OMERIGWE, EBI GRACE - University Of Nigeria Nsukka
97
OMERIGWE, EBI GRACE THE INFLUENCE OF BREAST CANCER CAMPAIGNS ON KNOWLEDGE, ATTITUDE AND PRACTICE AMONG WOMEN IN BENUE STATE ARTS DEPARTMENT OF MASS COMMUNICATION MADUFOR, CYNTHIA C. Digitally Signed by: Content manager‟s Name DN : CN = Webmaster‟s name O= University of Nigeria, Nsukka OU = Innovation Centre
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of OMERIGWE, EBI GRACE - University Of Nigeria Nsukka

0
OMERIGWE, EBI GRACE
THE INFLUENCE OF BREAST CANCER CAMPAIGNS
ON KNOWLEDGE, ATTITUDE AND PRACTICE
AMONG WOMEN IN BENUE STATE
ARTS
DEPARTMENT OF MASS COMMUNICATION
MADUFOR, CYNTHIA C.
Digitally Signed by: Content manager‟s Name
DN : CN = Webmaster‟s name
O= University of Nigeria, Nsukka
OU = Innovation Centre

1
THE INFLUENCE OF BREAST CANCER CAMPAIGNS ON
KNOWLEDGE, ATTITUDE AND PRACTICE AMONG WOMEN IN
BENUE STATE
OMERIGWE, EBI GRACE
PG/MA/10/57442
A RESEARCH PROJECT SUBMITTED TO THE DEPARTMENT OF
MASS COMMUNICATION, UNIVERSITY OF NIGERIA, NSUKKA, IN
PARTIAL FUFILMENT OF THE REQUIREMENTS FOR THE AWARD
OF MASTER OF ARTS DEGREE (M.A) IN MASS COMMUNICATION
DEPARTMENT OF MASS COMMUNICATION,
UNIVERSITY OF NIGERIA, NSUKKA
SEPTEMBER 2012

2
CERTIFICATION
We certify that this project has been read and approved as an original work submitted by
Omerigwe, Ebi Grace with registration number PG/MA/10/57442 to the Department of Mass
Communication, University of Nigeria, Nsukka, in partial fulfillment of the requirements for
the award of Master of Arts Degree (M.A) in Mass Communication.
……………………. ………… …………………………………….. ………..
DR. GREG EZEAH DATE DR. NNANYELUGO, M. OKORO DATE
(SUPERVISOR) (HEAD OF DEPARTMENT)
……………………………. ………………...
EXTERNAL EXAMINER DATE

3
DEDICATION
This research study is dedicated to God Almighty, the origin of knowledge from whom all
blessings flow and to the women folk.

4
ACKNOWLEDGEMENTS
First and foremost, I am grateful to God Almighty, who gave me strength and
inspiration, then to my supervisor, Dr. Ezeah, whose constructive criticism shaped the work a
great deal and then to the authors whose works were cited to give meaning to this study.
Also, to Mr. L.I. Anorue, whose suggestions set the pace for speed in this study. Not
forgetting, Alex Onyebuchi, who brainstormed to put me on the right track of thoughts for the
topic, and provided insight into the study and areas of focus. Thanks for being generous with
your knowledge and creative ideas. I also say thank you to Ekwe Okwudiri for suggesting
that I should delve into health communication. This has increased my personal health
interests. Also, I appreciate Dr. Udeajah, Dr. Ngwu and Dr. Okoro for being very jovial and
willing to impact knowledge to their students. And to other lecturers in the department, I say
thank you for sharing your knowledge.
A very big thank you to my parents who dimmed it fit to get me equipped with
knowledge to this level. May they reap where they have sown.
Furthermore, I appreciate my special friends, Eucheria and Maureen (Dr. Reen), and
the likes of Tochi, Orekye, Philip, Oke, Alhaji Abubakar, Ese, Onyi, Moses, Chiaha, I.g,
Mercy, Kefe, Alabo, Ifeanyi, Nonso, Aja, Okwy and all my course mates. Thanks for adding
spice to this academic period of study. My special thanks to Ekwe, for his moral and material
support. I am very happy to have met you.
I also acknowledge the support of my siblings Christy, Simon, Blessing and Patience.
Not forgetting my cousins Matthew, Sam, Felix, Joe, Ekpu, Igelle and Aemu. To my
esteemed Uncles Solomon, Steven and Austin; I say a very big thank you for being proud of
me, for standing up for me in prayers and for your great display of love.
Finally, I appreciate my special roommates and friends especially Aunty Betty, and
Aunty Ijeoma; Stella, Ijeoma and Aunty Rose. It was nice sharing in your life experiences.
Mummy Garos, Chinenye, Chioma, Chinelo and Okwy, God will be your strength and
refuge, a very present help in your time of need.

5
TABLE OF CONTENTS
Title Page…………………………………………………………………………….............0
Certification………………………………………………………………………………….1
Dedication……………………………………………………………………………............2
Acknowledgements………………………………………………………………………......3
Table of Contents…………………………………………………………………………….4
Abstract……………………………………………………………………………………....5
CHAPTER ONE: INTRODUCTION
1.1 Background of Study…………………………………………………………….6-10
1.2 Statement of Problem……………………………………………………………10-11
1.3 Objectives of the Study………………………………………………………….11-12
1.4 Research Questions………………………………………………………………….12
1.5 Significance of the Study……………………………………………………………13
1.6 Scope and Limitations of the Study…………………………………………………14
1.7 Operational definition of terms…………………………………………………...14-15
References………………………………………………………………………..16-17
CHAPTER TWO: LITERATURE REVIEW
2.1 Focus of Review……………………………………………………………………18
2.2 Breast Cancer: An Overview……………………………………………………18-21
2.3 Awareness, Knowledge and Exposure to Breast Cancer Campaigns …..………21-24
2.4 Practice of BSE, Other Screening Methods and Early Detection ……………..25-29
2.5 Theoretical Framework……………………………………………………..…..29-36
2.6 Summary of Literature……………………………………………………………...36
References………………………………………………………………………37-38
CHAPTER THREE: RESEARCH METHODOLOGY
3.1 Research Design………………………………………………………………....39
3.2 Population of Study……………………………………………………………..39-40
3.3 Sampling Size……………………………………………………………………40-43
3.4 Sampling Techniques…………………………………………………………….44-45
3.5 Measuring Instrument……………………………………………………………45
3.6 Validity and Reliability of Instrument……………………………………………46-47
3.7 Method of Data Collection and Analysis ………………………………………..48
References ……………………………………………………………………….49
CHAPTER FOUR: DATA PRESENTATION AND ANALYSIS
4.1 Data Presentation and Analysis………………………………………………..…50-70
4.2 Discussion of Findings…………………………………………………………...71-78
References………………………………………………………………………..79
CHAPTER FIVE: SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.1 Summary…………………………………………………………………………8 0-81
5.2 Conclusion……………………………………………………………………….82-83
5.3 Recommendations………………………………………………………………..83-84
References ………………………………………………………………………..85
BIBLIOGRAPHY ……………………………………………………………………....86-90
APPENDIX ……………………………………………………………………………...91-97

6
ABSTRACT
In Nigeria, 116 out of every 100,000 women have breast cancer. On the global scene,
annual, breast cancer (BRCA) incidence rate is over 1million cases and over 411,000 deaths.
Survival rate is less than 50% in developing countries, in contrast to 90% in developed
countries. This, as studies have revealed is due to late detection and diagnosis, poor
knowledge, attitude and practice towards breast cancer (BRCA), its causes, risk factors and
screening techniques. Consequently, MTN Foundation, National Breast Cancer Coalition,
Breast Cancer Action and the Miss University Nigeria campaigners have resorted to
aggressive awareness and sensitization programmes aimed at increasing knowledge,
changing attitudes and enhancing the practice of all necessary screening procedures; since
success is highly dependent on the influence of these campaigns to increase knowledge,
change unhealthy attitudes towards BRCA prevention and treatment and enhance practice of
screening methods. Using survey, personal interviews were used to find out the extent of
awareness and exposure, knowledge level, attitude and practice of screening among women
in Benue state. The Health Believe Model and Attitude Change theory gave explanation to the
reasons for unhealthy behaviours and subsequent results. Findings revealed superficial
knowledge about BRCA causes, symptoms, Genetic testing, BSE, and CBE. Also, that attitude
is influenced by strong negative emotional and psychological beliefs. The study, therefore,
emphasized the need for preventive rather than curative measures, noting the role of breast
cancer campaigns in advancing this cause.

7
CHAPTER ONE
INTRODUCTION
1.1 Background of the Study
The entire human race is at the brink of total destruction because of the increasing
susceptibility to cancer. Statistics emanating from different health organisations and agencies
around the world indicate that there are over 16 million new cases of cancer globally. This
figure, according to World Health Organization (WHO) 2011report, is likely to double in
2020 (Chustecka, 2011p.1). Over 16 million cancer cases have been predicted to occur in
2020 with 70 percent of these cases likely to take place in developing countries with Africa
accounting for over 57 percent incidence rate and one million cases of breast cancer
(Chustecka, 2011p.1).
The International Agency for Research on Cancer (IARC) gave an estimate of over
681,000 and 512,400 new cases of cancer in 2008 alone. These figures have increased to 1.4
million cases and 714,000 deaths in 2010 (IARC Report 2010 p.3). Unfortunately, it is
projected by IARC that these numbers will double before 2030, because of the aging and
growth of the population; unhealthy behaviours associated with lack of exercises, dieting,
smoking, economic development and urbanization. According to this report, the factors
mentioned above result in different types of cancers, such as cancer of the stomach, lungs,
liver, uterus, kidney (renal cell carcinoma), blood cancer known as leukemia, sinuses and
breast cancer. Breast cancer ranks the second most prevalent of all cancers worldwide after
cancer of the lungs (World Cancer Report, 2011p.4).
Globally, there are over 1.2 million cases of breast cancer with 411,000 deaths
annually. More than 56-60 percent of these deaths occur in developing countries including
Nigeria (Akpo, Akhator & Akpo 2010 p.3). It is estimated that in every 100,000 Nigerian
women, 116 of them have breast cancer and that more than half of the number have a very

8
high generic risk status and as such are vulnerable to the disease. (American Cancer Society,
2009 p.6). In addition, Akpo, Akhator and Akpo (2010 p.4), report that a recent oncological
review of cases in Nigeria revealed that, breast cancer survival rate is less than 50 percent in
Nigeria in contrast to 90 percent in developed countries. Bhopal (2002) refers to incidence as,
the calculated risk of acquiring a new state or becoming sick within a certain period of time.
He also notes that it is a frequency of occurrence of particular events at any given time.
Despite the high incidence rate, the good news, however, is that experts believe that the high
incidences of this disease can be reduced through aggressive enlightenment campaigns.
To this end, campaigns on breast cancer have been widely organized, not just in
Benue state, but in Nigeria, Africa and the world over. Worthy of note are the step-down
workshops at state levels developed by the wives of the Governors of the 36 states of the
Federation, as a follow up on the action plan by the United Nations Population Fund (UNFPA)
in April, 2008 at the Federal Capital Territory Abuja. The need to preserve lives and ensure a
steady decrease in the level of maternal mortality resulting from breast cancer has been very
salient. Also, the pet project of the Miss University Nigeria (MUN) which was an awareness
and sensitization campaign against breast cancer was hosted in Makurdi, the Benue State
capital in December, 2010. In fact, the MTN Foundation has breast cancer screening centers
located within Teaching hospitals, Federal Medical Centers (FMCs) and state General
hospitals across Nigeria (MTN Foundation, 2011 Report).
It is however, disheartening to note that despite several awareness and sensitization
campaigns on the need for regular self examination as a preventive measure for breast cancer,
so many women are still victims of the dreaded disease. As a matter of fact, breast cancer
statistics indicate an increase, especially in developing countries that previously enjoyed a
low incidence of the disease. It, therefore, means that accessibility to campaigns, awareness
and knowledge level of risk factors, attitude towards campaigns and practices are highly

9
questionable. If women are aware and exposed to campaigns, whether or not they practice
what they are taught is a determinant of the level of success of these campaigns.
A look at these significant campaigns organized by the National Breast Cancer
Coalition, tagged "Not Just Ribbons" with emphasis on substantive issues such as genetic
discrimination, access to medical care, patient‟s rights, and anti-pollution legislation as
against undue emphasis by business men on the pink ribbons; and Breast Cancer Action's
"Think Before You Pink" campaigns, give an understanding of what influence a well
structured campaign can exert on people. (Sulik, 2010 p.366–368).
Campaigns must be structured in such a way as to accommodate factors which are
vital in the fight against breast cancer. When access to the campaigns has been ensured,
exposure at the right time and place is the next consideration after which the structuring of
the campaign messages is done. These messages are meant to be the basic units of positive
influence in the campaigns, as they will determine the knowledge level, attitude and practices
of the target audience. It is the messages that will inform the women of the factors that cause
breast cancer, the types of breast cancer, the need for self examination and early detection,
the symptoms of breast cancer, treatment for it at the early stage and so on.
A good number of people might, therefore, underestimate or overestimate their
generic risk status based on their level of awareness of the possible genetic mutations that can
result in breast cancer. People who are not aware of generic factors will not understand that if
a member of the family is diagnosed of breast cancer, every other female member stands a
risk of developing breast cancer, thus the emphasis on periodic generic testing at the hospital,
besides the prescribed self examination.
That is why Ferrandis, Andreu and Galdón (2002 p.27), citing (Sattin et al., 1985),
explain that “a family history of breast cancer is a clear risk factor for developing the disease.
In effect, women who have a first degree relative with breast cancer have a 2- to 3-fold higher

10
risk of developing the disease, while women who have both the mother and a sister with
breast cancer are 14 times more likely to develop the disease than patients without a family
history of breast cancer”.
This brings us to the efficacy of awareness in the campaign against breast cancer, with
the view that efforts at raising awareness will lead to greater knowledge and invariably lead
to earlier detection and a greater survival rate. This awareness level, however, has the
information angle where according to a Chinese proverb: “the road to health is the road to
knowledge and ignoring knowledge is sickness”. Then there is the psychological angle where
too much of awareness causes guilt, fear, anxiety, depression and negative attitudes of self
isolation in breast cancer patients; where attitude developed is largely related to knowledge
acquired from social interactions, cultural values, personal interests and societal influence.
On this note, Eagly and Chaiken (1995 p.413) see attitude as a set of mental and neutral
readiness, organized through experience, which exerts a direct or dynamic influence upon a
response to all objects, and the situation with which it is related. Olson (2002 p.240–242),
Welch (2010 p.16) and Sulik (2010 p.74, 263), therefore, explain the attitude of women,
towards increased awareness on breast cancer thus:
An emphasis on educating women about lifestyle changes that may have
a small impact on preventing breast cancer often makes women feel
guilty if they do develop breast cancer. Some women decide that their
own cancer resulted from poor diet, lack of exercise, or other modifiable
lifestyle factor, even though most cases of breast cancer are due to non-
controllable factors, like genetics or naturally occurring background
radiation. Adopting such a belief may increase their sense of being in
control of their fate. Increased awareness inadvertently increases victim
blaming. Women who resist screening, mammography or breast self-
exams are subjected to social pressure, scare tactics, guilt, and threats
from some physicians to terminate the relationship with the patient.
Similarly, the emphasis on early detection results in women blaming
themselves if their cancer is not detected at an early stage.
The right attitude for women who have been diagnosed with breast cancer and those
who are free should, therefore, be captured in the campaigns, given that several factors

11
contribute in the formation of negative or positive attitudes. Like Sunder, Adarsh and Pankaj
(2009) explain, it is right to note that, society has cultural values and interests relating to
health and health services which determine attitudes towards these services, and that these
ideologies can be inimical to survival and so need to be addressed. Some women who are not
able to adapt to societal pressures, develop negative attitudes towards medical services. But
those who are able to adapt, resort to positive actions like being consistent with screening
methods and as reports have shown, most women also resort to taking up social roles and
advocacy in their fight against breast cancer, not only because of the health benefits but as a
way of promoting their emotional recovery.
1.2 Statement of Problem
Several campaigns such as those organized by MTN Foundation, National Breast
Cancer Coalition, Breast Cancer Action and the Miss University Nigeria have been organized
in the bid to fight breast cancer, yet the current statistical data of maternal mortality resulting
from breast cancer shows an increase. Cancer of the breast has the second highest cases of
cancers annually with an incidence rate of over one million cases and is still the second
principal cause of cancer mortality among women worldwide. (World Cancer Reports
2011p.4)
Breast cancer mortality rates are higher in developing countries as a result of late
detection and diagnosis. Another reason has been identified as due to lack of knowledge
about genetic risk factors for breast cancer. Also, social factors such as lack of awareness and
lack of knowledge about the disease, suspected poor attitudes towards Breast Self
Examination (BSE), Clinical Breast Examination (CBE), Mammography and other screening
methods. These explain the fact that breast cancer is not well understood by women. And as
such, there is the need for information and enlightenment to ensure early presentation at the

12
hospital. The increased mortality rate is, also, attributable to the lack of periodic practice of
early detection methods, like mammography and the lack of screening facilities. (Akpo,
Akhator & Akpo 2010 p.3)
The MTN Foundation, National Breast Cancer Coalition, Breast Cancer Action and
the Miss University Nigeria campaigners do not seem to know whether to attribute this
increase in death rate to inefficiency in campaign message delivery or timing for target
audience in campaign slots. Also, they do not know whether to blame it on audience
members‟ predispositions towards vital instructions and teachings adopted in the breast
cancer campaigns. However, some observers believe that any campaign aimed at fighting this
deadly disease must have all it takes to increase knowledge, change attitude and enhance
practice of screening methods among the audience. According to them, except there is a
significant change in the attitude of those exposed to breast cancer campaigns, the entire
exercise will amount to futility. This is the crux of the study. This study, therefore, was aimed
at finding out the extent to which women in Benue State are exposed to breast cancer
campaigns and how these campaigns have increased their awareness and knowledge level
about breast cancer risk factors, and preventive measures.
1.3 Objectives of the Study
The major purpose of this study is to discover how breast cancer campaigns have
influenced the knowledge, attitude and practice among women in Benue State towards breast
cancer prevention, detection and treatment. Therefore, the objectives of this study are to:
1. Determine the level of awareness about campaigns on the causes of breast cancer,
prevention, early detection and treatment among women in Benue State.
2. Find out the extent to which women in Benue State are exposed to breast cancer
campaigns.

