PAST PRESIDENTS - PSGPAK
83
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 3 HISTORY PAST PRESIDENTS 1. Prof. Khawaja Saadiq Husain 1985 – 1986 2. Prof. M. Sadiq Shah 1987 – 1988 3. Prof. Nazeer Chaudhry 1989 – 1990 4. Prof. Sibtul Hasnain Syed 1991 – 1992 5. Prof. Chengez Khan 1993 – 1994 6. Dr. S. J. Zuberi 1994 – 1996 7. Prof. Mohammad Musaddiq Khan 1996 – 1998 8. Prof. Muhammad Aslam Baloch 1999 – 2000 9. Prof. Muhammad Saeed Khokhar 2001 – 2002 10. Prof. Najib-ul-Haq 2003 – 2004 11. Prof. Jan Muhammad Memon 2005 – 2006 12. Prof. Muhammad Umar 2007 – 2008 13. Prof. Muzzam-ud-Din Ahmed 2009 – 2010 14 Prof. Arif M. Sidiqui 2011 – 2012
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of PAST PRESIDENTS - PSGPAK

Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 3
HISTORY
PAST PRESIDENTS
1. Prof. Khawaja Saadiq Husain 1985 – 1986
2. Prof. M. Sadiq Shah 1987 – 1988
3. Prof. Nazeer Chaudhry 1989 – 1990
4. Prof. Sibtul Hasnain Syed 1991 – 1992
5. Prof. Chengez Khan 1993 – 1994
6. Dr. S. J. Zuberi 1994 – 1996
7. Prof. Mohammad Musaddiq Khan 1996 – 1998
8. Prof. Muhammad Aslam Baloch 1999 – 2000
9. Prof. Muhammad Saeed Khokhar 2001 – 2002
10. Prof. Najib-ul-Haq 2003 – 2004
11. Prof. Jan Muhammad Memon 2005 – 2006
12. Prof. Muhammad Umar 2007 – 2008
13. Prof. Muzzam-ud-Din Ahmed 2009 – 2010
14 Prof. Arif M. Sidiqui 2011 – 2012

LIST OF PAST PRESIDENTS, PAST GENERAL SECRETARIES AND PAST VICE PRESIDENTS
4 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
PAST GENERAL SECRETARIES
1. Dr. Irshad Waheed 1985 – 1986
2. Dr. M. Aftab Anwar 1987 – 1988
3. Dr. Moiz-ud-Din 1989 – 1990
4. Dr. Zia-ud-Din Shamsi 1991 – 1992
5. Dr. Mumtaz Mehar 1993 – 1994
6. Dr. Wasim Jafri 1994 – 1996
7. Dr. Mohammad Irfan Daudi 1996 – 1998
8. Dr. Naheed Sultan 1999 – 2000
9. Dr. Muhammad Saeed Quraishy 2001 – 2002
10. Dr. Zaigham Abbas 2003 – 2004
11. Dr. Saad Khalid Niaz 2005 – 2006
12. Dr. Bader Faiyaz Zuberi 2007 – 2008
13. Dr. Saad Khalid Niaz 2009 – 2010
14. Dr. Hasnain Ali Shah 2011 – 2012

LIST OF PAST PRESIDENTS, PAST GENERAL SECRETARIES AND PAST VICE PRESIDENTS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 5
PAST VICE PRESIDENTS
1989 – 1990
1. Dr. Qudeerullah Qureshi (Sindh Chapter)
2. Dr. Sibtul Hasnain Syed (Punjab Chapter)
3. Dr. Humayun Zafar (NWFP Chapter)
1991 – 1992
1. Dr. Irshad Waheed (Sindh Chapter)
2. Dr. Arif Qayoom (Punjab Chapter)
3. Dr. Rahim Gul (NWFP Chapter)
1993 – 1994
1. Dr. Shafi Qureshi (Sindh Chapter)
2. Dr. Asif Abbas Naqvi (Punjab Chapter)
3. Dr. Sultan Mahmood (NWFP Chapter)
4. Dr. Javed Aslam Butt (Federal Chapter)
1994 – 1996
1. Dr. Jan Mohammad Memon (Sindh Chapter)
2. Dr. Irshad-ul-Haq (Punjab Chapter)
3. Dr. Pir Mohammad Khan (NWFP Chapter)
4. Dr. Shoaib Shafi (Federal Chapter)

LIST OF PAST PRESIDENTS, PAST GENERAL SECRETARIES AND PAST VICE PRESIDENTS
6 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
1996 – 1998
1. Dr. Iqbal Ahmed Memon (Sindh Chapter)
2. Dr. Arif Mahmood Siddiqui (Punjab chapter)
3. Dr. Mohammad Arif (NWFP Chapter)
4. Dr. Syed Irfan Ahmed (Federal Chapter)
5. Dr. Aslam Baloch (Baluchistan Chapter)
1999 – 2000
1. Dr. Wazir Muhammad Shaikh (Sindh Chapter)
2. Dr. Aftab Mohsin (Punjab Chapter)
3. Dr. Najeeb-ul-Haq (NWFP Chapter)
4. Dr. Waheed-uz-Zaman Tariq (Federal Chapter)
5. Dr. Sherzaman Jamaldini (Baluchistan Chapter)
2001 – 2002
1. Dr. Saeed Hamid (Sindh Chapter)
2. Dr. Altaf Alam (Punjab Chapter)
3. Dr. Syed Musanif Shah (NWFP Chapter)
4. Dr. Asghar Aurangzeb Durrani (Federal Chapter)
5. Dr. Muhammad Azam Mengal (Baluchistan Chapter)

LIST OF PAST PRESIDENTS, PAST GENERAL SECRETARIES AND PAST VICE PRESIDENTS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 7
2003 – 2004
1. Dr. Ibrar Shaikh (Sindh Chapter)
2. Dr. Moeed Ahmed (Punjab Chapter)
3. Dr. Humayun Zafar (NWFP Chapter)
4. Maj.Gen Tassawar Hussain (Federal Chapter)
5. Dr. Muzzam-ud-Din (Baluchistan Chapter)
2005 – 2006
1. Dr. Muhammad Saeed Qureshi (Sindh Chapter)
2. Dr. Ghias-un-Nabi Tayyab (Punjab Chapter)
3. Dr. Javed Iqbal Farooqi (NWFP Chapter)
4. Dr. Muhammad Umar (Federal Chapter)
5. Dr. Aziz-ur-Rehman (Baluchistan Chapter)
2007 – 2008
1. Dr. Hasnain Ali Shah (Sindh Chapter)
2. Dr. Aftab Mohsin (Punjab Chapter)
3. Dr. Noor Muhammad (NWFP Chapter)
4. Dr. Waseem Ahmed (Federal Chapter)
5. Dr. Muzzam-ud-Din Ahmed (Baluchistan Chapter)

LIST OF PAST PRESIDENTS, PAST GENERAL SECRETARIES AND PAST VICE PRESIDENTS
8 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
2009 – 2010
1. Dr. Zaigham Abbas (Sindh Chapter)
2. Dr. Wasim Amer (Punjab Chapter)
3. Dr. Aamir Ghafoor Khan (KPK Chapter)
4. Dr. Masood Siddiq (Federal Chapter)
5. Dr. M. Azam Mengal (Baluchistan Chapter)
2011 – 2012
1. Dr. Saad Khalid Niaz (Sindh Chapter)
2. Dr. Ghias-un-Nabi Tayyab (Punjab Chapter)
3. Dr. Mian Asadullah Jan (KPK Chapter)
4. Col. Shakeel Ahmed Mirza (Federal Chapter)
5. Dr. Shamimah Hanif (Baluchistan Chapter)

Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 9
ORIGINAL ARTICLE
EFFECT OF 1.5 LITRE INFUSIONS ON SERUM CREATININE AND OTHER FACTORS IN PATIENTS OF CIRRHOSIS
OF LIVER WITH RENAL IMPAIRMENT
MUHAMMAD IRFAN,1 MUHAMMAD ARIF NADEEM,2 HUDA GHULAM MIRZA3
ABDUL WAHEED1 ATTIQUE ABOU BAKR,1 AFTAB MOHSIN1 1Departments of Gastroenterology, 2Medicine, Services Institute of Medical Sciences / Services Hospital
and 3Department of Medicine, Lahore University Medical College, Lahore – Pakistan
ABSTRACT Objective: To determine the effect of 1.5 litre infusions on serum creatinine and other significant factors in patients of Liver Cirrhosis having renal impairment.
Study: Descriptive case series was carried out at Services hospital, Lahore.
Methodology: Patients of liver cirrhosis having renal impairment were recruited after informed consent. Diuretics were withdrawn, 1.5 liter of isotonic saline given, urine and blood examination were done. Ascitic fluid was graded via ultrasound. The data was analyzed and Chi-square test applied to find any significant association of factors at 5% level.
Results: Amongst 100 cirrhotic patients with serum creatinine above 1.5 mg/dl, a statistically significant decrease in serum creatinine was seen after infusing 1.5 litre isotonic saline solution (p = 0.000). The serum creatinine, of 45 patients (45%) with Hypovolemia – induced renal disease, came below 1.5 mg/dl while remaining 55 patients (55%) had Non-hypovolemia-induced renal dis-ease. Hypovolemia-induced renal disease had statistically significant association with younger age (p = 0.044), prior use of diuretics (p = 0.001), minimal ascites (p = 0.019), normal WBCs count (p = 0.028), low initial serum creatinine (p = 0.000), normalization of 24 hours urinary volume (p = 0.014) and number of patients discharged (p = 0.003). However it had no statistically signi-ficant association with gender, weight, residential area, history of diabetes mellitus, 24 hours uri-nary proteins, urine sodium, urine RBC and serum sodium.
Conclusion: 1.5 Litre infusions significantly improve serum creatinine in patients of liver cirr-hosis with renal impairment. Hypovolemia – induced renal disease is common in liver cirrhosis patients.
Key Words: Liver cirrhosis, Renal impairment, Hypovolemia-induced renal disease, Serum cre-atinine, Plasma expander.
INTRODUCTION Liver cirrhosis, the end – result of hepatocellular damages,1 is widespread menace in Pakistan due to high prevalence of hepatitis B and C viruses.2 Renal impairment is a common problem amongst these patients of Liver cirrhosis.3 It is caused by Hypovo-lemia – induced renal disease,4 intrinsic – renal dis-ease,5,6 drug toxicity,7-9 Hepatorenal syndrome,10 in-fection11,12 and obstructive uropathy. Hypovolemia-induced renal disease is one of its reversible causes, which if not identified and treated early, can culmi-nate in irreversible conditions like Hepatorenal syn-drome13 or intrinsic renal disease.14 Liver cirrhosis is itself a hypovolemic state. In addition to that, overuse of diuretics, vomiting, diarrhea, and over-
use of lactulose, Upper G.I. Bleed, Fluid / Sodium restriction, Peritoneal Paracentesis and Sepsis fur-ther worsen the Hypovolemia leading to Hypovo-lemia – induced renal disease. METHODOLGY This descriptive case series study was carried out at the Department of Medicine, Gastroenterology and Hepatology, Services hospital, Lahore over a period of one year from December 26, 2006 to December 25, 2007. A convenient sample of One hundred pati-ents of liver cirrhosis having renal impairment with any duration of illness, having age above 15 years and from both sexes were included. On the other hand patients with active upper gastrointestinal

MUHAMMAD IRFAN, MUHAMMAD ARIF NADEEM, HUDA GHULAM MIRZA et al
10 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
bleed and Co-morbid diseases (Respiratory failure, and pulmonary edema) were excluded from the stu-dy. Diagnosis of cirrhosis was made by prior liver biopsy or by combination of clinical and ultrasono-graphic findings, while renal impairment was defi-ned by serum creatinine of 1.5 mg/dl or more. Infor-med consent was obtained from patients recruited and their demographic data was recorded. The clinical as well as laboratory assessment was made. Diuretics were withdrawn in those pati-ents who were taking it. These patients were given 1.5 liter of normal saline intravenously and then serum creatinine was checked again to exclude hy-povolemia as cause of renal dysfunction. Urine was examined for sodium concentration, RBCs per HPF, 24 hours volume and urinary proteins. Blood exa-mination was done for WBC count and serum sodi-um. Ascitic fluid was graded via ultrasound. The co-llected data was entered on SPSS version 15. The descriptive analysis of the collected data was done. Gender, Residential Area, Current diure-tics use, History of diabetes mellitus, grades of asci-tes, Cause of renal impairment and hospitalization end result were the qualitative variables, while age, weight, initial serum creatinine, WBC count, 24 ho-urs urinary proteins, 24 hour urinary volume, urine sodium and serum sodium were quantitative vari-ables. Investigational data was interpreted in nega-tive or positive values. For quantitative variables, means and standard deviations were calculated and for qualitative variables, frequencies and percenta-ges were computed. Chi-square test was applied to find any association of factors at 5% level of signifi-cance. RESULTS One hundred patients of liver cirrhosis having se-rum creatinine more than 1.5 mg/dl were enrolled, 59% were males and 41% females. The mean age (years) of patients was 55.38 ± SD of 13.89, the mean weight (kilograms) was 62.30 ± SD of 7.61, the mean initial serum creatinine (mg/dl) was 2.95 ± SD of 1.64, the mean serum creatinine (mg/dl) after infusion of 1.5 liters of plasma expander was 2.13 ± SD of 1.57, the mean 24 hours urine volume (ml) was 744.54 ± SD of 471.18, the mean urine so-dium (mEq/L) was 58.80 ± SD of 54.32 and the mean serum sodium (mEq/L) was 136.24 ± SD of 5.75 (tables 1, 2). The area of distribution was mai-nly urban (82%) and majority of the patients had history of diuretics use (77%). Eleven patients were diabetic (table 2). A statistically significant decrease in serum cre-atinine was seen after infusing 1.5 litre isotonic Sali-ne solution (p = 0.000), (table 4). The serum creati-nine of 45 patients (45%) came below 1.5 mg/dl that
were labeled as having Hypovolemia-induced renal disease (HIRD) while remaining 55 patients (55%) were labeled as suffering from Non-hypovolemia – induced renal disease (NHIRD).
HIRD was statistically correlated with age of patients, gender, weight, residential area, use of diu-retics, grades of ascites, initial serum creatinine, 24 hours urinary volume, history of diabetes mellitus, 24 hours urinary proteins, urine sodium, urine RBC, serum sodium and end result of hospitalization.
HIRD was seen more in younger patients with age 50 years or below i.e., 57% (24 out of 42), while 64% patients of age more than 50 years (37 out of 58) were suffering from NHIRD. The association was statistically significant (p = 0.044).
HIRD was found more common in patients cur-rently using diuretics i.e., 54% (42 out of 77) had HIRD while among patients currently not using di-uretics, 87% patients (20 out of 23) had NHIRD. Amongst 45 patients of HIRD (93% i.e. 42) were currently using diuretics. The association was also statistically significant (p = 0.001).
The ascitic fluid was graded via ultrasound into 4 categories (No, Mild, Moderate, Severe). Out of 8 patients with no ascites, 75% (6) had HIRD, while 55% patients with mild ascites (11 out of 20), 47.6% with moderate ascites (10 out of 21) and 35.3% with severe ascites (18 out of 51) were also suffering from HIRD. In comparison, only 25% patients with no ascites, 45% with mild ascites, 52.4% with moderate ascites and 64.7% with severe ascites had NHIRD. Thus as the grade of ascites increases, the percenta-ges of patients suffering from HIRD decreases and the association was also statistically significant (p = 0.049).
Abnormal WBC count in our patients favored the possibility of NHIRD. WBC count was found normal in 40 patients (51%) with HIRD and 38 pat-ients (49%) with NHIRD. WBC count was found hi-gh in 5 patients (23%) with HIRD and 38 patients (77%) with NHIRD. The association was statistically significant (p = 0.028).
The initial serum creatinine values were divided in 3 groups (Table 3). Among patients with Initial Serum Creatinine up to twice of upper normal limit
( 1.8 mgdl), 17 patients (77%) had HIRD and 5 patients (23%) had NHIRD. Among patients with Initial Serum Creatinine two to three times of upper normal limit (1.9 – 2.7 mg/dl), 21 patients (55%) had HIRD and 17 patients (45%) had NHIRD. Amo-ng patients with Initial Serum Creatinine more than thrice of upper normal limit (> 2.7 mg/dl), 7 pati-ents (17%) had HIRD and 33 patients (83%) had NHIRD. As the values of Initial Serum Creatinine increases, the possibility for NHIRD also increases and this association was also statistically significant

EFFECT OF 1.5 LITRE INFUSIONS ON SERUM CREATININE AND OTHER FACTORS IN PATIENTS OF CIRRHOSIS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 11
Table 1: Quantitative Factors associated with Hypovolemia – induced Renal Disease (n = 100).
Quantitative Variables Mini-mum
Maxi-mum
Hypovolemia – Induced Renal Disease
Non-Hypovolemia Renal Disease p-
value Mean ± SD Mean ± SD
Age of patients (years) 21 85 51.60 ± 13.83 58.47 ± 13.28 0.013
Weight of patients (Kg) 45 86 61.58 ± 7.85 62.89 ± 7.42 0.393
Initial Serum Creatinine (mg/dl) 1.6 10.5 2.42 ± 1.49 3.39 ± 1.64 0.003
Serum creatinine after infusion of 1.5 L of Plasma expander (mg/dl)
0.5 11.8
WBC count (/mm3) 2100 26200 8006.67 ± 3667.57 10376.55 ± 4515.08 0.006
24 hours urinary Proteins (mg) 42 5619 815.69 ± 973.40 1017.62 ± 1085.32 0.335
24 hours urine volume (ml) 40 2130 888.11 ± 448.76 627.55 ± 467.70 0.006
Urine sodium (mEq/L) 5 254 62.89 ± 61.12 55.46 ± 48.38 0.499
Serum sodium (mEq/L) 112 150 136.51 ± 5.80 136.02 ± 5.76 0.672
Table 2: Qualitative Factors associated with Hypovolemia – induced Renal Disease (n = 100).
Qualitative Variables
Hypovolemia – Induced Renal Disease
(n = 45)
Non-Hypovolemia Renal Disease
(n = 55)
Likelihood Ratio
p-value
Gender:
Male
Female
16 (39%)
29 (50%)
25 (61%)
29 (50%)
1.007 0.414
Age (Years):
50
50
24 (57%)
21 (36%)
18 (43%)
37 (64%)
4.330 0.044
Weight (Kg):
60
> 60
21 (45%)
24 (45%)
26 (55%)
29 (55%)
0.004 1.000
Residential Area:
Rural
Urban
7 (39%)
38 (46%)
11 (61%)
44 (54%)
0.334 0.611
History of Diabetes mellitis:
No
Yes
41 (46%)
4 (36%)
48 (54%)
7 (64%)
0.378 0.750
Current use of Diuretics:
No
Yes
3 (13%)
42 (54%)
20 (87%)
35 (46%)
13.709 0.001
Grades of Ascites:
No
Mild
Moderate
Sever
6 (75%)
11 (55%)
10 (48%)
18 (35%)
2 (25%)
9 (45%)
11 (52%)
33 (65%)
5.817 0.019
WBC count:
Normal
High
40 (51%)
5 (23%)
38 (49%)
17 (77%)
5.966 0.028

MUHAMMAD IRFAN, MUHAMMAD ARIF NADEEM, HUDA GHULAM MIRZA et al
12 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
Table 3: Qualitative Factors associated with Hypovolemia – induced Renal Disease (n = 100).
Qualitative Variables
Hypovolemia – Induced Renal
Disease (n = 45)
Non-Hypovolemia Renal Disease
(n = 55)
Likelihood Ratio
p-value
Initial Serum Creatinine
24.690 0.000
Up to twice of upper normal limit
( 1.8 mg/dl) 17 (77%) 5 (23%)
Twice to thrice of upper normal limit (1.9 – 2.7 mg/dl)
21 (55%) 17 (45%)
More than thrice of upper normal limit (> 2.7 mg/dl)
7 (17%) 33 (83%)
24 Hours Urinary Proteins (mg):
3.107 0.931 Within normal range (< 150 mg) 4 (31%) 9 (69%)
More than normal but less than intrinsic renal disease range (150 – 500 mg)
22 (55%) 18 (45%)
In intrinsic renal disease range (> 500 mg) 19 (40%) 28 (60%)
24 hours Urine Volume:
7.097 0.014 Oliguria (< 500 ml) 12 (29%) 29 (71%)
Normal ( 500 ml) 33(56%) 26 (44%)
Urine Sodium:
0.832 0.386 < 20 mEq/L 11 (38%) 18 (62%)
20 mEq/L 34 (48%) 37 (52%)
Urine RBC Count:
3.627 0.073 No Hematuria (0 – 3 RBCs per HPF) 8 (30%) 19 (70%)
Hematuria (> 3 RBCs per HPF) 37 (51%) 36 (49%)
Serum Sodium:
0.020 1.000 < 130 mEq/L 7 (47%) 8 (53%)
130 mEq/L 38 (45%) 47 (55%)
Hospitalization End Result:
11.486 0.003 Death 0 (0%) 9 (100%)
Discharge 45 (49%) 46 (51%)
Table 4: Correlation between Initial serum creatinine and serum creatinine after infusing 1.5 liter plasma
expander (T-test) (n = 100).
Variables Minimum Maximum Mean ± SD 95% CI
p-value Low Up
Initial serum creatinine (mg/dl) 1.6 10.5
0.8200 ± 1.21 0.58 1.06 0.000 Serum creatinine after infusing 1.5 liter plasma expander (mg/dl)
0.5 11.8

EFFECT OF 1.5 LITRE INFUSIONS ON SERUM CREATININE AND OTHER FACTORS IN PATIENTS OF CIRRHOSIS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 13
Fig. 1: Graph between initial serum creatinine and serum creatinine after infusion of 1.5 L of plasma expander
(p = 0.000).
The association of 24 hours urine volume with HIRD was also statistically significant (p = 0.014). Up to 71% (29 out of 41) oligouric patients belong to NHIRD group while 56% (33 out of 59) patients having normal urine volume lies in HIRD group.
During hospitalization, 9 patients died and all belongs to NHRD group while 100% patients of HI-RD group were discharged. The association was also statistically significant (p = 0.003).
Hence, HIRD was statistically significantly ass-ociated with age of patients (p = 0.013), use of diu-retics (p = 0.001), grades of ascites (p = 0.049), WBCs count (p = 0.028), initial serum creatinine (p = 0.000), 24 hours urinary volume (p = 0.014) and end result of hospitalization (p = 0.003). How-ever there was no statistically significant association with gender (p = 0.317), weight (p = 0.952), resi-dential area (p = 0.565), history of diabetes mellitus (p = 0.542), 24 hours urinary proteins (p = 0.335), urine sodium (p = 0.499), urine RBC (p = 0.060) and serum sodium (p = 0.672), (tables 1, 2).
DISCUSSION In the present study, amongst the 8 patients with-out ascites, 6 patients (75%) had suffered hypovole-mia – induced renal disease (HIRD), while 55% pat-ients with mild, 47.6% with moderate and 35.3% with severe ascites had had it. Why more number of patients without ascites or mild ascites was hypovo-lemic, could be explained on the basis of overdiure-sis as 6 patients with no ascites and 13 patients with mild ascites were using diuretics. In 2001, a similar
study at Civil Hospital, Karachi, found hypovolemia induced renal disease only in 7.89% cirrhotic pati-ents.15 While Thabut and his colleagues found it in 34% patients when they classified the causes of re-nal failure among patients of Liver cirrhosis.16
Our patients currently on diuretics had statisti-cally significant HIRD (p = 0.001), strengthening the possible explanation of over – diuresis as the cause of the problem and making a pool of patients with HIRD leading to acute tubular necrosis (ATN), Intrinsic renal disease and Hepatorenal syndrome. Physicians should cautiously use diuretics especially if ascites is absent or mild. If it is necessary, then serial serum creatinine values should be monitored.
HIRD was statistically significantly associated with initial serum creatinine (p = 0.003), and was more common in patients with mild fluctuation in serum creatinine. As serum creatinine was increa-sed, possibility of hypovolemia – induced renal dis-ease was also decreased. It further strengthened our observation that serial monitoring of serum creati-nine is necessary in cirrhotic patients and if serum creatinine rises, then physicians should urgently re-evaluate their maneuvers making patient hypovo-lemic like overdiuresis and fluid restriction in an attempt to manage ascites and over-judicious use of lactulose in cirrhosis related gut care.
Association of 24 hours urine volume with HI-RD was also statistically significant (p = 0.014). Up to 71% (29 out of 41) oligouric patients belongs to non-hypovolemia renal disease group while 56% (33 out of 59) patients having normal urine volume lies in hypovolemia – induced renal disease group. This may be due to the fact that 24 hours urine collection was done after giving 1.5 liter plasma expander to all patients. Hence in hypovolemia-induced renal dise-ase patients not only serum creatinine be corrected but also urinary output became significantly adequ-ate. So infusion of 1.5 liter plasma expander in pati-ents of liver cirrhosis having renal impairment has a lot of significance.
During hospitalization, 9 patients died and all belongs to NHRD group while 100% patients of HI-RD group were discharged. The association was also statistically significant (p = 0.003) suggesting that HIRD is so benign that no death occurred in this group if managed timely.
In our study, hypovolemia – induced renal dise-ase was seen more in younger patients and associ-ation was statistically significant (p = 0.044). It mi-ght be due to more aggressive management of asci-tes with diuretics. Perhaps this younger age group was more concerned with ascitic fluid mobilization for cosmetic reason. Further studies may validate it more.

MUHAMMAD IRFAN, MUHAMMAD ARIF NADEEM, HUDA GHULAM MIRZA et al
14 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
CONCLUSION This study ascents the piece of information about 45% patients who had suffered from reversible hy-povolemia. If these patients are not properly trea-ted, could develop more complicated and irreversi-ble conditions like hepatorenal syndrome and intri-nsic renal disease, etc. Therefore, it is recommended that the clinicians should monitor their serum crea-tinine level more frequently and if increasing trend detected, then they should re-evaluate their therapy to avoid hypovolemia like over-diuresis and strict fluid restriction in an attempt to manage the ascites. Hence 1.5 Litre plasma expander has a significant role if renal impairment is found in liver cirrhotic patients. REFERENCES 1. Lawrence S, Friedman. Liver, biliary tract and pan-
creas. In: Lawrence M. Tierney, Stephen J, editors. Current medical diagnosis and treatment. 47th Ed. New York: Mc Graw-Hill; 2008: 584-6.
2. Khokhar N, Gill M, Malik G. General seroprevalence of hepatitis C and hepatitis B virus Infections in pop-ulation. J Coll Physicians Surg Pak 2004; 14: 534-6.
3. Gines P, Robert W, Schrier. Renal Failure in Cirrho-sis. N Engl J Med 2009; 361: 1279-90.
4. Hampel H, Bynum GD, Zamora E, El-Serag HB. Risk factors for the development of renal dysfunction in hospitalized patients with cirrhosis. Am J Gastroen-terol 2001; 96: 2206-10.
5. Meyers CM, Seeff LB, Stehman – Breen CO, Hoofna-gle JH. Hepatitis C and renal disease: an update. Am J Kidney Dis 2003; 42: 631-57.
6. Poole BD, Schrier RW. Glomerular disease in cirrho-sis. In: Ginès P, Arroyo V, Rodés J, Schrier RW, eds. Ascites and renal dysfunction in liver disease. 2nd ed.
Malden, MA: Blackwell, 2005: 360-71. 7. Salerno F, Badalamenti S. Drug induced renal failure
in cirrhosis. In: Ginès P, Arroyo V, Rodés J, Schrier RW, eds. Ascites and renal dysfunction in liver dis-ease. 2nd ed. Malden, MA: Blackwell, 2005: 372-82.
8. Ginès P, Cárdenas A, Schrier RW. Liver disease and the kidney. In: Schrier RW, ed. Diseases of the kidney and urinary tract. 8th ed. Philadelphia: Lippincott Williams and Wilkins, 2007: 2179-205.
9. McCullough PA. Contrast – induced acute kidney in-jury. J Am Coll Cardiol 2008; 51: 1419-28. (Erratum, J Am Coll Cardiol 2008; 51: 2197).
10. Salerno F, Gerbes A, Ginès P, Wong F, Arroyo V. Dia-gnosis, prevention and treatment of hepatorenal syn-drome in cirrhosis. Gut 2007; 56: 1310-8.
11. Fasolato S, Angeli P, Dallagnase L, et al. Renal failure and bacterial infections in patients with cirrhosis: epidemiology and clinical features. Hepatology 2007; 45: 223-9.
12. Tandon P, Garcia-Tsao G. Bacterial infections, sepsis, and multiorgan failure in cirrhosis. Semin Liver Dis 2008; 28: 26-42.
13. Kumar R, Ahmad R, Rath S, Sethar G. Frequency of Hepatorenal Syndrome among cirrhotics.J Coll Phy-sicians Surg Pak2005; 15: 590-3.
14. Wu, CC, Yeung, LK, Tsai, WS, et al. Incidence and factors predictive of acute renal failure in patients with advanced liver cirrhosis. Clin Nephrol 2006; 65: 28.
15. Kumar R, Ahmad R, Rath S, Sethar G. Frequency of Hepatorenal Syndrome among cirrhotics.J Coll Phy-sicians Surg Pak 2005; 15: 590-3.
16. Thabut D, Massard J, Gangloff A, et al. Model for End – Stage Liver Disease score and systemic inflam-matory response are major prognostic factors in pati-ents with cirrhosis and acute functional renal failure. Hepatology 2007; 46: 1872-82.

Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 15
ORIGINAL ARTICLE
EFFECT OF DIABETES MELLITUS (DM) ON THE EFFICACY OF STANDARD INTERFERON (SdIF) PLUS RIBAVIRIN COMBINATION THERAPY IN PATIENTS OF CHRONIC HEPATITIS C VIRUS (HCV) GENOTYPE – 3
MASROOR ALI QAZI,1 AHTISHAM ALI KHAN,1 SYED HASHIM RAZA1
ALI IMRAN,1 SABA QAZI,1 GHULAM MUHY-UD-DIN2 1Department of Medicine, Quaid-e-Azam Medical College/Bahawal Victoria Hospital, Bahawalpur
2Nishtar Medical College / Nishter Hospital, Multan
BACKGROUND Hepatitis C virus (HCV) infection is very common worldwide as well as in Pakistan. HCV is a major cause of chronic liver disease, cirrhosis, hepatocel-lular carcinoma. The estimated prevalence of HCV in world is 150 million whereas 3 – 4 million people get infected with HCV each year.1 Chronic hepatitis C develops in about 85% cases of acute hepatitis C.2 The estimated prevalence of HCV infection in Pakis-tan is around 5% – 6%, equating to about 9 – 11 mil-lion HCV infected cases.3,4 HCV has 6 genotypes worldwide named.1-6 Genotype 1 is probably the most common genotype world – wide however dif-ferent geographical regions have different predomi-nant genotypes. For example genotype 1 is the pre-dominant genotype in North and South America, Australia and Europe, genotype 4 is predominant genotype in Middle East, Genotype 5 in South Africa and genotype 3 is the predominant genotype in Pak-istan, India and Bangladesh.5 Relationship between diabetes mellitus (DM) and hepatitis C (HCV) infec-tion is very complex. HCV infection is more com-mon among diabetics compared to general popula-tion.6 Whether HCV infection leads to the develop-ment of DM or DM itself predisposes to the HCV in-fection yet needs to be determined.6 HCV and DM are independent risk factors of hepatocellular carci-noma. Presence of both increases the risk by several folds.7,8 HCV infected patients who also has DM has accelerated liver disease and progression to cirrho-sis compared to non-diabetics.7 HCV infection is treated with combination therapy of Interferon and ribavirin. However treatment schedule, disease cha-racteristics and several host and viral factors influ-ence treatment outcome in this patient population. Host factors adversely influencing treatment out-come include age more than 40 years, male gender, obesity, insulin resistance, ethnicity, TT genotype of Interleukin 28 B gene on chromosome 19, difference in T-cell response, normal alanine amino transfe-rase (ALT) level and presence of bridging fibrosis or
cirrhosis on liver histology.9 Viral factors associated with poor treatment outcome include high base line viral load and genotype 1 and 4. Baseline viral load and genotype are the strongest factors influencing outcome.9 Available evidence suggests that it is a potential host risk factor that may reduce the effi-cacy of interferon and ribavirin combination thera-py in HCV infected patients.10,11 So we performed this prospective study to find out that does diabetes has an influence on treatment outcome of hepatitis C infected patients treated with standard interferon (SdIF) and ribavirin as very little local data is avai-lable. We use SdIF because in our country especially in government hospitals standard interferon is still commonly being used because of its low price. MATERIALS AND METHODS: This was a prospective interventional / experimen-tal study conducted at Bahawal Victoria Hospital (BVH), Bahawalpur, Pakistan, from 30 May 2006 to 30 June 2008. All the patients coming to medical OPD for the treatment of hepatitis C were evaluated. Each patient was subjected to complete history and physical examination along with USG of abdomen and laboratory tests including anti HCV antibodyby ELISA, PCR for HCV RNA both qualitative and gen-otype determination, liver function tests, Complete blood counts, renal function tests, serum albumin, PT, INR, APTT, ANA and HBs Ag. The patients we-re then screened with following inclusion and ex-clusion criteria.
Inclusion Criteria
Patient with positive result of Qualitative PCR for HCV RNA.
Patient positive for genotype 3.
Exclusion Criteria
Age > 65 years.
Prior or current treatment of HCV infection with any interferon.
MASROOR ALI QAZI, AHTISHAM ALI KHAN, SYED HASHIM RAZA et al
16 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
Patients co-infected with other genotypes of HCV.
Current pregnancy or breast feeding.
Patient positive for HBs Ag.
Patient with advanced fibrosis as assessed with USG abdomen showing shrunken liver / irregu-lar margins.
Patient with decompensated cirrhosis.
Patient with other liver diseases such as Wil-son’s disease, autoimmune hepatitis, alcoholic liver disease, primary biliary cirrhosis, scleros-ing cholangitis, alpha one antitrypsin deficiency and hemochromatosis.
Thrombocytopenia (Platelet count < 50,000 / mm3).
Patients with neutropenia (Absolute neutrophil count < 750 cells / ml)
Serum creatinine more than 1.5 times the upper limit of normal value.
Current Intravenous drug abuse.
Sever cardiac, pulmonary, retinal, thyroid and psychiatric disease.
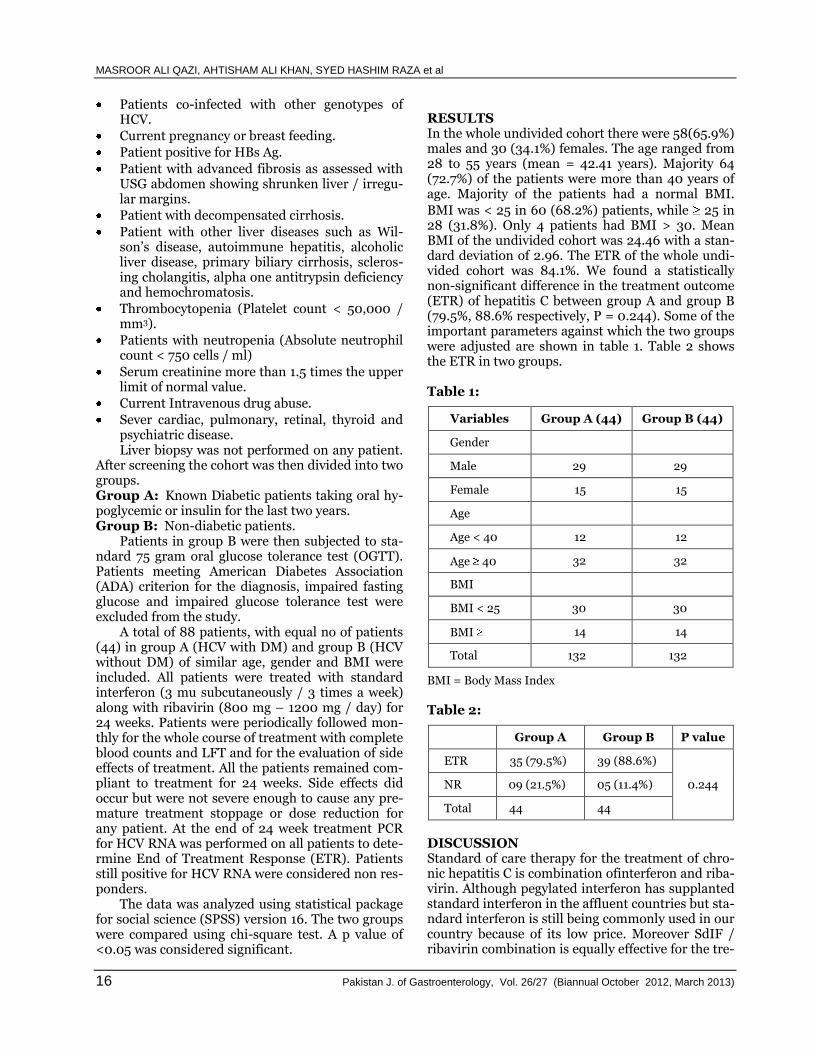
Liver biopsy was not performed on any patient. After screening the cohort was then divided into two groups. Group A: Known Diabetic patients taking oral hy-poglycemic or insulin for the last two years. Group B: Non-diabetic patients. Patients in group B were then subjected to sta-ndard 75 gram oral glucose tolerance test (OGTT). Patients meeting American Diabetes Association (ADA) criterion for the diagnosis, impaired fasting glucose and impaired glucose tolerance test were excluded from the study. A total of 88 patients, with equal no of patients (44) in group A (HCV with DM) and group B (HCV without DM) of similar age, gender and BMI were included. All patients were treated with standard interferon (3 mu subcutaneously / 3 times a week) along with ribavirin (800 mg – 1200 mg / day) for 24 weeks. Patients were periodically followed mon-thly for the whole course of treatment with complete blood counts and LFT and for the evaluation of side effects of treatment. All the patients remained com-pliant to treatment for 24 weeks. Side effects did occur but were not severe enough to cause any pre-mature treatment stoppage or dose reduction for any patient. At the end of 24 week treatment PCR for HCV RNA was performed on all patients to dete-rmine End of Treatment Response (ETR). Patients still positive for HCV RNA were considered non res-ponders. The data was analyzed using statistical package for social science (SPSS) version 16. The two groups were compared using chi-square test. A p value of <0.05 was considered significant.
RESULTS In the whole undivided cohort there were 58(65.9%) males and 30 (34.1%) females. The age ranged from 28 to 55 years (mean = 42.41 years). Majority 64 (72.7%) of the patients were more than 40 years of age. Majority of the patients had a normal BMI.
BMI was < 25 in 60 (68.2%) patients, while 25 in 28 (31.8%). Only 4 patients had BMI > 30. Mean BMI of the undivided cohort was 24.46 with a stan-dard deviation of 2.96. The ETR of the whole undi-vided cohort was 84.1%. We found a statistically non-significant difference in the treatment outcome (ETR) of hepatitis C between group A and group B (79.5%, 88.6% respectively, P = 0.244). Some of the important parameters against which the two groups were adjusted are shown in table 1. Table 2 shows the ETR in two groups. Table 1:
Variables Group A (44) Group B (44)
Gender
Male 29 29
Female 15 15
Age
Age < 40 12 12
Age 40 32 32
BMI
BMI < 25 30 30
BMI 14 14
Total 132 132
BMI = Body Mass Index
Table 2:
Group A Group B P value
ETR 35 (79.5%) 39 (88.6%)
0.244 NR 09 (21.5%) 05 (11.4%)
Total 44 44
DISCUSSION Standard of care therapy for the treatment of chro-nic hepatitis C is combination ofinterferon and riba-virin. Although pegylated interferon has supplanted standard interferon in the affluent countries but sta-ndard interferon is still being commonly used in our country because of its low price. Moreover SdIF / ribavirin combination is equally effective for the tre-

