Neuro-Oncology Single-Photon Emission CT: A Current Overview
13
FUNCTIONAL Neuro-Oncology Single-Photon Emission CT: A Current Overview Thomas C. Booth (1), Yenzhi Tang (2), Adam D. Waldman (3), Anne-Marie Quigley (4), David Lewis (5), Dimtri Soloviev (5), Malavika Nathan (4), Pervinder Bhogal (2), Sarah Jefferies (6), and John R. Buscombe (7) ABSTRACT There is increasing need for noninvasive biomarkers for glioma treatment-response evalu- ation and for distinguishing tumor progression and recurrence from treatment-related changes. Here, SPECT, particularly 201 Tl SPECT, plays an important role. SPECT takes ad- vantage of glioma cellular make-up. Specifically, Na /K pump expression, mitochondrial attenuation, and amino acid transporter expression are probed with 201 Tl, 99m Tc-MIBI, and 123 IMT radiotracers respectively. 201 Tl can be used to distinguish brain tumors and nontu- mors and to determine brain tumor type and grade gliomas. However, it is especially valuable in the detection of tumor recurrence in patients treated with radiation therapy for supratentorial glioma. Similarly, 99m Tc-MIBI can be used to distinguish recurrence from treatment residua. 99m Tc-TF is comparable with 99m Tc-MIBI, and both may allow clear identification of tumor boundaries. 123 IMT appears to be superior to 99m Tc-MIBI in deter- mining tumor recurrence and is particularly promising in detecting LGG recurrence. Addi- tionally, 123 IMT shows promise in treatment planning where there is a survival advantage. LGGs frequently express somatostatin receptors; however, because radiolabeled soma- tostatin analogs do not cross the BBB and because LGGs frequently do not disturb the BBB, somatostatin-receptor imaging is limited in glioma imaging. Among the non-natural amino acid class, 123 IPA is not preferable to the more established 123 IMT. In summary, most inter- national experience by using SPECT is with 201 Tl; however, other radiotracers are used with good effect in some clinics. INTRODUCTION In brain tumor imaging, conventional MR imaging provides essential structural information but limited physiologic de- tail. A rapidly enlarging enhancing lesion on MR imaging with or without clinical symptoms usually establishes a diagnosis of progressing tumor; this is nonspecific for differentiation of tumor and necro- sis. 1 Indeed, enhancing components re- flect only deficient BBB, and T2-weighted signal-intensity abnormality is biologi- cally nonspecific. Furthermore, anaplas- tic gliomas can often present as nonenhancing tumors, and even a glio- blastoma may present initially as a non- enhancing lesion, especially in older patients. Novel therapeutic agents, more sophis- ticated radiation therapy delivery, and ad- vances in neurosurgical techniques have been developed for the treatment of brain tumors. This has generated increasing need for noninvasive biomarkers for brain tu- mor treatment-response evaluation and for distinguishing tumor recurrence from treatment-related changes. 2 Advanced MR imaging and radionuclide imaging may ad- dress these needs. Coregistration of con- ventional MR imaging and radionuclide images or hybrid imaging allows the syner- gistic combination of anatomic and molec- ABBREVIATION KEY ADC apparent diffusion coefficient ATPase adenosine triphosphatase BBB blood brain barrier Cho choline 11 C MET L-methyl- 11 C methionine Cr creatine DTPA diethylenetriamine pentaacetic acid 18 F fluorine 18 18 FDG 18 F-fluorodeoxyglucose 18 FET O-(2-[ 18 F]fluoroethyl)-l- tyrosine GBM glioblastoma multiforme GLUT glucose transporter 201 Hg mercury 201 HGG high-grade glioma HMPAO hexamethypropyleneamine oxime 123 I iodine 123 123 IMT iodine-123--methyl tyrosine 111 In indium 111 123 IPA p-[(123)I]-iodo-L- phenylalanine LGG low-grade glioma MRS MR spectroscopy MRSI MR spectroscopic imaging MIBI hexakis-2-methoxyisobutyl isonitrile NAA N-acetyl aspartate Na / K sodium/potassium 201 Pb lead 201 PCV procarbazine, lomustine, and vincristine PET positron-emission tomography rCBV relative cerebral blood volume ROI region of interest SPECT single-photon emission CT SRS somatostatin receptor scintigraphy 201 Tl thallium 201 99m Tc technetium 99m TF 1,2-bis[bis(2- ethoxyethyl)phospino] ethane TI thallium index Received February 2, 2011; accepted August 24. From the Department of Biochemistry (T.C.B.), University of Cambridge, Cambridge, UK; Departments of Radiology (Y.T., P.B.) and Nuclear Medicine (A.-M.Q., M.N.), the Royal Free Hospital NHS Trust, London, UK; Department of Radiology (A.D.W.), Imperial College, London, UK; Cambridge Research Institute (D.L., D.S.), Cambridge, UK; and Departments of Clinical Oncology (S.J.) and Nuclear Medicine (J.R.B.), Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK. Please address correspondence to Thomas C. Booth, MRCP, FRCR, Department of Biochemistry, Uni- versity of Cambridge, Tennis Court Rd, Cambridge, UK CB2 1GA; e- mail: [email protected] http://dx.doi.org/10.3174/ng.3110014 108 Neurographics 01:108-120 December 2011 www.neurographics.com
Transcript of Neuro-Oncology Single-Photon Emission CT: A Current Overview

FUNCTIONAL
Neuro-Oncology Single-PhotonEmission CT: A Current OverviewThomas C. Booth (1), Yenzhi Tang (2), Adam D. Waldman (3),Anne-Marie Quigley (4), David Lewis (5), Dimtri Soloviev (5), Malavika Nathan (4),Pervinder Bhogal (2), Sarah Jefferies (6), and John R. Buscombe (7)
ABSTRACTThere is increasing need for noninvasive biomarkers for glioma treatment-response evalu-ation and for distinguishing tumor progression and recurrence from treatment-relatedchanges. Here, SPECT, particularly 201Tl SPECT, plays an important role. SPECT takes ad-vantage of glioma cellular make-up. Specifically, Na�/K� pump expression, mitochondrialattenuation, and amino acid transporter expression are probed with 201Tl, 99mTc-MIBI, and123IMT radiotracers respectively. 201Tl can be used to distinguish brain tumors and nontu-mors and to determine brain tumor type and grade gliomas. However, it is especiallyvaluable in the detection of tumor recurrence in patients treated with radiation therapy forsupratentorial glioma. Similarly, 99mTc-MIBI can be used to distinguish recurrence fromtreatment residua. 99mTc-TF is comparable with 99mTc-MIBI, and both may allow clearidentification of tumor boundaries. 123IMT appears to be superior to 99mTc-MIBI in deter-mining tumor recurrence and is particularly promising in detecting LGG recurrence. Addi-tionally, 123IMT shows promise in treatment planning where there is a survival advantage.LGGs frequently express somatostatin receptors; however, because radiolabeled soma-tostatin analogs do not cross the BBB and because LGGs frequently do not disturb the BBB,somatostatin-receptor imaging is limited in glioma imaging. Among the non-natural aminoacid class, 123IPA is not preferable to the more established 123IMT. In summary, most inter-national experience by using SPECT is with 201Tl; however, other radiotracers are used withgood effect in some clinics.
INTRODUCTIONIn brain tumor imaging, conventionalMR imaging provides essential structuralinformation but limited physiologic de-tail. A rapidly enlarging enhancing lesionon MR imaging with or without clinicalsymptoms usually establishes a diagnosisof progressing tumor; this is nonspecificfor differentiation of tumor and necro-sis.1 Indeed, enhancing components re-flect only deficient BBB, and T2-weightedsignal-intensity abnormality is biologi-cally nonspecific. Furthermore, anaplas-tic gliomas can often present asnonenhancing tumors, and even a glio-blastoma may present initially as a non-
enhancing lesion, especially in olderpatients.
Novel therapeutic agents, more sophis-ticated radiation therapy delivery, and ad-vances in neurosurgical techniques havebeen developed for the treatment of braintumors. This has generated increasing needfor noninvasive biomarkers for brain tu-mor treatment-response evaluation and fordistinguishing tumor recurrence fromtreatment-related changes.2 Advanced MRimaging and radionuclide imaging may ad-dress these needs. Coregistration of con-ventional MR imaging and radionuclideimages or hybrid imaging allows the syner-gistic combination of anatomic and molec-
ABBREVIATION KEY
ADC� apparent diffusion coefficientATPase� adenosine triphosphataseBBB� blood brain barrierCho� choline11CMET� L-methyl-11CmethionineCr� creatineDTPA� diethylenetriamine
pentaacetic acid18F� fluorine 1818FDG� 18F-fluorodeoxyglucose18FET�O-(2-[18F]fluoroethyl)-l-
tyrosineGBM� glioblastomamultiformeGLUT� glucose transporter201Hg�mercury 201HGG� high-grade gliomaHMPAO� hexamethypropyleneamine
oxime123I� iodine 123123IMT� iodine-123-�-methyl tyrosine111In� indium 111123IPA� p-[(123)I]-iodo-L-
phenylalanineLGG� low-grade gliomaMRS�MR spectroscopyMRSI�MR spectroscopic imagingMIBI� hexakis-2-methoxyisobutyl
isonitrileNAA�N-acetyl aspartateNa�/K� � sodium/potassium201Pb� lead 201PCV� procarbazine, lomustine, and
vincristinePET� positron-emission tomographyrCBV� relative cerebral blood volumeROI� region of interestSPECT� single-photon emission CTSRS� somatostatin receptor
scintigraphy201Tl� thallium 20199mTc� technetium 99mTF� 1,2-bis[bis(2-
ethoxyethyl)phospino] ethaneTI� thallium index
Received February 2, 2011;accepted August 24.
