
Neuroimaging Characteristics of Patients with Focal Hand Dystonia
10
Neuroimaging Characteristics of Patients with Focal Hand Dystonia Leighton B.N. Hinkley, PhD Department of Radiology, University of California, San Francisco, San Francisco, California Rebecca L. Webster, MS Physical Therapy and Rehabilitation Science, University of California, San Francisco, San Francisco, California Nancy N. Byl, PT, PhD Physical Therapy and Rehabilitation Science, University of California, San Francisco, San Francisco, California Srikantan S. Nagarajan, PhD Department of Radiology, University of California, San Francisco, San Francisco, California ABSTRACT Narrative Review: Advances in structural and functional imaging have provided both scientists and clinicians with information about the neural mechanisms underlying focal hand dystonia (FHd), a motor disor- der associated with aberrant posturing and patterns of muscle con- traction specific to movements of the hand. Consistent with the hypothesis that FHd is the result of reorganization in cortical fields, studies in neuroimaging have confirmed alterations in the topogra- phy and response properties of somatosensory and motor areas of the brain. Noninvasive stimulation of these regions also demon- strates that FHd may be due to reductions in inhibition between competing sensory and motor representations. Compromises in neuroanatomical structure, such as white matter density and gray matter volume, have also been identified through neuroimag- ing methods. These advances in neuroimaging have provided clinicians with an expanded understanding of the changes in the brain that contribute to FHd. These findings should provide a foundation for the development of retraining paradigms focused on reversing overlapping sensory representations and interactions between brain regions in patients with FHd. Continued collabora- tions between health professionals who treat FHd and research sci- entists who examine the brain using neuroimaging tools are imperative for answering difficult questions about patients with specific movement disorders. J HAND THER. 2009;jj:jej. Focal hand dystonia (FHd) is an idiopathic movement disorder characterized by abnormal, involuntary co-contractions of agonist and antagonist muscles in the affected limb. Patients with dystonia find it difficult to inhibit antagonist contractions. Thus, excessive muscle activation leads to end-range postures. Task-specific FHd is often referred to as occupational hand cramps, commonly associated with the performance of common tasks, such as writing, typing, or playing a musical instrument. When performing the target task, abnormal postur- ing and twisting can not only be observed in the fingers and the wrist but also in the entire upper limb and sometimes in the neck. In some cases, the condition can be bilateral, affecting both the left and right hands, and abnormal muscle contractions can also occur during other tasks involving the affected hand. 1e3 The purpose of this article is to review how neuroimaging techniques have been used to examine the neural substrates of FHd and how the same methods can be used to track changes in the brain that occur as the result of therapeutic intervention. CHARACTERISTICS OF FHD, CLINICAL MANAGEMENT, AND THE ROLE OF NEUROIMAGING Although the critical problem is decreased motor control, FHd may also be associated with decreased range of motion or hyperflexibility, decreased strength or excessive strength and muscle hypertro- phy, and/or impaired sensory processing. It is pri- marily the impairment of motor control that leads to an inability to perform the associated task and, in some cases, other activities of daily living, such as brushing one’s teeth, shaving, cutting nails, or but- toning a shirt. Current conservative interventions for FHd include psychological counseling, physical SPECIAL ISSUE Correspondence and reprint requests to Dr, Leighton B.N. Hinkley, Biomagnetic Imaging Laboratory, Department of Radiology, Box 0628, University of California, San Francisco, 513 Parnassus Avenue, S362, San Francisco, CA 94143-0628; e-mail: <leighton.hinkley@radio logy.ucsf.edu>. 0894-1130/$ e see front matter Ó 2009 Hanley & Belfus, an imprint of Elsevier Inc. All rights reserved. doi:10.1016/j.jht.2008.11.002 jej 2009 1 ARTICLE IN PRESS
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Neuroimaging Characteristics of Patients with Focal Hand Dystonia

ARTICLE IN PRESS
SPECIAL ISSUE
Neuroimaging Characteristics of Patients withFocal Hand Dystonia
Leighton B.N. Hinkley, PhDDepartment of Radiology, University of California,San Francisco, San Francisco, California
Rebecca L. Webster, MSPhysical Therapy and Rehabilitation Science, University ofCalifornia, San Francisco, San Francisco, California
Nancy N. Byl, PT, PhDPhysical Therapy and Rehabilitation Science,University of California, San Francisco, San Francisco,California
Srikantan S. Nagarajan, PhDDepartment of Radiology, University of California,San Francisco, San Francisco, California
Correspondence and reprint requests to Dr, Leighton B.N. Hinkley,Biomagnetic Imaging Laboratory, Department of Radiology, Box0628, University of California, San Francisco, 513 Parnassus Avenue,S362, San Francisco, CA 94143-0628; e-mail: <[email protected]>.
0894-1130/$ e see front matter � 2009 Hanley & Belfus, an imprintof Elsevier Inc. All rights reserved.
doi:10.1016/j.jht.2008.11.002
ABSTRACTNarrative Review:Advances in structural and functional imaging have provided
both scientists and clinicians with information about the neuralmechanisms underlying focal hand dystonia (FHd), a motor disor-der associated with aberrant posturing and patterns of muscle con-traction specific to movements of the hand. Consistent with thehypothesis that FHd is the result of reorganization in cortical fields,studies in neuroimaging have confirmed alterations in the topogra-phy and response properties of somatosensory and motor areas ofthe brain. Noninvasive stimulation of these regions also demon-strates that FHd may be due to reductions in inhibition betweencompeting sensory and motor representations. Compromises inneuroanatomical structure, such as white matter density andgray matter volume, have also been identified through neuroimag-ing methods. These advances in neuroimaging have providedclinicians with an expanded understanding of the changes in thebrain that contribute to FHd. These findings should provide afoundation for the development of retraining paradigms focusedon reversing overlapping sensory representations and interactionsbetween brain regions in patients with FHd. Continued collabora-tions between health professionals who treat FHd and research sci-entists who examine the brain using neuroimaging tools areimperative for answering difficult questions about patients withspecific movement disorders.
J HAND THER. 2009;jj:jej.