EFFECT OF DIABETES MELLITUS (DM) ON THE EFFICACY OF STANDARD INTERFERON (SdIF) PLUS RIBAVIRIN
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 17
atment of HCV genotype 3, the predominant geno-type in our country, compared to pegylated interfe-ron / ribavirin combination.12 The ETR for the who-le cohort is 84.1%. This result is comparable to other locally performed studies.13,14 Male gender also tur-ns out to be a bad prognostic factor in terms of tre-atment response. Out of 58, 14 (24.1%) males did not responded to treatment whereas 100% (n = 30) females achieved ETR. Many studies reported that patient with type 2 diabetes are less likely to achieve sustained virologic response (SVR) compared to non-diabetics. Moreover patient with type 2 diabe-tes are more likely to experience adverse effects of therapy than non-diabetics.10 However in this study we have found a statistically non-significant diffe-rence in ETR of diabetics compared to non-diabetics for the treatment of HCV genotype 3. El-Shazly et al also found similar result for genotype 4.15 The rea-son for this different result is multifactorial and pro-bably lies in ethnicity, a careful selection and adjus-tment of patients against important variables, num-ber of patients included, BMI, concomitant alcohol consumption, non-alcoholic fatty liver disease (NA-FLD), co morbidities, different grades of hepatic in-flammation and stages of liver fibrosis and HCV genotype. Majority of our patients in either group had a normal BMI, were non-alcoholic, had fewer co morbidities and no patient had advanced liver dise-ase. This signifies that host factors are also very im-portant in addition to viral factors in terms of treat-ment outcome of HCV infected patients. However, diabetes and HCV infection is an omi-nous association. Insulin resistance induces hepatic steatosis and hepatic steatosis is associated with more severe fibrosis in chronic HCV.16 HCV itself in-duces insulin resistance and also impairs the lipid oxidation as well as export of lipids as very low den-sity lipoproteins (VLDL) causing lipid accumulation in hepatocytes and leading to hepaticsteatosis.17,18 Steatosis is present in 73% of type 3 genotype and 50 % of type 1 genotype HCV infected patients.19 Hyper-insulinemia in type 2 diabetics causes exces-sive activation of hepatic stellate cells which leads to increase liver fibrosis.20 Hyperglycemia itself leads to increased hepatic fibrosis in HCV infected indivi-duals.36 Histologically the pattern of fibrosis (sub-sinusoidal and around the central vein) in chronic HCV infection is similar to seen in NAFLD suggest-ing that both may share some common mechani-sms.21 NAFLD is now considered the hepatic mani-festation of metabolic syndrome and is probably responsible for the diabetes associated liver cell injury. So both the diabetes and HCV cause hepatic injury (by some independent and some shared me-chanisms) and when present in the same individual lead to worsening of liver disease. Clinically this tra-nslates into worsening outcomes in HCV infected
patients who also has DM. For example diabetics with HCV infection have accelerated liver fibrosis. Moreover diabetics are at increased risk of hepato-cellular carcinoma and presence of HCV infection increases this risk by several folds.19,20 So every pat-ient with insulin resistance and chronic hepatitis C infection should strongly be advised to undergo an-tiviral therapy as early as possible provided they ful-fill the criteria for therapy.
In this study we had a relatively small sample size that might have reduce the statistical power to evaluate a difference in ETR rates of HCV genotype 3 infected patients with and without diabetes. How-ever it encourages appropriately designed larger scales studies for further evaluation of these results.
REFERENCES 1. http://www.who.int/mediacentre/factsheets/fs164/e
n/index.html 2. Lawrence S. Friedman. Current Medical Diagnosis
and Treatment. 51st Edition. Page 658. 3. Yasir Waheed, Talha Shafi, Sher Zaman Safi, Ishtiaq
Qadri. Hepatitis C virus in Pakistan: A systematic re-view of prevalence, genotypes and risk factors.World J Gastroenterol 2009 December 7; 15 (45): 5647-5653.
4. Pakistan Medical Research Council. National Survey on Prevalence of Hepatitis B & C in General Popula-tion of Pakistan. Information at: http://www.pmrc.org.pk/hepatitisbc.htm.
5. http://www.who.int/vaccine_research/diseases/viral_cancers/en/index2.html.
6. Naing C, Mak JW, Ahmed SI, Maung M. Relationship between hepatitis C virus infection and type 2 diabe-tes mellitus: Meta-analysis. World J Gastroenterol. 2012 Apr 14; 18 (14): 1642-51.
7. El-Serag HB, Tran T, Everhart JE. Diabetes increases the risk of chronic liver disease and hepatocellular carcinoma. Gastroenterology. 2004; 126: 460-468.
8. Hassan MM, Hwang LY et al. Risk factors for hepato-cellular carcinoma: synergism of alcohol with viral hepatitis and diabetes mellitus. Hepatology 2002; 36: 1206-1213.
9. Ghany MG, Strader DB, Thomas DL, Seeff LB. Diag-nosis, management, and treatment of hepatitis C: an update. American Association for the Study of Liver Diseases.Hepatology. 2009 Apr; 49 (4): 1335-74. doi: 10.1002/hep.22759.
10. Elgouhari HM, Zein CO, Hanouneh I, Feldstein AE, Zein NN. Diabetes mellitus is associated with impai-red response to antiviral therapy in chronic hepatitis C infection. Dig Dis Sci. 2009 Dec; 54 (12): 2699-705. doi: 10.1007/s10620-008-0683-2.
11. Konishi I, Horiike N, Hiasa Y, Tokumoto Y, Mashiba T, Michitaka K., et al. Diabetes mellitus reduces the therapeutic effectiveness of interferon – α2b plus ri-bavirin therapy in patients with chronic hepatitis C. Hepatology Research 2007; 37: 331–336.
12. Manns MP et al. Peginterferon alfa – 2b plus ribavirin compared with interferon alfa – 2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised
http://www.ncbi.nlm.nih.gov/pubmed?term=Elgouhari%20HM%5BAuthor%5D&cauthor=true&cauthor_uid=19148751

MASROOR ALI QAZI, AHTISHAM ALI KHAN, SYED HASHIM RAZA et al
18 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
trial. Lancet. 2001 Sep 22; 358 (9286): 958-65. 13. Jadoon SM, Jadoon S, Muhammad I.Response to sta-
ndard interferon A2b and ribavirin combination the-rapy in chronic hepatitis C treatment naive patients. J Ayub Med Coll Abbottabad. 2010 Oct – Dec; 22 (4): 164-6.
14. Nadeem A et al. Association of response to combined interferon alpha – 2b and ribavirin therapy in pati-ents of chronic hepatitis c with serum alanine amino-transferase levels and severity of the disease on liver biopsy. J Ayub Med Coll Abbottabad. 2009 Apr – Jun; 21 (2): 103-6.
15. Y. El – Shazly, M. Rafeek, R. Al-Swaff. Effect of well controlled diabetes mellitus on sustained virologic response in chronic HCV genotype 4 infected pati-ents. Journal of Diabetology, June 2012; 2: 3.
16. Hourigan LF, Macdonald GA, Purdie D, et al. Fibrosis in chronic hepatitis C correlates significantly with bo-dy mass index and steatosis. Hepatology 1999; 29: 1215-1219.
17. Alberstein M, Zornitzki T, Zick Y, Knobler H. Hepati-
tis C core protein impairs insulin downstream signal-ling and regulatory role of IGFBP1 expression. J Viral Hepat. 2012 Jan; 19 (1): 65-71. doi: 10.1111/j.1365-2893.2011.01447.x. Epub 2011 May 9.
18. Perlemuter G, Sabile A, Letteron P et al. Hepatitis C virus core protein inhibits microsomal triglyceride transfer protein activity and very low density lipopro-tein secretion: a model of viral-related steatosis. Fa-seb J 2002; 16: 185–94.
19. Asselah T, Rubbia – Brandt L, Marcellin P, Negro F. Steatosis in chronic hepatitis C: why does it really matter? Gut 2006; 55: 123e30.
20. Paradis V, Perlemuter G, Bonvoust F et al. High glu-cose and hyperinsulinemia stimulate connective tis-sue growth factor expression: a potential mechanism involved in progression to fibrosis in nonalcoholic steatohepatitis. Hepatology 2001; 34: 738–44.
21. Clouston AD, Jonsson JR, Purdie DM et al. Steatosis and chronic hepatitis C: analysis of fibrosis and stel-late cell activation. J Hepatol 2001; 34: 314–20.

Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 19
ORIGINAL ARTICLE
SAAG RATIO AS PREDICTOR OF ESOPHAGEAL VARICES IN PATIENTS WITH CIRRHOSIS AND ASCITES
MOMIN ALI, ZAFAR NIAZ, SAJID ABAIDULLAH
Department of Medicine, King Edward Medical University / Mayo Hospital, Lahore
ABSTRACT Introduction: Cirrhosis is a pathological entity that has cardinal features reflecting irreversible chronic injury to the hepatic parenchyma that results in extensive fibrosis in association with the formation of regenerative nodule. The most common causes of cirrhosis are chronic hepatitis C, B and chronic alcohol abuse.
Objective: Identify Serum Ascitic Albumin Gradient level of 1.1 g/dl or more as a predictor of oesophageal varices in patients with cirrhosis and ascites.
Study Design: Descriptive cross sectional study.
Setting: Mayo Hospital Lahore.
Duration with Dates: One year it’s mean from March 1, 2008 to February 28, 2009.
Methods: One hundred patients with liver cirrhosis and ascites were selected for this study. In-formed consent was obtained. All patients were interviewed and subjected to clinical examination, laboratory investigations, ultrasonography, ascitic tap and upper GI endoscopy.
Results: The mean value of serum albumin was 3.1 ± 0.66 gm/dl, serum prothrombin time was 21.9 ± 06.47 seconds and bilirubin was 1.99 ± 0.95 mg/dl. The mean value of SAAG ratio was 1.82
± 0.38 gm/dl. Out of hundred patients 81 (81%) had SAAG ratio 1.1 gm/dl while 19 (19%) patients had SAAG ratio < 1.1 gm/dl.On distribution of esophageal varices, there were 58 (58%) patients out of 82 patients with high SAAG had oesophageal varices while none out of 19 with low SAAG had varices. The sensitivity was 76%, sensitivity was 82%, positive predictive value 80.85%, nega-tive predictive value 77.3% and accuracy was 79.0%.
Conclusions: SAAG ratio is an important and an independent parameter associated with the presence of esophageal varices.
Key Words: Esophageal varices, liver cirrhosis, SAAG (serum ascites albumin gradient) ratio. INTRODUCTION Liver cirrhosis is prevalent world-over especially in Pakistan mainly due to chronic viral hepatitis.1 Por-tal hypertension is one of the major complications of liver cirrhosis leading to development of oeso-phageal varices (OV) and ascites.2 As high as 90% of the cirrhotic patients with portal hypertension can develop OV sometime in their life and up to 10% mortality occurs from first bleeding episode.3 Due to the ensuing life threatening complications, iden-tifying OV is an essential part of diagnostic as well as prognostic work up of patients with cirrhosis4 and this is done via upper GI endoscopy.5 However endoscopy is not much cost effective for OV screen-ing and being an invasive procedure it has its own risks.6 Also there has been an ever increasing work-load in our endoscopy units for variceal screening.
Many researchers have identified certain para-meters that can non invasively diagnose OV.7,8 Re-cently researchers have found that the difference of serum and ascites albumin levels, Serum Ascites Albumin Gradient (SAAG) is an important indicator of portal hypertension in patients with cirrhosis.9
Some researchers have also observed that SAAG levels equal to more than 1.1 g/dl indicated presence of portal hypertension10. The prevalence of oeso-phageal varices in cirrhosis is from 50% to 61%.11,12 In Pakistan prevalence of oesophageal varices is 65% and that of large varices is 15% in cirrhotic pat-ients.8 Several non invasive predictors of oesopha-geal varices have been proven to be helpful and effe-ctive in avoiding the too much burden on endo-scopic units. These include Platelet count to splenic size ratio, Serum albumin, Splenic index, Portal pre-
MOMIN ALI, ZAFAR NIAZ, SAJID ABAIDULLAH
20 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
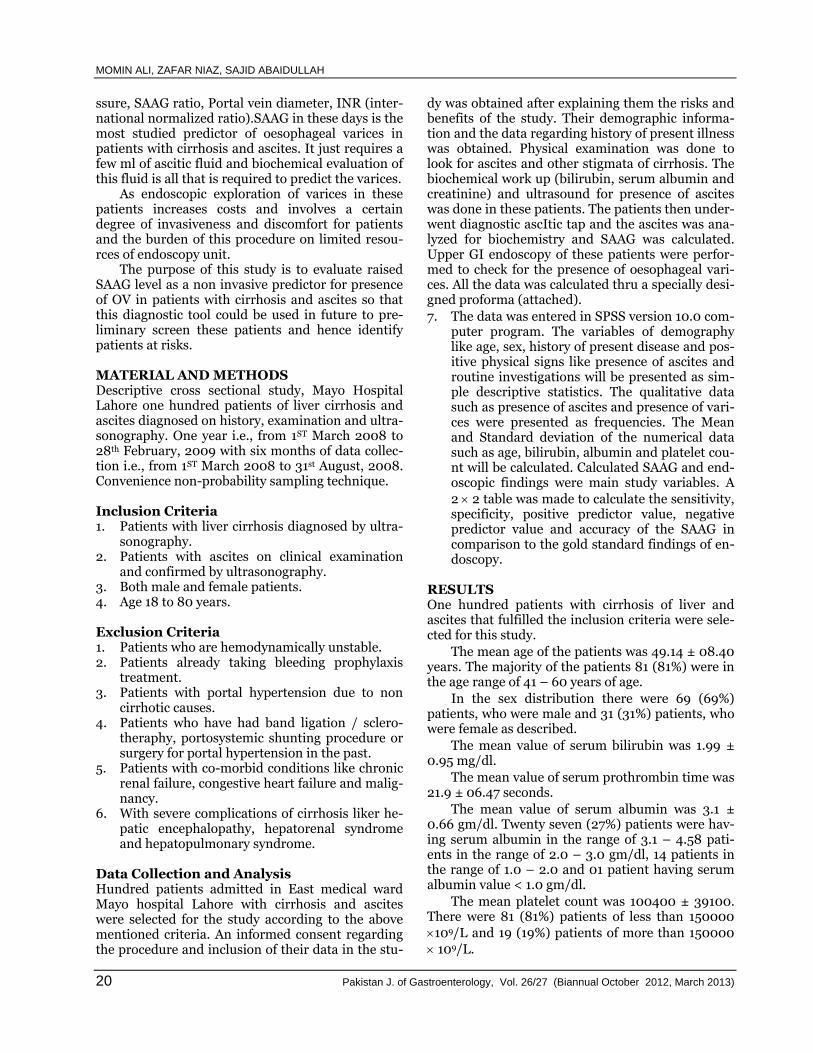
ssure, SAAG ratio, Portal vein diameter, INR (inter-national normalized ratio).SAAG in these days is the most studied predictor of oesophageal varices in patients with cirrhosis and ascites. It just requires a few ml of ascitic fluid and biochemical evaluation of this fluid is all that is required to predict the varices. As endoscopic exploration of varices in these patients increases costs and involves a certain degree of invasiveness and discomfort for patients and the burden of this procedure on limited resou-rces of endoscopy unit. The purpose of this study is to evaluate raised SAAG level as a non invasive predictor for presence of OV in patients with cirrhosis and ascites so that this diagnostic tool could be used in future to pre-liminary screen these patients and hence identify patients at risks. MATERIAL AND METHODS Descriptive cross sectional study, Mayo Hospital Lahore one hundred patients of liver cirrhosis and ascites diagnosed on history, examination and ultra-sonography. One year i.e., from 1ST March 2008 to 28th February, 2009 with six months of data collec-tion i.e., from 1ST March 2008 to 31st August, 2008. Convenience non-probability sampling technique. Inclusion Criteria 1. Patients with liver cirrhosis diagnosed by ultra-
sonography. 2. Patients with ascites on clinical examination
and confirmed by ultrasonography. 3. Both male and female patients. 4. Age 18 to 80 years. Exclusion Criteria 1. Patients who are hemodynamically unstable. 2. Patients already taking bleeding prophylaxis
treatment. 3. Patients with portal hypertension due to non
cirrhotic causes. 4. Patients who have had band ligation / sclero-
theraphy, portosystemic shunting procedure or surgery for portal hypertension in the past.
5. Patients with co-morbid conditions like chronic renal failure, congestive heart failure and malig-nancy.
6. With severe complications of cirrhosis liker he-patic encephalopathy, hepatorenal syndrome and hepatopulmonary syndrome.
Data Collection and Analysis Hundred patients admitted in East medical ward Mayo hospital Lahore with cirrhosis and ascites were selected for the study according to the above mentioned criteria. An informed consent regarding the procedure and inclusion of their data in the stu-
dy was obtained after explaining them the risks and benefits of the study. Their demographic informa-tion and the data regarding history of present illness was obtained. Physical examination was done to look for ascites and other stigmata of cirrhosis. The biochemical work up (bilirubin, serum albumin and creatinine) and ultrasound for presence of ascites was done in these patients. The patients then under-went diagnostic ascItic tap and the ascites was ana-lyzed for biochemistry and SAAG was calculated. Upper GI endoscopy of these patients were perfor-med to check for the presence of oesophageal vari-ces. All the data was calculated thru a specially desi-gned proforma (attached).
7. The data was entered in SPSS version 10.0 com-puter program. The variables of demography like age, sex, history of present disease and pos-itive physical signs like presence of ascites and routine investigations will be presented as sim-ple descriptive statistics. The qualitative data such as presence of ascites and presence of vari-ces were presented as frequencies. The Mean and Standard deviation of the numerical data such as age, bilirubin, albumin and platelet cou-nt will be calculated. Calculated SAAG and end-oscopic findings were main study variables. A
2 2 table was made to calculate the sensitivity, specificity, positive predictor value, negative predictor value and accuracy of the SAAG in comparison to the gold standard findings of en-doscopy.
RESULTS One hundred patients with cirrhosis of liver and ascites that fulfilled the inclusion criteria were sele-cted for this study.
The mean age of the patients was 49.14 ± 08.40 years. The majority of the patients 81 (81%) were in the age range of 41 – 60 years of age.
In the sex distribution there were 69 (69%) patients, who were male and 31 (31%) patients, who were female as described.
The mean value of serum bilirubin was 1.99 ± 0.95 mg/dl.
The mean value of serum prothrombin time was 21.9 ± 06.47 seconds.
The mean value of serum albumin was 3.1 ± 0.66 gm/dl. Twenty seven (27%) patients were hav-ing serum albumin in the range of 3.1 – 4.58 pati-ents in the range of 2.0 – 3.0 gm/dl, 14 patients in the range of 1.0 – 2.0 and 01 patient having serum albumin value < 1.0 gm/dl.
The mean platelet count was 100400 ± 39100. There were 81 (81%) patients of less than 150000
109/L and 19 (19%) patients of more than 150000
109/L.

SAAG RATIO AS PREDICTOR OF ESOPHAGEAL VARICES IN PATIENTS WITH CIRRHOSIS AND ASCITES
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 21
The mean value of SAAG ratio was 1.82 ± 0.38 gm/dl. Out of hundred patients 81(81%) had SAAG
ratio 1.1 gm/dl while 19 (19%) patients had SAAG ratio < 1.1 gm/dl (Table 1). Table 1: Distribution of patients by SAAG ratio (n = 100).
SAAG Ratio No. Percentage
< 1.1 18 18.0%
> 1.1 82 82.0%
Total 100 100.0%
Mean ± SD 1.82 ± 0.38
Key: SD: Standard deviation
On distribution of esophageal varices, 58 (58%)
patients out of 82 patients with high SAAG ( 1.1 g/dl) had oesophageal varices while none out of 19 with low SAAG (< 1.1 g/dl) had varices (Table 2). The sensitivity was 76%, specificity was 82%, positive predictive value 80.85%, negative predic-tive value 77.3% and accuracy was 79.0% (Table 4 and 5).
Table 2: Distribution of patients by Endoscopic findings (n = 100).
Varices No. Percentage
Present 58 58.0%
Absent 42 42.0%
Total 100 100.0%
Key: SD: Standard deviation
Table 3: Comparison of Esophageal varices ver-
sus SAAG ratio (n = 100).
Endoscopy (Gold Standard)
Total Positive Negative
Positive 76 (TP) 18(FP) 94
Negative 24 (FN) 82(TN) 106
Total 100 100 200
Key:
TP = True positive, FP = False positive
FN = False negative, TN = True negative
DISCUSSION In Pakistan chronic liver disease is a common disorder. With increasing incidence and high prevalence of hepatitis B and C, more and more people are being affected by chronic liver disease.13 There is a high prevalence of HCV in Pakistan.14 As a result of, a large pool of patients have develo-ped chronic liver disease and this number continues to grow further. Patients with chronic liver disease over the years develop portal hyper-tension and its associated complica-tions like esophageal varices, which not only affects the quality of life but may also lead to life threatening episodes of upper gastrointestinal bleedig.15-17 Severe upper gastrointestinal bleeding, as a complication of portal
SCREENING TESTS Table 4: Sensitivity, Specificity and Accuracy of Esophageal Vari-
ces.
Sensitivity rate = True Positive
100 True Positive + False Negative
= 76
100 = 76% 76 + 24
Specificity rate = True Negative
100 True Negative + False Positive
= 82
100 = 82% 82 + 18
Diagnostic Accuracy
=
True Positive + True Negative
100 True Positive + True Negative
False Positive + False Negative
= 76 + 82
100 = 79.0% 76 + 82 + 18 + 24
hypertension develops in about 30 – 40% of cirrho-tics. Despite significant improvement in the early diagnosis and treatment of oesophagogastric vari-ceal hemorrhage, the mortality rate of first variceal hemorrhage remains high (20% to 35%).18 Mortality resulting from variceal bleed can be minimized with effective pharmacological therapies and timely intervention. However, with limited acc-
ess to upper GI endoscopy for screening, there is a need to define a non-invasive parameter that can predict the presence or absence of esophageal vari-ces. To date several studies have been conducted outside Pakistan concerning the non-invasive diag-nosis of the presence of esophageal varices in pati-ents with liver cirrhosis19 and SAAG has been one of

MOMIN ALI, ZAFAR NIAZ, SAJID ABAIDULLAH
22 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
the recently studied parameter that has shown its worth in prediction of varices. This study was conducted to see whether the same is true for Pa-kistan.
The mean value of serum albu-min in our study was 3.1±0.66 gm/dl while in Demirel U et al9 the mean value of serum albumin was 2.53 ± 0.53 which is comparable with our results.
The mean value of SAAG was 1.82 ± 0.38 gm/dl. Out of hundred
patients 81(81%) had SAAG ratio
Table 5: Positive and Negative Predictive value of Esophageal Varices.
Positive Test = Predictive value of True Positive
100 True Positive + False Positive
= 76
100 = 80.85% 76 + 18
Negative Test = Predictive value of True Negative
100 True Negative + False Negative
= 82
100 = 77.3% 82 + 24
1.1 gm/dl while 19 (19%) patients had SAAG ratio < 1.1 gm/dl while in Demirel1 U et al9 the mean value of SAAG was 2.1 ± 0.51.4 patients had SAAG between 1.1 and 1.49. 15 patients with SAAG values between 1.5 and 1.99 and 16 patients with SAAG greater than 2.0. In another study Gurubacharya DL et al20 out of 32 patients 25 had SAAG greater than 1.1 g/dl while 7 had SAAG less than 1.1 g/dl. In study of Torres E et al21 out of 31 patients 25 had SAAG greater than 1.1 g/dl while 6 had SAAG less than 1.1 g/dl. In Das BB et al22 out of 26 patients 22 had SAAG greater than 1.1 g/dl while 4 had SAAG less than 1.1 g/dl. On distribution of esophageal varices, there were 58 (58%) patients having esophageal varices and 42 (42%) patients with no esophageal varices .58 out of 82 patients with SAAG greater than 1.1 g/dl had varices while none out of 18 patients with SAAG less than 1.1g/dl had varices. In Demirel1 U et al9 no patient with SAAG less than 1.1g/dl had varices while all patients with SAAG greater than 2 g/dl had varices while 15 out of 19 with SAAG bet-ween 1.1 and 2.0 g/dl had varices. In Gurubacharya DL et al20 18 out of 25 patients with > 1.1 g/dl had varices. No varices in patiens with SAAG < 1.1 g/dl. In Torres E et al21 17 out of 25 patients with > 1.1 g/dl had varices. No varices in patients with SAAG < 1.1 g/dl. In Das BB et al22 20 out of 22 patients with SAAG > 1.1 g/dl had varices. No varices in pati-ents with SAAG < 1.1 g/dl. All these results were comparable with results in our study. The study has shown a significant difference in the mean value between those with esophageal vari-ces and those who did not, therefore this can be used as a good discriminating parameter. In our study the sensitivity of SAAG was 76%, specificity was 82%, positive predictive value 80.85%, negative predictive value 77.3% and accu-racy was 79.0%. All these values clearly indicate the importance of SAAG in prediction of oesophageal varices. A large prospective study is needed to verify and
validate these findings and may allow identification of a group of patients who would most benefit from endoscopic screening for varices.23
CONCLUSION SAAG ratio is an important predictor and an inde-pendent parameter associated with the presence of esophageal varices. This will not only reduce the cost of treatment but will also help in identifying the patients who require primary prophylaxis for upper gastrointestinal bleeding.
REFERENCES 1. Ahmad K. Pakistan. A cirrhotic state? Lancet 2004
Nov 20-26; 364: 1843-4. 2. Farooqi RJ, Farooqi JI, Rehman M, Ahmad H,
Ahmad F, Gul S. Outcome after injection sclero-therapy for esophageal variceal bleeding in patients with liver cirrhosis and COPD J Postgrad Med Inst
Jan – Mar 2005; 19: 76-80. 3. Fontana RJ, Sanyal AJ, Mehta S, Doherty MC, Neu-
schwander – Tetri BA, Everson GT, Kahn JA, et al. Portal hypertensive gastropathy in chronic hepatitis C patients with bridging fibrosis and compensated cirrhosis: results from the HALT-C trial. Am J Gas-troenterol. 2006 May; 101: 983-92.
4. Fattovich G, Patalena M, Zagni I, Realdi G, Sehlam SW, Christensen E. European concerned action on viral hepatitis (EUROHEP). Effect of hepatitis B and C virus infections on the natural history of compen-sated cirrhosis: a cohort study of 297 patients. Am J Gastroenterol 2002; 97: 2886-95.
5. D Amico G, Garcia–Tsao G, Cales P. Diagnosis of portal hypertension: how and when. In: De Franchis R, (edi). Proceedings of the third Baveno Interna-tional Consensus Workshop on definitions, metho-dology and therapeutic strategies. Oxford: Blackwell science 2001: 36-63.
6. Brennan MRS, Targownik I, Gareth SD, Hetak AK, Ian MG.Endoscopic screening for esophageal varices in cirrhosis. Is it ever cost effective? Hepatology 2003; 37: 366-77.
7. Kakutani H, Hino S, Ikeda K, Sumiyama K, Uchi-yama Y, Kuramochi A, Kawamura M, Tajiri H. Pre-diction of recurrence of esophageal varices – special

SAAG RATIO AS PREDICTOR OF ESOPHAGEAL VARICES IN PATIENTS WITH CIRRHOSIS AND ASCITES
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 23
reference to a role for endoscopic ultrasonography. Hepatol Res. 2005 Dec; 33 (4): 259-66. Epub 2005 Oct 14.
8. Sarwar S, Khan AA, Alam A, Butt AK, Shafqat F, Malik K, Ahmad I, Niazi AK. Non-endoscopic predic-tion of presence of esophageal varices in cirrhosis. J Coll Physicians Surg Pak. 2005 Sep; 15: 528-31.
9. Demirel U, Karincaoğlu M, Harputluoğlu M, Ateş M, Seçkin Y, Yildirim B, Hilmioğlu F. Two findings of portal hypertension: evaluation of correlation bet-ween serum – ascites albumin gradient and esopha-geal varices in non-alcoholic cirrhosis. Turk J Gastro-enterol. 2003 Dec; 14 (4): 219-22.
10. Mene A, Sharma D, Raina VK. Correlation between serum – ascites albumin concentration gradient with gastrointestinal bleeding in patients of portal hyper-tension. Trop Doct. 2003 Jan; 33: 39-41.
11. Thomopoulos KC, Labropoulou KC, Mimidis KP, Kat-sakoulis EC, Ieonomou G, Nikolopoulou VN. Non-invasive predictors of the presence of large oesopha-geal varices in patients with cirrhosis. Dig Liver Dis 2003; 35: 473-8.
12. Giannini E, Botta F, Borro P, Risso D, Romagnoli P, Fasoli A, et al. Platelet count/spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of esophageal varices in pati-ents with liver cirrhosis. Gut 2003; 52: 1200-5.
13. Khokhar N. Spectrum of chronic liver disease in a tertiary care hospital. J Pak Med Assoc 2002; 52: 56-8.
14. Khokhar N, Gill ML, Malik GJ. General seropreva-lence of hepatitis C and hepatitis B virus infections in population. J Coll Physicians Surg Pak 2004; 14: 534-6.
15. Khokhar N, Niazi SA. Chronic liver disease related mortality pattern in Northern Pakistan. J Coll Phy-sicians Surg Pak 2003; 13: 495-7.
16. Atiq M, Gill ML, Khokhar N. Quality of life assess-ment in Pakistani patients with chronic liver disease. J Pak Med Assoc 2004; 54: 113-5.
17. De Franchis R, Primignani M. Natural history of por-tal hypertension in patients with cirrhosis. Clin Liver Dis 2001; 5: 645-63.
18. Giannini E, Botta F, Borro P, Risso D, Romagnoli P, Fasoli A, et al. Platelet count / spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of esophageal varices in pati-ents with liver cirrhosis. Gut 2003; 52: 1200-5.
19. Goh SH, Tan WP, Lee SW. Clinical predictors of blee-ding esophageal vairces in the ED. Am J Emerg Med 2005; 23: 531-5.
20. Gurubacharya DL, Mathura KC, Karki DB. Correla-tion between serum – ascites albumin concentration gradient and endoscopic parameters of portal hyper-tension. Kathmandu Univ Med J (KUMJ). 2005 Oct-Dec; 3: 327-33.
21. Torres E, Barros P, Calmet F. Correlation between serum-ascites albumin concentration gradient and endoscopic parameters of portal hypertension. Am J Gastroenterol. 1998 Nov; 93: 2172-8.
22. Das BB, Purohit A, Acharya U, Treskova E. Serum – ascites albumin gradient: a predictor of esophageal varices with ascites. Indian J Pediatr. 2001 Jun; 68 (6): 511-4.
23. Zaman A, Hapke R, Flora K, Rosen HR, Benner K. Factors predicting the presence of esophageal or gastric varices in patients with advanced liver dise-ase. Am J Gastroenterol 1999; 94: 3292-6.

24 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
ORIGINAL ARTICLE
IRREGULAR LIVER SURFACE ON AS A NON-INVASIVE MARKER OF ESOPHAGEAL VARICES IN CIRRHOTICS
SAJID NISAR, BILAL BUTT, AZHAR HUSSAIN
Medical Unit 4, Services Institute of Medical Sciences (SIMS) / Services Hospital, Lahore
ABSTRACT Introduction: Global burden of cirrhosis is likely to increase in subsequent years. Cirrhosis occurs as a result of chronic liver disease and is characterized by replacement of liver tissue by fib-rotic scar tissue and regenerative nodules which causes progressive loss of liver function. In Pakis-tani population mortality from cirrhosis and its complications is very common and causes fre-quent hospital admissions. Variceal bleeding is the major cause of mortality and morbidity in cirr-hosis and this is a consequence of portal hypertension. The prevalence of esophageal varices in pat-ients with chronic liver disease varies from 60% to 80%. 25% – 40% of patients with cirrhosis have variceal haemorrhage which is associated with a mortality rate of about 30%and up to 70% of tho-se who survive have one or more additional episodes of bleeding within following 2 years. Screen-ing for esophageal varices represents an important part in the diagnostic work up of cirrhotic patients. Current guidelines recommend that patients with cirrhosis who have large varices but have not had an episode of variceal bleeding should receive primary prophylaxis with a non-selec-tive β-blocker. Multiple esophagogastroduodenoscopy’s are carried out over the course of a pati-ent’s lifetime. It is better to limit upper gastrointestinal endoscopy to a subgroup of patients with high risks of bleeding and this is possible only if a simple non-invasive test to detect esophageal varices was available to select these at risk patients reducing both medical and financial burden on hospitals. To address this issue, liver surface on trans-abdominal ultrasonography is used as a non-invasive marker for presence of esophageal varices. Its application may reduce the need for endoscopy and may institute an early management to avoid life threatening upper gastrointesti-nal haemorrhage.
Objective: The objective of this study was to determine the Positive Predictive Value (PPV) of irregular liver surface on trans-abdominal ultrasonography for the non-invasive diagnosis of eso-phageal varices in cirrhotic patients keeping upper gastrointestinal endoscopy as Gold Standard.
Study Design: It was cross-sectional survey.
Setting: The study was conducted in Medical Unit IV, Services Hospital, Lahore.
Duration: The study was completed over a period of 6 months from January 28, 2012 to July 27, 2012.
Subjects and Methods: Three hundred twenty patients who had coarse echotexture of liver parenchyma and irregular liver surface on trans-abdominal ultrasound were selected from emer-gency of Services Hospital, Lahore. Informed Consent was taken from them for participation in the study. Ultrasound was done by the same single radiologist. These patients were then booked for diagnostic upper gastrointestinal endoscopy after Informed Consent. Upper gastrointestinal endo-scopy was performed in these selected patients after full preparation by a single endoscopist and presence or absence of esophageal varices was documented in each case.
Results: Irregular liver surface on transabdominal ultrasonography as a noninvasive marker for the presence of esophageal varices has a Positive Predictive Value (PPV) of 78.13%.
Conclusion: Our study showed that irregular liver surface on transabdominal ultrasonography is a simple and noninvasive method for diagnosis of esophageal varices and its application may decrease the need for performing upper gastrointestinal endoscopy in every cirrhotic patient.
Key Words: Cirrhosis, Esophageal Varices, Upper gastrointestinal endoscopy, Liver surface, Trans-abdominal ultrasonography, Radiologist, Endoscopist.

IRREGULAR LIVER SURFACE ON AS A NON-INVASIVE MARKER OF ESOPHAGEAL VARICES IN CIRRHOTICS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 25
INTRODUCTION Cirrhosis is a major cause of mortality and mor-bidity throughout the world. In Pakistani populat-ion mortality from cirrhosis and its complications is very common and it is a very frequent reason for admission in hospitals. Cirrhosis develops in about 10 – 20% of patients with chronic liver disease and this occurs within 5 – 30 years. The most common cause of cirrhosis in Pakistan and other under deve-loped countries is viral hepatitis as compared to developed countries where alcohol is more com-mon. Majority of patients (90%) with chronic liver disease have evidence of hepatitis B virus (HBV), hepatitis C virus (HCV) or co-infection. In its advan-ced stages cirrhosis is generally irreversible disease, and treatment focuses on preventing the progress-ion of cirrhosis and of its complications. In advan-ced stages of cirrhosis the only option is liver trans-plantation.1,2 In Pakistan, 10 million people are pre-sumed to be infected with HCV. Various studies have shown that prevalence of HCV in general Paki-stani adult population is 4.95% ± 0.53.3 Variceal bleeding is the major cause of mortality and morbidity in liver cirrhosis; this is a conseque-nce of portal hypertension. The prevalence of eso-phageal varices in patients with chronic liver disease varies from 60% to 80%.4,5 Twenty five percent to 40% of patients with cirrhosis have variceal haemo-rrhage which is associated with a mortality rate of about 30%6,7 and up to 70% of those who survive have one or more additional episodes of bleeding within the following 2 years.8,9 Active bleeding at endoscopy carries a high risk of mortality within 6 weeks of procedure.10 Current guidelines recommend that patients with cirrhosis who have large varices but have not had an episode of variceal bleeding should receive primary prophylaxis with a non-selective β-bloc-ker.11,12 Prophylactic uses of non-selective β-blockers in such patients with high risk of variceal haemorr-hage has been shown to decrease incidence of first episode of bleeding and death. The risk of bleeding from varices depends upon a number of factors including the size, shape, locat-ion, and appearance of the varices, as well as the severity of liver disease and previous history of ble-eding from varices. A treatment to reduce the risk of bleeding is recommended in selected patients with esophageal varices. Upper gastrointestinal haemorr-hage due to esophageal varices is a poor prognostic sign in cirrhosis.
OPERATIONAL DEFINITIONS Cirrhosis All patients who had coarse echotexture of liver par-enchyma on abdominal ultrasound were labelled as cirrhotics.
Liver Surface on Trans-abdominal Ultrasonography Liver surface was seen on trans-abdominal ultraso-nography and was termed as being irregular or smo-oth.
Positive Predictive Value
Positive Predictive Value
= True Positive
100 True Positive + False Positive
True Positives When irregular liver surface was present on ultra-sonography and esophageal varices were also pre-sent on endoscopy.
False Positives When irregular liver surface was present on ultra-sonography but esophageal varices were absent on endoscopy.
Esophageal Varices Esophageal varices were assessed by upper gastro-intestinal endoscopy and their presence or absence was observed. MATERIALS AND METHODS Setting The study was conducted in Medical Unit IV, Servi-ces Hospital, Lahore.
Duration with Dates The study was completed over a period of 06 mon-ths after the approval of synopsis i.e. from January 28, 2012 to July 27, 2012. Sample Size Sample size of 320 cases was calculated with 95% confidence level, 5.5% margin of error and taking Positive Predictive Value of irregular liver surface on trans-abdominal ultrasonography to be 56% in the diagnosis of esophageal varices in cirrhotic pati-ents keeping upper gastrointestinal endoscopy as Gold Standard. Sampling Technique Is non-probability consecutive sampling. Sample Selection Inclusion Criteria 1. Patients of chronic liver disease showing coarse
echotexture of the liver on abdominal ultra-sound.
2. Patients with irregular liver surface on trans-abdominal ultrasound.
3. Patients of 12 – 60 years of age and of both gen-ders.

