Management of adults with Wilms’ tumor: recommendations based on international consensus
9
r I l -------- ...•.. j I i .:'\·:1:-\1., EXPERT I I REVIEWS Heidi Seqers', Marry M van den Heuvel-Eibrink", Kathy Pritchard-Jones/ et al.; on behalf of the SIOP-RTSG and the COG-Renal Tumour Committee 'Department of Oncology/ Hematology, Erasmus MC-Sophia Children's Hospital. Or Molewaterplein, 603015 Gl, Rotterdam, The Netherlands 'UCL Institute of Child Health & Great Ormond Street Hospital, London, UK 'Autbor for correspondence: Tel.: +3110463 6691 Fax: +31 10 463 6801 m.vandenheuve/@erasmusmc.nl For the affiliations for all other authors, please see page 1115 Management of adults with Wilms' tumor: recommendations based on international consensus Expert Rev. Anticancer Ther. 11(7). 1105-1113 (2011) Since Wilms' tumor occurs rarely in adults, there are no standard treatments available. Most adult patients will be diagnosed unexpectedly following nephrectomy for presumed renal cell carcinoma. Outcome for adults is inferior compared with children, although better results are reported when treated within pediatric trials. Multiple factors, including the unfamiliarity of adult oncologists and pathologists with Wilms' tumors, lack of standardized treatment and consequent delays in initiating the appropriate risk-adapted therapy, may contribute to the poor outcome. A standardized approach for the management of adult Wilms' tumors is proposed with the aim to limit treatment delay after surgery and encourage a uniform approach for this rare disease and thereby improve survival. These recommendations are based on discussions held with representatives of the renal tumor committees of the Society of Paediatric Oncology and Children's Oncology Group, and have been updated with a review of more recently published institutional and trial experience of adults treated on pediatric protocols. They provide a critical evaluation of the current evidence for the management of adult Wilms' tumors and propose details of how current pediatric therapeutic guidelines could be adapted for use in adults. KEYWORDS: adult· management· Wilms' turnor \X1ilms' tumor or nephroblastorna, an embryonal type of kidney cancer, is the most common renal malignancy in children over 6 months of age and represents approximately 85% of all pediatric renal turnors [1.2]. Currently, using a combina- tion of surgery and chemotherapy for all chil- dren and additional radiotherapy for those with advanced-stage disease and/or with unfavorable histology (in International Society of Paediatric Oncology [SlOP] guidelines called 'high risk'), cure rates are high even for those with advanced stage disease [1.2]. In adults C~19 years of age), \X1ilms' turner is extremely rare, representing less than 1 % of all renal tumors [3-8]. The diagnosis ofWilms' tumor in adults is often unexpected following nephrectomy for presumed renal cell carcinoma (RCC), which is the most common (-85%) adult renal cancer (9]. Due to the fact that a Wilms' turnor is exceedingly rare in adults, no standard ther- apy has been developed. Consequently, phy- sicians faced with managing an adult with a \X1ilms' rurnor develop an individualized treatment plan deduced from the experience in children, numerous case reports and a few relatively small series of adult cases [4-8.10,11]. For many years the literature has suggested that the outcome for adults with a Wilms' turner is considerably worse than that for pediatric patients (3-8.10.11]. However, more recent data have indicated the potential for an improve- ment in outcome when adults are correctly diagnosed in time and treated according to (pediatric) protocols developed by the SlOP or the Children's Oncology Group (COG) [4.7]. Still, despite these reportS, the available infor- mation remains limited, making it difficult for surgeons and medical oncologisrs to manage an individual adult Wilms' turnor patient. Because protocolized therapies in children and adoles- cents with a Wilms' tumor currently result in high survival rates [1.2], pediarric oncologists are often consulted by medical oncologists for the management of an adult Wilms' turnor patient. This prompted several pediatric oncologists in Europe and North America with specific www.expert-ravlaws.com ISSN 1473-7140 1105 1O.l586/ERA. 11.76 © 2011 Expert Reviews Lrd Supplied by The British Library - "The world's knowledge"
Transcript of Management of adults with Wilms’ tumor: recommendations based on international consensus

r
I
l
-------- ...•..jI
i
.:'\·:1:-\1.,
EXPERT II REVIEWS
Heidi Seqers',Marry M van denHeuvel-Eibrink", KathyPritchard-Jones/ et al.;on behalf of theSIOP-RTSG andthe COG-RenalTumour Committee'Department of Oncology/Hematology, Erasmus MC-SophiaChildren's Hospital. Or Molewaterplein,603015 Gl, Rotterdam,The Netherlands'UCL Institute of Child Health & GreatOrmond Street Hospital, London, UK'Autbor for correspondence:Tel.: +3110463 6691Fax: +31 10 463 6801m.vandenheuve/@erasmusmc.nl
For the affiliations for all otherauthors, please see page 1115
Management of adultswith Wilms' tumor:recommendations based oninternational consensusExpert Rev. Anticancer Ther. 11(7). 1105-1113 (2011)
Since Wilms' tumor occurs rarely in adults, there are no standard treatments available. Mostadult patients will be diagnosed unexpectedly following nephrectomy for presumed renal cellcarcinoma. Outcome for adults is inferior compared with children, although better results arereported when treated within pediatric trials. Multiple factors, including the unfamiliarity ofadult oncologists and pathologists with Wilms' tumors, lack of standardized treatment andconsequent delays in initiating the appropriate risk-adapted therapy, may contribute to the pooroutcome. A standardized approach for the management of adult Wilms' tumors is proposedwith the aim to limit treatment delay after surgery and encourage a uniform approach for thisrare disease and thereby improve survival. These recommendations are based on discussionsheld with representatives of the renal tumor committees of the Society of Paediatric Oncologyand Children's Oncology Group, and have been updated with a review of more recently publishedinstitutional and trial experience of adults treated on pediatric protocols. They provide a criticalevaluation of the current evidence for the management of adult Wilms' tumors and proposedetails of how current pediatric therapeutic guidelines could be adapted for use in adults.
