Principles of Neuropsychology
603
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Principles of Neuropsychology
Second Edition
P R I N C I P L E SO F
N E U R O P S Y C H O L O G Y
Eric A. ZillmerDrexel University
Mary V. SpiersDrexel University
William C. CulbertsonDrexel University
Australia | Brazil | Canada | Mexico | Singapore | Spain | United Kingdom | United States

Acquisitions Editor: Erik EvansAssistant Editor: Gina KesslerEditorial Assistant: Christina D. GanimTechnology Project Manager: Lauren KeyesMarketing Manager: Sara SwangardMarketing Assistant: Melanie CreggerSenior Marketing Communications Manager: Linda YipContent Project Manager: Christy KruegerCreative Director: Rob HugelSenior Art Director: Vernon BoesSenior Print Buyer: Rebecca Cross
Permissions Editor: Robert KauserProduction Service: Graphic World Inc.Photo Researcher: Terri WrightCopy Editor: Graphic World Inc.Illustrator: International Typesetting and CompositionCover Designer: Denise DavidsonCover Image: © UHB Trust/Getty ImagesCover Printer: Thomson WestCompositor: International Typesetting and CompositionPrinter: Thomson West
© 2008, 2001 Thomson Wadsworth, a part of The ThomsonCorporation. Thomson, the Star logo, and Wadsworth aretrademarks used herein under license.
ALL RIGHTS RESERVED. No part of this work covered bythe copyright hereon may be reproduced or used in any formor by any means—graphic, electronic, or mechanical, includingphotocopying, recording, taping, Web distribution, informa-tion storage and retrieval systems, or in any other manner—without the written permission of the publisher.
Printed in the United States of America1 2 3 4 5 6 7 11 10 09 08 07
Library of Congress Control Number: 2007920598
ISBN-13: 978-0-495-00376-2ISBN-10: 0-495-00376-X
Thomson Higher Education10 Davis DriveBelmont, CA 94002-3098USA
For more information about our products, contact us at:Thomson Learning Academic Resource Center1-800-423-0563
For permission to use material from this text or product,submit a request online athttp://www.thomsonrights.com.Any additional questions about permissions can be submit-ted by e-mail to [email protected].
Principles of Neuropsychology, Second EditionEric A. Zillmer, Mary V. Spiers, William C. Culbertson

This book is dedicated to the memory ofCarl R. Pacifico
Drexel Alumnus, Class of ’44
Friend, Mentor, Benefactor
E.A.Z.
This book is dedicated to my father.
His guidance as a psychologist and his personal struggle with Parkinson’s disease have brought some of my greatest lessons.
M.V.S.
This book is dedicated to
my wife and daughter, my greatest gifts.
W.C.C.

This page intentionally left blank
BRIEF CONTENTS
Part One Introduction 1
Chapter 1 A History of Neuropsychology 3Chapter 2 Methods of Investigating the Brain 32Chapter 3 Neuropsychological Assessment and Diagnosis 62
Part Two The Functioning Brain 91
Chapter 4 Cells of Thought 93Chapter 5 Functional Neuroanatomy 114Chapter 6 Cerebral Specialization 154Chapter 7 Somatosensory, Chemical, and Motor Systems 176Chapter 8 Vision and Language 199Chapter 9 Memory, Attention, Emotion, and Executive Functioning 224
Part Three Disorders of the Brain 267
Chapter 10 Developmental Disorders of Childhood 269Chapter 11 Learning and Neuropsychiatric Disorders of Childhood 297Chapter 12 Cerebrovascular Disorders and Tumors 339Chapter 13 Traumatic Head Injury and Rehabilitation 369Chapter 14 Normal Aging and Dementia: Alzheimer’s Disease 399Chapter 15 Subcortical Dementias 423Chapter 16 Alterations of Consciousness 443
v

This page intentionally left blank
Part One I N T R O D U C T I O N 1
Chapter 1 A H i s t o r y o f N e u r o p s y c h o l o g y 3Keep in Mind 4Overview 4
The Brain in Antiquity: Early Hypotheses 5Ancient Greek Perspectives 6The Cell Doctrine 7Anatomic Discoveries and the Role of the Spiritual Soul 8Non-Western Attitudes 12
Localization Theory 13Phrenology and Faculty Psychology 13The Era of Cortical Localization 16Critics of Cortical Localization 18
Localization versus Equipotentiality 20
Integrated Theories of Brain Function 20Jackson’s Alternative Model 20Luria’s Functional Model 21
Modern Neuropsychology 24
Emerging Research Areas in Neuropsychology 27Forensic Neuropsychology 28Sports Neuropsychology 28Terrorism, Law Enforcement, and the Military 28
Summary 30Critical Thinking Questions 30Key Terms 30Web Connections 30
Neuropsychology in Action
1.1 The Brain of a Nazi 151.2 Paul Broca: A Manner of Not Speaking 171.3 Sigmund Freud: The Neurologist 191.4 The Walter Freeman Lobotomies: Mind over Matter? 22
Chapter 2 M e t h o d s o f I n v e s t i g a t i n g t h e B r a i n 32Keep in Mind 33Overview 33
Neurohistology Techniques 34Golgi Stain 34Nissl Stain 34Other Staining Techniques 35
CONTENTS
vii

Radiologic Procedures 35Skull X-Ray 36Air Encephalography (Pneumoencephalography) 36Computed Transaxial Tomography 36Angiography 38Sodium Amytal Injections (Wada Technique) 40
Electrophysiologic Procedures 40Electroencephalography 40Evoked Potential 44Electrical Stimulation 45Electromyography 47
Imaging of Brain Metabolism 47Regional Cerebral Blood Flow 47Single-Photon Emission Computed Tomography 48Positron Emission Tomography 49
Magnetic Imaging Procedures 51Magnetic Resonance Imaging 51Magnetoencephalography 56
Cerebrospinal Fluid Studies: Lumbar Puncture 56
Behavioral Examinations 56Neurologic Examination 56Neuropsychological Evaluation 57
New Advances in Imaging Techniques: Mapping the Brain 57Subtraction Procedures 57Image Analysis and Quantification (Three-Dimensional) 57Future Directions 58
Summary 60Critical Thinking Questions 61Key Terms 61Web Connections 61
Neuropsychology in Action
2.1 Case Example of Brainstem Auditory-Evoked Response 462.2 Undergoing a Magnetic Resonance Imaging Procedure 522.3 New Frontiers in Functional Magnetic Resonance Imaging 542.4 Diagnostic Neuroimaging and Neuropsychology 59
Chapter 3 N e u r o p s y c h o l o g i c a l A s s e s s m e n ta n d D i a g n o s i s 62Keep in Mind 63Overview 63
General Considerations in Neuropsychological Testing 63Why Testing? 64Rationale of the Neuropsychological Examination 65Appropriate Referrals for Neuropsychological Evaluation 66
Psychometric Issues in Neuropsychological Assessment 66Reliability 67Validity 67False Positives and Base Rates 67
viii Contents

Neuropsychological Tests 68Orientation (Arousal) 69Sensation and Perception 70Attention/Concentration 71Motor Skills 72Verbal Functions/Language 73Visuospatial Organization 74Memory 75Judgment/Problem Solving 76Neuropsychological Diagnosis 78Describing Function, Adaptation, and Prognosis 79
Interpreting Neuropsychological Assessment Data 79Approaches to Neuropsychological Interpretation 80Assessing Level of Performance 84Deficit Measurement 86Lateralizing Signs 88Pathognomonic Signs (Qualitative Observations) 88
Summary 89Critical Thinking Questions 89Key Terms 89Web Connections 89
Neuropsychology in Action
3.1 Case Example: The Neuropsychology of Lyme Disease 86
Part Two T H E F U N C T I O N I N G B R A I N 91
Chapter 4 C e l l s o f T h o u g h t 93Keep in Mind 94Overview 94
Neurons and Glial Cells 94Structure and Function of the Neuron 95Glial Cells 99
Communication within a Neuron: The Neural Impulse 102Resting Membrane Potential 102Action Potential 102
Communication among Neurons 105Structure of Synapses 105Synaptic Transmission 105Neurotransmitters 106
Regeneration of Neurons 110
Summary 112Critical Thinking Questions 112Key Terms 112Web Connections 113
Neuropsychology in Action
4.1 Short-Circuiting Neurons: Multiple Sclerosis 984.2 Neuronal Firing: Clinical Examples 104
Contents ix

4.3 What Can We Learn from Songbirds? 1094.4 Stem Cell Research: Science and Ethics 110
Chapter 5 F u n c t i o n a l N e u r o a n a t o m y 114Keep in Mind 115Overview 115
Anatomic and Functional Development of the Brain 116Neurogenesis and Cellular Migration 116Axon and Dendrite Development 117Synaptogenesis 117Myelination 117Pruning 118Regional Development 118Lobular and Convolutional Development 118Ventricular and Spinal Cord Development 119Postnatal Development 120
Organization of the Nervous System 121
Peripheral Nervous System 122
Central Nervous System 122Brain 122Spinal Cord 123
Gross Anatomy: Protection and Sustenance of the Brain 124Skull 125Meninges 125Ventricular System 127Vascular System 131Cerebral Arteries 132Venous System 133
Principal Divisions of the Brain 133
Brainstem and Cerebellum 134Lower Brainstem 137Upper Brainstem: Diencephalon 141Cerebellum 146
Telencephalon 147Basal Ganglia 147Limbic System 149Corpus Callosum 151
Summary 152Critical Thinking Questions 152Key Terms 152Web Connections 153
Chapter 6 C e r e b r a l S p e c i a l i z a t i o n 154Keep in Mind 155Overview 155
The Cerebral Hemispheres 155Structure 155
x Contents
Function 159Asymmetry, Lateralization, and Dominance 161
Hemispheric Anatomic and Functional Differences 163Neuropsychological and Behavioral Cerebral Differences 166
Sex Differences and Hemispheric Specialization 167Sexual Hormones 171
Summary 175Critical Thinking Questions 175Key Terms 175Web Connections 175
Neuropsychology in Action
6.1 The Evolution of the Brain: A Focus on Brain Size 1566.2 A Land Where Girls Rule in Math 172
Chapter 7 S o m a t o s e n s o r y , C h e m i c a l , a n d M o t o r S y s t e m s 176Keep in Mind 177Overview 177
Somatosensory Processing 178
Chemical Senses 184Taste 184Smell 187
Motor Systems 189Cortical Motor Processing 189The Cerebellum and Motor Processing 195Subcortical Motor Processing 195
Summary 197Critical Thinking Questions 197Key Terms 197Web Connections 198
Neuropsychology in Action
7.1 Synesthesia: Melded Sensory Integration 1797.2 Phantoms of Feeling 1847.3 Tourette Syndrome: Too Much Behavior 196
Chapter 8 V i s i o n a n d L a n g u a g e 199Keep in Mind 200Overview 200
Visual Processing 200Primary Visual Processing 201Higher Visual Processing: Object Recognition and Spatial Localization 204
Auditory and Language Processing 215Primary Auditory Processing 215Higher Auditory Processing: Speech and Language 215Aphasia: A Breakdown of Language 219
Contents xi

Summary 221Critical Thinking Questions 222Key Terms 222Web Connections 222
Neuropsychology in Action
8.1 Blindness: Helping Us See the Plasticity of the Brain 2058.2 The Case of Jonathan 2068.3 Case Study: Neglect 211
Chapter 9 M e m o r y , A t t e n t i o n , E m o t i o n ,a n d E x e c u t i v e F u n c t i o n i n g 224Keep in Mind 225Overview 225
Memory Systems 225A Framework for Conceptualizing Memory Systems 226Long-Term Memory 227Short-Term Memory and Working Memory 237
Attention 240Subcortical Structures Influencing Attention 240The Cerebral Cortex and Attention 241Models of Attention 242
Executive Functioning 246Development of Executive Functions 247Frontal-Mediated Functions and Dysfunctions 252
Relation of Memory, Attention, and Executive Function 258
Neuropsychology of Emotional Processing 259Brain Organization of Emotion 260
Summary 264Critical Thinking Questions 264Key Terms 265Web Connections 265
Neuropsychology in Action
9.1 Amnesia: The Case of N.A. 2279.2 Executive Function Tasks 2489.3 The Case of Phineas Gage 255
Part Three D I S O R D E R S O F T H E B R A I N 267
Chapter 10 D e v e l o p m e n t a l D i s o r d e r s o f C h i l d h o o d 269Keep in Mind 270Overview 270
Vulnerability and Plasticity of the Developing Brain 270
Child and Adult Brain: Structural and Functional Differences 273
Specific Developmental Disorders 274Abnormalities of Anatomic Development 274Genetic and Chromosomal Disorders 281Acquired Disorders 291
xii Contents
Summary 295Critical Thinking Questions 295Key Terms 295Web Connections 295
Neuropsychology in Action
10.1 Principles of Assessment in Pediatric Neuropsychology 275
Chapter 11 L e a r n i n g a n d N e u r o p s y c h i a t r i c D i s o r d e r so f C h i l d h o o d 297Keep in Mind 298Overview 298
Learning Disabilities 298Verbal Learning Disability: Dyslexia 299Nonverbal Learning Disability Syndrome 305
Pervasive Developmental Disorders 310Autism 311
Disruptive Behavioral Disorders 322Attention-Deficit/Hyperactivity Disorder 322
Tic Disorders 332Gilles de la Tourette’s Syndrome 332
Summary 337Critical Thinking Questions 337Key Terms 338Web Connections 338
Neuropsychology in Action
11.1 Genetics of Learning Disabilities 30011.2 Case Study of an Adolescent with Asperger’s Syndrome 31411.3 Case Study of a Child with an Attention-Deficit/Hyperactivity Disorder 327
Chapter 12 C e r e b r o v a s c u l a r D i s o r d e r s a n d Tu m o r s 339Keep in Mind 340Overview 340
Pathologic Process of Brain Damage 340Brain Lesions 340Anoxia and Hypoxia: Oxygen Deprivation to the Brain 341Hydrocephalus 342
Overview of Cerebrovascular Disorders 342Stroke Definition 343Impairment of Blood Supply to the Brain 344
Types of Cerebrovascular Disorders 344Transient Ischemic Attacks 344Infarctions 345Hemorrhage 346
Diagnosing Cerebrovascular Disease 347Computed Transaxial Tomography 349Angiography 349Other Tests 349
Contents xiii
Treatment and Prognosis of Vascular Disorders 349Factors Involved in Stroke Recovery 349Medical Treatment 350Preventing Stroke 350
Neuropsychological Deficits Associated with Stroke 351Neuropsychological Risk Factors 351Attention Deficits 352Memory Problems 353Deficits in Abstract Reasoning 353Cognitive Deficits Associated with Right Brain Strokes 353Cognitive Deficits Associated with Left Brain Damage 355Anterior versus Posterior Strokes 356Emotional and Behavioral Changes after a Stroke 356
Tumors of the Brain 357
Types of Intracranial Tumors 359Infiltrating Tumors 359Noninfiltrating Tumors 359Childhood Tumors 361Diagnosis of Brain Tumors 361Treatment of Brain Tumors 362
Brain Tumors and Neuropsychology 363
Other Neurologic Disorders 363Brain Abscess 363Infections 363Neurotoxins 365
Summary 367Critical Thinking Questions 367Key Terms 368Web Connections 368
Neuropsychology in Action
12.1 Migraine Headache: A Vascular Disorder of the Brain 34812.2 Case Example of a Left Stroke 35412.3 Neuropsychology of Treatments for Individuals with Brain Tumors 36412.4 Family and Child Adjustment to Cognitive Aspects of Cancer in Children 366
Chapter 13 Tr a u m a t i c H e a d I n j u r y a n d R e h a b i l i t a t i o n 369Keep in Mind 370Overview 370
Traumatic Head Injury 370
Epidemiology of Traumatic Head Injury 371
Mechanism of Impact: Neuronal Shearing, Stretching, and Tearing 371Penetrating Head Injury 373Closed Head Injury 373Assessing the Severity of Brain Injury 375
Complications of Moderate and Severe Brain Injury 376Edema 376Brain Herniation 376Extradural and Subdural Hemorrhage 377
xiv Contents
Intracranial Bleeding 378Skull Fractures 378Post-traumatic Epilepsy 379
Mild Head Injury: “Concussions” 379Sports-Related Concussions: A Neuropsychological Perspective 381Postconcussional Syndrome 385
Treatment of Head Injuries 385Neuropsychological Manifestations 386
Recovery, Rehabilitation, and Intervention of Traumatic Brain Injury 388
Adaptation and Recovery 388Diaschisis 388Brain Reorganization 389
Overview of the Rehabilitation Process 389Admission to Rehabilitation Programs 390Evaluation of Goals and Discharge Planning 393Treatment Planning 394Assessment of Everyday Activities 394
Treatment Methods for Neuropsychological Rehabilitation 395Psychotherapy in Rehabilitation 395
Summary 397Critical Thinking Questions 398Key Terms 398Web Connections 398
Neuropsychology in Action
13.1 Case Study: Penetrating Head Injury 37413.2 Can a Concussion Change Your Life? 38013.3 Consensual Sex after Traumatic Brain Injury: Sex as a Problem-Solving Task 38613.4 It Is More Than a Black Box 396
Chapter 14 N o r m a l A g i n g a n d D e m e n t i a : A l z h e i m e r ’ s D i s e a s e 399Keep in Mind 400Overview 400
Normal Aging 400
Cognitive Changes Associated with Aging 401Brain Changes Associated with Aging 404
Mild Cognitive Impairment 405Summary 406
Defining Dementia 406Diagnostic Criteria for Dementia 407Subtypes and Classifications of Dementia 408
Alzheimer’s Disease 409Diagnostic Problem of Alzheimer’s Disease 409Neuropathology of Alzheimer’s Disease 411Histologic Markers 411Clinical Presentation and Neuropsychological Profile of Alzheimer’s Disease 413
Treatment 420
Contents xv

xvi Contents
Treatments for Cognitive Enhancement 420Cognitive, Behavioral, and Psychiatric Symptom Control 421
Summary 421Critical Thinking Questions 421Key Terms 422Web Connections 422
Neuropsychology in Action
14.1 The Discovery of Alzheimer’s Disease 41014.2 Differentiating between Symptoms of Alzheimer’s Disease and Normal Aging 414
Chapter 15 S u b c o r t i c a l D e m e n t i a s 423Keep in Mind 424Overview 424
Parkinson’s Disease 424Neuropathology of Parkinson’s Disease 424Clinical Presentation and Neuropsychological Profile of Parkinson’s Disease 425Treatments for Parkinson’s Disease 431
Huntington’s Disease 434Neuropathology of Huntington’s Disease 434Clinical Presentation and Neuropsychological Profile of Huntington’s Disease 435
Creutzfeldt–Jakob Disease 436Neuropathology of Creutzfeldt–Jakob Disease 438Clinical Presentation and Neuropsychological Profile of Creutzfeldt–Jakob Disease 439
Summary 441Critical Thinking Questions 442Key Terms 442Web Connections 442
Neuropsychology in Action
15.1 Understanding Subcortical Dementia 42615.2 Pallidotomy Surgery: A Case Report 43215.3 Testing Fate: Would You Want to Know If You Were Going to Get
Huntington’s Disease? 43515.4 Creutzfeldt–Jakob Disease and Mad Cow Disease: What’s the Connection? 43815.5 The Neurologic Examination for Dementia 440
Chapter 16 A l t e r a t i o n s o f C o n s c i o u s n e s s 443Keep in Mind 444Overview 444
Understanding Consciousness 444Mind and Brain 445Anatomic Correlates of Consciousness 447
Rhythms of Consciousness 449
The Brain and Mind in Sleep 451Sleep Architecture 451Sleep Anatomy and Physiology 456Reticular Activating System and Rapid Eye Movement Sleep 456Functions of Rapid Eye Movement Sleep 459Sleep Disorders 461

Runaway Brain: Seizure Disorders 463Classification of Seizure Types 464Neuroanatomy and Neurophysiology of Seizures 467Neuropsychological Presentation 469Treatment of Epilepsy 472
Summary 474Critical Thinking Questions 474Key Terms 474Web Connections 475
Neuropsychology in Action
16.1 Self in the Mirror 44616.2 The Case of the Last Coronation 45016.3 Lucid Dreaming: A Paradox of Consciousness 45316.4 Déjà Vu and Epilepsy 46516.5 Epilepsy and the Case of the Sweeping Lady 468
References 477
Glossary 511
Answers to Critical Thinking Questions 539
Name Index 551
Subject Index 561
Contents xvii

This page intentionally left blank

How can behavior make neuropsychological sense? Thatis the question we try to answer when we teach neuropsy-chology to our students. Like many teachers, we have hadthe experience of observing instructors and examiningbooks on the topic of neuropsychology that presented thematerial in an esoteric manner removed from real-life sit-uations. Neuropsychology is an exciting and dynamicfield that readily stimulates and inspires students andteachers alike. It was with this goal in mind that we havewritten a progressive and accessible text on the study ofneuropsychology.
The goal of Principles of Neuropsychology was to writean undergraduate or beginning graduate-level psychologytextbook that teaches brain function in a clear, interest-ing, and progressive manner. The guiding thesis of Prin-ciples of Neuropsychology is that all interactions in dailylife, whether adaptive or maladaptive, can be explainedneuropsychologically. Thus, the text challenges the readerto consider behavior from a broader biological perspec-tive. This, in turn, leads to the conceptualization of amore neuropsychologically oriented discipline within psy-chology. In this respect, the text covers the role of thebrain in behavior as simple as a reflex and as complex aspersonality. Principles of Neuropsychology stresses the fol-lowing specific ideas:
1. An emphasis on human neuropsychology, experi-mental and clinical
Human neuropsychology is most appealing to psychologystudents, given that approximately half of all professionalpsychologists identify with a clinical or counseling spe-cialty. A major focus of Principles of Neuropsychology is tointegrate the relatively new field of human clinical neu-ropsychology and compare it with what is known aboutthe normal brain.
Rather than focus on a purely cognitive organization,which characterizes brain functioning and behavior ac-cording to specific aspects or components such as mem-ory, attention, or executive functioning, we chose to focuson disorders. Because neurologic disorders are multifacetedand usually involve overlapping and interacting cognitive
components, we believe it is most useful for aspiring prac-titioners and researchers to obtain a comprehensive viewof each neurologic disorder with its multiple cognitivecomponents.
2. An emphasis on integrating theory and research
The integration of theory with studies of neuroanatomicstructure and functioning is central to a dynamic under-standing of neuropsychology. In this respect, Principles ofNeuropsychology reviews general theories of brain functionand specific theories of higher cortical functioning. A con-ceptual understanding of brain function is important be-cause it provides a foundation on which to base the studyof complex behavioral syndromes as they correspond tobrain regions and neuronal networks. Otherwise, nothingmore than the memorization of brain anatomy and corre-sponding behavioral correlates is achieved, and an inte-grated understanding of neuropsychology remains out ofreach.
3. An emphasis on behavioral function
We give special attention to presenting the function ofspecific neuroanatomic structures. Students often do notabsorb the tremendous amount of information presentedin similar texts because the material is presented in isola-tion, out of a psychological context. In this text, we pres-ent basic neurobiology as it relates specifically to behav-ior. Using such a functional approach facilitates both theabsorption and comprehension of the material.
4. A focus on presenting real-life examples
To facilitate the reader’s understanding of complex mate-rial and to augment specific points, Principles of Neuropsy-chology includes numerous examples of clinical and nor-mal cases, procedures, and classic research findings atstrategic places in the text. Like many other teachers, wefind that didactic information is better understood when“real-life” situations are used. Many of the cases and proce-dures draw on our clinical and research experiences, whichwe accumulated in a variety of settings and services in-cluding state psychiatric hospitals, sleep centers, psychiatry
PREFACE
xix

departments, rehabilitation hospitals, and neurology andneurosurgery services. Throughout the text, we featurecase examples and Neuropsychology in Action boxes,written by prominent neuropsychologists, that focus oninteresting current issues related to brain functioning.
5. The presentation of didactic aids
Principles of Neuropsychology differs from other texts on thedidactic dimension, because it uses unique aids to facilitatelearning. These aids include an Instructor’s Manual, whichprovides outlines, class exercises, additional reference mate-rials, and didactic information; Web support, which in-cludes practice examinations, exercises, and additional refer-ence materials; more than 200 illustrations in the text; colorillustrations; boldfaced Key Terms throughout the text,which are listed at the end of each chapter and again in theGlossary at the end of the text; a Keep in Mind section atthe beginning of each chapter and Critical Thinking Ques-tions at the end of each chapter; and annotations on Websites, called Web Connections, at the end of each chapter.
The companion Web sites for students and instructorshave been updated and expanded for the new edition witha format that is easier to navigate. Now you will findchapter-by-chapter glossaries and interactive flash cards,plus videos and more practice exercises. To access thesefeatures and more, visit http://www.thomsonedu.com/psychology/zillmer. For instructors, the Instructor’s Manualwith Test Bank has been updated for the new edition andcontains even more sample test items. Many of the figuresand tables from the book are available for instructors asPowerPoint® electronic transparencies.
This second edition was revised related to the manysuggestions that we have received. Specifically, the authors
have integrated the latest studies and research to give stu-dents the most up-to-date information in this dynamicand expanding field. Furthermore, this edition includesan increased emphasis on neuroscience coverage to pro-vide empirical data in support of the discussions of neu-ropsychology. Clinical examples throughout the text areupdated in support of the new research in the developingfield of neuropsychology. This second edition also pro-vides additional chapters and coverage on topics of So-matosensory, Chemical and Motor Systems, Vision andLanguage, and Memory, Attention, and Executive Func-tioning. A reorganization of the material now places as-sessment methods of the brain, both medical and psycho-logical, at the beginning of the text to introduce studentsto this area early in their studies.
In summary, the intent of Principles of Neuropsychologyis to discuss brain functions, neurophysiology, and neu-roanatomy in an integrated and accessible format. An in-depth discussion on the relation among neuroscience,anatomy, and behavior is emphasized. Numerous exam-ples of clinical and real-life examples of neuropsychologyare provided, as is a focus on relevant scientific and theo-retical contributions in the field of neuropsychology.Unique to the study of neuropsychology is an organiza-tion of the material from history, assessment, neu-roanatomy, to clinical assessment that makes intuitive anddidactic sense. To facilitate a dynamic understanding ofthe field, the text emphasizes theory, functional process,case examples, and research, related to what has beenlearned about normal and neuropathological functioning.Approaching the field from this perspective challengesstudents to examine the field of neuropsychology as aframework for behavior.
xx Preface
Dr. Eric A. Zillmer, a licensed Clinical Psychologist,received his Doctorate in Clinical Psychology fromFlorida Tech in 1984 and was subsequently awarded the Outstanding Alumnus Award in 1995.Dr. Zillmer completed internship training at EasternVirginia Medical School and a postdoctoral fellowshipin clinical neuropsychology at the University of Vir-ginia Medical School. A member of Drexel Univer-sity’s faculty since 1988, Dr. Zillmer is a Fellow of theCollege of Physicians of Philadelphia, the AmericanPsychological Association, the Society for PersonalityAssessment, and the National Academy of Neuropsy-chology, for which he has also served as President. Hehas written extensively in the area of sports psychol-ogy, neuropsychology, and psychological assessment,having published more than 100 journal articles, bookchapters, and books, and he is a frequent contributorto the local and national media on topics rangingfrom sports psychology, forensic psychology, to thepsychology of terrorism. The Quest for the Nazi
Personality, published in 1995, has been summarizedas the definitive psychological analysis of Third Reichwar criminals. He is the coauthor of the d2 Test ofAttention and the Tower of London test. Dr. Zillmerserves on the editorial boards of Journal of PersonalityAssessment and Archives of Clinical Neuropsychology.His most recent book is entitled Military Psychology—Clinical and Operational Applications (2006). Dr.Zillmer currently serves as the Director of Athleticsat Drexel University.
Dr. Mary V. Spiers is Associate Professor of Psychol-ogy in the Department of Psychology at Drexel Uni-versity and is a licensed Clinical Psychologistspecializing in Neuropsychology. She earned herPh.D. in Clinical Psychology from the University ofAlabama at Birmingham, where she specialized inmedical psychology and neuropsychology. Dr. Spiers’sresearch and clinical expertise is in two areas. The firstarea is neuropsychological assessment with a focus on
ABOUT THE AUTHORS
xxi

everyday problems of memory. She has developedtests to assess memory and cognitive problems in dailymedication taking. Recently, she has focused on thedevelopment of ecologically valid spatial memory testswithin a virtual reality environment. Dr. Spiers’s secondarea of focus relates to cognitive performance and strat-egy differences related to sex and gender. She leads theWomen’s Cognitive Health Research Group at DrexelUniversity, whose aim is to investigate variation in brainfunctioning through the influence of sex and gender, themenstrual cycle, genetics/handedness, experience, andculture. She regularly teaches Neuropsychology on boththe undergraduate and graduate levels. In addition, shehas taught a variety of graduate courses related to clini-cal assessment and memory, including Neuropsycholog-ical Assessment, Neuropsychological Case Analysis, andModels of Memory in Neuropsychology.
Dr. William C. Culbertson is in private practice as aClinical Neuropsychologist who specializes in the
assessment and treatment of childhood and adolescentdisorders, particularly those with attention-deficit/hyperactivity disorder. He received his doctorate degreefrom Rutgers University and completed a postdoctoralfellowship in neuropsychology at Drexel University.Dr. Culbertson’s research interests are in the assess-ment of higher order problem-solving ability, specifi-cally as it relates to assessing frontal lobe damage, andexecutive functioning deficits. Dr. Culbertson has pub-lished in the field of neuropsychology (e.g., Assessment,Archives of Clinical Neuropsychology) and presented atprofessional conferences. He is an Associate VisitingScholar at the University of Pennsylvania and hastaught at Drexel University, both at the undergraduateand graduate level, including Counseling Psychology,Developmental Psychology, Cognitive Psychology,Theories of Personality, and various Seminars inNeuropsychology. He is a coauthor of the Tower ofLondonDX, now in its second edition, which is aneuropsychological measure of executive function.
xxii About the Authors

This book could not have been written without the coop-eration, assistance, and support of numerous individuals.Many students, scholars, and friends listened to us, of-fered suggestions, and provided encouragement along theway. Many reviewers helped shape the book from begin-ning to end. We are most grateful to the following review-ers for their generous contributions to this second edition:Joan Ballard, SUNY Geneseo; Jody Bain, University ofVictoria; Robert Deysach, University of South Carolina;Kenneth Green, California State University Long Beach;Julian Keenan, Montclair State University; Ann MarieLeonard-Zabel, Curry College; Jim Nelson, ValparaisoUniversity; Elizabeth Seebach, Saint Mary’s University ofMinnesota; Pamela Stuntz, Texas Christian University;Benjamin Walker, Georgetown University; Arthur Wing-field, Brandeis University; Nancy Zook, Purchase CollegeSUNY. We would also like to thank those who con-tributed to the previous edition: Timothy Barth, TexasChristian University; Richard Bauer, Middle TennesseeState University; Gary Berntson, Ohio State University;Thomas Fikes, Westmont College; Michael R. Foy, LoyolaMarymount University; Kenneth F. Green, CaliforniaState University Long Beach; Gary Hanson, Francis MarionUniversity; Barbara Knowlton, University of CaliforniaLos Angeles; Paul Koch, St. Ambrose University; MarkMcCourt, North Dakota State University; James Rose,University of Wyomong; Lawrence Ryan, Oregon StateUniversity; Bennett Schwartz, Florida International Uni-versity; Michael Selby, California Polytechnic Institute;Frank Webbe, Florida Institute of Technology; and finally,the many reviewers who did not wish to be named. Wewould also like to acknowledge those scholars who havecontributed Neuropsychology in Action boxes to this text.All of them are prominent neuropsychologists who have,going beyond the call of duty, given valuable time to makePrinciples of Neuropsychology “come alive.”
Drexel University psychology students played an im-portant role in this project. They read initial chapters andprovided feedback, were willing to use early versions ofthe manuscript as their textbook in class, and providedimportant research assistance. Simply put, this projectcould not have been accomplished without their diligent
efforts. Psychology undergraduate and graduate studentswho provided valuable research support on the first edi-tion included Barbara Holda, Priti Panchal, Dan Rosenberg,Holly Giordano, Stephanie Cosentino, Carrie Kennedy,Melissa Lamar, and Cate Price. Drexel University studentsin Dr. Spiers’s undergraduate and graduate neuropsychol-ogy classes provided valuable comments on both thestructure and content of this second edition. Specialthanks go to Karen Friedman, who coordinated referenceupdating in this second edition; to Heather McNiece,who coordinated the Key Terms and Glossary; and toMaiko Sakamoto, who assisted with the question bank.
Appreciation also goes to our colleagues Sepp Zihl andKarin Muenzel, both from the Ludwig-MaximiliansUniversity, Institute für Neuropsychologie, in Munich,Germany. Sepp and Karin allowed Dr. Zillmer to teachneuropsychology in an international forum. Our discus-sions on neuropsychology have been most stimulating andinspiring and have provided a springboard for many issuesdiscussed in this text. We also want to acknowledge our col-leagues Mark Chelder and Joelle Efthimiou, who have as-sisted us in the development of the Assessment of Impair-ment Measure (AIM), which we have used extensivelythroughout the text to demonstrate the principles of neu-ropsychological assessment.
Our friend Carl Pacifico played a special role in thisventure. He reminded us of how important it is to thinkabout brain-behavior functioning within the context ofevolution. Carl, ever the pragmatist, also shaped ourthinking about the functional and applied aspects of neu-ropsychology. We especially welcomed the occasions whenwe discussed neuropsychology and its relation to culture,religion, and philosophy.
Special recognition goes to key administrators atDrexel University. Former Dean of the College of Artsand Sciences Thomas Canavan provided encouragementfor our doctoral program in neuropsychology at Drexel andassistance for the successful APA accreditation process. Con-stantine “Taki” Papadakis, President of Drexel University, isacknowledged for revitalizing our university and, mostimportantly, making Drexel an exciting and fun place toteach and to do research.
ACKNOWLEDGMENTS
xxiii

Our department faculty served as an important discus-sion group, “think tank,” and sounding board; whether itwas around the copying machine, in the hallways, or overlunch, they allowed us to argue over the role of the brainand its relation to behavior. Thanks to Doug Porpora,David Kutzik, Tom Hewett, Elizabeth Petras, ArthurShostak, Doug Chute, Lamia Barakat, and Anthony Glas-cock. Dorota Kozinska, at the University of Warsaw,Poland, taught us the three-dimensional imaging of brainsand provided state-of-the-art brain electrical activity map-ping pictures. Erin D. Bigler, Professor of Psychology atBrigham Young University, and Frank Hillary, AssistantProfessor at Penn State University, generously providedthree-dimensional images of the brain. Frank Ruben C.Gur and his research group at the Department of Psychi-atry, University of Pennsylvania, allowed us to use cere-bral blood flow study pictures.
Any scholar with a family knows what it means towrite a book and attempt to maintain a normal familylife. Dr. Zillmer is grateful to his wife, Rochelle, and his
daughter, Kanya, for their support. Dr. Spiers thanksher husband, Sean, for his patience and understanding.Dr. Culbertson acknowledges his wife, Nancy, whoprovided countless hours of critical readings, tolerated hisabsences during those periods when he needed to write,and was unwavering in her support.
We cannot think of having had better editors for thisproject. We thank the production editor, Dan Fitzgerald,and the psychology editor, Erik Evans, assistant editor,Gina Kessler, and editorial assistant, Christina Ganim.They took our project seriously and forced us to focus onfinishing a product of the highest quality. The assistanceof many individuals has enabled us to publish this secondedition. We are grateful to all of them and have benefitedfrom their understanding, criticism, and advice. Thankyou.
Eric A. ZillmerMary V. Spiers
William C. Culbertson
xxiv Acknowledgments
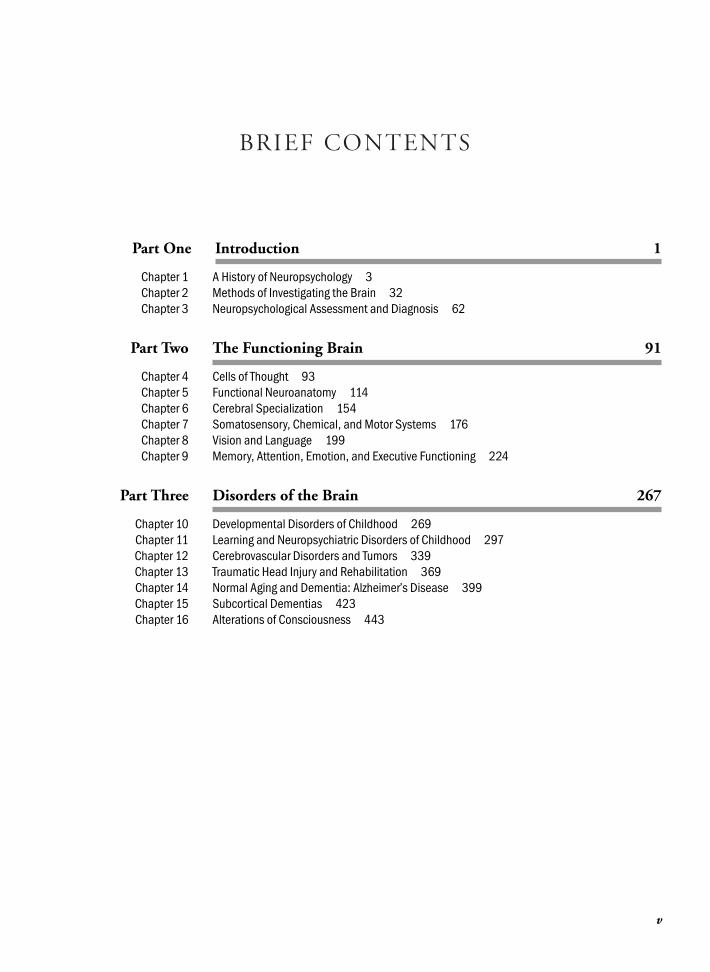
S T R U C T U R E - F U N C T I O N R E L A T I O N S H I P S
12345678123456789101112123451
Cervical
BrainC2
C3
C4C5
T2
C6
C7
T1C8
L1T12T11T10T9T8T7T6
T5T4T3
T2
L2
L3
L5
L4
S1
Thoracic
Lumbar
Sacral
a.
b.
c.2345
Sensory receptor
Dorsal root
Ventral root
Muscle
Parietal bone
Squamosal suture
Lambda
Occipital bone
Lambdoidal suture
External occipitalprotuberance
Temporal boneAsterion
External acoustic meatus
Mandible
Maxilla
Glabella
Sphenoid bone
Coronal suture
Frontal bone
BregmaPterion
NasionNasal bone
Zygomatic bone
Lacrimal boneEthmoid bone
Angleofmandible
Zygomatic archStyloidprocess
Mastoidprocess
(location ofintervertebraldisk)
spinal cord
ganglionnerve
meninges(protectivecoverings)vertebra
Anteriorcommunicating artery
Anteriorcerebral artery
Internal carotid arteryMiddle cerebral artery
Posterior communicatingarteryPosterior cerebral artery
Basilar arteryLabyrinthine arteryVertebral artery
Anteriorspinal artery
Posterior inferiorcerebellar artery
Superiorcerebellarartery
Pontinearteries
Anterior inferiorcerebellar artery
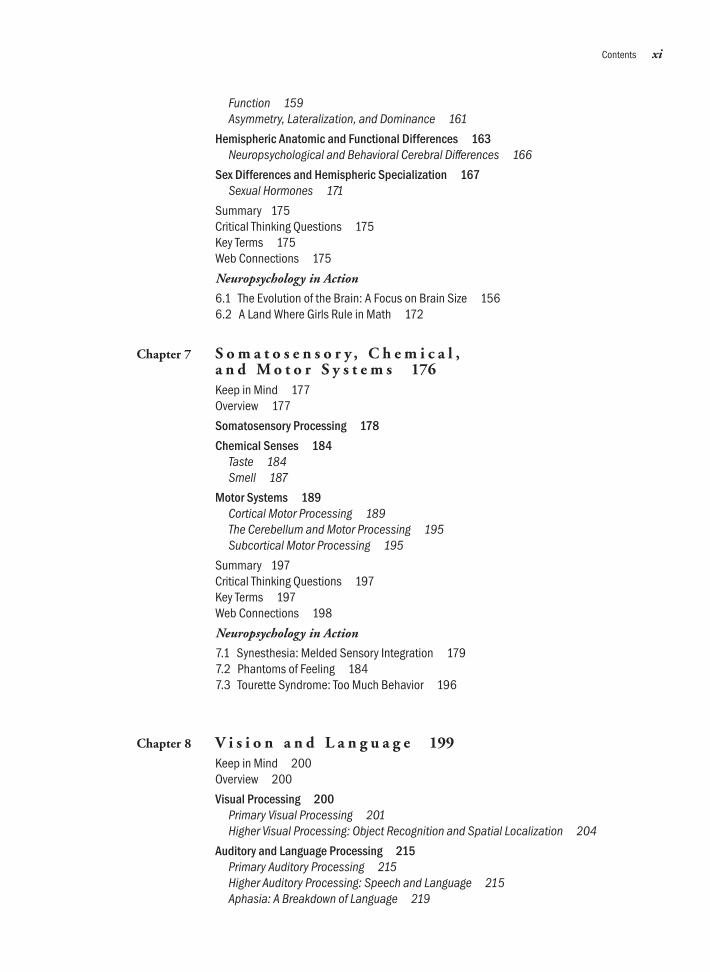
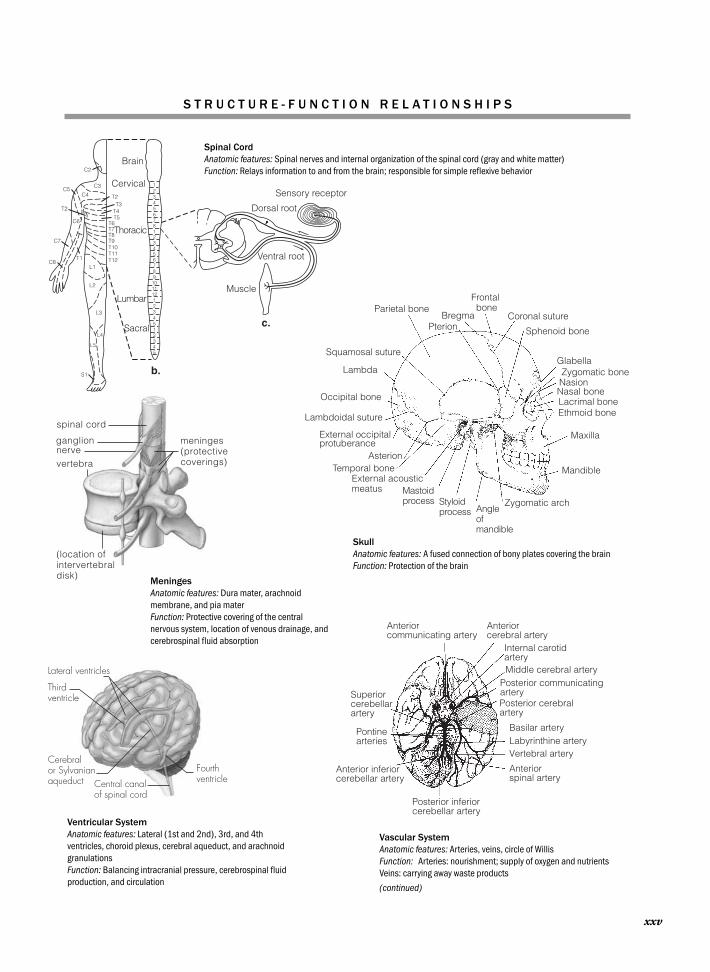
Spinal CordAnatomic features: Spinal nerves and internal organization of the spinal cord (gray and white matter)Function: Relays information to and from the brain; responsible for simple reflexive behavior
SkullAnatomic features: A fused connection of bony plates covering the brainFunction: Protection of the brain
MeningesAnatomic features: Dura mater, arachnoidmembrane, and pia materFunction: Protective covering of the centralnervous system, location of venous drainage, andcerebrospinal fluid absorption
Vascular SystemAnatomic features: Arteries, veins, circle of WillisFunction: Arteries: nourishment; supply of oxygen and nutrientsVeins: carrying away waste products
(continued)
Thirdventricle
Fourthventricle
Lateral ventricles
Cerebralor Sylvanianaqueduct Central canal
of spinal cord
Ventricular SystemAnatomic features: Lateral (1st and 2nd), 3rd, and 4thventricles, choroid plexus, cerebral aqueduct, and arachnoidgranulationsFunction: Balancing intracranial pressure, cerebrospinal fluid production, and circulation
xxv

Thalamus Pineal gland
Tectum
Pons
Medulla
Tegmentum
SuperiorcolliculusInferiorcolliculus
Midbrain
Posterolateralview ofbrainstem
Optic nerve(Cranial nerve II)
Cranial nerve IIICranial nerve V
Cranial nerve VIIIVIIVIIXX
XIXII
Spinal nerve Spinal cord
Medulla
Cranial nerve IV
Midbrain
PonsCerebellum
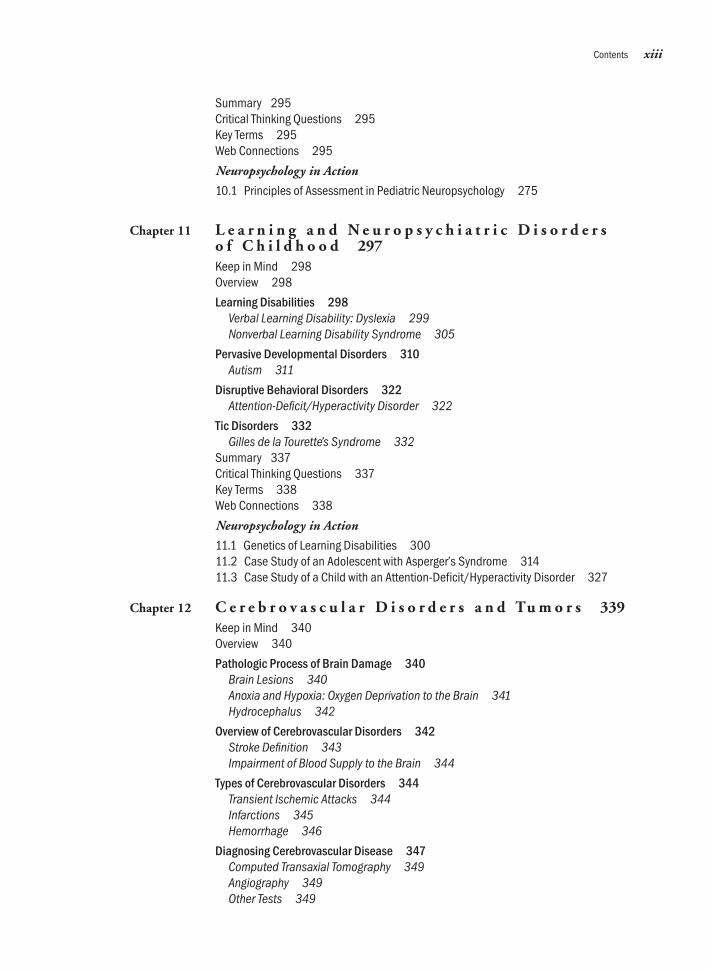
Lower BrainstemAnatomic features:Hindbrain: medulla oblongata (myelencephalon), pons (metencephalon)Midbrain: tectum and tegmentum, cranial nerves, reticularactivating systemFunction: Relays information to and from the brain; responsible for simple reflexive behavior
Cranial NervesAnatomic features: Located within the brainstemFunction: Conducting specific motor and sensory information
Pulvinar nucleus
Dorsomedialnucleus
Ventral lateral nucleus
Ventralposteriolateralnucleus
Lateral geniculate body
Dorsalhypothalamus
Dorsomedialhypothalamus
Posterior hypothalamus
Paraventricular nucleusof hypothalamus
Anterior commissureLateral hypothalamus(behind plane of view)Anterior hypothalamusPreoptic area
Supraoptic nucleus
Optic chiasm
Anterior pituitary
Mammillary body
Ventromedialhypothalamus
Posteriorpituitary
Cortex
Reticular formation
Suprachiasmaticnucleus
Brainstem
Cerebellum
Reticular FormationAnatomic features: Neural network within the lower brainstemconnecting the medulla and the midbrainFunction: Nonspecific arousal and activation, sleep and wakefulness
HypothalamusAnatomic features: Hypothalamic nuclei, major fiber systems, and thirdventricleFunction: Activates, controls, and integrates the peripheral autonomicmechanisms, endocrine activity, and somatic functions, including bodytemperature, food intake, and the development of secondary sexualcharacteristics
ThalamusAnatomic features: Thalamic nuclei and thalamocorticalconnectionsFunctions: Complex relay station—major sensory andmotor inputs to and from the ipsilateral cerebralhemisphere
S T R U C T U R E - F U N C T I O N R E L A T I O N S H I P S
xxvi
Cerebellarcortex
Deep cerebellarnuclei Pontine
nuclei
Fourthventricle
Globus pallidus(lateral part)
Caudate nucleus
Subthalamicnucleus
Substantia nigra
Putamen
Globus pallidus(medial part)
Thalamus
Corpus callosumFornix
Anteriornucleusof thalamus
Septum
Olfactory bulb
Mammillary bodyAmygdala
Hippocampus
Corpus callosum
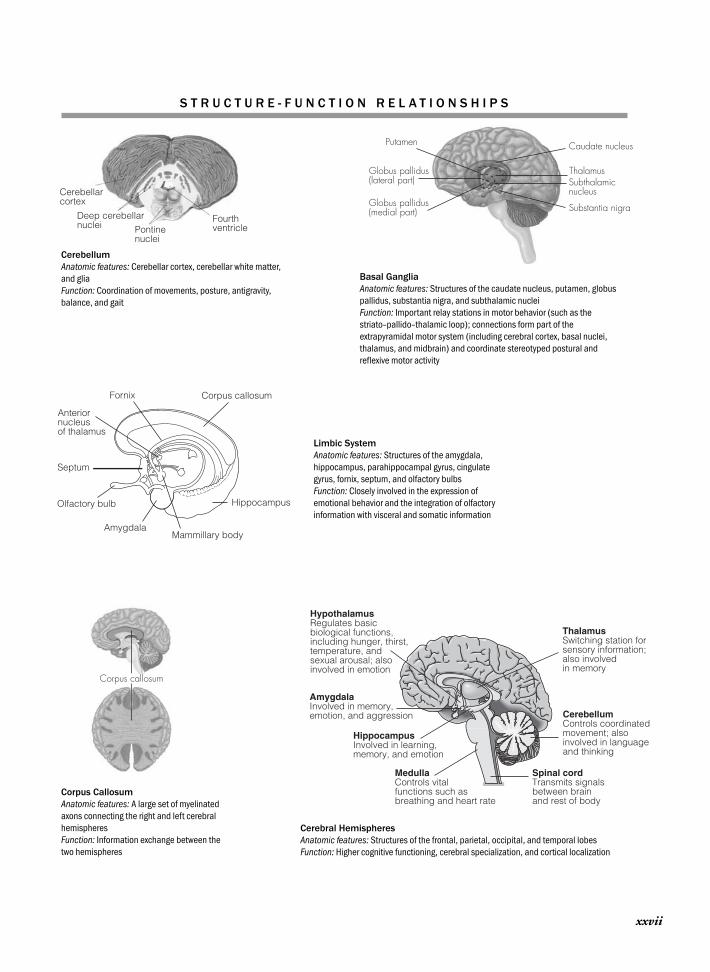
AmygdalaInvolved in memory,emotion, and aggression
HippocampusInvolved in learning,memory, and emotion
MedullaControls vital functions such as breathing and heart rate
ThalamusSwitching station forsensory information; also involved in memory
Spinal cordTransmits signalsbetween brainand rest of body
CerebellumControls coordinatedmovement; also involved in languageand thinking
HypothalamusRegulates basic biological functions, including hunger, thirst, temperature, and sexual arousal; also involved in emotion
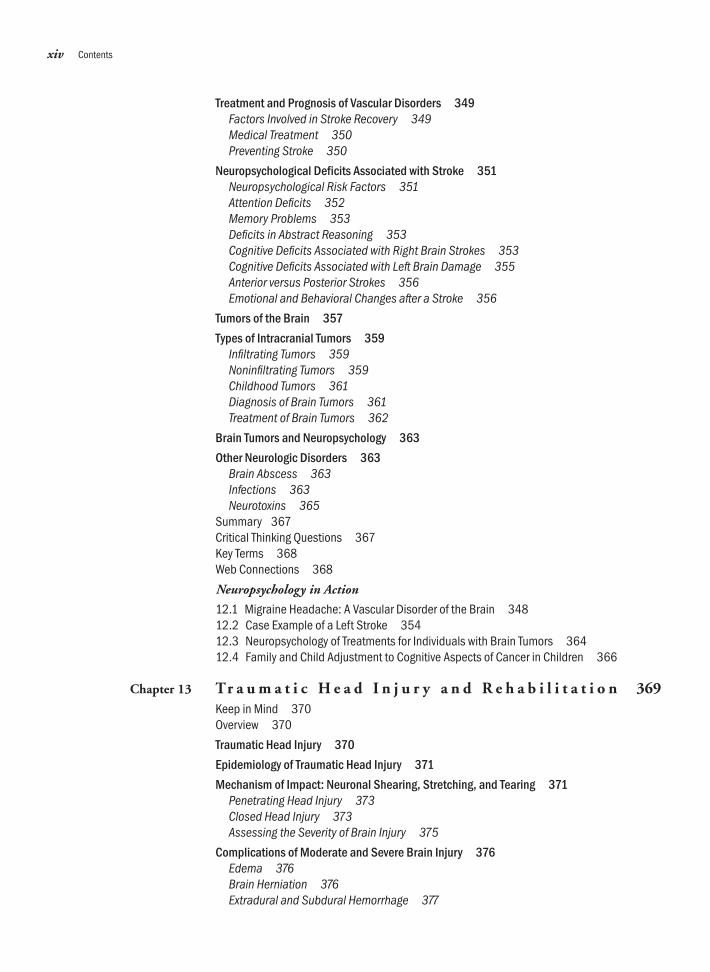
Cerebral HemispheresAnatomic features: Structures of the frontal, parietal, occipital, and temporal lobesFunction: Higher cognitive functioning, cerebral specialization, and cortical localization
CerebellumAnatomic features: Cerebellar cortex, cerebellar white matter,and gliaFunction: Coordination of movements, posture, antigravity,balance, and gait
Basal GangliaAnatomic features: Structures of the caudate nucleus, putamen, globuspallidus, substantia nigra, and subthalamic nucleiFunction: Important relay stations in motor behavior (such as thestriato–pallido–thalamic loop); connections form part of theextrapyramidal motor system (including cerebral cortex, basal nuclei,thalamus, and midbrain) and coordinate stereotyped postural andreflexive motor activity
Limbic SystemAnatomic features: Structures of the amygdala,hippocampus, parahippocampal gyrus, cingulategyrus, fornix, septum, and olfactory bulbsFunction: Closely involved in the expression ofemotional behavior and the integration of olfactoryinformation with visceral and somatic information
Corpus CallosumAnatomic features: A large set of myelinatedaxons connecting the right and left cerebralhemispheresFunction: Information exchange between thetwo hemispheres
S T R U C T U R E - F U N C T I O N R E L A T I O N S H I P S
xxvii

This page intentionally left blank
Part One
I N T R O D U C T I O N
Chapter 1 A History of Neuropsychology
Chapter 2 Methods of Investigating the Brain
Chapter 3 Neuropsychological Assessment and Diagnosis

This page intentionally left blank

Chapter 1
A HISTORY OF NEUROPSYCHOLOGY
I think, therefore I am.—René Descartes, Discourse on Method
There is no ghost in the machine.—Gilbert Ryle, The Concept of Mind
The Brain in Antiquity: Early HypothesesLocalization TheoryLocalization versus EquipotentialityIntegrated Theories of Brain FunctionModern NeuropsychologyEmerging Research Areas in Neuropsychology
Neuropsychology in Action
1.1 The Brain of a Nazi1.2 Paul Broca: A Manner of Not Speaking1.3 Sigmund Freud: The Neurologist1.4 The Walter Freeman Lobotomies: Mind over Matter?

OverviewAll the preceding questions concern the functions of the brain. The brain has evolved to play a particularlysignificant role in the human body, not only in sustaining life, but also in all thought, behavior, and reason-ing. It is the only organ completely enclosed by protective bony tissue, the skull, and it is the only organ thatcannot be transplanted and still maintain the person’s self. But how exactly does brain tissue generate andconstrain mental events?
Efforts to understand mind–body relationships and their relative contributions to health and well-beingextend back at least to the philosophies of Plato, Descartes, and Kant. Like many other sciences, neuropsy-chology has evolved from related fields, most notably psychology, neurology, neuroscience, biology, andphilosophy. Psychology is the study of behavior; specifically, it seeks to describe, explain, modify, and pre-dict human and animal behavior. Neuropsychology, a subspecialty of psychology, is the study of how com-plex properties of the brain allow behavior to occur. Neuropsychologists study relationships between brainfunctions and behavior; specifically, changes in thought and behavior that relate to the brain’s structural orcognitive integrity. Thus, neuropsychology is one way to study the brain by examining the behavior it pro-duces.
Humans read and write, compose music, and play sports. You would expect an organ that coordinatesand mediates all activity to have a huge number of components. And, in fact, the brain contains billions ofcells, or neurons, and an infinite number of possible connections among individual neurons, allowing us toexchange complex information. This amazing pattern of connections determines how and what the braindoes. Understanding this network of neurons is the central focus of neuropsychology.
Neuropsychology has grown tremendously since the 1970s, and in the 1990s, it was the fastest grow-ing subspecialty within psychology. Neuropsychologists lead the study of brain–behavior relationships andare involved in the design and development of technologies to treat diseases of the brain. They are involvedin patient care and research on the brain and work in universities, research institutes, medical and psychi-atric hospitals, correctional facilities, the armed forces, and private practice.
The study of neuropsychology currently is shaping our understanding of all behavior. But this has notalways been true. Many previous ideas about how the brain functions did not derive from scientificevidence. In general, two doctrines have emerged. The first doctrine, vitalism, suggests that many behav-iors, such as thinking, are only partly controlled by mechanical or logical forces—they are also partially self-determined and are separate from chemical and physical determinants. Extreme proponents of vitalismargue that spirits or psychic phenomena account for much observable behavior. Sigmund Freud’s psycho-analysis would be a good example of this doctrine. The second doctrine, materialism, suggests that logicalforces, such as matter in motion, determine brain–behavior functions. Materialism, in its simplest form,favors a mechanistic view of the brain (as a machine). Walter Freeman’s lobotomies embraced this idea.The history of neuropsychology is shaped by these two opposing principles.
This introductory chapter provides grounding in the historical, theoretical, and philosophical aspects ofneuropsychology. By charting the work of noted scholars, this chapter traces the development of neuropsy-chology from antiquity to the present.
4 PART ONE | Introduction
K e e p i n M i n d
Does our brain constitute a major aspect of who we are?
Is the brain the source of all behavior?
Where do we go when our brain dies?
What is a soul?

The Brain in Antiquity: Early Hypotheses
Evidence from as long ago as the time of cave draw-ings shows that people have long been aware of brain-be-havior relationships. The earliest neuropsychological in-vestigations recognized how diseases and blows to thebrain affect behavior. For example, trephination is an an-cient surgical operation that involves cutting, scraping,chiseling, or drilling a pluglike piece of bone from theskull. This procedure relieves pressure related to brainswelling. Archaeologists have recovered several thousandsuch skulls worldwide. Many who underwent trephina-tion clearly survived the operation, because many of theskulls show evidence of healing (new callus tissue); otherskulls show no signs of healing, so the patients died dur-ing or shortly after the operation. In some cases, the sameskull was trephined more than once. One recovered skullwas found with seven boreholes, at least some of whichwere made on separate occasions.
Why did our ancestors perform trephination (Figure 1.1)?Did they have a reasonable understanding of the brainand its relationship to behavior? Did they use this proce-dure for medical reasons, such as trauma with swelling, orfor other reasons? Did practitioners avoid certain areas ofthe brain because they knew that permanent behavioralproblems or death were likely to follow?
Much debate focuses on the reason for trephinations.Researchers have suggested that some cases may have in-volved a medical reason, such as a skull fracture. Such in-juries presumably occurred during hand-to-hand fightingwith stone-headed war clubs or perhaps as a result of a fallunconnected with warfare. On some skulls, however, trephi-nation was performed on intact crania with no sign of vio-lence. Thus, some investigators suggest that trephinationwas a “magical” form of healing, perhaps for displays ofbizarre behaviors, including what we would now recognizeas epilepsy or schizophrenia (Lisowski, 1967) (Figure 1.2).
Similar operations are important in modern neuro-surgery (Figure 1.3). Surgeons widely use two procedures.The first procedure, similar to the ancient Peruvian
CHAPTER 1 | A History of Neuropsychology 5
Figure 1.1 Trephination scene in Peru. (Image reprinted with permission from Department of Anthropology, NationalMuseum of Natural History, Smithsonian Institution, Washington, D.C. Photo courtesy of the San Diego Museum of Man.)

technique of drilling a number of small holes, involvesdrilling a hole next to a depressed skull fracture to facili-tate the elevation and removal of depressed bone frag-ments. Incidentally, modern neurosurgeons still use man-ual drills, which allow them more control during theoperation. The second surgical procedure drains internalbleeding after a blow to the head. With a special drill bit,the surgeon makes a hole over the site of the bleed. Thenthe surgeon screws a precisely machined bolt into the skull,allowing excessive blood to drain from within the cranium.This procedure reduces the intracranial pressure that is amajor cause of death after a head injury (see Chapter 13).
That surgeons today use an ancient surgical techniquethat even modern doctors once thought controversialunderscores that people have often misinterpreted the his-torical context in which ancient scientists proposed certainideas about the brain or performed specific procedures.Most ideas about the brain make more sense when consid-ered within the societal and cultural context in which theywere originally developed.
A N C I E N T G R E E K P E R S P E C T I V E S
Classical Greeks wrote the first accounts of brain–behaviorrelationships. Heraclitus, a philosopher of the sixth cen-tury B.C., called the mind an enormous space withboundaries that we could never reach. A group of schol-ars, including the geometer Pythagoras (about 580–500 B.C.), was the first to suggest that the brain is at thecenter of human reasoning and plays a crucial role in thesoul’s life. They described what is now called the brainhypothesis: the idea that the brain is the source of allbehavior.
Hippocrates (460–377 B.C.), a Greek physician hon-ored as the founder of modern medicine (Figure 1.4), alsobelieved the brain controls all senses and movements. Hewas the first to recognize that paralysis occurs on the sideof the body opposite the side of a head injury, followingthe areas governed by the right and left hemispheres ofthe brain. Hippocrates suggested that pleasure, merri-ment, laughter, and amusement, as well as grief, pain,anxiety, and tears, all arise from the brain (Haeger, 1988).Furthermore, Hippocrates argued that epilepsy, once con-sidered the “sacred disease” (because people thought thepatient was possessed by gods or spirits), is, in fact, nomore divine or sacred than any other disease, but has spe-cific characteristics and a definite medical cause. Thesewere bold propositions at a time when people thoughtbehavior was mostly under divine control. Hippocratesand his associates could not, however, discuss exactly howsuch brain–behavior relationships arose, perhaps because itwas then sacrilegious to dissect the human body, especiallythe brain.
Plato (420–347 B.C.) suggested in The Republic thatthe soul has three parts: appetite, reason, and temper. Thismay have served as the model for Freud’s psychoanalyticsubdivision of the psyche into the id, ego, and superego(see later discussion). Plato believed the rational part ofthe tripartite soul lay in the brain, because it is the organclosest to the heavens. Plato also discussed the idea thathealth is related to harmony between body and mind.Thus, historians credit Plato as being the first to proposethe concept of mental health.
6 PART ONE | Introduction
Figure 1.2 Adult male skull showing multiple trephina-tions by the scraping method. Evidence of inflammationindicates temporary survival. (Courtesy Mütter Museum,College of Physicians of Philadelphia.)
Figure 1.3 Modern trephination. A surgical hole isopened in the skull to relieve the intracranial pressure oftenassociated with consequences of head trauma. (CourtesyJeffrey T. Barth, PhD, University of Virginia.)
Not all ancient philosophers believed in the impor-tance of the brain to behavior. Aristotle (384–322 B.C.),a disciple of Plato, was a creative thinker in fields as var-ied as ethics, logic, psychology, poetry, and politics, andhe founded comparative anatomy. Aristotle, however, er-roneously believed the heart to be the source of all mentalprocesses. He reasoned that because the heart is warm andactive, it is the locus of the soul. Aristotle argued that be-cause the brain is bloodless, it functions as a “radiator,”cooling hot blood that ascends from the heart. The influ-ence of Aristotle’s so-called cardiac hypothesis proposingthe heart as the seat of such emotions as love and angercan still be seen in words such as heartbroken. Neverthe-less, Aristotle’s view of nature and his anatomic findingsdominated medical thinking and methods for the next500 years.
T H E C E L L D O C T R I N E
In Egypt, during the third and fourth centuries B.C., theso-called Alexandrian school reached its height. Well-known scientists worked in physiology and anatomy. Theygained considerable knowledge of the nervous system andneuroanatomy from performing public dissections, whichthe Ptolemaic rulers encouraged. Reports exist of scientistsactually vivisecting subjects—condemned criminals were atthe scientists’ disposal. These dissections allowed scientiststo notice different anatomic details, and they hypothesizedthat specific parts of the brain control different behaviors.Furthermore, they broke new ground by distinguishingbetween ascending (sensory) and descending (motor)nerves, and demonstrating that all nerves connect with thecentral nervous system.
An interesting development during this time was theerroneous suggestion that ventricular cavities within thebrain control mental abilities and movement. The ven-tricular localization hypothesis postulated that mentalas well as spiritual processes reside in the ventricularchambers of the brain. Indeed, gross dissection of thebrain shows that the lateral ventricles are the most strik-ing features. Thus, brain autopsies might have led investi-gators to conclude that these cavities contain animal spir-its and are in large part responsible for mental faculties.This hypothesis subsequently became known as the celldoctrine (“cell” meaning a small compartment or ventri-cle), a notion that endured for 2000 years. Leonardo daVinci (1452–1519), an Italian painter, sculptor, architect,and scientist, was a keen observer of anatomy. However,many of his early drawings were not guided by his keenscientific acumen, but instead by the inaccurate medievalconventions of his times. For example, Figure 1.5 showsone of his drawings based on a common, but inaccuratebelief about spherical ventricles. According to the cell doc-trine, foremost was the cell of common sense, where peo-ple thought the soul resided and that connected to nervesleading to the eyes and ears.
Today, people know that the cell doctrine is entirely in-accurate. The ventricles are actually the anatomic sitethrough which cerebrospinal fluid passes. This fluid pro-tects the brain and facilitates the disposal of waste material.It plays no role in thinking; in fact, a neurosurgeon friendof ours conceptualizes it poetically as “the urine of thebrain.” The cell doctrine was scientifically important pre-cisely because it was in error, and thus presented an obsta-cle to further inquiry that people did not overcome untilcenturies later. However, it did focus the medical commu-nity on the brain and stimulated discussion of how behav-ior, thought processes, and brain anatomy may be related.
CHAPTER 1 | A History of Neuropsychology 7
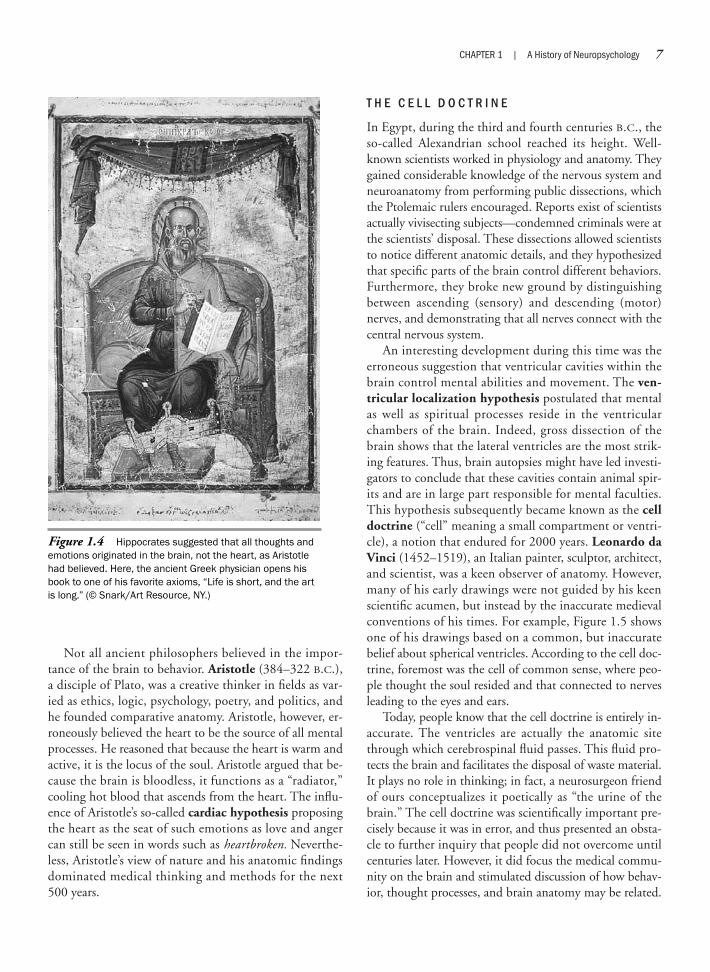
Figure 1.4 Hippocrates suggested that all thoughts andemotions originated in the brain, not the heart, as Aristotlehad believed. Here, the ancient Greek physician opens hisbook to one of his favorite axioms, “Life is short, and the artis long.” (© Snark/Art Resource, NY.)

Together with Hippocrates, Galen (A.D. 130–201), aRoman anatomist and physician, stands out as a supremefigure in ancient medicine (Figure 1.6). Galen was un-doubtedly the greatest physician of his time. By signifi-cantly advancing the anatomic knowledge of the brain,Galen distinguished himself as the first experimentalphysiologist and physician. He identified many of themajor brain structures and described behavioral changesas a function of brain trauma. It was Galen’s misfortune,however, that during his life the Roman authorities for-bade autopsies. He therefore based much of his clinicalknowledge on his experience as a surgeon appointed totreat gladiators; he remarked that war and gladiator gameswere the greatest school of surgery. Contemporary neu-ropsychologists have also made significant advances dur-ing periods of war, including World Wars I and II and theKorean and Vietnam conflicts, by studying the behavioraleffects of wounds to the brain.
Galen suggested that the brain is a large clot of phlegmfrom which a pump forced the psychic pneuma out intothe nerves. Perhaps he was comparing the brain to a major
technologic achievement of his time, the Roman systemof aqueducts, which relied on hydraulic principles. Al-though Galen believed the frontal lobes (Figure 1.7) arethe location of the soul, he supported the ventricular lo-calization hypothesis, describing in detail how he imag-ined human ventricles to look and function, based on hisstudies of the pig and the ox. Galen believed that all phys-ical function, including the brain, as well as the rest of thebody, depends on the balance of bodily fluids or humors,specifically blood, mucus, and yellow and black bile,which he related to the four basic elements—air, water,fire, and earth, respectively. Given that people thoughtthe agent that causes sickness resides in blood, doctorsoften bled patients as a curative procedure. Galen’s viewof humors became so ingrained in Western thought thatphysicians barely elaborated on the role of the brain andother organs, which remained largely unquestioned fornearly the next thousand years. We still say “good humor”or “bad humor” to describe someone’s mental disposition.Terms such as melancholic (having frequent spells of sad-ness) and choleric (having a low threshold for angry out-bursts) also remain in our vocabulary (Figure 1.8).
A N A T O M I C D I S C O V E R I E S A N D T H E R O L EO F T H E S P I R I T U A L S O U L
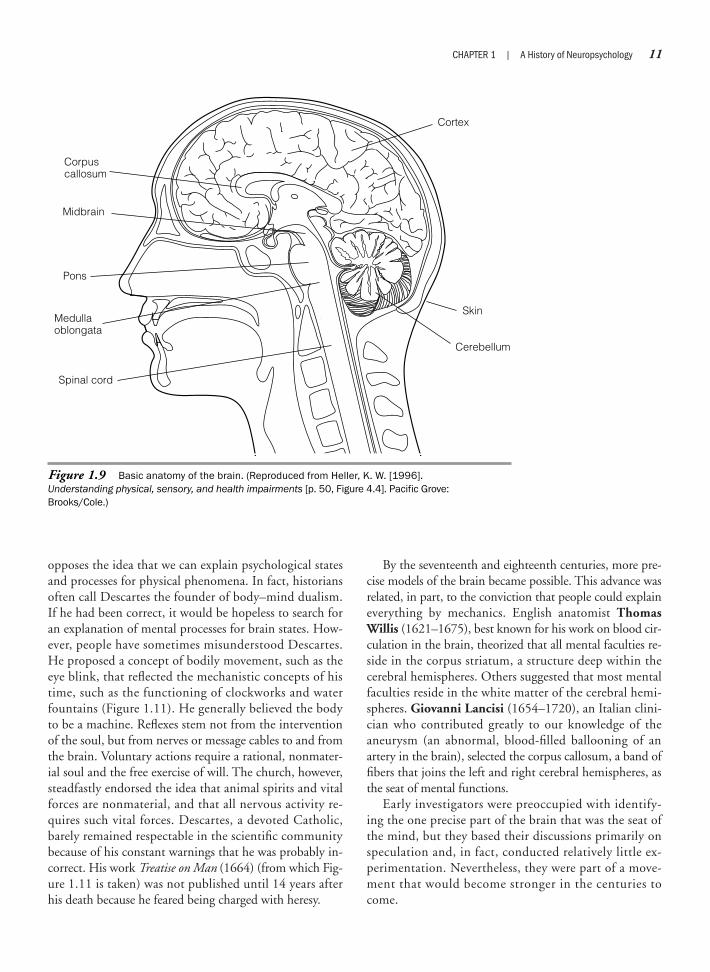
During the thirteenth century, scientists began to takeinitial steps away from the ventricular theory. For exam-ple, Albertus Magnus, a German Dominican monk, the-orized that behavior results from a combination of brainstructures that includes the cortex, midbrain, and cerebel-lum (Figure 1.9).
Not until scientific inquiry by Andreas Vesalius(1514–1564), however, were Galen’s anatomic mistakescorrected, particularly those related to the role of the ven-tricles and their effect on behavior. Galen had initiallydemonstrated the similar relative size of the ventricles inanimals and humans, whereas Vesalius placed more em-phasis on the relatively larger overall brain mass of hu-mans as responsible for mediating mental processes.Through continual dissections and careful scientific ob-servations, Vesalius demonstrated that Galen’s views wereinaccurate. Vesalius also pioneered the anatomic theater—a sort of performance dissection, where medical studentsand doctors could watch from a circular gallery. Despite aclimate of political and religious restrictions, Vesalius per-formed the first systematic dissections of human beings inEurope. Clearly, many opposed and objected to his exper-imental predilections. After all, the church retained au-thority over the soul, which was not subject to directinvestigation. But Vesalius proceeded to revolutionize
8 PART ONE | Introduction
Figure 1.5 Drawing by Leonardo da Vinci demonstrating,inaccurately, the placement of three spherical ventricles inaccordance with the cell doctrine. (The Royal Collection © 2007, Her Majesty Queen Elizabeth II.)
medicine through precise drawings of human anatomy(Figure 1.10). For the first time, surgeons could see whatthey were dealing with.
By the seventeenth century, scientists were looking fora single component of the brain as the site of mentalprocesses. René Descartes (1596–1650), for example,proposed a strict split or schism between mental processesand physical abilities. He hypothesized that the mind andbody are separate, but interact with each other. Descartestheorized that mental processes reside in a small anatomicfeature, the pineal gland. He reasoned that because thepineal gland lies in the center of the brain and is the onlystructure not composed of two symmetric halves, it wasthe logical seat for mental abilities. It is also close to theventricular system; thus, the “flow of the spirits” mightinfluence it. Today, the function of the pineal gland issomething of a mystery and is perhaps related tolight–dark cycles and the production of sleep-enhancingmelatonin.
Descartes has had an important philosophic influenceon the study of the brain, precisely because dualist thinking
CHAPTER 1 | A History of Neuropsychology 9
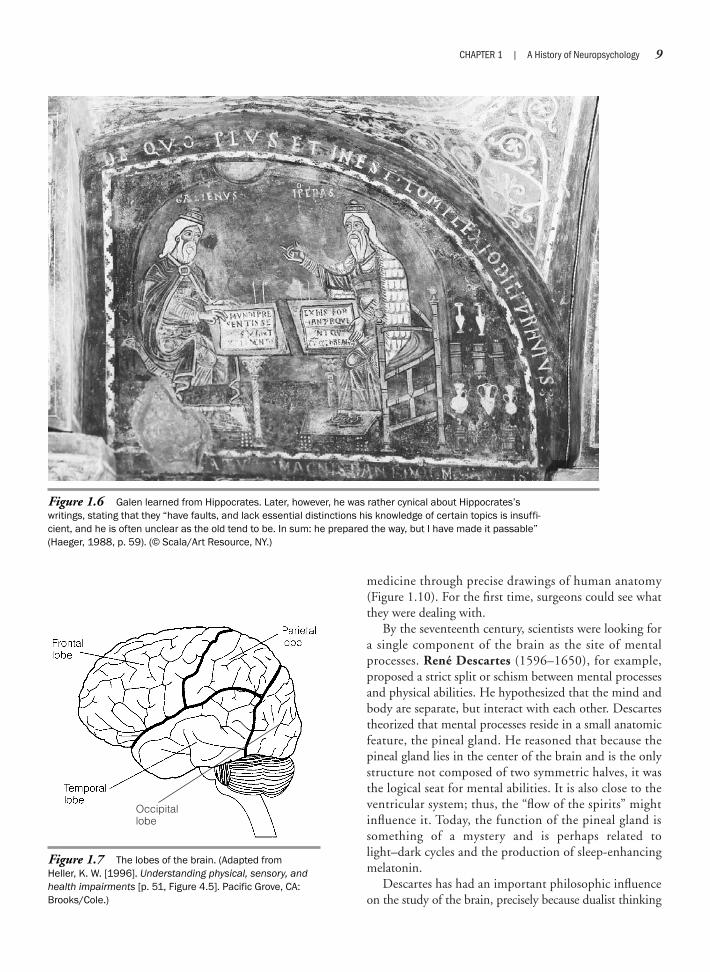
Figure 1.6 Galen learned from Hippocrates. Later, however, he was rather cynical about Hippocrates’swritings, stating that they “have faults, and lack essential distinctions his knowledge of certain topics is insuffi-cient, and he is often unclear as the old tend to be. In sum: he prepared the way, but I have made it passable”(Haeger, 1988, p. 59). (© Scala/Art Resource, NY.)
Occipitallobe
Figure 1.7 The lobes of the brain. (Adapted from Heller, K. W. [1996]. Understanding physical, sensory, andhealth impairments [p. 51, Figure 4.5]. Pacific Grove, CA:Brooks/Cole.)
10 PART ONE | Introduction
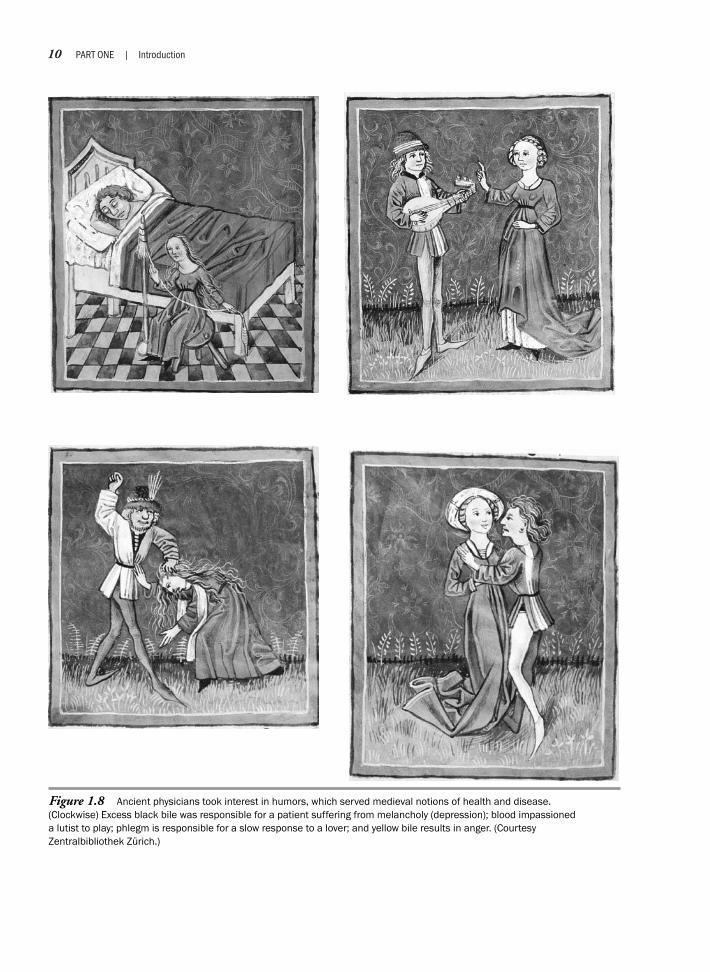
Figure 1.8 Ancient physicians took interest in humors, which served medieval notions of health and disease. (Clockwise) Excess black bile was responsible for a patient suffering from melancholy (depression); blood impassioned a lutist to play; phlegm is responsible for a slow response to a lover; and yellow bile results in anger. (Courtesy Zentralbibliothek Zürich.)
opposes the idea that we can explain psychological statesand processes for physical phenomena. In fact, historiansoften call Descartes the founder of body–mind dualism.If he had been correct, it would be hopeless to search foran explanation of mental processes for brain states. How-ever, people have sometimes misunderstood Descartes.He proposed a concept of bodily movement, such as theeye blink, that reflected the mechanistic concepts of histime, such as the functioning of clockworks and waterfountains (Figure 1.11). He generally believed the bodyto be a machine. Reflexes stem not from the interventionof the soul, but from nerves or message cables to and fromthe brain. Voluntary actions require a rational, nonmater-ial soul and the free exercise of will. The church, however,steadfastly endorsed the idea that animal spirits and vitalforces are nonmaterial, and that all nervous activity re-quires such vital forces. Descartes, a devoted Catholic,barely remained respectable in the scientific communitybecause of his constant warnings that he was probably in-correct. His work Treatise on Man (1664) (from which Fig-ure 1.11 is taken) was not published until 14 years afterhis death because he feared being charged with heresy.
By the seventeenth and eighteenth centuries, more pre-cise models of the brain became possible. This advance wasrelated, in part, to the conviction that people could explaineverything by mechanics. English anatomist ThomasWillis (1621–1675), best known for his work on blood cir-culation in the brain, theorized that all mental faculties re-side in the corpus striatum, a structure deep within thecerebral hemispheres. Others suggested that most mentalfaculties reside in the white matter of the cerebral hemi-spheres. Giovanni Lancisi (1654–1720), an Italian clini-cian who contributed greatly to our knowledge of theaneurysm (an abnormal, blood-filled ballooning of anartery in the brain), selected the corpus callosum, a band offibers that joins the left and right cerebral hemispheres, asthe seat of mental functions.
Early investigators were preoccupied with identify-ing the one precise part of the brain that was the seat ofthe mind, but they based their discussions primarily onspeculation and, in fact, conducted relatively little ex-perimentation. Nevertheless, they were part of a move-ment that would become stronger in the centuries tocome.
CHAPTER 1 | A History of Neuropsychology 11
Corpuscallosum
Midbrain
Pons
Medullaoblongata
Spinal cord
Cortex
Skin
Cerebellum
Figure 1.9 Basic anatomy of the brain. (Reproduced from Heller, K. W. [1996]. Understanding physical, sensory, and health impairments [p. 50, Figure 4.4]. Pacific Grove:Brooks/Cole.)
N O N - W E S T E R N A T T I T U D E S
Although Western ideologies predominantly shaped thebehavioral sciences, non-Western cultures also developedtheories to explain behavior. Although some of these the-ories certainly must have involved the role of the brain,we know little about how advanced people such as theEgyptians and Eastern cultures approached the brain, be-cause we lack detailed written accounts.
Common to eastern Mediterranean and African cul-tures was the belief that a god or gods sent diseases. Forexample, Egyptians viewed life as a balance between in-ternal and external forces. As a result, they treated manymental disorders as integrating physical, psychic, and spir-itual factors (Freedman, Kaplan, & Sadock, 1978). Theyconceptualized the brain as different from the mind. Asin Aristotelian theory, they considered the heart the cen-ter of mind, sensation, and consciousness. In India, oneof the earliest and most important medical documents,the Atharva-Veda (700 B.C.), proposed that the soul isnonmaterial and immortal.
During the Middle Ages, Arab countries demonstrateda humanist attitude toward the mentally ill, partly becauseof the Muslim belief that God loves the insane person.Because of this, the same treatments were available for therich and poor. The treatment of mental patients was hu-manist and emphasized diets, baths, and even musicalconcerts especially designed to soothe the patient.
Ancient Chinese medical texts also discussed psycho-logical concepts and psychiatric symptoms. For example,Chinese medical practitioners endorsed a mechanistic
12 PART ONE | Introduction
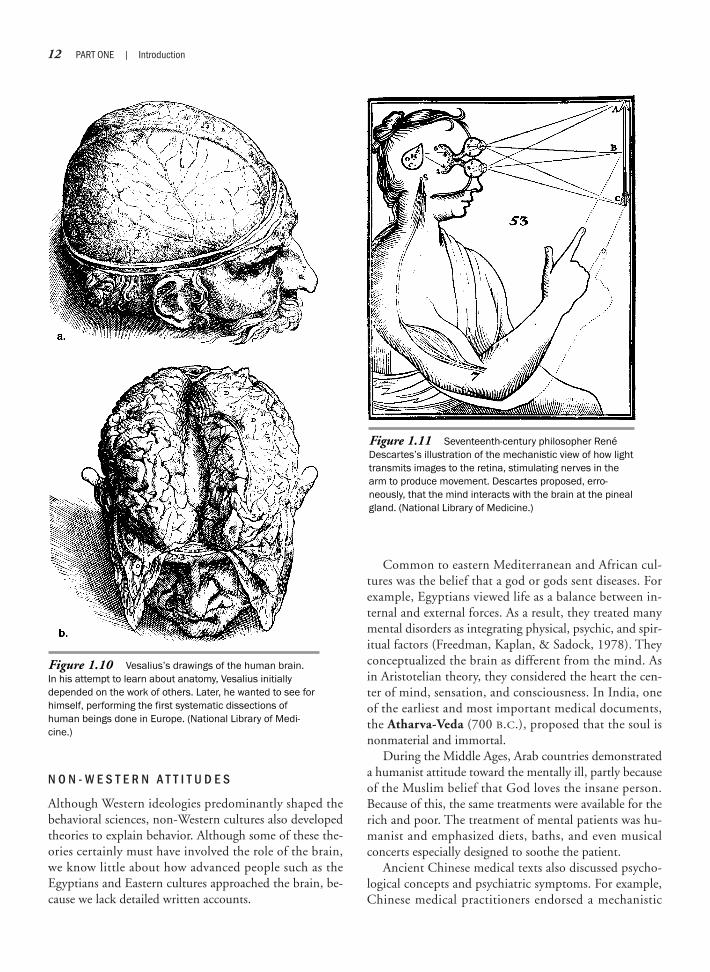
Figure 1.10 Vesalius’s drawings of the human brain. In his attempt to learn about anatomy, Vesalius initiallydepended on the work of others. Later, he wanted to see forhimself, performing the first systematic dissections ofhuman beings done in Europe. (National Library of Medi-cine.)
Figure 1.11 Seventeenth-century philosopher RenéDescartes’s illustration of the mechanistic view of how lighttransmits images to the retina, stimulating nerves in thearm to produce movement. Descartes proposed, erro-neously, that the mind interacts with the brain at the pinealgland. (National Library of Medicine.)

view of mental processes. They conceptualized manymental health disorders as illnesses or vascular disorders,as opposed to the prevailing European belief in demonicpossession. The ancient Chinese medical textbook TheYellow Emperor’s Classic of Internal Medicine (ca. 1000B.C.) includes references to dementia, convulsions, andviolent behavior. Confucian writings reflected early Chi-nese philosophical thought in proposing that mentalfunctions are not distinct from physical functions and donot reside in any part of the organism, although thesewritings give the heart special importance as a guide forthe mind. Surgeons practiced trephination in easternMediterranean and North African countries as early as4000 to 5000 B.C. There is no evidence of trephinationin ancient Japan, China, or Egypt. Because contributionsto the development of neuropsychology by non-Westernscholars remain unknown, we are left to wonder whetherthere may have been great discoveries or, alternatively,many of the same fallacies that Western cultures endorsedabout the role of the brain on behavior.
Localization Theory
P H R E N O L O G Y A N D F A C U L T Y P S Y C H O L O G Y
Not until the nineteenth century did modern neuropsy-chological theories on brain function begin to evolve.Thinkers formulated them, in part, from a need not onlyto recognize the brain as responsible for controlling be-havior, but more importantly, to demonstrate preciselyhow the brain organizes behavior. Early in the century,Austrian anatomist Franz Gall (1758–1828), borrowingperhaps from the concept of geography (the notion ofborders, at a time when people were discovering and map-ping new continents), postulated that the brain consistsof a number of separate organs, each responsible for abasic psychological trait such as courage, friendliness, orcombativeness. Gall, a distinguished Viennese physicianand teacher, suggested that mental faculties are innate anddepend on the topical structures of the brain. His theorysought to describe differences in personality and cognitivetraits by the size of individual brain areas. He hypothe-sized that the size of a given brain area is related to theamount of skill a person has in a certain field. Craniologyis the study of cranial capacity in relation to brain size,which indicated intelligence.
Gall’s work, however, was severely limited by facultypsychology, the predominant psychological theory of thattime, which held that such abilities as reading, writing, orintelligence were independent, indivisible faculties. Such
specific brain functions, therefore, were performed in iso-lation from functional systems in other parts of the brain.Gall also lacked statistical or methodologic theory thatwould have let him reliably measure the basic skills of in-terest to him. By assigning specific functions to particularplaces in the cerebral cortex, Gall formulated the basis ofthe localization theory of brain function (Table 1.1). Al-though Gall was wrong on most counts, he did help shapehow we currently perceive brain–behavior relationships.For example, Gall correctly suggested that because theircomplexity is greatest in humans, the most intellectualparts of the brain are the frontal lobes. He also argued thatthe brain is the organ of the mind and functions aregrouped within it.
From Gall’s basic theory of localization, the “science”of phrenology was born. This theory holds that if a givenbrain area is enlarged, then the corresponding area of theskull will also be enlarged. Conversely, a depression in theskull signals an underdeveloped area of the cortex. It isgenerally accurate that skull configurations closely followbrain configurations. Phrenology, in its most popularform, involves feeling the cranial bumps to ascertainwhich cerebral areas are largest (Figure 1.12). Sophisti-cated mechanical equipment was developed, such as thephrenology cap (Figure 1.13), to accurately identifybumps and indentations on the skull to make “precise”predictions about psychological strengths and weaknesses.
Although Gall made remarkable discoveries in neu-roanatomy, the theory of phrenology was entirely inaccu-rate. In Vienna and Paris, critics accused Gall of materialism
Selected “interpretations” corresponding to specific locations on the skull:
1. Amativeness: love between the sexes, desire to marry
2. Parental love: regard for offspring, pets, and so on
3. Friendship: adhesiveness, sociability, love of society
4. Inhabitiveness: love of home and country
5. Continuity: one thing at a time, consecutiveness
6. Combativeness: resistance, defense, courage, opposition
7. Destructiveness: executiveness, force, energy
8. Alimentiveness: appetite, hunger, love of eating
9. Acquisitiveness: accumulation, frugality, economy
10. Secretiveness: discretion, reserve, policy, management
Source: Wells, S. (1869). How to read character: New illustrated hand-book of phrenol-ogy and physiognomy (p. 35). New York: Fowler & Wells.
Table 1.1 Definition of the Organs
CHAPTER 1 | A History of Neuropsychology 13
and ultimately forced him to leave teaching. His studentJohann Spurzheim (1776–1832) carried on his phrenol-ogy teachings, lecturing extensively on phrenology in theUnited States. As a result, phrenology societies sprang upin the United States, and the movement became increas-ingly popular. To this day, people sometimes make attri-butions about an individual solely from specific physicalcharacteristics.
Gall also played an important role in developing de-terministic thought about the functions of the brain andthe mind; but in the final analysis, his critics accused himof having made the most absurd theories about the facul-ties of human understanding. Phrenology in its simplisticform had followers who made sweeping statements aboutthe brains and minds of men and women. Men, they sug-gested, have larger brain areas in the social region, with apredominance of pride, energy, and self-reliance, com-pared with women, whose brains reflect “inhabitiveness”(love of home) and a lack of firmness and self-esteem.Phrenologists also attempted cross-cultural comparisons,suggesting that the skulls of races and nations differ
widely in form (Neuropsychology in Action 1.1). Erro-neously, phrenologists (largely white individuals) sug-gested that the skulls of white people were superior, indi-cating great intellectual power and strong moralsentiment. The skulls from “less advanced races” did notfare as well, because those virtues were thought to be al-most invariably small in “savage” and “barbarous tribes”(Wells, 1869).
The promise of finding anatomic differences thatcould explain even complex social and intellectual be-haviors is, for some scientists, still quite tempting. Con-troversy exists whether the brains of murderers and ge-niuses are indistinguishable or different. Scientists in theformer Soviet Union preserved and studied the brains offamous communists to identify their “intellectual supe-riority.” In the United States, Albert Einstein has been
14 PART ONE | Introduction
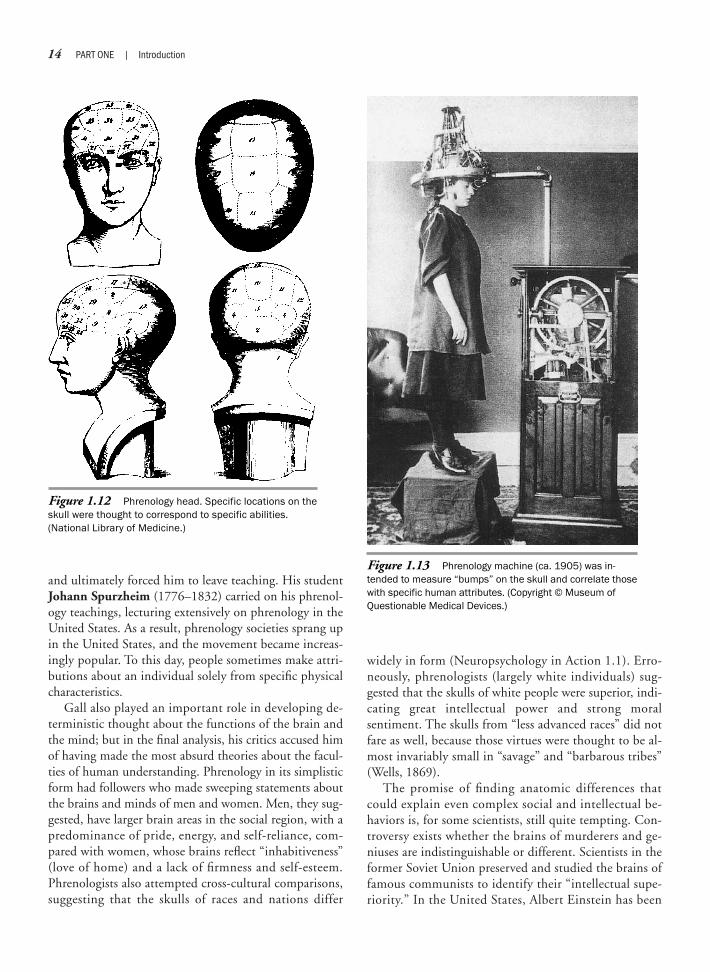
Figure 1.12 Phrenology head. Specific locations on theskull were thought to correspond to specific abilities.(National Library of Medicine.)
Figure 1.13 Phrenology machine (ca. 1905) was in-tended to measure “bumps” on the skull and correlate thosewith specific human attributes. (Copyright © Museum ofQuestionable Medical Devices.)

CHAPTER 1 | A History of Neuropsychology 15
Borrowing on ideas of Gall and Spurzheim,the Nazi propaganda leadership suggestedthat natural biological traits decide the totalbeing of a person, and they challenged thosewho sought to explain personality on anybasis other than a biological or racial one. Ofcourse, the Nazis erred in refusing to recog-nize complex contributing environmental andsocial influences that also shape and deter-mine behavior and individual differences.But U.S. armed forces leadership was alsoinvested in the same fallacy, trying todemonstrate that there may be somethingbiologically wrong with the Nazis. For exam-ple, in 1945, the U.S. Army ordered a post-mortem autopsy of Robert Ley’s brain, ahigh-ranking Nazi Labor Front boss, after hehad committed suicide while waiting tostand trial at the International MilitaryTribunal in Nuremberg. Allied doctors arguedthat deterioration in Ley’s frontal lobes as aresult of an old head injury explained hiscriminal behavior, which included violentanti-Semitism. Army pathologists concludedthat “the [brain] degeneration was of suffi-cient duration and degree to have impairedDr. Ley’s mental and emotional faculties andcould well account for his alleged aberra-tions in conduct and feelings” (“Dr. RobertLey’s Brain,” 1946, p. 188).
That the U.S. Army and the Americanpublic had an investment in the pathology ofLey’s brain is ironic, because the Nazis
themselves expended much effort todemonstrate, through pseudomedicalresearch using principles based on phrenol-ogy, that the skulls of Untermenschen(“subhumans”) were biologically inferior. Ina morbid display of unethical medicine, Nazidoctors at concentration camps routinelysent postmortem specimens of the targetedgroups to Berlin to exhibit and demonstrateinferiority (Lifton, 1986). In the same mode,the American public and media were in-vested in viewing the Nuremberg gang asbiologically and psychologically abnormal.After World War II, British and U.S. psychia-trists went so far as to suggest that onecould detect a Nazi by phrenology. Theyargued that Rudolf Hess, Hitler’s deputy, hadspecific anatomic features, including an“extreme primitive skull formation andmisshapen ears,” that could serve as possi-ble warning signals in spotting future Nazis(Rees, 1948).
The neuropathologic evidence that Ley’sbrain was abnormal actually turned out to beweak and undoubtedly distorted by thesignificant external pressure to find some-thing wrong with the Nazis at Nuremberg.Interestingly, after the execution of the 11high-ranking Nazi leaders at Nuremberg,scientists asked to perform additionalautopsies, particularly histologic studies ofthe Nazis’ brains (Zillmer, Harrower, Ritzler, &Archer, 1995). The authorities denied this
request, however, because the bodies wereto be cremated at the Dachau concentrationcamp and the ashes disposed of secretly.Currently, the remains of Ley’s brain are keptat the U.S. Army Institute of Pathology inWashington, DC.
Although a variety of functional andorganic disturbances may lead to aggressionand violent behavior, most violence (e.g.,domestic violence) is committed by peoplewith no diagnosable brain impairment.Phrenology has always been a temptingtheory, because it reduces complex racialviews to simple physical observations. Forexample, when my mother studied physics atthe University of Vienna during the early1940s, the Nazi authorities did not havemuch interest in the study of individualdifferences. A required course during theNazi occupation was Rassenkunde (RacialTheory), which replaced psychology andphilosophy.
The final analysis of the Nazi data sug-gested that the Nazis could not plead “braindamage” in the court of universal justice.There was no specific biological or evenpsychological inclination found towardviolence, aggression, or sadism. The Naziswere not deranged in a clinical sense. Crazywas not the answer. The Nazis came in avariety of stripes. Hitler’s men were moredifferent from each other than they werealike (Kennedy & Zillmer, 2006).
N e u r o p s y c h o l o g y i n A c t i o n 1 . 1
T h e B r a i n o f a N a z i
by Eric A. Zillmer
preserved in storage for later analysis. Einstein’s brain,the focus of several studies, may be anatomically larger instrategic areas that may partly explain his uncommonability for conceptual and multidimensional thinking(Witelson, Kigar, & Harvey, 1999). Most neuroscientists,however, agree that the idea of explaining a person’s per-sonality and abilities from neuroanatomic evidence ispremature (Figure 1.14.)
Faculty psychology and discrete localization theorycontinued to develop for a century. Many factors were
erroneous and simplistic, but three major developmentsrepresented significant progress. First, scientists were re-luctant to accept a single part or component of the brainas responsible for all behavior, as had proponents of ear-lier theories. Second, they placed more emphasis on therole of the cortex, which until then had not been seen asfunctioning neural tissue but as relatively unimportantprotective “bark” (“cortex” in Latin). Third, and perhapsmost important, scientists focused on the brain for theirstudy of behavior and the mind.
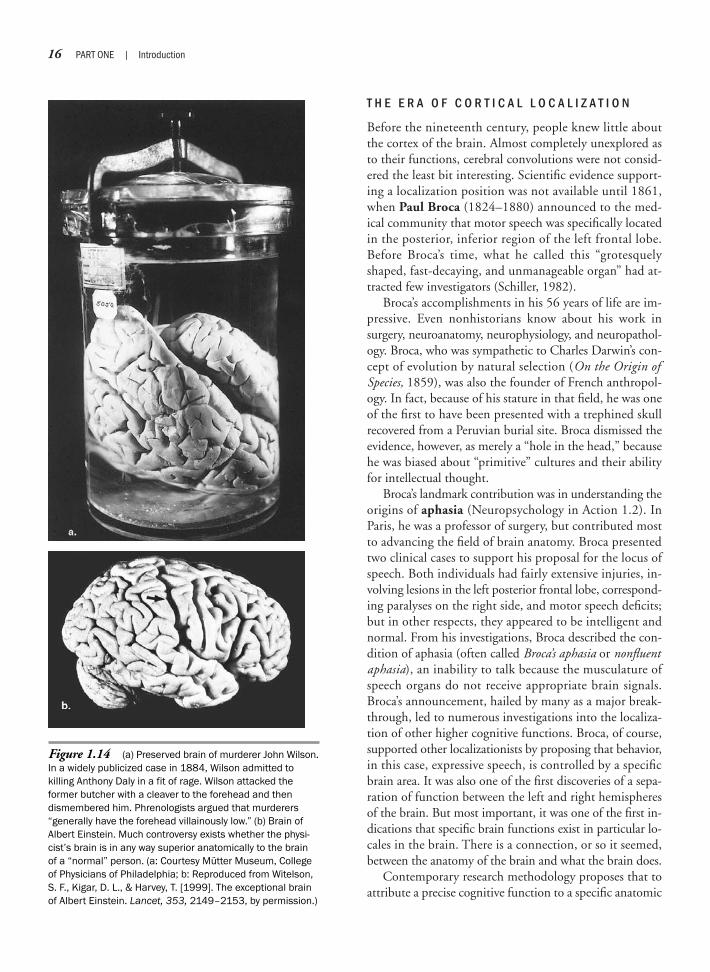
T H E E R A O F C O R T I C A L L O C A L I Z A T I O N
Before the nineteenth century, people knew little aboutthe cortex of the brain. Almost completely unexplored asto their functions, cerebral convolutions were not consid-ered the least bit interesting. Scientific evidence support-ing a localization position was not available until 1861,when Paul Broca (1824–1880) announced to the med-ical community that motor speech was specifically locatedin the posterior, inferior region of the left frontal lobe.Before Broca’s time, what he called this “grotesquelyshaped, fast-decaying, and unmanageable organ” had at-tracted few investigators (Schiller, 1982).
Broca’s accomplishments in his 56 years of life are im-pressive. Even nonhistorians know about his work insurgery, neuroanatomy, neurophysiology, and neuropathol-ogy. Broca, who was sympathetic to Charles Darwin’s con-cept of evolution by natural selection (On the Origin ofSpecies, 1859), was also the founder of French anthropol-ogy. In fact, because of his stature in that field, he was oneof the first to have been presented with a trephined skullrecovered from a Peruvian burial site. Broca dismissed theevidence, however, as merely a “hole in the head,” becausehe was biased about “primitive” cultures and their abilityfor intellectual thought.
Broca’s landmark contribution was in understanding theorigins of aphasia (Neuropsychology in Action 1.2). InParis, he was a professor of surgery, but contributed mostto advancing the field of brain anatomy. Broca presentedtwo clinical cases to support his proposal for the locus ofspeech. Both individuals had fairly extensive injuries, in-volving lesions in the left posterior frontal lobe, correspond-ing paralyses on the right side, and motor speech deficits;but in other respects, they appeared to be intelligent andnormal. From his investigations, Broca described the con-dition of aphasia (often called Broca’s aphasia or nonfluentaphasia), an inability to talk because the musculature ofspeech organs do not receive appropriate brain signals.Broca’s announcement, hailed by many as a major break-through, led to numerous investigations into the localiza-tion of other higher cognitive functions. Broca, of course,supported other localizationists by proposing that behavior,in this case, expressive speech, is controlled by a specificbrain area. It was also one of the first discoveries of a sepa-ration of function between the left and right hemispheresof the brain. But most important, it was one of the first in-dications that specific brain functions exist in particular lo-cales in the brain. There is a connection, or so it seemed,between the anatomy of the brain and what the brain does.
Contemporary research methodology proposes that toattribute a precise cognitive function to a specific anatomic
16 PART ONE | Introduction
Figure 1.14 (a) Preserved brain of murderer John Wilson.In a widely publicized case in 1884, Wilson admitted tokilling Anthony Daly in a fit of rage. Wilson attacked theformer butcher with a cleaver to the forehead and thendismembered him. Phrenologists argued that murderers“generally have the forehead villainously low.” (b) Brain ofAlbert Einstein. Much controversy exists whether the physi-cist’s brain is in any way superior anatomically to the brainof a “normal” person. (a: Courtesy Mütter Museum, Collegeof Physicians of Philadelphia; b: Reproduced from Witelson,S. F., Kigar, D. L., & Harvey, T. [1999]. The exceptional brainof Albert Einstein. Lancet, 353, 2149–2153, by permission.)

CHAPTER 1 | A History of Neuropsychology 17
Paul Broca identified a specific area on theconvoluted surface of the human brain,approximately 1 cubic centimeter (cm3) insize, as the central organ for expressivespeech. Broca’s famous discovery came at atime when he viewed the convolutions of thebrain as distinct organs. The evidence forthis, however, was particularly weak, andphrenology was receiving some criticism.Thus, it was not a coincidence that Brocamade such a discovery. He had been search-ing for some time for a patient just likeMonsieur Leborgne. In May 1861, Brocapresented the brain of Leborgne, alias “Tan,”a 51-year-old man who had died the previ-ous day under Broca’s care:
“I found one morning on my service a dyingpatient who 21 years ago had lost the facultyof articulate speech. I gathered his casehistory with the greatest care because itseemed to serve as a touchstone for the[localization] theory of my colleague. Thepatient died on April 17 [1861] at 11 A.M.The autopsy was performed as soon aspossible, that is to say within 24 hours. Thebrain was shown a few hours later in theSociété d’Anthropologie, then immediatelyput in alcohol.” (Schiller, 1982, pp. 177–178)
“The abolition of speech is a symptom ofsufficient importance, that it seems useful todesignate it by a special name.I have given itthe name aphemia [the term was laterchanged to aphasia by a colleague ofBroca’s, Professor Trousseau]. For what ismissing in these patients is only the faculty toarticulate words.” (Schiller, 1982, pp. 180)
“Although I believe in the principle of local-ization, I have been and still am askingmyself, within what limits may this principleapply? If it were demonstrated that thelesions, which abolish speech constantly,occupy the same convolution then one couldhardly help admitting that this convolution isthe seat of articulated speech.” (Schiller,1982, pp. 182)
Probably no other single preservedhuman brain has aroused more attentionthan the one Broca was describing. Somecriticized the manner of its preservation (inan unorthodox vertical position) and thedamage to the brain involving chronic andprogressive softening of the second andthird left frontal convolutions, as well as thespecimen’s unavailability for examination(Figure 1.15). Broca responded to his critics,“I have refrained from studying the deeperparts (of the brain), in order not to destroythe specimen, which I thought should bedeposited in the (Dupuytren) museum”(Schiller, 1982, p. 180).
Tan’s history has often been told, buthis basic disease has never been satisfac-torily diagnosed. Broca’s acquaintancewith this patient lasted barely a week.Neither the history nor the appearanceand description of the brain allow a confi-
dent clinical and pathologic interpretationin modern terms. Leborgne had beenepileptic since his youth and becameaphasic at the age of 30. He showedprogressive weakening on his right sidesince the age of 40, first in the arm. Hebecame hemiplegic and was bedridden for7 years. Leborgne deteriorated gradually,losing his intellect and vision, and finallydied at 51 of cellulitis with gangrene of theparalyzed right leg. His early history ofepilepsy arouses the suspicion that suc-cessive thrombotic infarcts might not havebeen the correct diagnosis, and thatperhaps a form of degenerative diseasemay be more plausible. He was also knownto have cursed when he was disturbed,which may also suggest that aphasia wasthe least of his problems (however, as wediscuss in later chapters, cursing andgrunts may be actually controlled by theright hemisphere, which does not domi-nate speech). In retrospect, Leborgne’shistory suggests that many other symp-toms accompanied his aphasia. It nowappears that Leborgne was a poor choiceas the prototype for Broca’s aphasia. IfBroca had had a statistical consultant, hewould have been advised not to make suchsweeping conclusions based on only onesubject!
Just as Broca preserved Leborgne’sbrain for safekeeping, he would have beenpleased to know that his own brain alsohas been stored in the Museum del’Homme (Museum of Man) in Paris. There,deep in the museum in a remote, mustycorner among abandoned cabinets andshelves hidden from the public, is a collec-tion of gray convoluted objects stored informaldehyde. Among them is the brain ofPaul Broca. If you look closely, you candetect the small region in the third convo-lution on the left frontal lobe of the cere-bral cortex that made him famous—Broca’sBroca’s area!
N e u r o p s y c h o l o g y i n A c t i o n 1 . 2
P a u l B r o c a : A M a n n e r o f N o t S p e a k i n g
by Eric A. Zillmer
Figure 1.15 Leborgne’s brain. Noteatrophy in Broca’s area. (Courtesy MuseéDupuytren.)
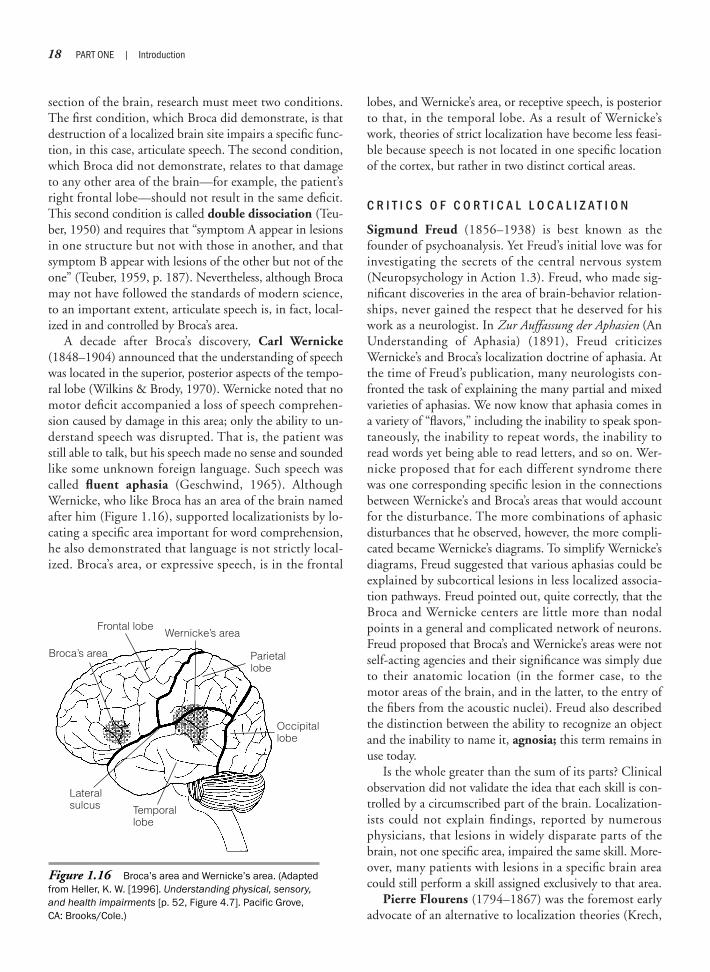
section of the brain, research must meet two conditions.The first condition, which Broca did demonstrate, is thatdestruction of a localized brain site impairs a specific func-tion, in this case, articulate speech. The second condition,which Broca did not demonstrate, relates to that damageto any other area of the brain—for example, the patient’sright frontal lobe—should not result in the same deficit.This second condition is called double dissociation (Teu-ber, 1950) and requires that “symptom A appear in lesionsin one structure but not with those in another, and thatsymptom B appear with lesions of the other but not of theone” (Teuber, 1959, p. 187). Nevertheless, although Brocamay not have followed the standards of modern science,to an important extent, articulate speech is, in fact, local-ized in and controlled by Broca’s area.
A decade after Broca’s discovery, Carl Wernicke(1848–1904) announced that the understanding of speechwas located in the superior, posterior aspects of the tempo-ral lobe (Wilkins & Brody, 1970). Wernicke noted that nomotor deficit accompanied a loss of speech comprehen-sion caused by damage in this area; only the ability to un-derstand speech was disrupted. That is, the patient wasstill able to talk, but his speech made no sense and soundedlike some unknown foreign language. Such speech wascalled fluent aphasia (Geschwind, 1965). AlthoughWernicke, who like Broca has an area of the brain namedafter him (Figure 1.16), supported localizationists by lo-cating a specific area important for word comprehension,he also demonstrated that language is not strictly local-ized. Broca’s area, or expressive speech, is in the frontal
lobes, and Wernicke’s area, or receptive speech, is posteriorto that, in the temporal lobe. As a result of Wernicke’swork, theories of strict localization have become less feasi-ble because speech is not located in one specific locationof the cortex, but rather in two distinct cortical areas.
C R I T I C S O F C O R T I C A L L O C A L I Z A T I O N
Sigmund Freud (1856–1938) is best known as thefounder of psychoanalysis. Yet Freud’s initial love was forinvestigating the secrets of the central nervous system(Neuropsychology in Action 1.3). Freud, who made sig-nificant discoveries in the area of brain-behavior relation-ships, never gained the respect that he deserved for hiswork as a neurologist. In Zur Auffassung der Aphasien (AnUnderstanding of Aphasia) (1891), Freud criticizesWernicke’s and Broca’s localization doctrine of aphasia. Atthe time of Freud’s publication, many neurologists con-fronted the task of explaining the many partial and mixedvarieties of aphasias. We now know that aphasia comes ina variety of “flavors,” including the inability to speak spon-taneously, the inability to repeat words, the inability toread words yet being able to read letters, and so on. Wer-nicke proposed that for each different syndrome therewas one corresponding specific lesion in the connectionsbetween Wernicke’s and Broca’s areas that would accountfor the disturbance. The more combinations of aphasicdisturbances that he observed, however, the more compli-cated became Wernicke’s diagrams. To simplify Wernicke’sdiagrams, Freud suggested that various aphasias could beexplained by subcortical lesions in less localized associa-tion pathways. Freud pointed out, quite correctly, that theBroca and Wernicke centers are little more than nodalpoints in a general and complicated network of neurons.Freud proposed that Broca’s and Wernicke’s areas were notself-acting agencies and their significance was simply dueto their anatomic location (in the former case, to themotor areas of the brain, and in the latter, to the entry ofthe fibers from the acoustic nuclei). Freud also describedthe distinction between the ability to recognize an objectand the inability to name it, agnosia; this term remains inuse today.
Is the whole greater than the sum of its parts? Clinicalobservation did not validate the idea that each skill is con-trolled by a circumscribed part of the brain. Localization-ists could not explain findings, reported by numerousphysicians, that lesions in widely disparate parts of thebrain, not one specific area, impaired the same skill. More-over, many patients with lesions in a specific brain areacould still perform a skill assigned exclusively to that area.
Pierre Flourens (1794–1867) was the foremost earlyadvocate of an alternative to localization theories (Krech,
18 PART ONE | Introduction
Temporallobe
Frontal lobeWernicke’s area
Parietallobe
Broca’s area
Occipitallobe
Lateralsulcus
Figure 1.16 Broca’s area and Wernicke’s area. (Adaptedfrom Heller, K. W. [1996]. Understanding physical, sensory,and health impairments [p. 52, Figure 4.7]. Pacific Grove,CA: Brooks/Cole.)

CHAPTER 1 | A History of Neuropsychology 19
Freud entered the University of Vienna in theautumn of 1873, at the early age of 17, andgraduated with a medical degree in 1881.Considering an academic research career inphysiology, he went to work in the laboratoryof the Brücke Institute. There he enjoyedlaboratory work and, initially, harbored anaversion to the clinical practice of medicine.Beset by financial difficulties, in May 1883,he began working under Meynert, a neuro-surgeon and psychiatrist, to gain additionalpractical experience. During this time, Freudcame closer to disorders of the brain, but herestricted his laboratory work to dissectingthe nervous system. At first, Freud investi-gated the cells of the spinal cord, the part ofthe nervous system that held his chiefinterest. For the next 2 years, he concen-trated on a specific area of the brainstem,the medulla, that resulted in three pub-lished articles. From October 1885 toFebruary 1886, Freud visited Paris to studywith the great neurologist Jean-MartinCharcot. Charcot was then at the zenith ofhis fame. No one, before or since, had sodominated the world of neurology, and forFreud to have been a pupil of his was apassport to distinction.
When Freud went to Paris, his anatomicinterests were still more in his mind than
any ambition as a clinician. On his return toVienna, he researched topics of visual fielddeficits, hemianopsia, in children and itslocalization. From correspondence, it isalso known that in 1887 and 1888 Freudwas working on a book on the anatomy ofthe brain, which he never finished (Jones,1981). His next publication in 1891 washis first book Zur Auffassung der Aphasien(An Understanding of Aphasia). Freudthought this text the most valuable of hisneurologic writings, although it proved notto be the one by which neurologic circlesremembered his name. Despite Freud’scritical and speculative monograph onaphasia, which ultimately achieved accep-tance, he did not have much luck with hisbook. Of the 850 copies printed, only 257had sold after 9 years, and Freud was paidonly $62 in royalties (Jones, 1981). Theneurologic community was not yet ready forhis insights, and all historical writings onaphasia omit any reference to the book. Yethis neurologic achievements were remark-able, especially for a young student, andthey illustrate his biological and geneticoutlook.
In retrospect, Freud’s psychoanalyticmodel can be loosely related to brainprocesses. For example, Freud’s id, the
unconscious “beast in the basement” thatoperates on the pleasure principle, mighthave developed out of the reptilian brain, aproduct of presocial evolutionary history.Freud’s superego, our conscience, is anevolutionarily more recent invention, con-ceptualized within prefrontal lobeprocesses that are involved in forming suchabstract concepts as morality, guilt, plan-ning, and inhibition. At this highest, mostcomplex level of brain structure, a majorfunction is to inhibit the spontaneousexpression of the more biologically pro-grammed patterns of behavior that arisefrom lower and evolutionary older struc-tures of the brain such as the id. The ego,based on the reality principle, is perhapsrelated to complex brain processes in the“middle,” that is, the cortex, excluding theprefrontal lobes (Wright, 1994). It is oftendifficult to trace threads between Freud’ssubsequent focus on unobservable, in-trapsychic events and his early investiga-tion of the nervous system. He never did,however, venture too far away from hisneurologic roots, as demonstrated in hiswork On Narcissism (1959), in which hesuggested that all provisional ideas onpsychology will one day be explained byorganic substrates.
N e u r o p s y c h o l o g y i n A c t i o n 1 . 3
S i g m u n d Fr e u d : T h e N e u r o l o g i s t
by Eric A. Zillmer
1962). Through an extensive number of experiments andlogical arguments, Flourens attempted to disprove Gall’slocalization theory. To support his beliefs, Flourens devel-oped the ablation experiment, in which removing anypart of the brain in birds led to generalized disorders ofbehavior. From his experiments, he reached several gen-eral conclusions. Sensory input at an elementary level islocalized, but the process of perception involves the wholebrain. Loss of function depends on the extent of damage,not on the location. All cerebral material is equipoten-tial; that is, if sufficient cortical material is intact, the re-maining material will take over the functions of any miss-ing brain tissue. Flourens suggested that the brain operatedin an integrated fashion, not in discrete faculties, and thatmental functions depend on the brain functioning as a
whole. Thus, the size of the injury, rather than its loca-tion, determines the effects of brain injury.
Flourens, however, was criticized on a number of dif-ferent points. First, he used animals with brains so smallthat any ablation would invade more than one functionalarea. Second, he observed only motor behavior—that is,behaviors such as eating or wing flapping—whereas thelocalizationists were mostly interested in more complexfaculties such as friendship or intellect. Flourens also er-roneously suggested that humans use only 10% of thebrain, an idea that laypeople still commonly hold today.Despite these scientific problems, many accept Flourensas having refuted localization theory. Nevertheless, thework of Broca and other localization theorists was the pre-dominant view of brain–behavior relationships and was

in large part accepted by the scientific community. Con-sequently, few people supported Flourens’s work until theearly 1900s, when equipotentialists again began to de-velop evidence and research to support their position.
Localizationversus Equipotentiality
Pierre Marie (1906) challenged Broca’s findings byexamining the preserved brains of the patients Broca hadused to support his hypothesis of localization. Mariefound that Leborgne had widespread damage, not a spe-cific lesion, as Broca had suggested. Marie attacked Broca’stheory, indicating that the patient could not speak be-cause the extensive lesion had caused a general loss of in-tellect, rather than a specific inability to speak. Other re-searchers soon expressed support for the equipotentialityposition. In general, these researchers proposed that, al-though basic sensorimotor functions may be localized inthe brain, higher cortical processes were too complex toconfine to any one area.
Two important neuropsychological findings alsochallenged strict localization theory. In 1881 (cited byBlakemore, 1977), Hermann Munk (1839–1912) foundthat experimental lesions in the association cortex of adog produced temporary mind-blindness: The animalcould see objects but failed to recognize their significance(e.g., as objects of fear). In the experiment, Munk first hadthe dogs learn to associate the shape of a triangle with fearby pairing them together with an electric shock. After thedogs learned the association, Munk lesioned parts of thecortex that were not primarily involved with vision. Af-terward, the dogs could see the object but could not per-ceive the meaning of the stimuli to which they were con-ditioned before the surgery. In 1914, Joseph Babinski(1857–1932), the founder of neurology, introduced theterm anosognosia, which means “no knowledge of thedisease,” to describe an inability or refusal to recognizethat one has a particular disease or disorder, thereby in-troducing the phenomenon of unawareness (Babinski &Joltran, 1924). Babinski observed patients who had le-sions, most often in the association cortex of the righthemisphere. These patients were capable of seeing andhearing, but denied that anything was wrong with themeven when they had severe neurologic damage such ashemiplegia.
Karl Lashley (1890–1958), a student of the famousbehaviorist John Watson, was a great exemplar of experi-mental neuropsychology and, according to Hebb (1983),
practically its founder. He was one of the first to combinebehavioral sophistication in experiments with neurologicsophistication. Lashley become America’s most eminentearly neuropsychologist, highly respected for his ingenu-ity in devising ways of disclosing the effects of brain oper-ations (Popplestone & McPherson, 1994). AlthoughLashley accepted the localization of basic sensory andmotor skills, he supported equipotential views with ex-periments on rats similar to those of Flourens on birds(Lashley, 1929). Lashley found that impairment in mazerunning in the rat was directly related to the amount ofcortex removed. He stated that the specific area removedmade little difference. From his experiments, Lashley for-mulated his famous principle of mass action: The extentof behavioral impairments is directly proportional to themass of the removed tissue. Lashley also emphasized themultipotentiality of brain tissue: Each part of the brainparticipates in more than one function (Teuber, Battersby,& Bender, 1960). Lashley believed that his results werehighly compatible with a view that brain tissue is equi-potential and can be involved in tasks other than thoseassigned by the localizationists.
In one form or another, localization and equipoten-tiality have dominated U.S. psychology, although neitherapproach has enjoyed universal acceptance because nei-ther can encompass all the collected scientific data andclinical observations. Clinical observers of medical pa-tients with very small lesions have often reported markedbehavioral deficits, even though the lesion may be micro-scopic. Thus, equipotentiality theory fails to account forthe specific deficits often seen in the absence of generalimpairment in intellect, abstract attitude, perception, orother global ability.
Integrated Theories of Brain Function
J A C K S O N ’ S A L T E R N A T I V E M O D E L
Unable to accept either the localization or equipotential-ity models of brain function, psychologists and neurolo-gists have searched for other alternative models. The cre-ation of one such model has been credited to the Englishneurologist Hughlings Jackson (1835–1911), whose pri-mary work was written during the second half of the nine-teenth century, but was not published in the United Statesuntil the 1950s. Jackson, a London neurologist, devotedhis research to the investigation of epileptic seizures andthe study of connections between limb movements and
20 PART ONE | Introduction

specific areas in the brain. Jackson observed that highermental functions are not unitary abilities, but consist ofsimpler and more basic skills. He suggested that one doesnot have a speech center; rather, one has the ability tocombine certain basic skills, such as hearing, discrimina-tion of speech sounds, and fine-motor and kinestheticcontrol of the speech apparatus, to create more complexhigher skills (Hebb, 1959). Consequently, the loss ofspeech can be traced to the loss of any one of a number ofbasic abilities or functional systems. It can be related to,for example, the loss of motor control, the loss of ade-quate feedback from the mouth and tongue, a defect inthe understanding and use of the basic parts of speech, orthe inability to decide to speak.
Thus, the loss of a specific area of the brain causes theloss or impairment of all higher skills dependent on thatone area. Furthermore, a lesion that causes the loss ofspeech does not necessarily indicate that the brain area re-sponsible for speech has been found. Jackson proposedthat localizing damage that destroys speech and localizingspeech are two different things. Jackson also believed thatbehavior can exist on many different levels within the ner-vous system. Thus, a patient may be unable to repeat theword “no” when asked to repeat it, even though the pa-tient is capable of saying, in exasperation, “No, Doctor, Ican’t say no!” (Luria, 1966). In the first instance, the pa-tient cannot say the word voluntarily. When the word isgiven as an automatic response, however, the patient isable to say it. The ability to say “no” exists as two separateskills: one voluntarily and one automatic. Each ability canbe impaired independently of the other. Because of this,Jackson noted, behavior rarely is lost completely unlessthe damage to the brain is severe (Golden, Zillmer, &Spiers, 1992).
Jackson suggested that, given his observations, be-havior results from interactions among all the areas ofthe brain. Even the simplest motor movement requiresthe full cooperation of all the levels of the nervous sys-tem, from the peripheral nerves and the spinal cord tothe cerebral hemispheres. In this regard, Jackson pointedtoward a more holistic, nearly equipotential view ofbrain function. But Jackson also argued that each areawithin the nervous system had a specific function thatcontributed to the overall system. Thus, his views alsohad a localizationist flavor. In actuality, of course, Jack-son’s views were those of neither school but reflected anintegration of significant empirical data. Jackson’s influ-ence can first be seen in British neurology of the earlytwentieth century, although many people overlooked theessential nature of what Jackson had proposed. They inter-preted his work as more supportive of an equipotentiality
view of higher mental functions than it actually was.Since World War II, many major theorists have pre-sented views compatible with Jackson’s. For example,Harlow (1952) concluded from his experimental mon-key studies that no cognitive ability is completely de-stroyed by any limited lesion, although there appears tobe some localization, a view entirely consistent withJackson’s beliefs. After reviewing much of the literature,Krech (1962) also reached two similar conclusions(Chapman & Wolff, 1959). First, no learning process orfunction depends entirely on any one area of the cortex.Second, each area within the brain plays an unequal rolein different kinds of functions. These conclusions,although contrary to either the localization or equipo-tentiality views, were also in accordance with Jackson’salternative approach.
L U R I A ’ S F U N C T I O N A L M O D E L
The most detailed adaptation of the principle first sug-gested by Jackson has appeared in the work of Russianneuropsychologist Alexander Luria (1902–1977). Luriawas responsible for the most profound changes in our ap-proach to understanding the brain and the mind. Luria,who earned doctoral degrees in psychology, medicine, andeducation, was the most significant and productive neu-ropsychologist of his time, and during the 1960s, heraised the field to a level that could not have been imag-ined. Luria realized that a viable brain–behavior theorymust not only explain data that fit both the localizationand equipotentiality hypothesis but also must account forfindings inconsistent with either theory. Luria—buildingon the work of his mentor and arguably the founder of cog-nitive psychology, Vygotsky (1965) as well as on Jackson’salternative approach (Hebb, 1959)—conceived each areain the central nervous system as being involved in one ofthree basic functions, which Luria labeled units. The firstunit, roughly defined as the brainstem and associatedareas, regulates the arousal level of the brain and the main-tenance of proper muscle tone. The second unit, includ-ing posterior areas of the cortex, plays a key role in the re-ception, integration, and analysis of sensory informationfrom both the internal and external environments. Thethird unit, the frontal and prefrontal lobes, is involved inplanning, executing, and verifying behavior (Luria, 1964,1966).
All behavior requires the interaction of those three basicfunctions. Consequently, all behavior reflects the brain op-erating as a whole. At the same time, each area within thebrain has a specific role in forming behavior. The impor-tance of any one area depends on the behavior to be
CHAPTER 1 | A History of Neuropsychology 21
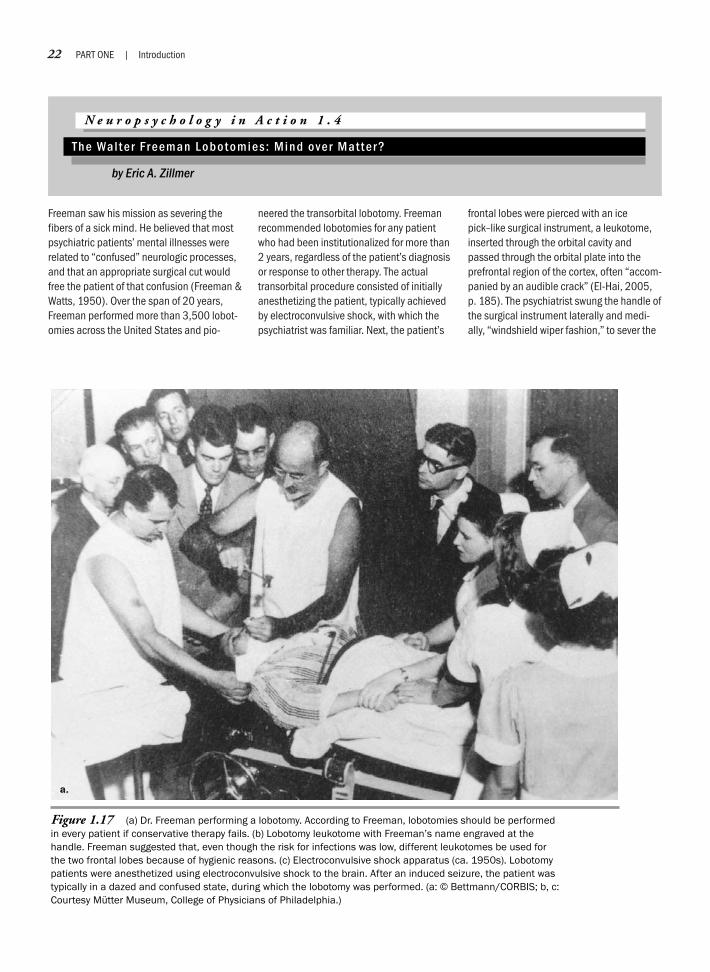
22 PART ONE | Introduction
Freeman saw his mission as severing thefibers of a sick mind. He believed that mostpsychiatric patients’ mental illnesses wererelated to “confused” neurologic processes,and that an appropriate surgical cut wouldfree the patient of that confusion (Freeman &Watts, 1950). Over the span of 20 years,Freeman performed more than 3,500 lobot-omies across the United States and pio-
neered the transorbital lobotomy. Freemanrecommended lobotomies for any patientwho had been institutionalized for more than2 years, regardless of the patient’s diagnosisor response to other therapy. The actualtransorbital procedure consisted of initiallyanesthetizing the patient, typically achievedby electroconvulsive shock, with which thepsychiatrist was familiar. Next, the patient’s
frontal lobes were pierced with an icepick–like surgical instrument, a leukotome,inserted through the orbital cavity andpassed through the orbital plate into theprefrontal region of the cortex, often “accom-panied by an audible crack” (El-Hai, 2005,p. 185). The psychiatrist swung the handle ofthe surgical instrument laterally and medi-ally, “windshield wiper fashion,” to sever the
N e u r o p s y c h o l o g y i n A c t i o n 1 . 4
T h e Wa l t e r Fr e e m a n L o b o t o m i e s : M i n d o v e r M a t t e r ?
by Eric A. Zillmer
Figure 1.17 (a) Dr. Freeman performing a lobotomy. According to Freeman, lobotomies should be performedin every patient if conservative therapy fails. (b) Lobotomy leukotome with Freeman’s name engraved at thehandle. Freeman suggested that, even though the risk for infections was low, different leukotomes be used forthe two frontal lobes because of hygienic reasons. (c) Electroconvulsive shock apparatus (ca. 1950s). Lobotomypatients were anesthetized using electroconvulsive shock to the brain. After an induced seizure, the patient wastypically in a dazed and confused state, during which the lobotomy was performed. (a: © Bettmann/CORBIS; b, c:Courtesy Mütter Museum, College of Physicians of Philadelphia.)
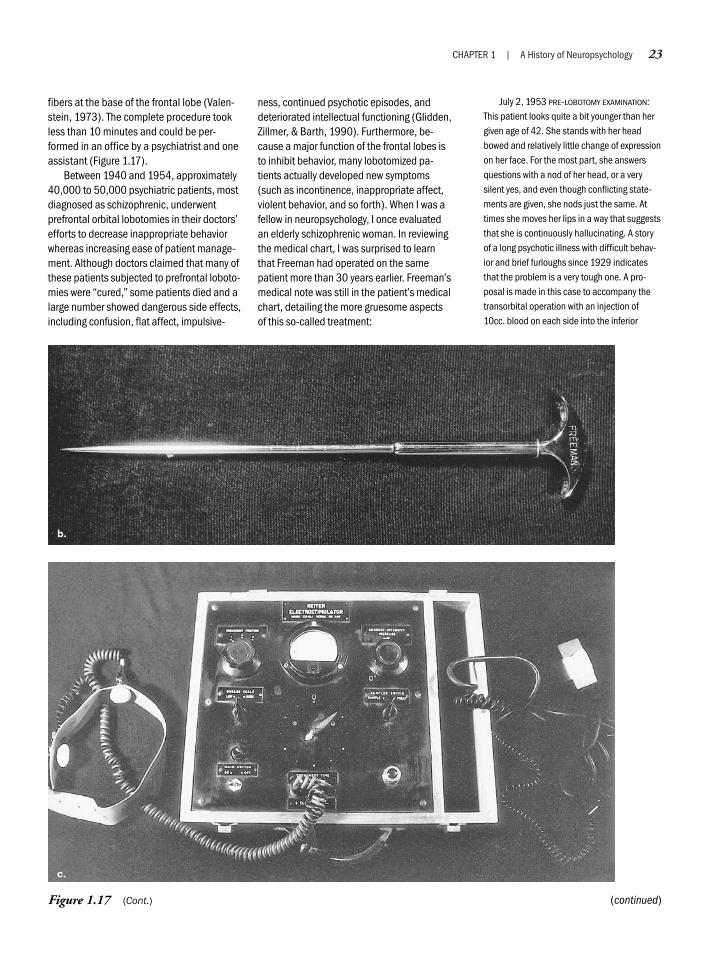
CHAPTER 1 | A History of Neuropsychology 23
fibers at the base of the frontal lobe (Valen-stein, 1973). The complete procedure tookless than 10 minutes and could be per-formed in an office by a psychiatrist and oneassistant (Figure 1.17).
Between 1940 and 1954, approximately40,000 to 50,000 psychiatric patients, mostdiagnosed as schizophrenic, underwentprefrontal orbital lobotomies in their doctors’efforts to decrease inappropriate behaviorwhereas increasing ease of patient manage-ment. Although doctors claimed that many ofthese patients subjected to prefrontal loboto-mies were “cured,” some patients died and alarge number showed dangerous side effects,including confusion, flat affect, impulsive-
ness, continued psychotic episodes, anddeteriorated intellectual functioning (Glidden,Zillmer, & Barth, 1990). Furthermore, be-cause a major function of the frontal lobes isto inhibit behavior, many lobotomized pa-tients actually developed new symptoms(such as incontinence, inappropriate affect,violent behavior, and so forth). When I was afellow in neuropsychology, I once evaluatedan elderly schizophrenic woman. In reviewingthe medical chart, I was surprised to learnthat Freeman had operated on the samepatient more than 30 years earlier. Freeman’smedical note was still in the patient’s medicalchart, detailing the more gruesome aspectsof this so-called treatment:
July 2, 1953 PRE-LOBOTOMY EXAMINATION:This patient looks quite a bit younger than hergiven age of 42. She stands with her headbowed and relatively little change of expressionon her face. For the most part, she answersquestions with a nod of her head, or a verysilent yes, and even though conflicting state-ments are given, she nods just the same. Attimes she moves her lips in a way that suggeststhat she is continuously hallucinating. A storyof a long psychotic illness with difficult behav-ior and brief furloughs since 1929 indicatesthat the problem is a very tough one. A pro-posal is made in this case to accompany thetransorbital operation with an injection of10cc. blood on each side into the inferior
(continued)Figure 1.17 (Cont.)

24 PART ONE | Introduction
external aspects of the lobe, in the hope ofeliminating to some extent the hallucinatoryactivities. The outlook for her release from thehospital is not good, but it may be possiblethat she will be more effectively able to adjuston the ward.
July 2, 1953 OPERATIVE NOTE: This patientpresents an exceptionally difficult problem:therefore, after a triple electroshock, theorbitoclasts were driven to a depth of 5 cm.
from the lid margin, parallel with the nose and3 cm. from the midline. The instruments werepulled far laterally then brought back halfwayand driven 2 cm. deeper. The handles weretouched over the nose, then separated a totalof 45 degrees and then elevated as firmly aspossible. On the right side, the orbitoclast wentthrough at an angle of about 60 degreessatisfactorily, but on the left side I met withsuch resistance that I was afraid for theinstrument and replaced it with a new instru-ment, upon which I could apply the utmost in
two-handed traction. Finally, the orbital plategave way, and a cut of something like 75 degrees was achieved on this side. Then Idrew 10 cc. blood from the right arm andinjected it into the outer lower portion of thefrontal lobe on the left side, and a similarquantity on the left side. The patient wascoming to by this time, and made known herdispleasure by her rather excited praying.When the blood injection had been completed,however, she was apparently in good condition.
—Walter Freeman, M.D.
(continued)
performed. For example, picking up the receiver when thephone rings—a simple, well-practiced act—requires littlearousal, planning, or evaluation. A more complex behav-ior, such as telling a caller what you will be doing nextTuesday evening, however, requires attention and arousal,as well as planning and evaluation. An injury that has lit-tle effect on the first behavior might be disastrous for thesecond, more complex one.
For each behavior, Luria formulated the concept offunctional systems, which represent the pattern of inter-action among the various areas of the brain necessary tocomplete a behavior. Each area in the brain can operateonly in conjunction with other areas of the brain. Fur-thermore, no area of the brain is singly responsible for anyvoluntary human behavior; thus, each area of the brainmay play a specific role in many behaviors. As with theequipotentiality theory, Luria regards behavior as the re-sult of interaction among many areas of the brain. As withthe localization theory, Luria assigns a specific role to eacharea of the brain. The multifunctional role of the brain iscalled pluripotentiality; any given area of the brain canbe involved in relatively few or many behaviors.
Luria suggested that behavior results from several func-tions or systems of brain areas, rather than from unitaryor discrete brain areas. A disruption at any stage is enoughto immobilize a given functional system. For example, anindividual without injury to what localizationists wouldcall the “reading center” is unable to read if there is dam-age to any of a number of parts of the functional systemsinvolved in reading. Each functional system, however, hassome plasticity and can change spontaneously or throughretraining. For example, sensory feedback is necessary forcontinually knowing the location of one’s fingers and armto direct motor movement. A person who loses sensoryfeedback from the arm loses an important link in complet-ing fine-motor tasks. The functional system, however, canbe altered by using visual feedback to locate the fingers of
the hand, something not previously needed. The patientcan thus reestablish fine-motor skills, despite the disrup-tion of the old functional system. Luria’s concept of alter-native functional systems accounts for the ability of higherlevel brain skills to compensate for lower level skills inbrain injury. This concept was demonstrated clearly in aninteresting case of ours. At age 3 months, the patient hadundergone a complete left hemispherectomy (removal ofa hemisphere). When we saw him at age 7, not only couldhe walk, but he also spoke fluently. This was undoubtedlyrelated to the plastic nature of the patient’s brain, in whichthe right side of the brain developed the organization nec-essary to execute behaviors, such as speech and control-ling the right side of the body.
Luria’s theories are particularly attractive and relevant toclinical neuropsychologists because they can account formost observations of patients with brain injuries. The the-ory also explains the observation that certain lesions gener-ally yield consistent deficits. In addition, through the con-cept of reorganization, Luria’s theory can account forindividuals who recover from brain trauma. Finally, the the-ory suggests ways to establish rehabilitation and treatmentprograms for the brain-injured patient and provides a strongtheoretical basis for understanding clinical neuropsychology.
Modern Neuropsychology
Herman Ebbinghaus (1850–1909) proposed thatpsychology has a long past but a short history. This is truefor modern neuropsychology as well. Since Broca madehis momentous discovery in the 1860s, a number of majorachievements and influential concepts led to the evolutionof neuropsychology as a discipline as we know it today. In1933, Kleist published his monumental work on wartimebrain injuries. Although his localization approach was ac-cepted in Germany, it was largely unknown outside that

country. In the United States and Britain, the findings andconclusions of Lashley, Marie, and Jackson set up a gen-eral antilocalization bias. In particular, the field of aphasiaremained divided between the “holists” and “diagrammakers” such as Wernicke (Benton, 1994). The birth ofmodern psychosurgery was in 1935, when Moniz andLima first attempted to alleviate mental suffering by oper-ating on the human frontal lobes. The novelty of his con-cept and the “quality” of Moniz’s results earned him a con-troversial Nobel Prize in medicine in 1949. In the 1940s,the apparently favorable effects of the surgery on the ma-jority of severely disturbed patients led to its introductionin the United States by psychiatrist Walter Freeman andhis surgical colleague James Watts. Currently, however,treating psychiatric patients with lobotomies is regarded asa step backward (Neuropsychology in Action 1.4).
Clinical neuropsychology originally emerged in themedical setting within traditional neurosurgery and neu-rology services. Early research was primarily concernedwith the cortical functioning of patients with penetratingmissile wounds or the diagnosis of neurologic disorderssuch as brain tumors or strokes. For example, a famousneurosurgeon who was advancing an understanding of therelationship between brain anatomy and behavior wasWilder Penfield (1891–1976). Penfield was educated atPrinceton, Johns Hopkins, and Oxford universities andwas the founder and director of the renowned MontrealNeurological Institute. He pioneered direct electrical stim-ulation of the brain during surgery by systematic mappingof the brain as a technique for finding damaged areas ofthe brain. He also used the services of psychologists as con-sultants to help him with the diagnosis of neurologic be-havioral conditions. In the 1930s, psychologists played alarge role in diagnosing brain lesions, including stroke andtumor. For example, a friend and mentor of ours, MollyHarrower, a professor emeritus at the University of Floridaand inventor of the Group Rorschach, was routinely askedin the 1930s to evaluate “organic patients.” In her autobi-ographical essay “Inkblots and Poems” (1991), she de-scribes how as a research fellow of noted neurologistWilder Penfield at the Montreal Neurological Institute,she was asked to perform regular diagnostic workups usingthe Rorschach test: “I was assigned to examine all incom-ing patients suspected of tumor, with re-testing 14 dayspostoperatively” (Harrower, 1991, p. 141). Currently, neu-ropsychologists play a smaller role in diagnosing neuro-logic disorders but an important part in evaluating func-tional impairment, prognosis, and recovery.
In the late 1930s, neuropsychology engaged the inter-est of only a few neurologists, psychiatrists, and psycholo-gists. Neuropsychology was loosely organized, and no
journals reflected a focused interest in this area. But anumber of scholars were working on issues that in timemade decisively important contributions to the field andshaped neuropsychology as we know it today.
The first neuropsychology laboratory in the UnitedStates was founded in 1935 by Ward Halstead at the Uni-versity of Chicago. Halstead worked closely with neuro-surgery patients and developed assessment devices that dif-ferentiated between patients with and without brain damage(Figure 1.18). Together with Ralph Reitan, Halstead laterdeveloped the popular Halstead-Reitan Neuropsychologi-cal Battery, an empirical approach to assessing brain dam-age (Halstead, 1947; Reitan & Wolfson, 1993).
The term neuropsychology itself is of recent origin andwas most likely first coined by Sir William Osler in 1913,when he used the word in an inaugural address for a newpsychiatric clinic at Johns Hopkins Hospital in Baltimore,Maryland (Bruce, 1985). In 1936, Karl Lashley also usedthe term when he addressed the Boston Society of Psychi-atry and Neurology (Bruce, 1985). Hans-Leukas Teuber(1916–1977) is credited for first using the term in a na-tional forum during a presentation to the American Psy-chological Association in 1948, during which he describeddifferent aspects of brain–behavior relationships in warveterans with penetrating brain wounds (Teuber, 1950).Then, in 1949, Canadian Donald Hebb published hisclassic, The Organization of Behavior: A NeuropsychologicalTheory. Neuropsychology has enjoyed tremendous growthever since. The study of neuropsychology has drawn infor-mation and knowledge from many disciplines, includinganatomy, biology, physiology, biophysics, and even philos-ophy. Thus, many interdisciplinary professionals, includingneurologists, neuropsychiatrists, linguists, neuroscientists,speech pathologists, and school psychologists, are inter-ested in the field of brain–behavior relationships and havecontributed to its development.
Nevertheless, until the 1960s and Luria’s writings, therewas no unifying theory of brain–behavior relationships. Infact, before the 1960s, few neuropsychology practitionersexisted. Those that did were primarily researchers in whatis now considered experimental neuropsychology.
Between 1960 and 1990 neuropsychology was charac-terized by a movement from the laboratory to the clinicand the establishment of distinct neuropsychological orga-nizations (e.g., The International Neuropsychological So-ciety in 1967; The National Academy of Neuropsychol-ogy in 1975; and the American Psychological Association,Division 40 of Clinical Neuropsychology, in 1980). Thisphase also marked the creation of many scientific journalsthat focused exclusively on advancing the science of neu-ropsychology (Table 1.2).
CHAPTER 1 | A History of Neuropsychology 25
Henry Hécaen (b. 1912) founded the journal Neu-ropsychologia. Hécaen, who earned his M.D. degree, madeimportant contributions to brain–behavior relationships inhealth and disease. One of his discoveries, which earnedhim an enduring place in the history of neuropsychology,
26 PART ONE | Introduction
Figure 1.18 Ward C. Halstead is recording eye movements (summer, 1940). (Courtesy Archives of the Historyof American Psychology, David P. Boder Museum Collection, Encyclopaedia Britannica.)
Applied Neuropsychology
Archives of Clinical Neuropsychology
Behavioral Brain Research
Brain and Cognition
Cortex
Journal of Clinical and Experimental Neuropsychology
Neuropsychology
Neuropsychologia
Table 1.2 Major Neuropsychology Journals
was his demonstration of the functional properties of theright hemisphere. In the 1940s and 1950s, most scientistsbelieved that the left hemisphere dominated the brain, be-cause it plays an important role in the mediation of lan-guage. Hécaen and his coworkers generated an irrefutablemass of evidence that the right, supposedly minor, hemi-sphere played a crucial role in mediating visuoperceptualand visuoconstructional processes. Much of Hécaen’s workwas not translated into English from French until the 1970s(e.g., see Hécaen & Albert, 1978), and as recently as theearly 1960s, scientists seldom discussed or researched issuesregarding the role of the right cerebral hemisphere. The U.S.neuropsychologist Arthur Benton continued to explore therole of the right cerebral hemisphere in behavior (Benton,1972). In the 1940s, Benton established one of the firstneuropsychology laboratories in the Neurology Departmentat the University of Iowa School of Medicine, which stillcarries his name; he also supervised dissertations in the newfield of neuropsychology and authored numerous booksand neuropsychological testing instruments, including theBenton Visual Retention Test (BVRT).

Oliver Zangwill (b. 1913) founded neuropsychologyin Great Britain. Zangwill, who received his M.A. fromCambridge University and saw no necessity to work forthe Ph.D. degree, transformed into a clinical neuropsy-chologist while working in the Edinburgh Injury Unit ofthe British military services during World War II. Therehe was called on to evaluate hundreds of patients withtraumatic brain lesions. Zangwill was also among the firstinvestigators to show that hemispheric specialization forspeech in left-handers did not conform to the then-accepted rule of right hemisphere dominance (Zangwill,1960). He also contributed significantly to understandingof the nature of neuropsychological deficits associatedwith unilateral brain disease or injury.
Norman Geschwind (1926–1984) is another impor-tant neuropsychologist who helped to shape his profes-sion’s focus and development. Geschwind received hisM.D. degree at Harvard and later single-handedly foundedbehavioral neurology. In 1958, he joined the staff of theneurologic service of the Boston Veterans AdministrationHospital, where he made many significant contributionsto neuropsychology. Among his contributions was his pro-posal that behavioral disturbances are based on the de-struction of specific brain pathways that he called discon-nections. He presented his idea in his now classic article“Disconnexion Syndromes in Animals and Man” (1965),which was largely responsible for reemphasizing the im-portant role of neuroanatomy in neuropsychology. Basedon his faith that anatomy must play a central role for thedescription and operation of many complex mental func-tions, Geschwind set out to prove that the dominance ofthe left hemisphere for speech must have an anatomicbasis. He and a young colleague set out to study the mor-phologic features of 100 brains and determined that, in-deed, there was a strong trend toward a larger auditory as-sociation cortex in the left hemisphere (Geschwind &Levitsky, 1968). This finding led to a continuing searchfor anatomic disparities that might be correlated withfunctional differences. His premature death at the age of58 deprived behavioral neurology of its preeminent figure.
The most recent phase of modern neuropsychology,the 1990s to the present, has enjoyed unprecedentedgrowth, and clinical neuropsychology has made impor-tant professional and theoretical contributions during the1990s; in fact, the U.S. Congress recognized the 1990s asthe “Decade of the Brain.” Muriel Lezak is one of sev-eral neuropsychologists who pioneered the assessmentapproach in clinical neuropsychology. Since the late1980s, neuropsychological assessment has played a majorrole in the development of clinical neuropsychology. Neu-ropsychological evaluations have become an importantprocedure, allowing the generation of useful behavioral,
cognitive, and clinical information about diagnosis andthe impact of a patient’s limitations on educational, so-cial, and vocational adjustment. In addition to the devel-opment of new testing methods to meet special needs indiagnostic evaluation, there has been a steady increasein the use of neuropsychological assessment techniques inneurology and psychiatry and an expansion of their scopeof application into other fields such as education, be-havioral medicine, and gerontology. Lezak proposed thatneuropsychological testing is clinically relevant and sug-gested a flexible approach to assessing the individual pa-tient. She also reminded those neuropsychologists whobecame interested in a rather narrow subspecialty withinpsychology that clinical neuropsychology is firmly rootedin clinical psychology. Her classic text NeuropsychologicalAssessment, originally published in 1976, is now in itsfourth edition (Lezak, Howieson, & Loring, 2004).
The popularity of neuropsychology did not occur in iso-lation, but was directly related to developments in otherfields, including clinical (e.g., behavioral neurology, biolog-ical psychiatry, and radiology) and experimental sciences(such as neurosciences and neurochemistry) (Table 1.3).
Emerging Research Areas in Neuropsychology
Many research areas of neuropsychology in whichneuropsychologists and neuropsychology students can par-ticipate are emerging. Three such areas are at the forefront of
CHAPTER 1 | A History of Neuropsychology 27
Psychologists study behavior. Education includes an undergraduate degree inpsychology and a doctoral degree (Ph.D. or Psy.D.) in an area of psychology.
Neuropsychologists are psychologists who study brain–behavior relation-ships. Education includes a doctoral degree in psychology and specialty(postdoctoral) training in neuropsychology.
Neurologists identify and treat clinical disorders of the nervous system,emphasizing the anatomic correlates of disease. Training includes a premedmajor at the college level, a doctoral degree from a medical school (M.D.),and residency training in neurology.
Neuropsychiatrists are medical doctors who have had residency training inpsychiatry and are mostly concerned with the organic aspects of mentaldisorders, such as schizophrenia or bipolar disorder.
Neurosurgeons are medical doctors who have specialized in the surgery ofnervous structures, including nerves, brain, and spinal cord.
Neuroscientists are researchers and/or teachers who have completeddoctoral training in biology or related fields. They are primarily interested inthe molecular composition and functioning of the nervous system.
Table 1.3 Professionals Who Study the Brain

applied neuropsychological science: forensic neuropsychol-ogy; sports neuropsychology; and the neuropsychology ofterrorism, law enforcement, and the military (Zillmer, 2004).
F O R E N S I C N E U R O P S Y C H O L O G Y
Forensic assessment is one of the fastest growing areas inthe field of clinical psychology, with an increasing num-ber of neuropsychologists presenting and/or evaluatingassessment results in the courtroom setting. Because ofthe expertise of neuropsychologists in psychological as-sessment, they have been at the forefront of performingevaluations relative to the determination of damages inpersonal injury cases and assistance in criminal cases.Most often, these have included the bread and butter offorensic neuropsychology, an assessment of brain injury.
Neuropsychologists have become increasingly more in-volved in evaluating the emotional sequelae of injury, cus-tody evaluations, and the complex appraisal of deceptionand malingering in assessments performed in the forensicdomain. In fact, it has become a common occurrence thata neuropsychologist is eventually confronted with somesort of forensic issue in his or her clinical work. Researchin forensic neuropsychology is important because it pro-vides the practicing clinician with scientific data and a sci-entific process that allows neuropsychologists to pursuehis or her work with increased precision. Also, as a scien-tist, the forensic expert must keep abreast of new scientifictechniques and research in the field of neuropsychology.The sophistication of forensic neuropsychology attests toits emergent maturity (Zillmer, 2003a). Examples of emerg-ing research areas in forensic neuropsychology include theneuropsychology of comprehending an individual’sMiranda rights; the evaluation and detection of attempts todeceive or malinger in evaluations performed in the foren-sic domain; and the assessment of competency to standtrial, of criminal responsibility, and of insanity (Zillmer &Green, 2006).
S P O R T S N E U R O P S Y C H O L O G Y
Much attention has been given to the study of sports-relatedconcussions, and great strides have been made in under-standing this health concern, including the cultivation ofneuropsychological assessment tools to diagnose concus-sions and the refinement of recovery curves after injury.Concussion injuries are now thought of as significant neu-ropsychological events with real long-term consequences.Nevertheless, many issues related to the diagnosis, assess-ment, and management of concussions are akin to puttinga complex puzzle together. What is the effect of age andsex in concussions? What neuropsychological tests are bestsuited for assessing concussions? What is the gold standard
for grading concussions? What return-to-play guidelinesare most practical? Most often, the neuropsychologist’srole in the area of sports-related concussions is that of aconsultant (Zillmer, 2003b).
Participation in competitive sports has increased world-wide, and sports-related concussions represent a signifi-cant potential health concern to all of those who partici-pate in contact sports. Given that there are approximately300,000 sports-related concussions reported each year, theneuropsychologist’s role in testing for concussions for pur-poses of diagnosis and symptom resolution is one that ourprofession should embrace. Moreover, for those neuropsy-chologists who love sports, it provides a unique opportunityto merge one’s professional skills with one’s affinity forsports. The neuropsychologist’s training and expertiseuniquely prepares him or her to play an important and re-warding role in this growing field. Examples of currentresearch interests in this area include the return to play deci-sions after concussive injuries in sports (Zillmer, Schneider,Tinker, & Kaminaris, 2006), the neuropsychology of per-formance enhancement in competitive athletics, and therelationship between cognitive and personality factors re-lated to sports injury and rehabilitation.
T E R R O R I S M , L A W E N F O R C E M E N T , A N D T H E M I L I T A R Y
The surprise terrorist attacks against the United States andthe devastating effects of hurricane Katrina have changedthe collective psychology of our nation. Thus, there is anincreased opportunity for the neuropsychology commu-nity to conduct behavioral research and consultation inlaw enforcement, disaster relief, and the armed forces.
Neuropsychologists have expertise that allows them toprovide insight into the cognitive operations of terrorism;they can play an important role in using research in thecognitive sciences to assist in understanding the psychologyof terrorism and the mindset of terrorists. In addition,neuropsychologists are in a unique position to studyhow the brain reacts in a crisis to investigate the opti-mal form of comprehending verbal information duringa catastrophe, to examine the effects of anxiety amonglaw-enforcement officials on their decision-making abilityduring a calamity, to understand the psychological im-pact of first responders, and to develop means for treatingvictims of terrorist attacks.
The most recent terrorism attacks and threats of chem-ical and biological warfare have also brought a new per-spective to the psychologist’s role in the military, in lawenforcement (e.g., in the search for the Washington, D.C.,sniper), and in the military’s role in enforcing peace (e.g.,Iraq, Bosnia, and Korea). The armed forces can provide
28 PART ONE | Introduction

some real-life experience, responsibility, and exposure formilitary neuropsychologists that are seldom available fortheir civilian counterparts. For example, each operatingU.S. Navy aircraft carrier has a “resident” psychologistonboard. Neuropsychologists are also deployed as part ofcombat stress units in Iraq, where they evaluate and man-age combat stress “on site.”
Neuropsychologists are experts in the science ofhuman decision making, and we believe that neuropsy-chological science can be put to good use in counterter-
rorism endeavors, law enforcement, and the military. Ad-vancing neuropsychological science directly and indirectlyin these areas benefits the security of our nation, as well asthe discipline of neuropsychology. Research examples in-clude military fitness for duty evaluations, preparing mili-tary members for the demands of captivity, the neuropsy-chology of terrorists, the neuropsychological effects ofweapons of mass destruction, and the assessment and se-lection of operational personnel for high-risk assignments(Kennedy & Zillmer, 2006).
CHAPTER 1 | A History of Neuropsychology 29
2000 B.C.: Early Brain Hypotheses
Peruvian and central European cultures practice trephination
Sixth to Fourth Centuries B.C.: Ancient Greek Influences
Heraclitus (sixth century B.C.): The mind is an unreachable, enormous space
Pythagoras (580–500 B.C.): The brain is the center of human reasoning
Hippocrates (460–377 B.C.): The brain controls all sense and movements
Plato (420–347 B.C.): The brain is the closest organ to the heavens
Aristotle (384–322 B.C.): The heart is the source of all mental processes
Third Century B.C. to Middle Ages: The Cell Doctrine
Alexandrian school (third to fourth century B.C.): Made advances inphysiology and anatomy
Galen (Italian, A.D. 130–201): Suggested ventricular hypothesis and roleof humors in health
Medieval and Renaissance Europe: Anatomic Discoveries and the Spiritual Soul
Albertus Magnus (German, ca. 1200): Deemphasized the role of the ventricles
Andreas Vesalius (Italian, 1514–1564): Corrected many historical mis-takes about brain anatomy
René Descartes (French, 1596–1650): Proposed a strict split betweenmental and physical processes
Thomas Willis (English, 1621–1675): Made contribution to understandingthe brain’s vascular structure
Giovanni Lancisi (Italian, 1654–1720): Highlighted the role of the corpuscallosum
Eighteenth and Nineteenth Centuries: Phrenology
Franz Gall (Austrian, 1758–1828): Personality is related to different sizesof specific brain areas
Johann Spurzheim (Austrian, 1776–1832): Intellectual capacity is relatedto brain size
Nineteenth-Century Europe: The Era of Cortical Localization
Paul Broca (French, 1824–1880): Motor speech is located in a smallregion of the left, frontal lobe.
Carl Wernicke (German, 1848–1904): Understanding of speech is locatedin the temporal lobe.
Nineteenth- and Twentieth-Century Critics of Cortical Localization
Sigmund Freud (Austrian, 1856–1938): Coined the term agnosia
Pierre Flourens (French, 1794–1867): Early advocate of an alternativetolocalization theories.
Hermann Munk (German, 1839–1912): Coined the term mind-blindness
Joseph Babinski (English, 1857–1932): Introduced the term anosognosia
Karl Lashley (American, 1890–1958): Formulated the principle of massaction in equipotentiality
Late Nineteenth- and Twentieth-Century Theories of Brain Function
Hughlings Jackson (English, 1835-1911): Claimed behavior exists ondifferent levels in the nervous system
Alexander Luria (Russian, 1902–1977): Formulated the concept offunctional systems of behavior.
Modern Neuropsychology
Karl Kleist (German, 1879–1960): Refined localization approach toneuropsychology
Wilder Penfield (Canadian, 1891–1976): Neurosurgeon who discovereddirect electrical stimulation of the brain
Ward Halstead and Ralph Reitan (American, ca. 1940s): Pioneeredneuropsychological testing
Donald Hebb (Canadian, 1904–1985): Published classic The Organiza-tion of Behavior
Henry Hécaen (French, ca. 1950s): Pioneered the role of the right hemi-sphere in neuropsychology
Arthur Benton (American, b. 1909): Continued to advance the role of theright hemisphere
Oliver Zangwill (British, ca. 1960s): Examined neuropsychology withtraumatic brain injury
Norman Geschwind (American, 1926–1984): Founded behavioral neurology
Edith Kaplan (American, 1970s): Pioneered the process approach
Muriel Lezak (American, 1970s): Refined clinical assessment in neuropsy-chology
Table 1.4 Time Line of Significant Developments in Neuropsychology
30 PART ONE | Introduction
SummaryNeuropsychology has had a particularly rich history (Table 1.4), and the future is promising as well. Philo-sophical thought, medical practice, and religious dogma have shaped human’s beliefs about the brain.Understanding “where we came from” and “where we are” shows how neuropsychology has evolved as adiscipline. Furthermore, recognizing different viewpoints encourages the neuropsychology student to com-pare and contrast different theories. Knowledge of brain–behavior relationships is a developing science,rather than an absolute fact. In addition, we propose that neuropsychology is a paradigm of how to explainand research behavior, not just a body of knowledge. Neuropsychology is also not a separate area of re-search to be pursued in isolation from other models of psychology. It is distinct from physiology, however,because its direct concern is not with synapses but with behavior. In 1983, Donald Hebb suggested: “[The]neuropsychologist of the future must be a psychologist as well as a neurologist. The complexities of psy-chology and the complexities of neurology are the same complexities” (p. 7). We propose that neuropsy-chology is a natural part of psychology. We still know relatively little about the 3-pound organ that definesus, but many significant advances in recent years have brought the field to a new threshold of knowledgethat has allowed researchers to identify many of the anatomic areas and functional systems within thebrain that help determine behavior. The next chapter examines procedures for investigating the brain.
C r i t i c a l T h i n k i n g Q u e s t i o n s
How does localization brain theory differ from equipotentiality brain theory? What are the lasting contributions of eachtheory?Has the quest for the search of the organ of the soul been completed?Why is Luria’s functional model of the brain such an important step in understanding brain functions?
K e y Te r m s
PsychologyNeuropsychologyNeuronsVitalismMaterialismTrephinationHeraclitusPythagorasBrain hypothesisHippocratesPlatoAristotleCardiac
hypothesisVentricular localization
hypothesis
Cell doctrineda Vinci, LeonardoGalenHumorsMagnus, AlbertusVesalius, AndreasDescartes, RenéWillis, ThomasLancisi, GiovanniAtharva-VedaGall, FranzLocalization theoryPhrenologySpurzheim, JohannBroca, PaulAphasia
Double dissociationWernicke, CarlFluent aphasiaFreud, SigmundAgnosiaFlourens, PierreAblation experimentEquipotentialMunk, HermannMind-blindnessBabinski, JosephAnosognosiaLashley, KarlMass actionJackson, HughlingsLuria, Alexander
Functional systemsPluripotentialityPenfield, WilderHalstead–Reitan
Neuropsychological BatteryTeuber, Hans-LeukasHebb, DonaldHécaen, HenryBenton, ArthurZangwill, OliverGeschwind, NormanLezak, Muriel
We b C o n n e c t i o n s
http://nanonline.orgNational Academy of Neuropsychology—The official home page of the National Academy of Neuropsychology(NAN). This site includes information on doctoral programs in neuropsychology, annual meetings, member-ship information, and more.
CHAPTER 1 | A History of Neuropsychology 31
http://www.the-ins.orgInternational Neuropsychological Society—The International Neuropsychological Society is a multidiscipli-nary organization dedicated to enhancing communication among the scientific disciplines that contributesto the understanding of brain-behavior relationships.
http://www.apa.orgAmerican Psychological Association—The official site of the American Psychological Association (APA) pro-vides links to student information, membership information, PsychNET, and career-planning information.
http://www.psychologicalscience.orgAmerican Psychological Society—The American Psychological Society is dedicated to the advancement ofscientific psychology and its representation at the national level. The Society’s mission is to promote, pro-tect, and advance the interests of scientifically oriented psychology in research, application, teaching, andthe improvement of human welfare.
Chapter 2
METHODS OF INVESTIGATING THE BRAIN
The most important advancement in the clinical neurosciences is the imag-ing of the living human brain.
—Erin Bigler
The brain is the last and greatest biological frontier.—James Watts
Neurohistology TechniquesRadiologic ProceduresElectrophysiologic ProceduresImaging of Brain MetabolismMagnetic Imaging ProceduresCerebrospinal Fluid Studies: Lumbar PunctureBehavioral ExaminationsNew Advances in Imaging Techniques: Mapping
the Brain
Neuropsychology in Action
2.1 Case Example of Brainstem Auditory-EvokedResponse
2.2 Undergoing a Magnetic Resonance ImagingProcedure
2.3 New Frontiers in Functional Magnetic ResonanceImaging
2.4 Diagnostic Neuroimaging and Neuropsychology

CHAPTER 2 | Methods of Investigating the Brain 33
OverviewThe primary constraint in unlocking the secrets of the brain has been the limit of available techniques andexamination procedures for investigating the brain. This was certainly true for early scientists, who struggledwith how inaccessible the living brain is to direct visualization. Short of performing in vivo neurosurgicalprocedures or postmortem examinations immediately after death, early scientists simply could not examinethe living brain. As a result, study of the brain was largely speculative and inferential, and researchers havemade many errors (see Chapter 1). Because of such difficulties, many famous psychologists, includingWilliam James and B. F. Skinner, insisted that the brain is not the province of psychologists. They suggestedthat the brain is like a “black box”—researchers cannot study the brain itself, but can associate certaininputs with specific outputs of behavior.
Since the 1970s, an explosion in technology has allowed more precise examination of the brain. Duringthe end of the nineteenth century, researchers developed staining techniques by which they could visualizeneurons. In the early part of the twentieth century, X-ray technology and pneumoencephalography allowedscientists to visualize the skull and the ventricles. The brain, however, remained elusive. This all changed inthe 1970s when researchers introduced computed transaxial tomography (CT), and then magnetic reso-nance imaging (MRI) in the mid-1980s. These two procedures, although crude in their initial stages of devel-opment, were soon refined so that visualizing specific and detailed brain structures became possible, in-cluding visualizing asymmetries in the living brain. At the same time, other technologies, includingelectroencephalography (EEG), single-photon emission computed tomography (SPECT), and positron emis-sion tomography (PET) advanced, allowing clinicians to view the brain from structural, metabolic, and elec-trophysiologic perspectives. For example, using PET, scientists can now measure, with three-dimensional(3-D) resolution, biochemical and physiologic processes in the human brain. More recently, the structuralimaging of brain anatomy has been correlated with functional parameters of the brain, which created a newdirection in brain research, namely, that of functional imaging.
These recent advances in neuroimaging dramatically changed how scientists investigate neural corre-lates of human behavior. These spectacular new developments are akin to changing filters in a camera,resulting in new and different images of the same picture. A “window to the brain” has opened, and so hasour understanding of the brain.
This chapter summarizes the major technologic methods of examining the brain, and Chapter 3 exam-ines neuropsychological techniques of studying the brain. We discuss advantages and disadvantages foreach procedure, particularly as they relate to understanding brain–behavior relationships and diseaseprocesses. This chapter provides the neuropsychology student with background on the various investiga-tional procedures he or she will likely encounter in the literature, research laboratory, or in clinical practice.Neuropsychologists should familiarize themselves with the basic information these techniques can provide.In fact, neuropsychologists play an important role in advancing this technology and are working side by sidewith radiologists and neurologists to unlock the secrets of the brain.
K e e p i n M i n d
What is the difference between a CT scan and an MRI?
What does an EEG measure?
What is functional imaging?
What is the difference between an invasive and a noninvasive procedure?
Are modern imaging techniques dangerous to the brain? Explain.
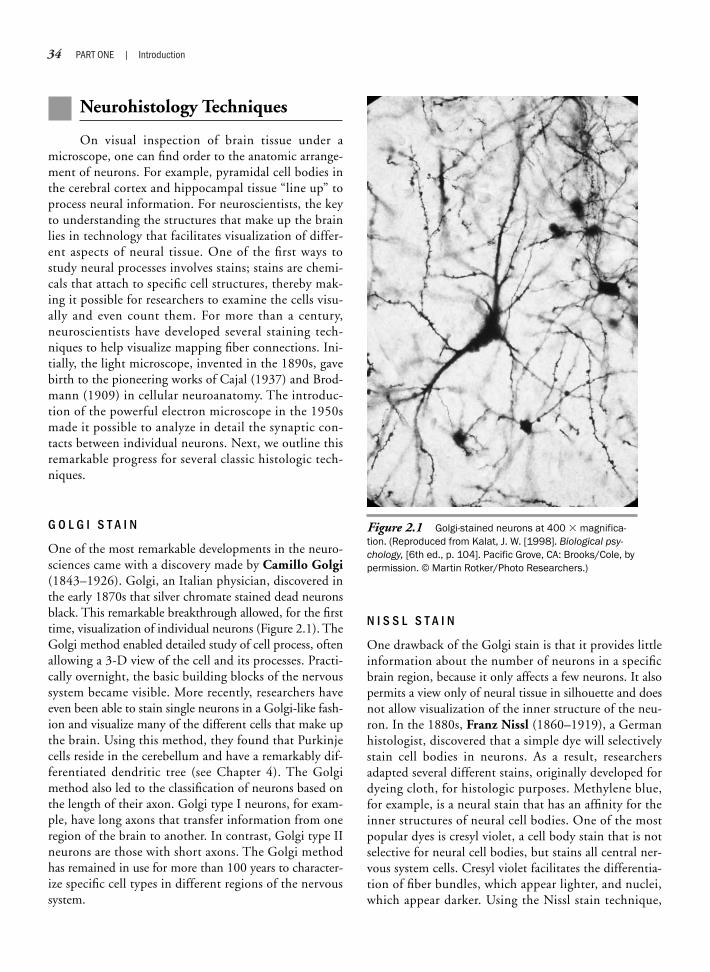
34 PART ONE | Introduction
Neurohistology Techniques
On visual inspection of brain tissue under amicroscope, one can find order to the anatomic arrange-ment of neurons. For example, pyramidal cell bodies inthe cerebral cortex and hippocampal tissue “line up” toprocess neural information. For neuroscientists, the keyto understanding the structures that make up the brainlies in technology that facilitates visualization of differ-ent aspects of neural tissue. One of the first ways tostudy neural processes involves stains; stains are chemi-cals that attach to specific cell structures, thereby mak-ing it possible for researchers to examine the cells visu-ally and even count them. For more than a century,neuroscientists have developed several staining tech-niques to help visualize mapping fiber connections. Ini-tially, the light microscope, invented in the 1890s, gavebirth to the pioneering works of Cajal (1937) and Brod-mann (1909) in cellular neuroanatomy. The introduc-tion of the powerful electron microscope in the 1950smade it possible to analyze in detail the synaptic con-tacts between individual neurons. Next, we outline thisremarkable progress for several classic histologic tech-niques.
G O L G I S T A I N
One of the most remarkable developments in the neuro-sciences came with a discovery made by Camillo Golgi(1843–1926). Golgi, an Italian physician, discovered inthe early 1870s that silver chromate stained dead neuronsblack. This remarkable breakthrough allowed, for the firsttime, visualization of individual neurons (Figure 2.1). TheGolgi method enabled detailed study of cell process, oftenallowing a 3-D view of the cell and its processes. Practi-cally overnight, the basic building blocks of the nervoussystem became visible. More recently, researchers haveeven been able to stain single neurons in a Golgi-like fash-ion and visualize many of the different cells that make upthe brain. Using this method, they found that Purkinjecells reside in the cerebellum and have a remarkably dif-ferentiated dendritic tree (see Chapter 4). The Golgimethod also led to the classification of neurons based onthe length of their axon. Golgi type I neurons, for exam-ple, have long axons that transfer information from oneregion of the brain to another. In contrast, Golgi type IIneurons are those with short axons. The Golgi methodhas remained in use for more than 100 years to character-ize specific cell types in different regions of the nervoussystem.
N I S S L S T A I N
One drawback of the Golgi stain is that it provides littleinformation about the number of neurons in a specificbrain region, because it only affects a few neurons. It alsopermits a view only of neural tissue in silhouette and doesnot allow visualization of the inner structure of the neu-ron. In the 1880s, Franz Nissl (1860–1919), a Germanhistologist, discovered that a simple dye will selectivelystain cell bodies in neurons. As a result, researchersadapted several different stains, originally developed fordyeing cloth, for histologic purposes. Methylene blue,for example, is a neural stain that has an affinity for theinner structures of neural cell bodies. One of the mostpopular dyes is cresyl violet, a cell body stain that is notselective for neural cell bodies, but stains all central ner-vous system cells. Cresyl violet facilitates the differentia-tion of fiber bundles, which appear lighter, and nuclei,which appear darker. Using the Nissl stain technique,
Figure 2.1 Golgi-stained neurons at 400 � magnifica-tion. (Reproduced from Kalat, J. W. [1998]. Biological psy-chology, [6th ed., p. 104]. Pacific Grove, CA: Brooks/Cole, bypermission. © Martin Rotker/Photo Researchers.)

scientists could then count the number of Nissl-staineddots that represented neurons in any area of the brain.
The Nissl method has become the classic microscopicmethod for studying the cell body and one of the most valu-able techniques for studying neurons in both normal andpathologic states. The Nissl stain outlines all cell bodies andselectively stains the nucleus but not the axon. Furthermore,Nissl patterns vary among different types of neurons. Forexample, motor neurons have larger Nissl bodies, and sen-sory neurons have smaller ones. The appearance of the Nisslsubstance also varies with cell activity; that is, Nissl bodiesdisintegrate when the axon of the neuron is injured.
O T H E R S T A I N I N G T E C H N I Q U E S
The Nissl and Golgi methods are selective in their affinityfor specific characteristics of neurons. The Nissl methodshows the cell body, specifically the cell nucleus. Thus, itmaps cell density. The Golgi method is particularly usefulfor investigating the distribution of dendrites and axons inindividual neurons, which appear pitch-black. Scientistshave developed other staining procedures specifically forstudying axons. For example, myelin staining selectivelydyes the sheaths of myelinated axons. As a result, whitematter, which consists of myelinated axons, is stainedblack, whereas other areas of the brain that consist primar-ily of cell bodies and nuclei are not (Figure 2.2).
Since the 1970s, researchers have introduced newtracing methods based on the principle of axonal trans-port to chart previously unexplored regions and circuitsof the brain. For example, the horseradish peroxidase(HRP) method (HRP is an enzyme found in horseradishroots) was introduced. Researchers inject HRP into a re-gion of the nervous system, and surrounding cell bodiesand axon terminals take it up. In neurons that have in-corporated HRP, axonal transport carries the enzyme toother interconnected cell bodies, where researchers candetect it with a simple staining procedure. Using the ax-onal transport technique, neuroscientists can study thetracing of pathways in the brain. Staining remains a vi-able method for studying the cellular function of the ner-vous system and helps neuroscientists in studying thespecialized contacts among neurons and their complexand often puzzling arrangements. Table 2.1 summarizesthe different staining techniques used in neuroscience.
Radiologic Procedures
From the initial X-ray of the head and the practicallyextinct air encephalogram to sophisticated CT, the rapidprogress of radiology has made a significant impact on the
field of clinical neurology and neuropsychology. This sec-tion discusses the techniques involved in neuroradiology,with special emphasis on computed tomography and an-giography.
CHAPTER 2 | Methods of Investigating the Brain 35
Nissl stain: A dye that stains the cell body of the neuron; this method isparticularly useful for detecting the distribution of cell bodies in specificregions of the brain
Golgi stain: A method of staining brain tissue that marks a few selectedindividual cells, differentiating the cell body, as well as its extensions
Myelin stain: Shows the myelin coating of axons, rendering it useful formapping pathways in brain tissue
Horseradish peroxidase: Allows mapping of neuronal pathways using axonaltransport mechanisms; this technique works in both directions, that is, fromthe axon back to the cell body, and vice versa
Table 2.1 Different Staining Techniques
Text not available due to copyright restrictions

36 PART ONE | Introduction
S K U L L X - R A Y
Physicist Wilhelm Conrad Röntgen (1845–1923) made aremarkable discovery that changed the science of medicineforever and earned him the 1901 Nobel Prize in physics.Röntgen (or Roentgen, to transliterate the German ö intoEnglish) quite serendipitously produced an invisible raythat, unlike heat or light waves, could pass through wood,metal, and other solid materials. This ray, also called theX-ray, created the field of radiology. The principle of X-raytechnology is the generation of Roentgen rays, electromag-netic vibrations of very short wavelength that can penetratebiological tissue and can be detected on a photographicplate. At the basis of its medical application was the prin-ciple that the diagnostic rays travel through the body atdifferent rates according to the density of organs. The re-sulting picture would show clear contrast between bonesand, to a lesser degree, soft parts. Researchers discovered thatX-rays pass easily though low-density tissue (water) but areabsorbed by high-density tissue (bone). In addition, theyfound that the possible harmful effects of X-rays coulddestroy diseased tissue, a discovery that led to radiotherapy.
Diagnostic X-ray films are useful for clinical work onvarious parts of the body, because they demonstrate thepresence and position of bones, fractures, and foreignbodies. A clinical disadvantage of X-ray films, specificallyof the head, is that they are two-dimensional (2-D). Thus,positive diagnosis of a 3-D clinical pathology is difficult.Second, an X-ray film of the head shows little differentia-tion between brain structures and cerebrospinal fluid(CSF), making clinical use of this procedure ineffective,with the exception of large and vascularized brain tumorsor massive bleeds. Furthermore, X-rays are potentiallydangerous, because they are cumulatively absorbed byhigh-density tissue. Thus, X-ray exposure entails a minorrisk. The advantage of X-raying the head is that it usesuniversally available technology, is inexpensive, and pro-vides good visualization of the skull. Thus, if there is thepossibility of a skull fracture, X-ray technology remains auseful diagnostic tool (Figure 2.3).
A I R E N C E P H A L O G R A P H Y( P N E U M O E N C E P H A L O G R A P H Y )
An air encephalogram, or pneumoencephalogram, isthe radiographic visualization of the fluid-containingstructures of the brain, the ventricles, and spinal column.It is similar to X-ray visualization, but it involves with-drawing CSF by lumbar puncture (see later); the CSF isthen replaced with a gas such as air, oxygen, or helium.The gas rises and enters the ventricular system, specifi-cally the four interconnecting cavities of the brain. Once
the gas has filled the ventricles, a technician takes a stan-dard X-ray film of the head. Because the gas is of muchlower density than the surrounding brain, the ventriclesappear as a dark shadow on the X-ray film and clearly out-line the surrounding brain tissue. Using this approach, aclinician can make a clinical diagnosis. The air encephalo-gram represented an advance on the standard X-ray filmbecause it allowed visualization of the ventricular system.
However, patients did not tolerate the procedure well.Attendants had to turn patients in various positions, oftenawkwardly, and invert them in 3-D space to advance thegas to a specific ventricle before the technician could takean X-ray film. Because gas had replaced the CSF, the cush-ioning aspects of the CSF had been compromised, whichoften resulted in excruciating headaches that could lastfor several days before the gas was reabsorbed. Today, themore modern CT scan has replaced both the traditionalX-ray image and the pneumoencephalogram.
C O M P U T E D T R A N S A X I A L T O M O G R A P H Y
Computed transaxial tomography (CT) is based on thesame principle as the X-ray examination. The medicalcommunity has widely embraced CT, making it the stan-dard technology for examining the brain.
H i s t o r y
CT scanning was invented in Great Britain in 1971 andintroduced to the United States in 1972 (Haeger,1988). Physicists developed the first model of transaxial
Figure 2.3 X-ray film of the head. (Courtesy Eric Zillmer.)

tomography in part by building on dramatic advances incomputer technology. Since its development, CT tech-nology has progressed from detecting only gross brain fea-tures to visualizing highly refined structural features. Be-fore this technology, precise neuropathologic diagnosiswas difficult.
T e c h n i q u e
After placing the patient’s head in the center of the CTscanner, the technician revolves an X-ray source around thehead as detectors monitor the intensity of the X-ray beampassed through the brain. The technician does not take theimages at a perfect horizontal perspective of the head.Rather, he or she slightly tilts the images at a 20-degreeangle to avoid scanning the air-containing sinuses, whichproduce distortion because of the combination of low(air) and high (bone) density (Figure 2.4). The first (low-est) image selected is usually at the level of the foramenmagnum, the base of the brain. Multiple sequential im-ages show the ventricles, basal ganglia, thalamus, and cere-bral cortex. Multiple transaxial images of the brain are ob-tained from many different angles. This requires a largeapparatus or X-ray tube, which can rotate 360 degreesaround the patient’s head (Figure 2.5). The detectors,which either rotate with the X-ray scanner or are placedin a circle around the patient, are more sensitive than thetraditional X-ray film. For comparison, X-ray film candetect difference of 10% to 15% in the density of softtissue, whereas CT can measure variations as small as 1%,often pinpointing density changes as small as 2 mm indiameter.
In contrast with the traditional X-ray visualization, inCT, the head is scanned using a very narrow beam. This al-lows for the segmentation of the brain into many differentslices. Depending on the nature of the study, the slices of
CHAPTER 2 | Methods of Investigating the Brain 37
Figure 2.4 X-ray image of the head demonstrating thevarious “slices” of which the images are calculated. Notethe absence of any differentiation of this patient’s brainusing X-ray technology. The 20-degree angle of the cuts isimplemented to avoid rays passing through the brain si-nuses at the front of the brain, which often causes distor-tion. (Courtesy Eric Zillmer.)
X–ra
y source
X–ray
detec
tor
a. b.
Figure 2.5 Computed transaxial tomography scanner. (a) The subject’s head is placed in the scanner, which isthen subjected to a rotating source of X-rays that pass through the brain at various angles. (b) A computer con-structs the final image of the brain. (Reproduced from Kalat, J. W. [1998]. Biological psychology [6th ed., p. 106,Figure 4.28]. Pacific Grove, CA: Brooks/Cole, by permission. Photo by Dan McCoy/Rainbow.)
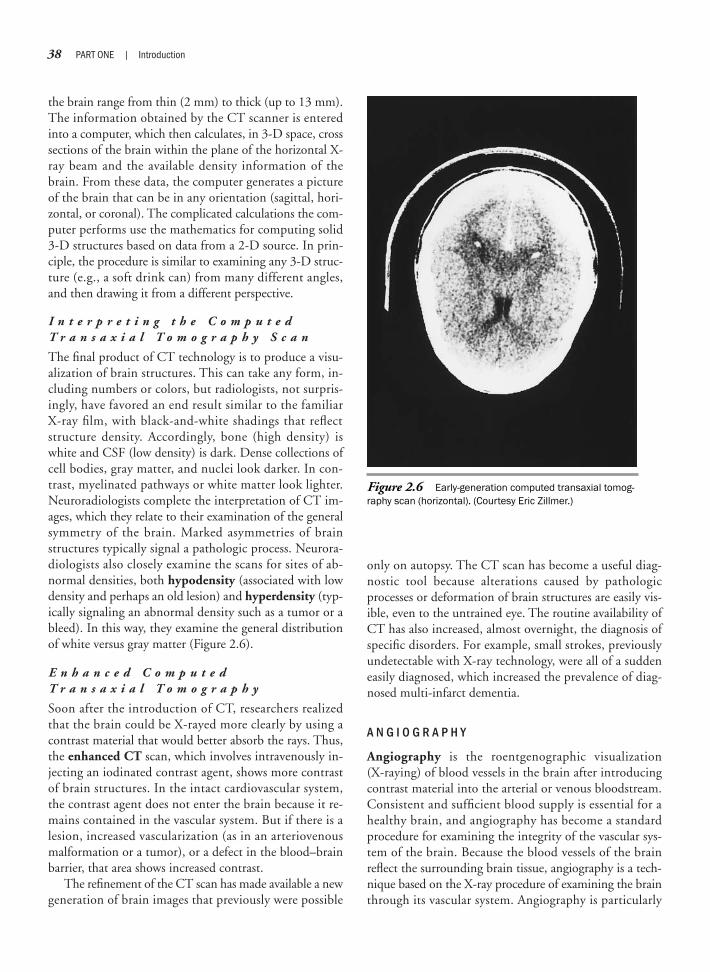
38 PART ONE | Introduction
the brain range from thin (2 mm) to thick (up to 13 mm).The information obtained by the CT scanner is enteredinto a computer, which then calculates, in 3-D space, crosssections of the brain within the plane of the horizontal X-ray beam and the available density information of thebrain. From these data, the computer generates a pictureof the brain that can be in any orientation (sagittal, hori-zontal, or coronal). The complicated calculations the com-puter performs use the mathematics for computing solid3-D structures based on data from a 2-D source. In prin-ciple, the procedure is similar to examining any 3-D struc-ture (e.g., a soft drink can) from many different angles,and then drawing it from a different perspective.
I n t e r p r e t i n g t h e C o m p u t e dT r a n s a x i a l T o m o g r a p h y S c a n
The final product of CT technology is to produce a visu-alization of brain structures. This can take any form, in-cluding numbers or colors, but radiologists, not surpris-ingly, have favored an end result similar to the familiarX-ray film, with black-and-white shadings that reflectstructure density. Accordingly, bone (high density) iswhite and CSF (low density) is dark. Dense collections ofcell bodies, gray matter, and nuclei look darker. In con-trast, myelinated pathways or white matter look lighter.Neuroradiologists complete the interpretation of CT im-ages, which they relate to their examination of the generalsymmetry of the brain. Marked asymmetries of brainstructures typically signal a pathologic process. Neurora-diologists also closely examine the scans for sites of ab-normal densities, both hypodensity (associated with lowdensity and perhaps an old lesion) and hyperdensity (typ-ically signaling an abnormal density such as a tumor or ableed). In this way, they examine the general distributionof white versus gray matter (Figure 2.6).
E n h a n c e d C o m p u t e d T r a n s a x i a l T o m o g r a p h y
Soon after the introduction of CT, researchers realizedthat the brain could be X-rayed more clearly by using acontrast material that would better absorb the rays. Thus,the enhanced CT scan, which involves intravenously in-jecting an iodinated contrast agent, shows more contrastof brain structures. In the intact cardiovascular system,the contrast agent does not enter the brain because it re-mains contained in the vascular system. But if there is alesion, increased vascularization (as in an arteriovenousmalformation or a tumor), or a defect in the blood–brainbarrier, that area shows increased contrast.
The refinement of the CT scan has made available a newgeneration of brain images that previously were possible
only on autopsy. The CT scan has become a useful diag-nostic tool because alterations caused by pathologicprocesses or deformation of brain structures are easily vis-ible, even to the untrained eye. The routine availability ofCT has also increased, almost overnight, the diagnosis ofspecific disorders. For example, small strokes, previouslyundetectable with X-ray technology, were all of a suddeneasily diagnosed, which increased the prevalence of diag-nosed multi-infarct dementia.
A N G I O G R A P H Y
Angiography is the roentgenographic visualization (X-raying) of blood vessels in the brain after introducingcontrast material into the arterial or venous bloodstream.Consistent and sufficient blood supply is essential for ahealthy brain, and angiography has become a standardprocedure for examining the integrity of the vascular sys-tem of the brain. Because the blood vessels of the brainreflect the surrounding brain tissue, angiography is a tech-nique based on the X-ray procedure of examining the brainthrough its vascular system. Angiography is particularly
Figure 2.6 Early-generation computed transaxial tomog-raphy scan (horizontal). (Courtesy Eric Zillmer.)

important in diagnosing structural abnormalities in theblood vessels themselves or in their arrangement. As a re-sult, angiography has become a useful tool in the earlyidentification of aneurysms (a ballooning of an artery; seeChapter 12) and the subsequent prevention of stroke. Toa lesser extent, clinicians can also identify other patholo-gies such as tumor, because they depend on increased vas-cularization or blood supply. Angiography also can detectshifts in cerebral arteries, which may indicate a mass-occupying lesion.
T e c h n i q u e
Femorocerebral angiography, developed in the mid-1950s, introduces a catheter into the arterial system. Pre-viously, physicians injected the contrast material directlyinto an artery, such as the internal carotid artery, but it issafer to insert a catheter via the femoral artery. The spe-cialist passes the preshaped, semirigid catheter through aneedle inserted in the femoral artery, and then guides itup the aorta to the aortic arch with the assistance of X-rayand television monitoring. The specialist can then placethe catheter into any of the three major arteries arisingfrom the aortic arch; the brachiocephalic artery, whichleads to the common right carotid artery or the right ver-tebral artery; the left common artery, which leads to theleft internal and external carotid artery; or the left subcla-vian artery, which connects to the left vertebral artery (seeChapter 12 for a more detailed discussion of the vascular
system of the brain). Using this technique, the specialistcan position or “park” the catheter tip at various strategicplaces of blood supply to the brain, to examine anterioror posterior cerebral arteries. Next, an automatic injectorsends an iodinated contrast agent through the catheter.At the same time, a technician takes rapid, serial X-rayfilms of the head over an 8- to 10-second interval in thefrontal and lateral planes, providing visualization of theinjected vessels and their complex intracranial branches.
Digital subtraction angiography, compared with con-ventional film angiography, is particularly effective in en-hancing visualization of blood vessels, including the mor-phologic and physiologic states of the arterial, capillary,and venous phases of the cerebral circulation (Figure 2.7).In this procedure, after the images of the contrast mate-rial have been acquired, the computer stores and subtractsthe X-ray image of the brain. The resulting visualizationof the vascular system is easily distinguished from that ofbrain tissue.
Intravenous angiography is somewhat more compli-cated than femorocerebral angiography; therefore, clini-cians do not use it as routinely. In intravenous angiogra-phy, the specialist inserts the catheter in the patient’sarm but must pass it through the heart, then the lungs,and then to the left side of the heart before it reaches theaortic arch. Thus, larger amounts of contrast mediummust be used, which increases the patient’s risk for renaltoxicity.
CHAPTER 2 | Methods of Investigating the Brain 39
a. b.
c.
Figure 2.7 Examples of angiography: (a) normal lateral view angiogram; (b) arteriovenous malformation fromcoronal perspective; and (c) aneurysm from lateral perspective. (a: SPL/Custom Medical Stock Photo; b: English/Cus-tom Medical Stock Photo; c: English/Custom Medical Stock Photo.)

40 PART ONE | Introduction
C l i n i c a l U s e
Angiography allows, from the puncture of a single artery,the maximum radiographic detail for diagnosing intrac-erebral lesions. Angiography is an invasive procedure, yetit is relatively safe and well tolerated by the patient, whois awake but slightly sedated. The risk from the procedureis related to the possibility of the catheter looseningplaques in the arteries that may then separate and travelto a smaller location in the arterial system, where they canblock the flow of blood, leading to an embolism. This is aconcern in patients with arteriosclerotic vascular disease.Few patients are allergic to the contrast medium, but theprocedure is contraindicated for these patients. In gen-eral, for initial diagnosis, clinicians prefer noninvasivetechniques, including CT scan and ultrasound (see Chap-ter 12 for a description of ultrasound used to examine thecarotid arteries). Angiography is, however, the most accu-rate diagnostic procedure for evaluating vascular anatomyand its abnormalities. Thus, it is particularly useful in di-agnosing cerebrovascular disorders.
S O D I U M A M Y T A L I N J E C T I O N S ( W A D A T E C H N I Q U E )
The Wada technique, named after its developer, is simi-lar to the angiogram in that the examiner places acatheter, typically in the left or right internal carotidartery. Then, a barbiturate sodium amytal is injected,which temporarily anesthetizes one hemisphere. Onlyone hemisphere is affected, even though vascular struc-tures connect the two hemispheres (Wada & Rasmussen,1960). This difference relates to that the pressure gradi-ents along cerebral arteries in both hemispheres are thesame; thus, there is no cross-filling (or crossover) of bloodfrom one hemisphere to the other, except if there is astroke or other damage to the vascular system. In thisway, neuropsychologists can study the precise functionsof one hemisphere while the other “sleeps” (see Chapter16 for a detailed discussion of the Wada technique).Table 2.2 provides an overview of the radiologic proce-dures discussed in this section.
Electrophysiologic Procedures
E L E C T R O E N C E P H A L O G R A P H Y
One of the most widely used techniques in neurology iselectroencephalography (EEG). The electroencephalo-gram is a recording of the electrical activity of nerve cells
of the brain through electrodes attached to various loca-tions on the scalp. The Austrian psychiatrist Hans Bergerfirst discovered in 1924 that patterns of electrical activitycan be recorded using metal electrodes placed on thehuman head (Brazier, 1959). Initially, Berger was inter-ested in finding physiologic evidence for telepathy, thescientifically unverified phenomenon of a mind commu-nicating with another by extrasensory means. Berger was,however, frustrated in his search to find support of men-tal telepathy, but he discovered that the electrical activityof the sleeping brain differed fundamentally from that ofthe awake brain. Researchers have used the resultingelectroencephalogram (“electrical brain writing”) to inves-tigate distinct patterns of electrical activity in both the nor-mal and pathologic brain. Its potential use for identifyingEEG correlates of behavior and personality have made ita popular research tool among behavioral scientists. Thus,EEG became the first dynamic way to measure brainfunction.
Skull X-ray: Two-dimensional representation of the head. Disadvantagesinclude low resolution of brain anatomy; advantages include low cost,availability, and its use in the diagnosis of skull fractures, which are easilyseen using this technique.
Air encephalography (pneumoencephalography): The radiographic visualiza-tion of the fluid-containing structures of the brain, which have been filled withgas. An improvement over the skull X-ray, but because of its invasive natureand side effects, it is not used in contemporary medicine.
Computed transaxial tomography (CT scan): CT renders an anatomic imageof brain density based on multiple X-ray images of the brain. CT, which isreadily available and can be used with almost anyone, provides a three-dimensional perspective of the brain with acceptable differentiation of brainstructures. Its disadvantages include the use of penetrating radiation andthat CT does not provide as much spatial resolution as does magneticresonance imaging.
Enhanced CT: A CT scan that involves injecting a contrast agent to providebetter visualization of brain structures, particularly bleeds. Disadvantagesare it is invasive and some patients may not tolerate the contrast agent well.
Angiography: The roentgenographic visualization of blood vessels in the brainafter introducing contrast material into the arterial or venous bloodstream.Angiography is the most useful technique for examining the blood supply toand from the brain. One disadvantage is that a catheter must be inserted intothe patient’s bloodstream, which requires an invasive medical procedure.
Sodium amytal injections (Wada technique): The injection of sodium amytaltemporarily anesthetizes one hemisphere. This is primarily a researchtechnique. It is used clinically to determine the lateralization of languagebefore temporal lobectomy is performed. It is a complicated medical proce-dure that requires placing an arterial catheter.
Table 2.2 Overview of Radiologic Procedures

T e c h n i q u e
To record an EEG, the technician places small metal elec-trodes, or leads, on the scalp and connects them via wiresto the electroencephalograph machine (Figure 2.8), whichamplifies the electrical potential of neurons recordingtheir activity on moving paper, a polygraph. Previously,electrodes were small needles that were inserted just belowthe skin of the scalp. Modern electrodes used with con-ductive gel have proved to be just as effective. In princi-ple, each pair of electrodes can act as its own recordingsite, measuring the electrical activity of millions of neu-rons close to the scalp. The neuronal activity of deeper,subcortical structures is not easily evaluated using EEG.Also, surface electrodes are placed at electrically inactivesites on the head, such as the mastoid bone behind theear (electrode placement A1 and A2), which act as groundleads. The EEG itself is generated primarily by neuronalactivity immediately below the cortex. Pyramidal nervecells, which have somewhat conical cell bodies, make upabout 80% of neurons in that region and exist in all areasof the cerebral cortex. Thus, EEG is mostly a measure ofcortical nerve cells of the pyramidal type.
The electrical signal of a neuron must penetratethrough different tissues to reach the electrodes, includingthe meninges, CSF, blood, the skull, and the scalp, to bemeasured. The electrical contribution of each neuron istiny, and it takes many thousands of neurons firing in con-cert to generate an electrical signal large enough for EEGto detect. Thus, the most easily visible EEG wave patternsdepend on the synchronicity of millions of neurons.
In general, brain wave patterns are either rhythmic orarrhythmic. Neurons typically fire in a rhythmic or syn-chronous pattern, leading to alpha, beta, theta, and delta
waveforms. In epilepsy, however, many neurons fire atonce, or in a burst or “spike” that corresponds with theamplitude that the EEG record shows. In principle, eachelectrode measures the summed signal of electrical activ-ity of groups of neuronal dendrites. EEG can be thoughtof as analogous to holding a microphone over New YorkCity to estimate the traffic by measuring the amount ofnoise from automobiles. Thus, EEG is a diagnostic toolmore sensitive to the “forest” than to the individual “tree.”
O v e r v i e w o f B r a i n W a v eA c t i v i t y
Brain wave activity may differ in polarity, shape, and fre-quency. The amplitude typically ranges from 5 to 100 mi-crovolts and is a measure of the signal strength of neuralactivity. The EEG records frequency of the waveformsfrom 1 to 100 Hz (signal frequency per second), meaningthat neural activity oscillates in a particular frequency. Thespecific shape of the waveform also interests the electroen-cephalographer. For example, during light sleep, the EEGshows a characteristic spindle activity and vertex (V)waves. Researchers have established a system of dividingbrain wave activity that is based on its frequency and am-plitude. To the neuropsychology student, frequency subdi-visions of the EEG may appear somewhat arbitrary, but ingeneral, they correlate with distinct divisions of subjectiveexperience of attention and arousal. Several different basictypes have been established that vary according to whethera person is alert, wakeful, drowsy, or sleeping (Table 2.3).
CHAPTER 2 | Methods of Investigating the Brain 41
Figure 2.8 Electromechanical electroencephalographicrecorder of the type used in the mid-1980s. (Courtesy Jeffrey T. Barth, University of Virginia.)
Gamma activity (35+ Hz) is a low-amplitude, fast-activity wave. Gammarhythms are the fastest and are often associated with peak performancestates and hyperarousal.
Beta is a low-amplitude, fast-activity wave with a frequency of more than12 Hz. Beta is often divided into high beta (18–35 Hz), typically associatedwith a narrow focus, overarousal, and anxiety; mid-beta (15–18 Hz), oftencorrelated with being active, alert, excited, or focused; and low beta (12–15 Hz),which has been associated with relaxed, external attention.
Alpha activity (8–12 Hz) is the predominant background activity in wakefulpersons. Alpha is most often associated with quiet, passive, resting, butwakeful states.
Theta activity ranges from 4 to 7 Hz and is most indicative of drowsiness,deeply relaxed states, and inwardly focused states.
Delta activity is the slowest frequency (<0.5–4 Hz). High-voltage, slow-frequency delta waves are never present in a wakeful, healthy person, butmostly occur during non–rapid eye movement (nondream) deep stage 4 sleep.
Table 2.3 Brain States and AssociatedSubjective Experience

42 PART ONE | Introduction
The pursuit of a specific brain state is a goal in itself.Because alpha and theta waves are characteristic of a per-son being relaxed, isolation flotation tanks and relaxationaudio cassette tapes, among other tools, have proved ef-fective in helping achieve such brain states. In athletics,researchers have demonstrated that peak performance isassociated with specific cortical arousal levels (Van Raalte& Brewer, 1996). Alpha waves, in contrast, are incompat-ible with being alert and focused. Thus, it is advantageousfor the competitive athlete to be in mid-beta rhythmwhen a difficult task is required, such as in ice hockeywhen the goalie faces a breakaway or in baseball when thebatter steps to the home plate to face a pitch. During betawaves, the cortex is most actively engaged via complexsensory input and external processing. The activity rate ofcortical neurons should be high, but also unsynchronized,because neurons may be involved in different aspects ofcomplex neuropsychological tasks. During beta waves,neurons fire rapidly, but not in concert with each other.However, it is difficult to sustain beta rhythm for long pe-riods; thus, successful athletes are skilled in switchingfrom alpha to beta rhythm and back “on command.”
S e i z u r e s a n dE l e c t r o e n c e p h a l o g r a p h y
Neurons can organize their rate of electrical activity in twofundamental ways. First, groups of neurons can fire in syn-chronized oscillations by taking cues from other cells, alsoknown as pacemaker cells or k neurons (k for constant). Cor-tical neurons also take cues from other brain structures suchas the thalamus, which can act as a powerful pacemaker,even when there is no external sensory input. For example,during non–rapid eye movement (NREM, or nondreamsleep), the thalamus generates rhythmic, self-sustaining dis-charge patterns that prevent organized information fromreaching the cortex. Thus, one’s brain is asleep, demonstrat-ing large, rhythmic delta waves. Second, neurons may firein a consistent rhythmic pattern in response to collectivebehavior, such as a large group of people clapping in a syn-chronized way without a cheerleader being present.
Seizures are the most extreme form of synchronousbrain activity, during which the whole brain (as in a grandmal seizure) or large portions of the brain (as in a partialseizure) fire with a defined and pronounced synchronythat never occurs during normal behavior (Figure 2.9).
Figure 2.9 Electroencephalogram example of spiking activity that accompanies epilepsy. (Courtesy EricZillmer.)

During seizures, most, if not all, cortical neurons partici-pate in excitation. Behavior is disrupted, and often con-sciousness is lost. Seizures themselves are best conceptual-ized as a symptom, not unlike a fever, and may betriggered by dozens of different causes. It is unlikely thatseizures have one underlying cause. The lifetime preva-lence for a single seizure is high, approximately 10%.Drugs that block gamma-aminobutyric acid (GABA) re-ceptors increase the possibility of a seizure. GABA hasstrong inhibitory properties and plays a major role in thebasic type of neuronal transmission that depends on rapidcommunication among neurons. Conversely, drugs thatprolong the inhibitory action of GABA (barbiturates orbenzodiazepines, e.g., Valium) suppress the possibility ofseizures. The brain is potentially always close to having aseizure, because runaway excitation is possible given theredundant feedback circuitry of the brain and its delicatebalance between inhibitory and excitatory potentials.Multiple seizures, however, are typical of a disorderknown as epilepsy (see Chapter 16 for a detailed discus-sion of epilepsy).
In patients with intractable (incurable) epilepsy, oneintervention is neurosurgery to remove, if possible, theprecise site or origin of the pathologic electric discharge.In such cases, a more precise EEG measurement isneeded, which can be obtained by placing electrodes di-rectly on the surface of the brain. This form of EEG,known as electrocorticography (ECoG), often is per-formed during temporal lobectomy surgery to isolate aprecise location of brain pathology. In addition, a sur-geon can place depth electrodes in the brain close to theprojected area of interest while the patient is awake andbeing monitored via 24-hour closed-circuit television.This is usually done to correlate seizure activity withEEG data. Depth electrodes and ECoG are invasive tech-niques and entail risks, including infection. These meth-ods are used only when the medical benefits greatly out-weigh the risks to the patient. Thus, surface scalpelectrode placement is the first and least invasive electro-physiologic study of the brain. EEG is also relatively in-expensive compared with CT and MRI procedures andis readily available.
C l i n i c a l U s e o fE l e c t r o e n c e p h a l o g r a p h y
The primary referral for a clinical EEG is to help with di-agnosis of a seizure disorder, sleep disorder, level of coma,or presence of brain death. In fact, EEG is the primarytool in diagnosing epilepsy and can often pinpoint thetype and location of seizure disorder. EEG is also usefulin diagnosing sleep disorders, because specific sleep states
are associated with particular forms of electrical activity.The primary abnormality seen on EEG recordings is aslowing of activity, as well as the presence of epileptiformactivity. For example, it is abnormal to find delta activityin a wakeful person. Typically, the slower the frequency inan awake patient, the more severe its abnormality. Peoplewith partial seizures often have EEG activity that slows to3 Hz. Epileptiform EEG activity consists of sharp waves(spike-and-wave discharge), which indicate a seizure dis-order. EEG diagnosis of epilepsy, however, produces fre-quent type II errors (misses). Thus, a normal EEG maynot indicate a normal brain.
Unfortunately, the EEG also demonstrates type I er-rors (false positive or false hits). That is, a mildly abnor-mal EEG may not necessarily reflect an abnormal brainunless the EEG indicates the specific profile of epilepsy,which, if present, has few false positives. Interpreting theEEG recording is something of an art because so manydifferent variables are introduced. These variables includeamplitude configuration of the polygraph, speed ofrecording paper, different electrode montages, a high in-cident of artifact caused by muscle movement that con-tributes to electrical activity, and inadequate electricalshielding of the examination room. Thus, different elec-troencephalographers often disagree on interpreting bor-derline abnormal EEGs, although they easily diagnose themore definite epileptic EEG patterns.
When a diagnostician suspects seizure disorder, severaltechniques can provoke epileptic discharges during theEEG recording, which is the absolute positive sign ofepilepsy. These methods include administering an EEGduring the patient’s sleep or when sleep deprived; that is,after the patient stays awake for one night, the diagnosti-cian administers the EEG in the morning. Other activa-tion techniques that provoke epileptic discharges duringthe EEG recording include hyperventilation and photicstimulation. The latter is the presentation of a strobe light,right in front of closed eyes, that is set at different fre-quencies to influence the base-rate activation pattern ofoccipital neurons. Diagnosticians also use serial EEGs and24-hour EEG recordings to monitor brain wave patternsover time. Once epilepsy is identified, doctors most com-monly treat it with anticonvulsant medication to reducespiking activity.
E l e c t r o e n c e p h a l o g r a p h y a n d N e u r o p s y c h o l o g y
EEG is a safe, painless, and relatively simple procedure.Its use in neuropsychology has been disappointing andlimited historically by a lack of relationship between EEGparameters and behavior, specifically indices of higher
CHAPTER 2 | Methods of Investigating the Brain 43

44 PART ONE | Introduction
cortical functioning. In fact, complex EEG waveforms donot change much during different kinds of sensory input,but appear to be most sensitive to the general arousal levelof the brain (Penfield & Jasper, 1954). This lack of con-vergence between EEG activity and behavior is probablycaused by the fact that the EEG is a relatively nonspecificmeasure of the underlying brain activity. Thus, using thetraditional eight-channel EEG, researchers have estab-lished only general relationships related to right versus lefthemisphere differences, or to posterior and anterior re-gions of the cortex.
EEG does not give an account of what a person isthinking; rather, it tells us if the person is thinking.Over recent years, more sophisticated recording equip-ment and computer analysis have refined the EEG. In-vestigators have been using increased numbers of elec-trodes (64, 128, and even up to 256) placed over thepatient’s entire head to correlate specific neural net-works involved in a particular neuropsychological task.Such enhanced EEGs have greatly improved signalquality and localization.
One invention that examines the more dynamic as-pects of electrophysiologic activity in the brain is brainelectrical activity mapping (BEAM) (Duffy, 1989). CTshows the structure of brain tissue, and PET scans (seelater) let researchers and clinicians examine the pattern ofbrain biochemistry and metabolism. BEAM, in contrast,uses computer technology to provide color-coded map-ping of the brain’s electrical activity in real time, that is, asquickly as it is occurring in the patient’s brain. In general,BEAM is nothing more than a way of enhancing theamount of information available on a standard EEG.Using an automated, integrated approach to EEG, thecomputer can calculate color-coded maps of electricalbrain activity (Figure 2.10). Then it codes computed EEGparameters as topographic displays showing neuroelectricactivity across the cortex while the patient is performing aneuropsychological task. BEAM is much more sensitiveto electrical correlates of cognitive tasks than the tradi-tional EEG. Quantitative EEG analysis also has shownsome promise in the diagnosis of clinical disorders such asdyslexia, a reading disorder.
Other improvements in EEG technology entail merg-ing the temporal resolution of EEG with the anatomic de-tail of MRI or the ability of PET to localize function. Suchcoregistration of different approaches to represent thefunctioning brain has resulted in multimodal approachesto neuroimaging, often providing new insights, as well ascorroborating established findings. For example, schizo-phrenics show abnormal, less active BEAMs and PETscans (less metabolism) in the frontal regions of the brain.
E V O K E D P O T E N T I A L
A further electrophysiologic diagnostic test is evoked po-tential (EP; also called event-related potential [ERP] ). EPinvolves artificial stimulation of sensory fibers that, inturn, generate electrical activity along the central and pe-ripheral pathways, as well as the specific primary receptiveareas in the brain. In contrast with EEG, EP is dependenton a stimulus and is most useful for assessing the integrityof the visual, auditory, and somatosensory pathways atspecific regions of the brain. EEG technology can recordthe electrical activity in response to a stimulus or event.During the traditional EEG, the overall background ac-tivity of the cerebral cortex hides specific sensory stimuli.In EP, a computer makes it possible to visualize thechanges in EEG responses to a specific stimulus (visual,auditory, or somatosensory), canceling out random elec-trical activity, but displaying electrical activity related tothe potential evoked by the stimulus. The resulting EPconsists of a series of positive and negative changes lastingfor about 500 milliseconds after the stimulus ceases. Thediagnostician analyzes the EP according to amplitude, la-tency, and the location of the specific brain region wherethe stimulus is processed.
B r a i n s t e m A u d i t o r y - E v o k e dR e s p o n s e
In brainstem auditory-evoked response (BAER), the ex-aminer presents clicks to each ear of the patient individu-ally via headphones. In response to the auditory stimulus,the auditory pathways generate an electrical signal along
Figure 2.10 Schizophrenic subject with history ofseizures was examined by electroencephalography andmagnetic resonance imaging (MRI) to observe extent ofabnormal activity during a seizure (left). Color-coded brainelectrical activity mapping (BEAM) presentation, with redindicating increased neuronal activity in the left frontal lobe(right). Results from BEAM superimposed over three-dimensional MRI cortex indicate abnormal discharge in leftfrontal lobe; note also widening sulci. See inside covers forcolor image. (Courtesy Dorota Kozinska, Ph.D., University of Warsaw, Warsaw, Poland.)

the central auditory pathways. EEG recording consists offive distinct waves that represent different latencies relatedto five nuclei groups where the auditory signal is beingintegrated. Although this delay is short, the examiner canmeasure and amplify it. Abnormal delays in responses,measured in milliseconds, often can pinpoint specific le-sions, but only along the pathways measured. The BAERcan diagnose a malfunction of the auditory nerve at thecochlear nucleus, the superior olive, the lateral lemniscus,and the inferior colliculus (Figure 2.11).
In BAER, five characteristic waves are recorded. Wave Ireflects activity of the vestibular nerve; wave II, the cochlearnucleus; wave III, the superior olivary complex; and wavesIV and V, the pons or lower midbrain. Decreased ampli-tudes, the absence of a wave, or prolonged interwave laten-cies may point to abnormal brainstem responses.
Approximately 50% of patients with multiple sclerosisdemonstrate a pathologic BAER typically at the level of thebrainstem. BAER has also aided in diagnosing patients withacoustic neuromas (tumors). Research using EP indicatesthat schizophrenics, compared with healthy subjects,demonstrate an abnormality that may indicate a deficit inthe “sensory gating” at the brainstem level, which may re-sult in impaired attention (Cullum et al., 1993). Research-ers can then confirm the finding using neuropsychologicalmeasures of attention, sustained concentration, and digitvigilance (e.g., digit cancelation). As with many of the other
imaging techniques featured in this chapter, there are inter-esting implications and a promising future in the interrela-tionships between neurophysiologic and neuropsychologi-cal indices of brain function. Neuropsychology in Action2.1 reviews a case example using BAER technology.
V i s u a l - E v o k e d R e s p o n s e
Similar to the auditory-evoked response procedure, invisual-evoked response (VER), the examiner presents a vi-sual stimulus separately to each eye of the patient. An al-ternating light/dark reversing checkerboard pattern pro-vides the visual stimulus. EEG responses are recordedfrom electrodes over the parietal and occipital regions.One wave originates in the receptive visual cortex and ismeasured using EEG technology. A normal delay fromthe presentation of the visual stimulus to the registra-tion of the electrodes over the occipital cortex is about100 milliseconds. Lesions along the visual nerve pathwaysresult in abnormal delays, decreased amplitude of therecorded response, or both.
S o m a t o s e n s o r y - E v o k e d R e s p o n s e
In somatosensory-evoked response (SER), the examinerstimulates peripheral nerves via an electrode placed overthe median nerve at the patient’s wrist. In addition, theexaminer places three electrodes for purposes of measure-ment, with the first two measuring peripheral electricalactivity of sensory pathways at the level of the patient’sarm and spinal cord. The third electrode is placed overthe patient’s contralateral somatosensory cortex. Abnor-malities in amplitude or latencies at the first two points ofmeasurement suggest peripheral nerve involvement. De-lays at the third wave suggest central sensory pathway in-volvement.
Figure 2.12 shows the graphic results of an SER exam-ination to evaluate somatosensory pathways in threedimensions. The technician delivers pulses transcuta-neously via a cup electrode to the median nerve at thepatient’s wrist. He or she adjusts the intensity of the stim-ulus to determine a painless muscle twitch of the thumb.Collected data are then transmitted to a computer foranalysis.
E L E C T R I C A L S T I M U L A T I O N
Historically, the electrical stimulation of nerve tissue isone of the oldest ways of investigating the living brain.Initially, scientists hoped that use of this technique couldchart a precise map of the cortex that would outline, akinto phrenology, the behavioral and cognitive properties ofthe brain, specifically the topography of the cortex.
CHAPTER 2 | Methods of Investigating the Brain 45
Auditorycortex
Medialgeniculate
++––
Superiorolive
Signalfromright ear
InferiorcolliculusCochlearnucleus
Signal fromleft ear
Figure 2.11 Auditory pathways from receptors in the earto the auditory cortex. Note the different nuclei along thepathways that form the basis for measuring integrationdelays, which can be measured and amplified using evokedpotential and electroencephalographic technology. (Repro-duced from Kalat, J. W. [1998]. Biological psychology[6th ed., p. 184, Figure 7.6]. Pacific Grove, CA: Brooks/Cole,by permission.)

46 PART ONE | Introduction
Surprisingly, this technique, which has been largely con-fined to the primary and sensory areas of the cortex, haselicited few positive responses (the generation of a mea-surable behavior). However, scientists have found a greatnumber of negative responses (disruption of function) asa result of electrical stimulation of the cortex.
For example, researchers easily demonstrated aphasia,a disruption of language functions, by numerous stimula-tions in different locations of the left hemisphere(Ojemann, 1980). More recently, neurologists have intro-duced electrical stimulation in the treatment of Parkin-son’s disease, based on the advances of stereotaxic opera-tions and knowledge of specific associations betweenelectrical stimulation and subcortical regions of the brain.Obviously, because of its invasive nature, direct electricalstimulation of the brain is not a routine diagnostic proce-dure. Primarily, researchers use it experimentally in clinicalcases for whom other interventions have not been suc-cessful. It can, however, provide great theoretical and clin-ical value in understanding the functions of the brain.
Figure 2.12 Sensory-evoked responses wereaveraged in a group of 10 healthy volunteersand superimposed onto the surface of a healthybrain. Images show electroencephalographicdistribution of sensory-evoked potential to rightmedian nerve, computed 18 milliseconds afterstimulus presentation. See inside covers forcolor image. (Courtesy Dorota Kozinska, Ph.D.,University of Warsaw, Warsaw, Poland.)
The patient is a 38-year-old man who wasemployed as a mechanic. Previously, he hadworked as a tile layer for 6 months, duringwhich he reported he was exposed to epoxy,alcohol, and other possibly toxic solvents.
Since then, he has reported dizziness andshort-term memory loss. Physicians subse-quently diagnosed him with chronic solventintoxication. An audiogram showed normalhearing bilaterally. An audiologist performedbrainstem auditory-evoked response (BAER)testing. Specifically, the tester presentedmonaural click stimulation in each ear at 70 dB using click rates of 11.4 and 57.7clicks/sec, with 2000 and 4000 repetitions,respectively. Absolute and interpeak latencies
in milliseconds at slow rate of 11.4 clicks/secfor waves I, III, and V were as follows:Note that the delays in milliseconds in-crease the further the signal is measuredfrom its initial detection in the ear (e.g., at
nuclei I, the vestibular nerve, the latency is1.5 milliseconds for the right ear; but atnuclei III, the superior olive, the signal wasmeasured 3.9 milliseconds after it was intro-duced to the right ear). Also, note the symmetrybetween right and left auditory processingroutes. BAER testing showed normal absoluteand interpeak latencies at slow and fast rates inthe right ear for waves I through III. Findings forthe left ear demonstrated delayed absolutelatencies for waves III and V at the fast and slow
rates. The audiologist measured interpeakdelays at waves I to III for the slow and fast rates,and waves III to V and I to V for the fast rate.Interear absolute and interpeak latency differ-ences are within normal limits. Even though
there were minor variations among the brainwave recordings, the audiologist concludedthat the test results suggested a normal BAERnot consistent with brainstem dysfunction.Subsequent neuropsychological testing didshow neuropsychological impairment onvarious tasks of new learning and memory.BAER, however, ruled out the possibility thatthose cognitive deficits were related to brain-stem impairment, and they were thus mostlikely related to cortical dysfunction.
N e u r o p s y c h o l o g y i n A c t i o n 2 . 1
C a s e E x a m p l e o f B r a i n s t e m A u d i t o r y - E v o ke d Re s p o n s e
by Eric A. Zillmer
I III V I–III III–V I–V
RIGHT 1.50 3.90 5.87 2.40 1.97 4.37
LEFT 1.60 4.14 6.10 2.54 1.87 4.42

E L E C T R O M Y O G R A P H Y
Electromyography (EMG) is the electrical analysis ofmuscles. In EMG, diagnosticians perform a nerve con-duction study of a specific muscle to diagnose neuromus-cular disorders. Patients undergoing EMG receive deep-needle stimulation of a muscle, which the technicianmeasures electrophysiologically ventral (closer to thespinal cord) to the stimulation. The technician delivers anelectrical potential to a muscle, using a wire insertedwithin a hollow needle. The electrical activity is amplifiedand displayed graphically via an oscilloscope. At the basisof EMG is that a relaxed muscle is electrically silent. Dur-ing voluntary contraction, muscle action potentials arepresent.
EMG is an important medical diagnostic techniquethat aids in diagnosing peripheral nerve damage, becauseit can isolate the dysfunction to a specific sensorimotorunit, including a motor or sensory neuron, neuromusculartransmission, or the muscle cell itself. The procedure alsohelps substantiate the presence of intact sensorimotorpathways—for example, when hysteria or malingering issuspected. If Sigmund Freud had had this diagnostic testavailable, he could have proved that Anna O., the patientof his first famous published case study, was truly hysteri-cal and did not suffer from a neuromuscular disorder asshe complained. Anna O. actually was treated by Freud’smentor Breuer, but Freud wrote up her case. Anna O.’smotor functioning was normal, even though she com-plained of partial paralysis. Freud suspected this normalityanyway and concluded that Anna produced the paralysisof the arm hysterically, because of her unconscious wish toremain in the role of a patient and to receive daily visits byfamous doctors. Nevertheless, using EMG technology, hecould have diagnosed this much more efficiently, withoutneeding to develop elaborate psychoanalytic theories.
A variation on the preceding techniques is recordingan electric shock stimulus of a peripheral nerve and mea-suring the subsequent muscle contraction. This techniquecan test both motor and sensory nerves. Results assist inthe differential diagnosis of muscle disease and peripheralnerve damage. For example, in carpal tunnel syndrome, arelatively common peripheral nerve disorder with accompa-nying sensory deficits in the first three digits and weaknessof the thumb, there is a characteristic latency of muscle andnerve action potentials. Although most patients toleratethis procedure well, EMG is mildly uncomfortable be-cause pain accompanies the insertion of the needle intothe muscle. Table 2.4 reviews the most popular electro-physiologic procedures currently in use.
Imaging of Brain Metabolism
Since the 1980s, researchers have developed tech-niques for analyzing the brain that focus on measuring para-meters of regional brain physiology. Such techniques are re-lated to the biological fact that neurons have an activemetabolism that the cerebral blood supply provides. Specifi-cally, the delivery of oxygen and glucose to neurons dependson cerebral blood flow (CBF). If the metabolic needs of theactive neurons are high, the rate of CBF is correspondinglyhigher. In this manner, neurologists can study regional bloodflow while the patient is performing neuropsychologicaltasks. In contrast with CT, which provides a static represen-tation of brain structures, measuring regional blood flow pro-vides dynamic data on CBF and metabolic activity. Theimaging of brain metabolism, therefore, permits a completelydifferent approach to examining the brain.
R E G I O N A L C E R E B R A L B L O O D F L O W
Blood flow in the cerebral hemispheres varies with metab-olism and activity. It can be a sensitive index of thechanges in cellular activity in response to cognitive tasks
Electroencephalography (EEG): EEG is one of the oldest brain-monitoringtechniques. It measures the general electrical activity of the cortex. It is mostuseful in assessing, in real time, the overall arousal state in a person.Increased electrode placements and computer integration capabilities haveresulted in high-resolution EEG and BEAM (brain electrical activity mapping),a promising assessment and research tool of the electrical activity of neu-rons.
Evoked potential (EP): EP, or event-related potential (ERP), is similar to EEGin that it assesses an electrical signal, but is related to a specific auditory(brainstem auditory-evoked response), visual (visual-evoked response), orsensory event (somatosensory-evoked response). Evoked potential assess-ment provides not an evaluation of general brain activity, but a millisecond-by-millisecond record of a specific sensory process.
Electrical stimulation: Researchers have used electrical stimulation of nervetissue to empirically map pathways of the cortex. More recently, clinicianshave introduced electrical stimulation in the treatment of Parkinson’s dis-ease. Direct electrical stimulation of the brain, an invasive medical proce-dure, is used only in those cases for whom other interventions or diagnosticprocedures have not succeeded.
Electromyography (EMG): EMG is the electrical analysis of muscles, adiagnostic procedure useful in diagnosing peripheral nerve damage. Theprocedure, however, is uncomfortable because it requires insertion of aneedle into the muscle.
Table 2.4 Electrophysiologic Procedures
CHAPTER 2 | Methods of Investigating the Brain 47
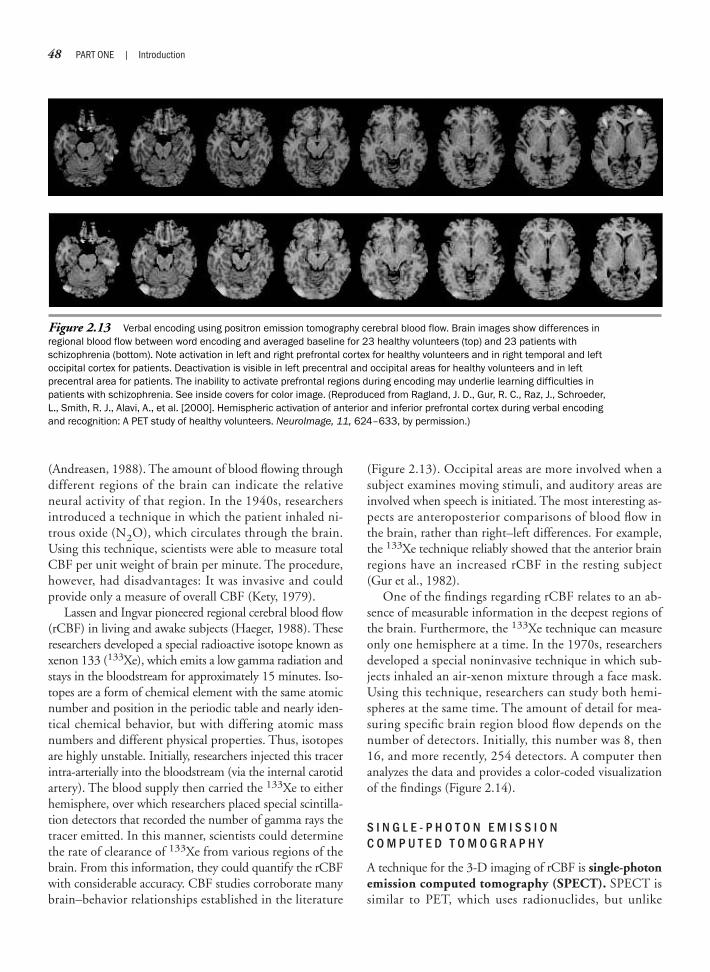
48 PART ONE | Introduction
(Andreasen, 1988). The amount of blood flowing throughdifferent regions of the brain can indicate the relativeneural activity of that region. In the 1940s, researchersintroduced a technique in which the patient inhaled ni-trous oxide (N2O), which circulates through the brain.Using this technique, scientists were able to measure totalCBF per unit weight of brain per minute. The procedure,however, had disadvantages: It was invasive and couldprovide only a measure of overall CBF (Kety, 1979).
Lassen and Ingvar pioneered regional cerebral blood flow(rCBF) in living and awake subjects (Haeger, 1988). Theseresearchers developed a special radioactive isotope known asxenon 133 (133Xe), which emits a low gamma radiation andstays in the bloodstream for approximately 15 minutes. Iso-topes are a form of chemical element with the same atomicnumber and position in the periodic table and nearly iden-tical chemical behavior, but with differing atomic massnumbers and different physical properties. Thus, isotopesare highly unstable. Initially, researchers injected this tracerintra-arterially into the bloodstream (via the internal carotidartery). The blood supply then carried the 133Xe to eitherhemisphere, over which researchers placed special scintilla-tion detectors that recorded the number of gamma rays thetracer emitted. In this manner, scientists could determinethe rate of clearance of 133Xe from various regions of thebrain. From this information, they could quantify the rCBFwith considerable accuracy. CBF studies corroborate manybrain–behavior relationships established in the literature
(Figure 2.13). Occipital areas are more involved when asubject examines moving stimuli, and auditory areas areinvolved when speech is initiated. The most interesting as-pects are anteroposterior comparisons of blood flow inthe brain, rather than right–left differences. For example,the 133Xe technique reliably showed that the anterior brainregions have an increased rCBF in the resting subject(Gur et al., 1982).
One of the findings regarding rCBF relates to an ab-sence of measurable information in the deepest regions ofthe brain. Furthermore, the 133Xe technique can measureonly one hemisphere at a time. In the 1970s, researchersdeveloped a special noninvasive technique in which sub-jects inhaled an air-xenon mixture through a face mask.Using this technique, researchers can study both hemi-spheres at the same time. The amount of detail for mea-suring specific brain region blood flow depends on thenumber of detectors. Initially, this number was 8, then16, and more recently, 254 detectors. A computer thenanalyzes the data and provides a color-coded visualizationof the findings (Figure 2.14).
S I N G L E - P H O T O N E M I S S I O N C O M P U T E D T O M O G R A P H Y
A technique for the 3-D imaging of rCBF is single-photonemission computed tomography (SPECT). SPECT issimilar to PET, which uses radionuclides, but unlike
Figure 2.13 Verbal encoding using positron emission tomography cerebral blood flow. Brain images show differences inregional blood flow between word encoding and averaged baseline for 23 healthy volunteers (top) and 23 patients withschizophrenia (bottom). Note activation in left and right prefrontal cortex for healthy volunteers and in right temporal and leftoccipital cortex for patients. Deactivation is visible in left precentral and occipital areas for healthy volunteers and in leftprecentral area for patients. The inability to activate prefrontal regions during encoding may underlie learning difficulties inpatients with schizophrenia. See inside covers for color image. (Reproduced from Ragland, J. D., Gur, R. C., Raz, J., Schroeder,L., Smith, R. J., Alavi, A., et al. [2000]. Hemispheric activation of anterior and inferior prefrontal cortex during verbal encodingand recognition: A PET study of healthy volunteers. NeuroImage, 11, 624–633, by permission.)

CHAPTER 2 | Methods of Investigating the Brain 49
positron emission, SPECT does not require an expensivecyclotron (a device that can generate radioactive chemicalswith a short half-life, also known as radioactive isotopes) fortheir production. Radiologists can label biochemicals ofinterest with a radioactive compound whose gamma rayscan be picked up by detectors surrounding the brain.Using SPECT, it is possible to three-dimensionallyimage the distribution of a radioactively labeled contrastagent. As in CT, a computer analyzes the data and recon-structs a 3-D cross section of the emissions pattern. Thetracer is injected intravenously and crosses into the braintissue based on CBF. Using this technique, analysts canestimate CBF and blood volume. Researchers can studysubjects undergoing SPECT while they are engaged in aneuropsychological task; however, the tracer has a longhalf-life, and it is difficult to keep a subject in the samemental state for a long period. A further limitation isthat the tracer takes approximately 2 days to clear fromthe brain; thus, it is possible to obtain only a single ex-posure of the brain using SPECT. An advantage ofSPECT is that it is relatively inexpensive (it is referred toas “the poor person’s PET”). A further advantage is that
individuals can be imaged while they are sleeping or se-dated, a useful option with young children or unmanage-able patients. Thus, imaging studies that require multipleconditions typically are investigated by using the morecostly positron emission tomography (PET) technique.
P O S I T R O N E M I S S I O N T O M O G R A P H Y
Emission tomography is a new visualization techniquethat detects a diverse range of physiologic parameters, in-cluding glucose and oxygen metabolism, in addition toblood flow, by distributing a radioactively labeled sub-stance in any desired cross section of the head. Themethod of PET technology is intravenous injection of aradioactive tracer (specifically positron-emitting sub-stances) and subsequent scanning of the brain for radioac-tivity. In contrast with SPECT, the radioactive isotopesinjected with the PET procedure have a short half-life andcan attach to specific agents, such as glucose. Glucose, thebody’s fuel, mixes with blood to reach the brain. As men-tioned earlier, the metabolism of the human brain variesin relation to its activity. The more active a specific area ofthe brain is, the more glucose it uses. Thus, the restingbrain differs metabolically from the active brain. PET isthe only procedure by which researchers can examinethree-dimensionally the regional cerebral glucose use andoxygen metabolism in the living brain. PET analysts donot view the brain as a static structure, but investigate thedynamic properties of the brain (Raichle, 1983).
T e c h n i q u e
In the PET procedure, technicians administer radionu-clides intravenously that the subject’s brain tissue takesup. The radionuclei are unstable, because they have an ex-cess positive charge. When the radioactive tracer decays,it emits a positron that then travels a short distance (a fewmillimeters) before colliding with an electron. This colli-sion results in the emission of two photons traveling inopposite directions, generating energy that detectorsaround the scalp can measure (Figure 2.15). When twodetectors calculate photon absorption at the same approx-imate time, the computer assumes they originate from thesame collision and can then calculate the exact positionshowing neural “hotspots.” PET functions by calculatingmillions of counts from detectors and estimating their ori-gin. Using a subtraction technique, investigators can iso-late blood flow patterns related to specific mental tasks.Computed tomography allows researchers to calculate acount and the locations of these collisions (depending onthe type of radionuclide used, such as carbon 11, nitro-gen 13, oxygen 15, or fluorine 18) to generate a visual
Figure 2.14 Topographic display of resting regionalcerebral blood flow (rCBF) using an early system. Darkerareas signal high rCBF; lighter areas suggest low rCBF.(Reproduced from Kalat, J. W. [1998]. Biological psychology[6th ed., p. 109, Figure 4.33]. Pacific Grove, CA:Brooks/Cole. Courtesy Karen Berman and Daniel Wein-berger, National Institute of Mental Health.)
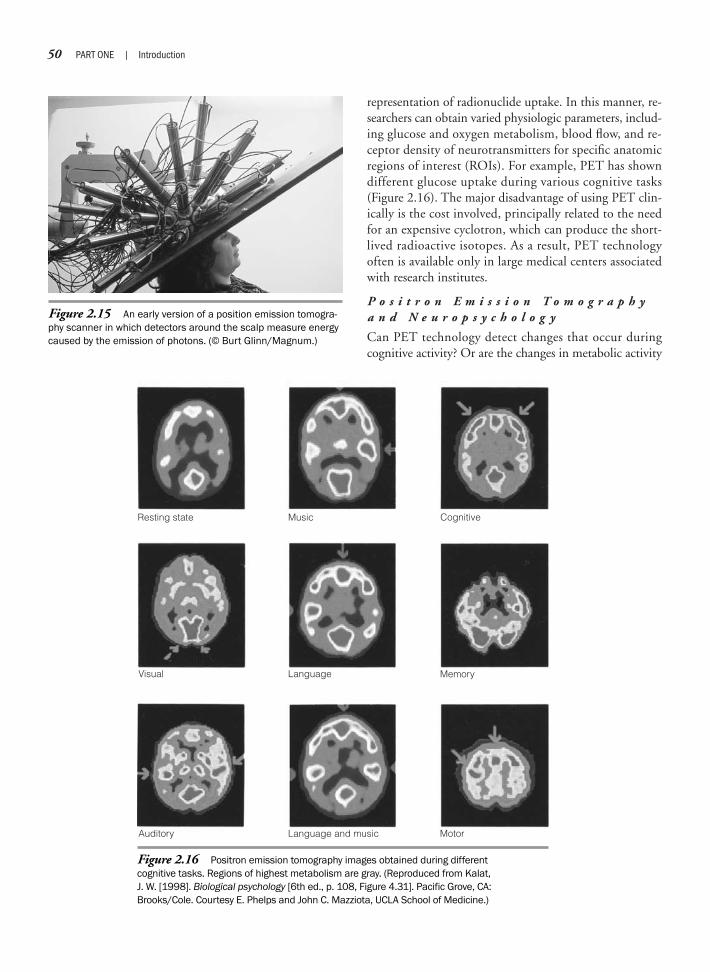
50 PART ONE | Introduction
representation of radionuclide uptake. In this manner, re-searchers can obtain varied physiologic parameters, includ-ing glucose and oxygen metabolism, blood flow, and re-ceptor density of neurotransmitters for specific anatomicregions of interest (ROIs). For example, PET has showndifferent glucose uptake during various cognitive tasks(Figure 2.16). The major disadvantage of using PET clin-ically is the cost involved, principally related to the needfor an expensive cyclotron, which can produce the short-lived radioactive isotopes. As a result, PET technologyoften is available only in large medical centers associatedwith research institutes.
P o s i t r o n E m i s s i o n T o m o g r a p h ya n d N e u r o p s y c h o l o g y
Can PET technology detect changes that occur duringcognitive activity? Or are the changes in metabolic activity
Figure 2.15 An early version of a position emission tomogra-phy scanner in which detectors around the scalp measure energycaused by the emission of photons. (© Burt Glinn/Magnum.)
Resting state Music Cognitive
Visual Language Memory
Auditory Language and music Motor
Figure 2.16 Positron emission tomography images obtained during differentcognitive tasks. Regions of highest metabolism are gray. (Reproduced from Kalat,J. W. [1998]. Biological psychology [6th ed., p. 108, Figure 4.31]. Pacific Grove, CA:Brooks/Cole. Courtesy E. Phelps and John C. Mazziota, UCLA School of Medicine.)

CHAPTER 2 | Methods of Investigating the Brain 51
too small to be detected? Measuring glucose metabolismrate is a more direct measure of neuron function thanis CBF. New tracers with a shorter half-life (such aspositron-labeled oxygen, O15) have led to investigationsof neuropsychological functions using PET, often withremarkable findings. Researchers use O15, which readilycrosses the blood–brain barrier, as a reference point forapproximate blood intake of various regions in the brain.PET research demonstrates that the effects of cognitiveeffort on regional brain activity can be detected andmeasured (e.g., a verbal task corresponds to the lefthemisphere and a spatial task to the right hemisphere).PET is also sensitive to individual differences, such assex, that affect the direction and degree of hemisphericspecialization for specific neuropsychological abilities.Thus, studies using imaging technology indicate that thereis a relationship between brain activity and behavior, andthat PET can detect these associations (Gur, Levy, &Gur, 1977).
A major finding using PET technology is that meta-bolic activity is suppressed in patients with a history ofhead trauma, brain tumors, and stroke, even thoughstructural representation of the brain, using MRI or CT,suggests intact brain anatomy. Thus, metabolic imagingof the brain can lead to a clearer understanding of thefunctioning brain, specifically where the pathology is un-clear, as in schizophrenics or epileptics. Although PET re-mains primarily a research tool because of its cost, it hasproved to be an important technique in measuring physi-ologic activity in the normal and damaged brain at rest orwhile engaging in behavior.
One of the most interesting research aspects of PETconcerns subjects performing various mental activities.Experimenters have taken PET scans of female and maleadult brains when subjects were either resting or solving arotating figure problem, a rather difficult spatial puzzle(Gur et al., 1982). Female subjects not only scored lowerthan male subjects, but there was a sex difference on thePET results. Even though the PET scans were not differ-ent while subjects were resting, when subjects were solv-ing the rotating figure problem, male brains showed max-imum neural activity in the right frontal area, whereasfemale brains demonstrated maximum activity in theright parietotemporal lobe. This suggests that men out-perform women on the rotation problem, and that theremay be a neural reason for this. There are, of course, tasksat which women outperform men. For example, womenare generally faster on tests that require perceptual speedand score higher than men on a test of verbal fluency inwhich one must list as many words as one can that beginwith the same letter (Lezak, Howieson, & Loring, 2004).
PET studies have generated much controversy regard-ing sex differences in the brain. Are there really functionaldifferences in the brain that arise from being male orfemale? The most recent studies indicate there are. Sometheorists suggest an evolutionary perspective by which sexdifferences in the brain might have come from differentskills needed by early humans. Male individuals withgood spatial skills, they argue, had an advantage in hunt-ing, and female individuals with good communicationskills had an advantage in child rearing (Springer &Deutsch, 1993).
But researchers have not established whether sex dif-ferences are related to differences in socialization andlearning experiences that are different for male and femaleindividuals, or whether the brains of female and male in-dividuals are organized differently and, therefore, func-tion differently. This controversy is not easily decided, butPET may shed light on this puzzle. Table 2.5 reviews themost frequently used imaging techniques based on brainmetabolism.
Magnetic Imaging Procedures
M A G N E T I C R E S O N A N C E I M A G I N G
Magnetic resonance imaging (MRI) is based on thework of Felix Bloch and Edward Purcell, who won theNobel Prize in physics in 1952 for their development of anew method of nuclear magnetic precision measurement.This led to the medical application of this technologycalled MRI during the early 1970s. Whereas CT usespenetrating X-ray radiation and PET uses radioactive
Single-photon emission computed tomography (SPECT): SPECT measuresblood flow, a correlate of brain activity. Because the radioactive tracer takesalmost 2 days to be eliminated from the body, researchers cannot use SPECTto monitor the brain’s mental activity “moment to moment.”
Positron emission tomography (PET): PET tracks blood flow, which isassociated with brain activity. It is primarily used to assess brain physiol-ogy, including glucose and oxygen metabolism, and the presence ofspecific neurotransmitters. The disadvantages of PET are that it is expen-sive, involves radiation, and renders low spatial resolution and data mustbe averaged over time (PET is not based on real time). The most promisinguse of PET has been its combined application with structural imagingtechniques, which can provide a remarkable tool for mapping brain loca-tion and function.
Table 2.5 Imaging of Brain Metabolism

52 PART ONE | Introduction
“Eric, your brain looks OK!” announces Dr. Jonathan “Yoni” Nissanov, ResearchProfessor of Biomedical Engineering andScience at Drexel University. It is 11:30 P.M.,and I am lying in a magnetic resonanceimaging (MRI) scanner at Drexel College ofMedicine in Philadelphia. Yoni has reservedthe million-dollar diagnostic tool for researchhe is conducting on functional imaging. Ihave agreed to be one of his test subjects.Because using the machine is expensive,research time is allotted only at night.
MRI is a relatively new diagnostic proce-dure that has been available for routine brainimaging only since the mid-1980s. Therefore,I am not surprised by the up-to-date, modernlook of the facility, a space age–like controlstation. Yoni and his research assistant, whoare operating the complex computerizedmachinery, greet me. My brain will be exposedto a strong magnetic field, so I must removeall metals that are on me, including my creditcards. The procedure is completely safe, I ambeing reassured. Yoni goes through his proto-col: “You don’t have a pacemaker? You don’thave an aneurysm clip? Is there any shrapnelin your head or metal plates in your skull?”Finally, Yoni asks, “You know the risks?” Yes,as a neuropsychologist I know them all toowell. The risks relate to the possibility that Imay find out something about my brain that Ido not necessarily want to know. The MRI willproduce textbook-quality anatomy pictures ofmy brain. Although the probability is small,there is the outside chance that the diagnosticprocedure may reveal a tumor or some otherabnormality of my brain. Just a month ago,one of my research colleagues learned thatshe had a malformation of her venous systemin her brain. She was also one of Yoni’s re-search participants. I repress these thoughtsas I enter the imaging suite. The layout of theMRI scanner consists of two rooms, which areconnected via intercom. The first one is thecontrol room, which features a rectangularwindow overseeing the second larger room,where an oversize, doughnut-shaped machineis placed. The control room has an assortment
of electronic gadgetry, the centerpiece being alarge TV-type console that controls the imagerand provides immediate visual feedback ofthe results. This is where Yoni and his assis-tant will remain during the procedure.
I lie on a stretcher-like surface, and at thepush of a button I am whisked via electricalmotors headfirst into the center of the largeelectromagnet. Yoni asked me earlier whetherI was claustrophobic, and now I understandwhy. There is only about an inch of spacearound my head, which is placed approxi-mately 4 feet within the center of the imager.
The small confines of the MRI machineare a significant problem for patients whosuffer from claustrophobia. I have been toldthat in the past such people were referred tothe animal MRI at the Philadelphia Zoo,which can accommodate large animals,before “open” MRI was developed. I amgrateful there is a small mirror positioned inan oblique angle right over my head, whichgives me the illusion of space, because I canlook out through the narrow opening towardmy feet. I can see Yoni behind the window inthe control room. “OK, we’re ready to start.”His voice reverberates through the intercomas a loud clicking noise begins.
For clinical diagnostic studies, theprocedure takes about 15 minutes, duringwhich the patient must remain as stationaryas possible. But Yoni wants to go through aseries of experiments during which I, oncommand, will clench my fists, right and leftalternately, to see how the MRI machinedetects functional activity in my brain. Yoniwill then superimpose the functional MRIdata, which reflect changes in blood oxy-genation in my motor cortex, over the struc-tural images of my brain. So I must keep myhead still all the time. Yoni constantly re-minds me of this over the intercom. I’veagreed to be in the imager for more than 90minutes. Given the confines of the space andthe incredibly loud, jackhammer-like, stac-cato noise, all of a sudden this does notseem like such a good idea, after all. The firsttask for Yoni is to establish a traditional MRI
study of my brain, a baseline. The loud clicksI hear are bombardments of radiofrequency(RF) on my brain, which has been placedunder a high magnetic field. The radio fre-quencies realign the magnetic fields ofbillions of hydrogen protons in my brain. TheMRI machine is tuned into the frequenciesthat the water molecules in my brain emitafter the external RF stops. The deflection orrealignment of this hydrogen map to themagnetic field can be detected, amplified,and recorded, and is the basis of the MRIprocess. Amazingly, I do not feel anything.
To be honest, I’ve thought about my MRIresults for some time. As a neuropsychologist,I know that my personality, my intellect—essentially who I am—depends on the integrityof my brain. What if they find somethingwrong? Wouldn’t a small change in the organi-zation of my brain almost guarantee an alteredsense of my reality? Haven’t I been actingrather eccentric lately? How would they breakthe news to me? Would a team of summoneddoctors rush in to announce, “There is aproblem with your brain”? I find myselfwondering how much training in psychologyphysicians receive for sharing diagnostic testresults with patients and their families.
After 15 minutes, Yoni steps into theimaging room to deliver his personal analysisof my brain. Although Yoni is a biomedicalengineer, I am greatly relieved when heannounces that my brain, on visual inspec-tion, looks “OK.” I have to remain in theincreasingly uncomfortable same positionfor the next 75 minutes as Yoni goes througha series of studies. But now I am excitedabout the thought of actually seeinganatomic pictures of my brain for the firsttime. I can hardly wait until the procedure isover and Yoni shows me the coronal imageson the control screen. Yes, everything is there,lateral ventricles, brainstem, cerebellum,and most importantly, my frontal lobes! I ama happy neuropsychologist as I leave thehospital at 1:30 A.M. with memory stick inhand, on which Yoni loaded an electroniccopy of my brain images.
N e u r o p s y c h o l o g y i n A c t i o n 2 . 2
U n d e r g o i n g a M a g n e t i c Re s o n a n c e I m a g i n g P r o c e d u r e
by Eric A. Zillmer

CHAPTER 2 | Methods of Investigating the Brain 53
isotopes, MRI is based on a fundamentally differentprocess, namely, that the hydrogen nucleus, which ispresent in high concentration in biological systems,generates alterations in a small magnetic field, whichcan be measured (Neuropsychology in Action 2.2).MRI provides pictures of anatomy superior to CT (Fig-ure 2.17), particularly for diagnosing underlying patho-logic disorders.
T e c h n i q u e
The principal technique involved in MRI is based onpatterns similar to the pattern a magnet makes on sur-rounding metal flakes. The metal flakes align themselvesaccording to the magnetic field. Similarly, when the headis subjected to a strong magnetic field, hydrogen pro-tons magnetize and align in the direction of the mag-netic field. A proton, which is an elementary particlepresent in all atomic nuclei, has a positive charge equalto the negative charge of an electron. A strong radio-frequency (RF) signal applied at a right angle to themagnetic field can alter the alignment of the hydrogenprotons. This radio wave sets the aligned hydrogen atomoscillating. The RF specifically selects only aligned hy-drogen atoms; other atoms will not react. Once the RFceases, the hydrogen “spins back” to its original
orientation as determined by the magnetic field, whichremains active.
The emission of a small RF signal accompanies thisdeflection, or spin back to equilibrium. That is, the re-turn of the hydrogen atoms to their previous orientationgenerates a magnetic field, which researchers can am-plify, measure, and record. Computer analysis can thenpresent a visualization of hydrogen density in various re-gions throughout the brain. Because water is present inmost biological tissue, this procedure can generate astrikingly accurate picture of the brain, or any otheranatomy.
The principle of MRI is that the hydrogen atom res-onates as a result of the combined effect of the radio wavesand the magnetic field. This frequency is specific for a givennuclear species in a magnetic field and allows scientists todetermine the origin of a given RF signal in space. For ex-ample, one measure of RF signal amplitude is hydrogendensity. Thus, variation of number of protons returning theRF signal is unique for different biological molecules, in-cluding fat, brain tissue, bone, and blood. This variationcontributes to the MRI contrast, allowing spatial detectionof signal data in 3-D space. As a result, researchers can accu-rately calculate brain tissue densities and can generate acomputer-constructed image, which is so spatially precisethat it can visualize structures as small as 1 mm.
There is one more major determinant of signal ampli-tude, namely, the magnetic relaxation times, also knownas T1 and T2. These are the time intervals necessary for anucleus to magnetize when placed in a magnetic field andthe delay before returning to its original equilibrium.Protons with short T1 values (solids) emit higher signalintensities and appear white on the MRI, whereas thosewith longer T1 values (fluids) appear dark. T2 measuresthe loss of the magnetic orientation (or spin) after RFperturbation. On T2-weighted images, nuclei with rela-tively long T2 values retain their signal strength, emit ahigher intensity signal, and appear brighter. Sometimes,the difference in T1 and T2 values may provide addi-tional visual information, such as differentiating tumorsand surrounding edema (swelling). More recently, 3-Dimages of the brain have been produced, based on MRItechnology. MR images are used as a starting point,specifically, MRI pixels in the X-Y plane resolution of thesubject’s original images. Using mathematic algorithms,a computer can generate a surface model of the scalp, aswell as the brain. The algorithms assume that a rigidbody transformation of objects can be matched. In thisway, it is suitable to align MRI data sets into one wholeobject. The result is an exact model of the brain in threedimensions (Figure 2.18).
Figure 2.17 Normal magnetic resonance image (coronalview). Note the symmetry of the lateral ventricles and den-sity differences between white and gray matter in the cortex.(Courtesy Eric Zillmer.)

54 PART ONE | Introduction
Blood oxygen level dependent (BOLD)magnetic resonance imaging (MRI) hasbecome synonymous with functional MRI(fMRI) and, largely because of its accessibil-ity, has grown to be the most widely usedfunctional neuroimaging technique in theexamination of human behavior. Put simply,fMRI is the measurement of blood flow inresponse to neural firing. The fMRI signal isbased primarily on the ratio of oxyhemoglo-bin to deoxyhemoglobin expressed as ahemodynamic response function, and thissignal is influenced by multiple factorsincluding blood flow, blood volume, andvessel size. fMRI provides excellent spatialresolution (on the order of millimeters) andgood temporal resolution (about 2000milliseconds). It is important to emphasizethat fMRI measures neither oxygen perfusionnor neural firing, but the hemodynamicresponse function that it does measure isreliable and well characterized.
Since the advent of fMRI, neuropsy-chology has been shaped and guided bynoninvasive means of accessing informa-tion about the brain. Understanding brainand behavior relationships has profitedgreatly from continued MRI advancements,including novel sequences that provideinformation about the structural, neu-rometabolic, and functional status of thebrain. The development of neuroimagingmethods that integrate information aboutboth structural and functional brain organi-zation in many ways has served to empha-size the role of neuropsychology in theclinical and cognitive neurosciences. Animportant reason for the integration ofneuropsychology and neuroimaging is thatinformation about brain status achievedthrough various imaging techniques isoften difficult to interpret without a behav-ioral reference point; that is, the criticaldependent variable is, and always has
been, human behavior. In functional imag-ing work, the role of the neuropsychologistis to provide expertise for the cognitive,motor, or sensory paradigm development,as well as the out-of-the-scanner interviewand assessment. These assessment com-ponents are critical to linking informationabout the cerebral substrate to humanbehavior. For these reasons, the neuropsy-chologist has become an important figurewithin many multidisciplinary teams usingneuroimaging techniques to better under-stand the effect of pathophysiology onhuman behavior. Moreover, although manynovel imaging techniques, such as fMRI,are only beginning to be used clinically, todate, the field of neuropsychology hasplayed an important role in the applicationand validation of these techniques inneurologically impaired samples (Figure 2.19).
N e u r o p s y c h o l o g y i n A c t i o n 2 . 3
N e w Fr o n t i e r s i n Fu n c t i o n a l M a g n e t i c Re s o n a n c e I m a g i n g
by Frank Hillary Ph.D., Pennsylvania State University
C l i n i c a l U s e
MRI of the central nervous system has provided behav-ioral scientists and neuroradiologists with revolutionaryquality of brain images in all planes (coronal, sagittal,and horizontal). As a result, MRI has become an im-portant diagnostic tool for detecting disease processes.This usefulness is related to that MRI is sensitive totissue alteration, including those seen in diseases associ-ated with demyelination (such as multiple sclerosis),hemorrhage (bleeding), and tumor. Because of its in-creased clinical use, MRI has become readily available,and mobile units have even been built that travel toremote hospitals.
MRI is a complex procedure based, in part, on molecu-lar physics and mathematics of imaging 3-D objects inspace. The principles underlying MRI sound complicated,and they are. Its scientific basis lies in physics and com-puter science; thus, an exact understanding of the proce-dure is not necessary for the neuropsychology student. But
Figure 2.18 Three-dimensional geometric align-ment of scalp surface. See inside covers for colorimage. (Courtesy Dorota Kozinska, Ph.D., University ofWarsaw, Warsaw, Poland.)

neuropsychologists are participating in the research usingthis technology because of their expertise in the functionalaspects of neuroanatomic structures, their knowledge ofneuropsychological tests, and their background in scien-tific methodology and design.
F u n c t i o n a l M a g n e t i c R e s o n a n c e I m a g i n g
Traditional MRI measures the frequencies of magneti-cally perturbed water molecules and provides a structuralrepresentation of the brain. More recent advances havefocused on detecting frequencies emitted from other mol-ecular species associated with cerebral metabolism. Effortshave concentrated on reconstructing images from glucosemetabolism and changes in blood oxygenation. A recentfinding is that oxygenated blood has slightly different mag-netic properties that special-sequence MRI scans can de-tect. In this manner, researchers can measure motor activ-ity and neuropsychological tests. The data from functionalMRI (fMRI) can then be superimposed (cross-sectioned
or co-registered) over the structural MRI for a precisemapping of structure and function. This combined use ofMRI and fMRI may revolutionize the study of the acti-vated brain, because it can provide almost continuousreal-time data on cerebral activity (Cohen, Noll, &Schneider, 1993).
The advantage of fMRI over SPECT, PET, and CT isthat there is no radiation exposure. Therefore, fMRI isless invasive. However, scientists do not completely knowthe effects of exposure of the brain to high magneticfields, which is higher in fMRI because molecules otherthan hydrogen are assessed. Furthermore, resolution offMRI is better than in PET images, which are recon-structed from thousands of calculations averaged over 90seconds, the half-life of the tracer. In contrast, fMRI canprovide independent images every few seconds or as fre-quently as the RF is turned on and off. This capabilitygives investigators a better picture-by-picture account ofthe neural correlates involved in specific tasks (Neuropsy-chology in Action 2.3).
CHAPTER 2 | Methods of Investigating the Brain 55
Figure 2.19 Functional magnetic resonance imaging signal response (percentagechange) from normal adult (a–c) and patient with severe traumatic brain injury (TBI) (d–f).(a, d) Motor response (i.e., finger tapping): note focal activation in healthy subject anddisorganization activation in TBI patient. (b, e) Normal cerebral blood flow: note diminishedcerebral blood flow in patient. (c, f) Corrected motor response based on baseline cerebralblood flow: note less organized activation in patient. See inside covers for color image.(Courtesy Frank Hillary, Ph.D., Pennsylvania State University.)

56 PART ONE | Introduction
M A G N E T O E N C E P H A L O G R A P H Y
Magnetoencephalography (MEG) involves measurementof changes in magnetic fields that are generated by under-lying electrical activity of active neurons. Neuronal activitygenerates not only electrical fields but also magneticfields. When neurons fire, the magnetic changes result-ing from the electrical fields, which reflect neural activ-ity, can be measured. Recording the magnetic fields thataccompany the electrical activity of neurons is known asMEG. MEG is the magnetic equivalent of EEG. Themagnetic field of neurons is small, and it requires specialsuperconducting coils, housed in elaborate magneticallyshielded rooms, to detect and measure the weak magneticfields. This specialized detector is called the superconduct-ing quantum interference device (SQUID), which is capa-ble of measuring tiny magnetic fields of the brain. MEGtraditionally has used systems with one to seven SQUIDsensors, although recent technology has made larger sensorarrays possible. The response of the brain to differentstimuli, similar to the EP technique, results in measur-able alterations in the magnetic field. A computer thencan calculate a 3-D location based on the source of themagnetic field in the brain. The physical location of themagnetic source can be improved by projecting the MEGonto MR images. MEG is more elaborate than EEG, butit can better localize the source of activity using isocon-tour maps of magnetic fields.
MEG is expensive and relies on complex technology;the SQUID is immersed in liquid helium to keep the sys-tem at a low temperature, which is necessary for super-conductivity. Currently, MEG is experimental and is notused for routine clinical diagnostic studies, althoughMEG is an added diagnostic tool in epilepsy, because itprovides more accurate seizure diagnosis than EEG tech-nology (Hari, 1994). Table 2.6 reviews current magneticimaging procedures.
Cerebrospinal Fluid Studies:Lumbar Puncture
The lumbar puncture, or spinal tap, is a medicaltechnique to collect a sample of CSF surrounding thespinal cord for diagnostic study. The patient lies on hisor her side in a fetal position, and the physician adminis-ters a local anesthetic. A long (3- to 3.5-inch) punctureneedle is inserted perpendicular between the third andfourth (or fourth and fifth) lumbar vertebrae. The needlepenetrates the dura and enters the spinal canal. Then thephysician collects CSF and checks CSF pressure (normal
range � 100 mm). In some cases, the physician adminis-ters radiopaque material or medication through the nee-dle, in which case, the CSF withdrawn is equal to thevolume of fluid introduced. At the end of the procedure,the physician withdraws the needle quickly. The lumbarpuncture is a relatively easy and routine way by which toobtain a CSF sample. Yet, lumbar puncture is invasiveand painful, requiring a local anesthetic, and infection isalways a concern.
On visual inspection, normal CSF is colorless and doesnot coagulate. After a subarachnoid hemorrhage (for ex-ample), the CSF may be stained with blood. Technicianstypically examine the CSF sample in a laboratory for cellcount, glucose levels, and protein content to detect CSFabnormalities. The lumbar puncture is a useful diagnosticaid for a variety of neurologic conditions in which theCSF has been “contaminated,” including acute and suba-cute bacterial meningitis, viral infections, brain abscess ortumor, multiple sclerosis, and hemorrhage.
Behavioral Examinations
N E U R O L O G I C E X A M I N A T I O N
The neurologic examination is a routine, introductory eval-uation that a neurologist performs. A neurologist is a physi-cian who has specialized in evaluating and treating neuro-logic disorders. Although there are many variations, inprinciple, the neurologic examination involves a detailed his-tory of the patient’s medical history and a careful assessmentof the patient’s reflexes, cranial nerve functioning, grossmovements, muscle tone, and ability to perceive sensory
Magnetic resonance imaging (MRI): MRI can provide the most detailedimages of brain structures. The obtained images are of excellent clarity, butindividuals who have metal in their bodies are contraindicated for theprocedure. Recent research focuses on the functional mapping of bloodflow or oxygenation using MRI. The advantage of functional MRI over otherfunctional procedures such as positron emission tomography is that itprovides good spatial resolution and images in short time periods or “realtime.”
Magnetoencephalography (MEG): MEG is the magnetic equivalent ofelectroencephalography, in which a computer can calculate a three-dimensional magnetic field of the brain. Superconducting quantum interfer-ence devices detect the small magnetic fields in the brain that are a markerof neural activity. A disadvantage of MEG is that it is expensive and notreadily available for clinical applications.
Table 2.6 Magnetic Imaging Procedures

CHAPTER 2 | Methods of Investigating the Brain 57
neuropsychological techniques. In addition, no imaging toolyet developed can indicate how patients will adapt with aspecific neurologic disorder, whether they will be able towork, or what quality of life they will have.
New Advances in ImagingTechniques: Mapping the Brain
S U B T R A C T I O N P R O C E D U R E S
Researchers often use the subtraction technique in imag-ing studies to isolate brain characteristics that are relevantduring a specific neuropsychological task. In principle, theprocedure uses two sets of data. The first set is obtainedusing the control condition. For example, to use PET instudying the neuronal aspects of a calculus task in the con-trol condition, researchers would ask subjects to recitenumbers that have no meaningful relationship to eachother. In the task condition, researchers obtain brain im-ages while subjects are performing calculus problems. Thelogic behind reciting numbers in the control task is thatboth tasks involve the neural mechanism of using num-bers, but only one condition uses numbers in a meaning-ful way. After researchers subtract the image of the noncal-culus condition from the second image they obtainedduring the calculus condition, the new picture shouldshow brain regions involved in the mathematical effort ofusing numbers in meaningful relationship to each other.
I M A G E A N A L Y S I S A N D Q U A N T I F I C A T I O N( T H R E E - D I M E N S I O N A L )
Recent advances in computer software have allowed 3-Dcomputer reconstruction of specific brain structures. Be-cause of recent advances in calculating volumetric analy-sis of specific brain structures, scientists applied segmen-tation methods to construct 3-D images, to visualize aspecific structure of the brain (such as ventricles) or aknown pathology (such as hemorrhage). Such 3-D im-ages advance the understanding of pathologic conditions,as well as brain structures, because scientists can now vi-sualize the site of the lesion from any angle or perspective.The ventricular system is difficult to appreciate in a 2-Dperspective, but in a 3-D model, it can be easily visual-ized. More recent quantitative imaging techniques haveautomated the evaluation of definable ROIs throughoutthe brain. Because normative data are not yet available,serial quantitative image examinations of individual caseshave proved useful. The correlation between quantitativeneuroimaging findings and neuropsychological indices ofbrain function has been only moderate.
stimuli. The neurologic examination typically includes anumber of brief cognitive procedures. These include lan-guage function, memory (e.g., remembering digits or mem-ory for words), visuospatial function (drawing), attention(reverse counting), and mental status (i.e., an assessment ofthe patient’s understanding of where he or she is, what timeit is, who he is, and why he is there). The neurologic exam-ination is not as detailed as a neuropsychological evalua-tion, because it is difficult to obtain an accurate compre-hensive assessment of higher cortical function during a briefexamination. More recently, a special focus in neurology,on behavior and higher cortical function (behavioral neu-rology), has overlapped more with neuropsychology. Ingeneral, the domains previously held by neurologists andby neuropsychologists are getting much closer, and bothdisciplines have much to learn from each other.
N E U R O P S Y C H O L O G I C A L E V A L U A T I O N
Whereas neurologists are interested in changes in the ner-vous system that occur within the clinical context (suchas lesions, disease, and trauma), neuropsychologists areprimarily interested in higher cognitive functioning. Luria(1990) suggests that neuropsychology is the most com-plex and newest chapter in neurology, without whichmodern clinical neurology would be unable to exist anddevelop. The neuropsychological evaluation providesadditional information about the patient’s health and isused, in conjunction with other pertinent information,for diagnosis, patient management, intervention, rehabil-itation, and discharge planning. Chapter 3 gives a detailedaccount of the role of the neuropsychological evaluation,its purpose, and its applications.
After reading this chapter, the student may wonderwhether modern imaging technology will soon replace neu-ropsychology. We strongly suggest that imaging technolo-gies and neuropsychology are compatible. In fact, we arenow in an era in which data from CT, for example, shouldbe used routinely with neuropsychology information. Notethat even though modern imaging technology has had spec-tacular success in depicting the brain’s anatomy, neuropsy-chological findings appear more sensitive to the progressionof degenerative diseases than either CT or MRI. Modernimaging technology is most useful in concert with neuropsy-chological studies. For example, consider a CT scan thatshows a large, marble-size tumor in the patient’s right pari-etal hemisphere. From a neurobehavioral view, we maymake certain assumptions about what cognitive functionsmay be compromised, based on the CT data. Such assump-tions, however, would be only hypothetical, and one wouldneed to assess the precise neurobehavioral sequelae using

58 PART ONE | Introduction
One procedure focuses on using volumetric MRIanalyses to estimate brain volume and ventricle-to-brainratio (VBR). A normal VBR is approximately 1.5%; thatis, about 1.5% of a normal, healthy, adult brain is dedi-cated to CSF. Increased VBR has been particularly consis-tent in subjects after traumatic brain injury, who havemuch higher VBR ratios, up to 4% (Johnson, Bigler,Burr, & Blatter, 1994). This increase is related to brainatrophy after the injury to the brain, with a correspond-ing increase of its ventricular space.
Furthermore, researchers can now digitize and super-impose serial MRI sections to create a 3-D picture of theentire head or brain or specific brain structures. This cur-rent technology can use 3-D representation of any isolatedbrain structure (Bigler, 1996). Other methods, includingSPECT, PET, quantitative EEG, and MEG, can also beused to generate 3-D images.
After establishing image analysis and quantification, thenext step was to address the interfacing of different imagingtechnologies to further explore structure and function inbrain-behavior relationships. For example, the high detail ofMRI-based images of the brain can be superimposed overimages derived from those obtained by PET. In this way, re-searchers can examine both structure and function simulta-neously. As technology develops further, it will be possibleto increase the combination and integration of imagingtechniques. Thus, one key focus in current imaging researchis integrating multifaceted data to understand regional brainfunction. In this manner, topographic information fromCT and MRI about the integrity of brain regions can com-plement information on regional brain physiologic activityderived from EEG, SPECT, and PET (Figure 2.20). How-ever, as with any research, neuropsychological theory isneeded to guide explorations of how brain activity relates tobehavior (Neuropsychology in Action 2.4).
F U T U R E D I R E C T I O N S
One of the greatest uncharted territories before thehuman species is the functional mapping of its own brain.Cartographers are scientists who use powerful technologyto examine the living brain right through the skull. Thetask is formidable: 100 billion neurons with a seeminglyinfinite number of interconnections. The human brain isthe most complex structure known in the entire universe.To make sense of this 3-pound “jungle” of cells, will it beenough to take pictures of the brain? Any new approachto brain mapping must move beyond simply visualizingstructure. The challenge before the cartographers of thenew millennium is to map function; that is, what brainstructures do what, and when. It is true that neuropsy-
chologists have identified many regions that specialize inparticular cognitive jobs, but they have gained much ofthis knowledge from people with brain pathology or in-jury. The new imaging technologies are capable of exam-ining the normal, healthy, functioning brain. We standon the brink of learning how the living, normal brain per-forms sophisticated mental functions.
The most exciting use of neuroimaging, we propose, isin combination with neuropsychological procedures. Thatneuroimaging measures and neuropsychological studiesdepend on shared neuroanatomy needs to be studied fur-ther. Thus, it is likely that scientists will combine mea-sures of neurophysiology and neuropsychology to unlockthe secrets of how the human brain functions. Further-more, imaging technologies will continue to be refined,with specific regard to the functional and structural as-pects of the brain. It will soon be possible to performbiochemical dissections on the human brain, to pinpointthe concentration of a neurotransmitter receptor withinthe brain of a living subject. It will be possible to examinethe effects of treatment of diseases known to be associatedwith disturbances in neurotransmitters or its receptors(e.g., schizophrenia, Parkinson’s disease, and Huntington’schorea).
New advances will also demonstrate brain activity frommoment to moment in real time with precise localization.
Figure 2.20 Sensory-evoked response examina-tion with magnetic resonance imaging. With thistechnique, electrical activity and anatomic detail canbe co-registered for clinical analysis. Image includesvisualization of right frontal tumor. See inside coversfor color image. (Courtesy Dorota Kozinska, Ph.D.,University of Warsaw, Warsaw, Poland.)
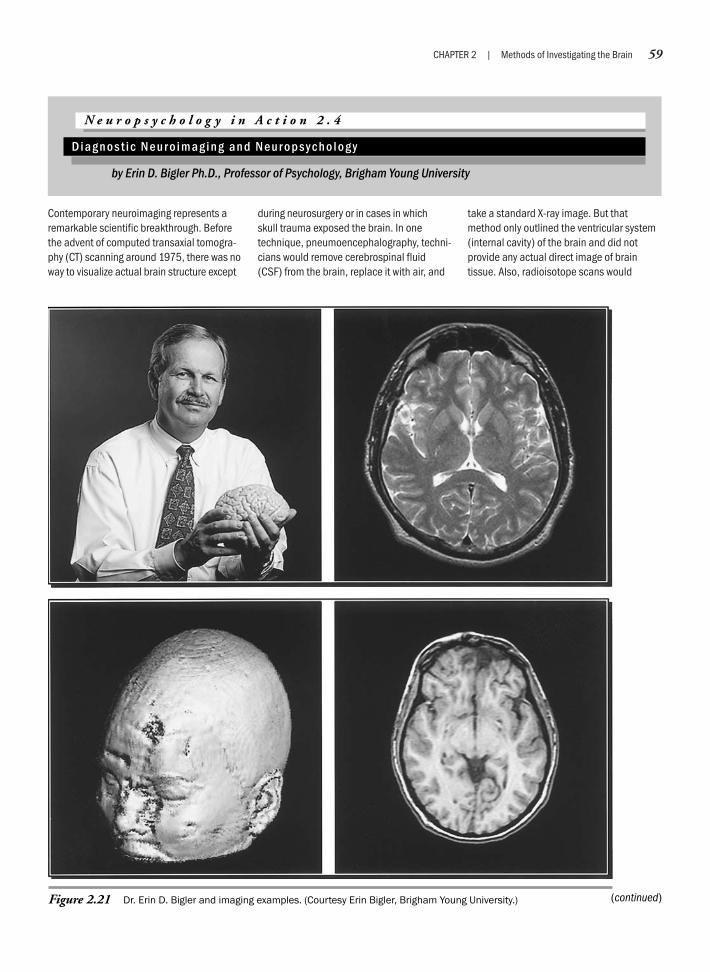
CHAPTER 2 | Methods of Investigating the Brain 59
Contemporary neuroimaging represents aremarkable scientific breakthrough. Beforethe advent of computed transaxial tomogra-phy (CT) scanning around 1975, there was noway to visualize actual brain structure except
during neurosurgery or in cases in whichskull trauma exposed the brain. In onetechnique, pneumoencephalography, techni-cians would remove cerebrospinal fluid(CSF) from the brain, replace it with air, and
take a standard X-ray image. But thatmethod only outlined the ventricular system(internal cavity) of the brain and did notprovide any actual direct image of braintissue. Also, radioisotope scans would
N e u r o p s y c h o l o g y i n A c t i o n 2 . 4
D i a g n o s t i c N e u r o i m a g i n g a n d N e u r o p s y c h o l o g y
by Erin D. Bigler Ph.D., Professor of Psychology, Brigham Young University
Figure 2.21 Dr. Erin D. Bigler and imaging examples. (Courtesy Erin Bigler, Brigham Young University.) (continued)

60 PART ONE | Introduction
measure uptake of a radiopharmaceutical,but could not visualize actual tissue. Thus, inthe early history of neurology and neuropsy-chology, the clinician had to rely on thepowers of inference to make conclusionsabout underlying brain pathology and neuro-logic disorders, because the brain could notbe viewed directly. Before the current state ofneuroimaging, knowing the patient’s history,an in-depth knowledge of brain anatomy andpathology, and examining the patients onstandard neurologic and neuropsychologicaltests allowed clinicians to make an inferenceabout particular brain regions that might beinvolved (damaged) or what type of diseaseprocess might be present. All this changedradically with the advent of modern brainimaging techniques. The CT scan was theforerunner for the development of magneticresonance imaging (MRI), which uses anentirely different technology. In scanning withCT technology, an X-ray beam passes throughthe head and various computer computations
create an index of tissue density. These tissuedensity values are then used to form an imageof the brain on a gray scale. MRI uses radiofre-quency waves that permit a reconstruction ofthe brain, essentially mimicking grossanatomy. The beauty of MRI is that scientistscan use it to acquire images of the brain in anyplane and in any angle or orientation.
For example, the first set of images inFigure 2.21 (top right) are of my brain(that’s me, holding a brain, in the top left).Viewing my brain in the horizontal (axial)position, you can see that the brain is asymmetric organ; therefore, a view of oneside should mirror the other side. In com-parison, just below my MRI scan is one froma patient who sustained severe traumaticbrain injury (TBI) in a motor vehicle acci-dent, with penetrating damage to thefrontal lobe. The lower left-hand quadrantshows the three-dimensional MRI recon-struction of the person’s head. You can seethe residual scars about the face and noseand the indentation that is in the frontal
region where the rearview mirror standpenetrated the skull and brain. Looking atthe horizontal (axial) view of this individ-ual’s brain in the bottom right-hand cornerand applying the principle of symmetry, youcan see the frontal (top) region of the brain,and on the right-hand side of the picture(the left side of the patient), a large area ofdegeneration in the frontal pole (areas inblack). This indicates necrosis or wasting ofthe brain. From the neuropsychologicalstandpoint, because the patient has pre-dominantly a frontal injury, you wouldexpect difficulties with complex reasoning,decision making, change in temperamentand personality, as well as alterations inmemory functioning. In fact, the patient’sneuropsychological studies demonstratesuch deficits. This is an excellent exampleof how brain imaging technology can inter-face with neuropsychological test findingsto establish the most accurate and specificassessment of behavioral and cognitivechanges in a patient with TBI.
The integration of different imaging technologies is onlyin its infancy. Scientists have yet to fully explore interrela-tionships among different neurodiagnostic procedures.The greatest potential of these tools may lie in assessingthe neuropsychological functions during neurophysiologic
procedures. The tools that appear most valuable at this timeare fMRI, MEG, quantitative EEG, PET, and SPECT. Thisdirection will lead to a multidimensional and increasinglycomprehensive approach to the functioning of the brain,bridging the gap between psychology and biology.
SummaryThe neuropsychology student may believe that the level of technology is so sophisticated that behavioraltechniques add little to the overall information about a human being. This is true to some extent, particu-larly in the area of diagnosis. The presence of tumors, stroke, and hydrocephalus is most easily, efficiently,and accurately discerned by modern imaging techniques. However, some diagnoses are so subtle and dif-fuse that only comprehensive neuropsychological tests can identify them. Although the neuropsychologist’srole in diagnosis has shrunk, behavioral techniques still play a major role in diagnosing early stages ofdementia or attention deficit disorder. Furthermore, sophisticated medical examination procedures cannotprovide a functional assessment of an individual, and certainly not an understanding of the patient’s qualityof life or perception thereof. A functional assessment is most effectively conducted by neuropsychologistsusing behavioral tools.
Moreover, remember that most of the outlined procedures provide a static picture of the brain, and thatneuropsychological dysfunction may extend considerably beyond the pathology that modern imaging tech-niques uncover. No doubt the alphabet soup of new imaging technologies has become a powerful tool in thestudy of brain–behavior relationships. But will this new technology fulfill what the phrenologists were unableto do, that is, create a precise functional map of the brain? Probably not. Many constraints hinder the use offunctional imaging in studying the human brain. For example, ultimately, the image rendered is not a directrepresentation of the mechanism involved in the mental activity, but some correlate. Furthermore, functional
(continued)
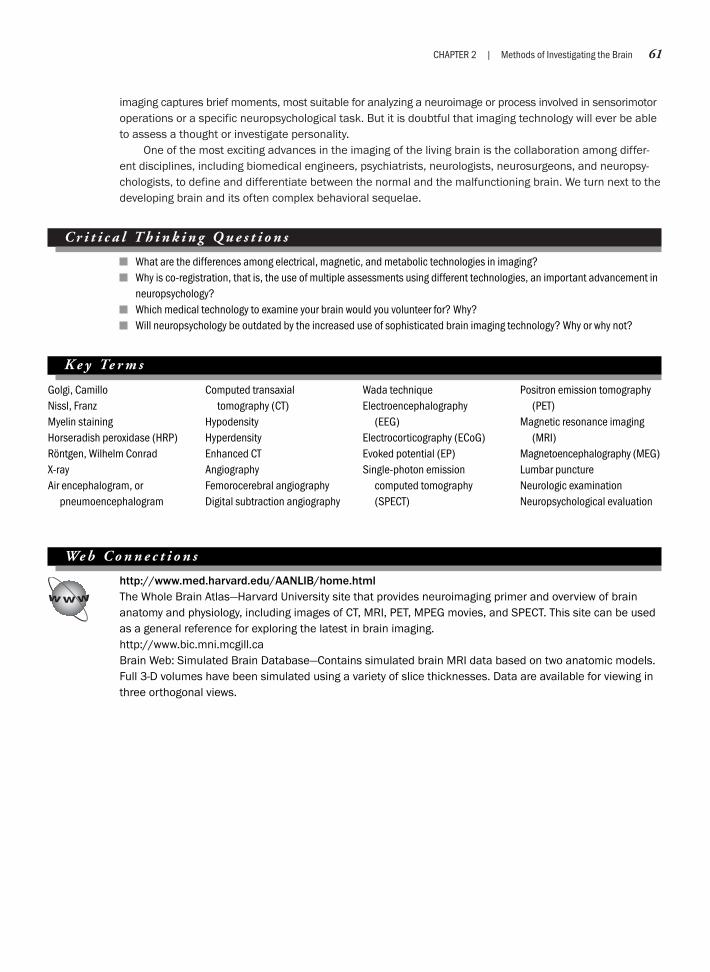
CHAPTER 2 | Methods of Investigating the Brain 61
imaging captures brief moments, most suitable for analyzing a neuroimage or process involved in sensorimotoroperations or a specific neuropsychological task. But it is doubtful that imaging technology will ever be ableto assess a thought or investigate personality.
One of the most exciting advances in the imaging of the living brain is the collaboration among differ-ent disciplines, including biomedical engineers, psychiatrists, neurologists, neurosurgeons, and neuropsy-chologists, to define and differentiate between the normal and the malfunctioning brain. We turn next to thedeveloping brain and its often complex behavioral sequelae.
C r i t i c a l T h i n k i n g Q u e s t i o n s
What are the differences among electrical, magnetic, and metabolic technologies in imaging?Why is co-registration, that is, the use of multiple assessments using different technologies, an important advancement inneuropsychology?Which medical technology to examine your brain would you volunteer for? Why?Will neuropsychology be outdated by the increased use of sophisticated brain imaging technology? Why or why not?
K e y Te r m s
Golgi, CamilloNissl, FranzMyelin stainingHorseradish peroxidase (HRP)Röntgen, Wilhelm ConradX-rayAir encephalogram, or
pneumoencephalogram
Computed transaxialtomography (CT)
HypodensityHyperdensityEnhanced CTAngiographyFemorocerebral angiographyDigital subtraction angiography
Wada techniqueElectroencephalography
(EEG)Electrocorticography (ECoG)Evoked potential (EP)Single-photon emission
computed tomography(SPECT)
Positron emission tomography(PET)
Magnetic resonance imaging(MRI)
Magnetoencephalography (MEG)Lumbar punctureNeurologic examinationNeuropsychological evaluation
We b C o n n e c t i o n s
http://www.med.harvard.edu/AANLIB/home.htmlThe Whole Brain Atlas—Harvard University site that provides neuroimaging primer and overview of brainanatomy and physiology, including images of CT, MRI, PET, MPEG movies, and SPECT. This site can be usedas a general reference for exploring the latest in brain imaging.http://www.bic.mni.mcgill.caBrain Web: Simulated Brain Database—Contains simulated brain MRI data based on two anatomic models.Full 3-D volumes have been simulated using a variety of slice thicknesses. Data are available for viewing inthree orthogonal views.

Chapter 3
NEUROPSYCHOLOGICAL ASSESSMENTAND DIAGNOSIS
The teacher is faced with the eternal dilemma, whether to present the clear,simple, but inaccurate fact, or the complex, confusing, presumptive truth.
—Karl Menninger
General Considerations in Neuropsychological TestingPsychometric Issues in Neuropsychological AssessmentNeuropsychological TestsInterpreting Neuropsychological Assessment Data
Neuropsychology in Action
3.1 Case Example: The Neuropsychology of Lyme Disease

CHAPTER 3 | Neuropsychological Assessment and Diagnosis 63
OverviewJeanne was a passenger on a motorcycle with her husband when at an intersection a car ran a stop sign andhit them. Although her husband received only minor injuries, Jeanne was thrown about 5 feet. Luckily, she waswearing a helmet. However, Jeanne thinks she must have been knocked out, because she does not rememberanything until the ambulance arrived. Emergency department personnel attended to her knee injury. She alsohad a terrible headache. Magnetic resonance imaging (MRI) did not detect any contusions or lesions. Thehospital released Jeanne that day and told her to see her general practitioner if she had any more problems.
Jeanne recovered for a week at home, and then went back to her job as a medical records clerk. Shealso returned to school to enroll in coursework for a nursing degree. First, she noticed that she often forgota client’s seven-digit medical record number between the time she looked at it and went next door to getthe chart. Her grades also started slipping. Before the accident, she was earning As and Bs; but on her firstbiology test a month after the accident, she received a D. She also continued to have headaches, which shehad not had before. Four months after her injury, after several visits to her general practitioner and a neu-rologist, neither of whom could find anything medically wrong with her, her practitioner referred her for aneuropsychological evaluation. The request was to evaluate Jeanne to determine whether she had suffereda brain injury as a result of her accident or if her symptoms might be a psychosomatic reaction, that is,related to increased stress in dealing with the accident and the aftermath.
What can neuropsychology offer Jeanne? Many people who have head injuries or suffer whiplash injuriesin car accidents, sports injuries, or falls may have a brief lapse of consciousness. They may feel temporarilyconfused or disoriented. They may or may not go to a doctor or to the hospital, and if they do, they are usuallyreleased after a brief observation. Computed transaxial tomography (CT) or MRI results are quite likely to benegative for any small or microscopic contusions or lesions. Only after going home and trying to resume thenormal tasks of working or going to school may someone such as Jeanne feel unable to concentrate or oftenforget things. The person may have other odd symptoms that he or she does not understand, such as becomingmore easily frustrated or just not feeling “herself.” If these problems do not resolve and the person is persistent,or the physician perceptive, then the physician should make a referral for neuropsychological testing.
K e e p i n M i n d
What do clinical neuropsychologists do?
How is clinical neuropsychology distinguishable from clinical psychology or from neurology?
What makes a neuropsychological test reliable and valid?
What different roles do neuropsychologists play?
What individual differences influence neuropsychological test interpretation?
How can a neuropsychologist improve a patient’s quality of life?
General Considerations in Neuropsychological Testing
This chapter describes the most frequently used as-sessment techniques in neuropsychology and outlines thescientific and theoretical principles of neuropsychologicalmeasurement. We stress that clinical neuropsychologists
use a number of different methods to evaluate and treatindividuals with brain dysfunction. Simply put, neu-ropsychologists are foremost clinical psychologists whohave specialized in neuropsychological conceptualizationsand methods. For neuropsychologists to understand theindividual, they must view psychology as the expressionof neuropsychology. From this perspective, neuropsychol-ogy is a broad field, and the neuropsychologist’s roles span
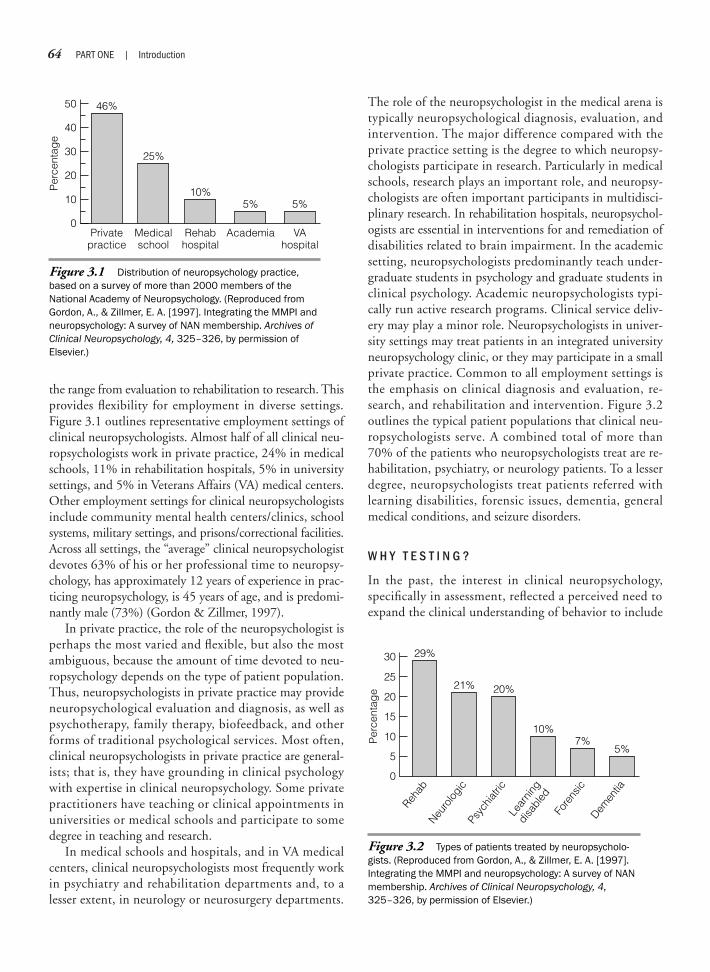
64 PART ONE | Introduction
the range from evaluation to rehabilitation to research. Thisprovides flexibility for employment in diverse settings.Figure 3.1 outlines representative employment settings ofclinical neuropsychologists. Almost half of all clinical neu-ropsychologists work in private practice, 24% in medicalschools, 11% in rehabilitation hospitals, 5% in universitysettings, and 5% in Veterans Affairs (VA) medical centers.Other employment settings for clinical neuropsychologistsinclude community mental health centers/clinics, schoolsystems, military settings, and prisons/correctional facilities.Across all settings, the “average” clinical neuropsychologistdevotes 63% of his or her professional time to neuropsy-chology, has approximately 12 years of experience in prac-ticing neuropsychology, is 45 years of age, and is predomi-nantly male (73%) (Gordon & Zillmer, 1997).
In private practice, the role of the neuropsychologist isperhaps the most varied and flexible, but also the mostambiguous, because the amount of time devoted to neu-ropsychology depends on the type of patient population.Thus, neuropsychologists in private practice may provideneuropsychological evaluation and diagnosis, as well aspsychotherapy, family therapy, biofeedback, and otherforms of traditional psychological services. Most often,clinical neuropsychologists in private practice are general-ists; that is, they have grounding in clinical psychologywith expertise in clinical neuropsychology. Some privatepractitioners have teaching or clinical appointments inuniversities or medical schools and participate to somedegree in teaching and research.
In medical schools and hospitals, and in VA medicalcenters, clinical neuropsychologists most frequently workin psychiatry and rehabilitation departments and, to alesser extent, in neurology or neurosurgery departments.
The role of the neuropsychologist in the medical arena istypically neuropsychological diagnosis, evaluation, andintervention. The major difference compared with theprivate practice setting is the degree to which neuropsy-chologists participate in research. Particularly in medicalschools, research plays an important role, and neuropsy-chologists are often important participants in multidisci-plinary research. In rehabilitation hospitals, neuropsychol-ogists are essential in interventions for and remediation ofdisabilities related to brain impairment. In the academicsetting, neuropsychologists predominantly teach under-graduate students in psychology and graduate students inclinical psychology. Academic neuropsychologists typi-cally run active research programs. Clinical service deliv-ery may play a minor role. Neuropsychologists in univer-sity settings may treat patients in an integrated universityneuropsychology clinic, or they may participate in a smallprivate practice. Common to all employment settings isthe emphasis on clinical diagnosis and evaluation, re-search, and rehabilitation and intervention. Figure 3.2outlines the typical patient populations that clinical neu-ropsychologists serve. A combined total of more than70% of the patients who neuropsychologists treat are re-habilitation, psychiatry, or neurology patients. To a lesserdegree, neuropsychologists treat patients referred withlearning disabilities, forensic issues, dementia, generalmedical conditions, and seizure disorders.
W H Y T E S T I N G ?
In the past, the interest in clinical neuropsychology,specifically in assessment, reflected a perceived need toexpand the clinical understanding of behavior to include
50
Per
cent
age
40
30
20
10
0Private
practice
46%
Medicalschool
25%
Rehabhospital
10%
Academia
5%
VAhospital
5%
Figure 3.1 Distribution of neuropsychology practice,based on a survey of more than 2000 members of theNational Academy of Neuropsychology. (Reproduced fromGordon, A., & Zillmer, E. A. [1997]. Integrating the MMPI andneuropsychology: A survey of NAN membership. Archives ofClinical Neuropsychology, 4, 325–326, by permission ofElsevier.)
30
Per
cent
age
0
Rehab
29%
Neuro
logi
cPs
ychi
atric
Lear
ning
disa
bled
Fore
nsic
Demen
tia
21% 20%
10%7%
5%
25
20
15
10
5
Figure 3.2 Types of patients treated by neuropsycholo-gists. (Reproduced from Gordon, A., & Zillmer, E. A. [1997].Integrating the MMPI and neuropsychology: A survey of NANmembership. Archives of Clinical Neuropsychology, 4,325–326, by permission of Elsevier.)
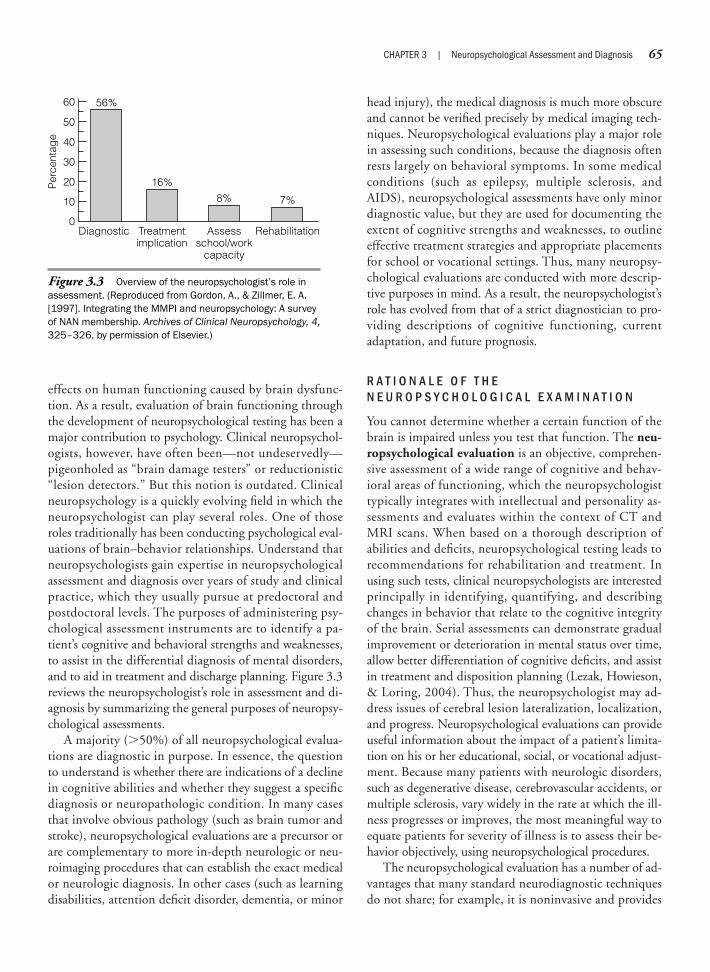
effects on human functioning caused by brain dysfunc-tion. As a result, evaluation of brain functioning throughthe development of neuropsychological testing has been amajor contribution to psychology. Clinical neuropsychol-ogists, however, have often been—not undeservedly—pigeonholed as “brain damage testers” or reductionistic“lesion detectors.” But this notion is outdated. Clinicalneuropsychology is a quickly evolving field in which theneuropsychologist can play several roles. One of thoseroles traditionally has been conducting psychological eval-uations of brain–behavior relationships. Understand thatneuropsychologists gain expertise in neuropsychologicalassessment and diagnosis over years of study and clinicalpractice, which they usually pursue at predoctoral andpostdoctoral levels. The purposes of administering psy-chological assessment instruments are to identify a pa-tient’s cognitive and behavioral strengths and weaknesses,to assist in the differential diagnosis of mental disorders,and to aid in treatment and discharge planning. Figure 3.3reviews the neuropsychologist’s role in assessment and di-agnosis by summarizing the general purposes of neuropsy-chological assessments.
A majority (�50%) of all neuropsychological evalua-tions are diagnostic in purpose. In essence, the questionto understand is whether there are indications of a declinein cognitive abilities and whether they suggest a specificdiagnosis or neuropathologic condition. In many casesthat involve obvious pathology (such as brain tumor andstroke), neuropsychological evaluations are a precursor orare complementary to more in-depth neurologic or neu-roimaging procedures that can establish the exact medicalor neurologic diagnosis. In other cases (such as learningdisabilities, attention deficit disorder, dementia, or minor
head injury), the medical diagnosis is much more obscureand cannot be verified precisely by medical imaging tech-niques. Neuropsychological evaluations play a major rolein assessing such conditions, because the diagnosis oftenrests largely on behavioral symptoms. In some medicalconditions (such as epilepsy, multiple sclerosis, andAIDS), neuropsychological assessments have only minordiagnostic value, but they are used for documenting theextent of cognitive strengths and weaknesses, to outlineeffective treatment strategies and appropriate placementsfor school or vocational settings. Thus, many neuropsy-chological evaluations are conducted with more descrip-tive purposes in mind. As a result, the neuropsychologist’srole has evolved from that of a strict diagnostician to pro-viding descriptions of cognitive functioning, currentadaptation, and future prognosis.
R A T I O N A L E O F T H EN E U R O P S Y C H O L O G I C A L E X A M I N A T I O N
You cannot determine whether a certain function of thebrain is impaired unless you test that function. The neu-ropsychological evaluation is an objective, comprehen-sive assessment of a wide range of cognitive and behav-ioral areas of functioning, which the neuropsychologisttypically integrates with intellectual and personality as-sessments and evaluates within the context of CT andMRI scans. When based on a thorough description ofabilities and deficits, neuropsychological testing leads torecommendations for rehabilitation and treatment. Inusing such tests, clinical neuropsychologists are interestedprincipally in identifying, quantifying, and describingchanges in behavior that relate to the cognitive integrityof the brain. Serial assessments can demonstrate gradualimprovement or deterioration in mental status over time,allow better differentiation of cognitive deficits, and assistin treatment and disposition planning (Lezak, Howieson,& Loring, 2004). Thus, the neuropsychologist may ad-dress issues of cerebral lesion lateralization, localization,and progress. Neuropsychological evaluations can provideuseful information about the impact of a patient’s limita-tion on his or her educational, social, or vocational adjust-ment. Because many patients with neurologic disorders,such as degenerative disease, cerebrovascular accidents, ormultiple sclerosis, vary widely in the rate at which the ill-ness progresses or improves, the most meaningful way toequate patients for severity of illness is to assess their be-havior objectively, using neuropsychological procedures.
The neuropsychological evaluation has a number of ad-vantages that many standard neurodiagnostic techniquesdo not share; for example, it is noninvasive and provides
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 65
60
Per
cent
age
0Diagnostic
56%
Treatmentimplication
16%
Assessschool/work
capacity
8%
Rehabilitation
7%
50
40
30
20
10
Figure 3.3 Overview of the neuropsychologist’s role inassessment. (Reproduced from Gordon, A., & Zillmer, E. A.[1997]. Integrating the MMPI and neuropsychology: A surveyof NAN membership. Archives of Clinical Neuropsychology, 4,325–326, by permission of Elsevier.)

66 PART ONE | Introduction
descriptive information about the patient. Specific testsused in neuropsychological assessment batteries may vary,although most assessments include objective measures ofintelligence, academic achievement, language function-ing, memory, new problem solving, abstract reasoning,constructional ability, motor speed, strength and coordi-nation, and personality functioning (Zillmer & Greene,2006).
You can conceptualize neuropsychological assessmentas a method of examining the brain by studying its be-havioral product. Because the subject matter of neuropsy-chological assessment is behavior, it relies on many of thesame techniques and assumptions as traditional psycho-logical assessment. As with other psychological assess-ments, neuropsychological evaluations involve the inten-sive study of behavior by means of standardized tests thatprovide relatively sensitive indices of brain–behavior rela-tionships. Neuropsychological tests have been used on anempirical basis in various medical and psychiatric settings,are sensitive to the organic integrity of the cerebral hemi-spheres, and can often pinpoint specific neurologic or psy-chological deficits. Neuropsychological assessment hasalso become a useful tool for clinical service delivery andfor research regarding the behavioral and cognitive aspectsof medical disorders.
A P P R O P R I A T E R E F E R R A L S F O RN E U R O P S Y C H O L O G I C A L E V A L U A T I O N
Because a neuropsychological workup may take from30 minutes to 8 hours of professional time, health practi-tioners should request consultations with some discrimi-nation for cost-effectiveness and utility. The interpreta-tion and diagnosis of the patient’s profile ultimatelydepends on the referral question, the neuropsychologist’stest selection, and the process by which the neuropsychol-ogist interprets the data. Referrals should specify exactlywhat questions or problems prompted the referral, whatthe referral source hopes to obtain from the consultation,and the purpose for which the referrer will use the infor-mation. The advanced student in neuropsychology oftenfeels frustrated by the failure of medical professionals togive a clear referral question. Note, however, that generat-ing appropriate referral questions, as well as questionsfrom the patient about the goals of the evaluation, is theresponsibility of the neuropsychologist. Thus, it is oftennecessary to educate the professional community aboutthe purpose and goals of a neuropsychological evaluation.Having the patients themselves ask specific questionsabout the goals of the evaluation (e.g., whether they cango back to work) often makes the evaluation process more
meaningful to patients, and typically motivates them toput forth a good effort.
In a medical setting, the neuropsychologist is mosthelpful to the treatment team as a neurobehavioral de-scriber of functional strengths and weaknesses, as well as aprovider of neurodiagnosis. As mentioned earlier, suchdisorders as mild head injuries, early stages of Alzheimer’sdementia, or learning disabilities may show no symptomsbeyond the cognitive dysfunction that formal neuropsy-chological testing assesses so well. Following is a listing ofinstances in which a neuropsychological consultation isgenerally useful:
Differential neurologic diagnosis
Acute versus static
Focal versus diffuse
Location of damage
Establishment of a baseline for neuropsychologicalperformance from which future evaluations can assessimprovement or deterioration
Descriptions of the effects of brain dysfunction onbehavior
Determinations of disability levels for compensationin personal injury litigation
Evaluation of vocational potential
Assessment of environmental needs after dischargefrom hospital (disposition planning)
Development of remedial methods for rehabilitationof the individual brain-damaged patient
Measurement of residual abilities during rehabilitation
Patient management
Psychometric Issues in Neuropsychological Assessment
The success of psychological testing procedures toassess and select individuals to become officers and under-take special assignments in World War I was the impetusfor some of the earliest recognition of psychology as a sci-entific field. Since then, the science of standardized clini-cal psychological testing has evolved to the point that thereare now hundreds of psychological assessment instrumentsin use today. It is important for the neuropsychology stu-dent to understand the scientific principles of psychologi-cal measurement before examining neuropsychologicalassessment instruments in more detail.

