
Neurologic features of horizontal gaze palsy and progressive scoliosis with mutations in ROBO3
10
DOI 10.1212/01.WNL.0000156349.01765.2B 2005;64;1196 Neurology T. M. Bosley, M. A.M. Salih, J. C. Jen, et al. ROBO3 scoliosis with mutations in Neurologic features of horizontal gaze palsy and progressive February 11, 2013 This information is current as of http://www.neurology.org/content/64/7/1196.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X. All since 1951, it is now a weekly with 48 issues per year. Copyright © 2005 by AAN Enterprises, Inc. ® is the official journal of the American Academy of Neurology. Published continuously Neurology
Transcript of Neurologic features of horizontal gaze palsy and progressive scoliosis with mutations in ROBO3
DOI 10.1212/01.WNL.0000156349.01765.2B 2005;64;1196Neurology
T. M. Bosley, M. A.M. Salih, J. C. Jen, et al.ROBO3scoliosis with mutations in
Neurologic features of horizontal gaze palsy and progressive
February 11, 2013This information is current as of
http://www.neurology.org/content/64/7/1196.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X.Allsince 1951, it is now a weekly with 48 issues per year. Copyright © 2005 by AAN Enterprises, Inc.
® is the official journal of the American Academy of Neurology. Published continuouslyNeurology

VIDEO Neurologic features of horizontal gazepalsy and progressive scoliosis with
mutations in ROBO3T.M. Bosley, MD; M.A.M. Salih, MD; J.C. Jen, MD, PhD; D.D.M. Lin, MD, PhD; D. Oystreck, OC(C);K.K. Abu-Amero, PhD; D.B. MacDonald, MD; Z. al Zayed, MD; H. al Dhalaan, MD; T. Kansu, MD;
B. Stigsby, MD, PhD; and R.W. Baloh, MD
Abstract—Objective: To review the neurologic, neuroradiologic, and electrophysiologic features of autosomal recessivehorizontal gaze palsy and progressive scoliosis (HGPPS), a syndrome caused by mutation of the ROBO3 gene on chromo-some 11 and associated with defective decussation of certain brainstem neuronal systems. Methods: The authors examined11 individuals with HGPPS from five genotyped families with HGPPS. Eight individuals had brain MRI, and six hadelectrophysiologic studies. Results: Horizontal gaze palsy was fully penetrant, present at birth, and total or almost total inall affected individuals. Convergence, ocular alignment, congenital nystagmus, and vertical smooth pursuit defects werevariable between individuals. All patients developed progressive scoliosis during early childhood. All appropriately studiedpatients had hypoplasia of the pons and cerebellar peduncles with both anterior and posterior midline clefts of the ponsand medulla and electrophysiologic evidence of ipsilateral corticospinal and dorsal column-medial lemniscus tract inner-vation. Heterozygotes were unaffected. Conclusions: The major clinical characteristics of horizontal gaze palsy andprogressive scoliosis were congenital horizontal gaze palsy and progressive scoliosis with some variability in both ocularmotility and degree of scoliosis. The syndrome also includes a distinctive brainstem malformation and defective crossing ofsome brainstem neuronal pathways.
NEUROLOGY 2005;64:1196–1203
Dretakis and Kondoyannis were the first to recog-nize the autosomal recessive syndrome of horizontalgaze palsy and progressive scoliosis (HGPPS; OMIM607313).1 The most complete neurologic descriptionto date2 was the 1975 review of a Hakka Chinesefamily, noting the absence of horizontal gaze in theexamined patients and the development of severe,progressive scoliosis during childhood.
We confirmed the autosomal recessive character ofthis syndrome in six affected individuals of two unre-lated consanguineous families and localized theproblem to chromosome 11q23–25.3 Recently, westudied 10 unrelated consanguineous HGPPS fami-lies and identified 10 different mutations in thehuman ROBO3 gene,4 a gene homologous to round-about genes in other species that are important inthe regulation of axonal midline crossing duringbrain development.5,6 We found electrophysiologic ev-idence of uncrossed corticospinal and dorsal column-
medial lemniscus pathways. Therefore, patients withHGPPS have a profound anatomic maldevelopmentof the brainstem, including failure of at least twolong neuronal tracts to decussate, violating a funda-mental principle of vertebrate neuroanatomy.
We describe neurologic, neuroradiologic, and elec-trophysiologic observations in 11 affected membersof five genotyped HGPPS families.
Methods. Patients. We interviewed five consanguineous fami-lies (figure 1) and examined 11 affected individuals (seven maleand four female subjects aged 2 months to 22 years) over a periodof up to 5 years (table 1). Four of these families were previouslyreported4 (Family A � Family 2; Family B � Family 1; Family C� Family 3; Family D � Family 4), and all affected individualsharbored homozygous mutations in ROBO3 (3325 � 1 G in FamilyA, G361E in Family B, R703P in Family C, and S705P in FamilyD). The remaining family (E) had the same frameshift mutation inROBO3 as Family A and proved to be distantly related. All indi-viduals signed informed consent approved by Institutional ReviewBoards at all participating institutions.
Clinical evaluation. All patients had a complete neuro-ophthalmologic and neurologic examination, including videotapingof eye movements. Near and distance visual acuity and near pointof accommodation were measured in most patients. Orthoptic as-sessment was performed on 10 individuals (not C-1), with observa-tions dependent on age and ability to cooperate. Fusional status
Additional material related to this article can be found on the NeurologyWeb site. Go to www.neurology.org and scroll down the Table of Con-tents for the April 12 issue to find the title link for this article.
