011; Liao et al., 2010a; Liao et al., 2010b; Liaoet al., 2011). Using independent component analysis, Liao
et al. (2010a) revealed altered connectivity in SAD patientsin seven out of the eight RS networks resulting from theiranalysis, including the DMN and a self-referential network.Noteworthy, a limbic network was not among these net-works. Subsequently, Liao et al. (2010b) used a seed-basedregion of interest analysis and demonstrated altered amyg-dala RS connectivity in social anxiety patients (Liao et al.,2010b). In their third study, Liao et al. (2011) combinedvoxel-based morphometry, RS functional connectivity(RSFC), and diffusion tensor imaging (Liao et al., 2011),and found decreased volumes and altered connectivity ofthe right inferior frontal gyrus and hippocampal areas.Finally, a whole-brain resting-state analysis was also per-formed, showing abnormal connectivity of frontal andoccipital lobes (Ding et al., 2011).
The group of Hahn et al. (2011) examined in one studyRSFC in SAD using a seed-based region of interest approachand found altered left amygdala connectivity. However, theinvestigated sample was heterogeneous, consisting of SADpatients as well as patients with comorbid panic disorder,and one panic disorder patient (Hahn et al., 2011). It istherefore difficult to ascertain whether the differenceswere solely attributable to SAD. Additionally, in four outof the five published RS studies patients were not usingmedication at the time of research, but were not drug-naive, thus possible effects of recent pharmacotherapycannot be ruled out. Since the effect of anti-anxietymedication on neuronal activity has been demonstrated inSAD patients (Furmark et al., 2005; Van der Linden et al.,2000), a drug-naive sample should preferably be used torule out such effects.
Here, we set out to investigate RSFC in drug-naive SADpatients without psychiatric comorbidity using a seed-basedcorrelation approach. Given the anatomical and functionalabnormalities found in previous MRI studies in SAD, suggest-ing a key role for the amygdala (Freitas-Ferrari et al., 2010;Kent and Rauch, 2003; Shin and Liberzon, 2010), and itskey role in emotion generation, fear and anxiety (LeDoux,2003), we hypothesized abnormalities in amygdala RSFC.Additionally, based on previous reports of involvement ofthe dorsal anterior cingulate cortex in SAD and based on thefunctions of the salience network (Seeley et al., 2007) andits relevance for anxiety disorders (Amir et al., 2005; Blairet al., 2011; Etkin et al., 2009; Etkin et al., 2010; Freitas-Ferrari et al., 2010) we also expected abnormalities in theconnectivity of the salience network. As the DMN showedaltered connectivity in many neuropsychiatric disorderssuch as depression (Broyd et al., 2009; Greicius et al.,2007), epilepsy, autism, attention deficit/hyperactivity dis-order, anxiety disorders (Broyd et al., 2009), and perhapsalso in SAD where it is thought to play a role in socialcognition (Gentili et al., 2009; Liao et al., 2010a), we alsohypothesized abnormalities in the connectivity of the DMNin social anxiety patients.
Resting-state functional connectivity abnormalities in limbic and salience networks 187

2. Experimental procedures
2.1. Participants
Subjects were selected from the MRI study within the large-scalelongitudinal multi-center cohort Netherlands Study of Depression andAnxiety (NESDA). NESDA is designed to investigate the long-termcourse and consequences of depression and anxiety disorders. Parti-cipants in NESDA were recruited from the community, and throughprimary care and specialized mental health institutions. The ratio-nales, methods and recruitment have been described in detail else-where; for an overview of diagnostics, inclusion and exclusion criteriasee: (Penninx et al., 2008; van Tol et al., 2010).
After receiving written information, all subjects provided writ-ten informed consent. Participants underwent MR imaging in one ofthe three participating centers (Academic Medical Center Amster-dam, Leiden University Medical Center, and University MedicalCenter Groningen) (van Tol et al., 2010). The study was approvedby the Medical Ethics Committees of all three centers and con-ducted in compliance with the Code of Ethics of the World MedicalAssociation (Declaration of Helsinki).
For the present study on SAD patients without comorbidity, MRIdata were available from 12 right-handed SAD patients (5 male) andfrom 12 healthy controls matched for age, gender, education,handedness, and scan-location (Table 1). All subjects were new tothis specific scanning situation. Patients were diagnosed with SAD andno other psychopathology using the DSM-IV-based Composite Interna-tional Diagnostic Interview, lifetime version 2.1 (American PsychiatricAssociation, 1994). At the time of scanning, anxiety and phobicsymptoms were also assessed using the Fear Questionnaire (FQ)(Marks and Mathews, 1979) and depressive symptoms were rated withthe Montgomery–Asberg Depression Rating Scale (Montgomery andAsberg, 1979). Demographic and clinical characteristics were analyzedusing SPSS 17.0 (SPSS Inc, Chicago, Illinois) with significance set atpo0.05.
2.2. Image data acquisition
Image acquisition took place at the Academic Medical CenterAmsterdam, the Leiden University Medical Center, and the Uni-versity Medical Center Groningen. Images were obtained on Philips3T magnetic resonance imaging systems (Philips Medical Systems,Best, The Netherlands), equipped with a SENSE-8 (Leiden UniversityMedical Center and University Medical Center Groningen) or SENSE-6 (Academic Medical Center Amsterdam) channel head coil.
