Towards people's experiences and behaviours within their ...
Upload
khangminh22Category
view
1download
0
1|P a g e
RAPID ASSESMENT ON YOUNG PEOPLE’S EXPERIENCES, CHALLENGES AND BEST PRACTICES ON DEMAND, ACCESS AND UTILIZATION OF YOUTH
FRIENDLY CONTRACEPTIVE SERVICES IN MBALE DISTRICT “I’m going to divulge my health problems, my everything, my what and what. I need a health worker I can trust to keep my issues. One who will not Judge me straight away” an adolescent
FGD participant in Mbale
May; 2020

2|P a g e
Acknowledgements The UYAHF gratefully acknowledges the valuable contribution of many individuals whose time, expertise and ideas made this research a success. Gratitude is extended to the Research Team Lead by Apio Winnie that consisted of Dabrine Kagalula, Sedrik Majakira, Kisakye Patricia and Nakato Joyce supported by a core team of research assistants, respondents; under the overall guidance of Mwesigye Patrick; the Key Informants for their valuable support and time to the research process. Lastly, UYAHF would like to acknowledge the invaluable input of the study report reviewer/consultant Patrick Ojulong for his insightful comments to the draft report.
Table of Contents Acronyms or Abbreviations.........................................................................................................................3Executive Summary.....................................................................................................................................41.0 Introduction...........................................................................................................................................71.2 Background............................................................................................................................................8
1.2.1 Purpose of the assessment..............................................................................................................9
1.2.2 Objectives.......................................................................................................................................9
1.2.3 Specific Objectives..........................................................................................................................9
2.0 Chapter Two: Methodology...................................................................................................................92.1 Assessment Approach........................................................................................................................9
2.2 Assessment sites.................................................................................................................................9
2.3 Sampling Method............................................................................................................................10
2.4 Data Collection Tools.......................................................................................................................10
2.5 Data Management and Analysis......................................................................................................10
2.6 Fieldwork Approach:.......................................................................................................................10
3.0 Chapter Three: Key Findings and Discussions....................................................................................113.1 Quality of care assessment indicators.............................................................................................11
3.2 Discussions on overall findings.......................................................................................................16
3.2.1 Health facility characteristic....................................................................................................16
3.2.2 Provider Characteristics...........................................................................................................17
3.2.3 Program Characteristics...........................................................................................................18
3.2.4 Adolescents SRH experiences in community............................................................................19
3.3 Service uptake for adolescent health...............................................................................................21
3.3.1 Family planning usage..............................................................................................................21

3|P a g e
3.3.1 Post Abortion Care Services recorded in Mbale.......................................................................22
4.0 Chapter Four: Conclusion, Challenges, recommendations and Lessons.............................................234.1 Conclusion.......................................................................................................................................23
4.2 Challenges........................................................................................................................................23
4.3 Recommendations............................................................................................................................24
4.4 Lessons.............................................................................................................................................25
Acronyms or Abbreviations CSOs Civil Society Organizations DHO District Health Office FDGs Focus Group Discussions HC Health Centre HSDP Health Sector Development Plan MoH Ministry of Health NGO Non-Governmental Organizations PWDs People with Disabilities RMNCAH Reproductive Maternal New born Child and Adolescent Health SDGs Sustainable Development Goals SRHR Sexual Reproductive Health and Rights STIs Sexually transmitted Infections STDs Sexually Transmitted Diseases UBOS Uganda Bureau of Statistics UDHS Uganda Demographic Household Survey YFS Youth Friendly Services

4|P a g e
Young girls in Mbale district advocating for their right to access safe contraceptives.
Executive Summary Adolescent health remains a worrying concern for Uganda and there is evident slow progress in most adolescent health related indicators performance. Uganda currently has a youthful population with 55% under 18 years of age (UBOs, 2016). Teenage pregnancy rates are at 25% up from 24.5% in 2011 (2016 UDHS) far from HSDP target of 14%. Uneducated girls account for 35% teenage pregnancies compared to 17% of girls with secondary education (UBOS 2016). HIV prevalence for adolescent girls 15-19 years is 3% versus 1.7% among men of same age, rises to 7.1% by age of 24 years with about 570 young women (15-24 years) getting infected with HIV each week (MoH 2011). Adolescents aged 15-19 contribute 17.6% maternal deaths due to pregnancy related conditions (AHSR 2016) and Uganda continues to

5|P a g e
have one of Africa’s highest unmet need for family planning among adolescents aged 15-19 years at 30.4% with total demand currently standing at 52.3% (UDHS, 2016).However, the last country assessment noted that oonly 5% of public health facilities provided what would qualify as youth friendly services in Uganda despite the policy provisions and SRHR service guidelines and standards. Promoting and protecting adolescents’ health is therefore critical to achieving the human development agenda, the Sustainable Development Goals (SDGs) and the Global Strategy for Women’s, Children’s and Adolescents’ Health. Uganda’s Ministry of Health (MoH) commits to ensuring that Adolescents and young people are given the information and services they need to remain healthy at all levels or care. It is upon this background that UYAHF conducted an assessment of Adolescent health friendly services in selected 09 health facilities in Mbale district. The assessment was carried out between January - February 2020 with a purpose of establishing the extent to which health facilities adhere and meet the national adolescent health service standards and guidelines. This report therefore provides a synoptic analysis of the findings in health facilities in Mbale district.
Key Assessment Findings
• Little focus on adolescent health at service delivery points for they are treated like the general population yet adolescents have peculiar health needs that require a significant special approach to their care at health facilities
• Although some of the adolescent health related information is collected routinely through the HIMS and DHIS, there is less evidence of utilization of the data to effectively plan interventions that are responsive to adolescents’ health needs.
• In some health facilities, efforts have been instituted to have peer educators and counselors though not fully institutionalized and poorly facilitated and as a result, don’t provide consistent services at the health facility.
• Even where adolescent health guidelines and standards exist, there is lack of implementation of the guidelines and documents are not sufficiently disseminated and implemented at district and health facility levels.
• Appropriate resources have also not been made available to support effective implementation of national adolescent health service standards and guidelines at health facilities neither are existing resources provided through PHC and RBF providing a clear set of targets for adolescents or support for delivery of adolescent health friendly focused services.
• There are no budgets specific to adolescent health at the district and facility levels and where there are at health facilities, they are largely partner supported through off budget support. Many of the health facilities with youth friendly corners or adolescent health clinics/days, they depend on partners to fund setting up adolescent friendly health services.
Gaps • Insufficient numbers of trained staff in provision of adolescent /youth friendly SRH
services. This study found a big gap in training of Health workers in Adolescent Health friendly service provision with less than 20% health workers in the sampled health facilities reporting being trained in adolescent care.
• There was very low utilization of Family Planning (FP) services among adolescents which is attributed to persistent social myths, lack of accurate information on family planning targeting adolescents.

