Peyronie's disease - Beyond the bend
141
University of Groningen Peyronie's disease - Beyond the bend Mohede, Daan DOI: 10.33612/diss.150703782 IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2021 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Mohede, D. (2021). Peyronie's disease - Beyond the bend: Historical, epidemiological, clinical, genetic and molecular biological aspects. University of Groningen. https://doi.org/10.33612/diss.150703782 Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 14-09-2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Peyronie's disease - Beyond the bend

University of Groningen
Peyronie's disease - Beyond the bendMohede, Daan
DOI:10.33612/diss.150703782
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2021
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Mohede, D. (2021). Peyronie's disease - Beyond the bend: Historical, epidemiological, clinical, genetic andmolecular biological aspects. University of Groningen. https://doi.org/10.33612/diss.150703782
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 14-09-2022

Peyronie’s Disease - Beyond the BendHistorical, epidemiological, clinical, genetic
and molecular biological aspects
Daan Carel John Mohede

Peyronie’s Disease - Beyond the BendHistorical, epidemiological, clinical, genetic and molecular biological aspects
ISBN: 978-94-6423-095-6 Cover art: Safira TaylorLayout and design: Wendy Schoneveld || www.wenzid.nlPrinted by: ProefschriftMaken || www.proefschriftmaken.nl
Financial support by the University of Groningen, University Medical Center Groningen and Kollf Institute is gratefully acknowledged.
Further financial support for printing of this thesis was kindly provided by ChipSoft, IPSEN and Prof. P.W. Boer Stichting.
© Daan Carel John Mohede, 2020. All rights reserved. No part of this thesis may be reproduced or transmitted in any form or by any means without prior written permission from the author. The copyright of the papers that have been published or have been accepted for publication has been transferred to the respective journals.

Peyronie’s Disease – Beyond the BendHistorical, epidemiological, clinical, genetic and molecular biological aspects
De ziekte van Peyronie – Voorbij de krommingHistorische, epidemiologische, klinische, genetische en moleculair biologische aspecten
Proefschrift
ter verkrijging van de graad van doctoraan de Rijksuniversiteit Groningen
op gezag van de rector magnificus prof. dr. C. Wijmengaen volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden opwoensdag 13 januari 2021 om 14:30
door
Daan Carel John Mohede
geboren 12-01-1991 te Enschede

Promotoren: Prof. dr. Igle Jan de Jong Prof. dr. Ruud A. Bank
Copromotor: Dr. Mels F. van Driel
Beoordelingscomissie: Prof. dr. E.J.H. Meuleman Prof. dr. M. Albersen Prof. dr. P. Olinga

Paranimfen: Dr. Sanne Vreugdenhil Dr. Dyaran S. Bansraj

Table of contents
General introduction9
Chapter 1 Peyronie’s disease – current perspectivesTranslated from: Mohede DCJ, van Driel MF, de Jong IJ, Beck J. Tijdschr Urol 2018;8:112-120
17
Chapter 2 Medical treatments of Peyronie’s disease: past, present, and futureMohede DCJ, de Jong IJ, van Driel MF. Urology 2019;125:1-5
31
Chapter 3 Patient reported outcomes on sexual function after surgical treatment of Peyronie’s diseasePublished as abstract: Mohede DCJ, Weidenaar AC, van Driel MF, van de Wiel HBM, de Jong IJ. J Urol 2018;199:e911
43
Chapter 4 Homosexuality and Peyronie’s diseaseSubmitted: Mohede DCJ, van de Wiel HBM, Meijer B, de Jong IJ, van Driel MF
57
Chapter 5 Prevalence of Peyronie’s and Ledderhose’s diseases in a series of 730 patients with Dupuytren’s diseaseMohede DCJ, Riesmeijer S, de Jong IJ, Werker PMN, van Driel MF. PRS 2020;145:978-984
67
Chapter 6 A genome-wide association study for Peyronie’s diseaseNot for publication: Mohede DCJ, van Driel MF, Riesmeijer S, de Jong IJ, Werker PMN, Nolte IM
79
Chapter 7 Verteporfin as a medical treatment in Peyronie’s diseaseMohede DCJ, de Jong IJ, Bank RA, van Driel MF. Sex Med 2018;6:302-308
91

Chapter 8 Summary and general discussion 103
Chapter 9 Nederlandse samenvatting 113
AppendicesDankwoord/AcknowledgementsCurriculum VitaeList of publications
124136139140


General introduction

General introduction
10
General introduction
Peyronie’s disease (PD) is named after the French surgeon Francois Gigot de la Peyronie (1678-1747), although early descriptions of it as an ‘obstacle for marital bliss’ go back as far as Theodoricus Borgognoni (1205-1298) and Nicolaes Tulp (1593-1674). (1) PD presents commonly with the bending of the penis. Many times, pain in the penis at erection is also one of the first complaints. Another early symptom is feeling a nodule, usually on the dorsal and/or lateral side, which is commonly called ‘plaque’. As a result, the patient is often anxious about malignancy. Furthermore, many patients worry about the real or imagined loss of their sexual capacity. Potential complications include insufficient rigidity (erectile dysfunction) and awkward vaginal intromission, in which the penis can be inserted only with great difficulty. The patient and his partner invariably ask questions about the cause of PD including possible heredity. As with all other disorders with a form of sexual impairment, PD is characterized by taboos. Because it is an uncomfortable topic, and therefore under-discussed in public, people tend to mistakenly believe PD is less prevalent than it actually is. (2)
Unfortunately, there is currently no cure for PD. Patients still have to depend on symptomatic medical and surgical treatments. In 2020, however, much more about its causes is known compared to previously. Fibrotic changes in the tunica albuginea (TA), the thick capsule surrounding the penile corpora cavernosa (CC), and genetic susceptibility both play a major role. At the beginning of the 1900s, the genetic association of PD with Dupuytren’s disease (DD) was already mentioned in the Dutch scientific medical literature. (3)
The tunica albuginea The TA is a two-layered structure of inner circular and outer longitudinal coats of connective tissue, encompassing the paired CC; it consists of elastin and collagen. An incomplete septum separates the CC and anchors dorsally to the circular inner layer of the TA.
Penile hemodynamics The hemodynamic process that leads to an erection comprises four physiological
mechanisms (Figures 1 and 2):- activation of parasympathetic, non-adrenergic and non-cholinergic nerves, releasing
nitric oxide through sexual stimulation;- flow to the corpora by dilation of cavernous arteries and the helicine arterioles; - expansion of the lacunar spaces and trapping of blood by compression of the draining
venules through relaxation of the trabecular smooth muscle; and- sufficient compression of the subtunical venules and reduction in blood outflow through
compliance of the TA and the connective tissue matrix. (4)

General introduction
11
i
The role of androgensIn the 1990s, androgen ablation by castration in animal models produced a marked increase in the extracellular matrix within the TA, with an approximately two-fold concomitant reduction of the smooth muscle to connective tissue ratio. (5, 6) According to clinicians, this reduction in tissue fibro-elastic properties compromised the cavernous tissue compliance and decreased the penile hemodynamics, resulting in erectile dysfunction by impairing the veno-occlusive function of the TA. (7)
In 2003, Shen and coworkers showed that androgens are also indispensable for the maintenance of a normal ultrastructure of the TA. (8) In castrated rats, they found a significant reduction in thickness of the TA. The TA of the intact animals was rich in elastic fibers, and the architecture showed typical regular arrangements, but the TA from castrated animals showed reduced density of elastic fibers and replacement by collagen. In 2005, it was suggested that androgens modulate the extracellular matrix through expression of growth factors. (9) Alongside this, case studies corroborated the restoration of erectile function in men with venous leakage after androgen treatment. (10, 11)
After 2010, several investigators showed that low testosterone levels could contribute to the pathogenesis of PD because of the androgens’ influence on collagen metabolism by modulating the activity of matrix metalloproteases and tissue inhibitors of these enzymes. (12, 13, 14) The aforementioned observations suggest that androgens play a major role in maintaining the architecture of the spongy tissue within the CC as well as the structure of the TA. This could explain why PD rarely occurs in young men.
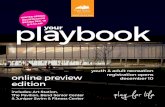
Figure I. In the flaccid state, the arteries, arterioles and sinusoids that make up the CC are contracted. Blood can flow freely through these spaces and can exit via the emissary veins. Figure II. Arteries, arterioles and sinusoids relax during the erect state. This causes the constriction of veins and venules, preventing outflow via the emissary veins by pressure of the TA. An erection is established by vascular inflow exceeding outflow.

General introduction
12
FibrosisFibrosis is the formation of excess connective tissue in an organ or tissue. This occurs in rare diseases such as idiopathic pulmonary fibrosis and systemic sclerosis, but also in more common disorders, such as liver cirrhosis, kidney disorders and inflammatory skin- and intestinal diseases. The deposition of collagen is an indispensable yet reversible part of the wound healing process. It can be disrupted, for example by repeated tissue damage in the same location or when the healing process, which normally is strictly regulated, destabilizes. Over the last few decades, there has been increasing evidence that stem cells play a major role in undisturbed wound healing. These cells counteract healing anomalies, accelerate wound contraction and reduce the density of extracellular matrix.
Fibrosis is characterized by an abnormal and increased proliferation of fibroblasts and an excessive accumulation of connective tissue, the so-called extracellular matrix. This concerns mainly collagen, but also glycosaminoglycans such as hyaluronic acid and glycoproteins such as fibronectin. In all forms of fibrosis, the differentiation and activation of cells leading to myofibroblasts is an important process. These blasts arise from locally-available fibroblasts, and from local epithelial or endothelial cells. The myofibroblasts are the main producers of collagen and other components of the extracellular matrix.
Overexpression of members of the TGF-β and other pro-fibrotic factors, such as myostatin and plasminogen activation inhibitor-2 have been found in PD plaques and are released during the acute inflammation subsequent to trauma. A fibrotic plaque then becomes apparent and can calcify or even ossify. (15) A suspected counteractor for pro-fibrotic factors is iNOS. As it leads to NO release, monocyte chemotactic protein 1 is attracted by the fibrin in the TA, probably inducing iNOS. This proposal is supported in animal experiments by the reverse correlation of pro-fibrotic factor levels and iNOS activity, regulated by gene transfer and L-N-(1-iminoethyl)-lysine acetate inhibition. (15)
Fibrocytes are circulating connective tissue progenitor cells and their transformation into myofibroblasts is influenced by various growth factors, cytokines and clotting factors. With the advance of the wound healing process, the myofibroblasts eventually disappear through apoptosis. There is evidence that epigenetic changes in fibroblasts or myofibroblasts could contribute to fibrosis formation. (16)
GeneticsPD, DD and Ledderhose’s disease (LD) are largely similar fibro-proliferative disorders, characterized by abnormal collagen deposition in the TA of the penis, palmar fascia of the hand and plantar fascia of the foot, respectively. In DD, nodules and cords can form in the

General introduction
13
iconnective tissue, the latter of which can cause debilitating flexion contractures of the digits. These diseases are thought to have a similar disease mechanism, indeed Abernathy (UK) first reported on their association in 1828. (17)
In the 1960s, one view was that PD patients had intercourse more frequently and more vigorously than age-matched cohorts, but in scientific practice it was impossible to prove this. However, there is no question that an accident during penetration when the penis bends excessively could induce PD. More recently, it was shown that the three disorders (PD, DD and LD) have a familial aggregation and several genetic risk variants are known to be associated. In 2004, Qian et al. already demonstrated that the patterns of gene expression alteration of certain genes in DD and PD were similar, indicating a common pathophysiology. (18) Gene expression, in this case messenger RNA is a derivative of family genetics. Biological cell studies identified an overlap in patterns of chromosomal aberrations in fibroblasts from PD and DD lesions. In 2012, our research group associated nine loci to DD in the first genome-wide association study (GWAS) of DD, and one of these nine loci could also be associated with PD. (19) A more recent GWAS discovered 17 additional loci for DD. (20) Our group will soon carry out a GWAS with the new data of approximately 63,000 individuals and perform a meta-analysis of DD with other cohorts to identify additional DD loci. This also provides the opportunity to further explore the genetic correlation of DD with PD.
This thesis discusses the following questions and issues:- What is the current knowledge about PD with regard to its history, epidemiology,
pathophysiology, pathogenesis and therapeutic options, and which of these areas shows the most significant gaps? (Chapter 1)
- Which nonsurgical treatments have been proposed for PD and related fibro-proliferative disorders throughout the ages? (Chapter 2)
- What are the long-term outcomes and complications of current treatment methods and how do they compare with each other? (Chapter 3)
- How does PD influence sexuality and do homosexual patients need a different approach? (Chapter 4)
- What is the prevalence of PD in patients with DD and LD? (Chapter 5)- Which aspects of PD (and DD) can be genetically explained and which genes are
responsible? (Chapter 6)- What are the effects of verteporfin on PD and which molecular biological pathways are
involved? (Chapter 7)- How can we improve future PD research and treatment? (Summary and general
discussion)

General introduction
14
References
1. Haneveld GT. Early Dutch contributions on Peyronie’s disease. Arch Chir Neerl 1979;31:123–129.2. van Driel MF. Manhood – the rise and the fall of the penis. London: Reaktion Books Ltd, 2009, p. 201.3. Schoonheid H. Induratio penis plastica. Ned T Gen 1907;25:1753-1755.4. Lue TF, Tanagho EA. Functional anatomy and mechanisms of penile erection. In: Contemporary
management of impotence and infertility. Eds. Tanagho EA, Lue TF, McClure RD. Baltimore: Williams & Wilkins, 1988, pp. 39-54.
5. Takahashi Y, Hirata Y, Yokoyama S, Ishii N, Nunes L, Lue TF, Tanagho EA. Loss of penile erectile response to intracavernous injection of acetylcholine in castrated dog. Tohoku J Exp Med 1991;163:85-91.
6. Traish AM, Park K, Dhir V, Kim NN, Moreland RB, Goldstein I. Effects of castration and androgen replacement on erectile function in a rabbit model. Endocrinology 1999;140:1861-1868.
7. Akkus E, Carrier S, Baba K, Hsu GL, Padma-Nathan H, Nunes L, Lue TF. Structural alterations in the tunica albuginea of the penis : impact of Peyronie’s disease, ageing and impotence. BJUI 1997;79:47-53.
8. Shen ZJ, Zhou XL, Lu YL, Chen ZD. Effect of androgen deprivation on penile ultrastructure. Asian J Androl 2003;5:33-36.
9. Natoli AK, Medley TL, Ahimastos AA, Drew BG, Thearle DJ, Dilley RJ, Kingwell BA. Sex steroids modulate human aortic smooth muscle cell matrix protein deposition and matrix metalloproteinase expression. Hypertension 2005;46:1129–1134.
10. Yassin AA, Saad F, Traish A. Testosterone undecanoate restores erectile function in a subset of patients with venous leakage: a series of case reports. J Sex Med 2006;3:727-735.
11. Kurbatov DG, Kuznetsky YY, Kitaev SV, Brusensky VA. Magnetic resonance imaging as a potential tool for objective visualization of venous leakage in patients with veno-occlusive erectile dysfunction. Int J Impot Res 2008;20:192-198.
12. Karavitakis M, Komninos C, Simaioforidis V, Kontos S, Lefakis G, Politis V, Koritsiadis Gonstantellou K, Doumanis G. The relationship between androgens, regulators of collagen metabolism, and Peyronie’s disease: A case control study. J Sex Med 2010;7:4011–4017
13. Cavallini G, Biagiotti G, Lo Giudice C: Association between Peyronie’s disease and low serum testosterone levels: detection and therapeutic considerations. J Androl 2012;33:381-388
14. Moreno SA, Morgentaler A.: Testosterone deficiency and Peyronie’s disease: pilot data suggesting a significant relationship. J Sex Med 2009; 6:1729-1735
15. Gonzalez-Cadavid NF, Rajfer J. Mechanisms of disease. New insights into the cellular and molecular pathology of Peyronie’s disease. Nat Clin Pract Urol, 2 (2005), pp.291-297.
16. Huang SK, Scruggs AM, McEachin RC, White ES, Peters-Golden M. Lung fibroblasts from patients with idiopathic pulmonary fibrosis exhibit genome-wide differences in DNA methylation compared to fibroblasts from nonfibrotic lung. PLoS ONE 2014;9:e107055.
17. Abernathy J. The consequences of gonorrhoea. Lecture on anatomy, surgery and pathology including observations on the nature and treatment of local diseases, delivered at the St. Bartholomew’s and Christ’s Hospitals. 1st ed. London, England: James Balcock; 1828:205.
18. Qian A, Meals RA, Rajfer J, Gonzalez-Cadavid NF. Comparison of gene expression profiles between Peyronie’s disease and Dupuytren’s contracture. Urology 2004;64:399-404.
19. Dolmans GH, Werker PM, de Jong IJ, Nijman RJ, LifeLines Cohort Study, Wijmenga C, Ophoff RA. WNT2 locus is involved in genetic susceptibility of Peyronie’s disease. J Sex Med 2012;9:1430-1434.
20. Ng M, Thakkar D, Southam L, Werker P, Ophoff R, Becker K, Nothnagel M, Franke A, Nurnberg P, Espirito-Santo AI, Izadi D, Hennies HC, Nanchahal J, Zeggini E, Furniss D. A genome-wise association study of Dupuytren disease reveals 17 additional variants implicated in fibrosis. Am J Hum Genet 2017;101:417-427.

15


Translated from:Mohede DCJ, van Driel MF, de Jong IJ, Beck
J. Tijdschr Urol 2018;8:112-120
Peyronie’s disease - current perspectives
Chapter 1

Chapter 1
18
Introduction
Knowledge concerning Peyronie’s disease (PD) has increased over the past decades. Unfortunately, a curative treatment is not yet possible. PD patients in the near future will have to depend on expectative or non-curative symptomatic treatment.We aim to discuss American and European guidelines and fill epidemiological, surgical, psychological, biological and genetic hiatuses. In the first part, we will discuss the disease, epidemiology, and historical aspects. We will then describe current perspectives on pathophysiology, pathogenesis and therapeutic options.
The disease and epidemiological aspectsPD is caused by changes in the tunica albuginea (TA), the connective tissue surrounding the corpora cavernosa in the penis. PD can cause painful erections, erectile dysfunction (ED), deformation, and shortening and curvature of the penis. (1) The so-called plaque, which is the fibrotic area in the TA, limits the expansion of the penis at the affected location, causing curvature, shortening, narrowing and/or hinging. The generally-accepted hypothesis is that PD is caused by a combination of microtrauma and a genetic predisposition to the disease. PD seems to appear most frequently in North-European Caucasians, less frequently in African-Americans and only sporadically in Asians. (2)
Demographic research shows a high prevalence (up to nine percent) of PD, especially in men older than fifty years. (3, 4) Globally, the prevalence seems to be increasing. This is probably explained by the presence of oral medication for men with ED, who would not have become aware of the deformity without therapy. Furthermore, there has been a rise in media attention for male sexual disorders. Epidemiological research has also shown correlations between PD and cardiovascular disease, depression and relationship problems. (5-7)
HistoryFrançois Gigot de la Peyronie (1678-1747) first described the disease in 1743. (8) The French surgeon was born in Montpellier, where he studied philosophy and surgery. In 1695, he received his diploma as a surgeon and continued his training in Paris assisting Georges Mareschal, who was surgeon at the Hôpital de la Charité. After Mareschals death in 1736, de la Peyronie was promoted to first surgeon to King Louis XV of France. He reorganized the surgical degree and played an important part in introducing the law that led to the ban on barbers executing surgical procedures. De la Peyronie was the first to provide a clear description of induratio penis plastica (the German designation). Centuries before, PD had been described as an obstacle to marital bliss by sages such as Theodoricus Borgognoni

Current perspectives
19
1
(1205-1298), Wilhelm of Salieto (1210-1276), Andreas Vesalius (1514-1564), Gabriele Falloppio (1523-1562), Julius Caesar Arantius (1530-1589), Nicolaas Tulp (1593-1674) and Frederik Ruysch (1638-1731). (9-11)
De la Peyronie believed PD was a sexually transmitted disease. He described plaques as painless ‘buds’, which were noticeable in the corpora cavernosa of older men either singularly or in a rosary-like formation. He also noticed that the curvature was always on the same side as the plaque. His remedy, among others, was to drink ‘holy’ water from the wells of Barège in the French Pyrenees.
Other important men in the history of PD are George McClellan (first surgical plaque-excision in 1828), Oswald Lowsley (plaque-excision with a fat-free graft in 1943), Reed Nesbit (procedure according to Nesbit for congenital penile curvature in 1965), John Pryor (the first to use the Nesbit-procedure in PD in 1979) and Tom Lue (plaque-incision with a venous graft in 1997).
PathophysiologyPD leads to fibrotic areas in the TA and causes a decrease in elasticity. (12) The normal TA consists of collagenous tissue and elastic fibers arranged in two layers: a horizontal outer layer enabling extension during erection and a circular inner layer enabling increase in circumference. The TA is separated from the erectile tissue of the corpora cavernosa by mobile connective tissue with a sophisticated network of blood and lymphatic vessels. Venous drainage of the spongy erectile tissue occurs through oblique venules in the TA, emerging in the vena dorsalis profunda. Movements of the two layers of the TA close the venules during erection.
PathogenesisThe most widely-accepted hypothesis is that the disease is caused by mechanic trauma of the TA during erection, followed by aberrant wound healing and scar tissue formation. In erection, the penis is filled with blood, and the TA and the septum between the corpora cavernosa stretch to the limit of their elasticity. This causes increase in length and circumference. The degree of elasticity is somewhat age dependent. When the penis meets resistance during sexual intercourse, the septal fibers can be subject to extreme tension causing small ruptures. This probably occurs more often in older men. They have a less elastic TA, which can cause the inner circular fibers to delaminate. (13) These ruptures cause hemorrhage and clots, fibrin depositions, fibroblast proliferation and increased vascular permeability. In addition, inflammatory cells are generated. An infiltrate of T-lymphocytes, macrophages and plasma cells arises, which surrounds the small vessels of

Chapter 1
20
the subtunicale layer. This leads to fibrotic areas that will eventually form the plaque. The process can take six to eighteen months. Most patients describe an aching pain, ‘as if the penis is bruised’. The plaque can calcify or even ossify. (14-16)
Without any doubt, a genetic susceptibility plays a part in PD because the disease often coexists with other fibrotic diseases, such as Dupuytren’s disease (DD) and Ledderhose’s disease. In 2011, the coexistence of PD and DD was investigated. Twenty-two percent of PD patients appeared to suffer from DD as well. (17) Previous studies had mentioned a coexistence of 0.1 to 58.8%, family occurrence of PD in 1 to 4% and of DD in 9.8%. (18-19) As with PD, DD is mostly seen in Caucasians. The disease is also known as Celtic disease. Some believe the prevalence of PD is even higher than that of DD because diseases of the external genitalia are often underreported.
A study in gene expression profiles of PD and DD patients has shown similar changes in genes responsible for collagen deposition, degradation, myofibroblast differentiation and ossification. (20) The way PD is inherited is unknown, but it seems to be heterogeneously. Autosomal dominance is often seen with variable penetrance. PD is rarely autosomal recessive or maternal, which suggests a mitochondrial inheritance. (21, 22) Dolmans et al. found significant correlation of PD with a single nucleotide polymorphism (SNP) rs 4730775 on the wingless-type mouse mammary tumor virus (MMTV) integration site family (WNT) 2 locus on chromosome 7. (23) WNT2 belongs to this WNT-family, which consists of genes coding for glycoproteins. These have an extracellular signaling function. The canonical pathway is the best defined; it activates the nuclear function of betacatenin. This subsequently changes gene expression, which influences the proliferation of myofibroblasts. (24) Research has shown enhanced beta-catenine, the end product of the WNT-pathway, in cells of PD plaques. (25) Research has also suggested an overstimulated WNT-cascade in PD.
Molecular biological research into compounds with anti-fibrotic properties has shown promising results. Verteporfin is such a compound and inhibits fibrotic effects of myofibroblasts on a protein level. (26)
Clinical and diagnostic aspectsPD can emerge at any point during adult life, with a median age of 53 years. It has a prevalence of three to nine percent of all adult men studied. (27) PD occurs in two phases: an inflammatory phase, lasting six to eighteen months, with painful erections and the development of plaques and deformation of the penis, followed by a chronic phase, characterized by ‘stable’ plaques that can calcify or ossify. The penis can also shorten and ED can occur. (28) After three months without changes, the disease is considered stable.