SAJID NISAR, BILAL BUTT, AZHAR HUSSAIN
26 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
Exclusion Criteria 1. Patients presenting with variceal bleed. 2. Patients taking non selective beta blockers and/
or nitrates on medical record. 3. Patients who had received any therapeutic in-
tervention for their varices like banding or inje-ction sclerotherapy.
4. Patients who refused to undergo upper gastro-intestinal endoscopy after informed consent.
Study Design It was a cross – sectional descriptive survey. Data Collection 320 patients who had coarse echotexture of liver parenchyma and irregular liver surface on trans-abdominal ultrasound were selected from emerge-ncy. Informed Consent was taken from them for participation in the study. Ultrasound was done by the same single radiologist. These patients were then booked for diagnostic upper gastrointestinal endoscopy at a later date after Informed Consent. Upper gastrointestinal endoscopy was performed in these selected patients after full preparation by a single endoscopist and presence or absence of eso-phageal varices was documented in each case. All this information was collected through a specially designed proforma (attached as Annexure I). DATA ANALYSIS Data was collected and compiled in the computer and analysed using SPSS version 16 for Windows. Demographic variables included age and gender. Gender and presence or absence of esophageal vari-ces were the qualitative variables and were presen-ted as frequencies and percentages. The Positive predictive value of irregular liver surface on trans-abdominal ultrasonography for the non-invasive diagnosis of esophageal varices in cirrhotic patients was calculated considering endoscopic findings (presence or absence of esophageal varices) as Gold Standard. Mean ± SD was calculated for all quanti-tative variables like age. RESULTS 320 patients who had coarse echotexture of liver parenchyma and irregular liver surface on transab-dominal ultrasound with ages between 12 – 60 yea-rs were selected from emergency department of Ser-vices Hospital, Lahore. Figure 1 shows gender distribution of 320 pati-ents, 50.3% (n = 161) were males and 49.7% (n = 159) were females. Table 1 shows age distribution of these 320 pati-ents. According to this, 10 patients (3.1%) were bet-ween 21 – 30 years of age, 30 patients (9.4%) were between 31 – 40 years, 116 patients (36.2%) were
between 41 – 50 years and 164 patients (51.2%) were between 51 – 60 years. Mean age was 49.86 ± SD8.60.
50.312
49.688
Male
Female
Fig. 1: Distribution of patients according to gender.
Table 1: Distribution of patients according to Age
(groups) n=320.
Age (Groups) Frequency Percentage %
21 – 30 10 3.1
31 – 40 30 9.4
41 – 50 116 36.2
51 – 60 164 51.2
Mean ± SD 49.86 ± 8.60
Minimum age: 25 years, Maximum age: 60 years
Table 2 shows patients according to the pre-sence or absence of esophageal varices. According to this table, 250 patients had esophageal varices (78.1%) and 70 patients did not have esophageal varices (21.9%). Bar chart of this is shown in Fig. 2.
Table 2: Distribution of patients according to eso-
phageal varices (EV) n = 320.
EV Frequency Percentage %
Present 250 78.1
Absent 70 21.9
Table 3: Distribution of patients according to
positivity n= 320.
Positivity Frequency Percentage %
True positives 250 78.1
False positives 70 21.9

IRREGULAR LIVER SURFACE ON AS A NON-INVASIVE MARKER OF ESOPHAGEAL VARICES IN CIRRHOTICS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 27
Positive Predictive Value = True Positive
100 True Positive + False Positive
Positive Predictive Value (PPV) =
78.13%
250
70
0
50
100
150
200
250
300
Present Absent
Fig. 2: Distribution of patients according to presence or absence of EV.
Table 4: Comparison of gender and presence or
absence of EV.
Gender EV Present
(%) EV Absent
(%) Total
Male 141 (87.6%) 20 (12.4%) 161
Female 109 (68.6%) 50 (31.4%) 159
Table 3 shows groups of patients according to positivity of patients. According to this table, 250 patients (78.1%) were true positives and70 patients (21.9%) were false positives. Table 4 shows comparison of gender and pre-sence or absence of esophageal varices. This shows that irregular liver surface on transabdominal ultra-sonography accurately predicted presence of eso-phageal varices in 141 (87.6%) males as compared to 109 (68.6%) females suggesting that it is better non-invasive marker in male gender. The research showed that the Positive Predic-tive Value (PPV) of this noninvasive marker for pre-sence esophageal varices is 78.13%.
DISCUSSION Cirrhotic patients must be screened for esophageal varices as a routine for diagnostic work up. Accord-ing to current consensus, every patient with cirrho-sis should be screened endoscopically for varices at the time of diagnosis.13-15 Diagnostic yield of upper gastrointestinal endoscopy is very high if the patient selection is done in a meticulous way. Upper gastro-
intestinal endoscopy is the gold standard for the diagnosis of esophageal varices.
Acute variceal bleeding continues to be associ-ated with significant mortality but this has decree-sed over the past two decades from 42% to 15%.This figure is still remarkably highespecially in subse-quent episodes of variceal bleeding.6,9
Periodic screening by endoscopy for esophageal varices is recommend in recent guidelines for all patients with cirrhosis.16
Cirrhotic patients have to undergo multiple endoscopies throughout life for diagnosis and sur-veillance of esophageal varices putting an enormous amount of burden in terms of cost, inconvenience and discomfort. Endoscopy is an invasive technique and often requires sedation to reduce pain and dis-comfort; therefore, many patients are reluctant to undergo this procedure and as a result are non-compliant with screening and surveillance recom-mendations. If a non-invasive, less distressing and cheap screening test is available for detection of eso-phageal varices this would reduce the financial, phy-sical and psychological burden on the patient and also reduce burden on endoscopy units. Endoscopy would then be limited only to patients with high risk of bleeding.
The concept of identifying esophageal varices in cirrhotic patients by non-invasive measures shows attraction because it will allow reduction in number of procedures and will ultimately improve health care.14
The aim of the study was to determine the Posi-tive Predictive Value (PPV) of Irregular liver surface on transabdominal ultrasonography for the non-invasive diagnosis of esophageal varices in patients with cirrhosis thereby allowing the clinicians to det-ect esophageal varices without having to perform upper gastrointestinal endoscopy.
REFERENCES 1. Almani SA, Memon AS, Memon AI, Shah MI, Rah-
poto Q, Solangi R. Cirrhosis of liver: Etiological fac-tors, complications and prognosis. J Liaquat Uni Med Health Sci 2008; 7: 61-6.
2. Abbasi A, Bhutto AR, Butt N, Lal K, Munir SM. Se-rum Cholesterol: Could it be a Sixth Parameter of Child – Pugh Scoring System in Cirrhotics Due to Viral Hepatitis? JCPSP 2012; 22 (8): 484-7.
3. Hayat AS, Shaikh N, Masood N. Study for frequency and aetiology of lymph-adenopathy during combina-tion therapy for chronic hepatitis C (pegylated inter-
Varices
Fre
qu
en
cy
Varices

SAJID NISAR, BILAL BUTT, AZHAR HUSSAIN
28 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
feron alpha plus ribavirin) at a tertiary care hospital in Hyderabad. JPMA 2011; 61: 986.
4. Frenette CT, Kuldau JG, Hillebrand DJ, Lane JJ, Pockros PJ. Comparison of esophageal capsule endo-scopy and esophagogastroduodenoscopy for diag-nosis of esophageal varices. World J Gastroenterol 2008; 14: 4480-5.
5. Mahassadi AK, Bathaix FY, Assi C, Bangoura AD, Allah – Kouadio E, Kissi HY et al. Usefulness of Non-invasive Predictors of Oesophageal Varices in Black African Cirrhotic Patients in Cˆote d’Ivoire (West Africa). Gastro Res Prac 2012; 10: 1155.
6. Flores PP, Lemme EM, Coelho HS. Esophageal motor disorders in cirrhotic patients with esophageal vari-ces non-submitted to endoscopic treatment. Arq Gas-troenterol 2005; 42: 213-20.
7. Sarangapani A, Shanmugam C, Kalyanasundaram M, Thangavelu BRP, Subbarayan JK. Non-invasive pre-diction of large esophageal varices in chronic liver disease patients. Saudi Gastroenterol 2010; 16: 38-42.
8. Sanyal AJ, Fontana RJ, Di Bisceglie AM, Everhart JE, Doherty MC, Everson GT et al. The prevalence and risk factors associated with esophageal varices in subjects with hepatitis C and advanced fibrosis. Gas-trointest Endosc2006; 64: 855-864.
9. McKay R, Webster NR. Variceal bleeding. Contin Educ Anaesth Crit Care Pain 2007; 7 (6): 191-4.
10. Bambha K, Kim WR, Pedersen R, Bida JP, Kremers WK, Kamath PS. Predictors of early re-bleeding and mortality after acute variceal haemorrhage in pati-ents with cirrhosis. Gut 2008; 57: 814-20.
11. Zaman A. Outcomes in Cirrhotic Patients with Vari-ceal Bleeding Despite Primary Prophylaxis with a β-Blocker. JWG2012; 2: 622.
12. de la Mora – Levy JG, Baron TH. Endoscopic mana-gement of the liver transplant patient. Liver Transpl 2005; 11: 1007-21.
13. Sharma SK, Aggarwal R. Prediction of large esopha-geal varices in patients with cirrhosis of the liver using clinical, laboratory and imaging parameters. J Gastroenterol Hepatol 2007; 22: 1909-15.
14. Garcia – Tsao G, Bosch J, Groszmann R. Portal hypertension and variceal bleeding – un-resolved issues. Hepatology 2008; 47: 1764-72.
15. Thomopoulos KC. Non-invasive prediction of eso-phageal varices: Is it possible? Saudi J Gastroenterol 2011; 17: 1-3.
16. Sharma SK, Aggarwal R. Prediction of large eso-phageal varices in patients with cirrhosis of the liver using clinical, laboratory and imaging parameters. J Gastroenterol Hepatol 2007; 22: 1909-15.

Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 29
ORIGINAL ARTICLE
UPPER GASTROINTESTINAL ENDOSCOPY – AN ANNUAL REVIEW OF CASES AT MEDICAL UNIT III (DEPARTMENT OF GASTROENTEROLOGY
AND HEPATOLOGY) SERVICES HOSPITAL LAHORE
SABEEN FARHAN,1 MUHAMMAD ARIF NADEEM,1 SHAHBAZ AHMAD QURESHI3 SAEED-UZ-ZAMAN,4 GHULAM ABBAS,2 AFTAB MOHSIN,1 MUTEE ULLAH KHAN1
Department of Medicine / Gastroenterology, 2Medical Unit III 1SIMS / Services Hospital, 3King Edward Medical University / Mayo Hospital, Lahore and 4Quaid e Azam Medical College, Bahawalpur
ABSTRACT Objective: To document various endoscopic findings in patients undergoing upper GI endoscopy in our endoscopy unit.
Design: Observational, retrospective case series.
Patients and Methods: The data of 998 patients who underwent upper gastrointestinal endo-scopy in Endoscopy Unit of Services Hospital Lahore from 1st January 2010 to 31st December 2010 was analyzed. Demographic features, reasons for referral and endoscopic diagnoses were noted.
Results: Among 998 patients, 46% were referred as follow up cases of esophageal banding for varices, 22% for upper gastrointestinal bleed, 17% for dysphagia and 12% for dyspepsia. Common endoscopic diagnoses were esophageal varices (40%), portal hypertensive gastropathy (44%), gas-tritis (22%), reflux esophagitis (13%), and peptic ulcer disease (10%).
Conclusion: The most common presenting complaint was upper GI bleeding and the most com-mon endoscopic finding was esophageal varices.
Key words: Upper GI endoscopy, esophageal varices, upper GI bleed, dyspepsia, dysphagia. INTRODUCTION Upper Gastrointestinal (UGI) symptoms are com-monest presenting complaints, both in indoor and outdoor patients, and may sometime create a diag-nostic dilemma. Therefore, UGI endoscopy has be-come the initial standard diagnostic approach to un-explained UGI symptoms. UGI bleeding is a common medical emergency1. Commonest causes are esophageal varices, peptic ulcer, gastric erosions and mucosal tears.1-3 UGI endoscopy is the diagnostic test of choice for UGI bleeding4 due to its therapeutic potential. The stric-tures of esophagus, hiatal hernias, portal hyperten-sive gastropathy, carcinoma esophagus and stomach are also common endoscopic findings. Medical Unit III of Services Hospital Lahore, being the recognized institution for training under-graduates and post graduate residents in the discip-lines of Gastroenterology and Hepatology, has a very large referral area from all over Punjab. The objective of the study was to find out com-mon reasons of referral for UGI endoscopy in our endoscopy unit, demographic features of referred patients and common endoscopic diagnoses.
PATIENTS AND METHODS The data of 998 patients who underwent UGI endo-scopy in our endoscopy unit from 1st January 2010 to 31st December 2010 was analyzed. Patients were referred from inpatient, outpatient and accident and emergency departments of the hospital. A written informed consent was taken from eve-ry patient before the procedure. Local anesthetic, 4% xylocaine solution, was used for gargles before the procedures. Midazolam IV was given to anxious and also in all patients who underwent dilatation. For obliteration of esophageal varices band ligation was done with Saeed’s Six Shooter band ligator. Dil-atation of esophageal strictures was done with Sava-ry Gilliard Dilators. Achalasia dilatation was done with achalasia balloon and pyloric dilatation was done with through the scope (TTS) balloon dilators. Injection histoacryl and lipiodol was used for oblite-ration of fundal varices. Bleeding duodenal ulcers were injected with 1:10,000 adrenaline and telan-gectasias were treated with the argon plasma coagu-lation (APC). The demographic data recorded were age and sex of the patients, indications, endoscopic diagno-
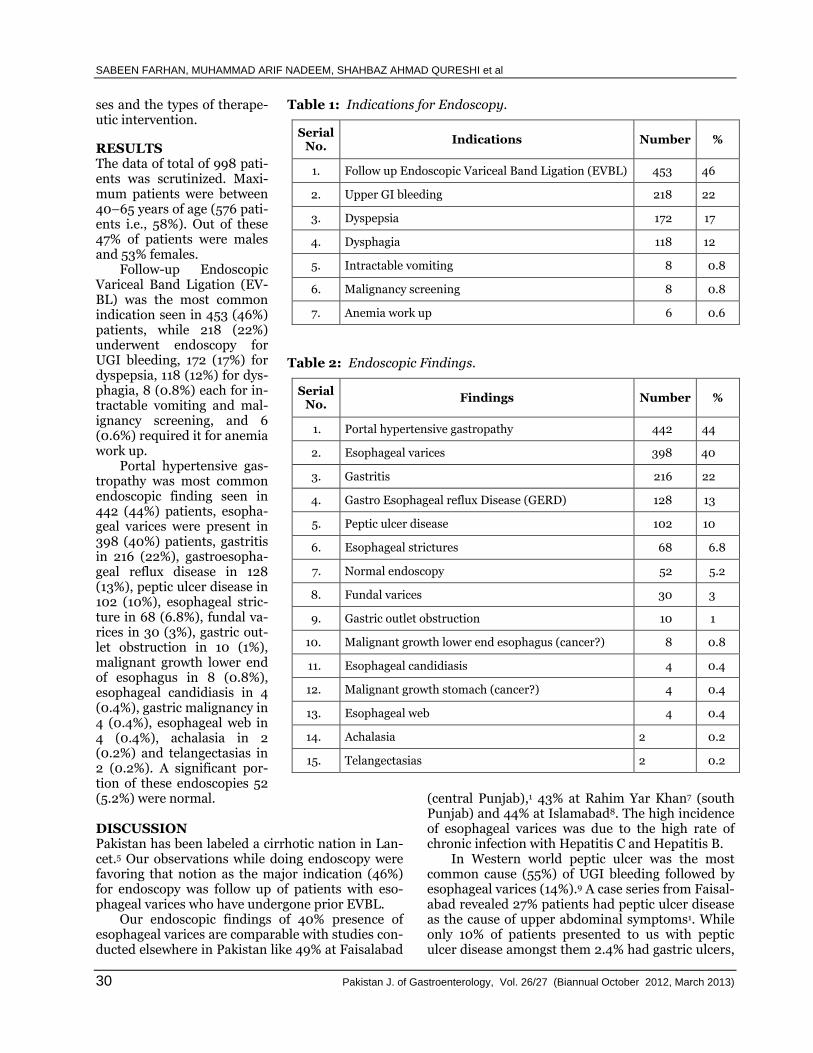
SABEEN FARHAN, MUHAMMAD ARIF NADEEM, SHAHBAZ AHMAD QURESHI et al
30 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
ses and the types of therape-utic intervention.
RESULTS The data of total of 998 pati-ents was scrutinized. Maxi-mum patients were between 40–65 years of age (576 pati-ents i.e., 58%). Out of these 47% of patients were males and 53% females. Follow-up Endoscopic Variceal Band Ligation (EV-BL) was the most common indication seen in 453 (46%) patients, while 218 (22%) underwent endoscopy for UGI bleeding, 172 (17%) for dyspepsia, 118 (12%) for dys-phagia, 8 (0.8%) each for in-tractable vomiting and mal-ignancy screening, and 6 (0.6%) required it for anemia work up. Portal hypertensive gas-tropathy was most common endoscopic finding seen in 442 (44%) patients, esopha-geal varices were present in 398 (40%) patients, gastritis in 216 (22%), gastroesopha-geal reflux disease in 128 (13%), peptic ulcer disease in 102 (10%), esophageal stric-ture in 68 (6.8%), fundal va-rices in 30 (3%), gastric out-let obstruction in 10 (1%), malignant growth lower end of esophagus in 8 (0.8%), esophageal candidiasis in 4 (0.4%), gastric malignancy in 4 (0.4%), esophageal web in 4 (0.4%), achalasia in 2 (0.2%) and telangectasias in 2 (0.2%). A significant por-tion of these endoscopies 52
Table 1: Indications for Endoscopy.
Serial No.
Indications Number %
1. Follow up Endoscopic Variceal Band Ligation (EVBL) 453 46
2. Upper GI bleeding 218 22
3. Dyspepsia 172 17
4. Dysphagia 118 12
5. Intractable vomiting 8 0.8
6. Malignancy screening 8 0.8
7. Anemia work up 6 0.6
Table 2: Endoscopic Findings.
Serial No.
Findings Number %
1. Portal hypertensive gastropathy 442 44
2. Esophageal varices 398 40
3. Gastritis 216 22
4. Gastro Esophageal reflux Disease (GERD) 128 13
5. Peptic ulcer disease 102 10
6. Esophageal strictures 68 6.8
7. Normal endoscopy 52 5.2
8. Fundal varices 30 3
9. Gastric outlet obstruction 10 1
10. Malignant growth lower end esophagus (cancer?) 8 0.8
11. Esophageal candidiasis 4 0.4
12. Malignant growth stomach (cancer?) 4 0.4
13. Esophageal web 4 0.4
14. Achalasia 2 0.2
15. Telangectasias 2 0.2
(5.2%) were normal. DISCUSSION Pakistan has been labeled a cirrhotic nation in Lan-cet.5 Our observations while doing endoscopy were favoring that notion as the major indication (46%) for endoscopy was follow up of patients with eso-phageal varices who have undergone prior EVBL. Our endoscopic findings of 40% presence of esophageal varices are comparable with studies con-ducted elsewhere in Pakistan like 49% at Faisalabad
(central Punjab),1 43% at Rahim Yar Khan7 (south Punjab) and 44% at Islamabad8. The high incidence of esophageal varices was due to the high rate of chronic infection with Hepatitis C and Hepatitis B. In Western world peptic ulcer was the most common cause (55%) of UGI bleeding followed by esophageal varices (14%).9 A case series from Faisal-abad revealed 27% patients had peptic ulcer disease as the cause of upper abdominal symptoms1. While only 10% of patients presented to us with peptic ulcer disease amongst them 2.4% had gastric ulcers,

UPPER GASTROINTESTINAL ENDOSCOPY – AN ANNUAL REVIEW OF CASES AT MEDICAL UNIT III
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 31
2.2% duodenal ulcers and 5.6% had severe duode-nitis. In other local studies from Islamabad and Peshawar revealed that peptic ulcer disease in 19.7% and 11.5% of patients respectively.6,8 Lower incide-nce of peptic ulcer as a cause of bleeding, because we had observed it 32% in 1998 at Mayo Hospital, Lahore,10 could be due to frequent use of acid sup-pressing drugs by medical practitioners in patients with symptoms of dyspepsia. Alcohol consumption appeared to play little role as a cause of UGI bleed-ing in this population, most likely due to religious prohibition of alcohol in the society. Amongst the dyspeptic patients, we observed the gastro esophageal reflux disease as the common finding (13%) on endoscopy after gastritis, while it was 32% in another study from Gang Ram Hospital, Lahore11, 9% in south Punjab (Rahim Yar Khan)12 and 23% at Peshawar.13 In contrary a study from Nigeria revealed 61% patients being referred with dyspepsia for endoscopy.14 Dysphagia was the fourth common reason for referral and the common findings were strictures and rarely there were esophageal webs, achalasia and candidiasis. In our hospital the commonest rea-son for esophageal strictures was the use of cor-rosives taken with suicidal intent. Tumors of the upper GI tract were found in 1.1%,6 even less common in our study and similar data is shown by other local studies.15-16 Normal upper GI examination on endoscopy accounted for 10.9% in the study from Islamabad6 as compared to our result where the frequency of normal endoscopy in patients with epigastric pain was 5.2%. These figures can further be minimized if a more strict criteria be laid down for endoscopy in patients with dyspepsia and endoscopy be done if their pain is intractable or if they develop alarm symptoms. CONCLUSION Upper GI endoscopy is the only reliable tool for cor-rectly determining the etiology of upper GI comp-laints and it also has therapeutic potential. A great bulk of referrals in our unit is of cirrhotic patients who are on follow up after EVBL. Portal hyperten-sive gastropathy and esophageal varices form the major bulk of endoscopic findings reflecting high prevalence of chronic liver disease. REFERENCES 1. Bilal A, Nagra H, Shahid M. Upper GIT bleeding: pre-
valence of peptic ulcer. The Prof Med J 2004; 11: 400-5.
2. Palmer KR, Penman ID. Diseases of the alimentary tract and pancreas. In: Haslett C, Chilvers ER, Hun-ter JAA, Boon NA. Davidson’s principles and practice of medicine. 19th edition. Edinburgh: Churchill Liv-ingstone, 2002: 747-830.
3. Farooqi JL, Farooqi RJ. Endoscopic management of bleeding peptic ulcer. JCPSP 2001; 11: 530-4.
4. McQuaid KR. Alimentary tract. In: Tierney LM, Mc-Phee SI, Papadakis MA, editors. Current Medical Diagnosis and Treatment, 45th edition. New York: McGraw Hill 2006: 573-5.
5. Ahmad K. Pakistan: a cirrhotic state? The Lancet 2004; 364: 9448.
6. Mahmood K, Saeedi MI, Muhammad R, Din Z. Upper gastrointestinal endoscopic findings in patients with dyspepsia. J Postgrad Med Ins 2006; 20 (1): 70-3.
7. Irfan Ahmad, Moazzam Ali Atif, Ghulam Mustafa. Upper gastrointestinal endoscopy: indications and outcome experience at Sheikh Zayed Hospital Rahim Yar Khan. J Sheikh Zayed Med Coll Jan – Mar 2010; 1 (1): 27-9.
8. Tashfeen Adam, Fatima Javid, Sharbat Khan. Upper Gastrointestinal bleeding: An etiological study of 552 cases J Pak Inst Med Sci Jul 2004; 15 (1): 845-8.
9. Jutabha R, Jensen DM. Management of severe upper gastrointestinal bleeding in the patient with liver dis-ease. Med Clin North Am 1996; 80: 1035.
10. Najam UN Nasir, Muhammad Arif Nadeem, Muham-mad Imran, Irshad Hussain, Nusrat Ullah Chaudhry. Oesophageal Varices vs. Peptic Ulcer: A Study of 100 Patients Presenting in Mayo Hospital with Upper Gastrointestinal Bleeding. Pak J Gastroenterol Jan 1998; 12 (1-2): 58-65.
11. Syed Asghar Naqi, Aamer Zaman Khan, Asim Kam-ran, Muhammad Nadeem Aslam, Abdul Rauf Arshad, Tariq Mahmood. Gastro Esophageal Reflux Disease: Incidence of GERD in 100 Consecutive Upper G.I. Endoscopies at Sir Ganga Ram Hospital Ann King Edward Med Uni Apr – Jun 1999; 5 (2): 165-6.
12. Irfan Ahmad, Moazzam Ali Atif. Upper GI Endoscopy-A review of 500 cases at Sheikh Zayed Medical Col-lege / Hospital Rahim Yar Khan Pak J Med Health Sci Dec 2007; 1 (4): 137-9.
13. Najmul Hassan Shah, Muhammad Sadiq Shah, Ikra-mullah Khan, Khalid Hameed. An audit of Diagnostic Upper GI Endoscopy and comparison of booked ver-sus open access cases J Coll Physicians Surg Pak Apr 1999; 9 (4): 174-6.
14. Olokoba A B, Olokoba L B, Jimoh A A G, Salawu F K, Danburam A, Ehalaiye B F. Upper gastrointestinal tract Endoscopy indications in northern Nigeria. J Coll Physicians Surg Pak May 2009; 19 (5): 327-8.
15. Adam T, Javed F, Khan S. Upper gastrointestinal ble-eding: An etiological study of 552 cases. J Pak Inst Med Sci 2004; 15 (1): 845-8.
16. Khurram M, Khaar HB, Hasan Z, Umar M, Javed S, Asghar T, et al. 12 year audit of upper gastrointestinal endoscopic procedures. JCPSP 2003; 13 (6): 321-4.

32 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
ORIGINAL ARTICLE
NON-ENDOSCOPIC PREDICTORS FOR THE PRESENCE OF ESOPHAGEAL VARICES IN PATIENTS WITH LIVER CIRRHOSIS SCREENED IN
GASTROENTEROLOGY DEPARTMENT LRH PESHAWAR
AAMIR GHAFOOR KHAN, MOEEN-UL-HAQ, ABBAS KHAN KHATTAK
HASHMATULLAH KHAN, MUHAMMAD NAZIR KHAN Department of Gastroenterology, Lady Reading Hospital, Peshawar
ABSTRACT Background and Study Aims: Current guidelines recommend screening cirrhotic patients whether compensated or decompensated with an upper GI endoscopy to detect esophageal varices and to institute prophylactic measures in patients with large esophageal varices. In this study, we aimed at identifying non-endoscopic parameters that could predict the presence of esophageal var-ices.
Patients and Methods: This observational and analytical study was carried out in Gastroente-rology Department of Lady Reading hospital Peshawar. Eighty two patients with established cirr-hosis referred to our department from various department or hepatitis clinic were evaluated. They had no previous history of variceal bleeding and were evaluated for predetermined variables and underwent upper GI endoscopy to look for esophageal varices. Subjects were put into two groups, Group A with varices and Group B with no varices. At the end of the study both groups were com-pared for predetermined variables.
Results: Eighty two patients were evaluated in the study out of whom 52 were men and 30 were women with male to female ratio of 1.73:1. 34 patients (41.46%) were having varices and 48 pati-ents (58.53%) were not having varices. Mean albumin in group A was 2.45 ± 0.49 while 3.8 ± 0.68 g/dl in Group B. Mean platelet count in Group A was 78000 ± 30000 while 170550 ± 70000 in Group B. Mean spleen size in Group A was 16.77 ± 2 cm and 13 ± 1.22 cm in group 2 while mean portal vein diameter was 12.2 ± 0.45 mm in Group A and 10 ± 1.18 mm in Group B. Threshold for best sensitivity and specificity were determined using ROC (Receiver Operated Curve) which sho-wed platelet count of < 72000 / ml Albumin < 2.3 g/dl, Portal vein diameter > 12.5 mm and spleen size > 19 cm is associated with varices having reasonable sensitivity and specificity.
Conclusion: Platelet count less than 72000 / ml, serum albumin less than 2.3 g/dl, portal vein diameter more than12.5 mm on ultrasound and spleen size 19 cm were found to be independent predictors of esophageal varices on endoscopy with reasonable sensitivity and specificity. So endo-scopy should be done in any patient with above mentioned parameters.
Key Words: Hepatitis C, Varices, Cirrhosis.
INTRODUCTION In compensated cirrotics varices are present in abo-ut 30 – 40% of patients and in 60% of those who present with asities,1 while in those cirrhotic pati-ents who present without varices, the annual inci-dence of new varices is about 5 – 10%.2 Once varices have been diagnosed, the overall incidence of vari-ceal bleeding is of the order of 25% at 2 years.3 Rup-tured esophageal varices cause 70% of all upper gas-trointestinal bleeding episodes in patients with por-tal hypertension.4 Mortality from variceal bleeding is currently 15 – 20%.
Because of these facts and poor outcome associ-ated with upper GI bleed, the identification of vari-ces in those who are at high risk and prevention of the first bleed is of utmost importance. According to current guide lines all patients should undergo scre-ening endoscopy at the time when cirrhosis is dia-gnosed. Patients with medium or large varices sho-uld be treated while all other patients should under-go periodic endoscopic surveillance. However at a given point in time a variable portion of the patients will not have varices. Thus screening all patients with upper GI endoscopy implies a no of un-neces-

NON-ENDOSCOPIC PREDICTORS FOR THE PRESENCE OF ESOPHAGEAL VARICES IN PATIENTS WITH LIVER CIRRHOSIS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 33
sary endoscopies which increases the workload of endoscopy units. It also means repeated upper GI endoscopies in asymptomatic patients, a procedure that is often perceived as unpleasant, requires cons-cious sedation and has small but not insignificant complications. These factors may decrease patient compliance and thus the effectiveness of screening program. The use of clinical features like platelet count, serum albumin, spleen size, platelet to spleen ratio, portal vein diameter may help physician to predict non-invasively which patients are likely to have lar-ge varices as indicated by various studies.5-7 Our health care system has limited facility of endoscopy even in tertiary care hospitals and the approach to screen every patient with cirrhosis for esophageal varices has its own limitation as well as is an economic burden.8 So non endoscopic predict-ion of esophageal varices in patient with cirrhosis is of great significance. The aim of our study is to evaluate platelet cou-nt, serum albumin, portal vein diameter and spleen size as non endoscopic predictors of varices and to calculate the threshold of above mentioned parame-ters at which these are significant in terms of sensi-tivity and specificity. If found to be significant this will guide us about the patients in whom screening OGD should be done while limiting the unnecessary endoscopies and economic burden. PATIENTS AND METHODS This observational and analytical study was carried out in Gastroenterology Department of Lady Read-ing hospital Peshawar from Sep 2011 to Dec 2011. Following patients were included in the study. 1. Patients having stigmata of chronic liver disea-
ses like palmer erythema, spider angioma, asi-ties, jaundice who have not bled previously.
2. Patients with coarse echotexture on ultrasound with no obvious signs of chronic liver disease and no prior history of upper GI bleed.
Following patients were excluded from the study. 1. Patients who are HbsAg or anti HCV positive
with normal ultrasound. 2. Patients of established cirrhosis with history of
previous upper GI bleed. 3. Patients already on primary prophylaxis. 4. Patients who had already undergone banding
and sclerotherapy. 5. Unstable patient. Patients fulfilling the abovementioned criteria referred to our department from various depart-ments or Hepatitis clinic were evaluated for pre-determined variables (platelet count, serum albu-min, portal vein diameter and spleen size) and underwent upper GI endoscopy to look for esopha-geal varices.
Subjects were put into two groups, Group A with varices and Group B with no varices. At the end of the study both groups were compared for pre-determined variables. RESULTS Eighty two patients were evaluated in the study out of whom 52 were men and 30 were women with male to female ratio of 1.73:1. 34 patients (41.46%) were having varices and 48 patients (58.53%) were not having varices. Mean age Group A was 46 years while 41 years in Group B. Out of 34 patients having varices 22 were having small esophageal varices while 12 were having large esophageal varices (Fig. 1).
27%
15%
58%
No Varices Small Varices Large Varices
Figure 1: Varices.
Mean albumin in Group A was 2.45 while 3.8 g/dl in Group B. Mean platelet count in Group A was 78000 while 170550 in Group B. Mean spleen size in Group A was 16.77 cm and 13 cm in Group B while mean portal vein diameter was 12.2 mm in Group A and 10 mm in Group B. Mean values ± SD are given in the table 1. Threshold for best sensitivity and specificity were determined using ROC (Receiver Operated Curve) curve which showed platelet count of Table 1: Comparison of Means between Two Gro-
ups.
Variable Group 1 Group 2
Age 46 ± 12 41 ± 11
Albumin 2.45 ± .49 3.8 ± .68
Platelet Count 78000 ± 30000 170550 ± 70000
Spleen Size 16.77 ± 2 13 ± 1.22
Portal Vein Diameter
12. 2 ± .45 10 ± 1.18
Parameter ± SD

AAMIR GHAFOOR KHAN, MOEEN-UL-HAQ, ABBAS KHAN KHATTAK et al
34 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
< 72000 / ml having sensitivity of 71% and specifi-city of 96%. Serum albumin < 2.3 g/dl has a sensi-tivity of 73% and specificity of 91%. Portal vein diameter > 12.5 mm has a sensitivity of 73% and specificity of 89% and spleen size >19cm has a sensitivity of 68% and 96%. Sensitivity, speci-ficity, positive predictive value and negative predic-tive values are given in table 2.
Table 2:
Variable Group 1 Group 2
Age 46 ± 12 41 ± 11
Albumin 2.45 ± .49 3.8 ± .68
Platelet Count 78000 ± 30000 170550 ± 70000
Spleen Size 16.77 ± 2 13 ± 1.22
Portal Vein Diameter
12.2 ± .45 10 ± 1.18
PPV = Positive predictor value, NPV = negative predictor value
DISCUSSION Although OGD is not a perfect gold standard for the diagnosis of esophageal varices, the search for a valid non–invasive method to replace it has so far given variable results. This is in part due to the fact that since OGD is considered as gold standard, when the result of an alternative method differ from the OGD it is automatically considered as false neg-ative (or false positive) of the alternative method even though in reality it might represent false posi-tive (or false negative) of OGD, and this puts any new method to disadvantage. Several studies in the past have shown indepen-dent parameters like splenomegaly,9-12 ascites,13 spi-der naevi,14 Child’s grade,15 platelet count,16,12 pro-thrombin time / activity,17 portal vein diameter,17 platelet count / spleen diameter ratio,18 serum albu-min,16 serum bilirubin,16 fibro test, CT scanning, video capsule endoscopy as significant predictors for the presence of esophageal varices. We tested platelet count, portal vein diameter, serum albumin and spleen size among them and found to be reliable predictors of esophageal vari-ces. Low platelet count, increased portal vein dia-meter and splenomegaly are found to be associated with esophageal varices.9,10,12,17 This is expected, as portal hypertension is the initial and most impor-tant factor leading to the development of varices while the presence of varices is proportional to the severity of liver disease and the degree of portal hypertension. Sarwar et al,6 and Zaman et al14 found
cutoff value of < 88 103 / µL for platelets to be independent risk factors for the presence of large
varices. In another study platelet count < 100,000 was found to be associated with any degree of eso-phageal varices while platelet count of <90000 with large esophageal varices.19 Splenic sequestration and antibody – mediated destruction of the platelets has been thought to be the cause of thrombocyto-penia in patients with cirrhosis. In our study the cutoff value is 72,000.
The measurement of the spleen bipolar diame-ter and portal vein diameter using ultrasonography is easily obtainable, reproducible and non-invasive and is routinely performed on patients with cirrho-sis as cirrhotic patients usually undergo annual / bi-annual abdominal ultrasonography as part of the surveillance program for hepatocellular carcinoma.
Low serum albumin is another predictor that has been found to be associated with the presence of esophageal varices. Sarwar et al[6] and Schepis et al17 found cutoff value of < 2.95 g/dl to be independent risk factors for the presence of esophageal varices. Low serum albumin is indicator of deranged hepatic function. The degree of hepatic dysfunction is likely to affects the development of portal hypertension via humoral factors and thus the development of varices. CONCLUSION Platelet count less than 72000, serum albumin less than 2.3 g/dl, portal vein diameter more than12.5 cm on ultrasound and spleen size 19 were found to be independent predictors of esophageal varices on endoscopy. So endoscopy should be done in any patient with above mentioned parameters. REFERENCES 1. D’Amico G. Esophageal varices: from appearance to
rupture;Natural history and prognostic indicators. In: Groszmann RJ, Bosch J (eds). Portal Hyperten-sion in the 21st Century. Dordrecht: Kluwer Acade-mic Publishers, 2004: pp. 147–154.
2. Christensen E, Fauerholdt L, Schlichting P et al. As-pects of the natural history of gastrointestinal bleed-ing in cirrhosis and the effect of prednisone. Gastro-enterology 1981; 81: 944–952.
3. D’Amico G, Pagliaro L, Bosch J. Pharmacological tre-atment of portal hypertension: an evidence – based approach. Semin Liver Dis 1999; 19: 475–505.
4. D’Amico G, De Franchis R. Upper digestive bleeding in cirrhosis. Post-therapeutic outcome and prognos-tic indicators. Hepatology 2003; 38: 599–612.
5. Javed Iqbal Farooqi, Hameed Ahmed, Qazi Ikra-mullah, Farooq Ahmed, Masood-ur-Rehman. Predic-tors of esophageal varices in patients of liver cirrhosis JPMI 2007; vol. 21, No.01: 60-64.
6. Sarwar S, Khan AA, Alam A, Butt AK, Shafqat F, Malik K, Ahmad I, Niazi AK. Non-Endoscopic pre-diction of presence of esophageal varices in cirrhosis. J Col Physicians Surg Pak 2005; 15: 528-31.
7. Ismail FW, Shah HA Hamid S, Jafri W. Non-invasive

NON-ENDOSCOPIC PREDICTORS FOR THE PRESENCE OF ESOPHAGEAL VARICES IN PATIENTS WITH LIVER CIRRHOSIS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 35
predictors of large varicrs in patients hospitalized with gastroesophageal variceal hemorrhage. Hepatol Int.2008; 2: 124-128.
8. Gralnek IM, Jenssen DM, Kovacs TO, Jutabha R, Ma-chicado GA, Gombein J, King. The economic impact of esophageal variceal hemorrhage: Cost-effective-ness implications of endoscopic therapy. Hepatology 1999; 29: 4.
9. Amarapurkar DN, Parikh SS, Shankaran K, Chopra K, Dhawan P, Kalro RH, et al. Correlation between splenomegaly and oesophageal varices in patients with liver cirrhosis. Endoscopy. 1994; 26: 563.
10. Chalasani N, Imperiale TF, Ismail A, Sood G, Carey M, Wilcox CM, et al. Predictors of large esophageal varices in patients with cirrhosis. Am J Gastroente-rol. 1999; 94: 3285–91.
11. Thomopoulos KC, Labropoulou – Karatza C, Mimidis KP, Katsakoulis EC, Iconomou G, Nikolopoulou VN. Non-invasive predictors of the presence of large oesophageal varices in patients with cirrhosis. Dig Liver Dis. 2003; 35: 473–8.
12. Pilette C, Oberti F, Aube C, Rousselet MC, Bedossa P, Gallois Y. Non-invasive diagnosis of esophageal vari-ces in chronic liver diseases. J Hepatol. 1999; 31: 867–73.
13. Sharma SK, Aggarwal R. Prediction of large esopha-geal varices in patients with cirrhosis of the liver using clinical, laboratory and imaging parameters. J Gastroenterol Hepatol. 2007; 22: 1909–15.
14. Ng FH, Wong SY, Loo CK, Lam KM, Lai CW, Cheng
CS. Prediction of oesophagogastric varices in patients with liver cirrhosis. J Gastroenterol Hepatol. 1999; 14: 785–90.
15. Pilette C, Oberti F, Aube C, Rousselet MC, Bedossa P, Gallois Y. Non-invasive diagnosis of esophageal vari-ces in chronic liver diseases. J Hepatol. 1999; 31: 867–73.
16. Zaman A, Becker T, Lapidus J, Benner K. Risk factors for the presence of varices in cirrhotic patients with-out a history of variceal hemorrhage. Arch Intern Med. 2001; 161: 2564–70.
17. Bressler B, Pinto R, El-Ashry D, Heathcote EJ. Which patients with primary biliary cirrhosis or primary sclerosing cholangitis should undergo endoscopic screening for oesophageal varices detection. Gut. 2005; 54: 407–10.
18. Schepis F, Camma C, Niceforo D, Magnano A, Pallio S, Cinquegrani M, et al. Which patients with cirrhosis should undergo endoscopic screening for esophageal varices detection? Hepatology 2001; 33: 333-8.
19. Giannini E, Zaman A, Kreil A, Floreani A, Dulbecco P, Testa E, et al. Platelet count / spleen diameter ratio for the noninvasive diagnosis of esophageal varices: Results of a multicenter, prospective, validat-ion study. Am J Gastroenterol 2006; 101: 2511-9.
20. Jijo V Cherian, Nandan Deepak, Rajesh Prabhu Pon-nusamy, Aravindh Somasundaram, V Jayanthi Non-invasive predictors of esophageal varices: Saudi J of Gastro2011; 17: 64-68.