Focal hand dystonia (FHd) is an idiopathicmovement disorder characterized by abnormal,involuntary co-contractions of agonist and antagonistmuscles in the affected limb. Patients with dystoniafind it difficult to inhibit antagonist contractions.Thus, excessive muscle activation leads to end-rangepostures. Task-specific FHd is often referred to asoccupational hand cramps, commonly associatedwith the performance of common tasks, such aswriting, typing, or playing a musical instrument.When performing the target task, abnormal postur-ing and twisting can not only be observed in thefingers and the wrist but also in the entire upper limband sometimes in the neck. In some cases, thecondition can be bilateral, affecting both the left andright hands, and abnormal muscle contractions can
also occur during other tasks involving the affectedhand.1e3 The purpose of this article is to review howneuroimaging techniques have been used to examinethe neural substrates of FHd and how the samemethods can be used to track changes in the brainthat occur as the result of therapeutic intervention.
CHARACTERISTICS OF FHD,CLINICAL MANAGEMENT, AND THEROLE OF NEUROIMAGING
Although the critical problem is decreased motorcontrol, FHd may also be associated with decreasedrange of motion or hyperflexibility, decreasedstrength or excessive strength and muscle hypertro-phy, and/or impaired sensory processing. It is pri-marily the impairment of motor control that leads toan inability to perform the associated task and, insome cases, other activities of daily living, such asbrushing one’s teeth, shaving, cutting nails, or but-toning a shirt. Current conservative interventions forFHd include psychological counseling, physical
jej 2009 1

ARTICLE IN PRESS
rehabilitation and retraining (including constraint-induced movement therapy, biofeedback, and senso-rimotor retraining techniques, such as Braille read-ing), and pharmaceutical agents, the most commonand effective of which being the injection of botuli-num toxin to weaken the muscles of the hand andforearm.4e7 In extreme cases, when the condition be-gins to affect tasks required for the activities of dailyliving and self-care, surgical treatment (includingthe implantation of deep brain stimulators) isconsidered.
Most researchers and clinicians agree that FHd is amultifactorial disorder, the result of an interactionbetween genetic, neurobiological, and environmentalfactors, including personal stress, musculoskeletallimitations, illness, and trauma to the upper extrem-ity. Although a combination of botulinum toxin andrehabilitative training may help manage the invol-untary movements to enable individuals to continueto perform their tasks, no treatment is consideredentirely successful in restoring normal motor control.Although there are testimonials from musicians whoclaim that they have been cured by using conserva-tive treatment and self-training, the critical elementsto ensure successful retraining are still elusive. Thedispute over the effectiveness of conservative man-agement may be due in part to the fact that thepathophysiology of FHd remains unknown.
Advances in noninvasive neuroimaging tech-niques have provided the means necessary to iden-tify multiple levels of changes in the brain that arelikely to contribute to the motor deficits present infocal dystonia. For example, structural magnetic res-onance imaging (MRI) allows us to examine thedetailed anatomy of the brain and deviations in thevolume, density, and morphology of cortical and sub-cortical structures in patients with focal dystonia. Amore recent application of MRI, diffusion tensorimaging (DTI), measures water diffusion across mye-linated structures in the central nervous system, andis currently used to reconstruct the white mattertracts that connect different areas of the brain.Other imaging techniques allow us to evaluatechanges in the functionality of brain structures.Positron emission tomography (PET) and functionalMRI (fMRI) indirectly measure neural activitythrough the consumption of oxygen in highly activebrain regions, highlighting areas that are active dur-ing specific behaviors. Advanced applications ofMR, such as spectroscopy, are used to identify certainbiochemical markers, such as the neurotransmittersgamma-aminobutyric acid (GABA) and glutamate,as they are used by neural structures. Functionalimaging methods such as electroencephalography(EEG) and magnetoencephalography (MEG) recordbrain activity through changes in electrical current(as in EEG) or changes in the magnetic fields (as inMEG) across the scalp induced by neural activity.
2 JOURNAL OF HAND THERAPY
Based on EEG and MEG findings, it is possible to re-construct changes in brain activity on the order ofmilliseconds. Collectively, these studies provide re-searchers and clinicians with a clearer picture aboutthe underlying neural mechanisms of FHd, andhow those mechanisms are modifiable as a result ofbehavioral intervention. However, it is challengingto determine if the changes in physiology and anat-omy defined in imaging are the result of, or con-versely contribute to, the motor deficits present inthis population. Integration of these data with infor-mation from work done in genetics, computationalmodeling, comparative neuroscience, and cortical ex-citation studies (using transcranial magnetic stimula-tion [TMS]) is imperative to our understanding ofwhat contributes to and is affected by the disorder.
SENSORIMOTOR LEARNINGHYPOTHESIS: EVIDENCE FORNEUROPLASTICITY IN FOCALDYSTONIA
Even though FHd is considered multifactorial, oneprevailing hypothesis for the development of FHd isbased on aberrant sensorimotor learning. Thishypothesis suggests that highly repetitive, rapid,attenuated movements associated with the onset ofFHd result in maladaptive changes in the represen-tation of the digits within the somatosensory andmotor cortices of the brain.8,9 Degradation of normalsomatotopy occurs as a result of an inability of thebrain to distinguish between near-simultaneoussensory inputs to the cortex, disrupting sensoryfeedback to the motor system and consequently finemotor movements.