Psychometrics, the science of measuring human traitsor abilities, is concerned with the standardization of psy-chological and neuropsychological tests. A standardizedtest is a task or set of tasks administered under standardconditions and designed to assess some aspect of a person’sknowledge or skill. Standardized psychological tests typi-cally yield one or more objectively obtained quantitativescores, which permit systematic comparisons to be madeamong different groups of individuals regarding some psy-chological or cognitive concept. Most neuropsychologistsagree that tests are rarely used alone and are not interpretedin a vacuum. Almost always, neuropsychological tests areonly one of multiple components of information used tomake important decisions about an individual. Neuropsy-chological assessment, therefore, depends on the complexinterplay among the neuropsychologist, the patient, thecontext of the assessment, and the data from neuropsycho-logical testing.
R E L I A B I L I T Y
For any psychological test to be useful, it must be bothreliable and valid. Reliability is the stability or depend-ability of a test score as reflected in its consistency on re-peated measurement of the same individual. A reliabletest should produce similar findings on each administra-tion. If test scores show a great deal of variation when ad-ministered to the same individual on several occasions,the test scores are unreliable and there is concern abouterror. Interpretation of the scores becomes difficult. Thereare several different forms of reliability, including test-retest reliability, split-half reliability (the correlation be-tween two halves of the test), or internal consistency (thedegree to which items of a scale measure the same thing,also known as Cronbach’s alpha). Thus, the concept of re-liability is not as simple as it first appears, and test devel-opers must present substantial detail when making claimsof test reliability.
V A L I D I T Y
The validity of a test is the meaningfulness of specific in-ferences made from the test scores; that is, does the testreally measure what it was intended to measure? If a testis unreliable, it cannot be valid. For example, if you takethe same language test on three different days and obtainthree different scores, it is easy to conclude that there isno consistency and, therefore, the test cannot possibly beused to predict anything about your language abilities. Areliable test is not necessarily a valid one. Let us say a testwas purported to measure how well you make organized
extemporaneous speeches. The test requires you to generateas many words as you can in 1 minute. On three differentdays you took the test, and on three days you got a similarscore. The test has high reliability. But is it telling us aboutyour ability to make impromptu speeches? Not necessarily.An analysis of the test’s validity may show that it is primar-ily measuring your ability to search and retrieve words frommemory. It may have little to do with your ability to putyour thoughts together and come up with a good speech.
Although the concept of a test accomplishing its pur-pose is easy to grasp, applying this concept often results inconfusion. Many tests that neuropsychologists use origi-nally were designed for purposes or diagnostic groupsother than those for which they are used now. Rather thandiscuss validity in overgeneralized terms, scrutinize an eval-uation of a test’s validity in relation to the specific purposeand the specific population it is used in. That is, never con-sider a test generically “valid” or “invalid.” The question toask is: “Is this test valid for this particular purpose?”
You can use several different strategies for determiningvalidity. Construct validity focuses primarily on the testscore as a measure of the abstract, psychological character-istic or construct of interest (such as memory, intelligence,impulsiveness, and so forth). Construct validity would bemost important if you wanted a demonstration of the cog-nitive or functional abilities a test measures (e.g., visuo-spatial problem solving or perceptual-motor functioning).
Content validity pertains to the degree to which asample of items or tasks makes conceptual sense or repre-sents some defined psychological domain. Various itemsof the test should correspond to the behavior the test isdesigned to measure or predict, such as measuring howfast someone can tap a finger, to assess upper extremitymotor speed. Finally, criterion validity demonstrates thatscores relate systematically to one or more outcome crite-ria, either now (concurrent validity) or in the future (pre-dictive validity). Criterion-related validity traditionallyhas been an area of prime concern in neuropsychology re-lated to the correct classification of diagnostic groups in-cluding brain-impaired, psychiatric, and normal individu-als. There is also the issue of whether the test is being usedas a measure to describe current everyday functioning.Criterion-related predictive validity is important if a test isdesigned to predict decline or recovery of function or fu-ture behavior of any type (such as medication managementor ability to drive a car).
F A L S E P O S I T I V E S A N D B A S E R A T E S
A false positive (also known as a type I error or false alarm)is a case in which a neuropsychological test erroneously
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 67

68 PART ONE | Introduction
indicates a pathologic condition—such as “brain dam-age”—in an individual who is actually “normal.” In set-ting a cutoff score on neuropsychological tests, statisticiansattend to the percentage of false rejects (or false positives),as well as to the percentages of successes and failures withinthe selected group. In most medical (life-threatening) situ-ations, statisticians set the cutoff point low enough to ex-clude all but a few false rejections (such as on tests that de-tect the presence of cancer). When the selection ratio isnot externally imposed, the cutting score on a test can beset at a point yielding the maximum differentiation be-tween criterion groups. You do so, roughly, by comparingthe distribution of test scores in the two criterion groups,including the relative seriousness of false rejections and ac-ceptances.
The validity resulting from the use of a test dependsnot only on the selection ratio but also on the base rateof the test. Base rate is the frequency with which apathologic condition is diagnosed in the populationtested. For example, if 10% of a psychiatric populationof a hospital has organic brain damage, then 10% is thebase rate of brain damage in this population. Althoughintroducing any valid test improves predictive or diag-nostic accuracy, the improvement is greater when thebase rates are closest to 50% (closest to chance). Withextreme base rates found in rare pathologic conditions(e.g., �1%), an improvement with a neuropsychologicaltest may be negligible. Under those conditions, the diag-nostic use of a neuropsychological test is unjustifiablewhen you take into account the cost of its administrationand scoring. When the seriousness of a condition makesits diagnosis urgent, as in Alzheimer's disease (AD), neu-ropsychologists may often use tests of moderate validity inearly stages of sequential decisions. Table 3.1 demonstratesa simple decision strategy for neuropsychological proce-dures. A single test is administered, and the decision toreject or accept a diagnosis is made with four possibleoutcomes.
Neuropsychological Tests
Table 3.2 reviews the most frequently used types ofneuropsychological measures currently in practice. Dif-ferent types of tests have different goals and applications.Achievement tests measure how well a subject has prof-ited by learning and experience, compared with others.Typically, achievement is most influenced by past educa-tional attainment. Achievement tests are not designed tomeasure the individual’s future potential, which is typi-cally measured by aptitude tests. Behavioral-adaptivescales examine what an individual usually and habituallydoes, not what he or she can do. Neuropsychologists mostfrequently use such scales in evaluating the daily skills ofindividuals who are quite impaired (such as the mentallyretarded or the severely brain injured). Intelligence testsare complex composite measures of verbal and perfor-mance abilities that are related, in part, to achievement(factual knowledge) and to aptitude (e.g., problem solv-ing). Neuropsychological tests traditionally have beendefined as those measures that are sensitive indicators ofbrain damage. Today, scientists consider a measure to bea neuropsychological test if a change in brain function issystematically related to a change in test behavior. Mostavailable neuropsychological tests, therefore, have abroader function (see later in this chapter for a moredetailed description of these tests). Another area of psy-chological testing concerns the nonintellectual aspectsof behavior. Tests designed for this purpose are com-monly known as personality tests—most often, measuresof such characteristics as emotional states, interpersonal
Decision Positive (presence of pathology) Negative (absence of pathology)
CORRECT Valid acceptance (hit) Valid rejection (correctrejection)
INCORRECT False positive (false alarm, False negativetype I error) (miss, type II error)
Table 3.1 Decision Making in Neuropsychological Assessment
Type of Test Characteristics Measured
Achievement Profit from past experience
Aptitude Profit from future training and educationalexperiences
Behavioral/adaptive Basic adaptive behaviors (e.g., self-care,communication, socialization)
Intelligence Ability to adapt to novel situations quickly
Neuropsychological Brain–behavior relationships
Personality Psychopathology and ability to adapt and copewith stress
Vocational Success in a specific occupation or profession
Table 3.2 Types of Tests Most Commonly Usedby Psychologists

relations, and motivation. Finally, vocational inventoriesassess opinions and attitudes that indicate the individual’sinterest in different fields of work or occupational settings.
Neuropsychologists generally recognize that there isconsiderable overlap among all types of psychologicaltests. For example, it is difficult to measure aptitude with-out measuring achievement, to measure vocational inter-est without measuring personality, or to measure intelli-gence without measuring neuropsychology. One way todeal with this overlap is to reduce the complexity to twobasic neuropsychological constructs: “crystallized” and“fluid” functions. Psychologists consider crystallizedfunctions to be most dependent on cultural factors andlearning. In contrast, they believe fluid functions to beculture free and independent of learning. Problem-solvingand abstract reasoning abilities are considered fluid,whereas spelling and factual knowledge are consideredcrystallized. Nevertheless, even this simple differentiationof psychological test properties is controversial. For exam-ple, much discussion concerns whether intelligence teststap mostly crystallized or fluid forms of behavior. Actu-ally, it is nearly impossible to measure all aspects of a com-plex skill or group of skills with a single test. As a result,neuropsychologists prefer to administer a number of dif-ferent tests, known as a test battery, that address differentareas of brain–behavior functioning. After all, testing be-havior, whether vocational or adaptive, is mediated bybrain function. Thus, neuropsychologists use the preced-ing tests to some degree to evaluate specific questionsabout an individual. The neuropsychological interview isalso an important part of the neuropsychological evalua-tion. The benefits of talking to the patient include an un-derstanding of the patient’s symptom presentation; thepatient’s awareness of his or her symptoms; and a reviewof the patient’s educational, marital, social, and develop-mental histories.
The best way to understand the purpose of the neu-ropsychological assessment is to examine the evaluationprocess. Because neuropsychological assessment batteriestypically evaluate a wide range of behaviors, they are con-sidered multidimensional in their approach to measuringhigher cortical functions. Thus, the neuropsychologicalexamination involves accurately evaluating multiple cog-nitive abilities (Table 3.3). The usual categories of theneuropsychological examination include the followingfunctional areas, which are listed hierarchically; that is,higher cognitive functions depend to a large degree on in-tact lower functions, which are listed first:
Let us examine each of these areas in greater depth. Foreach neuropsychological domain, we present an exampleto elucidate the construct measured and the method used
to do so. In addition, we present examples of frequentlyused neuropsychological tests for each neuropsychologicaldomain.
O R I E N T A T I O N ( A R O U S A L )
Brain impairment affects not only a person’s intellect ormuscle movement but all other aspects of performance aswell, including his or her level of consciousness. Patientswho are lethargic or tired all the time tend to performpoorly compared with patients who have good energy.Lethargy is sometimes a symptom of brain damage andsometimes a symptom of depression. It is the psycholo-gist’s job to determine which factors are at work in a givencase.
Alertness is the most basic aspect of cognition.Patients who cannot demonstrate adequate arousal mayhave difficulty participating in a neuropsychologicalevaluation and are, perhaps, unlikely to benefit from re-habilitation or psychological intervention. Orientationdescribes a patient’s basic awareness of himself or herselfto the world around them. Specifically, in neuropsychol-ogy, orientation refers to an individual’s knowledge ofwho he or she is (orientation to person), what the dateis (orientation to time), and where he or she is (orienta-tion to place). If a patient is fully oriented, the neu-ropsychologist will say that he or she is “oriented timesthree,” meaning that those three areas of awareness areintact.
N e u r o p s y c h o l o g i c a l I t e m s ( O r i e n t a t i o n )
The neuropsychological assessment typically involves thecommon evaluation of orientation in the three spheres;for example, “What is your full name?” (both first andlast names are required) “Where do you live?” (specifictown or city is required), or “How old are you?” In addi-tion, neuropsychologists may also ask additional ques-tions that relate to an individual’s ability to recall his orher specific whereabouts, the purpose of the hospitaliza-tion, and any part of his or her address: “What is thename of the place you are in now?” (a response indicatingthat the patient knows he or she is in a hospital is consid-ered correct) and “What town or city are you in now?”(any response indicating adequate orientation to the hos-pital’s location is scored). The following two examples areexamples of the patient’s orientation to well-known cur-rent facts involving famous individuals: “Who is Presi-dent of the United States right now?” and “Who was pres-ident before him?”
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 69

70 PART ONE | Introduction
N e u r o p s y c h o l o g i c a l T e s t s ( O r i e n t a t i o n )
To measure orientation, neuropsychologists frequentlyuse the Galveston Orientation and Amnesia Test (GOAT)(Levin, O’Donnell, & Grossman, 1979). This short men-tal status examination assesses the extent and duration ofconfusion and amnesia after traumatic brain injury. Likethe Glasgow Coma Scale (GCS; see Chapter 13), it wasdesigned for repeated measurements and can be used sev-eral times a day and repeated over days or week as neces-sary. The GOAT yields a score from 0 to 100, with a sug-gested cutoff score of 75 or better indicating relativelyintact orientation and the capacity of the patient to un-dergo formal neuropsychological testing. Both the GCSand the GOAT are simple to administer; therefore, thetreatment team often uses them. Because these scales quan-tify level of patient arousal, researchers have frequently
used them in examining outcome of brain injuries thatinvolve an alteration in consciousness.
S E N S A T I O N A N D P E R C E P T I O N
Sensation is the elementary process of a stimulus excit-ing a receptor and resulting in a detectable experience inany sensory modality; for example, “I hear something.”Perception depends on intact sensation and is the processof “knowing”; for example, “I hear music, it is Pearl Jam.”The perceptual process begins with arousal and orienta-tion, sensation is the second stage, and perception thethird. In assessing sensation and perception, the neuropsy-chologist is interested in quickly and grossly evaluating thepatient’s visual, auditory, and tactile functional levels.Screening for impaired sensation and perception yields im-portant information by ruling out the contributions of
OrientationArousalDegree of confusionDisorientationPlacePersonTimeAwareness of change/time
Sensation/PerceptionRecognitionFamiliarity of stimuliRelationship among featuresVisual acuityAuditoryTaste/smellTactile/proprioceptiveInternal/environmentalAwareness
AttentionSpanSelective attentionShiftingSustained attentionVigilanceNeglectFatigue
MotorCerebral dominanceInitiation and perseverationManual dexterity
Graphomotor skillsBalanceAmbulationMotor speedSpeech regulationMotor strength
VisuospatialConstructionRoute findingSpatial orientationFacial recognition
Language SkillsReceptive speech (following directions,reading comprehension)Expressive speech (verbal fluency, naming,writing, math)Articulation (stuttering, stammering, articu-lation voice, fluency)Speech production (articulation fluency, voice)Syntax and grammarAphasias: Broca’s, Wernicke’s, conduction,fluent, transcortical, subcortical
MemoryVerbalVisualImmediateShort termLong termRecognitionEncoding
StorageRetrievalChunkingDeclarativeProcedural
Abstract Reasoning/ConceptualizationComprehensionJudgmentCalculationsProblem solvingOrganizational abilitiesHigher level reasoningSequencing
Emotional/Psychological DistressDepressionAttitude toward rehabilitationMotivationLocus of controlFamily relationshipsGroup interactionOne-to-one interactionBehavioral impulsivityAggressive/confrontational
Activities of Daily LivingToiletingDressingBathingTransferringContinenceFeeding
Table 3.3 Common Areas of Neuropsychological Assessment Grouped Hierarchically by Function

dysfunctional visual or auditory sensation to test perfor-mance. In addition, discovering unilateral sensorydeficits aids in diagnosis of lateralized brain injury. It isimportant to understand that neuropsychologists are in-terested in a more or less general assessment of a patient’ssensory functioning. Specialists, including audiologists(hearing) or optometrist (visual), perform diagnosticevaluations.
N e u r o p s y c h o l o g i c a l I t e m s( S e n s a t i o n a n d P e r c e p t i o n )
Sample items of testing the sensory and perception do-main may include assessing the intactness of the patient’sleft and right visual fields (see Chapter 8 for a descriptionof visual field deficits). This is achieved by administeringa visual field examination, common in a neurologic ex-amination. For this procedure, the examiner must sit fac-ing the patient, at a distance of approximately 3 to 4 feet,and ask, “I would like you to look straight at my nose. Iam going to put my arms out like this, and I want you totell me which finger I am moving. You can point to it ifyou like.” The examiner extends the index finger of eachhand in a vertical fashion with arms spread out at shoul-der height and presents the stimuli by moving each fingerslightly, waiting for the patient’s response between trials.Discrimination of similar auditory, verbal stimuli may betested by the examiner saying, “I am going to say twowords, and I want you to tell me whether I am saying thesame word twice or two different words,” to assess audi-tory functioning:
house – house (same)people – peanut (different)bar – bar (same)first – thirst (different)
To assess the patient’s ability to sense or feel objects,the examiner may say, “I am going to place an object inone of your hands. I would like you to close your eyes,feel the object, and tell me what it is.” This proceduremeasures stereognosis, recognition of objects by touch.
N e u r o p s y c h o l o g i c a l T e s t s( S e n s a t i o n a n d P e r c e p t i o n )
Some neuropsychologists have standardized their proce-dures for examining sensory and perceptual functioningand developed scoring systems as well. For example, partof the well-known and often used Halstead–Reitan Neu-ropsychological Battery includes a sensory-perceptual ex-amination that tests for finger agnosia, skin writing recog-nition, and sensory extinction in the tactile, auditory, andvisual modalities (Reitan & Wolfson, 1993).
A T T E N T I O N / C O N C E N T R A T I O N
Attention is a critical requirement for learning. To remem-ber, you first have to pay attention. Some patients are in-capable of attending to their environment. Others may beable to attend to a learning task, but only for a limitedamount of time. Still others may be able to attend to a taskonly if there are no distractions in the environment. Psy-chologists divide the concept of attention into separatecategories such as sustained attention, paying attention tosomething over a prolonged period, and selective atten-tion, paying attention to more than one thing at a time.
N e u r o p s y c h o l o g i c a l I t e m s( A t t e n t i o n / C o n c e n t r a t i o n )
Tasks requiring mental control involve simple, over-learned information, but also require the person to main-tain an adequate level of attention throughout the item.Errors in this area may indicate extreme fatigue or impair-ment in concentration skills. For example,
“Count from 1 to 20 as quickly as you can.”“Recite the days of the week backward beginning with
Sunday.”“Say the alphabet (A, B, C . . .) all the way through.”“Count by threes, beginning with 1 and adding 3 to each
number. For example, 1, 4, 7, and so on. (Stop whenyou reach 22.)”
Another form of attention in this cognitive skill area isattention span. Here, the examiner asks the patient to at-tend to various verbal stimuli, then repeat them. Thestimuli become progressively more complex. In this man-ner, it is possible to evaluate a patient’s span of attentionfor unfamiliar combinations of stimuli.
“I am going to say some numbers, and after I finish, Iwould like you to repeat them.”
TRIAL 1 5 8 9
TRIAL 2 9 2 7 5
TRIAL 3 7 1 6 3 2
“Now I am going to say some more numbers; but thistime when I finish, I want you to say them backward.For example, if I say 3 – 6, you say 6 – 3.”
TRIAL 1 5 8
TRIAL 2 2 6 1
Sustained attention is the ability to concentrate over aperiod of time. For example, you can assess verbal atten-tion with the following task: “Tap on the table when youhear me say the number 4”:
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 71

72 PART ONE | Introduction
2 3 5 4 7 4 6 4 4 2
1 8 1 7 8 4 5 4 2 3
N e u r o p s y c h o l o g i c a l T e s t s( A t t e n t i o n / C o n c e n t r a t i o n )
Standardized tests of attention include the Symbol DigitModalities Test (SDMT) (Smith, 1982), which requiresthe respondent to fill in blank spaces with the numberthat is paired to the symbol above the blank space asquickly as possible for 90 seconds. The SDMT primarilyassess complex scanning, visual tracking, and sustainedattention. An interesting test of selective attention is thed2 Test of Attention (Brickenkamp & Zillmer, 1998).The d2 Test is a timed test of selective attention and is astandardized refinement of a visual cancelation test. It hasbeen translated into four languages and is the most fre-quently used test of attention in Europe. In response tothe discrimination of similar visual stimuli, the test mea-sures processing speed, rule compliance, and quality ofperformance, allowing estimation of individual attentionand concentration performance (Figure 3.4). The test wasoriginally developed in 1962 in Germany and Switzerlandas an assessment tool for driving efficiency. Subjects whofail the d2 task tend to have difficulty concentrating, in-cluding difficulty in warding off distractions.
M O T O R S K I L L S
Neuropsychologists are interested in assessing a person’sability to demonstrate motor control in the upper andlower extremities. Simple motor skills require little coordi-nation, whereas more complex items tap into higher motorprocesses. As items progress in difficulty, the patient mustshow more integration of cognitive skills to perform thetask successfully. The following neuropsychological
procedures measure varied aspects of a patient’s motorfunctioning. The hierarchic nature of the item presenta-tion can yield clues to the patient’s limits in motorfunctioning.
Neuropsychological items (motor) that involve gross-motor movement assess one of the most basic corticallymediated motor responses such as a response to a singlecommand; for example, “Raise your right hand,” or “Moveyour left leg.” You can evaluate motor speed from the pa-tient’s ability to “touch your thumb to your forefinger asquickly as you can,” and fine-motor ability can be evalu-ated from the command, “Touch your thumb to each fin-ger, one after the other.” These previous items assess theability to perform a particular response; the followingitems tap the patient’s ability to perform and inhibit motorbehavior: “If I clap once, you clap twice.” (Clap hands onetime.) “Now, I clap twice, you clap once.” (Clap handstwo times.) Neuropsychologists consider this a higher levelcognitive process, because it requires the patient to shiftbetween initiating and inhibiting behavior.
Neuropsychologists often examine graphomotor skills.The following items assess the ability to copy shapes withincreasing degrees of difficulty. They involve the integrationof visual perception (input) and a complex motor response(output). “Copy these designs. Take your time and do yourbest.” The patient’s drawings are scored related to the cor-rect shape, size, symmetry, and integration (Figure 3.5).
Motor apraxia items assess the intactness of commonmotor sequences. In general, the term apraxia refers to aninability to perform purposeful sequences of motor be-haviors. Although basic motor skills may be intact, thepatient may be unable to perform even overlearned motorsequences. The form of apraxia assessed here is motorapraxia or ideomotor apraxia. Impairments in this areamay stem from an inability to access a stored motor
Text not available due to copyright restrictions
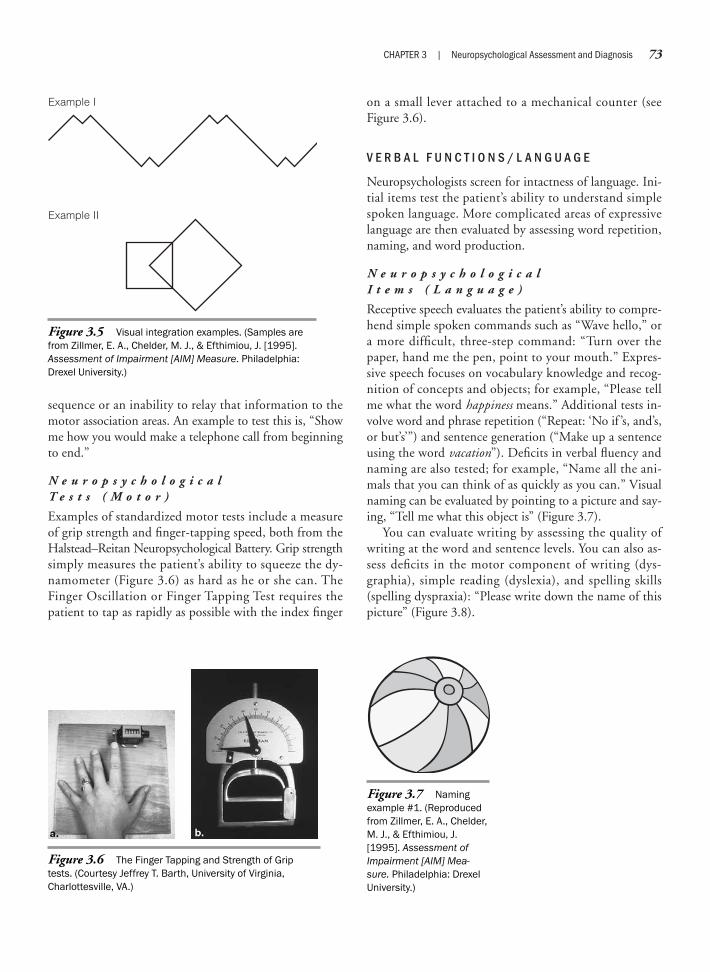
sequence or an inability to relay that information to themotor association areas. An example to test this is, “Showme how you would make a telephone call from beginningto end.”
N e u r o p s y c h o l o g i c a l T e s t s ( M o t o r )
Examples of standardized motor tests include a measureof grip strength and finger-tapping speed, both from theHalstead–Reitan Neuropsychological Battery. Grip strengthsimply measures the patient’s ability to squeeze the dy-namometer (Figure 3.6) as hard as he or she can. TheFinger Oscillation or Finger Tapping Test requires thepatient to tap as rapidly as possible with the index finger
on a small lever attached to a mechanical counter (seeFigure 3.6).
V E R B A L F U N C T I O N S / L A N G U A G E
Neuropsychologists screen for intactness of language. Ini-tial items test the patient’s ability to understand simplespoken language. More complicated areas of expressivelanguage are then evaluated by assessing word repetition,naming, and word production.
N e u r o p s y c h o l o g i c a l I t e m s ( L a n g u a g e )
Receptive speech evaluates the patient’s ability to compre-hend simple spoken commands such as “Wave hello,” ora more difficult, three-step command: “Turn over thepaper, hand me the pen, point to your mouth.” Expres-sive speech focuses on vocabulary knowledge and recog-nition of concepts and objects; for example, “Please tellme what the word happiness means.” Additional tests in-volve word and phrase repetition (“Repeat: ‘No if ’s, and’s,or but’s’”) and sentence generation (“Make up a sentenceusing the word vacation”). Deficits in verbal fluency andnaming are also tested; for example, “Name all the ani-mals that you can think of as quickly as you can.” Visualnaming can be evaluated by pointing to a picture and say-ing, “Tell me what this object is” (Figure 3.7).
You can evaluate writing by assessing the quality ofwriting at the word and sentence levels. You can also as-sess deficits in the motor component of writing (dys-graphia), simple reading (dyslexia), and spelling skills(spelling dyspraxia): “Please write down the name of thispicture” (Figure 3.8).
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 73
Example II
Example I
Figure 3.5 Visual integration examples. (Samples arefrom Zillmer, E. A., Chelder, M. J., & Efthimiou, J. [1995].Assessment of Impairment [AIM] Measure. Philadelphia:Drexel University.)
Figure 3.6 The Finger Tapping and Strength of Griptests. (Courtesy Jeffrey T. Barth, University of Virginia,Charlottesville, VA.)
Figure 3.7 Namingexample #1. (Reproducedfrom Zillmer, E. A., Chelder,M. J., & Efthimiou, J.[1995]. Assessment ofImpairment [AIM] Mea-sure. Philadelphia: DrexelUniversity.)

74 PART ONE | Introduction
N e u r o p s y c h o l o g i c a l T e s t s ( L a n g u a g e )
Many standardized neuropsychological tests assess verbaland language functioning. A simple but effective test ofauditory comprehension (receptive language) is the TokenTest (e.g., see Boller & Vignolo, 1966). Almost every non-aphasic person who has completed fourth grade shouldpass this test in its entirety. The test consists of a numberof commands (such as “Touch the small yellow circle.” or“Touch the green square and the blue circle.”) that relateto plastic tokens, which come in different shapes, sizes,and colors. This test is sensitive to disrupted linguisticprocesses that are central to aphasic disability.
The Controlled Oral Word Association (COWA) test(Benton & Hamsher, 1989) assesses the subject’s ability touse expressive speech. It measures verbal fluency by askingthe subject to name as many words as possible that startwith a specific letter. For example, within 60 seconds, anundergraduate or graduate student should be able to name15 words that start with the letter R. In the COWA, ex-aminers administer three word-naming trials using the let-ters C, F, and L. These letters were selected by Englishword frequency. That is, words beginning with C have arelatively high frequency; the second letter, F, a somewhatlower frequency; and the third letter, L, a still lower fre-quency. Word fluency is a sensitive indicator of generalbrain dysfunction and expressive language dysfunction.
V I S U O S P A T I A L O R G A N I Z A T I O N
In the visuospatial domain, neuropsychologists assess var-ious aspects of processing. They ask the patient to per-form tasks of map skills, route finding, spatial integrationand decoding, and facial recognition. The results of theseneuropsychological tests can provide information aboutspecific disorders of visuospatial organization.
N e u r o p s y c h o l o g i c a l I t e m s ( V i s u o s p a t i a l )
Neuropsychologists can evaluate spatial orientation withsimple directional skills and mazes, and then proceedthrough clock drawing and motor-free constructionaltasks: “If this were a compass on a map and you were fac-ing north, which direction would be behind you?” or“Draw the face of a clock, showing all the numbers, andset the hands to read 10 minutes after 11.” Testers mayevaluate visuospatial processing by asking, “Which ofthese sets of lines makes up this figure at the top: A, B, orC?” (Figure 3.9).
Facial recognition is the patient’s ability to recognize afamiliar face, as well as to compare similar faces and iden-tify facial affect. For example, the examiner may ask,“Show me ‘the happy face, the sad face, the angry face’”(Figure 3.10).
Visual sequencing also involves more integration andhigher order processing. The person must comprehendthe overall meaning of the activity, and then be able tocorrectly assemble the pictures to form the sequence ofsteps; for example, “This card has three pictures on it. Ifthe pictures are put in the right order, they tell a story.Look carefully at the pictures, tell me the story, and pointto the one you think comes first in the story. Now pointto the one that would come second, and the picture thatwould finish the story” (Figure 3.11).
N e u r o p s y c h o l o g i c a l T e s t s ( V i s u a l - S p a t i a l )
The Bender Gestalt test consists of nine geometric de-signs, which the patient must reproduce exactly (Bender,1938; Hutt, 1985). The “Bender,” as it is often called, is apopular measure of visuospatial construction. It measures
Figure 3.8 Naming exam-ple #2. (Reproduced fromZillmer, E. A., Chelder, M. J., &Efthimiou, J. [1995]. Assess-ment of Impairment [AIM]Measure. Philadelphia: DrexelUniversity.)
a. b. c.
Figure 3.9 Visuospatial test item. (Reproducedfrom Zillmer, E. A., Chelder, M. J., & Efthimiou, J.[1995]. Assessment of Impairment [AIM] Measure.Philadelphia: Drexel University.)
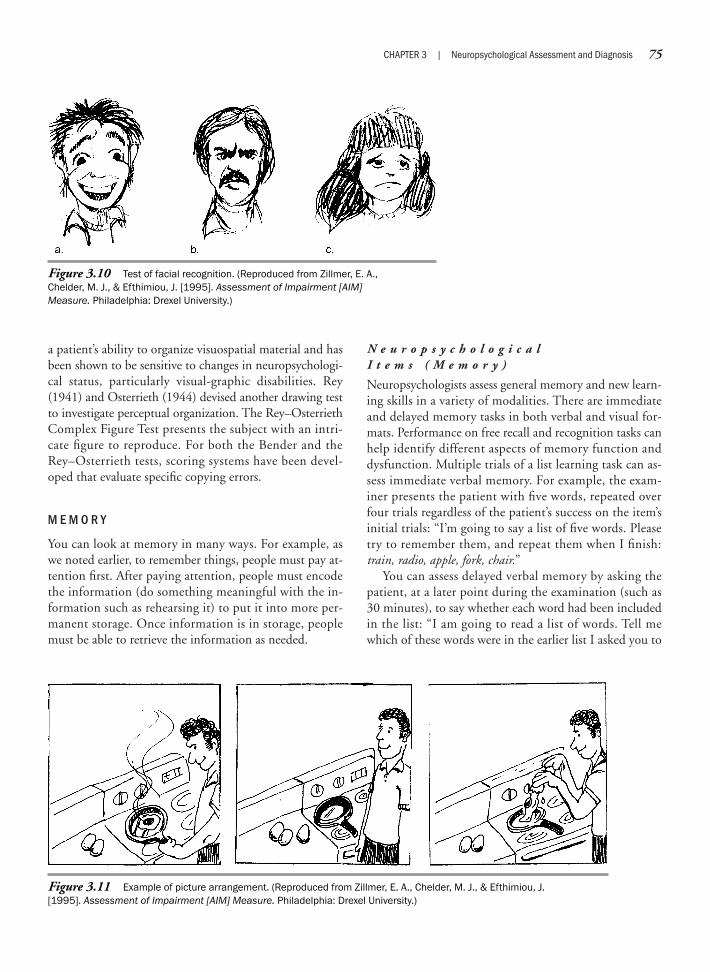
a patient’s ability to organize visuospatial material and hasbeen shown to be sensitive to changes in neuropsychologi-cal status, particularly visual-graphic disabilities. Rey(1941) and Osterrieth (1944) devised another drawing testto investigate perceptual organization. The Rey–OsterriethComplex Figure Test presents the subject with an intri-cate figure to reproduce. For both the Bender and theRey–Osterrieth tests, scoring systems have been devel-oped that evaluate specific copying errors.
M E M O R Y
You can look at memory in many ways. For example, aswe noted earlier, to remember things, people must pay at-tention first. After paying attention, people must encodethe information (do something meaningful with the in-formation such as rehearsing it) to put it into more per-manent storage. Once information is in storage, peoplemust be able to retrieve the information as needed.
N e u r o p s y c h o l o g i c a l I t e m s ( M e m o r y )
Neuropsychologists assess general memory and new learn-ing skills in a variety of modalities. There are immediateand delayed memory tasks in both verbal and visual for-mats. Performance on free recall and recognition tasks canhelp identify different aspects of memory function anddysfunction. Multiple trials of a list learning task can as-sess immediate verbal memory. For example, the exam-iner presents the patient with five words, repeated overfour trials regardless of the patient’s success on the item’sinitial trials: “I’m going to say a list of five words. Pleasetry to remember them, and repeat them when I finish:train, radio, apple, fork, chair.”
You can assess delayed verbal memory by asking thepatient, at a later point during the examination (such as30 minutes), to say whether each word had been includedin the list: “I am going to read a list of words. Tell mewhich of these words were in the earlier list I asked you to
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 75
Figure 3.10 Test of facial recognition. (Reproduced from Zillmer, E. A.,Chelder, M. J., & Efthimiou, J. [1995]. Assessment of Impairment [AIM]Measure. Philadelphia: Drexel University.)
Figure 3.11 Example of picture arrangement. (Reproduced from Zillmer, E. A., Chelder, M. J., & Efthimiou, J.[1995]. Assessment of Impairment [AIM] Measure. Philadelphia: Drexel University.)

76 PART ONE | Introduction
recall several times: clock, apple, book, train, table, fork,sandwich, truck, radio, chair.”
Delayed visual memory assesses the patient’s ability toremember visual information the examiner presented ear-lier in the testing (an intermediate delay), as well as theability to remember simple visual figures after a shortdelay. The examiner presents these items in a recognitionformat rather than a free recall format, so the patientchooses among similar stimuli, one of which is the cor-rect figure. “Earlier I asked you to copy four designs.Which of these designs was it?” (Figure 3.12).
You can assess contextual or logical memory, immedi-ate and delayed, by testing the patient’s free recall ability.The examiner presents a short story to the patient, testingmemory for information presented in a specific contex-tual structure. After an interference item, the examineragain asks the patient to tell the story. Slashes separateeach unit of information in the following example.
I am going to read to you a short story. When I finish, I wantyou to tell me as much of the story as you can remember. Try toremember it in the same words as I have used: “Joseph / Green /left his house / and headed for the subway. / He was on his way/ to the supermarket. / He purchased / wine, / steak, / and icecream. / Later that day / he had dinner / with his boss / fromthe office.” Now, tell me as much of the story as you can re-member.
A completely verbatim response is not necessary, be-cause neuropsychologists are mostly interested in whetherthe individual has formed a memory. For example, an ac-ceptable substitution for /steak/ is “meat” or “beef.”
N e u r o p s y c h o l o g i c a l T e s t s ( M e m o r y )
To provide thorough coverage of the varieties of memorydisabilities, researchers have developed batteries of mem-ory tests. One of the memory assessment instruments mostfrequently used by neuropsychologists is the WechslerMemory Scale (WMS; first introduced by Wechsler in1945), which is now in its third revision (WMS-III). TheWMS consist of seven subtests, which include personaland current information, orientation, mental control,
logical memory (which tests immediate recall of two ver-bal stories), digit span, visual reproduction (an immediatevisual memory drawing task), and associate learning(which requires verbal retention). The WMS is sensitiveto memory disorders and memory defects associated withaging.
J U D G M E N T / P R O B L E M S O L V I N G
A patient’s ability to use abstract reasoning relates, in part,to his or her capacity to understand concepts. In deter-mining a patient’s ability to use abstract reasoning, theneuropsychologist examines the patient’s ability to gener-alize from one situation to another. This skill is known as“transfer of learning.” For example, if a rehabilitation pa-tient can learn to transfer from the mat to the wheelchairwith minimal assistance during physical therapy, onewould normally expect the same patient to be able to gen-eralize that skill from the physical therapy wing of thehospital to the nursing wing. Otherwise, the patient’slearning is circumstantial.
Often, neuropsychologists are interested in evaluatinginsight specific to the patient’s capacity to realize the im-plications of his or her disorder. At times a patient pre-sents to a neuropsychologist, and says, “I’ll be fine as soonas I get home,” or “There is nothing wrong with me, I can drive a car.” Initially, the neuropsychologist will mea-sure his or her own evaluation against those by other teammembers. For example, if the patient has had a mildstroke and is hindered only by his or her own dislike ofthe hospital setting, it may be true that the patient will be“fine” on discharge. If the patient has experienced a mod-erate or more severe brain injury, the patient’s communi-cation may be evaluated as demonstrating lack of insight.One of the jobs of the neuropsychologist is to evaluatethe insight that a patient has regarding the nature and theimplications of his or her own disability.
N e u r o p s y c h o l o g i c a l I t e m s( P r o b l e m S o l v i n g )
You can evaluate higher order cognitive functioning andabstract thinking skills by asking the patient to interpretproverbs, solve everyday problems, or perform mentalarithmetic. For example, you can assess abstract reasoningby asking a patient to interpret a common proverb, scor-ing responses based on degree of abstraction. Proverb in-terpretations are a traditional feature of the neuropsycho-logical examination, assessing the ability to reason beyondthe concrete level. For example, “What does this sayingmean: ‘You can’t judge a book by its cover?’” An abstractanswer may be, “Don’t judge a person by their looks”; a
Figure 3.12 Example of design copy test.

concrete answer may be, “You don’t know what is insidethe book just by looking at its cover.”
A common way to assess concept formation is to use asimilarities/differences paradigm or analogies. The follow-ing items involve the abstract categorization of objects andconcepts. They assess whether the patient can determinethe appropriate abstract links between the objects and dis-criminate form and function: “How are an eagle and arobin alike?” or “Please complete this sentence: ‘Banana isa fruit, cat is an animal. Father is a man, mother is a . . .’”
Problem-solving tasks tap the patient’s ability to for-mulate solutions to a common, everyday situation. Re-sponses can often demonstrate impulsivity and poor socialjudgment, as well as decreased functional independence ora need for supervision. “What should you do if you can’tkeep an appointment?” Sometimes tests present absurdi-ties to evaluate reasoning skills, attention to abstract de-tails, and the ability to formulate an abstract verbal re-sponse: “What is strange about this sentence: ‘When thecook discovered that he had burned the meat, he put it inthe refrigerator to fix it’?” or “What is funny or strangeabout this picture?” (Figure 3.13).
N e u r o p s y c h o l o g i c a l T e s t s( P r o b l e m S o l v i n g )
Neuropsychologists have been creative in developing as-sessment procedures that evaluate executive abilities, andliterally dozens of tests measure this neuropsychologicaldomain. Only a few are mentioned here. The Trail Mak-ing Test B, part of the Halstead–Reitan Neuropsychologi-cal Battery, requires the participant to draw lines to con-nect consecutively numbered and lettered circles byalternating the two sequences (1 to A, A to 2, 2 to B, andso on). This timed task necessitates complex visual scan-ning, motor speed, mental flexibility, and attention.
The Wisconsin Card Sorting Test (WCST) (Berg,1948; Heaton, Chelune, Talley, Kay, & Curtis, 1993) iswidely used to study “abstract behavior” and “shiftingsets.” The examiner gives the subject a pack of 64 cardson which are printed 1 to 4 symbols—triangle, star, cross,or circle, in red, green, yellow, or blue. No two cards areidentical. The patient’s task is to place them one by oneunder four stimulus cards according to a principle that thepatient must deduce from the pattern of the examiner’sresponses to the patient’s placement of the cards. For ex-ample, if the principle is color, the correct placement of ared card is under one red triangle, regardless of the num-ber of symbols. Thus, the subject simply starts placingcards and the examiner tells him or her whether the place-ment is correct. After 10 cards have been placed correctlyin a row, the examiner shifts the principle, indicating theshift only to the patient by the changed patterns of “right”and “wrong” statements. A poor performance on this testoften suggests that the patient has trouble organizing hisor her own behavior or has difficulty applying one set ofrules to different situations. The WCST is a sensitive neu-ropsychological measure, particularly for injuries to thefrontal lobes.
Culbertson and Zillmer (2005) designed the Tower ofLondon–Drexel University (TOLdx) as a neuropsycholog-ical measure of executive planning and problem solvingbased on the original Tower of London (Shallice, 1982).The TOLdx measures executive planning that involves theability to conceptualize change, respond objectively, gen-erate and select alternatives, and sustain attention (Lezaket al., 2004). The frontal lobes, in systematic interactionwith other cortical and subcortical structures, support ex-ecutive planning. The TOLdx test materials include twoidentical tower structures (Figure 3.14), one for the sub-ject and one for the examiner to use. Each structure con-sists of three pegs of descending lengths and three coloredbeads that the patient can place on the pegs in differentconfigurations or patterns. The examiner asks the subjectto move the beads of his or her tower structure to match
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 77
Figure 3.13 Example of a visual absurdity. (Repro-duced from Zillmer, E. A., Chelder, M. J., & Efthimiou, J.[1995]. Assessment of Impairment [AIM] Measure.Philadelphia: Drexel University.)

78 PART ONE | Introduction
bead configurations that the examiner presents. In solvingthe bead patterns, the subject must adhere to two strictlyenforced problem-solving rules: Only move one bead at atime, and do not place more beads than fit on each peg.The examiner records number of moves, rule violations, andtime the subject uses in solving the bead patterns. Interpret-ing the subject’s performance involves an analysis of bothquantitative and qualitative variables. Empirical studies(Culbertson & Zillmer, 2005) show that the TOLdx is sen-sitive to a complex set of cognitive processes, including plan-ning computations, working memory, mental flexibility,attention allocation, and response inhibition.
S y m p t o m V a l i d i t y T e s t i n g i n F o r e n s i c N e u r o p s y c h o l o g y
Unlike traditional therapy clients, the potential monetarycompensation associated with personal injury or insur-ance claims may motivate patients tested to exaggerate ordistort their symptoms. For example, individuals suffer-ing from neuropsychological dysfunction as a result oftrauma frequently report problems in attention and mem-ory. Therefore, neuropsychologists learn to assess for aclient’s response bias. Psychologists have had a long andrich history of evaluating deception (e.g., polygraph proce-dures, assessing feigning of somatic symptoms). Throughthe use of their expertise in psychometrics and test theory,neuropsychologists have generated assessment proceduresto measure symptom validity.
Although symptom validity tests are commonly referredto as malingering tests, malingering is just one possible
cause of invalid or biased performance. Test bias on thepart of the client may range from outright malingeringand conscious distortion of test performance to subtler,nonoptimal approaches to his or her performance, suchas exaggeration. Thus, the neuropsychologist must also beexpert in evaluating the test-taking approach and motiva-tion of each individual. In some instances, these biasedtest-taking approaches actually stem from the patient’sneurologic symptoms. For example, patients with rightparieto-occipital stroke often have limited insight intotheir condition.
According to the Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition (DSM-IV) (AmericanPsychiatric Association, 1994, p. 683), malingering is “theintentional production of false or grossly exaggerated phys-ical or psychological symptoms, motivated by external in-centives such as avoiding military duty, avoiding work,obtaining financial compensation, evading criminal pros-ecution, or obtaining drugs.” Thus, it has become a stan-dard procedure for neuropsychologists to perform anassessment of malingering when performing independentneuropsychological evaluations (Zillmer, 2004; Zillmer &Greene, 2006), for example, using the Test of MemoryMalingering (TOMM) (Tombaugh, 1996, 2003).
N E U R O P S Y C H O L O G I C A L D I A G N O S I S
With the advent of modern medical diagnostic procedures(see Chapter 2), including single-photon emission com-puted tomography (SPECT), MRI, CT, positron emissiontomography (PET), angiography, and evoked potential,using behavior-based assessments to diagnose organic-functional causative factors has become less essential. Ithas become less important for neuropsychologists andpsychologists to act in the capacity of “lesion detectors”and more important to document the precise effects ofbrain dysfunction on behavior for purposes of remedia-tion and treatment (Zillmer & Perry, 1996). Nevertheless,clinical neuropsychologists continue to figure prominentlyin uncovering the behavioral syndromes that correspondto impaired brain regions and neuronal circuits and mayplay an important role in diagnosing neuropathologicconditions (e.g., see Goldman-Rakic & Friedman, 1991).
Medical teams still ask clinical neuropsychologists toaid in diagnosis, not merely confirming what might appearon PET or MRI images, but adding behavioral and descrip-tive information about a patient’s cognitive strengths andweaknesses. If a neurologist wants to know whether a pa-tient has had a left hemisphere stroke, a CT scan or anMRI can show this. Neuropsychological testing would beredundant and not as precise as sophisticated imaging
Figure 3.14 Administration of the Tower ofLondon–Drexel University test, which evaluates frontal lobefunctioning, that is, anticipatory-, pre-planning, and goal-oriented planning. (Courtesy Eric Zillmer.)

equipment for exactly locating the lesion within the brain.Imaging technology, however, does not provide informa-tion about how brain damage may affect behavior. Clini-cal neuropsychologists provide invaluable and uniquediagnostic information in areas where behavioral infor-mation provides an important piece of the diagnostic puz-zle. Those areas include the diagnoses of mild head injury,attention-deficit/hyperactivity disorder, learning disabil-ity, or AD. Currently available imaging techniques are notsufficient to diagnose AD. Brain biopsy after death is theonly certain method. Thus, Alzheimer’s dementia is a diag-nosis largely determined by behavioral methods. Throughcareful observation and history taking with the patient andfamily, the neuropsychologist documents the extent andprobable progression of the behavioral deterioration.Then, through repeated evaluations spread out over time,the neuropsychologist charts the severity and course of theneuropsychological impairments. If the team can rule outall other medical causes of dementia, then the person canbe diagnosed as having “possible” or “probable” AD. Infact, the diagnosis of most dementia subtypes requiresclose collaboration between neurologists and neuropsy-chologists (see Chapter 14).
Mild-to-moderate head injuries also present diagnosticissues that neuropsychology can help clarify. With manyhead injuries, particularly of the mild variety (such as con-cussion), it is not immediately evident whether the per-son has actually sustained a brain injury. In many cases,the diagnostic aim of the neuropsychological evaluation isto determine the presence and severity of brain injury.The diagnosis is made, not to answer the outdated ques-tion, “Is this patient ‘organic’?” but to answer the ques-tion, “Does this neuropsychological profile fit with whatis known about the neuropsychological pattern of impair-ment after closed head injury?” CT and MRI may notshow microscopic shearing, tearing, stretching, and bruis-ing of axons. Even if they did, you could not predict clearbehavioral symptoms from looking at radiologic or imag-ing data. As in AD, behavioral testing largely determinesthe diagnosis and severity of brain damage after closedhead injury. Thus, neuropsychologists play an importantrole in determining patterns of neuropsychological dys-function characteristic with a variety of central nervoussystem disorders. In addition, and to address the entirediagnostic picture, many neuropsychologists conductcomprehensive examinations of emotion and personality,to understand how the patient is adapting. For example,they not uncommonly diagnose depression or significantdeficits in stress tolerance in patients who have experi-enced a head injury. The neuropsychologist’s diagnosticskills as a psychologist helps differentiate between the
impact of emotional/personality problems and brain dys-function.
Neuropsychological diagnosis remains an importantcomponent of the neuropsychologist’s role. However, di-agnosis usually is not the only question of interest when apatient seeks neuropsychological testing. The next sectiondiscusses certain other issues that practicing neuropsy-chologists address.
D E S C R I B I N G F U N C T I O N , A D A P T A T I O N , A N D P R O G N O S I S
Describing behavioral functioning—that is, a patient’s cog-nitive strengths and weaknesses—puts the “psychology”into neuropsychology. Psychology is the science of behav-ior; neuropsychology is the science of brain–behaviorfunctioning. Although neuropsychology combines neuro-logic and psychological foci, the neurologic goal of de-tecting and classifying lesions dominated clinical neu-ropsychology through the 1970s. Since then, emphasishas shifted to a more behavioral focus, assessment of thehuman person, ranging from assessing cognitive abilitiesto evaluating quality-of-life indicators. In this approach,the goal as a clinical neuropsychologist is to describebrain–behavior functioning in such a manner as to accu-rately depict the current and future adaptive capabilitiesof the individual. Such information is important in evalu-ating the rehabilitation needs of a patient to facilitateadaptive functioning and prognosis, or in assessing the de-gree and type of assistance needed in the home and workenvironments. This chapter addresses these important is-sues in neuropsychological description, its similarities toand differences from generic psychological description,how it seeks to describe current adaptation in the realworld, and how neuropsychologists use it to predict thecourse of recovery or decline of an individual.
Interpreting NeuropsychologicalAssessment Data
By now it should be obvious that the neuropsycho-logical examination is a complex undertaking. Not only areno two patients alike, but how neuropsychologists adminis-ter the tests and which tests they select often differ. In addi-tion, many procedures we have reviewed measure more thanone functional domain, making it difficult to interpret theneuropsychological construct and cause underlying animpaired performance. This section presents an overviewof interpretative guidelines for the neuropsychologist.
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 79

80 PART ONE | Introduction
We provide quantitative and qualitative dimensions ofneuropsychological performance, as well as case studies;elucidate neuropsychological diagnosis; and detail evalua-tion. Although this depends on the specific referral ques-tion, the clinical neuropsychologist is primarily interestedin generating interpretive hypotheses about the patientand in answering specific questions about the test data,including the following:
Is there any cerebral impairment?Evidence of behavioral deficits?Behavioral changes caused by lesion?How severe is the injury?Is the injury medically significant?Does the injury impair the person’s ability to function in
his or her daily activities?Is the lesion progressive or static?Is the lesion diffuse or lateralized, or are there multiple
lesions?Is the impairment anterior or posterior? Can it be local-
ized?What is the most likely pathologic process? What is the
prognosis?What are the individual’s cognitive/behavioral strengths
and weaknesses, and how do they relate to daily livingskills, treatment, and rehabilitation?
Do the neuropsychological deficits influence the patient’squality of life?
What is the patient’s reaction to the injury and/or impair-ment?
A P P R O A C H E S T O N E U R O P S Y C H O L O G I C A LI N T E R P R E T A T I O N
Clinicians disagree somewhat in their approach to neu-ropsychological interpretation. These differences centeron both practical and theoretical test issues and have be-come a source of debate. In making determinations re-garding the evolution of a specific assessment and inter-pretation approach, practical and theoretical issues areoften intertwined. A typical example is test selection andtime needed for completing the neuropsychological ex-amination. Neuropsychologists usually broaden informa-tion regarding a patient by administering a wider range oftests (such as memory, motor, learning, and language);they deepen information by administering a number oftests examining varying aspects of the same cognitive do-main (such as selective attention or sustained attention).They must balance these theoretical considerationsagainst the practical reality of examination length. Manypatients cannot tolerate long testing sessions because of
fatigue effects. Given the current climate in which man-aged health care reduces specialized services to patients,most clinicians are also concerned about cost-effectivenessin time spent on evaluating the patient.
The approaches presented here include the majorstrategies of neuropsychological assessment and interpre-tation from which numerous variations have developed.We discuss the pros and cons of each approach in regardto both theoretical and practical issues.
S t a n d a r d B a t t e r y A p p r o a c h
Halstead (1947) and Reitan (1966) pioneered the use of astandard battery approach of tests for identifying braindamage. First, Halstead and Reitan identified tests thatwere sensitive to the integrity of cortical functioning.Then they sought to incorporate the evaluation of all themajor cognitive, sensory, motor, and perceptual skills thata neuropsychological examination should reflect. Thepurpose of the Halstead–Reitan Neuropsychological Bat-tery was to allow the development of various principlesfor inferring psychological deficit as applied to results ob-tained on individual subjects (Reitan & Wolfson, 1993).In this approach, the clinician gives the same tests to allpatients, regardless of his or her impression of an individ-ual patient or the referral question. Typically, a technicianadministers the neuropsychological procedures, ratherthan a doctoral-level psychologist, because the tests areadministered according to standardized rules of proce-dure, without variations. Using technicians allows moretesting for the same cost, because the more expensive timeof a doctoral-level neuropsychologist is not needed.
This standard battery approach has several advantages.First, it can ensure that all subjects are evaluated for allbasic neuropsychological abilities. This makes it unlikelythat the diagnosis could overlook a condition of impor-tance. Second, the neuropsychologist can use the data toidentify objective patterns of scores that he or she canconsider in diagnosing various neuropathologic condi-tions. Patterns within the data can help in diagnosing theprobability of certain causes of brain dysfunction. Knowl-edge of causes can be useful in providing the patient,physician, or treatment team with tentative diagnoses, aswell as in predicting the course of a disorder. Finally, thestandard battery approach lends itself to the teaching ofneuropsychological assessment and interpretation, becausethe beginning neuropsychology student need not makedecisions about test selection, and the interpretation isobjective and data driven. Finally, because the test instruc-tions, test selection, and test interpretation are all stan-dardized, this approach is particularly useful for empirical

studies and facilitates comparison across different researchprojects.
There are also drawbacks to the test battery approach.The time involved in testing any patient can be consider-able. Problems such as fatigue or loss of motivation maydevelop. The time involved forces the use of a testing tech-nician to ensure a reasonable cost and reasonable use ofthe neuropsychologist’s time. As a result, the neuropsy-chologist may have little contact with the patient outsideof the interview and, thus, loses the opportunity to make aqualitative analysis of the patient’s behavior. Obtainingqualitative impressions of the patient’s appearance and be-havior often is important, however. For example, we onceobserved a neuropsychologist who used the standard bat-tery approach make an interesting misdiagnosis. This par-ticular neuropsychologist strictly favored the neuropsy-chological battery approach and therefore typically did notinterview his patients. He claimed that the subjective pre-sentation of the case would “contaminate” his ability tomake an objective interpretation. During a neuropsycho-logical examination of a patient, the neuropsychologist’spsychometrician indicated on her data summary sheet thatthe patient’s performance on the Finger Tapping test waszero. The neuropsychologist proceeded to interpret thisscore as “severe, right-sided, upper extremity motor slow-ing with possible corresponding left hemisphere corticaldysfunction.” But visual inspection of the patient wouldhave made it obvious that the patient was not sufferingfrom motor slowing and “brain damage”—instead, hisright arm was amputated! The issue of using psychometri-cians to administer the neuropsychological tests remainscontroversial in contemporary neuropsychology.
The original choice of tests to include in the batteryheavily influences standard batteries. The theoretical be-liefs of the person doing the choosing often bias thechoice. A poorly chosen test battery, no matter how manytimes it is given, will continue to yield unsatisfactory re-sults. In different situations, alternate areas of assessmentmay be more effective in providing information. How-ever, because the user of a standard battery gives no addi-tional tests, he or she would never discover this. For ex-ample, the Halstead–Reitan Neuropsychological Batterydoes not include a memory test.
You can see a common problem of interpreting theempirical approach in composite tests that require the ex-aminee to have a number of cognitive skills. For example,the Hooper Visual Organization Test (Hooper, 1983) re-quires the subject to name or write more or less readilyrecognizable cut-up objects. The Hooper consists of 30stimuli. The maximum score is 30, and a score below 20
typically indicates “organic brain pathology.” Because ex-aminers think the measure primarily measures perceptualintegration, a function often associated with right hemi-sphere function, they often interpret low scores as percep-tual fragmentation most likely related to dysfunction ofthe right hemisphere. However, left hemisphere stroke pa-tients often make low scores on this test, not related toimpaired perceptual functioning, but related to the pa-tient’s impairment in naming objects. Thus, critiques ofthe battery approach often suggest that understandingwhy a patient failed a task is as valuable as that the personfailed (Luria, 1966). Such information, they argue, oftencan be more useful than test scores in making interven-tion and diagnostic decisions. Furthermore, opponents ofthe empirical approach argue that complex behavior can-not and should not be reduced to a single number or testscore. For example, the Hooper demands include com-prehending the instruction; visually scanning the stimu-lus figure; mentally rotating the cut-up parts of the objectto form a whole; and recognizing, naming, and articulat-ing the object, either in writing or orally. Thus, this seem-ingly simple task actually requires the person to integratea number of neuropsychological processes to generate acorrect response.
The standard battery method also fails to recognizethat altering a test procedure is sometimes valuable in de-termining a specific deficit. A standard battery may notbe appropriate for all patients, especially when there areperipheral deficits, such as injury to the limbs, a seriousvisual loss, or spinal cord injury. Such patients’ inabilityto complete a given test may reflect a peripheral motor orvisual problem, rather than a dysfunction of the centralnervous system. Consequently, data from such a patienton a standard battery may be useless for diagnosis, evalua-tion, and intervention. Finally, interpreting even a stan-dard battery requires considerable skill, knowledge, andexperience. Nevertheless, as standard rules and norms de-velop, standard batteries are somewhat easier to interpretand to teach.
Although the criticisms of the battery approach arevalid, many psychologists remain faithful to administer-ing a “core battery.” Approximately 55% of neuropsychol-ogists favor a flexible, modified battery approach, suggest-ing that the type of patient treated and the nature of thereferral question play important roles in test selection.
P r o c e s s A p p r o a c h
The process approach to neuropsychological testing,often called the hypothesis approach, rests on the idea thatthe neuropsychologist should adapt each examination to
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 81

82 PART ONE | Introduction
the individual patient. Rather than using a standard bat-tery of tests, the neuropsychologist selects the tests andprocedures for each examination, using hypotheses heor she has made from impressions of the patient andfrom information available about the patient. As a re-sult, each examination may vary considerably from pa-tient to patient for length and test selection. The clini-cian may use standard tests, or may alter and adapt testsas he or she tries to form an opinion on the nature ofthe deficits (Christensen, 1979; Lezak et al., 2004). Al-tering tests to discover the patient’s strategies is a popu-lar method within the process approach to neuropsycho-logical assessment (e.g., see Milberg, Hebben, & Kaplan,1986). Many conclusions reached in the examinationfollow the clinician’s qualitative interpretations of thetest results and the patient’s behavior. The clinician alsogrounds the conclusions on his or her experience andknowledge of the clinical literature. The principal devel-opers of the process approach are Alexander Luria andEdith Kaplan.
The process approach has several advantages. First, itacknowledges the individual nature of the patient’sdeficits and seeks to adapt the examination to this indi-viduality. Under the proper condition, such a techniquecan yield more precise measurements of a subject’s skillon a given ability than just the patient’s score on a giventest. Second, the examination can concentrate on thoseareas the neuropsychologist sees as most important for thepatient. It can ignore areas not important for the patient’sprognosis. Because the time for any examination is lim-ited, this enables the clinician to more thoroughly investi-gate significant areas.
Perhaps most important, the flexible/process approachemphasizes in what manner a patient fails or succeeds in aspecific cognitive task. For example, a patient is unable toanswer the question, “What is the capital of the UnitedStates?” Does this relate to the patient not understandingthe question (speech comprehension), does it indicate aninability to answer verbally (expressive aphasia), or doesthe patient not know the answer (poor factual knowl-edge)? The standard battery approach does not allow adeviation from the standard instructions of the test, be-cause deviating would invalidate the results. If the patientis unable to answer the question, the process approach al-lows for further investigation. For example, the examinercan show the patient a multiple-choice card with the an-swer and several wrong alternatives. If the patient pointsto the correct answer, “Washington, D.C.,” the neu-ropsychologist would interpret this response as meaningthat the patient knows this factual knowledge but cannotexpress this information either verbally or in writing.
Thus, the process approach lets the clinician concentrateon tasks related to the most important deficits that thepatient exhibits.
The process approach also has several disadvantages.Because the content of the examination emphasizes areasthat the clinician believes are important, the examinationmay selectively confirm the clinician’s opinion. Becausethe clinician may never test areas that he or she sees as ir-relevant, no one may realize that a deficit has been missed.Because the test’s focus is just on the patient and his orher expected problems, the data may be biased towardconfirming the original hypothesis. Thus, many neu-ropsychologists believe this more subjective approach re-lies willy-nilly on clinical experience, hunches, colleagues’anecdotes, intuition, common sense, folklore, and intro-spection (Meehl, 1973).
Using tests not standardized for a clinical population,or tests that have been adapted, also presents potentiallyserious problems. The interpretation of a test that has notbeen adequately standardized is always questionable. Theclinician’s subjective impression of what a score shouldmean for a given patient may be quite wrong. A test thatappears to measure one thing in a normal population maymeasure something entirely different in a brain-injuredpopulation. In each of these situations, the accuracy ofthe individual clinician’s judgment becomes the accuracyof the test. Thus, in the process approach, the opinion ofthe clinician is as good as his or her reputation. Currently,no measures of such accuracy exist, but probably thisvaries considerably among clinicians.
The use of different examinations and procedures foreach patient precludes the experimental validation of in-dividual tests in applied clinical settings. It also precludesevaluation of the process as a whole, because conclusionsdo not come from test scores, but from the clinician’sjudgments. Clinicians may, in such a situation, continueusing an ineffective test because it appears to work. Theprocess approach, therefore, does not lend itself to large-scale research, but often relies on case studies.
Structuring an examination on an individual basis maymean that it assesses only some of the basic functions me-diated by the brain. Rehabilitation and prognosis dependon the state of the brain as a whole; the lack of informa-tion on the entire brain can impede an interventionprogram or invalidate a prognosis. In practice, it is notunusual to see patients with secondary deficits that ap-pear unrelated to their primary referral problem and tothe impression that the patient gives. For example, it isnot unusual for a patient with a major stroke to have hadsmaller, secondary disorders of cerebral circulation. Thedeficits might have existed before the patient’s current

problem arose. Whatever the source of the deficits, theclinician must identify and consider them in making anyrecommendations for a client. Finally, the flexible/processapproach is more difficult to teach to students, becausefew “rules” and “procedures” exist. Test selection, adapta-tion, and interpretation depend largely on extensive clini-cal experience. This approach is also time-consuming, be-cause the neuropsychologist, rather than a technician,must perform the evaluation. Table 3.4 reviews the ad-vantages and disadvantages of the standard battery andprocess approaches.
Paul Meehl, a preeminent psychodiagnostician andformer president of the American Psychological Associa-tion, addressed the complex decision-making process in-volved in psychological assessment. In 1957, he wrote thenow-classic essay entitled “When Shall We Use OurHeads Instead of the Formula?” (1973). With this questionhe examined the rationale for when to use more empirical(psychometric) compared with more clinical approaches(qualitative) to psychological assessment, interpretation,and diagnosis. By the term formula, Meehl implied the sci-entific, empirical, and data-driven approach to psychol-ogy, consistent with those neuropsychologists who favorthe fixed battery approach. By “using our heads,” in con-trast, Meehl was referring to the more clinical, common-sense, approaches typically used by the process approachin neuropsychology. Meehl suggested that the two an-swers to his question—“Always” and “Never”—wereequally unacceptable. He also proposed that it would besilly to answer, “We use both methods; they go hand inhand.” If the formula and your head invariably yield the
same predictions about an individual, you should use theless costly method, because the more costly one is notadding anything. If the methods do not always yield thesame prediction—and most empirical studies show thatthey do not—then the psychologists cannot use both, be-cause they cannot predict in opposite ways for the samepatient.
This discussion remains a central theme in any type ofpsychological assessment, although the empirical approachhas been increasingly refined since Meehl wrote his fa-mous paper. Empirical and theoretic considerations sug-gest that the field of neuropsychology would be well ad-vised to continue to concentrate efforts on improvingactuarial techniques, rather than to focus on calibratingeach clinician for each of many different diagnostic prob-lems. In the meantime, neuropsychologists continue tomake descriptions, interpretations, and predictions abouthuman behavior. How should neuropsychologists bemaking interpretive decisions? Should they use theprocess approach, or should they follow the empirical,psychometric approach? Mostly, neuropsychologists willuse their heads, because researchers have not developedadequate empirical batteries for every type of neuropsy-chological problem. In those cases in which there are goodempirical approaches to neuropsychological problems (asin estimating intelligence), they should use an empiricalapproach. What if there is a case in which the formuladisagrees with the clinical opinion of the process ap-proach? Which approach should neuropsychologists usethen? Meehl, a staunch scientist, suggested that in such asituation, they should use their heads very, very seldom—
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 83
Standard Battery Approach Process Approach
Same tests or “core battery” given to all Examination administered by a neuropsychologistTests administered according to standardized rules Tests not administered in a standard wayInterpretation based on standardized norms Conclusions based on clinical experience
AdvantagesComprehensive evaluation of abilities Acknowledges the individuality of patientObjective interpretation based on normative data Examination focuses on most important deficitsFacilitates teaching because of standard rules/norms Emphasizes how a task is failed or solvedUseful for empirical studies Useful for clinical case studies
DisadvantagesTime demanding and labor intensive Test procedure may be biased by clinicianTests only as good as standardization Opinion of the clinician is subjectiveRelatively inflexible approach to testing Difficult to teach, because it requires experienceScores may not reflect a single cognitive process Does not lend itself to large-scale research
Table 3.4 Summary and Comparison of Approaches to Neuropsychological Interpretation

84 PART ONE | Introduction
except, of course, if the issue is as clear as a broken leg oramputated arm.
Considerable controversy has raged about the preced-ing approaches to performing and interpreting a neuropsy-chological evaluation. Although there are certainly schoolsof thought about this, almost 50% of neuropsychologistsreport using parts of both approaches (Figure 3.15). Thatis, a majority of neuropsychologists use a modified bat-tery approach, in which they choose specific tests to an-swer a referral question. They may interpret some tests inan empirical fashion and other test behavior in a morequalitative way. Approximately 25% report that theystrictly adhere to a standard/fixed battery approach or aprocess/qualitative approach.
We caution the neuropsychology student that diag-nostic and treatment decisions warrant integrating datadrawn from a number of sources, including neuropsy-chological measures, pertinent neuromedical findings,and the patient’s developmental and medical histories.Neuropsychologists typically do not render diagnosticdecisions based on a single neuropsychological mea-sure. Obviously, site, nature, and severity of the in-jury/disease process, premorbid personality, and a hostof other moderating variables affect neuropsychologicaltest performance. Interpreting the neuropsychologicaldata requires a thorough understanding of neuropsy-chological principles, developmental findings, andpsychopathology.
Interpretation of the neuropsychological protocol canthen proceed through several levels of analysis, includingthe following:
Overall level of impairment
Pattern of impairment
Lateralizing and localizing signsQualitative observations
Once interpretation proceeds through these levels, theneuropsychologist can then evaluate test data to deter-mine consistency with a patient’s known medical condi-tions and presenting diagnoses, as well as to predict func-tional abilities and limitations.
A S S E S S I N G L E V E L O F P E R F O R M A N C E
U s e o f N o r m s i n N e u r o p s y c h o l o g y
The use of norms in neuropsychology entails comparingan individual’s test scores and available normative data.This approach provides the neuropsychologist with infor-mation regarding an individual’s ability in comparisonwith others. This method compares the patient’s score ona test to an expected score, or norm. The method deter-mines the expected test score from the performance of anormative sample of patients and control subjects. Suchnorms may take into account such factors as age, sex, ed-ucation, and intelligence. Many neuropsychological testshave a cutoff score. A patient scoring worse than the cut-off score is labeled as impaired; a patient scoring better islabeled as within normal limits.
The selection of any specific cutoff point relates to fac-tors of test specificity and test sensitivity. When seeking toidentify people whose cognitive abilities are abnormal (e.g.,brain damage), neuropsychologists prefer a sensitive test. Insuch cases, they set the cutoff score so that as few errors aspossible arise in classifying a disease entity. However, sensi-tive tests that rely on measuring impaired cognitive func-tioning may also include false-positive errors, for example,erroneously identifying psychiatric patients as brain dam-aged. Such a test is of little value to the neuropsychologist,who wants to delineate the precise nature of a patient’sdeficits. Rather, the clinician needs tests that examine spe-cific aspects of neuropsychological functions; that is, teststhat have high specificity. Such tests may assess more gen-eral areas of cognitive functioning, including sustained at-tention or immediate memory. But they may miss patientswho have impairments outside of those specific areas of cog-nitive functions, which results in false-negative errors. Ofcourse, tests that have high sensitivity and high specificityare most useful in neuropsychology. In reality, there is al-ways a tradeoff between aspects of how specific a procedureis versus its usefulness as a sensitive test. Thus, neuropsy-chologists often set cutoff scores at an intermediate point atwhich the chances of misclassifying either impaired perfor-mance or normal performance are about equal.
50
Per
cent
age
40
30
20
10
0Modified/extended
48%
Process/qualitative
26%
Fixed battery/psychometric
22%
Figure 3.15 Approaches to neuropsychological testinterpretation. (Reproduced from Gordon, A., & Zillmer, E. A.[1997]. Integrating the MMPI and neuropsychology: A surveyof NAN membership. Archives of Clinical Neuropsychology, 4,325–326, by permission of Elsevier.)

S t a t i s t i c a l A p p r o a c h e s
When administering a battery of tests, it is important tobe able to compare performance on tests that measurewidely different skills. As you gain enough experiencewith a set of tests, this skill often becomes automatic.However, the easiest way to accomplish this task is to usestandardized scores rather than raw scores. A raw score isa score that is presented in terms of the original test units.It is simply the number of items passed or points earned.A standard score, in contrast, is a derived score that usesas its unit the standard deviation of the population onwhich the developers standardized the test. Thus, a stan-dard score is a deviation score. A standard deviation re-lates to the variability or scatter of test scores. This pat-tern is known as a distribution of test scores. The normalprobability distribution (also known as the bell-shapedcurve) represents the frequency with which many humancharacteristics are dispersed over the population. Forexample, intelligence and spatial reasoning ability are dis-tributed in a manner that closely resembles the bell-shaped curve.
In the normal distribution, 68.2% of all cases fall be-tween �1 standard deviation (SD) from the mean, 95.4%of the cases fall between �2 SD from the mean, and99.7% of the cases fall within �3 SD from the mean. Thenormal distribution is the basis for the scoring system onmany standardized tests. For example, on the ScholasticAptitude Test (SAT), the developers set the mean at 500and the standard deviation at 100. Hence, SAT scores re-flect how many SDs above or below the mean a studentscored. For example, a score of 700 means that you scored2 SDs above the mean, exceeding approximately 97% ofthe population on which the test is normed. Thus, testscores that place examinees in the normal distribution canalways be converted to percentile scores, which are ofteneasier to interpret. A percentile score indicates the per-centage of people who score below the score you obtained.For example, if you score at the 60th percentile, 60% ofthe people who take the test scored below you, and theremaining 40% scored above you. Tables are available thatpermit transformation from any SD placement in a nor-mal distribution to a percentile score.
Neuropsychologists use a variety of standard scores.They determine standard scores by a mathematical for-mula that can convert raw scores from tests to a standardscale. For example, Table 3.5 lists commonly used stan-dardized scores in clinical neuropsychology.
Once you know the test score frequency of a neuropsy-chological measure, you can easily compute a standardscore. For example, determine the standard score (SS) byfirst subtracting the mean score from a normative group
for a test from the person’s actual score. Divide the resultby the SD of the scores in the normative sample. Multi-ply this result by 15 (the SD), and add 100 (the mean) tothis answer. The formula for standard score is as follows:
SS � 100 � � 15.0
The standardized score approach to neuropsychologi-cal assessment has several advantages. First, all scores areroughly comparable. Second, you can make adjustmentsfor such factors as age and education. You do this by de-termining normative means and SDs for different age oreducational levels. You can then include the normativescores corresponding to a given person’s age or education.Of course, not all neuropsychological measures result innormal test distributions. Some distributions skew in onedirection or another. Some neuropsychological tests, par-ticularly those that the process approach favors, are rela-tively “easy.” That is, most “intact” individuals wouldhave few problems passing the test. For example, “On aplain piece of paper, draw a clock with all the numbersand the hands of the clock positioned at 10 minutes after11.” Most individuals would pass this task, but patientswith disturbances in visuospatial perception or planningability may “fail.” Thus, the resulting test score distributionis dichotomous (pass/fail) and does not present a normaldistribution. It is inappropriate to calculate standard scoresfrom such a test distribution. A great pitfall of the statisti-cal approach to neuropsychological interpretation is thatdevelopers have transformed to standard scores many teststhat are not normally distributed, thus providing inexactestimations of performance.
(Score obtained minus average normative score)�����
Standard deviation (normative sample)
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 85
Name of Standardized Mean Standard Deviation Tests UsedScore
Z-score 0 1 None
Sten score 5 1 16 personalityfactors
Scaled score 10 3 Wechsler subtests
T-score 50 10 Minnesota Multi-phasic PersonalityInventory, manynorms
Standard score (SS) 100 15 Wechsler IntelligentQuotient scores
Table 3.5 Examples of Different Standardized Scores

86 PART ONE | Introduction
David was an active, 66-year-old, righthand–dominant, married man who had com-pleted 11th grade before joining the U.S.Armed Forces. Before retiring, David wasemployed as a medical technician in a psychi-atric hospital. His wife, a nurse, was his super-visor. In August 1992, David began experienc-ing periods of blurred vision, headaches,nausea and “feeling ill all over, as if I wascoming down with the flu.” The family doctorsuspected a heart problem because David hada history of mild hypertension and anginabeginning in 1987, but a 24-hour electrocar-diogram (EKG) monitor showed no heartmalfunction. Over the next month, Davidexperienced five similar episodes. Then, inSeptember 1992, he awoke with numbnessand weakness on the right side, as well asslurred speech, and was subsequently hospi-talized. Initial neurologic findings indicatedthat David was awake and alert with dysarthriaand right hemiparesis. The examiner notedperiods of paralysis, with the comment that thepatient felt “locked in” when these occurred.Physicians at the hospital diagnosed him ashaving had a transient ischemic attack (TIA;see Chapter 12). After a 10-day course oftreatment, the patient was sent home. Hospitalrecords noted that he was “fully recovered” atthis point.
MRI of the brain suggested prominence ofthe ventricular system and subarachnoidspaces consistent with moderate atrophy. Thereport also noted mild white matter changeson the periventricular region. CT and MRI filmsof the coronal (Figure 3.16) planes showed asubacute cerebellar infarct (stroke). CT scans
of the head, without intravenous contrastinfusion, confirmed the atrophy and previ-ously visualized infarct in the left cerebellum.Repeat CT scan of the head without contrast 3 weeks later showed an additional new smallinfarction in the left thalamus (see Figure3.16). Intracranial and neck angiogramsequences revealed no stenosis of the right orleft carotid artery bifurcations. Taken together,radiologic data suggested moderate atrophy,postacute left cerebellar infarct, a small leftthalamic infarct, and minimal thickening ofthe common, internal, and external carotidarteries. The radiologic studies did not indi-cate the presence of intracranial hemorrhageor any significant stenosis or plaque in theright or left carotid system. Electroencephalo-gram showed no definite focal or epilepto-genic features.
David continued to have episodes ofnausea and blurred vision, and in October1992, he was again hospitalized with righthemiparesis, dizziness, and slurred speech.Initial diagnosis was that he had sufferedanother TIA. He was experiencing projectilevomiting and had episodes of high fever andbrief periods when he could move only oneeye. He also had behavioral digressions duringwhich he would not recognize anyone andwould pull out his IV tubes and exhibit otherstrange behaviors until he had to be restrainedto the bed. The medical staff was mystified asto the causes of David’s symptoms.
A few weeks into David’s treatment, theCenters for Disease Control and Prevention(CDC) notified the hospital that David hadtested positive for Lyme disease. Puzzled by
the cause of David’s symptoms, his familydoctor previously had taken a blood serol-ogy before the second hospitalization andforwarded samples to the CDC. David wasgiven a course of treatment appropriate for
N e u r o p s y c h o l o g y i n A c t i o n 3 . 1
C a s e E x a m p l e : T h e N e u r o p s y c h o l o g y o f Ly m e D i s e a s e
by Eric A. Zillmer
Figure 3.16 Horizontal computed axialtomography scan (top) showing infarction inleft thalamus. Coronal magnetic resonanceimage (bottom) demonstrating subacutecerebellar infarct, as well as moderateatrophy. (Courtesy Eric Zillmer.)
D E F I C I T M E A S U R E M E N T
Deficit measurement, as an approach, is standardizedand group oriented. It is useful for understanding generalconditions and disease states. By comparing a person with“the norm,” you can determine statistically probabledeficits. By examining a battery of tests, you can examinean individual’s pattern of strengths and weaknesses. You
can compare these with known, general profiles. But clin-icians are also concerned with the uniqueness and dy-namic qualities of each individual. The adaptive approachto neuropsychology mirrors developments in other areasof psychology. To paraphrase Howard Gardner, theHarvard psychologist, neuropsychologists should not beasking, “How smart is this person?” but “How is this personsmart?” In clinical neuropsychology, the focus is not only

CHAPTER 3 | Neuropsychological Assessment and Diagnosis 87
both stroke and Lyme disease. As a result,David’s strange symptoms abated and havenot returned, though the hemiparesis anddysarthria remain. The hospital physiciandid not agree that Lyme disease was re-sponsible for David’s symptoms. David wasdischarged to a rehabilitation hospital forcontinued care, where he was referred forneuropsychological testing to evaluate hiscognitive status and his ability to participatein speech and physical therapies. Table 3.6reviews the results of the neuropsychologi-cal battery.
David exhibited generalized deficits, withimpaired performance across cognitiveareas. His performance on the neuropsycho-logical tests indicated impaired attentionalcapacity, motor slowness, weakness in thenondominant upper extremity (the patientwas unable to use his dominant hand),impaired fine-motor ability, left auditorysuppressions, impaired visuoconstructionalability, deficient spatial memory, and poorexecutive functioning. David’s memoryperformance demonstrated slightly impairedverbal recall, moderately impaired visualrecall, and moderately to severely impaireddelayed recall for both verbal and visualmaterial. His intellectual performance, asmeasured by the Wechsler Adult IntelligenceScale, Third Edition (WAIS-III), was in the LowAverage range. David’s IQ scores indicatedslightly higher verbal than performanceability, again partially because of his righthemiplegia, but also because of impairedperception of visual material, especiallyvisual details. The visual impairment wasfurther documented by his borderline perfor-mance on the Hooper Visual OrganizationTest. On the Wisconsin Card Sorting Task,David failed to complete any categories andused the maximum possible number of trialsto complete the test. Results of clinical
personality testing (Minnesota MultiphasicPersonality Inventory [MMPI]) did not indi-cate significant psychopathology or psycho-logical dysfunction. However, factors re-flected in the protocol did suggestsusceptibility to developing psychologicalproblems including denial, somatic concern,and tension. Individuals with similar profilesare often mildly dysphoric, pessimistic aboutthe future, and difficult to engage in psycho-logical therapies because of their defensive-ness and lack of insight.
The neuropsychological evaluation did notshed any light on whether Lyme disease wasthe “culprit” for David’s medical problems (fora more detailed description of the clinical,radiologic, and neuropsychological manifes-tations of Lyme disease, see Bundick, Zillmer,Ives, & Beadle-Lindsay, 1995). David’s caseanalysis demonstrates that psychological andneuropsychological assessment may serve toaid in the more definitive diagnosis andimproved intervention/rehabilitation ofpatients exhibiting complex symptoms.
Age, years 66Sex MaleEducation, years 11Occupation Retired medical technician
Intellectual functioning (WAIS-III)Verbal IQ 91 (31)Performance IQ 84 (28)Full Scale IQ 87 (27)
Abstract reasoning, cognitive efficiency, mental flexibilityTMT A (seconds) 109 (26)TMT B (seconds) 255 (35)Wisconsin Card Sort (in perseveration errors) 65 (34)
Memory: WMS-RLogical Memory I 19 (36)Logical Memory II 5 (11)
Motor speed and coordinationFinger Oscillation DH Not attemptedFinger Oscillation NDH 31 (29)Grooved Pegboard (seconds) DH Not attemptedGrooved Pegboard (seconds) NDH 154 (34)
Note: WAIS-III = Wechsler Adult Intelligence Scale, Third Edition; IQ = intelligence quotient; TMT = Trail Making Test;WMS-R = Wechsler Memory Scale–Revised; DH = dominant hand; NDH = nondominant hand.
T-scores in parentheses from Heaton, Grant, and Matthews (1991).
Table 3.6 Neuropsychological Profile of Patient with Lyme Disease
on the level of deficits and strengths to describe function-ing; for example, “How adapted (normal) is this person?”but also, “How does this person adapt to his or her con-dition?” Neuropsychologists should question what is lostin terms of understanding the brain if they do not con-sider the range and extent of individual adaptations to in-jury, tumor, and disease.
D i f f e r e n t i a l S c o r e A p p r o a c h
The deficit measurement approach compares a patient’sscore on two tests. One test is theoretically highly sensi-tive to brain damage (e.g., a new problem-solving task);the second is theoretically insensitive to brain dysfunction(e.g., a measure of factual language). The insensitive testis supposed to reflect the individual’s ability before any

88 PART ONE | Introduction
brain injury occurred, whereas the sensitive test reflectsthe effects of brain damage. If the sensitive test score issignificantly worse, the neuropsychologist assumes thedifference is caused by a brain injury. In general, you com-bine two test scores to get a single score measuring theirdifference. You may accomplish this by simply subtract-ing or dividing one score by the other. Then analyze thissingle score by treating it as described in earlier in the As-sessing Level of Performance section.
P a t t e r n A n a l y s i s
A modification of the differential score approach is pat-tern analysis, which examines the relationships amongthe scores in a test battery. It seeks to recognize patternsconsistent with specific injuries and particular neurologicprocesses and has value in identifying mild disorders thatcause relatively little disturbance in level of performance.For example, in early stages of Alzheimer’s dementia, neu-ropsychologists would expect a deficit in memory func-tioning compared with performance on verbal tests,which may be relatively normal. If you plot all the neu-ropsychological data on a standardized norm worksheet, aprofile of cognitive skills may emerge. You can then ob-serve the interrelationships among these differing cogni-tive skills areas. A basic method of pattern analysis in-volves observing strengths and weaknesses in the highestand lowest scores. You can evaluate cognitive strengthsand weaknesses relative to the normative group by observ-ing which scores fall above, below, or within the averagerange. You can also determine strengths and weaknessesrelative to the individual’s specific profile. Again, high andlow scores are highlighted, but without regard for wherethey fall relative to the normative sample. Finally, you canintegrate information about cognitive strengths and weak-nesses with therapeutic suggestions to family and thetreatment team to improve the patient’s recovery.
The differential score method and pattern analysishave the advantage of recognizing that each individualstarts at a different level of performance. Thus, it avoidserror of misclassifying all people with low ability as“brain injured.” However, this approach has several po-tential sources of error. First, a sensitive test may fail toreflect the impairment present. Currently, no test is sen-sitive to all forms of brain dysfunction. Second, thebrain injury may lower a score on an insensitive test. Be-cause all abilities depend on the brain, brain damage canaffect all abilities. No test is fully insensitive to brain in-jury. Finally, relatively little is known about specific pat-terns of deficits that correlate with specific neurologicdisorders, or how to set any cutoff points to identifythose conditions.
L A T E R A L I Z I N G S I G N S
The two cerebral hemispheres control the contralateralsides of the body for most sensory and motor behaviors.If one side of the body performs significantly worse thanthe other, the opposite hemisphere may have been in-jured. Lateralizing signs are specific test results or behav-iors that suggest right or left cerebral hemisphere dys-function. This approach resembles the differential scoreapproach in that one side of the body serves as the con-trol for the other. Generally, you subtract the scores fromthe two sides of the body to obtain a single differencescore. You then treat this score as described in the level-of-performance approach. This approach may yield in-accurate conclusions, however, when an injury involvesboth hemispheres, or when an injury to the spinal cordis involved, because such injuries may also cause lateral-ized motor or sensory deficits or impair performancebilaterally.
P A T H O G N O M O N I C S I G N S ( Q U A L I T A T I V E O B S E R V A T I O N S )
Examining pathognomonic signs is a method that clini-cal neurologists commonly use. In the medical model, theclinical examination often assumes that specific, distinc-tive characteristics of a disease or pathologic conditioncan be detected. These signs or symptoms are often la-beled pathognomonic (derived from Greek meaning “fit togive judgment”), because often a specific diagnosis can bemade from them. The medical model is a causal model inwhich specific signs stem either from a specific medicalcondition or from the disease itself. Thus, a standard med-ical examination is often a series of medical tests forpathognomonic signs. Once a disease has been diagnosed,it can be treated. This model has served the field of medi-cine rather well. For example, the model attempts to fit(pigeonhole) the available information from the medicalexamination into often rigid and inflexible diagnostic cri-teria. Also, if the signs from the medical examination donot precisely fit, or are contradictory, and if some symp-toms are transient, the model does not work well, becauseno substantive diagnosis can be established; thus, no treat-ment can be offered.
Pathognomonic signs occur rarely in normal individ-uals. In clinical neurology, this includes such signs as aneye that will not move from side to side. In neuropsy-chology, examples of pathognomonic signs include therotation of a drawing or the failure to draw the left halfof a figure. You can count the number of pathognomonicsigns within a given test to get a summary number. You
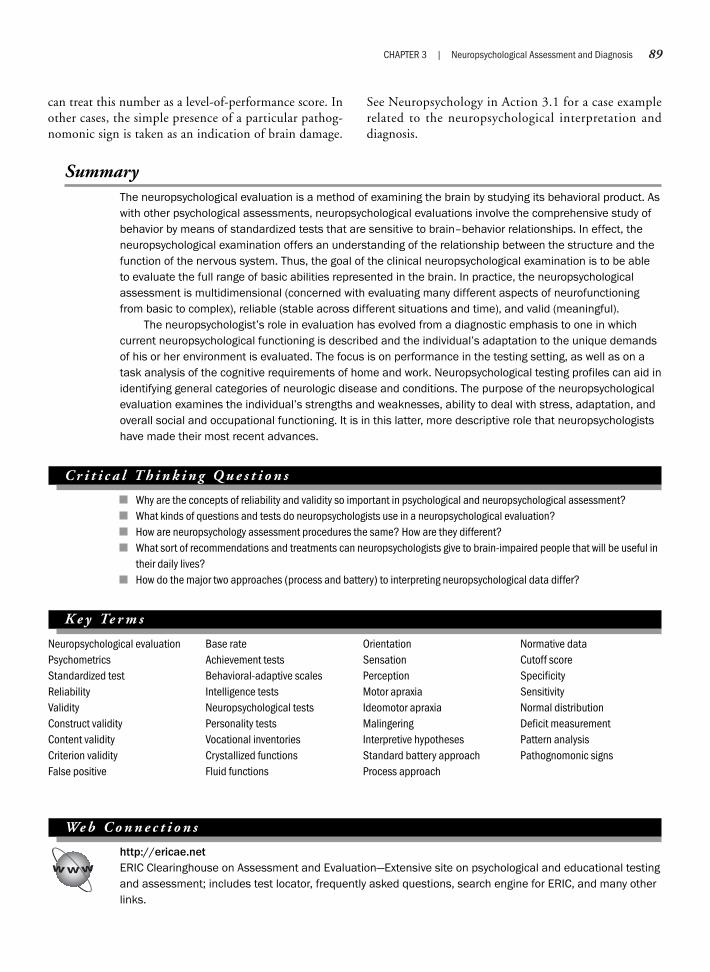
CHAPTER 3 | Neuropsychological Assessment and Diagnosis 89
SummaryThe neuropsychological evaluation is a method of examining the brain by studying its behavioral product. Aswith other psychological assessments, neuropsychological evaluations involve the comprehensive study ofbehavior by means of standardized tests that are sensitive to brain–behavior relationships. In effect, theneuropsychological examination offers an understanding of the relationship between the structure and thefunction of the nervous system. Thus, the goal of the clinical neuropsychological examination is to be ableto evaluate the full range of basic abilities represented in the brain. In practice, the neuropsychologicalassessment is multidimensional (concerned with evaluating many different aspects of neurofunctioningfrom basic to complex), reliable (stable across different situations and time), and valid (meaningful).
The neuropsychologist’s role in evaluation has evolved from a diagnostic emphasis to one in whichcurrent neuropsychological functioning is described and the individual’s adaptation to the unique demandsof his or her environment is evaluated. The focus is on performance in the testing setting, as well as on atask analysis of the cognitive requirements of home and work. Neuropsychological testing profiles can aid inidentifying general categories of neurologic disease and conditions. The purpose of the neuropsychologicalevaluation examines the individual’s strengths and weaknesses, ability to deal with stress, adaptation, andoverall social and occupational functioning. It is in this latter, more descriptive role that neuropsychologistshave made their most recent advances.
C r i t i c a l T h i n k i n g Q u e s t i o n s
Why are the concepts of reliability and validity so important in psychological and neuropsychological assessment?What kinds of questions and tests do neuropsychologists use in a neuropsychological evaluation?How are neuropsychology assessment procedures the same? How are they different?What sort of recommendations and treatments can neuropsychologists give to brain-impaired people that will be useful intheir daily lives?How do the major two approaches (process and battery) to interpreting neuropsychological data differ?
K e y Te r m s
Neuropsychological evaluationPsychometricsStandardized testReliabilityValidityConstruct validityContent validityCriterion validityFalse positive
Base rateAchievement testsBehavioral-adaptive scalesIntelligence testsNeuropsychological testsPersonality testsVocational inventoriesCrystallized functionsFluid functions
OrientationSensationPerceptionMotor apraxiaIdeomotor apraxiaMalingeringInterpretive hypothesesStandard battery approachProcess approach
Normative dataCutoff scoreSpecificitySensitivityNormal distributionDeficit measurementPattern analysisPathognomonic signs
We b C o n n e c t i o n s
http://ericae.netERIC Clearinghouse on Assessment and Evaluation—Extensive site on psychological and educational testingand assessment; includes test locator, frequently asked questions, search engine for ERIC, and many otherlinks.
can treat this number as a level-of-performance score. Inother cases, the simple presence of a particular pathog-nomonic sign is taken as an indication of brain damage.
See Neuropsychology in Action 3.1 for a case examplerelated to the neuropsychological interpretation anddiagnosis.
90 PART ONE | Introduction
http://www.unl.edu/burosBuros Institute of Mental Measurement—Home page of the Buros Mental Measurements Yearbook, tests inprint, test reviews, and test locators.
http://www.mindtools.com/page12.htmlPsychometric Testing—Interactive page that lets you discover your learning style; provides “IQ test,”Myers–Briggs Personality Test(R), and other measures.
http://www.toldx.comMore information on the Tower of London test.
http://www.sportsci.org/resource/stats/index.htmlA New View of Statistics—This site features a web-based book about the ins and outs of statistical proce-dures using simple sports analogies and common everyday problems. Within this site you can find concreteexamples of simple statistical terms and validity and reliability procedures on interpretation discussed inthis chapter.
Part Two
T H E F U N C T I O N I N G B R A I N
Chapter 4 Cells of Thought
Chapter 5 Functional Neuroanatomy
Chapter 6 Cerebral Specialization
Chapter 7 Somatosensory, Chemical, and Motor Systems
Chapter 8 Vision and Language
Chapter 9 Memory, Attention, Emotion, and Executive Functioning

This page intentionally left blank

Chapter 4
CELLS OF THOUGHT
Immense numbers of individual units, the neurons, completely indepen-dent, simply in contact with each other, make up the nervous system.
—Santiago Cajal
An invitation is offered to cross a bridge as vast as the infinite space sur-rounding us and as small as the width of a neuron’s membrane. This is ajourney into unknown territory, a voyage into the mind. To know the mindis to know the universe.
—Fred Alan Wolf
Neurons and Glial CellsCommunication within a Neuron: The Neural ImpulseCommunication among NeuronsRegeneration of Neurons
Neuropsychology in Action
4.1 Short-Circuiting Neurons: Multiple Sclerosis4.2 Neuronal Firing: Clinical Examples4.3 What Can We Learn from Songbirds?4.4 Stem Cell Research: Science and Ethics
OverviewCells are the building blocks of all living organisms. Evolutionarily old, one-celled creatures such as theamoeba show elementary responses to sensation and have decision-making capabilities. In their universeof a droplet of water, amoebas can move about, locate food, and engulf it. They can differentiate light fromdark and warmth from cold. This unicellular organism uses complex electrochemical processes, but has nonervous system and no brain. Moving up the evolutionary ladder, increased complexity of behavior corre-sponds with a more specialized nervous system, which is essential for speeded communication. The “jelly-fish,” for example, has a rudimentary nervous system, which allows coordinated movement, but still has nobrain.
The human central nervous system (CNS) contains billions of interconnected cells. Of the two maintypes of cells, neurons alone account for about 100 billion cells, and estimates suggest that glial cells out-number neurons by 10 to 1. Considering there are approximately 6 billion people on earth, the number ofcells in one human brain is more like the number of stars in the sky. The CNS is not connected in a simple,linear fashion, but in a densely packed tangle of interconnected networks. If 1 neuron connected only to100 others, the emerging network would be staggering in its size and complexity. However, evidence sug-gests that the number of connections actually ranges from 1000 to 100,000, averaging about 10,000 perneuron (Beatty, 1995; Hubel, 1988). Cells of the CNS are specialized and interact with each other in aunique manner. Their processing systems require a great deal of energy and consume the most oxygen andglucose of any bodily system.
This chapter focuses on the essential building blocks of thought and behavior: neurons and glial cells.Neurons and glia are classes of cells that contain subtypes based on their structure and function. Neuronsare considered the most important cells, and the basic electrical-chemical processes of neuronal communi-cation have been well described by scientists. Although glial cells traditionally have been described as hav-ing a supporting function for neurons, science now suggests that glial cells may have a larger role to play inthought and learning. The neuron can be studied as a universe unto itself, but neuropsychology is alsofocused on the effect of behavior related to neuronal disruption. Clinical problems such as multiple sclero-sis (MS) and spinal cord injury are the direct result of disease or injury at the neuronal level. The ability ofthe neuron to repair itself is intriguing because of the enormous implications for treatment.
94 PART TWO | The Functioning Brain
K e e p i n M i n d
How does the unicellular neuron differ from a one-celled creature?
What are the purposes of different cell types in the central nervous system?
How do neurons communicate?
Are damaged neurons able to regenerate?
Neurons and Glial Cells
The neuron differs from other cells in that it is spe-cialized for information processing. To some degree allfunctions that sustain life, as well as those that make ushuman, are coordinated and depend on the communica-tion of neurons. Neurons are anatomically independent;
they come very close to each other but do not touch. Thenervous system thus consists of separate units rather thanone continuous structure.
The neuron has often been studied by scientists withthe idea that by studying the fundamental parts, a betterunderstanding of the whole can be achieved. This reduc-tionistic view attempts to investigate complex phenomena

by dividing them into more easily understood compo-nents. Reductionists may describe their work as mappingthe brain. Everything, they argue, exists at a particular lo-cation (Churchland, 1993). The neuron hypothesis is inaccord with this viewpoint suggesting that (1) all neuralfunction is reflected in behavior, and (2) all behavior hasan underlying neural correlate (Pincus & Tucker, 1985).Reductionists argue that the healthy mature brain pro-duces the mind’s range of functions and experiences,which are perfectly correlated to precise biological phe-nomena. In other words, the reductionist viewpoint ar-gues that every human experience can be reduced to aphysical phenomenon. Although reductionism is consid-ered outdated and oversimplified because it is not possi-ble to correlate behavior with individual neurons, someneuropsychologists study the relation of behavior to as-semblies of neurons and interconnected neural networks.
The structure of neurons is similar to that of other bodycells in that they have a cell body that contains a nucleus,genes, cytoplasm, mitochondria, and other organelles nec-essary to conduct protein synthesis and energy production.However, neurons are quite different from other bodycells in several ways. For example:
1. They possess specialized extensions, dendrites andaxons, which allow for communication. Dendrites aretreelike or feathery extensions that branch from theneuron into the immediate neighborhood of the cellbody. The axon extends from the cell body to transmitinformation.
2. They possess specialized structures, particularly termi-nal buttons, which produce neurochemicals.
3. Neurons communicate through an electrochemicalprocess.
The structure of neurons allows them to communicatewith each other in an interesting way. Most body cellscommunicate with each other or the outside worldthrough energy exchange and intercellular transport,using the cellular membrane. Neurons, however, commu-nicate with each other by axonal firing, which allows elec-trochemical transmission across the synapse, the tiny gapbetween two neurons. The process of such communica-tion releases chemical neurotransmitters, permittinghighly sophisticated combinations of reactions that influ-ence downstream neuronal behavior.
Neurons also have properties of formation and regener-ation that differ from those of other body cells. In general,no new neurons form after birth (Cowan, 1990). In fact,during certain periods of development, massive pruningoccurs as important neural connections form in responseto learning and maturation. Excess neurons, which may
cause distracting associations, die off. An important ques-tion for brain science is to what extent neurons can re-generate once damaged. Neurons in the periphery canregenerate; for example, if surgeons reattach an ampu-tated finger, the finger may regain some mobility. Neu-rons in the spinal cord and brain do not heal sponta-neously. This is most evident in the complete severing ofneurons in the spinal cord, which leads to paralysis. Re-cent findings, however, suggest that some regrowth maybe possible. Research on reactivating damaged neurons isongoing, so perhaps some day scientists will be able to re-verse spinal cord damage (Naugle, Cullum, & Bigler, 1998).Later in this section (see Regeneration of Neurons) weexamine the question of neurogenesis, regeneration, andattempts to regain function after injury.
S T R U C T U R E A N D F U N C T I O N O F T H E N E U R O N
Neurons vary in shape and size, but have four commonfeatures (Figure 4.1):
1. A cell body with a nucleus2. Dendrites3. An axon4. Terminal synaptic buttons
Neurons are specialized to exchange information, specifi-cally the reception, conduction, and transmission of elec-trochemical signals.
C e l l B o d y
The functioning and survival of the neuron depend on theintegrity of the cell body that controls and maintains theneuronal structure. Because these cell bodies are gray, the term gray matter is used to describe areas of the brainthat are dense in cell bodies, such as the cortex. The cellsoma contains mitochondria, amino acids, and DNA, andit has the same properties of other cells in the body. Pro-tein synthesis cannot occur in the axon, so all axonal pro-teins come from the cell body.
D e n d r i t e s
Neurons generally receive chemical transmissions from oneanother through dendrites, feathery extensions that branchfrom the neuron into the immediate neighborhood of thecell body. There are often thousands of dendrites per neu-ron, and they differ in relation to the different functions ofthe neurons. The profuse branching of dendrites allowsthem to receive communication from a large number of ax-onal terminals across the synapse. The shapes of dendritic“trees” are often among the most characteristic morphologic
CHAPTER 4 | Cells of Thought 95

features of a neuron (Figure 4.2). For example, dendrites ofPurkinje cells (see Figure 4.2a), which are found in allareas of the cerebellar cortex, are characteristically spreadout in one plane and have thousands of dendritic spines.Many dendrites are covered with spines, or small knobs,that form the synaptic connection with communicatingneurons. Dendrites are tiny, only visible under an electronmicroscope, and are usually shorter than the axon, but theycan have up to thousands of synapses or contacts with otherneurons. Neuroscientists estimate that the total possibleconnectivity among neurons in the human brain is approx-imately 1015, or 10,000,000,000,000,000—more numer-ous than the known stars in the universe (Beatty, 1995;
Williams & Herrup, 1988). Dendrites comprise most ofthe receptive surface of a neuron.
A x o n
The axon extends away from the cell body. Its primary func-tion is to transmit electrochemical information from the cellbody to the synapse through microtubules along its length.Axons are anywhere from less than 1 millimeter (mm) inlength to 1 meter (m) or more. Large motor neurons havelong axons, some of them reaching from the lower end ofthe spinal cord to the foot muscles. Other neurons, includ-ing those that coordinate activity within a specific region ofthe CNS, have short axons. Unipolar axons proceed from
96 PART TWO | The Functioning Brain
Text not available due to copyright restrictions
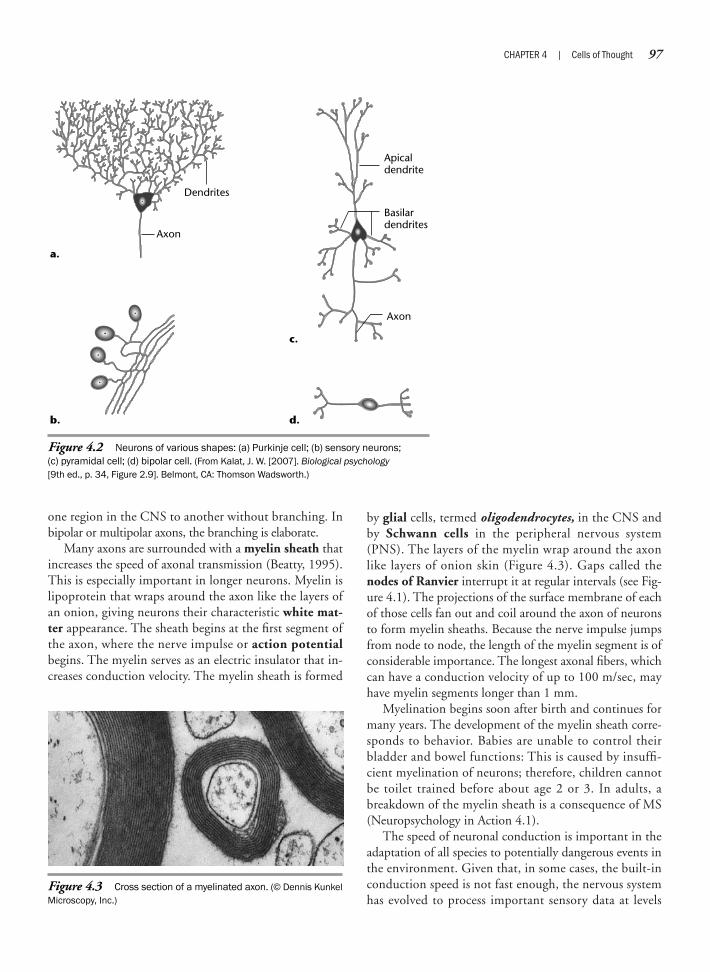
one region in the CNS to another without branching. Inbipolar or multipolar axons, the branching is elaborate.
Many axons are surrounded with a myelin sheath thatincreases the speed of axonal transmission (Beatty, 1995).This is especially important in longer neurons. Myelin islipoprotein that wraps around the axon like the layers ofan onion, giving neurons their characteristic white mat-ter appearance. The sheath begins at the first segment ofthe axon, where the nerve impulse or action potentialbegins. The myelin serves as an electric insulator that in-creases conduction velocity. The myelin sheath is formed
by glial cells, termed oligodendrocytes, in the CNS andby Schwann cells in the peripheral nervous system(PNS). The layers of the myelin wrap around the axonlike layers of onion skin (Figure 4.3). Gaps called thenodes of Ranvier interrupt it at regular intervals (see Fig-ure 4.1). The projections of the surface membrane of eachof those cells fan out and coil around the axon of neuronsto form myelin sheaths. Because the nerve impulse jumpsfrom node to node, the length of the myelin segment is ofconsiderable importance. The longest axonal fibers, whichcan have a conduction velocity of up to 100 m/sec, mayhave myelin segments longer than 1 mm.
Myelination begins soon after birth and continues formany years. The development of the myelin sheath corre-sponds to behavior. Babies are unable to control theirbladder and bowel functions: This is caused by insuffi-cient myelination of neurons; therefore, children cannotbe toilet trained before about age 2 or 3. In adults, abreakdown of the myelin sheath is a consequence of MS(Neuropsychology in Action 4.1).
The speed of neuronal conduction is important in theadaptation of all species to potentially dangerous events inthe environment. Given that, in some cases, the built-inconduction speed is not fast enough, the nervous systemhas evolved to process important sensory data at levels
CHAPTER 4 | Cells of Thought 97
Dendrites
Axon
Axon
Apicaldendrite
Basilardendrites
a.
c.
b. d.
Figure 4.2 Neurons of various shapes: (a) Purkinje cell; (b) sensory neurons; (c) pyramidal cell; (d) bipolar cell. (From Kalat, J. W. [2007]. Biological psychology[9th ed., p. 34, Figure 2.9]. Belmont, CA: Thomson Wadsworth.)
Figure 4.3 Cross section of a myelinated axon. (© Dennis KunkelMicroscopy, Inc.)

closer to their origin. The knee reflex is an example. Thesensory information that you are about to fall is sent to yourspinal cord, which relays it directly back with “instruc-tions” to extend your knee. This occurs without anyhigher cognitive processing. If the same sensory informa-tion traveled to the brain, the relay would take too longto process, which could result in a fall. Another exampleis the reflex arc in response to pain, such as a burn. Thesensation is relayed to your spinal cord, which gives theappropriate response: “Withdraw finger!” The informa-tion also reaches your brain, of course, although somewhatlater; it is then processed at that higher level: “Did I burnmy finger?”
In large animals, such as dinosaurs, to compensate forthe relatively long distances sensory and motor neuronshave to travel, large dinosaurs had a small additional brainat the level of the pelvis. Presumably, the brain integratedmany sensory and motor functions at this level so the di-nosaur could respond adaptively to the environment.
T e r m i n a l B u t t o n s
Near the end of the axon are branches with slightly en-larged ends called axonal terminals or terminal buttons.The site of interneuronal contact, where neurochemicalinformation transmits from one neuron to another, iscalled a synapse (see later in this section for a detailed dis-cussion of synapses). The terminal button is the presy-naptic portion of the synapse, the place where electrical
nerve impulses cause the release of a neurotransmitter.This chemical in turn affects another neuron or muscle ineither an excitatory or an inhibitory manner. Signals thattravel along the axon are electrical, and the transfer ofneurotransmitters across synapses, from one neuron toanother, is chemical. Researchers can therefore study andanalyze the brain through electrical means—for example,using the electroencephalograph, evoked potential, orelectrical stimulation—or through biochemical or meta-bolic techniques such as positron emission tomography.
N e u r o n C l a s s i f i c a t i o n a n d T e r m i n o l o g y
Neurologists commonly classify neurons either by mor-phology (shape) or by function. The three principal classesof neurons are defined by the number of processes ema-nating from their cell bodies. Most are multipolar neu-rons, with more than two processes, or extensions fromthe cell body (see Figures 4.2a, c). One of these is the axon,and the others are dendrites extending from various partsof the cell body. Bipolar neurons have two processes (seeFigure 4.2d ). Monopolar neurons have a single or unipo-lar process, and do not have dendrites originating directlyfrom the cell body or soma (see Figure 4.2b). Neuronswith short axons are called interneurons; they integrateneural activity within a specific brain region.
In classifying neurons by their function, motor neu-rons make muscles contract and change the activity of
98 PART TWO | The Functioning Brain
The destruction of the myelin sheatharound the axon can result in significantand often striking behavioral changes,including blindness and paralysis. Suchconditions are called demyelinating disor-ders, of which multiple sclerosis (MS) isthe best known. MS is the most commonneurologic illness in the United States,affecting 50 of every 100,000 youngadults. Symptoms are most often firstnoticed between the ages of 20 and 40.Because MS is more frequent in certaingeographic locations than in others (polarlatitudes), an environmental agent may beimplicated in the cause of the disease,
perhaps one related to a demyelinatingslow virus or an autoimmune process(Ebers & Sadovnick, 1993).
Although the contracting factor of MSremains an enigma, the course of the dis-ease is known; it is related to the localizedloss of myelin in the white matter of thebrain and subsequent neuronal death. Theloss of myelin initially results in “scrambled”electrical impulses, thus neuronal informa-tion slows or never reaches its target. Thesymptoms vary according to where thehardened patches, known as scleroticplaques, lie in the brain and spinal cord, butmost manifest visually (sudden unilateral
blindness), in the brainstem and cerebellum(wide-based gait, intention tremors), and inthe spinal cord (spastic gait, loss of positionsense, and paraplegia). Relapses areusually acute and persist for several weeks.Postmortem studies of MS patients haverevealed hundreds of lesions smaller than1.5 cm (Adams & Victor, 1993). Further-more, there is little potential for regrowth ofmyelin.
There is no known effective treatment orcure for MS. The prognosis is a gradualdeterioration of the patient’s condition overmany years. Death can result if the demyeli-nation affects vital centers of the brain.
N e u r o p s y c h o l o g y i n A c t i o n 4 . 1
S h o r t - C i r c u i t i n g N e u r o n s : M u l t i p l e S c l e r o s i s
by Eric A. Zillmer

glands; sensory neurons respond directly to changes inlight, touch, temperature, odor, and so on. The majorityof neurons are interneurons, or “between” neurons, be-cause they receive input from and send output to otherneurons.
Neurons are organized in collective structures; that is, behavior arises from the firing of many neurons, not a single neuron. These bundles—large collections ofneurons—are known as tracts, pathways, or fibers in theCNS and nerves in the PNS (Figure 4.4). The three majortypes of fibers all primarily consist of myelinated axonsthat appear as white matter:
1. Intracerebral (or association) fibers connect regionswithin one hemisphere.
2. Intercerebral (or commissural ) fibers connect struc-tures in the two hemispheres.
3. Projection fibers connect subcortical structures to thecortex and vice versa.
Anatomists often discuss pathways by the direction of theprojection and the systems they connect (England &Wakely, 1991). For example, the corticostriatal pathwayis where fibers connect cortical areas to the striatum. Like-wise, the hypothalamocerebellar tract projects from thehypothalamus to the cerebellum.
Aggregations of cell bodies—predominantly dendritesand terminal buttons—are grayish; their actual color in theliving state is pink. As noted earlier, gray matter is typicallyfound on the surface of the cerebral cortex, in the center ofthe spinal cord, and on large subcortical nuclei (e.g., in thethalamus). In the CNS, clusters of gray cell bodies arecalled nuclei (singular, nucleus), a term often used to des-ignate a group of nerve cells in direct relation to the fibersof a particular nerve. In the PNS, clusters of gray cell bod-ies are called ganglia (singular, ganglion). The presence ofnuclei in the brain is important to neuropsychologists be-cause nuclei often signal strategic clusters of neuronal cellbodies. Vital integration of neuronal information may be occurring at a specific neuroanatomic location. Somefunctional roles have been attributed to certain nuclei. Theprecise role of any one nucleus is, however, difficult todelineate, because the dendrites and axons may extend fora considerable distance outside of the boundary of the nu-cleus. In addition, some nuclei consist of different neuronswith different neurotransmitters from other neurons, whichincreases the complexity. In some cases, it may be more use-ful to conceptualize function according to neuronal regionsor networks rather than by nuclei. Nevertheless, mappingand identifying specific nuclei in the brain continues to oc-cupy brain scientists.
G L I A L C E L L S
Glial cells (also known as neuroglia or glia) outnumberneurons by a factor of 10, but because of their small size(1/10 that of a neuron), they make up about 50% of thevolume of the nervous system, with neurons comprisingthe other half. The term glia (derived from Greek gliok,meaning “nerve glue”) comes from an old notion that glialcells offer purely structural support to neurons. This isjust part of the story; glia have more functions. Glial cellsare often described as “servants” to neurons. They helpsupport neurons by physically and chemically bufferingthem from each other, and they supply nutrients and oxy-gen to neurons to support their very high metabolic rate,because neurons cannot store their own nutrients. Someglial cells act as housekeepers, metabolizing and removingthe carcasses of neurons destroyed by injury or disease,and as discussed earlier, certain glial cells form the protec-tive myelin sheath around axons. There is new evidence,however, that some glial cells (i.e., astrocytes) may func-tion more like “parents” than “servants” in directing andregulating neuronal behavior.
Glial cells are found throughout the CNS and PNS.The three main types of glial cells in the CNS are oligo-dendrocytes, microglia, and astrocytes. The primary
CHAPTER 4 | Cells of Thought 99
Figure 4.4 Bundles of myelinated neurons make up tracts,pathways, or fibers in the central nervous system and nerves inthe peripheral nervous system. (© SPL/Photo Researchers, Inc.)

Figure 4.5 Glia cells of the central and peripheral nervoussystems. Glia cells are of special interest to neurologists andneurosurgeons because they are the site of the principal tumorsof the brain and spinal cord. (From Kalat, J. W. [2007]. Biologicalpsychology [9th ed., p. 35, Figure 2.10]. Belmont, CA: ThomsonWadsworth. Photos: © Nancy Kedersha/UCLA/SPL/PhotoResearchers.)
Microglia
Axon
Schwanncell
Schwann cell Oligodendrocyte
Astrocyte
corresponding cell in the PNS is the Schwann cell(Figure 4.5).
Of tumors that invade the brain, the most prevalentarise from glial cells and are termed gliomas. Unfortu-nately, gliomas are often relatively fast-growing tumors.Astrocytes respond to brain injury by swelling or prolifer-ating to fill a damaged space. With injury, astrocytes canalso degenerate and form scar tissue.
As mentioned earlier, oligodendrocytes in the CNSand Schwann cells in the PNS are myelin-forming gliacells that envelope axons and neurons. These cells per-form a vital function in wrapping the nerve cell with alipid layer of myelin and increasing the speed with whicha neuron conducts its impulse along an axon. Schwanncells myelinate only a single segment of one cell, whereasoligodendrocytes may myelinate several segments of thesame axon or several different axons.
Microglia are small cells within the CNS that undergorapid proliferation in response to tissue destruction, mi-grating toward the site of injured or dead cells, where theyact as scavengers and metabolize tissue debris.
Astrocytes are fibrous, star-shaped cells (derived fromLatin astra, meaning “star”) with many small “feet” orprocesses that interpose themselves between neuronal cellbodies, dendrites, and the vasculature providing struc-tural support. The “servant,” or housekeeping, functionsof astrocytes are well known. These functions include: (1) “border patrol” of the brain via the blood–brain bar-rier to protect neurons from potential pathogens trans-ported by the blood, (2) maintenance of local ionic andpH balance between groups of neurons, and (3) deliveryof energy to neurons in the form of glucose and othermetabolic substances.
The border patrol via the blood–brain barrier is ac-complished because blood vessels in the CNS have a lin-ing of tightly joined endothelial cells, which the “feet” ofthe tightly joined astrocytes hold in place (Figure 4.6).This wrapping of blood vessels keeps large molecules outand permits only restricted transfer of soluble material be-tween blood and brain. The blood–brain barrier allowswater, gases, and small lipid-soluble substances to passacross. Certain substances (some drugs, for example) aretotally barred from the brain, and other substances re-quire an active transport system across the blood–brainbarrier.
Astrocytes help regulate the local intercellular ionicand pH balance. The receptor sites on the cellular mem-branes respond to ions such as calcium (Guthrie et al.,1999), and they restore the ion balance by removingexcess ions after neuronal firing. Astrocytes also clear neu-rotransmitters released through synaptic firing and cleanup intercellular metabolic waste.
Astrocytes also supply glucose to neurons through theblood–brain barrier. The “feet” of astrocytes, attached tocapillaries and blood vessels throughout the brain, act as asuction system, drawing glucose up from the bloodstreamvia astrocytes and into neurons. Before being passed on,glucose is partially metabolized by astrocytes into a formusable by neurons.
100 PART TWO | The Functioning Brain
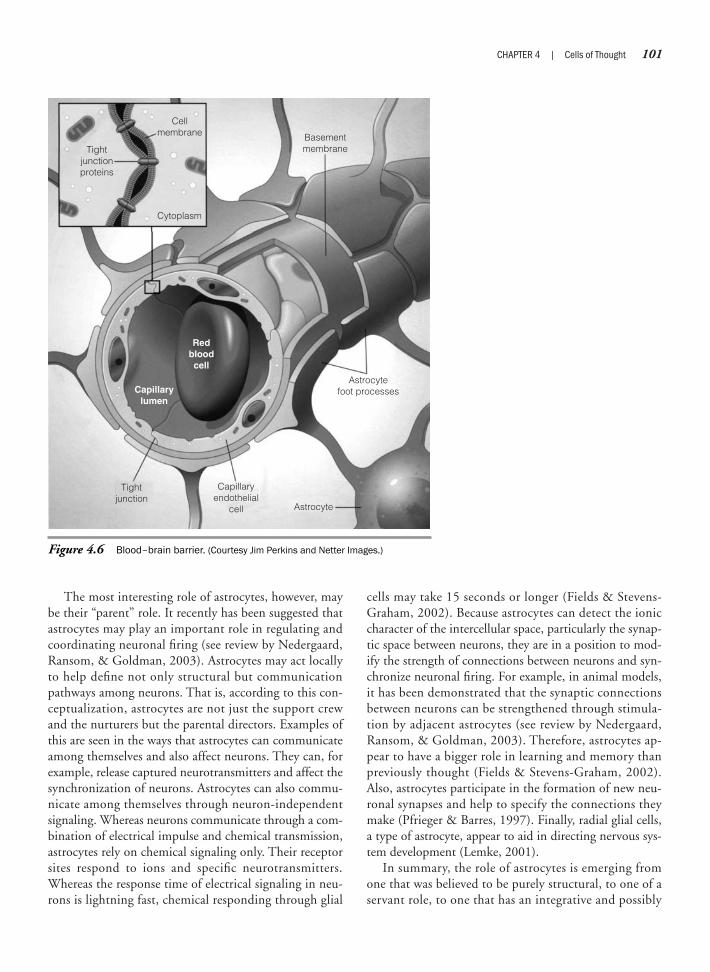
The most interesting role of astrocytes, however, maybe their “parent” role. It recently has been suggested thatastrocytes may play an important role in regulating andcoordinating neuronal firing (see review by Nedergaard,Ransom, & Goldman, 2003). Astrocytes may act locallyto help define not only structural but communicationpathways among neurons. That is, according to this con-ceptualization, astrocytes are not just the support crewand the nurturers but the parental directors. Examples ofthis are seen in the ways that astrocytes can communicateamong themselves and also affect neurons. They can, forexample, release captured neurotransmitters and affect thesynchronization of neurons. Astrocytes can also commu-nicate among themselves through neuron-independentsignaling. Whereas neurons communicate through a com-bination of electrical impulse and chemical transmission,astrocytes rely on chemical signaling only. Their receptorsites respond to ions and specific neurotransmitters.Whereas the response time of electrical signaling in neu-rons is lightning fast, chemical responding through glial
cells may take 15 seconds or longer (Fields & Stevens-Graham, 2002). Because astrocytes can detect the ioniccharacter of the intercellular space, particularly the synap-tic space between neurons, they are in a position to mod-ify the strength of connections between neurons and syn-chronize neuronal firing. For example, in animal models,it has been demonstrated that the synaptic connectionsbetween neurons can be strengthened through stimula-tion by adjacent astrocytes (see review by Nedergaard,Ransom, & Goldman, 2003). Therefore, astrocytes ap-pear to have a bigger role in learning and memory thanpreviously thought (Fields & Stevens-Graham, 2002).Also, astrocytes participate in the formation of new neu-ronal synapses and help to specify the connections theymake (Pfrieger & Barres, 1997). Finally, radial glial cells,a type of astrocyte, appear to aid in directing nervous sys-tem development (Lemke, 2001).
In summary, the role of astrocytes is emerging fromone that was believed to be purely structural, to one of aservant role, to one that has an integrative and possibly
CHAPTER 4 | Cells of Thought 101
Cellmembrane
Tightjunctionproteins
Cytoplasm
Basementmembrane
Astrocytefoot processes
Capillaryendothelial
cell Astrocyte
Tightjunction
Capillarylumen
Redbloodcell
Figure 4.6 Blood–brain barrier. (Courtesy Jim Perkins and Netter Images.)
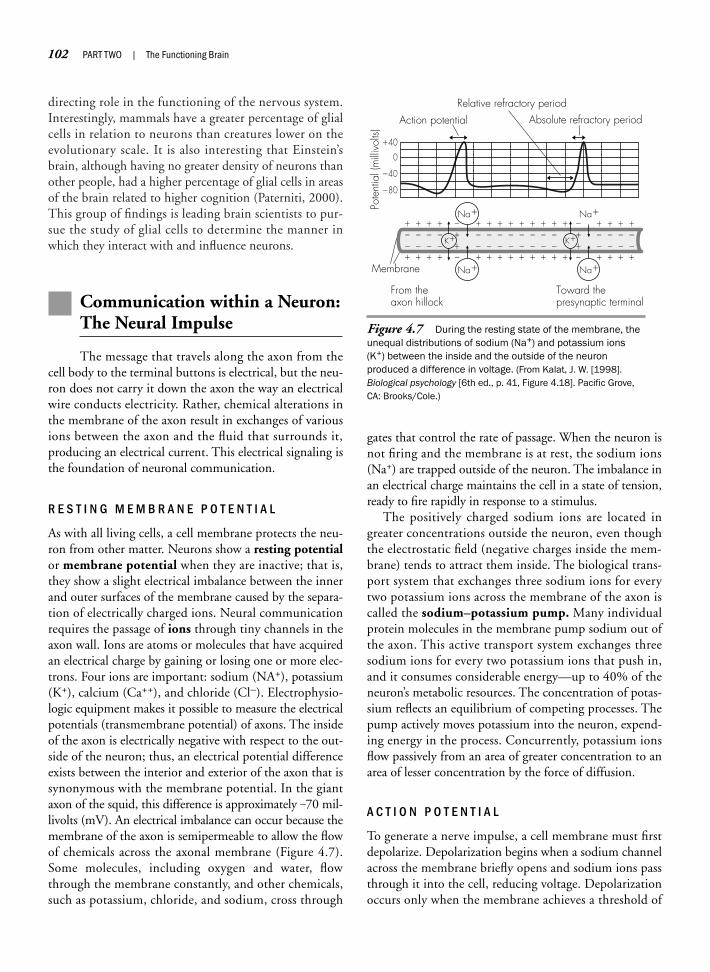
directing role in the functioning of the nervous system.Interestingly, mammals have a greater percentage of glialcells in relation to neurons than creatures lower on theevolutionary scale. It is also interesting that Einstein’sbrain, although having no greater density of neurons thanother people, had a higher percentage of glial cells in areasof the brain related to higher cognition (Paterniti, 2000).This group of findings is leading brain scientists to pur-sue the study of glial cells to determine the manner inwhich they interact with and influence neurons.
Communication within a Neuron:The Neural Impulse
The message that travels along the axon from thecell body to the terminal buttons is electrical, but the neu-ron does not carry it down the axon the way an electricalwire conducts electricity. Rather, chemical alterations inthe membrane of the axon result in exchanges of variousions between the axon and the fluid that surrounds it,producing an electrical current. This electrical signaling isthe foundation of neuronal communication.
R E S T I N G M E M B R A N E P O T E N T I A L
As with all living cells, a cell membrane protects the neu-ron from other matter. Neurons show a resting potentialor membrane potential when they are inactive; that is,they show a slight electrical imbalance between the innerand outer surfaces of the membrane caused by the separa-tion of electrically charged ions. Neural communicationrequires the passage of ions through tiny channels in theaxon wall. Ions are atoms or molecules that have acquiredan electrical charge by gaining or losing one or more elec-trons. Four ions are important: sodium (NA+), potassium(K+), calcium (Ca++), and chloride (Cl–). Electrophysio-logic equipment makes it possible to measure the electricalpotentials (transmembrane potential) of axons. The insideof the axon is electrically negative with respect to the out-side of the neuron; thus, an electrical potential differenceexists between the interior and exterior of the axon that issynonymous with the membrane potential. In the giantaxon of the squid, this difference is approximately _70 mil-livolts (mV). An electrical imbalance can occur because themembrane of the axon is semipermeable to allow the flowof chemicals across the axonal membrane (Figure 4.7).Some molecules, including oxygen and water, flowthrough the membrane constantly, and other chemicals,such as potassium, chloride, and sodium, cross through
gates that control the rate of passage. When the neuron isnot firing and the membrane is at rest, the sodium ions(Na+) are trapped outside of the neuron. The imbalance inan electrical charge maintains the cell in a state of tension,ready to fire rapidly in response to a stimulus.
The positively charged sodium ions are located ingreater concentrations outside the neuron, even thoughthe electrostatic field (negative charges inside the mem-brane) tends to attract them inside. The biological trans-port system that exchanges three sodium ions for everytwo potassium ions across the membrane of the axon iscalled the sodium–potassium pump. Many individualprotein molecules in the membrane pump sodium out ofthe axon. This active transport system exchanges threesodium ions for every two potassium ions that push in,and it consumes considerable energy—up to 40% of theneuron’s metabolic resources. The concentration of potas-sium reflects an equilibrium of competing processes. Thepump actively moves potassium into the neuron, expend-ing energy in the process. Concurrently, potassium ionsflow passively from an area of greater concentration to anarea of lesser concentration by the force of diffusion.
A C T I O N P O T E N T I A L
To generate a nerve impulse, a cell membrane must firstdepolarize. Depolarization begins when a sodium channelacross the membrane briefly opens and sodium ions passthrough it into the cell, reducing voltage. Depolarizationoccurs only when the membrane achieves a threshold of
102 PART TWO | The Functioning Brain
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
Action potentialRelative refractory period
Absolute refractory period
Membrane
Na�
Na�
Na�
Na�
K� K�
Pote
ntia
l (m
illivo
lts)
�40
0
�40
�80
From the axon hillock
Toward the presynaptic terminal
Figure 4.7 During the resting state of the membrane, theunequal distributions of sodium (Na+) and potassium ions(K+) between the inside and the outside of the neuron produced a difference in voltage. (From Kalat, J. W. [1998].Biological psychology [6th ed., p. 41, Figure 4.18]. Pacific Grove,CA: Brooks/Cole.)
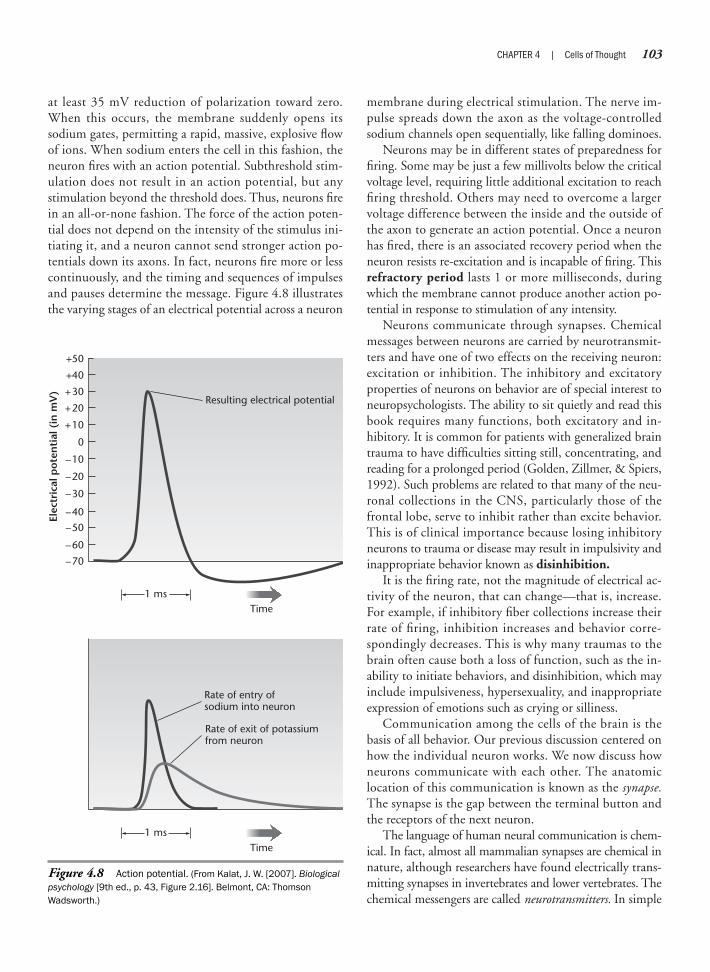
at least 35 mV reduction of polarization toward zero.When this occurs, the membrane suddenly opens itssodium gates, permitting a rapid, massive, explosive flowof ions. When sodium enters the cell in this fashion, theneuron fires with an action potential. Subthreshold stim-ulation does not result in an action potential, but anystimulation beyond the threshold does. Thus, neurons firein an all-or-none fashion. The force of the action poten-tial does not depend on the intensity of the stimulus ini-tiating it, and a neuron cannot send stronger action po-tentials down its axons. In fact, neurons fire more or lesscontinuously, and the timing and sequences of impulsesand pauses determine the message. Figure 4.8 illustratesthe varying stages of an electrical potential across a neuron
membrane during electrical stimulation. The nerve im-pulse spreads down the axon as the voltage-controlledsodium channels open sequentially, like falling dominoes.
Neurons may be in different states of preparedness forfiring. Some may be just a few millivolts below the criticalvoltage level, requiring little additional excitation to reachfiring threshold. Others may need to overcome a largervoltage difference between the inside and the outside ofthe axon to generate an action potential. Once a neuronhas fired, there is an associated recovery period when theneuron resists re-excitation and is incapable of firing. Thisrefractory period lasts 1 or more milliseconds, duringwhich the membrane cannot produce another action po-tential in response to stimulation of any intensity.
Neurons communicate through synapses. Chemicalmessages between neurons are carried by neurotransmit-ters and have one of two effects on the receiving neuron:excitation or inhibition. The inhibitory and excitatoryproperties of neurons on behavior are of special interest toneuropsychologists. The ability to sit quietly and read thisbook requires many functions, both excitatory and in-hibitory. It is common for patients with generalized braintrauma to have difficulties sitting still, concentrating, andreading for a prolonged period (Golden, Zillmer, & Spiers,1992). Such problems are related to that many of the neu-ronal collections in the CNS, particularly those of thefrontal lobe, serve to inhibit rather than excite behavior.This is of clinical importance because losing inhibitoryneurons to trauma or disease may result in impulsivity andinappropriate behavior known as disinhibition.
It is the firing rate, not the magnitude of electrical ac-tivity of the neuron, that can change—that is, increase.For example, if inhibitory fiber collections increase theirrate of firing, inhibition increases and behavior corre-spondingly decreases. This is why many traumas to thebrain often cause both a loss of function, such as the in-ability to initiate behaviors, and disinhibition, which mayinclude impulsiveness, hypersexuality, and inappropriateexpression of emotions such as crying or silliness.
Communication among the cells of the brain is thebasis of all behavior. Our previous discussion centered onhow the individual neuron works. We now discuss howneurons communicate with each other. The anatomic location of this communication is known as the synapse.The synapse is the gap between the terminal button andthe receptors of the next neuron.
The language of human neural communication is chem-ical. In fact, almost all mammalian synapses are chemical innature, although researchers have found electrically trans-mitting synapses in invertebrates and lower vertebrates. Thechemical messengers are called neurotransmitters. In simple
CHAPTER 4 | Cells of Thought 103
–70
–60
–50
–40
–30
+30
–20
–10
0
Resulting electrical potential
1 ms
Elec
tric
al p
ote
nti
al (
in m
V)
+10
+20
+40
+50
1 ms
Rate of entry ofsodium into neuron
Rate of exit of potassiumfrom neuron
Time
Time
Figure 4.8 Action potential. (From Kalat, J. W. [2007]. Biologicalpsychology [9th ed., p. 43, Figure 2.16]. Belmont, CA: ThomsonWadsworth.)

terms, a chemical message transfers across the synapse fromone neuron to another, where it influences the neuron orneurons to fire or not to fire. In reality, this particular ex-change is extremely complex, involving many different mol-ecules. The process is so intricate that a neuroscientist caneasily dedicate an entire career to the study of one neuro-transmitter exchange. But human brains, and minds, are af-fected not only by internally produced chemical messengersbut also by externally originating chemicals that find their way to the synapse. Such chemicals are known as
psychoactive drugs, and they include caffeine, cocaine, nico-tine, and alcohol, among many others.
Chemical transmission is very much at the center ofhuman behavior and emotions. In fact, many of the mostfascinating discoveries about the brain concern the chemi-cal nature of neuronal transmission. For example, research-ers have established that the large numbers of individualnerve cells or units in the nervous system are related to eachother through synapses in a more or less continuous fash-ion, creating a network (Neuropsychology in Action 4.2).
104 PART TWO | The Functioning Brain
The influence of neuronal firing on behavioris easily seen in a variety of related clinicalphenomena.
SeizuresSeizures, which are unusual electricalevents in the brain, have a wide range ofcauses, including trauma, tumors, andepilepsy. Seizures result from massivewaves of synchronized nerve cell activationthat may involve the entire brain. You canthus conceptualize them as “electricalstorms.” Seizures may have dramatic behav-ioral manifestations, including uncontrolledmuscle contractions, changes in perception,and alterations in mood and consciousness.
DrugsCertain drugs and poisons specifically alterthe flow of sodium and potassium through themembrane. Most drugs act at the level of thesynapse, but several substances directlyinfluence the firing rate of the axon, changingthe person’s perception or mood and, insome cases, causing death. For example,scorpion and black widow venoms overexcitethe nervous system by keeping sodiumchannels open and closing potassiumchannels, causing prolonged depolarizationthat renders the neuron helpless to conveyinformation. As a result, life-sustainingbehavior may cease (e.g., breathing maystop), or there may be a lack of disinhibition(such as a continuous involuntary flexing of a
muscle or tic). Novocain, a topical anestheticused by dentists, attaches itself to thesodium gates of the neuronal membraneand prevents sodium ions from entering.Consequently, the action potential is blockedand sensory nerve messages, including pain,cannot reach the brain because the neuronsthat typically convey this message cannotfire.
Chloroform decreases brain activity bypromoting the flow of potassium ions out of theneuron. This reduces the number of sodiumions that spontaneously pass through the cellmembrane and hyperpolarizes the neuronalmembrane, which reduces the responsivenessof the nervous system. Tetrodotoxin (T TX), apoison found in the Japanese blowfish, directlyblocks voltage-gated sodium channels.Lithium, a simple salt extracted from rock, isthe most effective treatment for bipolar disor-der (manic-depressive illness), which is char-acterized by severe mood swings (Freedman,Kaplan, & Sadock, 1978). Lithium stabilizesmood most effectively during the manic stage.Its overall effect on brain activity is not clearlyunderstood, but lithium is chemically similar tosodium and may partly take its place crossingthe membrane.
Electroconvulsive TherapyEarly in the twentieth century, a physiciannamed Ladislaus von Meduna noted thatpsychotic patients who had epilepsy im-proved in mood immediately after each
epileptic attack. Reasoning that the electri-cal storm of neural activity in the brainsomehow improved mental activity, Medunaapplied a large amount of electricity to theskull of depressed patients, causing thecollective firing of neurons—a seizure. Elec-troconvulsive therapy (ECT) sometimesimproves severe forms of depression within afew days. Although researchers do notclearly understand the mechanism, cur-rently, clinicians use ECT when it is importantto intervene quickly to prevent a patient fromacting on suicidal thoughts.
DeathWhen is a human considered dead? Whenthe heart stops beating? Or when the lungsstop breathing? Because the brain is theZentralorgan (German meaning “centralorgan”) that coordinates the beating of theheart and the breathing of the lungs, theclinical moment of death is precisely whenthe firing of the brain ceases. Thus, in moststates, once an unconscious patient hasbeen admitted to a hospital, the staff moni-tors brain electrical potential data with anelectroencephalograph. As long as there isbrain activity, the patient is considered alive.Interestingly, even after a brain has stoppedgenerating action potentials, the brain massitself can hold its own electrical charge for ashort time. This can be measured by placinga dead brain slice on an apparatus that issensitive to small electrical charges.
N e u r o p s y c h o l o g y i n A c t i o n 4 . 2
N e u r o n a l F i r i n g : C l i n i c a l E x a m p l e s
by Eric A. Zillmer
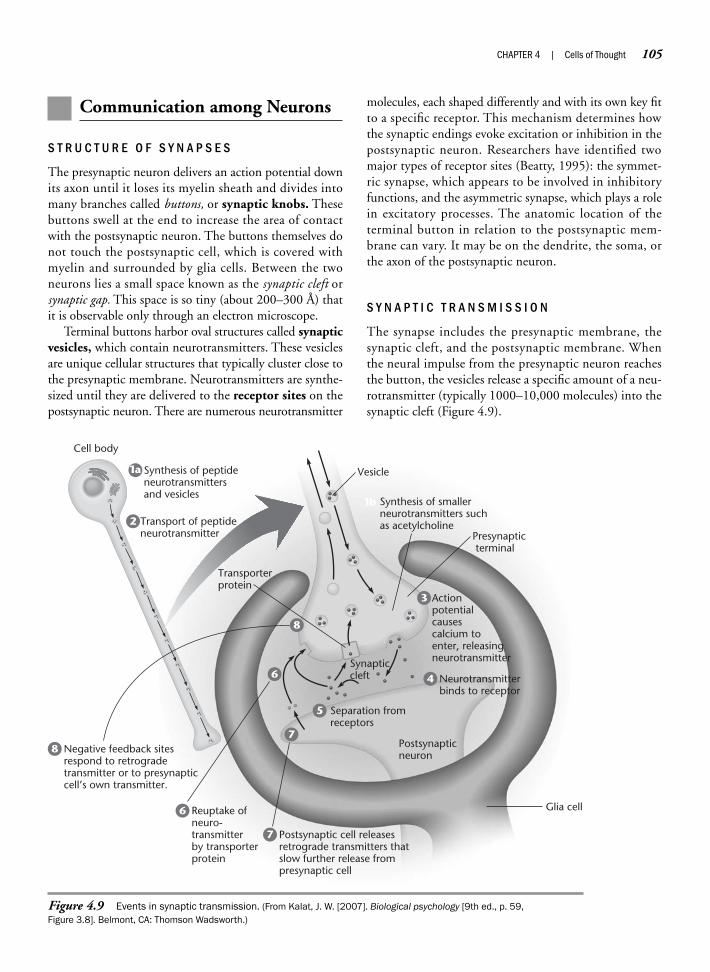
Communication among Neurons
S T R U C T U R E O F S Y N A P S E S
The presynaptic neuron delivers an action potential downits axon until it loses its myelin sheath and divides intomany branches called buttons, or synaptic knobs. Thesebuttons swell at the end to increase the area of contactwith the postsynaptic neuron. The buttons themselves donot touch the postsynaptic cell, which is covered withmyelin and surrounded by glia cells. Between the twoneurons lies a small space known as the synaptic cleft orsynaptic gap. This space is so tiny (about 200–300 Å) thatit is observable only through an electron microscope.
Terminal buttons harbor oval structures called synapticvesicles, which contain neurotransmitters. These vesiclesare unique cellular structures that typically cluster close tothe presynaptic membrane. Neurotransmitters are synthe-sized until they are delivered to the receptor sites on thepostsynaptic neuron. There are numerous neurotransmitter
molecules, each shaped differently and with its own key fitto a specific receptor. This mechanism determines howthe synaptic endings evoke excitation or inhibition in thepostsynaptic neuron. Researchers have identified twomajor types of receptor sites (Beatty, 1995): the symmet-ric synapse, which appears to be involved in inhibitoryfunctions, and the asymmetric synapse, which plays a rolein excitatory processes. The anatomic location of theterminal button in relation to the postsynaptic mem-brane can vary. It may be on the dendrite, the soma, orthe axon of the postsynaptic neuron.
S Y N A P T I C T R A N S M I S S I O N
The synapse includes the presynaptic membrane, thesynaptic cleft, and the postsynaptic membrane. Whenthe neural impulse from the presynaptic neuron reachesthe button, the vesicles release a specific amount of a neu-rotransmitter (typically 1000–10,000 molecules) into thesynaptic cleft (Figure 4.9).
CHAPTER 4 | Cells of Thought 105
Neurotransmitterbinds to receptor
Postsynapticneuron
Synapticcleft
Presynaptic terminal
Vesicle
Glia cell
Transporterprotein
Synthesis of smallerneurotransmitters suchas acetylcholineTransport of peptide
neurotransmitter
Synthesis of peptideneurotransmittersand vesicles
Cell body
1a
1b
2
Actionpotentialcausescalcium toenter, releasingneurotransmitter
3
6
Reuptake ofneuro-transmitterby transporterprotein
6
Negative feedback sitesrespond to retrogradetransmitter or to presynapticcell’s own transmitter.
8
Postsynaptic cell releasesretrograde transmitters thatslow further release frompresynaptic cell
7
7
Separation fromreceptors
5
4
8
Figure 4.9 Events in synaptic transmission. (From Kalat, J. W. [2007]. Biological psychology [9th ed., p. 59, Figure 3.8]. Belmont, CA: Thomson Wadsworth.)

Several scenarios are possible after the release of a neu-rotransmitter. The molecules may not fit a specific recep-tor site and, therefore, do not bind to the cell membrane.In this case, the neurotransmitter has no effect on a re-ceiving neuron, and no communication takes place. Or,neurotransmitters may be released in areas with no imme-diate postsynaptic receptors. In this case, the transmittermay diffuse over a wider area, affecting neurons far fromthe point of release. If the released neurotransmitter keysinto the receptor site, it will bind to the cell membrane.Depending on the type of neurotransmitter, it will affectthe ultimate firing or inhibition of the postsynaptic cellin one of two ways. Some neurotransmitters activate thepostsynaptic receptors, which triggers an alteration in theionic permeability of the cell membrane. Transmitters af-fecting the postsynaptic cell in this matter are consideredto be rapid transmitters, because the onset of ionic actionin the postsynaptic cell is fast, in the order of millisec-onds. Other neurotransmitters (e.g., serotonin) activatethe postsynaptic receptor to transmit a chemical messagethrough the cell membrane. The messenger, in turn, trig-gers a second messenger (intracellular molecule) that initi-ates a cascade of reactions within the postsynaptic cell.This intracellular activity produces a number of cellularchanges, including an alteration in the ionic permeability ofthe postsynaptic membrane. Second-messenger transmis-sion is considered to be slow with regard to onset of post-synaptic activity; that is, onset can range from hundredsof milliseconds to seconds (Schwartz & Kandel, 1991;Preston, O’Neal, & Talaga, 1997). The ionic changes ini-tiated by the two forms of neurotransmitter actions aresimilar. If the alteration in the permeability of the cell re-sults in increased levels of Na+ and Cl– moving into thepostsynaptic cell and smaller amounts of K+ moving out,the postsynaptic cell depolarizes. This depolarization,known as an excitatory postsynaptic potential (EPSP),increases the probability that the postsynaptic cell willreach its threshold. An EPSP makes it more likely that themembrane threshold will reach an action potential andthat the postsynaptic neuron will fire.
During an inhibitory exchange, the presence of a neu-rotransmitter increases the permeability of the postsynap-tic membrane, particularly to K+. This results in an ioniccurrent that hyperpolarizes the postsynaptic neuron.Thus, greater depolarization than normal is required toreach an action potential. This depolarization, called in-hibitory postsynaptic potential (IPSP), becomes lessprobable. Next, the synaptic vesicle either dissipates or isreabsorbed by the presynaptic membrane, which allowsthe recycling of neurotransmitters and completes thecycle. This summation of EPSPs and IPSPs, analogous to
yes/no messages, is the main principle of neural commu-nication. The nervous system is exceedingly complex, be-cause one single neuron may have many synaptic termi-nals on it that could influence the action potential ofthousands of other neurons.
N E U R O T R A N S M I T T E R S
Neurotransmitters permit the exchange of informationamong neurons and between neurons and other cells.Neurotransmitter types (Table 4.1) are classified accord-ing to molecular size. For example, the biogenic aminesand amino acids are small-molecule messengers, consistingof fewer than 10 carbon atoms, and the neuropeptides,which are larger molecules. Although smaller moleculeneurotransmitters, such as acetylcholine (ACh), sero-tonin, and the catecholamines, have traditionally re-ceived the most scientific study, neuropeptides are morenumerous in the brain, with more than 40 different neu-ropeptides currently identified (Kalat, 1998).
Just as each neurotransmitter has a specific shape,comparable with a key, each receptor site also has a spe-cific structure analogous to a lock. Thus, a specific neu-rotransmitter will attach itself only to a receptor with anappropriate fit. In some cases, a variety of neurotransmit-ters can adhere to a single type of receptor molecule:Many different keys may fit the same lock. At times, dif-ferent neurotransmitters may compete for the same re-ceptor molecule. For example, even though neurotrans-mitter A might have adhered to receptor Z at one time,in competition with neurotransmitter B, A may fail to
106 PART TWO | The Functioning Brain
Biogenic amines Acetylcholine (ACh)Serotonin (5-HT)
Catecholamines Dopamine (DA)Norepinephrine (NE) (noradrenalin)Epinephrine (EPI) (adrenalin)
Amino acids Gamma-aminobutyric acid (GABA)GlycineGlutamateAspartate
Peptides VasopressinOxytocinThyrotropin-releasing hormone (TRH)Corticotropin-releasing factorSubstance PTachykininsCholecystokinin
Table 4.1 Neurotransmitters

activate because B fits better. This scenario may occurthousands of times even at the individual level of oneneuron. Chemical transmission allows tremendous flexi-bility and refinement.
D i s t r i b u t i o no f N e u r o t r a n s m i t t e r s
Many distinct neurotransmitter pathways define the brainchemically and anatomically. The tracing of neuronalpathways along neurotransmitter systems has been at thecenter of the neurosciences since the development ofmodern staining methods. Investigations show that neu-rotransmitters are both localized to specific regions andwidely dispersed in the brain. The pathways of the cate-cholamine transmitters such as dopamine (DA) and nor-epinephrine are relatively specific in their targeting ofbrain regions, whereas other transmitters (e.g., glutamate)are widely distributed throughout the brain.
Acetylcholine—In the early 1900s, ACh (or choline) was thefirst neurotransmitter to be identified; researchers discov-ered that it stimulates the parasympathetic nervous sys-tem. It plays a prominent role in the PNS, influencingmotor control, and in autonomic nervous system func-tioning. ACh also is a predominant neurotransmitter atthe neuromuscular junction, stimulating muscular con-traction. In the CNS and brain, ACh affects a wide be-havioral repertoire. One of its most important functionsmight be to influence alertness, attention, and memory.
ACh has a simple chemical structure, but its method ofaction is complicated and is yet to be fully understood.One component necessary for synthesizing ACh is choline,which is supplied by foods such as liver, kidneys, egg yolks,seeds, and many vegetables and legumes. It is synthesizedin the liver and recycled in the brain. Choline easily crossesthe blood–brain barrier. There is evidence that shows aninflux of choline in the brain after eating and an outflowwhen plasma choline levels are lower, that is, betweenmeals (see Feldman, Meyer, & Quenzer, 1997). Like otherneurotransmitters, ACh binds to a variety of postsynapticreceptor subtypes. The two main subtypes of ACh aremuscarinic choline and nicotinic choline, named afterthe bitter botanical alkaloids that stimulate the receptors(muscarine from the fly agaric mushroom, Amanita mus-caria, and nicotine from tobacco, Nicotiana tabacum). Theimplication is that the action of ACh may differ from onereceptor subtype to another. Nicotinic receptor bindingcreates an excitatory response, whereas muscarinic re-sponses may be either excitatory or inhibitory. Therefore,in the PNS, for example, glands and muscles may be eitherexcited or inhibited, depending on the subtype of ACh
receptor. Certain drugs act on nicotinic receptors, and oth-ers are specific to muscarinic receptors.
As in the PNS, distribution of ACh is widespread in thebrain, where it has many possible behavioral functions. First,cholinergic (ACh) neurons in the striatum, a collection ofbrain structures named after their striped or striated appear-ance, influence motor system functioning. Degeneration ofstriatal neurons is associated with Huntington’s disease.
Second, ACh functions in arousal and in the sleep/wake cycle. The reticular activating system is a networkof neurons that arises from the brainstem and projectsthroughout the cortex. One of its primary functions is toregulate brain activation. For example, Sitaram, Moore,and Gillin (1978) report that an ACh antagonist such asscopolamine extends the normal interval (about 45 min-utes) between rapid eye movement (REM) sleep. Al-though many neurotransmitter systems are involved inthe sleep cycle, ACh appears to play a role in activatingthe cortex. Increased levels of ACh in the brainstem andbasal forebrain are associated with increased corticalarousal and wakefulness. Researchers can elicit REMsleep, which is characterized by increased cortical activity,by activating muscarinic ACh receptors.
Third, a major cholinergic system thought to influ-ence attention, memory, and learning emerges from thebasal forebrain and projects throughout the cortex and tostructures important for consolidating memory, such asthe hippocampus. An important cholinergic nucleus inthe basal forebrain is the nucleus basalis of Meynert(named after its discoverer). Its degeneration as a factor inAlzheimer’s disease became evident when researchers foundthat patients with this disorder had measurably lower thannormal levels of ACh in their brains. Alzheimer’s disease isassociated with severe memory dysfunction, and this obser-vation led researchers to wonder whether ACh plays a rolein memory functioning. Scopolamine, a drug that blocksACh at muscarinic receptor sites, causes deficits in encod-ing and consolidation into long-term memory (seePolster, 1993). Surgical patients given scopolamine oftenhave amnesia for the events before surgery. These findingsled to the development of drugs that serve as AChagonists binding to the same receptors as ACh and in-creasing ACh levels for use in clinical trials with patientswith Alzheimer’s disease. However, this intervention waslargely disappointing, perhaps in part because Alzheimer’sdisease involves much more than one neurotransmit-ter system. It is also possible that ACh has a less directinfluence on memory, and instead functions to main-tain a higher level of cortical alertness and attention that may be a necessary precursor to adequate memoryfunctioning.
CHAPTER 4 | Cells of Thought 107
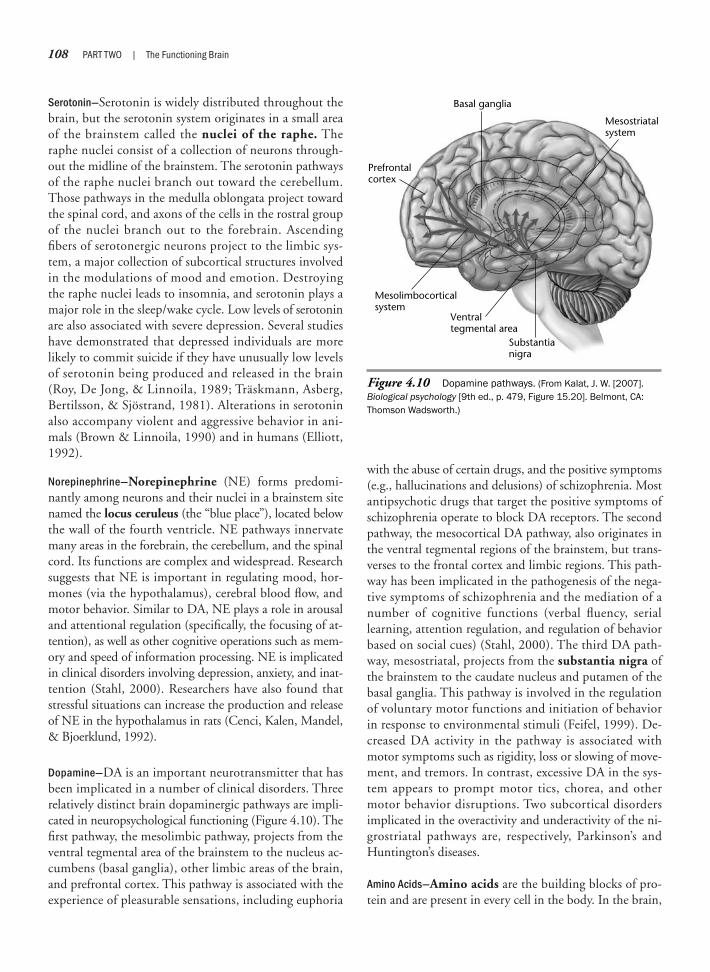
Serotonin—Serotonin is widely distributed throughout thebrain, but the serotonin system originates in a small areaof the brainstem called the nuclei of the raphe. Theraphe nuclei consist of a collection of neurons through-out the midline of the brainstem. The serotonin pathwaysof the raphe nuclei branch out toward the cerebellum.Those pathways in the medulla oblongata project towardthe spinal cord, and axons of the cells in the rostral groupof the nuclei branch out to the forebrain. Ascendingfibers of serotonergic neurons project to the limbic sys-tem, a major collection of subcortical structures involvedin the modulations of mood and emotion. Destroyingthe raphe nuclei leads to insomnia, and serotonin plays amajor role in the sleep/wake cycle. Low levels of serotoninare also associated with severe depression. Several studieshave demonstrated that depressed individuals are morelikely to commit suicide if they have unusually low levelsof serotonin being produced and released in the brain(Roy, De Jong, & Linnoila, 1989; Träskmann, Asberg,Bertilsson, & Sjöstrand, 1981). Alterations in serotoninalso accompany violent and aggressive behavior in ani-mals (Brown & Linnoila, 1990) and in humans (Elliott,1992).
Norepinephrine—Norepinephrine (NE) forms predomi-nantly among neurons and their nuclei in a brainstem sitenamed the locus ceruleus (the “blue place”), located belowthe wall of the fourth ventricle. NE pathways innervatemany areas in the forebrain, the cerebellum, and the spinalcord. Its functions are complex and widespread. Researchsuggests that NE is important in regulating mood, hor-mones (via the hypothalamus), cerebral blood flow, andmotor behavior. Similar to DA, NE plays a role in arousaland attentional regulation (specifically, the focusing of at-tention), as well as other cognitive operations such as mem-ory and speed of information processing. NE is implicatedin clinical disorders involving depression, anxiety, and inat-tention (Stahl, 2000). Researchers have also found thatstressful situations can increase the production and releaseof NE in the hypothalamus in rats (Cenci, Kalen, Mandel,& Bjoerklund, 1992).
Dopamine—DA is an important neurotransmitter that hasbeen implicated in a number of clinical disorders. Threerelatively distinct brain dopaminergic pathways are impli-cated in neuropsychological functioning (Figure 4.10). Thefirst pathway, the mesolimbic pathway, projects from theventral tegmental area of the brainstem to the nucleus ac-cumbens (basal ganglia), other limbic areas of the brain,and prefrontal cortex. This pathway is associated with theexperience of pleasurable sensations, including euphoria
with the abuse of certain drugs, and the positive symptoms(e.g., hallucinations and delusions) of schizophrenia. Mostantipsychotic drugs that target the positive symptoms ofschizophrenia operate to block DA receptors. The secondpathway, the mesocortical DA pathway, also originates inthe ventral tegmental regions of the brainstem, but trans-verses to the frontal cortex and limbic regions. This path-way has been implicated in the pathogenesis of the nega-tive symptoms of schizophrenia and the mediation of anumber of cognitive functions (verbal fluency, seriallearning, attention regulation, and regulation of behaviorbased on social cues) (Stahl, 2000). The third DA path-way, mesostriatal, projects from the substantia nigra ofthe brainstem to the caudate nucleus and putamen of thebasal ganglia. This pathway is involved in the regulationof voluntary motor functions and initiation of behaviorin response to environmental stimuli (Feifel, 1999). De-creased DA activity in the pathway is associated withmotor symptoms such as rigidity, loss or slowing of move-ment, and tremors. In contrast, excessive DA in the sys-tem appears to prompt motor tics, chorea, and othermotor behavior disruptions. Two subcortical disordersimplicated in the overactivity and underactivity of the ni-grostriatal pathways are, respectively, Parkinson’s andHuntington’s diseases.
Amino Acids—Amino acids are the building blocks of pro-tein and are present in every cell in the body. In the brain,
108 PART TWO | The Functioning Brain
Basal ganglia
Prefrontalcortex
Mesostriatalsystem
Substantianigra
Ventraltegmental area
Mesolimbocorticalsystem
Figure 4.10 Dopamine pathways. (From Kalat, J. W. [2007].Biological psychology [9th ed., p. 479, Figure 15.20]. Belmont, CA:Thomson Wadsworth.)

amino acids are involved in the basic neuronal transmis-sion that depends on rapid communication among neu-rons. Of the more than 20 amino acids, the most commonare gamma-aminobutyric acid (GABA), which hasstrong inhibitory properties, and glutamate, an excitatoryneurotransmitter. In fact, GABA is so common in theCNS that researchers believe one third of all synapses arereceptive to it. Glutamate also occurs in high concentra-tion throughout the nervous system and is the major ex-citatory neurotransmitter. The most prominent GABAer-gic projection system consists of the inhibitory Purkinjecells that extend into the deep portions of the cerebellarnuclei. Some of the major projecting systems of the basalganglia that are also inhibitory are the striatum, globuspallidus, and substantia nigra. The inability of patientswith Huntington’s disease to control their own motor be-havior perhaps relates to the loss of inhibitory GABAergicneurons in the basal ganglia.
Peptides—Peptides are short chains of amino acids; scien-tists have identified more than 60 peptides. High levels ofpeptides are present in the hypothalamus and the amyg-dala, and to a much lesser extent, in the cortex, the thala-mus, and the cerebellum. Naturally produced peptideswith opiate properties are called endorphins. Endorphinshave received much scientific attention for their analgesiceffects and their possible role in a pain-inhibiting neu-ronal system. Psychologists have always been interested innew procedures to alter the perception of pain, and re-search suggests that acupuncture and electrical stimula-tion of the brainstem arouse the pain-inhibiting endor-phin system. The nervous system has specific receptorsites that bind the drug morphine and related opiate com-pounds. The presence of opiate receptors suggests that thebrain itself can create opiate neurotransmitters, perhapsto produce a natural high after prolonged physical stressor in the event of a catastrophic injury. Endorphins that
CHAPTER 4 | Cells of Thought 109
Can the adult brain form new neurons? Thecommon wisdom has been that at birth thebrain has all the neurons it will ever possess.In fact, the brain goes through a necessaryprocess of pruning neurons as learningstrengthens certain neural associations andothers become unnecessary. There is evi-dence in some species of songbirds, how-ever, that new brain cells form in conjunctionwith seasonal changes in mating songs.Researchers Ball and Hulse (1998) havereviewed this literature and report intriguingfindings. Male canaries and sparrows, someof the most studied songbirds, have complexmating songs that show seasonal variation,being most prominent in spring. Neurobiolo-gists have precisely mapped the vocalsystem of these songbirds and have found aconsistent structure–function relation be-tween specific nuclei and singing behavior.
For example, the high vocal center (HVC)is responsible for vocal production, and therobust nucleus of the archistriatum (RA) aidsin coordinating respiration with singing.Within this circuit of nuclei are neurorecep-
tors that are specific for sex hormones, suchas androgens and estrogens. Receptors forthese steroid sex hormones are not presentin the vocal control circuitry of birds that arenot songbirds. The complexity of song pro-duction differs in male and female song-birds, with males singing more songs andmore complex songs. Researchers think thisgreater production in males serves as amating function, to attract females andestablish territory. This sex difference insinging behavior corresponds to structuraldifferences in the vocal control systems ofmales and females. Specifically, in malesongbirds, the HVC and RA are larger andcontain more hormonal receptor nuclei.These differences aroused the curiosity ofresearchers. Male song production is sea-sonal, so might there be seasonal changes inthe brains of males?
In fact, there were. In male canaries, theHVC had increased in size by nearly 100% inthe spring compared with the fall! The RAhad increased by a factor of about 75%(Nottebohm, 1981). The next question was,
“What was causing this increase?” Was thesize or volume of existing neurons changing?For example, might new dendritic connec-tions form during this time? Or were newneurons developing? Evidence showed thatthe nuclei that control singing increase involume when the blood levels of testos-terone rise. New staining techniques involv-ing a traceable radioactive tag of newlyforming cells indicated that new neuronsformed in the ventricles of canaries andmigrated to the vocal control system, specifi-cally the HVC and RA (Goldman & Nottebohm,1983). This was an astonishing finding.Further evidence indicates that adults ofother species also generate new neurons,and that this co-occurs with learning. Suchresearch has exciting implications for thestudy of human language. Will the findings ofneurogenesis in adult canaries generalize tohuman language or other types of learning?And if new neurons can be formed, what isthe implication for rehabilitation from braininjury and for lifetime adult learningprograms?
N e u r o p s y c h o l o g y i n A c t i o n 4 . 3
W h a t C a n We L e a r n f r o m S o n g b i r d s ?
by Mary V. Spiers

originate in the brainstem may interfere with pain im-pulses via their action on the spinal cord.
Regeneration of Neurons
To what extent a patient recovers from an injury tothe PNS or CNS pathways depends largely on the regen-erative capacity of the damaged neurons. The capacity forregeneration in the PNS is actually quite good; usefulfunction can often be restored with surgical nerve repair.Surgeons have reattached fingers and even completelimbs, and much sensory and motor function has beenrestored (Neuropsychology in Action 4.3).
The regeneration of neurons in the CNS is more com-plex. Once damaged, neurons do not heal spontaneouslyafter the developmental period. Generally speaking, hu-mans are born with as many neurons as they will everhave, although new research has suggested that adult hu-mans do generate new neurons from some stem cells invarious parts of the brain. This fact is related, in part, tothe structure of the CNS, which is infinitely more com-plicated than that of the PNS. As a result, the CNS has
little of the spontaneous cellular regeneration required toreconnect a damaged axon to its normal target. Mostoften, the projections of such neurons, as well as the tar-gets of other neurons, are lost. Later chapters discuss whythe brain can compensate when neurons are lost and alsohow neuronal plasticity and the reconfiguration of func-tional systems are important to the developing brain. Re-cently, a flurry of research activity has focused on estab-lishing procedures that facilitate neuronal growth throughstem cell research (Neuropsychology in Action 4.4) or byattempting to coax injured neurons into regrowing.
Injuries and diseases that result in neuronal loss or degen-eration are a major health concern and can significantly af-fect the quality of life in individuals with CNS disorders.For example, more than 100,000 people in the United Stateshave paraplegia or quadriplegia, a disabling condition thatresults from severed neurons in the spinal cord. Head in-juries—in which axonal shearing, a form of stretching causedby physical forces, is common—affect about 3 million peo-ple. Stroke, which is neuronal cell death due to insufficientoxygen, affects about 2 million people; degenerative condi-tions such as Alzheimer’s, Parkinson’s, and Huntington’sdiseases burden millions more. It is thus important for
110 PART TWO | The Functioning Brain
As scientific inquiry has evolved, so too haveethical dilemmas. Nowhere is this illustratedmore prominently than in the area of stemcell research. Stem cells are undifferentiatedcells; they do not yet have either an identi-fied or specialized function. They eventuallydifferentiate into the building blocks oftissues and organs. Another unique charac-teristic of stem cells that distinguishes themis their ability to proliferate or replicatethemselves for long periods.
Stem cells used for research typically areeither embryonic or adult stem cells (Com-mittee on the Biological and BiomedicalApplications of Stem Cell Research, 2002, p. 13). Embryos usually come as a donatedby-product of in vitro fertilization (NationalInstitutes of Health, 2002). Embryonic stemcells can be stimulated to differentiate intospecific cell types such as heart muscle
cells, blood cells, or nerve cells. Stimulationincludes changing “the chemical composi-tion of the culture medium,” altering “thesurface of the culture dish,” or modifying“the cells by inserting specific genes”(National Institutes of Health, 2002). Thegoal of such procedures is the future abilityto produce, on demand, specialized cellsthat can be used as a treatment for certaindiseases where there is degeneration ordestruction of cells.
Adult stem cells have been located in“bone marrow, peripheral blood, brain,spinal cord, dental pulp, blood vessels,skeletal muscle, epithelia of the skin anddigestive system, cornea, retina, liver, andpancreas” (Department of Health andHuman Services, 2001). It was not until the1990s that scientists discovered that thebrain contains stem cells. These stem cells
are able to generate the brain’s major celltypes: astrocytes and oligodendrocytes,which are nonneuronal glial cells, andneurons. Stem cells in adults have beenidentified in the subventricular zone of thetelencephalon (Alvarez-Buylla & Garcia-Verdugo, 2002) and in the dentate gyrus ofthe hippocampus (Gould & Gross, 2002;Song et al., 2002); these cells were demon-strated to differentiate into any type ofnervous tissue cell (Alvarez-Buylla & Lois,1995; Gage, 2000; Weiss et al., 1996).
The pluripotency, or plasticity, of embry-onic cells has been one of the touted advan-tages of embryonic stem cells comparedwith adult stem cells. However, recent re-search supports that at least some adultstem cells may also demonstrate thispluripotency, with the possibility that furtherresearch will uncover other adult stem cells
N e u r o p s y c h o l o g y i n A c t i o n 4 . 4
S t e m C e l l Re s e a r c h : S c i e n c e a n d E t h i c s
by Meghan L. Butryn, Danielle Kerns, and Heather W. Murray
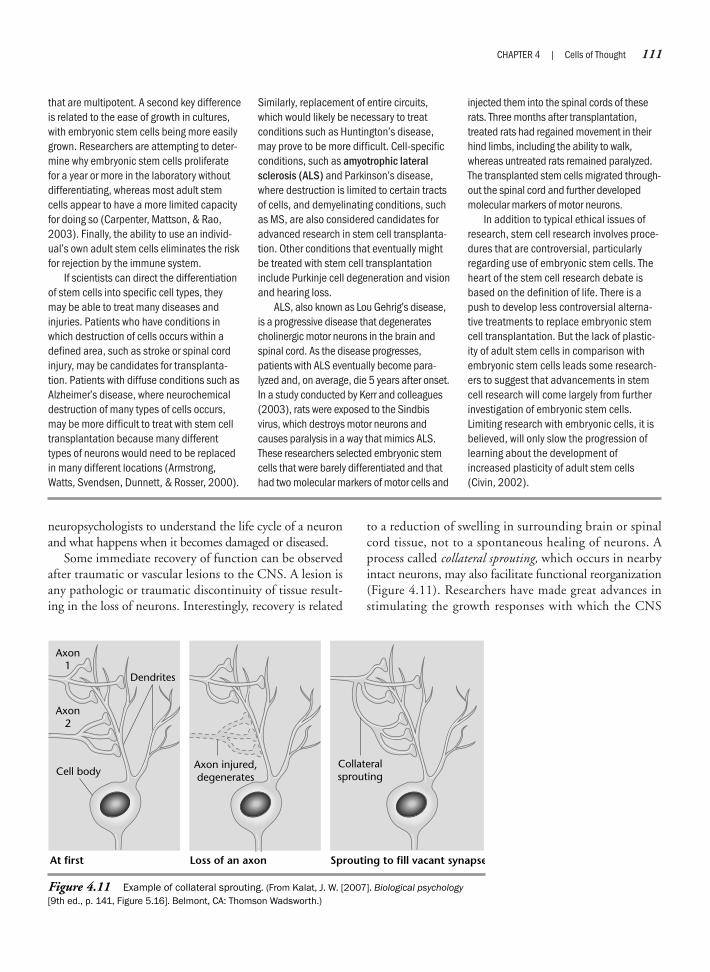
neuropsychologists to understand the life cycle of a neuronand what happens when it becomes damaged or diseased.
Some immediate recovery of function can be observedafter traumatic or vascular lesions to the CNS. A lesion isany pathologic or traumatic discontinuity of tissue result-ing in the loss of neurons. Interestingly, recovery is related
to a reduction of swelling in surrounding brain or spinalcord tissue, not to a spontaneous healing of neurons. Aprocess called collateral sprouting, which occurs in nearbyintact neurons, may also facilitate functional reorganization(Figure 4.11). Researchers have made great advances instimulating the growth responses with which the CNS
CHAPTER 4 | Cells of Thought 111
that are multipotent. A second key differenceis related to the ease of growth in cultures,with embryonic stem cells being more easilygrown. Researchers are attempting to deter-mine why embryonic stem cells proliferatefor a year or more in the laboratory withoutdifferentiating, whereas most adult stemcells appear to have a more limited capacityfor doing so (Carpenter, Mattson, & Rao,2003). Finally, the ability to use an individ-ual’s own adult stem cells eliminates the riskfor rejection by the immune system.
If scientists can direct the differentiationof stem cells into specific cell types, theymay be able to treat many diseases andinjuries. Patients who have conditions inwhich destruction of cells occurs within adefined area, such as stroke or spinal cordinjury, may be candidates for transplanta-tion. Patients with diffuse conditions such asAlzheimer’s disease, where neurochemicaldestruction of many types of cells occurs,may be more difficult to treat with stem celltransplantation because many differenttypes of neurons would need to be replacedin many different locations (Armstrong,Watts, Svendsen, Dunnett, & Rosser, 2000).
Similarly, replacement of entire circuits,which would likely be necessary to treatconditions such as Huntington’s disease,may prove to be more difficult. Cell-specificconditions, such as amyotrophic lateralsclerosis (ALS) and Parkinson’s disease,where destruction is limited to certain tractsof cells, and demyelinating conditions, suchas MS, are also considered candidates foradvanced research in stem cell transplanta-tion. Other conditions that eventually mightbe treated with stem cell transplantationinclude Purkinje cell degeneration and visionand hearing loss.
ALS, also known as Lou Gehrig’s disease,is a progressive disease that degeneratescholinergic motor neurons in the brain andspinal cord. As the disease progresses,patients with ALS eventually become para-lyzed and, on average, die 5 years after onset.In a study conducted by Kerr and colleagues(2003), rats were exposed to the Sindbisvirus, which destroys motor neurons andcauses paralysis in a way that mimics ALS.These researchers selected embryonic stemcells that were barely differentiated and thathad two molecular markers of motor cells and
injected them into the spinal cords of theserats. Three months after transplantation,treated rats had regained movement in theirhind limbs, including the ability to walk,whereas untreated rats remained paralyzed.The transplanted stem cells migrated through-out the spinal cord and further developedmolecular markers of motor neurons.
In addition to typical ethical issues ofresearch, stem cell research involves proce-dures that are controversial, particularlyregarding use of embryonic stem cells. Theheart of the stem cell research debate isbased on the definition of life. There is apush to develop less controversial alterna-tive treatments to replace embryonic stemcell transplantation. But the lack of plastic-ity of adult stem cells in comparison withembryonic stem cells leads some research-ers to suggest that advancements in stemcell research will come largely from furtherinvestigation of embryonic stem cells.Limiting research with embryonic cells, it isbelieved, will only slow the progression oflearning about the development ofincreased plasticity of adult stem cells(Civin, 2002).
At first
Axon2
Dendrites
Cell body
Axon1
Loss of an axon Sprouting to fill vacant synapse
Collateralsprouting
Axon injured,degenerates
Figure 4.11 Example of collateral sprouting. (From Kalat, J. W. [2007]. Biological psychology[9th ed., p. 141, Figure 5.16]. Belmont, CA: Thomson Wadsworth.)
typically reacts to trauma, replacing tissue lost to injury ordisease with neuronal transplants and developing assess-ment, prosthesis, and cognitive rehabilitation techniquesfor disrupted functional systems. One major finding by
neuropsychologists has been that an active training rehabil-itation program facilitates recovery of function. It is withinthis area of assessment and intervention that clinical neu-ropsychologists have made some of their greatest advances.
112 PART TWO | The Functioning Brain
SummaryThis chapter discusses the structure and function of the important “cells of thought.” Each of these classesof cells contain subtypes that are specialized for different types of information processing. Although scien-tists know most about the electrochemical processes of neurons, the chemical processes of glial cells aregaining more attention for their role in cognitive functioning. At its most fundamental level, all human be-havior originates from the basic processes mediated by the structural interconnections and the chemicalinfluences of neurons and glial cells with each other. Clinical disorders of neurons include diseases or con-ditions that physically damage the neuron or disrupt communication. In this chapter, we discuss multiplesclerosis and introduce disorders that will be examined in more depth in later chapters, such as epilepsyand spinal cord injury. Research related to the mechanisms of structural neuronal repair as well as a betterunderstanding of the chemical interplay of these cells is helping to inform treatment.
C r i t i c a l T h i n k i n g Q u e s t i o n s
Will it be possible one day to “map” the circuits of the human brain?Actor Christopher Reeve suffered a severe spinal cord injury and died without fulfilling his pledge to walk again. What is theoutlook for other people with paralysis caused by spinal cord injury?Is it possible for a drug to be effective if it does not activate a naturally occurring brain chemical receptor?What scientific and ethical questions will need to be resolved for research into neuronal repair and neurogenesis to besuccessful?
K e y Te r m s
DendritesAxonTerminal buttonsSynapseNeurotransmitterPruningGray matterPurkinje cellsDendritic spinesMyelin sheathWhite matterAction potentialGliaOligodendrocytesSchwann cellsNodes of RanvierMultipolar neuronsBipolar neuronsMonopolar neurons
InterneuronsMotor neuronsSensory neuronsTractsPathwaysFibersNervesIntracerebral fibersIntercerebral fibersProjection fibersNucleiGangliaMicrogliaAstrocytesGliomasBlood–brain barrierResting potentialMembrane potentialIons
Sodium–potassium pumpRefractory periodDisinhibitionSeizuresElectroconvulsive therapy (ECT)ElectroencephalographSynaptic knobsSynaptic vesiclesReceptor sitesExcitatory postsynaptic potential
(EPSP)Inhibitory postsynaptic potential
(IPSP)Acetylcholine (ACh)SerotoninCatecholaminesDopamineMuscarinic cholineNicotinic choline
StriatumReticular activating systemBasal forebrainHippocampusNucleus basalis of MeynertNuclei of the rapheNorepinephrineLocus ceruleusSubstantia nigraAmino acidsGamma-aminobutyric acid
(GABA)GlutamatePeptidesEndorphins Stem cellsAmyotrophic lateral sclerosis
(ALS)
We b C o n n e c t i o n s
http://psych.hanover.edu/Krantz/neurotut.htmlBasic Neural Processes TutorialsA good tutorial on the basics of neural processing. Includes a glossary of terms and quizzes on the structureof the neuron and the brain.
http://www.neuroguide.comNeurosciences on the InternetA searchable page that provides links to sites in neuroscience.
CHAPTER 4 | Cells of Thought 113

Chapter 5
FUNCTIONAL NEUROANATOMY
Anatomy is for physiology what geography is for the historian: It describesthe scene of action.
—Jean Fernel
The Brain—is wider than the sky—For—put them side by side—The one the other will containWith ease—and You—beside—
—Emily Dickinson
Anatomic and Functional Development of the BrainOrganization of the Nervous SystemPeripheral Nervous SystemCentral Nervous SystemGross Anatomy: Protection and Sustenance of the BrainPrincipal Divisions of the BrainBrainstem and CerebellumTelencephalon

CHAPTER 5 | Functional Neuroanatomy 115
OverviewNeuroanatomy is best understood within a conceptual framework of structure–function relationships. Inneuropsychology, a primary goal is to understand the psychological functions and systems of the brain.Rather than memorizing structures for structure’s sake, a more meaningful picture emerges from knowinghow the subdivisions of the brain are related, and what roles they play in initiating and regulating behavior.Neuroanatomy and neuroscience texts present slightly different variations of organization within the majorsubdivisions of the brain. Some authors focus on morphology as the organizing scheme, some on physiol-ogy, and some on embryonic and fetal development. Despite the daunting array of structures, the basiclogic of neuroanatomy is straightforward. The organization presented in this chapter shows the relationshipsbetween the often-confusing terms and groupings. This goal is accomplished by using the foundation of thedeveloping brain within the context of evolution, which provides a useful picture of functioning from basic tomore complex behaviors.
This chapter discusses individual structures and terminology, shows their location in the brain, andgives a brief overview of function. The material covered here is not a detailed review of the content oftencovered in courses on neuroscience or sensory motor systems, but rather constitutes an illustrated accountof the functional anatomy of the major components of the nervous system. With the foundation of the grossanatomy and functioning this chapter presents, you can appreciate the normal and abnormal phenomenaassociated with brain dysfunction. The structures are the important topographical features on which thevarious processing systems of the brain depend. This chapter is a stepping-stone for subsequent chaptersrelated to functional systems and, indeed, for the entire book. We develop these structures further as weexamine functional brain systems and neuropsychological disorders.
To set the stage for our discussion of the functional neuroanatomy of the brain, we discuss the prena-tal and postnatal development of the human brain. The gestation of the brain is a significant developmen-tal period when you consider that the rate of neuronal development is estimated at 250,000 neurons perminute, for a total, at birth, in excess of 100 billion (Cowan, 1979; Papalia & Olds, 1995). Despite thisastonishing rate of early brain development, the process is both orderly and systematic. That is, the braindevelops in accordance with genetically predetermined templates or “blueprints” that guide the unfoldingof structure and function. The developmental process does not stop and wait for better conditions such asoptimal maternal health and nutrition, nor does it reverse direction to repeat developmental stages thatare compromised by insults engendered by trauma, drugs, or environmental toxins. Accordingly, it is notsurprising that negative events during gestation account for a significant number of childhood neurologicdisorders.
The first section presents an overview of the anatomic development of the brain, followed by a presenta-tion of the major components of the nervous system. We also introduce the necessary terminology for acommon orientation to the geographical locations of structures. Next, we present structural features thatprotect and sustain the brain. Finally, we discuss principal divisions of the brain, from lower, evolutionarilyolder structures to higher order structures.
K e e p i n M i n d
What are the stages and processes of anatomic development?
How are the subsystems of the brain organized?
How does the brain protect and nourish itself?
Does brain structure follow brain function?
What are the major divisions of the brain?

Anatomic and FunctionalDevelopment of the Brain
Beginning as a hollow tube, the brain developssteadily through temporally distinct stages to its finalanatomic and functional state of well-delineated cellularlayers and regions. The development of the central ner-vous system (CNS) is orderly and systematic, generallyunfolding from head (cephalic) to tail (caudal), from near(proximal) to far (distal), and from inferior (subcortical)to dorsal (cortical). The earliest stage, neurogenesis, in-volves the proliferation of neurons of the neural tube andthe migration of these cells to predetermined locations. Thisstage is primarily genetically determined, although environ-mental influences can have an impact on this process. Sub-sequent stages include the growth of axons and dendrites,formation of synaptic junctures, myelination of axons, andsynaptic reorganization involving strengthening or loss ofsynaptic connections. The latter stages complete much oftheir maturation during postnatal development. In gen-eral, prenatal development is primarily concerned with theformation of the CNS, whereas postnatal development in-volves the increasing emergence of functionality.
N E U R O G E N E S I S A N D C E L L U L A RM I G R A T I O N
Both the CNS and peripheral nervous system (PNS) de-velop from the outer ectoderm layer of the fertilized egg atapproximately 18 days after conception. Ectodermal tissue(neural plate) rises, then subsequently folds and fuses atapproximately the fourth week to form the neural tube(Figure 5.1). The cavity of the neural tube gives rise to theventricular system of the CNS, and the cells lining the wallof the neural tube, termed precursor or progenitor cells,create the neurons and glial cells (astrocytes, oligoden-drocytes, and microglia) of the brain (Martin & Jessell,1991). Developing cells do not proliferate at the same ratealong the expanding neural tube. The timing and locationof these cells are genetically predetermined and relate totheir final placement and function in the mature brain.Once the proliferation of a specified group of neurons iscomplete, the migratory process commences and the cellsmove outward toward their genetically determined desti-nation in temporally different waves. As the cells reachtheir destination, they begin to develop the characteristicsof the cell types that are intrinsic to that particular brainregion (Kolb & Fantie, 1997). The process of increasingregional specialization of cells is referred to as differentia-tion. The migrating cells do not differentiate at the same
rate; for example, the cells destined for the hippocampusdifferentiate at a faster rate than the cells of the cortex(Monk, Webb, & Nelson, 2001).
The open ends of the neural tube close at approxi-mately the 26th day of gestation, with the anterior endsubsequently creating the brain, and the posterior endforming the spinal cord. The process of forming and clos-ing the neural tube is called neurulation. Failure of theneural tube to close during development can cause a num-ber of developmental disorders. For example, neuroscien-tists believe that spina bifida, a congenital developmentaldisorder characterized by an opening in the spinal cord,results from a disruption of the proliferation rate of neuralcells or from the failure of these cells to differentiate prop-erly in the neural tube. In contrast, when the anterior end
116 PART TWO | The Functioning Brain
Figure 5.1 Formation and closure of the neuraltube. (a) Start of neurulation, two cross-sectional views.(b) Late stage of neurulation, showing the anterior andposterior closing. (From Lemire, R. J., Loeser, J. D., Leech,R. W., & Alvord, E. C. [1975]. Normal and abnormal develop-ment of the human nervous system. Philadelphia: LippincottWilliams & Wilkins, by permission.)

of the tube fails to close, the brain fails to developanatomically, producing a condition termed anen-cephaly. In this condition, the brain is a vascular massand the infant does not survive.
The development of the cortex, corticogenesis, be-gins in the sixth to seventh embryonic week. The rapidlyproliferating cells along the wall of the neural tube mi-grate outward at different predetermined times. The neu-rons migrate in sheets (laminae) along nonneuronal (glial)fibers that span the cortical wall. Ultimately, these neu-ronal sheets constitute the six laminated layers of the cor-tex and the subcortical nuclei. The inner layer forms first,followed by the development of the outer layers of thecortex. Each successive generation of migrating cellspasses through the previously developed neuronal cells.Thus, the cortex develops from inside out, with migra-tion beginning earlier for the more anterior and lateralareas of the cortex (Rakic & Lombroso, 1998). By the18th week of gestation, virtually all cortical neurons havereached their designated locations and cell proliferationceases. The exceptions are the cells of the hippocampusand cerebellum that continue to proliferate after birth(Anderson, Anderson, Northam, Jacobs, & Catroppa,2001). After migration, many of the glia cells transform intoastrocytes, whereas others merely disappear (Monk et al.,2001).
Disruption in the migratory process can result in sig-nificant and extensive malformations of the developingbrain. For instance, abnormalities of cell migration canproduce developmental anomalies of the corpus callosumand other subcortical structures. Similarly, disruption ofcell migration during the first trimester of development isassociated with malformations of the cerebral cortex. Anexample is the condition of agyria, or lissencephaly, adisorder that occurs during the 11th to 13th weeks of ges-tation and involves the underdevelopment of the corticalgyri (Hynd, Morgan, & Vaughn, 1997). Severe neuro-logic problems accompany this condition, such as severemental retardation, motor retardation, seizures, and re-duced muscle tone. Most infants with agyria do not sur-vive beyond 2 years of age.
A X O N A N D D E N D R I T E D E V E L O P M E N T
As the neurons migrate along the glial fibers, axons beginto form rapidly and travel to other neurons of the brain,allowing for cortical–cortical, cortical–subcortical, andinterhemispheric communication. The intercommunica-tions afforded by axonal connections are crucial to the in-tegrative functioning of the brain. As the migrating neu-ronal cells reach their designated positions, dendrites
begin to sprout in a process called arborization. Subse-quently, little extensions called dendritic spines begin toextend out from the dendrites. The dendrites and den-dritic spines create synapses for gathering information totransmit to the neuron. Dendritic growth begins prena-tally and proceeds slowly, with the majority of arboriza-tion and spine growth actually occurring postnatally. Themost intensive period of dendritic growth occurs frombirth to approximately 18 months of age.
The development of the dendrites and dendritic spinesis highly sensitive to the effects of environmental stimula-tion. This sensitivity fosters the growth and differentia-tion of the brain; yet, it increases its vulnerability to dam-age. An example of this vulnerability is the discovery, forcertain groups of mentally retarded children, of abnor-malities of the dendritic spines that are not attributable togenetic factors. In these cases, neuroscientists suspectsome form of environmental insult as having producedthe anomaly.
S Y N A P T O G E N E S I S
Paralleling the growth of the axons and dendrites of thebrain is the formation of synapses, that is, synaptogene-sis. Synaptogenesis begins during the second trimesteras neuronal migration approaches completion. Thus, atthe 28th gestational week, synaptic density is low in allcortical regions, particularly the prefrontal cortex.Whereas the occipital lobe begins developing beforebirth and rapidly achieves near adult-level synaptic den-sity between ages 2 and 4, the more slowly developingprefrontal cortex does not reach adult levels until lateadolescence or adulthood. Likewise, the synaptic devel-opment of the motor speech cortex (Broca’s area) followsa slow trajectory paralleling that of the prefrontal cortex(Huttenlocher & Dabholkar, 1997). Regional increases insynaptic density accompany the emergence of function.For example, a rapid increase in synaptic density of thefrontal lobes during the latter part of the first year of lifecorrelates with the emergence of rudimentary executivefunctions.
M Y E L I N A T I O N
As cellular migration nears completion, oligodendrocytesbegin to encircle the axons, providing a protective whiteinsular sheath called myelin (see discussion in Chapter 4).The process of myelination begins in the spinal cord, pro-ceeds through the subcortical regions, and finally com-pletes the cortical circuitry. The cortical regions myelinateat different times, beginning in the posterior regions of
CHAPTER 5 | Functional Neuroanatomy 117

the brain and moving in an anterior direction, with theparietal and frontal lobes completing the process last. Themyelination of the latter two regions begins after birth,and in the case of the frontal regions, continues into ado-lescence and adulthood. The significant increase in brainweight in the postnatal years is primarily a function of thebrain’s increased myelination. Furthermore, the myelina-tion of regional circuitry generally correlates with theemergence of function. Thus, similar to synaptic density,myelination is a “marker” of increasing functional matu-rity of brain circuitry. For example, myelination of theoptic nerve begins at birth and is completed by the thirdmonth, consistent with the emergence of vision.
P R U N I N G
During the early months of neurodevelopment, the neu-rons and synaptic processes of the brain are initially over-produced. Researchers believe that the synaptic connec-tivity of the neurons is not completely geneticallypreprogrammed, and many of the initial connections maybe random, unnecessary, or poor. Subsequent develop-ment eliminates, or prunes, large numbers of neurons,with the process often beginning at the sites of the den-dritic spines. Pruning does not appear to be random, butrather to be a purposeful sculpting of the brain; that is,synaptic connections that are strengthened through sen-sory input and motor activity are spared. In contrast,pruning eliminates weakly reinforced or redundant con-nections, thus promoting neural efficiency. Economy instructure and function appears to be an overarching prin-ciple of evolutionary development. This process is exem-plified by the development of speech and language spe-cific to one’s culture. At birth, the infant is sensitive tothe range of sounds that are evident in all languages.However, the reinforcement of speech sounds unique toone’s culture results in the loss of sensitivity to sounds notevident in the language. Neuroscientists speculate thatneurons and synaptic processes representing the under-stimulated sounds are pruned. Functionally, this pruningpotentially accounts for the greater difficulty encounteredin learning a second language at an older age as opposedto at an earlier age.
Pruning is primarily a postnatal process, eliminating40% of the cortical neurons of the brain during child-hood. The remaining neurons are eliminated during ado-lescence, and possibly into early adulthood. The observedreduction in cortical gray matter during adolescence is be-lieved related to synaptic pruning (Gogtay, Giedd, Lusk,Hayashi, Greenstein, Vaituzis, et al., 2004). Pruning ofbrain regions proceeds at different times and rates. Thus,
reduction of the synapses in the visual cortex begins at1 year of age and is completed by age 12, whereas pruningof the prefrontal region proceeds from 5 to 16 years ofage (Pfefferbaum, Mathalon, Sullivan, Rawles, Zipursky,& Lim, 1994).
R E G I O N A L D E V E L O P M E N T
As noted earlier, the anterior, cranial end of the neuraltube expands to form the brain, and the posterior endevolves to form the spinal cord. Before neurulation iscomplete, three vesicles (dilations or expansions) developat the anterior end. These vesicles subsequently form theforebrain (prosencephalon), midbrain (mesencephalon),and hindbrain (rhombencephalon). In the fifth week ofdevelopment, the forebrain and hindbrain each subdivide,whereas the third vesicle, the midbrain, maintains its re-gional structure. The division of the prosencephalon resultsin the formation of the telencephalon and diencephalon.The rhombencephalon subdivides to form the meten-cephalon and myelencephalon. These regions, in turn,give rise to the cortical and subcortical structures of thebrain. The five subdivisions, in combination with the ven-tricular system and spinal cord, constitute the seven majordivisions of the CNS. Figure 5.2 presents the regionaldevelopment of the brain.
L O B U L A R A N D C O N V O L U T I O N A LD E V E L O P M E N T
As the cerebral cortex moves forward in development, itfirst expands anteriorly to form the frontal lobes, thendorsally to form the parietal lobes, and finally, posteriorlyand inferiorly to form the temporal and occipital lobes.The posterior and inferior expansion pushes the cortexinto a C-shape. As a result, this C form also shapes manyof the underlying structures, including the lateral ventri-cles, the head of the caudate of the basal ganglia, the hip-pocampus and fornix, and the cingulate and parahip-pocampal gyri (Martin & Jessell, 1991).
In the initial stages of prenatal development, the brainsurface is smooth, lacking both gyri and sulci. The gyri andsulci patterns of the cortex form after neuronal migration,and they reflect the processes of neuronal specialization,dendritic arborization, synaptic formation, and pruning.
The major sulci dividing the cerebral lobes appear first,whereas the gyri within the individual lobes emerge later.At approximately 14 weeks gestation, the longitudinal fis-sure dividing the two cerebral hemispheres and the Syl-vian (lateral) fissure demarcating the border of the pari-etal and frontal lobes are visible. Gyrification continues in
118 PART TWO | The Functioning Brain

an orderly and symmetric fashion through gestation, andby birth, the gyral patterns of the adult are present (Hynd& Hiemenz, 1997). Table 5.1 details this progression.
The formation of the gyri signals that intracortical con-nections are established. Although the gyri and sulci pat-
terns of each person differ slightly, unusual or extreme al-terations suggest deviations in cortical connections andpotential cognitive and behavioral deficits (Hynd &Hiemenz, 1997). For example, an insult to the brain (suchas intrauterine infection) during the fifth and sixth monthof gestation can produce polymicrogyria, a conditioncharacterized by the development of small, densely packedgyri. This anomaly is associated with learning disabilities,mental retardation, and epilepsy (Hynd et al., 1997).
V E N T R I C U L A R A N D S P I N A L C O R D D E V E L O P M E N T
As the CNS matures, the cavities within the cerebral vesi-cles of the neural tube subsequently form the ventricularsystem and the central canal of the spinal cord. The cavi-ties of cerebral vesicles differentiate into (1) the two lat-eral ventricles, formerly called the first and second ven-tricles of the forebrain; (2) the narrow cerebral aqueduct,or aqueduct of Sylvius, of the midbrain; and (3) thefourth ventricle of the hindbrain (Martin & Jessell,1991). The transformation of the ventricles into theircharacteristic C-shape begins at approximately 3 months.Cerebrospinal fluid (CSF) is produced in the ventricles,
CHAPTER 5 | Functional Neuroanatomy 119
Text not available due to copyright restrictions
Text not available due to copyright restrictions

cushions the brain and spinal cord within the skull andvertebral column, and removes waste products from thebrain.
The spinal cord does not divide; rather, it segmentsduring development. These units correspond to the cervi-cal, thoracic, lumbar, sacral, and coccygeal levels of themature spinal cord. Throughout early prenatal develop-ment, the spinal cord grows at the same rate as the verte-bral column and occupies the entire length of the verte-bral canal (space within the vertebral column). Later indevelopment, the growth of the vertebral column exceedsthat of the spinal cord. At birth, the caudal end of thespinal cord extends only to the lumbar vertebra (Martin,1996).
P O S T N A T A L D E V E L O P M E N T
During the last 3 months of prenatal life and the first 2 yearsof postnatal development, the brain changes rapidly. Atbirth, a baby’s brain is one-fourth the weight of its final adultweight of approximately 1300 to 1500 grams (Majovski,1997). By age 2, the brain has achieved three fourths ofits eventual adult weight and the cortical surface area ofthe hemispheres has doubled. During this rapid growthperiod, significant synaptic and dendritic interconnec-tions form, and pruning and myelination are occurring.Other maturational processes are also evident during thisperiod, including increases in neurotransmitters and re-lated biochemical agents and changes in electroencephalo-graphic wave patterns.
Positron emission tomography (PET) studies of in-fants are providing insights into the early postnatal de-velopment of the brain. Glucose is a primary energysource of the brain, and the rate at which glucose is used(metabolized) in various brain regions provides a mea-sure of the activation of these regions. PET imaging cancapture the glucose metabolism of brain structures.Moreover, the pattern of glucose metabolism of brainregions correlates with the behavioral, neurophysiologic,and neuroanatomic maturation of the brain (Chugani,Muller, & Chugani, 1996). In the newborn (5 weeks),four brain regions show the highest rate of glucose uti-lization. These areas include the sensorimotor cortex,thalamus, brainstem, and cerebellum. In contrast, glu-cose utilization is generally at low levels in other regionsof the cortex and basal ganglia. This pattern of regionalutilization indicates that the phylogenetically older brainstructures (primarily subcortical) are rapidly developing,consistent with the reflexive and limited behavioralrepertoire of the newborn. Cortical functions are at arudimentary level and are limited to the primary sen-
sory and motor areas. As the infant begins to demon-strate more coordinated visuomotor movements duringthe second to third month, increases in glucose metabo-lism are evident in the parietal, temporal, primary visualcortical regions, basal ganglia, and cerebellum. Primitiveneural reflexes become less prominent as subcortical andcortical regions integrate. Between 6 and 8 months, thefrontal and association cortices increase in activation.This increase correlates with the emergence of more ad-vanced cognitive behaviors. For example, by the eighthmonth, the infant is able to perform the delayed re-sponse task, a rudimentary measure of working memory(see Chapter 9). Continued changes in regional metabo-lism and associated behavioral maturation are evidentthrough childhood.
Total brain volume does not significantly increase after5 years of age. This stability of total brain volume beliesthe progressive and regressive growth of white and graymatter; that is, white matter volume increases are offsetby decreases in gray matter volume. White matter in-creases are evident throughout childhood into adulthood,although the growth varies across and within differentbrain regions. Cortical and subcortical gray matter ini-tially increases, with peak volumes being achieved at dif-ferent temporal points. For example, the peak in graymatter volume for the parietal lobes is between 10 and11 years of age, the temporal lobes by 16 years of age, andthe frontal lobes by 11 to 12 years of age (Casey, Giedd,& Thomas, 2000; Giedd, 2004). Progressive loss of graymatter occurs after these peaks. This loss of gray mattervolume reflects the developmental processes of pruningand cell death of neurons and glial cells. Among the lastmaturing cortical regions, as evidenced in achievement ofadult gray-to-white matter volumes, is the dorsolateralprefrontal cortex. The relatively late maturation of the dor-solateral prefrontal cortex is consistent with the protracteddevelopment of higher order or “executive” cognitive,emotional, and social processes and functions. The in-crease in white matter significantly enhances the speed ofneural transmission, whereas the reduction in gray matterrepresents a form of neural “streamlining” to support com-plex and efficient processing. Developmentally, the matu-ration of gray and white matter parallels the emergences ofever increasing cognitive, affective, and social behaviors.That is, brain regions associated with primary sensory andmotor functions mature first, followed by regions support-ive of higher order integrative (e.g., association brain areas)and executive functions (Gogtay et al., 2004).
This discussion of the anatomic development of thebrain completes our first step. We now examine the orga-nization and function of the nervous system.
120 PART TWO | The Functioning Brain
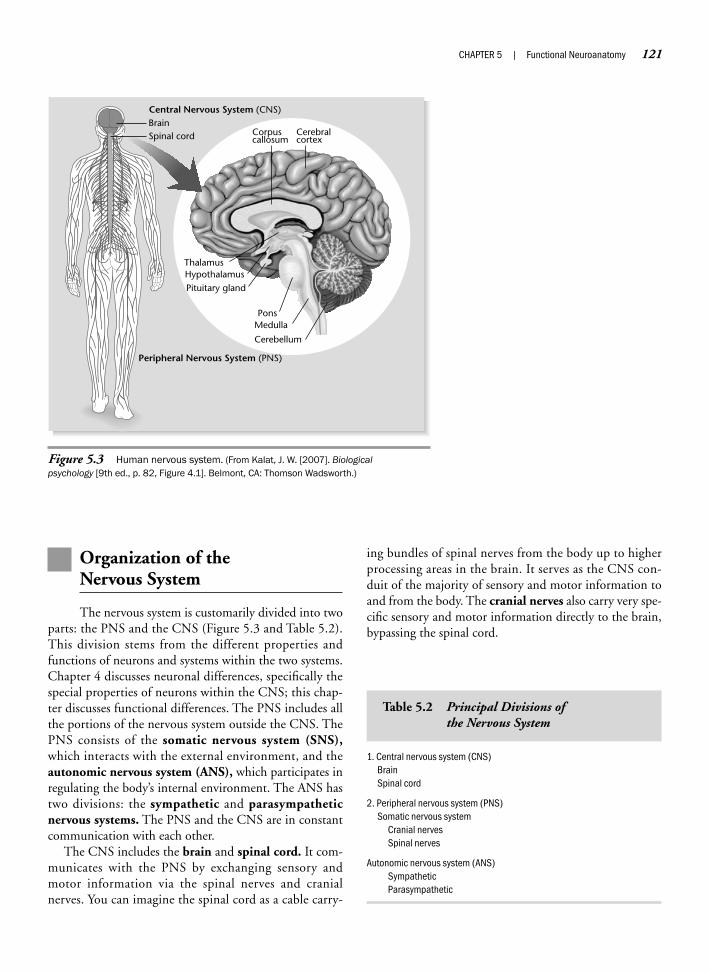
Organization of the Nervous System
The nervous system is customarily divided into twoparts: the PNS and the CNS (Figure 5.3 and Table 5.2).This division stems from the different properties andfunctions of neurons and systems within the two systems.Chapter 4 discusses neuronal differences, specifically thespecial properties of neurons within the CNS; this chap-ter discusses functional differences. The PNS includes allthe portions of the nervous system outside the CNS. ThePNS consists of the somatic nervous system (SNS),which interacts with the external environment, and theautonomic nervous system (ANS), which participates inregulating the body’s internal environment. The ANS hastwo divisions: the sympathetic and parasympatheticnervous systems. The PNS and the CNS are in constantcommunication with each other.
The CNS includes the brain and spinal cord. It com-municates with the PNS by exchanging sensory andmotor information via the spinal nerves and cranialnerves. You can imagine the spinal cord as a cable carry-
ing bundles of spinal nerves from the body up to higherprocessing areas in the brain. It serves as the CNS con-duit of the majority of sensory and motor information toand from the body. The cranial nerves also carry very spe-cific sensory and motor information directly to the brain,bypassing the spinal cord.
CHAPTER 5 | Functional Neuroanatomy 121
Peripheral Nervous System (PNS)
Corpuscallosum
Cerebralcortex
Cerebellum
ThalamusHypothalamusPituitary gland
PonsMedulla
BrainSpinal cord
Central Nervous System (CNS)
Figure 5.3 Human nervous system. (From Kalat, J. W. [2007]. Biologicalpsychology [9th ed., p. 82, Figure 4.1]. Belmont, CA: Thomson Wadsworth.)
1. Central nervous system (CNS)BrainSpinal cord
2. Peripheral nervous system (PNS)Somatic nervous system
Cranial nervesSpinal nerves
Autonomic nervous system (ANS)SympatheticParasympathetic
Table 5.2 Principal Divisions of the Nervous System

Peripheral Nervous System
In principle, all components of the PNS inform theCNS about events in the environment and transmit com-mands from the CNS to the body. The somatic nervoussystem consists of afferent nerves or sensory nerves thatconvey messages from the sense organs to the CNS (in-coming) and efferent nerves that carry motor signalsfrom the CNS to muscles (outgoing). Most nerves of thesomatic nervous system project at regular intervals to thespinal cord via the spinal nerves, except for 12 pairs ofcranial nerves, which synapse directly with the brain.
The function of the ANS is the neural control of in-ternal organs (e.g., heart and intestines). The ANS con-sists of both peripheral and central parts and includes asympathetic division that is involved in activities that ex-pend bodily energy. This expenditure most often occursin response to, or anticipation of, a stressful event. A sim-plified summary of the role of sympathetic activation isthat it prepares the body for action based on the “fight-or-flight” principle. Sympathetic activity mobilizes theenergy necessary for psychological arousal. It includes anincrease in blood flow, blood pressure, heart rate, andsweating, and a decrease in digestion and sexual arousal.
The parasympathetic division of the ANS acts to con-serve energy and is typically associated with relaxation. Itincreases the body’s supply of stored energy and facilitatesdigestion and gastric and intestinal motility. Most auto-nomic organs receive both sympathetic and parasympa-thetic input and are influenced by the relative level ofsympathetic and parasympathetic activity. For many bod-ily functions, the sympathetic and parasympathetic divi-sions act in opposite directions. You can think of the twobranches of the ANS as balancing each other, like twosides of a scale. People generally consider the functions ofthe ANS automatic, not under voluntary control. Theview that the response of the ANS to stress is not undervoluntary control provided the basis for the developmentof the lie detector test. However, biofeedback, medita-tion, hypnosis, and other forms of stress managementhave shown that these functions are not as “automatic” asonce thought, although some controversy has focused onthe degree to which humans can control them (Zillmer &Wickramaserkera, 1987).
Although it is useful to divide the nervous system asoutlined above, real functional anatomic circuits and sys-tems pay little heed to these boundaries. For example,many nerve cells described as part of the PNS have theircells of origin or terminal branches actually situated in theCNS. Consider the divisions within the nervous system as
somewhat flexible; they follow the organizational need toseparate complex phenomena into discrete and less com-plex units.
Central Nervous System
The brain and spinal cord form a continuous com-munication system of the CNS. The CNS has severalunique features. First, as discussed earlier, CNS neuronshave some properties that differ from PNS neurons inthat, for example, they do not show similar properties ofregeneration. Second, you can recognize the importanceof the CNS by the extra protection the body provides it.Structurally, it is located within the bony cavities of theskull and spine. Coverings called the meninges protect it,and it is surrounded by and floats in the protective CSF. TheCNS, and especially the brain, is the most well-nourishedarea of the body, being supplied with an intricate systemof arteries designed with “backup” systems. The bodygives it priority in receiving nutrients and oxygen, and atthe same time, gives it more protection, through theblood–brain barrier, from potentially harmful substancescirculating in the body.
B R A I N
Anatomically, the brain is continuous with the spinalcord, from which it emerges. From an exterior view, thebrain appears to be one organ with a left and a right hemi-sphere. It actually consists of several divisions with manyidentifiable structures.
How the brain is organized into subsystems that ulti-mately result in human behavior is a challenging ques-tion, one on which the rest of this text focuses. Considerthat the brain occupies a relatively small space of about1000 to 1500 cm3, roughly the size of a cantaloupe.Within this space functions an incredible array of differ-ent types of cells. There is also an almost infinite numberof possible connections that make up exceedingly com-plex networks. From this complexity a sense of order andorganization emerges that supports basic life, behavior,and consciousness. The human brain represents the mostadvanced stage of this integration.
A n a t o m i c T e r m s o f R e l a t i o n s h i p
Because the brain is a three-dimensional structure, neu-ropsychologists use a number of terms that describe spe-cific parts, planes, and directions. Unfortunately, the ter-minology is complex and not entirely standardized. This
122 PART TWO | The Functioning Brain

is related, in part, to the fact that we still use nomencla-ture proposed in Latin or Greek more than a century ago.In some instances, anatomists disagree about the bound-aries of a specific brain structure; thus, several terms maydescribe overlapping brain regions. Early anatomists usednames to describe structures simply because they re-minded them of something else. For example, the outerpart of the brain was named cortex, meaning “bark,” becauseit is a thin mantle or covering for the brain. Thus, wheneverwe use the original meaning of the names of brain structuresto help the reader form association about the nomenclature,we also provide precise anatomic terms to clear up any re-sulting confusion. Additionally, these precise anatomicterms will enable the reader to accurately communicateabout the geography and topology of the brain.
Descriptions usually divide the brain into one of thethree main planes (using the x-, y-, and z-axes). Table 5.3lists terms that describe the planes and orientation ofbrain anatomy.
S P I N A L C O R D
Overview
Gross anatomic features: spinal nerves, internal organi-zation of the spinal cord (gray and white matter)
Function: relays information to and from the brain,responsible for simple reflexive behavior
S t r u c t u r e
The spinal cord is continuous with the brain and extendsdownward along the back for about 46 cm. Like thebrain, it is protected by bone, meninges, and CSF. Thespinal cord is physically housed in the spinal column,which consists of alternating bony vertebrae and interver-tebral disks made up of cartilage that absorb mechanicalshocks sustained to the spinal column. The spinal cord it-self is considerably smaller than the vertebral canal andthe meninges. Fat, CSF, and veins combine to protectagainst contact with bony surroundings.
The spinal nerves consist of both sensory and motor neu-rons. At each of the 30 levels of the spinal cord, a pair of in-coming (afferent) dorsal root fibers signals incoming sen-sory information and a pair of outgoing (efferent) ventralroot fibers controls motor nerves and muscles (Figure 5.4).These nerves conduct information related to both the so-matic and autonomic nervous systems in the periphery. Inthe spinal cord, white matter (myelinated axons) makes upthe outside of the cord, whereas gray matter (cell bodies) islocated on the interior. Each area of the spinal cord corre-sponds to a specific body location and controls sensation
and movement of the associated body area: skin, mus-cle, and internal organs. There are 1 coccyx, 5 sacral (S),5 lumbar (L), 12 thoracic (T), and 8 cervical (C) spinalcord levels. The spinal nerves form ringlike innervationsaround the trunk of the body at each level of the spinalcord. The innervations of the limbs are extensions of thebody rings. For example, the nerves to the arms and handsare extensions of C-6, C-7, and C-8 innervations fromthe trunk.
F u n c t i o n
The spinal cord relays somatosensory information fromthe trunk and limbs to the brain. The cord also relays sim-ple motor messages from the brain to the trunk and limbs.
CHAPTER 5 | Functional Neuroanatomy 123
Planes bisecting the brain:
Horizontal plane—plane (x-axis) that shows the brain as seen from above orparallel to the ground.
Coronal plane—plane (y-axis) that shows the brain as seen from the front(frontal section). Typically, this plane is viewed from behind to provideconsistency for right and left directions of the brain and the picture.
Sagittal plane—plane (z-axis) that shows the brain as seen from the side orperpendicular to the ground, bisecting the brain into right and left halves(derived from Latin sagitta, meaning “arrow”).
Directional terms: Most often, directions in the human nervous system arerelated to the orientation of the spinal cord.
Anterior: toward the front or front end
Posterior: toward the back or tail
Inferior: toward the bottom, or below
Superior: toward the top or above
Medial: toward the middle/midline, away from the side
Lateral: toward the side, away from the midline
Rostral: toward the head
Caudal: toward the rear away from the head
Proximal: near the trunk or center, close to the origin of attachment
Distal: away from the center, toward the periphery, away from the origin of attachment
Dorsal: toward the back; the top of the brain is dorsal in humans
Ventral: toward the belly; the bottom of the brain is ventral in humans
Ipsilateral: on the same side
Contralateral: on the opposite side
Table 5.3 Planes of the Brain and Directionsof Orientation to the CentralNervous System
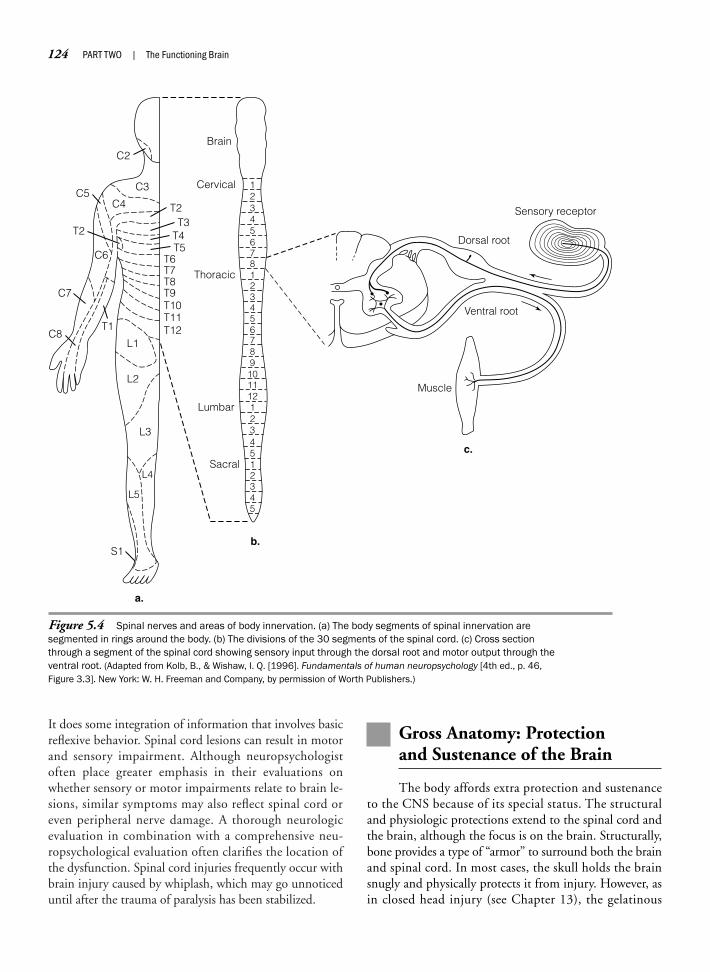
It does some integration of information that involves basicreflexive behavior. Spinal cord lesions can result in motorand sensory impairment. Although neuropsychologistoften place greater emphasis in their evaluations onwhether sensory or motor impairments relate to brain le-sions, similar symptoms may also reflect spinal cord oreven peripheral nerve damage. A thorough neurologicevaluation in combination with a comprehensive neu-ropsychological evaluation often clarifies the location ofthe dysfunction. Spinal cord injuries frequently occur withbrain injury caused by whiplash, which may go unnoticeduntil after the trauma of paralysis has been stabilized.
Gross Anatomy: Protection and Sustenance of the Brain
The body affords extra protection and sustenanceto the CNS because of its special status. The structuraland physiologic protections extend to the spinal cord andthe brain, although the focus is on the brain. Structurally,bone provides a type of “armor” to surround both the brainand spinal cord. In most cases, the skull holds the brainsnugly and physically protects it from injury. However, asin closed head injury (see Chapter 13), the gelatinous
124 PART TWO | The Functioning Brain
12345678123456789
101112123451
Cervical
BrainC2
C3
C4C5
T2
C6
C7
T1C8
L1T12T11T10T9T8T7T6
T5T4T3
T2
L2
L3
L5
L4
S1
Thoracic
Lumbar
Sacral
a.
b.
c.
2345
Sensory receptor
Dorsal root
Ventral root
Muscle
Figure 5.4 Spinal nerves and areas of body innervation. (a) The body segments of spinal innervation aresegmented in rings around the body. (b) The divisions of the 30 segments of the spinal cord. (c) Cross sectionthrough a segment of the spinal cord showing sensory input through the dorsal root and motor output through theventral root. (Adapted from Kolb, B., & Wishaw, I. Q. [1996]. Fundamentals of human neuropsychology [4th ed., p. 46,Figure 3.3]. New York: W. H. Freeman and Company, by permission of Worth Publishers.)

brain may accelerate and scrape against the bony projec-tions of the skull. It is important to understand theskull–brain relationship to understand how the brain maybe vulnerable to skull-related damage. Under the hardprotection of bone, protective membranes called meningesform a flexible structural but semipermeable protectivepad that completely surrounds the brain and spinal cord.The covering of the meninges forms another layer of pro-tection. However, certain types of tumors called menin-giomas may form here and impact on the brain. The CSFcirculates around and throughout the CNS via the ven-tricular system, which provides not only an additionalstructural fluid cushion but also physiologic protectionthrough its immunologic functions and its ability to actas a “waste disposal” system. The unique vascular systemof the brain not only supplies nutrients to the energy-demanding brain but also adds a layer of protection throughthe blood–brain barrier. The blood–brain barrier (see dis-cussion in Chapter 4) is formed by tightly formed endothe-lial cells in the walls of the capillaries of the brain, held inplace by astrocytes that prevent the passage of certain sub-stances into the brain.
S K U L L
Overview
Gross anatomic features: fused connection of bonyplates covering the brain
Function: protection of the brain
S t r u c t u r e
The skull consists of the frontal bone (in some individu-als, the frontal bone develops in two parts), two parietalbones, two temporal bones, the occipital bone, and thesphenoid bone (Figure 5.5). The cerebral lobes derivetheir names from the cranial plates of the skull, whosecorresponding outline they generally follow. This has ledto an imprecise nomenclature of the cortex because theexternal aspects of the skull are easily differentiated, un-like those of the cortical lobes. The skull provides groovesfor blood vessels in the roof (calvaria) of the cranium, con-spicuous ridges in the base of the skull, known as fossae,that hold the brain in place, and more or less symmetricorifices or foramina in the base of the skull that providepassage for nerves and blood vessels. The largest of theseorifices is the foramen magnum, which provides a largemedian opening in the occipital bone for the spinal cordto pass through to the brainstem.
In the newborn, the skull is a relatively large part of itsbody, accommodating the disproportionally large brain.
At birth, the brain is approximately 25% of its adult size,weighing about 500 grams, but will reach about 75% ofits mature size by its first year of maturation. Facilitatingthis rapid development of the brain, the bony plates thatcomprise the skull are not fused as they are in later years,but are separated by membranous, soft tissue. In the new-born, the membranous gaps are largest at the corners ofthe parietal bone. These soft openings are labeledfontanelles (“small fountains”) and may fluctuate withchanges in intracranial pressure. The largest of these open-ings is the anterior fontanelle, located at the top of thehead between the frontal and parietal bones. It does notfully close until 2 years after birth.
F u n c t i o n
The skull completely encases the brain, protecting itfrom external influences. Although normally the shell ofthe skull is an asset, in some instances, it can actually bea liability. The fact that the skull is rigid can become lifethreatening when the internal pressure of a swelling, in-jured brain cannot be released. Because the skull is notsmooth on the interior, but rather consists of bony pro-jections designed to hold the brain in place, injury to theareas around the bony projections of the frontal and tem-poral lobes is common with whiplash and other head in-juries, which cause the gelatinous brain to reverberate inthe skull. The skull varies in thickness; particularly, theareas around the temporal and sphenoid bones are rela-tively thin and are easily fractured by a blow to the sideof the head. Fractures to the base of the skull can lead toserious damage of the brain related to shearing of the cra-nial nerves, leakage of the CSF from the nose, and bleed-ing from the auditory canal.
M E N I N G E S
Overview
Gross anatomic features: dura mater, arachnoid mem-brane, pia mater
Function: protective covering of the CNS, location ofvenous drainage and CSF absorption
S t r u c t u r e
The brain and spinal cord are the only human structurescompletely enclosed in protective bone. In addition, theyare covered by the meninges, a set of thin membranes thathold the brain and spinal cord in place and act as a protec-tive buffer. The meninges of the CNS consist of threemeningeal membranes and completely surround the brainand the spinal cord. Inner to outer they can be remembered
CHAPTER 5 | Functional Neuroanatomy 125

126 PART TWO | The Functioning Brain
a.
Figure 5.5 Lateral (a) and basal (b) views of the skull. (From Chusid, J. G. [1982]. Correlative neuroanatomy& functional neurology [p. 256, Figure 19.3; p. 257, Figure 19.4]. New York: Appleton & Lange, by permission of theMcGraw-Hill Companies.)
with the mnemonic PAD: pia mater, arachnoid mem-brane, and dura mater (or simply dura) (Figure 5.6). Thethin pia mater (derived from Latin meaning “piousmother”) directly adheres to the surface of the CNS, fol-lowing its contours closely. The arachnoid membrane(spider web–like membrane) overlies the subarachnoidspace, which contains CSF. The dura mater (derivedfrom Latin meaning “tough mother”) is a dense, inelastic,double-layered membrane that adheres to the inner sur-face of the skull. The meningeal veins are in the outer por-tion of the dura. The space between the two dural layersis the epidural space. The space between the dura andthe arachnoid is the subdural space. Cerebral veins cross-ing the subdural space have little supporting structure
and, therefore, are most vulnerable to injury and bleedingas a result of trauma (e.g., subdural hematoma).
F u n c t i o n
The meninges provide a protective covering by encasingthe brain and spinal cord. They have no function in cog-nitive activity, but are of importance to neuropsycholo-gists because of clinical complications during injury. Forexample, a head trauma frequently tears large blood ves-sels in the subarachnoid space. In addition, the meningesare susceptible to inflammation, usually by bacterial in-fection, resulting in meningitis. Meningitis can be causedby both bacteria and viral infection. The disease is dan-gerous because it can progress quickly, within 24 hours,
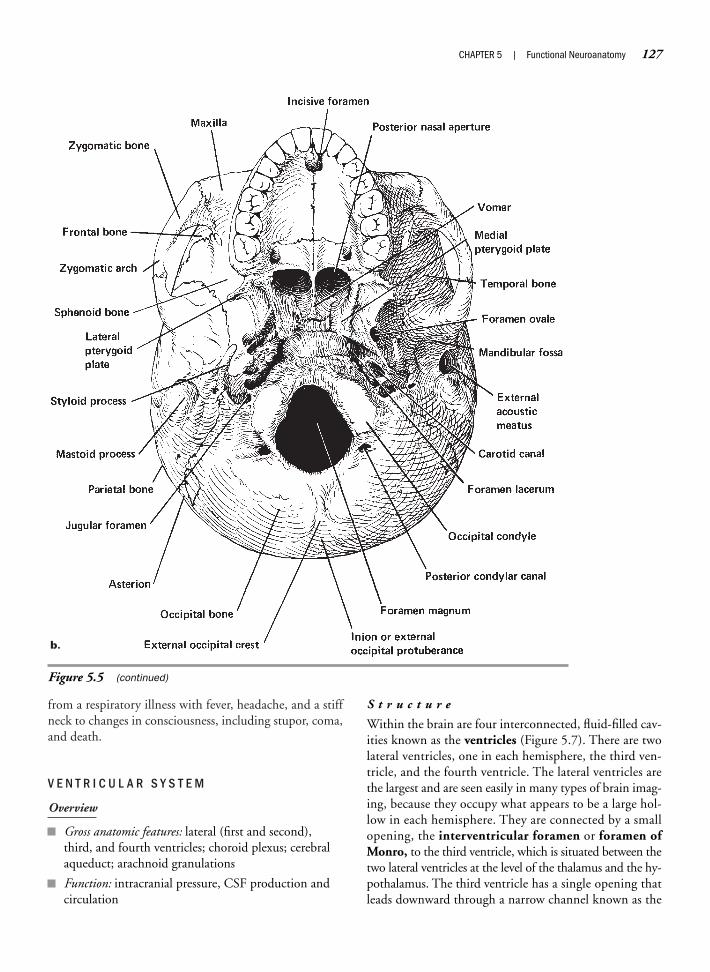
from a respiratory illness with fever, headache, and a stiffneck to changes in consciousness, including stupor, coma,and death.
V E N T R I C U L A R S Y S T E M
Overview
Gross anatomic features: lateral (first and second),third, and fourth ventricles; choroid plexus; cerebralaqueduct; arachnoid granulations
Function: intracranial pressure, CSF production andcirculation
S t r u c t u r e
Within the brain are four interconnected, fluid-filled cav-ities known as the ventricles (Figure 5.7). There are twolateral ventricles, one in each hemisphere, the third ven-tricle, and the fourth ventricle. The lateral ventricles arethe largest and are seen easily in many types of brain imag-ing, because they occupy what appears to be a large hol-low in each hemisphere. They are connected by a smallopening, the interventricular foramen or foramen ofMonro, to the third ventricle, which is situated between thetwo lateral ventricles at the level of the thalamus and the hy-pothalamus. The third ventricle has a single opening thatleads downward through a narrow channel known as the
CHAPTER 5 | Functional Neuroanatomy 127
b.
Figure 5.5 (continued)
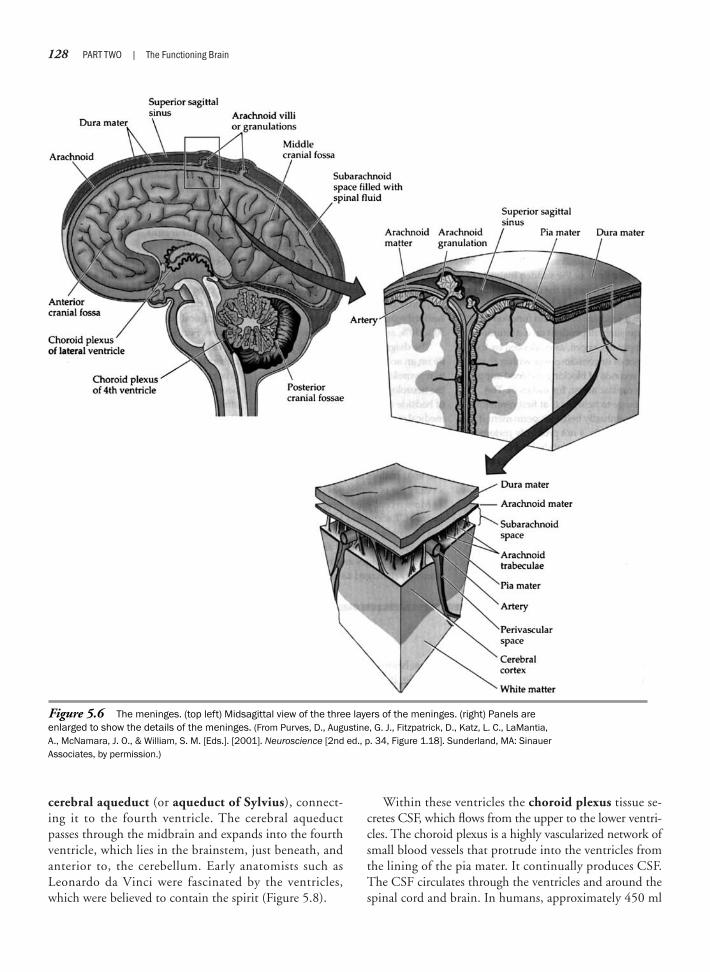
cerebral aqueduct (or aqueduct of Sylvius), connect-ing it to the fourth ventricle. The cerebral aqueductpasses through the midbrain and expands into the fourthventricle, which lies in the brainstem, just beneath, andanterior to, the cerebellum. Early anatomists such asLeonardo da Vinci were fascinated by the ventricles,which were believed to contain the spirit (Figure 5.8).
Within these ventricles the choroid plexus tissue se-cretes CSF, which flows from the upper to the lower ventri-cles. The choroid plexus is a highly vascularized network ofsmall blood vessels that protrude into the ventricles fromthe lining of the pia mater. It continually produces CSF.The CSF circulates through the ventricles and around thespinal cord and brain. In humans, approximately 450 ml
128 PART TWO | The Functioning Brain
Figure 5.6 The meninges. (top left) Midsagittal view of the three layers of the meninges. (right) Panels are enlarged to show the details of the meninges. (From Purves, D., Augustine, G. J., Fitzpatrick, D., Katz, L. C., LaMantia, A., McNamara, J. O., & William, S. M. [Eds.]. [2001]. Neuroscience [2nd ed., p. 34, Figure 1.18]. Sunderland, MA: Sinauer Associates, by permission.)
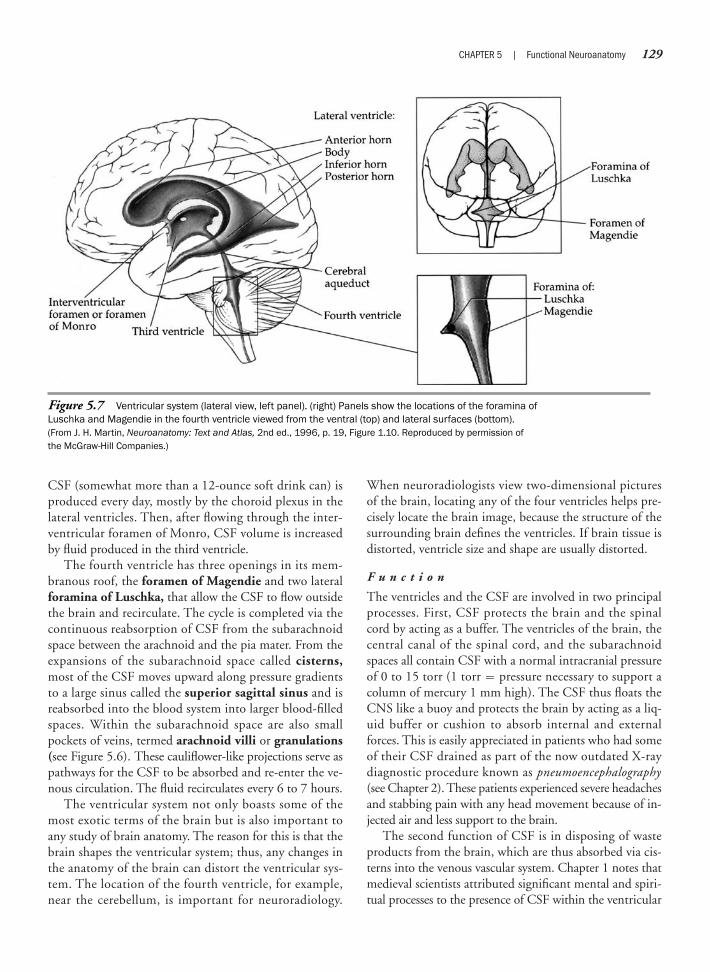
CSF (somewhat more than a 12-ounce soft drink can) isproduced every day, mostly by the choroid plexus in thelateral ventricles. Then, after flowing through the inter-ventricular foramen of Monro, CSF volume is increasedby fluid produced in the third ventricle.
The fourth ventricle has three openings in its mem-branous roof, the foramen of Magendie and two lateralforamina of Luschka, that allow the CSF to flow outsidethe brain and recirculate. The cycle is completed via thecontinuous reabsorption of CSF from the subarachnoidspace between the arachnoid and the pia mater. From theexpansions of the subarachnoid space called cisterns,most of the CSF moves upward along pressure gradientsto a large sinus called the superior sagittal sinus and isreabsorbed into the blood system into larger blood-filledspaces. Within the subarachnoid space are also smallpockets of veins, termed arachnoid villi or granulations(see Figure 5.6). These cauliflower-like projections serve aspathways for the CSF to be absorbed and re-enter the ve-nous circulation. The fluid recirculates every 6 to 7 hours.
The ventricular system not only boasts some of themost exotic terms of the brain but is also important toany study of brain anatomy. The reason for this is that thebrain shapes the ventricular system; thus, any changes inthe anatomy of the brain can distort the ventricular sys-tem. The location of the fourth ventricle, for example,near the cerebellum, is important for neuroradiology.
When neuroradiologists view two-dimensional picturesof the brain, locating any of the four ventricles helps pre-cisely locate the brain image, because the structure of thesurrounding brain defines the ventricles. If brain tissue isdistorted, ventricle size and shape are usually distorted.
F u n c t i o n
The ventricles and the CSF are involved in two principalprocesses. First, CSF protects the brain and the spinalcord by acting as a buffer. The ventricles of the brain, thecentral canal of the spinal cord, and the subarachnoidspaces all contain CSF with a normal intracranial pressureof 0 to 15 torr (1 torr � pressure necessary to support acolumn of mercury 1 mm high). The CSF thus floats theCNS like a buoy and protects the brain by acting as a liq-uid buffer or cushion to absorb internal and externalforces. This is easily appreciated in patients who had someof their CSF drained as part of the now outdated X-raydiagnostic procedure known as pneumoencephalography(see Chapter 2). These patients experienced severe headachesand stabbing pain with any head movement because of in-jected air and less support to the brain.
The second function of CSF is in disposing of wasteproducts from the brain, which are thus absorbed via cis-terns into the venous vascular system. Chapter 1 notes thatmedieval scientists attributed significant mental and spiri-tual processes to the presence of CSF within the ventricular
CHAPTER 5 | Functional Neuroanatomy 129
Figure 5.7 Ventricular system (lateral view, left panel). (right) Panels show the locations of the foramina of Luschka and Magendie in the fourth ventricle viewed from the ventral (top) and lateral surfaces (bottom). (From J. H. Martin, Neuroanatomy: Text and Atlas, 2nd ed., 1996, p. 19, Figure 1.10. Reproduced by permission of the McGraw-Hill Companies.)

chambers of the brain. This theory became known as theventricular localization hypothesis and later formed thebasis for the cell doctrine. On gross dissection of thebrain, the lateral ventricles are the most striking features;thus, this theory, although wrong, persisted robustly.
The ventricles have no direct role in cognitive func-tion. However, abnormal intracranial ventricular pressure(>15 torr) may lead to general cognitive deficits. A se-quence of events can occur in which the ventricles becomeenlarged with fluid, occupying greater space than usual.This results in brain swelling and an increase in intracra-nial pressure. The squeezing or displacing of brain tissue,in turn, leads to changes in behavior and cognition. Thisexpansion of the ventricles accompanied by increased in-tracranial pressure results in a medical condition calledhydrocephalus, which may be caused by an imbalance inthe rate of CSF production or absorption, or by blockage(such as by a tumor) of the circulation. The skull itself
may actually swell. If hydrocephalus occurs in childhoodbefore the cranial bones have closed, the skull may en-large to enormous size (Figure 5.9). Acute hydrocephaluscan be life threatening. Because the fused plates of theskull cannot accommodate the additional space, untreatedhydrocephalus among adults and older children results inchronic dilation of the ventricles and a thinning of thecortex. A variant of hydrocephalus in adulthood, particu-larly the elderly, is normal-pressure hydrocephalus(NPH), characterized by the presence of normal levels ofintracranial CSF. The term may actually be a misnomerinsofar as research (Vanneste, 2000) suggests that thereappears to be an initial stage of increased CSF pressurewith a subsequent enlargement of the ventricles. As theventricles expand, the CSF pressure returns to upper nor-mal to normal levels. However, there may be further tran-sient episodes of increased intraventricular pressure. It isbelieved that the mechanism of action that produces the
130 PART TWO | The Functioning Brain
Figure 5.8 Although many of Leonardo da Vinci’s (1452–1519) early brain anatomy drawings wereinaccurate, he later became a keen observer of neuroanatomy. For this drawing, which presented ananatomic breakthrough, he poured melted wax into the ventricles of an ox, then cut away the brain tissuesto determine the true shape of the ventricles. (The Royal Collection © 2007, Her Majesty Queen Elizabeth II.)
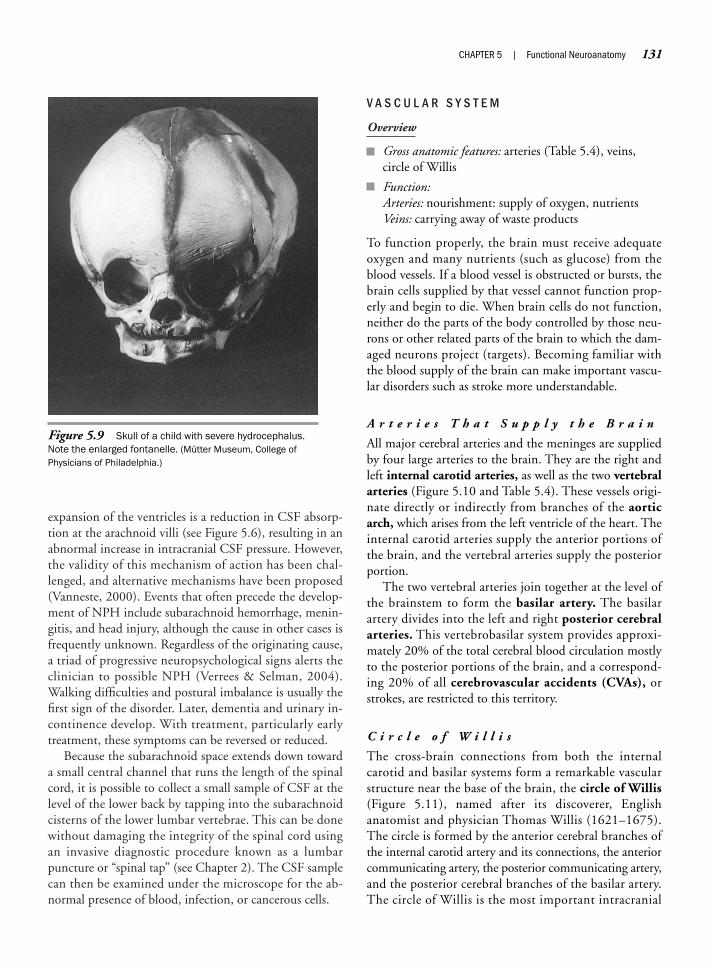
expansion of the ventricles is a reduction in CSF absorp-tion at the arachnoid villi (see Figure 5.6), resulting in anabnormal increase in intracranial CSF pressure. However,the validity of this mechanism of action has been chal-lenged, and alternative mechanisms have been proposed(Vanneste, 2000). Events that often precede the develop-ment of NPH include subarachnoid hemorrhage, menin-gitis, and head injury, although the cause in other cases isfrequently unknown. Regardless of the originating cause,a triad of progressive neuropsychological signs alerts theclinician to possible NPH (Verrees & Selman, 2004).Walking difficulties and postural imbalance is usually thefirst sign of the disorder. Later, dementia and urinary in-continence develop. With treatment, particularly earlytreatment, these symptoms can be reversed or reduced.
Because the subarachnoid space extends down towarda small central channel that runs the length of the spinalcord, it is possible to collect a small sample of CSF at thelevel of the lower back by tapping into the subarachnoidcisterns of the lower lumbar vertebrae. This can be donewithout damaging the integrity of the spinal cord usingan invasive diagnostic procedure known as a lumbarpuncture or “spinal tap” (see Chapter 2). The CSF samplecan then be examined under the microscope for the ab-normal presence of blood, infection, or cancerous cells.
V A S C U L A R S Y S T E M
Overview
Gross anatomic features: arteries (Table 5.4), veins,circle of Willis
Function:Arteries: nourishment: supply of oxygen, nutrientsVeins: carrying away of waste products
To function properly, the brain must receive adequateoxygen and many nutrients (such as glucose) from theblood vessels. If a blood vessel is obstructed or bursts, thebrain cells supplied by that vessel cannot function prop-erly and begin to die. When brain cells do not function,neither do the parts of the body controlled by those neu-rons or other related parts of the brain to which the dam-aged neurons project (targets). Becoming familiar withthe blood supply of the brain can make important vascu-lar disorders such as stroke more understandable.
A r t e r i e s T h a t S u p p l y t h e B r a i n
All major cerebral arteries and the meninges are suppliedby four large arteries to the brain. They are the right andleft internal carotid arteries, as well as the two vertebralarteries (Figure 5.10 and Table 5.4). These vessels origi-nate directly or indirectly from branches of the aorticarch, which arises from the left ventricle of the heart. Theinternal carotid arteries supply the anterior portions ofthe brain, and the vertebral arteries supply the posteriorportion.
The two vertebral arteries join together at the level ofthe brainstem to form the basilar artery. The basilarartery divides into the left and right posterior cerebralarteries. This vertebrobasilar system provides approxi-mately 20% of the total cerebral blood circulation mostlyto the posterior portions of the brain, and a correspond-ing 20% of all cerebrovascular accidents (CVAs), orstrokes, are restricted to this territory.
C i r c l e o f W i l l i s
The cross-brain connections from both the internalcarotid and basilar systems form a remarkable vascularstructure near the base of the brain, the circle of Willis(Figure 5.11), named after its discoverer, Englishanatomist and physician Thomas Willis (1621–1675).The circle is formed by the anterior cerebral branches ofthe internal carotid artery and its connections, the anteriorcommunicating artery, the posterior communicating artery,and the posterior cerebral branches of the basilar artery.The circle of Willis is the most important intracranial
CHAPTER 5 | Functional Neuroanatomy 131
Figure 5.9 Skull of a child with severe hydrocephalus.Note the enlarged fontanelle. (Mütter Museum, College ofPhysicians of Philadelphia.)
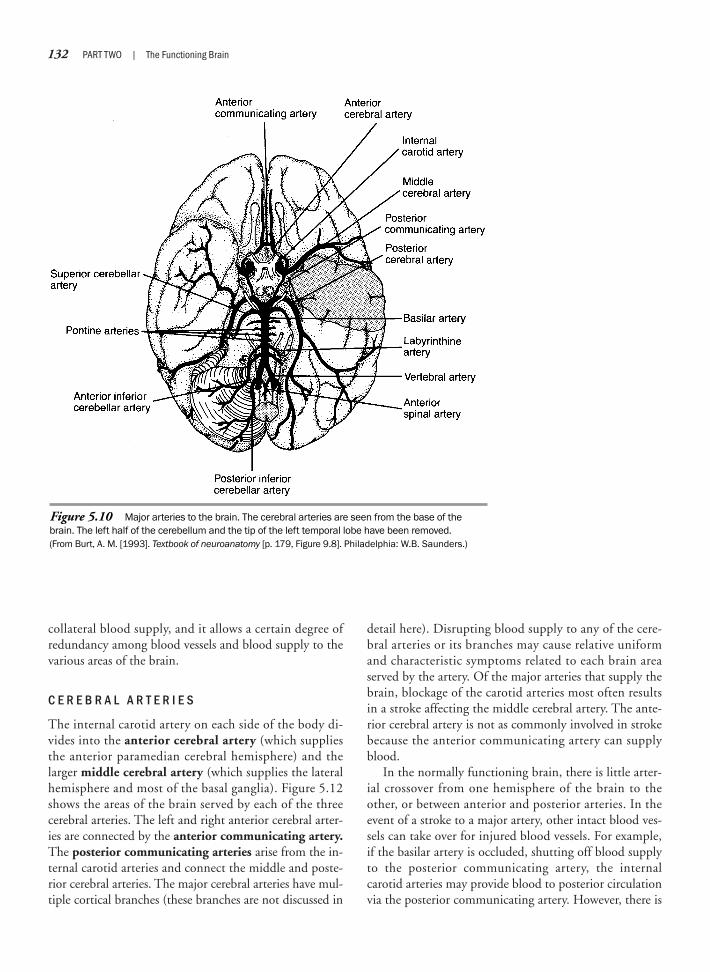
collateral blood supply, and it allows a certain degree ofredundancy among blood vessels and blood supply to thevarious areas of the brain.
C E R E B R A L A R T E R I E S
The internal carotid artery on each side of the body di-vides into the anterior cerebral artery (which suppliesthe anterior paramedian cerebral hemisphere) and thelarger middle cerebral artery (which supplies the lateralhemisphere and most of the basal ganglia). Figure 5.12shows the areas of the brain served by each of the threecerebral arteries. The left and right anterior cerebral arter-ies are connected by the anterior communicating artery.The posterior communicating arteries arise from the in-ternal carotid arteries and connect the middle and poste-rior cerebral arteries. The major cerebral arteries have mul-tiple cortical branches (these branches are not discussed in
detail here). Disrupting blood supply to any of the cere-bral arteries or its branches may cause relative uniformand characteristic symptoms related to each brain areaserved by the artery. Of the major arteries that supply thebrain, blockage of the carotid arteries most often resultsin a stroke affecting the middle cerebral artery. The ante-rior cerebral artery is not as commonly involved in strokebecause the anterior communicating artery can supplyblood.
In the normally functioning brain, there is little arter-ial crossover from one hemisphere of the brain to theother, or between anterior and posterior arteries. In theevent of a stroke to a major artery, other intact blood ves-sels can take over for injured blood vessels. For example,if the basilar artery is occluded, shutting off blood supplyto the posterior communicating artery, the internalcarotid arteries may provide blood to posterior circulationvia the posterior communicating artery. However, there is
132 PART TWO | The Functioning Brain
Figure 5.10 Major arteries to the brain. The cerebral arteries are seen from the base of thebrain. The left half of the cerebellum and the tip of the left temporal lobe have been removed. (From Burt, A. M. [1993]. Textbook of neuroanatomy [p. 179, Figure 9.8]. Philadelphia: W.B. Saunders.)

much individual variation in the circle of Willis; partsof the system may actually be missing in some people(e.g., in 15% of normal brains, the posterior cerebralartery is a direct extension of the posterior communicat-ing artery).
V E N O U S S Y S T E M
The veins are located in the outer portion of the dura andpass blood through vessels back to the heart. Venousdrainage starts with the superficial cerebral veins, whichoriginate in the brain substance within the pia mater andempty into the superior sagittal and transverse sinuses,the deep veins of the brain, and the straight sinus, whichconnects to the internal jugular vein. As noted earlier inthe discussion of the ventricular system, the subarachnoidspace contains pockets of veins called arachnoid granula-tions that serve as pathways for the subarachnoid CSF to beabsorbed and re-enter the venous circulation. Arachnoid
granulations first appear in childhood, around age 7, andincrease in size and number during adulthood. Unlike thearterial blood supply, the venous system of the brain doesnot have a right and left system. Thus, there is free circu-lation within the venous system, which may facilitate thespread of infectious agents from one hemisphere to theother. Chapter 12 gives a detailed description of vasculardisorders.
Principal Divisions of the Brain
The brain can be subdivided into three major divi-sions based on the development of the human embryo(see earlier). As the embryo’s neural tube closes, it beginsto differentiate into three bulges. The topmost becomesthe forebrain (prosencephalon), the middle is the midbrain(mesencephalon), and the third is the hindbrain (rhomben-cephalon). The remainder of the neural tube develops into
CHAPTER 5 | Functional Neuroanatomy 133
Artery Origin Distribution
Basilar Junction of right and left vertebral arteries Brainstem, internal ear, cerebellum, posteriorcerebrum
Carotid, common Brachiocephalic (right), aorta (left) Internal and external carotid
Carotid, external Common carotid artery Neck, face, skull
Carotid, internal Common carotid artery Middle ear, brain, choroid plexus of lateral ventricles
Cerebellar, inferior anterior Basilar artery Lower anterior cerebellum, inner ear
Cerebellar, inferior posterior Vertebral artery Lower part of cerebellum, medulla, choroid plexus of fourth ventricle
Cerebellar, superior Basilar artery Upper part of cerebellum, midbrain, pineal body, choroid plexus of third ventricle
Cerebral, anterior Internal carotid artery Orbital, frontal, and parietal cortex, corpus callo-sum, diencephalon, corpus striatum, internalcapsule, choroids plexus of lateral ventricles
Cerebral, middle Internal carotid artery Orbital, frontal, parietal and temporal cortex, corpus striatum, internal capsule
Cerebral, posterior Basilar artery Occipital and temporal lobes, basal ganglia, choroid plexus of lateral ventricles, thalamus, midbrain
Ophthalmic Internal carotid artery Eye, orbit, facial structures
Spinal, anterior Vertebral artery Spinal cord
Spinal, posterior Vertebral artery Spinal cord
Vertebral Subclavian artery, which arises from Neck muscles, vertebrae, spinal cord, brachiocephalic (right), aorta (left) cerebellum, cortex
Table 5.4 Arteries to the Brain
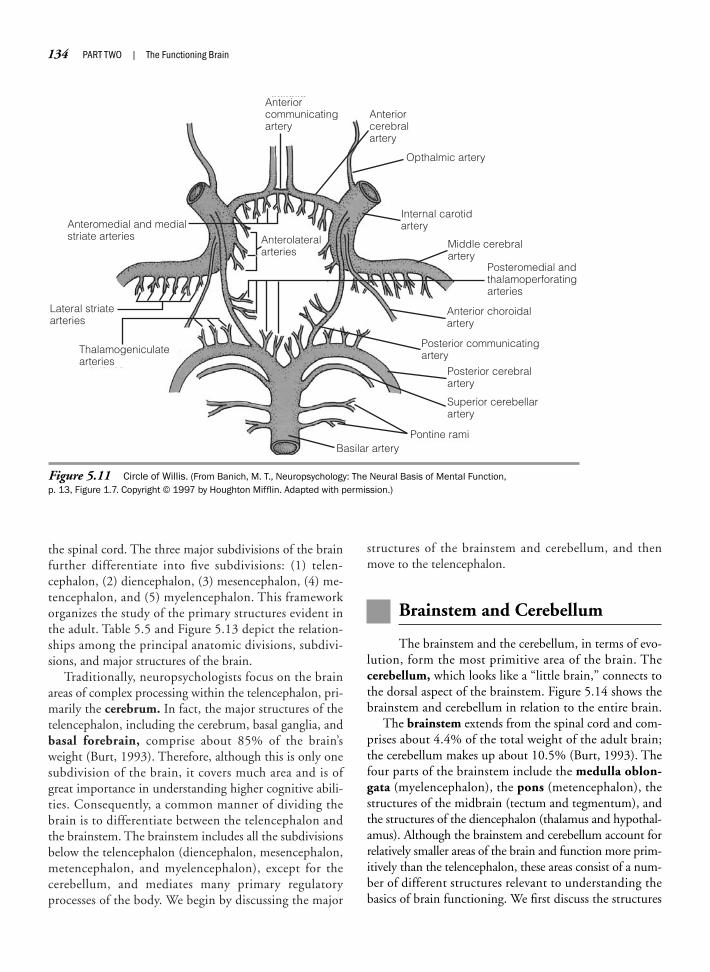
the spinal cord. The three major subdivisions of the brainfurther differentiate into five subdivisions: (1) telen-cephalon, (2) diencephalon, (3) mesencephalon, (4) me-tencephalon, and (5) myelencephalon. This frameworkorganizes the study of the primary structures evident inthe adult. Table 5.5 and Figure 5.13 depict the relation-ships among the principal anatomic divisions, subdivi-sions, and major structures of the brain.
Traditionally, neuropsychologists focus on the brainareas of complex processing within the telencephalon, pri-marily the cerebrum. In fact, the major structures of thetelencephalon, including the cerebrum, basal ganglia, andbasal forebrain, comprise about 85% of the brain’sweight (Burt, 1993). Therefore, although this is only onesubdivision of the brain, it covers much area and is ofgreat importance in understanding higher cognitive abili-ties. Consequently, a common manner of dividing thebrain is to differentiate between the telencephalon andthe brainstem. The brainstem includes all the subdivisionsbelow the telencephalon (diencephalon, mesencephalon,metencephalon, and myelencephalon), except for thecerebellum, and mediates many primary regulatoryprocesses of the body. We begin by discussing the major
structures of the brainstem and cerebellum, and thenmove to the telencephalon.
Brainstem and Cerebellum
The brainstem and the cerebellum, in terms of evo-lution, form the most primitive area of the brain. Thecerebellum, which looks like a “little brain,” connects tothe dorsal aspect of the brainstem. Figure 5.14 shows thebrainstem and cerebellum in relation to the entire brain.
The brainstem extends from the spinal cord and com-prises about 4.4% of the total weight of the adult brain;the cerebellum makes up about 10.5% (Burt, 1993). Thefour parts of the brainstem include the medulla oblon-gata (myelencephalon), the pons (metencephalon), thestructures of the midbrain (tectum and tegmentum), andthe structures of the diencephalon (thalamus and hypothal-amus). Although the brainstem and cerebellum account forrelatively smaller areas of the brain and function more prim-itively than the telencephalon, these areas consist of a num-ber of different structures relevant to understanding thebasics of brain functioning. We first discuss the structures
134 PART TWO | The Functioning Brain
Anteriorcommunicatingartery
Anteriorcerebralartery
Opthalmic artery
Internal carotidartery
Middle cerebralartery
Posteromedial andthalamoperforatingarteries
Anterolateralarteries
Anteromedial and medialstriate arteries
Lateral striatearteries
Thalamogeniculatearteries
Basilar arteryPontine rami
Superior cerebellarartery
Posterior cerebralartery
Posterior communicatingartery
Anterior choroidalartery
Figure 5.11 Circle of Willis. (From Banich, M. T., Neuropsychology: The Neural Basis of Mental Function, p. 13, Figure 1.7. Copyright © 1997 by Houghton Mifflin. Adapted with permission.)
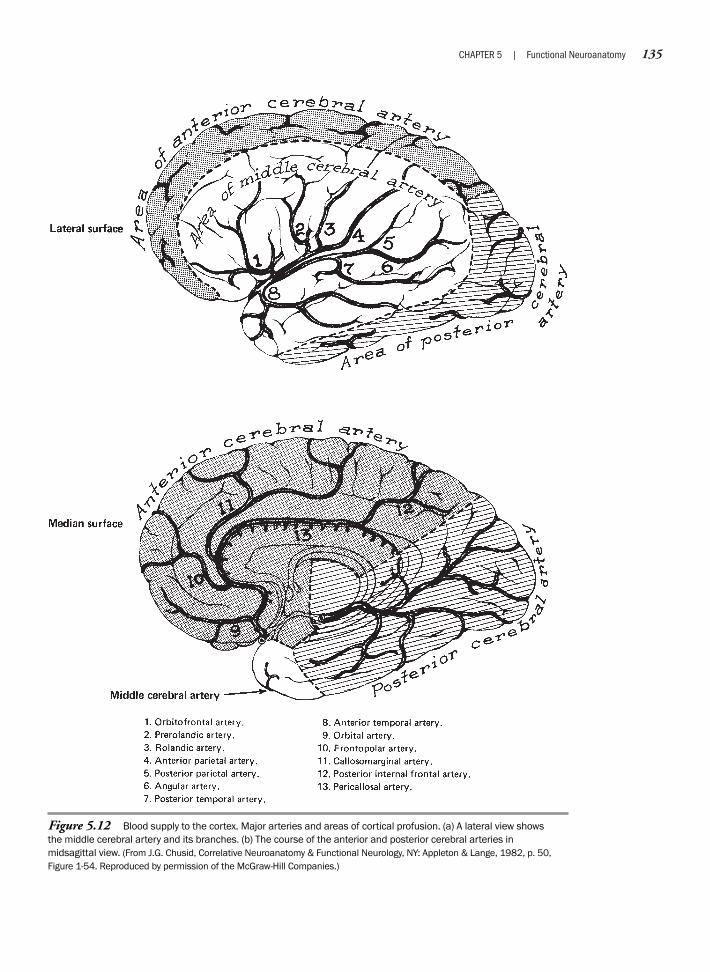
CHAPTER 5 | Functional Neuroanatomy 135
Figure 5.12 Blood supply to the cortex. Major arteries and areas of cortical profusion. (a) A lateral view shows the middle cerebral artery and its branches. (b) The course of the anterior and posterior cerebral arteries in midsagittal view. (From J.G. Chusid, Correlative Neuroanatomy & Functional Neurology, NY: Appleton & Lange, 1982, p. 50,Figure 1-54. Reproduced by permission of the McGraw-Hill Companies.)
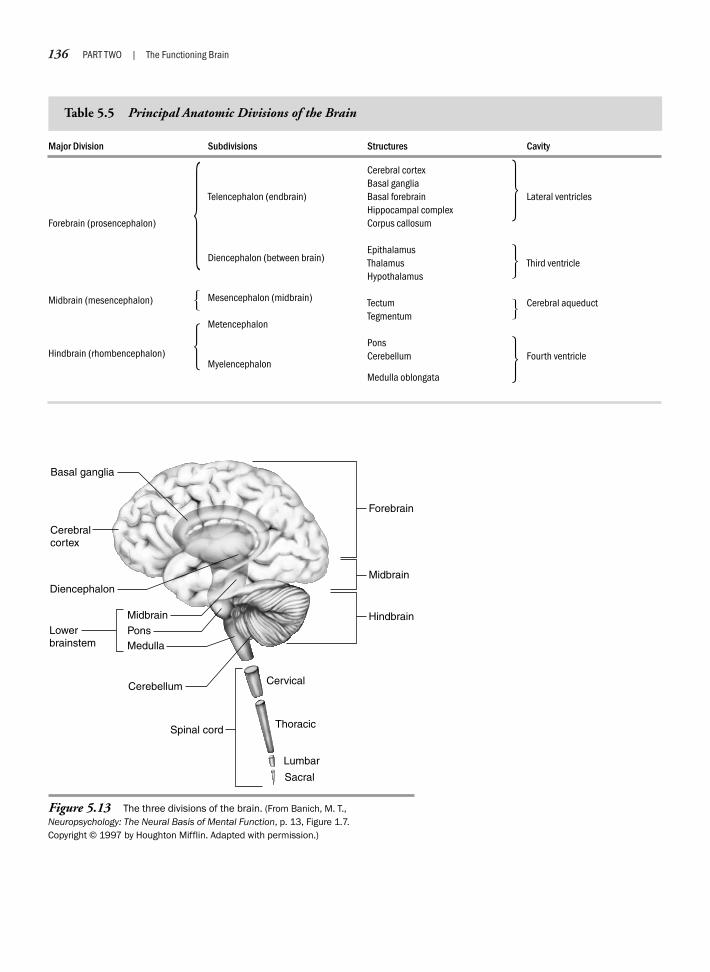
136 PART TWO | The Functioning Brain
Basal ganglia
Spinal cord
Medulla
Lowerbrainstem
Cerebellum
Pons
Midbrain
Diencephalon
Cerebralcortex
Cervical
Thoracic
Lumbar
Sacral
Hindbrain
Midbrain
Forebrain
Figure 5.13 The three divisions of the brain. (From Banich, M. T.,Neuropsychology: The Neural Basis of Mental Function, p. 13, Figure 1.7.Copyright © 1997 by Houghton Mifflin. Adapted with permission.)
Major Division
Forebrain (prosencephalon)
Midbrain (mesencephalon)
Hindbrain (rhombencephalon)
Subdivisions
Telencephalon (endbrain)
Diencephalon (between brain)
Mesencephalon (midbrain)
Metencephalon
Myelencephalon
Structures
Cerebral cortexBasal gangliaBasal forebrainHippocampal complexCorpus callosum
EpithalamusThalamusHypothalamus
TectumTegmentum
PonsCerebellum
Medulla oblongata
Cavity
Lateral ventricles
Third ventricle
Cerebral aqueduct
Fourth ventricle
Table 5.5 Principal Anatomic Divisions of the Brain
��
�
�
�
�
�
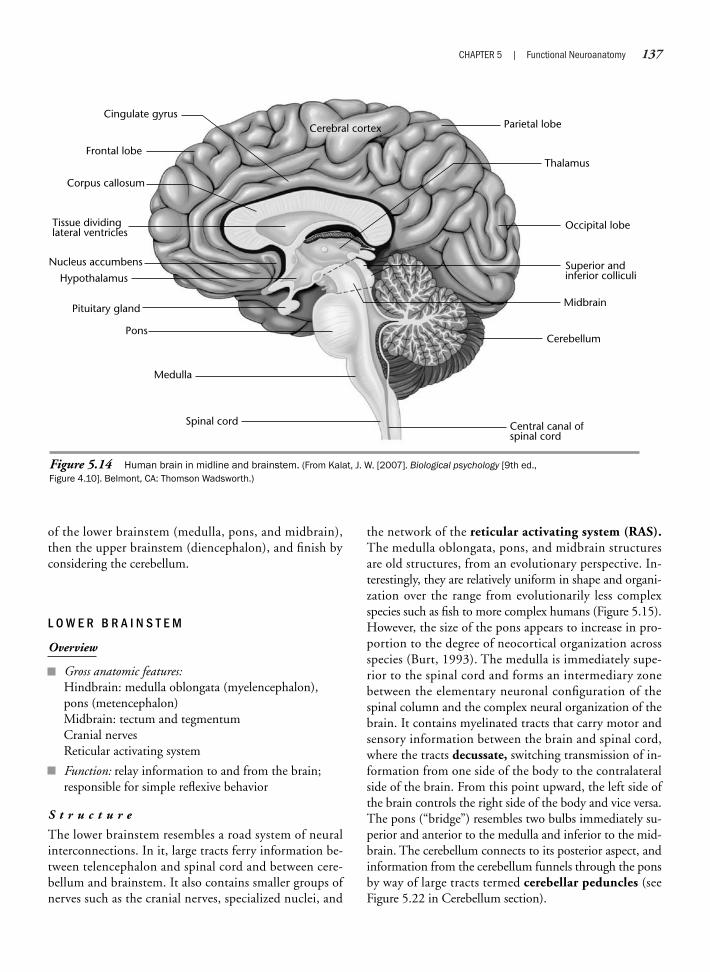
CHAPTER 5 | Functional Neuroanatomy 137
Cingulate gyrus
Frontal lobe
Corpus callosum
Tissue dividinglateral ventricles
Cerebral cortex Parietal lobe
Occipital lobe
Superior andinferior colliculi
Midbrain
Cerebellum
Central canal ofspinal cord
Thalamus
Nucleus accumbens
Hypothalamus
Pituitary gland
Pons
Medulla
Spinal cord
Figure 5.14 Human brain in midline and brainstem. (From Kalat, J. W. [2007]. Biological psychology [9th ed., Figure 4.10]. Belmont, CA: Thomson Wadsworth.)
of the lower brainstem (medulla, pons, and midbrain),then the upper brainstem (diencephalon), and finish byconsidering the cerebellum.
L O W E R B R A I N S T E M
Overview
Gross anatomic features:Hindbrain: medulla oblongata (myelencephalon),pons (metencephalon)Midbrain: tectum and tegmentumCranial nervesReticular activating system
Function: relay information to and from the brain;responsible for simple reflexive behavior
S t r u c t u r e
The lower brainstem resembles a road system of neuralinterconnections. In it, large tracts ferry information be-tween telencephalon and spinal cord and between cere-bellum and brainstem. It also contains smaller groups ofnerves such as the cranial nerves, specialized nuclei, and
the network of the reticular activating system (RAS).The medulla oblongata, pons, and midbrain structuresare old structures, from an evolutionary perspective. In-terestingly, they are relatively uniform in shape and organi-zation over the range from evolutionarily less complexspecies such as fish to more complex humans (Figure 5.15).However, the size of the pons appears to increase in pro-portion to the degree of neocortical organization acrossspecies (Burt, 1993). The medulla is immediately supe-rior to the spinal cord and forms an intermediary zonebetween the elementary neuronal configuration of thespinal column and the complex neural organization of thebrain. It contains myelinated tracts that carry motor andsensory information between the brain and spinal cord,where the tracts decussate, switching transmission of in-formation from one side of the body to the contralateralside of the brain. From this point upward, the left side ofthe brain controls the right side of the body and vice versa.The pons (“bridge”) resembles two bulbs immediately su-perior and anterior to the medulla and inferior to the mid-brain. The cerebellum connects to its posterior aspect, andinformation from the cerebellum funnels through the ponsby way of large tracts termed cerebellar peduncles (seeFigure 5.22 in Cerebellum section).
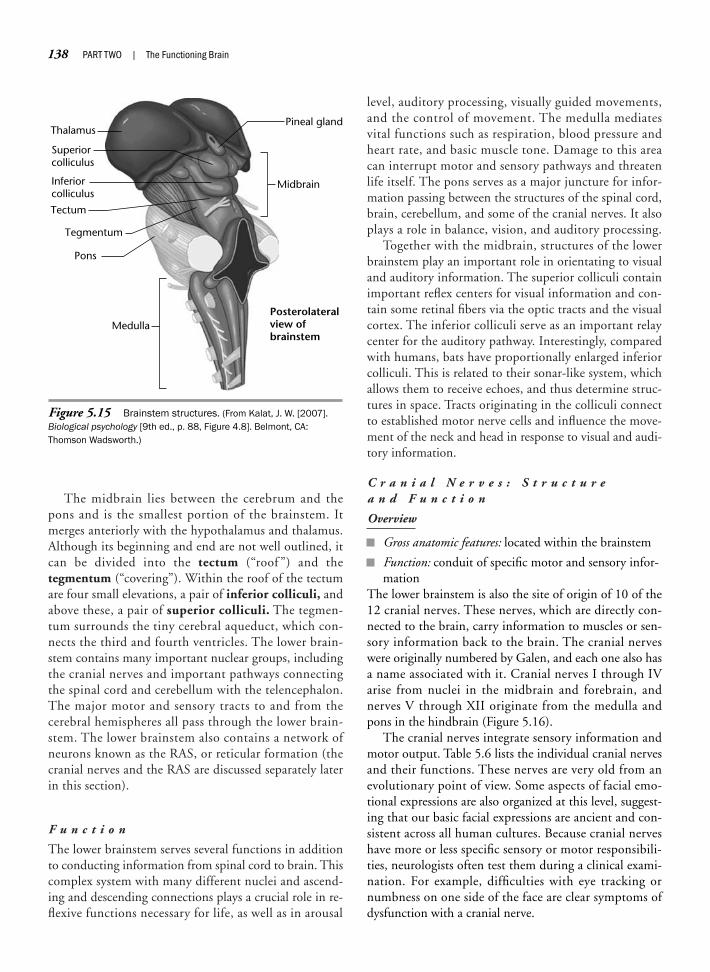
The midbrain lies between the cerebrum and thepons and is the smallest portion of the brainstem. Itmerges anteriorly with the hypothalamus and thalamus.Although its beginning and end are not well outlined, itcan be divided into the tectum (“roof ”) and thetegmentum (“covering”). Within the roof of the tectumare four small elevations, a pair of inferior colliculi, andabove these, a pair of superior colliculi. The tegmen-tum surrounds the tiny cerebral aqueduct, which con-nects the third and fourth ventricles. The lower brain-stem contains many important nuclear groups, includingthe cranial nerves and important pathways connectingthe spinal cord and cerebellum with the telencephalon.The major motor and sensory tracts to and from thecerebral hemispheres all pass through the lower brain-stem. The lower brainstem also contains a network ofneurons known as the RAS, or reticular formation (thecranial nerves and the RAS are discussed separately laterin this section).
F u n c t i o n
The lower brainstem serves several functions in additionto conducting information from spinal cord to brain. Thiscomplex system with many different nuclei and ascend-ing and descending connections plays a crucial role in re-flexive functions necessary for life, as well as in arousal
level, auditory processing, visually guided movements,and the control of movement. The medulla mediatesvital functions such as respiration, blood pressure andheart rate, and basic muscle tone. Damage to this areacan interrupt motor and sensory pathways and threatenlife itself. The pons serves as a major juncture for infor-mation passing between the structures of the spinal cord,brain, cerebellum, and some of the cranial nerves. It alsoplays a role in balance, vision, and auditory processing.
Together with the midbrain, structures of the lowerbrainstem play an important role in orientating to visualand auditory information. The superior colliculi containimportant reflex centers for visual information and con-tain some retinal fibers via the optic tracts and the visualcortex. The inferior colliculi serve as an important relaycenter for the auditory pathway. Interestingly, comparedwith humans, bats have proportionally enlarged inferiorcolliculi. This is related to their sonar-like system, whichallows them to receive echoes, and thus determine struc-tures in space. Tracts originating in the colliculi connectto established motor nerve cells and influence the move-ment of the neck and head in response to visual and audi-tory information.
C r a n i a l N e r v e s : S t r u c t u r e a n d F u n c t i o n
Overview
Gross anatomic features: located within the brainstem
Function: conduit of specific motor and sensory infor-mation
The lower brainstem is also the site of origin of 10 of the12 cranial nerves. These nerves, which are directly con-nected to the brain, carry information to muscles or sen-sory information back to the brain. The cranial nerveswere originally numbered by Galen, and each one also hasa name associated with it. Cranial nerves I through IVarise from nuclei in the midbrain and forebrain, andnerves V through XII originate from the medulla andpons in the hindbrain (Figure 5.16).
The cranial nerves integrate sensory information andmotor output. Table 5.6 lists the individual cranial nervesand their functions. These nerves are very old from anevolutionary point of view. Some aspects of facial emo-tional expressions are also organized at this level, suggest-ing that our basic facial expressions are ancient and con-sistent across all human cultures. Because cranial nerveshave more or less specific sensory or motor responsibili-ties, neurologists often test them during a clinical exami-nation. For example, difficulties with eye tracking ornumbness on one side of the face are clear symptoms ofdysfunction with a cranial nerve.
138 PART TWO | The Functioning Brain
ThalamusPineal gland
Tectum
Pons
Medulla
Tegmentum
Superiorcolliculus
Inferiorcolliculus
Midbrain
Posterolateralview ofbrainstem
Figure 5.15 Brainstem structures. (From Kalat, J. W. [2007].Biological psychology [9th ed., p. 88, Figure 4.8]. Belmont, CA:Thomson Wadsworth.)
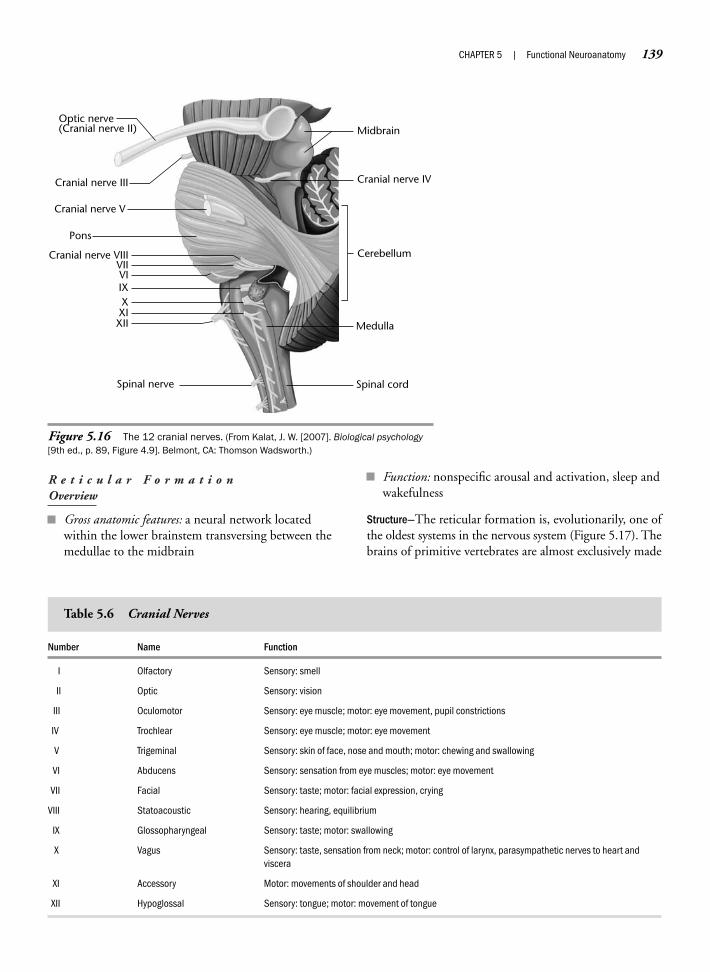
R e t i c u l a r F o r m a t i o n Overview
Gross anatomic features: a neural network locatedwithin the lower brainstem transversing between themedullae to the midbrain
Function: nonspecific arousal and activation, sleep andwakefulness
Structure—The reticular formation is, evolutionarily, one ofthe oldest systems in the nervous system (Figure 5.17). Thebrains of primitive vertebrates are almost exclusively made
CHAPTER 5 | Functional Neuroanatomy 139
Optic nerve(Cranial nerve II)
Cranial nerve III
Cranial nerve V
Cranial nerve VIIIVIIVIIXXXIXII
Spinal nerve Spinal cord
Medulla
Cranial nerve IV
Midbrain
Pons
Cerebellum
Figure 5.16 The 12 cranial nerves. (From Kalat, J. W. [2007]. Biological psychology[9th ed., p. 89, Figure 4.9]. Belmont, CA: Thomson Wadsworth.)
Number Name Function
I Olfactory Sensory: smell
II Optic Sensory: vision
III Oculomotor Sensory: eye muscle; motor: eye movement, pupil constrictions
IV Trochlear Sensory: eye muscle; motor: eye movement
V Trigeminal Sensory: skin of face, nose and mouth; motor: chewing and swallowing
VI Abducens Sensory: sensation from eye muscles; motor: eye movement
VII Facial Sensory: taste; motor: facial expression, crying
VIII Statoacoustic Sensory: hearing, equilibrium
IX Glossopharyngeal Sensory: taste; motor: swallowing
X Vagus Sensory: taste, sensation from neck; motor: control of larynx, parasympathetic nerves to heart andviscera
XI Accessory Motor: movements of shoulder and head
XII Hypoglossal Sensory: tongue; motor: movement of tongue
Table 5.6 Cranial Nerves
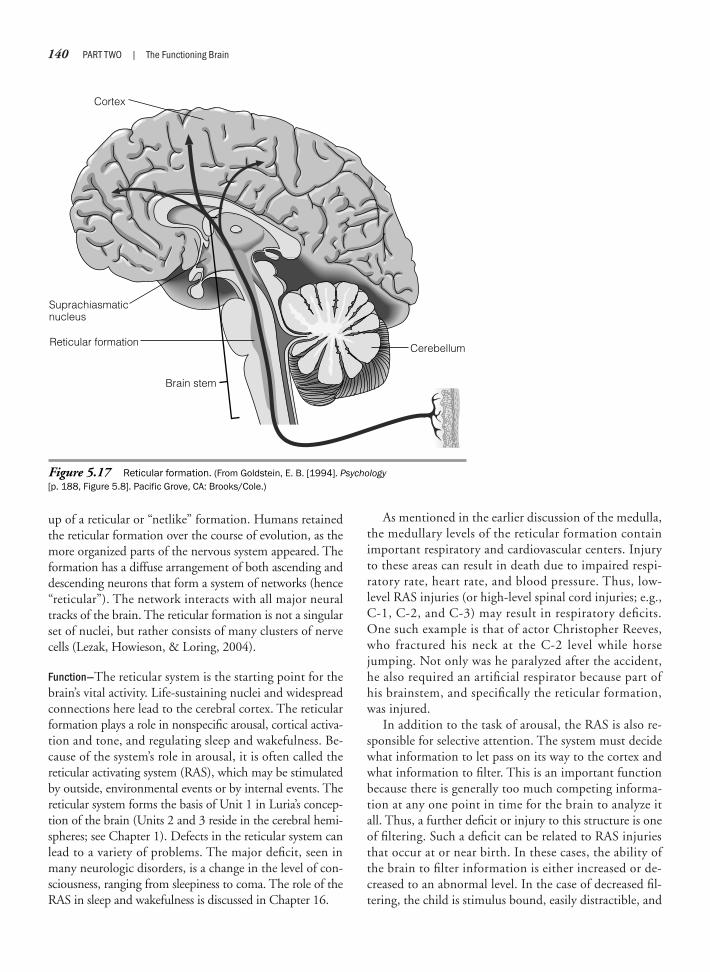
up of a reticular or “netlike” formation. Humans retainedthe reticular formation over the course of evolution, as themore organized parts of the nervous system appeared. Theformation has a diffuse arrangement of both ascending anddescending neurons that form a system of networks (hence“reticular”). The network interacts with all major neuraltracks of the brain. The reticular formation is not a singularset of nuclei, but rather consists of many clusters of nervecells (Lezak, Howieson, & Loring, 2004).
Function—The reticular system is the starting point for thebrain’s vital activity. Life-sustaining nuclei and widespreadconnections here lead to the cerebral cortex. The reticularformation plays a role in nonspecific arousal, cortical activa-tion and tone, and regulating sleep and wakefulness. Be-cause of the system’s role in arousal, it is often called thereticular activating system (RAS), which may be stimulatedby outside, environmental events or by internal events. Thereticular system forms the basis of Unit 1 in Luria’s concep-tion of the brain (Units 2 and 3 reside in the cerebral hemi-spheres; see Chapter 1). Defects in the reticular system canlead to a variety of problems. The major deficit, seen inmany neurologic disorders, is a change in the level of con-sciousness, ranging from sleepiness to coma. The role of theRAS in sleep and wakefulness is discussed in Chapter 16.
As mentioned in the earlier discussion of the medulla,the medullary levels of the reticular formation containimportant respiratory and cardiovascular centers. Injuryto these areas can result in death due to impaired respi-ratory rate, heart rate, and blood pressure. Thus, low-level RAS injuries (or high-level spinal cord injuries; e.g.,C-1, C-2, and C-3) may result in respiratory deficits.One such example is that of actor Christopher Reeves,who fractured his neck at the C-2 level while horsejumping. Not only was he paralyzed after the accident,he also required an artificial respirator because part ofhis brainstem, and specifically the reticular formation,was injured.
In addition to the task of arousal, the RAS is also re-sponsible for selective attention. The system must decidewhat information to let pass on its way to the cortex andwhat information to filter. This is an important functionbecause there is generally too much competing informa-tion at any one point in time for the brain to analyze itall. Thus, a further deficit or injury to this structure is oneof filtering. Such a deficit can be related to RAS injuriesthat occur at or near birth. In these cases, the ability ofthe brain to filter information is either increased or de-creased to an abnormal level. In the case of decreased fil-tering, the child is stimulus bound, easily distractible, and
140 PART TWO | The Functioning Brain
Cortex
Reticular formation
Suprachiasmaticnucleus
Brain stem
Cerebellum
Figure 5.17 Reticular formation. (From Goldstein, E. B. [1994]. Psychology[p. 188, Figure 5.8]. Pacific Grove, CA: Brooks/Cole.)

more pliable in low-stimulus sensory environments. Inthe case of increased filtering skills, the child shows symp-toms of sensory deprivation. This can result in a completewithdrawal from the external world, similar to the deficitseen in some autistic children.
In general, the brainstem, and the RAS in particular,plays a major and vital role in regulating wakefulness andin mediating and filtering ascending and descendingsensory and motor information. As such, the brainstemconstitutes the starting point of the brain’s analysis of in-formation. Disruption of the brainstem, specifically of theRAS, affects the level of arousal, orientation, and generalawareness of one’s surroundings. Neuropsychologists areinterested in the often profound symptoms associated withdysfunction of these areas. Neuropsychologists can system-atically assess general arousal when it is important to mon-itor the progress of people who are recovering from RASinjuries. Individuals with acute brainstem injuries may beplaced in inpatient medical care, because such patientsmay be in a stupor or coma, and thus dependent on exter-nal life support.
U P P E R B R A I N S T E M : D I E N C E P H A L O N
The diencephalon (also known as the interbrain or “betweenbrain”) is located at the head of the brainstem connectingthe cortex with lower structures of the brain. The dien-cephalon is part of the larger forebrain, and its evolution hasparalleled that of the cortex. The diencephalon consists oftwo prominent brain structures, the thalamus and the hy-pothalamus, which contain many nuclei that are of interestto neuropsychologists because of their functions in regulat-ing behavior. Phylogenetically, the thalamus consists of an-cient nuclei that may have originally reacted reflexively topleasant and unpleasant environmental stimuli before thecerebral cortex evolved. The hypothalamus, part of the lim-bic system, is considered instrumental in controlling the au-tonomic system. This system regulates emotional responsesand other functions such as thirst, appetite, digestion, sleep,temperature of the body, sexual drive, heart rate, andsmooth muscles of the internal organs.
H y p o t h a l a m u s
Overview
Gross anatomic features: structure of the hypothalamus,hypothalamic nuclei, major fiber systems, third ventricle
Function: activates, controls, and integrates the pe-ripheral autonomic mechanisms, endocrine activity,and somatic functions, including body temperature,food intake, and development of secondary sexualcharacteristics
Structure—The hypothalamus is the portion of the dien-cephalon that forms the floor and part of the lateral wallof the third ventricle. Anatomically, it is defined by theoptic chiasm rostrally and the mamillary bodies caudally.The boundaries of the hypothalamus are easily de-scribed, but it does not form a well-circumscribed re-gion and extends into surrounding parts. The hypothal-amus itself is small by weight (pea size, about 4 grams inadults), but contains a grouping of small and complexnuclei located at the junction of the midbrain and thethalamus (close to the roof of the mouth). Within thehypothalamus lie at least a dozen identifiable cell clus-ters named the hypothalamic nuclei (Figure 5.18). Theexact number depends on how the clusters are orga-nized, but is similar in most vertebrates, suggesting thatlittle has changed over time and across species. Origi-nally thought of as “a trifling part of the human brain,”the hypothalamic nuclei have become known over thepast half century as an important collection of nuclei,“the brain within the brain.” The hypothalamus playsan important role in regulating, activating, and integrat-ing peripheral autonomic processes, endocrine activity,and somatic functions.
In general, the hypothalamus has three longitudinalzones: lateral, medial, and periventricular. The medial as-pects of the hypothalamus have rich connections with thethalamus. The lateral nuclei have efferent and afferentconnections to and from regions outside the hypothala-mus, including brainstem fiber systems and preoptic andolfactory areas. In addition, the hypothalamus is an inter-action center for several neurotransmitter substances. Thehypothalamus, therefore, is a complex diencephalic struc-ture in terms of its communicating neurotransmitters anddendritic and axonal interconnectedness.
Function—The hypothalamus is interconnected to the ad-jacent “master gland” of the brain, the pituitary (alsoknown as hypophysis). The hypothalamus regulates theendocrine activity of the pituitary, both directly and in-directly (Kupfermann, 1991). The direct route involvesthe transport of hormones via axons from hypothalamicneurons extending downward to the posterior region ofthe pituitary. These axonal bundles constitute, in part, thepituitary stalk. Stimulation of these cells results in the re-lease of the hormones by the pituitary directly into thebloodstream. The direct route controls the release of theantidiuretic hormones and oxytocin, which are actuallyproduced by the hypothalamus, but are stored in the pi-tuitary gland. The antidiuretic hormones are involved inhomeostatic regulation, and oxytocin influences uterinecontractions at birth and lactation. The indirect track
CHAPTER 5 | Functional Neuroanatomy 141
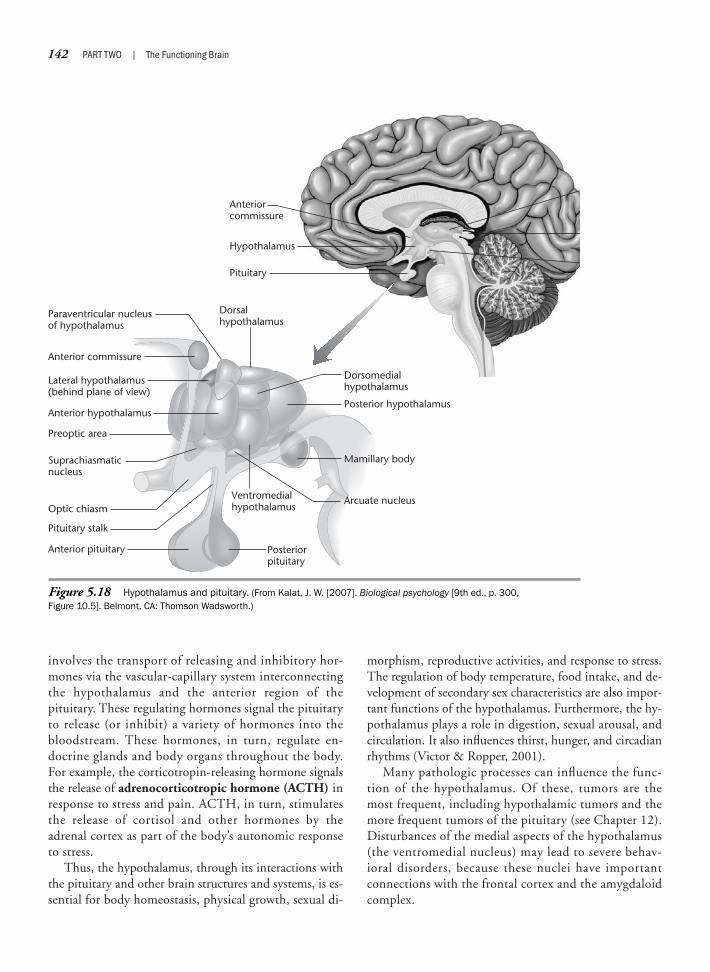
involves the transport of releasing and inhibitory hor-mones via the vascular-capillary system interconnectingthe hypothalamus and the anterior region of thepituitary. These regulating hormones signal the pituitaryto release (or inhibit) a variety of hormones into thebloodstream. These hormones, in turn, regulate en-docrine glands and body organs throughout the body.For example, the corticotropin-releasing hormone signalsthe release of adrenocorticotropic hormone (ACTH) inresponse to stress and pain. ACTH, in turn, stimulatesthe release of cortisol and other hormones by theadrenal cortex as part of the body’s autonomic responseto stress.
Thus, the hypothalamus, through its interactions withthe pituitary and other brain structures and systems, is es-sential for body homeostasis, physical growth, sexual di-
morphism, reproductive activities, and response to stress.The regulation of body temperature, food intake, and de-velopment of secondary sex characteristics are also impor-tant functions of the hypothalamus. Furthermore, the hy-pothalamus plays a role in digestion, sexual arousal, andcirculation. It also influences thirst, hunger, and circadianrhythms (Victor & Ropper, 2001).
Many pathologic processes can influence the func-tion of the hypothalamus. Of these, tumors are themost frequent, including hypothalamic tumors and themore frequent tumors of the pituitary (see Chapter 12).Disturbances of the medial aspects of the hypothalamus(the ventromedial nucleus) may lead to severe behav-ioral disorders, because these nuclei have importantconnections with the frontal cortex and the amygdaloidcomplex.
142 PART TWO | The Functioning Brain
Anteriorcommissure
Hypothalamus
Pituitary
Dorsalhypothalamus
Dorsomedialhypothalamus
Posterior hypothalamus
Ventromedialhypothalamus
Posteriorpituitary
Paraventricular nucleusof hypothalamus
Anterior commissure
Lateral hypothalamus(behind plane of view)
Anterior hypothalamus
Preoptic area
Suprachiasmaticnucleus
Optic chiasm
Anterior pituitary
Mamillary body
Arcuate nucleus
Pituitary stalk
Figure 5.18 Hypothalamus and pituitary. (From Kalat, J. W. [2007]. Biological psychology [9th ed., p. 300,Figure 10.5]. Belmont, CA: Thomson Wadsworth.)
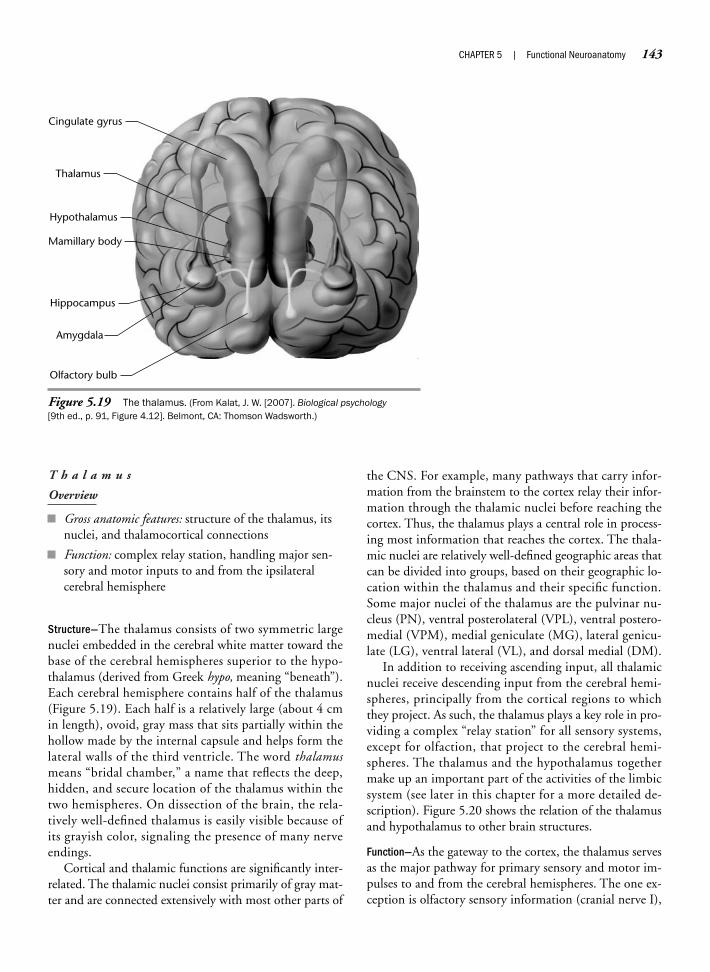
T h a l a m u s
Overview
Gross anatomic features: structure of the thalamus, itsnuclei, and thalamocortical connections
Function: complex relay station, handling major sen-sory and motor inputs to and from the ipsilateralcerebral hemisphere
Structure—The thalamus consists of two symmetric largenuclei embedded in the cerebral white matter toward thebase of the cerebral hemispheres superior to the hypo-thalamus (derived from Greek hypo, meaning “beneath”).Each cerebral hemisphere contains half of the thalamus(Figure 5.19). Each half is a relatively large (about 4 cmin length), ovoid, gray mass that sits partially within thehollow made by the internal capsule and helps form thelateral walls of the third ventricle. The word thalamusmeans “bridal chamber,” a name that reflects the deep,hidden, and secure location of the thalamus within thetwo hemispheres. On dissection of the brain, the rela-tively well-defined thalamus is easily visible because ofits grayish color, signaling the presence of many nerveendings.
Cortical and thalamic functions are significantly inter-related. The thalamic nuclei consist primarily of gray mat-ter and are connected extensively with most other parts of
the CNS. For example, many pathways that carry infor-mation from the brainstem to the cortex relay their infor-mation through the thalamic nuclei before reaching thecortex. Thus, the thalamus plays a central role in process-ing most information that reaches the cortex. The thala-mic nuclei are relatively well-defined geographic areas thatcan be divided into groups, based on their geographic lo-cation within the thalamus and their specific function.Some major nuclei of the thalamus are the pulvinar nu-cleus (PN), ventral posterolateral (VPL), ventral postero-medial (VPM), medial geniculate (MG), lateral genicu-late (LG), ventral lateral (VL), and dorsal medial (DM).
In addition to receiving ascending input, all thalamicnuclei receive descending input from the cerebral hemi-spheres, principally from the cortical regions to whichthey project. As such, the thalamus plays a key role in pro-viding a complex “relay station” for all sensory systems,except for olfaction, that project to the cerebral hemi-spheres. The thalamus and the hypothalamus togethermake up an important part of the activities of the limbicsystem (see later in this chapter for a more detailed de-scription). Figure 5.20 shows the relation of the thalamusand hypothalamus to other brain structures.
Function—As the gateway to the cortex, the thalamus servesas the major pathway for primary sensory and motor im-pulses to and from the cerebral hemispheres. The one ex-ception is olfactory sensory information (cranial nerve I),
CHAPTER 5 | Functional Neuroanatomy 143
Cingulate gyrus
Thalamus
Hypothalamus
Mamillary body
Hippocampus
Amygdala
Olfactory bulb
Figure 5.19 The thalamus. (From Kalat, J. W. [2007]. Biological psychology[9th ed., p. 91, Figure 4.12]. Belmont, CA: Thomson Wadsworth.)

which bypasses the thalamus and progresses directly fromolfactory receptors to olfactory bulbs to the cerebral cor-tex. Other neuronal fibers that do not pass through thethalamus are those that are involved in arousal.
The thalamus is analogous to the concept of a large,busy, commuter train station. It makes preliminary classi-fications, integrates information, and “sends” it on to thecortex for further processing. Specifically, each half of thethalamus sends information to, and receives informationfrom, the cerebral hemisphere on the same (ipsilateral)side of the brain. In this fashion, the descending projec-tions serve as a two-way system between each cortical re-gion and the corresponding thalamic nuclei.
The nuclei of the thalamus can be divided into twogroups by their structure, connections, and function. Thefirst group includes nonspecific nuclei, which are locatedprimarily toward the median portion of the thalamus.These nuclei project widely to other brain structures, in-cluding other thalamic areas, and to the cortex, particu-larly its frontal regions. They receive input from the spinal
cord and the reticular formation and appear to play a rolein monitoring the overall excitability of neurons in thecortex and the thalamus.
The second group of thalamic nuclei is referred to asspecific nuclei, which are involved in sensory and motorprocessing (Figure 5.21). Specific nuclei project to re-stricted regions of the cortex. For example, specific sen-sory nuclei include the VPL and VPM (not shown) nu-clei, which receive input from somatosensory relayneurons and project directly to the primary and secondarysomatosensory cortex. The LG body receives input fromthe optic tract and projects to the primary visual area inthe occipital cortex. The MG body receives input from theauditory relay nuclei and projects to the primary audi-tory cortex in the temporal lobe. Specific nuclei of thethalamus that are involved in controlling motor activityinclude the VL and ventral intermedial (VI; not shown)nuclei, which receive input from the cerebellum. The lat-eral portion of the ventral anterior (VA) nucleus receivesascending fiber tracts from the basal ganglia, which are
144 PART TWO | The Functioning Brain
AmygdalaInvolved inmemory, emotion,and aggression
HippocampusInvolved in learning,memory, and emotion
MedullaControls vital functionssuch as breathing andheart rate
ThalamusSwitching station forsensory information; also involved in memory
Spinal cordTransmits signalsbetween brainand rest of body
CerebellumControls coordinatedmovement; also involved in languageand thinking
HypothalamusRegulates basic biologicalfunctions,including hunger, thirst,temperature,and sexual arousal; also involved in emotion.
Figure 5.20 Subcortical structures of the brain. (From Goldstein, E. B. [1994]. Psychology [p. 89, Figure 3.8d].Pacific Grove, CA: Brooks/Cole.)

