Medical RPapplications Anh Methods Assembly Autiomation Journal
9
Research article Medical rapid prototyping applications and methods L.C. Hieu and N. Zlatov Cardiff School of Engineering, Cardiff University, Wales, UK J. Vander Sloten Department of Mechanical Engineering, Division of Biomechanics and Engineering Design, Heverlee, Belgium E. Bohez School of Advanced Technologies, Asian Institute of Technology, Bangkok, Thailand L. Khanh and P.H. Binh Department of Medical Imaging and Neurosurgery, Hanoi, Vietnam P. Oris Materialise Clinical Services Inc., Glen Burnie, Maryland, USA, and Y. Toshev Institute of Mechanics and Biomechanics, Bulgarian Academy of Sciences, Sofia, Bulgaria Abstract Purpose – Aims to investigate medical rapid prototyping (medical RP) technology applications and methods based on reverse engineering (RE) and medical imaging data. Design/methodology/approach – Medical image processing and RE are applied to construct three-dimensional models of anatomical structures, from which custom-made (personalized) medical applications are developed. Findings – The investigated methods were successfully used for design and manufacturing of biomodels, surgical aid tools, implants, medical devices and surgical training models. More than 40 medical RP applications were implemented in Europe and Asia since 1999. Research limitations/implications – Medical RP is a multi-discipline area. It involves in many human resources and requires high skills and know- how in both engineering and medicine. In addition, medical RP applications are expensive, especially for low-income countries. These practically limit its benefits and applications in hospitals. Practical implications – In order to transfer medical RP into hospitals successfully, a good link and close collaboration between medical and engineering sites should be established. Moreover, new medical applications should be developed in the way that does not change the traditional approaches that medical doctors (MD) were trained, but provides solutions to improve the diagnosis and treatment quality. Originality/value – The presented state-of-the-art medical RP is applied for diagnosis and treatment in the following medical areas: cranio- maxillofacial and dental surgery, neurosurgery, orthopedics, orthosis and tissue engineering. The paper is useful for MD (radiologists and surgeons), biomedical and RP/CAD/CAM engineers. Keywords Rapid prototypes, Modelling, Image processing, Medical equipment Paper type Research paper 1. Introduction Today reverse engineering (RE) and medical image-based modeling technologies allow construction of three-dimensional (3D) models of anatomical structures of human body based on anatomical information from scanning data such as computerized tomography (CT), magnetic resonance imaging (MRI), and laser (or structured light) scanning. RE and CT/ MRI scanners are, respectively, used for scanning data The Emerald Research Register for this journal is available at www.emeraldinsight.com/researchregister The current issue and full text archive of this journal is available at www.emeraldinsight.com/0144-5154.htm Assembly Automation 25/4 (2005) 284–292 q Emerald Group Publishing Limited [ISSN 0144-5154] [DOI 10.1108/01445150510626415] European Commission (EC), Flemish Interuniversity Council (VLIR), Belgium, and The Royal Society, United Kingdom, are acknowledged for the financial support of the following projects: PRIMACORPS CRAF- 99-70074 – Cost effective, realistic surgical trainer for “hands-on” endoscopic procedures through application of RP, CAD-CAM technology and a novel material; Medical Technology Transfer to ASEAN countries; and The Royal Society International Exchanges Joint – 3D human body modeling for medical and engineering applications. 284
Transcript of Medical RPapplications Anh Methods Assembly Autiomation Journal
Research article
Medical rapid prototyping applicationsand methods
L.C. Hieu and N. Zlatov
Cardiff School of Engineering, Cardiff University, Wales, UK
J. Vander SlotenDepartment of Mechanical Engineering, Division of Biomechanics and Engineering Design, Heverlee, Belgium
E. BohezSchool of Advanced Technologies, Asian Institute of Technology, Bangkok, Thailand
L. Khanh and P.H. BinhDepartment of Medical Imaging and Neurosurgery, Hanoi, Vietnam
P. OrisMaterialise Clinical Services Inc., Glen Burnie, Maryland, USA, and
Y. ToshevInstitute of Mechanics and Biomechanics, Bulgarian Academy of Sciences, Sofia, Bulgaria
AbstractPurpose – Aims to investigate medical rapid prototyping (medical RP) technology applications and methods based on reverse engineering (RE) andmedical imaging data.Design/methodology/approach – Medical image processing and RE are applied to construct three-dimensional models of anatomical structures,from which custom-made (personalized) medical applications are developed.Findings – The investigated methods were successfully used for design and manufacturing of biomodels, surgical aid tools, implants, medical devicesand surgical training models. More than 40 medical RP applications were implemented in Europe and Asia since 1999.Research limitations/implications – Medical RP is a multi-discipline area. It involves in many human resources and requires high skills and know-how in both engineering and medicine. In addition, medical RP applications are expensive, especially for low-income countries. These practically limit itsbenefits and applications in hospitals.Practical implications – In order to transfer medical RP into hospitals successfully, a good link and close collaboration between medical andengineering sites should be established. Moreover, new medical applications should be developed in the way that does not change the traditionalapproaches that medical doctors (MD) were trained, but provides solutions to improve the diagnosis and treatment quality.Originality/value – The presented state-of-the-art medical RP is applied for diagnosis and treatment in the following medical areas: cranio-maxillofacial and dental surgery, neurosurgery, orthopedics, orthosis and tissue engineering. The paper is useful for MD (radiologists and surgeons),biomedical and RP/CAD/CAM engineers.
Keywords Rapid prototypes, Modelling, Image processing, Medical equipment
Paper type Research paper
1. Introduction
Today reverse engineering (RE) and medical image-based
modeling technologies allow construction of three-dimensional
(3D) models of anatomical structures of human body based onanatomical information from scanning data such ascomputerized tomography (CT), magnetic resonance imaging(MRI), and laser (or structured light) scanning. RE and CT/MRI scanners are, respectively, used for scanning data
The Emerald Research Register for this journal is available at
www.emeraldinsight.com/researchregister
The current issue and full text archive of this journal is available at
www.emeraldinsight.com/0144-5154.htm
Assembly Automation
25/4 (2005) 284–292
q Emerald Group Publishing Limited [ISSN 0144-5154]
[DOI 10.1108/01445150510626415]
European Commission (EC), Flemish Interuniversity Council (VLIR),Belgium, and The Royal Society, United Kingdom, are acknowledged forthe financial support of the following projects: PRIMACORPS CRAF-99-70074 – Cost effective, realistic surgical trainer for “hands-on”endoscopic procedures through application of RP, CAD-CAMtechnology and a novel material; Medical Technology Transfer toASEAN countries; and The Royal Society International ExchangesJoint – 3D human body modeling for medical and engineeringapplications.
