Mycielski type constructions for hypergraphs associated with fractional colorings
36
CASE: OIT-49 DATE: 02/14/06 Lyn Denend prepared this case under the supervision of Professor Stefanos Zenios and Robert Chess as the basis for class discussion rather than to illustrate either effective or ineffective handling of an administrative situation. Copyright © 2006 by the Board of Trustees of the Leland Stanford Junior University. All rights reserved. To order copies or request permission to reproduce materials, e-mail the Case Writing Office at: [email protected] or write: Case Writing Office, Stanford Graduate School of Business, 518 Memorial Way, Stanford University, Stanford, CA 94305-5015. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means –– electronic, mechanical, photocopying, recording, or otherwise –– without the permission of the Stanford Graduate School of Business. GENOMIC HEALTH: LAUNCHING A PARADIGM SHIFT … AND AN INNOVATIVE NEW TEST The system has to recognize diagnostics with the same value proposition that they do therapeutics. Our business model depends on that changing paradigm. If we forced ourselves into the low- margin diagnostic world and accepted that diagnostics didn’t deserve the same level of recognition for the value they bring, then we would jeopardize our business model for the next decade, not just this one product. However, we also knew that we were taking on a bigger challenge by trying to do it this way. —Kim Popovits, President and COO of Genomic Health, reflecting on the launch of the company’s first product In late October 2003, Randy Scott and the Genomic Health team were jazzed. They had just received the results of Genomic Health’s first pivotal trial, and the outcome was even better than the group had hoped. The company’s product, Oncotype DX™, a first-of-its-kind genomic assay that quantified the likelihood of breast cancer recurrence, had exceeded the standard measures of patient age, tumor size, and tumor grade in predicting recurrence outcomes. The results of the study would be presented at the December 2003 San Antonio Breast Cancer Symposium and published in the New England Journal of Medicine in December of 2004. It had been Scott’s business strategy, as the co-founder, chairman, and CEO of Genomic Health, to develop high-value, information-rich diagnostics based on patient-level (gene expression) genomic testing to enable more personalized treatment decisions. Every year, more than 100,000 patients were diagnosed with early stage, node-negative, estrogen receptor positive breast cancer. Following surgery to remove the tumor, most of these individuals faced the decision of whether or not to receive chemotherapy in order to decrease the likelihood of recurrence, a costly treatment alternative that had disruptive short-term side effects and potentially serious long-term implications. While clinical studies had shown that chemotherapy improved patient survival rates in only 4 out of 100 patients, thousands of patients elected to receive the treatment with limited information that could tell them what their risk of recurrence was or how likely they were to personally respond to chemotherapy. Oncotype DX™, a 21-gene panel, would help provide
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Mycielski type constructions for hypergraphs associated with fractional colorings

CASE: OIT-49
DATE: 02/14/06
Lyn Denend prepared this case under the supervision of Professor Stefanos Zenios and Robert Chess as the basis for class discussion rather than to illustrate either effective or ineffective handling of an administrative situation. Copyright © 2006 by the Board of Trustees of the Leland Stanford Junior University. All rights reserved. To order copies or request permission to reproduce materials, e-mail the Case Writing Office at: [email protected] or write: Case Writing Office, Stanford Graduate School of Business, 518 Memorial Way, Stanford University, Stanford, CA 94305-5015. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means –– electronic, mechanical, photocopying, recording, or otherwise –– without the permission of the Stanford Graduate School of Business.
GENOMIC HEALTH: LAUNCHING A PARADIGM SHIFT …
AND AN INNOVATIVE NEW TEST
The system has to recognize diagnostics with the same value proposition that they do therapeutics. Our business model depends on that changing paradigm. If we forced ourselves into the low-margin diagnostic world and accepted that diagnostics didn’t deserve the same level of recognition for the value they bring, then we would jeopardize our business model for the next decade, not just this one product. However, we also knew that we were taking on a bigger challenge by trying to do it this way.
—Kim Popovits, President and COO of Genomic Health, reflecting on the launch of the company’s first product
In late October 2003, Randy Scott and the Genomic Health team were jazzed. They had just received the results of Genomic Health’s first pivotal trial, and the outcome was even better than the group had hoped. The company’s product, Oncotype DX™, a first-of-its-kind genomic assay that quantified the likelihood of breast cancer recurrence, had exceeded the standard measures of patient age, tumor size, and tumor grade in predicting recurrence outcomes. The results of the study would be presented at the December 2003 San Antonio Breast Cancer Symposium and published in the New England Journal of Medicine in December of 2004. It had been Scott’s business strategy, as the co-founder, chairman, and CEO of Genomic Health, to develop high-value, information-rich diagnostics based on patient-level (gene expression) genomic testing to enable more personalized treatment decisions. Every year, more than 100,000 patients were diagnosed with early stage, node-negative, estrogen receptor positive breast cancer. Following surgery to remove the tumor, most of these individuals faced the decision of whether or not to receive chemotherapy in order to decrease the likelihood of recurrence, a costly treatment alternative that had disruptive short-term side effects and potentially serious long-term implications. While clinical studies had shown that chemotherapy improved patient survival rates in only 4 out of 100 patients, thousands of patients elected to receive the treatment with limited information that could tell them what their risk of recurrence was or how likely they were to personally respond to chemotherapy. Oncotype DX™, a 21-gene panel, would help provide

Genomic Health OIT-49
p. 2
physicians and patients with individual tumor-based information to assist them in making more effective, individual treatment decisions. Scott was elated that the Genomic Health vision had resulted in a clinically validated test for analyzing breast cancer in patients, but he and the team now faced the challenge of determining how and when to launch this groundbreaking product. Convinced of the benefits of (and need for) Oncotype DX™, the team was eager to get the product to market as quickly as possible. Having spent nearly $30 million on research, development, and validation over more than three years (and anticipating that it might take as long as 18 to 24 months for the company to gain consistent reimbursement for the product), Scott also felt some urgency to get to market. However, as a result of extensive market research performed earlier in the year, Genomic Health realized it had less than 10 percent awareness in the physician community, and even less among consumers. When asked about what factors would influence their adoption, physicians overwhelmingly cited clinical validation studies⎯and lots of them⎯as being most important. While the results of the first pivotal trial were impressive, it was unlikely that a lone study would be persuasive to the oncology field. Some physicians felt that the legitimate use of genomics in making treatment decisions was still 10 to 20 years in the future. Furthermore, while initial market feedback had indicated adequate interest in a test that accurately predicted recurrence, physicians were increasingly telling the Genomic Health team that they wanted more information, including data that predicted how patients would respond to chemotherapy. While Oncotype DX™ was capable of producing this kind of data, this variable had not been included in the initial study so no clinical data was available to support this claim. Finally, while Genomic Health had been working on the reimbursement issue for the last six months, it still lacked firm commitments from any payers to reimburse for the use of Oncotype DX™. As Scott and his team celebrated the results of the clinical validation study, they never stopped looking forward. In preparation for the launch of their new test, they had to decide what marketing plan, pricing, and reimbursement strategy would give them the greatest chance of success in the market.
BACKGROUND: THE COMPANY’S INCEPTION
Randy Scott was passionate about the promise of personalized medicine. Fueled by the recent advancements in genomics, his vision was that personalized medicine would revolutionize healthcare the way that personal computers had changed the technology landscape. In his role as the co-founder of Incyte Corporation (see Exhibit 1 for a partial list of executive bios), Scott and his team had made massive databases of genomic information available to major pharmaceutical companies to aid their research and development efforts in identifying targeted therapies at the molecular level. However, as the cost of genomic information came down (due to what Scott called a kind of Moore’s Law effect in biotechnology), it would become possible to analyze genomic information on a patient-by-patient basis and develop truly personalized regimes to treat disease. While this prospect may have seemed impossible not even a decade earlier, by the late 1990s, Scott believed it to be attainable. He explained:
Genomic Health OIT-49
p. 3
To cure disease, you have to understand it in all of its detail. The beauty of the human genome project was that it declared biology to be a finite system. It's a finite system with a huge number of variables, but they are, nonetheless, finite. Once you've got a finite set of genes that basically regulates all of biology, the pace at which those genes come together is just like a finite puzzle. When you have a 1,000-piece puzzle, it can be very difficult to find the first two pieces that match. But, as they start to come together, the pieces fit faster and faster. And by the time you get to the end, the last 10 percent of the puzzle just zips together in no time at all. So I felt like the same thing was going to happen in biology. Having identified the complete set of genes, we could now start to systematically understand them relative to any given disease.1
Committed to the concept of developing personalized medicine and information-based business models, he took the basic idea to management and the board of directors at Incyte. However, his pitch met with a mixed response:
One of my more controversial views with the Incyte board at the time was that drugs would ultimately be commodities, and that greater value would come from genomic information about disease. I believed that there was more power in the information than in the solution because what's more important than understanding exactly, precisely what the molecular cause of a disease is? Once you have that information, there will be 10 potential therapies developed to treat it. These drugs will ultimately become generic, but the value in the diagnosis of that information will hold.
While Scott presented his view as a paradigm shift that would gradually be realized over the next 30 years, the board decided that this was not the appropriate direction for Incyte. As a result, Scott left Incyte in August of 2000 (see Exhibit 2 for a high-level timeline of major milestones). However, he did so with the company’s blessing, as well as its interest in investing in his next venture. Scott spent the next week or so writing a rough business plan that supported the role of genomic analysis in driving personalized medicine. With that plan in hand, he contacted his mentor, Joffre Baker, to seek advice. Baker, Scott’s thesis advisor during his PhD program at the University of Kansas, oversaw research discovery at Genentech. He was initially enthusiastic about the plan but wanted to consult with another colleague at Genentech, Steve Shak, who had recently led the clinical program for the successful breast cancer therapy Herceptin®. Scott recalled: “So Joff and Steve and I got together at my house in the fall of 2000 over Italian takeout and a bottle of red wine, and we just really hit it off. All three of us believed that this was absolutely the future of medicine. Once they got onboard and agreed this is what they wanted to do, that was really the launch of Genomic Health. I was going to do it no matter what, but it wouldn't have been done as well if they hadn't signed on.” Two others were quickly recruited by Scott to complete the founding team: Gene Early, to focus on organizational development, and Pat Terry to focus on the cancer advocacy community. The five founders 1 All quotations from representatives of Genomic Health are from interviews conducted by the authors in October and November 2005 unless otherwise cited.

