Promoting psychosocial well-being following a stroke: developing a theoretically and empirically...
12
Promoting psychosocial well-being following a stroke: Developing a theoretically and empirically sound complex intervention Marit Kirkevold a, *, Berit A. Bronken a,b , Randi Martinsen a,b , Kari Kvigne b a Institute of Health and Society, Department of Nursing Science, University of Oslo, P.O. Box 1153, Blindern, N-0318 Oslo, Norway b Hedmark University College, Norway International Journal of Nursing Studies 49 (2012) 386–397 A R T I C L E I N F O Article history: Received 30 January 2011 Received in revised form 5 September 2011 Accepted 2 October 2011 Keywords: Complex interventions Evaluation studies as topic Mental health Psychosocial factors Qualitative research Stroke A B S T R A C T Background: The psychosocial consequences of stroke are complex and comprehensive and include substantial and longlasting impacts on mood, identity, social relationships, return to work and quality of life. Many studies have explored possible interventions to prevent or treat psychosocial problems, but the results have generally been disappointing. Very few studies have provided adequate theoretical accounts of the mechanisms assumed to contribute to positive outcomes. Objectives: To describe the development of a psychosocial nursing intervention aimed at promoting psychosocial health and well-being and to stimulate dialogue about how to develop and report theoretically and empirically sound complex interventions in nursing. Design: A systematic, stepwise approach was used, consistent with the framework recommended for developing and evaluating complex interventions by the UK Medical Research Council. Data sources: Systematic reviews of empirical studies regarding the psychosocial consequences and needs of patients following stroke; qualitative, experiential studies of stroke and stroke recovery; theories of psychosocial well-being, coping, life skills, narrative approaches to rehabilitation and guided self-determination. Review methods: Each systematic review was examined to determine the major psychosocial challenges and needs experienced by stroke survivors, focusing on how these challenges and needs developed over the illness trajectory, how previous interventions had sought to address them and the effective mechanisms assumed to affect the level of success of interventions. Qualitative studies were examined to reveal the subjective experiences of stroke and stroke recovery, paying particular attention to the development of needs across time and context. A qualitative synthesis of the major characteristics of the trajectory of stroke rehabilitation and recovery during the first year was developed. Theories were examined to illuminate possible effective mechanisms and actions aimed at promoting psychosocial well-being during the stroke recovery process. Results: A dialogue-based intervention comprising eight encounters between stroke survivors and trained health care workers was designed, based on narrative theories, empowerment philosophy and guided self determination. Worksheets and a guiding topical outline were developed to support the dialogue. Conclusions: The UK Medical Research Council framework facilitated the systematic development of an empirically and theoretically informed complex nursing intervention aimed at promoting post-stroke psychosocial well-being. ß 2011 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +47 22 85 05 69. E-mail address: [email protected] (M. Kirkevold). Contents lists available at SciVerse ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns 0020-7489/$ – see front matter ß 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.ijnurstu.2011.10.006
Transcript of Promoting psychosocial well-being following a stroke: developing a theoretically and empirically...

Pth
Ma Inb H
International Journal of Nursing Studies 49 (2012) 386–397
A
Art
Re
Re
Ac
Ke
Co
Ev
Me
Psy
Qu
Str
*
00
do
romoting psychosocial well-being following a stroke: Developing aeoretically and empirically sound complex intervention
arit Kirkevold a,*, Berit A. Bronken a,b, Randi Martinsen a,b, Kari Kvigne b
stitute of Health and Society, Department of Nursing Science, University of Oslo, P.O. Box 1153, Blindern, N-0318 Oslo, Norway
edmark University College, Norway
R T I C L E I N F O
icle history:
ceived 30 January 2011
ceived in revised form 5 September 2011
cepted 2 October 2011
ywords:
mplex interventions
aluation studies as topic
ntal health
chosocial factors
alitative research
oke
A B S T R A C T
Background: The psychosocial consequences of stroke are complex and comprehensive and
include substantial and longlasting impacts on mood, identity, social relationships, return
to work and quality of life. Many studies have explored possible interventions to prevent or
treat psychosocial problems, but the results have generally been disappointing. Very few
studies have provided adequate theoretical accounts of the mechanisms assumed to
contribute to positive outcomes.
Objectives: To describe the development of a psychosocial nursing intervention aimed at
promoting psychosocial health and well-being and to stimulate dialogue about how to
develop and report theoretically and empirically sound complex interventions in nursing.
Design: A systematic, stepwise approach was used, consistent with the framework
recommended for developing and evaluating complex interventions by the UK Medical
Research Council.
Data sources: Systematic reviews of empirical studies regarding the psychosocial
consequences and needs of patients following stroke; qualitative, experiential studies
of stroke and stroke recovery; theories of psychosocial well-being, coping, life skills,
narrative approaches to rehabilitation and guided self-determination.
Review methods: Each systematic review was examined to determine the major
psychosocial challenges and needs experienced by stroke survivors, focusing on how
these challenges and needs developed over the illness trajectory, how previous
interventions had sought to address them and the effective mechanisms assumed to
affect the level of success of interventions. Qualitative studies were examined to reveal the
subjective experiences of stroke and stroke recovery, paying particular attention to the
development of needs across time and context. A qualitative synthesis of the major
characteristics of the trajectory of stroke rehabilitation and recovery during the first year
was developed. Theories were examined to illuminate possible effective mechanisms and
actions aimed at promoting psychosocial well-being during the stroke recovery process.
Results: A dialogue-based intervention comprising eight encounters between stroke
survivors and trained health care workers was designed, based on narrative theories,
empowerment philosophy and guided self determination. Worksheets and a guiding
topical outline were developed to support the dialogue.
Conclusions: The UK Medical Research Council framework facilitated the systematic
development of an empirically and theoretically informed complex nursing intervention
aimed at promoting post-stroke psychosocial well-being.
� 2011 Elsevier Ltd. All rights reserved.
Corresponding author. Tel.: +47 22 85 05 69.
E-mail address: [email protected] (M. Kirkevold).
Contents lists available at SciVerse ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
20-7489/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
i:10.1016/j.ijnurstu.2011.10.006

�
��
�
�
�
1
csratha2pp
c(Fdpwea(D
aa2dbTedddsemdafoadsb
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397 387
What is already known about the topic?
Psychosocial difficulties following stroke may impederehabilitation and recovery.
Few effective psychosocial interventions are available. The effective mechanisms of psychosocial interventionsare rarely described.
What this paper adds
An example of how to apply the systematic, stepwiseapproach suggested by the UK Medical Research Councilfor developing nursing interventions.
A proposed theoretical and empirical foundation for acomplex nursing intervention targeting psychosocialneeds post-stroke.
A description of the assumed effective components of acomplex psychosocial nursing intervention.
. Background
The psychosocial consequences of stroke can beomplex and comprehensive. Research has documentedubstantial and longlasting effects on mood, identity, socialelationships, return to work and participation in valuedctivities (Knapp et al., 2000). Approximately one third ofose affected report depressive symptoms, and 20% report
nxiety during the first few months or years (Barker-Collo,007; Ferro et al., 2009; Hackett et al., 2008a,b). Generalsychological distress and social isolation are alsorevalent (Knapp et al., 2000).
The psychosocial consequences of stroke may signifi-antly affect long-term functioning and quality of lifeerro et al., 2009; Teoh et al., 2009). Anxious and
epressed stroke survivors benefit less from rehabilitationrograms and have higher mortality rates than patientsithout such symptoms (Hackett et al., 2008a,b; Ferro
t al., 2009). Difficulties coping and loss of control isssociated with reduced functioning and well-being
onnellan et al., 2006).The causes and risk factors of psychosocial problems are
mbiguous. Two main theories of post-stroke depressionnd anxiety have been suggested (Whyte and Mulsant,002). The first proposes that depression and anxiety areirect effects of biological mechanisms, i.e., that ischemicrain lesions damage the nervous circuits regulating mood.his theory is supported by findings that the location andxtent of ischemic brain damage are associated withepression. The second theory proposes that post-strokeepression is caused by psychosocial mechanisms, i.e., thatepression and anxiety are reactions to overwhelmingtress, affective overload and an inability to cope with thextensive losses following a stroke. Post-stroke depressionay also be classified into early onset, or reactive,
epression, which develops hours or days after stroke,nd late onset depression, which occurs 3–6 monthsllowing the stroke. Early onset is more strongly
ssociated with spontaneous remission than later onsetepression. Whyte and Mulsant (2002) argue that post-troke depression is multifactorial and consistent with aiopsychosocial model. They suggest that a biological
mechanism may be particularly relevant for explainingearly-phase depression, whereas the psychosocialmechanism may be increasingly prominent in late-onsetdepression. Further research is needed to find effectivestrategies for the primary prevention of post-strokedepression, taking these different mechanisms intoaccount (Whyte and Mulsant, 2002).
