
Open randomized study of artesunate-amodiaquine vs. chloroquine-pyrimethamine-sulfadoxine for the...
10
Open randomized study of artesunate-amodiaquine vs. chloroquine-pyrimethamine-sulfadoxine for the treatment of uncomplicated Plasmodium falciparum malaria in Nigerian children A. Sowunmi, F. A. Fehintola, A. A. Adedeji, G. O. Gbotosho, E. Tambo, B. A. Fateye, T. C. Happi and A. M. J. Oduola Department of Pharmacology and Therapeutics, Institute for Medical Research and Training, University of Ibadan, Ibadan, Nigeria Summary background Artemisinin-based combination antimalarials are currently considered effective alternatives for the treatment of malaria in Africa, but there are few studies of such combinations in Nigerian children. We assessed the safety, treatment efficacy and effects on gametocyte carriage of the combination of artesunate plus amodiaquine and chloroquine plus pyrimethamine-sulfadoxine in children. methods We evaluated 153 children who were aged 12 years or younger who had uncomplicated Plasmodium falciparum malaria. Patients were randomly assigned a combination of artesunate (4 mg/kg of body weight daily for 3 days) plus amodiaquine (30 mg/kg over 3 days), or chloroquine (25 mg/kg over 3 days) plus pyrimethamine-sulfadoxine (25 mg/kg of the sulfadoxine component at presentation). The primary endpoints were the proportions of children with adequate clinical and parasitological response, late parasitological failure, late clinical failure and early treatment failure. The parasitological cure rates on days 14–28 were also used as the primary endpoints. results Both regimens were well tolerated; no child was withdrawn because of drug intolerance. All children treated with artesunate plus amodiaquine had adequate clinical and parasitological response (ACPR), while all but five children treated with chloroquine plus pyrimethamine-sulfadoxine had similar response. Fever clearance times were similar in the two treatment groups. However, the pro- portion of patients whose parasitaemia cleared by day 2 was significantly higher (100 vs. 50%, P ¼ 0.00001) and parasite clearance was significantly faster (1.7 ± 0.4 vs. 2.5 ± 0.8 days, P ¼ 0.0001) in children treated with artesunate plus amodiaquine. The cure rates on days 21 (100% vs. 94%, P ¼ 0.03) and 28 (100% vs. 90%, P ¼ 0.003) were also significantly higher in children treated with artesunate plus amodiaquine than in those treated with chloroquine plus pyrimethamine-sulfadoxine. Overall, a significantly higher proportion of children treated with chloroquine plus pyrimethamine- sulfadoxine carried gametocytes at least once during follow-up compared with those treated with artesunate plus amodiaquine [5 of 50 (10%) vs. 1 of 103 (0.97%), P ¼ 0.01]. conclusion The combination of artesunate plus amodiaquine is therapeutically superior to a combination of chloroquine plus pyrimethamine-sulfadoxine, and significantly reduced gametocyte carriage following treatment. keywords artesunate-amodiaquine, chloroquine-pyrimethamine-sulfadoxine, malaria, children, Nigeria Introduction Drug resistance in Plasmodium falciparum to chloroquine or pyrimethamine-sulfadoxine monotherapy (Sibley et al. 2001) is a major public health problem in much of sub-Saharan Africa and is a cause of recent increases in malaria–related morbidity and mortality in African children (Trape et al. 1998; Trape 2001). In Nigeria, despite the prevalence rates of chloroquine, pyrimethamine- sulfadoxine and chloroquine plus pyrimethamine-sulfa- doxine resistance of 35%, 17–25% and 0%, respectively (Sowunmi et al. 2001,2004a; Sowunmi 2002,2003), the public health policy is to treat uncomplicated malaria episodes with chloroquine, and to use pyrimethamine- sulfadoxine as the second line drug for those not responding to chloroquine. Tropical Medicine and International Health doi:10.1111/j.1365-3156.2005.01503.x volume 10 no 11 pp 1161–1170 november 2005 ª 2005 Blackwell Publishing Ltd 1161
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Open randomized study of artesunate-amodiaquine vs. chloroquine-pyrimethamine-sulfadoxine for the...

Open randomized study of artesunate-amodiaquine
vs. chloroquine-pyrimethamine-sulfadoxine for the treatment
of uncomplicated Plasmodium falciparum malaria in Nigerian
children
A. Sowunmi, F. A. Fehintola, A. A. Adedeji, G. O. Gbotosho, E. Tambo, B. A. Fateye, T. C. Happi andA.M. J. Oduola
Department of Pharmacology and Therapeutics, Institute for Medical Research and Training, University of Ibadan, Ibadan, Nigeria
Summary background Artemisinin-based combination antimalarials are currently considered effective
alternatives for the treatment of malaria in Africa, but there are few studies of such combinations in
Nigerian children. We assessed the safety, treatment efficacy and effects on gametocyte carriage of the
combination of artesunate plus amodiaquine and chloroquine plus pyrimethamine-sulfadoxine in
children.
methods We evaluated 153 children who were aged 12 years or younger who had uncomplicated
Plasmodium falciparum malaria. Patients were randomly assigned a combination of artesunate (4 mg/kg
of body weight daily for 3 days) plus amodiaquine (30 mg/kg over 3 days), or chloroquine (25 mg/kg
over 3 days) plus pyrimethamine-sulfadoxine (25 mg/kg of the sulfadoxine component at presentation).
The primary endpoints were the proportions of children with adequate clinical and parasitological
response, late parasitological failure, late clinical failure and early treatment failure. The parasitological
cure rates on days 14–28 were also used as the primary endpoints.
results Both regimens were well tolerated; no child was withdrawn because of drug intolerance. All
children treated with artesunate plus amodiaquine had adequate clinical and parasitological response
(ACPR), while all but five children treated with chloroquine plus pyrimethamine-sulfadoxine had
similar response. Fever clearance times were similar in the two treatment groups. However, the pro-
portion of patients whose parasitaemia cleared by day 2 was significantly higher (100 vs. 50%,
P ¼ 0.00001) and parasite clearance was significantly faster (1.7 ± 0.4 vs. 2.5 ± 0.8 days, P ¼ 0.0001)
in children treated with artesunate plus amodiaquine. The cure rates on days 21 (100% vs. 94%,
P ¼ 0.03) and 28 (100% vs. 90%, P ¼ 0.003) were also significantly higher in children treated with
artesunate plus amodiaquine than in those treated with chloroquine plus pyrimethamine-sulfadoxine.