36 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
ORIGINAL ARTICLE
LIVER DYSFUNCTION PART AND PARCEL OF DENGUE FEVER
HUDA G. MIRZA, IKRAM-UR-RAHIM, M. FAROOQ SAEED
MUTI-ULLAH KHAN, MUSSARAT AHMAD, RAZIA JAVAID, SAMEED ALI Department of Medicine, Akhtar Saeed Trust Teaching Hospital. (ASTTH), DHA EME Sector, Lahore
ABSTRACT Objective: To assess the effects of dengue virus on the liver enzymes in patients of Dengue fever.
Data Management: This retrospective observational study was conducted in the Medical depa-rtment of ASTTH Lahore between August to October 2011 in patients presenting to the OPD, Emer-gency and indoor who fulfilled the inclusion criteria. After taking history and clinical examination blood samples were tested for CBC, LFT’s Urea, creatinine, complete urine, Rapid IgG and IgM test for dengue virus. Positive results were confirmed by ELIZA method. According to the results, the patients were divided into different groups. Group1 comprised of patients with normal AST and ALT levels. In group 2 aminotransferases increased up to three times the normal value. Patients in whom there was an increase of enzymes 3 to10 times the reference values were classified as Group 3, while amino-transferase levels > 10 times the normal were included in group 4.
Results: Out of total 300 hundred confirmed patients, 54% were men, 48% were females and their mean age was 38.5 years. Two hundred twenty eight (76%) patients had Classical Dengue Fever and 72 (24%) patients had Dengue Haemorrhagic fever (DHF).The patients were grouped according to the increase in Amino-transferase levels. Among the 228 patients of Classic Dengue Fever highest number were in group 2 (51.75%) and the lowest were in group 4 (8.77%) In 72 pati-ents with DHF most patients were in group 4 (68%).
Conclusion: Dengue fever has a definite relationship with liver enzymes which increase with severity of the infection and is highest in DHF; therefore liver dysfunction is part and parcel of Dengue infection, so liver function tests must be checked along with hematology.
Key Words: Dengue fever, Liver Function tests, Dengue Haemorrhagic fever. INTRODUCTION Dengue Virus (DV) is an envelope, single – stran-ded, positive RNA virus and a member of the family Flaviviridae, genus flavivirus. There are four anti-genically related but distinct serologic subtypes; DV1, DV2, DV3 and DV4.1 Epidemic dengue fever (DF) was common in Asia and Pacific throughout the twentieth century.2 Dengue virus made its route geographically into Asia through South Asian countries.3 In Asia, the first outbreak of DHF began in the 1950s in the Phi-lippines and Thailand. However, in the next 20 yea-rs, the disease spread throughout South East Asia and by the mid 1970s, DHF was the leading cause of hospitalization and death among children in this region. Thereafter in the 1980’s and 1990s, dengue transmission intensified with regular epidemics every 3 – 5 years in hyper-endemic areas.4 In Pakis-tan, the first confirmed outbreak was due to sero-type DV2 reported in 1994 by Aga Khan University Hospital (AKUH).5 During September to December
2005, three major hospitals in Karachi had a sud-den increase in the number of patients with DHF.6 Genotyping of selected samples from the early part of the outbreak revealed the presence of DV3. This epidemic was probably a consequence of the intro-duction of DV3 in a population with prior sensitizat-ion to DV1 and DV2 resulting in severe disease. The-reafter, Pakistan experienced its largest and most severe outbreak of DHF in 2006 and DV2 and DV3 were identified as the predominant serotypes.7 Den-gue virus is now endemic in Pakistan, circulating throughout the year with a peak incidence in the post monsoon period. The symptomatology of dengue varies, generally consisting of the mild forms found in cases of classic dengue, the principal manifestations of which are high fever, arthralgias, myalgias, rash and gastroin-testinal disorders. Liver is an organ, which is effec-ted in most systemic diseases; dengue virus also tar-gets the liver. Hepatic dysfunction is common in dengue infection, and is attributed to a direct viral

LIVER DYSFUNCTION PART AND PARCEL OF DENGUE FEVER
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 37
effect on liver cells or as a consequence of dysregu-lated host immune responses against the virus, but the derangements in the trans-aminases range from mild and self-limiting disease to high levels indicat-ing varying degrees of acute hepatitis. There are iso-lated case reports of fulminant hepatic failure due to DV. Aspartate amino-transferase AST and ALT are liver enzymes involved in amino acid metabolism. The inflammatory process resulting from infection by the dengue virus leads to a parenchymatous les-ion that releases these markers into the blood. In the acute phase of the disease, an increase occurs in amino-transferases, the levels of which subsequen-tly decrease as the liver recovers. Purpose of our study is to see the relation of DV with the Liver enzymes in patients with Dengue fever in our local population as disturbed liver bio-chemistry is an integral part of DF and no previous data is available in our population. Data Management This retrospective study was conducted by the Medical Department at ASTTH, between August till October 2011.This study was conducted after appro-val by the Ethical Committee and after getting infor-med consent from the patients. A total of 300 pati-ents were included in the study, between the ages of 15 to 75 years. Both men and women were inducted presenting either in the Emergency or Outdoor / in-door department. History and clinical examination was done. Blood samples were collected for com-plete blood examination, complete liver profile, urea creatinine and complete urine examination. Initi-ally, the blood samples were tested by Rapid IgG and IgM Dengue Kit test and all positive results were confirmed by ELIZA to cut the costs. Thrombocytopenia was defined as a platelet count < 150,000 cells / mm3 blood. A hematocrit value > 45% was considered raised. Similarly, leuco-penia was defined as a white cell count < 4000 cells / mm3. Alanine aminotransferase (ALT) was conside-red raised if > 55 and > 33 IU/L for males and fema-les, respectively. Aspartate amino-transferase (AST) was defined as raised if > 46 and > 32 IU/L for males and females, respectively. Blood urea > 40 mg/dl and serum creatinine > 1.5 mg/dl were taken as cli-nically significant. Serology: Tests for the detection of anti-dengue antibodies were carried out in blood samples collected between the 7th and 11th days follo-wing the onset of symptoms. When the results of the tests were positive, patients were considered to be currently infected by the dengue virus, while cases in which the result samples were negative were con-sidered unconfirmed. Classical Dengue fever was suspected when two or more of the following symptoms were present: fever, retro-orbital pain, myalgias, arthralgias, along
with positive serology.
Dengue Hemorrhagic Fever (DHF): The diagno-sis of DHF was established according to the adapted World Health Organization (WHO) criteria: throm-bocytopenia < 100,000 / mm3, hemoconcentration and hemorrhagic manifestations such as spontane-ous petechiae, or a positive tourniquet test. Hemo-concentration was defined as hematocrit > 45% in men, > 40% in women
The patients were divided in different groups according the severity of disturbance of liver enzy-mes. Group1 comprised of patients with normal AST and ALT levels. In group 2 aminotransferases incre-ased up to three times the normal value. Patients in whom there was an increase in one or both enzyme 3 to 10 times the reference values were classified as Group 3, while aminotransferase levels > 10 times were included in group 4.
Exclusion Criteria
All patients were screened for Hepatitis B and HCV by ELIZA technique, Enteric fever by Typhidot me-thod and Malaria by thick and thin film slides. All patients with Positive results were not included in the study.
Data was entered in predesigned Performa, for subsequent processing and analysis, data was analy-zed on statistical package for social sciences (SPSS) version 13. Mean and standard deviations were cal-culated for age and sex. Frequency and percentages were computed for investigations.
RESULTS
A total of 300 patients were included in the study. Their mean age was 38.5 (ranging from 15 – 75 yea-rs) 160 (53.3%) were between the age of 30-45 years while infection in old age group 60 – 75 years is low (6.6%) Figure 1.
0
20
40
60
80
100
120
140
160
180
15 - 30 30 - 45 45 - 60 60 - 75
No. of Patients
Figure 1: Dengue Fever in different Age Groups.
No. of P
atients
Age

HUDA G. MIRZA, IKRAM-UR-RAHIM, M. FAROOQ SAEED et al
38 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
Among the total 162 (54%) were men and 138 (46%) women as shown in Figure 2.
0
50
100
150
200
250
300
350
Male Female Total
Series 1
Figure 2:
Among the 300, 228 (76%) patients had clas-sical dengue fever and 72(24%) patients had DHF. Among the 228 patients highest were in group 2 (51.75%) and the lowest were in group4 (8.77%) as shown in table 1.
Table 1: Dengue Fever 228 Patients (76%).
Liver Damage No. of Patients Percentage
Group 1 35 15.35%
Group 2 118 51.75%
Group 3 55 24.12%
Group 4 20 8.77%
In 72 patients with DHF more patients were in group 4 (68%) as in table 2.
Table 2: Dengue Hemorrhagic Fever 72 Patients
(24%).
Liver Damage No. of Patients Percentage
Group 1 0 0%
Group 2 0 0%
Group 3 23 32%
Group 4 49 68%
DISCUSSION Age: Dengue infection is generally considered to be a pediatric disease but is currently a growing prob-lem in adults throughout the tropics. Furthermore, dengue infection can be more severe in adults in whom early recognition of bleeding tendencies and signs of circulatory collapse would reduce mortality.
In our study most of the patients were young bet-ween the age of 30 – 45 (53.3%) While several inter-national studies from South – east Asian countries have shown that the average / mean age of reported dengue cases has increased from 5 – 9 years to older children and adults.8-10 In Thailand, affected adults over 15 years of age comprise 30 – 40% of dengue cases. At present, the average age of patients with dengue infection is increasing.11-12
Gender: In our study, out of total 300 patients men were predominantly affected 54% while only 46% females were inflicted. In a study of dengue inci-dence in Malaysia between 1973 and 1987 the majo-rity of reported cases were also found to be male.13 This pattern of male excess among older age groups agrees with previous studies in Singapore14-16 and has also been found in more recent dengue surveil-lance data from the Philippines for 2010 (the Philip-pines Department of Health, personal communicat-ion) and Singapore for 2009.17 Taken together, the-se findings suggest that there may be gender – rela-ted differences in dengue incidence, which might be due to exposure differences among older adolesce-nts and adults.
In our study conducted on 300 patients, 228 (76%) patients had classical dengue fever and 72 (24%) patients had DHF. Among the 228 patients highest number of patients were in group 2 (51.75%) In group 2 amino-transferases levels were increased up to three times the normal value and the lowest number of patients were in group 4 (8.77%) with aminotransferase levels > 10 times the normal val-ue. In international study conducted by Kuo et al.18 reported that approximately 90% of the patients in that study had abnormal AST levels, while abnormal levels of ALT, bilirubin, alkaline phosphatase and gamma-glutamyl transferase (GGT) were found in 80%, 7%, 16% and 83%, respectively, of patients with classic dengue. Liver involvement occurred through an inflammatory process in the paren-chyma provoked directly or indirectly by the virus, reducing the diameter of the lumen of the biliary canaliculus, causing obstruction and leading to bili-rubinemia or even jaundice, as reported in 3 cases of DHF.19,20 In a study carried out by Nguyen et al.21 AST values were reported to be frequently abnor-mal, reaching values higher than those of ALT, aro-und 97.7% and 37.3% above normal levels, respecti-vely. Levels of amino-transferases increases with severity of disease as suggested, In an another study the use of markers such as ALT and AST as parame-ters to evaluate severity in patients with dengue fever22 since grossly elevated liver enzymes are kno-wn to be an early warning sign for severe disease and clinical bleeding, vigorous follow up in such patients is warranted.23
No. of P
atients

LIVER DYSFUNCTION PART AND PARCEL OF DENGUE FEVER
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 39
CONCLUSION Dengue fever is more common in adults and male gender. It has a definite relationship with liver enzy-mes which increase with severity of the infection and is highest in DHF, therefore liver dysfunction is part and parcel of Dengue infection, so liver funct-ion tests must be checked along with hematology for dengue fever and this message must be implemen-ted during an Epidemic. REFERENCES 1. Guzman MG, Kouri G. Dengue and dengue hemor-
rhagic fever in the Americas: lessons and challenges. J Clin Virol. 2003; 27: 1–13.
2. Thomas SJ, Strickman D, Vaughn DW. Dengue epi-demiology: virus epidemiology, ecology, and emer-gence. Adv Virus Res. 2003; 61: 235–289.
3. Gubler DJ. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev. 1998; 11: 480–496.
4. Petersen LR, Marfin AA. Shifting epidemiology of Flaviviridae. J Travel Med. 2005; 12 (Suppl. 1): S3–11.
5. Chan YC, Salahuddin NI, Khan J, Tan HC, Seah CL, et al. Dengue haemorrhagic fever outbreak in Kara-chi, Pakistan, 1994. Trans R Soc Trop Med Hyg. 1995; 89: 619–620.
6. Jamil B, Hasan R, Zafar A, Bewley K, Chamberlain J, et al. Dengue virus serotype 3, Karachi, Pakistan. Emerg Infect Dis. 2007;13:182–183.
7. Khan E, Hasan R, Mehraj V, Nasir A, Siddiqui J, et al. Co-circulations of two genotypes of dengue virus in 2006 out – break of dengue hemorrhagic fever in Karachi, Pakistan. J Clin Virol. 2008; 43: 176–179.
8. Chareonsook O, Foy HM, Teeraratkul A, Silarug N. Changing epidemiology of dengue hemorrhagic fever in Thailand. Epidemiol Infect. 1999; 122: 161–6.
9. Pongsumpun P, Yoksan S, Tan IM. A comparison of the age distributions in the dengue hemorrhagic fever epidemics in Santiago de Cuba (1997) and Thailand (1998). Southeast Asian J Trop Med Public Health. 2002; 33: 255–8.
10. Kularatne SA, Gawarammana IB, Kumarasiri PR. Epidemiology, clinical features, laboratory investigat-ions and early diagnosis of dengue fever in adults: a descriptive study in Sri Lanka. Southeast Asian J Trop Med Public Health. 2005; 36: 686–92.
11. Patumanond J, Tawichasri C, Nopparat S. Dengue hemorrhagic fever, Uttaradit, Thailand. Emerg Infect
Dis. 2003; 9: 1348–50. 12. Simmons M, Burgess T, Lynch J, Putnak R. Protect-
ion against dengue virus by non-replicating and live attenuated vaccines used together in a prime boost vaccination strategy. Virology. 2010; 396: 280–8.
13. Shekhar KC, Huat OL. Epidemiology of dengue / dengue hemorrhagic fever in Malaysia – a retrospec-tive epidemiological study 1973 – 1987. Part I: Den-gue hemorrhagic fever (DHF). (Review). Asia – Paci-fic Journal of Public Health, 1992-1993, 6: 15–25.
14. Eong OE. Changing pattern of dengue transmission in Singapore.Dengue Bulletin, 2001; 25: 40.
(http://www.searo.who.int/LinkFiles/Dengue_Bulletin_Volume_25_ch7.pdf, accessed on 6 June 2011).
15. Ooi EE, Goh KT, Gubler DJ. Dengue prevention and 35 years of vector control in Singapore. Emerging In-fectious Diseases, 2006; 12 (6): 887–893.
pmid:16707042 16. Yew YW et al. Sero-epidemiology of dengue virus
infection among adults in Singapore. Annals of the Academy of Medicine, Singapore, 2009; 38: 667–675. pmid:19736569accessed on 26 December 2010).
17. Communicable Diseases Surveillance in Singapore 2009. Singapore Ministry of Health, 2010.
(http://www.moh.gov.sg/content/moh_web/home/Publications/Reports/2010/communicable_diseasessurveillanceinsingapore2009.html,accessed on 26 December 2010)
18. Kuo C.H., Tai D.I., Chang – Chien C.S., et al. Liver bio-chemical tests and dengue fever. Am J Trop Med Hyg 1992; 47 (3): 265-70.
19. Lum L.C., Lam S.K., George R., Devi S. Fulminant hepatitis in dengue infection. Southeast Asian J Trop Med Public Health 1993; 24 (3): 467-71.
20. Souza L.J., Lopes A.C., Bastos D.A. Icterícia na den-gue hemorrágica: relato de três casos. Rev Bras Clin Terap 2002; 28 (5): 198-201.
21. Nguyen T.L., Nguyen T.H., Tieu N.T. The impact of dengue hemorrhagic fever on liver function. Res Virol 1997; 148 (4): 273-7.
22. De Souza LJ, Nogueira RM, Soares LC, Soares CE, Ribas BF, et al. The impact of dengue on liver funct-ion as evaluated by aminotransferase levels. Braz J Infect Dis. 2007; 11: 407–410.
23. Murgue B, Deparis X, Chungue E, Cassar O, Roche C. Dengue: an evaluation of dengue severity in French Polynesia based on an analysis of 403 laboratory-confirmed cases. Trop Med Int Health. 1999; 4: 765–773.

40 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
ORIGINAL ARTICLE
PRECIPITATING FACTORS OF HEPATIC ENCEPHALOPATHY IN LIVER CIRRHOSIS
UMAIR AHMED, MIRZA AKMAL SHARIF, HUDA GHULAM MIRZA
TH RIZVI, AWAIS AHMED, UMER USMAN, AHSAN FAROOQ Medical Unit Allied / DHQ Hospital, Faisalabad
STRUCTURAL ABSTRACT Introduction: Hepatic encephalopathy is a well – recognized clinical complication of chronic liver disease. It is a reversible, complex neuropsychiatric syndrome characterized by disturbances in consciousness and behavior, personality changes, fluctuating neurologic signs and flapping tre-mors.
Objective: To find out the frequency distribution of precipitating factors of hepatic encephalo-pathy in post viral cirrhosis of liver.
Study Design: Cross sectional analytical study.
Setting: Study conducted in Medical Unit Allied / DHQ Hospital Faisalabad.
Duration with Date: Six months (1st July 2012 to 31st December 2012).
Subjects and Methods: Study conducted on 100 consecutive patients diagnosed as post viral cirrhosis of liver decompensated by hepatic encephalopathy of either sex between 20-70 years of age. All the patients were screened for different precipitating factors with history, examination and relevant investigations. History included drowsiness or deep coma preceded by haematemesis, melena, fever, constipation, sedative drugs, and use of high dose diuretics. Clinical examination revealed all signs of chronic liver disease and hepatic encephalopathy especially flapping tremor. Relevant investigations included TLC, serum potassium, ascitic fluid examination, urine C/E, and chest X-Ray for infection.
Results: Out of 100 patients, 52 were male while 48 were female. Thirty patients (30%) had upper GI bleed, 8 patients (8%) had Hypokalemia, 6 patients (6%) had used sedative drugs, 22 pat-ients (22%) had spontaneous bacterial peritonitis, 9 patients (9%) had history of high dose diure-tics, 15 patients (15%) had constipation, and 10 patients (10%) had others, or no identifiable preci-pitating causes of hepatic encephalopathy.
Conclusion: Upper GI bleed was on the top of list as a precipitating factor of hepatic encephalo-pathy followed by infection and constipation. A small percentage of Hypokalemia, sedative drugs, and diuretic induced encephalopathy were observed.
Key words: Hepatic encephalopathy, Liver Cirrhosis, Precipitating factors, upper GI bleed. INTRODUCTION Hepatic encephalopathy (HE) is a common neuro-psychiatric syndrome seen in patients with signifi-cant hepatic dysfunction in the absence of neurolo-gical disorders.1 It is a reversible, complex neuro-psychiatric syndrome characterized by disturbances in consciousness and behavior, personality changes, fluctuating neurologic signs, asterixis.2 It is seen in up to 30 – 45% of patients with cirrhosis and its lat-ent or sub clinical form (minimal hepatic encepha-lopathy can affect up to 60% of patients with liver disease.3 Many theories about the pathogenic mech-anism of hepatic encephalopathy exist, certain fac-
tors like hyper ammonia and increased blood-brain permeability to ammonia, increased brain concen-tration of manganese and inhibitor neurosteroids (alopregnanolone) have been documented to play important role in occurance of HE.4 HE is a severe prognostic sign. According to the results of a recent study, the survival probability after the first episode of overt encephalopathy in patients with chronic liver disease is 42% at one year of follow-up and 23% at 3 years.5 A precipitating factor of HE can be usually identified, and the treatment of the episode is directed towards the correction of this precipi-tant. Once the precipitating condition has been

PRECIPITATING FACTORS OF HEPATIC ENCEPHALOPATHY IN LIVER CIRRHOSIS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 41
resolved, the encephalopathy also subside usually.6 Multiple studies have been conducted worldwide determining the precipitating factors for HE. In multiple studies it was found that sepsis, gastroin-testinal bleeding, constipation, and diuretic use were the common precipitating factors of encepha-lopathy in patients with liver disease.7-9 Usage of drugs such as sedatives, tranquilizers, analgesics and diuretics, large volume paracentesis have all been considered to precipitate HE in otherwise sta-ble cirrhotic patient.10-12 In a recently published stu-dy, it was found that the most common precipitant of HE was spontaneous bacterial peritonitis (20.5%), constipation(18.3%) and urinary tract infe-ction (15.3%).6 In another study, it was found that the most common precipitating factors detected were infection (67%), constipation (49%) and gas-trointestinal bleeding (45%).13 Variations in disease pattern from time to time require the need for periodic studies to define the changing frequency distribution of precipitating fac-tors of hepatic encephalopathy for continuous medi-cal education and learning. The aim of the study was to ascertain the common precipitating factors and their frequency in patients presenting with HE so as to minimize and control the recurrent attacks of en-cephalopathy by early recognition of the precipitat-ing factors and therefore improve the prognosis in patients with cirrhosis of liver. MATERIAL AND METHODS The objective of this descriptive study was to deter-mine the frequency distribution of precipitating fac-tors of hepatic encephalopathy in post-viral cirrho-sis of liver. Study had conducted in Medical Unit Allied / DHQ Hospital Faisalabad from 1st July 2012 to 31 December 2012. 100 patients of cirrhosis of liver due to Hepatitis B, C or both were included in the study. Non-probability consecutive sampling technique was used as sampling technique. All patients with liver disease who were diagno-sed as having acute HE secondary to post viral liver cirrhosis and portal hypertension and classified as type C HE according to the working party classifi-cation of HE by Fereci et al14 were included in the study. Patients having Encephalopathy due to acute culminant hepatic failure (type A HE),14 Encephalo-pathy secondary to portal systemic bypass without intrinsic hepatocellular disease (type B HE),14 Ence-phalopathy with co-morbid conditions like diabetes mellitus and chronic renal failure were excluded from the study. Patients with diagnosis of cirrhosis of liver and hepatic encephalopathy on the basis of history and clinical examination and investigation were selected for study. They were screened for the precipitating factors like, drugs, upper GI bleed, Hypokalemia,
infection, constipation and diuretics. A question-naire was designed and used for data collection. A detailed clinical history of the patients was taken regarding their present and past illness, specifically enquired about fever, GI bleeding including haema-temesis and melena, constipation, high protein diet and loose motions ± vomiting. Detailed drugs his-tory especially about the use of diuretics, sedatives, nonsteroidal anti-inflammatory drugs and cough syrups was taken. Past history of jaundice, bleeding, edema and encephalopathy was also taken. Patients were examined for jaundice, anemia, fever, fetor hepaticus and asterixis. Hemodynamic status with signs of dehydration was also noted. Peripheral ede-ma and degree of ascites (if present) was recorded and Hepatic encephalopathy was graded according to the West Heaven criteria.14 All relevant investiga-tions including full blood count, Urine microscopy, serum electrolytes, blood urea and serum creati-nine, blood glucose and a chest radiograph were done. Serum bilirubin, Alanine Aminotransferase (ALT) levels, Serum Albumin and Prothrombin time were also done to help assess their Child-Pugh sco-re. An abdominal ultrasound was done in all cases for liver size, parenchymal echogenicity, portal vein diameter, spleen size and for the detection of asci-tes. In the presence of ascites a diagnostic ascitic tap was also done to look for any evidence of spontane-ous bacterial peritonitis. Data was analyzed with the help of SPSS version 15. Descriptive analysis of patients with hepatic en-cephalopathy was performed for demographic and laboratory parameters and results were presented as mean ± standard deviation for quantitative vari-ables. Frequency, percentages were calculated for all the qualitative variables including the precipitating factors. RESULTS The study showed 52 (52%) were male and 48 (48%) were female (Fig. 1).
52%
48% Male = 52
Female = 48
Fig. 1: Sex distribution of the patients (n = 100).
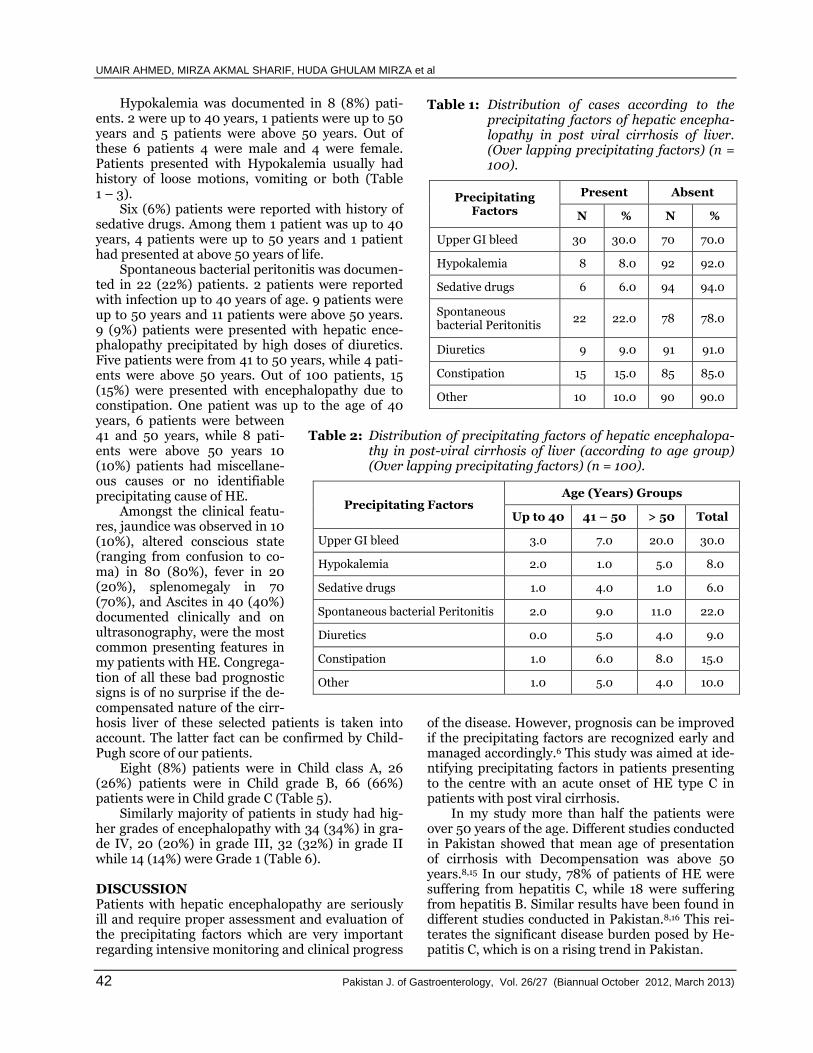
UMAIR AHMED, MIRZA AKMAL SHARIF, HUDA GHULAM MIRZA et al
42 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
Hypokalemia was documented in 8 (8%) pati-ents. 2 were up to 40 years, 1 patients were up to 50 years and 5 patients were above 50 years. Out of these 6 patients 4 were male and 4 were female. Patients presented with Hypokalemia usually had history of loose motions, vomiting or both (Table 1 – 3). Six (6%) patients were reported with history of sedative drugs. Among them 1 patient was up to 40 years, 4 patients were up to 50 years and 1 patient had presented at above 50 years of life. Spontaneous bacterial peritonitis was documen-ted in 22 (22%) patients. 2 patients were reported with infection up to 40 years of age. 9 patients were up to 50 years and 11 patients were above 50 years. 9 (9%) patients were presented with hepatic ence-phalopathy precipitated by high doses of diuretics. Five patients were from 41 to 50 years, while 4 pati-ents were above 50 years. Out of 100 patients, 15 (15%) were presented with encephalopathy due to constipation. One patient was up to the age of 40
Table 1: Distribution of cases according to the precipitating factors of hepatic encepha-lopathy in post viral cirrhosis of liver. (Over lapping precipitating factors) (n = 100).
Precipitating Factors
Present Absent
N % N %
Upper GI bleed 30 30.0 70 70.0
Hypokalemia 8 8.0 92 92.0
Sedative drugs 6 6.0 94 94.0
Spontaneous bacterial Peritonitis
22 22.0 78 78.0
Diuretics 9 9.0 91 91.0
Constipation 15 15.0 85 85.0
Other 10 10.0 90 90.0
years, 6 patients were between 41 and 50 years, while 8 pati-ents were above 50 years 10 (10%) patients had miscellane-ous causes or no identifiable precipitating cause of HE. Amongst the clinical featu-res, jaundice was observed in 10 (10%), altered conscious state (ranging from confusion to co-ma) in 80 (80%), fever in 20 (20%), splenomegaly in 70 (70%), and Ascites in 40 (40%) documented clinically and on ultrasonography, were the most common presenting features in my patients with HE. Congrega-tion of all these bad prognostic signs is of no surprise if the de-compensated nature of the cirr-
Table 2: Distribution of precipitating factors of hepatic encephalopa-
thy in post-viral cirrhosis of liver (according to age group) (Over lapping precipitating factors) (n = 100).
Precipitating Factors Age (Years) Groups
Up to 40 41 – 50 > 50 Total
Upper GI bleed 3.0 7.0 20.0 30.0
Hypokalemia 2.0 1.0 5.0 8.0
Sedative drugs 1.0 4.0 1.0 6.0
Spontaneous bacterial Peritonitis 2.0 9.0 11.0 22.0
Diuretics 0.0 5.0 4.0 9.0
Constipation 1.0 6.0 8.0 15.0
Other 1.0 5.0 4.0 10.0
hosis liver of these selected patients is taken into account. The latter fact can be confirmed by Child-Pugh score of our patients. Eight (8%) patients were in Child class A, 26 (26%) patients were in Child grade B, 66 (66%) patients were in Child grade C (Table 5). Similarly majority of patients in study had hig-her grades of encephalopathy with 34 (34%) in gra-de IV, 20 (20%) in grade III, 32 (32%) in grade II while 14 (14%) were Grade 1 (Table 6). DISCUSSION Patients with hepatic encephalopathy are seriously ill and require proper assessment and evaluation of the precipitating factors which are very important regarding intensive monitoring and clinical progress
of the disease. However, prognosis can be improved if the precipitating factors are recognized early and managed accordingly.6 This study was aimed at ide-ntifying precipitating factors in patients presenting to the centre with an acute onset of HE type C in patients with post viral cirrhosis. In my study more than half the patients were over 50 years of the age. Different studies conducted in Pakistan showed that mean age of presentation of cirrhosis with Decompensation was above 50 years.8,15 In our study, 78% of patients of HE were suffering from hepatitis C, while 18 were suffering from hepatitis B. Similar results have been found in different studies conducted in Pakistan.8,16 This rei-terates the significant disease burden posed by He-patitis C, which is on a rising trend in Pakistan.