13
3. Establish whether the knowledge level of women in Benue State, on breast cancer risk
factors, prevention, early detection and treatment has increased due to their exposure
to the campaigns.
4. Find out the attitude of women in Benue State towards breast cancer campaigns on
prevention, early detection and treatment.
5. Ascertain the extent to which they practice Breast Self Examination (BSE), Clinical
Breast Examination (CBE), Mammography and Genetic testing due to their exposure
to breast cancer campaigns.
1.4 Research Questions
The following research questions were directly drawn from the objectives of the study.
1. What is the level of awareness among women in Benue State, about campaigns on the
causes, prevention, early detection and treatment of breast cancer?
2. To what extent are women in Benue State exposed to breast cancer campaigns?
3. Has the knowledge level of women in Benue State, on breast cancer risk factors,
prevention, early detection and treatment increased due to their exposure to the
campaigns?
4. What is the attitude of women in Benue State towards breast cancer campaigns on the
prevention, early detection and treatment?
5. To what extent do they practice Breast Self Examination (BSE), Clinical Breast
Examination (CBE), Mammography and Genetic testing as a result of their exposures
to breast cancer campaigns?

14
1.5 Significance of the Study
The significance of this study to the media managers, health organization and
agencies, academic community and the general society cannot be over emphasized.
Drawing from this study, media professionals who are involved in breast cancer
campaigns will know the extent to which such campaigns influence knowledge, attitude and
practice of the audience towards prevention, early detection and treatment of breast cancer.
The study emphasized the need for aggressive campaigns relative to appropriate timing,
simplicity of campaign messages and influence of the campaigns.
The Ministry of Health and other health organizations and agencies (local and
international) will equally find the outcome of this study interesting. Given the scope of this
study, current statistics were provided on the knowledge, attitude and practice level of breast
cancer preventive measures among women in Benue State. Again, statistical data on mortality
rate might stir up concerns for better promotion of knowledge on self examination and early
detection; placing emphasis on prevention rather than cure. When this is achieved, increase in
death rate would have been reduced.
The study embraced both rural and urban populations in Benue State in contrast to
other works that dwelt only on rural and uneducated women. Also, studies surveying Benue
State on breast cancer awareness and sensitization are few. This study, therefore, gave
attention to health communication in the state.
Theoretically, this study provides an academic platform for testing claims put up by
some theories on attitude and behavioural change.
Finally the study is a contribution to the academia. It will serve as a reference tool for
further studies on the topic since one of the serious problems that have been identified in the
academic community in Nigeria is limited data base in research. In mass communication,
health communication related studies have not equally received serious attention despite the

15
huge resources thrown in this area. This study will, therefore, contribute to the limited pool of
literature in health communication.
1.6 Scope and Limitations of the Study
The study covers the women in Benue State from ages 15 and above. It looks at the
influence of breast cancer campaigns on knowledge, attitude and practice among these
women. The study covers a total of 11 local government areas, randomly selected from the 23
local government areas of the state drawn from the three senatorial zones of the state.
This study is, however, restricted to opinions from the questionnaire irrespective of
different individual motives in providing responses. Also, health responses on audience
breast cancer status were based on audience self believe and examination and were not at all
certified by medical doctors that they were free or infected. So based on what they felt, they
provided answers.
The study was also limited by time available to carry out the research. The available
time was not adequate given that several other activities had to be scheduled within the same
period.
1.8 Operational Definition of Terms
Breast Cancer: a disease condition that affects the breast of women in Benue State.
Campaigns: these are media programmes that are aimed at fighting against breast cancer by
informing women in Benue State on the dangers and how it can be prevented, detected or
treated
Influence: this refers to how the campaigns are able to bring about changes in the knowledge,
attitude and practices among the women in Benue State.

16
Attitudes: the disposition of women in Benue State towards breast cancer prevention, early
detection and treatment.
Knowledge: the level of technical know-how of women in Benue State on breast cancer
campaigns .relative to prevention, early detection and treatment.
Practices: all conscious efforts by the women in Benue State to fight breast cancer through
Breast Self Examination (BSE), Clinical Breast Examination (CBE), Mammography and
Genetic testing, as a result of their exposure to breast cancer campaigns.
Benue women: all females in Benue State between ages 15 and above

17
References
Akpo, E., Akpo, M. &Akhator, A. (2010). Breast cancer knowledge and screening practices
among Nigerian medical students. Delta: Delta State University. The International
Journal of Health. 11 (2).
American Cancer Society, (2009). Breast cancer: Early detection.. Retrieved April 18th 2012
fromhttp://www.cancer.org/docroot/CRI/content/CRI_2_6x_Breast_Cancer_Early_De
tection.asp.
Bhopal, R. (2002). Concepts of epidemiology. New York: Oxford University Press
Chustecka, Z. (2011). Cancer in Africa is 'Like a Runaway Train'. Medscape Medical
News 2011 WebMD, LLC. http://www.medscape.com/viewarticle/736870
Eagly, A.& chaiken, S. (1995). Attitude strength, attitude structure and resistence to change.
In R. Petty and J. Kosnic (Eds) Attitude strength. (PP 413- 415) Mahuah NJ: Erlbaum.
Ferrandis, E. D. Andreu, Y. & Galdón, M. J. (2002). The impact of information given to
patients’ families: Breast cancer risk notification. Análise Psicológica , 1 (20): 27-34.
http://www.scielo.oces.mctes.pt/pdf/aps/v20n1/v20n1a03.pdf. Retrieved April 18th,
2012
MTN Foundation, (2011). MTN foundation commissions a series of state-of-the-art dialysis
and mammography centers around Nigeria. 28th February, 2011 - 10:18 AM
http://www.mtnonline.com/mtnfoundation/content/mtn-foundation-commissions-
series-state-art-dialysis-and-mammography-centres-around-nigeriaRetrieved April 18th 2012
Olson, J. S. (2002). Bathsheba's breast: Women, cancer and history. Baltimore: The Johns
Hopkins University Press.
Park, K. (2009). Parks textbook of preventive and social medicine (20th ed). India:
Banarsidas Bhanot Publishers.
Sunder, L., Adarsh & Pankaj (2009). Textbook of community medicine; preventive and social
medicine (2nd ed). New Delhi, India: CBS Publishers and Distributors.
Sulik, G. (2010). Pink ribbon blues: How breast cancer culture undermines women's health.
New York: Oxford University Press.
The World Cancer Report, (2011). Global cancer rates could increase by 50% to 15 million
by 2020. http://www.who.int/mediacentre/news/releases/2003/pr27/en/.

18
The International Agency for Research on Cancer, (2010). World cancer report provides
clear evidence that action on smoking, diet and infections can prevent one third of
cancers, another third can be cured. http://www.who.int/mediacentre/news/releases/2003/pr27/en/ IARC reports.
UNFPA, (2010). UNFPA in Benue State: Annual report. http://nigeria.unfpa.org/benue.html
retrieved 6th May, 2012
Welch, H. G. (2010). "The Risk of Being Too Aware". The Los Angeles Times. ISSN 0458-
3035, 20th October. Retrieved April 18th, 2012 from
http://www.latimes.com/news/opinion/commentary/la-oe-welch-mammograms-
20101020,0,2961910.story.
World Health Organization (2011). WHO statistical information system. Geneva: World
Health Organization. Retrieved April 20, 2012 from http://www.who.int/whosis.
http://www.who.int/cancer/FINAL-Advocacy-Module%206.pdf

19
CHAPTER TWO
LITERATURE REVIEW
2.1 Focus of Review
The review provided insight into what breast cancer is, the various types of breast
cancer, factors that cause breast cancer and increase the mortality rate among young and old
women. It, furthermore, emphasized the need for preventive rather than curative measures
through early detection techniques, noting the role of breast cancer campaigns in advancing
this course. The Health Belief Model (HBM) and Attitude-Change Theory gave explanation
to the reasons why women still suffer and die from this disease despite some levels of
awareness generated through campaigns. To this end the review focused on the following:
Breast Cancer : An overview
Awareness, Knowledge and Exposure to Campaigns against Breast Cancer
Breast Self Examination, Other Screening Methods and Early Detection
Review of Empirical Works
Theoretical Framework
2.2 Breast Cancer: An Over View
Breast cancer is a dreaded disease and a principal cause of cancer mortality among
women worldwide and in Nigeria. It is the most common cancer among women and some
men who are hypogonadic (men with BRCA1 and BRCA2 genetic mutations). BRCA1 and
BRCA2 are human genes that belong to a class of genes known as tumor suppressors.
Changes in BRCA1 and BRCA2 genetic cells therefore result in breast cancer (National
Cancer Institute 2009 p.2&4). Cells in the breast begin to grow uncontrollably and invade
other normal cells and tissues, spreading to various parts of the body (invasive breast cancer)
in such a way that the normal body cells and tissues are obstructed from carrying out their

20
usual functions. When this happens, the normal cells that are being obstructed from
performing normally are said to have been strangulated to death. The uncontrollable cells
develop into tissues in a collection known as malignant tumours which are fatal. The ones,
however, that grow without spreading (non invasive breast cancer) and overtaking normal
cells are called benign tumours because they are not terminal.
A review of breast biopsies in the Lagos University Teaching
Hospital showed 34 per cent of all breast biopsies done over a10-
year period to be malignant. A report from Zaria described the mean
age at presentation of breast cancer as 42 years with 30 percent
occurring in women less than 25 years of age. At University College
hospital, Ibadan, 74 percent of breast cancer patients were pre
menopausal. A ten year review of breast cancer in Eastern Nigeria
revealed that patients with breast cancer constituted 30 per cent of all
patients with breast disease and that 69% of these patients were pre-
menopausal. (Salaudeen, Akande &Musa 2009 p.2)
Reports have also shown that of all malignancies typical of affluent societies, black
people appear to be at a greater risk than whites and the whites at higher risk than Asians.
Among Nigerian women, the peak age of breast cancer presentation is about 10-15years
earlier than what is observed in Caucasian women, where it occurs between the ages of 35-45
years (World Cancer Report 2011). This as we have come to understand is due to diverse
genetic risk factors and environmental factors that may affect each woman‟s susceptibility to
the disease. Life style and dieting are other factors that have been identified with
predispositions to the disease. A wrong eating habit without exercises to burn out or break
down huge fat levels of calories, results in an overall energy imbalance in the body system
and exposes one to breast cancer related diseases and breast cancer. Also, The World Cancer
Report (2011p.8) notes that, a highly caloric diet, rich in fat, refined carbohydrates and
animal protein, combined with low physical activity, is associated with a multitude of disease
conditions, including obesity, diabetes, cardiovascular disease, arterial hypertension and
cancer. Other causative factors have been identified as including reproductive history,
genetics and radiation (especially at times of breast development).

21
Breast cancer has been known and dreaded overtime. This is because its presentation
at the initial stage is as a painless lump that may not be detected without critical examination.
Again, treatments are often surgical and most times result in death. That is why advocacy
campaigns are geared towards early detection through the provision of awareness and
knowledge on genetic risk factors and other socio cultural factors that make women
vulnerable to the disease. Campaigns also emphasize the need for positive attitude and
periodic practice of Breast self examination (BSE), Clinical Breast Examination (CBE), and
other screening practices as preventive or early detection methods. Okobia, Bunker &
Okonofua (2006 p.13-19) therefore emphasize that for women to present early at the hospital
they need to be "breast aware"; and that they must be able to recognize symptoms of breast
cancer through routine practice of practicable screening.
Late detection and diagnosis are the result of increased Breast cancer mortality rates
in developing countries. Due to late presentations at the hospital, breast cancer accounts for
23% of all cancers in women with an annual occurrence of over one million cases of the
disease and 411,000 deaths (Akpo, Akhator & Akpo 2010 p.2). This, without any form of
doubts has been the reason for aggressive campaign efforts to fight the disease as far back as
the 19th century.
Early campaigns included the "Women's Field Army", run by the
American Society for the Control of Cancer (the forerunner of the
American Cancer Society) during the 1930s and 1940s. Explicitly
using a military metaphor, they promoted early detection and
prompt medical intervention as every woman's duty in the war on
cancer. In 1952, the first peer-to-peer support group, called Reach
to Recovery, was formed. Later taken over by the American
Cancer Society, it provided post-mastectomy, in-hospital visits
from women who had survived breast cancer, who shared their
own experiences, practical advice, and emotional support, but
never medical information. This was the first program designed to
promote restoration of a feminine appearance, e.g., through
providing breast prostheses, as a goal (Sulik 2010 p.37–38).

22
It is true to observe that previous campaign efforts to fight breast cancer dwelt on curative
measures rather than preventive. That was why programme planners had options of providing
artificial body parts for those who lost their breasts to surgery. The emphasis today, however,
rests on the need for prevention and early detection through aggressive and comprehensive
campaign policies and programmes that will promote the desired knowledge, attitude and
practice among women toward prevention and screening practices.
From a global perspective, there is strong justification for focusing cancer prevention
activities particularly on two main cancer-causing factors - tobacco and diet. The World
Cancer Report (2011p.5), citing Bengoa, Director, Management of Non-communicable
disease at WHO; explains the need to continue efforts to curb infections which cause cancers.
2.3 Awareness, Knowledge and Exposure to Campaigns against Breast Cancer.
The cause of breast cancer has not been completely ascertained. As a result, it cannot
be said with all certainty what the cause of breast cancer is. However, medical prognosis has
attributed the cause to certain genetic/hereditary factors, environmental factors and life style.
From this end, it can be stated categorically that breast cancer can be prevented and that your
life is in your hand since an individual‟s actions play a vital role in making lower cancer risk
a reality. This was properly captured in a statement made by Chris & Beng (2010 p.4) citing
Marilyn Gentry, the President of the American Institute of Cancer Research.
Know that cancer can be prevented and your actions play a vital
role in making lower cancer risk a reality to you and your family.
. . there are things you can do today to reduce your risk of cancer.
Not quick but basic lifestyle and dietary changes that will mean a
lower cancer risk for life
When people know that the factors that cause breast cancer are within their control, all they
need to know is what should be done at a given time and what should not be done. For

23
instance it has been emphasized that meals rich in calories and fat, animal protein and refined
carbohydrates should be consumed with caution. This is because they can be very harmful
especially when not backed up with activities to break down energy. With this knowledge the
women are empowered. All they need to do is control the levels of fat intake and consume
healthy diets. This control however will to a large extent be determined by their perception of
susceptibility to the disease and severity, benefits and barriers that can hinder positive
behaviour.
In the same light, perceived susceptibility to the threat of breast cancer, perceived
severity, coupled with modifying factors like age, knowledge, ethnicity, sex, personality and
socioeconomic factors will determine one‟s likely hood of attitude and actions based on
perceived benefits minus perceived barriers (Stretcher & Rosenstock 1997 p.34). Similarly,
Olweus (1993), identified variables such as age, gender, geographical location and level of
education as socio-demographic factors associated with certain harmful health behaviours.
In addition, two research studies conducted in 1980 and 1982 respectively by Leathar
and Roberts (1985 p.668-670), in 1985 gave a more elaborate report on attitudes towards
screening practices and made older women its central focus. The study was titled older
women‟s attitude towards breast disease, self examination and screening facilities:
implications for communication. Using Focus Group Discussion, the study identified
appropriate strategies for communication.
The results showed that knowledge of breast disease and screening facilities was poor
and that many psychological and emotional issues inhibited self examination.
It revealed, however, that increased information about BSE, CBE is unlikely to influence
attitude and practice unless it is presented together with emotional support, provided by
setting breast screening within general health screening rather than emphasizing the single
disease through mass media channels.

24
Results also revealed that, specific beliefs about breast cancer association with breast
feeding and pills were underdeveloped and not clear, awareness that women aged over 40
were more at risk was superficial although it was generally accepted that older women were
more susceptible to cancer. More so, the terminal nature of the disease dominated their
thoughts rather than early detection. And women concluded that any lump found was bound
to be malignant. Surgery was the only method of treatment they could mention.
It therefore identified, social class, poverty, age, poor knowledge and confusion about
the symptoms and extent of the disease, as psychological and emotional issues that inhibit
screening practices
The study illustrated that negative or positive attitudes were determined by
psychological and emotional issues since the dominant attitude expressed by respondents in
the focus group discussion showed that the topic was threatening. The psychology of losing a
breast owing to late detection felt abnormal and gave the affected woman a feeling of being
incomplete. Also, pity from friends and relations and the fear of possible death from the
disease greatly hindered thoughts of practicing screening. The thought of discovering a lump
could not be withstood by many because most of them concluded that any lump found was
bound to be malignant. There was uncertainty about what to look out for. They were also
pessimistic about learning or teaching the correct procedure.
Reasons for not using screening facilities were largely unrelated to factual knowledge,
though factual information was incomplete or inadequate. Wrong attitude towards screening
is emotionally based. The fear of a negative outcome is strong enough to make women refuse
screening.
The implication for communication therefore was that using media channels alone to
advocate for screening practices would only increase anxiety unless the means to resolve it
are provided; such means as emotional support. The study recommended that screening

25
should be carried out in the context of general health screening rather than emphasizing a
single disease. Since the policy that breast screening should be practiced as a single exercise
may not be quite appropriate for older women particularly those belonging to the working
class.
In a similar light, the knowledge of age factor in higher breast cancer risk is expected
to make women devoted to periodic screening and self examinations for early detection.
However, knowledge of age as a risk factor in the development of breast cancer is not enough
to influence practice of screening but the benefits of screening and threat of late detection
without screening, is more likely to prompt adoption of screening at older age. So the link
between knowledge, attitude and practice is thick. Knowledge influences attitude and positive
attitude culminates into practice.
It is, therefore, very important that campaigns inform adequately, paying particular
attention to barriers that hinder adoption of the desired behaviour. The World Cancer Report
(2011p. 8) provides that the following diet restrictions and controlled life style will enhance
lower cancer risk. The following practices can help protect you from breast cancer:
Restrict the amount of red meat in your diet
Increase your fiber intake by eating plenty of whole grain of cereals, fruits and
vegetable
Enjoy alcohol in moderation
Plan to have your first baby before the age of 30 years.
When you have babies, breast-feed them; the longer, the better.
Go for regular screening of your breasts
Perform self-breast examination monthly and regularly
Learn all that you can about breast cancer.

