Need for Pharmacopeial Quality Standards for Botanical ...
12
1/12 ABSTRACT Medicines from natural products have been used throughout human history. Because of growing interest, traditional medicine-based herbal medicines and botanical dietary supplements are popular among consumers. However, due to insufficient quality of many products, safety and efficacy are challenges from the modern medicine's point of view. This is particularly important at the global level because increased international commerce without the evidence of quality at global level makes consumers more prone to being exposed to low quality products. Efforts to ensure the quality of botanical products need the support of global public standards, and their proper use for quality assessments is also highly important. Differences in regulatory status among countries prompted the need for quality standards to include appropriate test methods and specifications. Pharmacopeial monographs define the specifications which herbal products need to show proper quality. Because of the complexity of the botanical materials, building quality standards in pharmacopeias needs careful consideration to include proper methods for identity, purity and strength, as well as appropriate acceptance criteria. Keywords: Dietary Supplements; Herbal Medicine; Quality; Standards; Pharmacopoeia HERBAL MEDICINES AND BOTANICAL DIETARY SUPPLEMENTS Nature has been a source of medicinal products for a long time. Chemical diversity and novel mechanisms of action made natural products valuable in many drug development and research programs, generating interesting and meaningful developments because of their ability to interact with numerous, varied biological targets, and some have become important drugs. 1 Natural products from plant origin are important in healthcare systems and many useful drugs have been developed from plant sources. 2,3 Many plant materials have been used as herbal medicines in traditional medicine systems worldwide. This includes Traditional Chinese Medicine, Korean Traditional Medicine, Kampo, Ayurveda, Unani, Siddha, and various systems from Africa and Latin America. 4-7 In the United States (US), herbal medicines were brought mainly by European immigrants Food Suppl Biomater Health. 2021 Mar;1(1):e10 https://doi.org/10.52361/fsbh.2021.1.e10 pISSN 2765-4362·eISSN 2765-4699 Review Article Received: Dec 15, 2020 Revised: Mar 12, 2021 Accepted: Mar 16, 2021 Correspondence: Nam-Cheol Kim, PhD Science Division, Department of Dietary Supplements and Herbal Medicines, United States Pharmacopeia, 12601 Twinbrook Parkway, Rockville, MD 20852, USA. E-mail: [email protected] © 2021 Health Supplements Future Forum This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https:// creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ORCID iDs Nam-Cheol Kim https://orcid.org/0000-0003-1959-4278 Disclosure The author has no potential conflicts of interest to disclose. Nam-Cheol Kim Science Division, Department of Dietary Supplements and Herbal Medicines, United States Pharmacopeia, Rockville, MD, USA Need for Pharmacopeial Quality Standards for Botanical Dietary Supplements and Herbal Medicines https://e-fsbh.org
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Need for Pharmacopeial Quality Standards for Botanical ...

1/12
ABSTRACT
Medicines from natural products have been used throughout human history. Because of growing interest, traditional medicine-based herbal medicines and botanical dietary supplements are popular among consumers. However, due to insufficient quality of many products, safety and efficacy are challenges from the modern medicine's point of view. This is particularly important at the global level because increased international commerce without the evidence of quality at global level makes consumers more prone to being exposed to low quality products. Efforts to ensure the quality of botanical products need the support of global public standards, and their proper use for quality assessments is also highly important. Differences in regulatory status among countries prompted the need for quality standards to include appropriate test methods and specifications. Pharmacopeial monographs define the specifications which herbal products need to show proper quality. Because of the complexity of the botanical materials, building quality standards in pharmacopeias needs careful consideration to include proper methods for identity, purity and strength, as well as appropriate acceptance criteria.
Keywords: Dietary Supplements; Herbal Medicine; Quality; Standards; Pharmacopoeia
HERBAL MEDICINES AND BOTANICAL DIETARY SUPPLEMENTSNature has been a source of medicinal products for a long time. Chemical diversity and novel mechanisms of action made natural products valuable in many drug development and research programs, generating interesting and meaningful developments because of their ability to interact with numerous, varied biological targets, and some have become important drugs.1 Natural products from plant origin are important in healthcare systems and many useful drugs have been developed from plant sources.2,3
Many plant materials have been used as herbal medicines in traditional medicine systems worldwide. This includes Traditional Chinese Medicine, Korean Traditional Medicine, Kampo, Ayurveda, Unani, Siddha, and various systems from Africa and Latin America.4-7 In the United States (US), herbal medicines were brought mainly by European immigrants
Food Suppl Biomater Health. 2021 Mar;1(1):e10https://doi.org/10.52361/fsbh.2021.1.e10pISSN 2765-4362·eISSN 2765-4699
Review Article
Received: Dec 15, 2020Revised: Mar 12, 2021Accepted: Mar 16, 2021
Correspondence:Nam-Cheol Kim, PhDScience Division, Department of Dietary Supplements and Herbal Medicines, United States Pharmacopeia, 12601 Twinbrook Parkway, Rockville, MD 20852, USA.E-mail: [email protected]
© 2021 Health Supplements Future ForumThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ORCID iDsNam-Cheol Kim https://orcid.org/0000-0003-1959-4278
DisclosureThe author has no potential conflicts of interest to disclose.