6|P a g e
• Stock out of key SRH commodities in health facilities and often discourages utilization of services among adolescents if each time they come and find them out of stock.
• The greatest barrier to access to services among adolescents and young people is stigma and discrimination that is re-enforced by social norms and cultural practices especially on family planning access to adolescents and young people.
• Other barriers at health facilities according to FGD participants and key informants include long waiting time at service points sometimes resulting from large numbers served. Adolescents often fear mixing in crowded waiting areas with adults especially in absence of specific adolescent health corners in health facilities
• Lower level health facilities particularly health centre IIs exhibited low levels of partner support and mentorship from high level health centre IIIs on provision of adolescent health services and as such though closer to communities – low utilisation of adolescent health services is evident at health centre IIs.
Recommendations • There is need for in-service training of Health Workers in adolescent health since
adolescents have not been perceived as a special group with specific needs by many service providers.
• Integration of adolescent services with SRH and ensuring revitalisation and intensification of School Health outreaches and programmes and community-based programmes that are focussed on adolescents and young people.
• Extra support and mentorship is needed for rural and lower level health facilities so that they enrol more adolescents. There is a need to lobby partners to support lower health facilities and rural ones
• District and health facility managers should plan, budget and equip health facilities with adolescent health corners and commodities to enhance SRH services for adolescents.
• There should be more deliberate training of all health workers and non-health staff at the health centres to ensure that they adopt adolescent and youth responsiveness in their approaches.

7|P a g e
1.0 Introduction Adolescence isoften described as not only a time of opportunity, but also one of risk. It presents a window of opportunity because actions could be taken during this period to set the stage for healthy adulthood and to reduce the likelihood of problems in the years that lie ahead. Over the past decade, there has been a global and national resurgence on adolescent health and young people’s well-being. Many countries have attempted to build health systems that take into consideration the unique needs of adolescents and young people through both policy and programmatic reforms. Uganda has quite an elaborate policy framework and strategies on adolescent health from the National Policy Guidelines and Service Standards for Sexual and Reproductive Health and Rights (MOH, 2014), the costed family planning implementation plan 2020, the national adolescent health policy and draft SRHR guidelines by ministry of health. These documents define adolescent health as core components of reproductive health package and considers sexuality as a central aspect of being human. They provide for family planning and contraceptive service delivery as a component of reproductive health to adolescents, establishment of youth friendly corners at health facilities and provision of integrated SRHR services to adolescents and young people. Some specifically seek to increase access and uptake to quality, affordable, acceptable and sustainable family planning services to the sexually active – adolescents inclusive. However, having good policies and strategies often does not translate into actual implementation. Statistics on adolescent health remain grim with adolescents expressing difficulty The Youth Engage and Take Action (YHA) project is a project whose overall goal is to mobilize, build capacity and amplify voices of young people in Uganda, Malawi, Zimbabwe, and Kenya to advocate for and demand from policy makers and duty bearers improved access to quality and youth friendly contraceptive services and information as a sexual reproductive right. Young people in Uganda are especially vulnerable to multiple sexual and reproductive health challenges that deter them from realizing their full potential. Among these are; limited access to sexual reproductive health services and information in addition to other social, cultural and economic obstacles that impede and compromise their quality of life, equity and dignity.

8|P a g e
1.2 Background Uganda’s RMNCAH sharpened plan estimates about 28% of maternal deaths in Uganda, 47% of 297,000 unsafe abortions annually as occurring among girls aged 15-24. Currently about 360,000 teenage pregnancies (25%) occur annually far from the health sector development plan (HSDP) target of 14% by 2020. Actually, going by the HSD target, thecurrent average rate of reduction in teenage pregnancies is so slow (about 3% per year)to be able to achieve the 14% reduction by 2020. One in every four girls aged 15 -19 years is already a mother or pregnant with her first child. The annual reduction should have yieldedat least 9.4% per year if the country was to reach the target of 14% set by 2020. Unmet need for family planning among adolescents aged 15-19 years is estimated at 30.4% with total demand of 52.3%.According to Uganda AIDS Commission and UNAIDS, 2 young women are getting infected with HIV in Uganda every hour while prevalence of HIV among adolescent girls stands at 9.1 percent, compared to the national prevalence rate of 7.3 percent. This has been attributed low comprehensive HIV knowledge among young people at 38% for women and 40% for males. A recent study by FAWE in 19 schools (six secondary and 13 primary) in Mbale showed of the 913 teenagers tested, 218 (177 females and 41 males) were found with gonorrhoea,135 females and 56 males had urinary tract infections (UTI) while 207 females had candida1 (FAWE, 2019). Teenage pregnancies in Mbaledistrict increased from 10% to 20% among girls of between 12 and 16 yearsbetween 2018 – 2020 leading to over 45% of the girls dropping out of school in Mbale District in 2018 alone.This points to high ssexual activity among adolescents and young people putting them at risk of HIV re-infection, getting sexually transmitted diseases (STDs), unwanted pregnancies and even infecting others. Despite all this, there is limited access and utilization of antenatal, prenatal and postnatal care among this age group (POPSEC, 2013). UYAHF therefore conducted a rapid assessment of09health centres to ascertain the readiness, quality and availability of adolescent/youth friendly SRH services in Mbale district. This will support UYAHF to generate robust evidence for engagement with duty bearers in Mbale district.
1Retrievedfromhttps://www.monitor.co.ug/News/National/STDs-on-the-rise-among-pupils-in-Mbale---survey/688334-5301612-33oftnz/index.htmlon17thMarch2020.

