“Michael's Game,” a card game for the treatment of psychotic symptoms
7
Intervention ‘‘Michael’s Game,’’ a card game for the treatment of psychotic symptoms Yasser Khazaal a, *, Je ´ ro ˆme Favrod b,c , Silke Azoulay e , Sophie Claude Finot j , Maria Bernabotto f , Ste ´ phane Raffard g , Joe ¨ l Libbrecht h , Karen Dieben a , David Levoyer i , Valentino Pomini c,d a Department of Psychiatry, Geneva University Hospitals, Geneva, Switzerland b La Source, Health Campus of the University of Applied Sciences of Western Switzerland, Lausanne, Switzerland c Community Psychiatry Service, Department of Psychiatry, University Hospital Centre and University of Lausanne, Switzerland d Institute for Psychotherapy, Department of Psychiatry, University Hospital Centre and University of Lausanne, Switzerland e Jura Bernois Psychiatric Services – Bienne Seeland, Biel, Switzerland f Esperance Centre, Var, Toulon, France g Adult Psychiatric Services, Montpellier University Hospital, Montpellier, France h Marronniers Centre, Tournai, Belgium i University Adult Psychiatric Centre, Guillaume Re ´gnier Hospital, Rennes, France j Male ´voz Psychiatric Hospital, Monthey, Switzerland 1. Introduction Despite the efficiency of anti-psychotic drugs in the treatment of psychotic disorders, a considerable proportion of patients endure residual symptoms, functional disturbance, and subjective distress [1,2]. It is also known that adherence to anti-psychotic drugs remains poor in many patients [3–5]. Persistent symptoms remain a major obstacle to recovery, because they often affect both insight towards illness and compliance to various types of interventions. The use of methods that try to alleviate persevering psychotic symptoms may contribute to the patients’ improvement. Among such methods, cognitive behavioural therapies (CBT) in group or individual format have proven to lead to a decrease in patients’ positive symptomatology [4,6–18], even if the decrease in symptoms is also modest [19], which is not surprising considering an illness as severe as schizophrenia. It appears that specific and important effects have been observed on insight, treatment adherence, as well as pathological behaviour consecutive to psychotic symptoms [14,15,18,20–23]. These effects could be of relevant importance when considering the fact that a large amount of persons presenting delusions do not spontaneously try to refute their beliefs, although the latter could appear peculiar to other people [24]. CBT aims at helping patients to develop alternative explanations to the evidences underlying their delusional ideas (for example through Socratic questioning or reality testing). The cognitive therapists assist their patients to explore more functional alternative interpretations of the situa- tions from which the delusions originated [25]. They also focus on the understanding of the relations existing between their thoughts, emotions, and behaviours, and promote emotional and beha- vioural modifications. Although the scientific data supporting the theoretical validity and practical efficiency of the cognitive therapy Patient Education and Counseling 83 (2011) 210–216 ARTICLE INFO Article history: Received 30 December 2009 Received in revised form 1 April 2010 Accepted 15 May 2010 Keywords: Cognitive therapy Behavioural therapy Psychosis Schizophrenia Delusions Insight ABSTRACT Objective: ‘‘Michael’s Game’’ is a card game which aims at familiarizing healthcare professionals and patients with cognitive therapy of psychotic symptoms. The present study tests the feasibility and the impact of the intervention in naturalistic settings. Methods: 135 patients were recruited in 11 centres. They were assessed pre- and post-tests with the Beck Cognitive Insight Scale (BCIS) and the Peters Delusion Inventory-21 items (PDI-21). Results: Data about 107 patients were included in the entire analyses. Significant improvements were observed on BCIS subscales as well as a reduction of severity of conviction and preoccupation scores on the PDI-21. The intervention has a moderate effect on the PDI-21 preoccupation and conviction as well as the BCIS subscales. Patients who benefit the most from the program are patients who have a low degree of self-reflectiveness and patients who are concomitantly preoccupied by their symptoms. Conclusion: The present study supports the feasibility and effectiveness of ‘‘Michael’s Game’’ in naturalistic settings. Practical implications: The game seems to be a useful tool for patients with psychotic disorders. ß 2010 Elsevier Ireland Ltd. All rights reserved. * Corresponding author at: Department of Psychiatry, Geneva University Hospitals, Rue Verte 2, 1205 Geneva, Switzerland. Tel.: +41 223725550; fax: +41 223202840. E-mail address: [email protected] (Y. Khazaal). Contents lists available at ScienceDirect Patient Education and Counseling journal homepage: www.elsevier.com/locate/pateducou 0738-3991/$ – see front matter ß 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.pec.2010.05.017
-
Upload
univ-montp3 -
Category
Documents
-
view
1 -
download
0
Transcript of “Michael's Game,” a card game for the treatment of psychotic symptoms

Patient Education and Counseling 83 (2011) 210–216
Intervention
‘‘Michael’s Game,’’ a card game for the treatment of psychotic symptoms
Yasser Khazaal a,*, Jerome Favrod b,c, Silke Azoulay e, Sophie Claude Finot j, Maria Bernabotto f,Stephane Raffard g, Joel Libbrecht h, Karen Dieben a, David Levoyer i, Valentino Pomini c,d
a Department of Psychiatry, Geneva University Hospitals, Geneva, Switzerlandb La Source, Health Campus of the University of Applied Sciences of Western Switzerland, Lausanne, Switzerlandc Community Psychiatry Service, Department of Psychiatry, University Hospital Centre and University of Lausanne, Switzerlandd Institute for Psychotherapy, Department of Psychiatry, University Hospital Centre and University of Lausanne, Switzerlande Jura Bernois Psychiatric Services – Bienne Seeland, Biel, Switzerlandf Esperance Centre, Var, Toulon, Franceg Adult Psychiatric Services, Montpellier University Hospital, Montpellier, Franceh Marronniers Centre, Tournai, Belgiumi University Adult Psychiatric Centre, Guillaume Regnier Hospital, Rennes, Francej Malevoz Psychiatric Hospital, Monthey, Switzerland
A R T I C L E I N F O
Article history:
Received 30 December 2009
Received in revised form 1 April 2010
Accepted 15 May 2010
Keywords:
Cognitive therapy
Behavioural therapy
Psychosis
Schizophrenia
Delusions
Insight
A B S T R A C T
Objective: ‘‘Michael’s Game’’ is a card game which aims at familiarizing healthcare professionals and
patients with cognitive therapy of psychotic symptoms. The present study tests the feasibility and the
impact of the intervention in naturalistic settings.
