Ongoing relationships with a personal focus: mothers' perceptions of birth centre versus hospital...
11
Ongoing relationships with a personal focus: mothers’ perceptions of birth centre versus hospital care Karen Coyle,Yvonne Hauck, Patricia Percival and Linda Kristjanson Objective: to describe women’s perceptions of care in Western Australian birth centres following a previous hospital birth. Design, setting and participants: an exploratory study was undertaken to examine the care experiences of women from three Western Australian birth centres. Data were obtained from 17 women whose interviews were audio-recorded and transcribed.The research focused upon women’s perceptions of their recent birth centre care as compared to previous hospital care during childbirth. Findings: four key themes emerged from the analysis: ‘beliefs about pregnancy and birth’, ‘nature of the care relationship’, ‘care interactions’and ‘care structures’. The themes of ‘care interactions’ and ‘care structures’ will be presented in this paper. Care interactions refer to women’s opportunities to develop rapport with their carers. Care structures involved the organisational framework in which care was delivered. The ¢rst two themes of ‘beliefs about pregnancy and birth’ and the ‘nature of the care relationship’ were discussed in a previous paper. Key conclusions and implications for practice: di¡erences in opportunities for care interactions and care structures were revealed between birth centre and hospital settings. Ongoing, cumulative contacts with midwives in the birth-centre setting were strongly supported by women as encouraging the development of rapport and perception of ‘being known’ as an individual. Additionally, care structures tailored to women were advocated over the systematised, fragmented care found in hospital settings. & 2001 Harcourt Publishers Ltd INTRODUCTION During the 1990s Australian maternity services followed trends in the UK and developed models of care which provided women with continuity of midwifery care (Brown & Lumley 1998). In the UK, the Changing Childbirth Report has pro- vided clear direction for the modification of maternity services, one of the key elements being continuity of carer (DoH 1993). These and other recommendations have resulted in many inno- vative models of maternity care being developed throughout the UK (Shields et al. 1998). In Australia, the major models developed to address the fragmented maternity services of- fered to women in the public health system have been birth-centre care and team midwifery (Brown & Lumley 1998, Waldenstrom & Lawson 1998). Both of these models incorporate mid- wifery care across the childbearing continuum, although they do not necessarily provide con- tinuity of carer. Continuity of ‘care’ versus continuity of ’carer’ is not clearly defined in the literature and has caused some confusion when assessing alterna- tive models of care. A systematic review to assess efficacy of alternative models of maternity care characterised by continuity of midwifery care Karen L. Coyle RN, RM, BHlthSc(Nur), MN, Family Birth Centre, King Edward Memorial Hospital, Bagot Road, Subiaco, WA, Australia 6008 Yvonne Hauck BScN, MSc, PhD, RM, Edith Cowan University, School of Nursing & Public Health, Pearson Street, Churchlands, WA, Australia 6018 E-mail: [email protected] Patricia Percival PhD, FRCNA, RN, RM Linda J. Kristjanson MN, PhD, RN, BN, Professor, Faculty of Communications, Health and Science, Edith Cowan University, Pearson St, Churchlands, WA, Australia 6018 (Correspondence to KC) Received 31 May 2000 Revised 6 October 2000 Accepted 22 February 2001 Published online 31 May 2001 Midwifery (2001) 17, 171^181 & 2001 Harcourt Publishers Ltd doi:10.1054/midw.2001.0258, available online at http://www.idealibrary.com on
Transcript of Ongoing relationships with a personal focus: mothers' perceptions of birth centre versus hospital...
Karen L.Coyle RN, RM,BHlthSc(Nur), MN, FamilyBirth Centre, King EdwardMemorial Hospital, BagotRoad, Subiaco,WA,Australia 6008
Yvonne Hauck BScN,MSc, PhD, RM, EdithCowan University, Schoolof Nursing & Public Health,Pearson Street,Churchlands,WA,Australia 6018E-mail:[email protected]
Patricia Percival PhD,FRCNA, RN, RM
Linda J.KristjansonMN,PhD, RN, BN, Professor,Faculty ofCommunications, Healthand Science, Edith CowanUniversity, Pearson St,Churchlands,WA,Australia 6018
(Correspondence to KC)
Received 31May 2000Revised 6 October 2000Accepted 22 February2001Published online 31May2001
Ongoing relationshipswitha personal focus: mothers’perceptions of birth centreversus hospital care
Karen Coyle,YvonneHauck,Patricia Percival andLinda Kristjanson
Objective: to describewomen’s perceptions of care inWestern Australian birth centresfollowing a previous hospital birth.
Design, setting and participants: an exploratory study was undertaken to examine the careexperiences of women fromthreeWestern Australian birth centres.Datawere obtainedfrom17 womenwhose interviewswere audio-recorded and transcribed.The researchfocused uponwomen’s perceptions of their recent birth centre care as compared toprevious hospital care during childbirth.
Findings: four key themes emerged fromthe analysis: ‘beliefs about pregnancy andbirth’,‘nature ofthe carerelationship’, ‘care interactions’and ‘care structures’. The themesof ‘careinteractions’and ‘care structures’ will be presented in this paper.Care interactions refer towomen’s opportunities to develop rapport with their carers.Care structures involved theorganisational framework inwhich carewas delivered. The ¢rst two themes of ‘beliefsabout pregnancy andbirth’and the ‘nature of the care relationship’ were discussed in aprevious paper.
Keyconclusions and implications for practice: di¡erences in opportunities for careinteractions and care structureswere revealedbetween birth centre andhospital settings.Ongoing, cumulative contactswithmidwives in the birth-centre setting were stronglysupported by women as encouraging the development of rapport andperception of ‘beingknown’as an individual. Additionally, care structures tailored towomenwere advocatedover the systematised, fragmented care found in hospital settings. & 2001HarcourtPublishers Ltd
INTRODUCTION
During the 1990s Australian maternity services
followed trends in the UK and developed models
of care which provided women with continuity of
midwifery care (Brown & Lumley 1998). In the
UK, the Changing Childbirth Report has pro-
vided clear direction for the modification of
maternity services, one of the key elements being
continuity of carer (DoH 1993). These and other
recommendations have resulted in many inno-
vative models of maternity care being developed
throughout the UK (Shields et al. 1998). In
Australia, the major models developed to
Midwifery (2001) 17, 171^181 & 2001Harcourt Publishers Ltddoi:10.1054/midw.2001.0258, available online at http://www.idealibrary.com on
address the fragmented maternity services of-
fered to women in the public health system have
been birth-centre care and team midwifery
(Brown & Lumley 1998, Waldenstrom & Lawson
1998). Both of these models incorporate mid-
wifery care across the childbearing continuum,
although they do not necessarily provide con-
tinuity of carer.