284

acquisition of the external and internal geometry of anatomicalstructures. From 3D models of anatomical structures, there aremany medical applications derived for surgical training,preoperative planning, surgical simulation, diagnosis andtreatments.
Physical models of anatomical structures can be fabricateddirectly from 3D digital data by rapid prototyping (RP)technology (Pham and Dimov, 2001). With the use of RP andrapid tooling (RT) technology, nowadays, we can fabricatecomplex 3D physical objects in a wide range of materials andsizes, from plastics and metals to biocompatible ones, andfrom big models to microstructures.
Medical RP technology is a multi-discipline area, whichapplies the biomedical modeling and RP to develop medicalapplications. It involves human resources from the fields ofRE, design and manufacturing, biomaterials and medicine.Medical RP has played an important role in diagnosis andtreatment; especially in preoperative planning, design andmanufacturing of implants and surgical aid tools.
In this paper, the main applications and solutions fordevelopment of medical RP applications are presented. Sincethe selection of the right modeling and design approaches isvery important to minimize the complexity and the lead timeof the product development process, geometrical modeling ofanatomical structures, medical application developmentprocedures and practical RT techniques are emphasized.
The paper is structured to reflect the following mainmedical RP applications:. biomodels, surgical aid tools and implants;. surgical training models and medical devices; and. tissue engineering scaffolds.
2. Applications
There are three main medical RP applications, including:1 design and manufacturing of biomodels, surgical aid tools
and implants;2 development of surgical training models and medical
devices; and3 design and manufacturing of scaffolds for tissue
engineering.
2.1 Biomodels, surgical aid tools and implants
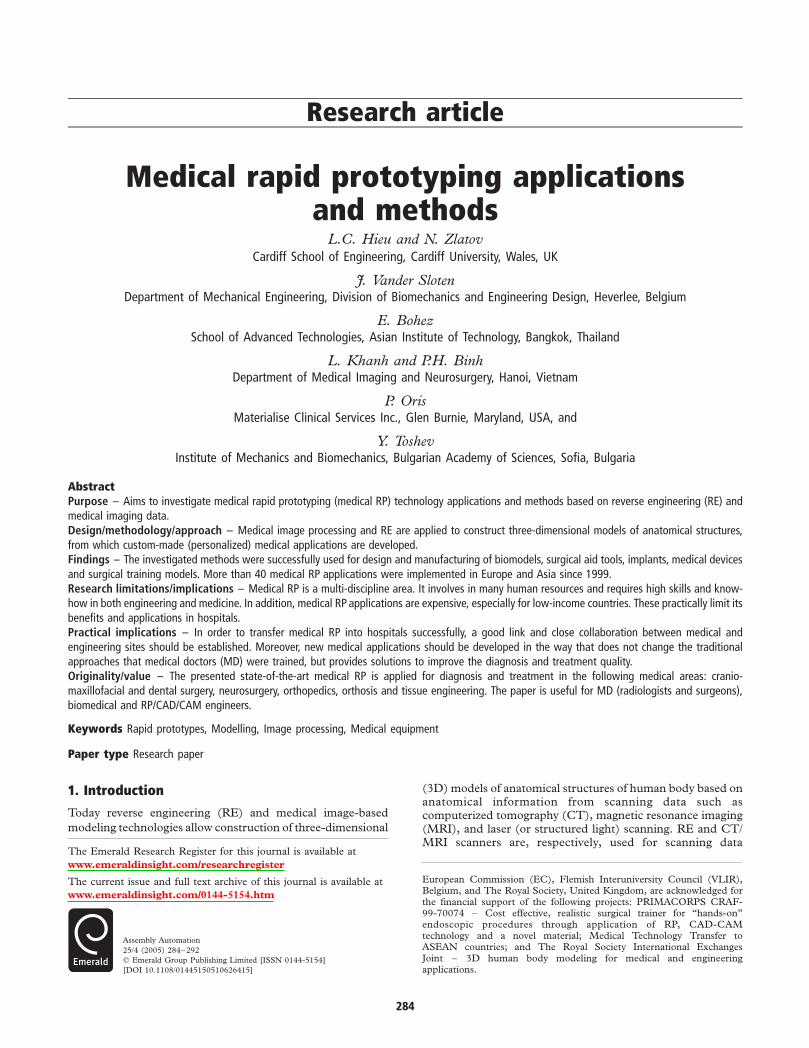
Biomodels are the physical models of anatomical structuresfabricated by RP from 3D digital anatomical data. Instead ofusing 2D images and 3D virtual computer models, medicaldoctors (MD) nowadays can use the accurate replica of partsor anatomical structures or region of interest (ROI) of thehuman body for preoperative planning, diagnosis andtreatment. Figure 1 shows the biomodels of a patient skull(A) and frontal-temporal area (B) with the defects.
The use of biomodels in preoperative planning, diagnosisand treatment were well documented (Kermer et al., 1998;Sailer et al., 1998; Joffe et al., 1999; D’Urso et al., 2000).Biomodels have been widely used in the field of cranio-maxillofacial, orthopedic and dental surgery. The benefits andmain applications of biomodels include:. enhancing the visualization of ROI and anatomical
features for better understanding of patient anatomy;. better communication in preoperative planning and
consultancy among surgical team members, radiologists,MD and patients;
. carrying out rehearsal procedures to improve surgeonsskills and optimize preoperative procedures; and
. prefabrication of custom-made implants and selection of
an optimal donor site for bone grafting.