From the Neuro-ophthalmology Division (Dr. Bosley) and Pediatric Ophthalmology Division (D. Oystreck), King Khaled Eye Specialist Hospital, Riyadh;Department of Neurology (Dr. Salih), King Khalid University Hospital, Riyadh; Neurology Department (Drs. Jen and Baloh), UCLA Medical Center, LosAngeles, CA; Radiology Department (Dr. Lin), Johns Hopkins Hospitals, Baltimore, MD; Genetics Department (Dr. Abu-Amero), Neuroscience Department(Drs. Bosley, MacDonald, al Dhalaan, and Stigsby), and Surgery Department (Dr. al Zayed), King Faisal Specialist Hospital and Research Centre, Riyadh,Saudi Arabia; and Neurology Department (Dr. Kansu), Hacettepe University Hospital, Ankara, Turkey.J.C.J. and R.W.B. are supported by NIH grant DC05524.Received July 13, 2004. Accepted in final form December 15, 2004.Address correspondence and reprint requests to Dr. Thomas M. Bosley, King Khaled Eye Specialist Hospital, PO Box 7191, Riyadh 11462, Saudi Arabia;e-mail: [email protected]
1196 Copyright © 2005 by AAN Enterprises, Inc.
was assessed at near with the Titmus stereoacuity test and Worth4-Dot test (hand-held flashlight) and at distance with Bagolinistriated lenses and a wall mounted Worth 4-Dot test. Ocularalignment was determined by modified cover test and prism cover
test in all positions of gaze, taking into account the inability ofthese patients to utilize a refixation reflex during occlusion ofeither eye. Versions and ductions were performed in addition toassessment of horizontal and vertical smooth pursuit, saccades,
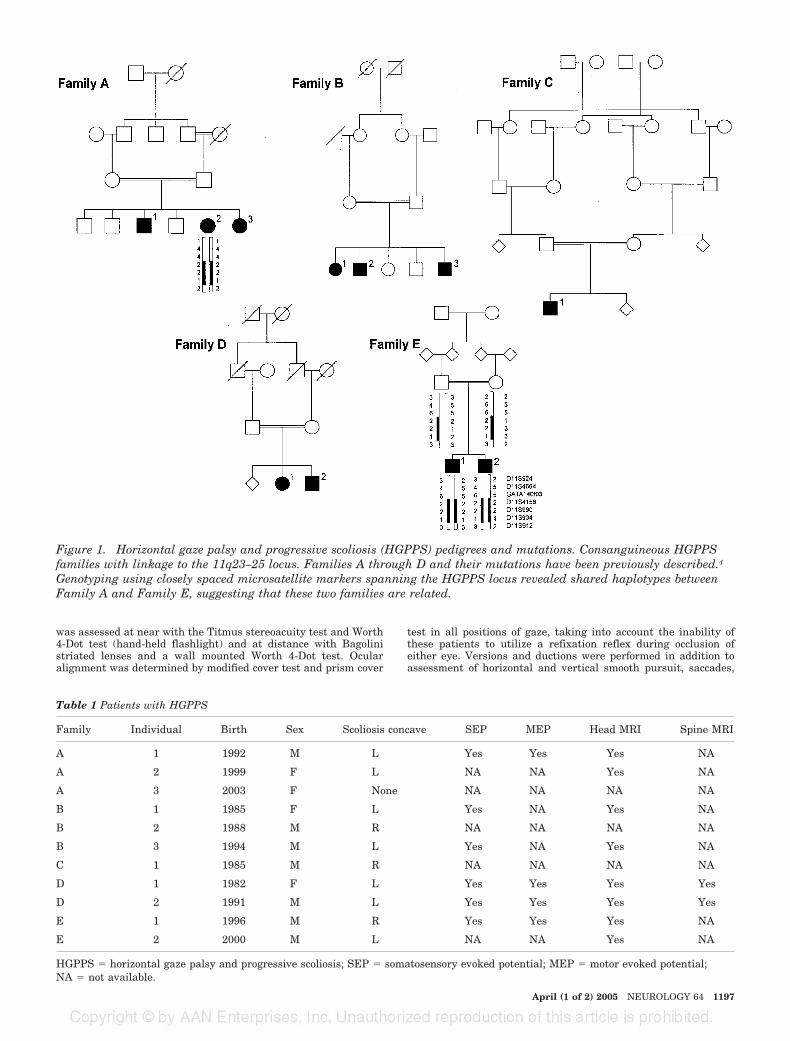
Figure 1. Horizontal gaze palsy and progressive scoliosis (HGPPS) pedigrees and mutations. Consanguineous HGPPSfamilies with linkage to the 11q23–25 locus. Families A through D and their mutations have been previously described.4
Genotyping using closely spaced microsatellite markers spanning the HGPPS locus revealed shared haplotypes betweenFamily A and Family E, suggesting that these two families are related.
Table 1 Patients with HGPPS
Family Individual Birth Sex Scoliosis concave SEP MEP Head MRI Spine MRI
A 1 1992 M L Yes Yes Yes NA
A 2 1999 F L NA NA Yes NA
A 3 2003 F None NA NA NA NA
B 1 1985 F L Yes NA Yes NA
B 2 1988 M R NA NA NA NA
B 3 1994 M L Yes NA Yes NA
C 1 1985 M R NA NA NA NA
D 1 1982 F L Yes Yes Yes Yes
D 2 1991 M L Yes Yes Yes Yes
E 1 1996 M R Yes Yes Yes NA
E 2 2000 M L NA NA Yes NA
HGPPS � horizontal gaze palsy and progressive scoliosis; SEP � somatosensory evoked potential; MEP � motor evoked potential;NA � not available.
