Troubled Abstraction: Whiteness in Charles Dana Gibson and George Du Maurier

Journal of Adolescence 2001, 24, 549–570doi:10.1006/jado.2001.0389, available online at http://www.idealibrary.com on
Mental health services in schools: the challenge oflocating a psychotherapy service for troubledadolescent pupils in mainstream andspecial schools
GEOFFREY BARUCH
In Part 1, the case is presented for school-based mental health services in terms of thelow utilization of community-based clinics and the high dropout rate among youngadolescents attending clinics in the community. The advantages and potential pitfallsof school-based services are also assessed. In Part 2, the paper discusses the lessonslearned from delivering psychotherapy services in mainstream and special schools totackle the mental health problems presented by troubled pupils. The author describesthe schools and discusses the expectations among teachers of the psychotherapist andpsychologist. The role of the psychotherapist and psychologist in the schools isoutlined. The types of treatment approach, the setting for treatment, method ofreferral, parental consent, and links with the wider network of adolescent mentalhealth services and evaluation of outcome are considered. Finally, the author discussesthe tensions that can arise between the psychotherapist and psychologist and schoolstaff and ways of overcoming them.
# 2001 The Association for Professionals in Services for Adolescents
Part 1: The rationale for mental health services in schools
IntroductionDespite the high prevalence of mental disorder and psychosocial impairment among youngpeople and the evidence of continuity of untreated psychopathology into adulthood only asmall proportion who require intervention receive help from a mental health service(Graham, 1986; Achenbach et al., 1995; Ferdinand et al., 1995; Smith and Rutter, 1995;Flaherty et al., 1996; Stanger et al., 1996; Achenbach et al., 1998; Wittchen et al., 1998).Graham (1986) estimates the overall prevalence of mental health problems in the adolescentpopulation at 20 per cent with 7–10 per cent having moderate to severe problems. In a studyof mental health need among young people and the take-up of mental health services in theU.S.A. 15–25 per cent of adolescents presented with emotional or behavioural problems butonly one third of this group were likely to attend a metal health service (Zahner et al., 1992;all quoted in Weist, 1999; Institute of Medicine, 1995; OTA 1991 quoted in Flaherty et al.,1996; Dryfoos, 1997). Similarly, in the UK there appears to be a vast gulf between the extentof diagnosable mental health problems (that are mostly co-morbid) in young people and theuse of appropriate mental health services [Kurtz, 1992; Health Advisory Service, 1995; AuditCommission, 1999; Office for National Statistics (ONS), 1999]. In the ONS study of themental health of children and adolescents aged 5–15 years, only about a quarter with mentalhealth disorders had been referred to a specialist mental health service.
Reprint requests and correspondence should be addressed to Geoffrey Baruch, Brandon Centre for Counsellingand Psychotherapy for Young People, 26 Prince of Wales Road, London NW5 3LG.
0140-1971/01/040549+22 $35�00/0 # 2001 The Association for Professionals in Services for Adolescents

550 G. Baruch
Although there is greater recognition of the mental health needs of troubled adolescents,adolescents’ needs have been relatively neglected compared to children and adults (Kazdin,1993; Health Advisory Service, l995; Audit Commission, l999). Kazdin cites three reasons.Firstly, adolescence has traditionally been viewed as a period of transition between childhoodand adulthood rather that a stage of development within its own right. Secondly, becauseadolescence is marked by considerable changeability in the behaviour and emotional state ofyoung people there is a tendency to take the view that their problems will disappear as aresult of the passage of time (Winnicott, 1966). Thirdly, within the adolescent stage ofdevelopment there are vast variations in psychosocial maturation that make the planning ofappropriate mental health services and interventions extremely hazardous compared toservices for children and adults.
In a study of adolescents who drop out of psychotherapy at the Brandon Centre, acommunity-based psychotherapy centre for young people, we found that those who droppedout were younger, had greater externalizing problems, school problems and presented withmoderate to severe hyperkinetic or conduct disorder. Those who continued were older, hadfewer externalizing problems and were self-referred (Baruch et al., 1998).
Findings from this study confirmed our clinical experience that young adolescents aged12–16 years are difficult to retain in psychotherapy and led us to consider alternative ways ofdelivering psychotherapy services to this age group. The most obvious alternative locus ofproviding psychotherapy for the younger adolescent is the school.
In Part 2 of the paper, I shall discuss the lessons learned by the Brandon Centre1 fromdelivering on-site psychotherapy services in mainstream and special schools to tackle themental health problems presented by troubled pupils. Before doing so, I shall briefly considerthe current development of mental health services in non-residential schools in thecommunity.
School-based mental health servicesIn the U.S.A., there has been a recent expansion of school-based mental health services thatadd to already existing services for pupils in special education and counselling for other pupils(Adelman and Taylor, 1999; Weist, 1999). The scope of these services, although includingpsychotherapy, is greater. The new expanded mental health input into schools includesassessment, multi-modal treatment, consultation and strategies for preventing mental illhealth that are available to all pupils in both special and mainstream education. As anindication of the significance attached to the expansion in school-based mental healthservices, two national centres dedicated to provide support and assistance for services inschools have been founded.
This expansion in school-based mental health services has occurred for a number ofreasons. Firstly, as cited above, there is the wide gap between young people who need mentalhealth input and those who actually receive specialist help. Outpatient and evencommunity-based mental health centres often fail to reach groups of young people ingreatest need, for instance refugee children and children from ethnic minority backgroundsand others from economically and socially disadvantaged backgrounds. Waiting lists are long.There are also high rates of young people not showing up for initial appointments and
1For over 30 years the Brandon Centre, a voluntary sector organization based in inner London, has been offeringfree psychotherapy and contraception to young people aged 12–25 years. The Centre’s outreach school-basedprojects for pupils at risk of school exclusion are cited as a service model in ‘‘National Service Framework for MentalHealth’’ (Department of Health, 1999).

Mental health services in schools 551
dropping out of treatment. Secondly, the high rate of demand for help with mental healthproblems from students using school-based health centres (of which there are over 1000throughout the U.S.A.) has given further impetus for dedicated school-based or linkedmental health services. Mental health problems among the young are the most significantreason for referral to a health centre. This use of resources is consistent with the finding fromepidemiological studies that mental health problems in young people ‘‘are more common andsignificant than physical health problems’’ (p. 132, Weist, 1999).
Finally, there are a number of perceived advantages of locating mental health services inschools that have spurred their expansion. Firstly, accessibility is improved so that take-up ofhelp is enhanced especially among hard-to-reach young people (Jepson et al., 1998; Weistet al., 1999). Secondly, mental health treatment is ‘‘normalized’’. There can be a stigmaattached to being referred to a mental health clinic in the community that deters the youngperson from seeking help. In school, the use of such help can be felt to be part of the ordinaryschool curriculum. Thirdly, by locating a service in school the practitioner can ensure thatthe benefits of treatment in terms of behaviour and internal well-being are generalizedbeyond the clinical setting. Moreover, the school-based practitioner is able to achieve greateraccuracy in recognizing and identifying the problems presented by the young person becauseshe/he can actually observe pupils’ behaviour and also learn directly from teachers’ reports.The availability of these sources of information can be enormously helpful to the on-sitepractitioner in formulating and assessing the impact of the treatment strategy. Fourthly, aschool-based mental health service also increases the opportunity to introduce strategies forthe prevention of mental health problems among young people so that these problems can betackled before they become pathological.
It is clear that in the U.S.A. a great deal of thought is going into developing ‘‘multifaceted,comprehensive and integrated school mental health programs’’ (p. 133, Weist, 1999) withthe aim of making them the cornerstone of mental health provision for children and youngpeople (Adelman and Taylor, 1999; Armbruster et al., 1999). An emerging trend is themovement from fragmented, narrowly focused and specialist oriented services tocomprehensiveness and cohesiveness in planning and delivering school-based services. Thisplanning includes considering how to integrate the school-based mental health service intothe organizational structure of the school so that the mental health practitioner, usually aclinical psychologist, is in a similar position to the teacher and school management tocontribute to the overall work of the school (Dryfoos, 1997; Flaherty et al., 1998).
Although schools are increasingly becoming a locus for mental health work with childrenand adolescents in the U.K. (Department of Health, 1999; Rutter, 1999), as yet such input,even more so than routine mental health services for adolescents (see Audit Commission,1999), is unevenly distributed throughout the country and highly variable in quality. School-based mental health input tends to be project oriented, initiated in a fragmentary way andoften not linked with the network of existing mental health services for children andadolescents. It is also highly insecure in terms of funding.
The type of input and practitioner are variable so that it would be inaccurate to talk interms of a practitioner who belongs to a single mental health profession, has a uniformtraining and implements a consistent approach to treatment. A person who has been trainedas a counsellor, a child and adolescent psychotherapist, a psychotherapist, a clinicalpsychologist, an education therapist, and an art therapist may carry out work in secondaryand special schools. There is also a tendency for people who are undergoing training in one ofthese professions to work in schools.

