
Prevention of running injuries by warm-up, cool-down, and stretching exercises
9
711 Prevention of running injuries by warm-up, cool-down, and stretching exercises WILLEM van MECHELEN,*† MD, PhD, HYNEK HLOBIL,* MD, HAN C. G. KEMPER,* PhD, WIM J. VOORN,‡ PhD, AND H. ROB de JONGH,§ PhD From the *Department of Health Science, Faculty of Human Movement Sciences, Vrije Universiteit, and the §Central Computer Department, and the ‡Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine, University of Amsterdam, Amsterdam, the Netherlands ABSTRACT The purpose of this study was to evaluate the effect of a health education intervention on running injuries. The intervention consisted of information on, and the sub- sequent performance of, standardized warm-up, cool- down, and stretching exercises. Four hundred twenty- one male recreational runners were matched for age, weekly running distance, and general knowledge of preventing sports injuries. They were randomly split into an intervention and a control group: 167 control and 159 intervention subjects participated throughout the study. During the 16-week study, both groups kept a daily diary on their running distance and time, and reported all injuries. In addition, the intervention group was asked to note compliance with the standardized program. At the end of the study period, knowledge and attitude were again measured. There were 23 injuries in the control group and 26 in the intervention group. Injury incidence for control and intervention sub- jects was 4.9 and 5.5 running injuries per 1000 hours, respectively. The intervention was not effective in re- ducing the number of running injuries; it proved signifi- cantly effective (P < 0.05) in improving specific knowl- edge of warm-up and cool-down techniques in the intervention group. This positive change can perhaps be regarded as a first step on the way to a change of behavior, which may eventually lead to a reduction of running injuries. The popularity of running as a form of exercise and recrea- tion has grown rapidly since the 1970s, first in North Amer- ica and later in Europe. Reasons for jogging include health and fitness, pleasure or relaxation, and competition or per- sonal performance.lo>3’ From a health point of view, benefits from regular physical activity include reduction of risk fac- tors for cardiovascular disease, such as obesity, hyperten- sion, and smoking.’ 5,18 28 38 On the other hand, runners, as any other athletes, sustain sports injuries. In the Netherlands, van Galen and Diederiks2° performed a telephone survey on sports injury incidence with a 4-week recall period. They used a repre- sentative sample of the Dutch population and included all self-reported injuries, both medically treated and not medi- cally treated. Based on their results, calculations were made for injury incident for the total Dutch population. The total number of sports injuries was estimated at 2,700,000. In absolute numbers, running was ranked 4th for the number of injuries incurred, with 126,000 injuries per year (54,000 medically treated), behind outdoor soccer, volleyball, and indoor soccer. If running exposure was taken into account, running was ranked as the 14th injury sport, with 3.6 injuries per 1000 hours of running (44% medically treated). Most running injuries are localized to the lower extremity, with a predominance in the knee .6 1,1 23 24,31,33,37,47,48 Running injuries are of a diverse nature and vary, as outlined by Powell et al.,39 from metabolic abnormalities such as anemia, amenorrhoea, hypothermia, and hyperthermia to extrinsic hazards such as dog bites and traffic collisions. However, most running injuries are musculoskeletal injuries associated with overuse. 2,1 15,17,29,36 This is understandable since run- ning involves the constant repetition of the same move- ments. According to Powell et al.,39 the etiologic factors related to musculoskeletal running injuries can be roughly divided into factors related to the runner, factors related to running, and factors related to the running environment. In relation to sports in general, some authors have sug- t Address correspondence and repnnt requests to Willem van Mechelen, MD, PhD, Department of Health Science, Faculty of Human Movement So- ences, Vnje Universiteit, van der Boechorststraat 7-9, 1081 BT Amsterdam, the Netherlands
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Prevention of running injuries by warm-up, cool-down, and stretching exercises

711
Prevention of running injuries by warm-up,cool-down, and stretching exercises
WILLEM van MECHELEN,*† MD, PhD, HYNEK HLOBIL,* MD,HAN C. G. KEMPER,* PhD, WIM J. VOORN,‡ PhD, AND H. ROB de JONGH,§ PhD
From the *Department of Health Science, Faculty of Human Movement Sciences, VrijeUniversiteit, and the §Central Computer Department, and the ‡Department of Clinical
Epidemiology and Biostatistics, Faculty of Medicine, University of Amsterdam,Amsterdam, the Netherlands
ABSTRACT
The purpose of this study was to evaluate the effect ofa health education intervention on running injuries. Theintervention consisted of information on, and the sub-sequent performance of, standardized warm-up, cool-down, and stretching exercises. Four hundred twenty-one male recreational runners were matched for age,weekly running distance, and general knowledge ofpreventing sports injuries. They were randomly splitinto an intervention and a control group: 167 controland 159 intervention subjects participated throughoutthe study. During the 16-week study, both groups kepta daily diary on their running distance and time, andreported all injuries. In addition, the intervention groupwas asked to note compliance with the standardizedprogram. At the end of the study period, knowledgeand attitude were again measured. There were 23injuries in the control group and 26 in the interventiongroup. Injury incidence for control and intervention sub-jects was 4.9 and 5.5 running injuries per 1000 hours,respectively. The intervention was not effective in re-ducing the number of running injuries; it proved signifi-cantly effective (P < 0.05) in improving specific knowl-edge of warm-up and cool-down techniques in theintervention group. This positive change can perhapsbe regarded as a first step on the way to a change ofbehavior, which may eventually lead to a reduction ofrunning injuries.