April (1 of 2) 2005 NEUROLOGY 64 1197

vestibulo-ocular response (VOR), optokinetic nystagmus (OKN),and vergences. One patient had forced ductions, and two patientshad electro-oculography of their nystagmus.
Neuroimaging. We reviewed MRI of the brain in eight af-fected individuals. Standard brain MR pulse sequences were ac-quired in five patients using a 1.5 Tesla GE Signa scanner (GEMedical Systems, Waukesha, WI) or 1.5 Tesla Siemens MagnetonVision (Siemens Medical Systems, Germany) including sagittalT1-weigted spin echo (350–500/10–15/1 [repetition time/echotime/number of excitations]), coronal fluid-attenuated inversionrecovery (8,800/130, inversion time, 2,200 msec), axial dual echo(3,500/119 and 17), and axial proton density inversion recoverysequences (8,700/29). MRI were obtained in three patients on a 3.0Tesla Siemens Magneton Allegra scanner (Siemens Medical Sys-tems, Germany) including sagittal T1-weighted (624/7), axialfluid-attenuated inversion recovery (8,000/80), and axial MP-RAGE (2,500/4.4, 1 mm thickness) through the brain, and axial3D FT constructive interference in steady-state (CISS) of the in-ner ear and cerebellopontine angle (11/5.6, 1 mm thickness). Twopatients also had MRI of the entire spine reviewed, includingsagittal and axial T1-weighted spin echo (500/9.8), T2-weightedfast spin echo (3,750–5,000/100–120), and coronal T2-weightedfast spin echo (5,000/120) sequences.
Electrophysiology. Somatosensory evoked potentials (SEP)were performed as described previously4,7 on six individuals.Transcranial motor evoked potentials (MEPs) were performed asdescribed previously7 on four individuals.
Results. Clinical observations. Table 2 details ocularmotility characteristics of these patients. All affected indi-viduals had no horizontal smooth pursuit, saccades, OKN,or VOR (figure 2, A through C). Horizontal ductions wereabsent except for one patient (Patient A-1) with small am-
plitude dysconjugate eye movements to the left (figure 2, Dthrough F) and mild narrowing of the palpebral fissure ofthe right eye on left gaze without retraction of the globe(see video E-1 on the Neurology Web site at www.neurology.org). This patient had normal forced ductions. Vertical ver-sions were normal in all except for saccadic smooth pursuitin five individuals.
Convergence was present in all individuals and rangedfrom poor to excellent. Two (Patients A-2 and B-1) wereable to converge on an approaching target to the end of thenose. Most patients had the ability to adduct each eyebeyond the midline by utilizing convergence, and threepatients (Patients A-1, B-3, and D-2) readily substitutedconvergence for momentary side gaze with a cross fixationpattern (figure 2, G through I; see video E-2).
Inability to abduct one or both eyes to primary positionfor distance was documented in the three siblings fromFamily B as indicated by the necessity of a slight face turntoward the fixating eye. Both eyes were spontaneously ad-ducted approximately 10 degrees in two siblings, while thethird sibling was able to bring one eye to the midline.These three individuals had an esotropia that was moder-ate at distance and somewhat less at near in two.
An intermittent 15 to 20 diopter comitant left hyper-tropia was present in the two brothers of Family E. Disso-ciation of the eyes did not readily elicit the manifestdeviation. Misalignment appeared mainly during times ofvisual attention at distance. Presence or absence of fusion
Table 2 Oculomotor abnormalities in patients with HGPPS
Family Member Horizontal Vertical Alignment Convergence Nystagmus
A 1 Minimal ductionsto left OD�OS
Normal Distance and nearorthophoria
Moderate; occasionallyused for horizontalgaze
Moderate horizontal pendular;head shaking
A 2 Absent Saccadic pursuit Distance and nearorthophoria
Excellent; not used forhorizontal gaze
Moderate horizontal pendular;head shaking
A 3 Absent Normal Distance and nearorthophoria
Excellent; not used forhorizontal gaze
Small horizontal pendularOS�OD; no head shaking
B 1 Absent Saccadic pursuitdownward
Distancemoderate ET;orthophoric atnear
Excellent Small horizontal pendular;dampened withconvergence; head shaking
B 2 Absent Normal Distance and nearmoderate ET
Poor cooperation Moderate horizontal pendularnystagmus; head shaking
B 3 Absent Normal Distancemoderate ET;near small ET
Present; occasionallyused for horizontalgaze
Modest horizontal pendulardampened by convergence;head shaking
C 1 Absent Saccadic pursuit Distanceorthophoria
Minimal None
D 1 Absent Saccadic pursuitdownward
Distance and nearorthophoria
Minimal None
D 2 Absent Saccadic pursuit Distance and nearorthophoria
Excellent; used forhorizontal gaze
None
E 1 Absent Normal Smallintermittentcomitant LHT
Good; not used forhorizontal gaze
Small elliptical; no headshaking
E 2 Absent Normal Smallintermittentcomitant LHT
Poor Small elliptical; no headshaking
HGPPS � horizontal gaze palsy and progressive scoliosis; OD � right eye; OS � left eye; ET � esotropia; LHT � left hypertropia.
1198 NEUROLOGY 64 April (1 of 2) 2005

could not be accurately determined given their inability toparticipate with subjective testing.