Methods: 135 patients were recruited in 11 centres. They were assessed pre- and post-tests with the
Beck Cognitive Insight Scale (BCIS) and the Peters Delusion Inventory-21 items (PDI-21).
Results: Data about 107 patients were included in the entire analyses. Significant improvements were
observed on BCIS subscales as well as a reduction of severity of conviction and preoccupation scores on
the PDI-21. The intervention has a moderate effect on the PDI-21 preoccupation and conviction as well as
the BCIS subscales. Patients who benefit the most from the program are patients who have a low degree
of self-reflectiveness and patients who are concomitantly preoccupied by their symptoms.
Conclusion: The present study supports the feasibility and effectiveness of ‘‘Michael’s Game’’ in
naturalistic settings.
Practical implications: The game seems to be a useful tool for patients with psychotic disorders.
� 2010 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Patient Education and Counseling
journa l homepage: www.e lsev ier .com/ locate /pateducou
1. Introduction
Despite the efficiency of anti-psychotic drugs in the treatmentof psychotic disorders, a considerable proportion of patientsendure residual symptoms, functional disturbance, and subjectivedistress [1,2]. It is also known that adherence to anti-psychoticdrugs remains poor in many patients [3–5]. Persistent symptomsremain a major obstacle to recovery, because they often affect bothinsight towards illness and compliance to various types ofinterventions. The use of methods that try to alleviate perseveringpsychotic symptoms may contribute to the patients’ improvement.
Among such methods, cognitive behavioural therapies (CBT) ingroup or individual format have proven to lead to a decrease in
* Corresponding author at: Department of Psychiatry, Geneva University
Hospitals, Rue Verte 2, 1205 Geneva, Switzerland. Tel.: +41 223725550;
fax: +41 223202840.
E-mail address: [email protected] (Y. Khazaal).
0738-3991/$ – see front matter � 2010 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.pec.2010.05.017
patients’ positive symptomatology [4,6–18], even if the decrease insymptoms is also modest [19], which is not surprising consideringan illness as severe as schizophrenia. It appears that specific andimportant effects have been observed on insight, treatmentadherence, as well as pathological behaviour consecutive topsychotic symptoms [14,15,18,20–23].
These effects could be of relevant importance when consideringthe fact that a large amount of persons presenting delusions do notspontaneously try to refute their beliefs, although the latter couldappear peculiar to other people [24]. CBT aims at helping patientsto develop alternative explanations to the evidences underlyingtheir delusional ideas (for example through Socratic questioning orreality testing). The cognitive therapists assist their patients toexplore more functional alternative interpretations of the situa-tions from which the delusions originated [25]. They also focus onthe understanding of the relations existing between their thoughts,emotions, and behaviours, and promote emotional and beha-vioural modifications. Although the scientific data supporting thetheoretical validity and practical efficiency of the cognitive therapy

Y. Khazaal et al. / Patient Education and Counseling 83 (2011) 210–216 211
of psychotic symptoms should lead to its wide use [16,26], thedissemination of this approach in naturalistic settings remainslimited [27]. Continuous efforts have to be oriented towards thecollection of new scientific evidence about the efficiency ofcognitive therapy in natural settings as well as towards theteaching of such methods among clinical staff members.
In this perspective, ‘‘Michael’s Game’’ [28], a training modulefor hypothetical reasoning, was conceived as a tool to promote thedissemination of cognitive therapies, by introducing and familiar-izing patients and staff to these specific intervention methods. Thegame is founded on the principles of cognitive therapy of psychoticsymptoms [14,25,29]. It proposes to use some of its methods [26]in a standardized and playful way. Through the game, staff andpatients are introduced to several active ingredients of cognitivetherapy, such as the normalization of psychotic symptoms,cognitive restructuring techniques that allow the creation ofalternative explanations to the evidences underlying the beliefs,the building of reality tests, and the establishment of connectionsbetween beliefs, emotions and behaviours.
In a preliminary study [28], 45 patients assessed with the PetersDelusion Inventory 21 items (PDI-21) [30] completed theintervention. A significant reduction of their level of convictionand preoccupation related to their delusional beliefs was observedat the end of the intervention. The present study aims to confirmthese results on a larger sample and to assess the impact of thegame on patients’ insight.
2. Methods
2.1. Participants and procedure
Participants were recruited in 11 outpatient centres, dayhospitals, or rehabilitation units in Switzerland, France, andBelgium. Three to seven patients were included in groups thattook part in 10–18 sessions (11.73 � 3.45). Participants gave oraland written informed consent. To be included in the study, patientshad to present persistent psychotic symptoms (presence of delusionsand/or hallucinations) and they had to be stabilized on anti-psychotic
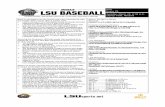
[(Fig._1)TD$FIG]Fig. 1. Examples of ‘‘Michael’s Game’’ cards. (1) A non-psychotic and non-emotional s
situation card.
medication (absence of acute agitation or severe disorganization). Thepatients were hence able to give informed consent and to participatein a group session.