From the Department of Biochemistry(T.C.B.), University of Cambridge,Cambridge, UK; Departments ofRadiology (Y.T., P.B.) andNuclearMedicine (A.-M.Q., M.N.), the RoyalFree Hospital NHS Trust, London, UK;Department of Radiology (A.D.W.),Imperial College, London, UK;Cambridge Research Institute (D.L.,D.S.), Cambridge, UK; andDepartments of Clinical Oncology(S.J.) andNuclear Medicine (J.R.B.),Addenbrooke’s Hospital, CambridgeUniversity Hospitals NHS FoundationTrust, Cambridge, UK.
Please address correspondence toThomas C. Booth, MRCP, FRCR,Department of Biochemistry, Uni-versity of Cambridge, Tennis CourtRd, Cambridge, UK CB2 1GA; e-mail: [email protected]
http://dx.doi.org/10.3174/ng.3110014
108 � Neurographics 01:108-120 December 2011 www.neurographics.com

ular information. One such radionuclide technique,SPECT, particularly 201Tl SPECT, plays an important butneglected complementary role to conventional MRimaging.
SPECT Compared with Advanced MR imagingMetabolic and physiologic information can be obtained byusing advanced MR imaging techniques while the patientundergoes conventional MR imaging. Such techniques canassess changes in metabolic tissue profile, tissue blood per-fusion, microvessel permeability, and water mobility,which are biomarkers for pathophysiologic changes relatedto tumor biology.3 Advanced MR imaging is performedmore commonly than SPECT (or PET),4 probably becauseof the improved spatial resolution for most techniques,lower cost, and wide availability compared with radionu-clide imaging.2 Perfusion and diffusion imaging are nowclose to being implemented by many centers for routineplanning of biopsy sampling, resection, radiation therapy,differentiation of radiation necrosis from tumor progres-sion, and follow-up of the effects of chemotherapy.3 How-ever, there are major limitations to advanced MR imaging.Perfusion imaging drawbacks include the semiquantitativenature of the technique, the need to establish optimal tim-ing, and the lack of standardization of acquisition and post-processing techniques. Diffusion imaging is limited by theeffect of edema on the ADC value, which can confoundgrade and assessment of therapeutic response. 1H-MRSpartial volume effects can limit differentiation of tumor andnecrosis in small lesions, and there are considerable chal-lenges in suppressing unwanted signal intensity.
To our knowledge, there are only a few small publishedstudies comparing SPECT with advanced MR imaging;thus, conclusions as to their relative benefits are limited.
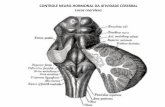
201Tl Production and Mechanism of Action201Tl is produced in a cyclotron from 201Pb, with a T1/2 of73 hours.5 201Tl decays by electron capture to 201Hg, emit-ting mainly characteristic x-rays in the 68- to 80- keV range(Fig 1). The chemical behavior of 201Tl is comparable withK�, both being monovalent with similar ionic radii. In nor-mal circumstances 201Tl cell influx (Fig 2) is reliant on themetabolic rate of the cell (ATPase-dependent) but is limitedby an intact BBB.
In gliomas, increased 201Tl uptake is correlated with pro-liferation (proliferating cell nuclear antigen)6 and may bedue to 3 factors: increased BBB permeability, increased re-gional blood flow, and increased Na�/K� ATPase pumpexpression.7 Here, the ATPase pump �1 subunit may proveto be a therapeutic target8 with implications for this imag-ing test.
201Tl Image EvaluationWith 201Tl SPECT, thallous chloride is usually administeredand given intravenously at a dose of 2–4 mCi (75–150MBq). Early imaging (5–10 minutes later) is usually suffi-
cient for clinical purposes. There is little background 201Tluptake in normal brain, though there is high uptake in thebase of the skull and in the orbital and hypophysealregions.5
Most important, even with concomitant steroid use,which can cause an apparent reduction of tumor size onMR imaging,9 there is high uptake of 201Tl in brain tumors.Evaluation by SPECT is usually by visual image inspection(ie, qualitative) with or without using the semiquantitativeTI (thalium index). The TI is a ratio describing tumor up-take in a ROI relative to uptake in the contralateral hemi-sphere, which may be a mirror image. The scalp can also bedesignated as the reference tissue when determining the TI.Regardless of choice of reference tissue, TI techniques haveintraclass correlation coefficients �0.80, indicating verygood observer agreement.10
201Tl Indications
Distinguishing Brain Tumors and Non-NeoplasticLesionsThere is increased 201Tl uptake in metastases, meningio-mas, and gliomas. Some non-neoplastic lesions have in-creased tracer uptake with false-positives occurring in hem-orrhagic infarction, epidural hematomas, and angiomas.11
However, SPECT is an adjunct to conventional MR imag-ing or CT, which, in most cases, would point the reader toan alternative diagnosis. In immunodeficient individuals,infections should also be considered in 201Tl-avid lesions,though malignancy can be distinguished from toxoplasmo-sis, the key differential diagnosis, by using a TI � 2 inlesions of �2 cm, yielding a sensitivity of 100% with aspecificity of 89%.12
Overall, the sensitivity for the detection of supratentorialbrain tumors is 72%, with a specificity of 81%. In the
Fig 1. 201Tl is produced in a cyclotron from 201Pb and then undergoesdecay by electron capture to 201Hg, emittingmainly characteristic x-raysin the 68- to 80-KeV range.
Fig 2. Influx of 201Tl into cells is through the Na�/K� ATPase pump. 201Tlis a K� analog.
Neurographics 01:108-120 December 2011 www.neurographics.com � 109

posterior fossa, the sensitivity is reduced; this reduction isprobably related to the size of these tumors compared withthe resolution of SPECT.11 However, a technique withworse resolution, MRS, actually gives a superior sensitivityof 85% and a specificity of 87% when Cho/NAA are usedto differentiate tumors from non-neoplastic lesions.13 Oneparticular limitation is that the spectroscopic and structuralMR imaging appearances of tumefactive demyelinatingplaques may closely resemble those of high-grade enhanc-ing neoplasms. The rCBV from perfusion imaging is prom-ising in this scenario because it is low in both plaques andabscesses and high in HGG.14,15 ADC from diffusion-weighted imaging is also highly effective (100% specificity)for addressing the specific question of whether a lesion is apyogenic abscess or a tumor.16 Compared with PET, 201TlSPECT appears more sensitive than 18FDG but is less sen-sitive than 11C MET.17 11C MET PET distinguishes braintumors and non-neoplastic lesions with 100% specificityand, therefore, appears to be the agent of choice ifavailable.18
Distinguishing Brain Tumor TypesMany types of tumors can be distinguished by using 201TlSPECT, though without judicious data acquisition, tumorsmay be indistinguishable.19 In 1 series, 201Tl SPECT per-formed at 10 minutes after tracer administration allowedHGGs, which have a TI of 2.9 � 0.5 (mean � SE), to bedistinguished from metastases, which a have a TI of 4.7 �0.9. Advanced MR imaging is also promising in this contextbecause rCBV values, as well as mean ADC values, arehigher within and surrounding HGGs compared with me-tastases20,21 and there are higher levels of Cho/Cr surround-ing HGGs.22 Although meningiomas can usually be diag-nosed with conventional MR imaging or CT,23 duralmetastases can be similar, and in these scenarios, the high TIof meningiomas (9 � 4.4) might allow discrimination.However, there is some overlap of the TI of meningiomasand metastases, and if diagnostic uncertainty remains, asuperdelayed scan (at 96 hours) can be performed. At 96hours, metastases have a TI washout rate (incorporates 10-minute and 96-hour values) of 0.1 � 0.1 and can be distin-guished from meningiomas, which have a TI washout rateof 0.5 � 0.1 as well as HGGs, which have a TI washout rateof 0.6 � 0.1.24 Clearly 2 examinations are inconvenient forsymptomatic patients, and more recently, dynamic imaginghas been developed. Analysis of tracer uptake for 15 min-utes gives an accuracy of 79% in distinguishing HGGs frombenign brain tumors (including meningiomas and LGGs),with a steeper slope observed in HGGs.19
Grading Gliomas201Tl uptake appears to correlate with survival,25,26 and, ina single report, was found to be more predictive of survivalthan glioma histopathologic grade alone, though this hasnot been verified in other studies.27 Nonetheless, gradingremains intrinsic to clinical management decisions; thus,
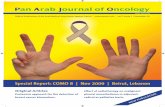
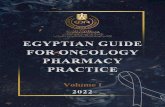
noninvasive grading is desirable. 201Tl uptake correlateswith grade according to many authors (Fig 3).5 However,other authors have found grade to be independent of201Tl uptake because tumors with central necrotic areasand moderate ring enhancement tend to be underesti-mated (Fig 4).28
To differentiate the broader categories of HGG andLGG, a TI threshold of 2.2 is 93% sensitive and 72% spe-cific25; alternatively, a TI threshold of 1.5 is 89% accu-rate,29 which is similar to the 91% accuracy obtained byusing 18FDG PET.30 These radionuclide methods comparefavorably with perfusion imaging, in which rCBV has asensitivity of 95% and a specificity of 58%. Interestingly,there is no added value from combining this perfusion tech-nique with MR spectroscopy.31 One reason that elevatedrCBV is limited in determining glioma grade is becauseoligodendrogliomas have significantly higher values thanastrocytomas.32 As an alternative to perfusion techniques,permeability imaging has been used to grade gliomas, but
Fig 3. 201Tl SPECTof gliomasof different grades. A,Grade2glioma,meanTI � 1.7 by using tumor ROI/contralateral mirror ROI. B, Grade 3 glioma,TI � 2.4. C, Grade 4 glioma, TI � 2.6.