The popularity of running as a form of exercise and recrea-tion has grown rapidly since the 1970s, first in North Amer-
ica and later in Europe. Reasons for jogging include healthand fitness, pleasure or relaxation, and competition or per-sonal performance.lo>3’ From a health point of view, benefitsfrom regular physical activity include reduction of risk fac-tors for cardiovascular disease, such as obesity, hyperten-sion, and smoking.’ 5,18 28 38On the other hand, runners, as any other athletes, sustain
sports injuries. In the Netherlands, van Galen and
Diederiks2° performed a telephone survey on sports injuryincidence with a 4-week recall period. They used a repre-sentative sample of the Dutch population and included allself-reported injuries, both medically treated and not medi-cally treated. Based on their results, calculations were madefor injury incident for the total Dutch population. The totalnumber of sports injuries was estimated at 2,700,000. Inabsolute numbers, running was ranked 4th for the numberof injuries incurred, with 126,000 injuries per year (54,000medically treated), behind outdoor soccer, volleyball, andindoor soccer. If running exposure was taken into account,running was ranked as the 14th injury sport, with 3.6 injuriesper 1000 hours of running (44% medically treated).Most running injuries are localized to the lower extremity,
with a predominance in the knee .6 1,1 23 24,31,33,37,47,48 Runninginjuries are of a diverse nature and vary, as outlined byPowell et al.,39 from metabolic abnormalities such as anemia,amenorrhoea, hypothermia, and hyperthermia to extrinsichazards such as dog bites and traffic collisions. However,most running injuries are musculoskeletal injuries associatedwith overuse. 2,1 15,17,29,36 This is understandable since run-
ning involves the constant repetition of the same move-ments.
According to Powell et al.,39 the etiologic factors relatedto musculoskeletal running injuries can be roughly dividedinto factors related to the runner, factors related to running,and factors related to the running environment.
In relation to sports in general, some authors have sug-
t Address correspondence and repnnt requests to Willem van Mechelen,MD, PhD, Department of Health Science, Faculty of Human Movement So-ences, Vnje Universiteit, van der Boechorststraat 7-9, 1081 BT Amsterdam,the Netherlands

712
gested stiffness of the muscles of the lower extremity andsubsequent lack of range of motion of adjacent joints as anathlete-related etiologic factor for musculoskeletal inju-ries. 1,11,19, 22, 36, 41,42 In terms of the prevention of lower extrem-ity injuries, it seems advisable to recommend stretchingexercises of muscles of the lower extremity. It is known thathip flexion can be improved by such exercises. 21
In line with stretching exercises, a lack of or improper useof warm-up and cool-down techniques is mentioned as a riskfactor for musculoskeletal overuse injuries of the lower ex-tremity in sports in general22,41 and for running in particu-lar. 35,39Sound epidemiologic evidence for the preventive effect of
warm-up, cool-down, and stretching exercises on lower ex-tremity running injuries is scarce and contradictory. Jacobsand Berson,24 as well as IJzerman and van Galen,23 foundinjured runners stretched significantly more before runningthan noninjured runners. Jacobs and Berson reported thatcertain stretching exercises, such as the hurdler stretch, canlead to injury of the medial collateral ligament and to themedial meniscus. Both studies suggested that runners, whoare at high risk of sustaining recurrent injury, stretch be-cause they have previous injuries, thereby biasing researchresults. Walter et al. 41 found runners who &dquo;sometimes&dquo;stretch to be at greater risk for injury, in contrast to runnerswho &dquo;always, usually, or never stretch.&dquo; They leave thisfinding unexplained. Blair et al.’ found that frequency ofstretching was not associated with running injuries. Maceraet al. 32 found that stretching before running was not asso-ciated with running injuries. With regard to warmup, Walteret al. 41 found that runners who say &dquo;they never warm up&dquo;had a significantly smaller risk of running injury comparedwith runners who say they &dquo;always, usually, or sometimes&dquo;warm up. In the same study, regular use of cool-downexercises was not related to running injuries at all. Theremay be a negative, rather then a positive, relation betweenthe above-mentioned preventive measures and the risk oflower extremity running injuries, although the findings areinconclusive.
The purpose of this study was to investigate the effect ofa health education intervention program by which runnerswere provided with information that encouraged them toperform standardized warm-up, cool-down, and stretchingexercises to reduce the incidence of injuries of the lowerextremity. Health education by providing information is
only effective if it is put forward as a planned strategy. Kokand Bouter2’ argued that such a planned strategy should beaimed at a favorable modification of the determinants ofhealth behavior.Kok and Bouter described attitude as an important deter-
minant of healthy behavior. They refer to attitude as theknowledge and beliefs of a person concerning the specificconsequences of a certain form of behavior. An attitude isthe weighing of all consequences of the performance of thebehavior as seen by the individual. Consequently, this studywas also aimed at the effect of the health education inter-vention on knowledge and attitude of runners with respect
to the prevention of running injuries in general and withrespect to warm-up, cool-down, and stretching exercises inparticular.
DESIGN AND SUBJECTS
Design
An experimental black-box design was chosen in which twogroups of subjects, a control and an intervention group, arecompared with respect to differences in running injury in-cidence as a direct effect of the health education interven-tion. Both groups were also compared with regard to differ-ences in knowledge and attitude toward the prevention ofrunning injuries in general and warm-up, cool-down, andstretching exercises in particular as intermediate effects ofthe health education intervention.We know that age and weekly running distance can be
considered important predictors of running injuries.39 Wetherefore decided to match control and intervention subjectsfor these two variables. If one assumes that a health educa-tion intervention by providing information will lead to theperformance of the standardized program of warm-up, cool-down, and stretching exercises, one should realize that thisrequires a modification of behavior. This process of behaviormodification comprises a number of stages that must becompleted if any modification is to be achieved.44 These
stages are as follows: knowledge modification leads to atti-tude modification leads to intention modification leads tobehavior modification.