552 G. Baruch
The relationship of the practitioner to the school is another feature that varies. Thepractitioner may be an employee of the school, may be self-employed, or may be employed byan external organisation in the NHS or voluntary sector that provides counselling,psychotherapy or psychology services in the community. The nature of the relationship isimportant because of the implications for practice. For instance, the counsellor employed bythe school and working on their own can be overwhelmed by demand from pupils and staffand may feel isolated from their professional base. The characterization of the interventionprovided in schools is as variable as the list of professions. This includes time-limitedcounselling from a variety of theoretical orientations, long-term psychoanalytic psychother-apy, time-limited group psychotherapy, time-limited cognitive-behavioural treatment on anindividual or group basis, art therapy and peer counselling.
Although there are advantages of psychotherapy services in school, there are also potentialpitfalls. Firstly, there is a danger that children’s right of privacy is ignored by teachers andmental health professionals who assume that psychotherapy or counselling are justifiedbecause they target a barrier to learning (Evans, 1999). The issue is not merely one ofensuring parental or child consent, important though this is. There is an underlyingphilosophical issue about the freedom of the child to be educated since that is their‘‘contract’’ with the school. The mixing of psychotherapy or counselling with learningviolates this contract and is an aspect of social control. There is every danger of teachersabandoning the routine approach of the school to behaviour problems and instead usingtherapy to control the child’s behaviour. Nonetheless a mental health perspective can helpteaching staff to recognize that underlying a pupil’s problematic behaviour is a mental healthproblem.
Secondly, there is the problem of confidentiality. Other pupils are likely to find out whenone of their peers is receiving psychotherapy or counselling. Moreover, knowing that they arereceiving psychotherapy or counselling may influence teachers’ evaluation of pupils’academic ability and character. Thirdly, there is the issue of parental participation indecisions about the application of mental health intervention to their child (Evans, 1999).As schools take on more and more welfare functions there may be a lack of meaningfulconsultation and involvement of parents and other relevant stakeholders. Also theassumption of welfare responsibilities by the school may convey to pupils that their parentsare unable to carry out basic support functions with their child.
Fourthly, in the rush to locate psychotherapy and counselling in schools because theyundoubtedly increase utilization especially by groups of hard-to-reach children (Fothergilland Ballard, 1998; Jepson et al., 1998; Kaplan et al., 1998; Grenberg et al., 1999; Weist et al.,1999), interventions may be implemented that are inappropriate to the problems presentedby young people or are empirically unsupported. In this regard, a further issue is raised thatconcerns demand by schools for counselling services. In the U.K., counselling is theintervention that schools demand and see as best practice in responding to the mental healthneeds of their pupils. Yet there is little evidence of the effectiveness of counselling other thanwith mild internalizing problems (Roth and Fonagy, 1996). The emotional and behaviouralproblems presented by pupils for whom teachers seek help for are mostly severe and co-morbid. Short-term counselling may be a valid means of assessment that leads to referral forother treatment modalities but often is not sufficient in its own right to ameliorate theproblems that severely troubled pupils present.
Fifthly, integrating the goals of psychotherapy and counselling with educational goals andobjectives can lead to tensions and conflict between mental health professional and teachers.

Mental health services in schools 553
For instance, there may be differences of opinion over whether priority should be given totherapeutic sessions over lessons or over a decision about whether to exclude a pupil. Indeedthe school’s exclusion policy may be at considerable variance with the practice of mentalhealth professionals. The therapeutic ethos of the mental health professional tends totolerate to aberrant behaviour but this may clash with the educational culture of the schoolwhich requires pupils to be co-operative in class.
Sixthly, the whole enterprise of locating psychotherapy and counselling in schools can beseverely undermined if teachers have unrealistic expectations of what can be achieved bymental health professionals and mental health professionals do nothing to ‘‘educate’’teaching staff about the limitations of their work as well as the potential benefits. Finally, apsychotherapy or counselling service is perhaps more vulnerable than a routine NHS clinicservice to funding being withdrawn because it is usually made available on a short-term basis.Obviously the premature termination of a service can be extremely disruptive and disturbingto young people who are receiving psychotherapy or counselling.
Our experience suggests that these potential pitfalls are part of the exciting challenge oflocating a psychotherapy service in schools and do not outweigh the advantages of theservice being delivered at a school.
Part 2: Delivering psychotherapy services for adolescentpupils in special schools and mainstream schools
IntroductionThis account is based on our experience of delivering psychotherapy since 1993 in threespecial schools and three mainstream schools located in north London. The services in theseschools have been funded by time-limited grants from Charitable Trusts and in one case, aone-off grant from the local Social Services Department. In most cases, the grants fromCharitable Trusts have been renewed. All the services, apart from one, are ongoing.
The schoolsMainstream school ‘‘A’’ is a boys’ secondary school. It is located in a district marked bysignificant social and economic deprivation. A high proportion of the local community iseither Asian or African-Caribbean and young people from these two ethnic backgroundscomprize the majority of pupils. An officer from the local education authority recommendedSchool ‘A’ to us because there were concerns about the high rate of school exclusion amongpupils. This problem was compounded because the school received pupils who had beenpermanently excluded from other local schools. The head teacher and deputy head teachersrecognized that disruptive behaviour that led to the exclusion of pupils was frequently causedby the impact of problems outside the school, particularly in the family. At the time westarted our psychotherapy service short-term counselling was being provided on one day perweek by a counsellor employed by the school.
Mainstream school ‘‘B’’ is a mixed secondary school. It is also located in an area of highsocial and economic deprivation where there is a concentration of people from ethnicminority backgrounds and latterly from refugee communities. The school had concerns aboutpupils who were troubled due to severe family problems. Often, disruptive and inappropriatebehaviour by some pupils brought their underlying problem to the attention of the teachingstaff that wished to deal with such difficulties in a sympathetic manner. There were also

