Preschool children's exposure to violence: Relation of behavior problems to parent and child reports
11
American Journal of Orthopsychiatry, 70(1), January 2000 © 2000 American Orthopsychiatric Association, Inc. Preschool Children's Exposure to Violence: Relation of Behavior Problems to Parent and Child Reports Ariana Shahinfar, Ph.D., Nathan A. Fox, Ph.D., Lewis A. Leavitt, M.D. A group of!55 parents and their preschool children attending Head Start reported on the children's exposure to community violence, level of distress symptoms, and behavioral problems. The behavioral correlates of exposure were found to differ according to exposure modality: internalizing problems were more likely in children who witnessed violence, and externalizing problems in those victimized by violence. Issues regarding self-reports by preschool children are highlighted, and clinical and research implications discussed. C ommunity violence has been recognized as epidemic in the United States (Rosenberg & Fenley, 1991; Rosenberg, O'Carroll, & Powell, 1992). With this public-health framing of the problem has come a growing concern for the number of children who are exposed to violent events. Community violence can be defined as the presence of violence and violence-related events within an individual's proximal environment, in- cluding home, school, and neighborhood; it may involve direct or threatened harm, be witnessed or experienced, and involve known or unknown per- petrators. In a survey conducted in Washington, D.C. (Richters & Martinez, 1993), 61% of a sam- ple of first- and second-grade children and 72% of fifth- and sixth-grade children reported witnessing violence in their community. In a similar survey (Bell & Jenkins, 1991) in Chicago, one-third of a sample of school-age children reported witnessing a homicide and two-thirds a serious assault. In New Orleans (Osofsky, Wewers, Hann, & Pick, 1993), 91% of 9-12 year-olds reported witnessing at least one violent incident. It is currently esti- mated that substantial numbers of children grow- ing up in these violent neighborhoods have also been the victims of community violence, often as innocent bystanders (Osofsky, 1995). As awareness of violence within the community has grown, the importance of research elucidating the correlates of such exposure for children has be- come especially urgent. Although the study of community violence has been informed by and is related to such other areas of trauma research as war and child maltreatment, several features distin- guish it from these other types of trauma. First, it is pervasive. Unlike maltreatment or family violence, which are usually limited to the home environ- ment, community violence infiltrates all ecological levels—in school, on the playground, and in the neighborhood, as well as in the home. Second, it presents a chronic threat, in contrast to the trauma of natural disaster, which is a time-limited event geographically unlikely to recur. Although not all children living in inner-city environments are con- tinuously exposed to violent incidents, the random nature of community violence presents a constant threat to the sense of safety of both children and their parents (Osofsky, 1995). Third, community violence is distinguished from other types of vio- lence by the alienation it engenders. For example, A revised version of a paper submitted to Hie Journal in August 1998. Research was supported by a grant from tlie Metropolitan Life Foundation, and by a post-doctoral fellmvship aiaarded by tlie National Institute of Child Health and Human Development to the first author. Authors are at: Center for Developmental Science, University of North Carolina at Chapel Hill (Shahinfar); Institute for Child Study, University of Maryland at College Park (Fox); and Waisman Center, University of Wisconsin at Madi- son (Leavitt). 115
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Preschool children's exposure to violence: Relation of behavior problems to parent and child reports

American Journal of Orthopsychiatry, 70(1), January 2000© 2000 American Orthopsychiatric Association, Inc.
Preschool Children's Exposure to Violence: Relationof Behavior Problems to Parent and Child Reports
Ariana Shahinfar, Ph.D., Nathan A. Fox, Ph.D., Lewis A. Leavitt, M.D.
A group of!55 parents and their preschool children attending Head Start reported on the
children's exposure to community violence, level of distress symptoms, and behavioral
problems. The behavioral correlates of exposure were found to differ according to exposure
modality: internalizing problems were more likely in children who witnessed violence, and
externalizing problems in those victimized by violence. Issues regarding self-reports by
preschool children are highlighted, and clinical and research implications discussed.
Community violence has been recognized asepidemic in the United States (Rosenberg& Fenley, 1991; Rosenberg, O'Carroll, &
Powell, 1992). With this public-health framing ofthe problem has come a growing concern for thenumber of children who are exposed to violentevents. Community violence can be defined as thepresence of violence and violence-related eventswithin an individual's proximal environment, in-cluding home, school, and neighborhood; it mayinvolve direct or threatened harm, be witnessed orexperienced, and involve known or unknown per-petrators. In a survey conducted in Washington,D.C. (Richters & Martinez, 1993), 61% of a sam-ple of first- and second-grade children and 72% offifth- and sixth-grade children reported witnessingviolence in their community. In a similar survey(Bell & Jenkins, 1991) in Chicago, one-third of asample of school-age children reported witnessinga homicide and two-thirds a serious assault. InNew Orleans (Osofsky, Wewers, Hann, & Pick,1993), 91% of 9-12 year-olds reported witnessingat least one violent incident. It is currently esti-mated that substantial numbers of children grow-ing up in these violent neighborhoods have also
been the victims of community violence, often asinnocent bystanders (Osofsky, 1995).
As awareness of violence within the communityhas grown, the importance of research elucidatingthe correlates of such exposure for children has be-come especially urgent. Although the study ofcommunity violence has been informed by and isrelated to such other areas of trauma research aswar and child maltreatment, several features distin-guish it from these other types of trauma. First, it ispervasive. Unlike maltreatment or family violence,which are usually limited to the home environ-ment, community violence infiltrates all ecologicallevels—in school, on the playground, and in theneighborhood, as well as in the home. Second, itpresents a chronic threat, in contrast to the traumaof natural disaster, which is a time-limited eventgeographically unlikely to recur. Although not allchildren living in inner-city environments are con-tinuously exposed to violent incidents, the randomnature of community violence presents a constantthreat to the sense of safety of both children andtheir parents (Osofsky, 1995). Third, communityviolence is distinguished from other types of vio-lence by the alienation it engenders. For example,
A revised version of a paper submitted to Hie Journal in August 1998. Research was supported by a grant from tlie MetropolitanLife Foundation, and by a post-doctoral fellmvship aiaarded by tlie National Institute of Child Health and Human Development tothe first author. Authors are at: Center for Developmental Science, University of North Carolina at Chapel Hill (Shahinfar);Institute for Child Study, University of Maryland at College Park (Fox); and Waisman Center, University of Wisconsin at Madi-son (Leavitt).