Continuity of ‘care’ versus continuity of ’carer’
is not clearly defined in the literature and has
caused some confusion when assessing alterna-
tive models of care. A systematic review to assess
efficacy of alternative models of maternity care
characterised by continuity of midwifery care

172 Midwifery
was recently undertaken by Waldenstrom and
Turnbull (1998). Seven randomised control trials
were included in this review (Flint et al. 1989,
MacVicar et al. 1993, Kenny et al. 1994, Rowley
et al. 1995, Harvey et al. 1996, Turnbull et al.
1996, Waldenstrom & Nilsson 1997). The review
highlighted the benefits of models that offer
continuity of midwifery care as reduced labour
interventions and increased levels of satisfaction
with care (Waldenstrom & Turnbull 1998).
Many of the trials do not indicate whether
women received care in labour from a known
midwife carer, so the findings may not necessa-
rily reflect continuity of carer, but rather a
continuity of philosophy of care.
In Australia, the birth-centre model is used by
about 5% of childbearing women (Waldenstrom
& Lawson 1998). Booking numbers in some
centres are nearing capacity and with the
increase in client numbers, midwife numbers
have also been increased proportionately. With a
focus on continuity of carer, some birth centres
are refining the model of care being offered by
modifying midwives’ work practices to minimise
the number of carers each client is exposed to
and guaranteeing a known carer at crucial times
such as during labour (Coyle 1997). This
refinement within the birth-centre context has
had limited evaluation, particularly from the
client’s perspective.
Consequently, the purpose of this study was to
address this issue and explore women’s percep-
tions of their experiences of care in the current
Western Australian birth-centre setting following
a previous hospital birth.
METHOD
The methods have been outlined in a previous
publication (Coyle et al. 2001). An exploratory
design guided by a modified grounded theory
approach involving the constant comparison
technique, was chosen to enable the principal
investigator to explore women’s perceptions of
the care they experienced in both birth-centre
and hospital settings (Strauss & Corbin 1998).
Women who had received care in three Western
Australian birth centres were interviewed. Data
collection involved face-to-face interviews with
seventeen women in their homes. The focus of
the interview was on women’s perceptions of the
care they received, not on their actual birth
experience. The interviewer explored women’s
perceptions of both their most recent care
experiences and previous hospital experiences.
Data were analysed from written narrative
communication transcribed from interviews.
Significant meanings of phrases, sentences and
paragraphs were coded and categorised into
groups allowing for the underlying meanings
within the communication to be identified within
the context of the entire interview (Field &
Morse 1990, Strauss & Corbin 1998).
Ethical approval for the study was given by
the university and hospital ethics committees.
FINDINGS ANDDISCUSSION
All seventeen participants in this study had
experienced at least one of their previous
pregnancies within a hospital setting, with one
participant also undergoing a previous home-
birth. All but one participant had achieved a
normal vaginal birth in their previous hospital
experience. Sixteen women were of Caucasian
background and one woman was of Maori
background. All participants had a current
partner. Participants’ ages ranged from 22 to
34 years with the number of children varying
from two to five. The socio-economic level of the
families varied across an income level of less than
$20 000 to greater than $50 000. The participants
represented a broad range of income levels as the
1996 census for Western Australia revealed that
the median household income was $34 000
(Australian Bureau of Statistics 2000). Eight
women had completed high-school requirements
and the remaining nine had achieved a post-
secondary qualification. Seven women described
their occupation as being in the service industry,
five as professionals and a further five solely
involved with home duties.
Participants shared their experiences of care in
both the hospital and birth-centre settings
providing a wealth of data about these two
different models of care. Final analysis of the
data resulted in the identification of four key
themes: ‘beliefs about pregnancy and birth’,
‘nature of the care relationship’, ‘care interac-
tions’ and ‘care structures’. Each of these themes
was comprised of two dimensions at either end of
a continuum, as outlined in Figure 1. The themes
‘beliefs about pregnancy and birth’ and ‘the
nature of the care relationship’ were presented in
a previous paper (Coyle et al. 2001). Care
interactions and care structures will be discussed
in this paper. Participant quotes will be utilised
to support the findings. A pseudo name is
presented following each quote and information
is given regarding parity, for example, [Ann, 2nd
baby].
Care interactions
The theme of ‘care interactions’ was defined as
opportunities that women have to develop
rapport with their carers. Interactions with
health-care providers were determined as either:
(a) cumulative interactions or (b) non-cumulative
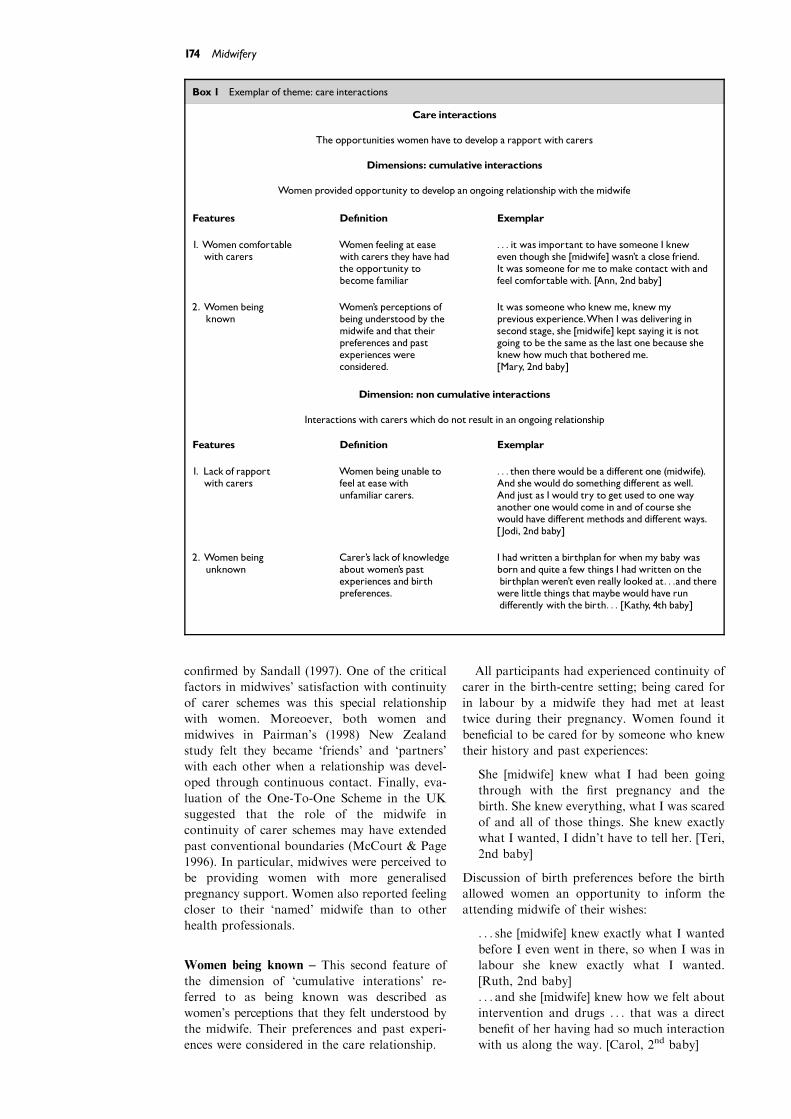
interactions. Box 1 provides an exemplar of this
theme.