As part of a fixed imaging protocol, resting-state functional MRIdata were acquired for each subject using T2
n-weighted gradient-
echo echo-planar imaging with the following scan parameters inAmsterdam and Leiden: 200 whole-brain volumes; repetition time2300 ms; echo time 30 ms; flip angle 801; 35 transverse slices; noslice gap; field of view 220! 220 mm; in-plane voxel size2.3! 2.3 mm; slice thickness 3 mm; duration 7.51 min. Parametersin Groningen were identical, apart from: echo time 28 ms; 39transverse slices; in-plane voxel size 3.45! 3.45 mm. In the dar-kened MR room participants were instructed to lie still with theireyes closed and not to fall asleep. After completion of the scan,subjects confirmed wakefulness during acquisition. A sagittal3-dimensional gradient-echo T1-weighted image was acquired forregistration purposes and gray matter analysis with the followingscan parameters: repetition time 9 ms; echo time 3.5 ms; flip angle801; 170 sagittal slices; no slice gap; field of view 256! 256 mm;1 mm isotropic voxels; duration 4.5 min.
No abnormalities were found upon inspection of the subjects’structural images by a neuroradiologist.
2.3. Preprocessing
FMRI data preprocessing and statistics were carried out using FEAT(FMRI Expert Analysis Tool) Version 5.98, part of FSL (FMRIB’sSoftware Library, http://www.fmrib.ox.ac.uk/fsl) (Smith et al.,2004). The following pre-statistics processing was applied: motioncorrection; non-brain removal; spatial smoothing using a 6 mmfull-width at half-maximum Gaussian kernel; grand-mean intensitynormalization of the entire 4D dataset by a single multiplicativefactor; high-pass temporal filtering (Gaussian-weighted least-squaresstraight line fitting, with a 0.01 Hz cut-off). Registration of the RSdata to high resolution T1-weighted, and the T1 to the 2 mm isotropicMNI-152 standard space image (T1 standard brain averaged over 152subjects; Montreal Neurological Institute, Montr!eal, QC, Canada) wascarried out (Smith et al., 2004). The resulting transformationmatrices were then combined to obtain a native to MNI spacetransformation matrix and its inverse (MNI to native space).
2.4. Statistical analysis
For the current study, a seed based correlation approach (Fox andRaichle, 2007) was employed to study functional connectivityduring rest (Roy et al., 2009). The following seed regions of interestwere selected: bilateral amygdala, bilateral dorsal anterior cingu-late cortex (dACC) (for the salience network), and bilateral poster-ior cingulate cortex (PCC) (for the DMN). We created a mask instandard space for the amygdala based on the Harvard–OxfordSubcortical Structural Probability Atlas in FSL (Veer et al., 2011).The coordinates for the dACC seeds were obtained directly from
Table 1 Demographic and clinical characteristics of patients with social anxiety disorder and healthy controls.
Social anxiety disorder patients (N=12) Healthy controls (N=12)
Gender 5 male/7 female 5 male/7 femaleScan location 2 AMC; 5 LUMC; 5 UMCG 3 AMC; 5 LUMC; 4 UMC
Mean SD Mean SD p
Age 34.8 8.8 (24–53 years) 34.0 7.2 (21–47 years) 0.821Education 11.8 3.2 (6–18 years) 13.7 2.4 (10–18 years) 0.123
20.8 8.2 (8–36) 4.5 4.3 (0–13) 0.001a
7.8 8.6 (0–25) 1.2 2.0 (0–5) 0.001a
SD=standard deviation; AMC=Academic Medical Center Amsterdam; LUMC=Leiden University Medical Center; UMCG=UniversityMedical Center Groningen; FQ=Fear Questionnaire; MADRS=Montgomery–Asberg Depression Rating Scale.
aMann-Whitney U Test.
J.N. Pannekoek et al.188

Table 1 of the study by Margulies et al. (2007), and PCC seed regioncoordinates were obtained from a study by Greicius et al. (2003).Table 2 contains the coordinates of the seed voxels. Spheres of4 mm radius were created around the seed voxels. They were thentransformed to native space by applying the inverse transformationmatrix obtained from the registration procedure, and spatiallyaveraged time series were extracted for each seed and for eachsubject. For each participant, and for each network of interest, weperformed a multiple regression analysis using the general linearmodel (GLM) (as implemented in FEAT) (Smith et al., 2004). Thetime courses that were extracted from the voxels in all of our seedregions were entered as a regressor in a GLM for each network.Apart from the two regressors describing the left and right seeds,nine nuisance regressors were included in the model: signal fromthe white matter, cerebrospinal fluid signal, and the global signal,as well as six motion parameters (three translations and threerotations). The global signal was included to reduce the influence ofartifacts caused by physiological signal sources (i.e., cardiac andrespiratory) on the results (Fox and Raichle, 2007).
After reslicing the resulting parameter estimate maps and theircorresponding within-subject variance maps into 2 mm isotropicMNI space, they were entered into a higher level within andbetween groups mixed effects analysis (one- and two-sample t-test).
As structural studies have indicated abnormalities in SAD, weused gray matter density information of each subject as a voxel-dependent covariate in our higher level model. By includingstructural information in the functional connectivity analysis,variance explained by potential differences in gray matter densityand/or possible misregistrations are taken into account (Oakeset al., 2007). Lower level contrasts were analyzed both withinand between groups were analyzed using the general linear modelin which age and scan location were also entered as regressors. Tocorrect for multiple comparisons, cluster correction was applied inall group analyses with significance set at a corrected po.05 and aninitial cluster-forming threshold of Z42.3 (Worsley, 2001).
3. Results
3.1. Questionnaires
At the time of scanning, SAD patients scored significantlyhigher than controls on the FQ social phobia sub-scores,and on the Montgomery–Asberg Depression Rating Scale(Table 1).
3.2. RSFC analysis
We first analyzed amygdala RSFC. Within both groupsthe connectivity pattern largely overlapped with areasdescribed to have functional and anatomical connections
with the amygdala in previous studies (Roy et al., 2009;Stein et al., 2007). Areas showing positive connectivity withthe amygdalae included the hippocampus, parahippocampalgyrus, insula, putamen, pallidum, thalamus, temporal pole,frontal orbital cortex, planum temporale, superior temporalgyrus, temporal fusiform gyrus, and brainstem. Areasshowing a negative resting-state connectivity were theprecentral gyrus, middle frontal gyrus, PCC/precuneus,supramarginal gyrus, angular gyrus, lateral occipital cortex,and cuneus.