554 G. Baruch
concerns about the emotional and behavioural problems of special needs pupils and refugeepupils. As well as our service, there is a counsellor who works at the school on a sessionalbasis. There is also input from two local NHS Centres of Excellence that provide mentalhealth services for children and adolescents. This input is focused exclusively on troubledrefugee pupils. Mental health professionals from these centres provide advice andconsultation to the teaching staff and also assist in running therapy groups.
Mainstream school ‘‘C’’ is in many respects similar to ‘‘A’’ and ‘‘B’’ in terms of the characterof its intake. ‘‘C’’ has many pupils who come from dysfunctional and disadvantagedbackgrounds. Recently there has been a large increase in from refugee backgrounds that havesuffered severe trauma. The school employs a counsellor on a part-time basis. Like ‘‘B’’, ‘‘C’’is linked to a Centre of Excellence that provides on-site advice and consultation to teachingstaff for helping troubled refugee pupils.
Special school ‘‘D’’ is a pupil referral unit that takes adolescent boys and girls from 14 yearsupwards who have been permanently excluded from mainstream education. The pupils havesevere behavioural problems particularly with unrestrained aggression. Many of them areyoung offenders. Same are ‘‘high tariff’’ offenders who have committed violent and otherserious crimes. Typically the pupils have severe learning difficulties. According to anassessment we carry out of their reading ability, it is not unusual for a pupil to have a readingage that is equivalent to six or more years behind their chronological age.
School ‘‘E’’ is a special school for boys who present with severe emotional and behaviouraldisorders and are unable to use mainstream education. The age range of pupils is from 11–16years. The intake is London-wide. Many of these pupils have had long-standing emotionaland behavioural problems. They come from highly dysfunctional families and it is not unusualfor them to have suffered emotional, physical and sexual abuse. Usually their families have along history of involvement with social services and have received input from mental healthservices in the community. Parents tend to have a negative perception of their experience ofsuch help which they feel has been of little benefit either to them or their child. The childrenexhibit anxiety and depressive disorders and problems with their attention and aggression.Some pupils assume hostile intent in relation to the behaviour of others towards them andthis leads to fighting and acts of violence in the school and delinquency outside school.Without exception, the statement of their educational needs identifies specialist mentalhealth treatment. Although there had been a mental health service at the school linked to alocal clinic, this no longer existed due to lack of resources when we linked up with the school.
School ‘‘F’’ is a special school for pupils aged 5–16 years with severe physical disabilitiessuch as cerebral palsy. Most of the children depend on the use of a wheelchair. The pupilsrequire an array of support such as speech therapy and physiotherapy. Many of the childrenhave learning difficulties and can only manage communication with the assistance of atechnical aid. Adolescence creates unique difficulties for this group of highly dependentchildren. They must find a way of coping with the adolescent process in the context of a bodythat restricts their opportunity to act on urges and wishes commonly experienced inadolescence. The teaching staff were aware that a number of children were depressed andanxious. They welcomed a psychotherapy service in order to address these difficulties. Theyparticularly welcomed being able to increase the accessibility of psychotherapy to their pupilswhose physical state can be a barrier to obtaining treatment in the community. Prior to ourrelationship with the school, there had been input from a local NHS clinic that had peteredout principally because the model was too oriented around consultation as opposed todirectly helping the children.

Mental health services in schools 555
The following vignettes are examples of typical referrals by teaching staff of pupils whomost concern.
Cathy (mainstream school ‘‘B’’)Cathy was aged 13 years when she was referred to the psychotherapist because she wassuicidal. Her mother was a diagnosed schizophrenic who had committed suicide. Her fatherhad alcohol problems and there were concerns that he was behaving in a sexuallyinappropriate way towards his daughter.
Ria (special school ‘‘F’’)Ria was aged 14 years when she started therapy for depression. She presented with a severephysical disability. Her mother who, although still living with Ria’s father, was having anaffair with another man in the family home, largely ignored her. Meetings between Ria’smother and her lover often took place in front of Ria. During the course of her therapy, Riaconfided that she was in love with a fellow female pupil. She was upset that the pupilalthough very friendly towards her, was not interested in being on intimate terms.
John (special school ‘‘E’’)John was aged 14 years when he started therapy. He was violent and unpredictable in hisbehaviour towards fellow pupils and teachers. Both parents regularly physically abused him.There were concerns that John’s parents openly engaged with pornographic materials in frontof their children.
Peter (special school ‘‘D’’)Peter had been excluded from several schools because of disruptive behaviour. He wasaggressive towards other pupils. He was unable to maintain attention for long and walked outof lessons. On several occasions he had been caught smoking marijuana at school. He wascharged with robbery and assault. Peter’s father, who was in prison, had been particularlyviolent towards him as a young child.
Referred pupils, like the ones briefly described, because of their past experience of mentalhealth services and other public services such as social services are mistrustful of mentalhealth professionals and social workers and have a negative perception of psychotherapy.They are therefore unlikely to attend a service, even one as easily accessible as the BrandonCentre. Yet they are in great need of help and the only way to reach out to them is by offeringa service in school.
The Brandon Centre’s service
Relationship of psychotherapists working in schools to the Brandon Centre.Careful thought has been given to fostering and maintaining the relationship between themember of staff who is working at the school and the Centre. This is especially importantbecause in all cases, apart from one, they are employed on a part-time basis. Without properconsideration being given to their relationship to the Centre, the member of staff could easilybecome detached and isolated in their work. All the members of staff receive weekly clinicalsupervision and, with the exception of one member staff, regularly attend a weekly clinicalmeeting. In the first part of the meeting, along with other Centre staff, they are able topresent clinical issues from ongoing work. In common with their colleagues working at the
556 G. Baruch
Centre, a member of staff working at a school has an opportunity once a term to use theentire second part of this clinical meeting to present their work at the school and to receivesupport from their colleagues. In addition, members of staff working at schools areencouraged to consult their colleagues informally about their work, which they are able to dosince they are present at the Centre at least on one day a week. The administrative duties ofmembers of staff working in schools also assist in binding them to the Centre. Like theircolleagues who work at the Centre, they are expected to keep an accurate recordin the Centre’s clinical diary of their appointments and to keep clinical files up to date.Furthermore they participate in the evaluation procedures that are used for thepsychotherapy service at the Centre. An underlying purpose of all these arrangements isto make members of staff who are working away from the Centre’s premises feel that theirstatus is the same as colleagues working at the Brandon Centre. Certainly it is my experiencethat the latter respect, are interested in and admire the work of members of staff at schools.By not splitting off the work in schools from the rest of the Centre’s activity, the former doesnot become a convenient focus for projecting the negative aspects of therapeutic work withyoung people.
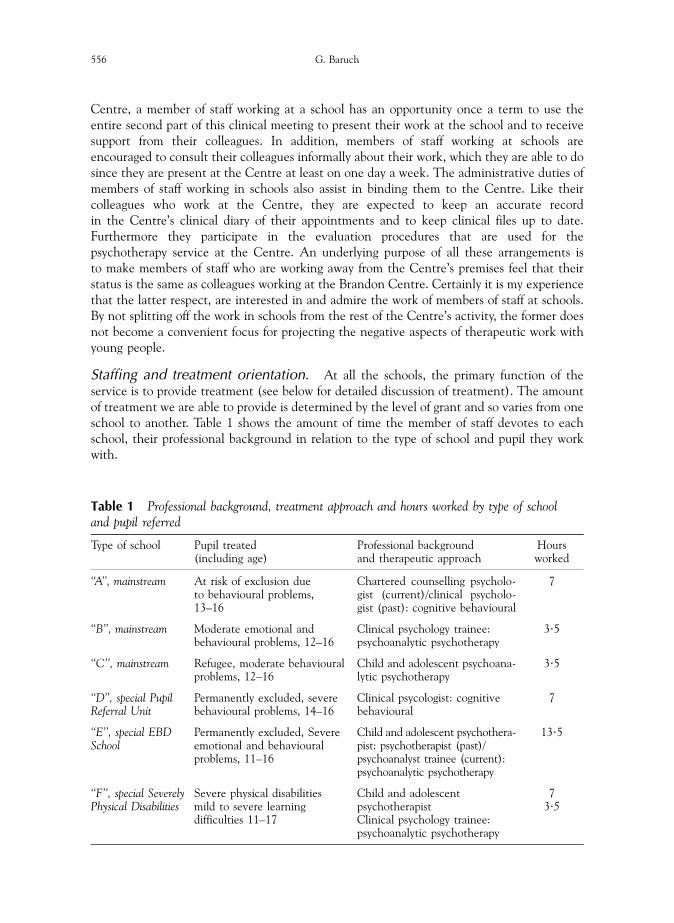
Staffing and treatment orientation. At all the schools, the primary function of theservice is to provide treatment (see below for detailed discussion of treatment). The amountof treatment we are able to provide is determined by the level of grant and so varies from oneschool to another. Table 1 shows the amount of time the member of staff devotes to eachschool, their professional background in relation to the type of school and pupil they workwith.
Table 1 Professional background, treatment approach and hours worked by type of schooland pupil referred
Type of school Pupil treated(including age)
Professional backgroundand therapeutic approach
Hoursworked
‘‘A’’, mainstream At risk of exclusion dueto behavioural problems,13–16
Chartered counselling psycholo-gist (current)/clinical psycholo-gist (past): cognitive behavioural
7
‘‘B’’, mainstream Moderate emotional andbehavioural problems, 12–16
Clinical psychology trainee:psychoanalytic psychotherapy
3?5
‘‘C’’, mainstream Refugee, moderate behaviouralproblems, 12–16
Child and adolescent psychoana-lytic psychotherapy
3?5
‘‘D’’, special PupilReferral Unit
Permanently excluded, severebehavioural problems, 14–16
Clinical psycologist: cognitivebehavioural
7
‘‘E’’, special EBDSchool
Permanently excluded, Severeemotional and behaviouralproblems, 11–16
Child and adolescent psychothera-pist: psychotherapist (past)/psychoanalyst trainee (current):psychoanalytic psychotherapy
13?5
‘‘F’’, special SeverelyPhysical Disabilities
Severe physical disabilitiesmild to severe learningdifficulties 11–17
Child and adolescentpsychotherapistClinical psychology trainee:psychoanalytic psychotherapy
73?5