Current perspectives
21
1
Patients are often concerned about losing sexual function and frequently worry about the future. Some are even afraid the disease has malignant properties. The deformation can make sexual intercourse impossible or very painful. Difficulties during intercourse are not only the result of the degree of curvature, but also of the partner relationship. A single, sexually-active man with a severe curvature suffers more from the disease than a man in a stable relationship. No research has been done into differences between hetero- and homosexual men.
PD can cause stress in patients and their partners. It is important to involve partners when explaining PD. Describing the situation in an objective manner at presentation is imperative, preferably by showing photographs taken from three perspectives. This can also be of great support in the follow-up period, especially when it comes to counseling about whether or not to undergo surgery. Photos of the erect penis from above show lateral deformation; photos from the sides show dorsal or ventral curvature; and frontal photos show possible rotation. A PDE-5 inhibitor or intracavernous injections with vasodilators (papaverine/phentolamine) can be used to treat coexisting ED. The exact angle of the curvature can be measured with a goniometer.
Physical examination has to be thorough. The glans penis must be held with between the thumb and index finger of the non-dominant hand to stretch the penis carefully and determine the remaining elasticity. The loss of elasticity indicates fibrosis. The length of the stretched penis is measured with a ruler from glans to the base of the penis. It is important to ensure this is objective because, in many cases, shortening occurs before any surgical intervention. The plaque is palpated with the dominant hand between thumb and index finger. It sometimes concerns minimal changes. Dorsal plaques are most common and can be easily distinguished from ventral plaques, which occur in less than five percent of PD patients. (1) Laterally-located plaques can cause severe coital problems. Deep penetration can lead to especially severe pain in partners, but the introduction can also be painful. Plaques circumventing the shaft can result in an hourglass deformity. The location of the plaque has to be noted, but this requires experience. A plaque size estimate by the hand of an inexperienced physician is unreliable. Indications of DD and Ledderhose’s disease also have to be examined. The Peyronie Disease Questionnaire (PDQ) can serve as guidance for anamnesis; further, physical examination is an important tool to render findings objective in case they are used in research. (29)
Thorough additional examination in the acute phase of the disease is rarely necessary. However, the diagnostic purpose of a duplex ultrasound is accepted by experts. Typical findings are a thickened TA, calcifications and septal fibrosis. In patients with coexisting

Chapter 1
22
ED, arterial and veno-occlusive dysfunction can be determined. This makes it important to combine the duplex ultrasound with an erection test, induced by phentolamine/papaverine or alprostadil injections. Magnetic resonance imaging (MRI) can take detailed pictures of plaques, but it is time-consuming, expensive and should be reserved for difficult cases, such as hourglass deformities.
Patients and partners should be aware that in approximately three to thirteen percent of patients, spontaneous remission occurs. (30) Since PD often coexists with diabetes and androgendeficiency, determining serum glucose, glycated hemoglobin (HbA1C), total testosterone, free testosterone and luteinizing hormone (LH) is recommended. (27)
TherapyCurrently, there is no consensus on an optimal treatment strategy. (1, 9, 19, 31) Even though pain reduces in most patients over the course of weeks or months, deformity is a much more manifest state.
Nonsurgical therapyOnly Collagenase Clostridium Histolyticum (CCH) is a registered pharmaceutical for the treatment of PD. Other oral drugs (pentoxyphylline and potassiumpara-aminobonzoate (PABA)); intralesional injections (verapamil, interferon, vitamin E and corticosteroids); as well as transcutaneous iontophoresis with verapamil and dexamethasone are described. These treatments are successful in some patients, but cannot be recommended according to European guidelines. (19)CCH was the first treatment for PD approved and registered by the Food and Drug Administration (FDA) and European authorities, albeit with certain restrictions.
Treatment with oral steroids, vitamin E and tamoxifen should be avoided whatsoever. Low-intensity shockwave treatment can be used to diminish pain, and traction devices can be used to counteract deformity and penile length. However, it can be painful and the effectiveness strongly depends on compliance. Radiotherapy has been empirically used with variable results and may be effective in the treatment of pain in the acute phase of the disease. (32) According to the European Society for Sexual Medicine (ESSM), there is no scientific proof for radiotherapy, but it increases the risk of local complications and should be considered obsolete. (27)
The results of nonsurgical therapy are difficult to interpret given the variety in study design, population, treatment period and dosage schemes. (27) A major limitation of comparing studies is the use of different end points. Reducing deformity of the erect penis (curvature, hinging, shortening) are the most common end points. A threefold study design (treatment

Current perspectives
23
1
vs. placebo vs. no treatment) over a period of at least eighteen months is preferred. (33) In practice, however, this is very difficult to organize.
Collagenase clostridium histolyticum (CCH)The fibrotic plaque consists of three types of collagen. CCH is a mix of two enzymes that block collagen types I and III, which are found in bones, scar tissue, connective tissue and plaques. CCH binds and unwinds or stretches the triple collagen helix and denaturizes protein compounds. (34) CCH in theory does not affect collagen type IV, which is mainly found in blood vessels and nerves. In-vitro and in-vivo research shows CCH to affect collagen type IV, which can explain the increase in pain and hematoma after CCH-injections compared to phentolamine/papaverine or alprostadil.
In 2013, results of the Investigation for Maximal Peyronie’s Reduction Efficacy and Safety Studies (IMPRESS) I and II were published. In these two identical, prospective, multicenter, randomized, double-blind, placebo-controlled, phase-III studies, 832 patients were included. The patients underwent four series of two injections, with six weeks between the series, and 24 to 72 hours between both injections per series. Patients were told to bend the plaque and stretch the penis three times a day. They were advised to straighten the penis during erection. The CCH-group showed a 34% improvement compared to 18% in the placebo group. (35)
Interestingly, the reduction in curvature led to an improvement in sexual satisfaction in 70% of all female partners. (36) Fifty-seven percent stated that their relationship had improved. A possible, but somewhat farfetched, explanation is that the plaque did not optically differ, but had become softer, thus causing the erect penis to be more flexible and less painful during intercourse.
Practical disadvantages of the original American treatment schedule are the number of injections (eight), high costs and difficult logistics. A trial in the United Kingdom combines three monthly injections with a traction device used twice a day for three months. Provisional results show no differences from the original schedule, but it does have financial and logistic advantages. (37) Disadvantages are needing to buy a traction device and the dependence on compliance. Unfortunately CCH was recently removed from the Asian, Australian and European markets for reasons that seem to have nothng to do with safety or efficacy.
Surgical therapyThe goal of surgery is to correct curvature and reduce coital problems. Surgery can only be considered in the stable phase and when severe difficulties with intercourse occur. Specific

Chapter 1
24
complications that have to be mentioned during counseling are the risk of ED, sensibility loss of the glans penis by neuropraxie of the dorsal nerve bundle, recurrence after surgery, palpable or painful knots under the skin, and further shortening of the penis. It is advised to determine penile length preoperatively, so patients realize shortening is also a result of the disease. (38) Having obtained informed consent, filing pre-, peri- and postoperative lengths is recommended.
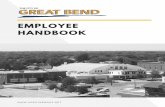
Nesbit-procedure and other shortening techniques.In 1965, Reed Nesbit was the first to report the excision of ellipses from the TA to treat patients with a congenital curvature. (39) Fourteen years later, the same technique was used in PD (Figure 1). (40) A penis with sufficient length is suitable for the Nesbit-procedure or another shortening technique, such as the Essed-Schröder (Figure 2), Yachia, Luc or the sixteen-dots cavernoplication according to Gholami (Figure 3). (41)
Figure 1.Procedure according to Nesbit. Top-left: the degloved penis after circumcision. Top-right: artifi cially in erection with a marked ellipse in the TA. Bottom-left: the earlier marked ellipse after excision, after which the defect is sutured. Bottom-right: the eventually straight and circumcised erect penis.

Current perspectives
25
1
The advantages of these procedures include the short operation time, the simplicity, the limited effect on hemodynamics of the erection and - most importantly - the effective straightening of the penis. Disadvantages include shortening, and the fact that they cannot correct hourglass and other complex deformities (rotation). In addition, sutures can rupture and lead to a recurrence of curvatures. The Nesbit-procedure and other shortening techniques should only be considered in patients with a penile length of at least 12 centimeters, measured on the convex side. In our experience, sexual intercourse otherwise becomes impossible because of the further loss of length.
Figure 2. Cavernoplication according to Essed-Schröder.
Figure 3. 16-dots-cavernoplication according to Gholami.

Chapter 1
26
Plaque incision or excision and grafting (PIEG)Patients with a severe curvature, calcification, hourglass and a short penis should be considered for a non-shortening procedure, such as PIEG (Figure 4). These procedures do not extend the penis. A major disadvantage is the loss of glandular sensibility caused by mobilizing the neurovascular bundle. This is often temporary.
Iatrogenic ED can be caused by an inflammatory reaction and fibrosis under the graft, thus damaging the smooth muscle tissue of the corpora and/or resulting in venous leakage. These techniques can be used in patients with pre-existing reduced erectile rigidity. However, they need to be prepared to use intracavernous injections with phentolamine/papaverine postoperatively, or - in the worst-case scenario - undergo a second procedure to implant a penile prosthesis.
Figure 4.PIEG (bovine pericard). Top left: the degloved penis after circumcision in artificial erec-tion. Top right: the defect in the TA after plaque incision. The neurovascular bundle is isolated by a yellow string.Bottom left: the covered defect with a bovine pericard graft. Bottom right: the eventually straight and circumcised erect penis.

Current perspectives
27
1
The most commonly-used autologous grafts are the vena saphena, skin, buccal mucosa, fascia of the m. rectus abdominus and fascia lata. Pericard of human and bovine cadavers, small bowel mucosa of pigs and fascia lata of cadavers are extracellular matrix graft materials that are used regularly. Synthetic grafts containing human fibrinogen and trombine or polytetrafluoro-ethylene are other possibilities. (42) The search for the ideal graft is far from over. Important criteria are availability, flexibility, infection insensitiveness and cost-effectiveness. The incentives for PIEG and CCH do not meet all these criteria. A substantial proportion of patients who have chosen PIEG regret their choice afterwards. It is recommended to discuss CCH as an alternative. An accepted treatment regimen is to perform monthly injections for three months combined with the use of a traction device twice a day. It is hoped that, in this way, PIEG can be averted or deferred.
Expectations and psychological aspectsPD can affect self-assurance, and counseling – preferably in multiple sessions – is important. (44) Many men have unrealistic expectations of treatment results. Patients and partners have to realize that the surgical goal is to functionally straighten the penis (within ten to twenty degrees of deviation) and that further shortening is linked with a procedure according to Nesbit or other shortening procedures.
Research has shown that PD can result in severe psychological problems. Depression and relationship issues are most common. (45) It is recommended to explore complaints, such as stress and depression, during the first outpatient clinic visit, whether or not with validated questionnaires. The course of psychological complaints and possible effects on the patient’s partner and relationship also deserve attention. In this aspect, homosexual men with PD are a special group and are difficult to categorize within current guidelines, which mostly relate to heterosexual men.
Concluding remarks
PD is a well-defined disorder. An increase in knowledge of genetics and molecular biology should improve therapeutic options. Adequate counseling and psychological support are a necessity in patients with PD.

Chapter 1
28
References
1. Ralph D, Gonzalez-Cadavid N, Mirone V, Perovic S, Sohn M, Usta M, et al. The Management of Peyronie’s Disease: Evidence-based 2010 Guidelines. J Sex Med. 2010;7(7):2359–74.
2. Sommer F, Schwarzer U, Wassmer G, Bloch W, Braun M, Klotz T, et al. Epidemiology of Peyronie’s disease. Int J Impot Res. 2002;14:379–83.
3. Mulhall JP, Creech SD, Boorjian SA, Ghaly S, Kim ED, Moty A, et al. Subjective and objective analysis of the prevalence of Peyronie’s disease in a population of men presenting for prostate cancer screening. J Urol. 2004;171(6, Part 1):2350–3.
4. Kumar B, Narang T, Gupta S, Gulati M. A clinico-aetiological and ultrasonographic study of Peyronie’s disease. Sex Health. 2006;3(2):113–8.
5. Rosen R, Catania J, Lue T, Althof S, Henne J, Hellstrom W, et al. Impact of Peyronie’s disease on sexual and psychosocial functioning: qualitative findings in patients and controls. J Sex Med 2008;5(8):1977–84.
6. Smith JF, Walsh TJ, Conti SL, Turek P, Lue T. Risk factors for emotional and relationship problems in peyronie’s disease. J Sex Med. 2008;5(9):2179–84.
7. Bjekic MD, Vlajinac HD, Sipetic SB, Marinkovic JM. Risk factors for Peyronie’s disease: A case-control study. BJU Int. 2006;97(3):570–4.
8. FG de la P. Sur quelques obstacles qui s’opposent à l’éjaculation naturelle de la semence. Mém Acad Roy Chir. 1743;1:318–33.
9. Hauck EW, Diemer T, Schmelz HU, Weidner W. A Critical Analysis of Nonsurgical Treatment of Peyronie’s Disease. Eur Urol. 2006;49(6):987–97.
10. Sergio Musitelli, MD, Maurizio Bossi, MD, and Hussein Jallous M. A Brief Historical Survey of “Peyronie’s Disease.” J Sex Med. 2008;5:1737–46.
11. Haneveld GT. Early Dutch contributions on Peyronie’s disease. Arch Chir Neerl. 1979;31(3):123–9.12. Gelbard MK, James K, Riach P, Dorey F. Collagenase versus placebo in the treatment of Peyronie’s disease:
a double-blind study. J Urol. 1993;149(1):56–8.13. Devine CJ, Somers KD, Jordan SG, Schlossberg SM. Proposal: trauma as the cause of the Peyronie’s lesion.
J Urol. 1997;157(1):285–90.14. Vermooten V. Metaplasia in the penis. The presence of bone, bone marrow and cartilage in the glans. N
Engl J Med. 1933;209:368–370.15. Bett WR. The os penis in man and beast. Ann R Coll Surg Engl. 1952;10:405-409.16. Sarma DP, Weilbaecher TG. Human os penis. Urology. 1990;35:349–350.17. Nugteren HM, Nijman JM, de Jong IJ, van Driel MF. The association between Peyronie’s and Dupuytren’s
disease. Int J Impot Res. 2011;23(4):142–5.18. Dolmans GH, de Bock GH, Werker PM. Dupuytren diathesis and genetic risk. J Hand Surg Am
2012;37:2106-11. 19. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, et al. EAU guidelines on
penile curvature. Vol. 62, Eur Urol. 2012. p. 543–52.20. Qian A, Meals RA, Rajfer J, Gonzalez-Cadavid NF. Comparison of gene expression profiles between
Peyronie’s disease and Dupuytren’s contracture. Urology. 2004;64(2):399–404.21. Wilma B. Bias PhD Leroy M. Nyberg Jr. Marc C. Hochberg Patrick C. Walsh John M. Opitz. Peyronie’s
disease: A newly recognized autosomal‐dominant trait. American Journal of Medical Genetics. 1982 June; 12-2.
22. Michou L1, Lermusiaux JL, Teyssedou JP, Bardin T, Beaudreuil J, Petit-Teixeira E. Genetics of Dupuytren’s disease. Joint Bone Spine. 2012 Jan;79(1):7-12.
23. Dolmans GH, Werker PM, Hennies HC, Furniss D, Festen EA, Franke L, et al. Wnt signaling and Dupuytren’s disease. N Engl J Med. 2011;365(4):307–17.
24. Moon RT, Kohn AD, De Ferrari G V, Kaykas A. WNT and beta-catenin signalling: diseases and therapies. Nat Rev Genet. 2004;5(9):691–701.
25. De Young LX, Bella AJ, O’Gorman DB, Gan BS, Lim KB, Brock GB. Protein Biomarker Analysis of Primary Peyronie’s Disease Cells. J Sex Med. 2010;7(1):99–106.
26. Mohede DCJ, Bank RA, van Driel MF, de Jong IJ. Anti-fibrotic effects of verteporfin on myofibroblasts in Peyronies disease. J Urol. Vol 199;4;912-913.

Current perspectives
29
1
27. Garaffa G, Trost LW, Serefoglu EC, Ralph D, Hellstrom WJG. Understanding the course of Peyronie’s disease. Vol. 67, International Journal of Clinical Practice. 2013. p. 781–8.
28. Mulhall JP, Schiff J, Guhring P. An analysis of the natural history of Peyronie’s disease. J Urol. 2006;175(June):2115–2118; discussion 2118.
29. Coyne KS, Currie BM, Thompson CL, Smith TM. Responsiveness of the Peyronie ’ s Disease Questionnaire ( PDQ ). J Sex Med. 2015;12(4):1072–9.
30. Bekos A, Arvaniti M, Hatzimouratidis K, Moysidis K, Tzortzis V, Hatzichristou D. The Natural History of Peyronie’s Disease: An Ultrasonography-Based Study. Eur Urol. 2008;53(3):644–51.
31. Nehra A, Alterowitz R, Culkin DJ, Faraday MM, Hakim LS, Heidelbaugh JJ, et al. Peyronie’s disease: AUA guideline. J Urol. 2015;194(3):745–53.
32. Mulhall JP, Hall M, Broderick GA, Incrocci L. Radiation therapy in Peyronie’s disease. J Sex Med. 2012;9(5):1435–41.
33. Pryor JP, Ralph DJ. Clinical presentations of Peyronie’s disease. Int J Impot Res. 2002;14(5):414–7.34. Cwikla DJ, Yafi FA. Intralesional collagenase Clostridium histolyticum in the management of Peyronie’s
disease: current best practice. Ther Adv Urol. 2018 Feb 8;10(4):139-153. 35. Gelbard M, Goldstein , Hellstrom WJ, McMahon CG, Smith T, Tursi J, Jones N, Kaufman GJ, Carson
CC. Clinical efficacy, safety and tolerability of collagenase clostridium histolyticum for the treatment of peyronie disease in 2 large double-blind, randomized, placebo controlled phase 3 studies. J Urol. 2013 Jul;190(1):199-207.
36. Goldstein I, Knoll LD, Lipshultz LI, Smith T, Kaufman GJ, McMahon CG. Changes in the Effects of Peyronie’s Disease After Treatment With Collagenase Clostridium histolyticum: Male Patients and Their Female Partners. Sex Med. 2017 Jun;5(2):e124-e130.
37. Abdel Raheem A, Johnson M, Abdel-Raheem T, Capece M, Ralph D. Collagenase Clostridium histolyticum in the Treatment of Peyronie’s Disease-A Review of the Literature and a New Modified Protocol. Sex Med Rev. 2017 Oct;5(4):529-535.
38. Smith JF, Walsh TJ, Lue TF. Peyronie’s disease: a critical appraisal of current diagnosis and treatment. Int J Impot Res. 2008;20(5):445–59.
39. Nesbit R. Congenital curvature of the phallus: report of three cases with description of corrective operation. J Urol. 1965;93:230–2.
40. Pryor JP FJ. A new approach to the correction of penile deformity in Peyronie’s disease. J Urol. 1979;122:622–3.
41. Gholami SS1, Lue TF. Correction of penile curvature using the 16-dot plication technique: a review of 132 patients. J Urol. 2002 May;167(5):2066-9.
42. Kadioglu A, Sanli O, Akman T, Ersay A, Guven S, Mammadov F. Graft materials in peyronie’s disease surgery: A comprehensive review. Vol. 4, J Sex Med. 2007. p. 581–95.
43. Anaissie J, Yafi FA. A review of surgical strategies for penile prosthesis implantation in patients with Peyronie’s disease. Transl Androl Urol. 2016;5(3):342–50.
44. Perneger T V. What is wrong with Bonferroni adjustments. Br Med J. 1998;316(7139):1236–8.45. Terrier JE, Nelson CJ. Psychological aspects of Peyronie’s disease. Transl Androl Urol. 2016;5(3):290–5.


Mohede DCJ, de Jong IJ, van Driel MFUrology 2019;125:1-5
Medical treatments of Peryonie’s disease:
past, present, and future
Chapter 2

Chapter 2
32
Introduction
Peyronie’s disease (PD) is a benign fibroproliferative disorder, which causes the formation of a plaque in the tunica albuginea of the corpora cavernosa in the penis. The disease is named after François Gigot de la Peyronie (1678-1747), although Fallopius and Vesalius had already described the disorder in 1561. (1)
Since the time of Peyronie, who sent his patients to the holy water of Baragès in the French Pyrenees (2), many nonsurgical empirical approaches have been tried, but still there is no effective cure. This is mainly due to a lack of understanding with regard to the biology and pathology of PD. (3) Once a calcified or even ossified plaque has developed, there is no nonsurgical treatment to make it disappear.
In 2004, Ralph and Minhas found 38 nonsurgical treatments of PD. (4) At the time of writing, none of them has received a grade A recommendation under the European guidelines. (5) Collagenase from Clostridium histolyticum is the only drug approved by the US Food and Drug Administration and the European Medicines Agency for intralesional injection in patients with a palpable plaque with dorsal or dorsolateral curvature greater than 30°.
The acute presentation of PD is treated conservatively and, in general, surgical approaches are only attempted after around one year in patients with stability for at least three months and a curvature that impedes sexual intercourse. During that waiting time, patients are often willing to undergo treatments. The effectiveness of these treatments, however, has not been proven in a three-arm study design (test treatment vs placebo vs no treatment) with a study duration of eighteen months. In this article, we reflect on the past, present and future of nonsurgical treatments of PD, with the emphasis being on oral treatments.
Material and methods
A wide literature search (The Cochrane Library, PubMed/MEDLINE, Web of Science, EMBASE and review of old German, Dutch, French and English medical books on male sexual functioning) was performed with the searches spanning until January 2018. The search included all medical interventions in patients with PD (or ‘cavernositis’, ‘penile fibrosis’, ‘fibrous sclerosis of the penis’, ‘induratio penis plastica’ or ‘Van Buren’s disease’), as reported in articles in any of the previously mentioned databases, or others found as references in articles and antiquarian books. We discuss our overall findings.

Medical treatments
33
2
Results
A total of 48 nonsurgical interventions were identified in articles from 1743 up until 2017 in all searched databases and relevant references. These included eleven external, twelve intralesional, seven topical and 22 oral interventions (table 1). Four of the treatments identified were used in two different ways.
Table 1. Historical overview of first reports about nonsurgical interventions for PD (E = external; I = intralesional; O = Oral; T = topical)
Year Therapy O/T/I/E Authors
1743 Mercury and mineral water O De la Peyronie (2)
1840 Potassium iodide O/T Ricord (6)*
1864 Electricity E Van Buren (7)*
1876
1878
Bromides and hyperthermia
Mercury and iodides
O/E
O/T
Hodgen (8)*
Curling (9)1890 Sulfur O Dubuc (10)*
1896 Copper sulfate O O’Zoux (11)*
1901
1901
Salicylate and thiosinamin
Mercury and iodides
O
I
Sachs (12)*
Walsham (13)1902 Arsenic O Reliquet (14)*
1907 Fibrinolysin O/T Waelsch (15)*
1910 Ionization E Lavenant: quoted by Zislin (16)*
1911 Milk O Van der Pool (17)*
1911 X-radiation E Bernasconi (18)*
1912 Ultraviolet light E LeFur (19)*
1922 Trypsin I Sonntag (20)*
1922 Radium E Kumer (21)*
1943
1943
Diathermy
Di-sodium phosphate
E
O
Wesson (22)
Wesson (22)1949 Vitamin E O Scardino (23)
1954 Cortisone I Teasly (24)
1954
1955
Hyaluronidase and steroid
Oestrogens
I
O
Bodner (25)
Minder (26)1959 Potassium para-aminobenzoate O Zarafonetis (27)
1960 Histamine iontophoresis T Whalen (28)
1963 Prednisolone O Chesney (29)
1967 Ultrasound E Heslop (30)

Chapter 2
34
Discussion
There is no generally accepted early treatment for PD, let alone the idea that prevention could be possible. The vast majority of the existing treatments are aimed at correcting the curvature, while in fact that is one of the complications of the disease. Nowadays, surgery is of very limited value in, for example, patients with peptic duodenal ulcers, pulmonary tuberculosis or anus carcinoma. Very effective nonsurgical treatments have replaced mutilating surgery. This is not yet the case for PD.
Throughout the past three centuries, many medical treatments have been tried, but nearly all were reported after clinical studies with a low number of patients and/or were based on
Year Therapy O/T/I/E Authors
1967 Dimethyl sulfoxide O Persky (31)
1967 Steroid iontophoresis T Rothfeld (32)
1970 Procarbazine O Aboulker (33)
1975 Parathyroid hormone I Morales (34)
1981 Orgoteine I Bartsch (35)
1983 Βeta-aminopropionitrile T Gelbard (36)
1985 Collagenase I Gelbard (37)
1985 Laser E Puente de la Vega (38)
1988 Prostacyclin I Strachan (39)
1989 Lithotrypsy E Bellorofonte (40)
1991 Interferon I Benson (41)
1992 Tamoxifen O Ralph (42)
1994 Verapamil I Levine (43)
1994 Colchicine O Akkus (44)
2001 Carnitine O Biagiotti (45)
2001 Traction devices E Scroppo (46)
2003 PDE5-I & arginine O Valente(47)
2006
2010
2016
2016
Pentoxifylline
Nicardipine
Superoxide-dismutase nicardipine and emu oil
Hyaluronic acid
O
I
T
I
Brant (48)
Soh (49)
Twidwell (50)
Zucchi (51)
*Cited in (52)
Table 1. Continued

Medical treatments
35
2
anecdotal experiences. In 1968, for example, Aron noted a regression of Dupuytren’s disease in a patient who was treated with the cytotoxic procarbazine for Hodgkin’s disease, and he suggested the use of this drug in fibroproliferative disorders. (53) In the 1970s, investigators from France reported excellent results in patients with PD, but in Belgium this treatment had disappointing results and became defunct. (54, 55) In this respect, it is remarkable that many titles of the articles about the treatment used the words ‘new therapy’. The modern era in the trial and error of medical therapy of PD began in 1949, with Scardino’s report on the use of tocopherols (23). Successful intralesional corticosteroid injections were first reported in 1954 by Teasly. (24) However, because a widely-accepted and effective medical treatment for PD was unavailable, research was primarily done by surgically-orientated urologists. They understandably focused on operation techniques, which led to them neglecting the pursuit of medical therapies. There was only one exception, which comprises the collagenase protocols of 1993 and the Collagenase Clostridium Histolyticum (CCH) injection therapy in the last decade. Collagenase really was the only subject of study in which the effects were evaluated in a randomized placebo-controlled, double-blind way, and moreover preceded by animal studies. (56) One of the few other animal studies showed reduction of fibrosis in the tunica albuginea, when the rats consumed pentoxifylline, L-arginine or any of three PDE-5 inhibitors (sildenafil, vardenafil, tadalafil) via drinking water. (47) The authors hypothesized that the increase in NO and/or cGMP/cAMP levels by chronic administration of nitrergic agents or PDE inhibitors could be effective in reversing the fibrosis of PD and, more speculatively, other fibrotic conditions.
In the European guidelines, none of the options depicted in the table carries a grade A recommendation. Today, drugs such as carnitine, arginine and dimethylsulphoxide (DMSO) belong to the domain of complementary and alternative medicine (CAM) in most European countries. Another alternative treatment available on the internet is bromelain, which is the crude extract of pineapple and has fibrinolytic, antithrombotic and anti-inflammatory properties. (57) However, there are no scientific data about its use by PD patients. According to the National Center for Complementary and Integrative Health in the US, bromelain is available as a powder, cream, tablet and capsule.
Overall, oral medical treatments are considered potentially effective in only the early phase of PD, namely, before plaque hardening and calcification occur. According to the current European guidelines, oral steroids, vitamin E and tamoxifen should be avoided completely. The remaining drugs for off-label use are pentoxifylline, a PDE- 5-inhibitor and/or arginine, or a combination of these.

Chapter 2
36
Current knowledge and new drugs for fibrosis In all fibroproliferative diseases, the differentiation and activation of myofibroblasts is one of the most important processes. These cells are the main producers of collagen and other extracellular matrix components. They also contain α-actin, which is a protein that causes cell contraction and thus contributes to distortion and dysfunction. (58) Myofibroblasts originate from locally-present fibroblasts or differentiated infiltrating fibrocytes. (59) Fibrocytes are circulating connective tissue progenitor cells. The transformation of precursor cells to myofibroblasts is influenced by various growth factors, cytokines and clotting factors. With the advancement of the healing process, the myofibroblasts will eventually disappear by apoptosis. It has been hypothesized that deregulation of this apoptotic process can occur, thus allowing more myofibroblasts to remain active. (60) In addition, there are indications that epigenetic changes in fibroblasts or myofibroblasts may contribute to fibrotic changes. (61, 62) Nowadays, as in PD, there are largely ineffective therapeutic options for patients with fibrotic diseases in general. New agents under investigation are pirfenidon, tyrosinekinase inhibitors, transforming growth factor-β, platelet- derived growth factor, interleukin-13 and lysyloxidase-2. (63)
Pirfenidon is an expensive, small molecule, available for oral use. The exact molecular mechanism of action is not completely explained. Based on in vitro studies, it is assumed that pirfenidon inhibits the proliferation and synthesis of pro- fibrotic and inflammatory mediators, and the collagen synthesis by fibroblasts and myofibroblasts. It is the first specific anti-fibrotic agent that is approved for the treatment of patients with idiopathic pulmonary fibrosis in Europe, Japan and the United States. (64) New studies may reveal whether pirfenidon works in patients with fibrotic diseases other than idiopathic pulmonary fibrosis.
The protein tyrosine kinase inhibitor nintedanib seems to be successful in the treatment of patients with idiopathic pulmonary fibrosis, while some forms of systemic sclerosis seem to decrease after treatment with the protein tyrosine kinase inhibitor imatinib mesilaat. (65, 66) However, these new treatment options are not yet beyond phase II studies in patients with idiopathic pulmonary fibrosis. It remains to be seen whether these therapies can also be applied in the treatment of patients with other fibrosing disorders.
Concluding remarks
Many of the old and new drugs reviewed have a reasonable basis for their use, but the lack of basic research on the biology and pathology in PD makes it difficult to understand the working mechanisms. The most important goal of medical therapy is to prevent or arrest

Medical treatments
37
2
the process of plaque formation and scarring. This means that a treatment should be initiated as soon as possible in the acute phase of PD. Patients typically present pain during this phase. If the plaque begins to harden, oral drugs will not be delivered. This is most likely due to the decreased vasculature.
Reviewers will continue to argue that there is a lack of standard assessment of severity, limited follow-up periods, absence of placebo or control groups, and a lack of standard definitions of outcome and so on. In a disease that can be self-limiting in five to thirteen per cent of patients, however, it will be difficult to prove the effectiveness of an early oral treatment. PD is not ordinarily a fibroproliferative disorder that solely affects the penis. In our view and as research shows, it is a local phenomenon of a systemic disease that is, among others, associated with Ledderhose’s and Dupuytren’s disease.
Surgery for PD is in itself a defeat of our therapeutic ingenuity, so the search for new, well-tolerated and effective medical therapy - oral drugs in the acute and intralesional agents in the more chronic phase - has to continue. In the end, the management of patients with PD should improve, with fewer of them needing surgery. In that respect, we strongly recommend a close collaboration with nonsurgical experts in fibrotic diseases.