Since knowledge is the starting point in the chain ofevents leading to behavior modification, we decided to matchcontrol and intervention subjects for their knowledge on theprevention of running injuries as well.
Subjects and matching
If one assumes a yearly running injury incidence rate of60%,’ and if the intervention should lead to a significant(25%) reduction of injury incidence rate,45 both the controland intervention groups should contain at least 237 subjectsby the end of the experiment if a one-tailed chi-square testwas to be applied.4° To recruit such a number of subjects forthis study, 32,506 questionnaires were sent to all civil ser-vants employed by the city of Amsterdam, with a request toparticipate in a study on running; 1057 questionnaires werereturned from 982 men and 75 women. For reasons of
homogeneity and because of the relatively small number ofresponding women, we decided to exclude all female volun-teers. The responses of 463 civil servants met the criteriaset to enter the study: healthy, no current injury, not homefrom work on sick leave, running at least 10 km/week allyear-round, not performing sports as a part of their profes-sion (police officers and firefighters were excluded), andwritten consent to participate in the study.Age and estimated weekly running distance for these
subjects were gathered from the questionnaire. To facilitatethe matching procedure, we had to first assess the level of
713
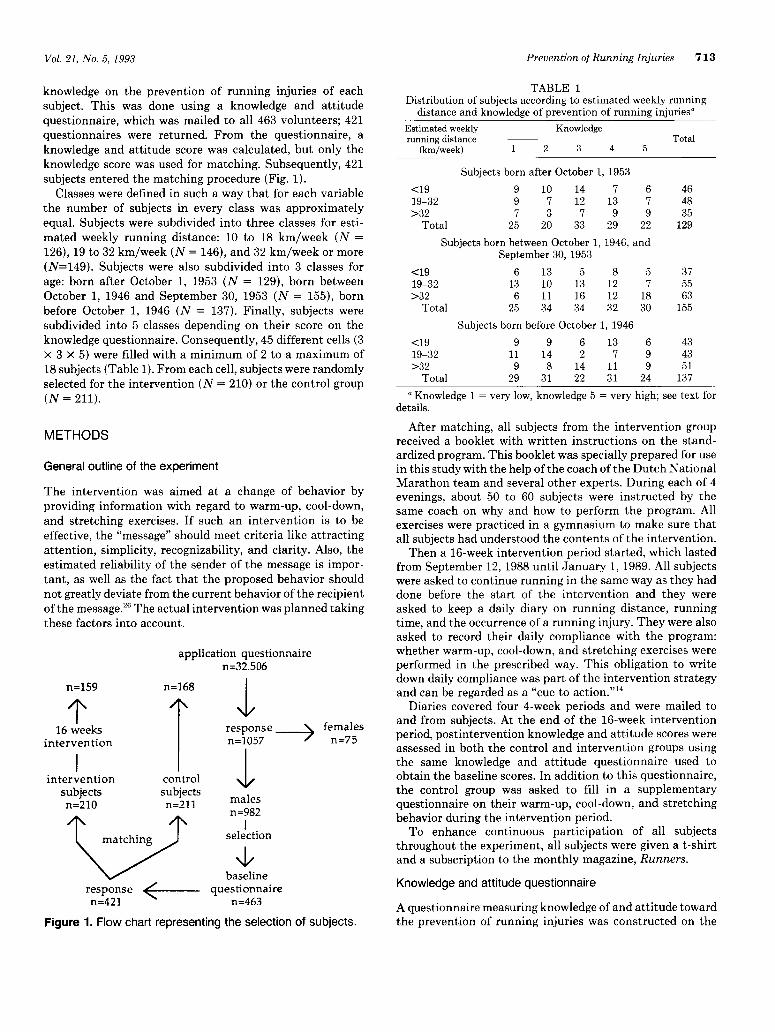
knowledge on the prevention of running injuries of eachsubject. This was done using a knowledge and attitudequestionnaire, which was mailed to all 463 volunteers; 421questionnaires were returned. From the questionnaire, aknowledge and attitude score was calculated, but only theknowledge score was used for matching. Subsequently, 421subjects entered the matching procedure (Fig. 1).
Classes were defined in such a way that for each variablethe number of subjects in every class was approximatelyequal. Subjects were subdivided into three classes for esti-mated weekly running distance: 10 to 18 km/week (N =126), 19 to 32 km/week (N = 146), and 32 km/week or more(N=149). Subjects were also subdivided into 3 classes forage: born after October 1, 1953 (N = 129), born betweenOctober 1, 1946 and September 30, 1953 (N = 155), bornbefore October 1, 1946 (N = 137). Finally, subjects weresubdivided into 5 classes depending on their score on theknowledge questionnaire. Consequently, 45 different cells (3x 3 x 5) were filled with a minimum of 2 to a maximum of18 subjects (Table 1). From each cell, subjects were randomlyselected for the intervention (N = 210) or the control group(N = 211).
METHODS
General outline of the experiment
The intervention was aimed at a change of behavior byproviding information with regard to warm-up, cool-down,and stretching exercises. If such an intervention is to be
effective, the &dquo;message&dquo; should meet criteria like attractingattention, simplicity, recognizability, and clarity. Also, theestimated reliability of the sender of the message is impor-tant, as well as the fact that the proposed behavior shouldnot greatly deviate from the current behavior of the recipientof the message.26 The actual intervention was planned takingthese factors into account.
Figure 1. Flow chart representing the selection of subjects.
TABLE 1
Distribution of subjects according to estimated weekly runningdistance and knowledge of prevention of running injuries&dquo;
a Knowledge 1 = very low, knowledge 5 = very high; see text fordetails.