115

116
war is based on ideological differences that lendpurpose to its violence and act as a unifying forcewithin each warring group. Liddell, Kemp, andMoema (1993) suggested that such purpose mayhave served as a protective factor for their sampleof South African boys in moderating the traumaticeffects of war. Community violence, on the otherhand, alienates individuals from the community,leaving them with neither an ideological frame-work nor a reference group by which to under-stand its occurrence or find support.
Several empirical studies have examined the in-cidence, prevalence, and correlates of exposure tocommunity violence in school-age children andadolescents (Attar, Guerra, & Tolan, 1994; Bell &Jenkins, 1993; DuRant, Cadenhead, Pendergrast,Slovens, & Under, 1994; Fitzpatrick & Boldizar,1993; Freeman, Mokros, & Poznanski, 1993; Glad-stein, Rusonis, & Heald, 1992; Martinez & Rich-ters, 1993; Osofsky, et al., 1993; Schubiner, Scott,& Tzelepis, 1993; Shakoor & Chalmers, 1991; Sin-ger, Anglin, Song, & Lunghofer, 1995). In general,their findings suggest that children exposed to vio-lence are more likely to display behavioral andpsychological problems than are their nonexposedpeers. For example, in a study of urban primary-and secondary-school students, Bell and Jenkinsfound reports of violence exposure to be associ-ated with increased fighting among boys andyounger children. Similarly, Schubiner et al. dem-onstrated that children who had been victims of vi-olence were at greater risk for involvement in itsperpetration than their nonvictim peers. In terms ofpsychological symptoms, Freeman and colleaguesdiscovered a significant positive relation betweenreports of exposure to violence and depression ina group of 6-12-year-old urban children. Othershave demonstrated significant associations be-tween parent or child reports of violence exposureand distress symptoms such as anger, anxiety,sleep problems, and increased fears (Fitzpatrick &Boldizar, 1993; Martinez & Richters, 1993; Singeret al., 1995). It has been noted that symptoms re-ported by children exposed to violence parallelthose of persons with post-traumatic stress disorder(Bell & Jenkins, 1993; Martinez & Richters, 1993).
To date, the literature on exposure to violencehas been concerned primarily with school-age andadolescent populations. Little research has focusedon its prevalence and correlates in younger chil-dren. As a result, there is little information regard-ing rates of exposure and effects of community vi-
Violence Exposure and Preschool Children
olence on children below school age. Althoughanecdotal reports (Garbarino, Kostelny, & Dub-row, 1991) and findings from a hospital screeningsurvey (Taylor, Zuckerman, Harik, & Groves, 1994)have suggested that infants and young childrenfrom large urban areas are indeed at risk for expo-sure to community violence, such exposure has notbeen examined using the sampling and methodol-ogy employed with older populations. Nor, itseems, have the psychological and behavioral cor-relates of preschool children's exposure been ex-plored in a systematic way.
The study reported here examined parent andchild perceptions of the rates and correlates of vio-lence exposure in a preschool sample. Children'sperceptions of frequency of exposure were ratedon a relatively new measure, the Violence Expo-sure (VEX) scale for children (Fox & Leavitt, 1995).Because preschool children are just beginning tograsp distinctions between fantasy and reality (Fla-vell, 1993; Woolley, 1998), information gatheredfrom their self-reports may not reflect discrete in-cidents of exposure; thus, the utility of the VEXwas as a tool for accessing these children's percep-tions of violence. In addition to exposure, the chil-dren were asked to report on their symptoms ofdistress. Parents were also asked to report theirchildren's exposure to violence, as well as thelevel of behavior problems they displayed. A studyhypothesis was that children exposed to commu-nity violence would evidence higher levels of be-havioral and distress symptomatology. Whetherpreschool children's exposure to community vio-lence would be similar in prevalence to that re-ported in the literature on older children and ado-lescents was also of interest.
METHODInstrument Development
A cartoon-based interview was developed to as-sess children's self-reports of exposure to vio-lence. The resulting instrument, the VEX scale(Fox & Leavitt, 1995), was based on a measure de-signed by Richters and Martinez (1990) to assesselementary-school children's self-reports of suchexposure. Whereas the Richters and Martinez in-strument utilizes verbal descriptions of violentevents, the VEX scale offers a cartoon depiction ofeach event in order to give the child a concrete ref-erence point. Eight of the pictures show a centralcharacter, Chris, witnessing violent events, and sixdepict Chris as the victim of violent events.
Shahinfar et al
The violent incidents assessed by the preschoolversion of the VEX scale are beating, chasing, rob-bery, threat with a weapon, shooting, stabbing,pushing or shoving, and slapping. The childrenwere asked about witnessing all of them, and aboutvictimization by all but shooting or stabbing,partly because of the low probability thatpreschoolers would be victims of such events,partly out of concern for keeping the traumatic va-lence of the cartoon depictions at a minimum.
Following the interviewer's explanation of whatChris is witnessing or experiencing in each picture,the children are asked how often they have beenexposed to the same incident. Below each cartoonis a picture of four thermometers, each with themercury at one of four labeled levels: never, once,a few times, and lots of times. For those incidentsto which the child responds positively, the inter-viewer probes for information regarding where theevent occurred, who was with the child at the time,and when the event occurred. The probing is in-tended to assess the veracity of the child's reporton the basis of its relevance to the cartoon depic-tion. At the same time, the questions are designedto allow comparison between specific parent- andchild-reported events.
Preliminary testing of the VEX scale was com-pleted with a pilot sample of 40 suburban, primar-ily Caucasian, preschool children in order to en-rich construction of the items. As a result, severalitems were dropped due to a lack of clarity, andseveral new questions were incorporated. The lat-ter were added to a) assess innocuous events towhich the child was likely to have been exposedwith varying frequency (e.g., watching televisionor seeing a child sitting on Santa's lap); b) providea "psychological break" from the high valenceitems; and c) act as an internal test of the children'sunderstanding of the questions. Finally, gender-differentiated versions of the scale were developedto minimize the possibility that response would beaffected by the children's inability to identify witha cross-gender character; except for the gender ofthe depicted character, the text remained the samein both versions.
