Neuropsychological Outcome of Head Injury Using a Short Battery
15
Archives of Clinical Neuropsychology, Vol. 15, No. 3, pp. 251–265, 2000 Copyright © 2000 National Academy of Neuropsychology Printed in the USA. All rights reserved 0887-6177/00 $–see front matter PII S0887-6177(99)00016-5 251 Neuropsychological Outcome of Head Injury Using a Short Battery Marie E. Volbrecht University of South Dakota John E. Meyers Northwest Iowa Rehab Consultants Jessica Kaster-Bundgaard University of South Dakota The purpose of this study was to demonstrate that a semi-flexible neuropsychological test battery would accurately identify and discriminate head trauma severity levels. In addition, it was in- tended to demonstrate that this same battery could discriminate head trauma individuals from in- dividuals with other diagnoses. Participants were patients referred for a neuropsychological eval- uation. All patients were administered a battery of tests taking approximately 3 hours. It was found that the semi-flexible battery was able to differentiate patients grouped into six different se- verity levels of loss of consciousness (LOC). In addition, the battery was able to differentiate pa- tients with diagnoses including mental health diagnosis, CVA, dementia, and head trauma. These results support previous findings, but utilized a semi-flexible test battery to do so. This shorter battery is beneficial to patient, neuropsychologists, and managed care providers alike. © 2000 National Academy of Neuropsychology. Published by Elsevier Science Ltd Russell (1998) recently published a defense of a critique of the Halstead-Reitan Neuro- psychological Test Battery (HRB). In this rebuttal, he stated that, with the exception of “the Luria-Nebraska Neuropsychological Battery (LNNB), there were no validation studies of any assessment methods using batteries, other than the HRB” (p. 374). Specif- ically, he pointed out the lack of published support for any sort of flexible battery. He pointed out, quite accurately, that not having proof a battery is invalid does not auto- matically make it valid. The current paper is an initial step toward filling in this missing piece in the field of neuropsychology. The authors would like to acknowledge the input of Mike Granaas, Ph.D. whose statistical advice is appreciated. Address correspondence to: John E. Meyers, PsyD, Northwest Iowa Rehab Consultants, Suite 340, 500 Jackson Street, Sioux City, Iowa 51101.
Transcript of Neuropsychological Outcome of Head Injury Using a Short Battery

Archives of Clinical Neuropsychology, Vol. 15, No. 3, pp. 251–265, 2000Copyright © 2000 National Academy of Neuropsychology
Printed in the USA. All rights reserved0887-6177/00 $–see front matter
PII S0887-6177(99)00016-5
251
Neuropsychological Outcome of Head Injury Using a Short Battery
Marie E. Volbrecht
University of South Dakota
John E. Meyers
Northwest Iowa Rehab Consultants
Jessica Kaster-Bundgaard
University of South Dakota
The purpose of this study was to demonstrate that a semi-flexible neuropsychological test batterywould accurately identify and discriminate head trauma severity levels. In addition, it was in-tended to demonstrate that this same battery could discriminate head trauma individuals from in-dividuals with other diagnoses. Participants were patients referred for a neuropsychological eval-uation. All patients were administered a battery of tests taking approximately 3 hours. It wasfound that the semi-flexible battery was able to differentiate patients grouped into six different se-verity levels of loss of consciousness (LOC). In addition, the battery was able to differentiate pa-tients with diagnoses including mental health diagnosis, CVA, dementia, and head trauma. Theseresults support previous findings, but utilized a semi-flexible test battery to do so. This shorterbattery is beneficial to patient, neuropsychologists, and managed care providers alike. © 2000National Academy of Neuropsychology. Published by Elsevier Science Ltd
Russell (1998) recently published a defense of a critique of the Halstead-Reitan Neuro-psychological Test Battery (HRB). In this rebuttal, he stated that, with the exception of“the Luria-Nebraska Neuropsychological Battery (LNNB), there were no validationstudies of any assessment methods using batteries, other than the HRB” (p. 374). Specif-ically, he pointed out the lack of published support for any sort of flexible battery. Hepointed out, quite accurately, that not having proof a battery is invalid does not auto-matically make it valid. The current paper is an initial step toward filling in this missingpiece in the field of neuropsychology.
The authors would like to acknowledge the input of Mike Granaas, Ph.D. whose statistical advice is appreciated.Address correspondence to: John E. Meyers, PsyD, Northwest Iowa Rehab Consultants, Suite 340, 500 Jackson
Street, Sioux City, Iowa 51101.
252 M. E. Volbrecht et al.
Dikmen, Machamer, Winn, & Temkin (1995) empirically demonstrated somethingthat apparently has been taken for granted in the field of neuropsychology. They dem-onstrated that various levels of severity in head injury patients led to differing levels ofexpected impairment as measured by an expanded version of the HRB. The current pa-per will first explain some of the basics of that study. Finally, this study will demonstratethat similar results can be obtained using a shorter semi-flexible neuropsychological testbattery.
The purpose stated by Dikmen, et al., (1995) was to “provide comprehensive infor-mation about brain—behavior relationships in traumatic head injury” (p. 80). This wasdone using 436 subjects representing a range of head injury severity and a comparisongroup consisting of trauma patients who experienced no head injury. Participants wereevaluated one month and one year post injury. Thirty-two of the head injury patientswere so severely injured that they were untestable at one year post-injury. As all datafrom the patients were rank ordered before statistical analyses, these patients were sim-ply given scores that were one point lower than the lowest testable person and includedin the analyses. The neuropsychological evaluation involved the administration of an ex-panded version of the Halstead-Reitan Neuropsychological Test Battery. The resultsshowed that level of severity and time since injury were significantly related to the neu-ropsychological test results.
There were several different measures of severity used by Dikmen, et al., (1995). Theone that will be employed in the current study is time to follow commands (referred toas loss of consciousness [LOC] here). They broke this variable down into six categories:
,
1 hr; 1–24 hrs; 25 hrs–6 days; 7–13 days; 14–28 days; and
$
29 days. This was found tobe significantly related to performance on the neuropsychological evaluation. They usedan ANOVA and Tukey’s pairwise comparisons to “discover at what level of head-injuryseverity the differences between the groups became significant” (p. 82). They found thatmost differences appeared between one full day and one week of loss of consciousness.