In SAD patients we found increased negative right amyg-dala connectivity with the left middle temporal gyrus, leftsupramarginal gyrus and left lateral occipital cortex(Figure 1; Table 3). No group differences were found onleft amygdala RSFC or when a contrast was made for the leftand right amygdala combined.
Next, we explored RSFC of the dACC, probing the saliencenetwork. The connectivity pattern for this seed in bothgroups also corresponded with areas described in previousresearch (Margulies et al., 2007). Areas showing positiveconnectivity in rest with the dACC included other parts ofthe ACC, the frontal pole, paracingulate gyrus, PCC, pre-central gyrus, supramarginal gyrus, parietal operculumcortex, central operculum cortex, inferior frontal gyrus,and middle frontal gyrus. Areas showing negative connec-tivity in rest included the subcallosal cortex, precuneus,cuneus, lateral occipital cortex, occipital fusiform cortex,parahippocampal gyrus, and lingual gyrus.
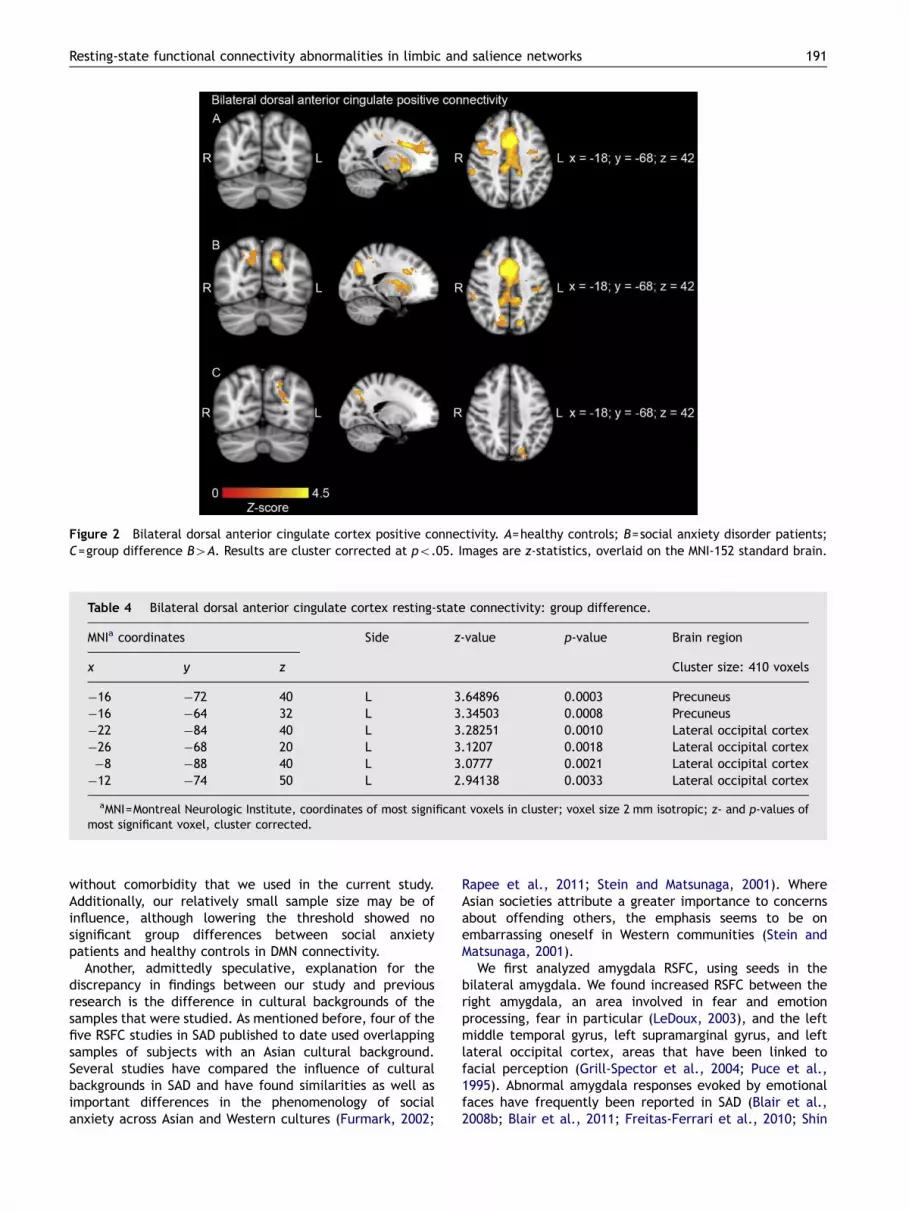
The combined bilateral dACC showed increased connec-tivity in SAD patients with the left precuneus and left lateraloccipital cortex (Figure 2; Table 4). Separate investigationsof the left and right dACC did not produce any significantgroup differences.
We investigated DMN connectivity with a seed in the leftand right PCC/precuneus. No group differences were foundin DMN connectivity (Figure 3).
3.3. Correlation of clinical and RS fMRI data
Post-hoc, fMRI data were correlated with FQ scores usingSPSS 17.0 (SPSS Inc., Chicago, Illinois, USA). If data did notmeet the assumptions required to perform parametricanalysis, and log-transforming did not resolve this problem,the appropriate non-parametric test was performed. The FQcontains a social phobia subscale that specifically focuses onfeared situations that are associated with SAD. We created amask of the resulting areas from our right amygdala analysis(the left middle temporal gyrus, left supramarginal gyrusand left lateral occipital cortex), and calculated theindividual z-scores from these areas using Featquery, partof FSL (Smith et al., 2004). Using non-parametric correla-tional analysis, we examined whether the strength of thefunctional connections was related to anxiety scores asmeasured with social phobia sub-scores on the FQ in the SADgroup. We followed the same approach for the resultingareas showing aberrant connectivity in our bilateral dACCanalysis (i.e., the left precuneus and lateral occipitalcortex). No association was found between strength of thefunctional connectivity and anxiety scores in any of theidentified regions.