PRECIPITATING FACTORS OF HEPATIC ENCEPHALOPATHY IN LIVER CIRRHOSIS
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 43
Table 3: Distribution of precipitating factors of hepatic encephalopathy in post viral cir-rhosis of liver. (According to sex) (Over lapping precipitating factors) (n= 100).
Precipitating Factors
Gender
Male Female Total
Upper GI bleed 22.0 8.0 30.0
Hypokalemia 4.0 4.0 8.0
Sedative drugs 4.0 2.0 6.0
Spontaneous bacterial peritonitis
11.0 11.0 22.0
Diuretics 4.0 5.0 9.0
Constipation 7.0 8.0 15.0
Other 4.0 6.0 10.0
Table 4: Frequency according to Viral markers
and Associated age and gender distribut-ion (n = 100).
Viral Markers No. % age
HCV 78 78.0
HBV 16 16.0
Both HCV and HBV 6 6.0
Total 100 100.0
Table 5: Frequency according to Child’s classifi-
cation and associated age and gender di-stribution (n = 100).
Child’s Class No. % age
A 8 8.0
B 26 26.0
C 66 66.0
Total 100 100.0
Table 6: Frequency acc. to grades of hepatic ence-phalopathy associated with age and gen-der distribution (n = 100).
Grades No. % age
1 14 14.0
II 32 32.0
III 20 20.0
IV 34 34.0
Hepatic encephalopathy was usually precipita-ted by different factors. Infection, gastrointestinal bleeding and constipation have been repeatedly demonstrated as important precipitating factors of HE,17 a fact also borne out by our study. A study on 100 patients in Rawalpindi showed that upper G I bleed was associated with 38% and infection was 26% which were similar to my study.18In our study SBP was found in 22% of patients. Patients in local setting are usually severely malnourished not only because of their disease but also because of food fa-ddism and taboos regarding their diet.19 Strict die-tary restrictions on these patients lead to anorexia and malnutrition, and eventually lowering their im-munity and making them more susceptible to infec-tions. Constipation probably is also the result of lack of consistent use of lactulose by our patients, which may be because it is costly and also because of lack of awareness in our population about constipation as important precipitating factor of HE. Electrolyte imbalance especially Hypokalemia which also corre-lates with the severity of the liver disease was found in 8 (8%) patients and may be considered, not only a precipitant but also a manifestation of advance na-ture of cirrhosis in our patients. Most of these pati-ents were associated with diarrhea and/or vomiting and two of patients had also undergone therapeutic paracentesis. Table 7 shows that findings of our study are comparable to different studies conducted locally as well as worldwide. Also indicating the fact that a lot
Table 7: Comparison of the studies of different precipitating factors.
Studies GI bleed (%) Constipation (%) Infection (%) Hypokalemia (%) Sedative Drugs
Faloon 20 33 6 -- 18 ----
Mumtaz K6 13.6 18.3 20.5 6.4 ----
Alam 16 22 32 24 18 ----
Khurram21 31 33 11 7 ----
Devrajani13 45 49 67 --- ----
Present study 30 15 22 8 6

UMAIR AHMED, MIRZA AKMAL SHARIF, HUDA GHULAM MIRZA et al
44 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
of work has to be done to decrease the percentage of these precipitating factors by proper assessment, early recognition and use of best available prophy-laxis so that the number of admission, morbidity and mortality related to these precipitating factors can be decreased.
CONCLUSION Precipitant – induced hepatic encephalopathy is a common complication of cirrhosis. Infections, cons-tipation and gastrointestinal bleeding were identi-fied as the major precipitants in this study. It is, the-refore, crucial that precipitating factors are identi-fied earlier, especially in patients with severe liver disease, and appropriate treatment initiated soon, with an aim to treat and manage them, and subse-quently ensuring better outcomes. It is also impor-tant to educate the patients and their families about these precipitants to ensure earlier presentation, diagnosis, and management of HE.
REFERENCES 1. Ferenci P, Lockwood A, Mullen K, Tarter R. Hepatic
encephalopathy – definition, nomenclature, diagno-sis, and quantification: Final report of the working party at the 11 th World Congresses of Gastroente-rology, Vienna, 1998. Hepatology 2002; 35: 716-21.
2. Chung RT, Podolsky DK. Cirrhosis and its complicat-ions. In: Kasper DL, Braunwald E, Fauci AS, Haiser SL, Lango DL, Jameson JL. editors Harrison’s Princi-ples of internal medicine. 16th ed. New York: Mc-Graw – Hill; 2005: 1858-69.
3. Poordad F. The burden of hepatic encephalopathy. Aliment Pharmacol Ther 2007; 25: 3-9.
4. Yergara – Gomez M, Flavia – Olivella M, Gil-Prades M, Dalmau – Obrador B. Diagnosis and treatment of hepatic encephalopathy in Spain: Results of a survey of hepatologist. Gastroenterology 2006; 29: 1-6.
5. Weissenborn K, Bokemeyer M, Krause J. Neurologi-cal and neuropsychiatric syndromes associated with liver disease. AIDS 2005; 19: 93-98.
6. Mumtaz K, Ahmed US, Abid S, Baig N, Hamid S, Jaf-ri W. Precipitating Factors and The Outcome of Hep-atic Encephalopathy in Liver Cirrhosis. JCPSP. 2010; 20: 514-8.
7. Butterworth RF. Pathophysiology of hepatic encepha-lopathy a new look at ammonia. Metab Brain Dis 2004; 17: 221-7.
8. Maqsood S, Saleem A, Iqbal A, Butt JA. Precipitating factors of hepatic encephalopathy: Experience at Pak-istan Institute of medical sciences Islamabad. J Ayub Med coll Abottabad 2006; 18: 58-62.
9. Ekanem EE, Etuk IS, Uniga AJ. Features of child-hood hepatic failure in Calabar, Nigeria. Niger Post-grad Med J 2001; 8: 86-9.
10. Dasarathy S, Mullen KD. Hepatic Encephalopathy. Current Treatment Options in Gastroenterology 2001; 4: 517-526.
11. Mas A. Hepatic encephalopathy: From Pathophysio-logy to treatment. Digestion 2006; 73: 86-93.
12. Fitz JG. Hepaticencephalopathy, hepatopulmonary syndromes, hepatorenal syndrome, coagulopathy and endocrine complications of liver disease. In: Feldman M, Friedman LS, Sleisenger MH. Editors. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease.7th ed. Philadelphia: WB Saunders, 2002: 1543-65.
13. Devrajani BR, Shah SZ, Devrajani T, Kumar D. Pre-cipitating factors of hepatic encephalopathy at a terti-ary care hospital Jamshoro, Hyderabad. J Pak Med Assoc. 2009; 59 (10): 683-6.
14. Ferenci P, Lockwood A, Mullen K, Tarter R, Weissen-born K, Blei A.Hepatic encephalopathy – definition, nomenclature, diagnosis, and quantification: final re-port of the working party at the 11thWorld Congres-ses of Gastroenterology, Vienna, 1998. Hepatology 2002; 35: 716-21.
15. Nadeem M, Yousaf MA, Zakaria M, Hussain T and Ali N. The value of clinical signs in diagnosis of cirrhosis. Pak J Med Sci 2005; 21: 121-4.
16. Alam I, Razaullah, Haider I, Humayun M, Taqweem A, Nisar M. Spectrum of precipitating factors of He-patic Encephalopathy in liver cirrhosis. Pakistan J Med Res. 2005; 44: 96-100.
17. Trom A, Griga T, Greving I, Hilden H, Schwegler H. Hepatic encephalopathy in patients with cirrhosis and upper GI bleeding. Hepatology 2000; 47: 473-7.
18. Sheikh A, Ahmed S I, Naseemullah M. Etiology of Hepatic Encephalopathy and Importance of Upper Gastrointestinal Bleeding and Infections as Precipita-ting Factors. J Rawal Med Coll Jun 2001; 5: 10-2.
19. Onuorah CE, Ayo AJ. Food taboos and their nutri-tional implications on developing nations like Nige-ria: a review. Nutr Food Sci 2003; 33: 235-40.
20. Faloon W W. Precipitating factors in the genesis of hepatic coma. N Y state J Med 1970; 23: 2891-96.
21. Khurram M, Khaar HB, Minhas Z, Javed S, Hassan Z, Hameed TA et al. An experience of cirrhotic hepatic encephalopathy at DHQ teaching hospital. J Rawal Med Coll 2001; 5: 60-4.

Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 45
ORIGINAL ARTICLE
EFFICACY AND SAFETY OF PEGYLATED INTERFERON ALPHA2A (PEGAFERON) AND RIBAVIRIN IN CHRONIC HEPATITIS C PATIENTS
GHIAS-UL-HASSAN, ISRAR-UL-HAQUE, GHIAS-UN-NABI TAYYAB
BILAL NASIR, MARIA ASLAM, ASIF MEHMOOD Division of Gastroenterology, Department of Medicine, Lahore General Hospital, Lahore
ABSTRACT Objective: Objective of the study was to see the efficacy and safety of Pegylated Interferon alpha 2a (Pegaferon) in chronic hepatitis C patients.
Materials and Methods: This was an open labeled, prospective, multicentre study done bet-ween June 2010 to June 2012. Study was designed to observe the achievement of sustained virolo-gical response with newly marketed pegylated interferon alpha 2a and ribavirin combination in genotype 3 patients, The enrolled patients were separated into Naïve (A), Relapsers (B) and Non Responders (C) based on the previous history of interferon exposure and its response. The RGT was followed on ALT and RVR, EVR, ETR and SVR and treatment adverse effects were noted at each follow up visit
Results: Out of total 153 treatment naïve patients, 85 (55%) were females and 68 (45%) were males, mean age was 38.2 ± 10.4 years, age ranged from 16 to 60 years. 77.8% (n 119) patients achieved RVR, 53% (n = 18/34) patients achieved EVR, 10.5% (n = 16/153) patients were non res-ponders. Those who achieved RVR continued the therapy for 24 weeks so ETR at week 24 was 96.6% (n = 115/119), ETR at week 48 was documented for those who achieved EVR and continued therapy for 48 weeks and it was 47.1% (n = 16/34), total of 3.9% (6/153) patients lost to follow up (4 patients lost to follow up after achieving RVR and 2 patients after achieving EVR). SVR at week 48 was 92.4% (n = 110/119), SVR at week 72 (for those who achieved the EVR and continued the-rapy for 48 weeks) was 41.2% (n = 14/34), so cumulative SVR was 81% (n = 124/153), total 7 pat-ients had post treatment relapse {4.2% (n = 5/119) patients were those who achieved RVR and 5.9% (2/34) patients were from the group who achieved EVR}. There were only 4 patients in group B (post standard interferon relapse) 2 patients achieved RVR, one patient achieved EVR and one of the patient remained non responder. Remaining three patients completed the therapy for 48 weeks and 2 of these achieved SVR. Out of total 5 patients who were non-responders to previous standard interferon treatment, 3 patients achieved RVR, one patient achieved EVR and one patient, who was non-responder at week 12, discontinued the therapy. Rest of the patients completed therapy for 48 weeks and 2 patients achieved SVR. No serious adverse event was noted during the treat-ment, fatigue was the commonest side effect (60%).
Conclusion: It is concluded that pegylated interferon alpha 2a (pegaferon) and ribavirin has good efficacy and safety in chronic hepatitis C patients.
Key words: RGT (Response guided therapy), SVR (sustained virological response), Hepatitis C. INTRODUCTION Hepatitis C viral infection is a major public health problem in Pakistan.1 Chronic HCV infection foll-ows a progressive course over 20 to 30 years and can ultimately result in cirrhosis, hepatic decom-pensation, hepatocellular carcinoma, and the need for liver transplantation. Studies with 10 to 20 years of follow-up suggest that cirrhosis occurs in up to 50 percent of chronically infected patients.2-4 Lower rates of disease progression have been described.
Antiviral therapy with pegylated interferon and ri-bavirin is the cornerstone of treatment of chronic hepatitis C virus (HCV) infection. The goal of anti-viral therapy in patients with chronic HCV is to era-dicate HCV RNA, which is predicted by attainment of a sustained virologic response (SVR). An SVR is associated with a 99 percent chance of being HCV RNA negative during long – term follow-up 5, and attaining an SVR has been associated with decreases in all – cause mortality, liver-related death, need for

GHIAS-UL-HASSAN, ISRAR-UL-HAQUE, GHIAS-UN-NABI TAYYAB et al
46 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
liver transplantation, hepatocellular carcinoma ra-tes, and liver – related complications.6-10 This study aims to study the efficacy and safety of newly marketed bio-similar pegylated interferon alpha 2a (Pegaferon) in CHC genotype 3 patients. MATERIALS AND METHODS This is an open labeled, prospective, multicentre study conducted between June 2010 to June 2012. Inclusion Criteria Both male and female patients between the age of 12 to 65 years with HCV RNA positive in serum and compensated liver disease (total serum bilirubin ≤ 1.5 g/dL; INR ≤ 1.5; serum albumin ≥ 3.4, platelet count ≥ 75,000 mm and no evidence of hepatic de-compensation (hepatic encephalopathy or ascites), patient should have acceptable hematological and biochemical indices (Hemoglobin 13 g/dL for men and 12 g/dL for women; neutrophil count ≥ 1500 / mm3 and serum creatinine ≤ 1.5 mg/dL, and patient must be willing to be treated and to adhere to treat-ment requirements. Exclusion Criteria 1) Severe concurrent medical disease such as sev-
ere uncontrolled hypertension, heart failure, significant coronary heart disease, poorly con-trolled diabetes (peglycated hemoglobin value > 8.5%), chronic obstructive pulmonary disease.
2) Hepatic decompensation (Child pugh score B7 or onwards).
3) Major uncontrolled depressive illness or a sev-ere psychiatric disorder, a seizure disorder or active substance abuse.
4) Autoimmune hepatitis or other autoimmune condition known to be exacerbated by peginter-feron and ribavirin.
5) Untreated thyroid disease. 6) Co-infection with human immunodeficiency
virus or hepatitis B, any other cause of liver dis-ease.
7) Morbid obesity (weight >125 kg). 8) Neoplastic disease. 9) Solid organ transplant (renal, heart, or lung). 10) Pregnant or unwilling to comply with adequate
contraception or lactating mothers. 11) Known hypersensitivity to drugs used to treat
HCV. 12) Age less than 12 years or more than 65 years. Data Collection Procedure The study was approved by ethical committees at each center, and all the patients provided with writ-ten informed consent. Patients who met the inclus-ion and exclusion criteria were included in the stu-dy. Patients were treated with subcutaneous inject-
ion of Pegylated interferon alpha 2a (Pegaferon) 180 mcg / week and oral weight based (15 mg/kg) Riba-virin in two to three divided doses daily, response guided therapy was started, patients with genotype 3 were followed up with qualitative PCR at week 4, 12 and 24/48 during the treatment and 24 weeks after the end of therapy. For genotype 3 treatment naïve patients, who achieved RVR were treated for 24 weeks, patients who failed to achieve RVR and achieve EVR they were treated for 48 weeks. Those who failed to achieve EVR were declared non res-ponders and treatment was stopped, for relapses and non responders to standard interferons durat-ion of treatment was one year irrespective of the fact whether they achieved RVR or EVR. A real-time PCR – based assay, with a lower limit of detection of 50 IU/ml was use. At each visit, the patients were assessed for clinical, hematological and bio-chemi-cal side effects of pegylated interferon alpha2 and ribavirin. These parameters were assessed at weeks 2 and 4 of therapy and at 4 to 8 week intervals the-reafter. Thyroid stimulating hormone (TSH) and free thyroxine levels were measured every 12 weeks while on therapy. Pregnancy tests were performed every 12 weeks for female subjects and spouses of male subjects. The protocol permitted dose modifi-cation (a 25%, 50%, or 75% reduction in the assig-ned dose) for patients who had clinically significant adverse events or important abnormalities in labo-ratory values. Patients were withdrawn from the study if they missed four consecutive weeks of tre-atment or if there was concerned about safety. Data was analysed by SPSS version 19. Definitions of Virological Responses a) Sustained Virological Response (SVR) is un-
dectable HCV RNA level (< 50 IU/ml), 24 weeks after treatment.
b) Rapid Virological Response (RVR) undetect-able HCV RNA in a sensitive assay (lower limit of detection 50 IU/ml) at week 4 of therapy, maintained up-to the end of treatment.
c) Early Virological Response (EVR) HCV RNA detectable at week 4 but undetectable at week 12, maintained up to end of treatment.
d) Delayed Virological Response (DVR): More than 2 log10 drop but detectable HCV RNA at week 12, HCV RNA undetectable at week 24, maintained up to end of treatment.
e) Null Response (NR): Less than 2 log 10 IU/ml decrease in HCV RNA level from baseline at 12 weeks of therapy.
f) Partial Response (PR): More than 2 log 10 IU/ ml decrease in HCV RNA level from baseline at 12 weeks of therapy but detectable HCV RNA at weeks 12 and 24.

EFFICACY AND SAFETY OF PEGYLATED INTERFERON ALPHA2A (PEGAFERON) AND RIBAVIRIN IN CHRONIC HEPATITIS C
Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013) 47
g) Breakthrough (BT): Reappearance of HCV RNA at any time during treatment after virolo-gical response.
RESULTS There were three groups in study, group A (treat-ment naïve), group B (Relapsers to standard inter-feron) and C (non responders to standard interfe-ron). Out of total 153 treatment naïve patients, 85 (55%) were females and 68 (45%) were males, mean age was 38.2 ± 10.4 years, age ranged from 16 to 60 years. 77.8% (n = 119) patients achieved RVR, 53% (n = 18/34) patients achieved EVR, 10.5% (n = 16/153) patients were non responders. Those who achieved RVR continued the therapy for 24 weeks so ETR at week 24 was 96.6% (n = 115/119), ETR at week 48 was documented for those who achieved EVR and continued therapy for 48 weeks and it was 47.1% (n = 16/34), total of 3.9% (6/153) patients lost to follow up (4 patients lost to follow up after achieving RVR and 2 patients after achieving EVR). SVR at week 48 was 92.4% (n = 110/119), SVR at week 72 (for those who achieved the EVR and conti-nued therapy for 48 weeks) was 41.2% (n = 14/34), so cumulative SVR was 81% (n = 124/153), total 7 patients had post treatment relapse {4.2% (n = 5/119) patients were those who achieved RVR and 5.9% (2/34) patients were from the group who achi-eved EVR}. There were only 4 patients in group B (post sta-ndard interferon relapse), 2 patients achieved RVR, one patient achieved EVR and one of the patient re-mained non responder, rest of three patients comp-leted the therapy for 48 weeks and 2 of these achie-ved SVR. Out of 5 patients who were non responders to
previous standard interferon treatment, 3 patients achieved RVR, one patient achieved EVR and one patient was non-responder at week 12 and disconti-nued the therapy. Rest of the patients completed therapy for 48 weeks and 2 patients achieved SVR. The adverse effects observed in our study were generally mild and tolerable, no patient disconti-nued treatment due to adverse effects, none of the patients had serious adverse event during the treat-ment. The neutrophil count during treatment decree-sed to less than 1500 per cubic millimeter in 30% patients. No serious infections were observed in patients even with a neutrophil count below 750 per cubic millimeter, and in none of the patients tre-atment was discontinued because of neutropenia. Platelet count of less than 50,000 per cubic milli-meter during treatment was uncommon, occurring in only four patients. No patient had platelet counts of less than 25,000 per cubic millimeter during tre-atment, and in none of the patients was treatment discontinued because of thrombocytopenia. Anemia was reported in 30% patients and 20% of patients required support by erythropoietin. DISCUSSION Pegylated interferon and ribavirin is the standard of care for treatment of patients with hepatitis C viral infection. We tested the efficacy and safety of newly marketed biosimilar pegylated interferon alpha 2a (Pegaferon) in our population, to test the efficacy response guided therapy was proposed and side effects of treatment were recorded at each follow up visit. In our study we included only patients with genotype 3, which is the predominant type of geno- type in Pakistan,11 among the treatment naïve group
Adverse events were as follows:
Anemia 30% Insomnia 50%
Neutropenia 30% Diarrhea 10%
Thrombocytopenia 8% Nausea 20%
Thyroiditis 1% Vomiting 5%
Headache 40% Decreased appetite 50%
Fatigue 60% Weight loss 50%
Pyrexia 40% Decreased concentration 5%
Myalgia 40% Injection site reaction 10%
Rigors 15% Pruritus 20%
Alopecia 30% Dry cough 15%
Depression 20%

GHIAS-UL-HASSAN, ISRAR-UL-HAQUE, GHIAS-UN-NABI TAYYAB et al
48 Pakistan J. of Gastroenterology, Vol. 26/27 (Biannual October 2012, March 2013)
119 patients out of total 153 achieved rapid virolo-gical response and 110 (92.4%) of these patients achieved sustained virological response, SVR for those who showed EVR was significantly low (41.2%) this shows the importance of early achieve-ment of virological response during the treatment and importance of prolonging the treatment accord-ing to the virological response. Over all cumulative SVR in treatment naïve patients was 81% which is comparable to the results of previously done studies internationally.12 Although SVR was achieved in patients who has had relapse or no response to previous interferon treatment but total number of patients in this co-hort was too small to draw any conclusion of clinical significance, so requires a larger cohort to see the efficacy in these groups. More number of patients with anemia (30%) were observed than what is reported in meta analy-sis (11%),13 which may be attributed to weight based dose of ribavirin as compared to fixed dose of 800 mg/day, these patients required the support of ery-thropoietin to maintain the hemoglobin during the treatment. It is worth noting that all those patients who de-veloped thyroiditis during the treatment achieved SVR. So it is concluded that pegylated interferon al-pha2a (Pegaferon) and ribavirin has good efficacy and safety for chronic hepatitis C patients. REFERENCES 1. Raja NS, Janjua KA. Epidemiology of hepatitis C
virus infection in Pakistan. J Microbiol Immunol Infect. 2008 Feb; 41 (1): 4-8.
2. Tong MJ, el-Farra NS, Reikes AR, Co RL. Clinical outcomes after transfusion-associated hepatitis C. N Engl J Med 1995; 332: 1463.
3. Takahashi M, Yamada G, Miyamoto R, et al. Natural course of chronic hepatitis C. Am J Gastroenterol 1993; 88: 240.
4. Yano M, Kumada H, Kage M, et al. The long – term
pathological evolution of chronic hepatitis C. Hepa-tology 1996; 23: 1334.
5. Swain MG, Lai MY, Shiffman ML, et al. A sustained virologic response is durable in patients with chronic hepatitis C treated with peginterferon alfa2a and ri-bavirin. Gastroenterology 2010; 139: 1593.
6. Backus L, Boothroyd DB, Phillips BR, et al. Impact of sustained virologc response to pegylated interferon/ ribavirin on all – cause mortality by HCV genotype in a large real – world cohort: The US Department of Veterans Affairs’ experience. Hepatology 2010; 52: 428A.
7. Russo MW. Antiviral therapy for hepatitis C is asso-ciated with improved clinical outcomes in patients with advanced fibrosis. Expert Rev Gastroenterol He-patol 2010; 4: 535.
8. Morgan TR, Ghany MG, Kim HY, et al. Outcome of sustained virological responders with histologically advanced chronic hepatitis C. Hepatology 2010; 52: 833.
9. Cardoso AC, Moucari R, Figueiredo – Mendes C, et al. Impact of peginterferon and ribavirin therapy on hepatocellular carcinoma: incidence and survival in hepatitis C patients with advanced fibrosis. J He-patol 2010; 52: 652.
10. Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sus-tained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fib-rosis. Ann Intern Med 2007; 147: 677.
11. Aziz H, Raza A, Murtaza S, Waheed Y, et al. Mole-cular epidemiology of hepatitis C virus genotypes in different geographical regions of Punjab Province in Pakistan and a phylogenetic analysis. Int J Infect Dis. 2012 Nov 22. S1201-9712 (12): 01275-1.
12. Manns MP, McHutchison JG, Gordon SC, et al. Peg-interferon alfa2b plus ribavirin compared with inter-feron alfa2b plus ribavirin for initial treatment of chr-onic hepatitis C: a randomised trial. Lancet. 2001 Sep 22; 358 (9286): 958-65.
13. Druyts E, Thorlund K, Wu P, Kanters S, Yaya S, Cooper CL, Mills EJ. Efficacy and Safety of Pegylated Interferon Alfa2a or Alfa2b Plus Ribavirin for the Tre-atment of Chronic Hepatitis C in Children and Adole-scents: A Systematic Review and Meta-analysis. Clin Infect Dis. 2012 Dec 27. [Epub ahead of print]

SUPPLEMENT PSG
2013
ABSTRACTS

57
ENDOSCOPY ABSTRACTS

58
Incidence of Post – Endoscopic Retrograde Cholangio (ERC) Sphincterotomy and Sphicteroplasty Pancreatitis
Asif Gull, Muhammad Shafiq, Ghias-ul-Hassan, Muhammad Amjid, Israr-ul-Haq, Ghias. N. Tayyab
Introduction: Post ERCP Acute pancreatitis is an uncommon complication with significant morbidity and chance of mortality. The chances of developing pancreatitis directly correlate with the complexity of the per ERC intervention. Per ERC sphincterotomy (ES) and large balloon Sphincteroplasty is done for to extract stones larger than 12 mm. Previously published incidence of post ERC sphincterotomy and large balloon Sphincteroplasty related pancreatitis is 0-45% and mild hyperamylasemia is 7 – 55%. This study has been done to find the risk of insignificant hyperamylasemia and clinical pancreatitis in our center.
Material and Methods: It is a prospective single center study conducted at Division of Gastroenterology, Medical unit. I, Lahore General Hospital / PGMI; Lahore carried out from September 2012 – December 2012. Patients meeting the standards of ERCP procedure and having CBD stones larger than 12 mm were enrolled in the study and evaluated for possibility of post procedure complications following ES and large balloon Sphincteroplasty. Patients were observed for post procedure abdominal pain and rise in Serum amylase for 4-6 hrs and persistence of abdominal pain longer than 24 hrs. Rise in serum Amylase was considered significant (> 300 U/L) or Insignificant (< 300 U/L).
Results: Thirty two eligible subjects were enrolled and analyzed. Male to Female ratio was 1: 4.33 and mean age was 47.63 yr. The indication for ES and large balloon Sphincteroplasty was CBD stones larger than 12mm (25 subjects; 78.12%), CBD stricture with large stones (5subjects; 15.62%) and post operative CBD fistula with retained stones (2 subject; 6.25%). Rise of Serum amylase > 300 U/L was observed in 7 subjects (21.7%) and Asymptomatic Hyperamyla-semia (Serum amylase < 300 U/L) observed in 14 subjects (43.75%). No enrolled subject died and all subjects were discharged within 24 hrs after procedure indicating mild pancreatitis only. In 28 patients complete ductal clearance was achieved and in remaining four a repeat procedure was done for a retained stone.
Conclusions: ERC Sphincterotomy and large balloon Sphincteroplasty is a safe procedure with insignificant hyper-amylasemia in 43.75% cases and mild pancreatitis in 21.7%. Although the number of patients with a rise in amylase level are higher in our study but could be due to stringent criteria used in our center.
Role of Intravenous Indomethacin in Prevention of Post Endoscopic Retrograde Cholangio (ERC) Sphincterotomy and Sphicteroplasty Pancreatitis
Asif Gull, Muhammad Shafiq, Ghias-ul-Hassan, Muhammad Amjid, Israr-ul-Haq, Ghias. N. Tayyab
Introduction: Post ERCP Acute pancreatitis is an uncommon complication with significant morbidity and chance of mortality. The chances of developing pancreatitis directly correlate with the complexity of the per ERC intervention. Per ERC sphincterotomy (ES) and large balloon Sphincteroplasty is done to extract stones larger than 12 mm. Previously published incidence of post ERC sphincterotomy and large balloon Sphincteroplasty related pancreatitis is 0 – 45% and mild hyperamylasemia is 7 – 50%. European society of endoscopy recommends per rectal use of diclofenac or Indo-methacin suppository for prevention of post ERC sphincterotomy but there is limited data in the studied group. This case controlled study has been conducted to evaluate the role of post procedure parenteral Indomethacin for prevention of Post-ERC Sphincterotomy and large balloon Sphincteroplasty related Pancreatitis.
Material and Methods: It is a single center prospective case-control study conducted at Division of Gastroenterology, Medical unit. I, Lahore General Hospital/PGMI; Lahore conducted between September 2012 to December 2012. Subjects with large CBD stone and meeting the standard inclusion/Exclusion criteria otherwise were assigned into drug study group and control group. 26 subjects were included in drug arm and were given 2 mg Indomethacin in 1000ml N/Saline over 4-6 hrs immediately after procedure. Control group (10 subjects) received 1000 ml N/Saline only. Subjects were followed on standard Performa documenting the abdominal pain and blood sample for serum amylase was taken 4-6 hrs after completion of procedure. Subjects were evaluated for possibility of post procedure complications that underwent ERC Sphincterotomy and large balloon Sphincteroplasty. Subjects were observed for post procedure abdominal pain and rise in Serum amylase for 4-6 hrs and persistence of abdominal pain longer than 24 hrs. Rise in serum Amylase was considered significant (> 300 U/L) or Insignificant (< 300 U/L).
Results:
Case Control
Total No. Patients 26 10
Male 3 (11.53%) 5 (50%)
Female 23 (88.46%) 5 (50%)
Male: Female 1 : 7.66 1:1

59
Mean Age 49.26 year 46 year
Post Procedure Pancreatitis 6 (23.07%) 2 (20%)
Asymptomatic Hyperamylasemia 11 (42.30%) 5 (50%)
Conclusion: Post ERC sphincterotomy (ES) and large balloon Sphincteroplasty procedure infusion of Indomethacin doesn’t reduce the incidence of Pancreatitis but it reduces the incidence of Post-ERCP Asymptomatic Hyperamylasemia. Though the number of the cases is small, it has been observed that Indomethacin infusion did not have any advantage on the standard post procedure care patients.
Annual Comparison of Audits of Colonoscopy in a Tertiary Care Hospital
Arsalan Jamil Raja, Imran syed, Syed Ansar Hussain, Salman Shakeel, Bilal Nasir Asif Gul, Ghias-ul-Hassan, Israr-ul-Haque Toor, Ghais-un-Nabi Tayyab
Objective: To determine/ compare the detailed colonoscopy data including demographic characters, indications, findings, cecal intubation rates ,causes of incomplete intubation rate of 2012 with the audit of colonoscopy year 2011.
Method: A retrospective analysis of the record of the patients who underwent Colonoscopy in Endoscopy unit of Medical Unit 1, Lahore General Hospital from Jan2012 to Dec 2012 was done and the results were compared to the previous colonoscopy audit done is same unit in year 2011.All the patients in the age range of 3 to 80 years, of both sexes,who underwent colonoscopy for various indications were included. Data was analyzed using SPSS version 19 and relevant descriptive analysis including mean, frequency and percentages were calculated and compared with the previous audit.
Results: Among the 310 patients who had their colonoscopy done for various indications, mean age was 38 and Sex distribution included 184 males (61.3 %) and 116 Females (38.7), which were fairly comparable with last year’s audit, mean age being 37.8 years with 62% males and 38% females. The most common indication in both the audits remained the same, i.e., bleeding per rectum in 42% (n = 126) in current and 41.2% in the last one. Other indications worth mentioning were chronic diarrhea in 17.7%, chronic abdominal pain in 17.3% almost same as the previous audit. Indications like anemia reduced from 6.9% to 5.3% and weight loss / mass rose from 2.1% to 7.3% in the current audit. Endoscopic findings included neoplastic lesions in various segments of colon in 11.3% which was higher than previous 7.6%,Ulcerative colitis in 15.4% compared to 7.4% last year, worms in 3.3%reduced than previous 7.2 %. Other minor findings like angiodyplasias, active bleeders or mild ulcers remained the same. Colonic preparation rate was considerable higher with adequacy of 94%than previous 90%.Cecal intubation ratesrose from previous 71% to current 80%. The most common reason for failure to intubate was due to termination of procedure due to patient intolerance of pain in 9.3% compared to 20% last year.
Conclusion: Compared to audit of year 2011, the trend towards neoplastic lesions of colon occurring at a younger age group has risen and warrants change in screening policy for CRC in our region for earlier detection of these lesions.
Annual Audit of Colonoscopy in a tertiary care Hospital 2012
Arsalan Jamil Raja, Imran Syed, Salman Shakeel, Shafiq Awan, Shafqat Rasool, Hafiz Ehsan Bilal Nasir, Ghais-ul-Hassan, Asif Gul, Israr-ul-Haque Toor, Ghias-un-Nabi Tayyab
Objective: To determine the demographic data, age and gender variations, indications, findings, cecal intubation rates and causes of incomplete intubation in patients undergoing colonoscopy.
Method: A retrospective analysis done from January to 31st Dec 2012conducted in endoscopy unit of Medical unit-I of Lahore General Hospital Lahore. Patients of all ages and gender were included with different indications for colonoscopy. Data was analyzed on SPSS version 19 with 12 variables and relevant descriptive analysis including mean, frequency and percentages were calculated.
Results: Total 310 patients were included with age range from 3-85 (Mean = 38)years having 61.3%( n=184) males and 38.7%( n = 116) females.
Indications for Colonoscopy:
Bleeding
P/R Chronic
Diarrhea Chronic
Abdominal Pain Weight
Loss Anemia
Ulcerative Colitis
Frequency 126 53 52 22 16 5
Percentage 42 17.7 17.3 7.3 5.3 1.7

60
Male (%) 63 57 56 73 50 80
Female (%) 37 43 44 37 50 20
Mean Age (years) 37.6 43 39 39 42 38
Colonoscopic Findings:
Ulcerative
Colitis Neoplastic
Lesions Polyps Proctitis Worms
Angio-dysplasis
Normal Colonscopy
Frequency 46 34 22 11 10 5 137
Percentage 15.4 11.3 7.3 3.7 3.3 1.7 45.7
Male 41 56 68 45 50 60 65
Female 59 44 32 55 50 40 35
Mean Age (Years) 37 42 30 42.45 29.3 52 40
Colon Viewed Up-to
Cecum (Cecal intubation Sigmoid Colon Ascending Colon Hepatic Flexure
Percentage 80% 10% 5.4% 4.6%
Colonic preparation was adequate in 94% and inadequate in 6 %. Failure of ceacal intubation was mainly due to termination of procedure due to pain intolerancein 9%, tight stricture/ growth in 8.3%, friable mucosa 7% and inade-quate preparation in 6.%.
Conclusion: According to audit analysis, most frequent findings were ulcerative colitis and neoplastic lesions of colon , with equal male and female distribution in formal and slight male predominance in the latter and mean age of presentation 37 and 42 years for ulcerative colitis and neoplastic lesion respectively. Considering the younger age of presentation for neoplastic lesions ( mean age 42 years), the CRC surveillance guidelines in our region needs to be revised and more studies and data is required from all the provinces for consensus regarding screening/surviellence for CRC especially at an earlier age group than previously defined.
Among the 290 patients who had their colonoscopy done for various indications, mean age was 37.75 and Sex distribution included 171 males (61.1%) and 108 Females (38.6%). Both, ean age and sex distribution were fairly comparable with last audit i.e 37.8 yrs and 62% males and 38% females. Regarding the most common indications for undergoing colonscopy, as compared to last audit where bleeding per rectum was the most frequent one(41.2%),this audit also showed bleeding per rectum to be the most common indication in our population of study, being 121 (43.2%). Other common presentations this year were chronic diarrhea 52 (18.6%) ,chronic abdominal pain 50 (17.9), constipation 14 (5%), Anemia in 9 (3.2%) which has reduced to half as compared previous audit of 6.9%,also worth mentioning is indication for unexplained wt loss in 19 (6.8%) patients. Endoscopic findings included.
Biliary Brush Cytology in the Assessment of Biliary Stricture at a Tertiary Care Center In Pakistan
Shafqat Mehmood, Muhammed Aasim Yusuf Shaukat Khanum Memorial Cancer Hospital and Research Centre (SKMCH & RC) Lahore
Purpose: Differentiation between benign and malignant biliary stricture is crucial. We evaluated the diagnostic value of biliary brushings and brush washings in this retrospective study. Patients and Methods: The medical records of the patients referred to gastroenterology department between January 2007 to October 2012 were reviewed in this retrospective study. Mean age, gender, indication for referral, ERCP findings and results of brush cytology were recorded and compared with the final histopathology. Those patients with negative brush cytology were subjected to additional procedures including endoscopic ultrasound guided fine needle aspiration or image guided biopsy. Results: A total of 71 patients had ERCP and brushings during the 5 year period. Mean age of the patients at pre-sentation was 61years (range, 30- 8 4 years; 58% males). The major indication for referral was to establish the etiology of obstructive jaundice. Cytological diagnoses obtained were malignancy, atypical/suspicious for malignancy and benign strictures. We were able to establish a diagnosis of malignancy in 50.7% (n: 36), atypical cells/likely malignant in 5.1 %( n: 4) and benign in 9 (7%) of the patients with 12 “false negative” cases. Two out of the four patients with atypical cells on brush cytology underwent EUS – FNA that confirmed the diagnosis of malignancy. Of the 31 patients with negative cytology, 12 patients were diagnosed as having malignancy on EUS-FNA or ultrasound guided biopsy. Unfortunately

61
84% of the patients had irresectable disease at presentation and so final histopathology, based on examination of a resected specimen, was available for only two patients, in both of whom a diagnosis of adenocarcinoma was confirmed. 9% (7/31) of the patients with negative cytology were diagnosed as having a benign structure after clinical follow up of 4-6 months. When patients with atypical / suspicious cytology were excluded from the study, the sensitivity of the brushings was 75% and when atypical / suspicious findings were taken into account, true positive sensitivity rose to 83%.
Conclusion: We feel that brush cytology is a safe, simple and valuable tool in establishing the diagnosis in patients with CBD strictures and should be performed in all patients undergoing ERCP for undiagnosed CBD strictures.
Capsule Endoscopy: is it Really Helpful in the Diagnosis of Small Bowel Lesions?
Yasir Abbas Zaidi, Kashif Malik, M. Joher Amin, Anwaar A Khan, Altaf Alam Arshad Kamal Butt, Waqar H. Shah, Akif Dilshad, Ali Hyder
Shaikh Zayed Hospital, Lahore, Pakistan
Objective: To determine the efficiency and safety of capsule endoscopy for small intestine diseases.
Methods: Given Imaging M2A capsule endoscopy (CE) was performed on 40 patients having various indications like obscure GI bleeding, anemia, abdominal pain or having clinical features of malabsorption. It is a case control study and was done, from February 2009 to March 2012, in the department of Gastroenterology, Shaikh Zayed Hospital, Lahore, Pakistan. All the patients having indications for the procedure were included. Patient having suspicion of intestinal obstruction, motility disorders and having pregnancy were excluded. Statistical Analysis was done using SPSS version 20.
Results: Out of 40 patients, 27 (67.5%) were male, while 13 (32.5%) were female. Mean age was 53 years with minimum 11 years and maximum of 80 years. Four (10%) patients showed negative finding, in the other 36 (90%) patients, intestinal lesions were detected. The findings consisted of 4 (10%) intestinal inflammation, 11 (27.5%) angioectasia, 2 (5%) protuberant lesions, 5 (12.5%) flattened intestinal mucosa, 5 (12.5) single or multiple ulcers, 1 ascarid in the intestine, 2 (5%) strictures, 4 (10%) visible vessels and the 1 intestinal Crohn's disease. Presence of blood resulted in poor visualization in 1 (2.5%) patient, while there was fresh blood in stomach in 1(2.5%) patient. Three patients were verified by surgical operation, while enteroscopy was done in two patients for the confirmation. Capsule impaction happened in two patients. All images of CE were good. Conclusion: Capsule endoscopy is a safe and effective procedure, with a good positive rate, and it can be used for small intestinal diseases.
Pattern of CBD stricture (An Endoscopic Finding)
Imran Ali Syed, Arsalan Jamil Raja, Ghias-ul-Hassan, Bilal Nasir Israr-ul-Haque, Zeeshan H. Khan, Ghias-un-Nabi Tayyab
Objective: To determine the cause, pattern of involvement, spectrum of age and gender variation in patients having common bile duct stricture.
Material and Methods: A cross sectional study conducted in the Division of Gastroenterology of Medical Unit-I of Lahore General Hospital, Lahore from January 2010 to December 2011.Data was analyzed on SPSS version19. Common bile duct stricture was classified into benign and malignant on the basis of history, CT imaging and ERCP appearance. Klatskin Tumors were classified according to the standard classification.
Results: Out of 149 patients 95.30% had malignant and 4.70% had benign stricture. Malignant strictures included cholangiocarcinoma (43.62%), ampullary tumor (36.24%), duodenal growth (7.38%), carcinoma head of pancreas (5.37%) and gall bladder cancer (2.68%).Benign Biliary Stricture secondary to an iatrogenic injury was an infrequent finding (4.68%). Cholangiocarcinoma had female: male of 1.16:1. The age ranged from 18-85 (mean 67.4) years having 24.62% (n = 16) below whereas 75.38% (n = 49) above fifty years. Distal CBD was involved in 41.54% (n = 27), mid CBD in 15.38% (n = 10), Klatskin type I in 30.77% (n = 20), type II in 3.08% (n = 2), type III bin 1.54%( n = 1) and type IV in 7.69% (n = 5). Ampullary carcinoma had a male preponderance with a male: female of 1.7: 1, age ranged from 45 – 83 (mean = 58.5) years having 11.11% (n = 6) below fifty years.
Conclusion: Malignant strictures are the main indication for ERCP with more males suffering from Ampullary tumor while more females suffered from proximal cholangiocarcinoma and majority presenting over fifty years of age.