26
2.4 Practice of Preventive Measures: BSE, CBE, Mammography and Genetic
Testing
There are so many things to look out for in BSE, CBE, Mammography, Genetic
testing and other screening methods. The following symptoms may suggest the onset of
breast cancer. Breast lump(s) or thickness, dimpling or puckering, unusual pain, a sore that
does not heal around the nipples, itching or rash, retracted (turned in) nipples, change of
shape or size, bloody discharge from the nipple, arms swelling or lump in the armpit (World
Cancer Report 2011p.10)
The essence of screening practices is to detect the symptoms that are not visible to the
eyes and those that cannot be detected by mere palpating of the breast. For instance,
mammography screening can detect breast lumps but might not pick out other breast diseases
like breast fibroid and cysts. In this case a breast biopsy screening test will be required to
check for other related diseases. When a lump or other abnormality is detected in the breast,
through BSE, or CBE the doctor will use many investigative techniques to arrive at a specific
diagnosis as possible. Detecting one or any of these symptoms therefore depends on women‟s
attitude towards detection and practice of screening.
The most successful advancement in the fight against cancer so far has been the early
detection of cervical cancer by cytology and of breast cancer by mammography. A recent
analysis by an International Agency for Research on Cancer (IARC) working group
concluded that under trial conditions, mammography screening may reduce breast cancer
mortality by 25-30% and that in nation-wide screening programmes a reduction by 20%
appears feasible (World Cancer Report 2011p.9)
The screening techniques available for detecting breast cancer include diagnostic
mammography, ultrasound scan, cutting-needle biopsy and open biopsy. In diagnostic
mammography, an X-ray procedure is used to detect any breast abnormalities in women. It is

27
advisable that all women should have a mammogram at least once every three years to help
them detect cancer early. Other studies prescribe an annual practice.
The ultrasound scan produces a photographic picture of soft tissues in great details. It
is used as a tool to detect lumps in the breasts. It is also widely used in gynecological
investigations. (Lagos State Ministry of Health 2009 p. 6)
Cutting-needle biopsy technique involves removing a small amount of tissue from a
lump for further investigation. Under local anesthetic a special needle is inserted into the
lump in order to withdraw a fine core of tissue from it. The open biopsy however is an
alternative to cutting-needle biopsy. This involves cutting the skin of the breast open to
remove the entire lump for further investigation. It is very appropriate for women over the
age of 30 years with an obvious breast lump to have it removed for further analysis. (Lagos
State Ministry of Health 2009 p.6)
Though cancer can be prevented, it can also be treated. This, however, depends on the
stage of presentation and the extent to which the disease has caused damage to the body. That
is why the emphasis of campaigns remains prevention. The extent to which late presentation
can destroy is fatal and cannot be overemphasized. When it is detected early before it
becomes terminal, it can be treated. The most common modes of treatment have been
identified as drugs, surgery, radiation therapy, or a combination of these modes of treatment.
(Lagos State Ministry of Health, 2009 p. 7)
For Genetic testing, looking out for mutation of Deoxyribonucleic Acid (DNA) genes
is the concern of experts since mutation is linked with development of hereditary breast and
ovarian cancer. They identify these changes and give appropriate treatments to ensure
normality. Normal cells, BRCA1 and BRCA2 help ensure the stability of the cell‟s genetic
material (DNA) and help prevent uncontrolled cell growth.
Men with these mutations also have an increased risk of breast cancer. Both men and

28
women who have harmful BRCA1 or BRCA2 mutations may be at increased risk of other
cancers. In other words, a woman who has inherited a harmful mutation in BRCA1 or
BRCA2 is about five times more likely to develop breast cancer than a woman who does not
have such a mutation. BRCA1 and BRCA2 are human genes that belong to a class of genes
known as tumor suppressors. Genetic tests are therefore available to check for BRCA1 and
BRCA2 mutations.
Several methods are available to test for breast cancer BRCA1 and BRCA2 mutations.
It has been established that most of these methods look for changes in BRCA1 and BRCA2
DNA, and changes in the proteins produced by these genes. Often times, a combination of
methods are used. (National Cancer Institute, 2009 p.14)
A blood sample is required for these tests, coupled with genetic counseling before and
after the tests. Screening methods, such as Magnetic Resonance Imaging (MRI), in women
with BRCA1 or BRCA2 mutations; Mammography, BSE, CBE can be used. (National
Cancer Institute, 2009 p.14)
It has, however, been observed that though there is a general awareness about the
disease, knowledge about the need for other preventive or early detection methods like
Genetic testing is minimal. Also people do not see the benefit of Genetic testing until more
than two family members present with the disease. Below is another review that found that
change in attitude and adoption of screening as a new behaviour was largely associated with
involvement of relations and friends in the practice or presentation of lump. This, perhaps,
explains their perception of susceptibility to the disease.
In this review of study conducted by Sule (2011 p.27-31), on the topic “Breast Cancer
Awareness and Breast Examination Practices Among Women in the Central Hospital Warri,
Delta State”, a population of women between ages 20-80 were interviewed, and the findings
revealed among other things that:

29
Breast cancer awareness was noted in 96.1% of the respondents.
43.6 % of the respondents knew breast cancer begins with a breast
lump. Self breast examination had been practiced in 45.5% of
respondents. Of this number, 83.3% of the practitioners did so at least
monthly. Clinical breast examination had been experienced in 15.6%
of the respondents. The practice of breast self examination was
significantly associated with previous breast complaints, a previous
breast procedure, previous clinical breast examination and having a
family member or acquaintance with breast cancer
The study recommended that health campaigns should be aimed at increasing the practice of
Breast Self Examination. And that training of nurses in regional centers with the art of
Clinical Breast Examination (CBE) will increase compliance of women in this useful
screening tool since less than 50% of respondents engaged in the practice of breast self
examination and the entire respondents considered CBE practice dismal.
Another review on the study: “Knowledge and Attitudes to Breast Cancer and Breast
Self Examination Among Female Undergraduates in Kwara State in Nigeria”; by Salaudeen,
Akande and Musa (2009 p.157-163), interviewed a sample population of seven hundred
people and demonstrated that majority of respondents were aware of breast cancer as a
disease entity, but that their knowledge and understanding of the disease was very low. The
study came up with the results below.
Six hundred and eighty two (97.2%) respondents had ever heard of
breast cancer. Only two hundred and fifty seven (36.7%) had good
knowledge of the cause of breast cancer among the respondents. Less
than half (45.5%) of respondents had good knowledge of symptoms of
cancer of the breast. Five hundred and twenty seven (75.3%)
respondents viewed breast cancer as a frightful disease. Five hundred
and seventy three (81.9%) respondents had heard of breast self
examination. Most respondents did not know what to look for during
breast self examination. Only 38.9% and 37.4% of respondents knew
that during breast self examination it is necessary to check the size of
the breast and colour. On the attitudes of respondents to breast self
examination, only one hundred and twenty eight (18.3%) respondents
care to seek for knowledge about breast self examination. Even
though more respondents had heard of breast self examination, only
two hundred and nine (29.8%) respondents claimed they know how to
perform it.

30
The study also showed that a good number of people are indifferent about knowing
what they should know about the disease. This in the researchers‟ view suggested that such
attitude was due to their belief that breast cancer is a rare disease and that they could never be
affected by it. According to the findings, only about 130 respondents cared to seek for or
increase their knowledge about the disease.
The study, therefore, recommended that Breast cancer awareness campaign is
necessary to improve early breast cancer detection. It also stressed the need for further studies
to address the knowledge gaps on breast cancer and breast self examination so that positive
attitudes can be developed by the young adults towards breast self examination.
Looking at the empirical reviews in this study, one very important fact seems
consistent in them. Levels of awareness were considerably high yet practice was grossly
inhibited. This means there is a need for campaigns to be strategically pointed towards
activating the emotional nodes of the people if attitude must change. The emotional factors
that inhibit screening practices must be duly attended to. And reasons for failure of campaign
programmes have been because the messages do not address the emotional barriers that
inhibit attitude change and practice. The Health Belief model and Attitude Theory which
form the theoretical frame work of the study, therefore, explain how these emotional factors
can be addressed to bring about change to a desirable extent.
2.5 Theoretical Framework
This study is anchored on The Health Belief Model and Attitude Change Theory.
The Health Belief Model
The Health Belief Model (HBM) is a social cognition model, developed by Irwin M.
Rosenstock in 1966. It is a health behaviour change and psychological model for studying
and promoting medical programmes of some public health services. In the 1970s and 1980s

31
the model was furthered by Becker and her colleagues. Subsequently, it was modified as late
as 1988, to accommodate emerging realities within the health community about the role that
knowledge and perceptions play in personal responsibility. Originally, the model was
designed to predict behavioural response to the treatment received by chronically ill patients,
but recently it has been used to predict more general health behaviours.
The HBM suggests that your belief in a personal threat together with
your belief in the effectiveness of the proposed behaviour will predict
the likelihood of that behaviour. The underlying concept of the
original HBM is that health behaviour is determined by Personal
beliefs or perception about a disease and the strategies available to
decrease its occurrence and that personal perception is influenced by a
whole range of intrapersonal factors affecting health behaviour.
(Taylor et. al 2007, as in Hochbaum, 1958)
Therefore, the original model had these constructs below which were subsequently
modified to explain other important issues and events that needed to be explained within the
concept of the constructs: Perceived susceptibility, Perceived severity, Perceived benefits and
Perceived barriers.
In perceived susceptibility an individual's assessment of their risk of getting the
condition, is determined by his knowledge about the risk. This, therefore, means that the
greater the perceived risk, the greater the likelihood of engaging in behaviours to decrease the
risk. Based on this perception, an individual will see the possibility of contracting breast
cancer especially males who believe it is entirely a disease condition for women while some
women will see the need for screening practices, because of the perception they have and the
knowledge that the disease can be treated if detected early. Based on this perceived
susceptibility, their attitude and practice will be informed. They will be motivated to go for
screening or not. It is expected that perception of increased susceptibility, will prompt healthy
behaviours while decreased susceptibility will increase unhealthy behaviours. However, some
people do not care about their susceptibility. They stick to unhealthy lifestyle and behaviour

32
whether or not it makes them predisposed to high breast cancer risk. (Taylor, et al 2007 p.34,
citing Maes & Louis 2003). Again, Nwana (2009), notes that certain health behaviours are
determined by one‟s sexuality and perception, of the characteristics of a particular sexuality;
given that in some parts of the world, drunkenness is synonymous to males. Also, women are
more prone to consumption of foods high in cholesterol.
In perceived severity, an individual's assessment of the seriousness of the condition
and its potential consequences is influenced by his medical information or knowledge and his
belief about the disease (Tailor et al, 2007 p.34, citing McCormick 1999). Some men might
perceive that the disease is not for men and that it is a condition associated only with females.
In this sense they do not perceive it as serious and so might not see the need for genetic
testing. However, medical sciences have identified men with BRCA1 and BRCA2 genetic
mutations with very high breast cancer risk and other cancers (National Cancer Institute,
2009 p.1).
When perceived susceptibility is combined with severity it becomes perceived
threat. The perceived threat that breast cancer cannot be treated except, detected early will
likely prompt positive attitude towards periodic screening. However, just as in perceived
susceptibility, threat does not always bring about change in attitude or practice. Some older
people will remain indifferent no matter the threat.
Also, in perceived benefits an individual's assessment of the positive consequences
of adopting the behaviour will bring about change. Also, knowing the usefulness of the new
behaviour in decreasing the risk of developing a disease will bring change. People will not
cut down on foods rich in calories, exercise or reduce intake of red meat if they do not know
the benefits they will derive from not eating it. Similarly, those who see early detection as
benefit for screening or BSE will undergo it than those who do not.

33
Again, perceived barriers refer to an individual's assessment of the influences that
facilitate or discourage adoption of the promoted behaviour. Change is a difficult thing for
some people who tend to be very resistant to new behaviours. So breaking the barriers that
hinder change is very tasking. So this is the most significant of all the constructs of the HBM
in determining behaviour change. Though the threat of breast cancer can motivate adoption of
Breast Self Examination (BSE) and other screening practices, the barriers to performing BSE
tend to exert a greater influence over practice than the threat of cancer itself. The benefits of
the new behaviour must, therefore, outweigh that of the old one for change to take place.
(Taylor et al 2007 p.33, citing Janz & Becker 1984; Champion & Menon 1997; Elingson
&Yarber 1997; Umeh & Rogan-Gibson 2001).
Shea and Remoker (2011 p.2) added two more constructs to the previous four namely:
Cues to action: instigators to readiness which include events, people and things that
move people to change their behaviour. For instance illness of a friend, family
member or even media reports etcetera (Taylor et al 2007 p.33, citing Graham 2002)
Self efficacy: belief in one‟s ability to take action to produce desired outcomes.
The concept of self efficacy was introduced by Bandura in the 1970s as task specific self-
confidence, and then other scholars took to better conceptualisations.
Taylor, et al (2007 p.34) broadened the constructs further as follows:
Expectations, which are the product/sum of perceived benefits, barriers and self-
efficacy. This may be seen as indicative of the extent to which the individual will try
to take a given action (Taylor et. al, 2007, citing Smedslund, 2000)
Cues to action: this refers to reminders or prompts to take actions consistent with an
intention, ranging from advertising to personal communications from health
professionals, family members and/or peers.

34
Demographic and socio-economic variables. These may include age, race, ethnicity
(cultural identity), education and income. These are an individual‟s personal factors
that affect whether the new behaviour is adopted.
Attitude-Change Theory
The Attitude Change Theory was developed from propaganda theories in the 1930s
during World War II (Baran & Davis 2012 p.175). The theory explains that there are pre-
existing attitudes, whether biological or psychological which have to be changed if selected
messages must have any effect on the target audience. Again, it explains that these pre-
existing attitudes are in-depth and, therefore, stand as barriers to effective penetration of
messages for desired change. Thus an intellectual and emotional strategy of communication
will influence change if properly channeled to do so. Change in evaluations and perceptions
of an individual‟s predispositions will take place if the required modification favours his
expectations, if it is tied to someone he admires, or if it is bound to be beneficial to him
(Wood, 2000 p.539).
According to Breckler and Wiggins (1992 p.407), attitude has a profound influence on
behavior. It influences the perception of objects and people‟s exposure to, and comprehension
of information. Eagly and Chaiken (1995 p.413), also view attitude from an angle of effects
and evaluation when they described attitude as a tendency or predisposition to evaluate an
object or symbol of that object in a certain way. Again, Park (2009) perceive attitude as more
or less a permanent way of behaviour acquired by social interactions. This means that, one‟s
attitude is affected by intrapersonal and inter personal factors relative to acquired knowledge.
This theory, therefore, explains three bases for attitude change, which include
compliance, identification, and internalization. These three processes demonstrate the
different levels of attitude change (Wood, 2000 p.539).

35
Compliance refers to a change in behaviour based on consequences, such as an
individual‟s hopes to gain rewards or avoid punishment from another group or person. The
individual does not necessarily experience changes in beliefs or evaluation towards an
attitude object, but he resorts to a change in behaviour due to the results he intends to get out
of his adoption of a new cognition. There is also awareness that he or she is being urged to
respond in a certain way perceived as positive (Wood, 2000 p.539).
Identification explains one‟s change of beliefs and actions in order to be similar to the
one he admires. In this case, the individual changes not because of what he intends to get
from the attitude but because it is associated with an admired one. This seems like
reinforcement theory where significant others have an influence in people‟s behaviour.
Internalization refers to adoption of an attitude due to the content of the perceived
attitude. At this level of attitude change, the individual‟s evaluation towards a perceived
attitude changes when he finds the content of the attitude to be intrinsically rewarding. The
new attitude or behaviour is consistent with the individual‟s value system, and tends to be
merged with the individual‟s existing values and beliefs. Therefore, behaviour towards some
object is a function of an individual‟s intent, which is a function of one‟s overall attitude
towards the action. The Expectancy-value theory is based on internalization of attitude
change (Wood, 2000 p.539).
When a group of people with different ways of thinking and biological make up are
made aware of a specific requirement there is bound to be obstacles in the way and manner
they receive and accept messages. So efforts must be made to achieve a unified attitude that
will favour a desired cause; and such efforts must appeal or activate the emotional nodes of
the people for positive attitude change. The war, therefore, provided a platform for the
warlords to reason that there are psychological barriers to persuasion and processes (ways
forward) that will enable a given set of messages to overcome those barriers. As such they

36
devised means of detecting these barriers to the practice of persuasive messages and assess
how effectively selected messages could overcome the barriers (Baran & Davis 2012 p. 175).
The theory identifies that existing attitudes or mental predispositions need to be
changed or channeled to a particular cause through an intellectually and emotionally binding
strategy (Baran & Davis 2012 p.175).
In the campaign against breast cancer, possible barriers to knowledge acquisition,
positive attitude and practice of campaign messages may include psychological, emotional
and physical. Psychological when women see issues with opening up to modern medicine
when they detect or observe body changes that may be harmful to their bodies and conceal
their observations due to shyness or cultural beliefs. Physical, when screening facilities are
not reachable or available, or medical specialists are limited. Emotional, when the fear of
being diagnosed of the disease overrides the need for early detection.
The campaign messages must, therefore, be structured to detect these obstacles to
effective communication and assess how effectively, selected messages can overcome them.
The strategy must appeal to the attitude of the people as this is a major determinant of
effective practice.
Baran and Davis (2012 p.184), submit the strengths and weaknesses of the attitude-
change theory as follows. On the positive note, they observe that the theory pays deep
attention to process in which messages can and cannot have effects. Again it provides insight
into influence of individual differences and group affiliations in shaping media influence.
Finally, attention to selective processes helps clarify how individuals process information.
On the negative, experimental manipulation of variables overestimates their power
and underestimates the media‟s. Also, it focuses on information in media messages, not on
more contemporary symbolic media and it uses attitude change as the only measure of effects
ignoring reinforcement and more subtle forms of media influence.