KEYWORDS: adult· management· Wilms' turnor
\X1ilms' tumor or nephroblastorna, an embryonaltype of kidney cancer, is the most common renalmalignancy in children over 6 months of age andrepresents approximately 85% of all pediatricrenal turnors [1.2]. Currently, using a combina-tion of surgery and chemotherapy for all chil-dren and additional radiotherapy for those withadvanced-stage disease and/or with unfavorablehistology (in International Society of PaediatricOncology [SlOP] guidelines called 'high risk'),cure rates are high even for those with advancedstage disease [1.2]. In adults C~19 years of age),\X1ilms' turner is extremely rare, representing lessthan 1% of all renal tumors [3-8]. The diagnosisofWilms' tumor in adults is often unexpectedfollowing nephrectomy for presumed renal cellcarcinoma (RCC), which is the most common(-85%) adult renal cancer (9].
Due to the fact that a Wilms' turnor isexceedingly rare in adults, no standard ther-apy has been developed. Consequently, phy-sicians faced with managing an adult witha \X1ilms' rurnor develop an individualized
treatment plan deduced from the experiencein children, numerous case reports and a fewrelatively small series of adult cases [4-8.10,11].
For many years the literature has suggested thatthe outcome for adults with a Wilms' turner
is considerably worse than that for pediatricpatients (3-8.10.11]. However, more recent datahave indicated the potential for an improve-ment in outcome when adults are correctlydiagnosed in time and treated according to(pediatric) protocols developed by the SlOP orthe Children's Oncology Group (COG) [4.7].
Still, despite these reportS, the available infor-mation remains limited, making it difficult forsurgeons and medical oncologisrs to manage anindividual adult Wilms' turnor patient. Becauseprotocolized therapies in children and adoles-cents with a Wilms' tumor currently result inhigh survival rates [1.2], pediarric oncologists areoften consulted by medical oncologists for themanagement of an adult Wilms' turnor patient.This prompted several pediatric oncologistsin Europe and North America with specific
www.expert-ravlaws.com ISSN 1473-7140 11051O.l586/ERA. 11.76 © 2011 Expert Reviews Lrd
Supplied by The British Library - "The world's knowledge"

Segers, van den HeuveI-Eibrink, Pritchard-Jones et al.
expertise in \V'ilms' tumors to develop a consensus 'best prac-tice' guideline for the management ofWilms' turner in adults.The aim of this international consensus recommendation isto further improve outcome by shortening adjuvant treatmentdelay and by using standardized treatment. The target group ofpatients who will benefit from these treatment recommendationsare patients above the age of 19 years (or >30 years in USA) whocan not be included in open pediatric clinical trials.
MethodsTo provide a summary of the known literature regarding Wilms'tumors in adults, a comprehensive search of the Pubmed data-base was performed for articles published until December 2010.Search-criteria relevant to adult \V'ilms' tumor patients wereused: adult, Wilms' turner, incidence, symptoms, management,treatment, outcome and toxicity. If not included initially, cross-references picked up during the review search were also selected.Only English articles were included.
The renal turners committees SlOP and COG brought togetherthose representatives 'of the major pediatric \V'ilms' tumortreatment groups Associazione ltaliana Ernarologia OncologiaPediatrica, Children's Cancer and Leukaemia group, COG RenalTumor Committee, Gesellschafc fUr Padiatrische Onkologie undHarnatologie (GPOH) and SlOP Renal Tumor Study Group(SIOP-RTSG) with expertise in the treatment of adults with aWilms' turner, whether in international trial group prorccols oron a national or institutional basis, to discuss how to adapt thepediatric therapeutic recommendations for use in adults. Thesediscussions were wide-ranging, multidisciplinary and based ona review of the available literature, as described previously, aswell as personal experiences. Adult urologists/surgeons, medicaloncologisrs and radiotherapists have reviewed the final recom-mendations to ensure their relevance for adult practice, which iswhere these patients present.
Review of the literatureEpidemiologyWilms' tumor is the most common renal malignancy in childrenover 6 months of age with an incidence rate of 8-10 per million peryear [1-2.6]. The median age at diagnosis for children is 3-4 yearsand 90% are diagnosed before the age of7 years [1,2,6]. In patients~IG years of age, it is a rarity with an incidence rate ofless than 0.2 permillion per year [3-8]. A population-based European epidemiologicalstudy from European Cancer Registries study on cancer patients'survival and care (EUROCARE) project, including data from years1983 to 1994 from G7 cancer registries that covered a combinedpopulation of 100 million in 22 European countries, demonstratedthat the median age at diagnosis for adult Wilms' tumor patients(defined as >15 years of age) was 34 years [6]. However, the rangewas wide with some patients even aged over GOyears [6].