62
ERCP in Patients with Mildly Raised Alkaline Phosphatase and Normal Biliary Imaging
Shahriyar Ghazanfar, Sajida Qureshi, Ali Taj, Saad Khalid Niaz, M. Saeed Quraishy Civil Hospital, Karachi
Objective: To evaluate the association of raised alkaline phosphatase with biliary pathology in the presence of normal imaging in patients with cholelithiasis
Methods: A retrospective descriptive study was conducted at Surgical Unit 4 of Civil Hospital Karachi, over a period of 5 yrs, from August 2006 to July 2012. Sixty five patients with altered LFT’s in terms of raised alkaline phosphatase and bilirubin and normal biliary tract on imaging were included in the study. Informed consent was taken from all patients and permission from hospital ethical committee was sought. All patients underwent standard ERCPs. And the findings and clinical data were entered on the special ERCP database. Results were analysed using SPSS version 11
Results: A total of 65 patients were included in the study. Mean age of study population was: 42.75 + 13.84 (20 – 75 years). Mean bilirubin level was: 1.04 + 1.03 (00.0 – 4.59). Mean alkaline phosphatase: 168.98c + 73.259 (110 – 714).
ERCP findings: Normal 50 patients (76.9%). Stones 10 patients (15.4%). Stricture 1 patient (1.5%). Failed ERCPS: 4 pts (6.2%) subsequently lost to follow-up. Successful duct clearance was achieved in 9 patients (13.8%). stents were placed in 2 patients (3.1%).
Conclusion: A minimally raised alkaline phosphatase may be associated with biliary obstruction so should not be ignored.
Prevention of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis by Diclofenac rectal suppository
Pervez Ashraf, Hafeezullha Shaikh, Nazim Arain, Nabiha Faisal, Shoaib Siddique, Shahid Mehmood Liaquat National Hospital, Karachi, Pakistan
Background: Acute pancreatitis is a serious and potentially fatal complication of endoscopic retrograde cholangio-pancreatography (ERCP) and occurs in 1 – 10% of patients, but may approach 30% or more depending on the presence of risk factors.1-2 Clinical trials evaluating the protective effect of non-steroidal anti-inflammatory drugs (NSAIDs) have
yielded inconclusive results. We performed study to evaluate the effect of prophylactic rectal NSAIDs for post-ERCP pancreatitis prevention.
Material and Method: In this uni-center, randomized controlled clinical trial; total 42 patients were included from Out Patient Department and Emergency, informed and written consent was taken and randomized as either control or to receive Diclofenac 100mg rectal suppository 60minutes before ERCP. Pre and post ERCP serum amylase were checked. Each patient receives IV midazolam and nulbuphin in incremental dose for comfort sedation. The primary outcome was post-ERCP pancreatitis, which was defined as new upper abdominal pain, an elevation of serum amylase to at least 3 times the upper limit of the normal range within 24 hours after the procedure, and hospitalization for atleast 2 nights. Whereas asymptomatic hyperamylasemia is defined as increase in serum amylase <3 times upper limit of normal range and absence of abdominal pain within 24 hours after the procedure.
Results: A total of 42 patients were enrolled with the mean age 53.52 years, 20 (47.6%)were male and 22 (52.4%)were female and completed follow-up. 21patients received rectal Diclofenac suppository while other taken as control and no drug was given. Post-ERCP pancreatitis developed in 3 (14.3%) out of 21patients in the Diclofenac suppository group and whereas in control group pancreatitis was noted in 4 (19.0%) out of 21 patients with non-significant P-value > 0.05. Whereas Asymptomatic hyper-amylasemia occurred in 1 (4.8%) out of 21patients in the diclofenac group and in con-trolled group 7 (33.3%) out of 21 patients with the significant P-value = 0.045.
Conclusions: Prophylactic administration of rectal NSAIDs significantly reduces the incidence of post-ERCP asympto-matic hyperamylasemia P-value0.045, but not reduces the incidence of pancreatitis. Further large randomized controlled trials are required before its introduction into routine care.
Key words: Nonsteroidal anti-inflammatory drugs, endoscopic retrograde cholangiopancreatography, Post-ERCP pan-creatitis
References: 1. Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc 2004;
59: 845-864. 2. Rabenstein T, Hahn EG. Post-ERCP pancreatitis: new momentum. Endoscopy 2002; 34: 325-329.

63
Frequency of Internal Hemorrhoids in All Patients Presenting with Lower Gastrointestinal Bleeding Undergoing Colonoscopy
Shahid Mahmood, Lubna Kamani, Mansoor ul haq, Pervez Ashraf Liaquat National Hospital, Karachi
Background: Lower gastrointestinal bleeding (LGIB) is a common medical emergency and remains a major cause of morbidity and mortality 1. Acute bleeding from the colon is usually less dramatic than upper gastrointestinal hemorrhage and is self – limiting in most cases 2. Lower gastrointestinal endoscopy is the primary modality to determine the cause and therapeutic intervention to stop bleeding.
Objective: To determine the frequency of internal hemorrhoids in all patients presenting with lower gastrointestinal bleeding undergoing colonoscopy.
Subject and Methods: This is a prospective cross – sectional study, performed in Gastroenterology Department, Liaquat National Hospital, Karachi on patients presenting with LGIB. History, examination and investigations were carried out. Colonoscopy was performed. Patient’s information was recorded on proforma and analyzed by using SPSS-17.0.
Results: Total 203 patients were included in this study. The mean age of the patients was 43.06 ±12.05 years. Out of 203 patients, there were 111 (54.7 %) males and 92 (45.3%) females, with 1.2:1 male to female ratio. Out of 203 patients, hemorrhoids was present in 76 (37.4 %) patients and it was the most common cause of lower GI bleed in which 35 pts (46.05%) were male and 41pts (53.94%) were females. 60 (78.94%) patients had bright red colour while 16 (21.06%) patients had maroon colour blood. Hemorrhoids were more prevalent in age group between 31 to 50 years of age. Bleeding related to rectum was present in 32 (23.1%) among which rectal ulcers were present in 14 (10.1%), rectal polyp in 9 (6.5%), proctitis in 6 (4.3%) and rectal growth in 3 (2.2%) patients. Bleeding related to colon was present in 38 (27.3%) patients, among which colitis was present in 8 (5.8%), ileitis was present in 6 (4.3%), illioceacal ulcers in 6 (4.3%), colonic ulcers in 5 (3.6%), ulcerative colitis 5 (3.6%), colonic growth in 5 (3.6%), diverticular disease in 2 (1.4%) and Crohn’s disease in 1 (0.7%) patient.
Conclusion: Majority of patients has internal hemorrhoids as a cause of LGIB. Proctoscopy or sigmoidoscopy can reveal the cause and unnecessary colonoscopic procedure can be avoided in younger patients with no alarm symptoms which will help in terms of time and cost effective.
Keywords: Lower GI Bleeding, hemorrhoids, Lower GI Endoscopy.
References 1. J.J. Farrell; L. S. Friedman Authors and Disclosures the Management of Lower Gastrointestinal Bleeding Posted:
06/14/2005; Alimentary Pharmacology and Therapeutics. 2005; 21 (11): 1281-1298. 2. Zia N, Hussain T, Salamat A. Diagnostic Evaluation of Patients Presenting With Bleeding Per Rectum by Colono-
scopy. J Ayub Med Coll Abbottabad. 2008 Jan-Mar; 20 (1): 73.
In Vision Pneumatic Dilatation of Achalasia without Fluoroscopic Guidance: Safety and Cost – Effectiveness
Asif J.Wakani, Pervez Ashraf, Hafeezullah Shaikh National Institute of Liver and GI Diseases (NILGID), Karachi
Objective: Aim of the study were to evaluate the technical feasibility, clinical efficacy, outcome, and complications of a new method of achalasia dilatation under direct endoscopic visualization, without fluoroscopic assistance.
Material and Methods: This study was conducted in the Department of Gastroenterology at Liaquat National Hospital, Institute for Postgraduate Medical Studies and Health Sciences, Karachi from January 2006 to Dec 2010. Patients with achalasia cardia were subjected to dilatation with a OLYMPUS (Swift achalasia balloon BA2) pneumatic dilator 35 mm at a pressure of 15 PSI with the new technique. The balloon was passed into the stomach over a guidewire, withdrawn across the gastroesophageal junction, and dilated with the endoscope positioned proximally. Patients were graded pre- and post treatment on the frequency of dysphagia, daytime regurgitation, nighttime symptoms, chest pain, and heartburn. Response was assessed by the improvement in dysphagia frequency.
Results: Forty – six patients (28 females, 18 males; mean age 42 yr) underwent 50 pneumatic dilations. The 30 – mm balloon was used in most cases (67%). The mean post dilation follow-up was 21.1 months (1.5 – 57.4 months). The range of inflation pressures was 8 – 18 PSI (median 15 PSI), and the duration of inflation was 30 – 120’s (median 90’s). Twenty eight of 46 patients (61%) had excellent or good results, fourteen (31%) had fair results, and four (8%) had poor results. There were no perforations related to balloon inflation. The initial success of the procedure was 92% in these patients.
Conclusions: In Vision Pneumatic balloon dilatation is the most effective nonsurgical cost-effective treatment modality to relieve dysphagia in patients with achalasia, avoiding the risk of radiation exposure and can be done as an office procedure, without the need of a fluoroscopy setup.

64
Manometric Pattern of Various Oesophageal Motility Disorders at Civil Hospital, Karachi
Babar Matin, Saad Khalid Niaz, M. Saeed Quraishy Dow Medical College and Civil Hospital, Karachi
Background: Oesophageal manometry has become the most reliable diagnostic tool to assess the oesophageal motor abnormalities. Aim of this study was to explore the frequency of various Oesophageal motility disorders referred for Oesophageal Manometry.
Methods: A prospective descriptive study. Patients with non obstructive dysphagia referred to our gastrointestinal physiology study unit at surgical unit 4, Civil Hospital, Karachi from December, 2009 to December, 2012 for motility studies were included. Sandhill Scientific, Inc. In SIGHT g2 system with a 6 channel Konigsberg esophageal manometry probe was used. A Performa was filled and readings were transferred on SPSS version 16.
Results: There were 115 patients out of whom 55 were males and 60 females. Age ranged from 18 to 75 years with a mean age of 40.65 years. Duration of dysphagia ranged from 1 month to 20 years with a mean of 3.60 years. There were 32(27.8%) patients with normal manometry while 46 (40.0%) had achalasia, ineffective oesophageal motility in 5 (4.3%), nutcracker oesophagus in 2 (1.7%), scleroderma in 2 (1.7%), postdilatation achalasia in 11(9.1%), post cardiomyotomy achalasia in 5 (4.3%), Hypertensive LES 1 (0.9%), diffuse oesophageal spasm 1(0.9%), frequent failed peristalsis 4 (3.5), failed peristalsis 4 (3.5) and as pre-operative evaluation for fundoplication 2 (1.7%).
Conclusion: Oesophageal manometry is an established tool for diagnosis of achalasia, impaired esophageal motility disorders, dysphagia of unclear etiology and pre-operative evaluation for fundoplication. In our experience, achalasia was the commonest disorder followed by ineffective oesophageal motility, frequent failed peristalsis, nutcracker oeso-phagus and scleroderma.
Mucinous Adenocarcinoma ovary; Diagnostic Delimma and the Usefulness of Colonoscopy Shafqat Mehmood, Muhammad Qayyum Khan
Shaukat Khanum Memorial Cancer hospital and Research Centre Lahore, Pakistan
Background: Differentiating primary from metastatic mucinous ovarian adenocarcinoma is often challenging. We assessed the usefulness of colonoscopy to sort out this delimma.
Patients and Method: This is a retrospective study carried out in the department of gastroenterology at a tertiary care hospital in Pakistan. The mean age, demographic details, indication for referral, tumor size and laterality, and the immunohistochemical stains were recorded for all the patients. Colonoscopy and upper GI endoscopy was performed in all the patients under conscious sedation after a written informed consent for the procedure.
Results: A total of 17 patients were referred to gastroenterology department between March 2009 and March 2012. Mean age of the patients was 36.7 years (range, 16 – 58 years) and the indication for referral was mucinous pathology. All of these patients had surgery at some outside hospital; histopathology was submitted at our pathology laboratory for review. Out of 17 patients, 16 had progressive abdominal distention as the primary symptom whereas one patient had a history of bleeding per rectum. 67% (12 out of 17) of the tumors were more than 10cm and 94% (16 out of 17) were unilateral. We were able to find the colorectal primary in 17.4% of the patients i.e. 3 out of 17 patients whereas upper GI endoscopies were unrevealing in almost all of the patients. CK – 7 was positive in two of these three and CK – 20 was positive in three out of three patients with colorectal primary. CEA was raised in all the patients with colorectal primary.
Conclusion: We were able to identify gastrointestinal primary in significant number of patients without GI symptoms on colonoscopy that showed immunohistochemical stain pattern of primary mucinous adenocarcinoma and had a tumor size of greater than 10cm and were unilateral.
Obstructive Jaundice – High Strictures and Low Strictures
Fayez Sandouk
Background: The basic therapy for malignancies in general is radical resection. However; in biliary malignancies, most of the cases come late and endoscopic palliative procedure is the ideal solution since it decreases the suffering and improves the quality of life of such patients with better cost effectiveness & less complications.
Strategy: The most important issues in biliary strictures are to be sure of the malignancy diagnosis, to locate the exact level of obstruction & staging. By all of these one can decide if the lesion is operable or decide the type and number of stents.
The malignancy diagnosis: can be achieved by many techniques. Taking biopsies and cytology brush from biliary strictures during ERCP has rather low sensitivity (55–60%) however; direct vision through the strictures like "SpyGlass" has very high sensitivity and specificity (98%). Tumor markers with the clinical pictures have also good sensitivity.

65
The location is very important to decide the type of surgery and also the type and number of stents in the non surgical cases. Lower half CBD strictures usually have better surgical resection results than upper half and hilar lesions. Klatskin Bismuth grade I responded very nicely to one stent, meanwhile we need two stents for stage II & III. On the other hand, stage IV is contraindicated for stenting and ERCP from the beginning. That is why it is very vital to stage the cases before endoscopy to avoid the very bad cholangitis complication. Nowadays; we do have very safe non invasive procedures for Staging. EUS is the best for staging ampullary tumor, CT Multislice may be the best for staging mid biliary portion and can discover the distal metastasis. Meanwhile, the MRCP is so good in mapping and staging Bismuth classification.
Types of stents: Stenting was proved as excellent alternative for surgery in palliating the non-surgical cases as it has similar result to surgery in clearing the jaundice, itching and improve the quality of life in addition to its cost effective-ness, morbidity and days of hospitalization. Most of the studies showed that Plastic and Self Expanding Metallic Stents (SEMS) have similar short term results. However; when the life expectancy of the patient is more than 4 months, SEMS have better patency, infection and cost effectiveness. Uncovered SEMS only are to be used for the Klaskin's II – III, meanwhile the recent ESGE guidelines showed that there is no difference between the covered and un-covered SEMS in the lower biliary strictures and Klatskin I. The right. Intrahepatic duct cannulation is usually easy, however; the Tricks to do selective Left IHD cannulation is to use cannulotome and bow it just below the bifurcation and manipulate the guide wire. This can be achieved by practicing training on a "Homemade Model" I invented.
Outcome of Upper GI Bleed in Patient who Had Early Endoscopy Compared with Late Endoscopy
Faizan Qaisar, Ayesha Memon, Syed Zafar Abbas
Background: Upper GI bleed (UGIB) is not an uncommon problem , it has various causes, esophageal varices is the commonest cause (42%) in our setup. Urgent endoscopy with intervention can improve morbidity, and may also reduce mortality which in the developed countries is still around 10 – 15%. There is no data available in our setup to determine the outcome of UGIB with and without urgent endoscopy.
Aims: To find out the outcome of UGIB and compare the effect of urgent vs. late or no endoscopies in these patients.
Methods: Retrospective study of all 50 consecutively admitted UGIB patient at MMCH their case note and endoscopy record were scrutinized.
Result: fifty patients (28 males, 22 females). Average age: 45.06 range: 22 – 85 years were admitted with history of melena or haemetemesis or both. They were divided into following groups.
Group A: Endoscopy done within 24 hours. Twenty four patients Out of them 14 males and 11 females having average age of 40.28
Outcome: all are discharged alive.
Group B: Endoscopy done within 24 – 48 hours. Eleven patients out of them 7 are males and 4 are females having average age of 44.09.
Outcome: All are discharged alive.
Group C: Endoscopy not done or done after 48 hours. Fifteen patients out of them 7 are males and 8 are females having average age of 50.81.
Outcome: thirteen were discharged alive 2 patients expired out of them one could not be resuscitated and died on the day of admission before Endoscopy could be arranged. The other one was in hepatic coma and died on 3rd day of admission.
Endoscopy Diagnosis:
Bleeding esopahageal varices 21
PUD = GU 02
DU 03
Gastritis \ Duodeniti 17
Mellory – Weiss tears 03
Upper GI cancers 01
Esophagitis 03
Intervention Performed:
Sclerotherapy 21
Biopsy 06
None 23

66
Conclusion: seventy percent of all patients admitted with UGIB, were subjected to Endoscopy within 48 hours. Out of the remaining 30% (15 patients), 2 died both had bleeding oesophageal varices.
Patterns of Endoscopic Findings in Patients Presenting with Dysphagia in Pakistan
Salman Shakeel, Ehsan Ullah, Maria Aslam, Rafia Javed, Hina Manzoor, Arsalan Jamil Ghias-ul-Hassan, Asif Gul, M. Asim Hameed, Israr-ul-Haque, Ghias un Nabi Tayyab
Introduction: To see the pattern of upper GI endoscopy findings in patients presenting with Dysphagia in relation with age, gender and duration of symptoms.
Material and Methods: It is a retrospective analysis that was conducted on 346 patients who presented at A&E Department and in GI OPD from January 2011 to November 2012 with history of dysphagia for solid or liquids. These selected patients were enrolled, an upper GI endoscopy was performed and findings were recorded. The data was analyzed on SPSS 19 and descriptive statistics recorded and results were analyzed as in given table.
Results: The pattern of pathologies on EGD is as shown in Table 1.
No. Endoscopic Finding Number Percentage Mean Age
(Years) Male : Female
Ratio
1. Esophageal Neoplasm 91 26.3 % 54 1.95:1
2. Post-Corrosive Esophageal Stricture 72 20.8% 28 1:1.46
3. Normal EGD 68 19.8% 38 1:1
4. Hiatus Hernia 51 15.3% 41 1.2:1
5. Achalasia Cardia 23 6.9% 42 1:1
6. Esophageal Candidiasis 18 4.3% 42 1:1.5
7. Esophageal Foreign Body 13 3.8% 45 1:1.2
8. Esophageal Web 05 1.4% 48 1:1.5
9. Tracheo-Esophageal Fistula 04 1.2% 29 1:0
10. Zenker’s Diverticulum 01 0.3% 43 1:0
In the patients above the age of 40 (n = 167, 48%), esophageal neoplasm was the predominant lesion (n=74, 44%) followed by Normal EGD (n =22, 13%). While in patients under the age of 40 years (n = 179, 52%), the predominant lesion is esophageal stricture (n = 60, 34%) followed by a normal EGD finding which comprises of (n = 45, 25%). In the patients suffering from esophageal neoplasm, the mean duration of onset of symptoms to the diagnosis was 4 months.
Conclusion: Although a good number of patients had a non mechanical etiology of dysphagia but majority of the patients had an underlying mechanical cause of obstruction. Majority of patients presenting with dysphagia and age above 40 had a neoplasia. Majority of patients presenting with dysphagia and age below 40 had post corrosive intake injury of the esophagus.
Abstract
Sajida Qureshi, Shahriyar Ghazanfar, Ali Taj, Saad Khalid Niaz, Saeed Quraishy
Objective: To evaluate our experience of endoscopic drainage of pancreatic pseudo cyst
Methods: A retrospective descriptive study was conducted at Surgical Unit 4 of Civil Hospital Karachi, over a period of 1 yr, from 1 August 2011 to 31 July 2012. Thirteen patients with pancreatic pseudo cyst confirmed on imaging were included in the study. Informed consent was taken from all patients and permission from hospital ethical committee was sought. All patients underwent standard ERCPs and endoscopic drainage of pseudo cyst. Findings and clinical data was entered on the special ERCP database. Results were analysed using SPSS version 11
Results: A total of 13patients were included in the study. Male to female ratio was: 4:9. Mean age of study population was: 30.46 + 10.890 (13 – 55 years). Mean bilirubin level was: 0.82 (0.30 – 3.8). Mean alkaline phosphatase: 207.69 (66 – 1026). Pancreatic duct Communication with cyst was seen in 3 patients. Eleven patients underwent successful drainage of cysts. Cysts were drained through stomach in 11 pts and duodenum in two. There was no major bleed but perforation was seen in one patient.
Conclusion: Endoscopic drainage of pancreatic pseudocyst is a safe and effective method preventing surgery in already morbid patients.

67
Strictures of GI tract, Endoscopic Management / Old and New
Fayez Sandouk
Background: The basic therapy for malignancies in general is radical resection. However; in Gastrointestinal mali-gnancies, most of the cases come late and endoscopic palliative procedure is the ideal solution since it decreases the suffering and improves the quality of life of such patients with better cost effectiveness & less complications than sur-gery. Stenting is more convenient, more cost effective and safer than repeated laser ablation or dilatation.
Strategy: The most important issue in GI Malignancy endoscopic stenting is to choose the proper stent, Covered or Uncovered as it is known that the uncovered SEMS has less migration tendency however, it has more in-growth obstruction incidence. Meanwhile, the covered SEMS has more migration incidence with better patency. Therefore; the ideal SEMS is that one which has uncovered net from outer surface and covered with mesh from the inner surface.
One classic strategy for SEMS in GI strictures is to choose the length at least 4 cm or more longer than the length of the stricture in order to keep at least 2 cm above and lower the stricture. Therefore; a proper GI series images are important to decide the length. One last strategy in the GI strictures especially the colonic is to consider the bending angles which demand increasing in the extra length and might need to use two overlapped SEMSs inside one inside the other to cover all the angle figure.
The gastric outlet stricture in specific has special strategy since the obstruction usually causes stretching of the stomach due to the stomach contents leading to elongation of it down to the pelvis in the advanced obstruction. This stretching will make the wall of the stomach very thin and easy to lacerate. That is why it very VITAL before the procedure whether endoscopic or surgical to insert Naso Gastric Tube for 2-3 days to return the stomach size and repair the electrolytes balance.
Endoscopic insertion of SEMSs proved itself as excellent palliative procedures for the non surgical cases of GI malignancies since they improve dramatically the quality of life of the patients and help their suffering and only 10-15 % of them might need re-stenting during the rest of their lives.
Therapeutic ERCP in Patient with Situs Inversus Totalis and Ampullary Diverticulum
Lubna Kamani, Raj Kumar, Shahid Mahmood, Sana Jafri, Faisal Siddiqui Liaquat National Hospital, Karachi
Background: Situs Inversus Totalis (SIT) is a rare entity with estimated incidence in the range of 1:10,000 to 1: 20,000.1 The clinical presentation of acute cholangitis or acute biliary pancreatitis secondary to bile duct stone2 is very rare in patients with SIT. Endoscopic retrograde cholangiopancreatography (ERCP) is the main treatment modality but it becomes very difficult and challenging in SIT patients due to malposition of visceras. We described a rare case of a male patient with SIT and ampullary diverticulum underwent therapeutic ERCP.
Case Report: A 55 – year – old male with known SIT, presented with obstructive jaundice and cholangitis. Abdominal CT confirmed situs inversus viscerum and dilatation of the intra- and extra-hepatic bile duct with common duct stones (Fig1). Therapeutic ERCP with sphincteroplasty was performed successfully with scope rotation to 180 degrees and shortening under fluoroscopic guidance despite difficulties of dual pathology.
Discussion: Endoscopic sphincterotomy and stone extraction are standard procedures for the removal of bile duct stones. SIT increases the technical difficulties and the possibilities of complications of therapeutic interventions. We started procedure with pt. in usual left semiprone position and able to negotiate scope from stomach till duodenum with 180 degree rotation and shortening. To our knowledge this is the first reported case of concomitant SIT and ampullary diverticulum in single patient with bile duct stones. In expert hands ERCP can be performed with some changes in scope positions with the help of fluoroscopy.
Key Words: Situs Inversus, Ampullary Diverticulum, Choledocholithiasis.
References 1. Al-Jumaily M, Hoche F. Laparoscopic cholecystectomy in situs inversus totalis: Is it safe? J Laparoendosc Adv Surg
Tech A 2001; 11: 229-31. 2. Crosher RF, Harnarayan P, Bremner DN. Laparoscopic cholecystectomy in situs inversus totalis. J R Coll Surg Edinb
1996; 41: 183-4.
69
GASTRO ABSTRACTS

70
A Survey of Ethics and Attitude in Regard to Environment among Iranian Medical Students
Ali Hamidian,1 Samaneh Hamidian2 1Faculty of Natural Resources, University of Tehran, Iran
2Faculty of Dentistry, Yerevan State Medical University, Republic of Armenia
Development of environmental education courses especially in developing countries is essential to conserve environment and also to decline environmental issues. In this paper, 150 undergraduate and postgraduate students at 1Tehran University of Medical Sciences were participated. The data were analyzed in Excel software. The results showed that 21% of the students do not attend environmental issues. According to the results, 88% of the students warn others to conserve the environment. The results showed that only 15% of the students have a satisfactory level of environmental knowledge. According to the results, 75% of the students are interested in passing environmental courses. Higher percentages of female students were observed for 4 indices (attention to environment, membership in NGOs, Environ-mental knowledge and interested in passing environmental courses). The results demonstrated that medical students are interested in environmental conservation programs. This is necessary to reconsider medical education curriculum according to sustainable development. Medical students, as future doctors and nurses should be aware of increasing environmental problems and like other citizen try to help the planet.
Key Words: Medical students, medical education curriculum, environment, sustainable development.
Correlation between Dyspepsia and Severity of Depression
Ommara Jamil, Zahid Hussain, Shahid Sarwar
Aims and Objectives: To determine the correlation between dyspepsia and severity of depression.
Patients and Methods: Study was carried out at department of medicine, Mayo hospital Lahore. After taking informed written consent patients with symptoms of dyspepsia fulfilling the rome III criteria were included in the study. All patients were evaluated for depression using Hamilton depression rating scale (HDRS) and upper gastrointestinal endoscopy was done.
Results: We included 101 patients with mean age of 35.81 (14.81) and male to female ratio of 1.41: 1 (54/47). Predominant symptoms noted were epigastric pain in 66 (65.3%), bloating in 50 (49.5%), early satiety in 73 (72.3%) patients, post parandial fullness in 41 (40.6%) and regurgitation in 41 (40.6%) patients. Alarm symptoms were positive in 44 (43.6%) patients. Patients of dyspepsia were classified as epigastric pain syndrome (EPS), 70 (69.3%) patients and post parandial distress syndrome (PDS) in 31 (30.7%) patients. Significantly more females had PDS (p 0.04), positive endoscopic findings were noted more in EPS (P 0.03). When study patients were evaluated for depression using HDRS, all patients except one had depression, mild in 23 (22.8%), moderate in 34 (33.7%), severe in 32 (31.7%) and very severe in 11 (10.9%) patients. When we compared patients with EPS and PDS for depression severe depression was seen in 32 (45.7%) patients of EPS while 11 (35.4%) patients of PDS had severe depression but difference was not significant (p-o.47).
Conclusion: Hence, female patients are more prone to develop PDS, while positive endoscopic findings were noted significantly more in patients with EPS. Interestingly all patients with very severe depression were suffering from EPS.
An Early Experience of Ligation of the Inter-sphincteric Fistula Tract (LIFT) to Treat Fistula in ANO
Objective: To evaluate the efficacy and safety of ligation of the inter-sphincteric fistula tract (LIFT) to treat fistula in ANO.
Methodology: This interventional study included 20 patients of fisula in ANO who underwent LIFT at SUII Liaquat University Hospital, Jamshoro Pakistan. This study was done prospectively from June 2010 to May 2011. All the patients of low anal fistula who consented for the study were included in the study and the complicated , recurrent and high type anal fistula were excluded. All Patients’ data recorded including history and physical examination findings, investiga-tions, operative procedure details and histopathology reports.
Results: Out of 20 cases 14 were males and 06 were females. Mean age was 42 years and median follow-up period was six months. Sixteen patients (80%) had complete healing of anal fistula and 4 patients (20%) had incomplete healing and required further intervention.
Conclusion: LIFT procedure is safe sphincter preserving procedure with increased primary healing rate and low recurrence rate.

71
Black Tongue Oral Hygiene or G.I. Upset Rural (Desert) Community is the Primary Health Care Challenge
Jewat Sunder, Satti Jewat Sindh United (N) Developmental Educational Rural Society Sindh
Aim: To provide facility to the rural (desert) community and to aware the community about the preventive measures of communicable diseases.
Background: Oral hygiene is also the primary health care issue especially in rural (desert) population, mouth ulceration, gum bleeding, dentalcries, bed breaths, along with h/o smoking, chewing of tobacco, nas, niswar, igonoring habit of the mouth wash, burshing, all things lead to oral health problems and black tongue is also one of them, which is commonly found rural (desert)community and hereditary of black tongue is also issue.
Methodology: Descriptive study on spss version 11.
Results: There were 94 cases of the black tongue, the results are: 23 (24.45%) males, 7 (7.44%) were boys children, 71 (75.53%) were females, 13 (13.82%) were girls. Mean age was: 15 – 45 years. Out of 94 cases: 23 (24.45%) were males with h/o smoking, 8 (8.51%), 3 (3.19%) h/o ATT in their life, 5(5.31) h/o G.I. upsets, (use of medicine), 7 (7.44%) h/abuse to supari, bhang. Out of 94 cases: 71 (75.53%) were females, h/o dentalcries 26 (27.65%), 13 (13.82%), h/o NASS abuse, 11 (11.70%), h/o smoking, 9 (9.57%), h/o (matt), 7 (7.44%), h/o G.I. upsets (use of medicine), 5 (5.31%), h/o ATT in their life. Out of 94 cases: 52 (55.31%) h/o on/off mouth wash (oral hygiene), 42 (44.68%) strong h/o mouth wash (oral hygiene) on festivals, eid, dewali. Out of 94 cases: 7(7.44%) families were hereditary, h/o of black tongue.
Conclusion: Though the black tongue may not major health issue but hereditary black tongue required further study. Oral hygiene does not required too money, there is more need of health education, awareness, realization to decrease the oral mucosa (or) Oral health issues.
Spectrum of Esophageal Mucosal Lesions in Pediatric Celiac Disease: A Prospective Controlled Study
Prasad KK, Thapa BR, Debi U, Sharma AK Singh K Postgraduate Institute of Medical Education and Research; Chandigarh – 160 012 (INDIA)
Introduction: Celiac disease (CD) may cause changes throughout the gastrointestinal tract. It is not known whether the esophageal mucosa is involved in CD. The purpose of this prospective study was to evaluate the spectrum of mucosal damage to the esophagus in patients with CD.
Materials and Methods: The spectrum of mucosal damage to the esophagus was investigated in 126 children with CD during 192 upper GI endoscopies performed to obtain duodenal biopsy specimens and was compared with findings in 49 children who underwent endoscopy for upper GI complaints without CD (non-CD patients) during last one year. Children were diagnosed as cases of CD based on the modified ESPGHAN criteria and positive serology. Duodenal histologic lesions were classified as proposed by our group.
Results: The mean age of CD children (M:F: 71:55) at presentation was 6.7 ± 3.3 years. 54/126 (42.9%) of CD and 23/49 (46.9%) of non-CD patients showed normal esophageal mucosa. The prevalence of lymphocytic esophagitis (LE) was higher in CD (11.9%) than non-CD (2.1%) patients. The prevalence of eosinophilic esophagitis, follicular esophagitis, reflux esophagitis and non-specific esophageal mucosal changes were similar in both groups. All but one child with LE showed classic duodenal histologic lesion.
Conclusions: Our findings showed that the esophageal mucosa can be damaged in CD patients and that the prevalence of LE is higher with CD. Awareness of potential coexistence of esophageal lesions in CD should promote optimal diagnosis of these conditions. Routine esophageal biopsies may be warranted when investigating for CD.
Celiac Disease: Gastrointestinal Symptoms and Beyond
Lubna Kamani, Shahid Mahmood, Mansoor Asad Liaquat National Hospital, Karachi
Background: Celiac disease (CD) is an autoimmune enteropathy triggered by the ingestion of gluten in susceptible individuals. The clinical spectrum is wide, including gastrointestinal (GI) or extra-intestinal (EI) features. Diagnosis is established with blood test including raised tissue trans-glutaminase antibodies (TTG IgA and IgG) and typical features on duodenal biopsies. There is dearth of literature regarding prevalence of extra-intestinal manifestation (EI) in this disorder.
Methods: This is an observational prospective cross-sectional study conducted at an outpatient Gastroenterology

72
Department of Liaquat National Hospital, Karachi. Total of 91 celiac disease patients were enrolled. Data including age, gender, clinical presentation, endoscopic findings, biochemical and serological values were collected. We report clinical spectrum of celiac disease and its EI manifestations.
Results: Out of 91 pt. 12 (10.9 %) were male and rest were females. GI manifestation were seen in 55 patients (60.4%). Epigastric pain was the most common mode of presentation accounting for 40 number pts out of 55 (70.6%) of patients followed by diarrhea in 30 number of pts out of 55 (54.5%), loss of appetite and weight loss in 26 number of pts out of 55 (47.2%). EI manifestation seen in 36 (39.5%) of patients in which anemia, short stature, symptomatic gallstones, migraine, oral ulcers, skin disorders, arthritis, vitamin B12 deficiency, oesophageal web, elevated SGPT, and thyroid disease were present in 30 (83.3%,), 4 (11.1%) , 5 (13.8%), 2 (5.5%), 2 (5.5%), 5 (13.8%), 2 (5.5%), 1 (3.6%), 2 (5.5%), 4 (11.1%), 5 (13.8%) patients respectively. Other gynecological manifestations in females were primary amenorrhea, secondary amenorrhea and infertility in 8 (8.7%), 10 (10.9%) and 5 (5.4%) patients respectively. 4 number of patients (11.1% out of 36) had more than one EI manifestation. Duodenal biopsy showed villous atrophy (19.7%), villous blunting (20.8%), raised intraepithelial lymphocyte (46%) and non specific in 13% of patients. Serology (i.e. TTG) was raised in 41(45%) patients only.
Conclusions: Celiac disease is a multi-system disorder. An awareness EI manifestation is necessary to avoid delay in diagnosis. It is imperative to consider both serological tests and histopathology of duodenum in diagnosing celiac disease.
References 1. Fasano A, Catassi C. Current approaches to diagnosis and treatment of celiac disease: an evolving spectrum. Gastro-
enterology. 2001; 120: 636–651. 2. Mustalahti K, Catassi C, Reunanen A, et al. The prevalence of CD in Europe: results of a centralized, international
mass screening project. Ann Med. 2010; 42: 587–595.
Chronic Pancreatitis – Medical and Endoscopic Management
Fayez Sandouk
Abstract: Chronic pancreatitis can cause real social problems because of the Recurrent Severe Pain, Weight Loss, Poor Appetite and Fatty Diarrhea. The pain in specific is usually very severe and might lead to disability, loos of Job and even drug addiction.
Alcohol is the main reason for chronic pancreatitis in the west, meanwhile biliary cholelethiasis is the first cause in the middle east. Other reasons are also known like high Triglycerids, Congenital Malformation like Pancreas Divisum, Hypercalcemia, specific medication in addition to hereditary familial Pancreatitis which is usually seen in children. There two common share of medical and endoscopic management of all causes of Chronic pancreatitis. The first is that we treat the cause, we might cure the disease once for all. The second is that we can markedly improve the patient quality of life by managing his severe pain and safe his social life, and the sooner we start our treatment the faster & better is the curing.
The strategy of the management of CP is to control the pain and let the patient re-gain his life by improving his bowel movement and more importantly relieving his severe pain. Also; to drain the pseudocysts. We do not touch the chronic pancreatitis unless it is symptomatic.
Medical management is usually helpful in the early stages and it is usually aim to relief the annoying, recurrent fatty diarrhea. High dose of pancreatic enzymes (…… unites) is very helpful in controlling this. However; the medical therapy for the pain symptoms has limited result and with time the patient might become addict to analgesics. Here endoscopic management has marvelous, satisfied result.
The pancreatic pain is usuallydue the strictures with or without stones in the pancreatic duct or due to pancreatic pseudocysts. Endoscopic therapy might need more than one session to achieve the ideal result. In all those cases a pancreatic sphincterotomyis to be performed first to facilitate the easy axis of the multiple sessions.
Although most of the chronic pancreatitis can be cured completely by dealing with the etiology like pancreas divisum and biliary stones, however; in some of other causes if the pain did not disappeared, we still can achieve very obvious decrease in the frequency and strength of pain episodes. The endoscopic management for chronic pancreatitis has three targets: the pancreatic strictures, the pancreatic stones and lastly the pseudocysts.
Strictures: Most of the strictures occurs at the ampullary orifice site which is usually cures by pancreatic sphincterotomy in 65%. The other strictures along the pancreatic duct is usually very tight and the best way to dilate them is by using the metallic Sohendra stent retrieval. After each dilatation we insert 7-10 F stent along the PD. Most of the cases cure after removal of stent after 6 month.
The pancreatic ductal stones usually crushed nicely by Extra Corporeal Shock Wave ECSW. The remained stones can be removed by small baskets or retrieval balloons. The pseudo cyst has become mainly an endoscopic technique and the Sandostatin.