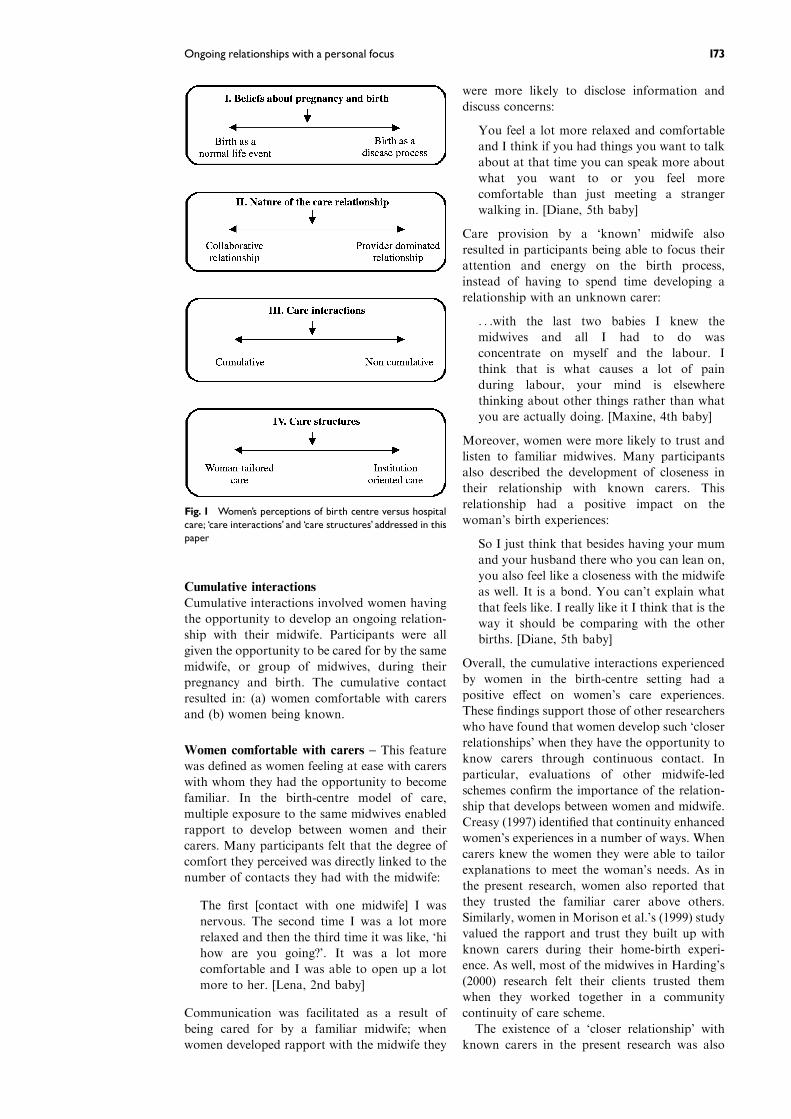
Fig. 1 Women’s perceptions of birth centre versus hospitalcare; ‘care interactions’ and ‘care structures’ addressed in thispaper
Ongoing relationships with a personal focus 173
Cumulative interactions
Cumulative interactions involved women having
the opportunity to develop an ongoing relation-
ship with their midwife. Participants were all
given the opportunity to be cared for by the same
midwife, or group of midwives, during their
pregnancy and birth. The cumulative contact
resulted in: (a) women comfortable with carers
and (b) women being known.
Women comfortable with carers – This feature
was defined as women feeling at ease with carers
with whom they had the opportunity to become
familiar. In the birth-centre model of care,
multiple exposure to the same midwives enabled
rapport to develop between women and their
carers. Many participants felt that the degree of
comfort they perceived was directly linked to the
number of contacts they had with the midwife:
The first [contact with one midwife] I was
nervous. The second time I was a lot more
relaxed and then the third time it was like, ‘hi
how are you going?’. It was a lot more
comfortable and I was able to open up a lot
more to her. [Lena, 2nd baby]
Communication was facilitated as a result of
being cared for by a familiar midwife; when
women developed rapport with the midwife they
were more likely to disclose information and
discuss concerns:
You feel a lot more relaxed and comfortable
and I think if you had things you want to talk
about at that time you can speak more about
what you want to or you feel more
comfortable than just meeting a stranger
walking in. [Diane, 5th baby]
Care provision by a ‘known’ midwife also
resulted in participants being able to focus their
attention and energy on the birth process,
instead of having to spend time developing a
relationship with an unknown carer:
. . .with the last two babies I knew the
midwives and all I had to do was
concentrate on myself and the labour. I
think that is what causes a lot of pain
during labour, your mind is elsewhere
thinking about other things rather than what
you are actually doing. [Maxine, 4th baby]
Moreover, women were more likely to trust and
listen to familiar midwives. Many participants
also described the development of closeness in
their relationship with known carers. This
relationship had a positive impact on the
woman’s birth experiences:
So I just think that besides having your mum
and your husband there who you can lean on,
you also feel like a closeness with the midwife
as well. It is a bond. You can’t explain what
that feels like. I really like it I think that is the
way it should be comparing with the other
births. [Diane, 5th baby]
Overall, the cumulative interactions experienced
by women in the birth-centre setting had a
positive effect on women’s care experiences.
These findings support those of other researchers
who have found that women develop such ‘closer
relationships’ when they have the opportunity to
know carers through continuous contact. In
particular, evaluations of other midwife-led
schemes confirm the importance of the relation-
ship that develops between women and midwife.
Creasy (1997) identified that continuity enhanced
women’s experiences in a number of ways. When
carers knew the women they were able to tailor
explanations to meet the woman’s needs. As in
the present research, women also reported that
they trusted the familiar carer above others.
Similarly, women in Morison et al.’s (1999) study
valued the rapport and trust they built up with
known carers during their home-birth experi-
ence. As well, most of the midwives in Harding’s
(2000) research felt their clients trusted them
when they worked together in a community
continuity of care scheme.