Although implants can be prepared preoperatively based on
biomodels, the implant design process is required for the ones
that are used for complex defects. From 3D anatomical data,
custom-made (or personalized) implants as well as surgical
aid tools can be exactly designed to avoid the mismatch of
using the standard ones for the patient. This is very useful for
the defect areas that need cosmetic surgery. The typical
examples are cranioplasty implants (Figures 2 and 3; Hieu
et al., 2003) and titanium membranes (Pattijn et al., 2000,
2002) for bone reconstruction.Surgical aid tools are very important for surgeons during
the operation. They are used for enhancing surgeon’s skills,
reducing the operation time, and increasing the accuracy and
safety of the operation. The most commonly used surgical aid
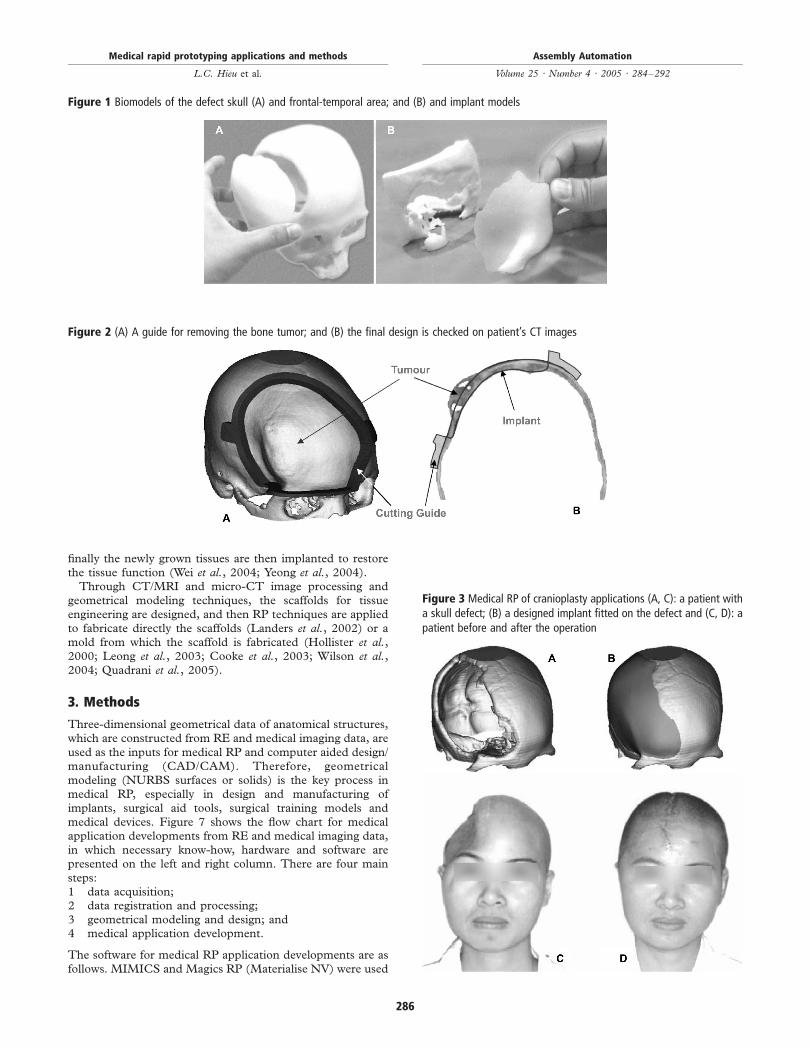
tools are the drilling guides (Figure 4(B)) for dental and spine
surgery (Van Brussel et al., 1996; Goffin et al., 2001; Van
Cleynenbreugel et al., 2002).The surgical aid tool for determining an optimal stem angle
in hip resurfacing anthroplasty (HAP) is shown in Figure 5. In
the traditional HAP surgical procedure, determining the stem
angle depends a lot on the experiences and skills of surgeons;
the risk and errors are therefore not avoided. Using 3D
models of the patient femur and computer simulations, an
optimal angle of the stem is calculated. The guide is then
designed for determining the right angle as well as increasing
the accuracy and minimizing the operation time.Figure 2 shows another surgical aid tool, which is used as a
guide for removing the bone tumor in one-step cranioplasty
operation. The implant is exactly designed and it is implanted
after the tumor is removed. In this way, in stead of using
two operations, surgeons need only one operation for the
treatment.
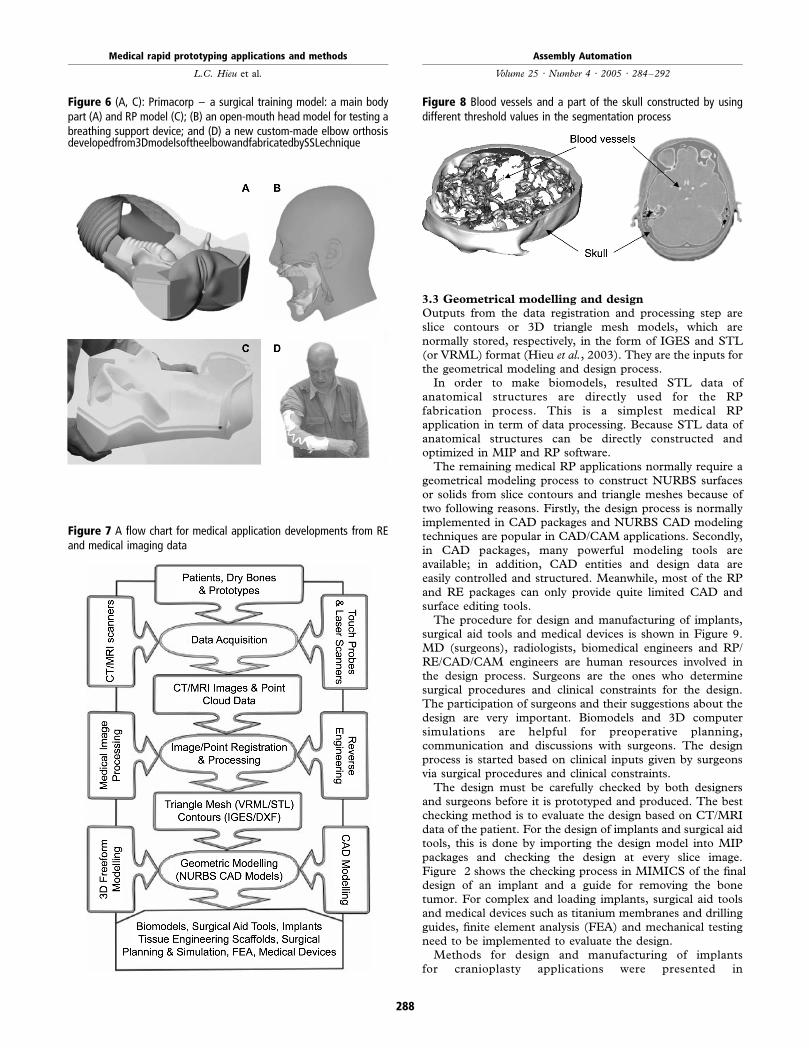
2.2 Surgical training models and medical devices
Medical RP and biomedical modeling technologies
evolutionally contribute to the development of new surgical
training models, which are playing an important role in
improvement of undergraduate and postgraduate training
skills in medical education. Components of the surgical
training model (called Primacorps) are shown in Figure 6(A)
and (C). Information produced from body scanning systems
(MRI) of live anaesthetized patients was used as reference for
the development of a training model. Therefore, the
Primacorps training model is very close to the human form,
has qualities of the human form and therefore replaces the
human form for the practice of surgery.Based on the patient data, custom-made medical devices
and external prostheses such as elbow and ankle-foot orthosis
are able to be designed and manufactured (Liliya et al.,2004a, b). Figure 6(D) shows a new custom-made elbow
orthosis developed from 3D models of the elbow and
fabricated by selective laser sintering (SLS) technique. An
open-mouth head model for testing a breathing support
device is shown in Figure 6(B); stereolithography (SLA)
technique was used to fabricate the model to allow
visualization of the inside structures.