Chapter 2
38
References
1. Hauck E, Weidner W, Nöske H. François Gigot de la Peyronie: the first complete clinical description of induration penis plastic. In: Schultheiss D, Musitelli S, Stief C, Jonas U, editors. Classical writings on erectile dysfunction An annotated collection of original texts from three millennia. Berlin: ABW Wissenschaftsverlag; 2005. p. 105–10.
2. De la Peyronie FG. Sur quelques obstacles qui s’opposent à l’éjaculation naturelle de la semence. Mém Acad Roy Chir. 1743;1:318–33.
3. Levine AL. Seeking answers on the quest for effective nonsurgical treatment of Peyronie’s disease. Eur Urol. 2007;51:601-4.
4. Ralph D, Minhas S. The management of Peyronie’s disease. B J Urol Int. 2004;93:208-15.5. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, et al. EAU guidelines on
penile curvature. Vol. 62, European Urology. 2012. p. 543–52. 6. Ricord. Gaz. Des Hôpitaux. Bull Gen Ther Paris.1840;19:222-6. 7. Van Buren K. 1875. In: Textbook, dis G-U Org, Arch F Dermat Syph. 1875th ed. 1874, p. 572. 8. Hodgen. No Title. Trans Med Soc, Missouri. 1876;28:31. 9. Curling TB. Impotency. In: Diseases of the testis, spermatic cord and scrotum. 4th ed. London: J & A
Churchill, 1878:460-5.10. Dubuc. No Title. Ann Des Mal Des Orgn G-U. 1890;181. 11. O’Zoux. No Title. Ann Des Mal Des Orgn G-U. 1896;14:38-41. 12. Sachs. No Title. Wien Klin Woch. 1901;14:111-8. 13. Walsham WJ, Spencer WG. Sores on the penis. In: Spencer WG. Surgery: its theory and practice. 8th ed.
London: J. & A. Curchill, 1903:1037.14. Reliquet. No Title. Ann Des mal Des Orgn G-U. 1890;181. 15. Waelsch. No Title. Deut Woch, Münch Med Woch. 1906;55:1427-30. 16. Lavenant, Zislin (Quoted by). No Title. These, Paris. 1911.17. Pool V der. No Title. Jour Of Cut G-U Dis. 1901;275 and 588. 18. Bernasconi. No Title. Rev Clin d’Urol, Paris,. 1912;1:53-6. 19. LeFur. No Title. 16th Sess l’Assoc Fr de l’Urol, Paris. October 1912. 20. Sonntag. No Title. Arch F Klin Chir. 1921;117:612-46. 21. Kumer. No Title. Dermat Woch. 1922;75:673-7. 22. Wesson M. Peyronie’s disease, cause and treatment. J Urol. 1943;49:350-6. 23. Scardino P, Scott W. The use of tocopherols in the treatment of Peyronie’s disease. N Y Acad Sci. 1949;52:390-6. 24. Teasly G. Peyronie’s disease: a new approach. J Urol. 1954;71:611-4. 25. Bodner H, Howard A, Kaplan J. Peyronie’s disease: cortisone- hyaluronidase-hydrocortisone therapy. J
Urol. 1954;72:400-3. 26. Minder J. Über die Wirkung des Oestrogen-Hormontherapie bei der Induratio Penis Plastica. Oncologia.
1955;8:19. 27. Zarafonetis C, Horrax T. Treatment of Peyronie’s disease with potassium para-amino benzoate (POTABA).
J Urol. 1959;81:770-2. 28. Whalen W. A new concept in the treatment of Peyronie’s disease. J Urol. 1960;83:851-2. 29. Chesney J. Plastic induration of the penis: Peyronie’s disease. Br J Urol. 1963;35:61-6. 30. Heslop RW, Oakland DJ, Maddox BT. Ultrasonic therapy In Peyronie’s Disease. Br J Urol. 1967;39:415-9. 31. Persky L, Stewart B. The use of dimethyl sulfoxide in the treatment of genitourinary disorders. Ann N Y
Acad Sci. 1967;141:551-4. 32. Rothfeld S, Murray W. The treatment of Peyronie’s disease with iontophoresis of C21 esterified
glucocorticoids. J Urol. 1967;97:874-875. 33. Aboulker P, Benassayag E. Traitement de l’induration plastique des corps caverneux par la procarbazine
(Natulan). J Urol. (French) 1970;76:499–503. 34. Morales A, Bruce A. The treatment of Peyronie’s disease with parathyroid hormone. J Urol. 1975;114:901-2. 35. Bartsch G, Menander-Huber KB, Huber W, Marberger H. Orgotein, a new drug for the treatment of
Peyronie’s disease. Eur J Rheumatol Inflamm. 1981;4:250-9.

Medical treatments
39
2
36. Gelbard M, Lindner A, Chvapil M, Kaufman J. Topical beta-aminopropionitrile in the treatment of Peyronie’s disease. J Urol. 1983;129:746-8.
37. Gelbard MK, James K, Riach P, Dorey F. Collagenase versus placebo in the treatment of Peyronie’s disease: a double-blind study. J Urol. 1993;149:56-8.
38. Puente de la Vega A, Calvo-Mateo M, Domenech M. Laser therapy in Peyronie’s disease. Actas Urol Esp. 1985;9:107-9.
39. Strachan Jr, Pryor JP. Prostacyclin in the treatment of painful Peyronie’s Disease. Br J Urol. 1988;61:516-7. 40. Bellorofonte C, Ruoppolo M, Tura M. Possibility of using piezoelectric lithtryptor in the treatment of severe
cavernous fibrosis. Arch Ital Urol Nefrol Androl. 1989;61:417-22. 41. Benson RJ, Knoll L, Furlow W. Interferon α2β in the treatment of Peyronie’s disease. J Urol. 1991;61:1342. 42. Ralph DJ, Brooks MD, Botazzo GF, Pryor JP. The Treatment of Peyronie’s disease with tamoxifen. Br J Urol.
1992;70:648-51. 43. Levine LA, Merrick PF, Lee RC. Intralesional verapamil injection for the treatment of Peyronie’s disease. J
Urol. 1994;151:1522-4. 44. Akkus E, Carrier S, Rehman J, Breza J, Kadioglu a, Lue TF. Is colchicine effective in Peyronie’s disease? A
pilot study. Urology. 1994;44:291-5. 45. Biagiotti G, Cavallini G. Acetyl-L-carnitine vs tamoxifen in the oral therapy of Peyronie’s disease: A
preliminary report. BJU Int. 2001;88:63–7. 46. Scroppo F, Mancini M, Maggi M. Can an external penis stretcher reduce Peyronie’s penile curvature? Int J
Imp Res. 2001;13(S21): 4th annual meeting of the European Society for Sexual Medicine. 47. Valente EGA, Vernet D, Ferrini MG, Qian A, Rajfer J, Gonzalez-Cadavid NF. L-Arginine and
phosphodiesterase (PDE) inhibitors counteract fibrosis in the Peyronie’s fibrotic plaque and related fibroblast cultures. Nitric Oxide Biol Chem. 2003;9:229-44.
48. Brant WO, Dean RC, Lue TF. Treatment of Peyronie’s disease with oral pentoxifylline. Nat Clin Pract Urol. 2006;3:111-115.
49. Soh J, Kawauchi A, Kanemitsu N, et al. Nicardipine vs. saline injection as treatment for Peyronie’s disease: a prospective, randomized, single-blind trial. J Sex Med. 2010;7:3743-49.
50. Twidwell J, Levine L. Topical treatment for acute phase Peyronie’s disease utilizing a new gel, H-100: a randomized, prospective, placebo-controlled pilot study. Int J Impot Res. 2016; 28:41-5.
51. Zucchi A, Constantini E, Cai T, Cavallini G, Liguori G, Favilla V, De Grande G, D’Achille G, Silvani M, Franco G, Palmieri A, Verze P, Mirone V. Intralesional injection of hyaluronic acid in patients affected with Peyronie’s disease: preliminary results from a prospective, multicenter, pilot study. Seks Med. 2016;4e85-e90.
52. Polkey H. Induratio penis plastica. Urol Cut Rev. 1928;287-308. 53. Aron E. Le traitement médical de la maladie de Dupuytren par un agent cytostatique (méthylhydrazine).
Presse Médical. 1968;76:1956.54. Sturm M, Lebeuf M. Résultats d’un traitement immunodépresseur dans la maladie de La Peyronie, la
maladie de Dupuytren et certaines sclérodermies. Bull de la Société Française de Dermatologie et de Syphiligraphie. 1971;78:523-5.
55. Oosterlinck W, Renders G. Treatment of Peyronie’s disease with procarbazine. B J Urol. 1975;47:219-20.56. Gelbard MK, Walsh R, Kaufman JJ. Collagenase for Peyronie’s disease experimental studies. Urol Res.
1982;10:135-40. 57. Sahbaz A, Aynioglu O, Isik Ha, Ozmen U, Cengil O, Dogan Gun O, Gungorduk K. Bromelain: a natural
proteolytic for intra-abdominal adhesion prevention. Int J Surg 2015;14:7-11.58. Hu B, Phan SH. Myofibroblasts. Curr Opin Rheumatol. 2013;25:71-7.) Myofibroblasts originate from
locally present fibroblasts or from differentiated infiltrating fibrocytes or by local epithelial or endothelial cells.
59. Kramann R, DiRocco DP, Humphreys BD. Understanding the origin, activation and regulation of matrix-producing myofibroblasts for treatment of fibrotic disease. J Pathol. 2013;231:273-89.
60. Ding BS, Cao Z, Lis R, et al. Divergent angiocrine signals from vascular niche balance liver regeneration and fibrosis. Nature. 2014;505:97-102.
61. Huang SK, Scruggs AM, McEachin RC, White ES, Peters-Golden M. Lung fibroblasts from patients with idiopathic pulmonary fibrosis exhibit genome-wide differences in DNA methylation compared to fibroblasts from nonfibrotic lung. PLoS ONE. 2014;9:e107055.

Chapter 2
40
62. Watson CJ, Collier P, Tea I, et al. Hypoxia-induced epigenetic modifications are associated with cardiac tissue fibrosis and the development of a myofibroblast-like phenotype. Hum Mol Genet. 2014;23:2176-88.
63. Dalm V, Dik WA, Thio HB, van den Blink B, van Hagen PM, van Daele PL. Fibrosing disorders: insights into pathogenesis and new treatment options. Ned Tijdschr Geneeskd. 2015;159:A8345.
64. Noble PW, Albera C, Bradford WZ, et al; CAPACITY Study Group. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377:1760-9.
65. Richeldi L, du Bois RM, Raghu G, et al; INPULSIS Trial Investigators. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370:2071-82.
66. Jang SW, Ihm SH, Choo EH, et al. Imatinib mesylate attenuates myocardial remodeling through inhibition of platelet-derived growth factor and transforming growth factor activation in a rat model of hypertension. Hypertension. 2014;63:1228-34.

41


Published as abstract:Mohede DCJ, Weidenaar AC, van Driel MF, van de Wiel HBM, de Jong IJ
J Urol 2018;199:e911
Patient reported outcomes on sexual function
after surgical treatment of Peyronie’s disease
Chapter 3

Chapter 3
44
Introduction
Peyronie’s disease (PD) is a consequence of changes in the composition of the tunica albuginea (TA). Fibrosis of the TA can lead to penile pain, deformation (that is, curvature and hourglass deformity), erectile dysfunction (ED) and shortening. (1) Whereas penile pain often decreases and disappears in time, deformity is more visible and long-lasting. The deformity develops during a six to eighteen month inflammatory phase and is considered ‘stable’ after three months without further changes. (2) Demographic studies show a relatively high prevalence of PD, specifically, up to 9% in men older than 50 years. (3, 4) Due to loss of length and penile pain, PD can have major impact on sexual function and cause serious psychological distress. (5) Measured with both validated and non-validated questionnaires, depression (48%) and relationship distress (>50%) are common. Loss of sexual confidence, reduced ability to initiate sex and decreased interest in sex are also often reported. Additionally, many men express social stigmatization and isolation.
No consensus about the optimal treatment strategy for PD has been reached. (1, 6–8) Pharmacotherapeutic options have no grade A recommendation in the European guidelines. (7) There is an indication for surgical correction if there are serious intercourse problems due to the penile deformity, but surgery should only be performed if the disease is stable.
The literature on the long-term outcomes of surgical interventions is mostly retrospective and the course of sexual function after treatment is underexplored territory. Therefore, our study aims to fill these gaps, which could improve counseling.
Objective To obtain long term results of Peyronie’s disease therapy and improve counseling.
Methods
Ethics statementAll research data were acquired after obtaining signed, informed consent from every individual patient and after approval of the Medical Ethics Committee (METc) of the University Medical Center Groningen (2016/561), in accordance with the Declaration of Helsinki.

Patient reported outcomes
45
3
Study populationData were retrospectively collected from all patients with PD who visited our outpatient clinic from 2007 until 2016. The data included patient-specific factors (age, demographics, (family) history, and sexual orientation) and the Dutch validated International Index of Erectile Function (IIEF) scores at presentation and follow-up (appendix A). The IIEF has fifteen questions concerning five domains of sexual function, including ‘erectile function (1-30 points)’, ‘orgasmic function (0-10)’, ‘sexual desire (2-10)’, ‘intercourse satisfaction (0-15)’, and ‘overall satisfaction (2-10)’. Patients nominated for a surgical procedure, as a result of sexual problems caused by the penile deformity, qualified for surgery according to the European guidelines. (7) The Nesbit procedure was reserved for patients with an adequate penile length of around twelve centimeters and a relatively mild curvature (< 60o). More complex deformities, for example, hourglass or a penile length of less than around twelve centimeters, justified plaque incision, and grafting (PIG) with bovine pericard. Patients suffering from co-existent ED who did not react to PDE5 inhibitors or intracavernous injections with vasodilators were advised to undergo erection prosthesis surgery. Acoording to our local protocol, after prosthesis surgery patients were told not to have sexual intercourse for six weeks and inflate their devices daily for 30 minutes, starting two weeks after surgery.
Retrospectively, the patients were divided into three groups: Nesbit, PIG, and prosthesis surgery. Patients who were not fit for surgery and those who had preferred a non-surgical approach (expectative treatment or a treatment with drugs such as pentoxyphylline, tadalafil, and/or analgetics), were all considered to be part of the conservatively treated group, irrespective of the stage of the disease. They served as controls with regard to the IIEF analysis. One senior urologist (MFvD) performed all surgeries and outpatient clinic contacts.
Patient questionnairesPatients were contacted by mail and asked to fill out the IIEF at follow-up, accompanied by additional questions regarding satisfaction, specific symptoms, and complications (Appendix A). The response rate was 56.6% (n = 170 out of 300). Patients were asked about outcomes such as loss of glandular sensibility, disabled intercourse, hindered intromission, pain experienced by partner, anorgasmia, need for psychological or psychiatric treatment, residual degree of rigidity, and partner satisfaction. Further, surgically treated patients were asked whether they experienced relapse, shortening, or post-surgical pain. They were also asked to depict the overall satisfaction rate with regard to the end result on a zero-to-ten scale, as well as whether or not they would be willing to undergo the same treatment with knowledge of the final outcome in their own case.

Chapter 3
46
Statistical analysisData were imported into the IBM SPSS 23 Statistics Data Editor. Cohort characteristics were analyzed descriptively using frequency distributions. Continuous data are presented as means ± standard deviation (µ ± ς) and ordinal data as median with interquartile ranges (IQR). An unpaired t-test was used for comparison of age (additionally, linear regression was used), follow-up, and degree of rigidity. Partner satisfaction and glandular sensibility loss were compared with the Mann-Whitney U test. The Chi-square test was used for comparison of disabled intercourse, hindered intromission, partner experienced pain, anorgasmia, and need for psychological treatment between surgical and conservative treatment. Differences in partner satisfaction, glandular sensibility loss, remaining degree of rigidity, whether patients would undergo intervention again, grade for end result, degree of shortening, and post-surgical pain between interventions were compared with the Kruskal-Wallis test. Disabled intercourse, hindered intromission, partner experienced pain, anorgasmia, need for psychological treatment, relapse, and shortening in those groups were analyzed using a Chi-square test. IIEF outcomes at presentation and follow-up were compared using the Wilcoxon rank sign test. Differences in IIEF outcomes between conservatively and surgically treated patients were evaluated using the Mann-Whitney U test. P < 0.05 was considered statistically significant and not corrected for multiple testing because research questions comprised specific inquiries.
Results
DemographicsThe 170 respondents had a mean age of 55 ± ten years, with a follow-up of 5.3 ± 3.7 years after the first presentation (Table 1). Seventy-seven of them had undergone surgical treatment and 93 had been treated conservatively. Of the 77 surgically treated, 56 were operated according to Nesbit, thirteen underwent a PIG, and eight primarily got an implant. At follow-up, three out of 93 (3.2%) conservatively treated patients stated that the symptoms had spontaneously vanished over the years. There were no significant differences regarding terms of age, follow-up, alcohol consumption, smoking, diabetes, liver disease, and epilepsy among groups.
Therapeutic outcomes of all respondents (n = 170)Of all respondents, 26.4% were no longer able to have intercourse and 53.5% experienced problems at intromission. A total of 9.2% experienced anorgasmia and the mean estimated residual maximal penile rigidity was 65.4 ± 30.3% (on a 0-100% scale). Over 7% of respondents had psychological or psychiatric treatment in the follow-up period. The

Patient reported outcomes
47
3
differences between the conservative approach and surgical treatments are summarized in Table 1. Loss of glandular sensibility was significantly higher in surgically treated patients (55.8% vs. 36.6%, p = 0.024). Partner satisfaction also differed significantly (p = 0.023) in favor of the conservatively treated. 46.7% of partners of respondents who had undergone surgery were unsatisfied, compared with 31.2% of partners of respondents who had not undergone surgery. Pain experienced by partners during intercourse was approximately 18% in both groups. Other investigated outcomes, including disabled intercourse, hindered intromission, partner experiencing pain, anorgasmia, psychological treatment, and residual degree of rigidity did not significantly differ between the conservatively and surgically treated groups.
Outcomes of surgically treated patients (n = 77)Due to the selection of patients (severe curvature and so on) and specific risks of the procedure, residual penile rigidity of patients treated with PIG was significantly lower than in those treated according to Nesbit (45.0% vs. 71.2%, p = 0.038). Patients who had prosthesis surgery experienced more intromission problems (87.5%) compared with those who had undergone other interventions (p = 0.011). Disabled intercourse, however, was not significantly different. 61.5% of the respondents after PIG stated they would not be willing to undergo the same procedure; this percentage was 23.2% (p = 0.007) for the Nesbit group. For patients with a penile prosthesis, this percentage was 50.0%. In addition, PIG patients gave lower grades for satisfaction with regard to the end result, albeit not significantly different from the other two surgical groups. In the follow-up period, 20.8% experienced a recurrent curvature and 91.5% experienced surgery-induced shortening of the penis (3.5 ± 2.5 centimeters), which did not significantly deviate in degree within the different groups.
Of all surgically treated patients, 24.7% experienced disabled intercourse, 18.2% of their partners suffered from pain during intercourse, 14.3% were unable to reach an orgasm, and 5.2% were at any point undergoing psychological or psychiatric treatment.

Chapter 3
48
Tabl
e 1.
Cha
ract
erist
ics,
trea
tmen
t out
com
es a
nd sa
tisfa
ctio
n of
the
resp
ondi
ng p
opul
atio
n. C
onse
rvat
ivel
y an
d su
rgic
ally
trea
ted
patie
nts w
ere
anal
yzed
stat
istic
ally,
as
wer
e pa
tient
s tre
ated
acc
ordi
ng to
the
diffe
rent
surg
ical
met
hods
. Cha
ract
erist
ics a
re d
ispla
yed
as µ
± ς
(age
, fol
low
-up,
resid
ual d
egre
e of
rigi
dity
, deg
ree
of
shor
teni
ng a
nd g
rade
for e
nd re
sult)
or m
edia
n (in
terq
uart
ile ra
nges
, day
s pos
t-su
rgic
al p
ain)
; n (%
). PI
G =
pla
que
inci
sion
and
graft
ing.
*p-v
alue
s rep
rese
nt
diffe
renc
es b
etw
een
Nes
bit a
nd P
IG; p
rost
hesis
gro
up w
as e
xclu
ded.
Cha
ract
eris
ticA
ll pa
tient
sC
onse
rvat
ive
Surg
ical
p-va
lue
Nes
bit
PIG
Pros
thes
isp-
valu
eN
o.17
093
7756
138
Age
at d
iagn
osis,
y55
±
10Fo
llow
-up,
y5.
3 ±
3.7
Ove
rall
trea
tmen
t out
com
e
Gla
ndul
ar se
nsib
ility
loss
, n (%
)75
(4
4.1)
34
(36.
6)43
(5
5.8)
0.02
428
(5
0.0)
10
(77.
0)7
(87.
5)0.
058
D
isabl
ed in
terc
ours
e, n
(%)
45
(26.
4)26
(2
8.0)
19
(24.
7)0.
353
12
(21.
4)7
(5
3.8)
2 (2
5.0)
0.30
3
Hin
dere
d in
trom
issio
n, n
(%)
91
(53.
5)47
(5
0.5)
45
(58.
4)0.
440
22
(39.
3)1
(7.7
)7
(87.
5)0.
011
P
artn
er e
xper
ienc
ing
pain
, n (%
)31
(1
8.2)
17
(18.
3)14
(1
8.2)
0.84
29
(1
6.1)
1 (7
.7)
3 (3
7.5)
0.41
7
Ano
rgas
mia
, n (%
)16
(9
.2)
6
(6.5
)11
(1
4.3)
0.28
610
(1
7.9)
0 (0
.0)
1 (1
2.5)
0.39
9
Psy
chol
ogic
al tr
eatm
ent,
n (%
)12
(7
.1)
8
(8.6
)4
(5
.2)
0.93
52
(3
.6)
1 (7
.7)
1 (1
2.5)
0.50
0
Res
idua
l deg
ree
of ri
gidi
ty (0
-100
%)
65.4
± 3
0.3
64.0
± 2
8.4
67.3
± 3
3.9
0.50
571
.2 ±
32.
145
.0 ±
34.
2-
0.03
8*Sa
tisfa
ctio
n pa
rtne
r0.
023
0.52
1
Sat
isfied
, n (%
)72
(4
2.4)
47
(50.
5)25
(3
2.5)
20
(35.
7)3
(23.
1)2
(25.
0)
Uns
atisfi
ed, n
(%)
63
(37.
1)29
(3
1.2)
36
(46.
7)24
(4
2.9)
9 (6
9.2)
4 (5
0.0)
U
nkno
wn,
n (%
)35
(2
0.5)
17
(18.
3)16
(2
0.8)
12
(21.
4)1
(7.7
)2
(25.
0)Su
rgic
al tr
eatm
ent o
utco
me
R
elap
se, n
(%)
16
(20.
8)12
(2
1.4)
4 (3
0.8)
0 (0
.0)
0.22
5
Sho
rten
ing
expe
rienc
ed, n
(%)
65
(91.
5)51
(9
4.4)
8 (8
4.6)
6 (7
5.0)
0.17
4
Deg
ree
of sh
orte
ning
, cm
3.5
± 2.
53.
2 ±
2.0
5.2
± 4.
33.
1 ±
2.8
0.51
3
Pos
t-su
rgic
al p
ain,
day
s7
(0-2
1)10
(0
-21)
26
(2.5
-90)
0 (0
-9)
0.05
2Sa
tisfa
ctio
n
Wou
ld u
nder
go in
terv
entio
n ag
ain
0.00
7*
Y
es, n
(%)
48
(62.
3)39
(6
9.7)
5 (3
8.5)
4 (5
0.0)
No,
n (%
)25
(3
2.4)
13
(23.
2)8
(61.
5)4
(50.
0)
I
n do
ubt,
n (%
)4
(5.2
)4
(7
.1)
G
rade
for e
nd re
sult
(0-1
0)6.
0 ±
2.4
6.2
± 2.
24.
6 ±
3.1
6.2
± 2.
50.
090*

Patient reported outcomes
49
3
IIEF analysisThe IIEF was obtained at the first presentation and, on average, five years later (Figure 1). Scores of surgically treated patients were compared with those of conservatively treated patients. At first presentation, only the median (IQR) IIEF scores for the domain ‘intercourse satisfaction’ were significantly lower in those who chose surgery (5 (0-8) vs. 9 (1-11), p = 0.035).
For the conservatively treated group, we compared the IIEF scores at follow-up with the baseline scores and found significant declines on ‘erectile function’ (22.5 (11.75-28) vs. 19 (6-28), p = 0.005), ‘orgasmic function’ (10 (5-10) vs. 8 (2.5-10), p < 0.001), ‘sexual desire’ (7 (6-8) vs. 7 (5-8), p = 0.008), and ‘intercourse satisfaction’ (9 (1-11) vs. 7.5 (0-11), p = 0.021). Within the surgically treated group, scores concerning ‘overall satisfaction’ increased significantly (6 (4-7) vs. 6 (3-8), p = 0.028) during follow-up.
Figure 1. Effect of conservative and surgical treatment on sexual function.Display of median scores (IQR) regarding sexual function domains of the IIEF, comparing scores at presentation (first IIEF) and follow-up (second IIEF) between conservatively and surgically treated patients. At presentation, ‘intercourse satisfaction’ was significantly lower in surgically treated patients compared with the conservatively treated patients. Comparing IIEF scores at presentation and after follow-up, ‘erectile function’, ‘orgasmic function’, ‘sexual desire’, and ‘intercourse satisfaction’ significantly decreased in conservatively treated patients whereas ‘overall satisfaction’ increased in surgically treated patients. At follow-up, there were no significant differences between conservatively and surgically treated patients. * indicates data with a p-value < 0.05. Box-and-whisker plot limits depict 75th and 25th percentiles and median values (box), and upper/lower quartiles ± (IQR) (upper and lower whiskers, respectively).