Nam-Cheol Kim
Science Division, Department of Dietary Supplements and Herbal Medicines, United States Pharmacopeia, Rockville, MD, USA
Need for Pharmacopeial Quality Standards for Botanical Dietary Supplements and Herbal Medicines
https://e-fsbh.org

and from Native Americans. The first edition of United States Pharmacopeia (USP) included 425 botanical substances.8 Herb and herbal product monographs reached their peak of 636 botanical substances in USP V in 1870, but by the time USP X was published in 1926, the total number of botanically-related monographs decreased to 203 botanical substances. This represents herbal medicines that were widely used in the US until herbals began to be replaced with non-herbal pharmaceutical drugs in the 1920s.9
Increasing interest in self-care in recent years especially during 1970s and 1980s, together with scientific and clinical developments, resulted in an increased growth in popularity of herbal-based remedies.10 Some consumers show positive attitudes towards herbal products, mostly because they are natural, and such products are more likely to be considered safe and used as part of a healthy lifestyle.11 In the US, Congress established the National Institutes of Health (NIH) Office of Alternative Medicine in 1992, then upgraded to the National Center for Complementary and Integrative Health (formerly National Center for Complementary and Alternative Medicine) in 1998.12 The NIH Office of Dietary Supplements was created in 1994 to conduct and coordinate research in herbs and supplements. The Dietary Supplement Health and Education Act (DSHEA), enacted in 1994, provided the current legal landscape for dietary supplements, including botanical dietary supplements. Regulations implemented under the authority granted under DSHEA recognized the need for quality specifications for dietary supplements marketed in the US.
While the perception of the general public is that herbal products are safe to use because they have been used traditionally for many years, there are issues to incorporate them into modern medicine's context. Traditional uses of herbal ingredients as an acute treatment, are now being utilized more for health promotion or disease prevention. Because insufficient information and different doses and concentrations in traditional uses, the efficacy and safety of many of these products has not been properly demonstrated using modern scientific investigation.11
ENSURING QUALITY OF HERBAL MEDICINES AND BOTANICAL DIETARY SUPPLEMENTSThe safety and quality of herbal materials and finished herbal products has become a concern for health authorities, pharmaceutical industries, and the public.13 Many herbal products remain untested and their use is also not properly monitored. This makes knowledge of their potential side effects very limited, and identification of the safe and effective therapies of herbal medicines as well as the promotion of their intended use more difficult.14
A report from World Health Organization (WHO) estimated that about 80% of its member countries use some form of traditional and alternative medicines.15 Large populations receive herbal medicines either from alternative and complementary medicine practitioners or from the open online global market. This allows consumers around the world to easily purchase traditional medicines from other countries. Many countries reported that the lack of appropriate mechanism for control of herbal medicines is one of the main regulatory difficulties.16 Opinions on the degree of necessary quality testing are often different among regulatory frameworks, and amongst health professionals and manufacturers.17 Countries develop frameworks that largely reflect national and regional priorities and needs, but because products are consumed internationally, it is necessary to have a consistent definition, especially for dietary supplements, and harmonized regulation for herbal
2/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

products in international countries as well as global quality public standards. This issue on quality for herbal medicines and botanical dietary supplements is emphasized in the WHO's Strategy on Traditional Medicines 2014–2023 where quality is still seen as a challenge in different countries.18 The quality of finished herbal products is influenced by the quality of the raw materials used. In case of botanical extracts, blends, and finished products, the quality faces even more challenges in misidentification and contamination, thus requirements and methods for quality control for these products are even more complex.13,17
Traditional use of herbal ingredients coupled with significant growth and international regulatory challenges have led to a need for a more relevant and accessible set of quality standards. There are issues associated with developing botanical standards based on the traditional botanical products, including the following:
• Very few systems of traditional medicines have much documentation or regulations in place.• There is a sustainability issue in terms of knowledge and resources. In many countries,
traditional medicine practices have been inherited mostly through undocumented practices.• Natural products are often used simultaneously for foods, functional foods, dietary
supplements and herbal medicines.• The opportunity for education is often limited due to the limited availability of expertise.• Lack of standards and deficient of standards.