37
2.6 Summary of Literature
The review looked at breast cancer on a general perspective, explaining the types of
breast cancer, the major causes which are genetic and environmental, and reasons for the high
incidence and mortality rates. It also looked at the major preventive or screening methods
known to women and emphasized the need for prevention using these methods, or the need
for treatment as the case may be.
The review equally examined the relationship between awareness, knowledge,
attitude and practice as determinants of positive or negative influence on the formation of
one‟s health behaviour and ability to make decisions on adopting an acceptable life style.
Four empirical works related to this study were reviewed and this brought about some
relevant findings on attitude and practice of screening methods: CBE, BSE, Mammography
and Genetic testing.
The study was given a theoretical support using the Health Belief Model and Attitude
Change theory. In addition, the four constructs on which the Health Belief Model was based
were explained, and the strengths and weaknesses of the attitude change theory were also
submitted in this review.

38
References
Akpo, E. & Akpo, M. Akhator, A. (2010). Breast cancer knowledge and screening practices
among Nigerian medical students. Delta: Delta State University. The Internet Journal
of Health. 11 (2). Retrieved April 18th, 2012 from http://www.ispub.com/journal/the-
internet-journal-of-health/volume-11-number-2/breast-cancer-knowledge-and-
screening-practices-among-nigerian-medical-students.html
Baran, S. J. & Davis, D. K. (2012), Mass communication theory: Foundations, ferment,
and future. (6th ed). United States: Wadsworth Cengage Learning
Breckler, S. J. & Wiggins, E. C. (1992). On defining attitude and attitude theory: once more
with feeling. In A.R. Pratkanis, S. J. Breckler, & A. C. Greenwald (Eds), Attitude
structure and function. Hillsdale, NJ: Erlbaum. P 407
Chris, K. H T. & Beng I. (2010). Knowing your breasts. minimizing breast cancer
risk! understand risk factors, preventive measures and early detection. Malaysia.
http://www.bookoncancer.com/productDetail.php?P_Id=8
Eagly, A.& chaiken, S. (1995). Attitude strength, attitude structure and resistence to change.
In R. Petty and J. Kosnic (Eds) Attitude strength. (PP 413- 415) Mahuah NJ: Erlbaum.
Health belief model, (2012). Retrieved May 5th, 2012 from
http://en.wikipedia.org/wiki/Health_belief_model
Lagos State Ministry of Health, (2009). Breast cancer. Lagos state: Breast Cancer
Organization. http://www.brecan.org /
Leathar, D. S., & Roberts. M. M. (1985). Older women's attitudes towards breast disease,
self examination, and screening facilities: Implications for communication.
Edinburgh: Springwell House. British Medical Journal. Vol. 290. March.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1417626/pdf/bmjcred00436-0016.pdf
Loewensten, G. (2007). Affect regulation and affective forecasting. In Gross, J. J. (Ed.)
Handbook of emotion regulation (pp. 180–203). New York: Guilford. http://en.wikipedia.org/wiki/Health_belief_model
National Cancer Institute. (2009). Cancer type risk factors and possible causes, prevention
detection and diagnosis. Espanol: NCI publications.
http://www.cancer.gov/cancertopics/factsheet/Risk/BRCA
Okobia M. N, Bunker, C. H., Okonofua F.E.,& Usifo O. (2006). Knowledge, attitude and
practice of Nigerian women towards breast cancer: a cross-sectional study. Edo state:
university of Benin. February 21, World J Surg PMCID: PMC1397833 Oncol.
doi: 10.1186/1477-7819-4-11
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1397833/ retrieved April 18th
2012
Park, K. (2009). Parks textbook of preventive and social medicine (20th ed). India:
Banarsidas Bhanot Publishers.

39
Sulik, G. (2010). Pink ribbon blues: How breast cancer culture undermines women's health.
New York: Oxford University Press. ISBN 0199740453
Salaudeen A. G., Akande T. M., Musa O. I. (2009). Knowledge and attitudes to breast
cancer and breast self examination among female undergraduates in a state in
Nigeria. Kwara state Nigeria: University of Ilorin. European Journal of Social
Sciences. 7 (3). http://www.eurojournals.com/ejss_7_3_15
Sule, E. A. (2011). Breast cancer awareness and breast examination practices among women
in a Niger delta hospital. Delta state: Wilolud Journals,
Continental J. Medical Research 5 (1) pp27 - 31, ISSN: 2141 – 4211
http://www.wiloludjournal.com
Stretcher, V., & Rosenstock, I.M. (1997). The Health Belief Model. In Glanz K., Lewis F. M.,
& Rimer B. K., (Eds). Health behaviour and health education: Theory, research and
practice. San Francisco: Jossey- Bass. PP 31-36. Retrieved on May 5th 2012
from http://www.health_belief_model.org
Shea, N., & Remoker C. (2011). The health belief model. PP 1-3.Retrieved on May 5th,
2012 http://www.Nicole_shea_and_catriona_Remoker_The_Health_Belief_Model
The World Cancer Report, (2011). Breast cancer statistics
http://canceraustralia.nbocc.org.au/breast-cancer/about-breast-cancer/breast-cancer-
statistics
Taylor, D., Bury M., Campling, N., Carter S., Garfied, S., Newbould, J., & Rennie, T.
(2007). A Review of the use of the health belief model (HBM), the theory of
reasoned action (TRA), the theory of planned behaviour (TPB) and the trans-
theoretical model (TTM) to study and predict health related behaviour change.
London: University of London. National Institute for Health and Clinical Excellence
(NIHCE). Retrieved on May 5th, 2012 from http://www.nice-
doh_draft_review_of_health_behaviour-theories.pdf
Wood, W. (2000). "Attitude Change: Persuasion and Social Influence". Annu. Rev.
Psychol 51: 539–570. Retrieved from http://en.wikipedia.org/w/index.php?title=Attitude_change&oldid=489610647

40
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Research Design
The research design considered apt for this study is survey. This is because the nature
of the study requires that the researcher solicits for audience response in order to determine
the level of awareness and knowledge level among women in Benue State about the causes of
breast cancer, prevention, early detection and treatment.
Personal interviews were, therefore, suitable to generate data which substantiated the
data from the questionnaire; while a well designed questionnaire was used to collect
quantitative data, which answered the research questions raised earlier.
Four persons were interviewed; three of them were females that fall within the
specified age range for this study, and the last was an oncologist. The questions structured for
the interview, answered the research questions substantially.
From the foregoing, it can be deduced that a research design is a laid down guide for
the researcher, with which he structures his study scientifically or systematically. It is a
strategy or blue print specifying which approach will be used for gathering and analyzing
data. (Ngwu 2011 p.62 citing Chukwuemeka 2002 p.31)
3.2 Population of the Study
The Population of the study was made-up of women in Benue State from age fifteen
and above who reside in the 23 local government areas in the State from which a
representative sample was drawn.
This population was 2,109,598 in the 23 local government areas in Benue State; who
were fifteen years and above (National Population Commission Census Report 2006).
The rationale for this selection includes the following:

41
Females within that age range have a greater susceptibility to breast cancer
They fall within the puberty stage when breast development starts,
reproductive and menopausal stages when the disease is most likely to present
They comprise of the group of people to whom the campaigns on knowledge,
attitude and practice towards screening are targeted.
3.3 Sampling Size
The percentage of the population of study to be sampled for objective analysis is the
sample size. Ngwu (2011p.51) explains that a sample is part of the entire population that is
selected for investigation. Samples are the actual elements that are observed or investigated
out of the entire elements within the Universe of study.
Using the Australian Calculator, by the National Statistical Service (NSS) the
following data were imputed and it automatically generated the sample size. According to
this formula, once the values for the following variables are provided, the calculator derives
the others. The variables supplied include:
Confidence level = 95percent
Proportion = 0.5
Population= 2,109,598
Confidence interval (standard error) = 0.05
In using the Australian calculator, it is expected that the researcher selects the
confidence level at which percentage error is estimated, enter the population size and the
proportion. The proportion is however taken to be 0.5 if left blank. It is also required that the
researcher fills in one of the confidence level, standard error, relative standard error or sample
size. Once these values are provided, the „calculate‟ button can be punched and the sample
size will be automatically generated.
42
The following explain the meaning of the variables used in the Australian calculator.
Confidence Level: This refers to the level of certainty at which the researcher estimates the
percentage error. Often times, the 95% confidence level is used.
Proportion: This shows the expected size of the population likely to have the desired
attribute sought for in the survey in a 50:50 probability rating which is one over two (½) or
50percent.
Confidence Interval: This allows that the researcher provides the desired accuracy expected
from the estimate.
Standard Error: This indicates the degree to which an estimate may differ from the actual
value derivable from a complete study.
Relative Standard Error: This is derived by comparing the ratio of standard error to the
actual estimate, expressed as a percentage.
From the Australian calculation, the minimum sample size for the study is 385. This is,
however, referred to as the basic sample size according to the National Statistical Service
(NSS); given that the basic sample size does not make provisions for eventualities that may
arise in the course of distributing the questionnaire. NSS therefore recommends the use of a
contingency in order to meet the need of enlarging the sample size to complement for the
possibility of lost copies of the questionnaire while on transit or during distribution.
Based on this, the researcher conducted an over sampling, in line with the
recommendation of some renowned scholars like Bertlett, Kotrlik and Higgins (2001 p.46),
citing Salkind (1997 p.107), Fink (1995 p.36) and Cochran (1977 p.396). In their opinion, the
sample size should be increased by 40% - 50% to account for „uncooperative subjects‟. Here,
the researcher is expected to estimate the anticipated response rate in percentage and divide
the basic sample size by that response rate.
Presented below is the calculation for contingency by Bertlett, Kotrlik and

43
Higgins (2001 p.46)
n2 = Minimum sample size
Anticipated response rate
Where anticipated return rate = 95%.
Where n2 = sample size adjusted for response rate.
Where minimum sample size = 385.
Therefore:
Minimum sample size 385
n2 = Anticipated response rate = 95%
n2 = 385/0.95 = 405.2632
The sample size for the study is therefore 405.
3.4 Sampling Techniques
The probability sampling technique was employed in the study, with particular
reference to the multi stage sampling technique. This technique requires that at each stage of
sampling, two or more techniques can be employed. Thus two major techniques were
employed: the cluster sampling and the simple random sampling techniques. Ikponmwosa
(2006 p.143) explains that the simple random sampling technique allows an equal chance for
each member of the defined population, appropriately, represented by a sample size, to be
selected. Again, Ikponmwosa (2006 p.148), explains that in a cluster, the population is
subdivided into defined segments in order to reduce it to such a size as would permit a
realistic and adequate representation of the population while reducing the cost of the research.
In this study, a cluster already exists from the three senatorial zones of the state. From
the three senatorial zones A, B and C, where there are 7, 7 and 9 Local Government Areas
(LGA) respectively, the researcher selected randomly, three LGAs each from zones A
(Vandeikya, Katsina-Ala, Kwande) and B (Gboko, Buruku and Makurdi); and 5 LGAs from

44
zone C (Ado, Otukpo, Apa, Ogbadigbo and Okpokwu). So from a total of eleven LGAs, the
copies of the questionnaire were distributed.
The copies of the questionnaire per zone were arrived at by dividing the number of
LGAs in each zone by the total number of LGAs in the state, multiplied by the sample size.
The copies of the questionnaire per zone were eventually divided by the number of randomly
selected LGAs of each zone. So, the six LGAs from zones A and B had 41 copies of the
questionnaire each, since 123.26 copies were the allocation for zones A and B each. The
5LGAs in zone C however had 31.70 copies of the questionnaire each, since 158.48 copies
were meant for the zone.
Table of Zones, LGA/Population and Copies of Questionnaire per Zone
ZONES LGAs POPULATION COPIES OF
QUESTIONNAIRE
PER
ZONE
ZONE A(NE) KATSINA-ALA 111378 7/23 X405=123.26
KONSHISHA 112300
KWANDE 123200
LOGO 83501
UKUUM 108255
USHONGO 95873
VANDEIKYA 117118
ZONE B (NW) BURUKU 102560 7/23 X405=123.26
GBOKO 180656
GUMA 96846
GWER WEST 60549
GWER EAST 83373
MAKURDI 146239
TARKA 39497
ZONE C (BS) ADO 92022 9/23 X405=158.48
AGATU 57119
APA 48122
OBI 49564
OJU 84271
OTUKPO 129799
OGBADIGBO 66141
OKPOKWU 86403
OHIMINI 34812
TOTAL 23 LGAs 2109598 405
SOURCE: NATIONAL POPULATION COMMISSION CENSUS REPORT 2006

45
3.5 Measuring Instrument
The questionnaire was carefully designed to accommodate the major variables in the
study; the variables being breast cancer campaigns, knowledge, attitude and practice.
Personal interviews were also used to substantiate the responses gathered from the
questionnaire
These were used as the measuring instruments and measurements ranged from access
to campaigns, awareness of breast cancer campaigns, to knowledge of breast cancer,
causative factors and screening practices as preventive measures.
3.8 Validity and Reliability of Instrument
The expected results tallied with previous empirical works. The questions were
structured to elicit response and make the analysis of data objective. Answers that were not
very well expressed on paper were covered for adequately by responses from the personal
interview. However, face validity technique was done to ensure the validity of the
questionnaire and interview questions. The instruments were given to the project supervisor
and some lecturers in the Department of Mass Communication, University of Nigeria Nsukka,
before distribution.
The concept of reliability is crucial in any study and even more crucial depending on
the research design selected. This is because, if a survey study is to be objective, its measures
and procedures must be reliable. Reliability is arrived at when repeated measurement of the
same material results in similar decisions or conclusions (Wimmer & Dominic 2011p.170).
Based on this a test-re-test was done as, the questionnaire was administered to 24
respondents twice at an interval of one week in a pilot study after they had been validated and
the data collected at both intervals were compared to see if they met the expected reliability
rate. Anaekwe (2002), explains that test-re-test method involves administering one test to the
same group of people on two different occasions and the two scores obtained, used to

46
compute a correlation co-efficient, which is interpreted as an estimate of reliability. The
formula for calculating reliability by Pearson is given below.
r= N∑XY - ∑X∑Y
-----------------------------------------
√N∑X2 – (∑X)
2 √N∑Y
2 – (∑Y)
2
Where X refers to the frequency figure on variable X, Y is a frequency figure on
variable Y and N is the number of subjects measured on both variables.
Table for Computing Correlation Coefficient
Number of
scale
measurement
Practice of screening
methods(test 1 )
X
Practice of screening
methods (test 2)
Y
(XY)
(N) (X) X2 (Y) Y
2 (XY)
01 10 100 9 81 90
02 6 36 6 36 36
03 8 64 9 81 72
Total 24 200 24 198 198
From the table above, N= 3, ∑X=24, ∑Y= 24, ∑XY= 198, ∑X2= 200,
∑Y2=198, (∑X)
2=576, (∑Y)
2=576
Computation:
r= N∑XY - ∑X∑Y
-----------------------------------------
√N∑X2 – (∑X)
2 √N∑Y
2 – (∑Y)
2
r= 3(198) – (24) (24)
-------------------------------------------
√3 (200) – 576 √3 (198) – 576
r= 594 – 576
------------------------------------
√600 – 576 √594 - 576
r= 18
----------------------
√24 √18

47
r= 18
---------------------
4.9 x 4.2
r= 18
------------------- = 0.87
20.58
In Osuala‟s opinion (2005p.149), a high correlation coefficient indicates high
reliability of measuring instrument. For this study, the reliability correlation co-efficient, of
the questionnaire, showed 0.87, so the instrument is considered reliable.
3.6 Method of Data Collection and Analysis
A self-administered questionnaire was developed and personal interviews were
conducted. Data were collected primarily from the respondents through the responses
provided on the questionnaire and the interview sessions. The instrument contained a total of
31 questions, consisting of structured questions on breast cancer awareness and knowledge,
screening practices and other descriptive characteristics. The descriptive characteristics
included age, religion, level of education, and occupation. The questions on breast cancer
knowledge and screening practices as well as those for descriptive characteristics consisted of
selected response items such as yes/no, don‟t know, and constructed response items. Results
were tabulated.
Data were analyzed using frequency distribution tables and simple percentages in a
descriptive analysis, to examine the characteristics of the population and correct responses to
questions on breast cancer, early detection by screening methods and prevention through
genetic testing and other screening methods. Also to examine their attitude and practices
towards prevention through the clinical techniques mentioned above and through others like
dietary control.