Genomic Health OIT-49
p. 4
were committed to organizational excellence and a consumer focus in addition to building state of the art technology and products Each of the five founders were to play a significant early role in building a balanced company dedicated to personalized medicine.
THE ENVIRONMENT
The diagnostics industry was typically considered part of the broad medical technology sector (along with medical devices). At their most basic, diagnostic offerings (devices or techniques used to identify a particular disease) were segmented into two primary types. In vitro diagnostics were tests that involved the analysis of bodily fluids or tissue samples and did not require the patient to be physically present (e.g., immunoassays, cytology, histology), whereas in vivo diagnostics involved tests done within the human body (e.g., x-rays, computer tomography (CT), molecular resonance imaging (MRI)). The in vitro diagnostics (IVD) market began growing rapidly in the 1960s with the discovery of new diagnostics markers (highly specific sites on chromosomes that could be used to help diagnose a particular disease) and the increased automation of diagnostics tests. By the end of 2002, the global IVD market totaled more than $23 billion, with approximately 40 percent of all sales generated in the U.S.2 In the industry, there were three primary types of participants: large pharmaceutical companies with diagnostic divisions (Johnson & Johnson, Roche, Abbott), diagnostics companies which focused on the manufacture, distribution, and marketing of diagnostic test kits and analyzers or services (Quest Diagnostics, Labcorp, Becton Dickinson), and biotechnology companies which focused on the development of novel technologies and innovative diagnostic methods (Affymetrix, Gen-Probe, Myriad Genetics).3 Initially, the diagnostics market was characterized by relatively high profit margins and low barriers to entry. However, as diagnostic technology became more complex and capital intensive and the effects of cost containment were felt in the sector, barriers to entry began to climb as margins decreased. In the 2002/2003 timeframe, profit margins varied significantly by type of diagnostic, but clustered around 5 to 10 percent. Accordingly, many diagnostic companies were dependent on selling hundreds of different tests, at low price points, in high volumes, while minimizing time and money spent on R&D for their businesses to be profitable. And, given the reimbursement environment, even this was no guarantee of success. After more than a decade of cost containment efforts, payers consistently cast a skeptical eye on the costs of diagnostic testing and, as a result of their reimbursement decisions, had a significant influence over which IVD technologies gained clinical and marketplace acceptance.4
Government Regulation
For years, medical devices and diagnostics in the U.S. were regulated by the Food & Drug Administration (FDA), under the Federal Food, Drug & Cosmetic (FD&C) Act, in much the same way as drugs were evaluated and approved. However, in 1976, the Medical Device Amendments to the FD&C Act were passed. These changes eliminated the need for “well-
2 “In Vitro Diagnostics Report,” Rensselaer: Lally School of Management & Technology, www.ceg.org, http://www.ceg.org/industryreports/Invitro%20Diagnostics.pdf (November 21, 2005). 3 Ibid. 4 Eileen Gorman, “Building a Diagnostics Market: One Molecule at a Time,” IVD Technology, September 2001.

Genomic Health OIT-49
p. 5
controlled clinical trials” on devices and diagnostics in favor of partially controlled trials, and even case studies, so long as they provided “reasonable assurance of safety and effectiveness” based on risk/benefit considerations.5 Specifically in the diagnostics arena, some tests were allowed to come on the market without undergoing any FDA review for safety and efficacy because they were considered homebrew in vitro diagnostics, or custom-made tests performed exclusively in the individual laboratories that created the tests. Companies providing homebrew diagnostics essentially sold the results of their tests as they were prohibited from transporting all or part of their tests (e.g., as a diagnostic kit) to prevent them from being administered by another party outside the company’s lab. While homebrew diagnostics were not governed by FDA regulations, the laboratories that developed and executed the tests were subject to certification under the Clinical Laboratory Improvement Amendment (CLIA) of 1988. According to the Centers of Medicare and Medicaid Services (CMS), which administered the program, CLIA required all laboratories that performed even one test on “materials derived from the human body for the purpose of providing information for the diagnosis, prevention or treatment of any disease or impairment of, or the assessment of the health of, human beings” to meet certain Federal requirements.6 CLIA’s objective was to establish quality standards for all laboratory testing to ensure the accuracy, reliability and timeliness of patient test results. The more complicated the test, the more rigorous the standards. To become CLIA certified, a laboratory had to submit an application, pass an evaluation, and then pay fees.7 While the CLIA certification process assessed the quality and standards of laboratory operations, it generally did not evaluate the efficacy of a test prior to its clinical use.
The “Genomics Revolution”
Despite its status as a relatively mature industry, the IVD sector got somewhat of a “second wind” with the initiation of the U.S. Human Genome Project (HGP). Launched in 1990, the HGP was a 13-year effort coordinated by the U.S. Department of Energy and the National Institutes of Health to identify all of the approximately 20,000-25,000 genes in human DNA, determine the sequences of the 3 billion chemical base pairs that make up human DNA, and store this information in databases where it could be utilized by the public and private sectors to fuel medical advancements.8 Relative to the diagnostics market, the Human Genome Project helped identify genetic diagnostic markers (specific genes linked to particular diseases) that would make possible significantly greater amounts of medical information from diagnostic tests. Among other benefits, genetic disease markers potentially allowed patients to be screened for hereditary diseases and counseled before the disease started to develop. They also enabled predisposing factors to be identified for diseases such as cancer and cardiovascular disease. Finally, they 5 Kshitij Mohan, “Devices Past and Future: Gauging the Pace of Change,” Medical Device Link, http://www.devicelink.com/grabber.php3?URL=http://www.devicelink.com/mddi/archive/99/06/014.html (November 21, 2005). 6 Centers for Medicare and Medicaid Services, “How to Apply for a CLIA Certificate,” www.cms.hhs.gov, http://www.cms.hhs.gov/clia/progdesc.asp (November 21, 2005). 7 Ibid. 8 Human Genome project Information, “About the Human Genome Project,” www.doegenomes.org, http://www.ornl.gov/sci/techresources/Human_Genome/project/about.shtml (November 21, 2005).

Genomic Health OIT-49
p. 6
supported the advancement of pharmacogenomics, or the analysis of how genetic variation in patients affected drug action, ultimately supporting the possibility of more personalized treatment of disease.9 Taken in combination, genomics-based diagnostics had the potential to provide a clear understanding of the true underlying cause of a patient’s condition, and pharmacogenomics the ability to determine whether that patient would respond to and tolerate a particular drug.10 For example, only those patients who over-expressed the genetic alteration for HER2 responded to the drug Herceptin®. By screening patients with a genetic diagnostic for this marker, physicians could make more personalized, effective treatment decisions and prescribe Herceptin® to only those patients with the greatest probability of benefiting from its effects. (See Exhibit 3 for more basic information about genomics and Exhibit 4 for a glossary of terms.) While all players in life sciences value chain were positioned to benefit from discoveries associated with the Human Genome Project and the advent of pharmacogenomics, some analysts believed that these forces were most likely to drive unprecedented, near-term growth in the diagnostics industry. If pharmacogenomics helped generate large numbers of tests, high demand for tests and the liability associated with not using them would help the market expand exponentially. In this scenario, the markets for gene-based diagnostics were forecast to potentially surpass revenues of $3 billion by 2005.11 Despite these promising growth predictions, the diagnostics sector as a whole had been relatively slow to embrace the potential of genomics as of the first part of the 2000s. A handful of major and niche diagnostic players had entered the market, but no single entity had established a leadership position. One of the few products available was the BRACAnalysis® test by Myriad Genetics, which assessed a woman's hereditary risk of developing breast or ovarian cancer based on detection of mutations in the BRCA1 and BRCA2 genes. Instead of diagnostics, much of the investment in genomics was being channeled toward technology designed to support targeted drug development and biotechnology research, where companies were attracted by double-digit growth rates, higher profit margins, and the promise of faster uptake in the marketplace. One consultant to companies in therapeutics and IVDs, Eileen Gorman, PhD, described the environment:
Lack of early participation by major IVD companies, for instance, created a field that was wide open for small, entrepreneurial biotechnology research companies—but without significant funding. In turn, when those companies whose original business plan was to identify genetic disease markers discovered that they could realize higher revenues by licensing their technologies for other applications, many chose to follow the money. Together, these factors have helped to create an ever-changing landscape of corporate participants in the field of molecular diagnostics.12
9 Smith, op. cit., pp. 106-107. 10 Ibid. p. 24. 11 Joseph F. Dooley, “The Genomics Outlook to 2005,” Business Insights, February 2005, p. 80. 12 Gorman, op. cit.

Genomic Health OIT-49
p. 7
Against this backdrop, and despite the many challenges in the industry, the diagnostics market was ripe for a revolution.
GETTING STARTED
Within the first several months following the inception of Genomic Health, Scott, Baker, and Shak faced a series of important decisions. First, they had to make the company’s business model more precise. Second, they had to prioritize their product development opportunities. Third, they had to raise money. In terms of Genomic Health’s business model, the founders believed it was a necessity to shatter industry norms. Shak explained, “The problem with the traditional diagnostics business was that it’s mostly about high-volume, low-margin testing. Since there’s not that much margin, you have to watch your costs, and so you can’t do much R&D. Instead, you traditionally need to focus on fulfillment.” Yet for Genomic Health to lead the paradigm shift that would ultimately position diagnostics ahead of pharmaceuticals in the life sciences value chain, it was essential to foster the company’s ability to develop high-value, information-rich diagnostics that would command premium pricing to support ongoing R&D. “What we’re talking about is a very high-tech, sophisticated, expensive test for the provider and for the buyer,” said Baker. “It’s expensive to buy and it’s expensive to produce. That is very different, by order of magnitude, than what people normally think of when they talk about measuring blood glucose or some other traditional diagnostic.” To support this unique business model, the founders recognized that each of the company’s products would need a compelling value proposition, to physicians, patients, and payers, to justify the cost of the test. They also agreed that they must develop not just a test but a laboratory service. As Kim Popovits, who joined the company in 2002 as its president and COO, put it, “Our science can be really exciting, but it only matters as much as we can deliver a value-added service to the physician and patient. What we’re selling,” she added, “is information.” To provide its service, the company would establish a central reference laboratory and manage all testing in-house. This approach would not only allow the company to maintain complete control over the quality of the results it provided, but would also enable it to pursue CLIA certification (which took significantly less time to complete then developing an FDA approved commercial kit) as a homebrew IVD. “This is how almost all other genetic tests come to market,” said Scott. “Initially, it was a fundamental part of the business model that we would have this fast track to market as a homebrew test.” However, the founders’ experience in the market made them question whether the adoption of a new genomic diagnostic would be dependent on the availability of rigorous validation studies that supported the safety and efficacy of the test. In particular, Steve Shak’s experience in clinical practice and drug development led him to strongly believe that clear demonstration of clinical validity and usefulness was key. There needed to be a compelling reason to order the test. The team sought input from the physician community and patient advocates on this subject and heard that clinical studies were critical to their plan. Scott explained:
We heard consistently that physicians wouldn’t use the test unless we could clinically prove to them that it was actually valid and it worked. We kept asking ‘Wouldn’t our test be better than having no information?’ But what we found is that the clinical community had been burned so many times that they were just