Clinical presentationWhile data on presenting symproms in adults with a Wilms'turn or are very limited [5,7], the few reported presenting clini-cal syrnproms commonly ,consist of abdominal or flank pain,
nonspecific symptoms such as malaise and weight loss and lessfrequently hemaruria and hypertension [5,7]. Although childhoodWilms' turners are often recognized on ultrasound, the radio-logical appearance of a Wilrns' tumor can be indistinguishablefrom the more common adult malignant renal neoplasm suchas RCC [9,12J,
GeneticsA genetic predisposition is described in up to 10% of pediat-ric \X'ilms' tumor patients. The more common syndromes thatpredisposeto \V'ilms' tumor are those associated with germlinemutations i~ the WTl gene that encodes a zinc finger nucleicacid-binding protein with multiple roles in gene regulation anddevelopment, and those associated with overgrowth typified byBeckwith-Wicdemann syndrome [1,2). However, these syndromesdo not seem ro be associated with the onset of a Wilms' tumor inadulthood. Although one case report of an adult \V'ilms' turnerpatient with a WTl mutation and one case report of an adult\V'ilms' tumor patient with hypospadias and cryptorchidism havebeen described [13,14]. Not only have germline aberrations beenidentified in pediatric Wilms' turners, but somatic mutations inseveral genes have also been reported. These include WTl muta-tions in approximately 15%, gain-of-function mutations in Wnt-signaling component CTNNBl (p-catenin) in approximately15% (usually in combination with WTl mutations) and WTXmutations in approximately 30% of sporadic pediatric Wilms'tumors [15]. TP53 mutations occur mostly in the relatively uncom-mon anaplastic Wilms' tumor subtype [IS]. Epigenetic abnormal-ities at l lpl S, affecting expression of Hl9 and IGF2, are alsofound in pediatric Wilms' turnors including those cases associatedwith Beckwith-Wiedernann syndrome [15]. Recurrent large scalegenomic changes, some associated with adverse outcome like Ipand IGq LOH, are also described in pediarric Wilms' tumors.Moreover, lp and IGq LOH are currently incorporated in theCOG treatment protocols, Another study of adults with a Wilms'tumor suggests a potential role for the dysregulation of the Wnt-
,signa ling pathway, as also demonstrated in some pediatric Wilms'tumors [16]. A further adult Wilms' turnor case showed isochro-mosome 7q as is sometimes seen in pediatric Wilms' tumors [17].
Thus far, the paucity of data available in adults makes it impos-sible to determine whether \V'ilms' turners in adults and childrenare biologically comparable and thus whether similar tumor enti-ties are occurring in a different age group, as suggested by theirmorphological similarities.
Stage & histologyAvailable adult series report a higher incidence of advanced Stagedisease (stage III or IV) ranging from 45 to 70% compared withpediarric series where approximately one-third of children are clas-sified as stage III or IV after primary nephrectomy 14-8.10,11] (stag-ing system in SUPPLE.\lE. xTARYTAlILE2; see online at: www.expertreviews.com/doi/suppl/lO.l586/era.l1.76). Thus far, only one adult casehas been reported with bilateral synchronous Wilms' turnor, incontrast to the 5-7% incidence stage V disease described in thepediatric Wilms' tumor population [10].
1106 Espcrs Rrv. Anticancer Tber. 11(7), (2011)
TlI
Supplied by The British Library - ''The world's knowledge"

Management or adults with Wilms' tumor: recommendations based on international consensus
Histologically, a Wilms' tumor is typically described as 'tripha-sic', consisting of blastema I, epithelial and stromal elements [18-20].
However, frequently, only two or even one component predomi-nate [18,19J. There are no histological differences between \'7ilms'turners occurring in children and adults. However, the diagnosisof a \'7ilms' tumor is somewhat complex and can represent a diag-nostic challenge not only for general pathologists who are usuallynot familiar with the histopathologic features and variants of thesetumor, but also for pediatric pathologists. This is illustrated inthe published SlOP experience: following central review by anexpert pediatric pathologist, 15-20% of renal turnor cases werereclassified [19). For that reason review of all cases by expert panelsof pathologists is standard in pediatric \'7ilms' turnor trials.
TreatmentA small number of reports are available to assess treatment andoutcome in adults with Wilms' tumors (TABLE 1) [4,5,7,8,10.11]. Mostpatients were treated with initial nephrectomy followed by stageadjusted chemotherapy with or without radiotherapy (TABLE 1)
[4,S,7,8,10,11). Only eight patients have been described who receivedpreoperative chemotherapy after biopsy prior to nephrectomy(TABLE I) [7,8). No cases receiving prcoperativc radiotherapy havebeen described (TABLE 1) [4,S,7,8,10,11]. The fact that so many adultsunderwent immediate nephrectomy, even in Europe where sur-gery is usually recommended after preoperative chemotherapy inchildren, is not surprising since immediate surgery is the mostcommon approach for RCC. Patients after nephrectomy weregenerally treated with chemotherapy and/or radiotherapy, overthe years more adapted according to stage and histology-appropri-ate regimens used in pediatric trials [4.5.7,8,10.11). In general, mostpatients with stage I favorable histology Wilms' tumor receivedactinomycin 0 (ActO) and vincristine (VCR), those with stage IIfavorable histology \'7i1ms' tumor received ActO, VCR with orwithout doxorubicine (OOX) and/or radiotherapy and those withstage III and IV disease mostly received ActO, VCR and OOX inaddition to radiation therapy. Available data indicate that 'excep-tions' were made, with many patients treated more intensively thantheir stage equivalent pediatric counterparts (TABLE I) [4.5,7.8.10.11).
Survival/prognosisAvailable series suggest that the outcome for adults with a Wilms'tumor has improved considerably owing to the use of multi-modality treatment prorocols adapted from the pediatric treat-ment prorocols [4.5,7,8.10.11]. The data clearly suggest that manyadults with Wilms' turnor, if treated appropriately, can expectedto be cured, in particular if the tumor has not spread and/or isresected completely. In 1982, the National Wilms' Tumor StudyGroup (NWTSG) reported for the first time. experience with31 adult Wilms' tumor patients (advanced stage: 51.7%) witha 3-year overall survival (OS) of 24% compared with 74% inchildhood patients at that time [11]. In 1990, the second reportfrom the NWTSG showed an important improvement with a3-year OS of 67% in 27 adults (median age: 24 years; advancedstage: 58%) by adopting the multimodal treatment protocolsused in children [10). In 2004, the third report from the NWTSG
group demonstrated a 5-year OS of 82.6% of23 adult patients(median age: 21.9 years; advanced-stage: 43%) treated simi-lar to their childhood counterparts according to the N\'7TSGprotocols [4]. This improved outcome is similar to the reportedoutcome in a cohort of 27 German adult patients (median age:25.4 years; advanced stage: 70%) treated according to the SlOPprotocols [7J.