The existence of a ‘closer relationship’ with
known carers in the present research was also
174 Midwifery
confirmed by Sandall (1997). One of the critical
factors in midwives’ satisfaction with continuity
of carer schemes was this special relationship
with women. Moreoever, both women and
midwives in Pairman’s (1998) New Zealand
study felt they became ‘friends’ and ‘partners’
with each other when a relationship was devel-
oped through continuous contact. Finally, eva-
luation of the One-To-One Scheme in the UK
suggested that the role of the midwife in
continuity of carer schemes may have extended
past conventional boundaries (McCourt & Page
1996). In particular, midwives were perceived to
be providing women with more generalised
pregnancy support. Women also reported feeling
closer to their ‘named’ midwife than to other
health professionals.
Women being known – This second feature of
the dimension of ‘cumulative interations’ re-
ferred to as being known was described as
women’s perceptions that they felt understood by
the midwife. Their preferences and past experi-
ences were considered in the care relationship.
All participants had experienced continuity of
carer in the birth-centre setting; being cared for
in labour by a midwife they had met at least
twice during their pregnancy. Women found it
beneficial to be cared for by someone who knew
their history and past experiences:
She [midwife] knew what I had been going
through with the first pregnancy and the
birth. She knew everything, what I was scared
of and all of those things. She knew exactly
what I wanted, I didn’t have to tell her. [Teri,
2nd baby]
Discussion of birth preferences before the birth
allowed women an opportunity to inform the
attending midwife of their wishes:
. . . she [midwife] knew exactly what I wanted
before I even went in there, so when I was in
labour she knew exactly what I wanted.
[Ruth, 2nd baby]
. . . and she [midwife] knew how we felt about
intervention and drugs . . . that was a direct
benefit of her having had so much interaction
with us along the way. [Carol, 2nd baby]
Box 1 Exemplar of theme: care interactions
Care interactions
The opportunities women have to develop a rapport with carers
Dimensions: cumulative interactions
Women provided opportunity to develop an ongoing relationshipwith themidwife
Features Def|nition Exemplar
1. Women comfortablewith carers
Women feeling at easewith carers they have hadthe opportunity tobecome familiar
. . . it was important to have someone I kneweven though she [midwife] wasn’t a close friend.It was someone forme tomake contact with andfeel comfortablewith. [Ann, 2nd baby]
2. Women beingknown
Women’s perceptions ofbeing understood by themidwife and that theirpreferences and pastexperiences wereconsidered.
It was someonewho knewme, knewmyprevious experience.When I was delivering insecond stage, she [midwife] kept saying it is notgoing to be the same as the last one because sheknew howmuch that botheredme.[Mary, 2nd baby]
Dimension: non cumulative interactions
Interactions with carers which do not result in an ongoing relationship
Features Def|nition Exemplar
1. Lack of rapportwith carers
Women being unable tofeel at easewithunfamiliar carers.
. . . then therewould be a di¡erent one (midwife).And shewould do something di¡erent as well.And just as I would try to get used to onewayanother onewould come in and of course shewould have di¡erentmethods and di¡erentways.[ Jodi, 2nd baby]
2. Women beingunknown
Carer’s lack of knowledgeabout women’s pastexperiences and birthpreferences.
I hadwritten a birthplan for whenmybaby wasborn and quite a few things I hadwritten on thebirthplanweren’t even really looked at. . .and therewere little things thatmaybewould have rundi¡erently with the birth. . . [Kathy, 4th baby]
Ongoing relationships with a personal focus 175
Many participants were eager to have their
‘named’ midwife carer present at the birth. As
one client outlined: ‘I really did want my own
midwife to be there because she knew me and she
knew how I wanted to give birth.’ [Maxine, 4th
baby]. Known midwives were also able to
determine how much support individual women
needed. Some women required minimal physical
input from the midwife: ‘The midwife very much
played the outer circle but came in as required.
But, not like doing lots of encouragement, I had
people for that and really appreciated that’
[Vivian, 3rd baby].
Other women needed a large amount of
physical and psychological support from the
midwife. Another participant described how the
birth-centre midwife provided individualised
support for her needs:
. . . she [midwife] was talking me through and
very often during the contractions I had to
hug her, to hold her, and she would look right
at me and say ‘you can do it, you can get
through it’. . . . she was like my tower, when I
look back on the birth, that was where my
strength was. My husband was not able to
provide that for me. He knew that. [Mary,
2nd baby]
Being known by the midwife also facilitated
participants’ perception of their ability to be in
control of their birth experience:
Having met her [midwife] before and
discussing what we would like to have
happen and the feeling that she was putting
me back in control, that really made a big
difference. Rather than the doctor being in
charge. [Ann, 2nd baby]
Overall, women perceived many positive benefits
when they had the opportunity to be cared for
throughout pregnancy and birth by a familiar
midwife. In particular, having the opportunity to
be cared for by a known carer throughout labour
was highly valued by those who experienced it.
These positive benefits of continuity of carer,
particularly during the birthing period, added
further evidence to the findings of a recent
Australian population-based survey undertaken
in Victoria (Brown & Lumley 1998). The research-
ers reported a strong correlation between satisfac-
tion and knowing the midwife prior to labour. In
another Australian study (Morison et al. 1999),
couples who birthed at home felt the ongoing care
from one midwife throughout the pregnancy, birth
and postnatal period was critical.
Other researchers have also emphasised the
benefits experienced by women who are able to
‘get to know’ the midwife/carer. For example, a
British grounded theory study of midwife-led
care by Walker et al. (1995) identified that
perceptions of support were enhanced when the
woman received care from a known carer;
someone they trusted and had confidence in.
Similarly, McCourt and Page (1996) identified
that being cared for throughout pregnancy and
birth by a familiar midwife resulted in the
midwife understanding the women’s individual
needs. British women in both this latter study
and in Garcia et al.’s (1998) research, felt more
confident and supported when they knew the
midwife. An interesting finding in Brown et al.’s
(1994) Australian survey was that women who
saw a private obstetrician throughout the an-
tenatal period were more satisfied than women in
the public hospital system who saw different
carers. However, this satisfaction did not extend
to the birth. Additionally, a comparative study
examining an English team midwifery scheme
found that women cared for under a traditional
model of care were more satisfied with antenatal
care (Farquhar et al. 2000). Again, these women
reported achieving a relationship with their
midwives due to greater exposure to named
midwives and higher continuity of carer.
Continuity of carer throughout the childbirth
cycle may also offer women other advantages.