9|P a g e
1.2.1 Purpose of the assessment To generate evidence on availability, access, quality and uptake of adolescent/ youth friendly services in selected health facilities in Mbale with a view of providing robust evidence based information to strengthen adolescent health friendly services in Mbaledistrict. 1.2.2 Objectives To assess the existence and quality of adolescent/youth friendly health services in selected health centres in Mbale district. 1.2.3 Specific Objectives 1. To assess the availability, access and quality of adolescent/youth friendly health services in
selected health facilities in Mbale district 2. Identify perceived barriers to access to quality adolescent/youth friendly services in
selected health facilities in Mbale district. 3. To advocate for strengthening of adolescent/youth friendly services in selected health
facilities in Busia district.
2.0 Chapter Two: Methodology This chapter describes the study design and approach, sampling method, study sites, methods and tools used to collect and analyze data for this study. 2.1 Assessment Approach The assessment used both qualitative and quantitative methods to collect data on adolescent health in the district and at health facilities using an array of tools. Specifically, the study team reviewed secondary data from health facility HIMS records, DHIS2 data base, administered a structured questionnaire aligned to the WHO health standards for adolescents and the national adolescent health quality of care standards, conducted focussed group discussions at community level with adolescent’s and key informant interviews with key district health personnel drawn from Mbale district. 2.2 Assessment sites The adolescent health assessment was conducted in Mbale district targeting health service providers and adolescents’ feedback in the community.A total of 08 health facilities ranging from the regional referral hospital, health centre IIIs and health centre IIs were reached and assessed with 86 participants interviewed (56F, 30M). Table 1: Health facilities assessed Health Facility Level Of Care Owner Ship
1. Mbale Regional Hospital RR Hospital GoU 2. Nakaloke Health Centre III GoU 3. Namatala Health Centre IV GoU 4. Mbale Epicentre Health Centre II GoU 5. Bufumbo Health Centre II GoU 6. Lwangoli Health Centre III GoU 7. Busiu Health Centre IV GoU 8. Maluku Health centre III GoU 9. Jewa Health Centre II GoU
10|P a g e
2.3 Sampling Method A simple random approach was used to select health facilities for the rapid assessment from existing health facilities in Mbale district. A list of health facilities was developed by category of care together with the district health office department and a random sample selected from each category of health care in Mbale district. 2.4 Data Collection Tools Interview tool Type of data collected Key Informant Interviews (KIIs) 27 KIIs were conducted with health facility in-charges,
senior midwives, records officers, district Biostatistician, to generate information about services,funding and expenditures in health
Focus Group Discussions (FGDs) 2 Focus Group Discussions (FGDs) were conducted with Adolescents between the ages of 10 -19 in the catchment of health facilities.to elicit community based feedback on quality, access and uptake of adolescent health services and also exploring challenges they experience while accessing adolescent health related services in health facilities.
Secondary data reviews An extensive desk review of various adolescent health related documents, HMIS reports, DHIS2 reports was conducted to obtain service delivery outputs for adolescents and used to triangulate with uptake analysis versus the perceived quality.
Structured interviewer administered questionnaire
9 structured interviewer administered interviews were conducted with health facility in-charges to assess the level of access availability and quality of youth friendly services using the national adolescent health service guidelines and service standards policy document 2014.
2.5 Data Management and Analysis For qualitative data, the FGD notes were transcribed and reviewed to aid in development of common themes for discussion in the report while quantitative data was analyzed using excel office windows to develop tally sheets and frequency tables based on individual yes or No matrix responses of health workers in target health facilities. Secondary data analysis focused on identifying quantitative trends in service uptake over time through a review of the HMIS and DHIS2 data for service uptake. 2.6 Fieldwork Approach: - Tools and study protocols were developed by staff and member organizations - Assessment protocol was shared and discussed with the DHO, reviewed and adopted - The scope of the assessment was agreed with the DHO and the role of the district health
office and UYAHF during and after the assessments. - A list of all health facilities by category of care (RRH, HCV, HCIV, III, III) was developed,
geographical distribution of health facilities reviewed and a random selection of facilities was taken by level of care.

11|P a g e
- The respondents were then derived from the list of health facility In-charges, Adolescent health focal persons and Peer Educators at selected health units as key respondents given their role in management and delivery of adolescent health services at the health facility.
- Interviews were then scheduled, task teams deployed and assessments conducted with selected participants
- Debriefing with the DHOs office was then undertaken after assessment and writing of the assessment report commenced.
- Dissemination meeting were then planned for with the district authorities.
3.0 Chapter Three: Key Findings and Discussions 3.1 Quality of care assessment indicators The assessment used a matrix of quality of care for adolescent health related services categorised according to health facility characteristics, provider characteristics and program characteristics. The discussion of the findings of the assessment is in the context of the WHO adolescent health and care standards and the country’s own national adolescent health service guidelines and standards developed by ministry of health of Uganda. Thematic area Indicators characteristics Provider characteristics
1. Availability of trained staff(s) accessible all the time to serve young people,
2. Should be non-judgmental and confidentiality maintained 3. Health facility staff respect young people’s SRHR 4. Adequate time for provider interaction 5. Peer educators and counselors available. 6. Should poses interpersonal skills to provide good provider
client interaction 7. Should be with positive attitudes and keen serve young people
Health facility characteristics
1. Youth friendly services should be integrated in the existing service.
2. Convenient location. 3. Adequate space 4. Promote Participation of Young People in service delivery 5. Comfortable environment to offer both visual and auditory
privacy, gender sensitive clean toilets and hand washing