After matching, all subjects from the intervention groupreceived a booklet with written instructions on the stand-ardized program. This booklet was specially prepared for usein this study with the help of the coach of the Dutch NationalMarathon team and several other experts. During each of 4evenings, about 50 to 60 subjects were instructed by thesame coach on why and how to perform the program. Allexercises were practiced in a gymnasium to make sure thatall subjects had understood the contents of the intervention.Then a 16-week intervention period started, which lasted
from September 12, 1988 until January 1, 1989. All subjectswere asked to continue running in the same way as they haddone before the start of the intervention and they wereasked to keep a daily diary on running distance, runningtime, and the occurrence of a running injury. They were alsoasked to record their daily compliance with the program:whether warm-up, cool-down, and stretching exercises wereperformed in the prescribed way. This obligation to writedown daily compliance was part of the intervention strategyand can be regarded as a &dquo;cue to action.&dquo;14
Diaries covered four 4-week periods and were mailed toand from subjects. At the end of the 16-week interventionperiod, postintervention knowledge and attitude scores wereassessed in both the control and intervention groups usingthe same knowledge and attitude questionnaire used toobtain the baseline scores. In addition to this questionnaire,the control group was asked to fill in a supplementaryquestionnaire on their warm-up, cool-down, and stretchingbehavior during the intervention period.To enhance continuous participation of all subjects
throughout the experiment, all subjects were given a t-shirtand a subscription to the monthly magazine, Runners.
Knowledge and attitude questionnaire
A questionnaire measuring knowledge of and attitude towardthe prevention of running injuries was constructed on the

714
basis of a literature survey.35 The initial knowledge ques-tionnaire contained 79 questions that were scored on a 3-point scale (3 points for &dquo;true,&dquo; 2 points for &dquo;don’t know,&dquo;and 1 point for &dquo;false&dquo;) and 45 attitude questions that werescored on a 5-point scale varying from 5 points for &dquo;total
agreement&dquo; to 1 point for &dquo;total disagreement&dquo; with anattitude statement. This questionnaire was tested for valid-ity and reliability in a pilot study 12 according to a methoddescribed by Swanborn.43 This method applies principles asdescribed by Ebel.16 The final version of the knowledge andattitude questionnaire as it was used in this intervention
study contained 56 knowledge questions and 31 attitudequestions. Neither part of the questionnaire contained ques-tions with an item-rest correlation coefficient of less than0.20 (this means that the correlation coefficient of each itemwith the total score was at least 0.2). Cronbach’s alpha ofthe knowledge part of the questionnaire was 0.89 and of theattitude part 0.79.From the questionnaire, the following seven scores were
calculated: 1) general knowledge of the prevention of run-ning injuries, 2) specific knowledge of warm-up exercises, 3)specific knowledge of stretching exercises, 4) specific knowl-edge of cool-down exercises, 5) general attitude toward theprevention of running injuries, 6) specific attitude towardwarmup, and 7) specific attitude toward cooldown.
Intervention
The content of the intervention, as described in the bookletand as explained during the instruction evening, was basedon a literature survey.35 The intervention consisted of awarmup of 6 minutes of running exercises, 3 minutes ofloosening exercises, and 10 minutes of stretching to beperformed before each running session. The stretching ex-ercises included three bouts (10 seconds each) of static
stretching of the iliopsoas and quadriceps muscles, the ham-strings, and the soleus and gastrocnemius muscles. A cool-down after each running session consisted of the inverse ofthe warmup. Stretching exercises were performed as outlinedabove twice a day regardless of running performance.
Injury registration
A running injury was defined as any injury that occurred asa result of running and caused one or more of the following:1) the subject had to stop running, 2) the subject could notrun on the next occasion, 3) the subject could not go to workthe next day, 4) the subject needed medical attention, or 5)the subject suffered from pain or stiffness during 10 subse-quent days while running. Any injury that met this defini-tion was to be noted in the daily running diary. Every injurywas also to be reported by a special postage-paid reply form.Every reported injury was seen by one of the two physi-
cians involved in the project. Location, injured structure,type of injury, and most likely medical diagnosis were noted.In case of a reported injury, a subject was excluded fromreentering the study. All diary data gathered after the re-
ported date of onset of injury were excluded from dataanalysis.
Data analysis
Incidence was calculated taking exposure into account andexpressed as the number of newly sustained running injuriesper 1000 hours of running. If applicable, overall differencesbetween the intervention and control group were analyzedby applying a two-tailed t-test, a chi-square test, or bycalculating a relative risk and its 95% confidence interval.
Differences in baseline attitude scores between the controland intervention group were tested by applying a two-tailedt-test.
The effect of the intervention was assessed by analyzingdifferences per cell by means of a one-tailed sign test be-tween the control and intervention group with regard toinjury incidence per exposure. The effect of the interventionwas also assessed by applying the same procedure for differ-ences between baseline and postintervention delta valueswith regard to knowledge and attitude scores. For all tests,P < 0.05 was considered statistically significant.
RESULTS
All materials (diaries and questionnaires) were returned by168 control and 159 intervention subjects. However, at theend of the intervention 1 cell contained only 1 control
subject, which made comparisons between control and in-tervention values for this cell impossible. For this reason,this cell and its subject were excluded from data analysis atcell level, thereby reducing the number of cells from 45 to44. Whenever data analysis was performed at group levelthe results of this subject were included. Consequently,results from 167 control and 159 intervention subjects dis-tributed over 44 cells were analyzed at cell level, and resultsfrom 168 control and 159 intervention subjects were ana-lyzed at group level. The total drop-out rate after 16 weekswas 94/421 x 100% = 22.3%.