Regulatory approaches vary internationally. In the US, botanical products are regulated as drugs, foods, or dietary supplements, depending on how they are intended to be used, and labeled for use, as applicable, and there is no regulatory category at the US federal level specifically for traditional medicines. “Botanical Drug Development: Guidance for Industry” describes a pathway for botanical articles to be legally marketed as botanical drugs.19 Herbal medicines in the US have a long history of use before the regulations for food and drugs were in place. DSHEA established the first comprehensive definition of dietary supplements, resulting in certain botanicals being considered foods based, in part, on intended use.20 A dietary supplement product cannot be marketed or portrayed as a product with therapeutic, medicinal, or pharmacological value. If it is marketed as a dietary supplement with a claim to cure, treat, diagnose, mitigate, or prevent a disease, US Food and Drug Administration considers the product to be a drug.21 However, dietary supplements can be produced, sold, and marketed without first demonstrating safety and efficacy, which is required for pharmaceutical drugs. In many other countries, botanical materials for medical use are regulated as drugs with no prescriptions are required. The permit for these herbal medicines is premarket authorization basis but the underlying premise is a preference for making these products available if they have a history of traditional use.
For many botanical articles that have been considered traditional medicines somewhere around the world, not all of them meet all the regulatory requirements in order to be legally marketed as drugs or dietary supplements in the US. As a result, consumers may choose botanical articles of questionable quality, purity, and strength. Thus, developing public standards for these articles is important to protect the US consumers from the exposure to such products. USP publishes public quality standards (monographs) in several compendia to include botanical articles. Only approved drugs (including herbal medicines) that are legally marketed can be included in USP-NF. Certain herbal medicines that have been grandfathered before Food, Drug, and Cosmetics Act in 1938 are also included in USP. For dietary supplements, since the passage of DSHEA in 1994, USP increasingly has focused attention on developing public monographs for dietary supplements and their ingredients.
3/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

USP included a separate section for dietary supplements in USP from 2003 and published first version of Dietary Supplements Compendium (DSC) in 2009. In order to admit newly recognized traditional medicine based botanical articles for the use of medicines, USP started to publish the Herbal Medicines Compendium (HMC) for herbal articles that (1) are approved by a national authority for use as ingredients of herbal medicines, or are included in a national pharmacopeia; and (2) are deemed appropriate for inclusion in the HMC by a USP Expert Committee.22
Public standards are valuable because they provide scientific basis for decision making, ensure a consistent approach to quality, and are useful for monitoring adulterants, substandard products, and quality generally. Therefore, they should include appropriate titles, useful definitions, validated methods and established limits.23 Quality public standards should be set by independent experts using a robust, transparent process that involves the evaluation and incorporation of public comments, and expertise drawn from diverse sectors, including academia, industry, and regulatory bodies. Public standards should also be set based on the development and submission of robust data, and intended to meet the needs of different manufacturers, regulators, suppliers, practitioners and consumers.24 A pharmacopoeia is a legally binding collection of standards and quality specifications for medicines used in a country or region.25 In 2019 survey, WHO reported that 110 countries around the world use national or other pharmacopoeia that includes herbal medicines and 65 of them stated the pharmacopoeia to be legally binding.15 The worldwide spread in the use of herbal products has produced various attempts to develop monographs to define quality standards. The German Commission E has been publishing therapeutic monographs since 1984. The European Scientific Cooperative for Phytotherapy has been developing therapeutic monographs since 1991 and the WHO has initiated a project to write monographs on widely used herbs around the world. In the United Kingdom herbal monographs have been published since 1983.26 In USP, monographs for traditional medicine based botanical articles are included in USP, HMC, and DSC.
PHARMACOPEIAL STANDARD DEVELOPMENT
Herbal pharmacopeias are intended to promote the responsible use of herbal medicines with the highest possible degree of efficacy and safety through the development of standards of identity, purity, and analysis for botanicals including the review of traditional and scientific data regarding their efficacy and safety.27 Previously, pharmacopeias for herbal medicines were focused primarily on plant source and the plant part, using macroscopic and microscopic descriptions. However, the gradual development of analytical techniques including chromatographic fingerprints and tests for impurities improved the quality of pharmacopoeial monographs.28 Herbal drugs with potent pharmacological activity made the inclusion of an assay important. The latest “Good Pharmacopoeial Practices: Draft Chapter on Monographs on Herbal Medicines” by WHO mentioned that the pharmacopoeial monographs for herbal medicines should contain information in the definition that is consistent with the monograph title followed by specifications for quality, including identity, purity and content.29 Individual monographs describe test procedures together with the corresponding specifications. The monograph may include official title, definition, identification section, tests/limits on contaminants, and an assay section determining constituents (compounds with known therapeutic activity, active markers or analytical markers). Analytical procedures can be selected from scientifically valid methods either from
4/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

existing compendial methods or methods from scientifically peer-reviewed journal articles. The method should be validated or verified for the intended purpose. Once the procedure is chosen for compendial method, it can be modified only if the modification is acceptable to meet system suitability. If the modified method is to be acceptable, validation or verification is necessary.