A large number of studies have explored possibleinterventions to prevent and/or treat psychosocial pro-blems (Hackett et al., 2008a,b; Knapp et al., 2000; Smithet al., 2008; Redfern et al., 2006). Although the results havegenerally been disappointing, a number of trials havedocumented modest positive outcomes. Pharmacologicaltreatment has been found to be effective in treating post-stroke depression, but not in preventing it (Hackett et al.,2008a,b). The research on psychosocial interventionssuggests that information, emotional support, practicaladvice and motivational support are important (Ellis et al.,2010; Smith et al., 2008; Redfern et al., 2006). The detailsof how the different elements of the interventionscontribute to positive outcomes and which elementswork best at different stages and in different subgroupsare not clear, however (Ellis et al., 2010; Smith et al., 2008;Redfern et al., 2006). The lack of clarity regarding theeffective mechanisms is attributed to the fact that veryfew studies have provided adequate theoretical accountsof the mechanisms assumed to contribute to positiveoutcomes (Ellis et al., 2010; Smith et al., 2008; Redfernet al., 2006).
Nurses are key professionals in the rehabilitation ofstroke patients and are ideally suited to address thepatients’ psychosocial needs and provide support andguidance to improve coping (Kirkevold, 2010). Never-theless, few nursing interventions have been developedthat specifically address the psychosocial well-being ofstroke survivors (Burton and Gibbon, 2005; Watkins et al.,2007). A recent review concluded that nursing interven-tions are underdeveloped and inadequately described(Forbes, 2009). In this paper, we respond to thesechallenges by describing the development of a psychoso-cial nursing intervention aimed at promoting psychosocialhealth and well-being. Specifically, we highlight the use ofempirical evidence and theoretical assumptions in guidingthe development. This intervention is assumed to addressthe psychosocial mechanism of post-stroke ill-being thatmay lead to depression and anxiety (Whyte and Mulsant,2002) by facilitating psychosocial adjustment. We hopethat this paper will stimulate a dialogue about how todevelop and report theoretically and empirically soundcomplex interventions in nursing.
2. Design and methods
We used a development approach consistent with theframework recommended for developing and evaluatingcomplex interventions proposed by the UK MedicalResearch Council (MRC) (Campbell et al., 2000; Craiget al., 2008). Complex interventions are ‘‘usually describedas interventions that contain several interacting compo-nents’’ (Craig et al., 2008, p. 979). Several dimensions ofcomplexity may be present, including the number of

inbeinlevataM20dedein‘thlinCoimMevFuofretotriarduusdeexphdeincowthveThou
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397388
teracting components, the number and difficulty of thehaviours required by those delivering or receiving thetervention, the number of groups or organisationalvels targeted by the intervention, the number andriability of outcomes and the degree of flexibility oriloring of the intervention (Craig et al., 2008, p. 979). TheRC framework has recently been recommended (Forbes,09) and found useful (Maindal et al., 2010) for thevelopment of nursing interventions. This frameworkscribes the development and testing of complex healthterventions in five phases, from the initial pre-clinicaleory and research review’ phase, through the ‘model-g’ and ‘exploratory trial’ phases into the ‘Randomizedntrolled Trial’ phase and, finally, the ‘long-termplementation’ phase. In the revised version of the
RC framework (Craig et al., 2008), the development andaluation process was described in a less linear fashion.rthermore, the importance of integrating a wide array
evidence, including knowledge from qualitativesearch and practical experience, has been emphasised underpin and optimise the intervention prior to anyal work. We have completed the first three phases ande currently analyzing the experiences and data collectedring these phases. We expect that this work will equip
with a sound theoretical and practical basis forsigning a follow-up, controlled trial in which theperiences and insights gained during the previousases are incorporated. We believe that the carefulvelopment of the theoretical foundations of ourtervention will help clarify how the different elementsntribute to positive outcomes. In the following sections,e present the theoretical and empirical foundations ofe intervention, practical deliberations and the inter-ntion. The design of this study is summarised in Fig. 1.is paper presents the results of the first two phases ofr study.
3. Phase 1: identifying evidence and theory
The MRC framework underscores the importance ofreviewing the research literature and clinical experience toidentify the specific needs for an intervention and relevantoutcomes, to review what we know about effectiveelements that may be integrated and to examinetheoretical perspectives that may explain the effectivenessof the intervention (Craig et al., 2008).
3.1. Methods for conducting needs assessment
The needs assessment for the intervention presented inthis paper was carried out using a number of steps. First,the need for psychosocial support was suggested by anumber of previous longitudinal studies by members ofthe research team, which focused on the subjectiveexperiences of people adjusting to substantial changesin life following a stroke (Eilertsen et al., 2010; Kirkevold,2002; Kvigne and Kirkevold, 2003; Kvigne et al., 2004). Asynthesis of these findings has been published previously(Kirkevold, 2010).
Second, a review of the literature sought to identifysystematic reviews of post-stroke psychosocial needs andthe effectiveness of interventions addressing these needs.We chose systematic reviews because there was extensiveliterature in this area, and a number of high quality reviewswere available. The strategy for the literature review issummarised in Box 1.
We identified 16 reviews, which were examined todetermine the major psychosocial challenges and needsexperienced by stroke survivors, how they developed overthe illness trajectory and how previous interventions hadsought to address them. We also looked for the effectivemechanisms of the interventions and the factors assumedto affect their level of success.
Fig. 1. Structure of intervention development process.

epTomacouap
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397 389
Third, theories were examined to illuminate possibleffective mechanisms and actions aimed at promotingsychosocial well-being during the stroke recovery process.he selection of theories was guided by the findingsbtained during the first two steps, which highlightedajor goals, factors and issues that needed to be taken into
ccount to promote psychosocial well-being. We specifi-ally sought theories that could help us conceptualise andperationalise psychosocial well-being and obtain a deepernderstanding of the psychosocial mechanisms related todjustment and coping following stroke. Based on ourrevious qualitative studies, we sought theories that could
guide us in developing strategies to support further under-standing of stroke and its ramifications and also strategiesthat could support participation and personal control.Finally, we sought theories regarding effective communica-tion with people suffering from aphasia.
The above steps led to the initial development of apsychosocial intervention aimed at promoting psychoso-cial well-being by reducing stress and uncertainty andimproving understanding, predictability and copingthrough goal-directed professional support. The proposedintervention was evaluated and critiqued by patient andrelative representatives, clinical experts and researchersduring several expert group meetings. The methods usedto recruit the participants and evaluate the interventionare summarised in Box 2.
The findings from the above steps, which are alignedwith phases 1 and 2 of the MRC framework, are presentedin the following sections.
3.2. Psychosocial challenges and needs following stroke
A substantial number of qualitative studies (Danielet al., 2009; Hafsteinsdottir and Grypdonck, 1997;
Box 1. Search and review strategies for the literature
review
Search strategy:
Literature searches were conducted in Medline,
Cochrane, Cinahl and Psychinfo, using various com-
binations of the search terms stroke and psychology,
depression, anxiety, psychosocial factors, psychoso-
cial well-being and qualitative. The major searches
were conducted during 2007 and 2008, with supple-
mentary searches conducted during 2010 and spring
2011. The searches were limited to English language
review articles, systematic reviews and evidence-
based reviews. These searches generated over 100
articles.
Selection procedure:
Titles and abstracts were reviewed, and the following
inclusion criteria were applied: stroke patients, non-
pharmacological, psychosocial needs and conse-
quences and psychosocial intervention. The following
exclusion criteria were used: non-empirical articles,
interventions not focusing on psychosocial needs and
consequences, and interventions directed towards
family and informal carers. The full text of articles that
met the initial inclusion criteria were read, leading to
the exclusion of additional articles that did not meet
the inclusion criteria.
Quality evaluation:
The included reviews were evaluated using the quality
criteria recommended by the EPOC (Effective Practice
and Organisation of Care) group in its guide for review
authors available at www.epoc.cochrane.org. Reviews
judged to be of high or moderate quality in terms of
documenting systematic searches, data extraction,
data analysis and reporting of findings were included.
The final sample included 16 systematic reviews.
Data extraction:
Data were extracted to answer the following ques-
tions: what are the major psychosocial challenges
and needs experienced by stroke survivors? How do
psychosocial challenges and needs develop over
time? How have previous interventions sought to
address them? What are the assumed effective
mechanisms of the interventions? Which factors
appear to affect the level of success? Reviews of
qualitative studies were examined to identify subjec-
tive experiences of the psychosocial consequences of
stroke and stroke recovery, and to determine how
psychosocial needs develop over time and across
contexts.