2.3 Scaffolds for tissue engineering applications
In tissue engineering, the sample cells can be cultured ex vivo
in which the scaffold is used for cell and tissue growth; and
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
285
finally the newly grown tissues are then implanted to restorethe tissue function (Wei et al., 2004; Yeong et al., 2004).
Through CT/MRI and micro-CT image processing andgeometrical modeling techniques, the scaffolds for tissueengineering are designed, and then RP techniques are appliedto fabricate directly the scaffolds (Landers et al., 2002) or amold from which the scaffold is fabricated (Hollister et al.,2000; Leong et al., 2003; Cooke et al., 2003; Wilson et al.,2004; Quadrani et al., 2005).
3. Methods
Three-dimensional geometrical data of anatomical structures,which are constructed from RE and medical imaging data, are
used as the inputs for medical RP and computer aided design/manufacturing (CAD/CAM). Therefore, geometricalmodeling (NURBS surfaces or solids) is the key process inmedical RP, especially in design and manufacturing ofimplants, surgical aid tools, surgical training models andmedical devices. Figure 7 shows the flow chart for medicalapplication developments from RE and medical imaging data,in which necessary know-how, hardware and software arepresented on the left and right column. There are four mainsteps:1 data acquisition;2 data registration and processing;3 geometrical modeling and design; and4 medical application development.
The software for medical RP application developments are asfollows. MIMICS and Magics RP (Materialise NV) were used
Figure 1 Biomodels of the defect skull (A) and frontal-temporal area; and (B) and implant models
Figure 2 (A) A guide for removing the bone tumor; and (B) the final design is checked on patient’s CT images
Figure 3 Medical RP of cranioplasty applications (A, C): a patient witha skull defect; (B) a designed implant fitted on the defect and (C, D): apatient before and after the operation
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
286
for processing CT/MRI images and STL data manipulations.CopyCAD & PowerShape (Delcam Inc.), Pro Engineer(PTC), UG (Unigraphics Solutions), and SolidWorks(SolidWorks Corp.) are used for RE data (points, trianglemesh) manipulations and geometrical modeling processes.
3.1 Data acquisition
The input data for 3D geometrical modeling of anatomicalstructures are RE data (point clouds) and CT/MRI images.
RE scanners are used to collect geometrical data formodeling of external shapes (face, foot, elbow, etc.), dentaltemplates (Figure 4(A)) and dry bones. The external shapesof the body can be directly scanned, or indirectly scanned viausing templates, which are fabricated by soft toolingtechniques. To avoid the undercuts and to completescanning of a whole object, different scanning angles anddirections are used.
Transmissive scanning methods are used for modeling theinternal structures, in which CT and MRI are well knownscanning technologies. Because different CT and MRIsystems from different vendors use their own native dataformats; to read CT/MRI images, a common digital imagingstandard – DICOM (digital imaging and communications inmedicine) is required. To construct accurate 3D anatomicalstructures for medical applications, the slice scanning
thickness are normally required from 1 to 2 mm, using a
spiral scanning mode.
3.2 Data registration and processing
RE data obtained from different scanning angles and
directions are then registered to merge into one single point
cloud (Figure 4(A)). Noise and redundant data are then
filtered to be an optimal one for constructing contours and
triangle mesh models (STL or VRML format).For medical imaging data, DICOM CT/MRI images are
imported into MIP packages. Based on the grayscale value of
image pixels, segmentation by thresholding techniques is used
to define ROI; and the resulted segmentation object will
contain only those pixels of the image with a value higher than
or equal to the threshold value. It is also possible to use two
thresholds in which the segmentation volume is defined by all
pixels with a gray value in between both threshold values. This
technique is used for segmentation of soft tissue in CT images
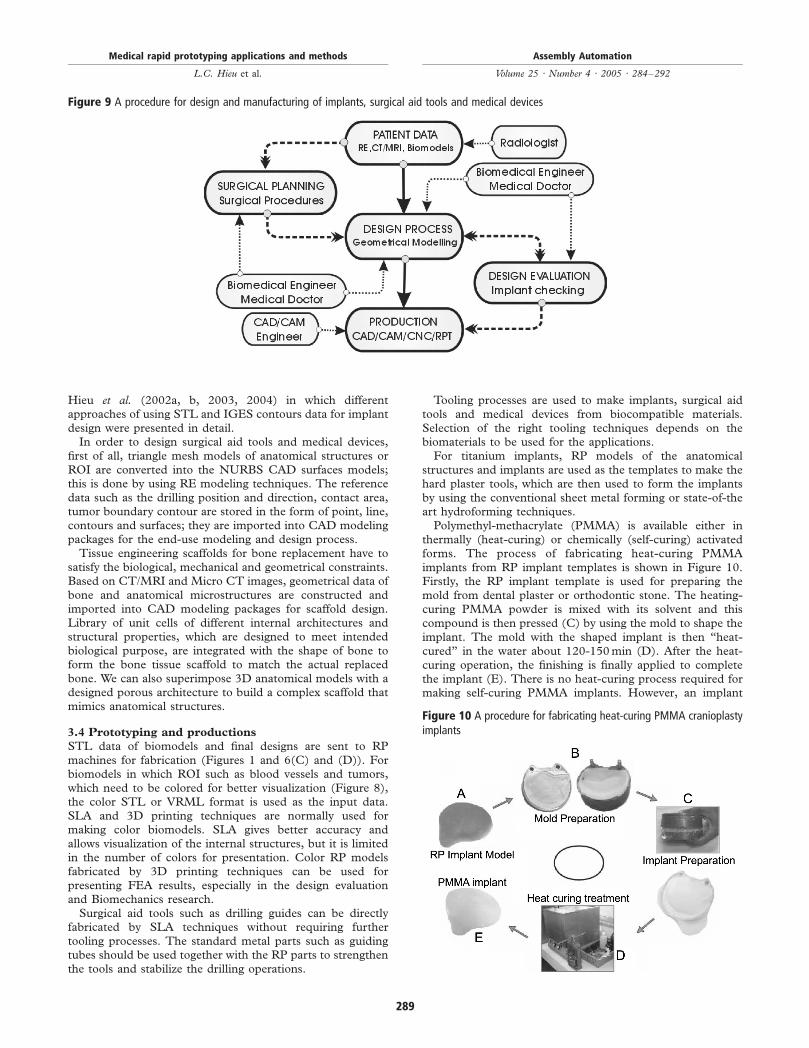
or for segmentation of several structures in MR images.Slice contours and 3D triangle mesh models are finally
constructed from segmented data. Figure 8 shows the blood
vessels and a part of the skull constructed by, respectively,
using the following threshold values: (155, 1,310) and (625,
2,375) in MIMICS.