110 � Neurographics 01:108-120 December 2011 www.neurographics.com
whether the contrast transfer coefficient is superior to rCBVremains unclear.33,34
One further advanced MR imaging technique deservesmention. Diffusion tensor imaging outside the region ofhigh T2-weighted signal intensity allows HGG to be differ-entiated from LGG with an impressive 100% specificity;however, this is limited by a sensitivity of 77%.35 11C METPET is similar to 201Tl in that it can accurately differentiateHGG and LGG, but not individual grades.36 In 1 study, 201Tlappears to be superior to both 11C MET and 18FDG.17 Insummary, 201Tl is equivalent to these PET tracers in differen-
tiating HGG and LGG but might be more practicable thanPET tracers for routine use as described below. Without adirect comparative series, it is unclear whether 201Tl is trulysuperior to advanced MR imaging in this context.
Distinguishing Brain Tumor Recurrence from RadiationNecrosis and Other ResiduaA typical indication for 201Tl SPECT is distinguishing gli-oma recurrence from radiation necrosis. A systematic re-view concluded that 201Tl SPECT is valuable in detectingsupratentorial glioma recurrence in patients treated withradiation therapy.37 Alternatively, dual isotope 201Tl and99mTc-HMPAO SPECT may improve the method. For ex-ample, by using this combination, 1 study showed that ra-diation necrosis can be distinguished from GBM recurrenceby using a 201Tl tumor/scalp TI � 2 and a 99mTc-HMPAOtumor/cerebellum ratio of �0.5.38
Following external beam radiation therapy, 201TlSPECT enables detection of glioma recurrence with 95%sensitivity and 60% specificity according to some authors.High detection rates are seen by using 201Tl after gammaknife therapy too, with respective values of 92% and67%.39 Likewise recurrence appears to be detected follow-ing brachytherapy; the few patients with histopathologiccorrelation showed 100% specificity and sensitivity.40
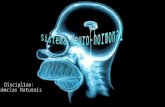
Most interest in using 201Tl SPECT to distinguish recur-rence from radiation necrosis is in the evaluation of treatedHGGs. In a visual inspection study of 7 patients treated forHGG, false-positive examinations occurred by using 201TlSPECT unlike in 11C MET PET.41 In a more recent study of19 patients treated for HGGs, visual inspection of SPECTimages showed an improved sensitivity and specificity of83% and 100%, respectively, for detecting HGG recur-rence (Fig 5).42 Another recent visual inspection study of 44patients treated for HGG also found no false-positive ex-aminations.43 Additionally, there was a 94% sensitivity byusing 201Tl SPECT alone, which is superior to 83% sensi-tivity using a combination of 18FDG PET and conventionalMR imaging. In a small study comparing 201Tl SPECT us-ing a TI of 1.4 with single-voxel MR spectroscopy per-formed at 1.5T, there was similar accuracy of 78% and82%, respectively.44 However, only 61% of MRS spectrawere usable due to degradation close to postoperative cav-ities and in the frontal region due to susceptibility artifacts.Additionally, the authors were constrained by poor repro-ducibility of voxel placement on successive studies andtherefore concluded that it was difficult to use MRS in thisscenario. In summary, the larger more recent studies, there-fore, demonstrate that 201Tl SPECT distinguishes recur-rence from radiation necrosis well.
Advanced MR imaging techniques, other than MRS, ap-pear more impressive than 201Tl SPECT. Substantial in-creases in intratumoral ADC 3 weeks after the start of che-motherapy or radiation therapy have been demonstrated byusing diffusion imaging.45 In this small study, ADC distin-guished, with 100% sensitivity and specificity, patients with
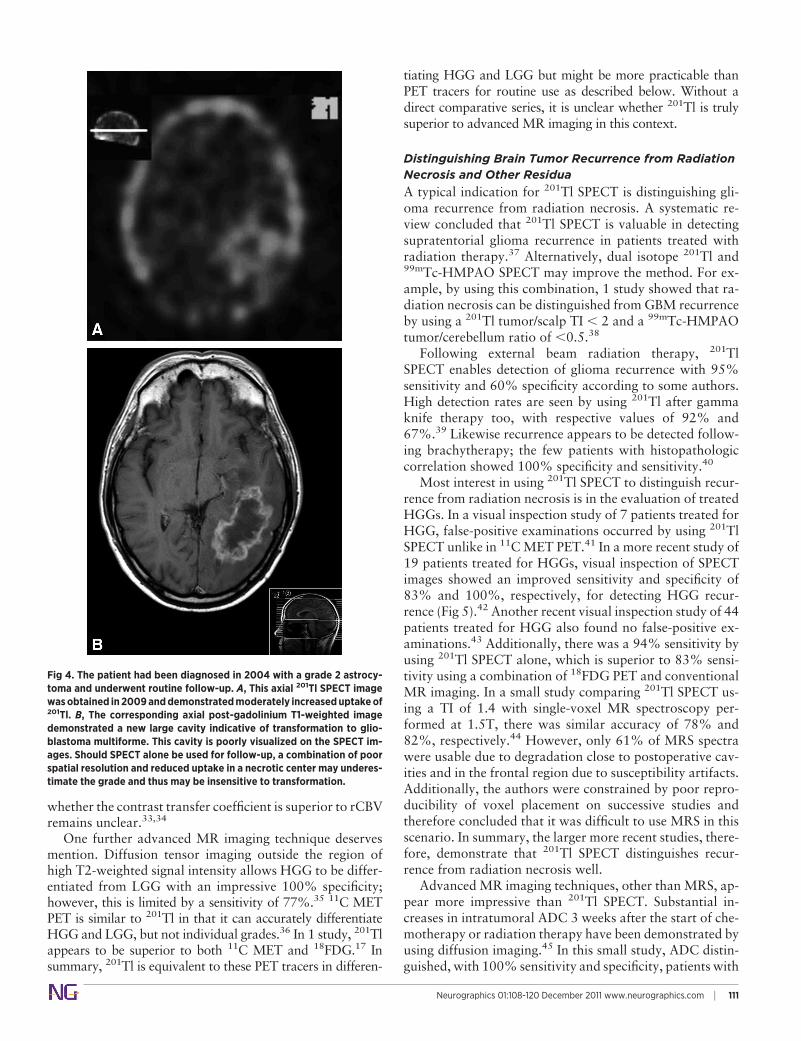
Fig 4. The patient had been diagnosed in 2004 with a grade 2 astrocy-toma and underwent routine follow-up. A, This axial 201Tl SPECT imagewasobtained in2009anddemonstratedmoderately increaseduptakeof201Tl. B, The corresponding axial post-gadolinium T1-weighted imagedemonstrated a new large cavity indicative of transformation to glio-blastoma multiforme. This cavity is poorly visualized on the SPECT im-ages. Should SPECT alone be used for follow-up, a combination of poorspatial resolution and reduced uptake in a necrotic center may underes-timate the grade and thus may be insensitive to transformation.
Neurographics 01:108-120 December 2011 www.neurographics.com � 111

HGGs who subsequently showed a partial response fromthose with stable or progressive disease. Perfusion imagingis also very promising with prolonged survival demon-strated in patients with HGG who have a decrease in thefractional volume of tumor with low rCBV 1 week intoradiation therapy.46 A sensitivity of 92% and a specificity of100% in distinguishing recurrence from radiation necrosishas since been demonstrated by using rCBV when perfusionimaging is performed during a wide range of time aftertreatment.47 Thus perfusion and diffusion imaging mayprove to be superior to 201Tl SPECT when used to detectHGG recurrence.
Although distinguishing glioma recurrence from radia-tion necrosis is the main indication for 201Tl SPECT, thereare potential indications for its use after chemotherapyalone or surgery. 201Tl SPECT may reveal early HGG re-currence after second-line chemotherapy. In this scenario,201Tl is an early treatment response biomarker followingtemozolomide48 and paclitaxel or PCV chemotherapy.26 Inthe postoperative setting (after 1–5 days), 201Tl SPECT willnot detect residual HGG using conventional early images(at 10 minutes). However, by using delayed images (at 3hours), residual tumor can be distinguished from postoper-ative radioactive accumulation.49
Treated LGGs have also been evaluated with 201TlSPECT. A TI threshold of 1.25 showed a sensitivity of 90%and a specificity of 80% in distinguishing LGG recurrencefrom radiation necrosis (Fig 6).50 Visual inspection resultsare similar, but when used as radionuclide adjuncts to con-ventional MR imaging, 201Tl SPECT is more sensitive than18FDG PET (95% and 70% sensitivity respectively) but lessspecific (83% and 92% respectively).43 201Tl SPECT hasalso been used to determine metastatic recurrence, where aTI threshold of 5 distinguished recurrence from radiationnecrosis with 91% sensitivity,51 a value superior to 82% or65% seen in two 18FDG PET studies.52,53 Although theevidence for 201Tl SPECT is limited because of low qualityand high heterogeneity of the studies included,37 it can beconcluded that 201Tl SPECT is a good technique to investi-gate recurrence, particularly in HGGs. When it comes todetection of LGG recurrence, 201Tl SPECT is less conclusiveand other SPECT tracers as well as PET imaging with aminoacids, discussed below, may be more promising.