A distress symptom inventory was developedthrough modification of the Levonn instrument(Richters, Martinez, & Valla, 1990) to includeonly those cartoon depictions of symptoms rele-vant to the preschool years. As described else-where in more detail (Martinez & Richters, 1993),the Levonn is a cartoon-based interview in which
117
the child is shown a picture of a character (namedLevonn) experiencing different types of distress.Below each cartoon is a picture of three ther-mometers, each with the mercury at one of threelabeled levels: never, some of the time, and a lot ofthe time. Children are asked to report how oftenthey have felt like Levonn by pointing to the ther-mometer that best represents the frequency withwhich they have experienced the same symptoms.
SampleThe subjects comprised 155 families with a
child between the ages of 3'A and 4'/2 living in alow-income, primarily African-American neigh-borhood near Washington, DC. Based on policecrime statistics, the neighborhood fell into themoderately violent range, and the majority ofcrimes into the categories of robbery, aggravatedassault, and larceny (Maryland State Police,1995). The neighborhood consisted of single-family dwellings, and public-assisted and privateapartment buildings. Of the families interviewed,52% resided in apartments and 48% in detachedhomes, with 38% of the latter living with extendedfamily. While green space and playgrounds wereavailable, several parents anecdotally reported thatchildren spent more time indoors due to safetyconcerns.
Families were identified by their eligibility toparticipate in the Head Start program. Of the 155children, 79 (51%) were boys and 76 (49%) fe-male, while 98.8% were African-American. Of theprimary caregivers, 141 (91%) were biologicalparents. The majority of the families (81.2%) wereheaded by a single caregiver, and 37% of the chil-dren received day-care. The average annual in-come for the sample was less than $7,200, and al-most 50% of the sample were entirely supportedby public assistance.
ProcedureDuring the summer months preceding the school
year, families were contacted either during HeadStart registration or over the phone and invited toparticipate in a one-hour interview to be conductedin their homes. The interview was part of a prelim-inary screening for inclusion in an aggression in-tervention program scheduled for the school year.The caregivers were told that the purpose of theinterview was to learn more about their child'sdaily behavior and experiences. The data pre-sented here concern the child behavior and vio-

118
lence exposure portions of the interview. All fami-lies were compensated $25 for their participationin the project, and 95% of those contacted agreedto participate.
Two interviewers visited the subjects' homesand independently (one from the children, theother from their primary caregiver) elicited infor-mation regarding the children's violence exposureand symptomatology. Interviewers and primarycaregivers were matched on race and gender in96% of the cases. After describing the interviewcontent and assuring of confidentiality (exceptwhere required by law to protect the safety of thechild or caregiver), informed consent was obtainedby the parent interviewer. Interviewers adminis-tered questionnaires by reading items aloud andrecording parents' verbal responses. The child in-terview was administered simultaneously, either inanother room or in a remote area of the same room.
MeasuresParent Reports
Child's exposure to violence. All primary care-givers completed a parent-report version of theVEX scale (Fox & Leavitt, 1995). The incidentsassessed paralleled those of the child-report mea-sure described above. For every event to which thecaregiver responded positively, the interviewerimmediately probed for information about wherethe event occurred, who the perpetrators and vic-tims were, who was with the child at the time, andhow long ago the exposure took place.
Child behavior problems. Caregivers completedthe Child Behavior Checklist (CBCL/4-18) (Achen-bach, 1991), a widely used questionnaire for as-sessing the behavior problems of children and ado-lescents. They were asked to report on the fre-quency of specific types of child behavior duringthe previous six months. The CBCL yields a totalbehavior problem score, as well as broad-bandscales for internalizing and externalizing prob-lems. Internalizing behavior problems comprisethe withdrawn, anxious/depressed, and somaticcomplaint CBCL subscales; externalizing behaviorproblems comprise the aggressive and delinquentsubscales of the CBCL.
Child Vocabulary AchievementAt the beginning of the children's interviews, re-
searchers spent approximately five minutes color-ing pictures with the children in order to build rap-port. They then announced that they had brought
Violence Exposure and Preschool Children
some picture games to play with the children. Thefirst of these was the Peabody Picture VocabularyTest-Revised (PPVT-R) (Dunn & Dunn, 1981), an-individually-administered, norm-referenced test ofreceptive vocabulary designed for persons above21/2 years of age. Because the child is required topoint to appropriate pictures in response to the ex-perimenter's words, the PPVT-R does not requirea baseline level of verbal ability; rather, it is an ap-titude test of the child's cognitive development inthe area of vocabulary achievement. It was in-cluded as part of the child interview to examinewhether differences in cognitive developmentwere related to children's ability to respond to theself-report format of the distress and exposurescales used in the study.
Child ReportsDistress symptoms. Children were next adminis-
tered the preschool version of the Levonn (Rich-ters et al, 1990), a cartoon-based interview tap-ping self-report of distress symptomatology. Afterbeing trained on the use of the thermometer re-sponse format with a sample question ("During thesummer, how many times do you eat ice cream?"),children were asked how often they had felt likethe cartoon character in each picture. The symp-toms assessed included sadness, lack of appetite,fear of going outside because of possible violence,intrusive traumatic memories, and having night-mares.
Exposure to violence. Each child completed theVEX scale (Fox & Leavitt, 1995) after the inter-viewer made the following statement:
I am going to show you some pictures that tell about a childwhose name is Chris. I will show you one picture at a time andtell you what is happening in that picture. Afterwards, I willask you questions about things you may have seen that are likewhat Chris saw or things that may have happened to you thatare like what happened to Chris.
Care was taken to ensure that the children under-stood they should report only things they had seenor experienced in real life, not things seen on tele-vision, video, or in the movies.
After completing the VEX scale, interviewersdebriefed the children by asking them how the vio-lence exposure pictures had made them feel. Inter-viewer and child then talked about what it is like tofeel scared, and about people in the child's supportnetwork who make them feel safe. This debriefingserved to ascertain whether children had been up-set by the VEX drawings and, if so, to connect
Shahinfar et al
them with the appropriate supports. Very few ofthe children in the sample indicated, verbally orbehaviorally, that they had been upset.