73
Effect of Helicobacter Pylori Infection on Gastric Juice Intrinsic Factor and R-Binder Levels in Patients with Dyspepsia
Shahid Rasool, Shahab Abid, Perwaiz Iqbal, Wasim Jafri Aga Khan University, Karachi
Introduction: Helicobacter pylori are a gram negative, microaerophilic human pathogen. H. pylori causes gastritis and is associated with development of peptic ulcer disease, gastric carcinoma, lymphoma, and many micronutrient deficiencies. Among micronutrient deficiencies, the most important association of H. pylori infection is with Iron and Cobalamin (Vit B12) deficiencies. Different studies have shown that H. pylori is a definite cause of B12 deficiency. Patho-genesis of micronutrient deficiencies and metabolic derangements caused by helicobacter pylori infection is not clear.
Aim: To determine the impact of H. pylori infection on gastric juice intrinsic factor and R-binder levels in patients with dyspepsia.
Methods: Eligible patients with dyspepsia were enrolled and variables like gender, eating habits, co-morbid disease, addiction and drugs were noted. Prior to gastroscopy, 5 ml of blood was taken to check serum B12 in all patients. During gastroscopy, 10 ml of gastric juice was aspirated from body of stomach by a Teflon catheter. H. pylori infection was diagnosed by histopathology of gastric biopsies and urea breath test. Gastric juice was collected in a sterile tube con-taining EDTA and gastric juice intrinsic factor and R-binder levels were measured in this sample within next seven days. Quantification of IF was carried out by the method described by Begley and Trachtenberg.
Results: Total of 125 patients with dyspepsia were enrolled with median age of 40.2 ± 11.5 years. Seventy four were male and 51 were females. 64% were H. pylori positive while 34% were negative. 24% patients had B12 deficiency (< 200 pg/ml). Median levels of intrinsic factor and R-binder levels in gastric juice of patients with dyspepsia were 13.2 vs 6.0, p = 0.003 and 9.0 vs 7.1, p = 0.269 respectively in H. pylori +ve and –ve group. There was a correlation between gastric juice B12 and IF levels.
Conclusion: Intrinsic factor and R-binder levels are high among H. pylori infected patients with dyspepsia. This may be used for further studies to reveal the pathophysiology of H. pylori related problems.
Evaluation of GERD and Dyspepsia Symptoms Improvement with Rabeprazole and Cinitapride Combination in Normal Clinical Setting
Background / Aims: GERD is one of the most prevalent gastrointestinal dysmotility disorders; PPI alone is half the treatment. Adding Prokinetic with PPI achieves significant improvement in patients overlapped with symptoms of GERD and dyspepsia. Our aim was to evaluate GERD symptoms improvement with Cinitapride & Rabeprazole combination in Pakistani population.
Methods: Using FSSG (Frequency scale for symptoms of GERD) patients were evaluated and enrolled on total score of more than 25. Newly diagnosed patients and patients on other PPIs were shifted to Cinitapride and Rabeprazole combi-nation given at 1mg TDS and 20mg OD respectively. Primary efficacy endpoint was 50% reduction in the mean intensity score of the symptom from baseline to final visit at week 6.
Results: Total of 978 patients were included. Efficacy was achieved in 771 (78.8%) patients. Significant reduction was seen in dyspeptic symptoms from 11.83±3.67 before treatment to 3.83 ± 2.81 and acid reflux symptoms from 16.06 ± 4.50 to 5.15 ± 3.61. Total score of patients was reduced from 27.89 ± 6.62 to 8.98 ± 5.84. Overall mean percentage reduction was 66.70% ± 21.82% and the combination was very well tolerated.
Conclusions: Cinitapride and Rabeprazole combination given at 1mg TDS & 20mg OD for 6 weeks showed an overall mean percentage reduction of 66.70% ± 21.82% and both were very well tolerated. Adding prokinetic is effective for patients dissatisfied with PPI monotherapy.
Before
Treatment After
Treatment Chi-square
Value p-value Significance
Dyspeptic symptoms 11.83 ± 3.67 3.83 ± 2.81 62.47 0.000 Significant
Acid Reflux related symptoms 16.06 ± 4.50 5.15 ± 3.61 67.78 0.000 Significant
Total score 27.89 ± 6.62 8.98 ± 5.84 73.11 0.000 Significant
Percentage reduction in score 66.70% ± 21.82% n/a n/a

74
27.89
8.98
0
10
20
30
40
Before Treatment After Treatment
Effect of Shunt Surgery on Small Intestinal Morphological and Functional Alterations in Patients with EHPVO
KK Prasad, A. Handu, BR Thapa, U. Debi, KLN Rao, K. Singh Postgraduate Institute of Medical Education and Research, Chandigarh-160012, INDIA
Introduction: Improvement of growth has been documented after porto-systemic shunt surgery in children with EHPVO. This study was undertaken to assess the effect of shunt surgery on small intestinal morphological and functional alterations in patients with EHPVO and to correlate it with the growth improvement.
Materials and Methods: Twenty patients who were operated for EHPVO were divided into two groups (Gp): Group A; Patients who underwent successful shunt surgery (n = 14) and Group B; Patients who underwent splenectomy with devascularisation (n = 1) and those with thrombosed shunts (n = 5). Growth parameters, endoscopy findings, gastric and duodenal mucosal histology, brush border enzyme activities, urinary D-xylose levels, stool steatocrit, fecal alpha-1 anti-trypsin, serum GH and IGF-1 levels and quality of life scores were assessed before surgery and at least 12 weeks after surgery.
Results: There was no significant difference between the pre- and post-operative gastric and duodenal mucosal histology. Pre-operative brush border lactase activities were significantly lower than normal and did not change signi-ficantly after surgery. EHPVO did not affect intestinal absorption or permeability and there was no significant change after surgery. Patients with successful shunt surgery showed significantly improved ‘z’ scores for height after surgery. Only one patient demonstrated growth hormone resistance. The quality of life scores improved significantly after sur-gery.
Conclusions: Children with EHPVO do not demonstrate any significant abnormality of small intestinal morphologic and function, which remains unaffected after shunt surgery. Thus, intestinal malabsorption does not appear to signi-ficantly contribute to the growth retardation seen in EHPVO. Although there is an improvement in growth after surgery, this may not be related to its effect on the gut.
Mean T
ota
l S
core
P-value=0.000

75
Presentation And Anthropometric Measurements of Coeliac Disease; Comparison of Australian with Pakistani Children
Brekhna Aurangzeb, Zaheer Abbassi, Nadeem Akhtar, Gulbin Shahid Yasir Bin Nisar, Steven Leach, Andrew S. Day, Avi Lemberg
Children’s Hospital, PIMS, Islamabad
Background: Coeliac disease (CD) is autoimmune enteropathy and has a variety of clinical presentations ranging from classical picture of sever undernutrition with chronic diarrhea and anemia to atypical presentation of resistant anemia, short stature.
Aims: To assess the presentation patterns and nutritional status of children with newly diagnosed CD in Australian and Pakistani children.
Methods: Twenty five newly diagnosed CD children at Sydney Children’s Hospital, Australia from Feb 2006 to April 2007 and 30 children at Children's Hospital, PIMS, Pakistan from Nov 2008 to Nov 2010 were enrolled. The pre-sentation patterns and nutritional status were assessed.
Results: No difference was observed in the mean age of the groups (6.98 years) in Pakistani cohort and (8.23 years) in Australian cohort. Most common presenting complaints in the Pakistani cohort were diarrhoea (84%), weight loss (64.5%), abdominal pain (61.3%), abdominal distension (61.3%) and vomiting (38.7%) whereas the most common pre-senting complaints in the Australian cohort were abdominal distension (100%), diarrhoea (36%), abdominal pain (36%), weight loss (32%) and constipation (32%). The mean height for age and weight for age scores of Pakistani children (-2.29 and -2.80 respectively) were significantly lower than the Australian children (-0.28 and -0.21 respectively) (p=0.0001 and 0.0001 respectively). Similarly, the mean hemoglobin value in the Pakistani cohort (8.47) was significantly lower (p=0.0001) than the Australian group (12.38).
Conclusions: Atypical presentation is more common in the Australian cohort compared to Pakistani. The Pakistani CD children are markedly undernourished and anemic at diagnosis than the Australian children. Public awareness of CD and availability of iron rich diet in Australia may explain these differences. Early detection of CD is important to prevent the adverse effects of under nutrition and anemia.
Key word: Coeliac disease, Anthropometry, Nutritional status.

77
HEPATOLOGY ABSTRACTS

79
12 Hours Terlipressin is as Effective as 72 Hours of Infusion in the Management of Bleeding Esophageal Varices
A. Salim, A. A. Khan, A. Alam, A. K. Butt, S. Anjum Gastroenterology, Shaikh Zayed Hospital, Lahore, Pakistan
Introduction / Objectives: To determine whether Terlipressin given for 12 hours is as effective as 72 hours of Terlipressin in preventing re-bleed after endoscopic control of variceal bleeding.
Aims and Methods: The aim of the study was to compare the efficacy and safety of 12 hour terlipressin treatment of bleeding eso-phageal varices to a 72 hour treatment period. Fifty patients with liver cirrhosis presenting with upper gastrointestinal bleed received Terlipressin starting with 2 mg I.V bolus, followed by 1mg 6 hourly for 12 hours until undergoing esophagogastroduodenoscopy. Patients with esophageal varices as primary cause of bleed underwent therapeutic band ligation. The patients were then randomized into two groups (A&B). Group A; continued to receive Terlipressin at a dose of 1mg 6 hourly for a total of 72 hours. Group B; received no Terlipressin after band ligation. Both groups were monitored for occurrence of re-bleeding for 5 days following band ligation. Re-bleeding was defined as a new bleeding episode, after initial control of bleeding, manifest as haematemesis, haematochezia, fresh blood in naso-gastric aspirate, drop in Haemoglobin ≥ 2 g/dL and circulatory instability.
Results: Re-bleeding occurred in 1 patient in Group-A (4%) and 2 patients in Group-B (8%) during the 5 day observation period (p-value >0.05. No statistical significance). Repeat endoscopy on the patients who re-bled showed ulcers over previous banding sites in the Group A patient and one of the Group B patients. These patients were managed conservatively as no active ooze was noted. The other Group B patient had visible varices (with red signs) which required repeat band ligation. One patient in Group A died due to persistent encephalopathy. No drug related adverse effects were seen in either group.
Conclusion: A lower dose and duration of Terlipressin, given only prior to endoscopic band ligation, shows similar results to a longer and more costly 3 day regime. This can result in significant cost reductions and decreased hospital stay with no increase in morbidity or mortality.
Validity of Alpha Fetoprotein for Diagnosis of Hepatocellular Carcinoma in Patients with Cirrhosis: A Case Control Study
Shahid Sarwar, Anwaar A. Khan Ramdev Chaudhary King Edward Medical University, Lahore
Objective: To determine the accuracy of serum alpha fetoprotein (AFP) for diagnosis of hepatocellular carcinoma (HCC) in patients with cirrhosis.
Patients and Methods: Consecutive patients, diagnosed with HCC by contrast enhanced CT, MRI or biopsy were included as cases. Patients of cirrhosis with no evidence of HCC were enrolled as control. Demographic, laboratory and radiological data were recorded. Serum AFP was determined in all patients at outset and was analyzed using ROC curve for its accuracy in diagnosing HCC.
Results: Total 275 patients were included, of these, 173 had HCC and 102 had cirrhosis, as control group. Predominant etiology of cirrhosis with HCC was hepatitis C, 139 (80.3%) of HCC and 86 (84.3%) in control group had Cirrhosis due to HCV. Stage of liver disease, as determined by Child Turcotte Pugh (CTP) score, was comparable among cases and control groups [mean CTP value 7.97 in HCC and 7.75 in control group (p value 0.51)]. Area under curve (AUC) for AFP was 0.85 (95% CI 0.80- 0.90) with optimum cut off value of 20.85 ng/ml which showed 72% sensitivity, 86.2% specificity, 94.6% positive predictive value (PPV), 47.8% negative pre-dictive value (NPV) and 75.4% overall accuracy in diagnosing patients with HCC.
Conclusion: Despite sub-optimal sensitivity, alpha fetoprotein is still a valid screening test for diagnosis of hepatocellular carcinoma.
Table: Diagnostic value of serum alpha fetoprotein as biomarker for HCC.
Cut-off Value (ng/ml)
Sensitivity (%)
Specificity (%)
*PPV (%) †NPV (%) Accuracy
(%)
10 79.1 70.5 82.03 66.6 76
20 72.2 86.2 89.9 64.7 77.45
50 59.5 98.03 98.09 58.82 73.8
100 50.2 100 100 54.25 68.7
200 45.6 100 100 52.04 65.8

80
400 42.7 100 100 50.7 64
*PPV: Positive predictive value †NPV Negative predictive value
Anemia as a Predictor of SVR during Treatment of Chronic Hepatitis C in Patients Undergoing Treatment with Interferon and Ribavirin
Chaudhry A., Nawaz A., Riaz M., Iftikhar M., Alvi A., Gujranwala Liver Foundation, Gujranwala, Pakistan
Fatima Memorial Hospital, Lahore, Pakistan
Background: Ribavirin is considered to be an important part of treatment of Chronic Hepatitis C. Optimal weight based dosing leads to better response rates albeit at the risk of developing clinically significant anemia. Patients who develop anemia during treatment may have higher sustained virologic response (SVR) rates. We studied the incidence of anemia and its effect on treatment outcome in genotype 3 patients treated with standard interferon α - 2b and ribavirin.
Objectives: To determine the incidence of anemia and its effect on treatment outcome in genotype 3 patients treated with standard interferon α - 2b and ribavirin.
Materials and Methods: We analyzed the data of all patients treated at Gujranwala Liver Foundation Hepatology clinic. Inclusion criteria; both sexes, age between 18 to 65, treatment naïve, any viral load, genotype 3, Child’s score < 7, baseline Hb > 13 g/dL. All patients received standard interferon α - 2b 3 MU sc thrice weekly and weight based ribavirin. Complete blood count was checked at week 2, 4, 8, 12 and 24. Additional tests were carried out where necessary. HCV RNA by PCR was tested at week 4, 12, 24 and 6 months after stopping the treatment. Anemia was classified as; Mild 10-11 g/dL; Moderate 8.5 to 10 g/dL; Severe < 8.5 g/dL.
Data was gathered by a standardized questionnaire and analyzed using SPSS.
Results: Total number of patients fulfilling the eligibility criteria was 406; male 179 [44%] and female 227 (56%). Amongst these 114 (28.07%) patients developed anemia; Male 32 (28%) and female 82 (72%). Anemia was mild in 58 (50.87%), moderate in 52 (45.61%) and severe in 4 (3.51%) patients. SVR rates were 69%, 60% and 100% in mild moderate and severe anemic patients respectively. Of 114 patients with anemia, 75 (65.78%) achieved SVR as compared with 174 (59.5%) of 292 patients who did not develop anemia. Treatment outcome in relation to onset of anemia during anti-viral therapy was also studied. The number of patients who developed anemia within 8 weeks therapy was 59 (51.75%) with 41 (69.5%) achieving SVR in this group; 55 (48.24) patients developed anemia after 8 weeks of therapy and their SVR rate was 36 (65.5%).
Conclusions:
1) Anemia does correlate with a better SVR in patients being treated for chronic hepatitis C with Interferon and Ribavirin.
2) Timing of onset of anemia, (8 weeks) did not however correlate with an improved SVR.
Number of Patients SVR (+) SVR (-)
With anemia 114 75 (65.78%) 39 (34.21%)
Without anemia 292 174 (59.5%) 118 (40.5%)
Calculate p-value=
Treatment outcome in relation to onset of anemia
Onset of anemia Number of Patients SVR (+) SVR (-)
Less than 8 weeks 59 23 (39%) 36 (61%)
More than 8 weeks 55 24 (43.63%) 31 (56.36%)
Calculate p-value =

81
Association between Baseline Parameters and End of Treatment Response to Conventional Interferon in Patients with Chronic Hepatitis C
Moeen-ul-haq, Muhammad Amin, Kamran hassan, Aamir Ghafoor, Abbas Khattak, Hashmat Ullah Lady Reading Hospital, Peshawar
Background: Several factors have been attributed with therapeutic response of CHC patients including host factors, viral factors, metabolic factors, histological factors, type of regimen used and duration of infection. A number of host-related factors have been associated with a lower likelihood of response to treatment, such as race, advanced liver fibrosis or cirrhosis, old age, male gender, obesity, transaminase levels, and host genetic polymorphisms. With regards to baseline virological factors, high viral loads, genotype, high levels of genetic variability within the E1 – E2 and NS5A regions, as well as mutations in the so-called interferon sensitivity deter-mining region (ISDR) and Core regions, have been related to therapeutic failure. Nevertheless, such findings have not been found in other studies and remain Controversial. Similar correlations are found between other virological responses like RVR and ETR. Among these several variables we have chosen age, sex, weight, viral load and ALT to see their association with ETR.
Objective: To study the association between baseline parameters and end of treatment response to conventional interferon treatment in patients with chronic hepatitis C.
Materials and Methods: This retrospective observational and analytical study was conducted in Gastroenterology department of LRH from January 2012 to June 2012. 145 chronic hepatits C patient, who were put on conventional anti viral therapy after proper evaluation and follow-up were included in the study when they reported with ETR. Various Baseline parameters included sex (male vs female), age (< 40 vs >40), weight(< 70 kg vs > 70 kg), viral load(< 400000 vs >400000) and ALT quotient (<3 vs >3). These variables were compared with ETR and Chi square test was applied to see for any significant association.
Results: About 145 patients were included in the study out of which 60 (41.4%) were male and 85 (58.6%) were females. Eighty six (59.3%) of the patient achieved ETR while 59 (40.7%) don’t. Among various variables tested weight < 70 (68.8% vs 40.8%) and female sex (63.5% vs 53.3%) were significantly associated with ETR with a p = .001 and p=.05 respectively. ALT quotient > 3 (66.7% vs 57.4%) although showing improved percentage was not statistically significant with a p = 0.1, While in patients with age< 40 (58.7% vs 60.7%), viral load < 400000 (58.7% vs 60.7%), there was no significant difference between two groups with a p =.13 for each.
Conclusion: Sex are low body weight are significantly associated with better ETR. Among these weight is modifiable factor and obese patients should be advised to lose weight before embarking them on anti viral therapy in order to improve their chances of viral clearance.
Awareness and Attitude of Barbers of Larkana Regarding Hepatitis B & C
Ahsan Buledi, Habib-ur-Rahman Qadri, Hakim Ali Abro Mumtaz Ali Chhutto, Majid Ahmed Shaih, Irshad Hussain Jokhio
Chandka Medical College Hospital, Larkana
Objective: To evaluate the level of awareness about the prevalence, transmission and consequences of Hepatitis B and C in the barbers (Hair dressers) of Larkana and their attitude towards their customers regarding hepatitis.
Study Design: Descriptive cross sectional KAP study.
Setting: study conducted by Department of Medicine, Unit I, CMC Larkana in the Larkana city during the month of March 2012.
Methodology: A structured pre-specified proforma / questionnaire was designed containing 19 questions regarding different aspects of awareness and attitude of barbers towards Hepatitis. That questionnaire was distributed randomly in the Barbers of Larkana city by the postgraduate students and after explaining the purpose of study and proper consent of them, the proforma was filled. Collected data was analyzed through SPSS 16 version.
Results: We evaluated 100 barbers, all were males. Their age ranged between 14-52 years. Their duration of serving as barbers was ranging as 1 – 35 years. About 70% of barbers know Hepatitis B & C virus as causative agent of jaundice. Above 65% Persons know that these viruses spread through common shaving material, while 78% of barbers think re-use of used blades. 95% of barbers are using separate blade for each customer while 5% do not practice such thing. About 65% of barbers are thinking that they can be infec-ted from already infected customers. 50% were telling that majority of their customers insist for fresh shaving blade / total shaving material. 64% of barbers are aware that hepatitis is fairly common in our area and is disastrous if not treated properly.
Conclusion: Awareness in the Barbers of the Larkana regarding hepatitis B and C is good. While majority of barbers of using sepa-rate shaving material for their customers.
Key words: Hepatitis – Awareness – Barbers – Shaving – Blades – Transmission – Juandice.

82
Characteristics of Responders and Non-Responders as Predictors of Pegylated Interferon Therapy in Chronic Hepatitis C
Amna Awan, Afifa Kulsoom, Muhammad Umar, Saima Ambreen, Sumaira Abbas, Wasiq Mumtaz
Objective: To determine the patient and virus related predictors of pegylated interferon therapy for chronic hepatitis C.
Method: Fifty nine patients having undergone pegylated interferon therapy (Peg-IFNα 180 mcg once a week and ribavirin, 800 mg per day for a period of 24 weeks) from 2008 to 2011 were included in the sample. Patient files were assessed and required variables were selected from them for analysis. We defined non-responders as the cases that did not clear serum HCV RNA as determined using PCR until 24 week of treatment. Other patients were defined as responders. We compared the virus and patient characteristics (genotype, gender, age, Hb, albumin, ALT levels at week 0 and 24, HCV RNA at week 4, 12, 24, 48,liver biopsy and previous treat-ment) during the therapy between non-responders and responders.
Results: There was not much difference observed in gender between responders and non-responders. The HCV RNA clearance rate was 55%, 70%, 71%, 21%, and 88.0% at 4, 12, 24, and 48wk, respectively. ALT levels at start of treatment and at week 24 were not significant in two groups (p > 0.5). Level of inflammation (grading) on liver biopsy was significant between the two groups .Patients with more than 5/18 grade on liver biopsy showed poor response to peg INF therapy (p = 0.005).
Conclusion: RVR and EVR are good predictors of response to peg INF therapy. Also liver biopsy can be used to select patients who can benefit most from the treatment.ALT levels need not be used for assessment of treatment response.
Clinical Presentation of Extrahepatic Portal Vein Obstruction and its Association with Portobiliopathy
Ghous Bux Soomro, Zaigham Abbas, Syed Mujahid Hassan, Nasir Hassan Luck, Sara Akhund Sindh Institute of Urology and Transplantation, Karachi, Pakistan
Background: Extrahepatic portal vein obstruction (EHPVO) is a common cause of non-cirrhotic portal hypertension (NCPH). Portal biliopathy (PB) is commonly present in patients with EHPVO. The primary objective of this study is to review the clinical presentation of non-cirrhotic portal hypertension and its association with PB.
Methods: Retrospective study of patients presenting with NCPH from 2003 to 2012. These patients were conservatively managed. Records were analyzed for presentation, clinical features, imaging, treatment, complications and outcome. Association with portal biliopathy was reported on the basis of ERCP.
Results: Our study included 29 patients; median age 12 years, range 3-50, 20 males (69%) and 9 females (31%). EHPVO was the cause in 27 and non-cirrhotic portal fibrosis (NCPF) in 2 patients. Etiology of EHPVO was idiopathic in 18 (62.1%), protein C or S deficiency in 3 (10.3%), and the rest had no definitive etiology. Most patients in our study underwent only endoscopic variceal band ligation (EVBL) n = 19 (65.5%) and 7 (24.1%) patients had EVBL plus injection sclerotherapy. Five (17.24%) patients had PB on the basis of ERCP; all of them had varices on endoscopy. Three patients were dealt with by stenting for strictures and recurrent cholan-gitis. Out of them one had multiple sessions of stone extractions after endoscopic shockwave lithotripsy as well as stent replacements. He later underwent open cholecystectomy. This patient expired in three years after diagnosis of PB. Four patients with PB underwent EVBL. Of all patients with NCPH, 19 patients are symptomless (65.5%) and 9 are still symptomatic (31%).
Conclusion: Our study suggested EHPVO to be the most prevalent cause of NCPH, with NCPF being less prevalent. Although vari-ceal ablation therapy provides good prognosis for patients with EHPVO, those with PB are difficult to treat due to reiterated stenting and frequent recurrence of cholangiopathic symptoms.
Efficacy and Safety of Pegylated Interferon Alpha 2a (Pegaferon) and Ribavirin in Chronic Hepatitis C Patients
Ghias ul Hassan, Israr ul Haque, Ghias-un-Nabi Tayyab, Bilal Nasir, Maria Aslam, Asif Mehmood Division of Gastroeneterolgy, Department of Medicine, Lahore General Hospital. Lahore
Objective: Objective of the study was to see the efficacy and safety of Pegylated Interferon alpha 2a (Pegaferon) in chronic hepatitis C patients.
Materials and Methods: This was an open labeled, prospective, multicentre study done between June 2010 to June 2012. Study was designed to observe the achievement of sustained virological response with newly marketed pegylated interferon alpha 2a and ribavirin combination in genotype 3 patients, The enrolled patients were separated into Naïve (A), Relapsers (B) and Non Responders (C) based on the previous history of interferon exposure and its response. The RGT was followed on ALT and RVR, EVR, ETR and SVR and treatment adverse effects were noted at each follow up visit.

83
Results: Out of total 153 treatment naïve patients, 85 (55%) were females and 68 (45%) were males, mean age was 38.2+/-10.4 years, age ranged from 16 to 60 years. 77.8% (n 119) patients achieved RVR, 53%(n 18/34) patients achieved EVR, 10.5%(n 16/153) patients were non responders. Those who achieved RVR continued the therapy for 24 weeks so ETR at week 24 was 96.6% (n 115/119), ETR at week 48 was documented for those who achieved EVR and continued therapy for 48 weeks and it was 47.1% (n 16/34), total of 3.9% (6/153) patients lost to follow up (4 patients lost to follow up after achieving RVR and 2 patients after achieving EVR). SVR at week 48 was 92.4% (n 110/119), SVR at week 72 (for those who achieved the EVR and continued therapy for 48 weeks) was 41.2%(n 14/34), so cumulative SVR was 81% (n 124/153), total 7 patients had post treatment relapse {4.2% (n 5/119) patients were those who achieved RVR and 5.9%(2/34) patients were from the group who achieved EVR}.
There were only 4 patients in group B (post standard interferon relapse) 2 patients achieved RVR, one patient achieved EVR and one of the patient remained non responder. Remaining three patients completed the therapy for 48 weeks and 2 of these achieved SVR. Out of total 5 patients who were non responders to previous standard interferon treatment,3 patients achieved RVR, one patient achieved EVR and one patient, who was non responder at week 12 ,discontinued the therapy. Rest of the patients completed therapy for 48 weeks and 2 patients achieved SVR. No serious adverse event was noted during the treatment, fatigue was the commonest side effect (60%).
Conclusion: It is concluded that pegylated interferon alpha 2a (pegaferon) and ribavirin has good efficacy and safety in chronic hepatitis C patients.
Key words: RGT (Response guided therapy), SVR (sustained virological response), Hepatitis C.
Extracorporeal Shock Wave Lithotripsy for Difficult Bile Duct Stones: a 5 Year Single Centre Experience
Syed Mujahid Hassan, Zaigham Abbas, Nasir Hassan Luck, Sabhita Shabir Munnawar Khaliq, Kapeel Raja, Syed Anwar Naqvi, Syed Adibul Hassan Rizvi
Sindh Institute of Urology and Transplantation, Karachi, Pakistan.
Objectives: Extracorporeal shock wave lithotripsy (ESWL) for common bile duct (CBD) stones has been used before but experience is limited. We herein report our experience with ESWL in the management of difficult biliary stones which could not be retrieved on initial ERCP.
Methods: From 2007 to 2011, 39 patients (age 47.56 ± 2.25 years); predominantly females (56.4%) were treated by ESWL for CBD stones. The indications of lithotripsy included large size of stone, more than 15 mm in 32 patients (82.05%), CBD stricture in 12 (30.8%), intrahepatic stones in 5 (12.8%) and cystic duct stones in 2 patients. Twenty five (64.1%) patients presented with jaundice while associated cholangitis in 14 (35.9%) cases. Nine (23.1%) of patients had previously undergone a cholecystectomy. Stone targeting was performed fluoroscopically in all the patients, following injection of contrast via nasobiliary drain in 38 patients and via T tube in one patient. Outcome was assessed by CBD clearance. Both early and late complications were noted.
Results: A total of 75 ESWL sessions were performed in 39 patients. Patients were submitted to 1.92 ± 0.17 session of lithotripsy (3866 ± 243 shockwaves). In 26 (66.7%) of the patients, the fragments were extracted endoscopically after shock – wave therapy; spontaneous passage was observed in 13 (33.3%) cases. Total CBD clearance was achieved in 26 (66.7%), partial CBD clearance in 7 (17.9%) while no response was seen in 6 (15.4%). The most frequent side effects were abdominal pain in 27 (69.2%), followed by vomiting in 5 (12.8%), macro or micro hematuria in 8 (20.5%), fever 3 (7.7%), hemobilia in 2 (5.1%) and cholangitis in 2 (5.1%) patients. Drain was displaced or removed by the patients in 4 (10.3%) cases while ESWL session could not be completed or tempo-rarily held in 9 patients due to development of complications. Total hospital stay was 9.49 ± 1.16 days (range 1 – 42).
Conclusion: ESWL for difficult biliary stones is safe and effective therapeutic alternative to surgical exploration.
Factors Predicting Survival after TACE
Farina M. Hanif, Sabhita Sheikh, Nasir Hassan Luck, Syed Mujahid Hassan, Zaigham Abbas Sindh Institute of Urology and Transplantation, Karachi, Pakistan
Background: Transarterial chemoembolization (TACE) is the preferred treatment for un-resectable, intermediate – stage hepato-cellular carcinoma (HCC). However, survival after TACE can be highly variable. The purpose of this study was to evaluate the efficacy of the factors as a predictor of overall survival with un-resectable HCC undergoing TACE as initial therapy.
Methods: Patient who underwent TACE in the last 2 years were included in study. Patient’s age, gender, cause of cirrhosis, Child Pugh’s score (CTP), MELD score, alpha fetoprotein level, number, site and size of tumor was recorded. Radiological response of TACE was assessed by Computer Tomography scan after 1 month and then 3 monthly

84
thereafter. Repeated sessions of TACE were done according to the response. Survival assessment was done and patients were censored at the last follow-up.
Results: Included in this study were 71 patients; male 57, median age 52 (range 18 -76). Median follow-up 8 months. Thirty-one patients had only one session of TACE, 17.2 sessions and rest 3 or more. On Univariate analysis serum bilirubin (p = 0.02), varices (p = 0.002), CTP class (p = 0.010) and size of tumor (p = 0.014) were significant. Cox regression analysis showed that tumor size less than 5 cm (p = 0.019), absence of varices (p = 0.004), Child class A (p = 0.009) were associated with better survival.
Conclusion: Our study demonstrates that absence of varices, small tumor size and Child class A are associated with better survival in patient undergoing TACE.
Frequency of Gallstones in Hepatitis C Virus Positive Patients at Chandka Medical College Teaching Hospital Larkana
Sultan Ahmed Chandio, Hakim Ali Abro, Fida Hussain Shaikh, Habib-ur-Rahman Qadri, Mumtaz Ali Chhutto, Majid Ahmed Shaikh
Chandka Medical College Hospital, Larkana
Introduction: Gallstones are a major public health problem. Its prevalence in HCV positive cases is found in 19.2% in USA. HCV infection is a global problem which not only causes chronic hepatitis, cirrhosis and hepatocellular carcinoma but also bile duct damage and hepatic steatosis have been found. Both HCV antigens and HCV RNA have been detected in biliary and gallbladder epithelium in patients with chronic HCV infection that correlates with biliary damage and gall stone formation.
Objectives: To Determine The Frequency of Gallstones In HCV Positive Patients at a Tertiary Care Hospital.
Design: Cross sectional study.
Place of Study: Department of medicine, Medical Unit-I Chandka Medical College Teaching Hospital, Larkana.
Duration of Study: From May21st to November 20th 2012. (06 Months)
Patients and Methods: Patients who visited medical OPD for treatment of HCV infection were advised for ultrasonologic examination, which was performed by a senior consultant radiologist, who specially looked for gallstones. Diagnosis of gallstones was made after views showing echos within galldladder and post acoustic shadowing.
Results: Total 160 patients were included in study among them 97 (60.6%) were male and 63 (39.4%) were female. Gallstones were present in 28 (17.5%) cases. Gallstones positive males were 11 (11.3%) and 17 (27%) were female. Gallstones were found more common in women and also in group of patients who did not know about the duration of acquiring HCV infection.
Conclusion: HCV infection is a risk factor to develop gallstones in younger patients. Duration of HCV positivity is directly pro-portional to the development of gallstones. Gallbladder wall thickness could be considered as an initial indicator to develop gallstones in future.
Mesh: Gallstones, HCV, Extraheptic Manifestations.
Frequency of Neuropathy in Hepatitis C Virus Positive Patients at Chandka Medical College Hospital Larkana, Sindh
Naheed Akhtar Shiakh, Hakim Ali Abro, Alam Ibrahim Sidiqui, Majid Ahmed Shaikh, Habib-ur-Rahman Qadri, Mumtaz Ali Chhutto
chandka Medical College Hospital, Larkana
Introduction: Peripheral neuropathy (PN) is described in 9% of patients chronically infected by HCV. The proposed mechanism causing neuropathy in HCV infection are presence of the virus RNA in nerve biopsies and even a direct viral aggression against the nerve. However, PN seems to the result from immunomediated mechanisms determined by the HCV in the nerve rather than related to direct viral infection with consequent in situ lesion in the nervous tissue.
Objectives: To determine the frequency of neuropathy in HCV positive patients at Chandka Medical College Hospital Larkana.
Study Design: Cross sectional study.
Study Setting: Department of Medicine, OPD of Medical Unit-I, Chandka Medical College Hospital, Larkana.
Study Duration: 1st October 2011 to 1st April 2012.

85
Patients and Methods: Patients who visited medical OPD for treatment of HCV infection were advised for The nerve conduction studies. In each patient sensory conduction velocity of the median, ulnar, fibular superficial is and sural nerves as well as motor velocities of median, ulnar, common fibular and tibial nerves was recorded.
Results: Total 156 patients were included in study among them 111 (71.2%) were male and 45 (28.8%) were female. Neuropathy were present in 22(14.1%) cases. Neuropathy positive male were 15 (13.5%) and 7 (15.5%) were female. Neuropathy was found more common in women and also in group of patients who were > 12 months about the duration of acquiring of HCV positivity infection and age group > 40 years.
Conclusion:
1. HCV is a risk factor to develop neuropathy especially in middle age patients.
2. Neuropathy is common in women as compared to men.
3. Duration of HCV positivity is directly proportional to the development of neuropathy.
Key Words: HCV, neuropathy.
Frequency of Nonresponders and its Common Genotypes among Patients with Chronic Hepatitis C Infection Undergoing Conventional Interferon Therapy
Nimatullah, Aamir Ghafoor Khan Gastroenterology Unit Lady Reading Hospital, Peshawar
Background: Hepatitis C infects around 170 million people, nearly 3% of world population and considered a worldwide public health problem. It is the most common cause of chronic liver disease and 20 to 30% patients develop cirrhosis liver with a risk of hepato-celular carcinoma. There are six major genotype of HCV virus. The combination of pegylated interferon with Ribavirin is the standard of care in chronic hepatitis C. Due to marked difference in cost, Conventional Interferon with Ribavirin is still the preferred therapy for genotype 2 and 3 in Pakistan. However, non response to conventional interferon is a major problem and genotype of HCV virus is one of the most important determinant of response to therapy.
Objective: To determine the frequency of Nonresponders and its common genotypes among patients with chronic hepatitis C virus infection undergoing conventional interferon and Ribavirine therapy.
Materials and Methods
Study Design: Descriptive cross-sectional study.
Study Setting: This study was conducted in Gastroenterology Unit of Postgraduate Medical Institute Government Lady Reading Hospital Peshawar.
Study Duration: The duration of the study was 09 months (1st Oct.2011 to 30th June 2012).
Sample Size: Two hundred five cases comprising 116 male and 89 female were included in the study.
Sampling Technique: Nonprobibility Consecutive Sampling.
Sample Selection
Inclusion Criteria
Both genders above the age of 18 years.
Patients with Chronic hepatitis C Infection.
Exclusion Criteria
Patients with co infection of HCV and HBV or HIV.
Patients with Decompensated Cirrhosis liver (diagnosed by ultrasound abdomen, albumin < 2.8 g/dl, bilirubine > 3 mg/dl and PT prolonged > 6 seconds).
Sampling Technique: All Patients fulfilling inclusion and exclusion criteria were started combination treatment. All patients were given 6 months interferon (INF 2b) 3 MIU Thrice weekly plus Ribavirin 400 mg TDS. All medicine were given from hospital Baitul mal fund .All patients were followed up closely and at the end of 6 months real time PCR for HCV RNA was done for each patient. Those Whose PCR for HCV RNA was negative were labeled responders and those whose PCR for HCV RNA was detected were labeled Nonresponders.
Results: Out of 205 patients, 116 (56.6%) were Male and 89 (43.4%) were Female. 133 (64.9%) patients were Responders and 72 (35.1%) patients were Nonresponders. Among the Nonresponders 4 (5.6%) had genotype 1A, 4 (5.6%) had genotype 2A, 57 (79.2%) had 3A, 1 (1.4%) had genotype 3B and 6 (8.3%) had untypeable genotype.

86
Conclusion: Conventional interferon Ribavirin therapy is an effective treatment for treatment naive patients of Chronic Hepatitis C but a significant number of patients don’t respond to this treatment. Among the non responders the most common genotype is 3A.
Keywords: Chronic hepatitis C, Interferon, Ribavirin, Genotype.
Frequency of Renal Impairment after Spontaneous Bacterial Peritonitis in Cirrhosis
Asif J. Wakani, Mansoor-ul-Haq, hafeezullah Shaikh Dow University of Health Sciences (DUHS), Karachi
Objective: To determine the frequency of renal impairment after spontaneous bacterial peritonitis (SBP-RI) in a population of cirrhotic patients admitted to a big tertiary care hospital.
Material and Methods: This study was conducted in the Department of Gastroenterology at Liaquat National Hospital, Institute for Postgraduate Medical Studies and Health Sciences, Karachi. A total 147 patients of liver cirrhosis were evaluated for the severity (Child-Pugh class) of cirrhosis. Etiology of cirrhosis was noted. Serum Blood Urea Nitrogen (BUN) and serum Creatinine in patients of liver cirrhosis was also calculated.
Results: Male to female ratio was 1.4: 1 and mean age was 50.69 ± 10.69 years. Child’s Pugh class – A was found in 29 (19.7%) patients, class – B in 68 (46.3%) and class – C in 50 (34%) patients. The mean blood urea nitrogen (BUN) was 22.4197 ± 11.64742 and serum creatinine was 1.2207 ± 0.92535. Renal impairment was observed in 40 (27.2%) patients while in 107 (72.8%) patients, renal function was normal. Frequency of renal impairment was higher in child’s Pugh class – B (23.5%) as compared to child’s Pugh class A, 5 (17.2%), and it was found to be highest in child’s Pugh class – C (38%).
Conclusion: The frequency of renal impairment after Spontaneous Bacterial Peritonitis among patients of liver cirrhosis is alar-mingly higher in the local set up as consistent with the reported literature. Thus, we recommend baseline renal functions and anti-cipating drug dosage reduction according to creatinine clearance and avoidance of nephrotoxic drugs in cirrhotic patients with Spon-taneous Bacterial Peritonitis and early identification of treatment strategies to reduce morbidity and mortality in these patients.
Keywords: Renal impairment, Cirrhosis, Child-Pugh class, Spontaneous Bacterial Peritonitis.
Is TAE a Valuable for Treatment of Spontaneous Rupture of Hepatocellular Carcinoma: A South – Asian Experience
Amna Subhan Butt, Nazish Butt, Saeed Hamid, Tanveer-ul-Haq, Wasim Jafri The Aga Khan University, Karachi
Introduction: Spontaneous rupture of hepatocellular carcinoma (HCC) is a potentially life-threatening complication. TAE has been found beneficial in the treatment of ruptured HCC in earlier studies. However, no data is available from Pakistan.
Objectives: To evaluate the Clinico-pathological characteristics, treatment outcome and survival of patients presented with spontaneously ruptured HCC treated with or without transarterial embolization(TAE).
Methods: This was a retrospective cross sectional study. Patients≥ 18 years, already diagnosed to have HCC, admitted to Aga Khan University Hospital during 2006-2011 were identified by using ICD code 1550. Those who presented with spontaneous rupture of HCC were analyzed. The primary outcome measure was control of bleeding. Secondary outcome measures were in-hospital mortality, 30-days mortality, overall survivaland factors associated with 30-day mortality.
Results: Out of 850 patients, 12 patients were diagnosed with spontaneously ruptured HCC. Mean age was 64.6±13.52years and 91.7% were males. The underlying cause of cirrhosis was HCV and HBV in 10(83.3%) and 1(8.3%) cases respectively. The mean Child-Pugh score was 10.17± 3.32 and MELD score was 17.58±5.97. Most of them presented with sudden abdominal pain (75%), abdominal distension with ascites(75%),hemoperitonium(58.3%), symptoms of acute anemia(83.3%) and hypovolemic shock(41.7%).The mean tumor diameter was 7.66±3.71cm (range 2.6-15cm). The lesion was solitary in 2(10%), paucifocal in 1(8.3%), multifocalin 7(58.3) and massive/infiltrative in2(16.7%). Furthermore, 9(75%)of patients had advanced HCC. PVT &extrahepatic spread was found in 5(41.7%) and 5(41.7%) cases respectively.
A total of 4(33.3%),6(50%) and 2(16.7%) patients were treated conservatively, underwent transcatheter arterial embolization(TAE) and transarterial chemoembolization (TACE). Success rate for control of bleeding via TAE/TACE was higher than conservative treatment(87.5%vs.25%).Overall median survival time was longer for patients treated with TAE/TACE(45days,range 2-240 vs.7.50days, range3-13) as compared to those who were treated conservatively. In-hospital mortality was significantly lower in TAE/TACE group(12.5% vs.100%, p 0.01).Although the difference was not statistically significant,30 days mortality was lower in patients treated with TAE/TACE (37.5%vs.100%, p 0.07).