In Table 2, overall descriptive values of running perform-ance are summarized for the control and intervention
groups. None of the variables show any statistically signifi-cant (Student’s t-test, P > 0.05) difference between thecontrol and intervention groups. The average runner in this
study ran about 2.7 times a week for 8.8 km per session at aspeed of 12.4 km/hr.Table 3 summarizes compliance with the prescribed inter-
vention as reported by daily diary by the intervention group.Table 4 summarizes information from the control group
on the performance of warm-up, cool-down, and stretchingexercises during the intervention period. This informationwas obtained at the end of the intervention period by ques-tionnaire.
Since the two methods of data collection with regard tothe performance of warm-up, cool-down, and stretchingexercises during the intervention period were different forboth groups, the results from Tables 3 and 4 can only beglobally compared. The tables show that in both groups a

715
TABLE 2Mean and standard deviation of running variables as written down
by subjects during the 16-week intervention period&dquo; a
° Differences between the intervention and control groups weretested by a two-tailed t-test. (No comparisons showed significantdifference, P > 0.05.)
TABLE 3
Compliance with intervention by the study group (N = 159)a
° Data derived from daily diaries.
TABLE 4Performance of warm-up, cool-down, and stretching exercises
among the control group (N = 167).....................
form of warmup and cooldown was performed by about 90%of the runners, whereas a form of daily stretching exerciseswas performed by about 58% of the runners.
Forty-nine injuries, 23 in the control group and 26 in theintervention group, were registered in the diaries. Of these49 injuries, 44 were also reported by means of a postage-paid injury reply form and subsequently evaluated. Thismeans that no information on the nature and location of
the injury was available from 5 subjects. From these 5
subjects, we know only the date on which they reportedthemselves in the daily diary as being injured.
Injury incidence analysis was performed using data refer-ring to the 49 injuries as registered in the diaries. Therewere no significant differences between these 2 groups (chi-square = 0.45, df = 1, P > 0.05).For both groups, injury incidence was calculated taking
exposure into account. In the control group, 4.9 injuries per1000 hours of running (95% confidence limit: 3.1 to 7.4)were calculated, and in the intervention group 5.5 injuries
per 1000 hours of running (95% confidence limit: 3.6 to 8.0);the relative risk for injury was 1.12 (95% confidence limit:0.56 to 2.72). To evaluate the effect of the interventionprogram, the injury incidence per 1000 hours of running wascalculated per cell for both the intervention and the control
groups. In 13 cells the injury incidence of the control subjectsexceeded the injury incidence of the intervention subjects,in 14 cells the opposite was found, and in 17 cells nodifference was found with regard to injury incidence betweengroups. By applying a one-tailed sign test, these differencesproved not significant (P > 0.05). We concluded that theintervention program did not result in a reduction of theincidence of running injuries per 1000 hours of running.
Differences in injury pattern between the control andintervention groups were analyzed by a chi-square test (P <0.05 is significant) using information from the 44 evaluatedinjuries. No differences were found between the interventionand control groups with regard to all registered variables:location of injury, injured anatomic structure, medical di-agnosis, and nature of injury (acute versus overuse andrecurrence of injury). The locations of the 44 evaluatedinjuries are presented in Table 5.
All injuries were equally distributed on the left and rightsides of the body. The injured anatomic structures were:muscle (11), tendon (9), joint (9), tendon-muscle (8), tendon-bone (4), bone (2), and skin (1). The distribution of the mostlikely medical diagnosis was as follows: strain (16), inflam-mation (11), sprain (3), blister (1), chondromalacia (3),miscellaneous (3), and diagnosis not clear (3). Seventy-fivepercent of the injuries were classified as overuse injuriesthat had developed over the course of hours or days; 25% ofthe injuries were classified as acute. Thirty percent of therunners had sustained a similar injury some time duringtheir running careers.Mean data of both groups were calculated for six knowl-
edge and attitude questionnaire scores. The general knowl-edge score is not included because the subjects were matchedon this score over the control and intervention groups.Analysis by means of a two-tailed t-test proved that thedifferences between the intervention and the control groupswere not significant (P > 0.05) concerning baseline scorefor which the two groups were not directly matched (baselinescore general attitude, baseline score specific knowledge ofwarming up, baseline score specific knowledge of coolingdown, baseline score specific knowledge of stretching exer-
TABLE 5Localization of 44 evaluated injuries

716
cises, baseline score specific attitude toward warming up,and baseline score specific attitude toward cooling down).We concluded that at baseline there were no differencesbetween the intervention and control groups with respect to
general attitude and specific knowledge and attitude scores.The effect of the intervention was also assessed by ana-
lyzing the difference per cell between the intervention andcontrol groups with respect to general and specific knowl-edge and attitude scores. For both groups per cell the meandifference (delta score) between the baseline and postinter-vention scores was calculated for each questionnaire vari-able. In Table 6, the mean difference (delta score) betweenbaseline and postintervention scores is summarized for eachvariable.From Table 6 we concluded that, except for specific knowl-
edge scores of stretching exercises by subjects in the inter-vention group, all knowledge and attitude scores in bothgroups had improved at the end of the intervention in
comparison with the score at baseline measurement. Theimprovement of scores of the intervention group with regardto specific knowledge about warming up, specific knowledgeabout cooling down, specific attitude toward warming up,and specific attitude toward cooling down was significantlygreater when compared with the improvement of scores ofthe control group.We identified, per cell, whether this mean difference (delta
score) was in favor of the intervention or the control groupor whether there was no difference between both groupswith respect to the mean difference (delta score) betweenbaseline and postintervention scores. The differences inmean difference (delta score) were then analyzed for signif-icance by means of a one-tailed sign test. The results of thisprocedure are summarized in Table 7. We concluded that,in comparison with the control group, the intervention pro-gram had led to a significant improvement of specific knowl-edge of warming up and cooling down in the subjects of theintervention group. ,
DISCUSSION
This study was aimed at a change of behavior of runnerswith regard to warm-up, cool-down, and stretching exercises.An important prerequisite in this study is the assumption
that there is a positive relationship between preventivebehavior (i.e., warm-up, cool-down, and stretching exercises)and injury prevention. If this prerequisite is valid, one mustconclude that the intervention in this study has not beensuccessful since there was no significant effect on the inci-dence of running injuries per 1000 hours of running at thelevel of the matched cells or at group level.
