Factors Affecting Consumers' Attitudes toward Online ... - CORE

Public attitudes toward the right to die
Stephen J. Genuis, MD, FRCSC, DABOG; Shelagh K. Genuis, BSc (OT); Wei-Ching Chang, PhD
Objective: To determine public attitudes toward the right to die, euthanasia and related end-of-life decisions.Design: Mail survey based on telephone numbers randomly selected by computer.Setting: Edmonton.Participants: Of 1347 computer-generated, randomly selected telephone numbers called be-tween February and June 1992, 902 individuals were reached, and 500 eligible contacts(55%) agreed to fill out the mailed questionnaire based on 12 vignettes involving end-of-lifedecisions. A total of 356 usable questionnaires (71%) were subsequently returned.Main outcome measures: Attitudes toward end-of-life decisions including withdrawal oflife support, euthanasia, chronic suffering and the right to die, living wills and family in-volvement in decision making for incompetent individuals. Comments and demographic datawere also solicited.Results: Of the respondents 84% supported a family's right to withdraw life support from apatient in a persistent coma, and 90% supported a mentally competent patient's right to re-quest that life support be withdrawn. Active euthanasia was supported by 65% for only pa-tients experiencing severe pain and terminal illness. There was marked opposition to eu-thanasia for patients in other circumstances, such as an elderly disabled person who feels heor she is a burden on relatives (opposed by 65%), a patient with chronic depression resistantto treatment (by 75%) or an elderly person no longer satisfied with life and who has variousminor physical ailments (by 83%). In all, 63% of the respondents felt that legalization of eu-thanasia for terminal illnesses would lead to euthanasia for many other, unsupported reasons,and 34% supported legislation to prohibit euthanasia in all situations.Conclusions: Public support for the right to die varies depending on the circumstances of thepatient. The single most significant factor determining attitudes was the level of religious ac-tivity. The family's wishes were an important factor in end-of-life decisions for patients un-able to communicate their desires. Both the general public and physicians should be primaryparticipants in determining legislation regarding the right to die.
Objectif: Determiner les attitudes du public a l'egard du droit de mourir, de l'euthanasie etdes decisions relatives 'a la fin de la vie.Conception: Sondage postal fonde sur des numeros de telephone choisis au hasard par ordi-nateur.Contexte : Edmonton.Participants: Entre fevrier et juin 1992, on a compose 1 347 numeros de telephone choisisau hasard par ordinateur, on a reussi 'a atteindre 902 personnes et 500 repondants admissibles(55 %) ont consenti 'a remplir le questionnaire postal en fonction de 12 vignettes comportantdes decisions relatives 'a la fin de la vie. Au total, 356 questionnaires (71 %) utilisables ontete renvoyes.Principales mesures de resultats: Attitudes 'a l'egard des decisions relatives 'a la fin de lavie, y compris le retrait des moyens d'assistance cardiorespiratoire, l'euthanasie, les souf-frances chroniques et le droit de mourir, les directives de mort naturelle et la participation desmembres de la famille 'a la prise de decisions pour le compte de personnes incapables. On aaussi demande des commentaires et des donnees demographiques.Rtesultats: Parmi les repondants, 84 % appuient le droit des membres de la famille de retirerles moyens d'assistance cardiorespiratoire 'a un patient qui a sombre dans un coma persistantet 90 % appuient le droit d'un patient mentalement competent de demander qu'on lui retireles moyens d'assistance cardiorespiratoire. Seulement 65 % des repondants sont d'accordavec l'euthanasie active, mais uniquement dans le cas des patients en grande souffrance et en
Dr. Genuis is an associate clinical professor at the University ofAlberta, Edmonton, Alta.; Ms. Genuis is an occupational therapist and is aneditor at KEG Publishing, Edmonton, Alta.; and Dr. Chang is coordinator of Utilization Management, the Caritas Health Group, Edmonton,Alta.
Reprint requests to: Dr. Stephen J. Genuis, 2911-66 St., Edmonton, AB T6K 4C1
v-For prescribing information see page 776 CAN MED ASSOC J 1994; 150 (5) 701

phase terminale. On s'oppose fermement 'a l'euthanasie dans d'autres circonstances commele cas d'une personne agee handicapee qui se croit un fardeau pour les membres de sa famille(65 %), celui d'un malade aux prises avec une depression chronique qui resiste aux traite-ments (75 %), ou celui d'une personne agee qui ne veut plus vivre et qui souffre de diversproblemes physiques mineurs (83 %). Dans l'ensemble, 63 % des repondants sont d'avis quela legalisation de l'euthanasie dans le cas des maladies terminales entrainerait l'euthanasiepour un grand nombre d'autres raisons non justifiees et 34 % appuient une mesure iegislativevisant 'a interdire totalement l'euthanasie.Conclusions: L'appui du public a l'egard du droit de mourir varie selon les circonstances dupatient. Le niveau d'activite religieuse est le facteur le plus important qui oriente les atti-tudes. Les desirs des membres de la famille sont un facteur important dans la decision rela-tive 'a la fin de la vie des patients incapables de communiquer leurs desirs. Le grand public etles medecins devraient etre des participants de premier plan dans l'detablissement d'unemesure legislative regissant le droit de mourir.