Box 2. Methods for recruiting and conducting expert
evaluation of the preliminary intervention
The preliminary evaluation was guided by an action-
oriented approach.
Recruitment procedure:
A wide range of health care professionals within stroke
care and rehabilitation (physicians, physiotherapists,
occupational therapists, nurses, speech therapists and
psychologists), leaders at different levels in hospitals
and community stroke care, stroke representatives
and family carers were invited to attend expert meet-
ings at three locations in the southern part of Norway
during 2007 and 2008. Two or three of the researchers
were usually present and facilitated the discussions,
applying a focus group approach.
Sample:
A total of 50 people were invited to participate in three
large groups (ranging from 10 to 18 members) and
three smaller groups (ranging from 4 to 8 members).
The groups met between one and 3 times.
Data collection:
The groups received written and oral information
regarding the intervention and were invited to discuss
the following aspects of the preliminary intervention:
the relevance and importance of the proposed content,
structure, approach and methods; issues/content lack-
ing coverage; how the intervention ought to be orga-
nized and integrated into existing health care structures;
feasibility and training needs.
Data analysis:
Written notes were taken at each meeting. The research
team systematically reviewed the preliminary interven-
tion in light of the comments. The suggestions from the
expert meetings were incorporated whenever appro-
priate. When conflicting suggestions/feedback were
provided, the research team sought to resolve the issue
by re-reviewing to the literature and consulting specific
Further detailed information is available upon request. experts on the issue at hand.

LaSaandethboemprtopaadresp
20fothwstrevvatiaidNosea mrothpsbeberewa limthtw
doetthexclops(Mrebem
3.3
he
thatprciaisobe
Ha
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397390
wrence, 2010; McKevitt et al., 2004; Murray et al., 2003;lter et al., 2008) have demonstrated that the recoveryd adjustment process following stroke is lengthy,manding and fraught with uncertainty. Patients andeir families struggle to make sense of their experiences;dily symptoms are unfamiliar and confusing, andotional reactions and functional progress are hard to
edict. Stroke patients express surprise at the time it takes improve despite their strong commitment and activerticipation in rehabilitation programs. The process ofjustment and recovery lasts well beyond the formalhabilitation period during which patients are offeredecialised rehabilitation services.In our studies (Eilertsen et al., 2010; Kirkevold, 2002,
10; Kvigne and Kirkevold, 2003; Kvigne et al., 2004), weund that patients went through different phases duringe first one to two years. Their concerns graduallyidened from being focused on bodily recovery, throughuggling to re-establish a functioning and meaningfuleryday life (in which they seek to assume previous roles,lued activities and significant relationships), to nego-ting their self-understanding and re-establishing their
entity in light of the changes brought about by the stroke.ne of the participants in these studies judged them-
lves fully recovered two years later, despite the fact thatajority of the participants had resumed most functions,
les and activities in which they were involved prior toe stroke. The patients seemed especially vulnerable toychological stress during periods of transition, i.e., whileing discharged from the stroke unit/acute care hospital,ing discharged from follow-up services, attempting tosume new roles and activities outside the home andhen acknowledging that the stroke would probably haveasting impact on their life. Most continued to struggle toprove and expressed insecurity and a lack of guidance ineir continued adjustment process throughout the firsto years.Systematic reviews of qualitative studies (Hafsteins-
ttir and Grypdonck, 1997; Lawrence, 2010; McKevitt al., 2004; Murray et al., 2003; Salter et al., 2008) supportese findings, although few studies have followedperiences of the recovery- and adjustment process assely as ours. In light of the high prevalence of
ychological difficulties and symptoms in stroke patientsurray et al., 2003), the findings from the literature
view suggest that targeted psychosocial support might needed to facilitate post-stroke adaptation and adjust-ent.
. Existing interventions aimed at promoting psychosocial
alth and well-being
A review of existing interventions aimed at addressinge psychosocial consequences of stroke indicate thattention has been directed towards specific psychologicaloblems such as depression and more general psychoso-l needs and challenges, e.g., a lack of information, sociallation and coping difficulties. These are summarisedlow.Preventing post-stroke depression has proved difficult.ckett et al. (2008a) reviewed ten randomised controlled
pharmacological trials and four psychotherapeutic trialsand found no significant effect of the pharmacologicalinterventions. There was some evidence for improvedmood following psychotherapeutic treatment, but theeffect size was limited.
Treating depression after stroke has also provedchallenging. Although a systematic review of 16 trials(12 pharmacological and 4 psychotherapeutic trials) foundevidence for a beneficial effect of pharmacological treat-ment, adverse effects also increased (Hackett et al., 2008b).The psychotherapeutic interventions showed no signifi-cant effect.
Psychosocial interventions focused on resolving psy-chosocial difficulties more generally have also had gen-erally disappointing effects. The provision of information,education, leisure therapy, support workers and counsel-ling has shown weakly positive or no effects (Knapp et al.,2000). These results were mostly attributed to weaknessesin study design; inadequate intensity, timing and trainingof therapists and a lack of attention to theoretical modelsthat could guide the development of psychosocial inter-ventions; the authors strongly recommend that this line ofresearch be pursued.
The systematic review by Smith et al. (2008) regardingthe provision of information to stroke patients and theircaregivers is slightly more promising. The authors con-clude that some benefits result from providing informa-tion, although these are clinically small. In particular, theirreview suggests that active approaches, combining teach-ing and the provision of knowledge with self-study,individualised counselling and support, are more effectivethan passive approaches for important outcomes such asrelieving depression and anxiety.
In a recent comprehensive review that specificallyfocused on complex interventions in stroke care, Redfernet al. (2006) reviewed 67 studies that tested complexinterventions intended to change knowledge, beliefs orbehaviours. Of these, 30 studies targeted adjustment andrecovery after stroke, and these involved education,training, counselling and social support. These interven-tions, particularly the informational and social supportinterventions, were less likely to succeed. Consistent withprevious studies, Redfern et al. concluded that fewcomplex interventions have been adequately developedor evaluated and recommended greater attention totheoretical development and methodological quality.
Ellis et al. (2010) responded to the repeated cry forfurther theoretical work with a systematic review of theeffect of stroke liaison workers on stroke patients andfamily members. They explored the relative effects ofvarious models and examined possible effective mechan-isms. They compared different types of liaison, informa-tional and educational and social support interventionsand classified them into three groups according to theirdegree of proactivity–reactivity, flexibility and structure,and scope (proactive and structured, reactive and flexible,and proactive and focused). Conducting an individual-levelmeta-analysis, the authors found little evidence of anoverall effect on patients and families regarding healthsatisfaction and level of independence, although patientsdid express satisfaction that ‘‘someone has really listened’’,
aethbaidthscseTT
pc(EtoH2mpdaHfroslaaFds
liaqle
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397 391
nd carers were satisfied with the information andducation they received. Subgroup analyses suggestedat persons with mild to moderate stroke seemed to
enefit most from this complex intervention, but theuthors cautioned that further research was needed toentify the specific aspects of this complex interventionat might be most effective and appropriate for different
ubgroups of stroke survivors and carers. Further researchomparing the effectiveness of the liaison service to earlyupported discharge services, which have shown positiveffects, was also recommended (Early Supported Dischargerialists, 2009; Larsen et al., 2006; Outpatient Servicerialists, 2003).
None of the above reviews specifically addressed thesychosocial needs of stroke survivors with aphasia, whoomprise approximately one third of stroke survivorsngelter et al., 2006). This group is particularly vulnerable anxiety, depression and social isolation (Code anderrmann, 2003; Code and Petheram, 2011; Kelly et al.,010). The language problems experienced by this groupay prevent them from talking to others about their
roblems and concerns, and they may have extensiveifficulties in accessing the services that they need (Hilarind Northcott, 2006; Parr et al., 2006; Shadden andagstrom, 2007). Frequently these patients are excludedom intervention studies due to their difficulties in fillingut questionnaires or participating in interviews. Sub-tantial research has been conducted to address thenguage and communication problems of people with
phasia (Lyon, 2004; Parr et al., 2003; Shadden, 2005).urther research is needed, however, regarding theevelopment of interventions that address their psycho-ocial needs more broadly.
The following observations recur frequently in theterature reviewed above: outcomes are modest, there is
lack of theoretically founded interventions, and inade-uate attention has been paid to methodological chal-nges. Despite these shortcomings, the literature
highlights the following important aspects that shouldbe considered in the next generation of research:
� the specific goals and outcomes to be targeted,� the timing and intensity of the intervention,� the active involvement of patients and carers,� the development of individually relevant coping skills,� close attention to the mechanisms that may facilitate
psychosocial well-being, and� the flexibility to adjust the intervention to the needs of
different subgroups.