For example, in a grounded theory study that
considered women’s experiences of transfer from
community-based to consultant-based commu-
nity care, the negative impact of transfer on
women’s experiences was reduced by the main-
tenance of midwife continuity from one care
setting to another (Creasy 1997). As well,
McCourt and Page (1996) found that the amount
of information given to women was increased
with known carers. In their evaluation, control
group women were more likely to feel they had
insufficient information. Moreoever, women in
the One-To-One Scheme felt more confident with
their knowledge level (McCourt & Page 1996).
Certainly, participants in the current research felt
communication was facilitated with known
carers.
As well as being of benefit to women, systems
allowing continuity of carer also have a number
of advantages for midwives. For example, as we
have previously discussed the ‘close relation-
ships’ or friendships and partnerships that can
develop also benefit midwives (Sandall 1997,
Fleming 1998, Pairman 1998, Walsh 1999).
Indeed, Sandall (1997) suggested that such
meaningful relationships can protect midwives
against burn-out. Other researchers have simply
concluded that it is easier, as well as more
satisfying, to know the person one is caring for.
However, some authors have cautioned against
midwives fostering over-dependency within such
relationships (Downe 1997, Leap 1997, Sandall
1997).
However, other researchers have disputed the
benefits of known carers. For example, Walden-
strom (1998) concluded that the philosophy of

176 Midwifery
carers may be more important than the indivi-
dual relationship with a particular midwife. The
satisfaction scores of birth-centre women, in the
Stockholm birth-centre trial, who received care
from a known versus unknown midwife carer
during the birth period were very high in both
groups. Care by a known midwife had no impact
on satisfaction rating. The birth-centre team was
comprised of ten midwives and the number of
contacts prior to labour with the known midwife
was not reported. Green et al. (1998) also argued
that the presence of a competent caring profes-
sional was more important to women during
labour than a known carer. Additionally, in the
research trails reviewed by Enkin et al. (1995)
and Hodnett (1998), in many instances the
positive outcomes were linked to a continuous
professional support from caregivers with whom
women had no previous social bond.
We feel, as do others, that there are certainly
difficulties in evaluating the positive effects of a
known carer across the childbearing continuum,
particularly using a quantitative approach. In
their evaluation of one-to-one practice, McCourt
et al. (1998) emphasised the difficulties of
assessing satisfaction using broad satisfaction
measures. The methods adopted in this study
produced data that provided greater insight into
the concept of continuity of carer from the
perspective of the care recipients, namely
mothers.
Non-cumulative interactions
Non-cumulative interactions were defined as
interactions with carers throughout pregnancy
which do not result in an ongoing relationship.
With previous births in the hospital system,
many women described meeting different carers
at each antenatal visit and during their birthing
experience. These non-cumulative contacts re-
sulted in: (a) lack of rapport and (b) women
being unknown.
Lack of rapport – The lack of rapport, as a
result of non-cumulative interactions, was de-
fined as women being unable to feel at ease with
unfamiliar carers. Having care provided by many
different carers throughout pregnancy and birth
culminated in the woman not having the
opportunity to develop rapport with carers.
Women felt a lot of time was spent covering
old ground:
I seem to remember, when you see different
people you always have to start the whole
story. You always have to talk your medical
history. And then they ask about the previous
deliveries, were they normal? You end up
doing that a lot. [Vivian, 3rd baby]
Many participants received care throughout
labour from unfamiliar carers during their
previous hospital experiences. Not being able to
develop rapport resulted in participants not
relating to carers:
. . . there seemed to be two people [staff]
around. I wasn’t that interested in looking
to be honest. But there seemed to be people
around but I couldn’t identify with anybody.
[Jodi, 2nd baby]
Some women also described carers they did not
know as strangers whose presence was a source
of anxiety:
It would have been nice to have everyone
around you that you knew, not just your
family. . .rather than all these strangers
around and then they change and you get
more strangers coming in. It’s a bit scary . . .
[Nicole, 2nd baby]
Experiencing a lack of trust was also mentioned
by some participants when care was provided by
unfamiliar carers:
. . . with the main hospital, when I had my first
baby and the people I didn’t know, I was
thinking to myself: ‘Did I really want to listen
to them?’ I wanted to do my own thing but
then again they were saying ‘no, no, no, you
have to do this’ and I really didn’t want to do
that. . . [Lena, 2nd baby]
For many women, control over the birth
experience was directly linked to the presence
of known carers. One participant described her
feelings when she was facing transfer to the main
hospital for induction of labour after having all
her pregnancy care in the birth centre:
. . . it was an absolutely enormous issue for me
that I would be transferred out...I would lose
control . . . [being cared for by] people I hadn’t
met and didn’t know [Kathy, 4th baby].
Overall, women described a lack of rapport with
unfamiliar carers as having a negative impact
upon their care experiences. This included feeling
ill at ease with carers and anxious about
constantly repeating information. More than
one-third of the 790 women in an Australian
survey by Brown et al. (1994) complained of
seeing different caregivers at each antenatal visit.
As in the present study, this prevented them
developing a rapport with caregivers. One
woman actually stated, ‘I felt we were being
treated like cattle’ (Brown et al. 1994, p. 37).
Moreoever, women often mentioned their con-
cern at having to frequently remind staff of their
needs and problems. Too many people at the
birth was also a recurring theme in Brown et al.’s
research (1994). As well, in the UK, Garcia et al.
(1998) found it was difficult for women to
constantly repeat the same information to

Ongoing relationships with a personal focus 177
different caregivers. Clients also felt their care
might suffer because of too many caregivers.
Woman being unknown – Being unknown was
defined as carer’s lack of knowledge about
women’s previous history and birth preferences.
As previously discussed, in the hospital system
women were exposed to multiple carers through-
out pregnancy and birth. When reflecting on
previous hospital experiences, many participants
said they felt unknown by carers. For one
participant, different carers at every antenatal
visit resulted in a failure to recognise her anxiety
related to a loss in her prior pregnancy:
It was seven months last time and I hadn’t got
one thing ready for the baby. . . it was like I
didn’t want to believe I was going to have a
baby. . .that is how I felt during the
pregnancy. . . I think if I had someone to
reassure me that nothing is wrong, they said
to me that things were fine, but that was
different people every time. . .I think I needed
someone to talk to. [Teri, 2nd baby]
In the hospital system, participants were often
encouraged to write a birth plan, but in many
cases that was not used. The written birth plan
seemed to have minimal impact as a tool to assist
women inform unfamiliar carers of their birth
preferences:
Actually, they sent out a questionnaire to
your home and you filled it out and that
allowed you to list all the choices and
preferences you wanted. But when I actually
went in it was never referred to and I
remember thinking later, I can’t remember
specifically what happened, but I remember
going home and thinking that they didn’t even
look at the care plan that I had written.