B eliefs and opinions about end-of-life decisionsvary greatly. However, given the technologic ca-pabilities that allow physicians to maintain and
extend life in previously unimagined ways, the need forfar-reaching discussion is becoming more evident. Al-though society has increasingly recognized "the right ofhopelessly ill patients to decline life-sustaining treat-ments",' the issue of euthanasia as it relates to individu-als, the medical profession and society continues to be acontentious dilemma. The term "euthanasia" as used inthis paper refers to the situation in which a physician orother agent knows about a patient's condition and desireto die and commits or assists in an act with the "primaryintention of ending the life of that patient," the act beingundertaken with compassionate motivation and withoutpersonal gain.'
Numerous courts of law have extended the rightsof seriously ill patients to withdraw from or refuse life-sustaining treatment, and these actions appear to haveextended the acceptance of euthanasia and have, per-haps, weakened previous societal prohibitions againstthe active termination of life in a therapeutic setting.' Inour society issues such as euthanasia are too complex tobe dealt with exclusively by one discipline.4 It is impor-tant that physicians, courts and government becomeaware of thoughtful public opinion, since it will be indi-viduals and families who will be personally facing manyof these difficult decisions.5
A number of polls attempting to elicit public atti-tudes toward euthanasia and assisted suicide have beenreported in the medical literature.6"' Respondents' sup-port for a terminally ill patient requesting physician as-sistance in dying varied from 54%9 to 75%." Two pollsshowed that 68% of respondents supported the permit-ting of terminally ill patients to end their own lives byactive means.8' Another poll found that 70% ofrespondents would be willing to have their own life-support system disconnected should they lapse into ir-reversible coma; a significant number, 46%, would stopshort of making that decision for another person.'2 Inthis same poll it was found that men more often thanwomen, and older people more often than younger,favoured the decision to disconnect life support. Polls
702 CAN MED ASSOC J 1994: 150 (5)
that explored more complex medical situations, beyondthe question of euthanasia for suffering, terminally illpatients, did not appear in the medical literature to anygreat degree.
Surveys of physicians' attitudes have shown thatcase vignettes are an effective way of eliciting opinions,particularly in ethically complex situations.' A profes-sionally written survey is also more likely to receivethoughtful response than is an unexpected telephonecall.6
We conducted a survey to determine public atti-tudes toward end-of-life decisions. The questionnairewas designed with four basic guiding questions inmind: What degree of support or opposition is there forwithdrawal of life support, assisted suicide and eu-thanasia? Is support or opposition to these practicesconsistent or does it vary depending on the patient'sclinical situation? Which demographic factors influ-ence the attitudes of respondents toward various end-of-life issues? What degree of support or opposition isthere for living wills and enactment of legislation inthis area, and who should be primarily involved in de-cision making?
Methods
The survey was confined to the city of Edmonton,whose population is 614 665 (Table 1). A list of 1347computer-generated, randomly selected telephone num-bers (covering all of the telephone exchanges in Edmon-ton) was obtained from the Population Research Labora-tory, Department of Sociology, University of Alberta,Edmonton. Each number was reviewed and called up to
four times between February and June 1992. Throughthis process 262 business numbers, fax numbers, out-of-town listings and not-in-service numbers were elimi-nated. In addition, 183 listings were excluded becauserepeated calls went unanswered.