Other SPECT RadiopharmaceuticalsMost SPECT performed to evaluate brain tumors uses the201Tl radiotracer. The usual indication is to distinguish gliomarecurrence from radiation necrosis. However, other SPECTmethods have been developed by using 99mTc, 123IMT, labeledsomatostatin analogues, and 123IPA radiotracers.
99mTc-MIBI Mechanism of Action99mTc-MIBI or 99mTc-sestamibi emits 140-keV �-rays,which are imaged more effectively than the lower energy201Tl �-rays; therefore, the image quality of 99mTc scans isoften better. Therefore this radiotracer has better imaging
Fig 5. The patient had undergone surgery and a course of radiation ther-apy for a HGG (anaplastic astrocytoma, grade 3 glioma). Distinguishingrecurrence from radiation necrosis was important. A and B, The postg-adoliniumT1-weighted imageswere insufficient tomake this distinction.C, Here, the 201Tl uptake is qualitatively high (ie, there is recurrence).
112 � Neurographics 01:108-120 December 2011 www.neurographics.com

properties than 201Tl. Furthermore, 99mTc has a short T1/2
of 6 hours, therefore allowing larger intravenous doses(10–30 mCi or 370–1110 MBq) without subsequent in-creases in the radiation dose to the patient. There is littlebackground 99mTc-MIBI uptake in normal brain, with highuptake in the scalp, pituitary gland, and choroid plexus (Fig7).54 A drawback of this radiotracer is that choroid plexusuptake interferes with paraventricular lesion detection.
MIBI is a lipophilic cation accumulating in cytoplasmand mitochondria as a result of passive diffusion across thenegatively charged cellular/organelle membrane.5 Like
201Tl, 99mTc-MIBI is excluded by the intact BBB. Increaseduptake of 99mTc-MIBI in brain tumors may be due to in-creased BBB permeability, increased regional blood flow,and high mitochondrial attenuation55 coupled with a highradiotracer uptake gradient in the mitochondria of malig-nant cells.54
Clinical Role of 99mTc-MIBI99mTc-MIBI may allow benign and malignant tumors to bedistinguished. Compared with 201Tl, 99mTc-MIBI uptake inmalignant tumors is equivalent to 201Tl uptake.56 99mTc-MIBI may also have higher uptake than 201Tl in residual orrecurrent disease, aiding detection.57 In children undergo-ing different treatment regimens for a range of brain tu-mors, 201Tl and 99mTc-MIBI uptake is equivalent.58 How-ever, clearer identification of boundaries by 99mTc-MIBImay be an advantage, for example, in radiation therapyplanning. 99mTc-MIBI also distinguishes glioma recurrencefrom radiation necrosis with a 90% sensitivity and 92%specificity.54 More specifically, LGG recurrence is detectedwith a 91% sensitivity and a 100% specificity, whereasHGG recurrence is detected with a 89% sensitivity and a83% specificity. One comparative study has been per-formed in which 99mTc-MIBI and single-voxel MRS de-tected HGG recurrence with the same sensitivity and spec-ificity (90% and 100% respectively).59 In addition toradiation therapy treatment response, 99mTc-MIBI has alsobeen used is an early treatment response biomarker of re-current HGG following temozolomide, PCV, or fotemus-tine chemotherapy.60 Overall, it appears that 99mTc-MIBI issimilar or superior in performance to 201Tl in detectingLGG recurrence and similar or inferior in detecting HGGrecurrence.
99mTc-TF99mTc-TF or 99mTc-tetrofosmin has also been used inSPECT. TF is a lipophilic cation with a similar mechanismof action to MIBI. 99mTc-TF has been used to grade gliomas
Fig 6. A, Making the distinction between LGG recurrence and radiationnecrosiswas the indication for this 201Tl SPECT. The axial postgadoliniumT1-weighted image (B) and the sagittal T2-weighted image (C) were in-sufficient to make this distinction. Here, the corresponding 201Tl SPECTimages demonstrate LGG recurrence.
Fig 7. Glioma demonstrated on 99mTc-MIBI SPECT. Note background up-take in the scalp, pituitary gland, and choroid plexus.
Neurographics 01:108-120 December 2011 www.neurographics.com � 113

and is equivalent to 99mTc-MIBI in distinguishing LGG andHGG.61 99mTc-TF has also been used to investigate a widerange of tumor types; the 99mTc-TF uptake is equivalent tothat found in 201Tl-avid brain tumors.62 However, similarto 99mTc-MIBI, clearer identification of boundaries by99mTc-TF compared with 201Tl may be an advantage in, forexample, radiation therapy planning. As might be expectedin a radiotracer similar to MIBI, 99mTc-TF can distinguishglioma recurrence from radiation necrosis.63 Overall, thereis limited systematic evidence to support routine use.5
99mTc-Glucohepatonate99mTc-glucohepatonate is an analog of glucose whose up-take is dependent on BBB disruption. Recently, it has beenshown to delineate recurrent HGG more clearly than201Tl,64 (though evidence from older acquisition methodsdoes not support this)7 and in a similar way to 99mTc-TF.65
Further studies are required before inferences concerningclinical application can be made.
123I-Labeled ProductsThe L-type amino acid transport systems take 123IMTacross the BBB and brain cell membranes. This transportsystem appears to be induced during rapid cell prolifera-tion, and there is equivalent uptake of 123IMT in SPECTand 11C MET in PET66 and more uptake than 18FDG PET,allowing clearer tumor delineation.67 Both 123IMT and 11CMET tracers do not appear to require BBB breakdown, thusadding extra information to that found with conventionalMR imaging.66,68 However, 123IMT is more practicablethan 11C MET for routine use as described below. 123IMTSPECT has a greater uptake in HGGs, which allows it to bedifferentiated from LGG with 71% sensitivity and 83%specificity,69 but further categorization into grades is morelimited than in 201Tl or 18FDG,70,71 adding little to conven-tional MR imaging,72 and a relationship has not been es-tablished between 123IMT uptake and survival unlike in201Tl.71 However, 123IMT SPECT shows particular prom-ise in treatment planning. Patients with recurrent HGG whoundergo treatment planning with 123IMT or 11C MET havea median survival of 9 months compared with 5 months inpatients whose treatment is planned conventionally.68 Inthis scenario, 123IMT might be more practicable than a PETtracer for routine use. Glioma treatment response to radia-tion therapy by using 123IMT SPECT has also been investi-gated but no relationship has been established.73
Following surgery, residual glioma can be distinguishedfrom postoperative inflammation in the operative site74;and after radiation therapy, glioma recurrence can be dis-tinguished from radiation necrosis with 78% sensitivity and100% specificity.75 In a similar study comparing 123IMTSPECT and MRS, a cutoff of 1.62 for 123IMT uptake gavea sensitivity and specificity of 95% and 100%, respec-tively.76 On the basis of metabolic ratios of Cho/Cr andCho/NAA as tumor criteria with cutoff values of 1.11 and1.17, single-voxel MRS performed at 3T gave an inferior
sensitivity and specificity of 89% and 83%, respectively. Ina study comparing 123IMT SPECT and 1H-MRSI, 123IMTwas superior at detecting tumor recurrence and also dem-onstrated higher spatial resolution.77 When 99mTc-MIBIand 123IMT were used to determine LGG recurrence, sen-sitivities were 53% and 94% and specificities were 75%and 100%, respectively. Thus in this setting, 123IMTSPECT is superior to 99mTc-MIBI SPECT, with positivepredictive values of 100% and 80% and negative predictivevalues of 90% and 46% respectively.78 Given that receiveroperating characteristic analysis demonstrates that 123IMTSPECT is also superior to 18FDG PET in the setting of LGGrecurrence (area under the receiver operating characteristicanalysis curve � 0.99 and 0.95, respectively), 123IMT mayprove to be a valuable tool in detecting LGG recurrence.79 IfFET, described below, becomes widely available, it may bepreferable to 123IMT SPECT because the sensitivity andspecificity of the 2 radiotracers appear to be equivalent yetthe tumor-to-brain contrast is superior with FET.80
IPAA radiotracer based on the amino acid phenylalanine hasrecently been investigated. The mechanism of action of123IPA is similar to that of 123IMT because much of thebiochemical structure is shared. However, when 123IPA and123IMT are compared, IMT has slightly higher uptake, es-pecially in LGG.81 Thus as a SPECT radiotracer, 123IMTremains preferable. Furthermore, these products have notbeen validated outside Japan and East Asia and are fre-quently more expensive than 201Tl and 99mTc MIBI, oftencosting the same or more than PET agents.