Mental health services in schools 557
A feature common to our work in all schools is the provision of long-term help. We try tobase our way of working in school on the model used at the Brandon Centre,2 which, inpsychoanalytic psychotherapy, essentially is to provide the young person with an opportunityto explore their problems without the hindrance of being limited by time. I think that thisapproach is in contrast to counselling services in schools, which tend to provide a short-termintervention. At school, the only constraints on the length of treatment we offer are fundingand if the pupil wishes to terminate treatment. A further constraint on the length oftreatment concerns the clinical psychology trainee whose length of employment at theCentre is for 12 months. However, pupils can be transferred from the outgoing psychologistto their successor.
Apart from the counselling psychologist who works at mainstream school ‘‘A’’ with pupilsat risk of exclusion due to disruptive behavior and the clinical psychologist who worked inthis school and the Pupil Referral Unit, the staff working at the other schools providepsychoanalytic psychotherapy. There is variation in the amount of adaptation of approachthat occurs. In the mainstream schools, there is little adaptation apart from sessions fittingaround the length of lessons, which involves shortening them from 50 to 40 minutes. Thepupils in these schools are able to communicate in a reasonably straightforward way.However the psychotherapist and clinical psychology trainee, where necessary, are active inthe sessions in prompting the pupil and in asking questions where the pupil is reticent andunfamiliar with talking about their thoughts and feelings. In the special schools, the problemof fostering therapeutic work is altogether different due to the severity of the pupils’emotional and behavioural problems and, in many cases, moderate to severe learningdifficulties.
For instance, the child psychotherapist in special school ‘‘F’’ works with some pupils whohave such profound learning difficulties that they can only communicate with the aid of aninstrument that decodes their communication. The therapist has to learn how to use theinstrument to make a dialogue possible. In some cases, with the pupil’s agreement, theirsupport worker is present at their sessions in order to assist the communication between thetherapist and the pupil. This arrangement may limit the pupil’s sense of being able to talksafely about private thoughts and feelings. On the other hand the intimate relationship thatdevelops between some support workers and pupils can be a focus of valuable therapeuticwork, for instance when the pupil is leaving the school and having to separate from thesupport worker.
Most pupils receiving psychotherapy in special education require an approach by the childpsychotherapist that takes account of shortcomings in their development. Sessions tend to beshorter and play, especially the use of games, is a strategy used in working with these pupils.The therapist hopes that through this medium the pupil can express their concerns andanxieties. A further function served by play is to ‘‘soften’’ the process of the pupils talkingabout themselves. Most pupils at the EBD school (special school ‘‘E’’) are extremely self-conscious and defensive about talking about themselves and their backgrounds. Progress isvery slow. They tend to react aggressively and provocatively towards the therapist as a way ofcontrolling her capacity to talk with them about uncomfortable and disturbing issues. Thechild psychotherapist (a woman) requires a great deal of patience and resilience especiallywith pupils who use sexually provocative and sexist language. She must retain a belief in the
2As well as long-term psychotherapy, the Brandon Centre also offers young people a time-limited six-sessionintervention. However at the end of this they can go back on to the waiting list for long-term psychotherapy.

558 G. Baruch
value of being emotionally available in the session with these psychologically damaged pupilswho expect to be rejected for their uncooperative behaviour. The difference with pupils intherapy at mainstream schools is striking. Since therapy is wholly voluntary most referredpupils in mainstream schools are motivated to engage in treatment. Moreover they are betterequipped than pupils in special education to reflect and think about their problems.Obviously there are issues that they may try to avoid but this avoidance can be commentedon by the therapist without engendering a hostile and aggressive response.
In the schools where our remit is to focus on problems of behaviour that are putting thepupil at risk of exclusion (mainstream school ‘‘A’’) or have led to permanent exclusion to thePupil Referral Unit (special school ‘‘D’’) the clinical psychologist and the counsellingpsychologist use a 20-session manual that combines programs on problem solving, angermanagement and moral reasoning with techniques of engagement that have been developedin psychotherapy work with young people at the Brandon Centre. A team that has beenrunning a randomized controlled trial testing interventions for young offenders hasdeveloped the manual.
The sessions on problem solving involve learning about problem identification andanalysis, formulating choices, consequential thinking, and decision-making. Behaviouraltechniques such as positive reinforcement, role-playing and modeling are used to help theyoung person internalize the skills imparted by the manual. Anger management helps theyoung person learn to identify the feelings associated with different types of anger, to consideranger-provoking situations and think about alternative responses to anger. The young personalso learns coping strategies to manage and control excessive anger. The aims of the sessionson moral reasoning are firstly to enable the young person to evaluate their behaviour, i.e. tothink about what behaviour is ‘‘right’’ or ‘‘good’’ and what behaviour is ‘‘wrong’’ or ‘‘bad’’,secondly to learn a framework that can be applied to judge ‘‘right’’ from ‘‘wrong’’, and ‘‘good’’from ‘‘bad’’, and thirdly to learn to apply the framework to situations they face in their lives,in particular situations in which other people are affected deleteriously by the young person’sactions.
We have mostly used an individual-based intervention. However, we piloted a groupversion of the manualized program in the Pupil Referral Unit. A teacher received training inthe manual so that they could work with the clinical psychologist in the pupil referral unit inimplementing the group intervention. Unfortunately, we were forced to abandon the groupformat. Kazdin (1997) has observed that groups comprised of delinquent adolescents cansustain their delinquency. We found that in the groups we ran that the behaviour of theyoung people was so problematic that it was impossible to deliver the manual. A furtherproblem concerned the teacher combining this role with a therapeutic one. Sometimes theteacher had to leave the group because there were disciplinary problems elsewhere in theschool. The group format of delivering therapy to young people in schools, hospitals andyoung offender institutions is very popular. However we would agree with Kazdin (1997) thatalthough there are conditions under which this format is beneficial, our experience withconduct disordered youth suggests that therapeutic change is not facilitated.
By varying the type of psychotherapy provided according to the principal reason forlocating a service in the school we are seeking to address the issue raised earlier in the paperabout implementing interventions that are appropriate for the problems presented by pupils.Nevertheless our ability to respond to the full range of needs presented by pupils in any oneschool is limited by the resources at our disposal. We therefore need to be clear about thelimitations of our contribution. Pupils may present with a whole range of mental health