A delay in starting adjuvant therapy after nephrectomy is com-mon in adults and seems to effect outcome adversely [8J. The pedi-arric \Vilms' turnor treatment protocols advise starting adjuvanttherapy within 7-14 days after nephrectomy. The 17 adults with aWilms' tumor reported by the Italian group started adjuvant ther-apy at a median of 59 days post-surgery [8). The ten patients whostarted treatment within 30 days of diagnosis had a 5-year event-free survival of 60% (± 15%) compared with 14.3% (± 13%) forthe seven patients with a delay greater than 30 days (p = 0.03).Their OS was 80% (± 12%) versus 28.6% (± 17%) (p = 0.05),respectively [SrREAFlcO F; UNPUBLISHED DATAl. No factors other thantime to start adjuvant therapy seemed to explain the worse sur-vival in this group of patients with a. delay of >30 days [8]. Bymaking a standardized approach available for this kind of turnor,we hope the time to start adjuvant therapy can be shortened andthat this will improve outcome.
Toxicity of treatmentA common late effect is cardiotoxicity owing to anthracyclines(TCO >300 mg/m2), which is more severe in combination withpulmonary irradiation. In addition, pulmonary irradiation canresult in restrictive lung disease, whereas abdominal radiotherapycan cause fertility problems, growth abnormalities and impairedrenal function. Renal dysfunction has been described after cyclo-fosfamide and carboplatin in adults, mostly as acute toxicity witha (slow) recovery [21-24]. Neurotoxicity owing to VCR as well ashepatotoxicity or veno-ccclusive disease (VOO) due to ActO are.like in children, also reported in adults [4.7J. In children. severeneurotoxicity due to VCR resulting in a change in dose or post-poning a dose orVeR is described in 1.7% [25J and 2.4% [26] ofa pediarric \'7ilms' turner study population, respectively. A smalladult study by a German group reported that 13 out of27 (48%)adults suffered from severe (grade 3-4) neurotoxicity, resultingin treatment delay, dose reduction, or even discontinuation oftreatment (40.7%) [7J. In most patients, however, the neuropathywas at least partially reversible [7J. In children, the incidence ofVOO ranges from 5 to 8% depending on the definition [27-29J.
If supportive management is initiated adequately and in a timelymanner, itis mostly reversible [27-29J. There are no large adult seriesthat described the incidence ofVOO or severe hepatotoxicity afterthe administration of ActO. The GPOH reported hepatotoxicityin one out of 30 (3%) adult renal tumor patients (27 Wilms'turnor and three clear cell sarcoma of the kidney) and severe VOOin one patient (3%), which resolved without residual effects [7]. ANorth American study reported 23 adult Wilms' tumor patientsof whom three (13%) died after treatment-related liver toxicity,3-6 months after treatment of ActO, in the absence of right flankirradiation [4).
www.cxperr-reviewe rorn 1107
Supplied by The British Library - "The world's knowledge"

Segers. van den Heuvel-Eibrink, Pritchard-Jones et al.
Expert commentaryRecommendations for the management of adultWilms'tumorDiagnostics & stagingBased on the available literature on adult Wilms' turnors com-bined with experience of the authors of this manuscript, stan-dardized recommendations for diagnostic work-up, stagingand treatment of adult \X'ilms' tumor patients are proposed inSCPPLBIEmARY TABLES 1-5. Patients that will benefit from these rec-ommendations are adult Wilms' turner cases above the age of19 years that are not eligible to be included in open pediatric trials.Our primary aim is to provide a 'best practice' guideline, basedon international consensus, thereby minimizing postoperativetreatment delay and improving survival.
Once the diagnosis is suspected, we advise, in order to avoiddelay in starting therapy, timely review by an expert pediarricpathologist thereby including immunohistochemistry and molec-ular biology studies to exclude more commonly found tumors inthis age group (ScrrmIENTARyTABlf 3). Recommended staging inves-tigations include a CT 'scan of the chest and abdomen, as thishas become a standard approach in adults to detect pulmonaryand hepatic rnetasrases and to assess tumor extension, vena cavainferior involvement and function of the contralateral kidneymuch more reliably than ultrasound (SuprLE"ENTARY TABLE 1). In thepast, pediatric Wilms' turner staging was largely dependent onultrasound and conventional chest x-ray. The clinical significanceof small pulmonary nodules detectable only on CT scan remainscontroversial in pediarric practice, but could be assumed to rep-resent metastatic (unless proven otherwise by histology) diseasein adults, although adult studies are lacking. Bone, bone marrowand CNS merasrases are extremely rare in pediatric patients [30]
and there are no data to suggest that this may be more commonin adults with a Wilms' tumor. Accordingly, screening for thesesites is not recommended in absence of suggestive symptoms.Moreover, in case of presence of these rare metastatic sites, recon-sideration of the accuracy of the diagnosis is necessary. Spermbanking in males or ovarian preservation in females could beconsidered immediately before starting chemotherapy withoutany delay, especially regimens containing cyclophosphamide orcarboplatin [31]. However, we have to remark that ovarian pres-ervation is not yet as successful as sperm banking in terms ofguaranteeing future offsprings.