SRSLGG frequently express somatostatin receptors; however,this is less common in HGG. Radiolabeled somatostatinanalogs do not cross the intact BBB, and because LGGsfrequently do not disturb the BBB, SRS is somewhat limitedin glioma imaging.55 However, unlike the other imagingmodalities described, there is the possibility of using thera-peutic radiolabeled somatostatic analogs such as 90YDOTA 0-D-Phe1-Tyr3-octreotide (DOTATOC) shouldthere be clear evidence for uptake on somatostatin imagingby using [111In-DTPA-d-Phe1]-octreotide (Fig 8).82 It is alsopossible to use innovative ways to deliver such therapeuticradiopeptides to the intra-axial tumors via intra-arterialcatheters placed in the carotid artery to improve localiza-tion with good results, including complete tumor resolu-tion.83,84 There is perhaps more potential for SRS in distin-guishing extra-axial lesions. Meningiomas usually expresssomatostatin receptors and are readily detected by usingSRS because they lie outside the BBB. Indeed, [111In-DTPA-d-Phe1]-octreotide may have a role in differentiating scartissue and recurrent meningiomas postoperatively.85 Fur-thermore, although meningiomas can usually be diagnosedwith conventional MR imaging or CT, some skull baselesions may be indistinguishable. SRS yields 0% sensitivity
114 � Neurographics 01:108-120 December 2011 www.neurographics.com

for schwannomas and 100% sensitivity for meningiomas,making this a useful technique to distinguish solitary lesionsin the cerebellopontine angle or multiple lesions in neurofi-bromatosis type II. Additionally, the authors of this studyhave postulated that SRS can distinguish optic nerve glio-mas from optic sheath meningiomas because LGGs demon-strate 0% sensitivity.
SPECT in a World Dominated by PETPET imaging has become more widely available in the de-veloped world and has become the main method for func-tional imaging of tumors in general. The sensitivity of thePET camera is in the range of 0.5�Ci/mL which can trans-late into subnanomolar (�nanomolar) ranges, dependingon the specific activity (curie/mol) of the radiopharmaceu-ticals.4 In comparison, SPECT is able to reliably detect ap-proximately 5 �Ci/mL. Therefore, PET is more efficient interms of images that can be acquired for any given radiationdose, and there is an improvement in resolution from 8- to10-mm in-plane resolution for SPECT to as low as 3 mmwith PET. However, in reality, even the sensitivity of PET isreduced in lesions �10 mm.86 Despite these differences, it ismisleading to make generalizations about SPECT or PET
superiority for disease applications because they have com-plementary roles both now and in the near future.4,87 Fornow, the advantages of clinical PET are mainly technicaland will likely be superseded. Indeed, some preclinicalSPECT scanners can provide a submillimeter spatial reso-lution, which can be further reduced to sub-half millimetersby using a specialized dedicated multipinhole geometry.88
These systems are not affected by physical and fundamentallimits that hinder the PET camera to reach submillimeterranges (ie, the positron range).89
A current advantage of PET over SPECT has been thatattenuation correction has been more straightforward toachieve in PET. However, recent developments in SPECTdesign attempt to accurately address this; therefore, the lat-est generation of SPECT cameras (or improved software forcurrent SPECT cameras) should be able to produce im-proved performance.90 Additionally, SPECT uses what isknown as an “Anger camera,” which relies on a collimator,a filtering device with pinholes, which inherently reducesthe efficiency of the system due to �-ray absorption and areduction of solid-angle coverage. By using a dual-layerCompton camera as an alternative to a traditional SPECTdetector type, it should be possible to improve efficiencythrough electronic collimation with an improved �100 sen-sitivity compared with current clinical SPECT.91 Moreover,Compton SPECT is unique in that it can be operated simul-taneously with MR imaging; this combination has neverbeen possible due to interaction with the strong magneticfield of the MR imaging system.. Thus PET-MR imaging,which can combine both functional and anatomical imag-ing, will not necessarily dominate hybrid imaging of braintumors in the future.
Currently, SPECT is widely available compared withPET and is less expensive5,92; and according to some, thereis a wider range of pharmaceuticals that can be used rou-tinely.55 This has influenced SPECT use globally—for ex-ample, all commercially available SPECT radiopharmaceu-ticals have been covered by National Health Insurance inJapan for more than a decade, unlike PET radiopharmaceu-ticals93; and in Europe, researchers are more likely to useSPECT than PET if they have small budgets.94 The corollaryis that access to PET has been constrained, even in devel-oped countries. In Europe, where there are differing health-care reimbursement systems, PET access can differ by �5between neighboring countries.95 In the United States, al-though PET imaging of brain tumors has been the standardof care at some institutions for at least half a decade,55 PETexamination of brain tumors has only been covered byMedicare since 2009 and routine cover is only for initialevaluation with 18FDG.
The premise of the glucose analog 18FDG is that malig-nant cells have highly elevated rates of glucose uptake andmetabolism compared with nonmalignant cells. In braintumors, there is overexpression of both GLUT-1 andGLUT-3 glucose transporters.96 Once phosphorylated byhexokinase in the intracellular space, FDG-6-phosphate is
Fig 8. Axial postgadolinium T1-weighted image (A) corresponding with111In-octreotide SPECT (B) in a patient with LGG, which frequently ex-presses somatostatin receptors. Because radiolabeled somatostatin an-alogs do not cross the intact BBB and because LGG frequently does notdisturb the BBB, somatostatin-receptor imaging is limited in gliomaimaging.
Neurographics 01:108-120 December 2011 www.neurographics.com � 115

essentially trapped because it is not metabolized further inthe glycolytic pathway. The advantage of 18FDG is demon-strated by a study of 117 patients with a range of braintumors who underwent post-treatment MR imaging and/orCT, which was unable to differentiate recurrence from ra-diation necrosis. Subsequent PET allowed tumor recurrenceto be determined with a positive predictive value of 96%.53
Despite this impressive result, there are some major chal-lenges in using 18FDG PET in the evaluation of brain le-sions. 18FDG is a nonspecific tracer with uptake in tumor aswell as normal glial and neuronal tissue. It is, therefore,difficult to distinguish tumors from normal brain.4,18 Sim-ilarly, increased uptake in inflammatory tissue can preventdifferentiation of malignant and benign lesions.55 In addi-tion, 18FDG is insensitive for some primary brain tumors, inparticular LGGs, which may be isometabolic with normalbrain. There are also timing constraints when using 18FDGafter treatment. For example, after radiotherapy, a focalarea of increased uptake of 18FDG may be nonspecific foreither tumor recurrence or radionecrotic inflammation, re-sulting in false-positive examination findings for up to 4months after treatment.97
With current evidence, the PET agent of choice is prob-ably 11C MET, which is much more specific and sensitivethan 18FDG, has excellent interobserver agreement, and hasthe advantages of 201Tl in that uptake is practically onlyseen in sites of active proliferation, representing viable tu-mor.18,98 Increased transport across the cell membrane andincorporation into proteins are the main mechanisms bywhich amino acid analogs such as 11C MET accumulate intumor cells.5 The main disadvantage of 11C MET is thatunlike 18F, its half-life is very short at 20 minutes and im-aging is only practicable in those centers with their owncyclotron and radiochemistry facilities.4 For now, this haslimited the use of this agent mainly to university centers;however, the 18F-labeled amino acid analogs, in particularFET99 and 3,4-dihydroxy-6-[18F]fluoro-l-phenylalanine,100
appear promising and might redress this logistical problemshould larger systematic studies be supportive.1 The role of18F-Cho, a phospholipid precursor increased in brain tu-mors, also shows potential.55,5 Unlike Cho and amino acidanalogs, the future roles of the thymidine analog [18F]fluoro-3-deoxy-3-L-fluorothymidine4 and the hypoxiamarker 18F-fluoromisonidazole are less clear.1
In the United Kingdom, a National Brain Tumor Path-way analysis did not conclude that PET (or advanced MRimaging) should be used in preference to SPECT.101 Theauthors stressed that a meta-analysis of such studies is prob-lematic because of small sample sizes, nonstandardizedtechniques, and differences in study populations. AlthoughSPECT has a lower resolution than PET and cannot be usedfor easy quantification of abnormal uptake, for many, it hasremained the most pragmatic method by which viable pri-mary brain tumors can be differentiated from nontumortissue. At present, the evidence supports continued routineuse of SPECT with further development of PET in several
key areas. This is particularly true when only 201Tl SPECTand 18FDG PET are available routinely (Table).