Genomic Health OIT-49
p. 8
completely skeptical of new data of uncertain utility. So they completely rejected the idea that a new test would be widely adopted without clinical validation.
As a result of this feedback, the founders accepted that clinical studies were essential to their business plan even though they were not required by any regulatory body in the U.S. The team estimated that the process of designing a rigorous clinical trial program and then working with collaborators to execute the trials and publish the results would add an additional one to two years to their time to market. It would also significantly increase the level of investment required. These realizations directly affected the inter-related decision of what product (or products) Genomic Health should focus on developing first. All three men had an initial bias for developing cancer diagnostics. Among other linkages, Shak and Baker had recently been integrally involved in Genentech’s efforts to bring the cancer drug Herceptin to market, and both remained passionate about medical needs in oncology. Baker explained it this way: “Basically, cancer is a genomic train wreck. It’s a highly personalized, fractured genome problem that can be very different from patient to patient. So it’s personalized, and what we were talking about was personalized medicine.” Scott was also enthusiastic about working in the cancer arena based on a recent experience of his own. When a friend was diagnosed with colon cancer, he accompanied her to a meeting with her oncologist and was overwhelmed by the lack of available information to help her make an appropriate treatment decision. As a result, according to Scott:
There was no doubt that we wanted to do cancer, but we wanted to be rigorous about it. So we talked to a lot of people and explored other areas. We even lined up about 10 different disease areas, such as infertility, cardiovascular disease, and other medical areas with relatively sophisticated consumers, and then rated and ranked them according to various criteria. It was your classic business school type analysis. But the bottom line was that we just kept coming back to cancer.
While the team was interested in exploring multiple types of cancer, including breast, lung, colon, and prostate cancers, this goal became increasingly unrealistic given the time and resources required to run a clinical trial program for each unique product. As Shak put it, “I think we were smart enough to know that you can’t do lots of different things, especially with a small group of people. You have to pick a couple of things⎯maybe even just one thing⎯and then do it really well.” Ultimately, the team decided to pursue breast cancer based on Shak and Baker’s experience in this field, as well as Shak’s extensive network in the breast cancer community. Scott elaborated: “Steve had developed strong scientific relationships in the breast cancer field, and there was an enormous need in this area. There was also a huge advocacy community and we knew that anything we did in breast cancer would get enormous media attention, which potentially meant that our customers would support us in marketing the product.” Of course, before much of this work could move forward, Genomic Health faced the important challenge of raising money. In November 2000, the company raised $7.9 million through a series A offering targeted at friends and family. In this initial round, the primary investments came from the co-founders, along with funds from Incyte. Shortly thereafter, in January 2001,

Genomic Health OIT-49
p. 9
Genomic Health sought additional funding from the venture capital community. “We basically put our own money in first,” said Scott. “Then when we went to talk to the venture capitalists, it would make it a little easier because we wouldn’t be waiting on them to get started and we would have a stronger value proposition for them.” While there was considerable risk associated with the company’s approach to the diagnostics market⎯including its use of leading-edge genomics technology, its unconventional business model, and its above-average time to market for diagnostics⎯Genomic Health had no trouble raising capital. “We went to a pretty narrow group of people who were pretty sophisticated thinkers,” recalled Scott. “I think the original investors would probably tell you they were investing almost more in the team than they were in the idea, although they loved the idea of personalized medicine.” Ultimately, the company raised a total of $29 million from its series B financing. In March 2001, Incyte invested another $5 million in the series C, and the series D concluded in November 2002 with an additional $9.3 million raised (see Exhibit 2).
RESEARCH, DEVELOPMENT, AND VALIDATION
With its direction set, the Genomic Health team was ready to focus on research, development, and validation of its first product. One of the earliest hurdles the company had to clear was determining whether or not it could use archived breast cancer tissue samples in the development and validation of its test. Historically, when tumors were removed by biopsy or by surgery, they were fixed and embedded in paraffin, and then archived in pathology labs across the country. This process, unique to cancer, was required as a result of government regulations. According to Baker, if Genomic Health could gain access to these tissue samples, “it meant we could do clinical trials with enormous numbers of patients, where we didn’t have to wait for patients to get well, experience a relapse, or die from the disease⎯that had already happened historically. This meant we could potentially move very, very fast to develop and test new products.” However, there were several challenges associated with this approach. First, said Shak, “The common belief was that the RNA in the tumor blocks was trashed. We had to prove that the signals we measured from the samples were meaningful.” Baker threw himself into the research and discovered multiple references that indicated the concept was feasible, but that nobody had ever implemented it in a broad program or scaled it to analyze more than one gene at a time. Genomic Health’s plan was to analyze hundreds to thousands of genes concurrently to increase the odds of identifying the right genes for its test. Baker and his team began experimenting with the approach to using archived tissue samples as soon as the company’s laboratory was ready for use in April 2001. According to Scott, “Once we got in the labs, everything started coming together. The first experiments worked beautifully and showed us that we could scale the approach to be able to look at hundreds of genes simultaneously.” An additional two years of work was required to optimize and refine the assay to work reliably with archival tissue. Reliable sources for all the reagents had to be obtained. The assay methods had to be shown to work with tumor blocks of varying age and methods of fixation. With the proof that RNA could be measured in tumor blocks, the company’s second challenge was gaining access to the historical tissue samples. Even though usefulness of the fixed paraffin embedded tumors was widely considered questionable, pathology labs were required to retain them because they served as the basis of each patient’s diagnosis. The Genomic Health team was uncertain how the archiving institutions would respond to its request to secure small samples

Genomic Health OIT-49
p. 10
from the tumors and, in particular, to gain access to the associated clinical records for each patient. “This is where the ‘Steve Shak factor’ came in to play,” said Scott. “I credit our success in securing access to archived tissues samples to Steve’s enormously positive reputation in the breast cancer field. Steve was able to go out to some of the same people he had worked with on the Herceptin trials, and obtain samples almost right off the bat, whereas I think people might have been relatively skeptical if it had been some unknown scientist approaching them.” One of the groups that was enthusiastic about collaborating with Genomic Health was the National Surgical Adjuvant Breast and Bowel Project (NSABP) in Pittsburgh. The NSABP, a world leader in breast cancer research over the last 30 years, had done more than 30 breast cancer studies in over 100,000 women. This group collaborated with Genomic Health in the development and validation of the assay. Genomic Health also began working with Kaiser Permanente in Northern California, the Providence Medical Center in Southern California, Indiana University, Rush University in Chicago, the MD Anderson Cancer Center at the University of Texas, Memorial Sloan-Kettering, and the Institute in Milan, with leaders in the breast cancer field from those institutions and other institutions providing the team with input and advice. The next step for the company was tackling the development of its test and the design of its clinical trial program. Baker led the effort in the lab while Shak spearheaded the medical strategy and clinical study design and analysis. To gain widespread acceptance among oncologists, Shak was convinced that the company needed to use a pharmaceutical blueprint for conducting its development and validation work. Leading physicians in the field understood and accepted this clinical model, and had come to expect the level of clinical evidence it produced in terms of evaluating new products for potential adoption. “Basically, we used the same strategy that I had used for drug development,” he said. “We leveraged the lessons and rigor of drug development and brought that to the development of diagnostics.” Roughly, Genomic Health’s Phase I trials corresponded to the proof of concept work that Baker and his team did in demonstrating that they could get meaningful signals from archived tissue samples, and determining that they did not have to modify existing technology to accomplish this. The Phase II trials would be focused on identifying the genes that mark clinical endpoints of interest. However, before this could be accomplished, Genomic Health needed to further refine the detailed scope and focus of its first product. According to Scott:
We were actually pretty far down the development path before we really honed in on this issue of looking just at early stage breast cancer and predicting recurrence. At first, we were exploring all the different drugs in breast cancer, what they did and didn’t do, and what tests we could develop to help increase their effectiveness. But, over time, we became fairly convinced that the ultimate baseline is understanding recurrence because so many breast cancer patients do very well without much therapy at all. This concept became part of our central dogma: Before we could predict drug response, we had to understand who even needed treatment.

Genomic Health OIT-49
p. 11
With a focus on breast cancer recurrence, Shak and Baker narrowed the initial target population for its first product (which would ultimately be called Oncotype DX™) to those patients with early stage, lymph node-negative (N-), estrogen receptor positive (ER+) breast cancer.
About the Target Patient Group
At the time Genomic Health was developing its test, approximately 200,000 new cases of breast cancer were diagnosed each year in the United States. In roughly 50 percent of the cases, the patients had early stage (stage I or II), N-, ER+ tumors. Lymph node-negative cancer meant that the disease had not yet spread to the patient’s axillary lymph nodes (under the arm). Estrogen receptor positive cancer meant that the patient’s cells were sensitive to the estrogen hormone, which had been shown to promote the growth of breast cancer cells. The more estrogen receptors present on the cancer cells, the more likely that anti-estrogen therapy (a common treatment alternative) would be effective. There were four common ways to treat early stage, N-, ER+ breast cancer. The primary course of action was surgery (removing the cancer from the breast via an operation). A lumpectomy (sometimes called excisional biopsy) was the removal of the lump in the breast and some of the tissue around it. A partial or segmental mastectomy involved the removal of the cancer as well as some of the breast tissue around the tumor and the lining over the chest muscles below the tumor.13 Based on clinical studies by the NSABP and other groups funded by the National Cancer Institute, it had been discovered that some women at the time of surgery already had small numbers of tumor cells that had traveled to other parts of the body, such as the bones, the liver, the lungs, or the brain. Surgery alone was not always effective, but no test was available to identify who already had small numbers of cancer cells at those distant sites. To prevent distant recurrence after surgery alone, a variety of adjuvant therapies, or treatments designed to prevent recurrence of the disease, were shown to be effective. These included radiation therapy (using high-dose x-rays to kill the cancer cells), hormone therapy (using hormones to stop the cancer cells from growing), and chemotherapy (using drugs to kill cancer cells). Beyond surgery, decisions about what other treatments to pursue were made between the patient and the oncologist based on tumor size, tumor grade, and patient history, as well as the patient/physician’s tolerance for risk. Given the qualitative, relatively subjective nature of these factors, treatment decisions varied significantly from patient to patient and from physician to physician, even in similar cases. Numerous studies documented “lack of consensus as to appropriate treatment for breast cancer coupled with a high confidence by individual clinicians in their own treatment decisions”14 From a patient’s perspective, information provided about treatment alternatives was not standardized so many felt overwhelmed and had difficulty determining the information most relevant to their personal situation.
13 “Breast Cancer,” www.cancer-info.com, http://www.cancer-info.com/breast.htm (November 29, 2005). 14 RB Deber and GG Thompson, “Variations in Breast Cancer Treatment Decisions and Their Impact in Mounting Trials,” www.pubmed.gov, http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1963129&dopt=Abstract (November 30, 2005).