CHAPTER 5 | Functional Neuroanatomy 145
Figure 5.21 Thalamocortical radiations. (a) Principal thalamocortical projections. (b) Relation of corticalareas to thalamic nuclei. (a: From J. G. Chusid, Correlative Neuroanatomy & Functional Neurology, NY: Appleton &Lange, 1982, p. 19, Figure 1.10 and p. 20, Figure 1.21. Reproduced by permission of the McGraw-Hill Companies;b: reproduced with permission from original drawings by Frank H. Netter, MD; first appeared in Ciba Clinical Sym-posia. Copyright ©1950, Ciba Pharmaceutical Co.)
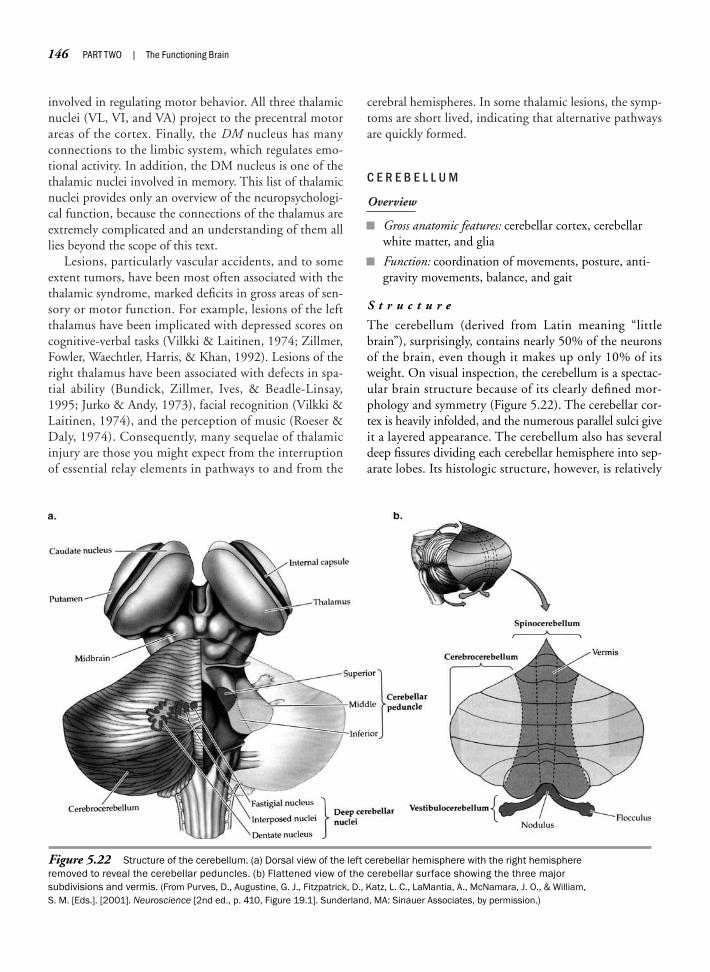
involved in regulating motor behavior. All three thalamicnuclei (VL, VI, and VA) project to the precentral motorareas of the cortex. Finally, the DM nucleus has manyconnections to the limbic system, which regulates emo-tional activity. In addition, the DM nucleus is one of thethalamic nuclei involved in memory. This list of thalamicnuclei provides only an overview of the neuropsychologi-cal function, because the connections of the thalamus areextremely complicated and an understanding of them alllies beyond the scope of this text.
Lesions, particularly vascular accidents, and to someextent tumors, have been most often associated with thethalamic syndrome, marked deficits in gross areas of sen-sory or motor function. For example, lesions of the leftthalamus have been implicated with depressed scores oncognitive-verbal tasks (Vilkki & Laitinen, 1974; Zillmer,Fowler, Waechtler, Harris, & Khan, 1992). Lesions of theright thalamus have been associated with defects in spa-tial ability (Bundick, Zillmer, Ives, & Beadle-Linsay,1995; Jurko & Andy, 1973), facial recognition (Vilkki &Laitinen, 1974), and the perception of music (Roeser &Daly, 1974). Consequently, many sequelae of thalamicinjury are those you might expect from the interruptionof essential relay elements in pathways to and from the
cerebral hemispheres. In some thalamic lesions, the symp-toms are short lived, indicating that alternative pathwaysare quickly formed.
C E R E B E L L U M
Overview
Gross anatomic features: cerebellar cortex, cerebellarwhite matter, and glia
Function: coordination of movements, posture, anti-gravity movements, balance, and gait
S t r u c t u r e
The cerebellum (derived from Latin meaning “littlebrain”), surprisingly, contains nearly 50% of the neuronsof the brain, even though it makes up only 10% of itsweight. On visual inspection, the cerebellum is a spectac-ular brain structure because of its clearly defined mor-phology and symmetry (Figure 5.22). The cerebellar cor-tex is heavily infolded, and the numerous parallel sulci giveit a layered appearance. The cerebellum also has severaldeep fissures dividing each cerebellar hemisphere into sep-arate lobes. Its histologic structure, however, is relatively
146 PART TWO | The Functioning Brain
Figure 5.22 Structure of the cerebellum. (a) Dorsal view of the left cerebellar hemisphere with the right hemisphereremoved to reveal the cerebellar peduncles. (b) Flattened view of the cerebellar surface showing the three majorsubdivisions and vermis. (From Purves, D., Augustine, G. J., Fitzpatrick, D., Katz, L. C., LaMantia, A., McNamara, J. O., & William,S. M. [Eds.]. [2001]. Neuroscience [2nd ed., p. 410, Figure 19.1]. Sunderland, MA: Sinauer Associates, by permission.)

simple compared with that of the cortex. The neurons ap-pear to be organized in repeating patterns. The cerebel-lum is located posteriorly and superiorly to the pons andmedulla, just inferior to the posterior portion of the cere-bral hemispheres. The cerebellum is attached to the brain-stem at the level of the pons (“bridge”) via the cerebellarpeduncles and consists of two large oval hemispheres con-nected by a single median portion, termed the vermis (de-rived from Latin meaning “worm”).
F u n c t i o n
The cerebellum is phylogenetically old and may have beenthe first brain structure to specialize in coordinatingmotor and sensory information. Observing patients withcerebellar disease makes clear the importance of this cen-ter for coordinating movement and postural adjustments.The cerebellum is heavily involved in basic processes nec-essary for general motor behavior, as well as in coordinat-ing movements. The oldest areas of the cerebellum areconcerned with keeping the body oriented in space mo-torically. The cerebellum also helps control muscles keep-ing the body upright despite the pull of gravity and mon-itors background muscle tone involved in voluntarymovement.
Lesions of the cerebellum, depending on location, maycause a variety of disorders, including deterioration of co-ordinated movement, irregular and jerky movements, in-tention tremor when attempting to complete a voluntarytask, static tremor when resting, impairment of alternat-ing movements, impairment in balance, disturbances ofgait, and uncontrolled nystagmic movements of the eyes.Evidence exists that people born without a cerebellum canfunction completely normally, because other brain struc-tures have adapted to take over its functions. Neuropsy-chologists often erroneously ignore the cerebellumbecause no obvious cognitive properties have been associ-ated with lesions of the cerebellum. However, it now ap-pears that the cerebellum stores memories for simplelearned motor responses and is involved in attentionalshifting, as well as other cognitive functions (Diamond,2000).
Telencephalon
The telencephalon, or endbrain, consists of the twocerebral hemispheres connected by a massive bundle offibers, the corpus callosum. The outer layer of the cortexconsists primarily of cell bodies (gray matter) and affectsthinking, memory, and voluntary behavior, as well as theregulation of motor behavior. Within each hemisphere is
a lateral ventricle and a collection of several large nucleiknown as the basal ganglia, which contain the cell bodiesof motor control neurons. The basal forebrain is also rec-ognized as a prominent division of the subcortical(below the cortex) aspect of the cerebrum. This area, sur-rounding the inferior tip of the frontal horn, is stronglyinterconnected with limbic structures, and some re-searchers (e.g., Crosson, 1992) consider it part of thelimbic system.
B A S A L G A N G L I A
The basal ganglia, also called the basal nuclei, are a col-lection of deep nuclei of the telencephalon (basal means“lowest level”; Figure 5.23) The basal ganglia communi-cate with motor regions in the cortex via the thalamus.With their complex interconnections and efferent out-puts and afferent inputs, the basal ganglia participate inthe control of higher order movement, particularly instarting or initiating movement.
Overview
Gross anatomic features: structures of the caudate nu-cleus, putamen, globus pallidus, substantia nigra, andsubthalamic nuclei
Function: important as relay stations in motor behav-ior (e.g., the striato-pallido-thalamic loop), coordi-nating stereotyped postural and reflexive motoractivity, and supporting higher order cognitive func-tions
S t r u c t u r e
Embedded deep within the cortex lies a group of symmet-ric subcortical gray matter structures known collectively asthe basal ganglia. They partially surround the thalamusand are themselves enclosed by the cerebral cortex andcerebral white matter. They have sensory projections tothe cerebral hemispheres, interconnections between partsof the cortex, and outflow from the cerebral cortex to othernervous system structures. Neuropsychologists most oftenconceptualize the basal ganglia within the context of themotor system and, thus, typically exclude the amygdala(located at the tail of the caudate nucleus) and a large partof the thalamus. However, the substantia nigra and thesubthalamic nucleus have important motor functionsand are usually included as part of the basal ganglia.
The two major structures of the basal ganglia are thecaudate nucleus and the putamen, with the adjacent me-dial and lateral globus pallidus. In general, these structures
CHAPTER 5 | Functional Neuroanatomy 147
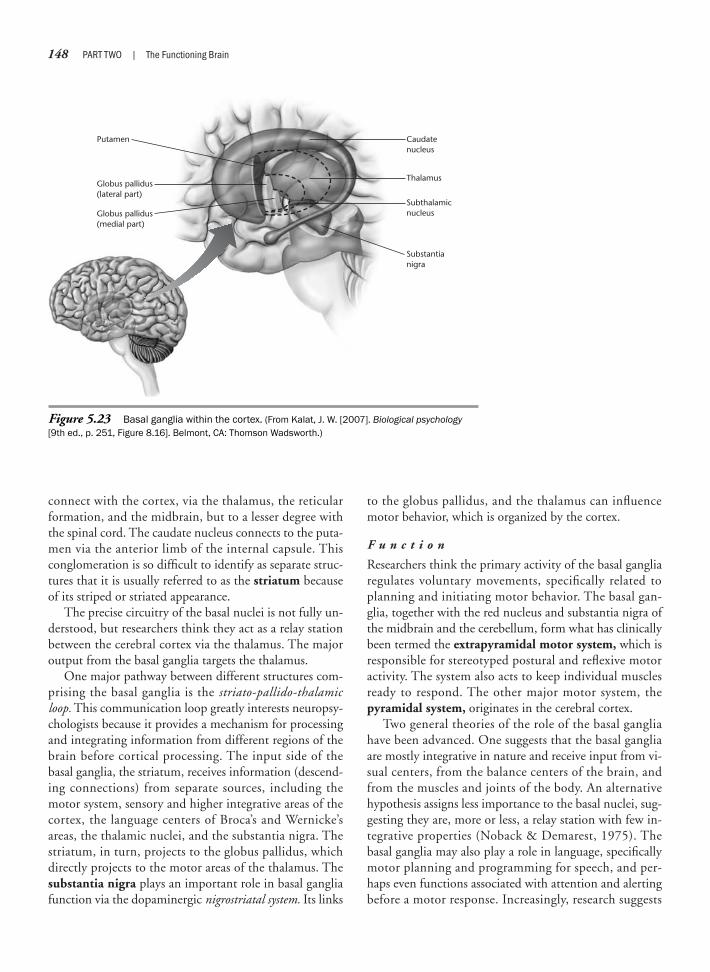
connect with the cortex, via the thalamus, the reticularformation, and the midbrain, but to a lesser degree withthe spinal cord. The caudate nucleus connects to the puta-men via the anterior limb of the internal capsule. Thisconglomeration is so difficult to identify as separate struc-tures that it is usually referred to as the striatum becauseof its striped or striated appearance.
The precise circuitry of the basal nuclei is not fully un-derstood, but researchers think they act as a relay stationbetween the cerebral cortex via the thalamus. The majoroutput from the basal ganglia targets the thalamus.
One major pathway between different structures com-prising the basal ganglia is the striato-pallido-thalamicloop. This communication loop greatly interests neuropsy-chologists because it provides a mechanism for processingand integrating information from different regions of thebrain before cortical processing. The input side of thebasal ganglia, the striatum, receives information (descend-ing connections) from separate sources, including themotor system, sensory and higher integrative areas of thecortex, the language centers of Broca’s and Wernicke’sareas, the thalamic nuclei, and the substantia nigra. Thestriatum, in turn, projects to the globus pallidus, whichdirectly projects to the motor areas of the thalamus. Thesubstantia nigra plays an important role in basal gangliafunction via the dopaminergic nigrostriatal system. Its links
to the globus pallidus, and the thalamus can influencemotor behavior, which is organized by the cortex.
F u n c t i o n
Researchers think the primary activity of the basal gangliaregulates voluntary movements, specifically related toplanning and initiating motor behavior. The basal gan-glia, together with the red nucleus and substantia nigra ofthe midbrain and the cerebellum, form what has clinicallybeen termed the extrapyramidal motor system, which isresponsible for stereotyped postural and reflexive motoractivity. The system also acts to keep individual musclesready to respond. The other major motor system, thepyramidal system, originates in the cerebral cortex.
Two general theories of the role of the basal gangliahave been advanced. One suggests that the basal gangliaare mostly integrative in nature and receive input from vi-sual centers, from the balance centers of the brain, andfrom the muscles and joints of the body. An alternativehypothesis assigns less importance to the basal nuclei, sug-gesting they are, more or less, a relay station with few in-tegrative properties (Noback & Demarest, 1975). Thebasal ganglia may also play a role in language, specificallymotor planning and programming for speech, and per-haps even functions associated with attention and alertingbefore a motor response. Increasingly, research suggests
148 PART TWO | The Functioning Brain
Globus pallidus(lateral part)
Caudatenucleus
Subthalamicnucleus
Substantianigra
Putamen
Globus pallidus(medial part)
Thalamus
Figure 5.23 Basal ganglia within the cortex. (From Kalat, J. W. [2007]. Biological psychology[9th ed., p. 251, Figure 8.16]. Belmont, CA: Thomson Wadsworth.)

that the basal ganglia, via their interconnections with thefrontal lobes, participate in the generation, inhibition,and execution of higher order behaviors (Lichter & Cum-mings, 2001). For instance, damage to the caudate nu-cleus of the basal ganglia can impair cognitive or mentalflexibility, a finding also evident with prefrontal damage.
Most understanding regarding the function of basalganglia is gained from knowledge of movement disordersassociated with basal ganglia dysfunction. Such abnor-malities, which also include disorders of the cerebellum,have been labeled extrapyramidal and are characterized byatypical movements and changes in muscle tone. In con-trast, pyramidal symptoms involve upper motor neurondisorders of the cortex and are more often associated witha loss of voluntary movement, including paralysis. Tworelatively common basal ganglia disorders are Parkinson’sdisease and Huntington’s disease (see Chapter 15).
Extrapyramidal symptoms also have been observed inschizophrenics who are treated with antipsychotic drugs.Those drugs, including Thorazine (chlorpromazine),Stelazine (trifluoperazine), and Haldol (haloperidol),block dopamine transmission. Although this reducespsychotic behavior and hallucinations, it has the side ef-fect of Parkinson-like symptoms, including writhingmovements of the mouth, face, and tongue. This neuro-logic presentation in schizophrenics who develop suchsymptoms is known as tardive dyskinesia and is irre-versible. In general, the overall connections and func-tions of the basal ganglia are not fully understood, al-though the principal function of this formation isassociated with motor behavior, specifically organizingease and flow of movement.
L I M B I C S Y S T E M
The anatomic term limbic (derived from the Latin wordlimbus, meaning “border”) was first coined by Paul Broca(Schiller, 1982). Broca noticed that a ring of cortical tis-sue forms a border around the brainstem and medial as-pects of the brain. Broca thought “le grand lobe limbique”was primarily involved with olfaction, because of its in-terconnections with the evolutionarily older rhinen-cephalon, or “smell brain.” In 1937, James Papez sug-gested the presence of a more precise circuit or “limbicsystem,” which he proposed was significantly involved inmediating emotional behavior. Indeed, proposing that aset of brain structures might be primarily involved in pro-cessing emotions was a bold statement at the time. Sincethen, however, the limbic system has received much at-tention for its major role in the expression of emotions, aswell as in olfaction, learning, and memory.
Overview
Gross anatomic features: structures of the amygdala,hippocampus, parahippocampal gyrus, cingulategyrus, fornix, septum, and olfactory bulbs
Function: the limbic system is closely involved in theexpression of emotional behavior and the integrationof olfactory information with visceral and somaticinformation
S t r u c t u r e
Broca defined the limbic lobe to include those structureson the medial and basal surfaces of the cerebral hemi-spheres. Because the limbic lobe is most developed inmammals, it is also known as the mammalian brain. Infact, in some primitive animals, such as the crocodile, theentire forebrain is limbic brain (the limbic cortex is partof the forebrain that developed first in evolution). Theprimary structures of the lobe include the medial cortexsurrounding the corpus callosum, termed the cingulategyrus (see Figure 5.14), and the medial cortex of the tem-poral lobes, or the parahippocampal gyrus, and the hip-pocampal formation (hippocampus, dentate gyrus, andsubiculum; see Figure 9.2). The structures of the limbicsystem are often debated, but usually also include thefornix, some brainstem areas, particularly the mammil-lary bodies of the hypothalamus, specific basal forebrainstructures, including the amygdala (“almond” because ofits shape), and the septum (Figure 5.24). Severalanatomic circuits have been described that include limbicsystem structures. The most likely role of the basolateralcircuit, which centers around the amygdala, is in emo-tional processing. The Papez circuit, which centersaround the hippocampus, is perhaps the most well-knownloop. We further discuss these functional systems inChapter 9.
F u n c t i o n
The limbic system is a most complex but important set ofbrain structures that has fascinated anatomists, neurolo-gists, and neuroscientists for more than 50 years. The lim-bic system is a bit misnamed because there is no one-to-one structure–function relationship, as is evident in manysensory systems that are discussed in Chapter 7. The roleof the limbic system in emotions and memory has gener-ated a great deal of interest in neuropsychology. Extensiveresearch has been conducted on several components ofthe highly interconnected limbic system. However, be-cause of the interconnectivity of the system, it is often dif-ficult to discern structure–function relationships. For ex-ample, the amygdala and hippocampus have specific
CHAPTER 5 | Functional Neuroanatomy 149

connections with other brain structures and also havebeen studied as separate entities. The activities of the lim-bic system in memory consolidation, emotional behavior,and olfactory processing are topics on which we furtherelaborate in Chapters 7 and 9.
The limbic system is closely related to the hypothala-mus, which researchers have singled out as the main brainstructure for integrating and organizing autonomicprocesses related to the emotional expression of behavior.In humans, limbic system dysfunction has been associ-ated with a variety of abnormalities, including emotionaland behavioral problems (Glaser & Pincus, 1969) andsexual dysfunction (Rosenblum, 1974).
The hippocampal formation has been specifically asso-ciated with memory acquisition (Douglas & Pribram,1966; Penfield & Milner, 1958; Scoville & Milner, 1957).The primary defect, seen after bilateral injury of the hip-pocampus, involves difficulty in learning new informa-tion. Such patients find themselves unable to retain newlylearned information, although immediate and old memo-ries remain relatively intact (Luria, 1971; Milner, 1968).
These effects on memory functioning are less profoundwhen only one hippocampal gyrus is affected (McLardy,1970). Lesions of the left hippocampal gyrus may causeproblems with verbal memory (Russell & Espir, 1961),whereas lesions of the right hippocampal gyrus may causegreater impairment in spatial memory, including mazelearning (Corkin, 1965).
The amygdala has ascending and descending connec-tions with the cerebral hemispheres, the thalamus, thehippocampus, and even the spinal cord. The amygdalaplays a specific role in fear conditioning and in impactingthe strength of stored memory (LeDoux, 1994). Theamygdala is discussed in greater detail in Chapter 9.
Numerous psychological disorders are characterized byemotional disturbances, and the limbic system has beenimplicated in many of them. Extreme violence in patientswho exhibit rage attacks and frequent aggressive behaviorcan follow damage to the amygdala and its connections.In fact, removal of the amygdala (amygdalotomy) has beenperformed on extremely violent and aggressive patients inan attempt to stem rage reactions. Balasubramanian and
150 PART TWO | The Functioning Brain
Corpus callosumFornix
Anterior nucleusof thalamus
Septum
Olfactory bulb
Mammillary body
Amygdala
Hippocampus
Figure 5.24 Limbic system with cortical area removed. (From Heller, K. W. [1996]. Understanding physical,sensory, and health impairments [p. 54, Figure 4.9]. Pacific Grove, CA: Brooks/Cole.)
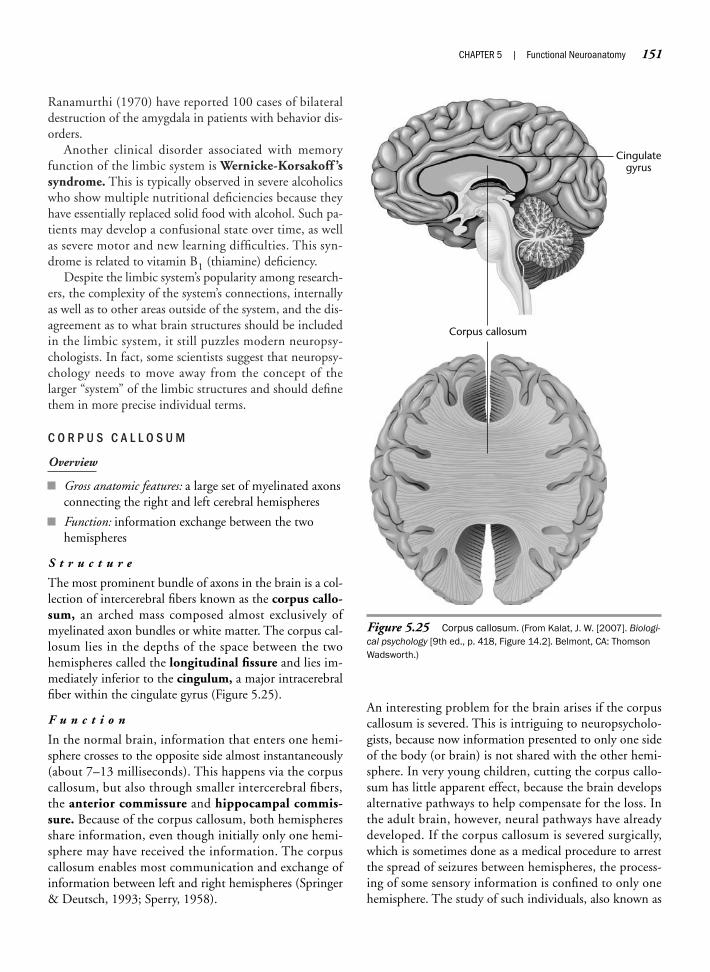
Ranamurthi (1970) have reported 100 cases of bilateraldestruction of the amygdala in patients with behavior dis-orders.
Another clinical disorder associated with memoryfunction of the limbic system is Wernicke-Korsakoff ’ssyndrome. This is typically observed in severe alcoholicswho show multiple nutritional deficiencies because theyhave essentially replaced solid food with alcohol. Such pa-tients may develop a confusional state over time, as wellas severe motor and new learning difficulties. This syn-drome is related to vitamin B1 (thiamine) deficiency.
Despite the limbic system’s popularity among research-ers, the complexity of the system’s connections, internallyas well as to other areas outside of the system, and the dis-agreement as to what brain structures should be includedin the limbic system, it still puzzles modern neuropsy-chologists. In fact, some scientists suggest that neuropsy-chology needs to move away from the concept of thelarger “system” of the limbic structures and should definethem in more precise individual terms.
C O R P U S C A L L O S U M
Overview
Gross anatomic features: a large set of myelinated axonsconnecting the right and left cerebral hemispheres
Function: information exchange between the twohemispheres
S t r u c t u r e
The most prominent bundle of axons in the brain is a col-lection of intercerebral fibers known as the corpus callo-sum, an arched mass composed almost exclusively ofmyelinated axon bundles or white matter. The corpus cal-losum lies in the depths of the space between the twohemispheres called the longitudinal fissure and lies im-mediately inferior to the cingulum, a major intracerebralfiber within the cingulate gyrus (Figure 5.25).
F u n c t i o n
In the normal brain, information that enters one hemi-sphere crosses to the opposite side almost instantaneously(about 7–13 milliseconds). This happens via the corpuscallosum, but also through smaller intercerebral fibers,the anterior commissure and hippocampal commis-sure. Because of the corpus callosum, both hemispheresshare information, even though initially only one hemi-sphere may have received the information. The corpuscallosum enables most communication and exchange ofinformation between left and right hemispheres (Springer& Deutsch, 1993; Sperry, 1958).
An interesting problem for the brain arises if the corpuscallosum is severed. This is intriguing to neuropsycholo-gists, because now information presented to only one sideof the body (or brain) is not shared with the other hemi-sphere. In very young children, cutting the corpus callo-sum has little apparent effect, because the brain developsalternative pathways to help compensate for the loss. Inthe adult brain, however, neural pathways have alreadydeveloped. If the corpus callosum is severed surgically,which is sometimes done as a medical procedure to arrestthe spread of seizures between hemispheres, the process-ing of some sensory information is confined to only onehemisphere. The study of such individuals, also known as
CHAPTER 5 | Functional Neuroanatomy 151
Corpus callosum
Cingulategyrus
Figure 5.25 Corpus callosum. (From Kalat, J. W. [2007]. Biologi-cal psychology [9th ed., p. 418, Figure 14.2]. Belmont, CA: ThomsonWadsworth.)
split-brain patients, has helped provide extensive and in-teresting data on the independent functioning of the twocerebral hemispheres (Gazzaniga, 1966; Geschwind,1965; Zaidel & Sperry, 1973). Researchers have learnedfrom such cases that each hemisphere can function and
process information in isolation. The idea that the brainmight be composed of two independently functioningbrain halves, perhaps even having two personalities or sep-arate minds, is a question we explore in our later discus-sion of consciousness (see Chapter 16).
152 PART TWO | The Functioning Brain
SummaryThis chapter reviews the development, major structures, and functions of the brain. This anatomy lesson isimportant for a variety of reasons. It is important to understand the functional aspects of the brain as theyrelate to brain anatomy. Knowledge of brain structures, in and of itself, is not very useful to neuropsycholo-gists. This is most interestingly demonstrated when students with little neuropsychological knowledge dis-sect a brain. They proceed in a most rapid manner with the dissection, naming each structure they are ableto detect as they go along. Once finished, they are typically perplexed with the mess they have made andhow little they have learned. They often ask, “Where has the brain gone?” Novices look at the brain as ananatomic object; neuropsychologists examine it as a functioning organ of interconnected systems.
This chapter serves as an overview of the basic neuroanatomic structures and functions of the CNS.However, it is typically the more integrated behaviors that interest neuropsychologists. Therefore, it is neces-sary to move from discussions of groupings of structures based on ontogeny to the idea of pluripotentialityof structures within functional systems. This concept, first introduced in Chapter 1, often transverses group-ings based on migration of structures during brain development. It is to the systemic organization of regionsof the cerebral hemispheres in support of behavior, particularly those involving higher order mental func-tions that we now turn.
C r i t i c a l T h i n k i n g Q u e s t i o n s
Why is an understanding of the stages and processes of brain development important to the neuropsychologist?If a child was born without the telencephalon region of the brain, would the child be able to orient to visual and auditorystimuli, perform reflexive movements, and sit up? Explain why or why not.To what extent can behavioral functions be localized to specific brain structures?What level of brain mapping is most useful to the neuropsychologist?
K e y Te r m s
Central nervous system (CNS)NeurogenesisPeripheral nervous system
(PNS)Neural tubePrecursor or progenitor cellsGlial cellsOligodendrocytesMicrogliaMigratory processDifferentiation processNeurulationSpina bifidaAnencephalyCorticogenesis
Agyria or lissencephalyAxonsDendritesArborizationDendritic spinesSynaptogenesisPrefrontal cortexMyelinPruningVisual cortexForebrain (prosencephalon)Midbrain (mesencephalon)Hindbrain (rhombencephalon)TelencephalonDiencephalon
MetencephalonMyelencephalonGyrus (gyri)Sulcus (sulci)Sylvian (lateral) fissurePolymicrogyriaCerebrospinal fluid (CSF)Vertebral columnSomatic nervous system (SNS)Autonomic nervous system
(ANS)Sympathetic nervous systemParasympathetic nervous
systemBrain
Spinal cordCranial nervesAfferent nervesEfferent nervesMeningesHorizontal planeCoronal planeSagittal planeAnteriorPosteriorInferiorSuperiorMedialLateralRostral
CaudalProximalDistalDorsalVentralIpsilateralContralateralMeningiomasVentricular systemVascular systemFossaeForaminaForamen magnumFontanellePia materArachnoid membraneSubarachnoid spaceDura materEpidural spaceSubdural spaceSubdural hematomaMeningitisVentriclesInterventricular foramen or
foramen of Monro
Cerebral aqueduct or aqueductof Sylvius
Choroid plexusForamen of MagendieForamina of LuschkaCisternsSuperior sagittal sinusArachnoid villi or granulationsHydrocephalusNormal-pressure hydrocephalus
(NPH)Internal carotid arteriesVertebral arteriesAortic archBasilar arteryPosterior cerebral arteriesCerebrovascular accident (CVA)Circle of WillisAnterior cerebral arteryMiddle cerebral arteryAnterior communicating arteryPosterior communicating
arteriesCerebrumBasal forebrain
CerebellumBrainstemMedulla oblongataPonsReticular activating system
(RAS)DecussateCerebellar pedunclesTectumTegmentumInferior colliculiSuperior colliculiThalamusHypothalamusPituitary stalkAdrenocorticotropic hormone
(ACTH)VermisBasal gangliaBasal nucleiSubthalamic nucleusCaudate nucleusPutamenGlobus pallidusStriatum
Substantia nigraExtrapyramidal motor systemPyramidal motor systemTardive dyskinesiaRhinencephalonCingulate gyrusParahippocampal gyrusHippocampal formationLimbic systemFornixMammillary bodiesAmygdalaSeptumBasolateral circuitPapez circuitWernicke-Korsakoff’s
syndromeCorpus callosumLongitudinal fissureCingulumAnterior commissureHippocampal commissure
CHAPTER 5 | Functional Neuroanatomy 153
We b C o n n e c t i o n s
http://www.meddean.luc.edu/lumen/MedEd/GrossAnatomy/h_n/cn/cn1/mainframe.htmThe Cranial NervesThis site provides excellent discussion of the cranial nerves.
http://www.neuropat.dote.huNeuroanatomyThis page features links to a number of resources in neuroanatomy.

Chapter 6
CEREBRAL SPECIALIZATION
Men are from Mars, and Women are from Venus.—John Gray
The Cerebral HemispheresHemispheric Anatomic and Functional DifferencesSex Differences and Hemispheric Specialization
Neuropsychology in Action
6.1 The Evolution of the Brain: A Focus on Brain Size6.2 A Land Where Girls Rule in Math

OverviewThis chapter focuses on the cerebral cortex with regard to structure, function, lateralization, and sex differ-ences. Our discussion of the cortex provides a foundation for subsequent chapters that explore the func-tional systems of the brain that support complex behavior such as language, memory, and emotions. Thecortical regions of the brain can be defined in a number of ways, although the most frequently used nomen-clature involves the divisions of the cortex into four lobes (occipital, temporal, parietal, and frontal).Although there is greater correspondence between region and primary sensory functions of the posteriorregions of the brain, higher order cognitive, emotional, and social functions are not specifically localized to aparticular lobe. Rather, multiple pathways and regions underpin functions, particularly those that involvecomplex behavior.
The human brain is composed of two hemispheres that interact in the support of behavior. The hemi-spheres differ regarding structure and function, with certain human attributes being lateralized to either theleft or right hemisphere. However, the lateralization of a function to one hemisphere does not mean that theother hemisphere is uninvolved in the support of the function. For example, speech and language are gener-ally lateralized to the left hemisphere in most people (both right- and left-handed individuals), but the righthemisphere is also intimately involved in speech and language functions.
It is generally recognized that each person’s brain is different from the brain of every other person.Putative cognitive and behavioral differences of male and female individuals have led to neuropsychologicalinvestigations to determine whether structural and functional differences exist between the brains of thetwo sexes. Significant attention has focused on the role of sex hormones in the organization and activationof the brain. You will soon realize that the relation of sex hormones to behavior is complex and not fullyunderstood.
CHAPTER 6 | Cerebral Specialization 155
The Cerebral Hemispheres
Overview
Gross anatomic features: structures of the frontal, pari-etal, occipital, and temporal lobes
Function: higher cognitive functioning, cerebral spe-cialization, and cortical localization
The cerebral hemispheres represent the most recentlyevolved brain structure in humans, although they are ap-proximately 1 to 3 million years old (see Neuropsychology
in Action 6.1). The complexity of the interhemisphericand intrahemispheric connections reflects this degree ofevolution, which allows humans to use such abstract con-cepts as symbols, language, and art.
S T R U C T U R E
The largest part of the brain consists of the cerebrum, orthe right and left cerebral hemispheres. The two hemi-spheres form a half globe with a flat basal surface. Thehemispheres are separated by a deep midline cleft, thelongitudinal fissure, and are connected via the corpus
K e e p i n M i n d
What is the relation of brain size to function?
Is there a one-to-one relationship between cerebral regions and function?
Why are the concepts of laterality, dominance, and asymmetry important in understanding brain–behavior functions?
Do sex differences exist in brain organization and activation? What are the implications of these differences?
How do you account for the presumed sex difference in mental rotation and verbal fluency?

156 PART TWO | The Functioning Brain
To understand the functioning brain, place itwithin the context of evolution. Two to threemillion years ago, humans living in East Africawere making stone tools, perhaps buildingsimple dwellings. Their brains would, in thecourse of a spectacular evolution, eventuallyenlarge to the size and complexity of today.Humans could not possibly perform thenumerous and complex behaviors that theydo without brain mechanisms that haveevolved over hundreds of thousands of years.Evolutionary psychology offers a coherenttheory that may begin to explain the strategicdifferences and similarities in the structuresand functions of the brain.
Central to the concept of evolution wasCharles Darwin’s (1809–1882) text On theOrigin of Species (1859). His historic 1835trip to the Galápagos Islands laid the foun-dation of his theory of biological evolution,even though he stayed for only 5 weeks.Darwin suggested that the mechanism forexplaining how species evolve from existingforms is a process based on natural selec-tion. He identified the process of naturalselection as the mechanism underlying theevolution of all organisms. He reasoned thatsome individuals were better able to surviveand reproduce than others, and that thecharacteristics that made these speciesmore successful could then be transmittedto the next generation. Perhaps the mostsignificant legacy of evolution is a powerfulbrain that has evolved to a degree allowinghumans to learn from experiences.
Basic human psychological mechanismsrelated to brain processes are likely to bespecies specific. For example, most or allhumans share certain psychological
processes, including fear of darkness;characteristic emotions such as anger, love,and humor; weapon making; sexual attrac-tion; and probably hundreds more (Wright,1994). People often call these processeshuman nature, but they must be related tobrain processes. One reason most humansshare many psychological mechanismsrelates to that natural selection tends toimpose relative uniformity in complex adap-tive designs, such as the brain. Thus, centralto any theory on brain evolution is thatcertain aspects of the CNS remain stable,whereas others must adapt over time. This ismost readily apparent at the level of humanphysiology and anatomy: All people have twoarms, a heart, and a brain; that is, they donot vary in possessing basic physiologicmechanisms. According to evolutionarypsychology, however, the brain must containa large number of specialized psychologicalmechanisms; each designed to solve adifferent or related adaptive problem. Thus,individuals also differ, and fundamentalindividual differences must be central to anycomprehensive brain theory.
One way that the human brain differs,compared with other species, is its size,particularly the size of the neocortex. Forexample, a general principle of neural orga-nization indicates that the size and complex-ity of a structure is related to its functionalimportance of the structure. The brain,through the meninges, is firmly attached tothe skull. Anthropologists measure theinternal volume of skulls, which is easilypreserved over time, to estimate the weightof the brain. Using this technique, re-searchers estimated the brains of our
earliest ancestors, dated approximately 5 million years ago, to be relatively small,about 400 cm3 (Changeux & Chavaillon,1995). Anthropologic evidence suggeststhat approximately 3 million years ago theanatomic organization of the CNS and itsassociated functions evolved at a spectacu-lar rate. Although the human brain wasalways relatively large in proportion to thebody, and presented a modern organization,the relative size of the brain rapidlyincreased in size. About 1 million years ago,the occipital lobes began to develop, fol-lowed by the frontal, parietal, and temporallobes. This new biological foundation en-abled increased memory capacity, morefrequent and specific spoken communica-tion (language), a more elaborate social life,and a more extensive exploration of theenvironment. Humans no longer dependedon gathering rocks, carcasses, and vegeta-bles, but became proficient in animal cap-ture. This evolution in the structural complex-ity and performance of the braincorresponded directly with the formation anddevelopment of diverse cultures.
Neanderthals are thought to have inhab-ited Europe and the Middle East as early as100,000 years ago. It is not clear exactly howsimilar they were to us, but they certainly hadan elaborate tool-using culture that includedritual burial (Changeux & Chavaillon, 1995).About 100,000 years ago, the growth in brainsize started to level off, probably related to thefact that the female pelvis, and the size of theskull that can fit through it, had not kept pacewith the evolution of the brain. This has madefor a remarkable state of affairs as it relates tobrain development in humans. At birth, the
N e u r o p s y c h o l o g y i n A c t i o n 6 . 1
T h e E v o l u t i o n o f t h e B r a i n : A F o c u s o n B r a i n S i z e
by Eric A. Zillmer
callosum. The surface of each hemisphere folds in on it-self in many places, creating grooves along the surface re-ferred to as sulci (singular, sulcus). Very deep grooves aretermed fissures. The irregularly shaped ridges betweensulci are known as gyri (singular, gyrus). No two brainsare exactly identical in the size or the shape of their gyri,
although the general gyral pattern is consistent enough tolocate major landmarks. The morphology of the brain’sgyri can be thought of as somewhat related to the idea ofa face, where the features such as the nose, eyes, andmouth are generally localizable but vary in shape accord-ing to the person. Perhaps, more like a fingerprint, each

person has his or her own “brain print.” So much varia-tion is evident between the brains of people that research-ers conducting imaging and histologic analyses must com-pensate for interindividual variability by standardizingand transforming formulas, rather than by comparing brainsdirectly (Mai, Assheuer, & Paxinos, 1997). Figure 6.1 pre-sents general gyral and sulcal features.
The surface of the cerebral hemispheres is covered bygray matter. As described in Chapter 4, the gray areas ofthe central nervous system (CNS) consist mainly of cellbodies of neurons that serve as the brain’s functional units.Underlying the cortex is white matter that links structureswithin the cerebral hemispheres and the CNS as a whole.The size, shape, and distribution of the cells and fibers vary
CHAPTER 6 | Cerebral Specialization 157
brain is approximately 1/4 its eventual size,compared with the rest of the body, which is1/20 its eventual size. Then, over the next 20 years of a human’s life, the brain maturesat an amazing rate, developing billions ofconnections and supporting cells. At age 16, itreaches a level of behavioral control andconscious realm (maturity) that the owner ofthe brain is allowed to drive himself or herselfaround in an automobile. At age 18, the brainis allowed to render an opinion, a vote, affect-ing other brains (through culture and society).
The basic brain structures are similar forall mammals, although brain size may varyconsiderably among different species. Oneof the many fascinating aspects of howhumans have evolved as a species is relatedto this extreme and unprecedented growthof the human brain, the cerebral cortex, andspecifically the prefrontal cortex, whichLuria named the “organ of civilization.” Tomany students, the size of an organism’sbrain may seem intuitively related to theintellectual properties of a species. Cer-tainly, if you compare animals with humans,there is a relation between brain size andintelligence. Aristotle commented on thathumans had proportionally the largest brainsof all animals.
Consider, for example, that gorillas,although physically larger than humans, onlyhave about one fourth of the brain size. Inhumans, the average adult brain size isabout 1300 cubic centimeters (cm3) andweighs about 1500 grams. But a bluewhale’s brain weighs 6000 grams, and anAfrican elephant’s brain 5700 grams. If,however, brain size is held constant as itrelates to body size, humans compare verywell. The brain of a whale accounts for only1/10,000 of its body weight, the elephant’sbrain 1/600, and the human brain 1/40.Thus, if the range of brain size with body sizeis held constant, the human brain is 21,000times larger and the neocortex is 142,000times larger than that of the shrew, a very
small, mouselike mammal. This means thatif a shrew were the size of a human, its brainwould weigh only 46 grams. The body/brainweight formula, however, does not work wellwith all small animals. For example, theferret’s brain makes up 1/12 of its bodyweight. In fact, the best ratio appears to bebetween an organism’s body surface (notbody weight) and brain size. Certainly, it islogical to assume that the surface of thebody, through which the organism hascontact with the environment, is more di-rectly related to brain function than is thetotal weight in bones and blood. When bodysurface is taken into consideration, thehuman comes in first among all vertebrates,with the chimpanzee and the dolphin follow-ing second and third (Changeux & Chavail-lon, 1995).
Large brains are not necessarily moreefficient or effective; in fact, absolute brainweight has no significance in itself. It mayrequire a larger brain more time to processinformation than a smaller one. There areeven differences in brain size among hu-mans. Big people tend to have larger brainsthan smaller people. This does not imply thatmen, who are, on average, taller and heavierthan women, are smarter. After correcting forbody size, men and women have brains ofapproximately equal size.
The size of a brain has been an object ofdebate and controversy for many centuries.Broca, for one, argued that the size of thebrains of human races had to account forsomething (1861). He proposed that “ingeneral, the brain is larger in mature adultsthan in the elderly, in men than in women, ineminent men than in men of mediocre talent,in superior races than in inferior races . . . .There is a remarkable relationship betweenthe development of intelligence and thevolume of the brain” (1861, pp. 188, 304).As evidence, Broca offered findings that 51unskilled workers had an average brainweight of 1365 grams, compared with the
brain weight of 24 skilled workers, which wasan average of 1420 grams. Any student ofstatistics knows that this finding may not bestatistically significant, given the largevariation of brain weights in humans and,presumably, in Broca’s sample as well.Furthermore, it is entirely possible that theunskilled workers were malnourished and,therefore, were smaller in stature than theskilled workers. In any case, Broca’s datahave not been confirmed by more recentstudies, suggesting that his findings weredue to chance. Nevertheless, Broca went togreat lengths to “prove” his theory. One hasto wonder what Gall himself must havethought of this—his brain measured “only”1100 grams.
The measurement (or mismeasurement)of human intellectual properties according tobrain size has been described by the evolu-tionary biologist Stephen J. Gould in TheMismeasure of Man (1981), in which hepresented a fascinating historical account ofphrenology and other pseudoscientific expla-nations of the size of the human brain and itsrelation to intelligence. What Broca andothers did not realize was that body size, aswell as many other factors, relates to thecomplexity of the brain and the nervoussystems of humans and other species. In fact,the complexity of the brain depends on manydimensions in addition to brain size, includingconnectivity, cell density, cell morphology,neurotransmitter complements, and perhapsthe most important variable, the rate andduration of neuronal sprouting. Among hu-mans, no brain size–intelligence relationexists.
The brain of Albert Einstein, the NobelPrize–winning physicist, underwent autopsyafter his death on April 18, 1955. Gall andBroca would have been surprised to learnthat the Princeton professor’s brain wasbasically normal in appearance and ofaverage size, although there were structuraldifferences in the parietal lobe.
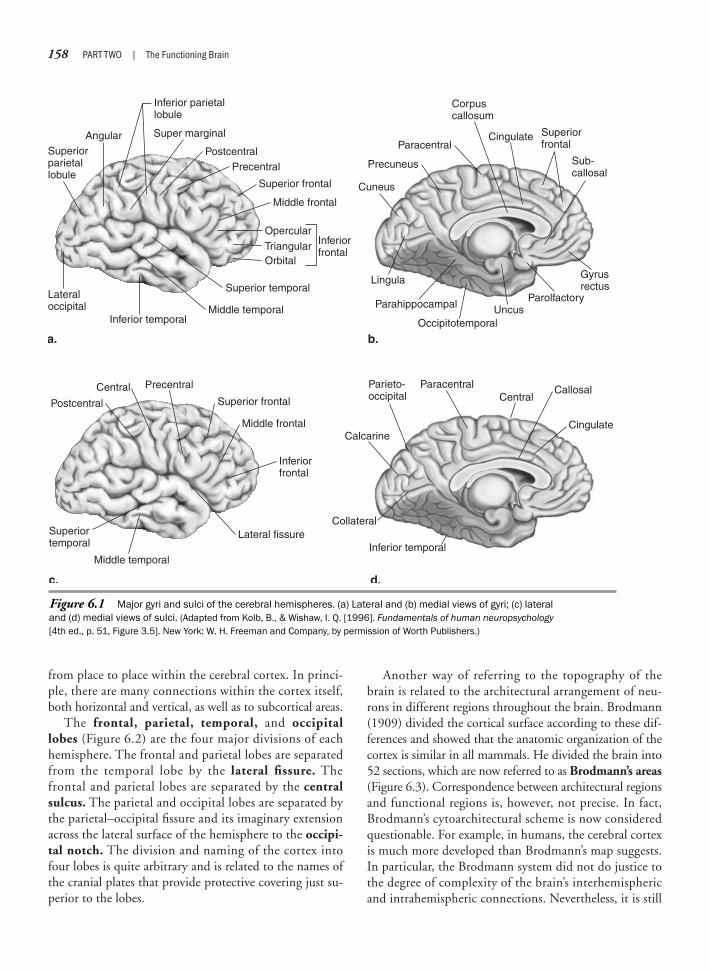
158 PART TWO | The Functioning Brain
from place to place within the cerebral cortex. In princi-ple, there are many connections within the cortex itself,both horizontal and vertical, as well as to subcortical areas.
The frontal, parietal, temporal, and occipitallobes (Figure 6.2) are the four major divisions of eachhemisphere. The frontal and parietal lobes are separatedfrom the temporal lobe by the lateral fissure. Thefrontal and parietal lobes are separated by the centralsulcus. The parietal and occipital lobes are separated bythe parietal–occipital fissure and its imaginary extensionacross the lateral surface of the hemisphere to the occipi-tal notch. The division and naming of the cortex intofour lobes is quite arbitrary and is related to the names ofthe cranial plates that provide protective covering just su-perior to the lobes.
Another way of referring to the topography of thebrain is related to the architectural arrangement of neu-rons in different regions throughout the brain. Brodmann(1909) divided the cortical surface according to these dif-ferences and showed that the anatomic organization of thecortex is similar in all mammals. He divided the brain into52 sections, which are now referred to as Brodmann’s areas(Figure 6.3). Correspondence between architectural regionsand functional regions is, however, not precise. In fact,Brodmann’s cytoarchitectural scheme is now consideredquestionable. For example, in humans, the cerebral cortexis much more developed than Brodmann’s map suggests.In particular, the Brodmann system did not do justice tothe degree of complexity of the brain’s interhemisphericand intrahemispheric connections. Nevertheless, it is still
Figure 6.1 Major gyri and sulci of the cerebral hemispheres. (a) Lateral and (b) medial views of gyri; (c) lateraland (d) medial views of sulci. (Adapted from Kolb, B., & Wishaw, I. Q. [1996]. Fundamentals of human neuropsychology[4th ed., p. 51, Figure 3.5]. New York: W. H. Freeman and Company, by permission of Worth Publishers.)
CentralCentral
Cingulate
Cingulate
Corpuscallosum
Postcentral
Postcentral
Precentral
Precentral
Paracentral
Paracentral
Superior frontal
Superior frontal
Superiorparietallobule
Super marginal
Inferior parietallobule
Superiorfrontal
Inferiorfrontal
Inferiorfrontal
Inferior temporal
Occipitotemporal
Parolfactory
Gyrusrectus
Middle frontal
Middle frontal
Middle temporal
Middle temporalInferior temporal
Superiortemporal
Superior temporal
a. b.
c. d.
Lateral fissure
Lateraloccipital
Collateral
Calcarine
Callosal
Sub-callosal
Parieto-occipital
Parahippocampal
Lingula
Cuneus
Precuneus
Uncus
Angular
Opercular
TriangularOrbital
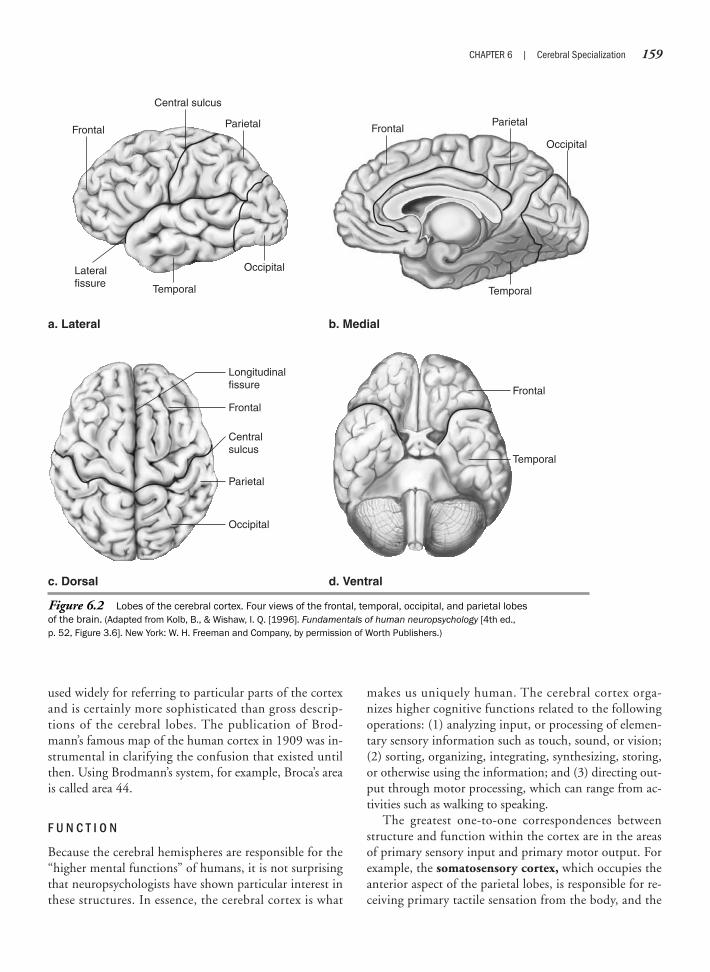
used widely for referring to particular parts of the cortexand is certainly more sophisticated than gross descrip-tions of the cerebral lobes. The publication of Brod-mann’s famous map of the human cortex in 1909 was in-strumental in clarifying the confusion that existed untilthen. Using Brodmann’s system, for example, Broca’s areais called area 44.
F U N C T I O N
Because the cerebral hemispheres are responsible for the“higher mental functions” of humans, it is not surprisingthat neuropsychologists have shown particular interest inthese structures. In essence, the cerebral cortex is what
makes us uniquely human. The cerebral cortex orga-nizes higher cognitive functions related to the followingoperations: (1) analyzing input, or processing of elemen-tary sensory information such as touch, sound, or vision;(2) sorting, organizing, integrating, synthesizing, storing,or otherwise using the information; and (3) directing out-put through motor processing, which can range from ac-tivities such as walking to speaking.
The greatest one-to-one correspondences betweenstructure and function within the cortex are in the areasof primary sensory input and primary motor output. Forexample, the somatosensory cortex, which occupies theanterior aspect of the parietal lobes, is responsible for re-ceiving primary tactile sensation from the body, and the
CHAPTER 6 | Cerebral Specialization 159
Figure 6.2 Lobes of the cerebral cortex. Four views of the frontal, temporal, occipital, and parietal lobesof the brain. (Adapted from Kolb, B., & Wishaw, I. Q. [1996]. Fundamentals of human neuropsychology [4th ed., p. 52, Figure 3.6]. New York: W. H. Freeman and Company, by permission of Worth Publishers.)
Frontal
Frontal
Lateralfissure
a. Lateral b. Medial
c. Dorsal d. Ventral
Frontal
Central sulcus
ParietalParietal
Occipital
Occipital
Occipital
Temporal
Temporal
Temporal
Parietal
Frontal
Longitudinalfissure
Centralsulcus
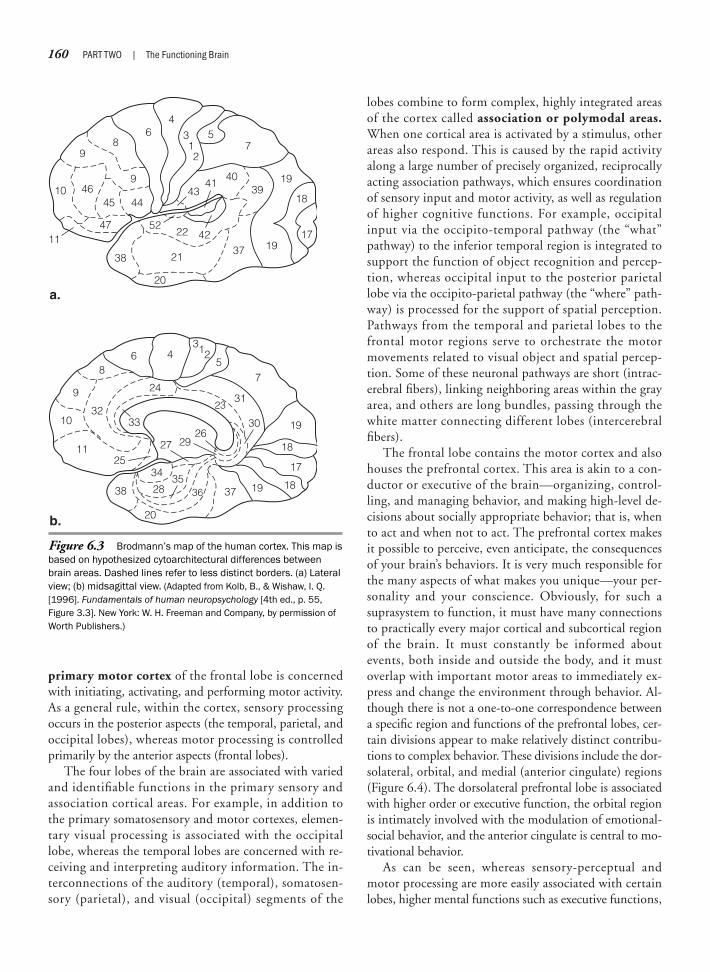
160 PART TWO | The Functioning Brain
primary motor cortex of the frontal lobe is concernedwith initiating, activating, and performing motor activity.As a general rule, within the cortex, sensory processingoccurs in the posterior aspects (the temporal, parietal, andoccipital lobes), whereas motor processing is controlledprimarily by the anterior aspects (frontal lobes).
The four lobes of the brain are associated with variedand identifiable functions in the primary sensory andassociation cortical areas. For example, in addition tothe primary somatosensory and motor cortexes, elemen-tary visual processing is associated with the occipitallobe, whereas the temporal lobes are concerned with re-ceiving and interpreting auditory information. The in-terconnections of the auditory (temporal), somatosen-sory (parietal), and visual (occipital) segments of the
lobes combine to form complex, highly integrated areasof the cortex called association or polymodal areas.When one cortical area is activated by a stimulus, otherareas also respond. This is caused by the rapid activityalong a large number of precisely organized, reciprocallyacting association pathways, which ensures coordinationof sensory input and motor activity, as well as regulationof higher cognitive functions. For example, occipitalinput via the occipito-temporal pathway (the “what”pathway) to the inferior temporal region is integrated tosupport the function of object recognition and percep-tion, whereas occipital input to the posterior parietallobe via the occipito-parietal pathway (the “where” path-way) is processed for the support of spatial perception.Pathways from the temporal and parietal lobes to thefrontal motor regions serve to orchestrate the motormovements related to visual object and spatial percep-tion. Some of these neuronal pathways are short (intrac-erebral fibers), linking neighboring areas within the grayarea, and others are long bundles, passing through thewhite matter connecting different lobes (intercerebralfibers).
The frontal lobe contains the motor cortex and alsohouses the prefrontal cortex. This area is akin to a con-ductor or executive of the brain—organizing, control-ling, and managing behavior, and making high-level de-cisions about socially appropriate behavior; that is, whento act and when not to act. The prefrontal cortex makesit possible to perceive, even anticipate, the consequencesof your brain’s behaviors. It is very much responsible forthe many aspects of what makes you unique—your per-sonality and your conscience. Obviously, for such asuprasystem to function, it must have many connectionsto practically every major cortical and subcortical regionof the brain. It must constantly be informed aboutevents, both inside and outside the body, and it mustoverlap with important motor areas to immediately ex-press and change the environment through behavior. Al-though there is not a one-to-one correspondence betweena specific region and functions of the prefrontal lobes, cer-tain divisions appear to make relatively distinct contribu-tions to complex behavior. These divisions include the dor-solateral, orbital, and medial (anterior cingulate) regions(Figure 6.4). The dorsolateral prefrontal lobe is associatedwith higher order or executive function, the orbital regionis intimately involved with the modulation of emotional-social behavior, and the anterior cingulate is central to mo-tivational behavior.
As can be seen, whereas sensory-perceptual andmotor processing are more easily associated with certainlobes, higher mental functions such as executive functions,
Figure 6.3 Brodmann’s map of the human cortex. This map isbased on hypothesized cytoarchitectural differences betweenbrain areas. Dashed lines refer to less distinct borders. (a) Lateralview; (b) midsagittal view. (Adapted from Kolb, B., & Wishaw, I. Q.[1996]. Fundamentals of human neuropsychology [4th ed., p. 55,Figure 3.3]. New York: W. H. Freeman and Company, by permission ofWorth Publishers.)
10 4645
4711
44
9
9
9
10
11
1819
17
18
19
86
24
23
36
2725
38
3435
37
303332
31
2926
28
20
4312
57
86
4
4341
4039
19
42
213837 19
17
18
20a.
753
12
2252
b.
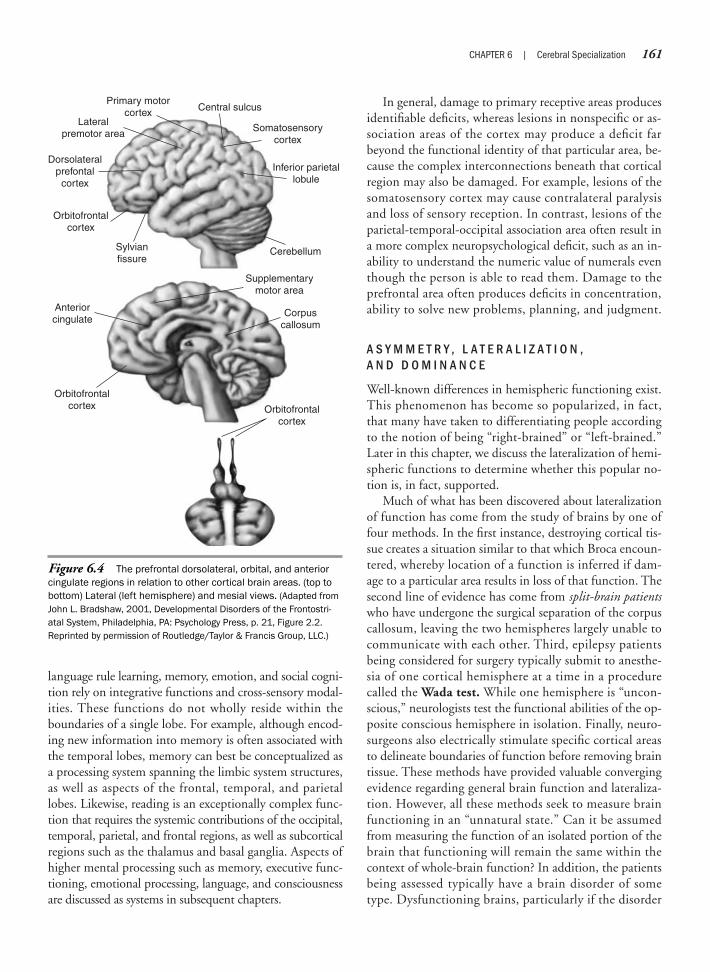
language rule learning, memory, emotion, and social cogni-tion rely on integrative functions and cross-sensory modal-ities. These functions do not wholly reside within theboundaries of a single lobe. For example, although encod-ing new information into memory is often associated withthe temporal lobes, memory can best be conceptualized asa processing system spanning the limbic system structures,as well as aspects of the frontal, temporal, and parietallobes. Likewise, reading is an exceptionally complex func-tion that requires the systemic contributions of the occipital,temporal, parietal, and frontal regions, as well as subcorticalregions such as the thalamus and basal ganglia. Aspects ofhigher mental processing such as memory, executive func-tioning, emotional processing, language, and consciousnessare discussed as systems in subsequent chapters.
In general, damage to primary receptive areas producesidentifiable deficits, whereas lesions in nonspecific or as-sociation areas of the cortex may produce a deficit farbeyond the functional identity of that particular area, be-cause the complex interconnections beneath that corticalregion may also be damaged. For example, lesions of thesomatosensory cortex may cause contralateral paralysisand loss of sensory reception. In contrast, lesions of theparietal-temporal-occipital association area often result ina more complex neuropsychological deficit, such as an in-ability to understand the numeric value of numerals eventhough the person is able to read them. Damage to theprefrontal area often produces deficits in concentration,ability to solve new problems, planning, and judgment.
A S Y M M E T R Y , L A T E R A L I Z A T I O N , A N D D O M I N A N C E
Well-known differences in hemispheric functioning exist.This phenomenon has become so popularized, in fact,that many have taken to differentiating people accordingto the notion of being “right-brained” or “left-brained.”Later in this chapter, we discuss the lateralization of hemi-spheric functions to determine whether this popular no-tion is, in fact, supported.
Much of what has been discovered about lateralizationof function has come from the study of brains by one offour methods. In the first instance, destroying cortical tis-sue creates a situation similar to that which Broca encoun-tered, whereby location of a function is inferred if dam-age to a particular area results in loss of that function. Thesecond line of evidence has come from split-brain patientswho have undergone the surgical separation of the corpuscallosum, leaving the two hemispheres largely unable tocommunicate with each other. Third, epilepsy patientsbeing considered for surgery typically submit to anesthe-sia of one cortical hemisphere at a time in a procedurecalled the Wada test. While one hemisphere is “uncon-scious,” neurologists test the functional abilities of the op-posite conscious hemisphere in isolation. Finally, neuro-surgeons also electrically stimulate specific cortical areasto delineate boundaries of function before removing braintissue. These methods have provided valuable convergingevidence regarding general brain function and lateraliza-tion. However, all these methods seek to measure brainfunctioning in an “unnatural state.” Can it be assumedfrom measuring the function of an isolated portion of thebrain that functioning will remain the same within thecontext of whole-brain function? In addition, the patientsbeing assessed typically have a brain disorder of sometype. Dysfunctioning brains, particularly if the disorder
CHAPTER 6 | Cerebral Specialization 161
Figure 6.4 The prefrontal dorsolateral, orbital, and anteriorcingulate regions in relation to other cortical brain areas. (top tobottom) Lateral (left hemisphere) and mesial views. (Adapted fromJohn L. Bradshaw, 2001, Developmental Disorders of the Frontostri-atal System, Philadelphia, PA: Psychology Press, p. 21, Figure 2.2.Reprinted by permission of Routledge/Taylor & Francis Group, LLC.)
Orbitofrontalcortex
Anteriorcingulate
Orbitofrontalcortex
Supplementarymotor area
Sylvianfissure
Corpuscallosum
Orbitofrontalcortex
Lateralpremotor area
Primary motorcortex Central sulcus
Dorsolateralprefontal
cortex
Somatosensorycortex
Inferior parietallobule
Cerebellum

162 PART TWO | The Functioning Brain
has existed over a long period, may not behave the sameway as intact brains. Now, through newer, noninvasivemethods of brain imaging, such as positron emission to-mography (PET), functional magnetic resonance imaging(fMRI), and single-photon emission computed tomogra-phy (SPECT), which show the dynamic workings of thebrain (see Chapter 2), researchers can test normal subjectsand pinpoint the centers of greatest brain activity for anyone type of task. In addition, two innovative neuroimag-ing techniques, magnetic resonance spectroscopy (MRS)and diffusion tensor imaging (DTI), allow for even “finer”analysis of brain functioning. MRS provides visualizationof the neurochemical activity of brain material, whereasthe DTI maps the axonal connectivity of brain regions(Nordahl & Salo, 2004). These latter two techniquesshould further increase our understanding of hemisphericand regional brain functioning.
The term hemispheric asymmetry refers to the differen-tiation in morphology and physiology of the brain betweenthe right and left hemispheres. The terms lateralizationand dominance refer to the differences in functional spe-cialization between the two hemispheres.
Probably the function most associated with lateralityis speech. Paul Broca first determined that damage to thefrontal operculum of the left hemisphere resulted in lossof speech (aphasia), whereas the right hemisphere ap-peared to play little or no role in language processing.Before Broca’s seminal finding, it was widely believed thatthe two hemispheres were redundant in function. Broca’sdiscovery led to the proposition that speech and languagewere properties of the left hemisphere. To say speech andlanguage are lateralized to the left hemisphere denotes afunctional dominance of the left hemisphere over theright hemisphere for language processing. Dominancedoes not mean that one hemisphere has complete or totalresponsibility for a function, but rather plays a primaryor major role in the support of a function. For example,although there is significant empirical support for the lat-eralization of language to the left hemisphere (for mostpeople), research has demonstrated that the right hemi-sphere is, in fact, able to perform a limited number oflanguage functions such as understanding and processingof rudimentary linguistic contents. It is unable, however,to process complex linguistic information, and only rarelyis able to communicate via speech. In addition, as discussedlater, the right hemisphere plays a major and complemen-tary role in regulating the nonverbal aspects of speech andlanguage.
Because of the decussation of the sensory and motortracks from the brain to the spinal cord, the right hemi-sphere shows greater involvement in the control of the
left hand, whereas the left hemisphere is associated withmodulation of the right hand. Broca (1861) proposedthat a person’s preferred handedness was opposite fromthe hemisphere specialized for language. Although theconcept of preferred handedness appears simple to as-certain, there continues to be disagreement over the def-inition of the concept. For example, some researchershave defined preferred handedness based on the handthe individual uses to write, whereas others prefer tolook to the hand the person uses across a number of ac-tivities to determine preference. The latter definitionlends to representing handedness as a differential vari-able that ranges on a bipolar continuum, with one ex-treme indicating complete right-handedness and theother extreme complete left-handedness. The midpointof the continuum would reflect mixed-handedness (am-bidexterity). Finally, preferred handedness has been de-fined by the relative efficiency or speed of the hands. Thelatter definition shifts the emphasis from “preference” to“proficiency” of hand use.
Consistent with Broca’s proposition, subsequent researchdemonstrates that the relation of preferred handedness tohemispheric lateralization is partially accurate when later-alization of right-handed individuals is considered. Forexample, an MRI study (Springer et al., 1999) of 100healthy right-handed participants (48% female, 52%male) reported that 94% were left hemisphere dominantfor language, whereas 6% showed bilateral, roughly sym-metric language representation. None of the healthy par-ticipants were found to be right hemisphere dominant. Inanother study (Knecht, Dräger, Deppe, Bobe, Lohmann,Flöel, et al., 2000) of 188 healthy right-handed participants(59% female, 41% male), left language lateralization wasidentified in 92.5% of the participants, whereas 7.5%demonstrated right hemisphere lateralization.
Left-handed individuals are also likely to show lefthemisphere lateralization for language, although to a lesserextent than right-handed individuals. Szaflarski et al.(2002) selected 50 healthy left-handed and ambidextrousparticipants for fMRI study. Predominately left hemi-sphere lateralization was found in 78% of the individuals,whereas 8% were predominantly right hemisphere lateral-ized, and 14% showed symmetric lateralization. In a largerstudy (Knecht, Dräger, Deppe, Bobe, Lohmann, Flöel,et al., 2000) with 326 healthy participants (198 females,128 males), handedness was determined by the EdinburghInventory (Oldfield, 1971), a self-rating scale. This mea-sure allows for a rating of handedness ranging from strongleft-handedness to strong right-handedness. Seven groupswere identified based on the Edinburgh Inventory. Thedetermination of language laterality was made by having

the participants perform word generation tasks while un-dergoing Doppler ultrasonography (fTCD). Overall re-sults demonstrated a linear relation: the greater the right-handedness, the higher the incidence of left hemispherelanguage dominance, and vice versa. In extreme left-han-ders, the incidence of right hemisphere dominance was27% compared with 4% for extreme right-handers withright hemisphere speech. The intermediate groups showeddecreasing right hemisphere lateralization as the degree ofright-handedness increased.
Initially, it was believed that “atypical” lateralization,particularly for right-handed people, was potentially anabnormal sign indicative of brain pathology or perturba-tions of brain organization. Support was drawn for thisview from the finding that a significant number of indi-viduals with brain abnormalities (e.g., epilepsy) demon-strated atypical lateralization. Yet, this assumption hasbeen challenged by empirical findings demonstrating thata significant proportion of healthy individuals also showatypical language specialization without neuropsychologi-cal impairments (Hartlage & Gage, 1997). When there isa family history of left-handedness, the likelihood thatleft-handedness of offspring will be associated with brainpathology is significantly reduced.
In summary, empirical and clinical studies suggest thatspeech is generally lateralized to the left hemisphere forright-handed individuals (about 95%). Although the ma-jority of left-handed individuals also show left hemispherespecialization for speech (about 70%), the incidence ofbilateral or right hemisphere lateralization is greater inleft-handed individuals.
Hemispheric Anatomicand Functional Differences
Although some structural differences between thehemispheres are known to correspond to functional dif-ferences in behavior, the relation between structure andfunction has not been fully determined. Table 6.1 out-lines the differences in morphology between the twohemispheres. Figure 6.5 depicts some of the major hemi-spheric differences in structure.
Gross inspection of the two hemispheres of the brainreveals a number of differences. If you first look at the en-tire brain from the top down, it appears askew. This is be-cause the right hemisphere often protrudes anteriorlyfrom the frontal lobes, and the left hemisphere protrudesposteriorly from the parietal-occipital area. Turning thebrain to the lateral surface of the cerebral hemispheres,
the Sylvian fissure (which is normally the large fissureseparating the frontal from the temporal and parietallobes) is steeper in the right hemisphere than in the left.This results in a larger parietal and temporal area withinthe right hemisphere. It is reasonable to speculate that thisallows higher level integration of visual, auditory, and pro-prioceptive information in the more spatially orientedright hemisphere. From an anterior view, the frontal op-erculum (Broca’s area) of the right hemisphere has a largersurface area, whereas the surface area of the left hemi-sphere is more pronounced in the subcortical area. Thismay reflect differences in the language production abili-ties between the two hemispheres. If you remove the tophalf of the brain, allowing a view of the horizontal sec-tioning of the two hemispheres (see Figure 6.5), you caneasily examine the area of the temporal lobes. Within thesuperior temporal lobes is Heschl’s gyrus, and posteriorto that is the planum temporale. The Heschl’s gyrus (alsoknown as the primary auditory cortex) of the right hemi-sphere is often larger than that of the left hemisphere,since it frequently consists of two gyri. In the left hemi-sphere, the planum temporale is larger than that of theright hemisphere. The structural differences here may ac-count for the functional differences in auditory process-ing between the two hemispheres: Heschl’s gyrus mayhave greater functional responsibility for the nonspeechaspects of language (pitch, tone, melody) and musicalprocessing, whereas the planum temporale plays a largerrole in speech comprehension. In addition to visible struc-tural differences, there are also differences in neuronal ar-chitecture and neurochemistry, dependent on the side ofthe brain.
CHAPTER 6 | Cerebral Specialization 163
Morphology Left Hemisphere Right Hemisphere
Size Greater density Larger and heavier
Lobes Parieto-occipital Frontal protuberanceprotuberance
Frontal Frontal operculum Frontal operculum larger subcortical larger surface
Temporal Larger planum temporale Larger Heschl’s gyrus (often 2)
Parietal Larger area
Sylvian fissure Longer and more Steeper slopehorizontal slope
Table 6.1 Anatomic and Physiologic Brain Asymmetries

164 PART TWO | The Functioning Brain
The gray and white matter composition of the twohemispheres provides clues to the type of processing as-sociated with each hemisphere. The right hemisphere isheavier and contains more white matter than the lefthemisphere. In contrast, the left hemisphere is composedof greater gray matter and more modality-specific sen-sory cortices. The composition of the left hemispheresuggests that it is more suited for single-modality and in-traregion or within-region processing. A greater conver-gence of sensory regions is evident in the right hemi-sphere, signaling an increased representation ofassociation regions. The increased association regions ofthe right hemisphere allows for multimodal and inter-regional processing (e.g., the association of the visual rep-resentation of an apple with its tactile representation).Because of these anatomic differences, it is hypothesizedthat the left hemisphere is better suited for processing in-formation that is linear, sequential, rule-governed, orconforms to specific codes, such as language. In contrast,the right hemisphere appears more suited for holistic or
global processing of information; for example, determin-ing the orientation of one’s body in space (propriocep-tive) or the spatial configuration and orientation ofobjects requires holistic or simultaneous processing ofrepresentative sensory input.
Empirical and theoretic efforts to associate hemi-spheric dominance to function have focused primarilyon the content to be processed or the mental operationto be performed. Thus, differences in hemispheric domi-nance are generally associated with the type of content(e.g., verbal versus visuospatial), characteristics of thecontent (e.g., abstract versus concrete), or the mentalfunctions recruited (e.g., analytic versus holistic opera-tions). Based on a review of approximately 1000 studiesof cerebral lateralization, Dean and Reynolds (1997)have summarized the functions and contents that areconsidered to show lateralization (Table 6.2). However,none of these characterizations of hemispheric domi-nance fully accounts for the functioning of the hemi-spheres. For example, Gazzaniga’s (2000) research with
Figure 6.5 Brain hemisphere asymmetries. (a) The sylvian fissure on the right (bottom) has a steeper slope thanon the left. (b) View cutting through the top portion of the brain at the level of the temporal lobes. (Adapted from Kolb,B., & Wishaw, I. Q. [1996]. Fundamentals of human neuropsychology [4th ed., p. 181, Figure 9.1]. New York: W. H. Freemanand Company, by permission of Worth Publishers.)
b.a.
Sylvian fissure
Sylvian fissure
Heschl'sgyrus
Planumtemporale
Planumtemporale
Heschl'sgyri

split-brain individuals demonstrates that the processingof certain inputs (contents) shows greater associationwith one or the other hemisphere; yet, the hemispheresalso differ in their processing orientation. The righthemisphere appears to show superiority to the left in“veridical processing” (accuracy of information represen-tation), whereas the left tends to process informationfrom an elaborative or explanatory perspective (interpre-tation and hypothesis generating), regardless of whetherthe content is verbal, facial, or abstract-figural.
There is a tendency to view the operations of the hemi-spheres as “either/or,” rather than as overlapping or com-plementary operations. The involvement of the hemi-spheres in the processing of language exemplifies thismutual functioning. As discussed earlier, language is consid-ered lateralized to the left hemisphere; however, neuroimag-ing studies (Vouloumanos, Kiehl, Werker, & Liddle, 2001)indicate that both hemispheres generally activate when lan-guage is processed, suggesting that complementary opera-tions are necessary to support the comprehension andexpression of language. Furthermore, individual differencesin lateralization of functions are frequently encountered,
which argues against the rigid mapping of specific func-tions or processes to either the left or right hemisphere.
As you are aware, the brain is composed of two hemi-spheres that are interconnected by major pathways (e.g.,corpus callosum). What factors would account for the lat-eralization of brain functions, and what are the advan-tages of hemispheric specialization? Although definitiveanswers to these questions are not evident, several relatedspeculations have emerged. First, the efficiency and speedof processing would be improved if a hemisphere was spe-cialized for processing. For example, speech involves therapid sequencing of complex motor commands that maybe better served by a single hemisphere, rather than bytwo hemispheres that are spatially and temporally sepa-rate. In essence, keeping functions “within house” wouldhave an advantage over the “between-house” processingof two hemispheres. Of course, lateralization of a func-tion poses a significant disadvantage when the designatedhemisphere is damaged. The degree of loss would begreater after unilateral damage to the hemisphere support-ing the function than if the function was representedasymmetrically. With asymmetric representation, the un-damaged hemisphere continues to provide some degree ofsupport of the function.
A second, although a variant of the previous proposal,relates to the differences in the manner and mode of pro-cessing of the left and right hemispheres. These differ-ences could lead to competition or conflict if the twohemispheres shared equally in control of processing. Sup-port for this view is provided by neuroimaging studies ofchronic stutters that show the presence of bilateral hemi-spheric activation associated with speech. Training forthe amelioration of stuttering appears to be associatedwith increased left dominance for speech (Fox et al.,1996).
Third, lateralization of one set of functions within ahemisphere frees the other hemisphere to specialize in adifferent set of functions. Gazzaniga (2000) notes that,as humans have evolved, the need for greater corticalspace has increased. Lateralization of functions to sepa-rate hemispheres provides the needed cortical space andalso reduces redundancy of cortical regions. The pres-ence of the corpus callosum enables the lateralized brainfunctions to contribute to the entire cognitive system.The importance of adequate cortical space to supportfunction is illustrated by the neuropsychological perfor-mance of young children who have undergone the re-moval of the left hemisphere (hemispherectomy). Some ofthese children are able to develop right hemisphere lan-guage. Yet, there appears to be a cost to the reorganization,as evidenced in the disruption of functions considered
CHAPTER 6 | Cerebral Specialization 165
Modes/Contents: Modes/Contents: Right Hemisphere Left Hemisphere
Simultaneous Sequential
Holistic Temporal
Global Local
Visual/Nonverbal Verbal analytic
Spatial reasoning Speech lateralization/verbal abilities
Depth perception Calculation/arithmetic
Melodic perception Abstract verbal thought
Tactile perception Writing (composition)
Haptic perception Complex motor functions
Nonverbal sound recognition Body orientation
Motor integration Vigilance
Visual constructive performance Verbal paired-associates
Pattern recognition Short-term verbal recall
Nonverbal memory Abstract and concrete words
Face recognition Verbal mediation
Complex motor functions
Table 6.2 Lateralized Functions of the Leftand Right Hemispheres

166 PART TWO | The Functioning Brain
lateralized to the right hemisphere, namely, spatial pro-cessing. It has been hypothesized that the transfer oflanguage to the right hemisphere “crowds out” certainspatial functions (Anderson, Northam, Hendy, &Wrennall, 2001).
N E U R O P S Y C H O L O G I C A L A N D B E H A V I O R A LC E R E B R A L D I F F E R E N C E S
To understand the difference in styles between right andleft hemisphere processing, consider how you would ap-proach the following tasks: When asking for directions,do you prefer verbal instructions directing you to go threeblocks to the first stop sign, then turn left and proceedthree blocks, then take a right, and so on, or do you pre-fer a spatial map with directions marked on it? When youcomplete a puzzle, do you attempt to match individualfeatures or concentrate on the overall gestalt? When learn-ing or listening to music, are you more attuned to therhythm or the melody? In math, are you more adept withmathematical calculations and algebra or with geometry?In each of these cases, the first preference corresponds tothe verbal-sequential processing typically associated withthe left hemisphere, and the second to right hemispherespatial-holistic processing. The stereotype of “left-brained” or “right-brained” individuals has resulted fromthe oversimplified notion that one set of hemisphericskills will become dominant in a particular person. Per-haps you feel you use one style more than another. But ina normally functioning brain, all capabilities are used tosome degree, although they may be developed to differentdegrees. Sometimes the contributions of various hemi-spheric abilities are not even noticed until their loss ismade evident through brain damage or disease. Whenneuropsychologists discuss lateralization and dominance,the reference is to the division of labor for a particularskill in the brain, rather than the dominance of “braintraits” in any one person.
A number of behavioral differences are evident in thefunctioning of the two hemispheres. The correspondencebetween structural asymmetries and functional lateraliza-tion depends, in some measure, on the complexity of thebehavior. The more simple primary sensory and motorfunctions show specific patterns of representation in eachhemisphere. In general, except for smell and taste, sen-sory processing is funneled from the site of the sensorystimulation to the contralateral, or opposite, hemisphere.For example, the somatosensory strip of the parietal lobeof the left hemisphere processes objects placed in the righthand. The primary occipital cortices of the left and righthemispheres are involved in the processing of informa-
tion in the right and left visual fields, respectively. Thesetwo senses are completely crossed, because the neuraltracts project only to one hemisphere, opposite from thebody site of stimulation. Audition is only partiallycrossed. The left hemisphere processes the majority of in-formation presented to the right ear, whereas the righthemisphere processes a smaller portion of this auditoryinput. Olfactory information, which evolutionarily repre-sents a more primitive sense, projects to the same (ipsilat-eral) hemisphere from each nostril; the right nostril isprocessed via the right olfactory bulb. Similarly, eachhemisphere receives taste sensations from its respectiveside (ipsilateral) of the tongue. On the output side, theprimary motor strip of the contralateral hemisphere con-trols primary motor processing. Thus, for instance, themotor strip of the left hemisphere controls motor move-ments of the right hand.
Higher order processing is, by definition, integrativein nature, involving multiple mental computations.Depending on the nature of the integration required,more or fewer brain areas are involved. Some may residein the domain of a single hemisphere, and some may re-quire both sides of the cortex. Although neuropsychologistsrecognize the integrative nature of higher order skills,some abilities demonstrate greater lateralization than oth-ers. As a general way of conceptualizing the differencesbetween the hemispheres, the side that is dominant forverbal abilities (often the left) is usually more proficientin speech production and understanding. It is facile inmanipulating the symbols of language, such as letters,words, and numbers. Both hemispheres are comparablein processing sound, with the left hemisphere (temporalregion) responding selectively to meaningful language(Giraud & Price, 2001). Of interest, neuroimaging (PET)shows that communicative signing by congenitally andprofoundly deaf individuals recruits similar left hemi-sphere regions (left inferior and middle frontal, and supe-rior temporal gyrus) as individuals with normal hearingwhen processing language (Petitto et al., 2000).
The right hemisphere is more adept at processing themelodic, or prosodic, aspects of sound. Furthermore, theright hemisphere holds the advantage for visuospatialtransformations, analysis of complex visual patterns, andemotional processing. Regarding emotional processing,the right hemisphere is thought to be more adept at read-ing emotions when expressed as gestures, tonal inflections,and facial expressions. When the right hemisphere is dam-aged, patients often speak in a monotone, fail to under-stand the emotional expressions of others, miss the gist ofconversations, have problems expressing emotions nonver-bally and verbally, and are limited in their understanding

of humor and sarcasm (Beeman & Chiarello, 1998; Heil-man, 2002; Meyers, 1999). Moreover, the right hemi-sphere, particularly the prefrontal cortex, exhibits prefer-ential control of attentional functions such as arousal,sustained and selective attention, response inhibition, andself-monitoring. Although the left hemisphere is less in-volved in attentional functions, it does play a significant rolein divided attention (Anderson, Jacobs, & Harvey, 2005).
Sex Differencesand Hemispheric Specialization
Virtually every discipline of behavior has investigatedthe two sexes in an effort to identify and determine theorigin and nature of putative behavioral and psychologi-cal differences. Neuropsychology and related professionshave joined these efforts from the perspective of deter-mining whether the sexes show brain-behavior differ-ences. Although significant neuropsychological literatureexists concerning sex differences, these empirical studiesare inconsistent and often contradictory, precluding un-equivocal conclusions. A number of morphologic (weight,volume, size, and composition) and functional differenceshave been identified through neuroimaging, electrophysi-ologic measures, and autopsy. Examples of structural andfunctional studies are presented in Tables 6.3 and 6.4, re-spectively. The most consistent findings relate to hemi-spheric differences, particularly in the morphology and ac-tivation of left temporal regions associated with language,as well as the anterior cingulate, corpus callosum, andgray/white matter ratios. However, not all studies haveidentified significant or similar differences (Sommer,Aleman, Bouma, & Kahn, 2004). For example, as presentedin Table 6.3, Good et al. (2001) found that healthy maleparticipants presented greater leftward asymmetry of theplanum temporale than healthy female participants, whereasthe opposite finding was evident in a study by Knaus,Bollich, Corey, Lemen, & Foundas (2004). Method-ologic differences and weaknesses likely contribute to theinconsistencies in findings. The identification and con-trol of moderating variables (age, handedness, hormonallevels, task type, method of administration, and so forth)and improved standardization of and advances in neu-roimaging and related techniques should help determinewhether, and under what circumstances, the brains of fe-male and male individuals differ.
It has been proposed that men are more likely to showstrongly lateralized speech functions, whereas women aremore likely to demonstrate bilateral or right representa-tion of speech. This came to light when researchers noticed
that, after suffering a left hemisphere stroke, women wereless likely to suffer the language impairment seen in men(see Levy & Heller, 1992). Support for this proposition isprovided by an fMRI study (Shaywitz et al., 1995) of menand women while performing a rhyming task. Brain acti-vation during the rhyming task was found to be more bi-lateral in women than men. Specifically, males demon-strated activation of the left lateralized inferior frontalgyrus, whereas females exhibited bilateral activation inthis brain region. Similarly, a study (Saucier & Elias,2001) of the relation of hand gestures to speech revealedthat males made significantly more hand gestures with theright hand when speaking, yet when listening to conver-sation, demonstrated an increase in gesturing with the lefthand. Females, in contrast, did not demonstrate asymme-tries in gesturing during either speech or listening. Thesefindings suggest that males are more functionally lateral-ized in speech than females. However, several subsequentinvestigations have challenged these findings. Frost andcolleagues (1999) determined that males and females didnot differ in their activation patterns in an fMRI studyinvolving the performance of a language comprehensiontask. Similarly, Knecht and colleagues (2000a) presenteda word fluency task to 188 healthy right-handed male andfemale participants while undergoing fTCD. The perfor-mance of the two groups did not differ in word fluencyperformance. Of importance, the distribution of languagelateralization was equivalent for males and females. Fi-nally, a recent study (Boles, 2005) of the relation of sex toperformance on measures of lateralized cerebral functionsdemonstrates several significant differences, but these dif-ferences were small, accounting for less than 9% of sharedvariance (commonality of measurement). The investiga-tor concludes that sex differences on measures of lateralityare so small as to preclude the use of these measures forclinical prediction.
Empirical investigations reveal that females show su-periority in language abilities, whereas males demonstrategreater proficiency in visuospatial skills (Gur et al., 1999;Voyer, Voyer, & Bryden, 1995). Before reviewing thisissue, however, several caveats are in order. First, the supe-riority of the respective sexes with regard to verbal and vi-suospatial skills does not pertain to all forms of verbal orvisuospatial tasks. Second, the differences in performancereflect group data and are not large in magnitude. In fact,there is substantial overlap in the performance of the twogroups. Based on a recent review of studies of sex differences,Hyde (2005) concludes that the research indicates that thesexes are significantly more alike than different. Specifically,the differences between the sexes across multiple domains(cognitive, memory, motor, social, and personality) were, at
CHAPTER 6 | Cerebral Specialization 167

168 PART TWO | The Functioning Brain
best, small in approximately 80% of the studies reviewed.Third, sex differences may relate more to differences insociocultural expectations, socialization, and experientialhistory than to neurobiological factors.
Differences in cognitive performance favoring femaleindividuals include verbal fluency and perceptual speed(Halpern, 1992; Kimura, 1999), delayed verbal memoryand retrieval efficiency (Drake et al., 2000), mathematiccomputation (Eals & Silverman, 1994; James & Kimura,1997), episodic olfactory memory (Öberg, Larsson, &Bäckman, 2002), and fine-motor dexterity (Agnew, Bolla-Wison, Kawas, & Bleecker, 1988). Females further excel inone form of spatial memory that involves the encoding and
retrieval of object location. However, the latter superiorityhas been related to the greater verbal facility of females,rather than to their spatial ability (Postma, Izendoorn,& De Haan, 1998). Conversely, males show an advantagewith tasks that involve mental rotation and spatial per-ception (Burton, Henninger, & Hafetz, 2005; Siegel-Hinson & McKeever, 2002), mathematic aptitude, mapreading, aiming at and tracking objects, geographic knowl-edge (Kolb & Whishaw, 1996), and three-dimensionalmaze performance (Grön et al., 2000; Kimura, 1999;Roberts & Bell, 2003). Voyer et al. (1995) performed ameta-analysis of 286 empirical studies that involved spatialabilities and sex differences. The findings of the analysis
Table 6.3 Comparisons of Female and Male Brain Structures
Sex Investigations
Female Smaller overall brain size (Kolb &Whishaw, 1996)
Higher percentage of overall graymatter; distribution of white matterand cerebrospinal fluid (CSF)symmetric for the hemispheres (Guret al., 1999)
Increased gray matter volumeadjacent to the depths of bothcentral sulci and in the left superiortemporal sulci, right Heschl’s gyrusand planum temporale, right inferiorfrontal and frontomarginal gyri, andcingulate gyrus (Good et al., 2001)
Leftward asymmetry of the planumtemporale (Knaus et al., 2004)
Greater density of neuronal materialin the left planum temporale(Witelson, Glezer, & Kigar, 1995)
Larger volume of gray matter in thedorsolateral prefrontal cortex andsuperior temporal gyrus (Schlaepferet al., 1995)
Greater cingulate sulcus volume(Paus et al., 1996)
Proportionally larger Broca andWernicke areas (Harasty, Double,Halliday, Kril, & McRitchie, 1997)
Larger isthmus of the corpuscallosum (Steinmetz et al., 1992)
Larger corpus callosum (Dubb, Gur,Avants, & Gee, 2003; Steinmetz etal., 1995)
Larger splenium of the corpuscallosum with increasing size withage (Dubb et al., 2003)
Increased volume of the hippocam-pus across childhood and adoles-cent development (Giedd, Castel-lanos, Rajapakse, Vaituzis, &Rapoport, 1997)
Male Higher percentage of overall whitematter and CSF; higher percentageof gray matter in left hemisphere,white matter symmetric, and greaterpercentage of CSF in the righthemisphere (Gur et al., 1999)
Increased leftward asymmetry inthe Heschl’s gyrus and planumtemporale; greater gray mattervolume, bilaterally in the mesialtemporal lobes, entorhinal andperirhinal cortex, and anterior lobesof the cerebellum (Good et al.,2001)
Symmetry of the planum temporale(Knaus et al., 2004)
Thicker cortex, higher neuronaldensity, and increased neurons inthe left temporal lobe (Rabinowics,Dean, Petetot, & de Courten-Meyers, 1999)
Greater hippocampal dendriticreduction in male rats with aging(Markham, McKian, Stroup, &Juraska, 2004)
Greater paracingulate sulcusvolume (Paus et al., 1996)
Greater asymmetry (L > R) of theanterior cingulate due to increasedfissurization (Yücel et al., 2001)
Larger genu and decreasing genusize with age (Dubb et al., 2003)
Increased volume of the lateralventricles and amygdala acrosschildhood and adolescent develop-ment (Giedd et al., 1997)
Longer corpus callosum anddecrease in width of the trunk andgenu of corpus callosum with age(Suganthy et al., 2003)

were as follows: males showed significantly greater profi-ciency relative to the performance of females with tasksthat involve mental rotation (ability to mentally rotatetwo- or three-dimensional figures quickly and accurately)and spatial perception (ability to determine spatial rela-tions despite the presence of distracting information).Further analysis demonstrated that sex differences gener-ally did not emerge until after 13 years of age, and themagnitude of sex differences in mental rotation and spa-tial perception increased with age. Of significance, sex dif-ferences were evident on only certain measures of mentalrotation and spatial perception, suggesting that (1) spatial
ability is not a unitary concept, but rather represents agroup of relatively distinct component skills; and (2) malesdo not demonstrate an advantage across all tasks that in-volve spatial abilities.
A number of studies have endeavored to determinewhether men and women recruit different brain circuitryduring spatial processing (Voyer et al., 1995). Illustratingthis research is a neuroimaging (fMRI) study by Grön andcolleagues (2000) that determined a significant overlap inthe neural circuitry activated while performing mazes, withexclusive activation in the left parahippocampal gyrus andleft hippocampus proper for males, and in the left superior
CHAPTER 6 | Cerebral Specialization 169
Table 6.4 Neuroimaging and Electrophysiologic Comparisons of Male and Female Brains
Sex Investigations
Female fMRI: Bilateral activation of theinferior frontal gyrus (rhyming task)(Shaywitz et al., 1995)
MRI: Bilateral activation of thesuperior and middle temporal gyri(linguistic listening) (Kansaku,Yamaura, & Kitazawa, 2000)
fMRI: Greater activation of the leftsuperior frontal gyrus and the rightmedial frontal gyrus, and rightprefrontal cortex, right inferior andsuperior parietal lobe (mazes)(Grön, Wunderlich, Spitzer, Tomczak, & Riepe, 2000)
fMRI: Greater activation of the leftventral premotor cortex (handsmental rotation) (Seurinck, Vinger-hoets, de Lange, & Achten, 2004)
PET: Greater activation of the rightinferior frontal gyrus and rightprecentral cortex (concrete nam-ing/face orientation) (Grabowski,Damasio, Eichhorn, & Tranel, 2003)
fMRI: Predominately left-sidedactivation (visual discriminationand construction tasks) (Georgopoulos et al., 2001)
EEG: Greater right parietal activa-tion than left (two-dimensionalmental rotation); greater rightparietal activation than left (three-dimensional mental rotation)(Roberts & Bell, 2003)
PET: Enhanced activation of the leftamygdala (emotional memory)(Cahill et al., 2001)
PET: Symmetric dorsal premotoractivation (tactile discrimination)(Sadato, Ibañez, Deiber, & Hallett,2000)
fMRI: Greater in the orbitofrontallobe in response to both happy andsad, relative to neutral, faces (Amin,Constable, & Canli, 2005)
Male fMRI: Activation of the left lateral-ized inferior frontal gyrus (rhymingtask) (Shaywitz et al., 1995)
MRI: Left activation of the superiorand middle temporal gyri (linguisticlistening) (Kansaku et al., 2000)
fMRI: Greater activation of the leftparahippocampal gyrus and lefthippocampus proper and righthippocampal gyrus and left poste-rior cingulate (mazes) (Grön et al.,2000)
fMRI: Greater activation of thelingual gyrus (hands mental rota-tion) (Seurinck, et al., 2004)
PET: Greater activation of leftinferotemporal regions and otherleft hemisphere regions (concretenaming/face orientation)(Grabowski et al., 2003)
fMRI: Primarily right hemisphereactivation (visual discriminationand construction tasks) (Georgopoulos et al., 2001)
fTCD: Comparable hemisphericactivation to females (word fluencytask) (Knecht, Deppe, Dräger,Bobe, Lohmann, Flöel, et al.,2000)
EEG: Greater left parietal activationthan right activation (two-dimensional mental rotation);greater right parietal activation thanleft (three-dimensional mentalrotation) (Roberts & Bell, 2003)
PET: Enhanced activation of theright amygdala (emotional memory)(Cahill et al., 2001)
fMRI: Greater activation in bilateralparietal to fearful, relative toneutral, faces (Amin et al., 2005)
fMRI: Comparable hemisphericactivation to males (languagecomprehension task) (Frost et al.,1999)
Note: fMRI = functional magnetic resonance imaging; PET = positron emission tomography; fTCD = Doppler-ultrasonography; EEG = electroencephalography.

170 PART TWO | The Functioning Brain
frontal gyrus and the right medial frontal gyrus for females.In addition, males showed greater activation of the righthippocampal gyrus and left posterior cingulate, as com-pared to females who demonstrated increased activity ofthe right prefrontal cortex, right inferior and superior pari-etal lobe. Finally, males were more proficient than femalesin solving the mazes. While males and females appear touse different neural circuitry during maze performance, thisdoes not rule out the possibility that other factors (for ex-ample, experiential history with spatial activities) may ac-count for the greater facility of males in maze performance.
A variety of explanations for the sex differences in spa-tial processing, particularly mental rotation, have been pro-posed. One explanation, consistent with our discussion,relates the male advantage in spatial processing to thegreater specialization of this function to the right hemi-sphere. A second proposal is that men have more experi-ence in spatial processing by virtue of socialization and roleexpectations. In a relatively recent lateralized tachistoscopicstudy (Siegal-Hinson & McKeever, 2002), males werefound to be more right hemisphere specialized (left visualfield superiority) and to have greater previous spatial activ-ity experience than females. The magnitude of right hemi-sphere specialization correlated significantly and positivelywith mental rotation ability. Further analysis determinedthat sex differences in spatial ability were primarily relatedto right hemisphere specialization, and experiences withspatial activity were of only secondary importance. Thus,experience with spatial activities was not supported as a pri-mary determinant of the difference in performance of thesexes. However, other lateralized tachistoscopic studies havenot identified male-related visual field superiority in spatialprocessing (Siegal-Hinson & McKeever, 2002), highlight-ing the current contradictions in this area of study.
Women have been found to work more carefully thanmen when performing mental rotation tasks, suggestingthat time may be a factor influencing overall performance(Voyer, 1997). Yet, when females and males were presenteda mental rotation task without time constraints (Voyer,Rodgers, & McCormick, 2004), males once again showedan overall advantage in performance. Thus, behavioralstyle (careful, time-consuming approach) did not accountfor the difference in mental rotation performance. Spatialexperiences and stylistic approach are but two of severalfactors that could account for sex differences in spatial per-formance. A multitude of social and cultural influencesshape and maintain sex differences. Unfortunately, the ul-timate impact of these sociocultural influences on sex arecomplex, often subtle, and not fully understood.
Adding to the complexity of determining whether sexdifferences exist in neuropsychological functioning is the
realization that task variations can prompt the recruit-ment of different neural circuits. For example, mental ro-tation of two-dimensional figures appears to recruit moreright parietal activation than left activation for females.The opposite pattern (left > right parietal activation) isevident for males. Yet, with three-dimensional figures,greater right parietal activation is evident for both malesand females (Roberts & Bell, 2003). Further exemplify-ing the effects of task differences on level of performanceand recruited neural processes is a recent fMRI study(Seurinck, Vingerhoets, de Lange, & Achten, 2004) thatcompares the performance of male and female healthyvolunteers in the mental rotation of tasks that involvehands and tools. The neuroimaging findings of the par-ticipants with comparable levels of mental rotation per-formance demonstrated that both sexes activated a com-mon neural substrate (superior parietal lobe, dorsolateralpremotor cortex, and extrastriate occipital regions). How-ever, activation differences were evident in the mental ro-tation of hands, with females showing greater involvementof the left ventral premotor cortex and males demonstrat-ing greater activation of the lingual gyrus. These, as wellas other studies, demonstrate the effects that task varia-tions might have on neuropsychological performanceboth across and between the sexes. Moreover, task varia-tions may contribute to the failure of investigators to repli-cate results and likely account for contradictory findings.
Although a number of studies report that females showgreater facility with verbal skills, particularly verbal flu-ency, conflicting studies are also evident. Similar to thefindings with spatial tasks, different verbal tasks may re-cruit different neural substrates for males and females. Forexample, men and women were asked to name concreteaspects of visually presented objects and perform a face ori-entation decision task while undergoing PET (Grabowskiet al., 2003). Males showed greater activation of the leftinferotemporal and other left hemisphere regions thanfemales. In contrast, females demonstrated greater activa-tion of the right inferior frontal gyrus and right precen-tral cortex, as compared to males who evidenced less acti-vation or actual deactivation of these regions. Thesedifferences suggest that men and women use differentstrategies in processing similar contents.
Increasingly, empirical efforts to control variables thatmay account for differences in sex-related neuropsycholog-ical performance are evident, as illustrated in Georgopou-los and colleagues’ (2001) study. Men and women werepresented two visual tasks: one task required visual discrim-ination and another required visual object construction.The same visual stimuli were used for both tasks, thus re-ducing the likelihood that task differences accounted for

performance. The visual discrimination task required theparticipants to judge whether pairs of square fragmentswere the same or different, whereas the visual object con-struction task required a determination of whether squarefragments, when visually assembled and related, wouldmake a “perfect square.” Blood oxygen level–dependent(BOLD) fMRI did not show differences in left versus righthemispheric activation for the sexes when performing thevisual discrimination task. However, the sexes did differwith respect to the visual object construction task, with fe-males showing predominately left-sided activation, andmales exhibiting both left and right hemisphere activation.The finding of increased right hemisphere activation wasspecific to the performance of men. The difference in per-formance between males and females could not be attrib-uted to the features of the task employed, and thus reflectedthe cognitive operations recruited. That is, the two sexesappeared to utilize different cognitive strategies to solve thevisual constructive tasks.
Sex differences have also been presented for emotional-ity. Wager, Phan, Liberzon, and Taylor (2003) conducteda meta-analysis of 65 neuroimaging studies related to sex,emotions, lateralization, and other relevant variables.These results indicate that the relationship between sex,brain activation, and emotional responses is much morecomplex than originally believed. Both sexes showed simi-lar lateralized activation patterns for emotion, althoughmen showed these patterns to a greater degree. Differencesin neural activation by sex were most evident at the re-gional, rather than the hemispheric, level. At the regionallevel, the sexes recruited relatively distinct but overlappingareas, with some regions lateralized left and others right.When processing emotions, males activated the left infe-rior frontal cortex and posterior cortex, and females morereliably involved the midline limbic regions, including thesubcallosal anterior cingulate, thalamus, midbrain, andcerebellum. Moreover, females showed left involvement inregions surrounding the amygdala (sublenticular nuclei),and males activated right-sided regions near the hippocam-pus. Based on these findings, Wager and colleagues specu-late that males may be more biased toward processing thesensory aspects of emotional stimuli with regard to action,whereas females direct more attention to the subjective ex-perience of emotion or, alternatively, show greater overtresponse to emotion. Finally, whether these regional andlateralized sex differences relate to actual or meaningfulbehavioral differences awaits further study.
The impact of sociocultural opportunities, resources,expectations, and attitudes regarding sex differences cannotbe underestimated. For example, greater facility with math-ematics has been attributed to males relative to females.
Although some have maintained that this greater facilityis sex determined, Neuropsychology in Action 6.2 clearlychallenges this supposition.
In summary, there are indications that females showan advantage in verbal abilities, while males tend todemonstrate superiority in visuospatial ability, particu-larly related to mental rotation tasks. However, these dif-ferences are not uniformly supported, and sex differencesmay be a consequence of sociocultural rather than neuro-biological influences, or the interaction of these factors.Finally, differences in emotional processing are evidentfor males and females that do not conform to a simple leftor right hemispheric specialization.
S E X U A L H O R M O N E S
Because of the pervasive effects of sex hormones on devel-opment and functioning, investigations have sought todetermine whether hormonal influences relate to sex dif-ferences in neuropsychological functioning. Much of thisfocus has been on the reproductive hormones (androgenand ovarian). An androgen hormone refers to any steroidhormone with a “masculinizing” effect. Up to 95% of an-drogens are produced by the testes. The principal func-tions of the androgen hormones include the masculiniza-tion of the fetus, production of sperm, and developmentof secondary sexual characteristics. The ovarian hormones(estrogens and progestins) are primarily secreted by theovaries. These hormones are responsible for the in utero“feminization” of the brain, regulation of the ovarian-reproductive cycle, secondary sexual characteristics, andmenopause. Sex hormones are believed to have both anorganizing and activating effect. The organization effectrelates to the effects of early exposure to hormones duringprenatal development, whereas the activation effect refersto the effects of hormones during later development; thatis, prenatal exposure to hormones organizes the way be-havior is activated by hormones later in development. Themasculinization and feminization of the prenatal brainexemplifies the organizing effects of sex hormones, whilethe physical and psychological changes associated withpuberty and menstruation illustrate the activating effects.Notably, male and female hormones are not restricted toeither sex in that both sexes produce androgen and ovarianhormones. Sex differences are evident in the hormonal-induced organization of the brain and the ratio of male-to-female circulating hormones in the respective sexes.
Efforts to determine whether reproductive hormonesaccount for visuospatial sex differences have involvedstudies of healthy individuals, individuals with develop-mental abnormalities affecting hormone levels, and those
CHAPTER 6 | Cerebral Specialization 171

172 PART TWO | The Functioning Brain
with surgically induced or naturally occurring reductionsin hormone levels (Erlanger, Kutner, & Jacobs, 1999). Stud-ies of healthy subjects show a possible inverted U-shapedcurve regarding the effects of androgens on spatial perfor-mance (Moffat & Hampson, 1996); that is, a positive
correlation is evident between testosterone levels and spa-tial task performance for females, but a negative correla-tion exists for males. Thus, males with elevated levels oftestosterone exhibit poorer spatial performance, whereasfemales with increased levels demonstrate enhanced
Text not available due to copyright restrictions

spatial performance. Additional investigations withhealthy participants indicate that average, not extreme,levels of testosterone relate to optimal spatial perfor-mance; that is, high levels of testosterone for males andlow levels for females are each associated with reducedspatial performance (McCormick & Teillon, 2001). Simi-larly, transsexuals undergoing cross-sex hormonal treat-ment also demonstrate differences in spatial performance.Individuals moving from a male to female gender demon-strate decreased spatial performance when administeredantiandrogens and estrogen, whereas those moving froma female to male gender demonstrate improved spatialperformance when treated with testosterone supplements(van Goozen, 1994; van Goozen, Cohen-Kettenis,Gooren, Frijda, & Van de Poll, 1995). Overall, these find-ings suggest that increased levels of male androgens en-hance the spatial performance of females, but have a “de-masculinizing” effect on male spatial performance. Notably,however, male androgens are not the only hormones thateffect spatial performance. For example, higher levels ofestrogen are associated with poorer spatial performance(Jones, Braithwaite, & Healy, 2003). Young women regu-larly taking oral contraceptives have near postmenopausallevels of estradiol and also perform more poorly on somespatial tasks than women not taking oral contraceptives(Mohn, Spiers, & Sakamoto, 2005).
The circulating levels of both male and female hormoneswarrant consideration when sex differences are the subject ofinvestigation. For example, one study (Drake et al., 2000)demonstrated that sex hormones may affect cognitiveabilities in a differential manner. In this study, the estro-gen, progesterone, androstenedione (natural hormonethat is a direct precursor to testosterone), and testosteronecirculating levels of healthy elderly women were comparedwith measures of neurocognitive functioning. The resultsshowed that high levels of estrogen were associated withbetter delayed verbal memory and retrieval, whereas lowlevels were correlated with better immediate and delayedvisual memory. Interestingly, testosterone levels were pos-itively associated with verbal fluency, but levels of proges-terone and androstenedione did not have any relationshipto cognitive performance.
In addition, circulating levels of female hormones mayinteract with brain organization. For example, as dis-cussed earlier, right-handers are largely considered lefthemisphere dominant for speech; however, sex may influ-ence bilateral expression of speech or other abilities. Itmay also be that other brain organizing factors, such asdegree of left-handedness in the family, termed familialsinistrality, may interact with the sexual organization ofthe brain. It has been suggested that right-handed women
with left-handed relatives (that is, familial sinistrals [FS�]women) may have shifted brain organization away fromthe “female” preference for high reliance on verbal strate-gies and toward more male strategies (Annett, 1985,2002). This has been supported in investigations of spa-tial performance on the Rey Complex Figure test (Rey,1941, translated by Corwin & Bylsma, 1993), where fa-milial sinistrality accounted for performance and strategyregardless of academic major, with FS� women perform-ing as well or better than men (D’Andrea & Spiers,2005a, 2005b). These investigators also report that acrossa range of spatial, verbal, and speeded motor tasks, famil-ial sinistrality interacted with the menstrual cycle suchthat FS� women performed better on all tasks duringmenses when ovarian hormone levels were low, whereaswomen without the hypothesized shift (FS� women)performed better on all tasks close to ovulation whenovarian levels were high (D’Andrea & Spiers, 2005a)
These various findings highlight the complexity of therelation of sex hormones to the performance of the sexes.Increasingly, we are realizing that the variables that inter-act with sex hormones and gender are multiple and notfully understood. Illustrating this issue is a relatively re-cent investigation (van Goozen, Gooren, Slabbekoorn,Sanders, & Cohen-Kettenis, 2002) in which individualsundergoing transsexual hormonal treatment did notdemonstrate the predicted shift in spatial performance.Previous studies have frequently used “mixed” transsexualgroups composed of right- and left-handed transsexualswho were either homosexual or heterosexual. In vanGoozen and colleagues’ study, the spatial performance ofonly right-handed, homosexual transsexuals was con-trasted with the performance of heterosexual participants.The transitioning transsexuals were treated with the ap-propriate sex hormone supplements and pretested andpost-tested with a battery of spatial measures. Post-testingwas undertaken 3 months after the sex hormone treat-ment. Results regarding levels of pretest and post-test spa-tial performance were as follows: heterosexual male con-trol participants showed a higher level of performancethan homosexual males transitioning to female gender,who, in turn, demonstrated greater proficiency than ho-mosexual females transitioning to male gender. Hetero-sexual female control participants achieved significantlylower scores than the previous three groups. Pretesting topost-testing did not demonstrate a significant effect of sexhormone treatment on spatial performance. The authorsspeculate that the failure to find the predicted effect mayhave been due to the unique composition of the transsex-ual group. They note that previous investigations havesuggested that homosexual transsexuals are biologically
CHAPTER 6 | Cerebral Specialization 173

174 PART TWO | The Functioning Brain
more similar to their desired sex, and their spatial perfor-mance tends to be similar to the opposite sex. Accord-ingly, their level of spatial performance would moreclosely approximate the opposite sex before sex hormonetreatment; thus, the degree or magnitude of possiblechange in performance would be limited (“ceiling effect”)after the introduction of sex hormones. Second, the au-thors report that left-handed individuals are more sensi-tive to neuroendocrinologic interventions, and the omis-sion of this group may have accounted for the failure tofind an activating effect of sex hormone treatment. Al-though replication and expansion of this study is war-ranted, it serves to capture the difficulty of disentanglingthe effects of sex hormones on gender performance.
Investigations of individuals with developmental disor-ders that affect reproductive hormones have identified simi-lar relations between androgen levels and visuospatial per-formance. For example, individuals with congenital adrenalhyperplasia (CAH; an endocrine disorder of prenatal origincharacterized by excessively high levels of androgen hor-mones) have been the subject of research. Hampson and col-leagues (1998) compared the visuospatial performance ofpreadolescent girls with CAH to unaffected control partici-pants and found that the visuospatial performance of theCAH group was significantly higher. In the same study, boyswith CAH hyperplasia showed lower visuospatial proficiencyrelative to the performance of unaffected control boys. In asimilar vein, individuals with androgen insensitivity (ge-netic males who produce androgens but whose androgen re-ceptors are not responsive to the hormone) demonstratelower performance relative to verbal intelligence when con-trasted with male and female control participants (Imperato-McGinley, Pichardo, Gautier, Voyer, & Bryden, 1991). Themeasure of performance intelligence involved tasks requir-ing visual, visuospatial, and visuomotor abilities.
For verbal abilities, a number of studies demonstratethat women, during the high-estrogen phase of their men-strual cycle, demonstrate enhanced cognitive skills in colornaming and color reading, mental flexibility, and paired-associate learning (see Erlanger et al., 1999 for review). Acomparison (Phillips & Sherwin, 1992) of the cognitive per-formance of women before and after hysterectomies whoreceived either an estrogen supplement or a placebo revealedthat the women who maintained their presurgical estrogenlevels demonstrated comparable memory recall (paragraphrecall). In contrast, those in the postsurgery placebo groupexhibited a significant decline in memory performance. Asimilar decrement in memory performance has been docu-mented in women who have been administered estrogen-suppressing agents (Sherwin & Tulandi, 1996). Shaywitzand associates (1999) investigated the fMRI activation pat-
terns of postmenopausal females when tested with tasks ofverbal and nonverbal memory. One group was treated for21 days with estrogen, and the second group received aplacebo. The estrogen-treated group showed greater lefthemisphere activation during encoding and increased acti-vation in the right frontal superior frontal gyrus during re-trieval. Increased activation of the inferior parietal lobe wasevident during storage of verbal information, and deceasedactivation of the inferior parietal lobe was observed duringthe storage of nonverbal information. Interestingly, the twogroups, despite their differences in regional activation, per-formed in a comparable manner on the measures of verbaland nonverbal memory. A number of studies (see Cameron’s[2001] review) have failed to support the enhancing effectsof hormone replacement therapy on cognitive performance.The mixed results suggest that certain hormone regimensmay have an enhancing (although subtle) effect on specificcognitive and memory processes.
Cognitive concerns are frequently voiced by womengoing through menopause. When the ovaries stop produc-ing estrogen, only estrone (a weaker sex hormone producedby the adrenal glands) remains. Initially, it was believed thatthe risk for stroke, heart disease, vascular dementia, and os-teoporosis were associated with decreased estrogen produc-tion. Although estrogen augmentation has been associatedwith improved cognitive performance in menopausalwomen, particularly in the area of verbal memory, otherstudies have provided contradictory results. A meta-analysisof studies (Yaffe, Sawaya, Lieberburg, & Grady, 1998) sug-gests that improved cognitive performance is evident onlyin women receiving estrogen therapy who were recentlymenopausal. More disturbing have been recent large-scalestudies (Nelson, Humphrey, Nygren, Teutsch, & Allan,2002; Shumaker et al., 2003, 2004; Wassertheil-Smolleret al., 2003) demonstrating that estrogen therapy for post-menopausal females may increase the risk for stroke, throm-boembolic events, breast cancer (with 5 or more years ofuse), and cholecystitis (inflammation of the gall bladder).An increased risk for dementia appears to be evident forwomen 65 years or older (Espeland et al., 2004). Related tothe latter finding, a recent study (Erickson et al., 2005) ofelderly women who were maintained on estrogen treatmentfor up to 10 years demonstrated spared gray matter in thefrontal cortex and increased performance on measures ofexecutive function. In contrast, elderly women who contin-ued estrogen treatment beyond 10 years exhibited increasedprefrontal deterioration and a greater rate of decline on themeasures of executive function. Currently, the increases inphysical and cognitive risk associated with prolonged estro-gen therapy in postmenopausal women appear to over-ridethe modest gains initially evident in cognitive functioning.

CHAPTER 6 | Cerebral Specialization 175
Cerebral hemispheresFissuresFrontal lobesParietal lobesTemporal lobesOccipital lobesLateral fissureCentral sulcus
Occipital notchBrodmann’s areasSomatosensory cortexPrimary motor cortexAssociation or polymodal areasWada testHemispheric asymmetryLateralization
DominanceDoppler ultrasonography
(fTCD)Sylvian fissureHeschl’s gyrusPlanum temporaleMeta-analysisMental rotation
Spatial perceptionSubcallosal anterior cingulateSublenticular nucleiAndrogen hormoneFamilial sinistralityCongenital adrenal
hyperplasiaAndrogen insensitivity
the participants. Notably, similar neural substrates areoften implicated in the cognitive processing of thesexes, and identified differences are often more of de-gree than type. In addition, differences in activated orrecruited neural substrates do not necessarily translateinto observable or meaningful differences in cognitiveperformance.
Overall, sex hormones appear to have an organizingand activating effect on brain development and func-tioning. Studies of varied gender groups show that sexhormones have either an enhancing or depressing effecton cognitive performance depending on such factors asthe levels of circulating hormones, the specific sex hor-mone manipulated, type of task introduced, and age of
SummaryIn this chapter, we examined the major structures and functions of the cortex, setting the stage for examiningthe systematic interaction of brain regions (cortical and subcortical) that support the complex behaviors thatare presented in subsequent chapters. Hemispheric differences exist, but they are not consistent with thesimple notion that people are either “right-brained” or “left-brained” in their behavior. Generally, the brainfunctions as a cohesive whole with interconnected pathways and regions performing both distinct andoverlapping functions. However, certain functions, such as speech, tend to be lateralized to one hemisphereor the other. Lateralization does not imply that the other hemisphere is not providing a complementaryfunction. For example, the left hemisphere is generally specialized for verbal speech, whereas the righthemisphere plays an equally important role in providing the prosodic aspects to speech.
Sex differences in the performance of neuropsychological tasks are evident, although the sexes over-lap in their performance and the actual differences are small. Morphologic and functional brain differenceshave been identified; however, there is a lack of empirical consensus. Because of the organizing and acti-vating influence of sex hormones, the relation of these hormones to neuropsychological performance hasbeen the subject of considerable investigation. Androgens appear to have an enhancing effect on visuospa-tial performance, whereas the bolstering effect of estrogen on verbal performance has received less sup-port. Certainly, the relation of sex hormones to neuropsychological performance is complex, and additionalstudies are warranted to identify the factors that mediate this relation.
C r i t i c a l T h i n k i n g Q u e s t i o n s
How would you explain the functional differences between the right and left hemispheres?Are there adaptive reasons why the cerebral hemispheres would gravitate toward either a bilateral or asymmetric organi-zation? Explain.What ecologic or evolutionary factors could account for the advantage of males in visuospatial abilities?
K e y Te r m s
We b C o n n e c t i o n s
Neuroanatomy
http://www.med.harvard.edu/AANLIB/hms1.html
Chapter 7
SOMATOSENSORY, CHEMICAL, AND MOTOR SYSTEMS
[W]e naturally came into conflict both with the naive mechanistic ideas oflocalization, in which mental functions are consigned to rigidly demarcatedareas of the brain, and with the idealistic concept that the higher mentalprocesses stand quite apart from the biological functions of the brain orresult from the indivisible activity of the “brain as a whole.”
—Alexander Luria
Somatosensory ProcessingChemical SensesMotor Systems
Neuropsychology in Action
7.1 Synesthesia: Melded Sensory Integration7.2 Phantoms of Feeling7.3 Tourette Syndrome: Too Much Behavior

CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 177
K e e p i n M i n d
How does the brain map incoming sensory information?
Is sensory information processed in the same manner by each system?
What happens when brain alteration causes malfunctions of ordinary experiences of perception?
OverviewA functional system is a circumscribed area of behavior that corresponds to a specific neuroanatomic path-way or network of pathways. Some systems are well defined and traceable, and others remain incompletelymapped. The sensory systems are among the most well delineated.
At times tracing systems through the brain may appear mechanistic, like the “leg bone connected tothe thigh bone” routine. Scientists have gained their current understanding of the brain by identifying indi-vidual functions and attempting to map them to structure hierarchically, from lower to higher order func-tions. However, many structures participate in multiple functions. A complex internetworking of functions isevident in the progression from the sensory and motor systems to higher functional systems where the workinvolves anatomic networks that are sometimes widely dispersed throughout the brain.
The brain is a dynamic biological network, but a small lesion in a strategic location can have devastat-ing effects on the system. It is therefore impossible to gain a thorough understanding of sensory and motorsystems by studying only intact brains. Russian psychologist Alexander Luria, whose pioneering work madepossible our understanding of functional brain systems, has argued that although higher mental functionsmay be disturbed by a lesion in any of the many different links of the system, they are disturbed differently bylesions in different links (Luria, 1966). Luria’s research profited greatly from his keen observations of neuro-logic patients. He noticed that anatomically different lesions were possible within the same behavioral syn-drome. He also noticed that a lesion in one area could affect a number of different behaviors.
The functional systems we focus on in this chapter may be broadly categorized as arising from sensoryinput and resulting in motor output. This chapter focuses on the somatosensory and motor systems, as wellas the chemical senses of taste and smell. In the next chapter, we examine the visual and auditory systems.We concentrate on how each system operates at the level of central brain mechanisms. Most sensory sys-tems are anatomically mapped to specific cortical areas devoted to primary sensory processing, whichprovide information that is then routed to secondary processing areas where it is “perceived” and meaningis attached. All sensory systems except smell follow a pathway through the thalamus, where they are di-rected to primary and secondary cortical processing areas (Figure 7.1). This chapter examines how eachsystem functions at the level of the brain, and what can happen when behavior goes awry because of injuryor disease. In general, we discuss disorders that illustrate a specific breakdown of a system rather thanbroad-based disorders. Also, the odd phenomenon of synesthesia is presented as an interesting possibleevolutionary mutation (Neuropsychology in Action 7.1). (We discuss disorders that involve multiple systemsin later chapters.)
Sensation is the body’s window to the world. The rangeof what humans can detect is unique to our species andbecomes the raw material of our perceptions and the stuffof our experiences. Information comes in fragments andrequires the central processor of the brain to literally “makesense” of the outside environment. Sensation begins with
the process of transduction (derived from the Latin trans-ducere, meaning to “lead across”). An environmental stim-ulus activates a specific receptor cell, creating energy,which is transduced into an electrical stimulus that is thencarried to neurons for the brain to process. (Receptor cellsare not technically neurons, although they do synapse with
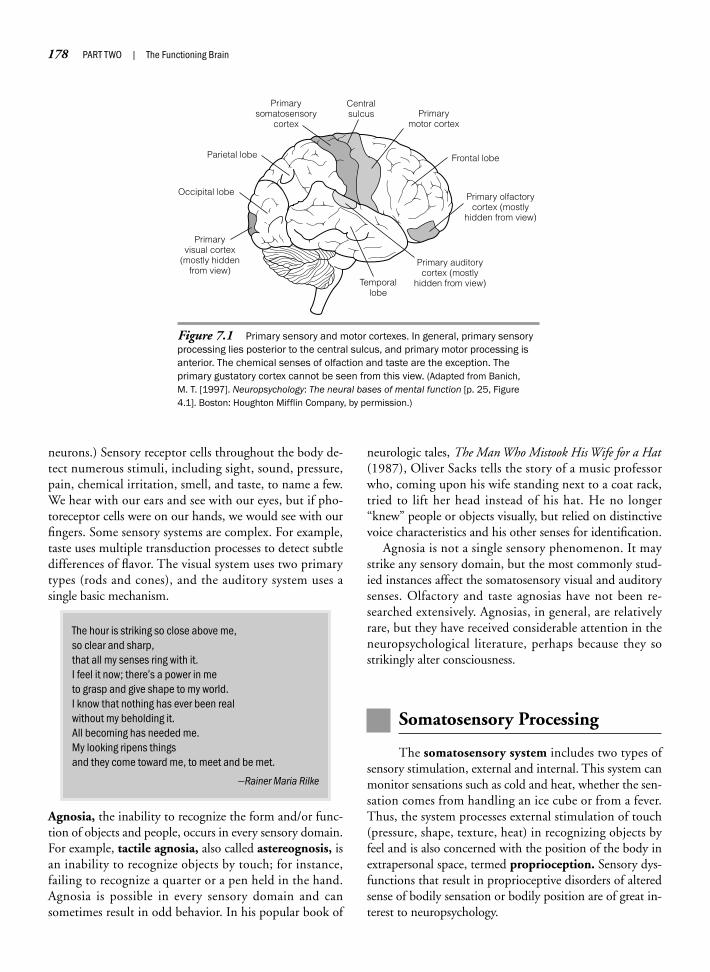
178 PART TWO | The Functioning Brain
neurons.) Sensory receptor cells throughout the body de-tect numerous stimuli, including sight, sound, pressure,pain, chemical irritation, smell, and taste, to name a few.We hear with our ears and see with our eyes, but if pho-toreceptor cells were on our hands, we would see with ourfingers. Some sensory systems are complex. For example,taste uses multiple transduction processes to detect subtledifferences of flavor. The visual system uses two primarytypes (rods and cones), and the auditory system uses asingle basic mechanism.
The hour is striking so close above me,so clear and sharp,that all my senses ring with it.I feel it now; there’s a power in meto grasp and give shape to my world.I know that nothing has ever been realwithout my beholding it.All becoming has needed me.My looking ripens thingsand they come toward me, to meet and be met.
—Rainer Maria Rilke
Agnosia, the inability to recognize the form and/or func-tion of objects and people, occurs in every sensory domain.For example, tactile agnosia, also called astereognosis, isan inability to recognize objects by touch; for instance,failing to recognize a quarter or a pen held in the hand.Agnosia is possible in every sensory domain and cansometimes result in odd behavior. In his popular book of
neurologic tales, The Man Who Mistook His Wife for a Hat(1987), Oliver Sacks tells the story of a music professorwho, coming upon his wife standing next to a coat rack,tried to lift her head instead of his hat. He no longer“knew” people or objects visually, but relied on distinctivevoice characteristics and his other senses for identification.
Agnosia is not a single sensory phenomenon. It maystrike any sensory domain, but the most commonly stud-ied instances affect the somatosensory visual and auditorysenses. Olfactory and taste agnosias have not been re-searched extensively. Agnosias, in general, are relativelyrare, but they have received considerable attention in theneuropsychological literature, perhaps because they sostrikingly alter consciousness.
Somatosensory Processing
The somatosensory system includes two types ofsensory stimulation, external and internal. This system canmonitor sensations such as cold and heat, whether the sen-sation comes from handling an ice cube or from a fever.Thus, the system processes external stimulation of touch(pressure, shape, texture, heat) in recognizing objects byfeel and is also concerned with the position of the body inextrapersonal space, termed proprioception. Sensory dys-functions that result in proprioceptive disorders of alteredsense of bodily sensation or bodily position are of great in-terest to neuropsychology.
Figure 7.1 Primary sensory and motor cortexes. In general, primary sensoryprocessing lies posterior to the central sulcus, and primary motor processing isanterior. The chemical senses of olfaction and taste are the exception. Theprimary gustatory cortex cannot be seen from this view. (Adapted from Banich, M. T. [1997]. Neuropsychology: The neural bases of mental function [p. 25, Figure4.1]. Boston: Houghton Mifflin Company, by permission.)
Centralsulcus Primary
motor cortex
Frontal lobeParietal lobe
Temporallobe
Occipital lobe
Primarysomatosensory
cortex
Primary olfactorycortex (mostly
hidden from view)
Primary auditorycortex (mostly
hidden from view)
Primaryvisual cortex
(mostly hiddenfrom view)

CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 179
One of the more exotic and seemingly rare(reported by 1 in 500,000) alterations insensory processing is the “cross-wiring” ofsenses called synesthesia. One womanreported that tasting lemon is like “pointspressing against the face,” and spearmintfeels like “cool glass columns.” The mostreported form of synesthesia is “auditioncolorée,” or colored hearing, described vividlyby the synesthete poet Arthur Rimbaud in hispoem “Les Voyelles” (“The Vowels”).
Probably the most completely describedcase of synesthesia was “S,” reported byLuria in his book The Mind of a Mnemonist(1968). Every sound, including tones, words,music, voices, and other noises, summonedup a vivid visual image. One tone could be a“velvet cord with fibers jutting out on allsides,” whereas another tone conjured up astrip, the color of “old tarnished silver.” Thesound of a voice could be “crumbly andyellow” or like a “flame with fibers.” Seeingsounds could often be so attention grabbingthat “S” could not follow the content of whatpeople were saying to him unless they spokevery slowly.
The melding of sensory perceptionsappears unique to each person, but theunderlying neural processes may be quitesimilar. Neurologist Richard Cytowic (1993)has suggested that the source of synesthe-sia emanates from the most primitivereaches of the brain, specifically the limbicsystem. In his early studies, Cytowic usedxenon inhalation to study the dynamic bloodflow activity within the brain of synesthetesin mid audition colorée. Contrary to hisinitial expectations, neural activity in thecortex did not increase, but actually de-creased an average of 18%. Surprisingly, itwas the limbic system that “lit up.” Cytowic
hypothesizes that the neocortex “turns off”during synesthetic processing whereas amore ancient, fundamental processingsystem takes over. Finding limbic systeminvolvement seems congruent in light of theway Luria’s patient S describes his ownexperiences:
S: I recognize a word not only by the images itevokes, but by a whole complex of feelings thatimage arouses. It’s hard to express . . . . UsuallyI experience a word’s taste and weight, and Idon’t have to make an effort to remember it—the word seems to recall itself. But it’s difficultto describe. What I sense is something oilyslipping through my hand . . . or I’m aware of aslight tickling in my left hand caused by a massof tiny, lightweight points. When that happens Isimply remember, without having to make theattempt. (Luria, 1968, p. 28)
Mood and memory are intimately linkedthrough the limbic system. In the case of S,auditory and visual sensation also appearlinked to this system. The final effect waseffortless and seemingly unlimited memorycapacity. A sound, once experienced, wouldalways recall an image. S went on to use thisstrange gift as a professional performer offeats of memory, astounding audiencesthroughout Russia.
Many viewed synesthesia as an abnormalmedical oddity. It is different from other “disor-ders” in that it is not an effect of acquired braindamage. This cross-wiring appears to be“hardwired” since birth. If, as Cytowic sug-gests, synesthesia is an evolutionarily moreprimitive form of processing sensory experi-ence, there may be remnants of synesthesia inmany of us. Do you ever feel blue?
N e u r o p s y c h o l o g y i n A c t i o n 7 . 1
S y n e s t h e s i a : M e l d e d S e n s o r y I n t e g r a t i o n
by Mary Spiers
Vowels
A black, E white, I red, U green, O blue: vowels,One day I will tell you latent birth.A, black hairy corset of shining fliesWhich buzz around cruel stench,
Gulfs of darkness; E whiteness of vapors and tents,Lances of proud glaciers, white kings, quivering of flowers;I, purples, spit blood, laughter of beautiful lipsIn anger or penitent drunkenness;
U cycles, divine vibrations of green seas,Peace of pastures scattered with animals, peace of the wrinkleswhich alchemy prints on heavy studious brows;
O supreme Clarion full of strange stridor,Silences crossed by worlds and angels:O, the Omega, violet beam from HIS eyes!
—Arthur Rimbaud
The somatosensory system contains a conglomerationof receptor types and sensory information. Receptors onthe skin are attuned to external sensations such as the pres-sure of a hand, a blast of wind, the pricking of a finger, thevibrational frequency of touch, the burn of a hot
stove, and the itching of poison ivy. Somatosensory recep-tors are also spread internally throughout the body tomonitor the stretching of the stomach during eating and di-gestion, the pain of muscle aches, and the spatial position ofarms and legs, to name a few examples. The receptor types
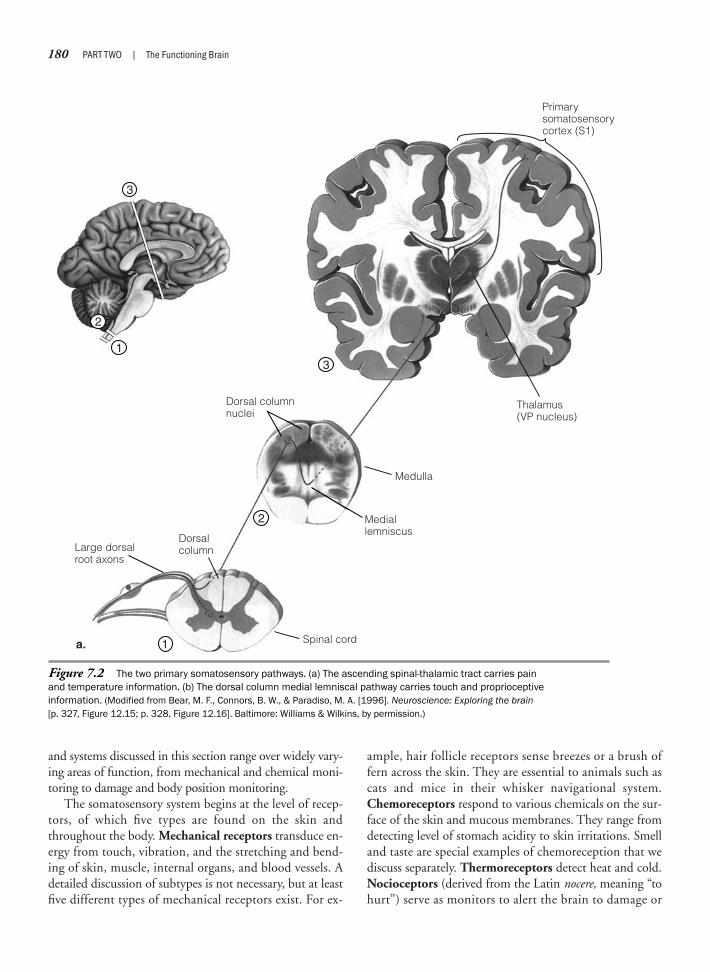
180 PART TWO | The Functioning Brain
and systems discussed in this section range over widely vary-ing areas of function, from mechanical and chemical moni-toring to damage and body position monitoring.
The somatosensory system begins at the level of recep-tors, of which five types are found on the skin andthroughout the body. Mechanical receptors transduce en-ergy from touch, vibration, and the stretching and bend-ing of skin, muscle, internal organs, and blood vessels. Adetailed discussion of subtypes is not necessary, but at leastfive different types of mechanical receptors exist. For ex-
ample, hair follicle receptors sense breezes or a brush offern across the skin. They are essential to animals such ascats and mice in their whisker navigational system.Chemoreceptors respond to various chemicals on the sur-face of the skin and mucous membranes. They range fromdetecting level of stomach acidity to skin irritations. Smelland taste are special examples of chemoreception that wediscuss separately. Thermoreceptors detect heat and cold.Nocioceptors (derived from the Latin nocere, meaning “tohurt”) serve as monitors to alert the brain to damage or
Figure 7.2 The two primary somatosensory pathways. (a) The ascending spinal-thalamic tract carries painand temperature information. (b) The dorsal column medial lemniscal pathway carries touch and proprioceptiveinformation. (Modified from Bear, M. F., Connors, B. W., & Paradiso, M. A. [1996]. Neuroscience: Exploring the brain[p. 327, Figure 12.15; p. 328, Figure 12.16]. Baltimore: Williams & Wilkins, by permission.)
2
3
13
2
1a.
Large dorsalroot axons
Dorsalcolumn
Mediallemniscus
Dorsal columnnuclei
Spinal cord
Primarysomatosensorycortex (S1)
Thalamus(VP nucleus)
Medulla

CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 181
threat of damage. They can be mechanical or chemical,but are specifically activated by potentially damaging stim-ulation such as heat or cold, painful pressure or pricking,or chemical damage such as exposure to noxious chemi-cals. They are present throughout the body, but they arenoticeably absent in the brain. This is how some types ofbrain surgery and brain mapping can be done while thepatient is conscious and alert. Proprioceptors (derivedfrom the Latin proprius, meaning “one’s own”) on skeletalmuscles detect movement via degree of stretch, angle, andrelative position of limbs. Proprioceptors on the handshelp identify the shapes of objects via touch.
These somatosensory receptors synapse with neuronsinto two primary pathways that transmit informationfrom the spinal cord to the thalamus (Figure 7.2). In eachcase, sensory information travels to the contralateralhemisphere from the point of origin. The first pathway,the ascending spinal-thalamic tract, carries sensory in-formation related to pain and temperature and runs par-allel to the spinal cord. It synapses over a wide region ofthe thalamus, and then to the somatosensory cortex. Thesecond pathway is the dorsal column medial lemniscalpathway, which carries information pertaining to touchand vibration. It is so named because it is routed up the
Figure 7.2 (Continued)
Primarysomatosensorycortex (S1)
Thalamus(intralaminarand VP nuclei)
3
2
3
2
1
1
DorsalcolumnSmall dorsal
root axons
Spinal cord
Spinothalamictract
Medulla
b.
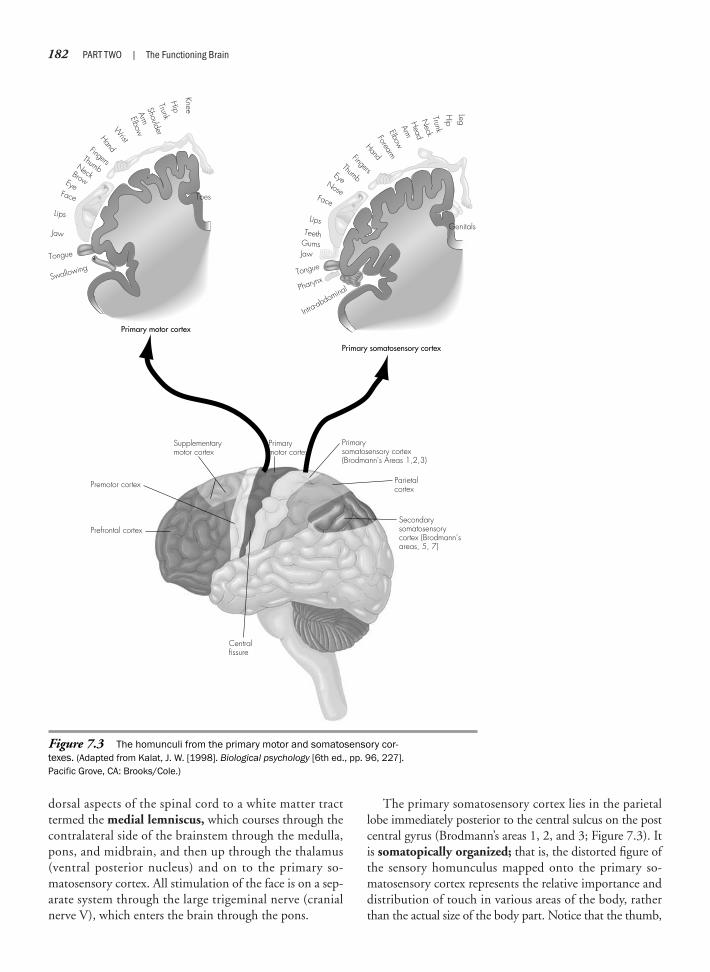
182 PART TWO | The Functioning Brain
dorsal aspects of the spinal cord to a white matter tracttermed the medial lemniscus, which courses through thecontralateral side of the brainstem through the medulla,pons, and midbrain, and then up through the thalamus(ventral posterior nucleus) and on to the primary so-matosensory cortex. All stimulation of the face is on a sep-arate system through the large trigeminal nerve (cranialnerve V), which enters the brain through the pons.
The primary somatosensory cortex lies in the parietallobe immediately posterior to the central sulcus on the postcentral gyrus (Brodmann’s areas 1, 2, and 3; Figure 7.3). Itis somatopically organized; that is, the distorted figure ofthe sensory homunculus mapped onto the primary so-matosensory cortex represents the relative importance anddistribution of touch in various areas of the body, ratherthan the actual size of the body part. Notice that the thumb,
Figure 7.3 The homunculi from the primary motor and somatosensory cor-texes. (Adapted from Kalat, J. W. [1998]. Biological psychology [6th ed., pp. 96, 227].Pacific Grove, CA: Brooks/Cole.)
Premotor cortex
Supplementarymotor cortex
Prefrontal cortex
Primarymotor cortex
Primarysomatosensory cortex(Brodmann's Areas 1,2,3)
Parietalcortex
Centralfissure
Secondarysomatosensorycortex (Brodmann’sareas, 5, 7)
Toes
Primary motor cortex
Hip
Knee
Trunk
Shoulder
ArmElbowWristHandFingersThumbNeckBrowEye
Face
Lips
Jaw
Tongue
Swallowing
Intra-abdominalPharynx
Tongue
Genitals
Primary somatosensory cortex
JawH
ip
LegGumsTeeth
Lips
Face
Nose
Eye
Thumb
Fingers
HandForearm
ElbowArm
Head
Neck
Trunk

Astereognosis/tactile agnosia: inability to recognize an object by touch
Finger agnosia: inability to recognize or orient to one’s own fingers
Paresthesia: spontaneous crawling, burning, or “pins and needles” sensation
Peripheral neuropathy: peripheral nervous system dysfunction causingsensory loss (for example, in diabetes)
Phantom limb pain: a feeling of pain in a nonexistent limb
Proprioceptive disorder: loss of body position sense
Tactile extinction/suppression/inattention: suppression of touch sensationon one side of body
Table 7.1 Examples of SomatosensoryDysfunction
fingers, and face represent proportionately the largest areas.These are the areas of most sensitive and discriminatingsensation in the body, having the largest proportion oftouch receptors. The somatosensory system is organizedcontralaterally, with the left hemisphere processing tactilesensation from the right side of the body and vice versa. Thework documenting the close correspondence of sensation tocortical mapping in the primary somatosensory cortexbegan in the early days of neurosurgery. In the 1940s,Wilder Penfield, a noted neurosurgeon at the MontrealNeurological Institute, started to use electrical stimulationto explore the functions of the cortex in patients undergo-ing neurosurgery for the relief of epilepsy. Applying electri-cal stimuli to different cortical areas in more than 1000 fullyconscious patients, Penfield mapped motor, sensory, lan-guage, and memory functions (Figure 7.4).
From the primary somatosensory cortex, sensory infor-mation is then integrated at the next level in the secondarysomatosensory cortex, which is immediately posterior(Brodmann’s areas 5, 7). There, the individual properties oftactile stimuli such as shape, weight, and texture are com-bined to form the perception of single and whole perceptssuch as “pencil,” “coin,” or “key” that can be recognized byfeel. Damage to this area may result in astereognosia, eventhough the person may readily recognize objects by sight.In this case, elementary powers of sensation are intact, butthe person cannot recognize things placed in the hand con-tralateral to the lesion. Neuropsychologists usually test for
this problem by blindfolding the patient, placing an objectin the hand, and asking the person to recognize and nameit by touch only. Damage interrupting higher level so-matosensory integration in the parietal area, particularlythe right parietal lobe, may result in a problem variouslyreferred to as tactile suppression, tactile extinction, or tactileinattention. In this instance of right parietal damage, a per-son does not report the sensation of touch on the left hand(that is, left-sided suppression) when the left and righthands are touched simultaneously, although he or she mayaccurately report a left-sided touch when that hand istouched in isolation. In this case, the problem involves sort-ing out competing tactile sensations. Left-sided touch is sup-pressed or extinguished when there is competing sensationfrom both sides of the body. Part of the Halstead–ReitanNeuropsychological Battery includes a sensory-perceptualexamination that tests for finger agnosia, skin writing recog-nition, and sensory extinction in the tactile, auditory, andvisual modalities (Reitan & Wolfson, 1993). Table 7.1 listsexamples of somatosensory disorders.
Disorders of proprioception represent the second type oftactile disorder in that the sensory problem is one of recog-nizing the relative position of your own body in space, ratherthan the recognition of objects external to yourself. This is aproblem of tactile integration, which is usually compro-mised by parietal lobe dysfunction. Because proprioceptorsrecord from the stretching of muscle, what you are receivingas sensory information is feedback from your own motormovements. This sensory information then is available tofeed back to fine-tune body movement. Normally, a combi-nation of vision, the vestibular organs, and the propriocep-tive sense supplies a kinesthetic sense of your physicalbody. Proprioception, like most elementary sensations, is sobasic and automatic that you take it completely for grantedunless it is disrupted or absent. Imagine, however, havingno sense of where your hands and legs are, or even of your
CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 183
Image not available due to copyright restrictions

184 PART TWO | The Functioning Brain
posture if your eyes are closed. In Oliver Sacks’s case of the“Disembodied Lady” (Sacks, 1987), a young woman of 37,suffering a sensory neuritis, had the feeling of “losing” partsof her body if she could not see them; that is, she experi-enced the feeling of total disembodiment. Having no nat-ural posture, her movements became a caricature of types,such as a dancer’s pose. Quite the opposite problem is ex-pressed in phantom limb pain. People with no external sen-sation entering the brain still have the curious experience ofpain or other sensation. Neuropsychology in Action 7.2 ex-plores this odd phenomenon.
Chemical Senses
Taste and smell evolutionarily are the oldest sensorysystems. They work in concert, and to most people, theyappear indistinguishable until a cold or other sinus condi-tion congests and diminishes the sense of smell. People arelikely to report that food does not “taste” so good or have asmuch flavor as usual, when it is actually blocked smell that
is affecting the pleasurability of food. It is easy to experiencethis condition by just holding your nose and sampling dif-ferent foods to see what “tastes” you actually experience.Taste and smell are also the least studied of the senses withinneuropsychology and neuroscience. This neglect may bedue, in part, to that other senses such as vision and auditionare well developed in humans, and thus have overshadowedthe chemical senses. The idea that the senses of taste andsmell may be vestigial and no longer of any real adaptive useto modern humans has also probably contributed to the lackof interest. However, these chemical senses are enjoying asurge of research attention that is pointing to connectionswith emotional behavior, hormones, immunology, andidentification of neurologic disease states.
T A S T E
The tongue contains numerous papillae or bumps onwhich lie from one to several hundred taste buds consist-ing of between 50 and 150 taste receptor cells. The bun-dles of receptor cells resemble onions, with the cilia at thetips of the cells protruding into the surface of the pore.
Phantoms are the experience of externalsensory experience in the absence of avail-able sensory input. This sounds strikingly likea hallucination. And perhaps had it not beenfor the widespread occurrence of phantomsfelt by what are considered otherwise “ratio-nal” people, phantoms might have beenconsidered psychosomatic experiences atbest and psychotic episodes at worst. Peoplemost commonly think of phantoms in respectto phantom limb pain after amputation, butthey can and do exist in any sensory modal-ity. The interesting questions here are, Howare phantoms experienced, and what aretheir causes? Finally, understanding phan-toms may also provide some clues to under-standing certain aspects of brain plasticityand reorganization.
Phantom limbs and phantom limb painare most commonly associated with ampu-tations. The amputee may feel a lost arm,feel that it swings in coordination with the
other arm while walking, or experience itsticking out so much as to necessitatemaneuvering through doors sideways. All thewhile, objective reality is shouting that it isnot there. Cold, heat, pressure, itching,tickling, and sweat can all be experienced inthe missing limb. Because as many as 70%of amputees experience pain in the ampu-tated part, psychologists specializing in painmanagement are striving to understandcauses and formulate treatments for thisproblem.
Phantoms may also be experienced insituations other than amputation and insenses other than tactile. Children bornwithout limbs, people who have sufferedparalysis after a spinal cord injury, and evenwomen in labor who have had spinal anes-thesia have also “felt” the presence of alimb. Some congenital amputees havereported being able to move nonexistentfingers or to experience the phantom emerge
and disappear from consciousness. Phan-tom seeing and hearing can occur in thecomplete or partial absence of vision andaudition. Auditory phantoms may be passedoff as tinnitus, or ringing in the ears, butsome people hear voices or music. Visualphantoms can also range from flashes oflight and color to fully formed images ofpeople and objects. In both cases, andperhaps a differentiating factor betweenthese types of “hallucinations” and thoseexperienced by schizophrenics, phantomsare quickly judged as separate from normalsensory-perceptual reality.
How can phantoms be described neuro-logically? Scientists know that phantomsemanate from central brain mechanismsrather than purely peripheral ones, althoughthe exact mechanism for the production ofphantoms is still a matter of some specula-tion. In the case of phantom limbs, amputa-tions leave exposed nerve endings that heal
N e u r o p s y c h o l o g y i n A c t i o n 7 . 2
P h a n t o m s o f F e e l i n g
by Mary Spiers

CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 185
Taste receptors are not neurons, but respond to the chem-ical qualities in food dissolved in saliva as they wash overthe tips of the receptors. In the course of eating, taste re-ceptors endure extremes of temperature, spicy food, andother chemical substances, which may cause damage. Per-haps because of this, taste receptors quickly wear out andare replaced on a cycle of about 10 days.
The traditional theory about how taste functions,presented in most general psychology textbooks, describesthe ability of the tongue to discriminate four primary tastesensations: sweet, salty, sour, and bitter. This schema isbased on specific taste bud receptor ability to detect thechemicals associated with each taste. For example, certainreceptors are attuned to sodium chloride (NaCl) andother salty chemicals, and likewise for the remaining pri-mary taste sensations. Some researchers have suggested afifth taste, umami (derived from the Japanese, meaning“delicious”). Deliciousness is operationally defined by theactivation of L-glutamate receptors that are attuned toglutamate-triggering substances such as monosodium glu-tamate (MSG). The primary tastes theory implies that, in
any mixture, individual taste sensations, such as saltiness,are identified by specific saltiness receptor types and trans-mitted to the brain along dedicated pathways, where theyare analyzed and labeled as salty. According to this theory,taste receptors of different types are grouped in variousareas of the tongue; the tip is specific for sweetness andsaltiness, the sides detect sourness, and the back is mostsensitive to bitterness.
The competing pattern theory suggests that taste isbest thought of as a pattern of sensation in which individ-ual receptors can process information about more thanone taste type. There is strong evidence that individualtaste fibers are not exclusive to one taste sensation, al-though they may roughly focus on one type (Smith &Vogt, 1997). The suggestion from the pattern theory isthat the experience of any particular taste, such as salti-ness, is carried to the brain, because the fibers are acti-vated to respond mostly to saltiness of the substance inthe mixture. The implication is that taste receptors mayhave multiple potentiality, rather than being dedicated torespond to a specific chemical.
as nodules called neuromas. Neuromascontinue to generate neural impulses. Forthis reason, initial treatments focus onsevering communication between the pe-ripheral sensory input and the spinal cord.However, this does not obliterate phantoms.Consequently, as an attempted treatment,surgeons have blocked or cut spinal nerves,and then central pathways feeding thesomatosensory cortex from the sensory relaystation of the thalamus. But phantoms stillexist. Traditional painkilling drugs are alsolargely ineffective, because phantom paindoes not seem to arise from the same painsystem.
From where in the brain do phantomsarise? Recent work in this area has led torethinking about the supposed lack ofplasticity of adult brains. A logical place tostart is to understand what happens in thesomatosensory strip when the correspondingsensory area on the body ceases to provideinput. Researchers have done deep-brainelectrode recordings on monkeys with anamputated finger. Surprisingly, sensory inputfrom adjacent fingers remapped itself ontothe somatosensory cortex so that it invadedthe area previously serving the amputatedfinger. This remapping occurred within weeksof the amputation. Neuroscientist Timothy
Pons demonstrated this sensory strip en-croachment in monkeys who had had theirsensory nerves cut more than 12 yearsearlier. In this case, massive territorialinvasion was seen; in one case, a hand andarm were now mapped onto the face. Recallthat we made the point earlier that neurons,once severed, are for all practical purposesdead and unable to regenerate; only par-tially severed axons can resprout. At least,this has been the common wisdom. Also,no brain reorganization is expected after acertain critical period of development.However, in the case of phantoms, there isno damage to neurons in the brain; all thedamage is peripheral. Somehow, healthyneurons are reorganizing themselves totake over an area of the brain that the bodyis no longer using. It is reasonable to expectthat healthy brain neurons may more easilyreorganize themselves than damaged ones.However, the mechanism by which this isdone is still a mystery. One aspect that haspuzzled scientists working on this problemis that if neurons were reorganizing them-selves on the homunculus of thesomatosensory strip itself, their growthwould have to cover long distances. Thismechanism seems unlikely, given that adultneurons can sprout over only short dis-
tances. One possible explanation is thatinstead of reorganization at the level of thesomatosensory cortex, reorganization isoccurring within the relay station of thethalamus, where all sensory inputs fromtouch, vision, and audition funnel through ina tight space. An axon merely has to reachacross a narrow stream to remap a finger tothe face or to even to the back. Odd as it mayseem, this phenomenon is now beingdemonstrated in human amputees. Ramachandran (Ramachandran, Rogers-Ramachandran, & Steward, 1992)tested a teenager who had recently lost hisleft arm in an auto accident. As the boy satblindfolded, Ramachandran touchedvarious parts of his body with a cottonswab. When he stimulated various areas ofhis lip and lower face, the boy felt hismissing thumb and fingers tingle. Sensa-tions from his hand were now remappedonto his face. Because acupuncture hashelped some people with phantom limbpain, it seems reasonable to speculate thatknowledge of remapping may dampen painif massage, acupuncture, or other meanscan be applied to the newly remappedareas of the body. In the case of this boy,odd as it may seem, face massage mayalleviate left arm and hand pain.

186 PART TWO | The Functioning Brain
Taste receptor cells synapse with sensory neurons thatcarry information via cranial nerves VII, IX, and X to themedulla of the brainstem (specifically the nucleus of thesolitary tract), where they are relayed via the thalamus(ventral posterior medial nucleus) to the primary gusta-tory cortex (Figure 7.5). Additional projections run fromthe thalamus directly to the somatosensory cortex amyg-dala, hypothalamus, and orbital prefrontal cortex. Thehypothalamus may code for pleasurability of food, be-cause it contains neurons that respond specifically tosweetness of food (Rolls, 1986).
The function of taste appears to be drawing us to cer-tain basic substances that the body needs and repelling usfrom potentially harmful chemicals. Certain receptors areattuned to sweet and salty foods, which the brain codes aspleasurable. Before the days of candy and salty fast foods,being drawn to sweet foods such as fruit provided needednutrition. Salt contains the body’s necessary sodium. It isalso adaptive to be repelled by bitter foods, which mightbe poisonous, and by sour foods, which might be spoiled.
Disorders of taste are rare in comparison with disor-ders of smell, although as mentioned earlier, people may
Figure 7.5 From taste buds to taste pathways in the brain. (Adapted from Kalat, J. W. [2004]. Biologicalpsychology [8th ed., p. 210, Figure 7.18a, p. 212 Figure 7.19]. Belmont, CA: Wadsworth/Thomson Learning.)
From taste buds on tongue
Nucleus of tractus solitarius
Somatosensory cortex
Ventralposteromedialthalamus
Hypothalamus
Orbitalprefrontalcortex
Amygdala
Corpuscallosum
Primary gustatorycortex
Foliate papilla
Taste bud close-up
Vallate (or circumvallate)papilla
Fungiformpapilla
Taste buds

report disorders of smell as disorders of taste because thetwo systems interact in flavor perception. Taste disordersmay range from a diminished sense of taste (hypogeusia)to a complete loss of taste (ageusia). Table 7.2 summarizestaste disorders. Phantogeusia is the experience of a taste“phantom” or hallucinatory taste. Taste phantoms oftencoincide with other disorders of taste. Most disorders oftaste appear to be caused by a problem in the central per-ception of taste, rather than a problem at the level of thetaste buds. For example, one of the more common reasonsfor taste distortion is medication usage. Other causes oftaste dysfunction include head injury, upper respiratoryinfection, and in the case of phantogeusia, sometimesdamage to the “taste nerve,” the chorda tympani (cranialnerve VII) if it is injured during ear or dental surgery (seeCowart et al., 1997).
S M E L L
Amble through a field on a summer afternoon, and theair is fragrant with smells of wildflowers, grasses, and aro-matic herbs. Inhale and microscopic molecules of scentwafting through the air are gradually taken in by your rel-atively slow olfactory detection system. The aromas youdetect and identify are, in part, a function of the ability ofthe odorant to dissolve in the moist mucous lining of thenose, but are also affected by age, sex, health, and braininjury.
Smell is the least understood sensory system, perhapsbecause scientists have considered it of little adaptive valueto humans. Certainly, it is the oldest sensory system evolu-tionarily, and it appears much more crucial to animals suchas bloodhounds and snakes, which are lower on the phylo-genetic scale. What function does scent serve for humans?Is it a vestigial sense? Many people appear to function wellin their lives having completely lost their sense of smell.However, the perfume industry is booming and aromather-apy is becoming a popular naturopathic approach to moodenhancement. This section examines the unique neu-roanatomy of the primary olfactory system. Unlike othersystems, olfactory neurons have regenerative qualities when
damaged. Finally, we also reflect on the potential implica-tions of links among mood, memory, and olfaction.
Inhalation (but actually just a sufficient sniff is needed)sends molecules of scent traveling up to the roof of thenasal cavity. These odorants dissolve in the olfactory ep-ithelium, a fine mucous lining consisting of odorant-binding proteins (OBPs), antibodies, and enzymes.Mucus is being continually produced; thus, the entire ep-ithelium is replaced about every 10 minutes. Scent mole-cules bound to OBPs activate the fine, hairlike cilia of ol-factory neurons waving within the olfactory epithelium.Researchers have discovered at least 500 to 1000 OBPgenes that appear to be coded for different odorants. Inhumans, the epithelium is small, about half the size of apostage stamp (5–10 cm2). Dogs, with their keen sense ofsmell, have an epithelium easily 10 times that of humans(100 cm2), with 100 times the neurons per square cen-timeter. Olfactory neurons in the epithelium synapse withthe right or left olfactory bulb through the thin cribri-form plate of the skull, where the central olfactory path-way (cranial nerve I) originates. So whereas three cranialnerves subserve taste, smell has only one pathway.
The olfactory system is unique in several ways. Notethat we have considered receptors when discussing othersensory systems. These receptors then synapse with den-drites of neurons. This is not the case with the olfactorysystem. The neurons themselves are directly exposed tothe environment. The health of the epithelial layer,where the dangling neurons lie, is crucial because someviruses, such as rabies, take advantage of this direct routeto the brain. This system is also interesting in that con-trary to the notion that new neural cells do not form inadults, the olfactory neurons compose a uniquely “plas-tic” system, continuing to reproduce and replace them-selves every 1 to 2 months throughout adulthood. Theolfactory neurons, however, are susceptible to traumaticinjury because they dangle through a opening in theskull, the cribriform plate. A blow to the head can easilysever these neurons. Although the neurons do regrow,they do not always reconnect with the olfactory bulbs(Figure 7.6).
The olfactory bulbs contain complex circuitry; the twobulbs even communicate with each other. Although themechanism is not completely understood, microelectroderecordings show that various aromas produce identifiablespatial maps on the bulbs, and these mosaics may changeeven during the sniffing of an odorant. The plasticity ofthe system has suggested to scientists that experience withsmell can easily modify the representational pattern ofstimulation on the olfactory bulb. The map on the bulbprojects to the areas of the brain that process and encode
CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 187
Ageusia: inability to recognize tastes
Dysgeusia: distorted taste sensation
Phantogeusia: experience of a phantom or hallucinatory taste
Hypogeusia: diminished taste sensitivity
Table 7.2 Disorders of Taste
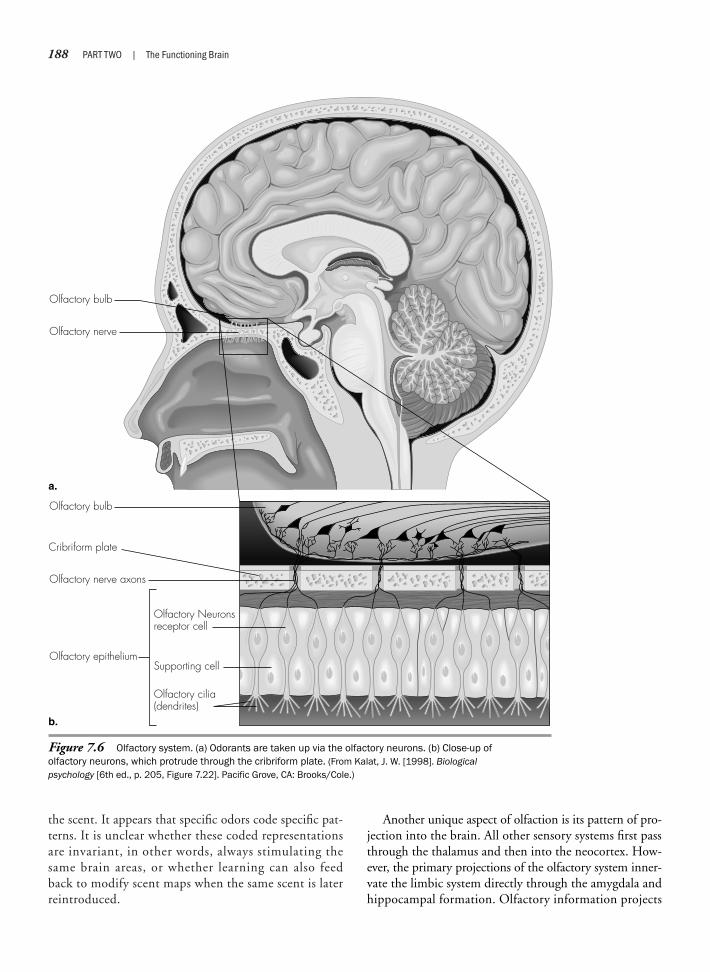
188 PART TWO | The Functioning Brain
the scent. It appears that specific odors code specific pat-terns. It is unclear whether these coded representationsare invariant, in other words, always stimulating thesame brain areas, or whether learning can also feedback to modify scent maps when the same scent is laterreintroduced.
Figure 7.6 Olfactory system. (a) Odorants are taken up via the olfactory neurons. (b) Close-up ofolfactory neurons, which protrude through the cribriform plate. (From Kalat, J. W. [1998]. Biologicalpsychology [6th ed., p. 205, Figure 7.22]. Pacific Grove, CA: Brooks/Cole.)
Olfactory bulb
Olfactory bulb
Olfactory nerve axons
Olfactory epithelium
Olfactory Neuronsreceptor cell
Supporting cell
Olfactory cilia(dendrites)
Olfactory nerve
a.
b.
Cribriform plate
Another unique aspect of olfaction is its pattern of pro-jection into the brain. All other sensory systems first passthrough the thalamus and then into the neocortex. How-ever, the primary projections of the olfactory system inner-vate the limbic system directly through the amygdala andhippocampal formation. Olfactory information projects

CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 189
into these primitive areas of the brain before passingthrough the relay station of the thalamus, and then intothe frontal cortex and onto other areas of the neocortex.Because of this connection, the effect of scent on emotionand mood is instantaneous and is most intensely processedpreconsciously. Secondarily, scientists believe that parallelthalamic projections to the frontal lobes are responsible forconscious recognition of scent. The cortex can then elabo-rate and refine the perception of aroma. The hippocampus,although not a memory storage center, is responsible forprocessing and coding memories before they are stored inthe neocortex. Together with the amygdala, these limbicsystem structures appear to be responsible for coding muchof the emotional tone of memories. This neural pattern ofprojection into the brain reflects the ancient evolution ofolfaction. Considering this brain anatomy, it is no wonderthat smell is so strongly tied to emotional memory.
In the early part of the nineteenth century, Freud sug-gested that disorders of smell and specific psychologicaldysfunctions may be connected (for types of olfactory dys-function, see Table 7.3). This idea remained largely unex-amined until a relatively recent resurgence of interest inolfaction occurred as it relates to certain brain diseases suchas Alzheimer’s disease, Parkinson’s disease, and schizophre-nia. For some time, people have observed that decreasedability to smell (hyposmia) is associated with aging, andthat both loss and distortion of smell (dysosmia) are asso-ciated with depression. With aging, the ability to perceivesour or bitter odors appears to diminish first, whereas theability to detect pleasant smells such as sweetness may per-sist well into old age. Interestingly, recent work has shownthat diminution of olfactory ability is an early sign of dis-eases of accelerated aging, such as Alzheimer’s disease andParkinson’s disease (for example, see Doty, 1990). Also,schizophrenics often have a distorted sense of smell. Clini-cal neuropsychologists are now using scratch-and-snifftests of odor identification and odor recognition thresh-old, such as the University of Pennsylvania Smell Identifi-cation Test (UPSIT) (Doty, Shaman, & Dann, 1984), totest for the presence of olfactory dysfunction in caseswhere clinicians suspect these diseases.
Partial or complete loss of smell is also a common oc-currence after traumatic injury to the brain. As noted ear-lier, because the olfactory neurons dangle through thecribriform plate, they are easily damaged or sheared off bysudden movements of the brain in relation to the skull.Even though olfactory neurons can regenerate, they oftendo not reconnect to the olfactory bulbs because they areblocked by scar tissue.
Motor Systems
The sensory systems provide a window to theworld, and the motor systems, in turn, provide the meansof acting on the world. Whereas control of sensory sys-tems occurs in posterior brain regions, the cortical con-trol of movement is largely anterior. Movement takes sev-eral forms, including reflex actions, automatic repetitiveactions such as walking, semivoluntary actions such asyawning, and voluntary actions such as deciding to pickup an object (Bradshaw & Mattingly, 1995).
Traditionally, scientists thought the motor systemwas organized hierarchically. Whereas sensory process-ing is thought to proceed in a bottom-up fashion,motor processing would follow a reverse path in a top-down manner. Sensory-perceptual processes build upfrom fragments analyzed in primary processing areasand are synthesized in secondary and higher order cor-texes. Then information that directs motor processingcomes into the system in the form of highly integratedsensory information from the sensory associationareas, such as the parietal lobes, and the subcorticalstructures of the basal ganglia and the cerebellum. Inaddition, internally generated motivation for action alsodirects movement. The system then directs this infor-mation to areas of secondary motor planning and pro-gramming before sending it to the primary motor cor-tex. According to this hierarchy theory, the primarymotor cortex sits at the top and funnels all informationabout movement to the body. However, a competingtheory suggests that the system works in a parallel pro-cessing mode, with several motor processing circuitsworking in coordination with the primary motor cortex(Haines, 1997).
C O R T I C A L M O T O R P R O C E S S I N G
Several cortical areas of the motor system are involved inmotor processing (Figure 7.7). The first of these is the pri-mary motor cortex. The next three motor areas are oftenreferred to as the secondary motor cortex and include the
Anosmia: total loss of smell
Dysosmia: distorted smell sensation
Phantosmia: experience of a phantom or hallucinatory smell
Hyposmia: diminished taste sensation
Table 7.3 Disorders of Smell

190 PART TWO | The Functioning Brain
supplementary motor area, the premotor area (PMA, orpremotor cortex), and the cingulate motor area (CMAor cingulate motor cortex). Finally, areas of the parietallobes and the dorsolateral prefrontal cortex are areas ofpremotor planning.
The role of the primary motor cortex is to managethe fine details required to perform movement. The pri-mary motor cortex lies in the precentral gyrus, or motorstrip of the frontal lobes, just anterior to the central sul-cus and the somatosensory strip. Neuronal input em-anates from the secondary motor areas and from the so-matosensory cortex. Neuronal output travels through theinternal capsule, and on to descending tracts of the spinalcord, and ultimately to the muscles of the body. The pri-mary motor cortex, like the somatosensory cortex, is so-matopically (or topographically) mapped as a homuncu-lus and allots area according to its degree of motorinnervation (see Figure 7.3). If the primary motor cortexis stimulated directly, typically through microstimulationin the course of neurosurgery, corresponding muscles inthe body move. For example, stimulating the thumb
causes the thumb to twitch or jerk. If the motor ho-munculus is compared with the sensory homunculus, it isevident that there are many similarities in the corticalmapping for motor control and sensory processing ofmovement. For example, the acute sense of touch on thefingers is also related to fine finger dexterity. However,some areas have proportionately more motor control abil-ities, or vice versa, so the maps appear somewhat differ-ent. The motor cortex, like the somatosensory cortex,controls the contralateral side of the body. Damage or dis-ease of the motor cortex results in hemiplegia, or the lossof voluntary movement, to the opposite side of the body.Hemiplegia is often a hallmark of stroke to the middlecerebral artery. So, for example, a common occurrence isto have a patient present with right-sided hemiplegia anddifficulty speaking due to a left-hemisphere stroke.
The primary motor cortex and the somatosensory cor-tex are in reciprocal communication with each otherthrough a reflex circuit. The primary motor cortex re-ceives feedback from the somatosensory cortex about theeffect of movement just initiated. So when your thumb
Text not available due to copyright restrictions

moves across the page to turn it, the sensation of the con-tact of the thumb on paper is immediately sent to the so-matosensory cortex and informs the primary motor cortex of the effect of its movement.
Each area of the secondary motor cortex has aslightly different role. The supplementary motor area(SMA, also supplementary motor cortex, or medialpremotor cortex) functions in organization and sequen-tial timing of movement. The internal intention to moveis also a function of this area. The SMA lies on the dorsaland medial portion of each frontal lobe (in Brodmann’sarea 6). It is posterior to the prefrontal cortex and ante-rior to the primary motor cortex. The SMA receivesinput from the parietal lobes (posterior parietal associa-tion area), the somatosensory strip, the secondary somatosensory areas, and subcortically from the basalganglia and the cerebellum. It also interconnects with thePMA. The SMA outputs to the primary motor cortex inboth the ipsilateral and contralateral hemisphere. It alsooutputs back to the basal ganglia and the cerebellum(Bradshaw & Mattingly, 1995). It functions specificallyas a planner of motor sequences. Like the primary motorcortex, it is also somatopically mapped to the muscula-ture in the body; however, the mapping is not as tightlyorganized. Electrical microstimulation of the SMA elicitsthe urge to make a movement, or the feeling of anticipa-tion of a movement (Bradshaw & Mattingly, 1995).Stimulation may also elicit muscle movement. But in-stead of the single-muscle flexion of the primary motorcortex, this stimulation activates groups of muscles and asequence of movement, and it can activate bilateralmovement (Haines, 1997).
Experiments with humans show a dissociation, orseparation, between the functional contributions of theprimary motor cortex and the SMA. In an early methodof studying areas of brain activity, researchers injected ra-dioactive xenon into the bloodstream. In this way, theycould measure increased areas of brain blood flow, andthus brain neuronal activity, as they were occurring.When the researchers asked volunteers to make randomfinger movements, the primary motor cortex “lit up,” butthe SMA remained relatively silent. When the experi-menters asked volunteers to make a sequence of move-ments with their fingers, such as drumming their fingersin a certain order, both the primary motor cortex and theSMA were active. Finally, when they asked the partici-pants to only imagine and rehearse the movements intheir minds, without doing anything, only the SMA wasactive (Roland, Larsen, Lassen, & Skinholf, 1980). Thisoffered strong evidence for the planning role of the SMAin sequential motor activities.
The PMA also plays a role in motor planning andsequencing and movement readiness. The PMA liesnext to the SMA in Brodmann’s area 6 of the frontallobes. Whereas the SMA is more medial, the PMA ismore lateral. The PMA receives neuronal input fromsome of the same general areas as does the SMA, butfrom slightly different places. For example, the PMAreceives parietal input from posterior parietal areas,rather than parietal association cortex. The PMA re-ceives input from the secondary somatosensory areas,rather than from both the primary and secondary so-matosensory areas, and receives more cerebellar input.As stated earlier, it is also reciprocally interconnectedwith the SMA and projects to the primary motor cortexand the reticular formation (Haines, 1997). The PMAis also somatopically organized. In a general way, thePMA performs similar premotor planning functions asthe SMA, such as the sequencing, timing, and properinitiation of voluntary movement, but it may functionmore in externally cued readiness for action, whereas theSMA provides more of an internal readiness cue (Brad-shaw & Mattingly, 1995). For example, when runnersline up for a race and hear the official say, “On yourmark . . . Get set . . . Go,” their PMA is most active be-tween “Get set” and “Go.” Studies with monkeys alsoindicate that the PMA is most active during this inter-val between cue and go (see Haines, 1997).
Less is known about the functioning of the thirdstructure of the secondary motor cortex, the CMA, al-though it likely plays a role in the emotional and moti-vational impetus for movement. The CMA is a medialinfolding of the frontal area of the cingulate gyrus. Re-call that the cingulate gyrus plays a role in the limbicsystem. The CMA lies next to the cingulate gyrus. TheCMA is organized somatopically in relation to thespinal cord. It projects both to the spinal cord and tothe primary motor area. Damage to the CMA results in alack of spontaneous motor activity (Bradshaw & Mattingly,1995). This apparent apathy is neurologic in origin andnot necessarily caused by a depressive state. People maybe able to say what they can do or should do, but oftendo not translate this into action. Together with theSMA, the anterior cingulate also appears to play a rolein the semantic premotor processing, or initiation, ofspeech.
Two additional cortical areas contribute to motor pro-cessing: the posterior parietal lobes and the dorsolateralprefrontal cortex. The posterior areas of the parietal lobes(Brodmann’s areas 5 and 7) are important in coordinatingspatial mapping with motor programming. These associationareas receive input from the somatosensory cortex, the
CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 191
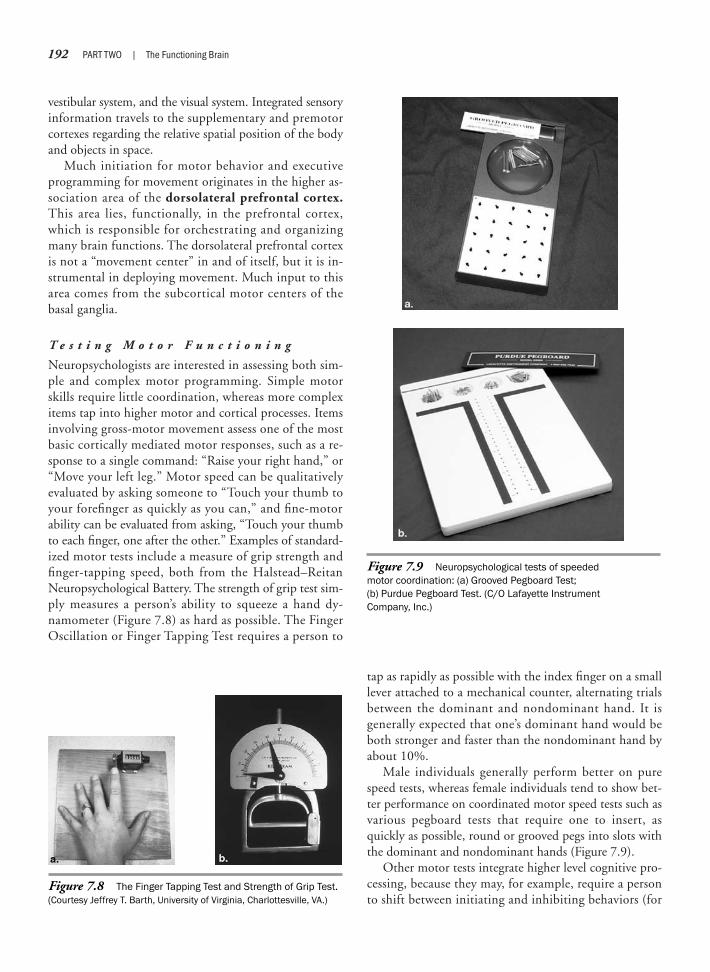
192 PART TWO | The Functioning Brain
vestibular system, and the visual system. Integrated sensoryinformation travels to the supplementary and premotorcortexes regarding the relative spatial position of the bodyand objects in space.
Much initiation for motor behavior and executiveprogramming for movement originates in the higher as-sociation area of the dorsolateral prefrontal cortex.This area lies, functionally, in the prefrontal cortex,which is responsible for orchestrating and organizingmany brain functions. The dorsolateral prefrontal cortexis not a “movement center” in and of itself, but it is in-strumental in deploying movement. Much input to thisarea comes from the subcortical motor centers of thebasal ganglia.
T e s t i n g M o t o r F u n c t i o n i n g
Neuropsychologists are interested in assessing both sim-ple and complex motor programming. Simple motorskills require little coordination, whereas more complexitems tap into higher motor and cortical processes. Itemsinvolving gross-motor movement assess one of the mostbasic cortically mediated motor responses, such as a re-sponse to a single command: “Raise your right hand,” or“Move your left leg.” Motor speed can be qualitativelyevaluated by asking someone to “Touch your thumb toyour forefinger as quickly as you can,” and fine-motorability can be evaluated from asking, “Touch your thumbto each finger, one after the other.” Examples of standard-ized motor tests include a measure of grip strength andfinger-tapping speed, both from the Halstead–ReitanNeuropsychological Battery. The strength of grip test sim-ply measures a person’s ability to squeeze a hand dy-namometer (Figure 7.8) as hard as possible. The FingerOscillation or Finger Tapping Test requires a person to
tap as rapidly as possible with the index finger on a smalllever attached to a mechanical counter, alternating trialsbetween the dominant and nondominant hand. It isgenerally expected that one’s dominant hand would beboth stronger and faster than the nondominant hand byabout 10%.
Male individuals generally perform better on purespeed tests, whereas female individuals tend to show bet-ter performance on coordinated motor speed tests such asvarious pegboard tests that require one to insert, asquickly as possible, round or grooved pegs into slots withthe dominant and nondominant hands (Figure 7.9).
Other motor tests integrate higher level cognitive pro-cessing, because they may, for example, require a personto shift between initiating and inhibiting behaviors (for
Figure 7.8 The Finger Tapping Test and Strength of Grip Test.(Courtesy Jeffrey T. Barth, University of Virginia, Charlottesville, VA.)
Figure 7.9 Neuropsychological tests of speededmotor coordination: (a) Grooved Pegboard Test; (b) Purdue Pegboard Test. (C/O Lafayette InstrumentCompany, Inc.)

D i s o r d e r s o f C o m p l e x M o t o r P r o c e s s i n g
A number of movement disorders may occur as a resultof brain damage or disease. If the primary motor area inone hemisphere is damaged by stroke or injury, hemi-plegia often results. Disorders of motor processing thatgo beyond the primary motor cortex can be classifiedunder two main types: disorders of when to act and dis-orders of how to act. For example, the motor system in-structs when to start and stop various behaviors. Akine-sia is a difficulty in initiating and maintaining behavior.Patients with akinesia may be extremely slow to start orperform a movement, may become rapidly fatiguedwhen performing repetitive movements, or may haveproblems in performing simultaneous or sequentialmovements. If a person continues in the same behavior,or constantly selects it in the presence of other choices,this is termed motor perseveration, another problem ofwhen to act. In addition, if a person behaves inappropri-ately, displaying a motor response when it is unwanted,this is termed defective response inhibition. These ex-amples of disorders of when to act can arise from a vari-ety of cortical and subcortical lesions and disorders. Forexample, patients with Parkinson’s disease show classicdeficits in motor initiation and motor perseveration.People with this affliction often display a slow, shuffling
example, “If I clap once, you clap twice.” [Clap hands onetime.] “Now, I clap twice, you clap once.” [Clap handstwo times.]). Neuropsychologists often examine grapho-motor skills. The following items assess the ability to copyshapes with increasing degrees of difficulty. They involvethe integration of visuoperception (input) and a complexmotor response (output).
Apraxia/dyspraxia: an inability or disability in performing voluntary actions
Akinesia: difficulty initiating and maintaining movement
Dyskinesia: uncontrolled involuntary movement
Chorea: involuntary, jerky, writhing, undulating “puppet-like” movements
Defective response inhibition: the inability to inhibit or an inappropriatemotor response.
Hemiplegia: loss of voluntary movement to one half of the body contralateralto the affected motor strip
Motor perseveration: an inability to stop a behavior or series of behaviors
Tremor: involuntary shaking, usually of a limb; tremors may be resting oroccur with intentional movement
Table 7.4 Examples of Motor Dysfunction
Example II
Example I
gate when they walk and may “freeze” and be unable tomove or back up when they enter a closet. People withHuntington’s chorea often show jerky, undulating, “pup-pet-like” movements of their limbs and grimacing,writhing movements of their faces. (Parkinson’s and Hunt-ington’s disease are discussed at length in Chapter 15.)Some examples of clinical motor dysfunction are de-scribed in Table 7.4.
Apraxia is the main type of disorder under the cate-gory of problems of how to act. Strictly defined, apraxiaimplies an absence of action, but neuropsychologists mostoften use it to describe a variety of missing or inappropri-ate actions that cannot be clearly attributed to primarymotor or sensory deficits, or lack of comprehension, at-tention, or motivation. Thus, the term apraxia refers toan inability to perform voluntary actions despite an ade-quate degree of motor strength and control. The adjective“voluntary” is key to understanding this disorder. A pa-tient may be able to spontaneously don a jacket, for in-stance, but be unable to do so on command. Therefore,family members who ask a patient to do something mayperceive him or her as being oppositional or stubbornwhen, in fact, he or she does not control the skills requiredto perform the action. A typical type of task that is givenif apraxia is suspected is to ask a patient to pantomime agoal-directed action or series of actions. For example, aperson may be asked, “Show me how you would use a keyto open a door.” Depending on the type of apraxia, a pa-tient may “misperform” this action in several ways.
There are several subtypes of apraxia, depending ona number of behavioral variables affecting movementand movement initiation. The types discussed in this chapter—limb-kinetic, ideomotor, conceptual, and
CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 193

194 PART TWO | The Functioning Brain
Figure 7.10 Two views of the cerebellum: (a) lateral view and (b) cutaway medial view. (Courtesy Mark DeSantis.)
Figure 7.11 Basal ganglia. (Modified from Bear, M. F., Connors, B.W., &Paradiso M. A. [2001]. Neuroscience: Exploring the brain [2nd ed., p. 389,Figure 14.11]. Baltimore, MD: Lippincott Williams & Wilkins, by permission.)
VL nucleus ofthalamuc
Caudatsenucleus
Putamen
Striatum
Globuspalidus
Subthalamicnucleus
Substantianigra

CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 195
dissociation (formerly ideational) apraxia—are the mostfrequently described.
People with limb-kinetic apraxia (also ideokinetic)appear clumsy and have poor motor control. In attempt-ing to show how a key would be used, limb-kineticapraxics may make large grasping motions, rather thanfine thumb-to-forefinger movements. Because limb-kinetic apraxia is defined as a problem in executing pre-cise, independent, or coordinated finger movements,people with this disorder are also likely to performquite poorly on the finger-tapping (see Figure 7.8) andpegboard tests (see Figure 7.9). The theories regardingthe brain areas implicated in limb-kinetic apraxia in-volve the corticospinal tract, basal ganglia, and the pre-motor cortex, as well as a larger frontoparietal circuit ofmotor control. A progression of gross- to fine-motorcontrol can be observed with the myelinization of thecorticospinal tract during development. As the corti-cospinal tract matures, children first grasp with the en-tire hand before being able to execute independent andcoordinated finger movements. However, limb-kineticapraxia goes beyond a corticospinal or basal gangliadeficit and involves aspects of grasping and fine-motormanipulation involved with the larger frontoparietal cir-cuit (Leiguarda, Merello, Nouzeilles, Balej, Rivero, &Nogues, 2003).
Ideomotor apraxia involves difficulties in the execu-tion of the idea of a movement, even though the knowl-edge of the action is preserved. For example, in responseto a request to pantomime use of a key, the person maymistakenly use the index finger as the key (body part astool error) or turn the whole arm in an unnatural fashion(movement orientation error). However, someone withideomotor apraxia may be able to use a key correctly if itis put in the hand and should recognize the correct ges-ture if it is performed by someone else, or if given achoice, can match tools with correct actions. Lesions tothe left parietal lobes are commonly associated with ideo-motor apraxia of either hand. It is believed that the leftparietal lobes have a special role in programming purpose-ful, skilled movements, especially in those who are lefthemisphere dominant for language (Meador, Loring, Lee,Nichols, & Heilman, 1999).
With conceptual apraxia, in contrast, the knowledgeof the action has been lost. For example, when asked togesture how to use the key, the person may perform anynumber of vague movements. When given a key, he orshe may try to use it as a pen or a toothbrush and, in ad-dition, may not be able to pick out the correct gesture ifshown by someone else. Conceptual apraxia is not associ-ated with damage to any one area, but is related to wider
loss of semantic knowledge of tools and actions. Thisproblem may be seen in the early stages of dementia, suchas Alzheimer’s disease.
Dissociation apraxia (formerly ideational apraxia) in-volves impairment in an action sequence. This type ofapraxia can be witnessed in a multistage request such as,“Show me how you would pour and serve tea.” Actionsmay be performed out of order, although the individualactions themselves are correct. Disorders of an action se-quence may be caused by executive or frontal lobe dys-function and a possible dissociation of action programsfrom language.
In summary, the apraxias, as disorders of the how sys-tem of motor control, represent problems with the men-tal representation of actions. Although we present apraxiasubtypes as independent entities, different types canoccur together in the same person. The apraxias repre-sent the most common type of motor problems treatedby neuropsychologists, because they can occur due to awide variety of cerebrovascular disorders (i.e., strokes), aswell as with tumors or disease states, and the disabilitythey produce interferes with many complex actions ofdaily life requiring higher cortical functioning.
T H E C E R E B E L L U M A N D M O T O R P R O C E S S I N G
The cerebellum permits seamless coordination and uncon-scious flow of movement. It coordinates reflex action andvoluntary movement, is concerned with the timing ofmovement, and can differentiate movement frequency at arate of 1/1000 of a second. The cerebellum aids in main-taining posture, balance, and muscle tone. It is also impli-cated in sequential aspects of motor learning, such as thesteps required to learn to play the piano. The cerebellum islocated posterior to the brainstem and inferior to the te-lencephalon (Figure 7.10) and reciprocally connects to thecortical sensory and motor systems, resulting in a constantfeedback loop coordinating the two areas. Cerebellarmotor disorders are most often caused by structural dam-age caused by trauma or stroke. They are characterized byirregular, jerky, and poorly coordinated movement. Mus-cle tone and strength, as well as motor resistance, may alsodecrease. Finally, in contrast with the resting tremor seenin Parkinson’s disease patients, cerebellar patients show anintention tremor.
S U B C O R T I C A L M O T O R P R O C E S S I N G
Cortical motor processing is largely concerned with volun-tary, conscious movement, whereas subcortical structures,

196 PART TWO | The Functioning Brain
namely, the basal ganglia and the cerebellum, function in amore automatic manner to regulate movement. The func-tion of the basal ganglia in movement largely controls thefluidity of overlearned and “semiautomatic” motor pro-grams (Bradshaw & Mattingly, 1995). The basal gangliareciprocally connect to the PMA and the SMA via the thal-amus. Also, an important brain circuit responsible for per-ceptual-motor learning and adaptation centers on the basalganglia. Specifically, this circuit includes the caudate nu-cleus, putamen, and globus pallidus. The nuclei of the stri-atal complex (caudate and putamen) receive projected in-formation from cortical sensory areas. From the striatum,information then funnels through the globus pallidus, and
then on to the thalamus, where it projects to the premotorand prefrontal areas (Mishkin, Malamut, & Bachevalier,1984) (Figure 7.11).
Some well-known motor disorders are associated withneurochemical abnormalities that affect the basal ganglia—Tourette syndrome is one of these (Neuropsychology inAction 7.3) as well as Parkinson’s disease, which specificallytargets the substantia nigra, and Huntington’s disease,which attacks the caudate nucleus. Although these two dis-orders attack structures within centimeters of each other,you can easily distinguish these motor disorders. You canrecognize Parkinson’s disease by its resting tremor and diffi-culty in initiating movement, whereas Huntington’s disease
George was a patient I saw for neuropsycho-logical evaluation. I knew that George, a 29-year-old left-handed man, was diag-nosed with Gilles de la Tourette syndrome(TS), but I was not prepared for his oddbehavior during my administration of theCategory test. The Category test measuresplanning and reasoning. I asked George tomatch a stimulus to one of four targets. Inessence, George had to figure out whichabstract category the stimulus fit best. Myresponsibility was to present each stimulusfigure, tell George whether he was correct,tell him when the category changed, andkeep score. In total, more than 200 stimulicards were presented, which fall into 7categories. The first stimulus card was easy,and I told George his response, “two,” wascorrect. As soon as I did so, he made apeculiar gesture, a kissing motion, in which helooked directly at me, raised his eyebrows, andshaped his mouth as if “blowing” me a kiss. Ifthis were not odd enough, I was dumbstruckwith George’s behavior when I told him he hadmade an error. He made an obscene gesturecommonly known as “flipping the bird”!
And so it went for the entire examination.When George was correct, he blew me a kiss,and when he made an error, he “gave me thefinger.” Like many neuropsychological tests,this one is staggered, so it becomes more
and more difficult. This resulted in Georgemaking more errors toward the end, a total of53. Midway through the examination, Idecided to continue with the test, but I didask George after the evaluation whether heknew he was engaging in these behaviorsand if he was somehow angry with me. Heinformed me that he was aware of what hedid, but that it seemed uncontrollable; “I justhad to do it,” he explained. He also told methat he was not angry with me and, in fact,enjoyed the testing and my company.
TS is a rare and fascinating disorder thathas puzzled scientists for more than acentury. TS occurs in less than 1% of thepopulation. Symptoms include facial andbodily tics, usually progressing from thehead to the torso and extremities, as well asrepetitive verbal utterances, including copro-lalia (uncontrollable cursing) in approxi-mately 50% of the cases (Newman, Barth, &Zillmer, 1986). Onset of the disorder istypically before age 10; symptoms vary inintensity over time and may be exacerbatedby stress. Most individuals with TS are maleand left-handed.
The specific cause of TS is unknown, butthe prevailing view is that there is a neuro-logic basis for the disorder, possibly involvingsubcortical structures that are responsiblefor motor coordination (Devinsky, 1983;
Bornstein, King, & Carroll, 1983). This viewis supported by findings of a high incidenceof motor asymmetries on clinical neurologicexaminations and abnormal electroen-cephalographic and computed tomographyscans (Newman, Barth, & Zillmer, 1986).However, no consistent or focalized neuro-logic deficits have emerged.
George, adopted in infancy, first dis-played bizarre motor symptoms—jerking ofhis shoulders—at age 2. Later, he developedshort barking sounds, repetitive movementsof his facial muscles and arms, and finally,loud shouting of profanities. The bouts ofimpulsive and sometimes assaultive behav-ior became so difficult to manage in theclassroom that George was taken out ofschool in the third grade. Subsequently, hewas in and out of psychiatric institutionsmost of his life. He was in a state psychiatricfacility when I evaluated him. He had beenhospitalized because he threw a brick at apassing car and chased it with an ax. Some-how, he thought that passengers in the carwere teasing him. Like George, many pa-tients with TS display peculiar motor symp-toms and psychiatric symptoms, includingdepression and impulsivity. Medicationsoften help patients with TS so that, in mostcases, they can lead a productive andsymptom-free life.
N e u r o p s y c h o l o g y i n A c t i o n 7 . 3
To u r e t t e S y n d r o m e : To o M u c h B e h a v i o r
by Eric Zillmer
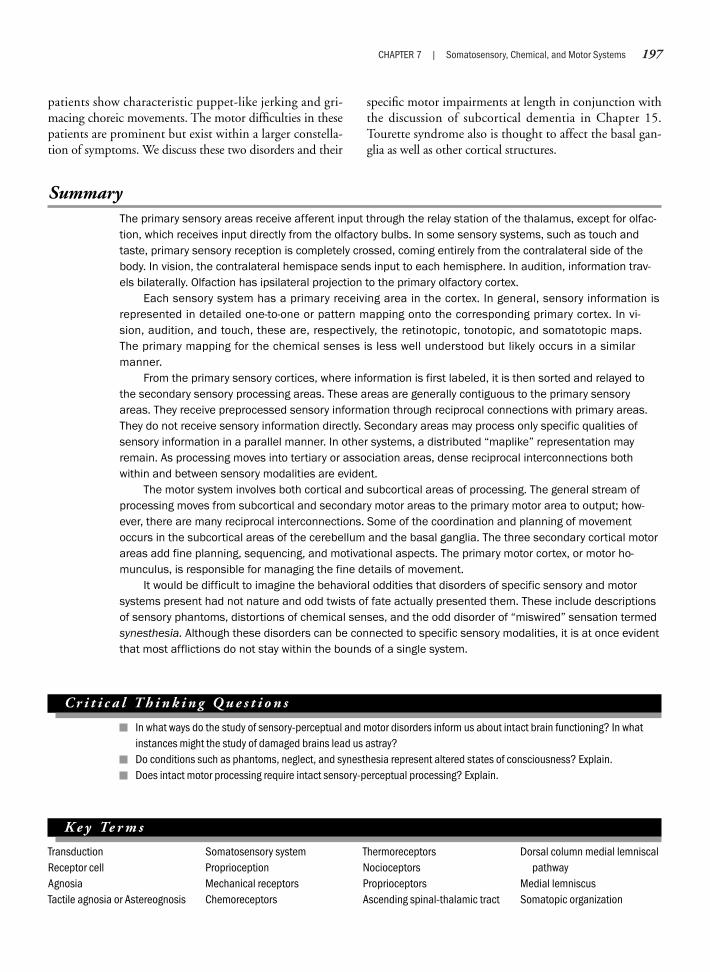
CHAPTER 7 | Somatosensory, Chemical, and Motor Systems 197
SummaryThe primary sensory areas receive afferent input through the relay station of the thalamus, except for olfac-tion, which receives input directly from the olfactory bulbs. In some sensory systems, such as touch andtaste, primary sensory reception is completely crossed, coming entirely from the contralateral side of thebody. In vision, the contralateral hemispace sends input to each hemisphere. In audition, information trav-els bilaterally. Olfaction has ipsilateral projection to the primary olfactory cortex.
Each sensory system has a primary receiving area in the cortex. In general, sensory information isrepresented in detailed one-to-one or pattern mapping onto the corresponding primary cortex. In vi-sion, audition, and touch, these are, respectively, the retinotopic, tonotopic, and somatotopic maps.The primary mapping for the chemical senses is less well understood but likely occurs in a similarmanner.
From the primary sensory cortices, where information is first labeled, it is then sorted and relayed tothe secondary sensory processing areas. These areas are generally contiguous to the primary sensoryareas. They receive preprocessed sensory information through reciprocal connections with primary areas.They do not receive sensory information directly. Secondary areas may process only specific qualities ofsensory information in a parallel manner. In other systems, a distributed “maplike” representation mayremain. As processing moves into tertiary or association areas, dense reciprocal interconnections bothwithin and between sensory modalities are evident.
The motor system involves both cortical and subcortical areas of processing. The general stream ofprocessing moves from subcortical and secondary motor areas to the primary motor area to output; how-ever, there are many reciprocal interconnections. Some of the coordination and planning of movementoccurs in the subcortical areas of the cerebellum and the basal ganglia. The three secondary cortical motorareas add fine planning, sequencing, and motivational aspects. The primary motor cortex, or motor ho-munculus, is responsible for managing the fine details of movement.
It would be difficult to imagine the behavioral oddities that disorders of specific sensory and motorsystems present had not nature and odd twists of fate actually presented them. These include descriptionsof sensory phantoms, distortions of chemical senses, and the odd disorder of “miswired” sensation termedsynesthesia. Although these disorders can be connected to specific sensory modalities, it is at once evidentthat most afflictions do not stay within the bounds of a single system.
C r i t i c a l T h i n k i n g Q u e s t i o n s
In what ways do the study of sensory-perceptual and motor disorders inform us about intact brain functioning? In whatinstances might the study of damaged brains lead us astray?Do conditions such as phantoms, neglect, and synesthesia represent altered states of consciousness? Explain.Does intact motor processing require intact sensory-perceptual processing? Explain.
patients show characteristic puppet-like jerking and gri-macing choreic movements. The motor difficulties in thesepatients are prominent but exist within a larger constella-tion of symptoms. We discuss these two disorders and their
specific motor impairments at length in conjunction withthe discussion of subcortical dementia in Chapter 15.Tourette syndrome also is thought to affect the basal gan-glia as well as other cortical structures.
K e y Te r m s
TransductionReceptor cellAgnosiaTactile agnosia or Astereognosis
Somatosensory systemProprioceptionMechanical receptorsChemoreceptors
ThermoreceptorsNocioceptorsProprioceptorsAscending spinal-thalamic tract
Dorsal column medial lemniscalpathway
Medial lemniscusSomatopic organization
198 PART TWO | The Functioning Brain
Kinesthetic senseFinger agnosiaParesthesiaPeripheral neuropathyPhantom limb painProprioceptive disorderTactile extinction/
suppression/inattention
PapillaeAgeusia
DysgeusiaPhantogeusiaHypogeusiaAnosmiaDysosmiaPhantosmiaHyposmiaSensory association
areasPremotor cortex or premotor
area (PMA)
Cingulate motor area (CMA) orcingulate motor cortex
Primary motor cortexHemiplegiaSecondary motor cortexSupplementary motor area
(SMA) or supplementarymotor cortex, medialpremotor cortex
DissociationDorsolateral prefrontal cortex
AkinesiaMotor perseverationDefective response
inhibitionApraxiaLimb-kinetic apraxiaIdeomotor apraxiaConceptual apraxiaDissociation apraxiaTremorStriatal complex
We b C o n n e c t i o n s
http://www.ninds.nih.gov/disorders/chronic_pain/detail_chronic_pain.htmThe National Institute of Neurological Disorders and Stroke site on Pain: Hope through research.
http://www.pbs.org/safarchive/3_ask/archive/qna/3294_peppers.htmlLinda Bartoshuk of Yale University discusses her research on supertasters.
http://www.cf.ac.uk/biosi/staff/jacob/teaching/sensory/olfact1.htmlTutorials on smell and what’s new in olfaction research.

Chapter 8
VISION AND LANGUAGE
I am part of all that I have seen.—Alfred Lord Tennyson
It is not often that we use language correctly; usually we use it incorrectly,though we understand each others meaning.
—St. Augustine
Visual ProcessingAuditory and Language Processing
Neuropsychology in Action
8.1 Blindness: Helping Us See the Plasticity of the Brain
8.2 The Case of Jonathan8.3 Case Study: Neglect

OverviewThe human visual and auditory systems cover more cortical area outside of their primary sites of processingthan the sensory systems discussed in Chapter 7. Humans rely greatly on vision and hearing, and the areasof the cortex devoted to each reflect this. In the areas of visual and auditory processing, we progress tohigher order functions such as visual object recognition, visuospatial processing, and speech and languagethat require an understanding beyond primary processing based on mapping of functions. This chapterdiscusses vision and audition from primary processing to higher integrative functions of vision and hearing.We also discuss representative disorders that can occur at each level of processing. As in Chapter 7, theseinclude agnosias, or in the case of language, aphasias. In the visual system, we also take an in-depth lookat the disorder of neglect as an example of a visuospatial problem, but also one that involves aspects ofattention and consciousness.
200 PART TWO | The Functioning Brain
K e e p i n M i n d
Does vision operate as a bottom-up or top-down process?
What would it be like to no longer be able to recognize your friends by their faces?
What is the difference between primary auditory and visual processing and higher order processing?
Visual Processing
Vision is one of our most important senses. In ad-dition to the occipital cortex, major portions of the tem-poral and parietal lobes are devoted to visual processing.Areas of the frontal lobes are involved in eye movementand higher processing of visuospatial working memory.The large areas devoted to vision reflect the human re-liance on sight and visual processing. Visual informationprocessing is also the most complex and best understoodsensory systems of the brain. However, for all of the at-tention, there are still debates about how vision works.
No one “master processor” integrates all visual infor-mation into perceptible form. Recognition of surround-ings, people, faces, and objects, though seemingly instan-taneous, is the culmination of separate but locallyconnected visual-perceptual processes. As a prerequisite torecognizing a friend walking through a crowd, you mustfirst have the necessary visual acuity, as well as adequatecolor and form perception. Visual acuity speaks to the abil-ity to perceive light, contrast between light and dark, re-solve a target, and have adequate visual fields. Receptorsfor form interpret shapes such as roundness or squareness,as well as orientation of lines to each other. Qualities oftexture and color such as feathery and blue are processed
by yet other primary visual areas. Although somewhatovergeneralized, at a higher perceptual level, the ventralvisual pathway to the temporal lobes serves as the “what”system largely responsible for object and face recognition.The dorsal pathway to the parietal lobes, or the “where”system, is specialized for spatial location. In building a vi-sual percept, some of these processes operate in sequence,and others may operate in parallel. Although we discussvisual processing as a “bottom-up” process of analyzingrudimentary or local bits of information that are built upinto coherent percepts, the issue of degree of impact of“top-down” or perceptual-driven processing on vision isan area of debate (Grill-Spector & Malach, 2004).
As complicated as this general characterization maybe, the human visual system is actually much more so-phisticated. In daily life you see under extremely “messy”visual conditions, through haze, from different perspec-tives, and from varying distances. Amazingly, visual per-ception of a tree stays constant, even though sometimes youmay see it through a fog, sometimes in the shade, partiallyobscured, from the north, from a distance, or from under-neath. Each time the image of the tree makes a differentimpression on your retina; yet, your brain’s perception of“tree” remains constant. Obviously, you do not simplymatch templates for a particular tree—there would be so
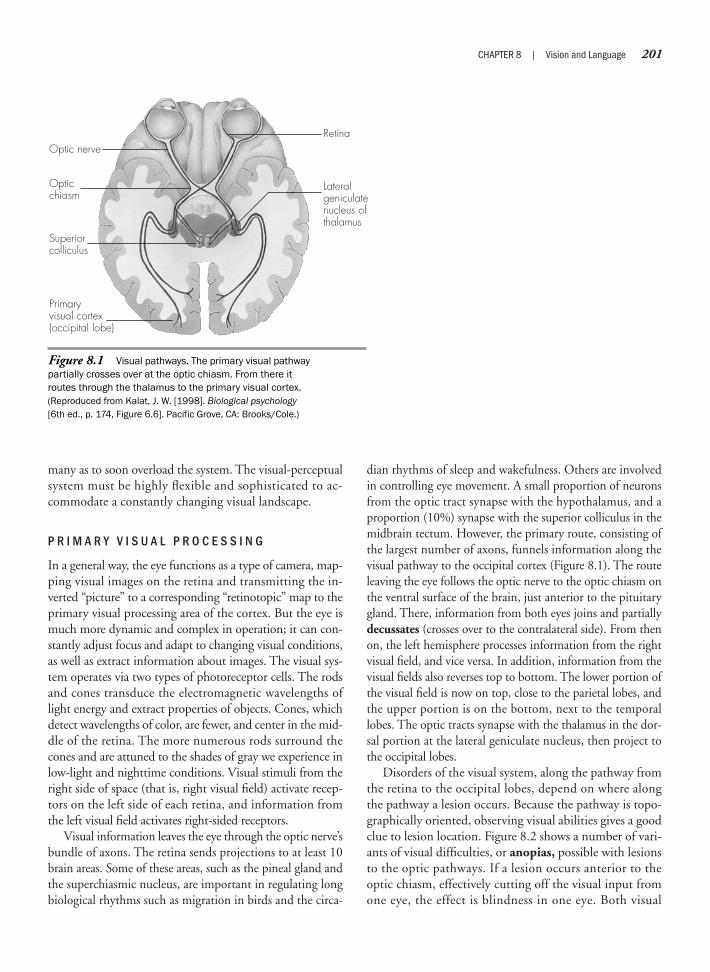
many as to soon overload the system. The visual-perceptualsystem must be highly flexible and sophisticated to ac-commodate a constantly changing visual landscape.
P R I M A R Y V I S U A L P R O C E S S I N G
In a general way, the eye functions as a type of camera, map-ping visual images on the retina and transmitting the in-verted “picture” to a corresponding “retinotopic” map to theprimary visual processing area of the cortex. But the eye ismuch more dynamic and complex in operation; it can con-stantly adjust focus and adapt to changing visual conditions,as well as extract information about images. The visual sys-tem operates via two types of photoreceptor cells. The rodsand cones transduce the electromagnetic wavelengths oflight energy and extract properties of objects. Cones, whichdetect wavelengths of color, are fewer, and center in the mid-dle of the retina. The more numerous rods surround thecones and are attuned to the shades of gray we experience inlow-light and nighttime conditions. Visual stimuli from theright side of space (that is, right visual field) activate recep-tors on the left side of each retina, and information fromthe left visual field activates right-sided receptors.
Visual information leaves the eye through the optic nerve’sbundle of axons. The retina sends projections to at least 10brain areas. Some of these areas, such as the pineal gland andthe superchiasmic nucleus, are important in regulating longbiological rhythms such as migration in birds and the circa-
dian rhythms of sleep and wakefulness. Others are involvedin controlling eye movement. A small proportion of neuronsfrom the optic tract synapse with the hypothalamus, and aproportion (10%) synapse with the superior colliculus in themidbrain tectum. However, the primary route, consisting ofthe largest number of axons, funnels information along thevisual pathway to the occipital cortex (Figure 8.1). The routeleaving the eye follows the optic nerve to the optic chiasm onthe ventral surface of the brain, just anterior to the pituitarygland. There, information from both eyes joins and partiallydecussates (crosses over to the contralateral side). From thenon, the left hemisphere processes information from the rightvisual field, and vice versa. In addition, information from thevisual fields also reverses top to bottom. The lower portion ofthe visual field is now on top, close to the parietal lobes, andthe upper portion is on the bottom, next to the temporallobes. The optic tracts synapse with the thalamus in the dor-sal portion at the lateral geniculate nucleus, then project tothe occipital lobes.
Disorders of the visual system, along the pathway fromthe retina to the occipital lobes, depend on where alongthe pathway a lesion occurs. Because the pathway is topo-graphically oriented, observing visual abilities gives a goodclue to lesion location. Figure 8.2 shows a number of vari-ants of visual difficulties, or anopias, possible with lesionsto the optic pathways. If a lesion occurs anterior to theoptic chiasm, effectively cutting off the visual input fromone eye, the effect is blindness in one eye. Both visual
CHAPTER 8 | Vision and Language 201
Figure 8.1 Visual pathways. The primary visual pathwaypartially crosses over at the optic chiasm. From there itroutes through the thalamus to the primary visual cortex.(Reproduced from Kalat, J. W. [1998]. Biological psychology[6th ed., p. 174, Figure 6.6]. Pacific Grove, CA: Brooks/Cole.)
Retina
Lateralgeniculatenucleus of thalamus
Optic nerve
Opticchiasm
Superiorcolliculus
Primaryvisual cortex(occipital lobe)

202 PART TWO | The Functioning Brain
Figure 8.2 Visual field defects. Numbers indicate interruptions of visual pathways and theircorresponding behavioral effects. In lesion 4, only the ventral temporal lobe fibers have been sev-ered. In lesion 5, only the dorsal parietal lobe fibers have been severed. (Reproduced from Peele, T. L.[1977]. The neuroanatomical basis for clinical neurology [3rd ed.]. New York: McGraw-Hill, by permission.)
Left visual field Right visual field
Left visual field right visual field Left visual field right visual field
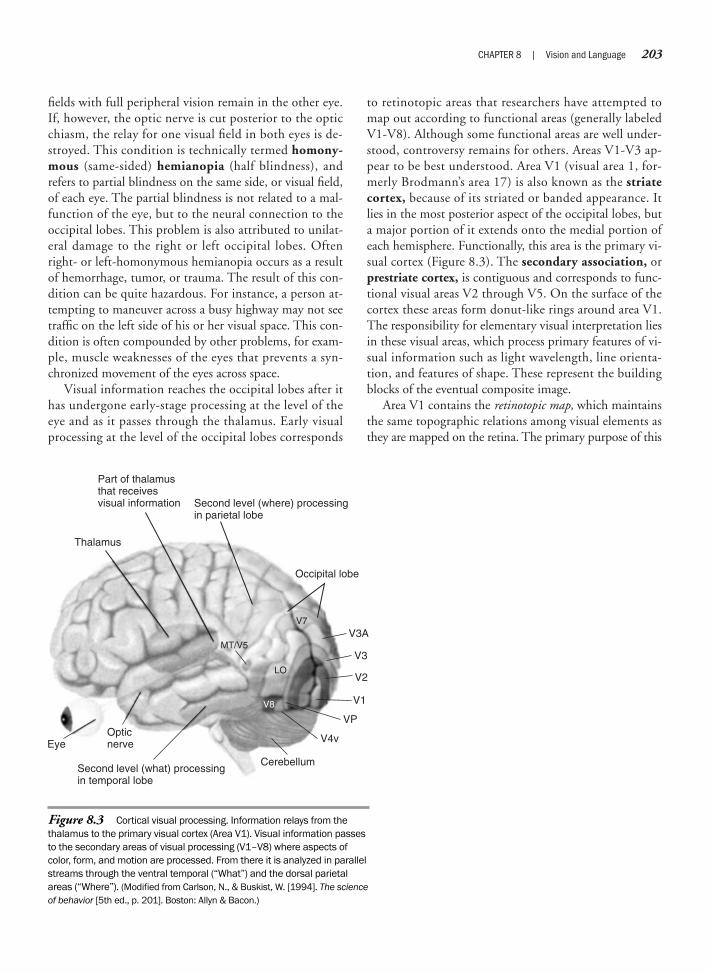
fields with full peripheral vision remain in the other eye.If, however, the optic nerve is cut posterior to the opticchiasm, the relay for one visual field in both eyes is de-stroyed. This condition is technically termed homony-mous (same-sided) hemianopia (half blindness), andrefers to partial blindness on the same side, or visual field,of each eye. The partial blindness is not related to a mal-function of the eye, but to the neural connection to theoccipital lobes. This problem is also attributed to unilat-eral damage to the right or left occipital lobes. Oftenright- or left-homonymous hemianopia occurs as a resultof hemorrhage, tumor, or trauma. The result of this con-dition can be quite hazardous. For instance, a person at-tempting to maneuver across a busy highway may not seetraffic on the left side of his or her visual space. This con-dition is often compounded by other problems, for exam-ple, muscle weaknesses of the eyes that prevents a syn-chronized movement of the eyes across space.
Visual information reaches the occipital lobes after ithas undergone early-stage processing at the level of theeye and as it passes through the thalamus. Early visualprocessing at the level of the occipital lobes corresponds
to retinotopic areas that researchers have attempted tomap out according to functional areas (generally labeledV1-V8). Although some functional areas are well under-stood, controversy remains for others. Areas V1-V3 ap-pear to be best understood. Area V1 (visual area 1, for-merly Brodmann’s area 17) is also known as the striatecortex, because of its striated or banded appearance. Itlies in the most posterior aspect of the occipital lobes, buta major portion of it extends onto the medial portion ofeach hemisphere. Functionally, this area is the primary vi-sual cortex (Figure 8.3). The secondary association, orprestriate cortex, is contiguous and corresponds to func-tional visual areas V2 through V5. On the surface of thecortex these areas form donut-like rings around area V1.The responsibility for elementary visual interpretation liesin these visual areas, which process primary features of vi-sual information such as light wavelength, line orienta-tion, and features of shape. These represent the buildingblocks of the eventual composite image.
Area V1 contains the retinotopic map, which maintainsthe same topographic relations among visual elements asthey are mapped on the retina. The primary purpose of this
CHAPTER 8 | Vision and Language 203
Figure 8.3 Cortical visual processing. Information relays from thethalamus to the primary visual cortex (Area V1). Visual information passesto the secondary areas of visual processing (V1–V8) where aspects ofcolor, form, and motion are processed. From there it is analyzed in parallelstreams through the ventral temporal (“What”) and the dorsal parietalareas (“Where”). (Modified from Carlson, N., & Buskist, W. [1994]. The scienceof behavior [5th ed., p. 201]. Boston: Allyn & Bacon.)
Occipital lobe
V7
LO
MT/V5
V8
V3A
V3
V2
V1
VP
V4v
CerebellumSecond level (what) processingin temporal lobe
Opticnerve
Thalamus
Part of thalamusthat receivesvisual information Second level (where) processing
in parietal lobe
Eye

area is to assemble and relay information to prestriateareas. In a reciprocal fashion, V1 also receives back pro-jections from information processed by these visual areaswithin the occipital lobes and continues to play a role inmaintaining spatial orientation between local bits of in-formation. Area V2, which is closely related to V1, is alsoa visual preprocessing area, assembling and mapping in-formation. Damage to area V1 causes cortical blindness,or hemianopia, in the opposite visual field. If area V1 isdamaged in both hemispheres, complete blindness willoccur. However, people with cortical blindness are some-times able to indicate that a stimulus is present, that it hasmoved, or that it is in a certain location, even though theyhave no conscious ability to “see” in the conventionalsense. This phenomenon is termed blindsight. Why doesthis happen? Although explanations are not definitive,part of the explanation may lie in that V1 may not becompletely damaged or that some visual information, per-taining to motion, for example, may be processed outsideof the striate (V1) cortex. However, the information isprocessed largely in an automatic or preconscious man-ner. No reports exist on the effect of damage to V2 alone.If V2 is damaged, V1 is also likely involved, because V2encircles V1 like a donut. Blindness, in general, raisesinteresting questions about the plasticity of the brain.Neuropsychology in Action 8.1 examines what mayhappen to the occipital cortex in the absence of visualstimulation. As we discussed in Chapter 7, with phan-tom limb, the brain may reorganize itself in interestingways.
The remaining functional visual areas in the occipi-tal lobes (areas V3-V8) are organized into four parallelsystems with reciprocal integration (Zeki, 1992). Thefour systems include motion, color, dynamic form(without color), and color plus dynamic form or shape.Area V3 appears specialized for dynamic form, or recog-nition of moving shapes, but does not code aspects ofcolor. It has been postulated that area V4 is selective forthe electromagnetic wavelengths of color, some aspectsof line orientation, and form (color-and-form area).Area V5 (also called area MT) lies on the occipitopari-etal juncture and receives input from a number of vi-sual cortical areas. It contains visual motion detectorcells that are specialized to respond to direction of mo-tion. Columns of cells within the layers of the cortexare responsive to different directions. Damage that tar-gets individual components of these secondary proces-sors leads to specific deficits in visual behavior. For ex-ample, damage to V4 has resulted in achromatopsia,the complete loss of ability to detect color. People withthis malady live in a black-and-white world. One man,
a successful painter of abstract art, experienced this asdifferent from watching black-and-white TV (Neu-ropsychology in Action 8.2). V4 and V8 are contiguousto each other, and some have also attributed color pro-cessing to area V8. Lesions to area V5 result in a verydifferent problem, akinetopsia, or the specific inabilityto identify objects in motion (Zihl, 1995). Damage toareas V3-V5 can result in a general inability to perceiveform. In this situation, patients may be able to make aperfect copy of a drawing, but are totally unable to un-derstand that the connection of lines corresponds to aspecific shape or object.
In summary, the occipital cortex processes elementaryaspects of vision. Although the functional types of pro-cessing are known, and some areas are mapped by cur-rently understood functional location, elementary visualprocessing is still not completely understood. Some wouldsuggest that visual processing, including color, proceedsin streams of processing that work in parallel fashion,rather than in localized or circumscribed structure-function maps. The next section further discusses the con-cept of processing streams.
H I G H E R V I S U A L P R O C E S S I N G : O B J E C T R E C O G N I T I O N A N D S P A T I A LL O C A L I Z A T I O N
Neuroscientists have identified at least 20 areas of sec-ondary or higher visual processing. However, for the pur-poses of this discussion, we focus on the following topics:(1) how visual elements are integrated so that the viewerappreciates the pieces of vision as a coherent whole, orobject; and (2) how objects are localized within a spatialframework. These two streams of visual processing are dif-ferentiated neuroanatomically, and they are often referredto as the “what” system, or ventral processing stream, ofobject recognition, in contrast with the “where” system,or dorsal processing stream, of object localization(Mishkin, Ungerleider, & Macko, 1983) (see Figure 8.3).The two anatomically distinct areas of the ventral anddorsal streams are probably coordinated through the thal-amus (Petersen, Robinson, & Morris, 1987). In the firstpart of this section, we discuss the behavioral functionsassociated with object recognition and object localizationand give an overview of the ventral and dorsal processingstreams.
One of the best ways to understand the differences be-tween the two systems is to examine the types of disor-ders that occur if each system is damaged. The disordersevident at this higher level of visual processing and per-ceptual integration involve the interaction of vision with
204 PART TWO | The Functioning Brain

CHAPTER 8 | Vision and Language 205
Does the brain’s “visual” cortex lie dormantin the absence of visual input? EsrefArmagan, a renowned Turkish painter, hasbeen blind from birth. He impresses audi-ences all over the world with his realisticrepresentations of objects and landscapes,complete with color, shadow, and perspec-tive. Although visual input has never reachedhis brain, Mr. Armagan’s occipital cortex hasnot atrophied, shrunk, disappeared, or evensimply remained inactive over his 52 yearswithout vision. In fact, research conducted atBeth Israel Deaconess Medical Center inBoston shows that while drawing objects thathe had previously explored tactilely, hisvisual cortex becomes activated as if he wereseeing. Current research on neuroplasticity ishelping us to understand how we can explain“visual” cortex activation in a man who hasnever seen with his eyes.
Traditionally thought to handle only vision,research now suggests the occipital cortexcan take on other duties ranging from so-matosensory processing to verbal memory. Inblind individuals, the occipital cortex is able toreorganize to accept nonvisual sensorimotorinformation. In an experiment using positronemission tomography scanning, occipital lobeactivation was measured during tactile dis-crimination tasks in sighted subjects and inBraille readers blinded in early life. Blindvolunteers showed activation of primary andsecondary visual cortical areas during tactiletasks, whereas sighted control subjectsactually showed reduced levels of regionalcerebral blood flow in the visual cortex(Sadato, Ibañez, Deiber, & Hallett, 1996).
Further research suggests that disruptingthe functioning of the occipital areas duringtactile tasks leads to correspondingbehavioral disruption in blind individuals. Ina study conducted by Dr. Leonardo Cohen,early-blind and sighted volunteers readtactile symbols (Braille and embossedRoman letters, respectively) while transcra-nial magnetic stimulation (TMS) was appliedto different scalp positions, transiently
disrupting the functioning of the correspond-ing cortical areas. In blind volunteers, TMSdelivered over midoccipital regions resultedin increased errors in Braille reading as wellas subjective accounts of distorted so-matosensory perceptions. They reportedmissing dots, faded dots, extra dots, anddots that did not make sense. In contrast,midoccipital stimulation in sighted subjectsdid not produce significant effects on identi-fication of embossed Roman letters orreports of abnormal perception of letters(Cohen, et al., 1997). This research suggeststhat the occipital or “visual” cortex is not onlyactive during the processing of somatosen-sory stimulation but is functionally relevantduring Braille reading for blind individuals.
Can neural plasticity also partially ex-plain the widely recognized superior verbalmemory abilities in the blind? A functionalmagnetic resonance imaging study con-ducted by Dr. Amir Amedi found occipitallobe activation during both verbal memorytasks and verb generation tasks in congeni-tally blind volunteers. During the same tasks,the extensive occipital activation was notobserved in sighted volunteers. The results ofthis study suggest that, in the case of visualdeprivation due to congenital blindness, theoccipital lobe becomes involved during tasksthat require verbal memory and may berelated to the superior verbal memory skillsreported in the blind. In fact, a functionalrole for the occipital cortex in verbal memorytasks is suggested by Amedi, as early visualcortex activity was correlated with verbal-memory scores (Amedi, 2003).
A growing body of evidence now con-tributes to the notion that brain regionstraditionally associated with one sensorymodality also participate in the processing ofother senses. In this way, the occipital cortexmay be viewed as being “metamodal,”meaning that it is capable of adapting andchanging in order to process informationregardless of the sensory modality it receives.The occipital cortex may have evolved to
become the “visual cortex” simply becausethis region of the brain may be best suited forthe processing of information supplied byvision; it may have qualities that provide itwith strengths in processing spatial informa-tion using retinal visual information(Pascual-Leone & Hamilton, 2001). Becauseof neural plasticity, in the event of loss of visualinput, the brain is able to adjust by recruiting theoccipital cortex for use in another capacity, orby unmasking pathways that may already bepresent in the blind and sighted alike (Pascual-Leone & Hamilton, 2001).
From this collection of studies thatsuggest the “visual cortex” plays a role intactile Braille reading and verbal memory inthe blind, we now know that the human brainis capable of reorganizing itself and readilyadjusts through adaptive recruitment of theoccipital cortex. Advances in the under-standing of this neuroplasticity have implica-tions for the development of visual prosthe-sis aimed at restoring vision in the blind.Historic accounts of attempts at the restora-tion of vision have been largely unsuccessful,with some ending in depression and wishesto become blind again, presumably becauseof the reorganization that takes place in thecortex (von Senden, 1960). For example,when vision has been restored in patients,many have exhibited difficulties with depthperception, causing incapacitating fears ofeveryday activities such as crossing thestreet because of the inability to judge theproximity of oncoming cars. Despite cuttingedge technology, restoration of functionalvision through visual prosthesis withoutregard to the way blindness affects the brainis not likely to result in meaningful visualperception (Merabet, et al., 2005). Indeed,success in developing technology that willallow blind individuals to see will depend onthe understanding of the neuroplasticity ofthe human brain and our ability to success-fully communicate with the brain that hasadjusted to blindness and that is readjustingto sight once again (Merabet, et al., 2005).
N e u r o p s y c h o l o g y i n A c t i o n 8 . 1
B l i n d n e s s : H e l p i n g U s S e e t h e P l a s t i c i t y o f t h e B r a i n
by Erin Abrigo
206 PART TWO | The Functioning Brain
Text not available due to copyright restrictions

other sensory-perceptual and higher order systems such asattention, memory, and consciousness. The problem ofvisual object recognition is best illustrated by the visualagnosias, and the problem of spatial location can be con-sidered by examining neglect.
T h e “ W h a t ” a n d “ W h e r e ”S y s t e m s o f V i s u a l P r o c e s s i n g
The ventral processing stream is perceptually specializedfor higher aspects of visual object recognition. It helps con-nect the visual perception of shape and form with the rep-resentation of that object’s meaning. The ventral process-ing stream contains interconnected regions from theoccipital lobes to the temporal lobes. The visual processingstream of the left hemisphere is more specific to recogniz-ing symbolic objects such as letters and numbers. The leftventral occipital lobe shows increased blood flow whenpeople process strings of letters (Snyder, Petersen, Fox, &Raichle, 1989). The right ventral system is more specificto the global recognition of objects and faces. Damage tothis system can result in visual agnosia. The next sectionprovides an in-depth discussion of the subtypes of visualagnosia (apperceptive and associate agnosia).
The dorsal processing stream is essential for visuallylocalizing objects in space and for appreciating the rela-tive relation of those objects to each other. Through reci-procal feedback to the motor system, this “where” systemalso helps in planning and coordinating motor move-ments. This stream of integrated structures connects theoccipital to the parietal lobes. Disorders of this systemcontribute to right–left discrimination problems, con-structional apraxia, and neglect.
Directional impairment, a form of spatial relations con-fusion, is usually referred to as a right–left discriminationproblem. Patients with this kind of difficulty routinely getlost if left on their own, particularly in a new environment.An inability to perform voluntary actions, termed con-structional apraxia, is the inability to perform actions thatrequire three-dimensional movement, such as building atower from blocks. (Apraxia is discussed in Chapter 7.)
D i s o r d e r s o f t h e “ W h a t ”S y s t e m : A p p e r c e p t i v e a n d A s s o c i a t i v e V i s u a l A g n o s i a
Agnosia is derived from the Greek, gnosis, meaning “ab-sence of knowing” and can occur in any sensory domain.In the modality of vision, people with visual object ag-nosia may fail to recognize objects at all, or in mildercases, confuse objects that they observe from different an-gles or in different lighting conditions. The term
prosopagnosia refers to the special case of inability to rec-ognize people by their faces, even though the person canoften recognize people by other means such as gait or toneof voice. People with visual agnosias can see. The disorderis less a pure sensory disorder than a higher perceptualdisorder of “knowing.” In The Man Who Mistook His Wifefor a Hat, Oliver Sacks describes the affliction of Dr. P, amusic teacher who can no longer recognize objects or peo-ple by sight. Presented with a red rose, Dr. P “took it likea botanist or morphologist given a specimen, not like aperson given a flower. ‘About six inches in length,’ hecommented. ‘A convoluted red form with a linear greenattachment.’” Dr. P was completely unable to name whathe had in his hand until it was suggested to him to smellit. “‘Beautiful!’ he exclaimed. ‘An early rose. What a heav-enly smell!’ He started to hum [the German tune] “DieRose, die Lilie. . . .” (Sacks, 1987, pp. 13–14). Dr. P’s af-fliction was that he was visually unaware of the totalityor gestalt of objects. He could see and identify form andcolor but could not combine these aspects into a highersense of meaning that is a rose. His only visual realitywas a mechanistic identification of features. This is typi-cal of how visual agnosia primarily involves the processesnecessary for object recognition or object meaning whileleaving intact elementary visual processes. Also, Dr. P’s ag-nosia, as is usually the case, was modality specific. Althoughhis visual knowing was impaired, a higher sense of know-ing was available through sense of smell. Dr. P also had noproblem in recognizing people by their voices.
Cognitive neuropsychologists often differentiate be-tween apperceptive visual agnosia and associative vi-sual agnosia. The essential difficulty in apperceptive vi-sual agnosia is object perception, or the inability tocombine the individual aspects of visual information suchas line, shape, color, and form together to form a “whole”percept. They seem to see in bits and pieces, like theproverbial blind men feeling the elephant. Their brainsare not synthesizing the entire picture. Associative visualagnosics have difficulty to varying degrees in assigningmeaning to an object. Even though they can, for instance,recognize differences in form between pictures of a pair ofscissors and a paper punch by matching the scissors to alike pair in a display of office objects (with which an ap-perceptive agnosic would have difficulty), they have lostthe link between the visual percept and the semanticmeaning. In both cases, if shown a pair of scissors, neitherthe apperceptive nor the associative agnosic can correctlyname “scissors.” But although the associative agnosic canpick out a pair of scissors, she or he shows difficulties notonly in naming but in explaining or demonstrating theuse for scissors.
CHAPTER 8 | Vision and Language 207

This distinction provides a useful conceptual frame-work and is used here; but in practice, the line betweenapperceptive and associative agnosias becomes cloudy,partly because the brain damage likely to cause theseproblems is often widespread and overlapping.
Apperceptive Agnosia—At first glance, those individuals, likeDr. P., with the apperceptive form of object agnosia maybe thought blind, because they tend to take no apparentnotice of objects and people in their vicinity. But on closerexamination, their sensory functions are clearly intact.Many people with this condition are aware that they canindeed see, but they have a problem correctly perceivingthings. Curiously, others with apperceptive agnosia arestrangely unaware of their condition. Only watching for aperiod of time might you catch them stepping over or avoid-ing objects. Awareness in this case is not an either/or phe-nomenon. Apperceptive agnosics may appear to disregardor show no concern for their problem until neuropsycho-logical testing reveals it to them. For example, visual recog-nition tasks of the type shown in Figure 8.4, in which anobject must be identified from fragments, is embedded, oris at an odd angle, are notoriously difficult. Apperceptiveagnosics also have difficulty copying objects. Because theyonly “see” pieces, their drawings are likely to appear as aset of unconnected fragments focusing on the detailsrather than on the entire gestalt of the object.
The most common site of damage in apperceptive ag-nosia is the parieto-occipital area of the right hemisphere.Sudden insults to the brain are the most common cause,often from carbon monoxide poisoning, mercury intoxi-cation, cardiac arrest, or stroke. In these cases, appercep-tive agnosia does not usually occur in isolation withoutother visuospatial impairment, because these brain insultsare likely to affect large areas of the cortex. Some cases ofapperceptive agnosia are caused by bilateral cortical atro-phy. If both hemispheres are involved, then the patientmay have Balint’s syndrome, which includes visual ag-nosia together with other visuospatial difficulties such asmisreaching and left-sided neglect.
Associative Agnosia—Associative agnosia is differentiatedbehaviorally from apperceptive agnosia in that the pri-mary difficulty is a loss of knowledge of the semanticmeaning of objects. Conceptually, the person can “recog-nize” objects at a perceptual level by picking them out,or correctly copying them, but perception breaks downat a higher level of meaning. For example, some peoplehave little apperceptive difficulty and can draw or copypictures of objects in great detail but cannot name them(for example, see Rubens & Benson, 1971). As Figure 8.5
shows, after making an accurate rendition of a bird, thepatient tentatively guessed it could be a “beach stump.”This represents a pure form of associative agnosia, butmany other patients also show aspects of apperceptive ag-nosia. For example, they may copy objects inconsistently,sometimes drawing them accurately and at other timesmaking perceptual mistakes. However, whereas the per-ceptual mistakes of the apperceptive agnosic are likely toshow inability to recognize the whole, the perceptualmistakes of the associative agnosic may show problemsof either recognition of the whole or of the details of anobject.
The research on the neurocorrelates of associative ag-nosia is confusing. A lateralized left hemisphere parieto-occipital lesion may be enough to cause an associative ag-nosia, although it can also occur in the presence of aunilateral right occipital lesion. Indeed, a number of struc-tural areas may produce associative agnosia. Farah (1990)suggests the variety of sites that produce associative ag-nosia may lead to heterogeneous perceptual impairments.Because assigning meaning is such a high-level corticalprocess, different lesion sites producing a similar effectalso speaks to the complexity of the perceptual-meaningsystem. We would venture, as have others, that, in gen-eral, the left hemisphere assigns meaning, whereas theright hemisphere governs the global aspects of perceptualintegration.
As stated earlier, many patients show both appercep-tive and associative aspects to their visual agnosia. For ex-ample, one artist who experienced a stroke resulting in bi-lateral medial occipital damage could name some objectsbut not others. Those he could name he could also drawwell. But those he did not recognize, he could only mech-anistically copy, feature by feature, first a square, then acircle, then connecting lines, without any inkling of whatthey represented (Wapner, Judd, & Gardner, 1978). Insummary, the differentiation between apperceptive andassociative agnosia is useful for descriptive and conceptualunderstanding, but it does not correspond to strictanatomic correlates that can be readily differentiated ordissociated.
D i s o r d e r o f t h e “ W h e r e ” S y s t e m : N e g l e c t
Certain types of brain damage can alter body experience.Damage to the right parieto-occipital or inferior parietalarea is the most common site of damage for an odd typeof inattention termed unilateral neglect, or simply ne-glect. (Unilateral spatial neglect has other aliases, such ascontralesional neglect, hemineglect, visuospatial or hemispa-tial agnosia, and visuospatial or hemispatial inattention.)
208 PART TWO | The Functioning Brain

Figure 8.4 Tests for apperceptive agnosia. Apperceptive agnosics have difficulty recognizing (a) fragmented objects, (b) entangled object, and (c) objects seen from unusual views. (Modified fromBradshaw, J. L., & Mattingly, J. B. [1995]. Clinical neuropsychology: Behavioral and brain science. San Diego:Academic Press, by permission.)
CHAPTER 8 | Vision and Language 209
People with neglect lose conscious awareness of an aspectof spatial or personal space despite adequately function-ing sensory and motor systems. Behaviorally, this prob-lem may first look like the result of a right hemispherestroke or lesion affecting the motor and somatosensorystrips on the contralesional side. The left limbs may ap-pear useless and hang limply. On closer examination, thearm or leg can clearly move and feel touch or pain—theyare simply being ignored by the conscious mind. This fail-ure of awareness extends beyond the body to the entire lefthemispace from the perspective of the afflicted person. It
is not unusual for people with neglect to collide with ob-jects and people on their left sides. Also, when reading, theymay leave out the left side of words or pages. Their copieddrawings focus on the right side of pictures. In one respect,neglect can be thought of as a forgetting or lack of con-scious attention to the left side; but even more so, it is as ifawareness is being pulled to the right. When trying to nav-igate, neglect patients frequently veer rightward and endup traveling in circles. The case study in Neuropsychol-ogy in Action 8.3 gives an in-depth illustration of thebehavioral manifestations of unilateral neglect. Although
210 PART TWO | The Functioning Brain
Text not available due to copyright restrictions

not in this case, many people with neglect think that theleft-sided part of their body does not belong to them.Protesting that it belongs to someone else, they may failto dress half of the body, put makeup on only one side ofthe face, or simply treat the neglected parts as objects withno personal meaning. What mechanisms disable body andspatial awareness? We will return to this question afterconsidering the neuropathologic and clinical presentationof neglect.
Neuropathology of Neglect—The classic picture of unilateralneglect that we have been discussing is most likely tooccur with lesions in the right inferior parietal lobe orgenerally in the posterior regions of the cortex. As men-tioned earlier, neglect cannot be solely attributed to sensoryprocessing deficits, implying that lesions in the somatosen-sory strip are not enough to produce neglect. Neglect can
also appear with other right hemisphere lesions, and muchless frequently, with left hemisphere lesions. Other righthemisphere locations reported to produce neglect includea variety of subcortical structures, the majority of whichimplicate the thalamus.
Classic neglect produces an abrupt alteration of con-sciousness most commonly occurring as a result of a rightparietal stroke, but sometimes coinciding with a trau-matic brain injury. In any case, the manifestation is typi-cally sudden and rarely seen in slow-growing tumors ordisease processes. Temporary and reversible neglect mayalso occur in conjunction with seizures, electroconvulsivetherapy, and intracarotid sodium amytal testing (Wadatesting) (see Bradshaw & Mattingly, 1995). Neglect mayalso stand out against the background of widespread righthemisphere damage. In this instance, there are accompany-ing motor, sensory, or attentional problems. For example, a
CHAPTER 8 | Vision and Language 211
One of the first cases of pure spatial ne-glect was published by Paterson and Zang-will in 1944. Their patient was a healthy 39-year-old right-handed man who, because ofan explosion, was hit by a projectile steelnut that penetrated his skull in the rightparietal occipital area. “Stereoscopic X-rays of the skull (28.9.43) showed a metal-lic foreign body consisting of a hexagonalnut about 1 in. in diameter with a shortlength of screw-headed bolt projecting fromits upper lateral surface” (Paterson &Zangwill, 1944, pp. 335–336). “The upperborders of the supramarginal and angulargyri on the right side were damaged on thesurface and their deeper connection inter-rupted by the in-driven bone fragments to adepth of just over 1 in. The lesion wascircumscribed and there was minimalcontusional damage” (p. 337). The resul-tant difficulties, as you would expect, werelargely confined to spatial and visual-perceptual functions. This man couldperceptually recognize objects, identifycolors, and discriminate right and left. He
also had no problems in spatial depthperception and size constancy. But thepatient himself alerted his doctors that hewas having trouble finding his way throughthe hallways on the way to the bathroomand was having trouble reading the time. Hesaid he had to read each hand of the clockseparately and then figure out the time.Staff observed him to collide “with objectson his left which he had clearly perceived afew moments before. He was liable at tableto knock over dishes on his left-hand sideand occasionally missed food on the left ofhis plate. He commonly failed to attend tothe left-hand page in turning the pages of abook and reading lines of disconnectedwords commonly omitted the first word ortwo” (Paterson & Zangwill, 1944, p. 339).On neuropsychological testing, when askedto draw, his figures showed a “piecemealperception” typical of right hemispherespatial problems. Interestingly, he couldslowly recognize objects placed in his leftvisual field, but if two designs were pre-sented simultaneously to the right and left
visual fields, he did not acknowledge theleft-sided design. In setting the time on aclock, he often transposed the minute handfrom the left- to the right-hand side. In apointing task, the authors arranged objectsaround the patient in a semicircle. “He wasinstructed to point to each object in turn.With eyes open no errors were made. Withhis eyes closed, on the other hand, therewas at once a general shift toward the right-hand side. Thus when asked to pointto the object on his extreme left the patientoften pointed straight ahead” (Paterson &Zangwill, 1944, p. 339). Unlike other casesof neglect, this man did not neglect the leftside of his own body, only his extrapersonalspace.
This case presents an interesting prob-lem of consciousness. How can this loss ofawareness be explained? On one level, thepatient was aware that he now disregardedthe left side of space. This shows someinsight into his problem. But on anotherlevel, no force of will could coax a full know-ing of his left-sided spatial world.
N e u r o p s y c h o l o g y i n A c t i o n 8 . 3
C a s e S t u d y : N e g l e c t
by Mary Spiers

variety of neglect-type problems are associated with motorweakness. In these cases, awareness of left-sided stimulimay be less impaired, but neglect-type symptoms becomeevident with the inability to perform or sustain motoracts on the side contralateral to the lesion (see Heilman,Watson, & Valenstein, 1993). If we include all the sub-types and derivations, we can best conceptualize neglectas a syndrome or general classification for a number of re-lated problems. However, we restrict this discussion toclassical unilateral spatial neglect, caused by right hemi-sphere damage, which is the best example of the neglectphenomenon.
Clinical Presentation—In clinically evaluating cases of uni-lateral neglect, neuropsychologists must disentangle thecontributions of spatial, motor, and attentional factors.This can only be done in a relative fashion, because eachof these systems contributes a portion to a sense of bodyand spatial consciousness. For example, although investi-gators agree that a functioning attentional system is cru-cial to spatial awareness, unilateral neglect and severeinattention can be differentiated. With both problemsthere can be a failure to detect an object, such as an apple,that is placed in the left visual field. However, the inat-tentive person becomes aware of the apple if forced toorient to it, whereas the person with neglect may con-tinue to insist that nothing is there. Neglect is also disso-ciable from visual field defects such as hemianopia, inwhich the person visually explores the left side of space(Hornak, 1992). Neglect may look similar to visual prob-lems, but it is actually a problem at a much higher levelof integration.
Because neglect is so obviously out of the range of or-dinary experience, measures to test for it do not rely onnorms, but rather on pathognomic signs. For example,we do not expect neglect to be evenly distributed in thepopulation in the form of a bell-shaped curve, with onlya few of us having no neglect, many of us having moder-ate neglect, and a few of us having profound neglect. In-stead, we expect all people with normally functioningbrains to be free of neglect. Therefore, the detection ofneglect and neglect-like symptoms is fairly straightfor-ward by observing performance on tasks such as drawingsand line bisection tasks. Figure 8.6 shows several clinicalexamples of neuropsychological tasks performed by peo-ple with neglect. Notice that in the drawings the left sideof the picture may be left out, sparse, or grossly distorted.In the line bisection and line cancellation tasks, the mid-point shifts to the right, leaving the left side of the line orthe page empty.
It is clear that unilateral neglect patients do not con-sciously acknowledge stimuli in the left side of space. Butdoes perception or a tacit recognition at an unconsciouslevel exist? Clinical investigations suggest that it does. Inan interesting series of studies, Vallar and his colleagues(Vallar, Sandroni, Rusconi, & Barbieri, 1991) tested au-tonomic responses such as galvanic skin conductance andbrain response via evoked potentials. In each case, the pa-tients with unilateral left-sided neglect failed to con-sciously recognize the presence of a stimulus presented tothe right side, although autonomic testing demonstratedthe patients were processing the stimulus implicitly at apreconscious level, without reaching awareness. Someclinical studies also suggest that people with neglect mayimplicitly process at a higher level, indicating acknowl-edgment of meaning or semantic awareness. In one of thefirst case studies to suggest implicit awareness in neglect,Marshall and Halligan (1988) gave their patient two pic-tures of a house, identical except for that in one the leftside of the house was obviously burning. The patient didnot acknowledge any discrepancies between the twohouses when asked to describe the pictures, nor did shesay they were different when forced to make a same–different choice. Curiously, however, when asked whichhouse she would prefer to live in, she consistently chosethe picture of the house that was not burning, althoughshe could not explain or give reasons for her choice. It isas though, from her perspective, the only explanation shecould give relied on an intuitive sense. Although not allneglect patients show this preservation of semantic knowl-edge (some actually chose the burning house; see Bisiach& Rusconi, 1990), studies using a variety of methodolo-gies confirm that higher order processing of various typesis possible in some patients with neglect (see Bradshaw &Mattingly, 1995).
Interestingly, the behavior of left unilateral neglectusually resolves somewhat over time if the damaged arearemains stable. Afflicted people gradually begin to ac-knowledge stimuli on the left side of their bodily space.Tests of tactile recognition, in which the researchertouches one hand or the other while the patient isblindfolded, show that he or she is recognizing bothhands. However, when both hands are touched at thesame time in a specific test of double simultaneous stim-ulation, residual neglect is often evident in that the pa-tient again suppresses or extinguishes perception of theleft hand.
Neglect, as can be imagined, is notoriously difficult totreat in the beginning stages. Patients who do not ac-knowledge their problem and who may believe their left
212 PART TWO | The Functioning Brain

side does not even belong to them are not motivated topay attention to their left side. Rehabilitation methodsoften try to direct attention to the neglected side. Thera-pists may use various methods such as forcing attentionto the left side via gradual movement of objects to the left,or even through the use of prism glasses. These methodsdo meet with some success, but often do not generalize todaily life.
Theories of Neglect—Two primary issues exist in conceptual-izing neglect. The first issue is understanding the asym-metric presentation of neglect between the two hemi-spheres. Why is neglect more prevalent with righthemisphere lesions? Any theory of neglect must explainwhy the overwhelming majority of cases show left-sidedneglect, and why right-sided neglect is so rare. The secondissue relates to the higher order or “conscious” processing
CHAPTER 8 | Vision and Language 213
Text not available due to copyright restrictions

problem that is neglect. If neglect is thought of as a net-work problem rather than as a dysfunction of an individ-ual system, it is easier to make sense of the variety of le-sion sites that may produce neglect.
Research has established that the right hemisphere ismore specialized for global spatial processing, whereasthe left hemisphere has a propensity for decoding spe-cific spatial features. Because the right hemisphere, andparticularly the right parietal lobe, plays a role in under-standing the gestalt or totality of space, disruptions thereare more likely to upset global spatial awareness. Also,the right hemisphere plays a larger role in arousal and at-tentional levels, which are prime factors in many explana-tory models of neglect. However, each of these problemscan occur in isolation without the patient losing con-sciousness of the left side of space. As with the man de-scribed in Neuropsychology in Action 8.3, no force ofwill could coax a “knowing” of his spatial world on theleft. Interestingly, it appears that patients may shift their“spatial axis” to the right so that midline is pulled orrepositioned within the right side of space relative to thebody (Mattingly, 1996). Marcel Kinsbourne (1993) haspostulated that this strong rightward orientation is less afunction of right hemisphere dysfunction per se than arelease of inhibition that lets the left hemisphere assertdominance in the presence of a now weakened righthemisphere. Perhaps some of the prime areas damaged,rendering the right hemisphere spatially ineffective, arelocations within the right parietal lobe having to dowith personal spatial frames of reference. Body positionwith respect to space is always egocentric, although peo-ple may have multiple frames with respect to bodies,heads, or position in relation to environment. Animalstudies support the contention that there are distinctneuronal centers for these spatial frames within the rightparietal cortex (for example, see Anderson, Snyder, Li, &Stricanne, 1993).
Do these findings explain why the midline shift inneglect is nearly always to the right? Bradshaw andMattingly (1995) suggest that each hemisphere plays aspecific role in spatial body position processing. Theleft hemisphere focuses on features and is strongly right-ward oriented. The right hemisphere takes a “globalview.” Normally, the two hemispheres hold each otherin balance, but when certain spatial positioning aspectsof the right hemisphere are damaged, the left hemi-sphere becomes overbearing, forcing a reorientation tothe right side of space. According to this view, damageto the left parietal lobe produces no corresponding left-ward shift because the spatial concerns of the left hemi-sphere are more feature oriented and language focused,
resulting in a “no specialized spatial position” sensewithin the left parietal lobes. If right neglect does occur,they suggest, together with other investigators (such asOgden, 1985), that the focus of the left hemisphere le-sion would be anterior to the parietal lobes. Unfortu-nately, partly because of the rarity of occurrence, no re-search has explained the mechanisms of right-sidedneglect.
Understanding neglect is not only a problem of dom-inance and asymmetry, it is also an issue of conceptualiz-ing the problem as a higher order network processingphenomenon. That unilateral neglect can occur withother nonparietal foci of damage is partial testament tothis claim. We mentioned earlier that the region of theright inferior parietal lobe is the area most commonlydamaged in cases of left unilateral neglect. As in other dis-orders discussed throughout this book, however, absenceof function associated with a lesion does not necessarilyimply that the lesioned area “contains” the function. Justas the hippocampus does not “contain” or store memorybut is one of the most crucial links in memory processingand consolidation, the right inferior parietal lobe does notin itself contain “body mindfulness” but may be a cruciallink. Neuroanatomically, left unilateral neglect also oc-curs with damage to a variety of subcortical structures,most notably the thalamus (see Bradshaw & Mattingly,1995). It is reasonable to speculate that neglect resultsfrom a disconnection in higher order processing that in-volves the coordination of many second-order systems,such as visual processing, attention, memory, and possi-bly other systems.
A number of theories attempt to provide models forunilateral neglect. They are beyond the scope of thisoverview, and excellent reviews exist elsewhere (for ex-ample, see Bradshaw & Mattingly, 1995). Most modelsdescribe the process of body and hemispace cognitionas including visual-perceptual processes, attention, andmotor action. Mesulam’s neural network model (for ex-ample, see Mesulam, 1985, 1990) is closely tied to neu-roanatomic functioning. He identifies three major func-tional areas that must interact for the body–spacesystem to work normally. Each of these areas corre-sponds to a cortical site. The parietal lobes control per-ceptual processing, the premotor and prefrontal cor-tices mediate exploratory-motor behavior, and thecingulate gyrus directs motivation. In turn, subcorticalstructures probably coordinate the orchestration of allthree areas. The reticular formation directs arousal, andthe thalamus (particularly the pulvinar of the thalamus)is postulated to focus and guide attention between spa-tial locations.
214 PART TWO | The Functioning Brain

Summary—The visual processing system reflects both thecomplexity and the reliance of humans on our visualsense. We discussed both features and streams of visualprocessing. The primary visual system, which serves as a“feature analyzer,” builds to the higher order systems ofobject recognition and spatial localization. Disorders suchas visual agnosia and neglect provide good examples ofhow each of these systems may malfunction. However,with vision, there is much reciprocal networking betweenparallel systems, so what appears hierarchical may not beentirely so. What is discussed in a bottom-up fashion mayalso be affected by top-down processing. Currently, brainscience has uncovered much of the structure and many ofthe functions of the visual road map through the brain.However, much work needs to be done in understandinghow the brain accommodates to varying visual experi-ences that represent the same precept. With an expansionof functional imaging techniques, a better understanding ofhigh-level integration of the fragmentary components ofvisual processing is occurring, especially in visual disor-ders, in which integration may be a product of systemsbeyond the visual system.
Auditory and LanguageProcessing
The human auditory system is a crucial sensory sys-tem, because it is the pathway to language, a uniquelyhuman development. This section examines the brain’scontrol of auditory processing, speech, and language byexploring the brain structures believed to be principal inlanguage functioning. Because no animal models of lan-guage exist, much knowledge of the neuropsychology oflanguage links closely to knowledge about the behavioraleffects of aphasia subtypes. Reliance on brain-damagedpatients to delineate systems can be tricky because lesionsmay not indicate site of damage, and many aphasics arestroke patients with a fairly wide area of damage.
P R I M A R Y A U D I T O R Y P R O C E S S I N G
Humans can detect a wide range of sound from the 30-Hzto the 20,000-Hz range. Difficulties in detecting the fea-tures of sound, such as how long a vowel versus a conso-nant sound might resonate, can result in higher levellanguage disturbance. One theory of autism considersthe idea that autistic people may not be tuned in to thefrequency of human speech, but instead have a propen-sity for lower frequency environmental sounds such as
those made by machines. If human speech is an aversiveand even fear-producing noise, then there would be awithdrawal from the sound of human speech. Many dif-ficulties can emerge if the primary building blocks ofsound detection and recognition are not intact.
The auditory system contains mechanical receptors de-signed to detect sound frequency. These hairlike receptorsare located in the fluid of the long, coiled, snail-likecochlea of the inner ear. As the mechanical mechanisms ofthe middle ear respond to external sound waves, they causevibrations in the fluid of the inner ear, thus vibrating thehairs of the auditory receptors. These receptors synapsewith the auditory nerve. The auditory nerve from eachear projects ipsilaterally to the cochlear nuclei of themedulla. From there, each pathway branches to projectauditory information to both the ipsilateral and contralat-eral superior olivary nuclei of the medulla. In this way,the auditory system differs from the visual system in thateach hemisphere receives input from both ears, resultingin bilateral representation of sound. This may help theperson localize sound in space. The auditory pathwaysthen course through the lower brainstem and ascendthrough the thalamus, where they are projected to the pri-mary auditory cortex (Figure 8.7).
The primary auditory cortex of each hemisphere liesdeep within the temporal lobe, largely on the medial as-pect of the superior temporal gyrus, within the valley ofthe lateral fissure. This area is commonly termed Heschl’sgyrus and corresponds to Brodmann’s area 41. Heschl’sarea is often larger in the right hemisphere, sometimesconsisting of two gyri to the left’s one gyrus. This corti-cal area processes the “fragments” of sound, much as thevisual system processes individual visual stimuli. Theprimary auditory cortex is organized into frequency-specific bands that parallel the layout of auditoryfrequency ranges mapped on the cochlea (see Figure 8.7).In this way, a tonotopic map projects onto the audi-tory cortex, similar to the retinotopic map of the visualsystem. Because the cortical bands can respond tomultiple frequencies, there is no strict one-to-onecorrespondence; rather, some bands are more attuned tocertain frequencies than others. The primary auditorycortex processes several elements of sound. In additionto frequency, the features of sound include loudness,timbre, duration, and change.
H I G H E R A U D I T O R Y P R O C E S S I N G : S P E E C H A N D L A N G U A G E
Speaking requires the ability to differentiate between speechsounds, or phonemes, such as vowels and consonants. For
CHAPTER 8 | Vision and Language 215
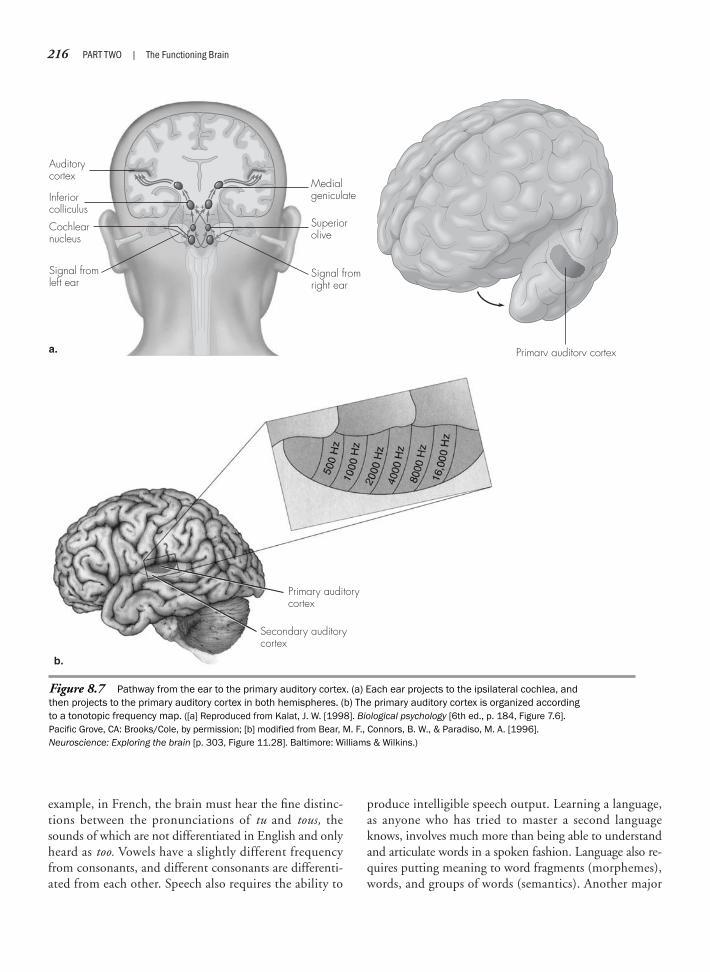
example, in French, the brain must hear the fine distinc-tions between the pronunciations of tu and tous, thesounds of which are not differentiated in English and onlyheard as too. Vowels have a slightly different frequencyfrom consonants, and different consonants are differenti-ated from each other. Speech also requires the ability to
produce intelligible speech output. Learning a language,as anyone who has tried to master a second languageknows, involves much more than being able to understandand articulate words in a spoken fashion. Language also re-quires putting meaning to word fragments (morphemes),words, and groups of words (semantics). Another major
216 PART TWO | The Functioning Brain
Figure 8.7 Pathway from the ear to the primary auditory cortex. (a) Each ear projects to the ipsilateral cochlea, andthen projects to the primary auditory cortex in both hemispheres. (b) The primary auditory cortex is organized accordingto a tonotopic frequency map. ([a] Reproduced from Kalat, J. W. [1998]. Biological psychology [6th ed., p. 184, Figure 7.6].Pacific Grove, CA: Brooks/Cole, by permission; [b] modified from Bear, M. F., Connors, B. W., & Paradiso, M. A. [1996]. Neuroscience: Exploring the brain [p. 303, Figure 11.28]. Baltimore: Williams & Wilkins.)
Auditorycortex
Medialgeniculate
++––
Superiorolive
Signal fromright ear
Inferiorcolliculus
Cochlearnucleus
Signal fromleft ear
a. Primary auditory cortex
b.
Primary auditorycortex
Secondary auditorycortex
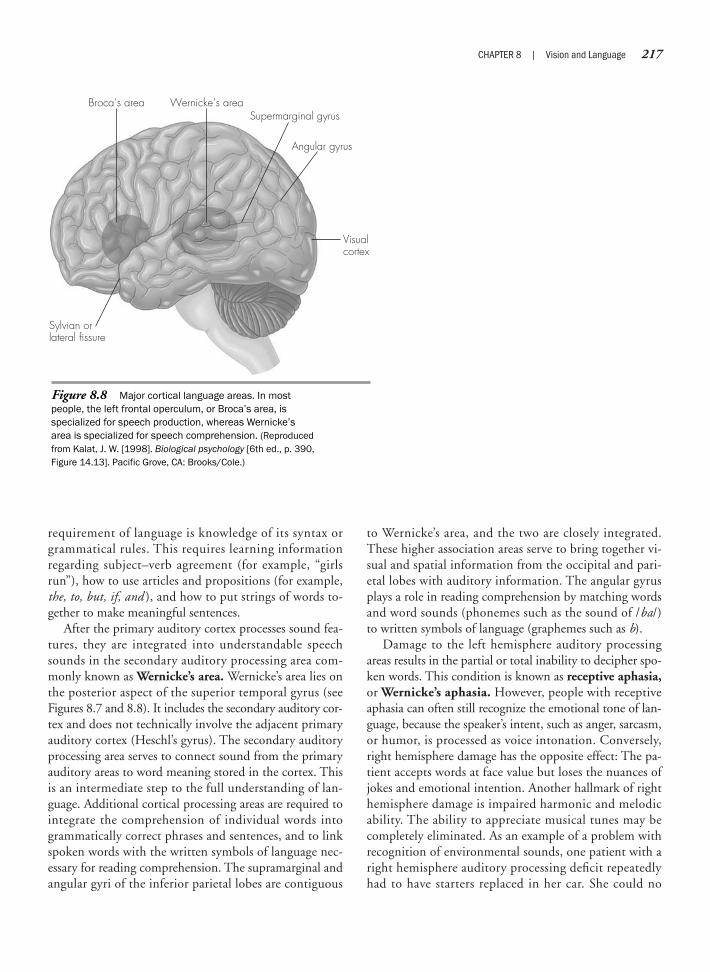
requirement of language is knowledge of its syntax orgrammatical rules. This requires learning informationregarding subject–verb agreement (for example, “girlsrun”), how to use articles and propositions (for example,the, to, but, if, and ), and how to put strings of words to-gether to make meaningful sentences.
After the primary auditory cortex processes sound fea-tures, they are integrated into understandable speechsounds in the secondary auditory processing area com-monly known as Wernicke’s area. Wernicke’s area lies onthe posterior aspect of the superior temporal gyrus (seeFigures 8.7 and 8.8). It includes the secondary auditory cor-tex and does not technically involve the adjacent primaryauditory cortex (Heschl’s gyrus). The secondary auditoryprocessing area serves to connect sound from the primaryauditory areas to word meaning stored in the cortex. Thisis an intermediate step to the full understanding of lan-guage. Additional cortical processing areas are required tointegrate the comprehension of individual words intogrammatically correct phrases and sentences, and to linkspoken words with the written symbols of language nec-essary for reading comprehension. The supramarginal andangular gyri of the inferior parietal lobes are contiguous
to Wernicke’s area, and the two are closely integrated.These higher association areas serve to bring together vi-sual and spatial information from the occipital and pari-etal lobes with auditory information. The angular gyrusplays a role in reading comprehension by matching wordsand word sounds (phonemes such as the sound of /ba/)to written symbols of language (graphemes such as b).
Damage to the left hemisphere auditory processingareas results in the partial or total inability to decipher spo-ken words. This condition is known as receptive aphasia,or Wernicke’s aphasia. However, people with receptiveaphasia can often still recognize the emotional tone of lan-guage, because the speaker’s intent, such as anger, sarcasm,or humor, is processed as voice intonation. Conversely,right hemisphere damage has the opposite effect: The pa-tient accepts words at face value but loses the nuances ofjokes and emotional intention. Another hallmark of righthemisphere damage is impaired harmonic and melodicability. The ability to appreciate musical tunes may becompletely eliminated. As an example of a problem withrecognition of environmental sounds, one patient with aright hemisphere auditory processing deficit repeatedlyhad to have starters replaced in her car. She could no
CHAPTER 8 | Vision and Language 217
Figure 8.8 Major cortical language areas. In mostpeople, the left frontal operculum, or Broca’s area, isspecialized for speech production, whereas Wernicke’sarea is specialized for speech comprehension. (Reproducedfrom Kalat, J. W. [1998]. Biological psychology [6th ed., p. 390,Figure 14.13]. Pacific Grove, CA: Brooks/Cole.)
Broca’s area
Sylvian orlateral fissure
Wernicke’s area
Visualcortex
Supermarginal gyrus
Angular gyrus

longer discriminate the difference in sound between thesound of the starter engaging and the sound of the engineturning over. Speech understanding, therefore, conveysword analysis, as well as emotional intentions, throughtone of voice, pitch, intensity, and rhythm.
Expressive speech links to the frontal operculum(Broca’s area), located in the left frontal lobe on the poste-rior portion of the third frontal gyrus (the inferior frontalgyrus). This area is adjacent to the facial area of the motorcortex. The inferior frontal gyrus is a premotor area of thefrontal lobes, and thus is concerned with aspects of speechplanning before output coordinated by the nearby motorstrip. In addition to mediating the fluency of speech,Broca’s area plays a role in the grammatical and syntacti-cal arrangement of words. Wernicke’s and Broca’s areasare linked by a band of white matter fibers called the ar-cuate fasciculus. This allows for close communication be-tween the two areas in expressive output. Words, whetherfrom external sources or from the self, are picked out formeaning in Wernicke’s area, and in parallel, the syntax ofthe phrase is constructed in Broca’s area. This is possiblebecause the arcuate fasciculus permits reciprocal interac-tion between the two areas (Yeterian & Van Hoesen, 1978).This interaction also makes logical sense, because syntaxdepends on the words used and the words selected also de-pend on the emerging syntax of the sentence (Bradshaw &Mattingly, 1995).
The basal ganglia and the thalamus have also been im-plicated in language functioning via their participation ina cortico-striato-pallido-thalamo-cortical loop (seeCrosson, 1992). This loop, or perhaps set of loops, con-nects the language centers of the cortex to the putamenand caudate nucleus of the striatum, to the globus pallidus,to specific nuclei in the thalamus, and back to the corticallanguage centers. The current thinking regarding the func-tion of these loops is that they play a role in regulating lan-guage; this role involves initiating language productionmore than constructing speech content (Crosson, 1992).
One hemisphere, usually the left, is dominant forspeech. This means that the left cerebral cortex prefer-entially processes speech sounds, whereas the rightprocesses nonspeech sounds. Not surprisingly, the func-tional dominance of the left hemisphere for speech cor-responds to preferential treatment for speech sound pro-cessing in the larger planum temporale of the lefthemisphere. After analysis of sound features, secondaryauditory information, such as phonemes, is integratedin the planum temporale, in the temporal area adjacentto the primary auditory cortex (Brodmann’s area 42).Although sound from each ear projects bilaterally, there
is an opposite hemisphere advantage; in this case, the lefthemisphere preferentially processes sound from the rightear. Because the left hemisphere shows a preference foranalyzing speech in most people, speech soundsprocessed through the right ear will be understood fasterand more accurately than speech sounds processed throughthe left ear.
The left hemisphere also has a propensity for rhythmof both speech and music as it codes for the sequence ofsounds. To check your left hemisphere dominance forrhythm, try keeping a metronome-like beat with yourleft hand and beat out the rhythm of a familiar tune, suchas Jingle Bells, with your right hand. Most people findthis easy if their left hemisphere, which controls theirright hand, is dominant for rhythm. After doing this, tryreversing what each hand is doing (right keeps the beat,and left taps out the rhythm) and see if you have more orless difficulty. The secondary auditory cortex of the righthemisphere, by contrast, is specific for aspects of tonality,including the melody of music and the intonation ofspeech, which is commonly referred to as speech prosody.The right hemisphere is adept at recognizing the relationbetween simultaneous sounds, such as the harmony ofchords, or the musical interval between notes. It alsoshows an advantage for recognizing nonspeech or environ-mental sounds such as those made by machines and cars, aswell as animals, birds, the pounding ocean surf, or a bab-bling creek.
The brain’s asymmetry for language processing andproduction is an extension of speech processing. The lefthemisphere specializes in processing word sounds, ormorphemes; semantics; and the grammatical rules oflanguage. The right hemisphere, long thought to be“mute,” plays a role in the emotional intention of bothvocalization and understanding. The right hemispheremay have no speech or understanding of grammaticalrules; however, a number of people, and more womenthan men, have some bilateral representation of speech.The right hemisphere is nonetheless capable of consider-able comprehension and expression. Although frankaphasia is rare after right hemisphere strokes, there can belinguistic impairments. These include a deficit in com-prehending tone and voice, producing similar emotionaltone, and understanding metaphors and jokes. We onceexamined a male adult patient who had undergone a com-plete left hemispherectomy. Although he was severelyaphasic, he could communicate somewhat using “grunts.”He was also able to curse, possibly because such commu-nication is more emotional in nature and, therefore, partlycontrolled by the right hemisphere.
218 PART TWO | The Functioning Brain

In summary, the complexity of speech and languagenecessitates specific brain systems, which in most peopleare lateralized. Beyond the discrete cortical componentscontrolling auditory reception (auditory cortices andWernicke’s area) and auditory speech production (Broca’sarea and motor cortex), language requires thought and,therefore, extensive interconnections to higher orderplanning and memory centers. The supramarginal gyrusand the angular gyrus of the parietal lobes are also im-portant to integrating verbal aspects of language withthe visual symbolic components involved in reading.Subcortical neural connections, including portions of thebasal ganglia and the thalamus, also play a role in lan-guage. Finally, cerebral lateralization exists for various lan-guage functions.
A P H A S I A : A B R E A K D O W N O F L A N G U A G E
Aphasia is a disturbance of language usage or comprehen-sion. It may impair the power to speak, write, read, gesture,or to comprehend spoken, written, or gestured language.Aphasia is a disturbance connecting speaking to thinking,and thus is differentiated from purely mechanical disor-ders of speech such as dysarthria or speech apraxiacaused by paralysis or incoordination of the musculatureof the mouth or vocal apparatus. Aphasic disorders alsodo not include pure mutism, that is, disturbances of lan-guage caused by severe intellectual impairment or loss ofsensory input (such as deafness or inability to see words).Aphasias are most frequently caused by vascular disorderssuch as stroke or by tumor or brain trauma. Although cor-tical damage to the frontal and temporal areas of the lefthemisphere causes most aphasias, damage to subcortical
structures of the basal ganglia (specifically the corpusstriatum) and the thalamus has also produced aphasia.
The two major types of aphasia are commonly referredto as Broca’s aphasia and Wernicke’s aphasia. Other classi-fications, subtypes, and combinations exist that may con-tain slightly different features or a mixture of some fea-tures of these two types (see Table 8.1). In seeing aphasiapatients, it is quickly evident that few patients fit neatlyinto one classification or the other. This is not surprising,because brain lesions and preexisting brain anatomy forlanguage varies among individuals, most notably betweenmen and women. Many clinicians find it most useful todescribe the features of the aphasia in behavioral terms,describing aphasia according to degree of fluency and thenature of the expressive and receptive problems involved.Fluent aphasia is characterized by fluent spontaneousspeech with normal articulation and rhythm, or fluencyin the repetition of words, phrases, or sentences. Nonflu-ent aphasia is difficulty in the flow of articulation, so thatspeech becomes broken or halting. Expressive aphasia isa disorder of speech output. Receptive aphasia implies adifficulty in auditory comprehension.
Often, patients experience not only a loss of spoken lan-guage but also a loss of written language and reading com-prehension. Writing is one of the most complex languageabilities. If it is disturbed as a result of impairment of thelimb to produce letters and words, the disturbance is notthought to be a disorder of language. Rather, words, letters,or numbers may appear foreign or incomprehensible be-cause of an inability to recall the form of letters. Attemptsat writing may be filled with real or imagined letters thatmake no sense to others. With time and training, the per-son may be able to understand simple written language (for
CHAPTER 8 | Vision and Language 219
Type of Aphasia Fluency, Content Repetition of Speech Comprehension of Speech Reading and Writing
Broca’s Confluent, agrammatical Impaired Normal Agrammatical, misspelling
Wernicke’s Normal, word salad Abnormal Poor Inaccuracies
Conduction Normal fluency, phonemic errors Abnormal Relatively intact Abnormal
Transcortical motor Halting Fluent Normal Reading normal,writing impaired
Transcortical sensory Normal Normal Poor Inaccuracies
Anomic Normal fluency, Normal Normal Normalword-finding errors
Global Abnormal Abnormal Abnormal Abnormal
Table 8.1 Aphasia Types

example, single words such as bath or food ) but not morecomplex written language, such as sentences or para-graphs. The extent of the recovery in this and other areaslargely depends on the degree of damage. Because readingcomprehension is based on prior mastery of auditory lan-guage, deficits in reading (alexia) often accompany deficitsin auditory comprehension. As with auditory defects, im-pairment in visual comprehension may involve a deficitin recognizing individual letters or words as being lettersor words, or an impairment in attaching the correctmeaning to the symbols written on a page. Deficits inwriting are most often associated with lesions to the an-gular gyrus, a cortical association area that provides cross-modal integration of visual, tactile, and verbal informa-tion. Reading deficits (alexia) are frequently related tolesions of the left fusiform and lingual areas.
B r o c a ’ s A p h a s i a
Broca’s aphasia is an expressive, nonfluent aphasia charac-terized by difficulties in speech production but relativelyadequate auditory verbal comprehension, as evidenced bythe ability to follow spoken commands (such as, “Pointto the cup”). Many forms of disorders of production exist,which can range from an inability to form words to an in-ability to place words together to form a spoken or writ-ten sentence. In simple expressive aphasia, the personknows what he or she wants to say but cannot find thewords to say it. It is like continually experiencing a situa-tion in which the word or words are on the tip of thetongue but are not quite connected to thought.
In mild cases of anomia, or word-finding difficulties,only a word or two here and there is lost, and the commu-nication can proceed quite normally. In more severe cases,most or all words can be lost. This problem in word find-ing is one that virtually all expressive aphasics suffer. Evenwhen the person produces words, he or she takes longerthan normal to do so. Difficulty in finding a word oftenresults in the person’s deliberately “talking around” a wordthat approximates the intended idea when he or she can-not find the intended word. For example, an aphasic mightsay, “I looked through that long pipe thing at the stars”(that is, a telescope). Aphasics may also make phonetic orlike-sounding errors, such as “I looked through that tele-phone at the stars,” or semantic meaning–related errors,such as “I looked through that barometer at the stars.”
Another problem experienced by many Broca’s apha-sics is one of articulation, or the ability to form phoneticsounds of vowels and consonants, which then are placedin different combinations to form words and sentences.People with severe deficits in articulating words often can-not produce simple sounds, even by imitation. If the
deficit in articulation is related to a motor impairment ofthe mouth, tongue, larynx, or pharynx, then it is notaphasia. The aphasic impairment is marked by the per-son’s confusion or deficit in choosing the desired soundfrom all those available in his or her repertoire. This some-times results in unintended strange-sounding syllables,words, or phrases (phonemic paraphasias) during the ef-fort to speak, or in noises being produced rather than lan-guage. Those with Broca’s aphasia may also show poorpronunciation and inappropriate speech rhythm, mani-fested by dysarthria, stuttering, and effortful speech.
Broca’s aphasia most commonly occurs with lesions tothe frontal operculum, but typically also includes lesionsto the motor cortex (precentral gyrus or motor strip) andunderlying white matter and subcortical structures of thebasal ganglia. Aphasia appears to resolve quickly if thefrontal operculum is the only structure involved, but ittends to be more persistent the more surrounding struc-tures are damaged (Bradshaw & Mattingly, 1995).
W e r n i c k e ’ s A p h a s i a
Wernicke’s aphasia is a receptive, fluent aphasia. This im-plies reduced comprehension of spoken language withthe continued ability to produce speech. If you stop toimagine this odd situation, you can see that Wernicke’saphasics, in addition to not understanding what otherssay, may not be able to understand what they themselvesare saying. This problem contributes to speaking in theform of a word salad of unconnected words and wordsounds. This feature of Wernicke’s aphasia is a deficit inputting words together in proper grammatical and syn-tactical form. This condition, more formally known asparagrammatism or extended paraphasia, refers to run-ning speech that is logically incoherent, often soundinglike an exotic foreign language. That is, the speech of aperson with Wernicke’s aphasia flows forth without hesi-tation and has appropriate intonation. Appropriate socialinteraction, such as speaking in turn and gesturing ap-propriately, remains intact. However, the words andphrases spoken are meaningless. Wernicke’s aphasics usu-ally do not realize their spoken language is meaninglessto others (anosognosia for speech). It is as if they knowexactly what is to be communicated, but their delivery isincoherent.
In mild cases of Wernicke’s aphasia, only a word or twohere and there sounds garbled or incomprehensible. In thiscase, communication can generally proceed because theperson is able to grasp the essence of the intention basedon the context within which the communication takesplace. With moderate disability, the patient can under-stand part, but not all, of the communication. In severe
220 PART TWO | The Functioning Brain

CHAPTER 8 | Vision and Language 221
cases, the patient may experience most or all speech as if itwere nonsense syllables or a foreign language. It is not un-common for others to misattribute behavior problems topeople with receptive aphasia. Sometimes noncomplianceis actually caused by the fact that the patient has misun-derstood the communication in the first place. Thus, a pa-tient may act as though a word was not heard at all (so-called word deafness) or as though only fragments of theword were heard. The most common defect, however, liesnot in failing to recognize that a word was spoken, butrather in failing to attach meaning to the word. In someaphasics, comprehension of individual words is intact, butgrammatical constructions are not.
Damage in Wernicke’s aphasia includes the secondaryauditory cortex (Wernicke’s area) and some involvementof surrounding structures. These often include the supra-marginal and angular gyri and portions of the middletemporal gyrus.
O t h e r A p h a s i a S u b t y p e s
The classification of aphasias into receptive and expressive isa useful didactic tool, but many people with left hemispherelesions have a combination of both symptoms, because ofdamage to the left middle cerebral artery, which serves bothexpressive and receptive areas. This section briefly reviewsthe symptoms of the various subtypes of aphasia beyond themore common Broca’s and Wernicke’s aphasias. Table 8.1summarizes the behavioral features of the aphasias.
Conduction Aphasia—The behavioral hallmark of conductionaphasia is a problem in repeating what others say. Thisproblem, obviously, may not become apparent except onformal testing. In ordinary conversation, expressive speechis fluent but marked with phonemic paraphasias, or er-rors of word usage of similar-sounding words (such asusing the word bark for tarp). Comprehension is relativelywell preserved but may suffer from minor errors. Readingaloud and writing are frequently impaired. Neuroanatom-ically, conduction aphasia is a result of separation of Broca’sarea from Wernicke’s area by damage of the arcuate fasci-culus, the connecting white matter fibers between the twoareas. The damage may also include lesions to the poste-rior portions of the lateral fissure responsible for aspects of
reading and writing, specifically the supramarginal and an-gular gyri.
Transcortical Motor Aphasia—Clinicians can recognize transcor-tical motor aphasia by the patient’s halting, nonfluentspontaneous speech; oddly, however, speech becomes flu-ent if the person merely repeats what another says. Inmany respects, except for the differences in repetition abil-ity, this deficit resembles Broca’s aphasia. Speech compre-hension is unimpaired and writing may also suffer. Read-ing comprehension, however, is generally intact. Lesionsto the area anterior or superior to Broca’s area are associ-ated with this aphasia type.
Transcortical Sensory Aphasia—Severe speech comprehensiondeficit marks transcortical sensory aphasia. Interestingly, de-spite being unable to comprehend speech, such aphasics canadequately repeat phrases and sentences presented to them.Lesions in the angular gyrus are the most likely culprits forthis aphasia; thus, reading and writing are also affected.
Anomic Aphasia—A problem in word finding, or anomia, isthe primary, and often only, difficulty in anomic aphasia.This aphasia is a frequent result of widespread brain im-pairment caused by conditions such as traumatic braininjury and dementias such as Alzheimer’s disease. As peo-ple age, an annoying concomitant often reported is a dif-ficulty in remembering people’s names or being unable toretrieve a word that is just on the “tip of the tongue.” Theact of “word finding” seems to be one of the most easilyaffected aspects of expressive language. Witness even theproblem of being “speechless” with anxiety. It is difficult,therefore, to distinguish what might be a temporary word-finding difficulty and a true aphasia.
Global Aphasia—Global aphasia is the most devastating ofthe aphasia subtypes because of its profound effect acrossall areas of speech functioning. There is marked disabilityin speech production, as well as speech comprehension.Reading, writing, and repetition are also impaired. Thisaphasia is caused by a massive lesion encompassing majorportions of the left hemisphere.
SummaryThe visual and auditory systems are two of the most important sensory systems for humans. Visual pro-cessing covers a wide cortical area beyond the occipital lobes when the meaning of visual material isconsidered. Likewise, auditory processing, because it also includes understanding and expression of the
222 PART TWO | The Functioning Brain
meaning of language, spreads out in a web that encompasses large portions of the cortex. One can con-ceptualize sensory-perceptual processing as a bottom-up process of sensory logic, because in each do-main the brain seeks to make “sense” of incoming information. But, it is becoming more evident that weimpose perceptions on sensory information from the top down as well. A fundamental question of con-sciousness is how the brain constructs perceptions of integrated wholes, such as an orange, for which youintegrate the visual features with the smell and taste. Brain scientists are beginning to ask how the dis-parate local elements bind to form a unified experience. This is referred to as “the binding problem ofconsciousness.”
A question related to the binding problem concerns how the brain accesses meaning. Some arguethat meaning is specific within each sensory system. In other words, there exists a specific visual mean-ing, auditory meaning, or even olfactory meaning. If this meaning is lost, as in various sensoryagnosias, the ability to access it through another sensory modality would be impossible. In discussingthe senses, it is quickly evident that basic sensory perception is anatomically and functionally distinct.However, meaning lost in one sensory modality can often be accessed through another. Exactly how anintegrated sense of meaning emerges remains unclear. Local interconnections may exist between sen-sory cortices or some sort of central integrative multimodal processor that allows multiple access fromthe sensory systems. Chapter 16 evaluates the problems of binding and how the mind constructsmeaning. Neuropsychology and neuroscience are still wrestling with the larger questions of how thissystem operates. Functionally, however, knowing that sensory-perceptual agnosias are modality specificlets rehabilitation professionals seek alternative “routes” for accessing meaning when one system isdamaged.
C r i t i c a l T h i n k i n g Q u e s t i o n s
What does the neuropsychology of sensory-perceptual processing have to contribute to the idea that there is an objectivereality related to object perception?How might it be possible to imagine or conjure up images in a sensory domains despite a lack of sensory input?Can one be “conscious” in one sensory domain but not in another?
K e y Te r m s
DecussatingAnopiaHomonymousHemianopiaStriate cortexSecondary association or
Prestriate cortexBlindsightAchromatopsia
AkinetopsiaVisual agnosiasVisual object agnosiaProsopagnosiaApperceptive visual agnosiaAssociative visual agnosiaBalint’s syndromeTonotopic mapWernicke’s area
Receptive aphasia or Wernicke’saphasia
Frontal operculumAphasiaDysarthriaSpeech apraxiaFluent aphasiaNonfluent aphasiaExpressive aphasia
AnomiaArticulationWord saladParagrammatism or extended
paraphasiaPhonemic paraphasias
We b C o n n e c t i o n s
http://serendip.brynmawr.edu/bbSee the exhibits related to vision: blindsight, blind spot, and tricks of the eye.
http://neuro.caltech.edu/~seckelHome page of illusions, perception, and cognitive science.

http://www.eyetricks.comThis site includes tons of optical illusion galleries, three-dimensional images, and brainteasers.
http://www.aphasia.orgThis site provides information on aphasia from the National Aphasia Association.
http://www.nidcd.nih.gov/health/voice/adultaphasia.aspThis site provides information on aphasia from the National Institute on Deafness and Other Communica-tion Disorders.
CHAPTER 8 | Vision and Language 223
Chapter 9
MEMORY, ATTENTION, EMOTION, AND EXECUTIVE FUNCTIONING
It is abundantly obvious here that for longer than we can tell, the truth isimmeasurably greater than all the tiny fragments we have so far been able todiscover.
—Attributed to Pavlov by Luria (1947)
Everything should be made as simple as possible, but not simpler.—Attributed to Albert Einstein
Memory SystemsAttentionExecutive FunctioningRelation of Memory, Attention, and Executive FunctionNeuropsychology of Emotional Processing
Neuropsychology in Action
9.1 Amnesia: The Case of N.A.9.2 Executive Function Tasks9.3 The Case of Phineas Gage

CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 225
OverviewThis chapter is devoted to higher functional systems that are not specific for sensory modalities. Languageand visual perception (see discussion in Chapter 8) are also considered higher functional systems becausetheir full expression depends on additional functional systems such as memory, attention, and executivefunctioning. However, language and visual perception emerge from sensory-perceptual systems; thus, it iseasier to follow their progression when they are discussed with these systems. The sensory and motorsystems represent the building blocks on which other systems are constructed and the raw material fromwhich other systems draw; they are the most straightforward and best mapped systems. The systems wediscuss in this chapter are integrated with the sensory-perceptual and motor systems but do not depend onany one modality. We refer to the systems here as higher order systems because, evolutionarily, the expres-sion in humans is complex and highly integrated. Most of these systems can be thought of as backgroundmanagement systems. Their functions are important for learning, organizing, setting priorities, planning,self-reflection, and self-regulation.
The systems discussed in this chapter include the classic systems or modules of cognitive neuropsy-chology, namely memory, attention, and executive functioning. In addition, we consider the brain and mindexpressions of emotional processing. For each system, we discuss the conceptual organization of the sys-tem, as well as known structure–function relations.
K e e p i n M i n d
What integrative and management functions do higher systems serve?
If short-term memory is impaired, can information be learned and consolidated into storage?
What are the similarities and differences of the models of attention?
Is there a cognitive function that could be considered the highest function?
What effects on behavior do disorders of “management” and “executive” functions have?
Memory Systems
Memory forms the basis of experience and percep-tions of self. It is dynamic and malleable. It allows peopleto travel back in time. How you see yourself, to a largedegree, is a product of the experiences of your life, thelessons you have learned, and what you remember asbeing important. Even what you tell yourself to remem-ber to do in the future must incorporate memory. Mem-ory pervades most aspects of human experience. Stories ofyour personal and cultural past are stored in memory;thus, it is a necessary foundation of social communica-tion. This section examines the various components ofmemory and what can happen when aspects of the mem-ory system malfunction.
When memory is working fluidly, there is little needto notice it. But consider the question from a neuropsy-
chological perspective: What do you lose if you lose yourmemory? One patient we evaluated, a man in his 70s withAlzheimer’s disease, could not remember that his wife haddied 2 years earlier. All his memories were still of herbeing there. Every time someone mentioned that his wifewas dead, he relived the grieving experience. It is scary toimagine waking up and not knowing who you are, whoyour friends are, and what has happened in your life.Consider also what it might be like if you could not en-code new information, if you could not remember whatsomeone said 10 minutes ago, or if you could not registerthe information you needed to take a test or learn a newskill.
Memory is an umbrella concept, and it is impossibleto say categorically that someone has an overall good orbad memory. It is simply not a single system. Memory isparceled into subsystems based on ideas of storage and

226 PART TWO | The Functioning Brain
processing. Neuropsychologists ask how the brain stores in-formation over the long term and how it encodes, orga-nizes, and then retrieves information from memory. Inmany disorders neuropsychologists treat on a daily basis,memory processing is at issue because memory is a “fragile”system, affected by many disorders, including most of thedementias, such as Alzheimer’s disease, toxic conditions,loss of oxygen, and head injury.
Scientific understanding of normal memory process-ing in the brain has profited greatly from the study of peo-ple afflicted with various memory disorders, especiallytypes of amnesia. However, the term amnesia can refer tomore than one type of condition. The “soap opera” ver-sion of amnesia occurs when one of the characters gets hiton the head and promptly forgets who she or he is and allthe specific episodes of her or his life. This character in-variably wanders off to make a new life, including thedevelopment of a new identity. Perhaps, after a time, astartling event occurs (possibly another blow to the head)and the character’s prior memory and identity floodsback. This type of memory deficit is reminiscent of a psy-chiatric dissociative state caused by severe emotionaltrauma, but it is not what occurs with neurologic injuryor disease.
Because neurologic patients acquire their memoryproblems in conjunction with a brain injury or disease, itis important to have terminology that marks the nature ofthe patient’s memory before the event and the effect onmemory after the event. Anterograde amnesia is the lossof the ability to encode and learn new information after adefined event (such as head injury, lesion, or diseaseonset). Retrograde amnesia is the loss of old memoriesfrom before an event or illness. For example, one of ourpatients, L.S., experienced a head injury as a result of acar accident and had moderate anterograde amnesia andmild retrograde amnesia. She had no memory of the caraccident and only vaguely remembered the paramedics.She did remember being in the hospital emergency room.After the accident, she had difficulty learning new infor-mation (anterograde amnesia). She often forgot her physi-cian’s name, and when she returned to college, she foundit hard to study and perform well on history tests forwhich she had to recall facts and dates. Her mild retro-grade amnesia is evidenced by her memory for driving outof the grocery store parking lot, which was about fiveblocks from the accident. However, she remembered noth-ing else of the short time preceding the accident. Amnesiasof this type are common in closed head injury (this con-dition is described further in Chapter 13). In general,anterograde (or a combination of anterograde-retrograde)amnesia is evident with brain injury. However, there are
instances of retrograde amnesia with relatively spared an-terograde learning and memory (Levine et al., 1998).Amnesia can be caused by a number of different prob-lems and can take several forms. An example of a circum-scribed lesion causing amnesia is the classic case of N.A.(Neuropsychology in Action 9.1).
A F R A M E W O R K F O R C O N C E P T U A L I Z I N GM E M O R Y S Y S T E M S
Psychology textbooks typically describe memory as hav-ing three main divisions: sensory memory, short-termmemory (STM), and long-term memory (LTM). Sen-sory memory is fleeting, lasting only milliseconds, but itscapacity is essentially unlimited in what may be taken in.STM is of limited capacity (7 � 2 bits of information)and degrades quickly over a matter of seconds if informa-tion is not held via a means such as rehearsal, or trans-ferred to LTM. LTM, theoretically, is of unlimited capac-ity and is relatively permanent except for models thatsuggest that loss of information through forgetting is pos-sible. Neuropsychologists are most concerned with LTMand its disorders because these are the problems most evi-denced by patients. Often, STM, as measured by neu-ropsychological tasks, is intact even when there are deficitsin LTM, although isolated disorders of STM exist. Neu-ropsychological conceptualizations of memory generallydo not consider sensory memory; rather, it is thought ofas a component of sensory processing.
Neuropsychology concerns itself with understandinghow memory systems work in correspondence withknown brain functioning. An important question con-cerns the possible existence of anatomically separate sys-tems in the brain for such concepts as STM, LTM,explicit-implicit memory, and episodic-semantic mem-ory. One way in which researchers can support the ideaof separate structures is by showing a double dissociationbetween behaviors. Research can demonstrate strong evi-dence for different systems if a lesion in an area of thebrain affects one system (LTM) but not the other (STM).Evidence is even stronger if researchers can show that adifferent lesion results in the opposite dissociation(affects STM but not LTM). This section focuses onconceptualizations of LTM and short-term workingmemory. We explore evidence for different memory sub-systems, a division between STM and LTM, and betweenpossible divisions of LTM such as separate declarative/ex-plicit versus procedural/implicit systems. As we exploreeach subsystem, we also discuss disorders that affect thatsystem.
L O N G - T E R M M E M O R Y
A problem that is inherently confusing in studying mem-ory is the multiple terms scientists use to describe the pos-sible subcomponents of LTM. Cognitive psychologists,neuropsychologists, neurologists, and the lay public usevarious, and sometimes conflicting, terms. For example,when referring to LTM, the lay public often thinks of theability to remember information from the distant past.However, neuropsychologists are referring to the specificability to register information (encode), organize the in-formation in a meaningful way (storage), and recall or rec-ognize the information when needed (retrieval). Accord-ing to this definition, LTM is the ability to learn andretain new information. Remote memory, by contrast,concerns memory for long-past events.
Various theoretical conceptualizations parcel LTM intosubsystems (Figure 9.1). Squire (Squire & Cohen, 1984;Squire & Butters, 1992) and other investigators advocatefor a structural–functional difference between declarativeand nondeclarative memory.
Declarative memory is explicit and accessible to con-scious awareness. Nondeclarative memory is usually im-plicit, and a person demonstrates it via performance.Squire and Butters (1992) maintain that the domain ofnondeclarative or procedural memory is that of rules andprocedures, rather than information that can be verbal-ized, although nondeclarative memory has not beenclearly operationally defined and often includes a hodge-podge of tasks such as motor skills learning, mirror read-ing, and verbal priming. Schacter (1987) differentiatesbetween explicit and implicit memories. Recall or
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 227
In 1960, N.A. was 22 years old and was amember of the U.S. Air Force. One day whileworking on a model airplane, he suffered anaccident that would affect him for the rest ofhis life. His roommate, apparently in a playfulmood, took a miniature fencing foil from thewall, tapped N.A. from behind, and as heturned around, thrust it forward. Unfortu-nately for N.A., the tiny foil penetrated thecribriform plate at the top of his nasal cavityand entered his brain. The foil pierced histhird cranial nerve, but more important, itmade a small lesion in the left dorsomedialnucleus of the thalamus. It was quicklydiscovered that N.A. was amnesic (retro-grade) for the past 2 years. In addition, thisminute injury left him with a devastatingimpairment in his ability to register newverbal memories (anterograde amnesia).
In meeting him, the casual observer maynot initially suspect there is anything wrong.N.A.’s intelligence quotient (IQ) is in the highaverage range and he exhibits good socialskills. Furthermore, he is friendly, polite, andhas a good sense of humor. But after talkingwith him for a few minutes, it becomesapparent that he does not remember details
of just a few minutes ago. If he is distractedby a passing thought or a passing car, thethread of conversation is lost. He has littlerecollection of the day’s events. If you meetagain the next day, he probably will notremember you or what transpired in yourprevious meeting with him.
N.A. likes to keep his room exactly thesame at all times and spends much timeobsessively arranging things. He becomesupset at his mother if she moves the tele-phone or one of his model airplanes. He likesthings exactly the same so he has a betterchance of finding them. Only after a longperiod and much repetition does he remem-ber something. If N.A. saw you every day, aftera period of time he might recognize you, butstill might not know your name. He has only asketchy memory of events that have tran-spired since 1960. For example, he has avague idea that Watergate was a politicalscandal in “Washington or Florida” but recallsno other details. Because N.A.’s injury is in theleft dorsomedial nucleus, he shows moreverbal than visual memory deficits. Interest-ingly, when he had to learn a new route fromhis house to the Veterans Administration
hospital for therapy, even after 4 years he wasunable to form a spatial map. He found hisway much like an adult returning to a child-hood neighborhood after years of absence. Aspieces of the visual scenery popped up beforehim, he decided if the landmark lookedfamiliar and turned accordingly. This haphaz-ard approach of seeing things sometimesrequired him to back up or retrace his stepsuntil something looked familiar.
N.A. recognizes that he has memoryproblems and is not confused. He knows whohe is and where he is, but may not know theday or year. As would be suspected, he haslittle social life. In a sense, he remains stuckin time. Most of his memories are from the1950s. When he fantasizes, he thinks ofBetty Grable. He does not know of the peopleor events since then. However, N.A. remainsoptimistic about his situation and rarely usesnotes because he wants to work on hismemory.
This case demonstrates that even a verysmall lesion, strategically placed, can causea devastating problem of memory. Kaushall,Zetin, and Squire (1981) have reported thecomplete case of N.A.
N e u r o p s y c h o l o g y i n A c t i o n 9 . 1
A m n e s i a : T h e C a s e o f N . A .
by Mary Spiers

228 PART TWO | The Functioning Brain
recognition, through verbal or nonverbal means, directlyindicates explicit memories. Conscious awareness is usu-ally implied, as is intention to remember. People demon-strate implicit memory by means in which consciousawareness is not always necessary, such as implicit prim-ing, skill learning, and conditioning. Yet another possibledistinction within LTM is between semantic and episodicmemory. Researchers consider both of these to be formsof explicit or declarative memory. Tulving (1972) intro-duced the distinction between an episodic memory,which refers to individual episodes, usually autobiograph-ical, that have specific spatial and temporal tags in mem-ory, and semantic memory, which refers to memory forinformation and facts that have no specific time tag refer-ence. For example, remembering the details and events ofyour first date involves episodic memory, whereas remem-bering the definition of a word relates to semantic mem-ory. With semantic memory, the context in which thememory was encoded is generally not present. Thus, mostof us do not remember the specific setting and people in-volved when we learned the name of the first president ofthe United States.
The most neuroanatomically defensible division be-tween LTM systems is that of declarative/explicit and
nondeclarative memory systems. Some also use the termsdeclarative versus procedural or explicit versus implicit in anearly synonymous manner. There is much debate overthe existence of separate episodic and semantic systems;in fact, although researchers first described these two sys-tems as clearly distinguishable conceptually, they now con-sider the systems to overlap with other memory concepts.
D e c l a r a t i v e M e m o r y
One of the first questions that come to mind when peo-ple begin thinking about memory is, “Where is memorystored in the brain?” This often implies the search for a“center” for memory storage in the brain. It also impliesthat if this center is removed, then all memory is removed.This would be like erasing the entire hard disk of a com-puter. (Please note that the brain does not operate like acomputer; in fact, brains build computers!) If all remotememory were removed from the brain, a person would beunable to remember his or her language, facts, episodes,names of people, or any other information previouslyencoded. From studies of brain-injured individuals, weknow that this does not happen. People may lose pieces ofremote memory, but their brains are not “erased.” There is noone memory storage center. Rather, most neuropsychologists
Figure 9.1 Long-term memory (LTM) taxonomy. Theories of anatomically separateLTM stores have included the noted distinctions. (From Weiten, W. [1998]. Psychol-ogy: Themes and variations [p. 291, Figure 7.28]. Pacific Grove, CA: Brooks/Cole.)
Memory
Declarative memorysystem(factual information, explicitmemories)
Nondeclarative/Proceduralmemory system(actions, perceptual-motor skills,conditioned reflexes, implicit memories)
Example: Riding a bicycle
Semanticmemorysystem(generalknowledge,storedundated)
Example:Lincoln gaveGettysburgAddress
Episodic memory system(dated recollections ofpersonal experiences)
Example: First kiss

think of memory as being ultimately stored in the areawhere it was first processed (for example, see Squire, 1987).This would imply, for example, that auditory memories arestored in primary, secondary, or auditory association areas,and likewise for other functional systems.
The function of the declarative memory system is toprocess information in such a way as to tag it or consoli-date it for storage in the brain. According to this model,when new declarative learning is occurring, informationfrom various cortical areas funnels into the structuresresponsible for declarative memory. After it is processed, re-turn neural pathways transmit information back to specificcortical areas.
Declarative Model of Encoding and Retrieval—Tulving andcoworkers (1994), based on neuroimaging studies ofhealthy individuals, developed a model of memory en-coding and retrieval, Hemispheric-Encoding-Retrieval-Asymmetry (HERA). The model proposes that the pre-frontal (dorsolateral) region of the left hemisphere isprimarily involved in episodic encoding, whereas theprefrontal area of the right hemisphere is prominentlyactivated for retrieval of episodic information. Subse-quently, a comprehensive review of 275 positron emis-sion tomography (PET) and functional magnetic reso-nance imaging (fMRI) studies by Cabeza and Nyberg(2000) provided partial support for the model. Analysisof these neuroimaging studies showed that the left pre-frontal region activated in verbal episodic encodingwhile retrieval of episodic information was right-later-alized (prefrontal region) for both verbal and nonverbalcontents. In contradiction with the prediction based onthe HERA model, encoding of nonverbal informationyielded bilateral and right-lateral prefrontal activation.Other regions activated during episodic retrieval in-cluded temporomedial, parietal, medial parietotempo-ral, temporal, occipital, and cerebellar areas, highlight-ing the multiplicity of regions and circuitry involved inmemory retrieval. Unlike episodic retrieval, the recall ofsemantic information is dependent on the left pre-frontal area for both verbal and nonverbal information(Cabeza & Nyberg, 2000). Similar to episodic retrieval,other brain regions are involved in semantic retrievalincluding temporal, anterior cingulate, and cerebellarregions.
Declarative Consolidation—Three major interconnected con-stellations of brain structures play a role in consolidatinginformation into LTM. The first memory centers aroundthe medial temporal lobes, the second around the dien-cephalon, and the third in the basal forebrain.
The medial temporal structures, which are important forlong-term declarative memory, center around the hip-pocampus and medial temporal lobe. The well-documentedcase of H.M. (Milner, Corkin, & Teuber, 1968; Scoville,1968) best exemplifies what occurs when these structuresare damaged. In 1953, at the age of 27 years, H.M. un-derwent brain surgery to reduce intractable seizures. Thesurgery involved bilateral removal of the hippocampusand portions of the surrounding area, which included thehippocampal formation (Figure 9.2). The hippocampalformation, or hippocampal complex, includes the hip-pocampus, the dentate gyrus, and the subiculum. In crosssection, the hippocampus has a distinctive “sea horse”shape. Information funnels into the hippocampus via theentorhinal cortex. In addition, the perirhinal and parahip-pocampal cortexes adjacent to the hippocampal forma-tion are believed to have a role in memory. At the time ofH.M.’s surgery little was known regarding the effects ofsuch surgery on memory. After the surgery, despite thepreservation of above-average intelligence, he was pro-foundly amnesic for new learning (anterograde amnesia),both episodic and semantic. He was able to recall oldmemories and facts, but new learning was no longer pos-sible. STM was preserved in that he could retain new in-formation for a few minutes. However, this informationcould not be consolidated into long-term storage. If hemet someone and then the person left, he would not haveany memory of the meeting a few minutes later. As a re-sult, if he met the person again, it was as if they had metfor the first time. H.M.’s amnesia was even more pro-found than N.A.’s, in that he also had difficulty learningnew visuospatial information.
The preservation of old memories with medial tempo-ral damage suggests that memories are not stored in thehippocampus; rather, this structure appears to be involvedin the movement of new information into long-term stor-age. PET and fMRI studies (Cabeza & Nyberg, 2000)show that the left medial temporal region activates duringthe encoding of verbal material, whereas bilateral activa-tion is evident for processing of nonverbal contents. Dam-age to the hippocampus can significantly disrupt declara-tive memory, but the extension of damage to theentorhinal and parahippocampal regions produces evenmore severe and long-lasting amnesia.
The specific functions of the regions of the medialtemporal lobe are not fully known, but research suggeststhat they make differential contributions to memory. Forexample, the visual association cortex shows significantprojections to the perirhinal cortex, whereas the parietalcortex projects to the parahippocampal cortex. These struc-tures appear to play specific roles in visual recognition and
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 229
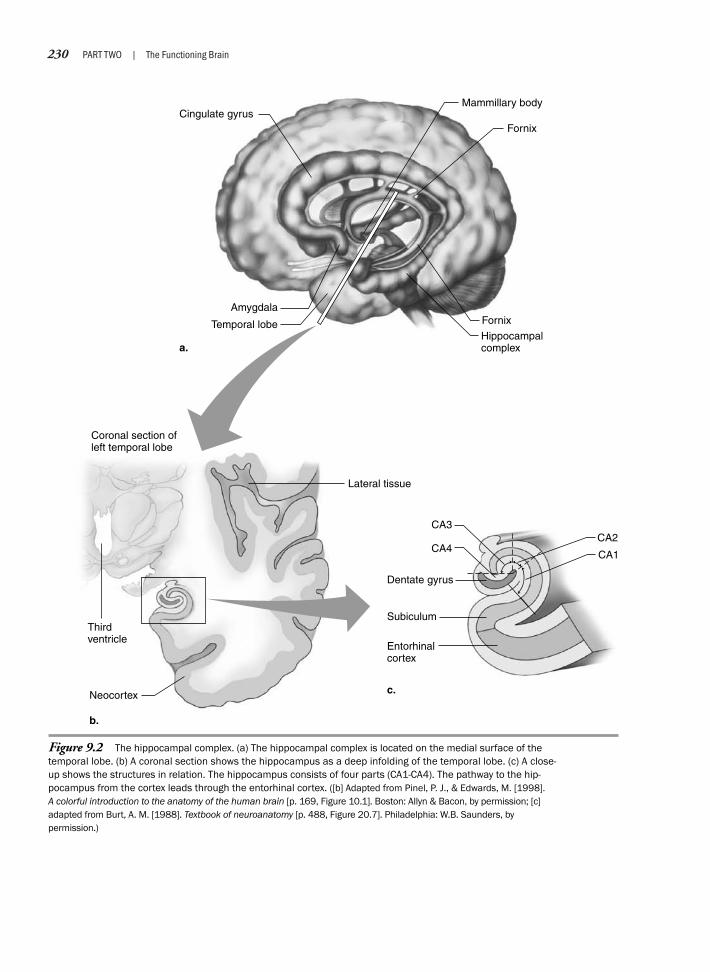
230 PART TWO | The Functioning Brain
Figure 9.2 The hippocampal complex. (a) The hippocampal complex is located on the medial surface of thetemporal lobe. (b) A coronal section shows the hippocampus as a deep infolding of the temporal lobe. (c) A close-up shows the structures in relation. The hippocampus consists of four parts (CA1-CA4). The pathway to the hip-pocampus from the cortex leads through the entorhinal cortex. ([b] Adapted from Pinel, P. J., & Edwards, M. [1998]. A colorful introduction to the anatomy of the human brain [p. 169, Figure 10.1]. Boston: Allyn & Bacon, by permission; [c]adapted from Burt, A. M. [1988]. Textbook of neuroanatomy [p. 488, Figure 20.7]. Philadelphia: W.B. Saunders, bypermission.)
Temporal lobe
a.
b.
c.
Lateral tissue
Dentate gyrus
Subiculum
Entorhinalcortex
Thirdventricle
Coronal section ofleft temporal lobe
Amygdala
Cingulate gyrus
Hippocampalcomplex
Mammillary body
Fornix
Fornix
Neocortex
CA3
CA4CA2
CA1

spatial memory, respectively (Squire & Knowlton, 2000).The hippocampus appears to have a special role in memorytasks that require the relating or combining of informationfrom different cortical sources, such as the relation of spe-cific objects or events in time and space.
The structures of the diencephalon involved in mem-ory center around specific nuclei of the thalamus and themammillary bodies of the hypothalamus (Figure 9.3).The thalamus consists of several nuclei, with the dorsalmedial nucleus of the thalamus the most often implicatedin memory disorders. Although the dorsal medial nucleusis involved in memory consolidation, there are sugges-tions that it may also assist in the initiation and monitor-ing of conscious retrieval of episodic memories (Wenk,2004). Damage to the dorsal medial nucleus is often im-plicated in Korsakoff ’s syndrome and in some cases of spe-cific amnesia, such as N.A.’s case (see Neuropsychology inAction 9.1). Korsakoff ’s syndrome is a consequence ofchronic alcoholism associated with vitamin deficiency(thiamine). As a result, degeneration of the thalamic dor-somedial nucleus and the mammillary bodies occurs.Patients with Korsakoff ’s syndrome exhibit significant an-terograde and retrograde amnesia, although certain formsof nondeclarative memory (for example, procedural mem-ory) are preserved. Moreover, there are cases of damagespecific to the diencephalon region resulting in amnesia,such as N.A.’s case (see Neuropsychology in Action 9.1).
The basal forebrain is the third area implicated in long-term declarative memory processing. As described inChapter 5, this area is a subcortical part of the telen-cephalon surrounding the inferior tip of the frontal hornand is strongly interconnected with limbic structures; someneuroscientists consider it part of the limbic system (for ex-ample, see Crosson, 1992). The basal forebrain represents amajor source of cholinergic output to the cortex. Some in-vestigators have suggested that extensive damage of basalforebrain structures may be needed to affect memory (Zola-Morgan & Squire, 1993); thus, looking at the contribu-tions of an individual nucleus to memory is probably notas profitable as regarding the system as a network. Becauseof its location surrounding the inferior tip of the frontalhorn and that the inferior communicating artery perfusesthis area, stroke easily affects the basal forebrain. This areais important to memory not only for the nuclei within butfor the fibers that traverse the area. The basal forebrain alsocontains numerous connections to the mediotemporal area.
The basal forebrain structures implicated in memoryinclude the nucleus basalis of Meynert, the medial septalnucleus, the nucleus of the diagonal band of Broca, andthe substantia innominata (Figure 9.4). The nucleusbasalis of Meynert includes a group of large neurons in-
terspersed within the substantia innominata. The substan-tia innominata is a gray and white matter area that sepa-rates the globus pallidus from the inferior surface of theforebrain. It interconnects with the frontal, parietal, andtemporal cortexes. An important tract coursing throughthe substantial innominata is the ventral amygdalofugalpathway, which connects the amygdala to the dorsal me-dial nucleus of the thalamus. The medial septal nucleuslies at the precommissural end of the fornix and projectsto the hippocampus through the fornix. It most likely af-fects memory when damage disrupts information flow tothe hippocampus. The nucleus of the diagonal band ofBroca is a white matter and cell body area located nearthe nucleus basalis. It also projects to the hippocampusthrough the fornix. Researchers think these structures areimportant cholinergic memory structures.
The major declarative memory system is the Papez cir-cuit. Papez originally proposed that this looping pathwaywas specific for emotional processing. He noticed that theclinical presentation of intense emotional symptoms inanimals with rabies (derived from Latin meaning “rage”)was associated with lesions in several limbic system struc-tures, specifically the hippocampus. Today, researchersknow this loop has more to do with consolidating infor-mation in memory than as a primary emotional proces-sor. Information from the cortex and higher cortical asso-ciation areas enters the circuit through the cingulategyrus, moves to the parahippocampal gyrus, and then intothe hippocampus through the hippocampal formation.The major output system of the hippocampal formationis the fornix. It contains nearly 1 million fibers and iscomparable in size with the optic tract (Nauta & Feirtag,1986). The fornix rises out of the hippocampal complexand arches anteriorly under the corpus callosum. Thefornix relays information to the mammillary bodies(specifically the medial mammillary nucleus) of the hypo-thalamus. From there information is projected to the ante-rior nucleus of the thalamus along the mamillo-thalamictract, from where it then goes to the cingulate gyrus tocomplete the circuit. Figures 9.2 and 9.5a show theanatomic location of the structures, and Figure 9.5b pre-sents a schematic of the loop.
It is readily apparent by examining amnesia cases suchas H.M. and N.A. that a break in the memory consolida-tion circuit can disrupt memory in a manner similar to di-rect removal of the hippocampus, which neurologists typi-cally consider the most crucial structure in the system.
N o n d e c l a r a t i v e M e m o r y
The term nondeclarative memory does not refer to a discretememory system as much as it acknowledges that some
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 231

232 PART TWO | The Functioning Brain
Text not available due to copyright restrictions
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 233
Text not available due to copyright restrictions

234 PART TWO | The Functioning Brain
memory functions operate outside the limbic circuitry ofexplicit or declarative memory. Researchers have variouslyreferred to the opposite of limbic circuitry–based memoryas “habit memory” (Mishkin, Malamut, & Bachevalier,1984), “procedural memory” (Cohen, 1984), and “im-plicit memory” (Graf & Schacter, 1985). The variety ofmemory functions this term encompasses most likely re-flects a collection of different abilities, not necessarily mu-tually exclusive, and perhaps dependent on different pro-cessing systems. For example, implicit memory impliesinfluence by prior experience without conscious aware-ness of the event. Procedural learning concerns the learn-ing of procedures, rules, or skills manifested through per-formance rather than verbalization, although consciousawareness may aid procedural learning. Because these
terms do not by themselves encompass the entire range ofnondeclarative memory, researchers prefer the less specificterm (see Squire, 1994). Neurologists also know that asingle lesion cannot erase all nondeclarative memory, as itmay for declarative new learning. Although it is prematureto present a neuroanatomic classification scheme, scien-tists can describe some aspects of nondeclarative memorywith respect to brain structures, particularly subcorticalbasal ganglia areas.
Researchers observing H.M. noticed that despite se-vere amnesia for declarative information, H.M. improvedwith practice on certain perceptual motor tasks (Milneret al., 1968; Scoville, 1968). He was learning, with prac-tice, without conscious recognition of this learning. If hisamnesia had been total, examiners would have expected
Text not available due to copyright restrictions

that each presentation of the task would be performed asif it were brand new. One area of nondeclarative memoryinvolves perceptual motor adaptation and skills acquisition.Many amnesiacs, such as H.M., show a normal learningcurve as they practice the pursuit rotor and reverse mirror-reading tasks. The pursuit rotor requires the examinee tokeep a stylus on a spinning disk, much like having to holda place on a record on a turntable. Reverse mirror readingrequires an individual to trace a maze while looking at itthrough a mirror. Perceptually, amnesiacs also show nor-mal adaptive behavior when wearing visual prisms. Be-cause prisms distort visual input, simple acts such asreaching for an object are misdirected at first. The visualmotor system must quickly learn to “retune” the systemso that it again correctly targets reaching according to thenew visual information. Interestingly, amnesiacs can dothis performance learning and adaptation despite severedeclarative amnesia. However, amnesiacs do not shownormal nondeclarative skill learning for all tasks. Forexample, investigations (Gabrieli, Keane, & Corkin,1987; Xu & Corkin, 2001) of H.M.’s performance on acomplex, nondeclarative, problem-solving task (Tower ofHanoi) did not find evidence of consistent improvementacross learning trials or mastery of the task.
Further support for a nondeclarative memory systemis provided by the differential performance of patientswith amnesia, Huntington’s disease, and Parkinson’s dis-ease on a measure of serial reaction-time skill learning(Schacter & Curran, 2000). The patients were requiredto press one of four keys when illumination occurredabove a key. The patient groups were not aware thatthere was a repeating sequence of illumination; yet,across learning trials, the patients with amnesia demon-strated improved performance as evidenced in decreasedkey press reaction times. In contrast, patients withHuntington’s and Parkinson’s diseases showed impairedlearning. Subcortical striatal pathology is central toboth Huntington’s and Parkinson’s diseases, suggestingthe involvement of this region in serial reaction-timelearning. Functional imaging studies have confirmedthat serial reaction-time skill learning is supported bythe striatal region and circuitry. Other regions that exhibitlearning-related changes during serial reaction-time skilllearning primarily involve the neocortex (primary motor,supplementary motor, premotor, parietal and occipital cor-tices). These changes suggest that serial reaction-timelearning involves changes in perceptual and motor areassupporting visually guided movements (Schacter & Curran, 2000).
Researchers also noticed that severely amnesic patientswith Korsakoff ’s syndrome showed a phenomenon known
as implicit priming. For example, in the word stem com-pletion priming paradigm, a list of words is first presented(for example, church, parachute, clarinet, and so on). Be-cause of the severe amnesia, the person’s memory is poorwhen examiners demand recall in a declarative task. Ex-aminers then give patients three-letter word stems (for ex-ample, chu____, par____, cla_____) and ask them tomake a word by completing the stems. “Primed” patientswith Korsakoff ’s syndrome were more likely to completethe stem with a word they had already seen than were un-primed examinees, despite the same level of declarativeamnesia for the words. Perceptual priming also appears inthe quicker recognition of fragmented objects (such asthose presented in Chapter 8 for testing apperceptive ag-nosics) or of words (see Figure 9.6 for examples of prim-ing stimuli). Similar to patients with Korsakoff ’s syn-drome, amnesic patients with damage to medial anddiencephalic brain areas often show unimpaired implicitperceptual priming.
Perceptually based implicit priming is associated withdecreased activity of the posterior neocortex. It has beentheorized that the decreased activation of the posterior neo-cortex reflects a reduction in neural resources needed toprocess the content when it recurs, because a visual traceremains from the original presentation of the material(Squire & Knowlton, 2000). Notably, implicit priming is
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 235
Figure 9.6 Amnesiacs who have deficient declarative memorymay still have intact implicit memory as they demonstrate byquickly recognizing fragments of previously presented words.(Reproduced from McCarthy, R. A., & Warrington, E. K. [1990]. Cogni-tive neuropsychology [p. 302, Figure 14.3]. San Diego: AcademicPress, by permission.)
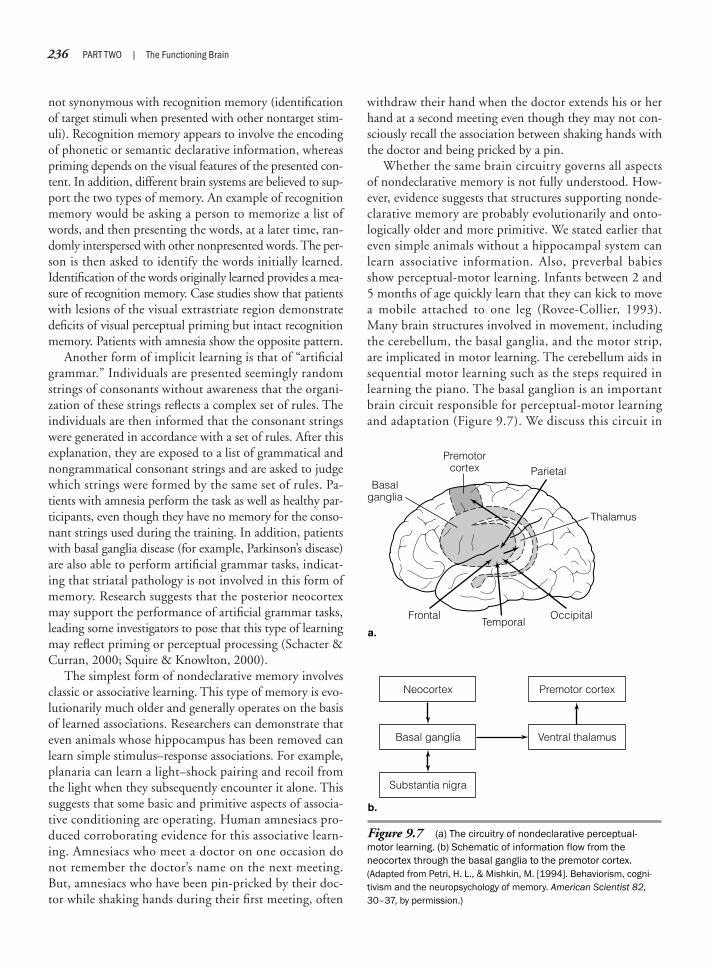
236 PART TWO | The Functioning Brain
not synonymous with recognition memory (identificationof target stimuli when presented with other nontarget stim-uli). Recognition memory appears to involve the encodingof phonetic or semantic declarative information, whereaspriming depends on the visual features of the presented con-tent. In addition, different brain systems are believed to sup-port the two types of memory. An example of recognitionmemory would be asking a person to memorize a list ofwords, and then presenting the words, at a later time, ran-domly interspersed with other nonpresented words. The per-son is then asked to identify the words initially learned.Identification of the words originally learned provides a mea-sure of recognition memory. Case studies show that patientswith lesions of the visual extrastriate region demonstratedeficits of visual perceptual priming but intact recognitionmemory. Patients with amnesia show the opposite pattern.
Another form of implicit learning is that of “artificialgrammar.” Individuals are presented seemingly randomstrings of consonants without awareness that the organi-zation of these strings reflects a complex set of rules. Theindividuals are then informed that the consonant stringswere generated in accordance with a set of rules. After thisexplanation, they are exposed to a list of grammatical andnongrammatical consonant strings and are asked to judgewhich strings were formed by the same set of rules. Pa-tients with amnesia perform the task as well as healthy par-ticipants, even though they have no memory for the conso-nant strings used during the training. In addition, patientswith basal ganglia disease (for example, Parkinson’s disease)are also able to perform artificial grammar tasks, indicat-ing that striatal pathology is not involved in this form ofmemory. Research suggests that the posterior neocortexmay support the performance of artificial grammar tasks,leading some investigators to pose that this type of learningmay reflect priming or perceptual processing (Schacter &Curran, 2000; Squire & Knowlton, 2000).
The simplest form of nondeclarative memory involvesclassic or associative learning. This type of memory is evo-lutionarily much older and generally operates on the basisof learned associations. Researchers can demonstrate thateven animals whose hippocampus has been removed canlearn simple stimulus–response associations. For example,planaria can learn a light–shock pairing and recoil fromthe light when they subsequently encounter it alone. Thissuggests that some basic and primitive aspects of associa-tive conditioning are operating. Human amnesiacs pro-duced corroborating evidence for this associative learn-ing. Amnesiacs who meet a doctor on one occasion donot remember the doctor’s name on the next meeting.But, amnesiacs who have been pin-pricked by their doc-tor while shaking hands during their first meeting, often
withdraw their hand when the doctor extends his or herhand at a second meeting even though they may not con-sciously recall the association between shaking hands withthe doctor and being pricked by a pin.
Whether the same brain circuitry governs all aspectsof nondeclarative memory is not fully understood. How-ever, evidence suggests that structures supporting nonde-clarative memory are probably evolutionarily and onto-logically older and more primitive. We stated earlier thateven simple animals without a hippocampal system canlearn associative information. Also, preverbal babiesshow perceptual-motor learning. Infants between 2 and5 months of age quickly learn that they can kick to movea mobile attached to one leg (Rovee-Collier, 1993).Many brain structures involved in movement, includingthe cerebellum, the basal ganglia, and the motor strip,are implicated in motor learning. The cerebellum aids insequential motor learning such as the steps required inlearning the piano. The basal ganglion is an importantbrain circuit responsible for perceptual-motor learningand adaptation (Figure 9.7). We discuss this circuit in
Figure 9.7 (a) The circuitry of nondeclarative perceptual-motor learning. (b) Schematic of information flow from the neocortex through the basal ganglia to the premotor cortex.(Adapted from Petri, H. L., & Mishkin, M. [1994]. Behaviorism, cogni-tivism and the neuropsychology of memory. American Scientist 82,30–37, by permission.)
Premotorcortex
Basalganglia
FrontalTemporal
a.
b.
Occipital
Parietal
Thalamus
Substantia nigra
Ventral thalamusBasal ganglia
Premotor cortexNeocortex

A moment in time. In the case of amnesiacs such as H.M.and N.A., this is everything they had. But healthy peoplealso travel from moment to moment in a “presence-chamber” of the mind, using this workspace to assembleinformation for storage and to connect and reconnect in-formation retrieved from LTM, to solve problems or tomake new associations. The difference is that N.A. couldno longer connect moments and store aspects of the pres-ent as new memory in LTM. The limited capacity andshort time frame of STM does not accommodate morethan a few thoughts, ideas, or bits of information at atime. As new bits arrive, they may take the place of othersor simply degrade. If there is no linkage between STMand LTM, STM floats as an island with only a small areaof possible habitation.
Researchers interested in memory have debated thequestion of the relation of STM to LTM. Cognitive tasks il-lustrate that the two appear to measure different areas ofmemory. STM is a limited-capacity, rapid-access, input-and-retrieval system analogous to computer RAM (random-access memory). LTM has unlimited capacity but with arestricted rate of input and retrieval much like ROM(read-only memory). The two systems are also coded dif-ferently. STM uses phonologic coding, relying on anacoustic code, whereas LTM heavily uses semantic cod-ing, or the associative meaning value of information to beremembered (for review, see Baddeley, 1986). Eventhough the two seemingly measure different aspects ofmemory functioning, a unitary view of memory function-ing would argue that LTM depends on STM. That is,these two systems are viewed as two components of onesystem linked in a serial fashion; thus, information enter-ing LTM must inevitably flow through STM. In contrast,a separate system view would argue that LTM and STMare dissociated, so someone could have an LTM deficitwith intact STM, whereas another person could have anSTM deficit but maintain adequate LTM. Patients withamnesia with severe LTM deficits often show intact STM.On formal testing, they can repeat increasingly longer se-ries of digits and perform well on other tasks presumed totest STM. However, other patients have a specific STMdeficit with preserved LTM. This is some of the most con-vincing evidence that STM and LTM are anatomicallyseparate.
Patients with a pure STM deficit are rare. However, re-searchers have reported cases with exactly this problem (forexample, see Shallice & Warrington, 1970; Basso, Spinnler,Vallar, & Zanobio, 1982). Shallice and Warrington (1970)reported the case of K.F., a patient who suffered a left pos-terior temporal lesion that left him with a greatly reducedSTM capacity for verbal information. He had a profound
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 237
Chapter 7 (see the section “Subcortical Motor Process-ing”). Specifically, this circuit includes the caudate nu-cleus, putamen, and globus pallidus. The nuclei of thestriatum (caudate and putamen) receive projected infor-mation from cortical sensory areas. From the striatum,information then funnels through the globus pallidus,and then on to the thalamus, where it projects to the pre-motor and prefrontal areas (see Figure 7.11) (Mishkin,Malamut, Bachevalier, 1984). Behaviorally, Huntington’sdisease best portrays the effect of caudate nucleus dys-function of the basal ganglia. Huntington’s disease devel-ops as a progressive subcortical dementia (see Chapter 15for a thorough description), but caudate nucleus degen-eration is the hallmark of Huntington’s disease and is oneof the first structural changes that computed tomogra-phy scans identify. The atrophic imaging change appearsat the onset of the choreiform movement disorder. Theeffect of this change appears to target perceptual-motorlearning tasks. In a series of studies spearheaded by Nel-son Butters (for review, see Squire & Butters, 1992), pa-tients with Huntington’s disease showed a dissociation inperformance from patients with Korsakoff ’s syndrome,amnesia, and Alzheimer’s disease. On declarative verbalmemory tasks, patients with Huntington’s disease per-formed relatively better than patients with Korsakoff ’ssyndrome and Alzheimer’s disease. However, on motorlearning tasks, the two cortically impaired groups out-performed the patients with Huntington’s disease. Thisdouble dissociation in functioning prompted the initialsuggestion for separate cortical and subcortical memorystructures. Since that time, animal studies and imagingstudies with healthy participants performing motorlearning tasks have added evidence for the role of thebasal ganglia in implicit memory.
S H O R T - T E R M M E M O R Y A N D W O R K I N G M E M O R Y
There seems to be a presence-chamber in my mindwhere full consciousness holds court, and where two orthree ideas are at the same time in audience, and anante-chamber full of more of less allied ideas, which issituated just beyond the full ken of consciousness. Out ofthis ante-chamber the ideas most nearly allied to thosein the presence chamber appear to be summoned in amechanically logical way, and to have their turn ofaudience.
—Francis Galton (1883)

238 PART TWO | The Functioning Brain
STM deficit, having a digit span length of about two,rather than the usual seven bits of information. He alsodemonstrated conduction aphasia whereby he could notrepeat sentences. Surprisingly, K.F. showed a normal ver-bal learning curve with practice, indicating intact storageof information in LTM. It is difficult to reconcile K.F.’sperformance with theories posing that verbal STM andLTM use the same anatomic structure, but in differentways. K.F.’s performance also challenges models that seri-ally link STM and LTM and, conversely, provides sup-port for models that postulate that verbal STM and LTMare separate or parallel systems.
The notion of STM as a component of LTM has grad-ually given way to ideas that now refer to working mem-ory (Baddeley, 1986) as a distinct system encompassingsome of the capacity limitations of STM, but that is a dy-namic system also influencing aspects of attention and ex-ecutive functioning. Several distinctions differentiate STM(sometimes called short-term span) from working mem-ory. First, a cognitive (mental) representation of informa-tion is held “on line” in temporary store (similar to STM).Second, the cognitive representations are subjected tosome form of mental manipulation or transformation.Third, attentional and inhibitory control is necessary forthe protection of the on-line cognitive representations,manipulations, and transformations from external or in-ternal inference. Fourth, the cognitive manipulations orcomputations often involve using information drawn fromlong-term storage. To understand working memory, con-sider the following: You are presented a multiplicationproblem to solve mentally such as multiplying 234 by 354.When performing this problem, you will hold a mentalrepresentation of the problem in short-term storage. Asyou maintain this mental representation while performingthe necessary computations to solve the problem, you willneed to intensely concentrate and, at the same time, blockout any internal or external stimuli that could disrupt yourfocus. Simultaneously, you will draw from LTM the ap-propriate multiplication facts and the mathematical opera-tions needed to solve the problem. Because of the dynamicand effortful cognitive processes involved in workingmemory, Moscovitch and Winocur (2002) believe that itwould be more aptly named “working-with-memory.”
Alan Baddeley’s (2001, 2002) seminal research and the-orization has substantially enhanced our understanding ofworking memory. Working memory is integral to a widerange of cognitive tasks from reading to math to problemsolving. Baddeley initially conceptualized working mem-ory as involving three components (Figure 9.8). The cen-tral executive is an attention-controlling system; it super-vises and coordinates slave systems and is the proposed
deficit in Alzheimer’s disease. The attention-controllingfunctions of the central executive system involve focusing,shifting, and dividing attention and interfacing with LTM.There are also two modality-specific “slave” systems. Thearticulatory phonologic loop stores speech-based infor-mation and is important in the acquisition of vocabulary.The visuospatial sketch pad manipulates visual and spa-tial images. Recently, Baddeley (2000, 2002) extended themodel to include a fourth component, the episodic buffer(see Figure 9.8). The episodic buffer is a temporary andlimited capacity storage system whose posited function isto hold and integrate information of different modalities(for example, visual and auditory) through linkage withLTM. The central executive controls this buffer and usesconscious awareness as a primary retrieval strategy. For ex-ample, if you are asked to recall a series of numbers pre-sented in word form, and you are able to categorize thenumbers into meaningful groups based on associations inlong-term storage, memory recall will be enhanced. Thus,if numbers are visually presented in word form—fourteen,ninety-two, nineteen, forty-one—and you draw fromLTM the numeric representation of historically significantdates and group the numbers as 1492 (Columbus discov-ers America) and 1941 (beginning of the World War II),you have integrated verbal and visual information throughlinkage with associative information held in LTM.
Neuropsychologically, the phonologic loop and the vi-suospatial sketch pad link to lateralized modalities in thebrain and to frontal lobe executive processes. The phono-logic loop involves auditory-verbal processing and de-pends on language-based left hemisphere processes. Like-wise, the visuospatial sketch pad is associated with the
Figure 9.8 A simplified representation of Baddeley’s workingmemory model. (Adapted from Baddeley, A. [2002]. Fractionating thecentral executive. In D. T. Stuss & R. T. Knight [Eds.], Principles offrontal lobe functioning [p. 256, Figure 16.4]. New York: Oxford Univer-sity Press, by permission.)
Visuo-spatialsketch-pad
Visualsemantics
CentralExecutive
EpisodicBuffer
Episodiclong-termmemory
Phonologicalloop
Language

right hemisphere. The neural substrates that support theepisodic buffer remain to be identified, although frontalarchitecture is believed to play a crucial role (Baddeley,2002). Goldman-Rakic’s (1988) groundbreaking work inprimate models of working memory points to the dorsolat-eral prefrontal cortex as the area that holds information “on
line” while it is processed. In these studies, Goldman-Rakictested monkeys’ abilities to recall the position of food inone of two food wells after a short delay of several sec-onds. Figure 9.9 shows the general paradigm of the study.Simultaneous recordings from neurons in the dorsolat-eral prefrontal area continued to fire during the delay
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 239
Text not available due to copyright restrictions

240 PART TWO | The Functioning Brain
until the action of food selection was completed. SinceGoldman-Rakic’s work, PET and fMRI studies have sup-plied confirmation in humans that the prefrontal cortexactivates during working memory tasks (Jonides et al.,1993; Smith, Marshuetz, & Geva, 2002). For example,based on neuroimaging research, Petrides (1998) has iden-tified two areas of the prefrontal cortex that are involvedin support of working memory. The first area, the ventro-lateral prefrontal cortex (Brodmann’s areas 45 and 47/12),activates when dynamic (strategic) retrieval of informa-tion from posterior brain regions is required; that is, whenthere is a conscious effort to retrieve specific informationin accordance with the individual’s intentions and plans.Thus, the ventrolateral cortex is actively involved in theselection, comparison, and judgment of information heldin memory. In contrast, the mid-dorsolateral frontal cor-tex (Brodmann’s areas 46 and 9) activates when informa-tion is to be maintained on line for the purpose of moni-toring and manipulation. Jointly, these two areas providethe foundation for higher order processes involved in theplanning and organization of behavior.
The move from conceptualizing STM as a storage ca-pacity system to that of working memory as a dynamic,integrated system entailing both lower and higher orderprocesses highlights the interrelated nature of brain sys-tems. Other memory processes such as prospective mem-ory (the memory for future intention), temporal memory(memory for information in time order), and source mem-ory (memory for context) also rely on frontal lobe and ex-ecutive functioning processes. The next section discussesattention, a major higher function that is essential to theefficiency of mental processing.
Attention
Everyone knows what attention is. It is the takingpossession of the mind in clear and vivid form of one outof what seem several simultaneous objects or trains ofthought.
—William James (1890)
Moving about the world, people confront a flood of infor-mation that the nervous system cannot treat equally. Yourbrain must target or “spotlight” specific material to processand tune out the irrelevant information. For example, whenyou stop to talk to a friend in a hallway, you may hear com-peting sounds of others talking and people walking downthe corridor. You may also be preoccupied by your own
inner thoughts. Nonetheless, if you “pay attention,” youcan orient to a small sample of the incoming informationand ignore most of the other input. In this way, attentionoperates as a gateway for information processing. Atten-tion allows orienting to, selecting, and maintaining focuson information to make it available for cortical processing.
The neuropsychology of attention historically hasbeen a confusing subject because there are so many sub-sets of attentional processing and many possible defini-tions of attention. The term attention can refer to a generallevel of alertness or vigilance; a general state of arousal;orientation versus habituation to stimuli; the ability tofocus, divide, or sustain mental effort; the ability to targetprocessing within a specific sensory arena (such as visualattention or auditory attention); or a measure of capacity.Researchers have also asked whether attention implies ageneral state of cortical tone or energy, or functions as anetwork or set of specific structures or networks withinthe brain. Attentional processing does not imply a unifiedsystem, and most researchers now view it as a multifac-eted concept that implies multiple behavioral states andcortical processes that various subsets of cerebral struc-tures control.
In many types of brain dysfunction, efficiency of thebrain to process information diminishes. Sometimes peo-ple cannot sustain attention to one particular stimulus forlonger periods or cannot select information (selective at-tention) from competing sources. This impairment maybe minimally present and detected only through formalneuropsychological testing, or may be profound and easilynoticeable by any observer.
Neuropsychological theories of attentional processing(for example, see Mesulam, 1981; Posner & Petersen,1990) usually consider the role of the reticular activatingsystem (RAS) in cortical arousal, subcortical and limbicsystem structures (particularly the cingulate gyrus) in reg-ulation of information to be attended to, the posteriorparietal lobe system in focusing conscious attention, andthe frontal lobes in directing attentional resources. Theyalso give the right hemisphere prominence as an atten-tional processor. Theorists have not yet worked out anyone-to-one correspondence between levels of attentionalbehavior and brain structures or networks. Rather, theycan describe general subsets of brain systems related to at-tentional functioning.
S U B C O R T I C A L S T R U C T U R E SI N F L U E N C I N G A T T E N T I O N
The RAS regulates the level of cortical activation orarousal—a necessary first step in attentional processing.