Based on the evidence reviewed above, we concludedthat there is a need to develop and test the effectiveness ofan intervention that seeks to promote psychosocial well-being during the recovery and adjustment process over thefirst year post-stroke. Such intervention must activelyengage the stroke survivors in the process and build ontheir available coping resources. In the next section, wedetail the theoretical deliberations that guided thedevelopment of the intervention.
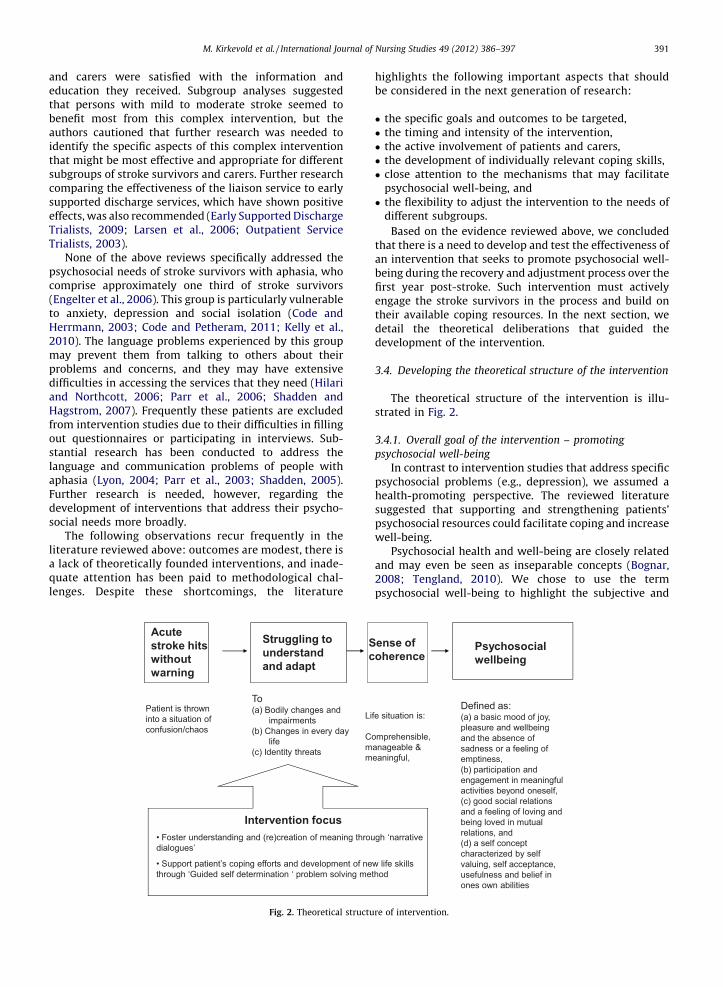
3.4. Developing the theoretical structure of the intervention
The theoretical structure of the intervention is illu-strated in Fig. 2.
3.4.1. Overall goal of the intervention – promoting
psychosocial well-being
In contrast to intervention studies that address specificpsychosocial problems (e.g., depression), we assumed ahealth-promoting perspective. The reviewed literaturesuggested that supporting and strengthening patients’psychosocial resources could facilitate coping and increasewell-being.
Psychosocial health and well-being are closely relatedand may even be seen as inseparable concepts (Bognar,2008; Tengland, 2010). We chose to use the termpsychosocial well-being to highlight the subjective and
Psychosoc ialwell being
Defin ed as: (a) a bas ic mood of joy, pleasure and wellbei ng and th e absen ce of sadnes s or a feelin g of empt ines s, (b) pa rticipa tion and engagement in mean ingful activ itie s be yond onese lf, (c) good soci al relat ions and a feeli ng of l oving and being lo ved in mutua l relations, an d (d) a se lf con cept cha racteri zed by se lf valui ng, se lf ac ceptance, usefulne ss and be lief in ones own abi lities
Struggling to understand and adap t
Acutestroke hits wit houtwarning
Inte rventio n focu s• Foster un derstandin g and (re )creation of mean ing th rough ‘nar rative dialogue s’
• Support patient ’s coping efforts and deve lop ment of ne w life skills through ‘Guided self de ter mina tion ‘ prob lem solvin g metho d
To(a) Bod ily change s and
impa irmen ts(b) Change s in ever y day
life (c) Identit y threat s
Patient is thrown into a sit uation of confusio n/chao s
Sense ofcoherenc e
Life situat ion is:
Compreh ensi ble, manageab le & meaningf ul,
Fig. 2. Theoretical structure of intervention.

inbe19exthinthreouwcoanan19beplfemrereacThacquvasolitstrthsioin
exathecoexnimanunacesCoindeof
3.4
m
inmadwPopubetoanid
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397392
teractive or social aspects of health. Theories of well-ing are often classified into three categories (Parfit,84; Brulde, 2007): hedonistic theories focus on theperience of pleasure or happiness, desire-fulfilmenteories emphasise the importance of desires or mean-gful goals in promoting well-being and objective listeories maintain that certain things are good for usgardless of whether or not they are wanted. We took asr point of departure the statement that psychosocial
ell-being ‘‘is high to the degree that the person’snscious cognitive and affective experiences are positived low to the degree that the person’s conscious cognitived affective experiences are negative’’ (Næss, 2001, p.40). According to this perspective, psychosocial well-ing has four dimensions: (a) a basic mood of joy,easure and well-being and the absence of sadness or aeling of emptiness, (b) participation and engagement ineaningful activities beyond oneself, (c) good sociallations and a feeling of loving and being loved in mutuallationship(s) and (d) a self-concept characterised by selfceptance, usefulness and a belief in one’s own abilities.is represents a hybrid conceptualization (Brulde, 2007),knowledging that psychosocial well-being is a conse-ence of intra-individual experiences, processes andlues, as well as external resources and factors such ascial relationships and support. Our review of theerature regarding the psychosocial consequences ofoke highlighted that each of these dimensions may bereatened following a stroke. Consequently, these dimen-ns were chosen as goals or outcomes to target with the
tervention (see Fig. 2).Major threats to well-being following stroke include
periences of chaos and a lack of control. This drew ourtention to Antonovsky’s theory (1987), which connectsalth and well-being to the experience of a sense ofherence in life. A sense of coherence is promoted byperiencing diverse life events as comprehensible (cog-tive), manageable (instrumental/behavioural) andeaningful (motivational) (Antonovsky, 1987; Erikssond Lindstrom, 2005, 2006). Because the literature reviewderscored that these aspects might be threatened byute stroke, they were seen as intermediate goalssential to the promotion of psychosocial well-being.nsequently these goals guided the development of the
tervention (see Fig. 2). In the two next sections, wescribe what we assume to be the effective components
the intervention that may help in reaching these goals.
.2. Storytelling as a means to promote understanding,
eaning, identity and self-esteem
As emphasised above, major issues following strokeclude the confusion and lack of comprehension andeaning experienced during the early phases of thejustment process. In attempting to address this issue,
e drew on ideas from narrative theory (McAdams, 2009;lkinghorne, 1988; Sarbin, 1986). Telling stories with therpose of explaining who we are, who we would like to, what values we cherish, which activities are important
us and with whom we socialise is a normal part of lifed contributes to the building and maintenance ofentity (Lieblich et al., 2004; McAdams, 2009). Narrative
theories emphasise that human beings create meaning intheir lives through the stories they tell about themselvesand others. Stories constitute our self-understanding,reflect our culture and contribute to the structuring andcreation of meaning in our lives (Polkinghorne, 1988;Sarbin, 1986). Furthermore, stories are essential in relatingto others. Through stories, we seek to position ourselveswithin the larger social and cultural fabric, relating ourpersonal narratives to the ‘master narratives’ that areavailable to us in our society. At the same time, otherpeople align us with master narratives that we maywelcome or oppose (McLeod, 2007), e.g., a handicap or achronically ill ‘master narrative’. Through narratives, weseek to negotiate a position within a given social contextthat gives meaning, direction, identity and value to ourlives (Taylor, 2007; Kraus, 2007). Research suggests thattelling one’s story is a fundamental need following atraumatic event and that this may actually promote healthin and of itself (Frank, 1995, 1998). Moreover, an inabilityor lack of opportunity to tell one’s story may lead to stressand psychological ill-being. Given the above, we assumedthat being encouraged and supported to tell one’s story,receiving responses from others and experiencing thatstories are shared would stimulate reflection and adjust-ment and strengthen identity, self-understanding and self-esteem.