Genomic Health OIT-49
p. 12
Radiation, a local adjuvant therapy, was typically recommended in cases where the tumor was large (greater than two centimeters in diameter) or the cancer was not well contained. Radiation usually began three to six weeks following surgery and could be performed in combination with hormonal therapy. If a patient intended to receive chemotherapy, this treatment was usually administered first, followed by radiation.15 Many doctors recommended the use of tamoxifen, an anti-estrogen hormonal therapy developed in the 1970s that had been shown in clinical trials to help prevent the original breast cancer from returning, alone or in combination with other adjuvant treatments. The drug, which was taken orally, also had been shown to prevent the development of new cancers in the opposite breast in many women. Most ER+ breast cancer patients were instructed to take tamoxifen for five-years following surgery. Potential side effects of the treatment included blood clots, depression, eye problems, uterine cancer, and possible problems with pregnancy, menstrual, and/or menopause. However, despite these risks the National Cancer Institute widely supported the use of tamoxifen as a treatment for breast cancer, citing that the benefits were firmly established and far outweighed the potential risks.16 Chemotherapy, which involved the systemic treatment of cancer using chemical toxins or drugs that were destructive to malignant cells and tissues, was another adjuvant treatment alternative.17 This treatment, which was administered orally or by injection, was usually given to patients over three to six months, in one-, two- or three-week cycles that allowed for a period of recovery between doses. Typically, oncologists recommended that patients begin chemotherapy within two to three weeks following surgery to increase the likelihood of all cancerous cells being destroyed. This meant that most patients had a relatively short period of time in which to make a decision about whether or not chemotherapy was right for them (see Exhibit 5). In most cases, chemotherapy was considered to be a disruptive treatment with significant short-term side effects, such as infection, pain in the mouth and throat, weight loss, fatigue, hair loss, rashes, and injection site reactions. In addition, the serious long-term effects of chemotherapy could include cognitive impairment, cardiac tissue damage, infertility, disease of the central nervous system, chronic fatigue, secondary malignancies, and personality changes. However, perhaps even more importantly, the benefits of chemotherapy in early stage N-, ER+ breast cancer patients had been shown to be relatively low by clinical standards. Brad Cole, Genomic Health’s CFO, explained:
There was a landmark study published in Lancet in 2004 which showed, after 12 years, only 4 out of 100 women with early stage node-negative, estrogen receptor positive breast cancer benefited from chemotherapy. Most people don’t know that. We all know people who have had breast cancer and gone through chemotherapy. It’s one of the few alternatives available to women who want to
15 “Adjuvant Therapy for Breast Cancer Guide,” MayoClinic.com, http://www.mayoclinic.com/health/breast-cancer-treatment/AT99999/PAGE=AT00005& (November 29, 2005). 16 “Breast Cancer: About Tamoxifen,” University of Maryland Medical Center, www.umm.edu, http://www.umm.edu/breast/tamox.htm (November 29, 2005). 17 “Chemotherapy,” www.dictionary.com, http://dictionary.reference.com/search?q=chemotherapy (November 28, 2005).

Genomic Health OIT-49
p. 13
do everything they can to have the best chance of beating it. But the doctors are kind of stuck because they have all of this data that shows only 4 out 100 women benefit. The problem is that they don’t know which 4 out of the 100 will improve their survival rate by going through chemotherapy.
Stated another way, the overall survival rate for N-, ER+ patients using tamoxifen hormonal therapy alone was approximately 83 percent, whereas the overall survival rate for those using tamoxifen and chemotherapy was approximately 87 percent. The implication was that thousands of women each year were being treated with risky and costly chemotherapy, which ranged from $15,000 to more than $40,000 per patient, but achieved no benefit from it. By providing a patient and her physician with factual data about her likelihood of recurrence, Genomic Health would potentially be able to help low-risk individuals avoid unnecessary treatment and give high-risk patients peace of mind that they were making the right decision in undergoing chemotherapy. In addition, there were other women who thought they were at low risk, and if found to have a high risk based on the test, could appropriately choose to take chemotherapy. The bottom-line payoff would come to payers each time chemotherapy was determined to be unnecessary based on the recurrence score of the individual patient. Payers could also be more confident that the women treated with chemotherapy were being well treated.
Developing the Test and Trials
To achieve these desired end results, the Genomic Health team developed a predictive gene panel by narrowing the field of the approximately 25,000 human genes down to 250 cancer-related genes through bioinformatic analysis of existing research literature and genomic databases. These 250 genes were further refined (through multiple Phase II clinical studies involving almost 500 patients) to a 21-gene panel whose composite gene expression profile could be represented by a single quantitative score, called a recurrence score. The higher the recurrence score, the more aggressive the tumor and the more likely it was to recur. The lower the recurrence score, the less aggressive the tumor and the less likely it was to recur. In determining recurrence scores, every gene was measured in triplicate to ensure the accuracy of all statistics. Another important development-related milestone that corresponded to the company’s Phase II trials included designing the testing process (see Exhibits 6 and 7). Genomic Health also set up the central reference lab according to CLIA regulations and “put together the infrastructure to be able to produce data with incredible accuracy and precision, day in and day out,” said Baker. “We spent two years doing lab work, developing the assay, and defining the testing process before we did a single validation study to evaluate its ability to correlate with clinical outcomes,” recalled Shak. But, in the end, the company ended up with “an assay where the accuracy and reproducibility were unbelievably great,” said Baker. At that point, the company was ready to embark on its first Phase III trial, or pivotal validation study. This work was performed in the fall of 2003 in collaboration with the NSABP. Its stated objective was to determine whether Oncotype DX™ predicted the likelihood of breast cancer recurrence over 10 years. The study involved archived tissue samples from 668 patients with N-, ER+ breast cancer who were enrolled in the NSABP Study B-14 between 1982 and 1988. Each patient sample was analyzed in a blinded fashion, against prospectively defined endpoints, and

Genomic Health OIT-49
p. 14
the results were provided back to the NSABP through a neutral party at the University of Pittsburgh for analysis. The recurrence score was used to prospectively define and assign patients into three risk groups: low, medium, and high. When the results were unblinded and evaluated against historical clinical outcomes, the recurrence score was determined to be a statistically significant predictor of breast cancer recurrence (p<0.00001). (See Exhibit 8 for more information about this pivotal validation study.) In October 2003, Genomic Health had groundbreaking results from its first pivotal study, which were scheduled to be announced at the San Antonio Breast Cancer Symposium in December 2003 (and published in the New England Journal of Medicine a year later). The company had completed its CLIA inspection of its lab and expected its certification shortly. Clinically, the company was ready to begin offering its Oncotype DX™ test.
COMMERCIALIZING ONCOTYPE DX™
More than a year and a half earlier, Genomic Health recognized the need to begin thinking about its emerging diagnostic offering in commercial terms and mapping a path to market that would enable the company to begin generating the revenues that would fuel its business model on an ongoing basis (see Exhibit 9 for a summary of consolidated financial information). Tapping into Shak and Baker’s network at Genentech, the company hired Kim Popovits as its new president and COO. Popovits, who had a background in pharmaceutical sales and marketing, had most recently launched four different therapeutic areas at Genentech. At Genomic Health, one of her first responsibilities would be to help the company prepare for the launch of its first product.
Market Readiness
In developing a launch strategy for Oncotype DX™, the company invested significant time and energy in performing both formal and informal market research. Popovits and her team conducted focus groups and surveys with various audiences, and Shak continually worked to collect feedback from his network in the physician community. Unfortunately, Genomic Health learned from nearly all of its sources that it faced low awareness, as well as low acceptance, among members of the oncology community. “When we actually went out and did some market surveys, it was a relatively small group of oncologists who had ever heard of our test or our company,” recalled Scott. “It was on the order of 10 percent.” The results were similar among patients, payers, and pathologists. Physicians in oncology were particularly skeptical of genomics-based diagnostics. “Many oncologists still thought that genomics-based diagnostics were 10 to 20 years off,” said Scott. “They didn’t understand the technology very well and I think we caught them a little by surprise.” Generally, the company encountered two types of physician responses. In the first, smaller group, there were individuals with the potential to be early adopters of the test. “They said, ‘Wow, we really need this type of molecular analysis to help guide us,’” explained Scott. However, others seemed more resistant to change. “We had other people who told us outright that they didn’t believe in it,” he said. “These doctors had been using tumor size, tumor grade, and patient age to make breast cancer treatment decisions for years, and they were reluctant to consider a new approach.” Added Popovits, “We realized that it would take serious evidence to make them believe there was a better way.”