Overall, a significantly higher proportion of children treated with chloroquine plus pyrimethamine-
sulfadoxine carried gametocytes at least once during follow-up compared with those treated with
artesunate plus amodiaquine [5 of 50 (10%) vs. 1 of 103 (0.97%), P ¼ 0.01].
conclusion The combination of artesunate plus amodiaquine is therapeutically superior to a
combination of chloroquine plus pyrimethamine-sulfadoxine, and significantly reduced gametocyte
carriage following treatment.
keywords artesunate-amodiaquine, chloroquine-pyrimethamine-sulfadoxine, malaria, children, Nigeria
Introduction
Drug resistance in Plasmodium falciparum to chloroquine
or pyrimethamine-sulfadoxine monotherapy (Sibley et al.
2001) is a major public health problem in much of
sub-Saharan Africa and is a cause of recent increases in
malaria–related morbidity and mortality in African
children (Trape et al. 1998; Trape 2001). In Nigeria,
despite the prevalence rates of chloroquine, pyrimethamine-
sulfadoxine and chloroquine plus pyrimethamine-sulfa-
doxine resistance of 35%, 17–25% and 0%, respectively
(Sowunmi et al. 2001,2004a; Sowunmi 2002,2003), the
public health policy is to treat uncomplicated malaria
episodes with chloroquine, and to use pyrimethamine-
sulfadoxine as the second line drug for those not responding
to chloroquine.
Tropical Medicine and International Health doi:10.1111/j.1365-3156.2005.01503.x
volume 10 no 11 pp 1161–1170 november 2005
ª 2005 Blackwell Publishing Ltd 1161

As alternatives to chloroquine or pyrimethamine-
sulfadoxine, particularly in areas where the parasite is
reasonably sensitive to chloroquine and pyrimethamine-
sulfadoxine, it has been suggested that both drugs be used
in combination, or in combination with other antimalarials
that have modes of action different from those of
chloroquine and pyrimethamine-sulfadoxine, with the aims
of slowing the progression of resistance to these drugs and
prolonging their lifespan (von Seidlein et al. 2000; Basco
et al. 2002; Sowunmi 2002; Drakeley et al. 2003; Gasasira
et al. 2003). An additional antipyretic effect is produced by
combining chloroquine with pyrimethamine-sulfadoxine
(Hugosson et al. 2003).
As a response to the World Health Organization
recommendation (WHO 2001), many African countries
are considering the use of artemisinin-based combinations
as alternatives to monotherapy with chloroquine or pyri-
methamine-sulfadoxine, requiring the revision of treatment
policies in endemic areas. Although artemisinin-based
combinations are effective and safe for use in children in
many countries in Africa (Adjuik et al. 2002), there is a
need to further study the efficacy and safety of these
combinations in different population groups.
Experience with the use of artemisinin-based combina-
tions is relatively limited in West Africa (von Seidlein et al.
2000,2001a,b; Adjuik et al. 2002) making it imperative to
evaluate their efficacies in other settings in sub-Saharan
Africa. Although the effects of artemisinin-based combi-
nations on asexual parasites have been assessed previously
in Nigeria (Sowunmi et al. 1998,2001), to date, in Nigeria,
no study has examined, clinically, the effects of artemis-
inin-based combinations on both asexual and sexual
parasites and compared it with a combination of chloro-
quine plus pyrimethamine-sulfadoxine. Such a study is
essential as it may influence policy and management of
drug resistance in the community.
The main aim of this study was to evaluate the safety,
antimalarial treatment efficacy, and effect on gametocyte
carriage of artesunate plus amodiaquine and chloroquine
plus pyrimethamine-sulfadoxine-combinations in children
aged 12 years or below with acute, symptomatic,
uncomplicated, falciparum malaria.
Materials and methods
Study area
The study was conducted in Ibadan, Southwest Nigeria
from July to December 2004. In this area of hyperendemic
malaria, transmission occurs all year round but is more
intense during the rainy season from April to October.
In the area, it is difficult, clinically, to distinguish
recrudescence from re-infection 14 days after commencing
antimalarial treatment, and traditionally, antimalarial
efficacy tests have usually been conducted for 14 rather than
the customary 28 days (Ekanem et al. 1987; Salako et al.
1990). The prevalence of chloroquine and pyrimethamine-
sulfadoxine resistance in the area (35% and 17–25%,
respectively) has been described recently (Sowunmi et al.
2004a). However, in vivo resistance to amodiaquine is low
(about 1–2%, Sowunmi et al. 2001; Sowunmi 2002).
Patients, treatment and follow up
Patients were eligible to join the study if they were: aged
12 years or younger, had symptoms compatible with acute
uncomplicated malaria, with pure P. falciparum parasitae-
mia >2000 asexual forms/ll, a body (axillary) temperature
>37.4 �C or history of fever in the 24–48 h preceding
presentation, absence of other concomitant illness, no his-
tory of antimalarial use in the 2 weeks preceding presenta-
tion, negative urine tests for antimalarial drugs (Dill-Glazko
and lignin), and written informed consent given by parents
or guardians. Patients with severe malaria (WHO 2000),
severe malnutrition, serious underlying diseases (renal, car-
diac or hepatic), and known allergy to study drugs were
excluded from the study. The protocol was approved by the
Ethics Committee of Oyo State Ministry of Health, Ibadan,
Nigeria. The disease history, taken by the attending physi-
cian, was recorded by asking patients or their parents when
the present symptomatic period had started, and was fol-
lowed by a full physical examination by the same physician.
Enrolled patients were randomly assigned artesunate
4 mg/kg of bodyweight daily for 3 days plus amodiaquine
(30 mg/kg over 3 days) (Larimal�, Ipca Pharmaceutical
Nigeria Plc) or chloroquine (May & Baker, Nigeria Plc)
25 mg/kg of body weight over three days plus pyrimeth-
amine-sulfadoxine (Fansidar�, Swipha Nigeria Plc)
25 mg/kg of body weight of the sulfadoxine component at
presentation (day 0). All drugs were given orally, as single
daily doses, and were administered in the clinic. All patients
waited for at least 3 h after drug administration to ensure
the drugwas not vomited. If it was, the patient was excluded
from the study. If necessary, patients were provided with
antipyrectics (paracetamol tablets, 10–15 mg/kg 8 h for
24–48 h). The randomization was computer-generated and
treatment codes were sealed in individual envelopes. Once
enrolled, study drugs were administered to patients by a
physician. Patient evaluation and follow up after drug
administration was performed by another physician blinded
to the drug treatment. The study nurse obtained thick and
thin blood films from each child as soon as they came to the
clinic. The slides were carefully labelled with the patients’
codes and were air dried before being stained.