People suffering from aphasia are restricted in theirnatural abilities to tell their stories through writing orspeech (Parr, 2004; Parr et al., 2006; Shadden and Hagstrom,2007). Nevertheless, research has highlighted the impor-tance of storytelling to maintain or recreate one’s identityfollowing aphasia (Hinckley, 2010; Moss et al., 2004;Shadden, 2005). In this intervention, we used an approachthat acknowledged the importance of narration andencouraged storytelling for people having language pro-blems. To overcome the challenges of providing psychoso-cial follow-up to people having aphasia, we used a methodtermed ‘‘Supported Conversation for Adults with Aphasia’’(Kagan et al., 1996; Simmons-Mackie et al., 2010).Emphasising the fundamental importance and value ofdialogue for all persons, this method was developed toimprove communication between persons with aphasia andpersons without communication challenges, therebyimproving access to social interaction. This method assignsa particular responsibility for facilitating social interactionsto the person without communication difficulties andprovides a number of different techniques that may enhancecommunication and understanding among persons withcommunication difficulties. These include the conscious useof non-verbal communication, pictures, writing and draw-ing to convey thoughts, feelings, experiences and actions,and the use of illustrated communication materials andkeywords to communicate written messages (Kagan et al.,1996; Simmons-Mackie et al., 2010). In applying thismethod, we sought to facilitate open and equal conversa-tions between people with aphasia and the health careprofessionals providing the psychosocial support interven-tion. At the same time, we developed particular commu-nication tools (detailed below) aimed at supporting thedevelopment of an identity-promoting narrative (Andersonand Marlett, 2004a,b).

3
th
foscmenawlicdthathpsZ
podphpthAwoaitminhPdsb
thid(pwinecpeth
4
rtimhpm
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397 393
.4.3. Promoting coping and the acquisition of new life skills
rough guided self-determination
As demonstrated by our review of the literature, copingllowing the advent of a serious, long-term illness, such as
troke, is a major issue. To deal effectively with theonsequences and accomplish recovery and adjustment, itay be necessary to support and strengthen the patient’s
xisting coping resources and support the development ofew life skills. We premised our intervention on thessumption that people are generally capable of dealingith life events and prefer being actively in control of theirves, yet may still need support when faced with new andhallenging life events such as the advent of seriousisease. We therefore sought to develop an interventionat acknowledged that patients are active partners and
gents in their own recovery process. This is in line withe ‘empowerment’ or ‘patient participation’ philosophies
roposed within the health promotion literature (Ander-on and Funnell, 2005, 2009; Leplege et al., 2007;offmann, 2004).
To address these issues, we drew on the theoreticalerspective of life skills development (Nutbeam, 1986),perationalised through the method termed ‘‘guided self-etermination’’ (Zoffmann, 2004). According to thiserspective, patients make decisions on issues related toealth and well-being depending on their own values anderspectives regarding the issues that are important toem and how they understand their needs and problems.
t the same time, certain life skills and abilities are neededhen faced with disease. These include insight into one’s
wn reactions towards the disease, the ability to identifynd describe the problems and challenges associated with, experience with diverse ways of reacting to andanaging it, and the ability to solve problems and conflicts
everyday life in ways that integrate the disease whileonouring important values, life goals and activities.revious research (Zoffmann and Lauritzen, 2006) hasemonstrated the effectiveness of supporting personsuffering from chronic conditions in developing life skillsased on this empowerment approach.
The theoretical strands briefly described above directede further development of the intervention by helping usentify the specific goals and aims of the interventionsychosocial well-being), the strategies used to promoteell-being (i.e., the use of story telling to supportterpretation, the recreation of meaning and the strength-
ning of psychosocial identity, and the development ofoping and life skills by promoting self-determinedroblem solving and value clarification, thereby strength-ning agency and control). In the next section, we describee intervention in greater detail.
. Phase 2: modelling process and outcome
Based on the empirical and theoretical findingseviewed above, we developed a dialogue-based interven-on. We planned the intervention to consist of eighteetings between the patient and a specially trained
ealth care professional (primarily a nurse or other healthrofessional with the relevant background) over sixonths following the stroke. The number of meetings
was based in part on previous effectiveness studies, inwhich the number of contacts varied from four to 28(Burton and Gibbon, 2005; Watkins et al., 2007), in partbased on findings from our qualitative, longitudinalstudies and in part based on pragmatic grounds (keepingthe number of meetings as low as possible while remainingsufficient to provide adequate support). Each meeting wasdesigned to last for approximately 1 h. The first meetingwas scheduled to occur as soon as possible after the stroke,usually within 4–8 weeks, and the last meeting wasscheduled to occur approximately 6 months post-stroke.The suggested times for each meeting were designed tocoincide with significant transition points and times ofincreased vulnerability in the recovery process as revealedby previous research. These included the time of dischargefrom a stroke rehabilitation unit, after the patient hadgained some experience of living with stroke at home, asthe physical recovery plateaued and when the lastingconsequences of the stroke had been fully acknowledged(Kirkevold, 2002; Kvigne et al., 2004; Eilertsen et al., 2010).
The meetings were to be conducted as informalconversations, but each meeting had a guiding topicaloutline determined by significant issues described in theresearch literature. We developed specific worksheets foreach meeting, which functioned as conversational startingpoints. The worksheets sought to encourage reflection,value clarification, goal setting and problem solving(Zoffmann, 2004), and focused on each of the topicsidentified during the literature review, including psycho-logical state/mood, daily life, activities, body, self-image,identity and social relationships. Each worksheet wascreated to invite participants to write down theirexperiences, thoughts, reflections, problems, needs andpossible solutions and actions. Together, the worksheetsmade up a workbook that was used as a pedagogical andmethodological tool intended to support the psychosocialrecovery and adjustment process of the participant andfacilitate conversations between the participant and healthcare professional. The worksheet design took the languageproblems of people with aphasia into account. We includedsimple language, pictures, colours and keywords tofacilitate reading and understanding.
Table 1 contains examples of the objectives, actions andcontent, along with the rationale and some supportiveresearch findings that were developed for each of the eightmeetings. These descriptions were developed to supportthe health care worker’s recollection of the basic theore-tical and empirical foundations of the intervention andconnect them to the objectives and actions proposed foreach meeting.
Because the literature is ambiguous with regard towhether psychosocial support is most effective whenprovided as individual one-on-one sessions or as profes-sionally facilitated peer group sessions (Smith et al., 2008),we decided to test both forms of administration. For thegroup format, the participants were to initially receive twoindividual conversations, followed by six group meetings.The focus, content and worksheets for each meeting wereotherwise planned to be identical for the two forms;however, the process had to be somewhat different bynecessity.

Table 1
Example of description of intervention meetings.
1. Meeting Place: (1) in hospital – if participant recruited from hospital, (2) at home – if participant recruited from primary care service
Purpose Activities Rationale Selected relevant research findings
Establish a
collaborative
relationship
Ensure a good
start on a 6 month
long collaborative
relationship
Support an early
start of the
recovery process
Health care worker (HCW) presents
self, the purpose of the intervention
and the ideas informing the nature of
the collaborative relationship
Invite patient to tell about what
happened in relation to the stroke to
get to know participant
For persons with aphasia, struggling
to convey their stories through
words, provide support through
other forms of expression, e.g.,
support from relatives, through
written expression, pictures,
drawings, other health care
professionals, speech therapist, etc.
Major content/elements are noted on
appropriate work sheet in the
participant’s workbook by HCW.
Work book is kept by HCW in this
phase. HCW writes own notes from
each meeting
Work sheet 1a:
Invitation to collaboration
(Zoffmann, 2004)
Work sheet 1b:
The stroke – what happened
A good relationship
is a necessary
prerequisite for
realizing the goals of
the intervention
Story telling is an
important strategy
for creating
meaning and
coherence in the
chaotic experiences
that is associated
with a stroke
Being allowed to tell
one’s story is an
important strategy
for dealing with/
coming to terms
with dramatic
experiences (Frank,
1995; Lundby,
1998)
Support from others
may contribute to
making the story
‘‘whole’’
Being hit by stroke is a dramatic situation that may be experienced
as a traumatic crisis. Several studies document experiences of
chaos, shock and uncertainty. The bodily changes in particular
appear to be scary (Kaufman 1988; Doolittle 1991, 1992; Becker,
1993)
There is a need that someone listens and contributes to an
understanding of what has happened (Byng et al., 2001). Paradiso
and Robinson (1998) discovered that during the first weeks
following the stroke twice as many women as men were
diagnosed with serious depression. The emotional changes seem
to be more apparent among women in this phase. Men seem to
focus on the physiological changes (Eilertsen, 2005; Flemming,
2002)
The need for the right amount/dosage and for repeated
information is emphasised by patients and relatives in this phase.