Genomic Health OIT-49
p. 15
The Genomic Health team also learned that physicians, as well as pathologists, were skeptical of the studies of patients treated in the past that it was conducting. Furthermore, they questioned the validity of the results derived from fixed paraffin-embedded tumor samples. Popovits elaborated on the problem: “It became clear that it would be a big hurdle to get physicians and oncologists to accept the way that we were doing our clinical trials. This was something that had never been done before⎯going back 20 years, taking archived tissue samples, and doing blinded analysis to bring a product out. It also didn’t naturally make sense to everybody why we were using a drug development approach to bring a diagnostic to market.” Another challenge stemming from the results of the company’s market research was related to the issue of recurrence. Early in the development of its product, the company had received feedback that a test which provided recurrence scores was compelling enough to physicians to get them interested in using it. However, as the potential launch approached, the team learned that physicians now wanted more information. Scott explained, “Initially, we thought we could just launch a recurrence product and then we would have a follow-on, second product which would predict chemotherapy response. But what we started to hear from clinicians was, ‘Well, that's great, but even if patients have a low probability of recurrence, we’re still going to give them chemotherapy if there’s a chance they’ll receive even a small benefit from it. So you need to tell us if patients are going to benefit from chemotherapy or not.’” Popovits added, “We thought it was unlikely that those low-risk patients were to have a large benefit from chemotherapy, but we hadn’t proven it by including it in our initial trials. So we were missing some data that was pretty critical.” As a result of its market research, Genomic Health understood that it needed additional data from multiple studies to help address physician concerns and build acceptance and adoption in the market. While the company was working on two studies at the time it collected this feedback (the initial NSABP trial, plus a similar study with Kaiser Permanente), the team recognized the need to launch additional trials, including those that would validate its product’s ability to predict chemotherapy response. However, such studies could take months to prepare and then complete. Additionally, because Genomic Health felt it was critical to execute its trials in partnership with well-known, neutral third-parties in oncology, it could be time consuming to get the results published since this responsibility was entrusted to the company’s collaborators. While this approach increased the credibility of the data, it significantly slowed down the process since these outside parties had multiple projects and different priorities to manage.
Pricing
As the company contemplated bringing Oncotype DX™ to market, it had to determine an appropriate price for the product. High volume diagnostics, such as blood tests, typically cost anywhere from $200 to $300 per test. “But the labs don’t do much R&D,” explained Cole, “and the tests don’t always have clinical validation correlated to patient outcomes.” Scott continued, “It was pivotal to our entire business to be able to get strong value-based pricing⎯not just to go after some low-end, cost-plus model, but to really make the argument that we were bringing a lot of value in the test. We knew that for the future of our business model, the test had to have reasonably strong margins, or investors simply wouldn’t be interested in funding additional tests in this space.”

Genomic Health OIT-49
p. 16
For guidance in this area, the company performed additional market research. According to Scott:
We did a market survey with 30 or 40 medical directors, and we got information from them about how they decide to reimburse tests. We asked specific questions around our technology and this specific test and what it would take to have it approved. We also used this as a pricing survey to get a sense of their price sensitivity and to test their knowledge of the economic impact of using chemotherapy in lots of patients who don’t need it.
Data from the study indicated that payers were relatively price insensitive after the cost of a test exceeded a certain threshold. “Once a test was more than $1,000 it was considered expensive,” recalled Popovits. “But their reaction wasn’t significantly different between price points of $1,500 and $4,500, assuming the test had clinical value and adequate validation to support high value pricing. They told us, ‘We’ll pay for innovation if you show that it really makes a difference.’” Given the absence of direct competitors in the market, one of the few benchmarks available to Genomic Health was Myriad Genetics’ BRACAnalysis® test for assessing a woman's hereditary risk of developing breast or ovarian cancer. This diagnostic had been priced at approximately $3,000 per test and was on its way to being reimbursed on a relatively broad scale. The Genomic Health team believed that the Oncotype DX™ test could potentially command a higher price than the Myriad Genetics offering because its results were more actionable. Popovits explained:
We clearly felt that our test offered more immediately valuable information because our patients had already been diagnosed with cancer and were being forced to make a treatment decision within two or three weeks of their surgery. The BRACAnalysis® test is wonderful, but the dilemma facing patients that find out they have this mutation is ‘What do you do about it?’ Do you wait for cancer to develop? Do you have radical surgery? Oncotype DX™ is a little bit different because we’re basically saying ‘You’ve got cancer and you’re trying to decide on a treatment. The expression analysis of your tumor signature can help you make that decision today.’
Reimbursement
Closely related to pricing was the issue of reimbursement. Genomic Health would potentially receive reimbursement for its product from third-party payers, such as insurance companies and health maintenance organizations, government payers, such as Medicare and Medicaid, and patients. However, given the innovative nature of the test and its potentially high cost, there were significant risks associated with the company’s ability to receive payment from each of these parties. Genomic health expected approximately 75 percent of its revenue to come from patients covered by private insurance companies. These payers would make reimbursement decisions based on a number of factors, including a payer’s determination that the test was:
• Not experimental or investigational
Genomic Health OIT-49
p. 17
• Medically necessary • Appropriate for the specific patient • Cost-effective • Supported by peer-reviewed publications
Since each payer made its own decision as to whether or not to establish a policy to reimburse for any given test, seeking approval could be a time-consuming and costly process. Genomic Health would have to seek contract reimbursement terms with each independent payer. In the absence of a contract, the company (or the individual receiving the test) would have to seek reimbursement, on an exception basis, for each individual claim. Government reimbursement, managed by CMS, would potentially account for an additional 20 percent of Genomic Health’s revenue. CMS could make a national coverage determination that would approve the company’s test for reimbursement across the United States. However, until that was achieved, coverage decisions would be left to the discretion of the local Medicare contractor in charge of the company’s claims. The final percentage of the company’s revenue (less than 5 percent) would come directly from patients, some of whom would not be able to afford the test in the absence of insurance coverage. To address the reimbursement challenge, Genomic Health hired a reimbursement and managed care expert in the first half of 2003. Under this individual’s guidance, the company began executing a targeted campaign to educate payers about its product. According to Shak, “One thing we did was develop a dossier to be used with medical directors that was created specifically to help payers understand the product, some of whom are not oncologists and need to be educated about cancer.” The team also conducted additional market research in the payer community and leveraged its network to gain access to key individuals in an effort to prepare them for the launch. However, as of October 2003 when the company received the results of its first clinical validation study, Genomic Health did not have a firm commitment from any private or governmental payer to reimburse its product on a consistent basis. Cole explained:
From the payer’s perspective, when something new comes along all it does is add cost to the system. They’ve been burned before when new treatment-altering products have come out but they can’t repeat their results in another study and then they never really go anywhere. So payers are unlikely to approve any test until there are multiple publications in peer reviewed medical journals and physicians demonstrate that they are behind it on a broad scale by starting to use it. Once the physician community is using it, then the payers become convinced. Small companies, like Genomic Health, actually have to be prepared to take an economic risk and start providing a service to physicians and patients, billing the insurance companies, and being rejected and told no if they ever intend to achieve reimbursement.
Scott concurred, “We originally expected that it might take 18 to 24 months or more to work through the reimbursement cycle before we would get to the state where the test was fully reimbursed as a robust, mature product.”
Genomic Health OIT-49
p. 18
Reimbursement was also a touchy subject with physicians and pathologists. According to Scott:
We heard some horror stories from pathologists and physicians who had also been burned in the past by taking on a new product or test, running it, and then being billed by the company. But when the patient’s insurance didn’t reimburse the test, the pathologist or physician ended up getting stuck with the bill. We found that that it was almost always the kiss of death for a product, because it immediately created a huge uproar and a backlash in the physician community. It became apparent very quickly that we had to eliminate the reimbursement risk to physicians, otherwise there would be a huge resistance to ordering our test.
One approach Genomic Health considered to address this issue was the possibility of managing the reimbursement process on behalf of patients, whether they were seeking reimbursement from CMS or a private payer. If the company could take on responsibility for filing claims and managing appeals, concurrent with its efforts to establish contract reimbursement terms with payers, it felt that it could minimize the risk to physicians while also demonstrating its commitment to helping patients. The question, of course, was whether the cost of such a program could be justified by the results. Additionally, while this approach would potentially help drive up adoption and the number of tests Genomic Health administered, it could also significantly lengthen the company’s accounts receivable cycle if it elected to seek reimbursement rather than billing patients directly and leaving this issue to them. The time and effort required to develop this capability was another concern. Even if Genomic Health outsourced the function, there was the risk that the time and resources dedicated to establishing these processes could distract the company from its desired core competencies of developing innovative diagnostics and providing high quality laboratory services. In cases where patient reimbursement ultimately was declined, Genomic Health would be faced with a bit of an odd situation. For patients covered by private insurance, Genomic Health would be required by law to bill those individuals directly and hold them responsible for the full cost of the test. Scott explained, “It would be considered Medicare fraud if we billed and got paid by Medicare, but then allowed people who weren’t in the Medicare system to forfeit payment.” However, for those individuals denied reimbursement under Medicare, the company would be unable to seek payment directly from the patients unless it had them complete an Advanced Beneficiary Notice (ABN) prior to completion of the test. The ABN stated that the patient promised to pay if Medicare did not decide to cover the procedure. “The rule under Medicare is that unless you have an ABN, which is optional to the company, you absolutely can’t bill the patient if reimbursement is declined,” said Scott. The Genomic Health team would have to decide whether or not it should require ABNs of its Medicare patients as part of its reimbursement strategy. Finally, in the area of reimbursement, Genomic Health had to decide on what strategy to use regarding its CPT Codes. CPT Codes described medical or psychiatric procedures performed by physicians and other health providers. The codes were developed by the Health Care Financing Administration (HCFA) to assist in the assignment of reimbursement amounts to providers by Medicare carriers. However, a growing number of managed care and other private insurance

Genomic Health OIT-49
p. 19
companies also based their reimbursements on the values established by HCFA.18 Popovits summarized the issue:
One way to get reimbursement is to go in and look at CPT codes that exist and just use them as currently defined. That would be the easiest way because we could take the 10 codes that best applied to our test, stack them on top of each other, and request reimbursement for the cumulative amount. Generally, something like that has a better chance of being approved because it works within the existing system and doesn’t require a lot of attention. For Oncotype DX™, we looked at that approach but we couldn’t find codes that reflected all of the important steps in our assay. So we had to make a decision: Do we try to force a square peg in the round hole by manipulating a system that works until we can get somewhere close to a price that reflects the value of our assay? Or, do we want to be more entrepreneurial and say, ‘Okay, everything else we’ve done to this point has never been done before. We’re not going to put the square peg in the round hole.’ In this scenario, we could use a miscellaneous code to tell the system that it doesn’t have a code that reflects what we do. But if we did that, every single claim we put in would get a manual review and we would have to defend each and every one.
While the prospect of facing manual reviews on every claim was daunting to the company, the team also worried that existing codes would only support a fraction of the work involved in performing the assay. "After a thorough review of the available codes, we could only account for about $1,700, which was not a price we felt was accurate or viable given the clinical value of the test, our cost of production, and the significant investment made in its development,” said Scott. Accordingly, the resolution of this issue would have to be closely linked to the company’s decision on how it would price its product.
The Marketing Plan
Consistent with the company’s approach to its development and validation work, the Genomic Health team was committed to planning and executing its product launch more like a pharmaceutical roll-out than a traditional diagnostic launch. “We had to take a different approach,” said Popovits, “because our whole model, our whole business concept depended on changing the way people think about a diagnostic product.” Rather than focusing solely on the pathology community and potentially partnering with a major lab, Genomic Health would broaden its efforts to include physicians (especially oncologists and surgeons), payers, and patients. As part of its marketing strategy, the company contemplated the need for a direct sales force. In the United States, there were 5,000 to 6,000 oncologists that could potentially order the Oncotype DX™ test. Within this population, approximately 1,000 to 1,500 were aligned with leading breast cancer institutions and/or considered thought leaders within the field. While the company was interested in reaching the entire audience, it had to carefully manage the financial 18 “CPT Codes Information Page,” American Academy of Child and Adolescent Psychiatry, www.aacap.org, http://www.aacap.org/clinical/cptcode.htm (November 28, 2005).