Chapter 3
50
When we analyzed differences in the entire cohort, ‘orgasmic function’ (9 (4-10) vs. 8 (2-10), p < 0.001) and ‘sexual desire’ (7 (5-8) vs. 6 (5-8), p = 0.003) significantly decreased during follow-up whereas the other scores did not show significant differences compared with those at first presentation. A comparison of IIEF scores at follow-up between surgically and conservatively treated patients no longer showed significant differences in sexual function domains.
Discussion
This study evaluates sexual functioning at presentation and long-term follow-up for surgically and conservatively treated patients with PD. Our results show a decrease in ‘sexual desire’ and ‘orgasmic function’ of the entire cohort over time, which is most likely caused by aging instead of PD itself. Remarkably, ‘erectile function’ did not decrease with age although, based on literature, it is likely to decrease to 15 points between the ages of 40 and 60. (9) However, the decrease in ‘sexual desire’ explains why ‘intercourse satisfaction’ and ‘overall satisfaction’ are stable: men and their partners may lose interest in intercourse, prioritize different things in life, or experience other sexual problems, which could all compensate for the decline in satisfaction rates. (10)
We focused on possible differences within and between surgically and conservatively treated patients. Regarding ‘intercourse satisfaction’, the surgically treated group showed worse starting conditions than the conservatively treated one. The latter group had qualitatively better starting conditions that lead to a conservative approach. Overall, the success of conservative therapy, for example the use of oral drugs such as pentoxyphylline and PDE5 inhibitors, is hard to predict and interpret because of differences in research methods, patient populations, and treatment. (11)
At follow-up, the conservatively treated patients showed a decrease in scores on ‘erectile function’, ‘orgasmic function’, ‘sexual desire’, and ‘intercourse satisfaction’. Progression of PD and aging partly explain the decrease in ‘intercourse satisfaction’. The fact that patients have knowledge of more (surgical) treatment options might contribute to the decline as well. Patients could believe that there are still unaddressed options that could possibly decrease their symptoms. They also report stable scores on ‘overall satisfaction’, which might be explained by a patient having learned to live with the disease and the fact that the decision to stay conservative was well thought out. (5) ‘Orgasmic function’ is another domain that is likely to decrease with age, as shown in previous reports. (10)

Patient reported outcomes
51
3
After surgical treatment, patients reported an increase in ‘overall satisfaction’ compared with the initial state. This may be indicative of a successful correction of the curvature, but also of the knowledge that every possible treatment was addressed. Most importantly, scores on ‘overall satisfaction’ indicate that one can expect improvement after surgical treatment based on current guidelines. In our opinion, indications for surgery should not be widened since scores of the surgically treated patients do not exceed those after a conservative approach.
Spontaneous remission occurred in 3.2% of patients, which corresponds to literature percentages (<13%). (2) This seems to concern milder variants of PD. Decreasing rigidity with age may also explain a milder curvature. In the future, genetic analysis of patients with milder and severe forms of PD could clarify spontaneous remission and provide tools for future research.
This study gives new insights into specific outcomes of different PD treatment methods, as reported by patients. At follow-up, rigidity as a percentage of the premorbid situation did not differ between surgically and conservatively treated patients. However, rigidity was significantly decreased in patients treated with PIG compared with those treated by a Nesbit procedure. Possible explanations for the rigidity-loss of PIG include poor starting conditions, but also the intervention itself, that is, bigger defects and detaching the neurovascular bundle. In other studies, loss of rigidity varied between zero and 53%. (11)In this study, penile shortening as a result of surgery was subjectively reported by all surgically treated patients, including the PIG ones. In the case of the Nesbit technique, this can be explained by the surgical technique and depends on the severity of the curvature. After PIG, other authors found a much milder or no shortening, albeit after shorter follow-up periods and measured by clinicians. (12,13) In this study, the PIG patients experienced shortening due to surgery, although this is difficult to explain except if due to recurrence in the follow-up period.
The overall recurrence of curvature in 20.8% of the surgically treated patients in this series is in accordance with findings in recent literature. (14)
Loss of glandular sensibility in the entire surgically treated group may be caused by circumcision. Subsequently, the glans has frequent contact with surrounding clothing and body parts and may subjectively lose sensitivity. Temporary loss of glandular sensitivity after PIG may be due to mobilization of the neurovascular bundle. The percentages vary from zero to 31%. (11)

Chapter 3
52
Hindered intromission in patients with an implant may be due to loss of control over the penis or a ‘floppy glans’ (figure 2) caused by implementation of foreign materials. A major finding within the surgically treated group was the fact that the majority of patients treated with PIG were dissatisfied and not willing to undergo this procedure again. The percentage of >60% is higher than in current literature; dissatisfaction rates might have been underestimated in previous reports. (15) Besides poor starting conditions in patients who need to be treated by PIG, further differences can be explained by variations in research methods, such as shorter follow-up periods. The Nesbit procedure showed satisfaction percentages comparable to those in literature. (1, 11, 16–20)
Partner dissatisfaction was higher among operated patients than the conservatively treated, and similar percentages were mentioned in literature. (21) Interestingly, these numbers represent the opinion of patients who indicate that they have a representative idea of whether their partners are affected by the disease. Clinicians should hence always encourage patients to involve their partner in decision-making processes over time. Depression symptoms have been described in approximately 50% of patients with PD. (5) However, only 7.1% in our cohort sought psychological help, which shows the importance of active attention to psychological referral in motivated patients. Psychological help can contribute to improving their quality of life. Patients did not always seek psychological help
Figure 2. ‘Floppy’ glans in the penis with prosthesis

Patient reported outcomes
53
3
as a direct result of PD, which made the determination of a possible correlation between patient and partner dissatisfaction far-fetched.
Over the past decade, novel approaches to managing the treatment of PD have emerged. The use of clostridial collagenase, however, is restricted to patients with stable PD, with a curvature of 30o-90o, without hourglass deformity, and with normal erectile function. (22) This specific treatment for such a group was enshrined in the 2015 American guidelines and was not used in the Netherlands during the course of this study. (23) Furthermore, medical treatments that have been used in this cohort are not recommended in the current guidelines.
One of the limitations of our non-randomized study was the partly-retrospective character. In the end, just over half of all patients completed follow-up. There were only two data points: at the patient’s initial visit and in 2016. Due to the likelihood that patients not choosing surgical treatment or patients who were advised by the surgeon to have conservative treatment, this likely could have led to significant differences from the surgically treated group. In addition, our study included a relatively low number of patients who underwent PIG or prosthesis implants, so propensity matching was not applicable. The differences between the three surgical treatments are therefore only descriptive. At the start of the study, a validated version of the Peyronie’s Disease Questionnaire was not yet available in Dutch. We were unable to test variations in surgical outcomes based on the physicians’ experience due to the fact that only one physician provided this care.
In conclusion, our study shows that sexual functioning in PD patients improved after surgery based on the current guidelines, leveling with the results of the conservatively treated patients. However, results varied between the different options. Surgery according to Nesbit is an effective option and can be safely considered. Worse starting conditions in PIG patients as well as the intervention itself could both lead to relatively high dissatisfaction over time. We advise being cautious with regards to this type of surgery, and providing realistic perspectives in terms of outcomes for patients as well as their partners. The limited number of patients that underwent implantation of a penile prosthesis was not sufficient to show small differences compared with other treatment groups.
Our findings could improve realistic preoperative counseling concerning sexual function and specific consequences of different treatment methods in patients with PD.

Chapter 3
54
References
1. Ralph D, Gonzalez-Cadavid N, Mirone V, Perovic S, Sohn M, Usta M, et al. The management of Peyronie’s disease: Evidence-based 2010 Guidelines. J Sex Med. 2010;7(7):2359–2374.
2. Mulhall JP, Schiff J, Guhring P. An analysis of the natural history of Peyronie’s disease. J Urol. 2006 June;175:2115–2118.
3. Mulhall JP, Creech SD, Boorjian SA, Ghaly S, Kim ED, Moty A, et al. Subjective and objective analysis of the prevalence of Peyronie’s disease in a population of men presenting for prostate cancer screening. J Urol. 2004;171(6, Part 1):2350–2353.
4. Kumar B, Narang T, Gupta S, Gulati M. A clinico-aetiological and ultrasonographic study of Peyronie’s disease. Sex Health. 2006;3(2):113–118.
5. Terrier JE, Nelson CJ. Psychological aspects of Peyronie’s disease. Transl Androl Urol. 2016;5(3):290–295. 6. Hauck EW, Diemer T, Schmelz HU, Weidner W. A critical analysis of nonsurgical treatment of Peyronie’s
disease. Eur Urol. 2006;49(6):987–997. 7. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, et al. EAU guidelines on
penile curvature. Eur Urol. 2012;62:543–552. 8. Nehra A, Alterowitz R, Culkin DJ, Faraday MM, Hakim LS, Heidelbaugh JJ, et al. Peyronie’s disease: AUA
guideline. J Urol. 2015;194(3):745–753. 9. Atan A, Basar MM, Tuncel A, Mert C, Aslan Y. Is there a relationship among age, international index
of erectile function, international prostate symptom score, and aging males’ symptoms score? Int Urol Nephrol. 2007;39(1):215–222.
10. Lindau S, Schumm L, Laumann E, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357:762–774.
11. Garaffa G, Kuehhas FE, Luca F De, Ralph DJ. Peyronie ’ s disease. Sex Med Rev. 2015;3(2):113–121. 12. Chung E, Ralph D, Kagioglu A, Garaffa G, Shamsodini A, Bivalacqua, et al. Evidence-based management
guidelines on Peyronie’s disease. J Sex Med. 2016;13(6):905–923. 13. Molina-Escudero R, Borda AP, Álvarez-Ardura M, Redón-Gálvez L, Martinez LC, Otaola Arca H.
Cavernoplastia con injerto de mucosa oral para el tratamiento quirúrgico de la enfermedad de La Peyronie. Actas Urol Esp. 2016;40(5):328–332.
14. Henry GD, Donatucci CF, Conners W, Greenfield JM, Carson CC, Wilson SK, et al. An outcomes analysis of over 200 revision surgeries for penile prosthesis implantation : a multicenter study. J Sex Med. 2012;9(1):309–315.
15. Hatzichristodoulou G. Grafting techniques for Peyronie’s disease. Transl Androl Urol. 2016;5(3):334–341. 16. Bokarica P, Parazajder J, Mazuran B, Gilja I. Surgical treatment of Peyronie ’ s disease based on penile
length and degree of curvature. Int J Impot Res. 2005;170–174. 17. Rolle L, Falcone M, Ceruti C, Timpano M, Sedigh O, Ralph DJ, et al. A prospective multicentric
international study on the surgical outcomes and patients ’ satisfaction rates of the “ sliding ” technique for end-stage Peyronie ’ s disease with severe shortening of the penis and erectile dysfunction. BJU Int. 2016; 117:814–820.
18. Savoca G, Scieri F, Pietropaolo F, Garaffa G, Belgrano E. Straightening corporoplasty for Peyronie ’s disease : A review of 218 patients with median follow-up of 89 months. Eur Urol. 2004;46:610–614.
19. Light MR, Lewis RW. Modified Nesbit procedure for the treatment of Peyronie’s disease: A comparative outcome analysis. J Urol. 1997;158(2):460–463.
20. Horstmann M, Kwol M, Amend B, Hennenlotter J, Stenzl A. A self-reported long-term follow-up of patients operated with either shortening techniques or a TachoSil grafting procedure. Asian J Androl. 2011;13(2):326–331.
21. Davis SNP, Ferrar S, Sadikaj G, Gerard M, Binik YM, Carrier S. Female partners of men with Peyronie’s disease have impaired sexual function, satisfaction, and mood, while degree of sexual interference is associated with worse outcomes. J Sex Med. 2016;13(7):1095–1103.
22. Gelbard M, Lipshultz LI, Tursi J, Smith T, Kaufman G, Levine LA. Phase 2b study of the clinical efficacy and safety of collagenase Clostridium histolyticum in patients with Peyronie’s disease. J Urol 2012;187:2268-2274.
23. Nehra A, Alterowitz R, Culkin DJ, Faraday MM, Hakim LS, Heidelbaugh JJ, et al. Peyronie’s disease: AUA guideline. J Urol. 2015; 194(3): 745-753.

55


Submitted:Mohede DCJ, van de Wiel HBM, Meijer B, de Jong IJ, van Driel MF
Homosexuality and Peyronie’s disease
Chapter 4

Chapter 4
58
Introduction
The penis is more than ‘just a body part’. Historically and today, it has mythical qualities which means that abnormalities often cause problems more than just the obvious functional difficulties that physicians are aware of. Muscularity, determination, effectiveness, penetration, directness, strength – the phallus underlies them all. (1)
Because of this special character of the penis, Peyronie’s disease (PD) is probably a particularly difficult condition. PD is, medically spoken, not a life-threatening or malignant disease, but it may have serious negative psychological consequences. This might even be more so the case in the homosexual community, where the penis often is perceived as a classical phallus, the iconic symbol of masculine identity.
In short, PD can be experienced as a functional problem, but can also lead to a wrecked personality and it is up to the urologist to respond in an appropriate way. The question is how. Literature, being the traditional support and assistant to a physician, offers no solution here. Besides pathophysiological knowledge and curative treatment options, there is a lack of information about how PD interferes with the quality of life in general, let alone with the quality of homosexual life.
In order to make a start with filling this lack of information, we decided to interview one of the homosexual patients in an ongoing research project into the psychological effects of PD. The aim was to explore the consequences of PD for his sexual life and to formulate questions for future research.
Method
Seven years post-diagnosis, we had three in-depth interviews with a 52-year-old homosexual man suffering erectile dysfunction (ED) and a relatively mild curvature due to PD. The conclusions were compared with data from the very limited PubMed-based literature as well as the conceptions of homosexual men with regard to PD on social media. Approval was obtained from the local medical ethical committee (METc 2016.683).

Homosexuality and Peyronie’s Disease
59
4
Results (Case-presentation)
Medical history A 44-year-old homosexual man was referred to our outpatient clinic by his general practitioner because of a curvature of his penis combined with ED. For the latter, he used intracavernosal self-injections with the combination of papaverine and phentolamine. Eighteen months before referral, he had noticed a hard spot on the dorsal side of his penis without the formation of a curvature. However, three months before the first consultation, his penis had once bent during anal sex, causing a small hematoma. After six weeks, a dorsal curvature became visible without any pain. He had no family history of PD, but his mother underwent surgery on both hands because of contractures due to Dupuytren’s disease (DD). At the time of the first visit, the patient had been together with his male partner for 15 years. They had unprotected sexual contact, both oral and penetrating (top and bottom). However, aside from this, the patient had unprotected active and passive oral sex and active protected penetrating (top and bottom) anal sex.
His medical history showed an episode of rectal blood loss, caused by hemorrhoids and a ciprofloxacin-resistant N. gonorrhoeae-based urethritis, for which he and his partner had been intravenously treated with ceftriaxone. He smoked a pack of cigarettes and consumed two units of alcohol a day. His answers on the International Index of Erectile Function (IIEF) showed no erectile dysfunction (29/30), some orgasmic dysfunction (5/10) and no dysfunction in sexual desire (9/10), intercourse satisfaction (14/15) and overall satisfaction (9/10).
Physical examination Physical examination at maximal extension revealed a three by two centimeter big ‘plaque’ on the dorsal side of a sixteen centimeter long, uncircumcised penis. Pictures of his erect penis showed a dorsal curve of 30o.
Diagnosis As the curvature developed at a later age, his mother suffered from DD and the evident plaque at the dorsal side, the most probable diagnosis was PD and not nodules due to the intracavernous injections. New scar tissue formation was possibly ongoing due to the preceding traumatic bending of the penis and a suspected small rupture of the thick capsule around the cavernous bodies of the penis.
Treatment regimen After thorough counseling, a conservative approach with regard of PD was accepted. The ED was already successfully treated by the intracavernous self-injections.

Chapter 4
60
At the second consultation, six months after our diagnosis, the curvature had increased to 45o and the penis had shortened. Besides the intracavernous injections, the patient had started using a vacuum pump, for pleasure and not as a necessity to develop an erection. A physical examination showed that the plaque had increased to five by two centimeters. The curvature did not seriously inhibit penetration.
However, the patient had developed severe psychological problems and was, as he said, no longer ‘proud’ of his penis. The PD negatively influenced his body satisfaction and self-esteem. He was suffering from a burnout, consumed too much alcohol and could not imagine that he would ever accept the deformation of his penis.
One year later, the curvature had not worsened. By then, he had accepted the help of a sexologist. His obsession with his penis was psychologically linked with his perfectionism and addictive personality, and it was characterized as a form of body dysmorphia. Through counseling, he became more conscious of his negative feelings and gradually his self-esteem improved. His compulsiveness and obsessiveness concerning his penis decreased. The sexological treatment was finished successfully after 30 months.
Patient evaluationThrough three in-depth interviews with the patient, we evaluated the entire treatment procedure. During the interviews, he expressed dissatisfaction concerning the questionnaires that had been used, especially because of their presumption of heterosexuality. For instance, he was displeased with terms used in the questionnaires such as ‘vaginal intercourse’, ‘vagina’ and ‘female’ or ‘read man, where woman is mentioned’ or ‘read anus, where vagina is mentioned’.
A more general complaint was the distant and ‘objective’ approach of sexuality. The way intercourse was described, as a structured process of optional foreplay, penetration and orgasm, was in his opinion too schematic. He pointed out an interesting distinction - or even paradox between - thinking of an orgasm as a process and/or result. Orgasm as a result is, in general, supposed to be a highly-valued positive outcome of sexual interaction. However, our patient replied that he was much less interested in an orgasm, as ‘it initiates the end of pleasure’. He cared more for the process of sexual interaction. PD restricted him in some sex positions, but his main complaint was that fun and uninhibitedness had gone.
According to him, homosexual men lead a more varied sex life than heterosexuals. His sex life had never been ‘average’. Together with his partner he often had visited sex parties. At these gatherings he had always gained a lot of attention because of his big penis. Since the existence of PD, this became much less common and, when he received this attention, he

Homosexuality and Peyronie’s Disease
61
4
could no longer take it seriously. According to his experience, there were `thousands of homo- and bisexual men living similar lives’ to his. He stated that homosexual men suffering PD are much more prone to social isolation than their heterosexual counterparts.
The fact that our patient had a penis above average in length could not console him. He experienced his deformity as ‘falling from a greater height’ in the gatherings he attended, causing the psychological effects to be more harming. In general, he thought that homosexual men may be more often dissatisfied with the looks of their penis than heterosexuals, possibly caused by the impact of comparison of the length and girth of other men’s penises.
Discussion
This case report was driven by curiosity on two possible relevant gaps: the gap between the medical-objective burden of PD; and the gap between the burden of hetero- and homosexual men suffering from PD.
In order to bridge both gaps, we decided to interview a homosexual patient who had participated in our more comprehensive research project on the impact of PD. We expected that, given the more important role of sexuality in general, and the penis as an iconic symbol of male sexuality in particular, the burden would be much bigger in homosexual men; a so-called interaction effect. We acknowledge the fact that the interviews conducted 7 years after diagnosis introduce a significant recall bias.
Although we only spoke to one patient, our expectations were confirmed. Our patient depicted a sexual context, being his part of the homosexual community, that indeed makes it understandable that in homosexual men the first gap, between medical (objective) and psychological (subjective) impact of PD will be wider than in most heterosexual men. Men who participate in sexual gatherings in, for example, saunas of locker rooms, where direct comparison of the ‘size and beauty’ of the penis may take place, are particularly at risk. Through this realization, we came up with a number of questions we would like to answer in future research: how do we measure the gap between medical simplicity and psychological invasiveness in PD? Are homosexual patients more susceptible to the psychological effects of PD than heterosexuals?
The answers to these questions will likely help formulate hypotheses that can be of help in the approach and treatment of PD patients in general, but particularly the homosexual

Chapter 4
62
ones. The moment a homosexual man presents himself to a urologist with symptoms of PD, it is vital not only to map the physical state, but also the psychological context. How does PD affect this patient’s sex life and identity? Although this advice also holds for heterosexual men, not discussing this kind of psychosocial issues seems to be less of a problem for them.
A bigger penis leads to higher satisfaction and self-assessment, especially in homosexual men. (7, 10) A penis longer than sixteen centimeters is considered as ideal. (6) The fact that our patient had a penis above average in length could not console him. He experienced his deformity as ‘falling from a greater height’, causing the psychological effects to be more harmful. In general, homosexual men may be more often dissatisfied with their looks than heterosexuals, possibly caused by the easier comparison of length and girth of their penis with other men. His perfectionism added to the negative psychological effects, but cannot be described as a homosexual characteristic. Obsession with the penis, however, may be more common in homosexual subjects. Not all homosexual PD patients will have such extreme psychological reactions to their condition, although there may be an interaction effect of being homosexual and being more susceptible to the negative psychological consequences. His other psychiatric diagnosis (body dysmorphia) adds to the susceptibility. Most interesting is the observation that PD can cause or exacerbate negative self-esteem or body image issues.
In general, sexual function is determined with the International Index of Erectile Function (IIEF), degree and progression with the Peyronie’s Disease Questionnaire (PDQ) and psychological effects by validated questionnaires such as the Hospital Anxiety and Depression Scale (HADS). (3, 11) Unfortunately, there is limited consideration of sexual orientation and the PDQ excludes all sexual intercourse other than vaginal. In general, questionnaires use heterosexual terms such as ‘vaginal intercourse’, ‘vagina’ and ‘female’. Sometimes they are addressed by additions such as ‘read man, where woman is mentioned’ or ‘read anus, where vagina is mentioned’. This could irritate respondents and therefore lead to potentially unreliable scores. Although this side effect probably occurs more often in our patients, given the described ‘gap’, it might be more important to take notice in the case of homosexual PD patients. Therefore, it is important to know that the IIEF was validated in only a small group of homosexual men. (4) Further, unexplained by any physical substrate, ED as qualified by the IIEF is more prevalent in homosexuals. (2) This finding might point out the inability of the IIEF to qualify ED in homosexuals.
The patient’s dysfunction on IIEF domains was largely based on intercourse failing to happen. Other criticism of questionnaires focus on their ‘black and white’ approach of

Homosexuality and Peyronie’s Disease
63
4
matters. They try to objectify sensitive parameters, such as psychological and sexual functioning, too extensively. They merely focus on the technical aspects of ‘having intercourse’ and determine to what degree respondents are able to get an erection, penetrate and reach an orgasm. In this way, sexual functioning is based on these parameters, while affection and emotions are not part of that equation. As it signified the end of pleasure, our patient stated that he was comparatively less interested in orgasm. He lamented the loss of excitement and freedom associated with sex positions that were now restricted by PD.
Inadequate counselling may result in the patient feeling guilty for potentially having caused PD through certain sexual acts, such as rough intercourse. On the internet, one finds advice with regard to choosing sex positions in case of PD. If there is for instance a dorsal curve, the anus should be approached from behind in standing position. Another recommendation is to choose a position that prevents the partner from viewing the deformed penis. An assertion in online circles is that a search for new sex positions can revive the sexual relationship. Our patient also believed that homosexual men are more inventive considering coping behavior with regard to sexual problems in general. Several toys and body parts had been used as substitutes for the erect penis. These substitutes had helped him in coping PD. In PubMed, we found only one study on psychological problems amongst homosexual men (n=27) with PD. (5) There appeared to be serious psychological stress, negatively influencing intimacy. However, no significant differences were found compared with heterosexual men, caused by the lack of power with the small number of patients.
Researchers recommend more attention for the psychological consequences of PD. (8, 9) If necessary, adequate referral for patient and his partner are of great importance. Patients will be advised to explore other ways of intimacy and, for some of them, peer contact can be helpful. In general, psychological stress in PD patients is high and seems not to decrease in time. In other words: for many of them, it is very difficult to learn to live with PD.
In conclusion, our in-depth interviews suggest that homosexual men are more susceptible to psychological effects of PD than heterosexuals. More research is needed to substantiate this statement. In clinical practice, it is important to ask for the sexual orientation at the first presentation, noticing the specific effects for the patient’s sex life and to provide adequate referral if necessary. Objective measurements or a questionnaire specifically for homosexuals should be developed, and if questionnaires such as the PDQ are being used, it is always important to notice their shortcomings for homosexual patients.

Chapter 4
64
References
1. van Driel MF. Manhood – The Rise and the Fall of the Penis. London: Reaction Books Ltd, 2009, p. 35.2. Breyer BN, Smith JF, Eisenberg ML, Ando KA, Rowen TS, Shindel AW. The impact of sexual orientation on
sexuality and sexual practices in North American medical students. J Sex Med. 2010 Jul;7(7):2391-2400.3. Chung E, Ralph D, Kagioglu A, Garaffa G, Shamsodini A, Bivalacqua T, et al. Evidence-Based Management
Guidelines on Peyronie’s Disease. J Sex Med. 2016;13(6):905–923 4. Coyne K, Mandalia S, McCullough S, Catalan J, Noestlinger C, Colebunders R et al. The International
Index of Erectile Function: development of an adapted tool for use in HIV-positive men who have sex with men. J Sex Med. 2010 Feb;7(2 Pt 1):769-774.
5. Farrell MR, Corder CJ, Levine LA. Peyronie’s disease among men who have sex with men: Characteristics, treatment, and psychosocial factors. J Sex Med. 2013;10(8):2077–2083
6. Hartzell R. Psychosexual symptoms and treatment of Peyronie’s disease within a collaborative model. Sex Med 2014; 2(4): 168-188.
7. Morrison MA, Morrison TG, Sager CL. Does body satisfaction differ between gay men and lesbian women and heterosexual men and women? A meta-analytic review. Vol. 1, Body Image. 2004. p. 127–138.
8. Smith JF, Walsh TJ, Conti SL, Turek P, Lue T. Risk factors for emotional and relationship problems in peyronie’s disease. J Sex Med. 2008;5(9):2179–2184.
9. Terrier JE, Nelson CJ. Psychological aspects of Peyronie’s disease. Transl Androl Urol. 2016;5(3):290–295. 10. Woertman L, Wit JMH de. Tevredenheid met het eigen lichaam en zelfwaardering van homoseksuele
mannen: Maakt een grote(re) penis een man gelukkig? Tijdschr voor Seksuol. 2005;29:181–188.11. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–
370.

65


Mohede DCJ, Riesmeijer S, de Jong IJ, Werker PMN, van Driel MFPRS 2020;145:978-984
Prevalence of Peyronie’s and Ledderhose’s diseases in a
series of 730 patients with Dupuytren’s disease
Chapter 5

Chapter 5
68
Introduction
Dupuytren’s (DD), Peyronie’s (PD) and Ledderhose’s disease (LD) are fibro-proliferative disorders characterized by abnormal collagen deposition in the palmar fascia of the hand, tunica albuginea (TA) of the penis and the plantar fascia of the foot, respectively. (Figure 1) In DD, nodules and cords can form in the connective tissue, of which the latter can cause debilitating flexion contractures of the digits. In LD, lumps in the sole of the foot can result in pain during walking. In PD, plaque formation results in penile pain, shortening, curvature and loss of rigidity. These diseases are thought to have a similar disease mechanism, and Abernathy (London, UK) first reported on their relation in 1828. (1)
The TA is a two-layered structure of inner circular and outer longitudinal layers of connective tissue encompassing the paired corpora cavernosa. An incomplete septum separates the corpora and anchors dorsally from the circular inner layer of the TA. Erection and bending of the rigid corpora cavernosa may lead to delamination at this location. (Figure 2) In practice, this means that >95% of the fibrotic ‘plaques’ are located on the dorsal site of the penis. Similarly, the ulnar metacarpals are more mobile than those at the radial site and are likely to be more vulnerable to tensile stress. The same holds for the distal medial border of the footpad, which is the typical location of LD.
In the 1960s, it was suggested that PD patients had intercourse more frequently and more vigorously than age-matched cohorts, but in scientific practice it was impossible to prove
Figure 1. Abnormal collagen deposition in the palmar fascia of the hand, tunica albuginea of the penis and the plantar fascia of the foot leading to DD, PD and LD respectively.

Peyronie’s, Ledderhose’s and Dupuytren’s Disease
69
5
this. (2) However, there is no question that an accident during penetration when the penis bends excessively may induce PD.
More recently, it was shown that the disorders have a familial aggregation and several genetic risk variants are known to be associated. In 2012, our research group associated nine loci to DD in the first GWAS of DD, and one of these nine loci could also be associated to PD. (3, 4) Nowadays, there are 26 risk variants known for DD, providing possibilities to further explore its genetic correlation with PD. In 2004, Qian et al. already demonstrated that the patterns of gene expression alteration of certain genes in DD and PD were similar, indicating a common pathophysiology. (5)
DD, PD and LD predominantly present in older men, and trauma seems to play a significant role. Interestingly, 51.7% of 169 Dutch field hockey players >65 years had DD (controls 13.8%). (6) Also with regard to PD, trauma to the TA in combination with a genetic susceptibility is the most widely-accepted etiological hypothesis. (7) The contracture characteristic of DD and PD appears to bear a relationship to the distribution of stress in the palmar fascia and the TA of the corpora cavernosa. (8) Age-related loss of tissue elasticity renders both structures susceptible to peaks of tensile stress. Biological cell studies identified overlap in patterns of chromosomal aberrations in fibroblasts from PD and DD lesions. (9)
Figure 2. Penile cross section shown left. On the right, the mechanism of trauma in the magnified vulnerable region is shown: I) The tunica albuginea is a two-layered structure of inner circular and outer longitudinal layers of connective tissue encompassing the paired corpora cavernosa. An incomplete septum separates the corpora and anchors dorsally from the circular inner layer of the tunica. II) Erection and bending of the rigid corpora cavernosa may lead to elastic tissue fatigue, subsequent ruptures and scar tissue. Persistent tension may lead to delamination of tunica albuginea layers, which fill with clots and turn into plaque in PD-susceptible individuals.