Of the 902 people contacted, 362 (40%) were unin-terested and 40 (4%) unable to participate because oflanguage or literacy problems. The remaining 500households contacted had someone 16 years of age orover who agreed to receive the questionnaire. The ques-
LE l" MARS 1994
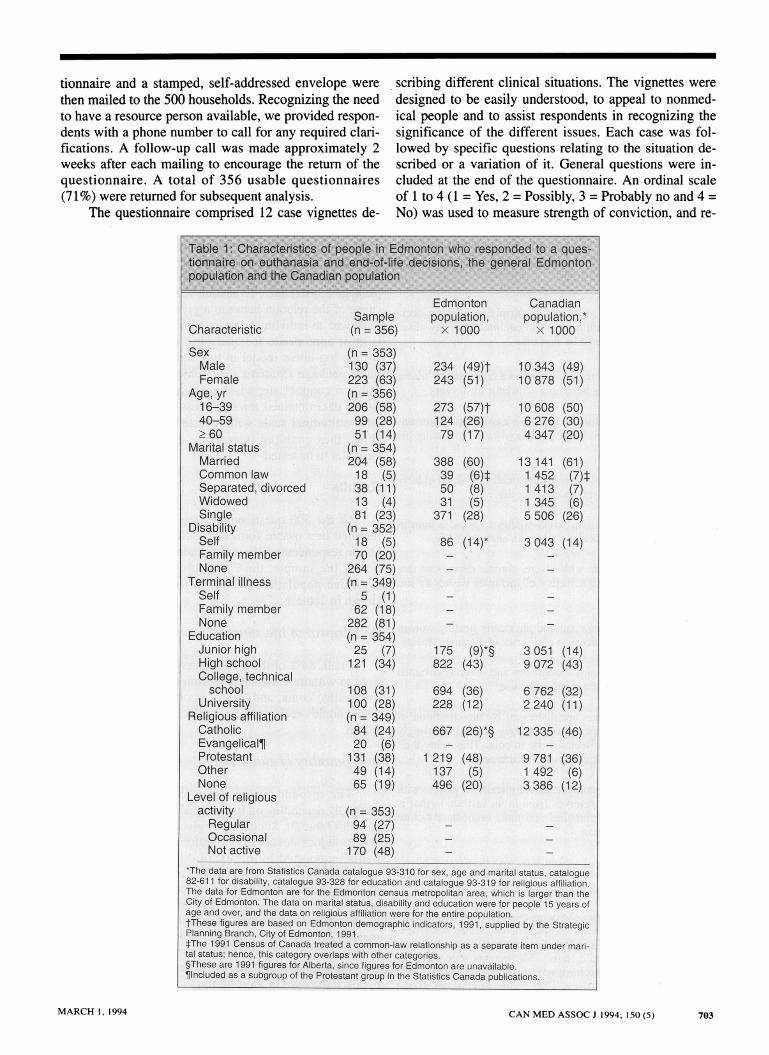
tionnaire and a stamped, self-addressed envelope werethen mailed to the 500 households. Recognizing the needto have a resource person available, we provided respon-dents with a phone number to call for any required clari-fications. A follow-up call was made approximately 2weeks after each mailing to encourage the return of thequestionnaire. A total of 356 usable questionnaires(71%) were returned for subsequent analysis.
The questionnaire comprised 12 case vignettes de-
Characteristc
SexMaleFemale
Age-,.yr16-3940-59.60-
Martal statusMarriedCommon lawSeparated, divorcedWidowedSingle
DisabilitySelfFamily memberNone
Terminal, illhessSelfFamily memberNone
EducationJunior highHigh schoolCollege, technicalschool
UniversityReligious affiliationCatholicEvangelicallProtestantOtherNone
Level of religiousactivityRegular
. OccasionalNot active
scribing different clinical situations. The vignettes weredesigned to be easily understood, to appeal to nonmed-ical people and to assist respondents in recognizing thesignificance of the different issues. Each case was fol-lowed by specific questions relating to the situation de-scribed or a variation of it. General questions were in-cluded at the end of the questionnaire. An ordinal scaleof 1 to 4 (1 = Yes, 2 = Possibly, 3 = Probably no and 4 =No) was used to measure strength of conviction, and re-
-tamonton CanadianSample population, population,*(n =356) X 1000 x 1000
(n 353)130 (37)223 (63)(n 356)206 (58)99 (28)51 (14)
(n = 354)204 (58)18 (5)38 (11)13 (4)81 (23)
(n= 352)18 (5)70 (20)
264 (75)(n - 349)
. 5 (1)62 (18)
282 (81)(ni. 354)25 (7)
121 (34)
108 (31)t10 (28)(n = 349)84 (24)20 (6)
131 (38)49 (14)65 (19)
(n = 353)94 (27)89 (t5)170 (48)
234 (49)t243 (51)
273 (57)t124 (26)79 (17)
388 (60)39 (6)t50 (8)31 (5)
371 (28)
86 (14)*
175 (9)*§822 (43)
694 (36)228 (12)
667 (26)*§
1 219 (48)137 (5)496 (20)
10 343 (49)10 878 (51)
10 608 (50)6276 (30)4347 (20)
13 141 (61)1 452 (7)t1 413 (7)1 345 (6)5506 (26)
3043 .(14)
3 051 (14)9072 (43)
6762 (32)2 240 (11)
12335 (46)
9 781 (36)1 492 (6)3386 (12)
*The data are from Statistics Canada catalogue 93-310 for sex, age and marital status, catalogue82-611 fo disability, catalogue 93-328 for education and catalogue 93-319 for religious affiliation.The data for Edmonton are for te Edmonton nsus m-etropolitan area, which is larger than theCity of Edmonton. The data on marital status, disability and education were for people 15 years ofage and over, and the data on retiglous affiliation were for the entire polation.tThee ligurs'are baed on Efeonton demographic indicators, 1991, suppHled by the StrategicPlanning :Branch, City of Edmontonf 1991.fThe 1991 Census of Canada treated a oommon-law relationship as a separate item under mari-tal status; hence, this cbategOy overlaps *9th other categories.§These are 1991 figures for Alberta, sinc.figures for lEdmonton are unavailable.¶lncluded asa ubgroup of the t nt group in the Statitcs Canada publications.