48
References
Bertlett, J. Kotrlik, J. & Higgins, C. (2001). Organisational research: Determining
appropriate sample size in survey research. Information Technology, Learning and
Performance Journal. 19 (1) pp.43-50
Chukwuemeka, E. O. (2002). Research methods and thesis writing: A multi- disciplinary
approach. Obiagu Enugu: Hope- Rising Ventures Publishers.
Ikponmwosa, O. (2006). Fundamentals of statistics in education and the social sciences.(3rd
ed) lagos, Accra: National book consortium
National Statistical Service, (2012). Australian calculator. Retrieved 6th May, 2012
from http://www.nss.gov.au/nss/home.nsf/NSS/0A4A642C712719DCCA2571AB00
243DC6?opendocument
National Population Commission, (2006). Census report. UNFPA in Benue State: Annual
report. http://nigeria.unfpa.org/benue.html. Retrieved 6th May, 2012
Ngwu, C. S. (2011). Nigerian newspapers coverage of the 78 days presidential vacuum
crisis under late President Umaru Musa Yar’adua: A study of the Daily sun,
Guardian, The Nation and Vanguard newspapers. Unpublished thesis Enugu State
University of Science and Technology, (ESUT), Enugu.
Nwodu, C. L. (2006). Research in communication and other behavioural sciences: Principles
methods and issues. Enugu: Rhyce Kerex publications
Osuala, E. C. (2005). Introduction to research methodology (3rd
ed.). Onitsha:
Africana-First Publishers Limited.
Wimmer, R. D. & Dominic, J. R. (2011). Mass media research: An introduction. (9th ed),
Wadsworth: Cengage

49
CHAPTER FOUR
DATA PRESENTATION AND ANALYSIS
4.1 Data Presentation and Analysis
The researcher sampled a total of 405 respondents; using simple percentages and
tables for data analysis. The questionnaire had a total of 31 questions consisting of
descriptive data and structured questions on breast cancer awareness and knowledge, attitude
and screening practices.
The following tables were used to analyze data generated from the questionnaire and
interview sessions.
Demographic Information
Table 1: Sex Distribution
Sex
Distribution
No. of
Respondents Percentage
Males 0 0%
Females 404 100%
Total 405 100%
Field survey 2012
Data in table one, show that none of the respondents was a male and 405 respondents
representing 100% were females. This is because the disease condition is rare amongst males
and more predominant among females.
Table 2: Occupation
Occupation
No. of
Respondents Percentage
Civil servants 81 20%
Business 58 14.3%
Students 203 50.1%
Any other 63 15.6%
Total 405 100%
Field survey 2012
Data in table 2 indicate that 81 or (20%) of the respondents were civil servants, 58 or
(14.3%) business women, 203 or (50.1%) were students and 63 or (15.6%) specified that they

50
were applicants and unemployed people. This data provided information on the level of
activity or involvement among women and how this might be a factor in attending clinical
breast examination (CBE) or carrying out breast self examination (BSE).
Table 3: Educational Qualification
Educational
Qualification
No. of
Respondents Percentage
None 63 15.6%
SSC 150 37%
Diploma 60 14.8%
B.A /B.Sc. 70 17.3%
M.A./M.Sc. 62 15.3%
Total 405 100%
Field survey 2012
Table 3 reveals that 63 respondents representing 15.6% of the total number of
respondents, do not have any form of educational qualification, 150 or (37%) have SSC
educational qualification, 60 respondents or (14.8%) have diploma qualification, 70
respondents or (17.3%) either have a B.A or B.Sc. and 62 respondents or (15.3%) are second
degree (M.A/M.Sc.) holders.
This reveals the fact that, education is not a barrier to their access to information on
breast cancer; as most of the respondents have had some levels of educational training. Thus
they can get information if they want to.
Table 4: Breast cancer status
Status
No. of
Respondents Percentage
Free 405 100%
Infected 0 0%
Total 405 100%
Field survey 2012
As presented in the table 4 above, the total number of respondents 405 or (100%)
sampled are not infected with the disease. This result, however, lacks authenticity from
medical diagnosis as their response is based on their personal body assessment and belief.

51
Table 5: Age Distribution
Age
distribution
No. of
Respondents Percentage
15-25 203 50.1%
26-36 70 17.3%
37-47 102 25.2%
48 and above 30 7.4%
Total 405 100%
Field survey 2012
This result shows that 203 or (50.1%) of the respondents were in the age bracket of
15- 25, 70 or (17.3%) of the respondents in the range of 26-36, 102 or (25.2%) fall within the
range of 37- 47 and 30 respondents or (7.4%) within range 48 and above.
This age representation tallies with the researcher‟s target age group which is 15 years
and above. People within these ranges, fall within the breast development stage, puberty and
menopausal stages when susceptibility to breast cancer is relatively high.
Awareness and Knowledge about Breast Cancer
Table 6: Awareness of breast cancer campaigns
Awareness
No. of
Respondents Percentage
Yes 300 74.1%
No 45 11.1%
Not sure 60 14.8%
Total 405 100%
Field survey 2012
The data as presented above explain that 300 or (74.1%) respondents were aware of
sensitization campaigns about breast cancer, 45 or (11.1%) respondents said they were not
aware of the campaigns while 60 or 14.8%) of the respondents said they were not sure
whether or not there were campaigns against breast cancer. This data indicate that, awareness
level about breast cancer campaigns is relatively high.

52
Table 7: Exposure to breast cancer campaigns
Exposure
No. of
Respondents Percentage
Yes 250 62%
No 100 24%
Not sure 55 14%
Total 405 100%
Field survey 2012
Table seven shows that 250 or (62%) of the respondents were exposed to breast
cancer campaigns, 100 or (24%) were not exposed while 55 or (14%) of the respondents were
not sure of their exposure to the campaigns. This data explain that awareness about campaign
programmes does not guarantee exposure to the programmes as people tend to be selective on
whether or not to participate in the programmes.
Table 8: Source of Information about Breast Cancer
Information source
No. of
Respondents Percentage
Friends/Street van shows 40 10%
Relations 62 15%
Media 223 55%
Doctors/Seminars 80 20%
Total 405 100%
Field survey 2012
From the above table, data can be represented as follows: that 40 respondents
representing 10% of the total number sampled referred to friends and street van shows as
their sources of breast cancer information, 62 or (15%) of the respondents said their relations
are their sources, 223 or (55%) named the media- print/electronic as their sources of
information and 80 or (20%) said medical doctors and medical seminars on the subject were
their sources of breast cancer information. This suggests that campaigns through the media
are not the only sources of information, even though they are the major sources.

53
Table 9: Aim of the campaigns
Aim of the
campaigns
No. of
Respondents Percentage
Early detection 70 17.3%
Prevention 155 38.3%
All of the above 180 44.4%
Total 405 100%
Field survey 2012
Table nine shows that 70 respondents or (17.3%) saw early detection as the sole aim
of breast cancer campaigns, 155 or (38.3%) of the respondents said prevention is the aim of
the campaigns while 180 or (44.4%) of the respondents said both prevention and early
detection cannot be separated as campaigns were aimed at achieving any of them. From the
above, some people emphasized prevention through avoidable actions while others placed
value on early detection. Whatever be the case, early detection remains the chief determinant
of a successful treatment
Table 10: Knowledge about breast cancer
Knowledge about breast cancer
No. of
Respondents Percentage
A breast disease that kills 284 70%
It can be treated if detected early 61 15%
It presents as a painless lump 40 10%
It is an uncontrolled growth of cells in the breast 20 5%
Total 405 100%
Field survey 2012
From table ten, we can state that 284 or (70%) respondents know that breast cancer is
a disease that kills; 61 or (15%) know that it can be treated if detected early, 40 or (10%)
know that it presents as a painless lump and 20 or (5%) know that it is an uncontrolled
growth of cells in the breast. This is an indication that, knowledge about breast cancer as a
disease condition is relatively high.

54
Table 11: Treatable Stage of Breast Cancer
Treatable stage of
breast cancer
No. of
Respondents Percentage
Early 284 70%
Middle - -
Late - -
Don‟t know 121 30%
Total 405 100%
Field survey 2012
The above table presents that, 284 or (70%) of the respondents know that breast
cancer (BRCA) can only be treated at its initial or early stage, while 121 or (30%) do not
know the stage at which BRCA can be treated. This is why the need for campaigns to
emphasize early detection in all screening procedures is important. This agrees with
information provided by the Lagos State Ministry of Health, (2009) that, though, cancer can
be prevented it can also be treated depending on the stage of its presentation (invasive or non
invasive stage), and the extent to which the disease has caused damage to the body. The
extent to which late presentation at the hospital can destroy is fatal and cannot be
overemphasized. When it is detected early before it becomes terminal, it can be treated using
the most common modes of treatment which have been identified as drugs, surgery, radiation
therapy, or a combination of these modes of treatment.
Table 12: Knowledge of Early Stage
Knowledge of early stage
No. of
Respondents Percentage
Shortly before symptoms become obvious 284 70%
Much later - -
When condition can no longer be treated - -
Don‟t know 121 30%
Total 405 100%
Field survey 2012
Data here show that, 284 or (70%) of the respondents know that before symptoms
become obvious, breast cancer stage is early and should be given appropriate treatment while
121 or (30%) respondents do not know when to say it is early or late. This data emphasizes

55
the need to enhance in-depth knowledge among women to ensure their safety.
Table 13: Relevance of Genetic Test
Need for genetic
test
No. of
Respondents Percentage
Yes 162 40%
No 81 20%
Not sure 162 40%
Total 405 100%
Field survey 2012
Data here represent that, 162 or (40%) of the respondents said „yes‟ to genetic test, 81
or (20%) said „no‟ and 162 or (40%), said they were not sure that genetic test should be done.
This shows that knowledge about genetic test is low; as a result most of the respondents
seemed indifferent about it. Also, it has not been ascertained that genetic testing is attainable
in Nigeria. However, it is important to note that a woman, who has inherited a harmful
mutation in BRCA1 or BRCA2 Deoxyribonucleic Acid (DNA), is about five times more
likely to develop breast cancer than a woman who does not have such a mutation. BRCA1
and BRCA2 are human genes that belong to a class of genes known as tumor suppressors.
Genetic tests are, therefore, available to check for BRCA1 and BRCA2 mutations (National
Cancer Institute, 2009 p.14)
Table 14: Knowledge of genetic factors as causative of BRCA
Knowledge of
genetic factors as
causative of BRCA
No. of
Respondents Percentage
Yes 162 40%
No - -
Not sure 243 60%
Total 405 100%
Field survey 2012
Again, table 14 indicates that 162 or (40%) of the respondents were knowledgeable
about genetic factors being causative of BRCA while 243 or (60%) were not sure whether or
not BRCA is caused by genetic factors. This explains the reason why most of the respondents

56
did not appreciate the need for genetic testing. The saying that knowledge is power is,
therefore, an understatement.
Table 15: Dieting/Nutrition, Breast Cancer Causative Factor
Dieting/nutrition,
BRCA causative
factor
No. of
Respondents Percentage
Yes 365 90%
No - -
Not sure 40 10%
Total 405 100%
Field survey 2012
From table 15, it is quite obvious that 365 or (90%) of the respondents said „yes‟ to
diet as a causative factor of BRCA and 40 respondents representing 10% of the respondents
said they were not sure of dieting being a cause of BRCA. This data indicate uncertainty
about the causes of the disease condition. This is an aspect that is, also, not known to medical
practitioners. As a result they simply restrain it to genetic and environmental causes.
Table 16: Control of Intake of Calories or Excess Fat in Diet
Control of intake of calories
No. of
Respondents Percentage
Reduced consumption of foods high in calories 90 22%
Reduced consumption of white flours 94 23%
High intake of vegetables 72 18%
Regular exercises 68 17%
Nothing 81 20%
Total 405 100%
Field survey 2012
Data from table 16 provides that 90 of the respondents or (22%) control intake of
calories by reducing the consumption of foods high in calories, 94 or (23%) reduce their
consumption of white flours, 72 or (18%) of the respondents consume high amounts of
vegetables instead, 68 or (17%) engage in regular exercises while 81 or (20%) do nothing to
control intake of calories. This data prove that despite some levels of knowledge and
awareness that consumption of foods high in calories is unhealthy; some group of people will

57
not make efforts to adopt healthy nutritional values. This is in contrast with the health belief
model where individuals adopt certain health behaviours based on perceived benefits that can
be derived from such new behaviours. Here perceived benefits do not stimulate attitude
change or adoption of a new health behaviour. In line with this, Olatunde (1979) opined that
perceived benefits and perception of admirable characteristics or health attitude in significant
others and oneself influences negative or positive health behaviours and attitudes. For
example the perception of one‟s self as possessing strong immunity against infections could
encourage negative health attitudes and behaviours
Table 17: Underestimation of Risks Status
Underestimating
risks status
No. of
Respondents Percentage
Yes 284 70%
No 40 10%
Not sure 81 20%
Total 405 100%
Field survey 2012
From the table above, 284 or (70%) of the respondents said that there were people
who underestimated their risk status, 40 or (10%) said „no‟, people did not underestimate
their risk status and 81 or (20%) of them said, they were not sure whether or not people
underestimated their risk status. It is, however, true that the level of knowledge of the cause
of BRCA can make people underestimate their risks status. There are people who do not feel
threatened even with the increasing knowledge of susceptibility resulting from genetic factors.
Such people seem to have certain belief that hinge on the fact that they cannot be infected.
Table 18: Over Estimation of Risks Status
Over estimating
risks status
No. of
Respondents Percentage
Yes 365 90%
No - -
Not sure 40 10%
Total 405 100%
Field survey 2012

58
From the table above, it can be interpreted that 365 or (90%) of the respondents said
that there were people who overestimated their risks status while 40 or (10%) of them said
they were not sure if people overestimated their risk status. This result, therefore, agrees with
the opinion by Olson (2002 p.240–242); Welch (2010 p.16); and Sulik (2010 p.74, 263) that
too much of awareness causes guilt, fear, anxiety, depression and negative attitudes of self
isolation in breast cancer patients. This implies that too much of awareness and knowledge
about breast cancer and the threat of susceptibility will agitate people to overestimate their
risks status
Table 19: Other Causes of Breast Cancer
Other causes of BRCA
No. of
Respondents Percentage
BRCA related infections (breast fibroid and cyst) 101 25%
Money or phone in the bra/exposure to radiation during
breast development 41 10%
Don‟t know 263 65%
Total 405 100%
Field survey 2012
In this table, 101 or (25%) of the respondents named BRCA related infections as other
causes of BRCA, 41 or (10%) named money or phone in the bra and exposure to radiation
during breast development as a factor that causes BRCA, while 263 or (65% ) said they did
not know other causes of BRCA. According to The World Cancer Report (2011p.8), a highly
caloric diet, rich in fat, refined carbohydrates and animal protein, combined with low physical
activity, is associated with a multitude of disease conditions, including obesity, diabetes,
cardiovascular disease, arterial hypertension and breast cancer. Other causative factors have
been identified as including reproductive history, genetics and radiation (especially at times
of breast development).

59
Table 20: Symptoms of Breast Cancer
Symptoms of BRCA
No. of
Respondents Percentage
Lumps, pains, swelling 300 74%
Reddening of nipples/dimpling 40 10%
Don‟t know 65 16%
Total 405 100%
Field survey 2012
Data here show that 300 or (74%) of the respondents know that BRCA presents as
lumps, pains and swelling, 40 or (10%) of them said it presents as reddening of nipples and
dimpling of the breast while 65 or (16%) of them said they did not know the symptoms of
BRCA presentation. This implies, therefore, that not every female knows how BRCA
presents itself. However, the following symptoms may suggest the onset of breast cancer.
Breast lump(s) or thickness, dimpling or puckering, unusual pain, a sore that does not heal
around the nipples, itching or rash, retracted (turned in) nipples, change of shape or size,
bloody discharge from the nipple, arms swelling or lump in the armpit (World Cancer Report
2011p.10)
Table 21: Audience Stand on Genetic Test for Hereditary Syndrome of Breast Cancer
Stand on genetic test for
hereditary syndrome of BRCA
No. of
Respondents Percentage
Yes 284 70%
No - -
Not sure 121 30%
Total 405 100%
Field survey 2012
Data from table 21 above show that, 284 or (70%) of the respondents agreed that
families that have hereditary syndrome predisposing to BRCA should go for genetic testing
while 121 or 30% of them said they were not sure whether or not such families should go for
genetic testing. However, to ease or reduce the fear of overestimating risk status and the
anxiety that every female in the family is not safe, it is wise for such families to go for
genetic testing. It will reveal risk status and may reduce the need for other forms of screening.

60
In line with the above, Ferrandis, Andreu and Galdón (2002 p.27), citing (Sattin et al.,
1985), explain that “a family history of breast cancer is a clear risk factor for developing the
disease. In effect, women who have a first degree relative with breast cancer have a 2- to 3-
fold higher risk of developing the disease, while women who have both the mother and a
sister with breast cancer are 14 times more likely to develop the disease than patients without
a family history of breast cancer”.
Table 22: Knowledge of Peak Age of Breast Cancer Presentation in Blacks
Knowledge of peak age of
BRCA presentation in blacks
No. of
Respondents Percentage
Yes 100 25%
No 150 37%
Not sure 155 38%
Total 405 100%
Field survey 2012
From the above, 100 respondents representing 25% of the total number of the
respondents know the peak age of BRCA presentation in blacks, 150 or (37%) of them, did
not know and 155 or (38%) were not sure of the peak age of BRCA presentation. This
explains the fact that most females do not know the peak periods when they should expect
BRCA presentation and thus look out for symptoms thoroughly. However, reports have
shown that of all malignancies typical of affluent societies, black people appear to be at a
greater risk than whites and the whites at higher risk than Asians. Among Nigerian women,
the peak age of breast cancer presentation is about 10-15years earlier than what is observed in
Caucasian women, where it occurs between the ages of 35-45 years (World Cancer Report
2011p.8).