No manifest deviation was present in primary gaze atdistance in the remaining three families (six individuals).Fusion was demonstrated at near and distance with 200seconds of near stereoacuity in one patient with ortho-tropia. Accurate sensory testing was not possible in threeindividuals because of poor subjective responses and wasnot assessed in the remaining two individuals. Variableside gaze incomitance was present in four individuals. Theone individual (Patient A-1) with some left gaze ability hada variable small angle esotropia on left gaze because ofasymmetric movement between the adducting and abduct-ing eye. The three individuals (Patients A-1, B-3, and D-2)who substituted convergence for side gaze had relativeconvergence of the visual axes during attempted side gaze.
Small to modest amplitude pendular nystagmus wasdocumented in eight individuals from three families. Nys-tagmus was horizontal in six individuals from two families(Families A and B) and elliptical in two individuals fromone family (Family E). Five individuals had associatedhead shaking; the three patients without head shakingincluded two brothers from one family (Family E) and theyoungest examined individual (A-3). Oculography in twoindividuals (Patients A-1 and A-2) confirmed small ampli-
tude conjugate pendular nystagmus (average amplitude 2degrees; average frequency 2 Hz).
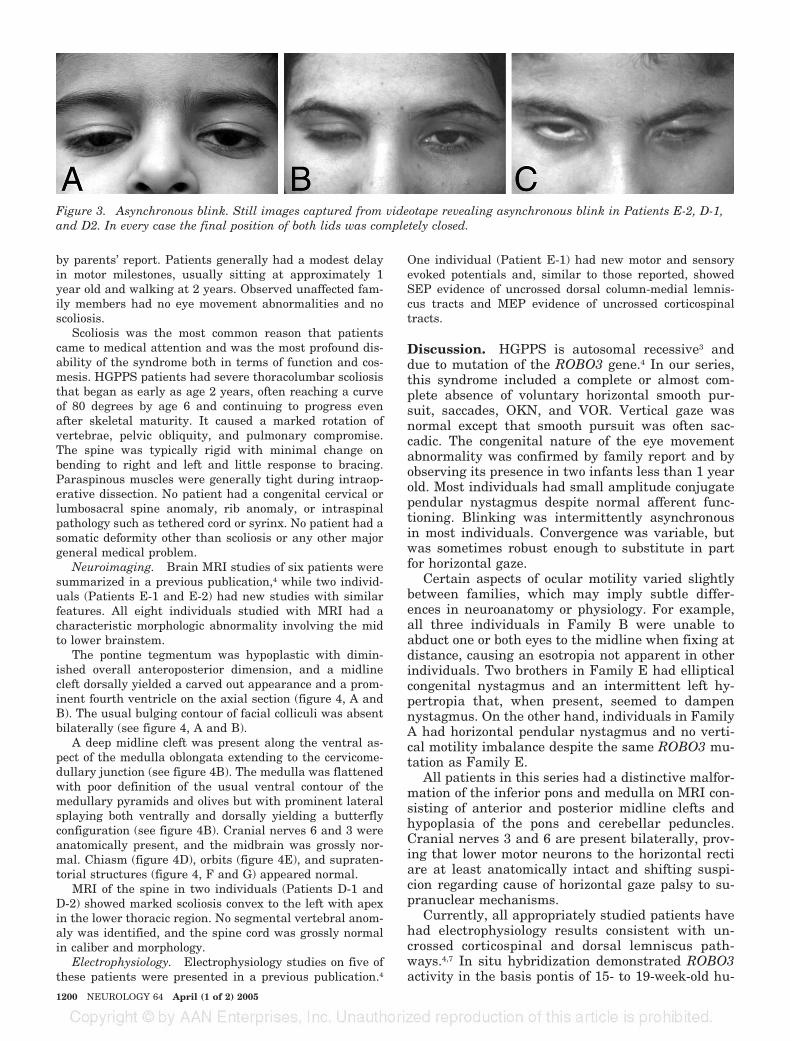
Static lid position was normal in all patients, but nineindividuals had observed intermittent slowed blink of oneor the other upper eyelid (figure 3). No patient had facialmyokymia.
The remainder of the ophthalmologic examination wasnormal in all individuals, including fundus examination,confrontation visual fields, pupils, and accommodation. Noindividual had amblyopia or significantly reduced visualacuity, although three individuals required spectacle cor-rection for a small myopic astigmatic refractive error. Pa-tients typically had a small improvement in theirbinocular visual acuity at near thought to be secondary todampening of nystagmus with convergence.
One patient (Patient B-2) was mentally retarded, butmental retardation was a recognized feature of this con-sanguineous family that segregated separately from HG-PPS except for this individual. Several individuals weredescribed as poor students, but intelligence was not for-mally tested. Hearing, speech, coordination, muscle toneand strength, abdominal reflexes, and sensation were nor-mal except for a gait disturbance typical of scoliosis and anincreased ankle jerk on the right in one individual (PatientB-1). All patients were right handed from early childhood
Figure 2. Montage of eye movements. Images B, E, and H are in primary position, while images A, D, and G are rightgaze and images C, F, and I are left gaze. Images A, B, and C are Patient C-1, who had no apparent horizontal eye move-ments. Images D, E, and F are of Patient A-1, who was unable to look right, was orthophoric in primary gaze, and wasable to look slightly to the left (right eye � left eye) with mild narrowing of palpebral fissure of the right eye but withoutretraction of globe. This was the largest horizontal excursion observed in this patient series. Images G, H, and I are ofPatient D-2. When attempting lateral gaze to either side he would tilt chin downward and converge, following the objectlaterally with the contralateral eye.