Given the complexity of the matrices of herbal products, attributes of an analytical method in dietary supplement and herbal medicines monographs that are fit for the intended purpose depend on the nature of the analyte, matrices, as well as the analytical objectives (qualitative, quantitative, or others).30 Botanical macroscopic/microscopic and DNA analyses can be used for plant materials or their powder forms, not for extracts or processed forms. In latter cases, analytical methods such as chromatographic or spectroscopic techniques should be utilized. To achieve more comprehensive qualification and quantification, these techniques are often used together in identification, composition, and detection of adulterants.
Components and considerations for herbal medicines and botanical dietary supplements monographs in USP and European Pharmacopoeia are well summarized and described.30-33 Table 1 shows components and associated General Chapters in typical USP herbal medicines and botanical dietary supplement monographs. Following are general consideration for composing botanical monographs.
5/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org
Table 1. Components in USP botanical monographMonograph section Description GC/guidelineMonograph title Standard common name or, Latin binomial without authority followed
by the name of the plant part(s) or plant product (e.g., latex, exudates, resin, gum-resin, oleo gum resin)
Nomenclature guidelines for dietary supplements
Definition • Full Latin binomial• Botanical characteristics of the plant (genus, species, variety,
chemotype), parts of the plants• Harvest/collection period• Synonyms, if applicable• Acceptance limits for the content of bioactive or marker compounds• HMC monographs provide additional information on synonyms, potential
confounding materials, common names, and constituents of interestIdentification • Phytochemical characteristics • GC <563> Identification of Article of Botanical Origin
• Profile/fingerprinting of the constituents • GC <203> HPTLC Procedure for Articles of Botanical Origin• Area ratio between constituents • GC <621> Chromatography
Composition/strength • Content of marker compounds • GC <621> Chromatography• Content ratio between constituents• Limits test for toxic constituents
Contaminants • Microbial levels• Aflatoxins• Elemental impurities• Residual solvents• Pesticide residues• Other adulterants
• GC <2021> Microbial Enumeration Tests• GC <2022> Absence of Specified Microorganisms Microbial
Enumeration Tests• GC <561> Articles of Botanical Origin• GC <2251> Screening for Undeclared Drugs and Drug
Analogues
Specific tests • Macroscopic and microscopic characterization • GC <563> Identification of Article of Botanical Origin• Foreign organic matter • GC <561> Articles of Botanical Origin• Total ash• Loss on drying• Acid-insoluble ash• Alcohol-soluble extractives• Water-soluble extractives
Labeling and packaging
• GC <565> Botanical Extracts
USP = United States Pharmacopeia, HMC = Herbal Medicines Compendium, HPTLC = high-performance thin layer chromatography, GC = General Chapter.

TitleThe monograph title should indicate accurately what is covered in the monograph and needs to be consistent with the Definition section in the monograph. Clear nomenclature is the key for the correct definition and identification. Botanical articles require accurate and universally accepted names of the contained botanicals. Common names are familiar to stakeholders, traders, and consumers, but may be used for different plants in different regions. Many botanical species can be found in specific regions around the world. However, due to the increase of international commerce, many species may be available in various places. Use of scientific names provides a greater degree of accuracy than common names. This limits the number of species that are acceptable, and provides appropriate tests for the botanical article to ensure the article of trade conforms to the proscribed quality standards.34 In USP, the monograph titles follow the guidelines for dietary supplements and herbal medicines.35,36
DefinitionThe definition correctly indicates the proposed article. It includes the accepted full Latin binomial, the plant family and parts, the harvest/collection period as well as the applicable processed form (e.g., powder, extract). Synonyms are also added if they are widely known for the particular plant material. The acceptance limits for the content of bioactive or characteristic marker constituents are included. In addition, the Definition may include the chemical names and molecular formulas of the constituents that were quantified.
IdentificationThe important purpose of the identification test is to make sure the target plant article for the monograph is in agreement with what is stated in the monograph title, definition, and package labeling. Compendial identification tests for herbal ingredients include macroscopic/microscopic, chemical, chromatographic, and spectroscopic methods. Since the objective of an identification test is to be able to discriminate between related species and/or potential adulterants or substitutes, the specific tests for a botanical ingredient usually include a combination of 2 or 3 procedures.