Is There a Role for SPECT in Pseudoprogression andPseudoresponse?Radiation therapy with concomitant and adjuvant temozo-lomide (the Stupp regimen) has lead to the phenomenon of“pseudoprogression,” which describes false-positive pro-gressive disease within 6 months after treatment typicallydetermined by MacDonald MR imaging criteria. Similarly,antiangiogenic treatment for recurrent disease has lead tothe early post-treatment phenomenon “pseudoresponse,”when there is false-positive responsive disease, again typi-cally determined by MacDonald MR imaging criteria. Bothphenomena can confound response assessment and maypresent real difficulties in clinical management. Any imag-ing technique that reliably distinguishes responders to treat-ment from nonresponders at an early stage will allow morerational treatment administration and early discontinua-
Summary of how SPECT and PET compare in the evaluation of gliomas
SPECTRadiotracer PET Radiotracer Evaluation Key Findings
201Tl 11C MET Detecting gliomas17 201Tl more sensitivethan 18FDG
18FDG 11C MET moresensitive than201Tl
201Tl 11C MET Distinguishinggliomarecurrence fromradiationnecrosis41
11C MET morespecific
201Tl 18FDG Distinguishing HGGrecurrence fromradiationnecrosis43
201Tl more sensitive
201Tl 18FDG Distinguishing LGGrecurrence fromradiationnecrosis43
201Tl more sensitive
18FDG more specific201Tl 18FDG & 11C MET Grading gliomas17 201Tl superior123IMT 18FDG Distinguishing LGG
recurrence fromradiationnecrosis79
123IMT superior
123IMT 18FDG Grading recurrentgliomas70
18FDG superior
123IMT 18FDG Detection anddelineation ofglioma67
123IMT superior
123IMT 18FET Detection anddelineation ofglioma80
18FET superior
116 � Neurographics 01:108-120 December 2011 www.neurographics.com

tion of ineffective treatment strategies.3 MacDonald criteriaare based on interval changes in contrast enhancement onT1-weighted images, which represent nonspecific BBB dis-ruption. It is only in the unusual situation in which newenhancement occurs outside the radiation field that pro-gression and pseudoprogression can be distinguished withconventional MR imaging.102 Therefore recent studies haveinvestigated advanced MR imaging for distinguishing pro-gression from pseudoprogression, though initial studies byusing rCBV have produced conflicting results.103,104 Mul-tiparametric MR imaging analysis, largely based on rCBVbut incorporating ADC as well as conventional MR imag-ing, may be more promising, with a sensitivity of 90% anda specificity of 94%.105
To our knowledge, no radionuclide imaging test has in-vestigated the phenomena of pseudoprogression and pseu-doresponse systematically, but similarities are likely be-tween 1) tests that distinguish recurrence from radiationnecrosis (described in detail above) and 2) tests that distin-guish progression from pseudoprogression. This is becausethere is overlap in the clinicoradiologic entities of radiationnecrosis and pseudoprogression, with pseudoprogressionrepresenting a mild and self-limiting variant of treatment-related necrosis.106 A key difference between the 2 entities isthat radiation necrosis typically occurs 18–24 months aftertreatment, whereas pseudoprogression occurs within 6months and represents more active inflammation. There-fore, inferences from previous 18FDG PET studies that dis-tinguished radiation necrosis from recurrence might be lim-ited in the context of the inflammatory pseudoprogressionbecause 18FDG is likely to be a less specific probe. On theother hand, the more specific 201Tl and amino acid analogsmay prove useful.
The Response Assessment in Neuro-Oncology WorkingGroup has proposed that pseudoresponse can be distin-guished from true response if there is enlargement of thenonenhancing portion of the lesion on T2-weighted andfluid-attenuated inversion recovery sequences on follow-upconventional MR imaging.102 Because this is nonspecific,the images can be examined for additional features thatsuggest infiltrating tumor, including mass effect, infiltrationof the cortical ribbon, and location outside of the radiationfield. Diffusion imaging at follow-up might play a limitedrole and might determine those patients who will surviveprogression-free at 6 months, albeit with a 58% accu-racy.107 As permeability of tumor vasculature is reduced byanti-angiogenic treatment, 201Tl SPECT is unlikely to be auseful method to differentiate pseudoresponse from trueresponse. This is in contrast to 123IMT, 18FET, and 11CMET, which are tracers that do not appear to require BBBbreakdown and therefore might play a future role.
CONCLUSIONSIn brain tumor imaging, radionuclide imaging is an adjunctto conventional MR imaging. SPECT reflects features ofglioma cellular make-up; specifically, Na�/K� pump ex-
pression, mitochondrial attenuation, and amino acid trans-porter expression are probed with 201Tl, 99mTc-MIBI, and123IMT radiotracers, respectively. 123IMT SPECT appearsto be particularly promising in detecting LGG recurrence.Additionally, 123IMT shows promise in treatment planningwhere there is a survival advantage. Most international ex-perience of SPECT is with 201Tl; however, other radiotrac-ers are used to good effect in some clinics. 201Tl SPECT isvaluable in the detection of tumor recurrence in patientstreated with radiation therapy for supratentorial glioma.However, high-quality evidence that would support widerclinical application is limited by the available data from anumber of small series on heterogenous patient groups per-formed to date. This limitation also applies to PET andadvanced MR imaging techniques that have shown promisein single institutions but have not been validated in multi-center prospective studies nor have been sufficiently widelyavailable to allow implementation in daily practice.3 Futurestudies are warranted to further explore the diagnostic po-tential of 201Tl SPECT, in particular to determine optimumthresholds for the detection of glioma recurrence.
REFERENCES1. Chen W, Silverman DH. Advances in evaluation of primary
brain tumors. Semin Nucl Med 2008;38:240–502. Waldman AD, Jackson A, Price SJ, et al. Quantitative imag-
ing biomarkers in neuro-oncology. Nat Rev Clin Oncol2009;6:445–54
3. Dhermain FG, Hau P, Lanfermann H, et al. Advanced MRIand PET imaging for assessment of treatment response inpatients with gliomas. Lancet Neurol 2010;9:906–20
4. Wong FC, Kim EE. A review of molecular imaging studiesreaching the clinical stage. Eur J Radiol 2009;70:205–11
5. Benard F, Romsa J, Hustinx R. Imaging gliomas with posi-tron emission tomography and single-photon emission com-puted tomography. Semin Nucl Med 2003;33:148–62
6. Ishibashi M, Taguchi A, Sugita Y, et al. Thallium-201 inbrain tumors: relationship between tumor cell activity inastrocytic tumor and proliferating cell nuclear antigen.J Nucl Med 1995;36:2201–06
7. Kaplan WD, Takvorian T, Morris JH, et al. Thallium-201brain tumor imaging: a comparative study with pathologiccorrelation. J Nucl Med 1987;28:47–52
8. Lefranc F, Kiss R. The sodium pump alpha1 subunit as apotential target to combat apoptosis-resistant glioblastomas.Neoplasia 2008;10:198–206
9. Watling CJ, Lee DH, Macdonald DR, et al. Corticosteroid-induced magnetic resonance imaging changes in patientswith recurrent malignant glioma. J Clin Oncol 1994;12:1886–89
10. Tony B, Vos MJ, Berkhof J, et al. Interobserver variability inthe semi-quantitative assessment of 201Tl SPECT in cere-bral gliomas. Nucl Med Commun 2005;26:45–48
11. Dierckx RA, Martin JJ, Dobbeleir A, et al. Sensitivity andspecificity of thallium-201 single-photon emission tomogra-phy in the functional detection and differential diagnosis ofbrain tumours. Eur J Nucl Med 1994;21:621–33
12. Young RJ, Ghesani MV, Kagetsu NJ, et al. Lesion size de-termines accuracy of thallium-201 brain single-photon emis-
Neurographics 01:108-120 December 2011 www.neurographics.com � 117

sion tomography in differentiating between intracranial ma-lignancy and infection in AIDS patients. AJNR Am JNeuroradiol 2007;26:1973–79
13. Butzen J, Prost R, Chetty V, et al. Discrimination betweenneoplastic and nonneoplastic brain lesions by use of protonMR spectroscopy: the limits of accuracy with a logistic re-gression model. AJNR Am J Neuroradiol 2000;21:1213–19
14. Cha S, Pierce S, Knopp EA, et al. Dynamic contrast-en-hanced T2*-weighted MR imaging of tumefactive demyeli-nating lesions. AJNR Am J Neuroradiol 2001;22:1109–16
15. Erdogan C, Hakyemez B, Yildirim N, et al. Brain abscess andcystic brain tumor: discrimination with dynamic susceptibil-ity contrast perfusion-weighted MRI. J Comput Assist To-mogr 2005;29:663–67
16. Nadal DL, Herlidou S, de MG, et al. Differential MRI diag-nosis between brain abscesses and necrotic or cystic braintumors using the apparent diffusion coefficient and normal-ized diffusion-weighted images. Magn Reson Imaging 2003;21:645–50