Mental health services in schools 559
problems like those seen in a population using a community-based clinic. These problemsadversely affect the whole life of the young person as well as being a barrier to learning. Inaddition to the diversity of problems presented by troubled pupils there is diversity of gender,social, cultural and ethnic background, disability and learning status. It is simply not possiblefor a service like ours to provide the range of interventions and personnel required to meetthis diversity. However, apart from the direct psychotherapy service we provide, we can makea further a contribution to meeting the needs of pupils by our contacts with local child andfamily consultation services and child and adolescent psychiatric services. There areexamples of pupils who have been referred to these services after the psychotherapist orpsychologist at the school has assessed the pupil and liaised with the relevant teaching staffand the pupil’s family. Such work by the psychotherapist and the psychologist is part of theirrole in ensuring that a troubled pupil receives appropriate treatment.
The treatment setting. In a community-based clinic or an outpatient department theavailability of a room dedicated to therapeutic work where privacy is guaranteed can betaken for granted. This is not the case in implementing psychotherapy in a school. Indeedfinding a proper location for therapeutic work can be extremely difficult. In most schoolsspace is at a premium and it is therefore inevitable that the therapist shares a room that hasmultiple functions. In some schools a classroom has been allocated for therapeutic sessions.Clearly this type of space can inhibit the pupil from sharing intimate details. The classroom isa public location. Classrooms usually have a door with a window and if they are on theground floor they have windows that can easily be peered into by other pupils. Thetherapeutic session in the classroom is likely to arouse a great deal of curiosity among otherpupils and so the therapist and pupil may find sustaining an atmosphere of privacy extremelydifficult. Pupils trying to enter the room, sometimes for genuine reasons as well as wanting tosatisfy their curiosity, may interrupt the session that takes place in a classroom. A furtherdisadvantage of the classroom is that the room can be easily ‘‘purloined’’ by a senior memberof the teaching staff who requires a room. However the public aspect of the classroom may bean advantage when working with pupils whose behaviour is unpredictable.
In some schools the psychotherapist or psychologist shares an office with other staff thatare providing ancillary services such as speech therapy. This location has the advantage ofbeing more private than a classroom. However there may be paraphernalia that can distractand tempt the pupil. In one instance, a hyperactive 12-year-old ran ahead of his childpsychotherapist and dashed into the room. By the time the child psychotherapist arrived thepupil had rung the emergency services and instructed them to attend the school immediately.Sharing with another discipline can raise other problems. In one of the schools, on twoseparate occasions, the children’s toys and drawings, drawing and writing materials that werekept in marked boxes were disposed of by the professional who shared their office with thechild psychotherapist. Naturally the loss was very distressing to the pupils she was helping.Such problems do not occur because of feelings of latent hostility to psychotherapy. Ratherthey occur because compared to other staff in the school the psychotherapist or psychologistspends less time there and so their presence can easily be overlooked and forgotten. We try toensure that the room and equipment for therapy is ‘‘ring fenced’’. This involves collaborationwith teaching and ancillary staff. The issue of collaboration is discussed below.
We have found that a further way in which a psychotherapy service in a school may departfrom the privacy afforded young people when they attend the Brandon Centre can be thevisible nature of the pupil going to the room for their session. Some pupils get into a routine

560 G. Baruch
whereby they make their own way to their appointment with the psychotherapist orpsychologist and in this way contribute to the privacy of their sessions. However others maybe ambivalent about having psychotherapy or are caught up in lessons or activities at breaktime and therefore forget to be available for their appointment. The dilemma for thepsychotherapist or psychologist is then whether to fetch the pupil from the classroom or theplayground. Inevitably this means exposing the pupil’s attendance at psychotherapy to theirpeers. Our psychotherapists and psychologists have not found it easy to resolve the dilemma.Their approach has been largely pragmatic: since they are at the school to providepsychotherapy and the pupil has agreed to therapy they collect the young person and in thesession raise the matter of voluntarily making themselves available for their appointments.Some pupils are then able to make their own way whereas others continue being collected.
In summary, one of the notable disadvantages of working in a school, unlike a clinic, is thelack of privacy. It can be very easy for other pupils to find out and to stigmatize a peer who isseeing a psychotherapist or psychologist. However we have little evidence of suchstigmatization occurring. Indeed, privacy being compromized by psychotherapy taking placeat school can have the reverse effect of stigmatization. For instance, at one of the mainstreamschools where we work we have learned from the teaching staff that a popular pupil who is inpsychotherapy and is looked up to by his peers has made psychotherapy ‘‘respectable’’ andeven desirable among his peers. The reduced privacy that is a feature of psychotherapy in theschools is to be balanced by the ‘‘normalizing’’ of psychotherapy. Therefore this disadvantageof reduced client privacy should not deter the provision of such help in schools.
Referral and consent. The process of referring a pupil is more complex than when aparent or professional refers a young person or they refer themselves to the Brandon Centre.For referrals, parental consent for assessment and treatment is axiomatic whereas a referralvia a teacher at school requires that parental consent is sought and obtained.
When we started providing psychotherapy in schools we were unclear and perhaps naı̈veabout how pupils were to be referred to the psychotherapist or psychologist. We were notclear about obtaining parental consent. To begin with, we agreed with the teaching staff toadopt a ‘‘laissez faire’’ approach: pupils would get to know of the existence of thepsychotherapist by coming into contact at break times and seeing the therapist sitting in ontheir class and would be able informally to refer themselves. This approach proved mostunsatisfactory in yielding referrals and was frustrating for the psychotherapist, the teachingstaff and the pupils. Moreover it did not address the issue of parents consenting to their childhaving psychotherapy. Eventually we evolved a clear procedure, which we implement in allthe schools where there is a psychotherapist or psychologist. There needs to be a seniorteacher who is the point of contact for referrals who is the key member of staff that thetherapist works with in obtaining referrals. In mainstream schools, this person communicatesto their colleagues about the availability of the service who can then make recommendationsof pupils who they feel are in need of help. Before doing so they are expected to elicit fromthe pupil whether they would be interested in ‘‘counselling’’. They may make the referralverbally or preferably by using a referral form (see Appendix 1). This form elicits from thereferring teacher relevant demographic details such as the pupil’s name, age, form, ethnicorigin, name and address of parent or carer, the name of the teacher making the referral, thereason for referral and space for additional information. The form may also elicit theavailability of the student for treatment although in practice the times of appointments arebest settled in dialogue with the referrer since sometimes they may vary from week to week