Chapter 5
70
Concurrent prevalences of LD and DD have been described by several authors in small to moderate sample sizes. (10-15) Coinciding prevalences of PD in DD, however, have only been described twice: in our preliminary results by Dolmans et al. in a sample of 361 patients, and recently by Shindel et al. in a sample of 85 patients. (4, 16) Since 2007, we have been gathering clinical information of patients suffering from DD, PD and LD. We report PD and LD prevalences in the largest sample size to date, consisting of 730 DD patients, in order to update our knowledge of prevalence rates and to create awareness. We also present doctor- and patient- (self) reported prevalences separately, to provide insight into the rate of reporting, as PD is known to be under-reported due to embarrassment. Since many patients with PD feel ashamed to talk about their condition, we reflect on the possible role of plastic and hand surgeons with regards to counseling their DD patients about possible concomitant PD.
Methods
Ethical approvalApproval for the Genetic Origin of Dupuytren Disease and Associated Fibromatosis (GODDAF) Study was acquired from the Medical Ethics Committee (METc) 2007/067 of the University Medical Center Groningen. All participants provided written informed consent.
Data and collectionThe GODDAF database contains patients affected by DD and/or PD and/or LD. The participants were recruited from 2007 to 2016 from the outpatient clinics for Plastic Surgery of several hospitals in the northern part of the Netherlands and from the department of Urology of the University Hospital in Groningen. For this study we used only patients recruited from the outpatient clinics for Plastic Surgery. DD was diagnosed by surgeons through physical examination. The database contains surgeons’ and patients’ completed questionnaires describing patient characteristics, demographics, diathesis factors and the extent of the fibro-proliferative disorder(s). Data on surgeon-reported concomitant LD and PD in DD patients were gathered during history taking. Patient-reported concomitant LD and PD was verified with questionnaires. An example of these questionnaires is attached as appendix (Appendix B). Patients answering “I think so” to whether or not they suffered from concomitant PD or LD, were part of the “yes” group in the data analysis.
StatisticsDescriptive statistics for continuous data on interval or ratio level of measurement are presented using means and standard deviations, and nominal data are presented as

Peyronie’s, Ledderhose’s and Dupuytren’s Disease
71
5
frequencies and percentages. We used chi-squared tests to control for allergies, alcohol consumption and smoking.
Results
Our total cohort of 1,725 DD patients consisted of 1,307 (75.8%) men and 415 women (24.1%). For three patients (1%), data on sex were missing. The mean age was 70.1 years (SD 10.7). Ninety-four per cent were Caucasians. Allergies, alcohol consumption and smoking did not significantly differ among groups.
Peyronie’s disease in Dupuytren’s patientsPD was determined by questionnaires, completed at the start of the study by both the participant and the surgeon. There were no patients referred by urologists. For 730 of the 1307 male DD patients, doctor-reported data on PD were available (577 missing). In 57 out of these 730, the surgeon noted the presence of PD, indicating a prevalence rate of 7.8% (Figure 3). According to the patients themselves, PD was present in 102 out of 1163 (8.8 %). Fifty of the 1,307 patients indicated not to know whether they had PD, and for 94 data were missing (Figure 4).
Ledderhose’s disease in Dupuytren’s patientsFor 619 of the 1725 patients, surgeons’ data on LD were missing. They reported the presence of LD in 178 of the remaining 1,106 DD cases, indicating a prevalence of 16.1% (Figure 5). According to the patients’ reports (n=1539), LD was present in 338 of them (24.0%). Sixty-nine indicated not to know if they had LD, and for 117 patients data were missing (Figure 6).
Figure 3. Doctor reported PD. Figure 4. Patient reported PD.

Chapter 5
72
Discussion
DD, PD and LD are common disorders in white people of Northwestern European origin. (9) In other parts of the world, they are regarded as much less common. (17) Here, we describe, as far as we know, one of few scientific reports that deal with the prevalence of LD in patients with DD and one of even fewer that report on the prevalence of PD in a population of men with DD (Table 1 and table 2). With a much larger sample size than previous studies (10), we updated the concurrent prevalences of PD and LD in DD patients, subdivided into surgeon- and patient-reported prevalence, which is a novelty compared to previous studies. As the present study is an update of our previous research by Dolmans et al., these samples partially overlap. (4)
Ledderhose’s diseaseA systematic review and meta-analysis in the general population of Western countries showed an LD prevalence rate of 1.4%. (17) In the preliminary analysis by Dolmans et al. of our cohort of patients affected by DD, we found a surgeon-reported LD prevalence of 13%. (8) In the present study, we found LD prevalence rates of 16.1% resp. 22.0%. These are similar to and confirm percentages found in Flanders, Belgium. (18) Patient reported data gathered by Schurer for the “International Dupuytren Society” showed a higher percentage (30%) in a large population. (19) Differences may be explained by the use of questionnaires and the uncertain diagnosis. Lumps on the sole of the foot can have many other causes than LD. (20)
Figure 5. Doctor reported LD. Figure 6. Patient reported LD.

Peyronie’s, Ledderhose’s and Dupuytren’s Disease
73
5
Peyronie’s disease A recent study from California hypothesized that the prevalence of PD in DD patients would be similar (i.e. approximately 22%) to the rate found previously in 415 consecutive PD patients in the northern part of the Netherlands. (21) Remarkably, the Californian study found that prevalence of PD in 85 men with DD was as high as 26%, as opposed to the present study (Table 2). (16) One explanation could be that in the Californian patients, the DD may have been more severe and for that reason showed a higher PD prevalence rate. In addition, the Californian group reports the prevalence of PD as the percentage of patients suffering from “PD-like symptoms”, possibly causing an overestimation of prevalence of the actual PD.
In the general male population, PD prevalence rates vary between three and nine per cent, with a median age of onset of 53 years. (22) The incidence of PD appears to be increasing, which is likely not the case in absolute figures, but indeed relatively and due to the availability of PDE-5-inhibitors (erection pills such as Sildenafil, Pfizer, Germany) for men with somatic erectile dysfunction, who would otherwise have been unaware of their penile
Table 1. Prevalence of Ledderhose disease (LD) in patients with Dupuytren disease.Reference Year Total (n) LD (%)Allen (10) 1955 unknown unknown 9.0Gordon (11) 1964 101 9 8.9Hueston (12) 1972 159 19 12.0Caroli (13) 1991 352 unknown 6.0Brenner (14) 2001 566 21 3.7De Greef (18) 2008 65 12 19.0Gudmundsson (15) 2012 137 18 13.2Dolmans (4) 2012 475 72 13Schurer (19) 2016 2235 624 30Shindel (16) 2017 85 9 10.6Present study 2019 1106
1539SR* 78PR** 338
16.122.0
*SR = surgeon reported**PR = patient reported
Table 2. Prevalence of Peyronie disease (PD) in patients with Dupuytren disease. Reference Year Total (n) PD (%)Dolmans (4) 2012 361 22 6.4Shindel (16) 2017 85 22 26Present study 2019 730
1163Surg 57Pts 102
7.88.8

Chapter 5
74
curvature. Furthermore, the PD prevalence is commonly underreported due to the sensitivity of the topic. (23) A review on the psychological aspects of PD suggest that as many as 81% of PD patients report emotional difficulties; 48% report a clinically meaningful depression (26% moderate; 21% severe); and 54% report relationship problems due to PD. (24) Regarding body image and self-esteem, PD patients describe themselves in qualitative terms such as ‘abnormal’, ‘ugly’, ‘disgusting’, ‘like a cripple’ and a ‘half man’, and some of them mention feelings of shame. (25) Many express a loss of sexual confidence and decreased sexual interest, and feel a sense of stigmatization and isolation leading to difficulties in speaking about their PD with sexual partners. Physicians should actively ask whether or not this is the case and provide solutions or help. Referral to a urologist to investigate medical (im)possibilities may be an outcome. Psychological support must be considered, keeping in mind an empathic attitude and always consider referral to a psychologist.
Remarkably, there are no data on possible psychological effects of LD. We identified only one study about the indirect psychological effects of DD on alcohol consumption and smoking. (26) With our ageing population and the increasing retirement age, DD poses an growing threat to ones capacity to work and thus the economy, and is likely to have its psychological burden. However, DD and LD probably do not impair partner relationships and self-confidence in the way PD does. (27)
Limitations of this studyA limitation of prevalence research in general is the heterogeneity in appearance of DD, PD and LD, and thus its diagnosis. As these are progressive diseases, the full extent of all three disorders may not have been present at the first presentation, when the questionnaires were filled out. Furthermore, some studies present doctor-reported data and others present patient-reported data or ‘disease-like’ symptoms. We differentiated between disease reported by patients and by surgeons, and concluded that a substantial number of patients did not report the presence of PD to the hand surgeon, which was probably because of embarrassment. We acknowledge that identification of disease through history taking, rather than confirmation on physical examination may introduce an element of either over- or underreporting. In general, a patient may misinterpret symptoms when reporting PD and LD, thus meaningful data on self-reported PD and LD requires surveys with an explicit description such as “curvature of the penis during erection” rather than simply asking whether the patient has ever had PD or LD.
As a result of the retrospective analysis of the data for this research, many questionnaires were unfortunately missing. Still, compared to other studies, our sample size is large. In

Peyronie’s, Ledderhose’s and Dupuytren’s Disease
75
5
addition, all participants originated from the same geographical location, making effect modification by genetic variability less likely. Undoubtedly, our DD cohort is more severely affected than men in the general population. Prevalence rates therefore may be higher in our cohort than in the general population as a more severe DD course is associated with increased PD and LD/ectopic disease prevalence rates. (28, 29, 30) This patient population, however, comprises the population presenting itself at the outpatient clinics, and thus is very relevant to hand surgeons.
For a urologist, it is a small effort to palpate the palmar fascia of the hands of PD patients and they therefore generally consider this examination as part of the routine exam at the first visit. (5) Understandably, plastic surgeons will be reluctant to examine the penis of their DD patients, as it is time-consuming and can be uncomfortable.
However, more than DD and LD, PD can have devastating psychological consequences. PD is often associated with erectile dysfunction and can therefore also have a negative impact on the wellbeing of the sexual partner. In daily life, most PD patients feel embarrassed to report their sexual complaints. This raises the question whether plastic surgeons need to actively ask their DD patients for symptoms of PD. In our opinion, they do not have to go into detail, but they can propose a referral to a competent urologist.
Conclusion
DD, PD and LD are very common disorders and very likely share (at least in part) a similar disease mechanism and overlapping genetic risk factors. In our DD patient cohort, the prevalence of PD was lower than described in literature. The prevalence of LD corresponded with the rates from literature. However, both were underreported by plastic surgeons, calling for a rise in awareness, recognition and referral to a urologist when bothersome or symptomatic.

Chapter 5
76
References
1. Abernathy J. The consequences of gonorrhoea. Lecture on anatomy, surgery and pathology including observations on the nature and treatment of local diseases, delivered at the St. Bartholomew’s and Christ’s Hospitals. 1st ed. London, England: James Balcock; 1828:205.
2. Lue TF, Melbard MK, Gueglio G, Jordan GH, Levine LA, Moreland R, Pryor J, Ralph D, Yachia D. Peyronie’s disease. In: Jardin A, Wagner G, Khoury S, Giuliano F, Padma-Nathan, Rosen R, eds. Erectile dysfunction – 1st International Consultation on Erectile Dysfunction – July 1-3, 1999, Paris. Plymouth: Health Publication Ltd; 2000, 439-76.
3. Dolmans GH, Werker PM, de Jong IJ, Nijman RJ, LifeLines Cohort Study, Wijmenga C, Ophoff RA. WNT2 locus is involved in genetic susceptibility of Peyronie’s disease. J Sex Med 2012;9:1430-4.
4. Dolmans GH, de Bock GH, Werker PM. Dupuytren diathesis and genetic risk. J Hand Surg Am 2012;37:2106-11.
5. Qian A, Meals RA, Rajfer J, Gonzalez-Cadavid NF. Comparison of gene expression profiles between Peyronie’s disease and Dupuytren’s contracture. Urology 2004 ;64:399-404.
6. Broekstra DC, van den Heuvel ER, Lanting R, Harder T, Smits, Werker PM. Dupuytren disease is highly prevalent in male field hockey players aged over 60 years. Br J Sports Med 2016;0:1-6.
7. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, Vardi Y, Wespes E; European Association of Urology. EAU guidelines on penile curvature. Eur Urol 2012;62:543-52.
8. Gelbard M. Peyronie’s disease. In: Hashmat AIDS, ed. The Penis. Philadelphia and London: Lea & Febiger; 1993,244-65.
9. Herati AS, Pastuszak AW. The genetic basis of Peyronie’s disease: a review. Sex Med Rev 2016;4:85-94. 10. Allen RA, Woolner LB, Ghormley RM. Soft tissue tumors of the sole. J Bone Joint Surg Am 1955;37A:14-26.11. Gordon SD. Dupuytren’s contracture: plantar involvement. B J Plast Surg 1964;17:412-3.12. Hueston JT.The incidence of Dupuytren’s contracture. Med J Aust 1960;6:999-1002.13. Caroli A. Zanasi S, Marcuzzi A, Guerra D, Christiani G, Ronchetti PI. Epidemiological and structural
findings supporting the fibromatous origin of dorsal nuckle pads. J Hand Surg 1991;16B:258-62.14. Brenner P, Krause-Bergmann A, Van VH. Dupuytren’s contracture in North-Germany. Epidemiological
study of 500 cases. Unfallchirurg 2001;104:303-11.15. Gudmundsson KG, Jónsson T, Arngrímsson R. Association of Morbus Ledderhose with Dupuytren’s
contracture. Foot and Ankle Int 2013;34:841-5. 16. Shindel AW, Sweet G, Thieu W, Durbin-Johnson B, Rothschild J, Szabo R. Prevalence of Peyronie’s disease-
like symptoms in men presenting with Dupuytren contractures. Sex Med 2017;5:e135-e141.17. Lanting R, Broekstra DC, Werker PM, van den Heuvel ER. A systematic review and meta-analysis on
the prevalence of Dupuytren disease in the general population of Western countries. Plast Reconstr Surg 2014;133:593-603.
18. De Greef I, De Smet L. A high prevalence of Dupuytren’s disease in Flanders. Acta Orthoped Belg 2010;76:316-20.
19. Schurer A, Manley G, Wach W. International patient survey (Part 2:Ledderhose disease). In: Werker PMN, Dias J, Eaton C, Reichert B, Wach W. (eds) Dupuytren Disease and Related Diseases – The Cutting Edge. Springer, Cham, 2016, pp 371-379.
20. Macdonald DJ, Holt G, Vass K, Marsh A, Kumar CS. The differential diagnosis of foot lumps: 101 cases treated surgically in North Glasgow over 4 years. Ann R Coll Surg Engl. 2007 Apr;89(3):272-5.
21. Nugteren HM, Nijman JM, de Jong IJ, van Driel MF. The association between Peyronie’s and Dupuytren’s disease. Int J Impotence Res 2011;23:142-5.
22. Porst H, Garaffa G, Ralph D (2012) Peyronie’s disease (PD) – Morbus de la Peyronie. Part 1: etiology, epidemiology, clinical evaluation and conservative therapy. In: Porst H, Reissman Y (eds) The ESSM Syllabus of Sexual Medicine. 1st edn. Medix, Amsterdam, 680-707.
23. Al-Thakafi S, Al-Hathal N. Peyronie’s disease: a literature review on epidemiology, genetics, pathophysiology, diagnosis and work-up. Transl Androl Urol 2016;5:280-9.
24. Nelson CJ, Mulhall JP. Psychological Impact of Peyronie’s Disease: a review. J Sex Med 2013;10:653–60. 25. Terrier JE, Nelson CJ. Psychological aspects of Peyronie’s disease. Transl Androl Urol 2016;5:290-5.

Peyronie’s, Ledderhose’s and Dupuytren’s Disease
77
5
26. Descatha A, Carton M, Mediouni Z, Dumontier C, Roquelaure Y, Goldberg M, Zins M, Leclerc A. Association among work exposure, alcohol intake, smoking and Dupuytren’s disease in a large cohort study (GAZEL). BMJ Open. 2014 Jan 29;4(1):e004214.
27. Bayat A and McGrouther DA. Plantar Management of Dupuytren’s Disease – Clear Advice for an Elusive Condition. Ann R Coll Surg Engl. 2006 Jan; 88(1): 3–8.
28. Dupuytren’s disease, Churchill Livingstone, Edinburgh, London, Melbourne and New York; 1985. p. 90.29. Werker PMN and Degreef I. Alternative and adjunctive treatments for Dupuytren disease. Hand Clin. 2018
aug; 34(3):367-375.30. Abe Y, Rokkaku T, Ofuchi S, Tokunaga S, Takahashi K and Moriya H. An objective method to evaluate the
risk of recurrence and extension of Dupuytren’s disease. J Hand Surg Br. 2004 Oct;29(5):427-430


Not for publication:Mohede DCJ, van Driel MF, Riesmeijer S, de Jong IJ, Werker PMN, Nolte IM
A genome-wide association study for Peyronie’s disease
Chapter 6

Chapter 6
80
Introduction
Peyronie’s disease (PD) in its classic form is the acquired curvature of the penis. In PD, the formation of plaque results in penile pain, shortening and loss of rigidity. Besides these discomforts, PD has extensive effects on the quality of life and psychological wellbeing of both patients and their partners. Due to insufficient knowledge of the pathological processes, we currently only have symptomatic treatment methods. (1) Underlying genetic mechanisms have been hypothesized, mostly in studies that also investigated the coexistence of Dupuytren’s disease (DD), a similar disease causing flexion contraction of the digits. (2, 3) Our research group previously presented the association of a single nucleotide polymorphism (SNP) rs4730775 at the WNT2 locus on chromosome 7, by comparing allele frequencies of 11 SNPs that had previously been associated with DD between 111 men with PD and healthy controls. (4, 5)
PD and DD are both fibro-proliferative disorders characterized by abnormal collagen deposition in the tunica albuginea (TA) of the penis and palmar fascia of the hand respectively. Already in 1828, Abernathy, from the UK, reported the idea of similar disease mechanisms in PD and DD. (6) More recently, it was shown that the two disorders aggregate within families and several genetic risk variants were shown to be associated with both diseases. (5) In 2004, Qian et al. already demonstrated that the patterns of expression alteration of certain genes in DD and PD were similar, indicating a common pathophysiology. (3) Furthermore, cell studies have identified overlap in patterns of chromosomal aberrations in fibroblasts from PD and DD lesions. (7)
Much is still unknown, however, regarding the genetic predisposition of PD. In this study, we aim to identify genetic variants for PD through the first genome-wide association study (GWAS). In addition, we perform a look-up of 26 SNPs currently found to be associated with DD and associate the genetic risk score composed of these 26 DD SNPs to PD in our samples. (8)
Methods
Study populationThe study was approved by the Medical Ethics Committee METc 2007/067 for the Genetic Origin of Dupuytren Disease (GODDAF) Study. Informed consent was obtained from all subjects.

Genome-wide association study
81
6
Three hundred and seventy two PD patients were recruited in the outpatient clinic of the Department of Urology of the University Medical Center Groningen (UMCG). They all were diagnosed by one senior urologist (MFvD). For this study, we used 5467 unrelated male Lifelines participants as healthy controls. Lifelines is a multi-disciplinary, prospective, population-based cohort study, examining in a unique three-generation design the health and health-related behaviors of 167,729 persons living in the northern part of the Netherlands. It employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioral, physical and psychological factors that contribute to the health and diseases of the general population, with a special focus on multi-morbidity and complex genetics. (9)
Genotyping and imputationWe collected blood samples at the outpatient clinic and isolated DNA by standard methods. We genotyped PD cases with the Illumina® 700k SNP GSA array. We excluded the following variants: SNPs with too much missing data (more than 5%), an MAF of less than 0.01 deviation from the Hardy-Weinberg equilibrium (p<0.0001), or with >15% deviation in allele frequency from that among 1,000 Genomes European individuals. We excluded samples when the percentage of missing genotypes was too high (>5%), they were duplicates, first or second degree relatives, heterozygosity deviated > 4SD from the mean, or when they came from a non-European individual. Lifelines participants (n=15,500) were genotyped with the Illumina Cytochip array. The same quality control checks were performed as for the cases. We performed quality control in PLINK v.1.9 and R v.3.3.1. (10, 11)
We combined cleaned genotype data of PD cases and Lifelines controls, and checked for relatedness. Duplicate samples and first- and second-degree relatives between the cohorts were excluded from the Lifelines database. We determined principal components from the resulting genotyping data.
PD cases and Lifelines controls were imputed separately using the 1,000 Genomes Phase 1 reference data. PD cases were imputed using the Michigan Imputation Server (URL: https://imputationserver.sph.umich.edu). Lifelines controls were phased using SHAPEIT and imputed using IMPUTE2. (12, 13)
Next, we combined imputed data while removing genetic variants with a low imputation quality (R2<0.8) in either dataset.

Chapter 6
82
Statistical methodsWe performed a GWAS using logistic regression in PLINK v.1.9 with disease status as the outcome; SNP as the independent variable using a multiplicative model; and five principle components as covariates to correct for population stratification. A p-value <5x10-8 was regarded as genome-wide statistically significant. (10)
Given the moderate sample size (power >80% for SNPs with a minor allele frequency of >13% and an odds ratio >2, we acknowledge that finding significantly associated variants for PD by performing a GWAS is not likely. Therefore we also investigated the 26 genetic loci identified for DD hypothesizing that these phenotypically similar diseases share a genetic background. (8) This strategy increases the prior probability of finding variants for the trait of interest (PD). For these candidate SNPs, a significance threshold of 0.05/26=0.0019 was adopted (Bonferroni correction). Additionally, we investigated the association of the weighted genetic risk score constructed from the 26 DD SNPs (equation 1).
Equation 1.
where i is the SNP, wi is the weight for SNP i, and xi is the number or dosage of the risk alleles that the patient carries for that SNP. Both the non-weighted GRS (with wi=1) and the weighted GRS (with wi equal to the log(odds ratio) for DD for SNP i) were calculated.
Results
During the quality control of the PD genotype data, 18 individuals were excluded: 6 because of too many missing genotypes, 0 because of a sex mismatch, 10 because they were non-European, 0 because of deviating heterozygosity and 2 because of duplicate samples, which yielded a final dataset of 354 PD cases. The quality control of the Lifelines samples was described in 2017. (12) For this study, we used the genetic data of the 5,598 male participants. Lifelines participants who were known as PD cases or who were a first or second degree relative to a PD case (n=131) were excluded from the Lifelines data, leaving a control dataset of 5,467 unrelated males. There was no selection based on age since the precise age at PD diagnosis was unavailable.
The imputed data was merged and checked for the quality of imputation. SNPs were excluded from the analysis when the imputation quality was < 0.8 in either dataset, thus leaving us with 1.77 million SNPs.

Genome-wide association study
83
6
We performed a GWAS with the remaining SNPs to compare genotype frequencies between the Lifelines controls and the PD cases. Of these, 195 SNPs showed a genome-wide significant p-value (i.e. <5E-8) (Figure 1). Most of these were single hits without any significant other SNPs near them. These were unlikely to have credible associations and were therefore regarded as false-positives. Three regions were left (Table 1; Figure 2). One of the significant loci was the WNT2 locus on chromosome 7 and two other regions were located on chromosome 15, all of which have been previously described in the GWAS on DD. (8)
An overview of the associations of previously-identified DD SNPs is shown in Table 2. Unfortunately, only 15 of the 26 SNPs were available in our dataset. Five SNPs were nominal significant, of which two on chromosome 7 remained significant after multiple testing correction (p<0.0019). The genetic risk scores (GRS) composed of the 15 available DD SNPs were both significantly associated with PD (8.8E-14 for the weighted and 3.0E-14 for the unweighted GRS) (Figure 3). With every additional SD, the risk in PD increased 1.49 (95% CI 1.34-1.65) times for the weighted GRS and 1.51 (95% CI 1.36-1.68) times for the unweighted GRS.
Figure 1. Manhattan plot of the PD GWAS

Chapter 6
84
Figure 2. Locus zoom plots of the three associated regions

Genome-wide association study
85
6
Discussion
In this study, we performed the first ever GWAS for PD. SNPs in three loci were found to be genome-wide significantly associated with PD. One of the hits (rs2402177) was a regulatory variant in WNT2, a gene that we previously also identified as a PD risk locus (Dolmans et al. 2011). This hit and the other two identified loci on chromosome 15 were also shown to be associated with DD, a phenotypically similar disease, in an earlier report. (8)
Figure 3. Distributions of (a) unweighted and (b) weighted genetic risk scores among PD cases and Lifelines controls.

Chapter 6
86
As mentioned, we were the first to perform a GWAS trying to identify genes for PD. Due to the sample size (n=354 PD cases), we unfortunately did not have much power. We therefore adopted a candidate SNP look-up to test the association of the 26 earlier identified SNPs for DD in our GWAS. Fifteen SNPs passed the stringent quality control of our GWAS data; five of them were nominally significantly associated with PD. This supports the theory that the two phenotypically similar diseases share a genetic background. A downside of this study was the use of two different chips for genotyping of cases and controls. However, new Lifelines data of approximately 36,000 individuals that were genotyped using the same genotyping chip as our PD cases (GSA, Illumina) will soon become available. This will
Table 1. Genome-wide significant associations with PD. The most significant SNP within each region is shown.Chr pos (hg19) SNP RA/CA Freq CA1 OR SE p-value
7 116915119 rs2402177 T/G 47 – 60 1.67 0.083 7.0E-10
15 35003398 rs1036460 T/C 82 – 74 0.55 0.094 2.9E-10
15 68973820 rs2415022 T/C 79 - 94 5.06 0.18 4.4E-20
Chr: chromosome; RA: reference allele; CA: coded allele; Freq: frequency; OR: odds ratio; SE: standard error.1The first is the percentage in the controls; the second is the percentage in the cases.
Table 2. Associations of the DD SNPs with PD. Only 15 were found that were of high quality.
Chr pos (hg19) SNP RA/CA OR SE p-value Info
1 22698447 rs7524102 A/G 0.97 0.108 0.79 1.02
1 162672011 rs17433710 T/C 1.08 0.13 0.53 0.98
5 108672946 rs246105 C/T 1.19 0.10 0.09 0.97
7 37973014 rs2598107 C/T 0.77 0.082 0.0011 0.99
7 37989095 rs16879765 C/T 0.84 0.12 0.14 0.98
7 116892846 rs38904 T/C 0.50 0.090 1.8E-14 0.86
8 25845675 rs10866846 G/A 1.02 0.085 0.78 0.94
8 70007938 rs629535 C/T 0.93 0.088 0.40 1.01
9 1201156 rs12342106 G/A 0.84 0.092 0.059 0.91
14 51074461 rs1032466 A/C 1.11 0.086 0.21 1.00
15 68628163 rs2306022 C/T 0.92 0.13 0.50 0.99
15 89238184 rs6496519 C/T 1.25 0.11 0.033 0.99
19 57678194 rs11672517 G/A 0.84 0.091 0.049 1.02
20 38300807 rs6016142 C/T 1.01 0.13 0.96 0.97
20 39320751 rs6102095 G/A 1.34 0.12 0.017 0.96
Chr: chromosome; RA: reference allele; CA: coded allele; Freq: frequency; OR: odds ratio; SE: standard error.1The first is the percentage in the controls; the second is the percentage in the cases.