With its genesis in the midbrain and its ability to projectto large cortical areas, the RAS sets a general cortical tone.Researchers can observe and categorize this arousal intobrain wave types (beta, alpha, theta, and delta) by theirfrequency as measured by an electroencephalograph(EEG). In a general way, sensory input “charges” the RAS.If the brainstem is processing sensory input, the RASmaintains high cortical activation. However, lack of sen-sory input does not necessarily make one drowsy. In fact,even with constant sensory input there can be habitua-tion. Those who live on a noisy street grow accustomedto the sound, but a sudden silence will cause the brain toorient to the change in sound patterning. Daily bio-rhythms of 90 minutes of relatively higher and loweralertness also cycle throughout the day, and circadianrhythms control the sleep/wake cycle through the RAS.We discuss these changing levels of cortical tone furtherin our discussion of sleep (see Chapter 16). If a person isawake and alert, general level of arousal is more of a back-ground issue than a central one in the neuropsychologyof attentional processing. However, the RAS also plays arole in anticipatory responding. Researchers have hypoth-esized that the RAS may send a preparatory signal to thecortex to alert it to receive stimuli, and thus put it in aheightened state of readiness to receive. Lesions to theRAS can result in lowered alertness or coma. Chapter 13discusses coma in greater detail.
Neuroscientists are also identifying the role of othersubcortical structures in attention. Although the precisefunctions that these structures play in attentional func-tioning remains to be specified, several interpretations havebeen posed. Moreover, these regions do not operate in iso-lation from one another or from other subcortical and cor-tical structures. For example, support of sustained atten-tion is ascribed to the right fronto-parietal-thalamic neuralnetwork (Sarter, Givens, & Bruno, 2001). With regard toselective visual attention, the thalamus, basal ganglia, andsuperior and inferior colliculi play a supporting role. Thethalamus receives activation from the reticular formationand projects this arousal to the cortex. Moreover, the thal-amus serves to select and relay information from subcorti-cal regions to the cortex and, conversely, conveys corticalneural signals to subcortical regions. Through its gatingfunction, it is in position to influence the selectivity of at-tention (Cohen, 1993). The superior colliculus of the mid-brain plays a role in the reflexive movement of the eyes andhead when orientating to visual stimuli, whereas the infe-rior colliculus is implicated when orientating to auditorystimuli. Researchers have historically attributed motorfunctions to the basal ganglia, but increasingly are recog-nizing their role in cognitive operations. Posner and
DiGirolamo (1998) pose that the basal ganglia is involvedin shifting or switching sets, and thus is a component ofthe act of orienting to stimuli.
T H E C E R E B R A L C O R T E X A N D A T T E N T I O N
The attentional issues of most interest to human neu-ropsychology generally concern the higher levels of atten-tional processing coordinated by the cerebrum, includingfocused attention, the ability to alternate and divide at-tentional processes, and the ability to sustain attention.Focused attention is the ability to respond and pick outthe important elements or “figure” of attention from the“ground” or background of external and internal stimula-tion. Focused attention also implies a measure of concen-tration or effortful processing. A basketball player whocan concentrate on making a free throw, while tuning outthe crowd, is a good example of high focus. However,even the most ordinary event of noticing requires cogni-tive focus. People are frequently called on to alternate anddivide attention in the course of daily activities. For ex-ample, a receptionist who must switch back and forth be-tween answering the phone and talking with customersmust use alternating attention while mentally holding aplace to return to the other activity. Divided attentionrequires partialing out attentional resources at the sametime rather than switching back and forth, howeverquickly. A good example is driving a car, listening to aradio, and talking with a passenger. Researchers have de-bated whether divided attention is, in fact, possible, orwhether people just manage to shift their attentionquickly between different stimuli. However, evidence in-dicates that people can divide attention to some degree.Sustained attention is the ability to maintain an effortfulresponse over time. It is related to the ability to persistand sustain a level of vigilance. People who work as airtraffic controllers or on assembly-line jobs must have ex-cellent abilities for sustaining attention.
Attention can be further characterized by task or in-formation-processing demands. Tasks that are routinelyprocessed or overlearned can be performed automaticallywith minimal conscious thought. Automatic processingplaces minimal demands on attentional resources, andsince processing demands are low, other tasks can be per-formed concurrently. In contrast, new, unfamiliar, or con-flicting tasks require the conscious deployment of mentaloperations. Controlled processing involves the executionof mental operations in a linear or serial manner with asignificant allocation of attentional resources. Parallel pro-cessing of additional tasks is generally not possible (Cohen,Aston-Jones, & Gilzenrat, 2004). An experienced driver
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 241

242 PART TWO | The Functioning Brain
does not need to attend to the mechanics of driving whileconversing with a passenger, because eye, hand, and footmovement associated with driving are well-practiced or“habitual.” A person driving for the first time must com-mit considerable attention to the mechanics of drivingand will find conversing with a passenger to be not onlydifficult but highly disruptive.
The disruption of attention is a common complaint ofpatients who have a variety of disorders. Table 9.1 providesa partial listing of disorders that include attentional dys-function as a prominent component of the symptom pat-tern. The range of disorders illustrates that attentionaldysfunction is easily compromised by neurologic, meta-bolic, and psychiatric disorders. Fatigue, or inability tosustain attention to an activity, frequently appears acrossa number of more generalized neuropsychological disor-ders. Patients with neurologic disease, as well as patientswho have suffered focal or generalized brain insults, oftendescribe mentally wearing out when engaged in tasks thatrequire persistent effortful attention. People with affectivedisorders frequently report attention and concentrationproblems. Depressed people often describe drifting off or“spacing out,” so that even when driving they may missan exit. Mania is associated with concentration problemsof another sort. Manic people may become so energeticwith a relentless “flight of ideas” passing through theirminds that they cannot accomplish anything, becausethey cannot concentrate on one thing at a time.
Attentional deficits are also a common concomitant ofschizophrenia. These include perseveration of thought
and action, inability to disengage attention, problems insustained attention or vigilance, distractibility, and an al-most random tendency to orient to both external and in-ternal stimuli. This set of deficits may cause the loose as-sociations in thought processes that schizophrenicscommonly show. Close to half of schizophrenics show nogalvanic skin conductance response (SCR), which is ordi-narily considered an orienting response to novel sensorystimuli (Dawson & Nuechterlein, 1984). Neuropsychol-ogists call this subgroup of schizophrenics electrodermalnonresponders. Nonresponders are more likely to show thenegative symptoms of schizophrenia including apathy,emotional and social withdrawal, and blunted affect.Nonresponders are also more likely to have cortical atro-phy than schizophrenic galvanic skin responders. Interest-ingly, the failure of a psychophysiological skin conduc-tance orienting response to sensory stimulation comesagainst a background of chronic elevation of autonomicresponses, which implies a generalized hyperarousal inthis subgroup. Some investigators suggest (see Cohen,1993, for review) that the attention deficit in schizophre-nia may be a primary cognitive dysfunction.
M O D E L S O F A T T E N T I O N
A myriad of models have been developed to conceptual-ize attentional functioning. Each model represents a dif-ferent theoretical orientation, type of attention, methodof study, and degree of empirical verification. We presentthe individual models that Mesulam, Posner, and Mirskydeveloped in order to provide familiarity with neuropsy-chological conceptualizations of attentional functioning.
M e s u l a m ’ s M o d e l o f S p a t i a l A t t e n t i o n
Mesulam (2000) presents a model of selective, spatial at-tention that has enhanced our understanding of neu-ropsychological manifestations of patients exhibitingsymptoms of attentional neglect. Based on clinical and em-pirical research, Mesulam poses that a neural network in-volving the frontal, parietal, and cingulate cortices supportsspatial attention to the extrapersonal world (Figure 9.10).Each of these regions makes a differential contribution tospatial attention. The parietal region generates an internalspatial representation (sensory map) of the extrapersonalenvironment, whereas the cingulate cortex assigns andregulates motivational and emotional significance to ex-trapersonal elements (Gitelman et al., 1999; Kim et al.,1999). The frontal cortex, particularly the frontal eyefields (Brodmann’s area 8) and surrounding areas, modu-lates and coordinates motor programs for exploration,
Attention-deficit/hyperactivity disorder
Neurologic diseaseMultiple sclerosisAlzheimer’s diseaseParkinson’s disease
Head trauma
Seizure disorders
Metabolic disorderHypoglycemic encephalopathyHyperthyroidism
Psychiatric disordersDepressionManiaSchizophrenia
Right hemisphere stroke: unilateral neglect
Table 9.1 Disorders That Show ProminentAttentional Dysfunction

scanning, foveating, fixating, and manipulating (reach-ing) extrapersonal stimuli. Spatial attention requires theintegrity of these three cortical areas, as well as their inter-connections with one another and with subcorticalregions in the thalamus and striatum. The model thusconceptualizes spatial attention in terms of sensory repre-sentation, motivational importance and expectancy, andmotor response.
Recently, Mesulam’s model (Nobre, Coull, Maquet,Frith, Vandenberghe, & Mesulam, 2004) was extended tospatial attention to information held within workingmemory. Research participants underwent neuroimaging(fMRI) while performing a spatial working memory taskand a spatial orientation task. The former task requiredthe orientation of attention to internalized representa-tions of previously encoded stimuli, and the latter re-quired attentional orientation to extrapersonal stimuli.Neuroimaging demonstrated that both tasks recruitedoverlapping networks involving the occipital, parietal, andfrontal cortices. While both spatial tasks activated the su-perior parietal lobe, only the right inferior parietal cortexwas selectively activated during extrapersonal attentionalorienting. With regard to the frontal lobes, orienting toextrapersonal stimuli activated the premotor and dorsalprefrontal cortex, while more anterior prefrontal regions
were selectively engaged in orienting attention to inter-nally represented stimuli. Previous research has associatedthese anterior prefontal regions with working memoryoperations. Overall, the findings suggest that overlap-ping neural networks are involved in orienting attentionto external and internal spatial representations.
Lesions in any of the neural components supportingspatial attention can lead to hemispatial neglect, that is,a failure to attend to the contralateral visual field. Hemis-patial neglect generally relates to right rather than lefthemisphere injury, suggesting hemispheric asymmetry inthe support of spatial attention. The right hemisphere ap-pears specialized for control of spatial attention across thevisual field, whereas the left hemisphere’s control is pri-marily limited to the contralateral right side visual field.
P o s n e r ’ s A n t e r i o r a n d P o s t e r i o r A t t e n t i o n M o d e l
Michael Posner presents a model of attention from the per-spective of cognitive psychology and neuroscience. Heposes that attention can be defined by three major func-tions: (1) orienting to events, particularly to locations in vi-sual space; (2) achieving and maintaining a vigilant or alertstate; and (3) orchestrating voluntary actions (Fernandez-Duque & Posner, 2001). Each attentional function is, inturn, supported by separate neural networks, namely, ori-enting, vigilance, and executive networks (Table 9.2).Moreover, these attention-neural networks operate inter-actively with each other and other cortical and subcorticalregions.
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 243
Figure 9.10 A theoretical schematic of the attentional sys-tem. (From Mesulam, M. M. [1985]. Principles of behavioral neurol-ogy. Philadelphia: E. A. Davis; reprinted from Cohen, R. A. [1993]. Theneuropsychology of attention [p. 334, Figure 14.2]. Reprinted by kindpermission of Springer Science and Business Media.)
Attention Networks Functions Neural Correlates
Posterior Orienting to stimuliorienting system
Disengage attention Temporoparietal, superior from a stimuli temporal, superior
parietal
Move to a stimuli Superior colliculusEngage new stimuli Thalamus
Vigilance attention Achieving and Right frontoparietal system maintaining an
alert state
Anterior or executive Orchestrating Anterior cingulate, attention system voluntary actions lateral and orbitofrontal
prefrontal cortex,basal ganglia, thalamus
Table 9.2 Posner’s Attention Networks

244 PART TWO | The Functioning Brain
When visually orienting to an event in the environ-ment, three basic cognitive operations—disengage, move,and engage—activate. Attention is first disengaged fromthe current event of focus and then moved to the newpoint of focus, where attentional resources are engaged.The operations of disengage, move, and engage are linkedto the parietal, midbrain, and thalamic region, respec-tively. Accordingly, the visual orienting system is termedthe posterior attention system. This system plays a rolein conscious attention to portions of your visuospatialfield and directs the attention of your eyes to a point inspace. The posterior parietal lobe mediates conscious at-tention to spatial targets, the midbrain superior colliculusplays a role in moving the eyes from one position to an-other, and the pulvinar of the thalamus helps select andfilter important sensory information for processing. Theorienting system is also activated in covert orientation.Covert orientation refers to the spatial engagement of at-tention to a target without moving the eyes or the head.For example, if you fixate your eyes on an object, you canalso attend to a peripherally located object without mov-ing your eyes or head.
Posner initially ascribed the disengage function to thesuperior parietal lobe. However, lesion studies showed thatdisruption of the disengage function was often associated
with lesions in the temporoparietal junction or superiortemporal lobe. This difference was resolved by the discov-ery that lesions of the temporoparietal junction or supe-rior temporal regions impair the ability to disengage froma stimulus, and then shift attention to a new or novelstimulus (Posner & Fan, in press). In contrast, lesions ofthe superior parietal lobe disrupt voluntary shifts of at-tention following a cue or when searching a visual target.
There are indications that the orienting system is mod-ulated, in part, by the cholinergic neurotransmitter ACh(acetylcholine). ACh is produced by the nucleus basalis ofthe brain forebrain and innervates many cortical areas, in-cluding the parietal lobes. Research with primates showsthat lesions of the nucleus basalis disrupt the disengage-ment of attention from an ipsilesional cue to engage a tar-get contralateral to the side of the lesion (Fernandez-Duque & Posner, 2001).
Patients with lesions to the right posterior orientingsystem frequently fail to attend to the opposite visualfield, a condition referred to as hemispatial neglect. Asdiscussed previously, hemispatial neglect is not a sensorydeficit to visual input, but rather a failure to attend to halfof the visual field (Figure 9.11). Posner (Posner & Petersen,1990) describes this as a problem of engaging, moving,and disengaging focus to objects in the contralateral field
Figure 9.11 A case of hemispatial inattention. (From Honoré Daumier, M. [1858]. Babinet prevenu par sa portiere de la visite de la comete. Le Charivari.Courtesy of Museum of Fine Arts, Boston, MA. Reprinted from Cohen, R. A. [1993]. Theneuropsychology of attention [frontispiece]. New York: Plenum Press, by permission.)

of vision. In this view, the system does not direct the eyesand the brain to engage the left side of space, or to disen-gage attention from the right side of space.
The vigilance attention system mobilizes and sus-tains alertness for processing high-priority targets and isimportant to attentional functioning. For example, ifyou were involved in an aerial search for survivors of aboating accident, you would have to maintain a highlevel of alertness and preparedness to identify a survivorin the expanse of the ocean. In addition, you would needto avoid processing irrelevant information (external orinternal) to avoid distraction. The neural network sup-porting the vigilance system includes the right frontaland parietal regions of the brain. The neurotransmitternorepinephrine, produced by the locus ceruleus of the mid-brain, is implicated in achieving an alert state and main-taining attention over time (Fan, McCandliss, Sommer,Raz, & Posner 2002).
The anterior or executive attention system controlsand coordinates other brain regions in the execution ofvoluntary attention. A hierarchy exists for attentional pro-cessing, with the anterior system passing control to theposterior system as needed. The executive attention sys-tem orchestrates higher order cognitive functions such astask switching, inhibitory control, conflict resolution,error detection, attentional resource allocation, planning,and the processing of novel stimuli. A number of corticaland subcortical substrates support the executive attentionnetwork, although Posner has focused much of his re-search and theorization on the anterior cingulate and lat-eral prefrontal cortex (Posner & DiGirolamo, 1998). Oneof the primary functions of the anterior cingulate relatesto the monitoring and resolution of conflict between op-erations occurring in different brain areas (Posner & Fan,in press). For example, if an overlearned (automatic) re-sponse to a stimulus is to be inhibited in favor of a lesssalient response, the anterior cingulate provides the top-down control necessary to initiate the operations of inhi-bition and response selection. Similarly, the anterior cin-gulate activates when a task requires error detection. Thus,if you were proofreading a recent paper that you had pre-pared for a class, the anterior cingulate would be activewith regard to identifying errors in the text.
Often, the lateral prefrontal cortex and anterior cingu-late are jointly activated, depending on the nature of thepresented demand or task. The involvement of the lateralprefrontal cortex in the executive attention system relatesto its role in holding mental representations of specific in-formation in temporary memory. This set of cognitive op-erations is consistent with the definition of working mem-ory. The Stroop test (1935) illustrates the roles of the
anterior cingulate and lateral prefrontal cortex in execu-tive attention. One of the trials of the Stroop test presentsthe examinee with the words red, green, and blue printedin an incongruous color. For example, the word red isprinted in green type. Reading is an overlearned (auto-matic) behavior for most adults, and when written text ispresented, decoding occurs quickly and automatically. Incontrast, naming the color of objects is a less rapid andautomatic process. When the words red, green, and blueare presented in incongruous color, reading the word isthe salient response. If you are asked not to read thewords, but to name the incongruous color of the printedwords, significant conflict is produced. The anterior cin-gulate activates, as discussed earlier, to provide the top-down inhibitory control and response selection. The lat-eral prefrontal region holds the mental representation ofthe “rule” (“Name the color, don’t read the word.”) inworking memory to guide the process.
Although norepinephrine and ACh are implicated inthe support of the alerting and orientating systems, re-spectively, dopamine is considered the primary neuralmodulator of the executive or anterior attention system(Fernandez-Duque & Posner, 2001). Disorders that in-volve disruption of dopaminergic modulation (for exam-ple, schizophrenia) frequently demonstrate dysfunctionsof executive attention. Furthermore, administration ofa dopamine agonist to patients with lesions of thefrontal lobes improves performance on measures ofexecutive function (McDowell, Whyte, & D’Esposito,1998).
M i r s k y ’ s E l e m e n t s o f A t t e n t i o n M o d e l
Allen Mirsky (National Institute of Mental Health,Bethesda, MD) developed a neuropsychological modelthat identifies the possible elements of attention and re-lates these elements to neuropsychological measures andthe underlying neural systems. Mirsky (1996) proposedthat there were three elements of attention: focus-execute,sustain, and shift. A battery of neuropsychological mea-sures considered sensitive to attentional functioning wascompiled (Table 9.3) and administered to adult neuropsy-chiatric patients and healthy control participants. The testdata revealed four factors, three of which correspondedwith the elements of attention proposed by Mirsky, andan additional element that was labeled encode. Subse-quently, the battery was extended to healthy children withmeasures appropriate to the younger age-group. Onceagain, four factors were identified, each similar to the ele-ments of attention identified in the adult studies.
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 245

246 PART TWO | The Functioning Brain
The four elements of attention, and their hypothesizedsupportive neural substrates, are presented in Table 9.3.In brief, the four elements are described as follows:
1. Focus-execute attention involves selective attentionand rapid perceptual-motor output.
2. Shifting attention describes the ability to move orchange attentional focus in a flexible and adaptivemanner.
3. Sustained attention pertains to the attention func-tion of vigilance.
4. Encode attention specifies the capacity to brieflymaintain information in memory (that is, “on line”)while performing other related computations oractions.
Recently, a fifth component of attention, stable, wasidentified, and represents the consistency of attentionaleffort. The five elements of attention are believed to besupported by relatively distinct neuroanatomic regions(see Table 9.3) that interconnect to form an attention sys-tem. The distribution of the attention system throughoutthe brain is widespread. Accordingly, the attention systemis quite vulnerable to disruption when brain injury is sus-tained; yet, it is also resilient. A specific attention func-tion may be compromised by injury, but undamagedneural regions can provide some degree of compensation.
Mirsky’s model has enhanced our understanding of thepotential difference in attentional regulation of variousclinical groups. Chapter 11 discusses the application ofMirsky’s model to the investigation of the attentional pro-cessing of children with attention-deficit/hyperactivitydisorder (ADHD).
The attention systems and structures presented hereare skewed toward visual attentional processing becausethis is the best understood and most widely studied sensoryprocessing system in relation to attention. Interestingly,studies of auditory spatial attention, similar to visuospa-tial attention, have been found to recruit the parietal cor-tex (Kim et al., 1999). There is agreement that, at a corti-cal level, the right hemisphere, particularly the parietaland frontal regions, plays a central role in attentional con-trol. Subcortically, the anterior cingulate, thalamus, colli-culi, and basal ganglia contribute to attentional function-ing. These cortical and subcortical regions do not operateindependently, but rather perform their functions via in-terconnecting neural systems.
Executive Functioning
Compared with all other areas of the cortex, the pre-frontal lobes are unique in organization and function. Formore than a century, controversy, confusion, and specula-tion have existed over the function(s) of the frontal lobes.Speculation has included conceptualizations of the frontallobes as structures that are “silent” (having limited func-tion), support a singular or global function (for example,abstract thinking), or underpin different classes of behav-iors (for example, impulse control, judgment, creativity,emotional regulation, and moral judgment). The functionsof the temporal, parietal, and occipital lobes follow straight-forward principles of organization built around sensory sys-tem processing. In contrast, frontal lobe pathology does not
Subject Group Factor 1: Focus-Execute Factor 2: Shift Factor 3/5: Sustain/Stable Factor 4: Encode
Adult WAIS-R Digit Symbol, WCST CPT WAIS-R Digit SpanStroop test, Letter and ArithmeticCancellation, and TMT-A and -B
Child WISC-R Coding and WCST CPT WISC-R Digit Span Digit Cancellation and Arithmetic
Supporting substrata Focus: Inferior parietal and Prefrontal cortex Rostral midbrain structures Hippocampus andsuperior temporal cortexes and brainstem amygdalaExecute: Inferior parietal and corpus striatum
Note: WAIS-R � Wechsler Adult Intelligence Scale-Revised (Wechsler, 1981); Stroop Test (Stroop, 1935); Letter Cancellation � Letter Cancellation Test (Talland, 1965); TMT-A and -B �Trail Making Test Parts A and B (Reitan & Davison, 1974); WCST � Wisconsin Card Sorting Test (Grant & Berg, 1948); CPT � Continuous Performance Test (Rosvold, Mirsky, Sarason,Bransome, & Beck, 1956); WISC-R � Wechsler Intelligence Scale for Children-Revised (Wechsler, 1974); Digit Cancellation (Mirsky, 1995).
Source: Adapted from Mirsky (1995, 1996).
Table 9.3 Mirsky’s Elements of Attention

CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 247
result in primary disorders of sensation or perception, motordisability, memory, or language. Rather, the frontal lobes,by virtue of their interconnections with almost all otherbrain regions—including the brainstem; occipital, temporaland parietal lobes; limbic regions; and subcortical areas—serve to guide, direct, integrate, and monitor goal-directedbehavior (Anderson, 2002; Anderson, Levin, & Jacobs,2002). If the brain is a symphony, the frontal lobes act asthe conductor—guiding, coordinating, and directing theseparate sections of the orchestra to produce a harmoniousand integrated musical performance.
The terms frontal lobe functioning and executive func-tioning are often used interchangeably. Although the termsoverlap, the former suggests that presented behaviors aredirectly linked to the frontal lobes, whereas the latter con-notes a class of behavioral manifestations that may be di-rectly or indirectly related to frontal lobe functioning. Be-cause of the significant afferent and efferent connectivityof the frontal lobes with other brain regions, disruption toany one these connecting systems can produce pathologicbehaviors similar to those caused by direct frontal damage.For example, lesions to the caudate nucleus of the basalganglia can result in pathologic behaviors similar to thoseseen with dorsolateral prefrontal damage. Although theterm executive functioning does not denote a specificanatomic basis for behavior, it does implicate the frontalcortex and its interconnective neural circuitry. Both termsconverge in the conceptualization of cortical functions thatrelate to the directing, controlling, and managing of be-havior, that is, higher order supervisory brain computa-tions. Functions attributed to the executive system includeplanning, flexible problem solving, working memory, at-tentional allocation, inhibition, and at the highest levels,the self-monitoring and self-assessment of behavior.Clearly, executive functioning refers to sets of higher orderbehavior, rather than a single type of behavior. Likewise,executive functioning is not limited to cognitive processes,but is intimately involved in emotional and social behav-ioral regulation. In fact, lesions of the prefrontal regions,and associated subcortical regions linked to emotional andsocial functioning, can produce some of the most devastat-ing impairments. Executive functioning impairments be-come more evident in the most complex aspects of humanconscious activity, or those activities of higher problemsolving, reasoning, abstraction, critical self-awareness, andsocial interaction that make us human.
D E V E L O P M E N T O F E X E C U T I V E F U N C T I O N S
The maturation of executive functions is crucial to psy-chological adaptation and adjustment across the life span
(Eslinger, Biddle, & Grattan, 1997). Initially, our under-standing of the development of executive functions laggedbehind that of the maturation of other cortically sup-ported functions such as intelligence. As discussed earlier,the lag was partially related to the belief in neuropsychol-ogy that prefrontal functions did not begin to emergeuntil late childhood or early adolescence. Although thisbelief delayed the initiation of active study and researchof childhood executive functions, significant progress hasbeen evident since the early 1980s. Accordingly, we pre-view here some of the advances in our understanding ofthe development of executive functions.
Empirical studies (Levin et al., 1991; Welsh, Pennington,& Groisser, 1991) suggest that basic executive functionsdevelop early in life and follow a protracted, multisteptrajectory to maturity in adulthood. The early appearanceof rudimentary executive functions and the later develop-ment of more complex functions, such as abstract reason-ing and judgment, parallel the lengthy development ofthe prefrontal cortex. Interestingly, the emergence of rudi-mentary executive functions correlates with the periods ofmaximum synaptic density of the frontal lobes. However,more complex functions continue to evolve long aftermaximum synaptic density is reached, and reflect a host of other developmental advances such as synapticpruning and sculpting, axonal myelination, and neuro-chemical and neurophysiologic changes.
Important advances in understanding the developmentof executive functions are due to the remarkable investi-gations of Goldman-Rakic (1987a,b), Diamond (1991),and others. Goldman-Rakic has studied the relation ofprefrontal development to the emergence of the cognitiveoperation of object permanence, that is, the capacity tostore in memory a representation of an object that is re-moved from view for the purpose of guiding future be-havior. Using a delayed response task (see Figure 9.9), theexperimenter required rhesus monkeys to maintain inmemory the spatial location or features of an object overdelays ranging from 0 to 10 seconds. By the age of 2 to4 months, the rhesus monkeys could perform the memorytasks at delay intervals of 2 to 5 seconds. During this 2- to4-month period, researchers observed maximum synapticdensity in the prefrontal lobes of the rhesus monkeys. Thecorresponding period of synaptic density in the human in-fant occurs between 8 and 24 months (Huttenlocher, 1990).The latter time interval also correlates with the infant’s abil-ity to perform a delayed response task (Neuropsychologyin Action 9.2), suggesting that the executive function ofworking memory has emerged.
Diamond (1991) conducted a series of infant studiesthat have helped clarify the development of executive
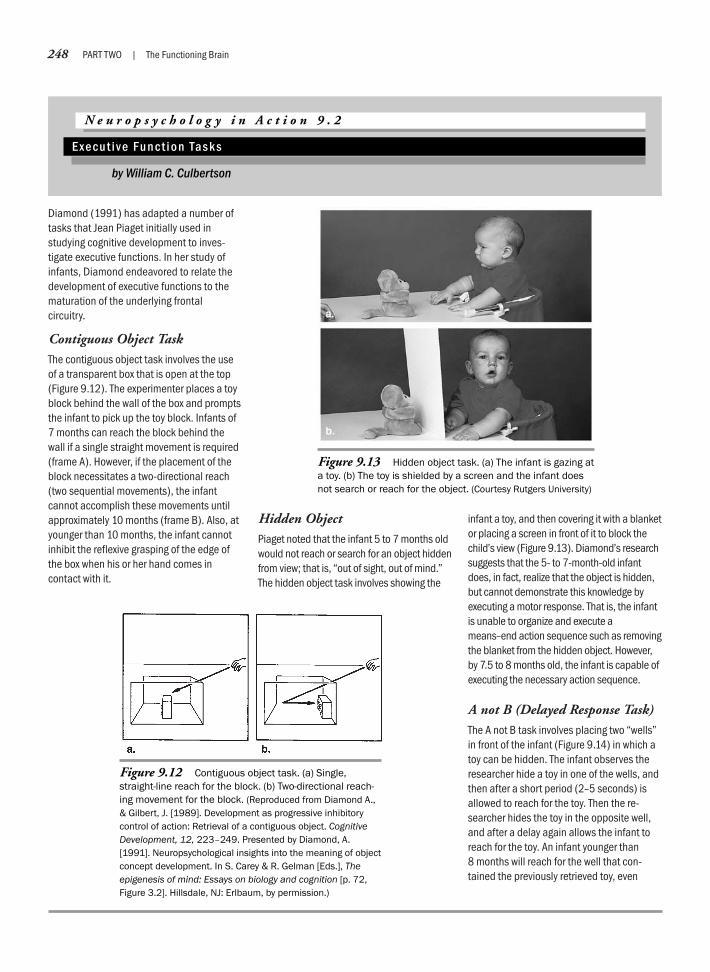
248 PART TWO | The Functioning Brain
Diamond (1991) has adapted a number oftasks that Jean Piaget initially used instudying cognitive development to inves-tigate executive functions. In her study ofinfants, Diamond endeavored to relate thedevelopment of executive functions to thematuration of the underlying frontal circuitry.
Contiguous Object TaskThe contiguous object task involves the useof a transparent box that is open at the top(Figure 9.12). The experimenter places a toyblock behind the wall of the box and promptsthe infant to pick up the toy block. Infants of7 months can reach the block behind thewall if a single straight movement is required(frame A). However, if the placement of theblock necessitates a two-directional reach(two sequential movements), the infantcannot accomplish these movements untilapproximately 10 months (frame B). Also, atyounger than 10 months, the infant cannotinhibit the reflexive grasping of the edge ofthe box when his or her hand comes incontact with it.
Hidden ObjectPiaget noted that the infant 5 to 7 months oldwould not reach or search for an object hiddenfrom view; that is, “out of sight, out of mind.”The hidden object task involves showing the
infant a toy, and then covering it with a blanketor placing a screen in front of it to block thechild’s view (Figure 9.13). Diamond’s researchsuggests that the 5- to 7-month-old infantdoes, in fact, realize that the object is hidden,but cannot demonstrate this knowledge byexecuting a motor response. That is, the infantis unable to organize and execute ameans–end action sequence such as removingthe blanket from the hidden object. However,by 7.5 to 8 months old, the infant is capable ofexecuting the necessary action sequence.
A not B (Delayed Response Task)The A not B task involves placing two “wells”in front of the infant (Figure 9.14) in which atoy can be hidden. The infant observes theresearcher hide a toy in one of the wells, andthen after a short period (2–5 seconds) isallowed to reach for the toy. Then the re-searcher hides the toy in the opposite well,and after a delay again allows the infant toreach for the toy. An infant younger than 8 months will reach for the well that con-tained the previously retrieved toy, even
N e u r o p s y c h o l o g y i n A c t i o n 9 . 2
E xe c u t i v e Fu n c t i o n Ta s k s
by William C. Culbertson
Figure 9.12 Contiguous object task. (a) Single,straight-line reach for the block. (b) Two-directional reach-ing movement for the block. (Reproduced from Diamond A.,& Gilbert, J. [1989]. Development as progressive inhibitorycontrol of action: Retrieval of a contiguous object. CognitiveDevelopment, 12, 223–249. Presented by Diamond, A.[1991]. Neuropsychological insights into the meaning of objectconcept development. In S. Carey & R. Gelman [Eds.], Theepigenesis of mind: Essays on biology and cognition [p. 72,Figure 3.2]. Hillsdale, NJ: Erlbaum, by permission.)
Figure 9.13 Hidden object task. (a) The infant is gazing ata toy. (b) The toy is shielded by a screen and the infant doesnot search or reach for the object. (Courtesy Rutgers University)

CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 249
though he or she has seen the researcherplace the toy in the opposite well.
In Figure 9.14, the infant has alreadysuccessfully retrieved the toy from the well tothe viewer’s right. The researcher then placedthe toy in the opposite well. In the first twoframes (top left and right), the infant is look-
ing at the well containing the toy. However,when allowed to reach for the toy, the infantuncovers the well that contained the toy onthe previous trial (bottom left and right).Success on this task requires the emergenceof working memory capability and the abilityto inhibit a previously reinforced response.
Detour Reaching TaskIn the detour reaching task, the experimenterrequires the infant to detour around a barrierto reach and retrieve an object. The taskinvolves a small transparent box that theexperimenter places in front of the infant withone of its sides open (Figure 9.15). If they cansee the toy through an open side, infants 6.5to 7 months of age will reach in to retrieve atoy. However, if the experimenter places thetoy directly in the child’s view, but behind aclosed side, the infant repeatedly and unsuc-cessfully tries to reach through the closedside. The infant is unable to inhibit reachingstraight for the toy. Also, the infant is unableto raise the box with one hand and reach atthe same time with the other hand. In Figure9.15, the child has lifted the box and isestablishing a direct line of sight to the toy. Asone hand moves down to reach into the box(second frame), the other hand holding thebox also moves down. At this point (thirdframe), the toy is in the child’s direct line ofsight through the top of the box. The childwithdraws her hand from the opening andtries, unsuccessfully, to reach for the toythrough the closed top of the box. Between 8and 12 months, the child develops the abilityto look through one side of the box whilereaching through another side. Similarly, thechild can raise the box with one hand, andsimultaneously reaching in with the other.
Figure 9.14 A not B task. (top) The infant is gazing at thetoy in the well. In the following frames, the infant continues togaze at the well holding the toy, yet lifts the cover from thewell that contained the toy on the previous trial. (Reproducedfrom Diamond, A. [1991]. Neuropsychological insights into themeaning of object concept development. In S. Carey & R. Gelman[Eds.], The epigenesis of mind: Essays on biology and cognition[p. 86, Figure 3.4]. Mahwah, NJ: Lawrence Erlbaum Associates, bypermission.)
Figure 9.15 Detour reaching task. (a) The child has lifted the box and is looking in at atoy. (b) As the child begins to reach for the toy, the box lowers. The toy is now in the child’sline of sight through the top of the box. (c) The child removes the hand from the box andtries to reach for the toy through the top of the box. (Society for Research in Child DevelopmentAbstracts, 3, 78, as presented in Diamond, A. [1991]. Neuropsychological insights into the mean-ing of object concept development. In S. Carey & R. Gelman [Eds.], The epigenesis of mind:Essays on biology and cognition [p. 90, Figure 3.5]. Mahwah, NJ: Lawrence Erlbaum Associates,by permission.)
a. b. c.
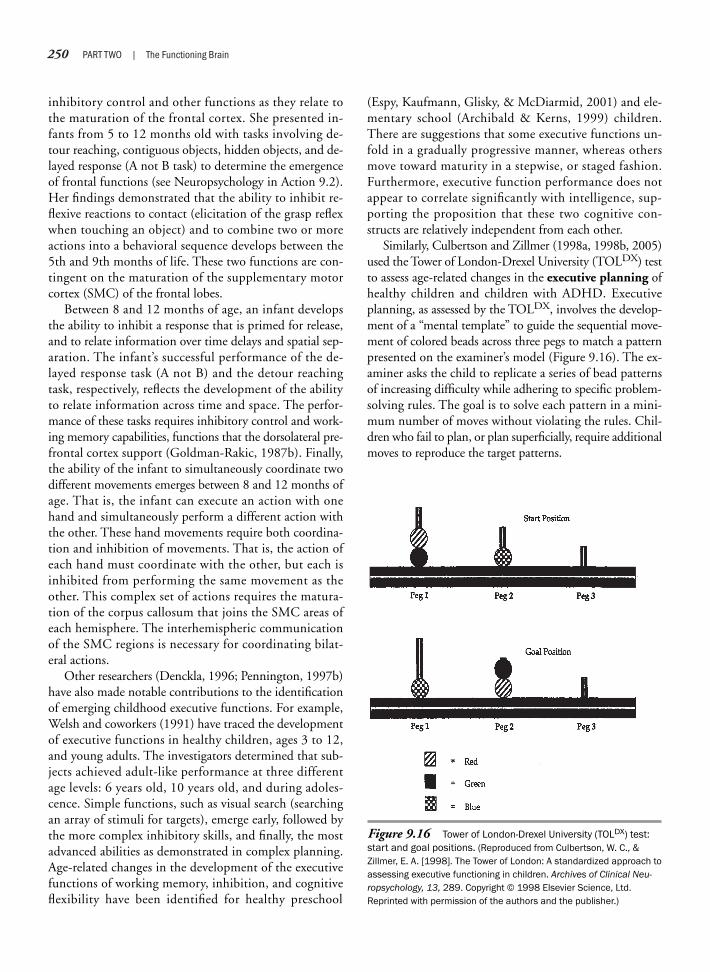
250 PART TWO | The Functioning Brain
Figure 9.16 Tower of London-Drexel University (TOLDX) test:start and goal positions. (Reproduced from Culbertson, W. C., &Zillmer, E. A. [1998]. The Tower of London: A standardized approach toassessing executive functioning in children. Archives of Clinical Neu-ropsychology, 13, 289. Copyright © 1998 Elsevier Science, Ltd.Reprinted with permission of the authors and the publisher.)
inhibitory control and other functions as they relate tothe maturation of the frontal cortex. She presented in-fants from 5 to 12 months old with tasks involving de-tour reaching, contiguous objects, hidden objects, and de-layed response (A not B task) to determine the emergenceof frontal functions (see Neuropsychology in Action 9.2).Her findings demonstrated that the ability to inhibit re-flexive reactions to contact (elicitation of the grasp reflexwhen touching an object) and to combine two or moreactions into a behavioral sequence develops between the5th and 9th months of life. These two functions are con-tingent on the maturation of the supplementary motorcortex (SMC) of the frontal lobes.
Between 8 and 12 months of age, an infant developsthe ability to inhibit a response that is primed for release,and to relate information over time delays and spatial sep-aration. The infant’s successful performance of the de-layed response task (A not B) and the detour reachingtask, respectively, reflects the development of the abilityto relate information across time and space. The perfor-mance of these tasks requires inhibitory control and work-ing memory capabilities, functions that the dorsolateral pre-frontal cortex support (Goldman-Rakic, 1987b). Finally,the ability of the infant to simultaneously coordinate twodifferent movements emerges between 8 and 12 months ofage. That is, the infant can execute an action with onehand and simultaneously perform a different action withthe other. These hand movements require both coordina-tion and inhibition of movements. That is, the action ofeach hand must coordinate with the other, but each isinhibited from performing the same movement as theother. This complex set of actions requires the matura-tion of the corpus callosum that joins the SMC areas ofeach hemisphere. The interhemispheric communicationof the SMC regions is necessary for coordinating bilat-eral actions.
Other researchers (Denckla, 1996; Pennington, 1997b)have also made notable contributions to the identificationof emerging childhood executive functions. For example,Welsh and coworkers (1991) have traced the developmentof executive functions in healthy children, ages 3 to 12,and young adults. The investigators determined that sub-jects achieved adult-like performance at three differentage levels: 6 years old, 10 years old, and during adoles-cence. Simple functions, such as visual search (searchingan array of stimuli for targets), emerge early, followed bythe more complex inhibitory skills, and finally, the mostadvanced abilities as demonstrated in complex planning.Age-related changes in the development of the executivefunctions of working memory, inhibition, and cognitiveflexibility have been identified for healthy preschool
(Espy, Kaufmann, Glisky, & McDiarmid, 2001) and ele-mentary school (Archibald & Kerns, 1999) children.There are suggestions that some executive functions un-fold in a gradually progressive manner, whereas othersmove toward maturity in a stepwise, or staged fashion.Furthermore, executive function performance does notappear to correlate significantly with intelligence, sup-porting the proposition that these two cognitive con-structs are relatively independent from each other.
Similarly, Culbertson and Zillmer (1998a, 1998b, 2005)used the Tower of London-Drexel University (TOLDX) testto assess age-related changes in the executive planning ofhealthy children and children with ADHD. Executiveplanning, as assessed by the TOLDX, involves the develop-ment of a “mental template” to guide the sequential move-ment of colored beads across three pegs to match a patternpresented on the examiner’s model (Figure 9.16). The ex-aminer asks the child to replicate a series of bead patternsof increasing difficulty while adhering to specific problem-solving rules. The goal is to solve each pattern in a mini-mum number of moves without violating the rules. Chil-dren who fail to plan, or plan superficially, require additionalmoves to reproduce the target patterns.
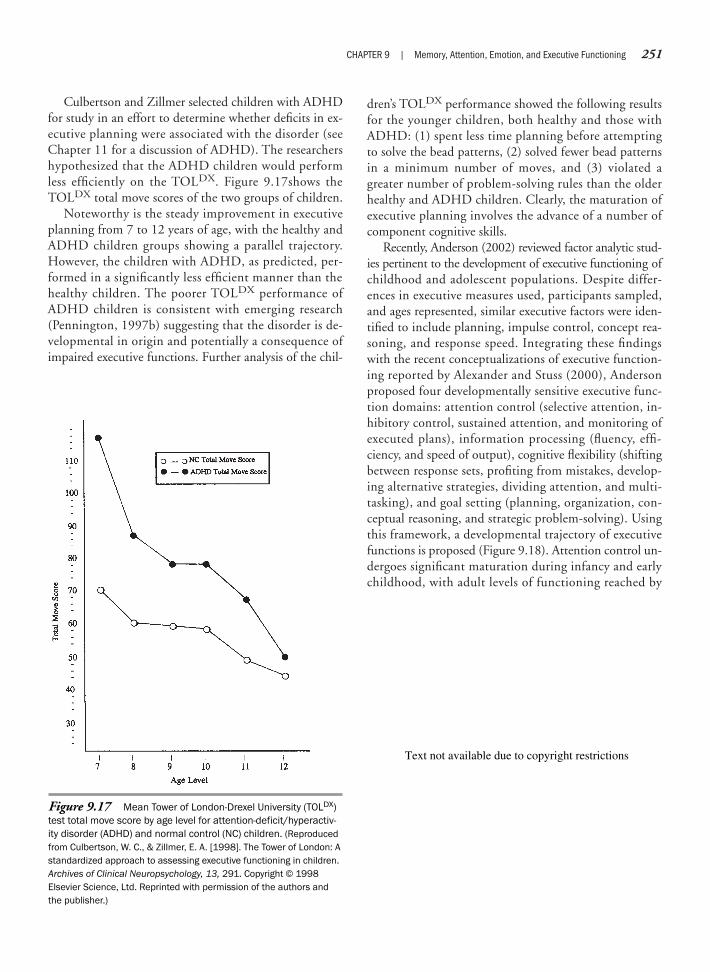
Culbertson and Zillmer selected children with ADHDfor study in an effort to determine whether deficits in ex-ecutive planning were associated with the disorder (seeChapter 11 for a discussion of ADHD). The researchershypothesized that the ADHD children would performless efficiently on the TOLDX. Figure 9.17shows theTOLDX total move scores of the two groups of children.
Noteworthy is the steady improvement in executiveplanning from 7 to 12 years of age, with the healthy andADHD children groups showing a parallel trajectory.However, the children with ADHD, as predicted, per-formed in a significantly less efficient manner than thehealthy children. The poorer TOLDX performance ofADHD children is consistent with emerging research(Pennington, 1997b) suggesting that the disorder is de-velopmental in origin and potentially a consequence ofimpaired executive functions. Further analysis of the chil-
dren’s TOLDX performance showed the following resultsfor the younger children, both healthy and those withADHD: (1) spent less time planning before attemptingto solve the bead patterns, (2) solved fewer bead patternsin a minimum number of moves, and (3) violated agreater number of problem-solving rules than the olderhealthy and ADHD children. Clearly, the maturation ofexecutive planning involves the advance of a number ofcomponent cognitive skills.
Recently, Anderson (2002) reviewed factor analytic stud-ies pertinent to the development of executive functioning ofchildhood and adolescent populations. Despite differ-ences in executive measures used, participants sampled,and ages represented, similar executive factors were iden-tified to include planning, impulse control, concept rea-soning, and response speed. Integrating these findingswith the recent conceptualizations of executive function-ing reported by Alexander and Stuss (2000), Andersonproposed four developmentally sensitive executive func-tion domains: attention control (selective attention, in-hibitory control, sustained attention, and monitoring ofexecuted plans), information processing (fluency, effi-ciency, and speed of output), cognitive flexibility (shiftingbetween response sets, profiting from mistakes, develop-ing alternative strategies, dividing attention, and multi-tasking), and goal setting (planning, organization, con-ceptual reasoning, and strategic problem-solving). Usingthis framework, a developmental trajectory of executivefunctions is proposed (Figure 9.18). Attention control un-dergoes significant maturation during infancy and earlychildhood, with adult levels of functioning reached by
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 251
Figure 9.17 Mean Tower of London-Drexel University (TOLDX)test total move score by age level for attention-deficit/hyperactiv-ity disorder (ADHD) and normal control (NC) children. (Reproducedfrom Culbertson, W. C., & Zillmer, E. A. [1998]. The Tower of London: Astandardized approach to assessing executive functioning in children.Archives of Clinical Neuropsychology, 13, 291. Copyright © 1998Elsevier Science, Ltd. Reprinted with permission of the authors andthe publisher.)
Text not available due to copyright restrictions

252 PART TWO | The Functioning Brain
middle childhood. Despite somewhat different trajecto-ries, information processing, cognitive flexibility, andgoal-setting functions achieve maturation by the end ofmiddle childhood. However, developmental refinementcontinues into mid-adolescence and early adulthood.
A more recent meta-analysis of relevant studies of ex-ecutive/frontal development (Romine & Reynolds, 2005)reported that abilities such as planning, verbal fluency,and inhibition of perseveration demonstrated pronouncedincreases between 5 and 8 years of age. Developmentalincreases were evident across all executive functions be-tween 8 and 11 years of age. Small incremental changeswere noted between 11 and 14 years of age for the inhibi-tion of perseveration and set maintenance. Planning andverbal fluency functions continue to develop throughoutadolescence and into early adulthood. The two reviewedmeta-analyses indicate that executive functions reach ma-turity at different points during development. It should beremembered that the development of executive functionsis, in part, contingent on the maturation of other brainregions and neural systems that support attention, lan-guage, emotions, and memory.
Research has also focused on the relation between thedevelopment of emotional regulation and maturation ofthe frontal region. Bell and Fox (1994) have found thatchanges in EEG activation associated with emotional ex-pression appear early in infant development. When astranger approached, 10-month-old infants exhibitedright frontal EEG activation, but the opposite pattern wasevident when the mother approached—that is, greater leftfrontal activation. Similarly, infants who appeared sad ordistressed, as assessed by facial expressions, showed greaterright frontal activation, whereas those expressing joydemonstrated greater left frontal activation. Of impor-tance was the finding that comparable frontal EEG acti-vation patterns continue to be evident in childhood andadulthood (Davidson, 1994).
Case studies of children who sustained damage to thefrontal cortex provide further insight into frontal lobe de-velopment and the regulation of emotional, moral, andsocial behavior. In a review of cases with varying ages oflesion onset (ranging from prenatal to age 16), Eslingerand colleagues (1997, 2004) found that the childrendemonstrated impairments in emotional regulation andinterpersonal relations, regardless of the age at which thedamage occurred. Both immediate and delayed deficitswere observed, suggesting that the development of socioe-motional regulatory control was ongoing. The progressiveemergence of delayed deficits indicated that the damagedfrontal system could not negotiate the increasing cogni-tive, social, and emotional demands of adolescence and
adulthood. For example, a boy who suffered damage tohis right frontal lobe at age 3 appeared to recover fully, al-though the mother did note alterations in his personalityafter the insult. During his early school years, he demon-strated problems in visuospatial performance, attentionalfocus, impulse control, and establishing friendships. Byadolescence, he exhibited limited facial expressions andmodulation of voice, interrupted the conversation of oth-ers, had not developed friendships or dated, and oftenfailed to understand the gist of intended communications.His social deficits reflected an inability to empathize orreciprocate emotionally with others, to understand socialcues and the pragmatics of language, and to accuratelyevaluate his own social strengths and weaknesses.
F R O N T A L - M E D I A T E D F U N C T I O N S A N D D Y S F U N C T I O N S
There is increasing evidence that the frontal lobes, inter-acting with cortical and subcortical circuitry, supportrelatively distinct but overlapping functions. Five pri-mary circuits have been identified—although evolvingresearch suggests that there may be at least two addi-tional circuits (Middleton & Strick, 2001). These cir-cuits project from different regions of the frontal lobesto designated regions of the basal ganglia and return viaspecific thalamic nuclei. The five neural circuits (Saint-Cyr, Bronstein, & Cummings, 2002) and their corticalorigination are skeletomotor (motor and premotor re-gions and parietal somatosensory cortex), oculomotor(frontal and supplementary eye fields), dorsolateral pre-frontal (dorsolateral prefrontal cortex), orbitofrontal(consists of two subcircuits that originate in the lateraland medial frontal cortex), and anterior cingulate (ante-rior cingulate cortex).
We focus on the three circuits that are often implicatedin neuropsychological and neuropsychiatric disorders.However, before we begin, several caveats are in order.The frontal lobes are, as previously discussed, richly inter-connected with other cortical and subcortical regions ofthe brain. Thus, the student should not consider the func-tions attributed to the frontal circuits to be solely local-ized or mediated by a specified region or circuit. The find-ing that damage to different regions of a circuit canproduce executive dysfunction comparable with that evi-dent when the frontal lobes are directly involved speaksto this caution. It is probably more accurate to describethe different frontal circuits as contributors, often major,to the mediation of certain types or forms of behavior. Sec-ond, a review of relevant studies shows that differentialprocessing biases for content (for example, verbal versus

nonverbal), modality, and types of mental operations areascribed to left versus right frontal architecture. However,there are notable exceptions to the putative specificity ofright versus left prefrontal systems. For example, verbalsemantic retrieval and episodic encoding activates the leftprefrontal region, whereas episodic retrieval instigatesright prefrontal computations (Cabeza & Nyberg, 2000).Moreover, it is not unusual to find bilateral activation ofthe frontal cortex for a given task, suggesting complemen-tary processing. Thus, care needs to be exercised when as-suming a one-to-one correspondence between task con-tent, input-output modality, or mental process recruitedand the implicated anterior laterality (left versus right).Third, despite significant research and study, we do notfully understand the functions of the frontal systems, nordo researchers and clinicians agree on the functions thatare associated with the different frontal circuits or regions.
D o r s o l a t e r a l C i r c u i t
The first circuit, dorsolateral prefrontal, is involved inhigher order cognitive operations. Often, this circuit is la-beled the “executive” circuit; however, with our realiza-tion that executive functioning is implicated in the medi-ation of emotional, motivational, and social behavior, weconsider the functions of each of the three circuits to beexecutive in nature. A sample of functions attributed tothe dorsolateral circuit includes working memory, cogni-tive flexibility, maintenance of behavioral sets, selectiveand sustained attention, generation of strategic and diver-gent responses, verbal and nonverbal fluency, planning andorganization, inhibitory control, abstract reasoning, mem-ory search and retrieval, temporal-spatial “tagging” (bind-ing time and spatial context to episodes), self-monitoring,insight, and judgment. Furthermore, the dorsolateralcircuit participates in emotional-motivational behavior,such that damage to the region may precipitate depres-sive symptoms, although these symptoms are more fre-quently associated with damage to the ventromedial pre-frontal region. The depressive symptoms associated withthe dorsolateral prefrontal cortex are characterized bydecreased initiative, apathy, indifference, psychomotor re-tardation, and social uneasiness (Anderson & Tranel,2002). This depressive presentation differs from clinicaldepression by the absence of vegetative functions, nega-tive cognition, and dysphoria. Some patients with dor-solateral damage demonstrate a decreased capacity toempathize with others, although this impairment ismore frequently associated with disruption of the or-bitofrontal circuit (Anderson & Tranel, 2002). The dor-solateral and orbital circuits may play complementaryroles in empathic processing, with the former mediating
the cognitive aspects of empathy, and the latter mediat-ing the emotional elements (Eslinger, 1998).
Luria (1990) gives an example of the cognitive diffi-culties of Patient U, who suffered from a progressivefrontal lobe tumor:
Patient U is presented the problem: One ABC book and one pencost 37 cents. One ABC book and two pens cost 49 cents. Howmuch do one ABC book and one pen cost separately?
The patient repeats the problem correctly but does notbegin to solve it.
(Dr. Luria): What should you do to solve the problem?(U): “37 and 49. . . . then it’s 86 all in all. . . .”(Dr. Luria): What did you add them for?(U): “To learn how much they paid all in all.”(Dr. Luria): What should you do next?(U): “Next. . . . I don’t know what next. . . . There is nothingelse. . . .”
In order to draw the patient’s attention to the final questionand help him distinguish the main solution elements, thestatement is presented in writing in the form of the followingequations:
One ABC book � one pen � 37 centsOne ABC book � two pens � 49 cents
(Dr. Luria): How much do one ABC book and one pen cost sepa-rately?
Patient U reads the equation, draws a line underneath andwrites down the result of simple summation:
“Two ABC books + three pens = 86 cents” saying, “I’velearned how many pens and ABC books, how much everythingcosts.”
It is evident that our attempt to show the difference betweenthe two equations and to prompt the proper logical sequenceended in failure. . . . [T]he investigator gives him the initialelement of the respective logical chain.
(Dr. Luria): First 37 cents were spent, then 49 cents. What is thedifference accounted for?(U): “It is accounted for by one pen! Then, 49 – 37 = 1 pen.”(Dr. Luria): What should you learn?(U): “How much do an ABC book and a pen cost separately.”(Dr. Luria): So?(U): So, a pen costs 12 cents. Now an ABC book. . . . 49 – 24 =25 cents. One ABC book costs 25 cents. (Luria, 1990, pp. 106–107)
In the above example, Patient U knows the arithmeticoperations necessary to solve problems but cannot discernthe important aspects of the problem without externalstructure. In fact, at first, he cannot initiate any response.His first, rather impulsive response is simply to sum thenumbers. He rigidly adheres to this strategy and is too cog-nitively inflexible to think of other possibilities. However,
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 253

254 PART TWO | The Functioning Brain
when he is guided, when the interviewer provides the im-portant aspects of the problem for him, he can arrive atthe correct answer. According to Stuss and Benson (1986),Patient U’s primary programs for math algorithms are in-tact, and they act in a fairly automatic or stereotyped man-ner. Unless organized by higher order executive functions,problem-solving behavior becomes chaotic—sometimesfailing to initiate, sometimes having no logical sequence,or sometimes perseverating on the first problem-solvingstrategy that comes to mind.
Joaquin Fuster (2002, 1997) has developed a theory ofprefrontal functioning that focuses significantly on therole of the dorsolateral cortex. He poses that the overar-ching function of the prefrontal architecture is the tem-poral organization of behavior, that is, the developmentand implementation of action sequences across time.Temporal organization of behavior extends to all volun-tary behavior including skeletal, ocular, speech, and inter-nal cognitive processes such as logical reasoning (Fuster,Van Hoesen, Morecraft, & Semendeferi, 2000). Four cog-nitive processes support the temporal organization of be-havior: attention, working memory, preparatory set, andmonitoring. These four cognitive processes are based onthe functional cooperation of the prefrontal cortex andthe subcortical and other cortical structures and circuits.
Attentional control relates to the cooperative activa-tion of the dorsolateral (selective, sustain, and orient-ing of attention), anterior cingulate (motivation anddrive aspects of attention), and orbital (inhibitorycontrol and filtering) cortices.
Working memory encompasses the processes dedi-cated to the maintenance and manipulation of infor-mation held in short-term storage to guide behavior.This function is supported by the dorsolateral pre-frontal areas. Working memory provides a retrospec-tive function in temporal organization. Its retrospec-tive function relates to the temporary retention ofmental representations of environmental (sensory)information pertinent to goal-directed behavior. Forexample, you need to hold “on line” the instructionsfor a test if you are to perform it correctly. The tem-poral organization of behavior requires both retrospec-tive memory and the preparation for action.
Preparatory motor set involves the preparation, tim-ing, and instigation of relevant goal-directed motorbehaviors. Once again, the dorsolateral cortex is impli-cated in the support of this function. Patients withfrontal lateral lesions often demonstrate deficits in plan-ning due to a failure to prepare for or to initiate a seriesof actions to achieve a goal. In essence, preparatory set
can be viewed as a failure in prospective memory, ormemory for future action.
Response monitoring determines whether currentgoal-directed behaviors should be maintained or mod-ified. This is important since sensory processing andmotor output operate across time, and environmentalchanges may occur that warrant alterations in goal-directed behaviors. Both the dorsolateral cortex andthe anterior cingulate are implicated in the support ofresponse monitoring.
These four functions support the diverse cognitive func-tions attributed to the dorsolateral prefrontal cortex. No-tably, Fuster recognizes that the dorsolateral cortex func-tions in concert with other cortical and subcorticalcircuitry in the support of behavior.
O r b i t o f r o n t a l ( L a t e r a l a n d M e d i a l ) C i r c u i t
The orbitofrontal circuit is involved in the mediation ofemotional and social responses. Initially, neuropsycholo-gists considered inhibitory processes as a primary func-tion of the orbitofrontal cortex. Converging research hasaltered this notion in that each region of the prefrontalcortex plays a role in behavioral inhibition (Roberts,Robbins, & Weiskrantz, 1998). However, the inhibitoryprocesses of the orbitofrontal circuit are relatively specificto the regulation of emotional and social behavior.
Impulsive, poorly modulated, and contextually inap-propriate behavior results when orbitofrontal inhibitoryfunctioning is impaired. For instance, one of our patients,a man in his 50s, provides a classic example of impulsivityafter a frontal lobe injury. Before his injury, T.J. was a suc-cessful businessman who traveled around the region mak-ing sales calls. One day, after the injury, he was to arriveat our office within a major medical center at 9 A.M. Hedrove around the parking garage trying to find a parkingspace. Unsuccessful in finding an empty spot, he becamefrustrated. Finally, he was stuck behind a car whose driverwas waiting for someone else to back out. Impulsively,T.J. rammed the car ahead of him. Relating this story, T.J.expressed dismay at himself for acting in a way he felt waswrong. Yet, he felt that at the moment, he just could nothelp himself.
Patients with orbitofrontal damage can show a rangeof negative or poorly modulated emotionality. Often, irri-table, angry, depressive, or manic-like emotions areprominent. Paradoxically, some patients exhibit a blunt-ing or dampening of affective responsivity and reducedinitiative. Accompanying characteristics of social disinhi-bition may include crude, coarse, and tactless behaviors.

There is often a disregard for rules of social decorum andrestraint; an excessive involvement in pleasure seeking; aminimal tolerance for frustration; a lack of sensitivity tofuture outcomes, both positive and negative (Bechara,Tranel, & Damasio, 2000); and a diminished or lost ca-pacity to empathize with others (Chow & Cummings,1999; Lichter & Cummings, 2001). Consequently, pa-tients with orbitofrontal damage are prone to make poor,and sometimes disastrous, life decisions (poorly conceivedbusiness ventures). Moreover, antisocial actions may re-sult and lead to criminal or legal difficulties (Zald & Kim,
2001). As in the tragic case of Phineas Gage (Neuropsy-chology in Action 9.3), family members and friends oftenreport that the “personality” of the patient, subsequent toorbitofrontal damage, has undergone significant change.
As you read the description of behaviors associatedwith orbital frontal damage, you might have noted thesimilarity between many of the behaviors associated withorbitofrontal damage and those exhibited by individualswith the diagnosis of “psychopath or sociopath” (cur-rently, the diagnoses of psychopath and sociopath havebeen replaced by the diagnosis of antisocial personality
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 255
In 1848, Phineas Gage was a 25-year-oldforeman employed by the Rutland andBurlington Railroad. On an autumn day inVermont, he and his crew were blastingthrough a rocky section when an accidentalexplosion sent a long metal bar, a tampingiron, shooting through his head. The pointedend of the rod entered under his left cheekand exited near the top middle of his skull,near the coronal and sagittal sutures. Therod was launched with such force that itlanded 30 meters away from him. Amazingly,although Gage was knocked flat, he was ableto get up and walk to the ox cart on which hesat while being driven into town. During theride he chatted and made an entry into hislogbook. Because he survived such a freak-ish accident, the case of Phineas Gage isarguably one of the most famous in the earlyhistory of neuropsychology.
Before the accident, Gage was seen aswell balanced emotionally and mentally,healthy and active. Immediately after theaccident, he fought postinjury infection torecover physically. He could walk and con-verse, recognized his friends and family, andappeared rational. To some he seemed fullyrecovered. But changes in his behavior soonemerged. His physicians noted, “Rememberspassing and past events correctly, as well asbefore the injury. Intellectual manifestationsfeeble, being exceedingly capricious andchildish, but with a will as indomitable as
ever; is particularly obstinate; will not yield torestraint when it conflicts with his desires”(Harlow, 1868, cited in Macmillan, 1996, p.246). As time went on, this behavior did notabate but endured. Six months later, hisphysician, John Martin Harlow, summarizedhis condition:
The equilibrium or balance, so to speak,between his intellectual faculties and hisanimal propensities, seems to have beendestroyed. He is fitful, irreverent, indulging attimes in the grossest profanity (which was notpreviously his custom), manifesting but littledeference for his fellows, impatient of restraintor advice when it conflicts with his desires, attimes pertinaciously obstinate, yet capriciousand vacillating, devising many plans of futureoperation, which are no sooner arranged thanthey are abandoned in turn for others appear-ing more feasible. A child in his intellectualcapacity and manifestations, he has theanimal passions of a strong man. Previous tohis injury, although untrained in the schools,he possessed a well-balanced mind, and waslooked upon by those who knew him as ashrewd, smart businessman, very energeticand persistent in executing all his plans ofoperation. In this regard his mind wasradically changed so decidedly that hisfriends and acquaintances said he was “nolonger Gage.” (Harlow, 1868, cited inMacmillan, 1996, p. 247)
Gage certainly suffered extensive damageto his left frontal lobe and probably alsosuffered damage to his right frontal lobe.Damasio and colleagues (Damasio,Grabowski, Frank, Galaburda, & Damasio,1994) have attempted to reconstruct thetrajectory and site of damage based onthree-dimensional computer modeling ofthe brain and skull. Their best estimate isthat the tamping rod impacted “the ante-rior half of the orbital frontal cortex . . . thepolar and anterior mesial frontal cortices . . .and the anterior-most sector of the anteriorcingulate gyrus” (p. 1104). Some righthemisphere damage was also implicated.It is interesting that Harlow implied Gagecould no longer “execute” his plans. Manybehaviors Gage exhibited are characteristicof people who have problems of executivefunctioning. Although his basic abilities toprocess information were intact, heshowed low frustration tolerance andimpulse control and a loss of ability tostructure and follow through on plans—somuch so, in fact, that he was seen as achanged person.
Source: The historical references for this case weresummarized from Macmillan, M. (1996). PhineasGage: A case for all reasons. In C. Code, C. Wallesch, Y. Joanette, & A. R. Lecours (Eds.),Classic cases in neuropsychology (pp. 243–262).Sussex, United Kingdom: Psychology Press, by permission.
N e u r o p s y c h o l o g y i n A c t i o n 9 . 3
T h e C a s e o f P h i n e a s G a g e
by Mary Spiers

256 PART TWO | The Functioning Brain
disorder (Diagnostic and Statistical Manual of MentalDisorders, Fourth Edition [DSM IV], 1994). In fact, thesimilarity between the two conditions prompted the la-beling of the orbitofrontal behavioral syndrome as“pseudopsychopathic” or “acquired sociopathy”(Blumer & Benson, 1975; Damasio, Tranel, & Damasio,1990). Unlike the true psychopath or sociopath, the pa-tient with orbitofrontal damage experiences remorse forinappropriate actions (Knight & Stuss, 2002) and doesnot demonstrate the intentional viciousness or planningwith regard to committing antisocial acts (Zald & Kim,2001).
With large lesions, particularly bilateral to the or-bitofrontal region, stimulus-bound behaviors or environ-mental dependency syndrome may be evident. Stimulus-bound behaviors or environmental dependency syndromesubsume a group of actions (utilization behavior, imita-tion behavior, grasp reflex, and manual groping;Archibald, Mateer, & Kerns, 2001) that are emitted with-out voluntary intent as the result of the loss of frontallymediated inhibitory control. This loss of inhibitory con-trol enables external stimuli to directly trigger thoughtsand actions. For example, utilization behavior relates touse of a presented object without intent or regard for thecontext. Thus, if pajamas are presented to a patient withorbitofrontal damage, she or he may undress and slip intothe garment, although the act is not “willed” or appropri-ate to the setting (for example, disrobing in the presenceof others).
Several theoretical explanations have been posed to ac-count for the social deficits associated with orbitofrontaldamage. First, the orbitofrontal circuit is intimately in-volved in the support of the capacity to empathize withothers. The diminishment or loss of the capacity for em-pathy appears to preclude an emotional appreciation ofothers, an essential prerequisite of social sensitivity andreciprocal interactions. Second, Damasio and colleagues(Damasio, 1994, 1998; Bechara, Tranel, & Damasio,2000, 2002) hypothesize that the orbitofrontal cortex(ventromedial) participates in the attachment of auto-nomic “tags” to events that, in turn, bias response selec-tion. These autonomic tags are termed somatic markersand represent “gut” reactions that covertly or overtly influ-ence behavior. Specifically, somatic markers are visceral-autonomic signals as to the valence (desirability or unde-sirability) of choices or decisions learned through previousexperiences with similar or related events. They assist indecision making by rapidly tagging those options thathave been associated with positive outcomes, and theyeliminate those alternatives that are likely to be associatedwith negative outcomes. They are particularly influential
when a presenting issue is novel or when uncertainty ex-ists as to the immediate or long-term consequences ofavailable decision or judgment options. In real-life situa-tions, we frequently encounter decision-making demandsin which the presenting situation is unfamiliar and/or un-certainty exists regarding which responses will or will notbring about desired consequences. In such situations, werely on a conflation of past knowledge, cognitive abilities,and intuition (hunch, “a sense,” or “best guess”). The lat-ter reflects a conscious awareness of somatic biasing, al-though such effects need not be conscious. Support forthe somatic marker hypothesis is evident in studies(Bechara, Tranel, Damasio, & Damasio, 1996; Becharaet al., 2000) showing that patients with bilateral or-bitofrontal damage (ventromedial) do not generate anSCR (indexing autonomic activity) when viewing emo-tionally arousing stimuli (pictures). Similarly, these pa-tients are able to recall these emotionally arousing images,but do so without the concomitant autonomic response.The latter suggests a disruption of the coupling of mem-ory content and somatosensory states. These patients arenot emotionless and are capable of evoking simple so-matic states in response to emotional stimuli. However,their ability to generate and couple complex somatic statesto events necessary for the guidance and constraint of de-cision making and judgment is impaired.
Third, Rolls’s (1998, 2002) research with nonhumanprimates and humans suggests that the orbitofrontal cor-tex is specialized for rapidly altering behavior in responseto changing reinforcement contingencies (reward, nonre-ward, and punishment). The alteration of behavior in re-sponse to changing reinforcing consequences is notrestricted to motor actions, but also pertains to emotionaland social behavior. The orbitofrontal cortex is uniquelysuited for its involvement in emotional-social processingbecause of its significant anatomic connections (direct andindirect) with the primary and association sensory cor-tices and limbic regions. Thus, the orbitofrontal cortexplays a crucial role in rapidly learning, modifying, and re-learning behavioral responses to changing contextual sig-nals, particularly those of a social nature. Rolls (2002)views emotions as a form of response elicited by reinforc-ing contingencies. In social situations, reinforcing contin-gencies are continually being exchanged and updatedbased on the presentation of interpersonal stimuli and theassociation of these stimuli with reward and punishment.As a function of this exchange, preexisting responses are maintained, altered, or extinguished, and new re-sponses are learned. With orbitofrontal damage, thecapacity to rapidly alter and learn emotional and re-lated responses in the face of changing contingencies is

CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 257
impaired. Consequently, emotional and social behaviorslack contextual regulation as evidenced by in impulsive,rigid, or inappropriate responses.
Interestingly, individuals with orbitofrontal (ventro-medial) lesions can demonstrate a relatively unimpairedneuropsychological profile when administered traditionalmeasures of executive functioning, perception, intelli-gence, memory, and language. Paradoxically, their social,vocational, and economic lives are often in shambles. Thecase of EVR (Barrash, Tranel, & Anderson, 2000) por-trays the consequences of such damage.
At age 35, EVR underwent resection of a bilateral orbitofrontalmeningioma. To achieve complete removal, orbital and lowermesial frontal cortices were excised along with the tumor.Profound personality changes ensued. Although his marriagehad previously been stable, he divorced his wife of many yearsand quickly entered into a second, short-lived marriage.Whereas formerly he had had a keen business sense with con-siderable financial success, postsurgically he entered into a seriesof disastrous business ventures over a brief period of time. Hehad been a respected community leader, but since the tumorresection he has never been able to maintain employment andnow lives in a sheltered environment. Despite generally superiorintellect, memory, and social knowledge by formal neuropsy-chological assessment, in real life he manifests severe defects indecision making, ability to judge the character of others, and inhis abilities to plan activities on a daily basis and into thefuture. (p. 356)
The finding that traditional executive measures fail toidentify the deficits of patients such as EVR has promptedthe development of measures that are potentially moresensitive to dysfunctions associated with orbital damage.Illustrating this advancement is the “gambling task” thatBechara and colleagues (2002) developed. The measureprovides a facsimile of decision-making in real life withregard to the weighting of potential rewards and punish-ments and the uncertainty of outcomes. The gamblingtask consists of four decks of cards (A, B, C, and D). Thepatient can select from any deck, and with each selectionreceives a reward (accrual of money) or penalty (loss ofmoney). Two of the decks are “disadvantageous” becausethey provide large rewards, but periodically assign unpre-dictably large penalties. Continued selection from the dis-advantageous decks culminates in a net loss. The two ad-vantageous decks provide smaller rewards and penaltiesand, if repeatedly selected, result in a net gain. Healthysubjects, over time, show a response pattern beginningwith a random selection from the four decks to a prefer-ence for the two advantageous decks. In contrast, the pa-tients with ventromedial lesions did not develop this pref-erence pattern and, in fact, were more likely to choose the
high-risk decks. Moreover, the SCRs of the healthy andventromedial subjects were monitored during the perfor-mance of the gambling task. Initially, the healthy subjectsgenerated SCRs as they won or lost money. Subsequently,as they gained experience with the decks, they began togenerate SCRs before the selection of any of the cards.These SCRs were more pronounced before picking a cardfrom a disadvantageous relative to an advantageous deck.In contrast, the patients with ventromedial damage didnot generate SCRs before selecting cards and continuedto show a preference for the disadvantageous decks.These findings suggest that decision making is guided bysomatic signals that are generated in anticipation of fu-ture consequences. With damage, insensitivity to the fu-ture consequences of behavior often results (Wagar &Thagard, 2004).
A n t e r i o r C i n g u l a t e C i r c u i t
The anterior cingulate is a relatively large neural substratewith widely distributed interconnections to other corticaland subcortical regions, implicating its functional in-volvement in neural circuits that support behavior. Notsurprisingly, it is implicated in both cognitive and affec-tive/motivational processing (Devinsky, Morrell, & Vogt,1995). The anterior cingulated is believed to support anumber of overlapping functions, including responsemonitoring, error detection, conflict resolution (incom-patible competing responses), inhibition when prepotent(primed) responses are to be overcome, selective and di-vided attention, and motivation or drive behavior. De-bate continues over whether the major role of the anteriorcingulate relates to the monitoring or regulation of neuralprocessing. Neuroimaging and event-related potentialstudies (Barch, Braver, Sabb, & Noll, 2000; Van Veen &Carter, 2002) show involvement of the anterior cingulatewhen (1) competing responses vie for release; (2) an erroroccurs in performance; or (3) a presented task is difficult,novel, complex or ambiguous. Moreover, its activationoften precedes or co-occurs with the activation of otherneural substrates. This latter activation pattern suggeststhat the anterior cingulate may monitor and coordinatethe engagement or amplification of control by otherneural systems. The purpose of this engagement or ampli-fication of control is to ensure efficient or optimal goal-directed performance (MacDonald, Cohen, Stenger, &Carter, 2000; Miller & Cohen, 2001).
The proximity and interconnectivity of the anteriorcingulate and orbitofrontal regions suggests that they mayinteract in support of executive functioning. Ullspergerand von Cramon (2004) pose that both are implicated in

258 PART TWO | The Functioning Brain
monitoring and decision-making behavior. The two re-gions appear to play complementary roles, with the ros-tral anterior cingulate implicated in monitoring self-generated actions and in signaling the need to quicklyalter neural processes to ensure optimal goal-directedmotor performance, whereas the orbitofrontal cortexmonitors the outcome of goal-directed actions by externalconsequences. The external consequence of action is, inturn, used to guide future decision making. Thus, the an-terior cingulate appears to be involved in the monitoringand alteration of ongoing actions, and the orbitofrontalcortex monitors the external consequences of these ac-tions to guide future actions.
Although the role of the anterior cingulate in responseinhibition is often stressed, it appears also to play an im-portant part in the initiation of behavior. For example,when confronted with conflicting response options, theanterior cingulate participates in both the suppression ofinappropriate responses and the initiation of appropriateones (Cabeza & Nyberg, 2000). Its role in initiating be-havior is further indexed by its activation when an indi-vidual is confronted with tasks that require semantic gen-eration, episodic memory retrieval, and working memory.In addition, evidence exists that the anterior cingulatemay be selectively activated when an individual’s move-ments are “willed” (volitional), as contrasted with actionsthat are determined by external stimuli. The effects of bi-lateral anterior cingulate damage dramatically illustratethe role of the anterior cingulate in behavioral initiation.With bilateral anterior lesions, the patient may experi-ence “akinetic mutism” or “abulia.” Akinetic mutismrefers to a syndrome involving profound apathy, reducedor absent verbal or motor behavior, a sense of psychologi-cal “emptiness,” reduced response to novelty, and indif-ference to pain, hunger, or thirst. Abulia refers to a simi-lar, although less severe syndrome of apathy, indifference,and minimally spontaneous verbal and motor activity(Lichter & Cummings, 2001). Damage to the orbitalfrontal cortex has also been associated with akineticmutism; however, research (Bechara, Tranel, & Damasio,2002) suggests that the damage has to extend into regionsof the anterior cingulate and/or basal forebrain for thesyndrome to be evident. Duffy and Campbell (2001) de-scribe the following case of akinetic mutism:
One patient, after a gunshot wound to both frontal lobes, wasessentially inert when left alone. When questioned, he related anawareness of personality change. He denied boredom and de-scribed it as a “loss of motivation” in that he entertained numer-ous ideas for activities but felt no impetus to act on them. Hisfacial expression was one of casual indifference, and he wouldoften respond with simple gestures instead of speaking. (p. 118)
Clearly, this patient portrays the amotivational state thatcharacterizes akinetic mutism.
Relation of Memory, Attention,and Executive Function
Memory, attention, and executive function repre-sent relatively distinct processes, although in some cases,there is disagreement whether a particular attentional ormemory process is better classified as an executive func-tion (for example, working memory). Clearly, theseprocesses are inter-related, but specifying the exact natureof this inter-relation is hindered by our limited under-standing of these domains, divergent definitions and con-ceptualizations, and varied theoretical perspectives. Whenexperts from the fields of memory, attention, and execu-tive function were asked to specify the behaviors denotedby the term executive function, no less than 33 differentterms were generated with only 40% agreement for 6 ofthe terms (self-regulation, sequencing of behavior, flexi-bility, response inhibition, planning and organization;Eslinger, 1996). Nonetheless, there is some agreement thatexecutive functions represent overarching controlling,organizing, integrating, and supervising computations.Attention and memory processes are subject to varyingdegrees of executive orchestration depending on the na-ture and type of attention and memory processes in-volved. From a neuroanatomic perspective, memory, at-tention, and executive functions are served by relativelydistinct, yet interconnected and overlapping, neural sys-tems. Neuroimaging investigations demonstrate that dif-ferent neural systems support executive, attention, andmemory functions; yet, these neural systems coactivate inthe performance of many executive, attentional, andmemory tasks, indicating shared or distributed process-ing. Furthermore, the inter-relation of these functions isevident when one realizes that executive functions wouldbe of little value if memory systems did not operate toregister, store, and enable the retrieval of life experiencesand knowledge, and if attentional systems did not supportthe processing of relevant or critical environmental andbody events. Jointly, attention, memory and executivefunctions play a central role in thinking, reasoning, prob-lem solving, language, and emotional and social behavior.Finally, human experience involves the capacity to repre-sent and relate past, present, and future events. Attentionalsystems are necessary for the processing of relevant ongo-ing and novel events, memory systems for the symbolicmaintenance of these experiences over time, and executive

CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 259
functions for the generation, guidance, and evaluation ofbehavior necessary to attain future goals (Eslinger, 1996).
As you reviewed the effects of damage to the atten-tional, memory, and executive systems, you likely realizedthat there is typically either a direct or indirect disruptionof emotional functioning. A review of Phineas Gage’s case(see Neuropsychology in Action 9.3) clearly portrays theprofound disruption to emotional regulation, arousal, andstyle that damage to the brain can engender. It is emotionthat gives direction, drive, and value to our personal andsocial behavior. Emotions intimately affect that which we attend to, remember, and strive to achieve (goals). It isto this fundamental aspect of human behavior that wenow turn.
Neuropsychology of Emotional Processing
Brain processing of emotion is an area that neu-ropsychology has largely ignored until recently. This ne-glect is partly a holdover from philosophical traditions ofrational empiricism and from conceptualizations of thebody and brain as being machine-like. People saw emo-tions as peripheral to understanding cognition, as beingof a lower order of evolutionary development, perhapseven vestigial. In other words, humans had evolved to be-come rational, logical beings somehow above emotion.Moreover, it is difficult to study subjective feeling states.Such research is not straightforward, as is presenting a vi-sual or auditory stimulus and recording activation of cor-responding brain regions. Also, animal models can pro-vide only limited information, because they cannotverbalize their feelings, and researchers must rely onmotor behaviors to infer the expression of emotions asrage and fear. The emotional repertoire of humans is enor-mous, subtle, and much more complicated than a re-sponse to external threats to physical safety, such as em-bodied in the fight-or-flight response.
Today, science views emotions as necessary for higherevolutionary adaptation. In the television show Star Trek(and its spinoffs), the ultralogical characters Mr. Spock,Data, and Seven of Nine show that being human entailshaving “emotional equipment.” People who are out oftouch with emotions and who have autistic-like qualities—like Temple Grandin, who describes herself as an “anthro-pologist on Mars” in Oliver Sacks’ book of the same name (1995)—have expressed a sense of alienation fromother humans on these grounds. Humans live in a socialcontext where self-understanding and social skills are
some of the most crucial factors in determining success insociety. Witness the surging interest in “emotional intelli-gence,” which stresses the ability to understand mood andemotion in self and others, to understand self and one’sown character, and then to act effectively on that knowl-edge. Researchers suggest that emotional intelligence ac-counts for just as much or more variance in determiningsuccess in life as traditionally measured general cognitiveintelligence.
One of the more interesting questions related to un-derstanding emotions is to ask whether emotional pro-cessing is a type of cognitive processing that the cortexinitiates, or whether emotion emerges without consciousthinking, and only secondarily becomes labeled. This di-chotomy is a variation on an old debate emanating fromthe early twentieth century. The James–Lange theory ofemotion, promoted by American psychologist WilliamJames and Danish psychologist Carl Lange (Lange, 1922),postulates that people consciously experience emotion asa reaction to physical sensory experience. That is, we feelfear because our hearts are racing; we are sad because weare crying. Although others saw this as an overstatement,the James–Lange theory does insist that sensory and cog-nitive experiences were intimately entwined and insepa-rable from each other. In other words, if all the physicalsensations of fear disappeared, so would the cognitiveexperience of fear. The opposing theory of the time wasthe Cannon–Bard theory (Cannon, 1927). WalterCannon, and later Philip Bard, argued that the consciousemotional experience is separate from bodily sensation orexpression. Although today most scientists agree thatcognitive experience of emotion corresponds to sensoryexperience, much variation exists among types of emo-tion, emotional intensity, and individual variation.
Joseph LeDoux (1992, 1996) describes emotion as asubjective state of awareness and suggests that only be-cause people have a cortex can they label emotion andthink about it, rather than just react to it as other animalsmight. Someone walking along in a forest might be star-tled by something that looks like a snake. It is adaptive ifthe mind signals the body in an immediate response ofdanger. Some scientists suggest that certain emotional re-sponses, such as reactions to certain movements andnoise, may be genetically “hardwired” as a protectivemechanism. According to LeDoux (1996), after that ini-tial lower order automatic processing, the cortex receivesand further processes the information, perceiving the ob-ject as a snake or a stick, weighing options, and direct-ing the body to take further action. The competing viewargues that the person must first recognize something cog-nitively as a threat for the emotion to develop. LeDoux

260 PART TWO | The Functioning Brain
and others have amassed convincing research suggestingthat basic fear conditioning can occur without a cortex.Some animals with their cortex removed still show basicfear responses. In this scenario, thought does not neces-sarily precede emotion. However, in addition to subcorti-cally initiated emotion, is it also possible to initiate anemotional response just by thinking? Certainly the expe-rience of most people would confirm this. Consideringan upcoming speech, thinking about running into asnake, feeling socially embarrassed, or anticipating a joy-ful reunion can all produce emotional responses in thebody separate from immediate external threats or joys.This section examines both subcortical and cortical con-tributions to emotional behavior.
B R A I N O R G A N I Z A T I O N O F E M O T I O N
Emotions involve complex physiological, cognitive, andmotor (action) processes that are supported by multiplecortical-subcortical architectures and circuitries. Differentand overlapping interconnected regions are involved inprocessing varied emotions, a clear indication that there isnot a single “emotional system.” Yet, these subsystems arecollectively referred to as the “limbic system” of the brain.The Papez’s circuit (see Figure 9.5) was initially proposedas the supporting system of emotional processing. Subse-quently, MacLean (1949, 1952) extended the system toinclude the amygdala, orbital prefrontal cortex, and re-gions of the striatum. Advances in neuroscience do notfully support these earlier conceptualizations of the lim-bic system because we now realize that the hippocampusis more intimately involved in nonemotional memoryprocessing, whereas the amygdala and related structuresplay a greater role in emotional processing. The two re-gions work in a complementary manner depending onthe event being processed. For example, patients with dam-age to the amygdala without co-occurring hippocampaldamage do not demonstrate a learned fear response to a con-ditioned stimulus. However, the patients are able to recallthat the conditioned stimulus was associated with an un-conditioned stimulus during training. In contrast, patientswith the opposite lesion profile (damaged hippocampus �preserved amygdala) exhibit a fear response to the condi-tioned stimulus without memory of the conditioned andunconditioned pairing (Armony & LeDoux, 2000).Thus, one region appears to underpin the learning of thedeclarative content (context), whereas the other supportsthe emotional learning associated with the event.
Investigations of the effects of emotion on memory re-tention provide further evidence of the complementaryrelation of the hippocampus and amygdala. Studies
(Cahill & McGaugh, 1998; McGaugh, 2004) of animalsand humans show that the degree of activation of the amyg-dala during encoding of emotionally arousing material(positive or negative) correlates significantly with subse-quent recall of the material. That is, as amygdala/emotionalarousal increases, the retention of declarative informationimproves. It has been hypothesized that the amygdalaenhances the consolidating processes of the hippocam-pus, and thus strengthens the retention of the declarativelearning. However, there is a limit to this enhancing ef-fect. With excessive or chronic emotion, memory reten-tion can actually be impaired. High levels of adrenocorti-cal hormones released during stress may account for thisimpairing effect.
P r i m a r y E m o t i o n s
Primary emotions are automatic, preorganized, arise fromsensory experience, and are processed through the limbicsystem before or parallel to being recognized consciously.Emotions such as fear, disgust, surprise, anger, and joyappear to be universal, because people express and recog-nize them across all cultures of the world. Damasio (1994)suggests that these emotions are innate and primarily con-trolled by the amygdala and anterior cingulate of the lim-bic system. As we have discussed, sensory information firstfunnels through the thalamus, is relayed to the cortex, andthen travels to the subcortical limbic system. Because ofthis anatomy, the general consensus was that consciousperception of an emotion preceded emotional limbic re-sponse. But LeDoux, who has studied fear conditioning,has suggested that projections from the thalamus to theamygdala provide a “shortcut” allowing the amygdala toprocess information directly, bypassing the cortical loop.This allows for an immediate, automatic, preconscious,and unconscious emotional response.
Fear is a well-researched primary emotion. In the hopethat the knowledge of fearful emotions can aid in treat-ing secondary emotions, such as human anxiety andpost-traumatic stress disorders, Joseph LeDoux, who hasdone extensive work in the area of fear conditioning withanimals, has studied how primary fear interacts withmemory. The neuroanatomy of the primary conditioned-fear response centers on the amygdala. Fearful behaviorsare easily conditioned to a tone via shock, trauma, orloud noise. Researchers have long known that severingconnections between the subcortical areas of the brain andthe cortex does not eliminate the conditioned-fear re-sponse. Therefore, the learning and maintenance of fearconditioning must occur in the subcortical structures. Re-searchers then demonstrated that lesioning the amygdalain certain places did interfere with fear conditioning.
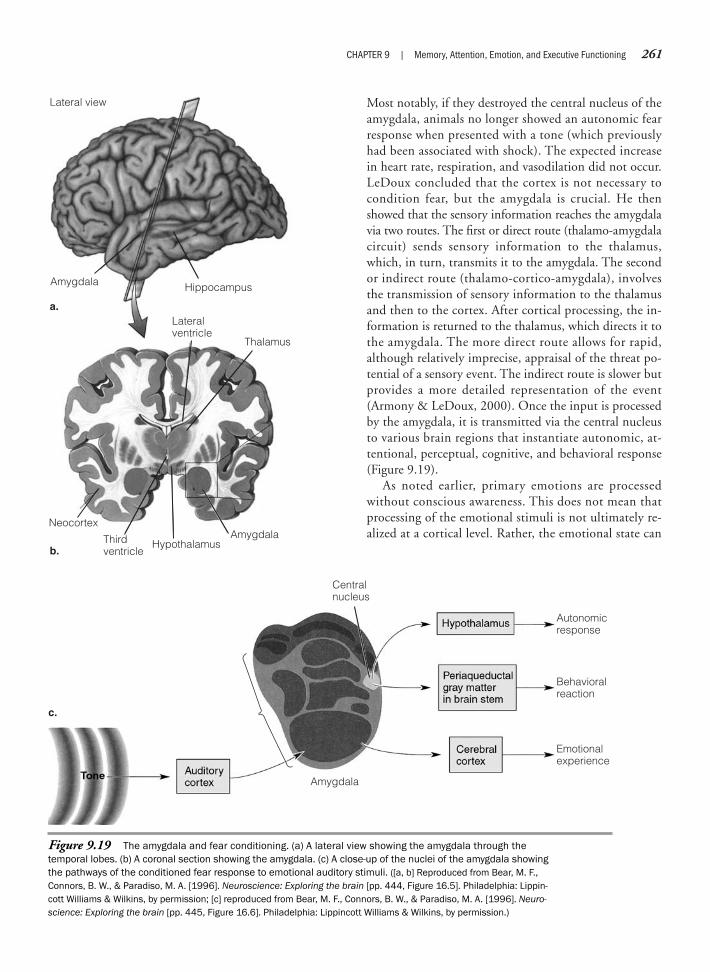
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 261
Most notably, if they destroyed the central nucleus of theamygdala, animals no longer showed an autonomic fearresponse when presented with a tone (which previouslyhad been associated with shock). The expected increasein heart rate, respiration, and vasodilation did not occur.LeDoux concluded that the cortex is not necessary tocondition fear, but the amygdala is crucial. He thenshowed that the sensory information reaches the amygdalavia two routes. The first or direct route (thalamo-amygdalacircuit) sends sensory information to the thalamus,which, in turn, transmits it to the amygdala. The secondor indirect route (thalamo-cortico-amygdala), involvesthe transmission of sensory information to the thalamusand then to the cortex. After cortical processing, the in-formation is returned to the thalamus, which directs it tothe amygdala. The more direct route allows for rapid,although relatively imprecise, appraisal of the threat po-tential of a sensory event. The indirect route is slower butprovides a more detailed representation of the event(Armony & LeDoux, 2000). Once the input is processedby the amygdala, it is transmitted via the central nucleusto various brain regions that instantiate autonomic, at-tentional, perceptual, cognitive, and behavioral response(Figure 9.19).
As noted earlier, primary emotions are processedwithout conscious awareness. This does not mean thatprocessing of the emotional stimuli is not ultimately re-alized at a cortical level. Rather, the emotional state can
Figure 9.19 The amygdala and fear conditioning. (a) A lateral view showing the amygdala through thetemporal lobes. (b) A coronal section showing the amygdala. (c) A close-up of the nuclei of the amygdala showingthe pathways of the conditioned fear response to emotional auditory stimuli. ([a, b] Reproduced from Bear, M. F.,Connors, B. W., & Paradiso, M. A. [1996]. Neuroscience: Exploring the brain [pp. 444, Figure 16.5]. Philadelphia: Lippin-cott Williams & Wilkins, by permission; [c] reproduced from Bear, M. F., Connors, B. W., & Paradiso, M. A. [1996]. Neuro-science: Exploring the brain [pp. 445, Figure 16.6]. Philadelphia: Lippincott Williams & Wilkins, by permission.)
Lateral view
Amygdala Hippocampus
a.
b.
Lateralventricle
HypothalamusAmygdalaThird
ventricle
Thalamus
Neocortex
Centralnucleus
Amygdala
Basolateralnuclei
c.
Emotionalexperience
Autonomicresponse
Behavioralreaction

262 PART TWO | The Functioning Brain
be triggered before there is conscious awareness. Supporthas been provided for the involvement of the amygdala inthe unconscious mediation of learned emotional re-sponses. For example, Morris, Ohman, & Dolan (1998)presented healthy participants with two angry faces, oneface (CS�) paired with a noxious stimuli (unconditionedstimulus, white-noise burst), and the other face (CS�)displayed without aversive stimulus pairing. After theconditioning training, the faces were presented to the par-ticipants either masked or unmasked. Masking enables astimulus to be processed, but without conscious aware-ness of the stimulus. The participants were instructed topress a button if they saw an angry face. None of the par-ticipants reported perceiving the masked faces, whereasall identified the unmasked faces. A measure of emotionalevocation (skin conductance) revealed that the CS� faceproduced a significantly greater emotional response thanthe CS� face for both the masked and unmasked condi-tions. Moreover, PET neuroimaging showed significantlygreater activation of the amygdala for the presentation ofthe CS� face relative to the CS� face, regardless ofwhether it was masked or unmasked. That is, fear learn-ing was evident with and without conscious awareness.Interestingly, the right amygdala showed greater activa-tion to the masked CS� face, while the activation of theleft amygdala was enhanced for the unmasked CS� face.This finding suggests greater involvement of right hemi-sphere regions in unconscious emotional facial process-ing, whereas left hemisphere regions appear preferentiallyinvolved in conscious or cortically mediated emotionalprocessing.
Damage to the amygdala can adversely impact on cor-tical processing of emotions. In essence, it leaves highercortical processing bereft of important input. Exemplify-ing this negative impact is a study (Adolphs, Tranel, &Damasio, 1998) of patients with complete bilateral amyg-dala damage. These patients were presented facial picturesand asked to rate the degree of positive/negative emotionsrepresented by each face and the degree of approachabil-ity and trustworthiness of the person represented by theface. When contrasted to patients without lesions of theamygdala, the patients with bilateral amygdala damagerated the faces as expressing more positive emotions andas more approachable and trustworthy. This positive biaswas particularly evident for faces considered to be mostnegative. The investigators pose that the positive bias re-lated to the role of the amygdala in processing threaten-ing and aversive stimuli. The loss of this input to corticalregions resulted in a shift to more positive ratings and in-creased approachability/trustworthy judgments by the bi-lateral amygdala group.
Fear learning is not limited to subcortical amygdalaaction (direct sensory conditioning). For example, onecan learn to fear a wild animal, such as a lion, without ex-periencing an attack by the animal. Support for involve-ment of the amygdala in fear learning without experienc-ing a noxious event is provided by Phelps and colleagues(2001), as well as other investigators. In Phelps’ study,participants were informed that the presentation of a spe-cific stimulus (blue square) would be associated with ashock, whereas a second stimulus (yellow square) wouldnot. Neither stimulus was ever paired with a shock. Yet,when the shock-specific stimulus was presented, there wassignificant activation of the amygdala, insular cortex, an-terior cingulate, premotor cortex, and striatum. A mea-sure of fear evocation (skin conductance) confirmed a fearresponse with the specified stimuli. The investigators posethat the insular cortex was central to the transfer of a cor-tical representation to the amygdala. Thus, fear learningwas produced by an imagined or anticipated cognitiverepresentation without actual contact with a negative sen-sory event. Clearly, fear learning can involve both subcor-tical and cortical processes.
S e c o n d a r y E m o t i o n s
Secondary emotions require higher cortical processing,and according to Damasio (1994), this processing is or-chestrated by the prefrontal cortical networks. There isalso a hemispheric asymmetry to higher emotional pro-cessing. People acquire secondary emotions throughlearning and experience. The perception of these states ishighly personal and individual. Social emotions such asembarrassment, pride, shame, and anxiety are highly de-pendent on learning and interact with one’s cognitiveperception of the social environment as it pertains tooneself. Secondary emotions do not necessarily imply aseparate “feeling” experience in the body. The feeling ofemotional experience remains linked through the limbicsystem. The difference is that secondary emotions aregenerated through higher cortical processes and arrive atthe limbic system over a different route from that takenby primary emotions generated through sensory experi-ence. Once in the limbic system, the brain processes theexperience of primary and secondary emotions in a simi-lar manner.
Secondary, or social, emotions mediated by the cere-bral hemispheres show lateralization of functioning. If aface is considered closely, you soon see that it is not sym-metric. In 1902, before the days of computer morphing,the German scientist Hallervorden (cited in Borod, Hay-wood, & Koff, 1997) cut pictures of faces in half at themidline. Taking the left half, he recreated the whole face

by using the original and its mirror image. He did thesame with the right half. Among other descriptors, he saw right-sided faces as more “lucid,” “sensible,” and “ac-tive,” and left-sided faces as more “perceptive” and “af-fective.” Because the right hemisphere controls the leftside of the lower face, and vice versa, lateralized facial dif-ferences in emotion basically reflect the activity of thecontralateral hemisphere. The general consensus acrosssubsequent studies confirms some of the early observa-tions in that the left side of the face (left hemiface) is more emotionally expressive than the right hemiface. Ingeneral, the right hemisphere seems to be dominant foremotional expression (for a review of the literature, seeBorod, Haywood, & Koff, 1997). The picture, however,is not completely cut and dry. Faces have an amazinglycomplex ability for emotional expression. The amount ofspace devoted to facial control on the motor homuncu-lus attests to this. Just in variations of smiles, there may be more than 18 different types. Psychologist Paul Ekman has described the cocktail party smile, the smile of relief, and the miserable smile, to name just a few. Some theorize that each hemisphere may be specificallyattuned to emotional type. Perhaps positive emotionsemanate from the left hemisphere and negative emotionsfrom the right (for review, see Borod, Haywood, & Koff,1997). The structure–function picture for emotion iscomplex, but many neuroanatomic theorists continue toassert that the right hemisphere plays the major integra-tive role in emotional processing. People with right hemi-sphere damage caused by stroke are usually less accurate atproducing emotions compared to those with left-sideddamage or healthy control individuals (Borod, 1993).
Observations of neurologically impaired patients haveprovided clues to an interesting issue in emotional pro-cessing, the anatomic differences between spontaneousand posed smiles. Posed facial expression appears largelycontrolled by contralateral cortical structures in the motorcortex. Spontaneous smiles and laughter, however, appearto be largely a function of subcortical limbic system struc-tures, including the cingulate gyrus, thalamus, and somestructures of the basal ganglia (such as the globus pal-lidus). Left hemisphere stroke patients, with damage tothe left motor cortex, have difficulty smiling for the cam-era because their facial muscles malfunction in responseto the brain command to produce a willful or social smile.The smile pulls to the left. A quite different pictureemerges if the person laughs spontaneously. The smile ap-pears natural. The limbic system and other subcorticalstructures, including the basal ganglia, control the spon-taneous smile (Figure 9.20). In any person, an observercan easily see a difference between these two types of
smiles. The true smile of enjoyment activates the orbicu-laris oculi muscles around the eyes; a fake smile does not.Another way of describing this is that smiling eyes showan activated limbic system. People with subcortical disor-ders, such as Parkinson’s disease, show the opposite prob-lem of stroke patients. Although they can show willfulemotion, much of their spontaneous emotion is damp-ened by a “masklike” face.
An area of research that has increased our understand-ing of cortical involvement in emotionality centers on theconsequences of frontal damage. As reviewed earlier, dam-age to the frontal cortical system can result in a wide rangeof emotional and behavioral dysfunctions. Some speci-ficity in the type of emotional dysregulation produced canbe traced to whether the dorsolateral, orbital, or medialfrontal region is preferentially damaged. In addition, cer-tain regions of frontal damage leave cognitive processesrelatively unimpaired, as verified by neuropsychologicalassessment, but result in significant social and emotionaldeficits. This pattern is often evident in patients who haveexperienced damage to the ventral and medial prefrontalcortices. Studies of the ventromedial cortex indicate thatthis region is implicated in emotional decision making(O’Doherty, Kringelbach, Rolls, Hornak, & Andrews,2001), recognition of emotions as represented in voice
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 263
Image not available due to copyright restrictions

264 PART TWO | The Functioning Brain
and facial expressions (Hornak, Rolls, & Wade, 1996), andprocessing of fear and anger (Blair, Morris, Frith, Perrett,& Dolan, 1999; Vuilleumier, Armony, Driver, & Dolan,2001). Anatomically, the ventromedial prefrontal cortexis interconnected with the hypothalamus, brainstem,amygdala, ventral striatum, and basal forebrain. These re-gions have been implicated in the mediation of attention,memory, and other cognitive functions in the processingof emotions.
Recently, an investigation (Kawasaki et al., 2005)sought to determine whether the ventromedial prefrontalcortex was involved in the processing of different cate-gories of emotions. Electrophysiologic monitoring viaimplanted electrodes allows for the assessment of neu-ronal responsiveness. However, because of ethical con-straints, this method is generally not condoned for usewith healthy individuals. Therefore, the investigatorsidentified patients with epilepsy who had electrodes im-planted in the ventromedial prefrontal cortex to monitortheir epilepsy. The epileptic foci of these patients did notinvolve the ventromedial prefrontal region. The patientswere presented emotional scenes of different emotionalvalence and arousal. Three categories of scenes (pleasant,aversive, and neutral) of high and low levels of emotionalarousal were used. More than 200 neurons in the left and
right ventromedial prefrontal regions were monitored.Results of the study showed that approximately 60 neu-rons in the left and right ventromedial prefrontal corticesparticipated in encoding the emotional significance ofthe visual scenes. These neurons were selective for pleas-ant and aversive scenes, with the largest number beingresponsive to the aversive scenes. The investigators hy-pothesize that the ventromedial prefrontal cortex, in co-ordination with other interconnected cortical-subcorticalregions, participates in associating visual stimuli withemotion and with the recognition (awareness) of thisemotion.
Emotional dysfunction often appears in conjunctionwith neurologic disorders, sometimes as normal reactionto loss of function, and sometimes as a direct result ofbrain dysfunction. For example, depression is a commonreaction to a life-altering injury or disease, but depressionis also common in people with cortical dysfunction andsome subcortical disorders such as Parkinson’s disease. Asdiscussed earlier, a frontal executive system called amoti-vational syndrome often appears behaviorally as indiffer-ence, apathy, or depression. On the other side of the emo-tional spectrum, euphoria or inappropriate labileemotional responses can occur with frontal and subcorti-cal syndromes.
SummaryThe systems presented in this chapter represent the highest level of brain integration. They depend on theinput of processed sensory information and, to a large extent, manage, organize, manipulate, and store thisinformation for further use. Many of the processes of these systems operate automatically or unconsciouslywithout apparent verbal awareness. Subcortical brain regions control many “unconscious” processes. Themore explicit and, therefore, more seemingly conscious aspects of higher order processing are representedin the cortical areas, most notably the frontal lobes. Cortical functions mediate our interactions with theexternal environment and support those behaviors that we consider to be “willed” or volitional.
This chapter, as well as the previous chapters, provides the foundation for the clinical issues and disor-ders presented later in this book. Whereas here we have considered functions and disorders by subsystem,we next examine cases of disorders that cut across functional areas.
C r i t i c a l T h i n k i n g Q u e s t i o n s
Do the higher cognitive functions discussed in this chapter represent more intelligent thought processes than those func-tions discussed in previous chapters? Explain.The memory, attention, and executive function systems interact. How would you explain this interaction?Do disorders of executive functioning represent a greater disability for humans than sensory-perceptual and motor disor-ders? Why or why not?Do emotions represent a higher cognitive function or a lower basic function? Explain.Are there advantages to multiple brain memory systems as contrasted to a single memory system?
CHAPTER 9 | Memory, Attention, Emotion, and Executive Functioning 265
Anterograde amnesiaRetrograde amnesiaShort-term memory (STM)Long-term memory (LTM)Remote memoryDeclarative memoryNondeclarative memoryProcedural memoryExplicit memoryImplicit memoryEpisodic memory
Semantic memoryImplicit primingWorking memoryCentral executiveArticulatory phonologic
loopVisuospatial sketch padEpisodic bufferFocused attentionAlternating attentionDivided attention
Hemispatial neglectPosterior attention systemVigilance attention systemAnterior or executive attention
systemFocus-execute attentionShifting attentionSustained attentionEncode attentionStable attentionObject permanence
Executive planningPseudopsychopathyAcquired psychopathyEnvironmental dependency
syndrome (stimulus-bound)Utilization behaviorSomatic markersAkinetic mutismAbuliaJames–Lange theoryCannon–Bard theory
We b C o n n e c t i o n s
http://www.lycaeum.org/drugs/other/brainMind-Body—great source for links to topics related to theories of the mind.
http://www.nimh.nih.gov/events/prfmri2.htmWorking Memory—site provides graphics for three-dimensional MRI reconstruction of the subject’s brain,including parietal and frontal areas, while holding a series of letters in working memory.
http://www.exploratorium.edu/memory/index.htmlMemory Web Site—features online exhibits and articles and lectures on memory. Page also shows demon-stration of memory for common objects such as a penny. The page asks the user to click on the penny thatactually looks like one.
K e y Te r m s

This page intentionally left blank
Part Three
D I S O R D E R S O F T H E B R A I N
Chapter 10 Developmental Disorders of Childhood
Chapter 11 Learning and Neuropsychiatric Disorders of Childhood
Chapter 12 Cerebrovascular Disorders and Tumors
Chapter 13 Traumatic Head Injury and Rehabilitation
Chapter 14 Normal Aging and Dementia: Alzheimer’sDisease
Chapter 15 Subcortical Dementias
Chapter 16 Alterations of Consciousness

This page intentionally left blank

Chapter 10
DEVELOPMENTAL DISORDERS OF CHILDHOOD
Sometimes even to live is an act of courage.—Seneca (died a.d. 65), Letters to Lucilius
Vulnerability and Plasticity of the Developing BrainChild and Adult Brain: Structural and Functional
DifferencesSpecific Developmental Disorders
Neuropsychology in Action
10.1 Principles of Assessment in PediatricNeuropsychology
or diffuse, and can result in minimal to complete loss offunction. Examples of potential teratogens are general dis-eases (such as rubella, influenza, and mumps), sexuallytransmitted diseases (such as syphilis, AIDS, and genitalherpes), drugs (such as alcohol, cocaine, barbiturates, andvaccines), environmental toxins (such as mercury, carbonmonoxide, lead, and polychlorinated biphenyls [PCB]),and radiation (such as from x-rays and exposure to ra-dioactive materials).
The precise impact of the teratogen on the unbornfetus varies with the nature of the insult and its proximityto a particular period of rapid brain growth, the geneticmakeup of the child/mother, the quality of the intrauter-ine environment, and the “dosage” and extent of exposure(Spreen, Risser, & Edgell, 1995). The prenatal brain ap-pears most vulnerable to morphologic damage duringearly organogenesis (weeks 2–8). Resultant malformationsare often so severe that the embryo is spontaneouslyaborted or presents at birth with conditions incompatiblewith life (Anderson, Northam, Hendy, & Wrennall, 2001).Although the probability of massive malformations de-creases during later periods of gestation, the brain continues
270 PART THREE | Disorders of the Brain
K e e p i n M i n d
What differences in the impact of brain injury are there for children compared with adults?
Is the brain of a child merely a small replica of the adult brain, differing only in size, or do the two brains differ insignificant ways?
How do children with Turner’s syndrome differ from children with Williams syndrome?
Can children with fetal alcohol syndrome outgrow their cognitive deficits?
OverviewThis chapter focuses on childhood developmental disorders that result from genetic and chromosomalalteration, and early environmental insults. Although these disorders can be traced to disruption of earlybrain development, the effects of the disruption persist throughout childhood, adolescence, and adulthood.We first discuss the vulnerability and plasticity of the young brain, then compare the child and the adultbrain. These topics are particularly significant in evaluating and predicting the immediate and long-termeffects of brain insult or injury. Next, we examine a number of developmental disorders to highlight theoften disabling consequences of anomalies in brain development. The disorders reviewed include hydro-cephalus (HC), Turner’s syndrome (TS), Williams syndrome (WS), and fetal alcohol syndrome (FAS). We dis-cuss these developmental disorders for prevalence and manifestations, pathogenesis and neuropsychologi-cal assessment, and current interventions to halt or ameliorate the negative effects of early neuraldisruption.
Vulnerability and Plasticity of the Developing Brain
The brain may fail to develop structurally and func-tionally as a consequence of inborn (genetic and chromo-somal) anomalies and environmental insults. Brain disor-ders, such as phenylketonuria (PKU), a genetic metabolicdisorder, can be inherited or result from alterations of cel-lular material, as evident in TS. Environmental causes re-late to damaging agents (such as alcohol) that preclude,alter, or halt natural brain development. The degree towhich a brain can recover from damage is complex andnot fully understood. Neuroscientists do know, however,that the plasticity of the brain allows for recovery of func-tion under certain conditions.
Teratogens are agents that, if introduced or presentduring certain periods of prenatal development, can pro-duce central nervous system defects. The defects caninclude agenesis, the failure of an organ to develop, or dys-genesis, the abnormal development of an organ. Further-more, the damaging effects of the teratogens can be focal
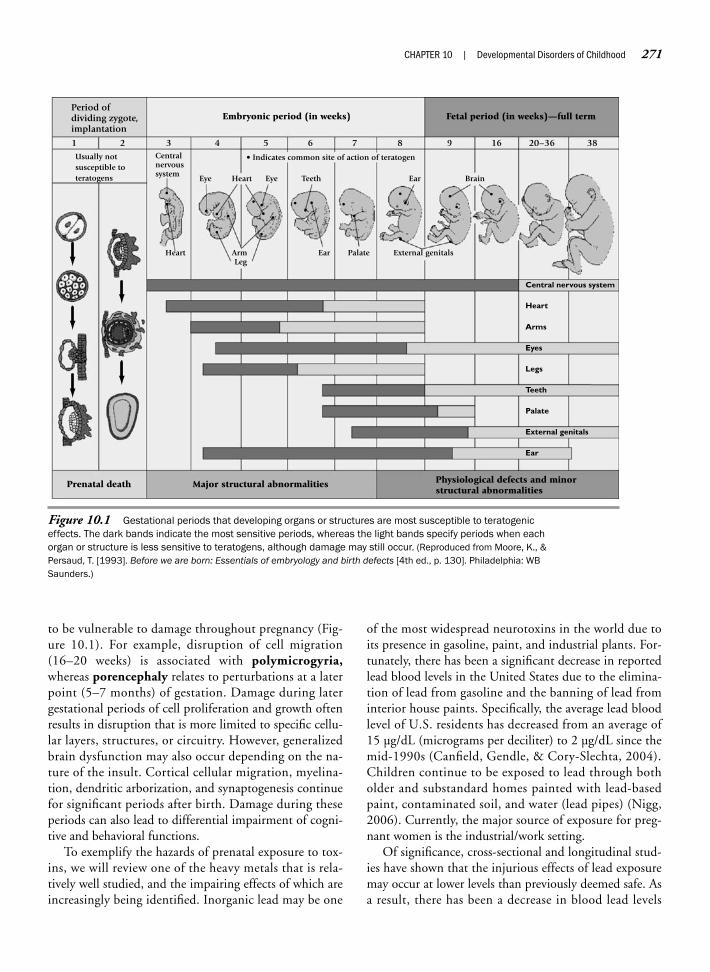
to be vulnerable to damage throughout pregnancy (Fig-ure 10.1). For example, disruption of cell migration(16–20 weeks) is associated with polymicrogyria,whereas porencephaly relates to perturbations at a laterpoint (5–7 months) of gestation. Damage during latergestational periods of cell proliferation and growth oftenresults in disruption that is more limited to specific cellu-lar layers, structures, or circuitry. However, generalizedbrain dysfunction may also occur depending on the na-ture of the insult. Cortical cellular migration, myelina-tion, dendritic arborization, and synaptogenesis continuefor significant periods after birth. Damage during theseperiods can also lead to differential impairment of cogni-tive and behavioral functions.
To exemplify the hazards of prenatal exposure to tox-ins, we will review one of the heavy metals that is rela-tively well studied, and the impairing effects of which areincreasingly being identified. Inorganic lead may be one
of the most widespread neurotoxins in the world due toits presence in gasoline, paint, and industrial plants. For-tunately, there has been a significant decrease in reportedlead blood levels in the United States due to the elimina-tion of lead from gasoline and the banning of lead frominterior house paints. Specifically, the average lead bloodlevel of U.S. residents has decreased from an average of15 µg/dL (micrograms per deciliter) to 2 µg/dL since themid-1990s (Canfield, Gendle, & Cory-Slechta, 2004).Children continue to be exposed to lead through botholder and substandard homes painted with lead-basedpaint, contaminated soil, and water (lead pipes) (Nigg,2006). Currently, the major source of exposure for preg-nant women is the industrial/work setting.
Of significance, cross-sectional and longitudinal stud-ies have shown that the injurious effects of lead exposuremay occur at lower levels than previously deemed safe. Asa result, there has been a decrease in blood lead levels
CHAPTER 10 | Developmental Disorders of Childhood 271
Figure 10.1 Gestational periods that developing organs or structures are most susceptible to teratogeniceffects. The dark bands indicate the most sensitive periods, whereas the light bands specify periods when eachorgan or structure is less sensitive to teratogens, although damage may still occur. (Reproduced from Moore, K., &Persaud, T. [1993]. Before we are born: Essentials of embryology and birth defects [4th ed., p. 130]. Philadelphia: WBSaunders.)
• Indicates common site of action of teratogenUsually notsusceptible toteratogens
Period ofdividing zygote,implantation
Heart
Eye Eye
Ear
Ear Brain
Palate External genitalsArmLeg
TeethHeart
Centralnervoussystem
1 2 3 4 5 6 7 8 9 16 20–36 38
Embryonic period (in weeks)
Prenatal death Major structural abnormalities Physiological defects and minorstructural abnormalities
Fetal period (in weeks)—full term
External genitals
Teeth
Legs
Arms
Central nervous system
Heart
Palate
Ear
Eyes

considered nonhazardous by the Centers for Disease Con-trol and Prevention and the World Health Organization.Before 1991, the safe blood lead level threshold was ≤25 µg/dL, whereas the current standard is ≤10 µg/dL.Yet, there is growing evidence that even this blood levelthreshold may be too high, as evident in the finding ofcognitive and behavioral impairments after blood lead lev-els of ≤10 µg/dL, leading some investigators (Canfield,Henderson, Cory-Slechta, Cox, Jusko, & Lanphear,2003) to propose that an even lower standard is war-ranted. At higher levels, there is clearer evidence regard-ing the negative impact of lead exposure on intellectualfunctioning; however, the findings for the negative effectsof lower levels of exposure on intelligence are less defini-tive. That is, not all studies (for review, see Kaufman,2001) report a decrease in intellectual performance atlower levels of exposure, and many report only small re-ductions, and often these reductions are related more topostnatal relative to prenatal lead exposure (Koller, Brown,Spurgeon, & Levy, 2004). Notably, many of these studiesfail to control for potential confounding factors (namely,mother’s intelligence quotient [IQ], education level,socioeconomic level, prenatal care, and use of other sub-stances) that could account for lower IQ scores.
Recent longitudinal and cross-sectional studies of chil-dren exposed to prenatal lead that have controlled forpotentially confounding variables report a reduction inintellectual performance. For example, Schnass and col-leagues (2006) observed children with prenatal lead expo-sure (pregnant mothers’ average blood lead levels were 8 µg/dL) through their first 10 years of life. The averagelead blood level for the children during their 1st to 5thyears of life was 9.8 µg/dL, and the level was 6.2 µg/dLwhen the children were 6 to 10 years of age. The investi-gators determined that lead exposure at approximately28 weeks gestation was negatively related to intellectualperformance. That is, the higher the maternal blood leadlevel, the lower the child’s assessed postnatal intelligence.A dose–response analysis indicated that the most signifi-cant impact on intelligence occurred within the first fewmicrograms of blood lead levels. The investigators con-cluded that prenatal lead exposure has a lasting and nega-tive impact on intellectual development.
Similarly, in an earlier well-controlled study (Ris,Dietrich, Succop, Berger, & Bornschein, 2004) of chil-dren exposed to prenatal lead, the effects on specific cog-nitive and motor skills were examined. Neurocognitiveassessments during childhood showed that the childrendemonstrated deficits in attentional control, fine-motorspeed and dexterity, and visuoconstructive abilities. Morealarming was the finding that the children’s deficits in
attentional control and visuoconstructive skills continuedto be evident when they were assessed as adolescents.
Empirical studies with animals suggest that lead expo-sure disrupts the mesocorticolimbic dopamine and gluta-mate neurotransmitter brain receptors, particularly thosereceptors in the nucleus accumbens of the basal ganglia.Other structures that have been implicated are the frontalcortex, hippocampus, amygdala, and cerebellum (Ris et al.,2004). However, the precise disruption of brain structureand function remains to be clarified.
Dangers to the developing brain are not limited to pre-natal teratogens. Potential dangers also threaten the peri-natal process of birth, including anoxia, medications in-troduced during labor and delivery, and mechanicalinjury to the skull and brain caused by trauma during de-livery. Intracranial hemorrhage and tissue damage are rec-ognized results of mechanical injury associated with thebirthing process (Spreen, Risser, & Edgell, 1995). Babiesof low birth weight are at particular risk for central ner-vous system damage. Furthermore, a wide range of poten-tial dangers threaten postnatal development. Traumatichead injury, toxins, radiation, malnutrition, tumors, infec-tions, and stroke all can cause significant injury to the de-veloping brain. Yet, there is resilience to the damaged brainrelated, in part, to protective factors such as a responsive,nurturing, and stimulating postnatal environment.
The term plasticity refers to the enduring changes inneural activity that accompany learning, or the recoveryof behavioral functioning after brain injury or disease(Frackowiak, 1996). Neuroscientists hypothesize that thebrain’s plasticity is greatest during developmental periodswhen synaptic density is highest; that is, when excessivenumbers of synapses exist, many of which have not com-mitted to function. These periods of maximum synapticdensity differ across cortical regions due to differentialrates of neuromaturation. For example, the window ofplasticity for the visual cortex is smaller than for the pre-frontal cortex. In the former case, synaptic density extendsuntil 5 years of age, whereas in the latter case, maximumdensity extends into late childhood (Huttenlocher, 1999;Huttenlocher & Dabholkar, 1997).
Initially, neuroscientists believed that the likelihood ofrecovery from a brain insult was greater if the injury oc-curred earlier rather than later in development. They laternamed this principle the Kennard principle in honor ofits originator, Margaret Kennard (Kolb, Gibb, & Gorny,2000). The Kennard principle suggests that the immaturebrain is more plastic than the mature brain. Some forms ofinsult do appear to follow this principle; for example, chil-dren with early focal brain injury often demonstrate milderand less extensive cognitive and emotional impairments
272 PART THREE | Disorders of the Brain

than adults with comparable lesions (Anderson, Northam,Hendy, Wrennall, 2001). However, the opposite effect isalso evident. That is, earlier brain lesions, particularly ifgeneralized, can have a pervasive impact on developingfunctions. In some cases, the early injury may initially ap-pear to have minimal effect if the cognitive or behavioralfunctions that the damaged region subserves do notemerge until a later point in development. As this devel-opment point is reached, significant functional impair-ments emerge. For example, the effects of early damage tothe auditory cortex may not be fully evident until languageskills fail to develop.
Some authors have proposed (Anderson, Northam,Hendy, Wrennall, 2001; Kolb, 1995) that the effect alesion has on the developing brain varies with the age atinsult. Lesions occurring before age 1, including prenataldevelopment, typically correlate with more global andlasting impairment than later injuries. Some degree ofneural reorganization and sparing of function is possiblewith lesions occurring between 1 and 5 years of age, de-pending on the nature, severity, and region of damage.During this period, most cortical regions reach maximumsynaptic-dendritic density. Finally, injuries after age 5 gen-erally predict minimal recovery of function. Thus, thereappears to be a “window” for optimum recovery extend-ing from the toddler through the preschool years. How-ever, not all studies support this set of generalities. For ex-ample, Bates (1999), in a review of studies, concludedthat worse outcomes were associated with damage occur-ring between 5 and 12 years of age as contrasted with in-jury during the prenatal period and subsequent earlychildhood years. Clearly, a simple linear association be-tween age of damage and cognitive and behavioral out-comes does not exist.
Child and Adult Brain: Structuraland Functional Differences
Neuroscientists are learning more and more aboutthe maturation of the central nervous system. An impor-tant realization is that the child’s brain differs in manysignificant ways from the adult brain. This section dis-cusses several of these differences to clarify this basic,though often forgotten, principle of the relation betweenbrain and behavior.
The brain of the adult is anatomically, physiologi-cally, and functionally mature, whereas that of the childis still developing. Accordingly, the effects of lesions tothe immature and mature brain differ significantly. In the
former case, injuries disrupt the acquisition of develop-mental abilities; in the latter case, previously acquiredabilities break down (Eslinger, Biddle, & Grattan, 1997).With the achievement of brain maturity, greater stabilityand predictability of behavior is evident. In comparison,the cognitive and behavioral functions of the developingbrain can vary dramatically. This variability depends on thecurrent developmental stage and on the nature and qualityof the child’s social-psychological-physical environment.
With lesions of the mature brain, assessing the degreeof functional loss and potential for recovery often involvesexamining the adult’s premorbid history. Young childrenhave an obviously abbreviated history from which to drawvariables necessary for prediction. Likewise, the youngchild has not developed a host of higher order functionssuch as reading and writing, thus severely hindering ef-forts to determine which functions are spared or compro-mised, both in the present and in the future.
Many pathologic signs of adult brain injury are devel-opmentally appropriate if the developing child exhibitsthem (Bernstein & Waber, 1997). For example, the prim-itive neural reflexes of the infant are obviously normal,but in adulthood, they are signs of frontal lobe or relatedneural damage. Likewise, early childhood damage to onecortical region may impact the development of otherbrain regions—a phenomenon not consistently observedwith adult injury. For example, Eslinger and coworkers(1997) report that childhood lesions to the left prefrontalcortex can disrupt development of the right prefrontal re-gions, an effect these researchers did not observe withcomparable damage to the mature brain.
One of the most striking examples of how the child’sbrain contrasts with that of the adult’s is the differing re-sponse to lesions in the language areas of the left hemi-sphere. Young children who experience such injury rarelyshow aphasia. Moreover, most children with early lefthemisphere damage acquire language abilities within thelower end of the average range (Stiles, 2000). In contrast,adults subject to similar lesions show a high prevalence ofaphasic disorders and recovery is often less robust. Inves-tigators initially attributed the difference to the brain’splasticity, and they posed that language transferred to theopposite hemisphere. However, the transfer of languageto the right hemisphere is at a cost due to the finding thatmany of the affected children show visuospatial deficitsand significant declines in intellectual performance. Re-searchers attributed the functional loss to a “crowding”effect. That is, language “crowds” into right hemisphereat the expense of other cognitive functions.
The posing of a transfer and crowding effect to accountfor the differences in language functioning of childhood
CHAPTER 10 | Developmental Disorders of Childhood 273

versus adulthood damage is being challenged. Emergingresearch suggests that the relationship between earlyhemispheric damage and language performance differs foryoung children as compared to adults with similar injury.In a series of studies (Bates & Roe, 2001; Stiles, 2000;Stiles, Bates, Thal, Trauner, & Reilly, 1998), the languagedevelopment of children with either early left or right uni-lateral damage was examined. During the initial assess-ment, when the children were between 10 and 17 monthsof age, the majority of children were delayed in early lan-guage acquisition. Noteworthy was the finding that re-ceptive language deficits were more common in the chil-dren with right hemisphere rather than with left hemisphereinjury. Furthermore, children with damage specific to theleft temporal injury were delayed in word production, butthey performed within the normal range on measures ofcomprehension and gestures. This profile is the oppositeof adults with left posterior injury, in whom language pro-duction is spared whereas comprehension is impaired. Incontrast, children with right hemisphere damage demon-strated visuoconstructive and emotional comprehensionand expression deficits similar to those demonstrated byadults with comparable damage. These findings suggestthat language acquisition is supported by widely distrib-uted brain regions of both hemispheres, and thus allowsfor the development of alternative pathways for neural me-diation of language. In contrast, there is greater neuralspecificity to the regions supporting spatial and affectiveprocesses. Accordingly, the visual constructive and emo-tional deficits associated with injury during early childhoodare more likely to be similar to those demonstrated byadults (Stiles, 2000). With age and commitment of brainregions and circuitry to language and other abilities, thebrain is less able to reorganize and redistribute functions toaccommodate to injury. However, brain plasticity is evi-dent in adulthood, although greatly constrained.
The impact of adult injury is generally apparent soonafter the lesion occurs, whereas the effects of injury to theimmature brain are less straightforward. Studies of pri-mates suggest that early lesions to the prefrontal and tem-poral cortexes can produce both immediate and delayedpresentation of impairments. Goldman-Rakic (1987a,b)conducted a series of studies to investigate the effects ofdamage to the prefrontal cortex. Lesions in the prefrontaldorsolateral region of the brain of mature monkeys impairedperformance on a delayed response task (see Figure 9.9),whereas infant monkeys with comparable lesions did notshow immediate impairment. However, as the infantmonkeys matured, a significant deficit emerged in delayedresponse performance. In contrast, lesions of the pre-frontal orbital cortex produced delayed response deficits
regardless of age at injury. Thus, age and region of pre-frontal cortex damage interacted to determine immediateor delayed impairment.
Similarly, case studies of children (Eslinger et al., 1997;Tranel & Eslinger, 2000) with early prefrontal damagesuggest that immediate and delayed impairments of cog-nitive and socioemotional executive functions can result.The emerging deficits in adolescence and early adulthoodappear most prominent in the development and regula-tion of socioemotional behaviors such as social awareness,interpersonal sensitivity, perspective taking, friendshipskills, and close emotional relationships. These emergingdeficits appear more disruptive to adjustment than similardeficits that occur in adulthood. The relation of immedi-ate and late-appearing deficits of age, affected hemisphere,specific cortical region of damage, and other mediatingvariables remains unclear and warrant further study.
Our discussion of the vulnerability and plasticity ofthe brain, as well as its difference from the adult brain,serves as a basic framework for understanding the neu-ropsychological assessment of childhood disorders.William Culbertson presents a case study of the effects ofan early frontal tumor and its subsequent cognitive im-pact (Neuropsychology in Action 10.1).
Specific Developmental Disorders
This section reviews several groups of neurodevelop-mental disorders that neuropsychologists frequently treat.These include abnormalities of anatomic development, ge-netic and chromosomal disorders, and acquired cerebral in-sults and diseases. We discuss a sample disorder from eachof these groups to acquaint the student with the clinical pre-sentation, neuropsychological pathogenesis, and treatmentof the disorder. The first disorder, HC, frequently co-occurswith many other disorders of anatomic malformation. Next,TS is one of the most commonly seen chromosomal disor-ders. We follow with a discussion of WS, a unique geneticdisorder that continues to spawn research because of its neu-rocognitive profile. Finally, FAS is a relatively common anddestructive disorder. Of the four disorders developmentaldisorders, FAS is completely preventable.
A B N O R M A L I T I E S O F A N A T O M I CD E V E L O P M E N T
Many conditions exist that reflect anomalies of neurodevel-opment. Hynd, Morgan, and Vaughn (1997) divide thesedisorders into five groups (Table 10.1). Each category reflectsa malformation of brain tissue with concurrent disruption
274 PART THREE | Disorders of the Brain

CHAPTER 10 | Developmental Disorders of Childhood 275
Case PresentationS.B. is an 8-year-old girl who was referred forneuropsychological evaluation after neuro-surgical removal of a right frontal tumor. Theevaluation was sought to determine hercurrent levels of cognitive functioning,establish a baseline for monitoring herrecovery, and provide appropriate educa-tional and management recommendations.The referral for evaluation was made 2 months after surgery.
During second grade, S.B. began tocomplain of headaches. These headachesbecame increasingly frequent and intense.Initial medical consultations did not identifythe basis for her headaches. Subsequently,her academic skill levels began to decline.Her headaches failed to abate and wereaccompanied by vomiting. She experiencedat least one night seizure. She was referredfor neuroimaging (magnetic resonanceimaging and computed axial tomography).The neuroimaging studies showed a massive(7 � 5 � 6 cm) nonfiltrating right frontallobe tumor. Subsequently, S.B. underwentneurosurgery for the excision of the tumor.Her postsurgical recovery was uneventful,and neither adjunctive radiation norchemotherapy was recommended.
Since the surgery, S.B. has continued toexperience headaches, although these areless frequent and intense than in the past.She fatigues quickly, appears to sleep more,and seems to struggle with sustainingattention to tasks. Her parents have wit-nessed no major sensory, motor, or cognitivealterations since her release from the hospi-tal. Similarly, no major changes or alter-ations in personality or social interactionshave been observed. She continues to beviewed by her parents as an active, ener-getic, and socially adept child.
Before the tumor, S.B.’s developmentaland medical history was unremarkable. Shewas an average student who was well likedby her teachers and peers. At the time of theevaluation, S.B. had returned to school on a
reduced day schedule and was makingsteady but slow academic progress. Herteacher reported inattentiveness, impulsivity,disorganization, and high levels of minormotor activity as areas of concern.
Behavior Observed During AssessmentS.B. is a dark-haired, well-developed childwho was appropriately attired in contempo-rary garb for the assessment. Her surgicalscar was clearly evident in the anterior regionof her skull. She did not appear to be con-cerned by the visibility of the scar to others.She related in a friendly, talkative, andspontaneous manner. Her verbal responsestended to be overly detailed, poorly orga-nized, and often tangential in nature. How-ever, her thinking was reality oriented, andemotional responses were appropriate to theevaluative context. She was prone to fatiguequickly and to report that she was develop-ing (or had developed) a headache. Accord-ingly, a number of relatively short sessionswere required to complete the assessment.
S.B. was motorically active acrossassessment sessions. This activity includedfidgety and restless behaviors and actionssuch as fiddling with her hair, the zipper onher jacket, objects on the desk, and a pieceof thread pulled from her shirt. It was notuncommon for her to sing or hum as sheworked on tasks. She was quick to reachout and manipulate test materials as theywere placed in front of her. Similarly, shewould often try to initiate her performanceof the assessment tasks before the exam-iner could complete the directions for thetasks.
When presented with new or difficulttasks, S.B. was prone to state, “I won’t beable to do this,” or to seek assistance. Hersense of self-efficacy appeared limited, asevident in frequent requests for feedback onthe adequacy of her performance (such as,“How many did I get right?” “Did I missany?”). Her tolerance for frustration was
limited, and support and coaxing was oftennecessary to maintain her comfort andperformance.
S.B. did not consistently monitor theaccuracy of her performance, resulting inneedless errors. She encountered difficultywith drawing/copying tasks due, in part, to aquick and uncritical approach. Her pencilgrasp (right hand) was unusual in that thebarrel of the pencil rested on her ring finger.
Neuropsychological AssessmentS.B.’s teacher completed rating scalespertinent to her observations of S.B.’s in-class behavior. The teacher provided ele-vated ratings (clinical range) on subscalessensitive to deficits in working memory,planning and organization, organization ofmaterials, and self-monitoring. The parentsalso completed rating scales related to theirobservations of S.B.’s behavior. Their ratingsshowed clinical elevations on subscalesassessing inattention, hyperactivity, rest-less-impulsive behaviors, psychosomaticcomplaints, and poor organization of materi-als. Borderline clinical ratings were pre-sented for problems with inhibition, workingmemory, planning and organization, andself-monitoring.
S.B.’s intelligence was determined to bewithin the average range, with a nonsignifi-cant discrepancy between verbal and perfor-mance intelligence. Her verbal subtestscores fell within the average range withoutany significant individual strengths or weak-nesses. In contrast, her performance subtestscores ranged from significantly belowaverage to above average. Her above-averageperformance was evident on a subtestassessing her ability to determine the appro-priate sequence of social stimuli. Below-average performance was demonstrated onsubtests assessing visual attention to detailsand visuoconstructive abilities (block designconstruction and puzzle assembly). Herachievement in reading, mathematics, and
N e u r o p s y c h o l o g y i n A c t i o n 1 0 . 1
P r i n c i p l e s o f A s s e s s m e n t i n P e d i a t r i c N e u r o p s y c h o l o g y
by William C. Culbertson
(continued)

276 PART THREE | Disorders of the Brain
of function. Several of these malformations are incompat-ible with life (for example, anencephaly and hydranen-cephaly), whereas others do not necessarily compro-mise the child’s survival, but do significantly impair oralter neuropsychological functioning. In many cases, agiven disorder may have multiple causes; in others, thepathogenesis is quite specific. However, the origin ofmost of the disorders is undetermined.
The extensiveness and severity of damage to the devel-oping brain tends to reduce life expectancy of childrenwith anatomic brain malformations. Surviving childrenshow a high rate of mental retardation, speech and lan-guage delays, learning disabilities, motor impairments,physical anomalies, and epilepsy. Children with severeand global neuropsychological deficits often require life-long supervision and assistance. We turn first to HC, arelatively frequent anomaly of the brain that can result inminimal to severe neuropsychological deficits.
H y d r o c e p h a l u s
Clinical Presentation and Incidence—Hydrocephalus (HC) canoccur during any developmental period and seriouslydamages the developing brain, disrupting both subcorti-cal and cortical functions. This condition results from anexcessive accumulation of cerebrospinal fluid (CSF) in thebrain’s ventricles (Figure 10.2). The increased volume ofCSF produces a concomitant increase in intracranial pres-sure and expansion of the ventricles. As the ventricles ex-pand, cerebral tissue is compromised and the cranium dis-torts. If untreated, the child may die or suffer severemental retardation. The actual incidence of HC is un-known because it is frequently associated with other con-genital disorders. However, it is estimated that 27 per100,000 newborns suffer from the condition (Kolb &Whishaw, 1996). The incidence of HC of mixed causesappears to be greater for boys (62%) than girls.
spelling was found to be consistent with herassessed level of intelligence.
S.B.’s working memory for verbal con-tents (mental arithmetic, repeating digitsbackward) was age appropriate. Similarly,when learning a list of words across repeatedtrials, she demonstrated an age-appropriatelearning curve and unimpaired memoryrecall. However, the introduction of analternative list of words for learning revealedinterference from the originally encoded list(words from the first list intruding into herrecall of the second list of words). Althoughher verbal fluency (letter and semantic)performance was within the average range,her design fluency performance fell withinthe impaired range.
Deficits were also evident when judgingthe spatial orientation of lines, imitatingsequences of movement in space, drawingfamiliar objects (for example, bicycle), andcopying developmental visuomotor forms.Furthermore, she demonstrated an impairedlevel of performance when rapidly shiftingbetween numbers and letters. Her fine-motordexterity with her dominant and nondomi-nant hand was below age expectancy, withsignificant impairment evident for her non-dominant left hand.
S.B.’s performance on measures ofsustained attention demonstrated poorattentional and inhibitory control. Althoughshe demonstrated age-appropriate perfor-mance on an executive task assessing ab-stract abilities and cognitive flexibility, shesignificantly faltered on a second measureassessing executive planning and problemsolving.
CommentaryThe impact of a major tumor on the develop-ing brain can result in a myriad of cognitive,emotional, and social deficits/excesses.Factors mediating the effects of the tumorare the child’s stage of development, natureand extent of the insult, cognitive resources(for example, intelligence), form of postsurgi-cal treatment (radiation and/or chemother-apy), and the availability and quality ofsupportive services. Despite the multiplicityof outcomes, a number of sequelae areassociated with right anterior damage,including poorly organized narrative dis-course, inattention/distractibility, disruptionof working memory, disinhibition, visualconstruction skill deficits, limited nonverbalfluency, and impaired monitoring. Moreover,memory disruption secondary to inattentionand interference effects is frequently evi-
dent. Executive planning and problemsolving can be markedly impaired. In con-trast, cognitive functions associated with leftfrontal circuitry can be relatively well pre-served. S.B.’s pattern of neuropsychologicalperformance is consistent with compro-mised cognitive functions supported by rightanterior brain circuitry.
S.B.’s neuropsychological strengths andweaknesses were presented to the parents.It was stressed that it was too early in herrecovery to determine precisely whichdeficits would persist or resolve, but herprogress should be monitored carefully,particularly because the impact of anteriordamage is often not fully evident untiladolescence. Recommendations weredeveloped to aid school personnel in provid-ing appropriate educational modificationsand interventions. An evaluation by a physi-cal therapist was recommended. The par-ents were further advised that if S.B.’sinattention, impulsivity, and minor motoractivity did not improve over time, theyshould consult with her neurologist todetermine the feasibility of introducingpsychostimulant medication. Supportivegroup therapy/counseling with children whohad undergone treatment for brain tumorswas recommended.
(continued)

CHAPTER 10 | Developmental Disorders of Childhood 277
Neuropathogenesis—HC is a disorder that occurs secondary toother pathologic events or processes. This pathogenesis canbe of prenatal, perinatal, or postnatal origin. Congenital(prenatal) disorders such as spina bifida, Dandy–Walkermalformation, Arnold–Chiari malformation, and stenosis ofthe aqueduct of Sylvius often result in HC (see Table 10.1).Of these congenital disorders, spina bifida is most fre-quently associated with HC (Mataró, Junqué, Poca, &Sahuquillo, 2001). The most common cause of perinataland postnatal HC is intraventricular hemorrhage (IVH),a condition that occurs in premature infants (see later).Other causes of HC, both prenatal and postnatal, includeinfections (meningitis and encephalitis), vascular abnor-malities, tumors, cysts, traumatic brain injury, and otherdisease processes (Erickson, Baron, & Fantie, 2001;Fletcher et al., 1996).
Physiological Dynamics—Any one of three underlying causescan produce an abnormal increase in the volume of ven-tricular CSF. These causative factors include oversecretionof CSF, obstruction of CSF passages, and impaired ab-sorption of CSF (Greenberg, Aminoff, & Simon, 2002;Fletcher et al., 1996). Oversecretion of CSF is rare and isgenerally a consequence of a secreting tumor of thechoroid plexus, the primary producer of CSF in the lat-eral ventricles.
The second cause of HC occurs within the ventricu-lar system and involves obstruction of the CSF pathwaysas a result of congenital malformation, tumors, or scar-ring. HC of this etiology is termed obstructive or non-communicating HC (Brookshire, Fletcher, Bohan,Landry, Davidson, & Francis, 1995; Marino, Fine, &McMillan, 2004). The aqueduct of Sylvius, also calledthe cerebral aqueduct of the third ventricle, is the mostcommonly obstructed ventricular pathway, because of itslong, narrow structure. Conditions obstructing the aque-duct of Sylvius include: (1) congenital narrowing (steno-sis) of the aqueduct; (2) a thin membrane lying on theaqueduct; (3) constriction of the aqueduct by pressurefrom an adjoining tumor; and (4) herniation of the cere-bellum and displacement of the fourth ventricle, as inArnold–Chiari malformation (Hynd et al., 1997). How-ever, the pathogenesis of obstructive or noncommunicatingHC may be idiopathic (unknown), and research findingssuggest that different familial forms may exist (Hynd &Willis, 1988).
The third form of HC results from disrupted reabsorp-tion of CSF into the bloodstream caused by obstructionin the basal subarachnoid cisterns or in the arachnoid villi(Fletcher et al., 1996; Marino et al., 2004; see Figure 10.2).
When spina bifida is excluded, the most common causeof HC in early development is IVH, a condition that,until relatively recently, occurred in 40% to 50% of pre-mature infants with birth weights less than 1800 g(Mataró et al., 2001; Willis, 1993). Recent medical ad-vances have reduced the incidence of IVH to 20% for pre-mature infants (Fletcher, Dennis, & Northrup, 2000).IVH is a result of breathing problems or pressure on thebrain during the delivery process causing vessels in thegerminal matrix (area around the ventricles) to ruptureand bleed into the ventricles. Blood and cellular debris clogthe arachnoid villa (which is responsible for reabsorbingCSF into the bloodstream) and CSF volume and pressureincrease, although its outward flow into the spinal canal isnot blocked. HC of this form is known as nonobstruc-tive or communicating HC.
Obstructive or noncommunicating HC is a congeni-tal disorder that develops early in gestation and is associ-ated with an ever-expanding impact on subsequent braindevelopment. In contrast, nonobstructive or communi-cating HC is primarily a consequence of perinatal andpostnatal insults to a brain that heretofore had developednormally.
Impact of Hydrocephalus on the Developing Brain—If unchecked,HC has a devastating impact on the developing brain andskull (Figure 10.3). As CSF volume increases, the ventri-cles progressively enlarge in a posterior to anterior direc-tion with corresponding disruption of brain anatomy andfunction. The ventricle lining suffers focal damage, cere-bral blood vessels distort and become dysfunctional, neu-rons are injured, and the concentration of neurotrans-mitters and cerebral fluid alters (Del Bigio, 2004;Dennis & Barnes, 1994). Increasing pressure extensivelydamages the underlying white matter of the brain.Specifically, the corpus callosum stretches and thins (hy-poplasia), midline projection fibers that connect thehemispheres to the diencephalon and caudal regionsstretch and distort, the internal capsule (fanlike whitefibers separating regions of the basal ganglia and dorsalthalamus) displaces, and the periventricular white mat-ter (white matter adjacent to the lateral ventricles) isdamaged (Dennis & Barnes, 1994; Ewing-Cobbs,Barnes, & Fletcher, 2003). Furthermore, the corticalmantle thins, often damaging the cerebral cortex andcompromising cognitive functions. Because of theposterior-to-anterior progression of HC, the cognitiveand motor functions supported by the posterior corticalregions, cerebellum, and midbrain structures with theirconnecting white matter tracks are most compromised

additional surgeries during the child’s life. Each surgeryincreases the risk for ventriculitis, or infection of the ven-tricles. Furthermore, introducing the shunt involves caus-ing a lesion to the brain, generally of the parietal lobe ofthe right hemisphere. The shunt track can irritate the sur-rounding brain tissue and increase the potential forseizures (Willis, 1993).
Although cognitive, motor, and sensory (visual) im-pairments frequently associate with HC, the precisesymptom presentation is highly individualistic. The pe-riod of developmental onset, the presence of other con-genital disorders and anomalies, surgery to introduce oradjust a shunt, and the nature of the child’s environmen-tal context are several variables that affect the array, sever-ity, and form of symptoms the child will experience.
278 PART THREE | Disorders of the Brain
Malformation Description Clinical Manifestations
Abnormalities of bulk growth
Micrencephaly Subnormal brain size associated with abnormally Size of face near normal; folded scalp, possible small head (<2 SD below mean for age and gender) epilepsy, and most typically intellectual retardation
Megalencephaly Abnormally large brain from overproduction of Associated with mental subnormality, normality, cerebral parenchyma. Males > females or (hypothetically) giftedness. Epilepsy may occur.
Dysplasias of cerebral hemispheres
Holoprosencephaly Two hemispheres fail to develop. A large fluid-filled Faciocerebral dysplasias, cebocephaly, apnea cavity results. No interhemispheric fissure present. spells, severe mental retardation, hypotelorism, 1:13,000 live births and other systemic deformities. Usually incom-
patible with life.
Agenesis of the corpus callosum Complete or partial failure of the corpus callosum Occasionally asymptomatic or found in associa-to develop. Males > females tion with spina bifida, facial and ocular deformities, micren-
cephaly, and hydrocephalus. Epilepsy and mental retardationmay occur.
Malformations of the cerebral cortex
Agyria/pachygyria Smooth lissencephalic surface of brain. Few Commonly found in association with agenesis of coarse gyri may be present corpus callosum, micrencephaly, epilepsy, severe mental
retardation, and early death
Polymicrogyria Development of many small gyri. Microscopically, Found in association with learning disabilities they may form an overlapping folded cortex (dyslexia), severe mental retardation, and epilepsy. Also appear
asymptomatically
Focal dysplasia Focal abnormalities in the cortical architecture Reported in cases of epilepsy and learning dis-usually consisting of disordered cells and layering abilities (dyslexia)of cortex
Malformations associated with congenital hydrocephalus
Dandy-Walker malformation Malformation of the cerebellum associated with a Hydrocephalus, agenesis of the corpus callosum, dilation of the fourth ventricle. Males > females Klippel-Feil and DeLange syndromes, and severe psychomotor
retardation
Table 10.1 Anatomic Disorders
(Mataró et al., 2001). As a result, children with HC fre-quently exhibit deficits in nonverbal (especially visu-ospatial) and motor performance.
As the ventricles continue to distend, the cerebralhemispheres mold into a balloon shape. Because suturesin the cranium of the fetus and infant have not yet fused,increasing pressure enlarges the skull to accommodate theincreased CSF volume. Once the sutures close, however,cranial volume is invariant, and the HC develops furtherat the expense of brain tissue (Rowland, Fink, & Rubin,1991).
Most children with symptoms of HC receive a shunt(see Figure 10.3). This medical procedure drains excessiveCSF away from the ventricular system into the stomach.A shunt that fails, or needs adjustment, may necessitate

Neuropsychological Assessment—Neuropsychological assess-ment of the child with HC focuses on clarifying bothspared and compromised functions. The extent and de-gree of impaired or spared cognitive functions differ foreach child. In general, greater overall impairment ofhigher order cognitive abilities accompanies more ad-vanced cases of HC. However, interaction of HC withother moderating variables, such as age, intelligence, andsocioeconomic status, potentially can lead to differentialeffects on cognitive functioning.
Before widespread use of the shunt, only a fourth ofuntreated HC children survived to adulthood, and manysurvivors were profoundly retarded (Hynd, Morgan, &Vaughn, 1997). In contrast, the cognitive performanceof early shunted children is significantly higher, span-ning the range of abilities from below to above average
CHAPTER 10 | Developmental Disorders of Childhood 279
(Willis, 1993). Some investigators suggest that childrenwith HC uncomplicated by other structural disruptions(such as multiple shunt operations or Arnold–Chiarimalformation) are likely to demonstrate less impairmentof overall cognitive ability (Erickson, Baron, & Fantie,2001). Yet, even in cases of relatively preserved overallintelligence, children with shunted HC frequentlydemonstrate deficits in visual-perceptual, visuospatial,motor (fine and gross), and memory performance(Ewing-Cobbs, Barnes, & Fletcher, 2003; Scott et al.,1998). The deficits in the visual-perceptual, visuospa-tial, and visuomotor domains are related to the disrup-tion of the posterior cortical regions, cerebellum, corpuscallosum, and other white matter pathways, whereaspoor motor skills are believed to be a consequence ofdamage to the cerebellum, basal ganglia, motor strip,
Malformation Description Clinical Manifestations
Malformations associated with congenital hydrocephalus (continued)
Arnold-Chiari malformation Congenital deformation of the brainstem and Congenital hydrocephalus, spina bifida, and cerebellum severe psychomotor retardation
Stenosis of the aqueduct of Sylvius Obstruction of the aqueduct and CSF circulation Often insidious onset of symptoms associated with hydro-cephalus. Shunted children may suffer learning/behavioralproblems. Nonverbal IQ < verbal IQ
Abnormalities of the neural tube and fusion defects
Spina bifida occulta Usually asymptomatic lesion discovered incidentally Can be associated with lipoma, dermal sinuses, and dimples
Spina bifida cystica Spinal defect that includes a cyst-like sac that Hydrocephalus a frequent complication. Cognitive may or may not contain the spinal cord deficits related to extent of hydrocephalus. Arnold-Chiari
malformation not uncommon
Cranium bifidum and encephalocele Fusion defects of skull referred to as cranium Many associated difficulties with hydrocephalus bifidum; myelomeningoceles or meningoceles including ataxia, cerebral palsy, epilepsy, and on the skull are referred to as encephaloceles. mental retardationMales < females
Anencephaly Vault of skull absent and brain represented by Condition incompatible with lifevascular mass. Face is grossly normal. 1 male:4 female
Hydranencephaly Cerebral hemispheres replaced by cystic sacs Difficult initially to distinguish from hydrocephalus. containing CSF Hypnoatremia, eye movement disturbances, and death
Porencephaly Large cystic lesion develops on the brain. May Occasionally asymptomatic but typically associ-occur bilaterally or unilaterally ated with mental retardation, epilepsy, and other neurodevel-
opmental malformations
Source: Modified and updated from Hynd, G., Morgan, A., & Vaughn, M. (1997). Neurodevelopmental anomalies and malformations. In C. Reynolds & E. Fletcher-Janzen (Eds.),Handbook of clinical child neuropsychology (2nd ed., p. 45). New York: Plenum Publishing Corporation. Reprinted by kind permission of Springer Science and Business Media.
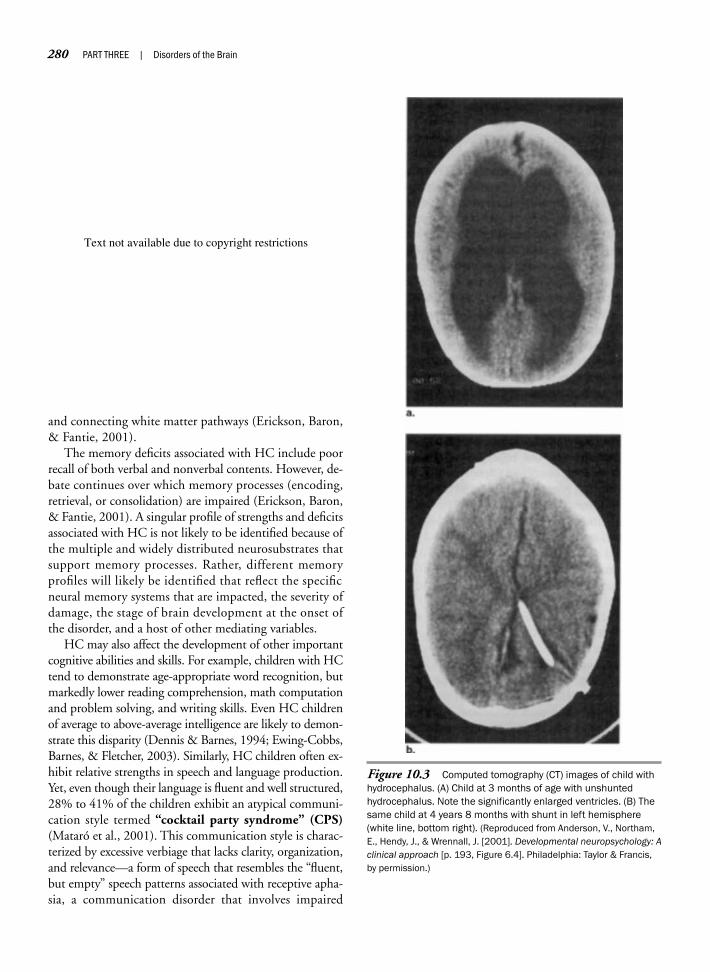
280 PART THREE | Disorders of the Brain
and connecting white matter pathways (Erickson, Baron,& Fantie, 2001).
The memory deficits associated with HC include poorrecall of both verbal and nonverbal contents. However, de-bate continues over which memory processes (encoding,retrieval, or consolidation) are impaired (Erickson, Baron,& Fantie, 2001). A singular profile of strengths and deficitsassociated with HC is not likely to be identified because ofthe multiple and widely distributed neurosubstrates thatsupport memory processes. Rather, different memoryprofiles will likely be identified that reflect the specificneural memory systems that are impacted, the severity ofdamage, the stage of brain development at the onset ofthe disorder, and a host of other mediating variables.
HC may also affect the development of other importantcognitive abilities and skills. For example, children with HCtend to demonstrate age-appropriate word recognition, butmarkedly lower reading comprehension, math computationand problem solving, and writing skills. Even HC childrenof average to above-average intelligence are likely to demon-strate this disparity (Dennis & Barnes, 1994; Ewing-Cobbs,Barnes, & Fletcher, 2003). Similarly, HC children often ex-hibit relative strengths in speech and language production.Yet, even though their language is fluent and well structured,28% to 41% of the children exhibit an atypical communi-cation style termed “cocktail party syndrome” (CPS)(Mataró et al., 2001). This communication style is charac-terized by excessive verbiage that lacks clarity, organization,and relevance—a form of speech that resembles the “fluent,but empty” speech patterns associated with receptive apha-sia, a communication disorder that involves impaired
Figure 10.3 Computed tomography (CT) images of child withhydrocephalus. (A) Child at 3 months of age with unshuntedhydrocephalus. Note the significantly enlarged ventricles. (B) Thesame child at 4 years 8 months with shunt in left hemisphere(white line, bottom right). (Reproduced from Anderson, V., Northam,E., Hendy, J., & Wrennall, J. [2001]. Developmental neuropsychology: Aclinical approach [p. 193, Figure 6.4]. Philadelphia: Taylor & Francis,by permission.)
Text not available due to copyright restrictions

language comprehension. Interestingly, deficits related tounderstanding and expressing abstract language are associ-ated with HC and are believed to contribute potentially tothe development of CPS. On a more positive note, manychildren who demonstrate CPS develop a more appropriatecommunication style with increasing age.
A particularly interesting finding concerns the relationof cognitive functioning to early- and late-occurring HC.Children with prenatal obstructive HC are prone to ex-hibit average verbal and language abilities, but below-average visuospatial and visuomotor abilities. This profileis similar to that of the nonverbal learning disability syn-drome (see discussion in Chapter 11). In contrast, chil-dren with HC resulting from perinatal and postnatal in-sults (such as IVH) are more likely to show comparableverbal and performance abilities, although both generallyfall within the low-average range (Willis, 1993).
The integrity of the executive functions of childrenwith HC has received less empirical attention than othercognitive domains. Executive functions refer to a wide rangeof higher order mental processes related to the generation,integration, control, and evaluation of goal-directed be-haviors that are supported by the frontal and frontal-cortical-subcortical networks of the brain (see Chapter 9).Preliminary studies of executive performance in childrenwith HC have identified executive deficits of attentionalallocation and control, concept formation, planning, cog-nitive flexibility, response inhibition, and self-regulation(Fletcher, Dennis, & Northrup, 2000; Willis, 1993).
Importantly, poor executive performance by childrenwith HC does not necessarily implicate damage or dis-ruption in the frontal cortex. For instance, in a recentstudy (Anderson, Anderson, Northam, Jacobs, &Mikiewicz, 2002), the executive performance of childrenwith HC, PKU, and frontal focal lesion and healthy con-trol children was examined. Both the HC and frontal le-sion groups performed poorly, relative to the healthy con-trol children, on an executive measure sensitive tovisuocontructive, planning, and organization skills (ReyComplex Figure; Rey, 1941, translated by Corwin &Bylsma, 1993). These findings leave unanswered the ex-tent to which the poor executive performance of the HCgroup related to visuospatial, motor, or executive plan-ning/organizational deficits, or some combination ofthese deficits. Because of the posterior-to-anterior pro-gression of damage associated with HC, posterior corticaland subcortical structures, as well as white matter path-ways, are generally disrupted before the frontal structures.This posterior disruption can, in turn, result in the trans-mission of distorted or incomplete visuospatial and/ormotor input to the frontal system. Thus, the poor perfor-
mance of the HC group could reflect an “executivedeficit” engendered by anomalies of nonfrontal structuresand pathways, rather than actual damage to the frontallobes. Additional empirical study is needed to clarify thespecific contributions of different neurosubstrates to theexecutive deficits of children and adolescents with HC.
Treatment—The prognosis for children with HC was direbefore the development of shunting. However, the adventof shunting has markedly increased the number of chil-dren who both survive and escape the significant destruc-tion of their cognitive functioning. Children with HCuncomplicated by the presence of other anomalies whoreceive early shunting often exhibit few, if any, cognitiveimpairments. Ultrasonography, a procedure that usessound waves to image internal structures, enables medicalpersonnel to identify HC in utero. This procedure allowsfor measurement of the ventricular expansion that pre-cedes the later enlargement of the cranium. From birthuntil age 2, HC is fairly easy to diagnose because the cra-nium quickly enlarges, developmental delays are evident,and eye movement abnormalities are present (Hynd,Morgan, & Vaughn, 1997).
G E N E T I C A N D C H R O M O S O M A LD I S O R D E R S
This section explores genetic and chromosomal disorders.Advances in the study of genetics, such as the mapping ofthe human genome, are accelerating at an exponential rate.More than 100 genetic and chromosomal disorders havebeen identified that, if untreated, can produce significantneuropsychological and physical deficits (see Table 10.2 forexamples). A multitude of factors can disrupt the geneticblueprint that defines the developing child. Genetic disor-ders can be a consequence of single-gene, chromosomal,parental imprinting, or molecular cytogenic anomalies.A discussion of the disorders associated with each of thesegenetic abnormalities is beyond the scope of this chapter.Accordingly, we focus on neurodevelopmental disordersassociated with chromosomal abnormalities.
Chromosomal disorders are a consequence of the mal-formation, deletion, addition, and/or dislocation of chro-mosomal material during the development of the oocyteor spermatocyte, or during conception and germinationof the egg (Marino, Fine, & McMillan, 2004; Spreen,Rissell, & Edgell, 1995). As a result, a genetic defect oc-curs even though the family history is negative for thedisorder. However, there are some families who have a his-tory of chromosomal disorders, suggesting direct genetictransmission from the parent to the offspring.
CHAPTER 10 | Developmental Disorders of Childhood 281

Chromosomal abnormalities can affect either autosomesor sex chromosomes. Autosomal abnormalities generallyproduce more severe birth defects than sex chromosome dis-turbances. More than 50% of first-trimester miscarriagesare due to chromosomal defects. In addition, congenital andcognitive deficits are frequently a consequence of this classof genetic disorder (Marino, Fine, & McMillan, 2004). Wediscuss two chromosomal disorders: TS and WS. TS is theconsequence of a missing or abnormal X sex chromosome,whereas WS is produced by a submicroscopic deletion onautosome 7. Studies of these two disorders have significantlyadvanced our understanding of the neuropsychological ef-fects of disturbances to the developing brain.
T u r n e r ’ s S y n d r o m e
Background and Clinical Presentation—In 1938, Turner pre-sented a syndrome characterized by a failure to developsecondary sexual characteristics, short stature, webbedneck, and cubitus valgus (an increased carrying angle atthe elbow). The disorder was subsequently namedTurner’s syndrome (TS). A previous case of the disorderhad also been reported by Otto Ullrich (1930); therefore,the syndrome is occasionally known as Ullrich–Turnersyndrome. TS was recognized as a chromosomal disorderaffecting female individuals in 1959, when Charles Fordand colleagues identified a missing X on the 45th chro-mosome. The karyotype—a visual representation of theconfiguration of a chromosome—is designated as 45,XO,
although there are other variations (see Web Connectionssection later in this chapter).
Consistent with Turner’s earlier description of the dis-order, an essential characteristic of TS is gonadal dysgene-sis, as evident in either the absence of the ovaries or thepresence of vestigial ovarian streaks. Short stature is an-other distinguishing characteristic, with achieved heightoften falling between 4 feet 6 inches and 4 feet 10 inches(Powell & Schulte, 1999). Physicians often identify in-fants with TS at birth due to characteristic edema of thehands and feet and loose skin folds at the nape of the neck.In childhood, physicians observe webbing of the neck,low-set ears, shield chest, deformed nails, cardiac andkidney malformations, and other features. Table 10.3
282 PART THREE | Disorders of the Brain
Genetic Chromosomal
Adrenoleukodystrophy Angelman’s syndrome
Friedreich’s ataxia Cornelia de Lange’s syndrome
Galactosemia Down’s syndrome
Hyperphenylalaninemia Fragile X syndrome
Krabbe’s disease Klinefelter’s syndrome
Lafora’s disease Prader-Willi syndrome
Lesch-Nyhan disease Sotos’ syndrome
Mucopolysaccharidosis Trisomy X syndrome
Phenylketonuria Tuberous sclerosis complex
Turner’s syndrome
Williams syndrome
Source: Harris, J. C. (1995). Developmental neuropsychiatry, vol. II: Assessment,diagnosis, and treatment of developmental disorders. New York: Oxford UniversityPress, by permission.
Table 10.2 Genetic and Chromosomal Disorders
Anatomic Abnormalities
Short stature
Webbed neck
Cubitus valgus
Broad chest
Prepubertal ovarian failure
Growth
Decreased mean birth weight
Lack of pubertal growth spurt
Skeletal
Curvature of the spine
Genu valgum (knock-knee)
Wrist deformity
Short hand and feet bones
Craniofacial
Premature closure of the skullsutures
Small jaw
Strabismus (cross-eyes)
Inner ear defects
Malrotation of ears
High arched palate
Cardiovascular
Aortic narrowing
Mitral valve prolapse
Septal defect (defect of the wall separating chambers of the heart)
Partial anomalous venous bloodreturn
Renal
Horseshoe kidney (abnormal tissueconnecting the kidneys) or ptotickidney (abnormal location in thepelvis)
Unilateral failure to develop orunderdeveloped kidney
Unilateral double ureter
Lymphatic
Dilation of the lymph vessels
Congenital swelling of thehands/feet
Hair and Skin
Low posterior hairline
Multiple moles
Finger/toenail deformities
Source: White, B. J. (1994). The Turner syndrome: Origin, cytogenetic variants, and factorsinfluencing the phenotype. In S. H. Broman & J. Grafman (Eds.), Atypical cognitive deficitsin developmental disorders (p. 185). Mahwah, NJ: Lawrence Erlbaum, by permission.)
Table 10.3 Physical and Medical Problems of Turner’s Syndrome

presents a sample of the physical characteristics and med-ical problems associated with TS. A distinctive cognitiveprofile for TS has been proposed and is discussed later inthis section (see Neuropsychological Assessment).
Incidence and Comorbidity—TS is one of the most commonchromosomal disorders, with an estimated female inci-dence rate of 1 in 2500 to 5000 births (Berch & Bender,2000). Researchers believe it occurs at conception, and99% of the affected fetuses spontaneously abort. The lifeexpectancy of individuals born with TS is not affected, al-though a number of physical conditions accompany thedisorder (see Table 10.3).
Frequent comorbid conditions of TS are learning dis-abilities and early symptoms of an attention-deficit/hyper-activity disorder (ADHD). Also, some researchers havesuggested that female individuals with TS are prone to de-pression, feelings of inadequacy, difficulty in concentrat-ing, poor peer relationships, and anxiety over sexuality andrelationships with male individuals. The factors that ac-count for these difficulties are unclear, but the small statureand sexual limitations of the individual with TS likely con-tribute to social difficulties and negative emotionality.
Chromosomal Defect and Turner’s Syndrome—TS is the result ofan anomaly of the female sex chromosome. The XX chro-mosome defines the developing embryo as female. In TS,the second X is either missing (monosomy X or 45,XO) orotherwise abnormal in formation or location. A wide vari-ety of karyotypes appear in liveborn TS children, with45,XO evident in approximately 50% of the cases.Isochromosome, the duplication of one arm of the X chro-mosome with the loss of the other arm, constitutes 10% to20% of cases. Mosaic karyotypes appear in 30% to 35%of children with TS (Temple, Carney, & Mullarkey, 1996).The mosaic karyotypes are characterized by the presence ofnormal chromosomes in some cells (46,XX) and abnormalchromosomes in others (Temple & Marriott, 1998). Themosaic karyotype, 45,X/46,XX, is associated with milderand less pervasive anomalies than the other karyotypes.
At birth, these children exhibit few distinguishing fea-tures, and short stature may be the first presenting symp-tom. In contrast, the small X-ring karyotype appears toincrease the risk for mental retardation, smaller head size,and greater growth-related retardation than the other TSkaryotypes. Note, however, that the TS physical pheno-type occasionally appears in children with apparently nor-mal karyotypes.
Neuropathogenesis—Neuroimaging studies provide supportfor right hemisphere (particularly posterior region)
involvement in the pathogenesis of TS. In an earlier mag-netic resonance imaging (MRI) study of TS and healthycontrol children, Reiss and coworkers (1995) determinedthat the ratios of gray to white matter for the right tem-poral and parietal areas were significantly lower for theparticipants with TS. In a more recent study (Brown et al.,2002) of children and adolescents with TS, MRI showedbilateral decreases in parietal gray and occipital white mat-ter and increased cerebellar gray matter. Moreover, apositron emission tomography (PET) study (Elliott,Watkins, Messa, Lippe, & Chugani, 1996) of childrenwith TS demonstrated significant bilateral parietal regionhypometabolism (reduced metabolism) relative to ahealthy control group. The researchers also observed atrend toward hypometabolic activity of the occipital re-gion. They hypothesized that the visuospatial and mathe-matic deficits associated with TS stemmed from parieto-occipital hypoactivation. Other regional differences inbrain volume or neuroactivation of patients with TS havebeen identified in the hippocampus, lenticular nucleus,thalamus, temporal cortex, and insula (Murphy et al.,1993, 1997). However, reduced tissue volume or atypicalactivation patterns for parietal and parieto-occipital areasare the most consistent findings across neuroimagingstudies.
Although posterior brain regions have received thegreatest empirical attention, increasing attention has fo-cused on the frontal system as it relates to executive per-formance associated with TS. Neuropsychological studieshave shown that individuals with TS demonstrate deficitsin verbal fluency, planning and organization, impulsiveregulation, strategic memory organization, cognitive flex-ibility, and attentional control (Buchanan, Pavlovic, &Rovet, 1998; Romans, Roeltgen, Kushner, & Ross, 1997;Temple, Carney, & Mullarkey, 1996). Haberecht and col-leagues (2001) subjected children and adolescents withTS and healthy control participants to function MRI(fMRI) while performing an executive function task,namely, a visuospatial working memory task. The chil-dren and adolescents with TS showed poorer perfor-mance than healthy control participants on the visuospa-tial working memory task. Moreover, fMRI showedsignificant bilateral hypoactivation (relative to healthy con-trol participants) of the dorsolateral prefrontal cortex, cau-date, and inferior parietal cortex while performing theworking memory task. The authors hypothesized that theworking memory deficits of TS relate to disruption ofthe frontal-striatal and frontal-parietal executive circuits.
In a more recent study (Tamm, Menon, & Reiss,2003), children and adolescents with TS and healthy vol-unteers underwent fMRI while performing a measure of
CHAPTER 10 | Developmental Disorders of Childhood 283

executive inhibitory control. The TS and healthy groupsdid not, contrary to prediction, differ in their inhibitoryperformance. Yet, the TS group was found to show acti-vation of additional regions of the superior and middleprefrontal cortices not demonstrated by the healthy con-trol group. The authors conclude that patients with TSdemonstrate altered (possibly compensatory) prefrontalcortical functioning with regard to response inhibition.Overall, neuroimaging studies have contributed to ourunderstanding of the brain-behavior relations of TS, butmuch remains to be discovered.
Neuropsychological Assessment—Originally, it was believedthat mental retardation was a common concomitant of TS.However, ongoing studies (Powell & Schulte, 1999) havedemonstrated that the intellectual functioning of childrenwith TS is generally within the low-average to averagerange. A smaller proportion of children fall within thebelow- or above-average range of intelligence (Swillen et al.,1993). Often, verbal intelligence exceeds performance in-telligence. That is, children with TS, when performing in-tellectual measures such as the Wechsler scales (1997,2002, 2003), tend to achieve higher scores on verbal lan-guage–related scales (for example, vocabulary) as con-trasted with performance scales (for example, block de-sign) that assess visual-perceptual and visuomotor abilities.
Several researchers have suggested that children withTS demonstrate a relatively distinct neurocognitive pro-file. The profile is characterized by intact verbal abilities incontrast with deficits in visuospatial, visuomotor, andarithmetic performance (Romans et al., 1997; Temple &Marriott, 1998). Table 10.4 summarizes the types of visu-ospatial and visuomotor deficits identified. Note that thesedeficits are generally associated with right parietal or dif-fuse right hemisphere dysfunction. Several investigatorshave drawn a parallel between the neurocognitive profile ofTS and that of the nonverbal learning disability syndrome(see discussion of the NVLD syndrome in Chapter 11).Alternatively, Pennington and Smith (1983) contend thatthe performance of individuals with TS suggests diffusebrain injury, rather than injury specific to either the right orleft hemisphere. Increasingly, investigators are realizing thatchildren with TS are at greater risk for the development ofspecific neurocognitive deficit patterns (such as preservedverbal abilities and visuospatial weaknesses), but thesedeficits are not universal for all children with TS.
Developmental Course—The incidence of prematurity forchildren with TS (45,XO) is high, with more than 25%of the infants born 2 to 4 weeks early, and approximately
30% born more than 4 weeks before their due dates(Harris, 1995). The body length of the infant at birth isbelow average. Measures (blood assays) of gonadotropinsassist in diagnosing the disorder. In the female individual,gonadotropins are hormones that stimulate the functionsof the ovaries. The majority of children with TS are diag-nosed before school age.
During the preschool years, children with TS are de-scribed as immature, overactive, distractible, and havingdifficulty sustaining attention. With increasing age, activ-ity appears to slow, and many children with TS later be-come normally active or hypoactive. Young children with TS do not exhibit behavioral problems and are gen-erally accepted by and involved with peers. However, byschool age, the peer interactions of many children withTS lessen and involvement in solitary activities increases.Temperamentally, children affected with TS tend to becompliant, unassertive, and conforming in their interac-tions with caretakers and peers. Peer interactions, how-ever, continue to decline during the elementary and mid-dle school years, and many youngsters with TS reportfeelings of loneliness and alienation (Powell & Schulte,1999; Swillen et al., 1993). With the onset of adolescence,teenagers with TS date less frequently and are involved infewer romantic and sexual relationships than their peers.Some investigators suggest that they may not be profi-cient at reading social cues, which negatively affects theirefforts to relate to peers. Growth retardation, physicalanomalies (such as webbing of the neck), medical prob-lems, social difficulties, and an awareness of their sexualdifference likely contribute to diminished self-esteem
284 PART THREE | Disorders of the Brain
Dysfunctions of:
Arithmetic
Design copying
Directional sense
Extrapersonal space
Left–right discrimination
Maze performance
Mental rotation
Motor learning
Part–whole perception
Route finding
Spatial reasoning
Visual discrimination
Spatial workingmemory
Visual sequencing
Visual-motor integration
Visual memory
Source: Buchanan, L., Pavolic, J., & Rovet, J. (1998). A reexamination of the visuospa-tial deficit in Tuner syndrome: Contributions of working memory. Developmentalneuropsychology (pp. 341–367). Mahwah, NJ: Lawrence Erlbaum, by permission.)
Table 10.4 Visuospatial and VisuomotorDeficits Associated with Turner’s Syndrome

(Bender, Linden, & Robinson, 1994). In light of thesefactors, it is not surprising that teenagers with TS are atrisk for development of anxiety, insecurity, and depres-sion. Despite deficits in the visuospatial and visuomotorareas, most children affected by the disorder (90%) at-tend regular school programs, although they may need re-medial interventions. Moreover, because of the physicalproblems associated with the condition (see Table 10.3),individuals with TS often need ongoing medical moni-toring and services. On a more encouraging note, TS doesnot preclude the establishment of stable personal relation-ships, marriage, or gainful employment.
Treatment—It is essential that adolescents with TS receive es-trogen therapy because of their gonadal dysgenesis. With-out proper medical interventions, youngsters with the dis-order do not mature sexually, which can cause significantdistress. Furthermore, the short stature associated with TSoften requires growth hormone therapy. Psychological orcounseling services may be needed, because the risk forteasing and lack of peer acceptance appears high for chil-dren with TS (Powell & Schulte, 1999; Rovet, 1993). Chil-dren and adolescents with TS who demonstrate inatten-tion, impulsivity, and hyperactivity encounter significantdifficulties within the classroom. Specialized educationalinterventions and, in many cases, the introduction of psy-chostimulant medications may assist the student. In addi-tion, spatial, executive, and academic weaknesses (mathe-matics) must be addressed to ensure appropriate academicprogress. Chapter 11 explores additional educational rec-ommendations relevant to the needs of the child with TS(see the Nonverbal Learning Disability Syndrome section).
W i l l i a m s S y n d r o m e
WS is an intriguing and enigmatic disorder. The disorder ischaracterized by physical abnormalities and low intellectualfunctioning, yet presents an uneven cognitive profile of rel-atively preserved strengths and distinct weaknesses. Ourunderstanding of the disorder is rapidly increasing due tothe surge in significant research since the mid-1980s.
Background and Incidence—In 1961, Williams, Barratt-Boyes,and Lowe described a neurodevelopmental disorder charac-terized by unusual facial features, cardiovascular defect, hy-percalcemia, and mental retardation that subsequently wasdesignated as Williams syndrome (WS). The disorder isalso referred to as Williams–Beuren syndrome because ofthe contributions of Beuren and colleagues (1964) to theunderstanding of the medical features of WS. Advances ingenetics and molecular biology reveal that WS is associated
with a submicroscopic genetic deletion on chromosome 7(band q11.23). WS equally affects male and female indi-viduals and does not appear to be overly represented in anyspecific ethnic groups. The disorder is relatively rare andoccurs at an estimated incidence rate of 1 per 20,000 to50,000 live births (Dykens, 2003; Karmiloff-Smith, 1997).
Clinical Presentation—WS is a unique neurodevelopmentaldisorder characterized by a recognizable pattern of dys-morphic facial features, cardiovascular and physical ab-normalities, mental retardation, specific cognitive profile,and distinct personality.
Table 10.5 presents a number of the physical andmedical features associated with WS (Morris & Mervis,
CHAPTER 10 | Developmental Disorders of Childhood 285
Visual and Ocular Gastrointestinal Renal
Stellate or lacy iris Infant feeding Kidney structural
Hyperopia (farsighted)difficulties abnormalities
Abnormal binocular Colic Renal artery stenosis
vision Vomiting Recurrent bladder
Strabismus Failure to thriveinfections
ConstipationEnuresis
Auditory/Voice Chronic abdominal painUrinary frequency
Chronic otitis media Umbilical and inguinal
Sound hypersensitivity hernias Dental
(hyperacusis) Obesity (adult) Small, widely spaced
Hoarse, low pitchedteeth
MusculoskeletalMalocclusion
Enamel hypoplasiaCardiovascular Hyperextensible joints
Supravalvar pulmonic Muscle hypotonia
stenosis Nocturnal leg pains
Peripheral pulmonic Compensatory posturestenosis
Kyphosis, lordosis, Generalized arteriopathy and scoliosis
Hypertension Joint contractors
Stiff, awkward gait
Metabolism/Growth Muscle hypertonia (Adult)
Hypercalcemia
Precocious puberty
Short stature
Table 10.5 Physical and Medical ConditionsAssociated with Williams Syndrome

1999). The distinctive facial dysmorphia of the childwith WS (Figure 10.4) has been called “elfin” due to abroad brow, puffy eyes, a stellate or lacy iris pattern, asmall upturned nose, a broad nasal bridge, full cheeks, awide mouth, prominent lips and ears, and small, widelyspaced teeth. As the child ages, the face narrows, thenose tip broadens, and asymmetry of facial features iscommon.
Cardiovascular anomalies, particularly supravalvaraortic stenosis (SVAS), are common. SVAS refers to theabnormal narrowing of the walls of the aorta, potentiallyleading to cardiac pathology. Approximately 65% to 75%of children and adults with WS are afflicted with SVAS(Morris & Mervis, 1999). Although aortic stenosis is ofsignificant concern, other arterial systems (for example,renal) are also affected. Because of the generalized arteri-opathology associated with WS, ongoing medical moni-toring and treatment are warranted.
During infancy and childhood, the hypercalcemia (ex-cessive calcium in the blood) of WS contributes to feedingdisturbances, vomiting, failure to thrive, constipation, andchronic abdominal pain. Individuals with WS are highly sen-sitive to sounds (hyperacusis), and young children demon-strate an exaggerated startle response to noise (Hagerman,1999). Similarly, older individuals with WS are often awareof sounds that others fail to detect and complain that cer-tain sounds produce a sense of apprehension. Childrenwith WS are prone to distractibility and hyperactivity, and
the extent to which hyperacusis contributes to these dis-turbances remains unclear.
Young children with WS exhibit hypotonia, whereasolder children and adults have problems with hyperto-nia. Joint instability and joint contractures adversely af-fect fine- and gross-motor movements. Due to poor mus-cle tone and joint anomalies, children with WSdemonstrate delays in motor development; a stiff, awk-ward gait; and abnormal posture.
Genetic Defect and Williams Syndrome—The microdeletion ofchromosome 7q11.23 can be transmitted by either par-ent, and the resulting physical and cognitive features ofthe disorder vary depending on the size of the deletion(Morris & Mervis, 1999). Seventeen genes have beenidentified in the 7q11.23 region that potentially relate toWS. The specific genes deleted and size of the deletionsare believed to affect the particular constellation of fea-tures that can be exhibited by individuals with WS. Sev-eral of these 17 contiguous genes are associated with spe-cific features of the WS phenotype. Of these genes,deletion of the elastin (ELN) gene has received the great-est support as pathogenic to WS (Schultz, Grelotti, &Pober, 2001). ELN is an important connective tissue pro-tein found in the skin, ligaments, organ walls, and wallsof arteries. The ELN deletion is believed to account for anumber of the physical anomalies associated with WS (seeTable 10.5), particularly those related to the cardiovascu-lar system. Currently, the chromosomal test fluorescentin situ hybridization (FISH) is the primary tool for de-termining whether an individual is afflicted with WS.Using this technique, 97% to 100% of individuals withWS demonstrate the deletion of the ELN gene (Morris &Mervis, 1999).
The second identified gene, LIM-Kinase (LIMK1), isa protein kinase that appears important in axon guid-ance during brain development (Osborne & Pober,2001). It is hypothesized that deletion in the LIMK1gene is associated with the significant visuospatial andvisuospatial construction deficits demonstrated by indi-viduals with WS. A third implicated gene, syntaxin 1A(STX1A), is a protein found in the membrane of cells,particularly neurons, and is necessary for neurotransmit-ter release. Hyperactivity and other behavioral problemsof individuals with WS are hypothesized to relate to thedeletion of this gene. Finally, the deletion of three othergenes—GTF2I (general transcription factor 2-I),GTF2IRD1 (general transcription factor 2-I repeat do-main containing protein 1), and CYLN2 (cytoplasmiclinker 2)—may be associated with the mental retardationassociated with WS. GTF2I and GTF2IRD1 are believed
286 PART THREE | Disorders of the Brain
Figure 10.4 The distinctive facial features of a 7-year-oldchild with Williams syndrome (right) and her normally develop-ing 4-year-old sister (left). (Reproduced from Morris, C. A., &Mervis, C. B. [1999]. Williams syndrome. In S. Goldstein & C. R.Reynolds [Eds.], Handbook of neurodevelopmental and geneticdisorders in children [p. 558, Figure 24.2]. New York: Guilford Press,by permission.)

to be involved in the regulation of gene expression, andCYLN2 is thought to perform linkage functions withinthe neurons (Osborne & Pober, 2001). Notably, the dis-cussed linkage of individual gene deletions to the specificfeatures of WS awaits future research for verification.Likewise, little currently is known of the functions of theremaining genes located at 7q.11.23 with regard to theWS phenotype.
Anatomic Brain Anomalies—Neuroimaging studies (Reiss et al.,2000; Schultz, Grelotti, & Pober, 2001) have reported areduction in the overall brain volume of individuals withWS, although regional brain reductions were not uni-form, with preserved volume of the temporal-limbicstructures, cerebellum, and gray matter noted. Further-more, Reiss and associates (2000) found that the de-creased volume was primarily in the white matter, al-though there was significant loss of gray matter evident inthe right occipital lobe. There were also indications ofgreater posterior (occipitoparietal) than anterior volumeloss. These anatomic differences are consistent with thecognitive profile of relatively preserved language and im-paired visuospatial abilities demonstrated by individualswith WS.
Likewise, cytoarchitectonic studies of individuals withWS have shown abnormal auditory cell packing density andneuronal size in the temporal lobe (Brodmann’s area 41),suggesting hyperconnectivity of the auditory cortex (Galaburda & Bellugi, 2000; Holiger, McMenamin,Sherman, & Galaburda, 2001). This finding may be re-lated to the relatively spared auditory functions (lan-guage and music) and unusual reactions to auditorystimuli such as hyperacusis (Levitin, Cole, Chiles, Lai,Lincoln, & Bellugi, 2004).
Neuropsychological Profile—The neuropsychological profileassociated with WS includes a unique constellation ofabilities, skills, and interests. This profile includes intel-lectual impairment, relatively preserved language skills,increased attention to facial processing, visuoconstructiveskill weaknesses, significant interest and relative profi-ciency in music, and high levels of sociability.
General Intellectual Performance and Language Abilities—Individuals with WS frequently demonstrate mild-to-moderate mental retardation; there is appreciable variabil-ity in intellectual performance, with cognitive scoresranging from significantly below average to low average(Robinson, Mervis, & Robinson, 2003). Particular weak-nesses are often evident in higher order conceptual reason-ing and problem solving (Levitin et al., 2004). Generally,
measures of verbal intelligence reveal higher levels of func-tioning than measures of nonverbal intelligence, particu-larly if visuospatial abilities are assessed.
Language skills are consistently reported to be an areaof relative strength for individuals with WS. Particularverbal strengths are evident in vocabulary development,phonologic processing, auditory short-term memory, au-ditory working memory, and verbal fluency (Robinsonet al., 2003; Volterra, Caselli, Capirci, Tonucci, &Vicari, 2003). In the normal population, language andglobal intelligence are generally highly correlated witheach other. Yet, the language abilities of individuals withWS are often more advanced than would be predictedby their cognitive ability performance. Increasingly,however, research shows that certain aspects of the lan-guage development associated with WS are far from nor-mal. Specifically, anomalies in the development of se-mantics, complex syntax, grammar, pragmatic language(Laws & Bishop, 2004), and comprehension of nonlit-eral language (Sullivan, Winner, & Tager-Flusberg,2003) are evident. Furthermore, indications exist thatthe precursors of language, as well as formal language,develop later and in different ways in children with WSrelative to healthy children. For example, the precursorto naming objects is referential pointing; yet, Mervis andBertrand (1997) found that naming precedes referentialpointing for young children with WS. Moreover, jointattention, another precursor of normal language devel-opment, is significantly reduced in toddlers with WScompared with healthy peers of comparable mental andchronologic age (Karmiloff-Smith, Brown, Grice, & Paterson, 2003). The emergence of formal language inchildren with WS is delayed approximately 2 years ascontrasted with healthy children of a similar age (Morris& Mervis, 1999). Furthermore, the onset of novel two-word combinations is even more delayed, ranging from26 to 50 months of age. However, once languageemerges, it develops at an increasing rate, often morerapidly than in children with other neurodevelopmentaldisorders such as Down’s syndrome (Mervis & Robinson,2000). The language of adolescents and adults with WScontinues to be an area of relative strength, althoughlanguage attainment is not comparable with that ofhealthy adolescents and adults.
A number of studies have indicated that children withWS differ in the manner in which they acquire language.For example, a series of recent studies (Robinson, Mervis,& Robinson, 2003; Volerra et al., 2003) has determinedthat children with WS rely more heavily on auditoryworking memory and short-term phonologic memory inlanguage acquisition, particularly grammar, than typically
CHAPTER 10 | Developmental Disorders of Childhood 287
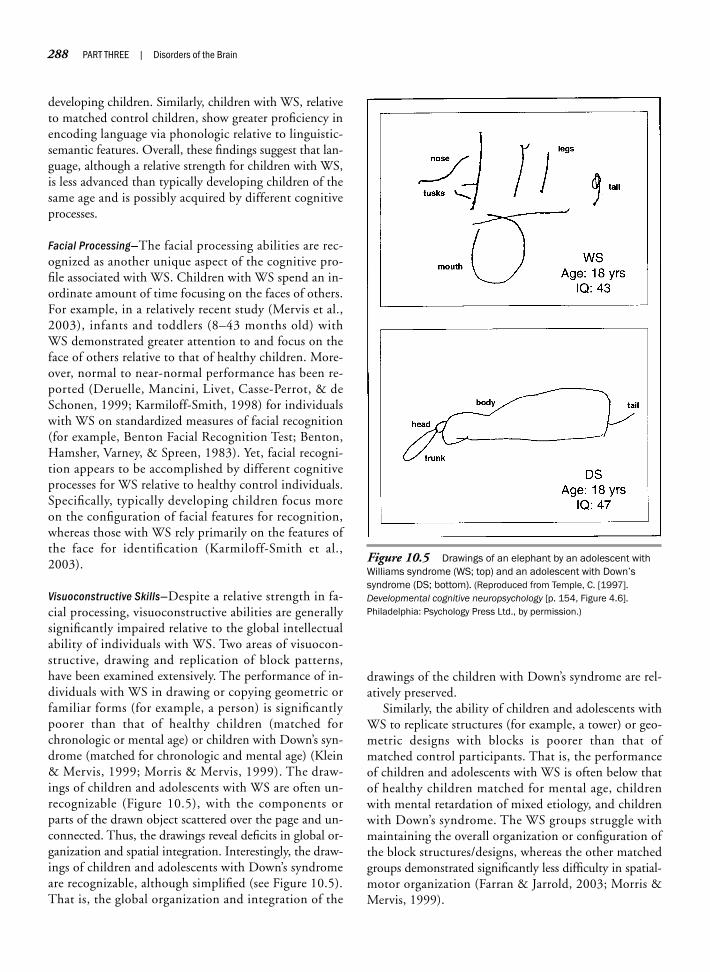
developing children. Similarly, children with WS, relativeto matched control children, show greater proficiency inencoding language via phonologic relative to linguistic-semantic features. Overall, these findings suggest that lan-guage, although a relative strength for children with WS,is less advanced than typically developing children of thesame age and is possibly acquired by different cognitiveprocesses.
Facial Processing—The facial processing abilities are rec-ognized as another unique aspect of the cognitive pro-file associated with WS. Children with WS spend an in-ordinate amount of time focusing on the faces of others.For example, in a relatively recent study (Mervis et al.,2003), infants and toddlers (8–43 months old) withWS demonstrated greater attention to and focus on theface of others relative to that of healthy children. More-over, normal to near-normal performance has been re-ported (Deruelle, Mancini, Livet, Casse-Perrot, & deSchonen, 1999; Karmiloff-Smith, 1998) for individualswith WS on standardized measures of facial recognition(for example, Benton Facial Recognition Test; Benton,Hamsher, Varney, & Spreen, 1983). Yet, facial recogni-tion appears to be accomplished by different cognitiveprocesses for WS relative to healthy control individuals.Specifically, typically developing children focus moreon the configuration of facial features for recognition,whereas those with WS rely primarily on the features ofthe face for identification (Karmiloff-Smith et al.,2003).
Visuoconstructive Skills—Despite a relative strength in fa-cial processing, visuoconstructive abilities are generallysignificantly impaired relative to the global intellectualability of individuals with WS. Two areas of visuocon-structive, drawing and replication of block patterns,have been examined extensively. The performance of in-dividuals with WS in drawing or copying geometric orfamiliar forms (for example, a person) is significantlypoorer than that of healthy children (matched forchronologic or mental age) or children with Down’s syn-drome (matched for chronologic and mental age) (Klein& Mervis, 1999; Morris & Mervis, 1999). The draw-ings of children and adolescents with WS are often un-recognizable (Figure 10.5), with the components orparts of the drawn object scattered over the page and un-connected. Thus, the drawings reveal deficits in global or-ganization and spatial integration. Interestingly, the draw-ings of children and adolescents with Down’s syndromeare recognizable, although simplified (see Figure 10.5).That is, the global organization and integration of the
drawings of the children with Down’s syndrome are rel-atively preserved.
Similarly, the ability of children and adolescents withWS to replicate structures (for example, a tower) or geo-metric designs with blocks is poorer than that ofmatched control participants. That is, the performanceof children and adolescents with WS is often below thatof healthy children matched for mental age, childrenwith mental retardation of mixed etiology, and childrenwith Down’s syndrome. The WS groups struggle withmaintaining the overall organization or configuration ofthe block structures/designs, whereas the other matchedgroups demonstrated significantly less difficulty in spatial-motor organization (Farran & Jarrold, 2003; Morris &Mervis, 1999).
288 PART THREE | Disorders of the Brain
Figure 10.5 Drawings of an elephant by an adolescent withWilliams syndrome (WS; top) and an adolescent with Down’ssyndrome (DS; bottom). (Reproduced from Temple, C. [1997]. Developmental cognitive neuropsychology [p. 154, Figure 4.6].Philadelphia: Psychology Press Ltd., by permission.)

Visuoconstructive tasks require that visuospatial infor-mation be processed and transmitted to the frontal sys-tem for action. Although the spatial deficits of WS havebeen associated with disturbances of the posterior regionsof the brain, the impact of the disorder on the executiveaction system and interconnecting pathways remains tobe elucidated. For example, Atkinson and associates(2003) presented a WS and a healthy control group ofchildren with three executive measures sensitive to the in-hibition of a prepotent response—holding in abeyance aresponse that is primed for release. The children with WS,in contrast with the healthy children, showed a dimin-ished ability to inhibit a prepotent spatially directed re-sponse. Yet, the two groups demonstrated comparableperformance related to inhibiting a pictorial-verbal (non-spatial) response. Although executive dysfunction is sug-gested, the basis of the deficit remains unanswered. As theauthors correctly conclude, the inhibitory deficit may re-late to a disturbance of the dorsolateral frontal region,parietal region, and/or interconnecting pathways of thetwo systems.
A potentially confounding factor in the studies of thevisuospatial processing of individuals with WS is pre-sented in Table 10.5. Children with WS frequently expe-rience visual sensory deficits such as binocular disorders,poor visual refraction, and decreased visual acuity. Thus,the visual sensory deficits associated with WS may ac-count for, or contribute to, poor visuoconstructive per-formance. To test this possible confound, Atkinson andcolleagues (2003) have investigated the relation of visualsensory deficits to visuospatial and visuoconstructive per-formance. Approximately 50% of the children and ado-lescents sampled for study exhibited some form of visualsensory deficit. The children and adolescents were admin-istered a battery of tests sensitive to visuospatial andvisuoconstructive abilities. The results demonstrated a neg-ligible relation between the occurrence of visual sensorydeficits and severity of spatial deficits. Accordingly, the vi-suospatial and visuoconstructive deficits associated withWS do not appear to relate to visual sensory impairments.
As discussed previously, individuals with WS demon-strate a local rather than global bias in face processing. Asimilar processing bias is proposed to account for, at leastin part, the visuoconstructive deficits associated with WS.However, Farran and Jarrold (2003), based on a review ofresearch of visual-perceptual and visuoconstructive per-formance of individuals with WS, conclude that individ-uals with WS are capable of global processing dependingon the nature of the task introduced. Specifically, individ-uals with WS show a global processing style on tasks ofvisual perception, but rely on a local processing approach
with tasks requiring visuoconstruction. That is, they relyon local processing when task performance involves themanipulation and construction of spatial elements. If theelements of the task are spatially invariant, and mental-motor manipulation is not required, they are able to use aglobal processing approach. Unfortunately, this interpre-tation does not account for the local preference of indi-viduals with WS in facial processing.
Dorsal versus Ventral Processing—Because of the significantdeficits in visuospatial relative to facial processing, neu-roscientists and neuropsychologists have sought to de-termine whether the disparity represents a dissociationbetween the ventral and dorsal streams of visual process-ing. The ventral stream (“what” processing; see Chapter 8)conveys visual object and face recognition to the tempo-ral lobes, whereas the dorsal stream (“where” processing)carries information to the parietal lobes necessary for theprocessing of spatial relations. Using tasks sensitive toventral and dorsal processing, investigations (Atkinsonet al., 1997, 2003) have shown that WS is generally as-sociated with deficits in dorsal relative to ventral pro-cessing, although a number children and adolescentswith WS show equally poor performance on both typesof tasks. Thus, there appears to be a subgroup of individ-uals with WS who demonstrate deficits in processing taskssupported by the dorsal stream, and another group whoshow deficits consistent with dorsal and ventral streamdisruption.
Recently, a National Institute of Mental Health(NIMH)–sponsored study (Meyer-Lindenberg et al.,2004) investigated the dorsal and ventral stream activa-tion of individuals with WS of normal intelligence. WSand control participants underwent neuroimaging (fMRIand MRI) while performing visual tasks requiring dorsalor ventral stream activation. The performance of the WSgroup with dorsal stream items showed isolated hypoacti-vation in the parietal portion of the dorsal stream. Controland WS participants did not differ in activation whenprocessing ventral stream items. Furthermore, structuralMRI revealed a reduction in gray matter volume in anarea immediately adjacent to the parieto-occipital intra-parietal sulcus for only the WS group (Figure 10.6).Analysis determined that the hypoactivation of the dorsalstream could be attributed to impaired input from thisisolated region. Clearly, the findings of the neuroimagingstudy are consistent with the deficits of individuals withWS on measures of visuospatial processing.
Musicality and Williams Syndrome—WS is associated with en-hanced interest, involvement, and proficiency in music.
CHAPTER 10 | Developmental Disorders of Childhood 289

Those with WS are as proficient at reproducing music,show comparable levels of achievement in music, and spon-taneously produce rhythmic sequences as often as typicallydeveloping individuals of the same age. Furthermore, indi-viduals with WS are more musical than Down’s syndromeand autistic individuals. Specifically, individuals with WSspend more time listening to music, show more interest inmusic-related activities, are more accurate in their repro-ductions of music, and play original music and rhythmsmore frequently those with other neurodevelopmentaldisorders (such as Down’s syndrome and autism). Fur-thermore, individuals with WS demonstrate a greateremotional response to music than other groups. For ex-ample, one child with WS began to weep with she hearda couple of notes played at a Mozart concert. The girl’s re-action was so strong that she had to leave the concert.When she tried to return, she once again began to weep.She later noted, “There are two kinds of Mozart: the kindthat hurts and the kind that does not hurt” (Levitin et al.,2004, p. 238).
Sociability and Emotionality—Children and adolescents withWS are characterized as highly sociable, interpersonallysensitive, and empathetic. They tend to be overly happyand friendly, yet are also prone to irritability (which ap-pears to abate with age) and moodiness. They are knownto approach and speak indiscriminately with others and
to be excitable, restless, and inattentive. In addition,they experience high levels of anxiety, worry, fearfulness,and somatic complaints. They are significantly moreanxious than children with other neurodevelopmentaldisorders (for example, Down’s syndrome) (Morris &Mervis, 1999), mental retardation of mixed etiology,and healthy developing children (Dykens, 2003). Although they are proficient at understanding the feel-ings of others, they find it difficult to recognize theirown fears (Lai, 1998). Interestingly, in contrast withhealthy children, they do not show an age-related reduc-tion in their fears.
Despite their social interest and affability, childrenand adolescents with WS are not fully accepted by peersbecause of their indiscriminate approach to others, im-maturity, and communication differences. The basis oftheir overfriendliness and sociability is unclear, but it isbelieved that their extreme focus on the faces of othersmay play a role in shaping these characteristics (Merviset al., 2003). In a recent study (Meyer-Lindenberg et al.,2005), the amygdala activation of individuals with WSand healthy control participants was investigated. Theparticipants underwent fMRI while processing facesportraying threatening feelings (anger and fear) andthreatening scenes (for example, burning building). Theamygdala is implicated in the support of a number ofemotion-related functions, including the monitoring ofenvironmental events for danger. For healthy controlparticipants, the amygdala showed greater activationwhen processing threatening faces than threateningscenes. The participants with WS showed the oppositepattern of greater activation for threatening scenes rela-tive to faces. The investigators hypothesize that the un-deractivation of the amygdala to threatening faces mayaccount for the diminished fear of strangers and socialdisinhibition demonstrated by individuals with WS.That is, the decreased activation may indicate an atten-uation of normal social fear or apprehension. In con-trast, the greater activation of the amygdala to threaten-ing scenes may underpin their high rates of nonsocialanxiety, worry, and fears.
Treatment—The first few months of the infant’s life can bequite trying for the parents and the infant. Infants withWS often feed poorly, vomit frequently, experience reflux,and fail to thrive. Hypercalcemia contributes to these gas-trointestinal disturbances, requiring medical attentionand dietary restrictions. When a child is identified withWS, a comprehensive examination should be undertakendue to the increased probability of medical complications,particularly cardiovascular disease.
290 PART THREE | Disorders of the Brain
Figure 10.6 A three-dimensional magnetic resonance imagerendering of the white matter of individuals with Williams syn-drome. A small anomaly (A) of the occipitoparietal region that maydisrupt the “downstream” activation of the “where” dorsalstream. The regional activation of the dorsal stream is evident invisuospatial processing of location (B) and construction (C). Drepresents regional overlap. (Karen Berman, M.D./NIMH.)
A
B
C D

Motor delays, muscle weakness, and hip contracturesbecome increasingly evident as the child moves into his orher toddler/preschool years. Orthopedic and physical/oc-cupational services are often needed to address these prob-lems. Although verbal skills are an area of relative strengthfor children with WS, the precursors to formal language,and the emergence of formal language itself, are delayed ordisturbed, warranting speech and language interventions.
The hyperacusis associated with WS may be a signifi-cant problem for the child. Accordingly, environmentalmodifications to reduce or alleviate the occurrence of loudand disturbing noises are needed. For example, the childmight be removed from the classroom in advance of a firedrill and placed in a room where the sound of the firealarm is muffled or be allowed to use ear plugs or earphones. Interestingly, as discussed earlier, individuals withWS often enjoy and show relative proficiency in the areaof music (Hopyan, Dennis, Weksberg, & Cytrynbaum,2001).
During the preschool and elementary school years, thechild often warrants special or remedial educational ser-vices because of general cognitive delays. These childrenfrequently demonstrate greater success in reading andspelling relative to math and handwriting. The academicinterventions used for children with nonverbal learningdisability syndrome (see Treatment of Nonverbal LearningDisability Syndrome in Chapter 11) are generally recom-mended for children or adolescents with WS (Hagerman,1999). Behavioral modification techniques and psychos-timulant medication may be warranted to address poorattentional focus, distractibility, and impulsivity. Socialskills training is important to facilitate social acceptanceby peers because of their overfriendliness and indiscrimi-nate approaching of others. The child or adolescent mayneed to learn verbal self-protective skills to cope with teas-ing or abuse by peers.
As discussed earlier, individuals with WS often experi-ence disruptive anxiety, depression, and other psychiatricissues. They can profit from psychotherapy due, in part,to their verbal strengths. Often, medications addressinganxiety or depression are needed to augment treatment;however, careful monitoring by medical professionals isimperative for those individuals with cardiovascular dis-ease or other significant medical issues.
A C Q U I R E D D I S O R D E R S
The number of agents, events, and processes that can po-tentially injure the prenatal and postnatal brain is stagger-ing. Environmental toxins, radiation, infections, anoxia,malnutrition, tumors, and traumatic head injuries can
result in anomalies of the developing brain. Of theseagents, traumatic head injuries, such as concussions, lac-erations, and contusions, are the cause of most braindamage in children and adolescents. Regardless of thenature of the insult, a one-to-one relation between braindisturbance and behavior is not evident. The predictionof functional outcomes is contingent on a host of factorsincluding: (1) age at which the lesion is incurred; (2) type,severity, and status (static or progressive) of the lesion; (3)premorbid personality and intelligence of the child; (4)quality and timeliness of medical attention; and (5) acces-sibility of acute and long-term services.
FAS is a specific condition that reflects the devastatingeffects of prenatal exposure to alcohol. Initially, it was sus-pected that impairments associated with FAS were re-stricted to mothers who chronically abused alcohol orwere “binge” drinkers. Increasingly, it is being realizedthat the prenatal embryo/fetus is at risk even with socialdrinking.
F e t a l A l c o h o l S y n d r o m e
Clinical Features—Fetal alcohol syndrome (FAS) is a long-lasting and debilitating disorder recognized in the medicaland neuropsychological fields since the early 1970s.Lemoine, Harrowsseau, Borteryu, and Menuet (1968) arecredited with being the first to describe the effects of alco-hol on a group of children with alcoholic parents. Jones,Smith, Ulleland, and Streissguth (1973) later identified theanomalies and characteristics that have come to define FAS.
Children with FAS frequently exhibit intrauterinegrowth retardation; characteristic facial features of widelyspaced eyes, shortened length of eyelids, elongated midface,flattened nose, underdeveloped upper lip (Figure 10.7), anddeficits associated with central nervous system involve-ment (Streissguth, 1997). Central nervous system deficitsinclude microcephaly (abnormally small head), infantileirritability, seizures, tremors, poor coordination, poor ha-bituation (difficulty in tuning out repeating stimuli), andreduced muscle tone. In addition, below-average intelli-gence, inattention, hyperactivity, learning disabilities, andpoor behavioral regulation commonly characterize chil-dren with FAS (Mattson, Riley, Gramling, Delis, & Jones,1998; Kerns, Don, Mateer, & Streissguth, 1997). AlthoughFAS is one of the most well-known causes of mental re-tardation, not all children affected with it are retarded.Table 10.6 presents frequently identified physical andmedical characteristics associated with FAS.
Children who are exposed to alcohol in utero, but whofail to exhibit growth deficits or other physical abnormali-ties of FAS, may still show functional impairments similar
CHAPTER 10 | Developmental Disorders of Childhood 291

to those of FAS. That is, the exposed children may mani-fest sensory and sensorimotor impairments, speech andlanguage delays, cognitive and learning weaknesses, andregulatory deficits such as inattention, impulsivity, andhyperactivity (Jacobson, Jacobson, Sokol, Martier, &Ager, 1993). These features are called fetal alcohol ef-fects (FAE) or alcohol-related neurodevelopmental dis-abilities (ARND).
Incidence—Estimates of the incidence rate of FAS in the gen-eral population range from 1 to 3 per 1000 live births. Re-searchers consider the incidence significantly higher, possi-bly two to three times greater, if children with FAE areincluded (Streissguth & Connor, 2001). The incidences ofFAS and FAE among alcoholic mothers (chronic users) aremarkedly greater, with estimates of 25 per 1000 and 90 per1000, respectively (Jenkins & Culbertson, 1996).
Neuropathogenesis—FAS is a consequence of alcohol use bythe pregnant mother during the baby’s prenatal develop-ment. The relation of the teratogenic effects of prenatalalcohol exposure to intake (amount, frequency, anddrinking patterns), period of brain development, and ma-ternal health/lifestyle variables during pregnancy remainspoorly understood.
The teratogenic effects of alcohol, as revealed in ani-mal and human studies, suggest a continuum of negativeeffects determined, in part, by a dose–response relation,that is, increasing amount and frequency of alcohol inges-tion correlates with greater injurious effects (Korkman,
292 PART THREE | Disorders of the Brain
Figure 10.7 The facial features of the developing FAS child (a–c): Unique features arethe widely spaced eyes, shortened length of eyelids, low nasal bridge, short and flattenednose, elongated midface, and thin upper lip. ([a, b] Reproduced from Hanson, J. W., Jones, K. L., & Smith, D. W. [1976]. Fetal alcohol syndrome: Experience with 41 patients. Journal of theAmerican Medical Association, 235[14], 1459, by permission of the American Medical Associa-tion; [c] reproduced from Streissguth, A. [1997]. Fetal alcohol syndrome [p. 53]. Baltimore: PaulBrookes, by permission.)
Kettunen, & Autti-Rämö, 2003). The children of moth-ers who consumed relatively low levels of alcohol are lesslikely to exhibit either physical or structural stigmata, butthey may still experience behavioral disturbances, socialmaladjustment, and cognitive deficits (Mattson et al.,1998). At the most severe end of the continuum, charac-terized by excessive alcohol abuse, there is a significantlygreater risk for the development of the full-blown FAS.
Although the risk to the developing embryo/fetus ismuch greater for pregnant mothers who chronically abusealcohol or frequently “binge” (multiple drinks consumedin a relatively short period), the point in brain gestationthat alcohol is introduced appears to have a differentiallydamaging impact. Alcohol exposure appears to causegreater damage to the developing brain during the earlymonths of gestation (first trimester). However, the great-est disruption occurs when the exposure spans the entirepregnancy (Carmichael Olson et al., 1997). There are in-dications that the introduction of alcohol during the stageof brain neurogenesis (weeks 6–18th week) may disturbcortical cell migration, resulting in global cognitivedeficits, whereas later prenatal exposure produces cogni-tive deficits that are more circumscribed in nature. Fra-ternal twin studies suggest that genetic factors may play arole in determining the vulnerability of the embryo/fetusto FAS. That is, maternal alcohol use can significantlyaffect one twin more than the other twin, despite theirsharing the same prenatal environment. Other factors,such as the mother’s health, psychiatric status, andlifestyle (for example, cigarette smoking and abuse of

CHAPTER 10 | Developmental Disorders of Childhood 293
other substances) and how efficiently she metabolizes al-cohol appear related to the risk for development ofFAS/FEA (Streissguth & Connor, 2001).
An often neglected but important factor mediating thephenotypic expression of FAS/FEA is the postnatal socialenvironment (particularly the home) of the child. TheFAS/FEA child is often raised by a mother who is copingwith the stresses of alcoholism and the demands of parent-ing a child. Children of alcoholics are subject to high levelsof neglect, abuse, inconsistent parenting, and out-of-homeplacements. The extent to which adverse environmentalevents shape and exacerbate the cognitive-emotional-
behavioral disturbances of the child with FAS/FEA remainspoorly understood (Streissguth & Connor, 2001).
Originally, researchers thought more severe neuropsy-chological deficits were specific to FAS. However, increas-ing evidence indicates that children, adolescents, andadults with FAE can display comparable functional deficits(Connor, Sampson, Bookstein, Barr, & Streissguth, 2000;Korkman et al., 2003). In one study (Mattson et al., 1998),for example, children with FAS and FAE underwent a com-prehensive neuropsychological evaluation. The assessmentresults showed that both groups, relative to healthy controlchildren, demonstrated impairment in language skills, ver-bal learning and memory, academic performance, fine-motor speed, and visuomotor integration skills. Of signifi-cance was the finding that children with FAE showed apattern of deficits comparable with those of FAS children,except in the areas of visuomotor integration and nonver-bal concept formation. In a more recent study of adultswith FAS and FEA (Connor et al., 2000), both the FASand FEA groups were found to be significantly impairedon a number of measures of executive function. Thus, indi-viduals with a history of prenatal alcohol exposure are likelyto demonstrate significant neuropsychological deficits, eventhough they appear physically normal.
Investigators have identified a number of neu-roanatomic alterations in the brains of FAS/FEA childrenthat reflect the destructive impact of alcohol on the devel-oping brain. Specifically, children with the disorder pres-ent with dysgenesis or agenesis of the corpus callosum,hippocampal damage, reduced basal ganglia volume, cere-bellar anomalies, expanded ventricles, and reduction in whitematter (Archibald, Mateer, & Kerns, 2001; Kaemingk & Paquette, 1999; Streissguth & Connor, 2001). The highproportion of FAS children with microcephaly indicatesthat brain size is reduced. Wass and colleagues (2001) stud-ied living fetuses exposed to alcohol with ultrasoundsonography and identified a reduction in size of the frontalcortex. Executive dysfunctions (Kaemingk & Paquette,1999) consistent with disturbances of the frontal circuitryhave been identified. Similarly, studies of animals exposedto prenatal alcohol report a wide range of brain anomalies,including reduction in brain weight and volume, andstructural disturbances or loss of neurons, dendritic spines,and subcortical and cortical white matter circuitry (Chen,Maier, Parnell, & West, 2004).
Neuropsychological Assessment—Children with FAS/FEA ex-hibit a broad spectrum of neuropsychological deficits. Inaddition to mental retardation, common FAS/FEAdeficits are evident in attentional regulation, response in-hibition, complex problem solving, spatial and object
Growth
Decreased fat tissue
Prenatal and postnatal growthdeficiency
Cardiac
Atrial septal defect (defect in thewall between the atria)
Ventricular septal defect (defect ofwall between the ventricles)
Craniofacial
Abnormally small jaw in adoles-cence
Microcephaly (abnormally smallhead)
Ptosis (droopy eyelid)
Short upturned nose
Shortened eyelid length
Underdeveloped lip features
Underdeveloped upper jaw
Skeletal
Altered palm crease patterns
Cervical spine abnormalities
Foot position defects
Joint alterations
Skeletal (continued)
Pectus excavatum (abnormallydepressed sternum)
Tapering terminal fingers, deformi-ties of finger/toenails
Union of the radius and ulnar bones
Other
Abnormal thoracic cage
Abnormally small eyes
Anomaly of the sex organs
Cleft lip and/or cleft palate
Dental malocclusion
Epicanthal folds
Excessive hair in infancy
Hearing loss, protuberant ears
Hernias of diaphragm, umbilicus, orgroin
Myopia, strabismus (cross-eyes)
Renal deformity
Small teeth with faulty enamel
Strawberry hemangiomata (blood-filled birthmarks or benign tumorsof small blood vessels)
Source: Harris, J. C. (1995). Developmental neuropsychiatry, vol. II: Assessment,diagnosis, and treatment of developmental disorders (p. 362, Table 12.1-1). New York:Oxford University Press, by permission.)
Table 10.6 Physical and Medical ConditionsAssociated with Fetal Alcohol Syndrome

memory, language skills, verbal learning and memory,speed of information processing, consistency of task per-formance, cognitive flexibility, planning, and academicperformance (Korkman, Kirk, & Kemp, 1998; Mattson,Riley, Delis, Stern, & Jones, 1996; Streissguth, Barr,Bookstein, Sampson, & Carmichael Olson, 1999). Fur-thermore, the array of deficits that accompany FAS/FEAoften exceeds what would be predicted based on level ofintelligence, suggesting that limited cognitive ability isnot the sole basis for these impairments (Kerns et al.,1997). Thus, multiple cognitive domains of functioningare vulnerable to in utero alcohol exposure including in-tellect, language, learning and memory, and executivefunctions (Lee, Mattson, & Riley, 2004).
Interestingly, the ratings of parents and teachers sug-gest that the primary behavioral difficulties of childrenwith FAS/FEA relate to attention deficits and social prob-lems (Streissguth & Connor, 2001). Empirical supportfor the observations of parents and teachers regarding thepoor attentional regulation associated with FAS/FEA isgrowing (Lee, Mattson, & Riley, 2004; Mattson, Lang, &Calarco, 2002). Moreover, there are indications that poorattention may be a more sensitive marker of prenatal al-cohol exposure than either low global intelligence or fa-cial stigmata (Mattson & Riley, 2000).
The myriad of behavioral, adaptive, and neuropsycho-logical characteristics of the child with FAS/FEA signalsthe need for a multidisciplinary approach to assessment.Clearly, a comprehensive neuropsychological evaluation isneeded to identify and interpret the cognitive, behavioral,and adaptive dysfunctions that characterize the child. Be-cause of the increased risk for cardiac, skeletal, and otherphysical conditions (see Table 10.6), a medical consulta-tion is certainly warranted. Finally, contingent on the child’spresenting issues, the evaluative services of a speech and lan-guage pathologist, educational specialist, social worker, andoccupational/physical therapist may be warranted.
Developmental Course—Longitudinal studies (Streissguth,1997) have revealed that the cognitive, behavioral, andadaptive deficits of FAS/FEA children do not fully resolvewith age. Thus, the negative effects of intrauterine expo-sure to alcohol generally endure. Infants with FAS/FEAoften present with low birth weight, feeding and sleep dis-turbances, poor habituation, and high levels of irritability(Jenkins & Culbertson, 1996). By 4 years of age, deficitsappear in gross- and fine-motor skills, attention, memory,academic achievement, and reaction time. In addition,enuresis (age-inappropriate bedwetting) and communi-cation disorders are quite frequent. By elementary schoolage, attention-deficit/hyperactivity disorder (ADHD)
symptoms of inattention, impulsivity, and hyperactivity,coupled with poor organization, communication deficits,behavioral problems, and disturbances of basic functions(sleeping, eating, and elimination) disrupt the adaptive ef-forts of FAS children (Steinhausen, Willms, & Spohr, 1993).Cognitive deficits, microcephaly, small physical stature, andpoor socialization skills often interfere with peer acceptance.Children affected by FAS/FEA with significant intellectualand learning deficits are often identified in their preschoolor elementary years and provided with early special educa-tion services.
With the advent of adolescence, communication dis-orders and disturbances of basic functions decline, al-though other cognitive and behavioral deficits persist. Re-ports that teenagers with FAS/FEA tend to manifest highrates of antisocial behaviors and substance abuse are ofconsiderable concern. Unfortunately, the multiple cogni-tive, behavioral, and adaptive deficits of FAS/FEA appearto continue into adulthood.
Treatment—It goes without saying that the best form oftreatment for an acquired disorder is prevention. Avoid-ing or significantly reducing alcohol consumption duringpregnancy eliminates or reduces the risk for FAS/FEA tothe unborn child. Although public awareness discouragesmany mothers from drinking during pregnancy, the alco-holic mother is of special concern. The physician, or otherpersonnel who encounter a pregnant women who abusesalcohol, should immediately apprise her of the risk to thefetus. In addition, the mother should be informed thatemerging research indicates that children of mothers whoappreciably reduce or cease drinking during the first orsecond trimester are at a reduced risk for development ofFEA/FAS (Korkman et al., 2003). A referral to persons oragencies that can assist the mother in altering her drink-ing behavior is a priority. Furthermore, the finding thatFAS/FEA children often experience high levels of neglect,abuse, inconsistent parenting, and out-of-home place-ments should prompt an assessment of the family’s needfor therapeutic, social, and economic assistance.
Children with FAS/FEA who are mentally retardedgenerally require specialized educational services eitherwithin the public schools or in a residential setting, de-pending on the severity of retardation and particular learn-ing needs of the child. Higher functioning children af-fected by FAS/FEA, despite average or above-averageintelligence, may also need supplemental or specialized ed-ucational services due to specific cognitive and achieve-ment weaknesses (Kerns et al., 1997). Furthermore, chil-dren with FAS/FEA with communication deficits shouldhave appropriate speech and language therapy. Behavioral
294 PART THREE | Disorders of the Brain
Phenylketonuria (PKU)
TeratogensAgenesisDysgenesisPolymicrogyriaPorencephalyKennard principleAnencephalyHydranencephalyHydrocephalus (HC)Spina bifidaIntraventricular hemorrhage
(IVH)
Obstructive ornoncommunicatinghydrocephalus
Nonobstructive orcommunicatinghydrocephalus
Shunt“Cocktail party syndrome” (CPS)UltrasonographySingle-gene disordersChromosomal disordersParental imprinting disordersMolecular cytogenic anomaliesAutosomes
Sex chromosomesCubitus valgusTurner’s syndrome (TS)KaryotypeVestigial ovarian streaksIsochromosomeMosaic karyotypesInhibitory controlGonadotropinsWilliams syndrome (WS)Supravalvar aortic stenosis
(SVAS)HypercalcemiaHyperacusis
HypotoniaHypertoniaJoint contracturesElastinFluorescent in situ hybridization
(FISH)Down’s syndromeFetal alcohol syndrome (FAS)MicrocephalyFetal alcohol effects (FAE) or
alcohol-relatedneurodevelopmentaldisabilities (ARND)
Enuresis
management systems are often needed within the homeand school, particularly if the child also displays symp-toms of ADHD. Medications can be introduced to helpregulate the child’s ADHD, particularly if the symptomsof inattention, impulsivity, and hyperactivity significantly
disrupt the child’s learning, family, and peer relationships.Social skills training may help improve peer acceptance.The aforementioned interventions must be continuedinto adolescence and modified in accordance with thechanging learning and behavioral needs of the teenager.
CHAPTER 10 | Developmental Disorders of Childhood 295
SummaryThe developing brain is vulnerable to a myriad of insults that can lead to damage and dysfunction. Yet, adegree of plasticity allows limited compensation, or return of function, after cerebral insults. However, thedynamics of this recovery process remain poorly understood. The clinical presentation, neuropathogenesis,neuropsychological assessment, and treatment of HC, TS, WS, and FAS illustrate the complex brain–behavior relations that define each of these neurodevelopmental disorders.
C r i t i c a l T h i n k i n g Q u e s t i o n s
In light of the devastating effects of many of the genetic and chromosomal disorders, do you think that potential parentsshould seek genetic counseling before having children? Explain.In recent years, an increasing number of teratogens have been identified in the environment. Are our children at greaterrisk for brain anomalies than children of earlier generations? Why or why not?What steps can be taken to prevent FAS?What do the neuropsychological profiles associated with TS and WS tell us about the organization of the brain?
K e y Te r m s
We b C o n n e c t i o n s
http://www.patientcenters.com/hydrocephalusHydrocephalus Center—provides information about hydrocephalus and its treatment.
http://gslc.genetics.utah.edu/units/disorders/karyotypeGenetic Science Center at the University of Utah—presents karyotypes for a number of genetic disordersincluding TS and WS.

http://www.turner-syndrome-us.orgTurner’s Syndrome Society of the United States—facts and information on TS.
http://www.williams-syndrome.orgWilliams Syndrome Association—provides information on the identification and treatment of individuals with WS.
http://www.nofas.orgNational Organization of Fetal Alcohol Syndrome—page dedicated to raising the public awareness of FAS;includes definition and strategies for working with children with FAS.
296 PART THREE | Disorders of the Brain

Chapter 11
LEARNING AND NEUROPSYCHIATRICDISORDERS OF CHILDHOOD
Youth, even in its sorrow, always has a brilliancy of its own.—Victor Hugo, Les Miserables (1862)
Learning DisabilitiesPervasive Developmental DisordersDisruptive Behavioral DisordersTic Disorders
Neuropsychology in Action
11.1 Genetics of Learning Disabilities11.2 Case Study of an Adolescent with Asperger’s
Syndrome11.3 Case Study of a Child with an
Attention-Deficit/Hyperactivity Disorder

OverviewThis chapter discusses learning, pervasive developmental, disruptive behavioral, and tic disorders of child-hood. These four classes of disorders can significantly disrupt a child’s developmental progression andadaption and often coexist with other conditions that further compromise the child’s functioning. Althoughthe pervasive developmental disorders occur less frequently, the impact of these conditions is profound,generally precluding self-sufficiency and independence and necessitating lifelong supervision.
The developmental disorders reviewed in Chapter 10 are often considered biological rather than psy-chological in origin because prominent anatomic brain defects and physical anomalies often accompanythe disorders. Moreover, the cause of these disorders is generally traceable to genetic/chromosomal de-fects or prenatal disruption. In contrast, the causes of childhood learning and neuropsychiatric disordersare not as easily linked to congenital anomalies. Accordingly, theorists have often proposed psychologicalfactors as determinants of these disorders. However, ongoing research and advances in neuroimaging areproviding evidence that brain disturbances may, in fact, play a prominent role in the etiology of both learningand neuropsychiatric disorders.
This chapter examines, in detail, specific disorders that represent learning, pervasive developmental,disruptive behavioral, and tic disorders. The first disorder, dyslexia, has received considerable attentionbecause of the importance of reading skills in our technologically advanced society. The second disorder,nonverbal learning disability syndrome (NVLD), reflects a major contribution of neuropsychology to the studyof learning disabilities. Byron Rourke (1989), through his extensive research, has identified a specific pat-tern of neurocognitive assets and deficits that differentiates the NVLD from reading disabilities. The thirddisorder, autism, is a pervasive developmental disorder that has attracted a voluminous body of research.Despite this research, the cause and brain–behavior relations of autism remain poorly understood. We thenreview attention-deficit/hyperactivity disorder (ADHD), one of the most prevalent childhood disruptive behav-ioral disorders, comprising about 50% of the population of child psychiatric clinics (Cantwell, 1996). Similarto autism, ADHD is the focus of considerable research that transverses diverse fields of study. Neuropsy-chology and related fields have identified a number of brain–behavior relations of ADHD that are enhancingour understanding of the pathogenesis of this disorder. Finally, we examine Gilles de la Tourette disorder, a childhood tic disorder, that waxes and wanes in severity and presentation over time.
7% and 15% of the school population (Gaddes & Edgell,1993) and are one of the largest childhood groups referredfor neuropsychological services (Culbertson & Edmonds,1996). Controversy persists regarding the definition, diag-nosis, etiology, and remediation of learning disabilities.
298 PART THREE | Disorders of the Brain
K e e p i n M i n d
What are the specific neurocognitive assets and deficits of children with verbal and nonverbal learning disabilities?
Can a nonverbal learning disability directly disrupt a child’s socioemotional adjustment?
Is Asperger’s syndrome a separate disorder, or merely high-functioning autism?
What treatment interventions are effective for children with attention-deficit/hyperactivity disorder (ADHD)?
Why is there such a high rate of comorbidity among ADHD, Gilles de la Tourette’s syndrome, and obsessive-compulsivedisorder?
Learning Disabilities
Learning disabilities adversely affect the ability of thechild to communicate and meet the challenges of educa-tion. Children with learning disabilities constitute between

Generally, professionals define learning disabilities asimpairments of one or more academic skills that cannot beaccounted for by sensory or motor deficits; mental retarda-tion; emotional disturbance; or environmental, cultural, oreconomic disadvantage (Hooper, Willis, & Stone, 1996).Common learning disabilities involve impairment ofreading (dyslexia), arithmetic (dyscalculia), and writtenexpression (dysgraphia).
Verbal learning disabilities, such as dyslexia, have re-ceived significantly more research and theoretical attentionthan the NVLD, which focuses on deficits in mathematics.We discuss dyslexia to help clarify, by contrast, the NVLD.An expanded coverage of the NVLD follows. This empha-sis acknowledges the greater disruptiveness of the NVLDto the child and the availability of a specific neuropsycho-logical model to guide identification and treatment of thedisorder (James & Selz, 1997).
V E R B A L L E A R N I N G D I S A B I L I T Y : D Y S L E X I A
Dyslexia may be acquired by insult to a previously nor-mal functioning brain or be developmental in origin.With acquired dyslexia (often referred to as alexia), thepatient, before brain insult, possessed reading skills. How-ever, after the insult, this ability is partially or fully lost.
In contrast, developmental dyslexia characterizes a lim-itation in the ability to acquire reading skills. Historically,the diagnosis of dyslexia has involved evidence of a signif-icant discrepancy between the child’s current readingachievement and grade level or intelligence. The discrep-ancy models that contrast reading to grade level or intelli-gence are currently under challenge, and alternative crite-ria for classification are being proposed (Siegel, 2003; Vanden Broeck, 2002).
Dyslexia is a prevalent disorder, as evident in the findingthat approximately 4% to 9% of school-age children are af-fected, with boys outnumbering girls 3 to 2 (Culbertson &Edmonds, 1996; Pliszka, 2003; Rumsey, 1996a). Similarto other developmental disorders, dyslexia tends to run infamilies, suggesting a genetic etiology. As Bruce Penning-ton reports in his discussion of the genetics of learningdisabilities (Neuropsychology in Action 11.1), a childwith parents affected with dyslexia is eight times morelikely to exhibit the disorder than children of parents whoare not reading disabled.
V i s u a l P r o c e s s i n g M o d e l o f D y s l e x i a
Despite a long history of research and investigation, thestudy of dyslexia continues to be fraught with divergentdiagnostic criteria, putative classifications, and a myriad
of theoretical explanations. However, a review of the re-search and theoretical models demonstrates increasingconvergence on two basic subtypes. The first subtype en-compasses children with significant reading deficitscaused by possible visual and visual-perceptual anomalies,whereas the second relates to children whose reading im-pairment stems from auditory-language dysfunction. Re-flecting this division are two forms of dyslexia: “surface”and “deep.” Surface dyslexia refers to impaired whole-word reading and an unimpaired ability to sound outwords, whereas deep dyslexia involves intact whole-wordreading and impaired ability to sound out words. The for-mer suggests an impairment of orthographic skills, andthe latter, an impairment of phonologic skills.
In studies of the visual domain, researchers have exam-ined eye movements and speed of visual processing (Eden,Stein, Wood, & Wood, 1995; Stein, 2001). Specifically,reading-disabled children and adults show slower flickerfusion rates when presented images of low spatial densityand contrast (brightness). Flicker fusion rate is the speedat which two separate visual images fuse into a singleimage when rapidly presented. The magnocellular visualsystem controls the processing of this form of visual input,prompting the magnocellular-deficit theory of dyslexia.
The magnocellular-deficit theory centers on the twovisual pathways of the human visual system, namely, themagnocellular and parvocellular pathways. Each of thesepathways processes information from the retina and, inturn, transfers the information to the visual cortex for fur-ther processing (Figure 11.1). The magnocellular visualsystem consists of large cells that are located in the infe-rior region of the lateral geniculate bodies and are highlysensitive to movement, rapid stimulus change, low con-trast, and spatial location. The parvocellular visual sys-tem involves smaller cells that are located dorsally in thelateral geniculate bodies and are responsive to stationaryobjects, color, high contrast, and fine spatial details (Birch& Chase, 2004; Skottun & Parke, 1999). The former sys-tem is activated during rapid saccadic eye movements,whereas the latter system is stimulated during eye fixationand is involved extensively in discriminating and identify-ing printed/written symbols. In reading, the individualmakes a series of brief fixations, separated by saccadic eyemovements. Neuroscientists hypothesize that the magno-cellular visual system inhibits the parvocellular system atthe time of each saccade, ensuring that the previous eyefixation image is terminated. In dyslexia, the magnocellu-lar visual system may fail to appropriately inhibit the par-vocellular system, resulting in a prolonged afterimage thatinterferes with reading; that is, letters seen in one fixationblur into the next fixation.
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 299

300 PART THREE | Disorders of the Brain
When I finished graduate school in clinicalpsychology in 1977, considerable controversyexisted about the validity of the construct oflearning disabilities. Some claimed theconstruct was a middle-class myth to excusethe poor performance of some children.Another possibility, offered by the psychoan-alytic paradigm that dominated clinical workat that time, reduced learning problems tolargely unconscious motivational problems.One of my supervisors only half-jokinglyinterpreted problems with addition as repre-senting conflicts over oral issues, problemswith subtraction as representing castrationanxiety, and so on. Partly because I hadminored in cognitive development in gradu-ate school, I was quite curious about whetherlearning disabilities existed, and if they did,how to understand and treat them.
Serendipity played a major role in focus-ing my curiosity. My first job after graduateschool was to help with a longitudinal studyof children with abnormal sex chromosomenumbers (the 45X, 47XXX, 47XXY, and 47XYYkaryotypes) initiated by Dr. Arthur Robinson,a pediatric geneticist. These children hadbeen observed since birth, and they werenow of school age. It soon became clear thatthese children had higher rates of learningdisabilities than either their siblings orchildren with abnormal numbers of sexchromosomes in only some of their cell lines(mosaics). Most interestingly, the type oflearning disability a child exhibited waslargely karyotype specific. These childrenprovided strong evidence that some learningdisabilities were influenced by geneticfactors, and that different genetic factorsaffected different aspects of cognitivedevelopment and academic skill.
Suddenly, a whole new vista opened onthe question of how valid the construct oflearning disabilities was. The fact of differen-tial genetic cause for at least some learningdisabilities convinced me of their validity, andalso gripped me with an intense curiosity to
understand in detail how the genetic alter-ation lead to the alteration in cognitivedevelopment. It was clear to me that one ofthe missing links in this causal chain was thebrain, and so I set out to learn all that I couldabout neuropsychology, as well as genetics.My new question was, How do the geneticalterations change brain development tocause specific changes in cognitive develop-ment? I also wondered whether geneticinfluences on learning disabilities were rareand limited to infrequent syndromes, such asabnormalities in sex chromosome number, orif they played a substantial role in learningdisabilities that currently had no known cause.
An opportunity to answer this secondquestion soon presented itself. Herbert Labsand Shelley Smith, both medical geneticists,invited me to help with their study of familialdyslexia by helping to define its cognitivephenotype. They had taken quite seriouslyHallgren’s (1950) classic study, which haddemonstrated a possible dominant geneinfluence on dyslexia, and were studyinggenetic linkage in extended families withdyslexia to find such genes. In 1983, wepublished an article in Science that pre-sented evidence for a gene influencingdyslexia located near the centromere ofchromosome 15. That same year, ShelleySmith and I published in Child Developmenta review of what was then known aboutgenetic influences on learning disabilitiesand speech and language disorders. Subse-quently, I published a number of articles onthe cognitive phenotype in familial dyslexia,finding that it was characterized by dyspho-netic spelling errors and an underlying deficitin phoneme awareness.
It eventually became clear that a largeproportion of the children who presentclinically with dyslexia have affected rela-tives, and that the recurrence rate amongfirst-degree relatives is quite high, about35% to 45%. This means that if a parent isdyslexic, the risk for having a dyslexic child is
about eight times greater than the risk in thegeneral population. Thus, genetic influenceson learning disabilities are not rare, butinstead account for a substantial portion ofthe etiology of the most common learningdisability, dyslexia.
The search for genes that influencedyslexia has continued. Shelley and I soonjoined forces with John DeFries and col-leagues at the Institute for Behavioral Genet-ics in Boulder, Colorado, who had indepen-dently conducted important family and twinstudies of dyslexia. Together, we eventuallyidentified the approximate location of asecond gene that influences dyslexia, thistime on the short arm of chromosome 6.Cardon and colleagues reported this discov-ery in Science in 1994. Three years later, aseparate team at Yale and Bowman Graymedical schools essentially replicated bothour linkage results, those on 15 and 6, in anindependent sample of families with dyslexia(Grigorenko et al., 1997). Taken together,these findings are essentially the first repli-cated genetic linkage results for a complexbehavioral disorder.
Therefore, some, but not all, of thequestions I began with have been answered.Learning disabilities exist in much the sameway that other complex medical phenotypes(such as obesity or heart disease) exist.There are genetic influences on them and asubstantial portion (about 50% according totwin studies) of the variance in the mostcommon learning disability, dyslexia, isattributable to genes. The approximatelocations of two of these genes influencingdyslexia are now known. Other disordershave shown us that understanding geneticmechanisms can illuminate the brain mech-anisms underlying learning disabilities. Thechallenge for the future (and for futuredevelopmental neuropsychologists) is tobetter understand both genetic and brainmechanisms in dyslexia and other learningdisorders.
N e u r o p s y c h o l o g y i n A c t i o n 1 1 . 1
G e n e t i c s o f L e a r n i n g D i s a b i l i t i e s
by Bruce Pennington Ph.D., Department of Psychology, Director of Developmental Cognitive Neuroscience Program,
University of Denver, Denver, CO

Initial support for anomalies of the magnocellular sys-tem in dyslexic persons stems from investigations (Galaburda & Livingstone, 1993) of the lateral geniculatebodies of normal-reading and reading-disabled adults.Brain autopsies revealed that the parvocellular cells of thetwo groups were similar, but the magnocellular cell bod-ies were generally smaller and more variable in size andshape in the dyslexic group. The investigators proposethat the structural differences in magnocellular cells areconsistent with slower visual processing.
In a more recent study (Demb, Boynton, Best, &Heeger, 1998) of young adults with a history of dyslexia,tasks were presented that required the visual detection of
moving stimuli. Dyslexic and healthy adults underwentfunctional magnetic resonance imaging (fMRI) whileperforming the tasks. The fMRI showed less activation inthe magnocellular pathway of the individuals withdyslexia relative to control participants. Furthermore,magnocellular-occipital areas of activation correlated sig-nificantly with reading speed, which is supportive of a re-lation between magnocellular deficits and reading perfor-mance. Although dyslexia may be causally related to thedisruption of magnocellular-parvocellular visual process-ing, it may also represent a more generalized deficit inrapid temporal processing.
P h o n o l o g i c M o d e l o f D y s l e x i a
Although dyslexia as a consequence of underlying deficitsin visual processing has received attention, impairment inphonologic processing as the central feature of the disor-der has received greater support (Swanson, Mink, & Bocian, 1999). The term phonologic processing refers to theapplication of rules for translating letters and letter se-quences into their corresponding speech–sound equiva-lents. This processing is supported by phonologic aware-ness, the awareness of and ability to differentiate betweenindividual phonemes, or speech sounds (Rumsey, 1996a).Children with dyslexia exhibit deficits in translating letterstrings into word sounds, also called word decoding.Deficits in this process cause reading to be slow andnonautomatic, disrupting efforts to identify and compre-hend presented words (Pennington, 1991). The wordrecognition deficits of the child with dyslexia are most ev-ident when he or she must read novel or unfamiliar words,that is, when the determination of letter–sound associa-tions is most critical. Moreover, children with dyslexiaoften have problems spelling because they are unable toefficiently translate the phonologic representation of aword to its visual configuration, a process that is the con-verse of reading. Despite these deficits, children withdyslexia frequently demonstrate preserved “listening com-prehension” when someone reads material to them. Fur-thermore, higher order cognitive functions such as gen-eral intelligence and reasoning, vocabulary, and syntax aretypically unimpaired (Shaywitz & Shaywitz, 2005).
Early deficits in phonologic processing are predictiveof later reading achievement, and interventions to reme-diate phonologic skill weaknesses facilitate the acquisitionof reading skills (Shaywitz & Shaywitz, 1999). Individu-als with severe phonologic deficits continue to show read-ing deficits into adolescence and adulthood, suggestingthat reading deficits are often a lifelong problem. Interest-ingly, adults who were dyslexic as children, but who showgood reading outcomes in adulthood, continue to exhibit
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 301
Figure 11.1 Magnocellular and parvocellular visual systems.The ventral magnocellular pathways are designated 1–2, and thedorsal parvocellular pathways are indicated by 3–6. (Adapted fromMason, C., & Kandel, E. [1991]. Central visual pathways. In E. Kandel,J. Schwartz, & T. Jessell [Eds.], Principles of neural science [3rd ed.,p. 425, Figure 29-6]. New York: Elsevier Science, by permission of theMcGraw-Hill Companies.)

phonologic deficits and a slow reading rate. For example,they continue to experience significant decoding deficitswhen required to read or spell nonwords, such as yite. Re-searchers believe their improvement in reading reflects acompensatory expansion of their sight vocabulary.
Deficits in phonologic processing are often accompa-nied by a second deficit, naming speed. Reduced namingspeed is commonly evident in dyslexic populations.Naming speed refers to the rate of retrieval of names forletters, digits, colors, and objects (Catts, Gillispie,Leonard, Kail, & Miller, 2002). Although debate contin-ues as to whether naming speed is independent of phono-logic awareness or a generalized deficit of cognitive pro-cessing, there are indications that naming speed is aprecursor to reading fluency. The identification of two pri-mary deficits associated with disabled reading has led tothe double-deficit hypothesis. The double-deficit hypoth-esis poses that reading disabilities can result from deficitsin either phonologic processing or naming speed. How-ever, children with both deficits are at the greatest risk forreading impairment (Schatschneider, Carlson, Francis,Foorman, & Fletcher, 2002; Waber, Forbes, Wolff, &Weiler, 2004).
In addition to phonologic and naming speed deficits,some children with dyslexia also demonstrate limitationsin working memory (a form of short-term memory inwhich information is both maintained and manipulated).As discussed earlier (see Chapter 9), working memory canbe conceptualized as a higher order central executive sys-tem that interacts with and regulates two “slave systems,”the articulatory phonologic loop and the visuospatialsketchpad (Baddeley & Hitch, 1994). The articulatoryphonologic loop is a temporary buffer for maintainingand manipulating auditory and verbal information,whereas the visuospatial sketchpad provides the samefunctions for visual and visuospatial information.
All three working memory components support read-ing performance, but disruption of the central executivesystem and phonologic loop are more strongly related toreading disabilities. Support for the involvement of theexecutive system is provided by studies of the memoryperformance of children with dyslexia. When performingmeasures of auditory and verbal working memory (sub-served by the phonologic loop), children with dyslexiashow significantly poorer performance than unimpairedreaders (Kibby, Marks, Morgan, & Long, 2004). Theyalso demonstrate deficits when performing tasks that as-sess temporal order memory (memory for the sequence ofevents across time). Temporal order memory involveshigher order cognitive processes supported by the execu-tive system (Howes, Bigler, Burlingame, & Lawson,
2003). Further support for the involvement of the execu-tive system includes the finding that under conditions ofhigh-processing demands, such as attempting to recall andmanipulate complex information, children with dyslexiademonstrate poorer memory for both verbal and visual in-formation than unimpaired readers (Swanson & Sachse-Lee, 2001). That is, the executive system fails to effec-tively allot attentional resources to coordinate the twoslave systems when confronted with high-processing de-mands. Despite these findings, it remains unclear whetherworking memory deficits are central or contributory tothe etiology of dyslexia.
N e u r o p a t h o g e n e s i s o f D y s l e x i a
The genetics of dyslexia is an area of significant study. Twinstudies demonstrate that reading deficits are highly herita-ble (h2 � 0.81), with a concordance rate of 83% for iden-tical twins (Alarcón, Pennington, Filipek, & DeFries,2000). Genetic studies have identified a linkage betweenreading disorders and genes on chromosomes 6 and 15.The heritability rate of phonologic processing is higherthan that of sight-reading, suggesting a greater geneticbasis for the former (Grigorenko et al., 1997). Althoughother genes are the focus of study, research investigationshave most consistently replicated the link between chro-mosome 6 and reading disabilities (Wood & Grig-orenko, 2001).
The primary emphasis of neuropsychological researchconcerning dyslexia has focused on the language cortex ofthe left hemisphere of right-handed individuals. Theplanum temporale of the left posterior temporal lobe(Figure 11.2) is one of the neural regions specifically im-plicated in phonologic processing (Hynd & Hiemenz,1997; Morgan & Hynd, 1998). For most people, theplanum temporales of the left and right hemispheres areasymmetric, with the left planum temporale being largerthan the right (L � R). Neuroimaging shows that indi-viduals with dyslexia often exhibit left-right planum tem-porale symmetry (L � R), or reversed normal asymmetry(R � L). However, the precise relation of atypical sym-metry to dyslexia awaits clarification.
Regional anomalies of the brains of dyslexic individu-als are also associated with differences in brain activationas revealed by cerebral blood flow. For example, a positronemission tomography (PET) study by Rumsey and col-leagues (1992) reported less activation of the left poste-rior temporal and temporoparietal cortices of individualswith dyslexia relative to normal-reading control individu-als when performing a task sensitive to phonologic aware-ness, namely, rhyme detection. A related PET study(Flowers, Wood, & Naylor, 1991) of dyslexic and normally
302 PART THREE | Disorders of the Brain

reading children found that the rate of cerebral blood flowto both the Wernicke’s area (region surrounding theplanum temporale) and angular gyrus related to readingperformance.
Further evidence for disruption of the temporal andtemporoparietal regions is provided by postmortem in-vestigations of the brains of dyslexic individuals. Post-mortem studies revealed neuronal ectopias (small loci ofabnormally placed neurons, sometimes referred to as“brain warts”) and cytoarchitectonic dysplasia (focalpathologic changes of cortical architecture) of the leftplenum temporale, suggesting abnormal neural develop-ment, most likely between the 5th and 7th month of fetalgestation (Hynd & Hiemenz, 1997). During this period,the gyri are rapidly forming, suggesting that the origin ofdevelopmental dyslexia, whether genetically determinedor a consequence of an insult, can be traced to a specificperiod of fetal development. However, not all studies havereplicated the finding of atypical planum temporale de-velopment (Filipek, 1996; Rumsey, 1998), suggesting thatother neural regions/systems may be involved in the etiol-ogy of dyslexia.
Greater specification of the neural substrates that sup-port phonologic processing is emerging (Horwitz, Rumsey,& Donohue, 1998; Pugh et al., 2000). PET studies of re-gional cerebral blood flow activation demonstrate that re-gions of the left angular gyrus, superior and middle tem-poral gyri (part of Wernicke’s area), inferior frontal cortex(near Broca’s area), and extrastriate and striate cortex (occipital) activate when individuals without dyslexia readirregular words (reading that requires orthographic famil-iarity) and pseudowords (reading that requires the use ofphonologic rules). The activation of these regions signifi-cantly correlates, suggesting a functional network support-ive of reading. In contrast, individuals with dyslexiademonstrate reduced activation across the functionalnetwork, and the left angular gyrus fails to significantlycorrelate with the activation patterns of the other reading-related regions. The latter finding prompted the investi-gators to conclude that the left angular gyrus of individu-als with dyslexia is functionally disconnected from theother regions of the network. Insofar as the angular gyrusis involved in the cross-modal transformation of visual(written) information into linguistic representations, thedisconnection would limit or distort input to the otherregions of the left hemisphere necessary for reading-related processing. Whether the functional disconnect isthe result of anomalies in the white matter interconnect-ing pathways that link the left angular gyrus with the otherreading-related regions of the left hemisphere, functionalanomalies specific to the angular gyrus, or some other un-known set of factors remains to be determined.
In a particularly well-designed study, Shaywitz and col-leagues (1998) endeavored to identify the neural sub-strates that correlated with reading performance. Hierar-chically arranged orthographic and phonologic tasks,progressing from simple to complex, were presented toadolescents and adults with dyslexia and participantswithout dyslexia while undergoing fMRI. The progres-sion and type of tasks presented were as follows: (1) judg-ment of line orientation (visuospatial processing withoutorthographic demands); (2) lowercase and uppercase letterdiscrimination (orthographic processing without phono-logic demands); (3) single-letter rhyming (orthographicto phonologic coding and analysis); (4) nonword rhyming(complex orthographic to phonologic coding and analy-sis); and (5) semantic categorization (orthographic,phonologic, and semantic analysis). As the presented tasksprogressed from lowercase and uppercase discriminationthrough nonword rhyming, unimpaired readers mani-fested increasing and systematic activation of the left pos-terior superior temporal gyrus, angular gyrus (parietal),and extrastriate and striate cortices (occipital), whereas
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 303
Images not available due to copyright restrictions

individuals with dyslexia did not demonstrate this pro-gressive activation. The dyslexic group showed greater ac-tivation of the right inferior frontal gyrus as phonologic de-mands became more complex. This increased activation ofthe right anterior regions suggests that individuals withdyslexia rely on alternative or “spared” circuitry to processreading contents. Thus, individuals with dyslexia demon-strated decreased activation of posterior brain regions thatencompassed both visual and language areas, and an in-creased activation of anterior brain regions. This activa-tion profile may provide a neural “marker” for identifyingindividuals with dyslexia.
Shaywitz and associates (2002) extended their study todyslexic and non–reading-impaired children and adoles-cents. The participants underwent fMRI while perform-ing the previously discussed hierarchically arranged or-thographic and phonologic tasks. The regional activationpatterns of the children and adolescents with dyslexia dif-fered from those of the nonimpaired readers. Further-more, the regional activation patterns paralleled thoseidentified in Shaywitz and colleagues’ (1998) earlierstudy. Based on the findings of these two studies and sub-sequent investigations (Shaywitz et al., 2003; Shaywitz& Shaywitz, 2005), three reading-related systems wereposed. Two of these systems involve the left posterior re-gion, and the third involves the left anterior region of thebrain. The first system, located in the left dorsal pari-etotemporal area (angular gyrus and posterior portions ofthe superior temporal gyrus), is believed to support themapping of visual print to its phonologic representation.This word analysis system operates on individual units ofwords (for example, phonemes), requires attentional allo-cation, and processes information slowly. The second sys-tem encompasses the left ventral occipitotemporal region(portions of the middle occipital and middle temporalgyrus) and operates on the whole word (visual wordrecognition). This visual word system requires minimalattentional allocation and serves the automatic and rapidrecognition of words. The final system is localized in theleft inferior frontal region of the brain (Broca’s area) andis implicated in articulation, silent reading, and naming.Disruptions of the two posterior systems are the primarydeterminants of dyslexia.
Two other neural regions, the corpus callosum andfrontal cortex, have received attention in the study ofdyslexia. Investigative studies of the structural integrity ofthe corpus callosum of dyslexic groups have producedcontradictory findings. Specifically, studies of the anterior(genu) and posterior (splenium) areas of the corpus callo-sum of individuals with dyslexia and individuals with pre-served reading skills have not shown consistent structural
differences in these regions (Hynd et al., 1995; Larsen,Hoien, & Odegaard, 1992). Causal explanations for therelation of the corpus callosum to dyslexia, when struc-tural differences are identified, center on increased or de-creased interhemispheric communication or inappropriateinhibition of one hemisphere by the other. Neuroscientistbelieve that these conditions disrupt the flow and integra-tion of information between the two hemispheres that isnecessary for reading.
The frontal cortex has also received attention, with re-searchers observing tentative differences between profi-cient and disabled readers. Children with either dyslexia orADHD presented bilaterally smaller frontal cortices than agroup of healthy children (Hynd, Semrud-Clikeman,Lorys, Novey, & Eliopulos, 1990). Moreover, the chil-dren with dyslexia differed from the other two compari-son groups by exhibiting greater symmetry of the anteriorregion because of the smaller width of the right frontallobe (R � L). Similarly, in a more recent pilot study(Semrud-Clikeman, Hooper, Hynd, Hern, Presley, &Watson, 1996), the smaller width of the right anteriorfrontal cortex was one of several anatomic variables thatdiscriminated among dyslexic, ADHD, and healthy con-trol children. The functional relation of the anatomic dif-ference of the frontal lobe to dyslexia is unclear. However,the frontal lobes mediate a number of executive functions,such as mental shifting, allocation of attention, and work-ing memory, that are crucial to reading (James & Selz,1997). Support for a relation between executive dysfunc-tion and dyslexia is emerging. For instance, in one study(Helland & Asbjørnsen, 2000), children with dyslexiashowed deficits on measures of attentional flexibility andshifting relative to the performance of healthy controlchildren.
In summary, reading is an exceptionally complexprocess that requires letter identification, phonologic andorthographic skills, naming speed, sequencing skills, at-tention, mental flexibility, and working memory. Further-more, the lexicon stores (our “internal dictionaries”) mustbe accessed to determine the meaning of words and tocomprehend what is being read. These myriad functionsrequire the support of multiple brain systems, with the leftposterior regions serving a central role in skilled reading.
The next section explores NVLD. Children exhibitingNVLD potentially manifest distinctly different neuropsy-chological profiles from those with verbal learning dis-abilities. Whereas verbal learning disabilities are generallyattributed to left hemisphere dysfunction and are impli-cated in reading disturbances, NVLD is attributed toright hemisphere dysfunction and is associated withdeficits in mathematics (dyscalculia).
304 PART THREE | Disorders of the Brain

N O N V E R B A L L E A R N I N G D I S A B I L I T Y S Y N D R O M E
C l i n i c a l P r e s e n t a t i o n a n d P r e v a l e n c e
The concept of NVLD as a neuropsychological disorderhas emerged from the ongoing investigations of ByronRourke, who has attempted to identify the neurocogni-tive, psychosocial, and adaptive characteristics of childrenwith learning disabilities. His investigative efforts revealedtwo basic subtypes of learning disability: one labeled R-S,for reading and spelling disability, and the other NVLD,for nonverbal learning disability syndrome. R-S childrendemonstrate weak psycholinguistic skills with relativelypreserved skills in visual-perceptual, tactile-perceptual,psychomotor, and nonverbal/novel problem solving(Table 11.1). Reading and spelling skills are poor, withgreater competency evident in mechanical arithmetic, al-though their performance is still below age expectancy.Rourke (1993) hypothesizes that the neuropsychologicaldeficits of the R-S group are associated with left hemi-sphere dysfunctions.
In contrast, children in the NVLD group present es-sentially the opposite pattern of strengths and deficits asthe R-S group (Table 11.2). That is, the NVLD groupshow relatively poor skills in visual-perceptual, tactile-perceptual, psychomotor, and nonverbal/novel problem-solving skills coupled with strengths in the psycholinguis-tic domain. They manifest major academic weaknesses inbasic arithmetic but demonstrate preserved linguisticskills such as sight word reading (Harnadek & Rourke,1994). Both groups exhibit comparable deficits in actualarithmetic achievement; however, Rourke (1993) attrib-utes the poor performance of the R-S group to verbaldeficits, and the low performance of the children withNVLD to weaknesses in visual-perceptual and nonverbalreasoning.
Researchers estimate the prevalence rate of NVLDwithin clinic populations at 5% to 10% (Rourke, 1989).Furthermore, NVLD represents between 0.1% and 1.0%of the entire learning disability population, with an over-all male-to-female ratio of approximately 1.2 to 1.0(Pennington, 1991).
N e u r o p s y c h o l o g i c a lP a t h o g e n e s i s
Rourke (1993) considers that NVLD reflects right hemi-sphere (particularly posterior) damage, or dysfunction,whereas R-S deficits more closely reflect problems in theleft, language-dominant, hemisphere system. Rourke hasadopted Goldberg and Costa’s (1981) theorization of
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 305
Neuropsychological Assets Neuropsychological Deficits
Primary assets Primary deficits
Motor and psychomotor Auditory perception
Novel material
Tactile perception
Visual perception
Secondary assets Secondary deficits
Tactile attention Auditory attention
Visual attention Verbal attention
Tertiary assets Tertiary deficits
Concept formation Auditory memory
Problem solving Verbal memory
Tactile memory
Visual memory
Verbal assets Verbal deficits
Pragmatics Phonology
Prosody Verbal association
Semantic > phonology content Verbal output (volume)
Verbal associations function Verbal reception
Verbal repetition
Verbal storage
Academic assets Academic deficits
Reading comprehension (late) Comprehension (early)
Mathematics Graphomotor
Reading Mechanical arithmetic
Science Reading
Spelling
Verbatim memory
Word decoding
Socioemotional/adaptive assets Socioemotional/adaptive deficits
Activity level Undetermined
Adaptive to novelty
Emotional stability
Social competence
Source: Rourke, B., & Fuerst, D. (1996). Psychosocial dimensions learning disabilitiessubtypes. Assessment, 3, p. 281, by permission.
Table 11.1 Core and Clinical Features of the Reading and Spelling Group

brain functioning in conceptualizing the neuropathogen-esis of NVLD. Goldberg and Costa propose that the righthemisphere, relative to the left, is more diffusely orga-nized, has more association regions, and shows greaterspecialization for inter-regional integration of informa-tion. Because of its capacity to integrate input from mul-tiple brain regions, the right hemisphere is more adeptat processing complex, novel, or ambiguous informa-tion. In contrast, the left hemisphere is more focally or-ganized, presents greater modality-specific cortical re-gions, and shows greater specialization for intraregionalintegration of input. The specialization of the left hemi-sphere is hypothesized to relate to the routine applicationof previously acquired cognitive strategies. The two hemi-spheres complement each other, with the right hemi-sphere showing prominence in establishing new rules, rou-tines, or strategies, and the left storing and applying thesenewly established computations in similar situations orwith comparable tasks in the future (Fisher, DeLuca, &Rourke, 1997).
Rourke (1995) maintains that the primary deficits oftactile-perceptual, visual-perceptual, and psychomotorabilities of NVLD are consistent with damage or dysfunc-tion of right hemisphere inter-regional integration,whereas assets of auditory-perceptual and verbal skills sug-gest a relatively intact left hemisphere. He also viewsdeficits such as poor problem solving in novel situations,or in the face of complexity, weaknesses in conceptualthinking, and impaired socioemotional skills as emanat-ing from right hemisphere involvement.
Rourke suggests that, although right hemisphere dam-age is sufficient to produce NVLD, it is the destruction ofthe white matter (myelinated circuitry) required for inter-regional integration that is necessary for producing the dis-order. That is, the development of NVLD can be causedby damage to white fibers (1) accessing the right hemi-sphere, (2) connecting cortical regions within the righthemisphere, or (3) linking cortical to subcortical regionswithin the right hemisphere (Rourke, 1995). Interest-ingly, Rourke hypothesizes that damage to these differentcommunicating fibers accompanies diverse disorders inassociation with NVLD. For example, early damage tothe association fibers of the right and left hemispherescould potentially cause both the primary features ofNVLD and the global linguistic deficiencies that charac-terize autism.
Although Rourke emphasizes the posterior right hemi-sphere as playing an important role in the pathogenesis ofNVLD, he proposes that the anterior brain regions mayalso be involved. For example, children with NVLD per-formed in a less efficient manner than children with
306 PART THREE | Disorders of the Brain
Neuropsychological Assets Neuropsychological Deficits
Primary assets Primary deficits
Auditory perception Complex psychomotor
Rote material Novel material
Simple motor Tactile perception
Visual perception
Secondary assets Secondary deficits
Auditory attention Exploratory behavior
Verbal attention Tactile attention
Visual attention
Tertiary assets Tertiary deficits
Auditory memory Concept formation
Verbal memory Problem solving
Tactile memory
Visual memory
Verbal assets Verbal deficits
Phonology Oral-motor praxis
Verbal association Phonology � semanticscontent
Verbal output Pragmatics function
Verbal reception Prosody
Verbal repetition
Verbal storage
Academic assets Academic deficits
Graphomotor (late) Graphomotor (early)
Spelling Mechanical arithmetic
Verbatim memory Reading comprehension
Word decoding Science
Socioemotional/adaptive assets Socioemotional/adaptivedeficits
Undetermined Activity level
Adaptive to novelty
Emotional stability
Social competence
Source: Rourke, B., & Fuerst, D. (1996). Psychosocial dimensions learning disabilitiessubtypes. Assessment, 3, p. 281, by permission.
Table 11.2 Core and Clinical Features of Nonverbal Learning Disability Syndrome

verbal learning disabilities when presented tasks requiringhigher order mental operations such as conceptual think-ing and mental flexibility (Fisher, DeLuca, & Rourke,1997). Moreover, Rourke (1995) indicates that the frontalsystem is necessary for (1) integrating lower level systems(such as sensorimotor) to formulate higher order levels ofabstraction; (2) responding to novelty and complexity;and (3) metacognition, that is, the ability to understandthe operation of one’s own cognitive processes. Rourkebelieves that damage to the interconnecting white mattertracks between the frontal lobes and the posterior regionsof the right hemisphere contributes to the deficits ofhigher order cognition evident in NVLD.
Many disorders and brain insults accompany NVLD,spanning genetic, chromosomal, structural, and environ-mental anomalies. Table 11.3 presents a partial list of im-plicated disorders. Although these disorders and insultsrepresent a varied and seemingly dissimilar set of causativefactors, clinical presentations, and developmental courses,Rourke and Del Dotto (1994) suggest that each shares acommon pathway to NVLD, namely, dysfunction of the
white matter of the brain. These disorders represent aspectrum of neurodevelopmental conditions that vary inthe severity of expression of NVLD, ranging from disor-ders that present virtually all the assets and deficits ofNVLD (such as hydrocephalus and Asperger’s syndrome),to those that display a majority of the assets and deficits(such as fetal alcohol syndrome and Turner’s syndrome),and finally, to those that exhibit only a subset of the assetsand deficits of the NVLD (such as autism). Thus, varyingnumbers of assets and deficits of NVLD are comorbidmanifestations of these disorders caused by damage to thewhite matter (Rourke, 1995).
N e u r o p s y c h o l o g i c a l A s s e s s m e n t
Harnadek and Rourke (1994) attempted to identify theprimary neuropsychological deficits of the NVLD and R-S groups. The neuropsychological test data of threegroups, NVLD, R-S, and healthy control children, wassubjected to statistical analysis to determine the most dis-criminating measures for classifying the children intotheir respective groups. Two sets of tests statistically dif-ferentiated the NVLD, R-S, and healthy control groups.The first set of measures assessed visuospatial organiza-tion, tactile-perceptual, and psychomotor skills, and thesecond, academic (reading) and auditory-perceptual skills.The measures of visuospatial-tactile-psychomotor skillscontributed significantly to the discrimination of theNVLD group from the R-S and healthy control groups,whereas the academic-auditory skill measures differenti-ated the R-S from the NVLD and healthy control groups.These two sets of measures accurately classified the chil-dren in their respective groups at an overall classificationrate of 98%. Recently, using a larger sample of childrenwith NVLD or reading/spelling deficits, the two sets ofmeasures once again accurately classified children with R-S and NVLD into their respective groups (Pelletier,Ahmad, & Rourke, 2001).
As noted earlier, children with NVLD frequently ex-hibit arithmetic deficits. Rourke and Conway (1997) hy-pothesize that during the initial learning of arithmeticskills in childhood, the novel, visuospatial, and concep-tual nature of the content recruit mainly right hemi-spheric systems. Once these skills are learned, however,they shift to the left hemisphere because of its greater fa-cility in processing and retrieving automatic information(Dool, Stelmack, & Rourke, 1993).
Examining the mathematics performance of childrenwith NVLD, researchers have identified seven overlappingerrors (Rourke, 1993): (1) errors in spatial organization,(2) misreading or omitting required mathematic symbols,(3) failure to apply or misapplication of mathematic
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 307
Asperger’s syndrome
Autism
Callosal agenesis (absence of the corpus callosum)
Congenital hypothyroidism
Cranial irradiation
Fetal alcohol syndrome
Hydrocephalus
Insulin-dependent diabetes mellitus
Intracranial tumors
Metachromatic leukodystrophy (genetic metabolic disorder)
Myelomeningocele (neural tube defect)
Sotos syndrome (growth disorder)
Traumatic brain injury
Triple X syndrome (genetic neurodevelopmental disorder)
Turner’s syndrome
Williams syndrome (genetic neurodevelopmental disorder)
Source: Adapted from Tsatsanis, K., & Rourke, B. (1995). Conclusions and futuredirections. In B. Rourke (Ed.), Syndrome of nonverbal learning disabilities: Neurodevel-opmental manifestations (p. 486), New York: The Guilford Press, by permission.
Table 11.3 Brain Disorders and InsultsAssociated with NonverbalLearning Disability Syndrome

procedures, (4) poorly formed or spaced numbers, (5) fail-ure to remember number facts or arithmetic rules, (6) dif-ficulties shifting from one set of arithmetic operations toanother, and (7) poor arithmetic judgment and reason-ing. The latter error involves production of unreasonablesolutions, or failure to generalize solutions, strategies, orplans for new or different arithmetic problems. Althoughchildren with other forms of learning and neuropsycho-logical deficits can show errors involving spatial and re-trieval deficits, several of the errors, particularly those dueto poor judgment and reasoning, discriminate childrenwith NVLD from other learning-disabled children. Er-rors in cognitive shifting, judgment, and reasoning po-tentially implicate deficits in executive function.
S o c i o e m o t i o n a l C h a r a c t e r i s t i c s
A broad set of adaptive and socioemotional disturbancesaccompany NVLD. Rourke believes these deficits are adirect consequence of the core deficits of the disorder (seeTable 11.2). Of these deficits, the most prominent lie inthe communication and interactional domains. The com-munication deficits appear in both verbal and nonverbalbehaviors. At the verbal level, children and adolescentswith NVLD tend to talk excessively, present tangentialcontents, and show a poor understanding of the pragmat-ics of language, that is, the emotional and social contentof a message. Moreover, they find it difficult to understandthe nonverbal behavior of others and to convey informa-tion through their own nonverbal behaviors (Rourke,Bakker, Fisk, & Strang, 1983).
Regarding social behavior, deficits in social sensitivity,interactional skills, social problem solving, and judgmentseriously hinder the efforts of individuals with NVLD torelate to others. They are prone to misread or fail to ap-preciate the social intents, perspectives, or feelings of oth-ers. In addition, they do not accurately assess social cause-and-effect relations (Rourke & Fuerst, 1996). Socialproblem solving of children with NVLD is particularlycompromised in new, changing, or complex social situa-tions, often resulting in rigid or stereotypic responses thatare inappropriate to the demands of the situation. Becauseof poor social judgment, caretakers and peers view the in-dividual with NVLD as lacking in common sense. Fre-quently, the child or adolescent encounters difficultiesgeneralizing social skills learned in one situation to an-other, even though the new situation is similar to the orig-inal learning context. Social conventions, such as main-taining eye contact and appropriate social distance, areoften violated. Finally, the poor psychomotor skills andclumsiness of children with NVLD can elicit teasing andtaunting from peers.
Although prone to acting-out behaviors and symptomsof ADHD while young (Voeller, 1996), children withNVLD tend to become shy and withdrawn with increas-ing age. Assessment by their mothers reveals that childrenwith NVLD often present internalizing symptoms suchas anxiety, depression, withdrawal, and poor social skills.Whether this is a direct response to their failures withinthe social sphere is unclear, although it is likely that socialfailings contribute to the emotional distress of childrenand adolescents with NVLD. The finding that childrenwith NVLD exhibit increasing and more severe internal-izing psychopathology (anxiety, depression, emotional la-bility, social isolation, and withdrawal) with age is of con-cern (Pelletier et al., 2001). In contrast, children with R-Sdeficits are less likely to demonstrate increased internalizingor externalizing (acting-out patterns) with advancing age.
N e u r o p s y c h o l o g i c a l M o d e l
Rourke’s model of learning disability, with regard to sub-types such as NVLD and R-S, is summarized as follows:
Subtypes of LD [learning disabilities] are manifestations ofdistinct profiles of neuropsychological assets and deficits; thesubtypes of LD may lead to specific problems in academicfunctioning, psychosocial functioning, or both; and, the rela-tionship between profiles of neuropsychological assets anddeficits, LD, and academic and social learning deficits can beunderstood fully only within a neurodevelopmental frameworkthat takes into consideration the changing nature of the acade-mic, psychosocial, and vocational demands that humans in aparticular society confront. (Rourke & Fuerst, 1996, p. 278)
A hierarchical organization is evident, with primaryneurocognitive assets and deficits leading to predictableand differential patterns of neuropsychological function-ing (secondary, tertiary, and linguistic) that, in turn, di-rectly affect academic, socioemotional, and adaptive func-tioning (see Tables 11.1 and 11.2). Thus, the adequacy ofthe child’s sensorimotor development sets the stage forsubsequent levels of cognitive development. The youngchild experiences the world through touch, movement,and vision. Contacting and exploring the environmentthrough the basic sensory modalities fosters the develop-ment of increasingly complex and higher level mentalstructures. The early deficits of the child with NVLD inthe tactile-perceptual, visual-perceptual, and psychomotordomains limit sensorimotor learning; and thus, hinder theformation of the basic building blocks necessary for the de-velopment of more advanced mental structures. Rourke andothers believe these early limitations bias the later develop-ment of conceptual thinking, creative problem solving, com-munication skills, and socioemotional interactions. As thechild moves into adolescence and developmental tasks
308 PART THREE | Disorders of the Brain

become increasingly complex, the functional deficits be-come more apparent. Unfortunately, the impairments ofthe adult are even more pronounced, as evident in thecommon finding of marginal adaptive success across be-havioral domains.
Little (1993) indicates that the primary deficits and as-sets of NVLD are a robust finding in the studies of learn-ing disabilities. However, support for the socioemotionalaspects of the disorder is less compelling. For example,Guy (1996) failed to find a greater prevalence of internal-izing psychopathology in children with NVLD relative tohealthy control children and children with verbal learningdisabilities.
D e v e l o p m e n t a l C o u r s e
The developmental course of NVLD is somewhat simi-lar to the natural history reported for Turner’s syndromeand higher functioning autistic/Asperger’s syndromechildren (see Pervasive Developmental Disorders sectionlater in this chapter). For the NVLD infant/toddler, ex-ploratory behavior and motor skills lag behind language development. With increasing age, delays hinder the devel-opment of self-help skills, and the child tends to dependtoo much on caretakers. Increasingly, the child encoun-ters difficulties in the social domain, with playmatesbeing either younger or older than the child withNVLD.
In the elementary years, children with NVLD are proneto act out, respond impulsively, exhibit hyperactivity, andencounter problems in sustaining attention (Rourke, Fisk,& Strang, 1986). Despite relatively advanced verbal skills,their communication patterns (both verbal and nonverbal)are often inappropriate. Misperceptions of social situationsimpair social problem solving and judgment, and poorsocial skills compromise efforts to relate successfully withpeers. The child develops few, if any, close friendships, andduring adolescence, peers often avoid teenagers withNVLD. Increasingly, teenagers with NVLD become sociallywithdrawn and isolated and show internalizing symptomsof anxiety and depression. Developmental patterns for adultswith NVLD await clarification. Unfortunately, NVLDadults show elevated rates of psychopathology, and their riskfor depression and suicidal behavior appears to be great.
T r e a t m e n t
Because of the communication and social deficits oftenassociated with NVLD, the child needs help developingverbal and nonverbal communication skills, basic socialskills (such as greeting), and more advanced social skills(social awareness, friendship skills, and social problemsolving). Early and ongoing interventions focused on the
development of communication and social skills may im-prove the child’s acceptance by peers. The young childwith NVLD who exhibits ADHD symptoms may benefitfrom increased structuring of home and school activities,and the introduction of psychostimulant or related med-ications. Furthermore, parents can profit from learningmanagement techniques to foster greater self-help skillsand independence by the child.
Children with NVLD are at risk for development ofpsychological difficulties. Parents and professionals shouldbe aware of this risk and prepare to provide early interven-tions if psychological problems arise. They should pay par-ticular attention to the NVLD youngster with depressivesymptoms that might signal an increased risk for suicide.
Rourke and Del Dotto (1994) have developed a com-prehensive intervention program for children and adoles-cents with NVLD. The program actively involves thecaretakers from its inception. A set of general principlesorganizes and guides treatment, with each program re-quiring individualization to accommodate the strengthsand deficits of each child. Initially, the program providesthe caretakers with information that helps them under-stand the nature and extent of the child’s disorder and de-velop realistic expectations. Then the program providesinterventions that will help the child (1) understand,learn, and generalize cognitive and social problem-solvingstrategies; (2) develop necessary communication skills; (3) engage and interact appropriately with others; (4) exploreand experience his or her environment; (5) use available aids(such as a digital watch for learning time concepts); and(6) gain a realistic view of his or her strengths and weaknesses.
School-age children with NVLD are at risk for acade-mic difficulties, particularly if spatial reasoning or execu-tive deficits are severe. Academic subjects that can be par-ticularly challenging to children with NVLD includehandwriting and mathematics. Since it is highly unlikelythat children with NVLD will outgrow these deficits, pro-grams should be directed toward helping them developcompensatory skills and strategies. For example, childrenwith NVLD often struggle with writing because of spatialand motor deficits. Accordingly, parents and professionalsshould encourage them, at an early age, to develop word-processing skills. Similarly, adolescents with NVLD needhelp in developing realistic academic and career goals inlight of their individual strengths and visuospatial andmathematic weaknesses.
E v o l u t i o n
NVLD, similar to other syndromes, is an evolving disorder.That is, the validity and clinical utility of the disorder isbeing evaluated based upon ongoing clinical investigations
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 309

and research. This process is clarifying the major tenets,as well as prompting the modification of defining features,diagnostic criteria, and specification of differences fromother disorders. For example, research is suggesting thatchildren with NVLD do not necessarily exhibit deficits inthe area of math calculation but rather in the visuospatialaspects of calculation. Venneri, Cornoldi, & Caruit(2003) determined that children with NVLD showknowledge of math facts and an understanding of calcula-tions similar to that of healthy control children. In con-trast, they made significantly more errors in the executionof written calculations, particularly when regrouping(“borrowing” or “carrying”) was involved. In addition,children with NVLD demonstrated significantly poorerperformance on measures of visuospatial skills and visu-ospatial working memory than healthy control children.The authors hypothesize that the poorer performance ofthe children with NVLD relates to visuospatial skilldeficits, including visuospatial working memory weak-nesses. Forrest (2004) has recently determined that chil-dren with NVLD were proficient in math operations(concepts and application) that allowed for the applica-tion of verbal abilities, but they faltered when confrontedwith mechanical arithmetic. The latter involved solvingwritten calculations (for example, 3 � 9 � 12), that is,problems that place greater demands on visual perceptualprocessing. Likewise, the author determined that visual-perceptual deficits were not generalized across all forms ofvisual and visuomotor tasks; rather, they appeared specificto the location of objects in space (spatial). Interestingly,children with NVLD did not demonstrate a greater preva-lence of internalizing psychopathology (namely, depres-sion or anxiety) than children with verbal disabilities andhealthy control youngsters. This finding conflicts with anearlier study (Carey, Barakat, Foley, Gyato, & Phillips,2001) of children treated for brain tumors who, upon as-sessment, demonstrated a profile consistent with NVLDincluding internalizing behavioral problems and socialdeficits. The children that participated in these two studies(Forrest, 2004; Carey et al., 2001) represent significantlydifferent clinical populations, and further investigations areneeded to determine under what conditions children withNVLD do or do not exhibit internalizing psychopathology.
Pervasive DevelopmentalDisorders
Pervasive developmental disorders encompass a set ofsevere neuropsychological deficits that are evident early inchildhood and have a poor prognosis for achieving normal
adaptive functioning. To varying degrees, each of the per-vasive developmental disorders involves impairment inone or more of the following domains of development:social interactions, verbal and nonverbal language, rangeof interests and activities, and flexibility of behavior. Thebehaviors manifested in these domains are age inappro-priate and are disproportionate to the child’s intelligenceand age, even though mental retardation is frequently acorrelate of the disorders. Researchers hypothesize that amyriad of central nervous system abnormalities play rolesin the etiology of the pervasive developmental disorders.However, in many cases, the origin of the disorder re-mains unknown. Table 11.4 summarizes the primary per-vasive developmental disorders and their associated be-havioral features.
310 PART THREE | Disorders of the Brain
Autistic Disorder
Impairment or delays in the domains of social interactions and communica-tions (including symbolic and imitative play), and repetitive and stereotypedpatterns of behavior, interests, and activities, with age of onset evidentbefore age 3.
Asperger’s Disorder
Symptom presentation similar to autism with regard to delays in developingage-appropriate social interactions and repetitive and stereotyped patternsof behavior, interests, and activities. Unlike autism, few significant develop-mental delays in language, cognitive, adaptive (other than social), self-help,and exploratory behaviors are evident.
Rett’s Disorder
Initial normal psychomotor development with normal head circumference.Between 5 and 48 months, head growth decelerates, accompanied by theloss of acquired hand motor movements, diminished social interest, emer-gence of poorly coordinated gait or trunk movements, and severely impairedlanguage development with psychomotor retardation. Present only in femalechildren.
Childhood Disintegrative Disorder
Normal development across behavioral domains is evident until 2 years ofage or later. Previously acquired skills deteriorate in two or more of thefollowing domains: language, social or adaptive behaviors, eliminationcontrol, play, or motor skills. The emergence of autistic-like symptoms insocial relatedness, communication, and repetitive and stereotypic behavioris evident. The loss of skills can plateau or continue to decline if accompa-nied by a degenerative neurologic disorder. Present in male and femalechildren, with greater prevalence in male children.
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders,Fourth Edition. Text Revision, Copyright 2000, American Psychiatric Association.
Table 11.4 Distinguishing Features ofPervasive Developmental Disorders

A U T I S M
B a c k g r o u n d a n d C l i n i c a lP r e s e n t a t i o n
Leo Kanner and Hans Asperger are credited with theidentification, first theoretical conceptualizations, and la-beling of the developmental disorder autism (Frith,1989). Autism entails severe impairments in social relat-edness and language development, and the presentationof unusual, repetitive, and/or stereotypic patterns of be-havior. Kanner, working in Baltimore, and Asperger,working in Vienna, each studied a group of disturbedchildren for whom there was little recognition, much lessunderstanding. Independently, each published their clas-sic articles (Asperger, 1944/1991; Kanner, 1943) withoutconsultation or reported awareness of the other. Remark-ably, both used the term autistic in characterizing the dis-order. Asperger’s work, largely ignored until recent years,is often associated with a higher functioning level or subtype of autism, Asperger’s syndrome, in which near-normal to normal functioning is evident in several behav-ioral domains (Frith, 1991).
The first area of disturbance in autism, impairment inthe ability to relate to others, particularly with regard tounderstanding and entering into reciprocal social relation-ships, is the cardinal symptom of the disorder. Kanner(1943) referred to this dramatic aspect of behavior as“autistic aloneness,” a psychological state of profoundseparation and disconnection from other people. At a be-havioral level, the child with autism exhibits this socialdisconnection by displaying the following characteristics:(1) a limited awareness of, or interest in, the desires, needs,distress, or presence of others; (2) an emotional remotenessor aloofness; (3) a failure to share activities, pleasures, andachievements with others; (4) a lack of understanding ofsocial convention; (5) an impairment in social perspectiveand empathetic role taking; (6) a restricted repertoire of so-cial skills, such as greeting behavior; and (7) awkward orstereotypic responses to others (Bailey, Phillips, & Rutter,1996). Moreover, children with autism often show deficitsin joint attention (reciprocal attention between the childand another), poor conversational skills, lack of eye con-tact, unusual body postures or gestures, and inappropri-ate facial expressions (Charman, 1997; Tanguay, 2000).
The second core characteristic of autistic behavior,deficits in communication, appears as impairments of lan-guage expression and comprehension. Spoken languagemay be delayed in onset or fail to develop altogether, andthe child makes little effort to compensate through non-verbal behaviors such as gestures or facial expressions.When language is used, the child may restrict it to the
repetitive use of stereotypic or idiosyncratic content.Caretakers see deficits in the understanding and use ofpragmatics of language (Rumsey, 1996b) and deviantforms of language such as echolalia (repeating the wordsor phrases of others), pronoun reversal, and neologisms(invention of words). The ability to understand languageis often impaired and is limited to the comprehension ofsimple, literal contents.
The ability to initiate and enter into symbolic, pre-tend, or imitative play is minimally developed (McDo-nough, Stahmer, Schreibman, & Thompson, 1997). Ini-tially, the child shows little interest in toys, suggestingdelayed or poor comprehension of the symbolic meaningof toys (Rutherford & Rogers, 2003). As interest devel-ops, the child manipulates toys repetitively as objectswithout symbolic or imaginative connotations. Insofar aspretend play is considered necessary for the developmentof social and communication skills, it is diagnosticallysignificant that the child with autism rarely partakes incomplex, imaginative, or cooperative play.
The third core feature of autism relates to one or moreof the following unusual behavioral patterns: (1) preoccu-pation with specific areas of interest, objects, or qualitiesof objects; (2) demands for environmental or behavioralsameness; and (3) stereotypic body movements or abnor-malities of posture (American Psychiatric Association[APA], 1994).
A fascination with and abnormal focus on areas of in-terest (such as geography), objects (fans, vacuum cleaners,and so on), parts of objects (such as buttons), movementof objects (such as spinning toys), or activities (such asdrawing) can dominate the child’s daily pursuits. More-over, the child may demand the maintenance of constancy(for example, the child’s room cannot be altered), order(toys must be lined up in a certain manner), or routine(the child must always walk the same route to the play-ground). Interference or disturbance of the child’s in-volvement in areas of interest or the child’s efforts tomaintain constancy can prompt a range of responses fromirritation, to overwhelming anxiety, to thunderous rage.Finally, disturbances of motility can encompass a widerange of movements such as rocking, spinning, twisting,or hand flapping. A variety of unusual postural move-ments may also be evident, such as a tendency to walk ontiptoe, holding the hands in an awkward manner, andwalking without moving the arms.
D e m o g r a p h i c a n d C o m o r b i dC o n d i t i o n s
Researchers estimate the prevalence rate of autism at 10affected children per 10,000, whereas the prevalence rate
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 311

for Asperger’s syndrome is 2 to 2.5 per 10,000 (Fombonne,2001, 2003a). Males outnumber females with autism bya 2:1 to 6:1 ratio.
Concern exists that the prevalence of pervasive devel-opmental disorders, particularly autism, is increasing atan alarming rate. A review of relevant epidemiologic stud-ies reports an increase in prevalence from 4.4 per 10,000for the years 1966 through 1991 to 12.7 per 10,000 forthe years 1992 through 2001 (Fombonne, 2003a). An ex-amination of the studies suggests that the increase may bespurious. Specifically, the increase may relate to the fol-lowing factors: (1) changes and broadening of the diag-nostic criteria for autism (for example, APA, 1994); (2) different methods used to identify individuals withautism; (3) increased focus and emphasis on identifica-tion, especially for the very young; (4) increased referralsfor services and interventions; and (5) diagnostic substi-tution (Fombonne, 2003a,b; Volkmar, Lord, Bailey,Schultz, & Klin, 2004). Concerning diagnostic substitu-tion, a study (Fombonne, 2003b) of the prevalence rateof autism in the state of California showed an increasefrom 5.8 to14.9 per 10,000 for the years 1987 to 1994,whereas the number of children diagnosed as mentally re-tarded during this same period decreased from 28.8 to19.5 per 10,000. The change in the two prevalence ratessuggests that greater numbers of individuals who, in ear-lier years, would have been classified as mentally re-tarded were being identified as autistic. There is a dearthof well-developed and comprehensive epidemiologicstudies concerning the incidence and prevalence rates forautism, and we await the development and results of fu-ture studies to determine whether the rates of autism areactually increasing.
Many children with autism (approximately 70%)function within the retarded range of intelligence, as ev-ident in intelligence quotient (IQ) scores below 70(Fombonne, 2003a). Interestingly, the ratio of male to fe-male individuals with autism is largest for those of nor-mal intelligence, but is approximately 2 : 1 (male/female)for those individuals with autism who are mentally re-tarded. An inverse relation exists between IQ and severityof autistic symptoms. That is, the higher the level of in-telligence, the less severe the autistic symptoms. Circum-scribed abilities and skills of exceptional levels (such ashyperlexia, or early acquisition of reading skills withoutcomprehension) may appear within the context of severemental retardation. The rate of savant skills—that is, ex-traordinarily developed skills within the context of limitedcognitive capability—in autism is estimated to be 10 timesthat of the normal population (Waterhouse, Fein, &Modahl, 1996). The risk for seizure disorders is high in
autistic groups, with a mean rate across studies of 16.8%and even higher for autistic children with IQs less than50 (Fombonne, 2001; Fein, Joy, Green, & Waterhouse,1996).
H i g h - F u n c t i o n i n g A u t i s m o r A s p e r g e r ’ s S y n d r o m e ?
Currently, controversy exists over whether the two pri-mary representatives of pervasive developmental disor-ders, autism and Asperger’s syndrome, are separate disor-ders, overlapping subtypes, or one disorder withAsperger’s syndrome representing individuals with autismwho are higher functioning, both cognitively and adap-tively. Before considering this controversy, we review thesymptom presentation of Asperger’s syndrome.
The term Asperger’s syndrome refers to a group of chil-dren, adolescents, or adults who exhibit autistic-likesymptoms but do not strictly fulfill the autism criteria.The criteria for autism and Asperger’s syndrome of theAmerican Psychiatric Association (1994) show a signifi-cant overlap in symptoms related to impairments in so-cial interactions and preoccupations with narrow, repeti-tive, and stereotypic patterns of behavior, interests, andactivities. Despite this overlap, the APA proposes severaldifferences. Specifically, children with autistic-like behav-ior are not to receive the diagnosis of Asperger’s syndromeif they exhibit the following characteristics: (1) significantimpairment in verbal and nonverbal communicationskills, (2) a lack of developmentally appropriate symbolicor imaginative play, (3) delayed language development orabsence of language, (4) cognitive deficits, (5) impairmentin self-help and adaptive skills (excluding those involvingsocial interactions), and (6) limited or absent exploratorycuriosity (Bailey et al., 1996). These exclusionary crite-ria are consistent with Asperger’s original behavioral de-scription of children exhibiting the disorder. That is,these children display poor social skills, odd and eccen-tric behaviors, and restrictive patterns of interests and ac-tivities, without significant delays in cognitive or languageabilities.
Research studies (Eisenmajer et al., 1996; Volkmar et al.,2004) have sought to further clarify the differences be-tween Asperger’s syndrome and autism. Children diag-nosed as exhibiting Asperger’s syndrome, as contrastedwith autism, show a greater (1) desire for social contactand friendship; (2) willingness to participate in play withother children centered on their special interest, such asdinosaurs; (3) likelihood of normal onset of language de-velopment and an absence of echolalia and pronoun re-versal; (4) use of odd words of speech, pedantic speech,and one-sided, repetitive conversations; (5) tendency to
312 PART THREE | Disorders of the Brain

pursue narrow and limited areas of interest, such as pre-occupation with clocks; and (6) likelihood of beinginattentive, impulsive, and overactive. However, thesedifferential characteristics have been challenged in re-cent studies (Macintosh & Dissanayake, 2004; Mayes& Calhoun, 2001).
The separation of the two disorders poses several chal-lenges. First, varied definitions and differential selectioncriteria artificially blur the boundaries between the twodisorders, hindering efforts to identify commonalities anddifferences in cognition and behavior, etiology, and re-sponsiveness to differential treatments. In addition to themajor diagnostic criteria of the DSM-IV (APA, 1994) andInternational Classification of Diseases (ICD-10; WorldHealth Organization, 1992), no less than five otherwidely publicized definitions of Asperger’s syndrome exist(Volkmar & Klin, 2000). Each definition leads to differ-ences in selection criteria, areas of study, and research re-sults, thus hindering efforts to determine whether the twodisorders are independent of one another.
Second, the reported difference between autism andAsperger’s syndrome may reflect the level of intellectualor language development of the two disorders. By defini-tion, one criterion for differentiating Asperger’s syndromefrom autism is the relative absence of language and cogni-tive impairment in Asperger’s syndrome. Thus, childrenwith Asperger’s syndrome may simply be brighter chil-dren with autism who show fewer language deficits.
Third, a number of studies are flawed by the failure ofthe investigators to use outcome measures that are inde-pendent of those used for the selection of the partici-pants. For instance, it is certainly appropriate for re-searchers who are interested in identifying the differentialcharacteristics of Asperger’s syndrome and high-function-ing autism to use a measure of motor functioning to formthe two groups. As a result of this selection criterion, onegroup would consist of children who exhibit motordeficits and the other group would include children whodid not. However, in the formal study of the two groups,it would then be inappropriate to assess them with motormeasures in an effort to determine whether motordeficits differentiated between the groups. The circular-ity of this approach is evident, because the groups wereoriginally selected based on their differences in motorfunctioning.
Fourth, young, higher functioning children with autismfrequently exhibit behaviors consistent with Kanner’s char-acterization of autism. However, with maturity, they oftenshow fewer differences in symptom presentation from indi-viduals with Asperger’s syndrome (Howlin, 2003; Volkmaret al., 2004). Accordingly, Asperger’s syndrome may
merely reflect the changing presentation, over time, ofhigher functioning individuals with autism.
The case study of Tom Z. familiarizes the student withAsperger’s syndrome (Neuropsychology in Action 11.2).The study details the symptoms, evaluative data, and fam-ily history of Tom Z., as well as some rather surprisingneuroimaging findings.
N e u r o p s y c h o l o g i c a lP a t h o g e n e s i s
Various researchers attribute the development of autismto a host of causative factors. There are indications thatthe disorder is either familial or genetic in origin; how-ever, the finding of high rates of perinatal complicationsin the history of children with autism also implicates en-vironmental factors. Some evidence exists for an autisticdiathesis, that is, a genetically mediated vulnerability forautism that interacts with an early environmental insultto produce the disorder (Pennington, 2002). However, adefinitive number of environmental risk factors for thedevelopment of autism have not been identified. For in-stances, there is public concern that the combinedmeasles-mumps-rubella (MMR) immunization (or sub-stances used as a preservative of the active immune agents)places children at risk for autism. Empirical studies, todate, have not supported a relation between autism andimmunizations (Fombonne, 2003b). For instance, inYokohama, Japan, the combined MMR immunization waswithdrawn beginning in 1988 with no child receiving thevaccine as of 1993 or thereafter. Single immunizations foreach of these diseases continued to be administered. Thecumulative incidence of autism increased significantly be-tween 1988 and 1993, with the highest increase evident in1993 (Honda, Shimizu, & Rutter, 2005). The findings in-dicate that the increased incidence of autism was unrelatedto the MMR vaccination. Unfortunately, the public con-cern over a possible relation between the MMR immuniza-tion and autism has prompted some parents to withholdMMR inoculations from their children. Clearly, such adecision increases the risk for the children to contract oneor more of these diseases.
Support for a familial/genetic component of autism isthe finding of relatively high rates of the disorder in thesiblings of children with autism. The rate is approximately3% to 6%, which is 25 to 50 times greater than the inci-dence in the normal population (Fombonne, Bolton,Prior, Jordon, & Rutter, 1997; Sutcliffe & Nurmi, 2003).Heritability studies of identical twins reveal co-occurrencerates of 60% to 92%, whereas rates for fraternal twinsrange from 0% to 10% (Tanguay, 2000). The substantial
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 313