61
Table 23: Frequency of Visit to Health Centers for Clinical Breast Examination (CBE)
Frequency of CBE
No. of
Respondents Percentage
Often 50 12%
Very often 10 2%
Not often 75 19%
Not at all 270 67%
Total 405 100%
Field survey 2012
Figures from table 23 make it obvious that, 50 or (12%) respondents visit health
centers for CBE, 10 or (2%) very often, 75 or (19%) not often, while 270 or (67%) of the
respondents do not visit health centers at all. This is an indication of low practice rate for
CBE. Olweus (1993) identified variables such as age, gender, geographical location and level
of education as socio-demographic factors associated with certain health behaviours whether
positive or negative.
Table 24: Practice of Breast Self Examination (BSE)
Practice of BSE
No. of
Respondents Percentage
Yes 324 80%
No 81 20%
Total 405 100%
Field survey 2012
Table 24 shows that 324 or (80%) of the respondents practiced breast self
examination while 81 or (20%) did not. This shows that though a good number of females did
not visit health centers for CBE, they practiced BSE conveniently. The World Cancer Report
(2011p.10), however, emphasizes that, the essence of screening practices is to detect the
symptoms that are not visible to the eyes and those that cannot be detected by mere palpating
of the breast. For instance, mammography screening can detect breast lumps but might not
pick out other breast diseases like breast fibroid and cysts. In this case a breast biopsy
screening test will be required to check for other related diseases, after which the doctor uses
several investigative techniques to arrive at a specific diagnosis as possible.
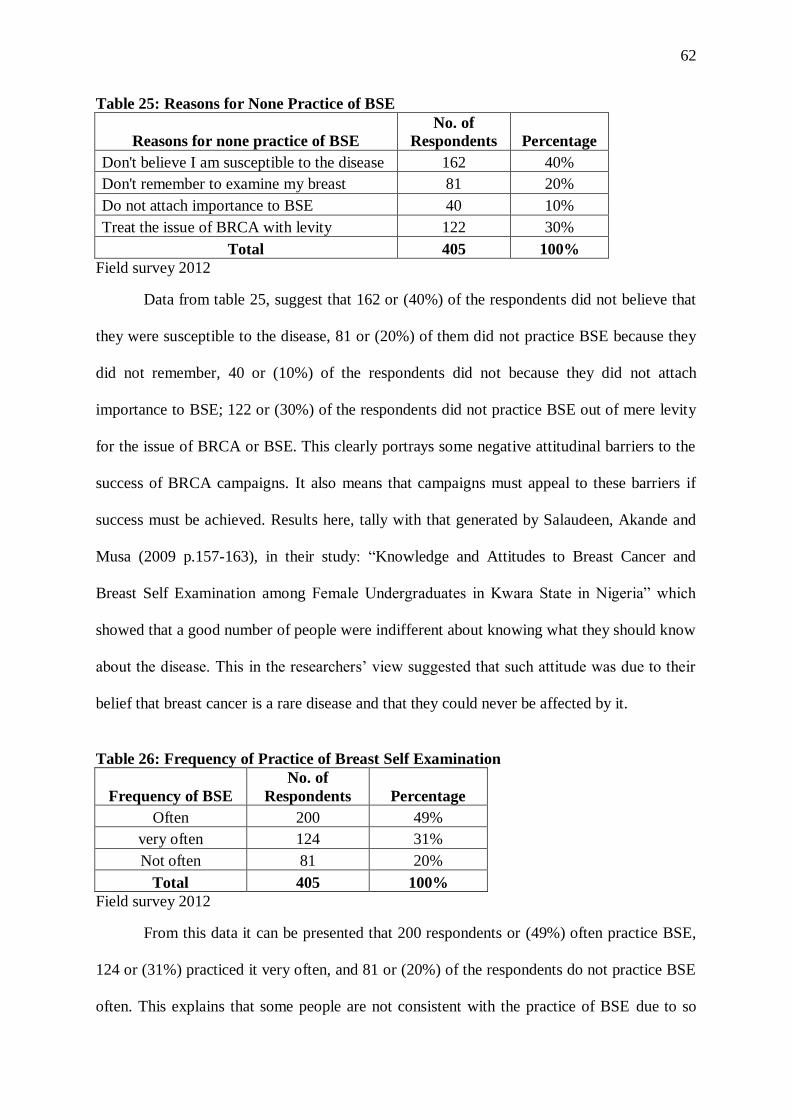
62
Table 25: Reasons for None Practice of BSE
Reasons for none practice of BSE
No. of
Respondents Percentage
Don't believe I am susceptible to the disease 162 40%
Don't remember to examine my breast 81 20%
Do not attach importance to BSE 40 10%
Treat the issue of BRCA with levity 122 30%
Total 405 100%
Field survey 2012
Data from table 25, suggest that 162 or (40%) of the respondents did not believe that
they were susceptible to the disease, 81 or (20%) of them did not practice BSE because they
did not remember, 40 or (10%) of the respondents did not because they did not attach
importance to BSE; 122 or (30%) of the respondents did not practice BSE out of mere levity
for the issue of BRCA or BSE. This clearly portrays some negative attitudinal barriers to the
success of BRCA campaigns. It also means that campaigns must appeal to these barriers if
success must be achieved. Results here, tally with that generated by Salaudeen, Akande and
Musa (2009 p.157-163), in their study: “Knowledge and Attitudes to Breast Cancer and
Breast Self Examination among Female Undergraduates in Kwara State in Nigeria” which
showed that a good number of people were indifferent about knowing what they should know
about the disease. This in the researchers‟ view suggested that such attitude was due to their
belief that breast cancer is a rare disease and that they could never be affected by it.
Table 26: Frequency of Practice of Breast Self Examination
Frequency of BSE
No. of
Respondents Percentage
Often 200 49%
very often 124 31%
Not often 81 20%
Total 405 100%
Field survey 2012
From this data it can be presented that 200 respondents or (49%) often practice BSE,
124 or (31%) practiced it very often, and 81 or (20%) of the respondents do not practice BSE
often. This explains that some people are not consistent with the practice of BSE due to so

63
many reasons. Leathar and Roberts (1985 p.668-670), in their two research studies conducted
in 1980 and 1982 respectively, gave a more elaborate report on attitudes towards screening
practices as they noted that some of the reasons for women‟s indifference to consistent
practice of BSE were that, the terminal nature of the disease dominated their thoughts rather
than early detection. Again, women concluded that any lump found was bound to be
malignant so, the thought of discovering a lump could not be withstood by many. They, also,
feared that surgery as a method of treatment was deadly. The researchers, therefore, identified
social class, poverty, age, poor knowledge and confusion about the symptoms and extent of
the disease, as psychological and emotional issues that inhibit screening practices.
Table 27: What to Look Out For When Conducting BSE
Focus of BSE
No. of
Respondents Percentage
Lumps, swelling and pains 300 74%
Reddening of nipples 20 5%
Dimpling of breast/ orange-like skin texture 20 5%
Not sure 65 16%
Total 405 100%
Field survey 2012
This result indicates that 300 or (74%) of the respondents looked out for lumps, pains
and swelling during BSE, 20 or (5%) of them looked out for reddening of nipples and breast
dimpling respectively, while 65 or (16%) were not sure of what to look out for. This reveals
that the most common symptoms females have knowledge about are, the presence of lumps,
swelling and pains. As such only a few of them have knowledge about reddening, dimpling
and an orange-like skin texture as symptoms of BRCA presentation.
Table 28: Ideal Period for Breast Self Examination
7-10 days AMP ideal for BSE
No. of
Respondents Percentage
Yes 305 75%
No - -
Not sure 100 25%
Total 405 100%
Field survey 2012

64
This table reveals that 305 or (75%) of the respondents said „yes‟ to 7-10days after
menstrual period as an ideal time for breast examination, 100 or (25%) of them said they
were not sure of the most suitable time for breast examination. Field surveys have shown that
some days after menstrual period is ideal to ensure that females do not confuse pains or
swelling associated with menstrual periods for BRCA symptoms
Table 29: Mammography as a Form of Early Breast Cancer Detection Technique
Stand on Mammography,
as a detection technique
No. of
Respondents Percentage
Yes 290 72%
No 65 16%
Don't know 50 12%
Total 405 100%
Field survey 2012
Results here reveal that 290 or (72%) of the respondents know that mammography is
a form of early breast cancer detection technique, 65 or (16%) of them said it was not a form
of early BRCA detection technique, and 50 or (12%) of them did not know whether or not it
was a form of early BRCA detection technique. This also emphasizes inadequate knowledge
of screening methods.
Table 30: Removal of Breast Lump Altering the Risks of Breast Cancer Recurrence
Removal of lump altering
BRCA risks
No. of
Respondents Percentage
Yes 284 70%
No 40 10%
Not sure 81 20%
Total 405 100%
Field survey 2012
Figures from the above table indicate that, 284 or (70%) of the respondents know that,
the removal of breast lump does not alter the risks of predisposition to breast cancer, 40 or
(10%) said that, it alters the risks of predisposition to BRCA while 81 or (20%) of them were
not sure whether or not removal of breast lump alters the risks of predisposition to breast

65
cancer. This also emphasizes the shallow nature of knowledge about the disease condition of
BRCA.
Table 31: Dimpling, Swelling, Redness and Lumps as signs of Breast cancer
Signs of BRCA
No. of
Respondents Percentage
Yes 340 84%
No - -
Don't know 65 16%
Total 405 100%
Field survey 2012
Field survey from table 31 above shows that, 340 or (84%) of the respondents know
the signs to look out for when palpating the breast, while 65 or (16%) of them did not know
what signs to look out for.
Interview Questions
First Segment of Interview: three females within the age bracket for this study.
Note that the text below are not the exact words of the interviewees as the texts were
paraphrased to ensure clarity, given that some of the interviewees were not familiar with
medical terminologies like breast self examination, even though they had an idea of it. Again,
one of the interviewees mixed her tenses with Pidgin English. In cases like that the researcher,
paraphrased with clearer words.
1. Number of Breast Cancer Campaigns Attended Since 2008
Exposure to campaigns Respondents
Since 2008, I have not attended any breast cancer campaigns but I stumbled
on an open van street campaign around Wadata market in June this year and
I stood by to get what they had to say. Patience
I have not attended any in Benue state since 2008 Mercy
None. Katherine
Field survey 2012

66
2. Knowledge level of BRCA risk factors, prevention, early detection and treatment due
to exposure to campaigns
Knowledge level due to exposure to campaigns Respondents
Due to my exposure to TV, newspapers and health magazines, I am kept
abreast of information about breast cancer. I also know that the major
treatment is surgery and that when lumps are detected they have to be
removed surgically too. Mercy
In my community development group, this subject was treated, coupled
with the street show I stumbled on. I also have doctor friends whom I gist
with about health issues including breast cancer. I know that there is a need
for early detection through self examination. Patience
I know about BSE, how to position my body for breast examination and
what to look out for. I got this information from a television programme
titled: „The Thrift Collector‟. Katherine
Field survey 2012
3. Knowledge of Breast Cancer
Knowledge of what BRCA is Respondents
It is a disease that affects the breast of females and it kills if not treated at an
early stage. Katherine
Is a disease condition that causes pains in the breast, lumps, swelling and
results in death if not detected early for treatment. Mercy
Breast cancer is a deadly breast disease. Patience
Field survey 2012
4. Knowledge of Screening Methods
Knowledge of screening methods
The three respondents had knowledge about Breast Self Examination (BSE) and Clinical
Breast Examination (CBE), even though they could not give it the actual name. They were
not aware of biopsy screening tests and mammography or even genetic test.
Field survey 2012

67
5. Knowledge of Ideal Frequency for Practice of BSE, CBE, Mammography and genetic
tests
Knowledge of ideal frequency for screening practice
As a result of the level of knowledge about screening methods, they could only say the ideal
periods to practice BSE and CBE; and as they rightly noted, these should be practiced
monthly and seven to ten days after menstruation to avoid confusing possible BRCA
symptoms with menstrual symptoms.
Field survey 2012
6. Relevance of Preventive Practices
Reason for Practice
Life is sacred. Women play dual roles in the family. As mothers they need to be breast
healthy for their babies and as wives they have to be healthy for their husbands and so that
they do not feel socially unaccepted due to mastectomy (entire breast removal) as the case
may result into.
Field survey 2012
Second Segment of Interview, with an Oncologist
In this segment of the interviews, a breast surgeon name with held for reasons he
would not disclose, provided answers to some of the questions raised. He works with the
Federal Medical Center in Makurdi, Benue state. He refused the recording of the interview
and said that he would prefer to be referred to as anonymous. The following are the responses
he gave. It is however important to note that the texts used were not his exact words. This is
because; the session was not recorded and then, some medical jargons had to be simplified
for better understanding.

68
Question 1: Causes of Breast Cancer
Causes of BRCA
In responding to this question, the doctor noted that there are no specific causes of BRCA
identified so far. However, he said that breast cancer (BRCA) mutations can be attributed to
basically genetic and environmental factors which can, also, be referred to as natural and
manmade. The genetic causes according to him are those that are concerned with
Deoxyribonucleic Acid (DNA) traits and how they are transferred by blood from generation
to generation. While the environmental causes are due to consumption of unhealthy diets,
like excess fats, polished carbohydrates, lack of physical exercises to enhance internal
balance, and exposure to radiation especially during early periods of breast development.
These environmental factors extend to unhealthy lifestyle, the use of cosmetics with some
harmful chemicals used in their production and so on
Field survey 2012
Question 2: Black Women and BRCA predisposition
Skin colour and predisposition to BRCA
The doctor expressed his contrary opinion to what the question actually suggests.
According to him, blacks are not more predisposed to BRCA and that there are no medical
facts to prove otherwise. He said that as a matter of fact, not until recently, statistics have
shown that blacks enjoyed a relatively low or no incidence rate of BRCA. He, therefore,
vehemently disagreed with the notion that blacks were more predisposed to BRCA.
However, some reports insist that blacks are more predisposed than whites and whites than
Asians, yet they do not provide reasons for their argument.
Field survey 2012
Question 3: Relevance of Genetic Testing
Relevance of genetic testing
It is necessary to ensure clarity of risks amongst relations and generations. Especially in
families where more than one or two first degree relations have shown obvious symptoms
or actually suffered from Breast cancer (BRCA). Though it is not yet certain that this is
obtainable anywhere in Nigeria, it is a very good idea to test for possible changes in BRCA
mutations.
Field survey 2012

69
Question 4: Breast Cancer Mortality Rate in Benue State
BRCA Mortality rate in Benue State
Generally, statistics have not provided specific figures for mortality rates in Benue state or
even Nigeria. It is however deducible from annual world reports that the estimated
incidence rate for Nigeria in 2010 and subsequent years is very high and this invariably
applies to the state too.
Field survey 2012
Question 5: Treatable Stages of Breast Cancer
Stages of BRCA
He also noted the types of breast cancer (BRCA) when he identified stages 0-IV of breast
cancer. Where zero is used to represent non-invasive breast cancer a type as he noted that
can be treated by lumpectomy which is removal of the infected tissues and a lymph node
biopsy might also be required to evaluate the state of the nodes since cancer travels fast
through them. All forms of breast cancers that have exceeded stage 0 are invasive and tend
to spread round the body. A type of invasive BRCA was identified as metastatic breast
cancer which, though, not as aggressive as the inflammatory type of invasive breast cancer,
is also deadly. He further explained that, the non-invasive BRCA develops in parts of the
breast and remain (sometimes) within that region without extending to other tissues or
regions of the body. Also, that the non-invasive types of cancers are mostly benign and can
be cured. On the other hand, the invasive cancers being that which invade a part of the body
and spread to other parts destructively cannot be cured. Finally, he emphasized that, unless
BRCA is detected at stage zero, treatment is never curable, as the disease will always have a
recurrence.
Field survey 2012
Question 6: Screening Centers in Benue State
Screening Centers in Benue State
He explained that he was not certain about the number of screening centers in the State but
identified some available at the Benue State Teaching Hospital in Makurdi, equipped by the
MTN Foundation; and others at the Federal Medical Center Api.
Field survey 2012

70
4.2 Discussion of Findings
The discussion was guided by the five research questions for the study. The following
are, therefore, answers to the research questions drawn from the objectives of the study in
chapter one. These answers were reached from the findings of the field survey research.
Research Question 1
What is the level of awareness among women in Benue State about campaigns on the
causes, prevention, early detection and treatment of breast cancer (BRCA)?
Questions six and 10 from the questionnaire were used to elicit for audience response on their
level of awareness about breast cancer campaigns.
The data as presented in table six explain that 300 or (74.1%) of the respondents were
aware of sensitization campaigns about breast cancer, 45 or (11.1%) of the respondents said
they were not aware of the campaigns while 60 or (14.8%) of the respondents said they were
not sure whether or not there were campaigns against breast cancer.
Results from table ten provide that, 284 or (70%) of the respondents were aware of
the fact that breast cancer is a disease that kills; 61 or (15%) knew that it could be treated if
detected early, 40 or (10%) were also aware that it presents as a painless lump and 20 or (5%)
knew that it is an uncontrolled growth of cells in the breast.
The findings here, therefore, indicate that awareness level about breast cancer (BRCA)
campaigns is relatively high and that, knowledge about breast cancer as a disease condition is
relatively high. In one way or the other a good number of the people have heard that BRCA is
a deadly disease condition that has to be prevented or detected early. So it is quite obvious
that the people are generally or superficially aware of the disease and the „fights‟ against it.

71
Research Question 2
To what extent are women in Benue State exposed to breast cancer campaigns?
Responses to this question came from field survey answers to questions seven and eight.
Data from table seven provide that, 50 or (12.3%) of the respondents were exposed to
breast cancer campaigns, 350 or (86.4%) were not exposed while 5 or (1.2%) of the
respondents were not sure of their exposure to the campaigns.
Evidence of exposure to campaigns was further presented as respondents provided
their sources of exposure. As seen in table eight above, 40 respondents representing 10% of
the total number sampled referred to friends and street van shows as their sources of breast
cancer information, 62 or (15%) of the respondents said their relations were their sources,
223 or (55%) named the media- print/electronic as their source of information and 80 or
(20%) said medical doctors and medical seminars were their sources of breast cancer
information.
These data provide findings that explain that awareness about campaign programmes
does not guarantee exposure to programmes but individual disposition to the programmes and
disposition to the credibility of sources. As a result, people tend to be selective of sources and
of whether or not to participate in these programmes. People, also, tend to perceive threats
and barriers to exposure differently; and depending on the direction that perception takes, the
action of exposure to campaign programmes will be defined. Findings, also, suggest that
campaigns through the media are not the only sources of information even though they are
the major sources.
Research Question 3
Has the knowledge level of women in Benue State on breast cancer (BRCA) risk
factors, prevention, early detection and treatment increased due to their exposure to the
campaigns?