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
1162 ª 2005 Blackwell Publishing Ltd

Follow up with clinical and parasitological evaluation
was done daily for 7 days (days 1–7) and then on days 14,
21 and 28. This consists of enquiry about the patient’s well
being, presence or absence of initial presenting symptoms,
presence of additional symptoms, measurement of body
temperature, heart and respiratory rates, and a blood
smear for the quantification of parasitaemia.
Side effects were defined as symptoms and signs that first
occurred or became worse after treatment was started. Any
new events occurring during treatment were also consid-
ered as side effects.
Thick and thin blood films prepared from a finger prick
were Giemsa-stained and were examined by light micros-
copy under an oil-immersion objective, at · 1000 magni-
fication, by two independent assessors who did not know
the drug treatment of the patient. A senior member of the
study team reviewed the slides if there was any disagree-
ment between the microscopists. In addition, the slides of
every third child enrolled in the study were reviewed by this
senior member. Parasitaemia (asexual or sexual) in thick
films was estimated by counting asexual or sexual parasites
relative to 1000 leukocytes, or 500 asexual or sexual
forms, whichever occurred first. From this figure, the
parasite density was calculated assuming a leukocyte count
of 6000/ll of blood.Routine haematological (haematocrit) and biochemical
tests (concentrations of alanine aminotransferase, aspartate
aminotransferase, bilirubin and creatinine) were performed
in 50 randomly selected children (using an autoanalyser),
pre-treatment and on day 14 to detect any drug-associated
effects.
Blood was spotted on filter papers on days 0, 3, 7, 14, 21
and 28, and at the time of treatment failures for parasite
genotyping. Parasite genotyping was done as previously
described (Happi et al. 2003,2004). PCR blots were
analysed for merozoite surface protein 2 (MSP 2) using
block 3 of MSP 2 in patients with recurrent parasitaemia
after day 14.
Response to drug treatment was assessed using WHO
1973 criteria as follows: S, sensitive, clearance of parasit-
aemia without recurrence; RI (mild resistance), parasitae-
mia disappears but reappears within 7–14 days, RII
(moderate resistance), decrease of parasitaemia but no
complete clearance from peripheral blood; RIII (severe
resistance), no pronounced decrease or increase in para-
sitaemia at 48 h after treatment. In those with sensitive or
mild resistance, parasite clearance time was defined as the
time elapsing between drug administration and absence of
detectable parasitaemia for at least 48 h. Fever clearance
time was defined as the time from drug administration until
the body temperature fell to or below 37.4 �C and
remained so for 48 h. Response to drug treatment was also
classified according to a modified version of the WHO
14-day in vivo clinical classification system (WHO 2003);
because not all patients were febrile at enrolment, a
temperature <37.5 �C was not an exclusion criterion for
enrolment. The modification also involved a follow up for
28 days in this area of intense transmission.
Cure rates were defined as the percentages of patients
whose asexual parasitaemia cleared from peripheral blood
and who were free of patent asexual parasitaemia on days
14, 21 and 28 of follow up. The cure rates on days 21 and
28 were adjusted on the basis of the PCR genotyping
results of paired samples for patients with recurrent
parasitaemia after day 14 of commencing treatment. In
patients with recurrent parasitaemia after day 14, those
with matching genotypes on day 0 and the day of
recurrence were classified as treatment failure; those with
mismatching genotypes were classified as cured.
Re-treatment of drug treatment failures
Patients failing treatment (within 14 days) with chloro-
quine plus pyrimethamine-sulfadoxine were re-treated with
artesunate plus amodiaquine and were followed for
another 28 days. Patients were re-treated whenever they
became symptomatic (usually between 14 and 21 days
after initial enrolment). Patients with profound clinical
(hyperpyrexia, oral fluid intolerance) and parasitological
deterioration during follow up were treated with
parenteral artemether (9.6 mg/kg, over 5 days) and were
regarded as treatment failures.
Data analysis
The sample size was calculated so that the study would be
able to detect a 20% absolute difference in parasitological
failure ‘rate’, between artesunate plus amodiaquine and
chloroquine plus pyrimethamine-sulfadoxine groups with
95% power and at a 5% significance level [The expected
treatment success ‘rates’ were 80% for artesunate plus
amodiaquine and 100% for chloroquine plus pyrimeth-
amine-sulfadoxine, based on a relatively recent study
(Sowunmi 2002)]. Randomization was done with a ratio
2:1, amodiaquine plus artesunate: chloroquine plus pyri-
methamine-sulfadoxine. Data were analysed using Version
6 of the Epi-Info software (Anonymous 1994). Variables
considered in the analysis were related to the densities of
P. falciparum gametocytes and trophozoites. Proportions
were compared by calculating chi2 with Yates’ correction
or by Fisher exact or by Mantel Haenszel tests. Normally
distributed, continuous data were compared by Student’s
t-tests and analysis of variance (anova). Data not con-
forming to a normal distribution were compared by the
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
ª 2005 Blackwell Publishing Ltd 1163

Mann–Whitney U-tests and the Kruskal–Wallis tests (or by
Wilcoxon ranked sum test). All tests of significance, except
where specifically indicated, were two-tailed. A P < 0.05
were taken to indicate significant differences. Data were
(double)-entered serially using the patients codes and were
only analysed at the end of the study.
Results
Patients’ characteristics
One hundred and fifty-five children were enrolled, 104
were treated with artesunate plus amodiaquine and 51
with chloroquine plus pyrimethamine-sulfadoxine. One
child from the artesunate plus amodiaquine group
was lost to follow up after day 7 because of parental
relocation. Another child in the chloroquine plus
pyrimethamine-sulfadoxine treatment group was given
amodiaquine by her mother on day 6. In both
children, parasitaemia cleared before day 3. These
children were excluded from the data analysis. Figure 1
shows the trial profile. Overall results are for 153
children. The demographic and clinical characteristics
of patients at enrolment are shown in Table 1.
These characteristics were similar in the two treatment
arms.
412 children screened
250 children with patent parasitaemia
155 children enrolled and randomized
104 assigned artesunate plus amodiaquine
51 assigned chloroquine plus pyrimethamine-sulfadoxine
1 excluded 1 excluded
0 treatment failure 2 treatment failures
103 evaluable on day 14 50 evaluable on day 14
0 treatment failure 1 treatment failure
103 evaluable on day 21 50 evaluable on day 21
0 treatment failures 2 treatment failures
103 evaluable on day 28 50 evaluable on day 28
Figure 1 Trial profile.