Genome-wide association study
87
6
allow for a GWAS of higher quality and less loss of SNPs because of the stringent filtering to control for potential batch effects between the case and control cohorts. In addition, our group will soon also carry out a new GWAS for DD using the same novel Lifelines data and will perform a meta-analysis of DD with four other cohorts (Lifelines approval number OV18_0461) in order to identify additional DD loci. This will provide possibilities to find more SNPs associated with PD and to further explore the genetic overlap of PD with DD. This research is necessary to provide a more comprehensive understanding of the landscape of genetic factors responsible for the development of PD. (7) The functional relevance of the identified loci can be explored and tested in in-vitro cell cultures. Moreover, such research will likely better define the links between malignancy and benign urologic conditions, such as PD, and ultimately facilitate the risk stratification, screening and treatment of PD patients. (15)
Conclusion
In conclusion, we have described the first GWAS to date in PD. We discovered three variants predisposing to PD and evidence for a shared genetic background of PD and DD. Analysis of the percentage of heritability of DD explained by these variants compared to that by all common autosomal variants, which is estimated to be ~11%, suggests that there are many more common variants affecting predisposition to DD, and thus likely also to PD, and that larger studies with greater power will detect further associated loci. (8)

Chapter 6
88
References
1. Nehra A, Alterowitz R, Culkin DJ, Faraday MM, Hakim LS, Heidelbaugh JJ, Khera M, Kirkby E, McVary KT, Miner MM, Nelson CJ, Sadeghi-Nejad H, Seftel AD, Shindel AW, Burnett AL; American Urological Association. Peyronie’s disease: AUA Guideline. J Urol 2015;194:745-753.
2. Dolmans GH, Werker PM, de Jong IJ, Nijman RJ, LifeLines Cohort Study, Wijmenga C, Ophoff RA. WNT2 locus is involved in genetic susceptibility of Peyronie’s disease. J Sex Med 2012;9:1430-1434.
3. Qian A, Meals RA, Rajfer J, Gonzalez-Cadavid NF. Comparison of gene expression profiles between Peyronie’s disease and Dupuytren’s contracture. Urology 2004;64:399-404.
4. Dolmans GH, Werker PM, Hennies HC, Furniss D, Festen EA, Franke L, Becker K, van der Vlies P, Wolffenbuttel BH, Tinschert S, Toliat MR, Nothnagel M, Franke A, Klopp N, Wichmann HE, Nürnberg P, Giele H, Ophoff RA, Wijmenga C, Dutch Dupuytren Study Group, German Dupuytren Study Group, LifeLines Cohort Study, BSSH-GODD Consortium. Wnt signaling and Dupuytren’s disease. J Hand Surg Am 2011;36:755-756; author reply 756;
5. Dolmans GH, Werker PM, de Jong IJ, Nijman RJ, Wijmenga C, Ophoff RA, LifeLines Cohort Study. WNT2 locus is involved in genetic susceptibility of Peyronie’s disease. J Sex Med 2012;9:1430-1434.
6. Abernathy J. The consequences of gonorrhoea. Lecture on anatomy, surgery and pathology including observations on the nature and treatment of local diseases, delivered at the St. Bartholomew’s and Christ’s Hospitals. 1st ed. London, England: James Balcock; 1828:205.
7. Herati AS, Pastuszak AW. The genetic basis of Peyronie’s disease: a review. Sex Med Rev 2016;4:85-94.8. Ng M, Thakkar D, Southam L, Werker PMN, Ophoff R, Becker K, Nothnagel M, Franke A, Nurnberg P,
Espirito-Santo AI,Izadi D,Hennies HC, Nanchahal J, Zeggini E, Furniss D. A genome-wide association study of Dupuytren disease reveals 17 additional variants implicated in fibrosis. Am J Hum Genet 2017;101:417-427.
9. Scholtens S, Smidt N, Swertz MA, Bakker SJL, Dotinga A, Vonk JM, van Dijk F, van Zon SKR, Wijmenga C, Wolffenbuttel BHR, Stolk RP. Cohort Profile: LifeLines, a three-generation cohort study and biobank. Int J Epidemiol 2015;44:1172-1180.
10. Chang CC, Chow CC, Tellier LCAM, Vattikuti S, Purcell SM, Lee JJ. Second-generation PLINK: rising to the challenge of larger and richer datasets. Gigascience 2015;4:7.
11. R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, 2019.
12. O’Connell J, Gurdasani D, Delaneau O, Pirastu N, Ulivi S, Cocca M, Traglia M, Huang J, Huffman JE, Rudan I, McQuillan R, Fraser RM, Campbell H, Polasek O, Asiki G, Ekoru K, Hayward C, Wright AF, Vitart V, Navarro P, Zagury JF, Wilson JF, Toniolo D, Gasparini P, Soranzo N, Sandhu MS, Marchini J. A general approach for haplotype phasing across the full spectrum of relatedness. PLoS Genet 2014; 10: e1004234.
13. Howie B, Marchini J, Stephens M. Genotype imputation with thousands of genomes. G3 (Bethesda) 2011;1:457-470.
14. Nolte IM, van der Most PJ, Alizadeh BZ, de Bakker PI, Boezen HM, Bruinenberg M, Franke L, van der Harst P, Navis G, Postma DS, Rots MG, Stolk RP, Swertz MA, Wolffenbuttel BH, Wijmenga C, Snieder H. Missing heritability: is the gap closing? An analysis of 32 complex traits in the Lifelines Cohort Study. Eur J Hum Genet 2017;25:877-885.
15. Lo EM, Hotaling JM, and Pastuszak AW. Urologic conditions associated with malignancy. Urol Oncol 2020;38:23-30.

89


.Mohede DCJ, de Jong IJ, Bank RA, van Driel MFSex Med 2018;6:302-308
Verteporfin as a medical treatment in Peyronie’s disease
Chapter 7

Chapter 7
92
Introduction
In 1743 François Gigot de la Peyronie (1678-1747) first provided a comprehensive description of induratio penis plastic, now known as Peyronie’s disease (PD). (1) PD is a benign fibroproliferative disorder of the penis, which causes the formation of a plaque in the tunica albuginea. Many pharmacological options have been proposed, but up till now none has received a grade A recommendation. Currently, collagenase from Clostridium histolyticum is the only drug approved by the American and European authorities for intralesional injection in patients with dorsal or dorsolateral curvature >30° with a palpable plaque. In the Netherlands the prescription of oral drugs for PD, for example pentoxyphilline, is only allowed if one informs the patient about its off-label use and possible adverse events.
Verteporfin (trade name Visudyne®; VP) is registered in the USA and Europe as a sensitizer for photodynamic therapy to eradicate abnormal blood vessels in the eye associated with the wet form of macular degeneration. The first report on photodynamic therapy with VP for choroidal neovascularization was already published in 1999. (2) VP accumulates in the abnormal blood vessels. When stimulated by non-thermal red light (wavelength 693 nm) in the presence of oxygen, VP produces reactive short-lived singlet oxygen and other oxygen radicals, locally damaging the endothelium and resulting in blockage of these vessels. In its inactivated form (i.e. VP that is not subjected to photo irradiation) VP is a small molecular inhibitor of the Hippo-Yes Activated Protein (YAP) pathway (Figure 1) and considered as a promising drug in the treatment of pancreatic cancer. (3) In that respect it is relevant to mention that Scandinavian studies showed that patients with Dupuytren’s disease (DD) in this part of the world have greater incidences of a variety of smoking related diseases as pancreatic, buccal and lung cancer. (4–6) DD and its related diseases are also a burden for societies in other parts of the world. (7) Especially severe and younger onset cases may be subject to increased cancer incidence and mortality. (8,9)
Inactive VP attenuates renal fibrosis in mice subjected to unilateral ureteral obstruction, probably by blocking the transcriptional activation of targets in the YAP cascade involved in fibrosis-related processes. (10) The objective of the present study was to determine whether VP would have similar effects on (myo)fibroblasts derived from plaques in patients with PD (being the cells responsible for the production of fibrotic lesions).

Verteporfin
93
7
Material and methods
Ethics statementPlaque tissue samples of PD patients were collected after informed written consent of the patient; our protocol was approved by the Medical Ethics Committee (METc) of the University Medical Center Groningen (2007/067; UMCG), in accordance with the Declaration of Helsinki.
Primary tissuesPlaque tissues were obtained from 5 PD patients with primary disease that underwent plaque incision and grafting or a Nesbit procedure by a senior urologist (M.F.vD.) in the UMCG.
Cell Culture Conditions (Myo)fibroblasts were obtained from dissected plaque tissue by culturing the small pieces in Dulbecco’s Modified Eagle’s Medium (DMEM, Lonza) containing 1% l-glutamine, 1% penicillin-streptomycin and 10% fetal bovine serum (FBS) at 37oC in a 5% CO2 incubator. Experiments were performed on cells from passage 8. In order to confirm the presence of
Figure 1. Simplified fibrosis-related processes in the YAP cascade. As a result of microtrauma and genetic susceptibility the YAP cascade comes into force causing ECM synthesis, myofibroblast differentiation, apoptosis resistance, migration and proliferation. These fibrotic processes lead up to plaque development and subsequent penile deformity. In red VP’s assumed point of engagement in the cascade. In fat markers of the different fibrotic processes.

Chapter 7
94
myofibroblasts (i.e. activated fibroblasts), immunofluorescent staining for α-SMA was performed before starting the VP experiments.
VP experimentStarvation of the cells took place for 16 hours overnight in culture medium consisting of DMEM containing 1% penicillin/streptomycin, 1% l-glutamine, 0.5% FBS and 17 mM ascorbic acid. Cells were kept at 37°C in 5% CO2. One day after starvation, the cells were exposed to VP (250 nM) in the previously mentioned culture medium containing 0.01% (v/v) dimethyl sulfoxide (DMSO; this was used as solvation vehicle for VP). The control group was exposed to 0.01% (v/v) DMSO. Lights were off when working with either VP or DMSO. The treatment took place for 24 and 48 hours in an incubator at 37°C in 5% CO2.
Immunostaining After treatment, cells were fixated in 1:1 acetone/methanol. The cells were then permeabilized with 0.5% Triton X-100 in phosphate-buffered saline (PBS), incubated with 10% serum of the secondary species and blocked with 1% bovine serum albumin (BSA) in PBS. Primary antibodies directed towards α-Smooth muscle actin (SMA) (Dako M0851 IgG2a) were diluted in 1% bovine serum albumin in PBS and incubated for one hour at room temperature. Secondary antibodies (GaMIgG2a-biotin) were diluted in 2% normal human serum in PBS and incubated for 30 min at room temperature, covered in tinfoil. Cells were then incubated with 1:100 streptavidin-Cy3 in 1:5000 4’,6-diamidino-2-phenylindole (DAPI) in tinfoil for 30 min at room temperature. DAPI was used to stain the nuclei. After every incubation step a washing step was performed, incubating the cells in fresh PBS three times for 5 min. Pictures were taken under a fluorescence microscope.
Real-Time Polymerase Chain Reaction (rt-PCR) After treatment, cells were lysed and stored in 350 μl of a mix with dithiothreitol (DTT) and FARB Buffer (10 μl DTT per 1 ml FARB Buffer) at -80°C. RNA was isolated using an RNA isolation kit (FavorPrep mini kit) according to the manufacturer’s instructions.
Complementary DNA (cDNA) was synthesized by priming with random hexamer primer (1 μl added to 11 μl concentrated RNA). After adding the primer, cells were incubated for 5 min in 65°C. A mixture of 4 μl reaction buffer 5x, 2 μl dNTP’S (10mM) mixture, 0.5 μl Ribolock RNAse inhibitor, 0.5 μl RNAse free H2O and 1 μl Reverse Transcriptase RevertAidTM M-MuLV was then added to each sample, making a total volume of 20 μl. Cells were subsequently incubated according to the next program: 5 min at 25°C; 60 min at 42°C; 5 min at 70°C and stored at -20oC. For the Real-Time PCR, triplicates of each sample were used.

Verteporfin
95
7
Primers (Table 1) were dissolved in MQ water, needing 0.25 μl of both forward and reverse primer per reaction (150 nM/primer). Mastermix per gene contains 5 μl SYBRgreen (Rouche; 2x) and 0.5 μl Prime Mix (6 μM). 5 μl diluted cDNA sample (5 ng/μl) and 5 μl Mastermix were added to each well in a 384 well plate, making a total volume of 10 μl. Plates were run on the ViiA 7 Real-Time PCR system (applied Biosystems). The relative gene expression was calculated using the ΔΔCt method, normalizing for the average expression of the household gene YWHAZ.
StatisticsExperiments were performed in triplicate. Statistics were performed using GraphPad Prism Software version 7. A Kruskal-Wallis test was used to determine whether there were differences in ranks between the three groups. Two-way ANOVA with Bonferroni post-test was used for statistics; a p < 0.05 was considered significant.
Results
Characterization of PD plaque cellsTo confirm the pathologic phenotype of cells isolated from PD plaques, baseline immunofluorescent stainings were performed which showed considerable levels of αSMA, being a marker for the presence of myofibroblasts (Figure 2). This findings confirmed the pathological nature of the obtained plaque samples.
Table 1. Sequences of the used primers. F = forward; R = reversed. A = adenine; C = cytosine; G = guanine; T = thymine. Sequences in 5’ to 3’ direction.
Primers SequenceF (5’ - 3’)
(5’ - 3’)
ACTA2 CTGTTCCAGCCATCCTTCAT TCATGATGCTGTTGTAGGTGGT
CCN2 AGCTGACCTGGAAGAGAACATT GCTCGGTATGTCTTCATGCTG
COL1A1 GCCTCAAGGTATTGCTGGAC ACCTTGTTTGCCAGGTTCAC
COL5A1 CCTGGATGAGGAGGTGTTTG CGGTGGTCCGAGACAAAG
EDA-FN AATCCAAGCGGAGAGAGTCA GGAATCGACATCCACATCAG
LOXL2 TGACCTGCTGAACCTCAATG TGGCACACTCGTAATTCTTCTG
PLOD2 GGGAGTTCATTGCACCAGTT GAGGACGAAGAGAACGCTGT
SERPINH1 TGGTGCTGATCTCATCCTTG AGAAACCCAGCAGCAGATTC
YAP AATCCCACTCCCGACAGG GACTACTCCAGTGGGGGTCA
YWHAZ GATCCCCAATGCTTCACAAG TGCTTGTTGTGACTGATCGAC

Chapter 7
96
Gene expression of fibrosis related genesMyofibroblasts derived from the plaque tissue responded to VP treatment for both 24 and 48 hours, resulting in significant decreases in gene expression levels of CCN2, COL1A1, COL5A1, EDA-FN, PLOD2 and LOXL2 (Figure 3). The mRNA level of SERPINH1 was decreased only at 48 h, whereas that of ACTA2 was reduced at 24 h only (Figure 2). As expected, VP did not affect mRNA levels of YAP. The control group (DMSO only) did not differ from the control group without DMSO, which showed that DMSO did not affect the cultures (data not shown). Compared with 24 h, the mRNA level of EDA-FN and SERPINH1 was even more decreased at 48 h, showing that VP has long-lasting anti-fibrotic effects (Figure 4).
Discussion
VP’s role in fibrosisThe lack of effective medical treatments of PD stems from a lack of understanding of its biology. However, today it is well known that tissue derived from PD plaques contains myofibroblasts, the cells responsible for the pathological fibrotic processes. Indeed, we
Figure 2. Characterization of PD plaque cells (passage 8). Part of the fibroblasts showed features of myofibroblasts, indicating the presence of activated cells in the PD plaques, Red αSMA; blue DAPI. Black scale bar represents 50 μm.

Verteporfin
97
7
found considerable amounts of myofibroblasts in our cell cultured derived from plaques. Furthermore, our study shows that in vitro exposure of VP to (my)fibroblasts inhibits the pathological processes by means of the down-regulation of fibrosis-associated genes. Fibrosis is characterized by excessive production, deposition and contraction of extracellular matrix (ECM), leading to significant organ dysfunction. (11) Here we show that VP is able to reduce the expression of the two major fibrillary collagens, i.e. collagen type I and type V, and the ECM component fibronectin (EDA-FN). This should lead to a less excessive deposition of ECM. It also helps that VP is able to decrease SERPINH1 levels (also known as HSP47), a chaperone needed for the proper transportation of collagen. In fibrosis the ECM stiffens, even before scarring occurs, due to an increased expression of enzymes involved in collagen cross-linking. In our study we found that the expression of at least two of these enzymes, LOXL2 and PLOD2, is inhibited by VP. This should lead to a less stiff ECM. In addition, collagen cross-linked by hydroxylysine residues mediated by PLOD2 is more difficult to degrade by matrix metalloproteinases. (12) Lower cross-links levels derived from PLOD2 most likely results in a faster degradation of collagen molecules, resulting in less ECM accumulation. Our findings suggest that VP might benefit patients mostly in the
Figure 3. Response of (myo)fibroblasts subjected to 250 nM VP for 24 and 48 hours. mRNA levels of YAP did not changed, whereas mRNA levels of extracellular matrix molecules (COL1A1, COL5A1, EDA-FN), collagen-modifying enzymes (SERPINH1, PLOD2, LOXL2), and the pro-fibrotic markers CCN2 and ACTA2 were attenuated by VP. * = p < 0.05.

Chapter 7
98
Figure 4. Response of (myo)fibroblasts subjected to 250 nM VP as a percentual difference after 24 and 48 hours. Compared with 24 h, the mRNA level of EDA-FN and SERPINH1 was even more decreased at 48 h, showing that VP has long-lasting anti-fibrotic effects. * = p < 0.05.

Verteporfin
99
7
acute phase of PD, but possibly also in the chronic phase. However important some of these mechanisms in certain malignancies are, our main foci for this study were PD and fibrosis related processes.
Pharmacokinetics and safetyFor its current indication (i.e. macular degeneration), VP is administered parenteral in the largest possible arm-vein in a dose of 6 mg/m2 and light-activated. This can be yearly repeated four times. No drug-drug interactions were ever described in patients treated with VP, but simultaneous use of photosensibilizing drugs as tetracyclines and thiazide diuretics may increase the risk of light-sensitivity reactions. Porphyria is an absolute contra-indication. During 48 hours, patients are photosensitive and advised not to come in contact with direct bright (sun)light and to cover themselves with sunglasses and clothes. (13) In animal studies, mild extravascular hemolysis and hematopoiesis were noted in inactivated daily doses 32-70 times (in dogs and rats) as high as advised in humans when administered for four weeks. (14) Fast admission of 2.0 mg/kg in pigs under general anesthesia led to hemodynamic instability and diphenhydramine decreased these effects, suggesting histamine related processes. Animal studies ruled out ocular toxicity. There was no teratogenicity reported in rabid fetuses that received 67 times the advised dosage in humans and no toxicity was seen in general genotoxic tests. In mice, beneficial effects were reported in immune mediated diseases. Normal immune reactions in the skin were decreased without causing skin reactivity or generalized non-specific immune suppression. An overview of preliminary clinical studies showed that VP was safe in humans with only minimal side effects. (15) Since VP is already FDA-approved, testing it as off-label treatment for PD may be an interesting step, but future research can better be focused on optimal administration and dosage schemes for possible treatment of PD. Up till now orally administered VP has not been tested, since parenteral administration is preferred for its current indication.
None of the options depicted in the European guidelines carry a grade A recommendation, but their assumed working mechanisms are worth taking into account considering the quest for new treatment strategies. (16) Combination therapy with historically proposed medical methods and up-and-coming ones such as verteporfin inhibiting disease related processes on different levels, can be considered for future trials. In that respect, we strongly recommend a close collaboration with biologists and experts in PD related fibrotic diseases.

Chapter 7
100
Recommendations and conclusion
With regard of PD urologists should focus on the disease before deformity, preferably in an internationally collaborative fashion. The search for new oral and intralesional agents, well-tolerated and effective in both the acute and chronic phase of PD, should be encouraged. As in DD new PD lab models (e.g. three-dimensional cell cultures) may be used to find novel therapeutic targets. To achieve these models, one obviously needs basic researchers. Human tissue-engineered models have already begun replacing animal models for preclinical drug testing. (17) Urologists with special interest in PD should organize brainstorming symposia with non-urologists as biologists and geneticists. Improved international collaboration will pave the way for funding and finding optimal research paths.
At the end the management of patients with PD undoubtedly will improve, with fewer of them needing surgery. In this respect verteporfin is one of the drugs that needs further investigation, because it apparently displays a wide spectrum of anti-fibrotic properties.

Verteporfin
101
7
References
1. De la Peyronie F. Sur quelques obstacles qui s’opposent à l’éjaculation naturelle de la semence. Mém Acad Roy Chir. 1743;1:318–33.
2. Miller JW, Schmidt-Erfurth U, Sickenberg M, Pournaras CJ, Laqua H, Barbazetto I, et al. Photodynamic therapy with verteporfin for choroidal neovascularization caused by age-related macular degeneration: results of a single treatment in a phase 1 and 2 study. Arch Ophthalmol. 1999;117(9):1161–73.
3. Wei H, Wang F, Wang Y, Li T, Xiu P, Zhong J, et al. Verteporfin suppresses cell survival, angiogenesis and vasculogenic mimicry of pancreatic ductal adenocarcinoma via disrupting the YAP-TEAD complex. Cancer Sci. 2017;108(3):478–87.
4. Wilbrand S, Ekbom a, Gerdin B. Dupuytren’s contracture and sarcoma. J Hand Surg Br. 2002;27(1):50–2. 5. Wilbrand S, Ekbom A, Gerdin B. A cohort study linked increased mortality in patients treated surgically
for Dupuytren’s contracture. J Clin Epidemiol. 2005;58(1):68–74. 6. Wilbrand S, Ekbom A, Gerdin B. Cancer incidence in patients treated surgically for Dupuytren’s contracture.
J Hand Surg Br. 2000;25(3):283–7. 7. Macaulay D, Ivanova J, Birnbaum H, Sorg R, Skodny P. Direct and indirect costs associated with Dupuytren’s
contracture. J Med Econ. 2012;15(4):664–71.8. Gudmundsson KG, Arngrimsson R, Sigfusson N, Jonsson T. Increased total mortality and cancer mortality
in men with Dupuytren’s disease. A 15-year follow-up study. J Clin Epidemiol. 2002;55(1):5–10. 9. Mikkelsen OA, Høyeraal HM, Sandvik L. Increased mortality in Dupuytren’s disease. J Hand Surg Br.
1999;24(5):515–8. 10. Szeto SG, Narimatsu M, Lu M, He X, Sidiqi AM, Tolosa MF, et al. YAP/TAZ Are Mechanoregulators of
TGF- -Smad Signaling and Renal Fibrogenesis. J Am Soc Nephrol. 2016;27(10):3117–28. 11. El-Sakka AI, Salabas E, Dinçer M, Kadioglu A. The pathophysiology of Peyronie’s disease. Vol. 11, Arab
Journal of Urology. 2013. p. 272–7. 12. Van Der Slot-Verhoeven AJ, Van Dura EA, Attema J, Blauw B, DeGroot J, Huizinga TWJ, et al. The type of
collagen cross-link determines the reversibility of experimental skin fibrosis. Biochim Biophys Acta - Mol Basis Dis. 2005;1740(1):60–7.
13. Verteporfin Roundtable Participants. Guidelines for using verteporfin (Visudyne) in photodynamic therapy for choroidal neovascularization due to age-related macular degeneration and other causes: update. Retina. 2002;25(2):119–34.
14. Adili F, Statius van Eps RG, Flotte TJ, LaMuraglia GM. Photodynamic therapy with local photosensitizer delivery inhibits experimental intimal hyperplasia. Lasers Surg Med. 1998;23(5):263–73.
15. Dougherty T. Photodynamic therapy for the treatment of cancer: current status and advances. In: Kessel D, editor. Photodynamic therapy of neoplastic disease. 1997;39:81. Boca Raton: CRC Press; 1989. p. 1–19.
16. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, et al. EAU guidelines on penile curvature. Vol. 62, European Urology. 2012. p. 543–52.
17. O’Gorman D. The future of basic Dupuytren disease research. In: Werker P, editor. Dupuytren disease and related diseases-the cutting edge. Switzerland: Springer International Publishing; 2017. p. 409–11.


Summary and general discussion
Chapter 8

Chapter 8
104
Summary
In spite of the increase of knowledge on Peyronie’s disease (PD) over the past decades, there is no curative treatment. Patients currently have to depend on symptomatic medical or surgical treatment. Chapter 1 summarises the most recent American and European guidelines and discusses the clinical picture, epidemiological and historical aspects, and describes current views on pathophysiology, pathogenesis and therapeutic options.
Chapter 2 gives an overview of nonsurgical treatments for PD and reflects on future developments. It includes a wide literature search on nonsurgical treatment of PD through the ages. In considering publications up until 2018, we found 48 nonsurgical interventions: 11 external, 12 intralesional, 7 topical and 22 oral. Four of these treatments were used in two of the aforementioned ways. Today, collagenase from clostridium histolyticum is the only drug approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of PD. All other nonsurgical treatments are off label. Unfortunately CCH was recently removed from the Asian, Australian and European markets for reasons that seem to have nothing to do with safety or efficacy.
Overall, oral medical treatments are thought to be effective in only the early phase of PD, before plaque hardening and calcification occur. According to the current European guidelines, oral steroids, vitamin E and tamoxifen should be avoided. The remaining drugs for off label use are pentoxifylline, a phosphodiesterase 5-inhibitor or arginine. There is, however, no generally-accepted early treatment for PD, before even considering the possibility of prevention. The vast majority of the existing treatments are aimed at correcting the curvature, which is one of the complications of the disease. Nowadays surgery is of very limited value in, for example, patients with peptic duodenal ulcers, pulmonary tuberculosis or anus carcinoma. More effective nonsurgical treatments have replaced this surgery. However, this approach is unfortunately not yet the case for PD. Surgery for PD is whatsoever a defeat of our therapeutic ingenuity, so the search for new, well-tolerated and effective medical therapy - oral drugs in the acute and intralesional agents in the more chronic phase - has to continue. In the end, the management of patients with PD will improve, with fewer of them needing surgery. In that respect, we strongly recommend close collaboration between urologists and non-surgical experts in fibrotic diseases.
Chapter 3 summarises the long-term outcomes of surgical interventions on the course of sexual function. The International Index of Erectile Function (IIEF) scores of new patients with PD were collected at first presentation between 2007 and 2016. In 2016, data was complemented by a questionnaire that included the IIEF. A total of 170 patients (56.1 per

Summary and general discussion
105
8
cent) responded with a mean follow up of 5.3 ± 3.7 years. The development of sexual function, satisfaction with the treatment and specific treatment outcomes (e.g. loss of penile sensitivity and shortening) were determined in conservatively- and surgically-treated patients. Of 170 patients, 93 were treated conservatively and 77 underwent surgical treatment, including 56 Nesbit corrections, 13 ‘plaque’ incisions and grafting (PIG) and 8 penile prostheses. Within the surgically treated group, more patients treated with PIG were dissatisfied (61.5 per cent) compared with Nesbit (30.9 per cent) and penile implant (50.0 per cent). Penile rigidity and sensitivity loss were higher in patients treated with PIG. Patients who received an implant were often troubled by hindered intromission due to a floppy glans. IIEF scores on the domain intercourse satisfaction at presentation were lower in surgically-treated patients than in the conservative group. Compared with the base line, orgasmic function and sexual desire decreased in the entire cohort. The conservatively-treated group showed a decline in erectile function, orgasmic function, sexual desire and intercourse satisfaction. On the contrary, overall satisfaction in the surgically-treated group had increased. At follow-up, no differences were seen in sexual function between surgically- and conservatively-treated patients in all IIEF domains. Overall, we concluded that after surgical treatment of PD, sexual function improves to a level equal to that of untreated patients. However, results varied between the different interventions in as much as patients after PIG reported high dissatisfaction rates compared with those undergoing a Nesbit procedure or a penile implantation.
For many homosexual men, penile erection is of utmost importance and is directly linked to self-esteem and body image. Seven years post-diagnosis, we had three in-depth interviews with a 52-year-old homosexual man suffering erectile dysfunction and a relatively mild curvature causing devastating psychological effects. Chapter 4 discusses these effects in relation to the limited literature, as well as the conceptions of homosexual men on social media. It shows that the psychological effects in homosexual PD patients could be more extensive than in heterosexual patients, even in mild cases.
PD, Dupuytren’s, and Ledderhose’s diseases (DD and LD) are related fibroproliferative disorders characterized by abnormalities in the connective tissue of the tunica albuginea of the penis, the palm of the hand and the sole of the foot, respectively. Coexistent prevalence rates of these diseases have only been described in a few small populations. Chapter 5 reports on a large population and raises awareness in surgeons treating DD. Patients diagnosed as having DD were recruited from outpatient clinics in the northern part of the Netherlands from 2007 to 2016. Patients and plastic surgeons completed questionnaires concerning demographics, clinical characteristics, the coexistence of LD and/or PD, and other factors. For 730 men with DD, the surgeons reported a prevalence rate of PD of 7.8

Chapter 8
106
per cent and 16.1 per cent for those with LD. The participants themselves reported prevalence rates of 8.8 per cent for PD and 22.0 per cent for LD. In the DD cohort, the prevalence of PD was lower than that described in the literature. The prevalence of LD corresponded with the already existing rates. However, both were underreported by plastic surgeons, which signifies the need for increased awareness, recognition and referral to a urologist when the conditions are bothersome or symptomatic.
Previously, our research group presented the association of a single nucleotide polymorphism (SNP) rs4730775 at the WNT2 locus on chromosome 7, by comparing allele frequencies of 11 SNPs that had previously been associated with DD between 111 men with PD and healthy controls. More recently, it was shown that the two disorders aggregate within families and several genetic risk variants were shown to be associated with both diseases. However, much is still unknown regarding the genetic predisposition of PD. Chapter 6 presents the first ever genome-wide association study (GWAS) for PD. SNPs within three loci were found to be genome-wide significantly associated with PD. One of the hits (rs2402177) was a regulatory variant in WNT2, a gene that we previously also identified as a PD risk locus. This hit and the other two identified loci on chromosome 15 were shown to be associated with DD. Due to the small sample size (n=354 PD cases), we unfortunately did not have much validity. New data of approximately 36,000 individuals that were genotyped using the same genotyping chip as our PD cases will soon become available. This will allow for a GWAS of higher quality and less loss of SNPs.
In Europe and the United States of America, verteporfin (Visudyne; VP) is registered and used in treating macular degeneration. Research shows that VP decreased the expression of fibrotic genes in fibroblasts collected from nodules of patients suffering from DD, possibly by deactivating transcription in the Yes Activated Protein (YAP) pathway. To analyse the effect of VP on myofibroblasts cultured from PD ‘plaque’, we took biopsies of five patients. By immunostaining, the presence of the pathologic myofibroblasts was determined. After culturing cells, VP was dispensed in starvation medium for 24 and 48 hours, and messenger (m)RNA levels of COL1A1, ACTA2, COL5A1, EDA-FN, LOXL2, CCN2, SER-PINH1, PLOD2, and YAP were quantified and compared with controls with real-time polymerase chain reaction. The pathologic phenotype of cells isolated from PD ‘plaque’ was confirmed with baseline immunostainings that showed considerable levels of a-smooth muscle actin, being a marker for the presence of myofibroblasts. The mRNA ratios of all the genes related to fibrosis (COL1A1, etc.) except YAP decreased significantly after treatment with VP within 24 and 48 hours. These results, described in chapter 7, suggest inhibition of fibrosis in the YAP cascade, downstream of YAP.