Information may be difficult to grasp due to shock, and cognitive
and language deficits. Ability to grasp oral and written information
may be severely impaired among persons with aphasia. Patients
and relatives request that someone tells them what is happening
and where to go to receive support and help without having to ask:
‘‘Remember I am new to this,’’ ‘‘Give me the tools’’ (Parr, 2004; Parr
et al., 2006)
Persons with aphasia often experience extreme frustration over
their lack of ability to express themsleves (Hafsteinsdottir, 1997;
Parr, 2004). Many persons with aphasia experience being ignored
and excluded from social interactions (Parr, 2004)
2. Meeting Place: (1) rehabilitation unit – 1 week before planned discharge, (2) at home – 1 week after discharge
Purpose Activities Rationale Selected relevant research findings
Person specific
knowledge about
patient is uncovered
as a common
starting point for
the collaborative
process
Identity and
self-esteem is
supported
and confirmed
Participant is mentally
prepared for the
further recovery
process when
discharged to home
Invite patient to talk
about the life that the
stroke is interfering with
Dialogue about who the
participant is, and the
values that have been
and continue to be
important and need to be
protected/promoted in
the future
Create a common
metaphor/picture of the
recovery process, taking
the metaphor of ‘‘The big
trial of strength’’ as a
point of departure
Uncover goals, plans,
thoughts and
expectations with regard
to life at home
Significant areas/topics
are noted on appropriate
work sheets in the work
book
Work sheet 2a:
Life line – who are you?
(Zoffmann, 2004)
Work sheet 2b:
Metaphor – ‘‘The big trial
of strength’’
Meaning is created through the stories people tell
about themselves. The stories will impact on what
we do, the choices and actions taken and they help
create continuity (Lundby, 1998). Reflection and
story telling about one’s life will contribute to create
meaning, structure and coherence in a chaotic
situation and thereby contribute to give direction
towards the future. Telling stories will also
contribute to conserve the identity of the patient
The consequences of a stroke are comprehensive and
diverse. The way a stroke impacts on different lives
will vary greatly depending on a wide range of
personal, relational and social/environmental
factors
The process of change is individual and
multidimensional. In order to preserve the goal of
self determination, participation, empowerment
and responsibility, person specific knowledge is a
prerequisite for a common understanding
(Zoffmann, 2004). Self-esteem and self respect are
dynamic phenomena that are influenced by
reflection, interaction and responses from others. A
stroke may impact on many different areas,
including function, sensibility, self esteem, roles,
relations, appearance and interactions
The work process, addressing the work sheets ‘‘Life
line – who are you?’’ (Zoffmann, 2004) and ‘‘The big
trial of strength’’ is part of preserving continuity in
life and tie past, present and future together. A
common metaphor can contribute to create a picture
with regard to where one is a the moment and what
may be required to achieve one’s goal
The transition from being in the hospital to
being discharged and encountering the
challenges in the home environment is
described as the real start point for
rehabilitation in several studies (Doolittle,
1992; Becker, 1993; Sisson 1998; Burton,
2000; Eilertsen, 2005)
The most common illness narratives are
those with restitution – content. These
describe illness as an inconvenient and
unpleasant condition, albeit a transitional
phase one can escape from through hard
work and a positive attitude (Frank, 1995)
Construction of narratives may create a
reality as much as refer to one. Metaphors
may impact on thoughts and actions in a
therapeutic way and be a useful tool for
collaboration between patient and therapist
(Mattingly, 1994)
Many persons with aphasia experiences
social exclusion. Many feel neglected and
not talked to in a normal (‘‘adult’’) way
(Pound, 2001). Dialogues may be changes
both in terms of content, quality and form:
From being an equal communication
partner, one is reduced to a person being
talked to, not talked with (Corneliussen et al.,
2006). Addresses are frequently directed
towards family and dialogues conducted
‘‘above the head’’ of the person with aphasia.
This may threaten the patient’s history,
identity and autonomy (Parr, 2004)
References may be provided upon request.
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397394

pr2seinpphaa(Hmpth
4
einathinoeBpreptiininsasoema
5
thinalismMFqeto
sbw
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397 395
Most of the meetings were planned to occur after thearticipant had been discharged from hospital and hadeturned to their homes or community services. However, 1–
meetings were to be conducted while the participant wastill hospitalised. The rationale for this was twofold: tostablish contact and prepare the participant for thetervention and to support the psychosocial adjustment
rocess as early as possible to prevent the development ofsychosocial ill-being (Whyte and Mulsant, 2002). The sameealth care professional was toconduct all the meetings with
given participant to secure continuity, security, predict-bility and trust, i.e., to develop a therapeutic relationship
inckley, 2010). The intervention was designed to supple-ent other rehabilitation services provided to the partici-
ant, and to be conducted in collaboration with the rest ofe participant’s treatment team.
.1. Critical review and consensus building
The purpose of this model development study was tonsure an empirically, theoretically and practically soundtervention. Although the above steps helped us develop
n intervention based on a broad range of empirical andeoretical evidence, the practical soundness of thetervention was less obvious. To strengthen this aspect
f the development process, we invited a wide range ofxperts to critically review the proposed intervention (seeox 2 for details). These discussions helped us specify andlan the details of the initial testing of the intervention andevise the content and layout of the worksheets and theducational instructions and program for the healthrofessionals who would conduct the intervention. Ques-ons such as who would be recruited to such antervention, what the organisational placement of thetervention would be and how it would be linked to other
ervices were raised during these focus groups, helping usnticipate some of the challenging issues we would have toolve when moving into the exploratory trial phase. Basedn the critical review and practical advice provided by thexpert groups, we finalised the intervention protocol andoved to the trial, the results of which will be presented as
separate paper.
. Discussion
In this paper, we have described the development of aeoretically and empirically informed complex nursingtervention aimed at promoting psychosocial well-being
fter stroke. The basis for this study was the finding from theterature that most previous intervention studies addres-ing psychosocial needs and problems have generally hadodest results (Hackett et al., 2008a,b; Knapp et al., 2000;urray et al., 2003; Smith et al., 2008; Redfern et al., 2006).
urthermore, it has been observed repeatedly that inade-uate attention has been directed towards identifying andxplaining the underlying theoretical mechanisms assumed
effect change (Smith et al., 2008; Redfern et al., 2006).The psychosocial consequences of stroke vary from mild
tress and general psychosocial ill-being to serious pro-lems, such as post-stroke depression and anxiety (Kou-enhoven et al., 2011; Whyte and Mulsant, 2002). There is
increasing consensus that more concerted efforts areneeded to address the psychosocial consequences of stroke.Our literature review highlighted the importance of payingclose attention to the mechanisms that may facilitatepsychosocial well-being. The intervention presented here isin line with one of the two major theories of post-strokedepression and anxiety, namely the psychosocial mechan-ism, which suggests that psychosocial problems occur as aresult of overwhelming stress, emotional overload andineffective coping strategies for dealing with the conse-quences of stroke (Whyte and Mulsant, 2002). According toWhyte and Mulsant (2002), this mechanism is particularlyrelevant to late onset depression, which is less likely to leadto spontaneous remission. Our intervention is aimed atpreventing serious psychosocial problems by strengtheningthe participants’ own, natural coping strategies. We assumethat through such a health-promoting approach, strokesurvivors might be supported in reducing their stress andemotional overload and increasing their sense of compre-hensibility, manageability and meaning.
The literature emphasises that specific goals and out-comes must be targeted in order to succeed in developingeffective psychosocial interventions. We aim to promotepsychosocial well-being, which we operationalised toinclude a general feeling of positive affect, engagement inmeaningful activities, good social relations and a positiveself-image. These outcomes are threatened by the con-sequences of stroke, and there is increasing evidence thatstroke survivors may need support to regain psychosocialwell-being (Murray et al., 2003; Salter et al., 2008).
The timing and intensity of the psychosocial interven-tions are frequently assumed to explain the lack ofsignificant outcomes in clinical trials (Knapp et al.,2000). However, the literature is unclear with regard tothis issue. Interventions vary greatly in terms of timing,intensity and duration (Knapp et al., 2000; Burton andGibbon, 2005; Watkins et al., 2007). In our intervention,the timing was guided primarily by the results ofqualitative, longitudinal studies, which indicate thattransition periods are particularly vulnerable times forstroke survivors. Furthermore, we included pragmaticdeliberations concerning the acceptability of an additionalpsychosocial intervention within a hard-pressed health-care service. We opted for eight meetings during the firstsix months, which we judged to be a realistic compromisebetween the ideal and pragmatically possible. However,in-depth evaluation of the intervention will explorewhether this is adequate or not.
Systematic reviews have found that the active involve-ment of patients and carers is paramount for successfulpsychosocial outcomes (Smith et al., 2008). We sought tomeet this requirement by inviting participants to tell theirstories in their own words, by actively encouraging them tochoose which issues to focus on in the dialogues and whichgoals to work towards and by supporting their own initiativeand problem-solving and coping skills. We believe that thisapproach facilitates the development of individually rele-vant coping skills by building on the values and goals ofparticular importance to the individual participant.