Empirical Justification
Dikmen, et al., (1995) demonstrated that a neuropsychological battery could discrim-inate head trauma patients of differing severity levels. In addition, they showed that thissame battery could differentiate head trauma patients from normal control patients.Like Russell (1998), our literature search did not reveal any studies that demonstratedthis same ability for a shorter semi-flexible battery. The current study attempted to doexactly that.
The current study used the same definition and break down for loss of consciousnessthat Dikmen, et al., (1995) used. Due to real-world constraints, there were some changesin the participants and measures used. One of the main purposes of this study was todemonstrate that sensitivity to differing levels of head injury severity was possible with asemi-flexible battery that was shorter than that used by Dikmen, et al., (1995). There-fore, the neuropsychological measures employed were different. In addition, the abilityof the semi-flexible battery to distinguish various patient groups was investigated in asecond experiment. The objective of these two experiments was to begin to validate theuse of this core battery of tests.
Measures Included in the Core Battery
The core battery used in this study generally takes about 3 hours to administer to individ-uals who have sustained a moderate head injury. When administered to “normal” indi-

Short Battery 253
viduals, it takes about 2 hours. The actual length of time per person is dependent on theamount of impairment. Very few, if any, people required four hours to complete theevaluation. A semi-flexible battery is defined as a core of assessments that most patientsreceive with additional assessments included as they were deemed useful for each indi-vidual referral question. For this study, all participants were administered the same coreof tests. For the sake of clarity, a brief explanation of the measures included in the corebattery will be given before description of the actual experiments.
Selections for inclusion in this neuropsychological battery were made based on re-view of literature regarding each test. Tests were selected based on their available nor-mative data, range of norms, sensitivity to brain injury and the need to have a wellrounded neuropsychological battery. Also, tests were selected on the basis of being rela-tively simple and requiring no expensive or cumbersome equipment. It is important tokeep in mind that no neuropsychological test measures a single cognitive ability. Themajor cognitive abilities tapped by the tests are presented and are not intended to be anexhaustive explanation of the neuropsychological characteristics of each test. See Spreen& Strauss (1998) and Lezak (1995) for more detailed descriptions of the tests.
The Wechsler Adult Intelligence Scale (Revised or III) (WAIS-R/III) was selectedfor inclusion in this battery of tests because of the research available to support the va-lidity of the seven subtest short form (Ward, 1990). The subtests included for the VerbalIQ were Information, Similarities, Digit Span, and Arithmetic. The subtests used for thePerformance IQ were Picture Completion, Block Design, and Digit Symbol. The sub-tests were selected not only because they formed a short form of the WAIS, but also be-cause each subtest individually has been identified as sensitive to brain injury. Informa-tion is used as a measure of long term memory recall and attention. Similarities is used toassess verbal abstraction. Digit Span and Arithmetic are used as measures of attentionand concentration. Picture Completion is used to assess visual perception and the abilityto identify essential from non-essential details. Block Design is a measure of visual spa-tial construction. Digit Symbol assesses a visual attention component, learning, and mo-tor speed.
Trails A and B were included in the battery as a measure of attention and concentra-tion, sequencing and visual motor skills (Reitan & Wolfson, 1985). Judgement of LineOrientation was included as a measure of visual perception that did not require a motorcomponent (Benton, Hamsher, Varney, & Spreen, 1983). Finger Tapping was includedas a measure of motor speed and persistence (Reitan & Wolfson, 1985). Finger Localiza-tion was used as a measure of tactile identification (Benton et al., 1983). Token Test wasused as a measure of simple direction following and receptive language. Sentence Repe-tition was included to assess not only a verbal attention component, but also expressiveand receptive language (Spreen & Strauss, 1991). Controlled Oral Word AssociationTest (COWAT) and Animal Naming were included as assessments of word fluency andmental flexibility. Boston Naming was used as an indication of naming ability (Spreen &Strauss, 1998). Dichotic listening was used as a measure of central auditory processing ofinformation. This test has been found sensitive to brain injuries that affect the deep cere-bral white matter pathways (Roberts et al., 1994). These types of injuries are oftentermed as axonal sheering or diffuse axonal injury. The Auditory Verbal Learning Test(AVLT) was included as a measure of verbal learning and memory. The AVLT has alearning curve measure, and immediate recall, delayed recall and recognition trials(Spreen & Strauss, 1998). The Rey Complex Figure Test (RCFT) was used as a measureof visual memory with immediate, delayed, and recognition trials (Meyers & Meyers,1995). The Victoria revision of the Category Test (Spreen & Strauss, 1991) was given inbooklet form. This test was given as a measure of reasoning and problem solving. A re-

254 M. E. Volbrecht et al.
cent study by Kozel & Meyers (1998) indicated that this short form of the Category Testis a good alternative to the full Category Test. This short form was chosen over the fullversion to help shorten the overall testing time. A Forced Choice (Brandt, Rubinsky, &Larson, 1985) measure was included in the battery as a measure of motivation.
EXPERIMENT 1
Hypotheses
Based on the results of Dikmen et al., (1995) it was hypothesized that the LOC wouldbe able to differentiate various severity levels of head trauma as measured by this partic-ular semi-flexible neuropsychological test battery.
Methods
Participants.
Participants’ data were drawn from the patient database of a practicingneuropsychologist. Criteria for inclusion were an identifiable head trauma and docu-mented loss of consciousness. All patients in the database were testable; therefore no es-timates of performance for untestable individuals were used in the analyses. This was be-lieved to be an improvement over the Dikmen et al., (1995) study because there was nological reason to try to predict performance for individuals who were untestable. If an in-dividual was referred who was untestable, the care and placement decisions about thatindividual were pretty obvious.