The sensorimotor learning hypothesis is supportedby an animal model of FHd developed by Byl et al. inwhich New World owl monkeys with no previoushistory of repetitive stress injury or repetitive motioninjury were trained in a behavioral task that involvedattending to a repetitive, rapid grasping movement toreceive a liquid reward.8,9 All animals continued train-ing until their ability to perform the task began to de-grade and they exhibited symptoms paralleling FHdin humans. After the development of the dysfunction,electrophysiological mapping of the representation ofthe hand in primary somatosensory cortex (S1) re-vealed robust dedifferentiation within the subdivisionsof S1 that receive inputs from the cutaneous mechano-receptors in the skin.10 Receptive fields for neurons in asubregion of S1, area 3a, that represent the hand weregreatly increased, and the receptive fields of many ofthese neurons overlapped the representations of twoor more neighboring digits (Figure 1). In addition, therepresentation of surfaces that remain generally sepa-rated in S1 (hairy and glabrous skin) became combinedin animals which developed this condition.8,9
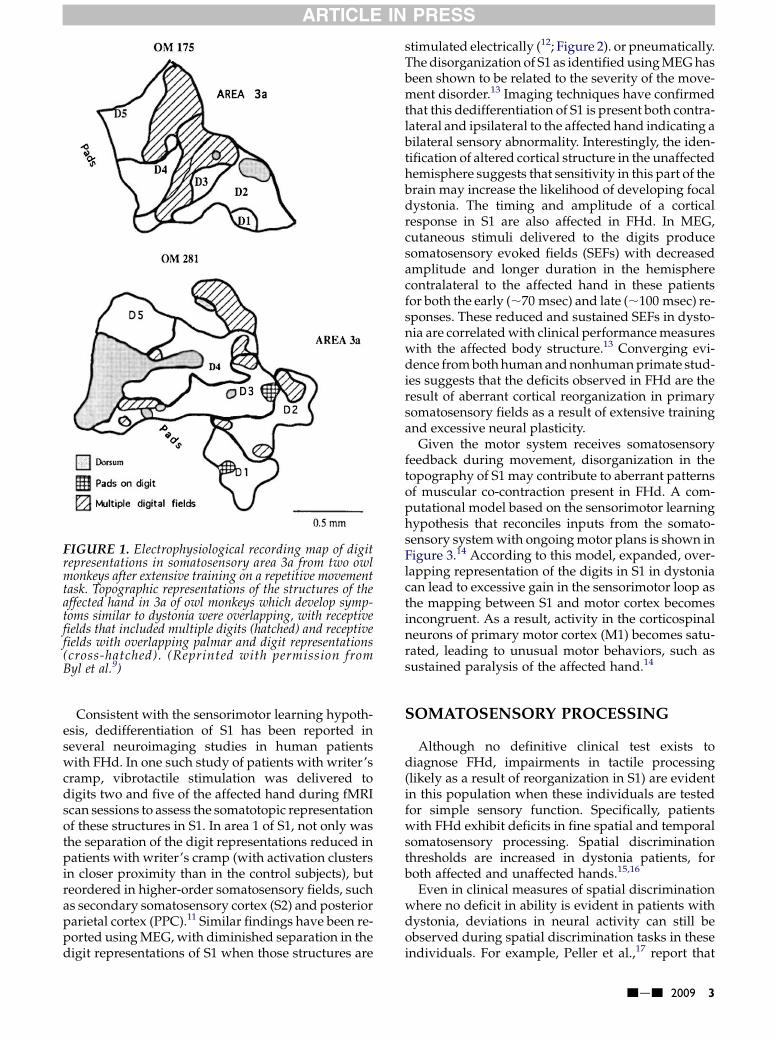
FIGURE 1. Electrophysiological recording map of digitrepresentations in somatosensory area 3a from two owlmonkeys after extensive training on a repetitive movementtask. Topographic representations of the structures of theaffected hand in 3a of owl monkeys which develop symp-toms similar to dystonia were overlapping, with receptivefields that included multiple digits (hatched) and receptivefields with overlapping palmar and digit representations(cross-hatched). (Reprinted with permission fromByl et al.9)
ARTICLE IN PRESS
Consistent with the sensorimotor learning hypoth-esis, dedifferentiation of S1 has been reported inseveral neuroimaging studies in human patientswith FHd. In one such study of patients with writer’scramp, vibrotactile stimulation was delivered todigits two and five of the affected hand during fMRIscan sessions to assess the somatotopic representationof these structures in S1. In area 1 of S1, not only wasthe separation of the digit representations reduced inpatients with writer’s cramp (with activation clustersin closer proximity than in the control subjects), butreordered in higher-order somatosensory fields, suchas secondary somatosensory cortex (S2) and posteriorparietal cortex (PPC).11 Similar findings have been re-ported using MEG, with diminished separation in thedigit representations of S1 when those structures are
stimulated electrically (12; Figure 2). or pneumatically.The disorganization of S1 as identified using MEG hasbeen shown to be related to the severity of the move-ment disorder.13 Imaging techniques have confirmedthat this dedifferentiation of S1 is present both contra-lateral and ipsilateral to the affected hand indicating abilateral sensory abnormality. Interestingly, the iden-tification of altered cortical structure in the unaffectedhemisphere suggests that sensitivity in this part of thebrain may increase the likelihood of developing focaldystonia. The timing and amplitude of a corticalresponse in S1 are also affected in FHd. In MEG,cutaneous stimuli delivered to the digits producesomatosensory evoked fields (SEFs) with decreasedamplitude and longer duration in the hemispherecontralateral to the affected hand in these patientsfor both the early (;70 msec) and late (;100 msec) re-sponses. These reduced and sustained SEFs in dysto-nia are correlated with clinical performance measureswith the affected body structure.13 Converging evi-dence from both human and nonhuman primate stud-ies suggests that the deficits observed in FHd are theresult of aberrant cortical reorganization in primarysomatosensory fields as a result of extensive trainingand excessive neural plasticity.