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
1164 ª 2005 Blackwell Publishing Ltd

Fever and parasite clearance and gametocyte carriage
Eighty-three children were febrile at enrolment, 56 in
artesunate plus amodiaquine and 27 in chloroquine plus
pyrimethamine-sulfadoxine groups. On the whole, 36 of
the children treated with artesunate plus amodiaquine, and
21 of those treated with chloroquine plus pyrimethamine-
sulfadoxine received paracetamol during the first 36 h. By
day 1, fever cleared in 53 children in the first group and in
26 children in the second group, without a significant
difference in the proportion of patients whose fever cleared
by day 1 (v2 ¼ 0.001, P ¼ 0.95). Overall, fever clearance
was similar in both treatment arms (1.1 ± 0.2 vs.
1.0 ± 0.2 days, P ¼ 0.7) (Table 2).
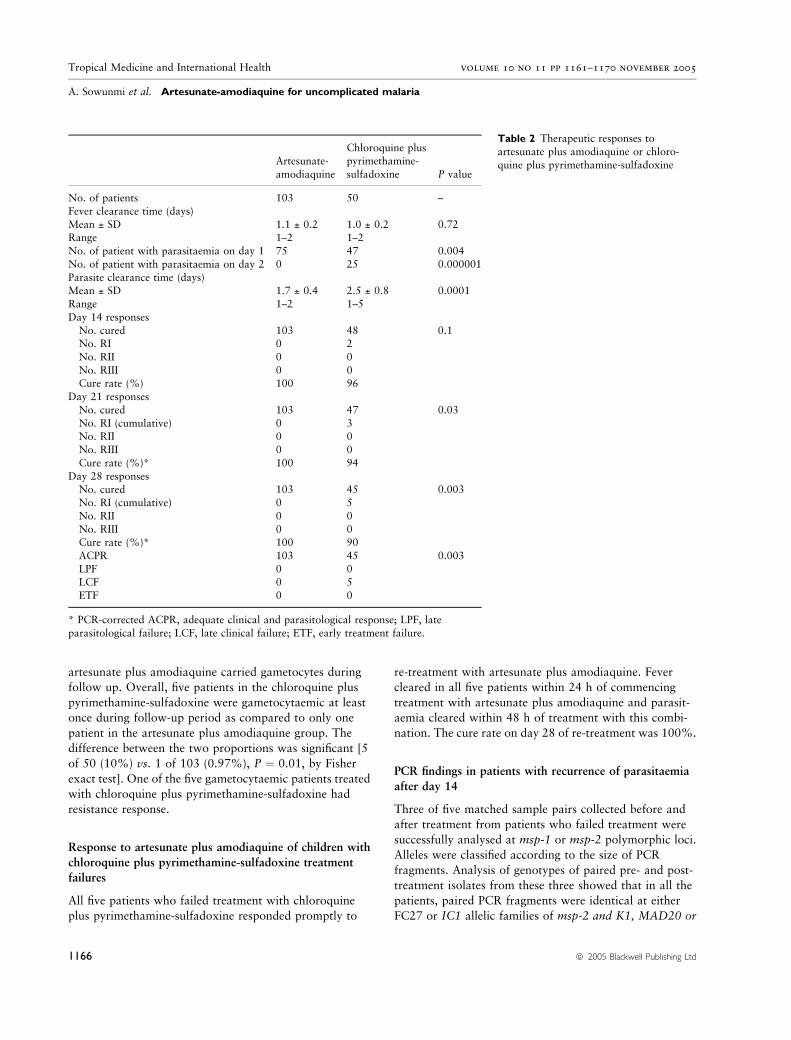
Compared with chloroquine plus pyrimethamine-sulfa-
doxine, artesunate plus amodiaquine substantially accel-
erated the clearance of parasitaemia. By day 2, all 103
children in the artesunate plus amodiaquine and 25 of the
50 children in the chloroquine plus pyrimethamine-sulfa-
doxine treatment arms had cleared their parasitaemias.
The difference in this proportion was significant
(v2 ¼ 57.9, P ¼ 0.000001). Overall, parasite clearance
was significantly shorter in those treated with artesunate
plus amodiaquine (1.7 ± 0.4 vs. 2.5 ± 0.8, P ¼ 0.0001)
(Table 2). The cure rate on day 14 was similar in the two
treatment arms (100% vs. 96%, P ¼ 0.1, by Fisher exact
test). However, cure rates in children treated with artesu-
nate plus amodiaquine were significantly higher on days 21
and 28 than in those treated with chloroquine plus
pyrimethamine-sulfadoxine (100% vs. 94%, P ¼ 0.03,
and 100% vs. 90%, P ¼ 0.003, respectively, by Fisher
exact test). Response to both treatment regimens was not
related to age: no child from the 26 and 77 <5 and ‡5-yearold, respectively treated with artesunate plus amodiaquine
failed treatment by day 28. Similarly, 2 and 3 children from
the 24 and 26 <5 and ‡5-year old, respectively treated with
chloroquine plus pyrimethamine-sulfadoxine failed treat-
ment by day 14 (P ¼ 0.6, by Fisher exact test).
All patients treated with artesunate plus amodiaquine
had ACPR. In those treated with chloroquine plus pyri-
methamine-sulfadoxine, 45 had ACPR and five had late
clinical failure (LCF).
Gametocyte carriage at enrolment in those treated with
artesunate plus amodiaquine was similar to those treated
with chloroquine plus pyrimethamine-sulfadoxine [1 of
103 (0.97%) vs. 1 of 50 (2%), P ¼ 0.5, by Fisher exact
test]. Similarly, carriage on day 7 was similar with both
treatment regimens [1 of 103 (0.97%) vs. 1 of 50 (2.0%),
P ¼ 0.5, by Fisher exact test). None of the patients without
gametocytaemia at enrolment who were treated with
Table 1 Demographic and clinical
characteristics of patients at enrolment Artesunate-
amodiaquine
Chloroquine plus
pyrimethamine-sulfadoxine P value
No. of patients 103 50 –
Male/female 56/47 23/27Age (years)
Mean ± SD 6.7 ± 3.1 5.9 ± 2.9 0.07
Range 1–12 0.9–11.5
No. <5 years 26 24Weight (kg)
Mean ± SD 19.3 ± 7.3 17.9 ± 6.7 0.16
Range 7–47 8–36
Duration of illness (days)Mean ± SD 2.8 ± 1.7 2.9 ± 1.3 0.72
Range 1–7 1–14
Temperature (�C)Mean ± SD 37.9 ± 1.2 38.0 ± 1.1 0.96
Range 36.0–40.5 36.2–40.7
Parasite count (per ll)Geometric mean 32173 43757 0.06Range 2024–395410 2196–1792000
Haematocrit (%)
Mean ± SD 31.1 ± 5.9 31.8 ± 4.7 0.56
Range 18–39 22–42No. <30% 19 11
Enlarged organ
Hepatomegaly 20 12Splenomegaly 36 15
Hepatosplenomegaly 15 5
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
ª 2005 Blackwell Publishing Ltd 1165
artesunate plus amodiaquine carried gametocytes during
follow up. Overall, five patients in the chloroquine plus
pyrimethamine-sulfadoxine were gametocytaemic at least
once during follow-up period as compared to only one
patient in the artesunate plus amodiaquine group. The
difference between the two proportions was significant [5
of 50 (10%) vs. 1 of 103 (0.97%), P ¼ 0.01, by Fisher
exact test]. One of the five gametocytaemic patients treated
with chloroquine plus pyrimethamine-sulfadoxine had
resistance response.