12|P a g e
facilities. 6. Contains information and education materials on the
following: - Body changes (secondary sexual characteristics) - Personal care and hygiene - Nutrition - Alcohol and substance abuse - RH/STI/HIV/AIDS - Life planning skills
7. Contains posters that are relevant, appealing in size, language and colour to young people.
8. Has case management guidelines 9. Simple data recording system for referrals with anonymous
data analysis. 10. Availability of job aides for service providers 11. Strong referral system (linkages with school, health facility) 12. Presence of education materials like posters, brochures and
pamphlets to give out to young people and where possible radios and TV shows with sexuality education
Program Characteristics
1. Adolescents participation in service delivery – supportive role or assigned a section to help adolescents
2. Adolescents involvement in monitoring SRH services 3. Adolescents being served without consent of parents or
spouses. 4. Availability of a range of RH services 5. Written guidelines for provision of adolescent health services 6. Condoms male and female mix 7. Posters specific for adolescent health issues
Provision of the youth friendly services programme assessment The main barriers identified to the provision of health services to young people reported by healthcare workers and adolescents were the limited number of trained staff in provision of adolescent health friendly services, the lack of a dedicated spaces/corners for young people in most health facilities, lack of prioritisation of adolescent health services in static settings and community outreaches for example school health outreaches aren’t as frequent as other community outreaches and sometimes health workers are not at liberty to discuss some specific topics like family planning during health education talks in schools. Additionally, some health workers do not see the peculiar needs of adolescents as significant and treat them just like as population categories neither were adolescents visible in service provision support either through peer educators or in service monitoring. Many health facilities did not see the necessity of engaging adolescents in service delivery. Health facilities performance Table 2: Malukhu Health Centre III Malukhu HC III Yes No Total Health Facility Characteristics 6 3 9 Provide Characteristics 6 1 7 Program Characteristics 9 0 9

13|P a g e
Table 3: Lwangoli HC III Lwangoli HC III Yes No Total Health Facility Characteristics 6 3 9 Provide Characteristics 2 5 7 Program Characteristics 6 3 9
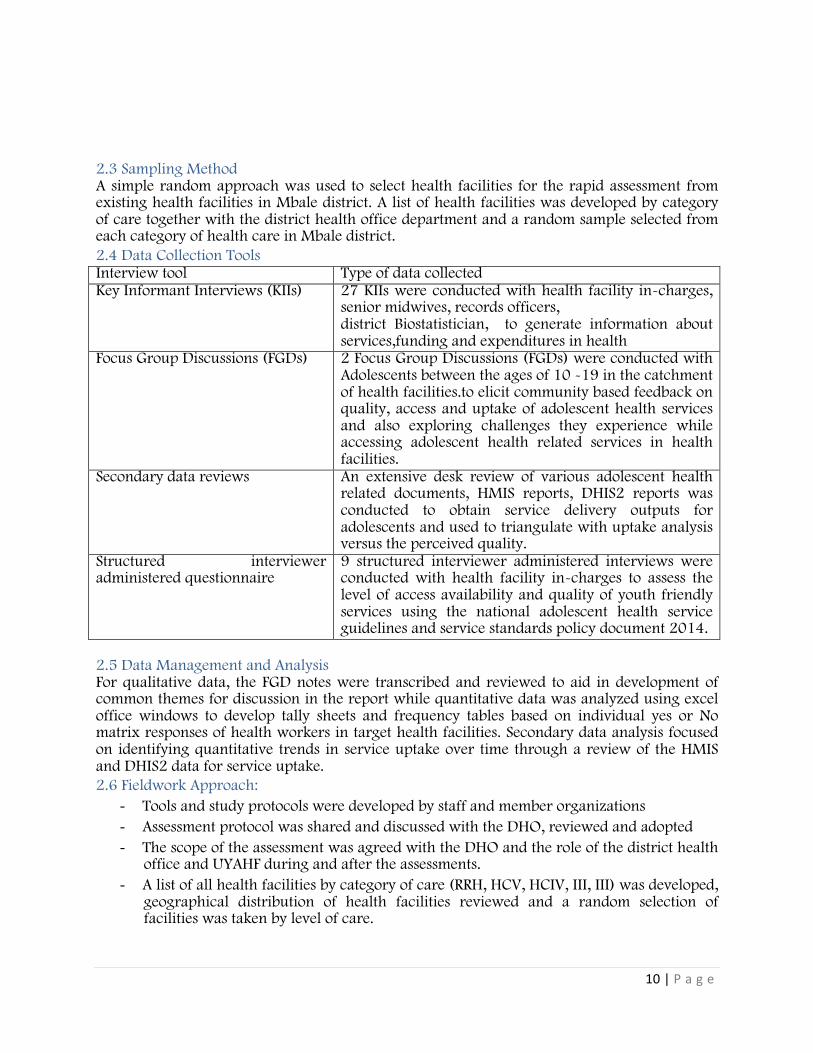
Table 4: Jewa HC III Jewa HC III Yes No Total Health Facility Characteristics 6 3 9 Provide Characteristics 5 2 7 Program Characteristics 8 1 9
6 6
9
3
1 0
HEALTH FACILITY CHARACTERISTICS
PROVIDE CHARACTERISTICS
PROGRAM CHARACTERISTICS
MALUKHUHC I I I
Yes No
6
2
6
3
5
3
HEAL TH FAC I L I T Y C HARAC TER I S T I C S
P ROV IDE C HARAC TER I S T I C S P ROGRAM CHARAC TER I S T I C S
LWANGOLI HC I I I
Yes No
14|P a g e
Table 5: Busiu Health Centre IV Busiu HC IV Yes No Total Health Facility Characteristics 5 4 9 Provide Characteristics 4 3 7 Program Characteristics 8 1 9
Table 7: Nakaloke Health Centre III Nakaloke HC III Yes No Total Health Facility Characteristics 8 1 9 Provide Characteristics 3 4 7 Program Characteristics 6 3 9
6 5
8
3 2 1
HEALTH FACIL ITY CHARACTER ISTI CS
PROVIDE CHARACTER ISTI CS
PROGRAM CHARACTER ISTI CS
JEWAHC I I I
Yes No
5 4
8
4 3
1
HEALTH FACIL ITY CHARACTER ISTI CS
PROVIDE CHARACTER ISTI CS
PROGRAM CHARACTER ISTI CS
BUSIUHC IV
Yes No