Figure 4 A dental template and a drilling guide constructed from laser scanning data (A) point cloud data; and (B) a template model and a drillingguide
Figure 5 (A) Hip resurfacing anthroplasty – HRA; and (B) a guide for determining the optimal stem angle in HRA surgery
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
287
3.3 Geometrical modelling and design
Outputs from the data registration and processing step areslice contours or 3D triangle mesh models, which are
normally stored, respectively, in the form of IGES and STL(or VRML) format (Hieu et al., 2003). They are the inputs forthe geometrical modeling and design process.
In order to make biomodels, resulted STL data ofanatomical structures are directly used for the RP
fabrication process. This is a simplest medical RPapplication in term of data processing. Because STL data ofanatomical structures can be directly constructed andoptimized in MIP and RP software.
The remaining medical RP applications normally require a
geometrical modeling process to construct NURBS surfacesor solids from slice contours and triangle meshes because oftwo following reasons. Firstly, the design process is normallyimplemented in CAD packages and NURBS CAD modelingtechniques are popular in CAD/CAM applications. Secondly,in CAD packages, many powerful modeling tools areavailable; in addition, CAD entities and design data areeasily controlled and structured. Meanwhile, most of the RP
and RE packages can only provide quite limited CAD andsurface editing tools.
The procedure for design and manufacturing of implants,surgical aid tools and medical devices is shown in Figure 9.MD (surgeons), radiologists, biomedical engineers and RP/
RE/CAD/CAM engineers are human resources involved inthe design process. Surgeons are the ones who determinesurgical procedures and clinical constraints for the design.The participation of surgeons and their suggestions about thedesign are very important. Biomodels and 3D computersimulations are helpful for preoperative planning,communication and discussions with surgeons. The designprocess is started based on clinical inputs given by surgeonsvia surgical procedures and clinical constraints.
The design must be carefully checked by both designersand surgeons before it is prototyped and produced. The bestchecking method is to evaluate the design based on CT/MRIdata of the patient. For the design of implants and surgical aidtools, this is done by importing the design model into MIP
packages and checking the design at every slice image.Figure 2 shows the checking process in MIMICS of the finaldesign of an implant and a guide for removing the bonetumor. For complex and loading implants, surgical aid toolsand medical devices such as titanium membranes and drillingguides, finite element analysis (FEA) and mechanical testingneed to be implemented to evaluate the design.
Methods for design and manufacturing of implantsfor cranioplasty applications were presented in
Figure 6 (A, C): Primacorp – a surgical training model: a main bodypart (A) and RP model (C); (B) an open-mouth head model for testing abreathing support device; and (D) a new custom-made elbow orthosisdevelopedfrom3DmodelsoftheelbowandfabricatedbySSLechnique
Figure 8 Blood vessels and a part of the skull constructed by usingdifferent threshold values in the segmentation process
Figure 7 A flow chart for medical application developments from REand medical imaging data
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
288
Hieu et al. (2002a, b, 2003, 2004) in which differentapproaches of using STL and IGES contours data for implantdesign were presented in detail.
In order to design surgical aid tools and medical devices,first of all, triangle mesh models of anatomical structures orROI are converted into the NURBS CAD surfaces models;this is done by using RE modeling techniques. The referencedata such as the drilling position and direction, contact area,tumor boundary contour are stored in the form of point, line,contours and surfaces; they are imported into CAD modelingpackages for the end-use modeling and design process.
Tissue engineering scaffolds for bone replacement have tosatisfy the biological, mechanical and geometrical constraints.Based on CT/MRI and Micro CT images, geometrical data ofbone and anatomical microstructures are constructed andimported into CAD modeling packages for scaffold design.Library of unit cells of different internal architectures andstructural properties, which are designed to meet intendedbiological purpose, are integrated with the shape of bone toform the bone tissue scaffold to match the actual replacedbone. We can also superimpose 3D anatomical models with adesigned porous architecture to build a complex scaffold thatmimics anatomical structures.
3.4 Prototyping and productions
STL data of biomodels and final designs are sent to RPmachines for fabrication (Figures 1 and 6(C) and (D)). Forbiomodels in which ROI such as blood vessels and tumors,which need to be colored for better visualization (Figure 8),the color STL or VRML format is used as the input data.SLA and 3D printing techniques are normally used formaking color biomodels. SLA gives better accuracy andallows visualization of the internal structures, but it is limitedin the number of colors for presentation. Color RP modelsfabricated by 3D printing techniques can be used forpresenting FEA results, especially in the design evaluationand Biomechanics research.
Surgical aid tools such as drilling guides can be directlyfabricated by SLA techniques without requiring furthertooling processes. The standard metal parts such as guidingtubes should be used together with the RP parts to strengthenthe tools and stabilize the drilling operations.
Tooling processes are used to make implants, surgical aidtools and medical devices from biocompatible materials.Selection of the right tooling techniques depends on thebiomaterials to be used for the applications.
For titanium implants, RP models of the anatomicalstructures and implants are used as the templates to make thehard plaster tools, which are then used to form the implantsby using the conventional sheet metal forming or state-of-theart hydroforming techniques.