Table 2 MNI coordinates of the seed regions.
Seed region MNI coordinates
x y z
Amygdala 722 "6 "16dACC 76 18 28PCC/precuneus 72 "52 26
MNI=Montreal Neurological Institute; dACC=dorsal anteriorcingulate cortex; PCC=posterior cingulate cortex.
Resting-state functional connectivity abnormalities in limbic and salience networks 189

4. Discussion
We investigated RSFC in drug-naive SAD patients withoutcomorbidity and pair-wise matched healthy controls, usingseed regions in the amygdala, the dACC and the PCC/precuneus. As expected, we found abnormalities in SAD inRS connectivity for the amygdala seeds and the seeds in thesalience network, but we found no differences in connec-tivity between patients and controls for the PCC/precuneusseeds probing the DMN. Specifically, in SAD we found alteredRS connectivity between the right amygdala and the leftmiddle temporal gyrus, left supramarginal gyrus, and leftlateral occipital cortex. Increased connectivity between thebilateral dACC seeds (salience network) with both the leftprecuneus and left lateral occipital cortex was also found.
Our results are generally in agreement with previousfindings of altered amygdala and anterior cingulate func-tional connectivity in SAD patients (Freitas-Ferrari et al.,2010; Liao et al., 2010b); however, our findings are notidentical to the abnormalities in connectivity patterns foundin other RS studies. Our results show some overlap with aprevious study in finding involvement of the supramarginalgyrus (Liao et al., 2010a) and middle temporal gyrus (Liaoet al., 2011), although these abnormalities concerneddifferent networks. Whereas a previous functional MRI study(Gentili et al., 2009) and a RS study (Liao et al., 2011) inSAD have reported abnormalities in the DMN, we did not.These discrepancies could be explained by the differentanalysis method used (i.e., model-free analysis versus seed-based region-of-interest) and/or the drug-naive cohort
Table 3 Right amygdala resting-state connectivity: group difference.
MNIa coordinates Side z-value p-value Brain region
x y z Cluster size: 536 voxels
"66 "44 4 L 3.78675 0.0002 Middle temporal gyrus, BAb 22"56 "54 2 L 3.55479 0.0004 Middle temporal gyrus"56 "68 0 L 3.50324 0.0005 Lateral occipital cortex, BA 19"56 "48 8 L 3.42287 0.0006 Middle temporal gyrus"62 "48 10 L 3.39525 0.0007 Supramarginal gyrus, BA 21"66 "46 14 L 3.32415 0.0009 Supramarginal gyrus
aMNI=Montreal Neurologic Institute, coordinates of most significant voxels in cluster.bBA=Brodmann area; voxel size 2 mm isotropic; z- and p-values of most significant voxel, cluster corrected.
Figure 1 Right amygdala negative connectivity. A=healthy controls; B=social anxiety disorder patients; C=group difference B4A.Results are cluster corrected at po.05. Images are z-statistics, overlaid on the MNI-152 standard brain.
J.N. Pannekoek et al.190
without comorbidity that we used in the current study.Additionally, our relatively small sample size may be ofinfluence, although lowering the threshold showed nosignificant group differences between social anxietypatients and healthy controls in DMN connectivity.
Another, admittedly speculative, explanation for thediscrepancy in findings between our study and previousresearch is the difference in cultural backgrounds of thesamples that were studied. As mentioned before, four of thefive RSFC studies in SAD published to date used overlappingsamples of subjects with an Asian cultural background.Several studies have compared the influence of culturalbackgrounds in SAD and have found similarities as well asimportant differences in the phenomenology of socialanxiety across Asian and Western cultures (Furmark, 2002;
Rapee et al., 2011; Stein and Matsunaga, 2001). WhereAsian societies attribute a greater importance to concernsabout offending others, the emphasis seems to be onembarrassing oneself in Western communities (Stein andMatsunaga, 2001).
We first analyzed amygdala RSFC, using seeds in thebilateral amygdala. We found increased RSFC between theright amygdala, an area involved in fear and emotionprocessing, fear in particular (LeDoux, 2003), and the leftmiddle temporal gyrus, left supramarginal gyrus, and leftlateral occipital cortex, areas that have been linked tofacial perception (Grill-Spector et al., 2004; Puce et al.,1995). Abnormal amygdala responses evoked by emotionalfaces have frequently been reported in SAD (Blair et al.,2008b; Blair et al., 2011; Freitas-Ferrari et al., 2010; Shin
Figure 2 Bilateral dorsal anterior cingulate cortex positive connectivity. A=healthy controls; B=social anxiety disorder patients;C=group difference B4A. Results are cluster corrected at po.05. Images are z-statistics, overlaid on the MNI-152 standard brain.
Table 4 Bilateral dorsal anterior cingulate cortex resting-state connectivity: group difference.
MNIa coordinates Side z-value p-value Brain region
x y z Cluster size: 410 voxels
"16 "72 40 L 3.64896 0.0003 Precuneus"16 "64 32 L 3.34503 0.0008 Precuneus"22 "84 40 L 3.28251 0.0010 Lateral occipital cortex"26 "68 20 L 3.1207 0.0018 Lateral occipital cortex"8 "88 40 L 3.0777 0.0021 Lateral occipital cortex"12 "74 50 L 2.94138 0.0033 Lateral occipital cortex
aMNI=Montreal Neurologic Institute, coordinates of most significant voxels in cluster; voxel size 2 mm isotropic; z- and p-values ofmost significant voxel, cluster corrected.