Participants in this study consisted of 150 adult head trauma individuals referred tothe neuropsychologist. Many individuals were hospital rehabilitation unit patients, somewere outpatients, some were acute inpatients, and some were lengthier vocational reha-bilitation follow-ups. None of the participants in this study were involved in litigation.The participants were representative of the population of head injured people normallyseen in this area of the Midwest. Patients were assessed at the time of the physicians’ re-ferrals. Therefore, there is a range of time post-injury. This was an unfortunate reality ofthe fashion in which patients are normally seen in practice. The varying time post-injurywas accounted for in the statistical techniques used.
Group 1 (
n
5
60) consisted of people with less than one hour of LOC. The mean age ofthis group was 33.55 years (SD
5
13.95) and the mean education was 12.82 years (SD
5
2.88). There was one left-handed individual, 16 women, 44 men, and all but one was Cau-casian. Group 2 consisted of 16 people who sustained an LOC between 1 hour and 1 day. Themean age of this group was 38.81 years (SD
5
14.27) and the mean education was 12.94years (SD
5
3.77). There were 2 left-handed individuals, all were men and Caucasian.Group 3 consisted of 31 people who had 25 hours to 6 days of LOC. The mean age of thisgroup was 28.84 years (SD
5
15.83) and the mean education was 12.00 years (SD
5
2.52).There were 4 left-handed individuals, 10 women, 21 men, and all but 2 were Caucasian.Group 4 consisted of 24 individuals who had 7 to 13 days of LOC. The mean age of thisgroup was 31.58 years (SD
5
16.67) and the mean education was 11.33 years (SD
5
2.18).There were 5 left-handed individuals, 12 women, 12 men, and all but 2 were Caucasian.Group 5 consisted of 9 individuals who had an LOC between 14 and 28 days. The meanage of this group was 32.44 years (SD
5
20.55) and the mean education was 10.44 years(2.46). There were 4 left-handed individuals, 5 women, 4 men, and all were Caucasian.Group 6 consisted of 10 individuals with 29 or more days of LOC. The mean age for thisgroup was 30.20 years (SD
5
11.43) and the mean education was 11.40 years (SD
5
2.27).There was 1 left-handed individual, 1 woman, 9 men, and all were Caucasian.
Short Battery 255
Measures.
All patients were given a short semi-flexible neuropsychological battery thatconsisted of the WAIS-R/III (seven subtest short form; Ward, 1990), Trail Making Test(Reitan & Wolfson, 1985), Judgment of Line Orientation (Benton, Hamsher, Varney, &Spreen, 1983), Finger Tapping (Reitan & Wolfson, 1985), Finger Localization (Bentonet al., 1983), Token Test (Spreen & Strauss, 1998), Sentence Repetition (Spreen &Strauss, 1998), COWAT (Spreen & Strauss, 1998), Animal Naming (Spreen & Strauss,1998), Boston Naming (Spreen & Strauss, 1998), Dichotic Listening (Roberts et al.,1994), AVLT (Spreen & Strauss, 1998), Rey Complex Figure Test (RCFT) (Meyers &Meyers, 1995), the Booklet Category Test (Victoria Revision; Spreen & Strauss, 1991;Kozel & Meyers, 1998) and a Forced Choice Task (FC) (Brandt, Rubinsky, & Larson, 1985).
Loss of consciousness information was gathered from the medical records of all pa-tients. This was used as a measure of severity of injury with the same breakdown as thatused by Dikmen et al. (1995).
Statistical analyses.
All raw data were converted to age, gender, or education correctedT scores as appropriate according to current norms. Data were inspected to ensure thatit met the assumptions required for statistical vigor.
F
-tests and Chi-squares were usedto determine if any demographic differences existed between the head trauma groups(as broken down by level of severity). A MANCOVA was used to assess whether thediffering time post-injury had an effect that covaried systematically with the assessmentresults. The dependent variables were the neuropsychological measures, the indepen-dent variable was the LOC, and the covariate was time since injury. It was not expectedthat the covariate would be significant because the time post-injury was expected to beequally distributed among the groups. If the covariate was significant, it could be addedto the interpretation to aid in later classification of patients. This relationship was thenfurther analyzed with a MANOVA to determine whether the performance on variousmeasures was affected by the LOC. Because a MANOVA is simply a multivariate ver-sion of an ANOVA, and therefore gives only information about whether or not any dif-ferences exist between the groups, it does not tell specifically between which groups thedifferences lie. Therefore, post-hoc analyses were used to investigate specifically wherethe differences existed. Finally, a Discriminant Function Analysis was utilized to deter-mine with what accuracy classification of severity could be made based on the assess-ment results. In a Discriminant Function Analysis, group membership is treated statisti-cally as a dependent variable because the procedure is trying to predict this membershipfrom the other variables. These other variables (in this study the neuropsychologicalmeasures) are treated statistically as independent variables. The statistical procedure re-sults in mathematical functions that are essentially formulas that can later be utilized topredict group membership of new patients based on test scores. With this techniquethere is always one less function possible than there are groups. Therefore, in this exper-iment, there are five functions possible. To aid in the interpretation of the resulting sig-nificant function(s), a plot of the resultant group centroid was used to indicate at whatpoint there was an obvious break in the scores.
Results
The
F
-tests and chi-squares revealed no significant differences in any of the demo-graphic variables (
p
’s
,
.05). The MANCOVA was significant (
F
(20, 109)
5
95.052,
p
,
.001). The effect of the covariate, time post-injury, was not significant (
F
(20, 109)
5
1.058,
p
5
.404), but the main effect of LOC was significant (
F
(20, 113)
5
3.88,
p
,
.001).This suggested that the variance in the variables was not due to the time since injury, butcould be accounted for by the length of loss of consciousness. To further investigate the

256 M. E. Volbrecht et al.
covariate, the significance levels of the effect of the covariate on each measure were ex-amined. This was to account for the fact that a few differences may have existed thatwere not sufficient to lead to a significant overall effect of the covariate. After using aBonferonni correction to account for the 20 comparisons, the only variable that was sig-nificantly affected by time since injury was the delayed trial of the Rey Complex FigureTest (
F
(1, 128)
5
10.379,
p
5
.002).On the MANOVA, using the same neuropsychological measures stated earlier as the
dependent variables and the LOC as the independent variable, the only variables thatwere not significantly different were: Finger Tapping–Dominant, Finger Localization–Dominant and Non-Dominant (
p
’s
.