..
p
CAN MED ASSOC J 1994; 150 (5) 703MARCH 1, 1994
spondents were encouraged to provide specific and gen-eral comments as well as demographic information.
Before distribution the questionnaire was critiquedat face value by a number of physicians involved in pal-liative care and by physicians doing research into eu-thanasia. It was then pretested to ensure participant un-derstanding.
The 12 vignettes were followed by specific ques-tions related to the right to die and the removal of lifesupport and therapy to cause death, the rights of familiesand institutions to make end-of-life decisions and therole of advance directives. The vignettes illustrated thefollowing clinical situations.
Case 1: A young man, rendered quadriplegic after an acci-dent, requires life-sustaining medical equipment to stay alive.He wishes the ventilator to be shut off.
Case 2: A middle-aged man has been in a coma after a motorvehicle accident and has been on a ventilator for 2 years.
Case 3: An elderly, terminally ill man is experiencing worsen-ing and intolerable pain. He requests assistance in ending hislife.
Case 4: A mentally competent, chronically disabled elderlyperson requests help in terminating her life.
Case 5: A young man with AIDS wishes to avoid a painfuldeath and requests medical assistance in ending his life.
Case 6: A young woman with severe, chronic depression thathas responded poorly to a variety of therapies wishes to endher life.
Case 7: A mentally competent and physically healthy womanhas lost the will to live because of a series of disappointments.
Case 8: A young woman is chronically and severely disabledafter a stroke due to oral contraceptive use.
Case 9: Family members are distressed by the condition oftheir elderly, mentally incompetent father, who is increasinglyuncontrollable and also seems to be in pain. They relay theirfather's previously indicated wish for euthanasia.
Case 10: A mentally incompetent, chronically ill patient withno family or financial reserves lives in an institution that isexperiencing financial pressures and must immediately closebeds to continue operation.
Case 1 1: Parents of a 4-year-old boy who is severely physi-cally and mentally handicapped feel that he has nothing to
look forward to and wish to have the child's life ended.
Case 12: A young couple is very upset when their first child isfound to have severe Down's syndrome associated with men-tal retardation as well as an intestinal abnormality that will re-
quire surgery for the child to live. The parents state that theydo not wish the child to have any treatment whatsoever andwish for him to die in peace. They refuse to consider giving
the child up for adoption, claiming that they love the child andfeel that his quality of life will not be in keeping with theirwishes.
We estimated the overall rate of acceptability bycombining the responses Yes and Possibly and then ad-justing for sex and age using a direct method (i.e., sex-and age-specific rates were calculated from the sampleand weighted by the corresponding population propor-tions to come up with the overall rate).`S The possibledemographic influences on attitudes were assessed intwo ways: (a) a bivariate method of Kruskal-Wallis one-way analysis of variance in the Systat microcomputerpackage (Systat Inc., Evanston, Ill.) to test the signifi-cance of the relation between a given 4-point attitudinalscale and an individual demographic factor (this methodis most appropriate for analysing ordinal scales)'4 and(b) the log-linear model in the Statgraphics microcom-puter package (Statistical Graphics Corp., Rockville,Md.) to conduct stepwise regression analysis on cat-egoric data obtained through cross-tabulation of a spe-cific attitudinal scale with selected demographic vari-ables, thus enabling interaction among demographicvariables to be tested.
Results
Of the 500 questionnaires mailed 356 (71%) werereturned in a usable form and included in the analysis.Of the respondents 63% were women. Other characteris-tics of the sample, the Edmonton population and theCanadian population, according to available data, areshown in Table 1.
Withdrawal of life support
In all, 84% of the respondents supported a family'sright to withdraw life support from a patient in a state ofirreversible coma, and 90% supported a mentally com-petent adult's request to die by having life support with-drawn.