Another inclusion criterion was a main DSM-IV diagnosis ofschizophrenia, schizoaffective disorder, or delusional disorder.Exclusion criteria were: (1) The inability to give informed consent,(2) evidence of organic brain disease, (3) main diagnosis of mentalretardation, (4) prior participation in the ‘‘Michael’s Game’’program or current cognitive therapy of psychotic symptoms.
Psychiatric diagnoses were established according to the DSM-IVcriteria following clinical interview by psychiatry residents and anattending senior psychiatrist before study inclusion. The presentstudy was approved by the ethical committee of the UniversityHospital Centre of Lausanne.
2.2. Intervention
‘‘Michael’s Game’’ is a group training module for hypotheticalreasoning. It comes in the form of a written card game, where eachcard corresponds to a situation that the central character, namedMichael, has experienced. Michael asks himself questions aboutthe encountered situations. The group of patients has the objectiveto answer Michael’s interrogations or to discuss the validity of hisinterpretations. Each card contains questions which help theparticipants through progressive stages, in order to formulatealternative hypotheses to Michael’s. Participants are led to identifythe behavioural and emotional consequences of the differentalternatives generated. The game is supervised by two caregivers.Sessions take place weekly and last from 60 to 90 min.
The game (see card examples on Figs. 1 and 2) was conceivedaccording the following progression: (1) non-psychotic and non-emotionally loaded situations (cards 1–11), (2) emotionally loadedbut non-psychotic situations (cards 12–32), (3) psychotic andemotionally loaded situations (cards 33–79).
The main technique brought out by the game is cognitiverestructuring. It is guided by the cards instructions which elicitSocratic questioning in participants, in order to find alternativeexplanation or behavioural experimentation to test the hypothe-
ituation card; (2) An emotional non-psychotic situation card; and (3) A psychotic

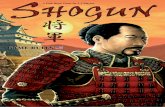
[(Fig._2)TD$FIG]
Fig. 2. Examples of objectives on the cards.
Y. Khazaal et al. / Patient Education and Counseling 83 (2011) 210–216212
ses. The program is designed to be playful and led in a non-judgemental and supporting atmosphere. Furthermore, theprogram involves active peer to peer interactions that are likelyvery useful [31] to improve patient participation. The game waswritten in French and has already been translated in English,German, Italian, and Spanish.
2.3. Game supervisors
The game supervisors were 15 nurses, 5 psychologists and 2social workers. They do not need to have a prior training incognitive therapy of psychotic symptoms; in fact, 5 of them did nothave any training on CBT and 15 others had minimal previoustraining. The game supervisors received a 2-h introduction to‘‘Michael’s Game,’’ either through a dedicated workshop or duringCBT training courses that lasted 2–3 days. The game supervisorswere trained by one of the first two authors. The workshopincluded a brief presentation of the rationale for cognitive therapyof psychotic symptoms, followed by a description of the game and1 h of role play. To ensure that therapists delivered theintervention as intended, supervision was provided during thestudy by telephone, email, group or individual sessions with one ofthe game authors.
2.4. Measures
All participants were assessed 1 week before and aftercompleting the intervention with the Beck Cognitive Insight Scale(BCIS) and the Peters Delusional Inventory (PDI-21). The BCIS [32]is a 15-item self-report scale measuring two constructs: The abilityto acknowledge fallibility, labelled ‘‘self-reflectiveness,’’ and thecertainty about belief and judgements, labelled ‘‘self-certainty.’’Participants rate the extent to which they agree with statementson a scale of 0 (do not agree at all) to 3 (agree completely). The 9items included in the ‘‘self-reflectiveness’’ subscale (minima andmaxima scores: 0–27) are relevant to the ability to remainobjective with regard to one’s own thoughts, to be open tocorrective feedback and capable to admit that one is wrong whenpresented with new points of view (for example, considering thatone’s beliefs can be due to particular inner emotional states, stressor imagination). The ‘‘self-certainty’’ scale (6-items; minima andmaxima scores: 0–18) assesses the degree of certainty about one’sown beliefs and judgements, addressed through questions aboutresistance to corrective information, dogmatism or overconfidencein one’s own conclusions despite opposite opinions. Higher scoresin self-reflectiveness indicate an increased ability to acknowledgefallibility, whereas higher scores in self-certainty indicate anincreased certainty about beliefs and judgements.
Beck et al. [32] show that the self-reflectiveness subscale issignificantly correlated with the awareness of delusions on theScale to Assess Unawareness of Mental Disorder [33]. Thisquestionnaire demonstrates good construct validity [32]. The
French translation was validated with an outpatient French-speaking sample suffering from schizophrenia [34] and shares asimilar factor structure with the original one.
The Peters Delusions Inventory (PDI-21) [30,35] is a self-reportquestionnaire dedicated to the measurement of delusions. 21delusional beliefs are investigated through three dimensions onthree 5-point Likert scales measuring: (1) The degree ofpreoccupation, (2) the degree of conviction, and (3) the degreeof anxiety (distress) related to the belief. This tool has good internalconsistency, good test–retest agreement, and good concurrentvalidity pertaining to schizotypy measures [36], magical ideation[37] and delusional ideation [38]. This questionnaire allows thedifferentiating of the general population from a group of patientsshowing psychotic symptoms. The latter can be distinguished fromthe former by the degrees of anxiety (distress), preoccupation, andconviction associated with the beliefs investigated in the scale [30].The scale was validated in French [39]. Since raw scores of PDI-21were usually related to the number of symptoms checked by thesubjects in a positive way (minimum: 0; maximum: 21), we optedto use instead proportional scores of distress, preoccupation orconviction associated with delusions (minima and maxima rawscore per dimension: 1–5). Patients who checked a lot of symptomsbut only felt moderate levels of distress or preoccupationassociated with them can be differentiated from those who onlychecked a few delusions that cause, however, a large amount ofdistress or preoccupation. In this sense, proportional PDI-21 scoresbetter reflect the mean burden and conviction associated with thepresence of delusional beliefs. PDI-21 proportional scores weresimply calculated by dividing raw scores obtained on distress,preoccupation or conviction scales by the total number ofsymptoms.