.05). The
F
-values and significance levels of allvariables are presented in Table 1. Tukey’s HSD was utilized for the post-hoc analyses.The means and standard deviations of the six groups on all measures are included in Ta-ble 2. As can be seen by inspection of this table, those patients sustaining a longer LOCobtained lower scores. The specific group differences that were significant in the posthoc analyses are indicated in Table 3.
A Discriminant Function Analysis was used to determine the classification ability of themeasures and to determine which groups could be best discriminated from which othergroups. The direct discriminant analysis was performed using 20 neuropsychological mea-sures as predictors of membership in the 6 groups based on LOC. Five functions were cal-culated, with a combined
x
2
(100)
5
135.45,
p
5
.011. After removal of the first function, noremaining functions were significant. Therefore, only one of the functions was significantlyuseful in differentiating among groups. This function accounted for 47.7% of the overallvariance in the sample. As seen in Figure 1, this function maximally discriminated Group 6and also lumped Groups 1 and 2 as being different from Groups 3, 4, and 5.
TABLE 1Significance Levels of the Measures
in the Omnibus MANOVA
Variable
F
-values
a
Significance
WAIS VIQ 5.255
,
.001WAIS PIQ 6.838
,
.001WAIS FSIQ 6.812
,
.001Trails A 3.901 .001Trails B 3.754 .003Judgement of Lines 4.602 .001Finger Tapping
Dominant 1.783 .121Non-dominant 3.227 .009
Finger LocalizationDominant 1.676 .145Non-dominant 2.184 .060
Token Test 4.332 .001Sentence Repetition 3.423 .006COWAT 2.365 .043Animal Naming 2.399 .041AVLT
Total 5.890
,
.001Recall 7.101
,
.001RCFT
Immediate Recall 5.196
,
.001Delayed Recall 4.679 .001Recognition 3.699 .004
Booklet Category Test 3.036 .013
a
All degrees of freedom
5
(5, 129).

Short Battery 257
The loading matrix of correlations, as seen in Table 4, suggested that the best predic-tors for differentiating between the LOC groups were AVLT (Recall and Total), WAISVIQ, PIQ, and FSIQ, RCFT (immediate and delayed recall and recognition), Judgmentof Line Orientation, Finger Tapping (Non-dominant), Sentence Repetition, Token Test,Trails A and B, and the Category Test (Victoria Revision). On all variables, the longerLOC groups obtained lower scores on the measures.
With the use of a classification procedure, 61.5% of the sample was correctly classi-fied. The extreme groups that were separated by the above function were classified morecorrectly than the middle groups (3 and 4). Misclassifications were usually the result ofindividuals being classified into the shorter LOC groups. The numbers and percentagesof the group classifications are presented in Table 5.
EXPERIMENT 2
Hypotheses
It was hypothesized that the neuropsychological measures would be able to differen-tiate between head injury patients and other patients with and without identifiable brainabnormalities/damage.
TABLE 2Group T Score Means and Standard Deviations for Different Lengths
of LOC on the Neuropsychological Measures
Variable
Groups
1 2 3 4 5 6
,
1 hr 1–24 hr 25 hr to 6 days 7–13 days 14–28 days
.
29 days
WAIS VIQ 47.86 (8.25) 49.14 (9.05) 45.12 (6.38) 41.76 (7.80) 38.14 (5.87) 39.30 (6.22)WAIS PIQ 48.74 (7.29) 47.71 (8.81) 45.54 (12.23) 42.29 (9.47) 35.71 (9.29) 34.50 (6.36)WAIS FSIQ 48.16 (7.85) 47.86 (8.56) 45.04 (9.29) 41.29 (8.01) 36.00 (7.19) 36.60 (6.20)Trails A 43.39 (9.49) 44.36 (7.41) 42.58 (12.62) 34.90 (13.11) 33.71 (11.90) 32.70 (13.73)Trails B 46.35 (10.29) 49.07 (6.66) 47.58 (12.73) 42.10 (13.74) 31.57 (14.18) 37.40 (14.06)Judgment of Lines 51.26 (7.79) 51.86 (6.68) 47.85 (7.13) 47.67 (9.78) 45.86 (10.37) 39.00 (9.80)Finger Tapping
Dominant 41.14 (9.27) 41.21 (6.44) 35.31 (12.72) 37.43 (10.04) 37.00 (7.64) 35.00 (12.97)Non-dominant 41.79 (10.44) 44.50 (6.25) 35.81 (16.41) 39.10 (11.93) 39.29 (11.48) 27.80 (14.84)
Finger LocalizationDominant 49.77 (9.83) 45.64 (10.54) 46.54 (9.07) 51.81 (9.65) 46.86 (7.65) 43.70 (10.35)Non-dominant 53.26 (6.99) 50.79 (8.61) 50.65 (7.23) 50.86 (8.77) 42.29 (17.65) 50.20 (11.85)
Token Test 52.19 (7.36) 53.86 (3.46) 47.65 (11.02) 45.67 (11.58) 39.86 (15.85) 44.80 (11.32)Sentence Repetition 41.25 (14.66) 40.71 (17.43) 31.54 (14.34) 33.00 (9.67) 28.71 (15.11) 28.60 (14.36)COWAT 37.19 (17.33) 40.00 (10.84) 34.04 (14.61) 26.71 (13.58) 31.00 (16.90) 26.30 (15.13)Animal Naming 47.81 (10.59) 43.43 (6.93) 45.77 (10.52) 41.48 (9.38) 40.86 (13.38) 38.70 (11.67)AVLT
Total 40.05 (13.18) 44.14 (9.31) 34.15 (15.54) 34.62 (14.74) 25.71 (22.43) 18.80 (8.53)Recall 43.12 (12.74) 40.43 (10.62) 35.50 (15.66) 34.90 (12.51) 28.71 (14.28) 19.30 (9.57)
RCFTImmediate 46.37 (12.76) 47.57 (13.15) 41.88 (16.10) 38.33 (14.76) 36.86 (16.86) 24.80 (8.24)Delayed 43.61 (12.63) 44.64 (12.16) 39.31 (14.98) 36.90 (16.00) 36.29 (16.14) 22.90 (7.16)Recognition 46.70 (8.94) 43.43 (7.64) 43.77 (15.13) 38.71 (13.66) 32.14 (14.36) 36.20 (12.11)
Category Booklet 43.11 (11.34) 45.64 (10.08) 41.46 (13.21) 36.71 (14.63) 36.00 (16.44) 29.80 (12.00)
WAIS
5
Wechsler Adult Intelligence Scale (Revised or III); COWAT
5
Controlled Oral Word AssociationTest; AVLT
5
Rey Auditory Verbal Learning Test; RCFT
5
Rey Complex Figure and Recognition Trial.