87
Conclusion: Ruptured hematoma is a life threatening complication requiring early diagnosis and treatment. Transcatheter arterial embolization is an effective and well-tolerated treatment in the management of hemoperitoneum associated with ruptured hepatocellular carcinoma.
Keywords Ruptured hepatocellular carcinoma, Transarterial embolization, Pakistan
In Hospital Mortality In Advanced Liver Disease
Objective: In hospital mortality is not been studied adequately in patient with advanced liver disease, we investigated predictors and factors that associated with mortality at 30 days .
Method: We analyzed prospectively the data of 120 advanced liver disease patient admitted from JAN 2011 to JAN 2012 at ISRA University Hospital Hyderabad.
Result: The rate of In hospital death was 12.5 % (n = 15 ) and 20 % were readmitted . The mortality rate was significantly higher in patient who has history of alcohol with p value 0.000 , patients with renal failure (p value 0.005 ), patients who were admitted with severe SBP ( p value 0.014 ) ,readmitted patients within 30 days (p value 0.000) , the other factors that are associated in hospital death with advanced liver disease are Bilirubin (p value 0.014 ), PT (p value 0.006) , creatinine (p value 0.002 ) and Sodium (p value 0.017 ).
Conclusion: Patients with advanced liver disease frequency readmitted in hospital with 30 days as in our study about 20 % and rate of hospital death were also significant 12.5 % especially in patients with renal impairment and severe SBP.
Incidence of spontaneous bacterial peritonitis in Cirrhotic patients with ascites and to assess its response to treatment with Ceftriaxone.
Nimatullah, Aamir Ghafoor khan Lady Reading Hospital Peshawar
Introduction: Spontaneous bacterial peritonitis is ascitic fluid infection in the absence of any recognizable secondary cause of infection. It is one of the common and potentially lethal complications of cirrhosis.
Objective: To find the incidence of spontaneous bacterial peritonitis in Cirrhotic patients with ascites and to assess its response to treatment with Ceftriaxone.
Study Design: Descriptive, case series.
Setting: This study was conducted in Gastroenterology Unit of Postgraduate Medical Institute Government Lady Reading Hospital Peshawar.
Duration: 07 months (from 1-05-11 to 01-12-11).
Subjects: Sixty patients of cirrhosis Liver with Ascites.
Methods: Cirrhotic patients with ascites admitted Gastroenterology Unit, LRH were included in the study. All these patients were subjected to ascites fluid tap according to standard protocol. Diagnosis of spontaneous bacterial peritonitis was based on an ascitic fluid neutrophilic count of > 250/mm3 without evidence of secondary peritonitis. All patients with spontaneous bacterial peritonitis were treated with ceftriaxone, 1gm IV, every 12h. Peritoneal paracentesis was then repeated after 48 hours to assess for treatment response.
Results: Out of 60 patients included, 36(60%) patients were males and 24(40%) were females. The mean age of the patients was 50.50 years and majority of the patients were in the age group of 41 to 65 years. Hepatitis C virus (HCV) infection was the most common cause of cirrhosis in 33 (55%) patients. Spontaneous bacterial peritonitis was diagnosed in 24 patients (40%), among these, 13 were males and 11 were females. In patients with spontaneous bacterial peritonitis, 21 patients (87.5%) responded to therapy after 48 hours of treatment with ceftriaxone, while in 03 patients (12.5%) treatment was ineffective.
Conclusion: Spontaneous bacterial peritonitis is a common complication of liver cirrhosis with ascites. Ceftraixone is an effective empirical therapy in the management of patients with spontaneous bacterial peritonitis.
Key words: Spontaneous bacterial peritonitis, Cirrhosis, Ascites, Ceftriaxone.

88
Left versus right liver lobe diameter albumin ratio as a predictor of esophageal varices in patients with cirrhosis
Syed Mudassir Laeeq1,Zaigham Abass1,Rajesh kumar1,Nasir Hassan Luck1,Syed Mujahid Hassan1 Sindh Institiute Of Urology &Transplantation
Introduction: Gold standard for diagnosing esophageal varices is upper gastrointestinal endoscopy, However, various non invasive markers have been studied to predict esophageal varices in cirrhotic patients. The aim of this study was to find out any significance of ratios of left and right lobe of liver with albumin as predictors of esophageal varices and compare both.
Methods: All patients diagnosed to have clinical cirrhosis were included while patients with portal vein thrombosis, history of shunt surgery, inferior vein thrombosis were excluded. Routine investigations included complete blood counts, bilirubin, alanine and aspartate transaminases, gamma glutamyl transferase, alkaline phosphatase, serum albumin, prothrombin time, and ultrasound abdomen with right and left liver lobe diameter measurements in the midclavicular line. Endoscopy was done to document presence of varices. The correlation between the calculated ratios and presence or absence of esophageal varices were estimated.
Results: One hundred and eleven subjects (80 males), mean age 40.3 years, were studied. Esophageal varices were seen in 68 (61.3%) patients; Child-Pugh class A accounted for 41.4%, class B 48.8%, and class C 12.6% cases of varices. The mean value of right lobe diameter/albumin ratio was 5.1± 1.9 in patients with varices versus 4.2± 1.6 in patients without varices (p=0.023). The mean value of left lobe diameter albumin ratio was 2.4± 0.9 in patients with varices versus 1.9± 0.6 in patients without varices (p<0.001). Areas under ROC curves were 0.377 and 0.69 respectively.
Conclusion: The left lobe diameter/albumin ratio is a better predictor of esophageal varices than right lobe diameter/albumin ratio in patients with liver cirrhosis.
Assessment Of Severity of Liver Injury in patients with Metabolic Syndrome.
Ehsan Ullah, Israr Ul Haque,Maria Aslam, Salman Shakeel, Imran Hassan Khan, Ghias Un Nabi Tayyab, Ghias ul Hassan, Israr ul Haq
Introduction: To evaluate the impact of metabolic syndrome on liver by measuring aminotransferase levels of the patients suffering from Metabolic Syndrome. Material and Methods: A Prospective cross-sectional study. Data was analyzed on spss10 with 16variables on which relevant details were noted. The study was conducted in 200 patients fulfilling the criteria of metabolic syndrome presenting at diabetes and endocrine clinic in Medical Unit-I, Lahore General Hospital, Lahore between August 2011 to November 2012. MS is defined as.waist cirumferance
≥ 90cm for men and ≥ 80cm for women for those of South and South-East Asian, Japanese, and ethnic South and Central American origins
plus any two of the following four factors:
- raised triglycerides: ≥ 1.7mmol/L
- reduced HDL-cholesterol: <1.03mmol/L in males and <1.29mmol/L in females, or specific treatment for these lipid abnormalities
- raised blood pressure: systolic BP ≥130 or diastolic BP ≥85mm Hg, or treatment of previously diagnosed hypertension
- impaired fasting glycaemia (IFG): fasting plasma glucose ≥5.6 mmol/L, or previously diagnosed type 2 diabetes
Degree of Liver Damage: The liver disease severity was classified into four groups according to AST and ALT levels (The laboratory reference values of AST & ALT for males and females are 28 & 26 IU and 30& 26IU/L, respectively) at the time of presentation. Grade A comprised of patients with normal AST and ALT levels. Grade B comprised of patients with one of the aminotransferases increased but no higher than two times the UNL. Group C comprised of patients with transaminitis 3 to 5 times the reference values. Group D comprised of transaminitis more than 5 times the reference values.
Results: 200 patients were included in the cohort .The mean age of the cohort was 45 years and 67% were females. The majority of the cohort was either overweight (32.4%) or obese (50.7%). Elevated ALT level was more prevalent in males than females. Obesity was a strong risk for abnormal ALT in both genders. Hypertriglyceridemia, hypercholesterolemia and young age were risks for elevated ALT in males only, whereas increased fasting plasma glucose was associated with elevated ALT in females only. Degree of liver enzymes rise indicating liver involvement was observed in 48.9% (Grade A), 34.5% (Grade B), 14.8% (Grade C) and 1.8% (Grade D).Grade C and D indicative of ongoing severe liver damage .

89
Conclusion: In this cohort of patients of metabolic syndrome, majority of patients had a rise in liver enzymes indicating liver injury. Grade C and D rise of enzymes in the studied cohort was relatively less common but may indicate the people at risk of developing NASH and its sequel requiring further research.
Prevalence And Risk Factors Of Nafld Among Native South Asian Pakistani Patient With Type 2 Dm
Amna Subhan Butt1, Saeed Hamid1, Zishan Haider2, Aatif Ahmad Khan3, Mohammad Salih1, JavedAkhter, Wasim Jafri1
Aga Khan University Hospital, Karachi
Introduction: Despite an increase in morbidity and mortality due to Diabetes (DM) and Metabolic syndrome (MS) in South-Asia and establishment of their association with Non-alcoholic fatty liver disease (NAFLD) in other part of world, scanty data is available regarding NAFLD from Pakistan. NAFLD is not only a precursor of cirrhosis & HCC but also associated with increased morbidity & early mortality.
Objective: To estimate the prevalence of NAFLD and to determine the predicting factors associated with NAFLD among native South Asian Pakistani patients with Type 2 DM & Metabolic Syndrome.
Method: This was a prospective, Cross-sectional study, conducted in outpatient clinics of the Aga Khan University hospital, Karachi, Pakistan during 2007 and 2010. Patients≥18 years of age diagnosed to have type 2 DM and MS were enrolled. Patients who have liver disease due to HBV, HCV, autoimmune and metabolic causes, taking hepatotoxic drugs or alcohol were excluded. NCEP, ATP III Criteria for MS with the exception of abdominal obesity (waist circumference >90 cm in men & 80 cm in women for Asian population) was used to define MS. Information was collected about demographics, BMI (KG/m2), waist circumference, components of MS, duration of DM, glycemic control and ALT. Ultrasound liver was performed by an experienced sonologist to identify NAFLD. Patients with elevated ALT were evaluated for HBV, HCV infection and for autoimmune and metabolic liver disease.
Results: Out of 180 patients 163 were eligible. Mean age was 54.3±11.1 years with 87(54%) males. Overall prevalence of NAFLD was 72.4%. Moreover, the NAFLD prevalence was higher among males as compared to females (51.3% vs.40.7%) and patients with HTN (73.6% vs. 53.6%), dyslipidemia (59.7% vs. 53.65%) and obesity (70% vs. 49.1%). Mean ALT was 27.0±15.9 IU/ml. ALT was higher above the normal limits in 15% cases and was associated with severe fatty changes in liver. Older age (p 0.02), obesity (p 0.01), higher waist circumference (p 0.03), longer duration of DM (p 0.01), dyslipidemia (0.04), poor glycemic control (p 0.03) were the factors significantly associated with NAFLD. Furthermore, prevalence of NAFLD was increased with increasing components of MS.
Conclusion: The prevalence of NAFLD was high in this cohort of South Asian Pakistani population with type 2 DM and Metabolic Syndrome. Moreover, NAFLD was not only strongly associated with the MS, the increasing components of MS were also found to be associated with higher risk of NAFLD.
Keywords: Diabetes Mellitus, Metabolic Syndrome, NAFLD
Optimal Utilization Of Prime Minister Funds For Treatment Of Hepatitis C
Dr. Muhammad Avais Khan, Dr. Kashif Malik, Dr. M. Johar Amin, Dr. Arshad K. Butt , Prof. Anwaar A. Khan, Prof. Altaf Alam, Prof. Zafar Iqbal, Dr. Waqar H. Shah, Dr. Farzana Shafqat.
, Sheikh Zayed Hospital, Lahore, Pakistan.
Introduction: Hepatitis C virus infection is one of the major causes of chronic liver diseases throughout the world. In Pakistan, 10 million people are presumed to be infected with this disease. In 2006, government of Pakistan started a program for hepatitis control and provided conventional interferon alpha to hepatitis C patients. Aims & Objectives: The primary objective is to evaluate the proper utilization of Government funded program for the treatment of hepatitis C. Also it was aimed to determine the type of HCV genotypes as well as sub-type in chronic hepatitis C patients, to check EVR, ETR and SVR in these patients, and to evaluate the cost effectiveness of these tests. A total of 1000 patients of hepatitis C virus were recruited. Results: Out of 1000 patients, 506 (50.6%) were males, while 494 (49.4%) were females. The age ranged from 16 to 67 years with a predominantly larger proportion of younger patients. HCV genotype was checked in 295 patients. Early Viral Response (EVR) was checked in 142 (14.2%) patients; it was achieved in 97 patients. End of treatment response (ETR) was checked in 609 (60.9%) patients, it was achieved in 405 (66.50). HCV RNA reports to confirm the SVR were available for only 60 (6%) of patients. Out of these 60, SVR was achieved in 46 (76.66%). Conclusion: Although 61% patients reported with HCV RNA reports at the end of treatment, but only 6% patients opted for follow up HCV RNA by PCR testing to look for SVR. Considering the huge cost of treatment of from

90
government funds, measures should be adopted to have a structured program for proper evaluation of these patients before, during and after the treatment.
Patterns Of Clinical Presentation And Outcome Of Budd Chiari Syndrome: Experience From A Tertiary Care Hospital In Pakistan
Abbas Ali Tasneem, Zaigham Abbas, Nasir Hassan Luck, Syed Mujahid Hassan
Introduction: Budd Chiari Syndrome (BCS) is characterized by hepatic venous outflow obstruction at the level of hepatic veins, intrahepatic or suprahepatic inferior vena cava or all. The aim of the study was to determine etiology, clinical presentation and outcome of such patients.
Methods: In this retrospective study, patients diagnosed to have BCS were evaluated for the cause, clinical presentation and outcome. Log rank test followed by Cox regression analysis was performed to identify independent predictors of survival.
Results: Twenty patients presented with BCS; male 14, age range at first presentation was 2-50 years (mean 14.9). Fourteen (70%) belonged to pediatric age group. Twelve (60%) patients had an acute presentation: tender hepatomegaly alone in 6, hepatomegaly with ascites in 5, and fulminant course in 1. Eight patients (40%) had chronic presentation: variceal bleeding in 4 and advanced cirrhosis in 4. The probable etiology was thrombosis secondary to hypercoagulable state in 17 followed by infiltrating renal cell carcinoma 1, abdominal tuberculosis 1 and liver abscess 1. Among hypercoagulable states protein C deficiency was commonest, present in 6 followed by combination of protein C and antithrombin III deficiency 5 and proteins C, S and antithrombin deficiency 4. Seven (35%) patients died; acute 4 and chronic 3. Causes of death included sepsis 4, fulminant hepatic failure 1, GI bleeding 1, and bleeding from site of liver biopsy 1. Poor survival was associated with serum albumin < 2.8 g/dl (p=0.022), bilirubin > 3mg/dl (p=0.025), and absence of varices (p=0.015). Cox regression analysis showed that low albumin and absence of varices were independent predictors of poor survival.
Conclusion: Budd Chiari Syndrome affects pediatric age group more frequently and is associated with high mortality. The commonest probable etiology was hypercoagulable state. Survival is poor with low albumin, high bilirubin and absence of varices suggesting an acute course.
Efficacy of biosimilar Pegylated Interferon Alpha 40 KD (Peg INF) in chronic hepatitis C infection
Ghias ul Hassan, Bilal Nasir, Imran Syed, Shafiq Awan, Israr ul Haq Toor, Ghias un Nabi Tayyab, Hammad Raza, S. Hassan Akhtar Bokhari, Khawar Saeed, Qazi Masroor, Muhammad Imran Nazir, K.M. Anjum
Introduction: Pegylated Interferons and Ribavirin combination is standard of care in the management of chronic HCV infected patients. Efficacy of the therapy is judged by the ability to achieve biochemical and virological response as judged by RVR, EVR, ETR and SVR.
Objective : To evaluate the efficacy of newly marketed biosimilar Pegylated Interferon Alpha 40KD (Peg INF) in chronic HCV patients.
Materials and methods: This was observational, prospective multicentre study to evaluate the ability of biosimilar pegylated interferon alfa 2a (40KD) along with Ribavirin (weight based) to achieve SVR. The enrolled patients were separated into Naïve(A), Relapsers(B) and Non Responders(C) based on the previous history of interferon exposure and its response. The RGT was followed on ALT and RVR, EVR, ETR and SVR.
Results:
RVR EVR ETR Week24
ETR Week48
SVR Week 48
SVR Week 72
Total SVR
Relapsers
NR Lost to follow up
Naïve (n 127)
77.9 % (99/127
57.7 % (15/26)
82 % (81/99)
54.2 % (13/24)
80.8% (80/99)
45.8 % 11/24
74% (91/123)
3.2% (3/94)
8.6% (11/127)
17.3% (22/127)
Relapsers to standard INF (N 61)
80% (49/61)
70 % (7/10)
-----------
78.6 % (44/56)
----------
89.4% (42/47)
4.3% (2/47)
5.1 % (3/59)
20% (12/61)
Non responders to standard IFN (N 21)
47.6% (10/21)
33.3% (3/9)
-----------
68 % (13/19)
----------
52.6% (10/19)
3/19 15.8%
31.6 % (6/19)
9.5% (2/21)

91
Conclusion: It is concluded that Bio-similar pegylated interferon alfa-2a (40kD) along with Ribavirin has good anti viral efficacy in Naïve, Relapsers and Nonresponders to standard IFN of chronic HCV infected patients requiring treatment.
Key words: SVR (Sustained virological response), NR(Nonresponders), Pegylated interferon
8 months follow up to evaluate survival patterns and quality of life in patients with Hepatocellular carcinoma since the initial diagnosis.
Maria Aslam, Israr Ul Haque, Ehsan Ullah,Salman Shakeel, Ghias Ul Hasan, Asif Gul, Ghias Un Nabi Tayyab, Altaf Alam
Introduction: To evaluate the survival pattern and quality of life in patients with HC after 8 months follow up.
Material and Methods: It is a prospective cross-sectional ongoing study conducted in 140 patients diagnosed to have HCC and presenting at GI departments of Lahore General Hospital and Sheikh Zayed Hospital, Lahore from January 2012 to April 2012 and have been followed for 8 months to check survival, the outcome of any treatment if there has been, quality of life, terminal event in case of death, and the date of death.
Results: Median age at the time of diagnosis of HCC is 57 years (range: 30–60), 100 males (71%) and 40 females (29%). At eight months follow up, 65 patients (46.4%) were alive, and 75 patients (53.5%) had died. Etiological cause of CLD and HCC was HCV in 67%(n.94), HBV in 14% (n.20) and 12% (n:17) had a co-infection of HCV and HBV. 9(6.4%) patients had a negative serology for viruses. Out of the patients suffering from HCC secondary to HCV, at 8 months follow up 50(53.1%) are alive and 44(46.8%) have died and the terminal event in HCV related cancer patients at the time of death was upper GI bleed in 17, Ascites and its complications in 11, lower GI bleeding in 6 and hepatic encephalopathy in 10 patients. The HBV related cancer patients were 20 (14% of total), out of which 09 are alive and 11 had died. In these HBV related HCC patients, 03 patients died due to upper GI bleed, 03 due to PSE,03 due to ascites and 02 due to lower GI bleeding. Seventy six percent (n.107) of patients received therapy, and 23.5% (n.33) received no specific therapy. Among patients who received therapy, surgical resection was the commonest procedure (n: 57 patients,53%) and 38(66.6%) are alive at 8 months of follow up, 38 patients (35.5%) received chemotherapy out of which only 11(29%) are alive, TACE has been done in 7(6.5%) out of which 3(43%) are alive , RFA was done in 2(1.8%),liver transplant in 3 patients(2.8%) and all are alive and stable at 6 months follow up. Rest of 35 patients (24.5%) received only supportive treatment and the death ratio in this group is 65% at 8 months. The average size of the tumor among deceased patients was >5cm and majority had multiple lesions or metastasis at the time of diagnosis n:41 (67% of the deceased).Statistical difference was found in survival of patients with single lesion or multiple lesions (p > 0.05).
Conclusion: It is concluded that HCC is a sinister diagnosis with grave prognosis and males are affected more commonly than females. The HCV related HCC are more prevalent in our community and portal hypertension related complications are the cause of death in most patients .However the early recognition and surgical resection can reduce the morbidity, improve the quality of life and survival of the patients. Liver transplantation and RFA are effective alternative remedies in suitable patients.
Risk factors for development of chronic HCV and HBV in the developing world- a study to determine the role of various risk factors in the development of chronic viral hepatitis and to
assess the level of awareness of these risk factors in the general population.
Nawaz A, Riaz M, Iftikhar M, Nawaz S, Nawaz M, Alvi A, Chaudhry A. Fatima Memorial Hospital, Lahore, Pakistan
Background: Hepatitis C is a parenterally transmitted virus. In Pakistan there is no national data for evaluating risk factors for hepatitis C. Most of the evidence available has been gathered from studies conducted in select areas of Pakistan. Different population subsets that have been shown to have a higher risk of acquiring chronic HCV include pregnant women (particularly after blood transfusion), multi-transfused patients with thalassemia major (34.8%-60%), Chronic renal failure patients on hemodialysis (23.7%-68.2%), healthcare professionals, IV drug users (60-94.3%), unsafe therapeutic injections, surgery/ dental work and sharing of objects.
Objectives:
1. To determine the role of various risk factors in development of chronic HCV
2. To study the population’s awareness of the risk factors of HCV.
Materials and Methods: The department of gastroenterology and Hepatology conducted a free camp for screening of hepatitis B & C on 30th July 2011. 435 persons were screened for hepatitis. Every person was asked about various risk factors associated with hepatitis transmission. The data was collected on questionnaire and analyzed in SPPS version 17

92
Results: Out of a total of 435 people who were screened at the camp, 12% had Hepatitis C and 3% had hepatitis B. Only one patient had both. 72% of the patients with hepatitis C were more than 30 years of age while Hepatitis B was more common in the younger age group. Male and female prevalence was 55% and 45% for HCV respectively. HCV and HBV did not appear to be more common in healthcare professionals. History of surgical procedure (15% vs 12%), deliveries (22% vs 12%), dental procedures (16% vs 12%), ear and nose piercing and shaving from the barber (19% vs 12%) increased the risk slightly for acquiring chronic hepatitis (B or C). Family history of chronic hepatitis (24% vs 12%), multiple blood transfusions ( 43% vs 12%) and frequent therapeutic injections (> 5 per year) (28 % vs 12%) significantly increased the risk of acquiring chronic hepatitis. 41% of the patients requested use of sterile instruments for surgery, 50% for dental procedures, 61% for barber shaving and only 18% asked for sterile instruments for body piercing. Hepatitis was more common with diabetes mellitus (41.2%) and asthma/ COPD (37.5%).
Conclusions:
Risk factors previously well known to correlate with chronic HCV were found in our study also including multiple blood transfusions, family history of chronic hepatitis and frequent therapeutic injections. Certain factors seen in previous studies to increase the risk of acquiring chronic hepatitis like surgical procedures, dental work, barber shaving and body piercing appeared to be less significant in our study population. In spites of awareness of the scale of the problem, only about half to one third of the population asked for use of sterile instruments during various procedures. Patients with Diabetes Mellitus and COPD/ Asthma had a very high prevalence of chronic hepatitis likely due to frequent therapeutic injections.
Role of biochemical tests in predicting common bile duct stone or strictures
Muhammad Osama Tariq Butt, Zaigham Abbas, Nasir Hassan Luck, Mujahid Sindh Institute 0f Urology and Transplantation, Karachi.
Background: Extrahepatic cholestasis associated with dilated bile ducts, is caused by bile duct stones or strictures. This study was done out to evaluate common liver function tests (LFTs) in the differential diagnosis of extrahepatic cholestasis separating patients with bile duct strictures from those with stones.
Methods: All consecutive patients with deranged LFTs and biliary dilatation on ultrasound were evaluated by endoscopic retrograde cholangiopancreatography (ERCP). Patients with biliary strictures were compared with bile duct stones. Complete blood counts, international normalization ratio, plasma alkaline phosphatase, gamma-glutamyltransferase, aminotransferases, and bilirubin values were determined in the same morning before doing ERCP.
Total patients evaluated were 227. 24 patients on ERCP were found to have mild biliary dilation without stone or stricture while 15 had both stone and stricture. Both groups were excluded. 8 patients who had previous stenting and 5 who had fistulous opening were also excluded from the final analysis leaving behind 175 patients for the study.
Results: Total number of patients were 175 out of which 84 were male. Mean age was 43.8 years in patients having CBD stone and 48.1 years in those having CBD stricture. Total Bilirubin (p = 0.003), Direct Bilirubin (p = 0.008), Alkaline phosphatase (p = 0.004), and International normalization ratio (p = 0.003) were found to be significantly higher by student t test in patients having CBD stricture while Alanine aminotransferase (ALT ) (p = 0.01) was significantly higher in patients having CBD stones.
Conclusion: Obstructive jaundice with CBD stricture is associated with more severe deranged LFTs while patients with CBD stones have higher ALT levels.
Role of intravenous antibiotic in variceal bleeding Ciprofloxacin V/S Third generation cephalosporin (Ceftriaxone)
Dr. Ramdev Chaudhary, Dr.Ommara Jamil,Dr.Sandeep Raj Kunwar, Dr.M Ayub, Dr. Shahid Sarwar, Prof. Dr. Tahira Murtaza Cheema.
Aims and Objective: To compare the efficacy of Ciprofloxacin and Ceftriaxone for control of in-hospital morbidity, mortality and prevention of infection in patients with variceal bleeding.
Setting: Gastroenterology unit, East Medical Ward, Mayo Hospital, Lahore.
Patients & Methods: We included all patients being admitted with haemtemesis and malena and found to have varices as source of bleeding on endoscopy. We performed clinical examination with baseline investigations in all patients. At admission, patients were randomized in two groups i.e. A and B. Group A recieved inj. Ceftriaxone while those in B had inj. Ciprofloxacin. All patients were followed for 7 days for outcome in terms of rebleeding, portosystemic encephalopathy (PSE), spontaneous bacterial peritonitis (SBP), systemic inflammatory response syndrome (SIRS) and septicemia. Chi square was used for comparing result.

93
Results: Total of 250 patients were included. Mean age of patients in group A was 51.54 (±12.087) with male to female ratio 1.23:1 (69/56) while in group B it was 50.21(±13.1) with male to female ratio 1.27:1 (70/55). On follow up, total 13 patients had rebleed, 6 from group A while 7 from group B (P value=0.776), 2 patients developed PSE one from each group, 5 developed SBP 1 from group A while 4 from group B (P value=0.399) and 16 patients developed SIRS, 6 from group A while 10 from group B (P value= 0.301) and 5 patients had positive blood culture, 1 from group A while 4 from group B. No patients died during one week follow up.
Conclusion: Ciprofloxacin and Ceftriaxone have similar efficacy in prevention of bacterial infection and sepsis in patients of variceal bleeding.
Role of oral antibiotics, “Ciprofloxacin vs Neomycin ” for secondary prophylaxis of Porto-systemic Encephalopathy (PSE) in patients with Liver Cirrhosis.
Shahzad Latif, Muhammad Ayub , Shahid sawar King Edward Medical University Lahore, Pakistan.
Objective: - To compare efficacy of Neomycin and Ciprofloxacin in secondary prophylaxis of porto systemic encephalopathy in Liver Cirrhosis.
Setting: - East Medical Ward Mayo Hospital Lahore .
Patients and method: - All patients being admitted with porto systemic encephalopathy were included after recovering conscious. Patients were randomized into two groups, group A which received Ciprofloxacin & group B who were given Neomycin at discharge. Patients were followed for relapse of PSE for 6 months; data were analyzed in SPSS 13.0.
Results: Total of 280 patients were included, mean age was 50.34 (± 6.901), male to female ratio was 1.47:1 (167/113).Malena was present in 226 (80.7%), while 241 (86.1%) patients had ascites at presentation.
One hundred thirty six (48.6%) patients received Neomycin while 144 (51.4%) patients received Ciprofloxacin for secondary prophylaxis.
Both groups were comparable with regards to stage of liver disease. After 6 months follow up 73, (80.69%) patients of Ciprofloxacin group had relapsed of PSE while 18 (13.23%) patients of Neomycin group developed encephalopathy. Difference was remarkably significant (P value <0.000).
Conclusions: - Neomycin is a superior drug for secondary prophylaxis of Encephalopathy due to better efficacy than Ciprofloxacin.
Key words: Liver Cirrhosis, porto systemic encephalopathy, Secondary prophylaxis.
Tattoo Mark Is Rural(Desert) Cultural tradition Or Spreading Of Viral Infection Jewat Sunder, Satti jewat
Institution: Sindh United (n) Developmental Educational Rural Society Sindh
Chief Minister Hepatitis Control Program Sindh
Back ground: Tatoo mark is the cultural /traditional mark or is the source of viral infection especially in the community of rural desert areas, viral infection - hepatitis, which is more serious health problem in our country.
Aim: Our aim to educate the rural (desert) community about hepatitis/causing factors and preventive measures, screening of HCV, HBsAg and vaccination of Hepatitis B. and treatment of the HCV+Cases.
Duration (Place): March 2012 to October 2012.
Methodology: Descriptive Study /Research Based on/ spss on version 11. There were 1000 cases Screened for HCVand HBsAg results as follow:
Females were (60.5%) and Males were (39.5%)
(31.25%) cases were positive and (68.75%) was negative.
Hepatitis B (HBsAg) out of 1000 cases (6%) positive.
Hepatitis C (HCV) out of 1000 cases -25% positive.
Total cases: 300 of screened for viral makers with tatoo marking:
Male: 134(45%) Male= HCV +ve were cases 25(8.33%)
Male =HBV+ve were cases 7(2.33%) Mean Age (15-45 years)
Female: 166(55%) Female:=HCV+ve were cases 35(11.6%)

94
Female =HBV+ve were cases 5(1.6%) Mean Age (15-45 years)
Conclusion: Health education is the key for the prevention of any health issue, by education awareness /literacy/we can break the rules by ethical way the traditional cultural myths which are the source of health problems also related with blood borne infection like tatoo mark.
To study the effectiveness of RVR in predicting SVR in HCV GT 3 patients treated with conventional interferon α2b and ribavirin
Asad Chaudhry, Altaf Alam, Muhammad Riaz, Muhamad Iftikhar Yousaf, Aftab Haider Alvi, Arif Nawaz
Background: HCV affects about 5 % of the population in Pakistan with 3 being the predominant genotype. IFN α (conventional) 3 MU sc thrice weekly with ribavirin is still widely used in Pakistan in view of good results against genotype 3 and significantly lower cost (approximately 20% of the cost of Pegylated Interferon). Response guided therapy (RGT) of HCV patients is being currently advocated for treatment of HCV with Pegylated Interferon as it leads to improved response rates along with early stoppage of treatment in non responders. The significance of RGT in treatment with conventional Interferon has not been studied. This study was done to address this question.
Objectives: 1) To evaluate RVR as a predictor of SVR with standard interferon and ribavirin in genotype 3 patients. 2) To study the relevance of RGT in treatment of HCV patients with conventional Interferon.
Methods; This is a retrospective analysis of data of genotype 3 patients treated with standard interferon α-2b and weight based ribavirin at the Gujranwala Liver Foundation Hepatology Clinic. Patients aged 18 to 65 years, detectable viral load, genotype 3, Childs’ score < 7 and negative HBsAg status were included in the study. Those with complete and partial EVR were continued on antiviral therapy. Treatment was stopped in patients who showed < 2 log reduction. Those who continued the treatment had their HCV RNA QL at week 24. Therapy was discontinued in patients whose HCV RNA was detected. In those with undetectable HCV RNA at week 24, antiviral therapy was stopped in patients who had favorable predictors of response while patients with poor predictors of response were assigned to 48 weeks’ treatment.
Results: SVR data on 124 patients was reviewed. 98 out of 124 patients (79%) had an ETR with an SVR of 60% overall. However the SVR increased to 79% in patients who had a RVR while it went down to 29% if patient did not have RVR. Interestingly however the relapse rate was higher in patients with a positive RVR. There were no non-responders amongst the 79 patients with a positive RVR.
SVR Relapser Non-responder
RVR+ (79) 62 [78.5%] 17 [21.5%] 0(0%)
RVR – (45) 13 [28.9%] 06 [13.3%] 26 [57.8%]
Conclusions:
RVR is an excellent predictor of SVR in genotype 3 pts treated with conventional interferon/Ribavirin.
Consideration may be given to switching patients who fail to achieve RVR to Pegylated interferon/Ribavirin- further studies are however needed in this area.
Vaccination status of the Health Care Workers of a Tertiary Care Hospital in Karachi.
Waquar uddin Ahmed, Javaria Waquar. Ejaz Haider and Ejaz Alam. Background: Vaccination status of the health care workers (HCW) against hepatitis B virus, working in the hospital is poorly known and efficacy of the vaccine provided by the Government is not known.
Objective: To determine the vaccination status of the HCW, working at Jinnah Postgraduate Medical Centre Karachi, and to vaccinate the unvaccinated HCW to determine the response of the vaccine provided by the Government.
Methods: An interview was conducted using a structured Performa from the HCW of Jinnah Postgraduate Medical Centre, Karachi at their working place. The data was entered in computer and analyzed. Unvaccinated HCW were checked for Anti HBs antibody titer as abase line and those with inadequate antibody titers, Catch up vaccination was done using vaccine received from the chief minister programme and its antibody response was checked after 1st,2nd and 3rd dose of vaccine, to determine antibody response.
95
Results: A total of 1584 HCW were interviewed, 950 (60%) were male and 634 (40%) female. Seven hundred sixty five (48.3) cases were never vaccinated against hepatitis B virus. Six hundred thirty cases (39.8%) were fully vaccinated, while 189 (11.9) cases were partially vaccinated. Seventy one (4.5) received only one shot of vaccine and 118 (7.5) received two shots of vaccine. Majority of the HCW were in the second and third decades of life, and were vaccinated with in less than 5 years duration. Reason for not being vaccinated were unawareness 355 (46.4%), unimportant 288 (37.6%), lack of fund 53 (6.9) and fear of needle 26 (3.4%). Only 384 (24.2%) cases checked their HBsAg status before vaccination.
Only 238 HCW turned up for vaccination, baseline antibody status was checked before vaccination 62 (26%) cases were already having Anti HBs positive, remaining 176 cases were vaccinated and Anti HBs titer was checked. After 1st dose Anti HBs was positive in 19%, after 2nd dose 35% and after 3rd dose 74% became Anti HBs positive.
Conclusion: Nearly half of the HCW are still unvaccinated due to unawareness and carelessness. Response to the vaccine provided by the Government is 74% which is compare able to the standard vaccine.
Validity of Aspartate aminotransferase to Platelet ratio index as Predictor of early Viral response in patients with Hepatitis C treated by Interferon-based therapy
Shaikh Samiullah1,1, Devrajai Bikharam2,1, Kalhoro Musarat3,2
Objective: To observe any change in value of aspartate aminotransferase to platelet ratio index from the baseline and to compare it with the Hepatitis C virus ribonucleic acid at 12 weeks after the start of interferon based treatment in patients with Hepatitis C.
Methods: The prospective study, conducted at the Department of Medicine, Liaquat University of Medical and Health Sciences Hospital, Jamshoro, Pakistan, from September 2009 to March 2010, included 158 consecutive, chronic patients of Hepatitis C with grade > 2 fibrosis on liver biopsy, or having aspartate aminotransferase/Platelet ratio index of > 1. The aspartate aminotransferase to platelet ratio index was determined as aspartate aminotransferase level (upper normal limit)/ platelets counts (109/L) x 100. Eligible patients were assigned to receive thrice weekly subcutaneous injection of 3MIU standard interferon >-2b and weight-base dosage of ribavirin. The early virological response was defined as undetectable Hepatitis C virus ribonucleic acid test at week 12 of the study. APRI <1 was considered to be the response to therapy. Paired sample t-test was applied to observe pre-and post-treatment mean ± SD of continuous variables, while Chi-square test was applied for comparing categorical variables. A p-value of 0.05 was considered statistically significant.
Results: Out of 158 patients enrolled, 90 fulfilled the inclusion criteria. The aspartate aminotransferase to platelet ratio index before treatment was 1.61 ± 1.00 and after treatment was 1.10 ± 1.08. Hepatitis C virus ribonucleic acid after 12 weeks of treatment was non-detectable (early viral response achieved) in 72 (80%) patients. A strong relation was found between aspartate aminotransferase to platelet ratio index and Negative polymerase chain reaction with early virological response as only 2 (4.5%) patients with negative polymerase chain reaction at 12 weeks had aspartate aminotransferase to platelet ratio index > 1 (p=0.001).
Conclusions: APRI can act as a predictor of early viral response in patients with Hepatits C.
Keywords: APRI, Early viral response, Hepatitis C