April (1 of 2) 2005 NEUROLOGY 64 1199
by parents’ report. Patients generally had a modest delayin motor milestones, usually sitting at approximately 1year old and walking at 2 years. Observed unaffected fam-ily members had no eye movement abnormalities and noscoliosis.
Scoliosis was the most common reason that patientscame to medical attention and was the most profound dis-ability of the syndrome both in terms of function and cos-mesis. HGPPS patients had severe thoracolumbar scoliosisthat began as early as age 2 years, often reaching a curveof 80 degrees by age 6 and continuing to progress evenafter skeletal maturity. It caused a marked rotation ofvertebrae, pelvic obliquity, and pulmonary compromise.The spine was typically rigid with minimal change onbending to right and left and little response to bracing.Paraspinous muscles were generally tight during intraop-erative dissection. No patient had a congenital cervical orlumbosacral spine anomaly, rib anomaly, or intraspinalpathology such as tethered cord or syrinx. No patient had asomatic deformity other than scoliosis or any other majorgeneral medical problem.
Neuroimaging. Brain MRI studies of six patients weresummarized in a previous publication,4 while two individ-uals (Patients E-1 and E-2) had new studies with similarfeatures. All eight individuals studied with MRI had acharacteristic morphologic abnormality involving the midto lower brainstem.
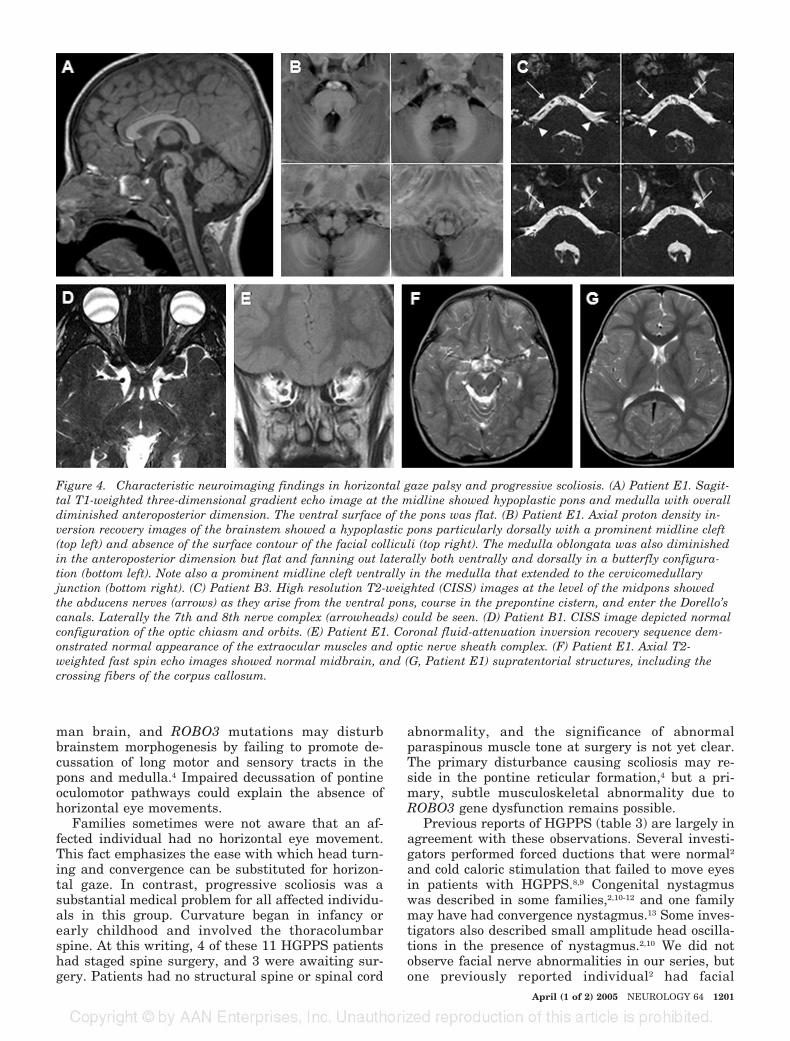
The pontine tegmentum was hypoplastic with dimin-ished overall anteroposterior dimension, and a midlinecleft dorsally yielded a carved out appearance and a prom-inent fourth ventricle on the axial section (figure 4, A andB). The usual bulging contour of facial colliculi was absentbilaterally (see figure 4, A and B).
A deep midline cleft was present along the ventral as-pect of the medulla oblongata extending to the cervicome-dullary junction (see figure 4B). The medulla was flattenedwith poor definition of the usual ventral contour of themedullary pyramids and olives but with prominent lateralsplaying both ventrally and dorsally yielding a butterflyconfiguration (see figure 4B). Cranial nerves 6 and 3 wereanatomically present, and the midbrain was grossly nor-mal. Chiasm (figure 4D), orbits (figure 4E), and supraten-torial structures (figure 4, F and G) appeared normal.
MRI of the spine in two individuals (Patients D-1 andD-2) showed marked scoliosis convex to the left with apexin the lower thoracic region. No segmental vertebral anom-aly was identified, and the spine cord was grossly normalin caliber and morphology.
Electrophysiology. Electrophysiology studies on five ofthese patients were presented in a previous publication.4
One individual (Patient E-1) had new motor and sensoryevoked potentials and, similar to those reported, showedSEP evidence of uncrossed dorsal column-medial lemnis-cus tracts and MEP evidence of uncrossed corticospinaltracts.