Resting-state functional connectivity abnormalities in limbic and salience networks 191

and Liberzon, 2010). The heightened RSFC of the amygdalain social anxiety patients may reflect an increased predis-position for the inaccurate interpretation of others’ facialexpressions.
We subsequently investigated bilateral dACC connectiv-ity, probing the salience network. The salience network,comprising the bilateral dACC and bilateral anterior insula,is purportedly involved in identifying the most relevantinternal and external stimuli, in order to guide behavior(Seeley et al., 2007). We found increased positive dACCseed connectivity in SAD patients with the left precuneusand left lateral occipital cortex. The anterior cingulate, oneof the structures of the salience network has, apart from itsrole in the salience network, also been associated with self-focused attention (Lemogne et al., 2010). The precuneus isthought to play a central role in self-reflection and self-processing features, like mental imagery and episodic/autobiographic memory retrieval (Cavanna, 2007; Cavannaand Trimble, 2006). Another proposed function of theprecuneus is the gathering of information on and represen-tation of the self and the external world (Cavanna, 2007).Strong self-focus has been previously reported in depres-sion, generalized anxiety disorder and SAD, specificallyattributing a role to public self-focus in the latter(Lemogne et al., 2010). The heightened connectivitybetween the bilateral dACC and the precuneus found inour study could underlie this raised awareness of the selfand the environment, in particular of other people. More-over, since the salience network is thought to be essential inidentifying the relevance of stimuli, a stronger connectivitybetween the dACC and the precuneus could reflect thetendency of social anxiety patients to attribute an exag-gerated significance to possible self-relevant stimuli fromthe external world (Blair et al., 2008a).
We observed that the strength of the RS functionalconnectivity was not related to anxiety scores as measuredwith the social phobia sub-scores of the FQ. Previous reportsdid show associations between abnormalities in connectivityand alterations in anxiety scores, as measured with the
Liebowitz Social Anxiety Scale (Ding et al., 2011; Liao et al.,2010a; Liao et al., 2010b; Liao et al., 2011) and with theSpielberger State and Trait Anxiety Scores (Hahn et al.,2011). Possibly, we did not find correlations due to metho-dological issues such as the characteristics of our sample,the sample size, or the use of the FQ social phobia sub-scores.
Overall, our results are in line with existing models ofSAD. Stein (1998) reviewed several animal and humanmodels of SAD and concluded that the neural circuitries ofanxiety and self-consciousness were likely to be involved inthe pathophysiology the disorder (Stein, 1998). Negativeself-appraisal had been linked to SAD before in two modelssuggesting an abnormal tendency of SAD patients to retro-spectively ruminate and to appraise themselves in a nega-tive manner (Clark and Wells, 1995; Rapee and Heimberg,1997). More recently, the role of circuitry underlying self-referential processing has also been emphasized by Blairet al. (2008a), who found that SAD patients show amygdalaand dorsal medial prefrontal cortex hyperresponsiveness tonegative, self-referential comments (Blair et al., 2008a).This heightened propensity to focus on the self couldpossibly also be represented in the increased RSFC thatwe found between the bilateral dACC and the left pre-cuneus. Clearly, the interpretation of abnormalities in RSFCis more speculative and should be done with caution, as therelation between abnormalities in RFSC and abnormalities intask related functional connectivity in SAD has not beendirectly studied yet.
Our study has several strengths. This is the first studyinvestigating RS functional connectivity in a group of drug-naive social anxiety patients without psychiatric comorbid-ity. There are also some noteworthy limitations to our study.Our sample size is relatively small and replication in other,larger samples is desirable in order to enable more con-clusive interpretation. It should also be noted that subjectsmay engage in different forms of cognitive action during theresting-state condition, which can influence resting-stateactivity patterns. We emphasize that RSFC data should be
Figure 3 Default mode network connectivity. A=healthy controls; B=social anxiety disorder patients. Results are cluster correctedat po.05. Images are z-statistics, overlaid on the MNI-152 standard brain.
J.N. Pannekoek et al.192

interpreted cautiously, and stress that any interpretationrefers only to functional connectivity between brain areasas opposed to the (dys)function of a distinct brain region.Also, by opting for a hypothesis-driven approach and thusonly exploring specific networks, abnormalities in othernetworks might have been missed. On the other hand, theuse of a seed-based region-of-interest approach allowseasier replication of our findings. Another limitation of thecurrent study was the possible influence of between-groupdifferences in heart rate variability and breathing on theresults. Since physiological activity was not monitored inthe current study, it remains unclear if any differencebetween the two groups has influenced the results, althoughprevious research shows that heart rate variability did notdiffer between anxiety patients and healthy controls in thelarger NESDA sample (Licht et al., 2009). Additionally,regressing out global signal changes has shown to at leastpartly filter out the effects of cardiac and respiratoryfluctuations (Birn et al., 2006; Fox and Raichle, 2007).Pooling data from different centers is another possiblelimitation. To account for this as much as possible, we havematched our groups based on scanning site and also added aconfound regressor for site in our statistical model. Afurther limitation is the absence of a specific questionnairefor the assessment of social anxiety. Use of a specific socialanxiety scale instead of the more generalized Fear Ques-tionnaire might prove to be more sensitive to identify anassociation between altered functional connectivity andextent of SAD symptoms. Finally, our RS fMRI data wereacquired at the end of a fixed imaging protocol, including afacial expression task, which could potentially have influ-enced RS connectivity (i.e., a spillover effect) with SADpatients still showing aberrant connectivity in areasinvolved in the processing of emotional faces while thefacial stimulus was no longer present.
In summary, we found altered RS connectivity in drug-naive SAD patients without comorbidity, between areasinvolved in the processing of fear and emotion and areasthat contribute to facial perception. Additionally, we foundaberrant connectivity between a key region of the saliencenetwork and areas involved in the processing of self-relevant stimuli, which has become a recent focus ofresearch in SAD.