Acceptability of euthanasia
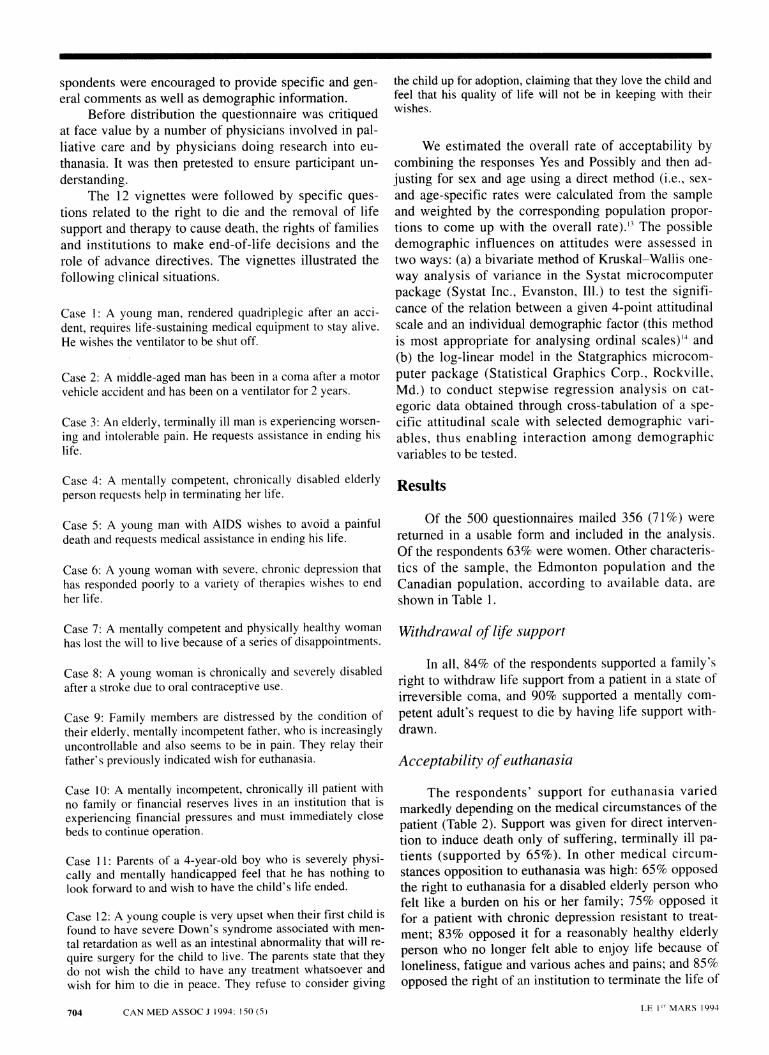
The respondents' support for euthanasia variedmarkedly depending on the medical circumstances of thepatient (Table 2). Support was given for direct interven-tion to induce death only of suffering, terminally ill pa-tients (supported by 65%). In other medical circum-stances opposition to euthanasia was high: 65% opposedthe right to euthanasia for a disabled elderly person whofelt like a burden on his or her family; 75% opposed itfor a patient with chronic depression resistant to treat-ment; 83% opposed it for a reasonably healthy elderlyperson who no longer felt able to enjoy life because ofloneliness, fatigue and various aches and pains; and 85%opposed the right of an institution to terminate the life of
LE V` MARS 1994704 CAN MED ASSOC J 1994; 150 (5)

a mentally incompetent, chronically ill patient for finan-
cial reasons.
Family's rights regarding euthanasia
The wishes of a patient's family members when thepatient is unable to express his or her own desires wasan important factor in the acceptability of life-support
withdrawal and euthanasia. Although 84% supported afamily's right to withdraw treatment from a patient inirreversible coma, 71% opposed the right of a hospitalto withdraw life support from such a patient if the fam-ily opposed the idea. The respondents indicated thatfamily members should be acting on the basis of someprevious directive from the patient. Only 20% of the re-spondents supported a family's right to request assis-
'"t'
ipAtf 9ptrn~( S V
ri'y' -toA. Cmrnaqi'.'pqi6t
I 4kk4a~renw~fl.~aitunah#I. ''J wit'.qujiiri.'u&w ' ''' -
w-10PO ~ 5061 59'
reqa~d*. help inYount>rrewiwith A17 4.v'3
V.I,c pneyp~'". '''
requests eulland.sia .1174
seiusly iladisabledchldrquest that thchild9bbeeoded . 35 34. 39
Paret refusemeiatreatment. require to.savte lfeofseeel anicpe
Child 39 35 39
70:. 76*.
'35
30'i1 i-
20
5
.10 .
2.0
55.
t.'140±----:ir
..1 ',
.1
3,8*.
'I'
<96>
77
:99
65
64.
27 2.
5 6
24*. '41 'V38
37§` ....41. . 1
MARCH 1, 1994 CAN MED150~~~~~~~~1.. 1 mcio705
were;erP s sIp6t 4wpeNte nmdYes: or Poetl.: Themrhenteexnsvd at;s
$pO01,basedbon KNKIWru tstj~c0.0,bedonMaclWUWet
---4 g' i .` 1.9o J i #'.+ +: 'i #w .1 +!.. S. i, +1..+ -- . M . -- . Q .i i., -
_.