In this study, we decided to primarily focus on strokesurvivors but encouraged the stroke survivors themselves

toasdesucodithmre
(Corin(2isssoca(epapaesveveprapar
tioBrasofmthdi20alsmarem
denurehasturefolittafrowsturetogithcuththnuef
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397396
invite informal carer(s) to some (or all) of the meetings they deemed appropriate. The rationale behind thiscision was to promote personal control in the strokervivor and keep the intervention at a manageable level ofmplexity to be able to evaluate the effectiveness of thefferent components of the intervention. We believe thate next logical step will be to extend the intervention toore systematically involve carers, should the initialsults warrant further development in this direction.
In our work, we were inspired by the MRC frameworkampbell et al., 2000; Craig et al., 2008), which wasiginally developed to support intervention development
primary health care settings. In line with Maindal et al.010), we found the MRC framework helpful in clarifyingues to take into account when developing our psycho-cial intervention. In particular, we found that payingreful attention to a wide range of available knowledgevidence), including findings from qualitative studies oftient experiences and the practical experiences oftients, family members and clinicians, helped to clarifysential issues that needed addressing during the inter-ntion. The many thorough reviews of previous inter-ntions available also helped guide the developmentocess, particularly by highlighting elements andproaches that have been found effective and identifyingeas in need of further specification.
Although this systematic way of developing interven-ns is by no means new within nursing (Sidani andaden, 1998), few frameworks have been available tosist in the development process thus far. One advantage
applying the MRC framework in intervention develop-ent is that it is used extensively in other disciplines,ereby facilitating communication and learning acrosssciplinary boundaries (Forbes, 2009; Campbell et al.,00; Craig et al., 2008). However, other frameworks areo available, such as intervention mapping (Bartholo-
ew et al., 1998; Kok et al., 2004), and nurse researcherse advised to review the various approaches when
barking on an intervention development study.This study had several limitations. It describes the
velopment of an empirically and theoretically informedrsing intervention. However, no empirical data has been
ported to support its merits thus far. Furthermore, weve relied heavily on systematic reviews of empiricaldies to underpin the intervention. Although these
views have been conducted using agreed-upon methodsr systematic reviews, they still represent secondaryerature. Furthermore, many studies, particularly quali-tive and non-experimental studies, have been excludedm these reviews. We have compensated for this
eakness by conducting a separate review of qualitativedies and building on our own program of qualitative
search regarding stroke recovery. We believe that, takengether, the applied empirical and theoretical literatureves sufficient support for the intervention presented inis paper. In the continuation of this study, which isrrently underway, we explore the impact and effects ofe intervention in a multiple case study. We believe thatis stepwise approach to developing and testing complexrsing interventions can facilitate the identification of the
6. Conclusion
Using the framework for developing and evaluatingcomplex interventions recommended by the UK MedicalResearch Council, this study has developed a complexpsychosocial intervention aimed at promoting psychoso-cial well-being through an improved ability to cope withstress, reduced emotional overload and increased com-prehensibility, manageability and meaning. The nextphase of this study, the intervention itself, which combinesa narrative approach and guided self-determination, iscurrently being tested in an exploratory trial to bepresented as a separate paper.
Acknowledgements
We acknowledge the important contributions ofpatients, health care professions and experts participatingin the development of the intervention. This project hasbeen financially supported by the Norwegian ExtraFoun-dation for Health and Rehabilitation through EXTRA funds,the Norwegian Aphasia association and The NorwegianWomen’s Public Health Association.
Conflict of interest: None.Funding: This study was supported by grants from the
Norwegian Extra Foundation for Health and Rehabilitationand Norwegian Women’s Medical Association. In addition,the study was supported by University of Oslo andHedmark University College.
Ethical approval: None.
References
Anderson, B., Funnell, M., 2005. The Art of Empowerment. AmericanDiabetes Association, Alexandria, Verginia.
Anderson, R.M., Funnell, M.M., 2009. Patient empowerment: myths andmisconceptions. Patient Education and Counseling 79, 277–282.
Anderson, S., Marlett, N.J., 2004a. Communication in stroke: the over-looked rehabilitation tool. Age and Ageing 33 (5), 440–443.
Anderson, S., Marlett, N.J., 2004b. The language of recovery: how effectivecommunication of information is crucial to restructuring post-strokelife. Topics in Stroke Rehabilitation 11 (4), 55–67.
Antonovsky, A., 1987. Unravelling the Mystery of Health. How PeopleManage Stress and Stay Well. Jossey-Bass, San Francisco.
Barker-Collo, S.L., 2007. Depression and anxiety 3 months post stroke:prevalence and correlates. Archives of Clinical Neuropsychology 22,519–531.
Bartholomew, L.K., Parcel, G.S., Kok, G., 1998. Intervention mapping: aprocess for developing theory- and evidence-based health educationprograms. Health Education & Behavior 25 (5), 545–563.
Bognar, G., 2008. Well-being and health. Health Care Analysis 16, 97–113.Brulde, B., 2007. Happiness and the good life. Introduction and conceptual
framework. Journal of Happiness Studies 8, 1–14.Burton, C., Gibbon, B., 2005. Expanding the role of the stroke nurse: a
pragmatic clinical trial. Journal of Advanced Nursing 52 (6), 640–650.Campbell, M., Fitzpatrick, R., Heines, A., Kinmonth, A.L., Sandercock, P.,
Spiegelhalter, D., Tyrer, P., 2000. Framework for design and evaluationof complex interventions to improve health. BMJ 321, 694–696.
Code, C., Herrmann, M., 2003. The relevance of emotional and psycho-social factors in aphasia to rehabilitation. Neuropsychological Reha-bilitation: An International Journal 13 (1), 109–132.
Code, C., Petheram, B., 2011. Delivering for aphasia. International Journalof Speech-Language Pathology 13 (1), 3–10.
Craig, P., Dieppe, P., MacIntyre, S., Mitchie, S., Nazareth, I., Petticrew, M.,2008. Developing and evaluating complex interventions: the newMedical Research Council guidance. BMJ 337, 979–983.
Daniel, K., Wolfe, C.D.A., Busch, M.A., McKevitt, C., 2009. What are the
social consequences of stroke for working-aged adults? Stroke 40 (6),e431–e440. fective elements of complex nursing interventions.
D
E
E
E
E
E
E
F
F
F
F
H
H
H
H
H
K
K
K
K
K
K
K
K
K
K
L
L
L
L
L
M. Kirkevold et al. / International Journal of Nursing Studies 49 (2012) 386–397 397
onnellan, D., Hevey, D., Hickey, A., O’Neill, D., 2006. Defining andquantifying coping strategies after stroke: a review. Journal of Neu-rology, Neurosurgery, and Psychiatry 77, 1208–1218.
ilertsen, G., Kirkevold, M., Bjørk, I.T., 2010. Recovering from a stroke: alongitudinal qualitative study of elderly Norwegian women. Journalof Clinical Nursing 19 (13–14), 2004–2013.
llis, G., Mant, J., Langhorne, P., Dennis, M., Winner, S., 2010. Stroke liaisonworkers for stroke patients and carers: an individual patient datameta-analysis. Cochrane Database of Systematic Reviews (5).
arly Supported Discharge Trialists, 2009. Services for reducing durationof hospital care for acute stroke patients. Cochrane Database ofSystematic Reviews (1).
ngelter, S.T., Gostynski, M., Papa, S., Frei, M., Born, C., Ajdacic-Gross, V.,Gutzwiller, F., Lyrer, P.A., 2006. Epidemiology of aphasia attributableto first ischemic stroke: incidence, severity, fluency, etiology, andtrombolysisis. Stroke 37 (6), 1379–1384.
riksson, M., Lindstrom, B., 2005. Validity of Antonovsky’s sense ofcoherence scale: a systematic review. Journal of Epidemiology andCommunity Health 59, 460–466.
riksson, M., Lindstrom, B., 2006. Antonovsky’s sense of coherence scaleand the relation with health: a systematic review. Journal of Epide-miology and Community Health 60, 376–381.
erro, J.M., Caeiro, L., Santos, C., 2009. Poststroke emotional and behaviorimpairment: a narrative review. Cerebrovascular Diseases 27 (Suppl.1), 197–203.
orbes, A., 2009. Clinical intervention research in nursing. InternationalJournal of Nursing Studies 46, 557–568.
rank, A.W., 1995. The Wounded Storyteller: Body Illness and Ethics.University Press, Chicago, IL.
rank, A., 1998. Just listening: narrative and deep illness. Families, Sys-tems and Health 16 (3), 197–212.