Role of the funding source
The infrastructure for the NESDA study is funded through theGeestkracht programme of the Netherlands Organization for HealthResearch and Development (ZonMw, grant number 10-000-1002) andis supported by participating universities and mental health careorganizations (VU University Medical Center, GGZ inGeest, Arkin,Leiden University Medical Center, GGZ Rivierduinen, UniversityMedical Center Groningen, Lentis, GGZ Friesland, GGZ Drenthe,IQ Healthcare, Netherlands Institute for Health Services Research(NIVEL) and Netherlands Institute of Mental Health and Addiction(Trimbos Institute). Part of this research was supported by a VIDIgrant from the Netherlands Organization for Scientific Research(NWO) to S.A.R.B. Rombouts. Part of this research was alsosupported through the Netherlands Organization for ScientificResearch—National Initiative Brain and Cognition (NWO-NIHC,project number 056-25-010).
Contributors
Nic van der Wee, Dick Veltman, Andr !e Aleman and Frans Zitmancontributed to the design of the NESDA study. Marie-Jos!e van Toland Liliana R. Demenescu contributed to the data acquisition.J. Nienke Pannekoek managed the literature searches and analyses.J. Nienke Pannekoek undertook the statistical analysis, withassistance from Ilya Veer, Serge Rombouts and Steven van derWerff. J. Nienke Pannekoek wrote the first draft of the manuscript.All authors contributed to and have approved the final manuscript.
Conflict of interest
None.
Appendix A. Supporting information
Supplementary data associated with this article can befound in the online version at http://dx.doi.org/10.1016/j.euroneuro.2012.04.018.
References
American Psychiatric Association, 1994. Diagnostic and StatisticalManual of Mental Disorders, 4th ed. (DSM-IV). American Psy-chiatric Association, Washington DC.
Amir, N., Klumpp, H., Elias, J., Bedwell, J.S., Yanasak, N., Miller,L.S., 2005. Increased activation of the anterior cingulate cortexduring processing of disgust faces in individuals with socialphobia. Biol. Psychiatry 57, 975–981.
Birn, R.M., Diamond, J.B., Smith, M.A., Bandettini, P.A., 2006.Separating respiratory-variation-related fluctuations from neu-ronal-activity-related fluctuations in fMRI. Neuroimage 31,1536–1548.
Biswal, B.B., Mennes, M., Zuo, X.N., Gohel, S., Kelly, C., Smith,S.M., Beckmann, C.F., Adelstein, J.S., Buckner, R.L., Colcombe,S., Dogonowski, A.M., Ernst, M., Fair, D., Hampson, M., Hopt-man, M.J., Hyde, J.S., Kiviniemi, V.J., Kotter, R., Li, S.J., Lin,C.P., Lowe, M.J., Mackay, C., Madden, D.J., Madsen, K.H.,Margulies, D.S., Mayberg, H.S., McMahon, K., Monk, C.S.,Mostofsky, S.H., Nagel, B.J., Pekar, J.J., Peltier, S.J., Petersen,S.E., Riedl, V., Rombouts, S.A., Rypma, B., Schlaggar, B.L.,Schmidt, S., Seidler, R.D., Siegle, G.J., Sorg, C., Teng, G.J.,Veijola, J., Villringer, A., Walter, M., Wang, L., Weng, X.C.,Whitfield-Gabrieli, S., Williamson, P., Windischberger, C., Zang,Y.F., Zhang, H.Y., Castellanos, F.X., Milham, M.P., 2010. Towarddiscovery science of human brain function. Proc. Nat. Acad. Sci.U.S.A. 107, 4734–4739.
Blair, K., Geraci, M., Devido, J., McCaffrey, D., Chen, G., Vythi-lingam, M., Ng, P., Hollon, N., Jones, M., Blair, R.J., Pine, D.S.,2008a. Neural response to self- and other referential praise andcriticism in generalized social phobia. Arch. Gen. Psychiatry 65,1176–1184.
Blair, K., Shaywitz, J., Smith, B.W., Rhodes, R., Geraci, M., Jones,M., McCaffrey, D., Vythilingam, M., Finger, E., Mondillo, K.,Jacobs, M., Charney, D.S., Blair, R.J., Drevets, W.C., Pine, D.S.,2008b. Response to emotional expressions in generalized socialphobia and generalized anxiety disorder: evidence for separatedisorders. Am. J. Psychiatry 165, 1193–1202.
Blair, K.S., Geraci, M., Korelitz, K., Otero, M., Towbin, K., Ernst,M., Leibenluft, E., Blair, R.J., Pine, D.S., 2011. The pathology ofsocial phobia is independent of developmental changes in faceprocessing. Am. J. Psychiatry.
Resting-state functional connectivity abnormalities in limbic and salience networks 193

Broyd, S.J., Demanuele, C., Debener, S., Helps, S.K., James, C.J.,Sonuga-Barke, E.J., 2009. Default-mode brain dysfunction inmental disorders: a systematic review. Neurosci. Biobehav. Rev.33, 279–296.
Cavanna, A.E., 2007. The precuneus and consciousness. CNS Spectr.12, 545–552.
Cavanna, A.E., Trimble, M.R., 2006. The precuneus: a review of itsfunctional anatomy and behavioural correlates. Brain 129,564–583.
Clark, D.M., Wells, A., 1995. A cognitive model of social phobia. In:Heimberg, R.G., Liebowitz, M.R., Hope, D.A., Schneier, F.R.(Eds.), Social Phobia: Diagnosis, Assessment, and Treatment.The Guilford Press, New York, pp. 69–96.
Damsa, C., Kosel, M., Moussally, J., 2009. Current status of brainimaging in anxiety disorders. Curr. Opin. Psychiatry 22, 96–110.