Response to artesunate plus amodiaquine of children with
chloroquine plus pyrimethamine-sulfadoxine treatment
failures
All five patients who failed treatment with chloroquine
plus pyrimethamine-sulfadoxine responded promptly to
re-treatment with artesunate plus amodiaquine. Fever
cleared in all five patients within 24 h of commencing
treatment with artesunate plus amodiaquine and parasit-
aemia cleared within 48 h of treatment with this combi-
nation. The cure rate on day 28 of re-treatment was 100%.
PCR findings in patients with recurrence of parasitaemia
after day 14
Three of five matched sample pairs collected before and
after treatment from patients who failed treatment were
successfully analysed at msp-1 or msp-2 polymorphic loci.
Alleles were classified according to the size of PCR
fragments. Analysis of genotypes of paired pre- and post-
treatment isolates from these three showed that in all the
patients, paired PCR fragments were identical at either
FC27 or IC1 allelic families of msp-2 and K1, MAD20 or
Table 2 Therapeutic responses to
artesunate plus amodiaquine or chloro-
quine plus pyrimethamine-sulfadoxineArtesunate-
amodiaquine
Chloroquine pluspyrimethamine-
sulfadoxine P value
No. of patients 103 50 –
Fever clearance time (days)
Mean ± SD 1.1 ± 0.2 1.0 ± 0.2 0.72Range 1–2 1–2
No. of patient with parasitaemia on day 1 75 47 0.004
No. of patient with parasitaemia on day 2 0 25 0.000001
Parasite clearance time (days)Mean ± SD 1.7 ± 0.4 2.5 ± 0.8 0.0001
Range 1–2 1–5
Day 14 responses
No. cured 103 48 0.1No. RI 0 2
No. RII 0 0
No. RIII 0 0Cure rate (%) 100 96
Day 21 responses
No. cured 103 47 0.03
No. RI (cumulative) 0 3No. RII 0 0
No. RIII 0 0
Cure rate (%)* 100 94
Day 28 responsesNo. cured 103 45 0.003
No. RI (cumulative) 0 5
No. RII 0 0
No. RIII 0 0Cure rate (%)* 100 90
ACPR 103 45 0.003
LPF 0 0LCF 0 5
ETF 0 0
* PCR-corrected ACPR, adequate clinical and parasitological response; LPF, late
parasitological failure; LCF, late clinical failure; ETF, early treatment failure.
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
1166 ª 2005 Blackwell Publishing Ltd

RO33, indicating genuine recrudescent infections after
treatment. In addition, these fragments indicated mono-
clonal infections in all the three patients. Although DNA
amplification in the remaining two patient isolates was not
successful, we considered resurgence of infections in these
patients as genuine recrudescence, because these two
patients re-presented clinical symptoms of malaria on day
14 when they would most likely have adequate blood
concentrations of the drug that could clear sensitive
infections.
Adverse events
Artesunate plus amodiaquine and chloroquine plus pyri-
methamine-sulfadoxine were well tolerated; no child was
withdrawn because of drug intolerance. Symptoms repor-
ted within the first week and during follow up were similar.
Pruritus, vomiting, abdominal pain, anorexia, cough and
headache were reported by 1, 8, 6, 2, 3 and 3 children,
respectively treated with artesunate plus amodiaquine. In
those treated with chloroquine plus pyrimethamine-sul-
fadoxine, 4, 2 and 1 child, reported pruritus, vomiting and
abdominal pain, respectively. Pruritus was significantly
more frequently reported by those treated with chloroquine
plus pyrimethamine-sulfadoxine (P ¼ 0.04) than by those
treated with artesunate plus amodiaquine. One child
treated with chloroquine plus pyrimethamine-sulfadoxine
had generalized macular eruptions on day 2 of treatment.
There was no mucosa involvement in this child, and there
was no family history of skin reaction to sulfonamides. The
eruptions resolved in 1 week without treatment. None of
the five children who failed initial treatment with chlo-
roquine plus pyrimethamine-sulfadoxine and were
re-treated with amodiaquine plus artesunate reported
adverse symptoms.
Haematological and biochemical parameters
Except for haematocrit values below 30% at enrolment in
19 and 9 children in artesunate plus amodiaquine and
chloroquine plus pyrimethamine-sulfadoxine, respectively,
and at day 7 in 10 and 4 children, respectively, haemato-
logical, biochemical and other parameters remained nor-
mal before and after treatment in all subjects (normal
biochemical parameters for the area: ALT 0–40 i.u/l; AST:
0–37 i.u/l; serum creatinine: 0.5–1.5 mg/dl; serum biliru-
bin: 0.5–1.0 mg/dl). Thrombocytopenia, defined as platelet
count <150 · 103 mm3, was present in 15 and 6 children
in artesunate plus amodiaquine and chloroquine plus
pyrimethamine-sulfadoxine, respectively, at enrolment, but
was not seen on day 14 in any child (normal value for the
area: 150–390 · 103 mm3).
Discussion
Artemisinin-based combination antimalarials are currently
favoured by the World Health Organization for use in
Africa (WHO 2001), but there are needs to consider
potential non-artemisinin-based combinations including
amodiaquine- or pyrimethamine-sulfadoxine-based com-
binations in resource poor African countries (Bloland et al.
2000; Sowunmi 2002; Bloland 2003; Gasasira et al. 2003).
In the current study, the combination of artesunate plus
amodiaquine was therapeutically superior to chloroquine
plus pyrimethamine-sulfadoxine, the individual compo-
nents of which are readily and widely available in Africa.