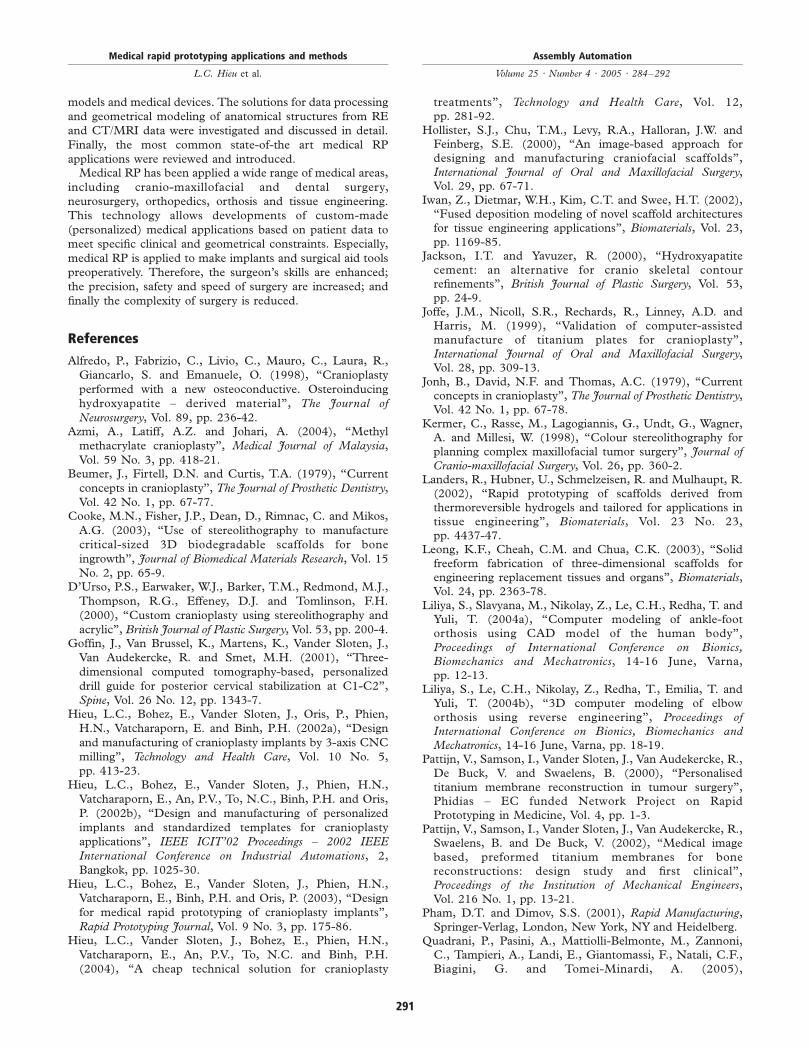
Polymethyl-methacrylate (PMMA) is available either inthermally (heat-curing) or chemically (self-curing) activatedforms. The process of fabricating heat-curing PMMAimplants from RP implant templates is shown in Figure 10.Firstly, the RP implant template is used for preparing themold from dental plaster or orthodontic stone. The heating-curing PMMA powder is mixed with its solvent and thiscompound is then pressed (C) by using the mold to shape theimplant. The mold with the shaped implant is then “heat-cured” in the water about 120-150 min (D). After the heat-curing operation, the finishing is finally applied to completethe implant (E). There is no heat-curing process required formaking self-curing PMMA implants. However, an implant
Figure 9 A procedure for design and manufacturing of implants, surgical aid tools and medical devices
Figure 10 A procedure for fabricating heat-curing PMMA cranioplastyimplants
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
289

needs to be shaped and contoured as quickly as possible,because the hardening time of self-curing PMMA is short.
For bone cement implants, room temperature vulcanization(RTV) tooling technique is the best solution; it is the mostoften used in manual casting processes. This technique is astandard method of making small quantities of (polymer)parts in industry, and it is considered as the best time and costprototyping (production) solution.
Tissue engineering scaffolds are directly fabricated by RPtechniques or using the RP model to make a mold from whichthe scaffold is fabricated (Iwan et al., 2002; Leong et al., 2003;Wilson et al., 2004; Quadrani et al., 2005). Among theavailable RP techniques, 3D printing and fuse depositionmodeling (FDM) are the most commonly used for fabricatingtissue engineering scaffolds because of versatility of usingscaffolding materials and they are able to overcome thelimitations of conventional manual-based fabricationtechniques.
4. Result and discussions
The presented medical RP methods were successfully applied,and more than 40 medical RP applications have been donesince 1999 in Europe and Asia, from fabricating biomodels(Figure 1) for surgical planning to making implants (Figure 3),surgical aid tools (Figures 2, 4 and 5), surgical trainingsystems and medical devices (Figure 6).
Based on patient data, medical RP allows custom-made(personalized) designs to meet both clinical and geometricalconstraints. It especially shows a superior benefit in complexsurgeries. In the field of cranio-maxillofacial surgery, theimplants are preoperatively made; therefore, the operationtime was saved about 30 min-1 h compared to the traditionalmethod in which an implant is manually intra-operativelyprepared.
Figure 3 shows a typical case of medical RP applications incranioplasty surgery. A patient with a defect on the headcaused by a traffic accident. It took about 4 working hours tocomplete the implant design using the presented medical RPmethods. The PMMA implant was preoperatively fabricatedand the operation time was about 2 h.
Since the errors from a segmentation process always exist.The image processing and segmentation process directlyinfluences the modeling and design accuracy. As shown inTable I, the human skull thickness was measured based ondifferent threshold values in MIMICS; the difference is up to1.12 mm. Finding an optimal threshold value depends on thepurpose of the modeling and design process, especiallyclinical requirements from surgeons. In order to assure thatthe design is correct and accurate; the final design data shouldbe checked directly on patient’s CT/MRI data (Figure 2).
Today, the accuracy of about 0.1 mm can be obtained byRP techniques. Therefore, the influence of RP processes tothe precision of making implants is acceptable. However, thetooling process, which is used to fabricate biocompatibleimplants from RP templates, is manually done; the influence
of this process to the implant accuracy is significant.