Mental health services in schools 561
to fit in with the pupil’s curriculum. The key member of staff makes contact with the parentor carer to discuss the reason for referral of their child and then arranges with thepsychologist or psychotherapist to send the parent a letter seeking their written permissionfor their child to receive treatment (see Appendix 2).
In the special schools, although the same system operates as in the mainstream school withtheir being a senior member of staff that is responsible for referrals, the lines of communicationare more fluid because the special school is much smaller than a mainstream school. All theteachers are likely to have contact with the psychotherapist or psychologist when they are onschool premises and in our experience talk informally to them about pupils who they think needpsychotherapy. It is also the case that most if not all pupils can have access to the psychotherapistor psychologist informally to discuss obtaining help unlike in a mainstream school because of itssize. It is sometimes possible to deal with the whole procedure of pupil and parental consentwhen the parents and child visit the school before the child’s intake into the school since it islikely that psychotherapy has been made a requirement in the statement of special needs. Thegreater opportunity for contact with the psychotherapist or psychologist among pupils and staffand the informality of that contact has led to pupils and teachers short-circuiting the referralprocess. For instance, there are occasions when a form teacher encourages a pupil to makecontact with the psychotherapist or psychologist and request help and psychotherapy hasproceeded without parental consent. Often, referrals on this basis end precipitously because themotivation for referral has not been exclusively to do with needs of the pupil. Thepsychotherapist or psychologist finds that they have been pulled into acting out a problematicaspect of the relationship between the pupil and the teacher, for instance, the teacher hasbecome over involved and identified with the pupil’s situation and needs to find a way ofextricating themselves from the relationship. I think that this is where the availability of weeklysupervision at the Brandon Centre can be so helpful to the psychotherapist and psychologist inminimizing their acting out and in assisting them in properly maintaining their role.
There are other circumstances that can complicate the process of referral, particularly inrelation to obtaining parental consent. As a result of the 1985 House of Lords ruling in theGillick case, children under the age of 16 years are entitled to receive medical treatmentwithout the knowledge of their parents so long as they are capable of understanding theimplications of what is proposed. We believe that this ruling must be applied cautiously in aschool environment because the teacher rather than the pupil initiates the referral. There istherefore a moral obligation for the teacher who is in locos parentis to inform the pupil’sparents or carers if they think therapy is recommended. However, in circumstances where achild reveals they want help because they are being abused, seeking parental consent wouldbe inappropriate although the teacher would be expected to act according to the school’schild protection procedure. A more common occurrence is when a pupil confides to ateacher or a school nurse problems at home or at risk behaviours such as deliberate self harm,severe alcohol and substance abuse or severe eating problems and requests help but only onthe condition that their parents or carers are not informed of their current vulnerability. Theteacher or school nurse may be persuaded to arrange psychotherapy without parental consentbecause of the perceived danger the child appears to be in. This is especially the case wherethe teacher has little confidence in the parents’ capacity to care for their child and the childcomplains about the home situation. In these instances we still insist that parental consent issought and obtained before offering the pupil psychotherapy. In practice, we find that whenthe referring teacher feels supported in negotiating the child’s agreement to their parentsbeing approached, consent is usually forthcoming. Nevertheless there are occasions when a
562 G. Baruch
pupil is clearly in need of psychotherapy but their parents refuse permission. Sadly it will notbe possible to help the child at this point in time and the role of the school-based therapistmay then involve supporting the teacher or school nurse who is providing the pupil withpastoral support.
By adhering to a formal referral procedure, as described, that is common to all the schoolswe work in we can reduce the possibility of factors emerging that undermine psychotherapywhen it is underway. The procedure, because it involves obtaining parental consent, meansthat the psychologist or psychotherapist can identify pupils who, perhaps unknown to theschool, are currently involved with a child and adolescent mental health service. Clearly it isimportant that before psychotherapy commences that the psychotherapist or psychologistinvestigates such involvement with the child’s parents. Contact needs to be made with theservice in order to establish whether assessment or treatment is being undertaken andwhether there is a role for psychotherapy at school.
Earlier we raised a problem that can arise with psychotherapy in schools whereby thepupil’s parents are ‘‘cut out’’ of meaningful involvement in the process of their child beingreferred for psychotherapy and when treatment is underway. This can occur when many ofthe children referred for help come from a highly dysfunctional background that has left anegative impression of the parents on the teaching staff. We have sought to ensure by ourreferral procedure that parents are consulted and meaningfully involved in their child’spsychotherapy. Indeed where parents are reluctant or unable to attend meetings at theschool the psychotherapist or psychologist who is working in a special school, timepermitting, makes a home visit.
Collaboration with school staff and integration in the school. We have foundthat unless the psychotherapist or psychologist is able to form a partnership with teachers andother relevant professional staff working in the school the tensions between them are likelyto lead to the psychotherapy service being undermined (Flaherty et al., 1998; Waxman et al.,1999). In discussing potential disadvantages of psychotherapy services in schools we havealready noted what some of these tensions consist of. We have encountered the followingtensions, conflicts and difficulties:
. Differences in professional responsibilities: with some teachers we have encounteredtensions regarding the timing of sessions when they involve the pupil missing part ofthe curriculum, which they teach. For instance, in special school ‘‘F’’, the Germanteacher objected to a pupil missing her lesson for a session even though a seniormember of staff responsible for enabling the psychotherapy service had sanctionedthe appointments for that lesson. This teacher took pride in her work and was notprepared to allow the pupil to miss lessons. Indeed, I think she felt her work wasbeing devalued.
. Different expectations of pupil behaviour: teachers need pupils’ behaviour toconform to a standard that allows them to deliver lessons and are therefore less likelyto be tolerant of disruptive behaviour than the psychotherapist or psychologist whoin any case only has contact with the pupil for 40 minutes per week. In special andmainstream schools where unacceptable behaviour by the pupil can triggerexclusion, psychotherapy can be undermined. In special schools ‘‘D’’ and ‘‘E’’there have been frequent instances of pupils being excluded without thepsychotherapist or psychologist being consulted and them only getting to know ofthe exclusion at the time the pupil’s appointment is due.
Mental health services in schools 563
. Different expectations regarding confidentiality: teachers are used to a far greaterdegree of open communication among their colleagues about pupils thanpsychotherapists and psychologists who restrict discussion of their clients forreasons of confidentiality.
The following are tensions, conflicts and difficulties that we have encountered withcounsellors employed by the school:
. The counsellor feeling threatened that their job is at risk and may wonder whetherthe school will want to continue employing them when a service is being providedusually at no cost to the school.
. The psychotherapist or psychologist being referred pupils who have been referredand are working with the counsellor.
. Rivalry and competitiveness between the counsellor and psychotherapist orpsychologist that undermine collaboration over referrals.
In all the schools where the Brandon Centre provides a psychotherapy service thepsychotherapist and psychologist have developed a common approach in establishing acollaborative relationship with education and counselling staff. This approach includes:
. Learning about and showing appreciation of the school’s culture and its distinctivecharacter: for instance special school ‘‘E’’ had been rapidly going downhill until thepresent head teacher had been drafted in. Although there were still undoubtedproblems she had brought the school through a bad period in very difficultcircumstances and it was important in establishing the psychotherapy service in theschool that the psychotherapist was able to appreciate the transformation that thehead teacher had made.
. Developing working relationships and friendships with teachers, administratorsand reception staff: probably this is the most important contribution of thepsychotherapist or psychologist in developing a successful service at a school. Thepsychotherapy and psychology staff that work in schools on behalf of the BrandonCentre have prior experience of working in schools and other organizationsproviding services for young people. For instance, one of the child psychotherapistshad been a social worker who worked in schools, another had been a dance therapistwho also worked in schools and one of the psychotherapists had been a youthworker. As a result of their professional background they have been able toempathize with school staff and reach out to them on a friendly basis withoutcompromizing their professional integrity. This capacity to develop relationships withthe staff of the school can extend to developing a friendly relationship withreception staff. For instance in school ‘‘C’’ the child psychotherapist had toovercome a somewhat hostile attitude from reception staff precipitated by requestshe needed to make in order to carry out his work. They reacted in this way becausethey did not want extra work. However over the period of two school terms heworked hard to win their confidence and co-operation, which he did successfully. Atthe same school and special school ‘‘F’’ he similarly worked hard to overcome theinitial antipathy of the caretakers whose help was needed because they held the keysthat he needed in order to get into the room where he works with pupils. Eventuallythey even arranged for a key to be cut for his use. The antipathy or hostility is rarelypersonal but rather a ‘‘knee jerk’’ response by these members of staff to further

564 G. Baruch
demands being made of them. I have observed how crucial the friendly demeanourof the psychotherapist and psychologist is to the successful implementation ofpsychotherapy especially when we have needed to replace a psychotherapist orpsychologist who has resigned. The teaching staff judge the candidate on the basis ofwhether that person will interact with them in an ordinary, friendly way. They aresimply put off if the candidate is detached and aloof. I have also observed that whengood relations exist, the teaching staff respect psychotherapy and trust thepsychotherapist and psychologist even though they may find our work in certainways somewhat alien and mysterious, particularly where the approach is non-directive.
. Having regular meetings with relevant staff: the crucial relationship that we havedeveloped in all the schools where we provide a psychotherapy service is with asenior member of staff, which usually is a deputy head teacher who is responsible forreferrals, for the incorporation of the service into the school and acts as the linkbetween the psychotherapist or psychologist and the rest of the teaching staff. Ineach school, we have established such a relationship and the psychotherapist orpsychologist and this key teacher usually meet once a week. At this meeting, thepsychotherapist or psychologist, as well as taking referrals, discusses treatment plansand offers feedback about pupils who are being assessed or treated without betrayingconfidentiality. The meeting also allows the senior member of the teaching staff toconvey their concerns about pupils. Finally, the meeting is used to agree andmaintain a consistent timetable that is acceptable to the teaching staff. Meetingteaching staff who have been involved in a referral, who are thinking of referring apupil, who are concerned about a pupil or who need to be seen both to give andobtain feedback about a pupil tends to occur on an informal basis, for instance atbreak times when the psychotherapist or psychologist is present in the staff room.We have found that such meetings are easier to affect in a special school by virtue ofits smaller size than in a mainstream school. Nevertheless, every effort is made bythe psychotherapist and the psychologist to make and retain contact with relevantteaching staff other than the key senior teacher. Contact is also made with teachingstaff by providing them with a letter that introduces them to the psychotherapist,and describes the service they are offering at the school and the method of referral(see Appendix 3).
. If possible the psychotherapist or psychologist attending one staff meeting a weekand assisting in teacher training events and the evaluation of the school by externalorganisations. In special schools ‘‘E’’ and ‘‘F’’ the psychotherapists happen to work atthe school on the day when there is a staff meeting and so regularly attend themeeting. All psychotherapy and psychology staff providing a service make everyeffort to make an input into a teacher-training event at least once a year and onbehalf of the school to provide a report on their work when the school it is beingreviewed by OFSTED. The presence of a psychotherapy service has been importantin promoting a positive evaluation of the school.
. In the schools where there is a school counsellor, the psychotherapist or psychologistmeet the counsellor regularly. We have found that in this way the concerns of thecounsellor, particularly the anxiety of their role being eroded can be met. Instead acollaborative relationship has been established that allows for a useful division oflabour. For instance, in school ‘‘C’’, the school counsellor is expected to provide