314 PART THREE | Disorders of the Brain
N e u r o p s y c h o l o g y i n A c t i o n 1 1 . 2
C a s e S t u d y o f a n A d o l e s c e n t w i t h A s p e r g e r ’ s S y n d r o m e
Tom Z. is a tall, stocky 15-year-old maleadolescent. He was born after an uncompli-cated pregnancy, and subsequent develop-mental milestones were achieved withinnormal limits. Tom talked before he walked.He taught himself to read by age 3 and wasreading adult-level books by age 4. By theage of 2.5 years, he had atypical intereststhat were pursued to the exclusion of otheractivities. Over the years, these interestshave included stop signs, arrows, stormdrains, windmills, clocks, mathematics, andcomputers.
In nursery school, he had poor peerrelations, talked incessantly about topics ofinterest only to himself, failed to listen to thecomments of others, and was often opposi-tional and impulsive. A clumsy and poorlycoordinated child, he often seemedmarkedly odd. A preschool psychologicalassessment recommended special educa-tion placement, and the parents tried variousprograms with limited success. They finallymoved him to homebound education. De-spite precocious academic achievements,Tom continued to have significant problemswith social interaction and in controlling hisbehavior.
At his first formal evaluation, when hewas 9.5 years old, Tom had no friends, poorinterpersonal skills, and signs of depression.His fascination with clocks pervaded allconversation. His poor social judgment wasclearly evident, particularly in his descriptionof interactions with peers. He showed limitednonverbal social behaviors, such as ges-tures, facial grimaces, emphasis of voice,and nonliteral communications. Interest-ingly, Tom’s father had a history of similarproblems. For example, Mr. Z. carried a smallnotebook to write down the names of impor-tant people he met because, “I can neverremember people’s faces; I can only remem-ber names when I write them down.”
Tom was evaluated again when he was12 years old. He continued to show amarkedly eccentric social style and engagedin one-sided conversations about computers
and mathematic concepts in a loud, poorlymodulated voice. His limited awareness ofsocial conventions was evident in his one-sided conversational style, his tendency tobelch and pass gas in public, and his use ofgraphic expletives without apparent intentionto shock others. He was preoccupied withthe subject of girlfriends and his sexualneeds.
Tom’s clinical presentation and assess-ment results were extreme in many respects.There was a significant discrepancy betweenhis Wechsler Intelligence Scale forChildren–Third Edition (WISC-III; Wechsler,1991) verbal and performance abilities(Verbal IQ � 139; Performance IQ � 127).He had superior scores in verbal reasoning,except for tasks involving social comprehen-sion. Although able to describe social demands, he could not translate thisknowledge into appropriate conduct. He alsoexhibited significant deficits in visuomotorskills, speed of processing, and motorfunctioning. Moreover, a large differenceexisted between his superior intelligencescore and his ratings on a measure of adap-tive skills. His adaptive rating score wassignificantly below average, indicating severedeficits in meeting the demands of everydaylife.
NeuroimagingFather and son underwent magnetic resonance imaging (MRI) of the brain. Thefather’s sagittal brain images showed a largeV-shaped wedge of missing tissue in thedorsolateral frontal region of the brain(Figure 11.3a). This region of tissue lossappeared in the same location of bothhemispheres, but was somewhat larger inthe left. Given the absence of a history oftrauma, the tissue loss likely represented anarea of focal dysmorphology of unknownorigin.
Tom showed a similar but noticeablysmaller region of structural anomalies inexactly the same area of both hemispheres.His abnormality, however, was somewhat
larger on the right, the reverse of the father’s(see Figure 11.3b). In addition, he showeddecreased tissue in the anteromesial regionof the left temporal lobe (see Figure 11.3c).The similarity of abnormalities in Mr. Z. andTom indicated potential familial transmission.
Discussion of Magnetic ResonanceImaging and Psychological TestingA three-dimensional rendering of the father’sbrain showed his neurodevelopmentalabnormality to be in the region of the middlefrontal gyrus (see Figure 11.3d). The deficitwas a recessed area of absent tissue. Fur-thermore, the three-dimensional imageshowed an abnormality that did not appearon the two-dimensional images: both rightand left frontal lobes showed an abnormalpattern of gyri and sulci. Normally, the frontallobe consists of three prominent horizontalgyri (the superior, middle, and inferior gyri)that run in parallel from anterior to posterior.Although the father’s superior frontal gyrusappeared normal, the middle frontal gyriwere vertical in both hemispheres. Thisaberrant pattern of surface structure mayhave originated from an abnormal prenataldevelopmental process.
Because of movement artifacts, a clearthree-dimensional representation of Tom’sbrain was not possible. However, researchersreconstructed coronal images by computermethods to evaluate his left temporal lobeabnormality. The images showed a largeregion of missing tissue and also an asymmetry of the lateral ventricles.
Any single case report must be inter-preted with caution, yet it is of interest thatTom’s neuropsychological deficits are under-standable in light of his brain abnormalitiesand other studies of individuals with autism,Asperger’s syndrome, and similar disorders(for example, see Piven et al., 1990). Asdescribed earlier, Tom’s psychological testing demonstrated significantly higherWISC-III Verbal IQ relative to Performance IQ.Consistent with his greater nonverbal difficul-ties, Tom’s frontal lobe abnormalities were

CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 315
more prominent on the right than the left side.The right hemisphere is also more prominentlyinvolved than the left hemisphere in regulatinglanguage prosody and pragmatics (Kolb &
Whishaw, 1990), two areas in which Tomperformed poorly. Moreover, the volume of hisleft hemisphere was somewhat larger than thatof the right. In a study published several years
ago, Willerman, Schultz, Rutledge, & Bigler(1992) found that a larger left than righthemisphere predicted a higher Verbal IQ thanPerformance IQ in male individuals.
(continued)
Images not available due to copyright restrictions

co-occurrence rates for identical twins suggest that geneticfactors play a significant role in the etiology of autism.Genetic research has implicated at least 20 genes as con-tributing to autism risk. Of these implicated genes, anom-alies of chromosome 15q11-q13 have been frequentlyreplicated across studies (Nurmi et al., 2003; Sutcliff &Nurmi, 2003).
The neural substrates considered to produce autismare numerous, but none has received unanimous support.Anatomic abnormalities, hypothesized or identified inautistic samples, have included most cortical and subcor-tical regions of the brain. In addition, empirical studiesreveal differences in neurochemical systems, brain vol-ume, proportion of white-to-gray matter, neuronal me-tabolism, and cellular migratory patterns of the cortex,prefrontal cortex, cerebellum, and limbic system (hip-pocampus, amygdala, and other limbic nuclei).
Studies have implicated abnormalities involving neu-rotransmitters as pathogenic of autism, with serotonin re-ceiving the most attention. Serotonin (5-HT) is involvedin regulating a number of brain functions, includinglearning, memory, sleep, pain responsiveness, mood, andinhibitory processes. In addition, there are indicationsthat excessive 5-HT can disrupt social affiliation and at-tachment. Children with autism show 25% to 50% in-crease in serotonin (hyperserotonemia), although theprecise role of 5-HT in the production of autistic symp-toms is unclear. Even more troublesome are studies show-ing that elevated levels of serotonin are not specific toautism, with other disorders such as mental retardationalso exhibiting hyperserotonemia (Anderson, 2002; Feinet al., 1996).
Converging evidence indicates that a large proportionof children with autism (14–30%) have a greater headcircumference than healthy control children. Brain size isalso larger (approximately 10%) in autistic populations(Volkmar et al., 2004). Of importance is the finding ofsmall brain size at birth, followed by two periods of ac-celerated growth occurring at 1 to 2 months and 6 to 14 months of age. Subsequently, brain size in autismreaches its maximum growth by ages 4 to 5 years and
thereafter begins to gradually decline. By adolescence andadulthood, brain size is similar to that of healthy adults(Courchesne, Carper, & Akshoomoff, 2003). Althoughthe underlying neurobiological factors accounting for thisdevelopmental pattern are unknown, this growth profilemay provide an early warning signal for the risk forautism. However, head or brain size enlargement may nothave a direct causative role in autism insofar as there is lit-tle relation between head/brain size and specific autisticsymptoms. In addition, other clinical populations showincreased head/brain size, specifically fragile X syndromeand tuberous sclerosis (Tanquay, 2000).
A second area of convergence relates to the finding ofatypical white-to-gray brain matter ratios in autistic pop-ulations (Schultz, Romanksi, & Tsatsanis, 2000). Al-though the pathogenic relation of disproportionate white-to-gray matter to autism remains to be clarified, it ishypothesized that it represents a disruption of the brain’sinterconnectivity (Volkmar et al., 2004). In turn, integra-tive brain functions are impaired. Interestingly, there isalso speculation that the atypical white-to-gray mattermay result in modularity of brain functions. Modularityrelates to brain functions that are specific to relatively sep-arate and independent brain regions or circuits. The highrate of savant capabilities in cognitively impaired autisticgroups is consistent with a modular organization—thatis, a set of neurally distinct, preserved, and self-containedmental functions.
Historically, the cerebellum has been thought to medi-ate motor behavior. Increasingly, clinical and researchstudies are reporting that the cerebellum is involved in anumber of cognitive operations including attentional be-havior, classical conditioning, and executive functions.Structural and functional abnormalities of the cerebellumin autistic populations are evident. For instance, studieshave identified hyperplasia or hypoplasia of the cerebellarvermis lobules (Courchesne, Townsend, & Saitoh, 1994;Filipek, 1995). Malformation of the cerebellar vermis lob-ules is believed to cause a disruption of attentional shift-ing and possibly other cognitive processes often evidentin autism. However, subsequent studies of cerebellar
316 PART THREE | Disorders of the Brain
(continued)The frontal lobe findings may clarify Tom’smotor difficulties and conceptual inflexibility.The structural abnormality was at the junctureof the primary motor strip, premotor area, anddorsolateral convexity, thus potentially affect-
ing the functions mediated by each of theseregions. The dorsolateral prefrontal cortex isknown to be involved in the executive functionsof working memory and shielding of cognitiveoperations from disruption by unwanteddistractions (Goldman-Rakic, 1987a).
Source: Adapted from Volkmar, F. R., Klin, A.,Schultz, R., Bronen, R., Marans, W. D., Sparrow,S., et al. (1996). Asperger’s syndrome. Journal ofthe American Academy of Child and AdolescentPsychiatry, 35, 118–123.

structure have produced negative results (Schultz et al.,2000). Furthermore, cerebellar anomalies are not specificto autism, as evident in similar malformations in thebrains of mentally retarded populations.
The temporal and limbic system structures, includingthe amygdala, hippocampus, and entorhinal cortex, ap-pear to play a major role in mediating human socioemo-tional behavior. Studies of the temporal lobe-limbic sys-tem of autistic populations reveal volumetric reductions,hypofunctional activity, and abnormalities in neuronalsize and density (Schultz et al., 2000). The importantfindings of atypical facial processing in autistic groups areof particular interest. Orienting to and focusing on thefaces of others initially occurs in early infancy and is animportant precursor of healthy emotional and social de-velopment. Children with autism show a lack of interestin human faces and, in contrast, a preferential interest inobjects as early as the first year of life.
The medial temporal-limbic system is intimately in-volved in facial and emotional processing. The fusiformand inferior temporal gyri (and possibly the lateral occipi-tal gyrus and parahippocampal gyrus) are preferentiallyinvolved in facial and object processing, respectively. Be-cause of its activation in facial processing, an area in themiddle region of the fusiform gyrus is referred to as thefusiform face area (FFA). At least seven different studiesof children, adolescents, and adults with autism (Piggotet al., 2004; Schultz et al., 2003; Wang, Dapretto, Hariri,Sigman, & Bookheimer, 2004) show reduced activationof the FFA to images of human faces. For instance,Schultz and associates (2000) have investigated the fMRIactivation patterns of autistic (autistic and Asperger’s syn-drome) and healthy young adults of normal intelligencewhen performing facial and object discrimination tasks.The study revealed that subjects with autism demon-strated decreased activation in the FFA and increased ac-tivation of the inferior temporal gyrus when performingthe facial discrimination task. In contrast, the healthycontrol participants showed significant activation of theFFA and decreased activation of the inferior temporallobe. Both healthy control participants and those withautism activated the inferior temporal gyrus when view-ing objects. Likewise, autistic groups have been found toshow reduced activation in the FFA when required tomatch emotional facial expressions or identify mentalstates based on facial details (Piggot et al., 2004; Schultzet al., 2003). Overall, these studies indicate that autism isassociated with atypical activation of a brain region re-lated to a basic building block of socioemotional behav-ior, namely, facial processing. A failure to attend to thefaces of significant others, and people in general, disrupts
normal socioemotional learning during development andpotentially contributes to the significant social disinterestand atypical interaction patterns that characterize autisticgroups.
There are indications that the FFA may have an evenbroader role in the mediation of socioemotional behavior.In an ingenious experiment, Klin (2000) used a task, theSocial Attribution Task, to assess the social cognitions ofyoung adults with autism. The Social Attribution Task in-volves the presentation of systematic movements of geo-metric shapes that, when viewed by healthy individuals, areimbued with social meaning. In contrast, individuals withautism do not impose social meaning on these movements;instead, they describe the physical features of the stimuli.In a recent fMRI study (Schultz et al., 2003), healthy con-trol participants were presented the Social AttributionTask, a face perception task, and control tasks. Of impor-tance to our discussion is the finding of marked activa-tion of the FFA for both the Social Attribution Task andface perception tasks, but not for the control tasks. Theauthors conclude that the FFA appears to have an impor-tant role in social attribution and judgment. However,the FFA is but one functional component of the limbicsystem, and attention by neuroscientists has also focusedon other limbic structures, such as the amygdala.
The amygdala is richly interconnected with the tem-poral cortex and other cortical and subcortical regions. Itis involved in emotional arousal, appraising the behav-ioral significance of environmental stimuli, attributingemotional valence to stimuli, and emotional learning(Schultz et al., 2003). Animal research demonstrates thatdamage to the limbic system, including the amygdala, canproduce autistic-like behaviors (Bachevalier, 1994). In addition, atypical neuroactivation of the amygdala is ap-parent in autistic groups when processing facial (Wang et al., 2004; Sparks et al., 2002) and theory of mind tasks(Baron-Cohen, O’Riordan, Stone, Jones, & Plaisted,1999).
Evidence also exists of anomalies in frontal lobe func-tioning associated with autism. Neuroimaging studiesshow atypical activation of the orbital and medial pre-frontal cortices and anterior cingulate in individuals withautism (Schultz et al., 2000). Because of the rich inter-connections of the frontal regions with limbic and otherbrain structures, the frontal cortices are in a position tointegrate and regulate the internal and external inputsnecessary for socioemotional behavior.
Increasingly, research and clinical work with autismand other populations has led to the theorization of a so-cial brain network. Interconnected orbital and medial pre-frontal cortices, anterior cingulate, amygdala, superior
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 317

temporal sulcus, and FFA are believed to underpin the so-cial brain. It is hypothesized that the orbital and medialprefrontal cortices play a role in integrating and regulat-ing affective and cognitive processes, whereas the dorso-medial prefrontal cortex and cingulate support social cog-nition (thinking about the thoughts, feelings, andintentions of others and social judgment). The amygdalaappears to be involved in modulating and interpreting theemotional significance of stimuli and in assisting the cor-tex with the integration of emotion and cognition forevaluation and action by the frontal lobes. The superiortemporal sulcus supports facial expressions, social ges-tures, eye gaze, and facial recognition, while the FFA as-sists in facial discrimination and social attribution. To-gether, the latter two structures support the perception ofsocial behavior (Schultz et al., 2000, 2003). Damage todifferent aspects of this distributed social brain networkmay account for the heterogeneity of cognitive, emo-tional, and social deficits of autistic populations. Obvi-ously, the social brain network warrants additional empir-ical verification and possible expansion to include otherlimbic structures.
N e u r o p s y c h o l o g i c a l A s s e s s m e n t
The diagnosis of autism requires a careful review of thechild’s developmental history and observations of thechild with family members, teachers, and peers. In addi-tion, a complete medical evaluation and review of perti-nent medical records should be standard practice becauseof the potential presence of genetic and chromosomal ab-normalities, the high likelihood of co-occurring medicalconditions (such as seizures), and the association ofautism with other neurodevelopmental disorders. More-over, assessments by other disciplines (such as speech andlanguage) are often needed to augment the evaluation.
The neuropsychological evaluation of the child withautism should involve a comprehensive assessment of cog-nitive and related behaviors. The selection of measuresdepends heavily on the unique presentation of the child.For example, the evaluation and selection of measuresmay be quite different for the child who has not devel-oped language than for the child who has rudimentarylanguage. Currently, the Autism Diagnostic Interview-Revised (Rutter, Le Couteur, & Lord, 2003) and AutismDiagnostic Observation Schedule (Lord et al., 2000) aretwo well-standardized measures that are considered the“gold standards” for the assessment of autism.
Cognitive Profiles—It was initially proposed that childrenwith Asperger’s syndrome and autism demonstrated dif-ferential cognitive patterns (Ehlers et al., 1997; Minshew,
1997). The Asperger’s syndrome profile involves greaterfacility in verbal relative to visuospatial or visuomotorproblem solving. This cognitive profile is consistent withthat demonstrated by children with NVLD (Rourke &Conway, 1997; see Nonverbal Learning Disability sectionearlier in this chapter). The autism cognitive profile is theconverse of the Asperger’s syndrome profile. That is, chil-dren with autism demonstrate relative strengths in visual-perceptual and visuospatial as contrasted with verbalproblem solving. The majority of subsequent studies(Macintosh & Dissanayake, 2004) are not supportive ofthese differential cognitive profiles. In fact, several of thesestudies have found no differences between the two groups,whereas others have shown the opposite cognitive pro-files, with autistic groups showing relatively advanced ver-bal relative to visuospatial and visual-perceptual abilities.
Although differential profiles for autism and Asperger’ssyndrome are not fully supported, they do highlight thevariability of performance that may be encountered in theneuropsychological assessment of this group, particularlyas contrasted with mentally retarded populations where amore uniform suppression of cognitive abilities is oftenevident. However, individuals with autism often demon-strate poor performance on tasks that require higher levelconceptual processes such as reasoning, inferring, inte-grating, and abstracting (Minshew, 1997). This deficitcuts across the domains of cognition involving language,memory, executive functions, and academic performance.In addition, individuals with autism tend to be more de-tail oriented and have difficulty with (1) integrating partsinto wholes, (2) identifying central elements or themes,(3) differentiating between relevant and irrelevant infor-mation, and (4) determining meaning (Ozonoff, 2001).Their thinking is often literal and concrete. The high rateof hyperlexia in autism exemplifies this disparity. Theautistic child with hyperlexia learns to read (decode) earlybut is impaired in comprehending the reading material.Interestingly, the cognitive and learning profile of autismis the converse of learning disabilities such as dyslexia.The dyslexic child cannot decode words but shows pre-served listening comprehension when another personreads the material aloud. In summary, deficits in higherorder thinking processes are evident across the autisticspectrum, including those individuals who are higher-functioning.
Executive Function—Similarities in the behaviors of individ-uals with autism and patients with prefrontal damagehave prompted speculation that executive dysfunctionmay be of causative significance in autism. Empirical ef-forts to determine the validity of this speculation, and to
318 PART THREE | Disorders of the Brain

identify differential patterns of executive performance,are growing.
Consistent with this line of investigation, Hughes,Russell, and Robbins (1994) have determined that chil-dren with autism perform in an inferior and differentialmanner on executive measures compared with healthycontrol children. Specifically, the autistic group exhibitedpoorer complex planning and mental shifting perfor-mance and also a unique type of executive deficit termed“stuck in set” perseveration. The researchers interpretedthe concept of “stuck in set” perseveration as a failure todisengage the current attentional focus from ongoing cog-nitive operations (Ciesielski & Harris, 1997). Such disen-gagement is necessary if the person is to shift attentionalfocus to a new set of demands, activities, or goals.
The most robust executive deficit associated withautism is that of higher order planning (Ozonoff, 2001).Executive planning involves complex, means–end prob-lem solving to achieve a behavioral goal and is supportedby a number of component processes to include workingmemory, mental flexibility, response inhibition (the abil-ity to delay a response), and the ability to project ahead intime. Research using tower tasks (Tower of London/Hanoi) to assess executive planning consistently showspoorer performance by autistic groups (both high- andlow-functioning) relative to healthy and other clinicalgroups (Pennington & Ozonoff, 1996). A set of studies byOzonoff and others (Ozonoff & Jensen, 1999; Ozonoff &Strayer, 2001) revealed distinct executive profiles for autis-tic, Gilles de la Tourette’s syndrome, and ADHD groups.Specifically, autistic groups showed impaired planning andmental flexibility, whereas ADHD groups exhibited defi-ciencies in response inhibition. The Gilles de la Tourette’ssyndrome and healthy control groups did not differ intheir performance across executive function tasks.
Ozonoff (2001) calls attention to the importance ofsubtle or overlooked factors that may affect the perfor-mance of individuals with autism. For instance, when ex-amining studies of executive performance, particularlythose that involved tower tasks, the performance of autis-tic groups varied from impaired to unimpaired. She dis-covered that most of the studies reporting unimpaired orimproved executive performance involved computerizedadministration of the executive measures. In contrast, im-paired performance was more likely to be evident whenthe measures were presented in a face-to-face format. Sub-sequent investigations indicated that the issue is muchmore subtle than type of test administration. The impor-tant variable appears to be the mode of feedback, humanversus nonhuman. Individuals with autism appear toshow poorer performance when feedback is presented
within a verbal, social-interactive, as contrasted to an im-personal, computer-generated context.
Social Cognition—Converging evidence is revealing thatautism is associated with deficits in social cognition. Socialcognition encompasses a diverse set of processes such as fa-cial perception, social orientation, joint attention, imita-tion, and theory of mind (TOM). We have reviewed facialprocessing in autism (see Neuropathogenesis earlier in thischapter). Deficits in social orientation (interest in and pref-erence for human contact over objects) and joint attention(sharing a common focus of attention with another) are ev-ident in autistic children. Likewise, imitation of others is akey component of social learning. Research reports thatchildren with autism often do not imitate the actions ofsignificant others and peers (Pennington, 2002).
TOM has received considerable empirical and theoret-ical attention. TOM, or “mentalism,” refers to the abilityto represent or infer mental states such as the beliefs, mo-tives, and intentions of others. This ability enables peopleto make attributions, to reason about mental states, and tounderstand and predict the behavior of others (Rowe, Bullock, Polkey, & Morris, 2001). It is posed to be in-volved in or support the social behaviors of perspective-taking, “mind-reading,” empathy, and the detection of de-ception, irony, humor, and faux pas (Baron-Cohen et al.,1999; Lawson, Baron-Cohen, & Wheelwright, 2004). Anexample of TOM would be observing a person and infer-ring what the person is “thinking” or predicting how theperson would respond. This example portrays a first-orderTOM. Higher levels of TOM are also evident. A second-order TOM would involve representing or inferring oneperson’s mental state about another person’s mental state(“Bill thinks that Mary believes that Joe believes . . .”).Young children are capable of performing first-ordertasks, whereas success with second-order TOM tasks isnot achieved until a later age, depending on the com-plexity and difficulty of the task presented. UnimpairedTOM processing is viewed as central to the develop-ment of appropriate interpersonal and communicationpatterns.
Investigations reveal deficits in TOM for autistic groupsrelative to healthy control participants (Jarrold, Butler,Cottington, & Jimenez, 2000; Ozonoff & Griffith, 2000;Rutherford & Rogers, 2003). Suggestions have been madethat TOM performance is supported, in part, by the or-bital prefrontal cortex (Baron-Cohen, Ring, Bullmore,Wheelwright, Ashwin, & Williams, 2000), a region impli-cated in higher order socioemotional regulation. A num-ber of imaging studies have also demonstrated a relationbetween TOM performance and the medial prefrontal
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 319

cortex activation (Shallice, 2001). In a relatively recent in-vestigation (Stuss, Gallup, & Alexander, 2001), patientswith lesions of the frontal and nonfrontal cortices werepresented with measures of TOM. In contrasting the per-formance of the different lesion groups, significantlypoorer TOM performance was associated right and bilat-eral frontal lesions, particularly lesions of the right medialprefrontal cortex.
Although TOM has enhanced our understanding ofautism, it has received its share of criticism. For example,TOM deficits are evident in other clinical groups, indi-cating a lack of specificity to autism (Pennington, 2002).Furthermore, TOM performance is related to verbal abil-ity and general cognitive level which undermines its util-ity as a specific index of social cognition. Finally, TOMhas been variously defined as a cognitive, language, emo-tional, or social construct, leading to confusion as to whatprocesses are actually encompassed by the theory. There-fore, we await further theoretical developments and re-search to clarify the meaning, boundaries, and utility ofTOM.
Although psychological constructs such as executivefunction and social cognition have enabled us to charac-terize and predict certain autistic behaviors, they lack thetheoretical breadth necessary to account for the diversecommunication, language, and social behaviors associ-ated with the disorder. We next turn to a theoreticalmodel that endeavors to provide a comprehensive neuro-functional model of autism.
C o m p r e h e n s i v e N e u r o f u n c t i o n a l M o d e l
Multiple theories and models are available to account forthe behavioral manifestations, core deficits, and cause ofautism. These conceptualizations focus on impairmentsof attention (shifting and selective), TOM, social attach-ment, socioemotional perception, memory, language, andexecutive function (Fein et al., 1996). The majority ofthese theoretical efforts are rather narrow with regard tothe specific autistic behavior that is interpreted or pre-dicted. Accordingly, most fail to account for the multiplebehavioral manifestations and proposed neural impair-ments of autism.
Waterhouse and coworkers (1996) propose a compre-hensive model to account for the heterogeneity of symp-toms and causes of autism. The comprehensive modelrests on a series of assumptions relating human social be-havior to brain functioning. It proposes four neurofunc-tional impairments that, in interaction, account for thesocial and related behavioral disruptions of autism:
1. Canalesthesia involves the fragmented processing ofincoming information from the different sensorymodalities. Because of this fragmentation, sensory in-formation in consciousness, working memory, and de-clarative memory fails to integrate properly, resultingin distorted representations of the information.
2. Impaired affective assignment is the disrupted link-ing of appropriate emotional meaning or significanceto novel and social stimuli. This disruption impairsappropriate responses to new situations and the socialactions of others.
3. Asociality is a profound disturbance of normal socialattachment and interdependence with others. Socialinterest and bonding motivation are minimal or lack-ing altogether.
4. Extended selective attention is an overextended at-tentional focus and inordinate delay in shifting atten-tion, resulting in a variety of inappropriate responsessuch as hypersensitivity to sensory input and persever-ative behaviors.
Waterhouse and coworkers (1996) link each of theaforementioned neurofunctional impairments to rela-tively distinct neural regions and circuitry. That is, dys-function of the hippocampus and amygdala of the tem-poral lobes produces canalesthesia and the impairedassignment of affective significance, respectively. Asocial-ity relates to the aberrant functioning of three interrelatedneurochemical systems: oxytocin and vasopressin neuropep-tide, endogenous opiate, and serotonin. Finally, the re-searchers consider extended selective attention to relate to adisruption of the temporal and parietal association areas.Although each of these supporting neural regions and cir-cuitry links to specific broad functions, they interact andoverlap to produce the deficits that the child with autismdisplays. Interestingly, Waterhouse and coworkers viewbrainstem, cerebellum, and frontal lobe damage—all ofwhich other researchers and theorists have considered of eti-ologic significance in autism—as only secondary causes orby-products of aberrant input from other neural systems.
An impressive body of supporting research based onneuroimaging, electrophysiology, neuropathology, andanimal studies supports the four neurofunctional impair-ments as pathogenic of autism. An individual with autismcan present all four of these impairments. However, someindividuals present three or fewer impaired neurofunc-tional systems. In such cases, the number and form of thesymptoms exhibited relate to damage to the individualsystem or group of systems. For example, if damage is re-stricted to the oxytocin-opiate system, the model predictsthat most of the autistic symptoms will be absent, except
320 PART THREE | Disorders of the Brain

for those behaviors associated with disrupted social at-tachment and lack of affiliation with others. Althoughthe validity and utility of the comprehensive model re-quires further empirical verification, it represents a boldeffort to integrate the theories and empirical findings ofautism.
D e v e l o p m e n t a l C o u r s e
Autism is a chronic, lifelong disorder that parents and pro-fessionals generally detect before the child reaches age 3. Anumber of distinguishing characteristics appear as thechild with autism develops, although individual differ-ences are evident. In infancy, the baby with autism maybe passive and unresponsive to being held and cuddled.Social or interactive behaviors directed to the infant bycaretakers often fail to elicit recognition or interest.
As the child with autism moves into the toddler andpreschool years, the onset of speech and language is oftendelayed or may fail to develop altogether. Moreover, aslanguage develops, echolalia, reversed pronouns, and ne-ologisms may emerge. Self-help skills lag in development.The child with autism is less likely than healthy childrento imitate the gestures or vocalizations of adults (Sigman,1994; Tanguay, 2000) and has only a limited desire orability to communicate with others.
The play of the child with autism lacks sophisticationin both structured and unstructured situations. The de-velopmental stages of parallel and cooperative play are de-layed or not attained at all. Stereotypic motor behaviors,unusual interests or preoccupations, demands for orderand sameness, and other peculiar behaviors may domi-nate the child’s daily activities. Unusual reactions, such ashypersensitivity to specific environmental stimuli (such asnoise) or advanced abilities or skills (such as hyperlexia),may also be apparent.
During the toddler and early preschool years, the par-ents begin to realize their child is not developing appropri-ately. Professional services are typically sought, and thechild is involved in a series of medical, psychological,speech, language, and related evaluations. At this point,there is a rendering of the diagnosis of autism for the first time, and comorbid conditions, such as mental retar-dation, are identified. Subsequently, the parents oftenenter the child into a preschool special education or treat-ment program with supportive services.
Autistic behavioral excesses and deficits continue to beevident during the child’s elementary school years. How-ever, as discussed earlier, improvement across behavioraldomains begin to be evident with increasing age, particu-larly for the higher functioning child with autism. Despite
this improvement, the child remains developmentally de-layed and continues to exhibit unusual behavioral pat-terns. Many of these children cannot enter a normal edu-cational program. Academic achievement is variable andpoor, particularly if cognitive or intellectual deficits arepronounced. Peer interactions are minimal, and mostchildren with autism never develop a close friendship.
Continued improvement may be evident with the ad-vent of adolescence, particularly for the higher function-ing child with autism. However, most individuals withautism continue to exhibit deficits in one or more of thecore impairment areas, and unfortunately, some teenagerswith autism regress (Piven, Harper, Palmer, & Arndt,1996). Low-functioning adolescents with autism oftenneed continued training in the more basic life skills andplacement in a program, such as a sheltered workshop,that emphasizes the development of rudimentary voca-tional skills. Higher functioning teenagers with autism,despite relative success in academics, lack social accep-tance by peers because of their ongoing deficits in social-ization and communication and their unusual interestsand patterns of behavior.
Approximately 80% of individuals with autism are un-able to move fully into the workforce, and up to half re-quire lifelong residential care (Pennington, 1991). Otherscan function effectively in a sheltered workshop or higherlevel of employment if the work environment is support-ive. Higher functioning individuals may be capable of lifein a group home or other assisted living program in thecommunity. Only about one-third are able to live inde-pendently.
T r e a t m e n t
Currently, the most significant treatments for autism andother pervasive developmental disorders include behav-ioral interventions, special education, and occasionally,pharmacotherapy. Despite early intervention and applica-tion of currently available treatment options, autistic andrelated disorders generally do not fully resolve.
Caretakers generally use behavior modification as anintervention in an autistic child’s comprehensive treat-ment program. Several investigators consider behaviormodification one of the more effective treatment optionsfor children with autism. Generally, the use of behavioralinterventions involves a functional analysis of targeted be-haviors to determine the relation of environmental an-tecedents and consequences to the child’s behavior. Usingthis analysis, psychologists develop a behavioral plan togenerate behaviors (such as social skills), strengthen appro-priate actions (such as increased eye contact), and reduce
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 321

or eliminate maladaptive behaviors (such as aggression orself-injury). Caretakers use both rewarding and aversivebehavior interventions to bring about desired change.Positive reinforcement and token systems are two exam-ples of rewarding interventions used to produce orstrengthen target behaviors. Aversive behavioral tech-niques incorporate the use of corrective feedback, time-out, response cost, and overcorrection to reduce inappro-priate behaviors. Response cost involves the loss of areinforcer contingent on the child demonstrating an in-appropriate behavior, whereas overcorrection involveshaving the child practice a positive response that is in-compatible with an inappropriate behavior. Overcorrec-tion is particularly effective in reducing self-stimulatingbehaviors, such as repetitive mouthing of objects.
Insofar as deficits in language and communicationskills are often dramatic, initial treatment efforts focusedon increasing language acquisition and production. Thatis, the interventions centered on prompting speech andreinforcing the child’s verbalizations. Although verbaliza-tions increased, the child’s actual ability to communicatedid not necessarily improve. The realization that verbalproduction does not equate with communication hasprompted a shift in treatment focus to increasing thechild’s spontaneous, communicative language. Moreover,social skills training is receiving increased attention as atreatment modality. These interventions target one of thecentral deficits of autism, the impaired ability to relate toothers. Finally, some children with autism benefit frompharmacologic interventions to reduce self-injurious behav-iors, hyperactivity, ritualistic behaviors, and aggressiveness.However, a number of the medications (such as haloperi-dol [Haldol]) require careful monitoring for potentiallyserious side effects. The advent of atypical antipsychoticmedications (for example, risperidone [Risperdal]) isreceiving support for treating severe behavioral distur-bances, significant agitation, and self-injurious orstereotypic behaviors (McDougle et al., 2000). Simi-larly, selective serotonin reuptake inhibitors (for exam-ple, fluoxetine hydrochloride [Prozac]) are efficaciousin treating compulsive, stereotypic behaviors and aggression.
In summary, children with autism frequently requirespecial educational services tailored to their individuallearning, social, and adaptive needs. In addition to acade-mic and daily living skills, many require ancillary servicessuch as speech, language, and physical therapy. Vocationaltraining and supervised job placement, often in a shel-tered workshop environment, provide meaningful em-ployment and the opportunity for social and recreationalactivities for individuals with autism.
Disruptive Behavioral Disorders
The APA (1994) currently classifies disruptive or ex-ternalizing behavioral disorders as psychiatric disorders.These disorders feature a variety of poorly controlled or acting-out behaviors that are developmentally inappropriateor violate societal dictates for acceptable behavior. The threeprimary representatives of this category are ADHD, opposi-tional defiant disorder (ODD), and conduct disorder (CD).As a developmental disorder, ADHD has generated an enor-mous number of theoretical and empirical studies since themid-1980s. It is to this disorder, the most prevalent of child-hood disruptive disorders, that we turn our attention next.
A T T E N T I O N - D E F I C I T/H Y P E R A C T I V I T YD I S O R D E R
C l i n i c a l B a c k g r o u n d a n d P r e s e n t a t i o n
The clinical manifestations of children exhibiting an attention-deficit/hyperactivity disorder (ADHD) arevariable, although clinicians generally agree that the coresymptom patterns include age-inappropriate inattention,impulsivity, and hyperactivity. These symptom patternsare chronic, cross situational in presentation, and devel-opmental in origin (APA, 1994). Thus, the behavioralsymptoms of ADHD are not transient in presentationand generally continue into adolescence and adulthood.Furthermore, these symptoms are typically observed be-fore school age and across multiple contexts such as home,school, and the community.
Since its inception in 1980, the diagnosis of ADHDhas undergone several revisions (Table 11.5). These revi-sions involve introducing different diagnostic models,changing exclusionary criteria, and delineating specificsubtypes. Despite these modifications, the diagnosis re-tains the core symptoms of inattention, impulsivity, andhyperactivity, although the combinations, relations, anddefinitions of these symptom patterns have altered.
D e m o g r a p h i c a n d C o m o r b i d C o n d i t i o n s
Currently, ADHD accounts for a third to half of all child-hood referrals for psychological services (Richters et al.,1995). Prevalence rates of 3% to 9% for childhood popula-tions are commonly cited (Spencer, 2002). The breakdownof ADHD figures by sex reveals that boys, compared withgirls, are more frequently diagnosed as exhibiting ADHD,with cited ratios ranging from 3:1 to 9:1 (Pennington,1997a). However, some researchers suggest that girls are
322 PART THREE | Disorders of the Brain

DSM Symptom Presentation
DSM-III (1980)
Attention-deficit with Inattention, impulsivity, hyperactivity and hyperactivity
Attention-deficit without Inattention and impulsivityhyperactivity
DSM-III-R (1987)
Attention-deficit/ Inattention, impulsivity, hyperactivity disorder and hyperactivity
Undifferentiated attention Inattentiondeficit disorder
DSM-IV (1994)
Attention-deficit/hyperactivity Inattention, impulsivity, disorder—combined type and hyperactivity
Attention-deficit/hyperactivity Inattentiondisorder—inattentive type
Attention-deficit/hyperactivity Impulsivity and hyperactivitydisorder—impulsive-hyperactive type
DSM-III � Diagnostic and Statistical Manual of Mental Disorders, Third Edition;DSM-III-R � Diagnostic and Statistical Manual of Mental Disorders, Third Edition,Revised; DSM-IV � Diagnostic and Statistical Manual of Mental Disorders, FourthEdition. Reprinted with permission from the Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition. Text Revision, Copyright 2000, American PsychiatricAssociation.
under-represented, partly because of the greater likelihoodthat boys will present with higher levels of overactivity andaggressive behaviors that quickly draw the attention of caretakers. Although a childhood disorder, 30% to 60%of diagnosed children continue to exhibit symptoms ofADHD in adulthood (Sheppard, Bradshaw, Purcell, &Pantelis, 1999). Currently, increased focus has been on theidentification and treatment of adults with ADHD.
There is a growing recognition that ADHD frequentlycoexists with other psychiatric and psychological disor-ders. ODD and CD are the most prevalent comorbid con-ditions of ADHD, with reported rates of occurrence rang-ing from 40% to 65% (Barkley, 1990; Wilens et al., 2002).ODD is characterized by chronic, age-inappropriate,angry mood and resistant, stubborn behaviors, and CDinvolves the repeated violations of the rights of others orof societal norms. Assaultive behaviors and illicit drug useare examples of the types of violations CD children ex-hibit. The basis for the high rates of comorbidity ofODD/CD with ADHD is unclear. However, evidencesuggests that social factors such as family sociopathy,
rather than genetic determinants, are contributors to thepathogenesis of these disorders.
ADHD also covaries with anxiety and depressive dis-orders at rates ranging from 18% to 51%, depending onthe childhood population sampled for study (Eiraldi,Power, & Nezu, 1997; Jensen, Martin, & Cantwell, 1997;Wilens et al., 2002). Estimates of the rate of comorbidityof ADHD and Gilles de la Tourette disorder range from25% to 50% (Cirino, Chapieski, & Massman, 2000). Fi-nally, from 15% to 20% of children with ADHD also ex-hibit learning disabilities (Richters et al., 1995). The highrates of comorbidity have led to speculation that ADHDis one disorder within a spectrum of related disorders.
N e u r o p s y c h o l o g i c a lP a t h o g e n e s i s
Neuropsychologists consider ADHD a neurobiologicallybased developmental disorder that responds to specifictypes of environmental and pharmacologic interventions.However, the etiology of ADHD is currently unknown.We review areas of investigation that are expanding ourknowledge of the pathogenesis and symptoms of ADHD.
Familial and Genetic Influence—Accumulating evidence suggeststhat ADHD is a familial disorder, possibly inheritable. Thefamilial nature of the disorder is clear from the elevated ratesof ADHD in first- and second-degree relatives. The presenceof familial ADHD does not necessarily signal that the disor-der is genetically determined because little is known of thepsychosocial environmental transmission of ADHD acrossgenerations. The finding of significant parental discord andpsychopathology in families of children with ADHD sug-gests that environmental factors may be of causative signifi-cance. However, the high rate of concordance of ADHD foridentical twins and the discovery of a potential linkage be-tween ADHD and genetic markers tips the balance in thedirection of a genetic component as the primary determi-nant of the disorder. Regarding the latter, researchers havelinked a thyroid gene to a narrow subgroup of children withADHD (Hauser et al., 1993) and have also identified a rela-tion between ADHD and a number of gene variants.
The D4 receptor gene on chromosome 11 has beenimplicated in the etiology of ADHD (Holmes et al.,2000; Smalley et al., 1998). One variant of the D4 gene,the 7-repeat allele (a segment of the DNA is repeatedseven times), has been associated with the personality traitof “novelty seeking” or “thrill seeking,” a characteristicoften evident in children with ADHD. Several studies havefound that children with ADHD are more likely to havethe 7-repeat allele than healthy children. However, only25% to 30% of children with ADHD carry the 7-repeat
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 323
Table 11.5 Changing Attention-Deficit/Hyperactivity Disorder Criteria

allele, indicating that the gene is neither necessary nor suf-ficient to produce the disorder (Barr, 2001; Pliszka, 2003).
The dopamine transporter gene (DAT1), located onchromosome 5, governs the reuptake of dopamine intothe neuron. The presence of one variant of the DAT1,10-repeat (segment of DNA repeated 10 times) allele, is as-sociated with greater risk for ADHD (Daly, Hawi, Fitzger-ald, & Gill, 1999; Waldman et al., 1998). The genetic re-search with “knockout” mice that examines the relation ofthe DAT1 gene to behavior is of interest. Knockout miceare bred without selected genes to study the effects of muta-tions and other genetic alterations. Investigations of knock-out mice without the (DAT1) gene reveal that the animalsdemonstrate hyperactivity, poor spatial performance, andother behaviors suggestive of disrupted inhibitory control.When administered a psychostimulant medication (for ex-ample, methylphenidate [Ritalin]), the mice showed a calm-ing response, similar to that evident with medicated chil-dren with ADHD (Gainetdinov & Caron, 2001).
Other genes implicated in ADHD are the dopaminereceptor D5, catechol O-methyltransferase (COMT;codes for the enzyme that catalyzes the breakdown ofdopamine and norepinephrine), and monoamine oxi-dase (MAO; codes for the enzyme that breaks downdopamine and norepinephrine after reuptake into theneuron). However, there are both confirmatory and con-tradictory studies regarding the association of thedopamine receptor (D5 ), COMT, MAO, and othergenes with ADHD (Pliszka, 2003), indicating the needfor further research to clarify and expand our knowledgeof the role of genetics in the pathogenesis of ADHD.
Neural Substrates—Numerous neural substrates have beenimplicated in the etiology and neuropsychological man-ifestations of ADHD, including most major corticaland subcortical systems, regions, and axes of the brain.Currently, four cortical-subcortical brain regions are thefocus of study. The first relates to possible abnormali-ties in the structure of the corpus callosum. Such anom-alies are believed to disrupt the transmission of impulsesbetween the cerebral hemispheres, thereby interferingwith the communication necessary for integrated be-havioral control. However, neuroimaging studies of thegenu (anterior portion) and splenium (posterior por-tion) of the corpus callosum of children with ADHDhave produced inconsistent results, with subjects dis-playing anatomic differences in both regions, in onlyone region, or in neither region, relative to healthy con-trol children (Hynd, Semrud-Clikeman, Lorys, Novey,& Eliopulos, 1991; Giedd et al., 1994; Semrud-Clikeman et al., 1994).
The second neural substrate considered of pathologicsignificance for ADHD is the frontal lobes. The parallelbetween the symptom patterns of patients with acquiredfrontal lobe damage and those of children with ADHDhas fostered speculation that disruption of the frontallobes may contribute to the etiology of the latter disorder(Bensen, 1991). Neuroimaging investigations have pro-vided some support for this speculation. The majority ofthese investigations (Castellanos et al., 1994; Filipek,Semrud-Clikeman, Steingard, Renshaw, Kennedy, & Biederman, 1997; Hynd et al., 1990) have found a lackof normal asymmetry (R � L) in the frontal lobes of chil-dren exhibiting ADHD, with the right prefrontal regionbeing anatomically smaller and, therefore, symmetric withthe left prefrontal lobe (R � L). In addition, there are in-dications that both left and right frontal lobes may besmaller for groups with ADHD relative to those withoutthe disorder (Sowell et al., 2004). The frontal lobes con-tribute to the control of attentional functioning, and thefinding of atypical symmetry and volume suggests a relationto ADHD. However, studies have not always replicatedthese findings of structural differences, nor have they deter-mined that differences in symmetry of the prefrontal lobesare specific to ADHD. For example, Hynd and colleagues(1990) have also identified atypical symmetry (R = L) ofthe prefrontal lobes in children exhibiting dyslexia.
Studies of cerebral blood flow within the frontal lobeshave revealed differences between individuals with ADHDand healthy volunteers. Zametkin and coworkers (1990),in a PET study of adults with ADHD, discovered that theparticipants exhibited hypofrontality in glucose use/cere-bral blood flow. Hypofrontality can reflect a disruptionin executive inhibitory control of behavior. However,subsequent studies of children and adolescents withADHD have not consistently replicated these findings,particularly when contrasting male and female adoles-cents (Ernst, Cohen, Liebenauer, Jons, & Zametkin,1997; Ernst, Liebenauer, Jons, & Zametkin, 1994; Zametkin et al., 1993).
Recently, a preliminary proton magnetic resonancespectroscopy (1H-MRS) and MRI study (Yeo et al., 2003)of children with ADHD and healthy control children ex-amined the relation of neurometabolite concentration,frontal volume, and attentional performance. For healthycontrol children, a significant relation between neu-rometabolite concentration, frontal volume, and atten-tional performance was not evident; however, a signifi-cant relation was evident for those children with ADHD.Specifically, concentration levels of Cre (sum of intracel-lular creatine and phosphocreatine indexing cellular energymetabolism) and N-acetylaspartate (a marker of neuronal
324 PART THREE | Disorders of the Brain
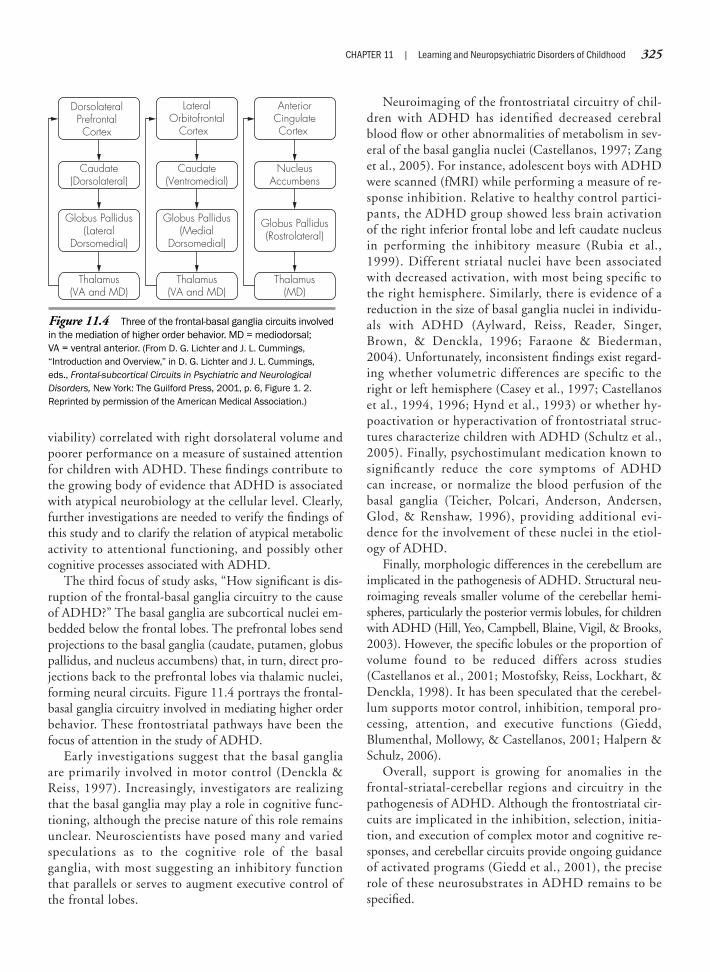
viability) correlated with right dorsolateral volume andpoorer performance on a measure of sustained attentionfor children with ADHD. These findings contribute tothe growing body of evidence that ADHD is associatedwith atypical neurobiology at the cellular level. Clearly,further investigations are needed to verify the findings ofthis study and to clarify the relation of atypical metabolicactivity to attentional functioning, and possibly othercognitive processes associated with ADHD.
The third focus of study asks, “How significant is dis-ruption of the frontal-basal ganglia circuitry to the causeof ADHD?” The basal ganglia are subcortical nuclei em-bedded below the frontal lobes. The prefrontal lobes sendprojections to the basal ganglia (caudate, putamen, globuspallidus, and nucleus accumbens) that, in turn, direct pro-jections back to the prefrontal lobes via thalamic nuclei,forming neural circuits. Figure 11.4 portrays the frontal-basal ganglia circuitry involved in mediating higher orderbehavior. These frontostriatal pathways have been thefocus of attention in the study of ADHD.
Early investigations suggest that the basal gangliaare primarily involved in motor control (Denckla &Reiss, 1997). Increasingly, investigators are realizingthat the basal ganglia may play a role in cognitive func-tioning, although the precise nature of this role remainsunclear. Neuroscientists have posed many and variedspeculations as to the cognitive role of the basalganglia, with most suggesting an inhibitory functionthat parallels or serves to augment executive control ofthe frontal lobes.
Neuroimaging of the frontostriatal circuitry of chil-dren with ADHD has identified decreased cerebralblood flow or other abnormalities of metabolism in sev-eral of the basal ganglia nuclei (Castellanos, 1997; Zanget al., 2005). For instance, adolescent boys with ADHDwere scanned (fMRI) while performing a measure of re-sponse inhibition. Relative to healthy control partici-pants, the ADHD group showed less brain activation of the right inferior frontal lobe and left caudate nucleusin performing the inhibitory measure (Rubia et al.,1999). Different striatal nuclei have been associatedwith decreased activation, with most being specific tothe right hemisphere. Similarly, there is evidence of areduction in the size of basal ganglia nuclei in individu-als with ADHD (Aylward, Reiss, Reader, Singer,Brown, & Denckla, 1996; Faraone & Biederman,2004). Unfortunately, inconsistent findings exist regard-ing whether volumetric differences are specific to theright or left hemisphere (Casey et al., 1997; Castellanoset al., 1994, 1996; Hynd et al., 1993) or whether hy-poactivation or hyperactivation of frontostriatal struc-tures characterize children with ADHD (Schultz et al.,2005). Finally, psychostimulant medication known tosignificantly reduce the core symptoms of ADHDcan increase, or normalize the blood perfusion of the basal ganglia (Teicher, Polcari, Anderson, Andersen,Glod, & Renshaw, 1996), providing additional evi-dence for the involvement of these nuclei in the etiol-ogy of ADHD.
Finally, morphologic differences in the cerebellum areimplicated in the pathogenesis of ADHD. Structural neu-roimaging reveals smaller volume of the cerebellar hemi-spheres, particularly the posterior vermis lobules, for childrenwith ADHD (Hill, Yeo, Campbell, Blaine, Vigil, & Brooks,2003). However, the specific lobules or the proportion ofvolume found to be reduced differs across studies (Castellanos et al., 2001; Mostofsky, Reiss, Lockhart, &Denckla, 1998). It has been speculated that the cerebel-lum supports motor control, inhibition, temporal pro-cessing, attention, and executive functions (Giedd, Blumenthal, Mollowy, & Castellanos, 2001; Halpern &Schulz, 2006).
Overall, support is growing for anomalies in thefrontal-striatal-cerebellar regions and circuitry in thepathogenesis of ADHD. Although the frontostriatal cir-cuits are implicated in the inhibition, selection, initia-tion, and execution of complex motor and cognitive re-sponses, and cerebellar circuits provide ongoing guidanceof activated programs (Giedd et al., 2001), the preciserole of these neurosubstrates in ADHD remains to bespecified.
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 325
Figure 11.4 Three of the frontal-basal ganglia circuits involvedin the mediation of higher order behavior. MD = mediodorsal; VA = ventral anterior. (From D. G. Lichter and J. L. Cummings,“Introduction and Overview,” in D. G. Lichter and J. L. Cummings,eds., Frontal-subcortical Circuits in Psychiatric and NeurologicalDisorders, New York: The Guilford Press, 2001, p. 6, Figure 1. 2.Reprinted by permission of the American Medical Association.)
Thalamus(VA and MD)
Globus Pallidus(Lateral
Dorsomedial)
Caudate(Dorsolateral)
DorsolateralPrefrontalCortex
Thalamus(MD)
Globus Pallidus(Rostrolateral)
NucleusAccumbens
AnteriorCingulateCortex
Thalamus(VA and MD)
Globus Pallidus(Medial
Dorsomedial)
Caudate(Ventromedial)
LateralOrbitofrontal
Cortex
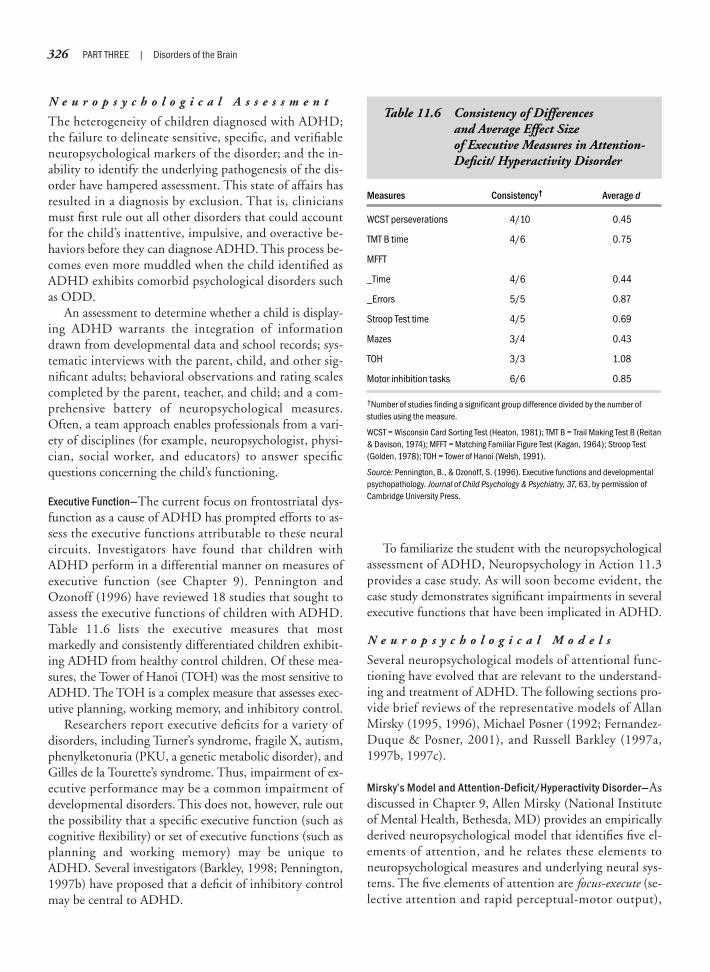
N e u r o p s y c h o l o g i c a l A s s e s s m e n t
The heterogeneity of children diagnosed with ADHD;the failure to delineate sensitive, specific, and verifiableneuropsychological markers of the disorder; and the in-ability to identify the underlying pathogenesis of the dis-order have hampered assessment. This state of affairs hasresulted in a diagnosis by exclusion. That is, cliniciansmust first rule out all other disorders that could accountfor the child’s inattentive, impulsive, and overactive be-haviors before they can diagnose ADHD. This process be-comes even more muddled when the child identified asADHD exhibits comorbid psychological disorders suchas ODD.
An assessment to determine whether a child is display-ing ADHD warrants the integration of informationdrawn from developmental data and school records; sys-tematic interviews with the parent, child, and other sig-nificant adults; behavioral observations and rating scalescompleted by the parent, teacher, and child; and a com-prehensive battery of neuropsychological measures.Often, a team approach enables professionals from a vari-ety of disciplines (for example, neuropsychologist, physi-cian, social worker, and educators) to answer specificquestions concerning the child’s functioning.
Executive Function—The current focus on frontostriatal dys-function as a cause of ADHD has prompted efforts to as-sess the executive functions attributable to these neuralcircuits. Investigators have found that children withADHD perform in a differential manner on measures ofexecutive function (see Chapter 9). Pennington andOzonoff (1996) have reviewed 18 studies that sought toassess the executive functions of children with ADHD.Table 11.6 lists the executive measures that mostmarkedly and consistently differentiated children exhibit-ing ADHD from healthy control children. Of these mea-sures, the Tower of Hanoi (TOH) was the most sensitive toADHD. The TOH is a complex measure that assesses exec-utive planning, working memory, and inhibitory control.
Researchers report executive deficits for a variety ofdisorders, including Turner’s syndrome, fragile X, autism,phenylketonuria (PKU, a genetic metabolic disorder), andGilles de la Tourette’s syndrome. Thus, impairment of ex-ecutive performance may be a common impairment ofdevelopmental disorders. This does not, however, rule outthe possibility that a specific executive function (such ascognitive flexibility) or set of executive functions (such asplanning and working memory) may be unique toADHD. Several investigators (Barkley, 1998; Pennington,1997b) have proposed that a deficit of inhibitory controlmay be central to ADHD.
To familiarize the student with the neuropsychologicalassessment of ADHD, Neuropsychology in Action 11.3provides a case study. As will soon become evident, thecase study demonstrates significant impairments in severalexecutive functions that have been implicated in ADHD.
N e u r o p s y c h o l o g i c a l M o d e l s
Several neuropsychological models of attentional func-tioning have evolved that are relevant to the understand-ing and treatment of ADHD. The following sections pro-vide brief reviews of the representative models of AllanMirsky (1995, 1996), Michael Posner (1992; Fernandez-Duque & Posner, 2001), and Russell Barkley (1997a,1997b, 1997c).
Mirsky’s Model and Attention-Deficit/Hyperactivity Disorder—Asdiscussed in Chapter 9, Allen Mirsky (National Instituteof Mental Health, Bethesda, MD) provides an empiricallyderived neuropsychological model that identifies five el-ements of attention, and he relates these elements toneuropsychological measures and underlying neural sys-tems. The five elements of attention are focus-execute (se-lective attention and rapid perceptual-motor output),
326 PART THREE | Disorders of the Brain
Measures Consistency† Average d
WCST perseverations 4/10 0.45
TMT B time 4/6 0.75
MFFT
_Time 4/6 0.44
_Errors 5/5 0.87
Stroop Test time 4/5 0.69
Mazes 3/4 0.43
TOH 3/3 1.08
Motor inhibition tasks 6/6 0.85
†Number of studies finding a significant group difference divided by the number ofstudies using the measure.
WCST = Wisconsin Card Sorting Test (Heaton, 1981); TMT B = Trail Making Test B (Reitan& Davison, 1974); MFFT = Matching Familiar Figure Test (Kagan, 1964); Stroop Test(Golden, 1978); TOH = Tower of Hanoi (Welsh, 1991).
Source: Pennington, B., & Ozonoff, S. (1996). Executive functions and developmentalpsychopathology. Journal of Child Psychology & Psychiatry, 37, 63, by permission ofCambridge University Press.
Table 11.6 Consistency of Differences and Average Effect Size of Executive Measures in Attention-Deficit/ Hyperactivity Disorder

shift (attentional flexibility), sustain (vigilance and persis-tence of attention), encode (working memory), and stable(consistence of attentional effort). The five componentsconstitute an attentional system that is widely distributedthroughout the brain. Accordingly, the system is quitevulnerable to disruption after brain injury; yet, it is alsoresilient. A specific attentional function may be compro-mised by injury, but undamaged neural regions may pro-vide some degree of compensation.
Support for the utility of the model for identifying andunderstanding the attentional processing of children withADHD is emerging. In an early study (Lowther &Wasserman, 1994), a battery of attentional measures se-lected to represent each element of attention was adminis-tered to children with ADHD and healthy control chil-dren. Each element of attention differentiated ADHD andhealthy children and correctly predicted group membership
with 91% accuracy. Recently, Kunin-Batson and associ-ates (2002), in a double-blind, placebo–control study ofchildren, determined that the introduction of psychos-timulant medication significantly augmented the “sus-tain” and “stable” components of attentional functioning,but not the “focus-execute” or “encode” elements of at-tention. Measures of the “shift” attentional componentwere not included for study in the investigation. Finally,as reviewed later, clinical childhood groups demonstratedifferential patterns of performance on measures sensitiveto Mirsky’s components of attention and the attentionalprocesses that Michael Posner poses.
Posner’s Model and Attention-Deficit/Hyperactivity Disorder—Asdiscussed in Chapter 9, Michael Posner has developed amodel of attention from the perspective of cognitive psy-chology and neuroscience. He hypothesizes that ADHD
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 327
B.C. is a 10-year-old boy with a history ofschool and home difficulties. His parentsand regular class teacher were concernedabout his inconsistent academic perfor-mance and poor behavioral control. Theteacher reported that B.C. frequently failedto complete his assignments, appeareddistracted, failed to follow directions, andrarely checked his work. Furthermore, he wasprone to call out in class, leave his seat, walkabout the room, and squirm when requiredto remain seated. Despite his classroomdifficulties, his group achievement testscores demonstrated average to above-average skill development.
At home, he was “always on the go,”could not sit quietly unless playing withbuilding blocks, and rushed when complet-ing chores or homework. It was difficult forB.C. to initiate or focus on his homeworkunless a parent sat with him to guide hisefforts. His ability to plan and organizeactivities (for example, picking up his toys,organizing game activities with friends, andso forth) was described as very poor. Despitehis behavioral difficulties, he was character-
ized as a gentle child who was rarely aggres-sive or noncompliant.
Neuropsychological FindingsBehavioral rating scales were completed bythe teacher and parents regarding B.C.’sbehavior. These ratings showed very high ratesof inattention, impulsivity, and hyperactivity.Formal neuropsychological results revealedthat B.C. was functioning within the averagerange of intelligence. Verbal and performanceintelligence were both comparably developedin the average range. Relative weaknesseswere evident on subtests sensitive to atten-tional weaknesses. His memory performancewas age appropriate. However, he demon-strated very poor sustained attention and highrates of impulsivity on auditory and visualmeasures of continuous performance. Relat-edly, he performed poorly on measuressensitive to selective attention and responseinhibition, goal persistence and impulsecontrol, and cognitive flexibility.
B.C. manifested very poor executiveplanning on the Tower of London-DrexelUniversity test (TOLDX) (Culbertson & Zillmer,
1998a, 1998b, 2005) relative to the perfor-mance of his peers. His planning attemptswere quick, without adequate forethought orreflection. From a qualitative perspective, hisproblem-solving approach was impulsive,rigid, and comparable with that of a muchyounger child.
The integration of the developmental,rating, and neuropsychological findingssupported the diagnosis of an attention-deficit/hyperactivity disorder–combined type.The neuropsychologist developed behavioralinterventions with B.C.’s teacher and family.These interventions focused on B.C.’s inat-tention, impulsivity, hyperactivity, and plan-ning deficits. Although he was responsive tobehavioral interventions, his behavioraldisinhibition remained high. Accordingly, theneuropsychologist sought a medical consul-tation to determine the feasibility of stimulanttherapy. Stimulant medication was intro-duced and gradually titrated to therapeuticlevels. A significant additive effect (behav-ioral interventions and medication) wasevident, with attention, impulse, and activitycontrol showing marked improvement.
N e u r o p s y c h o l o g y i n A c t i o n 1 1 . 3
C a s e S t u d y o f a C h i l d w i t h a n A t t e n t i o n - D e f i c i t / H y p e r a c t i v i t y D i s o r d e r
by William C. Culbertson

may result from disruption of the vigilance attention system,insofar as children with ADHD are impaired in their abil-ity to maintain attention over time. The study revealed thatchildren with ADHD showed deficits, relative to healthycontrol children, on measures sensitive to the functioning ofthe vigilance and anterior attention system (Pearson, Yaffee,Loveland, & Norton, 1995; Swanson et al., 1991). Thus,disruption of both the vigilance and anterior attentional sys-tems may play a key role in the etiology of ADHD.
The utility of Posner’s model was recently examined ina study (Brewer, Fletcher, Hiscock, & Davidson, 2001) ofthree groups of children (ADHD, congenital hydro-cephalus, and healthy control children). The childrenwere presented with measures sensitive to attentionalfocus, maintenance, and shifting. Furthermore, the mea-sures allowed for the separation of the disengage, move,and engage processes of Posner’s model of attention. Rel-ative to the control group, the children with hydro-cephalus demonstrated deficits in focusing and shiftingattention, whereas the children with ADHD were im-paired in sustaining and shifting attention. The difficul-ties of the hydrocephalus groups with focusing and shift-ing attention were related to impairments of disengagingand moving the focus of their attention. These impair-ments are consistent with disruption of the posterior at-tention system. In contrast, the shifting difficulties of theADHD group reflected preservative errors consistent withanterior system involvement. Likewise, poor sustained at-tention implicates impairment of the vigilance and anteriorsystems. The findings of greater posterior versus anteriorattentional dysfunction in the congenital hydrocephalusand ADHD groups correlate with the neuroanatomic and neurofunctional differences identified for the twogroups.
Recently, Swanson and colleagues (2000) have pro-posed a tentative model linking the symptoms ofADHD delineated in the DSM-IV (APA, 1994) to thecognitive processes and neural circuits that Posner pro-posed (Table 11.7). Different symptoms of inattentionreflect disruptions to the alerting and orienting processessupported primarily by the right frontal and posteriorparietal neural networks. Alerting symptoms relate todeficits in persistence of attention (sustained) and vigi-lance, whereas orienting symptoms define deficits of se-lective attention. The hyperactivity-impulsive symptomsare linked to perturbations of the executive controlprocesses underpinned by the anterior cingulate region ofthe brain. Although the neural circuits are relatively dis-tinct, they interact and overlap in their support of thecomplex behavioral manifestations associated withADHD. When considering the distribution of the neural
networks implicated in ADHD, damage within or be-tween networks could produce variability in the symp-tom presentation of children with the disorder. In fact,significant variability exists in the symptoms demon-strated by children with ADHD, and the proposedmodel may help clarify and further specify the behav-ioral manifestations of this disorder. We await the clinicaland empirical application of the model.
Barkley’s Model of Attention-Deficit/Hyperactivity Disorder—Russell Barkley (1997a,b,c) proposes a three-tiered execu-tive model of ADHD (Figure 11.5). The first tier, behav-ioral inhibition, is central to the model. Behavioralinhibition involves three inter-related processes: (1) the in-hibition of a prepotent response, (2) stopping an ongoingresponse, and (3) protecting an ongoing mental operationfrom disruption by competing external or internal events(interference control). These inhibitory processes are nec-essary for the effective operation of the four executive func-tions of tier 2: working memory; internalization of speech;regulation of arousal, emotions, and motivation; and re-constitution (recombining behavioral elements to create
328 PART THREE | Disorders of the Brain
Symptom Domains Cognitive Processes Neural Networks
Inattentive Alerting Frontal
Difficulty sustaining attention Right frontal cortex
Fails to finish Right posterior parietal
Avoids sustained efforts Locus ceruleus
Inattentive Orienting Posterior Parietal
Distracted by stimuli Bilateral parietal
Does not appear to listen Superior colliculus
Fails to pay close attention Thalamus
Hyperactive-Impulsive Executive control Anterior cingulate
Blurts out answers Anterior cingulate
Interrupts or intrudes Left lateral frontal
Cannot wait Basal ganglia
Source: Adapted from Swanson, J., Posner, M., Cantwell, D., Wigal, S., Crinella, F., Filipek, P., Emerson, J., Tuciker, D., & Nalcioglu, O. (2000). Attention-deficit/hyperactivity disorder: Symptom domains, cognitive processes and neural networks. InR. Parasuraman (Ed.), The attentive brain (p. 455, Table 20.2). Cambridge, MA: The MITPress, by permission.
Table 11.7 Diagnostic and Statistical Manualof Mental Disorders, Fourth Edition,Attention-Deficit/ HyperactivityDisorder Symptoms, CognitiveProcesses, and Neural Networks

new behaviors). Tier 2 functions, in turn, affect the con-trol, organization, and flexibility of the behavioral outputof tier 3. Although the brain as a whole supports theseprocesses, the prefrontal and frontal cortices are primarilyresponsible for the inhibitory and executive processes.
When inhibitory and executive processes are intact,the child develops the capacity to regulate behavior byusing internal representations of events in thought andimage. These internal representations enable the child tolink past learning and experience with both present de-mands and future consequences of actions. Furthermore,the capacity to internally manipulate and guide behaviorvia internal representations allows for the regulation ofemotion and motivation and the generation of new be-havioral patterns to augment goal-oriented behavior, par-ticularly when something thwarts intended actions. InADHD, impaired inhibitory control processes disrupt theoperation of the executive processes. The cascading effectof this impairment results in a host of behavioral excesses
and deficits, including poor impulse control, inattention,and hyperactivity.
Barkley’s model continues to spawn studies of in-hibitory control and executive function as they relate toADHD. Support is amply evident for poor inhibitorycontrol and executive functions deficits in ADHD popu-lations (Nigg, 2001; Purvis & Tannock, 2000), althoughthe verification is stronger for inhibitory weaknesses thanexecutive dysfunctions. Varieties of methodologic issuescloud recent efforts to determine the factors that accountfor differences in findings. A primary problem is the se-lection of developmentally appropriate tasks to assess ex-ecutive functions. Executive functions emerge at differentpoints in childhood, continue to develop in a multistepmanner, and reach final maturity in adolescence or earlyadulthood. Thus, the assessment of a specific executiveskill requires a measure sensitive to the stage/level of mat-uration of that particular skill. For example, the abilityto inhibit a motor response is more fully developed than
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 329
Text not available due to copyright restrictions

interference control (shielding a cognitive operation fromdistracting, nonrelevant intrusions) during the early child-hood years. Interference control has a more contracteddevelopmental trajectory that continues through theupper elementary years. Accordingly, comparing the per-formance of healthy preschool children with a group ofchildren with ADHD on a measure of interference con-trol will likely show minimal differences, because neithergroup fully possesses the executive skills to perform themeasure.
Recently, Berlin, Bohlin, Nyberg, and Janols (2004)presented children with ADHD and healthy control chil-dren (age 7–10 years) with a battery of developmentallyappropriate measures of inhibitory control and executivefunction. The measures were selected to target the execu-tive domains articulated in Barkley’s model. The resultsrevealed that the children with ADHD performed signifi-cantly poorer across the measures of inhibitory controland executive function, except for one, reconstitution.More importantly, when the measures that differentiatedthe two groups were combined for prediction (logisticregression), 86% of the children were correctly classifiedinto their diagnostic groups. The sensitivity (probabilitythat a child with ADHD would be correctly classified) andspecificity (probability that a healthy child would be cor-rectly classified) rates were 81% and 88%, respectively. Inaddition, inhibition, working memory, and self-regulationwere determined to be distinct predictors of group mem-bership. The latter finding indicates that the three execu-tive functions were each assessing a relatively unique setof abilities. Overall, the findings of the study are support-ive of Barkley’s model, but suggest that it be reduced tothree major components: inhibition, working memory,and self-regulation.
D e v e l o p m e n t a l C o u r s e
As a developmental disorder, ADHD is evident early inchildhood and, with maturation, shows changing symp-tom manifestations. In infancy, children displayingADHD tend to be highly active, overly responsive to stim-ulation, quick to anger, and show low adaptability tochange. During the toddler and preschooler years, chil-dren with ADHD are constantly “on the go,” seem “dri-ven by a motor,” continually manipulate objects, and shiftacross activities. Moreover, they constantly run and climb,often without apparent consideration for the consequencesof their actions. Preschoolers exhibiting ADHD are at riskfor accidental injury due to their inattention, impulsivity,and high activity levels. One 3-year-old, for example, wasso inattentive and hyperactive that he ran into walls, doors,and other stationary objects on a daily basis!
In a preschool setting, children with ADHD often findit difficult to remain seated, fail to listen to or follow di-rections, become too excited when stimulated, and talkloudly and incessantly. Peers describe classmates withADHD as bossy, uncooperative, and intrusive into theiractivities and games. The parents may be asked to removetheir child from the preschool program if the child is alsohighly oppositional or aggressive. The traditional elemen-tary school environment is referred to as the “showplace”for ADHD. The demands of school highlight the regula-tory deficits of children with ADHD. Specifically, the fol-lowing school requirements all tax the controlling efforts ofchildren displaying ADHD: (1) attention to work that canbe boring, tedious, and effortful; (2) organization of assign-ments and belongings; (3) completion of work withoutrushing; (4) remaining seated for long periods; (5) adher-ence to multiple classroom rules; (6) reflection before re-sponding; (7) refraining from talking unless permitted;and (8) cooperation with others. It is during the elemen-tary school years that children with ADHD begin to avoidhomework assignments, which inevitably leads to signifi-cant conflict with teachers and parents. Furthermore,peers often begin to move away from these children, find-ing their impulsivity, hyperactivity, and inattention torules of behavior difficult to tolerate.
As children with ADHD enter middle and highschool, their inability to meet the expectations for greaterindependence in managing the academic demands ofmultiple teachers leads to an ever-increasing sense of fail-ure and frustration. Perplexed, if not angry, teachers andparents continually confront these adolescents over theirfailure to live up to expected levels of academic perfor-mance. The normal adolescent strivings for independenceand self-direction fuel resistance to parental offers of assistance or attempts to provide structure to theteenager’s studying and homework habits. Ongoing rejec-tion by peers, particularly if the adolescent is aggressive,often results in the teenager gravitating toward peers whoare experiencing similar difficulties. Cumulatively, thesenegative experiences diminish the adolescent’s self-esteemand contribute to a growing realization that future educa-tional and vocational aspirations may be unattainable.
As adolescents who exhibit ADHD move into adult-hood, some show greater regulatory control and a relatedreduction or resolution of core symptoms of inattention,impulsivity, and hyperactivity. Unfortunately, a signifi-cant number of the adolescents (Weiss & Hechtman,1993) continue to manifest the core or residual symptomsas they enter adulthood. Early failings in school, rejectionby peers, and disappointed family members evolve intoproblems related to achieving success in work, marriage,
330 PART THREE | Disorders of the Brain

and family life. Not surprisingly, investigators report highrates of mood disorders, alcoholism, substance abuse, andantisocial personality disorders among adults withADHD (Barkley, 1998). Adults with ADHD are gener-ally gainfully employed and self-sufficient, although theytend to have poorer work records and lower vocationalstatus than their adult peers without ADHD. Clearly,many children and adolescents manifesting ADHD con-tinue to encounter adjustment difficulties in adulthood.
T r e a t m e n t
The treatment of children with ADHD warrants a com-prehensive, multimodal approach due to the multiplicityof deficits and difficulties that these children present.Each child presents a unique set of strengths and weak-nesses and, accordingly, warrants an individual treatmentplan tailored to his or her individual needs. When target-ing the ADHD child’s needs, the core symptoms of inat-tention, impulsivity, and hyperactivity serve as the pri-mary point of intervention. These core symptoms, asthey are manifested across contexts (family, educational,and social), expand and alter the specific treatment com-ponents. The presence of comorbid conditions (such asdepression) further modifies the treatment interventionsappropriate for the child. Typically, caretakers and teach-ers are involved in the process of implementing treatmentinterventions because of their key roles in engender-ing, exacerbating, or attenuating the child’s presentingsymptoms.
The two primary and most successful interventionswith ADHD are behavioral management and psy-chopharmacology. Behavioral management involves usinglearning principles to develop interventions to facilitateor inhibit behavior. Externally imposed interventions,such as token systems or response costs, appear more ef-fective for managing the child’s impulsivity, inattention,or overactivity than cognitive-behavioral interventionsthat focus on the child developing internal verbal self-control (Barkley, 1998).
Psychologists mold behavioral interventions to the spe-cific needs of the child in the home, school, and commu-nity. Such interventions frequently lead to significant pos-itive change in targeted ADHD core symptoms andcoexisting emotional-behavioral difficulties. Unfortu-nately, this improvement in behavioral control does notoften generalize beyond the specific context for which theinterventions were developed. For example, the improve-ment in impulse control brought about by behavioral in-terventions in a classroom may not transfer to the homeand community unless psychologists develop additionalbehavioral interventions for these contexts. A serious lim-
itation of behavioral management interventions is therapid reappearance of the child’s core ADHD symptomswhen the behavioral systems are faded out. In addition, itis difficult to implement behavioral management systemsfor older children and adolescents because they naturallyresist external structuring and control.
Various psychopharmacologic interventions currently areavailable for treating ADHD. The psychostimulant medica-tions (namely, methylphenidate [Ritalin], methylphenidatehydrochloride [Concerta], amphetamine [Adderall], anddextroamphetamine sulfate [Dexedrine] are the most fre-quently prescribed medications for ADHD. If the childis presenting other comorbid disorders, the physicianmay introduce additional medications in combinationwith the psychostimulants. For example, a depressedchild with ADHD may need an antidepressant medica-tion in conjunction with a psychostimulant medication.A relatively recent addition to the medication armamen-tarium of the physician is atomoxetine (Strattera). Atom-oxetine is a nonstimulant medication (norepinephrinereuptake inhibitor) that has been determined to signifi-cantly reduce the symptoms of ADHD (Weiss et al.,2005). It is a viable treatment option for children whoare nonresponsive to or unable to tolerate psychostim-ulant medications.
Several factors prompt the use of medication. As notedearlier, behavioral improvement often does not generalizebeyond the setting in which the training occurs. More-over, behavioral interventions may not fully manage themore seriously involved children who exhibit moderate tohigh levels of core symptoms. Finally, parents and educa-tors often find it difficult to use and maintain behavioralinterventions unless the psychologist who develops theinterventions closely supervises and supports them.
The behavioral improvements exhibited by childrentreated with psychostimulant medications can range fromslight to dramatic. Psychostimulant medications have en-abled children with ADHD to remain in the regular class-room due to the substantial improvement in their behavioralcontrol and academic achievement. Negative parent–childinteractions frequently decline as a consequence of thechild’s new ability to complete homework, follow homerules, and behave appropriately in public settings. Peers canoften identify when a child is medicated because of notice-ably improved behavioral control, although it is unclearwhether the medications actually contribute to increasedpeer acceptance. Interestingly, despite the widespread useand effectiveness of psychostimulant medications, neuro-scientists do not completely understand the neurochemicalactions of the drugs. Researchers have proposed a numberof hypothesized actions, most implicating the impact of
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 331

psychostimulant medication on the brain’s neurotrans-mitters, specifically dopamine and norepinephrine, result-ing in increased inhibitory control across cognitive andbehavioral systems.
Despite the positive effects of psychostimulant med-ications, these drugs also have several limitations: (1) sideeffects are common, such as temporary appetite suppres-sion and sleep disruption; (2) the therapeutic effective-ness of the medications vary from child to child; (3) thechild may show a brief intensification of core symptomsat the end of the last daily dose (“rebound effect”); (4) children often resist compliance with the medicationregimen; (5) the medications have minimal effect on cer-tain problems (such as learning disabilities); and (6) themedications do not “cure” the disorder. Regarding the lat-ter limitation, the core symptoms re-emerge when thechild is not medicated.
We now discuss Gilles de la Tourette’s disorder, a ticdisorder that can be baffling to observers and distressingto the affected child or adolescent. Unfortunately, Gillesde la Tourette’s disorder frequently co-occurs with ADHDand obsessive-compulsive disorder.
Tic Disorders
Motor and/or vocal tics can be transient, episodic, orchronic. Tics are particularly intriguing to neuroscientistsinsofar as they appear to represent a type of behavior that isboth voluntary and involuntary with regard to expression.Whether a tic condition constitutes a “disorder” depends ona number of factors such as chronicity; disturbance to acad-emic, social, or work performance; or degree of subjectivedistress. The most serious tic disorder is that of Gilles dela Tourette’s syndrome, which involves the presentationof both motor and vocal tics.
G I L L E S D E L A T O U R E T T E ’ S S Y N D R O M E
B a c k g r o u n d a n d C l i n i c a lP r e s e n t a t i o n
Gilles de la Tourette was a brilliant neurologist who stud-ied with Charcot at the Parisian Hôpital de la Saltpêtrièreduring the latter part of the seventeenth century. Becauseof his work, the disorder of multiple motor and vocal tics,Gilles de la Tourette’s syndrome (GTS), bears his name.Unfortunately, Gilles de la Tourette’s professional contri-butions were overshadowed by a series of tragedies duringhis life. He suffered gunshot wounds inflicted by a
psychiatric patient, struggled with bouts of depressionand mania in later life, and is believed to have died ofsyphilis (Bradshaw, 2001).
GTS is a developmental disorder that exemplifies thehazy boundary between neurology and psychiatry. Ini-tially, GTS was viewed as a psychiatric disorder and, con-sistent with the early development of psychiatry, consid-ered amendable to psychoanalytic interpretation andtherapeutic interventions (Cohen & Leckman, 1994).The APA (DSM IV, 1994) lists it as a “mental disorder,”despite advances in the neurosciences and related fieldselucidating the neuropathogenesis of the disorder. Moreaccurately, GTS appears to be a product of a complex andonly partially understood interplay of genetic, neurophys-iologic, and psychological factors.
Tics refer to repetitive, stereotypic, nonrhythmic, andreoccurring motor movements or vocal responses of briefduration (≤1 second). Tics are fragments of normalmotor/vocal behavior that are semivoluntary in expression.They occupy an intermediate point on the continuum ofmotor behavior, with one end represented by involuntarymovements (for example, resting tremor associated withParkinson’s disease) and the other end characterized byvolitional, deliberate, and purposeful actions. The semi-voluntary nature of tics relates to the fact that they can betemporarily either suppressed or expressed in an alteredor concealed manner (for example, integrating the tic intoa series of voluntary movements). An example of a semi-voluntary behavior that we all experience is yawning. Theurge to yawn can be temporarily suppressed or concealed(namely, covering one’s mouth), but if we are truly tired,it will ultimately emerge. Similarly, the tic is often pre-ceded by an urge or sensation (premonitory urge/sensa-tion) that can be suppressed, but this produces tension anddiscomfort that, in turn, compels the release of the move-ment or vocalization. Furthermore, the release of themovement/vocalization provides short-term relief fromthe tension and discomfort. Unfortunately, the relief isfollowed by renewed tension and discomfort, producing acycle of repeated tic behaviors.
Tics are classified as simple or complex. Table 11.8 pre-sents examples of each. Simple tics appear more reflexive,whereas complex tics appear more purposeful and coordi-nated. In extreme cases, motor or speech actions are per-formed compulsively.
Developmentally, tics are evident in healthy developingchildren, but resolve over time. Tic disorders are classified astransient, chronic, and GTS. A transient tic disorder refersto motor and/or vocal tics that are exhibited from 1 to 12 months. A chronic disorder relates to the presentation ofmotor or vocal tics for a period greater than 12 months.
332 PART THREE | Disorders of the Brain
Finally, GTS encompasses the expression of motor andvocal tics for a period exceeding 12 months. The tics asso-ciated with GTS are also required to cause significant dis-tress or interfere with the child’s or adolescent’s adjustmentto home, school, or community.
The onset of GTS can be gradual or rapid, with initialmotor tics involving the head and face, and later showinga caudal progression. The motor and vocal tics of GTSfluctuate (“wax and wane”) in their nature, location, fre-quency, severity, and duration of presentation. Thus, it isa condition that tends to be intermittent in its expres-sion—periods of tic behaviors that abate, only to reoccurat another point in time—through childhood and ado-lescence. The average age of onset is 7 years of age, al-though cases are known to occur both earlier and laterthan this age.
Tics tend to exacerbate with the onset of adolescence,but generally lessen or resolve by adulthood (Figure 11.6).Unfortunately, the public media often presents copro-praxia (obscene gestures) and coprolalia (obscene or inap-propriate speech) as representative of GTS. In fact, theseextreme behaviors are relatively rare, occurring in less than10% of the cases (APA, 1994).
Tic behaviors are exacerbated by stress, boredom, andexcitement. Conversely, they tend to diminish when thechild is relaxed, intensely focused on an activity, or emo-tionally calm. Interestingly, tics significantly abate whenthe child is asleep.
P r e v a l e n c e
The prevalence of GTS for school-age children is esti-mated to be 1 to 8 per 1000 children (Costello et al., 1996;
Hornsey, Banerjee, Zeitlin, & Robertson, 2001). Boys areaffected at a higher rate than girls, with estimated ratiosranging from l.8 to 8 boys to 0 to 6.6 girls (Leckman, Peterson, Anderson, Arsten, Pauls, & Cohen, 1997). Agenerally accepted estimate is a 4:1 ratio of boys to girls.GTS does not appear to have a disproportional affect onany specific racial or ethnic group.
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 333
Simple Motor Complex Motor Simple Vocal Complex Vocal
Blinking Jumping Throat clearing Repeating others’ speech
Facial twitches Touching others Sniffing Repeating one’s own words
Head or arm jerk Smelling Snorting Obscene words
Shoulder shrugs Facial expressions Yelping
Foot stomping Hand or head gestures Barking
Squatting Clicks
Twirling Grunts
Spinning in a circle Speech fragments
Imitating others’ behaviors Phrases
Obscene gestures Humming
Table 11.8 Simple and Complex Motor and Vocal Tics
Figure 11.6 Plot of mean tic severity for ages 2 to 18 years.Tic severity reaches its highest point between 10 and 12 years ofage and begins to decline thereafter. (Reproduced from Leckman,J., Peterson, B., Schultz, R., & Cohen, D. [2001]. Tics: When habit-forming neural systems form habits of their own. In C. Nelson & M.Luciana [Eds.], Handbook of developmental cognitive neuroscience[p. 557, Figure 35.5]. Cambridge, MA: The MIT Press, by permission.)
0 5 10 15
1
2
3
4
5
Rela
tive
TIC
Sev
erity
(ARR
TS)
Age (yrs)
Actual MeansEstimated Means

C o m o r b i d C o n d i t i o n s
Individuals with GTS often experience anxiety, depression,and aggression. Aggression can range from oppositional re-sponses to overt acting-out behavior. However, the twomajor conditions most likely to co-occur with GTS are obsessive-compulsive disorder (OCD) and ADHD.OCD is estimated to occur in approximately 30% to 60%of individuals with GTS, whereas 25% to 50% of childrenand adolescents with GTS exhibit a co-occurring ADHD(Cirino, Chapieski, & Massman, 2000; Leckman et al.,1997).
Obsessions are repetitive, intrusive, unwanted, and ofteninappropriate thoughts or images. Obsessive thoughts/images typically relate to themes of aggression, sexuality,contamination, cataclysmic events, symmetry, and exact-ness. Often, obsessions prompt compulsions that arethoughts or actions to resist, suppress, or neutralize the ob-sessions. Compulsive behaviors are many and varied, fre-quently involving checking, counting, ordering, washing,seeking reassurance, and ritualistic behaviors (Bradshaw,2001). Unfortunately, the anxiety reduction produced bycompulsions is short-lived. Obsessive thoughts/images re-occur and prompt, once again, the compulsive behaviors.
When GTS and OCD co-occur, it can be difficult todifferentiate complex motor tics from compulsive behav-iors. The two disorders can sometimes be differentiatedby the dynamics of the two conditions. The sequence ofevents in GTS is as follows: a premonitory urge or sensa-tion (sensorimotor prompting), followed by the release ofthe tic behavior and momentary relief of the tension andpress associated with the premonitory urge/sensation. Incontrast, OCD involves an unwanted image or thought(cognitive prompting) that engenders anxiety and distress.The compulsive behavior serves to alleviate the anxietyassociated with the obsessive thought/image.
As we have discussed, ADHD relates to the manifesta-tion of age-inappropriate inattention, impulsivity, andhyperactivity. The comorbidity of ADHD, OCD, andGTS is highly disruptive to the child or adolescent’s acad-emic performance, social acceptance, and self-valuing. Anumber of interpretations have been posed to account forthe comorbidity of OCD and ADHD with GTS. Of sig-nificance, however, are research findings indicating thatall three disorders appear to relate to perturbations of thefrontostriatal brain systems.
N e u r o p s y c h o l o g i c a lP a t h o g e n e s i s
GTS is one of the most familial of the neuropsychiatricdisorders and appears to be transmitted via autosomaldominant genes with incomplete penetrance (incompleteexpression in affected individuals) (Bradshaw, 2001;
Pennington, 2002). With monozygotic twins, the rate ofconcordance for GTS is 50% to 56%, and it increases to77% to 94% when GTS and chronic tic disorders arecombined. The concordance rate for dizygotic twins is8% to 18%, but increases to only 23% when combinedwith chronic tic disorder (Leckman et al., 1997; Leckman& Cohen, 1996; Pennington, 2002). The dopamine D2A1 allele and dopamine D3 and D4 receptor genes andchromosomal abnormalities (8, 18, and 22) have alsobeen implicated (Alsobrook & Pauls, 1999; Bradshaw,2001; Casey, Tottenham, & Fossella, 2002).
Alterations of neurotransmitters intrinsic to the frontos-triatal pathways have been posed as pathogenic to GTS(Bradshaw, 2001; Sheppard et al., 1999). The cate-cholamines (dopaminergic, serotonergic, and noradrenergicsystems) have received the greatest attention. Of these trans-mitters, dopamine appears to play the crucial role in GTS.In part, this is based on the effects of medications that eitherinhibit or facilitate dopamine activity. Dopamine (D2) re-ceptor antagonists such as haloperidol (Haldol) reduce motorand vocal tics. In contrast, dopamine agonists such as centralnervous system stimulants (for example, methylphenidate[Ritalin]) can exacerbate motor and vocal tics. It is unclearwhether striatal D2 receptors are hypersensitive to dopamineor whether there is a dopaminergic hyperinnervation of thestriatum (Leckman et al., 1997). The effectiveness of cloni-dine (Catapres) and guanfacine (Tenex) (2 noradrenergicreceptor agonists) in the treatment of the symptoms of bothGTS and ADHD further suggests a role of noradrenalin inthe modulating cortico-striatal-thalamo-cortical pathways.Support for the role of serotonin in the cause of GTS is lim-ited, although there is significant evidence for its role in OCD (Pennington, 2002). Currently, the role of othercentral neurotransmitters in the pathogenesis of GTS awaitsclarification.
Since the mid-1990s, ongoing research has focused onthe role of environmental factors that place a child at riskfor the development of tic disorders. Extensive research hasbeen directed toward determining whether there is a risk forthe development of tic disorders as part of an autoimmuneresponse. Clinical findings of a temporal relation between-hemolytic streptococci and the onset or exacerbation oftic disorders and/or OCD provided the impetus for this re-search. The National Institute of Mental Health labeled thisdisorder pediatric autoimmune neuropsychiatric disorders asso-ciated with streptococcal infections (PANDAS). Pathogeni-cally, it is hypothesized that the human body’s antibodiestargeting the streptococci also cross-react with the basal gan-glia, with resulting damage and production of tics andOCD behaviors. A number of studies have supported dif-ferences between increased levels of antistreptococcal anti-bodies for GTS relative to control groups; however, others
334 PART THREE | Disorders of the Brain

have not (Hoekstra, Kallenber, Korf, & Minderaa, 2002).Moreover, the mechanism of action of antistreptococcal an-tibodies with regard to the development or exacerbation of tics remains to be elucidated. Insofar as streptococcal in-fections are common among children and most do not de-velop tics and/or OCD, additional investigations are neededto determine what factors account for the development oftics and/or compulsions in a select few individuals.
Structural and functional neuroimaging studies have re-ported alterations of brain structure and metabolic activa-tion patterns associated with GTS. A consistent findingacross studies is reduced volume or atypical asymmetries ofthe caudate, putamen, and globus pallidus of the basal gan-glia (Peterson et al., 2003; Sheppard et al., 1999). Alteredactivations of the prefrontal cortex (lateral orbitofrontal andanterior cingulate), motor cortex, somatosensory associa-tion areas, and thalamus have also been reported (Jeffries,Schooler, Schoenbach, Herscovitch, Chase, & Braun,2002). Jointly, the neuroimaging studies provide growingevidence for the role of the frontostriatal pathways in thepathogenesis of GTS (Singer & Minzer, 2003). The motorand vocal tics of GTS are hypothesized to relate to disinhi-bition (possibly because of hypersensitivity of dopamine re-ceptors or hyperinnervation of the striatum) of the frontalmotor-striatal circuit, particularly at the level of the caudate,resulting in the release of motor programs. Notably, thefrontal motor circuit includes projections from the so-matosensory cortex, implicating its potential role in the gen-eration of premonitory urges. Hypoactivation at the level ofthe lateral orbitofrontal and anterior cingulated cortex sug-gests a disruption of top-down voluntary control.
While there are indications of hyperactivation and hy-poactivation of different frontostriatal circuits in OCD andADHD, the interactive pathogenic role of the circuits in co-occurring GTS, OCD, and ADHD is not well understood.The comorbidity of the three disorders implicates some levelor degree of dysfunction across the major frontostriatal cir-cuits; however, we await research findings explicating thenature and cause of this dysfunction.
N e u r o p s y c h o l o g i c a l A s s e s s m e n t
Because of the putative role of disinhibition in the expres-sion of motor and vocal tics, studies of inhibitory controlhave been undertaken. The evidence from these studieshas been inconsistent in supporting inhibitory weaknessesas specific to GTS (Channon, Pratt, & Robertson, 2003).Similarly, little evidence exists of deficits in executivefunctions supported by the dorsolateral prefrontal cortex,such as planning, rule finding, and set shifting (Ozonoff& Jensen, 1999). Lateral frontal regions are believed tocontribute to strategic, working, and procedural memory
processes, and at least one study (Stebbins, Singh, Weiner,Wilson, Goetz, & Gabrieli, 1995) has identified weak-nesses in this domain for adults with GTS participants.
Deficits related to visual-construction, visuomotor inte-gration, and motor performance are frequently evident inchildren and adults with GTS, possibly reflecting disrup-tion of the motor-striatal pathway (Leckman, Peterson,Schultz, & Cohen, 2001). Unfortunately, many of thesestudies have not controlled for the high frequency of co-morbid conditions that accompany GTS, potentially con-tributing to conflicting and equivocal results. However, se-lected studies controlling for comorbidity and GTS areavailable. For example, Silverstein, Como, Palumbo, West,and Osborn (1995) found that the poor attentional perfor-mance of adults with GTS is related to the presence ofADHD and OCD, and not a unique deficit associated withGTS. In a more recent study, Channon and colleagues(2003) compared GTS, GTS � ADHD, GTS � OCD,and healthy control children and adolescents on measuresof executive functioning, memory, and learning. Childrenand adolescents with only GTS differed from the healthycontrol youngsters on one measure of response initiation,whereas the GTS � ADHD group demonstrated deficitson several measures of executive function assessing responseinhibition, strategy generation, and multitasking. Further-more, the GTS � OCD group did not differ in their exec-utive performance from the healthy control group. Finally,none of the clinical groups differed from healthy controlindividuals in memory or learning performance.
Casey and colleagues (2002) have extensively studiedthe frontostriatal regions and circuitry of children with de-velopmental disorders and healthy children. Reflecting thisongoing research has been the development of a model ofcognitive control. One critical aspect of cognitive controlis the ability to suppress or override competing attentionaland behavioral responses to resolve conflict. The inhibi-tion of three forms of cognitive-motor processing (stimu-lus selection, response selection, and response execution)was studied with healthy control and clinic groups (chil-dren with GTS, ADHD, childhood onset schizophrenia,and Sydenham’s chorea). The Sydenham’s chorea groupwas selected because of the high rate of OCD (75%) asso-ciated with the disorder. The intent of the studies was todetermine whether the separate disorders demonstrateddifferent cognitive control deficits.
The children were administered a battery of tasks thatassessed the three cognitive control processes. The stimulusselection task requires the inhibition of attention to visualfeatures previously viewed in order to attend to a new fea-ture. The response selection task involved the learning of aseries of responses to specific stimuli, and then the produc-tion of a different (incompatible) set of responses to the
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 335

same stimuli. In the latter condition, the child was facedwith inhibiting the first learned response set in order to se-lect and generate the second response set. In contrast, thethird task, response execution, involved the creation of aprepotent response through the frequent association of theresponse with a specific stimuli and then periodically requir-ing the inhibition of the response to a different stimuli. Rel-ative to healthy children, the GTS group demonstrated sig-nificantly poorer performance in response-execution,whereas the ADHD group showed deficits in stimulus se-lection and response-execution. Furthermore, the childhoodschizophrenic group was impaired in stimulus-selection, andthe Sydenham’s chorea (OCD) group showed deficits inresponse-selection. Mapping of these cognitive processes tothe neural circuits is incomplete, although there are indica-tions that the right prefrontal cortex is primarily involved instimulus-selection, the right orbital/anterior cingulate cir-cuits are related to response execution, and the basal ganglia-thalamocortical circuits, at the level of the caudate,underpin response selection. Confirmation of these findingsshould increase our neuropsychological understanding ofGTS and other disorders and provide differential informa-tion to aid diagnosis and treatment.
T r e a t m e n t a n d D e v e l o p m e n t a lC o u r s e
The two primary treatment interventions for GTS are be-havioral modification and pharmacologic therapy. A widerange of behavioral interventions has been applied to GTSwith varying degrees of success. The techniques that havebeen introduced in the treatment of GTS include:(1) massed practice (rapid and repeated voluntary produc-tion of a tic); (2) operant conditioning (providing reinforce-ment for tic-free periods); (3) anxiety management training(for example, training in muscle relaxation for use in anxiety-engendering situations); (4) exposure plus response preven-tion (stimuli or conditions are presented that increase thelikelihood of premonitory urge, and the child is not allowedto release the tic); and (5) habit reversal (performing a com-peting and incompatible physical response contingent onthe urge to perform the tic). Of these techniques, habit re-versal has received the greatest support as an efficacious treat-ment (Piacentini & Chang, 2001). Although each of thesetechniques can lead to tic reduction, the treatment effectsoften fail to generalize to other situations and are frequentlyshort-lived.
The medications used for GTS treatment are generallydopamine antagonists, such as the neuroleptic haloperi-dol (Haldol), which are effective in the treatment of thedisorder. Unfortunately, the use of typical neurolepticscan result in a number of undesirable and sometimes se-
vere side effects. These side effects range from cognitiveslowing to Parkinsonian-like motor disturbances. The useof the newer atypical antipsychotic medications such asrisperidone (Risperdal) reduces the likelihood of side ef-fects, but their efficacy has not been fully established. Re-cently, there has been interest in the dopamine antagonistmetoclopramide, which has been found to be effective intic reduction without significant neuroleptic-like adverseside effects (Nicolson, Craven-Thuss, Smith, McKinlay,& Castellanos, 2005). However, further studies are war-ranted to assess its efficacy and safety over long periods ofuse. Clonidine (Catapres) and guanfacine (Tenex) are 2agonists and have been used with varying success in re-ducing tic behaviors. The precise mechanism of action of2 agonists is unknown, although there are indicationsthat dopamine utilization is increased in the frontal re-gions of the brain (Pennington, 2002).
The child or adolescent with GTS and comorbid OCDoften requires the introduction of behavioral and cognitivebehavioral interventions that target tic behaviors and dis-ruptive obsessions and compulsions. Often, these tech-niques are insufficient, and medication is introduced.Clomipramine (Anafranil), a tricyclic antidepressant, is ef-ficacious for the treatment of OCD. However, because ofthe potential for significant side effects associated withAnafranil, selective serotonin reuptake inhibitors (SSRIs)are currently the first line of pharmacologic intervention.Paroxetine (Paxil) is an SSRI that has been determined tobe helpful in reducing intrusive ideations and compulsivebehaviors for both children and adults. Importantly, SSRIsdo not typically exacerbate motor or vocal tics.
A particularly difficult presentation is the child withGTS and ADHD. The psychostimulants, although effec-tive for treating ADHD, can exacerbate the motor andvocal tics associated with GTS. However, not all childrenwho receive a psychostimulant medication experience ac-celeration of tic behaviors. For the child who is unable totolerate a psychostimulant, clonidine or guanfacine may beintroduced to reduce tics, as well as the hyperactivity andimpulsivity associated with ADHD. However, the 2 ago-nists are not always effective in the treatment of GTS orADHD. In addition, the child medicated with a 2 ago-nist warrants careful monitoring because of the potential for adverse cardiac effects. Recently, atomoxetine (Strattera)was approved for the treatment of ADHD. Atomoxetine isa noradrenaline reuptake inhibitor that, in addition to re-ducing ADHD symptoms, does not appear to exacerbateco-occurring motor and vocal tics. In more severe cases ofGTS with co-occurring OCD and/or ADHD, a combina-tion of medications is often needed to reduce disruptivesymptoms.
336 PART THREE | Disorders of the Brain

Neuropsychological strengths and weaknesses warrantconsideration when mapping out the child’s educationalcurriculum. The teacher and classmates of the child withGTS can profit from a discussion with the neuropsychol-ogist or other informed person concerning what tic be-haviors are and are not, the intermittent expression andpossible increasing severity of tic behaviors, and what theyare to do or not to do when the child is exhibiting tic be-haviors. This information is important for increasing theirunderstanding of GTS, disabusing misinterpretations,and reducing negative responses to the afflicted child. In-terventions to help the teacher and child to cope with ticswithin the classroom are important. For example, theteacher may need to allow the child to leave the classroomand go to the nurse’s office if a significant exacerbation oftic behavior occurs. While in the nurse’s office, the childcan be helped to initiate any techniques that have beenfound to be effective in reducing his or her tics. Seatingthe child in the front row of the class can reduce the de-tection of tics by classmates, because the majority of them
will be seated behind the child. Most important, theteacher and educational staff need to be alert and inter-vene quickly if they observe teasing or taunting of thechild by peers.
Adolescence can be a difficult period of development fora healthy teenager. The motor and vocal tics of GTS, cou-pled with ADHD and/or OCD comorbidity, can be disrup-tive to the adolescent’s efforts to affiliate with peers, initiatedating relationships, develop a positive body image, and es-tablish a healthy self-identity. Fortunately, as discussed ear-lier, motor and vocal tics of GTS begin to attenuate or re-solve during adolescence and early adulthood. Mostadolescents with GTS graduate from high school anddemonstrate appropriate adaptation to their disorder. In caseswhen GTS symptoms do not reduce, or even exacerbate, so-cial, vocational, and emotional adjustment in adulthood maybe compromised (Brown & Ivers, 1999). Hopefully, futurepharmacological advances and refinements will identify med-ications that will effectively address vocal and motor tics at allage levels while producing fewer negative side effects.
CHAPTER 11 | Learning and Neuropsychiatric Disorders of Childhood 337
SummarySeveral developmental disorders currently are the focus of extensive research by neuropsychology andother disciplines. The neuropsychological identification of the potential brain and behavior correlates ofdyslexia and NVLD have enhanced our understanding of learning disabilities. Although most theorizationand research has focused on disorders of reading and mathematics, other forms of learning disabilities,such as dysgraphia, await investigation. Autism has a profound and often global impact on the cognitiveand behavioral development of a child. Advances have been made in the understanding of the neuropatho-genesis, neuropsychological assessment, neuropsychological models, developmental course, and treatmentof autism. However, the cause of autism remains elusive, and treatment interventions often fail to signifi-cantly alter the symptoms of the disorder. ADHD is one of the most studied childhood disorders of our time.Researchers have redefined and relabeled the disorder, spawned numerous hypotheses and theories, andgenerated multiple interventions. Unfortunately, the etiology of ADHD remains unknown; the interplay ofmediating variables such as the child’s personality, environmental effects, and presence of comorbid disor-ders is also poorly understood; and the current treatment options are limited and often ineffective. Althoughthe entrance of neuropsychology into the study of ADHD is relatively recent, optimism remains high that itscontribution will provide new and much needed direction to the study and understanding of the disorder.Finally, GTS is a significantly disruptive and potentially embarrassing disorder that falls on the boundary ofvoluntary-involuntary behavior. The high frequency of comorbidity of other disorders with GTS highlights thediverse effects of frontostriatal dysfunction.
C r i t i c a l T h i n k i n g Q u e s t i o n s
Why are the symptoms of NVLD and ADHD so often displayed by children exhibiting a wide range of developmentaldisorders?Can a child with autism or Asperger’s syndrome develop normal social awareness and attachment? If so, how would thisbe accomplished?How would you respond to the comment, “ADHD does not exist, it is merely a diagnosis to excuse lazy and undisciplinedchildren?”
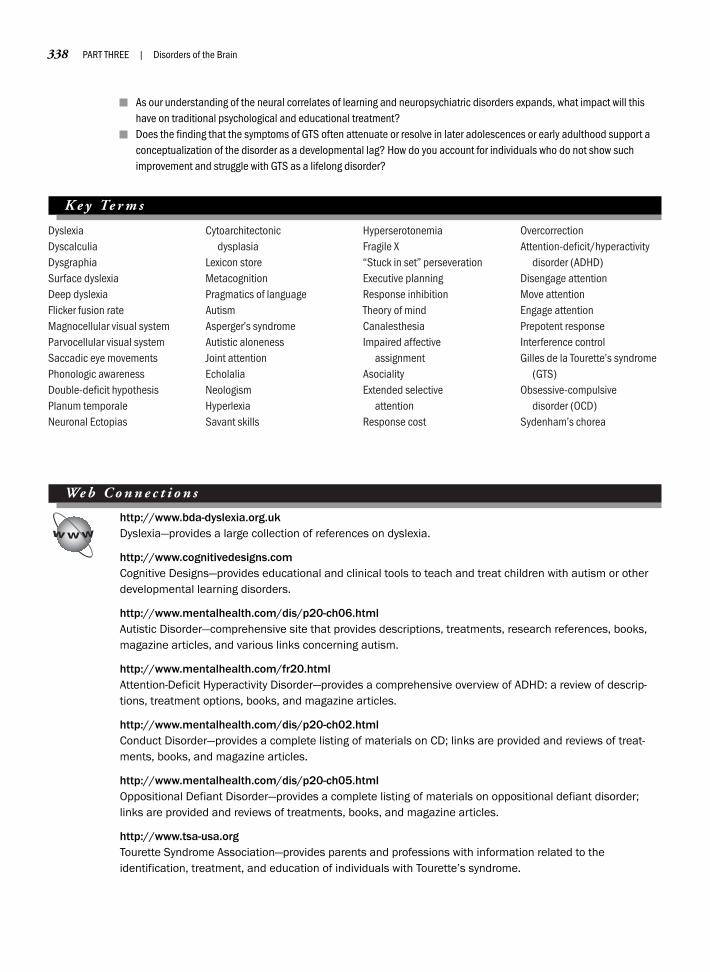
DyslexiaDyscalculiaDysgraphiaSurface dyslexiaDeep dyslexiaFlicker fusion rateMagnocellular visual systemParvocellular visual systemSaccadic eye movementsPhonologic awarenessDouble-deficit hypothesisPlanum temporaleNeuronal Ectopias
Cytoarchitectonic dysplasia
Lexicon storeMetacognitionPragmatics of languageAutismAsperger’s syndromeAutistic alonenessJoint attentionEcholaliaNeologismHyperlexiaSavant skills
HyperserotonemiaFragile X“Stuck in set” perseverationExecutive planningResponse inhibitionTheory of mindCanalesthesiaImpaired affective
assignmentAsocialityExtended selective
attentionResponse cost
OvercorrectionAttention-deficit/hyperactivity
disorder (ADHD)Disengage attentionMove attentionEngage attentionPrepotent responseInterference controlGilles de la Tourette’s syndrome
(GTS)Obsessive-compulsive
disorder (OCD)Sydenham’s chorea
We b C o n n e c t i o n s
http://www.bda-dyslexia.org.ukDyslexia—provides a large collection of references on dyslexia.
http://www.cognitivedesigns.comCognitive Designs—provides educational and clinical tools to teach and treat children with autism or otherdevelopmental learning disorders.
http://www.mentalhealth.com/dis/p20-ch06.htmlAutistic Disorder—comprehensive site that provides descriptions, treatments, research references, books,magazine articles, and various links concerning autism.
http://www.mentalhealth.com/fr20.htmlAttention-Deficit Hyperactivity Disorder—provides a comprehensive overview of ADHD: a review of descrip-tions, treatment options, books, and magazine articles.
http://www.mentalhealth.com/dis/p20-ch02.htmlConduct Disorder—provides a complete listing of materials on CD; links are provided and reviews of treat-ments, books, and magazine articles.
http://www.mentalhealth.com/dis/p20-ch05.htmlOppositional Defiant Disorder—provides a complete listing of materials on oppositional defiant disorder;links are provided and reviews of treatments, books, and magazine articles.
http://www.tsa-usa.orgTourette Syndrome Association—provides parents and professions with information related to the identification, treatment, and education of individuals with Tourette’s syndrome.
338 PART THREE | Disorders of the Brain
As our understanding of the neural correlates of learning and neuropsychiatric disorders expands, what impact will thishave on traditional psychological and educational treatment?Does the finding that the symptoms of GTS often attenuate or resolve in later adolescences or early adulthood support aconceptualization of the disorder as a developmental lag? How do you account for individuals who do not show suchimprovement and struggle with GTS as a lifelong disorder?
K e y Te r m s

Chapter 12
CEREBROVASCULAR DISORDERS AND TUMORS
In whatsoever house I enter, I will enter to help the sick.—Hippocrates (460–377 B.C.)
Pathologic Process of Brain DamageOverview of Cerebrovascular DisordersTypes of Cerebrovascular DisordersDiagnosing Cerebrovascular DiseaseTreatment and Prognosis of Vascular DisordersNeuropsychological Deficits Associated with StrokeTumors of the BrainTypes of Intracranial TumorsBrain Tumors and NeuropsychologyOther Neurologic Disorders
Neuropsychology in Action
12.1 Migraine Headache: A Vascular Disorder of the Brain
12.2 Case Example of a Left Stroke12.3 Neuropsychology of Treatments for Individuals
with Brain Tumors12.4 Family and Child Adjustment to Cognitive Aspects
of Cancer in Children

340 PART THREE | Disorders of the Brain
B R A I N L E S I O N S
What are lesions, and what effects do they have on thebrain? Brain lesions (derived from Latin laesio, meaning“to hurt”) are any pathologic or traumatic discontinuityof brain tissue. Lesions result in “holes” or “cavities” inthe brain and almost always entail loss of function. De-pending on their size and location, lesions result in minoror major behavioral effects. Lesions may be caused bytraumas, such as punctures from bullet wounds, frag-ments of skull fractures, or other foreign objects enteringthe brain. Other events that cause lesions include CVAs,surgical removal of tumors, or diseases such as multiplesclerosis or Creutzfeldt–Jacob disease.
Neurons that are completely severed often degener-ate. The tissue that surrounds the lesion shrinks and dies
K e e p i n M i n d
What is a stroke?
How long can the human brain function without oxygen?
How is the brain supplied with blood?
What are the lasting neuropsychological deficits after stroke?
What happens when a tumor grows in the brain?
OverviewThe normal functioning central nervous system (CNS) can be affected by a number of neurologic disordersand diseases. Some will result in similar types of damage, and some will be vastly different. Some result infocal effects, others result in diffuse damage. Physicians expect some, if not complete, recovery after manytypes of brain damage, such as mild head injuries. Other types of brain diseases are more severe and mayresult in lasting impairment, as is often the case in stroke, or may be even fatal, as is Alzheimer’s disease,with which there is an inevitable decline in health culminating in death. Thus, brain disorders may have awide-ranging impact on a person’s well-being. Often, significant neuropsychological deficits exist that resultin marked disabilities, alterations in personality, and a decline in quality of life.
This chapter discusses the most common neurologic problems and neuropsychological sequelae thatare associated with cerebrovascular accidents (CVAs) and tumors. Chapter 13 discusses the impact on thebrain and its recovery related to head injury. Chapters 14 and 15 present degenerative disorders, which aregood examples of diffuse and generalized involvement of brain pathology. Chapter 16 reviews disorders ofconsciousness, in which the typical clinical picture is also more generalized, with many behavioral adaptiveskills possibly affected.
For each disorder, we examine neuropathology, neuropsychological sequelae, appropriate treatments,and case examples of patients we have treated. We present the information within a neuropsychologicalperspective; that is, we describe the disorders with particular relevance to the relations among brainanatomy, biological processes of the brain, and their behavioral product.
Pathologic Process of Brain Damage
This section reviews examples of brain damage andtheir mechanisms of action within the brain. These exam-ples are not necessarily mutually exclusive, and many con-ditions may result in more than one problem. They alsoare not totally inclusive, but are meant to provide anoverview of some of the more common terms and condi-tions you will encounter as you read about variouspathologies throughout this book. Although some exam-ples result in specific behavioral effects, many terms, suchas “lesion,” are more generic, and their behavioral effectsoften depend on the specific location and extent of dam-age within the brain.

within hours. Cerebrospinal fluid (CSF) then fills thecavity. With time, surrounding brain tissue may collapsethe cavity, which may concomitantly distort other areasof the brain or ventricles, depending on the size of thelesion (Figure 12.1). Any dead neuronal debris is en-gulfed by the brain’s micro “cleaning machines,” thephagocytes, which are forms of glial cells (see Chapter 4).As a result, glial cells may be all that remains in the cav-ity of the lesion where neurons were once active. Thisobviously results in a blockage or interruption of neuraltransmission.
A N O X I A A N D H Y P O X I A : O X Y G E ND E P R I V A T I O N T O T H E B R A I N
Most readers will know that reduced flow of oxygen tothe brain is dangerous. CVAs or strokes imply by defini-tion a disruption or stoppage of blood to the brain.Strokes almost always result in neuronal loss or degenera-tion. Neurons need oxygen to break down glucose intocarbon dioxide and water. Furthermore, the brain has noreservoir of glucose or oxygen. Thus, the brain dependson a constant and immediate supply. An elaborate bloodsystem carries oxygen and important nutrients to thebrain. Although weighing less than 3 pounds, the brain is
rather demanding, requiring more than 20% of the body’soxygen to keep functioning effectively. As a result, thebrain is particularly vulnerable to oxygen depletion.
If a neuron lacks oxygen for some time, the neuronwill die. This necrosis, or neuronal cell death, is a directresult of a crucial interference with the cellular metabo-lism of the neuron. A complete absence of oxygen supplyto the brain is anoxia. The most common causes ofanoxia are cardiopulmonary failures associated with heartattacks, complications of anesthesia, accidents such asnear-drowning episodes, or other severe traumas to thebrain, such as are often seen in gunshot wounds to thehead. In these cases, where there may be respiratory orcardiac arrest, permanent brain damage follows unlessoxygen is restored quickly. Most anoxic episodes appearto result in damage to subcortical and limbic areas, thefrontal lobes, and the cerebellum.
In contrast, hypoxia describes a reduced, but notcomplete, oxygenation of brain. Hypoxia typically en-tails not cell death, but some possible interference in thefunctioning of the neuron. In general, 4 to 6 minutes ofanoxia may cause necrosis, although this is highly variable and depends on individual and environmentalcharacteristics. Hypoxia can occur at high altitude, dur-ing acute cardiac crisis, during the aftermath of open-heart surgery, and during exertion in deep-sea divers. Itmay also be seen in carbon monoxide poisoning, mayaccompany sleep in the aging brain, and is present inpeople with chronic obstructive pulmonary disease re-lated to chronic, intermittent lowered oxygen saturationin the blood.
A growing body of literature suggests that individualswho are otherwise healthy and who experience mild-to-moderate hypoxia may demonstrate significant diffi-culties in concentration, short-term memory, new learn-ing, and judgment. At extreme altitude—that is, morethan 22,000 feet—hypoxia can impair a human’s cogni-tive function, including motor speed, judgment, verbalfluency, learning, and short-term memory. Severe hypoxiaproduces more dramatic deficits, often resulting in irre-versible brain damage. However, under specific environ-mental conditions (such as cold water submersion), chil-dren may recover completely from acute hypoxia, even ifit has lasted as long as 20 minutes. The reasons for thisare unclear, but are probably related to young age and thepoorly understood effects of cold-water submersion onbrain metabolism.
Hypoxia can occur at high altitudes. For example,climbers refer to elevations above 25,000 feet as the “death zone,” because of the low oxygen level in theair (Krakauer, 1997). The air is so thin that even
CHAPTER 12 | Cerebrovascular Disorders and Tumors 341
Figure 12.1 Sagittal magnetic resonance imaging of brainwith small stroke in the superior portion of the cerebellum(bottom). Significant atrophy is associated with increased size ofthe lateral ventricles and intracranial space (top). See insidecovers for color image. (Courtesy Eric Zillmer.)

conditioned climbers may become hypoxic. In fact, ifone were to “pluck” a person from sea level and drophim or her on Mount Everest, which has an elevation of29,028 feet, death by anoxia would occur within min-utes. Even when adapted to extreme elevations, manyclimbers must use supplemental oxygen. Nevertheless,at such high altitudes, one becomes careless, sluggish,and fatigued. To conserve oxygen, the brain may dimin-ish oxygen supply to more distal parts of the body, in-creasing the risk for frostbite and hypothermia, andsometimes edema of the brain and death. Recent neu-ropsychological studies conducted on the ascent and thesummit of Mount Everest clearly indicate hypoxia inclimbers and a related dysfunction in memory and con-centration (for example, see Virues-Ortega, Buela-Casal,Garrido, & Alcazar, 2004).
Medical conditions can also affect oxygen uptake. Forexample, chronic obstructive pulmonary disease is a dis-order in which the lung has lost its capacity to efficientlyexchange oxygen with white blood cells. Sleep apnea(derived from Greek apnoia, meaning “negative breath-ing”) is a good example of chronic hypoxia during sleep.Breathing is disturbed throughout the night and oftencompletely stops for periods as long as a minute. Thesehypoxic episodes often occur with more severity duringrapid eye movement (REM) sleep, because the volun-tary muscles that assist in breathing are paralyzed duringdream sleep. Under normal circumstances, blood is 95%oxygenated, but in sleep apnea patients, this can de-crease to 50% and less. Consequently, people with sleepapnea often report morning headaches, poor attentionand concentration and, of course, sleepiness during theday (Zillmer, Ware, Rose, & Maximin, 1988). It is un-clear whether the effects of hypoxia reverse with in-creased oxygen saturation in the blood. To some extent,they appear to, because patients often completely recover. Reversibility is likely related to the length of deprivation.
H Y D R O C E P H A L U S
Hydrocephalus is a condition in which the ventricles en-large abnormally, because of increased CSF production,decreased CSF absorption, or a blockage of CSF flowthrough the ventricles. There are several medical reasonswhy this occurs. You may recall from Chapter 5 that theventricles produce and circulate CSF through and aroundthe brain and spinal cord. Spinal fluid and waste productsare then reabsorbed, in part by the ventricles. The pres-ence of blood or blood products mixing with the CSF,
perhaps as a result of hemorrhage or infection, may inter-fere with reabsorption. This condition is called commu-nicating hydrocephalus. Finally, blockage of the circula-tion of CSF is termed obstructive hydrocephalus. Inyoung children, obstructive hydrocephalus is often causedby a congenital narrowing or stenosis of the aqueduct ofSylvius between the third and fourth ventricles. In adults,obstructive hydrocephalus is most likely caused by braintumors protruding into the ventricles.
Damage to the brain caused by hydrocephalus resultsfrom the pressure of squeezing parts of the brain againstan immovable skull. If not corrected quickly, intensepressure can cut off the blood supply and result in celldeath. Behaviorally, hydrocephalus results in symptomsof increased cranial pressure, such as sleepiness, severeheadache, and nausea. Hydrocephalus is usually an acutecondition, but physicians can reverse it by releasing the pressure; they surgically insert a tube to shunt the CSFinto the peritoneal cavity of the body—the potential spacearound the lining of the abdominal and pelvic walls. Ifnot treated quickly, progressive hydrocephalus can be lifethreatening, because it impinges on vital brainstem func-tions such as respiration and arousal.
Overview of CerebrovascularDisorders
Bubbeh had to die, as you and I will one day have to die. Just asI had witnessed the decline of my grandmother’s life force, Iwas present when it gave the first signal of its finality. It wasearly on an ordinary morning; Bubbeh and I were doing ordi-nary things. Having finished breakfast a few minutes before, Iwas still hunched over the sports section of the Daily Newswhen I became aware that there was something very strange inthe way Bubbeh was trying to wipe clean the surface of thekitchen table. Even though we had long since realized that suchhousehold tasks were beyond her, she had never quite given uptrying, and seemed oblivious to the fact that one or another ofus always repeated the work after she laboriously shuffled out ofthe room. But when I looked up from the tabloid, I saw thather wide circular strokes were even more ineffectual than usual.Her sweeping hand had become aimless, as though acting on itsown with no plan or direction. The circles ceased to be circlesand soon became mere languid, useless drags of the moist cloththat was barely held in her flaccid hand, adrift on the tablewithout purpose or weight. Her face was turned straight ahead.She seemed to be looking at something outside the windowbehind my chair instead of at the table in front of her. Herunseeing eyes had the dullness of oblivion; her face was expres-sionless. Even the most impassive of faces betrays something,
342 PART THREE | Disorders of the Brain

but I knew at that instant of absolute blankness that I had lostmy grandmother. I shouted, “Bubbeh, Bubbeh!” but it made nodifference. She was beyond hearing me. The cloth slipped fromher hand and she crumpled soundlessly to the floor.
I bounded to her side and called her name again, but my shout-ing was as futile as my attempts to comprehend what washappening. Somehow, and I remember not a moment of it, Igathered her up and staggered to the room we shared. I laid herdown in my bed. Her breathing was stertorous and loud. Itblew in long, forceful blasts from only one corner of hermouth, and it flapped her cheek out like a buffeted wet saileach time she exhaled from that noisy bellows somewhere downdeep in her throat. I can’t recall which side it was, but oneentire half of her face seemed toneless and flaccid. I rushed tothe phone and called a doctor whose office was not far away.Then I contacted my aunt Rose at the Seventh Avenue dressfactory where she worked. Rose got there before the doctorcould free himself from a waiting room filled with early-morning patients, but we knew there was nothing he could doanyway. When he arrived, he told us Bubbeh had suffered astroke, and wouldn’t live more than a few days. She outsmartedthe doctor and hung on for the next 14 nights. (Nuland, 1993, p. 58–59)
Cerebrovascular disease is reported to be the mostcommon cause of neurologic disability in the Westernworld, the second leading cause of death among the old-est old (age �85), and the third most common cause ofdeath in the developed countries of the world. Only can-cer and heart attacks affect more people. Strokes are amajor health concern in the United States, and they cansignificantly affect the quality of life of those afflicted, aswell as their families.
In the United States, stroke affects approximately500,000 people each year, and it is the major cause of dis-ability among adults. The death rate associated withstrokes is approximately 5%, corresponding to approxi-mately 150,000 deaths each year in the United States. An-other 150,000 people are left with permanent severe dis-ability. Individuals suffering from a cerebrovascular disorderplace a significant financial and emotional burden on thefamilies who take care of their loved ones. The estimatedpublic health costs related to stroke amount to billions ofdollars per year and are expected to accelerate steadily asadvances in emergency medicine allow more stroke victimsto survive.
The average age of a stroke victim is approximately 70 years (see Zillmer, Fowler, Waechtler, Harris, & Khan,1992). As the population of the United States is growing,life expectancy is likewise increasing. Today, people areliving longer and into the age-groups that are more at riskfor CVAs. In fact, gerontologists have called the over 65
age-group the fastest-growing segment of the U.S. popu-lation. This increase in the elderly population greatlyswells the number of those at risk for strokes, creating asituation in which more people in the population will ac-tually be suffering from CVAs.
S T R O K E D E F I N I T I O N
The term stroke itself is not clearly defined and is not aprecise medical term. A more technical term for stroke iscerebrovascular accident (CVA), which describes a het-erogeneous group of vascular disorders that result in braininjury. The brain’s blood vessels are damaged, which candecrease blood flow within and to the brain. In simpleterms, stroke “suffocates” brain tissue and often producesan area of dead or dying brain tissue. A stroke always oc-curs in the brain and is the most common type of cere-brovascular disease. Thus, CVA or stroke is a commonlabel assigned to clinical syndromes that are caused byblockage in blood supply or by bleeding in the brain.Stroke can result from a wide variety of different vasculardiseases, but not all vascular disorders produce stroke. Al-though the onset of symptoms is rapid (hence the termstroke), the full development of the clinical picture maytake an appreciable time, sometimes hours, depending onthe rate of the bleed and its final cessation (Bannister,1992).
In the past, people have conceptualized stroke as a “faitaccompli”; That is, once it occurred, little could be done.Recent medical technology, however, has made advancesin treating the stroke patient immediately; therefore, earlydiagnosis and intervention have become a high priority.Physicians now treat stroke as a “brain attack,” a medicalemergency similar to a heart attack. Stroke can producean array of disorders of great complexity. Most strokesoccur, or are localized, in only one of the cerebral hemi-spheres, although in some instances, multiple strokes orone major subcortical stroke affects the entire brain. Ingeneral, the deficits directly relate to the location or thehemisphere where the stroke occurs.
Neuropsychologists play a crucial role in CVA diagno-sis and rehabilitation. They are at the forefront in manysignificant advances in long-term treatment and rehabili-tation of stroke patients. In addition, neuropsychologistsconduct research on CVA survivors because it providesthem with clinical data by which to examine localized le-sions, propose strategies for intervention and rehabilita-tion, and indirectly develop knowledge of the function-ing intact brain (Naugle, Cullum, & Bigler, 1998).
CHAPTER 12 | Cerebrovascular Disorders and Tumors 343

I M P A I R M E N T O F B L O O D S U P P L Y T O T H E B R A I N
The clinical presentation of a patient after stroke reflectsthe damage to the anatomic structures of the brain. Dis-ruption of major arteries can cause characteristic symp-toms according to the area of the brain that artery serves(the vascular system of the brain is reviewed in Chapter 5).For example, the symptoms of a right hemisphere strokeare quite different from those of a left hemisphere CVA.Almost always behavior is disrupted, and thus physi-cians often consult neuropsychologists to evaluatestroke patients. The following three related neuropsy-chological events often occur after a stroke, all of whichinterfere with normal brain functioning. Victims mayhave to contend with these three serious consequences ofstroke:
1. Disrupted blood supply decreases oxygenation, as inhypoxia or anoxia, of the involved brain tissue.
2. Related to bleeding (or hemorrhage), a space-occupyingmass or pocket of blood often develops, which maypress on nearby brain structures, affecting their in-tegrity. As a result, intracranial pressure (ICP) maysuddenly increase.
3. When blood spills out of the artery and into brainplasma, many toxins in the blood can interfere withnormal brain metabolism. In an intact vascular sys-tem, the blood–brain barrier (BBB) protects the sur-rounding tissue from any toxic properties contained inblood, but exposed blood outside of the artery irritatesbrain tissue.
Types of CerebrovascularDisorders
To effectively rehabilitate the patient and provideappropriate guidance to the family and patient, neuropsy-chologists differentiate among three different types andmechanisms of stroke:
1. “Temporary” strokes arise from insufficient blood sup-ply to an area of the brain. These events, collectivelycalled ischemia, often manifest in short-lasting attacksthat cause only transient deficits.
2. Blockage of an artery causes a more severe loss of bloodsupply. This infarction often results in more lastingneuropsychological deficits.
3. The third type of stroke is related to bleeding and todisplacement of the brain that arises from a hemor-
rhage. Hemorrhages are the most severe form ofstroke and often cause permanent brain damage ordeath.
Each cerebrovascular event is described in more detail inthe following paragraphs.
T R A N S I E N T I S C H E M I C A T T A C K S
Neuropsychologists call an acute, focal (localized) neuro-logic deficit, evidenced by a transient loss of function, atransient ischemic attack (TIA). Recovery should occurwithin 24 hours, but is often complete within a muchshorter time, often minutes. The attacks vary from infre-quent (that is, less than one a month) to very frequent(that is, several times a day).
Rudolf Virchow, a German physician and the founderof German medicine, coined the term ischemia (derivedfrom Greek ischein, meaning “to hold in check,” andhaima, meaning “blood”); literally, ischemia means “aholding in check of the flow of blood” to refer to the tem-porary disruption of blood flow. Deficits from TIAs healgradually, and the patient most often returns to normalneurologic and neuropsychological functioning. An im-portant assumption in a TIA is that no actual damage toany neurons has occurred, just a temporary insufficiencyof oxygen supply (Powers, 1990).
TIAs most commonly involve the internal carotid,middle cerebral, or the vertebral-basilar arteries. Clini-cally, neuropsychologists divide the deficits into the ante-rior circulation involving the carotid system and those affecting the posterior circulation involving the vertebral-basilar system. If the ischemic attack affects anterior cir-culation, the deficits manifested will most likely relateto brief clumsiness or weakness of a limb, dysarthria, oraphasia. If the attack affects the posterior circulation,deficits may include dizziness, neglect, double vision,and numbness or weakness of the extremities. Individu-als suffering from TIAs rarely lose consciousness com-pletely, and as mentioned earlier, cognitive and physicalfunctioning usually return to normal once the attackhas ceased.
Because one of the first “signs” of stroke is TIAs, theiroccurrence should be taken seriously. People sufferingfrom TIAs have a 20% to 35% greater risk for stroke thando unaffected individuals, and they go on to suffer obvi-ous infarction (see later). Little research has been con-ducted, however, to determine which individuals suffer-ing from TIAs go on to experience development of themore severe infarctions. Another third continue to haveTIAs without any permanent disability, and the remainder
344 PART THREE | Disorders of the Brain

have attacks that cease spontaneously. Two-thirds of thosesuffering from TIAs are male or hypertensive, or both(Powers, 1990). A neurologist or neuropsychologist easilyrecognizes symptoms of a TIA (Table 12.1). Unfortu-nately, the person suffering the TIA, because of confusionor an impaired capacity to use judgment, often does notrecognize the symptoms resulting from a TIA. In othercases, the TIA symptoms are so peculiar and vague thatclinicians find them difficult to establish, because of theirwaxing-and-waning, transient nature. This is particularlyfrustrating to the patient, who may be inadvertently re-ferred to a psychiatrist or psychologist because his or herpresentation does not appear to fit any established med-ical categories or because physicians can find nothingphysically wrong.
I N F A R C T I O N S
When ischemia is severe enough to kill the nerve cell,neurologists consider the neuron infarcted. Infarctions re-sult from an inadequate blood supply to an area of thebrain, causing tissue death or necrosis from the lack of oxygen. This event most often relates to obstruction ofthe local vascular circulation by blockage or occlusion ofa vessel, stopping blood flow. Occlusions are typicallycaused by either a blood clot or a fatty deposit lodged in avessel. The area of the brain in which this occlusion oc-curs depends on clot size. Occlusion can happen to thebrain as a whole, as in severe heart failure; in one of themajor arteries or their branches supplying blood to the brain; or in a small capillary. Cerebral infarction ismost likely the result of a thrombotic or an embolic vas-cular occlusion in blood flow. We discuss both ischemicevents in more detail in the following paragraphs.
T h r o m b o s i s
Thrombosis is the formation of a blood clot or thrombus(derived from Greek meaning “clot”) within the bloodvessel. A thrombosis at the heart is a heart attack. Athrombosis in the brain is a stroke. The most commonbasic neuropathologic process in infarction is that of ath-erosclerosis. In atherosclerosis, irregularly distributed yel-low fatty plaques are present in large- and medium-sizearteries. Fat deposits build up along blood vessel walls, re-ducing the size of the cerebral artery. In atherosclerosis,the blood clot lodging in the vessel reduces or completelyblocks blood flow through the vessel. Thus, atherosclerosisoften precipitates infarction due to occlusion. Atheroscle-rosis is not a uniform process throughout the cardiovas-cular system; it can affect certain parts of the arterial sys-tem more than others. The most common location foratherosclerosis is at the bifurcation of arteries (the pointwhere the division occurs), specifically at the commoncarotid artery. This condition is progressive, variable, anddifficult to predict, although it tends to become worse as aperson grows older. Atherosclerosis restricts blood supplyto the brain and results in inadequate oxygenation of braintissue. This produces a general decline in neuropsychologi-cal abilities of a diffuse nature. TIAs often, but not always,precede stroke that results from cerebral thrombosis.
The pathologic process underlying a thrombosis in-volves platelets. Platelets are disk-shaped cells found inthe blood of all mammals. They are important for theirrole in blood coagulation and are produced in large num-bers in the bone marrow. From there, they are releasedinto the bloodstream, where they circulate for approxi-mately 10 days. While circulating, these cells do not ad-here to each other or to the wall of a blood vessel. Whenthe endothelium, the layer of epithelial cells that line theblood vessels, is breached, however, the blood-clottingproperties of the platelets activate. That is, they changeshape and stick to the vessel wall, each other, and redblood cells. If this occurs pathologically—that is, in a nor-mal vessel—it leads to a thrombosis, ultimately occludingthe vessel. Aspirin is an important antithrombotic agent.
The middle cerebral artery on the left side is the mostcommonly reported site for an occlusion. Research hasshown that blood clot formation most frequently stemsfrom abnormality within the vessel wall and less fre-quently from an abnormality of the blood itself (Brown,Baird, & Shatz, 1986). If a thrombus forms and blocksthe flow of blood to the brain, a cerebral infarction oc-curs. The area of the brain in which this occlusion occursdepends on the size of the blood clot. If it is large, it maylodge in one of the major arteries; if smaller, it will lodge
CHAPTER 12 | Cerebrovascular Disorders and Tumors 345
Sudden tingling or numbness on one side of the face
Confusion as to time, place, or person
Loss or impairment of speech for understanding and/or communicating
Sudden slurring of speech, dizziness
Visual disturbances such as blurring or double vision
Other cognitive changes such as difficulty reading, writing, or thinking
Weakness on one side of the body (arm or leg)
Table 12.1 Symptoms of a Transient Ischemic Attack
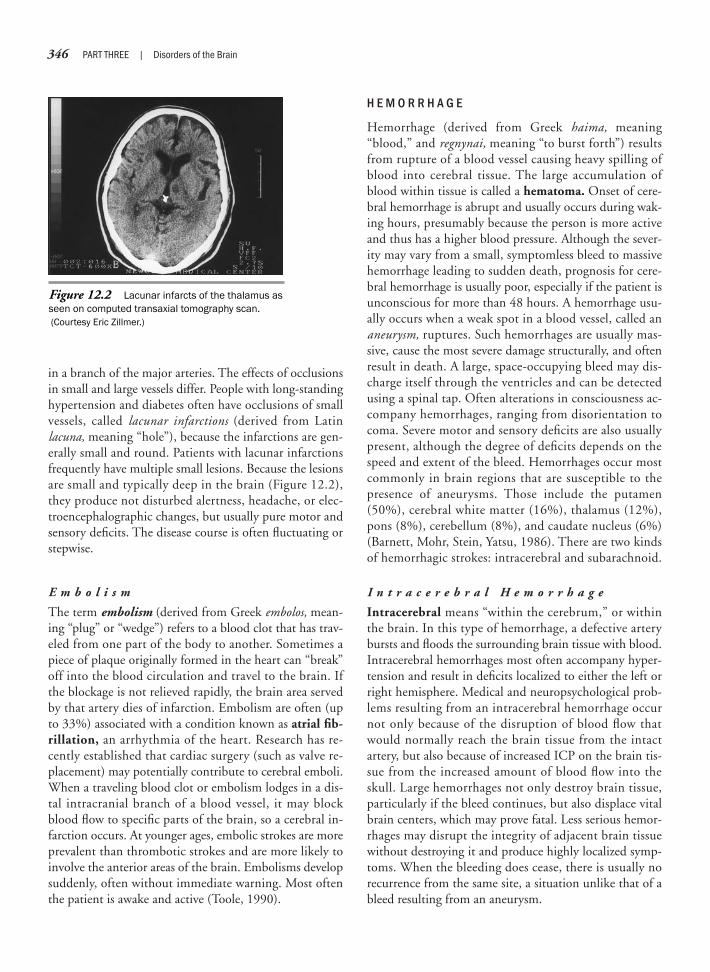
in a branch of the major arteries. The effects of occlusionsin small and large vessels differ. People with long-standinghypertension and diabetes often have occlusions of smallvessels, called lacunar infarctions (derived from Latin lacuna, meaning “hole”), because the infarctions are gen-erally small and round. Patients with lacunar infarctionsfrequently have multiple small lesions. Because the lesionsare small and typically deep in the brain (Figure 12.2),they produce not disturbed alertness, headache, or elec-troencephalographic changes, but usually pure motor andsensory deficits. The disease course is often fluctuating orstepwise.
E m b o l i s m
The term embolism (derived from Greek embolos, mean-ing “plug” or “wedge”) refers to a blood clot that has trav-eled from one part of the body to another. Sometimes apiece of plaque originally formed in the heart can “break”off into the blood circulation and travel to the brain. Ifthe blockage is not relieved rapidly, the brain area servedby that artery dies of infarction. Embolism are often (upto 33%) associated with a condition known as atrial fib-rillation, an arrhythmia of the heart. Research has re-cently established that cardiac surgery (such as valve re-placement) may potentially contribute to cerebral emboli.When a traveling blood clot or embolism lodges in a dis-tal intracranial branch of a blood vessel, it may blockblood flow to specific parts of the brain, so a cerebral in-farction occurs. At younger ages, embolic strokes are moreprevalent than thrombotic strokes and are more likely toinvolve the anterior areas of the brain. Embolisms developsuddenly, often without immediate warning. Most oftenthe patient is awake and active (Toole, 1990).
H E M O R R H A G E
Hemorrhage (derived from Greek haima, meaning“blood,” and regnynai, meaning “to burst forth”) resultsfrom rupture of a blood vessel causing heavy spilling ofblood into cerebral tissue. The large accumulation ofblood within tissue is called a hematoma. Onset of cere-bral hemorrhage is abrupt and usually occurs during wak-ing hours, presumably because the person is more activeand thus has a higher blood pressure. Although the sever-ity may vary from a small, symptomless bleed to massivehemorrhage leading to sudden death, prognosis for cere-bral hemorrhage is usually poor, especially if the patient isunconscious for more than 48 hours. A hemorrhage usu-ally occurs when a weak spot in a blood vessel, called ananeurysm, ruptures. Such hemorrhages are usually mas-sive, cause the most severe damage structurally, and oftenresult in death. A large, space-occupying bleed may dis-charge itself through the ventricles and can be detectedusing a spinal tap. Often alterations in consciousness ac-company hemorrhages, ranging from disorientation tocoma. Severe motor and sensory deficits are also usuallypresent, although the degree of deficits depends on thespeed and extent of the bleed. Hemorrhages occur mostcommonly in brain regions that are susceptible to thepresence of aneurysms. Those include the putamen(50%), cerebral white matter (16%), thalamus (12%),pons (8%), cerebellum (8%), and caudate nucleus (6%)(Barnett, Mohr, Stein, Yatsu, 1986). There are two kindsof hemorrhagic strokes: intracerebral and subarachnoid.
I n t r a c e r e b r a l H e m o r r h a g e
Intracerebral means “within the cerebrum,” or withinthe brain. In this type of hemorrhage, a defective arterybursts and floods the surrounding brain tissue with blood.Intracerebral hemorrhages most often accompany hyper-tension and result in deficits localized to either the left orright hemisphere. Medical and neuropsychological prob-lems resulting from an intracerebral hemorrhage occurnot only because of the disruption of blood flow thatwould normally reach the brain tissue from the intactartery, but also because of increased ICP on the brain tis-sue from the increased amount of blood flow into theskull. Large hemorrhages not only destroy brain tissue,particularly if the bleed continues, but also displace vitalbrain centers, which may prove fatal. Less serious hemor-rhages may disrupt the integrity of adjacent brain tissuewithout destroying it and produce highly localized symp-toms. When the bleeding does cease, there is usually norecurrence from the same site, a situation unlike that of ableed resulting from an aneurysm.
346 PART THREE | Disorders of the Brain
Figure 12.2 Lacunar infarcts of the thalamus asseen on computed transaxial tomography scan.(Courtesy Eric Zillmer.)

S u b a r a c h n o i d H e m o r r h a g e
A subarachnoid hemorrhage occurs when a blood vesselon the surface of the brain bursts and blood flows into thesubarachnoid space, the small cavity that surrounds thebrain. As with intracerebral hemorrhages, a major prob-lem that can occur from this type of stroke is increasedpressure on the brain. The extent of dysfunction seen withsubarachnoid hemorrhages depends, in part, on howmuch pressure is exerted on the brain. Acute symptomsinclude sudden headache, vomiting, and a possible inter-ruption of consciousness. Because of the diffuse effects onthe brain, localized symptoms, such as paralysis, typicallyare not present during a subarachnoid hemorrhage.
A n e u r y s m s
Aneurysms represent weak areas in the walls of an arterythat cause the vessel to balloon. These localized dilations ofblood vessels may be of congenital origin, but are also pres-ent after trauma, infection, and arteriosclerosis. Aneurysmscan produce more significant disorders when they begin tohemorrhage and are a major cause of stroke-related mortal-ity and disability. Aneurysm bleeds range from minor to acomplete rupture resulting in a hemorrhage, as describedearlier. Approximately 50% of aneurysms occur in themiddle cerebral artery and are most likely inherited or re-lated to a pathologic process that weakens arterial walls.Many vascular anomalies remain undetected only to begincausing problems when they rupture because of such fac-tors as high blood pressure. The base rate for adults is 4%;and among those who have aneurysms, 20% have multi-ple ones. Aneurysms, which expand with time, are mostoften less than 6 to 7 mm in diameter, with giantaneurysms expanding to 2.5 cm. It is relatively rare thatsmall aneurysms rupture (Bannister, 1992).
A r t e r i o v e n o u s M a l f o r m a t i o n s
Arteriovenous malformations (AVMs) represent directand essentially useless communications between arteriesand veins without an intervening capillary network.AVMs are typically congenital collections of abnormalvessels that result in abnormal blood flow. Because theyare inherently weak, AVMs may lead to stroke or to inad-equate distribution of blood in the regions surroundingthe vessels. Rupture of AVMs may produce intracerebraland subarachnoid bleeding. Like aneurysms, AVMs havea tendency for recurrent bleeding. The clinical symptomsof AVMs can include headache, which is similar to mi-graine in that it is related to the dilation of vessels, orother more vague cognitive complaints (Neuropsychol-ogy in Action 12.1). Often, AVMs have no identifiableclinical consequence and many individuals are not aware
they have the condition. The most serious complication ofAVMs is bleeding, typically at a very slow rate. Table 12.2summarizes the various types of cerebrovascular disordersreviewed in this chapter.
Diagnosing CerebrovascularDisease
Because of their sudden onset, infarctions are rela-tively easy to differentiate from other focal neurologic dis-orders such as tumors. Gradual obstruction of one vessel,however, may not produce an infarction at all. Becausethe occlusion develops over a long period, its eventualcourse into full occlusion may have few or mild effects,because alternative blood sources for the affected braintissues may have formed over time. The major diagnostictask in differentiating stroke from other neurologic con-ditions is to exclude other causes of lesions that producesimilar clinical pictures or cause a bleed. A precise diagnosis
CHAPTER 12 | Cerebrovascular Disorders and Tumors 347
Arteriovenous malformation—arteriovenous malformations (AVMs) representabnormal, often redundant vessels that cause abnormal blood flow. Becausethey have inherently weak vessel walls, AVMs may lead to slow bleeding orinadequate distribution of blood in the regions surrounding the vessels.
Embolism—a type of artery occlusion in which the clot forms in one area ofthe body and travels through the arterial system to another area, in this case,the brain, where the clot becomes lodged and obstructs cranial blood flow.Approximately 14% of all CVAs are caused by an embolus.
Hemorrhage—means bleeding, or literally, the escape of blood from thevessels. It is the most severe form of cerebrovascular accident (CVA), charac-terized by the rupturing of a blood vessel. Hemorrhages account for approxi-mately 10% of all strokes. Most hemorrhages stem from increased bloodpressure and the presence of abnormal formations of blood vessels, includ-ing aneurysms.
Migraine stroke—a rare type of stroke caused by severe transient ischemicattacks (TIAs), typically associated with classic migraine.
Thrombosis—a type of occlusion in which a clot or thrombus forms in anartery and obstructs blood flow at the site of its formation. This is the mostcommon form of stroke and accounts for approximately 65% of all CVAs.
Transient ischemic attack—a temporary (transient) lack of oxygen (ischemia)to the brain. This temporary lack of oxygen can cause a time-limited set ofneuropsychological deficits. TIAs technically are not considered a stroke,because neuronal death does not occur.
Table 12.2 Summary of Different Types of Vascular Disorders

348 PART THREE | Disorders of the Brain
Although the primary symptom of migraine isa seemingly subjective and excruciatingheadache, migraine is, in fact, a neurologicdisorder of the brain’s vascular structure.Symptoms consist of a moderate to severelateralized, “throbbing” headache, typicallybehind the eye, associated nausea, and anincreased sensitivity to light, odors, andsounds. Often, a family history shows similarheadaches, but the diagnosis is indicatedonly if no evidence of other organic disease,such as tumor or stroke, could account forthe symptoms. Migraines are common: 24 million or 1 of every 11 people in theUnited States suffer from migraine (Lezak,Howieson, & Loring, 2004). Migraines aremore prevalent among women than men (bya 3:1 ratio) and occur most often betweenages 30 and 45. The typical frequency ofmigraine is intermittent (about 2–5 permonth), and an attack lasts between 4 and72 hours. A migraine attack can incapacitatethe victim, so high labor costs arise fromdecreased work productivity and increasedabsenteeism. About 20% of migraine suffer-ers experience an aura, a neurologic eventthat occurs before the onset of pain and ismost likely caused by a TIA. The aura pre-sents usually as a visual symptom includingflashing lights, zigzag lines, or blurred orpartial loss of vision. Other neurologicsymptoms may also be present during anaura, including increased numbness of theskin (especially in the arms), difficulties inmotor coordination, and symptoms ofaphasia.
The trigeminal nerve, a large cranialnerve with three branches, has been impli-cated in migraine. The trigeminal nerveconveys sensory information including pain,touch, and temperature from most of theface and the scalp. A proposed mechanismfor migraine implicates the sensory “pain”fibers of the trigeminal nerve that surroundthe cranial arteries that supply blood to the
meninges. In people with migraine, thesenerve fibers sometimes release chemicalsknown as peptides. As a result, blood ves-sels become inflamed, and cranial bloodflow changes, first abnormally constrictingand then dilating.
Migraine auras occur during the constric-tion phase. This is such a common eventamong migraine sufferers that many patientsnotice this as a first sign of the oncomingmigraine. During the subsequent dilation,patients experience the symptoms of themigraine attack. Swollen blood vesselsstimulate surrounding nerve fibers to relayimpulses to the brain, where they are per-ceived as pain. The accompanying severenausea perhaps relates to a compromise inthe blood–brain barrier, which, in turn, allowstoxins naturally present in the blood to enterinto brain tissue. The neurotransmitterserotonin plays a major role in migraine(Figure 12.3). During migraine attacks,
serotonin levels decrease and medicationsor substances that deplete serotonin (suchas chocolate or the food additive MSG) oftentrigger a migraine. Conversely, administeringa serotonin agonist (such as sumatriptansuccinate [Imitrex]) often relieves theheadache.
Although many individuals with migrainesexperience development of transient ischemicattacks (TIAs), few go on to suffer from acerebrovascular accident (CVA). Althoughrare, migraine strokes do occur and seem toaccount for a small proportion of CVAs inpeople younger than 40 years, particularlyfemale individuals. Medical research hasdemonstrated that individuals suffering frommigraines are actually at less risk for strokethan the general population (Bannister,1992). This is because the migraine patient’scardiovascular system is inherently flexible,which allows the constriction and dilation ofarteries in the first place (Walton, 1994).
N e u r o p s y c h o l o g y i n A c t i o n 1 2 . 1
M i g r a i n e H e a d a c h e : A Va s c u l a r D i s o r d e r o f t h e B r a i n
by Eric A. Zillmer
Figure 12.3 The role of serotonin in migraine. (Courtesy Beth Willert © 2000. Reprinted by permission of theartist. From packaging display for GlaxoWellcome, Inc.)

is important to the medical team, as well as the neuropsy-chologist, to plan an appropriate rehabilitation programfor the stroke patient. The following sections review diag-nostic procedures that are used to document stroke.
C O M P U T E D T R A N S A X I A L T O M O G R A P H Y
Computed transaxial tomography (CT) is a powerful, al-most risk-free technique for imaging the structure of thebrain (see Chapter 2). The CT scan often provides thefirst evaluation in diagnosing stroke, particularly in dif-ferentiating between hemorrhagic and nonhemorrhagicstroke. On CT scans, hemorrhages appear initially asround, well-circumscribed lesions of uniform high den-sity. Over time, the circumference of the lesions becomesmore irregular and the lesion less dense. CT scans provideinformation not only about the location of a hemorrhage,but also size, possible edema (swelling), displacement ofother brain structures, and presence of blood in the ven-tricular system. Tumors, which appear on CT with a dif-ferent density, are easily differentiated. Contrast-enhancedCT typically does not increase detection of hemorrhages.TIAs are less easily monitored on CT because of theirsmall size.
A N G I O G R A P H Y
Angiography represents the most accurate diagnostic pro-cedure for vascular disorders. Angiography can also pro-vide an evaluation of collateral vessel potential and a diag-nosis of coexisting neurologic problems. Angiography isan invasive diagnostic procedure that entails some risk(see Chapter 2). Therefore, it is usually reserved as thefinal diagnostic test for stroke, and CT typically precedesangiography. The two most common routes for angiogra-phy are via the venous and arterial systems (see review inChapter 2). Arterial angiography is more popular in diag-nosing stroke, because it provides precise images of cere-bral arteries. This is because the specialist can pass thecatheter, which injects the contrast medium, up the aorticarch and selectively place it into the carotid or vertebralarteries. Angiography can also show whether the obstruct-ing lesion is significantly impairing carotid blood flowand whether the lesion can be removed surgically. Precisediagnosis of cerebral aneurysms, AVM, artery occlusion,and stenosis (narrowing of an artery) are all possible usingangiography.
O T H E R T E S T S
An alternative to angiography and imaging are noninva-sive tests, typically targeted at detecting anatomic and
physiologic information of the common and internal ar-teries. These devices, which use ultrasonic waves, func-tion on the principle that extensive lesions to the carotidarteries may produce distorted sound-wave feedback. Inaddition, pulse-wave Doppler imaging systems may besensitive to blood flow velocity. In most cases, a conclu-sive diagnosis is not made; rather, noninvasive devices forcarotid blood flow serve to screen for subsequent referralto the more invasive angiogram. CSF analysis using alumbar puncture is also of value in ruling out or confirm-ing a subarachnoid hemorrhage not seen on CT.
Treatment and Prognosis of Vascular Disorders
F A C T O R S I N V O L V E D I N S T R O K E R E C O V E R Y
Once an individual has had a stroke, the type of damageor lesion and associated neuropsychological symptoms de-pend on a number of medical and neuroanatomic factors.These include the extent of the lesion, the general healthof the cerebrovascular system, the presence of collateralcirculation in the brain, and the location of the lesion.These factors influence the extent and nature of associ-ated cognitive symptoms, as well as the possibility andprognosis for recovery and extent of rehabilitation.
S i z e o f B l o o d V e s s e l
If a small blood vessel (such as a capillary) is interrupted,the effects are more limited than the often devastatingconsequences of damage to a large vessel, such as the in-ternal carotid artery or other cerebral arteries. Strokes ofthese large arteries can result in lesions that include largeportions of the brain and produce serious behavioraldeficits, coma, and even death.
R e m a i n i n g I n t a c t V e s s e l s
If a CVA occurs in one restricted portion of the brain, theprognosis may be rather good, because healthy blood ves-sels in surrounding brain tissue often can supply blood toat least some of the deprived areas. In addition, the pres-ence of collateral blood vessels allows redundant bloodsupply to take more than one route to a given region. Theterm collateral is used to describe redundant blood flowpresent in the vascular network after occlusion of anartery. If one vessel is blocked, a given region may bespared an infarct because the blood has an alternativeroute to the affected brain area. Conversely, if a stroke oc-curs in a region surrounded by weak or diseased vessels
CHAPTER 12 | Cerebrovascular Disorders and Tumors 349

(as in arteriosclerosis), the effects may be much more seri-ous, because there is no possibility of compensating. Thesurrounding weak zones may also be at an increased riskfor stroke.
This communication between blood vessels by collat-eral channels is also known as anastomosis and providesan important defense against stroke. The properties ofcollateral communication that provides a sufficient bloodsupply to obstructed areas vary considerably among indi-viduals. Thus, damage to the same vessel in different peo-ple can produce symptoms that vary considerably. Anas-tomosis can provide some relief to blood-depleted brainareas, particularly if the primary vessel affected is gradu-ally blocked, rather than rapidly occluded.
P r e m o r b i d F a c t o r s
The presence of previous strokes is a strong predictor ofdisability. A small stroke in an otherwise healthy brainwill, in the long run, have a good prognosis for substan-tial recovery of function. However, the effects of an addi-tional lesion most often are cumulative. As a result, de-struction of a functional zone of brain tissue may produceserious consequences for the patient.
L o c a t i o n
The location of brain tissue involved in a vascular disor-der has neuropsychological significance. A lesion in thetemporal lobe can produce a deficit in understandingspeech; a stroke in the hippocampus can cause memorydeficits; and a lesion in the brainstem can trigger heartfailure, resulting in death. Thus, behavioral symptoms ofvascular disorder are important clues to the neuropsychol-ogist for locating the area of brain damage and assessingthe extent of damage.
M E D I C A L T R E A T M E N T
The initial treatment of the stroke patient involves med-ical stabilization and control of bleeding, if necessarythrough surgery. Common medications include anticoag-ulants to dissolve blood clots or prevent clotting, vasodila-tors to dilate or expand vessels, and blood pressure med-ication and steroids to control cerebral edema. Surgeonshave developed interventions to reduce the risk for bleed-ing for some aneurysms by “clipping” them (Figure 12.4).Other surgical procedures are used in the case of hemor-rhages when it may be necessary to operate to relieve thepressure of the blood from the ruptured vessel on the restof the brain. Small hemorrhages typically are not treatedsurgically, but rather are controlled by altering the pa-tient’s blood pressure.
Physicians typically treat infarctions by intravenouslyadministering heparin (a potent anticoagulant agent), butonly if diagnosis rules out a mass lesion from a trauma orhemorrhage (either intracerebral or subarachnoid). Ad-ministering an anticoagulant agent to a patient with a he-morrhage can be fatal; therefore, establishing a precise dif-ferential diagnosis is important. In medium-size bleeds,surgical draining is often effective, although this tech-nique may leave a surgical hole in the brain that may laterentail neuropsychological deficits. Other ways to decom-press the brain include artificial hyperventilation, corti-costeroids, and diuretics. In most cases, physicians artifi-cially lower the blood pressure. Treatment for TIAsymptoms, which is more difficult because the symptomsare ambiguous, is often restricted to pharmacologic inter-vention with anticoagulants. An obvious danger in usinganticoagulants is the inherent risk for an uncontrolled bleed.
AVMs are often surgically removed or are embolizedartificially. In the latter technique, the surgeon delivers anagent that blocks the blood vessel close to the lesion, insome cases permanently. The embolization agent is asponge, ball, coil, or balloon and entails certain risks. Thisdelicate technique uses highly selective catheterizationprocedures and close radiographic monitoring. The rea-son for this care is that the delivery system must advanceas close to the lesion as is possible; otherwise, healthy ar-teries may be embolized, or the embolus may migrate tothe lung or heart.
P R E V E N T I N G S T R O K E
Many people who have had a stroke say that it “struck outof nowhere”—there seemed to be no obvious warning.Typically, a stroke that occurs spontaneously results froman embolism or a hemorrhage. That one can have a strokewith little or no warning testifies to the importance of iden-tifying the many risk factors associated with stroke. Themost prominent risk factor is a history of stroke. In fact, asmentioned earlier, stroke recurrence is an important con-tributor to disability. In addition, common demographic
350 PART THREE | Disorders of the Brain
Figure 12.4 Aneurysm clip (approximate size � 6 mm). (Courtesy Eric Zillmer.)

factors predispose an individual to cerebrovascular dis-ease, including:
Heredity (cardiovascular disease in one’s family)Sex (men are at greater risk for stroke than women, a risk
related to their higher incidence of heart disease andhypertension)
Ethnicity (African Americans have one of the higheststroke rates, 40% greater among women and 10%greater among men)
Lifestyle indices also affect the probability of cardio-vascular disease. A well-known risk factor of CVA is hy-pertension. Elevated blood pressure means that the forceof the blood against the walls of the arteries is too high.As a result, over time the arteries become weakened andcan burst. If this happens in the brain, it results in a cere-bral hemorrhage. High blood pressure can also increasethe force of the blood against the artery walls and breakoff some plaque along those walls, which then travels as anembolus through the bloodstream until it clogs a narrowervessel. The dangerous part of hypertension is that mostpeople do not feel it, and thus do not seek medical help.
Other risk factors for stroke are diabetes and high cho-lesterol. Individuals with diabetes run a greater risk forstroke. Vascular diseases are most often related to prob-lems in artery linings, which become hardened by de-posits of cholesterol, fat, calcium, and other materialssuch as fibrin, a substance that encourages clot formation.Fat causes plaque to build up along the lining of bloodvessels, which can break off and lead to embolic stroke orcan become so built up that thrombotic stroke can occur.Because smoking is a vasoconstrictor, it is an additionalrisk factor for stroke. Smoking a cigarette constricts an al-ready too-narrow blood vessel.
Small amounts of alcohol may actually thin blood andcan serve the same purpose as one aspirin per day. Also,some evidence suggests that a glass of wine with dinnerreduced cholesterol. Alcohol becomes a risk factor whenconsumed in large quantities. Excessive consumptioncontributes to high blood pressure and may result inataxia (poor balance), which is often already a problemafter a stroke. Also, alcohol is a sedating drug and maynot interact well with other drugs. Finally, obesity con-tributes to the onset and maintenance of diabetes, hyper-tension, heart disease, and high cholesterol. Obesity ismedically defined as being 25% over your ideal weight.Approximately 26% of men and 30% of women in theUnited States are overweight. Cardiovascular complica-tions in obesity are related to the high correlation betweenbeing overweight and hypertension, a precursor of coro-nary heart disease.
Neuropsychological DeficitsAssociated with Stroke
Significant functional and cognitive impairmentsare often the result of stroke. These deficits can seriouslyimpair the patient’s ability to function independently andare often incapacitating and serious enough to lead to hos-pitalization in a rehabilitation facility. Typically, long-termhospitalization occurs because the patient is exhibitingsymptoms of inattentiveness, apraxia, communicationdifficulties, apathy, or general intellectual impairment.
Many factors influence cognitive changes as a result ofstroke. These factors include the patient’s age, interval be-tween the stroke onset and time of rehabilitation, natureof the stroke (infarction or hemorrhage), and size and lo-cation of lesion (such as right or left brain, anterior orposterior). The patient’s medical history is important, par-ticularly as it relates to the presence of previous strokes(such as lacunar strokes), prior CNS trauma or disease,and premorbid level of functioning. Many stroke-relatedcognitive deficits may resolve over time, sometimes im-mediately after the stroke. For example, the more local-ized the effects, the more positive the prognosis. But resid-ual deficits may remain that require an evaluation ofcognitive abilities and subsequent rehabilitation (Brown,Baird, & Shatz, 1986).
Because of their complexity and variability from pa-tient to patient, the cognitive deficits associated withstroke are not easily classified into simple categories. Fordidactic purposes, neuropsychologists correlate cognitivedeficits with the specific type of stroke. Correlating thelocation of an anatomic lesion with the stroke patient’scognitive impairments has been only modestly successful.Thus, the neuropsychology student should be careful notto rigidly adhere to specific patterns of deficits and recov-ery, but instead should realize that the disease course inindividual patients varies greatly (Weimar et al., 2002).
N E U R O P S Y C H O L O G I C A L R I S K F A C T O R S
Several important principles govern the properties of neu-ronal processes that are particularly relevant to under-standing the neuropsychology of cerebrovascular disor-ders. These principes are explained in the followingparagraphs.
N e c r o s i s
Neurons that have died as a result of necrosis do not spon-taneously regenerate. In most instances, lost neurons inthe CNS are incapable of healing after the developmental
CHAPTER 12 | Cerebrovascular Disorders and Tumors 351

period (see Chapter 4). Thus, no cellular regeneration ofthe neuron or regrowth of damaged neurons to their nor-mal target occurs. Neurons lost as a result of stroke arenot replaced. Fortunately, functional losses entailed bythese structural losses are not necessarily permanent, be-cause the brain has redundant pathways for supplyingblood to various areas. Specifically, redundant blood sup-ply in the brain may minimize neuronal death becausethere is sufficient blood supply to brain areas that havebeen damaged. Also, the process of rehabilitation allowssome compensation of functional losses with behaviorsthat have been left relatively intact. Rehabilitation mayalleviate enough disruption caused by stroke that the vic-tim regains some or nearly all of his or her premorbid levelof functioning. In fact, neuropsychologists have made sig-nificant headway recently in developing assessment, pros-thesis, and cognitive rehabilitation techniques to com-pensate for disrupted functional brain systems. Inaddition, neuroscientists are making some progress indesigning drugs that facilitate the regrowth of injuredneurons.
D i s i n h i b i t i o n
An important principle of neuronal processes relevant tounderstanding the neuropathology of stroke relates to thecapacity for inhibiting behavior after a stroke. As dis-cussed in previous chapters, many of the neuronal collec-tions, particularly in the frontal lobe, serve to inhibitrather than initiate behavior. This is important becauselosing inhibitory neurons to stroke may actually result inan inappropriate increase in behavior or disinhibition,and often causes striking behavioral and personalitychanges in stroke victims. Damage to an excitatory col-lection of fibers, of course, results in losing some func-tion. This is why many traumas to the brain, includingstroke, often show both loss of function (such as aphasiaand the inability to speak) and disinhibition (increasedlikelihood of inappropriate behavior) including impul-siveness, hypersexuality, and inappropriate feelings. Thiswas made painfully clear when a colleague of ours wasleading a stroke support group. All members of the sup-port group had sustained a stroke, and many had signifi-cant related cognitive deficits. Almost all membersdemonstrated poor judgment and disinhibition when itcame to operating an automobile, and they spent muchtime in the group discussing this. Nevertheless, they in-sisted on continuing to drive and drive poorly; in fact,many accidents happened in the parking lot before andafter group meetings. When group participants returnedfrom trips, they would discuss and bring along pictures oftheir recent accidents. They described these crashes with
some bravado, reflecting poor insight and a general lackof awareness of the dangers. This is a typical example ofdisinhibition because victims do not inhibit high-risk be-havior, as they may have done premorbidly, that is, beforethe stroke. The incapacity to drive after a stroke is one ofthe most sensitive issues facing health care workers, strokevictims, and their families.
D i s c o n n e c t i o n S y n d r o m e
Because the substructures of the brain connect so intri-cately, observed deficits in a stroke patient may not neces-sarily correspond to the lobe or site where the stroke oc-curred. For example, a stroke in the visual area of thecortex (occipital lobe) ordinarily results in some form ofvisual impairment. In addition, however, these visualdeficits may also disturb motor behavior or gait. Further-more, a stroke may disrupt important pathways of neu-rons that project to other centers of the brain. This is acommon problem when strokes occur near subcorticalstructures such as the striatum, a common stroke site. Sucha stroke commonly results in higher order cognitive deficits,because injury has severed projections to the cortex. Thisproblem is called disconnection syndrome, because impor-tant pathways in the brain have been “disconnected.”
A T T E N T I O N D E F I C I T S
Many types of brain dysfunction typically reduce effi-ciency of the brain in processing information. This is cer-tainly true for CVA. In milder cases, stroke victims can-not sustain their attention to one particular stimulus forlong periods or select information from competingsources (selective attention). This impairment may beminimally present and detectable only with formal neu-ropsychological testing, or it may be profound and easilynoticeable by any observer. Sometimes cognitive changesin stroke patients are so pervasive that the patient is con-siderably confused and disoriented as to time, place, andperson. Deficits of arousal typically relate to damage ofthe patient’s frontal lobe circuitry or the brainstem region.In contrast, deficits in attention may relate to local orglobal brain damage.
M o t o r a n d S e n s o r y I m p a i r m e n t
General behavioral slowing and a reduction of psychomo-tor activity can be dominant characteristics of stroke.Both the right and left hemispheres are associated withchanges in motor and sensory functioning from stroke.Such changes can be as benign as mild motor slowing oras debilitating as complete paralysis, particularly if the le-sions are in the thalamic area or the motor and premotor
352 PART THREE | Disorders of the Brain

areas of the frontal lobes. Motor deficits of the right brainresemble those of the left brain. Right hemisphere strokemotor deficiencies, however, are generally less severe, be-cause the nondominant left hand is not as important forskilled tasks.
Severe motor deficits are often apparent without for-mal testing and may involve impairment in motor speed,strength, steadiness, and fine-motor coordination. Evenmild deficits may significantly reduce the efficiency onhighly demanding manual tasks, interfere with self-careor light housework, deteriorate handwriting skills, and slowreaction times, which may require the victim to give updriving. Diminished sensory functioning is most likely inareas of visual acuity, visual field perception, and hearing.
M E M O R Y P R O B L E M S
Stroke survivors commonly report that their memory isnot as good as it was before the stroke, and on occasion,they may not recall a person’s name, even when they knowthat person well. Many stroke patients exhibit intactmemory for old learning, but not always for new learn-ing. That is, they can remember events that happenedyears ago, but may be unable to remember what they hadfor lunch today. Unless the lesion is extensive, CVAs donot typically cause loss of primary, immediate, or long-term memory, but are most pronounced in the area ofshort-term memory. This most likely relates to the strokepatient’s decreased capacity to organize and process largeamounts of information (“chunking”) in a fashion thatlends itself to easier memory storage or retrieval. Not un-commonly, these patients recall only a small amount ofnew material 30 minutes after it is presented to them.
Patients that have stroke-related hippocampal damageexperience significant memory difficulties, may requirerepetition of new information, and may show significantproblems with forgetfulness associated with a variety ofeveryday tasks. Such patients have frequent difficulty re-calling details of recent experiences, tend to misplacethings, fail to follow through on new obligations, andtend to get lost more easily in unfamiliar areas.
Stroke patients with the most severe memory deficitsare virtually unable to retain any information, particu-larly if their attention has been directed elsewhere. Suchindividuals also cannot profit from repeated exposures tostimuli. They need substantial assistance in daily livingand characteristically cannot take care of themselves, be-cause they may create fire hazards at home and cannotmanage financial affairs or keep track of scheduled activi-ties. For such patients, it helps to create an environmentwhere important objects are kept in the same place, the
same daily routines are maintained, and instructions areverbalized in the same sequence. A major concern relatedto memory impairment is the stroke patient’s ability tomanage his or her own medication schedule.
D E F I C I T S I N A B S T R A C T R E A S O N I N G
Impaired judgment, loss of insight, and diminished ca-pacity for abstract and complex thinking are commoncognitive changes among stroke victims, particularly ifanterior aspects of cortical areas are involved. People withmildly impaired abstract reasoning and new concept for-mation can often use their past accumulated knowledgeto exercise reasonable judgment for routine daily activi-ties. Those who show more serious cognitive decline oftenencounter difficulties with tasks that require complexplanning or organization and with novel situations. Suchpatients cannot assess new situations accurately anddemonstrate poor judgment, with serious consequencesto themselves or others.
C O G N I T I V E D E F I C I T S A S S O C I A T E D W I T H R I G H T B R A I N S T R O K E S
Researchers have directed much research attention towarddistinguishing the cognitive deficits between left versusright hemisphere brain damage. In general, patients withleft-sided brain damaged show markedly impaired lan-guage comprehension and communication, and stroke pa-tients with damage to the right hemisphere exhibit signifi-cantly more impairment in ability to process and executebehaviors that require visual-perceptual ability (Lezak,Howieson, & Loring, 2004; Reitan & Wolfson, 1993).
Deficits that affect the right cerebral artery involveareas responsible for spatial, rhythmic, and nonverbal pro-cessing. Right hemisphere symptoms, although serious inthe patient’s overall functioning, can be less striking in theacute phase, particularly if they do not involve motor dys-function. Right brain damage occurs as a consequence ofright-sided CVAs and is often associated with contralateralmotor and sensory impairment. Patients with right-sidedbrain injury present a variety of symptoms that pose a par-ticular challenge to the neuropsychologist. First, thedeficits often found among patients with right hemi-sphere brain damage are not as striking initially as thedeficits observed among patients with left hemisphere braindamage, in which case the patient is often aphasic.Second, many patients with right-sided brain damage dis-play a range of emotions from indifference to euphoria.This is in contrast with the depression often observedamong patients with left hemisphere brain damage.
CHAPTER 12 | Cerebrovascular Disorders and Tumors 353

Therefore, it is easy to assume that the deficits from rightbrain damage are not as serious as those from left braindamage. However, this is not true, because both types ofproblems can be highly disruptive to patient and familyalike, often even exceeding the problems associated withleft hemisphere CVAs.
For example, research has shown consistently that pa-tients with right hemisphere stroke remain longer in re-habilitation facilities than do patients with left hemi-sphere strokes (Zillmer et al., 1992). This difference isrelated to the pervasive deficits that patients with righthemisphere damage present in visuospatial abilities andthe extended rehabilitation required for dressing, ambu-lating, and other self-care behaviors.
Right hemisphere stroke patients are not diagnosed asrapidly as are left hemisphere stroke patients. This is prob-ably related to the difficulty that left hemisphere strokepatients display in using language—an obvious symptomthat helps a family member identify that something is“wrong” with their loved one. In contrast, patients withright-sided brain damage often use language fluently.Thus, on the surface, they “sound” okay. Furthermore,
patients with right-sided brain damage tend to be un-aware of their problems. Such patients often deny thatthere is anything wrong with them. As a result, patientsmay be blamed for being “rude,” “disruptive,” or “inap-propriate,” when they are actually exhibiting symptoms ofright brain injury, including impulsivity, verbosity, inat-tention, and poor judgment. Thus, although neuropsy-chological deficits in patients with right hemisphere strokemay be more subtle, they are equally and sometimes morefunctionally disabling than the more obvious language im-pairments typically associated with left hemisphere stroke.
V i s u o s p a t i a l D e f i c i t s
Deficits in right hemisphere stroke patients almost alwaysinclude visuospatial deficits—that is, the patient’s capac-ity to accurately perceive his or her surrounding world inits completeness. Neuropsychologists report that visu-ospatial deficits occur particularly after right hemispherestroke and include both visual-perceptual and visual-constructional abilities. Patients with problems in spatialrelations have difficulty estimating the distance betweendifferent objects, as well as between themselves and other
354 PART THREE | Disorders of the Brain
The patient is a 32-year-old, married, right-handed woman with 12 years of education.She worked as a manager for a fast foodrestaurant and lived with her husband andtwo young children in a two-story house. Onemonth before my evaluation, she sustained asudden onset of aphasia, right-sided weak-ness, and headache. Computed transaxialtomography (CT) scan showed an infarctionin the area of the left cerebral hemisphere. A carotid angiogram showed an occludedinternal carotid artery. Medical history wasunremarkable.
I tested her neuropsychologically 1 month after the stroke. In my clinicalinterview with the patient, her speech wasmarked by paraphasias (the substitution ofwrong words or phrases) and verbal perse-verative tendencies (unnecessary repeat-ing), which are signature symptoms for a lefthemisphere stroke. She was oriented toperson and could state her name, age, and
date of birth. She was somewhat oriented toplace; that is, she knew she was in a rehabili-tation hospital but could not give its name orlocation. She could write the correct date,but could not recall the current or last presi-dent. She showed a significant sensory andmotor deficit on her dominant right side. Shecould not feel light touch on her right handwith single or double simultaneous stimula-tion. On verbal tasks, she was able to per-form automatic tasks such as counting from1 to 20 and reciting the alphabet, but shecould not perform any other tasks thatrequired voluntary and purposeful speech.The patient’s gross- and fine-motor abilityand speed were intact on her nonaffectedleft side. However, on her dominant rightside, she showed a marked hemiparalysisand could not voluntarily move her rightshoulder, arm, hand, or fingers. She did notshow any evidence of motor apraxia andcould copy simple designs adequately with
her nondominant hand, suggesting intactright hemisphere functioning.
As expected, her verbal functions wereseverely impaired, consistent with the loca-tion of her cerebrovascular accident (CVA) inthe distribution of the left middle cerebralartery. Receptive language skills were mod-erately impaired, as she could follow onlyone-step commands without difficulty. Shebecame easily confused with two-stepcommands. Expressive speech was severelyimpaired. On the word fluency item, whichrequires the individual to name as manyanimals as possible in 30 seconds, she wasable to name only one and perseverated withthe word baseball, which was an incorrectresponse to a previous item. She was able tocorrectly repeat words and phrases after theexaminer, but was unable to initiate a correctresponse on her own. She also demon-strated alexia and agraphia for writtenlanguage.
N e u r o p s y c h o l o g y i n A c t i o n 1 2 . 2
C a s e E x a m p l e o f a L e f t S t r o ke
by Eric A. Zillmer

people or things. Common examples of mistakes that pa-tients make with this kind of disturbance include knock-ing items off a table when dusting, misplacing items ontables so that they are no longer centered or are in dangerof falling off, and misjudging steps or thresholds, whichputs them in danger of falling.
Obviously, patients with spatial relations disturbancemay have difficulty driving a car, and they may often needhelp in other areas of their lives such as stair climbing andactivities of daily life such as dressing, bathing, toileting,and eating. It is in unfamiliar environments and in novelsituations that driving is difficult for these patients. Incase of marginal impairment, it may be helpful to limitpatients to driving only in their own neighborhoods. Indifficult cases, a neuropsychological evaluation can aid inmaking this decision. Motor impersistence is also a com-mon sign—the stroke patient cannot persist with a motorresponse for any length of time (such as keeping eyesclosed or holding arms over the head). Often, others mayperceive the patient as being oppositional or stubborn,when, in fact, he or she is not in control of the skills re-quired to perform the action.
C O G N I T I V E D E F I C I T S A S S O C I A T E D W I T H L E F T B R A I N D A M A G E
In general, cognitive profiles are most robust when associ-ated with damage of the left versus the right brain hemi-sphere. For example, the middle cerebral arteries servemajor sensory and motor areas; thus, significant motorand sensory deficits often affect the side contralateral tothe stroke. One of the most common infarctions is thatof the left middle cerebral artery, in which deposits havetraveled up from the heart and then blocked the middlecerebral artery. Disorders of the left middle cerebral arterymost often involve cortical areas of the brain responsible forboth expressive and receptive speech. Thus, one of the mostdramatic symptoms of a left middle cerebral artery stroke isthe impairment in speaking or understanding speech, orboth. Deficits also include severe motor and tactile symp-toms on the contralateral right body side in addition to ex-pressive aphasia (Neuropsychology in Action 12.2).
Understanding and being understood by others is thegoal of most human interactions. When a stroke dam-ages that part of the brain that controls language and
CHAPTER 12 | Cerebrovascular Disorders and Tumors 355
The patient’s visuospatial functions werebasically intact. Figure–ground distinctions,spatial manipulation, visual sequencing,facial recognition, and spatial orientation alltested within normal limits. Her visual mem-ory appeared to be within normal limits forboth immediate and delayed recall proce-dures. However, verbal memory was severelyimpaired secondary to her receptive andexpressive aphasia. She was able to correctlyrepeat a list of five words for four separatetrials. However, on the recognition task (2 minutes later), she could identify only twowords and made five false positive responses.
Her judgment/problem solving appearedmoderately impaired secondary to herreceptive and expressive aphasia. Yet, shedid demonstrate some reasoning skills onthe purely visual problem-solving items suchas the visual analogies. She showed amoderate degree of psychological distress.
Overall, she showed a moderate degreeof cognitive impairment for left hemispherefunctions, which was consistent with the siteof her CVA. Interestingly, on casual observa-tion, she looked more impaired than she wason testing, given that laypeople almostalways evaluate a person’s cognitive statusbased on the vocabulary they use.
I retested the client 1 month later aftershe had completed her inpatient rehabilita-tion program. Overall, she showed significantimprovement in orientation, verbal functions,memory, judgment/problem solving, psycho-logical distress, and activities of daily livingskills. The client correctly responded verballyto all the orientation questions except forone, which asked what town the hospital waslocated in. Verbal functions improved dra-matically. The client showed good receptivespeech in that she was now able to followtwo-step commands easily. Verbal fluencyremained limited but still showed a dramaticimprovement. On the animal fluency item,she went from zero to five words and couldnow read and write sentences to dictation.Memory functions showed a significantimprovement in her verbal memory, becauseshe could now encode verbal information andretrieve it spontaneously. Judgment/problemsolving showed some problems with concretethinking, but generally good common sense,reasoning, and judgment. The reportedamount of psychological distress experiencedby this young woman decreased significantly,and she showed remarkable increase in herlevel of independent functioning in her activi-ties of daily living.
In summary, neuropsychological testingproved a valuable technique in tracking thisyoung woman’s recovery from stroke duringthe acute stage of recovery. It was alsoeffective in demonstrating the breadth ofimprovement this client made in cognitive,psychological, and physical skills, as well asdocumenting the residual areas of impair-ment in verbal functioning and verbal mem-ory. A follow-up evaluation as an outpatient12 months after stroke was recommended.The neuropsychology student should notethat the precise extent of this patient’sdeficits and partial recovery is not obviouseven to health care workers and the immedi-ate family. That is why neuropsychologicaltesting can be so important, not only inquantifying cognitive abilities but also insetting realistic expectations for recoveryand rehabilitation. In this case, the familywas focusing primarily on the patient’sresidual impairment in memory and lan-guage. In charting the patient’s remarkablerecovery, I was able to help the family re-frame their perceptions of the perceivedstrengths and weaknesses, thus helpingthem also cope with this potentially devas-tating disease.

communication, the effects can devastate both patientand family. Several types of communication problems canoccur with stroke, and neuropsychologists play an impor-tant role in diagnosing and rehabilitating specific formsof communication problems in stroke survivors. Manypatients also have apraxia, a loss of voluntary movementthat makes it difficult or impossible for patients to usegestures to communicate their needs. The presence ofapraxia is the main reason why speech pathologists do notroutinely attempt to teach aphasic patients sign languageto compensate for spoken language difficulties.
Often, patients lose not only spoken language butwritten language as well. Writing is one of the most com-plex of language abilities. If writing is disturbed by im-pairment to the limb that produces letters and words,neuropsychologists do not consider that a disorder of lan-guage. Rather, in written language deficits, words, let-ters, or numbers may appear foreign or incomprehensi-ble because the person cannot recall the form of letters.His or her attempts to write may be filled with real orimagined letters that make no sense to others. Withtime and training, the person may be able to understandsimple written language—for example, single wordssuch as bath or food—but still be unable to compre-hend more complex written language such as sentencesor paragraphs.
Many so-called behavioral problems seen with strokepatients with aphasia occur because of receptive aphasia.In moderate cases, the patient can understand part butnot all of the communication. Sometimes patients’ appar-ent noncompliance is actually caused by their misunder-standing the communication. Thus, a patient may act asthough he or she had not heard a word at all (so-calledword deafness) or as though he or she had heard only frag-ments of the word. The most common defect lies not infailing to recognize that someone spoke a word, but infailing to attach meaning to the word. Some patients withaphasia comprehend individual words, but not certaingrammatical constructions.
Often, stroke patients with visual disorders haveconsiderable difficulty reading because they are blind tocertain visual fields. This problem is not related to re-ceptive aphasia; rather, the patients cannot see theword—if they could, they would read it correctly—orare unaware of additional words that need to be read, asin unilateral inattention. The classification of aphasiasinto receptive and expressive is a useful didactic tool, butin reality, most left hemisphere stroke patients have acombination of both aphasia types, because the left mid-dle cerebral artery serves both expressive and receptiveareas.
A N T E R I O R V E R S U S P O S T E R I O R S T R O K E S
Disorders of the anterior cerebral artery may cause motoror sensory impairment involving the leg. Because the an-terior cerebral arteries serve the prefrontal lobes, deficitsconsistent with a prefrontal syndrome, including disinhi-bition and dysfunction of executive skills, are also charac-teristic. Strokes in the posterior cerebral artery are lesscommon and typically cause visual field loss and sensoryloss of one side. Basilar artery disorders may have a simi-lar effect as posterior cerebral arteries stroke if the poste-rior communicating artery provides insufficient bloodsupply. Those include blood flow disruption of the brain-stem, including cranial nerve involvement, the cerebel-lum (see Figure 12.1 for an example of a cerebellarstroke), and the occipital lobes.
E M O T I O N A L A N D B E H A V I O R A L C H A N G E S A F T E R A S T R O K E
After a stroke, it is common for patients to respond dif-ferently to people and events in terms of their emotionalreactions. This relates, in part, to the experience of signif-icant stress in the patient’s life, but also to that the in-tegrity of the brain has been compromised.
D e p r e s s i o n
Depression is a common and not surprising reaction tostroke. Depression may be indicated if patients feel over-whelmed with sadness, believe they have failed completely,blame themselves for their problems, and often feel likecrying. Poor sleep, decreased appetite, low self-esteem, andreduced efficiency are present as well. Whenever peopleexperience loss, depression is a natural response. Depres-sion is most likely to occur among patients with right-sided weakness and corresponding left hemisphere stroke.Often, a patient does not show signs of depression until 6to 12 months after a stroke, when the scope of the losshas sunk in and there is time to think about how life haschanged. Research and experience tells us that depressionis best treated with a combination of psychotherapy andantidepressant medication.
A p a t h y
Apathy, or indifference, involves lack of emotions. Theperson is not sad or happy. In fact, the person may notappear to have any emotions. The voice sounds monot-one, the face lacks expression, and if you ask the patientwhat he or she feels, the answer will be neutral, or withoutaffective tone. On occasion, patients who lack vocal and fa-cial expression nevertheless report that they feel depressed,
356 PART THREE | Disorders of the Brain

afraid, or angry. Both depression and apathy are quitecommon after a stroke, especially after anterior medialdamage. This is related, in part, to the loss of function thatcan accompany stroke, but also to reduced brain efficiencyafter such trauma. Thus, part of the depression or apathyin a stroke patient is related to the stroke itself. In this sense,the depression is more biological than psychological.
E u p h o r i a
Euphoria is an overriding positive emotional response thatis “too happy” given the circumstances. Euphoric peopleare not sad, indifferent, or apathetic; in fact, they are fullof ideas and energy. Patients with euphoria seem posi-tively happy about or despite their condition. Euphoriagoes beyond a capacity to overcome obstacles—it is as ifno obstacles existed. Apathy and euphoria are especiallycommon among patients with left-sided weakness—thatis, those suffering from right hemisphere stroke.
I m p u l s i v e E m o t i o n a l a n d B e h a v i o r a l D i s p l a y s
An impulsive emotional response is one that appears tocome without warning. Patients who have labile emotionswill cry or laugh in response to events or phrases that oth-ers around them might find only mildly arousing. For ex-ample, most people respond to the National Anthem be-fore a baseball game with a smile. The stroke patient mayrespond with seemingly uncontrolled tearfulness or laugh-ter. Labile emotional responses usually embarrass the pa-tient and upset the family members. As a consequence,family members often avoid talking about important fam-ily topics, lest the discussion “upset” the patient. It is im-portant to remember that labile emotional responses are aphysiological and not an emotional response to a stroke.In fact, patients often cry in response to happy events—aswhen a therapist compliments them.
Impulsivity of behavior also affects a person’s ability tostop motor actions. For example, a stroke survivor mayautomatically stand up and begin to walk on legs thatcannot support him or her. This is dangerous to the well-being of the stroke patient, and therapists spend muchtime in rehabilitation helping the patient to inhibit dan-gerous or inappropriate behaviors.
L a c k o f I n i t i a t i o n
On the other end of the spectrum, strokes can also impaira person’s ability to initiate (or start) a behavior (akine-sia). For example, the person may be hungry, and foodmay be sitting there ready to be consumed, but the per-son fails to bring the food to his or her mouth. In the ex-treme, the person may fail to chew once food has been
placed in his or her mouth. The inability to initiate be-havior may appear in the person’s verbal responses. Forexample, it may take a long time to answer questions. Adifficulty related to problems initiating actions is the per-severation of behavior. Perseveration is the inability tostop behaviors once they have started. A patient may per-form a motor movement over and over again, unable tostop it. Motor rigidity, perseveration, motor impersis-tence, and disinhibition are common problems in strokepatients and generally improve with rehabilitation.
P o o r J u d g m e n t
Many stroke victims demonstrate poor judgment, espe-cially with prefrontal cortical damage. Ironically, manysuch patients often can verbalize the appropriate actionsthey “should take,” but cannot follow through with thoseactions. For example, individuals with a spatial problemmay be able to verbalize the steps in preparing a cup ofcoffee, but nevertheless continue to let coffee overflowwhen pouring a cup. It is as if their words and actionswere not related. The brain trauma has impaired theirability to monitor their own behaviors and to understandthe consequences of their own actions.
Tumors of the Brain
When I was in graduate school my aunt (EAZ) wasdiagnosed with a brain tumor. The MRI suggested that itwas consistent in size and appearance with a malignanttumor. A decision was made to operate and remove asmuch of the tumor as was possible. Because the tumorwas the size of a baseball it had already displaced and in-vaded healthy brain tissue. As a result, my aunt’s speechwas severely impaired and she complained of headachesand dizziness. The brain surgery would immediately re-lieve many of my aunt’s symptoms and would allow for abiopsy to classify the exact type of tumor cell.
To reach such a tumor, a team of specialists first drill aseries of holes into the patient’s skull, not unlike the burrholes used in the ancient procedure of trephination (re-viewed in Chapter 1). Then the surgeon connects theholes with a surgical jigsaw. After he or she lifts the oval-shaped piece of skull the dura mater is exposed, a thickmembrane that protects the brain and spinal cord. Myaunt’s tumor was inside of the brain tissue and thus theneurosurgeon had to proceed through healthy brain tis-sue to reach the tumor. The neurosurgeon had to navi-gate carefully, dividing the tumor from the normal brain,cauterizing severed blood vessels along the way. Gradually
CHAPTER 12 | Cerebrovascular Disorders and Tumors 357

the tumor was cut, actually siphoned, away from myaunt’s brain and extracted. A lab autopsy verified the ini-tial diagnosis: a malignant glioma, a fast-growing anddangerous tumor (discussed later). By the following day,she would be walking the halls and feeling much better.Her long-term prognosis was poor, however, since re-search clearly demonstrated that similar patients only live6 to 12 months, even after a successful operation. Nomatter how careful the surgeon cuts out the malignanttumor, the few stray cancer cells that are inevitably leftbehind will begin to grow again. My aunt’s death sentencehad been postponed, perhaps by a year.
The term tumor refers to a morbid enlargement ornew growth of tissue in which cell multiplication is un-controlled and progressive. Tumors are also called neo-plasms, which means “new tissue.” The new cell growthresembles cells already normally present in the body. Thisgrowth is, however, often arranged in disorganized ways,does not serve any functional purpose, and often grows atthe expense of surrounding intact tissue. Brain tumorsmake up approximately 5% of all cancers and appear inapproximately 2% of all autopsies. Because cancer is thesecond most frequent cause of death, the actual numberof victims with brain tumors is actually quite high. Braintumors can occur at any age, but are most common inearly and middle adulthood (Golden, Zillmer, & Spiers,1992).
Brain tumors can be conceptualized according to twoprincipal forms:
1. Infiltrative tumors—take over (or infiltrate) neigh-boring areas of the brain and destroy its tissue
2. Noninfiltrative tumors—are encapsulated and differ-entiated (easily distinguished from brain tissue), butcause dysfunction by compressing surrounding braintissue
Tumors can be further classified according to two addi-tional descriptors:
1. Malignant—indicates that the properties of the tumorcells invade other tissue and are likely to regrow orspread
2. Benign—describes cell growth that is usually sur-rounded by a fibrous capsule, is typically noninfiltra-tive (noninvasive), and will not spread
The primary feature of malignant tumors is that theyare much more likely to reappear after surgical interven-tion. Because they are infiltrative, it is difficult to completelyremove malignant tumors surgically. Malignant tumors mayalso “travel” to other organs in the body through the blood-stream. This form of spreading is called metastasis.
Metastatic brain tumors typically originate from primarysites other than the brain, most frequently the lung or thebreast. Even benign tumors, however, are troublesome ifthey occur in the brain. This is because the skull completelyencloses the brain, and any mass-producing lesion displaceshealthy brain tissue. You may already realize that nerve cellsare not likely to cause brain tumors, because neurons donot grow or heal spontaneously. This is correct. Tumors ofthe brain arise mostly from the supporting cells of the brain.As a result, neurons are only indirectly affected. Neuromasare tumors or new growths that are largely made up of nervecells and nerve fibers.
One method of evaluating the malignant features of abrain tumor is to grade them from slow-growing neo-plasms to rapidly growing tumors. The grade of a tumoris determined by its malignancy, the tendency of a tumorto grow at a fast rate, causing severe destruction of braintissue and eventually death. Grading is from 1 to 4, with aGrade 1 tumor representing a slow-growing tumor accom-panied by few neuropsychological deficits. Grades 2 and 3represent intermediate rates of growth and neuropsycho-logical dysfunction. Grade 4 tumors grow fast and typi-cally have a poor prognosis for recovery. Table 12.3 reviewsthe different characteristics of brain tumors. Neurologicaland neuropsychological dysfunction results from the inva-sion and destruction of brain tissue by the tumor.Secondary effects include increased ICP and cerebralswelling (edema), which displace and compress brain
358 PART THREE | Disorders of the Brain
1. Characteristics of brain tumorsAtypical, uncontrolled growth of cellsCells do not serve functional purposeTumor grows at the expense of healthy cells
2. Infiltrating tumorsTake over and “invade” neighboring areas of the brain and destroysurrounding tissue
3. Noninfiltrating tumorsEncapsulated, well differentiated, and noninvasive
4. MalignantIndicates that the properties of the tumor cells invade other tissue andthat there is a propensity for regrowth
5. BenignDescribes abnormal cell growth that is usually surrounded by a fibrouscapsule and is noninfiltrative; a much smaller probability for regrowth
6. GradingA classification system of tumor growth; grading is in order of increasingmalignancy from Grades 1 to 4, depending on cell type.
Table 12.3 Characteristics of IntracranialTumors
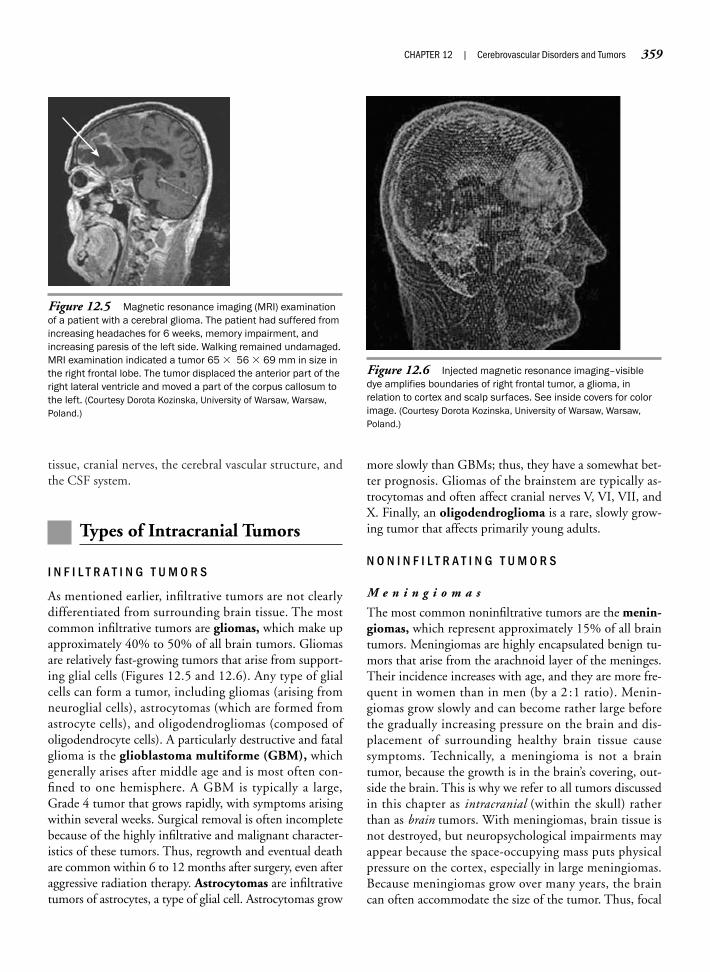
tissue, cranial nerves, the cerebral vascular structure, andthe CSF system.
Types of Intracranial Tumors
I N F I L T R A T I N G T U M O R S
As mentioned earlier, infiltrative tumors are not clearlydifferentiated from surrounding brain tissue. The mostcommon infiltrative tumors are gliomas, which make upapproximately 40% to 50% of all brain tumors. Gliomasare relatively fast-growing tumors that arise from support-ing glial cells (Figures 12.5 and 12.6). Any type of glialcells can form a tumor, including gliomas (arising fromneuroglial cells), astrocytomas (which are formed fromastrocyte cells), and oligodendrogliomas (composed ofoligodendrocyte cells). A particularly destructive and fatalglioma is the glioblastoma multiforme (GBM), whichgenerally arises after middle age and is most often con-fined to one hemisphere. A GBM is typically a large,Grade 4 tumor that grows rapidly, with symptoms arisingwithin several weeks. Surgical removal is often incompletebecause of the highly infiltrative and malignant character-istics of these tumors. Thus, regrowth and eventual deathare common within 6 to 12 months after surgery, even afteraggressive radiation therapy. Astrocytomas are infiltrativetumors of astrocytes, a type of glial cell. Astrocytomas grow
more slowly than GBMs; thus, they have a somewhat bet-ter prognosis. Gliomas of the brainstem are typically as-trocytomas and often affect cranial nerves V, VI, VII, andX. Finally, an oligodendroglioma is a rare, slowly grow-ing tumor that affects primarily young adults.
N O N I N F I L T R A T I N G T U M O R S
M e n i n g i o m a s
The most common noninfiltrative tumors are the menin-giomas, which represent approximately 15% of all braintumors. Meningiomas are highly encapsulated benign tu-mors that arise from the arachnoid layer of the meninges.Their incidence increases with age, and they are more fre-quent in women than in men (by a 2 :1 ratio). Menin-giomas grow slowly and can become rather large beforethe gradually increasing pressure on the brain and dis-placement of surrounding healthy brain tissue causesymptoms. Technically, a meningioma is not a braintumor, because the growth is in the brain’s covering, out-side the brain. This is why we refer to all tumors discussedin this chapter as intracranial (within the skull) ratherthan as brain tumors. With meningiomas, brain tissue isnot destroyed, but neuropsychological impairments mayappear because the space-occupying mass puts physicalpressure on the cortex, especially in large meningiomas.Because meningiomas grow over many years, the braincan often accommodate the size of the tumor. Thus, focal
CHAPTER 12 | Cerebrovascular Disorders and Tumors 359
Figure 12.5 Magnetic resonance imaging (MRI) examinationof a patient with a cerebral glioma. The patient had suffered fromincreasing headaches for 6 weeks, memory impairment, andincreasing paresis of the left side. Walking remained undamaged.MRI examination indicated a tumor 65 � 56 � 69 mm in size inthe right frontal lobe. The tumor displaced the anterior part of theright lateral ventricle and moved a part of the corpus callosum tothe left. (Courtesy Dorota Kozinska, University of Warsaw, Warsaw,Poland.)
Figure 12.6 Injected magnetic resonance imaging–visibledye amplifies boundaries of right frontal tumor, a glioma, inrelation to cortex and scalp surfaces. See inside covers for colorimage. (Courtesy Dorota Kozinska, University of Warsaw, Warsaw,Poland.)

or severe deficits usually do not accompany this type oftumor. Because the brain adapts to the slowly growingmeningiomas, tumors in the frontal area may grow rela-tively large before ICP produces behavioral symptoms.Therefore, meningiomas often cause no symptoms and re-main undiagnosed, only to be discovered later on autopsy.
The neurosurgeon finds meningiomas relatively easyto remove because they are encapsulated outside thebrain. Removal can, however, become complicated if thetumor is difficult to access, as when the lesion is in the in-trahemispheric fissure or the inferior parts of the brain.Meningiomas arising from the optic nerve sheath may be particularly difficult or impossible to remove, becausethey almost envelop the optic nerve. Nevertheless, be-cause they are encapsulated and benign, meningiomas offerthe best prognosis for complete recovery of any of the braintumors.
M e t a s t a t i c T u m o r
A malignant but encapsulated tumor is a metastatictumor. Metastasis is a medical term for the transfer of dis-ease from one organ or part not directly connected withit. The capacity to metastasize is a characteristic of all ma-lignant tumors. Metastatic tumors arise secondarily tocancerous tumors, which have their primary site in otherparts of the body, such as the lungs, breasts, or lymph sys-tem. The secondary growths arise because cancer cellsfrom the primary neoplasm detach. The bloodstream cancarry the cells to the brain, where they multiply. This iswhy early diagnosis in cancer is so important: to keeptumor tissue from “metastasizing.” Metastatic brain tu-mors typically have multiple sites and represent up to40% of all brain tumors seen in elderly adults. They gen-erally grow fast and typically occur at the junction of grayand white matter, close to the cortex surface, althoughthey can grow at any location in the brain. Metastaticbrain tumors in adults arise most frequently from bron-chogenic carcinoma (lung cancer), adenocarcinoma of thebreast (breast cancer), and malignant melanoma (skincancer).
A typical clinical picture in metastatic tumor is the di-agnosis of an elderly man with lung cancer related to along history of cigarette smoking. Examination of the pa-tient’s lymph nodes shows evidence of a tumor. Twelveweeks later, the patient develops a gait disturbance. Neu-ropsychological evaluation shows that the patient is cog-nitively intact but has motor slowing on the left side, anintention tremor, and difficulty walking in a straight line.Diagnostic imaging shows a metastatic tumor in the left
hemisphere of the cerebellum (recall that cerebellardeficits involve the ipsilateral arm and leg). Despite inten-sive chemotherapy and radiation therapy, the patient dies.The prognosis in metastatic brain cancer is typically poorbecause cancer invades multiple organs and producesmultiple growths in the brain. Neurosurgeons usually donot consider extracting metastatic tumors if multiple sitesare present. But as with any disease, there are exceptions,and disease progress is often difficult to predict. Forexample, U.S. cyclist Lance Armstrong was diagnosedwith testicular cancer. His cancer metastasized to his lungsand his brain, spawning multiple tumors. After surgery,Armstrong made a remarkable recovery and has not onlystayed cancer free, but went on to win the month-longTour de France, the most grueling bicycle race in theworld, a record seven times.
A c o u s t i c N e u r o m a
Acoustic neuromas are progressively enlarging, benigntumors within the auditory canal arising from Schwanncells of cranial nerve VIII, the auditory vestibular nerve,which sends sensory hearing and equilibrium informationto the brain. Initial symptoms include ringing in the ears(tinnitus), followed by partial deafness, such as in distin-guishing speech sounds and rhythmic patterns. Acousticneuromas typically begin to grow in the internal auditorycanal and then grow medially. They affect the cranialnerves V (the trigeminal nerve, which provides sensory in-formation of the face and motor control for chewing andswallowing) and VII (the facial nerve, which provides sen-sory information from the tongue and motor control offacial expressions and crying). As a result, the patient maylose his or her sense of hearing, followed by reports of aloss of taste on one side. Physicians often consult audiolo-gists in diagnosing acoustic neuromas.
P i t u i t a r y T u m o r s
The classification and neuropathology of pituitary tu-mors is complex because of the relation of the pituitarygland to the chemistry of the nervous and endocrine sys-tems. Scientists traditionally divide pituitary tumors intofunctioning and nonfunctioning adenomas. Pituitaryadenomas are benign neoplasms of the pituitary gland.Nonfunctioning adenomas produce symptoms caused bypressure on the pituitary and adjacent structures. As thetumor grows out of the sella—the bony capsule that holdsthe pituitary—headaches are common. Visual fielddeficits may also occur due to compression of the optic
360 PART THREE | Disorders of the Brain

chiasm (bitemporal hemianopsia). Hypothalamic com-pression usually causes diabetes insipidus.
Functioning pituitary tumors play an “uninvited” rolein the operation of the pituitary gland, often affecting therelease of the gland’s hormones. Functioning tumors ofthe pituitary gland include the acidophilic adenoma, atumor usually found in the anterior lobe of the gland. Theacidophilic adenoma provokes excessive secretion ofgrowth hormones, often resulting in giantism, a condi-tion featuring enlarged jaw, nose, tongue, hands, and feet.The chromophobic adenoma also appears in the ante-rior aspects of the pituitary gland and often produces hy-perpituitarism or hypopituitarism. Basophilic adenomasalso occur in the anterior lobe of the pituitary gland, butcause excessive secretion of adrenocorticotropic hormone(ACTH), which can cause Cushing’s syndrome. Thissyndrome, named after Boston surgeon Harvey Cushing(1869–1939), is a severe systemic illness most often seenin female individuals that includes neurologic symptomsand changes in bone structure, hypertension, and dia-betes. The ACTH-secreting tumor is the most seriouscondition encountered by any of the pituitary tumors andcan necessitate complete removal of the tumor, includingthe pituitary gland.
C H I L D H O O D T U M O R S
Childhood tumors are less frequent than brain tumors inadults. The most frequent is the medulloblastoma, arapidly growing and malignant tumor located in the infe-rior vermis close to the exit of CSF from the fourth ven-tricle. This type of tumor accounts for about two thirdsof all tumors in children and causes increased ICP due toobstructive hydrocephalus. Early symptoms include vom-iting and headache. Other common childhood tumors arecerebellar astrocytomas, gliomas of the brainstem andoptic nerve, and pinealomas. Pineal tumors are mostcommon in prepubescent boys. The tumor often com-presses the aqueduct of Sylvius, causing hydrocephalus,papilledema, and other signs of ICP. Table 12.4 summa-rizes the different types and features of brain tumors.
D I A G N O S I S O F B R A I N T U M O R S
The overall incidence of brain tumors for male and fe-male individuals is about equal, but cerebellar medul-loblastomas and GBM are more common in male indi-viduals, and meningiomas are more frequent in femaleindividuals. The overall frequency of various types of in-tracranial tumors is approximately 45% for gliomas, 15%
for pituitary adenomas, 15% for meningiomas, 15% formetastatic brain tumors, and 10% for other types.
Early behavioral symptoms in the diagnosis of tumorinclude a sudden onset of headaches, nausea, loss of cog-nitive function, or seizures. The ICP triad often accom-panies the growth of brain tumors and includes:
1. Headache2. Nausea and vomiting3. A positive papilledema, a swelling of the optic disk in
the eye
Of course, not every patient reporting a headache has abrain tumor, but headache often accompanies braintumor because of the enlarging tumor mass.
The introduction of the CT scan and the more recentmagnetic resonance imaging (MRI) has literally revolu-tionized diagnosis of tumors. High-resolution CT can vi-sualize even tiny tumors. Three-dimensional reconstruc-tion can often demonstrate the intimate relations of the
CHAPTER 12 | Cerebrovascular Disorders and Tumors 361
Acoustic neuroma—a benign tumor growing from the sheath of the acousticnerve at the cerebellopontine angle
Gliomas—a tumor composed of tissue representing neuroglia; the termglioma is often used to describe all primary, intrinsic neoplasms of the brainand the spinal cord
Glioblastoma—Malignant forms of astrocytoma
Glioblastoma multiforme—an astrocytoma of Grade 3 or 4, a rapidly growingtumor usually confined to one cerebral hemisphere and composed of amixture of spongioblasts, astroblasts, and astrocytes
Astrocytoma—a malignant tumor composed primarily of astrocytes
Ependymal glioma—a bulky, solid, firm vascular tumor of the fourth ventricle
Oligodendroglioma—a neoplasm derived from and composed of oligoden-drocytes
Optic glioma—a slowly growing glioma of the optic nerve or optic chiasm,associated with visual loss and loss of ocular movement
Meningioma—a typically benign tumor arising from arachnoid cells; producesneuropsychological deficits by exerting pressure on surrounding brainsubstances or cranial nerves
Metastatic tumor—a growth of a tumor, often multiple, distant from the siteprimarily involved in the morbid process
Pituitary adenoma—a tumor of the pituitary gland; pituitary adenomas areoften classified as functioning (changing the secretion of the pituitary gland)and nonfunctioning (benign)
Pinealoma—a tumor of the pineal body
Table 12.4 Types of Brain Tumors

tumor to its surrounding brain structure, facilitatingprecise removal of the tumor by surgeons. Today, neurol-ogists most efficiently diagnose brain tumor using CT orMRI, which often provides the definitive diagnosis (seeChapter 2 for a comprehensive review of medical diag-nostic procedures). Neurologists have used functionalMRI (fMRI) to differentiate brain tissue from tumor tis-sue, as well as to identify areas of the brain that are partic-ularly vital for cognitive functions. This is often impor-tant, because using fMRI neurologists can identify asafe corridor through the brain into the tumor, whichthe surgeon can then use. In addition, fMRI can helpdifferentiate whether the cancer itself contains vitalbrain tissue. Somatosensory-evoked responses and di-rect stimulation of the brain can also help separate im-portant brain tissue from brain tumor tissue. Neurolo-gists often use plain X-ray films in diagnosing andplanning surgery to remove meningiomas, because thistype of tumor can erode the skull in a high percentageof patients, as shown in radiographic changes on skullX-ray films.
Angiography occasionally can be useful in tumor diag-nosis to identify which primary branches of the cardiovas-cular system supply the tumor with its blood supply. Mod-ern imaging is most effective in diagnosing the presence ofa tumor, but not in diagnosing its type. Histologic exami-nation via brain biopsy is necessary to precisely diagnosethe type of tumor and to select the most appropriate inter-vention. Neurologists most frequently do this using CT-guided stereotaxic biopsy, which interfaces stereotacticframes that fasten to the patient’s head with steel pins. Abiopsy needle is affixed to the frame, which the neurosur-geon can move with precision in all three dimensions.Using this procedure and with the patient under localanesthesia, the neurosurgeon can take a brain specimenthrough a burr hole. Subsequent laboratory examinationcan then provide the exact diagnosis of the tumor.
T R E A T M E N T O F B R A I N T U M O R S
The preferred treatment for brain tumors is total surgicalexcision of the tumor whenever possible. The prognosisfor recovery after removing a brain tumor depends on twoprimary factors, the location and type of tumor. For ex-ample, a relatively simple surgical excision may involve awell-differentiated tumor, such as a meningioma, particu-larly if the tumor is in an easily accessible location (as insuperior aspects of the cortex). If the tumor is malignant,local radiation therapy typically follows surgical removalto prevent regrowth. If the tumor is inaccessible, for
example, in the region of the thalamus or brainstem, radi-ation therapy is the primary intervention. A fast-growingglioblastoma in a nonresectable location is often fatalwithin 12 months. Thus, the prognosis for GBMs is notgood, but combined treatments have a small success rate.For tumors that are difficult to access, located at the baseof the skull or covering the superior sagittal sinus, theneurosurgeon often uses a sophisticated operating micro-scope or a laser.
Chemotherapy for brain tumors is playing an increas-ingly important role in the battle against cancer.Chemotherapy is most effective in tumors that have ahigh growth fraction; that is, tumors that are actively di-viding and producing DNA. When a tumor is young,most of its cells are making DNA. When antitumor drugsreach tumor cells in the phases of cell cycling, the cellsdie. As the tumor ages, growth fraction decreases and drugsensitivity declines. Thus, the most effective form ofchemotherapy is when the tumor is young and 100% ofits cells are in the growth fraction—this again emphasizesthe importance of early diagnosis. However, the BBB,which protects the brain from foreign substances, compli-cates chemotherapy for brain tumors. The BBB preventscancer-killing drugs from entering brain tissue via thebloodstream. Thus, antitumor drugs targeting brain tu-mors are limited to agents easily transported across theBBB—typically, very lipid-soluble substances. In recentyears, however, researchers have discovered that somechemicals (such as the bradykinin agonist, RMP-7) arehighly effective in opening the BBB by making capillarywalls “leaky.” As a result, chemotherapy drugs can act di-rectly on the tumors, increasing their effectiveness asmuch as 10-fold.
Medicine will only achieve a cure in the fight againstbrain tumors, however, when it can enlist the patient’sown immune system to attack the cancer. Tumors pro-duce a chemical that tricks the immune system into ig-noring them. Recent genetic engineering research in an-imals has shown some promise in discovering substancesthat turn off the ability of the tumor cells to producetheir own vaccine. The tumor cells then become imme-diate targets of the immune system, which destroysthem.
Treating brain tumors is not only complicated froma scientific perspective, it also takes a psychological tollon the patient, as well as the patient’s family. As a re-sult, psychologists also play an important role in coun-seling patients undergoing cancer treatment or in hos-pice centers—health care centers that provide medicaland emotional support for the terminally ill and theirfamilies.
362 PART THREE | Disorders of the Brain

Brain Tumors and Neuropsychology
The neuropsychological manifestations of brain tu-mors depend on the location, size, and grade of thetumor, rather than on its histologic type. Smaller tumorsnear primary motor areas may cause seizures and loss ofmotor function, whereas deeper intracranial tumors maygrow rather large before focal clinical symptoms appear.Evaluations also find a general decline in adaptive areas,as well as in overall cognitive functioning, because thetumor displaces neighboring areas. The neuropsychologi-cal deficits of a GBM are profound. The destruction ofwhichever cerebral hemisphere is involved is severe andnearly complete. In the acute stages of GBM, neuropsy-chological evaluation typically is not undertaken, becausethe deficits are so severe and the overall medical conditionof the patient is of foremost concern. Patients with astro-cytomas may have longer histories of increasing problems,because of the slow growth of these neoplasms. Oligoden-drogliomas typically produce few neuropsychological ef-fects because they grow so slowly.
Focal neuropsychological symptoms of brain tumorsstem from localized destruction, compression of nervoustissue, or altered endocrine function. Tumors in thefrontal lobes are most commonly meningiomas andgliomas. They can produce both localized and generalizedcognitive deficits, including expressive aphasia (if locatedin the dominant hemisphere) or difficulties smelling(anosmia) related to a meningioma at the base of thefrontal lobe. Inattention and changes in motivation com-monly accompany tumors that affect both frontal hemi-spheres. Parietal lobe tumors may contralaterally impairsensory modalities, stereognosis, contralateral homony-mous hemianopsia, and apraxia. Speech disturbances,agraphia, and finger agnosia may appear if the left hemi-sphere is involved, and neglect is characteristic of patentswhose right hemisphere is affected.
Temporal lobe tumors may produce mixed expressiveand receptive aphasia of the dominant temporal lobe.Nondominant temporal tumors often do not have “obvi-ous” cognitive signs. Tumors deep in the temporal lobemay cause contralateral hemianopsia. Occipital lobe tu-mors most often entail visual deficits, typically a contralat-eral quadrant defect in the visual field or a hemianopiawith sparing of the macula. Subcortical tumors that in-volve the internal capsule produce contralateral hemiple-gia. Thalamic tumors produce contralateral sensory im-pairment. Basal ganglionic tumors often result in tremors.All brain tumors may produce seizures, which may be
preceded by an aura that may indicate the location of thetumor.
Metastatic tumors are often associated with neuropsy-chological test results indicating focal areas of deficits.Skills that the tumor does not affect may be relatively in-tact. Later stages of metastatic tumors with numerous sitesand sizes may produce a diffuse loss of most neuropsy-chological abilities. Acoustic neuromas typically do notentail severe cognitive loss, but rather a hearing impair-ment. A meningioma produces its behavioral effects bycompressing the brain. Meningiomas near the optic nerveresult in visual disturbances and are difficult to removebecause of their location. Pituitary tumors also producevisual field defects because of the close relation betweenthe optic chiasm and the pituitary gland.
Neuropsychological evaluations have proved most use-ful in establishing a cognitive baseline before neurosurgeryand in evaluating outcomes of patients after surgery. Asmentioned earlier, neuropsychologists also provide coun-seling and education to patients with brain tumor andtheir families. More recent research has focused on theneuropsychological implications of radiation therapy(Neuropsychology in Action 12.3).
Other Neurologic Disorders
B R A I N A B S C E S S
Brain abscesses are similar to tumors, both in appearanceand on visualization using imaging. Compared with atumor, however, a brain abscess arises from an infectionspreading to the brain or originating in the brain. Ab-scesses begin as an area of generalized inflammation andprogress to a “walled off,” localized pocket of pus withinthe brain. The abscess can gradually expand, destroyingand compressing brain tissue as it grows. Compared withbrain tumors, however, imaging typically shows an emptycenter within the abscess, differentiating it from a tumor,which appears more “solid.” In addition, the patient typi-cally presents with a history of prior infection.
I N F E C T I O N S
Infections and infectious diseases tend to attack specificbrain structures depending on the type. At least 20 differenttypes of infections affect the brain. Many are obscure andrare. Among the well studied are meningitis, herpes en-cephalitis, and human immunodeficiency virus (HIV).
CHAPTER 12 | Cerebrovascular Disorders and Tumors 363

Meningitis is a bacterial or viral infection of the meningesthat provide the protective covering of the brain. Menin-gitis can also be a result of brain surgery (there is an up to5% incidence rate); physicians routinely administer an-tibiotics to patients who have undergone intracranial pro-cedures to prevent such infections. Interestingly, such in-fections acquired during brain surgery vary, not only fromhospital to hospital depending on the thoroughness ofsterilization of the operating room but also among oper-ating rooms within a single hospital. Such data are, how-ever, not commonly published for the consumer, for
obvious reasons. Herpes encephalitis (not to be confusedwith genital herpes) aggressively attacks the medial tem-poral and orbital frontal areas. This appears to destroymuch of the limbic system, especially the hippocampus.The result is a near total inability to learn new informa-tion (anterograde amnesia). The HIV/AIDS virus haswider effects on the brain, because it progressively de-stroys the immune system. The virus itself may have di-rect consequences for the brain, but it also opens the brainto opportunistic infections and other diseases that can at-tack the brain.
364 PART THREE | Disorders of the Brain
Effective brain tumor treatment is always acompromise, involving the protection ofhealthy cells and the destruction of aggres-sive cancer cells that have infiltrated healthytissue. Treatment choices are complex andshould involve input from a team of onco-logic professionals, including neurosurgeon,oncologist–hematologist, radiation therapist,neuroradiologist, neurologist, and neuropsy-chologist. Surgical interventions range frombiopsy, or the removal of enough tissue formicroscopic determination of histologic typeand pathologic grade of tumor cells, to theresection of 100% of tumor tissue as amethod of preventing tumor regrowth. Brainsurgery may also involve Wada testing orfunctional magnetic resonance imaging (seeChapter 2), with the aid of the neuropsychol-ogist in determining hemispheric dominanceof movement and language, and help fromthe neuroradiologist in outlining blood flowpatterns in the brain. Specialists also mayuse brain mapping to localize function andpreclude resection of brain tissue crucial forlanguage or memory.
Besides surgical treatments for braintumors, medical professionals often giveradiation therapy and chemotherapy, eitheralone or in combination. The most commonmethod of radiotherapy involves externalphoton beam radiation; with this method,
technicians administer a total dose of radia-tion in fractions over a period of about 6 weeks, 5 days a week. If the treatment is toprevent metastasis or the seeding of tumorcells by blood- or lymph-based cancer, thenradiation may include the whole brain.However, to shrink or prevent the spread of aprimary tumor, radiation is focused on justparts of the brain. The best current alterna-tive therapies include conformal and stereo-tactic radiotherapy, surgical placement ofchemotherapy wafers in the tumor bed, andgene therapy.
The natural history of radiotherapyeffects is not well understood. Experimentalanimal studies demonstrate brain damageor decreased cell density from radiotherapy.Several studies in humans have associateddamage to the brain’s white matter withdelayed radiation effects (Corn et al., 1994).In addition, chemotherapy interacts withradiotherapy to exacerbate radiation dam-age. Although studies of children and severalretrospective studies have found alarmingeffects of radiation injury, some studies ofadults have not. The methodology used isoften the source of the discrepancies. Forexample, retrospective studies find abnor-mally high rates of white matter damage, lowIQ, memory impairment, and even dementiain both adults and children from 3 months to
many years after irradiation (DeAngelis,Delattre, & Posner, 1989). A late effect, upto 20 years after treatment, may result in anatherosclerotic-like disorder if carotid arter-ies were irradiated. Conclusions are con-founded when patients are tested at irregulartime periods, only brief neuropsychologicalevaluations are conducted, or no baselineneuropsychological testing (before treat-ment) is ordered.
Memory deficits have been implicated asthe most frequent and severe delayed effectof radiation therapy. Researchers considerthe early delayed effects, occurring 2 to 3 months after completion of radiationtreatment, to be mild and temporary. Thelate delayed effects of radiation therapy aremore severe, may progress, and are irre-versible. We compared longitudinal researchon patients who received radiation therapywith patients with similar tumor types butwho did not have radiotherapy. Patients withlow-grade, cortical, primary brain tumorsoften have long life expectancies and rela-tively few cognitive deficits. Neuropsycholo-gists give these patients a repeatable,comprehensive battery of tests that includesmany sensitive measures of attention andmemory processes. Evaluations occur justbefore irradiation, and then at 3-, 6-, and12-month intervals. Thus far we have learned
N e u r o p s y c h o l o g y i n A c t i o n 1 2 . 3
N e u r o p s y c h o l o g y o f Tr e a t m e n t s f o r I n d i v i d u a l s w i t h B r a i n Tu m o r s
by Carol L. Armstrong Ph.D., Department of Neurology, University of Pennsylvania and the Joseph Stokes Research Institute, Children’s
Hospital of Philadelphia, Philadelphia, PA
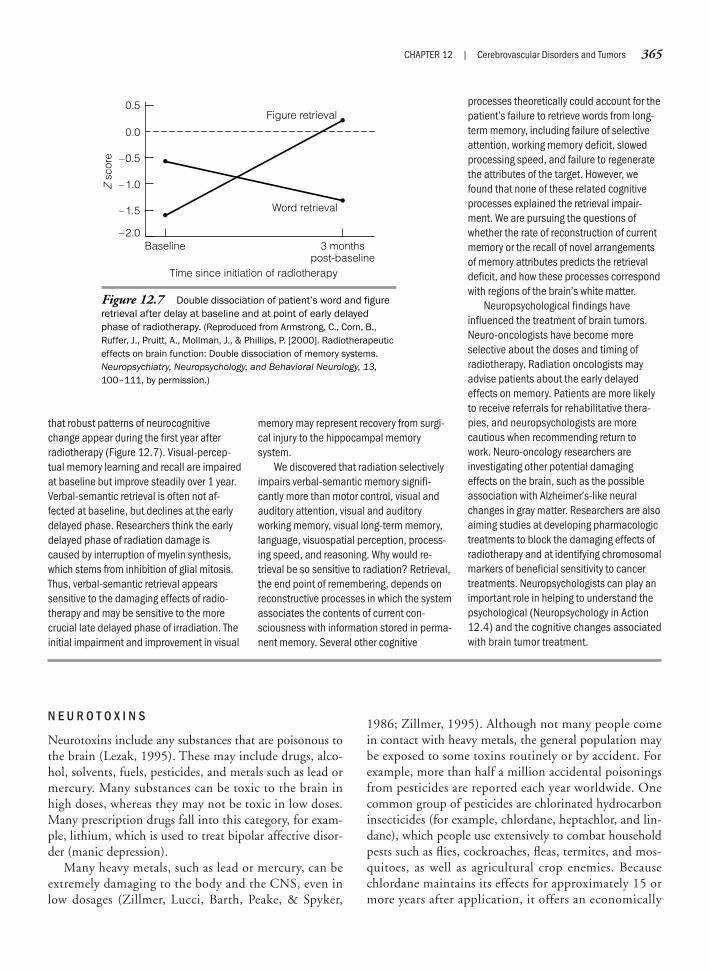
N E U R O T O X I N S
Neurotoxins include any substances that are poisonous tothe brain (Lezak, 1995). These may include drugs, alco-hol, solvents, fuels, pesticides, and metals such as lead ormercury. Many substances can be toxic to the brain inhigh doses, whereas they may not be toxic in low doses.Many prescription drugs fall into this category, for exam-ple, lithium, which is used to treat bipolar affective disor-der (manic depression).
Many heavy metals, such as lead or mercury, can beextremely damaging to the body and the CNS, even inlow dosages (Zillmer, Lucci, Barth, Peake, & Spyker,
1986; Zillmer, 1995). Although not many people comein contact with heavy metals, the general population maybe exposed to some toxins routinely or by accident. Forexample, more than half a million accidental poisoningsfrom pesticides are reported each year worldwide. Onecommon group of pesticides are chlorinated hydrocarboninsecticides (for example, chlordane, heptachlor, and lin-dane), which people use extensively to combat householdpests such as flies, cockroaches, fleas, termites, and mos-quitoes, as well as agricultural crop enemies. Becausechlordane maintains its effects for approximately 15 ormore years after application, it offers an economically
CHAPTER 12 | Cerebrovascular Disorders and Tumors 365
that robust patterns of neurocognitivechange appear during the first year afterradiotherapy (Figure 12.7). Visual-percep-tual memory learning and recall are impairedat baseline but improve steadily over 1 year.Verbal-semantic retrieval is often not af-fected at baseline, but declines at the earlydelayed phase. Researchers think the earlydelayed phase of radiation damage iscaused by interruption of myelin synthesis,which stems from inhibition of glial mitosis.Thus, verbal-semantic retrieval appearssensitive to the damaging effects of radio-therapy and may be sensitive to the morecrucial late delayed phase of irradiation. Theinitial impairment and improvement in visual
memory may represent recovery from surgi-cal injury to the hippocampal memorysystem.
We discovered that radiation selectivelyimpairs verbal-semantic memory signifi-cantly more than motor control, visual andauditory attention, visual and auditoryworking memory, visual long-term memory,language, visuospatial perception, process-ing speed, and reasoning. Why would re-trieval be so sensitive to radiation? Retrieval,the end point of remembering, depends onreconstructive processes in which the systemassociates the contents of current con-sciousness with information stored in perma-nent memory. Several other cognitive
processes theoretically could account for thepatient’s failure to retrieve words from long-term memory, including failure of selectiveattention, working memory deficit, slowedprocessing speed, and failure to regeneratethe attributes of the target. However, wefound that none of these related cognitiveprocesses explained the retrieval impair-ment. We are pursuing the questions ofwhether the rate of reconstruction of currentmemory or the recall of novel arrangementsof memory attributes predicts the retrievaldeficit, and how these processes correspondwith regions of the brain’s white matter.
Neuropsychological findings haveinfluenced the treatment of brain tumors.Neuro-oncologists have become moreselective about the doses and timing ofradiotherapy. Radiation oncologists mayadvise patients about the early delayedeffects on memory. Patients are more likelyto receive referrals for rehabilitative thera-pies, and neuropsychologists are morecautious when recommending return towork. Neuro-oncology researchers areinvestigating other potential damagingeffects on the brain, such as the possibleassociation with Alzheimer’s-like neuralchanges in gray matter. Researchers are alsoaiming studies at developing pharmacologictreatments to block the damaging effects ofradiotherapy and at identifying chromosomalmarkers of beneficial sensitivity to cancertreatments. Neuropsychologists can play animportant role in helping to understand thepsychological (Neuropsychology in Action12.4) and the cognitive changes associatedwith brain tumor treatment.
Figure 12.7 Double dissociation of patient’s word and figureretrieval after delay at baseline and at point of early delayedphase of radiotherapy. (Reproduced from Armstrong, C., Corn, B.,Ruffer, J., Pruitt, A., Mollman, J., & Phillips, P. [2000]. Radiotherapeuticeffects on brain function: Double dissociation of memory systems.Neuropsychiatry, Neuropsychology, and Behavioral Neurology, 13,100–111, by permission.)
Baseline–2.0
0.5
3 monthspost-baseline
Time since initiation of radiotherapy
Z s
core
0.0
–0.5
–1.0
–1.5 Word retrieval
Figure retrieval

366 PART THREE | Disorders of the Brain
Lisa, a 21-year-old woman, was referred to aconsulting psychologist by her pediatriconcologist because of depressed mood,behavioral manifestations of seizures with noassociated neurologic changes, and familyconflict. When she was 10 years old, Lisawas treated for acute nonlymphoblasticleukemia through bone marrow transplant,which included high-dose, whole-bodyradiation. Sequelae of the cancer and itstreatment included apparent seizures (par-ticularly when stressed); cognitive deficitsassociated with cranial radiation, includinglimitations in general intellectual functioning;and a pattern of deficits associated withnonverbal learning disability (Carey, Barakat,Foley, Gyato, & Phillips, 2001), cataracts,and infertility. At the time of referral, Lisalived with her parents and her youngerbrother. Although a high school graduate,she was not employed and spent most of hertime alone at home. Although her parentswere caring and protective, they did notencourage Lisa to branch out of the home,because they feared she would have aseizure in a public place, were uncertain ofher capabilities, and viewed the cancer andits consequences as severe and insurmount-able. Despite her current situation, Lisahoped to go to college, get married, andhave children.
The complexities of Lisa’s medical condi-tion placed a considerable burden on thefamily as a whole. The role of the patient’scognitive factors in family functioning iscomplex; some detrimental effects mayappear, but some families can cope withthese problems (Carlson-Green, Morris, &Krawiecki, 1995). A key to understandingthe relations among cognitive aspects ofchildhood cancer, child adjustment, andfamily functioning may be child and parentperceptions or appraisals of the impact ofthe illness. A series of studies on childhoodcancer survivors and their parents consis-tently relate perception of life threat associ-
ated with cancer, and its treatment in thepast and present, and appraisals of treat-ment intensity to child, parent, and familyadjustment (Barakat, Kazak, Meadows,Casey, Meeske, & Stuber, 1997; Foley,Barakat, Herman-Liu, Radcliffe, & Molloy,2000). However, objectively rated intensityof the treatment, severity of medical lateeffects, and history of cranial radiationtreatment are not consistently associatedwith adjustment in children treated forcancer.
These findings provide strong evidencefor the importance of child and parentsubjective appraisals or perceptions ofcognitive limitations in understanding childand family functioning after cancer diagnosisand treatment. Importantly, preventiveinterventions can modify child and parentappraisals of cognitive limitations and theimpact of the illness, to improve long-termfamily adaptation (Barakat & Kazak, 1999).It is essential to work with families from thepoint of cancer diagnosis to provide a realis-tic but optimistic framework for understand-ing children’s capabilities and needs. Theintervention must consider the child’s abilityto comprehend this information, givencognitive limitations.
Such interventions must also take intoaccount developmental process in families.As the children grow older, families mustreassess and reintegrate the meaning ofcognitive limitations for their child andfamily. For example, as children enter formalschooling, families must balance the need toaddress potential learning problems with theneed for children to engage in routine activi-ties with peers. As children reach adoles-cence and strive for autonomy, families mustbe able to set realistic goals with their chil-dren while allowing them to achieve inde-pendence in functioning. On the flip side,children and adolescents should gain guid-ance in choosing academic, vocational, andsocial goals that they can attain.
In addition to addressing perceptions, itis necessary to foster positive changes infamily interactions (such as interactionsaround homework, rules in the home, andpeer relationships) to promote children’scompetencies and, in turn, improve function-ing. In relation to this, frequent communica-tion among other systems, such as theschool, religious community, or medicaltreatment team, decreases conflicting infor-mation provided to families and improvescoordination of support. For instance, thechild, parents, and teachers may coopera-tively develop and implement a plan aimed athomework completion that provides structureand builds on the child’s cognitive strengths.
Finally, improving parent resources andcoping helps improve the functioning of fami-lies dealing with the long-term strains andmedical sequelae of cancer treatment, includ-ing cognitive changes. Family-to-family con-tact and support through multiple-familygroups is an integral part of bolstering chil-dren’s and their parents’ resources. Familieslearn from one another which coping strategiesmost facilitate healthy family developmentas the childhood cancer survivor moves intoadulthood.
After complete neurologic and psycho-logical evaluations, Lisa was diagnosed withgrand mal seizures, as well as unexplainedseizure activity, and major depression withdissociative features. Treatment entailedachieving a therapeutic dose of medicationfor her seizures and individual and familytherapy. The goal of family therapy was tohelp Lisa and her parents realistically assessher skills and recognize her potential. Ini-tially, through increasing her responsibility inthe home, trips to the mall (where she wasfree to shop on her own), and engagement inhobbies, Lisa’s sense of competence im-proved. Her parents’ perceptions of herabilities became more optimistic, and theirappraisals of her illness severity lightened.Lisa and her parents began to focus on
N e u r o p s y c h o l o g y i n A c t i o n 1 2 . 4
Fa m i l y a n d C h i l d A d j u s t m e n t t o C o g n i t i v e A s p e c t s o f C a n c e r i n C h i l d r e n
by Lamia P. Barakat Ph.D., Associate Professor of Psychology, Department of Psychology, Drexel University, Philadelphia, PA

appealing long-term treatment against termites. Chlor-dane is readily absorbed through the gastrointestinal tract,respiratory tract, or unbroken skin, and it is stored inbody fat. Once absorbed, chlordane is an axon poi-son, which disturbs the normal action of the sodium-potassium adenosinetriphosphatase (ATPase) pump,interfering with the transmission of nerve impulses. Be-cause of its chemical stability, chlordane can be detected inapproximately 70% of U.S. homes today and ranksamong the most ubiquitous neurotoxic materials beingreleased into the ecosystem (Zillmer, Montenegro, Wiser,Barth, & Spyker, 1996).
In general, toxic effects on the brain cannot be describedin simple terms, because the mechanisms of action are sovaried. Most common are cognitive deficits ranging frommild to severe on tasks that require speeded processing,problem solving, and delayed memory. Somatization, hys-terical features, and depression often dominate the clini-cal picture. Thus, the medical profession increasinglyrecognizes that chemicals can have significant neuropsy-chological effects (Hartman, 1995), and that neuropsychol-ogy offers promise in increasing knowledge of the effects oftoxins on the human CNS, describing specific patterns ofperformance, and monitoring the course of treatment.
CHAPTER 12 | Cerebrovascular Disorders and Tumors 367
increasing Lisa’s independent functioning.She successfully entered a vocational reha-bilitation program and made plans for aclerical position in the future. She began tomake friends and to attend social functions
through her rehabilitation program. Lisamade a number of overnight visits withsiblings, and her parents took a long-neededvacation without their daughter. Concur-rently, counselors gently guided Lisa through
cognitive interventions to understand andcome to terms with her limitations, particu-larly those relevant to her hopes for a collegeeducation and children. Lisa’s seizures anddepression remitted.
SummaryIn general, damage to the brain may result from either primary or secondary damage and may have eitheracute or long-term effects. In addition to damage within the immediate area, there may also be damage tomore distal areas because of disconnected neuronal pathways. The diagnosis of primary damage relates tothe initial injury or insult to the brain. If axons are completely severed or destroyed, the damage is oftenpermanent and that tissue is lost. Secondary brain damage, in contrast, may result in either permanent ortemporary damage. Secondary damage is caused by the aftereffects of the primary injury. Hemorrhage orbleeding causes oxygen deprivation and can lead to cell death known as necrosis. Edema, or “brainswelling,” hemorrhage, and infection may all cause increased cranial pressure. This pressure in the nonex-panding skull may effectively “cut off” areas of brain functions. If these secondary effects can be controlledquickly, the damage and functional effects may reverse in the acute stages of recovery. What is consideredprimary damage in one situation may be secondary damage in another. For example, a head injury (seediscussion in Chapter 13) may cause primary axonal severing, destruction of brain tissue, and secondaryswelling and hemorrhaging. The primary damage of a stroke may be caused by a hemorrhage, but theremay still be secondary swelling and ICP. Sudden traumas such as stroke tend to have more striking andnoticeable behavioral effects than slowly emerging processes. The most frequently encountered cerebro-vascular disorders may, at times, produce multiple cognitive disabilities; yet, often such dysfunction is rela-tively localized for the anatomic area involved, as well as the corresponding neuropsychological sequelae.However, more general neuropsychological disabilities are possible when, for example, larger areas of thebrain are infarcted. Brain tumors affect a significant proportion of the population and may lead to manydebilitating conditions. Neuropsychologists are at the forefront in researching cerebrovascular and tumortreatment and rehabilitation. In Chapter 13, we discuss other neurologic disorders of the brain, specificallythe neuropsychological consequences and rehabilitation of traumatic head injuries.
C r i t i c a l T h i n k i n g Q u e s t i o n s
What are the neurologic, behavioral, and emotional symptoms of a stroke?What are the major forms of treatment for stroke?Why do some stroke victims downplay their illness, whereas others go into a deep depression?
LesionsNecrosisAnoxiaHypoxiaSleep apneaHydrocephalusCommunicating hydrocephalusObstructive hydrocephalusStrokeCerebrovascular accident (CVA)Intracranial pressure (ICP)InfarctionHemorrhageTransient ischemic attack (TIA)IschemiaThrombosis
AtherosclerosisPlateletsEndotheliumEmbolismAtrial fibrillationHematomaIntracerebralSubarachnoid hemorrhageAneurysmsArteriovenous malformations
(AVMs)AuraMigraine strokeStenosisCollateral blood vesselAnastomosis
TumorNeoplasmInfiltrative tumorsNoninfiltrative tumorsMalignant tumorsBenign tumorsMetastasisNeuromasGrade of tumorGliomasGlioblastoma multiforme (GBM)AstrocytomasOligodendrogliomaMeningiomasMetastatic tumorsAcoustic neuromas
Pituitary tumorsFunctioning adenomasNonfunctioning adenomasPituitary adenomaAcidophilic adenomaChromophobic adenomaBasophilic adenomaCushing’s syndromeMedulloblastomaPinealomaOptic gliomaBrain abscessMeningitisHerpes encephalitisHuman immunodeficiency virus
(HIV)
We b C o n n e c t i o n s
http://www.med.harvard.edu/AANLIB/home.htmlHarvard Medical School: CVA Facts—This site for the Whole Brain Atlas has an excellent section of imagesdemonstrating various types of CVAs discussed in our text. A great way to visualize the extent of damagedifferent types of CVAs may manifest. Also shows MRI and single-photon emission computed tomographyimages of various neoplastic diseases, including glioma, metastatic tumors, and meningioma.
http://neurosurgery.mgh.harvard.eduBrain Aneurysm and AVM Center—Links you to the Harvard Brain Aneurysm and AVM Center at Mass Gen-eral, where you can find discussions of the latest treatment for these and other cerebrovascular disorders.
http://www.stanford.edu/group/neurology/strokeStroke Awareness—Stanford Medical Center’s site for stroke awareness and treatment information.
http://www.ninds.nih.govNational Institute on Neurological Disorders and Stroke—An excellent site for the most up-to-date informa-tion on CVAs and related disorders. Internal search engines allow you to be as specific as you would like inobtaining information.
Describe the most common neuropsychological deficits associated with stroke.Would you want to know what type of cell a tumor arises from if one of your family members had brain cancer? Why?Should physicians routinely inform their patients of such medical details?What is the neuropsychologist’s role in diagnosing and treating patients with brain tumors? What is his or her role with thepatient’s family?How do children who have brain tumors react differently to their disease from the way adults do? How do their familiesreact?
K e y Te r m s
368 PART THREE | Disorders of the Brain

Chapter 13
TRAUMATIC HEAD INJURY AND REHABILITATION
If you want to understand God, you study the anatomy of the brain.—Keith Black (neurosurgeon)
Traumatic Head InjuryEpidemiology of Traumatic Head InjuryMechanism of Impact: Neuronal Shearing, Stretching,
and TearingComplications of Moderate and Severe Brain InjuryMild Head Injury: “Concussions”Treatment of Head InjuriesRecovery, Rehabilitation, and Intervention of Traumatic
Brain InjuryAdaptation and RecoveryOverview of the Rehabilitation ProcessTreatment Methods for Neuropsychological
Rehabilitation
Neuropsychology in Action
13.1 Case Study: Penetrating Head Injury13.2 Can a Concussion Change Your Life?13.3 Consensual Sex after Traumatic Brain Injury:
Sex as a Problem-Solving Task13.4 It Is More Than a Black Box

370 PART THREE | Disorders of the Brain
Traumatic Head Injury
The Kennedy clan (that is, President John F.Kennedy’s family) engage in an annual family ritual dur-ing their skiing vacation in Aspen, Colorado. TheKennedy clan and friends gather at a mountaintop bar,waiting until the lifts shut down at about 4 P.M. Then,with few other skiers on the trails, they play football downthe slope, with skis but no poles. A cross between Frisbeeand touch football, “ski football” is an old Kennedy pas-time. They divide into two teams and start tossing amakeshift football through the thin mountain air toward
a goal, typically a trail marker. The rules of the game de-mand that a player must pass the ball to a teammatewithin 10 seconds or turn the ball over. This seems like alot of fun, but inherent in skiing, as is true for mostsports, is risk in the form of speed. Sports, in fact, accountfor 17% of all head injuries, second only to motor vehicleaccidents (MVAs). The most dangerous sports are eques-trian events, gymnastics, and cheerleading. Among inter-collegiate sports, gymnastics, football, lacrosse, and icehockey are the most likely to lead to head injuries. Skiing isactually a relatively safe sport—there is less than 1 deathper 1 million skied days. But that New Year’s Eve afternoon
K e e p i n M i n d
Do different injuries to the brain have similar effects on the brain, or should we expect a variety of effects?
What is the difference between a penetrating and a closed head injury?
What role do neuropsychologists play in the diagnosis and treatment of head injuries?
How do rehabilitation programs further the process of recovery and adaptation with traumatic brain injury?
What is the specific role of the neuropsychologist on the rehabilitation team?
OverviewNeurologists commonly differentiate neurologic disorders of the brain by whether they have a particularfocus or site, or are more generalized, affecting the brain as a whole. There are, however, many exceptionsto this simple classification paradigm. As discussed in Chapter 12, a stroke or a bleed in the brain is a focaldisorder because the damage occurred at a specific location. In contrast, many small bleeds or very largehemorrhages often present a diffuse clinical picture. Similarly, a single brain tumor may represent a precisefocal deficit, whereas a large tumor or multiple small tumors of the brain may leave the patient with morewide-reaching deficits, which typically entail diffuse neuropsychological deficits. For the most part, neu-ropsychologists consider tumors to be focal disorders of the brain, because most often they entail more orless circumscribed brain damage.
In contrast, diffuse disorders most often involve dysfunction of the entire brain and most frequentlyappear in closed head injuries (CHIs), toxic conditions, and degenerative disorders. This classification para-digm is not entirely accurate, but it helps the neuropsychologist make an overall determination of the sever-ity and extent of possible dysfunction. In a car accident, the rotational forces on the head often result inblunt trauma to the brain, and thus cause diffuse damage. In contrast, a gunshot wound to the head maypresent a relatively localized but devastating trauma to the brain and may have more localized deficits.Therefore, keep in mind that this categorization is not a hard-and-fast rule. In principle, focal disorders mayinterrupt a small area of brain functioning, whereas other areas of the brain remain relatively intact. Some-times the loss of brain tissue is so small that it may not be noticeable except with sophisticated neuropsy-chological testing or advanced imaging techniques.
This chapter discusses the more diffuse traumas of the brain related to head injury. Finally, less frequentlyencountered neurologic disorders are discussed, including brain abscesses, infections, and neurotoxins.

the conditions were getting worse, the slopes were slickand icy, and the sun was setting behind the mountains,making it hard to see in the shadows and flat light. Onthe quintessential “last run” on the last day of the year,Michael L. Kennedy, the 39-year-old son of Ethel and thelate Senator Robert, turned his head to catch the ball. Hehit a fir tree headfirst on the left side of the trail. Yes, itwas reckless to ski while playing a daring game of moun-tainside football. The ski patrol had warned against it.Tossing a makeshift football back and forth may have dis-tracted Kennedy just enough that he was not able to stopor swerve before striking the tree. According to eyewit-nesses, Kennedy—a good skier—first struck the tree witha tip of his ski, which caused him to catapult slightly andslam his head directly into its trunk without slowingdown. With his three youngest children watching in hor-ror, Michael Kennedy died of a severe head injury to theback of his fractured skull. His injury must have damagedhis brainstem, because his sister Rory, who was the first tohis side, noticed no pulse or breathing. The medulla ob-longata, a part of the lower brainstem, mediates vital func-tions necessary for life such as respiration, blood pressure,heart rate, and basic muscle tone. Damage to the medullacan interrupt motor and sensory pathways, as well asthreaten life itself. The death, ruled accidental, adds yetanother tragedy to America’s most famous clan.
Would a helmet have saved his life? Those who survivehead injuries often sustain significant brain damage,which can change them for a lifetime, both physically andemotionally. This can result in a markedly altered lifestylefor the survivor, those who take care of him or her, thefamily, and loved ones.
Epidemiology of Traumatic Head Injury
Human brains have evolved over hundreds of thou-sands of years, but only recently have people invented tech-nology, both recreational and occupational, that has putbrains in motion, often at high speeds. The skull and thedura mater protect the brain well, but they are no matchfor the physical forces unleashed on the brain during a headinjury, which often can result in brain damage. Head in-juries do not occur in isolation, and additional injuries arecommon; thus, most cases require additional medical at-tention to other seriously traumatized parts of the body,complicating the overall prognosis and intervention.
Accidents are the leading cause of death in people ages1 to 30. In the 1970s, the medical profession first recognized
head injuries, particularly those related to MVAs, as a na-tional epidemic. Researchers estimate that 500,000 peo-ple suffer brain injury every year. A majority of those arein the mild range, but millions of people in the UnitedStates are surviving and living with a moderate to severebrain trauma (Zillmer, Schneider, Tinker, & Kaminaris,2006). After MVAs, the causes of head injuries are, inorder, sports injuries, falls, violence, and industrial acci-dents. In individuals younger than 45 years, head injuriescause more deaths and disability every year than any otherneurologic illness. Those most at risk are young, underage 30, single, and male. The male/female ratio may be ashigh as 4:1. Young adults between ages 15 and 24, fol-lowed by children and adolescents aged 5 to 14, are atgreatest risk for traumatic brain injury (TBI). But no oneis immune. Studies implicate alcohol in one third to halfof all traumatic head injuries. In fact, head injuries aresuch a significant health problem among developed coun-tries that they play a role in approximately half of alldeaths related to trauma (Rimel, Giordani, Barth, Boll, &Jane, 1981).
Most often head injuries show no visible physical“scars.” However, significant changes in behavior andemotion follow head injuries, often most noticeable bypeople close to the victim. As recently as the mid-1980s,hospitals typically discharged survivors of head injuries,after recovering medically, without consideration ofwhether they had recovered cognitively or emotionally.Neuropsychologists now know that even mild head in-juries may entail a variety of learning and mood disorders.Head injuries also place a financial burden on society. Onaverage, each brain injury costs more than $100,000 inacute medical care and rehabilitation. Neuropsychologistsplay an important role in assessing survivors and in pro-viding rehabilitation. Because of the complexities of brainfunctions and the sequelae of TBI, the neuropsychologystudent must understand the pathophysiologic aspects ofhead trauma, as well as their neuropsychological correlates.
Mechanism of Impact: NeuronalShearing, Stretching, and Tearing
Bumps to the head are something everyone has en-dured. But when does a “bump” become a TBI? The patho-mechanism of head injuries relates to the physical forcesplaced on the neuron, specifically the axon and cell body(Figure 13.1). Neurologists have described these forces asshear and straining effects at the neuron level. The axonin particular can take only a certain amount of physical
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 371
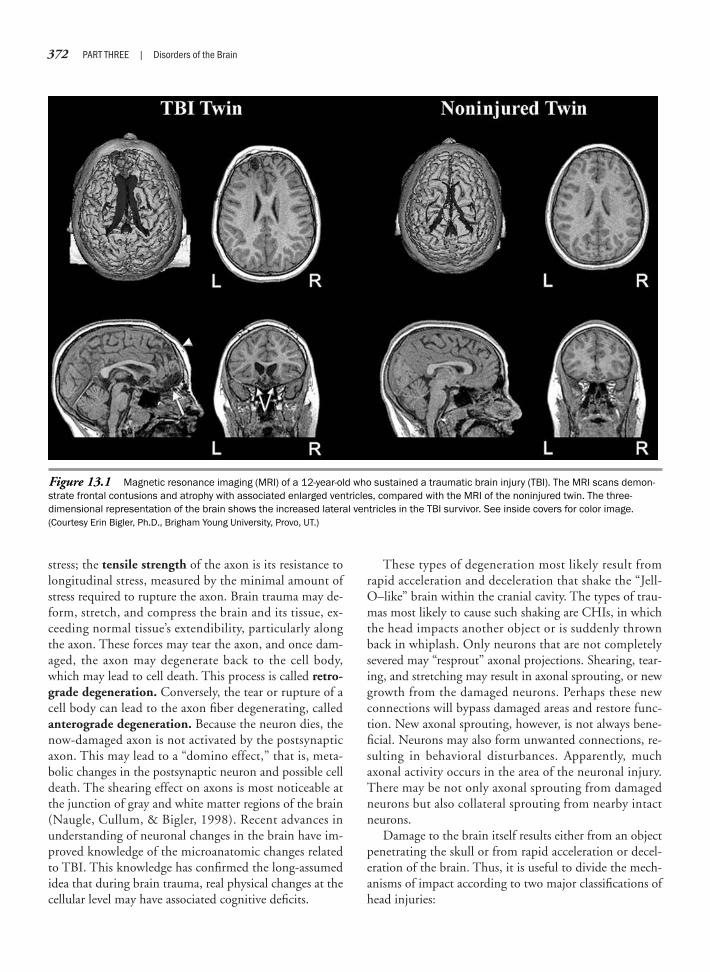
372 PART THREE | Disorders of the Brain
stress; the tensile strength of the axon is its resistance tolongitudinal stress, measured by the minimal amount ofstress required to rupture the axon. Brain trauma may de-form, stretch, and compress the brain and its tissue, ex-ceeding normal tissue’s extendibility, particularly alongthe axon. These forces may tear the axon, and once dam-aged, the axon may degenerate back to the cell body,which may lead to cell death. This process is called retro-grade degeneration. Conversely, the tear or rupture of acell body can lead to the axon fiber degenerating, calledanterograde degeneration. Because the neuron dies, thenow-damaged axon is not activated by the postsynapticaxon. This may lead to a “domino effect,” that is, meta-bolic changes in the postsynaptic neuron and possible celldeath. The shearing effect on axons is most noticeable atthe junction of gray and white matter regions of the brain(Naugle, Cullum, & Bigler, 1998). Recent advances inunderstanding of neuronal changes in the brain have im-proved knowledge of the microanatomic changes relatedto TBI. This knowledge has confirmed the long-assumedidea that during brain trauma, real physical changes at thecellular level may have associated cognitive deficits.
These types of degeneration most likely result fromrapid acceleration and deceleration that shake the “Jell-O–like” brain within the cranial cavity. The types of trau-mas most likely to cause such shaking are CHIs, in whichthe head impacts another object or is suddenly thrownback in whiplash. Only neurons that are not completelysevered may “resprout” axonal projections. Shearing, tear-ing, and stretching may result in axonal sprouting, or newgrowth from the damaged neurons. Perhaps these newconnections will bypass damaged areas and restore func-tion. New axonal sprouting, however, is not always bene-ficial. Neurons may also form unwanted connections, re-sulting in behavioral disturbances. Apparently, muchaxonal activity occurs in the area of the neuronal injury.There may be not only axonal sprouting from damagedneurons but also collateral sprouting from nearby intactneurons.
Damage to the brain itself results either from an objectpenetrating the skull or from rapid acceleration or decel-eration of the brain. Thus, it is useful to divide the mech-anisms of impact according to two major classifications ofhead injuries:
Figure 13.1 Magnetic resonance imaging (MRI) of a 12-year-old who sustained a traumatic brain injury (TBI). The MRI scans demon-strate frontal contusions and atrophy with associated enlarged ventricles, compared with the MRI of the noninjured twin. The three-dimensional representation of the brain shows the increased lateral ventricles in the TBI survivor. See inside covers for color image.(Courtesy Erin Bigler, Ph.D., Brigham Young University, Provo, UT.)

CHAPTER 13 | Traumatic Head Injury and Rehabilitation 373
1. Head injuries associated with a penetrating mecha-nism, called penetrating head injury
2. Closed head injuries (CHIs), associated with a blowto the head, but not penetrating the skull
P E N E T R A T I N G H E A D I N J U R Y
A penetrating head injury occurs when a small object haslodged in the brain, such as a knife, scissors, or a bulletfrom a gun. Penetrating head injuries are extremely dan-gerous to the cortical integrity of the brain because of twofactors. The first factor is the location and extent of thedamage. For example, a gunshot wound to the brainstemis almost always fatal. Conversely, damage to a cortical as-sociation area may entail “less” damage. The second fac-tor is the complications typically associated with pene-trating head injuries, which include infection andhemorrhaging.
Although most gunshot wounds to the head result infatal brain damage, survivors almost always receive a neu-ropsychological evaluation to outline the deficits andresidual strengths associated with the injury. We haveconsulted on many cases in which patients with seem-ingly fatal penetrating head injuries have survived, al-though with neuropsychological deficits (Neuropsychologyin Action 13.1).
Penetrating head injuries can greatly damage the brain,which is often incompatible with sustaining life. A large-caliber gunshot wound to the brain usually causes death,because there is significant tearing of blood vessels anddestruction of brain tissue along the bullet’s path throughthe brain. Small-caliber gunshot wounds can also be fatal,because they can “bounce” within the skull, fatally dam-aging a strategic area of the brain.
Self-inflicted gunshot wounds to the head are the pri-mary way men commit suicide, followed by jumping offhigh buildings and hanging. There are more than 25,000suicides in the United States every year, with a majoritybeing from gunshot wounds.
People who survive penetrating head injuries are oftendisabled for life. A well-documented case is James Brady,who was President Ronald Reagan’s press attaché. Duringan assassination attempt by John Hinckley, Jr., Brady wasstruck by bullets to his right frontal lobe. Hinckley used“killer bullets,” which, on impact, explode into hundredsof fragments. Surgeons completely removed Brady’s rightfrontal lobe, which was seriously damaged. Hinckley, aparanoid schizophrenic, later used the insanity defense toavoid prison; he is currently hospitalized in St. Elizabeth’sHospital in Washington, DC. Brady was left hemiplegic onthe left side of his body and has many other, more subtle,
neuropsychological symptoms. He and his wife have beenthe primary political forces behind the Brady Bill, whichseeks to control handgun purchases by former mental pa-tients and people with a criminal record. Countries thatmonitor gun purchases have shown dramatic success inreducing gun-related deaths and injuries. For example, inNorway, a small, northern European country of approxi-mately 5 million people, less than 10 deaths a year are at-tributed to gunshot wounds to the head. The latest statis-tics from the U.S. Department of Justice report that of allhomicides perpetrated in the United States in 1998, 52%or 14,000 were committed with handguns.
C L O S E D H E A D I N J U R Y
Closed head traumas have many different causes, butcommon to all is that the brain undergoes either markedacceleration or deceleration, or both. In acceleration, thebrain experiences a significant physical force that propelsit quickly from stationary to moving. Examples are thebrain being hit by a moving object such as a baseball bator a car, or a passenger in a rocket accelerating very fast.In deceleration, the brain is already in motion, travelingat a certain speed, and then stops abruptly, sometimes in-stantaneously. Examples include most MVAs and the ski-ing accident described earlier. The kinetic potential—thatis, the physical forces acting on the brain—can be ex-pressed mathematically for both types of injuries.
Let us first start with acceleration injuries. You canmeasure acceleration by noting the time elapsed from thestart of acceleration and multiplying it by the accelerationof gravity, or g � 9.8 m/sec2, and time, according to thefollowing formula: velocity (v) � the product of accelera-tion (g) and time (t) or v � gt. For example, think of your-self jumping off a 3-meter-high diving board. There aretwo ways you could get hurt. The first is related to acceler-ation from the forces (in this case, from gravity) that yourbrain is experiencing during the period of free fall. Inmathematical terms, you can calculate this using the pre-ceding formula. Thus, maximum impact velocity (v) for a3-meter board would be 12.94 m/sec, corresponding toapproximately 29 mph maximum impact speed (depend-ing how high you jump off the board; see Zillmer, 2003c).
The second type of injury you could receive is relatedto how fast your kinetic energy that you have acquired(29 miles/hour), as a result of the free-fall deceleration, isabsorbed by your body and brain. For example, you mayhave performed a jump in which you landed flat on yourstomach. In this case, you decelerate much more quicklythan you would if you entered the water feetfirst. You cancalculate deceleration (a) by dividing velocity over time

374 PART THREE | Disorders of the Brain
This case concerns a patient I treated in atrauma intensive care unit (ICU). The clientwas a 25-year-old, right-handed, unem-ployed, single mother with a 12th-gradeeducation. She was suffering from severedepression when she shot herself in theforehead with a small .32-caliber pistol. Shewas right-handed and held the pistol to herright temple, an inch above her right eye.With her two young children in the home, shethen pulled the trigger. The bullet pierced herright frontal skull, sending fragments of boneinto her right frontal and parietal lobe. Thebullet itself, sterilized by the heat from theacceleration from the gun barrel, came torest in the left frontal lobe (Figure 13.2).Damage to her brain was confined to herfrontal lobes. She did not injure subcorticalstructures and motor areas of the frontallobes, and no vital arteries or veins weresevered. In a way, she lobotomized herself,and surprisingly, she was actually consciousand responsive when she arrived in theemergency department!
She underwent a right frontal craniotomyfor debridement of the gunshot because thebone and skin fragments presented a risk forinfection. Surgeons inserted a metal plate inher right skull to repair the damage where thebullet had entered. The bullet itself was toodeeply lodged in the brain to be removed. Theneurosurgeon decided not to extract thebullet, because doing so would have requiredcutting through intact brain tissue to reachthe bullet. The bullet remained in her brain.
I conducted a neuropsychological evalu-ation while the client was still in the traumaICU, 3 days after trauma. It was not possibleto administer a complete neuropsychologicalexamination of the patient because of herlevel of fatigue and poor endurance. Theresults from the screening showed that shewas alert and oriented to person, place, andtime. She was aware that her speed ofprocessing was extremely slow and keptasking, “Why am I taking so long to respondto these questions?” Attention was mildly
impaired. She could repeat up to 5 digitsforward and could do automatism, such ascounting from 1 to 20 and reciting thealphabet. On tasks requiring more sustainedattention/concentration, however, sheshowed moderate problems, because shecould repeat only up to two digits backwardand made errors adding serial threes.
Her motor functions showed decreasedmotor speed and motor-sequencing prob-lems on the nondominant left hand. Visu-ospatial functions showed mild problems inspatial orientation and a left visual neglectsyndrome. Copying of designs showed aneglect of the left visual space. For example,her drawing of a clock was missing thenumbers from 6 to 10 on the left side.Receptive speech was adequate: She couldfollow two-step commands, but her process-ing speed was very slow. Expressive speechshowed markedly decreased fluency. Imme-diate visual and verbal memory were ade-quate. On delayed recall, however, sheshowed mild-to-moderate short-term mem-ory problems. Her overall abstract reasoningand planning were significantly impaired.
I include this evaluation hereto demonstrate the neuropsy-chologist’s role in a critical caresetting, as well as to documentthe neuropsychological func-tioning of a gunshot victim. Inmaking this neuropsychologicalevaluation, I established somecognitive impairment andidentified this client as a poten-tial rehabilitation patient. Therelatively mild degree of impair-ment, given the nature of thetrauma, suggests that theintegration centers of the brainwere spared from damage. Itcould have been a lot worseneuropsychologically and med-ically, although the patient contin-ued to struggle with depression.
Another account of penetrating gunshotwound from our clinical experience concernsa depressed man who tried to kill himself byusing a shotgun. He placed the shotgununderneath his chin, pointing the gunstraight up, and pulled the trigger. The blastremoved his chin, nose, mouth, and most ofthe prefrontal cortex. The suicide attemptalso left him blind. But vital areas of thebrain, including the brainstem, hypothala-mus, and subcortical structures, remainedintact, and the patient survived. Interest-ingly, the patient had inadvertently givenhimself a prefrontal lobotomy. His depres-sion was not present anymore, but he hadmany cognitive deficits and a bad temper.
In another, final example, during a prisonfight, one inmate plunged a pair of scissorsinto another inmate’s brain, straight down theparietal cortex. The scissors missed thesuperior sagittal sinus and must have beenshort enough to avoid penetrating subcorticalareas. The prisoner walked into the emer-gency department with the scissors stillimplanted in the skull—only the handlesshowed!
N e u r o p s y c h o l o g y i n A c t i o n 1 3 . 1
C a s e S t u d y : P e n e t r a t i n g H e a d I n j u r y
by Eric A. Zillmer
Figure 13.2 Computed transaxial tomography (CT)scan of .32-caliber bullet gunshot wound. CT scan showsthat the gunshot was to the right frontal area with bonefragments in the right frontal lobe. (Courtesy Eric Zillmer.)

(a � v/t). You have already calculated the velocity, so allyou need to establish is the time it takes to decelerate. Ifthat time period is instantaneous—if you were to hit theasphalt rather than the water—the deceleration would behigh and injury likely. If, however, it takes the diver 1 or2 seconds to decelerate, then the forces are much less. Thetime of deceleration is an important variable in the decel-eration equation. If very short, it corresponds to higherdeceleration. This is why downhill skiing or race carcrashes that take a “considerable” amount of time, al-though horrific to the observer, are actually safer, becausethe brain is decelerating more slowly.
Using the preceding formula, a springboard diver expe-riences approximately a corresponding deceleration of16.28 m/sec2 or approximately 2 g when jumping off a 3-meter board. If you were to hit asphalt from the sameheight, the approximate deceleration expressed in mathe-matical terms would be more than 50 g! In their cars, racecar drivers at the Indy 500 carry G-meters, which can cor-roborate the amount of gravity forces the driver experi-ences during a crash. In one crash during practice, a driverhit the retaining wall almost head-on. The G-meter indi-cated a force of 87 g, incompatible with sustaining life. Be-cause car racing is dangerous and drivers are at risk forCHIs, Indy race car drivers undergo preseason neuropsy-chological testing to establish a baseline in cognitive abili-ties if injuries occur during the season. This is also the casefor the National Hockey League (NHL), which has startedbaseline neuropsychological testing for all its players toevaluate the effects of mild CHIs (also called concussions),which have cut short some of the players’ careers.
In CHIs, the physical forces acting on the brain tissuemay occur at the point of impact (an impact injury) orits opposite pole, because the brain “tears” away from theskull (countercoup injury). Diffuse injury is also com-mon and most likely to occur at the frontal lobes and tem-poral poles, because of the uneven, “sandpaper-like” sur-face of the tentorial plates that hold those brain structuresin place. The physical forces may shear, tear, and rupturenerves, blood vessels, and the covering of the brain. In se-vere head injury, those forces are so strong that they re-duce the brain to a bloody, swollen pulp. As a result, theremay be severe complications associated with neuronal dis-ruption, ischemia, hemorrhaging, and edema.
A S S E S S I N G T H E S E V E R I T Y O F B R A I N I N J U R Y
The severity of a traumatic head injury has been most oftenassociated with corresponding scores on the GlasgowComa Scale (GCS) (Teasdale & Jennett, 1974). This mea-
sure gives the head injury trauma team a rapid, reliablemeasure of coma depth by assessing separate symptoms, in-cluding language, consciousness, and motor domains. Neu-ropsychologists generally accept the GCS as the standardmeasure for determining severity of injury in patients withcompromised consciousness, from the mildest confusionalstate (scores �13) to deep coma (scores �5; Table 13.1).Medically, coma is defined as a score of 8 or less, which cor-responds to a severe head injury. Thus, the standard defini-tion of coma is that a patient cannot open his or her eyes,make any recognizable sounds, and follow any commands(Levin, Benton, & Grossman, 1982). Depth of coma, to-gether with post-traumatic amnesia (PTA; described laterin this chapter), is a reliable measure of the overall level ofbrain damage and prognosis. The GCS has proved a goodoutcome measure after coma, with scores greater than 8 in-dicating a good recovery. Greater mortality is typically as-sociated with scores less than 7.
Coma is not the same as “being asleep.” In fact, elec-troencephalographic (EEG) monitoring shows that a co-matose patient has sleep–awake cycles even while in coma.Coma is directly associated with an injury to those areasof the brain, typically the lower brainstem and reticularactivating system (RAS), that are involved in brainarousal. Although it is not clear what precisely causescoma, researchers believe it is related to RAS damage. Inanimal experiments, researchers found that a linear accel-eration blow did not result in coma, but when the headwas free to move in a rotational plane, as in injuries fromMVAs, coma did appear. Coma is also not a binary phe-nomenon: It is incorrect to conceptualize the patient aseither in a coma or not. Rather, coma falls along a contin-uum. That is, patients can be in a deep coma or in a light,shallow coma, or somewhere in between. Alternatively,head injury survivors may not be in a coma at all, but maybe confused and disoriented. When patients recover fromcoma, they do not “suddenly awake” from it. Rather, theyslowly progress from deeper stages to more shallow stagesof coma. In this respect, the GCS has been a useful toolfor monitoring recovery of comatose patients. Limitationsof the GCS are twofold: First, incorrect assessment is pos-sible because of confounding factors including eyeswelling that prohibits assessment of eye opening and thepresence of an endotracheal tube and the use of drugs(such as barbiturates or anticonvulsants), both of whichcan prevent verbal response. The second limitation relatesto that a small lesion to the brainstem can cause coma, al-though most of the brain is not injured. In such a case,the coma, although serious and potentially life threaten-ing, is not a good indicator of overall brain damage, be-cause the cortex, for example, may be entirely intact.
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 375
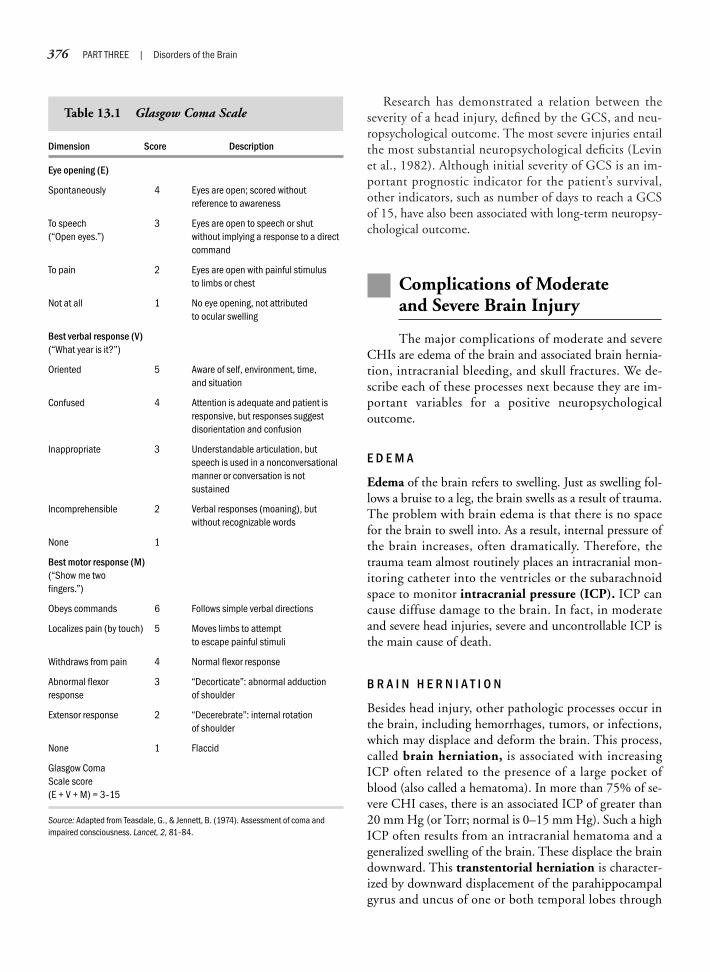
376 PART THREE | Disorders of the Brain
Research has demonstrated a relation between theseverity of a head injury, defined by the GCS, and neu-ropsychological outcome. The most severe injuries entailthe most substantial neuropsychological deficits (Levinet al., 1982). Although initial severity of GCS is an im-portant prognostic indicator for the patient’s survival,other indicators, such as number of days to reach a GCSof 15, have also been associated with long-term neuropsy-chological outcome.
Complications of Moderate and Severe Brain Injury
The major complications of moderate and severeCHIs are edema of the brain and associated brain hernia-tion, intracranial bleeding, and skull fractures. We de-scribe each of these processes next because they are im-portant variables for a positive neuropsychologicaloutcome.
E D E M A
Edema of the brain refers to swelling. Just as swelling fol-lows a bruise to a leg, the brain swells as a result of trauma.The problem with brain edema is that there is no spacefor the brain to swell into. As a result, internal pressure ofthe brain increases, often dramatically. Therefore, thetrauma team almost routinely places an intracranial mon-itoring catheter into the ventricles or the subarachnoidspace to monitor intracranial pressure (ICP). ICP cancause diffuse damage to the brain. In fact, in moderateand severe head injuries, severe and uncontrollable ICP isthe main cause of death.
B R A I N H E R N I A T I O N
Besides head injury, other pathologic processes occur inthe brain, including hemorrhages, tumors, or infections,which may displace and deform the brain. This process,called brain herniation, is associated with increasingICP often related to the presence of a large pocket ofblood (also called a hematoma). In more than 75% of se-vere CHI cases, there is an associated ICP of greater than20 mm Hg (or Torr; normal is 0–15 mm Hg). Such a highICP often results from an intracranial hematoma and ageneralized swelling of the brain. These displace the braindownward. This transtentorial herniation is character-ized by downward displacement of the parahippocampalgyrus and uncus of one or both temporal lobes through
Dimension Score Description
Eye opening (E)
Spontaneously 4 Eyes are open; scored without reference to awareness
To speech 3 Eyes are open to speech or shut (“Open eyes.”) without implying a response to a direct
command
To pain 2 Eyes are open with painful stimulus to limbs or chest
Not at all 1 No eye opening, not attributed to ocular swelling
Best verbal response (V)(“What year is it?”)
Oriented 5 Aware of self, environment, time, and situation
Confused 4 Attention is adequate and patient is responsive, but responses suggest disorientation and confusion
Inappropriate 3 Understandable articulation, but speech is used in a nonconversational manner or conversation is not sustained
Incomprehensible 2 Verbal responses (moaning), but without recognizable words
None 1
Best motor response (M)(“Show me two fingers.”)
Obeys commands 6 Follows simple verbal directions
Localizes pain (by touch) 5 Moves limbs to attempt to escape painful stimuli
Withdraws from pain 4 Normal flexor response
Abnormal flexor 3 “Decorticate”: abnormal adduction response of shoulder
Extensor response 2 “Decerebrate”: internal rotation of shoulder
None 1 Flaccid
Glasgow Coma Scale score (E + V + M) = 3–15
Source: Adapted from Teasdale, G., & Jennett, B. (1974). Assessment of coma andimpaired consciousness. Lancet, 2, 81–84.
Table 13.1 Glasgow Coma Scale

the tentorial hiatus. There is only one large opening inthe skull, the foramen magnum, which is the normalanatomic site of the lower brainstem. Brain herniationcan place extreme pressure on the lower brainstem, typi-cally cutting off the cranial nerve III (the oculomotornerve) and compromising the integrity of the brainstem.The cranial nerve symptom causes initial constriction, fol-lowed by dilation of the pupil on the herniation side. Fur-thermore, the patient may lose motor functions on thesame side as the herniation. Compression of the posteriorcerebral artery may obstruct blood circulation and even-tually cause necrosis. In the herniation syndrome, con-sciousness deteriorates to a state of deep coma withinminutes to hours. If left untreated, the patient goes into acoma and dies of respiratory failure because the brain cen-ters, among them the medulla oblongata, have been dam-aged and life-sustaining functions cease to operate.
Because edema thus progresses to brain herniation,controlling ICP is the main medical issue in acute CHI.Medical trauma personnel carefully monitor ICP, and if itis elevated, they treat it, often aggressively. Reducing thepatient’s blood pressure medically or by hyperventilationis often enough to stabilize ICP. In extreme cases, thetrauma staff artificially places the patient in a coma. Ofcourse, he or she is already in a coma related to the braininjury, but a pharmacologically induced coma addition-ally reduces brain metabolism, and hence swelling. A lastresort in controlling ICP is evacuation (surgical removal)of a lobe, such as the right frontal lobe, to make room forthe brain to swell into. This happened to one of our pa-tients, Frank, a 22-year-old college student. One night hejoined a friend to travel by car to a questionable locationof the city to buy marijuana. The drug dealers mistookFrank for someone else who, the night before, either didnot pay for drugs or started an altercation. His attackerswere never caught. They pulled Frank from the car, beathim up with a baseball bat, and left him for dead. Mirac-ulously, he survived, but with a severe CHI and in a coma.His ICP was so severe that he would have not lived hadnot the neurosurgeons removed his right frontal lobe, al-though there was no specific injury to that lobe. Theysimply removed it because Frank’s brain needed the addi-tional space to expand. Frank has now been through 10years of rehabilitation. He has severe cognitive deficits andneeds supervision 24 hours a day. His life has changeddramatically. He has had to learn all over again how towalk and talk. The rehabilitation hospital where Franknow lives has built a special room for him with softpadded walls, because of his uncontrollable temper. Tohis parents he is a completely different person from whohe was before the assault. His parents deal with the situa-
tion as if their son had died that night and as if the newFrank were their new son.
E X T R A D U R A L A N D S U B D U R A LH E M O R R H A G E
As a result of a head injury, cerebral blood vessels may te-ar, producing pools of blood within and between themeninges. Subdural and extradural bleeding frequentlycomplicate head injuries and are medically significant. Asubdural hematoma, in particular, may be associatedwith trivial bleeding only to cause problems weeks afterthe injury (Figure 13.3). Acute subdural or intracerebralbleeds most often appear in severe head injury. Togetherwith brain edema, they are present in most fatal cases. Theclassic symptom in the subdural is an initial period of un-consciousness, but because the dura adheres tightly to theskull, the bleeding delays and a prolonged interval occursduring which the patient is conscious and functioningmore or less normally. Once the bleed enlarges, it pushesthe brain laterally and downward, causing brain hernia-tion. As the hematoma enlarges, level of consciousnessdeteriorates quickly. This sequence of events is very dan-gerous, because the patient appears to have recoveredfrom the trauma to the head, only to deteriorate oncemore quickly—and often fatally.
The frequent subdural hematoma corresponds to ableed between the dura and the arachnoid space. A sub-dural hematoma is most likely caused by an acute venoushemorrhage related to rupture of a cortical vein, such asthe superior sagittal sinus. Subdural bleeding typically oc-curs over the outward surfaces of the frontal and parietallobes. Subdural hematomas are medical emergencies andtypically develop within 1 week after the injury (if thebleed is slow) to as quickly as within 1 hour. Skull frac-tures (of which MVAs are the most frequent cause) causemore than half of all subdurals. Alcohol is a major cata-lyst, because of its anticoagulant properties in blood. Leftuntreated, the brain pressure increases to such a degreethat the brain herniates, ultimately resulting in death.Symptoms of subdural hematoma include contralateralhemiparesis, ipsilateral pupil dilation, and changes in levelof consciousness. Radiologists can easily make the diagno-sis using computed transaxial tomographic (CT) imaging.
The less frequent extradural hematoma is a bleedthat occurs between the skull and the dura. Bleeding ofthe large middle meningeal artery most often causes anextradural hematoma. An epidural hematoma repre-sents a bleed between the meninges and the skull and isless common only occurring in 1% to 3% of majorCHIs. The cause of an epidural is most often related to
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 377
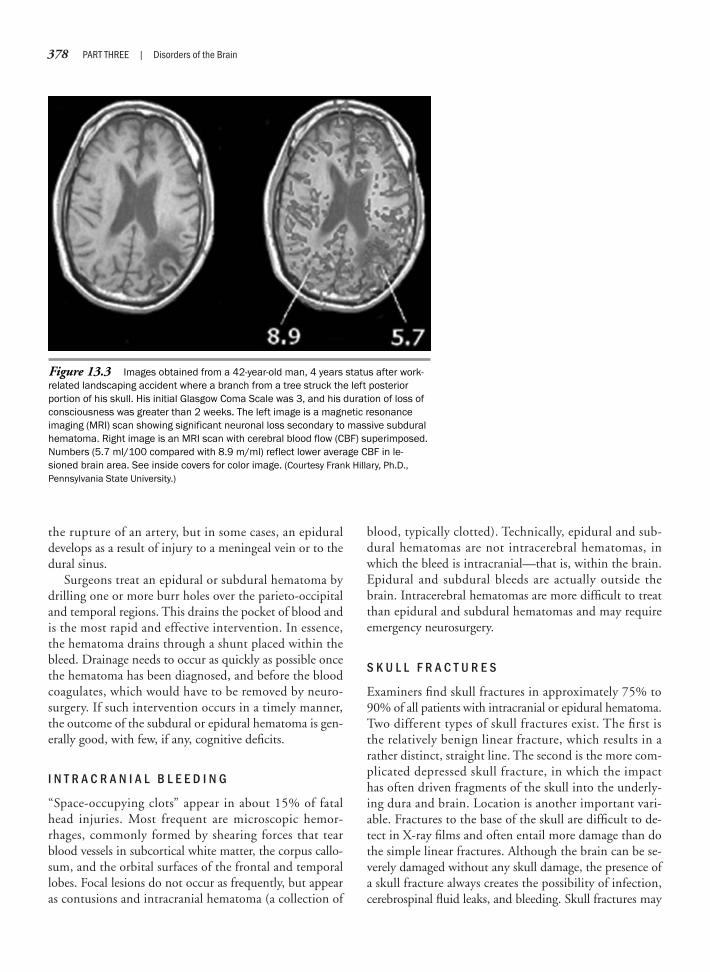
378 PART THREE | Disorders of the Brain
the rupture of an artery, but in some cases, an epiduraldevelops as a result of injury to a meningeal vein or to thedural sinus.
Surgeons treat an epidural or subdural hematoma bydrilling one or more burr holes over the parieto-occipitaland temporal regions. This drains the pocket of blood andis the most rapid and effective intervention. In essence,the hematoma drains through a shunt placed within thebleed. Drainage needs to occur as quickly as possible oncethe hematoma has been diagnosed, and before the bloodcoagulates, which would have to be removed by neuro-surgery. If such intervention occurs in a timely manner,the outcome of the subdural or epidural hematoma is gen-erally good, with few, if any, cognitive deficits.
I N T R A C R A N I A L B L E E D I N G
“Space-occupying clots” appear in about 15% of fatalhead injuries. Most frequent are microscopic hemor-rhages, commonly formed by shearing forces that tearblood vessels in subcortical white matter, the corpus callo-sum, and the orbital surfaces of the frontal and temporallobes. Focal lesions do not occur as frequently, but appearas contusions and intracranial hematoma (a collection of
blood, typically clotted). Technically, epidural and sub-dural hematomas are not intracerebral hematomas, inwhich the bleed is intracranial—that is, within the brain.Epidural and subdural bleeds are actually outside thebrain. Intracerebral hematomas are more difficult to treatthan epidural and subdural hematomas and may requireemergency neurosurgery.
S K U L L F R A C T U R E S
Examiners find skull fractures in approximately 75% to90% of all patients with intracranial or epidural hematoma.Two different types of skull fractures exist. The first isthe relatively benign linear fracture, which results in arather distinct, straight line. The second is the more com-plicated depressed skull fracture, in which the impacthas often driven fragments of the skull into the underly-ing dura and brain. Location is another important vari-able. Fractures to the base of the skull are difficult to de-tect in X-ray films and often entail more damage than dothe simple linear fractures. Although the brain can be se-verely damaged without any skull damage, the presence ofa skull fracture always creates the possibility of infection,cerebrospinal fluid leaks, and bleeding. Skull fractures may
Figure 13.3 Images obtained from a 42-year-old man, 4 years status after work-related landscaping accident where a branch from a tree struck the left posteriorportion of his skull. His initial Glasgow Coma Scale was 3, and his duration of loss ofconsciousness was greater than 2 weeks. The left image is a magnetic resonanceimaging (MRI) scan showing significant neuronal loss secondary to massive subduralhematoma. Right image is an MRI scan with cerebral blood flow (CBF) superimposed.Numbers (5.7 ml/100 compared with 8.9 m/ml) reflect lower average CBF in le-sioned brain area. See inside covers for color image. (Courtesy Frank Hillary, Ph.D.,Pennsylvania State University.)

also rupture meningeal arteries or large venous sinuses,resulting in epidural and subdural hematomas.
The relation between skull fractures and neuropsycho-logical functioning has been debated. Clearly, for the skullto fracture a significant force must have acted on the cra-nial plates. This force may have transferred to the brain,making actual brain damage more likely. The physics ofskull fractures are complicated. In a skull fracture, theskull itself may have absorbed much, if not most, of thekinetic energy, thereby protecting the brain from damage.This is analogous to falling off a bicycle while wearing ahelmet. The helmet absorbs much of the physical force,which transferred to the physical structure of the helmet(often destroying it), thereby protecting the head and thebrain. For these reasons, skull fractures may not be di-rectly related to specific levels of neuropsychological dys-function. However, brain damage is more likely in skullfractures because the initial forces that fractured the skullmust have been high, increasing the likelihood of braindamage.
P O S T - T R A U M A T I C E P I L E P S Y
Seizures are a major complication after head injury. Post-traumatic epilepsy follows about 10% of severe closedhead wounds and 40% of penetrating head injuries. Thecauses of the seizures relate to the presence of scar tissue,specifically alterations in neuronal membrane functionand its structure. Neurologists consider seizures stemmingfrom a head injury secondary, because they result from aknown pathologic lesion. It is difficult to predict whichhead injury survivor may experience development ofseizures, because onset can be delayed as much as 2 yearsafter the trauma. Risk factors that increase the likelihoodof for development of post-traumatic seizures includepenetrating type head injury, severity of brain damage,prolonged periods of coma, PTA (described later in thischapter), inflammation associated with the wound, andresidual neurologic symptoms. Seizures are such a fre-quent complication of head injury that patients receiveanticonvulsant medication prophylactically (routinely) tocontrol even the possibility of seizures.
Mild Head Injury: “Concussions”
The concept of a mild head injury is relatively re-cent. In the early 1980s, one of our mentors, Jeffrey T.Barth from the University of Virginia Medical School,was curious about what happens to patients who report
to the emergency department for a head injury complain-ing of a concussion. These patients typically have had noor a short loss of consciousness, followed by prompt re-covery without any localizing neurologic signs. They ex-hibit few immediate cognitive or physical complaints be-yond a headache, feeling dizzy, and vague memoryproblems. Together with a team of neurosurgeons andneurologists, Barth examined hundreds of patients whowere turned away from the emergency department, usu-ally with no referral follow-up, because their injury wasnot thought to be severe enough to hospitalize the pa-tient. The assumption was that there were no long-termproblems. In the early 1980s, concussions were not con-sidered a medical emergency.
Perhaps this indifference relates to how society dealswith mild head trauma. For example, in athletics, con-cussions are often tolerated with some bravado: “I washit in the head and didn’t know the score of the footballgame.” In fact, television football announcers recounthow “amusing” it was to have someone knocked out,only to return to the opponent’s sideline rather than hisown. They recall with great humor how a teammate,after being knocked out, proceeded to run with the foot-ball in the wrong direction. Similarly, the symptoms of“seeing stars” has not been thought of as a neurologicsymptom in this society, although it clearly is, but as arelatively benign, perhaps comic, event. In fact, manycomic strips use “stars” to characterize transient confu-sion (Figure 13.4).
Until recently, researchers have not studied and un-derstood the medical, neurologic, and psychologicalmanifestations of mild head injuries. Since the early1990s, an appreciation for milder forms of injuries to thehead has appeared in the scientific literature. Mild head in-juries often entail dizziness, fatigue, or headaches, with noloss or only brief loss of consciousness (Levin, Eisenberg,& Benton, 1989). The traditional literature often callsthis type of head injury a “concussion.” However, neu-ropsychologists now treat mild head injury as a signifi-cant medical event that has real, even long-term, conse-quences (Neuropsychology in Action 13.2). This findingis related not only to clinical evidence, in which patientshave described physical and cognitive symptoms, but alsoto experimental evidence. Research studies have demon-strated that earlier studies using only the light micro-scope were incorrect in finding no reliable associationbetween mild head injury and pathologic lesions in thebrain. Recent animal research, using histologic stainingtechniques, shows that neurons exposed to forces consis-tent with a mild head injury are damaged and die (Barthet al., 1983).
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 379

380 PART THREE | Disorders of the Brain
Three important findings have emerged from thisbody of research that are important to mild head injuries:
1. Mild head injuries usually go medically unnoticed.The medical community does not widely recognize theoften debilitating sequelae of such injuries.
2. During mild head injury, the physical energy trans-ferred to the brain is related to linear and rotationalmechanical forces associated with the sudden accelera-tion, deceleration, or both. These forces can result inshearing or stretching, and even in necrosis (cell death)
of neurons, which are the central building blocks of thecentral nervous system (for example, see Levin et al.,1982).
3. Head injuries, including the mild variety, are cumula-tive in effect. For example, Gronwall and Wrightson(1975) conducted one of the first investigations to es-tablish that after a second concussion the capacity ofadults to process information declined significantly.Thus, repeated blows to the head, such as those occur-ring in boxing and football, are especially dangerousto the athlete’s health.
After attending a research meeting in Vail,Colorado, on traumatic brain injuries, mycolleague, a 42-year-old neurosurgeon,decided to hit the ski slopes. While descend-ing a modest incline, he lost his balance andfell, striking his head. He was immediatelyknocked unconscious for a period of only 10to 15 seconds. On awakening, he experi-enced confusion that cleared within minutes,with the exception of a modest vertigo thatpersisted but did not interfere with his abilityto ski down the mountain. Because mymentor and friend, who is a renowned spe-cialist in brain trauma, continued to ski thatday, I thought this concussion had had noeffect on him. However, on returning home,he did report that he was a bit more dis-tractible and that his memory was flawed, forexample, when remembering the location ofhis Dictaphone, briefcase, and keys. He alsonoticed that when talking with colleaguesand residents, he could no longer quicklyrecall references to articles. His speed ofinformation processing was not affected, norwas his skill and judgment as a neurosur-geon; however, he did fatigue more quicklythan before.
What exactly is a concussion? The termconcussion refers to an injury to the brain,resulting either from a collision between thehead and an object or from a rapid, forcefulacceleration and deceleration. Neuropsy-
chologists typically diagnose a brain injurywhen the consequences include one or moreof the following: (1) an alteration or loss ofconsciousness, (2) a loss of memory for theevents immediately before and after theinjury, and (3) neurologic symptoms. Thedegree of injury can vary significantly, from amild concussion to death. The terms concus-sion and mild traumatic brain injury (TBI)frequently are used as synonyms, although Ifocus here on mild TBI. What features sepa-rate a mild from a moderate brain injury?Medical professionals generally accept thata “mild” rating should not involve a loss ofconsciousness that exceeds 30 minutes; inaddition, memory loss for events after thetrauma should not exceed 24 hours, and theneurologic symptoms should not lead to adeterioration of the patient’s Glasgow ComaScale (GCS) score to less than 13.
How many of us have sustained a mildTBI? Neurologists classify approximately twothirds of all brain injuries as mild. In theUnited States alone, researchers estimatethat approximately 1,300,000 peoplesustain a mild TBI each year. Approximatelyhalf are the result of motor vehicle accidents,and the rest involve assaults, falls, or sports-related injuries (such as in skiing, boxing,football, horseback riding, and ice hockey).What happens to the brain during mild TBI?Currently, the best data are derived from
studies of concussed animals or from hu-mans who, in addition to having concussions,died of other medical complications such aschest wounds. Particularly because of rota-tional forces, brain cells tear, and this shear-ing of axons most often occurs in subcorticaland frontotemporal regions. Because impactto the brain from the outside can vary sosignificantly, tearing and shearing of cells canalso vary among individuals. However, post-mortem examinations of concussed brainshave provided evidence of microscopicchanges, which can no doubt lead to neuro-physiological and neurochemical alterations.
What typical difficulties do patientsencounter? By evaluating patients in the firstphases after a mild TBI, researchers havedocumented frequent impairments onneuropsychological tests of sustainedattention, memory, and learning, and mea-sures that capture speed of informationprocessing. Most mild TBI survivors enjoy afavorable recovery in the 3 to 6 months afterthe injury. That is, these patients improve upto a level that is not statistically below that ofa control group. One study even found a wayto test patients before and after a mild TBI.Before the playing season, researcherstested college football players who had neversustained a brain injury and did follow-uptesting on those who later sustained a mildTBI. This retesting showed an initial decline
N e u r o p s y c h o l o g y i n A c t i o n 1 3 . 2
C a n a C o n c u s s i o n C h a n g e Yo u r L i f e ?
by Ronald M. Ruff Ph.D., Director of Neurobehavioral Rehabilitation, St. Mary’s Medical Center; Associate Adjunct Professor, Department of
Neurosurgery and Psychiatry, University of California at San Francisco, San Francisco, CA

S P O R T S - R E L A T E D C O N C U S S I O N S : AN E U R O P S Y C H O L O G I C A L P E R S P E C T I V E
Competitive sports participation has increased world-wide. Sports-related concussions represent a significantpotential health concern to those who participate in con-tact sports. In the United States alone, it is estimated thatapproximately 1.3 million individuals sustain a mild TBIeach year, approximately half of which result from MVAs.After MVAs, the causes of head injuries are, in order,
sports injuries, falls, violence, and industrial accidents.Thus, a high number of athletes are at risk for concus-sion, approximately 2% to 10% (Ruchinskas, Francis, &Barth, 1997), representing more than 300,000 sports-related head injuries annually (Moser & Schatz, 2002).
It has been recognized only recently that concussive in-juries present a significant neuropsychological event(Zillmer, 2003b). As a result, increasing emphasis has beenin providing protection to athletes. Those forms of pro-tection include rule changes to minimize concussion-type
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 381
on neuropsychological testing, with a posi-tive recovery in the subsequent weeks.However, a large body of literature hasunequivocally demonstrated that not all mildTBI patients enjoy a favorable recovery. Aminority continue to have not only persistentcognitive problems but also physical prob-lems, which typically include headache,vertigo, dizziness, energy loss, and in somecases, a heightened sensitivity to noise,light, alcohol, or medications. Emotionalreactions commonly include irritability,elevated anxiety, or depressive symptoms.These cognitive and physical problems can,in turn, lead to emotional, psychosocial, andvocational changes. Neuropsychologists usethe term postconcussive disorder for suchcases. In the literature, researchers haveestimated that postconcussive disordersoccur in 10% to 20% of all mild TBI cases(130,000–260,000 cases each year in theUnited States). Over the years, the impor-tance of a careful neuropsychological evalu-ation of patients with mild TBI has becomemore and more recognized.
What is the neuropsychologist’s role inevaluating mild TBI? The objective tools thatphysicians tend to rely on for diagnosingbrain injuries include computed transaxialtomography (CT) and magnetic resonanceimaging (MRI). However, for mild TBI, theseneuroimaging techniques lack sufficientsensitivity to visualize microscopic changes.Thus, CT and MRI scans are, as a rule, “nor-mal” in most mild TBI cases. Although thenewer dynamic neuroimaging techniquessuch as positron emission tomography (PET)and single-photon emission computedtomography (SPECT) scans have demon-strated greater sensitivity in case studies,
more research is required to determinewhether these newer techniques can objec-tify mild TBI conclusively. Because objectivetools cannot yet reliably evaluate the poten-tial brain damage involved in mild TBI,medical teams frequently assign to neu-ropsychologists, using subjective tools, thetask of providing answers. Using psychomet-ric tests, neuropsychologists are uniquelyqualified to delineate the upper thresholds ofcognitive functioning. Based on a patternanalysis across a neurocognitive test batterytogether with a psychodiagnostic evaluation,neuropsychologists can reach a diagnosis todetermine the extent to which brain damagehas contributed to the postconcussivedisorder. The three key challenges for makinga differential diagnosis are: (1) estimatingpreinjury functioning levels, (2) evaluatingcomorbid factors, and (3) exploring interac-tions among the postinjury problems. Esti-mating preinjury functioning is paramount forcapturing not only “deficits” but also anydecline in functioning.
To illustrate, let us return to the earlier-mentioned neurosurgeon who struck his headwhile skiing. Many neuropsychologists use animpairment index that largely represents acommon notion that a deficit is defined by ascore that falls two standard deviationsbelow the mean. However, this notion maylead to false negatives. For example, a 50%decrease in performance in an individualwhose preinjury functioning levels were at the95th percentile will result in a postinjuryperformance at the 45th percentile. Thisneurosurgeon commented, with respect tothe challenges neuropsychologists face:
Perceptions of a disease by one who has nothad the disease as a patient tend to be
modestly inaccurate. Recovery from a headinjury appears to be a long process, onerequiring innumerable strategies for compen-sation. Neurocognitive testing will indicatepart of the story, only if the results are abnor-mal; it leaves something to be desired inpredicting levels of performance for those whoare adequate competitors in a modernsociety. (Marshall & Ruff, 1989, p. 278).
In addition to capturing a relative lossbased on a comparison with the patient’sestimated preinjury functioning levels, it isalso crucial that the neuropsychologistbecome aware of preexisting medical riskfactors (history of alcohol or substanceabuse; prior concussion), as well as cogni-tive risk factors (preexisting learning disabili-ties) and emotional risk factors (such ashysteria, somatization, and secondary gain).Concurrent medical injuries are common inmild TBI cases, including neck, shoulder, andrib fractures, which can result in a painsyndrome. Excessive pain can interfere withsleep, and it always results in emotionalreactions that can, in turn, affect neurocog-nitive functioning. More systematic researchis called for to evaluate mild TBI cases withand without comorbid medical injuries.Finally, the interactions among postinjuryproblems require careful analysis. Postcon-cussive syndromes derail some patientsfrom their vocations as a result of a combina-tion of factors (such as headaches, vertigo,attentional difficulties, and mood changes).All of us who work in this field believe that wemust stress prevention. The mandatoryintroduction of helmets, safety belts, andairbags has reduced TBI rates. Be careful: Aconcussion has the potential to change yourlife!

382 PART THREE | Disorders of the Brain
injuries, as well as equipment changes, including improvedhelmets, mouth guards, and other face and head protectionto reduce the transfer of kinetic energy to the head duringan athletic contest (Figure 13.5). In the area of brain-behavior research, a concomitant focus has been on under-standing the neuropsychological manifestations of sports-related concussions. Neuropsychologists have directed their
attention to defining and grading concussions, as well as tounderstanding the neurometabolic changes associated withconcussions. In the area of clinical neuropsychology, ad-vancements have been made for concussion assessment anddiagnosis, as well as concussion management, rehabilita-tion, and return to play decisions. Accordingly, neuropsy-chologists have become an integral part of the sports medi-cine team involved in the care of athletes with sports-relatedconcussions. Today, neuropsychologists are playing a lead-ing role in the clinical and scientific aspects of sports-re-lated concussions.
T h e T w e n t i e t h C e n t u r y : A R e v o l u t i o n o f S c i e n c e a n d S p o r t s
The history of sports-related concussions is long, but itspast has been short. In the early part of the twentiethcentury, the frequent nature of collisions between foot-ball players called into question the safety of the sportand highlighted an awareness of head injuries in sports.Football helmets were not available until 1896, and be-cause of the physical properties of the helmets them-selves, as well as the nature of play, they were not effec-tive in the protection of athletes (Cantu & Mueller,2003). In fact, the 1905 college season ended with muchprotest over the brutality of football. On October 9,1905, midseason, President Roosevelt met with repre-sentatives from Harvard, Yale, and Princeton to discussmaking football less dangerous, in an effort to ulti-mately save the sport. Football was being publicly de-nounced as brutal and inappropriate for young menafter the Chicago Tribune published an injury report
Figure 13.5 Many sports have the potential for physicalcontact and collision. Sport is clearly a breeding ground for physi-cal injury. (Courtesy Drexel University, Philadelphia, PA, 2003, bypermission.)
Image not available due to copyright restrictions

listing 18 deaths and 159 serious injuries (Stewart,1995). Led by Henry M. MacCracken, the chancellor ofNew York University, the parties responsible for footballrules agreed to change the game. As a result, the Inter-collegiate Athletic Association was established, whichwould later become the National Collegiate Athletic As-sociation (NCAA), the current governing body for in-tercollegiate sports. The rule changes included outlaw-ing the “flying wedge” (Figure 13.6), one of football’smost violent offensive formations, during which a groupof lead offensive tacklers would provide protection forthe ball carrier. Overall, the consequences of head in-juries in football were the primary force underlying thecreation of the NCAA, which was established initially toensure the welfare of the student–athlete.
T h e 1 9 8 0 s V i r g i n i a F o o t b a l lS t u d i e s
Clinical and epidemiologic studies of mild head injury inthe 1980s reported neuropsychological deficits in new andrapid problem solving, attention and concentration, andmemory, which lasted up to 3 months after trauma(Barth, Macciocchi, Boll, Giordani, Jane, & Rimel, 1983;Rimel et al., 1981). At about the same time, Gennarelli(1983) and Ommaya (Ommaya & Gennarelli, 1974)were performing primate studies to evaluate the histologiceffects of mild acceleration/deceleration during headtrauma. They documented visible axonal shearing andstraining in the brainstem in experimentally induced mild
head injury. By the 1980s, there appeared to be a growingconsensus that mild head injury was not as innocuous aspreviously thought. Still, recovery curves lacked defini-tion and individual vulnerability of mild head injurieswere not well understood. Research was needed thatwould control preexisting factors and assess neurocogni-tive functions in a laboratory setting before and after theadministration of a controlled mild head injury to ahuman subject. In this way, the individual would act ashis or her own control.
Within this context, Jeff Barth and his colleague atthe University of Virginia (UVA) designed one of themost creative experiments in neuropsychology. They ap-proached college football players as the practical solu-tion to this research problem. Football players were atrisk to experience an acceleration/deceleration mildhead injury similar to the type of linear of rotationalbrain trauma experienced in MVAs within a natural yetcontrolled environment. The first landmark sports-relatedconcussion study therefore focused on the UVA foot-ball team. These early football studies suggested thatyoung, bright, healthy, and well-motivated student–athletes, who experience mild, uncomplicated headtrauma without loss of consciousness did demonstrateneuropsychological decline in areas of informationproblem solving and attention, but would likely followa rapid recovery curve and have no lasting disability(Barth et al, 1989).
Interestingly, these investigators at UVA also consultedwith professional football teams hoping to extend thesefindings beyond the college arena. But they found littleinterest in allowing scientists to study the potentially neg-ative effects of concussion, which were presumed to occur(Jeffrey Barth, personal communication, January 10,2004). A decade later, however, Mark Lovell and his col-leagues again spearheaded a movement aimed at imple-menting a program designed to educate and protect pro-fessional athletes. The Pittsburgh Sports ConcussionProgram initiated pilot baseline and postconcussiveneuropsychological testing of the Pittsburgh Steelers play-ers in the late 1980s through early 1990s. This programsuccessfully broke down many of the barriers regardingprofessional football players’ acknowledgment and accep-tance of concussive injuries, and in combination with theNFL Players Association’s growing concerns over career-ending injuries related to multiple concussions (for exam-ple, Troy Aikman and Steve Young), has now led to league-wide programs in both the National Football League(NFL; 1993) and NHL (1996) (Mark Lovell, personalcommunication, November 23, 2004; Pellman, Lovell,Viano, et al., 2004).
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 383
Figure 13.6 A bronze statue of the flying football wedge asseen at the NCAA museum in Indianapolis. The flying wedgerevolutionized the game but also led to numerous injuries andeven deaths on the field. (Courtesy NCAA Hall of Champions, Indi-anapolis, IN.)