2.5. Statistical analyses
Statistical analyses were carried out using SPSS for Windows(version 15.0). Descriptive statistics were used to summarizedemographic and clinical characteristics of the study participants.t-Tests for continuous variables and chi-squares tests forcategorical variables or Fischer exact tests, if appropriate, wereused to detect baseline differences between the groups. Effect sizeswere calculated using r [40] and Cohen’s d formula corrected forrepeated measure design [41]. Pearson r was used for thecorrelation analyses and a logistic regression with enter, forward,and backward stepwise methods were used for identifyingpredictors of outcome.
3. Results
3.1. Participants
135 subjects were included in a ‘‘Michael’s Game’’ group (64 inSwitzerland, 58 in France, and 13 in Belgium). 28 patients wereremoved from this initial sample because: (1) They dropped out ofthe program after less than 3 sessions (N = 7), (2) their maindiagnosis was not a psychotic disorder but mental retardation or abipolar disorder (N = 5), (3) they were missing data pertaining tooutcome scales (N = 16). As these latter participants representmore than 10% of the entire initial sample, and due to thenaturalistic and exploratory nature of our study, we decided toremove them rather than to conduct intent-to-treat analyses or touse other techniques to estimate the missing data.
Comparative statistical analyses between the sample ofincluded patients (N = 107) and those excluded from analyses(N = 28) did not reveal any particular differences on socio-demographic variables (see Table 1). As expected, given ourexclusion criteria, participating patients did have a higher number

Table 1Comparison between the samples of included and excluded patients.
Included patients (N = 107) Excluded patients (N = 28) Statistics
Age (mean; SD) 32.7a (9.2) 32.7 (8.4) t(130) = .02, p = .98
Women (freq, %) 40b (37.7%) 9 (32.1%) x2(1) = .30, p = .58
Country (freq, %) Switzerland: 50
France: 46
Belgium: 11
Switzerland: 14
France: 12
Belgium: 2
x2(2) = .28, p = .87
Patients living in a medical/assisted setting (freq, %) 35 (32.7%) 10 (35.7%) x2(1) = .09, p = .76
Patients with a diagnosis of schizophrenia 91 (85%) 18 (64.3%) x2(1) = 6.15, p = .01
PDI-21 symptoms (pre-test) 7.09 (4.72) 7.78 (4.81) t(133) = .69, p = .49
PDI-21 distress (pre-test) 18.39 (14.61) 21.54 (19.44) t(133) = .94, p = .35
PDI-21 preoccupation (pre-test) 19.92 (16.05) 23.54 (20.57) t(133) = 1.0, p = .32
PDI-21 conviction (pre-test) 23.66 (18.02) 26.75 (21.23) t(133) = .78, p = .44
BCIS self-reflectiveness (pre-test) 12.7 (5.88) 12.1c (5.36) t(132) =�.51, p = .61
BCIS self-certainty (pre-test) 9.0 (4.27) 9.48c (3.72) t(132) = .53, p = .59
Number of sessions 11.73d (3.45) 5.6e (4.86) t(22.4) =�5.31f, p< .0001
a N = 104.b N = 106.c N = 27.d N = 76.e N = 20.f Equal variances not assumed.
Y. Khazaal et al. / Patient Education and Counseling 83 (2011) 210–216 213
of sessions and were more likely to be diagnosed withschizophrenia than the excluded patients. The patients from bothsamples do not differ on the outcome scales at pre-test.
The sample that was retained (mean age: 32; SD = 8.4; range:17–53) consists of 40 women and 66 men (gender data of onesubject is missing), 50 coming from Swiss care centres, 46 fromFrance, and 11 from Belgium. Patients were living alone or incouples (N = 56), with their parents (N = 16), in sheltered homes –community apartments, or nursing homes – (N = 29), or had beenin forensic hospitals for over 6 months (N = 6).
91 of the participants were diagnosed with schizophrenia. 15were diagnosed with schizoaffective disorders and one wasdiagnosed with persistent delusional disorder. Pre-test meanscores for BCIS are reported in Table 1 and were quite similar tothose indicated for the schizophrenia group in the validation study[32]. Mean pre-test scores for the PDI-21 are also presented inTable 1. The total number of symptoms reported seems to be lowerin the present sample than in Peters et al.’s deluded sample [35](11.9 vs. 7.09 in the present sample). The proportional scores ofconviction, preoccupation and distress are, however, similar in thetwo samples.
3.2. Outcome
3.2.1. Sessions participation
Due to missing data about the patients’ participation in groupsessions, data about the participation to the program were fullyavailable for only 71% of the sample. The mean number of
Table 2Paired t-test between pre- and post-tests score on outcome scales.
Outcome scales Pre-test mean (SD) Post-test mean (SD)
BCIS self-reflectiveness 12.71 (5.37) 15.01 (5.70)
BCIS self-certainty 9.00 (4.28) 7.44 (3.53)
PDI-21 number of symptoms 7.09 (4.73) 6.28 (4.54)
PDI-21 distressd 2.43 (1.25) 2.25 (1.20)
PDI-21 preoccupationd 2.57 (1.23) 2.10 (1.12)
PDI-21 convictiond 3.07 (1.44) 2.58 (1.42)
a Paired t-tests.b Cohen’s d corrected for repeated measures designs (Dunlap et al., 1996 [41]): d ¼c Effect size r ¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi½t2=ðt2 þ dfÞ�
q(Rosenthal, 1994 [40]).
d Proportional score of PDI-21 distress, preoccupation and conviction were used (see
completed sessions is 11.7 (SD = 3.45). The mean participation rate(number of completed sessions by a participant � 100/totalnumber of session needed to complete the program in the samegroup) is 88.3% (SD = 15.7), which is relatively high. In fact, 47.4% ofthe patients participated in the program in its entirety (the totalnumber of sessions needed by a group to play with the totality ofthe cards). Furthermore, 81.6% present a participation rate equal orsuperior to 75%, an arbitrary benchmark chosen by the authors toreflect participation to a relatively high number of sessions.