Ding, J., Chen, H., Qiu, C., Liao, W., Warwick, J.M., Duan, X.,Zhang, W., Gong, Q., 2011. Disrupted functional connectivity insocial anxiety disorder: a resting-state fMRI study. Magn. Reson.Imaging 29, 701–711.
Etkin, A., Prater, K.E., Hoeft, F., Menon, V., Schatzberg, A.F., 2010.Failure of anterior cingulate activation and connectivity withthe amygdala during implicit regulation of emotional processingin generalized anxiety disorder. Am. J. Psychiatry.
Etkin, A., Prater, K.E., Schatzberg, A.F., Menon, V., Greicius, M.D.,2009. Disrupted amygdalar subregion functional connectivityand evidence of a compensatory network in generalized anxietydisorder. Arch. Gen. Psychiatry 66, 1361–1372.
Etkin, A., Wager, T.D., 2007. Functional neuroimaging of anxiety: ameta-analysis of emotional processing in PTSD, social anxietydisorder, and specific phobia. Am. J. Psychiatry 164, 1476–1488.
Fox, M.D., Raichle, M.E., 2007. Spontaneous fluctuations in brainactivity observed with functional magnetic resonance imaging.Nat. Rev. Neurosci. 8, 700–711.
Freitas-Ferrari, M.C., Hallak, J.E., Trzesniak, C., Filho, A.S.,Machado-de-Sousa, J.P., Chagas, M.H., Nardi, A.E., Crippa,J.A., 2010. Neuroimaging in social anxiety disorder: a systematicreview of the literature. Prog. Neuropsychopharmacol. Biol.Psychiatry 34, 565–580.
Furmark, T., 2002. Social phobia: overview of community surveys.Acta Psychiatry Scand. 105, 84–93.
Furmark, T., Appel, L., Michelgard, A., Wahlstedt, K., Ahs, F.,Zancan, S., Jacobsson, E., Flyckt, K., Grohp, M., Bergstrom, M.,Pich, E.M., Nilsson, L.G., Bani, M., Langstrom, B., Fredrikson,M., 2005. Cerebral blood flow changes after treatment of socialphobia with the neurokinin-1 antagonist GR205171, citalopram,or placebo. Biol. Psychiatry 58, 132–142.
Gentili, C., Ricciardi, E., Gobbini, M.I., Santarelli, M.F., Haxby, J.V.,Pietrini, P., Guazzelli, M., 2009. Beyond amygdala: default modenetwork activity differs between patients with social phobia andhealthy controls. Brain Res. Bull. 79, 409–413.
Greicius, M.D., Flores, B.H., Menon, V., Glover, G.H., Solvason,H.B., Kenna, H., Reiss, A.L., Schatzberg, A.F., 2007. Resting-state functional connectivity in major depression: abnormallyincreased contributions from subgenual cingulate cortex andthalamus. Biol. Psychiatry 62, 429–437.
Greicius, M.D., Krasnow, B., Reiss, A.L., Menon, V., 2003. Functionalconnectivity in the resting brain: a network analysis of thedefault mode hypothesis. Proc. Nat. Acad. Sci. U.S.A. 100,253–258.
Grill-Spector, K., Knouf, N., Kanwisher, N., 2004. The fusiform facearea subserves face perception, not generic within-categoryidentification. Nat. Neurosci. 7, 555–562.
Hahn, A., Stein, P., Windischberger, C., Weissenbacher, A., Spinde-legger, C., Moser, E., Kasper, S., Lanzenberger, R., 2011.Reduced resting-state functional connectivity between amyg-dala and orbitofrontal cortex in social anxiety disorder.Neuroimage.
Irle, E., Ruhleder, M., Lange, C., Seidler-Brandler, U., Salzer, S.,Dechent, P., Weniger, G., Leibing, E., Leichsenring, F., 2010.Reduced amygdalar and hippocampal size in adults with general-ized social phobia. J. Psychiatry Neurosci. 35, 126–131.
Kent, J.M., Rauch, S.L., 2003. Neurocircuitry of anxiety disorders.Curr. Psychiatry Rep. 5, 266–273.
LeDoux, J., 2003. The emotional brain, fear, and the amygdala. CellMol. Neurobiol. 23, 727–738.
Lemogne, C., Delaveau, P., Freton, M., Guionnet, S., Fossati, P.,2010. Medial prefrontal cortex and the self in major depression.J. Affect. Disorders.
Liao, W., Chen, H., Feng, Y., Mantini, D., Gentili, C., Pan, Z., Ding,J., Duan, X., Qiu, C., Lui, S., Gong, Q., Zhang, W., 2010a.Selective aberrant functional connectivity of resting state net-works in social anxiety disorder. Neuroimage 52, 1549–1558.
Liao, W., Qiu, C., Gentili, C., Walter, M., Pan, Z., Ding, J., Zhang,W., Gong, Q., Chen, H., 2010b. Altered effective connectivitynetwork of the amygdala in social anxiety disorder: a resting-state FMRI study. PLoS One 5, e15238.
Liao, W., Xu, Q., Mantini, D., Ding, J., Machado-de-Sousa, J.P.,Hallak, J.E., Trzesniak, C., Qiu, C., Zeng, L., Zhang, W., Crippa,J.A., Gong, Q., Chen, H., 2011. Altered gray matter morpho-metry and resting-state functional and structural connectivity insocial anxiety disorder. Brain Res..
Licht, C.M., de Geus, E.J., Van, D.R., Penninx, B.W., 2009.Association between anxiety disorders and heart rate variabilityin The Netherlands Study of Depression and Anxiety (NESDA).Psychosom. Med. 71, 508–518.
Margulies, D.S., Kelly, A.M., Uddin, L.Q., Biswal, B.B., Castellanos,F.X., Milham, M.P., 2007. Mapping the functional connectivity ofanterior cingulate cortex. Neuroimage 37, 579–588.