The tests can be used to determine the plant's botanical characteristics such as macroscopic and microscopic analyses to include morphological and histological characteristics: description of diagnostic morphological and anatomical features of vascular plants and the various plant parts including roots, stems, leaves, flowers, fruits and seeds. Diagnostic features in individual monograph may include the presence of particular tissue within an organ, the arrangement and type of cells within tissues, the presence and type of secretory canal, oil, orresin duct, or laticifers within an organ, the number of epithelial cells surrounding a secretory canal, the presence and type of ergastic substances such as starch, inulin, fat globules, essential oils, calcium oxalate crystals, cystoliths, polyphenols, fluids or materials occurring in the cytoplasm, organelles, vacuoles, cavities or cell wall.37
Modern chromatographic methods including high-performance liquid chromatography, ultra-high-performance liquid chromatography, high-performance thin layer chromatography (HPTLC), and gas chromatography are utilized because of their ability to determine unique fingerprints of the desired plant article in highly selective way. The chromatographic patterns can be used to distinguish closely related species, confounding materials, or adulterated/substituted plant articles. The acceptance range for fingerprinting tests should account for reasonable variability between different botanical article suppliers
6/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

and processors, and natural variability of the authentic article acquired under various cultivation and geographic conditions. The fingerprints must be able to distinguish these materials from other materials having potential for species substitution, particularly those with known toxic effects or existing safety concerns. The acceptance criteria for identification tests using chromatographic methods must contain a description of the critical features of the fingerprint chromatograms such as the presence of specified peaks, their order of elution, and, where possible, their relative magnitude. To the extent possible, efforts to assign these peaks to known constituents must be made. Acceptance criteria for peak ratios and elution order should be determined, taking into account the variability associated with the compendial article. For planar chromatographic tests, thin layer chromatography (TLC) and HPTLC, the description must include color and position of the characteristic bands under specified illumination modes. A color image of a typical TLC/HPTLC chromatogram for multiple samples should be provided. In addition to identification using specified markers, chromatographic identification may be achieved by describing the chromatographic profile without specific mention of markers, but with referencing of the chromatographic peaks or bands to known compounds.
With its advantage in botanical identification,38 USP recently introduced DNA-based methods for the identification of botanical articles in General Chapter <563> Identification of the Articles of Botanical Origin.37,39
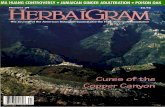
Different kinds of reference standards can be used depending on the type of identification test. For botanical identification, whole plant powdered plant materials can be used. For chemical identification, powdered plant materials, powdered extracts, purified fractions or pure compounds may be used. Powdered plant materials are used for the identification using DNA. Figs. 1 and 2 show examples of chemical fingerprinting for ginseng species.40
7/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org
UV 366 nm
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
White light
Fig. 1. HPTLC of ginseng species. 1: ginsenoside Ro; 2: ginsenoside Rb1; 3: ginsenoside Rb2; 4: ginsenoside Rc; 5: ginsenoside Rd; 6: Panax ginseng steamed root and rhizome dry extract; 7: Panax ginseng steamed root and rhizome; 8: Panax ginseng root and rhizome (Asian ginseng); 9: Panax quinquefolius root and rhizome (American ginseng); 10: Panax notoginseng root and rhizome (Tienchi ginseng); 11: ginsenoside Re; 12: notoginsenoside R1; 13: ginsenoside Rf; 14: ginsenoside Rg2; 15: ginsenoside Rg3; 16: ginsenoside Rg1. HPTLC = high-performance thin layer chromatography, UV = ultraviolet.

Composition/strengthQuantitative determination for marker constituents is important in quality monographs to represent the article's bioactivity. Proper marker component(s) should be carefully selected. If the content of bioactive components or marker constituents found in the desired plant article is too low, the component may not deliver the appropriate dose to achieve its intended biological effect. Quantitation is also important to track the presence and contents in the plant material in formulated products. The results of quantitative determinations are often expressed as the total amount of a class of constituents that are determined individually. Because of the complex biosystem, a single constituent cannot be responsible for specific plant bioactivity. Also, determination of single constituent may generate biased result because of the possibility of adulteration. Markers commonly found in other plants are not recommended unless they are present in distinctively high amounts in the plant of interest. In this case, additional markers need to be included to confirm the distinction from related plants or adulterants. For accurate analysis, chromatographic methods, such as liquid chromatographic and gas chromatographic method, are preferred over nonspecific methods, such as colorimetric or titration methods.