Given the motor system receives somatosensoryfeedback during movement, disorganization in thetopography of S1 may contribute to aberrant patternsof muscular co-contraction present in FHd. A com-putational model based on the sensorimotor learninghypothesis that reconciles inputs from the somato-sensory system with ongoing motor plans is shown inFigure 3.14 According to this model, expanded, over-lapping representation of the digits in S1 in dystoniacan lead to excessive gain in the sensorimotor loop asthe mapping between S1 and motor cortex becomesincongruent. As a result, activity in the corticospinalneurons of primary motor cortex (M1) becomes satu-rated, leading to unusual motor behaviors, such assustained paralysis of the affected hand.14
SOMATOSENSORY PROCESSING
Although no definitive clinical test exists todiagnose FHd, impairments in tactile processing(likely as a result of reorganization in S1) are evidentin this population when these individuals are testedfor simple sensory function. Specifically, patientswith FHd exhibit deficits in fine spatial and temporalsomatosensory processing. Spatial discriminationthresholds are increased in dystonia patients, forboth affected and unaffected hands.15,16
Even in clinical measures of spatial discriminationwhere no deficit in ability is evident in patients withdystonia, deviations in neural activity can still beobserved during spatial discrimination tasks in theseindividuals. For example, Peller et al.,17 report that
jej 2009 3

FIGURE 2. Neuromagnetic dipole localizations of digit representations in S1 of patients with FHd. (A) In the hemispherecontralateral to the nonaffected hand, digit representation is ordered, independent, and well separated. (B) Consistent withthe sensorimotor-learning hypothesis, sources localized in S1 in the hemisphere contralateral to the affected hand show littledistance between each other, with a digit topography that does not conform to the traditional ordering of these structures inS1. S1¼ primary somatosensory cortex; FHd¼ focal hand dystonia. (Reprinted with permission from John Wiley & Sons,Inc.12)
ARTICLE IN PRESS
although patients with writer’s cramp are able to per-form a simple spatial discrimination task of gratingsin either vertical or horizontal orientation as well ascontrol subjects, an increase in the amplitude of theblood oxygen level-dependent (BOLD) signal infMRI was greater in the basal ganglia and thalamusfor patients with writer’s cramp (when comparedwith changes in BOLD signal in healthy control sub-jects). This observation is consistent with the
FIGURE 3. Diagram of the computational model of sen-sory feedback in focal dystonia developed by Sanger andMerzenich (2000).14 Here, disorganized representationsin somatosensory cortex (S) contribute to excessive gainin a mapping from sensory to motor cortex (C), leadingto saturation in motor cortical activity (m) when combinedwith normal inputs from feedback through the basal gan-gliaecorticostriatal circuit (B) and the initial motor com-mand (u). (Reprinted with permission from Sanger andMerzenich.14)
4 JOURNAL OF HAND THERAPY
sensorimotor learning hypothesis, as expanded tac-tile receptive fields have been identified in subcorti-cal structures (such as the thalamus) in animalmodels of focal dystonia.8
In addition to deficits in tactile spatial processing,there is much evidence to suggest that there areabnormalities in temporal discrimination of somato-sensory stimuli in FHd. These impairments intemporal discrimination become evident duringassessments of somatosensory processing, such askinesthesia, graphesthesia, and stereognosis.18
Patients with FHd have difficulty discriminatingbetween two closely timed tactile stimuli.19
Impairments in temporal discrimination in focaldystonia may be due to inefficient processing in S1.Somatosensory-evoked potentials (SEPs) recordedin MEG are enhanced (greater amplitude withrespect to controls) in patients, which may contributeto an inability to discriminate between two rapidlypresented tactile stimuli.
Evoked responses in S1 will adapt when the stim-ulus presentation is coupled with a motor activity.Typically, performing a behavior with the hand (suchas writing or making circles with a toothbrush) willincrease the distance between the finger representa-tions in S1 localizations from MEG recordings.20 Thismechanism seems to be preserved in FHd. Although

ARTICLE IN PRESS
the distance between topographic representations inS1 are reduced in dystonia in response to passivetactile stimulation, this distance increases (and therepresentations stabilize) when the patient concur-rently executes a movement.21 This suggests thatsensory gating mechanisms may be spared in theseindividuals.
FIGURE 4. Functional magnetic resonance imaging time-series data from two regions of the basal ganglia, the puta-men (A) and globus pallidus (B) and two cortical areas,M1 (C) and S1 (D) during a simple finger-tapping task(E). Although activity increased in all regions during thetask, in patients with FHd (in red) this activity was increasedin amplitude, persistent and sustained after movement, apattern not seen in control subjects (in blue). (Reprintedwith permission from John Wiley & Sons, Inc.25) For inter-pretation of the references to color in this figure legend, thereader is referred to the web version of this article.
MOTOR PROCESSING
Although some aspects of sensorimotor integration(such as sensory gating) may remain uncompro-mised in patients with focal dystonia, it is wellestablished that aberrant patterns of activity exist inthe motor system of these patients, and this activityalso contributes to the condition. Motor processing iscomplex and involves the preparation, initiation, andexecution of movement followed by sensory feed-back. During movement preparation, regions of thefrontal lobe including premotor cortex (PMC) and thesupplementary motor area (SMA) are active beforeexecution of the behavior. In human fMRI studies,areas of PMC are active when an external signal (suchas a visual stimulus) is used to drive a motorresponse, whereas activity in the SMA is associatedwith motor imagery and internally driven move-ments.22,23 Higher-order motor areas, such as PMCand SMA, project directly to M1, where movementcommands are issued through the corticospinal tract.After movement onset, somatosensory feedback isprovided by processing in higher-order parietalfields, such as S2/parietal ventral area (PV) andPPC, to guide the action itself.
Functional neuroimaging techniques have beenused to identify alterations in the subcortical andcortical motor system of patients with focal dystonia.In the basal ganglia, fMRI activity (BOLD signalamplitude) is greater for FHd patients during a motortask when compared with normal individuals.24,25
This increase in the fMRI signal (when comparedwith a subject-specific baseline resting period) is sus-tained in specific structures of the basal ganglia(namely the putamen and globus pallidus) aftercompletion of the motor task, a pattern not identifi-able in the control population (25; Figure 4). In thebasal ganglia of these patients, an increase in thefMRI signal above what is normally seen duringmotor behavior is not specific to the affected task,and is present even when the patient performs a sim-ple grasping movement.26 Although it is difficult todiscern if abnormal overactivity in the basal gangliacontributes to or is the result of the motor impair-ments present in these patients, elevated activity inthis subcortical structure seems to be a primarycomponent of the disorder.