3.2.2. Impact of the program
Paired t-tests analyses were conducted to compare pre- andpost-tests outcome scores (see Table 2). If we set a Bonferronnicorrection of the error alpha for familywise error rate at .008 (for 6variables tested: 4 for PDI-21 and 2 for BCIS), the results of thepaired t-tests show that both BCIS subscales improved significantly(see Table 2). The PDI-21 preoccupation and conviction subscaleschanged significantly from pre- to post-tests assessments, but itwas not the case for the PDI-21 distress subscale and for the totalnumber of symptoms as assessed by the PDI-21. Moderate effectsizes were observed for all the statistically significant improve-ments (Table 2).
Another way to examine the impact of the program is to observehow many patients benefited from it. For this purpose wecalculated the threshold value of the Reliable Change Index(RCI) for each of our outcome measures [42]. The RCI is a statisticalmethod aiming to evaluate clinically significant change rather thanstatistically significant change. The threshold values (RCI criterion)
Mean difference SD ta df p db
�2.299 6.399 �3.716 106 0 0.415
1.561 4.155 3.885 106 0 0.395
�0.813 4.171 �2.016 106 .046 0.175
0.181 1.315 1.422 106 .158 0.148
0.473 1.198 4.087 106 0.401
0.483 1.718 2.906 106 .004 0.338
tffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi½2ð1� rÞ=n�
p.
text).

Table 3Values of RCI for outcome variables.
Outcome parameter Pre-test SD Reliability
measure
(alpha
Cronbach)
SE of
change
RCI
criterion
BCI self-reflectiveness 5.366 .73 3.943 7.729
BCIS self-certainty 4.276 .62 3.728 7.306
PDI-21 number
of symptoms
4.725 .78 3.134 6.143
PDI-21 distressa 1.250 .81 .771 1.510
PDI-21 preoccupationa 1.229 .81 .758 1.485
PDI-21 convictiona 1.441 .78 .956 1.873
a Proportional score of PDI-21 distress, preoccupation, and conviction were used
(see text).
Y. Khazaal et al. / Patient Education and Counseling 83 (2011) 210–216214
were reported in Table 3. The RCI for the BCIS was calculated usingthe Cronbach alpha found for the French version of this scale [34].For the PDI-21, values of test–retest reliability were obtained fromthe paper published by Peters et al. in 2004. We used the test–retest reliability measures because alpha Cronbach indices werenot specifically given for each subscale of the inventory. Patientswere then classified into two groups (benefit vs. no benefit fromthe program) for each outcome scale separately, depending onwhether the change values they exhibited were superior to thethreshold values or not. Table 4 presents the frequencies ofpatients who benefited from Michael’s Game in BCIS and PDI-21separately. Table 5 presents the frequencies of patients who
Table 4Frequency and percentage of patients who benefited from Michael’s Game in BCIS
and PDI-21 separately.
Frequency Percentage
Benefits in subscales of BCIS
No significant clinical change in any subscale 79 73.8
Significant clinical change in one subscale 23 21.5
Significant clinical change in both subscales
(self-reflectiveness and self-certainty)
5 4.7
Benefits in subscales of PDI-21
No significant clinical change in any subscale 85 79.4
Significant clinical change in one subscale 16 15.0
Significant clinical change in two subscales 3 2.8
Significant clinical change in the three subscales
(conviction, preoccupation, and distress)
3 2.8
Table 5Frequencies of patients who benefited from the program in at least one parameter
of BCIS or PDI-21.
Benefits in subscales of PDI-21 and BCIS Frequency Percentage
No significant clinical change in any subscale 58 54.2
Significant clinical change in one subscale 37 34.6
Significant clinical change in two subscales 9 8.4
Significant clinical change in three subscales 3 2.8
Table 6Correlations between pre-test and change scores with regard to main outcome variabl
Pre-test/change Self-reflectiveness change Self-certainty change Sym
BCIS self-reflectiveness �.542** .053 .02
BCIS self-certainty .135 �.650** �.14
PDI-21 total symptoms .058 .008 �.48
PDI-21 distress .246* �.269** �.03
PDI-21 preoccupation .401** �.165 �.10
PDI-21 conviction .307** �.174 �.13
Note: For the measurement of PDI-21 distress, preoccupation, and conviction, proporti* Correlation is significant at .05 level (2-tailed).** Correlation is significant at .01 level (2-tailed).
benefited with regard to at least one of the our five outcomeparameters (self-certainty and self-reflectiveness on BCIS, preoc-cupation, distress, and conviction on PDI-21). It appears that 45.8%of the patients benefit from the program with regard to at least one(or more) outcome parameters.
3.2.3. Who benefits from the program?
In order to deepen our analyses and try to better understandwhich kind of patients benefited the most from the program, wecalculated correlations between pre-test scores and degree ofchange.