72
In answering research question three above, questions nine, 11-16, 20, 22, 27-31 were
explicit about the knowledge level of women in Benue State on breast cancer risk factors,
prevention, early detection and treatment due to their exposure to the campaigns.
Table nine shows that, 70 respondents or (17.3%) saw early detection as the sole aim
of breast cancer campaigns, 155 or (38.3%) of the respondents said prevention was the aim of
the campaigns while 180 or (44.4%) of the respondents said both prevention and early
detection cannot be separated as campaigns are aimed at achieving any of them.
In table 11, 284 or (70%) of the respondents know that breast cancer (BRCA) can
only be treated at its initial or early stage, while 121 or (30%) did not know the stage at which
breast cancer can be treated. In addition to knowing that it has to be detected early some
people showed their understanding of the word early as data in table 12 show that, 284 or
(70%) of the respondents knew that before symptoms become obvious, breast cancer stage is
early and should be given appropriate treatment while 121or (30%) of the respondents did not
know when to say it is early or late.
Data from 13 above represents the fact that knowledge is superficial as genetic testing
is quite a new subject to most of the respondents. The figures indicate that only 162 or 40%
of the respondents saw the need for genetic testing, 81 or (20%) said no and 162 or (40%),
said they were not sure that genetic tests should be done.
Again, table 14 indicates that 162 or (40%) of the respondents were knowledgeable
about genetic factors being causative of breast cancer while 243 or (60%) were not sure
whether or not breast cancer was caused by genetic factors.
However, from table 15, it is quite obvious that 365 or (90%) of the respondents had
the correct knowledge of the fact that unhealthy dieting can be a causative factor of breast
cancer while 40 respondents representing 10% of the respondents said they were not sure of
dieting being a cause of breast cancer.

73
As a result of the above knowledge, data from table 16 provide that 90 of the
respondents or (22%) controlled intake of calories by reducing the consumption of foods high
in calories, 94 or (23%) reduced their consumption of white flours, 72 or (18%) of the
respondents consumed high amounts of vegetables instead, 68 or (17%) engaged in regular
exercises while 81 or (20%) did nothing to control intake of calories.
The most common symptoms known to the respondents are swelling, pains and lumps.
This is evident in data from table 20 which show that 300 or (74%) of the respondents knew
that breast cancer presents as lumps, pains and swelling, 40 or (10%) of them said it presents
as reddening of nipples and dimpling of the breast while 65 or (16%) of them said they did
not know the symptoms of breast cancer presentation.
Despite exposures to campaigns, knowledge about the peak age of breast cancer
presentation in blacks is low. From table 22, 100 respondents representing 25% of the
respondents knew the peak age of breast cancer presentation in blacks, 150 or (37%) of them,
did not know and 155 or (38%) were not sure of the peak age of breast cancer presentation.
Again, results from table 27 indicate that 300 or (74%) of the respondents looked out
for lumps, pains and swelling during BSE, 20 or (5%) of them looked out for reddening of
nipples, breast dimpling and an orange-like skin texture respectively, while 65 or (16%) are
not sure of what to look out for. In table 28, 305 or (75%) of the respondents said “yes” to 7-
10 days after menstrual period as an ideal time for breast examination, 100 or (25%) of them
said they were not sure of the most suitable time for breast examination.
Results from table 29, reveal that 290 or (72%) of the respondents knew that
mammography was a form of early breast cancer detection technique, 65 or (16%) of them
said it was not a form of early breast cancer detection technique, and 50 or (12%) of them did
not know whether or not it was a form of early breast cancer detection technique.

74
Figures from table 30 indicate that, 284 or (70%) of the respondents knew that,
removal of breast lump would not alter the risks of breast cancer recurrence, 40 or (10%) said
that, it would alter the risks of predisposition to breast cancer while 81or (20%) of them were
not sure whether or not the removal of breast lump would alter the risks of predisposition to
breast cancer.
Data from table 31show that, 340 or (84%) of the respondents knew the signs to look
out for when palpating the breast, while 65 or (16%) of them did not know what signs to look
out for.
Findings show that some people emphasize prevention through avoidable actions
while others place value on early detection. Early detection remains important as a
determinant of a successful treatment. There is the need, however, for campaigns to enhance
in-depth knowledge among women and emphasize prevention and early detection in all
screening procedures to ensure their safety.
Findings also reveal that knowledge about genetic testing is low; as a result most of
the respondents seemed indifferent about it. Also, that it has not been ascertained that genetic
testing is attainable in Nigeria. This explains the reason why most of the respondents do not
appreciate the need for genetic testing. It, therefore, means that knowledge is superficial since
genetic testing is quite a new subject to most of the respondents.
Discoveries, also, reveal uncertainty about the causes of the disease condition as an
aspect that is also not known to medical practitioners. As a result they simply restrict it to
genetic and environmental causes.
Furthermore, it was observed that despite some levels of knowledge and awareness
that consumption of foods high in calories is unhealthy; some group of people will not make
efforts to adopt healthy nutritional values. This agrees with the Health Belief Model (HBM)
that says health behaviour is determined by one‟s belief and perception about a disease and

75
the strategies available to decrease its occurrence and that personal perception is influenced
by a whole range of intrapersonal factors affecting health behaviour (Taylor et. al 2007),
citing (Hochbaum 1958). Based on the intrapersonal factors, Individuals adopt certain health
behaviours.
Additionally, observations are that not every female knows how breast cancer
presents itself. This explains why most females did not know the peak periods when they
should expect breast cancer presentation and thus look out for symptoms thoroughly.
Interestingly, the most common symptoms females have knowledge about are the
presence of lumps, swelling and pains. As such only a few of them have knowledge about
reddening, dimpling and an orange-like skin texture as symptoms of breast cancer
presentation.
Field surveys have shown that 7-10 days after menstrual period is ideal to ensure that
females do not confuse pains or swelling associated with menstrual periods for breast cancer
symptoms.
More so, findings emphasize the lack of adequate knowledge or the shallow nature of
knowledge about the disease condition of breast cancer.
Research Question 4
What is the attitude of women in Benue State towards breast cancer campaigns on the
prevention, early detection and treatment?
Responses to questions 17, 18, 19 and 21provide adequately for research question 4.
In table 17, 284 or (70%) of the respondents said that there were people who
underestimate their risk status, 40 or (10%) said that, people did not underestimate their risk
status and 81 or (20%) of them said, they were not sure whether or not people underestimated
their risk status.

76
From table 18, it can be interpreted that 365 or (90%) of the respondents said that
there were people who overestimated their risks status while 40 or (10%) of them said they
were not sure if people overestimated their risk status.
Data from table 21 above shows that, 284 or (70%) of the respondents agreed that
families that have hereditary syndrome predisposing to breast cancer should go for genetic
testing while 121 or (30%) of them said they were not sure whether or not such families
should go for genetic testing.
It was observed that the level of knowledge of the cause of breast cancer can make
people underestimate their risks status. It was also observed that there are people who do not
feel threatened even with the increasing knowledge of susceptibility resulting from genetic
factors. Such people seem to have certain beliefs hinged on the fact that they cannot be
infected.
From another angle, this result agrees with the opinion by Olson (2002: 240–242);
Welch (2010:16); and Sulik (2010: 74, 263) that too much of awareness causes guilt, fear,
anxiety, depression and negative attitudes of self isolation in breast cancer patients. This
implies that too much of awareness and knowledge about breast cancer and the threat of
susceptibility will agitate people to overestimate their risks status. However, to ease or reduce
the fear of overestimating risk status and the anxiety that every female in the family is not
safe, it is wise for such families to go for genetic testing. It will reveal risk status and may
reduce the need for screening.
Research Question 5
To what extent do they practice Breast Self Examination (BSE), Clinical Breast
Examination (CBE), Mammography and Genetic testing as a result of exposures to breast
cancer campaigns?

77
Responses to questions 23-26 provide answers to research question 5. Figures from
table 23 make it obvious that, 50 or (12%) of the respondents visit health centers for CBE, 10
or (2%) very often, 75 or (19%) not often, while 270 or (67%) of the respondents did not visit
health centers at all.
Table 24 shows that 324 or (80%) of the respondents practiced breast self
examination while 81 or (20%) did not.
Data from table 25, suggest that 162 or (40%) of the respondents did not believe that
they were susceptible to the disease, 81 or (20%) of them did not practice BSE because they
did not remember, 40 or (10%) of the respondents did not because they did not attach
importance to BSE; 122 or (30%) of the respondents did not practice BSE out of sheer levity
for the issue of breast cancer or BSE.
From table 26, data represent that 200 respondents or (49%) often practice BSE, 124
or (31%) practice it very often, and 81 or (20%) of the respondents did not practice BSE often.
Findings indicate low practice rate for CBE. These also show that though a good
number of females did not visit health centers for CBE, they practiced BSE conveniently and
most people were not even consistent with the practice of BSE.This clearly portrays high
levels of negative attitudinal barriers to the success of BRCA campaigns; and as such,
campaigns must appeal to these barriers if success must be achieved.

78
References
Field survey, (2012). Audience response to questions from the questionnaire and interviews.
received 28th June
Lagos State Ministry of Health, (2009). Breast cancer. Lagos state: Breast Cancer
Organization. http://www.brecan.org /
Leathar, D. S., & Roberts. M. M. (1985). Older women's attitudes towards breast disease,
self examination, and screening facilities: implications for communication.
Edinburgh: Springwell House. British Medical Journal. Vol. 290. March.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1417626/pdf/bmjcred00436-0016.pdf
National Cancer Institute. (2009). Cancer type risk factors and possible causes, prevention
detection and diagnosis. Espanol: NCI publications.
http://www.cancer.gov/cancertopics/factsheet/Risk/BRCA
Olatunde, A. (1979). Self medication, benefits, precaution and dangers. London: the
Macmillian Press.
Olweus, D. (1993). Victimization by peers: Antecedents and long term outcomes. In K. H.
Rubin & J. B. Asendorf (Eds). Social withdraswal, inhibition and shyness. Pp.315-
341. Hillsdale, New Jersey: Erlbaum.
Salaudeen A. G., Akande T. M., Musa O. I. (2009). Knowledge and attitudes to breast
cancer and breast self examination among female undergraduates in a state in
Nigeria. Kwara state Nigeria: University of Ilorin. European Journal of Social
Sciences. 7 (3).
Taylor, D., Bury M., Campling, N., Carter S., Garfied, S., Newbould, J., & Rennie, T.
(2007). A Review of the use of the Health Belief Model (HBM), the Theory of
Reasoned Action (TRA), the Theory of Planned Behaviour (TPB) and the Trans-
Theoretical Model (TTM) to study and predict health related behaviour change.
London: University of London. The Department of Practice and Policy, School of
Pharmacy. National Institute for Health and Clinical Excellence (NIHCE). Retrieved
on May 5th, 2012 from http://www.nice-doh_draft_review_of_health_behaviour-
theories.pdf

79
CHAPTER 5
SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.1 Summary
This study looked at the influence of breast cancer campaigns on knowledge, attitude
and practice among women in Benue state. Using the survey research design, quantitative and
qualitative data were gathered and these led to the following findings. The data gathered
indicate that, 300 or (74.1%) of the respondents were aware of sensitization campaigns about
breast cancer, 250 or (62%) of the respondents were exposed to breast cancer campaigns,
while 223 or (55%) named the media- print/electronic as their sources of information
It can also be stated that 284 or (70%) of the respondents know that breast cancer is a
disease that kills; and that 284 or (70%) of the respondents also know that breast cancer
(BRCA) can only be treated at its initial or early stage.
As a result of the above, 284 or (70%) of the respondents showed knowledge of the
fact that, breast cancer stage is early, before symptoms become obvious and should be given
appropriate treatment.
The knowledge level of the women was further measured, and 162 or (40%) of the
respondents said yes to genetic testing, given that they understood the relationship between
genetics as a risk factor in the cause of breast cancer (BRCA). However some of the women
could not mention other factors that can be linked to the causes of BRCA besides genetic
mutations.
It was also deduced that causes of BRCA were not known to many as 243 or (60%)
said they were not sure whether or not BRCA was caused by genetic factors. However, from
table15, it is quite obvious that 365 or (90%) of the respondents know that unhealthy dieting
is a causative factor of BRCA hence, the practice of preventive measures by 94 or (23%) of
the respondents who reduced their consumption of white flours.

80
Also, 284 or (70%) and 365 or (90%) of the respondents respectively, agreed that
knowledge influences attitude towards prevention or treatment, since people underestimate
their risk status, or overestimate their risks status based on the knowledge level they have
about the causes of breast cancer.
` It was also discovered that knowledge about the symptoms is limited to three common
symptoms as revealed in table 20 where 300 or (74%) of the respondents showed knowledge
about breast cancer presentation as lumps, pains and swelling.
Although, the subject of genetic testing is still quite new to the respondents, those
who saw a link between genetics and the cause of breast cancer, expressed their regard for it
as a screening method given that 284 or (70%) of the respondents said that, families that have
hereditary syndrome predisposing to breast cancer should go for genetic testing.
Knowledge about breast cancer is shallow, as the peak age of breast cancer
presentation is not quite known and 155 or (38%) respondents are not sure of the peak age of
breast cancer presentation.
Practice of Clinical Breast Examination is still on the low side, though some factors
seem to inhibit it, as suggested in table 25, where 162 or (40%) of the respondents do not
believe that they are susceptible to the disease. This is evident in the figures provided in table
23 that 270 or (67%) of the respondents do not visit health centers at all. On the other hand,
though 324 or (80%), of the respondents practice breast self examination, only 200
respondents or (49%) practice it often
Results also reveal that 290 or (72%) of the respondents know that mammography is a
form of early breast cancer detection technique, and 284 or (70%) of the respondents know
that, the removal of breast lump does not alter the risks of breast cancer recurrence, and so
caution should be taken.

81
5.2 Conclusion
In conclusion, the women in Benue State are aware of sensitization campaigns about
breast cancer, they are exposed to breast cancer campaigns, and the media- print/electronic
are their major sources of information. Females in Benue state also know that prevention and
early detection are vital aims of the campaigns.
They know that breast cancer is a disease that kills; and that it can only be treated at
its initial or early stage. Most of them acknowledged that before symptoms become obvious,
breast cancer stage is early and should be given appropriate treatment.
The subject of genetic testing is still quite new to the women in Benue State. Those
who understand the relationship between genetics as a risk factor in the cause of breast cancer,
agreed to genetic testing. Again, only a few of them know that mammography is a form of
early breast cancer detection technique
A good number of the women in Benue State attribute the cause of breast cancer to
unhealthy dieting and this is what is known. So, the major causes of breast cancer as provided
by medical prognosis are not known to many. However, the women‟s reduction of
consumption of white flours due to their knowledge of diet as a causative factor of breast
cancer proves that, knowledge influences attitude and positive attitude culminates into
practice.
Furthermore, attitudes of overestimating or underestimating one‟s risks status are
influenced by high or low levels of information acquired on the subject. Also, positive
attitude change is based on compliance of acquired knowledge with pre-existing beliefs,
connectivity of change messages with admired significant others and perception of derivable
benefits.
So many still do not know that other possible factors like having a breast cancer
related infection (breast fibroid, breast cyst) or actions like heating up the breast with

82
radiation can be associated with the disease.
Knowledge among women in Benue state about the symptoms is limited to three
common symptoms namely lumps, pains and swelling. Also, knowledge of the peak age of
breast cancer presentation is not quite known. Again, only a few of them know that, 7-10days
after menstruation is ideal for breast examination. They, however, know that removal of
breast lump does not alter the risks of breast cancer recurrence
Practice of CBE is still on the low side, and such factors as poor attitudes towards the
practice of preventive measures, and the belief that they are not susceptible to the disease
seem to account for it. Practice of breast self examination is, however, relatively high.
5.3 Recommendations
Since the study has revealed that practice of screening methods is highly inhibited by
emotional and psychological factors, it recommends that campaigns should be structured to
adequately accommodate these factors and effectively appeal to these negative attitudinal
barriers if success must be achieved.
Prevention of breast cancer should be emphasized paying serious attention to factors
that are responsible and how they can be effectively handled. This is very important, since the
cure of breast cancer is based on the type of cancer, the stage of diagnosis and the extent of
diagnosis; which could start from the last stage. If preventive measures are taken seriously,
survival rates will invariably increase since cure of cancer is not certain despite medical
techniques and treatments available.
The aim of cancer control is a reduction in both the incidence of the disease and the
associated morbidity and mortality, as well as improved life for cancer patients and their
families. In addition to substantial opportunities for primary prevention, the World Cancer
Report, also, emphasizes the potential of early detection, treatment and palliative care. It
urges all countries to establish comprehensive national cancer control programmes, aimed at

83
reducing the incidence of the disease and improving the quality of life for cancer patients and
their families. In developing countries in particular, where a large proportion of cancers are
detected late in the course of the disease, efforts to achieve earlier diagnosis and delivery of
adequate palliative care and pain relief deserve urgent attention (W.H.O. reports 2011).
The study, also, recommends that campaign planners, should lower the age for
screening and mammograms so that early detection and presentation at the hospital is
enhanced, even though it has been discovered that early detection is not a guarantee of
survival given that some types of breast cancers resist all forms of medications available as
they spread to the bones and brain. However, if screening is done at an earlier age, early
treatment could better reduce the risk of early death. A breast cancer statistics given by The
World Cancer Report (2011:1) revealed that about 24 per cent of new breast cancer cases
diagnosed in 2007 were in women younger than 50 years; 51 per cent in women aged 50-69;
and 25 per cent in women aged 70 and above. This suggests that early screening might just be
helpful in elongating life span. Early screening, particularly for cervical and breast cancers,
allows for successful treatment.
The study also recommends a healthy lifestyle as the best form of prevention.
Frequent consumption of fruits and vegetables and physical activity can make a difference.
Dietary recommendation also requires close coordination by campaign planners with
programs for the prevention of other related non-communicable diseases, mainly
cardiovascular diseases, chronic obstructive pulmonary diseases and diabetes (IARC 2011).
Policy makers should therefore make do with the latest information provided by the
independent Expert Report on diet and chronic disease, released in March 2003 by WHO and
FAO (Food and Agriculture Organization) in order to know which information will be most
appropriate for them to base advice on prevention of breast cancer and other related diseases
(World Cancer Report).