Because of developmental limitations, it waspossible that some of the children surveyed wouldnot be able to generalize from a pictured event toincidents that had actually occurred in their ownlives. To separate children not responding to themeasure with real-life recollections from thosewho were, interviewers took notes throughout theassessments on how well children appeared to un-derstand the VEX scale, based on their ability torespond to probes after responding positively to aviolence exposure item. Children were designatedas not understanding if they responded in any ofthree ways to the probe questions: 1) if theypointed to the picture when asked where they hadseen a particular incident, 2) if they named thecharacter in the picture as the person who was withthem at the time of exposure, or 3) if their answersto the probe questions were clearly based onevents not occurring in real life (e.g., to those ontelevision). Data from children whose responsesshowed that they understood the nature of thequestions were considered separately in the child-report analyses.
RESULTSPreliminary Analyses
Examination of children's responses to the VEXscale revealed three levels of understanding: chil-dren who (based on the criteria mentioned above)evidently understood the interview (W=73); chil-dren whose level of comprehension was either un-clear or variable (#=56); and children who wereunwilling or unable to complete the interview(N=26). With these three groups as factors, sepa-rate analyses of variance (ANOVAs) were com-puted on children's PPVT-R score (adjusted forage), CBCL score, distress symptomatology score,and parent- and child-reported VEX scale scores.Results revealed a main effect for group in whichchildren who understood the VEX scale scoredsignificantly higher on the PPVT-R than did thosein either of the other two groups (F(2, 150)=11.86;/?=.000). Children who understood the VEX scalealso reported significantly lower levels of total vio-lence exposure (7^2, 150)=125.202;/7=.000) and dis-tress symptomatology (F(2, 150)=14.87; p=.000)than did children in the other two groups. Nogroup differences were found for parent reports ofviolence exposure or CBCL behavior problems.
119
Data from the entire sample (#=155) were usedfor the parent-report analyses presented below.Only data from those children who gave clear indi-cation of understanding the violence exposurescale (#=73; 36 girls, 37 boys) were consideredfor the child self-report analyses. Where appropri-ate, however, data from the full sample were usedin examining relations among child-reported expo-sure and symptomatology, for the purposes ofcomparison.
Community Violence ExposureInter-item correlations, performed separately
within parent (#=155) and child (#=73) reports ofviolence exposure, revealed two statistically andconceptually related aggregate types of exposure:to mild violence, and to severe violence. Incidentsreflecting mild violence included exposure to beat-ing, chasing, pushing or shoving, and slapping.Those reflecting severe violence included expo-sure to robbery, threats with a weapon, shooting,and stabbing. Inter-item reliability was assessedfor children's reports of exposure to mild violence(8 items, Cronbach's tt=.80), parent's reports ofexposure to mild violence (8 items, Cronbach's«=.72), and children's reports of exposure to se-vere violence (6 items, Cronbach's «=.86). Becauseso few parents reported their child witnessing orvictimized by the severe violence items, there wasnot enough variability to assess the relation amongthe items that comprised this dimension.
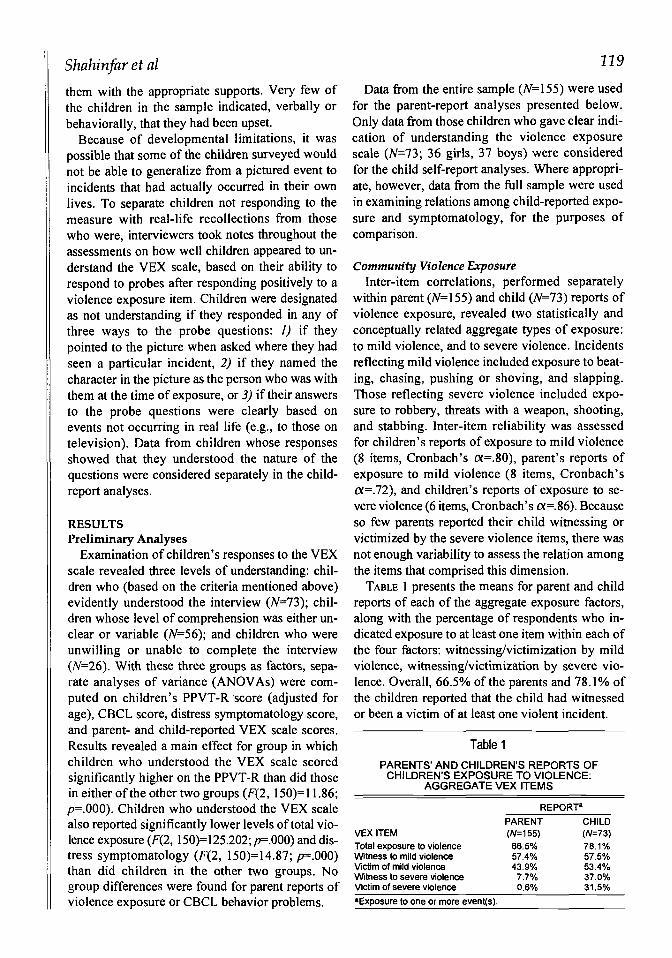
TABLE 1 presents the means for parent and childreports of each of the aggregate exposure factors,along with the percentage of respondents who in-dicated exposure to at least one item within each ofthe four factors: witnessing/victimization by mildviolence, witnessing/victimization by severe vio-lence. Overall, 66.5% of the parents and 78.1% ofthe children reported that the child had witnessedor been a victim of at least one violent incident.
Table 1
PARENTS' AND CHILDREN'S REPORTS OFCHILDREN'S EXPOSURE TO VIOLENCE:
AGGREGATE VEX ITEMS
REPORT"
VEX ITEMTotal exposure to violenceWitness to mild violenceVictim of mild violenceWitness to severe violenceVictim of severe violence
PARENT(W=155)66.5%57.4%43.9%
7.7%0.6%
CHILD(W=73)78.1%57.5%53.4%37.0%31.5%
•Exposure to one or more event(s).

120
Relation of Child and Parent Exposure ReportsPearson correlations computed between parent
and child reports showed no significant relationson the mild violence dimensions of the witnessingand victimization scores.
Because nearly half the children and even moreof the parents in this study reported that the childhad neither witnessed nor been a victim of severeviolence, parent-child concordance for these di-mensions was examined using chi-square analyses,with the witnessing and victimization dimensionsof exposure to severe violence grouped accordingto child (no/yes exposure) and parent (no/yes ex-posure) responses; no significant relations werefound.
Examination of qualitative responses to theprobe questions about the incidents reported byparents and children corroborated the statisticalfindings of discordance between parent and childreports of exposure. Thus, even when both parentsand children responded positively to a violence ex-posure item, the details of their probe responsesoften seemed to refer to different incidents.