15|P a g e
Table 10: Mbale RRH Mbale RRH Yes No Total Health Facility Characteristics 8 1 9 Provide Characteristics 6 1 7 Program Characteristics 9 0 9
Table 11: Namatala HC III Namatala HC III Yes No Total Health Facility Characteristics 7 2 9 Provide Characteristics 3 4 7 Program Characteristics 5 4 9
8
3
6
1
4 3
HEALTH FACIL ITY CHARACTER ISTI CS
PROVIDE CHARACTER ISTI CS
PROGRAM CHARACTER ISTI CS
KALYEBBI ALBERT
Yes No
8
6
9
1 1 0
HEALTH FACIL ITY CHARACTER ISTI CS
PROVIDE CHARACTER ISTI CS
PROGRAM CHARACTER ISTI CS
MBALERRH
Yes No

16|P a g e
Table 12: Mbale epicentreBusooba HC III EPI Busoba HC II Yes No Total Health Facility Characteristics 6 3 9 Provide Characteristics 3 4 7 Program Characteristics 4 5 9
3.2 Discussions on overall findings 3.2.1 Health facility characteristic The health facility characteristics are key physical features that a public health facility must have or exhibit to be attractive to adolescents and support service uptake. They are clearly elaborated in the national adolescent health service guidelines and standards (2014) and were adopted for this rapid assessment. Often adolescents or young people have poor health seeking behaviour whenever health services package are not adolescent friendly (Mbonye et al, 2003, Atuyambe et al, 2009). It is why deliberate efforts must be made to ensure services are attractive and responsive to the population in need. Adolescents are a unique population category with unique health needs and is the basis upon which the national service standards and guidelines were developed for all public and private health facilities providing adolescent health related services.
7
3
5
2
4 4
HEALTH FACIL ITY CHARACTER ISTI CS
PROVIDE CHARACTER ISTI CS
PROGRAM CHARACTER ISTI CS
NAMATALA HC III
Yes No
6
3
4
3
4
5
HEALTH FACIL ITY CHARACTER ISTI CS
PROVIDE CHARACTER ISTI CS
PROGRAM CHARACTER ISTI CS
EPI BUSOBAHC I I
Yes No
17|P a g e
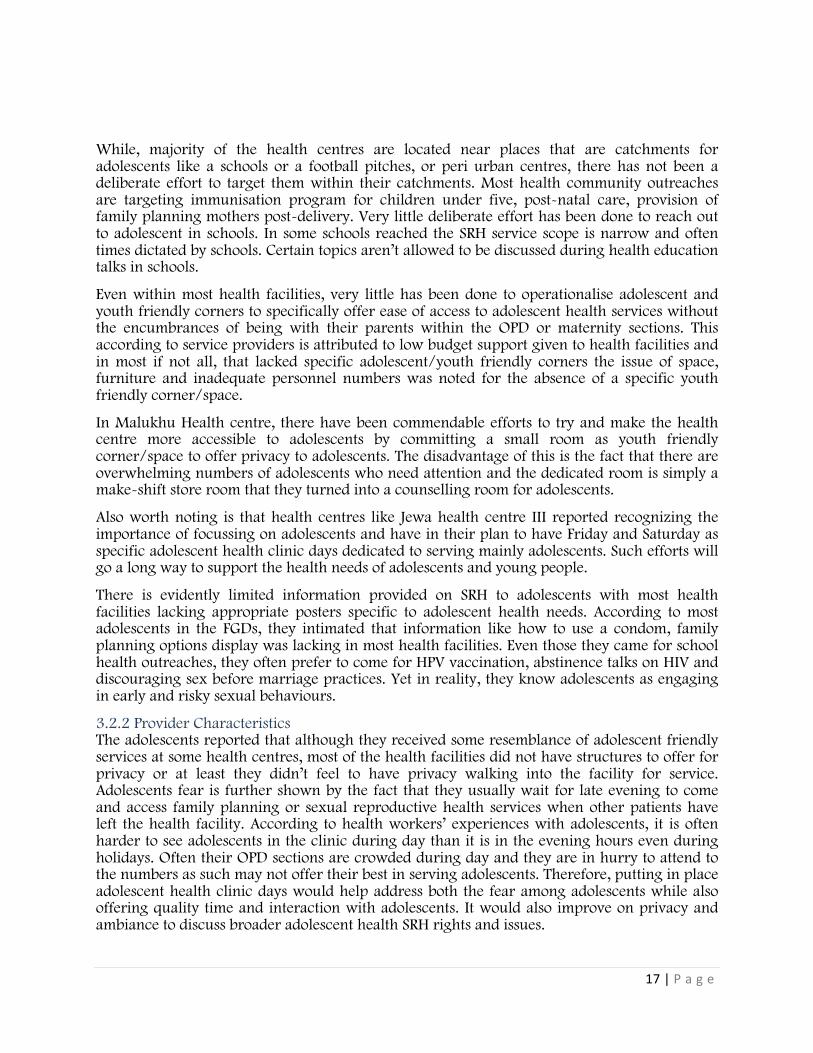
While, majority of the health centres are located near places that are catchments for adolescents like a schools or a football pitches, or peri urban centres, there has not been a deliberate effort to target them within their catchments. Most health community outreaches are targeting immunisation program for children under five, post-natal care, provision of family planning mothers post-delivery. Very little deliberate effort has been done to reach out to adolescent in schools. In some schools reached the SRH service scope is narrow and often times dictated by schools. Certain topics aren’t allowed to be discussed during health education talks in schools.
Even within most health facilities, very little has been done to operationalise adolescent and youth friendly corners to specifically offer ease of access to adolescent health services without the encumbrances of being with their parents within the OPD or maternity sections. This according to service providers is attributed to low budget support given to health facilities and in most if not all, that lacked specific adolescent/youth friendly corners the issue of space, furniture and inadequate personnel numbers was noted for the absence of a specific youth friendly corner/space.
In Malukhu Health centre, there have been commendable efforts to try and make the health centre more accessible to adolescents by committing a small room as youth friendly corner/space to offer privacy to adolescents. The disadvantage of this is the fact that there are overwhelming numbers of adolescents who need attention and the dedicated room is simply a make-shift store room that they turned into a counselling room for adolescents.
Also worth noting is that health centres like Jewa health centre III reported recognizing the importance of focussing on adolescents and have in their plan to have Friday and Saturday as specific adolescent health clinic days dedicated to serving mainly adolescents. Such efforts will go a long way to support the health needs of adolescents and young people.
There is evidently limited information provided on SRH to adolescents with most health facilities lacking appropriate posters specific to adolescent health needs. According to most adolescents in the FGDs, they intimated that information like how to use a condom, family planning options display was lacking in most health facilities. Even those they came for school health outreaches, they often prefer to come for HPV vaccination, abstinence talks on HIV and discouraging sex before marriage practices. Yet in reality, they know adolescents as engaging in early and risky sexual behaviours.
3.2.2 Provider Characteristics The adolescents reported that although they received some resemblance of adolescent friendly services at some health centres, most of the health facilities did not have structures to offer for privacy or at least they didn’t feel to have privacy walking into the facility for service. Adolescents fear is further shown by the fact that they usually wait for late evening to come and access family planning or sexual reproductive health services when other patients have left the health facility. According to health workers’ experiences with adolescents, it is often harder to see adolescents in the clinic during day than it is in the evening hours even during holidays. Often their OPD sections are crowded during day and they are in hurry to attend to the numbers as such may not offer their best in serving adolescents. Therefore, putting in place adolescent health clinic days would help address both the fear among adolescents while also offering quality time and interaction with adolescents. It would also improve on privacy and ambiance to discuss broader adolescent health SRH rights and issues.