Demonstrable differences in cortical activitybetween focal dystonia patients and healthy
individuals have also been identified using func-tional neuroimaging techniques. Similar to the basalganglia, cortical activity in M1 is greater in these
jej 2009 5

FIGURE 5. Percentage change in compound movementamplitude potential (%CMAP) in the little finger evokedby TMS during both a resting condition and a self-trig-gered movement of the second digit of the right hand.When TMS is applied over motor cortex during self-pacedmovement, MEPs of the little finger in patients with FHd(in white) are increased compared with when control sub-jects (in gray) perform the same movement (*p , 0.05).These data indicate that cortical mechanisms that nor-mally inhibit unwanted movements are compromised inpatients with focal dystonia. TMS¼ transcranial mag-netic stimulation; MEPs ¼motor-evoked potentials;FHd¼ focal hand dystonia. (Reprinted with permissionfrom John Wiley & Sons, Inc.38)
ARTICLE IN PRESS
patients when compared with control subjects duringa motor task with the affected body structure.27 Incontrast, cortical activity in regions such as PMCand the SMA is significantly reduced in thesepatients when they perform a manual task with theaffected hand.28 Although this pattern of hyperactiv-ity in M1 and hypoactivity in PMC/SMA are inagreement with computational models of focal dysto-nia, other studies have reported greater activity in M1during movement for control subjects when com-pared with FHd patients.29 A lack of agreement be-tween these findings may be due to the fact thatbaseline brain activity in M1 (in the absence of a mo-tor task, or after the movement itself) of these patientsis likely to be impaired, in a fashion seen in otherbrain regions, such as the basal ganglia.25
Interpretation across studies is also confounded byhow these areas are defined and subdivided by imag-ing researchers, particularly with how the same areasare identified across groups, as activity in one regionmay be influenced by ‘‘spreading’’ activity in alteredneighboring cortical fields.
One emerging explanation for cortical overactivity(in M1) and underactivity (in PMC and SMA) is thatmuscular co-contraction in dystonia is the result of abreakdown in mechanisms that inhibit unwantedmovement plans generated in motor cortex.30,31
Evidence to support this hypothesis has been gener-ated through studies that observe the effects of directstimulation of motor cortical areas, such as TMS.Generally, high-intensity stimulation of motor cortexthrough TMS will evoke movements that, when mon-itored through EMG, are of a larger amplitude(motor-evoked potentials [MEPs]) in dystoniapatients when compared with controls.32 Rapid(,5 msec) delivery of a second TMS pulse to motorcortex (paired-pulse stimulation) is known to resultin decreased MEPs that reflect intracortical inhibition(ICI), a process mediated by neurotransmitters (suchas GABA-A) that is designed to focus and selectappropriate responses and inhibit unwanted move-ments.33 MEPs evoked under multiple paired-pulseTMS stimulation paradigms remained unattenuatedin focal dystonia patients further supporting the positthat this process of motor cortex (ICI) is deficient inthis population.34e37 When a TMS pulse is triggeredby the flexion of one finger, MEPs recorded from aneighboring (stationary, and thus normally inhibited)digit are suppressed in control subjects and enhancedin dystonia patients (38; Figure 5). Studies using TMShave complemented data from functional neuroi-maging research that have previously identifiedincreased activity in M1 by suggesting that this over-activity in dystonia is the result of reduced ICI in M1.
Some evidence suggests that motor visualizationand imagery are also impaired in focal dystonia.Behaviorally, patients with writer’s cramp are slowerto respond to mental rotation tasks of the hands but
6 JOURNAL OF HAND THERAPY
not the feet, although accuracy is relativelypreserved, possibly due to an alteration of the repre-sentations of manual structures in S1.39 Additionallyit may be a result of dysfunction in the basal gangliaor motor cortices. When TMS is delivered to M1 inthese patients, enhanced MEP amplitudes persisteven when the movement is imagined and notreal.40 Visual processing areas may also play a moreprominent role in motor imagery in this population.In simple somatosensory spatial discriminationtasks, overactivation in fMRI (greater amplitude ofthe BOLD signal versus controls) of visual corticalfields was present suggesting a reliance on visualimagery for tactile discrimination.17
EFFECTS OF TRAINING
Knowledge about the underlying neural patho-physiology of FHd obtained through animal modelsand neuroimaging techniques have allowedclinicians to develop successful behavioral treatmentregimens. Some of these therapeutic interventions,such as constraint-induced movement therapy41 andlearning-based sensorimotor retraining13,42 havebeen successfully applied with the ultimate goal ofimproving the sensory representations of the affectedlimbs in the brain. Completion of these physical ther-apy programs can produce demonstrable changes incortical structure concurrent with the reduction ofdystonic symptoms. For example, subjective reportsof improvement after retraining with the handcoincide with changes in topographic organizationthat occur during the course of treatment.5 Imaging

ARTICLE IN PRESS
techniques with superior temporal resolution, suchas EEG and MEG, are ideal for examining training-induced neuroplasticity. These methods have beenused to identify changes in neural processing duringthe course of perceptual learning in healthy individ-uals. For example, activity in primary auditory cortexincreases after auditory temporal interval discrimina-tion training.43,44 Transformations in primary sensoryareas as a result of training can occur quite rapidly,with identifiable changes within the response proper-ties of auditory cortex over the course of a few days45
and can generalize across spatial location andsensory modality.46 Changes that occur in the brainas a result of treatment should extend outside of S1also. In many clinical conditions, including low-grade gliomas and stroke, changes in cortical func-tion occur bilaterally.47,48 Furthermore, recovery offine motor function in the affected hand is associatedwith changes in the ipsilateral hemisphere.49 Whole-brain coverage provided by most of the functionalimaging techniques allows imaging experts toexamine these changes as well.
To evaluate the extent to which neuroplasticitycontributed to this recovery, Byl et al.50 applied thetechniques of MEG to map the distribution, amplitude,and latency of somatosensory-evoked responses bothbefore and after learning-based sensorimotor retrain-ing. After treatment, significant functional changes inS1 were present (Figure 6). Sensorimotor retraining ex-panded representations of manual structures thatwere previously intermixed in S1 (Figure 6A). Digit re-ordering in S1, generally distinct in normal individ-uals, became normalized and more like the orderingin control subjects after treatment (Figure 6B). Lastly,temporal properties of the somatosensory-evoked re-sponse such as amplitude and latency became stabi-lized in patients who had completed the program,reducing the strength of the magnetic dipole and tight-ening the duration of the SEF to a level comparable tohealthy controls (Figure 6C).