Therefore, biomodels should be used to check the final
implants and surgical aid tools before they are sent to the
operation rooms. The influence of the sterilization process to
the accuracy should also be taken into account to avoid the
shrinkage of implants and surgical aid tools.The cost of medical RP is still expensive. Biomodels of a
full skull is about 1,500-2,000 USD. One PMMA
cranioplasty implant costs about 300-400 USD. However,
the presented medical RP methods can be applied to design
implants accurately. By using the computer simulations and
checking carefully the implant design, only implant template
needs to be fabricated. In this way, the treatment cost is
minimized (Hieu et al., 2003).Titanium (Joffe et al., 1999), Hydroxyapatite-derived
materials (Alfredo et al., 1998) and bone cements (Jackson
and Yavuzer, 2000) demonstrated a very good
biocompatibility; the infection rate is less than 2 percent
(Hieu et al., 2002a). However, they are quite expensive and
somewhat difficult to shape. The most commonly used
biomaterial for cranioplasty applications is PMMA (Jonh et al.,1979) with the infection rate of being about 1.7-12 percent
(Beumer et al., 1979; Remsen et al., 1986; Azmi et al., 2004).
The advantages of PMMA include radiolucency that is
necessary for patients requiring CT or MRI follow-up, poor
thermal and electrical conductivity, low cost, easy casting, and
acceptable biocompatibility. With the use of medical RP,
PMMA implants can be fabricated preoperatively, it therefore
avoids heat development and monomer-emission in the site of
the defect that always occurs when shaping the implant the
intra-operatively.A wide range of medical RP applications have been
introduced to improve the diagnosis and treatment quality.
However, the applications are still quite limited in many
hospitals. There are two main reasons that limit medical RP
applications in hospitals. Firstly, medical RP is a multi-
discipline area, biomedical engineers must be equipped a
good know-how, not only in design and manufacturing, but
also in the field of biomaterials, medical image processing and
medicine. This human resource is not always available in
hospitals. Secondly, the treatment cost is expensive; and it is
not convenient to change the old diagnosis and treatment
procedures by the new ones. Therefore, in order to transfer
medical RP into hospitals successfully, two following issues
should be taken into account.1 A good link and close collaboration between medical and
engineering sites should be established. There should be
units in which MD (surgeons), radiologist and biomedical
engineers are able to share the know-how and experiences
as well as to stimulate new medical applications.2 New medical applications should be developed in the way
that does not change the traditional approaches that MD
were trained, but provides solutions to improve the
diagnosis and treatment quality. Concretely new
procedures and solutions should enhance surgeon’s
skills, minimize the time and complexity of the
operation, and increase the safety for the patients.
5. Conclusions
Methods for medical RP were presented; they were
successfully used for design and manufacturing of
biomodels, surgical aid tools, implants, surgical training
Table I The human skull thickness measurement based on differentthreshold values
Threshold value 200 250 300 350 400 450 500
Skull thickness (mm) 6.64 6.36 6.18 5.97 5.81 5.70 5.52
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
290
models and medical devices. The solutions for data processing
and geometrical modeling of anatomical structures from RE
and CT/MRI data were investigated and discussed in detail.
Finally, the most common state-of-the art medical RP
applications were reviewed and introduced.Medical RP has been applied a wide range of medical areas,
including cranio-maxillofacial and dental surgery,
neurosurgery, orthopedics, orthosis and tissue engineering.
This technology allows developments of custom-made
(personalized) medical applications based on patient data to
meet specific clinical and geometrical constraints. Especially,
medical RP is applied to make implants and surgical aid tools
preoperatively. Therefore, the surgeon’s skills are enhanced;
the precision, safety and speed of surgery are increased; and
finally the complexity of surgery is reduced.
References
Alfredo, P., Fabrizio, C., Livio, C., Mauro, C., Laura, R.,
Giancarlo, S. and Emanuele, O. (1998), “Cranioplasty
performed with a new osteoconductive. Osteroinducing
hydroxyapatite – derived material”, The Journal of
Neurosurgery, Vol. 89, pp. 236-42.Azmi, A., Latiff, A.Z. and Johari, A. (2004), “Methyl
methacrylate cranioplasty”, Medical Journal of Malaysia,
Vol. 59 No. 3, pp. 418-21.Beumer, J., Firtell, D.N. and Curtis, T.A. (1979), “Current
concepts in cranioplasty”, The Journal of Prosthetic Dentistry,
Vol. 42 No. 1, pp. 67-77.Cooke, M.N., Fisher, J.P., Dean, D., Rimnac, C. and Mikos,
A.G. (2003), “Use of stereolithography to manufacture
critical-sized 3D biodegradable scaffolds for bone
ingrowth”, Journal of Biomedical Materials Research, Vol. 15
No. 2, pp. 65-9.D’Urso, P.S., Earwaker, W.J., Barker, T.M., Redmond, M.J.,
Thompson, R.G., Effeney, D.J. and Tomlinson, F.H.
(2000), “Custom cranioplasty using stereolithography and
acrylic”, British Journal of Plastic Surgery, Vol. 53, pp. 200-4.Goffin, J., Van Brussel, K., Martens, K., Vander Sloten, J.,
Van Audekercke, R. and Smet, M.H. (2001), “Three-
dimensional computed tomography-based, personalized
drill guide for posterior cervical stabilization at C1-C2”,
Spine, Vol. 26 No. 12, pp. 1343-7.Hieu, L.C., Bohez, E., Vander Sloten, J., Oris, P., Phien,
H.N., Vatcharaporn, E. and Binh, P.H. (2002a), “Design
and manufacturing of cranioplasty implants by 3-axis CNC
milling”, Technology and Health Care, Vol. 10 No. 5,
pp. 413-23.Hieu, L.C., Bohez, E., Vander Sloten, J., Phien, H.N.,
Vatcharaporn, E., An, P.V., To, N.C., Binh, P.H. and Oris,
P. (2002b), “Design and manufacturing of personalized
implants and standardized templates for cranioplasty
applications”, IEEE ICIT’02 Proceedings – 2002 IEEE
International Conference on Industrial Automations, 2,
Bangkok, pp. 1025-30.Hieu, L.C., Bohez, E., Vander Sloten, J., Phien, H.N.,
Vatcharaporn, E., Binh, P.H. and Oris, P. (2003), “Design
for medical rapid prototyping of cranioplasty implants”,
Rapid Prototyping Journal, Vol. 9 No. 3, pp. 175-86.Hieu, L.C., Vander Sloten, J., Bohez, E., Phien, H.N.,
Vatcharaporn, E., An, P.V., To, N.C. and Binh, P.H.
(2004), “A cheap technical solution for cranioplasty
treatments”, Technology and Health Care, Vol. 12,
pp. 281-92.Hollister, S.J., Chu, T.M., Levy, R.A., Halloran, J.W. and
Feinberg, S.E. (2000), “An image-based approach for
designing and manufacturing craniofacial scaffolds”,
International Journal of Oral and Maxillofacial Surgery,Vol. 29, pp. 67-71.