MARCH 1, 1994 CAN MED ASSOC J 1994; 150 (5) 705
tance in the death of a mentally incompetent familymember who had never expressed such a wish, whereas47% supported such a right if the incompetent familymember had indicated this wish orally when competentand 70% if the patient's wish had been expressed inwriting.
Parental rights regarding euthanasia
In all, 62% opposed giving parents the right to re-quest or assist in ending the life of a chronically andseverely ill or disabled child. As well, 59% opposedthe right of parents to refuse medical treatment re-quired to save the life of a severely handicapped child(Table 2).
Other related issues
Of the respondents 61% indicated that quality oflife should be an important consideration in decisions re-lated to euthanasia (Table 3). As well, 63% felt that le-galization of euthanasia for terminal illness would leadto euthanasia for many other reasons.
In all, 74% thought that a living will should belegally binding, although only 46% felt that hospitalsshould require patients to sign a living will on admission(Table 3).
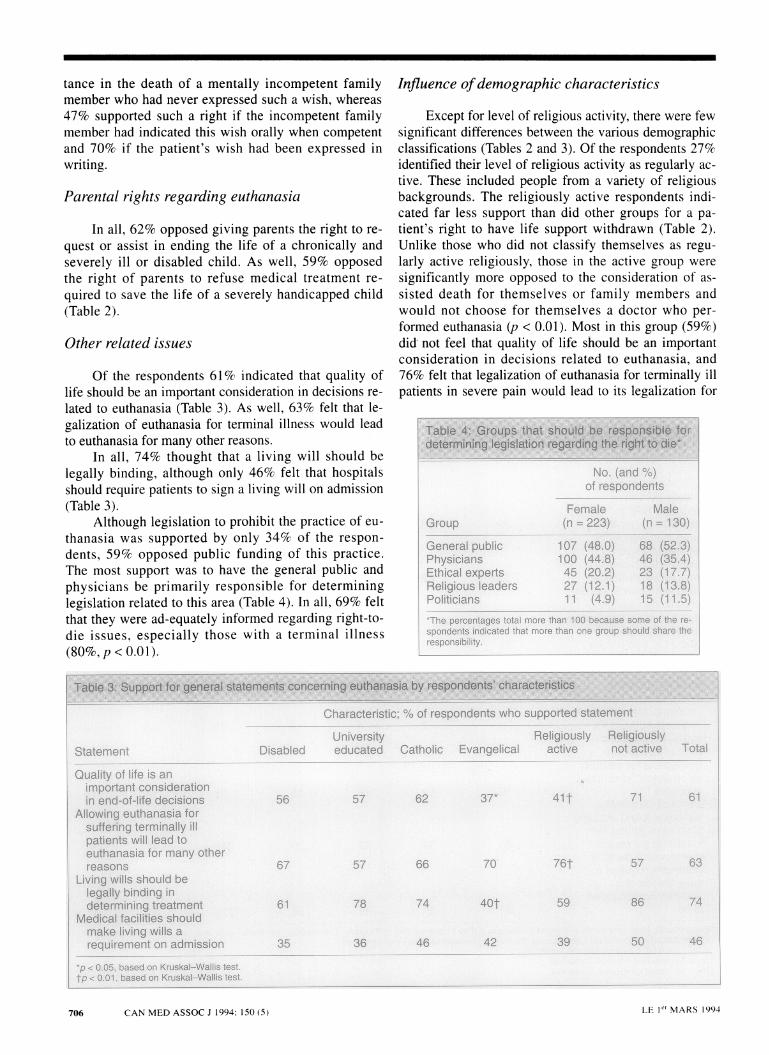
Although legislation to prohibit the practice of eu-thanasia was supported by only 34% of the respon-dents, 59% opposed public funding of this practice.The most support was to have the general public andphysicians be primarily responsible for determininglegislation related to this area (Table 4). In all, 69% feltthat they were ad-equately informed regarding right-to-die issues, especially those with a terminal illness(80%, p < 0.01).
Influence ofdemographic characteristics
Except for level of religious activity, there were fewsignificant differences between the various demographicclassifications (Tables 2 and 3). Of the respondents 27%identified their level of religious activity as regularly ac-tive. These included people from a variety of religiousbackgrounds. The religiously active respondents indi-cated far less support than did other groups for a pa-tient's right to have life support withdrawn (Table 2).Unlike those who did not classify themselves as regu-larly active religiously, those in the active group weresignificantly more opposed to the consideration of as-sisted death for themselves or family members andwould not choose for themselves a doctor who per-formed euthanasia (p < 0.01). Most in this group (59%)did not feel that quality of life should be an importantconsideration in decisions related to euthanasia, and76% felt that legalization of euthanasia for terminally illpatients in severe pain would lead to its legalization for
No. (and '/o)of respondets
Female(n=23) (n;.:(. )Group
Generalpublic 107 (4.O)i.Physicians 100 (44.8) 4 .4)Ethical experts 45 (20.2) 23 (17.7)Religious leaders 27 (12.1) 1:8(I38)Politicians 11 (4.9) 15 (11.5)*The percenteges total more than 100 b s em e respondents indicated that more than one group hul Share theresponsibility.