Summary and general discussion
107
8
General discussion
Diagnostics seem to be satisfactory, but undoubtedly a clearer assessment will improve both monitoring and researching PD. In the past, most medical treatments were proposed on a trial and error basis. Others were recommended because they were used in (possible) related diseases and a few were based on a specific pathophysiological mechanism. Today, intralesional collagenase injection therapy probably has some additional value. There is also growing interest in oral therapies with pentoxifylline, PDE-5-inhibitors and antioxidants, which are sometimes combined with surgery or mechanical appliances. A recent review suggests a serious role for penile stretching devices, but also points out that more research is needed.
“Who is the best candidate for which type of surgery?” and “how can we counsel properly?” are the most important questions for patients as well as clinicians. These questions are particularly raised by poor satisfaction rates, and even dissatisfaction regarding the current treatments based on European guidelines. For future research, it is important to use patient-rated outcome measures (PROMs) to measure the results of our interventions adequately. A PROM is not more than a clinical endpoint, which measures whether the patient is helped or harmed. However, comparing different techniques and options (surgical or non-surgical ones), often without having done an initial comparison between different groups, remains problematic. If one follows guidelines, patients undergoing non-surgical treatments will be different from patients undergoing, for example, a Nesbit procedure. They are different from PD patients, who are candidates for ‘plaque’ incision and grafting (PIG) or even the insertion of an inflatable penile prosthesis (IPP). The major issue remains the varied severity of PD.
Difficult vaginal intromission is a common complaint for PD patients as well as their partners. Our results show that patients who had prosthesis surgery experienced more intromission problems (87.5%) compared with those who had undergone other interventions. This could be due to a so-called floppy glans. Another disappointing result is that, contrary to data from literature, 50 per cent of our patients with an IPP stated they would not be willing to undergo the same procedure again.
According to a leading expert, there are serious difficulties regarding randomized, placebo-controlled, double blind investigations into PD patients: “clinics on their own cannot produce the numbers it takes and there is no established standard of care to use as a control.” (1) In addition, he states that most patients are reluctant to be treated by a placebo due to fear, and the practical and ethical limitations are generally significant.

Chapter 8
108
To answer the research questions more extensively, one needs to collect all the data regarding the patients in both pre- and postoperative state (pathological history, psychological aspects, sexual preferences and presence of a partner or not etc.). Meticulous methods and patience are the main components of a successful endeavor. Ultimately, the main goals are prevention and the replacement of surgery by less invasive interventions or drug therapy.
We found a high prevalence of PD in DD patients. We advise that handsurgeons who treat DD be aware of concomitant PD and its sometimes devastating psychological consequenses. In daily life, most PD patients feel too embarrassed to report their sexual complaints. This raises the question of whether plastic surgeons need to actively ask their DD patients for symptoms of PD. In our opinion, they do not have to go into detail, but they can propose a referral to a competent urologist.
We performed the first ever GWAS for PD patients. Unfortunately, the analysis did not have much power. New Lifelines data will allow for a GWAS of higher quality, which we will publish in the near future. The Lifelines biobank is an international recourse for health research, consisting of data and samples collected from a cohort study in the northern part of the Netherlands. This also means that our group will carry out a new GWAS for DD using this same new Lifelines data and will perform a meta-analysis of DD with other cohorts to identify additional DD loci. This will provide opportunities to find more SNPs associated with PD, including the overlap of PD with DD. This research will probably provide a more comprehensive understanding of the landscape of genetic factors responsible for the development of PD. (2) In addition, such research will likely better define the links between malignant and benign urologic conditions, such as PD, and will ultimately facilitate risk stratification, screening and the treatment of PD patients. (3)
We need researchers with cutting-edge skills in three areas: tissue engineering, computational biology and epigenetics. It could then be possible to find a biomarker for PD. In DD, the International Dupuytren Data Bank (IDDB) aims to identify predictive laboratory biomarkers of DD severity to facilitate the identification of a molecular target for drug development. The IDDB is an independent research project that uses crowdsourcing, new web technology and open access research. Similar initiatives from urologists or even collaboration with the IDDB could pave the way for more successful PD research.
In addition, we looked at the promising compound Verteporfin. This drug already has an important and registered place in the treatment of macular degeneration. Recently, it also appeared to have additional value in oncology. Given some overlapping pathways in oncological and fibrotic processes, we looked at the protein expression in cell cultures of

Summary and general discussion
109
8
‘plaques’ from PD patients. Verteporfin proved to have an anti-fibrotic effect. Dose-response studies, the optimal route of administration and clinical studies must show its true value for PD patients.
Conclusive remarks
There is a serious lack of knowledge about PD, so researchers can take a leading role in this field. Biologists, geneticists, plastic surgeons, psychologists and urologists must join forces to effectively investigate the disease. In general, urologists treat the curvature, but not the disease that caused it. The deformity, however, is a complication of the larger problem of PD. In the past, research was entirely deferred to urologists, who understandably focused on technical aspects. Most of them still tell their patients that the only options are either a surgical procedure or a ‘wait and see’ policy. Because PD is a chronic systemic disorder, investigators should use a chronic disease research model and this should be patient-guided, focusing on subsets of PD severity and quality of life, and using biomarkers to guide individualized treatments. This research typically is longitudinal and open-ended.
The aforementioned options would increase the patient’s understanding of his or her condition. The differences in expectations and options must always be properly discussed and recorded. To get a representative impression of their wishes and assessments, it would be a great advantage if patients with PD could come together in a formalized setting. As in DD patients, such an organization could help to understand what is really important and how patients can be helped in the best way. In science, one tries to make objective even the most subjective feelings. Quality of life measurements, however, do not correlate well with those of curvature severity. The former reflects what patients feel, think and believe. Collaboration with patients is not only important in determining the research agenda within a particular PD field, but also in the design and execution of future projects. The patient must be at the heart of our research and, as a urology resident, I am convinced that my discipline should be a leading one in this initiative, particularly as urologists have the closest contact with PD patients. We undoubtedly also need statisticians and experts in genetics, epidemiology, cell biology and medical engineering.
Papers usually have intriguing starting points, but there is often a notable methodological and clinical bias in study designs. “We mix what we know with what we think and in worst cases what we hope or believe,” as Levine already stated. (1) It is also important to publish research with negative results. Researchers who do so will not be remembered for a spectacular breakthrough treatment, but still deserve credit for addressing sensitive issues.

Chapter 8
110
Long-term outcomes regarding PD treatments have been stagnant for decades because the focus has been on managing the complications. Progress requires shifting the goal from treating the curvature to finding and treating the systemic basis of PD. Multidisciplinary research groups should develop protocols to assess multimodal treatments, such as combining pharmacotherapy, stretching devices and/or surgery. Researchers have to collaborate both nationally and internationally.

Summary and general discussion
111
8
References
1. Levine LA. Seeking answers on the quest for effective nonsurgical treatment of Peyronie’s disease. Eur Urol 2007;51:601-604.
2. Herati AS and Pastuszak AW. The genetic basis of Peyronie disease: a review. Sex Med Rev 2016;4:85-94.)3. Lo EM, Hotaling JM, Pastuszak AW. Urologic conditions associated with malignancy Urol Oncol
2020;38:23-30.


Samenvatting
Chapter 9

Chapter 9
114
Samenvatting
In de afgelopen decennia is de kennis over de ziekte van Peyronie aanzienlijk toegenomen. Toch is er geen curatieve behandeling mogelijk. Patiënten zijn vooralsnog aangewezen op symptomatische behandelingen. In hoofdstuk 1 worden de meest recente Amerikaanse en Europese richtlijnen besproken. Het betreft onder andere pathofysiologische en pathogenetische aspecten. Daarnaast komen de geschiedenis en de huidige inzichten aangaande klinische verschijnselen en therapeutische mogelijkheden aan bod.
In hoofdstuk 2 wordt niet alleen een overzicht geboden van de niet-chirurgische behandelingen voor de ziekte van Peyronie door de eeuwen heen, maar ook een blik op de toekomst geworpen met betrekking tot mogelijk nieuwe orale medicamenteuze behandelingen. In wetenschappelijke publicaties tot en met 2018 vonden we 48 niet-chirurgische interventies: 11 externe, 12 intralaesionale, 7 topische en 22 orale behandelingen. Vier van de laatstgenoemde werden op meerdere manieren toegepast. Anno 2020 is een serie intralaesionale injecties met collagenase verkregen uit de bacterie Clostridium histolyticum, de enige behandeling die door de Amerikaanse Food and Drug Administration en het in Amsterdam gevestigde Europees Geneesmiddelenbureau is goedgekeurd. Het medicijn is echter door de producent van de Europese, Australische en Aziatische markt gehaald, mogelijk om commerciele redenen. Alle andere niet-chirurgische behandelingen zijn off-label. Men spreekt van off-label gebruik als het geneesmiddel niet conform de geregistreerde indicatie wordt toegepast. Uit tuchtrechtelijke jurisprudentie wordt duidelijk dat off-label voorschrijven slechts geoorloofd is indien er overeenstemming met de patiënt (‘informed consent’) is verkregen en er in het dossier aantekening van is gemaakt.
Er wordt gedacht dat orale medicijnen alleen in de beginfase effectief zijn, vóórdat de plaque verkalkt. Volgens de huidige Europese richtlijn moeten orale steroïden, vitamine E en tamoxifen beslist niet voorgeschreven worden. De resterende orale medicatie betreffen pentoxifylline, één van de geregistreerde phosphodiësterase-5-remmers of arginine. Er is echter geen algemeen geaccepteerde vroege behandeling voor de ziekte, laat staan een mogelijkheid tot preventie.
De chirurgische behandeling is symptomatisch, gericht op correctie van de standsafwijking. De verkromming is feitelijk een complicatie van de ziekte. In vergelijking tot enkele decennia geleden is chirurgie voor bijvoorbeeld patiënten met een maagzweer, longtuberculose of anuskanker tegenwoordig van weinig betekenis meer. Meer effectieve behandelingen hebben de plaats ingenomen van chirurgische therapie. Voor de ziekte van Peyronie kan dit helaas nog niet gezegd worden. Chirurgie is hoe dan ook een gebrek aan

Samenvatting
115
9
therapeutisch vernuft, zo schreef de Italiaanse dichter, filosoof en essayist Guido Ceronetti (1927-2018). (1) De zoektocht naar effectieve niet-chirurgische therapie, orale medicatie in de acute en intralaesionale in de meer chronische fase, gaat echter door. In dat licht raden we een nauwe samenwerking van urologen met niet-chirurgisch georiënteerde experts op het gebied van fibrotische ziektes aan.
In hoofdstuk 3 bespreken we de lange termijn uitkomsten van chirurgische interventies in onze eigen kliniek. Tussen 2007 en 2016 werden alle nieuwe patiënten met de ziekte van Peyronie verzocht een vragenlijst aangaande het seksueel functioneren in te vullen. Het ging om de wereldwijd gevalideerde International Index of Erectile Function (IIEF). Eind 2016 werden zij opnieuw uitgenodigd een vragenlijst in te vullen, waarin ook de IIEF was opgenomen. 170 patiënten (56,1%) stuurden deze ingevuld terug. De gemiddelde follow-up bedroeg 5,3 ± 3,7 jaar. De ontwikkeling van seksuele functies, tevredenheid over de behandeling(en) en specifieke uitkomstmaten als verlies van gevoel in de eikel en verdere verkorting werden bepaald voor zowel de conservatief (niet-chirurgisch) als de chirurgisch behandelde patiënten. Van de 170 waren er 93 conservatief en 77 chirurgisch behandeld. Bij 56 van de laatstgenoemden ging het om een correctie volgens Nesbit, bij 13 om ‘plaque’ insnijding en grafting (PIG) met een matje en bij 8 om implantatie van een erectieprothese. De patiënten behandeld met PIG waren ontevredener (61,5%) dan degenen na een Nesbit procedure (30,9%) en die na het operatief inbrengen van een erectieprothese (50,0%). Stijfheidsproblemen en gevoelsverlies in de eikel kwamen ook vaker voor in de PIG-groep. Sommige mannen met een prothese bleken bij het inbrengen van de penis in de vagina last te hebben van een zogenaamde ‘floppy glans’.
De chirurgisch behandelde mannen hadden bij hun eerste polikliniekbezoek lagere IIEF scores op het domein `gemeenschapstevredenheid` dan de conservatief behandelden. Vergeleken met de eerste meting daalde de `orgasme functie` en `seksuele drive` voor alle proefpersonen. De conservatief behandelde groep liet een afname zien in `erectiele functie` en `gemeenschapstevredenheid`. In de chirurgisch behandelde groep nam de algehele tevredenheid over het seksleven toe.
Bij follow-up waren er alle IIEF domeinen bezien echter geen wezenlijke verschillen in het seksueel functioneren tussen de niet-chirurgische en chirurgisch behandelde mannen. We concludeerden dat chirurgische behandelingen in lijn met de geldende internationale richtlijnen in vergelijking met conservatief handelen niet tot een slechter seksueel functioneren leiden. Wel lopen de resultaten van chirurgie uiteen, want vooral na PIG rapporteerden de patiënten een hoge mate van ontevredenheid. Uiteraard dient daarbij opgemerkt te worden dat over het algemeen hun uitgangspositie beduidend slechter is, in de zin van een forsere kromstand met meer verkorting en verkalking.

Chapter 9
116
Voor homoseksuele mannen is een `normale` erectie wellicht van groter belang dan voor heteroseksuele. Zeven jaar na het stellen van de diagnose Peyronie interviewden we enkele malen een 52-jarige homoseksuele patiënt die te kampen had met erectiezwakte en een relatief milde verkromming. Deze verschijnselen hadden ernstig psychische gevolgen. De zeer beperkte wetenschappelijke literatuur en de conceptie van homoseksuele mannen op sociale media in ogenschouw nemend, bespreken we in hoofdstuk 4 deze gevolgen. Het laat zien dat de psychische effecten bij homoseksuele Peyronie patiënten verregaander kunnen zijn dan bij heteroseksuele, zelfs in milde gevallen.
De ziekten van Peyronie, Dupuytren en Ledderhose zijn verwante fibroproliferatieve aandoeningen, gekenmerkt door afwijkingen in bindweefsel van resp. de penis, de handpalm en de voetzool. Het tegelijk voorkomen van twee of drie van deze aandoeningen is alleen beschreven in kleine populaties. In hoofdstuk 5 gaat het echter om een relatief grote populatie. Tussen 2007 en 2016 werden patiënten met Dupuytren gerekruteerd op poliklinieken Plastische Chirurgie van enkele ziekenhuizen in het noorden van Nederland. Niet alleen deze patiënten, maar ook de behandelende plastisch chirurgen vulden vragenlijsten in over onder andere demografie, klinische karakteristieken en het tegelijkertijd bestaan van de ziekte van Ledderhose en/of Peyronie. Bij de 730 deelnemende patiënten met de ziekte van Dupuytren rapporteerden de chirurgen een prevalentie van 7,8% voor Peyronie en 16,1% voor Ledderhose. De patiënten zelf maakten melding van 8,8% voor Peyronie en 22,0% voor Ledderhose.
In dit cohort Dupuytren patiënten bleek de prevalentie van Peyronie lager dan die in de literatuur. De gelijktijdige aanwezigheid van de ziekte van Ledderhose was even hoog als eerder beschreven. Beide ziekten werden echter ondergerapporteerd door de plastisch chirurgen.
Onze onderzoeksgroep presenteerde eerder de associatie van een single nucleotide polymorfisme (SNP) rs 4730775 ter plaatse van het WNT2 locus op chromosoom 7, door allel frequenties van 11 SNPs geassocieerd met de ziekte van Dupuytren bij 111 mannen met de ziekte van Peyronie. Het is al geruime tijd bekend dat deze twee aandoeningen vaker voorkomen in bepaalde families. Er is echter nog veel onbekend over de genetische predispositie in geval van de ziekte van Peyronie. In hoofdstuk 6 wordt de eerste genome-wide association study (GWAS) gepresenteerd. SNPs op drie loci bleken significant geassocieerd met Peyronie. Een van de hits (rs2402177) bleek een variant van het al eerder geïdentificeerde Peyronie-risico locus WNT2. Deze hit en twee andere loci op chromosoom 15 waren eerder ook al geassocieerd met Dupuytren. Vanwege de relatief kleine sample grootte (n = 354 Peyronie cases), was er in onze studie helaas sprake van een beperkte

Samenvatting
117
9
validiteit. Nieuwe gegevens afkomstig van circa 36.000 mannen uit de Lifeline Study die werden gegenotypeerd met dezelfde chip, komen op korte termijn beschikbaar. Dit zal ongetwijfeld een GWAS met een hogere kwaliteit en met minder verlies van SNPs opleveren.
In Europa en de Verenigde Staten is verteporfin (Visudyne; VP) geregistreerd voor de behandeling van maculadegeneratie. VP bleek de expressie van fibrose-specifieke genen in fibroblasten afkomstig van patiënten met de ziekte van Dupuytren te verminderen. Dat gebeurde waarschijnlijk door het deactiveren van de transcriptie in de zogenaamde Yes Activated Protein (YAP) pathway. Om de effecten van VP op myofibroblasten uit de ‘plaque’ van Peyronie patiënten te analyseren, namen we biopten bij vijf patiënten. Middels immuun-specifieke kleuringen werd de aanwezigheid van pathologische myofibroblasten aangetoond. Na het kweken van deze cellen werd VP toegediend voor resp. 24 en 48 uur en werden de messenger (m)RNA gehalten van COL1A1, ACTA2, COL5A1, EDA-FN, LOXL2, CCN2, SER-PINH1, PLOD2 en YAP gekwantificeerd en vergeleken met een controlegroep middels een `real-time polymerase chain reaction`. De mRNA ratio’s van alle genen gerelateerd aan fibrose (COL1A1 etc.), behalve YAP, verminderden significant na toediening van VP gedurende de 24 en 48 uur. Deze in hoofdstuk 7 beschreven resultaten, wijzen erop dat VP fibrosering remt in de YAP cascade, stroomafwaarts van YAP.
Discussie
De huidige diagnostiek lijkt toereikend, maar een nog duidelijkere beoordeling, bijvoorbeeld in de vorm van kernspintomografie (MRI), zal zowel de monitoring als het wetenschappelijk onderzoek naar de ziekte van Peyronie verbeteren. In het verleden werden de meeste voorstellen voor medicamenteuze therapie gedaan op basis van trial and error. Andere ideeën werden aangedragen omdat ze veelbelovend waren bij patiënten met gerelateerde ziektebeelden. Slechts enkele waren gebaseerd op een specifiek pathofysiologisch mechanisme. Anno 2020 heeft behandeling, bestaand uit intralaesionele collagenase injecties, waarschijnlijk wel enige toegevoegde waarde. Er is groeiende interesse in orale therapie met pentoxifylline, PDE5-remmers en antioxidanten, welke soms gecombineerd worden met chirurgie of mechanische therapie. Penisstrekkende apparatuur wordt in dit verband het meest genoemd. Er is echter meer onderzoek dienaangaande nodig.
“Wie is de beste kandidaat voor welke type chirurgie?” en “hoe kunnen we het beste voorlichten?” zijn belangrijke vragen voor zowel patiënten als urologen. Deze rijzen vooral vanwege matige tevredenheidscijfers en zelfs ontevredenheid over de huidige behandelingen op basis van Europese richtlijnen. Met het oog op de toekomst is het belangrijk om

Chapter 9
118
zogenaamde door de patiënten zelf gescoorde uitkomsten (patient rated outcome measure; PROM) te gebruiken om de behandelingsresultaten juist in te schatten. Een PROM is niets anders dan een klinisch eindpunt, dat beschrijft of een patiënt al dan niet baat heeft bij een behandeling. Het vergelijken van verschillende technieken en opties (chirurgisch of niet-chirurgisch) zonder initiële correctie tussen groepen blijft problematisch. Als de richtlijnen worden gevolgd, zullen patiënten die een chirurgische ingreep hebben ondergaan verschillen van conservatief behandelde. Het grote probleem in het kader van onderzoek blijft de variatie in de ernst van de verschijnselen.
Bemoeilijkte vaginale intromissie is een veelgehoorde klacht van zowel Peyronie patiënten als hun partners. Onze resultaten tonen aan dat patiënten die prothesechirurgie ondergingen vaker intromissieproblemen ondervonden (87,5%) dan zij die een andere operatie ondergingen. Dit kan komen door een zogenoemde ‘floppy glans’. De eikel glijdt dan als het ware van de uiteinden van de met prothesemateriaal gevulde zwellichamen af. Een ander teleurstellend resultaat is dat maar liefst vijftig procent van onze patiënten met een prothese verklaarden niet dezelfde procedure te willen ondergaan mochten zij opnieuw voor de keuze komen te staan. Dat percentage is opvallend hoger dan de in de literatuur genoemde.
Er zijn serieuze moeilijkheden betreffende gerandomiseerde, placebo gecontroleerde, dubbelblinde onderzoeken bij patiënten met de ziekte van Peyronie. Om een erkend deskundige te parafraseren: één ziekenhuis alleen kan niet komen tot de benodigde aantallen patiënten en er is geen standaardbehandeling waarmee vergeleken kan worden. (2) Daarnaast stelt hij dat de meeste patiënten, veelal ingegeven door angstgevoelens, liever niet met een placebo willen worden behandeld én dat praktische en ethische bezwaren een rol spelen.
Om onderzoeksvragen nadrukkelijker te kunnen beantwoorden, zullen alle data betreffend de pre- en postoperatieve status van patiënten (voorgeschiedenis, psychische aspecten, seksualiteit, aanwezigheid van een partner etc.) verzameld moeten worden. Nauwkeurige methoden en geduld zijn daarbij van het grootste belang. Wij vonden dat er bij een behoorlijk aantal mannen met de ziekte van Dupuytren tegelijkertijd sprake was van de ziekte van Peyronie. Wij adviseren derhalve handchirurgen die deze mannen behandelen hier aandacht aan te schenken en daarbij de soms ernstige psychische gevolgen in het achterhoofd te houden. De meeste patiënten schamen zich om seksuele klachten te uiten. Dan rijst de vraag of plastisch chirurgen hun Dupuytren patiënten actief moeten vragen naar symptomen van Peyronie. Naar onze mening hoeven ze er niet in detail op in te gaan, maar dienen zij als de patiënt dat wenst naar een ter zake kundig uroloog te verwijzen.

Samenvatting
119
9
Wij voerden de eerste GWAS studie bij Peyronie patiënten uit. Helaas had de analyse een beperkte power. Nieuwe Lifelines data zullen leiden tot een GWAS van een hogere kwaliteit. De Lifelines biobank is een internationale bron voor geneeskundig onderzoek, bestaand uit data en samples verzameld uit een cohort studie in het noorden van Nederland. Dit betekent ook dat onze onderzoeksgroep een nieuwe GWAS voor Dupuytren uit zal gaan voeren met dezelfde data en dat daarnaast een meta-analyse van andere cohorten zal gaan plaats vinden om additionele loci te identificeren. Zo wordt de mogelijkheid geschapen om meer SNPs geassocieerd met Peyronie te vinden en meer inzicht te krijgen in de genetische overlap tussen de beide ziekten. (3) Daarnaast zal de mogelijke link tussen kwaadaardige ziekten en benigne urologische aandoeningen, zoals Peyronie, beter in kaart gebracht kunnen worden. Datzelfde geldt voor risicostratificatie, screening en behandeling. (4)
In dat verband zijn er onderzoekers nodig met vaardigheden op gebied van moleculaire biologie en epigenetica. Mogelijk kan er een biomarker voor Peyronie gevonden worden. In relatie tot de ziekte van Dupuytren is door plastisch chirurgen, revalidatieartsen, radiotherapeuten en basale wetenschappers de International Dupuytren Data Bank (IDDB) in het leven geroepen, juist om markers te vinden waarmee de ernst van de ziekte voorspeld kan worden én om een medicijn te vinden. De IDDB is een onafhankelijk onderzoeksinstituut dat crowdsourcing, nieuwe webtechnologie en open access onderzoek toepast. Vergelijkbare initiatieven van urologen of het samenwerken met instituties als de IDDB kunnen wellicht richting geven aan succesvol onderzoek naar de ziekte van Peyronie.Tot slot bestudeerden we Verteporfin. Dit officieel geregistreerde medicijn wordt al jaren toegepast bij de behandeling van maculadegeneratie. Ook heeft het de belangstelling gewekt vanuit de medische oncologie. Wij bekeken de eiwitexpressie in celkweken van ‘plaques’ van Peyronie patiënten. Verteporfin bewees een anti-fibrotisch effect te hebben. Dosis-respons studies, onderzoek naar de optimale toedieningsweg en klinische studies moeten de daadwerkelijke waarde voor patiënten met de ziekte van Peyronie aantonen.
Concluderende opmerkingen
Er is een serieus tekort aan kennis over de ziekte van Peyronie. Biologen, genetici, plastisch chirurgen, psychologen en urologen dienen hun krachten te bundelen teneinde de ziekte effectief te kunnen onderzoeken. Over het algemeen behandelen urologen de verkromming, maar niet de onderliggende ziekte die deze veroorzaakt. De vormafwijking is echter een complicatie van het wezenlijke probleem. In het verleden werd alleen onderzoek gedaan door urologen die zich logischerwijs in de eerste plaats richtten op de chirurgisch-technische aspecten. De meesten van hen vertellen hun patiënten tot op heden dat de enige twee opties ‘chirurgie’ of een ‘wait and see’ beleid zijn.