258 M. E. Volbrecht et al.
Methods
Participants.
The head trauma groups were part of the same sample as that used in theprevious experiment. This experiment used the results of the above Discriminant Func-tion in that the divisions found that separated out Group 6 by itself and combinedGroups 1 and 2 were utilized to create a long LOC group (
n
5
10) and a short LOCgroup (
n
5
71). This should help cut down on the variance that exists within the groups(because of the variance found in the head trauma population).
Group 1 (
n
5
76) consisted of the short LOC patients. The mean age of this groupwas 34.66 years (SD
5
14.09) and the mean education was 12.84 years (SD
5
3.06).There were three left-handed individuals, 60 men, 16 women, and all but 1 were Cauca-sian. Group 2 (
n
5
10) consisted of the long LOC patients. The mean age of this groupwas 30.20 years (SD
5
11.43) and the mean education was 11.40 years (SD
5
2.27).There was one left-handed individual, 9 men, 1 woman, and all were Caucasian.
The comparison groups consisted of individuals with mental health diagnoses, CVAs,Dementia (Alzheimer’s and subcortical types), and normals who were recruited specifi-cally for participation in research. Group 3 consisted of the patients with diagnoses ofCVA (
n
5
120). The mean age for this group was 65.33 years (SD
5
14.97) and the meaneducation was 11.97 years (SD
5
3.16). There were 9 left-handed individuals, 76 men, 44women, and all but 15 were Caucasian. Group 4 consisted of patients with no identifi-able structural abnormalities, the normals (
n
5
14) and those with mental health diag-
TABLE 3Significant Differences between LOC Groups
on Tukey’s HSD Post-Hoc Analyses
Groups to Compare
Variable 1 2 3 4 5 6
WAIS VIQ 4,5,6 5,6 1 1,2 1,2WAIS PIQ 5a,6b 5,6a 6 1 1a,2 1b,2a,3WAIS FSIQ 4,5a,6b 5,6 1 1a,2 1b,2Trails A 4,6 1 1Trails B 5 5 5 1,2,3Judgment of Lines 6b 6a 6 1b,2a,3Finger Tap—Non-dom. 6a 6 1a,2Finger Loc.—Non-dom. 5 1Token Test 5 5 1,2AVLT—Total 6b 5,6b 6 6 2 1b,2b,3,4AVLT—Recall 6b 6b 6 6 1b,2b,3,4Sentence Repetition 3 1CFT—Immediate 6b 6b 6 1b,2b,3CFT—Delayed 6b 6b 6 1b,2b,3CFT—Recognition 5 1Category Testc 6 6 1,2
The group membership is as follows: 1 5 ,1 hr; 2 5 1–24 hr; 3 5 25 hrto 6 days; 4 5 7–13 days; 5 5 14–28 days; 6 5 .29 days. No significantdifferences were found for the following: Finger Tapping (dominant),Finger Localization (dominant), COWAT, and Animal Naming. WAIS 5Wechsler Adult Intelligence Scale (Revised or III); COWAT 5 Con-trolled Oral Word Association Test; AVLT 5 Rey Auditory VerbalLearning Test; RCFT 5 Rey Complex Figure and Recognition Trial.All differences listed are at least at the .05 level (blank spaces indicateno differences are found for these comparisons).ap , .01.bp ,.001.cVictoria Revision.

Short Battery 259
noses (n 5 37). The mean age of this group was 42.16 years (SD 5 14.19) and the meaneducation was 12.69 years (SD 5 2.87). There was 1 left-handed individual, 23 men, 28women, and all but 2 were Caucasian. Finally, Group 5 consisted of those patients diag-nosed with some sort of dementia who demonstrated some abnormalities on brain scans(n 5 147). The mean age of this group was 75.01 years (SD 5 8.38) and the mean educa-tion was 11.54 years (2.72). There were 11 left-handed individuals, 50 men, 97 women,and all but 3 were Caucasian.
Those patients with CVAs or dementias had structural abnormalities in the brain thatwere unrelated to any identifiable trauma. These diagnoses and abnormalities were con-firmed via CT scans or MRIs. Those patients with mental health diagnoses (Somato-form, Conversion Disorder, or chronic pain), and the normals all had no evidence of anybrain abnormalities. No group comparable to the one used by Dikmen et al. (1995) wasavailable because patients who have no trauma involving the head are not often referredfor neuropsychological evaluation.
Measures. The neuropsychological measures used for this experiment were identical tothose used in Experiment 1.
Statistical analyses. F-tests and chi-squares were utilized to determine any demographicdifferences in age, education, race, or handedness between the groups. A DiscriminantFunction Analysis was performed to determine if the measures could differentiate suc-cessfully among the groups.
FIGURE 1. Bar graph showing the group centroids of the six LOC groups (Group 1 5 , 1 hr; Group 2 5 1to 24 hr; Group 3 5 25 hr to 6 days; Group 4 5 7 days to 13 days; Group 5 5 14 days to 28 days; and Group6 5 29 and over days).