THE ROLE OF NEUROIMAGINGIN THE DIAGNOSIS OF FHD
Although the behavioral manifestations of FHd areevident to the clinician, limited testing is available toconfirm such a diagnosis. A diagnosis of FHd istypically generated through behavioral testing by theclinician; however, neuroimaging tools can and doplay a powerful role in verification of the disorder.3
Although some genetic mutations, specifically thoseof the DYT1 and DYT7 genes, are associated withthe development of a focal dystonia,51e53 manycarriers of these genes do not develop the condition.Given the lack of a definitive genetic marker for focaldystonia, imaging methods such as MRI and MEGhave the potential to become important tools for clini-cians to assess and monitor the treatment of focal
dystonia. This is especially important as many otherforms of adult-onset primary dystonia share commongenetic mechanisms.30 Although MRI is commonlyused by clinicians to clear patients of other neurolog-ical conditions (such as tumor and stroke), it is also apowerful tool for assessment. The most commonapplication of these imaging methods is to identifyand track changes in the cortical representation ofthe affected body structure, generally done usingfMRI or MEG. Studies using structural MRIs havealso isolated specific anatomical changes in corticalvolume in FHd, such as the expansion of gray mattervolume in the putamen of patients with FHd.54 Thisis consistent with single photon emission computedtomography (SPECT) studies that have identified re-duced dopamine D2 receptor binding in structures ofthe basal ganglia.55 Some of these changes in anat-omy, such as increased gray matter volume aroundsensorimotor cortex, have been found to be specificto focal dystonia and absent in other forms of adult-onset dystonia.56e58
It is likely that neuroimaging will soon be used toidentify individuals who are at-risk for developingfocal dystonia. Many of the changes of functionalbrain activity identified in FHd are also present insome individuals who carry certain genes, such asDYT1. In a study done by Ghilardi et al. in 2003, indi-viduals who carry the DYT1 gene yet do not expressany clinical symptoms were impaired in the acquisi-tion of a motor sequence, and furthermore showedaberrant patterns of activity in higher-order motorareas (PMC and SMA) and the cerebellum duringthe training phase of the task.59,60 Also, in DYT1 car-riers, the integrity of the fiber tracts (as measured byDTI) connecting sensorimotor cortex with other corti-cal and subcortical brain structures is reduced,suggesting that even in the absence of motor impair-ment, aberrations in neuroanatomical structure stillexist.61 Changes in white matter integrity, specificallyin fiber tracts that connect the basal ganglia, can beidentified in the patient before treatment and canalso be tracked after a therapeutic intervention.62
Although it is difficult to determine if changes inthe behavior, neuroanatomy, and physiological func-tioning of the brain in both clinical patients and genecarriers are the cause of or are a result of FHd, agreater understanding of these characteristicsthrough applied neuroimaging will allow us tounderstand endophenotypic traits inherent to thecondition.30,31
FUTURE DIRECTIONS FORNEUROIMAGING AND FHD
Although many advances in the treatment ofFHd have been made through insights provided byneuroimaging, a considerable amount of workremains to be done in linking these motor
jej 2009 7

FIGURE 6. Changes in the response properties of primary somatosensory cortex (S1) recorded in magnetoencephalographyafter sensory discrimination training. After a comprehensive rehabilitation paradigm, observable changes in the volume ofactivity (A), digit order representation (B), and amplitude and latency of the S1 response (C) are stabilized in focal dystoniapatients in conjunction with alleviation of symptoms. (Reprinted with permission from Byl et al.50)
ARTICLE IN PRESS
impairments to underlying anatomical and physi-ological mechanisms. It is challenging to evaluatethe extent to which changes in brain anatomy andfunction are the result of primary versus secondaryeffects of the disorder, and this becomes critical tounderstand in the development of behavioral treat-ment regimens targeted to reverse neurobiologicalchanges. One of the stronger supports for impairedneural mechanisms as the source of FHd comesfrom demonstrations of deviant brain activity innonmanifesting genetic carriers.59e61 Here,changes in brain function can be observed in the ab-sence of any dystonic symptoms in the nonmani-festing carriers, suggesting that these alterationsin neurophysiology contribute to, and are not theresult of, the condition. However, given that thegenetic contributions to FHd are some of the mostcomplex and poorly understood of all dystonias,focal or otherwise,30,31 more work needs to bedone in this area. Conflicting reports in the litera-ture—such as why in some studies an increase inactivity in M1 is seen63 and in some reports adecrease is seen in the same region29,64—necessi-tate further investigations. Although this lack ofparsimony may be due to inherent differences inexperimental paradigms, it is equally likely dueto the fact that none of these brain regions act in iso-lation, and that further work in this area will needto focus on how interaction between these areas
8 JOURNAL OF HAND THERAPY
may contribute to the disorder. Alterations in thesemotor networks may become disentangled throughMEG and fMRI studies of functional connectivitycombined with MRI and DTI studies of anatomicalconnectivity.65,66 A greater understanding of theneural architecture that is affected in focal dystoniacan provide clinicians and scientists with informa-tion needed to develop accurate surgical interven-tions (such as the placement of deep brainstimulators) in addition to the opportunity to trackrecovery and guide retraining paradigms tailoredfor each individual patient.
CONCLUSION
Therapists, neuroscientists, neuroradiolo-gists, neurosurgeons, and neurologists have anexciting opportunity to work together to dis-cover more about the risk factors, etiology, andeffective intervention paradigms to facilitaterecovery of normal motor control in patientswith FHd. Although today, the application offunctional neuroimaging is most commonlyused for research purposes, neuroimaging maybegin to play a more important role in objec-tively documenting and guiding appropriateintervention strategies for patients with focaldystonia.

ARTICLE IN PRESS
REFERENCES
1. Sheehy MP, Mardsen CD. Writer’s cramp—a focal dystonia.Brain. 1982;105:461–80.
2. Marsden CD, Sheehy MP. Writer’s cramp. Trends Neurosci.1990;13:148–53.
3. Lin PT, Shamim EA, Hallett M. Focal hand dystonia. PractNeurol. 2006;6:278–87.
4. Das CP, Dressler D, Hallett M. Botulinum toxin therapy ofwriter’s cramp. Eur J Neurol. 2006;13:55–9.
5. Candia V, Wienbruch C, Elbert T, Rockstroh B, Ray W. Effectivebehavioral treatment of focal hand dystonia in musicians alterssomatosensory cortical organization. PNAS. 2003;100:7942–6.