[Kathy, 4th baby]
These findings support those of other researchers
who have found that women are disadvantaged
by not being known by their carers. McCourt et
al. (1998) found that many women not able to
have a carer who knew them expressed a need for
this service throughout the childbearing cycle. As
in the present study, some women in Garcia et
al.’s (1998) research, also compared present birth
experiences where they had continuity of carer
with previous births with unknown midwives:
women found the presence of strangers upsetting
particularly during the birth, but mentioned that
this did not happen when they knew their
midwife. Moreoever, in the present research a
critical pre-requisite for women feeling their care
was individual and personalised was knowing
their carer (discussed in greater detail in a
previous article Coyle et al. 2001). However, it
must be noted that other researchers have found
that continuity of carer models across the child-
bearing continuum do not always result in
increased maternal satisfaction with care (Wal-
denstrom 1998, Farquhar et al. 2000). Compar-
isons between studies continue to be problematic
due to inconsistent definitions regarding continu-
ity and the variety of research methods adopted.
Care Structures
The final theme of care structures was defined as
the organisational framework through which
care was delivered. Two dimensions of maternity
care were identified: (1) woman-tailored care and
(2) institution-oriented care. Women’s experi-
ences revealed that birth-centre care was more
likely to be woman tailored, while hospital care
was institution oriented. An exemplar of this
theme is presented in Box 2.
Woman-tailored care
Woman-tailored care was defined as the assis-
tance and attention provided to women during
their pregnancy and birth that focused on their
unique concerns, preferences and needs. This
dimension was characterised by three features:
(a) personalised care, (b) genuine caring and (c)
seeing-me-through.
Personalised care – Personalised care was
defined as attention and assistance provided by
midwives that revolved around women. When
women perceived they were the focus of care,
they felt they had received individualised care.
Care delivery in the birth centre was perceived as
woman focused:
But when they [midwives] talk to you, they
talk to you, not talk to you about something
else or someone else or what someone else did,
it was always your experience and what you
want and if you aren’t happy with that then
they change it because as far as they are
concerned you are the one having the baby
not them. . . [Ruth, 2nd baby]
Many participants described how they felt their
care was adjusted to suit them individually:
Everything went at its own pace. I didn’t feel
things were pushed on us. . .it was very very
nurturing care. . .there was no such thing as
the system taking over. [Vivian, 3rd baby].
Women’s birth centre experiences revealed that
preferences were accommodated by the midwives
caring for them. Midwives were perceived as
supporting women’s choices:
Everyone left me alone. left me to it which is
great, you know. It was really what I wanted
. . .I didn’t want to be poked and bothered,
and told to lay here and do this. [Sarah, 2nd
baby]

178 Midwifery
Genuine caring – Genuine caring is defined as
women’s perceptions that midwives provided
attention and assistance regarded as sincere.
The birth-centre setting allowed women to be
cared for by midwives with whom they had
developed a relationship. The nature of this care
relationship was perceived as very genuine. As
one participant outlined: ‘I was wondering
maybe they do care a different way when they
know someone’ [Bridgit, 2nd baby]. Birth-centre
midwives were also seen to spend more time with
women. This equated to caring: ‘. . .while they
[midwives] were here, that was your time. It
wasn’t looking at the watch all the time..’ [Ruth,
2nd baby].
Overall, when women felt their specific needs
were being met, they interpreted their care as
being personalised. Within the birth-centre
structure, midwives had the time to interact with
women without being rushed. This time invest-
ment made women feel carers were genuinely
interested in them as individuals.
Other researchers have also emphasised the
importance of woman-centred or personalised
care. Page et al. (2000) argue that for more than
two decades some hospitals have tried to provide
such woman-centred care. Moreover, a major
emphasis of the Changing Childbirth report
(DoH 1993) was that women must be the focus
of maternity care; that is their care should be
individual and personalised. Similarly, in Aus-
tralia a number of ministerial reviews have
emphasised the need for personalised and
individualised care during pregnancy and birth
(Health Department of Victoria 1990, Health
Department of Western Australia 1990, National
Health & Medical Research Council 1996).
Seeing-me-through – This third sub theme,
seeing-me-through, was defined as an assurance
Box 2 Exemplar of theme: care structures
Care structures
Def|ned as the organisational framework throughwhichmaternity care is delivered
Dimension: woman-tailored care
Assistance and attention provided towomen during their pregnancy and birth that focuses on their unique concerns,preferences and needs
Features Def|nition Exemplar
1. Personalised care The attention andassistance providedbymidwives that revolvesaroundwomen.
I felt at least they (midwives) tookmymeasureand letme bewhat I needed to be, does thatmakesense rather than treating people routinely.Or Ineed to tell you this because that’s the policy.[V|vian, 3rd baby]
2. Genuine caring Women’s perceptions thatmidwives provideattention and assistancethat was regarded assincere.
I was wonderingmaybe they do care a di¡erentway when they know someone. [Bridgit, 2nd baby]
3. Seeing-me-through An assurance that thesamemidwifewouldprovide all carethroughout labour andbirth.
. . . that was what she [midwife] said to me atmyvisits ‘‘whoever is with youwill bewith you thatentire time.We are not going to leave you, therewill be that same person there thewhole time’’.Like I say, when I look at it thatmade all thedi¡erence in being able to concentrate. . .[Mary, 2nd baby]
Dimension: institution-oriented care
Assistance and attention provided towomen during pregnancy and birth that focuses on the requirementsof the care setting.
Features Def|nition Exemplar
1. Systemised care The attention and assistanceprovided towomen by carerswhich revolves around theroutines and usual practices ofthe care setting.
I know withmy f|rst two sons [hospital births]therewere somany people popping in and out,and students, and all that stu¡ and you are a slabon that table and you are bringing a life intothis world. . . [Maxine, 4th baby]
2. Fragmented labour care The inability of the caresetting to assure one carer forwomen throughout labour.
But I think themain thing was I had likef|ve di¡erent people looking afterme all atonce. . . [Teri, 2nd baby]

Ongoing relationships with a personal focus 179
that the same midwife provided all care through-
out labour and birth. Labour was identified as an
important time for most participants, the birth-
centre model was able to accommodate one
midwife carer for the duration of labour. Many
participants felt this had a positive effect on their
care experiences: ‘if you had just one midwife
throughout that just makes a huge difference, it
really does’ [Bridgit, 2nd baby]. Women felt
positive about the assurance of one carer during
labour:
. . . that was what she [midwife] said to me at
my visits ‘whoever is with you will be with you
that entire time. We are not going to leave
you, there will be that same person there the
whole time’. Like I say, when I look at it that
made all the difference in being able to
concentrate. . . [Mary, 2nd baby]
The findings from the current study highlighted
not only the positive benefits of continuity of
carer throughout the child-bearing cycle, but also
emphasised the impact of having a single mid-
wife carer throughout the birth experience. Birth-
centre care in the present research allowed an
assurance of one carer being available for the
duration of the birth experience. This assurance
of one carer during labour was highly valued by
women, and positively affected their care experi-
ences.