18|P a g e
Highlighting the problem of lack of skilled human resource to handle cases of adolescents, the assessment team found out that most health centres did not have in place a sizeable number of health workers trained in provision of adolescent health friendly services and in some experiences of adolescents were not accorded priority during service provision. It was observed that adolescents would wait for long hours in the queue for services yet naturally, adolescents lack the patience to wait for longer hours especially for a service that is not related to any illness but could be in need of just family planning services or HIV and STU screening. Waiting with other patients sometimes people close to them makes them uncomfortable since there is often a habit of patients interacting and discussing what has brought them to the health facility.
“When the adolescent come today they see this one, tomorrow they see that one, they are not happy… Because maybe they trust you and then tomorrow they don’t get you.” KI in one health facility
The finding that facilities where some staff had received training in Youth Friendly Services still identified limited numbers of trained staff as a barrier to implementing this programme, indicates a need to train more, or ideally all, healthcare workers in each facility.
Some health workers who were interviewed revealed a lack of adequate knowledge in the full range of family planning methods and some help open biases and community myths about family planning access to adolescents. For example, a health worker in Lwangoli H/C held biases towards the use of a female condoms. It was such biases that seemed to offer hindrances to adolescents receiving non-judgemental SRH services at most of the health centres visited. Some out rightly opined that as health workers in health facilities, they were only willing to offer contraceptives to young people but not to those who are below 18 years old because they are ‘not yet married’. They reason that, sex outside marriage is sinful and early use of some family planning methods promotes promiscuity in society.
Furthermore, it was noted that whenever there any district led trainings for health workers on adolescent health friendly services, health facility in-charges often dominate such trainings and deny other critically cadres to benefit from such trainings. Even those that benefit from such trainings rarely translated such knowledge into practice at their health facilities or organise further knowledge sharing with fellow health workers at the health facility. The implication is that knowledge is rarely translated into practice at the health facility setting. it is most often the in-charges who are called and not the health workers who directly deal with the adolescents.
Even worse, some health workers pointed out the fact that adolescents fear some health workers due to their age difference or the fact that they know their parents and may not feel comfortable sharing their issues with them.
Issues of confidentiality are often more important to young people given cultural attitudes regarding pre-marital sexual relationships.
3.2.3 Program Characteristics All facilities provided family planning, treatment for minor ailments, HIV testing and counselling, pregnancy testing, antenatal care, health education, antiretroviral treatment, immunisation services, STI testing and treatment. The health centres as well provided laboratory testing for STIs, vaginal examinations for syndromic STI diagnosis. Legally

19|P a g e
adolescents can access health services, including, HIV testing and contraceptives, without parental consent
The health workers that were interviewed reported that they did not have access to any guidelines on adolescent health but that they had a clue based on what they learned in during their training in school.Even when the district goes for support supervision visits they hardly leave behind any printed hard copy guidelines specifically adolescent health care. Lwangoli Health centre reports having guidelines for adolescents but admits that they are not in regular use.
3.2.4 Adolescents SRH experiences in community. Multiple sexual partners; Definitely from the feedback from adolescents, many are actually sexually active with multiple sexual partners. The risky sexual behaviour is evident among the participants who were interviewed. Respondents Age at first sex Age of partner
at first sex Number of sex partners in life time
Number of sex intercourse in last three months
Girl 1 17 18 2 1 Girl 2 17 19 4 2 Boy 1 19 10 1 1 Boy 2 18 15 6 2 Boy 3 5 9 30 6 Boy 4 18 32 5 5 Boy 5 17 9 2 2 Boy 6 15 13 Like 25-30 About 6 All of the respondents had sex in last 3 months and all the respondents acknowledged having unprotected sex with their sexual partners. 06 of the 08 confessed not knowing how to use a condom while 02 or 08 sex with condoms was not pleasurable for them. Only one respondent ever attempted to discuss family planning options with her partner but threatened to chase her away if she took on family planning. First Sexual experiences among adolescents; Among the girls in the FGD who were sexually active, most of them reported that their first sexual encounter was a rape incident. It was observed that rape had become so normalized so much that most of their psychosocial well-being is not catered for. Many of the FGD participants (both boys and girls) had been lured into their first sexual encounter with especially older men and women through gifts or promise of a job in exchange for the sex. ‘We were 3 girls and they were 3 boys, they called us to visit them, my friends convinced me to go, we met them when they had organised food, soft drinks and alcohol for us. We enjoyed up to night and at the end each boy got a girl to sleep with without any protection.’ Mexi not her real name had this to say about her first sexual experience.