17. Sasaki M, Kuwabara Y, Yoshida T, et al. A comparativestudy of thallium-201 SPET, carbon-11 methionine PET andfluorine-18 fluorodeoxyglucose PET for the differentiationof astrocytic tumours. Eur J Nucl Med 1998;25:1261–69
18. Chung JK, Kim YK, Kim SK, et al. Usefulness of 11C-methi-onine PET in the evaluation of brain lesions that are hypo- orisometabolic on 18F-FDG PET. Eur J Nucl Med Mol Imag-ing 2002;29:176–82
19. Sugo N, Yokota K, Kondo K, et al. Early dynamic 201TlSPECT in the evaluation of brain tumours. Nucl Med Com-mun 2006;27:143–49
20. Rollin N, Guyotat J, Streichenberger N, et al. Clinical rele-vance of diffusion and perfusion magnetic resonance imag-ing in assessing intra-axial brain tumors. Neuroradiology2006;48:150–59
21. Lu S, Ahn D, Johnson G, et al. Diffusion-tensor MR imagingof intracranial neoplasia and associated peritumoral edema:introduction of the tumor infiltration index. Radiology2004;232:221–28
22. Chiang IC, Kuo YT, Lu CY, et al. Distinction between high-grade gliomas and solitary metastases using peritumoral 3-Tmagnetic resonance spectroscopy, diffusion, and perfusionimagings. Neuroradiology 2004;46:619–27
23. DeAngelis LM. Brain tumors. N Engl J Med 2001;4:114–2324. Kojima Y, Kuwana N, Noji M, et al. Differentiation of ma-
lignant glioma and metastatic brain tumor by thallium-201single photon emission computed tomography. Neurol MedChir (Tokyo) 1994;34:588–92
25. Comte F, Bauchet L, Rigau V, et al. Correlation of preoper-ative thallium SPECT with histological grading and overallsurvival in adult gliomas. Nucl Med Commun 2006;27:137–42
26. Vos MJ, Hoekstra OS, Barkhof F, et al. Thallium-201 single-photon emission computed tomography as an early predic-tor of outcome in recurrent glioma. J Clin Oncol 2003;21:3559–65
27. Higa T, Maetani S, Yoichiro K, et al. TI-201 SPECT com-pared with histopathologic grade in the prognostic assess-ment of cerebral gliomas. Clin Nucl Med 2001;26:119–24
28. Kallen K, Heiling M, Andersson AM, et al. Preoperativegrading of glioma malignancy with thallium-201 single-pho-ton emission CT: comparison with conventional CT. AJNRAm J Neuroradiol 1996;17:925–32
29. Black KL, Hawkins RA, Kim KT, et al. Use of thallium-201SPECT to quantitate malignancy grade of gliomas. J Neuro-surg 1989;71:342–46
30. Woesler B, Kuwert T, Morgenroth C, et al. Non-invasivegrading of primary brain tumours: results of a comparativestudy between SPET with 123I-alpha-methyl tyrosine andPET with 18F-deoxyglucose. Eur J Nucl Med 1997;24:428–34
31. Law M, Yang S, Wang H, et al. Glioma grading: sensitivity,specificity, and predictive values of perfusion MR imagingand proton MR spectroscopic imaging compared with con-ventional MR imaging. AJNR Am J Neuroradiol 2003;24:1989–98
32. Cha S, Tihan T, Crawford F, et al. Differentiation of low-grade oligodendrogliomas from low-grade astrocytomas byusing quantitative blood-volume measurements derivedfrom dynamic susceptibility contrast-enhanced MR imag-ing. AJNR Am J Neuroradiol 2005;26:266–73
33. Law M, Yang S, Babb JS, et al. Comparison of cerebralblood volume and vascular permeability from dynamic sus-ceptibility contrast-enhanced perfusion MR imaging withglioma grade. AJNR Am J Neuroradiol 2004;25:746–55
34. Cha S, Yang L, Johnson G, et al. Comparison of microvas-cular permeability measurements, K(trans), determined withconventional steady-state T1-weighted and first-pass T2*-weighted MR imaging methods in gliomas and meningio-mas. AJNR Am J Neuroradiol 2006;27:409–17
35. Price SJ, Burnet NG, Donovan T, et al. Diffusion tensorimaging of brain tumours at 3T: a potential tool for assessingwhite matter tract invasion? Clin Radiol 2003;58:455–62
36. Ceyssens S, Van Laere K, de Groot T, et al. [11C]methioninePET, histopathology, and survival in primary brain tumorsand recurrence. AJNR Am J Neuroradiol 2006;27:1432–37
37. Vos MJ, Tony BN, Hoekstra OS, et al. Systematic review ofthe diagnostic accuracy of 201Tl single photon emissioncomputed tomography in the detection of recurrent glioma.Nucl Med Commun 2007;28:431–39
38. Carvalho PA, Schwartz RB, Alexander E III, et al. Detectionof recurrent gliomas with quantitative thallium-201/techne-tium-99m HMPAO single-photon emission computerizedtomography. J Neurosurg 1992;77:565–70
39. Kline JL, Noto RB, Glantz M. Single-photon emission CT inthe evaluation of recurrent brain tumor in patients treatedwith gamma knife radiosurgery or conventional radiationtherapy. AJNR Am J Neuroradiol 1996;17:1–6
40. Koot RW, Habraken JB, Hulshof MC, et al. What is thevalue of emission tomography studies in patients with a pri-mary glioblastoma multiforme treated by 192Ir brachyther-apy? Acta Neurochir (Wien) 2008;150:345–49
41. Sonoda Y, Kumabe T, Takahashi T, et al. Clinical usefulnessof 11C-MET PET and 201Tl SPECT for differentiation ofrecurrent glioma from radiation necrosis. Neurol Med Chir(Tokyo) 1998;38:342–47
42. Tie J, Gunawardana DH, Rosenthal MA. Differentiation oftumor recurrence from radiation necrosis in high-grade glio-mas using 201Tl-SPECT. J Clin Neurosci 2008;15:1327–34
43. Gomez-Rio M, Rodriguez-Fernandez A, Ramos-Font C, etal. Diagnostic accuracy of 201 Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence.Eur J Nucl Med Mol Imaging 2008;35:966–75. Epub 2008Jan 3
44. Kallen K, Burtscher IM, Holtas S, et al. 201 Thallium SPECT
118 � Neurographics 01:108-120 December 2011 www.neurographics.com

and 1H-MRS compared with MRI in chemotherapy moni-toring of high-grade malignant astrocytomas. J Neurooncol2000;46:173–85
45. Moffat BA, Chenevert TL, Lawrence TS, et al. Functionaldiffusion map: a noninvasive MRI biomarker for early strat-ification of clinical brain tumor response. Proc Natl Acad SciU S A 2005;102:5524–29
46. Cao Y, Tsien CI, Nagesh V, et al. Survival prediction inhigh-grade gliomas by MRI perfusion before and duringearly stage of RT [corrected]. Int J Radiat Oncol Biol Phys2006;64:876–85
47. Hu LS, Baxter LC, Smith KA, et al. Relative cerebral bloodvolume values to differentiate high-grade glioma recurrencefrom post-treatment radiation effect: direct correlation be-tween image-guided tissue histopathology and localized dy-namic susceptibility-weighted contrast-enhanced perfusionMR imaging measurements. AJNR Am J Neuroradiol 2009;30:552–58
48. Vallejos V, Balana C, Fraile M, et al. Use of 201Tl SPECTimaging to assess the response to therapy in patients withhigh grade gliomas. J Neurooncol 2002;59:81–90
49. Sun D, Liu Q, Liu W, et al. Clinical application of 201TlSPECT imaging of brain tumors. J Nucl Med 2000;41:5–10
50. Gomez-Rıo M, Martınez Del Valle Torres D, Rodrıguez-Fernandez A, et al. (201)Tl-SPECT in low-grade gliomas:diagnostic accuracy in differential diagnosis between tumourrecurrence and radionecrosis. Eur J Nucl Med Mol Imaging2004;31:1237–43. Epub 2004 May 6
51. Serizawa T, Saeki N, Higuchi Y, et al. Diagnostic value ofthallium-201 chloride single-photon emission computerizedtomography in differentiating tumor recurrence from radia-tion injury after gamma knife surgery for metastatic braintumors. J Neurosurg 2005;10( suppl):266–71
52. Chao ST, Suh JH, Raja S, et al. The sensitivity and specificityof FDG PET in distinguishing recurrent brain tumor fromradionecrosis in patients treated with stereotactic radiosur-gery. Int J Cancer 2001;96:191–97
53. Wang SX, Boethius J, Ericson K. FDG-PET on irradiatedbrain tumor: ten years’ summary. Acta Radiol 2006;47:85–90
54. Le Jeune FP, Dubois F, Blond S, et al. Sestamibi technetium-99m brain single-photon emission computed tomography toidentify recurrent glioma in adults: 201 studies. J Neuroon-col 2006;77:177–83. Epub 2005 Nov 29
55. Workman RB, Wong TZ, Young W, et al. Neuro-oncology.In: Cook GJ, Maisey MN, Britton KE, et al, eds. ClinicalNuclear Medicine. 4th ed. London, UK: Hodder Arnold;2006:445–55
56. Nishiyama Y, Yamamoto Y, Fukunaga K, et al. Comparisonof 99Tcm-MIBI with 201Tl chloride SPET in patients withmalignant brain tumours. Nucl Med Commun 2001;22:631–39
57. Yamamoto Y, Nishiyama Y, Toyama Y, et al. 99mTc-MIBIand 201Tl SPET in the detection of recurrent brain tumoursafter radiation therapy. Nucl Med Commun 2002;23:1183–90
58. O’Tuama LA, Treves ST, Larar JN, et al. Thallium-201 ver-sus technetium-99m-MIBI SPECT in evaluation of child-hood brain tumors: a within-subject comparison. J NuclMed 1993;34:1045–51
59. Palumbo B, Lupattelli M, Pelliccioli GP, et al. Association of99mTc-MIBI brain SPECT and proton magnetic resonance
spectroscopy (1H-MRS) to assess glioma recurrence afterradiotherapy. Q J Nucl Med Mol Imaging 2006;50:88–93