Chapter 9
120
Aangezien Peyronie een chronisch systemische ziekte is, moet men ook een `chronische ziekte onderzoekmodel` gebruiken, dat patiëntgericht is en focust op kwaliteit van leven én het vinden van biomarkers waarmee behandelingen mogelijk zelfs geïndividualiseerd kunnen worden. Dit soort onderzoek is longitudinaal met een open eind.
De verschillen in verwachtingspatronen en behandelingsopties zullen altijd goed moeten worden besproken en vastgelegd. Om representatieve onderzoeksdoelen te kunnen formuleren, is het ongetwijfeld van meerwaarde als patiënten zich verenigen in een formele setting. Evenals bij Dupuytren patiënten kan een dergelijke organisatie helpen te begrijpen wat daadwerkelijk van belang is en hoe patiënten het best geholpen kunnen worden. In de wetenschap probeert men vaak de meest subjectieve gevoelens te objectiveren. Kwaliteit van leven correleert echter vaak niet met bijvoorbeeld de mate van kromstand gemeten met een gradenboog. Samenwerking met patiënten is niet alleen belangrijk bij het opstellen van een onderzoeksagenda, maar ook voor het ontwikkelen en uitvoeren van projecten. Patiënten vormen het hart van ons onderzoek. Als arts-assistent in opleiding tot uroloog ben ik ervan overtuigd dat mijn discipline in deze een leidende rol heeft, omdat wij nauw contact met hen hebben. Daarnaast zijn er uiteraard statistici en experts in genetica, epidemiologie, celbiologie en medische techniek nodig.
Artikelen hebben vaak intrigerende uitgangspunten, maar de methodologische en klinische bias in de onderzoeksopzet is over het algemeen aanzienlijk. `We mixen wat we weten, met wat we denken en in het ergste geval met wat we hopen of geloven,` zoals de uroloog Laurence Levine ooit schreef. (2) Het is daarom ook belangrijk negatieve resultaten te publiceren.
Tot slot: onderzoek naar de ziekte van Peyronie en de behandelingen ervan stagneerde, omdat de focus lag op het behandelen van de complicaties. Om wezenlijke vooruitgang te boeken zal men zich steeds meer gaan richten op de systemische oorzaken. Multidisciplinair samengestelde onderzoeksgroepen zullen protocollen gaan ontwikkelen om multimodale behandelingen te bestuderen, bijvoorbeeld het combineren van orale en intralaesionale farmacotherapie, mechanische apparatuur en/of chirurgie. En onderzoekers zullen moeten samenwerken, zowel nationaal als internationaal.

Samenvatting
121
9
Referenties
1. Ceronetti G. De stilte van het lichaam. Amsterdam: De Bezige Bij, 1995.2. Levine LA. Seeking answers on the quest for effective nonsurgical treatment of Peyronie’s disease. Eur Urol
2007;51:601-604.3. Herati AS and Pastuszak AW. The genetic basis of Peyronie disease: a review. Sex Med Rev 2016;4:85-94.)4. Lo EM, Hotaling JM, Pastuszak AW. Urologic conditions associated with malignancy Urol Oncol
2020;38:23-30.


Appendices
Dankwoord/Acknowledgements
Curriculum Vitae
List of publications

Appendices
124
Appendix A (translated from Dutch)
Questionnaire Surname:Peyronie’s disease Initials: Date of birth:
TO BE FILLED OUT BY THE PATIENT
This questionnaire considers sexual relationships and related language to be heterosexual. We do not mean to offend homosexual men. In case of homosexuality, please read anus or other substitute where vagina is mentioned.
What is the date today? ……… - ……… - 20……… (day-month-year)
In the passed you may or may not have undergone Peyronie’s disease related surgery. If this is not the case, please proceed to question 11.
What was the date of surgery? ……… - ……… - ……… (day-month-year)
1. Which procedure was performed? Please circle the correct procedure and if relevant the used grafting material. In case of multiple procedures please add the chronological order.
Surgery according to Nesbit with circumcision Excision or incision and grafting ( pericard/tachosil/gore-tex) with circumcision Semirigid penile prosthesis Inflatable penile prosthesis
2. Are you circumcized? Yes, during the above mentioned procedure Yes, previously Yes, after the above mentioned procedure No, because ………

Appendices
125
A
3. You underwent surgery because of Peyronie’s Disease. Would you be willing to undergo the same intervention with the knowledge of the end result?
Yes No
4. If a friend of yours would be in your situation before surgery. Would you advise him to undergo the same intervention you underwent?
Yes No I don’t know
5. Can you mark the end result (0-10)? 1 2 3 4 5 6 7 8 9 10 No
6. Does there remain to be a curvature after surgery? Direction (multiple answers possible): Up Left No Down Right ……… degrees
7. Has a new curvature developed since the intervention? Direction (multiple answers possible):
Up Left No Down Right ……… degrees
8. Did your penis shorten, because of surgery? Yes, … cm No
9. For how long did you experience pain after surgery? (Please circle and indicate the appropriate time in days/weeks/months)
None……… days/weeks/months
10. Did you develop any urinary tract symptoms since surgery and if so: which ones? No Yes ………
11. After being diagnosed with Peyronie’s Disese, did you ever undergo psychological/psychiatric treatment?
Yes, because of Peyronie’s Disease No Yes, because of something else

Appendices
126
12. How is your penile rigidity currently compared with before the disease (100%)? Please circle the right answer.
10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 13. Do you experience premature softening/loss of tumescence? Always Often Sometimes Almost never Never
14. Do you experience loss of penile sensibility and if so: where? No Glans Other part, ………
15. What caused the penile sensibility loss? Surgery Peyronie’s Disease Circumcision I don’t know Something different, ………
16. Are you capable of having sexual intercourse? Yes No Yes, but I’m restricted by ………
17. During sexual intercourse, does the penis often fall out of the vagina? Yes Not applicable No
18. Can you reach an orgasm? Yes, easily No Yes, but it’s not easy Yes, but it’s very hard to do so
19. Was that easier before you suffered from Peyronie’s Disease? Yes, it used to be easier No, it used to be the same No, it used to be harder
20. Do you have an exclusive (sexual) partner? Yes No

Appendices
127
A
21. Does your partner experience pain during sexual intercourse, because of the shape of your penis?
Yes No
22. Is your partner satisfied with your current sex life? Yes I don’t know No Not applicable
23. Do you use erection stimulating drugs? Levitra (vardenafil) Cialis (tadalafil) Viagra (sildenafil) Other, ………
Androskat injecties No
24. Do you experience any other Peyronie’s Disease related problems? No Yes, ………

Appendices
128
The International Index of Erectile Function
These questions ask about the effects that your erection problems have had on your sex life over the last four weeks. Please try to answer the questions as honestly and as clearly as you are able. Your answers will help your doctor to choose the most effective treatment suited to your condition. In answering the questions, the following definitions apply: - sexual activity includes intercourse, caressing, foreplay & masturbation- sexual intercourse is defined as sexual penetration of your partner- sexual stimulation includes situation such as foreplay, erotic pictures etc.- ejaculation is the ejection of semen from the penis (or the feeling of this)- orgasm is the fulfilment or climax following sexual stimulation or intercourse
The first five questions refer to erectile function Q1. Over the last month, how often were you able to get an erection during sexual activity? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always
Q2. Over the last month, when you had erections with sexual stimulation, how often were your erections hard enough for penetration? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always
Q3. Over the last month, when you attempted intercourse, how often were you able to penetrate your partner? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always
Q4. Over the last month, during sexual intercourse, how often were you able to maintain your erection after you had pentrated your partner? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always

Appendices
129
A
Q5. Over the last month, during sexual intercourse, how difficult was it to maintain your erection to completion of intercourse? 0. No sexual activity 2. Very difficult 4. Slightly difficult1. Extremely difficult 3. Difficult 5. Not difficult
The next three questions refer to satisfaction with intercourse Q6. Over the last month, how many times have you attempted sexual intercourse? 0. No attempts 2. 3-4 times 4. 7-10 times1. 1-2 times 3. 5-6 times 5. 11-20 times
Q7. Over the last month, when you attempted sexual intercourse how often was it satisfactory for you? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always
Q8. Over the last month, how much have you enjoyed sexual intercourse? 0. No intercourse 3. Fairly enjoyable1. No enjoyment 4. Highly enjoyable2. Not very enjoyable 5. Very highly enjoyable
The next two questions refer to orgasmic function Q9. Over the last month, when you had sexual stimulation or intercourse, how often did you ejaculate? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always
Q10. Over the last month, when you had sexual stimulation or intercourse, how often did you have the feeling of orgasm (with or without ejaculation)? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always

Appendices
130
The next two questions ask about sexual desire. In this context, sexual desire is defined as a feeling that may include wanting to have a sexual experience (for example masturbation or sexual intercourse), thinking about having sex, or feeling frustrated due to lack of sex. Q11. Over the last month, how often have you felt sexual desire? 0. No sexual activity 3. Sometimes (about half the time)1. Almost never or never 4. Much more than half the time2. A few times (much less than half the time) 5. Almost always or always
Q12. Over the last month, how would you rate your level of sexual desire? 1. Very low or not at all 4. High2. Low 5. Very high 3. Moderate
The next two questions refer to overall sexual satisfaction.Q13. Over the last month, how satisfied have you been with your overall sex life? 1. Very dissatisfied 4. Moderately satisfied2. Moderately dissatisfied 5. Very satisfied3. About equally satisfied and dissatisfied
Q14. Over the last month, how satisfied have you been with your sexual relationship with your partner? 1. Very dissatisfied 4. Moderately satisfied2. Moderately dissatisfied 5. Very satisfied3. About equally satisfied and dissatisfied
The last question refers to erectile function Q15. Over the last month, how do you rate your confidence that you can get and keep your erection? 1. Very low or not at all 4. High2. Low 5. Very high 3. Moderate

Appendices
131
A
Appendix B (translated from dutch)
Doctor questionnaire
Dupuytren’s disease
General - What is today’s date? - Which hand(s) are affected by Dupuytren’s disease? - Left/right/recurrence yes/no
Extension deficit (in degrees) - Extension deficit MCP of each ray of the left and right hand - Extension deficit PIP of each ray of the left and right hand - Extension deficit DIP of each ray of the left and right hand
Ectopic locations: - Knuckle pads of each ray of the left and right hand - Yes/no - Ledderhose’s disease - Yes/no/beginning - Peyronie’s disease - Yes/no/not checked
Patient questionnaire
Dupuytren’s disease
General - What is today’s date? - What is your date of birth? - What is your gender? - What is your highest level of education? - What is your ethnic background? - What is your current occupational status? - Have you performed physical labor involving your hands?

Appendices
132
- How long have you been performing this physical labor? - Do you have hobbies that involve manual labor? Dupuytren’s disease - Are you right-handed/left-handed/ambidextrous? - Do you have a positive family history for Dupuytren’s disease? - Yes/no/I don’t know - For how long have you been experiencing symptoms of Dupuytren’s disease? - 1 year/2 years/3 years/4 years/5 years/6 years/7 years/8 years/9 years/10-19 years/
over 20 years/I don’t know - At what age did you first notice nodules or flexion of the fingers? - 0-9 years/10-19 years/20-29 years/30-39 years/40-49 years/50-59 years/
60-69 years/70-79 years/ 80-89 years/over 90 years/I don’t know
As you may know, Dupuytren’s disease can also appear in different parts of the body: the fingers (knuckle pads), the soles of your feet (Ledderhose’s disease) and the penis (Peyronie’s disease). - Knuckle pads are nodules on the joint between the first and second phalanges. Do you
have knuckle pads? - Yes/I think so/no/I don’t know - Do you also have hardening or nodules on the sole of your foot? - Yes/I think so/no/I don’t know
The next question only applies to men. In Peyronie’s disease, hard plaques develop in the penis. These plaques can cause a curvature in erection. - Do you have Peyronie’s disease? - Yes/I think so/no/ I don’t know
Complaints and treatment of Dupuytren’s disease - Which complaints of Dupuytren’s disease apply to you (multiple answers possible)? - No complaints/difficulties pocketing hands/difficulties putting on gloves/difficulties with
daily activities/difficulties shaking hands/problems with work/pain/difficulties with hobbies/other
- Why would you consider surgery (multiple answers possible)? - Because it bothers me/because I’m afraid the disease will progress/on G.P.’s advice/plastic
surgeon’s advice/other - Have you ever been operated on before because of Dupuytren’s disease? If so, when? - No/left/right/both hands

Appendices
133
A
- Has your hand ever been operated on for reasons besides Dupuytren’s disease? If so, when? - No/left/right/both hands - What do you think caused Dupuytren’s disease in your case (multiple answers possible)? - No idea/manual labour/family history/hand injury/other - Have you suffered from any of these diseases? - Epilepsy/diabetes mellitus/liver disease - Do you use analgesics? - Do you use anticoagulants? - Do you use anti-diabetics? - Do you use anti-epileptic drugs? - Do you use any other drugs? Other questions - How many alcoholic beverages do you consume per week? - None/1-2 per week/3-5 per week/6-10 per week/11-15 per week/16-20 per week/
over 20 per week - Do you smoke tobacco? - No/yes/not anymore since ... - If you are currently a smoker: how many cigarettes do you smoke per day? - None/1-2 per day/3-5 per day/6-10 per day/11-15 per day/16-20 per day/
over 20 per day - Do you have any allergies? - Yes/no/I don’t know
Peyronie’s disease
General - What is today’s date? - What is your date of birth? - What is your highest level of education? - What is your ethnic background? - What is your current occupational status? Your complaints and treatment - For how long have you been experiencing symptoms of Peyronie’s disease? - 1 year/2 years/3 years/4 years/5 years/6 years/7 years/8 years/9 years/10-19 years/
over 20 years/I don’t know - At what age did you first notice hard plaques in the penis and/or a curvature? - 0-9 years/10-19 years/20-29 years/30-39 years/40-49 years/50-59 years/
60-69 years/70-79 years/ 80-89 years/over 90 years/I don’t know - Which complaints of Peyronie’s disease apply to you (multiple answers possible)?

Appendices
134
- No complaints/curvature of the penis during erection (upward/downward/to the left/to the right)/the penis does not become rigid enough/the penis becomes flaccid prematurely/entering the vagina with the penis is difficult/the penis is clearly shorter during erection/psychological burden/pain during erection/pain during intercourse/fear for cancer/not being able to aim well during urination/other
- Why would you consider surgery (multiple answers possible)? - Because it impedes me too much during intercourse/because it bothers my partner
during intercourse/for cosmetic reasons/on G.P.’s advice/against G.P.’s advice/on urologist’s advice/other
- Has your penis ever been operated on before? If so, when? - What do you think caused Peyronie’s disease in your case (multiple answers possible)? - No idea/trauma of the penis/family history/venereal disease/other - Have you suffered from any of these diseases? - Epilepsy/diabetes mellitus/liver disease - Do you use analgesics? - Do you use anticoagulants? - Do you use anti-diabetics? - Do you use anti-epileptic drugs? - Do you use any other drugs? - Do you use drugs that stimulate the erection? - Do you have a positive family history of Peyronie’s disease? - Yes/no/I don’t know - Do you also have hardening or nodules in the palm of the hand or fingers (Dupuytren’s
disease)? - Yes/I think so/no/I don’t know - To your knowledge, does Dupuytren’s disease occur in your family? - Yes/no/I don’t know - Knuckle pads are nodules on the joint between the first and second phalange. Do you
have knuckle pads? - Yes/I think so/no/I don’t know - To your knowledge, do knuckle pads occur in your family? - Yes/I think so/no/I don’t know - Do you also have hardening or nodules on the sole of your foot (Ledderhose’s disease)? - Yes/I think so/no/I don’t know - To your knowledge, does Ledderhose’s disease occur in your family? - Yes/no/I don’t know

Appendices
135
A
Other questions - How many alcoholic beverages do you consume per week? - None/1-2 per week/3-5 per week/6-10 per week/11-15 per week/16-20 per week/
over 20 per week - Do you smoke tobacco? - No/yes/not anymore since ... - If you are currently a smoker: how many cigarettes do you smoke per day? - None/1-2 per day/3-5 per day/6-10 per day/11-15 per day/16-20 per day/
over 20 per day - Do you have any allergies? - Yes/no/I don’t know

Appendices
136
Dankwoord/Acknowledgements
Dit proefschrift is tot stand gekomen met steun en bijdragen van een groot aantal mensen. In de eerste plaats betreft het de patiënten door en voor wie de onderzoeken uiteindelijk zijn gerealiseerd. Het delen van ervaringen en gevoelens over een intiem lichaamsdeel verdient veel respect.
Geachte prof. dr. Igle Jan de Jong, bedankt voor de mogelijkheden die u voor mij hebt gecreëerd. U hebt mij aangenomen als arts-onderzoeker en zaalarts in het UMCG, mijn eerste baan! De manier waarop u leiding geeft aan de afdeling Urologie verdient veel respect. Naast het vertrouwen dat u altijd in mij heeft gehad, waardeer ik vooral uw helikopterview en doelmatig handelen. Ik hoop deze vaardigheden te kunnen toepassen in mijn verdere loopbaan.
Geachte prof. dr. Ruud Bank, dank voor de begeleiding in het laboratorium. Deze periode, onderdeel van mijn verdiepingsstage in het laatste jaar van de studie Geneeskunde, is niet alleen zeer waardevol gebleken voor het bewerken van dit proefschrift, maar ook voor het ontwikkelen van praktische vaardigheden. Dank ook voor de prettige begeleiding.
Geachte dr. Van Driel, beste Mels. Alles begon bij jou. Een andrologie-poli (met palpabele plaques in alle soorten en maten) tijdens mijn eerste coschap maakte me enthousiast voor de urologie en ik was blij toen ik voor mijn stage wetenschap aan jou gekoppeld werd. Dat die stage tot dit proefschrift zou leiden had ik nooit durven dromen. Ik kan Sanne’s dankwoord kopierën: van de “alles komt goed” tot de “éénogen die koningen werden”. Je hebt de eerste jaren van mijn professionele leven gedefinieerd en hebt je opgeworpen als mijn mentor en vriend. Jouw reactie op mijn recente switch naar de opleiding Heelkunde spreekt wat dat betreft boekdelen. Ik kan mijn geluk niet op dat we dit proefschrift samen tot een goed einde hebben weten te brengen en wens jou, Getie, kinderen en kleinkinderen samen heel veel geluk. Zoals je oudste zoon zei toen we bij jou thuis de puntjes op de i aan het zetten waren: “Dit is de laatste?” Ik hoop dat ik je altijd om raad mag blijven vragen.
Daarnaast dank ik graag de leden van de leescommissie voor de beoordeling van dit proefschrift: prof. dr. Eric J.H. Meuleman, emeritus-hoogleraar Andrologie aan de Vrije Universiteit Amsterdam, prof. dr. Peter Olinga, hoogleraar Translationele Biofarmacie aan de Rijksuniversiteit Groningen en, in het bijzonder, prof. dr. Maarten Albersen, hoogleraar Urologie aan de Katholieke Universiteit Leuven. Laatstgenoemde had zeer waardevolle op- en aanmerkingen.

Acknowledgements (Dankwoord)
137
A
Mijn paranimfen Sanne Vreugdenhil en Dyaran Bansraj. Sanne, ik bewandelde ongeveer hetzelfde succesvolle, door Mels geplaveide pad als jij, maar heb toch een andere afslag genomen. Ik heb me altijd aan je kunnen optrekken en je stond altijd klaar als ik hulp nodig had. Dyaran, ik heb niet meer van zo’n sterk centrum deel uitgemaakt als toen in het A1 elftal. Dank voor je vriendschap door de jaren heen. Vanwege de pandemie is er voor jullie beiden helaas een minder grote rol weggelegd, maar toch, dank voor jullie hulp bij de afronding! Het echte feestje gaan we hopelijk nog vieren.
De afdeling Urologie mocht alweer lang geleden aansluiten bij onderzoek van de afdeling Plastische Chirurgie onder leiding van prof. dr. Paul Werker. Hij startte kort na zijn aantreden een zeer succesvol onderzoeksproject waarin de ziekte van Dupuytren centraal stond. Het onderzoek naar de ziekte van Peyronie sloot daar naadloos op aan. Ook Sophie Riesmeijer en dr. Evert-Jan ten Dam van genoemde afdeling hebben in de afgelopen jaren hulp geboden
Hetzelfde geldt voor prof. dr. Harry van de Wiel, dr. Alida Weidenaar, dr. Jack Beck, dr. Mistale Taylor, dr. Wouter van der Heide, Theo Borghuis en Alice Tigchelaar-Staghouwer. Dank voor jullie uiteenlopende bijdragen!
De urologen dr. Stijn Roemeling, Benjamin Doornweerd, Boaz Meijer, dr. Annemarie Leliveld-Kors, dr. Josine Quaedackers, dr. Emanuela Altobelli en dr. Rianne Lammers wil ik danken voor het in mij gestelde vertrouwen. Om naar Groningen te komen met de mededeling dat ik van opleiding wilde switchen is tot nu toe het moeilijkste moment geweest in mijn professionele leven. Jullie reacties en steun heb ik als erg prettig ervaren.
(Oud) A(N)IOS urologie van het UMCG. Ik heb veel plezier met jullie beleefd, zowel op de werkvloer als buiten het ziekenhuis. Jullie berichten en succeswensen na de ommezwaai hebben mij goed gedaan. Ik hoop jullie allen graag nog eens terug te zien.
Beste opleiders Chirurgie dr. Eric Sonneveld, dr Jan Willem de Waard en alle andere stafleden van de vakgroep Chirurgie in het Dijklander ziekenhuis, dank voor jullie vertrouwen en steun toen ik erachter kwam de overstap naar de heelkunde te willen maken. Dat geldt ook voor alle A(N)IOS Chirurgie van het Dijklander ziekenhuis. Ik ben blij van dit team deel uit te mogen maken!
Mijn ‘opleiders’ van de zij-instroom Geneeskunde, Gerard Terwisscha van Scheltinga en Tjalling Waterbolk wil ik danken voor de mogelijkheid alsnog arts te kunnen worden.

Appendices
138
Beste Claudio, Damien, Dyaran, Lars, Maarten en Salam, de boys, op het veld en erbuiten, dank voor alle gezelligheid en broederschap!
Beste Frans, Gino, Mike, Redha en Tim, wat een keiharde studententijd hadden we en wat mooi dat we dat af en toe vieren. Laten we die traditie nog lang in ere houden!
Lieve familie Mohede en Stolker, alle ooms, tantes, (achter)neefjes en nichtjes, wijlen opa Carel, opa John en oma Herma, lieve oma Meis en oma Buur, jullie wijsheden in acht nemend probeer ik mijn leven vorm en richting te geven. Dank voor jullie lessen in liefde, werklust, soberheid, gezelligheid, doorzettingsvermogen, loyaliteit, dankbaarheid en visie.
Dear Taylor family, thank you for always supporting us and making me feel so welcome. Rupert, Dagmar, Caspian and Mistale (again). Your lessons about living in the moment and doing things step by step, I hold very dear. I look forward to many more family holidays, dinners, drinks and other gatherings in places all around the world!
Lieve Stijn, Roos en Sophie. Ik ben zo trots dat ik jullie grote broer mag zijn en ben dankbaar voor jullie onvoorwaardelijke steun en gezelligheid. Als ik terugdenk aan onze jeugd word ik vanzelf vrolijk en realiseer me dat we er eigenlijk nog middenin staan, vooral op de momenten dat we met z’n allen op de hoekbank aan de Kolthofhorst zitten. Ik kan altijd op jullie rekenen en ga ervan uit dat dat gevoel wederzijds is. Lieve Redha, Stijn en John, ik ben blij dat jullie ons zessen zijn komen versterken.
Lieve papa en mama, over onvoorwaardelijke steun gesproken, wij vieren hebben zoveel geluk met jullie als ouders. Alles mocht en er moest niet zo heel veel. In alles heb ik me altijd gesteund gevoeld en, als er hulp nodig was, kwam die. Ik hou van jullie.
Lieve Safira, het leven is een groot avontuur sinds ik jou heb ontmoet. Nooit een saai moment. Samen hebben we de afgelopen jaren ups-en-downs beleefd. Samen komen we elke keer weer tot de beste keus. I’m so excited about the rest of our lives together. I love you.

Curriculum Vitae
139
A
Curriculum Vitae
Daan Carel John Mohede werd op 12 januari 1991 in Enschede geboren. Hij behaalde aldaar in 2009 aan het Bonhoeffer College het gymnasiumdiploma. Vervolgens ging hij Farmacie studeren aan de Rijksuniversiteit Groningen na uitgeloot te zijn voor Geneeskunde. De bachelor Farmacie succesvol afgerond hebbend, kreeg hij in 2013 via de Zij-instroom alsnog de kans Geneeskunde te studeren. Hij liep co-schappen in het Universitair Medisch Centum Groningen (UMCG) en het Isala ziekenhuis in Zwolle. De interesse in de urologie en andrologie werd tijdens het eerste coschap gewekt en tijdens het keuzeco-schap in het UMCG verder ontwikkeld. In de wetenschapsstage werd onder supervisie van dr. M.F. van Driel en prof. dr. I.J. de Jong het startsein gegeven voor dit proefschrift door verschillende onderzoeken op te zetten. De verdiepingsstage volgde hij in het laboratorium van de Medische Biologie onder supervisie van prof. dr. R.A. Bank. In 2017 behaalde hij zijn bul. Na zijn afstuderen ging hij als arts-assistent en arts-onderzoeker urologie in het UMCG aan de slag. Zo kon hij onder supervisie van dr. A.M. Leliveld-Kors klinische ervaring in de urologie opdoen en verder werken aan zijn proefschrift. Hij presenteerde de voortgang van zijn onderzoeken tijdens vergaderingen van de Nederlandse Vereniging voor Urologie in ‘s Hertogenbosch en Nieuwegein en in 2018 op het jaarlijkse congres van de American Urological Association te San Francisco.
In 2018 werd hij aangenomen voor de opleiding Urologie in de regio Groningen (opleider dr. S. Roemeling). In 2019 begon hij de vooropleiding Algemene Heelkunde in het Dijklander Ziekenhuis te Hoorn (opleiders dr. E. Sonneveld en dr. J.W. de Waard). Gedurende de vooropleiding rondde hij dit proefschrift af. In het najaar van 2020 besloot hij de switch te maken naar de opleiding Heelkunde en werd hij aangenomen in de Opleidings- en Onderwijsregio Amsterdam.
Sinds 2014 is Safira Taylor zijn levensgezellin.

List of publications
140
List of publications
This thesis1. Peyronie’s disease – current perspectives. Mohede DCJ, van Driel MF, de Jong IJ, Beck
J. Tijdschr Urol 2018;8:112-120.2. Medical treatments of Peyronie’s disease: past, present, and future. Mohede DCJ, de Jong
IJ, van Driel MF. Urology 2019;125:1-5.3. Patient reported outcomes on sexual function after surgical treatment of Peyronies
disease. Mohede DCJ, Weidenaar AC, van Driel MF, van de Wiel HBM, de Jong IJ. J Urol 2018;199:e911.
4. Homosexuality and Peyronie’s disease. Mohede DCJ, van de Wiel HBM, Meijer B, de Jong IJ, van Driel MF. Submitted
5. Prevalence of Peyronie and Ledderhose diseases in a series of 730 patients with Dupuytren disease. Mohede DCJ, Riesmeijer S, de Jong IJ, Werker PMN, van Driel MF. PRS 2020;145:978-984.
6. A genome-wide association study for Peyronie’s disease. Mohede DCJ, van Driel MF, Riesmeijer S, de Jong IJ, Werker PMN, Nolte IM. Not for publication
7. Verteporfin as a medical treatment in Peyronie’s disease. Mohede DCJ, de Jong IJ, Bank RA, van Driel MF. Sex Med 2018;6:302-308.
Other publicationUnexpected metal in the pelvis. DCJ Mohede, NF Casteleijn, ECC Cauberg. Nederlands Tijdschrift voor Geneeskunde. 2017;161(0):D1699.