20|P a g e
“When I was looking for a job, a boss undermined me, the boss told me to first have sex, at first I picked my letter and ran away. However, I came back because I wanted a job. I accepted, he broke my virginity. On that day I felt pain the whole day”. While many would think gifts for sex was only common to girls, a boy in the FGD revealed his first experience with sex and said “…the wife of my boss told me that if I do not play sex with her, she will tell my boss and I will no longer have a job” SRH information and use of contraceptives; The young people shared their sexual experiences and knowledge as pertains to use of contraceptives; with most of them noting that they had never had sex with a condom because they did not know how to use one. For those who knew how to use the condoms, they reported that they did not like using them because they found the experience to be unsatisfactory. Others also pointed out that they had heard that condoms cause cancer and therefore were reluctant to use them. This was mostly due to the lack of accurate knowledge on how to wear them and use them. The girls in the FGD reported that they lacked correct information on family planning and often let their partners decided on her behalf the choice of contraceptive method to use. Some even added that most of their partners threaten to leave them if they bring up the topic of child spacing and further shared that some of them want as many as 10 children because it is a sign of wealth even if they do not have the means to support these numbers. When asked whether they decided on contraceptive choices with their partners, one of the girls who was also a teenage mother, pointed out that her partner does not allow her to use contraceptives and has threatened to leave her or beat her if he ever finds out that she is using contraceptives. “Some methods are dangerous like pills. Why do they make the women bleed abnormally”? an adolescent boy asked during the FGD. Such notions continue to curtail women accessing family planning services since most of women have to seek for permission from the men to take on family planning. Part of such myths is what makes adolescents find it hard to access and use family planning methods without such prejudices. Additionally, the girls reported that another challenge with getting correct information on sexual reproductive health is that the posters that are in most health centres are in English yet majority of them cannot read in English. Furthermore, even for those that are in local languages, it poses as a challenge because some of them cannot read at all. They therefore depend on just their friends to get any information on sexual reproductive health. The issue is made worse for girls and boys with hearing impairments because they face challenges of access to information due to the lack of knowledge on sign language by the health workers. Stigma and discrimination especially when they attempt to access ANC, deliveries and family planning service; The girls also shared being afraid of getting antenatal services at the health

21|P a g e
centre because of the communication challenges and the already predetermined negative and judgemental biases of the nurses and midwives. Communication challenges for PWDs with hearing impairment;During an FGD with10 teenage girls with hearing disabilities, they shared their biggest problem as being the lack of sign language interpreters at all health facilities. The girls are required to along with a family member or friend with ability to communicate using sign language and often when they go un-accompanied, their health needs often seem not to be understood by the health workers because of the communication challenge. They emphasised some of their colleagues are molested and raped and find it difficulty seeking re-dress and whenever, they conceive, they are most often neglect. Additionally, as a practice in most health centres, health workers tell patients to wait until they are called into the consultation room and sometimes miss out being called because of the hearing impairment leading to longer stays at health facilities. Furthermore, they fear to go the hospital to test for HIV because they will have to go with a translator and yet this is meant to be a confidential issue discussed between the health worker and the patient. Majority of the girls reported that they have never gone for HIV tests because of the barrier of communication and yet they want their issues to be private. In most cases, they are asked to bring their partners to receive family planning services and ANC services yet their partners would not want to be seen with a PWD especially those without hearing impairment and as such limits their access to some of the essential adolescent health related services. 3.3 Service uptake for adolescent health 3 out of every 8 adolescents interviewed in the community had ever visited health facility for an HIV test, 2 out of every 8 went to health facility to get family planning services, 3 out of 8 went for counselling session on SRH.
3.3.1 Family planning usage The data on utilization of FP by adolescents was extracted using a tool which was filled in using the family planning register. The number of adolescents aged 10-19 years who received FP services were counted and compared to all women who received these services inJuly to September 2019 and October to December 2019. The same tool was completed using the HMIS register at the outpatient departments to find the proportion of adolescents receiving STI treatment in 2 quarters between July to September 2019 and October to December 2019.
In discussing their risky sexual behaviours in FGD M03, 3 out of 11 respondents reported that they have never had sex and they were girls of 9, 11, and 14 years old. In addition, they said that their preferred ages of first sexual encounter would be at 27, 25 and 20 years respectively.
Family planning Uptake in Mbale district
FP Method August September October New Revisit New Revisit New Revisit
Male condoms 263 153 188 196 140 193 Female condoms 5 10 3 8 70 35 UIDs 18 5 14 2 7 0 Injectable 277 158 228 155 186 108

22|P a g e
Implants - - - - - - Orals 40 31 35 33 11 12
3.3.1 Post Abortion Care Services recorded in Mbale Abortion is very prevalent among adolescents especially owing to social stigma and poverty levels and this pushes girls carry out unsafe abortions using crude meansand come to the hospital for post-abortion care. The health workers reported that this is often the case because girls fear that they will be taken to police if they are found to have aborted.
263
5
18
277
0
40
153
10 5
158
0
31
188
3 14
228
0
35
196
8 2
155
0
33
140
70
7
186
0 11
193
35
0
108
0
12
MA L E CONDOMS FEMAL E CONDOMS
U IDS IN J E C TAB L E IMP LANT S ORAL S
FAMILY PLANNING
AugustNew AugustRevisit SeptemberNew SeptemberRevisit OctoberNew OctoberRevisit
76
92
76
0 10 20 30 40 50 60 70 80 90 100
AUGUST
SEPTEMBER
OCTOBER
Post Abortion Care Services 2019