Discussion. HGPPS is autosomal recessive3 anddue to mutation of the ROBO3 gene.4 In our series,this syndrome included a complete or almost com-plete absence of voluntary horizontal smooth pur-suit, saccades, OKN, and VOR. Vertical gaze wasnormal except that smooth pursuit was often sac-cadic. The congenital nature of the eye movementabnormality was confirmed by family report and byobserving its presence in two infants less than 1 yearold. Most individuals had small amplitude conjugatependular nystagmus despite normal afferent func-tioning. Blinking was intermittently asynchronousin most individuals. Convergence was variable, butwas sometimes robust enough to substitute in partfor horizontal gaze.
Certain aspects of ocular motility varied slightlybetween families, which may imply subtle differ-ences in neuroanatomy or physiology. For example,all three individuals in Family B were unable toabduct one or both eyes to the midline when fixing atdistance, causing an esotropia not apparent in otherindividuals. Two brothers in Family E had ellipticalcongenital nystagmus and an intermittent left hy-pertropia that, when present, seemed to dampennystagmus. On the other hand, individuals in FamilyA had horizontal pendular nystagmus and no verti-cal motility imbalance despite the same ROBO3 mu-tation as Family E.
All patients in this series had a distinctive malfor-mation of the inferior pons and medulla on MRI con-sisting of anterior and posterior midline clefts andhypoplasia of the pons and cerebellar peduncles.Cranial nerves 3 and 6 are present bilaterally, prov-ing that lower motor neurons to the horizontal rectiare at least anatomically intact and shifting suspi-cion regarding cause of horizontal gaze palsy to su-pranuclear mechanisms.
Currently, all appropriately studied patients havehad electrophysiology results consistent with un-crossed corticospinal and dorsal lemniscus path-ways.4,7 In situ hybridization demonstrated ROBO3activity in the basis pontis of 15- to 19-week-old hu-
Figure 3. Asynchronous blink. Still images captured from videotape revealing asynchronous blink in Patients E-2, D-1,and D2. In every case the final position of both lids was completely closed.
1200 NEUROLOGY 64 April (1 of 2) 2005
man brain, and ROBO3 mutations may disturbbrainstem morphogenesis by failing to promote de-cussation of long motor and sensory tracts in thepons and medulla.4 Impaired decussation of pontineoculomotor pathways could explain the absence ofhorizontal eye movements.
Families sometimes were not aware that an af-fected individual had no horizontal eye movement.This fact emphasizes the ease with which head turn-ing and convergence can be substituted for horizon-tal gaze. In contrast, progressive scoliosis was asubstantial medical problem for all affected individu-als in this group. Curvature began in infancy orearly childhood and involved the thoracolumbarspine. At this writing, 4 of these 11 HGPPS patientshad staged spine surgery, and 3 were awaiting sur-gery. Patients had no structural spine or spinal cord
abnormality, and the significance of abnormalparaspinous muscle tone at surgery is not yet clear.The primary disturbance causing scoliosis may re-side in the pontine reticular formation,4 but a pri-mary, subtle musculoskeletal abnormality due toROBO3 gene dysfunction remains possible.
Previous reports of HGPPS (table 3) are largely inagreement with these observations. Several investi-gators performed forced ductions that were normal2
and cold caloric stimulation that failed to move eyesin patients with HGPPS.8,9 Congenital nystagmuswas described in some families,2,10-12 and one familymay have had convergence nystagmus.13 Some inves-tigators also described small amplitude head oscilla-tions in the presence of nystagmus.2,10 We did notobserve facial nerve abnormalities in our series, butone previously reported individual2 had facial
Figure 4. Characteristic neuroimaging findings in horizontal gaze palsy and progressive scoliosis. (A) Patient E1. Sagit-tal T1-weighted three-dimensional gradient echo image at the midline showed hypoplastic pons and medulla with overalldiminished anteroposterior dimension. The ventral surface of the pons was flat. (B) Patient E1. Axial proton density in-version recovery images of the brainstem showed a hypoplastic pons particularly dorsally with a prominent midline cleft(top left) and absence of the surface contour of the facial colliculi (top right). The medulla oblongata was also diminishedin the anteroposterior dimension but flat and fanning out laterally both ventrally and dorsally in a butterfly configura-tion (bottom left). Note also a prominent midline cleft ventrally in the medulla that extended to the cervicomedullaryjunction (bottom right). (C) Patient B3. High resolution T2-weighted (CISS) images at the level of the midpons showedthe abducens nerves (arrows) as they arise from the ventral pons, course in the prepontine cistern, and enter the Dorello’scanals. Laterally the 7th and 8th nerve complex (arrowheads) could be seen. (D) Patient B1. CISS image depicted normalconfiguration of the optic chiasm and orbits. (E) Patient E1. Coronal fluid-attenuation inversion recovery sequence dem-onstrated normal appearance of the extraocular muscles and optic nerve sheath complex. (F) Patient E1. Axial T2-weighted fast spin echo images showed normal midbrain, and (G, Patient E1) supratentorial structures, including thecrossing fibers of the corpus callosum.
April (1 of 2) 2005 NEUROLOGY 64 1201

myokymia and spasm, possibly implying parenchy-mal pontine dysfunction,14 and several additional pa-tients11,12 were reported to have facial weakness.