The relatively accelerated and sustained clearance of
parasitaemia by artesunate plus amodiaquine produced a
large parasite reduction ratio on day 2 and a cure rate of
100% at day 28 of follow up. These findings are similar to
those reported from other African countries (Adjuik et al.
2002). A similar proportion of patients allocated to each
treatment regimen received paracetamol during the first
36 h of the study. Therefore it would appear that the
similar fever clearance despite inferior efficacy of chlo-
roquine plus pyrimethamine-sulfadoxine at clearing para-
sitaemia may be due to the enhanced antipyretic effect of
chloroquine in the combination (Hugosson et al. 2003).
Recent studies from Nigeria showed that the combina-
tion of chloroquine plus pyrimethamine-sulfadoxine is
therapeutically superior to chloroquine or pyrimethamine-
sulfadoxine alone and the combination is effective in the
treatment of uncomplicated malaria infection, producing a
cure rate of 98–100% on day 14 (Sowunmi 2002; Pitmang
et al. 2005). However, when the findings of the current
study are compared with a previous study in children from
Ibadan, there appears to be significant decline in the
therapeutic efficacy of chloroquine plus pyrimethamine-
sulfadoxine: in 2002, the cure rate with the combination
was 100% on day 28 (Sowunmi 2002) and 90% in the
current study. This decline could be attributable to
increasing resistance in the parasite population to mono-
therapy with chloroquine or pyrimethamine-sulfadoxine.
However, despite increasing resistance to chloroquine
monotherapy, resistance to amodiaquine monotherapy
appears to be low in this endemic area (Sowunmi 2002).
The sensitivity of P. falciparum to the combination of
chloroquine plus pyrimethamine-sulfadoxine varies in
Africa and elsewhere. While sensitivity appears encour-
aging in many areas of West Africa (Bojang et al. 1998;
Sowunmi 2002; Pitmang et al. 2005), and at day 14
following treatment in many areas of East Africa (Gasasira
et al. 2003; Talisuna et al. 2004), this is not so in the east
on day 28 and elsewhere (Schwobel et al. 2003; Talisuna
et al. 2004).
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
ª 2005 Blackwell Publishing Ltd 1167

All of the chloroquine plus pyrimethamine-sulfadoxine
treatment failures were cured of their infections when they
were re-treated with artesunate plus amodiaquine. Overall,
this indicates a beneficial effect of the combination in
multidrug-resistant infections in children from this endemic
area.
The drug combinations used were well tolerated. The
reported adverse reactions were itching, presumably due to
the 4-aminoquinoline components of the combinations,
macular eruptions, in a 3-year-old child, presumably due to
the sulfadoxine component of pyrimethamine-sulfadoxine;
and gastrointestinal symptoms. The other reported symp-
toms, for example, those of gastrointestinal origin, were
not indistinguishable from the symptoms of malaria. Both
the sulfadoxine component of pyrimethamine-sulfadoxine,
and rarely, chloroquine (Cooper & Bunn 1991) can induce
haemolysis in Glucose 6 Phosphate Dehydrogenase
(G6PD)-deficient subjects, but no child, following treat-
ment, reported features suggestive of drug-induced hae-
molytic anaemia. Amodiaqune may induce leukopenia or
agranulocytosis when used repeatedly (or prophylactically)
(Hatton et al. 1986). In many endemic areas many people
with imagined malaria self-medicate with antimalarials
with a regularity that borders on prophylaxis (Sowunmi &
Salako 1992). Under this circumstance, the amodiaquine
component of artesunate amodiaquine combination can be
expected to induce leukopenia or agranulocytosis. There-
fore caution is required with the use of this combination in
many endemic areas.
Overall, a significantly higher proportion of children
treated with chloroquine plus pyrimethamine-sulfadoxine
carried gametocytes at least once during follow-up
compared with those treated with artesunate plus amo-
diaquine. Pyrimethamine-sulfadoxine monotherapy may
enhance gametocyte release into peripheral circulation
following treatment of malaria (Puta & Manyando 1997;
von Seidlein et al. 2001a; Sowunmi & Fateye 2003;
Sowunmi et al. 2004b). However, as shown in the present
study, it would appear the gametocyte releasing effect is
considerably reduced when the drug is used in combination
with 4-aminoquinolines (Sowunmi 2002; Sowunmi &
Fateye 2003) or as in other studies, with artesunate (von
Seidlein et al. 2001a,b). In other settings, after significant
resistance has developed to pyrimethamine-sulfadoxine
monotherapy, the gametocyte releasing effect may not be
modified by its combination with chloroquine (Tjitra et al.
2002).
Gametocyte carriage often peaks in children treated with
antimalarial monotherapy (for example, chloroquine or
pyrimethamine-sulfadoxine by day 7 following treatment
(Robert et al. 2000; Sowunmi et al. 2004b). In the
present cohort of children, gametocyte carriage following
treatment with artesunate plus amodiaquine was not seen
in children who did not carry gametocytes at enrolment.
Although artemisinin derivatives may be gametocytocidal,
the rapid clearance of asexual parasites by these drugs may
have prevented the progression of committed asexual
parasites to gametocytes in our cohort of children. The
latter is buttressed by the fact that delay in parasite
clearance greater than 2 days is associated with significant
risk of gametocyte carriage in children from this endemic
area (Sowunmi et al. 2004b). In other settings, for exam-
ple, in The Gambia and Thailand, artemisinin-based
combinations have significantly reduced gametocyte car-
riage (von Seidlein et al. 2001a,b) or reduced their infec-
tiousness to mosquitoes (Targett et al. 2001; Drakeley
et al. 2003) and may possibly interrupt transmission in
areas of low endemicity (Price et al. 1996).
Except in resource poor communities, there are few
justifications for the treatment of acute falciparum infec-
tions with chloroquine plus pyrimethamine-sulfadoxine in
Nigeria. First, the efficacy of the individual components of
the combination has declined significantly within the last
2 years; the prevalence of chloroquine and pyrimethamine-
sulfadoxine resistance is currently 50% and 25%,
respectively in under 5-year olds (Sowunmi et al. unpub-
lished). Second, and more importantly, when compared
with its efficacy 2 years ago, there has been a significant
decline in the efficacy of this combination in our area of
study. This decline in efficacy is confirmed by the finding
that comparison of the variant alleles in pre- and post-
treatment samples of the treatment failures indicates
genuinely recrudescent disease.