Yet, since the study concerned a health education inter-vention in which the provision of information played a majorrole, the effect of the intervention can also be judged at thelevel of the matched cells from changes in knowledge andattitude of the runners with respect to the prevention ofrunning injuries in general and from changes in knowledgeand attitude with respect to the specific preventive measuresrelated to the desired change in behavior. We can thereforeconclude that the intervention has been successful, giventhe significant improvement of the specific knowledge scoresof warmup and cooldown in the subjects of the interventiongroup compared with the control group. None of the othermeasured differences between baseline and postinterventionknowledge and attitude scores showed a significant differ-ence between the control and intervention groups. From the
standpoint of health education by providing information,&dquo;this improvement of knowledge of warmup and cooldowncan be regarded as a positive effect of the intervention.Some remarks with regard to the effects of the interven-
tion must be made. Damoiseaux 13 has argued that the extentof the modifying effect of health education by providinginformation depends on the way in which the informationis provided to the target group: on an individual (person-to-person) basis, on a group basis, or on a mass media basis(Table 8). In the present study, the information was providedon a group basis by means of a booklet and an evening ofinstruction. The improvement of knowledge with regard towarmup and cooldown, but not of attitude or of injuryincidence, is in line with the modifications one may expectif health education information is provided on a group basis.Other factors that influence the effect of this kind of
health education intervention are who provides the infor-mation and whether the provided information &dquo;appeals&dquo; tothe recipients. Ooijendijk and van Agt37 conducted a studyon running injury prevention. Two hundred fifty-six menand 60 women with an average age of 39 years and an
TABLE 6Mean value and standard deviation of the difference (A score) between the baseline and postintervention scores for each questionnaire
variable for both the control and intervention group’
° Small differences in numbers of subjects (N) within each group are because of missing values on some questionnaire scores.b P > 0.05 = not significant.

717
TABLE 7
Comparison of A scores between the control and the intervention groups’
° Figures given are number of cells in which the score differed.b NS, not significant.
TABLE 8Effect of modifying effecta
° The X indicates the maximal expected extent of the modifyingeffect of health education by providing information with respect tothe modification of knowledge, attitude or of behavior, dependingon how the subject is approached.
Adapted from Damoiseaux.l3
average weekly running distance of 30 km served as subjects.These runners were asked by questionnaire if they wantedto obtain information on injury prevention and, if so, inwhat way and from what person. Seventy-six percent of therunners were interested in information on injury prevention:78% wanted to obtain information from leaflets and 40% byoral instruction given by either a fellow runner (61%) or acoach (41%). In light of these results it seems valid toconclude that the way of providing information in our study(booklet in combination with an instructional group sessionusing a well-known coach as instructor) must have appealedto our subjects, thereby not hindering the transfer of infor-mation.The aim of our study was to bring about a reduction in
the incidence of running injuries by the performance of astandardized behavior concerning warm-up, cool-down, andstretching exercises. From the results as presented in Tables3 and 4, we concluded that in both the intervention andcontrol groups a form of warmup and cooldown was per-formed by about 90% of the runners, whereas a form of dailystretching exercises was performed by about 58% of therunners. On the basis of this finding, one should questionwhether the aim of the study in terms of a change in behaviorwith regard to warm-up, cool-down, and stretching exercisesto prevent running injuries, was a realistic one to start if thesame proportion of the control and intervention group showa more or less similar behavior.From the study of Ooijendijk and van Agt,37 we know that
most runners (93%) perform some sort of warmup. In theirstudy, 88% of the subjects performed stretching exercises asa part of the warmup, and 64% performed a cooldown.From a preventive point of view, it seems better to focus
future health education intervention strategies on behavior
that is not already conducted &dquo;naturally&dquo; to such an extentas warm-up, cool-down, and stretching exercises, such as theearly detection of symptoms of overuse injuries, full reha-bilitation after injury to avoid the recurrence of injury, andthe distribution of training load (running frequency, weeklyrunning distance, and running speed). These factors areimportant predictors of running injury.32,33,47We know of only 2 large-scale prospective studies con-
cerning running injuries. In the study by Macera et allmonthly diaries were used as a method of data collection. Intheir 1-year study, data were analyzed on all subjects whoreturned 80% of their monthly diaries, including the lastdiary. The drop-out rate in this study was 39% (310 malesubjects). In our study, with a drop-out rate of 22.3%, datawere analyzed only from subjects who had all diaries andquestionnaires present at the end of the study. When com-paring these two drop-out rates, it should also be noted thatthe Macera et al. study lasted 1 year and our study lasted 16weeks.