Exposure and DistressChild Reports
Pearson correlations were performed betweenchildren's total report of distress symptoms andthe self-reported violence exposure aggregates.Correlations were modest, but significant, for thewitnessing of mild violence (r=.29,p<.Q5), victim-ization by mild violence (r=.22, p=05), and wit-nessing of severe violence (r=.25, p<.05). No sig-nificant relation was found between child self-report of distress symptoms and victimization bysevere violence (r=.14, NS).
Parent Exposure and Child Distress ReportsAnalyses performed on the relation between par-
ent reports of violence exposure and child reportsof distress symptoms yielded no significant find-ings.
Exposure and Behavior ProblemsRelation of child gender and reported level of
violence exposure to behavioral outcome was ana-lyzed, and neither interaction nor main effects forgender were found. Also, no mean range differ-ences for either parent or child reports of exposureor symptomatology by gender were found. Ac-cordingly, gender was collapsed across subjects inthe analyses presented below.
Violence Exposure and Preschool Children
Child Report of Exposure andParent Report of Behavior Problems
Analysis of children's reports of exposure andparents' reports of child symptomatology wascompleted in two waves. First, analyses were car-ried out on the full sample, without regard to chil-dren's clinically judged response to the VEX scale.Second, the same analyses were computed usingonly data that were gathered from the 73 childrenjudged to have understood the interview. Thisstrategy demonstrated valid patterns of relationsbetween exposure and symptomatology that wereunique to the group of children who understoodthe interview.
Analyses of variance were performed separatelyon parent-reported behavior problems (internal-izing, externalizing, and total problems), withchild-reported violence exposure aggregates(no/yes exposure) as factors. On the full sample ofchild-reported exposure, no significant differenceswere found between groups in terms of parent-reported behavior problems.
On the data from children successfully respond-ing to the VEX scale, however, a different patternemerged. As indicated in FIGURE 1, children whoreported witnessing mild violence were rated bytheir parents as displaying more internalizingproblems than were children who did not reportsuch exposure. (F(l,71)=4.44,p<.05). Conversely,children who reported victimization by mild vio-lence were rated by their parents as displaying sig-nificantly more externalizing problems than werethose who reported none (F(l,71)=6.19, p=.0l).Analyses examining the relation between child re-port of exposure to severe violence and parent re-port of behavior problems did not produce signifi-cant findings.
Figure 1
CHILD BEHAVIOR PROBLEMS (CBCL) BY CHILDSELF-REPORT OF VIOLENCE EXPOSURE
Q INTERNALIZING
• EXTERNALIZING
YES

Shahinfar et al
Parent Reports of Exposure and Behavior ProblemsANOVAs were computed separately on behav-
ior problem scores (internalizing, externalizing,and total problems), with violence exposure aggre-gates (no/yes exposure) as factors. As depicted inFIGURE 2, and in accord with the pattern foundamong the child reports from the reduced sample,parents who reported that their child had witnessedmild violence also reported more internalizing be-havior problems than did parents who did not re-port such witnessing (F(l, 153)=7.54, p<.0\). Par-ents who reported that their child had been a vic-tim of mild violence also reported significantlyhigher externalizing behavior problems than didthose who reported no such victimization (F(l,153)=5.14, p<.05). Analyses of parent reports ofbehavior problems and exposure to severe vio-lence yielded no significant findings.
DISCUSSIONThe study reported here was designed to exam-
ine perceptions of prevalence, as well as corre-lates, of community violence exposure in a sampleof preschool children. Information was gatheredfrom parent reports of their children's experiencesand distress symptomatology, and from interviewswith the children themselves—a method that hasproved valuable in studies of elementary-schoolchildren's and adolescents' exposure to violence(Richters & Martinez, 1993). Because of the lowerage range investigated here, the findings con-tribute to the literature in both substantive andmethodological terms.
Consistent with the prevalence reported in stud-ies of older children, this study's data indicated adisturbing rate of exposure to violence: 78.1% ofthe children and 66.5% of parents reported chil-
Figure 2
CHILD BEHAVIOR PROBLEMS (CBCL) BY PARENTREPORT OF CHILD'S VIOLENCE EXPOSURE
14 ,
12
10
8 \
6
4
2
0
12.16D INTERNALIZING
• EXTERNALIZING
YES
222
dren's exposure to at least one incident of commu-nity violence. This suggests that the problem ex-tends below the age groups commonly studied inthis field, and that children are at risk for exposureto violence before they leave the protection of par-ents and home. Community violence appears to bepart of the experience of even very young children,who presumably spend most of their time in thepresence of parent or other adult caregivers.
Data from this study also suggested modest butsignificant relations between children's reports ofexposure to mild violence and of witnessing severeviolence, and their response to a self-report mea-sure of distress symptomatology. No such correla-tion, however, was found for children's reports ofvictimization by severe violence, perhaps becausethe reports were so few.
For both parent and child reports, the behavioralcorrelates of violence exposure differed accordingto the modality through which the exposure oc-curred. Specifically, children who were reportedby themselves or their parents as witnessing mildviolence (beating, chasing, pushing/shoving, andslapping) were rated by their parents as displayingsignificantly more internalizing (withdrawn, anx-ious/depressed) problems than were their nonwit-nessing peers. Children who were reported as vic-tims of mild violence evidenced a higher fre-quency of externalizing (aggressive, disruptive)behavior than did their nonvictim peers. Despitepoor parent-child concordance in terms of reportsof exposure, the pattern relating witnessing vio-lence to internalizing problems, and victimizationto externalizing behavior was evident for bothchild and parent reports of exposure. These pat-terns might be explained as different types of de-fense processes activated by witnessing versus vic-timization. For example, children who witness vio-lence rarely have the opportunity or resources tointervene in the event; rather, they must watchfrom the sidelines, recognizing their own inabilityto effect change in the situation. They may feelhelpless, and this, in turn, may lead them to thewithdrawal or anxiety characteristic of the inter-nalizing typology. On the other hand, children vic-timized by violence must deal with the situation bytending to their own physical or emotional painand, in a sense, this gives them a role in handlingthe exposure that the witnessing child lacks.Rather than withdrawing, victimized children maybe more likely to learn aggressive, externalizingbehavior as either a means of self-protection or a

322
way of relating to others. This link between modal-ity of exposure and type of problem behavior(internalizing or externalizing) has been reportedin a study investigating rural children's exposureto violence (Martin, Gordon, & Kupersmidt,1995), and may prove valuable for exploration inresearch with other populations, as well.