Genomic Health OIT-49
p. 20
and resource demands of developing a large sales force before the company had generated a consistent revenue stream. If it intended to proceed with a direct sales strategy, it had to decide how many reps to hire and precisely what audience to target. The Genomic Health team also considered what type of sales representatives would be potentially most effective selling into the oncology community. Because these physicians were used to interacting with pharmaceutical sales reps that typically had a strong understanding of the relevant clinical area, the company was attracted to this model for promoting Oncotype DX™. Given the resistance to change within some pockets of the target population, as well as the need for education about the advent of genomics, an experienced, well-trained sales force could be a key enabler of the company’s success. If it could attract and retain such a high caliber sales force, the next question was what that sales team should focus on during its first year on the job. How much education would be required in the physician community? How soon could the team realistically begin to expect sales? What messaging should the sales representatives use to address the numerous concerns that had been raised by physicians through the market research process? In terms of reaching consumers, the Genomic Health team had to determine what approach to take to direct-to-consumer (DTC) marketing. In recent years, DTC campaigns had become an integral component of many major pharmaceutical product launches and had resulted in significant demand generation. Because individuals affected by breast cancer tended to be highly motivated in terms of seeking out information and evaluating new diagnostic and treatment alternatives, the team felt that the target audience would be receptive to DTC marketing, particularly in the form of education, outreach, and PR. In support of this hypothesis, the team looked to Myriad Genetics. Myriad had implemented a DTC campaign when it launched its BRACAnalysis® test, which seemed to be well received among consumers. However, when consumers began requesting information about Myriad’s test before the physicians were fully educated, the doctors were put in an uncomfortable position which ended up having near-term negative effects on the company’s ability to gain market adoption. Genomic Health felt strongly about avoiding any sort of backlash within the oncology community, however, the team wondered to what extent a DTC campaign would be effective in helping drive demand. Finally, as Popovits and team worked on the launch plan, they contemplated what else to do to address the payer community. Until the company had more published data and greater demand among oncologists, what could it do to convince private and governmental payers of the value of Oncotype DX™? The company also needed a strategy for addressing the needs of uninsured patients. If there was no chance of reimbursement, what were the risks and benefits to the company of providing its test free of charge?
MOVING FORWARD
The Genomic Health team was eager to launch Oncotype DX™. Yet, there were significant challenges that stood between the group and the success of its first product. Scott wanted the input and consensus of his entire team to determine the right approach to the key pricing, reimbursement, and marketing issues facing the company, but he would ultimately entrust

Genomic Health OIT-49
p. 21
Popovits, with her extensive experience in launching commercial biotech products, with making the key commercial decisions.
Genomic Health OIT-49
p. 22
Exhibit 1 Partial List of Genomic Health Executive Bios
Randal W. Scott, PhD, has served as the Chairman of the Board and Chief Executive Officer of Genomic Health from its inception in August 2000; President from August 2000 until February 2002; Chief Financial Officer from December 2000 until April 2004; and Secretary from August 2000 until December 2000 and from May 2003 until February 2005. Dr. Scott was a founder of Incyte Corporation, a genomic information company, and served Incyte in various roles, including Chairman of the Board from August 2000 to December 2001, President from January 1997 to August 2000, and Chief Scientific Officer from March 1995 to August 2000. Dr. Scott holds a BS in Chemistry from Emporia State University and a PhD in Biochemistry from the University of Kansas. Kimberly J. Popovits has served as President and Chief Operating Officer of Genomic Health since February 2002 and as a director since March 2002. From November 1987 to February 2002, Popovits served in various roles at Genentech, Inc., a biotechnology company, most recently serving as Senior Vice President, Marketing and Sales, from February 2001 to February 2002, and as Vice President, Sales from October 1994 to February 2001. Prior to joining Genentech, she served as Division Manager, Southeast Region, for American Critical Care, a Division of American Hospital Supply, a supplier of health care products to hospitals. Popovits holds a BA in Business from Michigan State University. Joffre B. Baker, PhD, has served as the Chief Scientific Officer of Genomic Health since December 2000. From March 1997 to October 2000, Dr. Baker served as the Vice President for Research Discovery at Genentech. From March 1993 to October 2000, Dr. Baker oversaw Research Discovery at Genentech, which includes the Departments of Cardiovascular Research, Oncology, Immunology, Endocrinology, and Pathology. From July 1991 to October 1993, he served as Genentech’s Director of Cardiovascular Research. Prior to joining Genentech, Dr. Baker was a member of the faculty of the Department of Biochemistry at the University of Kansas. He holds a BS in Biology and Chemistry from the University of California, San Diego and a PhD in Biochemistry from the University of Hawaii. Steven Shak, MD, has served as the Chief Medical Officer of Genomic Health since December 2000. From July 1996 to October 2000, Dr. Shak served in various roles in Medical Affairs at Genentech, most recently as Senior Director and Staff Clinical Scientist. From November 1989 to July 1996, Dr. Shak served as a Director of Discovery Research at Genentech, where he was responsible for Pulmonary Research, Immunology, and Pathology. Prior to joining Genentech, Dr. Shak was an Assistant Professor of Medicine and Pharmacology at the New York University School of Medicine. Dr. Shak holds a BA in Chemistry from Amherst College and an MD from the New York University School of Medicine, and completed his post-doctoral training at the University of California, San Francisco. G. Bradley Cole has served as the Executive Vice President and Chief Financial Officer of Genomic Health since July 2004 and Secretary from February 2005. From December 1997 to May 2004, he served in various positions at Guidant Corporation, a medical device company, most recently as Vice President, Finance and Business Development, for the Endovascular
Genomic Health OIT-49
p. 23
Solutions Group from January 2001 until May 2004. He also served as Vice President and General Manager of the Vascular Surgery Business Unit from December 1998 until December 2000 and as Vice President, Finance and IT Systems of the Cardiac and Vascular Surgery Group from December 1997 until November 1998. From July 1994 to December 1997, Mr. Cole was Vice President, Finance and Chief Financial Officer of Endovascular Technologies, Inc., a medical device company that was acquired by Guidant Corporation. From December 1988 to February 1994, he was Vice President, Finance and Chief Financial Officer of Applied Biosystems Incorporated, a life sciences systems company. Mr. Cole holds a BS in Business from Biola University and an MBA from San Jose State University. Source: Information provided by Genomic Health.

Genomic Health OIT-49
p. 24
Exhibit 2 Timeline of Major Milestones
Timing Milestone August 2000 Scott leaves Incyte and develops rough business plan for Genomic
Health. October 2000 Scott, Baker, and Shak agree to co-found Genomic Health. November 2000 Genomic Health completes its series A funding; the company raises
$7.9 million from “friends and family,” including investments by the founders and Incyte.
January 2001 Genomic Health completes its series B funding; Baker-Tisch Investments, Kleiner, Perkins, Caufield & Byers, and Versant sign on as the primary investors and the company raises an additional $29 million.
March 2001 Genomic Health completes its series C funding, raising an additional $5 million from Incyte.
April 2001 Founders narrow the company’s focus to oncology. June 2001 Genomic Health completes proof of concept; company confirms its
ability to get profiles of gene expression out of tumor blocks. November 2001 Shak and team reach agreement with collaborators to access
archived tissue blocks. March 2002 Popovits joins as President and COO. November 2002 Management team decides on specific parameters for first diagnostic
product: early stage, node-negative, estrogen-receptor positive breast cancer.
November 2002 Genomic Health completes its series D funding. Raising an additional $9.3 million from 11 investors.
March 2003 Genomic Health completes phase II trials. March 2003 Genomic Health hires reimbursement specialist. August 2003 Genomic Health locks down assay parameters and completes
laboratory preparation. September 2003 Genomic Health initiates phase III trial in cooperation with NSABP. October 2003 Genomic Health completes market research with oncologists,
patients/advocacy groups, and payers. October 2003 Genomic Health receives results from phase III trial and achieves
defined end points. November 2003 Genomic Health completes CLIA inspection. December 2004 Genomic Health presents results of NSABP study at San Antonio
Breast Cancer Symposium. Source: Information provided by Genomic Health.