The proposed staging system in demonstrated in SUPPl-
EMENTARYTABLE 2 for adult \Vilms' tumor patients after immediatenephrectomy. For tumor staging after preoperative chemotherapy,all such turnors should be considered at least stage IH (becausethey have all had a biopsy) and therefore not eligible to be treatedwith the minimal therapy used for stage I Wilms' tumors (onlyVCR and ActD). SVPrlEmmARY TABLE 3A shows the histopathologi-cal classification system used after immediate nephrectomy. Twohistological risk groups can be identified: favorable and unfavor-able (focal and diffuse anaplasia) histology. In the rare instanceswhen nephrectomy is performed after chemotherapy in adultswith Wilms' tumor, we recommend using the SlOP WT 2001classification scheme (ScrpUME~"TAllYTABU 3B) [20]. For these very few
adult patients receiving pre-nephrecrorny chemotherapy, we rec-ommend treating cases with blastemal predominant histologyafter preoperative chemotherapy as in high-risk pediarric cases(Surrmlt~"TARYTABn4.3). We also advise consideration of patients withany anaplastic changes (diffuse or focal) as high risk or unfavorablehistology as no data are available in adults suggesting that focalanaplasia has a better outcome than diffuse anaplasia [32].
Treatment regimens
\X'ilms' rurnor is known to be a very chemosensitive turnor, withsuccessive clinical trials aiming to improve risk stratification andreduce rhc.burden of therapy. The backbone of pediatric chemother-apy regimens comprises VCR and ActD for low stage tumors, withDOX added in higher risk cases. Cyclophosphamide, etoposide,doxorubicin and carboplatin are used in the highest risk group.
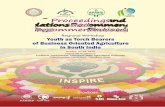
The therapeutic recommendations for adult patients who can'tbe included in officially open pediatric trials are described in FrCVRE 1
with detailed descriptions of the therapeutic regimens depicted inSUrPLDIu,"TARY TABLES 4.1-4.3. Although, we encourage the inclusionof adults in pediatric trials where possible, such as in the currentCOG trial where cases up to 30 years are eligible for registration.Only non-advanced stage patients with optimal staging and shorttime interval from nephrectomy to commencement of chemo-therapy are eligible for the minimum chemotherapy with VCR andActD, as in current pediatric SlOP and COG protocols. Althoughchildren with stage H favorable histology Wilms' tumor are treatedwithout DOX in the current COG protocol, to improve survival,the consensus recommendation here is to include DOX, based onthe lower survival rate and the average longer time from surgery topostoperative treatment in adult Wilms' tumor patients. Moreover,VCR intensity is decreased in these guidelines as compared withcurrent childhood prorocols, as adults frequently develop severeneurological toxicities [7]. However, these patients can always becritically discussed. In case of favorable histology by pediatricpathology review and rapid diagnosis with the start of cherno-therapy within 14 days after nephrectomy, treatment according topediatric COG protocol stage II favorable hisrologywithout DOXcould be acceptable. Metastatic or 'inoperable' cases diagnosedby preoperative biopsy should receive preoperative chemotherapybased on histology (favorable or unfavorable) with posrnephrec-tomy therapy based on stage, histology and response to preopera-tive chemotherapy. In the very rare instances when the diagnosisofWilms' tumor is first made on a biopsy and the tumor looksamenable to immediate nephrectomy, we also recommend givingpreoperative chemotherapy. This is because the 'added value' ofhistological response can be incorporated into the risk stratificationand because it reduces the risk of turner rupture, makes surgerysafer (in the pediatric setting) and hence should reduce the riskof needing either whole abdominal radiation or boosts to areas ofmacroscopic residue.
Surgical recommendations for nephrectomy are less detailed(SUl'PLEMU,"TARyTABU 1) because in the majority of patients the diagno-sis of\Vilms' tumor is made unexpectedly after nephrectomy forpresumed RCC. An adult Wilms' tumor patient, who has beentreated surgically by anything other than an immediate open rotal
1108
l
Supplied by The British Library - "The world's knowledge"

(f)C-0""Q..ro·0..0""'<-l::YCDOJ
~en::YC.0""--.III-<....:j
::YCD
~o20..en-»:::Io~CD0..
COCD:
,.
-- ----.~
"":<"><]
*-e".~no3
Tabre 1. Previous reports on the characteristics and outcomes of adult nephroblastomas."1 1°":'''': .' ;1.:'1: :"',:,..",•.I:
: ;,,\. .,~'I '.•.!~ : ,,! I ~
.1/
\ ~:- .
34 (15 to Localized: 15;>60) Regional
extension: 15
89 NAMitryeta/.(2004)
14Europe,Eurocare'
1983-1994
133(69/64)
NA NA NA NA NAIzawa eta/. Review' 1973- 128 26(2008) 2006 (15-73)
Terenziani Italy, 1983- 17 (11/6) 17.5et al. (2004) CNRI 2001 (16-29)
AIEOP
Kattan et al. France 1973- 22 24(1994) 1992 (14/8) (16-40)
Reinhard Germany, 1994- 27 25.4et al. (2004) SlOP 2001 (12/15) (15-62)~
93-011GPOH
Kalapurakal USA, 1988- 23 21.9et al. (2004) NWTS 2001 (13/10) (16.3-
4-5 51.3)
Arrigo et al. NWTS 1979- 27 (NA) 24(1990) 2-3 1987 (16-74)
51 FH: 16;UH: 1
8 4
4 8 3 7 FH: 21;UH: 1
LR: -;IR: 25;HR: 2;RCC:21t
FH: 23;UH: -
6 2 9' 10
8 6 45
4 11 FH: 23;UH: 4 (allstage IV)
6 5
",;1'
""r'
,." 'f': •• , •. 1· .-
NA NA NA NA NA 47.3 (relative) 5 years [6]
43 - 77 7 NA 68 4 years, [3]
6 months
7 7 2 45 62.4 10 years, (8)
11 months
6 1 15 - 41 55 8 years, (5)
(100 months) 4 months
13 14 - 57~ 83~ 4 years~ [7]
10 13 77.311 82,6'* 5 years1 months
5 19 3 NA . 67 (3 years)" 2 years,1 months
'Epidemiologic study.'Review with collected data from 128 adult WT patients. Six cases were from their two Canadian centres that have not been published before, the remaining 122 patients were from previous published case reportsor case series including 3,4, 5 and 6 patients.IStage IV patient with diagnostic biopsy who died before nephrectomy.'Calculated on the basis of 30 renal turners (25 WT; 2 WT) with RCC in the same kidney and three clear cell sarcomas of the kidney.'Stage 11 N+ is considered stage Ill. 7: Unknown."Two patients with RCC and WT in the same kidney."Analyses based on data from this report combined with data from 22 FHWTs stage HV previously reported in 1990 by the NWTSG [10].IIExclusion stage V patient.CNR-AIEOP: Consiglio Nazionale Ricerche/Asspcoazione Italiana Ematologia Oncologia Pediatrica; CT: Chemotherapy; FH: Favorable histology; HR: High risk; IR: Intermediate risk; LR: Low risk; NA: Not available;nephr: Nephrectomy; NWTS: National Wilms' Tumor Study; NWTSG: National Wilms' Tumor Study Group; OS: Overall survival; PA: Pathology/histology; RCC: Renal cell carcinoma; RT: Radiotherapy;SlOP: International Society of Pediatric Oncology; U H: Unfavorable histology; WT: Wilms' tumor. .