The correlations between pre-test and change scores for theBCIS and PDI-21 subscales are presented in Table 6. First of all, wesee that the diagonal presents the highest correlations. Every pre-test variable is negatively correlated with its change score. So thehigher the level of self-reflectiveness, self-certainty, distress,conviction, preoccupation, or number of symptoms the patientsdemonstrate at pre-test, the lower the changes pertaining to thatdimension. Second, cross-relationships between a pre-test scoreand changes in the other variables essentially concern PDI-21distress, preoccupation and conviction scores, and to a lesserextent, self-reflectiveness. Self-certainty and PDI-21 number ofsymptoms do not present significant cross-correlations with thechanges in the other variables. In general, the three PDI-21subscales mentioned correlate with change in self-reflectiveness,but not with change in self-certainty (except a correlation of �.27for distress). Preoccupation and conviction present the highestcorrelations with self-reflectiveness (.401 and .307, respectively).Preoccupation at pre-test negatively correlates with change indistress and conviction (r = �.38 for both scales, p < .05). The samepattern is observed with the conviction subscale, which positivelycorrelates with change in distress and preoccupation (r = �.38 and�.43, respectively, p < .05). Distress at pre-test also negativelycorrelates with change in preoccupation and conviction (r = �.32and �.29, p < .05). In other words, patients who have highpreoccupations or convictions about their delusions tend to changemore positively in their self-reflectiveness than patients lesspreoccupied or less convinced by their beliefs. But at the sametime, the preoccupation or conviction levels of these patients donot change that much.
We conducted a logistic regression with the six outcomeparameters measured at pre-test. Enter, forward and backwardstepwise methods for logistic regression were tested and theirresults compared. The results obtained with the backwardstepwise method are briefly summarized here, as this methodgave us the finest results. The Hosmer and Lemeshow test indicatesthat the model has a satisfactory goodness of fit (chi square = 6.54,p = .59). Cox & Snell and Nagelkerke R squares are both moderate(.223 and .298, respectively). This indicates an improvement of22.3–29.8% of the variance between the initial model (whereclassification occurs by chance) and the one including the threeretained predictors: PDI-21 preoccupation, PDI-21 conviction, andBCIS self-reflectiveness. Other predictors were removed from the
es.
ptom change Distress change Preoccupation change Conviction change
8 .164 .283** .256**
3 �.283** �.165 �.166
4** .067 �.075 �.079
9 �.566** �.320** �.287**
0 �.384** �.572** �.375**
9 �.370** �.433** �.610**
onal scores were used.

Table 7Logistic regression coefficients (backward stepwise method: Results at step 4a).
Variables in equation B SE Wald df Sig. Exp(B)
BCIS—Self-reflectiveness �.189 .049 14.896 1 .000 .828
PDI-21—Preoccupation .853 .280 9.282 1 .002 2.346
PDI-21—Conviction �.613 .232 6.993 1 .008 .542
Constant 1.875 .831 5.094 1 .024 6.521
a Variables entered on step 1: Self-reflectiveness: self-certainty, distress, preoccupation, conviction, symptoms; Variable removed on step 2: Symptoms (PDI-21); Variable
removed on step 3: Distress (PDI-21); Variable removed on step 4: Self-certainty (BCIS).
Y. Khazaal et al. / Patient Education and Counseling 83 (2011) 210–216 215
regression without lowering the adequacy of the model. Knowingthese three pre-test variables, the overall correct classification ofpatients in both groups is 72%, with 63.3% of the patients correctlycategorized in the benefit group (at least one reliable change) and79.3% of correct categorization in the no benefit group. Table 7shows the regression coefficients for the three variables kept at thefourth step. The odds ratio, Exp(B), is the highest for PDI-21preoccupation: An increase in preoccupation with psychoticsymptoms favours a beneficial participation in the program. Thereverse is observed for conviction and self-reflectiveness, where anincrease in these pre-test scores seems to be related to theprobability to take part in the no benefit group.
Finally, when running t-test to compare patients who benefit ornot from the program based on their pre-test variables, only theself-reflectiveness scale gives a statistically significant difference(t = 3.968, df = 105; p < .000): Patients with low self-reflectivenesswill benefit more from the program than patients with high self-reflectiveness. The benefit vs. no benefit groups are otherwise notdistinguishable on the PDI subscales measured at pre-test.
4. Discussion and conclusion
4.1. Discussion
The present study supports the feasibility of the approach basedon ‘‘Michael’s Game’’ in naturalistic clinical settings. After a shorttraining for the staff, the game was used in various psychiatricservices including services non-specialized in cognitive andbehaviour therapies of psychotic symptoms. The small dropoutrate found in the first study [28] is confirmed here. The highpercentage of session participation speaks in favour of a goodacceptability of the program by the patients.
The major impact of the ‘‘Michael’s Game’’ program seems to bethe improvement of the PDI-21 on the preoccupation andconviction scales and on both BCIS subscales. The effect sizesare moderate but quite similar to those previously observed in CBTfor psychotic symptoms [19]. These results can be considered assatisfactory, because ‘‘Michael’s Game’’ is a relatively brief groupgame intervention. In fact, ‘‘Michael’s Game’’ was conceived tointroduce patients and staff to cognitive therapy for psychoticsymptoms rather than to apply an individually tailored cognitivetherapy. In this sense, the program fully achieves its goals.
Since the program improves the patients’ cognitive insight andreduces their conviction or preoccupation towards delusionalideas, it could be considered as a preparatory or complementaryintervention to a more direct cognitive therapy. It might beinteresting to study the potential added effect of the programcombined with a more classical individual or group cognitivetherapy for psychotic symptoms.
Which patients should ‘‘Michael’s Game’’ target? We tried toraise this question through our correlation and logistic regressionanalyses. We saw that the pre-test levels of preoccupation withdelusion, conviction in the latter and cognitive self-reflectivenessappear as three interesting predictors of change. Patients with ahigh degree of self-reflectiveness (well disposed to discuss their
beliefs) will have a higher probability to show positive change inpreoccupation and conviction. Conversely, PDI preoccupation andconviction scores at pre-test have negative correlations withchange in the PDI-21 scores: Patients who are highly preoccupiedor convinced do not improve as much.
In parallel, we observed that approximately 45% of the patientsderive a clinically significant benefit from the program in at leastone of the outcome parameters. Through logistic regression wenoted that knowing the pre-test values of preoccupation, convic-tion and self-reflectiveness allowed to properly assign 72% of thepatients to either the benefit or the no benefit group. However,when the benefit vs. no benefit groups were compared directlywith regard to these pre-test parameters, only the value of self-reflectiveness was statistically different.