In terms of methodological contributions, thisstudy introduced the VEX scale (Fox & Leavitt,1995) as a new instrument for accessing percep-tions of violence exposure in children as young aspreschool age. With this advance, however, havecome a number of methodological problems thatdeserve mention, some of them specific to thesample studied, others common to violence re-search in general.
The first of these is related to the fact that not allchildren in the study were able to understand andcomplete the VEX scale. This raises questionsabout the utility of the instrument with a preschoolsample. It is important to note that half the samplewas clinically judged as able to respond appropri-ately, and could be distinguished from thosejudged unable to do so on the important indepen-dent measure of cognitive development as as-sessed by the PPVT-R. Thus, rather than disquali-fying the VEX scale for use with preschool chil-dren, the findings highlight the importance of con-sidering children's clinical cues, as well as theirlevel of cognitive development, in assessing po-tential for appropriate response to the instrument.
The accuracy, stability, and validity of measuresdesigned for preschool populations are presentlythe topic of much debate in other areas of the self-report literature (Beitchman, & Corradini, 1988;Ceci& Brack, 1993; Fantuzzo, McDermott, Manz,Hampton, & Burdick, 1996; Guralnick & Wein-house, 1983; Hughes, 1988). The work conductedso far suggests that the ability of preschool chil-dren to respond to self-report measures may be re-lated to such test construction variables as itemcontent (Eder. 1989; Eder, Gerlach, & Perlmutter,1987), as well as to individual child variables suchas memory capacity and suggestibility (Ceci &Bruck, 1993). Furthermore, although judging fre-quency of occurrence has been shown to be unaf-fected by the age, ability, education, or motivationof the reporting individual (Hasher & Zacks,1984), children's knowledge base may effect theirrecall of the frequency of particular stimuli(Harris, Mergler, Durso, & Jones, 1990). The pre-sent findings, which link level of cognitive devel-
Violence Exposure and Preschool Children
opment to children's ability to respond to the self-report instrument, may help in further elucidatingfactors related to children's developing ability togive reliable self-reports.
A second issue relevant to the limitations of us-ing the VEX scale with a preschool sample is thedevelopment of children's ability to distinguishbetween fantasy and reality. In a recent review,Woolley (1998) concluded that children are notfundamentally different from adults in this ability,and that "...from the research reviewed...childrenby the age of 3 have considerable knowledge aboutfantasy and reality" (p. 1007). She does, however,acknowledge that the ability begins at around agethree and improves steadily over the course of thenext five years of development. Children in thisstudy were between the ages of 3'/2 and 41/2—onthe cusp of emerging distinctions between fantasyand reality.
It is important to note that among the subsampleof children responding appropriately to the VEXscale, significant and meaningful relations werefound between child reports of exposure to vio-lence and parent reports of behavior problems.This pattern of findings, which mirrored thosefound when parent reports of both exposure andsymptomatology were considered, was not presentwhen the VEX scale responses from the entiresample of children's reports were considered. Thissuggests that meaningful data can be gatheredfrom preschool children's perceptions of violenceexposure if researchers are sensitive to variablesthat indicate children's levels understanding andresponses to the measure's self-report format. Al-though the validity of children's reports of expo-sure could not be absolutely corroborated by par-ent's reports, it is clear that children's perceptionswere linked to behavioral symptomatology.
Another important issue in analyzing the chil-dren's reports is the discordance found betweenparent and child reports. This problem has alsoplagued violence research with other populations.In studies of elementary and adolescent samplesthat considered both child and parent reports of vi-olence exposure, parent-child concordance wasfound to be low or even negatively correlated(Applebaum & Burns, 1991; Hill & Jones, 1997;Pynoos et al., 1987; Richters & Martinez, 1993;Schwarz & Kowalski, 1991). Richters and Mar-tinez suggested attribution of this poor concor-dance to several factors: parents may be unawareof their children's exposure to violence; they may

Shahinfar et al
repress violence exposure information as either apassive or an active coping strategy (e.g., parentsmay not report on violence in the home for fear thechild will be removed from the home by SocialServices); or, particularly with younger children,the accuracy of children's self-reports may becompromised by their inability to distinguish be-tween events they witnessed and those they onlyheard about. A fourth possibility is that childrenand parents construe what constitutes an act of vio-lence differently, and thus report different experi-ences when faced with questions about exposure.
It is possible that the discordance between par-ent and child reports in this study was related to acombination of the reasons ascribed to such dis-cordance in older populations. Young children arecommonly assumed to spend most of their timewith primary caregivers, but 1990 census data in-dicated that 51% of American children under theage of six receive day care outside of the home(Hernandez, 1995). In the present sample, 37% ofthe children were in day care of some type. It ispossible that reasons for the discord between par-ent and preschool child reports of exposure mir-rored those cited in other studies—parents andchildren, even young children, spend at least partof their days apart. If day-care providers, as well asprimary caregivers, had been interviewed, perhapsgreater concordance would have been found be-tween adult and child reports of exposure. Simi-larly, a higher level of concordance between re-porters of exposure to violence among older chil-dren might be procured if researchers interviewedteachers or peers, in addition to parents. However,such a wide range of sources might make it diffi-cult to judge which assessments of exposure werereliable.
Because young children's developmental capac-ity for self-reporting is uncertain, it seems morelikely that the discordance between parent andchild reports of exposure reflects differences inperception. Although nearly half the sample ofchildren could respond to probe questions and re-call incidents of exposure to aggressive or violentevents, very few of their reports paralleled those oftheir parents, even when both agreed that exposurehad occurred. Parents and preschool children mayhave different interpretations of what constitutes aviolent event. The fact that the preschool childrenoften responded with different particulars fromthose offered by their parents for the same eventsuggests that the children's view of what was most
123
salient and striking differed from that of their par-ents. At the same time, parent and child reports ofwitnessing of or victimization by violence werelinked to the same behavioral correlates, suggest-ing that particulars of the exposure were less im-portant than endorsement of the fact of exposure.As such, the data from this study must be viewedas representing parent and child perceptions of vi-olence exposure, the interpretation and reportingof which may or may not overlap. This reading ofthe data may also help explain discrepancies re-ported in the literature with older children and ado-lescents.