Quantitative tests use chromatographic methods that should meet the system suitability requirements. Suitable resolution is required to ensure that the peaks to be quantitated achieve baseline separation. Other requirements may include minimum number of theoretical plates to ensure sufficient retention and efficiency of the separation, maximum tailing factor to minimize integration issues caused by asymmetric peaks as well as relative standard deviation. Another important requirement for system suitability in USP botanical monograph testing is chromatogram similarity, which is needed to correctly identify
8/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org
Rg1 Rb1
Rb2Re Rf
Ro
Rc Rd
Rg1 Rb1
Rb2Re Rf
Ro
Rc Rd
Rg1 Rb1
Rb2Re
RoRc Rd
Rg1
Rb1
Rd
1
2
3
4
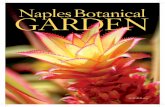
Fig. 2. HPLC of ginseng species. 1: Panax ginseng steamed root and rhizome; 2: Panax ginseng root and rhizome; 3: Panax quinquefolius root and rhizome; 4: Panax notoginseng root and rhizome. HPLC = high-performance liquid chromatography.

peaks of interest for the quantitation. Chromatogram similarity is determined against the authenticated reference botanical material or extract standard. To do this, a standard solution containing plant material or extract is injected, and the resulting chromatogram is then compared to a reference chromatogram provided in the USP certificate of that reference standard (RS) lot. The analyst is able to identify peaks for different components by comparison with the reference chromatogram.
To reduce the cost and simplify the analysis, a single RS of a purified isolated constituent is typically used to quantitate multiple compounds. If the analytes have response factors that are significantly different from the RS, the conversion factor for each analyte versus the RS should be used for the calculation. To obtain reliable conversion factors, fixed test conditions should be used, and test results should be statistically calculated from multiple determinations of an RS of known purity.
Quantitative analytical procedures should be validated. Typical validation parameters include accuracy, different levels of precision, specificity, detection limit, quantitation limit, linearity ranges, and robustness. USP follows the guideline in General Chapter <1225> Validation of Compendial Procedures.41
Purity (limit of contamination)Contaminants may be found in botanical materials and they can occur naturally or by human activities such as industrial waste and pollution. In addition, inappropriate post-harvesting practices could result the contamination of herbal materials, such as microbial and fungal contamination that can lead to mycotoxins such as aflatoxins. The limits for such contaminants should be appropriately set based on safety considerations according to the provisions in related General Chapters and other guidelines. Tests that are included in here are: elemental impurities, residual solvents, pesticides, microbial contamination, and aflatoxins.
Specific testsThere are quality parameters that apply to most pharmacopeial articles of botanical origin, including foreign organic matter, total ash, acid-insoluble ash, loss on drying or water determination, water-soluble extractives, and alcohol-soluble extractives. Certain tests are specific to certain herbal materials, such as the water-soluble extractives and alcohol-soluble extractives tests for bitterness, test for tannins, hemolytic tests for saponins, and some functionality testing for attributes such as swelling, foaming, and coloring intensity or coloring power. Submissions containing these tests must give the rationale and analytical test data in support of the suggested specifications.
Also, an individual botanical article may require specifications that are particular to that item, especially when safety or adulteration is an issue. Thus, limits may be set for certain constituents of the article that are considered undesirable negative markers, negative botanical characteristics, or markers of species substitution. If proposing a limit for undesirable substances that are either naturally present in the article or formed as a result of processing, the submission must be accompanied by toxicity data (if available), and specific procedures aimed at limiting or removing offending substances.
Additional requirementsPackaging and storage, labeling, and the RS used in the monograph may be included. The label statement of botanical monographs may include the Latin binomial name following
9/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

the authority; the plant part(s), plant product, or processed form contained in the article or from which the article was derived; and content, in percentage, of active principles or marker compounds. In addition to the labeling contained in the compendium, a botanical article is subject to compliance with such labeling requirements as may be promulgated by regulatory bodies. Particularly for botanical dietary supplements, a cautionary label statement may be included in some monographs based on the available information. USP has a system to evaluate dietary supplement admission to USP.42 This component acts as safeguard against inclusion of articles in USP and DSC that may give rise to safety concerns regardless of their legal marketing status. Reference materials included as a component of a monograph are authentic specimens that have been approved as suitable for use as comparison standards in the monograph tests.22 Reference standards are highly purified compounds for quantitative and qualitative determinations, and complex plant materials such as botanical extracts or authenticated plant powders for comparative references. They are designed to meet the monograph requirements of the particular ingredient and are used when testing a material for pharmacopoeial conformity, a requirement in the drug regulations of most countries.34 Pharmacopoeial reference materials are mainly intended for the use in compendial methods.43 When a reference standard is required within compendial methods, it is used to help ensure that the products are of appropriate identity, strength, quality and purity.