In short, it seems that the best patients for ‘‘Michael’s Game’’ arethose who are preoccupied by their symptoms and not so muchself-reflective. Highly self-reflective patients may benefit morefrom a cognitive therapy directly targeting their particulardelusions.
The present study has several limitations, such as its non-controlled nature, the use of self-report questionnaires, the lack ofblinding assessment, the non-controlled character of the pharma-cological treatments as well as the lack of long term follow-upmeasures. Furthermore, the consistency of the intervention wasnot controlled by audio recording. Therefore, the degree of fidelityof the ‘‘Michael’s Game’’ model cannot be fully verified. However,the initial training and the supervision (answers to game super-visors’ questions related to their group animations) by the first twoauthors probably ensure a correct game animation. A randomizedcontrolled study with blind assessments, sessions recording, and a6-month follow-up is currently in progress in order to alleviatethese limitations.
4.2. Conclusion
Despite several study limitations, ‘‘Michael’s Game’’ seems tohave a positive impact on the preoccupation and conviction scalesof the PDI-21 and on both BCIS subscales including patients whoare more difficult to treat such as those in the less reflectivesubgroup. Interesting effect sizes (moderate) were observed onthese main outcome parameters. The tool is relatively easy to useand disseminate. This characteristic, in association with the highproportion of patient participation, encourages further develop-ments in this field. However, the conclusion needs to be temperedby the fact that in spite of an interesting statistically significantchange and moderate effect sizes, 73.8% of the participants showedno clinically significant change on either subscales of the BCIS, and79.4% showed no clinically significant change on any of the PDI-21subscales. Nevertheless, it remains that approximately 45% of thepatients derive a clinically significant benefit from the program inat least one of the outcome parameters. In consideration of theseobservations, the clinical impact of the observed changes will befurther explored. The randomized controlled study currently inprogress may help through several other clinical measures andfollow-up assessments.

Y. Khazaal et al. / Patient Education and Counseling 83 (2011) 210–216216
4.3. Practical implications
This study shows the possible use of ‘‘Michael’s Game’’ innaturalistic settings. The game seems useful after a brief trainingand should be considered as a tool for a better dissemination ofcognitive therapy of psychotic symptoms in various psychiatricclinical settings. The game seems to have an interesting impact oncognitive insight and the patients’ attitudes towards theirsymptoms.
Authors’ contributions
‘‘Michael’s Game’’ was written by YK and JF. YK and JFparticipated in the design of the study. The manuscript wasdrafted by YK, JF, and VP. The statistical analysis was performed byVP. Other authors supervised the games and took part inrecruitment and data collection. The final manuscript was readand approved by all the authors.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgement
Many thanks to the patients who participated in this study aswell as to those who supervised the games.
References
[1] Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia.Schizophr Bull 1997;23:663–74.
[2] Lindenmayer JP. Treatment refractory schizophrenia. Psychiatry Q2000;71(Winter):373–84.
[3] Fenton WS, Blyler CR, Heinssen RK. Determinants of medication compliance inschizophrenia: empirical and clinical findings. Schizophr Bull 1997;23:637–51.
[4] Lecomte T, Leclerc C, Corbiere M, Wykes T, Wallace CJ, Spidel A. Groupcognitive behavior therapy or social skills training for individuals with arecent onset of psychosis? Results of a randomized controlled trial. J NervMent Dis 2008;196(December):866–75.
[5] Zygmunt A, Olfson M, Boyer CA, Mechanic D. Interventions to improvemedication adherence in schizophrenia. Am J Psychiatry 2002;159(Octo-ber):1653–64.
[6] Garety PA, Kuipers L, Fowler D, Chamberlain F, Dunn G. Cognitive behaviouraltherapy for drug-resistant psychosis. Br J Med Psychol 1994;67(Septem-ber):259–71.
[7] Gaudiano BA. Cognitive behavior therapies for psychotic disorders: currentempirical status and future directions. Clin Psychol Sci Pract 2005;12(Spring):33–50.
[8] Gould RA, Mueser KT, Bolton E, Mays V, Goff D. Cognitive therapy for psychosisin schizophrenia: an effect size analysis. Schizophr Res 2001;48(March):335–42.
[9] Kuipers E, Fowler D, Garety P, Chisholm D, Freeman D, Dunn G, et al. Hadley C.London-east Anglia randomised controlled trial of cognitive-behavioural ther-apy for psychosis. III. Follow-up and economic evaluation at 18 months. Br JPsychiatry 1998;173(July):61–8.
[10] Pilling S, Bebbington P, Kuipers E, Garety P, Geddes J, Orbach G, et al. Psycho-logical treatments in schizophrenia. I. Meta-analysis of family interventionand cognitive behaviour therapy. Psychol Med 2002;32(July):763–82.
[11] Rector NA, Beck AT. Cognitive behavioral therapy for schizophrenia: anempirical review. J Nerv Ment Dis 2001;189(May):278–87.
[12] Sensky T, Turkington D, Kingdon D, Scott JL, Scott J, Siddle R, et al. A random-ized controlled trial of cognitive-behavioral therapy for persistent symptomsin schizophrenia resistant to medication. Arch Gen Psychiatry 2000;57(Feb-ruary):165–72.
[13] Tarrier N, Beckett R, Harwood S, Baker A, Yusupoff L, Ugarteburu I. A trial oftwo cognitive-behavioural methods of treating drug-resistant residual psy-chotic symptoms in schizophrenic patients. I. Outcome. Br J Psychiatry1993;162(April):524–32 [see comment].
[14] Turkington D, Dudley R, Warman DM, Beck AT. Cognitive-behavioral therapyfor schizophrenia: a review. J Psychiatr Pract 2004;10(January):5–16.