......
l S. _..;:
[4]
[10)
s:o:Jo10<03ma~o0.Su;~.:r~3""'.C3o~iDoo33CD:J0.oo·:JenC-o'"(1)0.o:J::JiD39-o·:lQ.
oo:l'"<0:J'"C'"
.. ,
"

,-
;".,: \ i 'f:- \ 1~I Segers, van den Heuvel-Eibrink, Pritchard-Jones et al.
AdultWT
/ ~Immediate nephrectomy Metastatic disease/surgically 'inoperable' tumor
-:
'rStage 11
1
Stage 1IJstage 11/ VP161CARBO + AcWCRlDOXstage III CYCLO/DOX~= 'high risk' (SUPPLEMENTARYTADLE4.2)! (SUPPLEMENT;RY TABLE 4.3) +
RT§ . ~response as\sessment'ActDNCRlDOX(StJPPLEM[%'\'-ARY
TABLE 4.2)
+RT§
VP 16/CARBO + CYCLO/DOXu = 'high risk'(SUPPLEMENTARyTABlt 4.3)
+response assessment'/~ActDNCR
(SUPPLEMENTAl«
TABLE4.i)
Complete resolutionrnetastases
Complete resolutionmetastases
Incomplete resolutionmetastases
orsurgically 'inoperable' tumor
!
Incomplete resolutionmetastases
orsurgically 'inoperable' tumor
!ActDNCRlDOX
+RT lungs + flank/abd!
+••
Continue 'high risk'+
RT lungs + flank abd!+••
'High-risk'schedule+
RT lungs + flank abd!+
Consider surgicalresection lung metastases
+
"
'High-risk'schedule+
RT lungs + flank abd!+
Consider surgicalresection lung metastases
+"
Figure 1. Therapeutic guidelines for adult Wilms' tumor patients.'Only stage I favorable histology if all four criteria are met, that is:1. Stage and histology have been reviewed by a pediatric pathologist experienced in Wilms' turners:2, Histological examination and review has included at least one lymph node;3. Cf scan of the chest has excluded the presence of lung metastases;4. Chemotherapy can be started within 30 days of date of nephrectomy.
'All other stage I Wilms' tumor cases.§SeeSUPPLn'LYfARyTABlE5.
~'High risk' chemotherapy schedule.'Response assessment of metastases and operability of the primary tumor after 6 weeks by abdominal/pulmonary CT scan."Delayed nephrectomy should be considered after 6 weeks of preoperative chemotherapy if a nephrectomy has not been performed atinitial diagnosis. If the original diagnosis was made on biopsy only, then in the case of nonresponse or inadequate response topreoperative chemotherapy, the histological diagnosis should be reviewed again and a further biopsy may be warranted if there is anyuncertainty. Then in these cases where the Wilms' tumor (histologically confirmed again) remains surgically 'inoperable', we advise toconsider changing to the 'high-risk' schedule or go on with this schedule and assessoperability again after two to three coursesof chemotherapy.ActD: Actinomycin 0; CARBO: Carboplatin; CT: Computed tomography; CYCLO: Cyciofosfamide; DOX: Doxorubicin; FH: Favorablehistology; VCR: Vincristine; VP16: Etoposide; RT: Radiotherapy; UH: Unfavorable histology; WT: Wilms' tumor.
nephrectomy with adequate lymph nodes sampling and timelypathology review, is not eligible for the pediatric-style stage Itherapy (only VCR and ActO). Although, we realize that openpartial nephrectomy has become the gold standard for a single smallrenal turnor in adults [33], and moreover, that laparoscopic partialnephrectomy has emerged as a viable alternative to open partialnephrectomy in appropriately selected patients [33]. Cases of partialnephrectomy with clear margins should be discussed individu-ally with the national reference group for pediatric renal tumors.Laparoscopic nephrectomy should be considered as an experimental
approach and needs to be treated with the three-drug chemotherapyschedule and radiotherapy. When the diagnosis of\'V"ilms' turnorhas been made before nephrectomy, total nephrectomy is recom-mended according to adult nephrectomy guidelines for any renalcancer. We do emphasize the importance of adequate lymph nodessampling in case of a Wilms' tumor (SCPPU.\lL'<TARyTABLE I).
Recommendations for radiotherapy are described in(SCPPLEMENTARY TABLE 5). Radiotherapy, such as chemotherapy, shouldbe planned to start ideally by day 14 postnephrectomy although,starting by day 30 is acceptable.