There are implications for using artesunate-amodiaquine
combination in Nigeria. In order to prolong the clinical life
of this potentially useful combination, it is essential to
discourage the availability and use of the individual
components as monotherapy. The individual components
are now readily available in many communities. In addi-
tion, it is necessary to completely withdraw chloroquine for
the treatment of malaria. The latter is crucial since the
mutations in Pfcrt genes conferring resistance to chloro-
quine also confer resistance to amodiaquine (Ochong
et al. 2003). Indeed, Happi et al (unpublished data) have
shown that these mutations, in Nigerian isolates of
P. falciparum, also confer resistance to amodiaquine. The
use of artesunate alone may also encourage the develop-
ment, in Nigerian isolates of P. falciparum, of resistance to
the combination since a minority of these isolates show
reduced susceptibility to artemisinin, the parent drug from
which artesunate is derived (Oduola et al. 1992).
There are policy implications of the findings of this
study. Although there are effective alternatives to the two
combinations evaluated, for example, coartemether or
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
1168 ª 2005 Blackwell Publishing Ltd

pyrimethamine-sulfadoxine plus artesunate, these have not
been extensively evaluated in Nigeria. There are also cost
implications of using expensive combinations in resource-
poor communities, particularly in situations where the
diagnosis of malaria may be entirely presumptive.
Acknowledgements
The study received financial support from Ipca Pharma-
ceuticals Nigeria Plc. We are grateful to our clinic medical
officer Dr Olayiwola and clinic nurse Moji Amao for
assistance with running the study.
References
Adjuik M, Agnamey P, Babiker A et al. (2002) Amodiaquine-
artesunate versus amodiaquine for uncomplicated Plasmodium
falciparum malaria in African children: a randomized,
multicentre trial. Lancet 359, 1365–1372.
Anonymous (1994) Epi Info Version 6. A Word Processing
Data Base and Statistics Program for Public Health on IBM-
compatible Microcomputers. Centers for Disease Control and
Prevention, Atlanta, GA.
Basco LK, Same-Ekobo A, Ngane VF et al. (2002) Therapeutic
efficacy of sulfadoxine-pyrimethamine, amodiaquine and the
sulfadoxine-pyrimethamine-amodiaquine combination against
uncomplicated Plasmodium falciparum malaria in young
children in Cameroon. Bulletin of the World Health Organiza-
tion 80, 538–545.
Bloland PB, Ettling M & Meek S (2000) Combination therapy for
malaria in Africa: hype or hope? Bulletin of the World Health
Organization 78, 1378–1388.
Bloland PB (2003) A contrarian view of malaria therapy policy in
Africa. American Journal of Tropical Medicine and Hygiene 68,
125–126.
Bojang KA, Schneider G, Forck S et al. (1998) A trial of Fansidar
plus chloroquine or Fansidar alone for the treatment of
uncomplicated malaria in Gambian children. Transactions of
the Royal Society of Tropical Medicine and Hygiene 92, 73–76.
Cooper RA& Bunn HF (1991) Hemolytic anemias. In: Harrison’s:
Principles of Internal Medicine, Vol. 2 (eds Wilson JD,
Braunwald E, Isselbacher KJ, Petersdorf RG, Martin JB, Fauci
AS & Root RK) McGraw-Hill, New York, pp. 1531–1543.
Drakeley CJ, Jawara M, Targett GAT et al. (2003) Addition of
artesunate to chloroquine for the treatment of P. falciparum
malaria in Gambian children causes a significant but short-lived
reduction in infectiousness for mosquitoes. Tropical Medicine
and International Health 9, 53–61.
Ekanem OJ, Weisfeld JS, Salako LA et al. (1987) Sensitivity of
Plasmodium falciparum to chloroquine and sulphadoxine-
pyrimethamine in Nigerian children. Bulletin of the World
Health Organization 68, 45–52.
Gasasira AF, Dorsey G, Nzarubara B et al. (2003) Comparative
efficacy of aminoquinoline-antifolate combinations for the
treatment of uncomplicated falciparum malaria in Kampala,
Uganda. American Journal of Tropical Medicine and Hygiene
68, 127–132.
Happi TC, Thomas SM, Gbotosho GO et al. (2003) Point muta-
tions in the pfcrt and pfmdr-1 genes of Plasmodium falciparum
and clinical response to chloroquine, among malaria patients
from Nigeria. Annals of Tropical Medicine and Parasitology 97,
439–451.
Happi TC, Gbotosho GO, Sowunmi A et al. (2004) Molecular
analysis of Plasmodium falciparum recrudescent malaria
infections in children treated with chloroquine in Nigeria.
American Journal of Tropical Medicine and Hygiene 70, 20–26.
Hatton C, Peto T, Bunch C et al. (1986) Frequency of severe
neutropenia associated with amodiaquine prophylaxis against
malaria. Lancet i, 411–413.
Hugosson E, Tarimo D, Troye-Bloomberg M, Montgomery SM,
Premji Z & Bjorkmann A (2003) Antipyretic, parasitologic, and
immunologic effects of combining sulfadoxine/pyrimethamine
with chloroquine or paracetamol for treating uncomplicated
Plasmodium falciparum malaria. American Journal of Tropical
Medicine and Hygiene 69, 366–371.
Ochong EO, Van Den Broek IVF, Keus K & Nzila A (2003) Short
report: association between chloroquine and amodiaquine re-
sistance and allelic variation in the Plasmodium falciparum
multiple drug resistance 1 gene and the chloroquine resistance
transporter gene in isolates from the Upper Nile in southern
Sudan. American Journal of Tropical Medicine and Hygiene 69,
184–187.
Oduola AMJ, Sowunmi A, Milhous WK et al. (1992) Innate
resistance to new antiamalarial drugs in Plasmodium falciparum
from Nigeria. Transactions of the Royal Society of Tropical
Medicine and Hygiene 86, 123–126.
Pitmang SL, Thacher TD, Madaki JKA, Egah DZ & Fischer PR
(2005) Comparison of sulfadoxine-pyrimethamine with and
without chloroqunie for uncomplicated malaria in Nigeria.
American Journal of Tropical Medicine and Hygiene 72, 263–
266.
Price RN, Nosten F, Luxemburger C et al. (1996) Effects of
artemisinin derivatives on malaria transmissibility. Lancet 347,
1654–1658.
Puta C & Manyando C (1997) Enhanced gametocyte production
in Fansidar-treated Plasmodium falciparum malaria patients:
implications for malaria transmission control programmes.
Tropical Medicine and International Health 2, 227–229.
Robert V, Awono-Ambene HP, Le Hesran J-Y & Trape J-F
(2000) Gametocytaemia and infectivity to mosquitoes of
patients with uncomplicated Plasmodium falciparum malaria
attacks treated with chloroquine or sulfadoxine-pyrimethamine.