Mental health services in schools 565
short-term, time-limited interventions. With the agreement of the key seniormember of the teaching staff, she has been able to arrange that pupils who requirelong-term help be referred to the child psychotherapist.
We have found that the approach I have described addresses the pitfall I referred toearlier: namely teachers having unrealistic expectations about what a psychotherapy servicecan achieve. The effect of exclusion from school on psychotherapy remains the mostsignificant area that this approach has been unable to address. In schools that have to dealwith high levels of disruptive behaviour, for instance schools ‘‘A’’, ‘‘D’’ and ‘‘E’’, the use ofexclusion is a frequent response to excessive misbehaviour. Pupils who are receivingpsychotherapy are not spared this sanction when their behaviour becomes intolerable. Thusit has happened on a number of occasions that the psychotherapist or psychologist has cometo school expecting to work with a pupil who, without prior consultation, has been excluded.It seems as though that the schools where we run a service see the implementation ofexclusion as their sole prerogative. In the final analysis, I think teachers feel that were theuse of exclusion to be compromised by allowing a disruptive pupil to remain in schoolfor their psychotherapy session their capacity to control pupils would be fatally under-mined. However for the psychotherapist or psychologist the loss of sessions resultingfrom exclusion can be very frustrating in being able to address the actions that led tothe exclusion. To date we too have been excluded from the process of a pupil beingexcluded.
Evaluation. The perceived advantages of school-based services are the pivotal role of theschool in shaping the development of children, the increased accessibility of psychotherapyprovision for hard-to-reach young people and for less impaired adolescents who would nototherwise obtain help. However psychotherapy services in schools need to show that theirinterventions are at least as effective as those practised at a clinic-based service otherwiseimproved accessibility and utilization are meaningless. (Evans, 1999). Evaluation studies ofschool-based mental health services are beginning to appear that show promising outcomes(Kaplan et al., 1998). However a great deal more needs to be done in order to accumulateevidence of the effectiveness of psychotherapy services in schools.
At the very least there needs to be routine evaluation of mental health outcome as part ofthe overall evaluation of the psychotherapy service’s effectiveness. In the schools where werun a service, we use an adapted version of the approach to mental health outcome that hasbeen used at the Brandon Centre since 1993 (Baruch, 1995; Baruch et al., 1998a, b; Baruchand Fearon, 1999). Briefly this involves using the standardized measures developed byAchenbach (1991a, b). At intake, the young person completes the Youth Self Report Form, ateacher completes the Teacher’s Report Form, the therapist also completes the Teacher’sReport Form and a parent completes the Child Behaviour Checklist. This multipleperspective approach is designed to establish whether treatment gains are generalized acrosssettings other than school, for instance at home. The pupil is then reassessed at the end ofevery term during treatment and followed-up annually after they have completed treatmentuntil they leave school. We also use a standardized form to collect demographic anddiagnostic data at intake.
However we have yet to integrate our approach to evaluating the effectiveness oftreatment with the school’s views about how pupils are meant to benefit from therapy. Theschool’s perspective tends to be more pragmatic and concrete than that of the mental healthprofessional. For instance where disruptive behaviour is a barrier to learning a diminution of

566 G. Baruch
such behaviour may be expected so removing the threat of school exclusion class. Or where apupil has periodically been absent from school for unexplained reasons, a return to properattendance may be the goal of therapy from the point of view of the school.
Certainly establishing common ground between the perspective of the schools and mentalhealth professionals about the goals of treatment and their measurement is crucial.Otherwise psychotherapy services in schools are likely to be held up as the latest ‘‘cure-all’’for delivering mental health services for troubled young people only to be rejected whenanecdotal outcome evidence does not live up to expectations.
Conclusion
School-based services provided by counsellors, psychotherapists and psychologists are likelyto grow. The present U.K. government is committed to their expansion. There is no doubtthat they offer a unique setting in which the mental health needs of children and adolescentscan be addressed. They provide hard-to-reach young people an opportunity to access help,which they might not otherwise obtain. There is great scope for prevention of mental healthproblems as well as intervention. However an enormous amount of work needs to be donebefore they are no longer services isolated from mainstream child and adolescent mentalhealth services. Resources need to be earmarked. Policies on confidentiality and privacy needto be addressed. Stakeholder involvement and integration with the full range of child andadolescent mental health services need to be worked out if services in schools are to realisetheir undoubted potential to contribute to the alleviation of mental health problems ofyoung people.
References
Achenbach, T. M. (1991a). Manual for the Youth Self-Report and 1991 Profile. Burlington, VT: Universityof Vermont, Department of Psychiatry.
Achenbach, T. M. (1991b). Manual for the Teacher’s Report Form and 1991 Profile. Burlington, VT:University of Vermont, Department of Psychiatry.
Achenbach, T. A., Howell, C. T., McConaughy, S. H. and Stanger, C. (1995). Six-year predictors ofproblems in a national sample: III. Transitions to Young Adult Syndromes. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 34, 658–669.
Achenbach, T .M., Howell, C. T., McConaughy, S. H. and Stanger, C. (1998). Six year predictors ofproblems in a national sample: IV. Young adult signs of disturbance. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 37, 718–727.
Adelman, H. S. and Taylor, L. (1999). Mental health in schools and system restructuring. ClinicalPsychology Review, 19, 137–164.
Armbruster, P., Andrews, E., Couenhoven, J. and Blau, G. (1999). Collision or collaboration? School-based health services meet managed care. Clinical Psychology Review, 19, 221–238.
Audit Commission (1999). Children in Mind: Child and Adolescent Mental Health Services. London: theAudit Commission for Local Authorities and the National Health Service in England and Wales.
Baruch, G. (1995). Evaluating the outcome of a community-based psychoanalytic psychotherapyservice for young people between 12 and 25 years old: work in progress. PsychoanalyticPsychotherapy, 9, 243–267.
Baruch, G., Gerber, A. and Fearon, P. (1998a). Adolescents who drop out of psychotherapy at acommunity-based psychotherapy centre: a preliminary investigation of the characteristics of earlydrop-outs, late drop-outs and those who continue in treatment. British Journal of MedicalPsychology, 71, 233–245.