Some investigators have reported nonconsanguin-eous families with otherwise typical HGPPS individ-uals.2,8,10 Because the clinical syndrome described isso similar to autosomal recessive HGPPS, it is likelythat these families have unrecognized consanguinityor that affected individuals are compound heterozy-gotes with respect to ROBO3 mutations. Alterna-tively, it remains possible that a similar phenotypemay be caused by mutations in a different gene.
Uncrossed long tracts have been reported previ-ously in two individuals who probably had HGPPS.A man with “marked congenital scoliosis” had a “flatmedulla” and MRI evidence of corticospinal Walle-rian degeneration on the right that did not decussate10 months after a hypertensive right thalamic hem-orrhage that caused a moderate spastic right hemi-paresis.15 A similar man had “a marked congenitalscoliosis” and eye movements that were “mildly re-stricted in the horizontal direction bilaterally.”16 Tenmonths after a hypertensive right putaminal hemor-rhage causing a chronic right hemiparesis, his vibra-tion and position sense were still impaired on theright while light touch and pain sensation were de-creased on the left. Wallerian degeneration of theright corticospinal tract was visible only on the rightside of the brainstem, and functional MRI confirmedonly ipsilateral cortical activation after finger move-
ments. If these two patients had HGPPS, these re-ports add anatomic and physiologic evidence in favorof uncrossed corticospinal tracts.
ROBO3 activity has been detected in the spinalcord and brainstem of the developing mouse,17,18 andthese areas exhibit substantial morphologic distur-bance in a ROBO3 deficient mouse species.18 In con-trast, the spinal cord appears normal in patientswith HGPPS, and clinical examination of one patientwith a putaminal hemorrhage16 suggested normaldecussation of spinothalamic tracts in the spinalcord. Cerebral hemispheres also appear normal.
The human brainstem, however, is profoundly af-fected both anatomically and clinically by ROBO3mutation. No human pathology is available, but non-decussation of crossing axons in the pons and me-dulla probably results in anatomic medullary andpontine hypoplasia and midline clefts where crossingfibers are absent. The most obvious neurologic se-quela is the absence of all horizontal gaze reflexes,but asynchronous blinking, saccadic vertical smoothpursuit, and conjugate pendular nystagmus indicatethat additional brainstem axonal networks spanningthe midline are affected. Convergence and most as-pects of vertical gaze are largely unaffected, imply-ing that neuronal networks responsible for thesefunctions do not depend on crossing axons, dependon crossing axons not under ROBO3 control duringdevelopment, or are spared for other reasons.
The full HGPPS syndrome as currently formu-
Table 3 English language HGPPS references
Reference Origin Families/individuals Comment
10 Greek 5/8 Summary of previous reports plus new families;consistent EEG abnormalities; one family with nocomment about consanguinity
2 Chinese 1/4 Non-consanguineous family; one individual withfacial spasms; possibly progressive EOMabnormality
19 Chinese 1/4 Same family as in reference 2; described ptosis andprogressive ophthalmoplegia
20 American 1/2 One mentally retarded individual
9 Israeli 1/2 Non-consanguineous relatives with scoliosis
21 American 1/2 Non-consanguineous family
13 American 1/2 Possible convergence nystagmus; impaired verticalpursuit and VOR
11 Dutch 2/2 No comment regarding consanguinity; EOMrecording proved nystagmus to be conjugate andpendular; facial weakness
8 Japanese 2/2 One non-consanguineous family
22 German 1/2 No comment about consanguinity
3 Indian, Saudi 2/6 Families also included in reference 4
12 Italian 1/2 Family also included in reference 4
4 Saudi, Turkish, Indian, Greek,Pakistani, Italian
10 families All families consanguineous; uncrossed corticospinaland dorsal column pathways; previously publishedGreek, Indian, Italian, and Saudi families
HGPPS � horizontal gaze palsy and progressive scoliosis; EOM � extraocular motility; VOR � vestibulo-ocular reflex.
1202 NEUROLOGY 64 April (1 of 2) 2005

lated consists of 1) mutation of both copies of ROBO3on chromosome 11; 2) congenital complete or almostcomplete absence of conjugate horizontal gaze fol-lowed by progressive scoliosis during childhood; and3) a developmental malformation of the brainstemthat consists at least in part of uncrossed corticospi-nal and dorsal column pathways. All patients geno-typed thus far have these clinical and neuroanatomicfeatures, and thus far all of these clinical and radio-logic features are limited to the HGPPS syndrome. Itis not yet clear how a disturbance of brainstem ax-onal crossing during gestation precipitates horizon-tal gaze restriction, and functional studies of otherdecussating neuronal pathways have not been per-formed. It is also not clear how ROBO3 mutationsresult in progressive scoliosis, but this monogeneticdisorder may provide clues about neurogenic or mus-culoskeletal mechanisms involved in idiopathicscoliosis.
References1. Dretakis EK, Kondoyannis PN. Congenital scoliosis associated with
encephalopathy in five children of two families. J Bone Joint Surg Am1974;56:1747–1750.
2. Sharpe JA, Silversides JL, Blair RD. Familial paralysis of horizontalgaze associated with pendular nystagmus, progressive scoliosis, andfacial contraction with myokymia. Neurology 1975;25:1035–1040.
3. Jen J, Coulin CJ, Bosley TM, et al. Familial horizontal gaze palsy withprogressive scoliosis maps to chromosome 11q23–25. Neurology 2002;59:432–435.
4. Jen JC, Chan WM, Bosley TM, et al. Mutations in a human ROBO genedisrupt hindbrain axon pathway crossing and morphogenesis. Science2004;304:1509–1513.