[15] Turkington D, Kingdon D, Turner T, Insight into Schizophrenia Research Group.Effectiveness of a brief cognitive-behavioural therapy intervention in thetreatment of schizophrenia. Br J Psychiatry 2002;180(June):523–7.
[16] Bazzoni A, Morosini P, Polidori G, Rosicarelli ML, Fowler D. Group cognitivebehavior therapy in the routine care at a psychiatric ward of diagnosis andtreatment. Epidemiol Psychiatr Soc 2001;10(January–March):27–36.
[17] Chadwick P, Sambrooke S, Rasch S, Davies E. Challenging the omnipotence ofvoices: group cognitive behavior therapy for voices. Behav Res Ther2000;38(October):993–1003.
[18] Wykes T, Hayward P, Thomas N, Green N, Surguladze S, Fannon D, et al. Whatare the effects of group cognitive behaviour therapy for voices? A randomisedcontrol trial. Schizophr Res 2005;77(September):201–10.
[19] Zimmermann G, Favrod J, Trieu VH, Pomini V. The effect of cognitive behav-ioral treatment on the positive symptoms of schizophrenia spectrum disor-ders: a meta-analysis. Schizophr Res 2005;77(September):1–9.
[20] Kemp R, David A. Psychological predictors of insight and compliance inpsychotic patients. Br J Psychiatry 1996;169(October):444–50.
[21] Rathod S, Kingdon D, Smith P, Turkington D. Insight into schizophrenia: theeffects of cognitive behavioural therapy on the components of insight andassociation with sociodemographics–data on a previously published random-ised controlled trial. Schizophr Res 2005;74(May):211–9.
[22] Startup M, Jackson MC, Bendix S. North Wales randomized controlled trial ofcognitive behaviour therapy for acute schizophrenia spectrum disorders:outcomes at 6 and 12 months. Psychol Med 2004;34(April):413–22 [seecomment].
[23] Trower P, Birchwood M, Meaden A, Byrne S, Nelson A, Ross K. Cognitivetherapy for command hallucinations: randomised controlled trial. Br J Psychi-atry 2004;184(April):312–20.
[24] Freeman D, Garety PA, Fowler D, Kuipers E, Bebbington PE, Dunn G. Why dopeople with delusions fail to choose more realistic explanations for theirexperiences? An empirical investigation. J Consult Clin Psychol 2004;72(Au-gust):671–80.
[25] Beck AT, Rector NA. Cognitive therapy of schizophrenia: a new therapy for thenew millennium. Am J Psychother 2000;54:291–300.
[26] Turkington D, Kingdon D, Weiden PJ. Cognitive behavior therapy for schizo-phrenia. Am J Psychiatry 2006;163(March):365–73.
[27] Morrison AP, Renton JC, Williams S, Dunn H, Knight A, Kreutz M, et al.Delivering cognitive therapy to people with psychosis in a community mentalhealth setting: an effectiveness study. Acta Psychiatr Scand 2004;110(Ju-ly):36–44.
[28] Khazaal Y, Favrod J, Libbrecht J, Finot SC, Azoulay S, Benzakin L, et al. A cardgame for the treatment of delusional ideas: a naturalistic pilot trial. BMCPsychiatry 2006;6:48.
[29] Rector NA, Beck AT. Cognitive therapy for schizophrenia: from conceptualiza-tion to intervention. Can J Psychiatry 2002;47(February):39–48.
[30] Peters ER, Joseph SA, Garety PA. Measurement of delusional ideation in thenormal population: introducing the PDI (Peters et al. Delusions Inventory).Schizophr Bull 1999;25:553–76.
[31] Rummel-Kluge C, Stiegler-Kotzor M, Schwarz C, Hansen WP, Kissling W. Peer-counseling in schizophrenia: patients consult patients. Patient Educ Couns2008;70(March):357–62.
[32] Beck AT, Baruch E, Balter JM, Steer RA, Warman DM. A new instrument formeasuring insight: the Beck Cognitive Insight Scale. Schizophr Res2004;68(June):319–29.
[33] Amador XF, Flaum M, Andreasen NC, Strauss DH, Yale SA, Clark SC, et al.Awareness of illness in schizophrenia and schizoaffective and mood disorders.Arch Gen Psychiatry 1994;51(October):826–36.
[34] Favrod J, Zimmermann G, Raffard S, Pomini V, Khazaal Y. The Beck CognitiveInsight Scale in outpatients with psychotic disorders: further evidence from aFrench-speaking sample. Can J Psychiatry 2008;53:783–7.
[35] Peters ER, Joseph SA, Day S, Garety PA. Measuring delusional ideation: the21-item Peters et al. Delusions Inventory (PDI). Schizophr Bull 2004;30:1005–22.
[36] Claridge GA, McCreery C, Mason O, Bentall R, Boyle M, Slade P, et al. The factorstructure of ‘‘schizotypal’’ traits: a large replication study. Br J Clin Psychol1996;35:103–17.
[37] Eckblad M, Chapman LJ. Development and validation of a scale for hypomanicpersonality. J Abnorm Psychol 1986;95:217–33.
[38] Foulds GA, Bedford A. Hierarchy of classes of personal illness. Psychol Med1975;5:181–92.
[39] Verdoux H, van Os J. Psychotic symptoms in non-clinical populations and thecontinuum of psychosis. Schizophr Res 2002;54(March):59–65.
[40] Rosenthal R. Parametric measures of effect size. In: Cooper H, Hedges LV,editors. The handbook of research synthesis. New York: Russell Sage Founda-tion; 1994. p. 231–44.
[41] Dunlap WP, Cortina JM, Vaslow JB, Burke MJ. Meta-analysis of experimentswith matched groups or repeated measures designs. Psychol Methods1996;1:170–7.
[42] Jacobson NS, Truax P. Clinical significance: a statistical approach to definingmeaningful change in psychotherapy research. J Consult Clin Psychol1991;59:12–9.