260 M. E. Volbrecht et al.
Results
Inspection of the demographics for the groups used in this analysis demonstrated nosignificant differences in handedness, race, or education (all p’s . .05). There were sig-nificant differences found for gender (x2 (3) 5 46.79, p , .001) and age (F (3, 465) 5295.84, p , .001). These differences are not surprising given the diagnoses that thegroups were divided into. It was expected that the CVA and dementia groups would beolder than the other two groups. This also helps explain the gender differences aswomen generally live longer and so are over represented in these same two groups. Thisis not believed to affect any of the results because all comparisons on the neuropsycho-logical measures use T scores that take age and gender into account for those measuresthat have been shown to be influenced by these characteristics.
The direct discriminant analysis was performed using twenty neuropsychologicalmeasures as predictors of membership in the five groups defined above. Four functionswere calculated, with a combined x2(80) 5 455.84, p , .001. After removal of the firstfunction, the remaining association between the groups and the predictors was still sig-nificant with a x2(57) 5 196.25, p , .001. After removal of the second function, there wasstill a significant association with a x2(36) 5 83.83, p , .001. After removal of this func-tion, the remaining function was not significant. Therefore, 3 of the 4 possible functionswere significantly useful in differentiating among the groups. The 3 significant functions
TABLE 4Results of the Discriminant Function Analysis
for the LOC Groups
Variable Loading Coefficient
AVLT—Recall .630 .399AVLT—Total .583 .192WAIS PIQ .565 1.183WAIS FSIQ .546 21.453RCFT—Immediate .542 .113Judgment of Lines .525 .246RCFT—Delayed .519 2.020WAIS VIQ .473 .732Finger Tap (Non-dom) .434 .323Token Test .401 .082Sentence Repetition .402 .398Category Test (VR) .387 .177Trails A .364 2.096RCFT—Recognition .334 2.038Trails B .304 2.079COWAT .297 .010Finger Tap (Dom) .285 .102Animal Naming .267 2.284Finger Loc (Non-dom) .171 2.435Finger Loc (Dom) .158 .150
Lambda .326Eigenvalue .631R2 .622x2 135.45Significance .011
WAIS 5 Wechsler Adult Intelligence Scale (Revisedor III); COWAT 5 Controlled Oral Word Associa-tion Test; AVLT 5 Rey Auditory Verbal LearningTest; RCFT 5 Rey Complex Figure and RecognitionTrial; Dom 5 Dominant Hand; Nond 5 Non Domi-nant Hand.
Short Battery 261
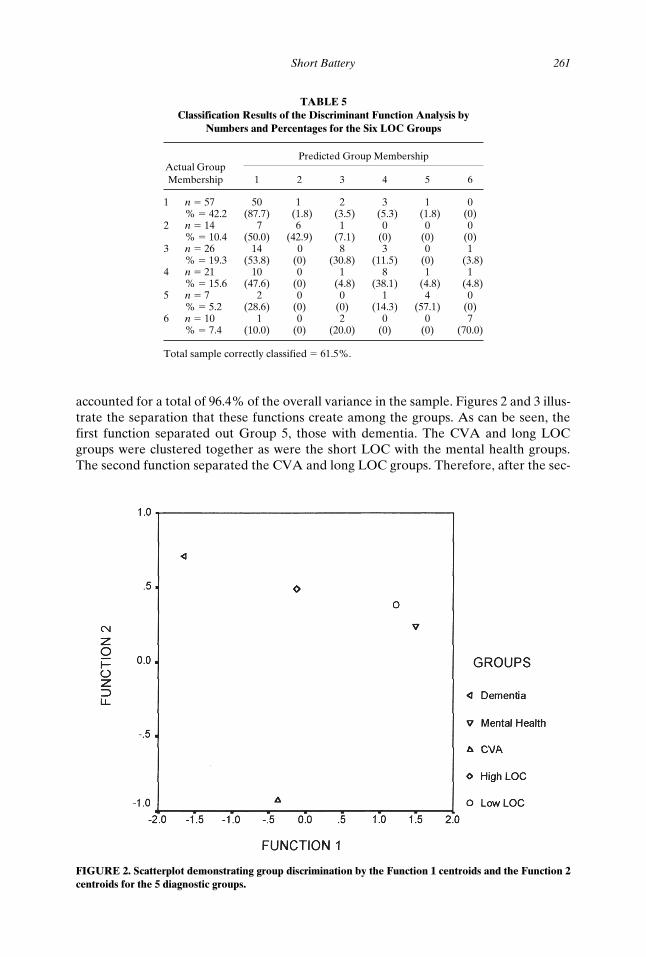
accounted for a total of 96.4% of the overall variance in the sample. Figures 2 and 3 illus-trate the separation that these functions create among the groups. As can be seen, thefirst function separated out Group 5, those with dementia. The CVA and long LOCgroups were clustered together as were the short LOC with the mental health groups.The second function separated the CVA and long LOC groups. Therefore, after the sec-
TABLE 5Classification Results of the Discriminant Function Analysis by
Numbers and Percentages for the Six LOC Groups
Actual Group Membership
Predicted Group Membership
1 2 3 4 5 6
1 n 5 57 50 1 2 3 1 0% 5 42.2 (87.7) (1.8) (3.5) (5.3) (1.8) (0)
2 n 5 14 7 6 1 0 0 0% 5 10.4 (50.0) (42.9) (7.1) (0) (0) (0)
3 n 5 26 14 0 8 3 0 1% 5 19.3 (53.8) (0) (30.8) (11.5) (0) (3.8)
4 n 5 21 10 0 1 8 1 1% 5 15.6 (47.6) (0) (4.8) (38.1) (4.8) (4.8)
5 n 5 7 2 0 0 1 4 0% 5 5.2 (28.6) (0) (0) (14.3) (57.1) (0)
6 n 5 10 1 0 2 0 0 7% 5 7.4 (10.0) (0) (20.0) (0) (0) (70.0)
Total sample correctly classified 5 61.5%.
FIGURE 2. Scatterplot demonstrating group discrimination by the Function 1 centroids and the Function 2centroids for the 5 diagnostic groups.