American Journal of Tropical Medicine and Hygiene 62,
210–216.
Salako LA, Ajayi FO, Sowunmi A & Walker O (1990) Malaria in
Nigeria: a revisit. Annals of Tropical Medicine and Parasitology
84, 435–445.
Schwobel B, Jordan S, Vanisaveth V et al. (2003) Therapeutic
efficacy of chloroquine plus sulphadoxine/pyrimethamine
compared with monotherapy with either chloroquine or
sulphadoxine/pyrimethamine in uncomplicated Plasmodium
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
ª 2005 Blackwell Publishing Ltd 1169

falciparum malaria in Laos. Tropical Medicine and Inter-
national Health 8, 19–24.
Sibley CH, Hyde JE, Sims PFG et al. (2001) Pyrimethamine-
sulfadoxine resistance in Plasmodium falciparum: what next?
Trends in Parasitology 17, 582–588.
Sowunmi A & Salako LA (1992) Evaluation of the relative efficacy
of various antimalarial drugs in Nigerian children under five
years of age suffering from acute uncomplicated falciparum
malaria. Annals of Tropical Medicine and Parasitology 86, 1–8.
Sowunmi A, Oduola AMJ, Ogundahunsi OAT et al. (1998)
Randomised trial of artemether versus artemether and mefloq-
uine for the treatment of chloroquine/sulfadoxine-pyrimetham-
ine-resistant falciparum malaria during pregnancy. Journal of
Obstetrics & Gynaecology 18, 322–327.
Sowunmi A, Sowunmi CO, Adedeji AA & Oduola AMJ (2001)
Comparison of artemether and artemether plus mefloquine in
children with malaria and effects on viability of Plasmodium
falciparum ex vivo. Clinical Drug Investigation 21, 33–40.
Sowunmi A (2002) A randomized comparison of chloroquine,
amodiaquine and their combination with pyrimethamine-sulfa-
doxine in the treatment of acute, uncomplicated, Plasmodium
falciparum malaria in children. Annals of Tropical Medicine and
Parasitology 96, 227–238.
Sowunmi A (2003) A randomized comparison of chloroquine, and
chloroquine plus ketotifen in the treatment of acute, uncom-
plicated, Plasmodium falciparum malaria in children. Annals of
Tropical Medicine and Parasitology 97, 107–117.
Sowunmi A & Fateye BA (2003) Plasmodium falciparum game-
tocytaemia in Nigerian children: before, during and after treat-
ment with antimalarial drugs. Tropical Medicine and
International Health 8, 783–792.
Sowunmi A, Fehintola FA, Adedeji AA et al. (2004a) Open
randomized study of pyrimethamine-sulphadoxine vs. pyri-
methamine-sulphadoxine plus probenecid for the treatment of
uncomplicated Plasmodium falciparum malaria in children.
Tropical Medicine & International Health 9, 606–614.
Sowunmi A, Fateye BA, Adedeji AA, Fehintola FA & Happi TC
(2004b) Risk factors for gametocyte carriage in uncomplicated
falciparum malaria in children. Parasitology 129, 255–262.
Talisuna AO, Nalunkuma-Kazibwe A, Bakyaita N et al. (2004)
Efficacy of sulphadoxine-pyrimethamine alone or combined
with amodiaquine or chloroquine for the treatment of uncom-
plicated falciparum malaria in Ugandan children. Tropical
Medicine and International Health 9, 222–229.
Targett G, Drakeley C, Jawara M et al. (2001) Artesunate reduces
but does not prevent posttreatment transmission of Plasmodium
falciparum to Anopheles gambiae. Journal of Infectious
Diseases 183, 1254–1259.
Tjitra E, Suprianto S & Anstey NM (2002) Higher gametocyte
prevalence following failure of treatment of Plasmodium
falciparum malaria with sulfadoxine-pyrimethamine and the
combination of chloroquine plus sulfadoxine-pyrimethamine:
implications for progression of anti-folate resistance.
Transactions of the Royal Society of Tropical Medicine and
Hygiene 96, 434–437.
Trape J-F, Pison G, Preziosi M-P et al. (1998) Impact of
chloroquine resistance on malaria mortality. Life Sciences 321,
689–697.
Trape JF (2001) The public health impact of chloroquine
resistance in Africa. American Journal of Tropical Medicine and
Hygiene 64 (Suppl. 1–2), 12–17.
von Seidlein L, Milligan P, Pinder M et al. (2000) Efficacy of
artesunate plus pyrimethamine-sulfadoxine for uncompli-
cated malaria in Gambian children. Lancet 355, 352–
357.
von Seidlein L, Drakeley C, Greenwood B, Walraven G & Targett
G (2001a) Risk factors for gametocyte carriage in Gambian
children. American Journal of Tropical Medicine and Hygiene
65, 523–527.
von Seidlein L, Jawara M, Coleman R, Doherty T, Walraven G &
Targett G (2001b) Parasitaemia and gametocytaemia after
treatment with chloroquine, pyrimethamine/sulfadoxine, and
pyrimethamine/sulfadoxine combined with artesunate in young
Gambians with uncomplicated malaria. Tropical Medicine and
International Health 6, 92–98.
World Health Organization (1973) Chemotherapy of Malaria and
Resistance to Antimalarials. Technical Report Series No. 529.
WHO, Geneva.
World Health Organization (2000) Severe falciparum malaria.
Transactions of the Royal Society of Tropical Medicine and
Hygiene 94 (Suppl. 1) 1–90.
World Health Organization (2001) Antimalarial Drug Combina-
tion Therapy. Report of a WHO Technical Consultation.
(WHO/CDS/RBM/2001.35) WHO, Geneva.
World Health Organization (2003) Asssessment and Monitoring
of Antimalarial Drug Efficacy for the Treatment of Uncompli-
cated Falciparum Malaria. (WHO/HTM/RBM/2003.50) WHO,
Geneva.
Authors
A. Sowunmi (corresponding author), F. A. Fehintola, A. A. Adedeji, G. O. Gbotosho, E. Tambo, B. A. Fateye, T. C. Happi
and A. M. J. Oduola, Department of Clinical Pharmacology, University College Hospital, Ibadan, Nigeria.
Tel.: +234-2-2412101, Fax: +234-2-2411843; E-mail: [email protected], [email protected]
Tropical Medicine and International Health volume 10 no 11 pp 1161–1170 november 2005
A. Sowunmi et al. Artesunate-amodiaquine for uncomplicated malaria
1170 ª 2005 Blackwell Publishing Ltd
