In a 1-year prospective study by Walter et al., 47 data werecollected by telephone survey 4, 8, and 12 months after thestart of the study. In their study, 88% of all planned tele-phone contacts took place. In light of these two prospectivestudies, the drop-out rate in our study seems acceptable.The drop-out rate may have been influenced by the fact thatthe intervention took place at the end of autumn and thebeginning of winter when weather condition are usually notas good as spring and summer. However, a recent nationalsurvey on sports participation conducted in the Netherlandsshowed that participation in recreational running is notmuch influenced by the season. 21The runners in this study were all men who ran on the
average about 2.7 times a week for 8.8 km per session at a
speed of 12.4 km/hr. If compared with the populations ofother studies, the average runner in our study can be con-sidered as representing the recreational runner who runs forpleasure and health rather than for competition, and whoparticipates in an organized roadrun every now andthen 6,20,28,32,33,37
Although many researchers in the field of sports etiologyresearch advise taking exposure to sports participation intoaccount,3,7,25.30,31,34,46.49 this is seldom the case. We know ofonly 3 studies regarding running that calculate injury inci-dence per 1000 hours of running. van Galen and Diederiks2°

718
found in their retrospective national survey an overall inci-dence for self-reporting running injuries of 3.6 per 1000hours of running. Lysholm and Wiklander 31 performed a 1-year prospective study with competitive male and femalerunners from various disciplines: sprint, middle-distance,and marathon. They found incidences for running injuriesvarying from 5.8 injuries per 1000 hours of running forsprinters to 2.5 injuries per 1000 hours of running for mar-athon runners. Finally, Bovens et al.’ found, in a prospectivestudy of 58 men (average age, 35 years), injury incidencesvarying with average weekly running distance from 12.1injuries per 1000 hours of running (average weekly runningdistance, 24 km/week) to 7.0 injuries per 1000 hours ofrunning (average weekly running distance, 44 km/week).The injury incidences in the present study fall within the
range of incidences found in the above-cited studies. How-
ever, it should be kept in mind that these figures may bedifficult to compare because of differences in definitions andresearch methods.3 No attempt was made to compare the
injury pattern found in this study with the pattern found inother studies since potential differences between studies canbe explained by differences in definitions and research meth-ods, as well as by research outcome.3 3
CONCLUSIONS
1. In a 16-week prospective intervention study in whichsubjects were matched for age, weekly running distance, andgeneral knowledge regarding the prevention of running in-juries, the running injury incidence was found to be 4.9injuries per 1000 hours of running for the control group and5.5 injuries per 1000 hours of running for the interventiongroup.
2. A health education intervention, consisting of providinginformation by means of booklet and an instructional groupsession aimed at a change of behavior with regard to warm-up, cool-down, and stretching exercises, did not result in areduction of running injury incidence expressed per hoursof running exposure. The intervention did lead to a positivechange of specific knowledge with regard to warmup andcooldown. No further knowledge or attitude changes wereobserved.
In terms of health education by providing information,this change can be regarded as a positive effect of the
intervention.
3. Regardless of the intervention, 90% of both the inter-vention and control group performed some form of warm-up and cool-down exercises, whereas some sort of dailystretching exercises was performed by about 58% of therunners. It therefore seems advisable not to focus the pre-vention of running injuries by a modification of behaviorwith regard to these measures, but by a modification ofbehavior with regard to the early detection of symptoms ofoveruse injuries, full rehabilitation after injury to avoid therecurrence of injury, and the distribution of training load.
ACKNOWLEDGMENTS
This study was funded by the Dutch Ministry of HealthWelfare and Cultural Affairs as the Dutch contribution to acoordinated research project of the Council of Europe:&dquo;Sports for All: Sports Injuries and Their Prevention.&dquo; Thisstudy was also financially supported by the MunicipalHealth Authority of the city of Amsterdam and by Sportcom,publisher of Runners monthly magazine.The authors express their gratitude to Mrs. Inge Crolla,
MSc, for her work as research assistant.
REFERENCES
1 Agre JC Hamstring injuries Proposed aetiological factors, prevention andtreatment. Sports Med 2 21-33, 1985
2 Andrews JR Overuse syndromes of the lower extremity Clin Sports Med2 137-148, 1983
3 Backx FJG, Inklaar H, Koornneef M, et al Draft FIMS position statementon the prevention of sports injuries Geneeskunde en Sport (Special Issue)May 1990, pp 22-27
4 Berlin JA, Colditz GA A meta-analysis of physical activity in the preventionof coronary heart disease Am J Epidemiol 132 612-628, 1990
5 Bijnen FCH, Zonderland ML, Enst GCv, et al Bewegen, fitheid en gezon-dheid Geneeskunde en Sport 24(6) 163-169, 1991
6 Blair SE, Kohl HW, Goodyear NN Rates and risks for running and exerciseinjuries Studies in three populations Res Q 58 221-228, 1987
7 Bol E, Schmickli SL, Backx FJG, et al Sportblessures onder de knie,NISGZ publication 38 Papendal, the Netherlands, Netherlands Institute ofSports Health Care, 1991