384 PART THREE | Disorders of the Brain
T w e n t y - F i r s t C e n t u r y a n d t h e R e f i n e m e n t o f S p o r t s N e u r o p s y c h o l o g y
Besides the advances that have been made in the neuro-scientific and neuropsychological community, experts onthe psychology of sports injuries have made significantadvances in how concussion injuries can be treated andconceptualized. Even though an injury is essentially a neg-ative experience, some unexpected benefits have beennoted; for example, the challenge in response to injury toreorder one’s life and lifestyle, to develop creative solu-tions in overcoming physical and mental deficits, and toforge new and meaningful relationships with others(Pargman, 1999). Thus, a renewed focus on the conceptof injury prevention and a multidisciplinary approach tothe rehabilitation of injured athletes has been made,which includes psychological intervention, as well as med-ical, mechanical, and social factors. This newly conceptu-alized multimodal approach appears especially appropri-ate in the context of making return-to-play decisions withconcussed athletes in view of the emergence of neuropsy-chology in sports medicine (Echemendia & Cantu,2003). In addition, neuropsychological profiles of ath-letes may help us understand their specific strengths andweaknesses and how they may cope with sports-relatedconcussions. As scientists and researchers provided in-creasing evidence for an organic basis to the clinical symp-toms of concussion, it became evident that the clinicalpicture reflects a dynamic state of affairs in which physi-cal, personal, social, competitive, and economic factorscontributed in varying degrees (Zillmer 2003b).
Contemporary sports-related concussion research isakin to putting a complex puzzle together: What is the ef-fect of age and sex in concussions? What is the epidemiol-ogy of the sports-related concussion injuries and how theydiffer by sport and sex (Figure 13.7). What neuropsycho-logical tests are best suited to assess concussions? What isthe gold standard for grading concussions? Who is mostsusceptible to sports-related concussion? What return-to-play guidelines are most practical?
We believe neuropsychologists play, and will continueto play, an important role in assembling this complex puz-zle. In the absence of any detectable abnormalities on tra-ditional magnetic resonance imaging (MRI) scans forcases with concussion (Bigler & Snyder, 1995), the objec-tive nature of neuropsychological testing has become a re-liable and valid approach to measuring cognitive impair-ment and symptom resolution for mild TBI. The futureof sports-related mild head injury research is expandingand will be best served by prospective neuropsychologicalstudy of athletes at high risk for multiple concussions. Bet-
ter protective equipment and devises, rule changes, andpooling of information into a comprehensive concussiondata bank to better define safe return-to-play criteria shouldbe the focus of sports medicine in the new millennium.
Future directions in the assessment and managementof sports-related concussion include: increased researchon prevalence rates and effects of concussions for femaleand young athletes, educating parents of youth athletesand family physicians on the importance of baseline andpostconcussion cognitive assessments, and further valida-tion of computerized assessment measures. Despite apaucity of research on female and youth athletes, there isevidence that female athletes are at greater risk for injurythan male athletes, and that concussions may affect chil-dren and young adolescents differently than older adoles-cents and adults. Sideline, baseline, and postconcussionassessments have become prevalent in documenting prein-jury and postinjury performance, recovery rates, andreturn-to-play decisions. New computerized assessmentprocedures are growing in popularity and are used in theNFL, NHL, NASCAR, and Formula 1.
The role of the neuropsychologist in the assessmentof concussions for purposes of diagnosis and symptomresolution is one that our profession should embrace.Moreover, for those neuropsychologists who love sports,it provides a unique opportunity to merge one’s profes-sional skills with one’s affinity for sports. Most often the
Figure 13.7 Female athletes are consistently found to be athigher risk for sustaining concussions than male athletes acrossall sports and all ages (Covassin, Swanik, & Sachs, 2003). Pic-tured are two college lacrosse players. In collegiate lacrosse menwear helmets, whereas women do not, which has initiated adebate regarding the use of head protection in the sport. (Courtesy Drexel University, Philadelphia, PA.)

role of the neuropsychologist in the area of sports-relatedconcussions will be that of a consultant and a researcher.In addition to being an expert in the neuropsychologicalassessment of concussions, the neuropsychologist mustunderstand the culture and epidemiology of the injuriesof the athletic arena and of various sports they may beasked to cover. We believe that the neuropsychologists’training and expertise uniquely prepares him or her toplay an important and rewarding role in this growing fieldin the future (Zillmer, Schneider, Tinker, & Kaminaris,2006).
P O S T C O N C U S S I O N A L S Y N D R O M E
Medical personnel often call the behavioral and cognitivesequelae of mild head injury “postconcussional syn-drome.” These sequelae range over a variety of somaticand neuropsychological symptoms, including headache,irritability, dizziness, lack of concentration, and impairedmemory. Researchers have documented the symptoms ofmild head injury most frequently with MVAs. However,analogous situations with acceleration/deceleration of thehead arise in the context of competitive sports. Manysports involve speed and the potential for collision. Infact, as mentioned earlier, 17% of all head injuries aresports related.
For example, research with football players suggeststhat many effects of sports-related collisions (such as tack-ling) that were originally thought to be relatively benign,actually have measurable neuropsychological conse-quences in college athletes. These collisions may not onlydiminish the performance of players on the field but canalso compromise their health off the field. Full apprecia-tion of impact injuries has only recently developed asmany NFL quarterbacks have reported the negative ef-fects of repeatedly being hit in the head. Frequent headimpact places them at risk for losing consciousness evenwhen experiencing relatively minor concussive forces tothe head. In some cases, this has resulted in cognitivechanges, including excessive dizziness and difficulty inconcentrating. Several players were forced to retire, andrules were changed, disallowing tackling with the helmetor “spearing” to the opposing player’s head.
Researchers have studied the neurologic aspects of pro-fessional boxing in more detail; these aspects are easily ap-preciated by the public because of the knockout (KO),which is a neurologic event synonymous with cerebral con-tusion. Only recently have researchers examined the neu-rologic aspects of amateur boxing, where duration offights, rules, and protective devices differ from profes-sional boxing. Other less obvious sports-related neurologic
effects appear in soccer players who frequently head theball. Findings indicate more EEG abnormalities amongprofessional players (Tysvaer, Storli, & Bachen, 1989) andthe presence of neuropsychological deficits among collegeplayers (Witol & Webbe, 1993). That football and soccercan involve potential mechanical forces to the head thatcan cause injury seems disturbing, particularly at the non-professional, “recreational” level. At that level, many ele-mentary school, high school, and college players are par-ticularly vulnerable to the developmental delays related tosuch head injuries (Levin et al., 1982).
Treatment of Head Injuries
An acute TBI often entails severe neurologic im-pairment. In severe head injuries, the patient is comatosewhen the medical emergency unit arrives. The initialmanagement of severe head injury follows the ABC as-sessment (airway, breathing, and circulatory status); themedics establish a respiratory airway, often freeing thepharynx from blood and other obstructions. If they donot establish an airway, anoxia will result, adding to thephysical injuries of the brain. After a clear airway has beenestablished, medics assess the patient’s breathing. Thenthe team establishes regular breathing, if necessary, artifi-cially, with sufficient oxygen, because hypoxia is commonin head injuries. Alterations in breathing may be relatedto brainstem dysfunction. Medics then evaluate circula-tory status by examining blood gases and blood pressure.They initiate intravenous infusion, including blood re-placement. Then, once the patient has been medically sta-bilized, they obtain diagnostic imaging using CT andMRI. Next, a neurologist conducts an evaluation to as-certain the level of consciousness and presence of neuro-logic symptoms. If the patient remains in a coma, theteam may hospitalize him or her in a neuro-intensive careunit, which has a specialized environment that facilitatescare of comatose patients.
As mentioned earlier, intracranial monitoring is thecornerstone of medical therapy. If ICP remains normal,the patient undergoes intensive supportive care. If ICP iselevated, medical personnel use aggressive measures toreduce it. These include controlled ventilation, which de-creases cerebral blood volume and constricts cerebral ves-sels, thus reducing ICP. Steroid therapy may prevent in-tracerebral edema. Patients are typically temperaturecontrolled with heating/cooling blankets, because ele-vated body temperature increases metabolic rate and hy-pothermia leads to other medical complications. Some-times medical personnel administer diuretics to reduce
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 385

386 PART THREE | Disorders of the Brain
John, age 24, and Theresa, age 22, are twoadults with traumatic brain injuries (TBIs).John suffered a head injury at age 17 in amotorcycle accident. At age 20, Theresasuffered a head injury when a drunk driverstruck her car as she waited at a red light. Asa result of their injuries, John and Theresacurrently live in a community-based rehabili-tation facility.
John experiences hemiplegia, difficulty inplanning for future events, and memory andattention deficits. Theresa experiencesseizures, as well as severe speech andmemory deficits. John and Theresa enjoyeach other’s company and often attendcommunity events together. More recently,John and Theresa have become interested ina physically intimate relationship.
The last issue is a concern for the agencythat provides their rehabilitative services.With their specific cognitive deficits, canJohn and Theresa consent to have sex? Can
they each make an informed decision usinginformation on sexual conduct, diseases,and pregnancy? Is either at a high risk forbeing victimized because of an inability toadequately protect himself or herself fromunwanted sexual advances? To explore theanswers to these questions, the issues of TBIand sexuality must be considered.
After a head injury, the often-ambiguousrules and rituals pertaining to sex can be-come even more difficult. Adverse effects ofTBI on sexuality range from sensorimotordeficits and bowel and bladder dysfunction,to changes in sex drive and various male andfemale genital sexual dysfunctions. In addi-tion to the neurologic, physical, and emo-tional effects on sexuality are cognitivechanges associated with TBI. Cognitivechanges can affect sexuality in a variety ofways, including impairment of the ability tomake safe choices regarding sexual behav-ior. The individual can be physically able to
engage in a sexual relationship, and even beinterested in pursuing one, but at the sametime be cognitively incapable of consenting.An inability to make decisions can result invictimization, unwanted pregnancies, anddiseases.
One hallmark of a moderate-to-severeTBI can be the loss of the ability to makecomplex decisions requiring judgment,insight, preplanning, reasoning, organiza-tion, and impulse control. Clearly, suchcognitive deficits can impair the ability toconsent to sex. When this issue arises, theneuropsychologist serves two main roles.First, the neuropsychologist, together withformal testing of cognitive and functionalstrengths and weaknesses, can assess anindividual’s capacity to consent to sex.Second, the neuropsychologist can recom-mend rehabilitative and educational strate-gies that are specially geared to a person’sfunctioning level and cognitive abilities and
N e u r o p s y c h o l o g y i n A c t i o n 1 3 . 3
C o n s e n s u a l S e x a f t e r Tr a u m a t i c B r a i n I n j u r y : S e x a s a P r o b l e m - S o l v i n g Ta s k
by Carrie H. Kennedy Ph.D., Lieutenant Commander, Navy Neuropsychology Fellow, University of Virginia, Charlottesville, VA
the ICP. If these measures do not control ICP, the prog-nosis is typically poor, and more aggressive measures aretaken, such as inducing barbiturate coma and surgery.Administering a large dosage of barbiturates decreasesthe cerebral metabolic rate and constricts cerebral vessels.Inducing barbiturate coma is controversial, because itmay contribute to additional neuropsychological seque-lae. A final measure is to remove part of the brain to makespace available.
N E U R O P S Y C H O L O G I C A L M A N I F E S T A T I O N S
Neuropsychological sequelae, of course, are prominentlyassociated with TBI. They range from patient reports ofmemory difficulty to problems with attention and con-centration, as well as alterations in mood. Neuropsychol-ogists play an important role in objectively assessingresidual ability after mild, moderate, and even severehead injuries, once the patient has been medically stabi-lized and is no longer in a coma or in acute medical care.
In addition to the cognitive effects of brain injury, per-sonality changes from frontal lobe damage may affect thepatient’s well-being and quality of life (Neuropsychologyin Action 13.3). Neuropsychologists routinely test headinjury survivors, because unless tested, cognitive deficits,especially memory, may at first go unnoticed, but causeproblems later when the patient returns home or to work.Most recovery after severe head injury occurs within thefirst 6 months, with smaller adjustments continuing forperhaps as long as 2 years. In the past, rehabilitation ex-perts have waited until the “natural” healing cycle hasfinished before initiating rehabilitation. More recentthinking has proved that rehabilitation is most effectivewhen started as early as medically possible (Levin et al.,1989).
A n t e r o g r a d e a n d R e t r o g r a d eA m n e s i a
Memory problems constitute a major deficit for peoplewho have sustained traumatic head injuries and are of

special interest to neuropsychologists. In fact, head in-jury experts grade the severity of a head injury partly onthe patient’s memory surrounding the accident. Suchmemory problems are called post-traumatic amnesia(PTA). Retrograde amnesia is the loss of memory forthe interval preceding the injury. Conversely, antero-grade amnesia is the loss of memory for events aftertrauma or disease onset. Although the patient may haveresidual short-term memory impairment from the headinjury, as well as other cognitive deficits, neuropsycholo-gists have established retrograde and anterograde amne-sia as a relatively robust measure of the severity of traumaand its associated cognitive symptoms. Because corticaland subcortical structures mediate memory, PTA hasproved a better overall indicator of brain damage thanlength and depth of coma, which may relate to isolateddamage of the brainstem. Neuropsychologists considerthese types of amnesia to relate mostly to anterior tem-poral lesions, an anatomic area particularly vulnerable tohead injuries, because of the bony features surroundingthis area of the brain.
N e u r o p s y c h o l o g i c a l E v a l u a t i o nOften other medical personnel ask neuropsychologists toevaluate head-injured patients at their bedside, close to thetime of their accident, while they are still hospitalized (seeNeuropsychology in Action 13.1). This examination istypically brief and serves to assess whether the patient cantolerate more formal, longer testing. It also establishes abaseline of overall cognitive abilities for future compar-isons. An example of such a neuropsychology consult is asfollows:
Neuropsychology Note. Results from brief neuropsychologicalprocedure, post-MVA with LOC (loss of consciousness) 30min, revealed a 33 yowm (year-old white male) who was ori-ented � 3 (to self, time, and place) and attentive/cooperativewith the exam. The patient was able to follow simple com-mands involving two-step learning. Memory appeared withinnormal limits (WNL) for immediate and short-term verbal/vi-sual material. Expressive/receptive speech were also WNL. Nosensory deficits including astereognosis, finger agnosia, neglect,right–left confusion, or hemianopsia, were observed. The patientdid manifest a bilateral resting hand tremor as well as motor
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 387
strengths. In this way, neuropsychologistscan optimize the decision making and safetyof TBI survivors, whereas facilitating thereturn of an important aspect of quality oflife, that of sexual intimacy.
Using an instrument such as the SexualConsent and Education Assessment (SCEA;see Kennedy, 1999), neuropsychologistsmake a capacity determination based onprescribed legal criteria for consent. Legalcriteria for sexual consent vary from state tostate, but a consensus of psychologists isthat individuals must have knowledge ofsexual conduct, knowledge of the conse-quences of sexual activity, and basic safetyskills to be deemed capable of consenting(Kennedy & Niederbuhl, 2001). Although,taken together, these criteria determine thecapacity of any given individual, each crite-rion is also a separate entity directly relatedto cognitive abilities that neuropsychologistscan measure.
The first two criteria for capacity forsexual consent, regarding the nature ofsexual conduct and consequences of sexualactivity, are a function of crystallized intelli-gence (knowledge that has been acquiredover the years) in most adults. That is,individuals who have had previous sexuality
education, sexual experience, or both aremore likely to retain general knowledge andinformation regarding sexuality. Later, suchadults who have experienced a TBI typicallyhave little difficulty communicating theirunderstanding of the nature of sexual con-duct and the various consequences of sexualactivity. However, individuals who have notyet obtained general knowledge aboutsexuality must learn it for the first time. AfterTBI, attentional, memory, and executivefunction deficits significantly hinder newlearning and can make a task such as learn-ing basic sexual knowledge daunting.
The third criterion, however, basic safetyskills, appears to be the most significanthurdle for individuals with moderate tosevere head injuries. This particular neu-ropsychological task appears to be anexecutive decision that involves a complexstring of decision making, reasoning, judg-ment, and planning. Preliminary findingssuggest that neuropsychological tasks thatassess those abilities, such as the Tower ofLondon–Drexel University (Culbertson &Zillmer, 2005), the Modified Wisconsin CardSorting Test, and word fluency are able tocorrectly classify cognitively impaired individ-uals who are and are not capable of consent-
ing to sexual activity (Kennedy, 2003).Additional research will provide furtherinformation regarding sexual consent andrelated neuropsychological requirements. Inturn, investigation of these questions will alsoprovide the basis for developing more effec-tive rehabilitative strategies to help peoplewith neurologic damage in regaining impor-tant parts of their lives, not least of which willbe sexual intimacy. This leads us back to ouroriginal questions about John and Theresa.
John and Theresa were both tested usingthe SCEA and a neuropsychological battery.Theresa easily passed all aspects of theassessment, whereas John showed signifi-cant difficulty with the concepts of sexuallytransmitted diseases and protection againstthem. John was declared not capable ofgiving consent until he could successfullycomplete an educational program dealingspecifically with diseases and methods ofprotection. The educational program, whichJohn completed, included methods oflearning that were optimal for John given hisneuropsychological test findings. Subse-quently, the rehabilitation facility workedwith John and Theresa about establishingprivacy, and their subjective quality of life isvastly improved.

388 PART THREE | Disorders of the Brain
incoordination, and difficulty in initiating specific motor move-ments. Perseveration of motor behavior was also apparent.Additional frontal lobe signs included poor reasoning abilityand judgment.
Results are consistent with mild to moderate head injury andbilateral frontal lesions as seen on MRI from revealing contu-sions in the inferior frontal regions. Psychologically, the pa-tient appears very distressed and depressed about his hospital-ization and MVA, with suicidal thoughts present (but nospecific plan). No other psychiatric symptoms were noted(hallucinations, delusions). Patient should be placed on sui-cide watch. Psychiatric consult should be ordered, and reloca-tion to psychiatric ward should be considered to better man-age suicide threats when the patient is medically stable. Otherrecommendations include comprehensive neuropsychologicaland psychological evaluation within the next four weeks toidentify functional strengths and weaknesses. Cognitive resid-ual effects that may hinder this patient’s ability to return tohis previous employment as a manager include his ability tofunction independently in life, and his need for outpatientpsychotherapy. This testing can be done on an inpatient oroutpatient basis and should be repeated over a 6- to 9-monthperiod to monitor his recovery. Once he is discharged I alsorecommend that he join our head injury group meetings,designed for individuals and families with histories of headinjuries.Signed: Dr. Eric A. Zillmer, Neuropsychologist
In general, the long-term neuropsychological effects ofhead trauma may vary considerably and depend on thestrength of the trauma and the medical condition of thepatient with the head injury. Not all head traumas pro-duce significant neuropsychological deficits. Others causepermanent and severe deficits. In general, neuropsycholo-gists consider CHIs a diffuse disorder of the brain, be-cause they may affect many different areas of the brain.Thus, differences in neuropsychological presentation in ahead-injured protocol typically relate to the patient’s levelof overall deficits.
Recovery, Rehabilitation, andIntervention of Traumatic BrainInjury
What is the potential for the human brain to re-cover or adapt after brain injury? First, insult to the braincan result in different effects depending on the site andmechanism of damage. What is remarkable, however, isthe brain’s amazing ability to try to adapt to damage. Ifdamage does not totally destroy neurons, the brain
attempts to restore functioning. If the injury was causedby shock or some other temporary mechanism, diaschisismay serve to “unmask” functioning neuronal systems.When neurons are damaged through processes such as tear-ing and shearing, they may reorganize through axonal re-sprouting, collateral sprouting, or developing supersensitiv-ities to neurotransmitters. When neuronal damage iscomplete, depending to a large degree on plasticity, thebrain may sometimes be able to substitute other function-ing neurons or neuronal systems or rely on some redun-dancy to take over. The neuropsychologist should con-sider the following factors when evaluating influences onrecovery:
1. Location and extent of damage2. Duration of time since injury3. Age (brain plasticity)4. Premorbid intellectual level5. Premorbid personality characteristics6. Premorbid functional level7. Medical health8. Emotional health9. Support system
10. Type of treatment
Behind most theories of neuropsychological recoveryand rehabilitation lies the premise that if functions arenot completely ablated, there is a chance that they canbe restored through the ability of the brain to heal andadapt. To what degree functions may spontaneously re-cover versus needing aid via neuropsychological rehabil-itation techniques remains unresolved. There is nodoubt that some spontaneous recovery can occur, buthow much does targeted training also help to restorefunction? What if a function is completely lost? In thiscase, most neurobehavioral rehabilitation focuses onsubstitution, or the use of other behavioral strategies ordevices to “work around” the problem or serve as an ex-ternal prosthetic device to help take the place of the lostfunction.
Adaptation and Recovery
D I A S C H I S I S
Diaschisis (first described by von Monakow, 1911) refersto an unmasking of function after temporary neuronaldisruption. Monakow’s theory of diaschisis (derived fromGreek schizein, meaning “to split”) described the loss offunction caused by cerebral lesions in areas that are remote

from the lesion, but that are neuronally connected to it. Adepression in neuronal functioning can occur due to neu-ronal shock, intercranial pressure, edema, metabolicchanges, or any condition that reduces blood flow. Thistransience of function inhibition implies that the neu-ronal systems have not been permanently damaged.Therefore, diaschisis differs from restitution in that it is apassive process of uncovering working systems rather thanan active process of repairing damaged systems. As thecondition causing the dysfunction is removed, the behav-ioral function re-emerges.
Researchers have proposed that diaschisis represents animbalance between excitatory and inhibitory mechanisms(Poppel & von Steinbuchel, 1992). An interesting demon-stration in animals (Poppel & Richards, 1974) provides anexample. If the right occipital lobe is damaged, blindnessin the left visual field results; however, if the left superiorcolliculus is destroyed, sight is restored. How is this so?Apparently, the colliculi of each hemisphere serve to in-hibit each other while each occipital lobe excites its ipsilat-eral colliculus. Thus, in the normal brain, all is balanced.However, when the right occipital lobe is damaged, theright superior colliculus, which no longer is receiving inputfrom its occipital lobe, cannot moderate the left superiorcolliculus. In fact, the right becomes overinhibited by therelative overactivity of the left. If the inhibitory input ofthe left is removed, the right becomes functional again andsome sight is restored. This complicated interplay betweenexcitatory and inhibitory functions repeats itself over andover again with different functional systems of the brain.According to the theory of diaschisis, this imbalance be-tween excitation and inhibition resolves spontaneously.
B R A I N R E O R G A N I Z A T I O N
Reorganization of brain function after injury has much todo with the plasticity of the brain. Plasticity, the behav-ioral or neural ability to reorganize after brain injury, ap-pears to be one of the more important factors contribut-ing to the speed and level of final recovery. Most researchon plasticity has tested animals, leaving the relation be-tween neuronal reorganization and behavioral organiza-tion unclear in humans. Immature nervous systems aremuch more plastic than those of adults; children showless behavioral effect and recover faster from brain injury.Some have suggested that recovery from aphasia in pre-pubescent children may be caused by the adaptability ofthe short-axon Golgi type II cells (Hirsch & Jacobson,1974; Kertesz & Gold, 2003). Whereas the long axon neu-rons of the brain appear to be preprogrammed genetically
for certain functions, the more flexible Golgi type II cellsappear to maintain flexibility until the onset of hormonalchanges associated with puberty.
A x o n a l a n d C o l l a t e r a lS p r o u t i n g
One way in which the brain reorganizes is through the re-growth of neurons that have been only partially damaged.As mentioned in Chapter 4, unlike axons in the periph-eral nervous system, those in the central nervous systemare not known to regenerate after total severing. However,axons that have been sheared may resprout, and collateralsprouting can occur from nearby intact neurons. Youngerorganisms appear to have the greatest potential for axonalregrowth. Theoretically, sprouting could replace the lostfunction. Although researchers have documented that ax-onal and collateral sprouting does occur, they do not yetknow whether the “reconnections” rebuild the previousfunction. Excessive sprouting may even hinder behavioralfunctioning.
D e n e r v a t i o n S u p e r s e n s i t i v i t y
If an area of the brain is lesioned, any remaining neuronsin that area may become hypersensitive to the neurotrans-mitters that act on them. The mechanism appears to actvia a proliferation of postsynaptic receptor sites. This mayresult in a greater excitatory or inhibitory potential, de-pending on the type of neuron.
Overview of the Rehabilitation Process
Rehabilitation seeks to retrain and re-educate peo-ple with disabling injuries, to improve level of daily func-tioning. The philosophy of a rehabilitation center is verydifferent from that of an acute care hospital. In the earlystages after an injury or trauma, the hospital’s goal is tomedically stabilize the patient. The hospital provides carefor the patient and does not require the patient to be ac-tive in treatment. Rehabilitation centers expect the pa-tient and family to take a more active role in retraining,and to become partners in treatment planning. Rehabili-tation settings also use rehabilitation teams of specialistswho work together in setting goals and implementingtreatment. This section considers the various specialties inmore detail. Traditionally, rehabilitation treatment was setup over a period of weeks to months on an inpatient unit,then followed periodically on an outpatient unit. Withthe advent of managed care, inpatient rehabilitation has
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 389

390 PART THREE | Disorders of the Brain
shortened, outpatient rehabilitation has lengthened, andthe role of the neuropsychologist has evolved to meet newdemands for services. The final goal of rehabilitation is toreintegrate people back into the community at the high-est level of functioning possible.
Rehabilitation psychology, like neuropsychology, is adistinct specialty area within psychology. Practicing re-habilitation psychologists may treat people who havesuffered non-neurologic problems such as burns,chronic pain, amputation, or blindness, as well as neu-rologic brain and spinal cord injuries and trauma. Thefocus is on applying psychological principles to recov-ery and adjustment to disability. More specifically, forthe psychologist working with brain disorders, neu-ropsychological rehabilitation—or brain injury rehabil-itation, as it is more commonly known—represents theintersection of neuropsychology and rehabilitation. Assuch, the focus is on the process of recovery, adjust-ment, and rehabilitation of brain disorders. The condi-tions most often seen on brain injury units of rehabilitationhospitals include TBI caused by head injuries from ac-cidents and falls and cerebrovascular accidents (CVAs).Less often, rehabilitation units treat patients recoveringfrom brain tumor or brain disease. With the increasingsurvival rate of heart attack victims, rehabilitation cen-ters are experiencing a greater influx of anoxic/hypoxicinjuries resulting from loss of oxygen to the brain be-fore resuscitation.
Rehabilitation hospitals are specialty hospitals, whichadmit patients who fit a restricted group of diagnoses,such as TBI. Length of inpatient stay varies but has short-ened dramatically since the advent of managed care. Asinpatient stays shortened, the focus of treatment evolvedto include a greater emphasis on outpatient treatmentwithin a person’s home, social, and occupational settings.
There are about 1600 TBI treatment programs in theUnited States (National Directory of Head Injury Ser-vices, 1992). A large proportion of neuropsychologistswork in rehabilitation settings where they apply knowl-edge of brain–behavior relations and neuropsychologicalevaluation to the process of recovery and communityreintegration. A challenge for neuropsychologists work-ing in these settings is to translate the patient’s level offunctioning to appropriate treatments regarding dailylife, since rehabilitation neuropsychologists spend themajority of their time treating the patient and family.Those involved in research constantly wrestle with theissue of ecologic validity—that is, with developing meansof evaluation and treatment specific to common issues ofrehabilitation such as driving, cooking, and return towork.
A D M I S S I O N T O R E H A B I L I T A T I O NP R O G R A M S
Although most neuropsychologists in rehabilitation workin specialty rehabilitation hospitals or treatment programsthat focus primarily on treatment, others work in large,acute-care hospitals that have rehabilitation units andfocus on early evaluation before transfer to a specializedfacility. Brain injury specialists working in acute-care hos-pitals get the earliest view of a person’s functioning, per-haps while emerging from coma or recovering from brainsurgery. They conduct the first evaluations of alertness,attention, sensorimotor, and cognitive skills over thecourse of the first few days and weeks of recovery beforebeing transferred to a longer term rehabilitation hospital.The GCS (see earlier) is a good example of a measure usedearly in the process of recovery from head injury. Also,acute care rehabilitation neuropsychologists conduct pre-operative and postoperative assessments to document thelevel of change in cognitive functioning. These first neu-ropsychological evaluations can serve as a valuable baselineand predictor of future level of recovery. Therefore, neu-ropsychological evaluation becomes a valuable part of theprescreening process. Neuropsychologists design the pre-screening process for entry into a rehabilitation programto select patients whom they consider to have potential fortreatment success and enough social support for postreha-bilitative care. In fact, admission to a rehabilitation programin itself suggests the absence of a medical life-threateningcrisis and the potential for further recovery.
The rehabilitation hospital is the primary setting forlearning the skills to return to a home setting. If rehabili-tation facilities did not exist, a large proportion of patientswith brain-damage would go directly from the acute-carehospital to a skilled nursing facility. This is because mostpatients admitted to rehabilitation hospitals cannot carefor themselves and may still be in a state of significantcognitive confusion, and their families do not yet under-stand the condition and the caretaking responsibilities.The rehabilitation hospital is an opportunity to take ad-vantage of the skills of others and to practice practicalskills with professional supervision. Therefore, it is quitenormal for patients to spend some time getting used tothe functioning and philosophy of a rehabilitation unit.The “team” approach is also a new concept for most peo-ple accustomed to acute-care hospitals.
As patients move from the acute-care hospital to a re-habilitation program, they must make the transition fromthe hospital environment to the rehabilitation environ-ment. Rehabilitation patients need time to orient to thephilosophy of empowerment that rehabilitation programs

advocate. The team teaches the means to maximize inde-pendence both for survivor and family caretaker. The goalfor a patient is not to live in the rehabilitation hospital,but to get back to community life. Thus, patients in a re-habilitation hospital are not relegated to the traditional“sick” role or to a self-perception that earlier experiencesin other acute-care medical units might have shaped.
A newly admitted patient must adapt to many factorsin the rehabilitation environment, such as structured re-habilitation programs and new expectations. In addition,the sheer variety of patients of different ages recoveringfrom myriad disorders can be overwhelming. Dependingon the size of the facility and the extent of services, thereare often separate units for orthopedic and brain injurypatients, although sometimes the patients are mixed to-gether. Where brain injury is involved, there is usually apreponderance of young men in their teens and 20s re-covering from head injuries, gunshot wounds, or spinalcord injury. Elderly heart attack and stroke victims arealso present, as well as tumor surgery patients. The pa-tients with brain injury can be expected to have signifi-cant cognitive compromise, often still involving confu-sion and PTA, as they arrive at a rehabilitation facility.
T h e R e h a b i l i t a t i o n T e a m : G o a l S e t t i n g , T r e a t m e n t , a n d E v a l u a t i o n
Once a patient is accepted for admission, the typical proto-col assigns him or her to a rehabilitation team. Teams usu-ally consist of specialists in rehabilitation nursing, social ser-vices, psychology/neuropsychology, physiatry, speechtherapy, occupational therapy, physical therapy, and thera-peutic recreation. Treatment teams are often directed by thephysiatrist, but may also be directed by psychologists orspeech therapists. A “physiatrist” is a physician who special-izes in physical medicine and rehabilitation. Other relatedspecialists may also become involved, including specialistsin audiology, nutrition, orthotics, optometrics, and den-tistry. A variety of medical specialists are also available to pa-tients, such as internists, urologists, cardiologists, ophthal-mologists, and pediatricians. These teams generally follow amultidisciplinary or transdisciplinary approach in whicheach discipline works together in a coordinated fashion toachieve specific treatment goals. More and more patientsand their families are becoming integral members of theirown treatment teams. This approach includes them in allareas of treatment planning and evaluation of progress.
Initial treatment planning routinely puts patients on aschedule of daily “therapies”; for example, 1 hour each ofphysical therapy, occupational therapy, and speech therapy.As noted earlier, patients who cannot endure this daily
training are generally not considered ready for compre-hensive rehabilitation and may be sent to a continuing carecenter until they are more able. Beyond the minimum re-habilitation requirement, many rehabilitation hospitalsprovide additional rehabilitation hours, which consist ofwhatever the patient needs most. Next, we explore the in-dividual contributions of neuropsychology, physical ther-apy, occupational therapy, speech therapy, and recreationaltherapy in greater detail. Although we discuss these as sep-arate disciplines, as a treatment team works together over aperiod of time, a degree of “cross-training” often occurs.In some rehabilitation hospitals, the lines between disci-plines become totally blurred as each person is referred toas a “brain injury therapist,” although their individual con-tributions may be somewhat different.
N e u r o p s y c h o l o g y
Neuropsychologists are active in the rehabilitation processfrom admission to discharge. As mentioned earlier, neu-ropsychologists on rehabilitation units of acute-care orcomprehensive hospitals may provide baseline evaluationsthat help determine an individual’s capability to partici-pate in a rehabilitation program. On a patient’s admissionto a rehabilitation unit, a neuropsychologist may conducta formal evaluation. He or she may also evaluate func-tional neuropsychological skills such as meal planning andpreparation, ability to plan and self-administer medica-tion, driving, or work-related tasks. The recommenda-tions generated specifically aim at helping the treatmentteam form workable goals and objectives given an indi-vidual’s pattern of cognitive and emotional strengths andweaknesses. These evaluations necessarily focus on thefunctional level of the individual and serve as a baseline todocument impairment. Notice that the focus of this evalu-ation is not only on the pattern of deficits exhibited buton the strengths that may aid the person in compensatingfor losses in other areas. During treatment planning, it isthe neuropsychologist’s role to discuss specific recommen-dations with the team regarding potential remediationstrategies. For example, would memory log training belikely to be successful? How will the person’s level of frus-tration tolerance impact his or her ability to participate invarious therapies? How feasible is this training, given thecognitive demands of the patient’s home environment?
During the treatment process, the neuropsychologistcontinues to assess progress toward goals of daily living inconjunction with other team members. Neuropsychologiststake part in individual patient counseling surrounding is-sues of loss and cognitive readjustment. Family educationand counseling regarding the effects of brain damage on be-havior and strategies to cope with cognitive and behavioral
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 391

392 PART THREE | Disorders of the Brain
deficits are also quite important to support the patient inreturn to the community. Finally, the neuropsychologistoften coordinates compensatory strategies across settingsfrom rehabilitation, home, community, work, and school.We discuss the neuropsychologist’s assessment and rehabili-tation methods in greater depth later in this chapter.
P h y s i c a l T h e r a p y
Physical therapists (PTs) focus on motor control with theaim of improving physical functioning to the highest de-gree possible. PTs evaluate each patient on admission to as-sess performance of functional activities related to strength,balance, coordination, physical endurance, and range ofmotion. The evaluation also considers the neurologic statusof the motor systems. For example, PTs evaluate activitiessuch as rolling, standing, sitting, transferring, using awheelchair, and walking. PTs develop and individualizetreatment programs for each patient according to specificstrengths and weaknesses. For example, treatment programsfor those with motor disability, weakness, or paralysis mayconsist of the following activities: mat activities, develop-mental sequences, balance training, hydro/pool therapy,strengthening exercises, transfer and wheelchair training,walking, and use of adaptive equipment. PTs accomplishgoals by teaching such activities as wheelchair managementand wheelchair propulsion. They instruct patients how totransfer from their wheelchairs, bed, toilet, and car. To walkagain may be a major goal. PTs determine when a patienthas sufficient strength, muscle control, and balance to at-tempt walking, and they assess the need for assistive devicessuch as walkers, canes, crutches, braces, or splints.
O c c u p a t i o n a l T h e r a p y
The term occupational therapy is confusing to some peo-ple who think that the training is specific to individualswho have an “occupation” and want to go back to work.This is not the only goal of occupational therapy. Occu-pational therapy is concerned with self-care activities suchas grooming, bathing, dressing, and feeding, commonlycalled activities of daily living (ADLs). Occupational ther-apists (OTs) also focus on work activities ranging fromhome management, meal preparation, money manage-ment, household chores, and activities involved with oc-cupations as well as avocations (that is, hobbies).
The OT evaluates and treats the performance compo-nents that are necessary for functioning in ADLs, work, andleisure. The performance components include many aspectsof human functioning. Of great importance to the OT is anassessment of sensory and perceptual-motor functioning.The use of muscles to bend, move, and perform purposiveaction (praxis) lies within the domain of occupational
therapy. Finally, issues of thinking, remembering, and prob-lem solving for daily life hold special importance for the OT.
Several ways exist to distinguish the difference in spe-cialization between PT and OT. Both are concerned withmuscle strength and coordination. However, in many hos-pitals, PTs work primarily on the lower extremities (allmuscles below the waist), and OTs work primarily on theupper extremities (everything above the waist). In thosehospitals that do not distinguish between upper and lowerextremity strength, the difference between PTs and OTsis usually broadly defined by strength (PT) and function(OT). In regard to the latter definition, for example, astroke survivor may be able to walk with strength and en-durance. That same patient, however, may not be able tojudge distances, determine left from right, or near fromfar. As a consequence, walking per se adds little to the pa-tient’s independence, because walking is not safe. The OTtakes on the job of applying strength gained from PT tousing that strength within everyday types of activities. Forexample, an occupational therapy session may focus onteaching the patient to discriminate between things that areclose and things that are far away (as in depth perceptiontraining) or things seen to the right versus things seen to theleft (as in left neglect training). This therapy is referred to asperceptual retraining, or perceptual remediation.
Another area of occupational therapy concerns amongbrain injury survivors is apraxia. Stroke victims often showthis lack of purposive action. In practical terms, the OTwill refer to, for instance, “dressing apraxia,” indicating thatthe patient cannot dress on command, or “on purpose.”This form differs somewhat from stroke patients who failto dress one side of their bodies because of neglect. If yousay to a stroke victim, “Let’s go outside,” she may automat-ically put on the sweater that is nearby. However, if you say,“Put on your sweater so we can go outside,” she may eithersimply go outside without regard for the sweater or may sitthere and fumble with the sweater because she can nolonger put it on. OTs try to use activities to meet goals;thus, in this case, the actions chosen will have the purposeor function of overcoming dressing apraxia.
S p e e c h T h e r a p y
Speech therapists provide therapy for patients experienc-ing a range of communication difficulties. These may in-clude mechanical speech difficulties involving speech pro-duction, expressive language, hearing and understandingspeech, reading, writing, and the social use of language.Speech therapists specifically trace communication prob-lems from the basic level of auditory acuity and speechproduction to higher level skills of communication andlinguistic integration.

The ultimate goal is to design interventions to aid inspeech production and understanding and to facilitatecommunication. This may be accomplished through prac-tice and retraining or with prosthetics aimed at assistingcommunication through artificial means.
The speech problems most commonly treated dealwith articulatory difficulties, or dysarthrias, caused byimproper muscle control of tongue, lips, or cheeks forpronouncing words. If either the left or right hemisphereis damaged, people with damage to the section of themotor strip controlling speech production will have con-tralateral impairment. Thus, half of the lips, cheeks, andtongue muscles used to articulate words may be weak-ened. Although it is not caused by a similar mechanism,if you have ever experienced slurred speech after a visit toa dentist who used Novocain, you will readily sympathizewith the problems stroke survivors face in articulatingspeech. In the extreme case, such speech may sound gar-bled or unintelligible.
Neuropsychologists often design higher order languageand communicative evaluations to assess the presence anddegree of aphasia, alexia, or agraphia. Speech therapistsmay specialize in evaluations to categorize aphasias (suchas expressive, receptive, transcortical, and global), and tounderstand the nature of reading and writing difficultiessuch as alexia and agraphia. At this level the interest is incognitive-linguistic integration.
T h e r a p e u t i c R e c r e a t i o n
Therapeutic recreation emphasizes the importance ofrecreational and leisure time activities. These activitiesserve a purpose beyond being just fun. For instance, pa-tients are encouraged to use skills learned in physical oroccupational therapy in completing craft projects. Thishelps in the “transfer” of learning. Therapeutic recreationalso allows patients to begin socializing with each other ina structured but less formal atmosphere than that affordedin other therapy settings.
At some facilities, the therapeutic recreational specialisttakes patients on community outings. Community out-ings allow patients to practice their skills in real-life set-tings, among nonhospital people. This can help patientson the first important step in their transition from the hos-pital setting back to their home, friends, and family. Theskills addressed in community outings may include:
1. Mobility: ramps, elevators, curbs, doorways, obstacles,transfers, and so on
2. Daily living skills: money management, safety aware-ness, personal energy pacing, nutritional awareness,and problem solving
E V A L U A T I O N O F G O A L S A N D D I S C H A R G EP L A N N I N G
The rehabilitation team begins planning discharge fromthe hospital and outpatient rehabilitation from day 1.This idea sometimes confuses patients and families, whobelieve they cannot make discharge plans until they ab-solutely know the final functioning level of the brain in-jury survivor. It is often difficult to realize that no one canguarantee the exact level of functioning a person will at-tain by the end of a rehabilitation program. However, re-habilitation teams are in the business of estimating rea-sonable goals and can give a solid ballpark estimate offunction level. Once this expected level of functioning isdetermined, then everyone can make appropriate plansfor what will happen after the hospital stay.
Many brain injury survivors living at home before theinjury choose to consider returning home after rehabili-tation. As they contemplate this option, everyone mustconsider the feasibility of living at home safely and hap-pily. The treatment team, patient, and family must con-sider the functional requirements of a person’s currentliving situation and his or her resources to cope with thatenvironment.
Increasingly, rehabilitation programs are incorporatingshorter inpatient stays and longer outpatient treatmentinto their programs. Some impetus for this, of course, isdue to the financial pressures of managed care. However,there is also a move to integrate people into the commu-nity as soon as possible. We return to a discussion of com-munity integration programs, with the example of jobcoaching, later in this chapter. Next, we turn to an in-depth look at the methods that neuropsychologists use inrehabilitation settings.
In summary, the philosophy of treatment in a rehabili-tation hospital requires that patients and families be ac-tive in rehabilitation. They are “trained” by multidiscipli-nary teams, which typically consist of specialists in areasof neuropsychology, as well as physical therapy, occupa-tional therapy, speech therapy, and therapeutic recreation.Each area contributes a unique expertise related to brain-behavior functioning. PTs focus on the motor system,OTs are concerned with applying motor functioning todaily life tasks and with other functional tasks of daily liv-ing, speech therapists evaluate and facilitate improvementin all aspects of communication, and therapeutic recre-ation specialists focus on leisure activities and on practic-ing skills in the community. Neuropsychologists provideinitial and ongoing evaluation, as well as treatment forcognition, mood, and behavior disorders. The trainingdone by each team member necessarily focuses on parallel
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 393

394 PART THREE | Disorders of the Brain
tracks: The first is to work directly with the patient to tryto restore function or compensate for lost function, and thesecond is to work with caregivers and family to ensure thattreatment will continue after rehabilitation ends. Duringoutpatient treatment, where community reentry is thefocus, the focus of the team turns to providing bridges toemployment or other vocational endeavors. The next sec-tions take an in-depth look at the role of neuropsycholo-gists in rehabilitation settings—first the role in assess-ment, then the role in treatment.
T R E A T M E N T P L A N N I N G
Successful treatment rests on appropriate evaluation. As-sessments need to answer questions related to the possi-bilities of success in treatment and in returning to the“real world.” What is the pattern of strengths and weak-nesses according to the functional areas of verbal process-ing, visuospatial processing, and so forth? Will the personbe able to absorb the purpose of therapy and rememberinstructions? Does the patient appreciate the need fortherapy? When deficits appear, what exactly is the natureof the problem? For example, in language, are there moreexpressive or receptive difficulties? How severe is the prob-lem? Are there residual abilities that indicate the deficitcan be strengthened through practice? Are there otherareas of strength that can be trained to compensate or sub-stitute for the problem? What is the likelihood that thisperson will be able to return home, return to work, returnto independent functioning? These questions, in additionto describing patterns of neuropsychological functioning,definitely require predictions. This forces the neuropsy-chologist to consider not only current level of function-ing but also the accumulated research and clinical knowl-edge regarding the probability and time course of recoveryfor the particular problem. Recovery depends on numer-ous factors: pattern of impairment, treatment program,degree of spontaneous recovery, physical and emotionalstate of the person, family support, and several other fac-tors. Prediction becomes quite a challenging task.
A S S E S S M E N T O F E V E R Y D A Y A C T I V I T I E S
Real-world tasks such as driving, cooking, balancing acheckbook, taking medication, or navigating an unfamil-iar route require numerous cognitive components. Neu-ropsychological assessment often attempts to isolate theeffects of functional areas such as divided attention, re-ceptive language, or memory encoding. Although this ishelpful in understanding the pattern of neuropsychologi-cal strengths and weaknesses, the “whole” of a process
such as preparing a meal may be more than the sum of itsgeneric cognitive “parts.” Cooking certainly requires sus-tained attention, the ability to read and follow recipes,the ability to organize preparation of different dishes sothey are finished at the same time, the necessity to moni-tor time so the cake will not burn, and of course, basic vi-suospatial abilities. A problem in any one of these areasmay lead to a dining disaster. But does the presence ofbasic skills ensure competence in cooking? A neuropsy-chological assessment that measures attention, reading,organization, and time monitoring may reveal deficits thatpose problems for independent meal preparation. But ifno problems are found, does this mean the person canprepare meals independently? Not necessarily. First of all,tests of general functional areas such as attention andmemory may be too nonspecific to shed light on the exactneuropsychological requirements that make up successfulmeal preparation. Does a general test of organizationalability adequately predict organization of meals? This is aquestion of ecologic validity. Second, even if we can iden-tify the basic cognitive components involved, do the de-mands of combining and integrating these componentsinto fluid action somehow change the nature of the task?
To deal with these issues, neuropsychologists who de-velop “ecologically valid” measures can take one of twoapproaches, and may take both. First, they may attempt atask analysis. This involves identifying all the relevant spe-cific neuropsychological requirements of the task. Thenthey must devise tasks that measure components. The ideais that if any deficits appear there is a strong likelihoodthat the person cannot perform the task. The advantageof this method is that it may use paper-and-pencil mea-sures and small, portable tasks to simulate the cognitivecomponents. These tests can also be standardized usinglarge populations. If the patient performs specific aspectsof the test poorly, that pinpoints the deficits, which canbe targeted for rehabilitation. The disadvantage is thatthis analytic approach may not totally capture the require-ments of the whole task. The second method is to actu-ally do the task or closely simulate it. Many rehabilitationhospitals use driving simulators to test driving skills. Theymay also build kitchens or apartments to directly test thefunctional skills of meal preparation or laundry, for exam-ple. If tasks can be recreated in a controlled environment,then the huge advantage is that they come closest to mim-icking real life. Then performance on the task as an inte-grated whole can be assessed. Of course, the primary dis-advantage is the initial expense of installing an entireworking kitchen or a driving simulator. In addition, un-less the key cognitive components of the task can beteased apart, doing poorly on a meal preparation task, for

example, may not yield much information on how to in-tervene in training. Finally, because each kitchen is differ-ent, and the components of meal preparation may differon any given day, success does not automatically translateinto success at home.
Treatment Methods forNeuropsychologicalRehabilitation
Neuropsychologists use two primary approaches tobrain injury rehabilitation that hearken back to our ear-lier discussion of restitution versus substitution of func-tioning: (1) approaches that stress retraining of an im-paired skill, such as attention or memory; and (2) thosethat focus on searching for adaptations to the person’s en-vironment in the context in which the person will usethem (Diller, 1994).
The first approach is cognitive remediation, or cogni-tive retraining. In this case, for example, computers maybe used to provide practice exercises to attempt tostrengthen memory or attention. In many instances, theunderlying hope is that the brain may be able to rebuildaxonal connections through retraining; that is, restitu-tion. Approaches to cognitive remediation, however, donot necessitate proving structural changes to achieve func-tional success. For those functions that appear lost, cogni-tive remediation may focus on finding adaptive means, or“work-arounds,” for lost memory or lost expressivespeech, for example. In other words, the idea is to findcompensatory strategies for the lost process. Cognitive re-mediation approaches are usually practiced in a labora-tory setting. They vary a great deal in the degree to whichthey seek to simulate real-life situations and in which sit-uations they might generalize.
Cognitive retraining rests on theories of learning andpedagogy. Learning or relearning a skill or behavior is abuilding process that depends on an adequate base for es-tablishing higher order skills. If the aim is restitution,some neuronal functioning must be left. Whyte (1986)provides a useful hierarchical conceptualization for train-ing. Basic mental activities such as focused attention or au-ditory processing represent the first level of cognitive oper-ations. Cognitive processes, the next step, are combinationsof cognitive operations. Flexible problem solving and wordfluency are two examples. A skill such as performing men-tal arithmetic or writing requires coordination of cognitiveprocesses. Even more complex are metaskills that requirethe ability to sequence skills together, or to apply old skills
to new situations. Finally, global functions such as work-ing, driving, or managing a household are the most com-plex and integrative activities that depend on the integrityof the lower functions. The idea is to train in sequencefrom lower to higher order operations.
Context-driven approaches (Diller, 1994) emphasizetreatments that either involve actually training the personin his or her home or work environment or are specificallytailored to the person’s future needs outside the hospital,even though he or she may practice them in the rehabilita-tion hospital. This is a relatively newer area of rehabilita-tion than is cognitive retraining. After it became evidentthat many people with brain injury fail to generalize ortranslate what they have learned in the laboratory environ-ment to their own home or work environment, neuropsy-chologists recognized the need to train specific skills rele-vant to an individual’s environment. Some of theapproaches that train “in place” include the use of jobcoaches and supported employment, driver training, fam-ily training to aid in the home, or computers to assist sched-uling or memory. Patients can also practice additional rele-vant skills for daily life in group therapy situations, inwhich groups of individuals with similar impairments mayconcentrate on social, orientation, or organizational skills(to name a few). Although, in some cases, the planners oftraining in the context where the skills will be used mayhope to restore function, usually the aim is compensatory.
Review of various treatment approaches makes ap-parent that practical, “ecologically valid,” or contextualapproaches to rehabilitation are increasingly the focus ofmany treatment programs. However, currently, there re-mains little outcome research to demonstrate their effec-tiveness. The largest number of studies has focused onsuch cognitive mediation efforts as documenting im-provements in deficits such as attention or memory(Diller, 1994). Also, most approaches to rehabilitationcombine deficit retraining and contextual methods in amore eclectic model. However, unless the neuropsycholo-gist takes a conceptual approach toward the rehabilitationprogram, a combination of methods may be criticized forits resemblance to a shotgun approach to treatment (throweverything at the problem and see if something hits).
P S Y C H O T H E R A P Y I N R E H A B I L I T A T I O N
Neuropsychological rehabilitation is concerned not onlywith rehabilitating cognition but also with personality,emotion, and awareness. Of course, the brain is also themediator of these functions. Altered self-awareness andpersonality after brain injury may, in fact, represent someof the most complicated and higher order brain processes
CHAPTER 13 | Traumatic Head Injury and Rehabilitation 395

396 PART THREE | Disorders of the Brain
that a neuropsychologist and rehabilitation team at-tempts to treat (for a case discussion, see Neuropsychol-ogy in Action 13.4). Psychotherapy can aid by discussingfrustrations in progress and providing motivationalstrategies. But more importantly, and more profoundly,individuals with brain damage who have suffered morethan mild impairment often report they no longer feel“normal” and have to go through a readjustment processto adapt to their new level of functioning. Those whohave suffered brain injuries report that their social lifehas declined (Elsass & Kinsella, 1987) and rank loneli-ness as their most frequent complaint (Thomsen, 1974).Relatives and significant others often describe a “person-ality change” (Jennett & Teasdale, 1981). Poor social in-teraction is evident in ratings of close others and directbehavioral observations (Newton & Johnson, 1985).These losses are perhaps the most tragic and far-reachingaspects of brain injury.
Frontal lobe damage, as we discussed earlier in thisbook, is a common result of moderate to severe head in-
jury due to bony skull projections and shearing. Frontallobe damage is typically suspect when certain qualities ofpsychosocial functioning are observed after injury. Amongthe difficulties co-occurring with frontal lobe injury areimpulsivity, disinhibition, lack of initiation, rigidity, lossof abstract attitude, poor social judgment, and loss of per-sonal and social awareness (Lezak, Howieson, & Loring,2004). Prigatano (1992; also see Prigatano, 1999) arguesthat self-awareness requires the highest integration of“thought” and “feeling” areas of the brain, combining in-puts from sensorimotor, limbic, and paralimbic areas. Thecommon perception that people with CHIs have an “ego-centric” or “unempathic” attitude is usually attributed tovarious manifestations of these and frontal lobe difficul-ties. The specific inability to see a situation from another’sviewpoint may be one of the cognitive dysfunctions un-derlying apparent egocentric or unempathic behavior.This skill, labeled cognitive perspective taking, variesamong moderately to severely injured people (Spiers,Pouk, & Santoro, 1994; Santoro & Spiers, 1994). The
N e u r o p s y c h o l o g y i n A c t i o n 1 3 . 4
I t I s M o r e T h a n a B l a c k B o x
Cecil R. Reynolds Ph.D., Department of Educational Psychology, Texas A&M University, College Station, TX
A popular means of treating disorders oflearning and behavior in children is behav-ioral therapy and derivative approaches thatcapitalize on changing behavior by imple-menting specific reinforcement programs.Clinically, this approach derived from work bythe Russian physiologist Ivan Pavlov onclassical conditioning (known sometimes asPavlovian conditioning) and the Americanpsychologist B. F. Skinner, who developedtheories of operant conditioning (Skinnerianconditioning). Pavlov is best known forteaching, quite by accident, a dog to salivateon hearing the sound of a bell. Skinnertaught rats to press levers for food andpigeons to peck keys to be fed. Early clini-cians such as Joseph Wolpe were able totake these phenomena and translate theminto methods to cause humans to alter theirbehavior by altering the so-called reinforce-ment systems they believe control a specificperson’s behavior.
As behavioral approaches to treatingdisorders of learning and behavior grew in
schools and clinics around the world, peak-ing in the late 1970s, understanding brainfunctioning faded into the background.Skinner and other radical proponents ofbehavior therapies argued that what went onin the brain was irrelevant. Only input andoutput were important, and people need notunderstand the brain’s function further; itwas treated as a black box, a euphemism fora space in which some transformation mayoccur through processes not understood butalso that are irrelevant to the understandingof behavior and learning. As late as 1977, Ihad a professor in graduate school, teachinga course in learning, make the pronounce-ment in class that “the brain has nothing todo with learning; learning is all accomplishedthrough change or continuance of reinforce-ment paradigms.” Such views were notuncommon.
Behavioral approaches to the manage-ment and alteration of behavior in childrenwith developmental disorders are often, butfar from always, effective. And as it turns out,
brain systems are crucial in mediatingreinforcement schedules and learning. Letme provide an example. At age 11, Deannaattended a program for gifted and talentedchildren at her local public school, with ameasured IQ in excess of 130. She playedpiano and had won a trophy as star player ofher soccer team a year earlier. In spring ofthat year, Deanna was riding in the passen-ger seat of her dad’s car when a drunk driverran a stop sign, striking the car at Deanna’sdoor. She suffered many injuries, including abroken pelvic bone and numerous cuts andbruises. Most devastating, however, was herhead injury. Deanna had suffered a massiveright frontal lobe injury, producing a largesubdural hematoma that was evacuated inneurosurgery. Her cerebral bleeding ex-tended through the right superior parietalareas, and much microscopic shearing andtearing of neurons occurred throughout herbrain. She spent 11 days in a deep coma,and her parents were warned that she mightnot even recognize them if she came out of

CHAPTER 13 | Traumatic Head Injury and Rehabilitation 397
general ability to recognize and appreciate one’s own func-tional and cognitive changes also varies over individualsand time since injury. However, those who have greaterawareness of their dysfunction typically show higher lev-els of emotional distress (Nockleby & Deaton, 1987).
Psychotherapy in the rehabilitation setting often targetsthese neuropsychology-based issues of self-awareness, ego-centricity, and empathy. Psychotherapy can be useful notonly to aid coping and adjustment but also for practical rea-
sons. Difficulty in psychosocial functioning and poor self-awareness is one of the prime reasons for poor vocationaloutcomes. If therapy targeting affective issues is provided,another 20% to 30% of patients may become productiveworkers (Prigatano, 1992). Beh-Yishay and Prigatano(1990) found that three factors largely predicted vocationaloutcome: involvement with others, ability to regulate affect,and acceptance of cognitive limitations. All three of thesefactors are mainly influenced by psychotherapy.
SummaryNeuropsychologists play an important role in evaluating the cognitive profile of patients who have sufferedfrom a TBI and are actively involved in the rehabilitation for these conditions. Neuropsychologists are mostinterested in how such conditions result in specific neuropsychological deficits and disabilities in adaptivebehaviors. Research in this area not only improves the patient’s care but also provides new knowledge on thenormal functioning brain. Rehabilitation is clearly becoming one of the major areas of practice for neuropsy-chology. The rehabilitation process is complex and depends on many mechanisms, including biological,
the coma at all. Deanna did revive and had amiraculous recovery.
After 6 months in a rehabilitation hospi-tal, Deanna returned to school. Over the next2 years, additional cognitive recovery wasevident. Her IQ, measured in the 60s (men-tally deficient) 6 months after injury, gradu-ally increased to nearly 100 (average), andher academic skills in reading, writing, andarithmetic came to grade level. A far cry fromtheir prior, or premorbid, status, but all in all,a positive outcome. However, this oncepopular, socially adept young girl was nowostracized by her peers due to her nowobnoxious behavioral patterns.
She had few social skills and just did notappear to know how to interact positivelywith others. She was extremely impulsive, asshe acted most often without thought, wasconstantly reaching out to touch whomevershe talked to, and had no clear sense ofpersonal space. Her social judgment wasseverely impaired, and she often blurtedinappropriate and embarrassing commentsto others. Deanna came to my attention aftera consult request from the University Clinic,where a doctoral student had been workingwith the family for more than a year to de-velop a behavioral treatment plan to changethese many socially inappropriate behaviors.Such problems are common among patients
of all ages with frontal lobe damage, espe-cially prefrontal and orbitomedial damage, allof which were present in this case. The earlyimages of her brain injury, taken via magneticresonance imaging (MRI) in the first fewweeks and months after her injury, docu-mented these lesions well. However, Deannaappeared resistant to behavioral intervention.
After a careful review of her case, anotherMRI scan was requested and obtained, nowmore than 30 months after injury. The newimages showed an injury that had not ap-peared before. Deanna had a lesion and scartissue on the posterior portion of her hip-pocampus just above the fourth ventricle ofthe brain. The importance of such a lesionmay not be immediately obvious; however,the hippocampus is a component of thelimbic system and is crucial to memoryfunctions. These brain systems, the fron-tolimbic system and particularly the hip-pocampus, are significantly involved inlearning reinforcement systems. Individualswith posterior hippocampal damage areespecially resistant to reinforcement sched-ules that are anything less than a one-to-oneratio reinforcement schedule.
The mediation systems that allow rein-forcement to be recalled and to mediatelearning had been irreparably damaged inDeanna. Despite the protestations of the
devotees of Skinnerian conditioning, thebrain does matter! Behavior therapies can beeffective in treating TBI and developmentallydisordered children with behavior problems,even with frontal lobe systems that areimpaired. However, once limbic system andspecifically hippocampal functions are alsodamaged, such interventions fail.
With this knowledge and evidence,Deanna’s insurance carrier was persuadedto fund a different, more intensive interven-tion. An in vivo therapeutic approach wasdevised in which a therapist went withDeanna to local shopping malls for severalhours several times a week. Deanna’s behav-ior was constantly monitored and redirectedin this setting by a therapist, who also de-vised a set of verbal cues and self-talkstrategies. In doing so, we took advantage ofher stronger verbal skills, given that most ofher injuries were in the right hemisphere, asDeanna learned social skills in real-lifesettings, in vivo, or “on the job,” so to speak.Being a teenager is a tough job; being ateenager with frontal lobe injury who doesnot respond to changes in the reward-and-punishment systems of life is nearly impossi-ble. Deanna did graduate from high school,a year late, and is now employed in a clericalassistant position at a university library. Shestill hopes to attend college.

398 PART THREE | Disorders of the Brain
Tensile strengthRetrograde degenerationAnterograde degenerationPenetrating head injuryClosed head injuryAccelerationDecelerationImpact injury
Countercoup injuryGlasgow Coma Scale
(GCS)ComaEdemaIntracranial pressure (ICP)Brain herniationTranstentorial herniation
Subdural hematomaExtradural hematomaEpidural hematomaPost-traumatic amnesia
(PTA)Retrograde amnesiaAnterograde amnesiaSubstitution
DiaschisisRestitutionPlasticityPhysical therapistOccupational therapySpeech therapistDysarthriaTherapeutic recreation
personal, and environmental factors. The assessment and evaluative methods used necessarily focus onfunctional or “real-life” tasks of daily living. Treatment requires that patients and families be active in reha-bilitation and work as “trainees” of the team. In rehabilitation, assessment is an ongoing process, monitor-ing the progress of treatment and aiding decision making regarding the effectiveness of interventions andthe prognosis for long-term outcome.
The methods of treatment currently being developed by neuropsychologists provide exciting and cre-ative ways to help ameliorate dysfunction of individuals with brain impairments. With specialized knowledgeof the brain and behavior, as well as technical advances, neuropsychologists are uniquely positioned toguide individuals and their families to their highest potential for recovery and functioning. Chapters 14, 15,and 16 focus on the relation between diffuse neuropsychological deficits and dementing conditions such asencountered in Alzheimer’s disease and disorders of consciousness.
C r i t i c a l T h i n k i n g Q u e s t i o n s
Can a head injury change a person’s life?What is the potential for the human brain to adapt and recover after brain injury?What are the challenges for rehabilitation in the twenty-first century?
K e y Te r m s
We b C o n n e c t i o n s
http://www.tbilaw.comBrain Injury Information Page—provides information about brain injury, concussion, and head injury.
http://www.neuropsychologycentral.comNeuropsychology Central—a great site that keeps you up to date on the latest in neuropsychological linksand resources. Internal search engine allows you to determine what topic you would like to focus on andprovides you with detailed summaries of each link that has been found. Provides links to neuropsychologi-cal assessment, forensics, treatment, and other related areas.
http://www.tbims.orgTraumatic Brain Injury (TBI) Model Systems—learn about TBI’s National Database, the diagnosis of TBI, theCenter for Outcome Measures, and more.
http://www.healthpsych.comHealth Psychology and Rehabilitation Web Site—comprehensive site that provides information on health andrehabilitation psychology.
http://www.neuro.pmr.vcu.eduNational Resource Center for Traumatic Brain Injury (TBI)—guide for TBI survivors; tips on rehabilitation andon living and working productively with TBI.

Chapter 14
NORMAL AGING AND DEMENTIA:ALZHEIMER’S DISEASE
In one’s youth every person and every event appear to be unique. With ageone becomes much more aware that similar events recur. Later on one is lessoften delighted or surprised, but also less disappointed than in earlier years.
—Albert Einstein
Normal AgingMild Cognitive ImpairmentDefining DementiaAlzheimer’s DiseaseTreatment
Neuropsychology in Action
14.1 The Discovery of Alzheimer’s Disease14.2 Differentiating between Symptoms of Alzheimer’s
Disease and Normal Aging

Normal Aging
Defining “normal aging” is a challenge. Stereotypesand concerns abound as people face getting older. So-cially, we may fear becoming isolated with adjustment to
retirement and death of friends or a spouse. Physically,age brings the threat of increased ailments and chronicillness. Cognitively, the possibility of memory problems,mental slowing, and dementia looms. These concerns areoften amplified by myths of aging, painting people older
400 PART THREE | Disorders of the Brain
OverviewElderly adults are the fastest growing segment of the U.S. population. In 1900, 4% of the population wasolder than 65. As of the 2000 census, this number has mushroomed to 12.4%, or 34.9 million people. Inthe year 2030, estimates suggest 20% of the population will be older than 65, constituting approximately70 million people (Administration on Aging, 2000). The 85-and-older group is expected to double its currentsize. This trend toward an aging population is found throughout Western industrialized countries. Thesenumbers reflect increased life expectancy and medical advances. However, diseases of aging become agreat concern.
Tremendous research effort is focused on understanding the neurologic conditions that target olderpeople. Among these conditions are a group of disorders, collectively known as the dementias, that causeglobal declines in cognitive and behavioral functioning. They have no one cause, and most causative factorsare still not fully understood. Moreover, many dementias have no known cure. Dementia is often progres-sive, eventually affecting numerous higher mental facilities. It is often considered a “thief of the mind,” firstrobbing one aspect of cognition such as memory, communication ability, or visuospatial skills, but thenreturning to steal other aspects of mental functioning.
With a top-heavy population of aging baby boomers, the problem of identifying dementia and providingmedical and psychological services to patients and families is becoming increasingly important. About 10%of Americans older than 65 live in specialized settings (such as residential care facilities or assisted living),and more than 1 million live in nursing homes. Older people account for more than 40% of hospitalizationdays in acute-care hospitals. They buy 25% of all prescription drugs and use 30% of the total health budget.Clinical neuropsychologists contribute valuable assessment skills to distinguish normal aging from demen-tia. They also play an important role in health care decision making, helping match level of care to an olderpatient’s actual needs.
This chapter examines the differences among normal aging, mild cognitive impairment (MCI), anddementia, and addresses questions regarding the aging brain and neuropsychological functioning. Forexample, is there an inevitable cognitive decline with age? This question can be addressed by consideringthe neuropsychological profiles of both healthy older adults and those with dementia. We examine demen-tias in both this and the next chapter. This chapter presents an in-depth evaluation of the most common de-mentia syndrome: Alzheimer’s disease (AD). This cortical dementia is examined from a neuropathologic, neu-ropsychological, and behavioral perspective. Chapter 15 presents the subcortical dementias of Parkinson’sdisease, Huntington’s disease, and Creutzfeldt–Jakob disease.
K e e p i n M i n d
Is dementia inevitable? How does healthy “normal” aging differ from dementia?
Are dementia and Alzheimer’s disease synonymous?
Does Alzheimer’s disease selectively affect “memory” structures of the brain?
Why is Alzheimer’s disease so difficult to diagnose?

than 65 as unattractive, dull, sickly, and unproductive(Dychtwald & Flower, 1989). Stereotypes of aging, how-ever, can be shattered by examples of highly functioningpeople. From rock performers such as Tina Turner torenowned scientists like Ruth Patrick (Figure 14.1), wewitness the great range of physical, social, and mentalability of people older than 65 and ask, What can we learnfrom those who age well?
One of the challenges for brain scientists is that therange of cognitive variation for people older than 65 iswide compared with people in their 20s, 30s, 40s, and50s. Some of this increased variation is due to the inci-dence of brain diseases of aging, such as the dementias orstrokes, and some of this may be due to “age-related” de-clines in cognition that affect people differentially as theyage. A large part of what clinical neuropsychologists areasked to do is to aid in determining the difference betweennormal cognitive declines due to the aging brain andbrain diseases. Inherent in this is whether problems suchas forgetting of names can be considered “normal age-related” or as the harbinger of AD. Scientists have won-dered whether age-related declines in cognition willinevitably lead to dementia (that is, is normal aging and de-mentia on a continuum?) or whether there is a qualitativedifference between a disease state and the aging brain. Thisissue is explored within this chapter and in Chapter 15.
This section reviews both cognitive and brain changesassociated with normal aging in humans. By consideringboth cross-sectional and longitudinal studies, as well asstudies that compare normal aging with dementia, a pic-ture of normal aging, cognition, and the brain emerges.
C O G N I T I V E C H A N G E S A S S O C I A T E D W I T H A G I N G
Why is there such a range of functioning in people olderthan 65? Does everyone lose some cognitive functionseven if they do not have degenerative brain disease? Is cog-nitive decline uniform, or are certain areas more likely todecline than others? What is the trajectory of cognitivedecline? Finally, are there protective factors against cogni-tive decline and disease?
Numerous examples exist of people who stay activeand working in their fields well past the age of retirement.Whether a scientist, a musician, or a mechanic, these peo-ple have developed an expertise and an accumulated bodyof knowledge related to their work. In fact, all people arelikely to develop areas of expertise over their lifetimes re-lated to work, hobbies, or talents. This crystallized intel-ligence consists of stored knowledge and habitual ways ofacting or solving problems built up over a lifetime. By re-hearsal, practice, and use, certain domains of knowledgebecome strengthened and are more easily accessible andperhaps less subject to decay. Verbal scales of intelligencetests typically measure general crystallized intelligence notrelated to a specific work domain. They measure factualknowledge, such as vocabulary definitions, or generalinformation learned in school. Crystallized intelligencerepresents an accumulation of acquired skills and general
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 401
Figure 14.1 (a) Tina Turner, one of the world’s most success-ful female rock artist, performs at age 65. (b) Dr. Ruth Patrick, oneof the world’s leading biologists, is still active at age 94. ([a] © HeinzAward photo/Lynn Keith; [b] REUTERS/Alexandra Beier.)

information and is more related to formal education or di-verse social experiences. Research using the Wechsler AdultIntelligence Scales (WAIS-R) suggests that levels of crys-tallized intelligence show only slight changes as we age(Kaufman, Reynolds, & McLean, 1989). It has also beentheorized that higher levels of crystallized intelligence orgeneral knowledge may provide a protective factor, or“functional reserve” (in this case, a “cognitive reserve”),against dementia that allows the brain to compensate inthe presence of declines presented by aging or disease.
Two series of studies lend credence to the idea that aprotective cognitive reserve may start early in life. Thefirst of these is provided by the longitudinal study of agingand AD called the Nun Study. David Snowdon of theUniversity of Kentucky has followed 678 Roman Catholicsisters who agreed to regular cognitive and medical assess-ments and brain donation at death. Snowdon and his col-leagues seek to shed light on the factors that lead to in-creased longevity, as well as on the determinants of ADand other brain disorders such as stroke. What is uniqueabout this research is the availability of records fromyoung adulthood and throughout the time each nunresided in the convent. In one study, Snowdon and col-leagues (1999) examined the linguistic complexity of au-tobiographies written as the nuns entered the convent be-tween ages 18 and 32. Women who scored lower on “ideadensity” (that is, the number of different ideas discussed)early in life also showed lower cognitive functioning afterage 75. Also, autopsies of a small sample of nuns indi-cated that the women who had brain markers of ADshowed lower “idea complexity” as young women thanthose who did not have brain pathology.
Snowdon’s studies used “idea density” as a proxy forintelligence, but researchers from Scotland (Whalley,Starr, Athawes, Hunter, Pattie, & Deary, 2000) were ableto actually assess the relation between a standardized gen-eral intelligence test, administered at age 11, and signs ofdementia more than 50 years later. Children who hadhigher mental ability were less likely to have dementiawhen they were located again at age 72. Interestingly,there was no relation between mental ability and declinefor those who had been diagnosed with an early-onset (be-fore age 65) dementia. Early-onset dementias, as discussedlater, may be caused by disease processes that are differentthan late-life cognitive decline.
Both the Nun studies and the Scottish studies show acorrelational link between early intelligence and the healthof the aging brain. One possible explanation is that a “cog-nitive reserve” serves as a reservoir to resist the effects ofaging. If this is so, it is not yet known whether cognitive re-serve is, for example, a reflection of having more neuronsand glial cells in crucial areas or the result of wider or more
efficient semantic networks. In addition, the positive corre-lation between intelligence and the aging brain may be re-lated to other factors associated with longevity. Those withhigher intelligence may be more likely to seek and followhealth information, have higher paying jobs, adhere to abetter diet, and have better access to health care.
Even people who show little signs of cognitive decline,however, are likely to notice changes in fluid intelligence.Areas of fluid intelligence involve novel reasoning and theefficiency of solving new problems or responding to ab-stract ideas. Fluid intelligence has also been conceptualizedas a measure of adaptability. Fluid intelligence is mostdirectly related to the influences of changing biological fac-tors and is relatively unaffected by higher levels of experi-ence or education. The most reliable declines in cognitionshow up in three areas of intellectual activity, all of whichare considered fluid markers of intelligence: (1) processingspeed, (2) abstract and complex new problem solving, and(3) memory and new learning.
Tests of fluid intelligence (for example, Wechsler’sDigit Symbol and Block Design) generally require bothnovel processing and the ability to complete a taskquickly. Studies of aging suggest that performance on testsof this type declines across the life span (Salthouse, 1991).Behavioral slowing also occurs and may partly contributeto poorer performance on a number of tests of fluid intel-ligence where speed is a factor, but age-related decline isstill observed on novel problem-solving tasks even in theabsence of speed demands.
Studies of aging suggest that older people are more likelyto have more difficulties in many aspects of memory. Earlyresearch in aging and memory suggested that the mainproblem for older people was information retrieval. Poorerperformance occurs with free recall, compared with recog-nition, with less contextualized information, and whenmore effort is involved. However, new learning may also bedifficult because of problems in encoding, particularly withintentional encoding. In fact, some of the retrieval issuesrelating to poorly remembered contextual information maybe due, in part, to poor encoding of context at the outset.Once information is encoded, however, healthy olderadults seem to show similar semantic storage in long-termmemory as younger adults. Semantic storage can be con-ceptualized as drawing more heavily on crystallized intelli-gence and knowledge structures (Bäckman, Small, Wahlin,& Larsson, 2000). There also appears to be little effect ofaging on procedural and implicit memory tasks, althoughthese may be performed more slowly.
It has been predicted that older adults would performmore poorly on prospective memory tasks because of ahigh degree of self-initiation required in remembering todo something in the future (for example, McDaniel &
402 PART THREE | Disorders of the Brain

Einstein, 2000). However, because prospective memoryrequires both remembering “what” is to be done and“when,” it appears that older people have more troublewith the “what” or content that may have more to do withbasic encoding, storage, and retrieval mechanisms in ret-rospective memory (for review, see Henry, MacLeod,Phillips, & Crawford, 2004). Although older people mayperform more poorly on laboratory prospective memorytasks, they do much better on real-life tasks, such as keep-ing appointments or remembering to post mail or returnphone calls; tasks for which motivation may be differentor external reminder aids may come into play (for review,see Henry et al., 2004).
A number of researchers suggest that working memory(WM) capacity declines with age. Interestingly, short-term memory, or the ability to recall strings of digits, doesnot appear to decline with age. However, this is a morepassive task than WM, where information must not onlybe held but also manipulated and processed in a morecomplex manner.
How stable is cognitive functioning among those 75,85, or older? Does the pattern look the same as one contin-ues to get older? Do initial losses of function stabilize, isthere a gradual decline, or is there an acceleration of loss insome areas of functioning? In a review of studies of longi-tudinal aging, it appears that the pattern of preserved crys-tallized intelligence over fluid intelligence does not hold inthose adults older than 75 (Bäckman et al., 2000), and allintellectual abilities show a decline in group studies.
However, a series of interesting studies conducted inSweden document the neuropsychological performanceof the oldest segment of the population. In one study, re-searchers gave neuropsychological tests twice, 2 yearsapart, to more than 300 people between the ages of 84and 90 (Johansson, 1991). This study of the oldest old(84–90 years old) found surprising stability in neuropsy-chological functioning between the first and second testsessions. Researchers expected that functioning of peopleat this advanced age would decline over 2 years. However,two thirds of the sample (66%) remained at the same cog-nitive level, whereas 31% declined (Johansson, Zarit, &Berg, 1992). Almost half (42%) remained in the normalrange of functioning during the 2-year time period. Thisfinding was surprising not only in that a large portion ofthe sample showed stability of cognitive function overtime but also that a significant portion of quite elderlyadults still had “normal” cognitive function.
Johansson and his colleagues (Johansson, 1991) sug-gest that cognitive changes were more related to terminaldecline, or proximity to death, than to chronologic age.Among other neuropsychological tests, these examinersadministered the digit span task, at regular intervals, to
normally aging Swedes older than 70. This requires re-peating increasingly longer series of digits either in se-quential or reverse order, respectively, until the testeemisses them. For the 70- to 88-year-olds studied overtime, Johansson examined two groups: those who diedbefore age 85 and those still living. Those alive at age 85showed a consistent performance as they aged; those whodied before age 85 started showing a drop in backwarddigit span by age 75 and marked declines in both forwardand backward span lengths by age 79.
What then is the secret of people who are active andproductive well into their later years? In recent years,much focus has been on what can be termed the “use itor lose it” hypothesis. This idea suggests that by keep-ing mentally active, or by increasing mental exercise,older people may be able to stave off mental decline anddiseases of aging. The question is, does mental exercise,such as doing crossword puzzles, starting a new hobby,or memory training help to slow or reverse the affectsof aging? This hypothesis has also been called thedifferential-preservation hypothesis (Salthouse, Babcock,Skovronek, Mitchell, & Palmon, 1990) because it is as-sumed that the large age differences in cognitive function-ing seen in the oldest adults are due to differences in theircurrent levels of mental activity and mental exercise. Thisis in contrast with the preserved-differentiation hypothesis(Salthouse et al., 1990) that is more in line with the ideaof “cognitive reserve” discussed earlier in this section. Inother words, it may be that the range of cognitive differ-ences found among older people are because those whoshowed higher cognitive ability to begin with continue toshow this pattern as they age. In a recent review and com-mentary on this issue, Salthouse (2006) suggests that theresearch on “mental exercise” or training as a strategy hasnot yet demonstrated convincing results. For example, re-search focused on training people on various cognitivetasks, although showing some immediate benefits in tar-geted task performance, has not shown to be generaliz-able to other tasks, often in the same cognitive domain.Also, the effects of training are not convincingly sustainedover time compared with those who were not trained.Therefore, although there is much optimism in the popu-lar press about our potential ability to stave off the gen-eral effects of aging through mental exercise, this idea doesnot yet appear to be supported.
Although the mechanisms are not yet known, peoplewho continue to be active well into their 70s, 80s, and90s may be the best at resisting both declines in fluid andcrystallized intelligence. They may have started out with ahigher level of crystallized intelligence, and thus are pro-vided with a certain degree of cognitive reserve. They mayhave learned a great deal in their life, which also provides
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 403

them with strong crystallized semantic networks. Althoughaspects of fluid intelligence such as speed and flexibility ofthought may decline, many older people do maintain anactive and independent lifestyle well into their later years.
B R A I N C H A N G E S A S S O C I A T E D W I T H A G I N G
Variation in functional abilities with aging is a clue thatthe brain may not decline in a uniform manner. But howdoes it age, and when is change noticeable? By reviewingboth global (structural and neuronal) and regional brainchanges affected by aging, as well as considering the tra-jectory of decline and factors that impact brain aging, apicture emerges of how the brain changes as people growolder.
The aging brain undergoes visually apparent grossstructural changes such as diminution in size and weight,flattening of the cortical surface, and expansion of thecerebral ventricles. The loss of weight and volume occursin a general linear trajectory (for review, see Raz, 2000).One of the first recognizable global indexes of brain healthor shrinkage is widening of the ventricles. If the brainloses volume in any area, the ventricles reflect this. How-ever, this gross marker does not necessarily imply that thebrain loses volume equally across all areas.
Concomitant changes occur at the neuroanatomic andbiochemical levels. Neurons undergo significant struc-tural changes with aging. Aging cells may shrink and die,lose some of their dendritic processes, and develop a yel-lowish brown pigment that accumulates in cells of thecortex and cerebellum and may have to do with “wear andtear” (Bourne, 1973; Kemper, 1994). Observations ofcortical thinning may have led to one of the myths ofhuman neurobiology, namely, that throughout adulthoodpeople lose a great number of neurons from their brainseach day. Better measurement methods indicate that thisis exaggerated, and that much cortical thinning may bedue to neuronal shrinkage rather than loss (for review, seeHaug, 1985). Although some markers of neuronal abnor-malities such as neurofibrillary tangles and senileplaques (see Figures 14.6 and 14.7) are hallmarks of ADand other dementias, they also occur in older people with-out frank evidence of cognitive dysfunction.
Images of aging brains often show white matter abnor-malities indicating attenuation of myelin around theaxons of neurons. This observation has led a number ofresearchers to question whether white matter (that is,myelinated axons) or gray matter (that is, cell bodies) maysuccumb more quickly to the aging process. Cerebrovascu-lar disease and hypertension, both more common in older
adults, are associated with white matter abnormalities (forexample, Strassburger et al., 1997), but these comorbidproblems of aging do not appear to fully explain whitematter aging. In an analysis of studies across the life span,gray matter suffers a linear decline from infancy throughold age, whereas white matter shows an inverted U-shaped function with increasing white matter into youngto middle adulthood, followed by a plateau and then adecline into old age (for review, see Raz, 2005).
The brain shows differential changes with aging. Al-though some brain areas appear more vulnerable to theeffects of aging, there are islands of relative preservation.The hippocampus, the frontal lobes, and specific associa-tion areas of the temporal and parietal lobes are more vul-nerable, whereas the occipital and somatosensory corticesare relatively preserved. The frontal cortex is one of thecortical areas most affected by aging. The most likely setof age-related neuronal changes specifically affects the pre-frontal cortex (Esiri, 1994). Neuronal loss in this area mayaccount for some of the fluid intelligence changes in cog-nitive functions occurring in older people.
Because cognitive functioning varies widely among olderpeople, it is also reasonable to assume that there is a range ofindividual variability in physical brain changes. When as-sessing the degree of cortical atrophy caused by advancingage, gross inspection of the brain demonstrates wide varia-tion (Figure 14.2). In the Swedish study (Johansson, 1991),85% of elderly adults’ brains appeared to have little to noevidence of cerebral atrophy. However, all did show someneuropathologic markers usually associated with dementia,including signs of ischemia (that is, insufficient blood sup-ply), neurofibrillary tangles, and senile plaque formations.In individuals older than 85, gray matter atrophy is oftenapparent on computed transaxial tomography (CT) in bothdemented and nondemented people. White matter attenua-tion (thinning of the white matter) relates to cognitivechanges associated with fluid intelligence, such as slowedspeed of behavior, poorer spatial ability, poorer arithmetic,and memory recognition skills (Johansson, 1991).
Genetic and environmental factors also play a role inan individual’s vulnerability to brain aging. A variety ofgenetic factors have been implicated in the dementias dis-cussed in this and the next chapter. Some of these geneticfactors may also prove to accelerate the aging process inpeople who do not develop a full-blown dementia. Forexample, a specific allele of apolipoprotein E (that is,ApoE4) has been implicated in some forms of AD. How-ever, ApoE4 may also be implicated in general problemsof white matter maintenance through its action on thecholesterol system of the fatty oligodendrocytes that makeup the myelin sheath and through a disruption in the
404 PART THREE | Disorders of the Brain
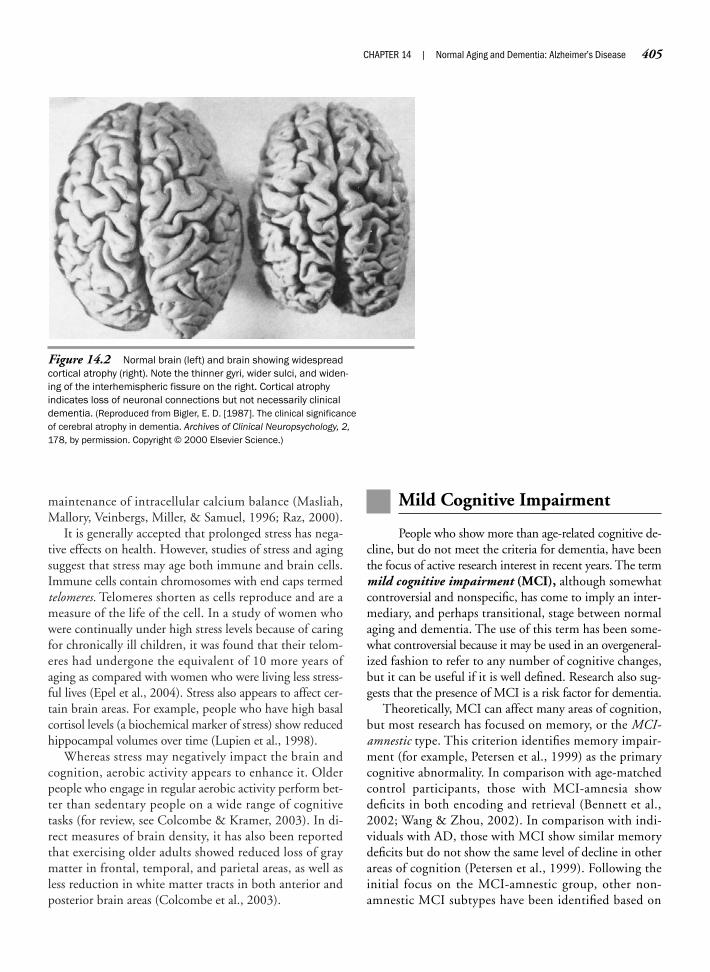
maintenance of intracellular calcium balance (Masliah,Mallory, Veinbergs, Miller, & Samuel, 1996; Raz, 2000).
It is generally accepted that prolonged stress has nega-tive effects on health. However, studies of stress and agingsuggest that stress may age both immune and brain cells.Immune cells contain chromosomes with end caps termedtelomeres. Telomeres shorten as cells reproduce and are ameasure of the life of the cell. In a study of women whowere continually under high stress levels because of caringfor chronically ill children, it was found that their telom-eres had undergone the equivalent of 10 more years ofaging as compared with women who were living less stress-ful lives (Epel et al., 2004). Stress also appears to affect cer-tain brain areas. For example, people who have high basalcortisol levels (a biochemical marker of stress) show reducedhippocampal volumes over time (Lupien et al., 1998).
Whereas stress may negatively impact the brain andcognition, aerobic activity appears to enhance it. Olderpeople who engage in regular aerobic activity perform bet-ter than sedentary people on a wide range of cognitivetasks (for review, see Colcombe & Kramer, 2003). In di-rect measures of brain density, it has also been reportedthat exercising older adults showed reduced loss of graymatter in frontal, temporal, and parietal areas, as well asless reduction in white matter tracts in both anterior andposterior brain areas (Colcombe et al., 2003).
Mild Cognitive Impairment
People who show more than age-related cognitive de-cline, but do not meet the criteria for dementia, have beenthe focus of active research interest in recent years. The termmild cognitive impairment (MCI), although somewhatcontroversial and nonspecific, has come to imply an inter-mediary, and perhaps transitional, stage between normalaging and dementia. The use of this term has been some-what controversial because it may be used in an overgeneral-ized fashion to refer to any number of cognitive changes,but it can be useful if it is well defined. Research also sug-gests that the presence of MCI is a risk factor for dementia.
Theoretically, MCI can affect many areas of cognition,but most research has focused on memory, or the MCI-amnestic type. This criterion identifies memory impair-ment (for example, Petersen et al., 1999) as the primarycognitive abnormality. In comparison with age-matchedcontrol participants, those with MCI-amnesia showdeficits in both encoding and retrieval (Bennett et al.,2002; Wang & Zhou, 2002). In comparison with indi-viduals with AD, those with MCI show similar memorydeficits but do not show the same level of decline in otherareas of cognition (Petersen et al., 1999). Following theinitial focus on the MCI-amnestic group, other non-amnestic MCI subtypes have been identified based on
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 405
Figure 14.2 Normal brain (left) and brain showing widespreadcortical atrophy (right). Note the thinner gyri, wider sulci, and widen-ing of the interhemispheric fissure on the right. Cortical atrophyindicates loss of neuronal connections but not necessarily clinicaldementia. (Reproduced from Bigler, E. D. [1987]. The clinical significanceof cerebral atrophy in dementia. Archives of Clinical Neuropsychology, 2,178, by permission. Copyright © 2000 Elsevier Science.)

other variations in cognitive decline (Petersen, 2004,2005). Imaging studies also suggest that this MCI groupshows hippocampal and brain atrophy that is worse thanwould be expected in normal aging but is not as markedas that seen in AD (Jack et al., 2000, 2004, 2005).
A major reason for targeting those with MCI is to de-termine their risk for progressing to AD or another de-mentia. Indeed, longitudinal research has suggested thatthe MCI-amnestic group is at a greater risk for develop-ment of a dementia at an accelerated rate (Bennett et al.,2002; Daly et al., 2000; Flicker, Ferris, & Reisberg, 1991;Ganguli, Dodge, Shen, & DeKosky, 2004; Lopez et al.,2003). Through the identification of this group, at a highrisk for dementia, therapeutic interventions can poten-tially be started earlier and biomarkers for various typesof dementias can be studied.
S U M M A R Y
The findings from various researchers in aging and cogni-tion suggest that both crystallized and fluid intelligenceare important for successful functioning in advanced age.Ability, level of education, and knowledge gained early inlife appear to provide some buffer against later brain dis-orders. Not everyone ages cognitively at the same rate,and many people retain high abilities into advanced age.Some individuals may suffer devastating effects, bothphysical and cognitive, whereas others suffer relatively feweffects. Therefore, among groups of older people, age isnot the only, or best, predictor of cognitive decline ormortality. The process of aging increases the probabilityof cognitive problems. Aging also results in brain and neu-ronal changes, but physical changes do not by themselvesalways differentiate between normal aging and dementiabecause of a wide range of individual differences and dif-ferences in functional cognitive reserve. Different mea-sures of functional capacity may well be the key to identi-fying those at greatest risk for cognitive impairment.Advanced imaging methods correlated with neuropsycho-logical functioning hold promise for more precisely relat-ing structure to function. This will also aid in identifyingpeople at greatest risk for development of dementia, suchas those with MCI, and in ultimately answering the fol-lowing question: What is the difference between normalaging and dementia?
Defining Dementia
With public and scientific attention focused on de-mentia, one might expect general agreement when refer-ring to dementia and subtypes of dementia such as AD.Given the cornucopia of terms used to refer to dementia
and subtypes of dementia, however (Table 14.1), there canbe confusion. Professionals and laypeople alike may confusedementia—the behavioral syndrome—with one particularcondition, such as AD. Patients and families often label de-menting conditions as “hardening of the arteries,” “senility,”or “old-timers’ disease,” which often reflects a perceptionthat the problem is inevitable in aging. In the most genericsense, dementia refers to a behavioral syndrome, and notone disease or cause. It denotes conditions that may have avariety of causes. Some dementias may be treatable, and oth-ers may not be treatable. Some stem from disease processesthat inevitably become worse, and some from toxic expo-sure or injury, resulting in a behavioral decline that plateaus.
The dementia syndrome is a cluster of behavioralsymptoms that may or may not point to a disease, but de-mentia is not a disease entity in and of itself. The varioussubcategories of dementia usually relate to the suspecteddisease, cause, or primary site of damage (for example,cortical versus subcortical). Researchers have found wellover 50 causes of dementia (see Table 14.1). Among the
406 PART THREE | Disorders of the Brain
Progressive Dementias
Cortical dementiasAlzheimer’s diseaseMotor neuron diseasePick’s diseaseProgressive aphasiaWilson’s disease
Subcortical dementiasHuntington’s diseaseParkinson’s diseaseProgressive supranuclear palsyAIDS dementiaCreutzfeldt–Jakob disease
Mixed dementiasLewy body dementiaVascular dementiasBinswanger’s disease
Potentially Static Dementias
Toxic conditionsAlcoholic dementiaHeavy metal poisoning (such as
lead and mercury)
Infectious conditionsHerpes encephalitis
Miscellaneous conditionsTumorNormal pressure hydrocephalusTrauma
Potentially Reversible Dementias
Systemic illnessSevere anemiaUremia
Deficiency statesB12 deficiency
Endocrine disordersAddison’s diseaseThyroid disorders
Drug toxicityAnticholinergicsAntipsychotics
Table 14.1 Representative Causes of Dementia

most well known are the degenerative dementias causedby a progressive and unrelenting disease process such asAD or Parkinson’s disease. Neurologists traditionally havecategorized these disease processes as cortical, subcortical,or mixed, depending on the degree to which they affectgray or white matter areas of the brain. Vascular, infectious,and toxic conditions, as well as a variety of other brainconditions, may also result in dementia.
Some of these conditions are progressive, whereas oth-ers, such as the dementia resulting from herpes encephali-tis, may be static, rarely worsening over time. Althoughmost dementing conditions encountered by neuropsychol-ogists represent persistent or progressive states, or both, re-searchers have also documented “reversible” or temporarydementias. Reduced metabolic efficiency accompaniesaging, making older adults especially susceptible to condi-tions and substances that they might have tolerated whenyounger. For example, symptoms of dementia can stemfrom adverse reactions to medications (such as sedative-hypnotics and anticholinergic drugs), nutritional disor-ders (such as thiamine deficiency and pernicious anemia),metabolic disorders (hypoglycemia, hypercalcemia, kidneyfailure), psychiatric disorders (severe mood disorders, psy-chosis), and other conditions such as anesthesia or surgery.However, when these conditions are treated, the dementiais usually reversible and the patient returns to baseline.
D I A G N O S T I C C R I T E R I A F O R D E M E N T I A
No one set of criteria represents definitive agreement re-garding the diagnosis of dementia. Somewhat varying di-agnostic standards are described in the Diagnostic and Sta-tistical Manual (4th ed., revised; DSM-IV-R) and by theNational Institute of Neurological and CommunicativeDisorders and Stroke-Alzheimer’s Disease and Related Dis-orders Association (NINCDS-ADRDA) (McKhann et al.,1984) (Table 14.2). However, experts agree about some ofthe major features of dementia. The first is that dementiaresults in a loss of cognitive or intellectual function. This fea-ture implies a decline that is acquired and unusual. It isacquired because people born with impaired intellectualfunction, having developmental disorders such as mentalretardation, do not have dementia simply by virtue ofpoor intellect, although they too can experience develop-ment of dementia. The loss of cognitive or intellectualfunctioning must also be unusual or outside of the realmof what would be expected with normal aging. As we havediscussed, aging may bring about some cognitive decline,particularly in memory and areas of fluid intelligence. Butthe decline associated with dementia represents a markedchange from previous levels of intellectual and memory abil-ity. Although the most well known subtypes of dementia
have a predilection for the elderly and result in progres-sive deterioration, this broad definition of dementia couldhypothetically refer to the sudden loss of intellectual func-tion from head injury in a 17-year-old.
Although patterns of impairment may differ, the secondarea of diagnostic agreement in dementia involves multipleareas of cognitive impairment. The abilities impaired in de-mentia may represent all cognitive functions or may pres-ent different patterns of neuropsychological disability. Bothsets of criteria for dementia identify memory impairmentas a prominent and necessary feature. However, it is themultiple and often diffuse cognitive decline that character-izes dementia. It is not uncommon to see impairment inabstract thinking and problem solving, impaired judgment,and other problems of higher cortical functioning.
In summary, the term dementia in its broadest senserefers to a group of conditions and diseases that sharesome similar neuropsychological and behavioral symp-toms, although the underlying causes may vary widely.The prime identifying feature is a decline in multiple areasof cognitive functioning, including memory. Beyond thisinitial definition of dementia, however, lies what is probablymost important in working with patients with dementia—an understanding of the different neuropsychological pre-sentations of dementia subtypes.
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 407
Criteria DSM-IV-R NINCDS-ADRDA
Memory impairment R R
Impairment of additional area of R Dcognition (such as language, construction, praxis, or executive functioning)
Confirmed on mental status tests NS R
Impaired/decline in social or R NS occupational function
State of consciousness unclouded R R
Evidence of specific organic factor R NSetiologically related to the disorder or absence of conditions other than organic mental syndrome
Note: DSM-IV-R = Diagnostic and Statistical Manual of Mental Disorders, FourthEdition, Revised; NINCDS-ADRDA = National Institute of Neurological and Communica-tive Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association; R = required; D = desirable but not required; NS = not specified.
Source: Adapted from Rebok, G. W., & Folstein, M. F. (1993). Dementia. Journal ofNeuropsychiatry and Clinical Neurosciences, 5, 265–276; and Katzman, R., Lasker, B.,& Bernstein, N. (1988). Advances in the diagnosis of dementia: Accuracy of diagnosisand consequences of misdiagnosis of disorders causing dementia. In R. D. Terry (Ed.),Aging and the brain (Vol. 32, pp. 17–61). New York: Raven Press.
Table 14.2 Diagnostic Criteria for Dementia

S U B T Y P E S A N D C L A S S I F I C A T I O N S O F D E M E N T I A
C o r t i c a l v e r s u s S u b c o r t i c a l
Traditionally, the primary demarcation among subtypesof dementia has followed the attempt to distinguish be-tween cortical and subcortical dementias. Cortical de-mentias primarily affect, or start out by affecting the cere-bral cortex, or gray matter. AD is typically includedwithin this category. With subcortical dementias, thedisease state predominantly affects the white matter, orneuronal connections between cortical areas, and graymatter structures below the cortex. The term subcorticalwas first used to describe the neuropathology and accom-panying pattern of cognitive deficits associated with pro-gressive supranuclear palsy (Albert, Feldman, & Willis,1974). Since that time, it has expanded to include Hunt-ington’s and Parkinson’s diseases and may also refer to dis-eases such as acquired immune deficiency syndrome(AIDS)–related dementia and some depressions. The dif-ficulty with this differentiation, both neuroanatomicallyand behaviorally, is that these disorders do not conformto strict cortical–subcortical boundaries in the brain. Forexample, AD typically causes significant cortical neuronalloss and atrophy, but also specifically attacks the hip-pocampus, a subcortical limbic system structure. In con-trast, diagnosticians usually identify Parkinson’s diseaseby the subcortical structure that it targets, the substantianigra, although evidence suggests that it also affects somehigher cortical functions such as executive functioning.Even when evidence indicates that a disease targets onlysubcortical structures, “cortical” effects may appear be-cause of the disconnection of neural pathways in thewhite matter that connect the gray matter areas. Althoughwe use the terms cortical and subcortical dementia as gen-eral categories, you must loosely interpret them to implya major or primary area of damage rather than an exclu-sive area of damage.
S t a t i c v e r s u s P r o g r e s s i v e
All dementias that result from a disease process are pro-gressive. Diseases such as AD, Pick’s, Huntington’s, orCreutzfeldt–Jakob inevitably follow a continuous cogni-tive and behavioral decline. Other conditions, however,may cause a static or steady-state cognitive disorder. Aneurotoxic substance (such as lead or alcohol) or infec-tion (such as herpes encephalitis) continues to cause braindamage as long as it is present. But when the condition isarrested, the resultant dementia usually plateaus.
Both static and progressive dementias can begin with asudden change of functioning, over days or weeks, or a
more insidious or gradual onset, over the course ofmonths or years. Lead poisoning may impact the brainfor a period of years before obvious impairment appears.Herpes encephalitis, in contrast, is an acute infectiouscondition with sudden and dramatic effects on the brain.Progressive dementias can also vary in their course. Theprogression, as in the case of AD, is gradual. However,there may be long periods during which the declineplateaus. Vascular dementias often produce a stepwiseprogression, as multiple infarcts (multi-infarct demen-tia) or strokes occur at different times. Only repeatedneuropsychological testing and keen observation by theneuropsychologist, patient, or family can demonstrate theprogression of the dementia.
R e v e r s i b l e v e r s u s I r r e v e r s i b l e
Researchers have focused primarily on irreversible andprogressive dementias. However, clinicians are likely tosee a variety of patients with dementia-like symptomsthat may remit with time. Part of the diagnostic problemwith the so-called reversible dementias is that these peo-ple may actually have delirium rather than dementia.Delirium does not signal dementia, but rather is a tran-sient cognitive problem associated with an acute confu-sional state. Typically, individuals with delirium havepoor attention, disorganized thinking, perceptual disrup-tion, disorientation, memory impairment, and an alteredstate of consciousness. Because delirium and dementiashare memory impairment and disorientation, they canbe easily confused. However, with delirium, the symp-toms develop over a period of days or hours and arecaused by specific organic problems such as overmedica-tion or an acute or worsening medical condition. Manymedical problems listed in Table 14.1 as potentially re-versible dementias cause delirium. Moreover, it is not un-common for patients with dementia to experience devel-opment of delirium. For example, a person might beadmitted to the hospital to have surgery or to be treatedfor an acute medical condition. Perhaps an already re-duced cognitive capacity causes vulnerability to the cog-nitive effects of general metabolic dysfunction. Peoplewho become delirious for short periods and then recovershould not be diagnosed with dementia, even a reversibleone. One difference in presentation is that people withdementia, other than in the late stages, are alert and canrespond to what is going on around them. People withdelirium are grossly confused and disoriented to theirsurroundings. A true “reversible dementia” should meetthe behavioral criteria for dementia discussed earlier; thatis, the individual must show dementia in the absence ofa delusional state.
408 PART THREE | Disorders of the Brain

Research continues on the question of reversibility.Several possibilities exist. For example, anticholinergicdrugs impair memory functioning. Perhaps, reduced cog-nitive functioning caused by large doses of a medicationcan, indeed, permanently reverse when the person stopstaking the medication. Or perhaps, dementia symptomsstemming from overmedication indicate the early stagesof dementia in an already compromised brain, so that dis-continuing the drug only temporarily increases cognitivefunctioning.
The remainder of this chapter focuses on AD. Thisrepresents the most scrutinized and researched dementia.We focus on the epidemiology of AD, diagnostic issues,clinical presentation, and neuropsychological profile andtreatment.
Alzheimer’s Disease
Alzheimer’s disease (AD), named after its discov-erer, Alois Alzheimer (Neuropsychology in Action 14.1),is a progressive cortical dementia that is irreversible andthus results in an inevitable decline. It is the most devas-tating and prevalent of the dementias, representing theeighth leading cause of death overall for people older than65 (Hoyert & Rosenberg, 1997) and more than 50% ofdiagnosed dementia cases (Kay, 1995). The number ofnew cases of AD increases with age from 1% of the popu-lation aged 65 to 75 years to 6% to 8% of adults olderthan 85. The rate of survival varies widely between 2and 20 years with a median survival rate of between 3 and4 years after diagnosis (Helmer et al., 2001; Wolfson etal., 2001). The prevalence, or number of people livingwith AD at any one time, increases with age and survivalrate. It is estimated that between 10% and 30% of peoplearound the world older than 85 have AD (for example,Bowirrat, Treves, Friedland, & Korczyn, 2001; Gurlandet al., 1999; Stevens et al., 2002; Wang et al., 2000).Based on the 2000 census, it is estimated that between 3and 4 million people older than 65 have AD (Mayeux,2003).
There appears to be no single cause for AD, and inmost cases, the causative factor remains unknown. AD islinked to increased age, which has led some to speculatethat it is a disease of “accelerated aging”—implying that ifwe all lived long enough, AD would be inevitable. Over alifetime, women are about twice as likely to experiencedevelopment of dementia or AD as men (Seshadri et al.,1997), but this may be partly accounted for by thatwomen have a longer life expectancy (Mayeux, 2003).People with more education appear less likely to experi-
ence development of AD, but again, this is probably amarker of larger cognitive reserves acting as a buffer be-tween neuropathology and disease manifestation.
AD does not have a clearly identified genetic compo-nent in most cases. A variation exists that is autosomaldominant, meaning the family pedigree shows about 50%of the family members as having AD, but this type proba-bly affects less than 150 families worldwide. The mostlikely chromosomal culprits in genetically established ADappear to be chromosomes, 1, 14, and 21. Interestingly,people born with Down’s syndrome, or trisomy 21(named because the disorder results from an abnormalityon chromosome 21), inevitably develop a dementia, usu-ally by age 40. The associated brain changes correspondingto AD (neurofibrillary tangles and senile plaques) appearyears before clinical diagnosis. In summary, although thebiomedical research searching for causes and markers ofthe disease appears promising, scientists still know littleabout the actual causes of AD.
D I A G N O S T I C P R O B L E M O F A L Z H E I M E R ’ S D I S E A S E
A definitive diagnosis of AD requires the behavioral pres-ence of dementia and the identification of neuropatho-logic markers of AD. No single medical test, imaging pro-cedure, or behavioral test can positively identify AD (forexample, Mayeux, 2003), short of a brain biopsy showingthe characteristic neurofibrillary tangles and neuriticplaques, which are most predominant in the hippocam-pus and cortical association areas. Because biopsy is not aprocedure to which most people would submit, a defini-tive diagnosis cannot be made until autopsy. AD is diffi-cult to diagnosis because there are other dementias thathave may have similar symptoms, especially in the laterstages of the disease. In diagnostic accuracy studies, wherephysicians have to choose the correct diagnosis amongseveral types of dementias, AD disease tends to be over-diagnosed, meaning that other progressive dementias maybe misdiagnosed as AD (Lopez et al., 1999). A recent Chi-nese study that analyzed both the clinical features andbrain markers of various dementias at autopsy found thatthe agreement rate between clinical diagnosis of dementiaand pathologic findings was 64.5% of cases (Wang, Zhu,Gui & Li, 2003). Concordance between clinical and bio-logical findings was strongest for vascular dementias(66.7%) and less strong for degenerative dementias(40%).
The clinical diagnosis of AD depends largely on evi-dence related to behavioral and neuropsychological profiles
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 409
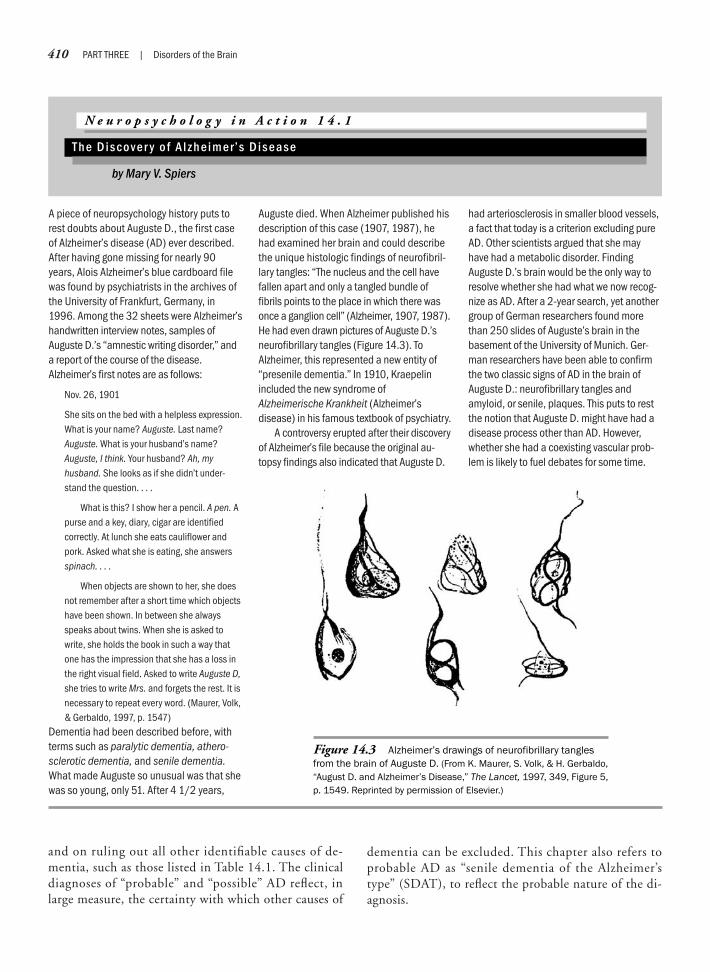
and on ruling out all other identifiable causes of de-mentia, such as those listed in Table 14.1. The clinicaldiagnoses of “probable” and “possible” AD reflect, inlarge measure, the certainty with which other causes of
dementia can be excluded. This chapter also refers toprobable AD as “senile dementia of the Alzheimer’stype” (SDAT), to reflect the probable nature of the di-agnosis.
410 PART THREE | Disorders of the Brain
A piece of neuropsychology history puts torest doubts about Auguste D., the first caseof Alzheimer’s disease (AD) ever described.After having gone missing for nearly 90years, Alois Alzheimer’s blue cardboard filewas found by psychiatrists in the archives ofthe University of Frankfurt, Germany, in1996. Among the 32 sheets were Alzheimer’shandwritten interview notes, samples ofAuguste D.’s “amnestic writing disorder,” anda report of the course of the disease.Alzheimer’s first notes are as follows:
Nov. 26, 1901
She sits on the bed with a helpless expression.What is your name? Auguste. Last name?Auguste. What is your husband’s name?Auguste, I think. Your husband? Ah, myhusband. She looks as if she didn’t under-stand the question. . . .
What is this? I show her a pencil. A pen. Apurse and a key, diary, cigar are identifiedcorrectly. At lunch she eats cauliflower andpork. Asked what she is eating, she answersspinach. . . .
When objects are shown to her, she doesnot remember after a short time which objectshave been shown. In between she alwaysspeaks about twins. When she is asked towrite, she holds the book in such a way thatone has the impression that she has a loss inthe right visual field. Asked to write Auguste D,she tries to write Mrs. and forgets the rest. It isnecessary to repeat every word. (Maurer, Volk,& Gerbaldo, 1997, p. 1547)
Dementia had been described before, withterms such as paralytic dementia, athero-sclerotic dementia, and senile dementia.What made Auguste so unusual was that shewas so young, only 51. After 4 1/2 years,
Auguste died. When Alzheimer published hisdescription of this case (1907, 1987), hehad examined her brain and could describethe unique histologic findings of neurofibril-lary tangles: “The nucleus and the cell havefallen apart and only a tangled bundle offibrils points to the place in which there wasonce a ganglion cell” (Alzheimer, 1907, 1987).He had even drawn pictures of Auguste D.’sneurofibrillary tangles (Figure 14.3). ToAlzheimer, this represented a new entity of“presenile dementia.” In 1910, Kraepelinincluded the new syndrome ofAlzheimerische Krankheit (Alzheimer’sdisease) in his famous textbook of psychiatry.
A controversy erupted after their discoveryof Alzheimer’s file because the original au-topsy findings also indicated that Auguste D.
had arteriosclerosis in smaller blood vessels,a fact that today is a criterion excluding pureAD. Other scientists argued that she mayhave had a metabolic disorder. FindingAuguste D.’s brain would be the only way toresolve whether she had what we now recog-nize as AD. After a 2-year search, yet anothergroup of German researchers found morethan 250 slides of Auguste’s brain in thebasement of the University of Munich. Ger-man researchers have been able to confirmthe two classic signs of AD in the brain ofAuguste D.: neurofibrillary tangles andamyloid, or senile, plaques. This puts to restthe notion that Auguste D. might have had adisease process other than AD. However,whether she had a coexisting vascular prob-lem is likely to fuel debates for some time.
N e u r o p s y c h o l o g y i n A c t i o n 1 4 . 1
T h e D i s c o v e r y o f A l z h e i m e r ’ s D i s e a s e
by Mary V. Spiers
Figure 14.3 Alzheimer’s drawings of neurofibrillary tanglesfrom the brain of Auguste D. (From K. Maurer, S. Volk, & H. Gerbaldo,“August D. and Alzheimer’s Disease,” The Lancet, 1997, 349, Figure 5,p. 1549. Reprinted by permission of Elsevier.)

N E U R O P A T H O L O G Y O F A L Z H E I M E R ’ S D I S E A S E
M a j o r B r a i n S t r u c t u r e sA f f e c t e d b y A l z h e i m e r ’ s D i s e a s e
Two interesting facts exist regarding the neuropathologyand pathophysiology of AD. First, the disease targets spe-cific regions of the brain. Second, disease-targeted struc-tures sustain neuronal loss and atrophy. Although AD is a“cortical dementia,” because major areas of the cerebralcortex show brain shrinkage, this disease does not respectcortical boundaries. It greatly affects major subcorticallimbic system structures such as the hippocampus andamygdala. Most pathologic changes occur in the corticaltemporoparietal association areas and the subcortical lim-bic cortexes. Specifically, the disease destroys the majorpathways to and from the hippocampus, cutting off di-rect connections to association cortices.
Gross postmortem inspection of the brain often findscortical atrophy. In Figure 14.4, the most marked atrophyis in the frontal, temporal, and parietal areas. The gyri arethinned, and the sulci are noticeably widened. Researchersestimate that in AD about half of the large neurons deteri-orate (Terry, Peck, deTeresa, Schecter, & Horoupian,1981), resulting in a loss of volume. Specifically, theseneurons lose dendritic arborization, or branching. Theventricles also enlarge, because of cortical thinning (Fig-ure 14.5). Although dementia severity increases with in-creased cell death, longitudinal comparisons of globalcerebral atrophy with dementia severity do not reliablyindicate dementia (Bigler, 1987; Johansson, 1991).
A closer look at specific structures reveals that they sus-tain massive cell loss. In fact, SDAT appears to followstructural borders. Chief among these are the parietal andtemporal cortices, the hippocampus and the structures lead-ing to it (entorhinal cortex and the perforant neural path),the amygdala, and specific nuclei of the thalamus (VanHoesn & Damasio, 1987). In addition, certain subcortical
frontal areas are implicated, such as the nucleus basalis ofMeynert and the olfactory areas. Noticeably spared arethe primary motor and sensory areas (tactile, auditory, vi-sual) and the basal ganglia. The affected structures corre-spond to areas of higher cognitive functioning and mem-ory, leaving relatively untouched more basic sensory andmotor abilities.
H I S T O L O G I C M A R K E R S
The two neuropathologic findings that Alzheimer (1907,1987) identified, still considered the primary markers ofthe disease, are neurofibrillary tangles and neuritic, or se-nile, plaques. These are evident by microscopic inspec-tion of brain tissue obtained at autopsy. Neurofibrillarytangles resemble entwined and twisted pairs of ropewithin the cytoplasm of swollen cell bodies (see Figures14.3 and 14.6). Tangles consist of proteins, termed tauproteins, that are believed to accumulate as a result of ab-normal phosphorylation. The excessive collection createstangles that are dispersed throughout the brain but dis-proportionately in the areas just listed, including the tem-poroparietal areas and the hippocampal complex. Thespecificity of structural deterioration in AD extends to thecellular layers of the cortex. For example, within the six-layered isocortex of the cortical association areas, tanglesand plaques devastate layers 3 and 5, whereas other layersare relatively spared (Van Hoesn & Damasio, 1987).
Alzheimer described neuritic plaques as “clump-likedeposits in the neuropil.” They are round aggregates of“cellular trash” that have a particular affinity for the re-gions where the majority of synapses lie (the neuropil).
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 411
Images not available due to copyright restrictions
Image not available due to copyright restrictions

The synapses eventually disintegrate, leaving holes andneurites (that is, pieces of axons and dendrites) wherethere were once active connections (Figure 14.7). Plaquesare likely to concentrate in the frontal and temporal re-gions (Zubenko, Moossy, Martinez, Rao, Kopp, &Hanin, 1989) and are numerous around the hippocampalformation. As we discussed earlier, tangles and plaquesare not specific to AD. They also appear in normally agingindividuals without evidence of dementia, as well as inother degenerative diseases. It is the pattern and quantityof these markers that defines AD.
An exciting recent discovery is that the substance ofneuritic plaques and tangles may lead to hypotheses re-garding possible causes of and treatments for AD. Theneuritic plaques found in AD contain an amino acid pep-tide protein core termed beta-amyloid (�-amyloid). As
a result, these neuritic plaques are also called amyloidplaques. Bradshaw and Mattingly (1995) review severalpossibilities for how β-amyloid may operate. First, it iscoded on chromosome 21, the same chromosome respon-sible for Down’s syndrome. The behavioral significanceof this is that if they live past 30 years, people withDown’s syndrome often show AD-like dementia symp-toms. Therefore, chromosome 21 may be responsible forboth problems. Second, there is debate on the functionof β-amyloid. Is it a cause of the disease, a by-product of thedisease, a “protective reactant,” or an autoimmune response?
As we discussed earlier in this chapter, genetic researchhas focused on the protein ApoE4, which may be associ-ated with both WM aging and AD. This additional pro-tein in plaques and tangles has been studied for its impor-tance in AD. ApoE4 is one of four possible variants, oralleles, of the protein ApoE. Seventy-five percent of peo-ple in the population have the ApoE3 variant (Corder etal., 1993), but risk for development of AD increases to90% if a person inherits the ApoE4 variant from bothparents. In addition, a double set of ApoE4 alleles also re-duces the mean age of onset. ApoE4 is responsible for fer-rying cholesterol into the brain; however, researchers arecurrently investigating how this protein may operate inAD. It appears on yet another chromosome, chromosome19, which binds with β-amyloid in cerebrospinal fluid.The exact mechanism for this binding process is not yetknown; however, researchers hypothesize that ApoE4 maynot be the direct or sole cause of the disease (see Bradshaw& Mattingly, 1995); rather, the protective factors thatApoE2 or ApoE3 provide may be lost. However, there isnot yet consensus whether it can serve as a specific or sen-sitive marker of the disease (Mayeux et al., 1998), andthere are no genetic markers of AD that have yet been es-tablished for diagnostic purposes (Knopman et al., 2001).Researchers have also examined the CSF of patients withpotential AD to examine potential β-amyloid deficienciesor the presence of tau proteins in cerebrospinal fluid. Al-though a combination of some of these biomarkers holdspromise in aiding diagnosis, that some biomarkers aresensitive to more than one condition precludes their rou-tine use in determining the diagnosis of AD (Knopmanet al., 2001).
N e u r o t r a n s m i t t e r S y s t e m sA l t e r e d b y A l z h e i m e r ’ s D i s e a s e
AD may impact multiple neurotransmitter systems.However, the most consistent evidence of a neurotrans-mitter with a direct effect on memory processes in AD isacetylcholine (ACh).
412 PART THREE | Disorders of the Brain
Image not available due to copyright restrictions
Image not available due to copyright restrictions

In the brain, ACh is synthesized in a group of neuronscalled the basal forebrain cholinergic complex (BFCC). Thecell bodies of these neurons lie in the basal forebrain struc-tures of the nucleus basalis of Meynert, the diagonal bandof Broca’s area, and the globus pallidus. These axons proj-ect to the hippocampus and the cerebral cortex, primarilythe frontal and temporal cortexes. The BFCC is a subcor-tical component of the limbic system and the majorsource of choline for the hippocampus and cortex (Coyle,1985). Researchers have long known that ACh plays a rolein memory. Drachman (1977) demonstrated that block-age of receptors causes memory loss even in young adults.In AD, the devastation of the BFCC neurons profoundlydepresses brain levels of ACh, perhaps as much as 60% to90% (Terry & Davies, 1980; Bowen, Benton, Spillane,Smith, & Allen, 1982).
Some of the other neurotransmitters implicated in ADare the catecholamines, the amino acid glutamate, andthe neuropeptides somatostatin and corticotrophin. How-ever, at this juncture, none of these neurotransmitters ap-pears to play a clear role in AD. Researchers have reportedthat all are reduced in AD, but their reduction may besecondary to the disease process. For example, generalstress also reduces somatostatin. As you might imagine,research in this area is progressing quickly because of thepush to find appropriate pharmacologic treatments.
N e u r o i m a g i n g i n A l z h e i m e r ’ sD i s e a s e
Gross neuroimaging of the brain in patients with AD mayindicate cerebral atrophy on CT or magnetic resonanceimaging (MRI). The electroencephalograms of patientswith AD are likely to show generalized slowing (LaRue,1992). Degree of atrophy or slowing taken in isolation isnot reliably associated with degree of neuropsychologicalimpairment (for example, see Bigler, 1987), but the de-gree of ventricular enlargement seen over time as the cor-tex atrophies accompanies increasing cognitive impair-ment (Burns, Jacoby, & Levy, 1991) but is only a grossindex of general brain health. Special imaging proceduresdemonstrate the enlarged hippocampal fissure that resultsfrom neuronal loss, tangles, and plaques that begin earlyin the disease process. Also characteristic of AD is a pat-tern of metabolic or vascular insufficiency, or both, seenin the temporoparietal area, which shows up on positronemission tomography (PET) and single-photon emissioncomputed tomography (SPECT) scans. This hypometab-olism can be either unilateral or bilateral and depends onfactors such as severity of illness, sex, and age at onset (forreview, see Forstl & Hentschel, 1994).
CTs and MRIs are primarily useful, not to confirm adiagnosis of AD, but to rule out other conditions such astumor or vascular causes of dementia seen as multiplesmall strokes or ischemic attacks. However, promisingnew methods of analyzing volume and ratio of specificstructures through structural imaging may help confirmdiagnosis of AD. PET and SPECT scans appear most sen-sitive for detecting the characteristic patterns of SDAT.These imaging measures are then correlated with neu-ropsychological measures to provide a dynamic picture ofthe disease process.
C L I N I C A L P R E S E N T A T I O N A N D N E U R O P S Y C H O L O G I C A L P R O F I L E O F A L Z H E I M E R ’ S D I S E A S E
The clinical presentation of patients with AD can vary,but many share characteristic patterns (Neuropsychologyin Action 14.2). The most consistent deficits across pa-tients with autopsy-documented AD are memory and flu-ent anomic aphasia (for example, see Price et al., 1993).Visuospatial difficulties are also characteristic. Thesedeficits correspond with neuroimaging studies showingpatterns of hypometabolism in limbic and associationareas in early stages of the disease. In this classic presenta-tion, some frontal areas of the brain appear relativelyspared. This also corresponds with neuropsychologicaltesting and clinical observation indicating that, despitesevere memory impairment, many patients with AD re-tain an appropriate “social facade,” do not have a Broca-type (nonfluent) aphasia, and retain normal strength andsimple motor speed until the end stages of the disease.However, the impairments progress over time, graduallyaffecting all higher mental functions of the brain. Whatfollows is a description of the neuropsychological and be-havioral performance, according to functional area, typi-cal of those with the SDAT variant. Because memory dys-function is the hallmark of AD, we devote more discussionto this problem than to the other functional areas.
M e m o r y
AD globally and profoundly impairs memory. New de-clarative learning problems at all levels (encoding, stor-age, and retrieval) and retention over time are usually no-ticed first. In addition, structures of the brain that holdpreviously well-learned semantic knowledge informationin organized associational frameworks begin to deterio-rate. Finally, short-term memory span, names of familymembers, and familiar stories fragment. The only type oflearning that appears to persist lies outside the corticolim-bic system, with certain types of nondeclarative learning.
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 413

414 PART THREE | Disorders of the Brain
Although memory impairment is the hall-mark of Alzheimer’s disease (AD), thoseolder than 65 (the time of life when AD ismost likely to manifest) often decline inmemory ability. The key is to differentiatebetween general complaints of forgetfulnessand lowered cognitive functioning thataccompany normal aging and cognitiveindicators of incipient dementia. Considerthe following two scenarios, which arecompilations of cases seen by the authors.
Case 1: Mrs. C
Mrs. C is a 90-year-old woman from a smallmidwestern town who has lived by herself forthe past 10 years since her husband died.She is active in her church and volunteers ata local thrift shop. At home she spends mostof her time reading, keeping up with corre-spondence to family and friends, and talkingwith neighbors on the phone. She drove hercar until a year ago, when after increasingrestrictions on night driving due to failingeyesight, she agreed with her physician thatshe should give it up. She tells her familythat her memory is quite poor. She can readthrough a whole book, but says if she pickedit up again it would be “just like reading anew book.” She watches the news daily andis interested in following the elections andcandidates for office. Mrs. C has a definiteopinion regarding who she likes, althoughshe does not remember many of the detailsof current events and says the news “goes inone ear and out the other.” However, shedoes remember major life events, if askedabout them by her children. She can recountepisodes from her teens and 20s quite welland tells old family stories from her child-hood with incredible detail and animation.For the first time in her life she has had tostart taking several prescription medicinesfor heart problems. At first she needednearly constant prompting to remember totake her three daily doses at the right times.However, over the course of 2 to 3 months,
she learned her medication routine. Shealways remembered to take her pills whenshe got up and before bed, but frequentlyforgot the 11 A.M. pill.
Case 2: Mrs. R
Mrs. R is a 75-year-old woman who is marriedand lives with her husband. Mr. and Mrs. R have always had an active social life,getting together with friends quite often to godancing or play bridge in their retirementcommunity. Within the past several years, Mr.R has noticed that his wife does not seem tobe paying attention when they play bridgeanymore. She has made wrong bids andmakes mistakes keeping score. She usuallymakes a joke about these things, saying to herfriend, “Lucy, you’re just trying to distract meso you’ll win.” Everyone has a big laugh, whichseems to just egg her on. Mrs. R particularlylikes to tell stories of when she was young, andshe has a lot of them to entertain everyone.When the conversation turns to the day’snews, Mrs. R seems to have little comment oncurrent events, although she and her husbandhave always watched the news together everynight. She seems to get news stories mixedup. Mrs. R says she just does not have toomuch use for the news and that “it goes in oneear and out the other.” A new couple hasjoined their dancing club, and much to Mr. R’sembarrassment, Mrs. R keeps reintroducingherself to them even after 4 months. After awhile it became comical, and Mrs. R says shedoes it on purpose for a joke. Mrs. R has takenmedication for the past 15 years and hasalways managed well. But now her husbandfeels like he must remind her to take her pillsbecause he noticed she often does not put itout by her plate as she used to do. Sheresents being reminded and says accusingly,“I put it out. Are you sure you didn’t just take itand put it away when you cleared the table?”This behavior is upsetting to Mr. R, but thething that bothers him most is that his wife,who had been a good cook, is now very
disorganized in the kitchen. After he noticedthat a cake tasted salty, he watched her asshe prepared other things. She often addedingredients twice or totally left out essentialsof her recipes.
Both Mrs. C and Mrs. R have troubleremembering in areas in which they werepreviously more able, and they appear tohave declined from their own former levelsof ability. In some respects, both show asimilar pattern of memory loss in thatremote memory, or information learnedmany years ago, such as stories from child-hood or facts related to work or homepersist remarkably well in comparison withnew learning. Difficulty remembering whatthe news commentator said or learning anew medication routine or a new namepresents more of a problem in both cases.These similarities between normal aging anddementia can prompt dread in people whosee themselves as less able to rely on theirpowers of memory. However, these twocases have several notable differences.First, Mrs. C appears to have some insightinto her memory difficulties, whereas Mrs. Rrationalizes, jokes, and blames others forher poor memory. Second, Mrs. C learns andretains some new things, even though thelearning may take longer.
Mrs. R, in contrast, not only is showingdifficulty learning new things but appears tobe losing her ability to perform previouslywell-learned tasks, such as cueing herself totake her own medication or to cook. Finally,there is a suggestion that Mrs. R’s problemsseem more pervasive, in that she may alsohave problems in concentration, attention,calculation skills, and name finding. Mrs. R’smemory difficulties are characteristic ofdementia, possibly AD, and may appearparadoxic to patients’ families, who can seethat their family member is socially appropri-ate and retains remote and overlearnedinformation quite well. It is easy to discountthe importance of cognitive problems.
N e u r o p s y c h o l o g y i n A c t i o n 1 4 . 2
D i f f e r e n t i a t i n g b e t w e e n S y m p t o m s o f A l z h e i m e r ’ s D i s e a s e a n d N o r m a l A g i n g
by Mary V. Spiers

Long-Term Declarative Memory—As in other conditions thatproduce “amnesia,” SDAT results in profound difficultiesin learning new declarative information. As discussed inChapter 9, declarative memory can be loosely dividedinto episodic and semantic memory; people with SDAThave deficits in both. One of the first and most promi-nent symptoms of AD is a deficit in new declarative learn-ing (sometimes termed anterograde amnesia to differenti-ate it from retrograde amnesia [deficit in remote recall]).On neuropsychological testing, patients with SDAT inthe mild to moderate stages of the disease typically showmarked impairment on both verbal and visual learningtasks, although the progression may begin with one areabeing of greater deficit. Performance on list learning overtrials usually does not progress much beyond an immedi-ate memory span length. That is, if a person has a mem-ory span of four or five items, five attempts to learn anine-word list often reveals a flat learning curve begin-ning with recall of four to five items and ending with re-call of four to five items. Verbal recall of stories and wordlists shows a large number of perseveration and intrusionerrors (among others, see Butters et al., 1988). For exam-ple, the person may repeat words from the same list as ifrecalling them for the first time or may recall one aspect ofa design that is presented, such as a dot in a box as fiveor six dots in a box. The person may recall specific eventsor stimuli across situations, intruding elements from onestory into another story or remembering elements of onedesign as part of another. Although all people with classi-cal amnesia show profound difficulties in new learning,this repeating and confusion of memory differs from mostother amnestic dysfunctions that the corticolimbic circuitcauses. Intrusions and perseverations are most commonin two conditions, AD and Korsakoff ’s amnesia, whichalso involve similar patterns of frontal lobe involvement.Butters (for example, see Butters et al., 1988) hypothe-sizes that the similar pattern of intrusion and persevera-tion errors in SDAT and alcoholic Korsakoff ’s amnesiamay be caused by a significant loss of cholinergic neuronsin the basal forebrain area.
Although many healthy elderly people may forget,they can often remember lost thoughts with the help ofretrieval cues. This facilitation of memory by retrieval cuesalso characterizes Huntington’s disease, but the memoryproblem in AD is more global and profound. People withAD show impairment in encoding, consolidation, and re-trieval. The constellation of memory deficits in ADgreatly hinders retrieval because it depends on proper en-coding, organization, and consolidation of material to beremembered. Thus, retrieval cues will not aid AD pa-tients’ recall of information, suggesting that encoding and
consolidation have not occurred. Besides that patientswith SDAT show flat learning curves (demonstrating lit-tle to no ability to profit from practice), any informationthat the patient may have remembered immediately afterpresentation quickly disappears. As the disease progresses,information is lost faster and faster. Although many peo-ple benefit from practice over days and weeks, patientswith SDAT do not appear to show this consolidation ofdeclarative learning.
Breakdown of Semantic Knowledge—People afflicted with ADhave another fundamental problem of memory, whichpervades the entire organization of knowledge. As dis-cussed earlier in this book, the brain stores information atthe site where it was first processed. That is, most visu-ospatial information is stored in the posterior areas of thecortex, primarily the parietal and posterior temporallobes. Auditory information is stored in the temporallobes, and so on. The dominant theory of memory con-solidation, simply put, is that the hippocampus, whichhas afferent and efferent projections to most areas of thecortex receives to-be-remembered information, codes itfor storage, and sends it back to the original processingsite (Squire, 1987). Researchers believe memory for infor-mation and facts is not stored as separate and completeunits (for example, all information about robins stored inone node). Rather, they hypothesize that the brain con-tains associations of meaning, “semantic networks,”whose individual nodes may contain pieces of informa-tion or attributes, such as “bird,” “wings,” “small,” and“red breast,” which when activated as a pattern lead to therecognition of “robin.”
Most amnestic patients, although they cannot encodenew information, have an intact semantic organizationalnetwork for information. In AD, the memory disorder ismuch more pervasive, involving a progressive disintegra-tion of this associational network, eventually even for oldlearned information. The evidence for this loss of knowl-edge through semantic degradation rests on several find-ings. First, neuropsychologists noticed that patients withAD do not organize new information semantically as theyare attempting to learn it. Thus, if presented with wordlists that have inherent semantic categories, such as fruits,vegetables, and items of clothing, most people learn andrecall information within semantic categories, clusteringthe information together. This “semantic clustering” isdeficient or nonexistent among patients with AD, whoinstead show a serial ordering or primacy/recency effect.Second, patients with AD appear to lose conceptualknowledge. Fluency tasks often reveal an interestingpattern. Asked to name as many animals as possible in
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 415

60 seconds, people with AD often can retrieve superordi-nate and high-frequency category exemplars such as cator bird, but show difficulty retrieving subordinate cate-gory exemplars such as leopard or robin. This degrada-tion appears to be more than just a problem in retrievingsemantic information from long-term memory. Thisdegradation has been shown to be consistent across tasks,so that the patient may also have difficulty in defining“robin” or naming a picture of a robin (Hodges, Salmon,& Butters, 1991). These difficulties represent neu-ropathologic changes of higher order intermodal associa-tion cortices strongly involved in semantic networking(for example, posterotemporal, inferior parietal), ratherthan classical language problems associated with thefrontal operculum (Broca’s area), superior temporal gyrus,or supramarginal gyrus. As the disease progresses, theseconnected memories or knowledge structures appear tobreak down to such a degree that even the identity andassociation of family members eventually become con-fused in the patient’s mind.
In this discussion of memory in AD, we have focusedprimarily on the encoding, storage, and retrieval processesof declarative long-term memory. These are undoubtedlythe areas of the most recognizable and profound memorydifficulty. Two areas of memory that appear less affectedby AD are short-term memory span and nondeclarativelong-term memory.
Relatively Spared Memory Systems—On short-term memorytasks such as length of digit span forward, patients withAD perform relatively well in the early stages of the dis-ease. In later stages, short-term memory retention declines.However, if the examiner looks closely at short-term mem-ory capacity, or WM, it is typically compromised.
Patients with AD perform relatively well on some non-declarative memory tasks. Separate nondeclarative mem-ory systems exist outside of the subcortical limbic system.The workings of these systems for the most part appearimplicit, or outside consciousness. Learning skills with alarge motor and practice component, such as riding abike or typing, or learning psychomotor tests, such aspursuit rotor or mirror tracing, appear to be part of amotor skills learning system. It is not yet clear whetherother systems controlling classically conditioned re-sponses and priming represent yet other nondeclarativememory networks, or if they are subcomponents of asingle nondeclarative network.
People with AD show normal performance on somenondeclarative tasks and impairment on others. Soliveri(Soliveri, Brown, Jahanshahi, & Marsden, 1992) describesthe pattern of nondeclarative memory performance in
various neurologically impaired groups. Most people withAD perform well on motor learning tasks that researchersthink represent an unimpaired striatal system. However,the picture is different with priming tasks. The method-ology of priming, discussed in Chapter 9 with the discus-sion of memory, assumes that previous exposure to anitem will facilitate its future processing. Word stem com-pletion priming tasks typically first present a list of words,such as there, church, and leaf. Later, they present three-letter stems such as the___, chu___ and lea__. Typicallyamnestics—even though they have not been able todemonstrate learning of the words through declarativemeans, namely, spontaneous recall—are likely to producethe targeted words on word stem completion tasks. Peo-ple with AD usually cannot perform these tasks well. In-terestingly, on perceptual priming tasks that present com-plete and incomplete figures, patients with AD appear toperform better in some instances. Because of this pattern,researchers suggest that patients with AD confront a spe-cific difficulty in implicit verbal priming whereas main-taining nondeclarative learning abilities in perceptualpriming and in attaining motor skills. Why would this beso? Verbal implicit priming tasks are probably anotherpointer to the AD breakdown of the semantic network.Motor skill learning is intact because it is controlled bythe striatum, which is relatively unaffected in AD. Per-ceptual priming appears to point to a relatively more in-tact visual object recognition system, which may not beaffected until late in the disease process.
L a n g u a g e / S p e e c h
Patients with AD do show language problems, but thesecannot be neatly characterized with other classic aphasias.In fact, the aphasia progressively worsens both in degreeand type. Early in the disease process, AD patients showan anomic aphasia, characterized chiefly by word-findingand naming difficulties (Cummings, Benson, Hill, &Read, 1985). A confrontation naming test (such as theBoston Naming Test), in which the person must retrievethe exact name of an item from line drawings, often re-sults in semantic and circumlocution (talking around) er-rors. A patient with AD is more likely to say “tool” for“hammer” or “some type of musical instrument” for “har-monica,” indicating that he or she recognizes the seman-tic category but can retrieve only the general category orthe wrong exemplar from the same category (for example,see Hodges, Salmon, & Butters, 1991). This type ofanomia, together with the difficulty in semantic fluencytasks discussed earlier, suggests a semantic anomic apha-sia. As the dementia progresses, language problems be-come more profound. Comprehension problems begin to
416 PART THREE | Disorders of the Brain
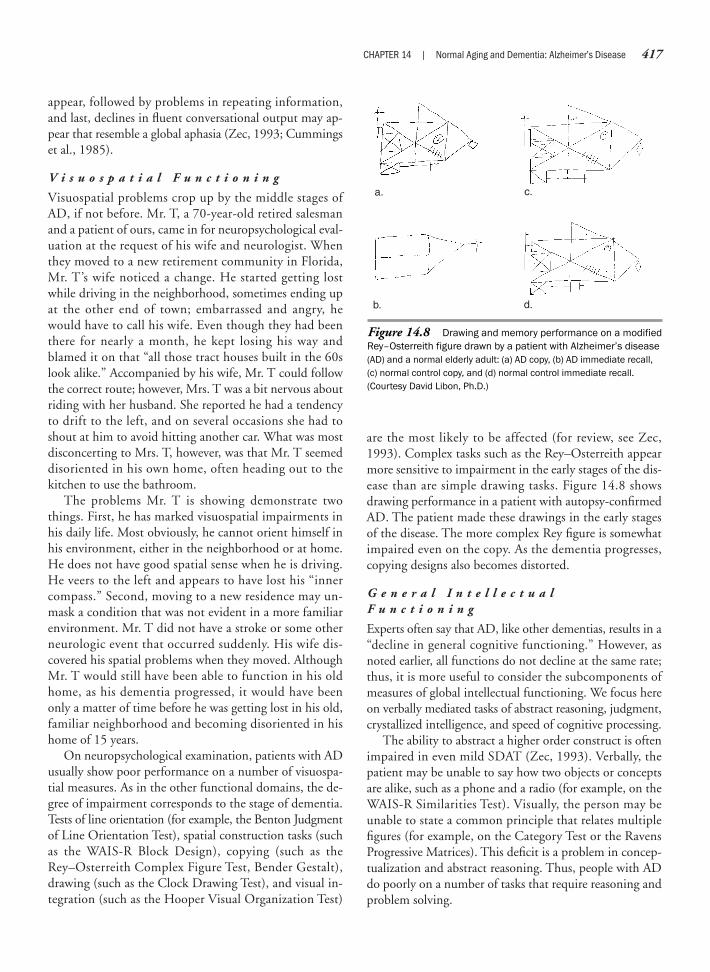
appear, followed by problems in repeating information,and last, declines in fluent conversational output may ap-pear that resemble a global aphasia (Zec, 1993; Cummingset al., 1985).
V i s u o s p a t i a l F u n c t i o n i n g
Visuospatial problems crop up by the middle stages ofAD, if not before. Mr. T, a 70-year-old retired salesmanand a patient of ours, came in for neuropsychological eval-uation at the request of his wife and neurologist. Whenthey moved to a new retirement community in Florida,Mr. T’s wife noticed a change. He started getting lostwhile driving in the neighborhood, sometimes ending upat the other end of town; embarrassed and angry, hewould have to call his wife. Even though they had beenthere for nearly a month, he kept losing his way andblamed it on that “all those tract houses built in the 60slook alike.” Accompanied by his wife, Mr. T could followthe correct route; however, Mrs. T was a bit nervous aboutriding with her husband. She reported he had a tendencyto drift to the left, and on several occasions she had toshout at him to avoid hitting another car. What was mostdisconcerting to Mrs. T, however, was that Mr. T seemeddisoriented in his own home, often heading out to thekitchen to use the bathroom.
The problems Mr. T is showing demonstrate twothings. First, he has marked visuospatial impairments inhis daily life. Most obviously, he cannot orient himself inhis environment, either in the neighborhood or at home.He does not have good spatial sense when he is driving.He veers to the left and appears to have lost his “innercompass.” Second, moving to a new residence may un-mask a condition that was not evident in a more familiarenvironment. Mr. T did not have a stroke or some otherneurologic event that occurred suddenly. His wife dis-covered his spatial problems when they moved. AlthoughMr. T would still have been able to function in his oldhome, as his dementia progressed, it would have beenonly a matter of time before he was getting lost in his old,familiar neighborhood and becoming disoriented in hishome of 15 years.
On neuropsychological examination, patients with ADusually show poor performance on a number of visuospa-tial measures. As in the other functional domains, the de-gree of impairment corresponds to the stage of dementia.Tests of line orientation (for example, the Benton Judgmentof Line Orientation Test), spatial construction tasks (suchas the WAIS-R Block Design), copying (such as theRey–Osterreith Complex Figure Test, Bender Gestalt),drawing (such as the Clock Drawing Test), and visual in-tegration (such as the Hooper Visual Organization Test)
are the most likely to be affected (for review, see Zec,1993). Complex tasks such as the Rey–Osterreith appearmore sensitive to impairment in the early stages of the dis-ease than are simple drawing tasks. Figure 14.8 showsdrawing performance in a patient with autopsy-confirmedAD. The patient made these drawings in the early stagesof the disease. The more complex Rey figure is somewhatimpaired even on the copy. As the dementia progresses,copying designs also becomes distorted.
G e n e r a l I n t e l l e c t u a lF u n c t i o n i n g
Experts often say that AD, like other dementias, results in a“decline in general cognitive functioning.” However, asnoted earlier, all functions do not decline at the same rate;thus, it is more useful to consider the subcomponents ofmeasures of global intellectual functioning. We focus hereon verbally mediated tasks of abstract reasoning, judgment,crystallized intelligence, and speed of cognitive processing.
The ability to abstract a higher order construct is oftenimpaired in even mild SDAT (Zec, 1993). Verbally, thepatient may be unable to say how two objects or conceptsare alike, such as a phone and a radio (for example, on theWAIS-R Similarities Test). Visually, the person may beunable to state a common principle that relates multiplefigures (for example, on the Category Test or the RavensProgressive Matrices). This deficit is a problem in concep-tualization and abstract reasoning. Thus, people with ADdo poorly on a number of tasks that require reasoning andproblem solving.
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 417
Figure 14.8 Drawing and memory performance on a modifiedRey–Osterreith figure drawn by a patient with Alzheimer’s disease(AD) and a normal elderly adult: (a) AD copy, (b) AD immediate recall,(c) normal control copy, and (d) normal control immediate recall.(Courtesy David Libon, Ph.D.)
a.
b.
c.
d.

Crystallized intelligence (see earlier discussion) refersto accumulated knowledge over the life span. Often, neu-ropsychologists measure this via tests of vocabularyknowledge (for example, WAIS-R Vocabulary) or over-learned information. For example, someone who has livedin the United States for several years should know in whatmonth Memorial Day falls. However, few formal testsmeasure specific areas of expertise that may accumulatefrom a person’s line of employment. This knowledge storeis one of the few areas that remain preserved until the laterstages of the disease.
Although patients with SDAT are slower on speededcomplex tasks (for review, see Zec, 1993), they do not ex-hibit the bradyphrenia, or extremely slow informationprocessing speed characteristic of patients with subcorti-cal dementias.
E x e c u t i v e F u n c t i o n i n g
Although deficits are subtle early on, difficulties in execu-tive control are evident to caregivers. For example, in an at-tempt to compensate for memory loss, a person may keepnotes. But without an adequate executive strategy, increaseddisorganization may show up in notes found in variousplaces around the house and in tasks started but left un-finished. Family members often notice perseveration ofthought because the person tells stories over and over or asksquestions repeatedly. The person may be less flexible thanbefore. Many apparent “personality” changes may actuallystem from frontal impairment. Repeated behaviors, such aschecking and rechecking, may emerge from the combinedeffect of a poor memory and increased perseveration.
An interesting aspect of dysfunctional executive abilityis that many patients with AD appear to lose metacogni-tive awareness, or the inability to self-monitor their ownbehavior and performance. Many clinicians describe pa-tients with AD as having little insight into their owndeficits. Often, they appear generally unaware or uncon-cerned about the magnitude or consequences of theirdeficits. Is this psychological response understandable as adefense mechanism against the devastating effects of thedisease? Not in the typical sense. Many patients with ADappear truly unaware of their difficulties, and consistentlyoverestimate their abilities to accomplish things.
Problems in the ability to organize, plan, and use ap-propriate strategies for problem solving in patients withAD often appear on tests designed for evaluating strategicprocessing (such as Tower of London or Tower of Hanoi)and qualitatively on tests designed for other purposes suchas visuospatial problem solving (such as the Block DesignTest of WAIS-R). Intrusions and perseverations oftenshow up on memory tests. Perseveration is evident as an
418 PART THREE | Disorders of the Brain
inability to shift sets on tests that require flexible problemsolving (for example, Wisconsin Card Sorting Test orTrails Making Test B).
O r i e n t a t i o n , A t t e n t i o n , a n d L e v e l o f C o n s c i o u s n e s s
AD is not an altered state of consciousness, such as delir-ium. General orientation and selective attention persistuntil late in the course of the disease. However, morecomplex forms of attention such as divided and alternat-ing attention decline from the early stages. Orientationfor person, time, and place is generally intact until themoderate to severe stages of AD.
M o t o r a n d S e n s o r y F u n c t i o n
In relation to other areas of functioning, motor and sen-sory abilities are relatively preserved throughout thecourse of AD. Simple motor speed and strength persistuntil late in the course of the dementia. However, morecomplex motor behavior, which may involve coordina-tion or skilled movement, declines earlier.
The disease process appears to spare sensory function-ing—that is, visual, auditory, and tactile acuity. Olfactionis the only primary sensory area affected; sense of smell iscompromised even in the mild stages of the disease (Jones& Richardson, 1990). Many patients with AD report vi-sual disturbances such as difficulty in reading, interpret-ing pictures, and recognizing familiar people. Althoughophthalmologists often find good acuity and full visualfields, neuropsychological testing often reveals visual-perceptual and visuospatial deficits, which may cause theself-reported visual disturbances.
M o o d , E m o t i o n , P e r s o n a l i t y ,a n d I n s i g h t
As with Alzheimer’s (1907, 1987) famous patient, clini-cians may first refer people for psychiatric symptoms. Insome cases, these symptoms stem from the cognitive diffi-culties that accompany AD, but in other cases, the symp-toms, such as depression, may represent an additional dis-order. Suspiciousness of others and frank paranoiddelusions can manifest memory dysfunction. One 70-year-old woman tearfully related that her husband hadbegun accusing her of stealing his glasses and other per-sonal items. After 50 years of marriage, he also accused herof having an affair. On questioning, it became apparentthat he was accusing her of taking things he was misplac-ing. Because of his impaired time estimation, not uncom-mon in AD, 5 minutes could seem like an hour, or anhour like 5 minutes. So when she went to the grocerystore on a quick errand, it seemed like an eternity to him.

He had little insight into his memory difficulties, and intrying to make sense of a frustrating situation, he exter-nalized the problem and blamed his wife.
Symptoms that herald a significant about-face in per-sonality usually raise a red flag for family members. Suchpatients are most likely to be seen by mental health pro-fessionals. However, psychiatric symptoms that are exacer-bations of premorbid personality styles make recognizingchange extremely difficult. A woman always consideredimpulsive and distractible, flighty or disorganized, may atfirst appear simply eccentric when she begins to lose trackof daily memories. When attempting to deal with mem-ory loss, the person is likely to carry on with coping stylesand defense mechanisms characteristic of earlier times. Asmemory becomes less reliable, a person concerned withorder, timeliness, or organization may obsessively checkdates, doctor’s appointments, medications, memos, andlists.
Depression and Dementia—A common problem in making adifferential diagnosis of behavioral disturbances amongthe elderly is to distinguish psychological depression fromglobal loss of intellectual function. The most effective wayto make these diagnostic determinations is to obtain for-mal psychometric testing from a neuropsychologist, whocan describe the patient’s cognitive functioning in detail,recognize normal and abnormal patterns of performance,and establish a baseline of performance against which tomeasure any changes over time. In addition, more subjec-tive guidelines may include the depressed patient’s ten-dency to exaggerate memory problems when comparedwith the demented patient’s tendency to deny or mini-mize them. It is important to query for information re-garding any situational/environmental life crisis thatmight have precipitated a depressive reaction, but thatwould not be expected to trigger a dementia process. Be-cause some elderly patients are heavily medicated, it isalso important to review all prescriptions to determinewhether any, alone or in combination, interfere with op-timal cognitive functioning. Of course, depression mayalso coexist with a cognitive disorder. Approximately 40%of people with AD may also suffer from depression orsymptoms of depression, although major depressiveepisodes are relatively rare (Cummings, 1994).
A common differential diagnostic issue with whichconsulting neuropsychologists deal is the referral to dis-tinguish between depression and dementia in elderly pa-tients. Following is a possible scenario:
When asked about her husband’s behavior during aninitial interview, Mrs. S related that her husband nolonger appears interested in his daily activities and hobbies.
CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 419
He used to tinker with their cars and had a hobby ofbuilding wooden clocks. He has gradually given both ofthese up over the past year and a half and says he is nolonger interested in them. He spends much more of hisday sleeping than he used to, although he is up a lot atnight. He has also lost weight and doesn’t seem to have astrong interest in eating. In fact, says his wife, Mr. S does-n’t seem to have a strong interest in anything. “If it wasn’tfor me,” she says, “he’d probably spend his whole day sit-ting in his chair. I try to give him things to do, like cross-word puzzles or little things to fix, but when I come back,he hasn’t gotten anywhere. We don’t see our friends any-more because he just doesn’t seem to have much to say.”Mr. S agreed that he had given up most of his former hob-bies, saying he just wasn’t interested in them anymore, al-though he wasn’t sure why. He didn’t admit to feeling par-ticularly sad or discouraged about these or any other events.Largely, he appeared to be apathetic, not particularly movedin any direction either to be excited and motivated to ac-complish things, or to be despondent about his situation.Although he didn’t seem to display internal motivation,Mrs. S did say that her husband would accompany her onoutings when she planned them. Recently, they had goneto New England on a four-day chartered bus trip withmembers of their church. Mr. S went along on all the ac-tivities and did not spend time sleeping during the day.
At first glance, Mr. S appears to suffer from symptomssuggestive of depression: He has lost interest in previouslyenjoyable hobbies and activities, and his eating and sleep-ing habits have changed. Curiously, however, he does notadmit to depressed mood or show other subjective or af-fective signs of depression. He also will become involvedin some activities. At this point, three possibilities need tobe considered: (1) Mr. S may have primary depression,(2) a dementing process may explain Mr. S’s depressivesymptoms, or (3) Mr. S may have both progressive de-mentia and depression. Further discussion of depressivesymptoms and testing for depression may show motiva-tional and affective difficulties, perhaps a reaction to amore sedentary lifestyle after retirement, or problems re-lated to his current life situation over the past severalyears. Chronic medical problems, if they exist, are likelyto result in decreased energy, a loss of vitality, and de-pressed mood. However, it is also possible that thesesymptoms may be largely explained by dementia. Mr. Smay have given up former hobbies such as clock buildingbecause he no longer has adequate visuospatial functioningor the organizational and planning abilities to successfullyapproach novel or complex problems. He also may sufferfrom “cognitive inertia.” If this is the case, what appearsto be poor motivation may be an inability to structure

and organize in such a manner as to accomplish tasks. Al-though at first only complex projects may be affected,later in the disease, even straightforward tasks such aswashing dishes or taking out the garbage may be difficultto begin, because the affected person does not knowwhere to start. Other possibilities to consider, consistentwith AD, are that he may have little insight into his diffi-culties and thus may appear vague and somewhat de-tached when speaking about himself. Certainly, furtherinterviewing and testing concerning memory and othercognitive problems are warranted. The primary objectivehere is not to differentiate between dementia and depres-sion based on a brief description of Mr. S’s difficulties.Rather, the point is to consider that, especially when psy-chiatric symptoms present themselves for the first time inolder patients, these may signal underlying cognitiveproblems. Although changes in personality and moodoccur with some frequency in AD, they are not necessaryor particular to this disease.
Treatment
No currently available treatments can reverse, halt,or slow the progression of AD. We simply do not yetknow enough about the neurophysiology and causes ofthe disease to develop medical treatments tailored to at-tack the underlying mechanisms. What, then, does treat-ment focus on? First, there is a big push for psychophar-macologic investigators to develop drugs that will enhancecognitive functioning. Many drugs are in the experimen-tal stages, and a few have made it to market. Most targetthe cholinergic system, and therefore memory. Second,both pharmacologic and behavioral interventions areaimed at ameliorating psychiatric symptoms and excessdisability (that is, additional cognitive and psychiatric im-pairment not directly attributable to the disease). Witheach of these treatments, the goal is to improve quality oflife for both the AD sufferers and their caregivers. Thissection provides an overview of psychopharmacologic andbehavioral approaches to intervention.
T R E A T M E N T S F O R C O G N I T I V EE N H A N C E M E N T
As discussed earlier, ACh is the neurotransmitter systemthat holds the most promising physiological link to AD.Many drugs that target the cholinergic system seek toincrease its production or action and, therefore, to com-pensate for the impaired cholinergic production in thebasal forebrain, including the nucleus basalis. Researchershave tried varied approaches to augment levels of brain
ACh. One approach is to increase the availability of AChprecursors such as choline. Because large quantities ofcholine are found in lecithin, a substance contained infoods such as egg whites and chocolate, researchers oncethought that by increasing dietary choline, they mightalso elevate brain levels of ACh. However, no clear im-provements in memory have materialized from this orother approaches. Other pharmacologic approaches haveattempted to target the synaptic transmission itself. Onemethod increases ACh by blocking its breakdown by in-hibiting acetylcholinesterase. Other methods strive to di-rectly increase the output of ACh or stimulate the post-synaptic cholinergic (muscarinic) receptors to increasefiring. Physostigmine (Synapton) was one of the firstcholinergic augmenting drugs that clinical trials tested withAD patients in the mid-1980s. Although some studies sug-gested improvement, this gain appeared minimal in lightof overall declining functioning. But there is some indica-tion that longer term use may result in more gain (for re-view, see Ashford & Zec, 1993). In the mid-1990s, tacrine(Cognex), which is a long-acting acetylcholinesterase in-hibitor, received a flurry of attention. It appeared to showsome positive effects, but also resulted in a side effect ofliver toxicity. To date, no fewer than 10 drugs have beendesigned specifically to enhance cholinergic activity in thebrain. At this point, however, the search is still on to findthe right combination of noticeable memory enhancementcoupled with tolerable side effects.
Alternative experimental approaches aimed at under-standing the pathophysiology of AD hold the promise offuture therapeutic benefit. Nerve growth factor (NGF) is amethod being researched to increase cholinergic neuronalfunctioning. NGF is part of a family of neurotrophins, orneuron-feeding nutrients, that researchers have longknown sustain neural viability in the autonomic nervoussystem. The cholinergic system neurons in the basal fore-brain also have specific receptors for NGF. In animals, an-tibodies to NGF result in neuronal shriveling and death.Also in animals, introducing NGF appears to increaseACh functioning and learning and memory behavior inthose with lesioned brains. NGF may prove therapeutic inAD if it can sustain life and promote growth of survivingcholinergic neurons. Methods suggested include intraven-tricular infusion of NGF through a pump (Olson, 1990),attachment of NGF to a gene that can specifically targetthe ACh system through a retrovirus, and direct neural im-plants of tissue with active NGF (Dunnet, 1991).
A pharmacologic treatment to halt or reverse the mem-ory and cognitive loss suffered in AD is likely to emergeas our understanding of the underlying pathophysiol-ogy develops. Probably this will involve a multifaceted
420 PART THREE | Disorders of the Brain

CHAPTER 14 | Normal Aging and Dementia: Alzheimer’s Disease 421
approach to treatment, because large areas of the brainare affected. The treatments reviewed here primarily tar-get the most common and prominent symptom of newlearning. A truly effective solution will have to conquerthe pervasive cognitive decline.
C O G N I T I V E , B E H A V I O R A L , A N D P S Y C H I A T R I C S Y M P T O M C O N T R O L
The other avenue of treatment for AD aims at symptomcontrol. Behavioral, psychiatric, and cognitive difficultiescan emerge either associated with the progression of thedisease itself or attributable to processes above and be-yond those symptoms that can be explained by the dis-ease itself—a condition termed excess disability. Attemptsto manage these symptoms use either pharmacologic orbehavioral tools.
Common behavioral and affective symptoms associ-ated with dementia include depression, insomnia, perse-cutory ideation, hallucinations, apathy, agitation, irritabil-ity, and purposeless or inappropriate activity patterns.Minor tranquilizers or antidepressants may aid depressionand insomnia, but pharmacologic treatment of psychoticsymptoms such as delusions or hallucinations may causeserious unwanted side effects. Neuroleptics may further
impair cognition, increase agitation, and cause other un-wanted motor symptoms.
Patients with AD are also susceptible to illness andconditions associated with aging such as respiratory orurinary tract infections and hearing and vision problems.The associated behavioral problems associated with this“excess disability” can include decreased or increased ac-tivity levels, delirium, or hallucinations. In the case of ill-ness, when the condition resolves the behavioral problemlikewise should subside. Visual or hearing problems mayalso amplify hallucinations or sensory illusions.
Because of the severe memory deficit, behavioral man-agement strategies based on learning and responding toreinforcement paradigms can easily prove futile. Instead,most management strategies seek to restructure the envi-ronment to ensure safety, provide appropriate stimula-tion, and redirect inappropriate behavior. As the diseaseprogresses, the person needs more constant supervision.Many nursing homes have specially designated Alzheimer’sunits because of the difficulties of behavioral manage-ment. If a patient is living at home, the burden on care-givers can be enormous. Respite care in the form of de-mentia “day care” programs serves the purpose of providingappropriate activity and behavioral management, as wellas a needed break for caregivers.
SummaryPsychological studies of the elderly have established that aging itself does not necessarily cause dementia.Instead, aging produces predictable changes in patterns of abilities in crystallized and fluid intelligence.Healthy and active individuals in their 60s, 70s, and 80s do not necessarily differ substantially from theirpast level of functioning in the level of their crystallized cognitive skills or abilities. Relatively stable skillsinclude well-learned verbal abilities such as reading, writing, and speaking; simple arithmetic ability; andimmediate and long-term memory. In contrast, fluid intelligence, including short-term memory, abstract andnovel problem solving, and behavioral slowing are examples of types of functioning that normal aging maycompromise. Health care costs, the aging of the U.S. population, and a renewed concern for well-being ofolder people have hastened inquiries and interest in this area. Although elderly people are at high risk fordiseases that impair cognitive functioning (such as AD), cognitive impairment is potentially reversible in 5%to 20% of dementia cases (for example, in nutritional deficiencies). An understanding of precise neuropsy-chological deficits can improve the medical management even of patients with irreversible dementia. Neu-ropsychologists play an important role in comprehensive medical, functional, psychosocial, and neuropsy-chological assessment. Assessment of mental status and cognitive abilities yields valuable informationabout prognosis, and it is important in monitoring a patient’s health or illness and helping the patient makefurther life plans (Zillmer & Passuth, 1989; Zillmer, Fowler, Gutnick, & Becker, 1990).
C r i t i c a l T h i n k i n g Q u e s t i o n s
Will exercising one’s mind help ward off dementia? Must one “use it or lose it”?How is Alzheimer’s disease best identified in life?How can a neuropsychological profile aid dementia sufferers and their families?How does the concept of self of the patient with Alzheimer’s disease change with the progression of the disease?

DementiaCrystallized intelligenceFluid intelligenceNeurofibrillary tanglesSenile plaques
AtrophyMild cognitive impairment
(MCI)Cortical dementiaSubcortical dementia
Multiple infarcts (multi-infarctdementia)
DeliriumAlzheimer’s disease (AD)Beta-amyloid (-amyloid)
Acetylcholine (ACh)BradyphreniaMetacognitive
awarenessNeurotrophins
K e y Te r m s
422 PART THREE | Disorders of the Brain
We b C o n n e c t i o n s
http://www.mc.uky.edu/nunnetOfficial site of the “Nun Study,” a longitudinal study of aging and AD funded by the National Institute on Aging.
http://www.agelessdesign.comAgeless Design: Smarter, Safer Living for Seniors—Site of the first organization to dedicate its resources,imagination, and heart to creating smarter, safer living for seniors. By recommending logical, cost-effectivehome modifications, unique ideas, and products, homes can accommodate those dealing with age-relatedconditions and embrace the special needs of people as they age.
http://www.un.org/esa/socdev/ageingThe United Nations Program on aging around the world.
http://www.alzforum.orgAlzheimer’s Forum—a nonprofit foundation that has established this site to serve the scientific and clinicalresearch community.
http://www.informatik.fh-luebeck.de/icd/icdchVF-D-Index.htmlICD-10 Codes for Dementing Disorders—provides a classification system (the ICD-10) of mental and physicaldisorders used by the World Health Organization. This site includes a brief description and diagnostic crite-ria for most major brain diseases.
http://pni.med.jhu.eduJohns Hopkins University Division of Psychiatric Neuro-Imaging—these pages describe quantitative brainanalyses of neuropsychiatric disorders such as AD, using MRI, functional MRI, and SPECT imaging.
http://dementia.ion.ucl.ac.ukDementia Web—site is based at the National Hospital for Neurology and is supported by The Institute ofNeurology and the Division Imperial College School of Medicine. This site provides updates on dementiaresearch, a virtual chat room, a dementia support group, and other links.
http://www.neurologychannel.com/dementiaNeurology Channel—has information about dementia and other neurologic disorders.
http://www.mentalhealth.com/dis/p20-or05.htmlInternet Mental Health: Dementia—provides diagnosis, treatment, and research reports for caregivers andspecialists.
http://tv.cbc.ca/national/pgminfo/memory/index.htmlThe National Online: In Search of Memory—provides information on three forms of memory: semantic, procedural, and episodic memory. It relates these memory forms to different dementia disorders.
Chapter 15
SUBCORTICAL DEMENTIAS
Age is not determined by years, but by trouble and infirmities of mind and body.
—Mark Twain
Parkinson’s DiseaseHuntington’s DiseaseCreutzfeldt–Jakob Disease
Neuropsychology in Action
15.1 Understanding Subcortical Dementia15.2 Pallidotomy Surgery: A Case Report15.3 Testing Fate: Would You Want to Know If You
Were Going to Get Huntington’s Disease?15.4 Creutzfeldt–Jakob Disease and Mad Cow
Disease: What’s the Connection?15.5 The Neurologic Examination for Dementia

Checkoway & Nelson, 1999). PD rarely occurs beforeage 40, and the public case of actor Michael J. Fox, whodeveloped PD at age 29, is highly unusual. PD appearsmore common in men than women, although no differ-ences in risk factors have been identified. Dementia inPD, however, does appear to be age related. Between 24%and 31% of those with PD meet the criteria for dementia(for review, see Aarsland, Zaccai, & Brayne, 2005). How-ever, only about 12% of patients with PD who are in their50s have dementia, compared with about 70% of thoseolder than 80 (Mayeux et al., 1992). Younger patientswith PD are likely to function well, but dementia is morelikely with increased age and disease severity. People mostlikely to have dementia appear to be those who have ei-ther had the disease for a longer period or are older at thetime of diagnosis (Kay, 1995).
N E U R O P A T H O L O G Y O F P A R K I N S O N ’ SD I S E A S E
PD is marked by a degeneration of dopaminergic cells andpigmentation in the substantia nigra (black substance)(Figure 15.2). It is also characterized by Lewy bodies,which are small, tightly packed granular structures with
424 PART THREE | Disorders of the Brain
K e e p i n M i n d
How do the cortical and subcortical dementias differ from each other?
How do behavioral motor presentations differ among subcortical disorders?
What are the symptoms and progression of Huntington’s and Parkinson’s diseases?
How is Creutzfeldt–Jakob disease acquired?
OverviewSubcortical dementias are so named because, although these conditions often affect cortical areas andfunctioning, the structures that are prominently damaged are subcortical. Parkinson’s disease (PD) andHuntington’s disease (HD) attack the basal ganglia; PD targets the substantia nigra, and HD targets thecaudate nucleus. Creutzfeldt–Jakob disease (CJD) affects yet another noncortical structure, the cerebellum.The common behavioral feature characterizing these and most subcortical dementias is slowed cognitiveand motor dysfunction (Neuropsychology in Action 15.1: Understanding Subcortical Dementia). What isinteresting is the manner in which each disease affects the motor system in a different way. You can trulyappreciate the complexities of the motor system by examining these diseases. Motor problems presentgreat physical limitations and hardship. These dementias, however, do not represent only motor systemdysfunction. The dementias we present in this chapter are progressive and involve multiple functional sys-tems. We present PD in greater detail than the other disorders because it is more common, and thesepatients are more likely to be seen by clinical neuropsychologists.
Parkinson’s Disease
Parkinson’s disease (PD) is a slowly progressivedisease of the dopaminergic system that, like Alzheimer’sdisease (AD), largely affects older adults. Later stages ofthe disease are associated with dementia. PD, or idio-pathic parkinsonism as it is also known, is the most com-mon manifestation of parkinsonism. Parkinsonism, likedementia, does not refer to a particular disease, but ratherto a behavioral syndrome marked by the motor symptomsof tremor, rigidity, and slowness of movement. This clus-ter of motor symptoms may be caused by PD but also bydrugs, encephalitis, toxins such as carbon monoxide andmanganese, and injury. Mohammed Ali, the famous boxer,experienced parkinsonian symptoms (called dementiapugilistica) after repeated blows to the head (Figure 15.1).Parkinsonism occurring in the absence of PD can be a sta-tic condition. Although the cause of PD is unknown, andthe disease is therefore called idiopathic, it is known to se-lectively affect the substantia nigra and the dopaminergicsystems of the brain.
PD affects an estimated 1% of the population of theUnited States that is older than 50 years, with the incidenceof new cases increasing with age (Bennett et al., 1999;

CHAPTER 15 | Subcortical Dementias 425
ringlike filaments found within dying cells. Althoughneurodegeneration and Lewy bodies are pathognomonicmarkers in cells of the substantia nigra, patients with PDmay also have concentrations of them in other pigmentedsubcortical areas such as the locus ceruleus or unpigmentedareas such as the nucleus basalis of Meynert, hypothalamus,cerebral cortex, cranial nerve motor nuclei, and compo-nents of the autonomic nervous system (for review, seeOlanow & Tatton, 1999). Although the pattern of con-centration of Lewy bodies in the substantia nigra indi-cates PD, the presence of Lewy bodies in the brain is notspecific to PD. They may also appear in normally agingpeople, individuals with AD, and those with other pro-gressive neurodegenerative conditions. This leads to spec-ulation that Lewy bodies are either (1) indicators of a gen-eral disease process or (2) markers of cell death.
The darkly pigmented, or melanized, substantia nigrais a midbrain structure that is part of a group of subcor-tical structures that collectively make up the basal gan-glia. The basal ganglia, which reciprocally connect to thepremotor cortex and the supplementary motor areas viathe thalamus, largely function to control the fluidity of over-learned and “semiautomatic” motor programs (Bradshaw& Mattingly, 1995). The loss of dopamine from the sub-stantia nigra is directly related to the problems of move-
ment initiation and motor rigidity in PD (Bradshaw &Mattingly, 1995). Aging itself takes a toll on thedopamine system, and some cell loss is expected. But thedopaminergic degeneration in PD is several times thatof normal aging. Perhaps the reason that noticeableparkinsonian symptoms do not appear in older adults isbecause there is a “dopamine threshold,” estimated tobe breached at between 50% and 80% cell loss (Bradshaw& Mattingly, 1995), before symptoms appear.
C L I N I C A L P R E S E N T A T I O N A N D N E U R O P S Y C H O L O G I C A L P R O F I L E O F P A R K I N S O N ’ S D I S E A S E
When a physician refers patients with PD to a consult-ing neuropsychologist, the diagnosis has usually beenwell established from the characteristic resting tremorand allied motor symptoms. In this case, the referral isusually to help determine the presence or extent of cog-nitive decline. However, physicians may refer patients toeither a psychotherapist or a neuropsychologist to aid indiagnosis before the “classic” symptoms appear. Unlikestroke, which presents with sudden motor weakness, PDis insidious, slowly sneaking up on its victim. The pa-tient may first sense vague aches and pains and wonderwhether arthritis is developing. A general feeling of tired-ness or malaise may come first, which could easily be at-tributed to overwork or “burnout.” Other patients withPD may first report feeling irritable or depressed. Thesesymptoms may be met with assurances, a suggestion toundertake medical tests, or a referral to a psychologist toinvestigate possible psychosomatic problems or depres-sion. As the disease continues to progress, subtle motor
Figure 15.1 Mohammed Ali, who experienced developmentof Parkinsonian symptoms from injuries that occurred during hisboxing career, lit the flame in the 1996 Summer Olympics. (© AP/Wide World Photos.)
Image not available due to copyright restrictions

symptoms begin to appear. Perhaps the person noticesweakness in an arm or leg, including problems in writ-ing, holding a pen, or typing. Voice quality becomes
softer and more monotone, and facial expression appearsflat to others. If the symptoms are limited to one side ofthe body, it may appear that the person has suffered a
426 PART THREE | Disorders of the Brain
Subcortical dementia is a clinical syndromecharacterized by slowness of cognitive pro-cessing, executive dysfunction, difficultyretrieving learned information, and abnormali-ties of mood and motivation. The syndrome isproduced by disorders affecting frontal-subcortical circuits, including lesions of thestriatum, globus pallidus, and thalamus.
Kinnier Wilson (1912), in his originaldescription of Wilson’s disease, recognizedthe clinical features of subcortical dementia,which von Stockert (1932) described againin the context of discussing postencephaliticParkinson’s disease (PD). Martin Albert andcolleagues (Albert, Feldman, & Willis, 1974)reintroduced the syndrome into clinicalneurology in descriptions of the subcorticaldementia of progressive supranuclear palsyat Boston University in 1975. Substantialcontroversy centered on this syndrome whenresearchers first introduced it. Critics of theconcept suggested that most dementiasyndromes include both cortical and subcor-tical abnormalities, and that the clinicalphenomenology was not distinctive enoughto guide differential diagnosis. Subsequentexperiences have helped to remold theconcept and to account for these criticisms.For example, the subcortical changes in AD inthe nucleus basalis of Meynert lead to acholinergic deficiency that manifests at thecortical level. Thus, although the pathology issubcortical in location, the dysfunctionprimarily affects the cerebral cortex. Likewise,although there are cortical changes in Hunt-ington’s disease, they are minor comparedwith the marked subcortical abnormalities,and the mental status changes correlate withthe subcortical rather than the corticalabnormalities. Thus, even within these mixedsyndromes, it is possible to identify corticaland subcortical patterns of dysfunction.
Researchers have increasingly docu-mented the clinical features of subcorticaldementia (Cummings, 1986). Slowing ofcognition stems from the increased centralprocessing time imposed by subcorticaldisorders. Patients have prolonged re-sponse latencies and slowed complexreaction times. They show executive dys-function, including difficulty with set shift-ing, as measured by tests such as theWisconsin Card Sorting Test or Trails B ofthe Trail Making Test; reduced verbal flu-ency on tests of word list generation, suchas the number of animals that can benamed in 1 minute; impoverished motorprogramming, as measured by tests suchas execution of serial hand sequences; andpoor abstracting abilities when asked tointerpret proverbs or to distinguish amongsimilar concepts. Memory abnormalitiesare primarily of a retrieval deficit type.Patients store information at nearly normalrates but have difficulty retrieving theinformation in a timely way. Thus, on testsof recall they perform poorly, but on tests ofrecognition memory they may perform inthe normal range. This recall deficit in-cludes both recent and remote information.Patients with subcortical dementia showneuropsychiatric and neuropsychologicalabnormalities. Apathy and depression areparticularly prominent. Less common areirritability, disinhibition, mania, and psy-chosis. Motor abnormalities also accom-pany most subcortical dementias when thedisease involves striatal structures, thesubstantia nigra, or globus pallidus. Parkin-sonism and chorea are the predominantmotor manifestations in patients withsubcortical dementia.
Recent advances in neuroanatomy con-tribute to neuropsychological understanding
of subcortical dementia syndromes. Fivefrontal subcortical circuits link regions of thepremotor cortex to areas of the striatum,globus pallidus, and thalamus. The dorsolat-eral prefrontal subcortical circuit mediatesexecutive function and projects from dorsolat-eral prefrontal regions to the head of thecaudate nucleus, globus pallidus, dorsome-dial thalamus, and back to the prefrontalcortex. The anterior cingulate region in themedial prefrontal region mediates motivatedbehavior via a frontal subcortical circuitincluding the nucleus accumbens, globuspallidus, dorsomedial thalamus, and anteriorcingulate. An orbitofrontal subcortical circuitmediates the social governance of behaviorand includes orbitofrontal cortex, inferiorcaudate nucleus, globus pallidus, anddorsomedial thalamus. Dysfunction in thelateral prefrontal-subcortical circuit producesexecutive dysfunction; abnormalities of theanterior cingulate-subcortical circuit result inapathy; and abnormalities of theorbitofrontal-subcortical circuit producedisinhibited, tactless behavior (Cummings,1993).
Treatment of patients with subcorticaldementia depends on the specific cause oftheir syndrome. Parkinsonian disorders andPD are treated with levodopa and otherdopaminergic agents. The depressionsyndrome in many patients with subcorticaldementia typically responds to antidepres-sant agents such as selective serotoninreuptake inhibitors. The apathetic syn-drome may respond to dopaminergicagonists or psychostimulants such asmethylphenidate. Cognitive dysfunction inpatients who have a cholinergic distur-bance, such as those with PD, may respondto cholinergic therapies such ascholinesterase inhibitors.
N e u r o p s y c h o l o g y i n A c t i o n 1 5 . 1
U n d e r s t a n d i n g S u b c o r t i c a l D e m e n t i a
by Jeffrey L. Cummings M.D., Professor of Neurology and Psychiatry, UCLA School of Medicine, Los Angeles, CA

tude. Semiautomatic movements such as walking, armswinging, blinking, swallowing, and facial expressivenessmay appear almost frozen, as if the person is robot-likeand must consciously think to move. The description of apatient with PD as having “masked facies”—denoting amasklike face—captures the essence of an emotionlessface. The person’s demeanor may seem depressed; a va-cant stare may be produced by the combination of re-duced facial emotion, slow speech, and decreased eyeblinking. In addition to slowness, many movements de-cline in magnitude. Patients with PD do not take longsteps and swing their arms high in the air, but rather ex-hibit a rapid, small, shuffling, festinating gait. Hand-writing also gets slower and smaller (micrographia), andthe voice becomes softer as the ability to project the soundof one’s voice becomes increasingly difficult. Patients withPD also describe difficulty in initiating movement, or hy-pokinesia, and may have to consciously think to beginwalking, to turn around, or to lift a fork. During themovement, the person may also freeze and may need to
mild stroke. It is nearly impossible to diagnose PD at thisstage because the classic motor symptoms have not yetemerged. It would also be rare to even suspect PD, be-cause these initial symptoms could herald a multitude ofdifferent problems.
The cognitive profile of those diagnosed with PD issomewhat heterogeneous depending on the presence ofdementia and the stage of the disease. Raskin and col-leagues (Raskin, Borod, & Tweedy, 1990) suggest twopossibilities for the occurrence of dementia in patientswith PD. First, demented PD patients may represent aqualitatively different subgroup, experiencing a later onsetof symptoms and showing more subcortical and frontalatrophy. The second explanation is that this group maydiffer only in degree, with a more pronounced progres-sion of cognitive decline. Dementia in patients with PDhas been contrasted and compared with both AD andLewy body dementia (LBD). In LBD, Lewy bodies areprominent throughout the cortex and present a patternsimilar to that seen in AD. A magnetic resonance imaging(MRI) study comparing patients with PD with and with-out dementia with patients with LBD showed that pa-tients with PD with dementia and patients with LBD hadwidespread cortical atrophy, but patients with PD with-out frank dementia had atrophy primarily in the frontallobes (Burton et al., 2004).
This section examines the cognitive profile of non-demented patients with PD. Some authors suggest thatthe cognitive profile is heterogeneous; that is, there maybe several subgroups of PD, possibly pointing to sub-groups of neuropathology (Dubois, Boller, Pillon, &Agid, 1991). Others have also raised questions aboutlateralization of cognitive deficits. Do cognitive deficitsin any way parallel the type and degree of motor symp-tomatology?
Just as memory dysfunction is the hallmark of AD,motor dysfunction is characteristic of PD. Our reviewof functional systems begins with the clinical presenta-tion and neuropsychological dysfunction of the motorsystem.
M o t o r S y m p t o m s
The motor symptoms of PD generally fall into groups ofpositive and negative symptoms (Table 15.1). Positivesymptoms indicate an excess of motor behavior, or abnor-mal motor reactivity, whereas negative symptoms indicatea diminution or loss of motor functioning. Some expertsbelieve that negative symptoms may manifest before thepositive symptoms, although they may be frequentlymissed. You can think of bradykinesia as a poverty ofmovement that is not only slowed but reduced in magni-
CHAPTER 15 | Subcortical Dementias 427
Positive Symptoms
Resting tremor
Rigidity (cogwheel)
Stooped posture
Impaired righting reflex/poor balance
Negative Symptoms
Bradykinesia: slowness of movement
Hypokinesia: reduced motor initiation
Gait disturbance
Slow
Festinating (rapid small steps)
Freezing
Masked facies: reduced facial expression
Slowed speech
Decreased voice amplitude
Ocular disturbances
Decreased blink rate
Decreased light accommodation
Slowed saccades
Table 15.1 Motor Symptoms of Parkinson’sDisease

“will” the action to continue. Ironically, it may also bedifficult to stop an action such as walking or writing,which has led to the suggestion that PD results in a fun-damental deficit in initiating and terminating semiauto-matic motor programs (for example, see Bradshaw &Mattingly, 1995).
Despite the debilitating effect of the negative symp-toms of PD, the positive symptoms of PD are perhapsmore noticeable, and most people recognize them as thehallmarks of the disease. Chief among these are a restingtremor and rigidity. Resting tremor, as opposed to a cere-bellar intention tremor, is often characterized as “pillrolling.” This rhythmic shaking, often first occurring inone hand or the other, looks as if the person might be rub-bing or rolling a coin or pill between thumb and forefinger.The tremor stops or lessens with voluntary movementssuch as reaching, swinging the arm, grasping, or manipu-lating objects. When the person is sleeping, the tremorusually disappears.
However, with heightened states of alertness, concen-tration, or nervousness, the tremor is likely to increase.The degree of tremor at any one time is partly due to thevoluntary–involuntary nature of the movement, the levelof alertness, and the level of stress. It is not always pre-dictable, coming in bursts, but it does increase in speedand may become more violent as the disease progresses.In the early stages of PD, it is not uncommon for thetremor to influence only one side of the body, affectingthe hand and foot first and maybe one side of the face.Eventually, it moves to the contralateral side and affectsall extremities.
Rigidity, the other major positive symptom, occurs asa tightening of muscles and joints. When a neurologisttries to move the person’s wrist, elbow, or knee, there ispersistent resistance to this passive movement. Sometimesthis resistance appears as a ratcheting movement, as if theperson’s joint were a cogwheel (cogwheel rigidity). Mus-cles may appear tense and feel contracted to touch, evenwhen the person is relaxing. This increasing rigidity mayresult in the characteristic stooped or hunched posture ofPD. In addition to a more rigid posture, poor balance andthe inability to adjust posture may be evident. The inabil-ity to catch oneself quickly, or impaired righting reflex,may appear if the person is pushed or missteps.
On neuropsychological testing of the motor system,patients with PD are extremely slow, with poor reactiontimes. This is certainly evident on basic tasks that may re-quire simple speeded movement, such as finger tapping.Poor motor performance is also evident on many othertasks that have a speeded motor component such as copy-ing geometric designs with blocks within a specified time
limit (such as WAIS-R, Wechsler Adult Intelligence Scale,Revised [WAIS-R] Block Design).
Because PD usually begins as a lateralized motor dis-order, some investigators have speculated that the cogni-tive profile may also show lateralized impairment. Indeed,this may be the case. People with hemiparkinsonism oftendo show a neuropsychological profile consistent withwhat would be expected from lateralized cortical damage(Raskin et al., 1990). Exclusively left-sided motor symp-toms link to more right hemisphere deficits. Raskin alsosuggests that this profile may reflect unilateral damage tobasal-cortical pathways, resulting in disconnection, ratherthan unilateral lesions of the basal ganglia.
Motor symptoms may result in lateralized neuropsycho-logical profiles—but is there a relation between the degreeof motor impairment and the severity of cognitive dysfunc-tion? Patients with PD followed for up to 10 years did notshow evidence of such correspondence (Portin & Rinne,1986). Although drugs that targeted the motor symptoms,such as levodopa (L-dopa), had great impact on motor per-formance, they had little effect on cognitive performance.
V i s u o s p a t i a l D e f i c i t s
Of nonmotor, higher cognitive functions, visuospatialdeficits in nondemented PD are among the most com-monly reported in the literature and among the most con-troversial. Many studies have found that patients with PDperform poorly on spatial tasks that have a motor compo-nent. This is not surprising because evidence exists for im-pairment on visuospatial tasks regardless of whether thereis a motor component (for review, see Raskin et al., 1990).However, enough studies show mixed results, or no im-pairment on visuospatial tasks, to throw the issue of spa-tial impairment into doubt (for review, see Dubois et al.,1991). To what can we attribute this discrepancy? It maybe caused, in part, by the heterogeneity of presentation inpatients with PD. Different patients may have somewhatdifferent pathology, and thus different clinical presenta-tions. As discussed earlier, those with more left-sidedmotor impairment may show more right hemispheredamage (visuospatial deficits). Some studies include pa-tients in more advanced stages of the disease. Some pa-tients with PD may have a comorbid dementia. In anycase, factors having to do with possible subgroups of pa-tients with PD continue to cloud the picture of visuospa-tial functioning.
In nondemented PD sufferers who have visuospatialdysfunction, does such dysfunction point to parietal im-pairment or some other mechanism? First, patients withPD may report having difficulty orienting themselves inspace. For example, when having to walk around the
428 PART THREE | Disorders of the Brain

house in the dark without the aid of visible landmarks oroutside in a fog, one person relates, “I used to walk alonein the wood, fog or no fog, but when the symptoms ofPD appeared, I noticed that I could not orient myself anymore, and in case of fog, I got lost” (Dubois et al., 1991,p. 203). Spatial abilities require the person to visualize therelative position of objects in three-dimensional space,and to make a motor response to orient himself or herselfor other objects in that space. Therefore, the visual-spatial-motor aspects link in an overall spatial framework.Disease could theoretically disrupt this network in theparietal lobes or anywhere along the visuomotor system.Some investigators have suggested that the basal gangliaplay a role in the visuomotor aspects of visuospatial prob-lems in patients with PD (Danta & Hilton, 1975; Duboiset al., 1991). But what about patients who have visual-perceptive difficulty, but no visuomotor problems? Forexample, a popular test used by neuropsychologists, Ben-ton’s Judgment of Line Orientation Test (Benton et al.,1983), requires matching drawings of lines in various ori-entations to a template (Figure 15.3). It does not requiredrawing or movement of the body. Yet, many nondementedPD patients have difficulty with this task (Goldenberg,Wimmer, Auff, & Schnaberth, 1986). One explanation isthat any disruption in the visual-spatial-motor circuit mayimpair performance. Another suggestion is that even intasks in which a person does not use a motor response, he
or she still has an internal representation of a perceptual-motor response (Villardita, Smirni, LaPira, Zappala, &Nicoletti, 1982).
In summary, although it is not clear whether all pa-tients with PD experience visuospatial dysfunction, a siz-able proportion does. Certain subgroups of patients, orthose in more advanced stages of the disease, for example,may show the most difficulty. The parietal lobes per se donot appear chiefly responsible for the problem. Rather,the basal ganglia are implicated in a larger visuospatialnetwork.
E x e c u t i v e F u n c t i o n i n g
Many patients with PD have executive functioning diffi-culties. Difficulties with specific executive functions can beevident, although most do not have difficulty with abstractthinking (Raskin et al., 1990). These deficits show up earlyin the disease process, and thus appear to result directlyfrom the disease (for review, see Dubois et al., 1991).
Among executive dysfunctions reported in the litera-ture are difficulties with changing mental sets, maintain-ing mental sets, and temporal structuring. The inabilityto switch mental set in response to environmental de-mands, or perseveration, shows most clearly on neuropsy-chological testing through measures that require strategyshifts to solve problems (such as the Wisconsin Card Sort-ing Test) or an alternating response between two differenttypes of stimuli (such as the Trail Making Test B or theStroop Test). Someone who has set-shifting problems re-peatedly tries to use the same strategy, even if it is notworking. Investigators have found that patients with PDdo not make more total errors on these types of tasks, butthe errors they do make are perseverative (Raskin et al.,1990; Dubois et al., 1991). The perseverative problem inmaintaining set occurs after the patient tries a new or dif-ferent strategy. It is a tendency to revert back to a previ-ous strategy after switching “mental set.” Some authorshave also explained the verbal fluency difficulties of thisgroup as a problem of set maintenance (Dubois et al.,1991). Verbal fluency tasks typically require the person tolist as many words as possible that begin with a specifiedletter or belong to a specified category. The problem ap-pears most evident when the person uses several differentletters. First, the task is to name as many words, within a1-minute time period, that start with the letter F, then toname all the possibilities that begin with A, then with S.In such tasks, during the middle of the S sequence, pa-tients with PD may revert to words that begin with F orA (Lees & Smith, 1983).
A difficulty in “time tagging” events is a problem in tem-poral structuring. Researchers have reported patients with
CHAPTER 15 | Subcortical Dementias 429
Text not available due to copyright restrictions

PD may have memory for news events without associatedmemory for the event order (Sagar, Sullivan, Gabrieli,Corkin, & Growdon, 1988). In daily life this can trans-late into problems remembering “when” medications havebeen taken or learning the sequence of new tasks. Tempo-ral ordering is an executive problem that interacts withmemory.
Not all of the frontal lobe is involved in the dysexecu-tive problems of PD; rather, the premotor area and thebasal ganglia with its associated projections to the frontallobes are implicated.
L a n g u a g e / S p e e c h
PD typically does not produce classical aphasia. Also, few,if any, linguistic impairments appear involving grammarand sentence structure (Dubois et al., 1991). Thus, gen-eral language processing and comprehension are intact.Some researchers indicate that more subtle problems inunderstanding grammatic complexity may be evident onmore sophisticated neuropsychological tests (Levin,Tomer, & Rey, 1992). However, close to 70% of patientswith PD have difficulties with articulation and the neuro-mechanical aspects of speech production (Levin et al.,1992). We have mentioned that patients with PD losevoice amplitude and vocal emotional expression (dyspho-nia), which results in monotonous voice. Other speechirregularities may include segmented accelerated bursts ofspeech (tachyphemia) and compulsive word or phraserepetition (palilalia).
Tests that measure aspects of expressive or receptiveaphasia show little impairment in patients with PD. How-ever, patients may perform poorly on semantic fluencyand word-finding tasks (such as the Boston Naming Test).However, as discussed earlier, these tasks are better con-ceptualized as belonging in another domain (executivefunctioning). Behavioral assessment of speech is themethod that will demonstrate the characteristic disarticu-lation problems.
M e m o r y
Compared with AD, memory functioning is relativelyspared in PD, even in patients with PD with dementia(Sagar et al., 1988). Digit repetition and block-tappingrepetition are usually preserved (for review, see Duboiset al., 1991). On tests involving episodic memory, pairedassociate learning, auditory verbal learning, and visual re-production of geometric designs, patients with PD doshow a recall deficit but demonstrate encoding and regis-tration of declarative material through recognition tasks(for reviews, see Dubois et al., 1991; Levin et al., 1992).The implication of this pattern is that strategic memory
processes for organization and retrieval of declarative in-formation are defective.
Nondeclarative learning presents a mixed bag in PD.Verbal priming and perceptual-motor adaptation arelargely unimpaired in patients with PD without dementia(Crosson, 1992; Heindel, Salmon, Shults, Wallcke, &Butters, 1989). However, nondeclarative learning, whichrelies on intact motor or executive functioning, is oftendeficient. The ability to learn new motor skills declines asthe disease progresses (Crosson, 1992). This is not sur-prising, considering the general dysregulation of themotor system. Procedural learning, measured by rule-learning tasks, such as the Tower of London, may be defi-cient, but results are mixed. At times, patients with PDperform poorly because of a problem in maintaining men-tal set for the rule, again pointing more to a problem inexecutive functioning than to a memory registrationproblem.
Most of the apparent memory difficulties experi-enced by patients with PD stem from interactionsamong the executive, the memory registration, and themotor systems. Patients with PD may show difficulty inmotor skill acquisition. Patients with PD without de-mentia can passively register declarative information inshort- and long-term memory. However, many havetrouble using this information effectively. This includeseffectively organizing information to be recalled, main-taining a consistent mental set when trying to learn orretrieve information, and time tagging or knowing notonly that something has occurred but “knowing when”it happened.
M o o d , E m o t i o n , P e r s o n a l i t y ,a n d I n s i g h t
A large proportion of patients with PD suffer from de-pression. Debate continues whether the mood disorder isa primary dysfunction of the disease or a secondary resultof the medications used to treat the disease. To those suf-fering from depression, the debate may seem academic.Some researchers also suggest that depression may be anatural reaction to realizing that the patient has PD. Al-though this probably occurs to some degree, it does notseem to adequately explain the occurrence of depression.Patients with PD appear to be more depressed than pa-tients with many other chronic diseases (Raskin et al.,1990).
Although few standardized neuropsychological testsmeasure expression of emotion, researchers have studiedthis in patients with PD. The findings are somewhatequivocal, but some suggest that patients with PD have adysfunction in emotional expression associated with a
430 PART THREE | Disorders of the Brain

right-frontal focus (for example, see Ross, 1985). Thesepatients may have difficulty in showing an angry face or asurprised face but may be able to recognize emotionalexpression. Does this finding suggest a cortical deficit inemotional expression? Or rather, a problem in the moremechanical aspects of emotional expression? Because ofthe “masked facies,” it is difficult to determine whetheremotional expression is lost or just diminished in fre-quency and intensity. Future research may help answerthis question.
T R E A T M E N T S F O R P A R K I N S O N ’ S D I S E A S E
Without treatment, patients with PD are souls trapped inthe cages of their bodies, unable to command or coax theirmutinous muscles into action. Out of the tragedy of thisdisease, however, has emerged a palette of treatments thatare worth examining, not only for addressing PD but be-cause they represent creative and forward-thinking ap-proaches to the treatment of aging-related brain disordersin general. Interestingly, the treatment for PD appears tobe traveling full circle from surgery to drugs to surgery. Inaddition, gene therapies, tissue implants, and various ap-proaches to prevention are on the horizon.
The first surgical approaches to PD in the late 1950swere based on the idea of alleviating symptoms by inter-fering with what was thought to be “malfunctioning cir-cuitry” in the basal ganglia through heat-induced surgicallesioning of the global pallidus. By 1960, a group ofSwedish researchers could demonstrate motor improve-ment in a significant number of their patients. However,this treatment preceded the advent of computed transax-ial tomography (CT) scans, MRIs, and the precisionstereotaxic and electrode recording tools needed to locatespecific neurons. The imprecision of this surgery madenegative side effects likely.
The discovery of L-dopa as a possible treatment for PDin 1961 (Birkmayer & Hornykiewicz, 1961) was revolu-tionary and heralded a new approach to the treatment ofneurodegenerative diseases. With the advent of a seemingmiracle drug, surgical approaches fell by the wayside bythe late 1960s. Today, there exists a menu of drugs thatact not only on the dopaminergic system but also on re-lated neurotransmitter systems.
In Paris in the 1860s, anticholinergics extracted fromplant sources (such as scopolamine from jimsonweed,black henbane, or deadly nightshade) were the first treat-ments used for PD. Although the mechanism of actionwas not known initially, these solanaceous alkaloids actedby blocking the action of acetylcholine, offering somesymptomatic control of motor systems for tremor and
rigidity. However, the side effects of “anticholinergic in-toxication” limit their usefulness. Possible systemic effects,including dry mouth, blurred vision, constipation, weakbladder, and cognitive effects such as memory problems,confusion, slurred speech, and visual hallucinations, cancreate more than a small nuisance for patients. Physiciansnow prescribe synthetic anticholinergics of different types,if at all, during the early stages of the disease, and usuallyin combination with levodopa.
L-Dopa is the left (levo) form of the dopa molecule, asimple amino acid. Prepared as a drug, it is called lev-odopa. Plants and animals manufacture it, and it appearsnaturally in fava beans and other legumes. Levodopa,being a dopamine precursor, directly metabolizes intodopamine. Cousins of levodopa include dopamine ago-nists and analogs that mimic the action of dopamine bystimulating its release, whereas reuptake blockers work bypreventing reuptake at the synapse to retard metabolic re-moval. Drugs acting on the dopaminergic neurotransmit-ter system are still the best family of drugs found to alle-viate tremor, bradykinesia, and rigidity. The difficultywith these orally ingested drugs, however, is that they con-vert to dopamine in the body and do not easily penetratethe blood–brain barrier. Probably less than 1% actuallycrosses over to be useful to the striatum, causing systemicbuildup of dopamine in organs such as the liver and kid-neys. Therefore, medications usually combine L-dopawith a decarboxylase inhibitor (such as carbidopa) to pre-vent the conversion to dopamine until it crosses theblood–brain barrier. Because carbidopa cannot cross theblood–brain barrier, it acts as a protector against conver-sion in the body until it releases the levodopa into thebrain. This arrangement delivers about five times thedopamine to the targeted area, greatly enhancing the ef-fectiveness of the drug.
Physicians may also use other drugs to treat PD, eitheras adjuncts or to counteract side effects of long-termdopaminergic drug usage. Doctors may add monoamineoxidase B (MAO-B) inhibitors, antidepressants, andagents to counteract the effect of dyskinesia to the com-plex menu, which must be taken at intervals as frequentlyas every 4 hours. These drugs are extending the survivalof patients with PD, but not without a price. The side ef-fects of dopaminergic drugs, including vivid nightmares,disturbed sleep, perceptual illusions, and hypomania canbe very disturbing. Also, after a long course of treatment,usually 10 years or so, the drugs lose effectiveness,dopaminergic neurons become hypersensitive, and thetherapeutic window becomes shorter in duration, result-ing in a severe on/off syndrome. During the “on” phase,the drug exerts its action but may overshoot, resulting in
CHAPTER 15 | Subcortical Dementias 431

432 PART THREE | Disorders of the Brain
The following case report profiles one “typi-cal” patient who underwent right pallidotomyin an attempt to alleviate some of his ad-verse motor fluctuations. M.J. is a 56-year-old, right-handed man with a 16-year historyof Parkinson’s disease (PD). His symptomsfirst began on the left side of his body withabnormal spontaneous movements of hisfoot, including a rhythmic tapping and aninvoluntary curling up of his toes. After about10 years, his motor deficits worsened and hesuffered from significant bilateral symptomsincluding bradykinesia, rigidity, and motorfluctuations. He had dyskinesias when hismedication was “on” and freezing when “off.”Other than PD, M.J. had no other majormedical or psychiatric problems. He wasforced to go on medical disability 3 yearsago. He has few hobbies, spending his daysmaintaining the house, walking the dog,doing yard work, and some cooking. M.J.acknowledges a feeling of depression, whichincreases when he does not feel well.
When he arrived for his presurgicalneuropsychological assessment, M.J. pre-sented as an alert, oriented, pleasant, andcooperative man with a stiff, slow gait.Dystonic posturing of his head and uppertorso was evident when sitting. Although hisfacial expression was fixed, he displayed arange of affect. A moderate tremor, whichwas greater on the left, was also evident. Hisspontaneous speech was soft in volume,with a choppy cadence, but his languagewas intact.
No disturbance in thinking was notedduring the interview. Results of neuropsycho-logical testing indicated a few areas of mildimpairment that were consistent with PD.These included problems with speed ofmental processing, working memory for bothauditory-verbal and visuospatial information,visual scanning, graphomotor control, andretrieval of verbal and visuospatial material.Recognition memory was intact. Consistentwith his self-reported history, M.J. wasdepressed, socially isolated, and withdrawn.
N e u r o p s y c h o l o g y i n A c t i o n 1 5 . 2
P a l l i d o t o my S u r g e r y : A C a s e Re p o r t
by Barbara L. Malamut Ph.D.
Figure 15.4 In the pallidotomy surgery for Parkinson’s disease, the surgeon isusing the triangulation of three coordinates of the frame to pinpoint the patient’sglobus pallidus. (Reproduced from Ueckert, S. [1996, January 22]. In R. SoRelle, “Newprocedure slows effects of Parkinsons: Surgery can restore balance to system.” HoustonChronicle, 4a, by permission.)
(continued)

an effect akin to an overdose. In this phase, severe dyski-nesia resembling choreic movements and dystonia involv-ing muscular posturing may result. This may cycle quicklyto “off ” symptoms, which include the disease symptoms,particularly freezing, severe tremor, and panic.
L-Dopa could not live up to the hopes that pharmaco-logic substitution of missing dopamine would be sufficienttreatment. The debilitating “on/off” drug phenomena ledto the return of surgical techniques. These operations cur-rently are intended for those for whom the drug treatmentsare no longer effective. Now, however, high-tech precisionimaging of the brain results in a greater chance of locatingthe offending neurons. Currently, two types of operationsare being conducted. The first operations focus on surgicallesioning of offending neurons. The second wave of surg-eries, deep brain stimulation operations, involves nonde-structive electrical interference.
Pallidotomy, the PD surgery of the late 1950s, was re-vived in the early 1990s. Surgeons use it in an attempt toalleviate the abnormal uncontrolled movement of dyski-nesia and the frequent on/off symptoms. In pallidotomy,surgeons lesion the ventral (that is, the internal portion)of the globus pallidus by heat-coagulating the neurons.
Studies have shown that the decreased dopamine in thebasal ganglia causes the motor portions of the pallidum tobecome overactive. This hyperfiring, in turn, inhibits thethalamus and portions of the brainstem (which causesbradykinesia and dyskinesia). Lesioning the posteroven-tral portion of the pallidum arrests this excessive outputto the thalamus and brainstem (Neuropsychology in Ac-tion 15.2). Surgeons use a second lesioning procedure ona portion of the thalamus, thalotomy, to attack tremor.Interestingly, they also use this procedure for patients withtremor caused by multiple sclerosis, essential tremor ofold age, cerebellar tremor, and poststroke tremor. Thesetwo operations are typically unilateral and not done incombination. In fact, the lesion sites for the two opera-tions are only millimeters apart. Bilateral lesions done atthe same time appear to greatly increase the risk for cog-nitive deficits. In pallidotomy, the risk may be greatest formemory difficulty and confusion. For thalotomy, speechdysfunction appears to be the greatest risk.
Deep brain stimulation procedures represent the newestvariation of these surgeries. The target site is the same as inthalotomy, except that instead of a destructive lesion, sur-geons transmit electrical interference to the neurons via a
CHAPTER 15 | Subcortical Dementias 433
M.J. was a good candidate for pallido-tomy because he was generally in goodphysical and mental health, his neuropsy-chological profile did not indicate cognitivedecline or dementia, and his medicationshad lost much of their effectiveness. The dayof M.J.’s surgery, he was injected with a localanesthetic and fitted with a stereotacticframe necessary to locate the area to belesioned (Figure 15.4). With the frame inplace, a computed transaxial tomographyscan was done and compared with his previ-ous magnetic resonance image, to identifythe precise placement of critical brain struc-tures. After drilling a tiny hole through M.J.’sskull, the surgeon inserted a small canula, ortube, through the dura mater and snaked amicroelectric probe through his brain towardhis right pallidum. As the probe approachedthe area of neuronal hyperactivity, soundbursts became more frequent. The surgeonfirst stimulated the area to observe motorresponse. (M.J. was conscious so his re-sponses to stimulation could be tested andany adverse affects on vision or speech couldbe noted before actual lesions were made.)Being careful not to affect the nearby optic
tract, the surgeon then made a small heat-induced lesion to permanently destroy theoveractive neurons of the pallidum. After thissurgery, M.J. needed a few stitches and wasreleased within 24 hours. M.J. experiencedno surgical complications.
Six months later, M.J. returned for aneuropsychological re-evaluation to monitorhis cognitive status. He reported that sincesurgery, his left-sided rigidity had disap-peared and he no longer had pain or involun-tary movements when walking. On observa-tion, he no longer had dystonic posturing butdid continue to walk with a slow, shufflinggait. In addition, his speech was now normalin volume, but he had developed a mildstammer. Overall, M.J. was pleased with theresults of his surgery, although he realizedthis was not a cure. Improvement relative tohis preoperative neuropsychological evalua-tion was noted in speed of mental process-ing, working memory for both auditory-verbaland visuospatial information, and grapho-motor control. M.J.’s problems with depres-sion remained, and he began taking antide-pressant medication and agreed to beginpsychotherapy.
This case raises several critical andcommon issues regarding pallidotomysurgery. Although pallidotomy effectivelyalleviates many motor symptoms and painassociated with later stages of PD, it doesnot cure the disease or return the patient topreinjury functioning. The long-term benefitsand risks of pallidotomy are unknown.Studies currently under way are examiningthe cognitive sequelae of the pallidotomyprocedure in comparison with the naturalprogression of the disease. The newestprocedure, approved by the U.S. Food andDrug Administration in July 1997, is deepthalamic stimulation, which works as a typeof electronic pacemaker interfering with theventral intermediate thalamic nucleus. Thesurgery, performed like pallidotomy, primarilyreduces tremor but may have little effect onthe other PD symptoms. This surgery, unlikepallidotomy, does not result in permanentlesions. Other treatment modalities currentlybeing explored, such as gene therapy andfetal implant surgery, may be promisingavenues for the future. These procedures mayactually arrest or reverse PD, rather than justameliorate some of its motor symptoms.

permanently implanted lead. An implanted adjustableneurostimulator operates somewhat like a pacemaker andcan be turned on and off by the patient.
Although these surgeries represent new hope for pa-tients for whom drugs are no longer effective, they are pal-liative, not curative. Patients experience relief of symp-toms, and about 80% may improve, but they must stilltake medication. The progression of the disease continues.
Huntington’s Disease
Huntington’s disease (HD), although rare, hasbeen well studied in the last quarter of the 20th century.Why the resurgent interest in a disease that physicians de-scribed more than a century ago and then seemingly leftto languish until the 1960s? From 1872, when GeorgeHuntington described this “hereditary chorea,” until the1960s, researchers paid little attention to this neurologicdisease, which causes adults in the prime of their lives toseemingly “go insane,” develop a tendency toward suicide,and suffer devastating motor impairment in the form ofchorea. Families of HD sufferers have spearheaded thesearch for the gene that controls the disease. For neu-ropsychology, the specificity of this disease offers a win-dow to learn about the widespread behavioral effects ofcaudate nucleus deterioration.
George Huntington was not the first to describe thetwisting, writhing, grimacing choreic movements, whichare reminiscent of a puppet at the hands of a sinister mas-ter. In the 16th century, “peculiar” families were de-scribed, but the hereditary nature of the disease did notappear to come into the medical consciousness until evo-lutionary theory emerged in the mid-1800s (Wexler,1995). Other physicians before Huntington hypothesizedabout the hereditary nature of the disease, but it wasyoung George Huntington, just 22 years old, who in his1872 article described the disorder most clearly and mostcompletely. He emphasized the emotional and psycholog-ical aspects of the disease, describing “the tendency to in-sanity, and sometimes that form of insanity that leads tosuicide.” This became the classic account of the disorder,forever after associated with the name Huntington.
The story of the search for the “Huntington’s gene”begins in the late 1960s. After years of relatively little sci-entific interest in this apparently incurable disorder, twofamilies picked up the torch. Marjorie Guthrie, ex-wife ofthe singer Woody Guthrie, who had HD, founded an or-ganization of HD families to raise money for research.The Wexlers, whose story is told in the book Mapping
Fate (Neuropsychology in Action 15.3) were instrumentalin pushing basic scientific research toward the search forthe gene. Nancy Wexler, at risk for HD herself, was activein the study of colonies of HD families in Venezuela.Largely through the energy generated by these and otherat-risk families, researchers pinpointed the offending genein 1993. This discovery does not translate into an imme-diate cure or treatment. However, it does provide the firsthopeful step in that direction.
HD is a progressive subcortical dementia. This raredisease, which affects about 5 to 10 in 100,000 people, islinked to the gene ITI5 on chromosome 4 and is passedon by one parent in an autosomal dominant inheritancepattern. As far as genes go, ITI5 is a big one, with morethan 300,000 base pairs, and it is evident in all tissues ofthe body. People with normal versions of the gene havebetween 11 and 34 repeats of the trinucleotide CAG (cy-tosine, adenine, guanine), which codes the gene. How-ever, those with the HD-positive gene have 37 to as manyas 100 or more repeats. More repeats entail earlier onsetand greater severity of symptoms. Some overlap exists be-tween normal and abnormal functioning, making 35 to40 a borderline range. When operating normally, ITI5produces the amino acid glutamine. It is not clear howthe body uses glutamine, or the exact function of ITI5,but researchers do know that expanded gene sequence re-peats on other genes characterize inherited diseases suchas myotonic dystrophy and spinobulbar muscular dystro-phy, which affected President Kennedy.
Autosomal dominance translates into a 50% chance ofacquiring the disease. Because this disorder runs in fami-lies, HD is not suspect unless there is a family history. Inthose with a family history, a simple genetic test can de-termine the presence of the disease, but much to the sur-prise of many scientists, most people at risk have chosennot to be tested (see Neuropsychology in Action 15.3).
N E U R O P A T H O L O G Y O F H U N T I N G T O N ’ SD I S E A S E
Deterioration of the caudate nucleus bilaterally plays aprimary role in the neuropathology of HD, although ul-timately, HD affects multiple brain systems. The cau-date nucleus is one of the structures that comprise thestriatum, together with the globus pallidus and puta-men. The striatum is part of the basal ganglia, which isresponsible for modulating motor activity. However, therole of the striatum is somewhat different from that ofthe substantia nigra, which is primarily affected in PD.Although the substantia nigra is responsible for theproper initiation and termination of movements, the
434 PART THREE | Disorders of the Brain

striatum controls the proper timing, ordering, and se-quencing of movement patterns (Bradshaw & Mattingly,1995). The caudate nucleus has reciprocal projections(afferent and efferent neurons) to a number of limbicand prefrontal areas. Although HD primarily affects thecaudate, it may also affect the putamen, other areas ofthe striatum, and possibly other limbic system structuressuch as the hippocampus. By the end stages of the dis-ease, the frontal lobes may also shrink by 20% to 30%(Vonsattel, 1992).
In patients with HD who are showing the symptomsof the disease, structural neuroimaging techniques such asCT or MRI clearly reveal the loss of cell mass in the cau-date and a widening of the ventricles. On MRI, the vol-ume of the caudate and other basal ganglia structures isclearly reduced. The apparent structural deterioration ofthe caudate corresponds to a downward progression ofbehavioral functioning. Functional neuroimaging viapositron emission tomography scan is more sensitive toearly changes and can show hypometabolism in thefrontal and striatal regions before deterioration is evident
structurally (Hasselbalch et al., 1992) and before a clini-cal diagnosis (Penny & Young, 1993).
C L I N I C A L P R E S E N T A T I O N A N DN E U R O P S Y C H O L O G I C A L P R O F I L E O F H U N T I N G T O N ’ S D I S E A S E
How do the symptomatology and neuropsychologicalfunctioning of the HD sufferers differ from profiles ofAD or PD? HD results in a unique pattern of impairmentin which difficulties associated with frontal lobe function-ing and motor functioning are prominent. Although PDalso results in frontal executive system and motor impair-ment, the presentation differs in some ways. The caudatenucleus, rather than the substantia nigra, is the main cul-prit in HD.
Many of the cognitive difficulties of patients with HDlikely stem from a breakdown in premotor frontal lobefunctioning and the connectivity of the caudate-frontalsystem. Early in the disease process, patients with HDshow characteristic frontal signs of rigidity, perseveration,
CHAPTER 15 | Subcortical Dementias 435
Would you take a test to determine whetheryou would develop an inherited brain dis-ease in the future? This is the questionfacing family members of people withHuntington’s disease (HD), a subcorticaldementia with devastating motor andcognitive consequences. Fortunately, thedisease is rare, but if it runs in your family,you have a 50% chance of acquiring thisautosomal dominant genetic disease. Thereis no cure and there is no treatment, and ifyou do have it, you may pass it on to yourchildren. You are also likely to die while inyour 50s. Would knowing this help you toplan? Plan not to have children, perhapsplan not to even marry, or perhaps try topack a lot of living into a short time? Wouldknowing lessen your worry? Or would know-ing be a traumatic experience? Would youconsider suicide? Would you always be onguard watching and waiting for the firstsymptoms to appear?
These questions face the 125,000people at risk for the disease in the UnitedStates. In 1983, researchers discovered agenetic marker that paved the way for thefirst testing for HD. Then 10 years later, in1993, researchers located the gene ITI5(named “Interesting Transcript”) on the shortarm of chromosome 4, and the test becamemuch more accurate. Only a simple bloodtest is required. Scientists predicted a floodat testing centers, but there has been only atrickle of people, about 6% of those at risk.Why is this? The answers come from those atrisk. Alice Wexler, author of the book Map-ping Fate, describes the story of her ownfamily, and of her mother, who died of HD.After her mother’s diagnosis in 1968, theWexler family, led by her father and sister,spearheaded one of the most innovativeapproaches to scientific investigation,bringing scientists and families together incollaborative efforts to search for the HD
gene. The book chronicles the scientific andpersonal odyssey of the discovery of thegene. Alice Wexler describes her own am-bivalence and the feelings of others whohave struggled with the idea of gettingtested. Some have taken the test, mention-ing control and relief from uncertainty asmajor reasons. Others are concerned aboutconfidentiality of their medical records andpossible denial of insurance coverage. Forthose who have tested positive, the experi-ence is often traumatic and, surprisingly,may not alleviate the anxiety because thereis no certainty as to when the symptoms maydevelop. Even for those who test negative,the result may come as a shock as theyrealize they have built their lives around thepossibility that they might acquire a fataldisease. Alice Wexler, like so many others,has decided against being tested. If you wereat risk, you could test your fate. But wouldyou want to?
N e u r o p s y c h o l o g y i n A c t i o n 1 5 . 3
Te s t i n g Fa t e : Wo u l d Yo u Wa n t t o K n o w I f Yo u We r e G o i n g t o G e t H u n t i n g t o n ’ s D i s e a s e ?
by Mary V. Spiers

and difficulty switching mental set in daily life, as well ason neuropsychological testing. Some dysfunctions stemfrom the impacts that poor executive organizational abili-ties and attention/concentration problems have on cogni-tive functioning. For example, the memory difficulties ofpatients with HD appear largely attributable to poor execu-tive functioning. Capacity for learning new information de-clines in HD, but the picture differs from the AD profile.Patients with HD demonstrate low levels of free recall butimprove greatly if given a recognition test. Why? Apparentlythey encode new information, or multiple-choice recogni-tion tests would not aid performance. Patients with HD ap-pear to suffer primarily from a retrieval problem caused byineffective memory search operations. They may have apoor ability to differentiate what they know from what theydo not know (for review, see Brandt & Bylsma, 1993). Thisproblem in strategic memory processing and metamemory(knowledge of one’s own memory) appears attributablelargely to frontal lobe and executive functioning difficultiesrather than to hippocampal involvement, although bothmay interact to some degree. Executive difficulties probablyalso interact with other cognitive processes such as verbaland spatial conceptualization and processing.
The final manner by which the striatofrontal lobecomplex may exert its effects on cognitive functioning isthrough multiple connections to other areas of the brain.Patients with HD appear to have difficulty orientingthemselves in space, which may be a parietal dysfunction.For example, the old-time child’s game of blind man’sbluff, in which one child is spun around blindfolded andthen required to tag others by sound alone as they callout, would be difficult for patients with HD. Potegal(1971) has explained this egocentric spatial disorder as aproblem in readjusting, or the ineffectiveness of the cau-date in modulating changes in spatial position. Althoughresearch has not yet confirmed this interpretation, it ap-pears reasonable, given the role of the striatum in modu-lating other motor activity.
The emotional difficulties experienced by many pa-tients with HD likely result from prefrontal and limbicsystem interactions. Patients with HD exhibit a dispro-portionately high degree of affective disturbance, in theform of depression and manic depression. The suicide rateof 6% (Farrer, 1986) in HD is greater than in other de-generative disorders. Are these emotional disturbances aresponse to a desperate situation, or perhaps a symptomof frontal-subcortical impairment? Suicide may be an un-derstandable response, given the severe cognitive devasta-tion that people in the early stages of the disease can an-ticipate. HD sufferers are no strangers to what will befallthem. They have seen a parent, a grandparent, aunts, and
uncles succumb to the same horrible disease. However,the rate of emotional disturbance in HD is greater thanexpected. Depression is the most common affective dis-turbance (Brandt & Bylsma, 1993), but the literature re-ports a wide range of affective and psychiatric distur-bances in patients with HD. These include anxiety,apathy, irritability, impulsivity, aggression, sexual distur-bance, schizophreniform thought disorder, and psychosisinvolving hallucinations and delusions (for reviews, seeBrandt & Bylsma, 1993; Bradshaw & Mattingly, 1995).Interestingly, the emotional disturbances often precedemotor symptoms. At this point, the affected individualmay not even be aware of his or her diagnosis. These emo-tional symptoms can be best conceptualized as a symp-tom of the disease, or a predisposition toward symptomssuch as depression. However, this is not to say that reac-tions to the illness do not contribute to the picture ofemotional disturbance. A reaction to the severity of thedisease can compound a predisposition to depression.
The motor difficulties of HD are characterized bychorea: twisting, writhing, undulating, grimacing move-ments of the face and body. Interestingly, overmedicatedPD patients also show choreic movements. This has ledto the hypothesis that the dopamine system lies at the rootof both these problems. Obviously, this gross-motor dys-function seriously hinders everyday activity. Like patientswith PD, patients with HD are slow motorically (bradyki-nesia). Also, as in PD, the chorea tends to disappear withsleep and increase with stress. Unlike PD, patients withHD walk with a wide-based gait. Their speech isdysarthric, becoming increasingly erratic in its rate of pro-duction and staccato with intermittent pauses. They be-come clumsy and uncoordinated, unable to do fine-grained work. In testing patients with HD, these severemotor difficulties disrupt performance on other tests thathave a motor component, even if the test is designed tomeasure other functions such as visual problem solving.In assessing the cognitive performance of patients withHD, motor-free tests provide the clearest picture. Cur-rently, no cure exists for HD, and the treatments that existfocus primarily on the relief of emotional symptoms suchas depression and hallucinations.
Creutzfeldt–Jakob Disease
Creutzfeldt–Jakob Disease (CJD), a dementialong hidden in obscurity because of its rarity (one thatmost neuropsychologists have never seen personally inone of their patients), has suddenly leaped into the lime-light because of its connection to “mad cow disease” and
436 PART THREE | Disorders of the Brain

because of the fear that its incidence is increasing. CJD isa compelling disease, unlike the other dementias we haveconsidered, because of both its speed of progression andmode of transmission. With a malignantly cascading de-cline over 3 to 4 months, it is the most quickly progress-ing dementia. Scientists have long known that humanscan transmit this disease via transplants of affected neuraltissue, cornea transplants, or contamination via medicalprocedures, but it is now also becoming clear that CJDand its variants can cross species through the consump-tion of tainted meat containing neural tissue. Extensivespongelike holes appear in the brains of its victims, givingit the fitting name “spongiform encephalopathy” (SE).The mechanism by which the brain becomes infected haseluded scientists for decades because CJD does not mani-fest the symptoms of typical acute infections. Virologists,biologists, and chemists are joining clinicians to unravelthe mysteries of this disease.
In the early 1900s, Bertha, a 23-year-old Germanwoman, was a patient of Hans Gerhard Creutzfeldt.Creutzfeldt, an assistant of Alois Alzheimer at the MunichPsychiatric Clinic, was, like Alzheimer, trying to clarifythe differences and similarities between behaviors under-stood as “psychiatric” and “neurologic.” Creutzfeldt no-ticed that Bertha showed many behaviors typical of othermental illnesses, such as believing she was possessed bythe devil, neglecting her hygiene, and posturing strangely.However, other symptoms suggested frank brain impair-ment. Bertha also had an unsteady gait, twitchy eyes, avoluntary tremor, and a tendency to giggle inappropri-ately. These latter symptoms, which we now recognize asindicating subcortical motor and emotional dysfunction,were Creutzfeldt’s clues. After Bertha died, Creutzfeldtexamined her brain tissue under the microscope. Whathe saw were the little “stars” of astrogliosis (Figure 15.5)dotting her brain. In 1920, he published his article thatdescribes Bertha. With the synchronicity that often oc-curs in science, Dr. Jakob reported a similar case in1921. Creutzfeldt and Jakob thus share the distinctionof discovery.
CJD is a quickly progressive subcortical dementia esti-mated to affect only 1 person in 1 million people per year.This is extremely rare even in comparison with HD,which affects 5 to 10 per 100,000 people. CJD appearsaround the world with the same prevalence and does notappear to vary across groups or cultures. AlthoughCreutzfeldt’s patient was young, most cases have been intheir 50s or 60s. For the most part, researchers have hy-pothesized that CJD spontaneously arises as a randommutation. As long as it is not passed on to others, the dis-ease dies out with its victim. Some variants of CJD may
manifest themselves differently in the behavior of those itafflicts. For example, the extremely rare familial CJD vari-ant termed Gerstmann-Straussler-Scheinker syndrome(GSS), reported in only a handful of families, results in a“fatal insomnia.” This is the only reported incidence oftransmission other than through external infection. Re-searchers believe that in older people CJD incubates foryears before manifesting.
One of the most alarming aspects of this disease, andthe reason it has been catapulted out of obscurity, is itsrelation to other SEs. Variations of SE, as mentioned ear-lier, are aptly named: Portions of the brain actually resem-ble a sponge, because of the microscopic pattern of holes.Researchers have identified SEs in species from minks tosheep (scrapie) to cows (bovine spongiform encephalopa-thy [BSE] or “mad cow disease”) to humans (CJD andkuru). In his book Deadly Feasts, Richard Rhodes chroni-cles the history of the SEs. He describes the history andcurrent status of research into CJD and kuru. Kuru is aSE that the Fore people of Papua New Guinea contract,which presented itself when they began ritually cannibal-izing their dead at the beginning of the 1900s. Rhodes(1997) also describes the history of the research, whichsuggests that SEs can easily leap across species, and thatthey are probably variations of the same disease process.
CHAPTER 15 | Subcortical Dementias 437
Figure 15.5 The dark stars of astrogliosis.(Courtesy D. Carlton Gajdusek.)

In his book he predicts an alarming increase in the inci-dence of CJD (Neuropsychology in Action 15.4).
N E U R O P A T H O L O G Y O FC R E U T Z F E L D T – J A K O B D I S E A S E
The cause of CJD has eluded scientists until recently be-cause it is a transmissible or infectious agent with none ofthe usual symptoms of acute infection. In fact, scientistsfirst thought that kuru could be genetic, because it oc-curred primarily among the women and children of theFore people. However, only the women and children wereeating the dead in a mortuary love feast. Men believedcontact with women weakened them, and they did notpartake in the ritual. Acute infections are easily identifiedby noticing the body’s defensive immune system response.Inflammation, increased numbers of lymph cells in cere-brospinal fluid, and fever are typical, yet none of thesesymptoms occurs in CJD or any of the SEs.
No one knows from where this infectious agent origi-nally arose. Perhaps it originated from a randomly occur-
ring mutation. This might account for the rarity in thepopulation at large and that CJD occurs with equal fre-quency throughout the world. However, in the last cen-tury, SE has also been transmitted by eating infected neuraltissue. This has happened both within species such as cows(BSE or mad cow disease) and across species. SE has de-veloped in mice, hamsters, and even primates injected withkuru. CJD has developed in humans who have eaten in-fected meat (see Neuropsychology in Action 15.4). Manyscientists now believe CJD to be a slow virus that incu-bates over years, perhaps in the spleen, and is camouflagedin cells so as not to be recognized as an invader. Some havealso hypothesized that slow viruses are responsible for AD,PD, and amyotrophic lateral sclerosis (ALS).
What exactly do SEs, specifically CJD, do to the brain?Certain areas of the brain look spongy, taking on a charac-teristic spongiform pattern. CJD, like kuru, attacks the cere-bellum, but it also damages the cerebrum. Microscopically,the “stars” of astrogliosis that Creutzfeldt found were the re-sult of the glial cells, or the “cleanup machines” of the brain,filling in after neuronal tissue had died. Astrogliosis is the
438 PART THREE | Disorders of the Brain
In his book Deadly Feasts (1997), RichardRhodes traces the history of spongiformencephalopathies (SEs) in humans and otherspecies. He reflects scientists’ views thatthese diseases are variations of the sameinfectious process, and that the ingestion orinjection of diseased neural tissue canspread many SEs within or across species. Healso forecasts an alarming increase in humanencephalopathies over the next few years ifpeople do not contain and eliminate thedisease in the animal food supply.
How exactly did mad cow disease(bovine spongiform encephalopathy [BSE])arise and become a threat to humans?Farmers routinely give cattle protein supple-ments: dairy cows all through their life, andbeef cattle for end-stage fattening. As longas farmers fed cattle largely vegetableprotein (such as soy) or fish protein togetherwith their diet of grass or hay, and no trans-mission from randomly affected cattle
occurred, BSE did not arise. However, duringthe 1980s, a series of events in Great Britaintriggered a BSE epidemic. One factor wasthat, because the pound was devalued, theprice of soy and fish meal increased, so theagricultural industry began to rely moreheavily on animal sources of protein. Animalprotein typically comes from the by-productsof slaughterhouses—bones and offal (guts,heads, tails, and blood) are processed intobonemeal pellets or powder and fed to othercattle. As long as the rendering processkilled any disease, bonemeal was a goodsource of protein. During the 1980s inBritain, changes in the rendering processdecreased the bonemeal processing temper-ature and abandoned fat removal, no longerdestroying BSE in tissue. By the late 1980s,BSE had spread throughout Great Britainand had infected more than 2000 cattle.Farmers noticed that their cattle were “be-coming aggressive, rather nervous, knocking
other cows. . . . and becoming dangerous tohandle. . . . If you shooed her, she wouldstumble, particularly on the back legs, andgo down, and then scrabble along” (p. 172).In 1988, the British government ordered milkfrom affected cows destroyed. However, notuntil an outbreak in humans occurred in1996 were massive amounts of beef cattledestroyed. The base rate for CJD is 1 in 1million people older than 50. CJD casesdeveloping under that age are extremelyrare. In the world, there had been only 10known adolescent cases. Only with kuru-associated cannibalism did researchersnotice that young people acquired spongi-form encephalopathy with a shortenedincubation period. Between 1991 and 1996,10 cases of a CJD variant of people youngerthan 40 emerged in Great Britain. Accordingto statistical probability, this is an epidemic.Only time will tell whether awareness hasstopped the spread of this disease.
N e u r o p s y c h o l o g y i n A c t i o n 1 5 . 4
C r e u t z f e l d t – J a ko b D i s e a s e a n d M a d C o w D i s e a s e : W h a t ’ s t h e C o n n e c t i o n ?
by Mary V. Spiers

aftereffect, not the cause of the disease. Amyloid plaques arealso numerous, but as discussed earlier, these are not specificto CJD but are also found in other diseases such as AD.
Patricia Merz, with the aid of her electron microscope,first found small, twisted, sticklike fibers in the cells oftissue samples of sheep with the sheep version of SE,called “scrapie” (Merz, Somerville, Wisneiwski, & Iqbal,1981). Interestingly, she could then correctly distinguishbetween healthy control subjects and affected victimswith CJD from these scrapie-associated fibrils (SAFs) inspleen and neural tissue samples. Merz hypothesizes thatSAFs may be the disease agent, which incubates in thespleen over years before affecting the brain. SAFs havebeen found in kuru and CJD brains, but not in AD, PD,or ALS brains. This was the first indication of a diseaseagent specific to SEs such as CJD.
The name that has become popular in referring toSAFs is prions (Pruisiner, 1982). Currently, several differ-ent variations or strains have been identified. Prion pro-teins (PrPs), the protein components of prions, which arepresent in both normal and afflicted individuals, havebeen the target of research interest in CJD. However, in-fected PrP resists normal protein digestion via enzymes.Interestingly, both diseased and normal PrP have the sameDNA specifications. This helps explain the riddle of whythe body’s immune system does not attack the infectedprotein. It does not recognize the protein as foreign! How-ever, one of the unsolved mysteries of this disease is to un-derstand how a normal protein changes to an abnormalprotein with the same structural DNA. Several hypothe-ses exist to explain the mechanism of action. One is thatthere may be a small virus, termed a virion, that has notyet been identified. Proteins are not known to mutate ontheir own, but perhaps small bits of “naked” nucleic acidinfected with the virion, divorced from their cells, attachthemselves to proteins and force the mutation. Anotherexplanation involves an interesting nonbiological form ofreplication. Carleton Gajdusek (1988), who won the NobelPrize in Medicine, has postulated that something else mustbe transporting the infectious agent, because even whenthe nucleic acid is destroyed by radiation, the “infection”persists. He explains this as a crystal nucleation process.Similar to how crystals such as diamonds form in nature,the infection provides the pattern that is the nucleus, orcatalyst, for the reaction. Successive proteins then mutateby patterning themselves after the original. If this soundslike science fiction, scientists have already dubbed this the“Ice-9” metaphor after a Kurt Vonnegut novel in which allthe water on earth turns to ice, in a crystallization process.
Whether a yet undiscovered virion, nuclear crystalliza-tion, or some other process is causing CJD, scientists are
CHAPTER 15 | Subcortical Dementias 439
pursuing this disease with renewed vigor because of itsunfortunate recent resurgence. We now turn to the clini-cal aspects of CJD.
C L I N I C A L P R E S E N T A T I O N A N DN E U R O P S Y C H O L O G I C A L P R O F I L E O F C R E U T Z F E L D T – J A K O B D I S E A S E
Even though emotional symptoms may be first evident,the hallmark of CJD, as well as other SEs such as kuru, ismotor symptomatology. The motor symptoms are thoseexpected of cerebellar and subcortical dysfunction. Move-ments become uncoordinated, walking resembles adrunken stagger, and speech is slurred and inarticulate.Involuntary tremors and choreiform grimaces emerge,and finally victims cannot swallow and thus may die ofstarvation. Visual function alters, eventually leading toblindness in some people. These cerebellar and subcorti-cal motor problems may follow initial, emotionally re-lated complaints of mood disorders such as anxiety, de-pression or hypomania, fatigue, difficulty sleeping, andattention/concentration problems. As with the confusionover Creutzfeldt’s patient Bertha, these symptoms maylead one to first believe that a pure mood disorder is pres-ent, or in Bertha’s case, which was more advanced, a delu-sional or psychotic disorder. However, the classic motorsymptoms quickly reveal themselves.
The dementia of CJD and its variants has a rapid pro-gression, typically less than a year and usually within 3 to4 months. Kuru has a similar progression. The Fore peo-ple of Papua New Guinea categorized the disease (usingpidgin) in five stages: (1) kuru laik i-kamap now (“kurulike he come up now”), the first stage before motor symp-toms are present; (2) wokabout yet (“walk-about yet”),motor and gait problems apparent; (3) sindaun pinis (“sitdown finish”), inability to walk; (4) slip pinis (“sleep fin-ish”), stuporous state; and (5) klostu dai nau (“close to dienow”), final stage during which swallowing is lost(Rhodes, 1997). Some have likened the progression toclassical advanced parkinsonism, but it certainly has fea-tures of HD as well.
Neuropsychological testing of patients with CJD israrely done, not only because of the rarity of the disease,but also because of its circumstances. By the time the dis-order is identified, patients are untestable. Unfortunately,at this time, there are no treatments and no cure. Perhapsthe only fortunate aspect is that the disease dies out if it isnot passed along. The level of kuru in the Fore people hasdecreased dramatically since they have stopped eating in-fected tissue.

440 PART THREE | Disorders of the Brain
Watching a neurologist at bedside can beperplexing. A process of inference is at workthat is not apparent to the onlooker. It beginswith history taking, which incorporates asdata every symptom the patient describesand the form and pattern of the descriptiveprocess. The physical aspects of examinationare selective in some respects and elabo-rated in others, to serve an incipient processof hypothesis testing at work during theexamination. An active set of principlesworking inwardly guides the conduct of theneurologist. I undertake here to make thoseinferential processes and those principlesexplicit, in a general form.
The neurologist examines the centralnervous system (CNS) with an attitude thatdiffers from the common attitude toward thebody and its symptoms. The neurologistapplies an invisible reference “map” derivedfrom neuroanatomy and neurophysiology,and from encounters with past patients andsyndromes. She or he seeks to define andlocalize a symptom as an epiphenomenonof unwitnessed internal mechanisms,respecting the rules of nervous tissuefunction rather than the culturally validatedrules of somatic experience. In the examina-tion of aging and dementia, the neurologistis, in addition, sensitized to a number ofpivotal issues in history taking, and pivotalphysical signs that narrow the selection ofpossible causes. A set of diagnostic hy-potheses, ranked by priority, is the goal ofthe examination, then (most often) to beexplored by laboratory and neuroimaginginvestigations, before the neurologist rec-ommends treatments.
The neurologist’s attitude is “phenome-nologic” in the sense that he or she must“bracket” or hold uninterpreted the symptomthe patient presents until a precise neuro-logic meaning can be attributed to thesymptom (we will call these “symptomhypotheses”). Therefore, most of the exami-nation effort focuses on the adept taking of ahistory, often from observers and family, aswell as the patient. The neurologist applies
the tools of physical examination to clarifysymptoms, achieve more precise localiza-tion, and select a favored hypothesis.
The model yielding symptom hypothesesalways includes attention to the followingseven issues:
1. Clinical CourseSudden onset (suggesting vascular or phar-macologic causes)Insidious progression (suggesting metabolic,neoplastic, inflammatory, infectious, ordegenerative causes)Episodic or paroxysmal occurrence (suggest-ing epileptic or vascular causes)Exacerbating–remitting course (suggestinginflammatory or demyelinating causes, ordisorders deriving from variable systemicillness, or related to neuromuscular junctionfatigue)
2. Hierarchical Level of AdvancementWithin the nervous system as a whole,symptoms localize to a “level of organiza-tion”: muscle, neuromuscular junction,peripheral nerve, spinal root, spinal cord,brainstem, or brain. Within the brain “level,”symptoms will vary from simple (for example,segmental loss of light perception) to com-plex (smelling colors, misattributing meaningto objects), from unimodal (for example,primary motor outputs or primary sensoryinputs) to heteromodal (for example, con-verging complex functions, personality, or theflexibility, anticipation, and organizingexecutive functions of the frontal lobe). The“level” and “complexity” of the symptom leadthe inferential process selectively to parts ofthe nervous system in which these qualitiesmust necessarily be generated.
Within the CNS, where neuropsychologi-cal dysfunction will arise, elicited historyamplifies these issues:
3. “Central Quality” of SymptomsThe presentation of a system may direct theinferential process away from the peripheral
nerves to the CNS, the spinal cord andbrain. A patient may describe a limb asdisobedient or clumsy, rather than weak orlimp, and may describe a limb sensory deficitas a regional perversion of normal sensation,rather than numbness. In the visual system,lateralized inattention or distortions (forexample, metamorphosis, color alteration,movement or space misperception, or appari-tions) are central in origin. Paroxysmal intru-sive experiences, seizures, unrealistic experi-ences, failure of reality testing, or anysymptom reporting the disruption of theindividual’s normal connection to the social orsensory environment raises the specter ofbrain disease.
4. LateralizationCo-occurrence of dysfunction in the same-side arm and face may place a suspectlesion contralaterally above the pons, anddysfunction in the same-side leg and armmay place a suspect lesion above the level ofsynapse within the cervical spinal cord. Thepresence of “crossed symptoms” (such asright face with left arm) invites exploration oflocalization within regions of anatomiccrossing of specific projections, such as thecrossing of paths in the brainstem. Coinci-dence of multiple lesions may imitate, insome cases, a single lesion in a complexregion. Therefore, neuropsychologists mustrewrite the logic of inference to entertain allpossibilities. Neuroimaging and electro-physiologic tests can corroborate the infer-ence of a focal lateralized hemisphericsyndrome, and lateralized neuropsychologi-cal findings can substantiate and clarify thediagnosis.
5. Heritable and Risk FactorsPast nervous system insults (such astrauma), vascular disease outside thenervous system (such as coronary diseaseand cardiac arrhythmia), systemic illnesses(such as immune system compromise,hyperlipidemia, diabetes mellitus, andautoimmune diseases) all narrow the
N e u r o p s y c h o l o g y i n A c t i o n 1 5 . 5
T h e N e u r o l o g i c E x a m i n a t i o n f o r D e m e n t i a
by Allen J. Rubin M.D.

CHAPTER 15 | Subcortical Dementias 441
SummarySubcortical dementias primarily target subcortical structures in the brain. The hallmark of these dementiasis motor system disorder, but the behavioral impairment also targets many higher cognitive functions.Patients with PD are more likely to experience development of dementia as they age, although dementia isnot inevitable. This chapter has examined the neuropsychological profile of patients with PD withoutdementia. In addition to the characteristic motor symptoms, patients with PD often show lateralized motor
guesswork in selecting a specific pathologicprocess in brain. Occurrence of CNSdiseases in preceding generations (such asdementias, Huntington’s disease) renderscertain diagnoses more likely.
6. Confluence, Association,Dissociation, DisconnectionConfluence of symptoms (such as ipsilat-eral motor and sensory findings), associa-tion (such as right-sided weakness withaphasia, chronic vertigo with loss of facialsensation, right–left confusion withagraphia), or dissociation (such as preser-vation of pain sensation only on the rightand preservation of vibratory sensationonly on the left; loss of voluntary facialmovement but preservation of automaticemotional facial mimicry) all point to aCNS localization. Last, history or examina-tion can identify disconnection of cerebralprocesses, which may be identified byhistory or examination (for example, alexiawithout agraphia, conduction aphasia withisolated loss of language repetition) andcan place lesions in the interconnectingbrain white matter connections.
7. Syndrome Recognition,Including NeurobehavioralProfilesA neuropsychologist may advance a “diag-nostic hypothesis” of a distinct diseasesyndrome, subject to confirmation withselected laboratory tests (genetic DNAstudies, metabolic-hematologic studies,computed transaxial tomography or mag-netic resonance neuroimaging, Doppler orcontrast angiography, electroencephalogra-phy, sensory-evoked responses, cerebralfluid examination, quantitative visualperimetry, and brain biopsy) and neuropsy-chological consultation.
The following three cases of progressivediseases among the elderly illustrate how
the symptoms and findings converge to allowdiagnostic hypotheses.
Case 1At 62, a female patient retired from her workas an effective office manager; at that timeshe was involved in dancing and was acompetitive bridge player as recreation. At75, she presented with an insidious courseof handwriting shrinkage, tremor at rest,stooping, and shuffling in gait. At 79, shehad the onset of tiredness and discourage-ment with lack of motivation and failure ofinitiative, dysphoric mood, and agoraphobia.
Pertinent examination: Her mental statewas normal, with the exception of verbalmemory, which benefited by cuing. Orthosta-tic hypotension was present. She exhibitedmasked facies and bradykinesia. A restingtremor was observed. Rigidity was present inpassive movements. She required the aid ofher arms to rise from a chair and walked withdiminished arm swing and shortened steps.Coordinated movements were slow butaccurate. Reflexes were normal.
Summary: An insidious CNS disorder withpredominantly motor impairment respectinga specific degenerative pattern. A disorder ofmemory retrieval may be emerging.
Principal diagnostic hypothesis: Parkin-son’s disease with secondary depressionand anxiety disorder. Possibly has an earlysubcortical dementia.
Case 2At 58, a financial planner found himselftaking additional time to perform routinetasks, and found that he could not managephone transactions. His personality becameirritable and obsessive, with reduced frustra-tion tolerance and temperamental flares overtrivial matters. He found he could not plan ororganize as before, and he had several “nearmisses” in driving over a short period.
His examination showed slowed velocityof ocular refixation movements (saccades),
motor impersistence of tongue protrusion,and poorly sustained grip. His speech wasgrammatic and expressive, but dysrhythmic.With mental effort, he showed choreicmovement in the face and all extremities. Hisgait was slightly widened in base. His musclestretch reflexes were hyperactive.
Summary: An insidious progressive braindisorder with frontal executive functionalimpairment and evolving irritable personal-ity, accompanied by an adult-onset choreicmovement disorder. Frontal-subcorticallocalization is suspected.
Principal diagnostic hypothesis: Hunting-ton’s disease. If the family history is negativefor this genetic disorder, confirmation of thediagnosis can be sought through DNA testing.
Case 3A 65-year-old retired judge experiencesslowly progressive impairment. He hasdifficulty in word finding and adopts a“circumlocutory” speech. He misplacesobjects and cannot retain the content of hisreading. He loses direction when he walks inunfamiliar places, and he finds that hecannot continue his hobby of constructingmodels. After several years, he loses insightthat he is impaired, and accuses his wife ofbeing a malevolent impostor. His memoryimpairment is not helped by cues or reminders.
The neurologic examination, other than themental status, is entirely normal, although hehas difficulty cooperating with the examiner.
Summary: A progressive disorder mani-festing anomic aphasia, visuospatial impair-ment, and apraxia, all cortical dysfunctions.Memory encoding is impaired and notbenefited by recognition. The absence of anymotor impairment is striking.
Principal diagnostic hypothesis: A corticaldegenerative dementia such as Alzheimer’sdisease is likely. The medical team will under-take a search for treatable and reversibleconditions that imitate this pattern.
Subcortical dementiaParkinson’s disease (PD)ParkinsonismRigidityLewy bodiesResting tremor
BradykinesiaMasked faciesFestinating gaitMicrographiaHypokinesiaDysphonia
TachyphemiaPalilaliaAnticholinergicsDyskinesiaPallidotomyThalotomy
Huntington’s disease (HD)ChoreaCreutzfeldt–Jakob disease (CJD)Gerstmann-Straussler-Scheinker
syndrome (GSS)Kuru
dysfunction. Visuospatial and executive dysfunction often are evident. Language difficulties are typicallyminor, and memory difficulties, in comparison with AD, primarily involve executive aspects of memory. Pa-tients with PD also frequently suffer from a concomitant mood disorder. The pharmacologic and surgicaltreatments for PD are among the most promising treatments for any of the dementias.
HD is a good example of a contrasting subcortical dementia with motor difficulties different from thoseof PD. It is also a good example of a progressive hereditary disease. The neuropsychological profile of HDillustrates the executive functioning problems caused by compromise of the striatofrontal lobe complex.Interestingly, patients with HD also show a significant affective disturbance. Finally, CJD, although quiterare, is a good example of a fast-acting dementia that is transmissible via infected neural tissue.
Differential diagnosis among dementia subtypes can be quite complex. This chapter, as well asChapter 14, discusses only some of the major exemplars of dementia. Practicing neuropsychologists mustcome to recognize and differentiate many more subtypes. The study and recognition of dementias requiresmuch experience with a number of dementia subtypes, and careful assessment and observation of behav-ioral differences. In this endeavor, neuropsychologists work in close conjunction with neurologists whospecialize in geriatrics. We end this chapter with a look at how neurologists approach evaluation and diag-nosis in differentiating dementia subtypes (Neuropsychology in Action 15.5).
C r i t i c a l T h i n k i n g Q u e s t i o n s
It may soon be possible to test for many neurologic diseases. Would you want to be tested for the possibility of futuredementia?How is the behavioral quality of subcortical motor disorders presented in this chapter similar or different from the corticalmotor disorders such as apraxia presented in Chapter 7?How do the subcortical and cortical motor systems work together?What are the ethical and scientific issues in the treatment of dementias?
K e y Te r m s
442 PART THREE | Disorders of the Brain
We b C o n n e c t i o n s
http://www.parkinson.org/site/pp.asp?c=9dJFJLPwB&b=71117National Parkinson’s Foundation—PD information and research.
http://www.ninds.nih.gov/disorders/huntington/huntington.htmNational Institute of Neurological Disorders and Stroke (NINDS) Huntington’s Disease Information Page.
http://www.ninds.nih.gov/disorders/cjd/cjd.htmNINDS Creutzfeldt–Jakob Disease Information Page.

Chapter 16
ALTERATIONS OF CONSCIOUSNESS
Each mind fabricates itself. We sense its limits, for we have made them.—Rainer Maria Rilke
If we cannot understand such global and major changes in the state of thebrain-mind as occur in sleep, what chance will we have with the far moresubtle changes in consciousness that trouble our patients?
—Attributed to Edward Evarts, by J. Alan Hobson (1995)
Understanding ConsciousnessRhythms of ConsciousnessThe Brain and Mind in SleepRunaway Brain: Seizure Disorders
Neuropsychology in Action
16.1 Self in the Mirror16.2 The Case of the Last Coronation16.3 Lucid Dreaming: A Paradox of Consciousness16.4 Déjà Vu and Epilepsy16.5 Epilepsy and the Case of the Sweeping Lady

experience? Is self-awareness a mind process, as WilliamJames thought, or a mind state? These questions have tan-talized philosophers, theologians, and scientists through-out time. Brain science has taken up the challenge of de-ciphering consciousness. This was once the domain of
444 PART THREE | Disorders of the Brain
K e e p i n M i n d
Can “brain” states differ from “mind” states?
How can awareness and consciousness be defined?
What brain mechanisms are responsible for the “paradox” of rapid eye movement sleep?
What alterations of consciousness are represented by different seizure types?
Do alterations in conscious alertness result from similar biological mechanisms?
OverviewConsciousness can be conceptualized in a number of ways. Awareness, level of mental alertness, and levelof attention are common representations. Consciousness can also imply the mind’s subjective experience ofbrain states and processes that are available to perception. These various definitions point to a number ofdifferent functional anatomic areas depending on the aspect of consciousness under consideration. Disor-ders of these disparate functional systems also result in a variety of disorders of consciousness. For exam-ple, we have discussed alterations in conscious “knowing,” or agnosias of the visual system. The total un-awareness of one side of the body, or neglect, is a dramatic dysfunction of normal conscious awareness. Thesedisorders of lowered, distorted, or piecemeal awareness can occur in any sensory modality. Synesthesia, or theabnormal melding of sensory-perceptual experiences, represents yet another alteration of consciousnesscovered in this book.
This chapter revisits questions of brain and mind by considering conceptualizations of consciousnessparticularly for awareness and alertness. We discuss both normal and disordered aspects of consciousnessthrough a discussion of normal sleep, sleep disorders, and seizure disorders. Throughout the day and night,alertness fluctuates according to preset circadian (derived from Latin, meaning “about a day”) rhythms. Thestudy of these daily rhythms, as people move from waking to sleeping and dreaming, offers lessons in thelimits of normal brain alterations of consciousness. Disrupted flow of these brain rhythms can result in avariety of sleep disorders. Some, such as the rare circadian rhythm disorder (see Neuropsychology inAction 16.2) can threaten life itself. Others, such as narcolepsy, show major disruptions of the REM (rapideye movement sleep) cycle and result in sleep intrusions into wakefulness. Most sleep disorders disruptcognition in some way. In sleep apnea, for example, memory and concentration difficulties are prevalent.
Seizures represent another set of disorders of consciousness. Seizure events of various types repre-sent alterations of daytime alertness and awareness. These internally generated brainstorms of activitymanifest differently, largely according to the location of the seizure focus in the brain. Typically, neurologistscategorize them as either generalized or partial seizures, depending on the extent of brain involvementduring the seizure episode. We present these in the context of a general seizure classification scheme.Seizures can occur as a result of a variety of causes. Neurologists consider most people with repeatseizures to have an epileptic syndrome. This, of course, is potentially more threatening to brain functionthan is an isolated seizure event. We discuss the neuroanatomy and neurophysiology of epilepsy, as well asthe neuropsychological consequences and types of treatments available.
Understanding Consciousness
What is consciousness? What makes human con-sciousness different from that of other animals? Whatsorts of brains or brain activity are necessary for conscious

psychology, spearheaded by Wilhelm Wundt and the earlystructuralists at the turn of the century; the strong behav-ioral movement in U.S. psychology later cast aside thestudy of consciousness as too subjective for serious study.Observable behavior was now paramount, and the brainwas merely a “black box.” Psychologists now know thatconsciousness is fundamentally important to understand-ing the human condition. Conscious experience, how-ever, is difficult to measure and observe because of itshighly private nature. Nobel prize laureate Francis Crick(Crick and James Watson discovered the structure ofDNA) admonishes scientists not to worry too much overaspects of the problem that they cannot solve scientificallyor, more precisely, cannot solve solely by using existing sci-entific ideas. Perhaps the only sensible approach is to pressthe experimental attack until scientists confront dilemmasthat call for new ways of thinking (Crick & Koch, 1990).
Here we are concerned with defining the concept ofconsciousness, the mind–brain relation, and current the-ories related to how the brain represents consciousness.After considering the “how” of consciousness, we turn totheorist David Chalmer’s question related to the “why” ofconsciousness. Even if we can explain how the brain rep-resents conscious experience, we need to know why this isimportant to human functioning. Why are we not un-thinking and unfeeling automatons?
To begin, most people agree that consciousness impliesawareness. This is the primary dictionary definition. Theterm consciousness also refers to a certain level of mentalalertness and attention. It also connotes what one’s innerself knows or feels. Consciousness is above all a subjectiveand highly personal reckoning of external and internalevents. Measuring it has also relied largely on the person’sability to manifest internal experiences through verbal ex-pression. The issue of awareness raises interesting ques-tions for neuropsychology. If the mind is the subjectiveexperience of brain states and processes, then the mindreflects awareness of brain and body functioning. Becauseof either external or internal stimulation, sometimes themind may be able to show more awareness, whereas atother times it seems totally oblivious to the workings ofthe physical brain and body. One of the main questionsthat brain science must answer (to put it in what is nowthe common vernacular) is, What distinguishes the con-scious mind from the subconscious or unconscious mind?
M I N D A N D B R A I N
Popular culture often represents the brain in mechanisticterms, like a type of giant computer, reminiscent of New-tonian physics. However, machines can self-regulate behav-ior but do not have self-awareness or a subjective experience
of consciousness. Another interesting question is to whatextent do animals show self-awareness (Neuropsychologyin Action 16.1). An interesting theoretical question re-lates to whether computers will someday imitate thehuman brain, and presumably become conscious. Willartificial intelligence (AI) mimic human consciousness, asin the imagined character HAL, the supercomputer in thescience fiction movie 2001: A Space Odyssey? During aspace shuttle to Mars, HAL starts to display “his” ownawareness and decision-making capability, finally killingoff the shuttle crew.
Conceptualizing the brain as a computer has only lim-ited usefulness. After all, brains have built computers, notthe other way around. It appears more useful to concep-tualize the brain as attached to the person, as a biologicalentity. The level of consciousness of biological entitiespartly responds to biological and cosmic rhythms, as evi-denced in the sleep/wake cycle and the rhythm of the sun.Consciousness also changes in response to internal physi-ology and chemistry, with inputs from food and drugs.The term mind is used to reflect subjective experience,and therefore consciousness, of the emanations of thebrain and the body together. Can we assume that everystate of mind links to a brain state, and that every state ofbrain reflects a mind state, be it conscious or unconscious?
Scientists have often wondered whether split-brain pa-tients, who have had the two hemispheres of their brainsurgically disconnected, are “of two minds.” In an oldermethod of treating seizures, surgeons cut the half-billionaxons that allow interhemispheric cross-talk in many pa-tients with intractable seizures. Are these two hemispheresstill conscious of each other? Do split-brain patients re-tain one consciousness, or do two separate realities or eventwo separate personalities exist? Immediately after surgery,some split-brain patients report having two competinghemispheres. When getting dressed, the right hand mayreach for a blue shirt whereas the left hand is grabbing ared shirt. These apparently competing programs, how-ever, usually resolve within a matter of weeks. After that,split-brain patients typically report a unified consciousexperience. In daily life their actions are not recognizablydifferent from their presurgery state. Only specialized test-ing that presents information to only one hemisphere at atime continues to show differences. In effect, this testingappears to reveal more differences between right and lefthemisphere processing than it shows a fundamental divi-sion of consciousness in those who have had a split-brainoperation.
The stumbling block is that we usually documentawareness via our ability to verbalize, a province largelyof the left hemisphere. In individuals with an intact cor-pus callosum, the right hemisphere—and therefore the
CHAPTER 16 | Alterations of Consciousness 445

consciousness of the right hemisphere—is accessible toleft hemisphere verbalizations. Split-brain patients mustreformulate a sense of completeness by making their ex-periences accessible to both halves of their brains throughexternal cross talk. They can largely do this by movingtheir eyes to capture both visual fields and verbalizing outloud so that each hemisphere hears what is available tothe other hemisphere. Within us, many brain and bodyprocesses are either automatic or unavailable, and thus
typically remain unconscious to the mind. For split-brainpatients, the hemispheres are physically unavailable toeach other. The brain is not communicating internally,but the subjective experience is of one mind. The chal-lenge for the split-brain patient is to consciously integrateeach half of the cerebral hemispheres that have been madesurgically unconscious of each other.
Most people with intact brains agree that large areas ofpotential experience remain below the level of conscious
446 PART THREE | Disorders of the Brain
Have you ever caught your cat (or dog) shav-ing? Have you ever wondered why your (male)pet might not shave? Well outside of the factthat it is likely difficult to shave with noopposable thumb and challenging to balanceyourself on two limbs when you are used tomoving about on four, there is another,neurocognitive reason why your pets do notshave. They cannot recognize themselves inthe mirror! That’s right, your pet (that isunless you own a pet chimpanzee) does nothave the cognitive capacity to recognize itselfin the mirror; in fact, your pet likely sees itsmirror reflection as another member of thesame species and reacts as such (for exam-ple, hisses, piloerection for cats).
In 1970, a comparative psychologistnamed Gordon Gallup (Gallup, Nash, Potter,& Donegan, 1970) was investigating thebehavior of animals in front of mirrors as away to measure social behavior systemati-cally when he stumbled on the fact that mostorganisms react to their mirror reflection as ifit were a member of the same species; thatis, they responded to their mirror reflectionwith species-specific social behaviors(threats, attempts to mate, spitting, barking,feces throwing, among other reactions). Toscientifically test this notion, Gallup devel-oped the “mark test,” which entails markingareas of an animal’s body that cannot beseen without the mirror. Animals that canrecognize themselves in mirrors ought to usethe mirror to examine their newly markedanatomy. It turns out that only our closest
living relatives—the great apes(chimpanzees, orangutans, and gorillas)—posses the ability to use their mirror reflec-tion like humans do (Gallup, 1982).
What is the importance of mirror self-recognition for neuropsychology, and whocares whether chimps can do it? It turns outthat the ability to recognize yourself in amirror is strongly related to your sense ofself, or self-awareness, which allows you toengage in a number of adaptive socialbehaviors, for example, empathy, sympathy,deception, and so on (Gallup, 1982). Inaddition, great apes’ frontal lobes are themost encephalized, second only to humans.Meaning relative to other parts of their brainand their body, great ape frontal lobes arelarger than would be expected by chance.Therefore, the investigation of self-recognitionin nonhuman primates provides us withinsights into the neuropsychological andpossible clinical underpinnings of self andconsciousness in humans.
If I were to ask you: “Does everyonerecognize themselves in a mirror?” You’dlikely answer, “Of course!” Not true. In fact,there are several neuropsychological condi-tions that are marked by deficits in self-processing. The most notable is a conditionknown as “mirror sign,” or mirror self-misidentification syndrome (Breen, Caine, &Coltheart, 2001). Patients with mirror signare able to use mirrors to recognize objects,and even other people, but when askedabout their own reflection, they often
respond as if their mirror reflection was astranger who was following him or heraround. Usually untroubled by their disorder,family members report that patients act“funny” or “strange” at home, often surpris-ing themselves as they walk past mirrors.Some patients do complain that their newcounterpart does not talk to them, whichdoes create some frustration. Neuropsycho-logically, these patients are marked primarilyby right hemisphere dysfunction, whichsuggests that the capability to processinformation about the self may be localizedto regions of the right frontal lobe. Thisnotion has recently been confirmed byseveral functional magnetic resonanceimaging investigations of self-face recogni-tion (Platek, Keenan, Gallup, & Mohamed,2004; Platek et al., 2005).
Several other neuropsychological condi-tions are marked by subtler deficits in self-processing. For example, patients withschizophrenia make many errors when askedto distinguish their own face from familymembers’ faces and are more likely thancontrol subjects to classify unknown faces asbeing their own face.
Collectively. these data—from compara-tive, nonhuman studies to neuropsychiatricpatient findings—suggest that the frontallobes, and perhaps specifically the rightfrontal lobe, are involved in self-processingand when damaged or compromised mightresult in impairments in self-awareness andcorresponding social intelligence.
N e u r o p s y c h o l o g y i n A c t i o n 1 6 . 1
S e l f i n t h e M i r r o r
by Steven M. Platek

experience. The common saying “we only use 10% of ourbrain” might be better thought of as “our conscious mindmay be aware of only a percentage of what our brains doand are capable of.” Our brains control and monitor theentire nervous system of our bodies and respond to physi-ological mechanisms in the body, such as those of the en-docrine system, to maintain a state of brain–body home-ostasis. Many of these processes are automatic andreflexive. They are unconscious. But they can be broughtinto awareness via techniques such as biofeedback, andcan then be modified by the conscious mind. Many havewondered what might be possible if aspects of the uncon-scious mind became conscious. What hidden potentialcould people then develop, such as becoming consciousduring the “unconscious” state of sleep or developingsenses and perception beyond what is now commonlythought possible? This may sound like the stuff of sciencefiction, but researchers have documented lucid dreaming(see later). It is also reasonable to assume that scientistswill find ways to study the limits of sensory-perceptualexperiences. Boundaries between the concepts of the con-scious mind and the unconscious mind are blurring. Thechallenge now before brain science is to understand theworkings of these aspects of mind and to relate them tobrain states and processes.
A N A T O M I C C O R R E L A T E S O F C O N S C I O U S N E S S
How are states of consciousness represented in brainanatomy and physiology? René Descartes thought thepineal gland was the center of conscious experience, butresearchers have found no single location for conscious-ness. After several hundred more years, this question maystill be somewhat premature, because brain science hasnot yet clearly defined the operations and boundaries ofconsciousness. Different areas of the brain may play rolesin specific aspects of conscious perception and alertness.Brain science is also now providing interesting clues tohow the brain “binds” disparate fragments of informationfrom different cortical and subcortical regions into a sub-jective sense of coherent unity.
The candidates for brain regions or functional areasthat have a role in conscious behavior have, depending onthe behavior in question, included numerous areas of thebrain, both cortical and subcortical. The various defini-tions of consciousness suggests that different brain corre-lates are implicated depending on whether the focus is onnotions of awareness or perception, notions of alertnessor attention, or notions of what is felt or known by one’s
inner self. Perceptual awareness, “knowing,” and therefore,perceptual consciousness, build up through modality-specific sensory systems of vision, audition, proprioception,olfaction, and taste. The brain correlates of sensory-perceptual consciousness depend on the integrity of eachof these systems. Therefore, it is possible for one sensorymodality to block access to “knowing,” whereas still show-ing awareness through other sensory modalities. Such is thecase with the agnosias, as we have discussed in Chapters 7and 8, which can occur after damage to any of the sensorysystems. When speaking of level of consciousness, or alert-ness, researchers often identify the reticular activatingsystem (RAS) in the midbrain as responsible for arousal,which we discuss in regard to sleep. Finally, if the self-referential, self-evaluative, and metacognitive aspects of con-sciousness are the focus, then researchers can consideraspects of executive system and frontal lobe functioning.
Brain researchers and theorists have been most in-trigued by how the brain creates a unitary experience ofconsciousness at one particular moment in time. This canbe referred to as the binding problem. What is the mecha-nism that binds disparate neural elements together? Aunitary experience of consciousness is an operation of thehighest order and, therefore, requires a cortex. Thus, themore sophisticated the cortex, theoretically, the greaterthe ability for subjective experience and self-awareness.
Let us examine the role of the cortex in consciousnessmore closely. Neuroscientists commonly describe experi-ences represented in the cortex as stable spatial patterns.For example, vision is a complex constructional processresulting in object recognition by building and bindingelements related to color, form, movement, and spatialposition. This binding may occur as a simple structuralpattern. Experience in seeing your grandmother increas-ingly hardwires the synaptic conjunctions between theneurons from various cortical areas forming the patternthat defines “grandmother.” This way of thinking is anadvance over conceptualizations that first postulated theexistence of single “grandmother” cells in which therecognition of grandmother, although the culmination ofmany processes, was ultimately embodied in one neuronor neuron group. Brain scientists soon realized that themodel of single cumulative grandmother cells was grosslyinefficient, because separate cells would have to be avail-able for every possible combination and permutation ofpeople and objects. Even though the brain consists ofbillions of neurons, it would soon run out of neurons forevery possible permutation of a memory. Having grand-mother represented in a large cortical neuronal assembly isa more efficient conceptualization in terms of processing.Individual neurons can participate in different assemblies,
CHAPTER 16 | Alterations of Consciousness 447

one representing grandmother, another father, another ateacher, and so on. The firing pattern within the web ofneurons takes precedence over any individual neuron. Ifthe pattern is disrupted at crucial points, the brain losesrecognition of the person.
The neocortex unquestionably plays a major role inevaluating external and internal experiences, but subcorti-cal structures, and particularly the thalamus, may play acrucial role in orchestrating the higher cortical symphony.Francis Crick and Christof Koch (1990), in their study ofvisual consciousness, have postulated that the upper lay-ers of the cortex are largely unconscious, whereas the pyra-midal neurons in layer 5 may be “conscious.” Their rea-soning is that this is the only layer that “projects right outof the cortical system.” Layer 5 also shows an unusualpropensity to fire in bursts. Others have also noted thisimportant observation that groups of neurons fire to-gether in bursts, which appears to be an important clue tothe binding problem. Researchers know that many cellassemblies throughout the brain fire in synchronous oscil-lations. For example, in the motor system, the inferiorolive of the brainstem sends information in packets ofbursts at an oscillation of 10 cycles/sec to the cerebellum.Much as with frames of a movie, the movement only ap-pears fluid because we cannot discriminate the fine breaksin continuity.
The thalamus, the sensory relay station of the brain,may also play a crucial role in synchronizing corticalprocesses. In an alert state, an electroencephalograph(EEG) records in the gamma frequency range (35–80cycles/sec), averaging 40 cycles/sec from the cortex. Thisnormal frequency decreases with relaxed wakefulness to 8to 10 cycles/sec and with deep sleep and coma to 0.5 to 4cycles/sec. Faster frequencies are asynchronous, whereasslower frequencies become increasingly synchronized andrhythmic. Rodolfo Llinas of New York University (citedin Becker & Seldon, 1985) postulates that the EEG fre-quency represents a binding wave that continuouslysweeps the cortex like a huge radar arm. As the wave scansthe brain, the brain synchronizes and interprets all infor-mation in that sweep as a unified experience. This action,then, could bind packets of information from widely dis-tributed and noncontiguous regions of the cortex by syn-chronizing them in time. The implication is that morehardwired spatial patterns of neurons do not act as theprime binding mechanism. Researchers have postulatedthis theory as a general explanation for how consciousnessoperates, as well as a specific explanation for how aspectsof visual consciousness such as visual object recognitionwork (Bressler, Coppola, & Nakamura, 1993; Crick &Koch, 1990).
If there is a “binding wave,” from where does this fre-quency emanate? It appears as if the intralaminar nucleusof the thalamus generates a cortical binding signal every12.5 thousandths of a second (that is, every 0.0125 sec-ond) (Llinas cited in Becker & Seldon, 1985). As men-tioned earlier, nearly all sensory and motor systems routethrough the thalamus. The thalamus is in constant two-way communication with the cortex through a feedbacksystem of millions of thalamocortical loops. A number ofinvestigators believe this system, which reaches through-out the cortex, is intimately involved with conscious ex-perience. Because nearly all information channels throughthe thalamus, it can act as the integrator, selecting, pack-aging, and tagging information that occur together intime from all areas of the brain, and sending it back forthe cortex to record as an object or an event. The thala-mus and the thalamocortical projection system play animportant role in arousal, sleep, and seizure disorders. Itmay also play a role in remapping phantom sensations. Atemporal binding system, whether through the thalamusor other structures, would be highly efficient, because itcould register any number of novel neural code combina-tions together and be experienced instantly without rely-ing on the hardware of contiguous, linear cortical con-nections. These findings suggest that, indeed, there is nosingle organ of consciousness; instead, the frequencies oftemporal binding may coordinate experience. This wouldindicate that the whole brain can contribute to awarenessdepending on which systems activate at any one time tosignal the effect of an experience. This view implies a dy-namic quality to the brain and conscious experience thatis infinitely more flexible than former conceptualizations.
According to theorist David Chalmers (1996), the“how” question of consciousness is not the difficult ques-tion. The difficult question is not how conscious processesbind together, but how a subjective experience of mindarises from the functioning brain and its synchronizedand bundled oscillations. By looking deeper into people’sdirect subjective experiences, some of which are explicitand some of which are implicit, researchers will learnmore about the relation of brain to mind.
People customarily link consciousness of externalevents with the tangible. Even our vocabulary reflects this:“I know something to be true because I saw it with myown eyes, I can feel it, I can sense it.” Most of what peo-ple experience they know by way of senses of smell, taste,sight, sound, and touch—the springtime smells of lilacsand freshly mown grass, the sight of children runningacross the yard, the sound of laughter, and the squeeze ofa hand. But external realities exist that most of us cannotperceive directly through our senses. At the turn of the
448 PART THREE | Disorders of the Brain

20th century, people were just becoming aware that soundcould travel through long distances, even through bodies,yet people cannot perceive such sound directly without alittle box called a radio. In the animal world, whales, dogs,and bats communicate within their own species on differ-ent frequencies than humans can “consciously” perceive.We now know that low- and high-frequency sound exists,because we have instruments that can measure and trans-mit these “unconscious” ranges of sound. In the samevein, people know that electrical fields and microwave en-ergy exist. In 1933, Enrico Fermi, a physicist, predictedthe presence of neutrinos, or energy particles, which per-meate the universe and freely flow through bodies with-out leaving a trace. In 1956, physicists definitively identi-fied neutrinos. What else might exist that people cannotconsciously perceive? Modern science may be just begin-ning to unravel the mysteries that lie beyond limitedhuman sensory abilities.
The Western empirical, materialistic tradition of sci-ence takes the stance that if something cannot be observedand measured it does not exist. To study the full range ofconsciousness, this archaic and human-centered viewmust give way to the possibility that the range of realityextends beyond ordinary human sensory-perceptual expe-rience. Brain dysfunction can truncate, extend, or other-wise bend sensory-perceptual experience. Many cases wepresent in this book certainly stretch the bounds of ordi-nary conscious experience. Supersensory abilities may alsobe possible. Some Chinese health practitioners diagnoseand heal by working with only the energy fields of thebody. Fortunately, new technologies may bring intoawareness many aspects of sensory experience that are outof range to the “naked senses.” Scientists may now experi-mentally verify awareness of both pathologically alteredand exceptional sensory perception, although few studieshave considered these issues.
Previously, the limited means of measuring subjectiveexperience have hampered scientists in studying con-sciousness. Primarily, they have had to rely on direct ex-perience of the senses and on language to reveal con-sciousness. In other words, people could demonstrateawareness if they could hear, see, taste, smell, or touchsomething and be able to describe it. Because the lefthemisphere is more specialized for spoken words, somehave characterized it as the seat of consciousness. But thatsimplistic notion equates awareness with an ability to de-scribe the phenomenon. Many people can probably recallexperiences in which they had a sense of knowing with-out the ability to verbalize or touch what they felt.
Also, some processes that are now implicit may bemade explicit. People can demonstrate implicit knowl-
edge through their actions based on that knowledge. Sci-entists also know that subliminal sound and scent, underthe level of detectable awareness, can affect brains in apredictable manner. Similarly, scientists will also be ableto determine whether some individuals can detect electri-cal energy fields of which most are not conscious. On theinternal side of the coin, many of what are considered au-tomatic processes, such as breathing and heart rate, churnalong without conscious awareness or control. But themeans already exist to bring many of these processes intoconscious awareness through various biofeedback tech-nologies such as heart-rate monitoring, galvanic skin re-sponse measurement, and EEG. Although these technolo-gies present a recent tool for more conscious body andmind control, masters of meditation have long exertedamazing control over many brain and body states. Giventhe increased ability to gain a window into automatic andsubconscious processes through vivid functional brainimaging techniques, whole new areas of research are open-ing up that may now allow neuropsychologists to learnnot only about the workings of the brain but also how toconsciously control various brain states. The possibilitiesavailable for extending the range of normal conscious ex-perience represent an exciting frontier in brain science.
This chapter visits daily aspects of consciousness, aswell as disorders of consciousness. What happens whenthe fundamental experiences of consciousness run amokbecause of brain dysfunction? The daily rhythms of alert-ness and arousal people all move through from waking tosleeping and dreaming provide directions for studying thelimits of normal brain alterations of consciousness. Dis-rupted flow of these brain rhythms can cause a variety ofsleep disorders, of which one of the more interesting isnarcolepsy. Finally, seizures represent an alteration of con-sciousness that also affects level of alertness—an inter-nally generated brainstorm of synchronized activity.
Rhythms of Consciousness
Cyclic changes are inherent in the passing of sea-sons, in weather patterns, in tidal ebbs and flows, and inthe rising and setting of the sun. In humans, mood andenergy levels respond to seasonal shifts, menstruation cy-cles follow monthly rhythms, and sleep and wakefulnesscycles oscillate daily in a circadian rhythm. Humans alsorespond to shorter ultradian 90-minute cycles of height-ened and lowered brain arousal. The autonomic system ofthe brain controls the rhythms of heart rate and respira-tion. The brain itself is a web of neuronal circuitry with afrequency measured in cycles per second on an EEG (see
CHAPTER 16 | Alterations of Consciousness 449

Chapter 2 for a detailed discussion of EEG). It alternatesbetween periods of brain asynchronicity, usually indica-tive of an alert brain state, and periods of “altered con-sciousness” synchronicity, in which groups of neurons os-cillate rhythmically. Some of these synchronous oscillations,such as those occurring during sleep, represent normalvariations. Others, which occur during seizures and coma,may suggest pathology. Many of the normal internalrhythms of the body and brain, such as sleep, are cali-brated in response to external environmental changes suchas the light/dark cycle. Scientists do not yet understand agreat deal about the complex interplay between the manyhuman rhythms and external environmental rhythms thataffect human functioning.
In addition to these questions, neuropsychology is in-terested in how brain states, measurable via dynamicimaging means such as EEG and positron emission to-mography, correspond to mind states in both ordinaryand pathological functioning. In absence seizures, slow-wave synchronous activity abruptly interrupts the nor-mally asynchronous waking state. It would appear, then,that slow synchronous brain activity heralds pathology.But absence seizures in children, which are marked bybrief lapses in consciousness, show the same 3 cycles/sec
synchronous brain waves characteristic of normal delta-stage sleep. The EEGs of people in coma also show thisslow synchronous wave. Masters of meditation, however,can produce delta waves and remain seemingly “conscious.”Although the EEG can record similar brain states in twodifferent people, mind states and awareness can range con-siderably. Therefore, similar brain-wave frequencies canimply pathologic “unconscious” mind states, normal sleep-ing mind states, or fully conscious mind states. Althoughthe EEG provides clues as to whether one is thinking, itdoes not capture the subjective experience of the mind.
Many interesting questions of consciousness revolvearound alertness and level of arousal. We examine sleep insome depth in this chapter because of its rhythmic brainactivity and the paradoxical and fascinating nature of thedreaming REM (rapid eye movement) stage. Deep withinthe hypothalamus, a biological clock—in conjunctionwith the visual system—calibrates the sleep/wake cycle. Acase example illustrates how chaotic sleep and health canbecome without this clock (Neuropsychology in Action16.2). Sleep disorders such as narcolepsy also illustratethe manner in which sleep/wake rhythms may becomeconfused, resulting in daytime sleep intrusions and frag-mented nighttime sleep.
450 PART THREE | Disorders of the Brain
He was Italian, 53 years old, and an indus-trial manager whose health had been fineexcept for some problems with high bloodpressure. Much to his misfortune, he wasdestined to show researchers how dire thingscan get when the body’s internal clock runsamok.
In 1985, the man experienced develop-ment of insomnia. His sleep fell to only 2 or 3 hours a night, he became impotent, and hebegan to have difficulties with his digestionand developed a high temperature. Within 2 months, he could sleep for only 1 hour anight and was often observed rising from hisbed, standing, and giving a military salute.He told his family that he was dreaming of acoronation. By the time the man was admit-ted to the hospital in Bologna, he had
ceased to sleep normally at all. He was alertwhen spoken to, but when left alone woulddrift into a stupor in which he would gestureas if communicating in a dream. His doctorstried to treat him with a variety of strongdrugs, none of which had a lasting effect. Inthe eighth month of his illness, the man’sstupor was relieved only by episodes inwhich he screamed and thrashed about. In the ninth month, he died.
Examining his otherwise normal brain,doctors found that certain regions of thethalamus had degenerated. The man’s raredisease supported suspicions that sleep, atleast nondreaming NREM (non–rapid eyemovement sleep) sleep, is affected bychemical processes in the thalamus. Justbelow that structure, near the base of the
brain, is a bean-sized region known as thehypothalamus. The hypothalamus sends outsignals that regulate basic processes suchas hunger and sex and affect emotions suchas anger. It is also a central control for thebiological clock that controls sleep; when thehypothalami of mice are damaged, the micelose any semblance of orderly or regularsleep.
This man’s misfortune also displayed thegenetic nature of this sleep disorder. Thedoctors learned from one of the man’srelatives, also a doctor, that in the last 6generations of the man’s family at least 14relatives, including his sisters, had died ofthe same bizarre condition.Source: Adapted from The Case of the LastCoronation. (1988, March–April). Hippocrates.
N e u r o p s y c h o l o g y i n A c t i o n 1 6 . 2
T h e C a s e o f t h e L a s t C o r o n a t i o n
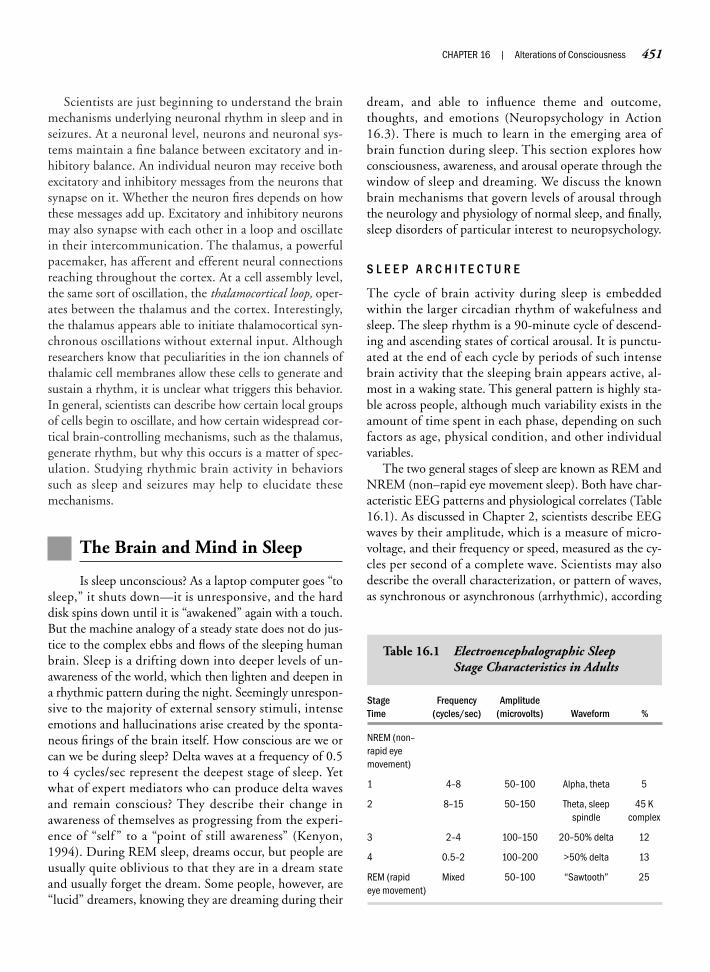
Scientists are just beginning to understand the brainmechanisms underlying neuronal rhythm in sleep and inseizures. At a neuronal level, neurons and neuronal sys-tems maintain a fine balance between excitatory and in-hibitory balance. An individual neuron may receive bothexcitatory and inhibitory messages from the neurons thatsynapse on it. Whether the neuron fires depends on howthese messages add up. Excitatory and inhibitory neuronsmay also synapse with each other in a loop and oscillatein their intercommunication. The thalamus, a powerfulpacemaker, has afferent and efferent neural connectionsreaching throughout the cortex. At a cell assembly level,the same sort of oscillation, the thalamocortical loop, oper-ates between the thalamus and the cortex. Interestingly,the thalamus appears able to initiate thalamocortical syn-chronous oscillations without external input. Althoughresearchers know that peculiarities in the ion channels ofthalamic cell membranes allow these cells to generate andsustain a rhythm, it is unclear what triggers this behavior.In general, scientists can describe how certain local groupsof cells begin to oscillate, and how certain widespread cor-tical brain-controlling mechanisms, such as the thalamus,generate rhythm, but why this occurs is a matter of spec-ulation. Studying rhythmic brain activity in behaviorssuch as sleep and seizures may help to elucidate thesemechanisms.
The Brain and Mind in Sleep
Is sleep unconscious? As a laptop computer goes “tosleep,” it shuts down—it is unresponsive, and the harddisk spins down until it is “awakened” again with a touch.But the machine analogy of a steady state does not do jus-tice to the complex ebbs and flows of the sleeping humanbrain. Sleep is a drifting down into deeper levels of un-awareness of the world, which then lighten and deepen ina rhythmic pattern during the night. Seemingly unrespon-sive to the majority of external sensory stimuli, intenseemotions and hallucinations arise created by the sponta-neous firings of the brain itself. How conscious are we orcan we be during sleep? Delta waves at a frequency of 0.5to 4 cycles/sec represent the deepest stage of sleep. Yetwhat of expert mediators who can produce delta wavesand remain conscious? They describe their change inawareness of themselves as progressing from the experi-ence of “self ” to a “point of still awareness” (Kenyon,1994). During REM sleep, dreams occur, but people areusually quite oblivious to that they are in a dream stateand usually forget the dream. Some people, however, are“lucid” dreamers, knowing they are dreaming during their
dream, and able to influence theme and outcome,thoughts, and emotions (Neuropsychology in Action16.3). There is much to learn in the emerging area ofbrain function during sleep. This section explores howconsciousness, awareness, and arousal operate through thewindow of sleep and dreaming. We discuss the knownbrain mechanisms that govern levels of arousal throughthe neurology and physiology of normal sleep, and finally,sleep disorders of particular interest to neuropsychology.
S L E E P A R C H I T E C T U R E
The cycle of brain activity during sleep is embeddedwithin the larger circadian rhythm of wakefulness andsleep. The sleep rhythm is a 90-minute cycle of descend-ing and ascending states of cortical arousal. It is punctu-ated at the end of each cycle by periods of such intensebrain activity that the sleeping brain appears active, al-most in a waking state. This general pattern is highly sta-ble across people, although much variability exists in theamount of time spent in each phase, depending on suchfactors as age, physical condition, and other individualvariables.
The two general stages of sleep are known as REM andNREM (non–rapid eye movement sleep). Both have char-acteristic EEG patterns and physiological correlates (Table16.1). As discussed in Chapter 2, scientists describe EEGwaves by their amplitude, which is a measure of micro-voltage, and their frequency or speed, measured as the cy-cles per second of a complete wave. Scientists may alsodescribe the overall characterization, or pattern of waves,as synchronous or asynchronous (arrhythmic), according
CHAPTER 16 | Alterations of Consciousness 451
Stage Frequency Amplitude Time (cycles/sec) (microvolts) Waveform %
NREM (non–rapid eye movement)
1 4–8 50–100 Alpha, theta 5
2 8–15 50–150 Theta, sleep 45 K spindle complex
3 2–4 100–150 20–50% delta 12
4 0.5–2 100–200 >50% delta 13
REM (rapid Mixed 50–100 “Sawtooth” 25eye movement)
Table 16.1 Electroencephalographic SleepStage Characteristics in Adults
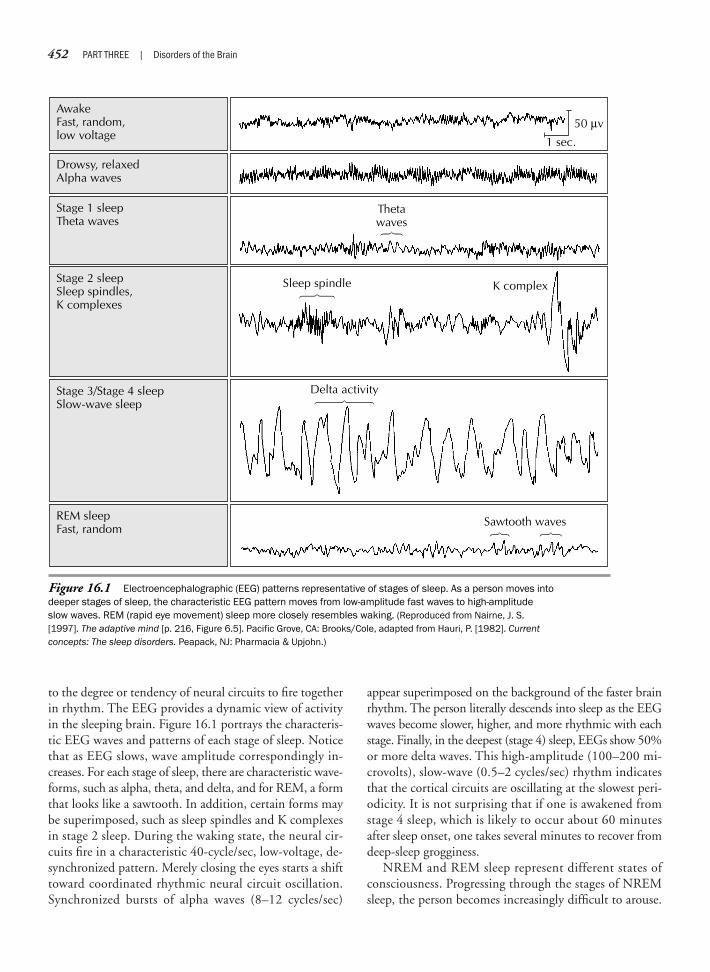
to the degree or tendency of neural circuits to fire togetherin rhythm. The EEG provides a dynamic view of activityin the sleeping brain. Figure 16.1 portrays the characteris-tic EEG waves and patterns of each stage of sleep. Noticethat as EEG slows, wave amplitude correspondingly in-creases. For each stage of sleep, there are characteristic wave-forms, such as alpha, theta, and delta, and for REM, a formthat looks like a sawtooth. In addition, certain forms maybe superimposed, such as sleep spindles and K complexesin stage 2 sleep. During the waking state, the neural cir-cuits fire in a characteristic 40-cycle/sec, low-voltage, de-synchronized pattern. Merely closing the eyes starts a shifttoward coordinated rhythmic neural circuit oscillation.Synchronized bursts of alpha waves (8–12 cycles/sec)
appear superimposed on the background of the faster brainrhythm. The person literally descends into sleep as the EEGwaves become slower, higher, and more rhythmic with eachstage. Finally, in the deepest (stage 4) sleep, EEGs show 50%or more delta waves. This high-amplitude (100–200 mi-crovolts), slow-wave (0.5–2 cycles/sec) rhythm indicatesthat the cortical circuits are oscillating at the slowest peri-odicity. It is not surprising that if one is awakened fromstage 4 sleep, which is likely to occur about 60 minutesafter sleep onset, one takes several minutes to recover fromdeep-sleep grogginess.
NREM and REM sleep represent different states ofconsciousness. Progressing through the stages of NREMsleep, the person becomes increasingly difficult to arouse.
452 PART THREE | Disorders of the Brain
Figure 16.1 Electroencephalographic (EEG) patterns representative of stages of sleep. As a person moves intodeeper stages of sleep, the characteristic EEG pattern moves from low-amplitude fast waves to high-amplitudeslow waves. REM (rapid eye movement) sleep more closely resembles waking. (Reproduced from Nairne, J. S.[1997]. The adaptive mind [p. 216, Figure 6.5]. Pacific Grove, CA: Brooks/Cole, adapted from Hauri, P. [1982]. Currentconcepts: The sleep disorders. Peapack, NJ: Pharmacia & Upjohn.)
Drowsy, relaxedAlpha waves
AwakeFast, random,low voltage
50 µv
1 sec.
Stage 1 sleepTheta waves
Thetawaves
Stage 3/Stage 4 sleepSlow-wave sleep
Delta activity
Stage 2 sleepSleep spindles,K complexes
Sleep spindle K complex
REM sleepFast, random
Sawtooth waves

CHAPTER 16 | Alterations of Consciousness 453
Often when one is asleep, there is somethingin consciousness which declares that whatthen presents itself is but a dream.
—Aristotle
Can one be simultaneously conscious anddreaming? Although an ancient phenome-non, documented in stories throughouthistory, lucid dreaming has only recentlycaught the attention of scientists who areexploring the frontiers of human conscious-ness. Throughout history, most of the majorreligions have used lucid dreaming as aspiritual practice. Examples within Christian-ity, Islam, Hinduism, and Tibetan Buddhismshow how to use lucid dreaming as a path toenlightenment. The assertions are that themeditative masters can maintain consciousawareness throughout sleep. This ability mayemanate from incredible mental control inwaking life and from long years of practice inthe meditative arts. However, many ordinarypeople also report lucid dreams. Childrenhave lucid dreams more naturally, withoutspecial training, but prevalence declines withage. Among 10-year-olds, 63% in one studyreported lucid dreaming on a monthly basis,58% of 11-year-olds, and 36% of 12-year-olds (Armstrong-Hickey, 1991).
Most dreams occur in a state of unaware-ness of their illusory nature. In fact, sleep itselfis generally characterized as unconscious.Lucid dreaming is the ability, while dreaming,to become conscious of the fact that one is ina dream state. The following is a description ofthe first lucid dream of one man:
I was standing in a field in an open areawhen my wife pointed in the direction of thesunset. I looked at it and thought, “How odd;I’ve never seen colors like that before.” Then itdawned on me: “I must be dreaming!” Neverhad I experienced such clarity and perception—the colors were so beautiful and the sense offreedom so exhilarating that I started racingthrough this beautiful golden wheat fieldwaving my hands in the air and yelling at thetop of my voice, “I’m dreaming! I’m dreaming!”Suddenly, I started to lose the dream; it must
have been the excitement. I instantly woke up.As it dawned on me what had just happened, Iwoke my wife and said, “I did it, I did it!” I wasconscious within the dream state and I’ll neverbe the same. Funny isn’t it? How a taste of itcan affect one like that. It’s the freedom, Iguess; we see that we truly are in control of ourown universe. (LaBerge, 1990, pp. 1–2)
At once it is evident that lucid dreams differfrom ordinary dreams. Lucid dreamerstypically report vivid sensation and height-ened imagery and clarity, not only visualsensation, but auditory and kinesthetic aswell. Hearing music, seeing bright light, andflying are common. Joy and exhilaration oftendistinguish these dreams. What often triggerslucidity is awareness of inconsistency oroddity. The dreamer abruptly shifts into con-scious awareness, sometimes accompaniedby a feeling of mind expansion and greaterself-knowledge. What is interesting in com-parison with ordinary dreams is that luciddreams are not disjointed, lacking in judg-ment, or irrational. The dreamer has controland free will in the sense of deciding where togo and what to do, but cannot totally controlthe plot or outcome. For example, thedreamer may decide to travel to a certainplace or meet various people, but may besurprised by what occurs. The person mayalso decide to use the dream to face prob-lems of living, which has ramifications for thestudy of lucid dreams in a healing or thera-peutic manner. A person with a fear of waterreported the following dream:
In reality I have a great fear of water, andswimming was one of the possible choices forme to try in a lucid dream. In the dream I’m inmy backyard and am immediately aware thatI’m dreaming. I decide that it would be great funto swim. Instantly there is water all around me. Iswim several hundred feet and make manyadjustments to my swimming form.
I start to stand up in what is chest deepwater and start to feel fearful. I remind myselfthat in a dream there is no reason to fear. Iimmediately feel comfortable and start to
walk back around the house, when I observethat the water has disappeared. (LaBerge,1990, p. 260)
The study of lucid dreams has revealedthat dreams occur in real time, not in aninstant or a blink of the eye. As dreamers,people may take shortcuts and transportthemselves from place to place, but thestory line of dream action occurs at ordinaryspeed. This is known because sleep re-searchers, such as the group at StanfordSleep Research Center, have been able tocorrelate eye movement during lucid dreamswith dream reports. First, a prearrangedsignal is set—for example, a light embeddedin eye shades worn by the sleeper will flashthree times when EEG recordings detectREM sleep. If the dreamer detects the lightand becomes aware that this is the signal,he or she returns a signal by moving theeyes in a pattern that was practiced beforesleep onset. This methodology is quiteingenious, because during the benignparalysis of REM sleep, the only way for thedreamer to signal to the external world isthrough the eyes. One lucid dreamer re-ported that in his dream he was walkingalong a beach when suddenly he saw thesun rise and set, rise and set, rise and set.He kept walking, and then suddenly thoughthow odd that was. In an “aha” experience,he recognized that this was the prearrangedsignal and was able to signal back to theresearchers with his eyes. His report of thedream and the time period between thesignal and the dreamer’s response corre-sponded to the eye movement tracings.
Are lucid dreams a melding of theconscious and unconscious mind states?During lucid dreams, the dreamer hasknowledge of normally available wakingthoughts and memories, as well as anawareness of the dream illusion. What isnormally unconscious has become con-scious. Lucid dreams have been described,and they may reasonably be thought of as
(continued)
N e u r o p s y c h o l o g y i n A c t i o n 1 6 . 3
L u c i d D r e a m i n g : A P a r a d o x o f C o n s c i o u s n e s s
by Mary V. Spiers

It takes a bit of commotion to wake someone from stage4 NREM sleep. The brain is less active and becomes lesscapable of organized activity. Some individuals may vo-calize, but this speech usually does not seem logical. Somemotor behavior may occur as well, and sleepwalkingsometimes accompanies NREM sleep. Although NREMsleep is associated with a sleeping brain, curiously thebody is “awake,” twitching and turning. Sometimes thetwitching is so strong that the person may kick. This iscalled nocturnal myoclonus (restless leg syndrome) andcan be so strong that it may wake up the person.
After the first descent into deep sleep, there is a pro-gressive lightening that culminates at 90 minutes aftersleep onset in the first REM period (named for the promi-nence of rapid eye movements). REM sleep shows manycontrasts with NREM sleep (Table 16.2). The most strik-ing feature is the relatively high level of alertness duringREM sleep, much like stage 1 sleep. In fact, the first timesleep researchers measured REM sleep via EEG theythought the subject had awakened.
The characteristic REM EEG pattern of low-voltage,random, fast “sawtooth” waves is a dynamic representa-tion of the sleeper’s internally generated heightened cor-tical arousal and is associated with intensive processingof the internal mind state of dreaming. The first REMperiod may be quite short, lasting less than 5 minutes.Thus, in REM sleep, the brain is active and seeminglyawake. A person awakened during REM sleep often re-ports dreams. However, the body is immobile duringREM sleep. In fact, all voluntary muscles are temporarily“paralyzed” from the neck down. Both female and maleindividuals show sexual response (lubrication or erec-tion). As the night progresses, Figure 16.2 illustrates howREM periods lengthen at the end of each 90-minutecycle. Correspondingly, sleep stages 3 and 4 taper off inthe early morning hours. In general, normal sleepersspend 75% in NREM and 25% in REM sleep over anight’s sleep.
What we have just described is normal adult sleep.Variability in this cycle depends on age and several otherfactors (Figure 16.3). Infants, in contrast, spend 50% oftheir sleep time in REM sleep, and a large proportion oftheir NREM sleep in stage 4 sleep. By late middle age,most people have lost all of this physiologically restorative
stage 4 sleep and retain only a small proportion of REMsleep. Why this tremendous variation in the developmen-tal qualities of sleep? The answer may lie in the functionsvarious types of sleep serve in growth and development.
Among other phasic events, the pituitary gland, undercontrol of the hypothalamus, releases somatotrophin(growth hormone) during stage 4 sleep, and the immunesystem is particularly active. During rapid growth anddevelopment, stage 4 sleep may be more necessary. Stage 4sleep is often termed restorative sleep because it also
454 PART THREE | Disorders of the Brain
Event NREM REM
Occurrence Greater in first Greater in second half of night half of night
Eye movement Slow, rolling Rapid, conjugate
Mentation Short, ordinary Dreams
Fragmented Vivid, emotional
Sensory processing Lowered Inhibited
Motor response Relaxed Atonic
Benign paralysis
Autonomic nervous Low Highsystem variability
GSR variability High Low
CNS temperature Decreases Increases
Sexual response Low High
Neurotransmitter activity
Aminergic High Low
Cholinergic acetylcholine Low High
Hormonal secretion rate
Growth hormone High Low
Parathyroid hormone High Low
Luteinizing hormone Low High
NREM = non–rapid eye movement; REM = rapid eye movement; GSR = galvanic skinresponse; CNS = central nervous system.
Table 16.2 Comparison of NREM and REMSleep Events
(continued)a cocreation between the two mind states,
sometimes marked by intense pleasure,but with a different twist from the Freudian
idea of a naughty “id” in that the dreameroften experiences these as mind-expandinggrowth opportunities filled with personalinsight and a sense of personal accomplish-
ment. The scientific study of lucid dreamingmay well represent the next wave of researchin understanding the brain processesrelated to levels of consciousness.
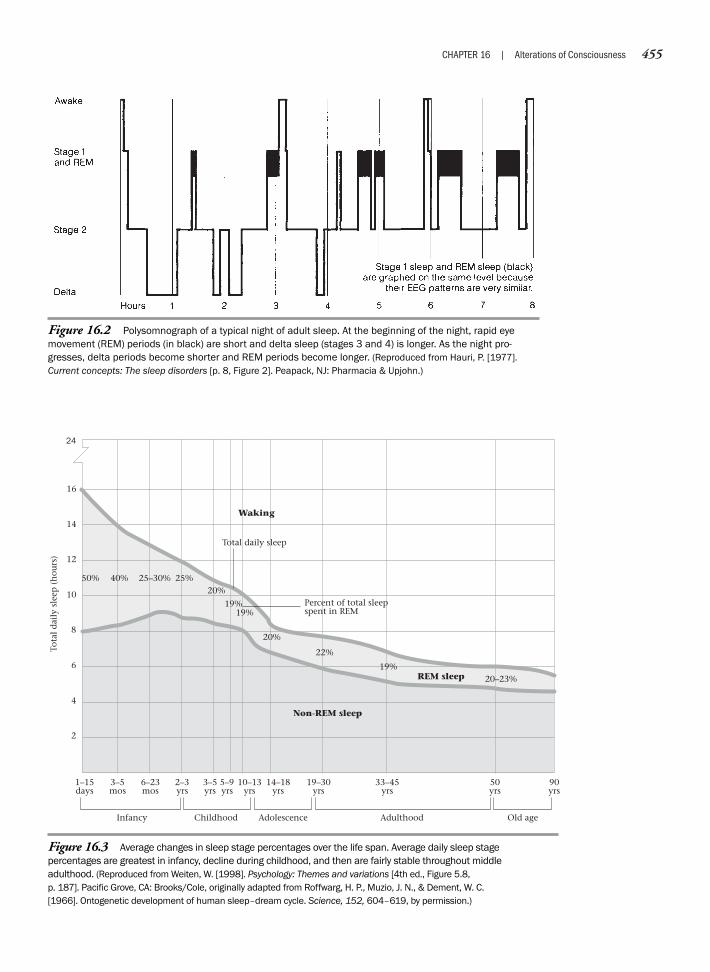
CHAPTER 16 | Alterations of Consciousness 455
Figure 16.2 Polysomnograph of a typical night of adult sleep. At the beginning of the night, rapid eyemovement (REM) periods (in black) are short and delta sleep (stages 3 and 4) is longer. As the night pro-gresses, delta periods become shorter and REM periods become longer. (Reproduced from Hauri, P. [1977].Current concepts: The sleep disorders [p. 8, Figure 2]. Peapack, NJ: Pharmacia & Upjohn.)
Figure 16.3 Average changes in sleep stage percentages over the life span. Average daily sleep stagepercentages are greatest in infancy, decline during childhood, and then are fairly stable throughout middleadulthood. (Reproduced from Weiten, W. [1998]. Psychology: Themes and variations [4th ed., Figure 5.8,p. 187]. Pacific Grove, CA: Brooks/Cole, originally adapted from Roffwarg, H. P., Muzio, J. N., & Dement, W. C.[1966]. Ontogenetic development of human sleep–dream cycle. Science, 152, 604–619, by permission.)
Percent of total sleep spent in REM
Non-REM sleep
Childhood AdolescenceInfancy
1–15days
Adulthood Old age
3–5mos
6–23mos
2–3yrs
3–5yrs
10–13yrs
14–18yrs
19–30yrs
33–45yrs
50yrs
90yrs
5–9yrs
50% 40% 25–30% 25%20%
19%
20%
22%
19%20–23%
Total daily sleep
Waking
REM sleep
16
14
12
10
8
6
4
2
Tota
l d
aily
sle
ep (
hou
rs)
24
19%

increases in adults in response to intense physical exer-tion. At older ages, this growth-and-tissue-repair functionof growth hormone becomes less available.
S L E E P A N A T O M Y A N D P H Y S I O L O G Y
Circadian clocks (derived from Latin, meaning “about aday,” as noted earlier), which set the daily pattern of sleepand wakefulness, are intrinsic to most living organisms.This clock might have been patterned in ancient timesand embedded in DNA as all life on earth learned to re-spond to the rhythms of the cycles of days, months,seasons, and years. Even plants have a rudimentary circa-dian triggering mechanism. The heliotrope folds its leavesat night and opens them in the morning, but it is not di-rectly guided by the light of the sun. Even in a dark roomit continues opening and closing, according to daily cy-cles and according to some internal timing mechanism.
In humans, and all mammals, a more specialized circa-dian clock nestles in the suprachiasmic nucleus (SCN)of the hypothalamus. If the SCN is removed from thebrain, the neurons continue to fire according to the pro-grammed daily rhythms. However, if the SCN were to-tally dependent on genetic programming, what wouldhappen when traveling to the other side of the world?The daily internal clock must have a way to resynchro-nize according to the light/dark cycle. That, indeed, isthe case. In fact, if left without any natural light cues,humans will revert to about 25-hour/day cycles of wakingand sleeping. Natural light, or in some cases an alarm clock,apparently resynchronizes the human circadian clock eachday for functioning in accord with a 24-hour day. Thehalves of the SCN lie just above the optic chiasm and receivelight via neural input from the two visual fields as they crosshemispheres to the opposite sides of the brain (Figure 16.4).When this internal clock runs amok, sleep patterns can begreatly, even fatally, disrupted (see Neuropsychology inAction 16.1).
Scientists do not yet know how the human circadianclocks signal sleep onset each night and awakening eachmorning—perhaps through qualitatively different signals,or via a gradual change in the release of neurotransmittermolecules. Clifford Saper, of Harvard University, and hiscolleagues (Saper, Chou, & Scammell, 2001) have sug-gested that the ventrolateral preoptic area of the hypo-thalamus may be the “master switch” to arousal (seeFigure 16.3). Researchers have observed this somnolenceregion to be the only brain center that is more active dur-ing sleep than wakefulness. Other researchers have identi-fied a peptide molecule named “factor S” and claim it may
be one of the neurotransmitters most directly responsiblefor setting off the downward drift into sleepiness. Injectedinto the hypothalamus, factor S induces sleep and in-creases body temperature. It also appears to trigger the re-lease of interleukin-1, which raises many interesting ques-tions about the immunoprotective function of sleep. Thiscollective evidence points to a strong role for the hypo-thalamus as the “biological sandman.”
When activated, the hypothalamus sends its molecularmessage to the thalamus and the RAS of the lower brain-stem. Gradually, the brain moves from a state of processingexternal sensory information to a closing off of inputsfrom vision, hearing, and touch. During alertness, thethalamus relays inputs from most sensory systems, exceptfor smell. The thalamus constantly communicates withthe cortex through a feedback system of millions of thala-mocortical loops. With high alertness, neuronal firing isfrequent and finely tuned. Any external sensory “noise”against this background is easily picked up because thebrain discriminates it from the high-frequency back-ground rhythm by its irregularity or novelty. As alertnessdrops, at a certain point the thalamocortical loops startoscillating to their own rhythm, in a sort of internal dancebetween the thalamus and the cortex.
On an EEG, this is also when the sleep spindles(12–14 cycles/sec) emerge, typical of stage 2 sleep. Withthe slowed frequency of thalamocortical firing, orientationto and processing of external stimuli is less likely. The brainturns inward, attention drifts, and the sleeper becomesoblivious to his or her surroundings. Currently, the thala-mocortical loop stands as the primary mechanism in sleeponset and in maintenance of reduced attention to exter-nal stimuli. As sleep continues to deepen, responsivenessto the outward environment lessens even further. Yetmany parents of newborns apparently maintain vigilanceto their baby’s stirrings while sleeping. Perhaps future re-search will reveal whether another mechanism monitorsthe environment during sleep, or whether sleep remainslighter for those who must remain alert. Animals in thewild, which must retain more alertness to danger, showlighter and more fragmented sleep than zoo and domesticanimals. Perhaps this is also the case with humans.
R E T I C U L A R A C T I V A T I N G S Y S T E M A N D R A P I D E Y E M O V E M E N T S L E E P
Approximately every 90 minutes, and lengtheningthroughout the night, a sleeper enters REM stage sleep.The cortical activity of high-frequency sawtooth EEG
456 PART THREE | Disorders of the Brain
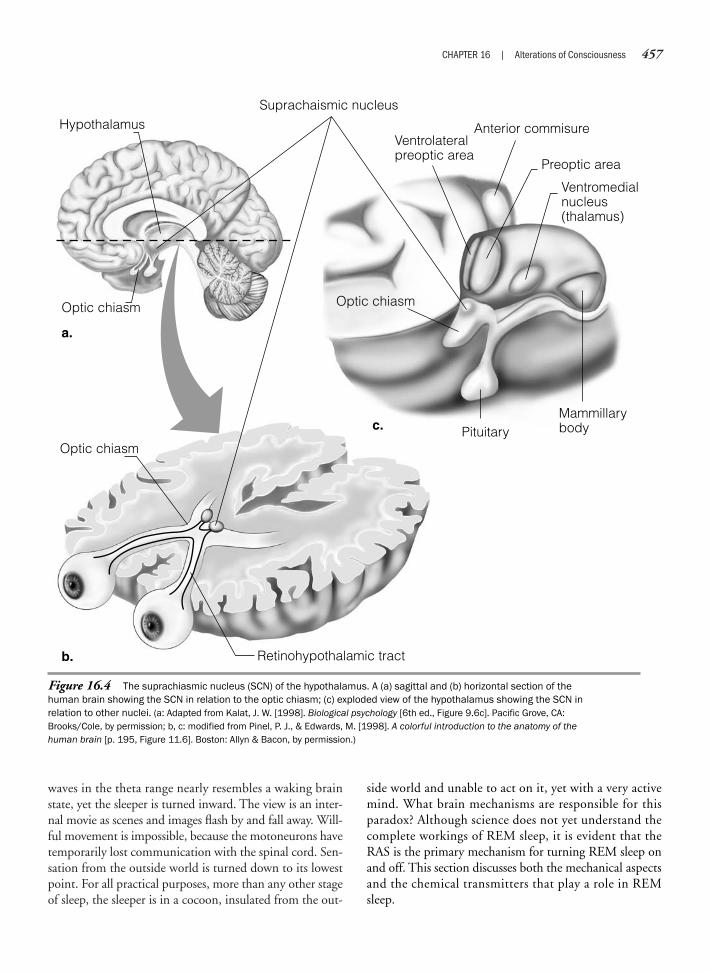
waves in the theta range nearly resembles a waking brainstate, yet the sleeper is turned inward. The view is an inter-nal movie as scenes and images flash by and fall away. Will-ful movement is impossible, because the motoneurons havetemporarily lost communication with the spinal cord. Sen-sation from the outside world is turned down to its lowestpoint. For all practical purposes, more than any other stageof sleep, the sleeper is in a cocoon, insulated from the out-
CHAPTER 16 | Alterations of Consciousness 457
Figure 16.4 The suprachiasmic nucleus (SCN) of the hypothalamus. A (a) sagittal and (b) horizontal section of thehuman brain showing the SCN in relation to the optic chiasm; (c) exploded view of the hypothalamus showing the SCN inrelation to other nuclei. (a: Adapted from Kalat, J. W. [1998]. Biological psychology [6th ed., Figure 9.6c]. Pacific Grove, CA:Brooks/Cole, by permission; b, c: modified from Pinel, P. J., & Edwards, M. [1998]. A colorful introduction to the anatomy of thehuman brain [p. 195, Figure 11.6]. Boston: Allyn & Bacon, by permission.)
Optic chiasm
Retinohypothalamic tract
Optic chiasm
a.
Optic chiasm
Pituitary
HypothalamusSuprachaismic nucleus
Anterior commisureVentrolateralpreoptic area
Preoptic area
Ventromedialnucleus(thalamus)
Mammillarybody
b.
c.
side world and unable to act on it, yet with a very activemind. What brain mechanisms are responsible for thisparadox? Although science does not yet understand thecomplete workings of REM sleep, it is evident that theRAS is the primary mechanism for turning REM sleep onand off. This section discusses both the mechanical aspectsand the chemical transmitters that play a role in REMsleep.
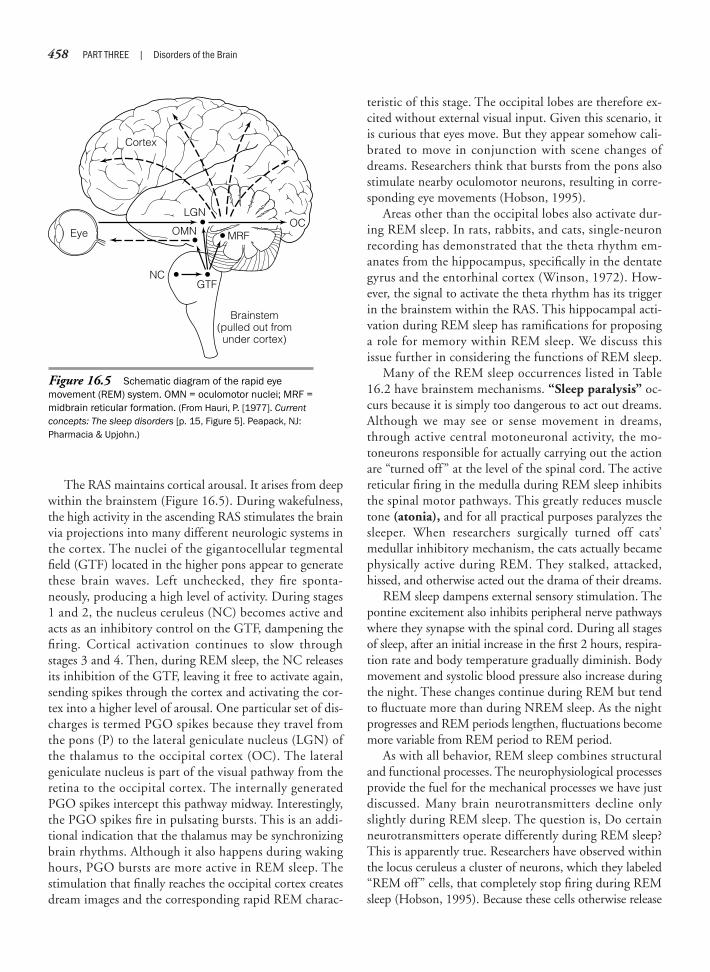
The RAS maintains cortical arousal. It arises from deepwithin the brainstem (Figure 16.5). During wakefulness,the high activity in the ascending RAS stimulates the brainvia projections into many different neurologic systems inthe cortex. The nuclei of the gigantocellular tegmentalfield (GTF) located in the higher pons appear to generatethese brain waves. Left unchecked, they fire sponta-neously, producing a high level of activity. During stages1 and 2, the nucleus ceruleus (NC) becomes active andacts as an inhibitory control on the GTF, dampening thefiring. Cortical activation continues to slow throughstages 3 and 4. Then, during REM sleep, the NC releasesits inhibition of the GTF, leaving it free to activate again,sending spikes through the cortex and activating the cor-tex into a higher level of arousal. One particular set of dis-charges is termed PGO spikes because they travel fromthe pons (P) to the lateral geniculate nucleus (LGN) ofthe thalamus to the occipital cortex (OC). The lateralgeniculate nucleus is part of the visual pathway from theretina to the occipital cortex. The internally generatedPGO spikes intercept this pathway midway. Interestingly,the PGO spikes fire in pulsating bursts. This is an addi-tional indication that the thalamus may be synchronizingbrain rhythms. Although it also happens during wakinghours, PGO bursts are more active in REM sleep. Thestimulation that finally reaches the occipital cortex createsdream images and the corresponding rapid REM charac-
teristic of this stage. The occipital lobes are therefore ex-cited without external visual input. Given this scenario, itis curious that eyes move. But they appear somehow cali-brated to move in conjunction with scene changes ofdreams. Researchers think that bursts from the pons alsostimulate nearby oculomotor neurons, resulting in corre-sponding eye movements (Hobson, 1995).
Areas other than the occipital lobes also activate dur-ing REM sleep. In rats, rabbits, and cats, single-neuronrecording has demonstrated that the theta rhythm em-anates from the hippocampus, specifically in the dentategyrus and the entorhinal cortex (Winson, 1972). How-ever, the signal to activate the theta rhythm has its triggerin the brainstem within the RAS. This hippocampal acti-vation during REM sleep has ramifications for proposinga role for memory within REM sleep. We discuss thisissue further in considering the functions of REM sleep.
Many of the REM sleep occurrences listed in Table16.2 have brainstem mechanisms. “Sleep paralysis” oc-curs because it is simply too dangerous to act out dreams.Although we may see or sense movement in dreams,through active central motoneuronal activity, the mo-toneurons responsible for actually carrying out the actionare “turned off ” at the level of the spinal cord. The activereticular firing in the medulla during REM sleep inhibitsthe spinal motor pathways. This greatly reduces muscletone (atonia), and for all practical purposes paralyzes thesleeper. When researchers surgically turned off cats’medullar inhibitory mechanism, the cats actually becamephysically active during REM. They stalked, attacked,hissed, and otherwise acted out the drama of their dreams.
REM sleep dampens external sensory stimulation. Thepontine excitement also inhibits peripheral nerve pathwayswhere they synapse with the spinal cord. During all stagesof sleep, after an initial increase in the first 2 hours, respira-tion rate and body temperature gradually diminish. Bodymovement and systolic blood pressure also increase duringthe night. These changes continue during REM but tendto fluctuate more than during NREM sleep. As the nightprogresses and REM periods lengthen, fluctuations becomemore variable from REM period to REM period.
As with all behavior, REM sleep combines structuraland functional processes. The neurophysiological processesprovide the fuel for the mechanical processes we have justdiscussed. Many brain neurotransmitters decline onlyslightly during REM sleep. The question is, Do certainneurotransmitters operate differently during REM sleep?This is apparently true. Researchers have observed withinthe locus ceruleus a cluster of neurons, which they labeled“REM off” cells, that completely stop firing during REMsleep (Hobson, 1995). Because these cells otherwise release
458 PART THREE | Disorders of the Brain
Figure 16.5 Schematic diagram of the rapid eyemovement (REM) system. OMN = oculomotor nuclei; MRF =midbrain reticular formation. (From Hauri, P. [1977]. Currentconcepts: The sleep disorders [p. 15, Figure 5]. Peapack, NJ:Pharmacia & Upjohn.)
Cortex
LGN
OMN
GTFNC
OC
Brainstem(pulled out fromunder cortex)
Eye MRF

norepinephrine and serotonin, the consequence is a rela-tive unavailability of these substances to the brain duringREM. J. Alan Hobson (1995) hypothesizes that the lower-ing of these aminergic transmitters plays a role in the “lackof self-reflective awareness, disorientation, and logical fal-lacy” in verbal reports of dreaming during REM sleep.Hobson also postulates that serotonin and norepinephrineact as long-term neuromodulators on the brain. As NREMsleep commences, “REM off” cells begin to slow their fir-ing rate, with the functional result of slowly releasing theirhold on the “rational” cortex. The mind becomes moredisinhibited during sleep but is especially free to wanderduring REM because of a now complete lack of aminergictransmission. At the end of the REM cycle, the cells “turnon,” activating at a higher level of serotonin and norepi-nephrine. This level then tapers off, leading to the nextREM period. From this information, it is possible to spec-ulate that lengthening REM periods during the night mayresult from progressively lower levels of aminergic neuro-transmitter release during the night.
Another neurotransmitter of interest in REM sleep isacetylcholine (ACh). Interestingly, ACh increases duringREM sleep in animals and can trigger “spectacularly longand intense” REM periods when administered in highdoses. As discussed in Chapters 4 and 9, ACh is impor-tant in facilitating memory processing. The next sectionexplores the role of REM in memory consolidation.
F U N C T I O N S O F R A P I D E Y E M O V E M E N T S L E E P
Scientists know that slow-wave delta sleep is physicallyrestorative, but the debate over the purpose of REM sleephas ranged from postulations that it serves as a type of men-tal “garbage dump” to Freud’s assertion that dreams are the“royal road to the unconscious.” Science is now aware of atleast two behavioral functions that REM sleep may serve.The first is memory consolidation. The second function isthe intrapsychic function of dreaming. With a nod toFreud, neuropsychologists now conceptualize the psycho-logical function of dreaming somewhat differently fromFreud. Because scientists have again blessed the study ofpersonal internal conscious processes, the study of dreamfunction is once more opening up. Next, we introduce anarea of study that is likely to provide many insights into thefunctioning of the conscious and subconscious minds.
M e m o r y C o n s o l i d a t i o n a n dR a p i d E y e M o v e m e n t S l e e p
The physiological means by which long-term memory stor-age occurs is most likely through long-term potentiation
(LTP) of special glutamate neurotransmitter receptors(N-methyl-D-aspartate [NMDA] receptors) in the hip-pocampus. Memory consolidation may also be inhibitedby gamma-aminobutyric acid (GABA). The hippocampusactively produces theta waves during REM sleep, as wellas during stage 1 and 2 sleep. The important link betweensleep and memory is that LTP in the hippocampus occursduring the production of theta rhythms (Larson & Lynch,1986). Researchers have long thought that memory con-solidates during sleep, because people can remember moreafter sleep. Sleeping pills may interfere with this process.However, it has been difficult to know whether sleep orREM itself accounts for the memory boost, or whetherpeople just remember better when other information doesnot interfere. Now animal and human experiments haveprovided more evidence that memory is processed duringsleep. Using rats, a team of researchers have recorded fromindividual neurons of the hippocampus (Pavlides & Win-son, 1989). While the rats were awake, and moving aboutlearning their position, only specific spatial coding neu-rons fired. Later during sleep, and particularly during pro-duction of the theta rhythm, these same neurons, andonly these same neurons, fired at an even higher rate thanduring waking learning. This finding suggests that ratswere reprocessing and strengthening the information dur-ing sleep.
In another experiment, a group of Israeli researchersstudied memory consolidation and sleep under three dif-ferent conditions. The task involved having to identifyperceptual targets embedded in a visually noisy back-ground. With learning and practice, people can usuallyimprove their speed in picking out targets. In the firstcondition, researchers let people sleep normally after theirinitial practice session. In the second condition, research-ers awakened people each time they entered REM sleep,effectively depriving them of REM sleep. In the samemanner, in the third condition, researchers deprived peo-ple of delta sleep within stages 3 and 4. The two groupsthat were allowed REM sleep showed enhanced tasklearning on awakening. All those who underwent REMsleep deprivation, in contrast, showed either less im-provement or an actual decrement in performance(Karni, Tanne, Rubenstein, Askenasy, & Sagi, 1994). To-gether, the findings from both animal and human re-search suggest that stage REM sleep plays a role in mem-ory consolidation. However, whether REM plays aunique role in memory consolidation is still a matter ofdebate. This is a promising area of research for neuropsy-chologists and neuroscientists interested in the relationsamong REM, ACh, and hippocampal consolidationthrough LTP.
CHAPTER 16 | Alterations of Consciousness 459