5. Kidd T, Brose K, Mitchell KJ, et al. Roundabout controls axon crossingof the CNS midline and defines a novel subfamily of evolutionarilyconserved guidance receptors. Cell 1998;92:205–215.
6. Sabatier C, Plump AS, Ma L, et al. The divergent Robo family proteinRig-1/Robo3 is a negative regulator of Slit responsiveness required formidline crossing by commissural axons. Cell 2004;117:157–169.
7. MacDonald DB, Streletz LJ, Al-Zayed Z, Abdool S, Stigsby B. Intraop-erative neurophysiologic discovery of uncrossed sensory and motorpathways in a patient with horizontal gaze palsy and scoliosis. ClinNeurophysiol 2004;115:576–582.
8. Hamanishi C, Tanaka S, Kasahara Y, Shikata J. Progressive scoliosisassociated with lateral gaze palsy. Spine 1993;18:2545–2548.
9. Granat M, Friedman Z, Aloni T. Familial infantile scoliosis associatedwith bilateral paralysis of conjugate gaze. J Med Genet 1979;16:448–452.
10. Dretakis EK. Scoliosis associated with congenital brain-stem abnormal-ities. A report of eight cases. Int Orthop 1984;8:37–46.
11. Kruis JA, Houtman WA, v. Weerden TW. Congenital absence of conju-gate eye movements. Doc Ophthalmol 1987;67:13–18.
12. Pieh C, Lengyel D, Neff A, Fretz C, Gottlob I. Brainstem hypoplasia infamilial horizontal gaze palsy and scoliosis. Neurology 2002;59:462–463.
13. Yee RD, Duffin RM, Baloh RW, Isenberg SJ. Familial, congenital paral-ysis of horizontal gaze. Arch Ophthalmol 1982;100:1449–1452.
14. Sogg RL, Hoyt WF, Boldrey E. Spastic paretic facial contracture. Neu-rology 1963;13:607–612.
15. Hosokawa S, Tsuji S, Uozumi T, et al. Ipsilateral hemiplegia caused byright internal capsule and thalamic hemorrhage: demonstration of pre-dominant ipsilateral innervation of motor and sensory systems by MRI,MEP, and SEP. Neurology 1996;46:1146–1149.
16. Terakawa H, Abe K, Nakamura M, et al. Ipsilateral hemiparesis afterputaminal hemorrhage due to uncrossed pyramidal tract. Neurology2000;54:1801–1805.
17. Camurri L, Mambetisaeva E, Sundaresan V. Rig-1 a new member ofRobo family genes exhibits distinct pattern of expression during mousedevelopment. Gene Expr Patterns 2004;4:99–103.
18. Sabatier C, Plump AS, Le M, et al. The divergent Robo family proteinrig-1/Robo3 is a negative regulator of slit responsiveness required formidline crossing by commissural axons. Cell 2004;117:157–169.
19. Crisfield RJ. Scoliosis with progressive external ophthalmoplegia infour siblings. J Bone Joint Surg Br 1974;56B:484–489.
20. Riley E, Swift M. Congenital horizontal gaze palsy and kyphoscoliosisin two brothers. J Med Genet 1979;16:314–316.
21. Ehrenberg M, Jay WM, Sidrys LA, Fritz KJ. Congenital bilateral hori-zontal gaze palsy in a brother and sister. J Pediatr Ophthalmol Strabis-mus 1980;17:224–226.
22. Thomsen M, Steffen H, Sabo D, Niethard FU. Juvenile progressivescoliosis and congenital horizontal gaze palsy. J Pediatr Orthop B 1996;5:185–189.
ACTIVATE YOUR ONLINE SUBSCRIPTIONAt www.neurology.org, subscribers can now access the full text of the current issue of Neurology and back issues to 1999.Select the “Login instructions” link that is provided on the Help screen. Here you will be guided through a step-by-step ac-tivation process.
Neurology online offers:• Access to journal content in both Adobe Acrobat PDF or HTML formats• Links to PubMed• Extensive search capabilities• Complete online Information for Authors• Examinations on designated articles for CME credit• Access to in-depth supplementary scientific data
April (1 of 2) 2005 NEUROLOGY 64 1203
DOI 10.1212/01.WNL.0000156349.01765.2B 2005;64;1196Neurology
T. M. Bosley, M. A.M. Salih, J. C. Jen, et al.ROBO3mutations in
Neurologic features of horizontal gaze palsy and progressive scoliosis with
February 11, 2013This information is current as of
ServicesUpdated Information &
http://www.neurology.org/content/64/7/1196.full.htmlincluding high resolution figures, can be found at:
Supplementary Material
DC1.htmlhttp://www.neurology.org/content/suppl/2005/04/09/64.7.1196.
DC2.htmlhttp://www.neurology.org/content/suppl/2005/04/28/64.7.1196.Supplementary material can be found at:
Referenceshttp://www.neurology.org/content/64/7/1196.full.html#ref-list-1This article cites 19 articles, 8 of which can be accessed free at:
Citations
rlshttp://www.neurology.org/content/64/7/1196.full.html#related-uThis article has been cited by 13 HighWire-hosted articles:
Subspecialty Collections
http://www.neurology.org/cgi/collection/ocular_motilityOcular motility
http://www.neurology.org/cgi/collection/all_geneticsAll Geneticsfollowing collection(s):This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.neurology.org/misc/about.xhtml#permissionstables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.neurology.org/misc/addir.xhtml#reprintsus
Information about ordering reprints can be found online:




