The positive effects of providing continuous
trained support during labour have been well
documented by other researchers (Enkin et al.
1995, Hodnett 1998). In their review of social
and professional support in childbirth, it was
concluded that a critical feature of such support
is the promise or assurance that women in labour
will not be left alone. A consistent finding of the
trials reviewed by Enkin et al. (1995) and
Hodnett (1998) was that the continuous presence
of a trained support person led to a reduction in
pain relief medication, operative deliveries (both
vaginal and caesarean), and an Apgar score of
more than seven at five minutes.
However, as in the present research, continuity
of carer may well be an important pre-requisite
in assuring women of a constant presence during
labour. For example, in McCourt and Page’s
(1996) study, almost all the women with a known
midwife had continuous professional support
during labour compared to only half of the
control group. In the present research the effects
of a ‘known carer’ versus a continuous profes-
sional presence (with no previous social relation-
ship with the women) cannot be separated, as
women in the birth centres had all met their
midwife before labour.
Institution-oriented care
Institution-oriented care was defined as the
assistance and attention provided to women
during pregnancy and birth that focused on the
requirements of the institution. Care delivery in
the hospital was experienced as institution
oriented by many participants in this study. This
dimension was characterised by two features: (a)
systemised care and (b) fragmented labour care.
Systemised care – Systemised care was defined
as the attention and assistance provided to
women by carers that revolved around the
routines and usual practices of the care setting.
Many women perceived that the organisational
structure of the hospital setting dictated the type
of care they received; they felt they were ’just a
number’ in a large system. As one participant
described: ‘I was sitting there . . . no one to talk
to, no-one really cares, you are just a patient’
[Ruth, 2nd baby]. The hospital system did not
allow women to become familiar with carers.
Having intimate procedures performed by un-
known carers resulted in a perception of
impersonal care: ‘. . . the doctor who actually
examined me [vaginal examination] . . . I had
never met him. I found it very impersonal’
[Sharon, 2nd baby].
Hospital care often involved a doctor being
called in for the birth of the baby. One
participant described how she felt when her
doctor attended the birth of her first child. The
doctor’s lack of involvement in labour care made
the woman feel he did not have any under-
standing of what she had been through up to that
point. The conversations going on around the
woman resulted in her feeling that she was
unimportant:
I thought, well you haven’t been with me the
past 20 hours... he [doctor] just walks in and I
remember him talking to one of the nurses
and she asked what he had been doing and he
said he had just had some friends for dinner
and his dinner party had been interrupted or
something and that has stayed on my mind. It
seemed he was feeling oh she is just another
woman in labour, she’s in another world, she
doesn’t really know what’s going on. [Ann,
2nd baby]
The hospital’s inability to offer choices resulted
in women perceiving care as inflexible and
impersonal:
With my first child that is what I had. This is
what we’ve got, this is what you get. I didn’t
like that because I didn’t have a choice. I just
turned up for the experience. [Ruth, 2nd
baby]
Women were also expected to endure long waits
prior to being seen in hospital antenatal clinics,
and carers often had little time available to
discuss concerns with the women.

180 Midwifery
At the hospital I was sitting there waiting for
2 or 3 hours and never saw the same doctor
twice. . .I felt like no one really cared. . . they
didn’t have time to talk. . . you waited 3 hours
and then you were given 10minutes and then
you were out. [Diane, 5th baby]
The hospital structure, where women had pre-
viously birthed, allowed little time for carers to
address individual concerns. This resulted in
women perceiving that carers were lacking in
empathy and that care was system focused rather
than woman centred. These findings suggest, that
despite an increasing emphasis on woman-
centred care, in practice care often remains
depersonalised. Many respondents in Brown
et al.’s (1994) Australian survey of 790 women
also felt they were not treated as individuals by
those working in antenatal, labour and postnatal
settings.
Fragmented labour care – The second sub theme
of fragmented labour care was defined as the
inability of the care setting to assure one carer
for women throughout labour. The hospital shift
system often resulted in women being exposed to
multiple carers within a short time frame. A
woman would often become familiar with her
carers and then a shift change would mean new
staff would appear:
I liked the first lot and I was just starting to
get used to them and then all of a sudden, I
had an epidural, went to sleep a bit, woke up
and I had different ones, and it was like, oh
OK. [Nicole, 2nd baby]
Women were aware that midwives were due off
shift, and this caused them anxiety. Some
participants did not feel it was appropriate for
carers to leave them halfway through labour:
I think, me myself if I was a midwife and I
came in to somebody who was going into
labour I would stay with them through to the
end instead of OK I have to clock off now,
run out and another lady come in and it is OK
right what are we doing. For myself I would
want to see it through to the end and that is
what I felt they should have done instead of
half way through. [Lena, 2nd baby]
Overall, a lack of continuity of carer throughout
labour within hospital settings was perceived to
have a negative impact on many women’s birth
experiences. Too many carers during this crucial
time was a source of anxiety for many women. In
the hospital context, organisational constraints
such as rigid shift work systems, meant women
could not be assured of continuity of carer
throughout labour. These finding support those
of a large Australian survey (Brown & Lumley
1998) that found women experienced fragmented
care during their birth. A UK survey (Garcia et
al. 1998) also found that women giving birth in
hospital were more likely to receive fragmented
care. As in the present study, this fragmented
care was upsetting for women.
The findings of the present research to some
extent support Page et al’s (2000) contention that
the place of care is the most important determi-
nant of the way a midwife practices. As we have
discussed, women in the present study certainly
felt their most recent care in birth centres was
quite different from their previous hospital-care
experiences. The underlying philosophy of the
midwives giving this care is perhaps best summed
up by Brodie (1997) when she discusses the
differences between allegiance to institutions
rather than to women. Systems of care that
encourage a continuous relationship between the
woman and her carer (such as that found in birth
centres in the present research) alter the mid-
wives’ allegiance from the institution to the
individual woman.
CONCLUSION
In summary, in the current study we have been
able to provide a detailed description of how
women perceive continuity of midwife carer, in
the birth-centre context. The benefits of con-
tinuity of carer identified by women in this study
are well supported by other empirical findings. In
the birth-centre setting, cumulative interactions
with a consistent midwife provided women with
the opportunity to develop rapport with their
carer and feel truly known as an individual.