T h e D r e a m i n g M i n dThe aspects of consciousness discussed thus far involve themind looking out. Dreams reflect the mind looking in.There is almost no physical input or output. Brains andminds are temporarily suspended from bodies. This is anamazing state, seemingly disjointed and illogical. Except forthose who are “lucid” dreamers, dreaming minds wanderfrom scene to scene with no conscious guidance. Dreamersare detached from their own self-consciousness and morecritical selves. Dreams may be intensely emotional tostrangely devoid of emotion. After a history of much debateon the function that dreams may serve, scientists are return-ing to the premise that dreams have a psychological core.
Aspects of the mind state of dreams may correlate withthe physical aspects of a brain temporarily divorced from abody. Noted sleep researcher J. Alan Hobson (1995) hassuggested that dreamers may feel they move effortlesslyduring dream states because they are being moved orguided by internally generated states and active central mo-toneurons. Perhaps in some measure, dream experiences offloating or flying also result from the brain being allowedto “float free” from the body, or perhaps in combinationwith, as Hobson suggests, spontaneous stimulation of ori-entation and position control centers in the brain. Hobsonnotices that when dreamers try to “will” dream movementwhile trying to escape from a pursuer, their feet and bodiesmay become leaden because of the conflicting motor mes-sages of “voluntarily commanded movement (saying go)and the involuntarily clamped muscles (saying stop).” Hefurther suggests that this standoff may suddenly break offthe dream, thrusting the person into wakefulness and vividdream recall. Awakening from a particular terrifying dreamis called a “sleep anxiety attack.” In fact, a large percentageof reported dreams are “hostile,” and the most frequentthemes are those of being chased and falling.
Many other correspondences probably exist betweenbrain–body states and mind states in dreaming. This is aninteresting area of study in its own right, and work in itwill help to explain “how” people dream. Another ques-tion fundamental to understanding consciousness is“why” people dream. The brain activity occurring duringREM sleep, such as memory consolidation, does not re-quire conscious awareness. Biological functions of thebrain could all occur without being brought to waking at-tention. Many dreams are not recalled. But why do somedreams bubble to the surface? This has been a matter oftheoretical interest since Freud’s revolutionary The Inter-pretation of Dreams, written in 1899. Since Freud’s time,the history of dream theory has gone through a cycle fromFreud’s ideas that dreams represented unconscious sexualand aggressive urges, to the behaviorist movement totally
turning away from the study of subjective states. FrancisCrick’s utilitarian housekeeping notion that dreams mayjust be the images that float by as the brain rids itself ofthe day’s mental garbage suggests that dreaming is noth-ing more than a random firing of neurons. But manydream researchers have come back to a version of psycho-logical interpretations.
Freud laid some of the basic groundwork in thinkingabout the psychological function of dreams from whichother theories could spring. Today, most dream theorists donot attribute the same negative sexual and aggressive moti-vations to dream images that Freud did, but some of hismethods and ideas may still be useful in uncovering the psy-chological meaning of dreams for the dreamer. With expan-sion from recent conceptualizations, researchers may becloser to a neuropsychological understanding of dreaming.Freud divided mental processing into conscious and uncon-scious processes. He saw unconscious processes as primitive,ancient, and disguised. Dreams, he felt, arose from these“unconscious” areas of the brain. This conceptualization isnot unlike recent ideas of explicit versus implicit informa-tion processing. That which is explicit is available to verbalconscious awareness. However, as in memory processing andin some disorders such as neglect, a level of processing andrecognition may exist outside conscious awareness. Is thisnot unlike the unconscious or the subconscious? Freud didnot have the ability to look deep into the brain, but his ideasthat unconscious thoughts emerge from more primitiveareas of the brain are not inconsistent with theories of im-plicit processing taking place in the more primitive subcor-tical and limbic centers of the brain.
Perhaps where modern dream interpretive approacheshave advanced most is in moving away from Freud’s ideathat even remembered dream content is unavailable psy-chologically to the dreamer unless interpreted by some-one, such as an analyst, who can slice through the mani-fest content, defense mechanisms, and symbols, to uncoverthe latent meaning. This is not to say that the perspectivesof others regarding the meaning of one’s dreams are use-less. In fact, such perspectives may be quite revealing andhelpful. However, some of the greatest understandingavailable of the meaning in a dream involves self-interpre-tation in light of personal current life circumstances. Afterall, the dream was generated by the person dreaming it.Self-interpretation may involve not only the content, butthe associated emotion that the dream invokes.
Troubling life circumstances provide the fodder for sleepresearcher Rosalind Cartwright (Cartwright, Lloyd, Knight,& Trenholme, 1984; Cartwright, Kavits, Eastman, &Wood, 1991). Her volunteers, all going through separationor divorce, agreed to go through psychological testing that
460 PART THREE | Disorders of the Brain

examined coping styles, and they consented to be awakenedduring REM sleep to report their dreams. Cartwright foundthat dream content and topics differed among subjects, butthe themes were congruent with the waking response to theproblem. Indeed, the content and themes of dreams may beuseful in helping to solve many personal problems. Butsometimes dreams accompany remarkable changes in wak-ing life. We once treated depression in a patient who wasalso a smoker trying to kick the habit. During one therapysession he reported a dramatic dream he had had. In hisdream, his whole body was turned grotesquely inside out,showing his lung, which was full of tumors and pus, to theoutside world. After this dream the patient quit smoking.
An interesting exercise in exploring your own “dreamconsciousness” is to keep a dream journal for collectingand analyzing the content and themes of your dreams.What sensory processes are operating? Do you see, hear,feel, taste, or smell things in your dreams? As we men-tioned earlier, sleep researcher J. Alan Hobson reminds usthat the absurdity of dreams and the temporary “impair-ment” of judgment and cognition that occur duringdreaming are common phenomena. Temporary disinhibi-tion of the cortex may very well represent a physiologicaldisconnection of aspects of the frontal lobes from othercortical and limbic centers. This may help to explain ouroften bizarre logic and lack of self-reflection duringdreams. But what of those brain-impaired individualswho have structural damage resulting in waking disinhi-bition? Will we find that their dreams are even more dis-inhibited? This is a question for future research.
S L E E P D I S O R D E R S
For most people, sleep is a pleasurable event. For somepeople, however, sleeping can become a medical emer-gency, as during sleep apnea, or intrude into wakefulness,as in narcolepsy.
S l e e p A p n e a
Sleep apnea has become the most common disorder thesleep literature describes and the most common presentingproblem that sleep disorder centers evaluate (Guilleminault,1982). Sleep apnea syndrome (SAS) is a serious disorderresulting from frequent episodes of apnea (cessation ofairflow) during sleep. Apnea literally means “lack ofbreath.” It is normal for muscles to relax during REMsleep. In some people, however, excessive muscle relax-ation may disrupt breathing. The sleep apnea patient mayactually stop breathing while asleep. This, of course, pre-sents an immediate crisis for the body, because of the dan-ger of hypoxia and of increased rapid heart rate and bloodpressure. The apnea finally stops when, in an effort tobreathe, the patient arouses, gasping for air. Each gasp forair is associated with a mini-awakening, as recorded onthe EEG. If repeated apnea and awakening occur morethan five times an hour, the patient is diagnosed withsleep apnea (Figure 16.6).
Patients with SAS may actually experience hundredsof apnea episodes per night, lasting up to a minute orlonger. Serious cases may show more than 500 apneas pernight, each one lasting more than 10 to 120 seconds andterminating with at least partial arousal. In addition tomarkedly disrupted sleep characterized by a significantabsence of the normal progression of sleep stages, danger-ously low levels of oxygen to the brain may result. Apneaperiods usually produce declines in sleep-related bloodoxyhemoglobin saturation and increases in carbon dioxide.This condition, known as hypoxia, is associated withbelow-average levels of oxygenated blood, often below 60%(normal is 95%). These changes have a profound impacton numerous body systems. It is impossible to hold one’sbreath indefinitely, even when a person is sleeping. Essen-tially, a reflex controls breathing. But in young children,this reflex has not yet developed, and cessation of breathing
CHAPTER 16 | Alterations of Consciousness 461
Figure 16.6 An electroencephalogram (EEG)-recorded episode of sleep apnea. The patient is fully awake atpoint 1 (EEG alpha waves). At point 2, he is starting to fall asleep (EEG theta waves). At point 3, the patient is fullyasleep (notice the relaxation of the chin electromyogram and absence of breathing). At point 4, the patient awakensand breathing resumes. The cycle then repeats. (Reproduced from Hauri, P. [1977]. Current concepts: The sleep disor-ders. Peapack, NJ: Pharmacia & Upjohn.)
4
K-ComplexK-Complex
21
ThetaWaves
AlphaWaves
AlphaWaves
AlphaWaves
ThetaWaves
321431
4
2LefteyeRighteyeChinEMGEEG(C /ear)
Respiration

during sleep may result in death. This is one of the possiblecauses of sudden infant death syndrome (SIDS); SIDSmost often occurs between the ages of 2 and 4 months.
Two primary mechanisms are involved in sleep apnea.The first one is the more common obstructive sleepapnea. Apneas occur most often during REM sleep wheneither the upper airway collapses, not allowing air to pass,or the body weight of the patient on the chest compro-mises respiratory effort. In each case, the consequence isdisordered breathing. In the second mechanism of sleepapnea, central sleep apnea, disordered breathing is re-lated to the brain failing to send the necessary signals tobreathe. This may reflect brainstem abnormalities thatmanifest only during sleep. In either case, the disorder isserious and often associated with severe O2 desaturation.The terms central and obstructive do not represent a strictdichotomy, because obstructive sleep apnea may impairCNS control of muscles, and episodes of obstructive sleepapnea often precede central apnea. Such episodes arecalled mixed apnea. Complications of apnea result in poorphysical health and associated neuropsychological deficitsof poor concentration and memory (Barth, Findley,Zillmer, Gideon, & Surrat, 1993).
The cause of sleep apnea is not well understood, al-though age, obesity, and being male are all risks. Generally,researchers consider sleep apnea episodes to be caused by acomplex interaction of physiologic and anatomic factors.Clinical features that are characteristic of the syndrome in-clude excessive daytime sleepiness, heart failure, hyperten-sion, headaches, disturbing snoring, irritability, sleep dis-ruption, and personality changes. The hypoxia of sleepapnea markedly affects central neurotransmitter functionand cellular metabolism, disrupting the biochemical andhemodynamic (pertaining to blood circulation) state of theCNS. Hypoxia may also lead to disturbed fluid and elec-trolyte distribution within the sodium-potassium pump,and it alters brain adenosine levels in animals. In addition,in patients with sleep apnea, cerebral blood flow studiesdemonstrate abnormally decreased blood flow, which mayfurther compromise neuropsychological functioning be-cause of decreased neuronal activity (Guilleminault &Dement, 1978). Sleep apnea can have serious psychosocialeffects as well, including significant changes in adaptivefunctioning (Zillmer, Ware, Rose, & Bond, 1989).
Most treatment efforts focus on relief of apneas throughsurgical and mechanical means. The most effective treat-ment is continuous positive airway pressure (CPAP),which is a mask that “forces” air through the nose ormouth while sleeping. CPAP is not considered a “cure,”but it abolishes sleep apnea by maintaining upper airwayflow during sleep. One of the most successful and least in-vasive treatments for SAS, CPAP acts as a pneumatic splint
to prevent upper airway collapse during the night. CPAPmust be used every night by the patient but has few sideeffects as long as one can actually sleep (one patient de-scribed CPAP as analogous to holding your head out ofthe car window while driving at 50 miles/hour). Losingweight can also help, because obesity is a major risk factorin sleep apnea. More controversial treatments includesurgery to increase the dimensions of the pharynx via uvu-lopalatopharyngoplasty (UPPP) and tracheotomy, tocompletely bypass the upper airway obstruction duringsleep (Williams & Karacan, 1978). UPPP involves remov-ing the uvula, the small, fleshy tissue hanging from thecenter of the soft palate, which may relax and sag, ob-structing the upper airway. However, this treatment is notas successful as CPAP and may also alter the subject’s voice.Patients who have undergone treatment for SAS often re-port an improvement in their cognitive functioning.
N a r c o l e p s y
The most notable disorder resulting from impaired CNScontrol of the sleep/wake cycle is narcolepsy (derived fromGreek meaning “a taking hold of numbness”). Narcolepticsare afflicted with irresistible daytime “sleep attacks.” Theycan fall asleep while at work, while driving a car, or dur-ing a conversation. Such sleep attacks can last from a fewseconds to more than 30 minutes. Excessive daytimesleepiness is the primary symptom of narcolepsy, al-though patients are also subject to narcoleptic sleep at-tacks, cataplexy, sleep paralysis, and hypnagogic hallu-cinations. Narcolepsy is a central nervous system disorderof the region in the brainstem that controls and regulatessleep and wakefulness. Once the disorder is established, ittypically persists for one’s entire life. Narcolepsy occurs in1 of 1000 people. Symptoms typically begin to appear be-tween the onset of puberty and age 25.
Excessive Daytime Sleepiness—Pathologic daytime sleepinessis often the first sign to emerge in narcolepsy, typically as-sociated with normal amounts of sleep at night. Manynarcoleptics are asleep or sleepy during much of the day.They often report poor concentration and memory. Espe-cially during the afternoon, after a meal, or when watch-ing TV, narcoleptics are at risk for falling asleep. It is as ifno amount of sleep could satisfy the patient’s frequent andirresistible need for sleep. Excessive daytime sleepiness isthe most prominent and troublesome component of nar-colepsy. The patient is typically miserable and fatigued,often demonstrating inappropriate sleep.
Cataplexy—Cataplexy is the most debilitating of the nar-coleptic symptoms. Cataplexy is a brief (seconds to
462 PART THREE | Disorders of the Brain

minutes) episode of muscle weakness, actual paralysis, orboth. In a benign form of cataplexy, only the face and thehead may droop. In a severe attack, all the muscles maybecome limp, resulting in the victim falling to the floor.After the attack, the patient quickly regains alertness andmuscle tone. Cataplectic attacks occur during periods ofsudden excitement and emotional change, includinglaughter, anger, and athletic activity. The sleep paralysis ofcataplexy is always associated with pathologic REM sleep.If a cataplectic attack lasts long enough, it often becomesfull-blown REM sleep. Thus, you can think of cataplexyas an inappropriate attack of REM sleep. The pathologicintrusion of REM sleep and associated motor inhibitionrelates to a variety of nervous system dysfunctions, includ-ing massive nonreciprocal excitation of spinal inhibitoryinterneurons and active inhibition of motoneurons.
Hypnagogic Hallucinations—Hypnagogic hallucinations arealso a symptom of narcolepsy and occur in the transitionbetween wakefulness and sleep onset. Most people do notexperience imagery during the transition from waking tosleep, because they are moving into NREM sleep, a periodof little imagery. Narcoleptics, in contrast, can experiencehypnagogic hallucinations during their shorter transitionfrom waking to REM sleep. Thus, narcoleptics may expe-rience vivid, dreamlike intrusions into wakefulness. Thehallucinations can be mundane or nightmarish, and theycan cause great anxiety.
Sleep Paralysis—Sleep paralysis is the momentary paralysison awakening or at sleep onset. Although the person maybe able to see what is happening in the room, the body istotally unable to move for seconds to minutes. Peoplewithout narcolepsy have also described this sleep paralysison awakening from a REM period in the early morninghours. To “break out” of this paralysis, they may start bymoving their eyes, then willfully moving a finger. As soon
as the voluntary muscles engage, the person breaks out ofthe REM-controlled sleep paralysis.
Narcolepsy can be best conceptualized as an imbalanceamong the wake, REM, and NREM systems. In such pa-tients, wakefulness is weak, and REM sleep, or partsthereof, can intrude into it. This imbalance among thethree stages can range from mild to severe. Narcolepsy isnot a psychological disorder, although the socioeconomicand psychological toll on the patients can be great. The ca-sual observer often thinks narcoleptic attacks are related toepilepsy, but they are not. The cause is generally unknown,although a minority of patients manifests parts of the syn-drome after encephalitis, severe head injury, or braintumor. Clinicians often make the differential diagnosis ina sleep disorder center using a procedure known as themultiple sleep latency test (MSLT). Interestingly, narcolep-tics are asked to arrive at the sleep disorder center, not inthe evening, but during the morning. Around 10 A.M.they are put to “rest.” The reason for this is that the earlymorning would be the least likely time for most well-restedpeople to fall asleep and proceed into REM sleep. The sub-ject must fall asleep in less than 5 minutes (normal sleeplatency is 15 minutes at nighttime) and must show at leasttwo sleep-onset REM periods to diagnose narcolepsy (Fig-ure 16.7). Treatment of narcolepsy includes counseling forpatient and family, developing good sleep habits includingfrequent naps, and the administration of medication, typi-cally stimulants (such as amphetamines) for sleepiness andtricyclics (such as imipramine) for cataplexy. Althoughnarcolepsy cannot be cured, its symptoms can be con-trolled with proper behavioral and medical therapy.
Runaway Brain: Seizure Disorders
Seizures, like sleep, are reversible alterations of con-sciousness. But seizures occur suddenly during periods ofexpected wakefulness and are abnormal. For reasons not
CHAPTER 16 | Alterations of Consciousness 463
Figure 16.7 The narcoleptic goes quickly into rapid eye movement sleep. (Reproduced from Hauri, P. [1977].Current concepts: The sleep disorders. Peapack, NJ: Pharmacia & Upjohn.)
Sawtooth Waves
EEG(C /ear)4
ChinEMG
Lefteye
Righteye
Fully Awake
Narcoleptic Subject
REM Sleep
RapidEye
Movements
EMG Inhibition

fully explainable, groups of neurons fire excessively in syn-chronous oscillation, as opposed to their normal pattern ofrelatively independent electrical activity. During a seizure,the firing rate of neurons may be as high as 500 times asecond, which is more than 6 times faster than the normalrate of 80 firings per second (National Institute of Neuro-logical Disorders and Stroke [NINDS], 2004). Seizures aretransient alterations in consciousness and can be provokedby external stimuli such as pulsing lights or sounds, or inter-nal triggers such as psychological and physical stress, sleepdeprivation, high fever, and hormonal changes. Althoughthere are many types of seizures that can be categorizedby focus, behavior, and the extent of abnormal brain ac-tivity, there are two main categories of seizures. If the ab-normal firing is confined to a particular brain area, theresult will be a partial or focal seizure. If the abnormaldischarge involves both hemispheres, the event is termeda generalized seizure. Episodes can also begin as a par-tial seizure and secondarily generalize to involve thewhole brain.
The causes of seizures are varied. Seizures that first ap-pear in infants and young children may manifest due togenetic and developmental abnormalities of the brain, in-fections, fever, or other disorders in metabolism. In peo-ple of all ages, seizures may also be caused by traumaticbrain injury, brain infections, tumors, vascular abnormal-ities, alcohol and drug use or withdrawal, or environmen-tal toxins. In about half of the seizures reported, however,there is no clearly identifiable cause.
Epilepsy is not a disease itself, but a syndrome in whichbrain seizure activity is a primary and chronic symptom.Older diagnostic schemes stated epilepsy could be diagnosedonly if the seizures were recurrent (at least two separateseizures) and unpredictable. Newer consensus definitionsstate that people can be diagnosed with epilepsy after suffer-ing only one seizure if they also have an “enduring” alter-ation of the brain that makes it highly likely they will sufferfuture seizures (Fisher et al., 2005). Many people who havehad a seizure, in fact, do not show the full epileptic syn-drome (Hauser, 1992). Adults may suffer “nonepilepticepisodes” from such events as hyperventilation breath hold-ing, migraines, ischemic attacks, drug toxicity, narcolepsy,and extreme emotion such as anger. In summary, a personmust have at least two seizures, or the high potential for morethan one seizure, that cannot be attributed to another med-ical condition to be diagnosed with epilepsy.
Epilepsy affects approximately 1% of the U.S. popula-tion (NINDS, 2004) with an age-related increase in inci-dence to 3% by age 75. Many more people or approxi-mately 10% of the population may suffer a seizure duringtheir life (Epilepsy Foundation, n.d.).
C L A S S I F I C A T I O N O F S E I Z U R E T Y P E S
Previously, classification of seizures was based on the origi-nal French classification scheme and was categorized ac-cording to behavioral observations of what happened dur-ing a seizure. For example, grand mal or “big bad” seizureswere named for the most violent motoric abnormalities ofstiffening (tonic) and jerking (clonic) episodes and theaccompanying loss of consciousness. The petit mal or“little bad” seizures, in contrast, were considered seizuresthat do not result in violent physical loss of control butdo cause an altered state of consciousness. Current seizureclassifications depend on what is known of the origin orfocus of the seizure within the brain. The current tax-onomies are divided into two primary classifications: gen-eralized and partial seizures. Generalized seizures involveboth cortical hemispheres at the onset, whereas partialseizures are confined to a specific area. Partial seizures maybe further divided into two types: simple partial and com-plex partial. In simple partial seizures, consciousness is pre-served, whereas in complex partial seizures, consciousnessis impaired. In addition, a partial seizure can spread out,resulting in a secondary generalized seizure, which is aseizure that started being partial—limited to a specific brainarea—and later generalized to both hemispheres. As youmay imagine, besides the consciousness factor that dividespartial seizures into simple or complex, there are many dif-ferent variations of partial seizures, depending on the siteof origin. Generalized seizures can also be classified intodifferent types. The epilepsy classification scheme presentedin Table 16.3 shows the seizure types of both groups.
Regardless of the primary seizure type, up to 70% ofpeople report having an aura before a seizure. This hap-pens in prodromal phase, or precursory phase, of theepisode, in which one may experience odd transientsymptoms such as nausea, dizziness, or numbness. Sensory
464 PART THREE | Disorders of the Brain
Generalized Seizures Partial or Focal Seizures
1. Absence 1. Simple: focal motor, somatosensory or special-sensory, psychic, and autonomic
2. Myoclonic 2. Complex partial: psychomotor, temporal lobe
3. Clonic 3. Secondarily generalized
4. Tonic
5. Tonic-clonic
6. Atonic
Table 16.3 Seizure Classification

alterations or hallucinations in any sensory domain mayappear. For example, chemical sense disruptions maymanifest as unpleasant metallic tastes or foul odors. Somepeople recognize their aura as an emotional change suchas fear or anxiety. Others experience a temporary aphasiaor a sense of forced thinking. Yet others describe auras asan otherworldly or surreal dream state, or a sense of déjà vu(Neuropsychology in Action 16.4). These symptoms arehighly idiosyncratic but are likely to be consistent within
a person. Most seizure sufferers become adept at recog-nizing their own auras; however, some auras occur with-out awareness, although they may be recognized by oth-ers. Auras may point to the genesis, or the epileptogenicfocus, of the seizure within the brain (Cascino, 1992).Interestingly, some people are also able to arrest the pro-gression of a seizure during this prodromal phase by learn-ing to counteract the sensation with its opposite. For ex-ample, if a foul smell is part of an aura, a strong pleasant
CHAPTER 16 | Alterations of Consciousness 465
We have all some experience of a feeling, thatcomes over us occasionally, of what we aresaying and doing having been said and donebefore, in a remote time—of our having beensurrounded, dim ages ago, by the same faces,objects, and circumstances—of our knowingperfectly what will be said next, as if wesuddenly remember it!
—Charles Dickens, David Copperfield
Have you ever been in a situation wheresuddenly everything seems familiar, theplace, the objects, the layout of the setting . . .even the movements taking place. . . andthen, when you are still perplexed by such abizarre feeling, it goes away? Then youprobably are like the two thirds of the popu-lation who has experienced at least one déjàvu experience in their lifetime.
The phenomenon of déjà vu caught theattention of philosophers and writers forages, and more recently has become thesubject of scientific study. The most commondefinition for déjà vu (“already seen” inFrench) was proposed by V. M. Neppe(1983): “Any subjectively inappropriateimpression of familiarity of a present experi-ence with an undefined past.” This definitionimplies that there is a certain insight into thenature of the impossibility of the situation.
Interestingly, a considerable number ofpatients with temporal lobe epilepsy reportdéjà vu auras. In the late 1800s, HughlingsJackson first observed that seizures thatarose in the medial temporal lobe couldresult in a “dreamy state” described as vivid
memory-like hallucinations and/or the senseof having previously lived through the exactsame situation. Later, other researchers havetried to evoke that “dreamy state” by electri-cally stimulating different regions of thetemporal lobe such as the lateral temporalneocortex, the hippocampal formation, andthe amygdala (Mullan & Penfield, 1959;Halgren, Walter, Cherlow, & Crandall, 1978).Gloor (1990) proposes that this dreamy statecould be evoked by lateral temporal lobestimulation, but only if the brain activityspread medially toward the limbic system,thus emphasizing the importance of limbicrather than temporal neocortical structures.After much debate, in 1994, Bancaud andhis colleagues studied 16 patients withtemporal lobe epilepsy with presurgicallyimplanted electrodes; measured the electri-cal activity of the temporal lobe, the amyg-dala, and the hippocampus; and at the sametime, attempted to stimulate those areas ofthe brain. They found that déjà vu could beexperimentally evoked by stimulation of anyof those three sites, and that there was noone single place that was solely responsiblefor the experience in every epilepsy patient.However, they did find that the stimulation ofthe deeper structures (amygdala and hip-pocampus) was 10 times more likely to evokethose states, concluding that the temporalneocortex probably plays a secondary butstill important role in the déjà vu experience.
Another area of interest in the field of déjàvu and epilepsy is that of lateralization,
because the presentation of a déjà vu couldeventually help neurologists diagnose the siteof seizure onset for those who present thistype of aura. Mullan and Penfield (1959)suggest that déjà vu occurs in the nondomi-nant temporal lobe—usually, but not always,the right temporal lobe for right handedpeople. In accordance with this idea, Gloor(1990) asserts that having an aura of déjà vuwould be sufficient to localize the focus of theseizure to the right temporal lobe. However,Weinand and colleagues (1994) later foundthat right-handed seizure patients withpreictal déjà vu all had seizures arising intheir left hemispheres. They concluded thathandedness rather than language domi-nance appears to be a more consistentpredictor of ictal déjà vu lateralization.
Many people have experienced at leastone déjà vu experience, and this does notimply that they have epilepsy. However, aconnection to the temporal lobe and limbicstructures may exist, as well as a brief abnor-mal firing, which gives a false sense offamiliarity. Researchers have suggested apositive correlation of déjà vu with highersocioeconomic level, more education, moretravel, and better dream recall (Brown,2003). The range of possible explanationsfor this fascinating phenomenon is extensivebut not yet fully understood. Perhaps bybetter understanding déjà vu we will be ableto discover more about the oddities of thebrain and how our memories and experi-ences are processed and retrieved.
N e u r o p s y c h o l o g y i n A c t i o n 1 6 . 4
D é j à Vu a n d E p i l e p s y
by Karen B. Friedman

smell may halt the seizure (Efron, 1957). We explore thisaspect of seizure control further in our discussion ofepilepsy treatment.
After a seizure episode is a postictal phase in whichthe person gradually emerges into full consciousness.Often symptoms of confusion, disorientation, depression,headache, or fatigue follow. Less common, the personmay bite his or her tongue or lose bladder control. Thisphase may be momentary or may last for hours, some-what depending on seizure type.
The following sections discuss seizure types accordingto the epilepsy classification scheme of Table 16.3. Clini-cal descriptions correlate with what is known of their neu-rologic counterparts. A more generalized discussion of thebrain mechanisms responsible for seizure activity follows.
G e n e r a l i z e d S e i z u r e s
Generalized seizures, formally known as grand mal seizures,are bilaterally symmetric episodes characterized by a tem-porary lack of awareness. The brain origin of these seizureshas traditionally been considered unknown or generalized.Behaviorally, they typically have a motor component thatonlookers consider frightening. The motor discharge islikely to consist of any combination of a tonic or clonic form.Some seizures have only the tonic component, others onlythe clonic component, and a number of seizures involveboth aspects. In these tonic-clonic seizures, the behavior thatalerts others to a seizure onset is the tonic stage. Patients de-scribe passing out, and onlookers are likely to witness a stiff-ening of the person’s whole body, jaw clenching, and a blueappearance to the face. The blueness may look like a respi-ratory arrest, but during a seizure this actually occurs be-cause peripheral blood vessel constriction allows moreblood to flow to the brain. In any case, breathing stops onlytemporarily. After seconds to minutes, the second clonicstage appears. The body begins a rhythmic jerking of limbsand may involve the whole torso. This is followed by abruptlimpness (or atonia) and a gradual regaining of consciousawareness. Generalized seizures may take several forms, butusually include components of irregular motor discharge inthe form of tonic and/or clonic movement.
Other types of generalized seizures resulting in abnor-mal muscular symptoms are myoclonic and atonicseizures. Myoclonic seizures manifest in arrhythmicbursts of jerky motor movements that usually do not lastmore than a second and tend to occur in clusters over ashort period. People who experience them sometimes de-scribe them as “jumps.” Atonic seizures, in contrast, arecharacterized by a sudden loss of muscle tone and may re-sult in a fall. They last no longer than 15 seconds whilethe person remains conscious.
Absence seizures appear in some classification schemesas a partial seizure and in others as a generalized seizure.This may represent differences related to the brain areasresponsible and the extent of cortical involvement. Asseen in the following case example described by a neu-rologist, the typical gross-motor involvement of general-ized absence seizures is not present and is replaced byictal automatisms.
[A] mother brought her delightful red-headed eight-year-olddaughter to see me. Because the girl seemed so attentive, intelli-gent, and well-behaved, it was hard for me to believe that shewas having a difficult time at school. Her teacher reported thatshe made frequent mistakes on the blackboard and was oftenunable to answer simple questions. In my office, I asked her totake some rapid shallow breaths. After thirty seconds, she staredvacantly into space with her eyelids fluttering. Ten seconds later,she was back to her usual self. I had witnessed a classic absenceseizure. Her EEG showed a pattern of 3 cycles/sec spike anddome activity during overbreathing, typical of absence epilepsy.(Richard & Reiter, 1990, p. 30)
In the above case, the doctor precipitated a seizure byhaving the girl hyperventilate. This girl’s fluttering eyelidsare an important behavioral clue to seizure activity. Addi-tional automatisms may include stereotyped hand move-ments or facial tics. Less typical for this type of seizure is asudden myoclonic jerk or atonic loss of muscle tone. Atthe approach of an attack, some individuals may just stoptalking midstream, stare blankly into space for the dura-tion of the attack, and then resume without noticing anylapse in consciousness. Absence attacks characteristicallyaffect children from age 4 to 14. Interestingly, many chil-dren with absence attacks “outgrow” them, suggesting thata delay or anomaly in brain development plays an impor-tant role in their occurrence. It is rare for adults with noseizure or trauma history to develop absence attacks.
P a r t i a l S e i z u r e s
Partial or focal seizures may take several forms, but theyalways begin as a local neuronal discharge that may gen-eralize across the corpus callosum, eventually involvingthe entire brain in a secondarily generalized seizure. Thisseizure category represents the most common type, affect-ing about 800,000 people in the United States (Cascino,1992). These seizures can be more frequently localizedthan generalized seizures, but still only a third of those af-flicted have identifiable causes. Head trauma, stroke, andviral brain diseases such as meningitis and encephalitis area few of the conditions that may lead to partial seizures.
Partial seizures consist of three main types. First, sim-ple seizures are focal events that may involve sensorimo-tor expression or psychic expression (mood, emotion, or
466 PART THREE | Disorders of the Brain

altered consciousness). The behavior experienced reflectsthe area from which the seizure emanates. For example,discharges from the motor strip can cause sudden orstereotypic movement, such as jerking or twitching. Peo-ple have reported that their eyes may move to a certainposition or that they turn their heads involuntarily. Occipi-tal lobe foci can result in seeing vivid images or flashinglights. Memory and personality alterations can be a resultof temporal lobe foci, and intensive mood experiences canoccur with limbic system foci. The behavioral results varywidely from person to person but are closely tied to the siteof seizure focus. Because there is no further involvement,the person can also experience these events as an aura.
The second type of partial seizure is complex partialseizures, the most common forms being psychomotor ortemporal lobe epilepsy. These are more “complex” thansimple partial seizures in that they have an element of al-tered psyche or awareness in addition to sensory or motorcomponents. About half of those with complex partialseizures experience an aura (Cascino, 1992). Complexpartial seizures typically emanate from the temporal lobesbut can also occur as the result of a frontal lesion. The al-teration of consciousness can take several forms. It mayinclude a sense of déjà vu (“already seen”) in new environ-ments or jamais vu (“never seen”) in a familiar place. Theperson may experience a sense of forced thinking, illusions,panic, terror, or even ecstasy. The motor changes duringthe ictal phase often take the form of odd, catatonic-likeposturing and automatisms such as lip smacking or undo-ing buttons. The shift into the ictal phase is abrupt, usu-ally commencing with a motionless stare. The postictal pe-riod of confusion and drowsiness can be quite long withcomplex partial seizures. The case of the “sweeping lady” isa good example of what may happen with complex partialseizures (Neuropsychology in Action 16.5).
The third type of partial seizure, a secondarily general-ized seizure, is actually a variation of the first type. If a sim-ple seizure spreads, this spreading can generalize throughoutthe whole brain as in the case of Jacksonian seizures. Jack-sonian seizures involve motor areas and have been called“marching seizures,” because they begin with jerking or tin-gling of a single body area and spread to other areas. Thesymptoms reflect their corresponding brain regions; thus,diagnosticians consult maps of the motor homunculus.
N E U R O A N A T O M Y A N D N E U R O P H Y S I O L O G YO F S E I Z U R E S
Partial and secondarily generalized seizures are the mostlikely to be localized because both the aura and the behav-ior during a seizure can point to a seizure’s epileptogenic
focus (the anatomic site of onset). Generalized seizures aredifficult to localize, because they quickly disrupt the entirerange of behavior involving all cortical neurons and may arisefrom a central mechanism capable of having a global effecton the brain. If there is an identifiable seizure focus, EEGrecording is useful in locating it if a seizure occurs sponta-neously or can be induced during EEG monitoring.
Seizures are a symptom, similar to the concept of fever,that something is going on in the brain. A seizure may belocalized to a particular anatomic area of the brain, andtechnicians may be able to image a corresponding struc-tural pathology such as a lesion, a tumor, a vascular disease,or other anomaly. For example, the cause of some child-hood seizures may be malformed brain tissue (Figure 16.8).
Because seizures also arise from metabolic disturbancesand infections that affect the delicate physiological balanceof the brain, neurologists cannot always find a structurallocation of injury or neuronal destruction in the brain. Al-though many normal people may experience a seizure, theoccurrence may indicate significant brain pathology andmedical consultation should always be sought.
Normally, the brain maintains a balance of neuronalfiring between excitatory discharges and inhibitory con-trol of excessive firing. Single neurons and neuronal cir-cuits fire according to their own direction and processingin what appear to be random patterns. Because so manydifferent patterns are occurring simultaneously, and be-cause the EEG represents a summation of neuronal fir-ing, the resultant EEG tracing is fast and asynchronous.Seizures occur due to excessive excitatory synchronousneuronal firing. If you have ever been caught up in a“wave” in a packed football stadium, the analogy to thebrain is similar. All the people represent individual neu-rons and are initially involved in their own behaviors. Atfirst, although small groups of people may be involved ina rhythmic “give and take,” the summation of “stadiumbehavior” appears random, with occasional synchronousbursts of cheering from one side or the other. But if asmall group of people successfully initiate a wave, beforelong the entire stadium of 50,000 people synchronizes ina rhythm that sweeps through the crowd.
Absence seizures provide a good example of a general-ized seizure that arises from a central mechanism. EEGsof classical absence seizures show characteristic synchro-nous bilateral spike-and-wave discharge with a 3cycles/sec frequency. This EEG frequency is within thesame range as delta waves, characteristic of deep sleep. Areasonable description of absence seizures is that theyforce a temporary disconnection within the arousal sys-tem of the RAS, thus pushing the whole cortex into atemporary sleeplike state.
CHAPTER 16 | Alterations of Consciousness 467

Both animal and human studies point to the thalamo-cortical circuitry as the source for the primary aberrantmechanism involved in absence attacks. As we have dis-cussed, during an alert state, neurons in the thalamocorti-cal loop are involved in continuous tonic firing. This al-lows signals from the external environment to pass throughthe thalamus to the cortex. External transmission to thecortex dampens when neurons begin firing according to aninternally generated oscillating rhythm. Neurologists thinkthat a group of neurons within the thalamus, the nucleusreticularis thalami (NRT), regulates oscillatory behaviorof the thalamocortical loop. Direct recordings indicatethat this is the source of rhythmic burst firing when theEEG becomes synchronized and also is a source of asyn-chronous firing during wakefulness. The NRT also proj-ect to the contralateral dorsal thalamus, and thus havethe ability to influence both hemispheres. The NRTmainly consist of GABAergic neurons that project to eachother within the NRT and other areas of the thalamus.
One of their main functions is in controlling cerebral ex-citability. Researchers report that during earlydevelopment, one form of GABA receptors—the GABA-btype—increases and later is pruned to adult levels.Researchers also know that GABA agonist drugs makeabsence seizures worse. Some investigators believe thatabsence seizures in children may result from an error indevelopment, resulting in a temporary overabundance ofGABA receptors and, therefore, a temporary imbalance inthe excitatory/inhibitory forces of the brain (Snead, 1995).They think what happens within this system of neuronsthat affects a shift between asynchronous and synchronousrhythms is a change in the calcium potential of the cellularmembrane. This may explain why some antiepileptic drugssuch as ethosuximide and trimethadione, which act on thecalcium current of the membrane, are effective.
In addition to the GABAergic neurons within the thala-mus, numerous neurotransmitter systems may be involvedin generalized absence seizures, because the ascending
468 PART THREE | Disorders of the Brain
Epilepsy is a common neurologic disorder,currently affecting more than 2 millionpeople in the United States (for a detaileddiscussion of epilepsy, see Bennett, 1992).Diagnosis of epilepsy depends on clinicalinterview and EEG assessment showingabnormality in the interictal (betweenseizures) scalp electrode EEG tracings. Theinterictal spike is a marker for this disorder(McIntosh, 1992).
When psychic alterations occur, theseizures are called complex partial seizures.For neuropsychologists, these are the mostinteresting epileptic disorders (Bennett,1987). They may be associated with motorautomatisms consisting of stereotyped,repetitive movements such as chewing,blinking, lip smacking, pointing, or picking atone’s clothes. Complex partial seizures,because of their frequent temporal lobe andlimbic system focus, may have an emotional
component to the psychic alterations. Themost common emotion is fear, but theperson may also report pleasure, sadness,or vague familiarity. Individuals with complexpartial seizures also commonly report sen-sory hallucinations or misperceptions. Thesesensations may range throughout the spec-trum of visual, gustatory, olfactory, auditory,or somatic perceptions. Olfactory sensationsare the most common type of sensory aurareported. These are typically quite displeas-ing (such as the smell of burning or rottingflesh), but may on occasion be pleasant(such as the smell of roses).
In the course of a complex partial seizure,the person may utter meaningless speech,laugh, or cry. Complex motor responses mayalso occur, including compulsive, purpose-less writing and even running. During acomplex partial seizure, a person may beunaware of or unresponsive to her or his
environment, failing to respond to questionsby others. The person may be vaguely awareof what is going on but unable to control it.While in a state of altered consciousnessduring a seizure, he or she may go into an-other room, wander through a public place, orleave a store and wander down the street.Imagine how upset you would be to findyourself in a different place from where you“just” were and to have lost several minutesor even hours of time, not knowing what youdid during the interim. This is illustrated bythe case of the sweeping lady.
This individual—let us call her Alice—hasbeen a client of mine for almost 15 years. We meet on occasion as she continues todeal with the impact of her epilepsy on herlife. Alice’s epilepsy has never been com-pletely controlled by antiepileptic drugs, a fartoo common experience for those with com-plex partial seizures. She has had to alter her
N e u r o p s y c h o l o g y i n A c t i o n 1 6 . 5
E p i l e p s y a n d t h e C a s e o f t h e S w e e p i n g L a d y
by Thomas L. Bennett Ph.D., Professor of Psychology, Colorado State University, Clinical Director, Brain Injury Recovery Program,
Fort Collins, CO

neuronal pathways to the cortex involve cholinergic, no-radrenergic, dopaminergic, and serotonergic neurons.ACh and cholinergic projections emanating from the nu-cleus basalis to the cortex have an effect on arousal apartfrom the thalamocortical loop. Thus, the regulation andcontrol of arousal, and therefore seizures, represent acomplex interaction of anatomic and physiologic systems.
N E U R O P S Y C H O L O G I C A L P R E S E N T A T I O N
Although neurologists may diagnose many seizures viaEEG and other imaging measures, this is not always pos-sible because seizures do not occur “at will.” The interic-tal intervals can range from minutes to months to years.Neuropsychological evaluation can help determine theprobability, by level and extent, that functional deficitsare caused by seizure activity, and can therefore aid in di-agnosis. A neuropsychological assessment can help iden-tify areas of the brain that may not be working properlyand, therefore, provide an estimate of a possible area of
seizure onset. For example, if a person shows impairedmemory for a list of words, this may indicate an abnor-mality in the left temporal region. Testing can also helpdetermine the extent to which emotional components andstress may stem from seizures and help discriminate be-tween neurologically based epilepsy and pseudoseizuresarising from a somatoform disorder. As with any otherneurologic disorder, neuropsychological testing candemonstrate a pattern of individual cognitive strengthsand weaknesses to make appropriate recommendationsfor better adjustment to daily life.
One of the most frequent uses of a neuropsychologicalevaluation in epilepsy is in the context of a presurgicalevaluation. When medication or other treatment hasproved ineffective to reduce or eliminate the seizures, thenthe resection of the possible epileptogenic focus is consid-ered. To perform a surgery of this type, the neurosurgeonneeds to perform a series of tests to determine with preci-sion the site of the focus and to assess whether the personwould not suffer undue loss of function from removal of
CHAPTER 16 | Alterations of Consciousness 469
lifestyle and goals in life significantly; butoverall, she has adapted well to her disability.Before the onset of her seizure disorder in herearly 20s, she was active in sports and thecommunity, and she planned to return tocollege to complete a bachelor’s degree.Alice has two daughters. She has worked in acouple of settings, but overstimulation andfatigue can increase seizure frequency, andshe currently is not working. Diagnosticelectroencephalograms (EEGs) have pro-duced some normal and some abnormalresults. (Normal EEGs are also observed inothers with complex partial seizures, showingthat a normal EEG does not rule outepilepsy.) Her seizure pattern is interesting,because it typically contains many of thephenomena I have discussed.
Early in the development of her epilepsy,and when the seizures were less frequent witha fairly long interictal interval, Alice typicallyexperienced epigastric sensations (“butter-flies in the stomach”) and nausea during theday before her seizures. This phenomenon,which was a seizure event, actually led her toseek evaluation from a gastrointestinalspecialist before complex partial seizureswere diagnosed. During this interval, her timeperception was distorted so that everythingseemed to slow down around her. She feltdetached from her surroundings.
As the abnormal electrical activity spreadand overt signs of the seizure pattern beganto develop, Alice experienced olfactory/gustatory sensations, including detecting theodor of putrid, burning flesh, olfactorysensations, and the taste of soap. A blankstare preceded her motor automatisms, andshe lost clear awareness of her surroundingsat this point. She then began purposelesspacing and hand rubbing for 2 to 3 minutes.She reported that she was vaguely aware ofthese things happening, but she could notcontrol them. She would typically emit aseries of grunting and gasping sounds,which sounded to others as if she werehaving trouble getting enough air. Grimac-ing contorted her face. She laughed uncon-trollably for several minutes, and then criedand rocked back and forth for severalminutes more. The sequence ended whenthe spread of epileptic activity caused ageneralized tonic contraction and she lostconsciousness. This case illustrates thewealth of events that can occur during acomplex partial seizure episode.
Several times Alice lost all awareness ofwhat she had done for several hours. Thishappened when she went into a grocerystore or large department store during theday when things were busy, noisy, andvisually overstimulating. She later discovered
that she must have just aimlessly wanderedthrough the store, perhaps repeatedlyexamining objects, because she had lost upto 2 to 3 hours of time for which she had norecollection. One of the most unusual experi-ences she had during a complex partialseizure occurred several years ago. I havethought of this as the “great fugue,” or the“case of the sweeping lady.”
It was the middle of the day in late springor early summer, and Alice was home alone.She remembers that she was in her kitchenand had decided to sweep the floor. Shevaguely remembers starting to sweep thefloor, but nothing of the next 45 to 60 min-utes. Apparently, she swept across thekitchen, down the hall, through the entryway,and out the front door! Her next memory wasthat she was lying on a stranger’s porch. Atfirst, she did not know who she was or whereshe was. Over the next few minutes, shebecame reoriented and realized she was onsomeone’s porch. She stood up, walkeddown the sidewalk into the street, andrecognized a friend’s house several housesaway. That enabled her to reorient to whereshe was. It turned out that she had walkedseveral blocks from her home, crossingseveral intersections, without awareness,while in an extended complex partial seizurefugue!

the affected brain area. A neuropsychological evaluation isin order; first, because it provides a baseline of the person’slevel of performance, and second, because as mentionedearlier, it can help by providing clues as to where the focusof the seizures might be through analysis of the patterns of
dysfunction. To determine and localize brain impairment,the neuropsychologist will analyze the facts obtained bysuch an evaluation in conjunction with other sources ofinformation such as clinical observation and structural andfunctional brain imaging. A procedure that is usually per-formed in a presurgical evaluation is inpatient video EEGmonitoring (Figure 16.9). EEG monitoring is either donethrough noninvasive scalp electrodes (such as those used forsleep EEGs) or through depth electrodes that are surgicallyimplanted. EEG and behavior (via video recording) arethen continuously recorded together 24 hours a day. Thepurpose is to localize the seizure onset and learn as muchas possible about the individual behavioral seizure charac-teristics. Even though the ultimate goal is to eliminate theseizures, this is a point in the treatment course where allinvolved want a seizure to happen! If a seizure does notoccur spontaneously (as we mentioned earlier, interictalperiods can take months, even years), actions can be takenwithin this controlled environment to provoke a seizure,such as reduce the antiepileptic medication or induce sleepdeprivation or hyperventilation.
The presurgical neuropsychological evaluator is alsolooking for any fluctuations in consciousness or behaviorthat may herald a seizure. If seizures occur during testing,and if the patient is conscious and not in danger of in-jury, an assessment of consciousness and memory can bemade. For example, after the seizure is over, the personcan be asked to recall what happened or to rememberwhat was said or shown to them during the episode.Sometimes an evaluation can be continued after aseizure if the person recovers quickly and does not expe-rience many postictal symptoms; but on some occasions,the person may show signs of confusion, and thereforethe evaluation needs to be continued at another time.
Neuropsychologists are also typically involved in theadministration of a specialized presurgery evaluation com-monly called the Wada test (it is also referred to as the in-tracarotid amobarbital procedure [IAP]). This is particu-larly useful before surgeries for partial complex seizuresinvolving the temporal lobe (temporal lobe epilepsy/partialcomplex seizures), to determine the likely effect of remov-ing brain tissue on the functions of language and mem-ory. Named after its developer, Juhn Wada (Wada &Rasmussen, 1960), this procedure involves the injectionby a radiologist of a barbiturate, sodium amytal, throughthe patient’s carotid artery to anesthetize one hemisphereat a time. Even though the two hemispheres are connectedand irrigated by arteries, the sodium amytal reaches onlyone side because of equal pressure on both sides of thebrain. The blood pressure on one side makes the barbitu-rate stay on the other side. The aim is to test the function
470 PART THREE | Disorders of the Brain
Figure 16.8 Malformed tissue, present and growing frombirth, was the cause of seizures. After removal this person hasbeen seizure free and able to attend college. (Courtesy H. McNiece.)

of each hemisphere individually for its relative dominancefor language and its ability to support memory function-ing before temporal lobectomy. During the 6 to 8 minuteswhile one hemisphere remains “paralyzed,” the neuropsy-chologist tests the functioning of the “awake” hemisphereto model functioning without the other hemisphere. Thisis a gross measure of loss of function, typically focusing onspeech and memory. If, for example, the Wada test showsthat speech is atypically represented in the right hemi-sphere, then right temporal lobectomy is contraindicated.
Many variations of the procedures are used during theWada test, but the core involves brief testing of both ex-pressive and receptive language and short- and long-termmemory in both the verbal and visuospatial domains. Thepremise behind this assessment procedure is that the neu-ropsychological testing shows the distribution of brainfunction and can help predict the sparing of memory andlanguage functioning after temporal lobe resection. Thisaspect is usually quite helpful; however, some controversyexists over whether sodium amytal injections indeed anes-thetize memory functions. For one reason, the injectioninto the anterior carotid artery only perfuses into the ante-rior portion of the hippocampus, leaving posterior aspectsfree to function. To handle this problem, some medical
centers also selectively inject the middle or posterior cere-bral artery, although this is more risky. The change in a pa-tient undergoing a Wada procedure is usually quite dra-matic, in that the brain anesthetizes quickly and speechabruptly halts if the dampened hemisphere is dominantfor speech. Because many patients being considered forepilepsy surgery have a long-standing history of epilepsy,often dating back to early developmental years, cerebralrepresentation of speech can show a variety of patterns,presumably because the brain, responding to seizures, mayhave developed atypically. For example, there could be re-versed dominance for speech with both expressive andreceptive aspects controlled by the right hemisphere, equaldisruption in each hemisphere, or a dissociation of expres-sive speech in one hemisphere and receptive speech in theother (for review, see Jones-Gotman, 1996).
Neuropsychological presentation of seizures is highlyindividualistic, depending on seizure locus, type of seizure,and chronicity of disorder. No typical pattern of cognitivedysfunction is associated with epilepsy, and some patientsmay show few to no discernible problems. However, manyseizure sufferers exhibit attention and memory problems.This is particularly evident in tests that require sustainedor divided attention. In general, cognitive functioning
CHAPTER 16 | Alterations of Consciousness 471
Figure 16.9 Inpatient electroencephalographic and video monitoring of a patient during aseizure. (Courtesy Astro-Med, Inc.)

tends to be more impaired with longer duration (youngerage of onset) and increased frequency of seizures (Haynes& Bennett, 1990). Lowered cognitive functioning is alsolinked with greater EEG abnormality. In general, the typeof seizure activity parallels the functional deficits expected.For example, generalized tonic-clonic seizures are morelikely to result in widespread functional impairment ofboth hemispheres. Partial seizures (which have not gener-alized) are most likely to be associated with lateralized im-pairment related to the side of abnormal discharge. Asmentioned earlier, behavior during auras and the type ofmotor or sensory behavior evident during a seizure canalso provide clues to seizure locus and are likely to corre-spond to neuropsychological assessment.
People with complex partial seizures that involve thetemporal lobe show the most consistent neuropsychologicaland behavioral pattern. This group most commonly re-ports problems with learning, memory, and language andis less affected by attentional difficulties. Verbal fluencyand verbal retrieval deficits are common manifestations ofthe interaction between memory and language. However,all aspects of memory encoding, organization, and re-trieval may be affected. Emotional and behavioral distur-bances, although prevalent among seizure sufferers in gen-eral, are most common with those who have complexpartial seizures that involve the temporal lobe.
T R E A T M E N T O F E P I L E P S Y
The treatment of epilepsy is a collaborative effort betweenthe patient and various health care professionals. As inmany chronic diseases, patients are often the best expertson the symptoms of their conditions and the situationsmost likely to provoke a seizure. The various treatmentsavailable for epilepsy range from behavioral management,to nutritional therapy, to pharmacologic treatments, toneurosurgery; however, medication remains the mostwidely used form of treatment, and for most patients,seizures can be controlled with medication.
The decision to take regular medication for seizures re-quires a neurologist’s full evaluation as to its necessity, aswell as a commitment from the patient. As we have dis-cussed, seizures may occur in isolation, but epilepsy de-notes a pattern of seizure activity. If a neurologist can es-tablish a diagnosis of epilepsy, then a physician oftenprescribes specific drugs according to seizure type. For ex-ample, generalized tonic-clonic seizures often respond toanticonvulsants that prolong the inhibitory action ofGABA in the brain. These drugs include phenytoin(Dilantin), carbamazepine (Tegretol), or sodium valproate(Depakote) barbiturates and benzodiazepines. As de-
scribed earlier, absence seizures appear to involve a mecha-nism that is pharmacologically different from GABA. Ab-sence seizures are worsened by GABAergic drugs such asDilantin, Tegretol, or barbiturates (Snead, 1995) and aretreated by GABA-b antagonists ethosuximide (Zarontin),but may also be treated with Depakote. Physicians maytreat partial seizures with the preceding drugs or, forseizures involving motor disturbances, often use clon-azepam (Klonopin) or acetazolamide (Diamox). In in-stances when drugs have not effectively controlled seizures,surgery as a treatment method has also been used. Thepathologic brain area, if it can be localized, is simply cutout. This is where the neuropsychological evaluation, andspecifically the Wada test, can be particularly useful in ad-vising the surgeon as to areas of function, such as speechand memory, that might be affected by the procedure.
In recent years, a dietary treatment called the “keto-genic diet” has been gaining popularity. It was first devel-oped in the 1920s based on anecdotal reports about theeffectiveness of strict dietary regimens that date back evento Biblical times. It was not until the early 1990s when in-terest in this diet was renewed after a 2-year-old boy withintractable seizures was treated successfully at the JohnHopkins Hospital. This diet mimics the effects of biochem-ical changes that occur during fasting (acidosis, dehydra-tion, and ketosis). It is mainly a very “low-carb” diet, basedon an intake of proteins, fat, and little carbohydrates. Itsmechanism of action is not fully understood yet, but scien-tists consider that calorie restriction, acidosis, ketosis, ordehydration may be possible mediators of its effect onseizure control. This treatment is generally used whenseizures are difficult to control; when the patient respondspoorly to medication; or when there is adequate control,but the drug’s side effects are not well tolerated. A recentstudy has shown that 37% of patients have a 90% reduc-tion in seizures and an additional 30% experience a 50%to 90% reduction (Thiele, 2003). It has also been suggestedthat even though this treatment works for adults, it appearsto be more effective in children (Vining, 1999).
Some people with seizures have also learned to con-trol their attacks by noticing their auras and arresting theseizure before the ictal episode fully materializes. One pi-oneer in seizure research, Wilder Penfield, made the fol-lowing observation: “When an attack is just beginning,strong stimulation of the part threatened may avert thefurther development of a seizure” (Penfield, 1975, p. 39).Sensory auras including smell, touch, and taste appear par-ticularly amenable to natural arrest. For example, if theaura involves the sensation of a putrid smell, countering thiswith a pleasant smell may interrupt the progression of aseizure. In an early case study, Robert Efron (1957) reports
472 PART THREE | Disorders of the Brain

that one of his patients, a concert singer, had seizures pre-ceded by the aura of a bad smell. He gave her a vial of es-sential oil of jasmine to sniff at the onset of her aura. Thejasmine served as a natural counteractant to the halluci-nated bad smell and apparently stopped the seizure.Through behavioral conditioning, Efron also taught thepatient to arrest her seizures by imagining the odor of jas-mine. In a similar vein, some patients find that they canhalt gustatory auras such as metallic tastes by eating some-thing pleasant tasting. Tactile auras have been stopped bysuch methods as tickling and squeezing. It is reasonable toassume that because the type of aura experienced by anyone person is highly individual, patients would need toexperiment to find what works for them. Efron’s patientwas able to control her seizures well enough that her med-ications could be reduced. In another interesting example(Pritchard, Holmstrom, & Giacinto, 1985), a patient withcomplex partial seizures developed his own technique ofblinking or shutting his eyes and visualized himself fishing.What was most striking was that EEG monitoring corrobo-rated that he could arrest his seizure through this specific vi-sualization, but not through other mental tasks suggested tohim such as mental arithmetic or reading.
In addition to these self-control methods, other behav-ioral techniques have been explored to control seizures.These involve stress reduction measures, as well asbiofeedback. Because seizures have often been associatedwith increased levels of stress, progressive relaxation tech-niques have offered some effectiveness (Rousseau,Hermann, & Whitman, 1985). This technique involvestightening and relaxing isolated muscle groups and alsolearning how to apply this procedure when facing situa-tions and feelings that are associated with a high risk forseizure activity (Dahl, Melin, & Lund, 1987). Besides thenotion that stress can, on some occasions, precipitateseizures, it has also been suggested that sudden changes inarousal may be associated with seizure upsurge. There-fore, a technique called “countermeasures” has been ap-plied to fight the onset of seizures. With this technique,the goal is to change the arousal level when early signs ofa seizure appear. For example, if a person experiencesdrowsiness at the time of the seizure onset, the objectiveof the countermeasure technique would be to teach theperson to heighten the arousal level at this point to pre-vent the progression of the seizure (Dahl, Brorson, &Melin, 1992). Biofeedback based on galvanic skin re-sponse has also been used to reduce seizure frequency.This practice is based on the notion that an increase insympathetic arousal (galvanic skin response) is associatedwith reduced abnormal cortical activity present inepilepsy (Nagai, Goldstein, Fenwick, & Trimble, 2004).
EEG biofeedback is another method that has beenused to attempt seizure reduction, particularly for thosewho do not respond to conventional drug treatments. Theidea of neurofeedback is for the person to learn to iden-tify the EEG patterns that may lead to seizures. The EEGsignals occurring in real time are “fed back” to the personin a form that is easily understood. While being monitored,a person could, for example, receive feedback via a tonethat would sound lower on the musical scale if the direc-tion of the neuronal pattern was to de-emphasize seizureactivity and sound higher if seizure activity was morelikely. By training people to recognize their brain andmind states, the idea is that they can also learn to controlthem. The purpose of this technique is to apply “operantconditioning” principles to brain activity. In addition totones, this is often done by presenting to the patient hisor her own brain activity in a creative way and providingrewards whenever the brain signals move in the desireddirection. For example, some protocols of neurofeedbackfor children use spaceship races in which each spaceshiprepresents a type of brain wave captured by the EEG andthe goal is to make the desired spaceship “win the race,”which, in fact, means that the targeted brain activity mea-sured by the EEG is moving in the desired direction.Overall, EEG biofeedback or “neurofeedback” for thetreatment of epilepsy has shown positive results along theyears; however, no consensus has been reached as to whichparticular protocol works the best, because few studies areavailable, and the ones that exist are quite variable in sub-ject selection and also lack rigorously controlled designs.Nevertheless, recent improvements in quantitative EEG(qEEG) may facilitate this endeavor. qEEG uses digitaltechnology to capture brain-wave activity, which isrecorded and converted into a color map of brain func-tions. The advantages of qEEG as compared with a regu-lar EEG are that data can be more easily interpreted and apatient’s performance can be compared statistically withits own or with that of a large population database. Withthis technology a new window of opportunity is openedfor the development of neurofeedback, because it be-comes easier to target and quantify particular sites of ab-normal brain activity for each individual and also detectincoherences in neuronal firing between different brainlocations that may contribute to seizure activity. A pre-liminary study by Walker and Kozlowski (2005) has re-ported several cases for whom qEEG biofeedback was ap-plied where seizures decreased considerably and many ofthe subjects even become medication free. Controllingseizures by learning how to recognize and manipulatebrain activation is an exciting field that deserves furtherexploration.
CHAPTER 16 | Alterations of Consciousness 473

ConsciousnessCircadian rhythmNarcolepsySeizuresPartial seizuresEpileptic syndromeEpilepsyLucid dreamingReticular activating system
(RAS)
UltradianAbsence seizuresREM (rapid eye movement)
sleepNREM (non–rapid eye
movement) sleepNocturnal myoclonusSuprachiasmic nucleus (SCN)Sleep paralysisAtonia
Sleep apnea syndrome (SAS)
ApneaHypoxiaSudden infant death syndrome
(SIDS)Obstructive sleep apneaCentral sleep apneaUvulopalatopharyngoplasty
(UPPP)
Excessive daytime sleepiness
CataplexyHypnagogic hallucinationsGeneralized seizureGrand mal seizureTonicClonicPetit mal seizureComplex partial seizure
SummaryConsciousness is a frontier of brain science that presents some of the most intriguing puzzles of the humanmind. Although issues of changing alertness, such as sleep and sleep disorders, may be easier to map outand understand within the workings of the brain, issues of awareness, particularly understanding of thebrain mechanisms of self-awareness and unity of experience, still present many mysteries. Throughout thisbook, we have considered many brain disorders that result in altered states of awareness. In this chapter,we went further into defining normal consciousness and considered two types of disorders of conscious-ness: sleep disorders and seizure disorders.
With normal alertness, circadian peaks and valleys occur on about a 24-hour cycle in accordancewith the sleep/wake cycle. In general, EEG indicates level of alertness, as seen in normal sleep andwakefulness patterns. However, EEG, which is the outward measure of brain rhythm, is not necessarilyan accurate indicator of mind state. Two people may show similar EEG patterns but have very differentlevels of conscious alertness. For example, although sleep is often called “unconscious,” some peopleshow “lucidity” during REM sleep. Slow delta waves accompany deep sleep and coma, but accomplishedmeditators can also produce this “deep” brain state whereas maintaining a more alert “mind” state. Themind state of dreaming during the brain state of REM has fascinated philosophers and scientists alikeas they endeavor to understand potential connections to problem solving, memory, and psychologicaladjustment.
The hypothalamus, the thalamus, and the RAS are particularly important in the sleep/wake cycle. Whenthis clocklike rhythm is disrupted, sleep disorders such as life-threatening insomnia or narcolepsy can occur.Excessive daytime sleepiness occurs with most sleep disorders, often associated with patient reports ofpoor memory and concentration.
Seizures suddenly alter consciousness during wakefulness and often result in abnormal movementand mentation. Seizures are the outward behavioral manifestation of excessive excitatory synchronousneuronal firing. The behavioral symptoms of seizures relate to the scope and the location of the brain focus,and the classifications of generalized and partial seizures are well documented. Neuropsychologists assessseizure patients for treatment planning and surgical evaluations. Although treatment of seizures primarilyrelies on medications, behavioral interventions may also be possible in the future as scientists and individu-als learn more about controlling aspects of their own consciousness.
C r i t i c a l T h i n k i n g Q u e s t i o n s
What is the biological or psychological function of “rhythms” of consciousness?How fluid are the boundaries between conscious and subconscious awareness?How do REM sleep and dreaming change in people who have various neurologic disorders?In what ways might neuropsychology be able to contribute to treatments for people with sleep disorders or epilepsy?
K e y Te r m s
474 PART THREE | Disorders of the Brain
We b C o n n e c t i o n s
http://www.stanford.edu/~dement/sleepinfo.htmlStanford University Sleep Center—a complete guide to various sleep disorders including all the disordersdiscussed in the text. In addition, discussions of the relation of sleep disorders to specific psychiatric andmedical diagnosis may provide an interesting link between previously discussed disorders and sleepdisturbances.
http://www.sleepnet.com/disorder.htmSleepNet—provides an overview of sleep, including sleep disorders, research, sleep labs, and more.
http://www.efa.orgEpilepsy Foundation—presents research as well as advocacy information.
http://neuro.med.cornell.edu/NYH-CMC/ne-general.htmlCornell University Epilepsy Center—this overview of epilepsy covers the basics, such as the definition of aseizure, to more advanced discussions of treatment options and surgical procedures available for patientswith epilepsy.
http://neurosurgery.mgh.harvard.edu/epilepsy.htmHarvard Epilepsy Site—not only is this site an excellent source for discussions of surgical options in epilepsy,it also provides general resources and other links on this topic, as well as the more general topic of epilepsyas a whole.
CHAPTER 16 | Alterations of Consciousness 475
AuraProdromal phaseEpileptogenic focusPostictal phase
Myoclonic seizuresAtonic seizuresAutomatismsSimple seizure
Psychomotor or temporal lobeepilepsy
Secondarily generalized seizure
Jacksonian seizureNucleus reticularis thalami
(NRT)Benzodiazepines

This page intentionally left blank

Aarsland, D., Zaccai, J., & Brayne, C. (2005). A systematicreview of prevalence studies of dementia in Parkinson’sdisease. Movement Disorders, 20(10), 1255–1263.
Adams, R. D., & Victor, M. (1993). Principles of neurology(4th ed.). New York: McGraw-Hill.
Administration on Aging. (2000). A profile of older Americans.Washington, DC: Author.
Adolphs, R., Tranel, D., & Damasio, A. R. (1998). The humanamygdala in social judgment. Nature, 393, 470–474.
Agnew, J., Bolla-Wilson, K., Kawas, C., & Bleeker, M. L.(1988). Purdue Pegboard age and sex norms for ages fortyand older. Developmental Neuropsychology, 4, 29–35.
Alarcón, M., Pennington, B. F., Filipek, P. A., & DeFries, J. C.(2000). Etiology of neuroanatomical correlates of readingdisability. Developmental Neuropsychology, 17, 339–360.
Albert, M. L., Feldman, R. G., & Willis, A. L. (1974). The “sub-cortical dementia” of progressive supranuclear palsy. Journalof Neurology, Neurosurgery, and Psychiatry, 37, 121–130.
Alexander, M. P., & Stuss, D. T. (2000). Disorders of frontallobe functioning. Seminars in Neurology, 20, 427–437.
Alsobrook, J. P., & Pauls, D. L. (1999). Molecular genetics ofchildhood psychiatric disorders. In D. S. Charney, E. J.Nestler, & B. S. Bunney (Eds.), Neurobiology of mentalillness (pp. 749–760). New York: Oxford University Press.
Alvarez-Buylla, A., & Garcia-Verdugo, J. M. (2002).Neurogenesis in adult subventricular zone. Journal ofNeuroscience 22(3), 629–634.
Alvarez-Buylla, A., & Lois, C. (1995). Neuronal stem cells inthe brain of adult vertebrates. Stem Cells, 13(3), 263–272.
Alzheimer, A. (1907). Über eine eigenartige Erkrankung derHirnrinde. Allgemeine Zeitschrift für Psychiatrie, 64, 146–148.
Alzheimer, A. (1987). About a peculiar disease of the cerebralcortex. Alzheimer’s Disease and Associated Disorders, 1, 7–8.
Amedi, A., Raz, N., Pianka, P., Malach, R., & Zahory, E.(2003). Early visual cortex activation correlates with supe-rior verbal memory performance in the blind. NatureNeuroscience, 6, 758–766.
American Psychiatric Association. (1980). Diagnostic and statis-tical manual of mental disorders (3rd ed.). Washington,DC: Author.
American Psychiatric Association. (1987). Diagnostic and statis-tical manual of mental disorders (3rd Rev. ed.). Washington,DC: Author.
American Psychiatric Association. (1994). Diagnostic and statis-tical manual of mental disorders (4th ed.). Washington,DC: Author.
Amin, Z., Constable, R. T., & Canli, T. (2005). Gender differ-ences in the implicit processing of emotional faces: Aregion of variance approach. Journal of CognitiveNeuroscience, B141(Suppl.), 65–66.
Andersen, R. A., Snyder, L. H., Li, C. S., & Stricanne, B.(1993). Coordinate transformations in the representationof spatial information. Current Opinions in Neurobiology,3, 171–176.
Anderson, G. M. (2002). Genetics of childhood disorders:XLV. Autism, part 4: Serotonin in autism. Journal of theAmerican Child and Adolescent Psychiatry, 41, 1513–1516.
Anderson, S. W., & Tranel, D. (2002). Neuropsychologicalconsequences of dysfunction in human dorsolateral pre-frontal cortex. In F. Boller, J. Grafman (Series Eds.), &J. Grafman (Vol. Ed.), Handbook of neuropsychology: Thefrontal lobes (Vol. 7, 2nd ed., pp. 145–156). New York:Elsevier.
Anderson, V., Jacobs, R., & Harvey, A. S. (2005). Prefrontallesions and attentional skills in childhood. Journal of theInternational Neuropsychological Society, 11, 817–831.
Anderson, V., Levin, H. S., & Jacobs, R. (2002). Executivefunctions after frontal lobe injury: A developmental per-spective. In D. T. Stuss & R. T. Knight (Eds.), Principlesof frontal lobe function (pp. 504–527). New York: OxfordUniversity Press.
Anderson, V., Northam, E., Hendy, J., & Wrennall, J. (2001).Developmental neuropsychology: A clinical approach.Philadelphia: Taylor & Francis.
Anderson, V. A., Anderson, P., Northam, E., Jacobs, R., &Catroppa, C. (2001). Development of executive functionsthrough late childhood and adolescence in an Australiansample. Developmental Neuropsychology, 20, 385–406.
Anderson, V. A., Anderson, P., Northam, E., Jacobs, R., &Mikiewicz, O. (2002). Relationships between cognitiveand behavioral measures of executive function in childrenwith brain disease. Child Neuropsychology, 8, 231–240.
Andreasen, N. C. (1988). Brain imaging: Applications in psy-chiatry. Science, 239, 215–226.
Annett, M. (1985). Left, right, hand and brain: The right shifttheory. London: Lawrence Erlbaum Associate.
Annett, M. (2002). Handedness and brain asymmetry: The rightshift theory. East Sussex, United Kingdom: PsychologyPress.
Archibald, S. J., & Kerns, K. A. (1999). Identification anddescription of new tests of executive functioning in chil-dren. Child Neuropsychology, 5, 115–129.
REFERENCES
477

Archibald, S. J., Mateer, C. A., Kerns, K. A. (2001). Utilizationbehavior: Clinical manifestations and neurological mecha-nisms. Neuropsychology Review, 11, 117–130.
Armony, J. L., & LeDoux, J. E. (2000). How danger is encoded:Toward a systems, cellular, and computational under-standing of cognitive-emotional interactions in fear. In M. S. Gazzaniga (Ed.), The new cognitive neurosciences(2nd ed., pp. 1067–1079). Cambridge, MA: MIT Press.
Armstrong, C., Corn, B., Ruffer, J., Pruitt, A., Mollman, J., &Phillips, P. (2000). Radiotherapeutic effects on brainfunction: Double dissociation of memory systems.Neuropsychiatry, Neuropsychology, & Behavioral Neurology,13(2), 101–111.
Armstrong, R. J., Watts, C., Svendsen, C. N., Dunnett, S. B., &Rosser, A. E. (2000). Survival, neuronal differentiation, andfiber outgrowth of propagated human neural precursorgrafts in an animal model of Huntington’s disease. CellTransplantation, 9, 55–64.
Armstrong-Hickey, D. (1991). A validation of lucid dreamingin school age children. Lucidity, 10, 250–254.
Ashford, J. W., & Zec, R. F. (1993). Pharmacological treat-ment in Alzheimer’s disease. In R. W. Parks, R. F. Zec, &R. S. Wilson (Eds.), Neuropsychology of Alzheimer’s diseaseand other dementias. New York: Oxford University Press.
Asperger, H. (1991). “Autistic psychopathy” in childhood (U. Frith, Trans.). In U. Frith (Ed.), Autism and Asperger’s syndrome (pp. 32–97). New York: Cambridge UniversityPress.
Atkinson, J., Braddick, O., Anker, S., Curran, W., Andrew, R.,Wattam-Bell, J., et al. (2003). Neurobiological models ofvisuospatial cognition in children with Williams syn-drome: Measures of dorsal-stream and frontal function.Developmental Neuropsychology, 23, 139–172.
Atkinson, J., King, J., Braddick, O., Nokes, L., Anker, S., &Braddick, F. (1997). A specific deficit of dorsal visualstream function in Williams syndrome. NeuroReport, 8,1919–1922.
Aylward, E. H., Reiss, A. L., Reader, M. J., Singer, H. S.,Brown, J. E., & Denckla, M. B. (1996). Basal ganglia vol-umes in children with attention-deficit hyperactivity dis-order. Journal of Child Neurology, 11, 112–115.
Babinski, J., & Joltran, E. (1924). Un nouveau cas d’anosog-nosie. Revue Neurologique, 31, 638–640.
Bachevalier, J. (1994). Medical temporal lobe structure andautism: A review of clinical and experimental findings.Neuropsychologica, 32, 627–648.
Backman, L., Small, B. J., Wahlin, A., & Larsson, M. (2000).Cognitive functioning in very old age. In F. I. M. Craik& T. A. Salthouse (Eds.), Handbook of aging and cognition(2nd ed., pp. 499–558). Mahwah, NJ: Erlbaum.
Baddeley, A. (1986). Working memory. New York: OxfordUniversity Press.
Baddeley, A. D. (2000). The episodic buffer: A new compo-nent of working memory? Trends in Cognitive Sciences, 4,417–423.
Baddeley, A. D. (2001). Alan D. Baddeley award for distin-guished scientific contributions. American Psychologist, 56,849–864.
Baddeley, A. D. (2002). Fractionating the central executive. InD. T. Stuss & R. T. Knight (Eds.), Principles of frontallobe function (pp. 246–260). New York: OxfordUniversity Press.
Baddeley, A. D., & Hitch, G. J. (1994). Developments in theconcept of working memory. Neuropsychology, 8, 485–493.
Bailey, A., Phillips, W., & Rutter, W. (1996). Autism: Towardsan integration of clinical, genetic, neuropsychological, andneurobiological perspectives. Journal of Child Psychologyand Psychiatry, 37, 89–126.
Balasubramanian, V., & Ranamurthi, B. (1970). Stereotaxicamygdalotomy in behavior disorders. Confinia Neurology,32, 367.
Ball, G. F., & Hulse, S. H. (1998). Birdsong. AmericanPsychologist, 53, 37–58.
Bancaud, J., Brunet-Bourgin, F., Chauvel, P., & Halgren, E.(1994). Anatomical origin of deja vu and vivid ‘memories’in human temporal lobe epilepsy. Brain, 117(Pt 1), 71–90.
Banich, M. T. (1997). Neuropsychology: The neural basis of men-tal function. New York: Houghton Mifflin.
Bannister, R. (1992). Disorders of the cerebral circulation. InR. Bannister (Ed.), Brain and Bannister’s clinical neurology(7th ed.). New York: Oxford University Press.
Barakat, L. P., & Kazak, A. E. (1999). Family issues. In R. T.Brown (Ed.), Cognitive aspects of chronic illness in children(pp. 333–354). New York: Guilford Press.
Barakat, L. P., Kazak, A. E., Meadows, A. T., Casey, R.,Meeske, K., & Stuber, M. L. (1997). Families survivingchildhood cancer: A comparison of posttraumatic stresssymptoms with families of healthy children. Journal ofPediatric Psychology, 22(6), 843–589.
Barch, D. M., Braver, T. S., Sabb, F. W., & Noll, D. C. (2000).Anterior cingulated and the monitoring of response con-flict: Evidence from an fMRI study of overt verb genera-tion. Journal of Cognitive Neuroscience, 12, 298–309.
Barkley, R. A. (1990). Attention deficit hyperactivity disorder.New York: Guilford Press.
Barkley, R. A. (1997a). ADHD and the nature of self-control.New York: Guilford Press.
Barkley, R. A. (1997b). Behavioral inhibition, sustained atten-tion, and executive functions: Constructing a unifyingtheory of ADHD. Psychological Bulletin, 121, 65–94.
Barkley, R. A. (1997c). Update on a theory of ADHD and itsclinical implications. The ADHD Report, 5, 10–16.
Barkley, R. A. (1998). Attention deficit hyperactivity disorder(2nd ed.). New York: Guilford Press.
Barnett, H. J., Mohr, J. P., Stein, B. M., & Yatsu, F. M. (1986).Stroke: Pathophysiology, diagnosis, and management (Vols. 1& 2). New York: Churchill Livingstone.
Baron-Cohen, S., O’Riordan, M., Stone, V., Jones, R., &Plaisted, K. (1999). Recognition of faux pas by normally
478 References
developing children and children with Asperger syndromeor high-functioning autism. Journal of Autism andDevelopmental Disorders, 29, 407–418.
Baron-Cohen, S., Ring, H. A., Bullmore, E. T., Wheelwright,S., Ashwin, C., & Williams, S. C. (2000). The amygdalatheory of autism. Neuroscience and Biobehavioral Reviews,24, 355–364.
Baron-Cohen, S., Ring, H. A., Wheelwright, S., Bullmore, E.,Brammer, M., Simmons, A., et al. (1999). Social intelli-gence in the normal and autistic brain: An fMRI study.European Journal of Neuroscience, 11, 1891–1898.
Barr, C. L. (2001). Genetics of childhood disorders: XXII.ADHD, part 6: The dopamine D4 receptor gene. Journalof the American Child and Adolescent Psychiatry, 40, 118–121.
Barrash, J., Tranel, D., & Anderson, S. W. (2000). Acquiredpersonality disturbances associated with bilateral damageto the ventromedial prefrontal region. DevelopmentalNeuropsychology, 18, 355–381.
Barth, J. T., Alves, W. M., Ryan, T. V., Macciocchi, S. N.,Rimel, R. E., Jane, J. A., et al. (1989). Mild head injuryin sports: Neuropsychological sequelae and recovery offunction. In H. S. Levin, H. M. Eisenberg, & A. L.Benton (Eds.), Mild head injury. New York: OxfordUniversity Press.
Barth, J. T., Findley, L. J., Zillmer, E. A., Gideon, D. A., &Surrat, P. M. (1993). Obstructive sleep apnea, hypoxemia,and personality functioning: Implications for medical psy-chotherapy assessment. Advances in Medical Psychotherapy,6, 29–36.
Barth, J. T., Macciocchi, S. N., Boll, T. J., Giordani, B., Jane,J. A., & Rimel, R. W. (1983). Neuropsychological seque-lae of minor head injury. Neurosurgery, 13, 529–533.
Basso, A., Spinnler, H., Vallar, G., & Zanobio, M. E. (1982).Left hemisphere damage and selective impairment ofauditory verbal short-term memory: A case study.Neuropsychologia, 20, 263–274.
Bates, E. (1999). Plasticity, location and language develop-ment. In S. Broman, & J. Fletcher (Eds.), The changingnervous system (pp. 214–253). New York: OxfordUniversity Press.
Bates, E., & Roe, K. (2001). Language development in chil-dren with unilateral brain injury. In C. A. Nelson & M.Luciana (Eds.), Handbook of developmental cognitive neu-roscience (pp. 281–308). Cambridge, MA: MIT Press.
Bear, M. F., Connors, B. W., & Paradiso, M. A. (1996).Neuroscience: Exploring the brain. Baltimore: Williams &Wilkins.
Beatty, J. (1995). Principles of behavioral neuroscience. Chicago:Brown & Benchmark.
Bechara, A., Tranel, D., & Damasio, A. R. (2002). The somatic marker hypothesis and decision-making. In F. Boller, J. Grafman (Series Eds.), & J. Grafman (Vol. Ed.),Handbook of neuropsychology: The frontal lobes (Vol. 7, 2nded., pp. 117–144). New York: Elsevier.
Bechara, A., Tranel, D., & Damasio, H. (2000). Characterizationof the decision-making deficit of patients with ventromedialprefrontal cortex lesions. Brain, 123, 2189–2202.
Bechara, A., Tranel, D., Damasio, H., & Damasio, A. R.(1996). Failure to respond autonomically to anticipatedfuture outcomes following damage to prefrontal cortex.Cerebral Cortex, 6, 215–225.
Becker, R. O., & Seldon, G. (1985). The body electric:Electromagnetism and the foundation of life. New York:William Morrow.
Beeman, J. J., & Chiarello, C. (1998). Complementary right-and left-hemisphere language comprehension. CurrentDirections in Psychological Science, 7, 1–8.
Beh-Yishay, Y., & Prigatano, G. P. (1990). Cognitive remedia-tion. In E. Griffith & M. Rosenthal (Eds.), Rehabilitationof the adult and child with traumatic brain injury (2nd ed.).Philadelphia: F. A. Davis.
Bell, M. A., & Fox, N. A. (1994). Brain development over thefirst year of life: Relations between electroencephalograph-ic frequency and coherence and cognitive and affectivebehaviors. In G. Dawson & K. W. Fischer (Eds.), Humanbrain and the developing brain (pp. 314–345). New York:Guilford Press.
Bender, B. G., Linden, M. G., & Robinson, A. (1994).Neurocognitive and psychosocial phenotypes associatedwith Turner syndrome. In S. H. Broman & J. Grafman(Eds.), Atypical cognitive deficits in developmental disorders(pp. 197–216). New York: Oxford University Press.
Bender, L. (1938). A visual motor gestalt test and its clinical use.New York: American Orthopsychiatric Association.
Benes, F. M. (1997). Corticolimbic circuitry and the develop-ment of psychopathology during childhood and adoles-cence. In N. A. Krasnegor, G. R. Lyon, & P. S. Goldman-Rakic (Eds.), Development of the prefrontal cortex:Evolution, neurobiology, and behavior (pp. 211–240).Baltimore: Paul H. Brookes.
Bennett, D. A., Beckett, L. A., Murray, A. M., Shannon, K. M.,Goetz, C. G., Pilgrim, D. M., & Evans, D. A. (1996).Prevalence of parkinsonian signs and associated mortalityin a community population of older people. New EnglandJournal of Medicine, 334, 71–76.
Bennett, D. A., Wilson, R. S., Schneider, J. A., Evans, D. A.,Beckett, L. A., Aggarwal, N. T., et al. (2002). Natural his-tory of mild cognitive impairment in older persons.Neurology, 59(2), 198–205.
Bennett, T. L. (1987). Neuropsychological aspects of complex partial seizures: Diagnostic and treatment issues.International Journal of Clinical Neuropsychology, 9, 37–45.
Bennett, T. L. (1992). The neuropsychology of epilepsy. NewYork: Plenum Press.
Bensen, D. F. (1991). The role of frontal dysfunction in atten-tion-deficit hyperactivity disorder. Journal of ChildNeurology, 6, S9–S12.
Benton, A. L. (1972). The “minor” hemisphere. Journal ofHistory of Medicine and Allied Sciences, 27, 5–14.
References 479
Benton, A. L. (1994). Four neuropsychologists. NeuropsychologyReview, 4, 31–44.
Benton, A. L., & Hamsher, K. D. (1989). Multilingual aphasiaexamination. Iowa City, IA: AJA Associates.
Benton, A. L., Hamsher, K. D., Varney, N. R., & Spreen, O.(1983). Contributions to neuropsychological assessment. NewYork: Oxford University Press.
Berch, D. B., & Bender, B. G. (2000). Turner syndrome. In K. O. Yeates, M. D. Ris, & H. G. Taylor (Eds.), Pediatricneuropsychology: Research, theory and practice (pp. 252–274).New York: Guilford Press.
Berg, E. A. (1948). A simple objective treatment for measuringflexibility in thinking. Journal of General Psychology, 39,15–22.
Berlin, L., Bohlin, G., Nyberg, L., & Janols, L. O. (2004).How well do measures of inhibition and other executivefunctions discriminate between children with ADHD andcontrols? Child Neuropsychology, 10, 1–13.
Bernstein, J. H., & Waber, D. P. (1997). Pediatric neuropsy-chological assessment. In T. E. Feinberg & M. J. Farah(Eds.), Behavioral neurology and neuropsychology(pp. 721–728.). New York: McGraw-Hill.
Beuren, A. J., Schulze, C., Eberle, P., Harmjanz, D., & Apitz,J. (1964). The syndrome of supravalular aortic stenosis,peripheral pulmonary artery stenosis, mental retardationand similar facial appearance. American Journal ofCardiology, 13, 471–483.
Bigler, E. D. (1987). The clinical significance of cerebral atrophy indementia. Archives of Clinical Neuropsychology, 2, 177–190.
Bigler, E. D. (1996). Neuroimaging (Vols. 1 & 2). New York:Plenum.
Bigler, E. D., & Snyder, J. L. (1995). Neuropsychological out-come and quantitative neuroimaging in mild head injury.Archives of Clinical Neuropsychology, 10(2), 159–174.
Birch, S., & Chase, C. (2004). Visual and language processingdeficits in compensated and uncompensated college stu-dents with dyslexia. Journal of Learning Disabilities, 37,389–410.
Birkmayer, W., & Hornykiewicz, O. (1961). Der L-dioxyphenalalanin L-DOPA Effekt bei der ParkinsonAkinese. Wiener Klinische Wochenzeitschrift, 73, 787–793.
Bisiach, E., & Rusconi, M. L. (1990). Break-down of perceptualawareness in unilateral neglect. Cortex, 26(4), 643–649.
Blair, R. J., Morris, J. S., Frith, C. D., Perrett, D. I., & Dolan,J. R. (1999). Dissociable neural responses facial expres-sions of sadness and anger. Brain, 122, 883–893.
Blakemore, C. (1977). Mechanics of the mind. Cambridge,United Kingdom: Cambridge University Press.
Blumer, D., & Benson, D. F. (1975). Personality changes withfrontal and temporal lobe lesions. In D. F. Benson & D. Blumer (Eds.), Psychiatric aspects of neurological disease(pp. 151–170). New York: Grune & Stratton.
Boles, D. B. (2005). A large-sample study of sex differences infunctional cerebral lateralization. Journal of Clinical andExperimental Neuropsychology, 27, 759–768.
Boller, F., & Vignolo, L. A. (1966). Latent sensory aphasia inhemisphere-damaged patients: An experimental studywith the Token Test. Brain, 89, 815–831.
Bornstein, R. A., King, G., & Carroll, A. (1983). Neuro-psychological abnormalities in Gilles de la Tourette’s syndrome. Journal of Nervous and Mental Disease, 171,497–502.
Borod, J. C. (1993). Cerebral mechanisms underlying facial,prosodic and lexical emotional expression: A review ofneuropsychological studies and methodological issues.Neuropsychology, 445–463.
Borod, J. C., Haywood, C. S., & Koff, E. (1997). Neuro-psychological aspects of facial asymmetry during emotionalexpression: A review of the normal adult literature.Neuropsychology Review, 7, 41–60.
Bourne, G. H. (1973). Lipofuscin. In D. H. Ford (Ed.),Neurobiological aspects of maturation and aging(pp. 189–201). Amsterdam: Elsevier.
Bowen, D. M., Benton, J. S., Spillane, J. A., Smith, C. C., &Allen, S. J. (1982). Choline acetyltransferase activity andhistopathology of frontal neocortex from biopsies of dementedpatients. Journal of Neurological Science, 57, 191–202.
Bowirrat, A., Treves, T. A., Friedland, R. P., & Korczyn, A. D.(2001). Prevalence of Alzheimer’s type dementia in anelderly Arab population. European Journal of Neurology,8(2), 119–123.
Bradshaw, J. L. (2001). Developmental disorders of the frontostri-atal system: Neuropsychological, neuropsychiatric and evolu-tionary perspectives. Philadelphia: Taylor & Francis.
Bradshaw, J. L., & Mattingly, J. B. (1995). Clinical neuropsy-chology: behavioral and brain science. San Diego, CA:Academic Press.
Brandt, J. A., & Bylsma, F. W. (1993). The dementia ofHuntington’s disease. In R. W. Parks, R. F. Zec, & R. S.Wilson (Eds.), Neuropsychology of Alzheimer’s disease andother dementias (pp. 265–282). New York: OxfordUniversity Press.
Brazier, M. A. (1959). The historical development of neuro-physiology. In J. Field, H. W. Magoun, & V. E. Hall(Eds.), Handbook of physiology (Vol. 1). Washington, DC:American Physiological Society.
Breen, N., Caine, D., & Coltheart, M. (2001). Mirrored-selfmisidentification: Two cases of focal onset dementia.Neurocase, 7(3), 239–254.
Bressler, S. L., Coppola, R., & Nakamura, R. (1993). Episodicmultiregional cortical coherence at multiple frequenciesduring visual task performance. Nature, 366, 153–156.
Brewer, V. R., Fletcher, J. M., Hiscock, M., & Davidson, K. C.(2001). Attention processes in children with shuntedhydrocephalus versus attention deficit-hyperactivity disor-der. Neuropsychology, 15, 185–198.
Brickenkamp, R., & Zillmer, E. A. (1998). d2 Test of Attention.Göttingen, Germany: Hogrefe & Huber.
Broca, P. (1861). Perte de la parole. Bulletin de la SociétéAnthropologique, 2, 235–238.
480 References

Brodal, A. (1981). Neuroanatomy in relation to clinical medicine(3rd ed.). New York: Oxford University Press.
Brodmann, K. (1909). Vergleichende Lokalisationslehre derGrosshirnrinde in ihren Prinzipien dargestellt auf Grund desZellenbaues. Leipzig: Barth.
Brookshire, B. L., Fletcher, J. M., Bohan, T. P., Landry, S. H.,Davidson, K. C., & Francis, D. J. (1995). Verbal andnonverbal skill discrepancies in children with hydro-cephalus: A five-year longitudinal follow-up. Journal ofPediatric Psychology, 20, 785–800.
Brown, A. S. (2003). A review of the deja vu experience.Psychological Bulletin, 129(3), 394–413.
Brown, G., Baird, A. D., & Shatz, M. W. (1986). The effectsof cerebrovascular disease and its treatment on higher cor-tical functioning. In I. Grant & K. M. Adams (Eds.),Neuropsychological assessment of neuropsychiatric disorders.New York: Oxford University Press.
Brown, G. L., & Linnoila, M. I. (1990). CSF serotoninmetabolite 5-HIAA studies in depression, impulsivity, andviolence. Journal of Clinical Psychiatry, 54, 31–41.
Brown, R. T., & Ivers, C. E. (1999). Gilles de la Tourette syn-drome. In S. Goldstein & C. R. Reynolds (Eds.),Handbook of neurodevelopmental and genetic disorders inchildren (pp. 185–215). New York: Guilford Press.
Brown, W. E., Kesler, S. R., Eliez, S., Warsofsky, I. S.,Haberecht, M., Patwardhan, A., et al. (2002). Brain devel-opment in Turner syndrome: A magnetic resonance imag-ing study. Psychiatry Research: Neuroimaging, 116, 187–196.
Bruce, D. (1985). On the origin of the term “neuropsychology.”Neuropsychologia, 28, 813–814.
Buchanan, L., Pavlovic, J., & Rovet, J. (1998). A reexamina-tion of the visuospatial deficit in Turner syndrome:Contributions of working memory. DevelopmentalNeuropsychology, 14, 341–368.
Bundick, W. T., Zillmer, E. A., Ives, D., & Beadle-Lindsay, M.(1995). Neurobehavioral sequelae and neurological compli-cations of acute Lyme disease: Case studies of two adults.Advances in Medical Psychotherapy and Psychodiagnosis, 8,145–160.
Burns, A., Jacoby, R., & Levy, R. (1991). Computed tomogra-phy in Alzheimer’s disease: A longitudinal study.Biological Psychiatry, 29, 383–390.
Burt, A. M. (1993). Textbook of neuroanatomy. Philadelphia: W. B. Saunders.
Burton, E. J., McKeith, I. G., Burn, D. J., Williams, E. D., &O’Brien, J. T. (2004). Cerebral atrophy in Parkinson’sdisease with and without dementia: A comparison withAlzheimer’s disease, dementia with Lewy bodies andcontrols. Brain, 127(Pt 4), 791–800.
Burton, L. A., Henninger, D., & Hafetz, J. (2005). Genderdifferences in relations of mental rotation, verbal fluency,and SAT scores to finger length ratios and hormonalindexes. Developmental Neuropsychology, 28, 493–506.
Butters, N., Salmon, D. P., Munro Culum, C., Cairns, P.,Troster, A. I., Jacobs, D., et al. (1988). Differentiation of
amnestic and demented patients with the WechslerMemory Scale-Revised. The Clinical Neuropsychologist, 2,133–148.
Cabeza, R., & Nyberg, L. (2000). Imaging cognition II: Anempirical review of 275 PET and fMRI studies. Journal ofCognitive Neuroscience, 12, 1–47.
Cahill, L., Haier, R. J., White, N. S., Fallon, J., Kilpatrick, L.,Lawrence, C., et al. (2001). Sex-related difference inamygdala activity during emotionally influenced memorystorage. Neurobiology of Learning and Memory, 75, 1–9.
Cahill, L., & McGaugh, J. L. (1998). Mechanisms of emotionalarousal and lasting declarative memory. Trends inNeuroscience, 21, 294–299.
Cajal, R. (1937). Recollections of my life. Memoirs of theAmerican Philosophical Society (Vol. 8). (Original workpublished 1901–1917.). Boston: MIT Press.
Cameron, J. L. (2001). Effects of sex hormones on brain devel-opment. In C. A. Nelson & M. Luciana (Eds.),Handbook of developmental cognitive neuroscience(pp. 59–78). Cambridge, MA: MIT Press.
Canfield, R. L., Gendle, M. H., & Cory-Slechta, D. A.(2004). Impaired neuropsychological functioning in lead-exposed children. Developmental Neuropsychology, 26,513–540.
Canfield, R. L., Henderson, C. R., Cory-Slechta, D. A., Cox,C., Jusko, T. A., & Lanphear, B. P. (2003). Intellectualimpairment in children with blood lead concentrationsbelow 10 µg per deciliter. New England Journal ofMedicine, 348, 1517–1526.
Cannon, W. B. (1927). The James-Lange theory of emotion: Acritical examination and an alternative theory. AmericanJournal of Psychology, 39, 106–124.
Cantu, R. C., & Mueller, F. O. (2003). Brain injury-relatedfatalities in American football, 1945–1999. Neurosurgery,52(4), 846–853.
Cantwell, D. P. (1996). Attention deficit disorder: A review ofthe past 10 years. Journal of Child and AdolescentPsychiatry, 35, 978–987.
Cardon, L. R., DeFries, J. C., Fulker, D. W., Kimberling, W. J., Pennington, B. F., & Smith, S. D. (1994).Quantitative trait locus for reading disability on chromo-some 6. Science, 265, 276–279.
Carey, M. E., Barakat, L. P., Foley, B., Gyato, K., & Phillips, P. C.(2001). Neuropsychological functioning and social func-tioning of survivors of pediatric brain tumors: Evidence ofnonverbal learning disability. Child Neuropsychology, 7(4),265–272.
Carlson, N., & Buskist, W. (1994). The science of behavior (5thed.). Boston: Allyn & Bacon.
Carlson-Green, B., Morris, R. D., & Krawiecki, N. (1995).Family and illness predictors of outcome in pediatricbrain tumors. Journal of Pediatric Psychology, 206,769–784.
Carmichael Olson, H., Streissguth, A. P., Sampson, P. D., Barr,H. M., Bookstein, F. L., & Thiede, K. (1997). Association
References 481

of prenatal alcohol exposure with behavioral and learningproblems in early adolescence. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 36,1187–1194.
Carpenter, M. K., Mattson, M., & Rao, M. S. (2003). Sourcesof cells for CNS therapy. In T. Zigova, E. Snyder, & R. Sanberg (Eds.), Neural stem cells for brain and spinalcord repair (pp. 1–44). Totowa, NJ: Humana Press.
Cartwright, R. D., Kravits, D. O., Eastman, C. I., & Wood, E. (1991). REM latency and the recovery from depression:Getting over divorce. American Journal of Psychiatry, 148,1530–1535.
Cartwright, R. D., Lloyd, S., Knight, S., & Trenholme, I.(1984). Broken dreams: A study of the effects of divorceand depression on dream content. Psychiatry, 47,251–259.
Cascino, G. D. (1992). Complex partial seizures: Clinical fea-tures and differential diagnosis. Psychiatric Clinics of NorthAmerica, 152, 373–382.
Casey, B. J., Castellanos, F. X., Giedd, J. N., Marsh, W. L.,Hamburger, S. D., Schubert, A. B., et al. (1997).Implication of right frontostriatal circuitry in responseinhibition and attention-deficit hyperactivity disorder.Journal of Child Psychology and Psychiatry, 36, 374–383.
Casey, B. J., Giedd, J. N., & Thomas, K. M. (2000).Structural and functional brain development and its rela-tion to cognitive development. Biological Psychology, 54,241–257.
Casey, B. J., Tottenham, N., & Fossella, J. (2002). Clinical, imag-ing, lesion, and genetic approaches toward a model of cog-nitive control. Developmental Psychobiology, 40, 237–254.
Castellanos, F. X. (1997). Toward a pathophysiology ofattention-deficit hyperactivity disorder. Clinical Pediatrics,36, 381–393.
Castellanos, F. X., Giedd, J. N., Berquin, P. C., Walter, J. M.,Sharp, W. Tran, T., et al. (2001). Quantitative brain mag-netic resonance imaging in girls with attention-deficit/hyperactivity disorder. Archives of GeneralPsychiatry, 58, 289–295.
Castellanos, F. X., Giedds, J. N., Eckburg, P., Marsh, W. L.,Vaituzis, C. V., Kaysen, D., et al. (1994). Quantitativemorphology of the caudate nucleus in attention deficithyperactivity disorder. American Journal of Psychiatry, 151,279–281.
Castellanos, F. X., Giedds, J. N., Marsh, W. L., Hamburger, S. D., Vaituzis, A. C., Dickstein, D. P., et al. (1996).Quantitative brain magnetic resonance imaging inattention-deficit hyperactivity disorder. Archives of GeneralPsychiatry, 53, 607–616.
Catts, H. W., Gillispie, M., Leonard, L. B., Kail, R. V., &Miller, C. A. (2002). The role of speed of processing, rapidnaming, and phonological awareness in reading achieve-ment. Journal of Learning Disabilities, 35, 510–525.
Cenci, M. A., Kalen, P., Mandel, R. J., & Bjoerklund, A.(1992). Regional differences in the regulation of dopamine
and noradrenaline release in the medial frontal cortex,nucleus accumbens and caudate-putamen: A microdialysisstudy in the rat. Brain Research, 581, 217–228.
Centers for Disease Control and Prevention. (1997). Sport-relatedrecurrent brain injuries—United States. JAMA: The Journalof the American Medical Association, 277, 1190–1192.
Chalmers, D. J. (1996). The conscious mind: In search of a fun-damental theory. New York: Oxford University Press.
Changeux, J. P., & Chavaillon, J. (1995). Origins of the humanbrain. Oxford, United Kingdom: Clarendon Press.
Channon, S., Pratt, P., & Robertson, M. M. (2003). Executivefunction, memory, and learning in Tourette’s syndrome.Neuropsychology, 17, 247–254.
Chapman, L. F., & Wolff, H. (1959). The cerebral hemi-spheres and the highest integrative functions of man.Archives of Neurology, 1, 357.
Charman, T. (1997). The relationship between joint attentionand pretend play in autism. Development andPsychopathology, 9, 1–16.
Checkoway, H., & Nelson, L. M. (1999). Epidemiologicapproaches to the study of Parkinson’s disease etiology.Epidemiology, 10(3), 327–336.
Chen, W. J., Maier, S., Parnell, S. E., & West, J. R. (2004).Alcohol and the developing brain: Neuroanatomical studies.Retrieved September 2005, from the National Institute ofAlcohol Abuse and Alcoholism of the National Institute ofHealth Web site: http://pubs.niaaa.nih.gov/publications/arh27-2/174-180.htm
Chow, T. W., & Cummings, J. L. (1999). Frontal-subcorticalcircuits. In B. L. Miller & J. L. Cummings (Eds.), Thehuman frontal lobes: Functions and disorders (pp. 3–26).New York: Guilford Press.
Christensen, A. L. (1979). Luria’s neuropsychological investiga-tion (2nd ed.). Copenhagen: Munksgaard.
Chugani, H., Muller, R., & Chugani, D. (1996). Functionalbrain organization in children. Brain & Development, 18,347–356.
Churchland, P. S. (1993). Neurophilosophy: Toward a unifiedscience of the mind/brain. Cambridge, MA: MIT Press.
Chusid, J. G. (1982). Correlative neuroanatomy and functionalneurology. Los Altos, CA: Lange Medical.
Ciesielski, K. T., & Harris, R. J. (1997). Factors related to per-formance failure on executive tasks in autism. ChildNeuropsychology, 3, 1–12.
Cirino, P., Chapieski, L., & Massman, P. (2000). Card sortingperformance and ADHD symptomatology in childrenand adolescents with Tourette syndrome. Journal ofClinical and Experimental Neuropsychology, 22, 245–257.
Civin, C. I. (2002). Commitment to biomedical research:Clearing unnecessary impediments to progress. Stem Cells,20(6), 482–484.
Cohen, D. J., & Leckman, J. F. (1994). Developmental psy-chopathology and neurobiology of Tourette’s syndrome.Journal of the Academy of Child and Adolescent Psychiatry,33, 2–15.
482 References

Cohen, J. D., Aston-Jones, G., & Gilzenrat, M. S. (2004). A system-level perspective on attention and cognitive con-trol: Guided activation, adaptive gating, conflict monitor-ing, and exploitation versus exploration. In M. I. Posner(Ed.), Cognitive neuroscience of attention (pp. 74–76). NewYork: Guilford Press.
Cohen, J. D., Noll, D. C., & Schneider, W. (1993).Functional magnetic resonance imaging: Overview andmethods for psychological research. Behavior ResearchMethods, Instruments, & Computers, 25, 101–113.
Cohen, L. G., Celnik, P., Pascual-Leone, A., Corwell, B., Falz, L., Dambrosia, J., et al. (1997). Functional relevance of cross-modal plasticity in blind humans. Nature, 389, 180–183.
Cohen, N. J. (1984). Preserved learning capacity in amnesia:Evidence for multiple memory systems. In L. R. Squire &N. Butters (Eds.), Neuropsychology of memory. New York:Guilford Press.
Cohen, R. A. (1993). The neuropsychology of attention. NewYork: Plenum Press.
Colcombe, S., & Kramer, A. F. (2003). Fitness effects on thecognitive function of older adults: A meta-analytic study.Psychological Science, 14(2), 125–130.
Colcombe, S. J., Erickson, K. I., Raz, N., Webb, A. G.,Cohen, N. J., McAuley, E., et al. (2003). Aerobic fitnessreduces brain tissue loss in aging humans. Journals ofGerontology. Series A, Biological Sciences and MedicalSciences, 58(2), 176–180.
Committee on the Biological and Biomedical Applications ofStem Cell Research. (2002). Stem cells and the future ofregenerative medicine. Retrieved October 17, 2006, fromhttp://www.nap.edu/openbook/0309076307/html/7.html.
Connor, P. D., Sampson, P. D., Bookstein, F. L., Barr, H. M.,& Streissguth, A. P. (2000). Direct and indirect effects ofprenatal alcohol damage on executive function.Developmental Neuropsychology, 18, 331–354.
Corder, E. H., Saunders, A. M., Strittmatter, W. J., Schmechel,D. E., Gaskell, P. C., Small, G. W., et al. (1993). Gene doseof apolipoprotein E type 4 allele and the risk of Alzheimer’sdisease in late onset families. Science, 261, 921–923.
Corkin, S. (1965). Tactually guided maze learning in man.Effects of unilateral cortical excisions and bilateral hip-pocampal lesions. Neuropsychologia, 3, 339.
Corn, B. W., Yousem, D. M., Scott, C. B., Rotman, M.,Asbell, S. O., Nelson, D. F., et al. (1994). White matterchanges are correlated significantly with radiation dose.Cancer, 74, 2828–2835.
Corwin, J., & Bylsma, F. W. (1993). Translations of excerptsfrom André Rey’s Psychological examination of traumaticencephalopathy and P. A. Osterrieth’s Complex FigureCopy Test. The Clinical Neuropsychologist, 7, 3–15.
Costello, E. J., Angold, A., Burns, B. J., Stangl, D. K., Tweed,D. L., Erkanli, A., et al. (1996). The Great SmokeyMountains study of youth, goals, design, methods, andthe prevalence of DSM-III-R disorders. Archives ofGeneral Psychiatry, 53, 1129–1136.
Courchesne, E., Carper, R., & Akshoomoff, N. (2003).Evidence of brain overgrowth in the first year of life inautism. Journal of the American Medical Association, 290,337–344.
Courchesne, E., Townsend, J. P., & Saitoh, O. (1994). Thebrain in infantile autism: Posterior fossa structures areabnormal. Neurology, 44, 214–223.
Covassin, T., Swanik, C. B., & Sachs, M. L. (2003).Epidemiological considerations of concussions amongintercollegiate athletes. Applied Neuropsychology, 10(1),12–22.
Cowan, W. C. (1979). The developing brain. In W. C. Cowan(Ed.), The brain (pp. 56–69). San Francisco: W. H. Freeman.
Cowan, W. M. (1990). The development of the brain. In R. R. Llinas (Ed.), The workings of the brain: Development,memory, and perception. New York: W. H. Freeman.
Cowart, B. J., Young, I. M., Feldman, R. S., & Lowry, L. D.(1997). Clinical disorders of smell and taste. In G. K. Beauchamp & L. Bartoshuk (Eds.), Tasting andsmelling. San Diego: Academic Press.
Coyle, J. T. (1985). The cholinergic systems in psychiatry. InR. E. Hales & A. J. Frances (Eds.), Psychiatry update:American Psychiatric Association annual review (Vol. 4).Washington, DC: American Psychiatric Press.
Crick, F., & Koch, C. (1990). Towards a neurobiological theoryof consciousness. Seminars in the Neurosciences, 2, 263–275.
Crosson, B. (1992). Subcortical functions in language and mem-ory. New York: Guilford Press.
Culbertson, J. L., & Edmonds, J. E. (1996). Learning disabili-ties. In R. L. Adams, O. A. Parsons, J. L. Culbertson, &S. J. Nixon (Eds.), Neuropsychology for clinical practice:Etiology, assessment, and treatment of common neurologicaldisorders (pp. 331–408). Washington, DC: AmericanPsychological Association.
Culbertson, W., & Zillmer, E. A. (2005). TOL-DX Tower ofLondon-Drexel University (2nd ed.). Toronto, Ontario:Multi-Health Systems.
Culbertson, W. C., & Zillmer, E. A. (1998a). The constructvalidity of the Tower of London-Drexel University as ameasure of the executive functioning of ADHD children.Assessment, 5, 215–226.
Culbertson, W. C., & Zillmer, E. A. (1998b). The Tower ofLondonDX: A standardized approach to assessing execu-tive functioning in children. Archives of ClinicalNeuropsychology, 13, 285–301.
Cullum, C. M., Harris, J. G., Waldo, M., Smernoff, E., Madison, A., Nagamoto, H., et al. (1993).Neurophysiological and neuropsychological evidence forattentional dysfunction in schizophrenia. SchizophreniaResearch, 10, 131–141.
Cummings, J. L. (1986). Subcortical dementia: Neuropsychology,neuropsychiatry, and pathophysiology. British Journal ofPsychiatry, 149, 682–697.
Cummings, J. L. (1993). Frontal-subcortical circuits andhuman behavior. Archives of Neurology, 50, 873–880.
References 483

Cummings, J. L. (1994). Depression in neurologic diseases.Psychiatric Annals, 24, 525–531.
Cummings, J. L., Benson, D. F., Hill, M., & Read, S. (1985).Aphasia in dementia of the Alzheimer type. Neurology, 35,394–397.
Cytowic, R. E. (1993). The man who tasted shapes: A bizarremedical mystery offers revolutionary insights into reasoning,emotion, and consciousness. New York: Putnam.
Dahl, J., Brorson, L. O., & Melin, L. (1992). Effects of abroad-spectrum behavioral medicine treatment programon children with refractory epileptic seizures: An 8-yearfollow-up. Epilepsia, 33(1), 98–102.
Dahl, J., Melin, L., & Lund, L. (1987). Effects of a contingentrelaxation treatment program on adults with refractoryepileptic seizures. Epilepsia, 28(2), 125–132.
Daly, E., Zaitchik, D., Copeland, M., Schmahmann, J.,Gunther, J., & Albert, M. (2000). Predicting conversionto Alzheimer disease using standardized clinical informa-tion. Archives of Neurology, 57(5), 675–680.
Daly, G., Hawi, Z., Fitzgerald, M., & Gill, M. (1999).Mapping susceptibility loci in attention deficit hyperactiv-ity disorder: Preferential transmission of parental alleles atDAT1, DBH, and DRD5 to affected children. MolecularPsychiatry, 4, 192–196.
Damasio, A. R. (1994). Descartes’ error. New York: Putnam.Damasio, A. R. (1998). The somatic marker hypothesis and the
possible functions of the prefrontal cortex. In A. C.Roberts, T. W. Robbins, & L. Weiskrantz (Eds.), The pre-frontal cortex: Executive and cognitive functions (pp. 36–50).New York: Oxford University Press.
Damasio, A. R., Tranel, D., & Damasio, H. (1990).Individuals with sociopathic behavior caused by frontaldamage fail to respond autonomically to social stimuli.Behavioural Brain Research, 41, 81–94.
Damasio, H., Grabowski, T., Frank, R., Galaburda, A. M., &Damasio, A. M. (1994). The return of Phineas Gage:Clues about the brain from the skull of a famous patient.Science, 264, 1102–1105.
D’Andrea, E. A., & Spiers, M. V. (2005a). The effect of famil-ial sinistrality and academic experience on cognition inright-handed women. Neuropsychology, 19, 657–663.
D’Andrea, E. A., & Spiers, M. V. (2005b, October 27).Hormones, cognitive performance, and individual differences.Paper presented at the Graylyn Conference on Women’sCognitive Health, Winston-Salem, NC.
Danta, G., & Hilton, R. (1975). Judgement of the visual verti-cal and horizontal in patients with Parkinsons. Neurology,25, 43–47.
Darwin, C. (1968). On the origin of species. (Originally pub-lished in 1859.) New York: Penguin Books.
Davidson, R. J. (1994). Temperament, affective style, and frontallobe asymmetry. In G. Dawson & K. W. Fischer (Eds.),Human brain and the developing brain (pp. 518–537). NewYork: Guilford Press.
Dawson, M. E., & Nuechterlein, K. H. (1984). Psycho-physiological dysfunctions in the developmental course of
schizophrenic disorders. Schizophrenia Bulletin, 102,204–232.
Dean, R. S., & Reynolds, C. R. (1997). Cognitive processingand self-reported lateral preference. NeuropsychologyReview, 7, 127–142.
DeAngelis, L., Delattre, J. Y., & Posner, J. (1989). Radiation-induced dementia in patients cured of brain metastases.Neurology, 39, 789–796.
Del Bigio, M. R. (2004). Cellular damage and prevention inchildhood hydrocephalus. Brain Pathology, 14, 317–324.
Demb, J. B., Boynton, G. M., Best, M., & Heeger, D. J.(1998). Psychophysical evidence for a magnocellular pathway deficit in dyslexia. Vision Research, 38,1555–1560.
Denckla, M. B. (1996). A theory and model of executive func-tion: A neuropsychological perspective. In G. R. Lyon &N. A. Krasnegor (Eds.), Attention, memory, and executivefunction (pp. 263–278). Baltimore: Paul H. Brookes.
Denckla, M. B., & Reiss, A. L. (1997). Prefrontal-subcorticalcircuits in developmental disorders. In N. A. Krasnegor,G. R. Lyon, & P. S. Goldman-Rakic (Eds.), Developmentof the prefrontal cortex: Evolution, neurobiology, and behav-ior (pp. 283–294). Baltimore: Paul H. Brookes.
Dennis, M., & Barnes, M. (1994). Developmental aspects ofneuropsychology: Childhood. In D. W. Zaidel (Ed.),Neuropsychology (2nd ed., pp. 219–246). New York:Academic Press.
Department of Health and Human Services. (2001). Stemcells: Scientific progress and future research directions.Retrieved October 17, 2006, from http://stemcells.nih.gov/info/scireport/2001report.htm
Deruelle, C., Mancini, J., Livet, M. O., Casse-Perrot, C., & de Schonen, S. (1999). Configural and local processing offaces in children with Williams syndrome. Brain andCognition, 41, 276–298.
Devinsky, O. (1983). Neuroanatomy of Gilles de la Tourette’ssyndrome. Archives of Neurology, 5, 447–453.
Devinsky, O., Morrell, M. J., & Vogt, B. A. (1995).Contributions of anterior cingulated cortex to behaviour.Brain, 118, 279–306.
Diamond, A. (1981). Retrieval of an object from an open box:The development of visual-tactile control of reaching inthe first year of life. Society for Research in ChildDevelopment Abstracts, 3, 78.
Diamond, A. (1991). Neuropsychological insights into themeaning of object concept development. In S. Carey &R. Gelman (Eds.), The epigenesis of mind: Essays on biologyand cognition (pp. 67–110). Hillsdale, NJ: Erlbaum.
Diamond, A. (2000). Close interrelation of motor develop-ment and cognitive development of the cerebellum andprefrontal cortex. Child Development, 71, 44–56.
Diamond, A., & Gilbert, J. (1989). Development as progres-sive inhibitory control of action: Retrieval of a contiguousobject. Cognitive Development, 12, 223–249.
Dickens, C. (1849). David Copperfield. Oxford: Oxford WorldClassics.
484 References

Diller, L. (1994). Finding the right treatment combinations:Changes in rehabilitation over the past five years. In A. Christensen & B. P. Uzzell (Eds.), Brain injury andneuropsychological rehabilitation: International perspectives.Hillsdale, NJ: Erlbaum.
Dool, C. B., Stelmack, R. M., & Rourke, B. P. (1993). Event-related potentials in children with learning disabilities.Journal of Clinical Child Psychology, 22, 387–398.
Doty, R. L. (1990). Olfaction. In F. Boller & J. Grafman (Eds.),Handbook of neuropsychology (Vol. 4). Amsterdam: Elsevier.
Doty, R. L., Shaman, P., & Dann, M. (1984). Development ofthe University of Pennsylvania Smell Identification Test: A standard microencapsulated test of olfactory function.Physiology of Behavior, 32, 489–502.
Douglas, R. J., & Pribram, K. H. (1966). Learning aids andlimbic lesions. Neuropsychologia, 4, 197.
Dr. Robert Ley’s brain. (1946). Medical Record, 159, 188.Drachmann, D. A. (1977). Memory function in man: Does
the cholinergic system have a specific role? Neurology, 27,783–790.
Drake, E. B., Henderson, V. W., Stanczyk, F. Z., McCleary, C. A., Brown, W. S., Smith, C. A., et al. (2000).Associations between circulating sex steroid hormones andcognition in normal elderly women. Neurology, 54, 599.
Dubb, A., Gur, R., Avants, B., & Gee, J. (2003). Character-ization of sexual dimorphism in the human corpus callosum. NeuroImage, 20, 512–519.
Dubois, B., Boller, F., Pillon, B., & Agid, Y. (1991). Cognitivedeficits in Parkinson’s disease. In S. Corkin, J. Grafman,& F. Boller (Eds.), Handbook of neuropsychology (Vol. 5,pp. 195–240). Amsterdam: Elsevier.
Duffy, F. H. (1989). Clinical value of topographic mappingand quantified neurophysiology. Archives of Neurology, 46,1133–1135.
Duffy, J. D., & Campbell, J. J. (2001). Regional prefrontalsyndromes: A theoretical and clinical overview. In S. P.Salloway, P. F. Malloy, & J. D. Duffy (Eds.), The frontallobes and neuropsychiatric illness (pp. 113–123).Washington, DC: American Psychiatric Publishing.
Dunnet, S. B. (1991). Neural transplants as a treatment forAlzheimer’s disease? Psychological Medicine, 21, 825–830.
Dychtwald, K., & Flower, J. (1989). Age wave: The challengesand opportunities of an aging America. Los Angeles: Tarcher.
Dykens, E. M. (2003). Anxiety, fears, and phobias in personswith Williams syndrome. Developmental Neuropsychology,23, 291–316.
Eals, M., & Silverman, I. (1994). The hunter-gatherer theoryof spatial sex differences: Proximate factors mediating thefemale advantage in recall of object arrays. Ethology andSociobiology, 15, 95–105.
Ebers, G. C., & Sadovnick, A. D. (1993). The geographic dis-tribution of multiple sclerosis. Neuroepidemiology, 12, 1–5.
Echemendia, R. J., & Cantu, R. C. (2003). Return to play fol-lowing sports-related mild traumatic brain injury: Therole for neuropsychology. Applied Neuropsychology, 10(1),48–55.
Eden, G. F., Stein, J. F., Wood, M. H., & Wood, F. B. (1995).Verbal and visual problems in reading disability. Journalof Learning Disabilities, 28, 272–290.
Efron, R. (1957). The conditioned inhibition of uncinate fits.Brain, 80, 251–262.
Ehlers, S., Nyden, A., Gillberg, C., Sandberg, A. D., Dahlgren,S. O., Hjlemquist, E., et al. (1997). Asperger’s syndrome,autism and attention disorders: A comparative study ofthe cognitive profiles of 120 children. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 38,207–217.
Eiraldi, R. B., Power, T. J., & Nezu, C. M. (1997). Patterns ofcomorbidity associated with subtypes of attention-deficit/hyperactivity disorder among 6- to 12-year-old children.Journal of the American Academy of Child and AdolescentPsychiatry, 36, 503–514.
Eisenmajer, R., Prior, M., Leekam, S., Wing, L., Gould, J.,Gelham, M., et al. (1996). Comparison of clinical symp-toms in autism and Asperger’s disorder. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 35,1523–1531.
El-Hai, J. (2005). The lobotomist: A maverick medical geniusand his tragic quest to rid the world of mental illness.Hoboken, NJ: John Wiley & Sons.
Elliott, F. A. (1992). Violence-the neurologic contribution: Anoverview. Archives of Neurology, 49, 595–603.
Elliott, T. K., Watkins, J. M., Messa, C., Lippe, B., &Chugani, H. (1996). Positron emission tomography andneuropsychological correlations in children with Turner’ssyndrome. Developmental Neuropsychology, 12, 365–386.
Elsass, L., & Kinsella, G. (1987). Social interaction followingsevere closed head injury. Psychological Medicine, 17,67–78.
England, M. A., & Wakely, J. (1991). Brain and spinal cord:An introduction to normal neuro-anatomy. Aylesbury,United Kingdom: Mosby-Wolfe.
Epel, E. S., Blackburn, E. H., Lin, J., Dhabhar, F. S., Adler, N. E., Morrow, J. D., et al. (2004). Accelerated telomereshortening in response to life stress. Proceedings of theNational Academy of Sciences of the United States ofAmerica, 101(49), 17312–17315.
Epilepsy Foundation. (n.d.). Epilepsy and seizure statistics, 2005, from www.epilepsyfoundation.org/answerplace/statistics. cfm.
Erickson, K., Baron, I. S., & Fantie, B. D. (2001). Neuro-psychological function in early hydrocephalus: Reviewfrom a developmental perspective. Child Neuropsychology,7, 199–229.
Erickson, K., Colcombe, S., Elavsky, S., McAuley, E., Korol,D., Scalf, P., et al. (2005). Interactive effects of fitness and duration of hormone treatment on prefrontal cortexvolume and executive function. Journal of CognitiveNeuroscience, D101(Suppl.), 123.
Erlanger, D. M., Kutner, K. C., & Jacobs, A. R. (1999).Hormones and cognition: Current concepts and issues inneuropsychology. Neuropsychology Review, 9, 175–207.
References 485

Ernst, M., Cohen, R. M., Liebenauer, M. A., Jons, P. H., &Zametkin, A. J. (1997). Cerebral glucose metabolism inadolescent girls with attention-deficit/hyperactivity disor-der. Journal of the American Academy of Child andAdolescent Psychiatry, 36, 1399–1406.
Ernst, M., Liebenauer, L. L., Jons, P. H., & Zametkin, A. J.(1994). Cerebral glucose metabolism in adolescent girlswith attention-deficit/hyperctivity disorder. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 36,1399–1406.
Ernst, M., Liebenauer, L. L., King, A. C., Fitzgerald, G. A.,Cohen, R. M., & Zametkin, A. J. (1994). Reduced brain metabolism in hyperactive girls. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 33,858–868.
Esiri, M. (1994). Dementia and normal aging: Neuropathology.In F. A. Huppert, C. Brayne, & D. W. O’Connor (Eds.),Dementia and normal aging (pp. 385–436). Cambridge,United Kingdom: Cambridge University Press.
Eslinger, P. J. (1996). Conceptualizing, describing, and measuringcomponents of executive function: A summary. In G. R.Lyon & N. A. Krasnegor (Eds.), Attention, memory, and exec-utive function (pp. 367–396). Baltimore: Paul H. Brookes.
Eslinger, P. J. (1998). Neurological and neuropsychologicalbases of empathy. European Neurology, 39, 193–199.
Eslinger, P. J., Biddle, K. R., & Grattan, L. M. (1997).Cognitive and social development in children with pre-frontal cortex lesions. In N. A. Krasnegor, G. R. Lyon, &P. S. Goldman-Rakic (Eds.), Development of the prefrontalcortex: Evolution, neurobiology, and behavior (pp. 295–336).Baltimore: Paul H. Brookes.
Eslinger, P. J., Flaherty-Craig, C. V., & Benton, A. L. (2004).Developmental outcomes after early prefrontal cortexdamage. Brain and Cognition, 55, 84–103.
Espeland, M. A., Rapp, S. R., Shumaker, S. A., Brunner, R.,Manson, J. E., Sherwin, B. B., et al. (2004). Conjugatedequine estrogens and global cognitive function in post-menopausal women. Journal of the American MedicalAssociation, 291, 2959–2968.
Espy, K. A., Kaufmann, P. M., Glisky, M. L., & McDiarmid, M. D. (2001). New procedures to assess the executive func-tions in preschool children. The Clinical Neuropsychologist,15, 46–58.
Ewing-Cobbs, L., Barnes, M. A., & Fletcher, J. M. (2003). Earlybrain injury in children: Development and reorganizationof cognitive function. Developmental Neuropsychology, 24,669–704.
Fan, J., McCandliss, B. D., Sommer, T., Raz, A., & Posner, M. I. (2002). Testing the efficiency and independence ofattentional networks. Journal of Cognitive Neuroscience,14, 340–347.
Farah, M. J. (1990). Visual agnosia: Disorders of object visionand what they tell us about normal vision. Cambridge, MA:MIT Press/Bradford.
Faraone, S. V., & Biederman, J. (2004). Neurobiology of atten-tion deficit hyperactivity disorder. In D. S. Charney &
E. J. Nestler (Eds.), Neurobiology of mental illness (2nded., pp. 979–999). New York: Oxford University Press.
Farran, E. K., & Jarrold, C. (2003). Visuospatial cognition inWilliams syndrome: Reviewing and accounting for thestrengths and weaknesses in performance. DevelopmentalNeuropsychology, 23, 173–200.
Farrer, L. A. (1986). Suicide and attempted suicide inHuntington’s disease: Implications of preclinical testingfor persons at risk. American Journal of Medical Genetics,24, 305–311.
Feifel, D. (1999). Neurotransmitters and neuromodulators infrontal-subcortical circuits. In B. L. Miller & J. L.Cummings (Eds.), The human frontal lobes: Functions anddisorders (pp. 174–186). New York: Guilford Press.
Fein, D., Joy, S., Green, L. A., & Waterhouse, L. (1996).Autism and pervasive developmental disorders. In B. S.Fogel, R. R. Schiffer, & S. M. Rao (Eds.), Neuropsychiatry(pp. 571–614). Philadelphia: Williams & Wilkins.
Feldman, R. S., Meyer, J. S., & Quenzer, L. F. (1997).Principles of neuropsychopharmacology. Sunderland, MA:Sinauer Associates.
Fernandez-Duque, D., & Posner, M. I. (2001). Brain imagingof attentional networks in normal and pathological states.Journal of Clinical and Experimental Neuropsychology, 23,74–93.
Fields, R. D., & Stevens-Graham, B. (2002). New insights intoneuron-glia communication. Science, 298, 556–562.
Filipek, P. A. (1995). Quantitative magnetic resonance imagingin autism: The cerebellar vermis. Current Opinion inNeurology, 8, 134–138.
Filipek, P. A. (1996). Structural variations in measures of developmental disorders. In R. W. Thatcher, G. R. Lyon, J. Rumsey, & N. Krasnegor (Eds.), Developmental neuroimaging: Mapping the development of brain andbehavior (pp. 169–186). San Diego, CA: Academic Press.
Filipek, P. A., Semrud-Clikeman, M., Steingard, R. J., Renshaw,P. F., Kennedy, D. N., & Biederman, J. (1997).Volumetric MRI analysis comparing subjects havingattention-deficit hyperactivity disorder with normal con-trols. Neurology, 48, 589–601.
Fisher, N. J., DeLuca, J. W., & Rourke, B. P. (1997).Wisconsin Card Sorting Test and Halstead Category Testperformances of children and adolescents who exhibit thesyndrome of nonverbal learning disabilities. ChildNeuropsychology, 3, 61–70.
Fisher, R. S., van Emde Boas, W., Blume, W., Elger, C.,Genton, P., Lee, P., & Engel, J. (2005). Epileptic seizuresand epilepsy: definitions proposed by the InternationalLeague Against Epilepsy (ILAE) and the InternationalBureau for Epilepsy (IBE). Epilepsia, 46(4), 470–472.
Fletcher, J. M., Brookshire, B. L., Landry, S. H., Bohan, T. P.,Davidson, K. C., Francis, D. J., et al. (1996). Attentionskills and executive functions in children with earlyhydrocephalus. Developmental Neuropsychology, 12, 53–76.
Fletcher, J. M., Dennis, M., & Northrup, H. (2000). Hydro-cephalus. In K. O. Yeater, M. D. Ris, & H. G. Taylor
486 References
(Eds.), Pediatric neuropsychology: Research, theory, andpractice (pp. 25–46). New York: Guilford Press.
Flicker, C., Ferris, S. H., & Reisberg, B. (1991). Mild cogni-tive impairment in the elderly: Predictors of dementia.Neurology, 41(7), 1006–1009.
Flowers, D. L., Wood, F. B., & Naylor, C. E. (1991). Regionalcerebral blood flow correlates of language processes inreading disability. Archives of Neurology, 48, 637–643.
Foley, B., Barakat, L. P., Herman-Liu, A., Radcliffe, J., &Molloy, P. (2000). The impact of childhood hypothalamic/chiasmatic brain tumors on child adjustment and familyfunctioning. Children’s Health Care, 29, 209–223.
Fombonne, E. (2001). Ask the editor: What is the prevalenceof Asperger disorder? Journal of Autism and DevelopmentalDisorders, 31, 363–364.
Fombonne, E. (2003a). Epidemiological surveys of autism andother pervasive developmental disorders: An update. Journalof Autism and Developmental Disorders, 33, 365–382.
Fombonne, E. (2003b). The prevalence of autism. Journal ofthe American Medical Association, 289, 87–89.
Fombonne, E., Bolton, P., Prior, J., Jordon, H., & Rutter, M. (1997). A family study of autism: Cognitive patternsand levels in parents and siblings. Journal of ChildPsychology and Psychiatry, 38, 667–684.
Ford, C. E., Jones, K. W., Polani, P. E., de Almeida, J. C., &Briggs, J. H. (1959). A sex-chromosome anomaly in acase of gonadal dysgenesis Turner syndrome. Lancet, 2,711–713.
Forrest, B. J. (2004). The utility of math difficulties, internalizedpsychopathology, and visual-spatial deficits to identify chil-dren with nonverbal learning disability syndrome: Evidencefor a visual-spatial disability. Child Neuropsychology, 10,129–146.
Forstl, H., & Hentschel, F. (1994). Contribution to the differ-ential diagnosis of dementias: Neuroimaging. Reviews inClinical Gerontology, 4, 317–341.
Fox, P. T., Ingham, R. J., Ingham, J. C., Hirsch, T. B., Downs,J. H., Martin, C., et al. (1996). A PET study of the neur-al systems of stuttering. Nature, 382, 158–161.
Frackowiak, R. S. (1996). Plasticity and the human brain:Insights from functional imaging. In E. L. Bjork & R. A. Bjork (Eds.), Memory. New York: Academic Press.
Freedman, A. M., Kaplan, H. I., & Sadock, B. J. (1978).Modern synopsis of comprehensive textbook of psychiatry II.Baltimore: Williams & Wilkins.
Freeman, W., & Watts, J. W. (1950). Psychosurgery in the treat-ment of mental disorders and intractable pain. Springfield,IL: Charles C. Thomas.
Freud, S. (1891). Zur Auffassung der Aphasien. Vienna:Deuticke.
Freud, S. (1959). On narcissism: An introduction. In S. Freud(Ed.), Collected papers (pp. 30–59). New York: BasicBooks.
Frith, U. (1989). Autism: Explaining the enigma. Cambridge,MA: Blackwell.
Frith, U. (1991). Asperger and his syndrome. In U. Frith (Ed.),Autism and Asperger syndrome (pp. 1–36). New York:Cambridge University Press.
Frost, J. A., Binder, J. R., Springer, J. A., Hammeke, T. A.,Bellgowan, P. S., Rao, S. M., Cox, R. W. (1999). Languageprocessing is strongly left lateralized in both sexes:Evidence from functional MRI. Brain, 122, 199–208.
Fuster, J. M. (1997). The prefrontal cortex: Anatomy, physiology,and neuropsychology of the frontal lobe (3rd ed.). New York:Lippincott-Raven.
Fuster, J. M. (2002). Physiology of executive functions: Theperception-action cycle. In D. T. Stuss & R. T. Knight(Eds.), Principles of frontal lobe function (pp. 96–108).New York: Oxford University Press.
Fuster, J. M., Van Hoesen, G. W., Morecraft, R. J., &Semendeferi, K. (2000). Executive systems. In B. S. Fogel,R. B. Schiffer, & S. M. Rao (Eds.), Synopsis of neuropsy-chiatry (pp. 229–244). Philadelphia: Lippincott Williams& Wilkins.
Gabrieli, J. D., Keane, M. M., & Corkin, S. (1987). Acquisitionof problem-solving skills in global amnesia. Society forNeuroscience Abstract, 13, 1455.
Gaddes, W. H., & Edgell, D. (1993). Learning disabilities andbrain function (3rd ed.). New York: Springer.
Gage, F. H. (2000). Mammalian neural stem cells. Science,287, 1433–1438.
Gainetdinov, R. R., & Caron, M. G. (2001). Genetics of child-hood disorders: XXIV. ADHD, Part 8: Hyperdopaminergicmice as an animal model of ADHD. Journal of theAmerican Child and Adolescent Psychiatry, 40, 380–382.
Gajdusek, D. C. (1988). Transmissible and non-transmissibleamyloidoses: Autocatalytic post-translational conversionof host precursor proteins to beta-pleated configuration.Journal of Neuroimmunology, 20, 95–110.
Galaburda, A., & Bellugi, U. (2000). Multi-level analysis ofcortical neuroanatomy in Williams syndrome. Journal ofCognitive Neuroscience, 12, 74–88.
Galaburda, A., & Livingstone, M. (1993). Evidence for a mag-nocellular defect in developmental dyslexia. Annals of theNew York Academy of Sciences, 682, 70–82.
Gallup, G. G., Jr. (1982). Self-awareness and the emergence ofmind in primates. American Journal of Primatology, 2,237–248.
Gallup, G. G., Jr., Nash, R. F., Potter, R. J., & Donegan, N. H. (1970). Effect of varying conditions of fear onimmobility reactions in domestic chickens (Gallus gallus). Journal of Comparative & Physiological Psychology,73(3), 442–445.
Ganguli, M., Dodge, H. H., Shen, C., & DeKosky, S. T.(2004). Mild cognitive impairment, amnestic type: anepidemiologic study. Neurology, 63(1), 115–121.
Gazzaniga, M. S. (1966). Interhemispheric communication ofvisual learning. Neuropsychologia, 4, 183.
Gazzaniga, M. S. (2000). Cerebral specialization and inter-hemispheric communication: Does the corpus callosumenable the human condition? Brain, 123, 1293–1326.
References 487

Gennarelli, T. A. (1983). Head injury in man and experimentalanimals: Clinical aspects. Acta Neurochirugica, 32(Suppl.),1–13.
Georgopoulos, A. P., Whang, K., Georgopoulos, M. A.,Tagaris, G. A., Amirikian, B., Richter, K., et al. (2001).Functional magnetic resonance imaging of visual objectconstruction and shape discrimination: Relations amongtask, hemispheric lateralization, and gender. Journal ofCognitive Neuroscience, 13, 72–89.
Geschwind, N. (1965). Disconnexion syndromes in animalsand man. Brain, 88, 237–294.
Geschwind, N., & Levitsky, W. (1968). Human brain: Left-right asymmetries in temporal speech region. Science, 161,186–187.
Giedd, J. N. (2004). Structural magnetic resonance imaging ofthe adolescent brain. Annals of the New York Academy ofSciences, 1021, 77–85.
Giedd, J. N., Blumenthal, J., Mollowy, E., & Castellanos, F. X.(2001). Brain imaging of attention deficit/hyperactivity dis-order. Annals New York Academy of Sciences, 931, 33–49.
Giedd, J. N., Castellanos, F. X., Casey, B. J., Kozuch, P., King,A. C., Hamburger, S. D., et al. (1994). Quantitative mor-phology of the corpus callosum in attention deficit hyper-activity disorder. American Journal of Psychiatry, 151,665–669.
Giedd, J. N., Castellanos, F. X., Rajapakse, J. C., Vaituzis, A. C., & Rapoport, J. L. (1997). Sexual dimorphism of the developing human brain. Progress inNeuropsychopharmacology and Biological Psychiatry, 21,1185–1201.
Gilman, S., & Newman, S. W. (1996). Essentials of clinicalneuroanatomy and neurophysiology (9th ed.). Philadelphia:F. A. Davis.
Gilman, S., & Newman, S. W. (1996). The cerebrospinal fluid.In Manter & Katz’s Clinical neuroanatomy and neuropsy-chology (9th ed.) (pp. 259–263). Philadelphia: F. A. Davis.
Giraud, A. I., & Price, C. J. (2001). The constraints func-tional neuroimaging places on classical models of audi-tory word processing. Journal of Cognitive Neuroscience,13, 754–765.
Gitelman, D. R., Nobre, A. C., Parrish, T. B., LaBar, K. S.,Kim, Y. H., Meyer, J. R., et al. (1999). A large-scale dis-tributed network for covert spatial attention: Furtheranatomical delineation based on stringent behavioural andcognitive controls. Brain, 122, 1093–1106.
Glaser, G. H., & Pincus, J. H. (1969). Limbic encephalitis.Journal of Nervous Mental Disorder, 149, 59.
Glidden, R. A., Zillmer, E. A., & Barth, J. T. (1990). Thelong-term neurobehavioral effects of prefrontal lobotomy.The Clinical Neuropsychologist, 4, 301.
Gloor, P. (1990). Experiential phenomena of temporal lobeepilepsy: Facts and hypotheses. Brain, 113(Pt 6),1673–1694.
Gogtay, N., Giedd, J. N., Lusk, L., Hayashi, K. M., Greenstein,D., Vaituzis, A. C., et al. (2004). Dynamic mapping ofhuman cortical development during childhood through
early adulthood. Proceedings of the National Academy ofSciences, 101, 8174–8179.
Goldberg, E. (2001). The executive brain: Frontal lobes and thecivilized mind. New York: Oxford.
Goldberg, E., & Costa, L. (1981). Hemispheric differences inthe acquisition and use of descriptive systems. Brain andLanguage, 14, 14–22.
Golden, C. J. (1978). The Stroop Color and Word Test. Chicago:Stoelting.
Golden, C. J., Zillmer, E. A., & Spiers, M. V. (1992).Neuropsychological assessment and intervention.Springfield, IL: Charles C. Thomas.
Goldenberg, G., Wimmer, A., Auff, E., & Schnaberth, G.(1986). Impairment of motor planning in patients withParkinson’s disease: Evidence for ideomotor apraxia.Journal of Neurology, Neurosurgery, and Psychiatry, 49,1266–1272.
Goldman, S., & Nottebohm, F. (1983). Neuronal production,migration, and differentiation in a vocal control nucleus ofthe adult female canary brain. Proceedings of the NationalAcademy of Sciences of the United States of America, 80,2390–2394.
Goldman-Rakic, P. S. (1987a). Circuitry of primate prefrontalcortex and representation of behavior by representationalmemory. In F. Plum (Ed.), Handbook of physiology: Thenervous system (Vol. V). Bethesda: American PhysiologicalSociety.
Goldman-Rakic, P. S. (1987b). Development of cortical circuitryand cognitive function. Child Development, 58,601–622.
Goldman-Rakic, P. S. (1988). Topography of cognition:Parallel distributed networks in primary association cortex. Annual Review of Neuroscience, 11, 137–156.
Goldman-Rakic, P. S. (1993). Working memory and the mind.In Mind and brain: Readings from Scientific American.New York: W. H. Freeman.
Goldman-Rakic, P. S., & Friedman, H. R. (1991). Thecircuitry to working memory revealed by anatomy andmetabolic imaging. In S. Levin, H. M. Eisenberg, & A. L.Benton (Eds.), Frontal lobe functioning and dysfunction.New York: Oxford University Press.
Goldstein, E. B. (1994). Psychology. Pacific Grove, CA:Brooks/Cole.
Good, C. D., Johnsrude, I., Ashburner, J., Henson, R. N. A.,Friston, K. J., & Frackowiak, R. S. J. (2001). Cerebralasymmetry and the effects of sex and handedness on brainstructure: A voxel-based morphometric analysis of 465normal adult human brains. NeuroImage, 14, 685–700.
Gordon, A., & Zillmer, E. A. (1997). Integrating the MMPIand neuropsychology: A survey of NAN membership.Archives of Clinical Neuropsychology, 4, 325–326.
Gould, E., & Gross, C. G. (2002). Neurogenesis in adultmammals: Some progress and problems. Journal ofNeuroscience 22(3), 619–623.
Gould, S. J. (1981). The mismeasure of man. New York:Norton.
488 References

Grabowski, T. J., Damasio, H., Eichhorn, G. R., & Tranel, D.(2003). Effects of gender on blood flow correlates of nam-ing concrete entities. NeuroImage, 20, 940–954.
Graf, P., & Schacter, D. L. (1985). Implicit and explicit mem-ory for new associations in normal and amnesic subjects.Journal of Experimental Psychology: Learning Memory &Cognition, 2, 501–518.
Grant, D. A., & Berg, E. A. (1948). A behavioral analysis ofdegree of reinforcement and ease of shifting two newresponses in a Weigl-type card sorting problem. Journal ofExperimental Psychology: Learning Memory & Cognition,38, 404–411.
Greenberg, D. A., Aminoff, M. J., & Simon, R. P. (2002).Clinical neurology (5th ed). New York: McGraw-Hill/Appleton & Lange.
Grigorenko, E. L., Wood, F. B., Meyer, M. S., Hart, L. A.,Speed, W. C., Shuster, A., et al. (1997). Susceptibility locifor distinct components of developmental dyslexia onchromosome 6 and 15. American Journal of HumanGenetics, 60, 27–39.
Grill-Spector, K., & Malach, R. (2004). The human visual cor-tex. Annual Review of Neuroscience, 27, 649–677.
Grön, G., Wunderlich, A. P., Spitzer, M., Tomczak, R., &Riepe, M. W. (2000). Brain activation during human nav-igation: Gender-different neural networks as substrate ofperformance. Nature Neuroscience, 3, 404–408.
Gronwall, D. M. A. (1977). Paced Auditory Serial-AdditionTask: A measure of recovery from concussion. Perceptualand Motor Skills, 44, 367–373.
Guilleminault, C. (1982). Sleeping and waking disorders:Indications and techniques. Menlo Park, CA: Addison-Wesley.
Guilleminault, C., & Dement, W. C. (1978). Sleep apnea syndromes and related sleep disorders. In R. L. Williams &I. Karacan (Eds.), Sleep disorders: Diagnosis and treatment.New York: Wiley.
Gur, R. C., Gur, R. E., Obrist, W. D., Hungerbuhler, J. P.,Younkin, D., Rosen, A. D., et al. (1982). Sex and hand-edness differences in cerebral blood flow during rest andcognitive activity. Science, 217, 659–660.
Gur, R. C., Turetsky, B. I., Matsui, M., Yan, M., Bilker, W.,Hughett, P., et al. (1999). Sex differences in brain grayand white matter in healthy young adults: Correlationswith cognitive performance. Journal of Neuroscience, 19,4065–4072.
Gur, R. E., Levy, J., & Gur, R. C. (1977). Clinical studies ofbrain organization and behavior. In A. Frazer & A.Winokur (Eds.), Biological bases of psychiatric disorders.New York: Spectrum.
Gurland, B. J., Wilder, D. E., Lantigua, R., Stern, Y., Chen, J., Killeffer, E. H., et al. (1999). Rates of dementia inthree ethnoracial groups. International Journal of GeriatricPsychiatry, 14(6), 481–493.
Guthrie, P. B., Kanappenberger, J., Segal, M., Bennett, M. V. L.,Charles, A. C., & Kater, S. B. (1999). ATP release fromastrocytes mediates glial calcium waves. Journal ofNeuroscience, 19(2), 520–528.
Guy, S. C. (1996). Social and emotional responsivity of chil-dren with nonverbal learning disabilities. DissertationAbstracts International: Section B: The Science andEngineering, 57, 6573.
Haberecht, M. F., Menon, V., Warosfsky, I. S., White, C. D.,Dyer-Friedman, J., & Glover, G. H. (2001). Functionalneuroanatomy of visual-spatial working memory inTurner syndrome. Human Brain Mapping, 14, 96–107.
Haeger, K. (1988). The illustrated history of surgery. New York:Bell.
Hagerman, R. J. (1999). Neurodevelopmental disorders:Diagnosis and treatment. New York: Oxford UniversityPress.
Haines, D. E. (1997). Fundamental neuroscience. New York:Churchill Livingstone.
Halgren, E., Walter, R. D., Cherlow, D. G., & Crandall, P. H.(1978). Mental phenomena evoked by electrical stimula-tion of the human hippocampal formation and amygdala.Brain, 101(1), 83–117.
Hallgren, B. (1950). Specific dyslexia (congenital word blind-ness): A clinical and genetic study. Acta Psychiatrica etNeurologica, 65(Suppl.), 1–28.
Halpern, D. F. (1992). Sex differences in cognitive abilities (2nded.). Hillsdale, NJ: Erlbaum.
Halpern, J. M., & Schulz, K. P. (2006). Revisiting the role ofthe prefrontal cortex in the pathophysiology of attention-deficit/hyperactivity disorder. Psychological Bulletin, 132,560–581.
Halstead, W. C. (1947). Brain and intelligence: A quantitativestudy of the frontal lobes. Chicago: University of ChicagoPress.
Hampson, E., Rovet, J. F., & Altmann, D. (1998). Spatial rea-soning in children with congenital adrenal hyperplasiadue to 21-hydroxylase deficiency. DevelopmentalNeuropsychology, 14, 299–320.
Hanson, J. W., Jones, K. L., & Smith, D. W. (1976). Fetalalcohol syndrome: Experience with 41 patients. Journalof the American Medical Association, 235, 1459.
Harasty, J., Double, K. L., Halliday, G. M., Kril, J. J., &McRitchie, D. A. (1997). Language-associated corticalregions are proportionally larger in the female brain.Archives of Neurology, 54, 171–176.
Hari, R. (1994). Human cortical functions revealed by magne-toencephalography. Progress in Brain Research, 100, 163–168.
Harlow, H. F. (1952). Functional organization of the brain inrelation to mentation and behavior. In M. M. Fund (Ed.),The biology of mental health and disease. New York: Hoeber.
Harlow, J. M. (1868). Recovery from the passage of an ironbar through the head. Publications of the MassachusettsMedical Society, 2, 327–347.
Harnadek, M. C. S., & Rourke, B. P. (1994). Principal identi-fying features of the syndrome of nonverbal learning dis-abilities in children. Journal of Learning Disabilities, 27,144–154.
Harris, J. C. (1995). Developmental neuropsychiatry. New York:Oxford University Press.
References 489

Harrower, M. (1991). Inkblots and poems. In C. D. Walker(Ed.), Clinical psychology in autobiography (pp. 125–170).Pacific Grove, CA: Brooks/Cole.
Hartlage, L. C., & Gage, R. (1997). Unimanual performanceas a measure of laterality. Neuropsychology Review, 7,143–156.
Hartman, D. E. (1995). Neuropsychological toxicology:Identification and assessment of human neurotoxic syndromes(2nd ed.). New York: Plenum.
Hasselbalch, S. G., Oberg, G., Sorensen, S., Andersen, A. R.,Waldemar, G., Schmidt, J. F., et al. (1992). Reducedregional cerebral blood flow in Huntington’s disease stud-ied by SPECT. Journal of Neurology, Neurosurgery, andPsychiatry, 55, 1018–1023.
Haug, H. (1985). Are neurons of the human cerebral cortexreally lost during aging? A morphometric examination. InJ. Tarber & W. H. Gispen (Eds.), Senile dementia ofAlzheimer type (pp. 150–163). New York: Springer-Verlag.
Hauri, P. (1977). The sleep disorders. Kalamazoo, MI: UpjohnCompany.
Hauser, P., Zametkin, A. J., Martinez, P., Vitiello, B., Matochik,J. A., Mixon, A. J., et al. (1993). Attention deficit-hyper-activity disorder in people with generalized resistance tothryroid hormone. New England Journal of Medicine, 328,997–1001.
Hauser, W. A. (1992). Seizure disorders: The changes with age.Epilepsia, 33(Suppl. 4), S6–S14.
Haynes, S. D., & Bennett, T. L. (1990). Cognitive impairmentsin adults with complex partial seizures. InternationalJournal of Clinical Neuropsychology, 12, 74–81.
Heaton, R. K. (1981). Wisconsin Card Sort manual. Odessa,FL: Psychological Assessment Resources.
Heaton, R. K., Chelune, G. J., Talley, J. L., Kay, G. G., &Curtis, G. (1993). Wisconsin Card Sorting Test manual:Revised and expanded. Odessa, FL: PsychologicalAssessment Resources.
Heaton, R. K., Grant, I., & Matthews, C. G. (1991).Comprehensive norms for an extended Halstead-Reitan bat-tery: Demographic corrections, research findings, and clinicalapplications. Odessa, FL: Psychological AssessmentResources.
Hebb, D. O. (1949). The organization of behavior: A neuropsy-chological theory. New York: Wiley.
Hebb, D. O. (1959). Intelligence, brain function and the theo-ry of mind. Brain, 82, 260.
Hebb, D. O. (1983). Neuropsychology: Retrospect andprospect. Canadian Journal of Psychology, 37, 4–7.
Hécaen, H., & Albert, M. L. (1978). Human neuropsychology.New York: Wiley.
Heilman, K. M. (2002). Matter of mind: A neurologist’s view ofbrain-behavior relationships. New York: Oxford UniversityPress.
Heilman, K. M., Watson, R. T., & Valenstein, E. (1993).Neglect and related disorders. In K. M. Heilman & E.Valenstein (Eds.), Clinical neuropsychology (3rd ed.). NewYork: Oxford University Press.
Heindel, W. C., Salmon, D. P., Shults, C. W., Wallcke, P. A.,& Butters, N. (1989). Neuropsychological evidence formultiple implicit memory systems: A comparison ofAlzheimer’s and Parkinson’s disease patients. Journal ofNeuroscience, 9, 582–587.
Helland, T., & Asbjørnsen, A. (2000). Executive functions indyslexia. Child Neuropsychology, 6, 37–48.
Heller, K. W. (1996). Understanding physical, sensory, andhealth impairments. Pacific Grove, CA: Brooks/Cole.
Helmer, C., Joly, P., Letenneur, L., Commenges, D., &Dartigues, J. F. (2001). Mortality with dementia: Resultsfrom a French prospective community-based cohort.American Journal of Epidemiology, 154(7), 642–648.
Henry, J. D., MacLeod, M., Phillips, L., & Crawford, J. R.(2004). A meta-analytic review of prospective memoryand aging. Psychology and Aging, 19, 27–39.
Hill, D. E., Yeo, R. A., Campbell, R. A., Blaine, H., Vigil, J., &Brooks, W. (2003). Magnetic resonance imaging correlatesof attention-deficit/hyperactivity disorder. Neuropsychology,17, 496–506.
Hirsch, H. V. B., & Jacobson, M. (1974). The perfect brain.In M. S. Gazzaniga & C. B. Blakemore (Eds.),Fundamentals of psychobiology. New York: Academic Press.
Hobson, J. A. (1995). Sleep. New York: Scientific AmericanLibrary.
Hodges, J. R., Salmon, D. P., & Butters, N. (1991). Thenature of the naming deficit in Alzheimer’s andHuntington’s disease. Brain, 114, 1547–1558.
Hoekstra, P. J., Kallenber, C. G. M., Korf, J., & Minderaa, R. B.(2002). Is Tourette’s syndrome an autoimmune disease?Molecular Psychiatry, 7, 437–445.
Holiger, D. P., McMenamin, D., Sherman, G. F., &Galaburda, A. (2001). Williams syndrome: Cell packingdensity and neuronal size in primary auditory cortex[Abstract]. Society for Neuroscience Annual Meeting, SanDiego, CA, 986.4.
Holmes, J., Payton, A., Barrett, J. H., Hever, T., Fitzpatrick,H., Trumper, A. L., et al. (2000). A family-based and acase-control association study of the dopamine D4 recep-tor gene and dopamine transporter gene in attentiondeficit hyperactivity disorder. Molecular Psychiatry, 5,523–530.
Honda, H., Shimizu, Y., & Rutter, M. (2005). No effect ofMMR withdrawal on the incidence of autism: A totalpopulation study. Journal of Child Psychology andPsychiatry, 46, 572–579.
Hooper, H. E. (1983). Hooper Visual Organization Test VOT.Los Angeles: Western Psychological Services.
Hooper, S. R., Willis, W. G., & Stone, B. H. (1996). Issuesand approaches in the neuropsychological treatment ofchildren with learning disabilities. In E. S. Batchelor & R. S. Dean (Eds.), Pediatric neuropsychology: Interfacingassessment and treatment in rehabilitation (pp. 211–248).Boston: Allyn & Bacon.
Hopyan, T., Dennis, M., Weksberg, R., & Cytrynbaum, C.(2001). Music skills and the expressive interpretation of
490 References

music in children with Williams-Beuren syndrome: Pitch,rhythm, melodic imagery, phrasing, and musical affect.Child Neuropsychology, 7, 42–53.
Hornak, J. (1992). Ocular exploration in the dark by patientswith visual neglect. Neuropsychologia, 30, 353–384.
Hornak, J., Rolls, E. T., & Wade, D. (1996). Face and voiceexpression identification in patients with emotional andbehavioral changes following ventral frontal lobe damage.Neuropsychologia, 34, 247–261.
Hornsey, H., Banerjee, S., Zeitlin, H., & Robertson, M.(2001). The prevalence of Tourette syndrome in 13–14-year-olds in mainstream schools. Journal of ChildPsychology and Psychiatry and Allied Disciplines, 42,1035–1039.
Horwitz, B., Rumsey, J. M., & Donohue, B. C. (1998).Functional connectivity of the angular gyrus in normalreading and developmental dyslexia. Proceedings of theNational Academy of Sciences, 95, 8939–8944.
Howes, N. L., Bigler, E. D., Burlingame, G. M., & Lawson, J. S.(2003). Memory performance of children with dyslexia: Acomparative analysis of theoretical perspectives. Journal ofLearning Disabilities, 36, 230–246.
Howlin, P. (2003). Outcome in high-functioning adults withautism with and without early language delays:Implications for the differentiation between autism andAsperger syndrome. Journal of Autism and DevelopmentalDisorders, 33, 3–13.
Hoyert, D. L., & Rosenberg, H. M. (1997). Alzheimer’s diseaseas a cause of death in the United States. Public HealthReports, 112(6), 497–505.
Hubel, D. H. (1988). Eye, brain, vision. New York: ScientificAmerican Library.
Hughes, C., Russell, J., & Robbins, T. W. (1994). Evidence forexecutive dysfunction in autism. Neuropsychologia, 32,477–492.
Hutt, M. L. (1985). The Hutt adaptation of the Bender-GestaltTest: Rapid screening and intensive diagnosis (4th ed.).Orlando, FL: Grune & Stratton.
Huttenlocher, P. R. (1990). Morphometric study of humancerebral cortex development. Neuropsychologia, 28,517–527.
Huttenlocher, P. R. (1999). Dendritic and synaptic develop-ment in human cerebral cortex: Time course and criticalperiods. Developmental Neuropsychology, 16, 347–368.
Huttenlocher, P. R., & Dabholkar, A. S. (1997). Developmentalanatomy of prefrontal cortex. In N. A. Krasnegor, G. R.Lyon, & P. S. Goldman-Rakic (Eds.), Development of theprefrontal cortex: Evolution, neurobiology, and behavior(pp. 69–84). Baltimore: Paul H. Brookes.
Hyde, J. S. (2005). The gender similarities hypothesis.American Psychologist, 60, 581–592.
Hynd, G. W., Hall, J., Novey, E. S., Eliopulos, D., Black, K.,Gonzales, J. J., et al. (1995). Dyslexia and corpus callo-sum morphology. Archives of Neurology, 52, 32–38.
Hynd, G. W., Hern, K. L., Novey, E. S., Eliopulos, D.,Marshall, R., Gonzalez, J. J., et al. (1993). Attention
deficit-hyperactivity disorder and asymmetry of the cau-date nucleus. Journal of Child Neurology, 8, 339–347.
Hynd, G. W., & Hiemenz, J. R. (1997). Dyslexia and gyralmorphology variations. In C. Hulme & M. Snowling(Eds.), Dyslexia: Biology, cognition and intervention(pp. 38–58). London: Whurr.
Hynd, G. W., Morgan, A. E., & Vaughn, M. (1997).Neurodevelopmental anomalies and malformations. In C. R. Reynolds & E. Fletcher-Janzen (Eds.), Handbook ofclinical child neuropsychology (2nd ed., pp. 42–61). NewYork: Plenum Press.
Hynd, G. W., Semrud-Clikeman, M., Lorys, A. R., Novey, E. S., & Eliopulos, D. (1990). Brain morphology indevelopmental dyslexia and attention deficitdisorder/hyperactivity. Archives of Neurology, 47, 919–926.
Hynd, G. W., Semrud-Clikeman, M., Lorys, A. R., Novey, E. S., Eliopulos, D., & Lyytinen, H. (1991). Corpus cal-losum morphology in attention deficit-hyperactivity dis-order: Morphometric analysis of MRI. Journal of LearningDisabilities, 24, 141–146.
Hynd, G. W., & Willis, W. G. (1988). Pediatric neuropsychology.Boston: Allyn & Bacon.
Imperato-McGinley, J., Pichardo, M., Gautier, T., Voyer, D., &Bryden, M. P. (1991). Cognitive abilities in androgen-insensitive subjects: Comparisons with control males andfemales from the same kindred. Clinical Endocrinology,34, 341–347.
Jack, C. R., Jr., Petersen, R. C., Xu, Y., O’Brien, P. C., Smith,G. E., Ivnik, R. J., et al. (2000). Rates of hippocampalatrophy correlate with change in clinical status in agingand AD. Neurology, 55(4), 484–489.
Jack, C. R., Jr., Shiung, M. M., Gunter, J. L., O’Brien, P. C.,Weigand, S. D., Knopman, D. S., et al. (2004).Comparison of different MRI brain atrophy rate measureswith clinical disease progression in AD. Neurology, 62(4),591–600.
Jack, C. R., Jr., Shiung, M. M., Weigand, S. D., O’Brien, P. C., Gunter, J. L., Boeve, B. F., et al. (2005). Brainatrophy rates predict subsequent clinical conversion innormal elderly and amnestic MCI. Neurology, 65(8),1227–1231.
Jacobson, S. W., Jacobson, J. L., Sokol, R. J., Martier, S. S., &Ager, J. W. (1993). Prenatal alcohol exposure and infantinformation processing ability. Child Development, 64,1706–1721.
James, E. M., & Selz, M. (1997). Neuropsychological bases ofcommon learning and behavior problems in children. InC. R. Reynolds & E. Fletcher-Janzen (Eds.), Handbook ofclinical child neuropsychology (2nd ed., pp. 157–189). NewYork: Plenum Press.
James, T. W., & Kimura, D. (1997). Sex differences in remem-bering the locations of objects in an array: Location-shiftsversus location-exchanges. Evolution and Human Behavior,18, 155–163.
Jarrold, C., Butler, D. W., Cottington, E. M., & Jimenez, F.(2000). Linking theory of mind and central coherence bias
References 491

in autism and in the general population. DevelopmentalPsychology, 36, 126–138.
Jeffries, K. J., Schooler, C., Schoenbach, C., Herscovitch, P.,Chase, T. N., & Braun, A. R. (2002). The functionalneuroanatomy of Tourette’s syndrome: An FDG PETstudy III: Functional coupling of regional cerebral meta-bolic rates. Neuropsychopharmacology, 27, 92–104.
Jenkins, M. R., & Culbertson, J. L. (1996). Prenatal exposureto alcohol. In R. L. Adams, O. A. Parsons, J. L.Culbertson, & S. J. Nixon (Eds.), Neuropsychology forclinical practice: Etiology, assessment, and treatment of com-mon neurological disorders (pp. 407–452). Washington,DC: American Psychological Association.
Jennett, B., & Teasdale, G. (1981). Management of headinjuries. Philadelphia: F. A. Davies.
Jensen, P. S., Martin, D., & Cantwell, D. P. (1997).Comorbidity in ADHD: Implications for research, prac-tice, and DSM-V. Journal of the American Academy ofChild and Adolescent Psychiatry, 36, 1065–1079.
Johansson, B. (1991). Neuropsychological assessment in theoldest-old. International Psychogeriatrics, 3(Suppl.), 51–60.
Johansson, B., Zarit, S. H., & Berg, S. (1992). Changes incognitive functioning of the oldest old. Journal ofGerontology Psychological Sciences, 47, 75–80.
Johnson, S. C., Bigler, E. D., Burr, R. B., & Blatter, D. D.(1994). White matter atrophy, ventricular dilation, andintellectual functioning following traumatic brain injury.Neuropsychology, 8, 307–315.
Jones, A. W. R., & Richardson, J. S. (1990). Alzheimer’s dis-ease: Clinical and pathological characteristics.International Journal of Neuroscience, 50, 147–168.
Jones, C. M., Braithwaite, V. A., & Healy, S. D. (2003). Theevolution of sex differences in spatial ability. BehavioralNeuroscience, 117, 403–411.
Jones, E. (1981). The life and work of Sigmund Freud: The for-mative years and the great discoveries (Vol. 1). New York:Basic Books.
Jones, K. L., Smith, D. W., Ulleland, C. N., & Streissguth, A. P. (1973). Pattern of malformation in offspring ofchronic alcoholic mothers. Lancet, 1, 1267–1271.
Jones-Gotman, M. (1996). Psychological evaluation for epilep-sy surgery. In S. Shorvon, F. Dreifuss, D. Fish, & D. Thomas (Eds.), The treatment of epilepsy. Oxford,United Kingdom: Blackwell Science.
Jonides, J., Smith, E. E., Koeppe, R. A., Awh, E., Minoshima,S., & Mintun, M. A. (1993). Spatial working memory inhumans as revealed by PET. Nature, 363, 623–625.
Jurko, M. F., & Andy, O. J. (1973). Psychological changes cor-related with thalamotomy site. Journal of Neurology,Neurosurgery, and Psychiatry, 36, 846.
Kaemingk, K., & Paquette, A. (1999). Effects of prenatal alco-hol exposure on neuropsychological functioning.Developmental Neuropsychology, 15, 111–140.
Kagan, J. (1964). The Matching Familiar Figures Test.Cambridge, MA: Harvard University.
Kalat, J. W. (1998). Biological psychology (6th ed.). PacificGrove, CA: Brooks/Cole.
Kalat, J. W. (2004). Biological psychology (8th ed.). Belmont,CA: Wadsworth/Thomson Learning.
Kandel, E. R., Schwartz, J. H., & Jessell, T. H. (1991).Principles of neural science (5th ed.). New York: ElsevierScience.
Kanner, L. (1943). Autistic disturbances of affective contact.Nervous Child, 2, 9–33.
Kansaku, K., Yamaura, A., & Kitazawa, S. (2000). Sex differ-ences in lateralization revealed in the posterior languageareas. Cerebral Cortex, 10, 866–872.
Karmiloff-Smith, A. (1997). Crucial differences betweendevelopmental cognitive neuroscience and adult neuropsychology. Developmental Neuropsychology, 13,513–524.
Karmiloff-Smith, A. (1998). Development itself is the key tounderstanding developmental disorders. Trends inCognitive Sciences, 2, 389–398.
Karmiloff-Smith, A., Brown, J. H., Grice, S., & Paterson, S.(2003). Dethroning the myth: Cognitive dissociation andinnate modularity in Williams syndrome. DevelopmentalNeuropsychology, 23, 227–242.
Karni, A., Tanne, D., Rubenstein, B. S., Askenasy, J. J. M., & Sagi, D. (1994). Dependence on REM sleep ofovernight improvement of a perceptual skill. Science,265, 679–682.
Katzman, R., Lasker, B., & Bernstein, N. (1988). Advances inthe diagnosis of dementia: Accuracy of diagnosis and con-sequences of misdiagnosis of disorders causing dementia.In R. D. Terry (Ed.), Aging and the brain (Vol. 32, pp. 17–61). New York: Raven Press.
Kaufman, A. S. (2001). Do low levels of lead produce IQ lossin children? A careful examination of the literature.Archives of Clinical Neuropsychology, 16, 303–341.
Kaufman, A. S., Reynolds, C. R., & McLean, J. E. (1989). Age and WAIS-R intelligence in a sample of adults in the20–74-year age range: A cross sectional analysis with edu-cational level controlled. Intelligence, 13, 235–253.
Kaushall, P. I., Zetin, M., & Squire, L. R. (1981). Single casestudy: A psychosocial study of chronic, circumscribedamnesia. Journal of Nervous and Mental Disease, 169,383–389.
Kawasaki, H., Adolphs, R., Hiroyuki, O., Kovach, C.,Damasio, H., Kaufman, O., et al., (2005). Analysis ofsingle-unit responses to emotional scenes in human ven-tromedial prefrontal cortex. Journal of CognitiveNeuroscience, 17, 1509–1518.
Kay, D. W. K. (1995). The epidemiology of age-related neuro-logical disease and dementia. Reviews in ClinicalGerontology, 5, 39–56.
Kemper, T. L. (1994). Neuroanatomical and neuropathologicalchanges in normal aging and in dementia. In M. Albert &J. Knoefel (Eds.), Clinical neurology of aging (pp. 3–78).New York and Oxford: Oxford University Press.
492 References
Kennedy, C. H. (1999). Assessing competency to consent tosexual activity in the cognitively impaired population.Journal of Forensic Neuropsychology, 1, 17–33.
Kennedy, C. H. (2003). Legal and psychological implicationsin the assessment of sexual consent in the cognitivelyimpaired population. Assessment, 10(4), 352–358.
Kennedy, C. H., & Niederbuhl, J. (2001). Establishing criteriafor sexual consent capacity. American Journal of MentalRetardation, 106(6), 503–510.
Kennedy, C. H., & Zillmer, E. A. (2006). Military psychology:Clinical and operational applications. New York: GuilfordPress.
Kenyon, T. (1994). Brain states. Naples, FL: United StatesPublishing.
Kerns, K. A., Don, A., Mateer, C. A., & Streissguth, A. P.(1997). Cognitive deficits in nonretarded adults with fetalalcohol syndrome. Journal of Learning Disabilities, 30,685–693.
Kerr, D. A., Lladó, J., Shamblott, M. J., Maragakis, N. J.,Irani, D. N., Crawford, T. O., et al. (2003). Humanembryonic germ cell derivatives facilitate motor recoveryof rats with diffuse motor neuron injury. Journal ofNeuroscience, 23, 5131–5140.
Kertesz, A., & Gold, B. T. (2003). Recovery of cognition (pp. 617–639). In K. M. Heilman & E. Valenstein (Eds.),Clinical neuropsychology. New York: Oxford University Press.
Kety, S. S. (1979). Disorders of the human brain. ScientificAmerican, 241, 202–214.
Kibby, M. Y., Marks, W., Morgan, S., & Long, C. J. (2004).Specific impairments in developmental reading disabili-ties: A working memory approach. Journal of LearningDisabilities, 37, 349–363.
Kim, Y. H., Gitelman, D. R., Nobre, A. C., Parrish, T. B.,LaBar, K. S., & Mesulam, M. M. (1999). The large-scalenetwork for spatial attention displays multifunctional over-lap but differential asymmetry. NeuroImage, 9,269–277.
Kimura, D. (1999). Sex and cognition. Cambridge, MA: MITPress.
Kinsbourne, M. (1993). Orientational bias model of unilateralneglect: Evidence from attentional gradients within hemi-space. In H. Robertson & J. C. Marshall (Eds.),Unilateral neglect: Clinical and experimental studies(pp. 63–86). Hove, United Kingdom: Erlbaum.
Klein, B. P., & Mervis, C. B. (1999). Contrasting patterns ofcognitive abilities of 9- and 10-year-olds with Williamssyndrome or Down syndrome. DevelopmentalNeuropsychology, 16, 177–196.
Kleist, K. (1933). Gehirnpathologie. Leipzig: Barth.Klin, A. (2000). Attributing social meaning to ambiguous visual
stimuli in higher functioning autism and Asperger syn-drome: The social attribution task. Journal of ChildPsychology and Psychiatry, 41, 831–846.
Knaus, T. A., Bollich, A. M., Corey, D. M., Lemen, L. C., &Foundas, A. L. (2004). Sex-linked differences in the
anatomy of the perisylvian language cortex: A volumetricMRI study of gray matter volumes. Neuropsychology, 18,738–747.
Knecht, S., Deppe, M., Dräger, B., Bobe, L., Lohmann, H., Ringelstein, E. B., et al. (2000a). Language lateraliza-tion in healthy right-handers. Brain, 123, 74–81.
Knecht, S., Dräger, B., Deppe, M., Bobe, L., Lohmann, H.,Flöel, A., et al. (2000). Handedness and hemispheric language dominance in healthy humans. Brain, 123,2512–2518.
Knight, R. T., & Stuss, D. T. (2002). Prefrontal cortex: Thepresent and the future. In D. T. Stuss & R. T. Knight(Eds.), Principles of frontal lobe function (pp. 573–598).New York: Oxford University Press.
Knopman, D. S., DeKosky, S. T., Cummings, J. L., Chui, H., Corey-Bloom, J., Relkin, N., et al. (2001). Practiceparameter: Diagnosis of dementia (an evidence-basedreview). Report of the Quality Standards Subcommitteeof the American Academy of Neurology. Neurology, 56(9),1143–1153.
Kolb, B. (1995). Brain plasticity and behavior. Mahwah, NJ:Erlbaum.
Kolb, B., & Fantie, B. (1997). Development of the child’sbrain and behavior. In C. R. Reynolds & E. Fletcher-Janzen (Eds.), Handbook of clinical child neuropsychology(2nd ed., pp. 17–41). New York: Plenum Press.
Kolb, B., Gibb, R., & Gorny, G. (2000). Cortical plasticityand the development of behavior after early frontal cortical injury. Developmental Neuropsychology, 18,423–444.
Kolb, B., & Whishaw, I. Q. (1990). Fundamentals of humanneuropsychology (3rd ed.). New York: W. H. Freeman.
Kolb, B., & Whishaw, I. Q. (1996). Fundamentals of humanneuropsychology (4th ed.). New York: W. H. Freeman andCompany.
Koller, K., Brown, T., Spurgeon, A., & Levy, L. (2004). Recentdevelopments in low-level lead exposure and intellectualimpairment in children. Environmental HealthPerspectives: Annual Review, 112, 987–994.
Korkman, M., Kettunen, S., & Autti-Rämö, I. (2003).Neurocognitive impairment in early adolescence followingprenatal alcohol exposure of varying duration. ChildNeuropsychology, 9, 117–128.
Korkman, M., Kirk, U., & Kemp, S. (1998). NEPSY: A devel-opmental neuropsychology assessment manual. San Antonio,TX: Psychological Corporation.
Krakauer, J. (1997). Into thin air. New York: Villard.Krech, D. (1962). Cortical localization of function. In
L. Postman (Ed.), Psychology in the making. New York:Knopf.
Kunin-Batson, A., Primeau, M., Zelko, F., Glanzman, M.,Martini, D. R., & Erwin, R. (2002). Effects ofmethylphenidate on neuropsychological functioning inchildren with ADHD. Journal of the InternationalNeuropsychological Society, 8, 309–310.
References 493

Kupfermann, I. (1991). Hypothalamus and limbic system:Peptidergic, neurons, homeostasis, and emotional behav-ior. In E. R. Kandel, J. H. Schwartz, & T. M. Jessell(Eds.), Principles of neural science (pp. 736–749). New York: Elsevier.
LaBerge, S. (1990). Exploring the world of lucid dreaming. NewYork: Ballantine Books.
Lai, Z. (1998). Emotional expression and perception inWilliams syndrome. Paper presented at the CognitiveNeuroscience Society, San Francisco, CA.
Lange, C. G. (1922). The emotions. Baltimore: Williams &Wilkins.
Larsen, J. P., Hoien, T., & Odegaard, H. (1992). Magnetic res-onance imaging of the corpus callosum in developmentaldyslexia. Cognitive Neuropsychology, 9, 123–134.
Larson, J., & Lynch, G. (1986). Induction of synaptic potenti-ation in hippocampus by patterned stimulation involvestwo events. Science, 232, 985–988.
LaRue, A. (1992). Aging and neuropsychological assessment. NewYork: Plenum Press.
Lashley, K. S. (1929). Brain mechanisms and intelligence.Chicago: University of Chicago Press.
Laws, G., & Bishop, D. (2004). Pragmatic language impair-ments and social deficits in Williams syndrome: A com-parison with Down’s syndrome and specific languageimpairment. International Journal of CommunicationDisorders, 39, 45–64.
Lawson, J., Baron-Cohen, S., & Wheelwright, S. (2004).Emphathising and systemising in adults with and withoutAsperger syndrome. Journal of Autism and DevelopmentalDisorders, 34, 301–309.
Leckman, J. F., & Cohen, D. J. (1996). Tic disorders. In M.Lewis (Ed.), Child and adolescent psychiatry: A comprehen-sive textbook (2nd ed., pp. 622–629). Baltimore: Williams& Wilkins.
Leckman, J. F., Peterson, B. S., Anderson, G. M., Arsten, A. F.,Pauls, D. L., & Cohen, D. J. (1997). Pathogenesis ofTourette’s syndrome. Journal of Child Psychology andPsychiatry and Allied Disciplines, 38, 119–142.
Leckman, J. F., Peterson, B. S., Schultz, R. T., & Cohen, D. J.(2001). Tics: When habit-forming neural systems formhabits of their own. In C. A. Nelson & M. Luciana(Eds.), Handbook of developmental cognitive neuroscience(pp. 549–560). Cambridge, MA: MIT Press.
LeDoux, J. E. (1992). Brain mechanisms of emotion and emo-tional learning. Current Opinion in Neurobiology, 2,191–197.
LeDoux, J. E. (1994). Emotion, memory and the brain.Scientific American, 270(6), 50–57.
LeDoux, J. (1996). The emotional brain: The mysterious under-pinnings of emotional life. New York: Touchstone.
Lee, K. T., Mattson, S. N., & Riley, E. P. (2004). Classifyingchildren with heavy prenatal alcohol exposure using mea-sures of attention. Journal of the InternationalNeuropsychological Society, 10, 271–277.
Lees, A. J., & Smith, E. (1983). Cognitive deficits in the earlystages of Parkinson’s disease. Brain, 106, 257–270.
Leiguarda, R. C., Merello, M., Nouzeilles, M. I., Balej, J.,Rivero, A., & Nogues, M. (2003). Limb-kinetic apraxiain corticobasal degeneration: Clinical and kinetic features.Movement Disorders, 18(1), 49–59.
Lemire, R. J., Loeser, J. D., Leech, R. W., & Alvord, E. C.(1975). Normal and abnormal development of the humannervous system. New York: Harper & Row.
Lemke, G. (2001). Glial control of neuronal development.Annual Review of Neuroscience, 24, 87–105.
Lemoine, P., Harrowsseau, H., Borteryu, J. P., & Menuet, J. C.(1968). Les enfants de parents alcoholiques: Anomaliesobservees a propos de 127 cas. Quest Medicale, 21, 476–482.
Levin, B. E., Tomer, R., & Rey, G. J. (1992). Cognitiveimpairment in Parkinson’s disease. Neurologic Clinics, 2,471–485.
Levin, H. S., Benton, A. L., & Grossman, R. G. (1982).Neurobehavioral consequences of closed head injury. NewYork: Oxford University Press.
Levin, H. S., Culhane, K. A., Hartmann, J., Evankovitch, K.,Mattson, A. J., Harward, H., et al. (1991). Developmentalchanges in performance on tests of purported frontal lobefunction. Developmental Neuropsychology, 7, 377–395.
Levin, H. S., Eisenberg, H. M., & Benton, A. L. (1989). Mildhead injury. New York: Oxford University Press.
Levin, H. S., O’Donnell, V. M., & Grossman, R. G. (1979).The Galveston Orientation and Amnesia Test: A practicalscale to assess cognition after head injury. Journal ofNervous and Mental Disease, 167, 675–684.
Levine, B., Black, S. E., Cabeza, R., Sinder, M., McIntosh, J. P.,Toth, J. P., et al. (1998). Episodic memory and the self in a case of isolated retrograde amnesia. Brain, 121,1951–1973.
Levitin, D. J., Cole, K., Chiles, M., Lai, Z., Lincoln, A., &Bellugi, U. (2004). Characterizing the musical phenotypein individuals with Williams syndrome. ChildNeuropsychology, 10, 223–247.
Levy, J., & Heller, W. (1992). Gender differences in humanneuropsychological function. In A. A. Gerall, H. Moltz, &I. L. Ward (Eds.), Handbook of behavioral neurobiology:Sexual differentiation. New York: Plenum.
Lezak, M. D. (1995). Neuropsychological assessment (3rd ed.).New York: Oxford University Press.
Lezak, M. D., Howieson, D. B., & Loring, D. W. (2004).Neuropsychological assessment (4th ed.). New York: OxfordUniversity Press.
Lichter, D. G., & Cummings, J. L. (2001). Introduction andoverview. In D. G. Lichter & J. L. Cummings (Eds.),Frontal-subcortical circuits in psychiatric and neurologicaldisorders (pp. 1–43). New York: Guilford Press.
Lifton, R. J. (1986). The Nazi doctors: Medical killing and thepsychology of genocide. New York: Basic Books.
Lisowksi, F. P. (1967). Prehistoric and early historic trepana-tion. In D. Brothwell & A. T. Sandison (Eds.), Diseases in
494 References

antiquity (pp. 651–672). Springfield, IL: Charles C.Thomas.
Little, S. S. (1993). Nonverbal learning disabilities and socioe-motional functioning: A review of recent literature.Journal of Learning Disabilities, 26, 653–665.
Lopez, O. L., Jagust, W. J., DeKosky, S. T., Becker, J. T.,Fitzpatrick, A., Dulberg, C., et al. (2003). Prevalence andclassification of mild cognitive impairment in theCardiovascular Health Study Cognition Study: part 1.Archives of Neurology, 60(10), 1385–1389.
Lopez, O. L., Litvan, I., Catt, K. E., Stowe, R., Klunk, W.,Kaufer, D. I., et al. (1999). Accuracy of four clinical diagnostic criteria for the diagnosis of neurodegenerativedementias. Neurology, 53(6), 1292–1299.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Jr., Leventhal,B. L., DiLavore, P. C., et al. (2000). Autism DiagnosticObservation Schedule-Generic: A standard measure ofsocial and communication deficits associated with thespectrum of autism. Journal of Autism & DevelopmentalDisorders, 30, 205–223.
Lowther, J. L., & Wasserman, J. D. (1994, November). Use ofMirsky’s neurocognitive model of attention in identifyingDSM-IV disorders of attention. Poster presented at theannual meeting of National Academy of Neuropsychology,Orlando, FL.
Lupien, S. J., de Leon, M., de Santi, S., Convit, A., Tarshish,C., Nair, N. P., et al. (1998). Cortisol levels duringhuman aging predict hippocampal atrophy and memorydeficits. Nature Neuroscience, 1(1), 69–73.
Luria, A. R. (1964). Neuropsychology in the local diagnosis ofbrain injury. Cortex, 1, 3.
Luria, A. R. (1966). Higher cortical functions in man. NewYork: Basic Books.
Luria, A. R. (1968). The mind of a mnemonist. New York: BasicBooks.
Luria, A. R. (1971). Memory disturbances in local brainlesions. Neuropsychologia, 9, 367.
Luria, A. R. (1990). The neuropsychological analysis of problem-solving. Orlando, FL: Paul M. Deutsch Press.
MacDonald, A. W., Cohen, J. D., Stenger, V. A., & Carter, C. S.(2000). Dissociating the role of the dorsolateral prefrontaland anterior cingulated cortex in cognitive control.Science, 288, 1835–1838.
Macintosh, K. E., & Dissanayake, C. (2004). Annotation: The similarities and differences between autistic disorderand Asperger’s disorder: A review of the empirical evidence. Journal of Child Psychology and Psychiatry, 45,421–434.
MacLean, P. D. (1949). Psychosomatic disease and the “visceralbrain”: Recent developments bearing on the Papez theoryof emotion. Psychosomatic Medicine, 11, 338–353.
MacLean, P. D. (1952). Some psychiatric implications of phys-iological studies on frontotemporal portion of limbic sys-tem (visceral brain). Electroencephalography and ClinicalNeurophysiology, 4, 407–418.
Macmillan, M. (1996). Phineas Gage: A case for all reasons. InC. Code, C. Wallesch, Y. Joanette, & A. R. Lecours(Eds.), Classic cases in neuropsychology (pp. 243–262).Sussex, United Kingdom: Psychology Press.
Mai, J. K., Assheuer, J., & Paxinos, G. (1997). Atlas of thehuman brain. San Diego, CA: Academic Press.
Majovski, L. V. (1997). Mechanisms and development of cere-bral lateralization in children. In C. R. Reynolds & E.Fletcher-Janzen (Eds.), Handbook of clinical child neu-ropsychology (2nd ed., pp. 102–119). New York: PlenumPress.
Marie, P. (1971). Pierre Marie’s papers on speech disorders.New York: Hafner.
Marino, B. S., Fine, K. S., & McMillan, J. A. (2004). Blueprintspediatrics (3rd ed.). Malden, MA: Blackwell Publishing.
Markman, J. A., McKian, K. P., Stroup, T. S., & Juraska, J. M.(2004). Sexually dimorphic aging of dendritic morphologyin CA1 of hippocampus. Hippocampus, 15, 97–103.
Marshall, J. C., & Halligan, P. W. (1988). Line bisection in acase of visual neglect. Nature, 336, 766–777.
Marshall, L. F., & Ruff, R. M. (1989). Neurosurgeon as a victim.In H. S. Levin, H. M. Eisenberg, & A. L. Benton (Eds.),Mild head injury. New York: Oxford University Press.
Martin, J. H. (1996). Neuroanatomy text and atlas (2nd ed.).Stamford, CT: Appleton & Lange.
Martin, J. H., & Jessell, T. M. (1991). Development as a guideto the regional anatomy of the brain. In E. R. Kandel, J. H. Schwartz & T. M. Jessell (Eds.), Principles of neuralscience (3rd ed., pp. 296–308). New York: Elsevier Science.
Masliah, E., Mallory, M., Veinbergs, I., Miller, A., & Samuel,W. (1996). Alterations in apolipoprotein E expressionduring aging and neurodegeneration. Progress inNeurobiology, 50(5–6), 493–503.
Mason, C., & Kandel, E. R. (1991). Central visual pathways.In E. R. Kandel, J. H. Schwartz, & T. M. Jessell (Eds.),Principles of neural science (3rd ed., pp. 420–439). NewYork: Elsevier.
Mataró, M., Junqué, C., Poca, M. A., & Sahuquillo, J. (2001).Neuropsychological findings in congenital and acquiredchildhood hydrocephalus. Neuropsychology Review, 11,169–178.
Mattingly, J. B. (1996). Paterson & Zangwill’s (1944) case ofunilateral neglect: Insights from 50 years of experimentalinquiry. In C. Code, C. Wallesch, Y. Joanette, & A. R. Lecours (Eds.), Classic cases in neuropsychology(pp. 243–262). Brighton, United Kingdom: PsychologyPress.
Mattson, S. N., Lang, A. R., & Calarco, K. E. (2002).Attentional focus and attentional shift in children withheavy prenatal alcohol exposure. Journal of theInternational Neuropsychological Society, 8, 295.
Mattson, S. N., & Riley, E. P. (2000). Parent ratings of behav-ior in children with heavy prenatal alcohol exposure toalcohol. Alcoholism: Clinical and Experimental Research,24, 226–231.
References 495
Mattson, S. N., Riley, E. P., Delis, D. C., Stern, C., & Jones,K. L. (1996). Verbal learning and memory in childrenwith fetal alcohol syndrome. Alcoholism: Clinical andExperimental Research, 20, 810–816.
Mattson, S. N., Riley, E. P., Gramling, L., Delis, D. C., &Jones, K. L. (1998). Neuropsychological comparison ofalcohol-exposed children with or without physical featuresof fetal alcohol syndrome. Neuropsychology, 12,146–153.
Mattson, S. N., Riley, E. P., Sowell, E. R., Jenigan, T. L.,Sobel, D. F., & Jones, K. L. (1996). A decrease in the sizeof the basal ganglia in children with fetal alcohol syn-drome. Alcoholism: Clinical and Experimental Research, 20,1088–1093.
Maurer, K., Volk, S., & Gerbaldo, H. (1997). Auguste D. andAlzheimer’s disease. Lancet, 349, 1546–1549.
Mayes, S. D., & Calhoun, S. L. (2001). Non-significance ofearly speech delay in children with autism and normalintelligence and implications for DSM-IV Asperger’sdisorder. Autism, 5, 81–94.
Mayeux, R. (2003). Epidemiology of neurodegeneration.Annual Review of Neuroscience, 26, 81–104.
Mayeux, R., Denaro, J., Hemenegildo, N., Marder, K., Tang,M. X., Cote, L. J., & Stern, Y. (1992). A population-based investigation of Parkinson’s disease with and without dementia. Archives of Neurology, 49,492–497.
Mayeux, R., Saunders, A. M., Shea, S., Mirra, S., Evans, D.,Roses, A. D., et al. (1998). Utility of the apolipoprotein E genotype in the diagnosis of Alzheimer’s disease.Alzheimer’s Disease Centers Consortium on ApolipoproteinE and Alzheimer’s Disease. New England Journal ofMedicine, 338(8), 506–511.
McCarthy, R. A., & Warrington, E. K. (1990). Cognitive neu-ropsychology. San Diego, CA: Academic Press.
McCormick, C. M., & Teillon, S. M. (2001). Menstrual cyclevariation in spatial ability: Relation to salivary cortisol lev-els. Hormones and Behavior, 39, 29–38.
McDaniel, M. A., & Einstein, G. O. (2000). Strategic andautomatic processes in prospective memory retrieval: Amultiprocess framework. Applied Cognitive Psychology, 14,S127–S144.
McDonough, L., Stahmer, A., Schreibman, L., & Thompson,S. J. (1997). Deficits, delays, and distractions: An evalua-tion of symbolic play and memory in children withautism. Development and Psychopathology, 9, 17–41.
McDougle, C. J., Scahill, L., McCracken, J. T., Aman, M. G.,Tierney, E., Arnold, L. E., et al. (2000). Research units onpediatric psychopharmacology (RUPP) autism network:Background and rationale for an initial controlled studyof risperidone. Child and Adolescent Psychiatric Clinics ofNorth America, 9, 201–224.
McDowell, S., Whyte, J., & D’Esposito, M. (1998).Differential effects of a dopaminergic agonist on pre-frontal function in head injury patients. Brain, 121,1155–1164.
McGaugh, J. L. (2004). The amygdala modulates the consoli-dation of memories of emotionally arousing experiences.Annual Review of Neuroscience, 27, 1–28.
McIntosh, G. C. (1992). Neurological conceptualizations ofepilepsy. In T. L. Bennett (Ed.), The neuropsychology ofepilepsy. New York: Plenum.
McKhann, G., Drachman, D., Folstein, M., Katzman, R.,Price, D., & Stadlan, E. M. (1984). Clinical diagnosis ofAlzheimer’s disease: Report of the NINCDS-ADRDAWork Group. Neurology, 34, 939–944.
McLardy, T. (1970). Memory function in hippocampal gyribut not in hippocampi. International Journal ofNeuroscience, 1, 113.
Meador, K. J., Loring, D. W., Lee, G., Nichols, M., &Heilman, K. M. (1999). Cerebral lateralization: relation-ship of language and ideomotor praxis. Neurology, 53,2028–2031.
Meehl, P. (1973). Psychodiagnosis: Selected papers. New York:Norton Press.
Merabet, L. B., Rizzo, J. R., Amedi, A., Somers, D. C., &Pascual-Leone, A. (2005). What blindness can tell usabout seeing again: Merging neuroplasticity and neuro-prostheses. Nature Reviews Neuroscience, 6, 71–77.
Mervis, C. B., & Bertrand, J. (1997). Developmental relationsbetween cognition and language: Evidence from Williamssyndrome. In L. B. Adamson & M. A. Rornski (Eds.),Research on communication and language acquisition:Discoveries from atypical development (pp. 75–106). New York: Brookes.
Mervis, C. B., Morris, C. A., Klein-Tasman, B. P., Bertrand, J.,Kwitny, S., Appelbaum, L. G., et al. (2003). Attentionalcharacteristics of infants and toddlers with Williams syn-drome during triadic interactions. DevelopmentalNeuropsychology, 23, 243–268.
Mervis, C. B., & Robinson, B. F. (2000). Expressive vocabu-lary ability of toddlers with Williams syndrome or Downsyndrome: A comparison. Developmental Neuropsychology,17, 111–126.
Merz, P. A., Somerville, R. A., Wisneiwski, H. M., & Iqbal, K.(1981). Abnormal fibrils from scrapie-infected brain. ActaNeuropathologica, 54, 63–74.
Mesulam, M. M. (1981). A cortical network for directed attentionand unilateral neglect. Annals of Neurology, 10, 309–325.
Mesulam, M. M. (1985). Principles of behavioral neurology.Philadelphia: F. A. Davis.
Mesulam, M. M. (1990). Large-scale neurocognitive networksand distributed processing for attention, language andmemory. Annals of Neurology, 28, 597–613.
Mesulam, M. M. (2000). Principles of behavioral and cognitiveneurology (2nd ed.). New York: Oxford University Press.
Meyer-Lindenberg, A., Hariri, A. R., Munoz, K. E., Mervis, C. B., Mattay, V. S., Morris, K. E., et al. (2005). Normalcorrelates of genetically abnormal social cognition inWilliams syndrome. Nature Neuroscience, 8, 991–993.
Meyer-Lindenberg, A., Kohn, P., Mervis, C. B., Kippenhan, J. S., Olsen, R. K., Morris, C. A., et al. (2004). Neural
496 References
basis of genetically determined visuospatial constructiondeficits in William syndrome. Neuron, 43, 623–631.
Meyers, P. S. (1999). Right hemisphere damage: Disorders ofcommunication and cognition. San Diego: SingularPublishing Group.
Middleton, F. A., & Strick, P. L. (2001). Revised neuroanato-my of frontal-subcortical circuits. In D. G. Lichter & J. L. Cummings (Eds.), Frontal-subcortical circuits inpsychiatric and neurological disorders (pp. 44–58). New York: Guilford Press.
Milberg, W. P., Hebben, N., & Kaplan, E. (1986). The Bostonprocess approach to neuropsychological assessment. In I. Grant & K. M. Adams (Eds.), Neuropsychological assess-ment of neuropsychiatric disorders. New York: OxfordUniversity Press.
Miller, E. K., & Cohen, J. D. (2001). An integrative theory ofprefrontal cortex function. Annual Review of Neuroscience,24, 167–202.
Milner, B. (1968). Visual recognition and recall after righttemporal lobe excision in man. Neuropsychologia, 6,191.
Milner, B., Corkin, S., & Teuber, S. C. (1968). Further analy-sis of the hippocampal amnesic syndrome: 14 year follow-up study of H.M. Neuropsychologia, 6, 215–234.
Minshew, N. J. (1997). Pervasive developmental disorders:Autism and similar disorders. In T. E. Feinberg & M. J.Farah (Eds.), Behavioral neurology and neuropsychology(pp. 817–826). New York: McGraw-Hill.
Mirsky, A. F. (1995). Perils and pitfalls on the path to normalpotential: The role of impaired attention. Homage toHerbert G. Birch. Journal of Clinical and ExperimentalNeuropsychology, 17, 481–498.
Mirsky, A. F. (1996). Disorders of attention: A neuropsycho-logical perspective. In G. R. Lyon & N. A. Krasnegor(Eds.), Attention, memory, and executive function(pp. 71–96). Baltimore: Paul H. Brookes.
Mishkin, M., Malamut, B., & Bachevalier, J. (1984). Memoriesand habits: Two neural systems. In G. Lynch, J. L. McGaugh, & N. M. Weinberger (Eds.), Neurobiologyof learning and memory. New York: Guilford Press.
Mishkin, M., Ungerleider, L., & Macko, K. A. (1983). Objectvision and spatial vision: Two cortical pathways. Trends inNeurosciences, 6, 414–417.
Moffat, S. D., & Hampson, E. (1996). A curvilinear relation-ship between testosterone and spatial cognition inhumans: Possible influences of hand preference.Psychoneuroendocrinology, 21, 323–337.
Mohn, K., Spiers, M. V., & Sakamoto, M. (2005, November).Oral contraceptive use and cognitive functioning inyoung women presented at the annual meeting of theNational Academy of Neuropsychology [Abstract].Archives of Clinical Neuropsychology, 20, 846.
Monk, C. S., Webb, S. J., & Nelson, C. A., (2001). Prenatalneurobiological development: Molecular mechanisms andanatomical change. Developmental Neuropsychology, 19,211–236.
Moore, K. L., & Persaud, T. V. N. (1993). Before we are born:Essentials of embryology and birth (4th ed.). Philadelphia:W. B. Saunders.
Morgan, A. E., & Hynd, G. W. (1998). Dyslexia, neurolin-guistic ability, and anatomical variation of the planumtemporale. Neuropsychology Review, 8, 79–93.
Morris, C. A., & Mervis, C. B. (1999). Williams syndrome. InS. Goldstein & C. R. Reynolds (Eds.), Handbook of neurodevelopmental and genetic disorders of childhood(pp. 555–590). New York: Guilford Press.
Morris, J. S., Öhman, A., & Dolan, R. J. (1998). Consciousand unconscious emotional learning in the human amygdala. Nature, 393, 467–470.
Moscovitch, M., & Winocur, G. (2002). The frontal cortexand working with memory. In D. T. Stuss & R. T. Knight(Eds.), Principles of frontal lobe function (pp. 188–209).New York: Oxford University Press.
Moser, R. S., & Schatz, P. (2002). Enduring effects of concus-sion in youth athletes. Archives of Clinical Neuropsychology,17(1), 91–100.
Mostofsky, S. H., Reiss, A. L., Lockhart, P., & Denckla, M. B.(1998). Evaluation of cerebellar size in attention-deficithyperactivity disorder. Journal of Child Neurology, 13,434–439.
Mullan, S., & Penfield, W. (1959). Illusions of comparativeinterpretation and emotion; production by epileptic dis-charge and by electrical stimulation in the temporal cor-tex. AMA Archives of Neurology and Psychiatry, 81(3),269–284.
Murphy, D. G., DeCarli, C., Daly, E., Haxby, J. V., Allen, G., White, B. J., et al. (1993). X-chromosome effects onfemale brain: A magnetic resonance imaging study ofTurner’s syndrome. Lancet, 342, 1197–2000.
Murphy, D. G. M., Mentis, M. J., Pietrini, P., Grady, C., Haxby,J. V., De La Granja, M., et al. (1997). A PET study ofTurner’s syndrome: Effect of sex steroids and the X chro-mosome on brain. Biological Psychiatry, 41, 285–298.
Nagai, Y., Goldstein, L. H., Fenwick, P. B., & Trimble, M. R.(2004). Clinical efficacy of galvanic skin response biofeed-back training in reducing seizures in adult epilepsy: A pre-liminary randomized controlled study. Epilepsy andBehavior, 5(2), 216–223.
Nairne, J. S. (1997). Psychology: The adaptive mind. PacificGrove, CA: Brooks/Cole.
National Directory of Head Injury Services. (1992).Southbridge, MA: National Head Injury Foundation.
National Institute of Neurological Disorders and Stroke(NINDS). (2004). Seizures and epilepsy: Hope throughresearch. Retrieved December 28, 2005, fromwww.ninds.nih.gov/disorders/epilepsy/epilepsy.htm.
National Institutes of Health. (2002). Stem cells information.Retrieved from http://stemcells.nih.gov/info/basics/defaultpage.asp.
Naugle, R. I., Cullum, C. M., & Bigler, E. D. (1998).Introduction to clinical neuropsychology: A casebook. Austin,TX: Pro-Ed.
References 497
Nauta, W. J. H., & Feirtag, M. (1986). Fundamental neu-roanatomy. New York: W. H. Freeman.
Nedergaard, M., Ransom, B., & Goldman, S. A. (2003). Newroles for astrocytes: Redefining the functional architectureof the brain. Trends in Neurosciences, 26(10), 523–530.
Nelson, H. D., Humphrey, L. L., Nygren, P., Teutsch, S. M.,& Allan, J. D. (2002). Postmenopausal hormone replace-ment therapy. Journal of the American Medical Association,288, 872–881.
Neppe, V. M. (1983). The concept of déjà vu. ParapsycholigcalJournal of South Africa, 4, 25–35.
Newman, A. C., Barth, J. T., & Zillmer, E. A. (1986). Serialneuropsychological assessment in an adult with Tourette’ssyndrome. International Journal of ClinicalNeuropsychology, 9, 135–139.
Newton, A., & Johnson, D. A. (1985). Social adjustment andinteraction after severe head injury. British Journal ofClinical Psychology, 24, 225–234.
Nicolson, R., Craven-Thuss, B., Smith, J., McKinlay, B. D., &Castellanos, F. X. (2005). A randomized double-blind,placebo-controlled trial of metoclopramide for the treat-ment of Tourette’s disorder. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 44, 640–646.
Nigg, J. (2001). Is ADHD a disinhibitory disorder?Psychological Bulletin, 127, 571–598.
Nigg, J. T. (2006). What causes ADHD? Understanding whatgoes wrong and why. New York: Guilford Press.
Noback, C. R., & Demarest, R. J. (1975). The human nervoussystem. New York: McGraw-Hill.
Nobre, A. C., Coull, J. T., Maquet, C. D., Frith, C. D.,Vandenberghe, R., & Mesulam, M. M. (2004). Orientingattention to locations in perceptual versus mental repre-sentations. Journal of Cognitive Neuroscience, 16, 363–373.
Nockleby, D. M., & Deaton, A. V. (1987). Denial versus dis-tress: Coping patterns in post head trauma patients.International Journal of Clinical Neuropsychology, 9,145–148.
Nordahl, T. E., & Salo, R. (2004). Selected neuroimaging top-ics in psychiatric disorders. In S. C. Yudofsky & H. F.Kim (Eds.), Neuropsychiatric assessment (pp. 155–190).Washington, DC: American Psychiatric Publishing.
Nottebohm, F. (1981). A brain for all seasons: Cyclicalanatomical changes in song-control nuclei for the canarybrain. Science, 214, 1368–1370.
Nuland, S. B. (1993). How we die. New York: Vintage.Nurmi, E. L., Dowd, M., Tadevosyan-Leyfer, O., Haines, J. L.,
Folstein, S. E., & Sutcliffe, J. S. (2003). Exploratory sub-setting of autism families based on savant skills improvesevidence of genetic linkage to 15q11-q13. Journal of theAmerican Child and Adolescent Psychiatry, 42, 856–863.
Öberg, C., Larsson, M., & Bäckman, L. (2002). Differentialsex effects in olfactory functioning: The role of verbalprocessing. Journal of the International NeuropsychologicalSociety, 8, 691–698.
O’Doherty, J., Kringelbach, M. L., Rolls, E. T., Hornak, J., &Andrews, C. (2001). Abstract reward and punishment
representatives in the human orbitofrontal cortex. NatureNeuroscience, 4, 95–102.
Ogden, J. A. (1985). Anterior-posterior interhemispheric dif-ferences in the loci of lesions producing visual hemine-glect. Brain and Cognition, 4, 59–75.
Ojemann, G. A. (1980). Brain mechanisms for language:Observation during neurosurgery. In J. S. Lockard & A. A. J. Ward (Eds.), Epilepsy: A window to brain mecha-nisms. New York: Raven Press.
Olanow, C. W., & Tatton, W. G. (1999). Etiology and patho-genesis of Parkinson’s disease. Annual Review ofNeuroscience, 22, 123–144.
Oldfield, R. C. (1971). The assessment and analysis of handed-ness: The Edinburgh inventory. Neuropsychologia, 9, 97–113.
Olson, L. (1990). Grafts and growth factors in CNS. Basic sci-ence with clinical promise. Stereotactic FunctionalNeurosurgery, 54, 250–267.
Ommaya, A. K., & Gennarelli, T. A. (1974). Cerebral concus-sion and traumatic unconsciousness. Brain, 97, 633–654.
Osborne, L., & Pober, B. (2001). Genetics of childhood disor-ders: XXVII. Genes and cognition in Williams syndrome.Journal of the American Child and Adolescent Psychiatry,40, 732–735.
Osterrieth, P. A. (1944). Le test de copie d’une figure com-plexe. Archives de Psychologie, 30, 206–356.
Ozonoff, S. (2001). Advances in the cognitive neuroscience ofautism. In C. A. Nelson & M. Luciana (Eds.), Handbookof developmental cognitive neuroscience (pp. 537–548).Cambridge, MA: MIT Press.
Ozonoff, S., & Griffith, E. M. (2000). Neuropsychologicalfunction and the external validity of Asperger syndrome.In A. Klin, F. R. Volkmar, & S. S. Sparrow (Eds.),Asperger syndrome (pp. 72–96). New York: Guilford Press.
Ozonoff, S., & Jensen, J. (1999). Specific executive functionprofiles in three neurodevelopmental disorders. Journal ofAutism and Developmental Disorders, 29, 171–177.
Ozonoff, S., & Strayer, D. L. (2001). Further evidence ofintact working memory ability in autism. Journal ofAutism and Developmental Disorders, 31, 257–263.
Papalia, D. E., & Olds, S. W. (1995). Human development(6th ed.). New York: McGraw-Hill.
Papez, J. W. (1937). A proposed mechanism of emotion.Archives of Neurology & Psychiatry, 38, 725–743.
Pargman, D. (1999). Psychological bases of sport injuries (2nded.). Morgantown, WV: Fitness Information Technology.
Pascual-Leone, A., & Hamilton, R. (2001). The metamodalorganization of the brain. Progress in Brain Research, 134,427–445.
Paterniti, M. (2000). Driving Mr. Albert: A trip across Americawith Einstein’s brain. New York: Random House.
Paterson, A., & Zangwill, O. L. (1944). Disorders of visualspace perception associated with lesions of the right cerebral hemisphere. Brain, 67, 331–358.
Paus, T., Otaky, N., Caramanos, Z., MacDonald, D.,Zijdenbos, A., d’Avirro, D., et al. (1996). In vivo mor-phometry of the intrasulcal gray matter in the human
498 References

cingulate, paracingulate, and superior-rostral sulci:Hemispheric asymmetries, gender differences and proba-bility maps. Journal of Comparative Neurology, 376,664–673.
Pavlides, C., & Winson, J. (1989). Influences of hippocampalplace cell firing in the awake state on the activity of thesecells during subsequent sleep episodes. Journal ofNeuroscience, 9, 2907–2918.
Pearson, D. A., Yaffee, L. S., Loveland, K. A., & Norton, A. M. (1995). Covert visual attention in children withattention deficit hyperactivity disorder: Evidence for devel-opmental immaturity? Development and Psychopathology, 7,351–367.
Pelletier, P. M., Ahmad, S. A., & Rourke, B. P. (2001).Classification rules for basic phonological processing dis-abilities and nonverbal learning disabilities: Formulationand external validity. Child Neuropsychology, 7, 84–98.
Pellman, E. J., Lovell, M. R., Viano, D. C., Casson, I. R., &Tucker, A. M. (2004). Concussion in professional foot-ball: Neuropsychological testing. Neurosurgery, 55,1290–1303.
Penfield, W. (1975). The mystery of the mind. Princeton, NJ:Princeton University Press.
Penfield, W., & Jasper, H. H. (1954). Epilepsy and the function-al anatomy of the human brain. Boston: Little, Brown.
Penfield, W., & Milner, B. (1958). Memory deficit producedby bilateral lesions in the hippocampal zone. Archives ofNeurology Psychiatry, 79, 475.
Pennington, B. F. (1991). Diagnosing learning disorders: A neu-rological framework. New York: Guilford Press.
Pennington, B. F. (1997a). Attention deficit hyperactivity dis-order. In T. E. Feinberg & M. J. Farah (Eds.), Behavioralneurology and neuropsychology (pp. 803–807). New York:McGraw-Hill.
Pennington, B. F. (1997b). Dimensions of executive functionsin normal and abnormal development. In N. A.Krasnegor, G. R. Lyon, & P. S. Goldman-Rakic (Eds.),Development of the prefrontal cortex: Evolution, neurobiolo-gy, and behavior (pp. 265–282). Baltimore: Paul H.Brookes.
Pennington, B. F. (2002). The development of psychopathology:Nature and nurture. New York: Guilford Press.
Pennington, B. F., Heaton, R. K., Karzmark, P., Pendleton, M. G., Lehman, R., & Shucard, D. W. (1985). The neu-ropsychological phenotype in Turner syndrome. Cortex,21, 391–404.
Pennington, B. F., & Ozonoff, S. (1996). Executive functionsand developmental psychopathology. Journal of ChildPsychology and Psychiatry, 37, 51–87.
Pennington, B. F., & Smith, S. (1983). Genetic influences onlearning disabilities and speech and language disorders.Child Development, 54, 369–387.
Penny, J. B., & Young, A. B. (1993). Huntington’s disease. InJ. Jankovic & E. Tolosa (Eds.), Parkinson’s disease andmovement disorders (2nd ed., pp. 205–216). Baltimore:Williams & Wilkins.
Petersen, R. C. (2004). Mild cognitive impairment as a diag-nostic entity. Journal of Internal Medicine, 256(3),183–194.
Petersen, R. C. (2005). Mild cognitive impairment: Where arewe? Alzheimer Disease Association Disorders, 19(3),166–169.
Petersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J.,Tangalos, E. G., & Kokmen, E. (1999). Mild cognitiveimpairment: Clinical characterization and outcome.Archives of Neurology, 56(3), 303–308.
Petersen, S. E., Robinson, D. L., & Morris, J. D. (1987).Contributions of the pulvinar to visual spatial attention.Neuropsychology, 25, 97–105.
Peterson, B. S., Thomas, P., Kane, M. J., Scahill, L., Zhang,H., Bronen, R., et al. (2003). Basal ganglia volumes inpatients with Gilles de la Tourette syndrome. Archives ofGeneral Psychiatry, 60, 415–424.
Petitto, L. A., Zatorre, R. J., Gauna, K., Nikelski, E. J., Dostie,D., & Evans, A. C. (2000). Speech-like cerebral activityin profoundly deaf people processing signed languages:Implications for the neural basis of human language.Proceedings of the National Academy of Sciences, 97,13961–13966.
Petri, H. L., & Mishkin, M. (1994). Behaviorism, cognitivismand the neuropsychology of memory. American Scientist,82, 30–37.
Petrides, M. (1998). Specialized systems for the processing ofmnemonic information within the primate frontal cortex.In A. C. Roberts, T. W. Robbins, & L. Weiskrantz (Eds.),The prefrontal cortex: Executive and cognitive functions(pp. 103–116). New York: Oxford University Press.
Pfefferbaum, A., Mathalon, D. H., Sullivan, E. V., Rawles, J. M., Zipursky, R. B., & Lim, K. O. (1994). A quantita-tive magnetic resonance imaging study of changes inbrain morphology from infancy to late adulthood.Archives of Neurology, 51, 874–887.
Pfrieger, F. W., & Barres, B. A. (1997). Synaptic efficacyenhanced by glial cells in vitro. Science, 277(5332),1684–1687.
Phelps, E. A., O’Connor, K. J., Gatenby, J. C., Gore, J. C.,Grillon, C., & Davis, M. (2001). Activation of the leftamygdala to a cognitive representation of fear. NatureNeuroscience, 4, 437–441.
Phillips, S. M., & Sherwin, B. B. (1992). Effects of estrogenon memory function in surgically menopausal women.Psychoneuroendocrinology, 17, 485–495.
Piacentini, J., & Chang, S. (2001). Behavioral treatments forTourette syndrome and tic disorders: State of the art. InD. J. Cohen & C. G. Goetz (Eds.), Tourette syndrome(pp. 319–331). Philadelphia: Lippincott Williams &Wilkins.
Piggot, J., Kwon, H., Mobbs, D., Blasey, C., Lotspeich, L.,Menon, V., et al. (2004). Emotional attribution in high-functioning individuals with autism spectrum disorder: Afunctional imaging study. Journal of the American Childand Adolescent Psychiatry, 43, 473–480.
References 499
Pincus, J. H., & Tucker, G. J. (1985). Behavioral neurology.New York: Oxford University Press.
Pinel, P. J., & Edwards, M. (1998). A colorful introduction tothe anatomy of the human brain. Boston: Allyn & Bacon.
Piven, J., Berthier, M. L., Starkstein, S. E., Nehme, E.,Pearlson, G., & Folstein, S. (1990). Magnetic resonanceimaging evidence for a defect of cerebral cortical develop-ment in autism. American Journal of Psychiatry, 147,734–739.
Piven, J., Harper, J., Palmer, P., & Arndt, S. (1996). Course ofbehavioral change in autism: A retrospective study ofhigh-IQ adolescents and adults. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 35, 523–529.
Platek, S. M., Keenan, J. P., Gallup, G. G., Jr., & Mohamed, F. B.(2004). Where am I? The neurological correlates of selfand other. Cognitive Brain Research, 19(2), 114–122.
Platek, Steven M; Loughead, James W; Gur, Ruben C; Busch,Samantha; Ruparel, Kosha; Phend, Nicholas; Panyavin,Ivan S; Langleben, Daniel D. (2006). Neural Substratesfor Functionally Discriminating Self-Face From PersonallyFamiliar Faces. Human Brain Mapping, 27(2), 91–98.
Pliszka, S. R. (2003). Neuroscience for the mental health clini-cian. New York: Guilford Press.
Polster, M. R. (1993). Drug-induced amnesia: Implication forcognitive neuropsychological investigations of memory.Psychological Bulletin, 114, 477–493.
Poppel, E., & Richards, W. A. (1974). Light sensitivity in cor-tical scotomata contralateral to small islands of blindness.Experimental Brain Research, 21, 125–130.
Poppel, E., & vonSteinbuchel, N. (1992). Neuropsychologicalrehabilitation from a theoretical point of view. In N.vonSteinbuchel, D. Y. von Cramon, & E. Poppel (Eds.),Neuropsychological rehabilitation (pp. 3–19). Berlin:Springer.
Popplestone, J. A., & McPherson, M. W. (1994). An illustratedhistory of American psychology. Madison, WI: Brown &Benchmark.
Portin, R., & Rinne, U. (1986). Predictive factors for cognitivedeterioration and dementia in Parkinson’s disease.Advances in Neurology, 45, 413–416.
Posner, M. I. (1992). Attention as a cognitive and neural sys-tem. Current Directions in Psychological Science, 1,11–14.
Posner, M. I., & DiGirolama, G. J. (1998). Executive control:Conflict, target detection, and cognitive control. In R.Parasuraman (Ed.), The attentive brain (pp. 401–424).Cambridge, MA: MIT Press.
Posner, M. I., & Fan, J. (2004). Attention as an organ system.In J. Pomerantz (Ed.), Neurobiology of perception and com-munication: From synapse to society the IVth De Lange con-ference. Cambridge, United Kingdom: CambridgeUniversity Press.
Posner, M. I., & Petersen, S. E. (1990). The attention systemof the human brain. Annual Review of Neuroscience, 13,25–42.
Postma, A., Izendoorn, R., & De Haan, E. H. F. (1998). Sexdifferences and object location memory. Brain andCognition, 36, 334–345.
Potegal, M. (1971). A note on spatial motor deficits in patientswith Huntington’s disease: A test of a hypothesis.Neuropsychologia, 9, 233–235.
Powell, M. P., & Schulte, T. (1999). Turner syndrome. In S.Goldstein & C. R. Reynolds (Eds.), Handbook of neurode-velopmental and genetic disorders of childhood (pp. 277–297).New York: Guilford Press.
Powers, W. J. (1990.). Stroke. In A. L. Pearlman & R. C.Collins (Eds.), Neurobiology of disease. New York: OxfordUniversity Press.
Preston, J. D., O’Neal, J. H., & Talaga, M. C. (1997).Handbook of clinical psychopharmacology for therapist (2nded.). Oakland, CA: New Harbinger Publications.
Price, B. H., Gurvit, H., Weintrub, S., Geula, C., Leimkuhler,E., & Mesulam, M. (1993). Neuropsychological patternsand language deficits in 20 consecutive cases of autopsy-confirmed Alzheimer’s disease. Archives of Neurology, 50,931–937.
Prigatano, G. P. (1992). Neuropsychological rehabilitation andthe problem of altered self-awareness. In N.vonSteinbuchel, D. Y. von Cramon, & E. Poppel (Eds.),Neuropsychological rehabilitation. Berlin: Springer.
Prigatano, G. P. (1999). Principles of neuropsychological rehabili-tation. New York: Oxford University Press.
Pritchard, P. B., Holmstrom, V. L., & Giacinto, J. (1985). Self-abatement of complex partial seizures. Annals ofNeurology, 18, 265–267.
Pruisiner, S. B. (1982). Novel proteinaceous infectious particlescause scrapie. Science, 216, 136–144.
Pugh, K. R., Mencl, W. E., Jenner, A. R., Katz, L., Frost, S. J.,Lee, J. R., et al. (2000). Functional neuroimaging studiesof reading and reading disability (developmental dyslexia).Mental Retardation and Developmental Disabilities ResearchReview, 6, 207–213.
Purves, D., Augustine, G. J., Fitzpatrick, D., Katz, L. C.,LaMantia, A., McNamara, J. O., & Williams, S. M.(Eds.) (2001). Neuroscience (2nd ed.) Sunderland, MA:Sinauer Associates.
Purvis, K. L., & Tannock, R. (2000). Phonological processing,not inhibitory control, differentiates ADHD and readingdisability. Journal of the American Academy of Child andAdolescent Psychiatry, 39, 485–494.
Rabinowicz, T., Dean, J. M.-C., Petetot, J. M. C., & deCourten-Myers, G. M. (1999). Gender differences in thehuman cerebral cortex: More neurons in males; moreprocesses in females. Journal of Child Neurology, 14,98–107.
Ragland, J. D., Gur, R. C., Raz, J., Schroeder, L., Smith, R. J.,Alavi, A., et al. (2000). Hemispheric activation of anteriorand inferior prefrontal cortex during verbal encoding andrecognition: A PET study of healthy volunteers.NeuroImage, 11, 624–633.
500 References

Raichle, M. E. (1983). Positron emission tomography. AnnualReview of Neuroscience, 6, 249–267.
Rakic, P., & Lombroso, P. J. (1998). Development of the cere-bral cortex: I. forming the cortical structure. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 37,116–117.
Ramachandran, V. S., Rogers-Ramachandran, D., & Steward,M. (1992). Perceptual correlates of massive cortical reor-ganization. Science, 258, 1159–1160.
Raskin, S. A., Borod, J. C., & Tweedy, J. (1990).Neuropsychological aspects of Parkinson’s disease.Neuropsychology Review, 1, 185–221.
Raz, N. (2000). Aging of the brain and its impact on cognitiveperformance: Integration of structural and functionalfindings. In F. I. M. Craik & T. A. Salthouse (Eds.),Handbook of aging and cognition (2nd ed., pp. 1–90).Mahwah, NJ: Erlbaum.
Raz, N. (2005). The aging brain observed in vivo: Differentialchanges and their modifiers. In R. Cabeza, L. Nyberg, &D. Park (Eds.), Cognitive neuroscience of aging. New York:Oxford.
Rebok, G. W., & Folstein, M. F. (1993). Dementia. Journal ofNeuropsychiatry and Clinical Neurosciences, 5, 265–276.
Rees, J. R. (1948). The case of Rudolf Hess: A problem in diag-nosis and forensic psychiatry. New York: Norton.
Reiss, A. L., Eliez, S., Schmitt, J. E., Straus, E., Lai, Z., Jones,W., et al. (2000). Neuroanatomy of Williams syndrome:A high-resolution MRI study. Journal of CognitiveNeuroscience, 12(Suppl.), 65–73.
Reiss, A. L., Mazzocco, M. M. M., Greenlaw, R., Freund, L. S., & Ross, J. L. (1995). Neurodevelopmental effect on X monosomy: A volumetric imaging study. AmericanNeurological Association, 38, 731–738.
Reitan, R. M. (1966). A research program on the psychologicaleffects of brain lesions in human beings. In N. R. Ellis(Ed.), International review of research in mental retardation(pp. 153–218). New York: Academic Press.
Reitan, R. M., & Davison, L. A. (1974). Clinical neuropsychol-ogy: Current status and applications. Washington, DC: V. H. Winston.
Reitan, R. M., & Wolfson, D. (1993). The Halstead-ReitanNeuropsychological Test Battery: Theory and clinical inter-pretation (2nd ed.). Tucson, AZ: Neuropsychology Press.
Rey, A. (1941). Psychological examination of traumaticencephalopathy. Archives de Psychologie, 28, 286–340.
Rhodes, R. (1997). Deadly feasts. New York: Simon andSchuster.
Richard, A., & Reiter, J. (1990). Epilepsy: A new approach.New York: Prentice Hall.
Richters, J. E., Arnold, L. E., Jensen, P. S., Abikoff, H.,Conners, C. K., Greenhill, L. L., et al. (1995). NIMHcollaborative multisite multimodal treatment study ofchildren with ADHD: Background and rationale. Journalof the American Academy of Child and AdolescentPsychiatry, 34, 987–1008.
Rilke, R. M. (1996). Rilke’s book of hours: Love poems to God(A. Burrows & J. Macy, Trans.). New York: RiverheadBooks.
Rimel, R. W., Giordani, B., Barth, J. T., Boll, T. J., & Jane, J. A.(1981). Disability caused by minor head injury.Neurosurgery, 9(3), 221–228.
Ris, M. D., Kietrich, K. N., Succop, P. A., Berger, O. G., &Bornschein, R. L. (2004). Early exposure to lead and neu-ropsychological outcomes in adolescence. Journal of theInternational Neuropsychological Society, 10, 261–270.
Roberts, A. C., Robbins, T. W., & Weiskrantz, L. (1998).Discussions and conclusions. In A. C. Roberts, T. W.Robbins, & L. Weiskrantz (Eds.), The prefrontal cortex:Executive and cognitive functions (pp. 221–242). NewYork: Oxford University Press.
Roberts, J. E., & Bell, M. A. (2003). Two- and three-dimensional mental rotation tasks lead to different pari-etal laterality for men and women. International Journalof Psychophysiology, 50, 235–246.
Robinson, B. F., Mervis, C. B., & Robinson, B. W. (2003).The roles of verbal short-term and working memory inthe acquisition of grammar by children with Williamssyndrome. Developmental Neuropsychology, 23, 13–32.
Roeser, R. J., & Daly, D. D. (1974). Auditory cortex deconnec-tion associated with thalamic tumor. Neurology, 24, 555.
Roland, P. E., Larsen, B., Lassen, N. A., & Skinholf, E. (1980).Supplementary motor area and other cortical areas inorganization of voluntary movements in man. Journal ofNeurophysiology, 43, 118–136.
Rolls, E. T. (1986). Neuronal activity related to the control offeeding. In R. Ritter & S. Ritter (Eds.), Neural andhumoral controls of food intake. New York: Academic Press.
Rolls, E. T. (1998). The orbitofrontal cortex. In A. C. Roberts,T. W. Robbins, & L. Weiskrantz (Eds.), The prefrontalcortex: Executive and cognitive functions (pp. 67–86). NewYork: Oxford University Press.
Rolls, E. T. (2002). The functions of the orbitofrontal cortex.In D. T. Stuss & R. T. Knight (Eds.), Principles of frontallobe function (pp. 354–375). New York: OxfordUniversity Press.
Romans, S. M., Roeltgen, D. P., Kushner, H., & Ross, J. L.(1997). Executive function in girls with Turner’s syn-drome. Developmental Neuropsychology, 13, 23–40.
Romine, C. B., & Reynolds, C. R. (2005). A model of thedevelopment of frontal lobe functioning: Findings from a meta-analysis. Applied Neuropsychology, 12,190–201.
Rorschach, H. (1942). Psychodiagnostics: A diagnostic test basedon perception. Bern, Switzerland: Huber.
Rosenblum, J. A. (1974). Human sexuality and cerebral cortex.Disorder of the Nervous System, 35, 268.
Ross, E. (1985). Modulation of affect and nonverbal commu-nication by the right hemisphere. In M. M. Mesulam(Ed.), Principles of behavioral neurology (pp. 239–257).Philadelphia: F. A. Davis.
References 501
Rosvold, H. E., Mirsky, A. F., Sarason, I., Bransome, E. D., &Beck, L. H. (1956). A continuous performance test of braindamage. Journal of Consulting Psychology, 20, 343–350.
Rourke, B. B., & Del Dotto, J. E. (1994). Learning disabilities:A neuropsychological perspective. Thousand Oaks, CA: Sage.
Rourke, B. P. (1989). Non-verbal learning disabilities: The syn-drome and the model. New York: Guilford Press.
Rourke, B. P. (1993). Arithmetic disabilities, specific and oth-erwise: A neuropsychological perspective. Journal ofLearning Disabilities, 26, 214–226.
Rourke, B. P. (1995). The NLD syndrome and the white mat-ter model. In B. P. Rourke (Ed.), Syndrome of nonverballearning disabilities: Neurodevelopmental manifestations(pp. 1–26). New York: Guilford Press.
Rourke, B. P., Bakker, D. J., Fisk, L. J., & Strang, J. D. (1983).Child neuropsychology: An introduction to theory, research,and clinical practice. New York: Guilford Press.
Rourke, B. P., & Conway, J. A. (1997). Disabilities of arith-metic and mathematical reasoning: Perspectives from neu-rology and neuropsychology. Journal of LearningDisabilities, 30, 34–46.
Rourke, B. P., Fisk, J. L., & Strang, J. D. (1986).Neuropsychological assessment of children: A treatment-oriented approach. New York: Guilford Press.
Rourke, B. P., & Fuerst, D. E. (1996). Psychosocial dimensionsof learning disability subtypes. Assessment, 3, 277–290.
Rousseau, A., Hermann, B., & Whitman, S. (1985). Effects ofprogressive relaxation on epilepsy: Analysis of a series ofcases. Psychology Reports, 57(3 Pt 2), 1203–1212.
Rovee-Collier, C. (1993). The capacity for long-term memoryin infancy. Current Directions in Psychological Science, 2,130–135.
Rovet, J. F. (1993). The psychoeducational characteristics ofchildren with Turner syndrome. Journal of LearningDisabilities, 26, 333–341.
Rowe, A. D., Bullock, P. R., Polkey, C. E., & Morris, R. G.(2001). ‘Theory of mind’ impairments and their relation-ship to executive functioning following frontal lobe exci-sions. Brain, 124, 600–616.
Rowland, L. P., Fink, M., & Rubin, L. (1991). Cerebrospinalfluid: Blood-brain barrier, brain edema, and hydrocephalus.In E. R. Kandel, J. H. Schwartz, & T. M. Jessell (Eds.),Principles of neural science (3rd ed., pp. 1050–1060).New York: Elsevier Science.
Roy, A., De Jong, J., & Linnoila, M. (1989). Cerebrospinalfluid monoamine metabolites and suicidal behavior indepressed patients. Archives of General Psychiatry, 46,609–612.
Rubens, A. B., & Benson, D. F. (1971). Associative visualagnosia. Archives of Neurology, 24, 304–316.
Rubia, K., Overmeyer, S., Talyor, E., Brammer, M., Williams,S. C. R., Simmons, A., et al. (1999). Hypofrontality inattention deficit/hyperactivity disorder during higher-order motor control: A study with functional MRI.American Journal of Psychiatry, 156, 891–896.
Ruchinskas, R. A., Francis, J. P., & Barth, J. T. (1997). Mildhead injury in sports. Applied Neuropsychology, 4(1),43–49.
Rumsey, J. M. (1996a). Neuroimaging in developmentaldyslexia. In G. R. Lyon & J. M. Rumsey (Eds.),Neuroimaging: A window to the neurological foundations oflearning and behavior in children (pp. 57–78). Baltimore:Paul H. Brookes.
Rumsey, J. M. (1996b). Neuroimaging studies of autism. In G. R. Lyon & J. M. Rumsey (Eds.), Neuroimaging: A win-dow to the neurological foundations of learning and behaviorin children (pp. 119–146). Baltimore: Paul H. Brookes.
Rumsey, J. M. (1998). Brain imaging of reading disorders.Journal of the American Academy of Child and AdolescentPsychiatry, 37, 12.
Rumsey, J. M., Andreason, P., Zametkin, A. J., Aquino, T.,King, A. C., Hamberger, S. D., et al. (1992). Failure toactivate the left temporoparietal cortex in dyslexia.Archives of Neurology, 49, 527–534.
Russell, W. R., & Espir, M. L. E. (1961). Traumatic aphasia.London: Oxford University Press.
Rutherford, M. D., & Rogers, S. J. (2003). Cognitive under-pinnings of pretend play in autism. Journal of Autism andDevelopmental Disorders, 33, 289–302.
Rutter, M., Le Couteur, A., & Lord, C. (2003). ADI-R AutismDiagnostic Interview-Revised. Los Angeles, CA: WesternPsychological Services.
Sacks, O. (1987). The man who mistook his wife for a hat. NewYork: Harper & Row.
Sacks, O. (1995). An anthropologist on Mars. New York: Knopf.Sadato, N., Ibañez, V., Deiber, M.P., & Hallett, M. (2000).
Gender differences in premotor activity during active tac-tile discrimination. NeuroImage, 11, 532–540.
Sadato, N., Pascual-Leone, A., Grafmani, J., Ibañez, V., Deiber,M-P., Dold, G., & Hallett, M. (1996). Activation of theprimary visual cortex by Braille reading in blind subjects.Nature, 380, 526–528.
Sagar, H., Sullivan, E., Gabrieli, J., Corkin, S., & Growdon, J.(1988). Temporal ordering and short-term memorydeficits in Parkinson’s disease. Brain, 111, 525–539.
Saint-Cyr, J. A., Bronstein, Y. L., & Cummings, J. L. (2002).Neurobehavioral consequences of neurosurgical treat-ments and focal lesions of frontal-subcortical circuits. InD. T. Stuss & R. T. Knight (Eds.), Principles of frontallobe function (pp. 408–427). New York: OxfordUniversity Press.
Salthouse, T. A. (1991). Theoretical perspectives on cognitiveaging. Hillsdale, NJ: Lawrence Erlbaum Associates.
Salthouse, T. A. (2006). Mental exercise and mental aging:Evaluating the validity of the “use it or lose it” hypothesis.Perspectives on Psychological Science, 1, 68–87.
Salthouse, T. A., Babcock, R. L., Skovronek, E., Mitchell, D. R. D., & Palmon, R. (1990). Age and experienceeffects in spatial visualization. Developmental Psychology,26, 128–136.
502 References
Santoro, J. M., & Spiers, M. V. (1994). Social cognitive factors inbrain injury associated personality change. Brain Injury, 8,265–276.
Saper, C. B., Chou, T. C., Scammell, T. E. (2001). The sleepswitch: Hypothalamic control of sleep and wakefulness.TRENDS in Neurosciences, 24, 726–731.
Sarter, M., Givens, B., & Bruno, J. P. (2001). The cognitiveneuroscience of sustained attention: Where top-downmeets bottom-up. Brain Research Reviews, 35, 146–160.
Saucier, D. M., & Elias, L. J. (2001). Lateral and sex differ-ences in manual gesture during conversation. Laterality:Asymmetries of Body, Brain, and Cognition, 6, 239–245.
Schacter, D. L. (1987). Implicit memory: History and currentstatus. Journal of Experimental Psychology: Learning,Memory and Cognition, 13, 501–518.
Schacter, D. L., & Curran, T. (2000). Memory withoutremembering and remembering without memory:Implicit and false memories. In M. S. Gazzaniga (Ed.),The new cognitive neurosciences (2nd ed., pp. 829–840).Cambridge, MA: MIT Press.
Schatschneider, C., Carlson, C. D., Francis, D. J., Foorman,B. R., & Fletcher, J. M. (2002). Relationship of rapidautomatized naming and phonological awareness in earlyreading development: Implication for the double-deficithypothesis. Journal of Learning Disabilities, 35, 245–256.
Schiller, F. (1982). Paul Broca: Explorer of the brain. New York:Oxford University Press.
Schlaepfer, T. E., Harris, G. J., Tien, A. Y., Peng, L., Lee, S., &Pearlson, G. D. (1995). Structural differences in the cere-bral cortex of healthy female and male subjects: A mag-netic resonance imaging study. Psychiatry Research:Neuroimaging, 61, 129–135.
Schnass, L., Rothenberg, S. J., Flores, M. F., Martinez, S.,Hernandez, C., Osorio, E., et al. (2006). Reduced intel-lectual development in children with prenatal lead expo-sure. Environmental Health Perspectives, 114, 791–797.
Schultz, K. P., Tang, C. Y., Fan, J., Marks, D. J., Cheung, A. M., Newcorn, J. H., et al. (2005). Differential prefrontalcortex activation during inhibitory control in adolescentswith and without childhood attention-deficit/hyperactivitydisorder. Neuropsychology, 19, 390–402.
Schultz, R. T., Gauthier, I., Klin, A., Fulbright, R. K., Anderson,A. W., Volkmar, F., et al. (2000). Abnormal ventral tempo-ral cortical activity during face discrimination amongindividuals with autism and Asperger syndrome. Archivesof General Psychiatry, 57, 331–340.
Schultz, R. T., Grelotti, D. J., Klin, A., Kleinman, J., Van derGaag, C., Marois, R. (2003). The role of the fusiform facearea in social cognition: Implications for the pathology ofautism. Philosophical Transactions of the Royal Society ofLondon, 358, 415–427.
Schultz, R. T., Grelotti, D. J., & Pober, B. (2001). Genetics ofchildhood disorders: XXVI. Williams syndrome andbrain-behavior relationships. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 40, 606–609.
Schultz, R. T., Romanski, L. M., & Tsatsanis, K. D. (2000).Neurofunctional models of autistic disorder and Aspergersyndrome: Clues from neuroimaging. In A. Klin, F. R.Volkmar, & S. S. Sparrow (Eds.), Asperger syndrome(pp. 172–209). New York: Guilford Press.
Schwartz, J. H., & Kandel, E. R. (1991). Synaptic transmis-sion mediated by second messengers. In E. R. Kandel, J. H. Schwartz, & T. M. Jessell (Eds.), Principles of neuralscience (3rd ed., pp. 173–193). New York: Elsevier.
Scott, A. M., Fletcher, J. M., Brookshire, B. L., Davidson, K. C., Landry, S. H., Bohan, T. C., et al. (1998).Memory functions in children with early hydrocephalus.Neuropsychology, 12, 578–589.
Scoville, W. B. (1968). Amnesia after bilateral mesial temporal-lobe excision: Introduction to case H.M. Neuropsychologia,6, 211–213.
Scoville, W. B., & Milner, B. (1957). Loss of recent memoryafter bilateral hippocampal lesions. Journal of Neurology,Neurosurgery, and Psychiatry, 20, 11.
Semrud-Clikeman, M., Filipek, P. A., Biederman, J., Steingard,R., Kennedy, D., Renshaw, P., et al. (1994). Attention-deficit hyperactivity disorder: Magnetic resonance imagingmorphometric analysis of the corpus callosum. Journal ofthe American Academy of Child and Adolescent Psychiatry,33, 875–881.
Semrud-Clikeman, M., Hooper, S. R., Hynd, G. W., Hern, K., Presley, R., & Watson, T. (1996). Prediction of groupmembership in developmental dyslexia, attention deficithyperactivity disorder, and normal controls using brainmorphometric analysis of magnetic resonance imaging.Archives of Clinical Neuropsychology, 11, 521–528.
Seshadri, S., Wolf, P. A., Beiser, A., Au, R., McNulty, K.,White, R., et al. (1997). Lifetime risk of dementia andAlzheimer’s disease: The impact of mortality on risk esti-mates in the Framingham Study. Neurology, 49(6),1498–1504.
Seurinck, R., Vingerhoets, G., de Lange, F. P., & Achten, E.(2004). Does egocentric mental rotation elicit sex differ-ences? NeuroImage, 4, 1440–1449.
Shallice, T. (1982). Specific impairments of planning.Philosophical Transactions of the Royal Society of London B,298, 199–209.
Shallice, T. (2001). ‘Theory of mind’ and the prefrontal cortex.Brain, 124, 247–248.
Shallice, T., & Warrington, E. K. (1970). Independent func-tioning of verbal memory stores: A neuropsychologicalstudy. Quarterly Journal of Experimental Psychology, 22,261–273.
Shallice, T., & Warrington, E. K. (1977). The possible role ofselective attention in acquired dyslexia. Neuropsychologia,15, 31–41.
Shaywitz, B. A., Shaywitz, S. E., Pugh, K. R., Constable, R. T.,Skudlarski, P., Fulbright, R. K., et al. (1995). Sex differ-ences in the functional organization of the brain for lan-guage. Nature, 373(6515), 607–609.
References 503
Shaywitz, B. A., Shaywitz, S. E., Pugh, K. R., Mencel, W. E.,Fulbright, R. K., Skudlarski, P., et al. (2002). Disruptionof posterior brain systems for reading in children withdevelopmental dyslexia. Society of Biological Psychiatry, 52,101–110.
Shaywitz, S., & Shaywitz, B. (1999). Dyslexia. In K. Swaiman& S. Ashwal (Eds.), Pediatric neurology: Principles & practice (Vol. 1, pp. 576–584). St. Louis, MO: Mosby.
Shaywitz, S. E., & Shawitz, B. A. (2005). Dyslexia (specificreading disability). Biological Psychiatry, 57, 1301–1309.
Shaywitz, S. E., Shaywitz, B. A., Fulbright, R. K., Skudlarski,P. M., Mencl, W. E., Constable, R. T., et al. (2003).Neural systems for compensation and persistence: Youngadult outcome of childhood reasoning disability.Biological Psychiatry, 54, 25–33.
Shaywitz, S. E., Shaywitz, B. A., Pugh, K. R., Fulbright, R. K.,Constable, R. T., Mencl, W. E., et al. (1998). Functionaldisruption in the organization of the brain for reading indyslexia. Proceedings of the National Academy of Sciences,95, 2636–2641.
Shaywitz, S. E., Shaywitz, B. A., Pugh, K. R., Fulbright, R. K.,Skudlarski, P. M., Mencl, W. E., et al. (1999). Effect ofestrogen on brain activation patterns in postmenopausalwomen during working memory tasks. Journal of theAmerican Medical Association, 281, 1197–1202.
Sheppard, D. M., Bradshaw, J. L., Purcell, R., & Pantelis, C.(1999). Tourette’s and comorbid syndromes: Obsessivecompulsive and attention deficit hyperactivity disorder. A common etiology? Clinical Psychology Review, 19, 531–552.
Sherin, J. E., Shiromani, P., McCarley, R. W., & Saper, C. B.(1996). Ventrolateral preoptic neurons that innervate thetuberomammillary nucleus are activated during sleep.Science, 271, 216–219.
Sherwin, B. B., & Tulandi, T. (1996). “Add-back” estrogenreverses cognitive deficits induced by a gonadotropinreleasing-hormone agonist in women with leiomyomatauteri. Journal of Clinical Endocrinology and Metabolism,81, 2545–2549.
Shumaker, S. A., Legault, C., Kuller, L., Rapp, S. R., Thal, L.,Lane, D. S., et al. (2004). Conjugated equine estrogensand incidence of probable dementia and mild cognitiveimpairment in postmenopausal women. Journal of theAmerican Medical Association, 291, 2947–2958.
Shumaker, S. A., Legault, C., Rapp, S. R., Thal, L., Wallace, R. B., Ockene, J. K., et al. (2003). Estrogen plus prog-estin and the incidence of dementia and mild cognitiveimpairment in postmenopausal women. Journal of theAmerican Medical Association, 289, 2651–2662.
Siegel, L. S. (2003). IQ-discrepancy definitions and the diag-nosis of LD: Introduction to the special issue. Journal ofLearning Disabilities, 36, 2–3.
Siegel-Hinson, R. I., & McKeever, W. F. (2002). Hemisphericspecialization, spatial activity experience, and sex differ-ences on tests of mental rotation ability. Laterality:Asymmetries of Body, Brain, and Cognition, 7, 59–74.
Sigman, M. (1994). What are the core deficits in autism? In S. H. Broman, & Grafman, J. (Eds.), Atypical cognitivedeficits in developmental disorders (pp. 139–158). NewYork: Oxford University Press.
Silverstein, S. M., Como, P. G., Palumbo, D. R., West, L. L.,& Osborn, L. M. (1995). Multiple sources of attentionaldysfunction in adults with Tourette’s syndrome:Comparison with attention deficit-hyperactivity disorder.Neuropsychology, 9, 157–164.
Singer, H. S., & Minzer, K. (2003). Neurobiology of Tourette’ssyndrome: Concepts of neuroanatomic localization andneurochemical abnormalities. Brain Development,25(Suppl.), 70–84.
Sitaram, N., Moore, A. M., & Gillin, J. C. (1978).Experimental acceleration and slowing of REM ultradianrhythm by cholinergic agonist and antagonist. Nature,274, 490–492.
Skottun, B. C., & Parke, L. A. (1999). The possible relation-ship between visual deficits and dyslexia: Examination ofa critical assumption. Journal of Disabilities, 32, 2–5.
Smalley, S. L., Bailey, J. N., Palmer, C. G., Cantwell, D. P.,McGough, J. J., Del’Homme, M. A., et al. (1998).Evidence that the dopamine D4 receptor is a susceptibili-ty gene in attention deficit hyperactivity disorder.Molecular Psychiatry, 3, 427–430.
Smith, A. (1982). Symbol Digit Modalities Test SDMT. Manualrevised. Los Angeles: Western Psychological Services.
Smith, D. V., & Vogt, M. B. (1997). The neural code andintegrative processes of taste. In G. K. Beauchamp & L. Bartoshuk (Eds.), Tasting and smelling. San Diego, CA:Academic Press.
Smith, E. E., Marshuetz, C., & Geva, A. (2002). Workingmemory: Findings from neuroimaging and patient stud-ies. In F. Boller, J. Grafman (Series Eds.), & J. Grafman(Vol. Ed.), Handbook of neuropsychology. The frontal lobes(Vol. 7, 2nd ed., pp. 55–72). New York: Elsevier.
Snead, O. C. (1995). Basic mechanisms of generalized absenceseizures. Annals of Neurology, 37, 146–157.
Snowdon, D. A., Greiner, L. H., Kemper, S. J., Nanayakkara,N., & Mortimer, J. A. (1999). Linguistic ability in earlylife and longevity: Findings from the Nun Study. In J. M.Robine, B. Forette, C. Franceschi, & M. Allard (Eds.),The paradoxes of longevity. Berlin: Springer.
Snyder, A. Z., Petersen, S., Fox, P., & Raichle, M. E. (1989).PET studies of visual word recognition. Journal ofCerebral Blood Flow and Metabolism, 9(Suppl. 1), S576.
Soliveri, P., Brown, R. G., Jahanshahi, M., & Marsden, C. D. (1992). Procedural memory and neurological disease. European Journal of Cognitive Psychology, 4,161–193.
Sommer, I. E. C., Aleman, A., Bouma, A., & Kahn, R. S.(2004). Do women really have more bilateral languagerepresentation than men? A meta-analysis of functionalimaging studies. Brain, 127, 1845–1852.
504 References
Song, H. J., Stevens, C. F., & Gagge, F. H. (2002). Neuralstem cells from adult hippocampus develop essentialproperties of functional CNS neurons. NaturalNeuroscience, 5, 438–445.
Sowell, E. R., Thompson, P. M., Welcome, S. E., Henkenius,A. L., Toga, A. W., & Peterson, B. S. (2004). Corticalabnormalities in children and adolescents with attentiondefict hyperactivity disorder. Lancet, 362, 1699–1707.
Sparks, B. F., Friedman, S. D., Shaw, D. W., Aylward, E. H.,Echelard, D., Artru, A. A., et al. (2002). Brain structuralabnormalities in young children witrh autism spectrumdisorder. Neurology, 59, 184–192.
Spencer, T. J. (2002). Attention-deficit/hyperactivity disorder.Archives of Neurology, 59, 314–316.
Spiers, M. (1995). The cognitive screening for medication self-management. Unpublished test, Drexel University,Philadelphia, Pennsylvania.
Spiers, M. V., & Kutzik, D. M. (1995). Self-reported memoryof medication use by the elderly. American Journal ofHealth-System Pharmacy, 52, 985–990.
Spiers, M. V., Pouk, J. A., & Santoro, J. M. (1994). Examiningperspective-taking in the severely head-injured. BrainInjury, 8, 463–473.
Spreen, O., Risser, A. T., & Edgell, D. (1995). Developmentalneuropsychiatry. New York: Oxford University Press.
Springer, J. A., Binder, J. R., Hammeke, T. A., Swanson, S. J.,Frost, J. A., Bellgowan, P. S. F., et al. (1999). Languagedominance in neurologically normal and epilepsy sub-jects. Brain, 122, 2033–2046.
Springer, S. P., & Deutsch, G. (1993). Left brain, right brain(4th ed.). New York: W. H. Freeman.
Squire, L. R. (1987). Memory and brain. New York: OxfordUniversity Press.
Squire, L. R. (1994). Declarative and nondeclarative memory:Multiple brain systems supporting learning and memory.In D. L. Schacter & E. Tulving (Eds.), Memory systems(pp. 203–232). Cambridge, MA: MIT Press.
Squire, L. R., & Butters, N. (1992). Neuropsychology of memory(2nd ed.). New York: Guilford Press.
Squire, L. R., & Cohen, N. J. (1984). Human memory andAmnesia. In G. Lynch, J. L. McGaugh, & N. M.Weinberger (Eds.), Neurobiology of learning and memory.New York: Guilford Press.
Squire, L. R., & Knowlton, B. J. (2000). The medial temporallobe, the hippocampus, and the memory systems of thebrain. In M. S. Gazzaniga (Ed.), The new cognitive neuro-sciences (2nd ed., pp. 765–779). Cambridge, MA: MITPress.
Stahl, S. M. (2000). Essential psychopharmacology:Neuroscientific basis and practical application (2nd ed.).Cambridge, United Kingdom: Cambridge Press.
Stebbins, G. T., Singh, J., Weiner, J., Wilson, R. S., Goetz, C. G., & Gabrieli, J. D. E. (1995). Selective impairmentsof memory functioning in unmedicated adults with Gillesde la Tourette’s syndrome. Neuropsychology, 9, 329–337.
Stein, J. (2001). The sensory basis of reading problems.Developmental Neuropsychology, 20, 509–534.
Steinhausen, H. C., Willms, J., & Spohr, H. L. (1993). Long-term psychopathological and cognitive outcome of chil-dren with fetal alcohol syndrome. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 32, 990–994.
Steinmetz, H., Jancke, L., Kleinschmidt, A., Schlaug, G.,Volkmann, J., & Huang, Y. (1992). Sex but no hand dif-ference in the isthmus of the corpus callosum. Neurology,42, 749–752.
Steinmetz, H., Staiger, J. F., Schlaug, G., Huang, Y., & Jancke,L. (1995). Corpus callosum and brain volume in womenand men. NeuroReport, 6, 1002–1004.
Stevens, T., Livingston, G., Kitchen, G., Manela, M., Walker,Z., & Katona, C. (2002). Islington study of dementiasubtypes in the community. British Journal of Psychiatry,180, 270–276.
Stewart, B. (1995). American football. American History, 30,29–69.
Stiles, J. (2000). Neural plasticity and cognitive development.Developmental Neuropsychology, 18, 237–272.
Stiles, J., Bates, E. A., Thal, D., Trauner, D., & Reilly, J.(1998). Linguistic, cognitive, and affective developmentin children with pre- and perinatal focal brain injury: Aten-year overview from the San Diego longitudinal proj-ect. In C. Rovee-Collier, L. P. Lipsitt, & H. Hayne (Eds.),Advances in infancy research (pp. 131–163). Stamford, CT:Ablex Publishing.
Strassburger, T. L., Lee, H. C., Daly, E. M., Szczepanik, J.,Krasuski, J. S., Mentis, M. J., et al. (1997). Interactiveeffects of age and hypertension on volumes of brain struc-tures. Stroke, 28(7), 1410–1417.
Streissguth, A. (1997). Fetal alcohol syndrome. Baltimore: PaulH. Brookes.
Streissguth, A. P., Barr, H. M., Bookstein, F. L., Sampson, P. D., & Carmichael Olson, H. (1999). The long-termneurocognitive consequences of prenatal alcohol exposure:A 14-year study. Psychological Science, 10, 186–190.
Streissguth, A. P., & Connor, P. D. (2001). Fetal alcohol syn-drome and other effects of prenatal alcohol: Developmentalcognitive neuroscience implications. In C. A. Nelson & M.Luciana (Eds.), Handbook of developmental cognitive neuro-science (pp. 505–518). Cambridge, MA: MIT Press.
Stroop, J. R. (1935). Studies of interference in serial verbalreactions. Journal of Experimental Psychology: LearningMemory & Cognition, 18, 643–662.
Stuss, D. T., & Benson, D. F. (1986). The frontal lobes. NewYork: Raven Press.
Stuss, D. T., Gallup, G. G., & Alexander, M. P. (2001). Thefrontal lobes are necessary for ‘theory of mind.’ Brain,124, 279–286.
Suganthy, J., Raghuram, L., Antonisamy, B., Vettivel, S.,Madhavi, C., & Koshi, R. (2003). Gender- and age-related differences in the morphology of the corpus callosum. Clinical Anatomy, 16, 396–403.
References 505

Sullivan, K., Winner, E., & Tager-Flusberg, H. (2003). Canadolescents with Williams syndrome tell the differencebetween lies and jokes? Developmental Neuropsychology,23, 85–104.
Sutcliffe, J. S., & Nurmi, E. L. (2003). Genetics of childhooddisorders: XLVII. Autism, part 6: Duplication and inher-ited susceptibility of chromosome 15q11-q13 genes inautism. Journal of the American Child and AdolescentPsychiatry, 42, 253–256.
Swanson, H. L., Mink, J., & Bocian, K. M. (1999). Cognitiveprocessing deficits in poor readers with symptoms of read-ing disabilities and ADHD: More alike than different?Journal of Educational Psychology, 91, 321–333.
Swanson, H. L., Posner, M., Potkin, S., Bonforte, S., Youpa,D., Fiore, C., et al. (1991). Activating tasks for the studyof visual-spatial attention in ADHD children: A cognitiveanatomic approach. Journal of Child Neurology, 6,S119–S127.
Swanson, H. L., & Sachse-Lee, C. (2001). A subgroup analysisof working memory in children with reading disabilities:Domain-general or domain-specific deficiency? Journal ofLearning Disabilities, 34, 249–263.
Swanson, J., Oosterlaan, J., Murias, M., Schuck, S., Flodman,P., Spence M. A., et al. (2000). Attention deficit/hyperactivity disorder children with a 7-repeat allele ofthe dopamine receptor D4 gene have extreme behaviorbut normal performance on critical neuropsychologicaltests of attention. Procceedings of the National Academy ofSciences, 97, 4754–4759.
Swanson, J., Posner, M. I., Cantwell, D., Wigal, S., Crinella,F., Filipek, P., et al. (2000). Attention-deficit/hyperactivitydisorder: Symptom domains, cognitive processes, andneural networks. In R. Parasuraman (Ed.), The attentivebrain (pp. 445–460). Cambridge, MA: MIT Press.
Swillen, A., Fryns, J. P., Kleczkowska, A., Massa, G.,Vanderschueren-Lodeweyck, M., & Van den Berghe, H.(1993). Intelligence, behaviour and psychosocial develop-ment in Turner syndrome: A cross-sectional study of 50preadolescent and adolescent girls 4–20 years. GeneticCounseling, 4, 7–18.
Szaflarski, J. P., Binder, J. R., Possing, E. T., McKiernan, K. A.,Ward, B. D., & Hammeke, T. A. (2002). Language later-alization left-handed and ambidextrous people: FMRIdata. Neurology, 59, 238–244.
Talland, G. A. (1965). Deranged memory. New York: AcademicPress.
Tamm, L. Menon, V., & Reiss, A. L. (2003). Abnormal pre-frontal cortex function during response inhibition inTurner syndrome: Functional magnetic resonance imagingevidence. Society of Biological Psychiatry, 53, 107–111.
Tanguay, P. E. (2000). Pervasive developmental disorders: A10-year review. Journal of the American Academy of Childand Adolescent Psychiatry, 39, 1079–1095.
Teasdale, G., & Jennett, B. (1974). Assessment of coma andimpaired consciousness. Lancet, 2, 81–84.
Teicher, M. H., Polcari, A., Anderson, C. M., Andersen, S. L.,Glod, C. A., & Renshaw, P. (1996). Dose-dependenteffects of methylphenidate on activity, attention, andmagnetic imaging measures in children with ADHD[Abstract]. Society for Neuroscience Abstracts, 22, 1191.
Temple, C., & Marriott, A. J. (1998). Arithmetical ability anddisability in Turner’s syndrome: A cognitive neuropsycho-logical analysis. Developmental Neuropsychology, 14, 47–67.
Temple, C. M., Carney, R. A., & Mullarkey, S. (1996). Frontallobe function and executive skills in children withTurner’s syndrome. Developmental Neuropsychology, 12,343–363.
Terry, R. D., & Davies, P. (1980). Dementia of the Alzheimertype. Annual Review of Neuroscience, 3, 77–95.
Terry, R. D., Peck, A., DeTeresa, R., Schechter, R., &Horoupian, D. S. (1981). Some morphometric aspects ofthe brain in senile dementia of the Alzheimer type. Annalsof Neurology, 10, 184–192.
Teuber, H. L. (1950). Neuropsychology. In M. R. Harrower(Ed.), Recent advances in psychological testing (pp. 30–52).Springfield, IL: Charles C. Thomas.
Teuber, H. L. (1959). Some alterations in behavior after cere-bral lesions in man. In A. D. Bass (Ed.), Evolution of ner-vous control. Washington, DC: American Association forthe Advancement of Science.
Teuber, H. L., Battersby, W. S., & Bender, M. B. (1960).Visual field defects after penetrating missile wounds.Cambridge, MA: Harvard University Press.
Thiele, E. A. (2003). Assessing the efficacy of antiepileptictreatments: the ketogenic diet. Epilepsia, 44(Suppl. 7),26–29.
Thomsen, I. V. (1974). The patient with severe head-injury andhis family: A follow-up study of 50 patients. ScandinavianJournal of Rehabilitation Medicine, 6, 180–183.
Tombaugh, T. (2003). The test of memory malingering(TOMM) in forensic psychology. Journal of ForensicNeuropsychology, 2(3/4), 69–96.
Tombaugh, T. N. (1996). Test of Memory Malingering(TOMM). New York: Multi-Health Systems Inc.
Toole, J. F. (1990). Cerebrovascular diseases (4th ed.). NewYork: Raven.
Tranel, D., & Eslinger, P. J. (2000). Effects of early onset braininjury on the development of cognition and behavior:Introduction to the special issue. DevelopmentalNeuropsychology, 18, 273–280.
Träskmann, L., Asberg, M., Bertilsson, L., & Sjöstrand, L.(1981). Monoamine metabolites in CSF and suicidalbehavior. Archives of General Psychiatry, 38, 631–636.
Tsatsanis, K. D., & Rourke, B. P. (1995). Conclusions andfuture directions. In B. P. Rourke (Ed.), Syndrome of non-verbal learning disabilities: Neurodevelopmental manifesta-tions (pp. 476–496). New York: Guilford Press.
Tulving, E. (1972). Episodic and semantic memory. In E.Tulving & W. Donaldson (Eds.), Organization of memory(pp. 381–403). New York: Academic Press.
506 References

Tulving, E., Kapur, S., Craik, F. I. M., Moscovitch, M., &Houle, S. (1994). Hemisphere encoding/retrieval asym-metry in episodic memory: Positron emission tomographyfindings. Proceedings of the National Academy of Sciences,91, 2016–2020.
Turner, H. H. (1938). A syndrome of infantilism, congenitalwebbed neck, and cubitus valgus. Endocrinology, 23,566–574.
Tysvaer, A. T., Storli, O. V., & Bachen, N. I. (1989). Soccerinjuries to the brain: A neurologic and electroencephalo-graphic study of former players. Acta NeurologicaScandinavica, 80, 151–156.
Ullrich, O. (1930). Uber typicke kombinationsbilder multiplerabartungen. Zeitschrift fur kinderheilkunde, 49, 271–276.
Ullsperger, M., & von Cramon, D. Y. (2004). Decision mak-ing, performance and outcome monitoring in frontal cor-tical areas. Nature Neuroscience, 7, 1173–1174.
Valenstein, E. S. (1973). Brain control. New York: Wiley.Vallar, G., Sandroni, P., Rusconi, M. L., & Barbieri, S. (1991).
Hemianopia, hemianesthesia, and spatial neglect: A studywith evoked potentials. Neurology, 41, 1918–1922.
Van den Broeck, W. (2002). The misconception of theregression-based discrepancy operationalization in the def-inition and research of learning disabilities. Journal ofLearning Disabilities, 35, 194–204.
van Goozen, S. H. (1994). Male and female: Effects of sex hor-mones on aggression, cognition and motivation. Amsterdam:University of Amsterdam Press.
van Goozen, S. H., Cohen-Kettenis, P. T., Gooren, L. J.,Frijda, N. H., & van de Poll, N. E. (1995). Gender dif-ferences in behavior: Activating effects of cross-sex hor-mones. Psychoneuroendocrinology, 20, 343–363.
van Goozen, S. H. M., Gooren, L. J. G., Slabbekoorn, D.,Sanders, G., & Cohen-Kettenis, P. T. (2002). Organizingand activating effects of sex hormones in homosexualtranssexuals. Behavioral Neuroscience, 116, 982–988.
Van Hoesen, G., & Damasio, A. R. (1987). Neural correlatesof cognitive impairment in Alzheimer’s disease. In V. B.Brooks (Ed.), Handbook of physiology: The nervous system(Vol. V). Bethesda, MD: American Physiological Society.
Vanneste, J. A. L. (2000). Diagnosis and management of nor-mal-pressure hydrocephalus. Journal of Neurology, 247,5–14.
Van Raalte, J. L., & Brewer, B. W. (1996). Exploring sport andexercise psychology. Washington, DC: AmericanPsychological Association.
van Veen, V., & Carter, C. S. (2002). The timing of action-monitoring processes in the anterior cingulate cortex.Journal of Cognitive Neuroscience, 14, 593–602.
Venneri, A., Cornoldi, C., & Caruit, M. (2003). Arithmeticdifficulties in children with visuospatial learning disability(VLD). Child Neuropsychology, 9, 175–183.
Verrees, M., & Selman, W. R. (2004). Management of normalpressure hydrocephalus. American Family Physician, 70,1071–1078.
Victor, M., & Ropper, A. H. (2001). Adams and Victor’s prin-ciples of neurology (7th ed.). New York: McGraw-Hill.
Vilkki, J., & Laitinen, V. (1974). Differential effects of left andright ventrolateral thalamotomy on receptive and expres-sive verbal performances and face matching.Neuropsychologia, 12, 11.
Villardita, C., Smirni, P., LaPira, F., Zappala, G., & Nicoletti,F. (1982). Mental deterioration, visuoperceptive disabili-ties and constructional apraxia in Parkinson’s disease. ActaNeurologica Scandinavica, 66, 112–120.
Vining, E. P. (1999). Clinical efficacy of the ketogenic diet.Epilepsy Research, 37(3), 181–190.
Virues-Ortega, J., Buela-Casal, G., Garrido, E., & Alcazar, B. (2004). Neuropsychological functioning associatedwith high-altitude exposure. Neuropsychol Rev, 14(4),197–224.
Voeller, K. K. S. (1996). Brief report: Developmental neurobi-ological aspects of autism. Journal of Autism andDevelopmental Disorders, 26, 189–193.
Volkmar, F. R., & Klin, A. (2000). Diagnostic issues inAsperger syndrome. In A. Klin, F. R. Volkmar, & S. S.Sparrow (Eds.), Asperger syndrome (pp. 25–71). New York:Guilford Press.
Volkmar, F. R., Klin, A., Schultz, R., Bronen, R., Marans, W. D., Sparrow, S., et al. (1996). Asperger’s syndrome.Journal of the American Academy of Child and AdolescentPsychiatry, 35, 118–123.
Volkmar, F. R., Lord, C., Bailey, A., Schultz, R. T., & Klin, A.(2004). Autism and pervasive developmental disorders.Journal of Child Psychology and Psychiatry, 45, 135–170.
Volterra, V., Caselli, M. C., Capirci, O., Tonucci, F., & Vicari,S. (2003). Early linguistic abilities of Italian children withWilliams syndrome. Developmental Neuropsychology, 23,35–59.
von Monakow, C. (1911). Lokalisation der Hirnfunktionen.Journal of Psychiatry and Neurology, 17, 185–200.
Von Senden, M. (1960). Space and sight: The perception ofspace and shape in the congenitally blind before and afteroperation. Urbana-Champaign, IL: Free Press ofIllinois.
von Stockert, F. G. (1932). Subcortical dementia. Archives ofPsychiatry, 97, 77–100.
Vonsattel, J. P. (1992). Neuropathology of Huntington’s disease. In A. B. Joseph & R. R. Young (Eds.), Movementdisorders in neuropathology and neuropsychiatry(pp. 186–194). Oxford, United Kingdom: BlackwellScientific.
Vouloumanos, A., Kiehl, K. A., Werker, J. F., & Liddle, P. F.(2001). Detection of sounds in the auditory stream:Event-related fMRI evidence for differential activation tospeech and nonspeech. Journal of Cognitive Neuroscience,13, 994–1005.
Voyer, D. (1997). Scoring procedures, performance factors,and magnitude of sex differences in spatial performance.American Journal of Psychology, 110, 259–276.
References 507
Voyer, D., Rodgers, M. A., & McCormick, P. A. (2004). Timingconditions and the magnitude of gender differences onthe Mental Rotations Test. Memory and Cognition, 32,72–82.
Voyer, D., Voyer, S., & Bryden, M. P. (1995). Magnitude ofsex differences in spatial abilities: A meta-analysis andconsideration of critical variables. Psychological Bulletin,117, 250–270.
Vuilleumier, P., Armony, J. L., Driver, J., & Dolan, R. J. (2001).Effects of attention and emotion on face processing in thehuman brain: An event-related fMRI study. Neuron, 30,829–841.
Vygotsky, L. S. (1965). Psychology and localization of func-tions. Neuropsychologia, 3, 381.
Waber, D. P., Forbes, P. W., Wolff, P. H., & Weiler, M. D. (2004).Neurodevelopmental characteristics of children with learn-ing impairments classified according to the double-deficithypothesis. Journal of Learning Disabilities, 37, 451–461.
Wada, J., & Rasmussen, T. (1960). Intracarotid injection ofsodium amytal for the lateralization of cerebral speechdominance: Experimental and clinical observations.Journal of Neurosurgery, 17, 266–282.
Wagar, B. M., & Thagard, P. (2004). Spiking Phineas Gage: Aneurocomputational theory of cognitive-affective integra-tion in decision making. Psychological Review, 111,67–79.
Wager, T. D., Phan K. L., Liberzon, I., & Taylor, S. F. (2003).Valence, gender, and lateralization of functional brainanatomy in emotion: A meta-analysis of findings fromneuroimaging. NeuroImage, 19, 513–531.
Waldman, I. D., Rowe, D. C., Abramowitz, A., Kozel, S. T.,Mohr, J. H., Sherman, S. L., et al. (1998). Association andlinkage of the dopamine transporter gene and attention-deficit hyperactivity in children: Heterogeneity owing todiagnostic subtype and severity. American Journal ofHuman Genetics, 63, 1767–1776.
Walker, J.E., & Kozlowski, G. P. (2005). Neurofeedback treat-ment of epilepsy. Child and Adolescent Psychiatric Clinicsof North America, 14, 163–176, viii.
Walt, V. (2005, March 7). A land where girls rule in math.Time, 165, 56–57.
Walton, J. N. (1994). Brain’s diseases of the nervous system (10thed.). Oxford, United Kingdom: Oxford University Press.
Wang, A. T., Dapretto, M., Hariri, A. R., Sigman, M., &Bookheimer, S. Y. (2004). Neural correlates of facial affectprocessing in children and adolescents with autism spec-trum disorder. Journal of the American Child andAdolescent Psychiatry, 43, 481–490.
Wang, L. N., Zhu, M. W., Gui, Q. P., & Li, X. H. (2003).[An analysis of the causes of dementia in 383 elderlyautopsied cases]. Zhonghua Nei Ke Za Zhi, 42(11),789–792.
Wang, Q. S., & Zhou, J. N. (2002). Retrieval and encoding ofepisodic memory in normal aging and patients with mildcognitive impairment. Brain Research, 924(1), 113–115.
Wang, W., Wu, S., Cheng, X., Dai, H., Ross, K., Du, X., et al.(2000). Prevalence of Alzheimer’s disease and otherdementing disorders in an urban community of Beijing,China. Neuroepidemiology, 19(4), 194–200.
Wapner, W., Judd, T., & Gardner, H. (1978). Visual agnosia inan artist. Cortex, 14, 343–364.
Wass, T. S., Persutte, W. H., & Hobbins, J. C. (2001). Theimpact of prenatal alcohol exposure on frontal cortexdevelopment in utero. American Journal of Obstetrics andGynecology, 185, 737–742.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G.,Kooperberg, C., Baird, A., et al. (2003). Effect of estrogenplus progestin on stroke in postmenopausal women. Journalof the American Medical Association, 289, 2673–2684.
Waterhouse, L., Fein, D., & Modahl, C. (1996). Autism.Psychology Review, 103, 457–489.
Wechsler, D. (1944). The measurement of adult intelligence (3rded.). Baltimore: Williams & Wilkins.
Wechsler, D. (1945). A standardized memory scale for clinicaluse. Journal of Psychology, 19, 87–95.
Wechsler, D. (1974). Wechsler Intelligence Scale for Children–Revised. New York: Psychological Corporation.
Wechsler, D. (1981). Wechsler Adult Intelligence Scale–Revised.New York: Psychological Corporation.
Wechsler, D. (1991). Manual for the Wechsler Intelligence Scalefor Children, Third Edition, WISC-III. San Antonio, TX:Psychological Corporation.
Wechsler, D. (1997). Wechsler Adult Intelligence Scale–III. SanAntonio, TX: The Psychological Corporation.
Wechsler, D. (2002). Wechsler Primary and Preschool Scale–III.San Antonio, TX: The Psychological Corporation.
Wechsler, D. (2003). Wechsler Intelligence Scale for Children–IV.San Antonio, TX: The Psychological Corporation.
Wehman, P. H. (1991). Cognitive rehabilitation in the work-place. In J. S. Kreutzer & P. H. Wehman (Eds.), Cognitiverehabilitation for persons with traumatic brain injury.Baltimore: Paul H. Brookes.
Weimar, C., Kurth, T., Kraywinkel, K., Wagner, M., Busse, O.,Haberl, R. L., et al. (2002). Assessment of functioning anddisability after ischemic stroke. Stroke, 33(8), 2053–2059.
Weinand, M. E., Hermann, B., Wyler, A. R., Carter, L. P.,Oommen, K. J., Labiner, D., et al. (1994). Long-termsubdural strip electrocorticographic monitoring of ictaldeja vu. Epilepsia, 35(5), 1054–1059.
Weiss, G., & Hechtman, L. T. (1993). Hyperactive childrengrown up (2nd ed.). New York: Guilford Press.
Weiss, M., Tannock, R., Kratochvil, C., Dunn, D., Velez-Borras, J., Thomason, C., et al. (2005). A randomized,placebo-controlled study of once-daily atomoxetine in theschool setting in children with ADHD. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 44,647–655.
Weiss, S., Dunne, C., Hewson, J., Wohl, C., Wheatley, M.,Peterson, A. C., & Reynolds, B. A. (1996). MultipotentCNS stem cells are present in the adult mammalian spinal
508 References

cord and ventricular neuroaxis. Journal of Neuroscience,16, 7599–7609.
Weiten, W. (1994). Psychology: Themes and variations (2nd ed.).Pacific Grove, CA: Brooks/Cole.
Weiten, W. (1998). Psychology: Themes and variations (4th ed.).Pacific Grove, CA: Brooks/Cole.
Wells, S. (1869). How to read character: New illustrated hand-book of phrenology and physiognomy. New York: Fowler &Wells.
Welsh, M. C. (1991). Rule-guided behavior and self-monitoring on the Tower of Hanoi disk-transfer task.Cognitive Development, 6, 59–76.
Welsh, M. C., Pennington, B. F., & Groisser, D. B. (1991). Anormative-developmental study of executive function: Awindow on prefrontal function in children.Developmental Neuropsychology, 7, 131–149.
Wenk, G. L. (2004). Functional neuroanatomy of learning andmemory. In D. S. Charney & E. J. Nestler (Eds.),Neurobiology of mental illness (2nd ed., pp. 807–812).New York: Oxford University Press.
Wexler, A. (1995). Mapping fate: A memoir of family, risk, andgenetic research. New York: Random House.
Whalley, L. J., Starr, J. M., Athawes, R., Hunter, D., Pattie, A.,& Deary, I. J. (2000). Childhood mental ability anddementia. Neurology, 55(10), 1455–1459.
White, B. J. (1994). The Turner syndrome: Origin, cytogeneticvariants, and factors influencing the phenotype. In S. H.Broman & J. Grafman (Eds.), Atypical cognitive deficits indevelopmental disorders (pp. 183–196). New York: OxfordUniversity Press.
Whyte, J. (1986). Outcome evaluation in the remediation ofattention and memory deficits. Journal of Head TraumaRehabilitation, 1, 43–53.
Wilens, T. E., Biederman, J., Brown, S., Tanguay, S.,Monuteaux, M. C., Blake, C., et al. (2002). Psychiatriccomorbidity and functioning in clinically referredpreschool children and school-age youths with ADHD.Journal of the American Child and Adolescent Psychiatry,41, 262–268.
Wilkins, R. H., & Brody, I. A. (1970). Wernicke’s sensoryaphasia. Archives of Neurology, 22, 279.
Willerman, L., Schultz, R., Rutledge, N., & Bigler, E. (1992).Hemisphere size asymmetry predicts relative verbal andnonverbal intelligence differently in the sexes: An MRIstudy of structure-function relations. Intelligence, 16,315–328.
Williams, J. C. P., Barratt-Boyes, B. G., & Lowe, J. B. (1961).Supravalvular aortic stenosis. Circulation, 24, 1311–1318.
Williams, R. L., & Karacan, I. (1978). Sleep disorders:Diagnosis and treatment. New York: Wiley.
Williams, R. W., & Herrup, K. (1988). The control of neuronnumber. Annual Review of Neuroscience, 11, 423–453.
Willis, K. E. (1993). Neuropsychological functioning in chil-dren with spina bifida and/or hydrocephalus. Journal ofClinical Child Psychology, 22, 247–265.
Wilson, S. A. K. (1912). Progressive lenticular degeneration: Afamilial nervous disease associated with cirrhosis of theliver. Brain, 34, 296–508.
Winson, J. (1972). Interspecies differences in the occurrence oftheta. Behavioral Biology, 7, 479–487.
Witelson, S. F., Glezer, I. I., & Kigar, D. L. (1995). Womenhave greater density of neurons in posterior temporal cor-tex. Journal of Neuroscience, 15, 3418–3428.
Witelson, S. F., Kigar, D. L., & Harvey, T. (1999). The excep-tional brain of Albert Einstein. Lancet, 353, 2149–2153.
Witol, A., & Webbe, F. (1993). Neuropsychological deficitsassociated with soccer play. Archives of ClinicalNeuropsychology, 9, 204–205.
Wolfson, C., Wolfson, D. B., Asgharian, M., M’Lan, C. E.,Ostbye, T., Rockwood, K., et al. (2001). A reevaluation ofthe duration of survival after the onset of dementia. NewEngland Journal of Medicine, 344(15), 1111–1116.
Wood, F. B., & Grigorenko, E. L. (2001). Emerging issues inthe genetics of dyslexia: A methodological preview.Journal of Learning Disabilities, 34, 503–511.
World Health Organization. (1992). The ICD-10 classificationof mental and behavioral disorders: Clinical descriptions anddiagnostic guidelines. Geneva, Switzerland: World HealthOrganization.
Wright, R. (1994). The moral animal. New York: Vintage.Xu, Y., & Corkin, S. (2001). H. M. revisits the Tower of
Hanoi puzzle. Neuropsychology, 15, 69–79.Yaffe, K., Sawaya, G., Lieberburg, I., & Grady, D. (1998).
Estrogen therapy in postmenopausal women. Journal ofthe American Medical Association, 279, 688–695.
Yeo, R. A., Hill, D. E., Campbell, R. A., Vigil, J., Petropoulos,H., Hart, B., et al. (2003). Proton magnetic resonance spec-troscopy investigation of the right frontal lobe in childrenwith attention-deficit/hyperactivity disorder. Journal of theAmerican Child and Adolescent Psychiatry, 42, 303–310.
Yeterian, E. H., & Van Hoesen, G. W. (1978). Cortico-striateprojections in the rhesus monkey: The organization ofcertain cortico-caudate connections. Brain Research, 139,43–63.
Yücel, M., Stuart, G. W., Maruff, P., Velakoulis, D., Crowe, S. F., Savage, G., et al. (2001). Hemispheric and gender-related differences in the gross morphology of the anteriorcingulate/paracingulate cortex in normal volunteers: AnMRI morphometric study. Cerebral Cortex, 11, 17–25.
Zaidel, D., & Sperry, R. W. (1973). Performance on Raven’sColored Progressive Matrices Test by subjects with cere-bral commissurotomy. Cortex, 9, 34.
Zald, D. H., & Kim, S. W. (2001). The orbitofrontal cortex.In S. P. Salloway, P. F. Malloy, & J. D. Duffy (Eds.), Thefrontal lobes and neuropsychiatric illness (pp. 33–70).Washington, DC: American Psychiatric Publishing.
Zametkin, A. J., Liebenauer, L. L., Fitzgerald, G. A., King, A. C., Minkunas, D. V., Herscovitch, P., et al. (1993). Brainmetabolism in teenagers with attention-deficit hyperactivitydisorder. Archives of General Psychiatry, 50, 333–340.
References 509

Zametkin, A. J., Nordahl, T. E., Gross, M., King, A. C., Semple,W. E., Rumsey, J., et al. (1990). Cerebral glucose metabo-lism in adults with hyperactivity of childhood onset. NewEngland Journal of Medicine, 323, 1362–1365.
Zang, Y. F., Jin, Z., Weng, X. C., Zhang, L., Zeng, Y. W., Yang,L., et al. (2005). Functional MRI in attention-deficithyperactivity disorder: Evidence for hypofrontality. Brainand Development, 27, 544–550.
Zangwill, O. L. (1960). Cerebral dominance and its relation topsychological function. Edinburgh, United Kingdom:Oliver & Boyd.
Zec, R. F. (1993). Neuropsychological functioning inAlzheimer’s disease. In R. W. Parks, R. F. Zec, & R. S.Wilson (Eds.), Neuropsychology of Alzheimer’s disease andother dementias. New York: Oxford University Press.
Zeki, S. (1992). The visual image in mind and brain. Readingsfrom Scientific American. New York: W. H. Freeman.
Zihl, J. (1995). Eye movement patterns in hemianopic dyslexia.Brain, 118, 891–912.
Zillmer, E. A. (1991). Rorschach Interpretation AssistanceProgram-Version 2 Review. Journal of PersonalityAssessment, 572, 381–383.
Zillmer, E. A. (1995). The case of Aaron B. In D. L. Chute &M. E. Bliss (Eds.), Exploring psychological disorders(pp. 115–124). Pacific Grove, CA: Brooks/Cole.
Zillmer, E. A. (1996, November). Mind over matter: Brainresearch in the next millennium. Invited paper toCongressional staff on Capitol Hill, Washington, D.C.
Zillmer, E. A. (2003a). The neuropsychology of repeated 1- and 3-meter springboard diving among college athletes.Applied Neuropsychology, 10(1), 23–30.
Zillmer, E. A. (2003b, editor-special edition). Introduction tospecial issue on psychological and neuropsychologicalassessment in the forensic arena: Art or science?Assessment, 10(4), 318–320.
Zillmer, E. A. (2003c, editor-special edition). Sports-relatedconcussions. Applied Neuropsychology, 10(1), 1–3.
Zillmer, E. A. (2004). National Academy of Neuropsychology:President’s address. The future of neuropsychology.Archives of Clinical Neuropsychology, 19(6), 713–724.
Zillmer, E. A., Chelder, M. J., & Efthimiou, J. (1995).Assessment of Impairment AIM Measure. Philadelphia:Drexel University.
Zillmer, E. A., Fowler, P. C., Gutnick, H. N., & Becker, E.(1990). Comparison of two cognitive bedside screeninginstruments in nursing home residents: A factor analyticstudy. Journal of Gerontology: Psychological Sciences, 45,69–74.
Zillmer, E. A., Fowler, P. C., Waechtler, C., Harris, B., &Khan, F. (1992). The effects of unilateral and multifocallesions on the WAIS-R: A factor analytic study of strokepatients. Archives of Clinical Neuropsychology, 7, 29–41.
Zillmer, E. A., & Greene, H. (2006). Neuropsychologicalassessment in the forensic setting. In R. P. Archer (Ed.),Clinical assessment instruments in forensic settings: Uses andlimitations. Mawah, NJ: Lawrence Erlbaum.
Zillmer, E. A., Harrower, M., Ritzler, B., & Archer, R. P.(1995). The quest for the Nazi personality: A psychologicalinvestigation of Nazi war criminals. Hillsdale, NJ:Erlbaum.
Zillmer, E. A., Lucci, K., Barth, J. T., Peake, T., & Spyker, D.(1986). Neurobehavioral sequelae of subcutaneous injec-tion with metallic mercury. Journal of Toxicology: ClinicalToxicology, 24, 100–110.
Zillmer, E. A., Montenegro, L., Wiser, J., Barth, J. T., &Spyker, D. (1996). Neuropsychological sequelae in suba-cute home chlordane poisoning: Ten case studies. Archivesof Clinical Neuropsychology, 11, 77–89.
Zillmer, E. A., & Passuth, P. M. (1989). Predicting functionalability from mental status among nursing home residents.The Gerontologist, 29, 142A.
Zillmer, E. A., & Perry, W. (1996). Cognitive-neuropsychologicalabilities and related psychological disturbance: A factormodel of neuropsychological, Rorschach, and MMPIindices. Assessment, 3, 209–224.
Zillmer, E., Schneider, J., Tinker, J., & Kaminaris, C. (2006).A history of sports-related concussions: a neuropsycholog-ical perspective. In R. Echemendia (Ed.), Sports neuropsy-chology: Assessment and management of traumatic braininjury. New York: Guilford Press.
Zillmer, E. A., Ware, J. C., Rose, V., & Bond, T. (1989). Anexamination of the Symptom Checklist 90-Revised SCL-90-R in the assessment of personality function insleep disorders. Sleep Research, 18, 189.
Zillmer, E. A., Ware, J. C., Rose, V., & Maximin, A. (1988).MMPI characteristics of patients with different severity ofsleep apnea. Sleep Research, 17, 136.
Zillmer, E. A., & Wickramaserkera, I. (1987). Biofeedback andhypnotizability: Initial treatment considerations. ClinicalBiofeedback and Health, 10, 51–57.
Zola-Morgan, S., & Squire, L. R. (1993). Neuroanatomy ofmemory. Annual Review of Neuroscience, 16, 547–563.
Zubenko, G. S., Moossy, J., Martinez, A. J., Rao, G. R., Kopp,U., & Hanin, I. (1989). A brain regional analysis of mor-phologic and cholinergic abnormalities in Alzheimer’s dis-ease. Archives of Neurology, 46, 634–639.
510 References
Ablation experiment Developed by Pierre Flourens,and involved removing parts of the brain of pigeonsand hens. Flourens reported that excising any partof the brain in birds led to generalized, not local-ized, disorders of behavior.
Absence seizures Occur when the normally asyn-chronous waking state is abruptly interrupted bylow-wave synchronous activity; characterized bysynchronous bilateral spike-and-wave discharge.
Abulia A syndrome similar to that of akineticmutism, but of lesser severity. The syndrome ischaracterized by significant reduction in drive,interest, and spontaneous behavior. The syndromeis associated with medial damage to the frontallobes.
Acceleration The brain experiencing a significantphysical force that propels it quickly, from station-ary to moving.
Acetylcholine (ACh) Also called choline; the first neu-rotransmitter to be identified; plays a prominentrole in the peripheral nervous system, influencingmotor control, and in autonomic nervous systemfunctioning.
Achievement tests Most influenced by past education-al attainment; measures how well a subject has profited by learning and experience compared withothers.
Achromatopsia The complete loss of ability to detectcolor.
Acidophilic adenoma A functioning type of pituitarytumor that usually appears in the anterior lobe ofthe pituitary gland. The acidophilic adenoma cre-ates excessive secretion of growth hormones oftenresulting in giantism (excessive growth of hands and feet).
Acoustic neuroma Progressively enlarging, benigntumor within the auditory canal arising fromSchwann cells of the VIIIth cranial nerve.
Acquired sociopathy See Pseudopsychopathy.Action potential An electrical potential across the
neuron membrane. The action potential spreadsdown the axon as the voltage-controlled sodium
channels open up sequentially, like falling dominoes.
Adrenocorticotropic hormone (ACTH) A hormonesecreted by the anterior pituitary gland that mediatesthe release of hormones from the adrenal cortex.Increased and decreased secretions of ACTH have beenassociated with a various disorders and disease states.
Affective significance of stimuli The binding orattachment of emotion to novel and social stimuli.
Afferent nerves (sensory nerves) Convey incomingmessages from the sensory receptors to the centralnervous system.
Agenesis Complete or partial failure of an organ todevelop.
Ageusia Inability to recognize tastes.Agnosia An absence of knowing. The distinction
between the ability to recognize an object and theinability to name it. Term first coined by SigmundFreud.
Agyria, or lissencephaly A congenital disorder inwhich the normal gyri and sulci of the brain fail todevelop. Believed to occur between the third andfourth month of gestation.
Air encephalogram or pneumoencephalography Theradiographic visualization of the fluid-containingstructures of the brain, the ventricles, and spinalcolumn. It is similar to the X-ray, but it involves thewithdrawal of cerebrospinal fluid by lumbar punc-ture, which is then replaced with a gas including air,oxygen, or helium.
Akinesia A difficulty in initiating and maintainingbehavior. Patients with akinesia may be extremelyslow to start or perform a movement, may becomerapidly fatigued when performing repetitive move-ments, or may have problems in performing simul-taneous or sequential movements.
Akinetic mutism A syndrome associated with medialfrontal damage involving a loss of initiative, apathy,reduced verbal and motor behaviors, and profoundindifference.
Akinetopsia The specific inability to identify objectsin motion.
GLOSSARY
511
Alcohol-related neurodevelopmental disabilities(ARND) See Fetal alcohol effect.
Alternating attention The ability to switch back andforth between tasks.
Alzheimer’s disease (AD) An irreversible corticaldementia, not due to an identifiable cause, that ischaracterized by neuropathologic markers includingneurofibrillary tangles and senile plaques.
Amino acids A group of neurotransmitters that plays amajor role in the more basic type of neuronal trans-mission that depends on rapid communicationamong neurons.
Amygdala Literally “almond,” because of its shape; hasa specific role in fear conditioning and impacts thestrength of stored memory.
Amyotrophic lateral sclerosis (ALS) Disease of themotor system in which people experience a gradualto total loss of muscle control and muscle function.
Anastomosis Communication between blood vesselsby collateral channels. See Collateral blood vessel.
Androgen hormone Any steroid hormone, primarilyproduced by the testes, that has a “masculinizing”effect on development. Effects include the masculin-ization of the fetus, production of sperm, and devel-opment of secondary sexual characteristics.
Androgen insensitivity Refers to a set of genetic dis-orders resulting from mutation of the gene encodingfor the androgen receptor. Affected males demon-strate varying degrees of under-development ofmale-sex physical characteristics.
Anencephaly A congenital condition characterized bya failure in development of the two hemispheres,mesencephalon, and diencephalon of the brain. Thebrain is represented by a vascular mass. The condi-tion produces severe neurologic deficits and isincompatible with life.
Aneurysms Weak areas in the walls of an artery thatcause the vessel to balloon.
Angiography X-raying blood vessels in the brain afterintroducing contrast material into the arterial or venousbloodstream. Angiography is the most useful techniquefor examining the blood supply to and from the brain.
Anomia Problems in word finding. Only a word ortwo, here and there, is lost, and the communicationcan proceed pretty much as normal. In more severecases, most or all words can be lost.
Anopias Term for visual difficulties.Anosmia Total loss of smell.Anosognosia A term first coined by Babinski to indi-
cate the inability or refusal to recognize that one hasa particular disease or disorder.
Anoxia The complete cessation of oxygen supply tothe brain. Anoxia often occurs with stroke or othersevere traumas of the brain, such as are often seen ingunshot wounds to the head.
Anterior Toward the front or front end.Anterior attention system (executive attention system)
An attentional system of the brain mediating thevoluntary control of attention that is supported bythe frontal and medial cortices of the brain.
Anterior cerebral artery Resulting from half of thedivision of an internal carotid artery, it supplies theanterior medial portion of its corresponding cerebralhemisphere.
Anterior commissure Minor intercerebral fibers.Anterior communicating artery Connects the left and
right anterior cerebral arteries.Anterograde amnesia The loss of memory for events
after trauma or disease onset.Anterograde degeneration The degeneration of the
axon after the cell body has been damaged.Anticholinergics Treatment for Parkinson’s disease; act
by blocking the action of acetylcholine.Anton’s syndrome Actual denial of cerebral blindness;
a behavioral mirror of apperceptive agnosia.Aortic arch Arises from the left ventricle of the heart.Aphasia A disturbance of language usage or compre-
hension. It may involve the impairment of thepower to speak, write, read, gesture, or comprehendspoken, written, or gestured language.
Apnea The cessation of airflow; literally means “a lackof breath.”
Apperceptive visual agnosia A visual problem withobject perception as the primary difficulty.
Apraxia An absence of action, but the term is mostoften used to describe a variety of missing or inap-propriate actions that cannot be clearly attributed toprimary motor deficits or the lack of comprehensionor motivation. Thus, apraxia refers to an inability toperform voluntary actions despite an adequateamount of motor strength and control.
Arachnoid granulations Small “pockets” of cauliflower-like veins within the subarachnoid space, whichserve as pathways for the subarachnoid cere-brospinal fluid to be absorbed and re-enter thevenous circulation.
Arachnoid membrane A “spiderlike” avascular mem-brane of the meninges.
Arborization The sprouting and branching of den-drites during brain development.
Aristotle (Greek, 384–322 B.C.) a disciple of Plato;erroneously believed that the heart is the source of
512 Glossary

all mental processes. Aristotle argued that becausethe brain is bloodless, it fills the function of a “radi-ator,” cooling hot blood ascending from the heart.
Arteriovenous malformations (AVM) Abnormal,often redundant vessels that result in abnormalblood flow. Because AVMs have inherently weakvessel walls, they may lead to slow bleeding or inad-equate distribution of blood in the regions sur-rounding the vessels.
Articulation The ability to form phonetic sounds ofvowels and consonants, which then are placed indifferent combinations to form words and sen-tences.
Articulatory phonologic loop A working memory“slave system” that stores speech-based informationand is important in the acquisition of vocabulary.
Ascending spinal-thalamic tract Carries sensoryinformation related to pain and temperature andruns in parallel to the spinal cord. It synapses over awide region of the thalamus, primarily on theintralaminar and ventral posterior nuclei of the thal-amus, and then to the somatosensory cortex.
Asociality Denotes a lack of social interest and related-ness. This anomaly is hypothesized to be one of themechanisms responsible for autistic behaviors.
Asperger’s syndrome A pervasive developmental disor-der characterized by symptoms of autism, includingimpairments in social relatedness and atypical pat-terns of behavior, interest, or activity. However, incontrast with autism, impairment in language,adaptive skills (with the exception of social skills),and curiosity about the environment are not pro-nounced. The disorder tends to have a later age ofonset than autism.
Association or polymodal areas Brain regionsinvolved in the integration of sensory informationfrom different sensory cortices and linking the sen-sory cortices to the motor cortices. These associativecortices support complex mental and behavioralfunctions.
Associative visual agnosia A visual problem having todo with difficulty in assigning meaning to an object.
Astereognosia Inability to recognize an object bytouch.
Astereognosis See Tactile agnosia.Astrocytes Non-neural, star-shaped glia cells that are
highly branched and occupy much space betweenneurons in the gray matter. Their multiple functionsinclude supporting neurons by interweaving amongnerve fibers, contributing to the metabolism ofsynaptic transmitters, and regulating the balance of
ions. Astrocytes join together to provide a barrierbetween parts of the central nervous system (CNS)and non-CNS tissue.
Astrocytomas A form of malignant tumors primarilycomposed of astrocytes, a type of glia cell.
Atharva-Veda 700 B.C. Indian text that proposed thatthe soul was nonmaterial and never died.
Atherosclerosis A neuropathologic process character-ized by irregularly distributed yellow fatty plaques inlarge and medium-sized arteries.
Atonia Lack or reduction of muscle tone.Atonic seizures Are characterized by a sudden loss of
muscle tone and may result in a fall. They last nolonger than 15 seconds while the person remainsconscious.
Atrial fibrillation A disorder that upsets the heart’srhythm, which may cause it to not pump enoughblood to meet the body’s needs. A normal heartcontracts and relaxes to a regular beat. In atrial fib-rillation the heart contracts at a very irregular andsometimes very rapid rate, which results in an irreg-ular heart rhythm.
Atrophy Brain shrinkage.Attention-deficit/hyperactivity disorder (ADHD) A
neuropsychological developmental disorder charac-terized by age-inappropriate inattention, impulsivi-ty, and overactivity.
Aura A neurologic event that occurs before the onsetof a migraine or a seizure. The aura presents usuallyas a visual symptom including flashing lights, zigzaglines, or blurred or partial loss of vision.
Autism Previously referred to as infantile autism orKanner’s autism. A pervasive developmental disorder,evident before age 3, involving impaired communi-cation, socialization, and behavioral adaptation.Atypical behaviors, preoccupations, or interests arefrequently evident. The cause of the disorder isunknown, and the prognosis is poor.
Autistic aloneness A term proposed by Leo Kanner inhis description of autistic children, referring to oneof the central symptoms of the disorder, namely, theprofound separation and disconnection of autisticindividuals from other people.
Automatisms Stereotyped hand movements or facialtics often seen during an absence seizure.
Autonomic nervous system (ANS) Provides the“automatic” neural control of internal organs (suchas heart, intestines). Most autonomic organs receiveboth sympathetic and parasympathetic input.
Autosomes A non-sex chromosome. Humans generallyhave 22 pairs of autosomes in each cell of the body.
Glossary 513