Clinical SignificancePerceptions may be particularly important from
a clinical standpoint. For example, studies of chil-dren growing up in violent environments havedemonstrated that it is the child's interpretation ofa violent event, not the event itself, that may ex-plain patterns of symptomatology and coping(Gibson, 1987; Liddell et al, 1993). Reports bypreschool children in the current sample systemati-cally varied with the degree of both child and par-ent reports of symptomatology, suggesting that thechildren's reports reflected some environmentalstimulus related to either the presence or the per-ception of violence in their community. At thevery least, the data offer a glimpse of the informa-tion that might be gathered about young children'sexperiences with community violence. Under-standing children's perception and interpretationof events is critical toward helping them deal withtrauma. The VEX scale may prove a useful tool inopening a dialogue with children about their per-ceptions of and experiences with community vio-lence.
Implications for ResearchThe goal of this study was to provide data on
perceptions of prevalence and correlates of com-munity violence exposure among very young chil-dren, a group about which little is known. This isnot to imply an attempt to uncover the causality ofrelations among exposure, distress symptoms, andbehavior problems. For example, it is possible thatexternalizing behavior problems were related tovictimization by violence because aggressive chil-dren prompted aggressive responses from their en-vironments, not because environmental violencecontributed to aggression in the children. Simi-larly, children with internalizing problems may
124
have been more sensitive to violent stimuli in theenvironment and their reports of violence were,thus, a manifestation rather than a cause of dis-tress. A much more detailed examination of con-textual issues (e.g., place of exposure, parentalprocessing of the event) would be necessary toachieve a full understanding of the impact of vio-lent events on children. New models for under-standing the relevance of the contextual features ofexposure have been recently articulated by Lynchand Cicchetti (1998) and will, ideally, inform fu-ture generations of researchers.
The role of such factors as family functioningand the quality of the parent-child relationship inameliorating or exacerbating children's responsesto violence exposure should also be considered.For example, if parents are the perpetrators of theviolence, the children may not receive supportfrom them in reporting their exposure or associ-ated symptomatology. Not all parents are unam-bivalent, beneficent caretakers. It is essential to in-vestigate which features of family functioning andparent-child relationships can help resilient chil-dren avoid a negative outcome. This issue has beeninvestigated in the child abuse and neglect litera-ture, but is only beginning to be explored with re-gard to children's exposure to the broader dimen-sions of community violence (Gorman-Smith &Tolan, 1998).
Finally, further research is needed to explore thedifferent links between particular modalities of vi-olence exposure and specific behavioral symp-tomatology. The social-learning model of behav-ioral development (Bandura, 1973, 1986) positsthat exposure to aggressive role models increaseschildren's chances of developing aggressive be-havior problems. The findings of the present studyand of others that have revealed differences be-tween children's witnessing of and victimizationby violence (Fitzpatrick, 1993; Martin, Gordon, &Kupersmidt, 1995; Schubiner, Scott, & Tzelepis,1993) indicate that particular modalities of expo-sure may be associated with specific behaviorproblems. When considering prevention effortsdesigned to reduce aggressive and delinquent be-havior, it may be especially important to identifythose children who have been victims of violence.
CONCLUSIONNational data indicate that community violence
is an important social problem, but whether andhow such violence touches the lives of young chil-
Violence Exposure and Preschool Children
dren has not yet been fully addressed in the litera-ture. This study is among the first to attempt a sys-tematic examination of the prevalence of exposure •to violence among a preschool population, sincemost of the research in this area has been primarilydirected at school-age and adolescent populations.The current results support the notion that violenceexposure represents a significant experience forchildren as young as preschoolers in some areas ofthe United States, and suggest that serious atten-tion must be given to further research on the preva-lence and remediation of this important socialproblem.
ReferencesAchenbach, T.M. (1991). Manual for the Child Behavior
Checklist. Burlington: Department of Psychiatry, Universityof Vermont.
Applebaum, D.R., & Burns, G.L. (1991). Unexpected child-hood death: Posttraumatic stress disorder in surviving sib-lings and parents. Journal of Clinical Child Psychology, 20,114-120.
Attar, B.K., Guerra, N.G., & Tolan, P.H. (1994). Neighbor-hood disadvantage, stressful life events, and adjustment jnurban elementary-school children. Journal of Clinical ChildPsychology, 23, 391-400.
Bandura, A. (1973). Aggression: A social learning theoryanalysis. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (1986). Social foundations of thought and action.Englewood Cliffs, NJ: Prentice Hall.
Beitchman, J.H., & Corradini, A. (1988). Self-report measuresfor use with children: A review and comment. Journal ofClinical Child Psychology, 44, 477-490.
Bell, C.C., & Jenkins, E.J. (1991). Traumatic stress and chil-dren. Journal of Health Care for the Poor and Underserved,256(1), 175-185.
Bell, C.C., & Jenkins, E.J. (1993). Community violence andchildren on Chicago's Southside. Psychiatry, Interpersonaland Biological Processes [Special Issue], 56(7,1,47-54.
Ceci, S., & Bruck, M.'(1993). Suggestibility of the child wit-ness: A historical review and synthesis. Psychological Bul-letin. 773,403-439
Dunn, L.M., & Dunn, L.M. (1981). Peabody picture vocabu-lary test revised. Circle Pines, MN: American GuidanceService.
DuRant, R.H., Cadenhead, C., Pendergrast, R.A., Slavens, G.,& Linder, C.W. (1994). Factors associated with the use ofviolence among urban Black adolescents. American Journalof Public Health, <W, 612-617.
Eder, R. (1989). The emergent personologist: The structureand content of 3'/i, 5'/2, and 7'/i year-olds' concepts of them-selves and other persons. Child Development, 60,1218-1228.
Eder, R., Gerlach, S.G., & Perlmutter, M. (1987). In search ofchildren's selves: Development of the specific and generalcomponents of the self concept. Child Development, 58,1044-1050.
Fantuzzo, J., McDermott, P.A., Manz, P.H., Hampton, V.R., &Burdick, N.A. (1996). The pictorial scale of perceived com-petence and social acceptance: Does it work with low-income urban children? Child Development, 67,1071-1084.
Fitzpatrick, K.M. (1993). Exposure to violence and presenceof depression among low-income African-American youth.