84
References
The World Cancer Report, (2011). Global cancer rates could increase by 50% to 15 million
by 2020 http://www.who.int/mediacentre/news/releases/2003/pr27/en/
The International Agency for Research on Cancer, (2010). World cancer report provides
clear evidence that action on smoking, diet and infections can prevent one third of
cancers, another third can be cured.
http://www.who.int/mediacentre/news/releases/2003/pr27/en/ IARC reports
World Health Organization (2011). WHO statistical information system. Geneva: World
Health Organization. Retrieved April 20, 2012 from http://www.who.int/whosis.
http://www.who.int/cancer/FINAL-Advocacy-Module%206.pdf

85
Bibliography
Books Anaekwe, M. C. (2002). Basic research methods and statistics in education and social
sciences. Onitsha, Anambra State: Sofie Publicity and printing Ltd
Baran, S. J. & Davis, D. K. (2012), Mass communication theory: Foundations, ferment, and
future. (6th ed). United States: Wadsworth Cengage Learning
Bardsley, C. H. (2009). Opiods. In J. A. Marx(Ed). Rosen’s emergency medicine: concept
and clinical practice. (7th ed). Philadelphia, PA: Mosby Elsevver.
Bhopal, R. (2002). Concepts of epidemiology. New York: Oxford University Press
Chukwuemeka, E. O. (2002). Research methods and thesis writing: A multi- disciplinary
approach. Obiagu Enugu: Hope- Rising Ventures Publishers.
Errosnman, H. (1998). Tropical physical and health education. USA: Fildman Publishers
Green, L. W. & Kreuter, M. W. (1999). Health promotion planning: An educational and
ecological approach. Canada: CA, Mayfiled.
Haro, M. S., Percel, G. S. & Wirege, J. R. (2001). Explanation in personal health. USA:
Houghton Mifflin Company.
Ikponmwosa, O. (2006). Fundamentals of statistics in education and the social sciences. (3rd
ed) lagos, Accra: National book consortium
Linus, I. O. (2006). Understanding research methods and thesis writing. Enugu: Linco
enterprises. ISBN: 978-059-216-4
Lindberg, L. D., Bogess, S. & Williams, S. (2000). Multiple threats: the co-occurrence of
teen health risks behaviours. USA: Urban Institute: Office of the Assistant Secretary
for Planning and Evaluation (ASPE)
Mcquail, D. (2010).Mass communication theory: An introduction. Netherlands: Sage
Publishers
Nwana, O. C. (1990). Research in Health Communication at University of Nigeria Nsukka. In
P. Obanya (Ed). Aspects of Nigerian educational literature.
Nwodu, C. L. (2006). Research in communication and other behavioural sciences: Principles
methods and issues. Enugu: Rhyce Kerex publications
Olatunde, A. (1979). Self-medication, benefits, precaution and dangers. London: the
Macmillian Press.
Olson, J. S. (2002). Bathsheba's breast: Women, cancer and history. Baltimore: The Johns
Hopkins University Press. ISBN 0-8018-6936-6
86
Osuala, E. C. (2005). Introduction to research methodology (3rd
ed.). Onitsha:
Africana-First Publishers Limited.
Park, K. (2009). Parks textbook of preventive and social medicine (20th ed). India:
Banarsidas Bhanot Publishers.
Sulik, G. (2010). Pink ribbon blues: How breast cancer culture undermines women's health.
New York: Oxford University Press. ISBN 0199740453
Sunder, L., Adarsh & Pankaj (2009). Textbook of community medicine; preventive and social
medicine (2nd ed). New Delhi, India: CBS Publishers and Distributors.
Wimmer, R. D. & Dominic, J. R. (2011). Mass media research: An introduction. (9th ed),
Wadsworth: Cengage
Journals
Bertlett, J. Kotrlik, J. & Higgins, C. (2001). Organisational research: Determining
appropriate sample size in survey research. Information Technology, Learning and
Performance Journal. 19 (1) pp.43-50
Breckler, S. J. & Wiggins, E. C. (1992). On defining attitude and attitude theory: once more
with feeling. In A.R. Pratkanis, S. J. Breckler, & A. C. Greenwald (Eds), Attitude
structure and function. Hillsdale, NJ: Erlbaum. P 407
Eagly, A.& chaiken, S. (1995). Attitude strength, attitude structure and resistence to change.
In R. Petty and J. Kosnic (Eds) Attitude strength. (PP 413- 415) Mahuah NJ: Erlbaum.
Olwues, D. (1993). Victimization by peers: Antecedents and long term outcomes. In K. H.
Rubin & J. B. Asendorf (Eds). Social withdraswal, inhibition and shyness. Pp.315-
341. Hillsdale, New Jersey: Erlbaum.
Oyero, O. (2010). Child Rights and Media Democratization: An Agenda for Realization of
the MDGS in Nigeria. In N. Okoro, S.O. Idemili, P.C. Agba, N.F. Iyama, N.
Udoakah, H.G. Igben etal (Eds) International journal of communication: An
interdisciplinary journal of communication studies. Number 11. Nsukka:
Communication Studies Forum.ISSN: 1597-4324
Thesis
Akwuba, S.E. (2012). Attitude to caesarean delivery among mothers attending antenatal
clinics at general hospitals in Anambra State. Unpublished thesis, University of
Nigeria Nsukka
Aleke, C.O. (2012). Incidence of drug abuse and cigarette smoking among secondary school
students in Ezza North local government area, Ebonyi State. Unpublished thesis,
University of Nigeria Nsukka
Ngwu, C. S. (2011). Nigerian newspapers coverage of the 78 days presidential vacuum
crisis under late President Umaru Musa Yar’adua: A study of the Daily sun,

87
Guardian. The Nation and Vanguard newspapers. Unpublished thesis Enugu State
University of Science and Technology, (ESUT), Enugu.
Online Books and Journals
Akpo, E.; Akpo, M. &Akhator, A. (2010). Breast cancer knowledge and screening practices
among nigerian medical students. Delta: Delta State University. The Internet Journal
of Health. 11 (2). Retrieved April 18th, 2012 from http://www.ispub.com/journal/the-
internet-journal-of-health/volume-11-number-2/breast-cancer-knowledge-and-
screening-practices-among-nigerian-medical-students.html
American Cancer Society, (2009). Breast cancer: Early detection.. Retrieved April 18th 2012
fromhttp://www.cancer.org/docroot/CRI/content/CRI_2_6x_Breast_Cancer_Early_De
tection.asp.
Chustecka, Z. (2011). Cancer in Africa is 'Like a Runaway Train'. Medscape Medical
News 2011 WebMD, LLC. http://www.medscape.com/viewarticle/736870
Chris, K. H T. & Beng I. (2010). Knowing your breasts. minimizing breast cancer
risk! understand risk factors, preventive measures and early detection. Malaysia.
http://www.bookoncancer.com/productDetail.php?P_Id=8
Ferrandis, E. D. Andreu, Y. & Galdón, M. J. (2002). The impact of information given to
patients’ families: Breast cancer risk notification. Análise Psicológica , 1 (20): 27-34.
http://www.scielo.oces.mctes.pt/pdf/aps/v20n1/v20n1a03.pdf. Retrieved April 18th,
2012
Health belief model, (2012). Retrieved May 5th
, 2012 from
http://en.wikipedia.org/wiki/Health_belief_model
Lagos State Ministry of Health, (2009). Breast cancer. Lagos state: Breast Cancer
Organization. http://www.brecan.org /
Leathar, D. S., & Roberts. M. M. (1985). Older women's attitudes towards breast disease,
self examination, and screening facilities: implications for communication.
Edinburgh: Springwell House. British Medical Journal. Vol. 290. March.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1417626/pdf/bmjcred00436-0016.pdf
Loewensten, G. (2007). Affect regulation and affective forecasting. In Gross, J. J. (Ed.)
Handbook of Emotion Regulation (pp. 180–203). New York: Guilford.
http://en.wikipedia.org/wiki/Health_belief_model
MTN Foundation, (2011). MTN foundation commissions a series of state-of-the-art dialysis
and mammography centers around Nigeria. 28th February, 2011 - 10:18 AM
http://www.mtnonline.com/mtnfoundation/content/mtn-foundation-commissions-
series-state-art-dialysis-and-mammography-centres-around-nigeriaRetrieved April 18th 2012
National Cancer Institute. (2009). Cancer type risk factors and possible causes, prevention
detection and diagnosis. Espanol: NCI publications.
http://www.cancer.gov/cancertopics/factsheet/Risk/BRCA

88
National Statistical Service, (2012). Australian calculator. Retrieved 6th May, 2012
from http://www.nss.gov.au/nss/home.nsf/NSS/0A4A642C712719DCCA2571AB00
243DC6?opendocument
National Population Commission, (2006). Census report. UNFPA in Benue State: Annual
report. http://nigeria.unfpa.org/benue.html. Retrieved 6th May, 2012
Okobia M. N, Bunker, C. H., Okonofua F.E.,& Usifo O. (2006). Knowledge, attitude and
practice of nigerian women towards breast cancer: a cross-sectional study. Edo state:
university of Benin. February 21,World J Surg PMCID: PMC1397833 Oncol.
doi: 10.1186/1477-7819-4-11
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1397833/ retrieved April 18th
2012
Salaudeen A. G., Akande T. M., Musa O. I. (2009). Knowledge and attitudes to breast
cancer and breast self examination among female undergraduates in a state in
nigeria. Kwara state Nigeria: University of Ilorin. European Journal of Social
Sciences. 7 (3). http://www.eurojournals.com/ejss_7_3_15
Shea, N., & Remoker C. (2011). The health belief model. PP 1-3.Retrieved on May 5th,
2012 http://www.Nicole_shea_and_catriona_Remoker_The_Health_Belief_Model
Stretcher, V., & Rosenstock, I.M. (1997). The Health Belief Model. In Glanz K., Lewis F. M.,
& Rimer B. K., (Eds). Health Behaviour and Health Education: Theory, Research
and Practice. San Francisco: Jossey- Bass. PP 31-36. Retrieved on May 5th 2012
from http://www.health_belief_model.org
Sule, E. A. (2011). Breast cancer awareness and breast examination practices among women
in a nigerdelta hospital. Delta state: Wilolud Journals,
Continental J. Medical Research 5 (1) pp27 - 31, ISSN: 2141 – 4211
http://www.wiloludjournal.com
The World Cancer Report, (2011). Breast cancer statistics
http://canceraustralia.nbocc.org.au/breast-cancer/about-breast-cancer/breast-cancer-
statistics
Taylor, D., Bury M., Campling, N., Carter S. et al (2007). A Review of the use of the Health
Belief Model (HBM), the Theory of Reasoned Action (TRA), the Theory of Planned
Behaviour (TPB) and the Trans-Theoretical Model (TTM) to study and predict health
related behaviour change. London: University of London. The Department of Practice
and Policy, School of Pharmacy. National Institute for Health and Clinical Excellence
(NIHCE). Retrieved on May 5th, 2012 from http://www.nice-
doh_draft_review_of_health_behaviour-theories.pdf
The World Cancer Report, (2011). Global cancer rates could increase by 50% to 15 million
by 2020. http://www.who.int/mediacentre/news/releases/2003/pr27/en/.
The International Agency for Research on Cancer, (2010). World cancer report provides
clear evidence that action on smoking, diet and infections can prevent one third of

89
cancers, another third can be cured. http://www.who.int/mediacentre/news/releases/2003/pr27/en/ IARC reports.
UNFPA, (2010). UNFPA in Benue State: Annual report. http://nigeria.unfpa.org/benue.html
retrieved 6th May, 2012
Welch, H. G. (2010). "The Risk of Being Too Aware". The Los Angeles Times. ISSN 0458-
3035, 20th October. Retrieved April 18th, 2012 from
http://www.latimes.com/news/opinion/commentary/la-oe-welch-mammograms-
20101020,0,2961910.story.
World Health Organization (2011). WHO statistical information system. Geneva: World
Health Organization. Retrieved April 20, 2012 from http://www.who.int/whosis.
http://www.who.int/cancer/FINAL-Advocacy-Module%206.pdf
Wood, W. (2000). "Attitude Change: Persuasion and Social Influence". Annu. Rev.
Psychol 51: 539–570.
http://en.wikipedia.org/w/index.php?title=Attitude_change&oldid=489610647

90
Appendix I
Questionnaire
Department of Mass
Communication, University of
Nigeria Nsukka
19th April, 2012
Dear Respondent,
I am a post graduate student of the department of mass communication, conducting a
research study on Breast Cancer Campaigns. The motive for the study is purely academic.
Under no situation is the researcher intending to transfer the information that would be
generated to any other person. I therefore solicit for your response to the questions provided
below.
You may want to know that all answers will be treated confidentially. Thanks for your
cooperation.
Yours faithfully,
Grace, Ebi Omerigwe

91
Appendix II
A Questionnaire on Breast Cancer Campaigns
Part A
Instruction: please tick (√) as appropriate in the boxes below
PERSONAL DATA
1. Sex: male ( ) female ( )
2. Occupation: civil servant ( ) business ( ) student ( ) any other
specify ……………………………………………………………………..
3. Educational Qualification: None ( ) SSCE ( ) DIPLOMA ( ) B.SC ( ) MA. /M.SC.
( )
4. What is your status? Free ( ) infected ( )
5. Age 15 - 25 ( ) 26 - 36( ) 37 – 47( ) 48 and above ( )
Part B: Awareness, Knowledge, Attitude and Practice
6. Are you aware of breast cancer campaigns? Yes ( ) No ( ) Not sure ( )
7. Are you exposed to breast cancer campaigns? Yes ( ) No ( ) Not sure ( )
8. What is your source of information about breast cancer? Friends and street van
shows( ) relations( ) media print/electronic ( ) medical doctors and medical seminars
( )
9. What do you think is the sole aim of the campaigns? Early detection ( ) prevention ( )
all of the above ( )
10. What do you know about breast
cancer? …………………………………………………………………………………
………………………………………………………………………….
………………………………………………………………………………….
11. At what stage is breast cancer treatable? Early stage ( ) middle ( ) late stage ( )
Don‟t know ( )

92
12. When is the early stage? Shortly after identifying symptoms( ) much later ( ) when
the condition can no longer be treated ( ) Don‟t know ( )
13. Should women go for genetic testing? Yes( ) No( ) Not sure ( )
14. Do you know that genetic factors can cause breast cancer? Yes ( ) No( ) Not sure( )
15. Do you know that dieting/nutrition is also a causative factor of breast cancer? Yes( )
No( ) Not sure( )
16. How do you control calories or excess fat in your
diet?..................................................................................................................................
......................................................................................................................
Attitude and knowledge
17. Are there people who underestimate their risks status? Yes( ) No( ) Not sure( )
18. Are there people who over estimate their risk status? Yes( ) No( ) Not sure( )
19. Beside the genetic mutations what do you think can cause breast
cancer?...................................................................................................................... ........
.....................................................................................................................
20. What are the symptoms of breast cancer?
Lumps, swelling, pains ( ) Reddening of nipples/Dimpling ( ) Don‟t know ( )
21. Do you agree that families that most likely present a hereditary syndrome
predisposing to breast cancer should go for genetic testing? Yes( ) No( )
Not sure ( )
22. Do you know that among Nigerian women, the peak age of breast cancer presentation
is about 10-15years earlier than what is observed in Caucasian(white) women, where
it occurs between the ages of 35-45 years? Yes( ) No( ) Not sure( )

93
Practice and Knowledge
23. How often do you visit health centers for clinical breast examination (CBE)?
Often ( ) very often ( ) Not often ( ) Not at all ( )
24. Do you practice breast self examination (BSE)? Yes ( ) No ( )
25. If no, why don‟t you practice it? ...........................................................................
…………………………………………………………………………………..
26. How often do you self examine your breast? Often( ) very often( ) Not often( )
27. What do you look out for when conducting breast self examination?
Lumps, swelling, pains ( ) Reddening of nipples ( )Dimpling( ) Not sure( )
28. Are Periods between seven to ten days after menstrual period (AMP) ideal for breast
examination? Yes ( ) No ( ) Not sure ( ).
29. If no, what periods are most ideal? ........................................................................
…………………………………………………………………………………...
30. Is mammography a form of early breast cancer detection technique? Yes ( ) No ( )
don't know ( ).
31. Do you know that removal of breast lump does not alter the risks of breast cancer
recurrence? Yes ( ) No ( ) not sure ( )

94
Appendix III
Interview Questions
First segment of interview
3 Females within the specified age range
1. How many breast cancer campaigns have you attended since 2008? RQ 1
2. How has your knowledge level of breast cancer, risk factors, prevention, early
detection and treatment, increased due to exposure to the campaigns? RQ3
3. What is breast cancer?
4. What are the various screening methods known to you? RQ2
5. To what extent do you think women should carryout BSE, CBE, Mammography and
Genetic testing? RQs 4 & 5
6. Why should women take these preventive practices seriously? RQ4 &5
Second segment of interview
An Oncologist
1. What are the causes of breast cancer?
2. Why are black women said to be more predisposed to breast cancer than the
Caucasians (whites)?
3. Why do women need genetic testing?
4. What is the breast cancer mortality rate in Benue State?
5. At what stage would breast cancer no longer be treatable?
6. Where in Benue state are breast cancer screening practices performed?

95
Appendix IV
Breast Cancer Stages
Surgery: partial mastectomy and removal of lymph nodes
Source: Hasham, posted in Breast cancer causes, women problem breast cancer. Retrieved
on the 13th of August, 2012

96
Appendix V
Symptoms of Breast Cancer