These chromosomes are involved in transmitting allgenetic traits and conditions other than those thatare sex-linked.
Axon Extends from cell body. Its main function is totransmit information in the form of an actionpotential.
Babinski, Joseph (1857–1932) Founder of Britishneurology.
Balint’s syndrome Related to damage of the parieto-occipital area of both hemispheres; includes visual agnosia together with other visuospatial difficulties such as misreaching and left-sidedneglect.
Basal forebrain Structure of the telencephalon, sur-rounding the inferior tip of the frontal horn;strongly interconnects with limbic structures;includes various structures such as the amygdalaand the septum.
Basal ganglia Also called the basal nuclei; deep nucleiof the telencephalon. Structures include the caudatenucleus, putamen, globus pallidus, substantia nigra,and subthalamic nuclei. Important relay stations inmotor behavior (for example, the striato-pallido-thalamic loop). Coordinate stereotyped postural andreflexive motor activity.
Basal nuclei See Basal ganglia.Base rate The frequency with which a pathologic con-
dition is diagnosed in the population.Basilar artery Formed from a joining of the two verte-
bral arteries at the level of the brainstem.Basolateral circuit Anatomic circuit centered around
the amygdala; its most likely role is in emotionalprocessing.
Basophilic adenomas A functioning type of tumor ofthe pituitary gland in the anterior lobe of the pitu-itary gland, which causes excessive secretion ofadrenocorticotropic hormone, which can causeCushing’s syndrome.
Behavioral-adaptive scales Tests that examine whatan individual usually and habitually does, not whathe or she can do. Such scales are most frequentlyused in evaluating the daily self-care skills of peoplewho are quite impaired.
Benign Describes cell growth that is usually surroundedby a fibrous capsule, is typically noninfiltrative (thatis, noninvasive), and will not spread to other partsof the body.
Benton, Arthur American neuropsychologist who pio-neered the role of the right cerebral hemisphere inbehavior.
Benzodiazepines A family of sedating drugs used totreat anxiety and sleep disorders.
Beta-amyloid Amino acid peptide protein core found inthe center of senile plaques. Also written as �-amyloid.
Bipolar neurons Neurons with two axons.Blindsight The ability in those with cortical blindness
to indicate that a stimulus is present, that it hasmoved, or that it is in a certain location, eventhough they have no conscious ability to “see” inthe conventional sense.
Blood–brain barrier Affords protection from potentiallyharmful substances circulating in the body throughthe bloodstream. It bars certain drugs totally fromthe brain, and other substances require an activetransport system across the blood–brain barrier.
Bradykinesia A poverty of movement that is not onlyslowed but reduced in magnitude; negative motorsymptom of Parkinson’s disease.
Bradyphrenia Extremely slow information processingspeed characteristic of patients with subcorticaldementias.
Brain The anterior portion of the central nervous sys-tem located within the skull. It is continuous withthe spinal cord and comprised of white/gray matter.
Brain abscesses A “walled-off,” localized pocket of puswithin the brain often related to an infection.
Brain herniation A pathologic process associated withincreasing intracranial pressure that occurs in thecranium, which may result in a displacement anddeformation of the brain.
Brain hypothesis Suggests that the brain is the sourceof all behavior.
Brainstem Evolutionary old brain structure involvedin regulating brain activation. It emerges from theuppermost portion of the spinal cord and includesall the subdivisions below the telencephalon (that is,the diencephalon, the mesencephalon, the meten-cephalon, and the myelencephalon), except for thecerebellum.
Broca, Paul (1824–1880) French anthropologist andscientist who advanced surgery, neuroanatomy, neu-rophysiology, and neuropathology.
Brodmann’s areas Cytoarchitectural scheme dividingthe cortex into 52 sections.
Canalesthesia The fragmentation of the processing ofincoming information from the sensory modalities.The anomaly is believed to be one of the causativefactors of autistic behaviors.
Cannon–Bard theory Opposite of James–Lange theory.Walter Cannon, and later Philip Bard, argued the
514 Glossary
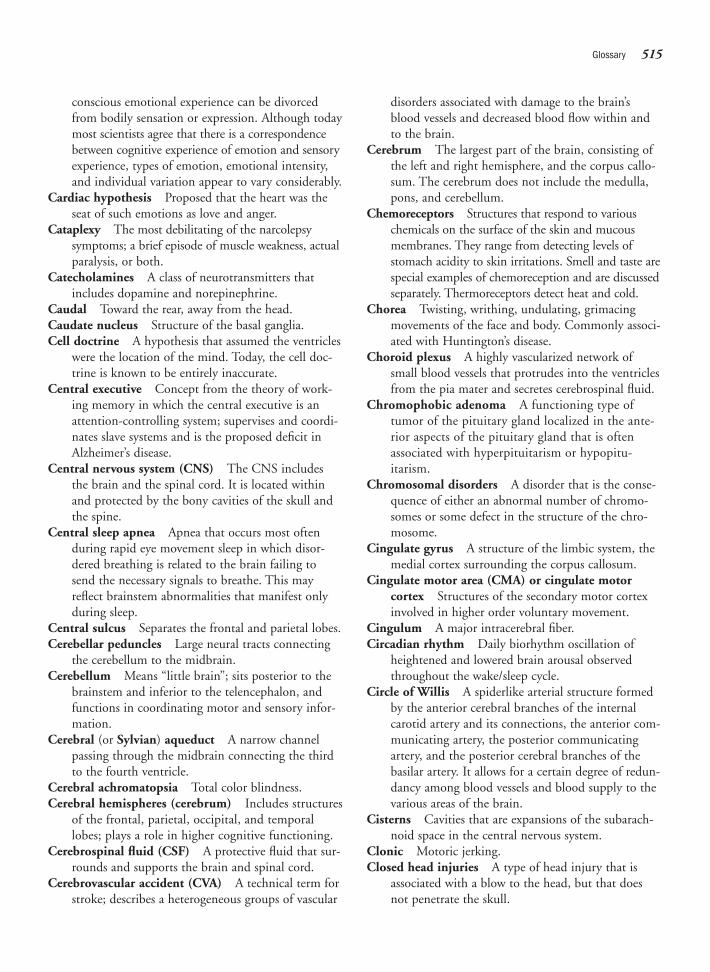
conscious emotional experience can be divorcedfrom bodily sensation or expression. Although todaymost scientists agree that there is a correspondencebetween cognitive experience of emotion and sensoryexperience, types of emotion, emotional intensity,and individual variation appear to vary considerably.
Cardiac hypothesis Proposed that the heart was theseat of such emotions as love and anger.
Cataplexy The most debilitating of the narcolepsysymptoms; a brief episode of muscle weakness, actualparalysis, or both.
Catecholamines A class of neurotransmitters thatincludes dopamine and norepinephrine.
Caudal Toward the rear, away from the head.Caudate nucleus Structure of the basal ganglia.Cell doctrine A hypothesis that assumed the ventricles
were the location of the mind. Today, the cell doc-trine is known to be entirely inaccurate.
Central executive Concept from the theory of work-ing memory in which the central executive is anattention-controlling system; supervises and coordi-nates slave systems and is the proposed deficit inAlzheimer’s disease.
Central nervous system (CNS) The CNS includesthe brain and the spinal cord. It is located withinand protected by the bony cavities of the skull andthe spine.
Central sleep apnea Apnea that occurs most oftenduring rapid eye movement sleep in which disor-dered breathing is related to the brain failing tosend the necessary signals to breathe. This mayreflect brainstem abnormalities that manifest onlyduring sleep.
Central sulcus Separates the frontal and parietal lobes.Cerebellar peduncles Large neural tracts connecting
the cerebellum to the midbrain.Cerebellum Means “little brain”; sits posterior to the
brainstem and inferior to the telencephalon, andfunctions in coordinating motor and sensory infor-mation.
Cerebral (or Sylvian) aqueduct A narrow channelpassing through the midbrain connecting the thirdto the fourth ventricle.
Cerebral achromatopsia Total color blindness.Cerebral hemispheres (cerebrum) Includes structures
of the frontal, parietal, occipital, and temporallobes; plays a role in higher cognitive functioning.
Cerebrospinal fluid (CSF) A protective fluid that sur-rounds and supports the brain and spinal cord.
Cerebrovascular accident (CVA) A technical term forstroke; describes a heterogeneous groups of vascular
disorders associated with damage to the brain’sblood vessels and decreased blood flow within andto the brain.
Cerebrum The largest part of the brain, consisting ofthe left and right hemisphere, and the corpus callo-sum. The cerebrum does not include the medulla,pons, and cerebellum.
Chemoreceptors Structures that respond to variouschemicals on the surface of the skin and mucousmembranes. They range from detecting levels ofstomach acidity to skin irritations. Smell and taste arespecial examples of chemoreception and are discussedseparately. Thermoreceptors detect heat and cold.
Chorea Twisting, writhing, undulating, grimacingmovements of the face and body. Commonly associ-ated with Huntington’s disease.
Choroid plexus A highly vascularized network ofsmall blood vessels that protrudes into the ventriclesfrom the pia mater and secretes cerebrospinal fluid.
Chromophobic adenoma A functioning type oftumor of the pituitary gland localized in the ante-rior aspects of the pituitary gland that is oftenassociated with hyperpituitarism or hypopitu-itarism.
Chromosomal disorders A disorder that is the conse-quence of either an abnormal number of chromo-somes or some defect in the structure of the chro-mosome.
Cingulate gyrus A structure of the limbic system, themedial cortex surrounding the corpus callosum.
Cingulate motor area (CMA) or cingulate motor cortex Structures of the secondary motor cortexinvolved in higher order voluntary movement.
Cingulum A major intracerebral fiber.Circadian rhythm Daily biorhythm oscillation of
heightened and lowered brain arousal observedthroughout the wake/sleep cycle.
Circle of Willis A spiderlike arterial structure formedby the anterior cerebral branches of the internalcarotid artery and its connections, the anterior com-municating artery, the posterior communicatingartery, and the posterior cerebral branches of thebasilar artery. It allows for a certain degree of redun-dancy among blood vessels and blood supply to thevarious areas of the brain.
Cisterns Cavities that are expansions of the subarach-noid space in the central nervous system.
Clonic Motoric jerking.Closed head injuries A type of head injury that is
associated with a blow to the head, but that doesnot penetrate the skull.
Glossary 515
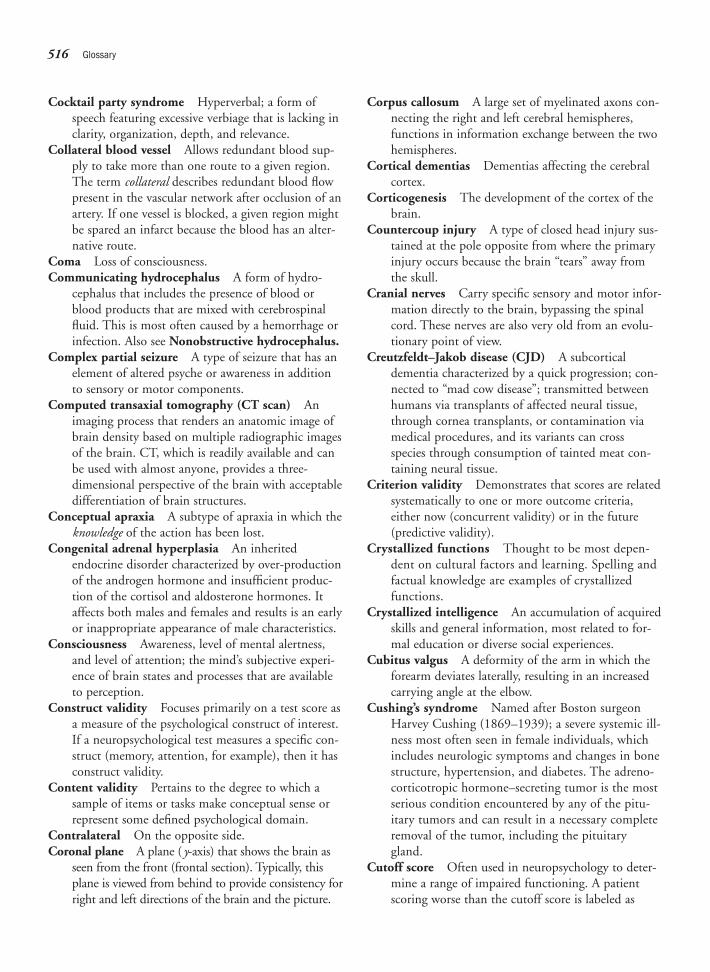
Cocktail party syndrome Hyperverbal; a form ofspeech featuring excessive verbiage that is lacking inclarity, organization, depth, and relevance.
Collateral blood vessel Allows redundant blood sup-ply to take more than one route to a given region.The term collateral describes redundant blood flowpresent in the vascular network after occlusion of anartery. If one vessel is blocked, a given region mightbe spared an infarct because the blood has an alter-native route.
Coma Loss of consciousness.Communicating hydrocephalus A form of hydro-
cephalus that includes the presence of blood orblood products that are mixed with cerebrospinalfluid. This is most often caused by a hemorrhage orinfection. Also see Nonobstructive hydrocephalus.
Complex partial seizure A type of seizure that has anelement of altered psyche or awareness in additionto sensory or motor components.
Computed transaxial tomography (CT scan) Animaging process that renders an anatomic image ofbrain density based on multiple radiographic imagesof the brain. CT, which is readily available and canbe used with almost anyone, provides a three-dimensional perspective of the brain with acceptabledifferentiation of brain structures.
Conceptual apraxia A subtype of apraxia in which theknowledge of the action has been lost.
Congenital adrenal hyperplasia An inheritedendocrine disorder characterized by over-productionof the androgen hormone and insufficient produc-tion of the cortisol and aldosterone hormones. Itaffects both males and females and results is an earlyor inappropriate appearance of male characteristics.
Consciousness Awareness, level of mental alertness,and level of attention; the mind’s subjective experi-ence of brain states and processes that are availableto perception.
Construct validity Focuses primarily on a test score asa measure of the psychological construct of interest.If a neuropsychological test measures a specific con-struct (memory, attention, for example), then it hasconstruct validity.
Content validity Pertains to the degree to which asample of items or tasks make conceptual sense orrepresent some defined psychological domain.
Contralateral On the opposite side.Coronal plane A plane ( y-axis) that shows the brain as
seen from the front (frontal section). Typically, thisplane is viewed from behind to provide consistency forright and left directions of the brain and the picture.
Corpus callosum A large set of myelinated axons con-necting the right and left cerebral hemispheres,functions in information exchange between the twohemispheres.
Cortical dementias Dementias affecting the cerebralcortex.
Corticogenesis The development of the cortex of thebrain.
Countercoup injury A type of closed head injury sus-tained at the pole opposite from where the primaryinjury occurs because the brain “tears” away fromthe skull.
Cranial nerves Carry specific sensory and motor infor-mation directly to the brain, bypassing the spinalcord. These nerves are also very old from an evolu-tionary point of view.
Creutzfeldt–Jakob disease (CJD) A subcorticaldementia characterized by a quick progression; con-nected to “mad cow disease”; transmitted betweenhumans via transplants of affected neural tissue,through cornea transplants, or contamination viamedical procedures, and its variants can crossspecies through consumption of tainted meat con-taining neural tissue.
Criterion validity Demonstrates that scores are relatedsystematically to one or more outcome criteria,either now (concurrent validity) or in the future(predictive validity).
Crystallized functions Thought to be most depen-dent on cultural factors and learning. Spelling andfactual knowledge are examples of crystallizedfunctions.
Crystallized intelligence An accumulation of acquiredskills and general information, most related to for-mal education or diverse social experiences.
Cubitus valgus A deformity of the arm in which theforearm deviates laterally, resulting in an increasedcarrying angle at the elbow.
Cushing’s syndrome Named after Boston surgeonHarvey Cushing (1869–1939); a severe systemic ill-ness most often seen in female individuals, whichincludes neurologic symptoms and changes in bonestructure, hypertension, and diabetes. The adreno-corticotropic hormone–secreting tumor is the mostserious condition encountered by any of the pitu-itary tumors and can result in a necessary completeremoval of the tumor, including the pituitarygland.
Cutoff score Often used in neuropsychology to deter-mine a range of impaired functioning. A patientscoring worse than the cutoff score is labeled as
516 Glossary

impaired; a patient scoring better is labeled as with-in normal limits (WNL).
Cytoarchitectonic dysplasia A focal pathologicchange of the cellular organization of brain cells.
da Vinci, Leonardo (1452–1519) Italian painter,sculptor, architect, and scientist.
Deceleration Describes an event in which the brain isin motion traveling at a certain speed and thenstops abruptly.
Declarative memory A form of memory that isexplicit, verbalizable, and accessible to consciousawareness.
Decussating Switching the transmission of informa-tion from one side of the body to the contralateralside of the brain.
Deep dyslexia A reading disorder characterized by animpaired ability to sound out words, while whole-word skills are unimpaired.
Defective response inhibition The act of inappropri-ately, displaying a motor response when it isunwanted.
Deficit measurement An approach to neuropsycho-logical assessment for understanding general condi-tions and disease states about a patient by examin-ing scores that are impaired and comparing themwith other factors known about the patient.
Delirium A transient cognitive problem associatedwith a confused state caused by specific organicproblems.
Dementia A pattern of impairment with varying causescharacterized by a deteriorating progression in mem-ory, as well as other areas of cognitive functioning.
Dendrites Feathery extensions that branch from theneuron into the immediate neighborhood of the cellbody.
Dendritic spines Short outgrowths on the dendritesthat contain synapses for gathering information tobe sent to the neurons.
Descartes, René (French, 1596–1650); proposed astrict split or schism between mental processes andphysical abilities. He hypothesized that the mindand body are separate, but interact with each other.
Diaschisis A passive process of uncovering workingneural systems after temporary neuronal disruptionin areas far removed from the lesion site.
Diencephalon Composed primarily of the thalamusand hypothalamus and a structure of the brainstem,also known as the interbrain or “between brain.”
Differentiation process A phase of prenatal centralnervous system development that commences when
migrating neural cells reach their predetermined des-tinations within the brain. As the neural cells reachtheir destination, they develop the unique character-istics of the cells specific to that brain region.
Digital subtraction angiography A procedure inwhich the x-ray image of the brain is stored andsubtracted after the images of the contrast materialhave been acquired. The process is particularly effec-tive in enhancing the visualization of blood vessels,including the morphologic and physiologic states ofthe arterial, capillary, and venous phases of the cere-bral circulation.
Disengage attention The withdrawal or decoupling ofattentional focus from a stimulus.
Disinhibition Impulsivity and inappropriate behavior;may result from losing inhibitory neurons to traumaor disease.
Dissimulation A form of malingering in which thepatient is consciously denying that there is anythingwrong with him or her, to achieve some secondarygain (for example, to avoid hospitalization, to gainemployment).
Dissociation A separation between functional contri-butions of two different brain areas.
Distal Away from the center, toward the periphery,away from the origin of attachment.
Divided attention Partialing out one’s attentionalresources at the same time rather than switchingback and forth, however quickly.
Dominance Hand (and to a lesser extent, eye andfoot) preferences and proficiencies in performingtasks or to the cerebral organization of the brain.
Dopamine A neurotransmitter that plays an importantrole in the organization of motor behavior.
Doppler-ultrasonography (fTCD) A noninvasivediagnostic procedure that uses an ultrasound scan-ner to convert sound waves into images of bloodflow within body tissue and organs. It is used toassess the direction, velocity, and turbulence ofblood flow.
Dorsal Toward the back. The top of the brain is dorsalin humans.
Dorsal column medial lemniscal pathway Carriesinformation pertaining to touch and vibration. It isso named because it is routed up the dorsal aspectsof the spinal cord to a white matter tract termed themedial lemniscus that courses through the contralat-eral side of the brainstem through the medulla,pons, and midbrain to be routed up through thethalamus (ventral posterior nucleus) and on to theprimary somatosensory cortex.
Glossary 517

Dorsal simultagnosia A visual disorder related todamage of the parieto-occipital area of both hemi-spheres. Even though parts of a picture may be rec-ognized, the whole is not perceived.
Dorsolateral prefrontal cortex This area is located,functionally, in the prefrontal cortex, which isresponsible for orchestrating and organizing manyfunctions of the brain. The dorsolateral prefrontalcortex is not a “movement center” in and of itselfbut is instrumental in deploying movement. Sensoryinformation from the integrative association area ofthe parietal lobes is relayed to this motor planningarea.
Double-deficit hypothesis Poses that reading disor-ders can be traced to deficits in phonological pro-cessing and/or naming speed. The presence of botha deficit in phonological processing and slow nam-ing speed is predictive of the most severe readingproblem.
Double dissociation A logical progression of scientificassumptions in localizing functional areas in thebrain. For example, if symptom A appears withlesions in brain structure X, but not with those in Y,and symptom B appears with lesions of Y, but notof X, then those specific areas of the brain each havea specific function.
Down’s syndrome Also referred to as trisomy 21. Agenetic disorder due to an extra chromosome on the21st pair. The disorder is characterized by recogniz-able facial features, short stature, and mild to severecognitive deficits.
Dura mater “Tough mother”; a dense, inelastic, double-layered, vascularized membrane of the meningesthat adheres to the inner surface of the skull.
Dysarthria A specific motor apraxia involving thevocal musculature. People with dysarthria differfrom pure aphasiacs, although the two conditionsmay occur together in that such patients know whatthey want to say but are unable to formulate wordsbecause of a problem with motor control.
Dyscalculia A disorder of mathematics involvingimpaired ability to comprehend number concepts,spatially orient numbers, reason mathematically, orperform mathematical operations.
Dysgenesis Abnormal or defective development of anorgan.
Dysgraphia An impairment of the ability to write orexpress oneself in writing. Deficits are evident inone or more of the following areas: (1) letter forma-tion, speed of writing, and spatial organization ofwriting; (2) written expression; (3) mechanical
knowledge of spelling, grammar, punctuation, andcapitalization; and (4) organization and thematicconstruction of written expression.
Dysgeusia Distorted taste sensation.Dyskinesia Uncontrolled involuntary movement.Dyslexia A developmental or acquired disorder of
reading involving the disruption of one or more ofthe component skills of reading. Central readingskills include letter identification, phonologic aware-ness and processing, and decoding of the writtenword.
Dysosmia Distorted smell sensation.Dysphonia Loss of vocal emotional expression result-
ing in a monotonous voice tone.
Echolalia An atypical communication behavior char-acterized by the repetition or “echoing” of the wordsor phrases just spoken by another person. Often dis-played by children with pervasive developmentaldisorders.
Ectopias Also referred to as “brain warts.” Small areasof abnormally placed brain neurons.
Edema The swelling of the brainEfferent nerves Motor nerves carry outgoing signals
for action from the central nervous system to themuscles.
Elastin A protein within elastic fibers of connectivetissue accounting for the elasticity of structures suchas the skin, blood vessels, heart, lungs and tendons.
Electroconvulsive therapy (ECT) Shock therapy;administering a large amount of electricity to theskull causing the collective firing of neurons: aninduced seizure. ECT sometimes improves severeforms of depression within a few days. Although themechanism is not clearly understood, therapists useECT when it is important to intervene quickly toprevent the patient from acting on suicidalthoughts.
Electrocorticogram (ECoG) A form of EEG in whichelectrodes are placed directly on the exposed cortexduring surgery to isolate a precise location of brainpathology.
Electroencephalography (EEG) One of the mostwidely used techniques in neurology. In EEG, theelectrical activity of nerve cells of the brain arerecorded through electrodes attached to variouslocations on the scalp.
Epileptogenic focus The anatomic site of onset.Embolism Derived from Greek embolos, meaning
“plug” or “wedge”; a type of occlusion of an arteryin which the clot forms in one area of the body
518 Glossary
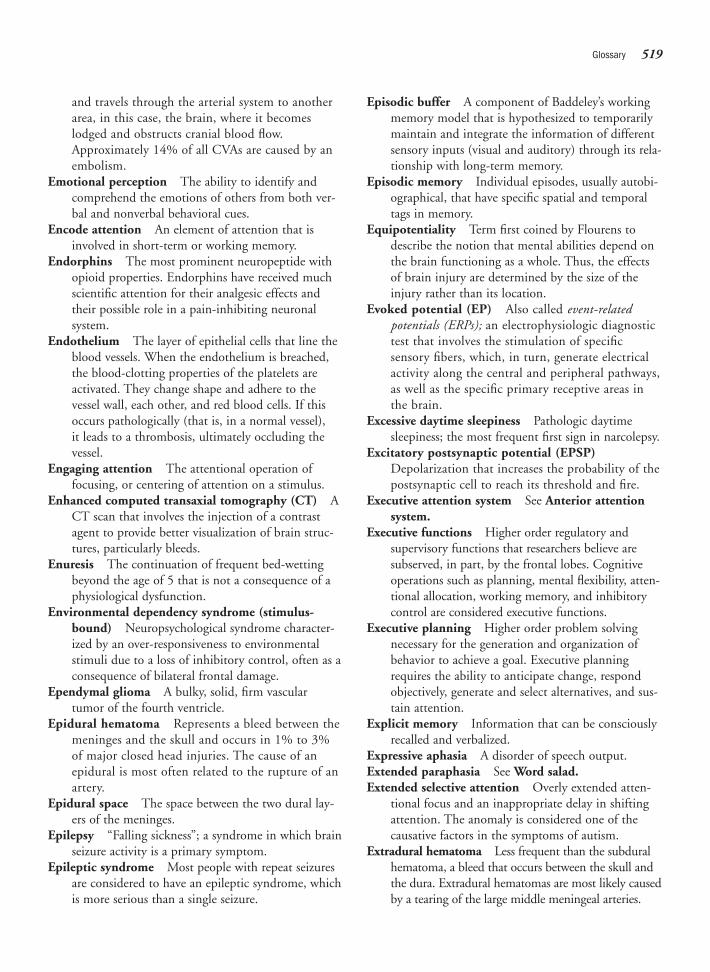
and travels through the arterial system to anotherarea, in this case, the brain, where it becomeslodged and obstructs cranial blood flow.Approximately 14% of all CVAs are caused by anembolism.
Emotional perception The ability to identify andcomprehend the emotions of others from both ver-bal and nonverbal behavioral cues.
Encode attention An element of attention that isinvolved in short-term or working memory.
Endorphins The most prominent neuropeptide withopioid properties. Endorphins have received muchscientific attention for their analgesic effects andtheir possible role in a pain-inhibiting neuronal system.
Endothelium The layer of epithelial cells that line theblood vessels. When the endothelium is breached,the blood-clotting properties of the platelets areactivated. They change shape and adhere to the vessel wall, each other, and red blood cells. If thisoccurs pathologically (that is, in a normal vessel), it leads to a thrombosis, ultimately occluding the vessel.
Engaging attention The attentional operation offocusing, or centering of attention on a stimulus.
Enhanced computed transaxial tomography (CT) ACT scan that involves the injection of a contrastagent to provide better visualization of brain struc-tures, particularly bleeds.
Enuresis The continuation of frequent bed-wettingbeyond the age of 5 that is not a consequence of aphysiological dysfunction.
Environmental dependency syndrome (stimulus-bound) Neuropsychological syndrome character-ized by an over-responsiveness to environmentalstimuli due to a loss of inhibitory control, often as aconsequence of bilateral frontal damage.
Ependymal glioma A bulky, solid, firm vasculartumor of the fourth ventricle.
Epidural hematoma Represents a bleed between themeninges and the skull and occurs in 1% to 3%of major closed head injuries. The cause of anepidural is most often related to the rupture of anartery.
Epidural space The space between the two dural lay-ers of the meninges.
Epilepsy “Falling sickness”; a syndrome in which brainseizure activity is a primary symptom.
Epileptic syndrome Most people with repeat seizuresare considered to have an epileptic syndrome, whichis more serious than a single seizure.
Episodic buffer A component of Baddeley’s workingmemory model that is hypothesized to temporarilymaintain and integrate the information of differentsensory inputs (visual and auditory) through its rela-tionship with long-term memory.
Episodic memory Individual episodes, usually autobi-ographical, that have specific spatial and temporaltags in memory.
Equipotentiality Term first coined by Flourens todescribe the notion that mental abilities depend onthe brain functioning as a whole. Thus, the effectsof brain injury are determined by the size of theinjury rather than its location.
Evoked potential (EP) Also called event-relatedpotentials (ERPs); an electrophysiologic diagnostictest that involves the stimulation of specificsensory fibers, which, in turn, generate electricalactivity along the central and peripheral pathways,as well as the specific primary receptive areas inthe brain.
Excessive daytime sleepiness Pathologic daytimesleepiness; the most frequent first sign in narcolepsy.
Excitatory postsynaptic potential (EPSP)Depolarization that increases the probability of thepostsynaptic cell to reach its threshold and fire.
Executive attention system See Anterior attentionsystem.
Executive functions Higher order regulatory andsupervisory functions that researchers believe aresubserved, in part, by the frontal lobes. Cognitiveoperations such as planning, mental flexibility, atten-tional allocation, working memory, and inhibitorycontrol are considered executive functions.
Executive planning Higher order problem solvingnecessary for the generation and organization ofbehavior to achieve a goal. Executive planningrequires the ability to anticipate change, respondobjectively, generate and select alternatives, and sus-tain attention.
Explicit memory Information that can be consciouslyrecalled and verbalized.
Expressive aphasia A disorder of speech output.Extended paraphasia See Word salad.Extended selective attention Overly extended atten-
tional focus and an inappropriate delay in shiftingattention. The anomaly is considered one of thecausative factors in the symptoms of autism.
Extradural hematoma Less frequent than the subduralhematoma, a bleed that occurs between the skull andthe dura. Extradural hematomas are most likely causedby a tearing of the large middle meningeal arteries.
Glossary 519

Extrapyramidal motor system Responsible for stereo-typed postural and reflexive motor activity. The sys-tem also acts to keep individual muscles ready torespond.
False positive Also known as a Type I error or falsealarm. Refers to a case in which a neuropsychologi-cal test erroneously indicates the presence of apathologic condition.
Familial sinistrality The degree of left-handednesswithin the nuclear and extended family.
Femorocerebral angiography Angiography that intro-duces a catheter into the arterial system via thefemoral artery.
Festinating gait The rapid, shuffling gait characteristicof Parkinson’s disease.
Fetal alcohol effect (FAE) A developmental disorderthat involves the cognitive and behavioral deficitsassociated with FAS, but without the physical stig-mata of FAS. Also see Fetal alcohol syndrome.
Fetal alcohol syndrome (FAS) A developmental disor-der caused by the pregnant mother ingesting alco-hol. The disorder is characterized by recognizablephysical stigmata, neurologic abnormalities, andcognitive and behavioral impairments. Unlike manyof the congenital disorders, FAS is preventable.
Fibers See Tracts.Finger agnosia Inability to recognize or orient to one’s
own fingers.Fissure A very deep sulcus in the cortex.Flicker fusion rate Denotes the speed at which two
separate visual images appear to fuse visually into asingle image.
Flourens, Pierre (French, 1794–1867) The foremostearly advocate of an alternative to localization theories.
Fluent aphasia A disorder of speech in which thepatient remains able to talk, but his or her speechmakes no sense, often sounding like some unknownforeign language.
Fluid functions Believed to be culture-free and inde-pendent of learning. Problem solving and abstractreasoning are considered fluid functions.
Fluid intelligence Novel reasoning and the efficiencyof solving new problems or responding to abstractideas.
Fluorescent in situ hybridization (FISH) A labora-tory technique in which a DNA probe is labelledwith a fluorescent dye to detect chromosomalabnormalities.
Focus-execute attention The ability to respond andpick out the important elements or “figure” of
attention from the “ground” or background ofexternal and internal stimulation. Also implies ameasure of concentration or effortful processing.
Focused attention A form of selective attentioninvolving the restriction of attention to a specificfeature, or set of features, to the exclusion of otherfeatures.
Fontanelles Literally “small springs or fountains”;membranous gaps between the bony skull platesthat are evident in newborns.
Foramen of Magendie The middle opening, of three,of the membranous roof of the fourth ventricle,allowing the cerebrospinal fluid to flow outside thebrain and recirculate.
Foramen magnum The largest of the foramina; pro-vides a large median opening in the occipital bonefor the spinal cord to pass through to the brain-stem.
Foramen of Monro See Interventricular foramen.Foramina More-or-less symmetric orifices in the base
of the skull that provide passage for nerves andblood vessels.
Foramina of Luschka The two lateral openings, ofthree, of the membranous roof of the fourth ventri-cle, allowing the cerebrospinal fluid to flow outsidethe brain and recirculate.
Forebrain, or prosencephalon The topmost divisionof the developing brain.
Fornix A structure of the limbic system that containsnearly 1 million fibers; it rises out of the hippocam-pal complex and arches anteriorly under the corpuscallosum. The fornix relays information to themammillary bodies.
Fossae Conspicuous ridges in the base of the skull thathold the brain in place.
Fragile X A genetic disorder frequently associatedwith mental retardation and other cognitivedeficits and distinctive physical features. The disor-der is related to a compression or break of the X chromosome.
Freud, Sigmund (Austrian, 1856–1939) Best knownas the founder of psychoanalysis and the father ofclinical psychology. Freud’s initial love was neurologyand investigating the secrets of the central nervoussystem.
Frontal lobe One of the four cortical lobes; containsthe primary motor cortex and the prefrontal lobe.Its functions are motor processing and executive,including planning, inhibition, and formulation ofbehavior.
Frontal operculum Broca’s area.
520 Glossary

Functional systems A concept first formulated byLuria in which behavior results from interactionamong many areas of the brain.
Functioning adenomas Pituitary tumors that play an“uninvited” role in the operation of the pituitarygland, often affecting the release of the gland’s hor-mones.
Galen (A.D. 129–201) Roman anatomist and physi-cian who identified many of the major brain struc-tures and described behavioral changes as a functionof brain trauma.
Gall, Franz (1758–1828) Austrian anatomist who pos-tulated that mental faculties were innate and relatedto the topical structures of the brain.
Gamma-aminobutyric acid (GABA) One of morethan 20 amino acids, GABA is a neurotransmitterknown to have strong inhibitory properties.
Ganglia (singular, ganglion) A strategic collection ofnerve cells in the peripheral nervous system.
Generalized seizure A seizure caused by an abnormalrhythm of the entire brain; formally known as “grandmal”; bilaterally symmetric episodes characterized bya temporary lack of awareness, or what appears onobservation to be a complete loss of consciousness.
Gerstmann-Straussler-Scheinker syndrome (GSS)An extremely rare familial Creutzfeldt–Jakob diseasevariant that results in a “fatal insomnia.”
Geschwind, Norman (1926–1984) American neurolo-gist who proposed that behavioral disturbances werebased on the destruction of specific brain pathwaysthat he called disconnections.
Gigantocellular tegmental field (GTF) Located in thehigher pons; appears to generate brain waves. Leftunchecked, the neurons fire spontaneously, produc-ing a high level of activity. One particular set of dis-charges is termed PGO spikes because they travel fromthe pons (P) to the lateral geniculate (G) nucleus ofthe thalamus and to the occipital (O) cortex.
Gilles de la Tourette syndrome See Tourette’s syn-drome.
Glasgow Coma Scale (GCS) A three-item scale oftenused in the medical setting to assess the severity ofcoma. The GCS ranges from 3 to 15 points, withlower scores indicating severe coma and higherscores suggesting a confusional state.
Glia Greek meaning “glue”; glia cells outnumber neu-rons and provide supportive structure and metabolicfunction to the neuron.
Glioblastoma multiforme (GBM) A particularlydestructive and fatal glioma.
Gliomas A type of brain tumor, gliomas are a rela-tively fast growing brain tumor that arises fromsupporting glia cells. Gliomas are the most com-mon infiltrative brain tumor, which make upapproximately 40% to 50% of all brain tumors.The term glioma is often used to describe all pri-mary, intrinsic neoplasms of the brain and thespinal cord.
Globus pallidus A structure of the basal ganglia.Glutamate One of more than 20 amino acids, gluta-
mate is the major excitatory neurotransmitter of thebrain.
Golgi, Camillo (1843–1926) Italian physician whomade the discovery in the early 1870s that silverchromate stained dead neurons black. This allowedpeople to visualize individual neurons for the firsttime.
Gonadotropins Hormonal substances that stimulatethe functions of the testes and ovaries.
Grading of tumors A method of evaluating themalignant features of brain tumors. Grading isfrom 1 to 4, with a grade 1 tumor representing aslow-growing tumor accompanied by few neu-ropsychological deficits. Grades 2 and 3 representintermediate rates of growth and neuropsycholog-ical dysfunction. Grade 4 tumors are fast grow-ing and typically have a poor prognosis forrecovery.
Grand mal seizure Literally “big bad” seizure; consistof violent motoric abnormalities of stiffening andjerking episodes and the accompanying loss of con-sciousness.
Gray matter Areas of the brain that are dense in cellbodies such as the cortex and that appear gray.
Gyri (singular, gyrus) Ridges of the cortex betweensulci.
Halstead–Reitan Neuropsychological Battery(HRNB) The first neuropsychology laboratoryin the United States was founded in 1935 byWard Halstead at the University of Chicago.Halstead worked closely with neurosurgerypatients and developed assessment devices thatdifferentiated between patients with and withoutbrain damage. Halstead later developed, withRalph Reitan, the HRNB, which represented anempirical approach to the assessment of braindamage.
Hebb, Donald Publisher of the classic The Organizationof Behavior: A Neuropsychological Theory. This bookbrought much growth to the field of neuropsychology.
Glossary 521
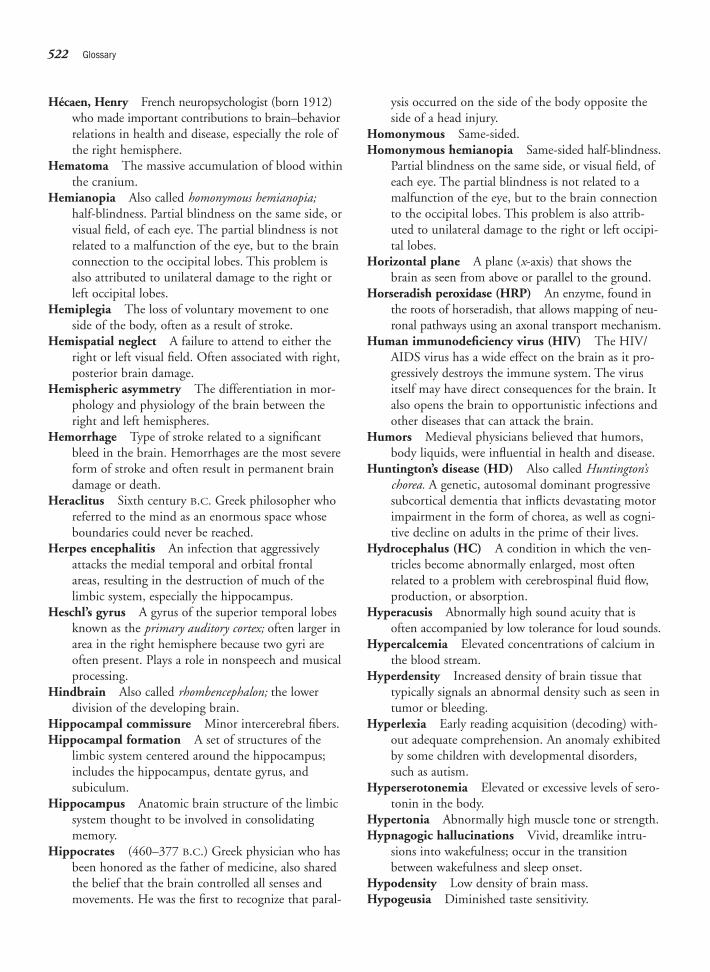
Hécaen, Henry French neuropsychologist (born 1912)who made important contributions to brain–behaviorrelations in health and disease, especially the role ofthe right hemisphere.
Hematoma The massive accumulation of blood withinthe cranium.
Hemianopia Also called homonymous hemianopia;half-blindness. Partial blindness on the same side, orvisual field, of each eye. The partial blindness is notrelated to a malfunction of the eye, but to the brainconnection to the occipital lobes. This problem isalso attributed to unilateral damage to the right orleft occipital lobes.
Hemiplegia The loss of voluntary movement to oneside of the body, often as a result of stroke.
Hemispatial neglect A failure to attend to either theright or left visual field. Often associated with right,posterior brain damage.
Hemispheric asymmetry The differentiation in mor-phology and physiology of the brain between theright and left hemispheres.
Hemorrhage Type of stroke related to a significantbleed in the brain. Hemorrhages are the most severeform of stroke and often result in permanent braindamage or death.
Heraclitus Sixth century B.C. Greek philosopher whoreferred to the mind as an enormous space whoseboundaries could never be reached.
Herpes encephalitis An infection that aggressivelyattacks the medial temporal and orbital frontalareas, resulting in the destruction of much of thelimbic system, especially the hippocampus.
Heschl’s gyrus A gyrus of the superior temporal lobesknown as the primary auditory cortex; often larger inarea in the right hemisphere because two gyri areoften present. Plays a role in nonspeech and musicalprocessing.
Hindbrain Also called rhombencephalon; the lowerdivision of the developing brain.
Hippocampal commissure Minor intercerebral fibers.Hippocampal formation A set of structures of the
limbic system centered around the hippocampus;includes the hippocampus, dentate gyrus, andsubiculum.
Hippocampus Anatomic brain structure of the limbicsystem thought to be involved in consolidatingmemory.
Hippocrates (460–377 B.C.) Greek physician who hasbeen honored as the father of medicine, also sharedthe belief that the brain controlled all senses andmovements. He was the first to recognize that paral-
ysis occurred on the side of the body opposite theside of a head injury.
Homonymous Same-sided.Homonymous hemianopia Same-sided half-blindness.
Partial blindness on the same side, or visual field, ofeach eye. The partial blindness is not related to amalfunction of the eye, but to the brain connectionto the occipital lobes. This problem is also attrib-uted to unilateral damage to the right or left occipi-tal lobes.
Horizontal plane A plane (x-axis) that shows thebrain as seen from above or parallel to the ground.
Horseradish peroxidase (HRP) An enzyme, found inthe roots of horseradish, that allows mapping of neu-ronal pathways using an axonal transport mechanism.
Human immunodeficiency virus (HIV) The HIV/AIDS virus has a wide effect on the brain as it pro-gressively destroys the immune system. The virusitself may have direct consequences for the brain. Italso opens the brain to opportunistic infections andother diseases that can attack the brain.
Humors Medieval physicians believed that humors,body liquids, were influential in health and disease.
Huntington’s disease (HD) Also called Huntington’schorea. A genetic, autosomal dominant progressivesubcortical dementia that inflicts devastating motorimpairment in the form of chorea, as well as cogni-tive decline on adults in the prime of their lives.
Hydrocephalus (HC) A condition in which the ven-tricles become abnormally enlarged, most oftenrelated to a problem with cerebrospinal fluid flow,production, or absorption.
Hyperacusis Abnormally high sound acuity that isoften accompanied by low tolerance for loud sounds.
Hypercalcemia Elevated concentrations of calcium inthe blood stream.
Hyperdensity Increased density of brain tissue thattypically signals an abnormal density such as seen intumor or bleeding.
Hyperlexia Early reading acquisition (decoding) with-out adequate comprehension. An anomaly exhibitedby some children with developmental disorders,such as autism.
Hyperserotonemia Elevated or excessive levels of sero-tonin in the body.
Hypertonia Abnormally high muscle tone or strength.Hypnagogic hallucinations Vivid, dreamlike intru-
sions into wakefulness; occur in the transitionbetween wakefulness and sleep onset.
Hypodensity Low density of brain mass.Hypogeusia Diminished taste sensitivity.
522 Glossary

Hypokinesia Reduced motor initiation; negativemotor symptom of Parkinson’s disease.
Hyposmia Diminished smell sensation.Hypothalamus A structure of the diencephalon, part of
the limbic system; considered instrumental in con-trolling the autonomic system. Activates, controls,and integrates the peripheral autonomic mecha-nisms, endocrine activity, and somatic functions,including body temperature, food intake, and devel-opment of secondary sexual characteristics.
Hypotonia Abnormally low muscle tone or strength.Hypoxia The reduced oxygenation of brain. Hypoxia
is typically not associated with cell death, but somepossible interference in the functioning of the neu-ron. Hypoxia is usually related to inadequatebreathing, such as experienced during sleep apnea,can occur at high altitude, or is related to carbonmonoxide poisoning.
Ideomotor apraxia See Motor apraxia.Impact injury A type of closed head injury in which
the physical forces act on the brain tissue at thepoint of impact.
Impaired affective assignment A failure to link theappropriate emotional meaning to both internal andexternal stimuli. Considered a key deficit of autism.
Implicit memory Demonstrated by means wherebyconscious awareness is not always necessary, such asimplicit priming, skill learning, and conditioning.
Implicit priming The phenomenon in which, if“primed” with three-letter word stems, people aremore likely to complete the stem with a word theyhave already seen.
Infarction A severe loss of blood caused by a blockageof an artery, often resulting in more lasting neu-ropsychological deficits.
Inferior Toward the bottom, or below.Inferior colliculi Two elevations within the roof of the
tectum, which serve as an important relay center forthe auditory pathway.
Infiltrative tumors Tumors that take over or infiltrateneighboring areas of the brain and destroy its tissue.
Inhibitory control Inhibition of behavior throughinvoluntary and voluntary neuropsychologicalprocesses. At a voluntary level, this capacity is consid-ered an executive function and connotes the volitionalcapacity to withhold behavior, particularly wheninvoking environmental contingencies are evident.
Inhibitory postsynaptic potential (IPSP) The pres-ence of an ionic current flow that hyperpolarizes thepostsynaptic neuron. As a result, a greater depolar-
ization than normal is required for excitation andthere is only a small probability that there will be anaction potential.
Intelligence The aggregate or global capacity involvingan individual’s ability to act purposefully, to thinkrationally, and to deal effectively with the environment.
Intelligence tests Complex composite measures of ver-bal and performance abilities that are related partlyto achievement (for example, factual knowledge)and partly to aptitude (for example, problem solv-ing). Although there are well over 100 different testsof intelligence, the scales that David Wechsler devel-oped have become widely used throughout theworld and typically include a variety of scales mea-suring verbal-comprehension skills and tests tappingperceptual-organization abilities.
Intercerebral fibers Connect structures between twohemispheres.
Interference control The ability to screen or block outinternal or external distractions that could intrudeinto and disrupt attentional focus.
Interictal Between seizures.Internal carotid arteries Two of the four major arter-
ies to the brain, supplying the anterior portions ofthe brain.
Interneurons Neurons with short axons or no axons.Interpretive hypotheses Inferences about the patient’s
cognitive status that the neuropsychologist makes inthe process of interpreting neuropsychologicalassessment data.
Interventricular foramen (foramen of Monro) Asmall opening connecting the lateral ventricles.
Intracerebral “Within the cerebrum” or brain.Intracerebral fibers Fibers that connect regions within
one hemisphere.Intracranial pressure (ICP) Related to the presence
of a bleed (or hemorrhage) within the cranium(skull) usually associated with the development of aspace-occupying mass or pocket of blood, whichmay press on nearby brain structures, affecting theirintegrity.
Intraventricular hemorrhage (IVH) Bleeding withinthe ventricles of the brain. A common cause ofhydrocephalus in premature infants. Vessels in thearea surrounding the ventricles rupture, and theblood and cellular debris obstruct the structures thatallow for the reabsorption of the cerebrospinal fluidinto the bloodstream.
Ions Atoms or molecules that have acquired an electri-cal charge by gaining or losing one or more elec-trons. Four ions that are important in neuronal
Glossary 523
communication are sodium (NA+), potassium (K+),calcium (Ca++), and chloride (Cl–).
Ipsilateral On the same side.Ischemia A restriction or insufficiency of blood supply
to an area of the brain, with possible damage or dysfunction depending on the duration of theischemia. These events can also be short-lasting,with transient deficits.
Isochromosome An abnormal karyotype characterizedby identical arms on the X (female) chromosome.The chromosomal anomaly is associated withTurner’s syndrome.
Jackson, Hughlings British neurologist (1835–1911)who wrote on the integration of the localization andequipotentiality models of brain function. He sug-gested that behavior resulted from interactionsamong all areas of the brain, but that each area inthe nervous system had a specific function that con-tributed to the overall system.
Jacksonian seizure Involves motor areas; such eventshave been called marching seizures because theybegin with jerking or tingling of a single body areaand spread to other areas.
James–Lange theory of emotion Promoted byAmerican psychologist William James and Danishpsychologist Carl Lange, postulating that emotion isconsciously experienced as a reaction to physicalsensory experience. In other words, we feel fearbecause our hearts are racing; we are sad because weare crying. Although critics saw this as an overstate-ment, the James–Lange theory did correctly insistthat sensory and cognitive experiences were inti-mately entwined and could not be separated fromeach other.
Joint attention The reciprocal attention evident in theinteraction of individuals. Disruption of this inter-actional capacity of mother and child has been asso-ciated with autism.
Joint contractures An abnormal shortening of theelastic tissue of a joint resulting in distortion ordeformity.
Karyotype A visual representation of an individual’schromosomes that displays the structural compo-nents and integrity of the chromosomes.
Kennard principle A principle of neural recoverythat bears the name of its originator, MargaretKennard. The principle holds that earlier braininjury is associated with less impairment and bet-ter recovery of functions than injury occurring
later in development. Subsequent clinical andexperimental studies have not fully supported thisprinciple.
Kinesthetic sense A sense of one’s physical body issupplied by a combination of vision, the vestibularorgans, and the proprioceptive sense.
Kuru A spongiform encephalopathy suffered by theFore people of Papua New Guinea.
Lancisi, Giovanni (1654–1720) Italian clinician whocontributed greatly to the knowledge of aneurysm:abnormal blood-filled ballooning of an artery in thebrain.
Lashley, Karl (1890–1958) American neuropsycholo-gist who was one of the first to combine behavioralsophistication in experiments with neurologicsophistication, thereby creating the field of experi-mental neuropsychology.
Lateral Toward the side, away from the midline.Lateral fissure Separates the frontal and parietal lobes.Lateralization With dominance, refers to the differ-
ences in functional specialization between the twobrain hemispheres.
Lesions Derived from Latin laesio, meaning “to hurt”;any pathologic or traumatic discontinuity of braintissue. Depending on their size and location, lesionsresult in minor or major behavioral effects.
Lewy bodies Small, tightly packed granular structureswith ringlike filaments, found within dying cells.
Lexicon store A “storehouse” of words that an individ-ual knows or understands.
Lezak, Muriel American neuropsychologist who pio-neered the assessment approach in clinical neu-ropsychology.
Limb-kinetic apraxia A subtype of apraxia involvingproblems in executing precise, independent, orcoordinated finger movements.
Limbic system Includes the fornix; some brainstemareas, particularly the mammillary bodies of thehypothalamus; and specific basal forebrain struc-tures, including the amygdala (“almond” because ofits shape) and the septum.
Lissencephaly See Agyria.Localization theory Assigns specific functions to par-
ticular places in the cerebral cortex.Locus ceruleus Located below the wall of the fourth
ventricle, it has been implicated as an importantnorepinephrine pathway.
Longitudinal fissure The space between the twohemispheres.
Long-term memory (LTM) Theoretically of unlimitedcapacity and relatively permanent except for models
524 Glossary

suggesting that loss of information through forget-ting is possible.
Lucid dreaming The ability while dreaming tobecome conscious of that one is in a dream state.
Lumbar puncture Also known as a spinal tap; a med-ical technique for collecting a specimen of cere-brospinal fluid surrounding the spinal cord for diag-nostic study.
Luria, Alexander (1902–1977) Russian neuropsychol-ogist who was responsible for the most profoundchanges in the scientific understanding of the brainand mind.
Magnetic resonance imaging (MRI) A visualizationprocedure that provides the most detailed images ofbrain structures. The advantage of functional MRIover other functional procedures, such as positronemission tomography, is that it provides good spa-tial resolution and images in short time periods, or“real time.”
Magnetoencephalogram (MEG) The magneticequivalent of the electroencephalogram in which athree-dimensional magnetic field of the brain canthen be calculated. Superconducting quantuminterference device (SQUID) detects the smallmagnetic fields in the brain that are a marker ofneural activity. A disadvantage of MEG is related tothat it is expensive and not readily available forclinical applications.
Magnocellular visual system One of the two visualsystems that extends from the eyes to the visual cor-tex. It consists of large cells that are inferiorly locatedin the lateral geniculate bodies that are highly sensi-tive to movement, low contrast, and spatial location.
Magnus, Albertus (German, ca. 1200–1280) De-emphasized the role of the ventricles in brain func-tioning.
Malignant tumors Tumors whose cells invade othertissues and are likely to regrow or spread.
Malingering The intentional exaggeration or presenta-tion of neuropsychological symptoms.
Mammillary bodies Two small nuclei on the floor ofthe posterior hypothalamus.
Masked facies Used to describe the masklike expres-sion of patients with Parkinson’s disease.
Mass action The extent to which behavioral impair-ments are directly proportional to the mass of theremoved brain tissue.
Materialism A theory that brain–behavior functionsare produced by matter in motion, favoring a mech-anistic view of the brain as a machine.
Mechanical receptors Structures that transduce energyfrom touch, vibration, and the stretching and bend-ing of skin, muscle, internal organs, and blood vessels.
Medial Toward the middle/midline, away from the side.
Medial lemniscus A white matter tract that coursesthrough the contralateral side of the brainstemthrough the medulla, pons, and midbrain to berouted up through the thalamus (ventral posteriornucleus, VP) and on to the primary somatosensorycortex.
Medulla oblongata Myelencephalon; a structure ofthe brainstem.
Medulloblastoma A brain tumor seen most frequentlyin children; rapidly growing and very malignant;located in the inferior vermis close to the exit ofcerebrospinal fluid from the fourth ventricle. Thistype of tumor accounts for about two thirds of alltumors in children and produces increased intracra-nial pressure caused by obstructive hydrocephalus.
Membrane potential See Resting potential.Meninges Protective covering of the brain and spinal
cord consisting of the pia mater, the arachnoidmembrane, and the dura mater.
Meningiomas Highly encapsulated, benign tumorsthat arise from the arachnoid layer of the meninges.Meningiomas represent approximately 15% of allbrain tumors.
Meningitis Inflammation of the meninges caused by bacterial infection or viral infection. It canprogress quickly, within 24 hours, from a respira-tory illness, with fever, headache, and a stiff neck,to changes in consciousness including stupor,coma, and death.
Mental rotation Refers to the ability to mentally visu-alize and rotate forms, objects, or scenes in two- orthree-dimensional space.
Mesencephalon One of the five principal divisions ofthe brain, part of the brainstem.
Meta-analysis A statistical technique designed to ana-lyze the results from a number of different and inde-pendent studies. The technique allows for the identi-fication of significant relationships and outcomes.
Metacognition A higher order cognitive ability thatenables an individual to examine and analyze themanner in which he or she thinks, solves problems,encodes and retrieves information, and performscognitive operations.
Metacognitive awareness An ability to monitor one’sown behavior and performance.
Glossary 525

Metastasis A form of tumor spreading in which tissuefrom a malignant tumor “travels” to other organs inthe body through the bloodstream. The capacity formetastasis is a characteristic of all malignant tumors.Metastatic brain tumors typically originate fromsites other than the brain, most frequently the lungor the breast.
Metastatic tumors Growths that arise secondarily tocancerous tumors that have their primary site inother parts of the body, such as the lungs, breasts, orthe lymphatic system. The secondary growths arisebecause cancer cells from the primary neoplasmdetach and travel to other sites through the bloodsystem.
Metencephalon One of the five principal divisions ofthe brain, part of the brainstem.
Microcephaly A congenital disorder characterized byan abnormally small head in relation to the rest ofthe body. The head is more than two standard devi-ations below the average circumference for a childof a similar age and sex. The size of the brain is alsosubnormal, and the condition is associated withmental retardation.
Microglia Small cells within the CNS that undergo rapidproliferation in response to tissue destruction, migrat-ing toward the site of injured or dead cells, where theyact as scavengers and metabolize tissue debris.
Micrographia Small handwriting; a common motorsymptom of Parkinson’s disease.
Midbrain (mesencephalon) The middle division of thedeveloping brain.
Middle cerebral artery Resulting from half of thedivision of an internal carotid artery, it supplies thelateral hemisphere and most of the basal ganglia ofits corresponding cerebral hemisphere.
Migraine stroke A rare type of stroke in which atransient ischemic attack, typically associated withclassic migraine, is severe enough to cause astroke.
Migratory process A phase of prenatal central nervoussystem development characterized by the movementof neural cells along the wall of the neural tube togenetically predetermined locations.
Mild cognitive impairment (MCI) Implies an inter-mediary, and perhaps transitional, stage betweennormal aging and dementia.
Mind-blindness A neuropsychological deficit in whichan animal’s behavior suggests that it can “see”objects—that is, the test subjects do not bump intothe object—but fail to recognize its significance (forexample, as an object of fear).
Molecular cytogenic disorders Disorders or diseasesrelated to chromosome abnormalities (extra, miss-ing, or rearranged).
Monopolar neurons Unipolar neurons; neurons witha single axon.
Mosaic karyotypes The presence of both structurallynormal and abnormal female chromosomes thatproduces one form of Turner’s syndrome.
Motor apraxia Ideomotor apraxia; an inability toaccess a stored motor sequence or an inability torelay that information to the motor associationareas. An example is the inability to show me howyou would make a telephone call from beginning toend.
Motor neurons Neurons responsible for contractingmuscles or changing the activity of a gland.
Motor perseveration The act of continuing in thesame motor behavior, or constantly selecting it inthe presence of other choices.
Move attention A cognitive-attentional operationinvolving the shifting or movement of attentionalfocus from one stimuli to the next.
Multi-infarct dementia A dementia caused by multi-ple small strokes or ischemic attacks.
Multipolar neurons Neurons with more than twoaxons.
Munk, Hermann (German, 1839–1912) Found thatexperimental lesions in the visual association cortexproduced temporary mind-blindness in dogs.
Muscarinic choline One of two main subtypes ofacetylcholine, a neurotransmitter known to stimu-late receptors.
Myelencephalon One of the five principal divisions ofthe brain; part of the brainstem.
Myelin A lipid sheath that surrounds and insulates theaxons of the central and peripheral nervous systems.It serves to increase the speed of nerve conduction.
Myelin sheath Fatty-type covering of axons thatincreases the speed of axonal transmission.
Myelin staining Selectively dyes the sheaths of myeli-nated axons. As a result, white matter, which con-sists of myelinated axons, stains black, unlike otherareas of the brain that consist mostly of cell bodiesand nuclei.
Myoclonic seizures Manifest in arrhythmic bursts ofjerky motor movements that usually do not lastmore than a second and tend to occur in clustersover a short period.
Narcolepsy A disorder that consists of irresistible day-time “sleep attacks”; a central nervous system disor-
526 Glossary
der of the region of the brainstem that controls andregulates sleep and wakefulness. The primary symp-tom of this disorder is excessive daytime sleepiness.
Necrosis (or neuronal cell death) A direct result of acritical interference with the cellular metabolism ofthe neuron. In general, a period of 4 to 6 minutesof anoxia may cause necrosis.
Neologism Atypical language characterized by the gen-eration or production of words that are meaningless.
Neoplasm Literally “new tissue.” The neurologic termfor tumor.
Neostriatum This structure, also known as the striatalcomplex, includes the caudate and putamen andreceives projected information from cortical sensoryareas. From the neostriatum, information is thenfunneled through the globus pallidus, then on tothe thalamus, where it projects to the premotor andprefrontal areas.
Nerves A large collection of axons located in theperipheral nervous system, primarily composed ofwhite matter.
Neural tube The embryonic tube that develops intothe central nervous system, specifically the brainand spinal cord. The neural tube develops duringthe third week of gestation. Abnormalities in neuraltube development can lead to congenital develop-mental disorders.
Neurofibrillary tangles Excessive collections of tauproteins resembling entwined and twisted pairs ofrope within the cytoplasm of swollen cell bodies inthe brain. These are pathologic markers ofAlzheimer’s disease.
Neurogenesis The congenital process by which theneurons of the brain develop.
Neurologic examination A routine introductory evalu-ation performed by a neurologist—a physician whohas specialized in evaluating and treating neurologicdisorders. Although there are many variations, inprinciple, the neurologic examination involves adetailed history of the patient’s medical history and acareful assessment of the patient’s reflexes, cranialnerve functioning, gross movements, muscle tone,and ability to perceive sensory stimuli.
Neuromas Tumors or new growths that are largelymade up of nerve cells and nerve fibers.
Neuronal ectopias Also known as “brain warts.” Anabnormal placement and development of neuralcells often associated with a disruption of the migra-tory phase of brain development.
Neurons Specialized nerve cells that allow complexinformation exchange.
Neuropsychological evaluation Involves a detailedexamination, often using standardized tests, todescribe an individual’s cognitive strengths andweaknesses. Often used in conjunction with otherpertinent information, for diagnosis, patient man-agement, intervention, rehabilitation, and dischargeplanning.
Neuropsychological tests Traditionally defined asthose measures that are sensitive indicators of brainfunctioning.
Neuropsychology The study of the relations betweenbrain functions and behavior; specifically, changes inthoughts and behaviors that relate to the structuralor cognitive integrity of the brain.
Neurotransmitters Chemicals that influence neuronalbehavior.
Neurotrophins Neuron-feeding nutrients.Neurulation The congenital process involving the
formation and closure of the neural tube that sub-sequently develops into the brain and spinalcord.
Nicotinic choline One of two main subtypes ofacetylcholine, a neurotransmitter named after nico-tine (from tobacco, Nicotiana tabacum), a bitter-tasting alkaloid that stimulates receptors.
Nissl, Franz (1860–1919) German histologist whodiscovered in the 1880s that a simple dye can stainthe cell bodies in neurons. The Nissl method is par-ticularly useful for detecting the distribution of cellbodies in specific regions of the brain.
Nocioceptors Derived from Latin nocere, meaning“to hurt.” Receptors that serve as monitors to alertthe brain to damage or threat of damage. They canbe mechanical or chemical but are specifically acti-vated by potentially damaging stimulation such asheat or cold, painful pressure or pricking, or chem-ical damage such as exposure to noxious chemicals.
Nocturnal myoclonus Restless leg syndrome; twitch-ing of muscles that occurs during non–rapid eyemovement sleep. In severe cases, this will wake upthe subject.
Nodes of Ranvier Regular gaps along the axon wherethe myelin is interrupted.
Noncommunicating hydrocephalus See Obstructivehydrocephalus.
Nondeclarative memory Knowledge that is implicitand inaccessible to conscious recall or verbalization.This form of memory is demonstrated through per-formance (e.g., riding a bicycle).
Nonfluent aphasia A difficulty in the flow of articula-tion, so that speech becomes broken or halting.
Glossary 527

Nonfunctioning adenomas Benign neoplasms of thepituitary gland.
Noninfiltrative tumors Invasive tumors; encapsulatedand differentiated (easily distinguished from braintissue); cause dysfunction by compressing surround-ing brain tissue.
Nonobstructive hydrocephalus Also referred to ascommunicating hydrocephalus. A form of hydro-cephalus produced by blockage that disrupts reab-sorption of cerebrospinal fluid into the blood-stream.
Norepinephrine (NE) A neurotransmitter that isimportant to the regulation of mood, memory, hor-mones (via the hypothalamus), cerebral blood flow,and motor behavior.
Normal distribution A frequency distribution inwhich the values or scores group around a mean. Inneuropsychological testing, many test scores displaysuch distributions.
Normal-pressure hydrocephalus (NPH) A neuro-logic condition involving ventricular enlargementin the absence of elevated intracranial pressure.Most frequently evident in older adults and char-acterized by a triad of progressive neurologic signs(postural imbalance, dementia, and urinary incon-tinence).
Normative data These data compare the patient’sscore on a test to an expected score, or norm. Theexpected test score is determined from the perfor-mance of a normative sample of patients and con-trol subjects.
NREM sleep (non–rapid eye movement sleep)Includes sleep stages 1 through 4.
Nuclei (singular, nucleus) A strategic collection ofnerve cells in the central nervous system.
Nuclei of the raphe A collection of neurons locatedthroughout the midline of the brainstem; implicatedin serotonin pathways.
Nucleus basalis of Meynert Named after its discoverer;a collection of neurons implicated in Alzheimer’sdisease.
Nucleus reticularis thalami (NRT) A group of neu-rons within the thalamus that regulates oscillatorybehavior of the thalamocortical loop.
Object permanence A cognitive capacity described bythe developmental psychologist Jean Piaget, which isinitially absent in the infant, but subsequently devel-ops. The infant is unable to store in memory a repre-sentation of an object that is removed from view. Inessence, what is out of sight is “out of mind.”
Objective personality tests Typically use the question-naire technique of measurement (for example,true/false or multiple-choice questions).
Obsessive-compulsive disorder A psychiatric disordercharacterized by recurrent thoughts or images(obsessions) that are intrusive and anxiety producingwhich prompt or compel overt or mental behaviors(compulsions) to reduce this anxiety. Althoughobsessive-compulsive behaviors are viewed by thepatient as irrational and excessive, this awarenessdoes not alter the symptoms.
Obstructive hydrocephalus Also referred to as noncom-municating hydrocephalus. A form of hydrocephalusproduced by obstruction within the ventricular systemof the brain. The obstruction can be a consequence ofcongenital malformation, tumors, or scarring.
Obstructive sleep apnea Apnea that occurs mostoften during rapid eye movement sleep when eitherthe upper airway collapses, not allowing air to pass,or the body weight of the patient on the chest com-promises respiratory effort.
Occipital lobe One of the four cortical lobes, primari-ly dedicated to visual processing.
Occipital notch Sulci within the medial occipital lobe.Occupational therapy Rehabilitation specialty that
focuses on improving self-care activities such asgrooming, bathing, dressing, and feeding, as well asactivities concerned with a person’s occupation andavocation.
Oligodendrocytes A type of non-neural cell; theprojections of the surface membrane of each suchcell fan out and coil around the axon of neuronsin the central nervous system to form the myelinsheath.
Oligodendroglioma A rare, slowly growing tumorthat mostly affects young adults and is derived fromand composed of oligodendrogliocytes.
Optic gliomas A slowly growing glioma of the opticnerve or optic chiasm; associated with visual lossand loss of ocular movement.
Orientation A patient’s basic awareness of himself orherself in relation to the world around.
Orthotic Customizable cognitive adjunct, such as acomputer, used in rehabilitating people with braininjury.
Overcorrection An aversive behavior modificationtechnique that involves having a child practice apositive response that is incompatible with an inap-propriate behavior. Overcorrection is particularlyeffective in reducing self-stimulating and other inap-propriate behaviors.
528 Glossary

Palilalia Compulsive word or phrase repetition.Pallidotomy A surgical treatment for Parkinson’s dis-
ease; in this technique, the ventral, or internal por-tion, of the globus pallidus is lesioned via heat coag-ulation of the neurons.
Papez circuit Anatomic circuit centered around thehippocampus; plays a role in declarative memoryprocessing.
Papillae Bumps on which lie from one to several hun-dred taste buds consisting of between 50 to 150taste receptor cells.
Paragrammatism See Word salad.Parahippocampal gyrus Structure of the limbic system.Parasympathetic nervous system Division of the auto-
nomic nervous system; functions to store energy byfacilitating functions such as digestion through gastric and intestinal motility.
Parental imprinting disorders Also known as genomicimprinting. A child receives two sets of chromosomes,one set from the mother, and the other from thefather. The expression of the genes in each set is inaccordance with the parent of origin. If the childreceives both sets of chromosomes from the same par-ent, there will be a loss of expression of the genes ofthe other parent. This abnormal imprinting has beenassociated with several neurodevelopmental disorders.
Paresthesia Spontaneous crawling, burning, or “pinsand needles sensation.”
Parietal lobe One of the four cortical lobes, concernedwith the integration of information from sensoryareas.
Parkinson’s disease (PD) A progressive disease processcharacterized by a dopamine deficiency of the sub-stantia nigra; results in resting tremors and alliedmotor symptoms; may cause a subcortical dementia.
Parkinsonism A behavioral syndrome marked bymotor symptoms including tremor, rigidity, andslowness of movement.
Partial seizure A seizure caused by an abnormalrhythm confined to a particular brain area; alsoknown as focal seizures; always begins as a localneuronal discharge; the most common type ofseizure.
Parvocellular visual system One of the two visual sys-tems extending from the eyes to the visual cortex. Itconsists of small cells dorsally located in the lateralgeniculate bodies that are sensitive to viewing sta-tionary objects, high contrasts, and fine spatialdetails.
Pathognomonic signs Neurologic symptoms fromwhich a specific diagnosis can be made.
Pathways See Tracts.Pattern analysis Examines the relations among the
scores in a test battery.Penetrating head injury A type of head injury associ-
ated with a penetrating mechanism such as a bulletfrom a gun, a knife, or scissors.
Penfield, Wilder Famous neurosurgeon who madeadvancements in the understanding of the relationbetween brain anatomy and behavior.
Peptides A group of neurotransmitters, peptides areshort chains of amino acid. More than 60 neuroac-tive peptides have been identified.
Perception The process of “knowing”; depends onintact sensation.
Peripheral nervous system (PNS) The PNS includesall the portions of the nervous system outside thecentral nervous system. The PNS consists of thesomatic and the autonomic nervous systems.
Peripheral neuropathy Peripheral nervous system dys-function causing sensory loss (as in diabetes).
Personality tests Measures of such characteristics asemotional states, interpersonal relations, and moti-vation.
Petit mal seizure Literally “little bad” seizure; causesan altered state of consciousness but lacks the vio-lent physical loss of control seen during the grandmal seizure.
Phantogeusia Experience of a phantom or hallucina-tory taste.
Phantom limb pain A feeling of pain in a nonexistentlimb.
Phantosmia Experience of a phantom or hallucinatorysmell.
Phenylketonuria (PKU) A genetic disorder affecting themetabolism of phenylalanine. If untreated, mentalretardation and other cognitive deficits can result.Dietary control, particularly if started early, can reduceor eliminate the negative effects of the disorder.
Phonemic paraphasias Errors of word usage of similar-sounding words (for example, using the word barkfor tarp).
Phonologic awareness The awareness of and ability todifferentiate between individual phonemes or speechsounds.
Phonologic processing The application of codes fortranslating letters and letter sequences into theappropriate speech–sound equivalents. Deficits inthis processing have been linked to dyslexia.
Phrenology An obsolete theory proposing that if agiven brain area was larger in an individual, thenthe corresponding skull at that point should be
Glossary 529

enlarged, indicating a well-developed area of thebrain. Conversely, a depression signaled an underde-veloped area of the cortex. Phrenology involved, inits most popular form, the reading of cranial bumpsto ascertain which of the cerebral areas were largest.
Physiatry The medical specialty of combining physicalmedicine and rehabilitation.
Physical therapy A rehabilitation specialty thatfocuses on improving motor control and physicalfunctioning.
Pia mater Literally “pious mother”; a vascularized partof the meninges that directly adheres to the surfaceof the central nervous system.
Pinealoma A type of tumor of the pineal body.Pituitary adenoma Tumors of the pituitary gland that
are often classified into functioning (changing thesecretion of the pituitary gland) and nonfunctioning(benign).
Pituitary stalk Also known as the infundibular stalk.It is the axon bundle extending from the hypothala-mus to the posterior region of the pituitary. Thisconnection mediates the release of oxytocin andantidiuretic hormone directly into the bloodstream.
Pituitary tumors Tumors that arise from the pituitarygland. It is traditional to divide pituitary tumorsinto functioning and nonfunctioning adenomas.
Planum temporale Region of the posterior surface ofthe temporal lobes between the Heschl’s gyrus andthe Sylvian fissure. The planum temporale of theleft hemisphere is involved in mediating phonologicprocessing and language comprehension.
Plasticity Behavioral or neural ability to reorganizeafter brain injury.
Platelets Disk-shaped cells found in the blood of allmammals. They are important for their role inblood coagulation and are produced in large num-bers in the bone marrow. From there they arereleased into the bloodstream, where they circulatefor approximately 10 days.
Plato (Greek, 420–347 B.C.) Suggested that the soulcan be divided into three parts: appetite, reason,and temper. Plato also discussed the concept ofhealth as being related to the harmony between thebody and the mind. Thus, he has been credited asbeing the first to propose the concept of mentalhealth.
Pluripotentiality The multiple, functional role of thebrain. That is, any given area of the brain can beinvolved in relatively few or relatively many behaviors.
Polymicrogyria A congenital disorder that can be tracedto a disruption of the structure of the developing
brain during the fifth to sixth month of gestation.As a consequence of this disruption, the gyri fail to develop appropriately. On inspection, the gyri are found to be small and crowded together.Learning disorders, mental retardation, epilepsy, andother neuropsychological anomalies are linked tothe disorder.
Pons Metencephalon; a “bridge” resembling two bulbs,a structure of the brainstem.
Porencephaly A congenital disorder of brain forma-tion in which cystic lesions are on the surface of thebrain.
Positron emission tomography (PET) A visualiza-tion technique that tracks blood flow, which isassociated with brain activity. It is mostly used toassess brain physiology, including glucose and oxy-gen metabolism, and the presence of specific neuro-transmitters.
Posterior Toward the back or tail.Posterior attention system One of the attentional sys-
tems of the brain that mediates visuospatial orient-ing and is supported by the parietal, midbrain, andthalamic regions.
Posterior cerebral arteries Formed by a division ofthe basilar artery.
Posterior communicating arteries Arise from theinternal carotid arteries and connect the middle andposterior cerebral arteries.
Postictal phase Phase in which the person graduallyemerges into full consciousness; follows the seizureepisode.
Post-traumatic amnesia (PTA) A patient’s memory ofevents surrounding an accident.
Pragmatics of language Aspects of language thatextend beyond the literal.
Precursor or progenitor cells Early cells lining theneural tube that proliferate to create the neuronsand glia cells of the brain.
Prefrontal motor cortex Section of the frontal lobe.This area is considered to be the “conductor” or“executor” of the brain. Also called prefrontal cortex.
Premorbid functioning The cognitive and neuropsy-chological status occurring before the developmentof disease or trauma.
Premotor area (PMA) See Premotor cortex.Premotor cortex Also known as premotor area. Located
in Brodmann’s area 6 of the frontal lobes; receivesneuronal input from posterior parietal areas, sec-ondary somatosensory areas, and cerebellum; plays arole in motor planning and sequencing, and may aidin the procedural aspects of carrying out motor plans.
530 Glossary
Prepotent response A response that has been “primed”to occur through reinforcement, repeated use, habit,or reflex.
Prestriate cortex See Secondary association.Primary motor cortex Part of the frontal lobe, con-
cerned with the initiation, activation, and perfor-mance of motor activity.
Procedural memory Memory that is usually implicitand is demonstrated via performance. Proceduralmemory’s domain is that of rules and proceduresrather than information that can be verbalized,although procedural memory has not been clearlyoperationally defined and includes a hodgepodge oftasks such as motor skill learning, mirror reading,and verbal priming.
Process approach Also known as the “hypothesisapproach”; based on the idea that each examinationshould be adapted to the individual patient. Ratherthan using a standard battery of tests, the neuropsy-chologist selects the tests and procedures for eachexamination, based on hypotheses made fromimpressions of the patient and from informationavailable about the patient. As a result, each exami-nation may vary considerably from patient topatient for length and test selection.
Prodromal phase A phase before the seizure, in whichan aura occurs; odd, transient symptoms such asnausea, dizziness, or numbness may occur, as well assensory alterations or hallucinations in any sensorydomain.
Progenitor cells See Precursor cells.Projection fibers Neurons that connect sets of brain
structures to each other (e.g. subcortical structuresto the cortex and vice versa).
Projective personality test Tests that rely on relativelyambiguous, vague, and unstructured stimuli, such asinkblots.
Proprioception The position of the body in extraper-sonal space. Sensory dysfunctions that result in pro-prioceptive disorders include altered sense of bodilysensation and bodily position.
Proprioceptive disorder Loss of body position sense.Proprioceptors Derived from Latin proprius, meaning
“one’s own”; structures on skeletal muscles thatdetect movement via degree of stretch, angle, andrelative position of limbs. Proprioceptors on thehands help identify the shapes of objects via touch.
Prosencephalon See Forebrain.Prosody An aspect of speech that conveys meaning
through intonation, tempo, pitch, word stress, flu-ency, and rhythm. It augments the meaning of spo-
ken language and is important in communicatingthe emotional content of language.
Prosopagnosia The special case of inability to recog-nize people by their faces.
Prospective memory The intention to remember toperform an action in the future.
Prosthetic Cognitive replacement, such as a computer,used in the rehabilitation of people with braininjury.
Proximal Near the trunk or center, close to the originof attachment.
Pruning The process of eliminating excessive neuronsand synapses in the developing brain. The elimina-tion appears to reflect a purposeful “sculpting” ofthe brain to promote neural efficiency.
Pseudopsycopathy Also known as “acquired sociopa-thy.” The emergence of uninhibited and poorlymodulated behavior, poor judgment and violationof social norms following orbitofrontal damage.Unlike the true psychopath or sociopath, the patientwith orbitofrontal damage experiences remorse forinappropriate actions and does not demonstrate theintentional viciousness or planning with regard tocommitting antisocial acts.
Psychology The study of describing, explaining, pre-dicting, and modifying behavior.
Psychometrics The science of measuring human traitsor abilities. Concerned with the standardization ofpsychological and neuropsychological tests.
Psychomotor epilepsy See Temporal lobe epilepsy.Purkinje cells A specific type of neuron that is found
in the cerebellum. The dendrites characteristicallyspread out in one plane.
Putamen Structure of the basal ganglia.Pyramidal cells A specific type of neuron that is
found in all areas of the cerebral cortex. Thesecells have bodies that are pyramidal or conical inshape.
Pyramidal motor system This system originates inthe cerebral cortex and controls voluntary move-ment.
Pythagoras (ca. 580–500 B.C.) Greek scholar whosuggested that the brain is at the center of humanreasoning and plays a central role in the “soul’s life.”
Receptive aphasia A difficulty in auditory comprehen-sion. Also see Wernicke’s aphasia.
Receptor cells Receptor cells detect numerous stimuli,including sight, sound, pressure, pain, chemical irri-tation, smell, and taste. Not technically neurons,although they create energy that is transduced into
Glossary 531

an electrical stimulus that is carried to neurons andthen processed in the brain.
Receptor sites Sites on the postsynaptic neuron towhich neurotransmitters are delivered.
Reductionism Investigating complex phenomena bydividing them into more easily understood compo-nents. Related to brain research, reductionists arguethat behavior is no more than the results of chemi-cal and structural relation among neurons.
Refractory period A recovery period after a neuronhas fired. During this period, which lasts one ormore milliseconds, the neuron resists re-excitationand is incapable of firing.
Reliability The stability or dependability of a testscore as reflected in its consistency on repeated mea-surement of the same individual. A reliable testshould produce similar findings on each administra-tion.
REM sleep Rapid eye movement sleep; state of sleepwhere dreams occur.
Remote memory Memory for long-past events.Response cost A behavioral modification technique
that involves removing or taking away an alreadypresent positive reinforcer contingent on thedisplay of a specific undesirable behavior. Thetechnique is used to inhibit or suppress a specificbehavior.
Response inhibition Three interrelated controlprocesses: (1) stopping an ongoing response, (2) blocking or screening out distractions, and (3) restraining a response primed for release.
Resting potential Membrane potential; a slight electri-cal imbalance between the inner and outer surfacesof the membrane caused by the separation of electri-cally charged ions.
Resting tremor Rhythmic shaking that often occurs inone hand first; positive motor symptom ofParkinson’s disease; characterized as “pill rolling.”
Restitution One of two primary approaches to braininjury rehabilitation; stresses the retraining of animpaired skill in the hope that the brain can rebuildaxonal connections through retraining.
Reticular activating system (RAS) Also called reticu-lar formation; a neural network located within thelower brainstem transversing between the medullaand the midbrain. Functions in nonspecific arousaland activation, sleep and wakefulness.
Retrograde amnesia In this disorder, the patient has no recollection of the interval preceding theinjury; the loss of old memories before an event or illness.
Retrograde degeneration The degeneration of theaxon back to the cell body, once the axon has beendamaged. This process may lead to cell death.
Rhinencephalon Evolutionarily old “smell brain.”Rhombencephalon See Hindbrain.Rigidity Tightening of muscles and joints; positive
motor symptom of Parkinson’s disease.Ring X karyotypes A relatively rare karyotype that is
associated with one variant of Turner’s syndrome.Mental retardation frequently occurs in this form ofTurner’s syndrome.
Röntgen, Wilhelm Conrad (1845–1923) Physicistwho made a remarkable discovery that an invisibleray that, unlike heat or light waves, could passthrough wood, metal, and other materials. This ray,also called X-ray, gave rise to radiology.
Rostral Toward the head.
Saccadic eye movements Quick eye movements madewhen the eye moves from one point of fixation tothe next.
Sagittal plane Derived from Latin sagitta, meaning“arrow.” A plane (z-axis) that shows the brain asseen from the side or perpendicular to the ground,bisecting the brain into right and left halves.
Savant skills Extraordinary skills possessed by an indi-vidual who otherwise displays limited capacity. Forexample, the ability of a retarded child to mentallycalculate complex square roots is a savant skill.
Schwann cells Type of non-neural cells. The projec-tions of the surface membrane of each of those cellsfan out and coil around the axons of neurons in theperipheral nervous system to form myelin sheaths.
Secondarily generalized seizure A simple seizure thatcrosses the corpus callosum and eventually involvesthe entire brain.
Secondary association Prestriate cortex; processes pri-mary features of visual information such as lightwavelength, line orientation, and features of shape.
Secondary motor cortex Functions in strategic plan-ning of the specific aspects of movement. The inten-tion to move is also a function of this area.
Seizures Massive waves of synchronized nerve cell acti-vation that can involve the entire brain. Seizures mayhave dramatic behavioral manifestations, includinguncontrolled muscles contractions, changes in per-ception, and alterations in mood and consciousness.
Semantic memory Memory for information and factsthat have no specific time-tag reference.
Senile plaques Also called neuritic plaques. Roundaggregates of beta-amyloid that on disintegration
532 Glossary
leave holes and misshapen neurons where there oncewere active connections.
Sensation The elementary process when a stimulus hasexcited a receptor and results in a detectable experi-ence in any sensory modality.
Sensitivity How sensitive a test is in measuring a par-ticular neuropsychological construct.
Sensory association area An area of the cortex thatfunctions to integrate information from differentsensory areas.
Sensory neurons Neurons that respond directly tochanges in light, touch, temperature, or odor.
Septum In general, refers to a thin plate of brain tis-sue separating two cavities or tissue areas. The sep-tal area stretches between the fornix and the cor-pus callosum, forming one of the walls of thefrontal horn of the lateral ventricle. The septal areainterconnects with the hippocampus and the hypo-thalamus.
Serotonin A neurotransmitter that is involved in sleep,depression, memory, and other neurologic processes.
Sex chromosomes A chromosome that determines thesex of a person. Humans have two sex chromo-somes, X and Y, with the former determiningfemale sexual characteristics, and the latter, malesexual characteristics. A male is defined by the pair-ing of XY chromosomes, and a female, by the pair-ing of XX chromosomes.
Shifting attention An element of attention involvingthe movement of attentional focus from one stimulior task to another.
Short-term memory (STM) Memory of limitedcapacity (7 ± 2 bits of information); degrades quicklyover a matter of seconds if information is not heldvia a means such as rehearsal or transfer to long-term memory.
Shunt A medical procedure to drain excessive cere-brospinal fluid from the ventricular system to thestomach. The procedure is used with people whohave acquired hydrocephalus.
Simple seizures Focal events that may involve sensori-motor expression or psychic expression (mood,emotion, altered consciousness).
Simulation A form of malingering in which thepatient is faking or exaggerating an illness or theseverity of the symptoms, usually to gain some sec-ondary gain (such as attention, hospitalization, or afinancial settlement).
Single-gene disorders A disease or disorder that is dueto a mutation of a single gene. An example of asingle gene disorder is Tay-Sachs disease.
Single-photon emission computed tomography(SPECT) A visualization technique that measuresblood flow, a correlate of brain activity. Because ittakes the radioactive tracer almost 2 days to be elimi-nated from the body, SPECT cannot be used to mon-itor the brain’s mental activity “moment to moment.”
Sleep apnea Derived from Greek a pnoia, meaning“negative breathing”; refers to breathing that is dis-turbed while sleeping and often completely stops forperiods as long as a minute.
Sleep apnea syndrome A serious sleeping disorderresulting from frequent episodes of apnea.
Sleep paralysis Momentary paralysis on awakening orat sleep onset; the body is totally unable to move forseconds to minutes.
Social emotional learning disability Disturbed socio-emotional behavior that is directly related to neu-ropsychological processing deficits and does notreflect a secondary reaction to a learning disabilitysuch as dyslexia.
Sodium–potassium pump An active transportsystem across the membrane of the axon thatexchanges three sodium ions for every two potassiumions.
Somatic nervous system (SNS) That part of theperipheral nervous system that provides “voluntary”neural control with the external environment.Communicates with the central nervous systemthrough spinal and cranial nerves.
Somatopic organization Organization that followsthe distorted figure of the sensory homunculusmapped onto the primary somatosensory cortex,which represents the relative importance and distri-bution of touch in various areas of the body ratherthan the actual size of the body part.
Somatosensory cortex Structure found in the anteriorportion of the parietal lobe, concerned with primarytactile sensory processing.
Somatosensory system Body system that involves twotypes of sensory stimulation, external and internal.The somatosensory system can monitor sensationssuch as cold and heat, whether the sensation comesfrom the handling of an ice cube or from a fever.So the system processes external stimulation oftouch (pressure, shape, texture, heat) in recognizingobjects by feel and is also concerned with theposition of the body in extrapersonal space(proprioception).
Spatial perception Refers to the ability to mentallyvisualize forms, objects or scenes in two- or three-dimensional space.
Glossary 533
Specificity A factor in setting a cutoff score on a test.Neuropsychological tests with high specificity exam-ine specific aspects of neuropsychological functions;that is, they are not correlated with other tests orfactors.
Speech apraxia See Dysarthria.Speech therapy A rehabilitation specialty that focuses
on communication difficulties such as deficits inspeech production, understanding speech, reading,and writing.
Spina bifida A congenital developmental disorder char-acterized by an opening in the spinal cord, commonlyfound in the lower region of the cord. The disorderis a consequence of a failure of the posterior end ofthe neural tube to close during gestation.
Spinal cord Part of the central nervous system thatacts as the conduit for the majority of sensory andmotor information to and from the body.
Spurzheim, Johann (1776–1832) Austrian student ofGall; lectured extensively on phrenology in theUnited States.
Stable attention An element of attention referring tothe consistency of attentional performance over time.
Standard battery approach In this approach, the sametests are given to all patients, regardless of the clini-cian’s impression of the patient or the referral question.Typically, a technician gives the tests and administersthem according to standardized rules of procedures.
Standardized test A task or set of tasks administeredunder standard conditions. Designed to assess someaspect of a person’s knowledge or skill. Standardizedpsychological tests typically yield one or more objec-tively obtained quantitative scores, which permitsystematic comparisons to be made among differentgroups of individuals regarding some psychologicalor cognitive concept.
Stem cells Undifferentiated cells; they do not yet haveeither an identified or specialized function. Theyeventually differentiate into the building blocks oftissues and organs.
Stenosis Narrowing of an artery.Striatal complex This group of structures includes the
caudate and putamen and receives projected infor-mation from cortical sensory areas. From the stria-tum, information then funnels through the globuspallidus, then on to the thalamus, where it projectsto the premotor and prefrontal areas. Also seeNeostriatum.
Striate cortex A collection of brain structures involvedin the motor system named after their striped or stri-ated appearance. It is located in the most posterior
aspect of the occipital lobes, but a major portion ofit extends onto the medial portion of each hemi-sphere. Also see Striatal complex.
Striatum A collection of brain structures (includingthe caudate nucleus and the putamen) involved inthe motor system; named after their striped or stri-ated appearance. It is located in the most posterioraspect of the occipital lobes, but a major portion ofit extends onto the medial portion of each hemi-sphere.
Stroke A neurologic event, also known as cerebrovascu-lar accident (CVA), that always occurs in the brainand is the most common type of cerebrovasculardisease.
Stuck-in-set perseveration Maintenance of a problem-solving approach when changing demands signal theneed for an altered or modified approach orresponse.
Subarachnoid hemorrhage Occurs when a blood vessel on the surface of the brain bursts and bloodflows into the small cavity that surrounds the brain,the subarachnoid space.
Subarachnoid space Space containing cerebrospinalfluid; below the arachnoid membrane.
Subcallosal anterior cingulate The subcallosal gyruscovers the inferior aspects of the rostrum of the cor-pus callosum. It continues posteriorly as the cingu-late and parahippocampal gyrus. It is consideredpart of the limbic system of the brain.
Subcortical Below the cortex.Subcortical dementia Dementia that primarily affects
subcortical areas of the brain; characterized by slow-ness of cognitive processing, executive dysfunction,difficulty retrieving learned information, and abnor-malities of mood and motivation; examples includeParkinson’s, Huntington’s, and Creutzfeldt–Jakobdiseases.
Subdural hematoma Bleeding into the subduralspace; often encountered after a head injury.
Subdural space The space between the dura and thearachnoid parts of the meninges.
Sublenticular nuclei Nuclei of the extended amyg-dala, a forebrain continuum, that projects into thecentromedial amygdala.
Substantia nigra Structure of the basal ganglia. A col-lection of neurons and nuclei known to be impor-tant dopamine pathways.
Substitution One of two primary approaches to braininjury; focuses on searching for adaptations to theperson’s environment in the context in which theywill be used.
534 Glossary

Subthalamic nucleus Structure of the basal ganglia.Sudden infant death syndrome (SIDS) Death caused
by the cessation of breathing during sleep.Sulci (singular, sulcus) Valleys formed by infolding of
the cortex.Superior Toward the top or above.Superior colliculi Two elevations within the roof of
the tectum functioning as important reflex centersfor visual information.
Superior sagittal sinus Large sinus of the brain.Supplementary motor area Located on the dorsal
and medial portion of each frontal lobe; functionsas a motor sequencer and planner. It receivesinput from the somatosensory strip and the basalganglia.
Suprachiasmic nucleus (SCN) A nucleus of the hypo-thalamus, hypothesized to be a biological clock thatcalibrates the sleep/wake cycle.
Supravalvar aortic stenosis (SVAS) An acquired orcongenital condition in which there is a narrowingof the aortic value impeding the flow of blood fromthe left ventricle to the arteries. The resulting car-diac problem can be life threatening.
Surface dyslexia A developmental or acquired readingdisorder characterized by impaired whole-wordreading, but preserved phonological skills.
Sustained attention The ability to maintain an effort-ful response over time. A form of attention involv-ing the maintenance of attentional focus over time.Sometimes referred to as “time-on-task perfor-mance,” or “behavioral persistence.”
Sydenham’s chorea (SC) A neurologic movement dis-order characterized by chorea of the face, neck,trunk, and limbs; diminished muscle tone andstrength; and psychological disturbances, especiallyobsessive-compulsive behaviors. The disorder fre-quently affects children and adolescents after astreptococcal infection (a beta-hemolytic). It hasbeen proposed that the disorder is caused by anabnormal autoimmune response to the streptococcalbacteria that reacts against the basal ganglia. Thedisorder often resolves spontaneously, and treatmentis generally reserved for severe or chronic cases.
Sylvian aqueduct See Cerebral aqueduct.Sylvian fissure The large fissure separating the frontal
from the temporal and parietal lobes.Sympathetic nervous system Division of the auto-
nomic nervous system that mobilizes the energynecessary for psychological arousal in response to, oranticipation of, a stressful event based on the “fight-or-flight” response. Sympathetic activation includes
an increase in blood flow, blood pressure, heart rate,and sweating, and a decrease in digestion and sexualarousal.
Synapse The tiny gap between the terminal buttonand the receptors of the two neurons. Neuronscommunicate through synapses. The anatomiclocation of this communication is known as thesynapse.
Synaptic knobs Ends of neurons that have characteris-tic swelling to increase the area of contact with thepostsynaptic neuron.
Synaptic vesicles Oval structures within the termi-nal that typically cluster close to the presynapticmembrane and where neurotransmitters aresynthesized.
Synaptogenesis The developmental process by whichthe synapses and dendrites of the brain form.
Tachyphemia Segmented accelerated bursts of speech.Tactile agnosia Also called astereognosis; a disorder in
which there is an inability to recognize objects bytouch.
Tactile extinction/suppression/inattention Suppressionof touch sensation on one side of body.
Tardive dyskinesia A disorder with Parkinson-likesymptoms, including writhing movements of themouth, face, and tongue, often develops in schizo-phrenics after long-term medication use.
Tectum “Roof”; structure of the midbrain.Tegmentum “Covering”; a structure of the midbrain
that surrounds the cerebral aqueduct.Telencephalon Also called the endbrain; one of the
five principal divisions of the brain; consists of thetwo cerebral hemispheres, which are connected by amassive bundle of fibers, the corpus callosum.
Temporal lobe One of the four cortical lobes, con-cerned with the reception and interpretation ofauditory information; also plays a role in memory.
Temporal lobe (psychomotor) epilepsy A form ofseizure originating from the temporal lobe; emotionalsymptoms often present (such as changes inmood).
Tensile strength The amount of physical, longitudinalstress that an axon can withstand before it ruptures.
Teratogen Any agent that disrupts the normal devel-opment of the embryo and fetus.
Terminal buttons Also called axon terminals. The siteof interneuronal contact, where neurochemical infor-mation is transmitted from one neuron to another.
Teuber, Hans-Lukas (American, 1916–1977) Creditedfor first using the term neuropsychology in a national
Glossary 535

forum during a presentation to the AmericanPsychological Association in 1948.
Thalamus A structure of the diencephalon, an impor-tant sensory relay station.
Thalotomy A surgical treatment for Parkinson’s diseaseand other disorders causing tremor; used to attacktremor by lesioning the thalamus.
Theory of mind The cognitive capacity to under-stand, attribute, and predict the mental state of oth-ers, and the relation of these mental states to behav-ior. Deficits in this capacity have been observed inautistic children and other developmental disorders.
Therapeutic recreation An approach to treatment thatemphasizes the importance of recreational and leisuretime activities in brain injury rehabilitation, to helpin the “transfer” of learning. Therapeutic recreationalso allows patients to begin socializing with eachother in a structured, but less formal, atmospherethan that afforded in other therapy settings.
Thermoreceptors Receptors that serve as monitors todetect heat and cold throughout the body.
Thrombosis A type of occlusion in which a clot orthrombus (Greek meaning “clot”) forms in an arteryand obstructs blood flow at the site of its formation.This is the most common form of stroke andaccounts for approximately 65% of all cerebrovascularaccidents.
Tonic Motorically stiffened.Tonotopic map Projected onto the auditory cortex in
a manner similar to the retinopic mapping of thevisual system. Because the cortical bands canrespond to multiple frequencies, there is no strictone-to-one correspondence, but bands are moreattuned to certain frequencies than others.
Tourette’s syndrome A tic disorder defined by multi-ple involuntary motor and vocal tics. The disorderappears familial in origin. The cause is unclear, butdysfunction of the basal ganglia has been implicated.Also called Gilles de la Tourette syndrome.
Tracts Also known as pathways or fibers. Large collec-tion of axons located in the central nervous system.Primarily composed of white matter.
Transduction Derived from Latin transducere, mean-ing “to lead across.” An environmental stimulusactivates a specific receptor cell, and this energy istransduced into an electrical stimulus, which isthen carried to neurons to be processed by thebrain.
Transient ischemic attack (TIA) A temporary (tran-sient) lack of oxygen (ischemia) to the brain, whichmay cause a time-limited set of neuropsychological
deficits. TIAs are technically not considered a stroke,because neuronal death typically does not occur.
Transtentorial herniation Associated with highintracranial pressure and generalized swelling of thebrain. As a result, the brain is displaced downward.
Tremor Involuntary shaking, usually of a limb,tremors may be resting or occur with intentionalmovement.
Trephination An ancient procedure in which smallholes were scraped or cut into the skull deliberatelyfor either surgical or mystical reasons.
Tumor The morbid enlargement or new growth of tis-sue in which the multiplication of cells is uncon-trolled and progressive. The tumor growth is oftenarranged in nonorganized ways, does not serve anyfunctional purpose, and often grows at the expenseof surrounding intact tissue.
Turner’s syndrome (TS) A syndrome characterized by afailure to develop secondary sexual characteristics,short stature, webbed neck, and cubitus valgus. It iscaused by an anomaly in the X chromosome (female).
Ultradian rhythm Ninety-minute cycles of heightenedand lowered brain arousal observed throughout thewake/sleep cycle.
Ultrasonography A procedure for imaging the internalstructures of the body by introducing and recordingthe reflection of high-frequency sound waves.
Utilization behavior A characteristic behavior of envi-ronmental dependency syndrome that involves the ten-dency to grasp and use objects that are within reach.The use of the object is in accordance with its func-tion, but inappropriate for the situation. It is oftenassociated with bilateral frontal damage.
Uvulopalatopharyngoplasty (UPPP) The removal ofthe uvula, the small, fleshy tissue hanging from thecenter of the soft palate, which may relax and sag,obstructing the upper airway. A surgical approach tothe treatment of sleep apnea.
Validity The validity of a test is the meaningfulness ofthe test scores. Validity gauges whether a specifictest really measures what it was intended to mea-sure. There are different types of validity: construct,content, and criterion validity.
Vascular system The blood supply system of arteriesand veins.
Ventral Toward the belly. The bottom of the brain isventral in humans.
Ventricles Four interconnected, fluid-filled cavities inthe brain.
536 Glossary
Ventricular localization hypothesis Theory thatpostulated that mental and spiritual processes werelocated in the ventricular chambers of the brain.
Ventricular system Four interconnected, fluid-filledcavities in the brain.
Vermis A structure of the cerebellum; two large, ovalhemispheres connected by a single median portion.
Vertebral arteries Two of the four major arteries to thebrain, supplying the posterior portions of the brain.
Vertebral column The bony structure that extends fromthe cranium to the coccyx and encloses the spinal cord.
Vesalius, Andreas (1514–1564) Belgian-born anato-mist who advanced neuroanatomy through continualdissections and careful scientific observations.
Vestigial ovarian streaks A failure of gonadal develop-ment characteristic of Turner’s syndrome.Reproductive cells are evident in the gonads ofTurner’s syndrome embryos but begin to deterioratelate in fetal development. By early childhood, thegonads consist only of fibrous streaks.
Vigilance attention system One of the attentional sys-tems of the brain that mediates sustained attention.
Visual agnosia Inability to recognize a person orobject by sight.
Visual cortex The cerebral cortex of the occipital lobeof the brain that is responsible for vision.
Visual object agnosia Failing to recognize objects atall, or in milder cases, confusing objects if they areobserved from different angles or in different light-ing conditions.
Visuospatial sketch pad A working memory “slavesystem” that manipulates visual and spatialimages.
Vitalism A theory that suggests that behavior is onlypartly controlled by mechanical or logical forces.
Vocational inventories Tests that measure opinionsand attitudes indicating an individual’s interest indifferent fields of work or occupational settings.
Wada technique Also known as the Wada test, after itsdeveloper. Similar to the angiogram in that it placesa catheter, typically in the left or right internalcarotid artery. Then sodium amytal, a barbiturate, isinjected, which temporarily anesthetizes one hemi-sphere. In this way, neuropsychologists can studythe precise functions of one hemisphere whereas theother one “sleeps.” Also called the intracarotid sodium amytal procedure (IAP).
Wada test A technique for determining language later-alization and memory functions that involves anes-thetizing one cerebral hemisphere, and then present-
ing cognitive tasks to the patient. The process isthen repeated with the other hemisphere. Impairedperformance of the cognitive tasks specific to theanesthetized hemisphere suggests the lateralizationor presentation of language/memory functions inthat hemisphere.
Wernicke, Carl (German, 1848–1904) Announcedthat the understanding of speech was located in thesuperior, posterior aspects of the temporal lobe.Wernicke noted that a loss of speech comprehensiondue to damage in this area was not accompanied byany motor deficit; only the ability to understandspeech was disrupted.
Wernicke’s aphasia Damage to the left hemisphereauditory processing areas results in the partial ortotal inability to decipher spoken words. This con-dition is also known as receptive aphasia.
Wernicke’s area A structure that includes the sec-ondary auditory cortex and is located on the poste-rior aspect of the superior temporal gyrus. It isresponsible for auditory processing of speech.
Wernicke–Korsakoff ’s syndrome A disorder associatedwith memory function of the limbic system, typicallyobserved in severe alcoholics who show multiplenutritional deficiencies. Such patients may develop aconfusional state over time, as well as severe new-learning and motor difficulties.
White matter Myelinated axons. Areas of the brainthat are mostly made up of myelinated axons, suchas neuronal tracts and pathways, which are charac-teristically white in appearance.
Williams syndrome (WS) A neurodevelopmental dis-order characterized by a recognizable pattern of dys-morphic facial features, cardiovascular and physicalabnormalities, mental retardation, a specific cogni-tive profile, and a distinct personality.
Willis, Thomas (1621–1675) English anatomist bestknown for his work on the blood circulation of thebrain.
Word salad Unconnected words and word sounds.This feature of Wernicke’s aphasia is a deficit in plac-ing words together in proper grammatical and syn-tactical form. This condition is more formallyknown as paragrammatism or extended paraphasia,and it is characterized by running speech that is logi-cally incoherent, often sounding like an exotic for-eign language.
Working memory A concept introduced by AlanBaddeley, also referred to as short-term memory, or“working on memory.” Working memory directs thetemporary storage of information being processed in
Glossary 537
538 Glossary
any range of tasks from reading to math to problemsolving. It includes the concepts of the central execu-tive, the articulatory phonologic loop, and the visu-ospatial sketch pad.
X-rays A type of light ray that is useful for clinical workof various parts of the body, because they show thepresence and position of bones, fractures, and foreignbodies. A clinical disadvantage of X-rays, and specifi-
cally X-ray films of the brain, is that there is little dif-ferentiation between the brain structures and thecerebrospinal fluid, making the clinical use of thisprocedure ineffective.
Zangwill, Oliver (1913–1987) British neuropsycholo-gist who contributed significantly to an understand-ing of the nature of neuropsychological deficits asso-ciated with unilateral brain disease or injury.
C H A P T E R 1
How does localization brain theory differ from equipoten-tiality brain theory? What are the lasting contributions ofeach theory?Localization brain theory assumes that detailed brain processesin specific anatomic locations cause specific mental processes.Phrenology is a good example of localization theory. Equipoten-tiality brain theory assumes that the brain functions more or lessas a unit. One proponent of equipotentiality brain theory isFlourens, who suggested that the entire brain is greater than thesum of its parts. The lasting contribution of localization theoryis that, indeed, some brain functions appear to be localized to aspecific brain region. For example, Broca’s area specifically con-trols verbal motor output. However, many functions, such asthinking and problem solving, do not appear to have a strict orprecise anatomic representation in the brain. The lasting contri-bution of equipotentiality theory is the idea that redundancy maybe built into the brain and that if one area of the brain is dam-aged, another area may be able to compensate for the function.
Has the quest for the search of the organ of the soul beencompleted?Yes and no. Yes, the search for the organ has been completed.There is no question that the healthy brain gives rise to the mindand the soul. The question that is not yet answered is, How ex-actly does the brain accomplish this? Much has been learnedfrom recent research involving neuropsychology and modernimaging technology, but the precise mechanism—that is, howthe soul arises from brain matter—has remained elusive.
Why is Luria’s functional model of the brain such an impor-tant step in understanding brain functions?Luria combined both the localization and equipotentiality ap-proaches to neuropsychology into one model. As with equipo-tential theory, Luria regards behavior as the result of an interac-tion of many different areas of the brain. As with localizationtheory, Luria also assigns a specific role to each area of the brain.In Luria’s functional model, each function depends on the inter-action of specific brain systems. Luria suggests that behavior isthe result of the brain operating as a whole. At the same time,each area within the brain has a specific role in the formation ofbehavior. The importance of any one area depends on the be-havior to be performed. This model has been useful in rehabili-tating patients with neuropsychological disorders, such as strokeand brain trauma, where one function may be damaged, but an-other function may compensate for the loss.
C H A P T E R 2
What are the differences among electrical, magnetic, andmetabolic technologies in imaging?Electrical measures record the electrical activity of nerve cellsof the brain through electrodes attached to various locationson the scalp. This procedure, known as electroencephalography(EEG), is most sensitive to the actual firing rate of large collec-tions of neurons. Magnetic imaging measures the concentra-tion of the hydrogen nucleus, which is present in high concen-tration in biologic systems and generates a small magneticfield. This procedure is known as magnetic resonance imaging(MRI). With MRI researchers can accurately calculate braintissue densities and can generate a computer-constructedanatomic representation. The imaging of brain metabolismprovides a completely different approach to the examinationof the brain. For example, measuring glucose metabolism is adirect correlate of neuronal activity and can lead to a clearerunderstanding of the functioning brain. Medical technologiesthat use this approach are single-photon emission computedtomography (SPECT) and positron emission tomography(PET).
Why is co-registration, that is, the use of multiple assess-ments using different technologies, an important advance-ment in neuropsychology?A major advancement in imaging technology has been to mergedifferent assessment technologies, such as the anatomic detail ofMRI with the ability of PET to localize function using the imag-ing of brain metabolism. Such co-registration of different ap-proaches has resulted in multimodal approaches to neuroimag-ing, often providing new insights, as well as corroboratingestablished findings.
Which medical technology to examine your brain would youvolunteer for? Why?We personally do not mind having our brains imaged using dif-ferent technologies. A risk is always associated with this, how-ever, namely, that some previously unknown pathology may bedetected, but those chances are relatively small. The only otherrisk, then, is the inconvenience of an invasive procedure. On acontinuum from least to most invasive, those procedures are(in our opinion): radiography, EEG, EP, MRI, MEG, SPECT,PET, EMG, lumbar puncture, and angiography. Because MRIis relatively noninvasive but allows for precise anatomic pic-tures of the brain, it would be the procedure we would volun-teer for first.
ANSWERS TOCRITICAL THINKING QUESTIONS
539

Will neuropsychology be outdated by the increased use ofsophisticated brain imaging technology? Why or why not?No. Modern imaging technologies and the study of neuropsy-chology are compatible. Certainly, the advances in modernimaging technology have been spectacular in showing theanatomy of the brain. Furthermore, the domains previously heldby neurologists and that by neuropsychologists are getting muchcloser, and both disciplines have much to learn from each other.But neuropsychologists are bringing special knowledge to thearea of brain research and are participating in the research usingthis technology because of their expertise in the functional as-pects of neuroanatomic structures, their knowledge of neuropsy-chological tests, and their background in scientific methodologyand design. Thus, neuropsychologists play an important role inproviding functional assessments of patients with brain injuries.Neuropsychologists also diagnose conditions (such as concus-sions) that are not easily detected using modern imaging tech-nologies, and they evaluate a patient’s potential for adapting to aspecific neurologic disorder, their capacity to work, and theirquality of life.
C H A P T E R 3
Why are the concepts of reliability and validity so importantin psychological and neuropsychological assessment?If a test is not repeatable, it is not reliable and thus can pro-vide no consistent score on a specific dimension. Think ofweighing yourself on a scale that gives you a different weightevery time you step on it. Such a scale could not be trusted,could it? Validity is important because it relates to the mean-ingfulness of a psychological test score. What if a psychologi-cal measure of depression does not really measure depression,but something else, such as stress? Such a scale would not bean appropriate measure of depression. Let us go back to theexample of the scale. This time it is reliable. (Remember, if atest is not reliable, it cannot be valid.) A scale would not be avalid measure for anything other than estimating weight. Forexample, you would not use the scale to determine the roomtemperature. This is the assumption of validity, that is,whether a psychological or neuropsychological test measureswhat it is intended to measure.
What kinds of questions and tests do neuropsychologists usein a neuropsychological evaluation?Neuropsychologists use primarily standardized tests and ques-tions in a neuropsychological examination. That is, they mayuse specific tests and scales that have questions that every sub-ject receives more or less in the same way. As a result, the neu-ropsychologist knows what it means if a person does not knowthe answer to a particular set of questions. Neuropsychologistsuse many different tests, tasks, puzzles, and questions to get anoverview of an individual’s cognitive strength and weaknesses.Thus, it is not uncommon to have a battery of tests that includemeasures of memory, attention, intelligence, personality func-tioning, and so on. The neuropsychologist uses a specific set of
procedures to answer the referral question. For example, he orshe may treat a referral question about diagnosis differently froma referral question about employment capacity, in terms of se-lecting neuropsychological tests.
How are neuropsychology assessment procedures the same?How are they different?All neuropsychological assessment procedures are similar in thatthe same rules of reliability and validity apply. Also, almost allneuropsychological tests are given in a standardized format andenvironment, and are administered to the patient individually.They are different in that they measure different aspects of be-havior. Tests can measure memory, problem solving, and atten-tion, to name just a few aspects. Some tests measure personalityfunctioning, adaptive skills, intelligence, vocational skills, andeducational attainment. These types of tests are strictly not neu-ropsychological tests, even though they depend on brain func-tioning, because they are not sensitive indicators of cortical dys-function. A test is considered to be a neuropsychological test if achange in brain function systematically relates to a change intest behavior.
What sort of recommendations and treatments can neu-ropsychologists give to brain-impaired people that will beuseful in their daily lives?How to make recommendations to individuals about their every-day lives has become an important issue in neuropsychologicalassessment. This is important because many neuropsychologicaltests appear to be somewhat abstract on the surface. For exam-ple, a test of driving capacity has not been developed yet, so neu-ropsychologists rely on traditional measures of attention, mem-ory, and eye-hand coordination to make inferences aboutwhether a person with brain injury should be allowed to drive.In addition to driving, there are many instances in which neu-ropsychologists can help their patients regarding activities thathave a cognitive component, but are performed almost every day.Those activities can range from balancing a checkbook, goingshopping, and finding one’s way around, to more basic activitiessuch as getting dressed, taking a bath, or brushing one’s teeth.Neuropsychologists can determine which everyday tasks patientswith brain injuries may have problems performing. Neuropsy-chologists then recommend what task may be strengthenedthrough rehabilitation or through compensation of other intactskills. For example, if a right hemisphere patient has trouble find-ing his or her way around a hospital and often gets lost, the pa-tient may learn specific right/left directions and also compensateby learning to ask bystanders for directions. The patient may alsorely on a notepad that always reminds him or her what the desti-nation is. Thus, neuropsychologists play an important role intreating and rehabilitating patients with brain injuries.
How do the two major approaches (process and battery) tointerpreting neuropsychological data differ?The two approaches are different in a variety of ways (seeTable 3.4); therefore, it is almost a philosophical difference interms of neuropsychological assessment. The principal difference isthat the battery approach is a standardized approach to assessment,
540 Answers to Critical Thinking Questions

whereas the process approach is a clinical analysis of a patient.The former is akin to having a patient undergo a series of testsand standardized questions to understand his or her abilities anddeficits. The latter is based on the idea that each patient’s pre-sentation is so unique that it is of most importance to under-stand the unique problems for which the patient is seeking treat-ment, and thus to tailor the examination to the individual. Thestandard battery approach has evolved through empirical analy-sis and the extensive testing history of psychological testing. Theprocess approach has evolved in the clinical setting. Althoughproponents of the process approach would disagree with thisconclusion, research supporting the process approach is not asrobust as the empirical foundation of the standard battery ap-proach. As with many issues that are so polarized, most neu-ropsychologists borrow certain aspects from each approach intheir own approach to neuropsychological assessment.
C H A P T E R 4
Will it be possible one day to “map” the circuits of thehuman brain?Various “mapping systems” of the brain are discussed in thechapters that deal with brain anatomy. Mapping systems gener-ally have focused on major structures of the brain as they per-tain to function, or to various “architectural” layers of the brainand cortex. From these the correspondence of various structureswith their functions has been demonstrated. However, here weare asking about mapping brain circuits that revolve around neu-ronal pathways and interconnections. As discussed in this chap-ter, there are billions of neurons and glial cells with multipleconnections. It has been estimated that the human brain per-forms more than 1 quadrillion operations per second, which ismore than a thousand times faster than the current supercom-puters. The shear size and power of the human brain still makesit the most complex structure in the known universe. Attemptsat mapping circuitry of simple organisms, such as the honeybee,have been accomplished. So is this just a matter of scale thatcomputing power will one day be able to conquer? The answerto this question also lies in considering that there are vast indi-vidual differences in the way each person’s brain is “wired,” andthat brain communication networks can modify themselves andchange with experience, development, and learning. Mappingthe circuitry of the human brain is not only extremely complex,it is a moving target.
Actor Christopher Reeve suffered a severe spinal cord injuryand died without fulfilling his pledge to walk again. What isthe outlook for other people with paralysis caused by spinalcord injury?Not long ago, the traditional wisdom on neuronal damage to thespinal cord presumed that little healing occurs once a neuron inthe brain or the spinal cord has been damaged. At best, theprocess called collateral sprouting, which occurs in nearby intactneurons, might facilitate a functional reorganization. The com-plexities involved in the regrowth of neurons and their millions
of projections to other neurons are daunting. All these connec-tions can be lost within a split second due to brain trauma. Thelikelihood that these connections regrow spontaneously wasthought to be quite small. Although Christopher Reeve neverwalked again, through intensive rehabilitation aimed at keepinghis muscles toned and moving his limbs as he normally wouldin walking or cycling, he did recover some sensation even after5 years. Was this actual neuronal repair, regrowth, or functionalreorganization? The answer is unknown. However, it is nowknown that some function can return long after what was previ-ously believed. In addition, current research in neuronal repair,either through stem cell research or in coaxing CNS neurons toact like PNS neurons, is promising. The current outlook is muchmore promising for people with paralysis caused by spinal cordinjury.
Is it possible for a drug to be effective if it does not activatea naturally occurring brain chemical receptor?The human brain is affected not only by internally producedchemical messengers, but also by externally originating chemi-cals that find their way to the synapse. The discovery that thebrain has receptors for endogenous opiates, such as endorphins,which produce similar behavioral responses as external opiates,provides the fodder for this question. Why do substances suchas caffeine, cocaine, nicotine, and alcohol affect the brain? Thenervous system has specific receptor sites that bind drugs suchas nicotine and opiate compounds. Others may work becausethey are a close enough mimic, or act as a blocking agent. Certaindrugs, however, are totally barred from the brain, and other sub-stances require an active transport system to cross the blood–brain barrier. In general, drugs at the synapse either increase ordecrease the likelihood of neuronal transmission. Therefore,drugs can exert their actions in various ways, but it appears thatbrain receptors must react to them even if they are not perfectmimics.
What scientific and ethical questions will need to be resolvedfor research into neuronal repair and neurogenesis to be suc-cessful?Scientifically, the primary question pertaining to neuronal repairis, “What is different about the growth and repair mechanisms be-tween a CNS and a PNS neuron?” Current research suggests thatsome characteristics of myelin may be part of the issue, and muchattention has focused on this. Interestingly, because myelin is anissue, research in multiple sclerosis and spinal cord injury may helpto inform each other. One of the main questions pertaining to neu-rogenesis is, “What causes neurons to grow and die?” Both of theseissues raise many other questions such as, “At what developmentalstage do neurons decide to quit replicating?” and “What are theadaptative and maladaptive implications of naturally occurringand induced neurogenesis?” Ethically, for treatment of injury anddisease, the questions revolve around a debate between the extentthat science could be helpful in intervening to find cures for dis-eases and disorders against the issues of using embryonic stem cellsto advance the research. Unfortunately, the debate is often framedas an “either/or” question. Scientists and the public will benefit
Answers to Critical Thinking Questions 541

from creative ways to solve this problem if informed solutionsand ethical decision making is encouraged.
C H A P T E R 5
Why is an understanding of the stages and processes of braindevelopment important to the neuropsychologist?The stages and processes of brain development are important tothe neuropsychologist for a number of reasons. First, knowledgeof the stages and timing of brain maturation allows for the iden-tification of emerging cognitive-behavioral functions. Second, arecognized association exists between specific disorders and dis-ruption/retardation at specific stages of brain development. Forexample, lissencephaly (absence of cortical sulci and gyri) iscaused by disruption of neural cell migration during the 11th to13th week of brain development. This knowledge can increaseour understanding of the etiologies of the disorders and poten-tially shape preventive interventions. Third, knowledge of therelation between brain maturation and behavior provides a yard-stick for determining whether the child’s observed behaviors areconsistent with healthy brain development. Fourth, studies ofthe interplay between environmental influences and brain de-velopment allow for a determination of conditions that support,enhance, or retard cognitive-behavioral development. Finally,knowledge of the stages and processes of brain maturation canprompt the development of restorative and rehabilitative inter-ventions for treating those who have suffered early brain injury.
If a child was born without the telencephalon region of thebrain, would the child be able to orient to visual and audi-tory stimuli, perform reflexive movements, and sit up? Ex-plain why or why not.Removal of the telencephalon would result in the loss of the fol-lowing brain structures: cerebral cortex, basal ganglia, limbicsystem, and olfactory bulbs. Despite this loss, the child wouldbe able to orient to visual and auditory stimuli, demonstrate re-flexive movements, and sit up because of the preservation of sub-cortical and spinal structures and systems. For example, auto-matic orientation to visual and auditory stimuli is supported bythe superior and inferior colliculi, respectively, of the midbrain.In addition, the child would be able to perform most elemen-tary functions such as ambulation, eating, drinking, and sleep-ing. However, the ability to link automatic movements to vol-untary movements and to respond flexibly and adaptively toenvironmental demands would be compromised. Furthermore,the ability to provide meaning, value, emotion, and voluntaryintent to behavior would be lost.
To what extent can behavioral functions be localized to spe-cific brain structures?The structures presented in this chapter represent importanttopographic features on which the various processing systems ofthe brain depend. Aspects of behavior can be attributed directlyto many of these structures. In general, the structures describedin depth here, such as the brainstem structures, are responsiblefor rudimentary aspects of behavior. Many of the structures arenecessary for sustaining life, for controlling wakefulness and
sleep, and for controlling other drive states. As a general rule,more basic and fundamental aspects of behavior are more easilytraced to specific structures. In the following chapters it will be-come evident that as behavior becomes more complex, there is amove from specific structure-function correspondence to an em-phasis on larger functional systems that subserve the complexi-ties of human behavior.
What level of brain mapping is most useful to the neuropsy-chologist?When it comes to understanding the relationship of the humanbrain to behavior, mapping at the level of the cell or the neuronis usually considered too minuscule to provide an accurate pic-ture of the complexity of human behavior. Also, some functionsare basic and automatic, and of less interest related to their psy-chological functions, such as the role of CSF as a waste productremover. Finally, understanding the complex organization of thebrain, as a whole, would not provide useful information for neu-ropsychologists, who are often asked to respond to questionssuch as, “What effect does an injury to the basal ganglia have onbehavior?” or “If a person has poor motor coordination, whichareas of the brain are most likely to be affected?” In general, re-searchers tend to think of behavior related to its function, so itis most useful to consider the brain structures and systems thatrelate to that function. In this chapter, basic structures were pre-sented with ties to function. However, in the following chap-ters, more complex functions such as visual perception or mem-ory, as well as more complex and interconnected systems withinthe brain, emerge as the most useful level in describing mosthuman behaviors.
C H A P T E R 6
How would you explain the functional differences betweenthe right and left hemispheres?Several points should be made when describing the functionaldifferences of the two brain hemispheres. First, although gener-alizations can be drawn, it is important to remember that thereare notable exceptions. For example, although speech is gener-ally considered to be lateralized to the left hemisphere, some in-dividuals possess bilateral or right-lateralized speech. Second,hemispheric functional differences relate to the interaction of anumber of variables to include the nature of the stimulus (e.g.,visual vs auditory), mental computations required (e.g., detail vsglobal processing), routine or novel nature of processing de-mands, and manner of task presentation. Third, hemisphericfunction is rarely “either/or”; that is, both hemispheres functionin a complementary manner to support a given function. Forexample, the left hemisphere is typically involved in the verbalaspects of speech, while the right hemisphere provides the affec-tive or prosodic aspects to speech. Fourth, there are indicationsthat the left hemisphere is more proficient in linear, sequential,and rule-bound processing, whereas the right hemisphere showsgreater proficiency in holistic, simultaneous, and integrative per-formance. However, other conceptualizations provide equally
542 Answers to Critical Thinking Questions

meaningful descriptions of the functional differences of thehemispheres. Finally, we await further research to clarify thefunctioning of the brain as a whole, as well as the individualcontributions of the respective hemispheres.
Are there adaptive reasons why the cerebral hemisphereswould gravitate toward either a bilateral or asymmetric or-ganization? Explain.Although science does not provide a definitive answer to thisissue, to approach this question it is important to think aboutwhat factors lead to differences in hemispheric organization.One of these factors is handedness. About 90% of the popu-lation is right-handed, with a tendency toward left hemispheredominance for speech. Another factor is sex. Sex hormonesaffect brain organization starting during fetal development.Women tend to be more bilaterally organized than men. Con-sidering these two factors, it is interesting to speculatewhether, for example, men needed to have more lateralizedbrains for stereotypically “male” activities such as visuospatialabilities, and women needed to have more bilaterally orga-nized brains for stereotypically “female” activities such as su-perior language function. And what advantages might right-handers have, if any?
What ecologic or evolutionary factors could account for theadvantage of males in visuospatial abilities?From an evolutionary perspective, a number of hypotheseshave been posed to account for the advantage of male relativeto female individuals in visuospatial abilities. Each of these hy-potheses has met with criticism and countering interpreta-tions. The hunter role of early man has been posed as a reasonfor the advanced visuospatial performance of the male sex.Specifically, the use of weapons (such as throwing a spear tokill game) is hypothesized to account for the visuospatial pro-ficiency of the male sex. Another hypothesis that relates to thehunter role of early man proposes that the distances thathunters would have to travel in the pursuit of game would fa-cilitate the development of visuospatial abilities. Similarly,wars throughout the ages (early clans through modern wars)have generally been fought by men, experiences that may haveserved to reinforce the development of spatial abilities. Froman early age, male and female individuals encounter differentsocialization experiences regarding their roles as male or fe-male. Male individuals are more likely to involve themselves inplay involving active and spatially related activities. Whetherthis preference is solely a function of socialization continues tobe an area of debate. However, it is clear, from a historical per-spective, that the male sex has been expected to show more in-terest and involvement in play and work activities (e.g., sports,construction) that emphasize visuospatial abilities. Thus, maleindividuals have been provided greater exposure, experience,and training in visuospatial activities. As the distinction be-tween male and female roles with regard to academic, voca-tional, athletic, and other life pursuits become less distinct(and limiting), it would be expected, from a socialization per-spective, that the difference between male and female visu-ospatial abilities would be reduced or eliminated.
C H A P T E R 7
In what ways do the study of sensory-perceptual and motordisorders inform us about intact brain functioning? In whatinstances might the study of damaged brains lead us astray?The study of patients with damaged brains has provided impor-tant clues to the workings of brain systems. For example, by ex-amining patients with lesions in Broca’s or Wernicke’s areas, ordamage to area V4 (occipital cortex), functions of language andvision, respectively, have been mapped. However, this strategycan lead to erroneous information in that a lesioned area doesnot always “contain” the function, but it may, instead, act as a“cable” in the network that serves to join two or more functions.
Do conditions such as phantoms, neglect, and synesthesiarepresent altered states of consciousness? Explain.Phantoms, such as phantom limbs, appear as sensory-perceptual“hallucinations.” A neglect patient can show a total unawarenessof the left side of the body and even deny the ownership of alimb. A synesthete can feel jaggedness when eating chocolate.These examples appear to be distortions from the “norm” ofconscious awareness. Yet, these deviations of “reality testing” arenot labeled as psychotic processes. Why not? Perhaps the mostinteresting fact here is the variations one can experience in con-scious awareness. And for some, such as synesthetes, the meld-ing of sensory perceptions may have constituted a “nornal” real-ity since birth.
Does intact motor processing require intact sensory-perceptual processing? Explain.Consider the example of speech presented in this chapter. Towhat extent does speaking require the ability to understandspeech? This chapter discusses the extent to which expressivespeech is damaged in those with Wernicke’s aphasia. Would thisbe more or less of a problem in a child who is born with a diffi-culty in understanding speech? Do you think this is the case inall sensory modalities? Can you think of any exceptions?
C H A P T E R 8
What does the neuropsychology of sensory-perceptual pro-cessing have to contribute to the idea that there is an objec-tive reality related to object perception?This question is the fodder for philosophical debate. However,from a neuropsychological point of view, consider that the chap-ter began by saying, “The range of what humans can detect isunique to our species.” The sensory detectors of other speciesmay result in detection of different stimuli or experiences in awider or narrower range than for humans. For example, manyanimals do not detect color, but can detect faint smells or havevisual acuity that is far superior to humans. Whose actuality isreal? Even if this question is limited to human experiences, con-sider that being “objective” implies being unbiased by personalexperience. Sensory information comes in fragments; for exam-ple, an object’s name, the intensity of pain, or the pleasantness ofa smell must be attached at secondary and higher processing cen-ters. At each level of processing, more aspects of interpretation
Answers to Critical Thinking Questions 543

are required. So, are there aspects of sensory perception wheregeneral agreement can constitute objective reality? Where wouldyou draw a line between the seeming “realness” of sensation andthe “personal experience” of perception?
How might it be possible to imagine or conjure up imagesin all sensory domains despite a lack of sensory input?Although the mechanisms are not fully understood, it is knownthat one can have a sensory illusion or hallucination in any sen-sory domain. This most commonly occurs with psychiatric ill-nesses such as schizophrenia. In schizophrenia, the most com-mon type of hallucination is auditory. This question alsoforeshadows a future discussion of consciousness to be presentedin Chapter 16, which discusses seizures and epilepsy. Abnormalbrain firing in regions concerned with sensory functioning oftenproduces a sensory aura before a seizure. This may be an oddtaste or smell, a tingling feeling in a part of the body, or unusualvisual or auditory sensations. Thus, the brain can produce sen-sory “feeling” without external input. In the case of normal brainfunctioning, does this also happen? Take dreaming, for example.When you sleep, you conjure up visual images with your eyesclosed. How does this happen? (Look ahead to Chapter 16.)
Can one be “conscious” in one sensory domain but not inanother?Yes. This chapter explores the example of neglect. Unilateralneglect is a condition in which the impaired individual loses“conscious awareness of an aspect of spatial or personal spacedespite adequately functioning sensory and motor systems.”Also, in any type of agnosia, by definition, there is a “not know-ing.” Chapter 7 introduces this term and states that agnosia canoccur in any sensory domain. Thus, for example, astereognosisis an inability to recognize or “know” objects by touch. Chap-ter 7 also discusses smell and taste agnosias. This chapter dis-cusses language and vision. Although when discussing languagewe do not refer to a hearing agnosia but rather aphasia, the ideais the same. If damage occurs to a specific area, it is possible tolose conscious awareness in just one sensory domain while re-taining a sense of meaning or awareness in the other sensorymodalities.
C H A P T E R 9
Do the higher cognitive functions discussed in this chapterrepresent more intelligent thought processes than thosefunctions discussed in previous chapters? Explain.The implication is that “higher” cognitive processes indicate thepinnacle of intellectual functioning, given that we often equateabstract and complex thought with the highest levels of humanachievement. This may well be the case from the human pointof view. Can you think of examples to dispute this statementfrom what you have read in previous chapters?
The memory, attention, and executive function systems interact. How would you explain this interaction?Memory, attention, and executive function represent relativelydistinct processes, although in some cases, disagreement existswhether a particular attentional or memory process is better
classified as an executive function (e.g., working memory).Clearly, these processes are interrelated, but specifying the exactnature of this interrelation remains to be defined and specified.Nonetheless, some agreement exists that executive functions rep-resent overarching controlling, organizing, integration, and su-pervisory computations. Attention and memory processes aresubject to varying degrees of executive orchestration dependingon the nature and type of attention and memory processes in-volved. From a neuroanatomic perspective, memory, attention,and executive functions are served by relatively distinct yet in-terconnected and overlapping neural systems. Furthermore, theinterrelation of these functions is evident when one realizes thatexecutive functions would be of little value if memory and at-tentional systems were not present. Jointly, attention, memory,and executive functions play a central role in thinking, reason-ing, language, visuoconstruction skills, and sensorimotor andperceptual motor skills. Finally, attentional systems are neces-sary for the processing of relevant ongoing and novel events,memory systems for the symbolic maintenance of these experi-ences over time, and executive functions for the generation,guidance, and evaluation of behavior necessary to attain futuregoals (Eslinger, 1996).
Do disorders of executive functioning represent a greater dis-ability for humans than sensory-perceptual and motor dis-orders? Why or why not?Although some may answer unequivocally yes, it can also be ar-gued that with sensory-perceptual and motor disorders, thebuilding blocks of functioning may be so compromised that in-tact higher functions may not be able to be expressed adequately.What arguments can you make for each case?
Do emotions represent a higher cognitive function or a lowerbasic function? Explain.In many ways, emotions represent the most basic of functionsevolutionarily. Fear, anger, and other primary emotions areshared with the most primitive of creatures. We included emo-tions in the chapter on higher cognitive functioning because inhumans, the interpretation and higher perception of emotions,particularly social emotions, by the cortex requires a high degreeof cortical processing.
Are there advantages to multiple brain memory systems ascontrasted to a single memory system?Since it is highly unlikely that a single brain memory systemcould accommodate all the different types and processes ofmemory that have been identified, there are clear advantages tomultiple brain memory systems. That is, differential memorysystems allow for the support of a wide range of memory formsand computations. Furthermore, multiple memory systems arepotentially an asset if an individual suffers injury to a neural net-work that supports a relatively specific memory system. Al-though this would result in the disruption of certain memoryfunctions, other forms of memory supported by the uninjuredmemory systems would be preserved. Also, the knowledge ofwhich memory systems are compromised and which are unim-paired provides the neuropsychologist with a framework for de-veloping individualistic rehabilitation interventions.
544 Answers to Critical Thinking Questions

C H A P T E R 1 0
In light of the devastating effects of many of the genetic andchromosomal disorders, do you think that potential parentsshould seek genetic counseling before having children?Explain.Genetic and chromosomal disorders can have devastating effectson the developing brain and other body systems of the child.Many of these disorders are not currently detectable before thechild’s conception, so genetic counseling would not necessarilyprevent their occurrence. Fortunately, only a small percentage ofchildren are afflicted. However, it is advisable that individualswith family histories of genetic/chromosomal disorders or ofethnic or regional origins often associated with specific disorderssuch as Tay-Sachs disease, seek genetic counseling.
In recent years, an increasing number of teratogens havebeen identified in the environment. Are our children atgreater risk for brain anomalies than children of earlier gen-erations? Why or why not?An increasing number of teratogens have been identified, sug-gesting, at first glance, greater risk to our children. Althoughmany of these teratogens have been present for years, the injuri-ous effects to the unborn child have only recently been recog-nized. The identification of previously existing and new agentshelps reduce birth defects by prompting appropriate control,avoidance, or elimination of these agents. Ideally, greater atten-tion should be given to identifying and regulating potential ter-atogens before they are released into the environment. Unfortu-nately, identifying and regulating teratogens does not necessarilyprevent their impact on our children. For example, the in-trauterine teratogenic effects of alcohol have been documentedfor years; yet, children affected with FAS/FAE continue to beborn.
What steps can be taken to prevent FAS?The use of alcohol is an established fact in our society, andmoderate use does not necessarily lead to deleterious effects.Unfortunately, some women fail to make the necessary modi-fications in drinking patterns when pregnant because theylack awareness or understanding of the potential effects of al-cohol consumption on the developing child. In other cases,women continue drinking because alcohol consumption is alifestyle preference or because they are struggling with alco-holism. Improving prevention would involve increasing pub-lic awareness of FAS, starting with early and appropriate edu-cation provided by medical agencies, schools, social agencies,and public health alerts. Women with chronic drinking prob-lems require special attention because of difficulty in alteringestablished drinking patterns. These individuals should be ad-vised to forestall pregnancy until they can abstain from alco-hol, and treatment options should be provided. If pregnancyhas occurred, the risks of continued drinking to the fetusshould be explained and treatment options quickly identifiedand provided.
What do the neuropsychological profiles associated with TSand WS tell us about the organization of the brain?
The studies of TS and WS have expanded our understanding ofthe organization of the brain. The relatively unique neurocogni-tive profiles of these two disorders suggest the following: (1) anumber of cognitive functions are relatively independent of gen-eral cognitive ability, whereas others are strongly related to over-all ability; (2) similar behaviors can be supported by differentanatomic regions/circuitry; (3) the development of comparableskills and abilities by individuals with TS or WS are achieved bydifferent processes; (4) there is significant intraindividual vari-ability in the neurocognitive performance of individuals withTS and WS, indicating that factors other than genetic/chromo-somal abnormalities affect performance outcomes; and (5) theneurocognitive profiles do not support a “modular” organiza-tion of the brain. For the latter, a modular view of brain organi-zation proposes the presence of inborn, behaviorally designated,and independently functioning brain units. Injury to a givenmodule results in the disruption of neurocognitive functionssupported by that unit, while functions specific to other mod-ules remain unaffected. In essence, the modular view of an in-jured brain is that of a normal brain with some “components”impaired and others preserved (Karmiloff-Smith, Brown, Grice,& Paterson, 2003). Several findings argue against the neurocog-nitive profiles of TS and WS as validating evidence for a modu-lar conceptualization of brain functioning. First, the neurocog-nitive dissociations of TS and WS are “relative” and not“absolute.” That is, preserved functions are “relative” rather than“absolute” strengths. For example, the language skills of a childwith WS or TS may be more advanced than their visuoconstruc-tive skills; however, both sets of skills are generally lower thanthose of typically developing children. A cognitive dissociationconsistent with a modular conceptualization would predict thatthe aforementioned language skills would be unimpaired. Sec-ond, as noted earlier, similar neurocognitive behavior can besupported by different brain circuitry/regions and develop indifferent ways. Thus, neurocognitive behaviors are not localizedto specific brain units or follow invariant steps or processes dur-ing their development.
C H A P T E R 1 1
Why are the symptoms of NVLD and ADHD so often dis-played by children exhibiting a wide range of developmentaldisorders?As we have discussed, Rourke and associates hypothesize thatwhite matter tissue damage causes NVLD. Insofar as white mat-ter damage is evident across a number of developmental disor-ders, NVLD symptoms would be expected to occur, varying innumber and intensity, depending on the extent and location ofthe impairment. Likewise, the functional neural systems thatsupport attention and behavioral regulation are distributedthroughout the brain, and accordingly, the injurious effects todifferent regions or circuits of the brain could result in behav-iors of inattention, impulsivity, and overactivity. Thus, thesymptoms of ADHD could potentially be evident across a vari-ety of developmental disorders.
Answers to Critical Thinking Questions 545

Can a child with autism or Asperger’s syndrome develop nor-mal social awareness and attachment? If so, how would thisbe accomplished?A primary impairment of both autism and Asperger’s syndromeis a significant deficit in social awareness and attachment. Un-fortunately, these social deficits are rarely, if ever, fully resolved.Although therapists have used social skills training and other in-terventions, they have met little success. The amelioration of so-cial impairments of autism and Asperger’s syndrome is ham-pered by lack of understanding of the neuropsychological basisand determinants of social functioning. Specifically, neuropsy-chologists need to identify the developing relations of neuralsystems to special classes of social behavior (such as attachment),the effects of environmental influences on neural-social devel-opment, the causative factors specific to different types andforms of social impairments, and the malleability of and meansof modifying neural-social behaviors necessary for altering socialdeficits. Once they gain this knowledge, people should be ableto develop interventions necessary for the development of nor-mal social relatedness and interaction.
How would you respond to the comment, “ADHD does notexist, it is merely a diagnosis to excuse lazy and undisci-plined children?”Some challenge the very existence of ADHD as an excuse for lazyand undisciplined children. To counter this challenge, cite thevoluminous research that supports the existence of the disorder,the converging clinical and empirical studies that delineate thekey symptoms and potential etiologies of the disorder, and theoutcome studies that show significant improvement in regula-tory control for children with ADHD who receive appropriatemedical and psychological treatment. Finally, present specific be-cause differences between the child who is exhibiting ADHDand one who is showing lazy and undisciplined behaviors.
As our understanding of the neural correlates of learningand neuropsychiatric disorders expands, what impact will thishave on traditional psychological and educational treatment?As researchers increasingly identify neural correlates of learningand neuropsychiatric disorders, significant changes will becomeevident in psychological and educational interventions. Al-though the potential changes are both numerous and unknown,several have been predicted. First, the discovery of genetic andchromosomal links to specific developmental disorders and ac-companying neurogenetic interventions will enable children tobe born relatively free of neuropsychological deficits. The needfor traditional medical and psychological services specific tothese disorders will be rendered virtually obsolete. Second, neu-rogenetic, molecular, and chemical advances will guide the de-velopment of medical interventions to repair and regeneratedamaged brain tissue. In such cases, neuropsychological treat-ment will primarily focus on developing plans and interven-tions to enable parents and other caretakers to provide theexperiences necessary to stimulate development and recovery offunctions. Third, advances in the understanding of brain–behavior relations will encourage the development of increas-ingly complex neuropsychological models to predict appropriate
treatment options for specific brain disorders as affected bysocioenvironmental factors, age, sex, health status, cognitiveabilities, and other variables. Fourth, as understanding of brain–cognitive functioning expands, people will be able to developspecific educational strategies and interventions that will ex-pand and maximize the learning of children, both disabled andnondisabled.
Does the finding that the symptoms of GTS often attenuateor resolve in later adolescence or early adulthood support aconceptualization of the disorder as a developmental lag?How do you account for individuals who do not show suchimprovement and struggle with GTS as a lifelong disorder?The concept of developmental lag indicates a delay in the onsetor rate of development of motor, communication, socialization,or other expected behaviors. The concept further assumes that amature level of functioning ultimately will be achieved, and thusdoes not denote a disability. Clearly, the attenuation or resolu-tion of GTS during late adolescence or early adulthood does notmeet the standard of a slowly emerging or developing set of ex-pected behaviors. Yet, inhibitory (motor) control is a develop-mental phenomenon that begins in infancy and continues tomaturity in adolescence/adulthood. If research determines thattic behaviors are a function of a lag in the maturation of motorcontrol, greater support will be provided for conceptualizingGTS as a developmental delay. However, the finding that a num-ber of individuals with GTS do not show improvement withage, the complexity of behaviors that can constitute a “tic,” theinvoluntary-voluntary quality of some tics, and the “waxing andwaning” nature of tic behaviors argues against a simple causativeexplanation for GTS, such as developmental delay. The factorsthat determine whether an individual will or will not recoverfrom GTS remain unclear. It is possible that there are yet to beidentified subtypes of GTS that differ with regard to the pro-gression and resolution of tic behaviors. Other factors that mayaffect the chronicity of GTS are tic severity, age at onset, pres-ence of other comorbid conditions, and types and duration oftreatment.
C H A P T E R 1 2
What are the neurologic, behavioral, and emotional symp-toms of a stroke?The initial neurologic symptoms of stroke include a suddenheadache, nausea, and loss of behavioral function, which maybe relatively specific in nature. Because a stroke can affect manydifferent areas of the brain, the neurologic symptoms may vary,but there can be an associated loss of consciousness. Behavioralsymptoms relate to the precise area of the brain that has been af-fected. For those affected with left-hemisphere stroke, a com-mon behavioral symptom is difficulty in understanding and ex-pressing speech. Visual symptoms indicate posterior or basilarinvolvement, but a precise understanding of the behavioralsymptoms is often not possible until a comprehensive neuropsy-chological evaluation is completed. Emotional symptoms caninclude depression for left-hemisphere stroke or irritability for
546 Answers to Critical Thinking Questions

right-hemisphere stroke. Again, a comprehensive neuropsycho-logical evaluation may include a measure of emotional and per-sonality functioning.
What are the major forms of treatment for stroke?The acute treatment of the stroke patient involves medical sta-bilization and control of bleeding, through medication orsurgery. Common medications include anticoagulants to dis-solve blood clots or prevent clotting, vasodilators to dilate or ex-pand the vessels, and blood pressure medication and steroids tocontrol cerebral edema. Surgery can include clipping a bleedinganeurysm or evacuating blood to control the intracranial pres-sure often associated with a hemorrhage. Treatment for TIAsymptoms is more difficult because of the ambiguous nature ofthe symptoms and is often restricted to pharmacologic interven-tion with anticoagulants. Long-term treatment of stroke patientsmay include intensive rehabilitation, including speech therapy,occupational training, and vocational training. Often, basic ac-tivities of daily living must be “relearned.” Periodic re-evalua-tion by a neuropsychologist may determine treatment and reha-bilitation progress and outcome.
Why do some stroke victims downplay their illness, whereasothers go into a deep depression?The symptoms of a right-hemisphere stroke are quite differentfrom those of a left-hemisphere CVA because of the lateraliza-tion of many functions in the brain. A right-hemisphere strokemay result in a “lack of awareness” associated with poor insightand disinhibition. Patients with right brain damage tend to beunaware of their dysfunction associated with the consequencesof the stroke. In fact, such patients often deny that there is any-thing wrong with them. Many patients with right brain damagedisplay a range of emotions from indifference to euphoria. Thiscontrasts with the depression that patients with left brain dam-age often show. Therefore, it is easy to assume that deficits fromright brain damage are not as serious as those from left braindamage. As a result, right-hemisphere stroke patients may beblamed for being “rude,” “disruptive,” or “inappropriate” whenthey are actually exhibiting symptoms of right brain injury, in-cluding impulsivity, verbosity, inattention, and poor judgment.Obviously, these problems can be highly disruptive to the pa-tient and family alike, often even exceeding the problems associ-ated with left-hemisphere CVAs. Because right-hemispherestroke patients and their families underestimate the severity ofthe condition, those patients are not diagnosed as rapidly as areleft-hemisphere stroke patients.
Describe the most common neuropsychological deficitsassociated with stroke.Almost always, neuropsychological disruption appears in strokesurvivors; thus, neuropsychologists often evaluate stroke pa-tients. Both the right and left hemispheres are associated withchanges in motor and sensory functioning after a stroke. Thosechanges can be as benign as mild motor slowing to effects as de-bilitating as complete paralysis, particularly if there are lesionsin the thalamic area or the motor and premotor area of thefrontal lobes. Right-hemisphere stroke motor deficiencies, how-ever, are generally less severe, because the nondominant left
hand is not as important for skilled tasks. Deficits that affect theright cerebral artery involve areas responsible for spatial, rhyth-mic, and nonverbal processing. Right-hemisphere symptoms,although serious in the patient’s overall functioning, can be lessstriking in the acute phase, particularly if they do not involvemotor dysfunction. Research has shown consistently that pa-tients with right-hemisphere stroke are hospitalized longer in re-habilitation facilities than are patients with left-hemispherestrokes. This fact is related to the pervasive deficits that right-hemisphere patients present with in the area of visuospatial abil-ities and the extended rehabilitation process that is required inrehabilitating these patients in areas of dressing, ambulating,and other self-care behaviors. The capacity to drive after a strokecontinues to be one of the most sensitive issues facing healthcare workers, as well as the stroke patients and their families.
Would you want to know what type of cell a tumor arisesfrom if one of your family members had brain cancer? Why?Should physicians routinely inform their patients of suchmedical details?Yes, I (E.A.Z.) would like to know. The reason for knowing isthat the more information the patient and family has, the easierit is to make personal decisions, such as estate management, is-sues of quality of life, and life expectancy. The specific type ofbrain tumor, and the type of cell it has arisen from, often signalsa clear course of the disease. For example, the glioblastoma mul-tiforme (GBM) is a particularly destructive and fatal glioma.Conversely, the presence of a meningioma often has little conse-quence to one’s long-term well-being. Many physicians sharedetailed medical information with their patients and treat themas educated consumers. But many do not. My Aunt Edna diedof a brain tumor, but the doctors never told her or her familywhat kind of tumor she had, even though clearly (to me) it wasa GBM. As a result, the family had great hopes for her recovery,which unfortunately was not realistic; she passed away within8 months. Would you like to know?
What is the neuropsychologist’s role in diagnosing and treat-ing patients with brain tumors? What is his or her role withthe patient’s family?Since the advent of modern imaging technologies, neuropsy-chologists play only a minor role in the diagnosis of brain tu-mors. CT and MRI technology can often pinpoint the preciselocation and size of a brain tumor. If the tumor is thought to befatal, neuropsychologists often provide counseling and educa-tion to patients with brain tumor and their families. If the braintumor is operable and recovery is likely, neuropsychologists canprovide a baseline assessment to which future evaluations (aftersurgery) can be compared. Treatment choices are complex andshould have input from a team of oncologic professionals in-cluding neurosurgeon, oncologist-hematologist, radiation thera-pist, neuroradiologist, neurologist, and neuropsychologist. Ingeneral, neuropsychologists can play an important role in as-sessing brain tumor survivors and in providing rehabilitationcare and intervention. As with other neurologic disorders, neu-ropsychologists can play an important role in helping people tounderstand the cognitive changes associated with brain tumor
Answers to Critical Thinking Questions 547

diagnosis and treatment, and assist families in coping with thismedical illness.
How do children who have brain tumors react differently totheir disease from the way adults do? How do their familiesreact?In general, children are quite resistant to the psychological con-sequences of life-threatening diseases. When they are adoles-cents, the burden on them physically and psychologically maymanifest itself by experiencing depressed mood and irritability.But young children seem to cope surprisingly well when con-fronted with cancer. The parents of those children seem to ab-sorb much of the psychological distress, however, often feelingguilty and being overprotective. Families often view the cancerand its consequences as severe and insurmountable. As a result,when a child is diagnosed with a brain tumor, it has become es-sential to work with the entire family to understand the subjec-tive appraisals or perspectives of the child and the family and toprovide a realistic but optimistic framework. This crisis is notonly the child’s but also the entire family’s. Thus, diagnosis andtreatment of cancer in children affects family functioning in sub-tle ways, and family functioning affects cancer and its treatmentin children. Psychologists play an important role in managingthe emotional consequences of the families and children withbrain tumor.
C H A P T E R 1 3
Can a head injury change a person’s life?Yes, often dramatically. The consequences of moderate and se-vere traumatic head injury can be profound, with obvious emo-tional and cognitive changes in the patients who survive headinjuries. It is not unusual in such cases that a spouse reports thata head injury victim is not the person that he or she married.The patient’s quality of life, marital status, and employment sta-tus often change significantly. The consequences of mild headinjury (MHI) and concussions are more subtle, even to the pa-tients themselves. Nevertheless, they can change a person’s life,because the mild cognitive deficits that are often associated withMHI affect the person’s quality of life. Often, depression andsomatic complaints appear in MHI patients, as do cognitivedeficits in memory and attention. However, many individualswho have sustained an MHI completely recover. Often, neu-ropsychologists can determine the level of recovery by making aneuropsychological assessment.
What is the potential for the human brain to adapt and re-cover after brain injury?In this chapter, as well as in previous chapters, we have presentedcases in which patients had to adapt to the devastating effects ofbrain injury. Some patients have adapted well even in the face oflittle to no recovery. Other patients, particularly younger chil-dren, have made dramatic recoveries of function. The practicingneuropsychologist must weigh multiple factors, including injuryseverity, age, previous level of functioning, available resources, aswell as the patient’s psychological state and level of motivation inpredicting potential for recovery. This remains an inexact science,
but neuropsychologists are often surprised by the ability of peo-ple to adapt to their injuries.
What are the challenges for rehabilitation in the twenty-firstcentury?After reading this chapter, where do you think neuropsychologi-cal rehabilitation should head in this century? Should it be inthe area of technology? Inpatient treatment? Community rein-tegration and job skills? Family and patient counseling relatedto adapting to the injury or illness? The practicing neuropsy-chologist must weigh multiple factors, including injury severity,age, previous level of functioning, available resources as well asthe person’s psychological state and level of motivation in pre-dicting potential for recovery. The biggest potential for rehabili-tation may, however, be in the area of research and development.Right now scientists can program the nervous system of onlythe simplest invertebrates. However, changes in technology areoccurring at lightning speed. For example, will those paralyzedfrom the neck down walk again through the aid of technology?
C H A P T E R 1 4
Will exercising one’s mind help ward off dementia? Must one“use it or lose it”?Debate continues among researchers that maintaining flexibilityof thought and keeping mentally active contributes to one’s cog-nitive reserve. However, even researchers who have not foundconfirming results are still hopeful that an active, healthylifestyle, both mentally and physically, may help ward off somedisorders of aging.
How is Alzheimer’s disease best identified in life?Because Alzheimer’s disease (AD) is a diagnosis of exclusion,only confirmed later by biopsy at autopsy, behavioral and cogni-tive profiles are crucial to the differential diagnosis of AD and ofvarious dementia subtypes. In addition to differentiating be-tween AD and normal aging, Chapter 14 makes clear that dif-ferent dementia subtypes show distinct neuropsychological pro-files. Knowing the behavioral and cognitive profile is one of thebest means of differentiating between some types of cortical(AD) and vascular dementias and normal aging. This is becauseonce all other medical causes have been ruled out, imaging andphysiologic testing often cannot detect minute vascular changesor patterns of brain necrosis. This is also because, as we havesaid, degree of cortical shrinkage is not reliably associated withdeclines in cognitive functioning. Changes in behavioral func-tioning, however, are the hallmark of dementia and they mustbe documented carefully.
How can a neuropsychological profile aid dementia sufferersand their families?As is evident from the previous question, in addition to aidingin diagnosis, one of the best things a cognitive profile can pro-vide is a picture of the person’s pattern of strengths and weak-nesses, and an estimation of degree of decline from former abili-ties. This picture is a “snapshot in time,” but it serves to educatepatients and caretakers about the degree to which the person is
548 Answers to Critical Thinking Questions

currently able to manage independently and in what areas he orshe is likely to need assistance. The neuropsychological profilecan also serve as a planning aid for future caretaking and treat-ment needs. Although there is no “cure” for AD, ameliorativetreatments can help the AD patient. Knowing, for example, thatan AD patient has preserved nondeclarative motor skill learningmeans that the patient may be taught relaxation techniques thatrequire progressive muscle relaxation, even though they retainno declarative knowledge of learning. Such behavioral treat-ments used by psychologists show promise in calming restless-ness and agitation that can occur in later stages of the disease. Insum, the neuropsychological profile helps show the problematicbrain functioning, educate regarding strengths and weaknesses,plan for individualized caretaking needs, and suggest possiblebehavioral treatments.
How does the concept of self of the patient with Alzheimer’sdisease change with the progression of the disease?This question allows speculation, given what has been presentedof the neuropsychological profile of the patients withAlzheimer’s disease (AD). If you look at each area where declineis evident, how do you think this would affect a person’s self-concept? New learning deficits and declarative memory loss arehallmarks of the disease. Considering the possibility that aspectsof our selves are built on memories of our own experiences, doyou think a person’s self-concept would change as he or she lostaspects of his or her memory, as the person has increasing trou-ble learning, or as the person is having trouble doing certainthings he or she once did well? Are there certain people whosesense of self may be more affected by AD than others would?
C H A P T E R 1 5
It may soon be possible to test for many neurologic diseases.Would you want to be tested for the possibility of future de-mentia?A positive genetic test for Huntington’s disease (HD) indicatesalmost certain manifestation of the disease. But what aboutother neurologic diseases, where a positive test could indicatemuch lower odds of disease certainty? There are cases of AD pa-tients with normal identical twins. Factors other than inheri-tance play into whether dementia develops in a person. Wouldyou want to know about your tendency toward a certain dis-ease? Would you want others to know? Why do you think mostpeople at risk for HD have declined to be tested?
How is the behavioral quality of subcortical motor disorderspresented in this chapter similar or different from the corti-cal motor disorders such as apraxia presented in Chapter 7?Is the behavioral quality of the motor dysfunction of Parkin-son’s, Huntington’s, or Creutzfeldt–Jakob disease different fromthat of, say, apraxia (see Chapter 7)? Most clinicians would sayyes. With subcortical motor problems, the movement is usuallynot orchestrated or regulated well, but apraxia is a problem ofnot “knowing.” For example, if asked to pantomime “pouringand serving tea,” an apraxic patient may have no idea of how todemonstrate this or may mime an incorrect action. In contrast,
a patient with Parkinson’s disease is more likely to demonstratethe correct movement, but may have trouble initiating themovement or show slowness in performing the movement(tremor may be evident in later stages of the disease during in-tentional movements). In what other ways might the behavioralquality of subcortical motor disorders differ from that of corti-cal motor disorders?
How do the subcortical and cortical motor systems worktogether?Chapter 7 describes two theories of how the motor system maywork. First, the hierarchy theory states that the primary motorcortex sits at the top and is the funnel for all bodily informa-tion. A competing theory suggests that the motor system worksin a parallel processing mode with several motor processingcircuits working in coordination with the primary motor cor-tex. Although these theories remain debatable, we also knowthat much of the initiation for motor behavior and executiveprogramming for movement originates in the higher associa-tion area of the prefrontal cortex, which is responsible for or-chestrating and organizing motor behavior. The dorsolateralprefrontal cortex (contained within) is not a “movement cen-ter” in and of itself, but it is instrumental in deploying move-ment. Much of the input to this area comes from the subcorti-cal motor centers. Therefore, the subcortical and corticalmotor functions must coordinate and may do so through thedorsolateral prefrontal cortex. Although there appears to besome hierarchy of functioning, it may also be that parallel cir-cuits relate to different aspects of motor behavior within thishierarchy.
What are the ethical and scientific issues in the treatment ofdementias?This chapter and Chapter 14 discuss a number of different treat-ments for dementias. These treatments include drug, behavioral,and even surgical interventions. The most ethically controversialtreatments include genetic treatments and surgical interventionswith “fetal” brain tissue. Also, to what extent should society seekto develop drugs to ameliorate symptoms of dementia? Whatare the costs versus the benefits?
C H A P T E R 1 6
What is the biological or psychological function of “rhythms”of consciousness?This chapter discusses the idea that there are preset circadianrhythms of human consciousness. It also discusses how theseoperate in normal waking, sleeping, and dreaming. It is also ap-parent that narcolepsy disrupts the flow of this rhythm so thatsleep attacks may occur during wakefulness. Also, the rare circa-dian rhythm disorder can be life threatening (see “The Case ofthe Last Coronation,” Neuropsychology in Action 16.2). Givenwhat you know of this, can you speculate on the biological rea-sons for daily and 90-minute periods of relatively more active tomore quiet brain activity? Does this somehow “tone” the brain,as some suggest? Psychologically, is it adaptive for humans to al-ternate between periods of activity and quiet?
Answers to Critical Thinking Questions 549

How fluid are the boundaries between conscious and sub-conscious awareness?This question concerns not only this chapter, but also ideas ofconscious awareness, which have been presented throughout thebook, as well as general ideas of consciousness debated in psy-chology. To approach this issue, first one must conceptualizeand operationalize a definition of “conscious awareness” withparticular attention to how conscious awareness is demon-strated. Must this always be in a verbal manner? Can onedemonstrate awareness just through performance of an action?When one is in a state of consciousness, which is other thanbeing “fully awake,” what sense of awareness can there be? Howdoes your knowledge of the functional and dysfunctional brainhelp to inform your ideas of consciousness?
How do REM sleep and dreaming change in people whohave various neurologic disorders?This issue presents an exciting and relatively underexplored areain neuropsychology. A number of case reports of people withabnormalities in dreaming from global cessation of dreaming, todecreased or odd qualities of dreaming, to problems in remem-
bering dreams are in the literature. How do you think dreams ofpeople with frontal lesions differ from those of people with pari-etal lesions? Do you think that people with motor problems willalso have motor problems in their dreams?
In what ways might neuropsychology be able to contributeto treatments for people with sleep disorders or epilepsy?If you consider the range of behavioral treatments of clinicalpsychology and the neuropsychological problems represented bythe disorders presented in this chapter, you can see that a num-ber of treatment strategies are possible. For example, memoryand concentration problems are common in sleep apnea and, toa certain extent, in narcolepsy. Do you think strategies that aidmemory will be useful for sleep apnea patients? Narcolepsy pa-tients may have sleep attacks in response to emotional stimuli.Might relaxation techniques help them? With seizure patients, ifauras are related to the foci of the seizure, might visualizationtechniques help to ward off visual auras, and therefore theseizure? What else can you think of? These areas are ripe forfuture investigation.
550 Answers to Critical Thinking Questions

Aarsland, D., 424Abikoff, H., 322, 323Abramowitz, A., 324Abrigo, E., 205Achten, E., 169, 170Adams, R. D., 98Adler, N. E., 405Adolphs, R., 262, 264Ager, J. W., 292Aggarwal, N. T., 405Agid, Y., 427, 429, 430Agnew, J., 168Ahmad, S. A., 307, 308Akshoomoff, N., 316Alarcón, M., 302Albert, M., 406Albert, M. L., 26, 408, 426Alcazar, B., 342Aleman, A., 167Alexander, M. P., 251, 320Allan, J. D., 174Allen, G., 283Allen, S. J., 413Alsobrook, J. P., 334Altmann, D., 174Alvarez-Buylla, A., 110Alves, W. M., 383Alvord, E. C., 116Alzheimer, A., 410, 418, 437Aman, M. G., 322Amedi, A., 205Amin, Z., 169Aminoff, M. J., 277Amirikian, B., 169, 170Andersen, A. R., 435Anderson, A. W., 317, 318Anderson, C. M., 325Anderson, G. M., 251, 316, 333Anderson, P., 117, 281Anderson, R. A., 214Anderson, S. L., 325Anderson, S. W., 253, 257Anderson, V. A., 117, 166, 167,
247, 270, 273, 280, 281Andrew, R., 289Andrews, C., 263Andy, O. J., 146Angold, A., 333Anker, S., 289Annett, M., 173Appelbaum, L. G., 288, 290Archer, R. P., 15Archibald, S. J., 250, 256, 293Aristotle, 7Armony, J. L., 260, 261Armstrong, C. L., 364–365Armstrong, Lance, 360
Armstrong, R. J., 111Armstrong-Hickey, D., 453Arndt, S., 321Arnold, L. E., 322, 323Arsten, A. F., 333, 334Artru, A. A., 317Asbell, S. O., 364Asberg, M., 108Asbjornsen, A., 304Asgharian, M., 409Ashburner, J., 167Ashford, J. W., 420Ashwin, C., 319Askenasy, J. J. M., 459Asperger, H., 311Assheuer, J., 157Aston-Jones, G., 241Athawes, R., 402Atkinson, J., 289Au, R., 409Auff, E., 429Augustine, G. J., 128, 146Autti-Rämö, I., 292, 294Awh, E., 240Aylward, E. H., 317, 325
Babcock, R. L., 403Babinski, J., 20Bachen, N. I., 385Bachevalier, J., 196, 234, 237Bäckman, L., 168, 402, 403Baddeley, A. D., 237, 238, 239,
302Bailey, A. D., 311, 312, 313, 316Bailey, J. N., 323Bailey, P., 135Baird, A. D., 174, 345, 351Bakker, D. J., 308Balasubramanian, V., 150–151Balej, J., 195Ball, G. F., 109Banerjee, S., 333Banich, M. T., 136Bannister, R., 343, 347Barakat, L. P., 310, 366–367Barbieri, S., 212Barch, D. M., 257Bard, P., 259Barkley, R. A., 323, 326, 329, 331Barnes, M. A., 277, 279Barnett, H. J., 346Baron, I. S., 277, 279–280Baron-Cohen, S., 317, 319Barr, H. M., 292, 293, 294, 324Barrash, J., 257Barratt-Boyes, B. G., 285Barres, B. A., 101
Barrett, J. H., 323Barth, J. T., 23, 41, 73, 192, 196,
365, 367, 371, 379, 381, 383,462
Basso, A., 237Bates, E., 273Battersby, W. S., 20Beadle-Lindsay, M., 87, 146Bear, M. F., 180, 194, 261Beatty, J., 96, 105Bechara, A., 255, 256, 257, 258Beck, L. H., 246Becker, J. T., 406Becker, R. O., 448Beckett, L. A., 405, 424Beeman, J. J., 167Beh-Yishay, Y., 397Beiser, A., 409Bell, M. A., 168, 169, 170, 252Bellgowan, P. S. F., 162, 167, 169Bellugi, U., 287, 290Bender, B. G., 283, 285Bender, M. B., 20Bennett, D. A., 405, 424Bennett, M. V. L., 100Bennett, T. L., 468–469, 472Benson, D. F., 208, 256, 324,
416, 417Benton, A. L., 25, 26, 74, 252,
288, 375, 376, 379, 380, 385,429
Benton, J. S., 413Berch, D. B., 283Berg, E. A., 246Berg, S., 77, 403Berger, H., 40Berger, O. G., 272Berlin, L., 330Berman, K., 49Bernstein, J. H., 273Berquin, P. C., 325Berthier, M. L., 314Bertilsson, L., 108Berttrand, J., 287, 288, 290Best, M., 301Biddle, K. R., 247, 273, 274Biederman, J., 324, 325Bigler, E. D., 58, 59, 95, 302,
315, 343, 372, 384, 405, 411,413
Bilker, W., 167Binder, J. R., 162, 167, 169Birch, S., 299Birkmayer, W., 431Bishop, D., 287Bisiach, E., 212Bjoerklund, A., 108
Black, K., 304Black, S. E., 226Blackburn, E. H., 405Blaine, H., 325Blake, C., 323Blakemore, C., 20Blasey, C., 317Blatter, D. D., 58Bleeker, M. L., 168Bloch, F., 51Blume, W., 464Blumenthal, J., 325Blumer, D., 256Bobe, L., 162, 167, 169Bocian, K. M., 301Boeve, B. F., 406Bohan, T. P., 277Bohlin, G., 330Boles, D. B., 167Boll, T. J., 371, 383Bolla-Wilson, K., 168Boller, F., 74, 427, 429, 430Bollich, A. M., 167Bolton, P., 313Bond, T., 462Bonfort, S., 328Bookheimer, S. Y., 317Bookstein, F. L., 292, 293, 294Bornschein, R. L., 272Bornstein, R. A., 196Borod, J. C., 262, 263, 427, 428Borteryu, J. P., 291Bouma, A., 167Bourne, G. H., 404Bowen, D. M., 413Bowirrat, A., 409Boynton, G. M., 301Braddick, O., 289Bradshaw, J. L., 161, 189, 191,
196, 209, 211, 212, 213, 214,218, 220, 323, 332, 334, 412,425, 428, 435, 436
Brady, James, 373Braithwaite, V. A., 173Brandt, J. A., 436Bransome, F. D., 246Braun, A. R., 335Braver, T. S., 257Brayne, C., 424Brazier, M. A. B., 40Bressler, S. L., 448Brewer, B. W., 42Brewer, V. R., 328Brickenkamp, R., 72Briggs, J. H., 282Broca, P., 16, 149, 162Brodal, A., 35
NAME INDEX
Note: Names of patients are listed under Patient.
551
Brodmann, K., 158Brody, I. A., 18Broman, S. H., 282Bronen, R., 315, 316, 335Bronstein, Y. L., 252Brooks, W., 325Brookshire, B. L., 277Brorson, L. O., 473Brown, A. S., 465Brown, G. L., 108, 345, 351Brown, J. E., 325Brown, R. G., 416Brown, R. T., 337Brown, S., 325Brown, T., 272Brown, W. E., 283Brown, W. S., 168, 173Bruce, E., 25Brunner, R., 174Bruno, J. P., 241Bryden, M. P., 167, 168, 169, 174Buchanan, L., 283, 284Buela-Casal, G., 342Bullmore, E. T., 319Bullock, P. R., 319Bundick, W. T., 87, 146Burlingame, G. M., 302Burns, A., 413Burns, B. J., 333Burr, R. B., 58Burt, A. M., 132, 134, 137Burt. A. M., 230Burton, L. A., 168Busch, S., 446Buskist, W., 203Busse, O., 351Butler, D. W., 319Butryn, M. L., 110–111Butters, N., 227, 237, 415, 416,
430Bylsam, F. W., 173, 281, 436
Cabeza, R., 226, 229, 253, 258Cahill, L., 169, 260Cairns, P., 415Cajal, R., 34Calarco, K. E., 294Calhoun, S. L., 313Campbell, J. J., 258Campbell, R. A., 324, 325Canfield, R. L., 271, 272Canli, T., 169Cannon, W., 259Cantu, R. C., 382, 384Cantwell, D. P., 323, 328Capirci, O., 287Cardon, L. R., 300Carey, M. E, 310, 366Carey, S., 249Carlson, C. D., 302Carlson, N., 203Carlson-Green, B., 366Carmichael Olson, H., 292, 294Carney, R. A., 283Caron, M. G., 324Carpenter, M. K., 111Carper, R., 316Carroll, A., 196
Carter, C. S., 257Carter, L. P., 465Cartwright, R. D., 460Caruit, M., 310Cascino, G. D., 465, 466, 467Caselli, M. C., 287Casey, B. J., 120, 325, 334, 335Casey, R., 366Casse-Perrot, C., 288Casson, I. R., 383Castellanos, F. X., 324, 325, 336Catroppa, C., 117Catt, K. E., 409Catts, H. W., 302Celnik, P., 205Cenci, M. A., 108Chalmer, D., 445Chalmers, D., 448Changeux, J. P., 156, 157Channon, S., 335Chapieski, L., 323, 334Chapman, L. F., 21Charcot, J-. M., 19Charles, A. C., 100Charman, T., 311Chase, C., 299Chase, T. N., 335Chavaillon, J., 156, 157Checkoway, H., 424Chelder, M. J., 73, 74, 75, 77Chelune, G. J., 77Chen, J., 409Chen, W. J., 293Cherlow, D. G., 465Cheung, A. M., 325Chiarello, C., 167Chiles, M., 287, 290Chou, T. C., 456Chow, T. W., 255Christensen, A. L., 82Chugani, D., 120Chugani, H., 120, 283Chui, H., 412Churchland, P. S., 95Chusid, J. G., 135, 145Ciesielski, K. T., 319Cirino, P., 323, 334Civin, C. I., 111Cohen, D. J., 315, 332, 333, 334,
335Cohen, J. D., 55, 241, 257Cohen, L. G., 205Cohen, N. J., 227, 234Cohen, R. A., 241, 242, 243, 244Cohen, R. M., 324Cohen-Kettenis, P. T., 173Colcombe, S., 174, 405Cole, K., 287, 290Commenges, D., 409Como, P. G., 335Conners, C. K., 322, 323Connor, P. D., 292, 293, 294Connors, B. W., 180, 194, 261Constable, R. T., 167, 169, 304Convit, A., 405Conway, J. A., 307, 318Cook, E. H., Jr., 318Copeland, M., 406
Coppola, R., 448Corder, E. H., 412Corey, D. M., 167Corey-Bloom, J., 412Corkin, S., 150, 235, 430Cornoldi, C., 310Corwell, B., 205Corwin, J., 173, 281Cory-Slechta, D. A., 271, 272Costa, L., 305–306Costello, E. J., 333Cote, L. J., 412, 424Cottington, E. M., 319Coull, J. T., 243Courchesne, E., 316Covassin, T., 384Cowan, W. C., 115Cowan, W. M., 95Cowart, B. J., 187Cox, C., 272Cox, R. W., 167, 169Coyle, J. T., 413Craik, F. I. M., 229Crandall, P. H., 465Craven-Thuss, B., 336Crawford, J. R., 403Crawfrod, T. O., 111Crick, F., 445, 448, 460Crinella, F., 328Cron, B. W., 364Crosson, B., 147, 218, 430Culbertson, J. L., 292, 294, 298,
299Culbertson, W. C., 77, 78,
250–251, 275–276, 327Culhane, K. A., 247Cullum, C. M., 45, 95, 343, 372Cummings, J. L., 252, 255, 258,
325, 412, 416, 417, 419, 426Curran, T., 235, 236Curran, W., 289Curtis, G., 77Cytowic, R., 179Cytrynbaum, C., 291
D’Andrea, E. A., 173D’Esposito, M., 245da Vinci, L., 7, 128, 130Dabholkar, A. S., 117, 272Dahl, J., 473Dahlgren, S. O., 318Daly, D. D., 146Daly, E. M., 283, 404, 406Daly, G., 324Damasio, A. M., 255, 256Damasio, A. R., 257, 258, 260,
262, 263, 411Damasio, H., 169, 170, 255, 256,
264Dambrosia, J., 205Dann, M., 189Danta, G., 429Dapretto, M., 317Dartigues, J. F., 409Darwin, C., 16, 156Davidson, K. C., 277, 328Davidson, R. J., 252Davies, P., 413
Davis, E. A., 243Davis, M., 262Davision, L. A., 246Dawson, M. E., 242de Almeida, J. C., 282De Haan, E. H. F., 168De Jong, J., 108De La Granja, M., 283de la Tourette, G., 332de Lange, F. P., 169, 170de Leon, M., 405de Schonen, S., 288Dean, R. S., 163DeAngelis, L., 364Deary, I. J., 402Deaton, A. V., 397DeCari, C., 283DeFries, J. C., 300, 302Deiber, M. P., 205DeKosky, S. T., 406, 412Del Bigio, M. R., 277Del Dotto, J. E., 307, 309Del’Homme, M. A., 323Delattre, J. Y., 364Delis, D. C., 291, 292, 293, 294DeLuca, J. W., 306, 307Demarest, R. J., 148Demb, J. B., 301Dement, W. C., 455, 462Denaro, J., 412, 424Denckla, M. B., 250, 325Dennis, M., 277, 280, 281, 291Deppe, M., 162, 167, 169Derns, D., 110–111Deruelle, C., 288DeSantis, M., 194Descartes, R., 4, 9–10, 447DeTeresa, R., 411Deutsch, G., 51, 151Devinsky, O., 196, 257Dhabhar, F. S., 405Diamond, A., 147, 247–249Dieber, M. P., 169DiGirolamo, G. J., 241, 245DiLavore, P. C., 318Diller, L., 395Dissanayake, C., 313, 318Dodge, H. H., 406Dolan, R. J., 262Don, A., 291, 294Donohue, B. C., 303Dool, C. B., 307Dostie, D., 166Doty, R. L., 189Douglas, R. J., 150Dowd, M., 316Downs, J. H., 165Drachman, D. A., 413Dräger, B., 162, 167, 169Drake, E. B., 168, 173Dubois, B., 427, 429, 430Duffy, F. H., 44Duffy, J. D., 258Dulberg, C., 406Dunne, C., 110, 331Dunner, S. B., 420Dunnett, S. B., 111Dykens, E. M., 285
552 Name Index

Eals, M., 168Eastman, C. I., 460Ebbinghaus, H., 24Ebers, G. C., 98Echelard, D. A., 317Echemendia, R. J., 384Eckburg, P., 324, 325Eden, G. F., 299Edgell, D., 270, 272, 281, 298Edmonds, J. E., 298, 299Edwards, M., 230, 232–233, 457Efron, R., 466, 472, 473Efthimiou, J., 73, 74, 75Ehlers, S., 318Eichhorn, G. R., 169, 170Einstein, G. O., 403Eiraldi, R. B., 323Eisenberg, H. M., 379Eisenmajer, R., 312El-Hai, J., 22Elavsky, S., 174Elger, C., 464Elias, L. J., 167Eliez, S., 283, 287Eliopulos, D., 304, 324Elliott, F. A., 108Elliott, T. K., 283Elsass, L., 396Emerson, J., 328Engel, J., 464England, M. A., 99Epel, E. S., 405Erickson, K., 174, 277, 279–280Erickson, K. I., 405Erkanli, A., 333Erlanger, D. M., 172, 174Ernst, M., 324Erwin, R., 327Esiri, M., 404Eslinger, P. J., 247, 252, 253, 258,
273, 274Espeland, M. A., 174Espir, M. L. E., 150Espy, K. A., 250Evankovitch, K., 247Evans, A. C., 166Evans, D. A., 405, 424Ewing-Cobbs, L., 277, 279
Fallon, J., 169Falz, L., 205Fan, J., 244, 245, 325Fantie, B. D., 116, 277, 279–280Farah, M. J., 208Faraone, S. V., 325Farran, E. K., 288, 289Farrer, L. A., 436Feifel, D., 108Fein, D., 312, 316, 320Feirtag, M., 231Feldman, R. G., 408, 426Feldman, R. S., 107, 187Fenwick, P. B., 473Fermi, E., 449Fernandez-Duque, D., 243, 244,
245, 326Ferris, S. H., 406Fields, R. D., 101
Filipek, P. A., 302, 303, 324, 328Findley, L. J., 462Fine, D., 277, 281, 282, 312Fink, M., 278Fiore, C., 328Firth, C. D., 243Fisher, N. J., 306, 307Fisher, R. S., 464Fisk, L. J., 308, 309Fitzgerald, M., 324Fitzpatrick, A., 406Fitzpatrick, D., 128, 146Fitzpatrick, H., 323Flaherty-Craig, C. V., 252Fletcher, J. M., 277, 279, 281,
302, 328Fletcher-Janzen, E., 279Flicker, C., 406Flodman, P., 328Flöel, A., 162, 169Flourens, P., 18–20Flowers, D. L., 302Foley, B., 310, 366Folstein, M. F., 407Folstein, S. E., 314, 316Fombonne, E., 312, 313Foorman, B. R., 302Ford, C. E., 282Forrest, B.J., 310Forstl, H., 413Fossella, J., 334, 335Foundas, A. L., 167Fowler, P. C., 146, 343, 354Fox, P. T., 165, 207, 252Frackowizk, R. S. J., 167Francis, D. J., 277, 302Francis, J. P., 381Frank, R., 255Freedman, A. M., 12Freeman, W., 22–24, 25Freidman, S. D., 317Freud, S., 4, 18–19, 460Freund, L. S., 283Friedland, R. P., 409Friedman, H. R., 78Friedman, K. B., 465Frijda, N. H., 173Friston, K. J., 167Frith, U., 311Frost, J. A., 162, 167, 169Fuerst, D., 305, 306, 308Fuerst, D. E., 308Fulbright, R. K., 167, 169, 317,
318Fulker, D. W., 300Fullbright, R. K., 303, 304Fuster, J. M., 254
Gabrieli, J. D. E., 235, 335, 430Gaddes, W. H., 298Gage, P., 110Gage, R., 163Gainetdinov, R. R., 324Gajdusek, D. C., 437, 439Galaburda, A. M., 255, 287, 301Galen, 8Gall, F., 13–14Gallup, G. G., Jr., 320, 446
Galton, F., 237Ganguli, M., 406Garcia-Verdugo, J. M., 110Gardner, H., 86, 208Garrido, E., 342Gaskell, P. C., 412Gatenby, J. C., 262Gauna, K., 166Gauthier, I., 317, 318Gautier, T., 174Gazzaniga, M. S., 163, 165Geiman, R., 249Gendle, M. H., 271Gennarelli, T. A., 383Genton, P., 464Georgopoulos, A. P., 169, 170Georgopoulos, M. A., 169, 170Gerbaldo, H., 410Geschwind, M., 27Geschwind, N., 18Geva, A., 240Giacinto, J., 473Gibb, R., 272Gideon, D. A., 462Giedd, J. N., 118, 120, 324, 325Gill, M., 324Gillberg, C., 318Gillin, J. C., 107Gillispie, M., 302Gilman, S., 280Gilzenrat, M. S., 241Giordani, B., 371Giraud, A. I., 166Gitelman, D. R., 242, 246Givens, B., 241Glanzman, M., 327Glaser, G.H., 150Glidden, R. A., 23Glisky, M. L., 250Glod, C. A., 325Gloor, P., 465Goetz, C. G., 335, 424Gogtay, N., 118, 120Goldberg, E., 305–306Golden, C. J., 21, 103, 358Goldenberg, G., 429Goldman, S. A., 101, 109Goldman-Rakic, P. S., 78,
239–240, 247, 250, 274, 316Goldstein, E. B., 140, 144Goldstein, L. H., 473Goldstein, S., 286Golgi, C., 34, 35Gonzales, J. J., 304Good, C. D., 167Gooren, L. J., 173Gooren, L. J. G., 173Gordon, A., 64, 65, 84Gore, J. C., 262Gorny, G., 272Gould, J., 312Gould, S. J., 157Grabowski, T. J., 169, 170, 255Grady, C., 283Grady, D., 174Graf, P., 234Grafman, J., 282Gramling, L., 291, 292, 293
Grant, D. A., 246Grattan, L. M., 247, 273, 274Green, L. A., 312, 316, 320Greenberg, D. A., 277Greene, H., 28, 66, 78Greenhill, L. L., 322, 323Greenlaw, R., 283Greenstein, D., 118Greiner, L. H., 402Grelotti, D. J., 286, 287, 317, 318Griffith, E. M., 319Grigorenko, E. L., 300, 302Grill-Spector, K., 200Grillon, C., 262Groisser, D. B., 247, 250Grön, G., 168, 169Gronwall, D. M. A., 380Grossman, R. G., 70, 375, 376,
380, 385Growdon, J., 430Gui, Q. P., 409Gunter, J. L., 406Gur, R. C., 48, 51, 167, 446Gur, R. E., 48, 51Gurland, B. J., 409Guthrie, P. B., 100Guy, S. C, 309Gyato, K., 310, 366
Haberecht, M. F., 283Haberl, R. L., 351Haeger, K., 36, 48Hafetz, J., 168Hagerman, R. J., 286, 291Haier, R. J., 169Haines, D. E., 189, 191Hainse, J. L., 316Halgren, E., 465Hall, J., 304Hallervorden, J., 262Hallett, M., 169, 205Hallgren, B., 300Halligan, P. W., 212Halpern, D. F., 168Halpern, J. M., 325Halstead, W., 25, 80Hamburger, S. D., 325Hamilton, R., 205Hammeke, T. A., 162, 167, 169Hampson, E., 172, 174Hamsher, K. D., 74, 288Hamshet, K. D., 429Hanin, I., 412Hanson, J. W., 292Hari, R., 56Hariri, A. R., 317Harlow, H. F., 21Harlow, J. M., 255Harnadek, M. C. S., 305, 307Harper, J., 321Harris, B., 146, 343, 354Harris, J. C., 282, 293Harris, J. G., 45Harris, R. J., 319Harrower, M., 15, 25Harrowsseau, H., 291Hart, B., 324Hart, L. A., 300, 302
Name Index 553

Hartlage, L. C., 163Hartmann, J., 247Harvey, A. S., 167Harvey, T., 15Harward, H., 247Hasselbalch, S. G., 435Haug, H., 404Hauri, P., 452, 455, 458, 461, 463Hauser, P., 323Hauser, W. A., 464Hawi, Z., 324Haxby, J. V., 283Hayaski, K. M., 118Haynes, S. D., 472Haywood, C. S., 262, 263Healy, S. D., 173Heaton, R. K., 77Hebb, D. O., 20, 21, 25Heben, N., 82Hécaen, H., 26Hechtman, L. T., 330Heeger, D. J., 301Heilman, K. M., 167, 195, 210,
212Heindel, W. C., 430Heiss, G., 174Helland, T., 304Heller, K. W., 11, 18, 167Helmer, C., 409Hemenegildo, N., 412, 424Henderson, C. R., 272Henderson, V. W., 168, 173Hendrix, S., 174Hendy, J., 166, 270, 273, 280Henkenius, A. L., 324Henninger, D., 168Henry, J. D., 403Henson, R. N. A., 167Hentschel, F., 413Heraclitus, 6Herman-Liu, A., 366Hermann, B., 465, 473Hern, K., 304Herrup, K., 96Herscovitch, P., 335Hever, T., 323Hewson, J., 110, 331Hiemenz, J. R., 302, 303Hill, D. E., 324, 325Hill, M., 416Hillary, F., 55, 378Hilton, R., 429Hinckley, John Jr., 373Hippocrates, 6, 8Hiroyuki, O., 264Hirsch, H. V. B., 389Hirsch, T. B., 165Hiscock, M., 328Hitch, G. J., 302Hjlemquist, E., 318Hobbins, J. C., 293Hobson, J. A., 458, 459, 460, 461Hodges, J. R., 416Hoekstra, P. J., 335Hoien, T., 304Holiger, D. P., 287Holmes, J., 323Holmstrom, V. L., 473
Honda, H., 313Hooper, H. E., 81Hooper, S. R., 299, 304Hopyan, T., 291Hornak, J., 212, 263, 264Hornsey, H., 333Hornykiewicz, O., 431Horoupian, D. S., 411Horwitz, B., 303Houle, S., 229Howes, N. L., 302Howieson, D. B., 27, 51, 65, 82,
140, 353, 396Howlin, P.Hoyert, D. L., 409Hughes, C., 319Hughett, P., 167Hulse, S. H., 109Humphrey, L. L., 174Hungerbuhler, J. P., 48Hunter, D., 402Huntington, G., 434Hutt, M. L., 74Huttenlocher, P. R., 117, 247, 272Hyde, J. S., 167Hynd, G. W., 117, 274, 277, 279,
281, 302, 303, 304, 324
Ibañez, V., 169, 205Imperato-McGinley, J., 174Ingham, J. C., 165Ingham, R. J., 165Iqbal, K., 439Irani, D. N., 111Ivers, C. E., 337Ives, D., 87, 146Ivnik, R. J., 405, 406Izendoorn, R., 168
Jack, C. R., Jr., 406Jackson, H., 20–21, 465Jacobs, A. R., 172, 174Jacobs, D., 415Jacobs, R., 117, 167, 247, 281Jacobson, J. L., 292Jacobson, M., 389Jacobson, S. W., 292Jacoby, R., 413Jagust, W. J., 406Jahanshahi, M., 416James, E. M., 299, 304James, T. W., 168James, W., 259, 444Jane, J. A., 371, 383Janols, L-O., 330Jarrold, C., 288, 289, 319Jasper, H. H., 44Jeffires, K. J., 335Jenkins, M. R., 292, 294Jennett, B., 375, 376, 396Jensen, J., 319, 335Jensen, P. S., 322, 323Jessell, T. M., 116, 118, 301Jimenez, F., 319Joanette, Y., 255Johansson, B., 403, 404, 411Johnson, D. A., 396Johnson, S. C., 58
Johnsrude, I., 167Joly, P., 409Jones, A. W. R., 418Jones, C. M., 173Jones, E., 19Jones, K. L., 291, 292, 293, 294Jones, K. W., 282Jones, R., 317, 319Jones, Z., 287Jones-Gotman, M., 471Jonides, J., 240Jons, P. H., 324Jordon, H., 313Joy, S., 312, 316, 320Judd, T., 208Junqué, C., 277, 278, 280Jurko, M. F., 146Jusko, T. A., 272
Kaemingk, K., 293Kahn, R. S., 167Kail, R. V., 302Kalat, J. W., 34, 37, 49, 97, 100,
103, 105, 106, 111, 121, 137,138–139, 142, 143, 148, 151,182, 186, 188, 201, 216, 217,234, 457
Kalen, P., 108Kallenber, C. G. M., 335Kaminaris, C., 28, 371, 385Kanappenberger, J., 100Kandel, E., 301Kandel, E. R., 106Kane, M. J., 335Kanner, L., 311Kansaku, K., 169Kant, I., 4Kaplan, E., 82Kaplan, H. I., 12Kapur, S., 229Karacan, I., 462Karmiloff-Smith, A., 285, 288Karni, A., 459Kater, S. B., 100Katona, C., 409Katz, L. C., 128, 146Kaufer, D. I., 409Kaufman, A. S., 272, 402Kaufman, O., 264Kaufmann, P. M., 250Kaushall, P. I., 227Kawas, C., 168Kawasaki, H., 264Kay, D. W. K., 409, 424Kay, G. G., 77Kaysen, D., 324, 325Kazak, A. E., 366Keane, M. M., 235Kedersha, N., 100Keenan, J. P., 446Kemp, S., 294Kemper, T. L., 404Kemper,S. J., 402Kennard, M., 272Kennedy, C. H., 15, 29, 386–387Kennedy, D., 324Kennedy, Michael, 371Keraclitus, 6
Kerns, K. A., 250, 256, 291, 293,294
Kerr, D. A., 111Kertesz, A., 389Kesler, S. R., 283Kettunen, S., 292, 294Kety, S. S., 48Khan, F., 146, 343, 354Kibby, M. Y., 302Kiehl, K. A., 165Kietrich, K. N., 272Kigar, D. L., 15Killeffer, E. H., 409Kilpatrick, L., 169Kim, S. W., 255, 256Kim, Y. H., 242, 246Kimberling, W. J., 300Kimura, D., 168King, G., 196Kinsbourne, M., 214Kinsella, G., 396Kippenhan, J. S., 289Kirk, U., 294Kitazawa, S., 169Kitchen, G., 409Klatt, E. C., 411, 412, 425Klein, B. P., 288Klein-Tasman, B. P., 288, 290Kleinman, J., 317, 318Kleist, K., 24Klin, A., 312, 313, 315, 316, 317,
318Klunk, W., 409Knaus, T. A., 167Knecht, S., 162, 167, 169Knight, R. T., 238, 256Knight, S., 460Knopman, D. S., 406, 412Knowlton, B. J., 231, 235, 236Koch, C., 445, 448Koeppe, R. A., 240Koff, E., 262, 263Kohn, P., 289Kokmen, E., 405Kolb, B., 116, 124, 158, 159, 160,
163, 168, 272, 273, 276, 315Koller, K., 272Kooperberg, C., 174Kopp, U., 412Korczyn, A. D., 409Korf, J., 335Korkman, M., 292, 294Korol, D., 174Kovach, C., 264Kozel, S. T., 324Kozinska, D., 44, 46, 54, 58, 359Kozlowski, G. P., 473Krakauer, J., 341Kramer, A. F., 405Krasuski, J. S., 404Kravits, D. O., 460Krawiecki, N., 366Kraywinkel, K., 351Krech, D., 18–19, 21Kringelbach, M. L., 263Kuller, L., 174Kunin-Batson, A., 327Kunkel, D., 97
554 Name Index
Kupfermann, I., 141Kurth, T., 351Kushner, H., 283, 284Kuter, K. C., 174Kutner, K. C., 172Kwitny, S., 288, 290Kwon, H., 317
LaBar, K. S., 242, 246LaBerge, S., 453Labiner, D., 465Lai, Z., 287, 290Laitinen, V., 146LaMantia, A., 128LaMantia, L. C., 146Lambrecht, L., 318Lanbphear, B. P., 272Lancisi, G., 11Landry, S. H., 277Lane, D. S., 174Lang, A. R., 294Lange, C., 259Langleben, D. D., 446Lantigua, R., 409LaPira, F., 429Larsen, B., 191Larsen, J. P., 304Larson, J., 459Larsson, M., 168, 402LaRue, A., 413Lashley, K., 20Lassen, N. A., 191Lawrence, C., 169Laws, G., 287Lawson, J. S., 302, 319Le Courteur, A., 318Leckman, J. F., 332, 333, 334,
335Lecours, A. R., 255LeDoux, J. E., 150, 259–260, 261Lee, G., 195Lee, H. C., 404Lee, K. T., 294Lee, P., 464Leech, R. W., 116Leekam, S., 312Lees, A. J., 429Legault, C., 174Leiguarda, R. C., 195Lemen, L. C., 167Lemire, R. J., 116Lemke, G., 101Lemoine, P., 291Leonard, L. B., 302Letenneur, L., 409Leventhal, B. L., 318Levin, B. E., 430Levin, H. S., 70, 247, 375, 379,
380, 385Levine, B., 226Levitin, D. J., 287, 290Levitsky, W., 27Levy, J., 51, 167Levy, L., 272Levy, R., 413Lezak, M. D., 27, 51, 65, 82, 140,
353, 365, 396Li, C. S., 214
Li, X. H., 409Liberzon, I., 171Libon, D., 417Lichter, D. G., 258, 325Liddle, P. F., 165Liebenauer, M. A., 324Lieberburg, I., 174Lifton, R. J., 15Lim, K. O., 118Lima, 25Limacher, M., 174Lin, J., 405Lincoln, A., 287, 290Linden, M. G., 285Linnoila, M. I., 108Lippe, B., 283Lisowski, F. P., 5Litchter, D. G., 255Little, S. S., 309Litvan, I., 409Livet, M. O., 288Livingston, G., 409Livingstone, M., 301Lladó, J., 111Llinas, R., 448Lloyd, S., 460Lockhart, P., 325Loeser, J. D., 116Lohmann, H., 162, 167, 169Lois, C., 110Lombroso, P. J., 117Long, C. J., 302Lopez, O. L., 406, 409Lord, C., 318Lord,C., 312, 313, 316Loring, D. W., 27, 51, 65, 82,
140, 195, 353Lorys, A. R., 304, 324Lotspeich, L., 317Loughead, J. W., 446Loveland, K. A., 328Lovell, M. R., 383Lowe, J. B., 285Lowry, L. D., 187Lucci, K., 365Lund, L., 473Lupien, S. J., 405Luria, A. R., 21–22, 24, 81, 82,
150, 179Lusk, L., 118Lynch, G., 459Lyon, G. R., 303
M’Lan, C. E., 409Macciocchi, S. N., 383MacDonald, A. W., 257Macintoch, K. E., 313, 318Macko, K. A., 204MacLean, P. D., 260MacLeod, M., 403Macmillan, M., 255Madison, A., 45Magnus, A., 8Mai, J. K., 157Maier, S., 293Majovski, L. V., 120Malach, R., 200, 205Malamut, B., 196, 234, 237
Malamut, B. L., 432–433Mallory, M., 405Mancini, J., 288Mandel, R. J., 108Manela, M., 409Manson, J. E., 174Maquet, C. D., 243Maragakks, N. J., 111Marans, W. D., 315, 316Marder, K., 412, 424Marie, P., 20Marino, B. S., 277, 281, 282Marks, D. J., 325Marks, W., 302Marois R., 317, 318Marriott, A. J., 283, 284Marsden, C. D., 416Marsh, W. L., 324, 325Marshall, J. C., 212Marshall, L. F., 380Marshuetz, C., 240Martier, S. S., 292Martin, C., 165Martin, D., 323Martin, J. H., 116, 118, 120Martinez, A. J., 412Martinez, P., 323Martini, D. R., 327Masliah, E., 405Mason, C., 301Massman, P., 323, 334Mataró, M., 277, 278, 280Mateer, C. A., 256, 291, 293,
294Mathalon, D. H., 118Matochik, J. A., 323Matsui, M., 167Mattingly, J. B., 189, 191, 196,
209, 211, 212, 213, 214, 218,220, 412, 425, 428, 435, 436
Mattson, A. J., 247Mattson, M., 111Mattson, S. N., 291, 292, 293,
294Maurer, K., 410Maximin, A., 342Mayes, S. D., 313Mayeux, R., 409, 412, 424Mazziota, J. C., 50Mazzocco, M. M. M., 283McAuley, E., 174McCandliss, B. D., 245McCleary, C. A., 168, 173McCormick, C. M., 173McCormick, P. A., 170McCracken, J. T., 322McDaniel, M. A., 402McDiarmid, M. D., 250McDonough, L., 311McDougle, C. J., 322McDowell, S., 245McGaugh, J. L., 260McGough, J. J., 323McIntosh, G. C., 468McIntosh, J. P., 226McKeever, W. F., 168, 170McKinlay, B. D., 336McLardy, T., 150
McLean, J. E., 402McMenamin, D., 287McMillian, J. A., 277, 281, 282McNamara, J. O., 128, 146McNulty, K., 409McPherson, M. W., 20McxCarthy, R. A., 235Meador, K. J., 195Meadows, A. T., 366Meehl, P., 82, 83Meeske, K., 366Melin, L., 473Mencel, W. E., 304Menon, V., 283, 317Mentis, M. J., 283, 404Menuet, J. C., 291Merabet, L. B., 205Merello, M., 195Mervis, C. B., 285–286, 287, 288,
289, 290Merz, P. A., 439Messa, C., 283Mesulam, M. M., 214, 240, 242,
243, 246Meyer, J. R., 242Meyer, M. S., 300, 302Meyer-Lindenberg, A., 289Meyer. J. S., 107Meyers, P. S., 167Middleton, F. A., 252Mikiewicz, O., 281Milberg, W. P., 82Miller, A., 405Miller, C. A., 302Milner, B., 150Minderaa, R. B., 335Mink, J., 301Minoshima, S., 240Minshew, N. J., 318Mintun, M. A., 240Minzer, K., 335Mirsky, A. F., 242, 245, 246, 326,
327Mishkin, M., 196, 204, 234, 236,
237Mitchell, D. R. D., 403Mixon, A. J., 323Mobbs, D., 317Modahl, C., 312, 320Moffat, S. D., 172Mohamed, F. B., 446Mohn, K., 173Mohr, J. H., 324Mohr, J. P., 346Mollowy, E., 325Molloy, P., 366Moniz, A. C. E., 25Monk, C. S., 116, 117Montenegro, L., 367Monuteaux, M. C., 323Moore, A. M., 107Moore, K., 271Moossy, J., 412Morecraft, R. J., 254Morgan, A. E., 117, 274, 277,
279, 281, 302Morgan, S., 302Morrell, M. J., 257
Name Index 555
Morris, C. A., 285–286, 288, 289,290
Morris, J. D., 204Morris, J. S., 262Morris, R. D., 366Morris, R. G., 319Morrow, J. D., 405Mortimer, J. A., 402Moscovitch, M., 229, 238Moser, R. S., 381Mostofsky, S. H., 325Mueller, F. O., 382Mullan, S., 465Mullarkey, S., 283Muller, R., 120Munk, H., 20Munro Culum, C., 415Murias, M., 328Murphy, D. G., 283Murray, A. M., 424Murray, H. W., 110–111Muzio, J. N., 455
Nagai, Y., 473Nagamoto, H., 45Nair, N. P., 405Nakamura, R., 448Nalcioglu, O., 328Nanayakkara, N., 402Naugle, R. I., 95, 343, 372Nauta, W. J. H., 231Naylor, C. E., 302Nedergaard, M., 101Nehme, E., 314Nelson, C. A., 116, 117Nelson, D. F., 364Nelson, H. D., 174Nelson, L. M., 424Neppe, V. M., 465Netter, F. H., 145Newcorn, J. H., 325Newman, A. C., 196Newman, S. W., 280Newton, A., 396Nezu, C. M., 323Nichols, M., 195Nicoletti, F., 429Nicolson, R., 336Nigg, J. T., 271, 329Nikelski, E. J., 166Nissanov, J., 52Nissl, F., 34–35Noback, C. R., 148Nobre, A. C., 242, 243, 246Nockleby, D. M., 397Nogues, M., 195Noll, D. C., 257Nordahl, T. E., 162Northam, E., 117, 166, 270, 273,
281Northrup, H., 277, 280Norton, A. M., 328Nottebohm, F., 109Nouzeilles, M. I., 195Novey, E. S., 304, 324Nuechterlein, K. H., 242Nuland, S. B., 343Nurmi, E. L., 313, 316
Nyberg, L., 229, 253, 258, 330Nyden, A., 318Nygren, P., 174
O’Brien, P. C., 406O’Connor, K. J., 262O’Doherty, J., 263O’Donnell, V. M., 70O’Neal, J. H., 106O’Riordan, M., 317, 319Öberg, C., 168Oberg, G., 435Obrist, W. D., 48Ockene, J. K., 174Odegaard, H., 304Ogden, J. A., 214Öhman, A., 262Ojemann, G. A., 46Olanow, C. W., 425Oldfield, R. C., 162Olds, S. W., 115Olsen, R. K., 289Olson, L., 420Ommaya, A. K., 383Oommen, K. J., 465Oosterlaan, J., 328Osborn, L. M., 335Osborne, L., 286, 287Osler, W., 25Ostbye, T., 409Osterrieth, P. A., 75, 77Ozonoff, S., 318, 319, 326, 335
Palmer, C. G., 323Palmer, P., 321Palmon, R., 403Palov, I., 396Palumbo, D. R., 335Pantelis, C., 323, 334, 335Panyavin, I. S., 446Papalia, D. E., 115Papez, J. W., 231Paquette, A., 293Paradiso, M. A., 180, 194, 261Pargman, D., 384Parke, L. A., 299Parnell, S. E., 293Parrish, T. B., 242, 246Pascual-Leone, A., 205Paterniti, M., 102Paterson, A., 211Patient Alice, 468–469Patient Anna O., 47Patient Auguste D., 410Patient B. C., 327Patient Bertha, 437Patient David, 86–87Patient Dr. P., 207Patient Frank, 377Patient George, 196Patient H. M., 229, 234–235Patient Jeanne, 63Patient John, 386–387Patient Jonathan, 206Patient K. F., 237–238Patient Leborgne, 17Patient Lisa, 366–367Patient M. J., 432–433
Patient Mr. S., 419Patient Mr. T, 417Patient Mrs. C., 414Patient Mrs. R., 414Patient N. A., 227, 231Patient Phineas Gage, 255, 259Patient S. B., 275–276Patient T. J., 254Patient Theresa, 386–387Patient Tom Z., 313, 314–316Patient U., 253–254Patrick, R., 401Pattie, A., 402Patwardham, A., 283Pauls, D. L., 333, 334Pavlides, C., 459Pavlovic, J., 283Pavolic, J., 284Paxinos, G., 157Payton, A., 323Peake, T., 365Pearlson, G., 314Pearson, D. A., 328Peck, A., 411Peele, T. L., 202Pelletier, P. M., 307, 308Pellman, E. J., 383Penfield, W., 25, 44, 150, 183,
465, 472Pennington, B. F., 247, 250, 251,
284, 299, 300, 301, 302, 305,313, 319, 320, 321, 322, 326,334, 336
Penny, J. B., 435Perry, W., 78Persaud, T., 271Persutte, W. H., 293Petersen, R. C., 405, 406Petersen, S. E., 204, 207, 240Peterson, A. C., 110, 331Peterson, B. S., 324, 333, 334,
335Petitto, L. A., 166Petri, H. L., 236Petrides, M., 240Petropoulos, H., 324Pfefferbaum, A., 118Pfrieger, F. W., 101Phan, K. L., 171Phelps, E., 50Phelps, E. A., 262Phend, N., 446Phillips, L., 403Phillips, P.C., 310, 366Phillips, S. M., 174Phillips, W., 311Piaget, J., 248Pianka, P., 205Pichardo, M., 174Pietrini, P., 283Piggot, J., 317Pilgrim, D. M., 424Pillon, B., 427, 429, 430Pincus, J. H., 95, 150Pinel, P. J., 190, 230, 232–233,
457Piven, J., 314, 321Plaisted, K., 317, 319
Platek, S. M., 446Plato, 4, 6Pliszka, S. R., 299, 324Pober, B., 286, 287Poca, M. A., 277, 278, 280Polani, P. E., 282Polcari, A., 325Polkey, C. E., 319Polster, M. R., 107Pons, T., 185Poppel, E., 389Popplestone, J. A., 20Portin, R., 428Posner, J., 364Posner, M. I., 240, 243, 244, 245,
326, 327, 328Postma, A., 168Potegal, M., 436Pouk, J. A., 396Powell, M. P., 284, 285Power, T. J., 323Powers, W. J., 344, 345Pratt, P., 335Presley, R., 304Preston, J. D., 106Pribram, K. H., 150Price, C. J., 166Prigatano, G. P., 396, 397Primeua, M., 327Prior, J., 313Prior, M., 312Pritchard, P. B., 473Pruisiner, S. B., 439Pugh, K. R., 167, 169, 303, 304Purcell, E., 51Purcell, R., 323, 334, 335Purves, D., 128, 146Purves, K. L., 329Pythagoras, 6
Quenzer, L. F., 107
Radcliffe, J., 366Raichle, M. E., 49, 207Rakic, P., 117Ranamurthi, B., 150–151Ransom, B., 101Rao, G. R., 412Rao, M. S., 111, 167, 169Rapp, S. R., 174Raskin, S. A., 427, 428Rasmussen, T., 40, 470Rawles, J. M., 118Raz, A., 245Raz, N., 205, 404, 405Read, S., 416, 417Reader, M. J., 325Reagan, Ronald, 373Rebok, G. W., 407Rees, J. R., 15Reilly, J., 274Reisberg, B., 406Reiss, A. L., 283, 287, 325Reitan, R. M., 25, 71, 80, 183,
246, 353Reiter, J., 466Relkin, N., 412Renshaw, P., 324, 325
556 Name Index
Rey, G. J., 75, 173, 281, 430Reynolds, B. A., 110, 331Reynolds, C. R., 163, 252, 279,
286, 396–397, 402Rhodes, R., 437Richard, A., 466Richardson, J. S., 418Richter, K., 169, 170, 323Richters, J. E., 322Riepe, M. W., 168, 169Riley, E. P., 291, 292, 293, 294Rimel, R. W., 371, 383Ring, H. A., 319Ringelstein, E. B., 167Rinne, U., 428Ris, M. D., 272Risi, S., 318Risser, A. T., 270, 272, 281Ritzler, B., 15Rivero, A., 195Rizzo, J. R., 205Robbins, T. W., 254, 319Robert, A. C., 254Roberts, J. E., 168, 169, 170Robertson, M. M., 333, 335Robinson, A., 285Robinson, B. F., 287Robinson, B. W., 287Robinson, D. L., 204Rockwood, K., 409Rodgers, M. A., 170Roe, K., 274Roeltgen, D. P., 283, 284Roffwarg, H. P., 455Rogers, S. J., 311, 319Roland, P. E., 191Rolls, E. T., 186, 256, 263, 264Romans, S. M., 283, 284Romanski, L. M., 316, 317Romine, C. B., 252Röntgen, W. C., 36Ropper, A. H., 142Rose, V., 342, 462Rosen, A. D., 48Rosenberg, H. M., 409Rosenblum, J. A., 150Ross, E., 431Ross, J. L., 283, 284Rosser, A. E., 111Rosvold, H. E., 246Rotman, M., 364Rourke, B. P., 298, 305, 306, 307,
308, 309, 318Rousseau, A., 473Rovee-Collier, C., 236Rovet, J. F., 174, 283, 284, 285Rowe, A. D., 319Rowe, D. C., 324Rowland, L. P., 278Roy, A., 108Rubens, A. B., 208Rubenstein, B. S., 459Rubin, A. J., 440–441Rubin, L., 278Ruchinskas, R. A., 381Ruff, R. M., 380–381Rumsey, J. M., 299, 301, 303,
311
Ruparel, K., 446Rusconi, M. L., 212Russell, J., 319Russell, W. R., 150Rutherford, M. D., 311, 319Rutledge, N., 315Rutter, M., 313, 318Rutter, W., 311Ryan, T. V., 383
Sabb, F. W., 257Sach, M. L., 384Sache-Lee, C., 302Sacks, O., 184, 206, 207, 259Sadato, N., 169, 205Sadock, B. J., 12Sadovnick, A. D., 98Sagar, H., 430Sagi, D., 459Sahuquillo, J., 277, 278, 280Saint-Cyr, J. A., 252Saitoh, O., 316Sakamoto, M., 173Salmon, D. P., 415, 416, 430Salo, R., 162Salthouse, T. A., 403Sampson, P. D., 292, 293, 294Samuel, W., 405Sandberg, A. D., 318Sanders, G., 173Sandroni, P., 212Santi, S., 405Santoro, J. M., 396Saper, C. B., 456Sarason, I., 246Sarter, M., 241Saucier, D. M., 167Saunders, A. M., 412Sawaya, G., 174Scahill, L., 322, 335Scalf, P., 174Schacter, D. L., 227, 234, 235,
236Schatschneider, C., 302Schatz, P., 381Schechter, R., 411Schiller, F., 17, 149Schmahmann, J., 406Schmechel, D. E., 412Schmidt, J. F., 435Schmitt, J. E., 287Schnaberth, G., 429Schneider, J. A., 28, 371, 385, 405Schneider, W., 55Schoenbach, C., 335Schooler, C., 335Schreibman, L., 311Schubert, A. B., 325Schuck, S., 328Schulte, T., 284, 285Schultz, K. P., 325Schultz, R. T., 286, 287, 312, 313,
315, 316, 317, 318, 325, 333,335
Schwartz, J. H., 106, 301Scott, C. B., 364Scoville, W. B., 150Segal, M., 100
Seldon, G., 448Selman, W. R., 131Selz, M., 299, 304Semendeferi, K., 254Semrud-Clikeman, M., 304, 324Seshadri, S., 409Seurinck, R., 169, 170Shallice, T., 237, 320Shaman, P., 189Shamblott, M. J., 111Shannon, K. M., 424Sharp, W., 325Shatz, M. W., 345, 351Shaw, D. W., 317Shaywitz, B. A., 167, 169, 301,
303, 304Shaywitz, S. E., 167, 169, 301,
303, 304Shen, C., 406Sheppard, D. M., 323, 334, 335Sherman, G. F., 287Sherman, S. L., 324Sherwin, B. B., 174Shimizu, Y., 313Shiung, M. M., 406Shults, C. W., 430Shumaker, S. A., 174Shuster, A., 300, 302Siegel, L. S., 299Siegel-Hinson, R. I., 168, 170Sigman, M., 317, 321Silverman, I., 168Silverstein, S. M., 335Simon, R. P., 277Sinder, M., 226Singer, H. S., 325, 335Singh, J., 335Sitaram, N., 107Sjöstrand, L., 108Skinholf, E., 191Skinner, B. F., 396Skottun, B. C., 299Skovronek, E., 403Skudlarski, P., 167, 169, 304Slabbekoorn, D., 173Small, B. J., 402Small, G. W., 412Smalley, S. L., 323Smernoff, E., 45Smirni, P., 429Smith, A., 72Smith, C. A., 168, 173Smith, C. C., 413Smith, D. W., 185, 291, 292Smith, E. E., 240, 429Smith, G. E., 405, 406Smith, J., 336Smith, S., 284Smith, S. D., 300Snead, O. C., 468, 472Snowdon, D. A., 402Snyder, A. Z., 207Snyder, J. L., 384Snyder, L. H., 214Sokol, R. J., 292Soliveri, P., 416Somers, D. C., 205Somerville, R. A., 439
Sommer, I. E. C., 167Sommer, T., 245Sorensen, S., 435Sowell, E. R., 324Sparks, E. R., 317Sparrow, S., 315, 316Speed, W. C., 300, 302Spence, M. A., 328Spencer, T. J., 322Sperry, R. W., 151Spiers, M. V., 21, 103, 109, 173,
179, 184–185, 211, 227, 358,396, 410, 414, 435, 438,453–454
Spillane, J. A., 413Spinnler, H., 237Spitzer, M., 168, 169Spohr, H. L., 294Spreen, O., 270, 272, 281, 288,
429Springer, J. A., 162, 167, 169,
255Springer, S. P., 51, 151Spurgeon, A., 272Spurzheim, J., 14Spyker, D., 365, 367Squire, L. R., 227, 231, 234, 235,
236, 237Squrie, L. R., 415Stahl, S. M., 108Stahmer, L., 311Stanczyk, F. Z., 168, 173Stangl, D. K., 333Starkstein, S. E., 314Starr, J. M., 402Stebbins, G. T., 335Stein, B. M., 346Stein, J. F., 299Steingard, R., 324Steinhausen, H. C., 294Stelmack, R. M., 307Stenger, V. A., 257Stern, C., 294Stern, Y., 409, 412, 424Stevens, T., 409Stevens-Graham, B., 101Stewart, B., 383Stiles, J., 273, 274Stone, B. H., 299Stone, V., 317, 319Storili, O. V., 385Stowe, R., 409Strang, J. D., 308, 309Strassburger, T. L., 404Straus, E., 287Streissguth, A. P., 291, 292, 293,
294Stricanne, B., 214Strick, P. L., 252Strittmatter, W. J., 412Stroop, J. R., 246Stuber, M. L., 366Stuss, D. T., 238, 251, 256, 320Succop, P. A., 272Sullivan, E. V., 118, 430Sullivan, K., 287Surrat, P. M., 462Sutcliffe, J. S., 313, 316
Name Index 557

Svendsen, C. N., 111Swanik, C. B., 384Swanson, H. L., 301, 302, 328Swanson, J., 328Swanson, S. J., 162Szczepaik, J., 404
Tadevosyan-Leyfer, O., 316Tagaris, G. A., 169, 170Tager-Flusberg, H., 287Talaga, M. C., 106Talley, J. L., 77Tamm, L., 283Tang, M. X., 325, 412, 424Tangalos, E. G., 405Tanguay, P. E., 311, 313, 316,
321, 323Tanne, D., 459Tannock, R., 329Tarshish, C., 405Tatton, W. G., 425Taylor, S. F., 171Teasdale, G., 375, 376, 396Teicher, M. H., 325Teillon, S. M., 173Temple, C. M., 283, 284, 288Terry, R. D., 407, 411, 413Teuber, H. L., 18, 20, 25Teutsch, S. M., 174Thagard, P., 257Thal, D., 274Thal, L., 174Thiede, K., 292Thiele, E. A., 472Thomas, K. M., 120Thomas, P., 335Thompsen, I. V., 396Thompson, P. M., 324Thompson, S. J., 311Tierney, E., 322Tinker, J., 28, 371, 385Toga, A. W., 324Tombaugh, T. N., 78Tomczak, R., 168, 169Tomer, R., 430Tonucci, F., 287Toole, J. F., 346Toth, J. P., 226Tottenham, M., 334, 335Townsend, J. P., 316Tran, T., 325Tranel, D., 169, 170, 253, 255,
256, 257, 258, 262Träskmann, L., 108Trauner, D., 274Trenholme, I., 460Treves, T. A., 409Trimble, M. R., 473Troster, A. I., 415Trumpter, A. L., 323Tsatsanis, K. D., 316, 317Tucher, A. M., 383Tuciker, D., 328Tucker, G. J., 95Tulandi, T., 174Tulving, E., 228, 229Turetsky, B. I., 167Turner, Tina, 401
Tweed, D. L., 333Tweedy, J., 427, 428Tysvaer, A. T., 385
Ueckert, S., 432Ulleland, C. N., 291Ullrich, O., 282Ullsperger, M., 257Ungerleider, L., 204
Vaituzis, A. C., 118Vaituzis, C. V., 324, 325Valenstein, E., 23, 210, 212Vallar, G., 212, 237van de Poll, N. E., 173Van den Broeck, W., 299Van der Gaag, C., 317, 318van Emde Boas, W., 464van Goozen, S. H., 173Van Hoesen, G. W., 218, 254,
411Van Raalte, J. L., 42Vandenberghe, R., 243Vanneste, J. A. L., 130, 131Varney, N. R., 288, 429Vaughn, M., 117, 274, 277, 279,
281Venneri, A., 310Verrees, M., 131Vesalius, A., 8–9Viano, D. C., 383Vicarti, S., 287Victor, M., 98, 142Vienbergs, I., 405Vigil, J., 324, 325Vignolo, L. A., 74Vilkki, J., 146Villardita, C., 429Vingerhoets, G., 169, 170Vining, E. P., 472Virchow. R., 344Virues-Ortega, J., 342Vitiello, B., 323Voeller, K. K. S., 308Vogt, B. A., 257Vogt, M. B., 185Volk, S., 410Volkmar, F. R., 312, 313, 315,
316, 317, 318Volterra, V., 287von Cramon, D. Y., 257von Monakow, C., 388von Senden, M., 205von Stockert, F. G., 426Vonsattel, J. P., 435von Steinbuchel, N., 389Vouloumanos, A., 165Voyer, D., 167, 168, 169, 170,
174Voyer, S., 167, 168, 169Vygotsky, L. S., 21
Waber, D. P., 273Wada, J., 40, 470Wade, D., 264Waechtler, C., 146, 343, 354Wagar, B. M., 257Wager, T. D., 171, 257
Wagner, M., 351Wahlin, A., 402Wakely, J., 99Waldemar, G., 435Waldman, I. D., 324Waldo, M., 45Walker, J. F., 473Walker, Z., 409Wallace, R. B., 174Wallcke, P. A., 430Wallesch, C., 255Walt, V., 172Walter, J. M., 325Walter, R. D., 465Walton, J. N., 348Wang, A. T., 317Wang, L. N., 409Wang, Q. S., 405Wapner, W., 208Ware, J. C., 342, 462Waring, S. C., 405Warosfsky, I. S., 283Warrington, E. K., 235, 237Warsofsky, I. S., 283Wass, T. S., 293Wassertheil-Smoller, S., 174Waterhouse, L., 312, 316, 320Watkins, J. M., 283Watson, J., 20, 212, 445Watson, T., 304Wattam-Bell, J., 289Watts, C., 111Watts, J. W., 22, 25Webb, A. G., 405Webb, S. J., 116, 117Webbe, F., 385Wechler, D., 246Weigand, S. D., 406Weimar, C., 351Weinand, M. F., 465Weinberger, D., 49Weiner, J., 335Weiskrantz, L., 254Weiss, G., 330Weiss, M., 331Weiss, S., 110Weiten, W., 228, 455Weksberg, R., 291Welch, M. C., 247, 250Welcome, S. E., 324Wells, S., 14Weng, X-C, 325Werker, J. F., 165Wernicke, C., 18, 25West, J. R., 293West, L. L., 335Wexler, A., 434Whalley, L. J., 402Whang, K., 169, 170Wheatley, M., 110, 331Wheelwright, S., 319Whishaw, I. Q., 168, 276, 315White, B. J., 283White, C. D., 283White, N. S., 169White, R., 409Whitman, S., 473Whyte, J., 245, 395
Wickramaserkera, I., 122Wigal, S., 328Wilder, D. E., 409Wilens, T. E., 323Wilkins, R. H., 18Willerman, L., 315William, S. D., 146William, S. M., 128Williams, J. C. P., 285Williams, R. L., 462Williams, R. W., 96Williams, S. C., 319Willis, A. L., 408, 426Willis, K. E., 278, 279,
281Willis, T., 11, 131Willis, W. G., 277, 299Willms, J., 294Wilson, R. S., 335, 405Wilson, S. A. K., 426Wimmer, A., 429Wing, L., 312Winner, E., 287Winocur, G., 238Winson, J., 458, 459Wiser, J., 367Wishaw, I. Q., 124, 158, 159,
160, 163Wisneiwski, H. M., 439Witelson, S. F., 15Witol, A., 385Wohl, C., 110, 331Wolf, P. A., 409Wolff, H., 21Wolfson, C., 409Wolfson, D. B., 25, 71, 80, 183,
353, 409Wood, E., 460Wood, F. B., 299, 300, 302Wood, M. H., 299Wrennall, J., 166, 270, 273,
280Wright, R., 19Wrightson, P., 380Wunderlich, A. P., 168, 169Wundt, W., 445Wyler, A. R., 465
Xu, Y., 406
Yaffe, K., 174Yaffee, L. S., 328Yamura, A., 169Yan, M., 167Yang, L., 325Yao, R. A., 325Yatsu, F. M., 346Yeo, R. A., 324Yeterian, E. H., 218Young, A. B., 435Young, I. M., 187Youpa, D., 328Yousem, D. M., 364Yunkin, D., 48
Zaccai, J., 424Zahory, E., 205Zaichik, D., 406
558 Name Index
Zald, D.H., 255, 256Zamerkin, A. J., 323Zametkin, A. J., 324Zang, Y-F., 325Zangwill, O. L., 27, 211Zanobio, M. F., 237Zappala, G., 429Zarit, S. H., 403
Zatorre, R. J., 166Zec, R. F., 417, 420Zeitlin, H., 333Zeki, S., 204Zelko, F., 327Zeng, Y-W., 325Zetin, M., 227Zhang, H., 335
Zhou, J. N., 405Zhu, M. W., 409Zihl, J., 204Zillmer, E. A., 15, 19, 21, 22, 23,
28, 29, 36, 37, 38, 42, 52, 53,64, 65, 66, 72, 73, 74, 75, 77,78, 84, 86–87, 98, 103–104,122, 146, 156–157, 196,
250–251, 327, 341, 342, 343,346, 348, 354–355, 358, 365,367, 371, 373–374, 381, 384,462
Zin, Z., 325Zipursky, R. B., 118Zola-Morgan, S., 231Zubenko, G. S., 412
Name Index 559

This page intentionally left blank
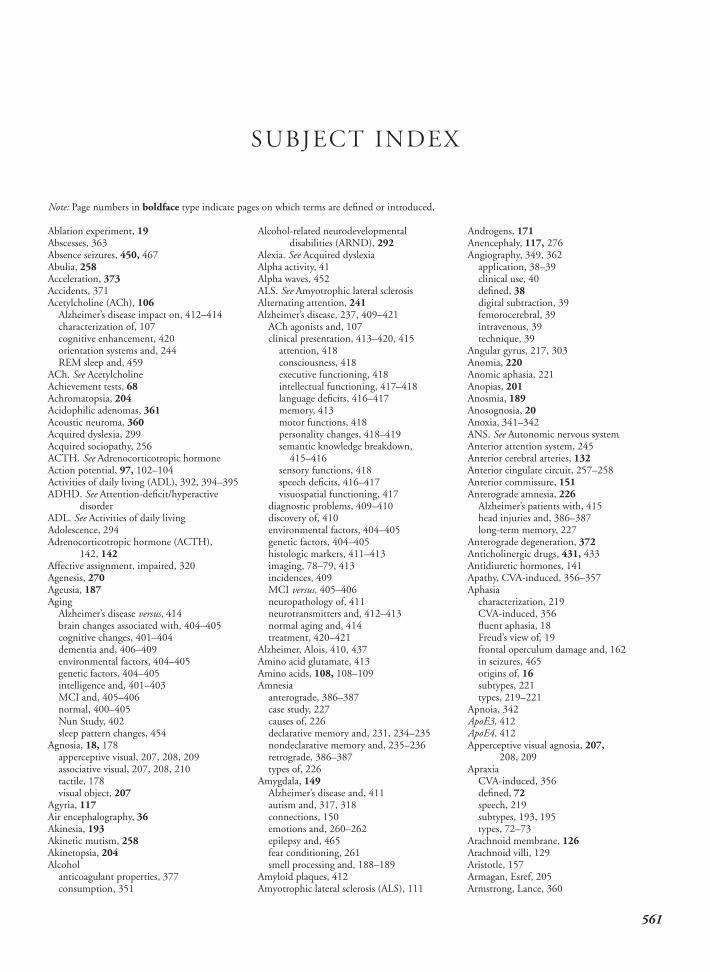
Ablation experiment, 19Abscesses, 363Absence seizures, 450, 467Abulia, 258Acceleration, 373Accidents, 371Acetylcholine (ACh), 106
Alzheimer’s disease impact on, 412–414characterization of, 107cognitive enhancement, 420orientation systems and, 244REM sleep and, 459
ACh. See AcetylcholineAchievement tests, 68Achromatopsia, 204Acidophilic adenomas, 361Acoustic neuroma, 360Acquired dyslexia, 299Acquired sociopathy, 256ACTH. See Adrenocorticotropic hormoneAction potential, 97, 102–104Activities of daily living (ADL), 392, 394–395ADHD. See Attention-deficit/hyperactive
disorderADL. See Activities of daily livingAdolescence, 294Adrenocorticotropic hormone (ACTH),
142, 142Affective assignment, impaired, 320Agenesis, 270Ageusia, 187Aging
Alzheimer’s disease versus, 414brain changes associated with, 404–405cognitive changes, 401–404dementia and, 406–409environmental factors, 404–405genetic factors, 404–405intelligence and, 401–403MCI and, 405–406normal, 400–405Nun Study, 402sleep pattern changes, 454
Agnosia, 18, 178apperceptive visual, 207, 208, 209associative visual, 207, 208, 210tactile, 178visual object, 207
Agyria, 117Air encephalography, 36Akinesia, 193Akinetic mutism, 258Akinetopsia, 204Alcohol
anticoagulant properties, 377consumption, 351
Alcohol-related neurodevelopmentaldisabilities (ARND), 292
Alexia. See Acquired dyslexiaAlpha activity, 41Alpha waves, 452ALS. See Amyotrophic lateral sclerosisAlternating attention, 241Alzheimer’s disease, 237, 409–421
ACh agonists and, 107clinical presentation, 413–420, 415
attention, 418consciousness, 418executive functioning, 418intellectual functioning, 417–418language deficits, 416–417memory, 413motor functions, 418personality changes, 418–419semantic knowledge breakdown,
415–416sensory functions, 418speech deficits, 416–417visuospatial functioning, 417
diagnostic problems, 409–410discovery of, 410environmental factors, 404–405genetic factors, 404–405histologic markers, 411–413imaging, 78–79, 413incidences, 409MCI versus, 405–406neuropathology of, 411neurotransmitters and, 412–413normal aging and, 414treatment, 420–421
Alzheimer, Alois, 410, 437Amino acid glutamate, 413Amino acids, 108, 108–109Amnesia
anterograde, 386–387case study, 227causes of, 226declarative memory and, 231, 234–235nondeclarative memory and, 235–236retrograde, 386–387types of, 226
Amygdala, 149Alzheimer’s disease and, 411autism and, 317, 318connections, 150emotions and, 260–262epilepsy and, 465fear conditioning, 261smell processing and, 188–189
Amyloid plaques, 412Amyotrophic lateral sclerosis (ALS), 111
Androgens, 171Anencephaly, 117, 276Angiography, 349, 362
application, 38–39clinical use, 40defined, 38digital subtraction, 39femorocerebral, 39intravenous, 39technique, 39
Angular gyrus, 217, 303Anomia, 220Anomic aphasia, 221Anopias, 201Anosmia, 189Anosognosia, 20Anoxia, 341–342ANS. See Autonomic nervous systemAnterior attention system, 245Anterior cerebral arteries, 132Anterior cingulate circuit, 257–258Anterior commissure, 151Anterograde amnesia, 226
Alzheimer’s patients with, 415head injuries and, 386–387long-term memory, 227
Anterograde degeneration, 372Anticholinergic drugs, 431, 433Antidiuretic hormones, 141Apathy, CVA-induced, 356–357Aphasia
characterization, 219CVA-induced, 356fluent aphasia, 18Freud’s view of, 19frontal operculum damage and, 162in seizures, 465origins of, 16subtypes, 221types, 219–221
Apnoia, 342ApoE3, 412ApoE4, 412Apperceptive visual agnosia, 207,
208, 209Apraxia
CVA-induced, 356defined, 72speech, 219subtypes, 193, 195types, 72–73
Arachnoid membrane, 126Arachnoid villi, 129Aristotle, 157Armagan, Esref, 205Armstrong, Lance, 360
SUBJECT INDEX
Note: Page numbers in boldface type indicate pages on which terms are defined or introduced.
561
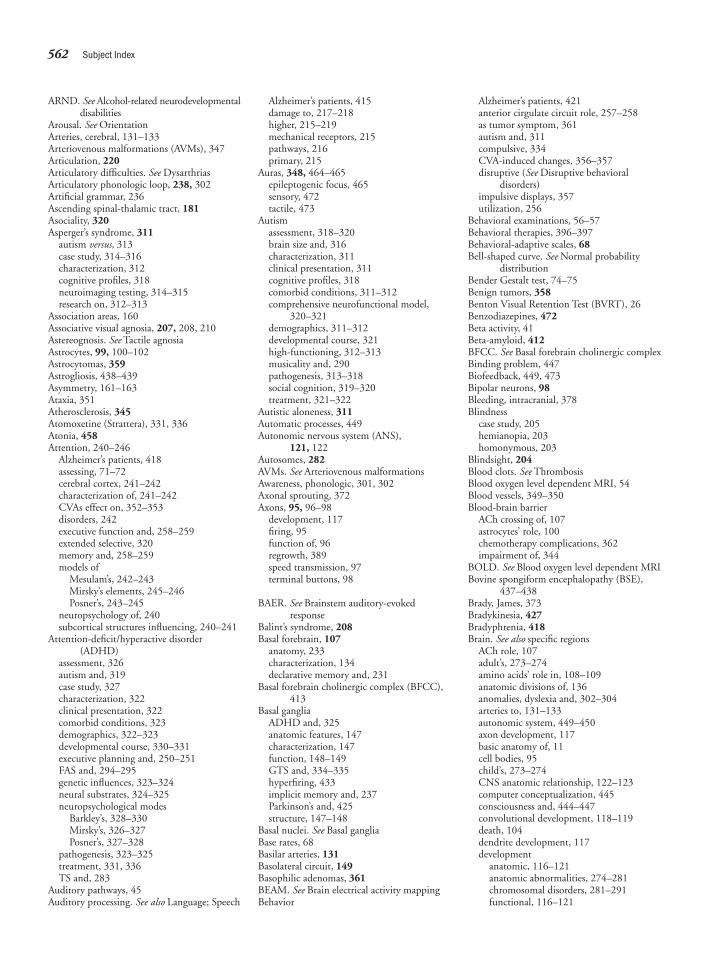
ARND. See Alcohol-related neurodevelopmentaldisabilities
Arousal. See OrientationArteries, cerebral, 131–133Arteriovenous malformations (AVMs), 347Articulation, 220Articulatory difficulties. See DysarthriasArticulatory phonologic loop, 238, 302Artificial grammar, 236Ascending spinal-thalamic tract, 181Asociality, 320Asperger’s syndrome, 311
autism versus, 313case study, 314–316characterization, 312cognitive profiles, 318neuroimaging testing, 314–315research on, 312–313
Association areas, 160Associative visual agnosia, 207, 208, 210Astereognosis. See Tactile agnosiaAstrocytes, 99, 100–102Astrocytomas, 359Astrogliosis, 438–439Asymmetry, 161–163Ataxia, 351Atherosclerosis, 345Atomoxetine (Strattera), 331, 336Atonia, 458Attention, 240–246
Alzheimer’s patients, 418assessing, 71–72cerebral cortex, 241–242characterization of, 241–242CVAs effect on, 352–353disorders, 242executive function and, 258–259extended selective, 320memory and, 258–259models of
Mesulam’s, 242–243Mirsky’s elements, 245–246Posner’s, 243–245
neuropsychology of, 240subcortical structures influencing, 240–241
Attention-deficit/hyperactive disorder(ADHD)
assessment, 326autism and, 319case study, 327characterization, 322clinical presentation, 322comorbid conditions, 323demographics, 322–323developmental course, 330–331executive planning and, 250–251FAS and, 294–295genetic influences, 323–324neural substrates, 324–325neuropsychological modes
Barkley’s, 328–330Mirsky’s, 326–327Posner’s, 327–328
pathogenesis, 323–325treatment, 331, 336TS and, 283
Auditory pathways, 45Auditory processing. See also Language; Speech
Alzheimer’s patients, 415damage to, 217–218higher, 215–219mechanical receptors, 215pathways, 216primary, 215
Auras, 348, 464–465epileptogenic focus, 465sensory, 472tactile, 473
Autismassessment, 318–320brain size and, 316characterization, 311clinical presentation, 311cognitive profiles, 318comorbid conditions, 311–312comprehensive neurofunctional model,
320–321demographics, 311–312developmental course, 321high-functioning, 312–313musicality and, 290pathogenesis, 313–318social cognition, 319–320treatment, 321–322
Autistic aloneness, 311Automatic processes, 449Autonomic nervous system (ANS),
121, 122Autosomes, 282AVMs. See Arteriovenous malformationsAwareness, phonologic, 301, 302Axonal sprouting, 372Axons, 95, 96–98
development, 117firing, 95function of, 96regrowth, 389speed transmission, 97terminal buttons, 98
BAER. See Brainstem auditory-evokedresponse
Balint’s syndrome, 208Basal forebrain, 107
anatomy, 233characterization, 134declarative memory and, 231
Basal forebrain cholinergic complex (BFCC),413
Basal gangliaADHD and, 325anatomic features, 147characterization, 147function, 148–149GTS and, 334–335hyperfiring, 433implicit memory and, 237Parkinson’s and, 425structure, 147–148
Basal nuclei. See Basal gangliaBase rates, 68Basilar arteries, 131Basolateral circuit, 149Basophilic adenomas, 361BEAM. See Brain electrical activity mappingBehavior
Alzheimer’s patients, 421anterior cirgulate circuit role, 257–258as tumor symptom, 361autism and, 311compulsive, 334CVA-induced changes, 356–357disruptive (See Disruptive behavioral
disorders)impulsive displays, 357utilization, 256
Behavioral examinations, 56–57Behavioral therapies, 396–397Behavioral-adaptive scales, 68Bell-shaped curve. See Normal probability
distributionBender Gestalt test, 74–75Benign tumors, 358Benton Visual Retention Test (BVRT), 26Benzodiazepines, 472Beta activity, 41Beta-amyloid, 412BFCC. See Basal forebrain cholinergic complexBinding problem, 447Biofeedback, 449, 473Bipolar neurons, 98Bleeding, intracranial, 378Blindness
case study, 205hemianopia, 203homonymous, 203
Blindsight, 204Blood clots. See ThrombosisBlood oxygen level dependent MRI, 54Blood vessels, 349–350Blood-brain barrier
ACh crossing of, 107astrocytes’ role, 100chemotherapy complications, 362impairment of, 344
BOLD. See Blood oxygen level dependent MRIBovine spongiform encephalopathy (BSE),
437–438Brady, James, 373Bradykinesia, 427Bradyphrenia, 418Brain. See also specific regions
ACh role, 107adult’s, 273–274amino acids’ role in, 108–109anatomic divisions of, 136anomalies, dyslexia and, 302–304arteries to, 131–133autonomic system, 449–450axon development, 117basic anatomy of, 11cell bodies, 95child’s, 273–274CNS anatomic relationship, 122–123computer conceptualization, 445consciousness and, 444–447convolutional development, 118–119death, 104dendrite development, 117development
anatomic, 116–121anatomic abnormalities, 274–281chromosomal disorders, 281–291functional, 116–121
562 Subject Index
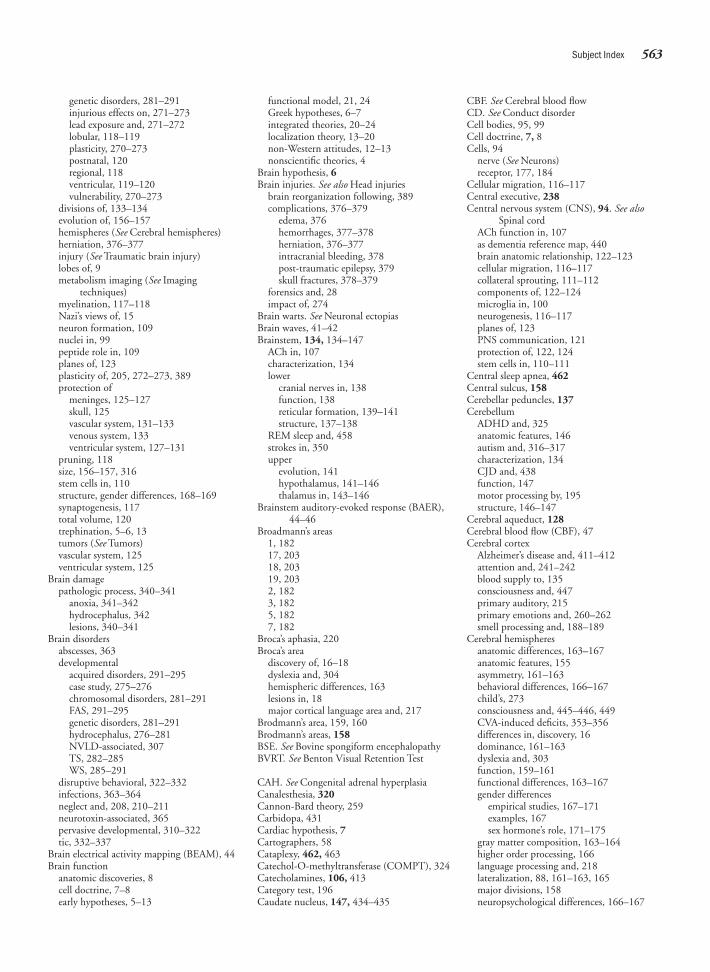
genetic disorders, 281–291injurious effects on, 271–273lead exposure and, 271–272lobular, 118–119plasticity, 270–273postnatal, 120regional, 118ventricular, 119–120vulnerability, 270–273
divisions of, 133–134evolution of, 156–157hemispheres (See Cerebral hemispheres)herniation, 376–377injury (See Traumatic brain injury)lobes of, 9metabolism imaging (See Imaging
techniques)myelination, 117–118Nazi’s views of, 15neuron formation, 109nuclei in, 99peptide role in, 109planes of, 123plasticity of, 205, 272–273, 389protection of
meninges, 125–127skull, 125vascular system, 131–133venous system, 133ventricular system, 127–131
pruning, 118size, 156–157, 316stem cells in, 110structure, gender differences, 168–169synaptogenesis, 117total volume, 120trephination, 5–6, 13tumors (See Tumors)vascular system, 125ventricular system, 125
Brain damagepathologic process, 340–341
anoxia, 341–342hydrocephalus, 342lesions, 340–341
Brain disordersabscesses, 363developmental
acquired disorders, 291–295case study, 275–276chromosomal disorders, 281–291FAS, 291–295genetic disorders, 281–291hydrocephalus, 276–281NVLD-associated, 307TS, 282–285WS, 285–291
disruptive behavioral, 322–332infections, 363–364neglect and, 208, 210–211neurotoxin-associated, 365pervasive developmental, 310–322tic, 332–337
Brain electrical activity mapping (BEAM), 44Brain function
anatomic discoveries, 8cell doctrine, 7–8early hypotheses, 5–13
functional model, 21, 24Greek hypotheses, 6–7integrated theories, 20–24localization theory, 13–20non-Western attitudes, 12–13nonscientific theories, 4
Brain hypothesis, 6Brain injuries. See also Head injuries
brain reorganization following, 389complications, 376–379
edema, 376hemorrhages, 377–378herniation, 376–377intracranial bleeding, 378post-traumatic epilepsy, 379skull fractures, 378–379
forensics and, 28impact of, 274
Brain warts. See Neuronal ectopiasBrain waves, 41–42Brainstem, 134, 134–147
ACh in, 107characterization, 134lower
cranial nerves in, 138function, 138reticular formation, 139–141structure, 137–138
REM sleep and, 458strokes in, 350upper
evolution, 141hypothalamus, 141–146thalamus in, 143–146
Brainstem auditory-evoked response (BAER),44–46
Broadmann’s areas1, 18217, 20318, 20319, 2032, 1823, 1825, 1827, 182
Broca’s aphasia, 220Broca’s area
discovery of, 16–18dyslexia and, 304hemispheric differences, 163lesions in, 18major cortical language area and, 217
Brodmann’s area, 159, 160Brodmann’s areas, 158BSE. See Bovine spongiform encephalopathyBVRT. See Benton Visual Retention Test
CAH. See Congenital adrenal hyperplasiaCanalesthesia, 320Cannon-Bard theory, 259Carbidopa, 431Cardiac hypothesis, 7Cartographers, 58Cataplexy, 462, 463Catechol-O-methyltransferase (COMPT), 324Catecholamines, 106, 413Category test, 196Caudate nucleus, 147, 434–435
CBF. See Cerebral blood flowCD. See Conduct disorderCell bodies, 95, 99Cell doctrine, 7, 8Cells, 94
nerve (See Neurons)receptor, 177, 184
Cellular migration, 116–117Central executive, 238Central nervous system (CNS), 94. See also
Spinal cordACh function in, 107as dementia reference map, 440brain anatomic relationship, 122–123cellular migration, 116–117collateral sprouting, 111–112components of, 122–124microglia in, 100neurogenesis, 116–117planes of, 123PNS communication, 121protection of, 122, 124stem cells in, 110–111
Central sleep apnea, 462Central sulcus, 158Cerebellar peduncles, 137Cerebellum
ADHD and, 325anatomic features, 146autism and, 316–317characterization, 134CJD and, 438function, 147motor processing by, 195structure, 146–147
Cerebral aqueduct, 128Cerebral blood flow (CBF), 47Cerebral cortex
Alzheimer’s disease and, 411–412attention and, 241–242blood supply to, 135consciousness and, 447primary auditory, 215primary emotions and, 260–262smell processing and, 188–189
Cerebral hemispheresanatomic differences, 163–167anatomic features, 155asymmetry, 161–163behavioral differences, 166–167child’s, 273consciousness and, 445–446, 449CVA-induced deficits, 353–356differences in, discovery, 16dominance, 161–163dyslexia and, 303function, 159–161functional differences, 163–167gender differences
empirical studies, 167–171examples, 167sex hormone’s role, 171–175
gray matter composition, 163–164higher order processing, 166language processing and, 218lateralization, 88, 161–163, 165major divisions, 158neuropsychological differences, 166–167
Subject Index 563
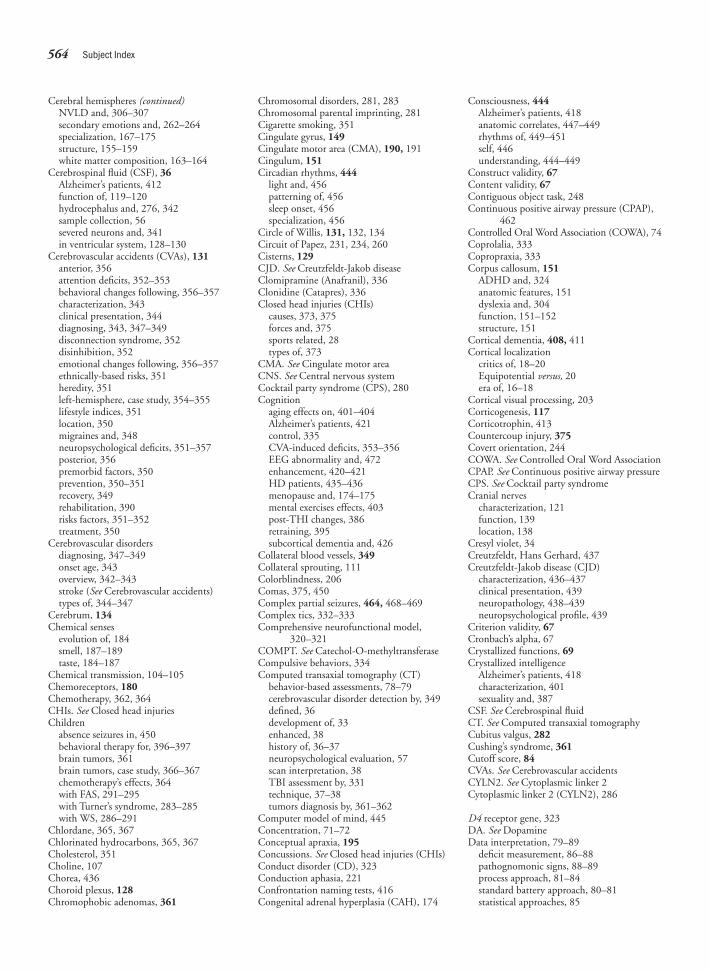
Cerebral hemispheres (continued)NVLD and, 306–307secondary emotions and, 262–264specialization, 167–175structure, 155–159white matter composition, 163–164
Cerebrospinal fluid (CSF), 36Alzheimer’s patients, 412function of, 119–120hydrocephalus and, 276, 342sample collection, 56severed neurons and, 341in ventricular system, 128–130
Cerebrovascular accidents (CVAs), 131anterior, 356attention deficits, 352–353behavioral changes following, 356–357characterization, 343clinical presentation, 344diagnosing, 343, 347–349disconnection syndrome, 352disinhibition, 352emotional changes following, 356–357ethnically-based risks, 351heredity, 351left-hemisphere, case study, 354–355lifestyle indices, 351location, 350migraines and, 348neuropsychological deficits, 351–357posterior, 356premorbid factors, 350prevention, 350–351recovery, 349rehabilitation, 390risks factors, 351–352treatment, 350
Cerebrovascular disordersdiagnosing, 347–349onset age, 343overview, 342–343stroke (See Cerebrovascular accidents)types of, 344–347
Cerebrum, 134Chemical senses
evolution of, 184smell, 187–189taste, 184–187
Chemical transmission, 104–105Chemoreceptors, 180Chemotherapy, 362, 364CHIs. See Closed head injuriesChildren
absence seizures in, 450behavioral therapy for, 396–397brain tumors, 361brain tumors, case study, 366–367chemotherapy’s effects, 364with FAS, 291–295with Turner’s syndrome, 283–285with WS, 286–291
Chlordane, 365, 367Chlorinated hydrocarbons, 365, 367Cholesterol, 351Choline, 107Chorea, 436Choroid plexus, 128Chromophobic adenomas, 361
Chromosomal disorders, 281, 283Chromosomal parental imprinting, 281Cigarette smoking, 351Cingulate gyrus, 149Cingulate motor area (CMA), 190, 191Cingulum, 151Circadian rhythms, 444
light and, 456patterning of, 456sleep onset, 456specialization, 456
Circle of Willis, 131, 132, 134Circuit of Papez, 231, 234, 260Cisterns, 129CJD. See Creutzfeldt-Jakob diseaseClomipramine (Anafranil), 336Clonidine (Catapres), 336Closed head injuries (CHIs)
causes, 373, 375forces and, 375sports related, 28types of, 373
CMA. See Cingulate motor areaCNS. See Central nervous systemCocktail party syndrome (CPS), 280Cognition
aging effects on, 401–404Alzheimer’s patients, 421control, 335CVA-induced deficits, 353–356EEG abnormality and, 472enhancement, 420–421HD patients, 435–436menopause and, 174–175mental exercises effects, 403post-THI changes, 386retraining, 395subcortical dementia and, 426
Collateral blood vessels, 349Collateral sprouting, 111Colorblindness, 206Comas, 375, 450Complex partial seizures, 464, 468–469Complex tics, 332–333Comprehensive neurofunctional model,
320–321COMPT. See Catechol-O-methyltransferaseCompulsive behaviors, 334Computed transaxial tomography (CT)
behavior-based assessments, 78–79cerebrovascular disorder detection by, 349defined, 36development of, 33enhanced, 38history of, 36–37neuropsychological evaluation, 57scan interpretation, 38TBI assessment by, 331technique, 37–38tumors diagnosis by, 361–362
Computer model of mind, 445Concentration, 71–72Conceptual apraxia, 195Concussions. See Closed head injuries (CHIs)Conduct disorder (CD), 323Conduction aphasia, 221Confrontation naming tests, 416Congenital adrenal hyperplasia (CAH), 174
Consciousness, 444Alzheimer’s patients, 418anatomic correlates, 447–449rhythms of, 449–451self, 446understanding, 444–449
Construct validity, 67Content validity, 67Contiguous object task, 248Continuous positive airway pressure (CPAP),
462Controlled Oral Word Association (COWA), 74Coprolalia, 333Copropraxia, 333Corpus callosum, 151
ADHD and, 324anatomic features, 151dyslexia and, 304function, 151–152structure, 151
Cortical dementia, 408, 411Cortical localization
critics of, 18–20Equipotential versus, 20era of, 16–18
Cortical visual processing, 203Corticogenesis, 117Corticotrophin, 413Countercoup injury, 375Covert orientation, 244COWA. See Controlled Oral Word AssociationCPAP. See Continuous positive airway pressureCPS. See Cocktail party syndromeCranial nerves
characterization, 121function, 139location, 138
Cresyl violet, 34Creutzfeldt, Hans Gerhard, 437Creutzfeldt-Jakob disease (CJD)
characterization, 436–437clinical presentation, 439neuropathology, 438–439neuropsychological profile, 439
Criterion validity, 67Cronbach’s alpha, 67Crystallized functions, 69Crystallized intelligence
Alzheimer’s patients, 418characterization, 401sexuality and, 387
CSF. See Cerebrospinal fluidCT. See Computed transaxial tomographyCubitus valgus, 282Cushing’s syndrome, 361Cutoff score, 84CVAs. See Cerebrovascular accidentsCYLN2. See Cytoplasmic linker 2Cytoplasmic linker 2 (CYLN2), 286
D4 receptor gene, 323DA. See DopamineData interpretation, 79–89
deficit measurement, 86–88pathognomonic signs, 88–89process approach, 81–84standard battery approach, 80–81statistical approaches, 85
564 Subject Index
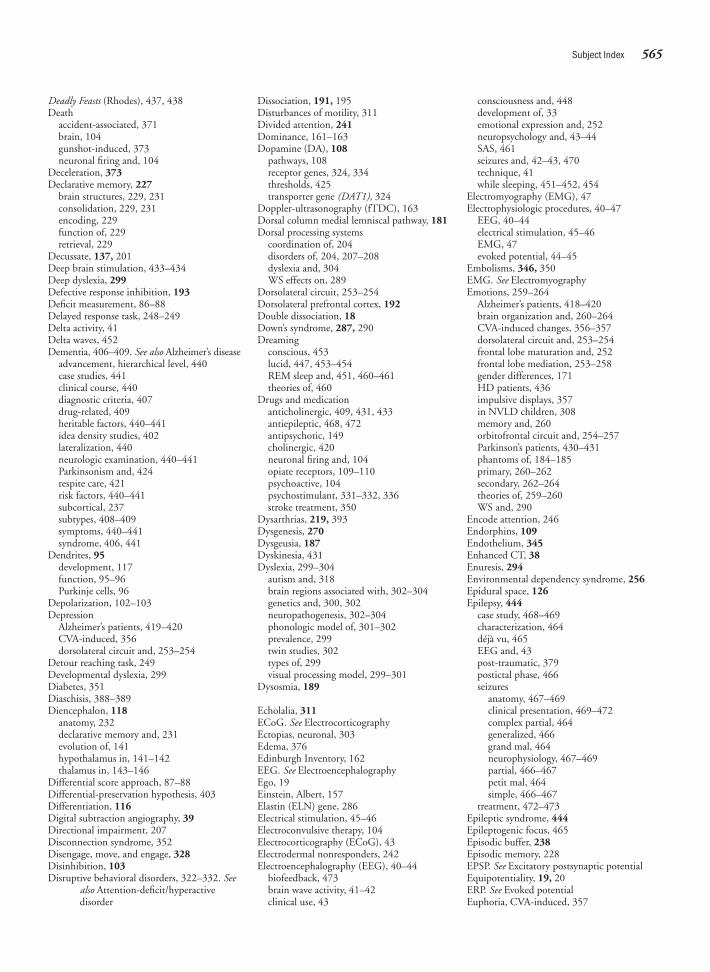
Deadly Feasts (Rhodes), 437, 438Death
accident-associated, 371brain, 104gunshot-induced, 373neuronal firing and, 104
Deceleration, 373Declarative memory, 227
brain structures, 229, 231consolidation, 229, 231encoding, 229function of, 229retrieval, 229
Decussate, 137, 201Deep brain stimulation, 433–434Deep dyslexia, 299Defective response inhibition, 193Deficit measurement, 86–88Delayed response task, 248–249Delta activity, 41Delta waves, 452Dementia, 406–409. See also Alzheimer’s disease
advancement, hierarchical level, 440case studies, 441clinical course, 440diagnostic criteria, 407drug-related, 409heritable factors, 440–441idea density studies, 402lateralization, 440neurologic examination, 440–441Parkinsonism and, 424respite care, 421risk factors, 440–441subcortical, 237subtypes, 408–409symptoms, 440–441syndrome, 406, 441
Dendrites, 95development, 117function, 95–96Purkinje cells, 96
Depolarization, 102–103Depression
Alzheimer’s patients, 419–420CVA-induced, 356dorsolateral circuit and, 253–254
Detour reaching task, 249Developmental dyslexia, 299Diabetes, 351Diaschisis, 388–389Diencephalon, 118
anatomy, 232declarative memory and, 231evolution of, 141hypothalamus in, 141–142thalamus in, 143–146
Differential score approach, 87–88Differential-preservation hypothesis, 403Differentiation, 116Digital subtraction angiography, 39Directional impairment, 207Disconnection syndrome, 352Disengage, move, and engage, 328Disinhibition, 103Disruptive behavioral disorders, 322–332. See
also Attention-deficit/hyperactivedisorder
Dissociation, 191, 195Disturbances of motility, 311Divided attention, 241Dominance, 161–163Dopamine (DA), 108
pathways, 108receptor genes, 324, 334thresholds, 425transporter gene (DAT1), 324
Doppler-ultrasonography (fTDC), 163Dorsal column medial lemniscal pathway, 181Dorsal processing systems
coordination of, 204disorders of, 204, 207–208dyslexia and, 304WS effects on, 289
Dorsolateral circuit, 253–254Dorsolateral prefrontal cortex, 192Double dissociation, 18Down’s syndrome, 287, 290Dreaming
conscious, 453lucid, 447, 453–454REM sleep and, 451, 460–461theories of, 460
Drugs and medicationanticholinergic, 409, 431, 433antiepileptic, 468, 472antipsychotic, 149cholinergic, 420neuronal firing and, 104opiate receptors, 109–110psychoactive, 104psychostimulant, 331–332, 336stroke treatment, 350
Dysarthrias, 219, 393Dysgenesis, 270Dysgeusia, 187Dyskinesia, 431Dyslexia, 299–304
autism and, 318brain regions associated with, 302–304genetics and, 300, 302neuropathogenesis, 302–304phonologic model of, 301–302prevalence, 299twin studies, 302types of, 299visual processing model, 299–301
Dysosmia, 189
Echolalia, 311ECoG. See ElectrocorticographyEctopias, neuronal, 303Edema, 376Edinburgh Inventory, 162EEG. See ElectroencephalographyEgo, 19Einstein, Albert, 157Elastin (ELN) gene, 286Electrical stimulation, 45–46Electroconvulsive therapy, 104Electrocorticography (ECoG), 43Electrodermal nonresponders, 242Electroencephalography (EEG), 40–44
biofeedback, 473brain wave activity, 41–42clinical use, 43
consciousness and, 448development of, 33emotional expression and, 252neuropsychology and, 43–44SAS, 461seizures and, 42–43, 470technique, 41while sleeping, 451–452, 454
Electromyography (EMG), 47Electrophysiologic procedures, 40–47
EEG, 40–44electrical stimulation, 45–46EMG, 47evoked potential, 44–45
Embolisms, 346, 350EMG. See ElectromyographyEmotions, 259–264
Alzheimer’s patients, 418–420brain organization and, 260–264CVA-induced changes, 356–357dorsolateral circuit and, 253–254frontal lobe maturation and, 252frontal lobe mediation, 253–258gender differences, 171HD patients, 436impulsive displays, 357in NVLD children, 308memory and, 260orbitofrontal circuit and, 254–257Parkinson’s patients, 430–431phantoms of, 184–185primary, 260–262secondary, 262–264theories of, 259–260WS and, 290
Encode attention, 246Endorphins, 109Endothelium, 345Enhanced CT, 38Enuresis, 294Environmental dependency syndrome, 256Epidural space, 126Epilepsy, 444
case study, 468–469characterization, 464déjà vu, 465EEG and, 43post-traumatic, 379postictal phase, 466seizures
anatomy, 467–469clinical presentation, 469–472complex partial, 464generalized, 466grand mal, 464neurophysiology, 467–469partial, 466–467petit mal, 464simple, 466–467
treatment, 472–473Epileptic syndrome, 444Epileptogenic focus, 465Episodic buffer, 238Episodic memory, 228EPSP. See Excitatory postsynaptic potentialEquipotentiality, 19, 20ERP. See Evoked potentialEuphoria, CVA-induced, 357
Subject Index 565

Evoked potentialBAER, 44–46SER, 45technique, 44VER, 45
Evolutionbrain size, 156–157chemical senses, 184diencephalon, 141medulla oblongata, 137midbrain, 137upper brainstem, 141
Excessive daytime sleepiness, 462Excitatory postsynaptic potential (EPSP), 106Executive attention system, 245Executive functioning, 246–258
ADHD children and, 250–251, 326Alzheimer’s patients, 418anterior cingulate circuit, 257–258attention and, 258–259autism and, 318–319case study, 255development, 247, 250–252dyslexia and, 302, 304frontal lobe mediation
anterior cingulate circuit, 257–258dorsolateral circuit, 253–254orbitofrontal circuit, 254–257
HC effects on, 281memory and, 258–259Parkinson’s patients, 429–431subcortical dementia and, 426tasks, 248–249
Executive planning, 319Explicit memory, 227–228Expressive aphasia, 219Extended paraphasia. See ParagrammatismExtended selective attention, 320Extradural hematomas, 377Extrapyramidal motor system, 148, 148
Facial expressionsautism and, 317secondary emotions and, 263WS and, 288
Faculty psychology, 13–20FAE. See Fetal alcohol effectsFalse positives, 67–68Familial sinistrality, 173Family therapy, 355–367FAS. See Fetal alcohol syndromeFear conditioning, 261Feelings. See EmotionsFemorocerebral angiography, 39Festinating gait, 427Fetal alcohol effects (FAE), 292
assessment, 293–294development course, 294treatment, 294–295
Fetal alcohol syndrome (FAS), 291assessment, 293–294clinical features, 291–292comorbid conditions, 293development course, 294incidence, 292neuropathogenesis, 292–293treatment, 294–295
FFA. See Fusiform face areaFibers, 99Fibrin, 351FISH. See Fluorescent in situ hybridizationFissures, 1565-HT. See SerotoninFlicker fusion rate, 299Fluency tasks, 415–416Fluent aphasia, 18, 219Fluid functions, 69Fluid intelligence, 402, 403–404Fluorescent in situ hybridization (FISH), 286Focus-execute attention, 246Focused attention, 241Fontanelles, 125Football injuries, 382–383Foramen of Magendie, 129Foramen magnum, 125Foramen of Monro, 127Foramina, 125Forebrain (prosencephalon), 118Forensic neuropsychology, 28, 78Fornix, 149, 231Fossae, 125Fragile X syndrome, 316Frontal lobes, 158
ADHD and, 324–325aging and, 404anterior cingulate circuit, 257–258autism and, 317dyslexia and, 304function, 160functioning (See Executive functioning)injury to, 396orbitofrontal circuit, 254–257stroke-damage, 352
Frontal operculum, 162fTCD. See Doppler-ultrasonographyFunctional MRI, 54, 55Functional systems, 24Functioning adenomas, 360Fusiform face area, 317, 318
G-meters, 375GABA. See Gamma-aminobutyric acidGalveston Orientation and Amnesia Test
(GOAT), 70Gamma activity, 41Gamma-aminobutyric acid (GABA), 43
memory consolidation and, 459properties of, 109seizures and, 468, 472
Ganglia, 99GBM. See Glioblastoma multiformeGCS. See Glasgow Coma ScaleGender differences
Alzheimer’s disease rates, 409autism, 312emotions, 171GTS, 333hemispheric specialization
examples of, 167sex hormone’s role, 171–175studies of, 167–171
math skills, 172meningioma incidences, 359sexual hormones and, 171–175
spatial processing, 169–170sports injury risks, 384verbal ability, 174
General transcription factor 2-1 (GTF21),286–287
GeneticsADHD, 323–324autism and, 313, 314, 316brain aging and, 404HD and, 434learning disabilities, 300, 302WS and, 286–287
Gerstmann-Straussler-Scheinker syndrome(GSS), 437
Gigantocellular tegmental field (GTF), 458Gilles de La Tourette syndrome. See Tourette
syndromeGlasgow Coma Scale (GCS), 375–376Glial cells, 94
characterization, 99myelin sheath formation and, 97tumors (See Gliomas)types of, 99–100
Glioblastoma multiforme (GBM), 359gender differences, 361neuropsychological deficits, 363
Gliomas, 100, 359Global aphasia, 221Global processing, 289Globus pallidus, 147Glucose, 120Glutamate, 109GOAT. See Galveston Orientation and
Amnesia TestGolgi stain, 34Gonadotropins, 284Grade of tumor, 358Grand mal seizure, 464Grandmother cells, 447Granulations. See Arachnoid villiGray matter, 95
autism and, 316cerebral hemispheres and, 164
Group therapy, 395GSS. See Gerstmann-Straussler-Scheinker
syndromeGTF. See Gigantocellular tegmental fieldGTF21. See General transcription factor 2-1GTS. See Tourette syndromeGuanfacine, 336Guanfacine (Tenex), 336Gunshot wounds, 373Gyrification, 118, 119
Haldol (haloperidol), 149Hallucinations, hypnagogic, 463Haloperidol (Haldol), 334, 336Halstead-Reitan Neuropsychological Battery, 77Handedness, 162HC. See HydrocephalusHD. See Huntington’s diseaseHead injuries. See also Brain injuries
adaptation, 388–389mild, 379–385
impact of, 380postconcussional syndrome, 385postconcussive syndromes, 381
566 Subject Index
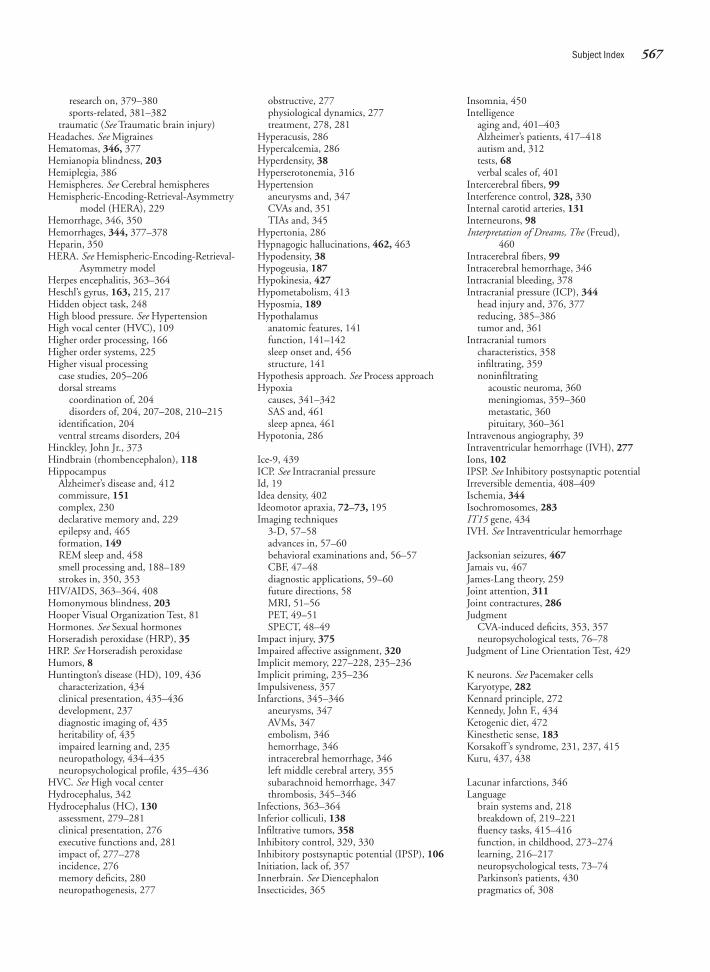
research on, 379–380sports-related, 381–382
traumatic (See Traumatic brain injury)Headaches. See MigrainesHematomas, 346, 377Hemianopia blindness, 203Hemiplegia, 386Hemispheres. See Cerebral hemispheresHemispheric-Encoding-Retrieval-Asymmetry
model (HERA), 229Hemorrhage, 346, 350Hemorrhages, 344, 377–378Heparin, 350HERA. See Hemispheric-Encoding-Retrieval-
Asymmetry modelHerpes encephalitis, 363–364Heschl’s gyrus, 163, 215, 217Hidden object task, 248High blood pressure. See HypertensionHigh vocal center (HVC), 109Higher order processing, 166Higher order systems, 225Higher visual processing
case studies, 205–206dorsal streams
coordination of, 204disorders of, 204, 207–208, 210–215
identification, 204ventral streams disorders, 204
Hinckley, John Jr., 373Hindbrain (rhombencephalon), 118Hippocampus
Alzheimer’s disease and, 412commissure, 151complex, 230declarative memory and, 229epilepsy and, 465formation, 149REM sleep and, 458smell processing and, 188–189strokes in, 350, 353
HIV/AIDS, 363–364, 408Homonymous blindness, 203Hooper Visual Organization Test, 81Hormones. See Sexual hormonesHorseradish peroxidase (HRP), 35HRP. See Horseradish peroxidaseHumors, 8Huntington’s disease (HD), 109, 436
characterization, 434clinical presentation, 435–436development, 237diagnostic imaging of, 435heritability of, 435impaired learning and, 235neuropathology, 434–435neuropsychological profile, 435–436
HVC. See High vocal centerHydrocephalus, 342Hydrocephalus (HC), 130
assessment, 279–281clinical presentation, 276executive functions and, 281impact of, 277–278incidence, 276memory deficits, 280neuropathogenesis, 277
obstructive, 277physiological dynamics, 277treatment, 278, 281
Hyperacusis, 286Hypercalcemia, 286Hyperdensity, 38Hyperserotonemia, 316Hypertension
aneurysms and, 347CVAs and, 351TIAs and, 345
Hypertonia, 286Hypnagogic hallucinations, 462, 463Hypodensity, 38Hypogeusia, 187Hypokinesia, 427Hypometabolism, 413Hyposmia, 189Hypothalamus
anatomic features, 141function, 141–142sleep onset and, 456structure, 141
Hypothesis approach. See Process approachHypoxia
causes, 341–342SAS and, 461sleep apnea, 461
Hypotonia, 286
Ice-9, 439ICP. See Intracranial pressureId, 19Idea density, 402Ideomotor apraxia, 72–73, 195Imaging techniques
3-D, 57–58advances in, 57–60behavioral examinations and, 56–57CBF, 47–48diagnostic applications, 59–60future directions, 58MRI, 51–56PET, 49–51SPECT, 48–49
Impact injury, 375Impaired affective assignment, 320Implicit memory, 227–228, 235–236Implicit priming, 235–236Impulsiveness, 357Infarctions, 345–346
aneurysms, 347AVMs, 347embolism, 346hemorrhage, 346intracerebral hemorrhage, 346left middle cerebral artery, 355subarachnoid hemorrhage, 347thrombosis, 345–346
Infections, 363–364Inferior colliculi, 138Infiltrative tumors, 358Inhibitory control, 329, 330Inhibitory postsynaptic potential (IPSP), 106Initiation, lack of, 357Innerbrain. See DiencephalonInsecticides, 365
Insomnia, 450Intelligence
aging and, 401–403Alzheimer’s patients, 417–418autism and, 312tests, 68verbal scales of, 401
Intercerebral fibers, 99Interference control, 328, 330Internal carotid arteries, 131Interneurons, 98Interpretation of Dreams, The (Freud),
460Intracerebral fibers, 99Intracerebral hemorrhage, 346Intracranial bleeding, 378Intracranial pressure (ICP), 344
head injury and, 376, 377reducing, 385–386tumor and, 361
Intracranial tumorscharacteristics, 358infiltrating, 359noninfiltrating
acoustic neuroma, 360meningiomas, 359–360metastatic, 360pituitary, 360–361
Intravenous angiography, 39Intraventricular hemorrhage (IVH), 277Ions, 102IPSP. See Inhibitory postsynaptic potentialIrreversible dementia, 408–409Ischemia, 344Isochromosomes, 283IT15 gene, 434IVH. See Intraventricular hemorrhage
Jacksonian seizures, 467Jamais vu, 467James-Lang theory, 259Joint attention, 311Joint contractures, 286Judgment
CVA-induced deficits, 353, 357neuropsychological tests, 76–78
Judgment of Line Orientation Test, 429
K neurons. See Pacemaker cellsKaryotype, 282Kennard principle, 272Kennedy, John F., 434Ketogenic diet, 472Kinesthetic sense, 183Korsakoff ’s syndrome, 231, 237, 415Kuru, 437, 438
Lacunar infarctions, 346Language
brain systems and, 218breakdown of, 219–221fluency tasks, 415–416function, in childhood, 273–274learning, 216–217neuropsychological tests, 73–74Parkinson’s patients, 430pragmatics of, 308
Subject Index 567
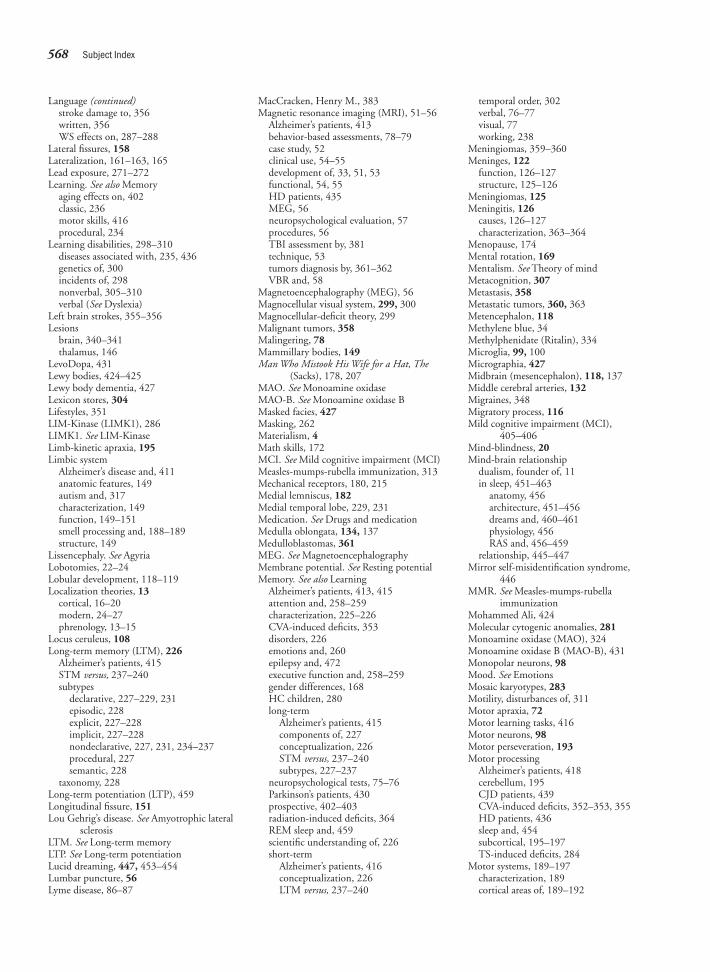
Language (continued)stroke damage to, 356written, 356WS effects on, 287–288
Lateral fissures, 158Lateralization, 161–163, 165Lead exposure, 271–272Learning. See also Memory
aging effects on, 402classic, 236motor skills, 416procedural, 234
Learning disabilities, 298–310diseases associated with, 235, 436genetics of, 300incidents of, 298nonverbal, 305–310verbal (See Dyslexia)
Left brain strokes, 355–356Lesions
brain, 340–341thalamus, 146
LevoDopa, 431Lewy bodies, 424–425Lewy body dementia, 427Lexicon stores, 304Lifestyles, 351LIM-Kinase (LIMK1), 286LIMK1. See LIM-KinaseLimb-kinetic apraxia, 195Limbic system
Alzheimer’s disease and, 411anatomic features, 149autism and, 317characterization, 149function, 149–151smell processing and, 188–189structure, 149
Lissencephaly. See AgyriaLobotomies, 22–24Lobular development, 118–119Localization theories, 13
cortical, 16–20modern, 24–27phrenology, 13–15
Locus ceruleus, 108Long-term memory (LTM), 226
Alzheimer’s patients, 415STM versus, 237–240subtypes
declarative, 227–229, 231episodic, 228explicit, 227–228implicit, 227–228nondeclarative, 227, 231, 234–237procedural, 227semantic, 228
taxonomy, 228Long-term potentiation (LTP), 459Longitudinal fissure, 151Lou Gehrig’s disease. See Amyotrophic lateral
sclerosisLTM. See Long-term memoryLTP. See Long-term potentiationLucid dreaming, 447, 453–454Lumbar puncture, 56Lyme disease, 86–87
MacCracken, Henry M., 383Magnetic resonance imaging (MRI), 51–56
Alzheimer’s patients, 413behavior-based assessments, 78–79case study, 52clinical use, 54–55development of, 33, 51, 53functional, 54, 55HD patients, 435MEG, 56neuropsychological evaluation, 57procedures, 56TBI assessment by, 381technique, 53tumors diagnosis by, 361–362VBR and, 58
Magnetoencephalography (MEG), 56Magnocellular visual system, 299, 300Magnocellular-deficit theory, 299Malignant tumors, 358Malingering, 78Mammillary bodies, 149Man Who Mistook His Wife for a Hat, The
(Sacks), 178, 207MAO. See Monoamine oxidaseMAO-B. See Monoamine oxidase BMasked facies, 427Masking, 262Materialism, 4Math skills, 172MCI. See Mild cognitive impairment (MCI)Measles-mumps-rubella immunization, 313Mechanical receptors, 180, 215Medial lemniscus, 182Medial temporal lobe, 229, 231Medication. See Drugs and medicationMedulla oblongata, 134, 137Medulloblastomas, 361MEG. See MagnetoencephalographyMembrane potential. See Resting potentialMemory. See also Learning
Alzheimer’s patients, 413, 415attention and, 258–259characterization, 225–226CVA-induced deficits, 353disorders, 226emotions and, 260epilepsy and, 472executive function and, 258–259gender differences, 168HC children, 280long-term
Alzheimer’s patients, 415components of, 227conceptualization, 226STM versus, 237–240subtypes, 227–237
neuropsychological tests, 75–76Parkinson’s patients, 430prospective, 402–403radiation-induced deficits, 364REM sleep and, 459scientific understanding of, 226short-term
Alzheimer’s patients, 416conceptualization, 226LTM versus, 237–240
temporal order, 302verbal, 76–77visual, 77working, 238
Meningiomas, 359–360Meninges, 122
function, 126–127structure, 125–126
Meningiomas, 125Meningitis, 126
causes, 126–127characterization, 363–364
Menopause, 174Mental rotation, 169Mentalism. See Theory of mindMetacognition, 307Metastasis, 358Metastatic tumors, 360, 363Metencephalon, 118Methylene blue, 34Methylphenidate (Ritalin), 334Microglia, 99, 100Micrographia, 427Midbrain (mesencephalon), 118, 137Middle cerebral arteries, 132Migraines, 348Migratory process, 116Mild cognitive impairment (MCI),
405–406Mind-blindness, 20Mind-brain relationship
dualism, founder of, 11in sleep, 451–463
anatomy, 456architecture, 451–456dreams and, 460–461physiology, 456RAS and, 456–459
relationship, 445–447Mirror self-misidentification syndrome,
446MMR. See Measles-mumps-rubella
immunizationMohammed Ali, 424Molecular cytogenic anomalies, 281Monoamine oxidase (MAO), 324Monoamine oxidase B (MAO-B), 431Monopolar neurons, 98Mood. See EmotionsMosaic karyotypes, 283Motility, disturbances of, 311Motor apraxia, 72Motor learning tasks, 416Motor neurons, 98Motor perseveration, 193Motor processing
Alzheimer’s patients, 418cerebellum, 195CJD patients, 439CVA-induced deficits, 352–353, 355HD patients, 436sleep and, 454subcortical, 195–197TS-induced deficits, 284
Motor systems, 189–197characterization, 189cortical areas of, 189–192
568 Subject Index
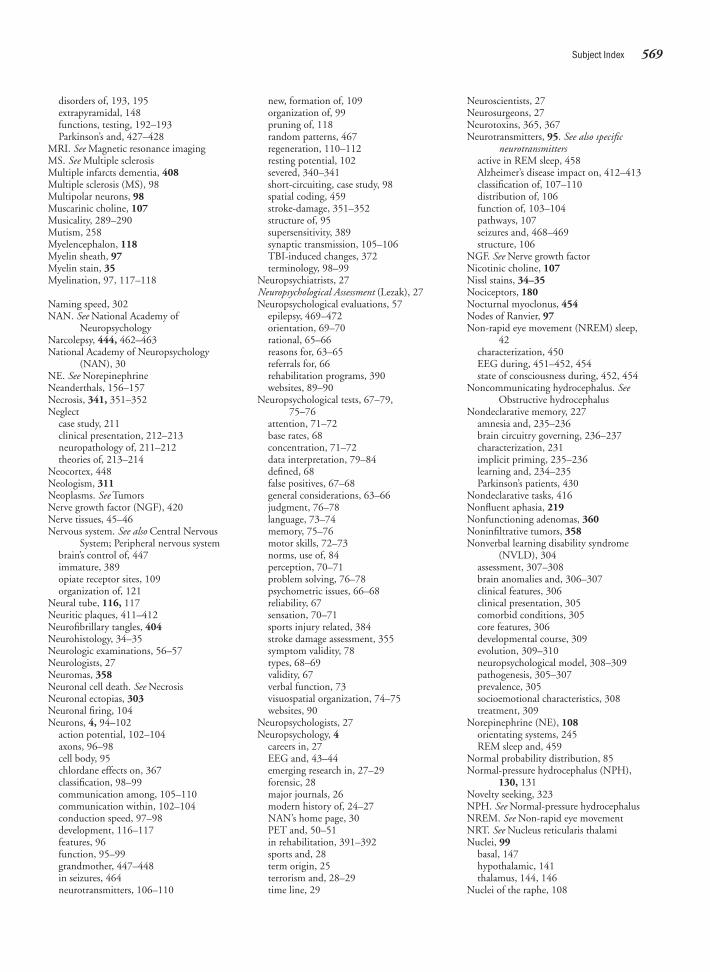
disorders of, 193, 195extrapyramidal, 148functions, testing, 192–193Parkinson’s and, 427–428
MRI. See Magnetic resonance imagingMS. See Multiple sclerosisMultiple infarcts dementia, 408Multiple sclerosis (MS), 98Multipolar neurons, 98Muscarinic choline, 107Musicality, 289–290Mutism, 258Myelencephalon, 118Myelin sheath, 97Myelin stain, 35Myelination, 97, 117–118
Naming speed, 302NAN. See National Academy of
NeuropsychologyNarcolepsy, 444, 462–463National Academy of Neuropsychology
(NAN), 30NE. See NorepinephrineNeanderthals, 156–157Necrosis, 341, 351–352Neglect
case study, 211clinical presentation, 212–213neuropathology of, 211–212theories of, 213–214
Neocortex, 448Neologism, 311Neoplasms. See TumorsNerve growth factor (NGF), 420Nerve tissues, 45–46Nervous system. See also Central Nervous
System; Peripheral nervous systembrain’s control of, 447immature, 389opiate receptor sites, 109organization of, 121
Neural tube, 116, 117Neuritic plaques, 411–412Neurofibrillary tangles, 404Neurohistology, 34–35Neurologic examinations, 56–57Neurologists, 27Neuromas, 358Neuronal cell death. See NecrosisNeuronal ectopias, 303Neuronal firing, 104Neurons, 4, 94–102
action potential, 102–104axons, 96–98cell body, 95chlordane effects on, 367classification, 98–99communication among, 105–110communication within, 102–104conduction speed, 97–98development, 116–117features, 96function, 95–99grandmother, 447–448in seizures, 464neurotransmitters, 106–110
new, formation of, 109organization of, 99pruning of, 118random patterns, 467regeneration, 110–112resting potential, 102severed, 340–341short-circuiting, case study, 98spatial coding, 459stroke-damage, 351–352structure of, 95supersensitivity, 389synaptic transmission, 105–106TBI-induced changes, 372terminology, 98–99
Neuropsychiatrists, 27Neuropsychological Assessment (Lezak), 27Neuropsychological evaluations, 57
epilepsy, 469–472orientation, 69–70rational, 65–66reasons for, 63–65referrals for, 66rehabilitation programs, 390websites, 89–90
Neuropsychological tests, 67–79, 75–76
attention, 71–72base rates, 68concentration, 71–72data interpretation, 79–84defined, 68false positives, 67–68general considerations, 63–66judgment, 76–78language, 73–74memory, 75–76motor skills, 72–73norms, use of, 84perception, 70–71problem solving, 76–78psychometric issues, 66–68reliability, 67sensation, 70–71sports injury related, 384stroke damage assessment, 355symptom validity, 78types, 68–69validity, 67verbal function, 73visuospatial organization, 74–75websites, 90
Neuropsychologists, 27Neuropsychology, 4
careers in, 27EEG and, 43–44emerging research in, 27–29forensic, 28major journals, 26modern history of, 24–27NAN’s home page, 30PET and, 50–51in rehabilitation, 391–392sports and, 28term origin, 25terrorism and, 28–29time line, 29
Neuroscientists, 27Neurosurgeons, 27Neurotoxins, 365, 367Neurotransmitters, 95. See also specific
neurotransmittersactive in REM sleep, 458Alzheimer’s disease impact on, 412–413classification of, 107–110distribution of, 106function of, 103–104pathways, 107seizures and, 468–469structure, 106
NGF. See Nerve growth factorNicotinic choline, 107Nissl stains, 34–35Nociceptors, 180Nocturnal myoclonus, 454Nodes of Ranvier, 97Non-rapid eye movement (NREM) sleep,
42characterization, 450EEG during, 451–452, 454state of consciousness during, 452, 454
Noncommunicating hydrocephalus. SeeObstructive hydrocephalus
Nondeclarative memory, 227amnesia and, 235–236brain circuitry governing, 236–237characterization, 231implicit priming, 235–236learning and, 234–235Parkinson’s patients, 430
Nondeclarative tasks, 416Nonfluent aphasia, 219Nonfunctioning adenomas, 360Noninfiltrative tumors, 358Nonverbal learning disability syndrome
(NVLD), 304assessment, 307–308brain anomalies and, 306–307clinical features, 306clinical presentation, 305comorbid conditions, 305core features, 306developmental course, 309evolution, 309–310neuropsychological model, 308–309pathogenesis, 305–307prevalence, 305socioemotional characteristics, 308treatment, 309
Norepinephrine (NE), 108orientating systems, 245REM sleep and, 459
Normal probability distribution, 85Normal-pressure hydrocephalus (NPH),
130, 131Novelty seeking, 323NPH. See Normal-pressure hydrocephalusNREM. See Non-rapid eye movementNRT. See Nucleus reticularis thalamiNuclei, 99
basal, 147hypothalamic, 141thalamus, 144, 146
Nuclei of the raphe, 108
Subject Index 569

Nucleus ceruleus, 458Nucleus reticularis thalami (NRT), 468Nun Study, 402NVLD. See Nonverbal learning disability
syndrome
Obesity, 351Object permanence, 247Observations, qualitative, 88–89Obsessions, 334Obsessive-compulsive disorder (OCD)
characterization, 334effects of, 337treatment for, 336
Obstructive hydrocephalus, 277Obstructive sleep apnea, 462Occipital lobes, 158
blindness and, 205, 389function, 160REM sleep and, 458seizures and, 467visual processing and, 203–204
Occipital notch, 158Occlusion, 345Occupational therapy, 392, 393OCD. See Obsessive-compulsive disorderODD. See Oppositional defiant disorderOlfactory information processing, 166Olfactory system, 187–189Oligodendrocytes, 97Oligodendrogliomas, 359, 363On Narcissism (Freud), 19On the Origin of Species (Darwin), 16, 156Opiate receptors, 109–110Oppositional defiant disorder (ODD), 323,
326Orbitofrontal circuit, 254–257Organization of Behavior, The: A
Neuropsychology Theory (Hebb), 25Organs, definitions of, 13Orientation
GOAT, 70spheres, 69–70testing, 69
Overcorrection, 322Oxygen uptake. See NecrosisOxygen, positron-labeled, 51Oxytocin, 141
Pacemaker cells, 42Pallidotomy, 433–434PANDAS, 334Papez circuit, 149Papillae, 184Paragrammatism, 220Parahippocampal gyrus, 149Parasympathetic Nervous System (PNS),
121Parietal lobes, 158Parkinson’s disease (PD), 424–434
case study, 432–433characterization, 424clinical presentation, 425–431
executive functioning, 429–431language, 430memory, 430motor system, 427–428personality changes, 430–431
speech, 430visuospatial deficits, 428–429
impaired learning and, 235neuropathology, 424–425symptoms, 424treatments, 431–434
Paroxetine (Paxil), 336Partial seizures, 444, 466–467Parvocellular visual system, 299Pathognomonic signs, 88–89Pathways, 99
auditory, 45, 216DA, 108neurotransmitter, 107somatosensory, 181–182visual, 201
Patrick, Ruth, 401Pattern analysis, 88Pattern theory of taste, 185PD. See Parkinson’s diseasePenetrating head injuries, 373, 374Peptides, 109, 110Perception, 70–71Performance, assessing level of, 84–86Peripheral nervous system (PNS)
ACh function in, 107ANS function in, 122cellular migration, 116–117CNS communication, 121components of, 122ganglia in, 99neurogenesis and, 116–117Schwann cells in, 97, 100stem cells in, 110
Personality tests, 68Pervasive developmental disorders, 310–322
autismclinical presentation, 311comorbid conditions, 311–312demographics, 311–312developmental course, 321neurofunctional model, 320–321neuropsychological assessment, 318–320pathogenesis, 313–318treatment, 321–322types, 312–313
distinguishing features, 310etiology, 310
PET. See Positron emission tomographyPetit mal seizure, 464Phantogeusia, 187Phantoms, 184–185Phantosmia, 189Phenylketonuria (PKU), 270Phonemic paraphasias, 221Phonologic awareness, 301, 302Phonologic model of dyslexia, 301–302Phrenology, 13–20Physical therapy, 392, 393Physostigmine (Synapton), 420Pia mater, 126Pinealomas, 361Pittsburgh Sports Concussion Program, 383Pituitary stalk, 141Pituitary tumors, 360–361, 363PKU. See PhenylketonuriaPlanum temporale, 163, 302Plaques
amyloid, 412neuritic, 411–412sclerotic, 98
Plasticity, 272, 389Platelets, 345Pluripotentiality, 24PMA. See Premotor areaPneumoencephalography. See Air
encephalographyPNS. See Peripheral nervous systemPolymicrogyria, 271Polymodal areas. See Association areasPons, 134, 137Porencephaly, 271Positron emission tomography (PET), 33
Alzheimer’s patients, 413behavior-based assessments, 78–79characterization, 49neuropsychology and, 50–51postnatal development studies, 120subtraction procedures, 57technique, 49–50verbal encoding using, 48
Positron-labeled oxygen, 51Post-traumatic amnesia (PTA), 387Post-traumatic epilepsy, 379Posterior attention system, 244Posterior cerebral arteries, 131Posterior communicating arteries, 132Postictal phase, 466Postnatal development, 120–121Pragmatics of language, 308Precursor cells, 116Prefontal cortex, 117Pregnancy, 292Premotor area (PMA), 190, 191Prepotent response, 328Preserved-differentiation hypothesis, 403Prestriate cortex. See Secondary associationPrimary auditory cortex. See Heschl’s gyrusPrimary emotions, 260–262Primary motor cortex, 160
anatomy of, 178role of, 190somatosensory cortex and, 190–191
Primary sensory cortex, 178Primary visual processing, 201–204
characterization, 201disorders of, 201–203functional areas, 203–204retinotopic map, 203–204
Priming tasks, 416Prion proteins (PrPs), 439Problem solving tests, 76–78Procedural learning, 234Procedural memory, 227Process approach, 81–84Progenitor cells, 116Progressive dementia, 408Projection fibers, 99Proprioception, 178, 183Proprioceptors, 181Prosopagnosia, 207Prospective memory, 402–403PrPs. See Prion proteinsPruning, 95, 118Pseudopsychopathic sociopathy. See Acquired
sociopathy
570 Subject Index
Psychoactive drugs, 104Psychologist, 27Psychology, 4Psychometrics, 67Psychomotor epilepsy, 467Psychostimulant medication, 331–332Psychosurgery, 25Psychotherapy, 395–397PTA. See Post-traumatic amnesiaPurkinje cells, 96Putamen, 147Pyramidal system, 148
Quantification analysis, 57–58
RA. See Robust nucleus of the archistriatumRadiation damage, 364–365Radio-frequency (RF) signal, 53Radiologic procedures, 35–40
air encephalography, 36angiography, 38–40CT, 36–38skull x-ray, 36Wada technique, 40
Rapid eye movement (REM), 450ACh role, 107cataplexy and, 463dreaming and, 451EEG during, 451–452, 454function of, 459–461hypoxia and, 342reticular activating system and, 456–459state of consciousness during, 452, 454
RAS. See Reticular activating systemReceptors
auditory, 215cells, 177mechanical, 180sites, 105on skin, 179–181
Recognitiondisorders, 207–208processing systems, 204tests, 209
Refractory period, 103Regional CBF, 47–48Rehabilitation, 389–397
admission to programs, 390–395discharge planning, 393–394everyday activities assessment, 394–395goal evaluation, 393–394outpatient treatment, 394specialties
neuropsychology, 391–392occupational therapy, 392physical therapy, 392speech therapy, 392–393therapeutic recreation, 393
stroke, 352team approach, 391treatment methods, 395–397treatment planning, 394
Reliability, 67REM. See Rapid eye movementRepublic, The (Plato), 6Response cost, 322Resting potential, 102Resting tremor, 425
Restless leg syndrome. See Nocturnalmyoclonus
Restorative sleep, 454, 456Reticular activating system (RAS), 107
comas and, 375cortical arousal, 458function, 240–241location, 137REM sleep and, 456–459stimulation, 140
Reticular formationanatomic feature, 139function, 140–141structure, 139–140
Retrograde amnesia, 226, 386–387Retrograde degeneration, 372Reversible dementia, 408–409Rey-Osterrieth Complex Figure Test, 75RF. See Radio frequencyRhinencephalon, 149Right brain strokes, 353–355Rigidity, 424Risperidone (Risperdal), 336Robust nucleus of the archistriatum (RA), 109Roosevelt, Theodore, 382
Saccadic eye movement, 299SAFs. See Scrapie-associated fibrilsSAS. See Sleep apneaSCEA. See Sexual Consent and Education
AssessmentSchizophrenia
attentional deficits in, 242drug treatments, 149lobotomy and, 23
Schwann cells, 97acoustic neuroma-associated, 360function of, 100
Sclerotic plaques, 98SCN. See Suprachiasmic nucleusScopolamine, 107Scrapie-associated fibrils (SAFs), 439SDAT. See Senile dementia of the
Alzheimer’s typeSDMT. See Symbol Digit Modalities TestSecondarily generalized seizures, 467Secondary association, 203Secondary emotions, 262–264Seizures, 444, 463–473
anatomy, 467–469causes, 464, 467characterization, 464classification
complex partial, 464generalized, 466partial, 466–467petit mal, 464simple, 466–467
classifications, 464–467clinical presentation, 469–472EEG and, 42–43neuronal firing and, 104neurophysiology, 467–469postictal phase, 466
Semantic knowledge breakdown, 415–416Semantic memory, 228Senile dementia of the Alzheimer’s type
(SDAT), 410–411, 413, 418
Senile plaques, 404Sensation, 70–71, 177Sensitivity, 84Sensory association areas, 189Sensory auras, 472Sensory neurons, 99Sensory system
Alzheimer’s patients, 418chemical senses, 184–189CVA-induced deficits, 352–353somatosensory processing, 178–184
Septum, 149SER. See Somatosensory-evoked responseSerotonin (5-HT), 106
CVAs and, 348distribution, 108function, 316GTS and, 334REM sleep and, 459
Serotonin reuptake inhibitors (SSRIs), 336Set-shifting problems, 4297-repeat allele, 323–324Sex chromosomes, 282Sexual Consent and Education Assessment
(SCEA), 387Sexual hormones
cerebral specialization and, 171–175circulating levels, 173effects of, 171menopause and, 174
Sexuality, 386–387Shifting attention, 246Short-term memory (STM), 226
Alzheimer’s patients, 416deficits, 237–238LTM versus, 237–240working memory and, 238–240
SIDS. See Sudden infant death syndromeSimple drawing tasks, 417Simple seizures, 466–467Simple tics, 332–333Single-gene, 281Single-photon emission computed
tomography (SPECT)Alzheimer’s patients, 413development, 33technique, 48–49
Skulls, 125anatomy, 126, 127fractures, 378–379newborn, 125x-ray, 36
Sleepanatomy, 456architecture, 451–456mechanisms, 450–451normal, 454NREM, 42
characterization, 450EEG during, 451–452, 454state of consciousness during, 452, 454
onset, 456phasic events, 454, 456physiology, 456REM, 450
ACh role, 107cataplexy and, 463dreaming and, 451
Subject Index 571

Sleep (continued)EEG during, 451–452, 454function of, 459–461hypoxia and, 342reticular activating system and,
456–459state of consciousness during, 452, 454
rhythms, 451–452stages of, 451–452
Sleep apnea (SAS), 342, 461–462Sleep disorders
case study, 450narcolepsy, 462–463SAS, 461–462
Sleep paralysis, 458, 463Sleepwalking, 454SMA. See Supplementary motor areaSMDT. See Symbol Digit Modalities TestSmell
characterization, 187disorders of, 189olfactory system, 187–189
Smell Identification Test (UPSIT), 189SNS. See Somatic nervous systemSociability
autism and, 311GTS, 337in NVLD children, 308WS and, 290
Social brain network theory, 317–318Social cognition, 319–320Sociopathy, 255–256Sodium amytal injections, 40
hemisphere dominance evaluations, 161speech, 470–471
Sodium-potassium pump, 102Somatic markers, 256Somatic nervous system (SNS), 121Somatosensory cortex, 159, 190–191Somatosensory system
dysfunctions of, 183–184pathways, 181–182primary cortex, 182–183receptors, 179–181types of sensory stimulation and, 178
Somatosensory-evoked response (SER), 45Somatostatin, 413Songbirds, 109Soul
non-Western views, 12parts, Plato’s views, 6spiritual, 8
Space-occupying clots, 378Spatial ability
Alzheimer-induced deficits, 413, 417,428–429
CVA-induced deficits, 354–355disorders, 208, 210–215egocentric disorder, 436gender differences, 169–170processing system, 204, 207TS-induced deficits, 284
Spatial coding neurons, 459Spatial perception, 169Specificity, test, 84SPECT. See Single-photon emission computed
tomography
Speechapraxia, 219brain systems and, 218Broc’s area, 16–18disorders, 219–221locus of, 16loss of, 21Parkinson’s patients, 430requirements, 215–216stroke damage to, 355–356Wernicke’s area, 18
Speech therapyconditions treated by, 393goal, 393specialties, 392
Spina bifida, 116, 277Spinal cord
development, 119–120function of, 123–124protection of, 125–127segmentation of, 120structure of, 123
Spinal tap. See Lumbar punctureSplit-brain patients, 445–446Sports neuropsychology, 28Sports-related concussions
CHI, 28contemporary research, 384history of, 382–383mild THI, 381–382prevention efforts, 383–385Virginia football studies, 383
SQUID. See Superconductoring quantuminterference device
SSRIs. See Serotonin reuptake inhibitorsStains
Golgi, 34myelin, 35Nissl, 34–35
Standard battery approach, 80–81Standardized scores, 85Static dementia, 408Stelazine (trifluoperazine), 149Stem cells, 110, 111Stenosis, 349STM. See Short-term memoryStress and aging studies, 405Striatal complex, 196Striate cortex, 203Striatum, 107, 148Strokes. See Cerebrovascular accidentsStroop test, 245Stuck-in-set perseveration, 319STX1A. See Syntaxin 1ASubarachnoid hemorrhage, 347Subarachnoid space, 126Subcallosal anterior cingulate, 171Subconscious processes, 449Subcortical dementias, 237
characterization of, 408CJD as, 436–438HD as, 434–436PD as, 424–434regions associated with, 411understanding, 426
Subcortical motor processing, 195–197, 448Subdural hematomas, 377
Subdural space, 126Substantia nigra, 108
functions, 147–148HD and, 434–435Parkinson’s and, 425
Subthalamic nucleus, 147Subtraction procedures, 57Sudden infant death syndrome (SIDS), 462Summer, Larry, 172Superconductoring quantum interference
device (SQUID), 56Superego, 19Superior colliculi, 138Supplementary motor area (SMA), 191Suprachiasmic nucleus (SCN), 456, 457Supravalvar aortic stenosis (SVAS), 286Surface dyslexia, 299Sustained attention, 241, 246SVAS. See Supravalvar aortic stenosisSydenham’s chorea, 335Sylvian (lateral) fissure, 118Sylvian aqueduct. See Cerebral aqueductSylvian fissures, 163Symbol Digit Modalities Test (SMDT), 72Symptom validity testing, 78Synapses, 103
structure of, 105transmissions, 105–106
Synaptic cleft, 105Synaptic knobs, 105Synaptic vesicles, 105Synaptogenesis, 117Synchronous brain activity. See SeizuresSynesthesia, 179Syntaxin 1A (STX1A), 286
Tactile agnosia, 178, 183Tactile auras, 473Tangles, 411–412Tardive dyskinesia, 149Taste
disorders of, 186–187function of, 186receptor cells, 184theories of, 185
Tau proteins, 411, 412TBI. See Traumatic brain injuryTectum, 138Tegmentum, 138Telencephalon, 118, 147–152
basal ganglia, 147–149corpus callosum, 151–152hemispheres, 147limbic system, 149–151
Telomeres, 405Temporal lobes, 158
autism and, 317dyslexia and, 302epilepsy and, 465, 467function, 161strokes in, 350
Temporal order memory, 302Tensile strength, 372Teratogens, 270Terminal buttons, 95, 98Terrorism, 28–29Test battery, 69
572 Subject Index
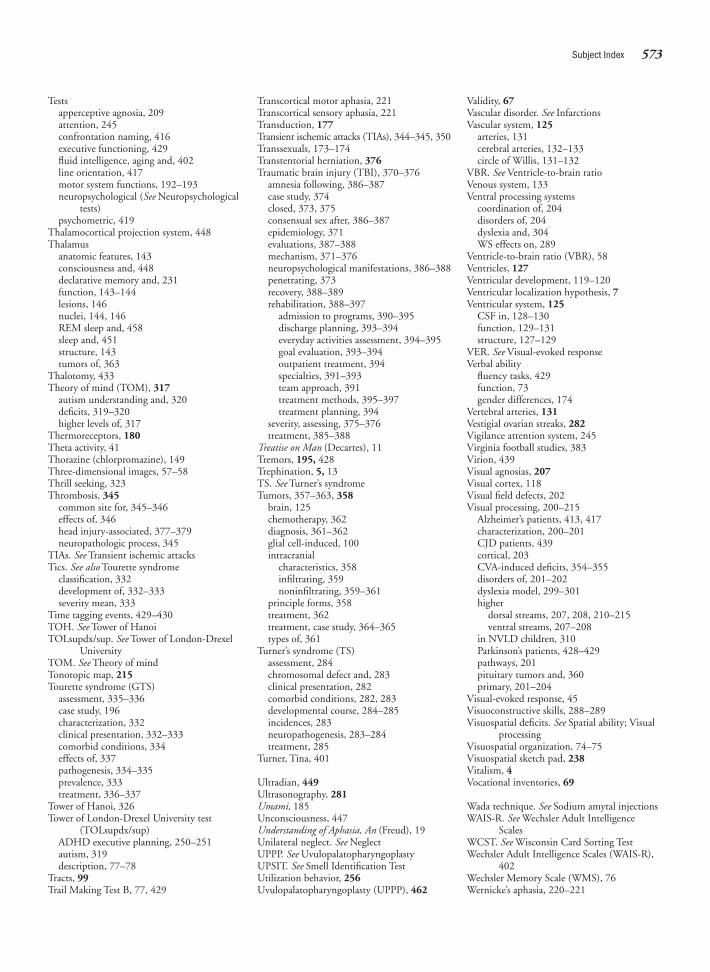
Testsapperceptive agnosia, 209attention, 245confrontation naming, 416executive functioning, 429fluid intelligence, aging and, 402line orientation, 417motor system functions, 192–193neuropsychological (See Neuropsychological
tests)psychometric, 419
Thalamocortical projection system, 448Thalamus
anatomic features, 143consciousness and, 448declarative memory and, 231function, 143–144lesions, 146nuclei, 144, 146REM sleep and, 458sleep and, 451structure, 143tumors of, 363
Thalotomy, 433Theory of mind (TOM), 317
autism understanding and, 320deficits, 319–320higher levels of, 317
Thermoreceptors, 180Theta activity, 41Thorazine (chlorpromazine), 149Three-dimensional images, 57–58Thrill seeking, 323Thrombosis, 345
common site for, 345–346effects of, 346head injury-associated, 377–379neuropathologic process, 345
TIAs. See Transient ischemic attacksTics. See also Tourette syndrome
classification, 332development of, 332–333severity mean, 333
Time tagging events, 429–430TOH. See Tower of HanoiTOLsupdx/sup. See Tower of London-Drexel
UniversityTOM. See Theory of mindTonotopic map, 215Tourette syndrome (GTS)
assessment, 335–336case study, 196characterization, 332clinical presentation, 332–333comorbid conditions, 334effects of, 337pathogenesis, 334–335prevalence, 333treatment, 336–337
Tower of Hanoi, 326Tower of London-Drexel University test
(TOLsupdx/sup)ADHD executive planning, 250–251autism, 319description, 77–78
Tracts, 99Trail Making Test B, 77, 429
Transcortical motor aphasia, 221Transcortical sensory aphasia, 221Transduction, 177Transient ischemic attacks (TIAs), 344–345, 350Transsexuals, 173–174Transtentorial herniation, 376Traumatic brain injury (TBI), 370–376
amnesia following, 386–387case study, 374closed, 373, 375consensual sex after, 386–387epidemiology, 371evaluations, 387–388mechanism, 371–376neuropsychological manifestations, 386–388penetrating, 373recovery, 388–389rehabilitation, 388–397
admission to programs, 390–395discharge planning, 393–394everyday activities assessment, 394–395goal evaluation, 393–394outpatient treatment, 394specialties, 391–393team approach, 391treatment methods, 395–397treatment planning, 394
severity, assessing, 375–376treatment, 385–388
Treatise on Man (Decartes), 11Tremors, 195, 428Trephination, 5, 13TS. See Turner’s syndromeTumors, 357–363, 358
brain, 125chemotherapy, 362diagnosis, 361–362glial cell-induced, 100intracranial
characteristics, 358infiltrating, 359noninfiltrating, 359–361
principle forms, 358treatment, 362treatment, case study, 364–365types of, 361
Turner’s syndrome (TS)assessment, 284chromosomal defect and, 283clinical presentation, 282comorbid conditions, 282, 283developmental course, 284–285incidences, 283neuropathogenesis, 283–284treatment, 285
Turner, Tina, 401
Ultradian, 449Ultrasonography, 281Umami, 185Unconsciousness, 447Understanding of Aphasia, An (Freud), 19Unilateral neglect. See NeglectUPPP. See UvulopalatopharyngoplastyUPSIT. See Smell Identification TestUtilization behavior, 256Uvulopalatopharyngoplasty (UPPP), 462
Validity, 67Vascular disorder. See InfarctionsVascular system, 125
arteries, 131cerebral arteries, 132–133circle of Willis, 131–132
VBR. See Ventricle-to-brain ratioVenous system, 133Ventral processing systems
coordination of, 204disorders of, 204dyslexia and, 304WS effects on, 289
Ventricle-to-brain ratio (VBR), 58Ventricles, 127Ventricular development, 119–120Ventricular localization hypothesis, 7Ventricular system, 125
CSF in, 128–130function, 129–131structure, 127–129
VER. See Visual-evoked responseVerbal ability
fluency tasks, 429function, 73gender differences, 174
Vertebral arteries, 131Vestigial ovarian streaks, 282Vigilance attention system, 245Virginia football studies, 383Virion, 439Visual agnosias, 207Visual cortex, 118Visual field defects, 202Visual processing, 200–215
Alzheimer’s patients, 413, 417characterization, 200–201CJD patients, 439cortical, 203CVA-induced deficits, 354–355disorders of, 201–202dyslexia model, 299–301higher
dorsal streams, 207, 208, 210–215ventral streams, 207–208
in NVLD children, 310Parkinson’s patients, 428–429pathways, 201pituitary tumors and, 360primary, 201–204
Visual-evoked response, 45Visuoconstructive skills, 288–289Visuospatial deficits. See Spatial ability; Visual
processingVisuospatial organization, 74–75Visuospatial sketch pad, 238Vitalism, 4Vocational inventories, 69
Wada technique. See Sodium amytal injectionsWAIS-R. See Wechsler Adult Intelligence
ScalesWCST. See Wisconsin Card Sorting TestWechsler Adult Intelligence Scales (WAIS-R),
402Wechsler Memory Scale (WMS), 76Wernicke’s aphasia, 220–221
Subject Index 573
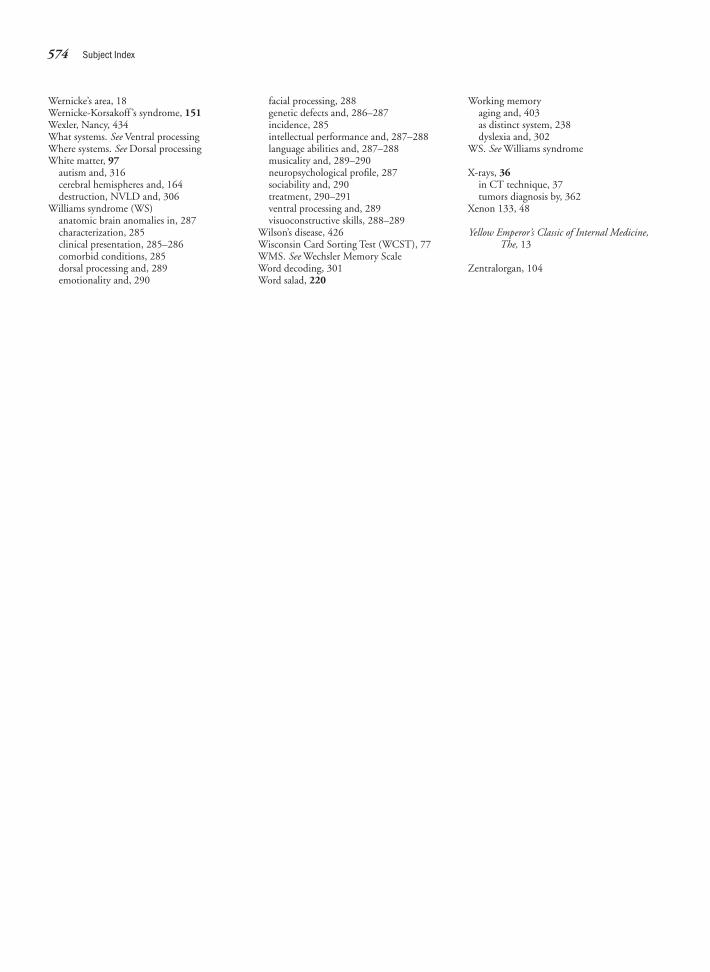
Wernicke’s area, 18Wernicke-Korsakoff ’s syndrome, 151Wexler, Nancy, 434What systems. See Ventral processingWhere systems. See Dorsal processingWhite matter, 97
autism and, 316cerebral hemispheres and, 164destruction, NVLD and, 306
Williams syndrome (WS)anatomic brain anomalies in, 287characterization, 285clinical presentation, 285–286comorbid conditions, 285dorsal processing and, 289emotionality and, 290
facial processing, 288genetic defects and, 286–287incidence, 285intellectual performance and, 287–288language abilities and, 287–288musicality and, 289–290neuropsychological profile, 287sociability and, 290treatment, 290–291ventral processing and, 289visuoconstructive skills, 288–289
Wilson’s disease, 426Wisconsin Card Sorting Test (WCST), 77WMS. See Wechsler Memory ScaleWord decoding, 301Word salad, 220
Working memoryaging and, 403as distinct system, 238dyslexia and, 302
WS. See Williams syndrome
X-rays, 36in CT technique, 37tumors diagnosis by, 362
Xenon 133, 48
Yellow Emperor’s Classic of Internal Medicine,The, 13
Zentralorgan, 104
574 Subject Index