60. Prigent-Le JF, Dubois F, Perez S, et al. Technetium-99msestamibi brain SPECT in the follow-up of glioma for eval-uation of response to chemotherapy: first results. Eur J NuclMed Mol Imaging 2004;31:714–19
61. Choi JY, Kim SE, Shin HJ, et al. Brain tumor imaging with99mTc-tetrofosmin: comparison with 201Tl, 99mTc-MIBI,and 18F-fluorodeoxyglucose. J Neurooncol 2000;46:63–70
62. Soricelli A, Cuocolo A, Varrone A, et al. Technetium-99m-tetrofosmin uptake in brain tumors by SPECT: comparisonwith thallium-201 imaging. J Nucl Med 1998;39:802–06
63. Alexiou GA, Fotopoulos AD, Papadopoulos A, et al. Evalu-ation of brain tumor recurrence by (99m)Tc-tetrofosminSPECT: a prospective pilot study. Ann Nucl Med 2007;21:293–98
64. Barai S, Rajkamal, Bandopadhayaya GP, et al. Thallium-201 versus Tc99m-glucoheptonate SPECT for evaluation ofrecurrent brain tumours: a within-subject comparison withpathological correlation. J Clin Neurosci 2005;12:27–31
65. Barai S, Bandopadhayaya GP, Julka PK, et al. Imaging usingTc99m-tetrofosmin for the detection of the recurrence ofbrain tumour: a comparative study with Tc99m-glucohep-tonate. J Postgrad Med 2004;50:89–93
66. Langen KJ, Muhlensiepen H, Holschbach M, et al. Trans-port mechanisms of 3-[123I]iodo-alpha-methyl-L-tyrosinein a human glioma cell line: comparison with [3H]methyl]-L-methionine. J Nucl Med 2000;41:1250–55
67. Weber W, Bartenstein P, Gross MW, et al. Fluorine-18-FDGPET and iodine-123-IMT SPECT in the evaluation of braintumors. J Nucl Med 1997;38:802–08
68. Grosu AL, Weber WA, Franz M, et al. Reirradiation of re-current high-grade gliomas using amino acid PET (SPECT)/CT/MRI image fusion to determine gross tumor volume forstereotactic fractionated radiotherapy. Int J Radiat OncolBiol Phys 2005;63:511–19
69. Kuwert T, Morgenroth C, Woesler B, et al. Uptake of iodine-123-alpha-methyl tyrosine by gliomas and non-neoplasticbrain lesions. Eur J Nucl Med 1996;23:1345–53
70. Bader JB, Samnick S, Moringlane JR, et al. Evaluation ofl-3-[123I]iodo-alpha-methyltyrosine SPET and [18F]fluoro-deoxyglucose PET in the detection and grading of recur-rences in patients pretreated for gliomas at follow-up: a com-parative study with stereotactic biopsy. Eur J Nucl Med1999;26:144–51
71. Schmidt D, Gottwald U, Langen KJ, et al. 3-[123I]Iodo-alpha-methyl-L-tyrosine uptake in cerebral gliomas: rela-tionship to histological grading and prognosis. Eur J NuclMed 2001;28:855–61
72. Riemann B, Papke K, Hoess N, et al. Noninvasive grading ofuntreated gliomas: a comparative study of MR imaging and3-(iodine 123)-L-alpha-methyltyrosine SPECT. Radiology2002;225:567–74
73. Kuczer D, Feussner A, Wurm R, et al. 123I-IMT SPECT forevaluation of the response to radiation therapy in high gradegliomas: a feasibility study. Br J Radiol 2007;80:274–78
74. Weber WA, Dick S, Reidl G, et al. Correlation betweenpostoperative 3-[(123)I]iodo-L-alpha-methyltyrosine up-take and survival in patients with gliomas. J Nucl Med 2001;42:1144–50
75. Kuwert T, Woesler B, Morgenroth C, et al. Diagnosis of
Neurographics 01:108-120 December 2011 www.neurographics.com � 119

recurrent glioma with SPECT and iodine-123-alpha-methyltyrosine. J Nucl Med 1998;39:23–27
76. Plotkin M, Eisenacher J, Bruhn H, et al. 123I-IMT SPECTand 1H MR-spectroscopy at 3.0 T in the differential diag-nosis of recurrent or residual gliomas: a comparative study.J Neurooncol 2004;70:49–58
77. Lichy MP, Henze M, Plathow C, et al. Metabolic imaging tofollow stereotactic radiation of gliomas: the role of 1H MRspectroscopy in comparison to FDG-PET and IMT-SPECT[in German]. Rofo 2004;176:1114–21
78. Henze M, Mohammed A, Schlemmer H, et al. Detection oftumour progression in the follow-up of irradiated low-gradeastrocytomas: comparison of 3-[123I]iodo-alpha-methyl- L-tyrosine and 99mTc-MIBI SPET. Eur J Nucl Med Mol Im-aging 2002;29:1455–61
79. Henze M, Mohammed A, Schlemmer HP, et al. PET andSPECT for detection of tumor progression in irradiated low-grade astrocytoma: a receiver-operating-characteristic anal-ysis. J Nucl Med 2004;45:579–86
80. Pauleit D, Floeth F, Tellmann L, et al. Comparison of O-(2–18F-fluoroethyl)-L-tyrosine PET and 3–123I-iodo-alpha-methyl-L-tyrosine SPECT in brain tumors. J Nucl Med2004;45:374–81
81. Hellwig D, Romeike BF, Ketter R, et al. Intra-individualcomparison of p-[123I]-iodo-L-phenylalanine and L-3-[123I]-iodo-alpha-methyl-tyrosine for SPECT imaging ofgliomas. Eur J Nucl Med Mol Imaging 2008;35:24–31
82. Merlo A, Hausmann O, Wasner M, et al. Locoregional reg-ulatory peptide receptor targeting with the diffusible soma-tostatin analogue 90Y-labeled DOTA0-D-Phe1-Tyr3-oc-treotide (DOTATOC): a pilot study in human gliomas. ClinCancer Res 1999;5:1025–33
83. Turner N, Amlot P, Platts A, et al. Type-1 histiocytosis re-sponse to 90Y-lanreotide. Lancet Oncol 2004;5:193–94
84. Buscombe JR, Pigott K. New approaches in targeting intra-cerebral tumours with 90Y-labelled radiopeptides. EurJ Nucl Med Mol Imaging 2002;29:1697–98
85. Schmidt M, Scheidhauer K, Luyken C, et al. Somatostatinreceptor imaging in intracranial tumours. Eur J Nucl Med1998;25:675–86
86. Ozawa Y, Hara M, Sakurai K, et al. Diagnostic accuracy of(18)F-2-deoxy-fluoro-D-glucose positron emission tomogra-phy for pN2 lymph nodes in patients with lung cancer. ActaRadiol 2010;51:150–55
87. Rahmim A, Zaidi H. PET versus SPECT: strengths, limita-tions and challenges. Nucl Med Commun 2008;29:193–207
88. van der HF, Vastenhouw B, Ramakers RM, et al. U-SPECT-II: an ultra-high-resolution device for molecular small-ani-mal imaging. J Nucl Med 2009;50:599–605
89. Khalil MM, Tremoleda JL, Bayomy TB, et al. MolecularSPECT imaging: an overview. Int J Mol Imaging 2011;2011:796025. Epub 2011 Apr 5
90. Madsen MT. Recent advances in SPECT imaging. J NuclMed 2007;48:661–73
91. Harkness LJ, Boston AJ, Boston HC, et al. Optimisation of adual head semiconductor Compton camera using Geant4.Nuclear Instruments and Methods in Physics Research Sec-
tion A: Accelerators, Spectrometers, Detectors and Associ-ated Equipment. 2009;604:351–54
92. Herholz K, Coope D, Jackson A. Metabolic and molecularimaging in neuro-oncology. Lancet Neurol 2007;6:711–24
93. Saji H. PET and SPECT applications in medicine and phar-macology in Japan. Ann Nucl Med Sci 2000;113:225–32
94. Herholz K, Perani D, Fazekas F, et al. A survey of neuroim-aging research in European neurological departments. EurJ Neurol 2001;8:111–17
95. Facey K, Bradbury I, Laking G, Payne E. Overview of theclinical effectiveness of positron emission tomography imag-ing in selected cancers. Health Technol Assess 2007;11:iii-267
96. Nishioka T, Oda Y, Seino Y, et al. Distribution of the glu-cose transporters in human brain tumors. Cancer Res 1992;52:3972–79
97. Minn H. PET and SPECT in low-grade glioma. Eur J Radiol2005;56:171–78
98. Van LK, Ceyssens S, Van CF, et al. Direct comparison of18F-FDG and 11C-methionine PET in suspected recurrenceof glioma: sensitivity, inter-observer variability and prognos-tic value. Eur J Nucl Med Mol Imaging 2005;32:39–51
99. Langen KJ, Hamacher K, Weckesser M, et al. O-(2-[18F]fluoroethyl)-L-tyrosine: uptake mechanisms and clini-cal applications. Nucl Med Biol 2006;33:287–94
100. Chen W, Silverman DH, Delaloye S, et al. 18F-FDOPA PETimaging of brain tumors: comparison study with 18F-FDGPET and evaluation of diagnostic accuracy. J Nucl Med2006;47:904–11
101. National Institute for Health and Clinical Excellence. Im-proving outcomes for people with brain and other CNS tu-mours. www.nice.org.uk.
102. Wen PY, Macdonald DR, Reardon DA, et al. Updated re-sponse assessment criteria for high-grade gliomas: responseassessment in neuro-oncology working group. J Clin Oncol2010;28:1963–72
103. Mangla R, Singh G, Ziegelitz D, et al. Changes in relativecerebral blood volume 1 month after radiation-temozolo-mide therapy can help predict overall survival in patientswith glioblastoma. Radiology 2010;256:575–84. Epub2010 Jun 7
104. Tsien C, Galban CJ, Chenevert TL, et al. Parametric re-sponse map as an imaging biomarker to distinguish progres-sion from pseudoprogression in high-grade glioma. J ClinOncol 2010;28:2293–99
105. Hu X, Wong KK, Young GS, et al. Support vector machinemultiparametric MRI identification of pseudoprogressionfrom tumor recurrence in patients with resected glioblas-toma. J Magn Reson Imaging 2011;33:296–305
106. Hygino da Cruz LC Jr, Rodriguez I, Domingues RC, et al.Pseudoprogression and pseudoresponse: imaging challengesin the assessment of post-treatment glioma. AJNR Am JNeuroradiol 2011 Mar 31. [Epub ahead of print]
107. Pope WB, Kim HJ, Huo J, et al. Recurrent glioblastomamultiforme: ADC histogram analysis predicts response tobevacizumab treatment. Radiology 2009;252:182–89
120 � Neurographics 01:108-120 December 2011 www.neurographics.com