262 M. E. Volbrecht et al.
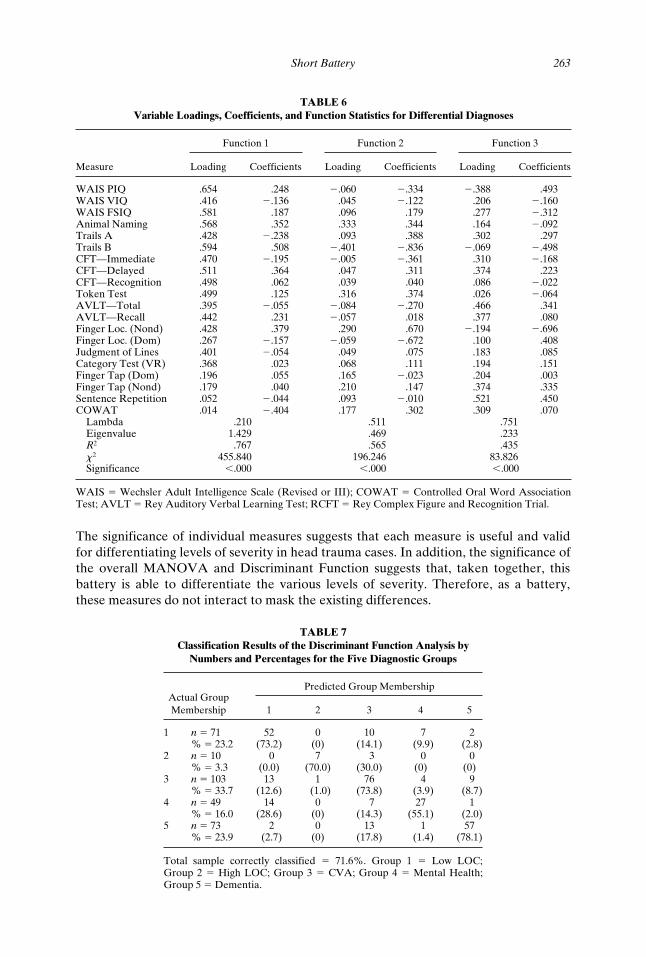
ond function dementia, CVAs, and head trauma with long LOC were differentiated.This left the short LOC group and mental health patients clustered. The third functiondid somewhat separate these two groups so they could be differentiated. The informa-tion on the functions, including the variables that best contributed to each differentia-tion, are displayed in Table 6.
With the use of a classification procedure, 71.6% of the sample was correctly classi-fied. As can be seen in Table 7, misclassifications were congruent with the above resultsin that the long LOC group was more difficult to differentiate from the CVA group.Likewise, the misclassifications for the mental health diagnostic group were most oftenmisclassified as short LOC. The lowest classification ability was with the mental healthgroup, with a correct classification rate of 55.1%.
DISCUSSION
The length of LOC was found to be correlated to different response levels on the as-sessment measures. The results of Experiment 1 show that this battery can help discrim-inate different severity levels of head trauma. In addition, the length of time between theinjury sustained and the testing session affected only one variable in the battery. Thissuggests that the time since injury variable was evenly distributed among the groups so itdid not differentially affect the group results on these measures. As in Dikmen et al.(1995), patients with longer LOC achieved lower scores on several measures. This mayindicate that the length of LOC affects the prognosis for patients sustaining head injury.
FIGURE 3. Scatterplot demonstrating group discrimination by the Function 2 centroids and the Function 3centroids for the 5 diagnostic groups.
Short Battery 263
The significance of individual measures suggests that each measure is useful and validfor differentiating levels of severity in head trauma cases. In addition, the significance ofthe overall MANOVA and Discriminant Function suggests that, taken together, thisbattery is able to differentiate the various levels of severity. Therefore, as a battery,these measures do not interact to mask the existing differences.
TABLE 6Variable Loadings, Coefficients, and Function Statistics for Differential Diagnoses
Function 1 Function 2 Function 3
Measure Loading Coefficients Loading Coefficients Loading Coefficients
WAIS PIQ .654 .248 2.060 2.334 2.388 .493WAIS VIQ .416 2.136 .045 2.122 .206 2.160WAIS FSIQ .581 .187 .096 .179 .277 2.312Animal Naming .568 .352 .333 .344 .164 2.092Trails A .428 2.238 .093 .388 .302 .297Trails B .594 .508 2.401 2.836 2.069 2.498CFT—Immediate .470 2.195 2.005 2.361 .310 2.168CFT—Delayed .511 .364 .047 .311 .374 .223CFT—Recognition .498 .062 .039 .040 .086 2.022Token Test .499 .125 .316 .374 .026 2.064AVLT—Total .395 2.055 2.084 2.270 .466 .341AVLT—Recall .442 .231 2.057 .018 .377 .080Finger Loc. (Nond) .428 .379 .290 .670 2.194 2.696Finger Loc. (Dom) .267 2.157 2.059 2.672 .100 .408Judgment of Lines .401 2.054 .049 .075 .183 .085Category Test (VR) .368 .023 .068 .111 .194 .151Finger Tap (Dom) .196 .055 .165 2.023 .204 .003Finger Tap (Nond) .179 .040 .210 .147 .374 .335Sentence Repetition .052 2.044 .093 2.010 .521 .450COWAT .014 2.404 .177 .302 .309 .070
Lambda .210 .511 .751Eigenvalue 1.429 .469 .233R2 .767 .565 .435x2 455.840 196.246 83.826Significance ,.000 ,.000 ,.000
WAIS 5 Wechsler Adult Intelligence Scale (Revised or III); COWAT 5 Controlled Oral Word AssociationTest; AVLT 5 Rey Auditory Verbal Learning Test; RCFT 5 Rey Complex Figure and Recognition Trial.
TABLE 7Classification Results of the Discriminant Function Analysis by
Numbers and Percentages for the Five Diagnostic Groups
Actual Group Membership
Predicted Group Membership
1 2 3 4 5
1 n 5 71 52 0 10 7 2% 5 23.2 (73.2) (0) (14.1) (9.9) (2.8)
2 n 5 10 0 7 3 0 0% 5 3.3 (0.0) (70.0) (30.0) (0) (0)
3 n 5 103 13 1 76 4 9% 5 33.7 (12.6) (1.0) (73.8) (3.9) (8.7)
4 n 5 49 14 0 7 27 1% 5 16.0 (28.6) (0) (14.3) (55.1) (2.0)
5 n 5 73 2 0 13 1 57% 5 23.9 (2.7) (0) (17.8) (1.4) (78.1)
Total sample correctly classified 5 71.6%. Group 1 5 Low LOC;Group 2 5 High LOC; Group 3 5 CVA; Group 4 5 Mental Health;Group 5 5 Dementia.