CONCLUSION
Global consumers concerned about health need quality standards because of the challenges of using traditional based herbal medicines and botanical dietary supplements. To address these concerns, pharmacopeias, including USP, provide the quality standards by setting the specifications for identity, strength and purity to reflect the quality of the products. The current regulatory status for botanical products in many countries may not appropriately address quality without appropriate standards. Proper application of pharmacopeial specifications is strongly recommended to ensure the quality of botanical herbal medicines and dietary supplements.
ACKNOWLEDGEMENTS
The author thanks Dr. Kit Goldman in USP for reviewing the manuscript.
REFERENCES
1. Yuan H, Ma Q, Ye L, Piao G. The traditional medicine and modern medicine from natural products. Molecules 2016;21(5):559-78. PUBMED | CROSSREF
2. Cragg GM, Newman DJ. Natural products: a continuing source of novel drug leads. Biochim Biophys Acta 2013;1830(6):3670-95. PUBMED | CROSSREF
3. Newman DJ, Cragg GM. Natural products as source of new drug from 1981-2014. J Nat Prod 2016;79(3):629-61. PUBMED | CROSSREF
4. Abdullahi AA. Trends and challenges of traditional medicine in Africa. Afr J Tradit Complement Altern Med 2011;8(5 Suppl):115-23. PUBMED | CROSSREF
10/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

5. Guido PC, Ribas A, Gaioli M, Quattrone F, Macchi A. The state of the integrative medicine in Latin America: the long road to include complementary, natural, and traditional practices in formal health systems. Eur J Integr Med 2015;7(1):5-12. CROSSREF
6. Jaiswal YS, Williams LL. A glimpse of Ayurveda - The forgotten history and principles of Indian traditional medicine. J Tradit Complement Med 2016;7(1):50-3. PUBMED | CROSSREF
7. Park HL, Lee HS, Shin BC, Liu JP, Shang Q, Yamashita H, et al. Traditional medicine in China, Korea, and Japan: A brief introduction and comparison. Evid Based Complement Alternat Med 2012;2012:429103. CROSSREF
8. United States Pharmacopeia (USP). The Pharmacopoeia of the United States of America: 1820. Boston, MA: Wells and Lilly; 1820.
9. Blumenthal M. Introduction. In: The ABC Clinical Guide to Herbs. New York, NY: American Botanical Council/Thieme; 2003, xvii-xxiv.
10. Tyler VE. Herbal medicine: from the past to the future. Public Health Nutr 2000;3(4A):447-52. PUBMED | CROSSREF
11. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Some traditional herbal medicines, some mycotoxins, naphthalene and styrene. IARC Monogr Eval Carcinog Risks Hum 2002;82:1-556.PUBMED
12. Institute of Medicine (US). Complementary and Alternative Medicine in the United States. Washington, D.C.: National Academic Press; 2005.
13. World Health Organization (WHO). Annex 1. In: WHO Expert Committee on Specifications for Pharmaceutical Preparations. 51st Report. Geneva: WHO; 2017.
14. World Health Organization (WHO). Traditional Medicine Strategy 2002–2005. Geneva: WHO; 2002.
15. World Health Organization (WHO). WHO Global Report on Traditional and Complementary Medicine 2019. Luxembourg: WHO; 2019.
16. World Health Organization (WHO). National Policy on Traditional Medicine and Regulation of Herbal Medicines: Report of a WHO Global Survey. Geneva: WHO; 2005.
17. Dwyer JT, Coates PM, Smith MJ. Dietary supplements: regulatory challenges and research resources. Nutrients 2018;10(1):41. PUBMED | CROSSREF
18. World Health Organization (WHO). WHO Traditional Medicine Strategy 2014–2023. Hong Kong: WHO; 2013.
19. U.S. Department of Health and Human Services; U.S. Food and Drug Administration; Center for Drug Evaluation and Research (CDER). Botanical Drug Development: Guidance for Industry. Revision 1. Silver Spring, MD: U.S. FDA; 2016.
20. Institute of Medicine (US); National Research Council (US) Committee on the Framework for Evaluating the Safety of Dietary Supplements. Dietary Supplements: a Framework for Evaluating Safety. Washington, D.C.: National Academies Press; 2005.
21. Bent S. Herbal medicine in the United States: review of efficacy, safety, and regulation: grand rounds at University of California, San Francisco Medical Center. J Gen Intern Med 2008;23(6):854-9. PUBMED | CROSSREF
22. Herbal Medicines Compendium. Herbal Medicines Compendium general notices. Version 1.0: May 20, 2013. https://hmc.usp.org/sites/default/files/documents/General_Notices/2014-09-30%20HMC%20GN%20Update.pdf. Updated 2013. Accessed May 14, 2020.
23. Giancaspro GI. Role of public standards in the international regulatory framework for dietary supplements. Health Functional Food Scientific Symposium. Pangyo: Korea Health Supplements Association; 2019.