1110 Expert Rrv. Anticancer Tbrr. 11(7). (2011)
Supplied by The British Library - "The world's knowledge"

:"~~•i ~I~, IIIManagement of adults with Wilms' tumor: recommendations based on international consensus
Toxicity & tumor monitoringToxicity monitoring should comprise of blood COUntSand liverfunction tests prior to the administration of each dose of ActDor DOX. Disproportionate thrombocytopenia and signs ofhepatotoxicity will alert the physician to the possibility ofVOD,a potential complication of ActD. Monitoring for impaired renalfunction (both glomerular and tubular) as well as possible cardiacstress/failure (especially in cases with lung irradiation in combina-tion with DOX) or impaired lung function is recommended inpatients bearing this risk.
During and after therapy, tumor monitoring by chest andabdominal imaging is recommended every 3 months for 2 years,since most of the relapses occur within 2 years of completion oftherapy [1.5.7.8.10].
RegistrationWe strongly recommend the registration of each adult \X'ilms'turn or patient within a pediatric renal turnor trial where possibleaccording to each national regulatory situation. Although, we real-ize it is difficult to register patients who are treated at institutionswhere the pediatric trial is not open. This is a global problem andcan really only be overcome by building a truly international data-base such as has been done successfully in the international pleuro-pulmonary blastoma registry. To achieve this, it requires a morespecific endeavour by the academic community as well as funding.
Five-year viewOur aim is that these recommendations build the basis for collect-ing uniform and accurate data on clinical characteristics, treat-ment, outcome and toxicity in this rare group of adult patientswith a pediatric cancer. Moreover, within 5 years we hope thatthe many international efforts ongoing to address the problems of
research and improvements in clinical practice for very rare dis-eases (e.g., RARECARE in Europe) might achieve the necessaryregulatory framework approval processes that would make thisfeasible. Thus, the registration of all adult Wilms' tumor patientswill be implemented. An international database with a coordinat-ing centerwill then also facilitate the development of a biobank ofadult Wilms' tumors with the possibility for biology studies. Theknowledge from these registry data, possibly in combination withdata from biology studies, will help us to assess whether Wilms'turners in adults are any different than those occurring in children.Then, more evidence based guidelines for diagnosis and treatmentof adult \X'i1ms' tumor patients with the aim to improve outcomea~d reduce toxicity can be developed in the future.
ConclusionA standardized approach to the diagnosis, staging and treatment ofadults (~19 years) with a Wilms' tumor is proposed based on theavailable literature and international consensus from the field ofpediatric Wilms' tumors. Although we realize that with increasingage the tumor may reflect a more aggressive biological behavior andtaken into account the risk of toxicity, we envisage that these con-sensus recommendations will facilitate decrease in postoperativetreatment delay and thereby an improvement in outcome.
Financial & competing interests disclosureThis is aposition paper by the Renal Tumour Stl/dy Group ofthe IntemationalSociety of Paediatric Oncology (SlOP) and the Renal Tumars Committee(RTC) of the Children': Oncology Group (COG). Tbe authors have no otherrelevant affiliations orfinancial involvement with any organization or entitywith a financial interest in or financial conflict with the subject matter OT
materials discussed in th« manuscript apart from thou disclosed.No writing assistance was utilized in the production of this manuscript.
Key issues• Consult a pediatric oncology colleague with experience in treatment of Wilms' tumors as soon as histological diagnosis is suspected.
• Pathological review by a pediatric pathologist expert in Wilms' tumors (if Wilms' tumor is suspected do not delay until other renaltumors are excluded by immunohistochemical and molecular studies).
• Avoid delay in starting chemotherapy. Chemotherapy, including radiotherapy if necessary, should be planned to start ideally by day 14postnephrectomy, although delaying the start until day 30 is acceptable.
• Be alert for toxicity of vincristine (neurotoxicity) and actinomycin D (hepatic toxicity) in adults.
• Register patients in pediatric renal tumor trials where possible according to each national regulatory situation.
ReferencesSpreafico F, Bellani FF. Wilms' tumor:past, present and (possibly) future. ExpertRev. Anticancer Tber. 6(2), 249-258(2006).
2 McLorie GA. Wilrns' turnor(nephroblasroma). CUTT. Opin. UTa/. 11(6),
567-570 (2001).
3 Izawa JI, Al-Ornar M, Winquist E et al.Prognostic variables in adult Wilms'tumour. Can.]. SIITg. 51(4),252-256(2008).
4 Kalapurakal IA, Nan B, Norkool Petal.Treatment outcomes in adults withfavorable histologic type Wilms' tumor-anupdate from the National \V'ilms' TumorStudy Group. Int.], Radial. Oncol. BioI.Phyr. 60(5), 1379-1384 (2004).
Katran J, Tournade MF, Culine S,Terrier-Lacornbe MJ, Droz JP. AdultWilrns' tumour: review of22 cases.EIIT.]. Cancer 30A(I2), 1778-1782 (1994).
6 Mitry E, Ciccolallo L, Coleman MP, GattaG, Pritchard-jones K. Incidence of andsurvival from Wilms' tumour in adults in
Europe: data from the EUROCARE study.Eur.J. Canm42(14), 2363-2368 (2006).
7 Rcinhard H, Aliani S, Ruebe C, Stocklc M,Leuschner I. Graf N, Wilms' turner inadults: results of the Society ofPcdiatricOncology (SlOP) 93-01/Society forPediatric Oncology and Hematology(GPOH) study.]. Cfin. Oncol.22(22),4500-4506 (2004).
8 Terenziani M, Spreafico F. Collini P (t al.Adult Wilms' turner: a rnonoinstitutionalexperience and a review of the literature.Cancer 101(2), 289-293 (2004).
www.expert-rcviews.corn 1111
J
Supplied by The British Library - ''The world's knowledge"

.~ 11
I ' ;- I ,/ i:~\ i;! Segers, van den Heuvel-Eibrink, Pritchard-Jones ef al.