23|P a g e
Teenage ANC attendance and deliveries in target health facilities
4.0 Chapter Four: Conclusion, Challenges, recommendations and Lessons 4.1 Conclusion The adolescent and youth friendly services have the potential to improve not only access to key adolescent health services but as well health outcomes for young people. Government of Uganda recognises provision of adolescent health friendly services asa successful model to meet the specific needs of adolescents and young people male its health systems adolescent. The national adolescent health service standards and guidelines for creation of youth-friendly clinic programmes in terms of the achievement of standards relating to clinic policies and the clinic environment.
4.2 Challenges • Lack of youth friendly corners and in a few health facilities that had them, they were not
up to standard. Yet such corners are supposed to act as attraction points for adolescents to come for complete complimentary SRH services.
August Sep Oct August Sep Oct August Sep Oct August Sep Oct August Sep OctANC 33 45 52 47 47 0 12 10 6 18 15 12 26 30 23Deliveries 9 17 23 18 19 24 2 10 4 7 5 10 7 5 6
NamatalHCIV NakalokeHCIII LwangoliHCIII BusiuHCIV BufumboHCIII
0
10
20
30
40
50
60
August Sep Oct August Sep Oct August Sep Oct August Sep Oct August Sep Oct
NamatalHCIV NakalokeHCIII LwangoliHCIII BusiuHCIV BufumboHCIII
ANCsandDeliveriesinselectedHFs2019
ANC Deliveries

24|P a g e
• Limited scope of SRH information and materials provided and sometimes very selective information is provided especially to school students during school health outreaches. Most schools limit health workers from providing family planning related information to sexually active adolescents to avert teenage pregnancy.
• Most health facilities have not embraced peer approach to support delivery of adolescent health friendly services. In most health facilities visited, non-reported having peer educators to support service provision to adolescents and young people.
• Low number of health workers trained in provision of adolescent health friendly services in health facilities. This limits the number of health personnel with attitude and zeal to provide adolescent health responsive services.
• Many of the health facilities lack interpreters for PWDs adolescents that visit health facilities and sometimes affects communication between the service provider and the service user seeking health care.
• Lack of peer counselors/educators in most health facilities yet the country rolled out peer to peer guidelines for health facilities to adopt and ensure reach of adolescents with key SRH services.
• Frequent stock out of some SRH commodities at health facilities. Of particular mention were STi drugs, mam kits, family planning options like IUDs
• Social norms, customs and religious beliefs continue to influence practice of some health workers and attitude of communities in supporting adolescents to access SRH services. Some health workers shared theirreservations with providing family planning services to younger adolescents while others saw it as a gateway to promoting promiscuity among adolescents.
4.3 Recommendations • There is need to intensify in-service training of Health Workers in provision of adolescent
health friendly services. Health workers need to recognize adolescents first as a peculiar group from other population categories and design appropriate service packages and interpersonal communication mechanisms to reach them.
• Integration of adolescent services with SRH and ensuring revitalization and intensification of School Health outreaches and programmes and community-based programmes that are focused on adolescents and young people.
• Extra support and mentorship is needed for rural and lower level health facilities to develop appropriate service packages and modify health facility environments to make services attractive to adolescents and increase uptake of key adolescent health services.
• Health facilities should explore partnerships with nonprofit organizations to build capacity of health workers on provision of adolescent health friendly services and can work together to modify the health facility to make them more appealing to adolescents.
• District and health facility managers should set some targets upon which district and health facility plans and budgets can be integrated to equip and operationalize the national adolescent health service standards and guidelines in health facilities with adolescent health corners and commodities to enhance SRH services for adolescents.

25|P a g e
• Health facilities should gazette youth friendly corners where the young people can feel confident to express themselves in regards to their sexuality and sexual issues/challenges
• Awareness should be created about the health facilities that offer YFS in order to increase uptake of the services by adolescents.
• Peer educators identified, trained, attached and facilitated to provide support to health facilities reach adolescents with critical SRH services, this will most likely increase reach and the uptake of the SRH services by particularly adolescents.
• Health facilities should establish condom dispensers in strategic areas where adolescents frequent to increase accessibility of the contraceptive them.
• Widen the scope of services for school health outreaches and make them more routine to effectively reach out to a large number of adolescents in- school.
4.4 Lessons • Many health workers have social prejudices on some SRH service components like
contraceptives for adolescents. This in tandem creates a secondary fear among adolescents to come for such services in health facilities
• Often there is an assumption that in-service health workers have inherent knowledge and skills of serving adolescents having acquired during their training. however, often experience has showed that additional in-service training of health workers in adolescent friendly health services is required for adolescents are a special group with specific needs from rest of population.
• Integration of adolescent services with SRH and ensuring revitalisation and intensification of School Health outreaches and programmes and community-based programmes that are focussed on adolescents and young people is urgently required. Most of the current adolescent health outreaches are focused on pregnancy testing for those in school, HPV vaccination in schools while at community, focus is on immunisation, ANC, PNC, and family planning for mothers with children younger than 2 years.
• Extra support and mentorship is needed for rural and lower level health facilities so that they enrol more adolescents. There is a need to lobby partners to support lower health facilities and rural ones.
• District and health facility managers should plan, budget and equip health facilities with adolescent health corners to enhance SRH services.

26|P a g e
References 1. Health sector Development Plan 2016 – 2020 2. RMNCAH sharpened plan Investment case 2016 – 2020 3. Annual Health Sector Performance Report 2018/19 4. The National Adolescent Health Service Standards and Guidelines 2014
Copyright © 2022 FDOKUMEN