8 Bovens AMP, Janssen GME, Vermeer HGW, et al Occurrence of runninginjuries in adults following a supervised training program Int J Sports Med10 S186-S190, 1989
9 Clement DB, Taunton JE A guide to the prevention of running injuriesAustr Fam Physician 10 156-164, 1981
10 Clough PJ, Dutch S, Maugham RJ, et al Pre-race drop-out in marathonrunners Reasons for withdrawal and future plans Br J Sports Med 21148-149, 1987
11 Cornelius WL, Hinson MM The relationship between isometric contractionsof hip extensors and subsequent flexibility in males J Sports Med PhysFitness 20 75-80, 1980
12 Crolla I, Cuppens C Het meten van kennis en attitude ten aanzien vanpreventie van hardloopblessures: de ontwikkeling van twee vragenlijsten,doktoraalonderzoeksverslag Master’s thesis Vakgroep Gezondheid-kunde Faculteit der Bewegngswetenschappen, Virje Universiteit, Amster-dam, 1988
13 Damoiseaux V Sportblessure-preventie via massamediale voorlichting, inRijsewijk van M, Wieberdink EAM, Zuurbier MA (eds) Voorlichting enSportblessures Utrecht, Handelijle Centrum GVO, 1986, pp 59-67
14 Dishman RK (ed) Exercise Adherence Its Impact on Pubhc Health Cham-paign, IL, Human Kinetics Books, 1987
15 Dressendorfer RH, Wade ChE The muscular overuse syndrome in long-distance runners Physician Sportsmed 11(11) 116-130, 1983
16 Ebel RL Essentials of Educational Measurement New York, Prentice HallInc, 1972
17 Eggold JF Orthotics in the prevention of runners’ overuse injuries Physi-cian Sportsmed 9(3) 125-131, 1981
18 Eichner ER Exercise and heart disease Epidemiology of the "exercisehypothesis " Am J Med 75 1008-1023, 1983
19 Ekstrand J, Wiktorsson M, Oberg B, et al Lower extremity goniometricmeasurements A study to determine their reliability Arch Phys MedRehabil 63 171-175, 1982
20 Galen W van, Diederiks J Sportblessures breed uitgemeten Haarlem, DeVneseborch, 1990
21 Hardy L Improving active range of hip flexion Res Q 56 111-114, 198522 Hess GP, Cappiello WL, Poole RM, et al Prevention and treatment of
overuse tendon injuries Sports Med 8 371-384, 198723 IJzerman JC, Galen WCC van Blessures bij lange afstandlopers The
Hague, The Royal Dutch Athletic Association, 198724 Jacobs SJ, Berson BL Injuries to runners A study of entrants to a 10,000
meter race Am J Sports Med 14 151-155, 198625 Kennedy MC, Vanderfield GK, Kennedy JR Sport Assessing the risk Med
J Austr 2: 253-254, 197726 Kok GJ GVO en sportletsels, in Rijsewjjk MV, Wieberdinck EAM, Zuurbier

719
ZA (eds) Voorlichting en sportblessures Rijswijk, Ministry of Health, 1986,pp 41-49
27 Kok G, Bouter LM On the importance of planned health educationPrevention of ski injury as an example Am J Sports Med 18 600-605,1990
28 Koplan JP, Powell KE, Sikes RK, et al An epidemiological study of thebenefits and risks of running JAMA 248. 3118-3121, 1982
29 Lehman WL. Overuse syndromes in runners Am Fam Physician 29 157-161,1984
30 Loes M de, Goldie K Incidence rate of injuries during sport activity andphysical exercise in a rural Swedish municipality Incidence rates in 17
sports Int J Sports Med 9 461-467, 198831 Lysholm J, Wiklander J Injuries in runners Am J Sports Med 15 168-
171,198732 Macera CA, Pate RR, Powell KE, et al Predicting lower-extremity injuries
among habitual runners Arch Intern Med 149 2565-2568, 198933 Marti B, Vader JP, Minder CE, et al On the epidemiology of running
injuries Am J Sports Med 16 285-294, 198834 Mechelen WV 25 jaar schade door sport Geneeskunde en Sport 23(5)
196-198,199035 Mechelen WV, Hlobil H, Kemper HCG How Can Injuries Be Prevented?
NISGZ publication no 25E Oosterbeek, Netherlands Institute of SportsHealth Care, 1987
36 Mirking G The prevention and treatment of running injuries J Am PodiatrMed Assoc 66 880-884, 1976
37 Ooijendijk WTM, van Agt L Preventie van hardloopblessures Genees-
kunde en Sport 23(4) 146-151, 1990
38 Paffenbarger RS, Hyde RT Exercise in the prevention of coronary heartdisease Prev Med 13 3-22, 1984
39 Powell KE, Kohl HW, Caspersen CJ, et al An epidemiological perspectiveon the causes of running injuries Physician Sportsmed 14(6) 100-114,1986
40 Rumke CL, With C de De grootte van groepen bij het vergelijken vantwee percentages of twee kansen NTVG 121 944-949, 1977
41 Safran MR, Seaber AV, Garrett WE Warm-up and muscular injury preven-ton. An update Sports Med 8 239-249, 1989
42 Shellock FG, Prentice WE Warming-up and stretching for improved phys-ical performance and prevention of sports-related injuries Sports Med 2:267-278,1985
43 Swanborn PG Schaaltechnieken, Theone en praktijk van acht eenvoudigeprocedures Meppel, Boom, 1982
44 Vent de TGM, Hlobil H, Mechelen WV Sports injuries prevention byinformation and education—a preparative study Report No 51, ConsumerSafety Institute, Amsterdam, November 1988
45. Vulpen AV Sport for All Sport Injuries and Their Prevention Oosterbeek,Council of Europe, Netherlands Institute of Sports Health Care, Ooster-beek, 1989
46 Wallace RB Application of epidemiologic principles to sports injury re-search Am J Sports Med 16 S22-S24, 1988
47 Walter SD, Hart LE, Mcintosh JM, et al The Ontano Cohort Study ofrunning-related injuries Arch Intern Med 149 2561-2564, 1989
48 Watson MD, DiMartino PP Incidence of injuries in high school track andfield athletes and its relation to performance ability Am J Sports Med 15251-254, 1987
49 Wiktorsson-Moller M, Oberg B, Ekstrand J, et al Effects of warming up,massage, and stretching on range of motion and muscle strength in thelower extremity Am J Sports Med 11 249-252, 1983




