Woman-tailored care also ensured that women
received personalised, genuine care that trans-
cended the entire childbearing continuum. The
perceived success of this model has been the
removal of the organisation barriers, which in
the traditional medical model, have inhibited
continuity of carer due to systemised fragmented
care.
ACKNOWLEDGMENTS
The authors would like to acknowledge the generous
financial assistance provided by the Nurses Board of
Western Australia, Edith Cowan University and the Olive
Anstey Nursing Fund who supported this study.
REFERENCES
Australian Bureau of Statistics 2000 1996 Census of
population and housing. Online. Available: http://
www.abs.gov.au
Brodie P 1997 Being with women: the experiences of
Australian team midwives. Inpublished thesis. Uni-
versity of Technology Sydney
Brown S, Lumley J, Small R et al. 1994 Missing voices the
experience of motherhood. Oxford University Press,
Melbourne Victoria

Ongoing relationships with a personal focus 181
Brown S, Lumley J 1998 Changing childbirth: lessons
from an Australian survey of 1336 women. British
Journal of Obstetrics & Gynaecology 105: 143–155
Coyle KL 1997 Report on the clinical audit used to
evaluate the group practice model of care at the
Family Birth Centre – King Edward Memorial
Hospital. Unpublished report. King Edward Memor-
ial Hospital. Perth. Western Australia
Coyle K, Hauck Y, Percival P et al. 2001 Normality and
collaboration: mothers’ perceptions of birth centre
versus hospital care. Midwifery doi: 10.1054/
midw.2001.0256
Creasy J 1997 Women’s experience of transfer from
community-based to consultant-based maternity care.
Midwifery 13: 32–39
Department of Health 1993 Changing childbirth. Part 1:
Report of the expert maternity group. OHMS,
London
Downe S 1997 The less we do, the more we give. British
Journal of Midwifery 5: 43
Enkin M, Keirse M, Renfrew M et al. 1995 A guide to
effective care in pregnancy and childbirth 2nd ed.
Oxford University Press, New York
Farquhar M, Camilleri-Ferrante C, Todd C 2000 Con-
tinuity of care in maternity services: women’s views of
one team midwifery scheme. Midwifery 16: 35–47
Fleming VE 1998 Women-with-midwives-with-women: a
model of interdependence. Midwifery 14: 137–143
Field PA, Morse JM 1990 Nursing research: The
application of qualitative approaches. Chapman and
Hall, New York
Flint C, Poulengeris P, Grant A 1989 The ‘Know Your
Midwife’ scheme: A randomised trial of continuity of
care by a team of midwives. Midwifery 5: 11–16
Garcia J, Redshaw M, Fitzsimmons B et al. 1998 First
class delivery: a national survey of women’s views on
maternity care. Audit Commission, London
Green J, Curtis P, Price H et al. 1998 Continuing to care.
The organisation of midwifery services in the UK:
a structured review of the evidence. Books for
Midwives Press, Hale
Harding D 2000 Making choices in childbirth. In: Page L
(Ed.) The new midwifery science and sensitivity in
practice. Churchill Livingstone, London
Harvey S, Jarrell J, Brant R et al. 1996 A randomised
controlled trial of Nurse-Midwifery care. Birth 23:
128–135
Health Department of Victoria 1990 Having a Baby in
Victoria. Final Report of the Ministerial Review of
Birthing Services in Victoria, Melbourne
Health Department of Western Australia 1990 Report of
the Ministerial Task Force to Review Obstetric
Neonatal and Gynaecological Services in Western
Australia. Volume 1. Summary and Recommenda-
tions
Hodnett E 1998 Continuity of caregivers during preg-
nancy and childbirth. Cochrane Review, Cochrane
Library Issue 3 Update Software, Oxford
Kenny P, Brodie P, Eckerman S et al. 1994 Westmead
hospital team midwifery project evaluation. Centre
for health economics research and evaluation West-
mead Hospital, Westmead, New South Wales,
Australia
Leap N 1997 Caseload practice that works. MIDIRS
Midwifery Digest 7: 416–418
MacVicar J, Dobbie G, Owen Johnstone L et al. 1993
Simulated home delivery in hospital: a randomised
controlled trial. British Journal of Obstetrics and
Gynaecology 100: 316–323
McCourt C, Page L (Eds) 1996 Report on the evaluation
of One-to-One midwifery. Thames Valley University,
London
McCourt C, Page L, Hewison J et al. 1998 Evaluation of
one-to-one midwifery: women’s responses to care.
Birth 25: 73–80
Morison S, Percival P, Hauck Y et al. 1999 Birthing at
home: the resolution of expectations. Midwifery 15:
32–39
National Health and Medical Research Council 1996
Options for Effective Care in Childbirth for effective
care in childbirth. Australian Government Publishing
Service, Canberra
Page L, Cooke P, Percival P 2000 Providing one to one
practice and enjoying it. In: Page L (Ed.) The new
midwifery science and sensitivity in practice. Church-
ill Livingstone, London
Pairman S 1998 The midwifery partnership: an explora-
tion of the midwife/women relationship. Unpublished
thesis University of Wellington, New Zealand
Rowley MJ, Hensely MJ, Brinstead MW et al. 1995
Continuity of care by a midwife team versus routine
care during pregnancy and birth: A randomised trial.
The Medical Journal of Australia 163: 289–293
Sandall J 1997 Midwives’ burnout and continuity of care.
British Journal of Midwifery 5: 106–11
Shields N, Turnbull D, Reid M et al. 1998 Satisfaction
with midwife-managed care in different time periods:
a randomised controlled trial of 1299 women.
Midwifery 14: 85–93
Strauss A, Corbin J 1998 Basics of qualitative research:
techniques and procedures for developing grounded
theory. Sage Publications, London
Turnbull D, Holmes A, Shields N et al. 1996 Randomised
controlled trial of efficacy of midwife managed care.
The Lancet 348: 213–218
Waldenstrom U 1998 Continuity of carer and satisfaction.
Midwifery 14: 207–213
Waldenstrom U, Nilsson C 1997 A randomised controlled
trial of birth centre care versus standard maternity
care: effects on women’s health. Birth 24: 17–26
Waldenstrom U, Lawson J 1998 Birth Centre Practices in
Australia. Australian & NZ Journal of Obstetrics and
Gynaecology 38: 42–50
Waldenstrom U, Turnbull D 1998 A systematic review
comparing continuity of midwifery care with standard
maternity services. British Journal of Obstetrics and
Gynaecology 105: 1160–1170
Walker JM, Hall S, Thomas M 1995 The experience of
labour: a perspective from those receiving care in a
midwife-led unit. Midwifery 11: 120–129
Walsh D 1999 An ethnographic study of women’s
experience of partnership caseload midwifery prac-
tice: the professional as a friend. Midwifery 15:
165–176