Genomic Health OIT-49
p. 25
Exhibit 3 Genomic Basics
What is a gene? A genome is the entire set of hereditary instructions for building, running, and maintaining an organism, and passing life on to the next generation. The genome is made of deoxyribonucleic acid (DNA). The genome is made up of genes, which are packaged in chromosomes and affect specific characteristics of the organism. Each of Earth's species has its own distinctive genome: the dog genome, the wheat genome, the genomes of the cow, cold virus, bok choy, Escherichia coli, and so on. The genome contains all of the information necessary to produce a specific organism. Whilst genomes belong to species, they also belong to individuals. With the exception of identical twins and other clones, every person has a unique genome, in the same way as does every deer, oak tree, and eagle. Genomes are different between individuals as well as species. The genes of an organism, whether animal, plant or microbe, determine its physical and chemical characteristics. Genes consist of organized units of molecules called DNA, which themselves consist of four different chemical bases, called nucleotides. Each nucleotide unit pairs with its complementary nucleotide in the double helix structure of DNA, forming a base pair. The precise sequence of the nucleotides in a gene determines the physical and chemical activity that the gene produces in an organism. When a gene is expressed, it acts alone or in combination with other expressed genes to synthesize structural proteins and enzymes. The activity of these proteins causes the cell to perform biological functions, which influence the physical and chemical characteristics of the organism. A modification in a gene sequence may lead to the over- or under-production of a protein, modifying the normal biological function of the cell, and potentially affecting the physical and chemical characteristics of the entire organism. There are a number of useful ways to examine a genomic structure. Genes can be analyzed for the sequence of a gene, the function of a gene, the parts of the genome that regulate genes, or the DNA outside of genes, where genes are located in the genome, or how different genes work together.
Genes and Disease Increased awareness of the role of genes in regulating the functions of living organisms has generated a worldwide effort to identify and sequence genes and genomes of many organisms, including the estimated 3 billion nucleotide pairs of the human genome. This effort is being led by the Human Genome Project and related academic, government and industry research projects. Although a rough draft of the human genome sequence indicates that it comprises approximately 30,000 genes, it is anticipated that many years of additional research will be required to understand the specific functions and roles in disease of each of these genes and their patterns of interaction. This research, commonly referred to as genomics, is expected to lead to a new healthcare paradigm where disease is understood at the molecular level, allowing patients to be diagnosed according to their genomic profile and then treated with drugs designed to work on specific molecular targets. Ultimately, in addition to diagnosis and treatment, prevention and cure of disease might also be possible based on genomic information. Source: Excerpts from “The Genomics Outlook to 2005” by Joseph F. Dooley, PhD, FACB, Business Insights, February 1999.

Genomic Health OIT-49
p. 26
Exhibit 4 Glossary of Important Terms
Archived Tumor Sample: A tumor sample that has been preserved and stored. Tumor tissue is commonly preserved for storage by being treated with a preservative called formalin and then embedded in paraffin (wax). Biopsy: A procedure where tumor tissue is removed from the body for laboratory examination to determine whether or not cancer or some other disease is present. A biopsy can be performed using a needle to extract a small amount of cells or as a surgical procedure to remove a larger piece of tissue. Cancer: A condition in which abnormal cells divide without control. Cancer cells can invade nearby tissues and can spread through the bloodstream and lymphatic system to other parts of the body. Chemotherapy: Treatment with cytotoxic drugs to destroy cancer cells. Chemotherapy may be used in addition to surgery and is sometimes used in combination with other therapies such as radiation. Clinical Trial: A research study to test drugs, procedures, or testing technologies to determine how well they work compared to other practices. Core Biopsy: A procedure which uses a needle to extract a very small sample of tissue from an identified breast mass in order to obtain a preliminary diagnosis. Diagnosis: Identification of a condition, such as breast cancer, by its signs, symptoms, and the results of laboratory tests. Distant Recurrence: Breast cancer that recurs, or returns, in the bones, liver, lungs, or other organs after an entire treatment protocol has been completed. DNA (Deoxyribonucleic Acid): A long linear polymer found in the nucleus of a cell and formed from nucleotides and shaped like a double helix; associated with the transmission of genetic information. DNA has been called “the king of molecules.” Early Stage Breast Cancer: A term that can be used to describe stage I and II, lymph node-negative breast cancer. ER (Estrogen Receptor): A feature (protein) that may be present on certain cells to which estrogen molecules can attach. The term "ER positive" means that a woman's cells are sensitive to estrogen hormone. Gene: The functional and physical units of heredity that are passed from a parent to their offspring.

Genomic Health OIT-49
p. 27
Gene Expression: The process by which a gene's coded information is translated into the structures present and operating in the cell. DNA is first translated into RNA; some RNA then encodes the information to make proteins. Gene Expression Profile: A picture of the expression of multiple genes from a single specimen. Genome: The complete genetic material of a living thing. Genomics: The study of complex sets of genes and their effects on biology. Human Genome Project: An international research and technology-development effort aimed at mapping and sequencing the entire genome of human beings. Immunoassay: A laboratory test based on an “antigen-antibody” reaction. The presence of specific antigens and antibodies in the body can be a very clear indication of specific diseases or functional disorders. This test allows specific information to be obtained on the quality and quantity of these substances. In Situ (carcinoma in situ): Pre-cancerous cells that are isolated in the lobes or milk ducts of the breast. In Vitro Diagnostics: While “diagnostics” on its own refers to the process of disease screening, the addition of “in-vitro” clearly identifies where this takes place. Translating from the Latin, this means “in glass”, i. e. outside the body in the lab – usually on the basis of body fluid and tissue samples. In Vivo Diagnostics: This method of tracking down diseases is also characterized by its location. “In-vivo” translates as “in a living being,”, i.e., directly on the body. Examples include x-rays or ultrasound scans. Lumpectomy: A surgical procedure that removes a localized mass of tissue including the breast cancer tumor and a small amount of tissue surrounding the tumor. Marker: A marker labels a very specific location. A text marker, for example, highlights an important passage in a text. In the medical sense, the marker refers to a highly specific site on a chromosome. This could be a gene or a sequence repetition or cleavage site in the DNA. Markers can also be used in the diagnosis of diseases, e. g., the marker for chronic heart insufficiency is proBNP. Mastectomy: A surgical procedure to remove all or part of the breast. Metastatic Breast Cancer: Breast cancer that has spread beyond the breast to other parts of the body. Monoclonal Antibodies: Manufactured compounds specifically designed to find targets on cancer cells for diagnostic or treatment purposes.

Genomic Health OIT-49
p. 28
Node-Negative Breast Cancer: Breast cancer that has not spread to the lymph nodes under the arms (axillary lymph nodes). Node-Positive Breast Cancer: Breast cancer that has spread to the axillary lymph nodes under the arms. Oncotype DX™: A unique diagnostic test that looks at the genomic profile of a breast tumor to quantify the likelihood that breast cancer will return, or recur. Pharmacogenomics: A branch of research that investigates whether individual genes influence the reactions of drugs in the body – and if so, which. Radiation Therapy: The use of radiation to destroy cancer cells. Radiation therapy may be used before surgery or after surgery and is sometimes used in combination with chemotherapy. Recurrence: A return of cancer after treatment. Recurrence Score™: The results of the Oncotype DX™ assay are presented as a recurrence score. This is a number between 0 and 100 that correlates to a specific likelihood of breast cancer recurrence within 10 years of the initial diagnosis. RNA (Ribonucleic Acid): A long linear polymer of nucleotides found in the nucleus but mainly in the cytoplasm of a cell where it is associated with microsomes. It transmits genetic information from DNA to the cytoplasm and controls certain chemical processes in the cell. Screening: Monitoring for masses or suspicious areas in breast tissue. Staging: A classification system for breast cancers based on the size of the tumor, whether the cancer has spread to the lymph nodes, and whether the cancer has spread to other sites in the body (metastasis). Stage I Breast Cancer: The tumor is ≤ 2 cm in diameter and has not spread beyond the breast. Stage IIA Breast Cancer: The tumor is ≤ 2 cm and has spread to the lymph nodes under the arm (axillary lymph nodes) or the tumor is > 2-5 cm and has not spread to the lymph nodes. Stage IIB Breast Cancer: The tumor is > 2-5 cm and has spread to the lymph nodes under the arm or the tumor is > 5 cm in diameter and has not spread to the lymph nodes. Stage IIIA Breast Cancer: The tumor is > 5 cm in diameter and has spread to the lymph nodes under the arm or the tumor is any size and has spread more extensively in the lymph nodes. Stage IIIB Breast Cancer: The tumor is any size and has extended to other tissues near the breast; the tumor may or may not have spread to the lymph nodes.
Genomic Health OIT-49
p. 29
Stage IV Breast Cancer: Cancer that has spread to other locations in the body (metastasized). Surveillance/Follow-Up: An ongoing assessment by the medical team, once treatment has been completed, to assess the cancer's remission and look for any evidence of recurrence. Treatment Monitoring: An ongoing and frequent assessment by the medical team, during the time of treatment, to monitor how the patient is tolerating the treatment and how the cancer is responding. Tumor: Tissue growth where the cells that make up the tissue have multiplied uncontrollably. A tumor can be benign (non-cancerous) or malignant (cancerous). Source: Information provided by Genomic Health and other information available via public sources.

Genomic Health OIT-49
p. 30
Exhibit 5 About Oncotype DX™
Target Audience
Timing of Use
Source: Information provided by Genomic Health.