Shahinfar et al
Journal of Consulting and Clinical Psychology, 61,528-531.
Fitzpatrick, K.M., & Boldizar, J.P. (1993). The prevalence andconsequences of exposure to violence among African-American youth. Journal of the American Academy of Childand Adolescent Psychiatry, 32, 424-430.
Flavell, J.H. (1993). Young children's understanding of think-ing and consciousness. Current Directions in PsychologicalScience, 2, 40-43.
Fox, N.A., & Leavitt, L.A. (1995). The Violence ExposureScale for Children-VEX (preschool version). College Park:Department of Human Development, University of Mary-land.
Freeman, L.M., Mokros, H., & Poznanski, E.O. (1993). Vio-lent events reported by urban school-aged children: Charac-teristics and depression correlates. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 32, 419-423.
Garbarino, J., Kostelny, K., & Dubrow, N. (1991). Noplace tobe a child. Lexington, MA: Lexington Books.
Gibson, K.(1987). Children in political violence. Social Sci-ences and Medicine, 28, 659-667.
Gladstein, J., Rusonis, E.S., & Heald, F.P. (1992). A compari-son of inner-city and upper-middle class youths' exposureto violence. Journal of Adolescent Health, 13, 275-280.
Gorman-Smith, D., & Tolan, P. (1998). The role of exposureto community violence and developmental problems amonginner-city youth. Development and Psychopathology, 10,101-116.
Guralnick, M.J., & Weinhouse, E. (1983). Child-child socialinteractions: An analysis of assessment instruments foryoung children. Exceptional Children, 50, 268-271
Harris, J., Durso, F., Mergler, N., & Jones, S. (1990). Knowl-edge base influences on judgments of frequency of occur-rence. Cognitive Development, 5, 223-233.
Hasher, L., & Zacks, R.T. (1984). Automatic processing offundamental information: The case of frequency of occur-rence. American Psychologist, 39, 1372-1388.
Hernandez, D.J. (1995). Changing demographics: past andfuture demands for early childhood programs. The fu-ture of children: Long-term outcomes of early childhoodprograms (Vol. 5, No. 3, David and Lucille PackardFoundation).
Hill, H.M., & Jones, L.P. (1997). Children's and parents' per-ceptions of children's exposure to violence in urban neigh-borhoods. Journal of the National Medical Association, 89,270-276.
Hughes, H.M. (1988). Psychological and behavioral correlatesof family violence in child witnesses and victims. AmericanJournal of Orthopsychiatry, 58, 77-90.
Liddell, C., Kemp, J., & Moema, M. (1993). The young lions:South African children and youth in political struggle. InL.A. Leavitt & N.A. Fox (Eds.), The psychological impactof war and violence on children. Hillsdale, NJ: LawrenceErlbaum.
Lynch, M., & Cicchetti, D. (1998). An ecological-transactionalanalysis of children and contexts: The longitudinal interplayamong child maltreatment, community violence, and chil-dren's symptomatology. Development and Psychopathol-ogy, 10, 235-258.
125
Martin, S., Gordon, T., & Kupersmidt, J. (1995). Survey ofexposure to violence among the children of migrant andseasonal farmworkers. Public Health Reports, 110,268-276.
Martinez, P., & Richters, J.E. (1993). The NIMH CommunityViolence Project II: Children's distress symptoms associ-ated with violence exposure. Psychiatry, Interpersonal andBiological Processes [Special Issue], 56(1), 22-35.
Maryland State Police (1995), Crime in Maryland: 1994 Uni-form crime report. Pikesville, MD: Author.
Osofsky, J.D. (1995). The effects of exposure to violence onyoung children. American Psychologist, 50, 782-788.
Osofsky, J.D., Wewers, S., Hann, D.M., & Fick, A.C. (1993).Chronic community violence: What is happening to ourchildren? Psychiatry: Interpersonal and Biological Pro-cesses [Special Issue], 56(1), 36-45.
Pynoos, R.S., Frederick, C.J., Nader, K., Arroyo, E., Steinberg,A., Eth, S., Nunez, F., & Fairbanks, L. (1987). Life threatand posttraumatic stress in school age children. Archives ofGeneral Psychiatry, 44, 1057-1063.
Richters, J.E., & Martinez, P. (1990). Things I have seen andheard: An interview for young children about exposure toviolence. Rockville, MD: National Institute for MentalHealth.
Richters, J.E., & Martinez, P. (1993). The NIMH CommunityViolence Project I: Children as victims and witnesses to vi-olence. Psychiatry, Interpersonal and Biological Processes[Special Issue], 56(1), 7-21.
Richters, J.E., Martinez, P., & Valla, J.P. (1990). Levonn: Acartoon-based measure of children's distress symptoms.Washington, IX: National Institute of Mental Health.
Rosenberg, M.L., & Fenley, M.A. (1991). Violence in Amer-ica: A public health approach. New York: Oxford Univer-sity Press.
Rosenberg, M.L., O'Carroll, P., & Powell, K. (1992). Let's beclear: Violence is a public health problem. Journal of theAmerican Medical Association, 267, 3071-3072.
Schwarz, E.D., & Kowalski, J.M. (1991). Malignant memo-ries: PTSD in children and adults after a school shooting.Journal of the American Academy of Child and AdolescentPsychiatry, 30, 936-944.
Schubiner, H., Scott, R., & Tzelepis, A. (1993). Exposure toviolence among inner-city youth. Journal of AdolescentHealth, 14,214-219.
Shakoor, B.H., & Chalmers, D. (1991). Co-victimization ofAfrican-American children who witness violence: Effectson cognitive, emotional, and behavioral development. Jour-nal of the National Medical Association, 83, 233-238.
Singer, M.I., Anglin, T.M., Song, L., & Lunghofer, L. (1995).Adolescents' exposure to violence and associated symp-toms of psychological trauma. Journal of the AmericanMedical Association, 273, 477-482.
Taylor, L., Zuckerman. B., Harik, V., & Groves, B.M. (1994).Witnessing violence by young children and their mothers.Journal of Developmental and Behavioral Pediatrics,15(2), 120-123.
Woolley, J. (1998). Thinking about fantasy: Are children fun-damentally different thinkers and believers from adults?Child Development, 68, 991-1011.
For reprints: Ariana Shahinfar, Ph.D., Dept. of Psychology, La Salle University, 1900 West Olney Ave., Philadelphia, PA, 19141