24. Kim NC. Value of standards in herbal product developments. The 50th Annual Meeting and Symposium of the Korean Society of Pharmacognosy. Seoul: Korean Society of Pharmacognosy; 2019.
25. World Health Organization (WHO). The International Pharmacopoeia. Geneva: WHO; 2013.
26. Blumenthal M. Herbal monographs initiated by numerous groups. HerbalGram 1997;40:30-8.
27. Alamgir AN. Pharmacopoeia and herbal monograph, the aim and use of WHO's herbal monograph, WHO's guide lines for herbal monograph, pharmacognostical research and monographs of organized, unorganized drugs and drugs from animal sources. In: Therapeutic Use of Medicinal Plants and Their Extracts. Volume 1. Cham: Springer Nature Switzerland AG; 2017, 259-353.
28. Länger R, Stöger E, Kubelka W, Helliwell K. Quality standards for herbal drugs and herbal drug preparations – appropriate or improvements necessary? Planta Med 2018;84(6-07):350-60. PUBMED | CROSSREF
11/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org

29. World Health Organization (WHO). Good Pharmacopoeial Practices: Draft Chapter on Monographs on Herbal Medicines. Geneva: WHO; 2017.
30. Sarma N, Giancaspro G, Venema J. Dietary supplements quality analysis tools from the United States Pharmacopeia. Drug Test Anal 2016;8(3-4):418-23. PUBMED | CROSSREF
31. Bouin AS, Wierer M. Quality standards of the European Pharmacopoeia. J Ethnopharmacol 2014;158 Pt B:454-7. PUBMED | CROSSREF
32. Ma C, Oketch-Rabah H, Kim NC, Monagas M, Bzhelyansky A, Sarma N, et al. Quality specifications for articles of botanical origin from the United States Pharmacopeia. Phytomedicine 2018;45:105-19. PUBMED | CROSSREF
33. Schiff PL Jr, Srinivasan VS, Giancaspro GI, Roll DB, Salguero J, Sharaf MH. The development of USP botanical dietary supplement monographs, 1995-2005. J Nat Prod 2006;69(3):464-72. PUBMED | CROSSREF
34. Upton R, David B, Gafner S, Glasl S. Botanical ingredient identification and quality assessment: strengths and limitations of analytical techniques. Phytochem Rev 2020;19:1157-77. CROSSREF
35. Herbal Medicines Compendium. Guideline for assigning titles to USP Herbal Medicines Compendium monographs. Version 1.0: May 7, 2014. https://hmc.usp.org/sites/default/files/documents/Nomenclature_guideline/HMC%20Nomenclature%20Guidelines%20v.%201.0.pdf. Updated 2014. Accessed May 14, 2020.
36. United States Pharmacopeia (USP). Guideline for assigning titles to USP dietary supplement monographs. https://www.usp.org/get-involved/donate/submission-guidelines. Updated 2019. Accessed May 14, 2020.
37. United States Pharmacopeia (USP). General Chapters <563> Identification of Articles of Botanical Origin. North Bethesda, MD: USP; 2020.
38. Parveen I, Gafner S, Techen N, Murch SJ, Khan IA. DNA barcoding for the identification of botanicals in herbal medicine and dietary supplements: strengths and limitations. Planta Med 2016;82(14):1225-35. PUBMED | CROSSREF
39. Okunji C, Giancaspro GI, Sarma N, Reynaud DH, Littlec DP. DNA-based methods for authentication of articles of botanical origin-compendial applications. Pharmacop Forum 2012;39(5) ):1-14.
40. Herbal Medicines Compendium. Panax ginseng steamed root and rhizome. https://hmc.usp.org/monographs/panax-ginseng-steamed-root-and-rhizome-0-2. Updated 2016. Accessed May 14, 2020.
41. United States Pharmacopeia (USP). General Chapters <1225> Validation of Compendial Procedures. North Bethesda, MD: USP; 2020.
42. United States Pharmacopeia (USP). Guideline for the admission of dietary supplement ingredients to the USP-NF monograph development process. https://www.usp.org/sites/default/files/usp/document/get-involved/submission-guidelines/guideline-for-the-admission-of-dietary-supplement-ingredients.pdf. Updated 2017. Accessed May 26, 2020.
43. United States Pharmacopeia (USP). 5.80. USP reference standards. In: General Notices and Requirements: Applying to Standards, Tests, Assays, and Other Specifications of the United States Pharmacopeia. North Bethesda, MD: USP; 2020.
12/12https://doi.org/10.52361/fsbh.2021.1.e10
Quality Standards Botanical Dietary Supplements Herbal Medicines
https://e-fsbh.org