Iwan, Z., Dietmar, W.H., Kim, C.T. and Swee, H.T. (2002),“Fused deposition modeling of novel scaffold architectures
for tissue engineering applications”, Biomaterials, Vol. 23,
pp. 1169-85.Jackson, I.T. and Yavuzer, R. (2000), “Hydroxyapatite
cement: an alternative for cranio skeletal contourrefinements”, British Journal of Plastic Surgery, Vol. 53,
pp. 24-9.Joffe, J.M., Nicoll, S.R., Rechards, R., Linney, A.D. and
Harris, M. (1999), “Validation of computer-assisted
manufacture of titanium plates for cranioplasty”,
International Journal of Oral and Maxillofacial Surgery,Vol. 28, pp. 309-13.
Jonh, B., David, N.F. and Thomas, A.C. (1979), “Currentconcepts in cranioplasty”, The Journal of Prosthetic Dentistry,Vol. 42 No. 1, pp. 67-78.
Kermer, C., Rasse, M., Lagogiannis, G., Undt, G., Wagner,A. and Millesi, W. (1998), “Colour stereolithography for
planning complex maxillofacial tumor surgery”, Journal ofCranio-maxillofacial Surgery, Vol. 26, pp. 360-2.
Landers, R., Hubner, U., Schmelzeisen, R. and Mulhaupt, R.
(2002), “Rapid prototyping of scaffolds derived fromthermoreversible hydrogels and tailored for applications in
tissue engineering”, Biomaterials, Vol. 23 No. 23,
pp. 4437-47.Leong, K.F., Cheah, C.M. and Chua, C.K. (2003), “Solid
freeform fabrication of three-dimensional scaffolds forengineering replacement tissues and organs”, Biomaterials,Vol. 24, pp. 2363-78.
Liliya, S., Slavyana, M., Nikolay, Z., Le, C.H., Redha, T. andYuli, T. (2004a), “Computer modeling of ankle-foot
orthosis using CAD model of the human body”,
Proceedings of International Conference on Bionics,Biomechanics and Mechatronics, 14-16 June, Varna,
pp. 12-13.Liliya, S., Le, C.H., Nikolay, Z., Redha, T., Emilia, T. and
Yuli, T. (2004b), “3D computer modeling of elbow
orthosis using reverse engineering”, Proceedings ofInternational Conference on Bionics, Biomechanics andMechatronics, 14-16 June, Varna, pp. 18-19.
Pattijn, V., Samson, I., Vander Sloten, J., Van Audekercke, R.,
De Buck, V. and Swaelens, B. (2000), “Personalised
titanium membrane reconstruction in tumour surgery”,Phidias – EC funded Network Project on Rapid
Prototyping in Medicine, Vol. 4, pp. 1-3.Pattijn, V., Samson, I., Vander Sloten, J., Van Audekercke, R.,
Swaelens, B. and De Buck, V. (2002), “Medical image
based, preformed titanium membranes for bone
reconstructions: design study and first clinical”,Proceedings of the Institution of Mechanical Engineers,Vol. 216 No. 1, pp. 13-21.
Pham, D.T. and Dimov, S.S. (2001), Rapid Manufacturing,Springer-Verlag, London, New York, NY and Heidelberg.
Quadrani, P., Pasini, A., Mattiolli-Belmonte, M., Zannoni,C., Tampieri, A., Landi, E., Giantomassi, F., Natali, C.F.,
Biagini, G. and Tomei-Minardi, A. (2005),
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
291

“High-resolution 3D scaffold model for engineered tissuefabrication using a rapid prototyping technique”, Medical &Biological Engineering and Computing, Vol. 43 No. 2,pp. 196-9.
Remsen, K., Lawson, W. and Biller, H.F. (1986), “Acrylicfrontal cranioplasty”, Head and Neck Surgery, Vol. 9,pp. 32-41.
Sailer, H.F., Haers, P.E., Zollikofer, C.P.E., Warnke, T.,Carls, F.R. and Stucki, P. (1998), “The value ofstereolithographic models for preoperative diagnosis ofcraniofacial deformities and planning of surgicalcorrections”, International Journal of Oral and MaxillofacialSurgery, Vol. 27, pp. 327-33.
Van Brussel, K., Vander Sloten, J., Van Audekercke, R. andFabry, G. (1996), “Internal fixation of the spine intraumatic and scoliotic cases. The potential of pediclescrews”, Technology and Health Care, Vol. 4 No. 4,pp. 365-84.
Van Cleynenbreugel, J., Schutyser, F., Goffin, J., Van Brussel,K. and Suetens, P. (2002), “Image-based planning andvalidation of C1-C2 transarticular screw fixation usingpersonalized drill guides”, Computer Aided Surgery, Vol. 7No. 1, pp. 41-8.
Wei, S., Andrew, D., Binil, S. and Jae, N. (2004), “Computer-aided tissue engineering: overview, scope and challenges”,Biotechnology and Applied Biochemistry, Vol. 39, pp. 29-47.
Wilson, C.E., de Bruijn, J.D., van Blitterswijk, C.A., Verbout,
A.J. and Dhert, W.J. (2004), “Design and fabrication of
standardized hydroxyapatite scaffolds with a defined macro-
architecture by rapid prototyping for bone-tissue-
engineering research”, Journal of Biomedical Materials
Research A, Vol. 68 No. 1, pp. 123-32.Yeong, W.Y., Chua, C.K., Leong, K.F. and Chandrasekaran,
M. (2004), “Rapid prototyping in tissue engineering:
challenges and potential”, Trends Biotechnol, Vol. 22
No. 12, pp. 643-52.
Further reading
Peckitt, N.S. (1999), “Stereoscopic lithography: customized
titanium implants in orofacial reconstruction”, British
Journal of Oral and Maxillofacial Surgery, Vol. 37,
pp. 353-69.Popat, A.H. (1998), “Rapid prototyping and medical
modeling”, Phidias – EC funded Network Project on
Rapid Prototyping in Medicine, Vol. 1, pp. 10-12.Santler, G., Karcher, H. and Ruda, C. (1998a), “Indications
and limitations of three-dimensional models in cranio-
maxillofacial surgery”, Journal of Cranio-maxillofacial
Surgery, Vol. 26, pp. 11-16.
Medical rapid prototyping applications and methods
L.C. Hieu et al.
Assembly Automation
Volume 25 · Number 4 · 2005 · 284–292
292