Genomic Health OIT-49
p. 31
Exhibit 6 High Level Genomic Health Testing Process
Patient is diagnosed with breast cancer.
Following surgery, physician orders Onco type DX™ test.
Pathology lab sends fixed paraffin-embedded tumor block or six thin sections from the biopsy specimen to Genomic Health using the specimen collection and transportation kit.
Genomic Health receives, tracks, and analyzes the tissue samples using its 21-gene panel to determine the patient’s recurrence score.
Genomic Health delivers results to the treating physician, by fax, overnight mail, and/or secure online access, within 10 to 14 days of receipt of the tissue sample.
Genomic Health OIT-49
p. 32
Important Notes: • The Genomic Health solution fits within current clinical practice and therapeutic protocols
(analyzing tissues as they are currently handled, processed and stored by clinical pathology laboratories).
• Because the specimens are formalin fixed, they require no special handling and can be sent by overnight mail to the Genomic Health laboratory in Redwood City, California.
• Results are provided to physicians within the crucial two-to-three week decision window after the tumor has been surgically removed and before the patient and the treating physician discuss additional treatment options. Typically, treatment does not begin within this time period to give the patient time to heal and to reduce the risk of infection.
• In cases where the complete tumor block has been provided to Genomic Health, it is promptly returned to the pathology lab as soon as the test has been completed.
Source: Information provided by Genomic Health.
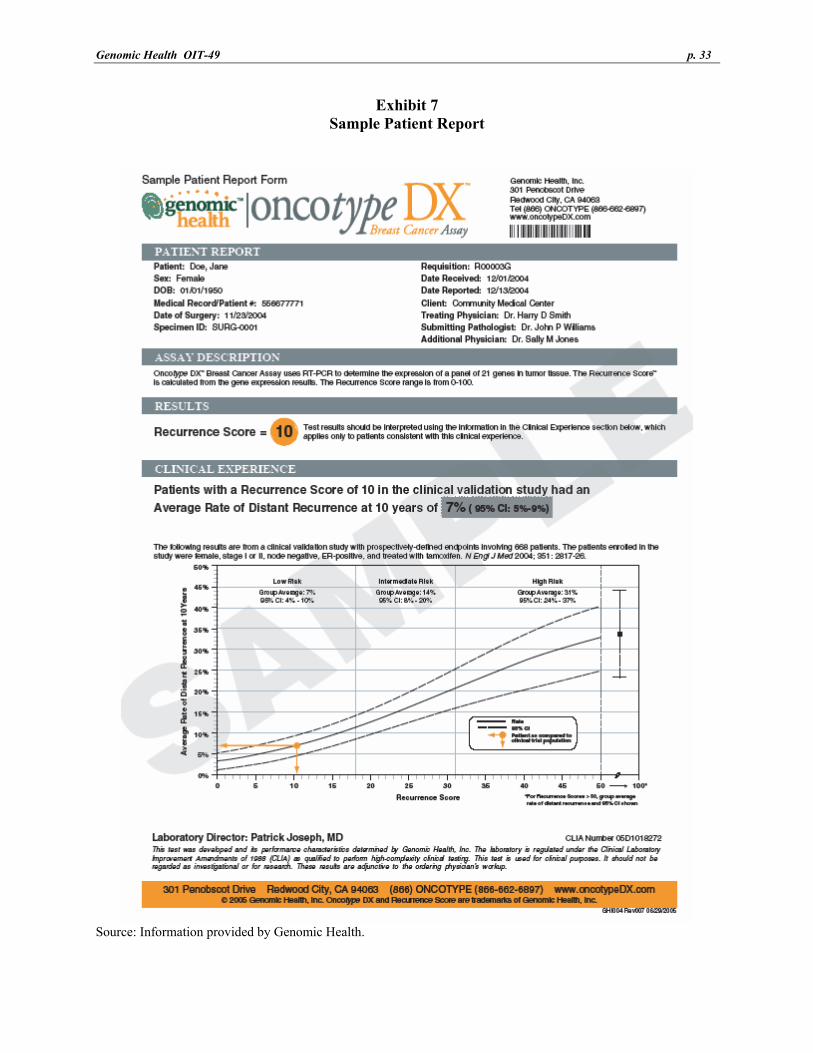
Genomic Health OIT-49
p. 33
Exhibit 7 Sample Patient Report
Source: Information provided by Genomic Health.
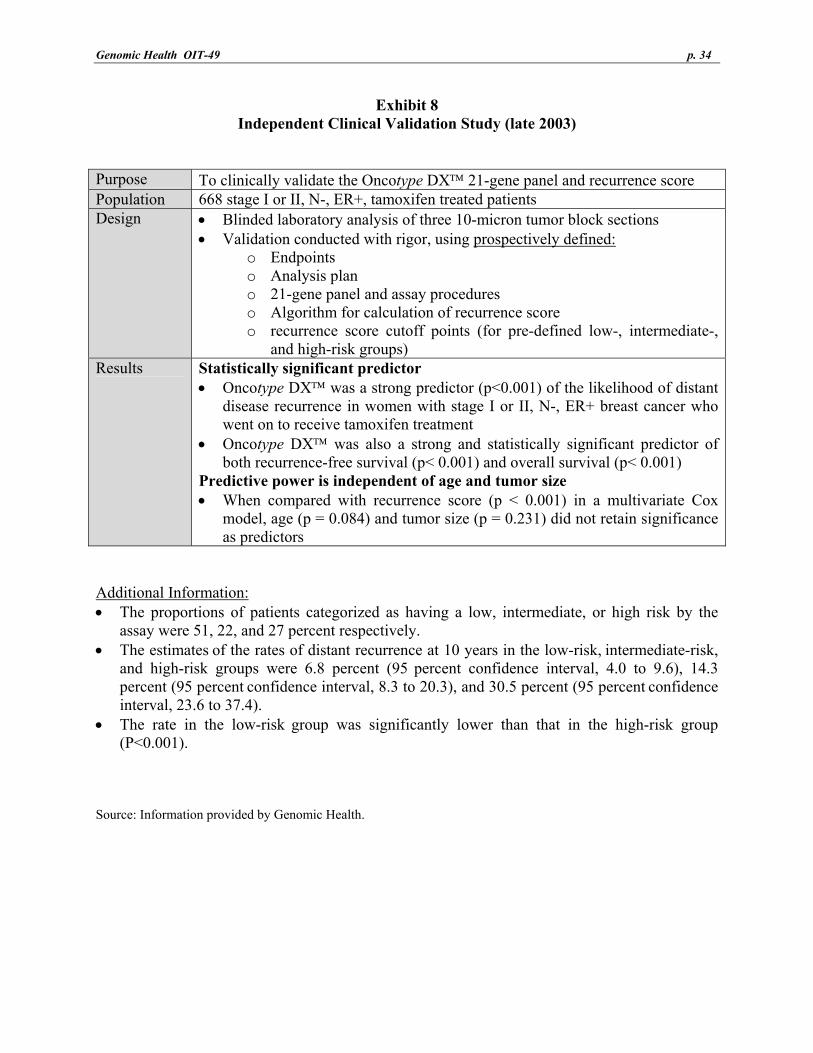
Genomic Health OIT-49
p. 34
Exhibit 8 Independent Clinical Validation Study (late 2003)
Purpose To clinically validate the Oncotype DX™ 21-gene panel and recurrence score Population 668 stage I or II, N-, ER+, tamoxifen treated patients Design • Blinded laboratory analysis of three 10-micron tumor block sections
• Validation conducted with rigor, using prospectively defined: o Endpoints o Analysis plan o 21-gene panel and assay procedures o Algorithm for calculation of recurrence score o recurrence score cutoff points (for pre-defined low-, intermediate-,
and high-risk groups) Results Statistically significant predictor
• Oncotype DX™ was a strong predictor (p<0.001) of the likelihood of distant disease recurrence in women with stage I or II, N-, ER+ breast cancer who went on to receive tamoxifen treatment
• Oncotype DX™ was also a strong and statistically significant predictor of both recurrence-free survival (p< 0.001) and overall survival (p< 0.001)
Predictive power is independent of age and tumor size • When compared with recurrence score (p < 0.001) in a multivariate Cox
model, age (p = 0.084) and tumor size (p = 0.231) did not retain significance as predictors
Additional Information: • The proportions of patients categorized as having a low, intermediate, or high risk by the
assay were 51, 22, and 27 percent respectively. • The estimates of the rates of distant recurrence at 10 years in the low-risk, intermediate-risk,
and high-risk groups were 6.8 percent (95 percent confidence interval, 4.0 to 9.6), 14.3 percent (95 percent confidence interval, 8.3 to 20.3), and 30.5 percent (95 percent confidence interval, 23.6 to 37.4).
• The rate in the low-risk group was significantly lower than that in the high-risk group
(P<0.001). Source: Information provided by Genomic Health.
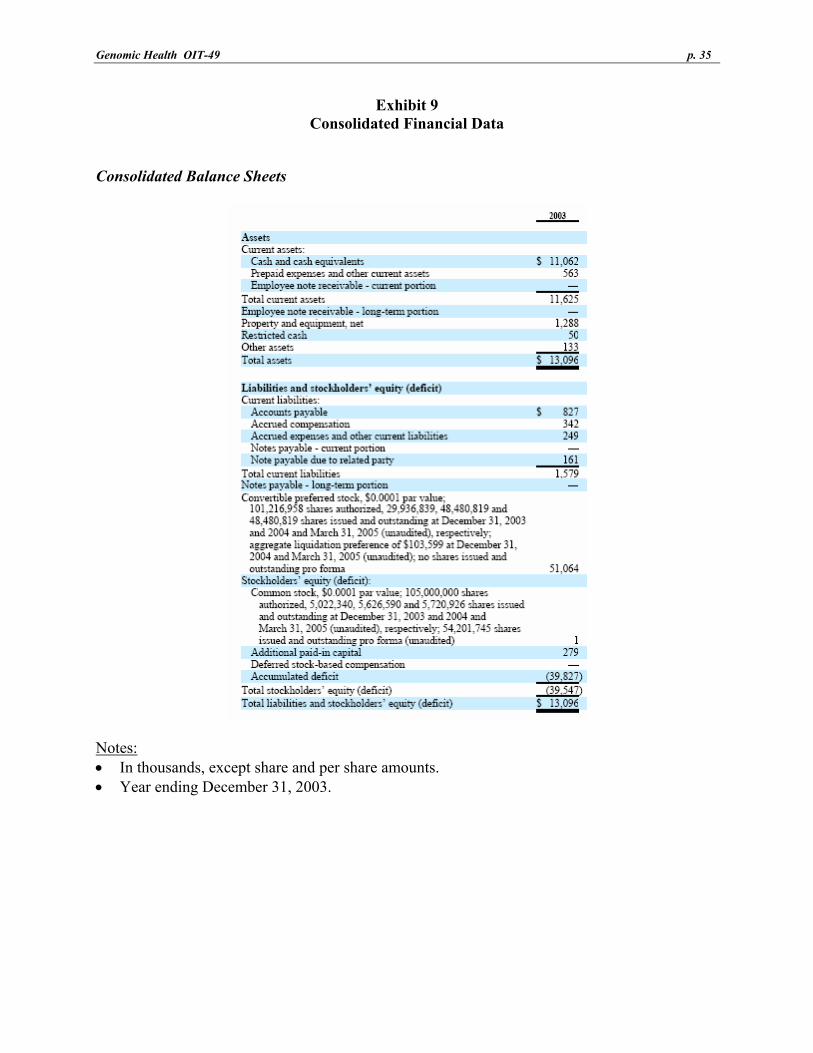
Genomic Health OIT-49
p. 35
Exhibit 9 Consolidated Financial Data
Consolidated Balance Sheets
Notes: • In thousands, except share and per share amounts. • Year ending December 31, 2003.

Genomic Health OIT-49
p. 36
Consolidated Statement of Operations
Notes: • In thousands, except share and per share amounts. • Year ending December 31, 2003.
Source: Information provided by Genomic Health.