706 CAN MED ASSOC J 1994; 150 (5) LE I'rMARS 1994

other reasons. The religiously active were also the mostconsistently opposed to public funding of euthanasia(82%); 64% felt that government should prohibit suchpractices through legislation. When compared with otherdemographic categories, a significantly higher propor-tion of the religiously active respondents (41%) were op-posed to the idea of making living wills legally binding(Table 3) (p < 0.01).
Discussion
Our findings indicate that public acceptance of eu-thanasia varies depending on the circumstances. Majori-ty acceptance of this practice was limited to situations ofpainful terminal illness. Most people were concernedabout quality of life and felt that legalization of euthana-sia for the terminally ill would eventually lead to its le-galization for other reasons not generally supported.There is strong evidence that both the general public andphysicians should be the primary participants in deter-mining legislation regarding the right to die.
A degree of bias resulted through the two-stageprocess of telephone and mailing; the main sources ofbias identified were as follows.
* Nonresponse due to lack of interest (40% of peo-ple contacted), literacy or language problems (4%) orfailing to return a mailed survey (16% of the 902 peoplecontacted).
* Self-selection: once the questionnaire was mailedout the respondent within the household was large-ly self-selected. Although a degree of bias did resultthrough the two-stage process of telephone contact andmailing (females, young adults and educated peoplewere the most likely to respond), a thoughtful responsewould not have been facilitated by the brief and immedi-ate format of a telephone survey because of the length ofthe questionnaire and the complexity of the issues.
* The views of Edmontonians do not necessarilyrepresent the views of all Canadians.
The bias toward younger women may be partiallydue to the fact that women in general tend to take pri-mary responsibility for the care of other family mem-bers. Gilligan'5 described the "ethic of care" as it relatesto women's relationships, and other authors have inte-grated this approach with the care of the dying: "We areconvinced that an ethic of care provides a vital perspec-tive to the moral enterprise of caring for dying per-sons."'6 Although the survey did not reveal significantdifferences between the opinions of women and men, thegreater interest of women, as shown by the higher partic-ipation rate, may have been due in part to their greaterinvolvement in caregiving.
The respondents indicated support for the with-drawal of life-support systems from a comatose patientfor whom there was little chance of any positive change.These results concur with the findings of one author,who stated that "we couldn't use life-sustaining technol-
ogy unless we were able to stop using it too."'7 This is acritical principle, since the results of resuscitation are notalways predictable. Without the ability to withdraw un-successful treatment society would necessarily reach thestage of prioritizing who would be resuscitated, with re-sultant discrimination against people not meeting thespecified criteria.
Although there was opposition to euthanasia for avariety of non-life-threatening reasons, and althoughmost of the respondents felt that legalization of euthana-sia for the terminally ill would eventually lead to its le-galization for other reasons, most did not favour legisla-tion outlawing euthanasia. Therefore, although peoplemay not favour prohibitive legislation in this area, theymay wish to have standards and criteria in place to limitthe use of euthanasia. This raises the concern that stan-dards can shift on the basis of medical practice and caselaw. This has been illustrated in the Netherlands, wheredespite criteria that euthanasia be consistently and freelyrequested by the patient,'8 there is "official recognitionof the fact that involuntary active euthanasia is regularlypractised ... not as sporadic punishable acts committedby some outcasts, but as a justifiable part of commonmedical practice."'9 In areas where common practiceamong health care professionals contradicts legislatedcriteria, the differences need to be re-evaluated.
In addition, our results indicated that the respon-dents' level of religious activity had a significant impacton their views related to euthanasia. This is not surpris-ing, because end-of-life decision making challenges notonly our views of certain medical technologies and treat-ments but also our definitions of life and death and themeaning we give to these events. When seeking societaldirection in such a bioethically complex area, it is im-portant to remember that "theology and religious tradi-tion play major roles in developing value consensus in apluralistic society".20
In our study the only support for active euthanasiawas found for suffering, terminally ill patients. Many au-thors have suggested that if patients are provided withadequate pain relief, physical support and compassion,and control over treatment decisions in the setting ofphysician-supervised palliative or hospice care, the de-mand for euthanasia would be greatly reduced.2'23 Wedid not explore programs such as palliative care andcommunity rehabilitation services and cannot assumethat respondents were fully aware of these alternatives.Before euthanasia gains a higher profile, it is imperativethat genuine access to comprehensive palliative and hos-pice care become a reality for all dying people and theirfamilies.24
Although physicians play a pivotal role in the careof elderly or dying patients, their role in the area of eu-thanasia is as yet undefined in Canada. The public's rolein establishing policy is also unresolved, particularlywhen the personal knowledge and involvement of indi-viduals may be limited; however, physicians must be-
CAN MED ASSOC J 1994; 150 (5) 707MARCH 1, 1994
come aware of public attitude and fully explore the rolethat they, as individuals and as a professional group,wish to play in this controversial area.