ackett, M.L., Anderson, C.S., House, A., Halteh, C., 2008a. Interventionsfor preventing depression after stroke. Cochrane Database of Sys-tematic Reviews (3).
ackett, M.L., Anderson, C.S., House, A., Xia, J., 2008b. Interventions fortreating depression after stroke. Cochrane Database of SystematicReviews (4).
afsteinsdottir, T.B., Grypdonck, M., 1997. Being a stroke patient: areview of literature. Journal of Advanced Nursing 26, 580–588.
ilari, K., Northcott, S., 2006. Social support in people with chronicaphasia. Aphasiology 20 (1), 17–36.
inckley, J., 2010. Hope for happy endings: stories of clients and clin-icians. Stroke Rehabilitation 17 (1), 1–5.
agan, A., Winckel, J., Shumway, M.A., 1996. Supported Conversation forAdults with Aphasia. Aphasia Center, Toronto, North York, Canada.
elly, H., Brady, M.C., Enderby, P., 2010. Speech and language therapy foraphasia following stroke. Cochrane Database of Systematic Reviews (5).
irkevold, M., 2002. The unfolding illness trajectory of stroke. Disabilityand Rehabilitation 24 (17), 887–898.
irkevold, M., 2010. The role of nursing in the rehabilitation of strokesurvivors. Advances in Nursing Science 33 (1), e27–e40.
napp, P., Young, J., House, A., Forster, A., 2000. Non-drug strategies toresolve psychosocial difficulties after stroke. Age and Ageing 29, 23–30.
ok, G., Schaalma, H., Ruiter, R.A., van Empelen, P., Brug, J., 2004. Inter-vention mapping: protocol for applying health psychology theory toprevention programmes. Journal of Health Psychology 9 (1), 85–98.
ouwenhoven, S., Kirkevold, M., Engedal, K., Kim, S.H., 2011. Depression inacute stroke: prevalence, dominant symptoms and associated factors. Asystematic literaturereview. Disability& Rehabilitation33(7),539–556.
raus, W., 2007. The narrative negotiation of identity and belonging. In:Bamberg, M. (Ed.), Narrative – State of the Art. John BenjaminsPublishing Company, Amersterdam, pp. 123–132.
vigne, K., Kirkevold, M., 2003. Living with bodily strangeness: women’sexperiences of their changing and unpredictable body following astroke. Qualitative Health Research 13 (9), 1291–1310.
vigne, K., Kirkevold, M., Gjengedal, E., 2004. Fighting back – struggling tocontinue life and preserve the self following a stroke. Health Care forWomen International 25 (4), 370–387.
arsen, T., Olsen, T.S., Sorensen, J., 2006. Early home-supported dischargeof stroke patients: a health technology assessment. InternationalJournal of Technology Assessment in Health Care 22 (3), 313–320.
awrence, M., 2010. Young adults’ experience of stroke: a qualitativereview of the literature. British Journal of Nursing 19 (4), 241–248.
eplege, A., Gzil, F., Cammelli, M., Lefeve, C., Pauchoud, B., Ville, I., 2007.Person-centeredness: conceptual and historical perspectives. Disabil-ity and Rehabilitation 29 (20–21), 1555–1565.
ieblich, A., McAdams, D.P., Josselson, R., 2004. Healing Plots. The Basis ofPsychotherapy. American Psychological Association, Washington, DC.
yon, J., 2004. Evolving treatment methods for coping with aphasiaapproaches that make a difference in everyday life. In: Duchan, J.F.,
Byng, S. (Eds.), Challenging Aphasia Therapies. Psychology Press,New York, pp. 54–82.
Maindal, H.T., Kirkevold, M., Sandbæk, A., Lauritzen, T., 2010. Lifting thelid of the ‘‘black intervention box’’ – the systematic development of anaction competence programme for people with screen-detected dys-glycaemia. BMC Health Services Research 10, 114., http://www.biomedcentral.com/1472-6963/10/114.
McAdams, D.P., 2009. The Person. An Introduction to the Science ofPersonality Psychology, 5th rd. J. Wiley & Sons, Hoboken, NJ.
McKevitt, C., Redfern, J., Mold, F., Wolfe, C., 2004. Qualitative studies ofstroke. A systematic review. Stroke 35 (6), 1499–1505.
McLeod, J., 2007. Narrative thinking and the emergence of postpsycho-logical therapies. In: Bamberg, M. (Ed.), Narratives – State of the Art.John Benjamins Publishing Company, Amsterdam/Philadelphia, pp.237–248.
Moss, B., Parr, S., Byng, S., Petheram, B., 2004. ‘‘Pick me up and not a downdown, up up’’: how are the identities of people with aphasia repre-sented in aphasia, stroke and disability websites? Disability & Society19 (7), 753–768.
Murray, J., Ashworth, R., Foster, A., Young, J., 2003. Developing a primarycare-based stroke service: a review of the qualitative literature.British Journal of General Practice 53, 137–142.
Nutbeam, D., 1986. Health promotion glossary. Health Promotion(Oxford, England) 1 (1), 113–127.
Næss, S., 2001. Livskvalitet som psykisk velvære.(Quality of life as psy-chological well-being). Tidskr Nor Lægeforen 121 (16), 1940–1944.
Outpatient Service Trialists, 2003. Therapy-based rehabilitation services forstroke patients at home. Cochrane Database of Systematic Reviews (1).
Parfit, D., 1984. Reasons and Persons. Oxford University Press, New York.Parr, S., 2004. Living with Severe Aphasia – The Experience of Commu-
nication Impairment After Stroke. Joseph Rowntree Foundation,Pavillion.
Parr, S., Pound, C., Hewitt, A., 2006. Communication access to health andsocial care services. Language Disorders 26 (3), 189–198.
Parr, S., Duchan, J., Pound, C., 2003. Aphasia Inside Out: Reflections onCommunication Disability. Open University Press.
Polkinghorne, D., 1988. Narrative Knowing and the Human Sciences. StateUniversity of Redfern, New York Press, Albany.
Redfern, J., McKevitt, C., Wolfe, C.D.A., 2006. Development of complexinterventions in stroke care. A systematic review. Stroke 37, 2410–2419.
Salter, K., Hellings, C., Foley, N., Teasell, R., 2008. The Experience of Livingwith Stroke: A Qualitative Meta-Synthesis. Journal of RehabilitationMedicine 40, 595–602.
Sarbin, T.R., 1986. Narrative Psychology: The Storied Nature of HumanConduct. Praeger, New York.
Shadden, B.B., 2005. Aphasia as identity theft. Aphasiology 19 (3/4/5),211–223.
Shadden, B., Hagstrom, F., 2007. The role of narrative in the life participationapproach to aphasia. Topics in Language Disorders 27 (4), 324–338.
Sidani, S., Braden, C.J., 1998. Evaluating Nursing Interventions: A Theory-driven Approach. Sage, Thousand Oaks, CA.
Simmons-Mackie, N., Raymer, A., Armstrong, E., Holland, A., Cherney, L.R.,2010. Communication partner training in aphasia: a systematicreview. Archives of Physical Medicine and Rehabilitation 91 (12),1814–1837.
Smith, J., Forster, A., House, A., Knapp, P., Wright, J.J., Young, J., 2008.Information provision for stroke patients and their caregivers.Cochrane Database of Systematic Reviews (2).
Taylor, S., 2007. Narrative as construction and discursive resource. In:Bamberg, M. (Ed.), Narratives – State of the Art. John BenjaminsPublishing Company, Amsterdam/Philadelphia, pp. 113–122.
Teoh, V., Sims, J., Milgrom, J., 2009. Psychosocial predictors of quality oflife in a sample of community-dwelling stroke survivors: a long-itudinal study. Topics in Stroke Rehabilitation 16 (2), 157–166.
Tengland, P.A., 2010. Health promotion and disease prevention: a realdifference for public health practice? Health Care Analysis 18, 203–221.
Watkins, C.L., Auton, M.F., Deans, C.F., Dickinson, H.A., Jack, C.I.A., Light-body, C.E., Sutton, C.J., van den Broek, M.D., Leathley, M.J., 2007.Motivational interviewing early after acute stroke (RCT). Stroke 38(3), 1004–1009.
Whyte, E.M., Mulsant, B.H., 2002. Post stroke depression: epidemiology,pathophysiology, and biological treatment. Biological Psychiatry 52,253–264.
Zoffmann, V., 2004. Guided self-determination. A life skills approachdeveloped in difficult type 1 diabetes. Avhandling for graden. PhDThesis. University of Aarhus, Denmark.
Zoffmann, V., Lauritzen, T., 2006. Guided self-determination improves lifeskills with type 1 diabetes and A1C in randomized controlled trial.Patient Education & Counseling 64 (1–3), 78–86.




