Mental health services in schools 567
Baruch, G., Fearon, P. and Gerber, A. (1998b). Evaluating the outcome of a community-basedpsychoanalytic psychotherapy service for young people: one-year repeated follow-up. In RethinkingClinical Audit, R. Davenhill and M. Patrick (Eds). London: Routledge.
Baruch, G., Fearon, P. and Gerber, A. (1999). Emotional and behavioural problems in adolescents/young adults receiving treatment at a community-based psychotherapy centre for young people: apreliminary study of the correspondence among adolescent/young adult and significant otherreports. British Journal of Medical Psychology, 72, 251–265.
Department of Health (1999). National Service Framework for Mental Health: Modern Standards &Service Models. London: Department of Health.
Dryfoos, J. G. (1997). School-based youth programs: Exemplary models and emerging opportunities. InIntegrated Services for Children and Families: Opportunities for Psychological Practice, R. J. Illback,C. T. Cobb and H. M. Joseph (Eds). Washington, DC: American Psychological Association,pp. 23–52.
Evans, S. W. (1999). Mental Health Services in Schools: utilization, effectiveness and consent. ClinicalPsychology Review, 19, 165–174.
Flaherty, L. T., Garrison, E. G., Waxman, R., Uris, P. F., Keys, S. G. Glass Siegel, M. and Weist M. D.(1998). Optimizing the roles of school mental health professionals. Journal of School Health, 68,420–424.
Ferdinand, R. F., Verhulst, F. C. and Wiznitzer, M. (1995). Continuity and change of self-reportedbehaviors from adolescence into young adulthood. Journal of the American Academy of Child andAdolescent Psychiatry, 34, 680–690.
Fothergill, G. and Ballard, E. (1998). The school-linked health center: a promising model ofcommunity-based care. Journal of Adolescent Health, 23, 29–38.
Graham, P. J. (1986). Behavioural and intellectual development in childhood epidemiology. BritishMedical Bulletin, 42, 155–162.
Grenberg Garrison, E., Roy, I. S. and Azar, V. (1999). Responding to the mental health needs of Latinochildren and families through school-based services. Clinical Psychology Review, 19, 199–220.
Health Advisory Service. (1995). Child and Adolescent Mental Health Services: Together We Stand.London: HMSO.
Institute of Medicine. (1995). Report Card on the National Plan for Research on Child and AdolescentMental Disorders: The Midway Point. Washington, DC: Institute of Medicine.
Jepson, L., Juszczak, L. and Fisher, M. (1998). Mental health care in a high school based health service.Adolescence, 33, 1–15.
Kaplan D. W., Calogne B. N., Guernsey B. P. and Hanrahan M. B. (1998). Managed care and school-based health centres: use of health services. Archives of Pediatric and Adolescent Medicine, 152,25–33.
Kazdin A. E. (1997). Practitioner review: psychosocial treatments for conduct disorder in children.Journal of Child Psychology and Psychiatry, 38, 161–178.
Kurtz, Z. (1992). With Health in Mind: Mental Health Care for Children and Young People. London: Actionfor Sick Children.
Office for National Statistics (1999). Mental health of children and adolescents. London: GovernmentStatistical Service.
Roth, A. and Fonagy, P. (Eds). (1996). What Works for Whom? A Critical Review of PsychotherapyResearch. London: The Guilford Press.
Rutter, M. (1999). Services for children with mental health problems: how should they be developed?Presentation made on 2nd February 1999 at Conference on ‘Developing Effective Child andAdolescent Mental Health Services: Current Initiatives and Innovations’. Organized by FOCUSat the Royal College of Psychiatrists’ Research Unit in collaboration with: the Audit Commission,The Health Advisory Service and Young Minds.
Smith, D. J. and Rutter, M. (1995). Psychosocial Disorders in Young People: Time Trends and Their Causes.Chichester: John Wiley & Sons.
Stanger, C., MacDonald, V. V., McConaughy, S. H. and Achenbach, T. M. (1996). Predictors of cross-informant syndromes among children and youths referred for mental health services. Journal ofAbnormal Child Psychology, 24(5), 597–614.
Waxman, R. P., Weist, M. D. and Benson, D. M. (1999). Toward collaboration in the growingeducation–mental health interface. Clinical Psychology Review, 19(2), 239–253.
568 G. Baruch
Weist, M. D. (1999). Challenges and opportunities in expanded school mental health. ClinicalPsychology Review, 19, 131–136.
Weist, M. D., Myers, C. P., Hastings, E., Ghunman, H. and Han, Y. L. (1999). Psychosocial functioningof youth receiving mental health services in the school versus community mental health centers.Community Mental Health, 35, 69–81.
Winnicott, D. W. (1996). Adolescence: struggling through the doldrums. In The Family and IndividualDevelopment. London: Tavistock Publications, pp. 79–87.
Wittchen, H.-U., Nelson, C. B. and Lachner, G. (1998). Prevalence of mental disorders andpsychosocial impairments in adolescents and young adults. Psychological Medicine, 28,109–126.
Zahner, G. E., Pawelkiewicz, W., Di Francesco, J. J. and Adnopoz, J. (1992). Children’s mental healthservice needs and utilization patterns in an urban community: an epidemiological assessment.Journal of the American Academy of Child and Adolescent Psychiatry, 31, 951–960.
Appendix 1
Counselling Referral Request for Psychologist/Psychotherapist (Brandon Centre)
Name of Student _____________________ Date of Birth ______________
Form _____________________ Ethnic Origin ______________
Religion _____________________ Name of Parent(s)/Carer ______________
Address __________________________________________________________
__________________________________________________________
__________________________________________________________________________Please note: The name and address of the parent/carer given above will be the person whomthe school contacts regarding agreement for the counselling to take place.__________________________________________________________________________
Name of teacher making referral ____________________________________
Date _____________________
Reason for Referral _____________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
Mental health services in schools 569
Has this student previously received counselling YES NO DON’T KNOW (Please circle)
Additional Information__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
Appendix 2
Dear Parent.
I am writing in order to seek your agreement for . . .. . .. . .. . .. . .. . .. . .. . . to take part in aprogramme designed to help some students overcome difficulties they are experiencing atschool.
The programme takes place once a week for 45 minutes and is administered by a CounsellingPsychologist. Each session will make use of a variety of exercises designed to help students todevelop areas that complement their general studies. Two main areas of focus will beimproving reasoning and problem solving skills and developing further abilities to formpositive relationships with both peers and teachers.
If you agree to . . .. . .. . .. . .. . .. . .. . .. . . taking part, please complete and return the attachedslip to me as soon as possible. In the meantime if you have any questions you wish to ask thenplease do not hesitate to contact me.
Yours sincerely
Charles WellsCounselling Psychologist
__________________________________________________________________________
I/we give permission for . . .. . .. . .. . .. . .. . .. . . to receive counselling at the school. I/weunderstand that the counselling is provided at no cost to me/us.
570 G. Baruch
Name of parent (please print) _________________________________________________
Signature _________________________________________________
Date _________________________________________________
Appendix 3
School Based psychotherapy for high-priority groups of young people
Dear Teacher:I would like to take this opportunity to introduce myself and to describe the service that isbeing offered to support the efforts of teachers in tackling disruptive behaviour within theclassroom and in the school.
I am a Counselling Psychologist based at the Brandon Centre in Kentish Town. The Centrehas a renowned reputation for its psychotherapy work with young people who haveemotional and behavioural problems. This reputation has been established over the last 30years working with young people from all parts of London.
Our aim is to provide psychotherapy for high-priority groups of young people who may bewary of attending a clinic, and this has led to the development of school based services inpartnership with a number of schools.
I am offering a programme of individual treatment for boys between the ages of 13 and 16whose behaviour is sufficiently disruptive to cause concern, and who risk possible schoolexclusion if the behaviour persists or worsens.
The programme uses a cognitive behavioural approach that is tailored to the needs of eachboy and addresses the cognitive difficulties behind his behavioural problems. The aim is toequip him to deal with these problems in a constructive way. Within the programme two keyareas of psychological functioning are addressed: deficits in problem-solving skills and poorsocial perspective taking skills. The young person will be expected to attend twenty sessionsheld once weekly at the school with each session lasting no more that 45 minutes. Thisenables the process of problem solving and social perspective taking to be taught in a highlysystematic way.
If you know of any pupil who you think might benefit from this programme then pleasecomplete one of the attached referral forms and give it to . . .. . .. . .. . .. . . I am also at theschool each Thursday should you wish to discuss a possible referral with me in person.
Yours sincerely
Charles WellsCounselling Psychologist
Copyright © 2022 FDOKUMEN