Marks, I.M., Mathews, A.M., 1979. Brief standard self-rating forphobic patients. Behav. Res. Ther. 17, 263–267.
Montgomery, S.A., Asberg, M., 1979. A new depression scaledesigned to be sensitive to change. Br. J. Psychiatry 134,382–389.
Oakes, T.R., Fox, A.S., Johnstone, T., Chung, M.K., Kalin, N.,Davidson, R.J., 2007. Integrating VBM into the general linearmodel with voxelwise anatomical covariates. Neuroimage 34,500–508.
Penninx, B.W., Beekman, A.T., Smit, J.H., Zitman, F.G., Nolen, W.A.,Spinhoven, P., Cuijpers, P., De Jong, P.J., Van Marwijk, H.W.,Assendelft, W.J., Van Der Meer, K., Verhaak, P., Wensing, M., De,G.R., Hoogendijk, W.J., Ormel, J., Van, D.R., 2008. The Nether-lands Study of Depression and Anxiety (NESDA): rationale, objec-tives and methods. Int. J. Methods Psychiatry Res. 17, 121–140.
Potts, N.L., Davidson, J.R., Krishnan, K.R., Doraiswamy, P.M., 1994.Magnetic resonance imaging in social phobia. Psychiatry Res. 52,35–42.
Puce, A., Allison, T., Gore, J.C., McCarthy, G., 1995. Face-sensitiveregions in human extrastriate cortex studied by functional MRI.J. Neurophysiol. 74, 1192–1199.
Raichle, M.E., MacLeod, A.M., Snyder, A.Z., Powers, W.J., Gusnard,D.A., Shulman, G.L., 2001. A default mode of brain function.Proc. Nat. Acad. Sci. U.S.A. 98, 676–682.
Rapee, R.M., Heimberg, R.G., 1997. A cognitive-behavioral modelof anxiety in social phobia. Behav. Res. Ther. 35, 741–756.
Rapee, R.M., Kim, J., Wang, J., Liu, X., Hofmann, S.G., Chen, J., Oh,K.Y., Bogels, S.M., Arman, S., Heinrichs, N., Alden, L.E., 2011.Perceived impact of socially anxious behaviors on individuals’ livesin Western and East asian countries. Behav. Ther. 42, 485–492.
Roy, A.K., Shehzad, Z., Margulies, D.S., Kelly, A.M., Uddin, L.Q.,Gotimer, K., Biswal, B.B., Castellanos, F.X., Milham, M.P., 2009.Functional connectivity of the human amygdala using restingstate fMRI. Neuroimage 45, 614–626.
Seeley, W.W., Menon, V., Schatzberg, A.F., Keller, J., Glover, G.H.,Kenna, H., Reiss, A.L., Greicius, M.D., 2007. Dissociable intrinsic
J.N. Pannekoek et al.194

connectivity networks for salience processing and executive
control. J. Neurosci. 27, 2349–2356.Shah, S.G., Klumpp, H., Angstadt, M., Nathan, P.J., Phan, K.L.,
2009. Amygdala and insula response to emotional images in
patients with generalized social anxiety disorder. J. Psychiatry
Neurosci. 34, 296–302.Shin, L.M., Liberzon, I., 2010. The neurocircuitry of fear, stress, and
anxiety disorders. Neuropsychopharmacology 35, 169–191.Smith, S.M., Jenkinson, M., Woolrich, M.W., Beckmann, C.F.,
Behrens, T.E., Johansen-Berg, H., Bannister, P.R., De, L.M.,
Drobnjak, I., Flitney, D.E., Niazy, R.K., Saunders, J., Vickers,
J., Zhang, Y., De, S.N., Brady, J.M., Matthews, P.M., 2004.
Advances in functional and structural MR image analysis and
implementation as FSL. Neuroimage 23 (Suppl 1), S208–S219.Stein, M.B., 1998. Neurobiological perspectives on social phobia:
from affiliation to zoology. Biol. Psychiatry 44, 1277–1285.Stein, D.J., Matsunaga, H., 2001. Cross-cultural aspects of social
anxiety disorder. Psychiatry Clin. North Am. 24, 773–782.Stein, J.L., Wiedholz, L.M., Bassett, D.S., Weinberger, D.R., Zink,
C.F., Mattay, V.S., Meyer-Lindenberg, A., 2007. A validated
network of effective amygdala connectivity. Neuroimage 36,736–745.
Van der Linden, G., van, H.B., Warwick, J., Wessels, C., van, K.J.,Zungu-Dirwayi, N., Stein, D.J., 2000. Functional brain imagingand pharmacotherapy in social phobia: single photon emissioncomputed tomography before and after treatment with theselective serotonin reuptake inhibitor citalopram. Prog. Neurop-sychopharmacol. Biol. Psychiatry 24, 419–438.
van Tol, M.J., van der Wee, N.J., van den Heuvel, O.A., Nielen,M.M., Demenescu, L.R., Aleman, A., Renken, R., Van Buchem,M.A., Zitman, F.G., Veltman, D.J., 2010. Regional brain volumein depression and anxiety disorders. Arch. Gen. Psychiatry 67,1002–1011.
Veer, I.M., Oei, N.Y., Spinhoven, P., van Buchem, M.A., Elzinga,B.M., Rombouts, S.A., 2011. Beyond acute social stress:increased functional connectivity between amygdala and corti-cal midline structures. Neuroimage 57, 1534–1541.
Worsley, K.J., 2001. Statistical analysis of activation images. In:Jezzard, P., Matthews, P.M., Smith, S.M. (Eds.), Functional MRI:An Introduction to Methods. Oxford University Press Inc.,New York, pp. 251–270.
Resting-state functional connectivity abnormalities in limbic and salience networks 195




