264 M. E. Volbrecht et al.
In addition, the results reveal that one function in the discriminant analysis was ableto account for about 48% of the differences among the 6 LOC groups. This function wasable to separate those patients with a LOC longer than 29 days as being different fromall other groups on the battery. The function also grouped patients with a LOC of lessthan 1 hr with those patients who had a LOC of between 1 and 24 hr. Finally, these pa-tients could be differentiated from patients with a LOC between 25 hr and 28 days.
Finally, 61.5% of the sample was correctly classified into LOC groups. Those patientsin the extreme groups were more consistently classified correctly, suggesting that classi-fication is more precise in the extreme groups. More difficult to classify were the middlegroups, that did not seem to differ from each other significantly or consistently. There-fore, this semi-flexible neuropsychological battery can be utilized to distinguish variousbroad levels of severity of head injury based on LOC.
In addition, this semi-flexible neuropsychological battery could correctly distinguishhead trauma patients from people with mental health diagnoses, strokes, and dementiasas described in Experiment 2. Although differences were found in age between thegroups this was not believed to explain the differentiation that was found. This is be-cause the appropriate T scores were used in all analyses—any measures that have beenfound in the past to be affected by age differences utilized the age corrected norms.
The longer LOC group was better differentiated from other diagnoses than were theshorter LOC patients. This is similar to the finding of Dikmen et al. (1995) in that theHRB they employed was better able to differentiate longer LOC patients than shorterLOC patients from normal controls. The first function that helped to differentiate thegroups seemed to do so on the basis of functioning level/severity of difficulties. The sec-ond function that separated long LOC from CVAs, seems to be making a distinction be-tween the more localized damage seen in CVAs versus the more diffuse damage typi-cally seen in more severe head injuries. Finally, the last function separated the shortLOC group from the mental health/normal group. This seems to be on the lines of or-ganic versus non-organic difficulties. These results support the effectiveness of thisshorter semi-flexible battery in helping to determine these diagnoses in patients who areseen in practice. As in any study, results should be replicated by others to ensure that theresults are not due to variations in the data that are unique to this group of patients.
The current study also begins to answer the call of Russell (1998) for some proof thatbatteries other than the HRB and LNNB are valid. Russell commented on the need toidentify the validity of a battery of tests, not just the individual tests, when testifying incourt. This is a step in that direction for this particular battery. It is suggested that moreresearch be completed with this core of tests as they seem to be promising as a battery.In addition, professionals with a different core already in use are encouraged to publishstudies that validate those batteries.
The results of this study also demonstrate that sensitivity to the brain damage that re-sults from head injury is possible to achieve with a semi-flexible test battery that isshorter than the one used in the Dikmen et al. (1995) study. A shorter battery is advan-tageous to the field of neuropsychology for several reasons. First, Medicare and HMO’slook more favorably upon brief interventions and are therefore more willing to pay forservices. Second, neuropsychologists ultimately will be able to serve more patients in thesame amount of time it used to take to serve one patient. Third, a shorter battery is morehumane when testing people who are likely to have a tendency to fatigue and frustrateeasily. Therefore, more patients will be able to be helped in a manner that is easier onthem and more likely to be cooperated with. There is no reason to unnecessarily frus-trate patients when the needed neuropsychological information can be obtained in halfthe usual time.
Short Battery 265
REFERENCES
Benton, A., Hamsher, K., Varney, N., & Spreen, O. (1983). Contributions to Neuropsychological Assessment:A Clinical Manual. Oxford University Press: New York.
Brandt, J., Rubinsky, E., & Larson, G. (1985). Uncovering malingered amnesia. Annals of the New YorkAcademy of Science, 44, 502–503.
Dikmen, S. S., Machamer, J. E., Winn, H. R., & Temkin, N. R. (1995). Neuropsychological outcome at 1-yearpost head injury. Neuropsychology, 9, 80–90.
Kozel, J. J. & Meyers, J. E. (1998). A cross-validation study of the Victoria Revision of the Category Test.Archives of Clinical Neuropsychology, 13, 327–332.
Lezak, M. (1995). Neuropsychological Assessment (3rd ed). Oxford University Press: New York.Mack, W., Freed, D., Williams, B., & Henderson, V. (1992). Boston Naming Test: Short versions for use in
Alzheimer’s disease. Journal of Gerontology: Psychological Sciences, 47, 154–158.Meyers, J. & Meyers, K. (1995). Rey Complex Figure and Recognition Trial: Professional Manual. Psycholog-
ical Assessment Resources: Florida.Reitan, R. & Wolfson, D. (1985). The Halstead-Reitan Neuropsychological Test Battery: Theory and Clinical
Interpretation. Neuropsychology Press: Arizona.Roberts, M., Persinger, M., Grote, C., Evertowski, L., Springer, J., Tuten, T., Moulden, D., Franzen, K., Rob-
erts, R., & Baglio, C. (1994). The Dichotic Word Listening Test: Preliminary Observations in Americanand Canadian Samples. Applied Neuropsychology, 1, 45–56.
Russell, E. W. (1998). In defense of the Halstead-Reitan Battery: A critique of Lezak’s review. Archives ofClinical Neuropsychology, 13, 365–381.
Spreen, O., & Strauss, E. (1991). A Compendium of Neuropsychological Tests: Administration, Norms andCommentary. Oxford University Press: New York.
Spreen, O., & Strauss, E. (1998). A Compendium of Neuropsychological Tests: Administration, Norms andCommentary. Oxford University Press: New York.
Ward, L. (1990). Prediction of verbal, performance and full scale IQs from seven subtests of the WAIS-R.Journal of Clinical Psychology, 46, 436–440.