6. Priori A, Pesenti A, Cappellari A, Scarlato G, Barbieri S. Limbimmobilization for the treatment of focal occupational dysto-nia. Neurology. 2001;57:405–9.
7. Zeuner KE, et al. Motor training as treatment in focal handdystonia. Mov Disord. 2005;20:335–41.
8. Blake DT, et al. Sensory representation abnormalities thatparallel focal hand dystonia in a primate model. SomatosensMot Res. 2002;19:347–57.
9. Byl NN, Merzenich MM, Jenkins WM. A primate genesismodel of focal hand dystonia and repetitive strain injury: 1.Learning-induced dedifferentiation of the representation ofthe hand in the primary somatosensory cortex in adult mon-keys. Neurology. 1996;47:508–20.
10. Sur M, Merzenich MM, Kaas JH. Magnification, receptive-fieldarea, and ‘‘hypercolumn’’ size in areas 3b and 1 of somatosen-sory cortex in owl monkeys. J Neurophysiol. 1980;44:295–311.
11. Butterworth S, Francis S, Kelly E, McGlone F, Bowtell R, SawieGV. Abnormal cortical sensory activation in dystonia: an fMRIstudy. Mov Disord. 2003;186:673–82.
12. Meunier S, et al. Human brain mapping in dystonia revealsboth endophenotypic traits and adaptive reorganization. AnnNeurol. 2001;50:521–7.
13. McKenzie AL, Nagarajan SS, Roberts TP Merzenich MM BylNN. Somatosensory representation of the digits in clinical per-formance in patients with focal hand dystonia. Am J Phys MedRehabil. 2003;82(10):737–49.
14. Sanger TD, Merzenich MM. Computational model of the roleof sensory disorganization in focal task-specific dystonia.J Neurophysiol. 2000;84:2458–64.
15. Sanger TD, Tarsy D, Pascual-Leone A. Abnormalities of spatialand temporal sensory discrimination in writer’s cramp. MovDisord. 2001;16:94–9.
16. Molloy FM, Carr TD, Zeuner KE, Dambrosia JM, Hallett M.Abnormalities of spatial discrimination in focal and general-ized dystonia. Brain. 2003;126:2175–82.
17. Peller M, et al. The basal ganglia are hyperactive during thediscrimination of tactile stimuli in writer’s cramp. Brain.2006;129:2697–708.
18. Byl NN, et al. Sensory dysfunction associated with repeti-tive strain injuries of tendonitis and focal hand dystonia:a comparative study. J Ortho Sports Phys Ther. 1996;23:234–44.
19. Bara-Jimenez W, Shelton P, Sanger TD, Hallett M. Sensory dis-crimination capabilities in patients with focal hand dystonia.Ann Neurol. 2000;47:377–80.
20. Braun C, Heinz U, Schweizer R, Wiech K, Birbaumer N,Topka H. Dynamic organization of the somatosensory cortexinduced by motor activity. Brain. 2001;124:2259–67.
21. Braun C, Schweizer R, Heinz U, Wiech K, Birbaumer N,Topka H. Task-specific plasticity of somatosensory cortex inpatients with writer’s cramp. Neuroimage. 2003;20:1329–38.
22. Toni I, Thoenissen D, Zilles K. Movement preparation andmotor intention. Neuroimage. 2001;14:S110–7.
23. Lotze M, et al. Activation of cortical and cerebellar motor areasduring executed and imagined hand movements: an fMRIstudy. J Cogn Neurosci. 1999;11:491–501.
24. Preibisch C, Berg D, Hofmann E, Solymosi L, Naumann M. Ce-rebral activation patterns in patients with writer’s cramp: afunctional magnetic resonance imaging study. J Neurol. 2001;248:10–7.
25. Blood AJ, et al. Basal ganglia activity remains elevated aftermovement in focal hand dystonia. Ann Neurol. 2004;55:744–8.
26. Obermann M, et al. Increased basal-ganglia activation per-forming a non-dystonia-related task in focal dystonia. Eur JNeurol. 2008;8:831–8.
27. Lerner A, Shill H, Hanakawa T, Bushara K, Goldfine A, HallettM. Regional cerebral blood flow correlates of the severity ofwriter’s cramp symptoms. Neuroimage. 2004;21:904–13.
28. Ibanez V, Sadato N, Karp B, Deiber MP, Hallett M. Deficient acti-vation of the motor cortical network in patients with writer’scramp. Neurology. 1999;53:96–105.
29. Oga T, et al. Abnormal cortical mechanisms of voluntarymuscle relaxation in patients with writer’s cramp: an fMRIstudy. Brain. 2002;125:895–903.
30. Breakefield XO, Blood AJ, Li Y, Hallett M, Hanson PI, StandaertDG. The pathophysiological basis of dystonias. Nat Rev Neu-rosci. 2008;9:222–34.
31. Defazio G, Berardelli A, Hallett M. Do primary adult-onsetfocal dystonias share aetiological factors? Brain. 2007;130:1183–93.
32. Ikoma K, Samii A, Mercuri B, Wassermann EM, Hallett M. Ab-normal cortical motor excitability in dystonia. Neurology. 1996;46:1371–6.
33. Di Lazzaro V, et al. Direct demonstration of the effect oflorazepam on the excitability of the human motor cortex.Clin Neurophysiol. 2000;111:794–9.
34. Ridding MC, Sheean G, Rothwell JC, Inzelberg R, Kujirai T.Changes in the balance between motor cortical excitation andinhibition in focal, task specific dystonia. J Neurol NeurosurgPsychiatry. 1995;59:493–8.
35. Abbruzzese G, Marchese R, Buccolieri A, Gasparetto B, Trom-petto C. Abnormalities of sensorimotor integration in focaldystonia: a transcranial magnetic stimulation study. Brain.2001;124:537–45.