Many aspects of end-of-life decisions were pre-sented in this survey. We hope that the results will serveas an impetus for further discussion and research. Be-cause palliative and hospice care is not yet universallyavailable one cannot predict how public opinion wouldbe affected by the full access and availability of suchcomprehensive care. A national survey involving casestudies and including alternatives such as palliative andhospice care would be helpful in determining consis-tency of thought and attitude across the country. Giventhe increasing complexity of end-of-life decisions, re-search into the benefits and harms of health care proxiesin conjunction with or in contrast to a written living willwould also be very beneficial to patients, health careprofessionals and institutions.
We thank Vernie Wynnyk for her excellent assistance in di-recting the survey and Sheila Fynn for all the efficient andprompt help in acquiring the necessary literature.
References
1. Orentlicher D: Physician participation in assisted suicide. JAMA1989; 262: 1844-1845
2. Sawyer DM, Williams JR, Lowy F: Canadian physicians and eu-thanasia: 2. Definitions and distinctions. Can Med Assoc J 1993;148: 1463-1466
3. Caralis PV, Hammond JS: Attitudes of medical students, house-staff, and faculty physicians towards euthanasia and terminationof life-sustaining treatment. Crit Care Med 1992; 20: 683-690
4. Reed J: Interdependence in euthanasia. Humane Med 1992; 8: 97-98
5. Lo B, Rouse F, Dornbrand L: Family decision making on trial:Who decides for incompetent patients? N En,gl J Med 1990; 322:1228-1232
6. Kuhse H, Singer P: Doctors' practices and attitudes regarding vol-untary euthanasia. Med J Aust 1988; 148: 623-627
7. Wanzer SH, Federman DD, Adelstein SJ et al: The physician's re-
sponsibility toward hopelessly ill patients. N Enigl J Med 1989;320: 844-849
8. Rosenblum VG, Forsythe CD: The right to assisted suicide: Pro-
tection of autonomy or an open door to social killing? Issues LawMed 1990; 6: 3-31
9. Battin MP: Assisted suicide: Can we learn from Germany? Hast-ings Cent Rep 1992; Mar-Apr: 44-51
10. Smith R: Euthanasia: time for a royal commission. BMJ 1992;305: 728-729
11. Smith ML, Orlowski J, Radey C et al: A good death: Is euthanasiathe answer? Cleve Clin J Med 1992; 59: 99-109
12. Steiber SR: Right to die: public balks at deciding for others. Hos-pitals 1987; 10: 72
13. Iezzoni L: Severity standardization and hospital quality assess-ment. In Couch JB (ed): Health Care Quality Management for the21st Century, American College of Physician Executives, Tampa,Fla, 1991: 177-231
14. Moses LE, Emerson JD, Hosseini H: Analyzing data from orderedcategories. N Engl J Med 1984; 311: 442-448
15. Gilligan C: In a Different Voice, Harvard U Pr, Cambridge, Mass,1982: 24-63
16. Dossetor JB, Wright DE, Burgess MM: Ethical issues in caringfor the dying [E]. Humane Med 1993; 9: 7-9
17. Scofield GR: Physician-assisted suicide: Part of the problem orpart of the solution? Trends Health Care Law Ethics 1992; 7:15-18
18. Sprung CL: Changing attitudes and practices in forgoing life-sus-taining treatments. JAMA 1990; 263: 2211-2215
19. Fenigsen R: The report of the Dutch government committee oneuthanasia. Issues Law Med 1991; 4: 339-344
20. O'Rourke K: Assisted suicide: an evaluation. J Paini SymptonManiage 1991; 6: 317-324
21. Daikos GK: The terminal quality of life and passive or active eu-thanasia. Qual Assur Health Care 1990; 2: 375-386
22. Rehm D, Martin E: The hospice response to proposals of assistedsuicide. RI Med J 1992; 75: 127-128
23. McIntyre RL: Editors' round-table: physician-assisted dying.Trends Health Care Law Ethics 1992; 7: 28-31
24. Byock IR: Final exit: a wake-up call to hospice. Hospice J 1991;7:51-66
708 CAN MED ASSOC J 1994; 150 (5) LE 1c` MARS 1994
Copyright © 2022 FDOKUMEN