36. Stinear CM, Byblow WD. Impaired modulation ofcorticospinal excitability following subthreshold rTMS in focalhand dystonia. Hum Mov Sci. 2004;23:527–38.
37. Stinear CM, Byblow WD. Elevated threshold for intracorticalinhibition in focal hand dystonia. Mov Disord. 2004;19:1312–7.
38. Sohn YH, Hallett M. Disturbed surround inhibition in focalhand dystonia. Ann Neurol. 2004;56:595–9.
39. Fiorio M, Tinazzi M, Aglioti SM. Selective impairment of handmental rotation in patients with focal hand dystonia. Brain.2006;129:47–54.
40. Quartarone A, et al. Corticospinal excitability during motorimagery of a simple tonic finger movement in patients withwriter’s cramp. Mov Disord. 2005;22:1488–95.
41. Taub E, Uswatte G, Mark VW, Morris DM. The learned nonusephenomenon: implications for rehabilitation. Eura Medico-phys. 2006;42:241–55.
42. Byl NN, Nagarajan S, McKenzie AM. Treatment effectivenessof patients with a history of repetitive strain injury and focalhand dystonia: a planned, prospective follow-up study.J Hand Ther. 2000;13:289–301.
43. Cansino S, Williamson SJ. Neuromagnetic fields reveal corticalplasticity when learning an auditory discrimination task. BrainRes. 1997;764(1e2):53–66.
44. Bosnyak DJ, Eaton RA, Roberts LE. Distributed auditory corti-cal representations are modified when non-musicians aretrained at pitch discrimination with 40 Hz amplitude modu-lated tones. Cereb Cortex. 2004;14:1088–99.
45. van Wassenhove V, Nagarajan SS. Auditory cortical plasticityin learning to discriminate modulation rate. J Neurosci. 2007;27:2663–72.
46. Nagarajan SS, Blake DT, Wright BA, Byl N, Merzenich MM.Practice-related improvements in somatosensory interval dis-crimination are temporally specific but generalize across skinlocation, hemisphere, and modality. J Neurosci. 1998;18:1559–70.
47. Wunderlich G, Knorr U, Herzog H, Kiwit JC, Freund HJ,Seitz RJ. Precentral glioma location determines the displace-ment of cortical hand representation. Neurosurgery. 1998;42:18–26.
jej 2009 9

ARTICLE IN PRESS
48. Cao Y, D’Olhaberriague L, Vikingstad EM, Levine SS, WelchKM. Pilot study of functional MRI to assess cerebral activationof motor function after poststroke hemiparesis. Stroke. 1998;29:112–22.
49. Cramer SC, Nelles G, Schaechter JD, Kaplan JD, Finklestein SP,Rosen BR. A functional MRI study of three motor tasks in theevaluation of stroke recovery. Neurorehabil Neural Repair.2001;15:1–8.
50. Byl NN, Nagarajan S, McKenzie AL. Effect of sensory discrim-ination training on structure and function in patients with focalhand dystonia: a case series. Arch Phys Med Rehabil. 2003;84:1505–14.
51. Gasser T, Windgassen K, Bereznai B, Kabus C, Ludolph AC.Phenotypic expression of the DYT1 mutation: a family withwriter’s cramp of juvenile onset. Ann Neurol. 1998;44:126–8.
52. Dhaenens CM, et al. Clinical and genetic evaluation in a Frenchpopulation presenting with primary focal dystonia. MovDisord. 2005;20:822–5.
53. Bhidayasiri R, Jen JC, Baloh RW. Three brothers with a very-late-onset writer’s cramp. Mov Disord. 2005;20:1375–7.
54. Black JK, Ongur D, Perlmutter JS. Putamen volume in idio-pathic focal dystonia. Neurology. 1998;51:819–24.
55. Horstink CA, Praamstra P, Horstink MW, Berger HJ, Booij J,Van Royen EA. Low striatal D2 receptor binding as assessedby [123I]IBZM SPECT in patients with writer’s cramp. J NeurolNeurosurg Psychiatry. 1997;62:672–3.
56. Draganski B, et al. ‘‘Motor circuit’’ gray matter changes inidiopathic cervical dystonia. Neurology. 2003;61:1228–31.
10 JOURNAL OF HAND THERAPY
57. Garraux G, Bauer A, Hanakawa T, Wu T, Kansaku K, Hallett M.Changes in brain anatomy in focal hand dystonia. Ann Neurol.2004;55:736–9.
58. Etgen T, Muhlau M, Gaser C, Sander D. Bilateral gray-matterincrease in the putamen in primary blepherospasm. J NeurolNeurosurg Psychiatry. 2006;77:1017–20.
59. Ghilardi MF, et al. Impaired sequence learning in carriers of theDYT1 dystonia mutation. Ann Neurol. 2003;54:102–9.
60. Carbon M, Ghilardi MF, Argyelan M, Dhawan V, Bressman SB,Eidelberg D. Increased cerebellar activation during sequencelearning in DYT1 carriers: an equiperformance study. Brain.2008;131:146–54.
61. Carbon M, et al. Microstructural white matter changes incarriers of the DYT1 gene mutation. Ann Neurol. 2004;56:283–6.
62. Blood AJ, Tuch DS, Makris N, Makhlouf ML, Sudarsky LR,Sharma N. White matter abnormalities in dystonia normalizeafter botulinum toxin treatment. Neuroreport. 2006;17:1251–5.
63. Hu XY, Wang L, Liu H, Zhang SZ. Functional magnetic reso-nance imaging study of writer’s cramp. Chin Med J. 2006;119:1263–71.
64. Pujol J, et al. Brain cortical activation during guitar-inducedhand dystonia studied by functional MRI. Neuroimage. 2000;12:257–67.
65. Rykhlevskala E, Gratton G, Fabiani M. Combining structuraland functional neuroimaging data for studying brain connec-tivity: a review. Psychophysiology. 2008;45:173–87.
66. Guye M, Bartolomei F, Ranjeva JP. Imaging structural andfunctional connectivity: towards a unified definition of humanbrain organization? Curr Opin Neurol. 2008;21:393–403.




