I 19 Vujanic GM, Sandsredr B, Kelsey A, 26 Pritchard-jorics K, Kelsey A, Vujanic G,McLaughlin JK, Lipworth L, Tarone RE.
Sebire NJ. Central pathology review in Irneson ], Hutton C, Mitchell C. Older agei Epidemiologic aspects of renal cell1 multicentcr trials and studies: lessons is an adverse prognostic factor in stage I,1 carcinoma. Semin. Oncol. 33(5),527-533I from the nephroblastorna trials. Cancer favorable histology Wilms' tumor treated1 (2006). 115(9), 1977-1983 (2009). with vincristine monochemotherapy: a11
i' 10 Arrigo S, Beckwirh JB, Sharples K,20 Vujanic GM, Sandsredt B, Harms D, study by the United Kingdom Children's
D'Angio G, Haase G. Better survival after Kelsey A, Leuschner I. de Kraker J. Cancer Study Group, Wilm's Tumorcombined modality care for adults with Revised International Society of Working Group';' Clin. Oncol. 21(17).Wilms' tumor. A report from the National Paediatric Oncology (SlOP) working 3269-3275 (2003).Wilms' Tumor Study. Cancer 66(5), classification of renal turnors of 27 Bisogno G, de Kraker J. Weirich A et al.827-830 (1990). childhood. Med. Pediatr. Oncol. 38(2), Vcno-occlusive disease of the liver in
11 Byrd RL. Evans AE. D'Angio G]. Adult 79-82 (2002). children treated for Wilms' tumor. Med.Wilms' tumor: effect of combined therapy
21 Beyer J, Rick 0, Weinknecht S. Kingrcen Pediatr. Oncol. 29(4). 245-251 (1997).on survival.]. Urol. 127(4),648-651
D, Lenz K, Siegert W. Nephrotoxicity 28 Czauderna P. Katski K, Kowalczyk J et al.(1982).
after high. dose carboplatin, etoposide and Venoocclusive liver disease (YOD) as a12 Lowe LH. Isuani BH. Helier RM et al. ifosfamide in germ-cell turnors: incidence complication ofWilms' tumour
Pediarric renal masses: Wilms' tumor and and implications for hematologic recovery management in the series of consecutivebeyond. Radiographies 20(6), 1585-1603 and clinical outcome. Ban, Marrow 206 patients. Eur.]. Pediatr. Surg. 10(5),(2000). Transplant. 20(10), 8\3-819 (\997). 300":'303 (2000).
13 Trappe RU. Rim H. Lippek F et al. 22 Chauvergne J. Chiner-Charror P. Stock le 29 Ludwig R. Weirich A. Abel U, HofmannEffective use of high-dose chemotherapy E. Thomas L. Toulouse C. [Carbcplarin W, GrafN, Tournade MF. Hepatotoxicityand autologous stcrrr cell rescue for relapsed and etoposide combination for the in patients treated according to theadult Wilms' tumor and a novel alteration treatment of recurrent epithelial ovarian nephroblastorna trial and studyin intron 1 of the WTl gene.]. Pediatr. cancer]. Bull. Canar83(4), 315-323 SIOP-9/GPOH. M,d. Pediatr. Oncol.Hematol. Oncol. 26(12), 820-823 (2004). (1996). 33(5),462-469 (1999). ,
14 Hsiao HL. Chang TH, Wu WJ. Huang 23 Thatcher N, Qian W, Clark PI a al. 30 van den Heuvel-Eibrink MM. GrafN, Pein I,CH. Adult Wilms' turner with hypospadias Ifosfamide. carboplarin, and etoposide F et al. Intracranial relapse in Wilms'and cryptorchidism: a case report. with midcycle vincristine versus standard tumor patients. Pediatr. Blood Cancer. ,.Kaobsiung ]. Md Sci. 23(1l). 584-589 chemotherapy in patients with small-cell 43(7),737-741 (2004).(2007). lung Cancer and good performance status: 31 van Casteren Nj, Dohle GR, Romijn jc,
15 Williams RD. Al-Saadi R. Chagtai T a al. clinical and quality-of-life results of the de Muinck Keizer-Schrama SM, Weber RF.Subtype-spccific FBXW7 mutation and British Medical Research Council van den Heuvel-Eibrink MM. SemenMYCN copy number gain in Wilms multicenter randomized LU21 trial. cryopreservation in pubertal boys beforeturner. Clin. Cancer R". 16(7).2036-2045 }. Clin. Oncol. 23(33). 8371-8379 (2005). gonadotoxic treatment and the role of(2010). 24 White SC. Lorigan p, Middleton MR endocrinologic evaluation in predicting
16 Su MC, Huang WC, Lien HC. p-catenin et al. Randomized phase II study of sperm yield. Fmi!. Steril. 90(4).1119-1125expression and mutation in adult and cyclophosphamide. doxorubicin, and (2008).pediatric Wilms' turners. APMIS 116(9). vincristine compared with single-agent 32 Faria P, Beckwirh JB. Mishra K et al. Focal771-778 (2008). carboplatin in patients with poor versus diffuse anaplasia in Wilrns
17 Rubin BP, Pins MR. Nielsen GP a al. prognosis small cell lung carcinoma. tumor--new definitions with prognosticIsochromosome 7q in adult Wilms' tumors: Cancer 92(3),601-608 (2001). significance: a report from the Nationaldiagnostic and pathogenetic implications. 25 de Kraker J, GrafN, van Tinrercn H et al. Wilms' Turner Study Group. Am.}. Slag.Am.]. Surg. Patbol. 24(12), 1663-1669 Reduction of postoperative chemotherapy Patbol. 20(8). 909-920 (1996).(2000). in children with stage I intermediate-risk 33 Gill IS. Kavoussi LR, Lane BR a al.
18 Vujanic GM. Sandstedt B. The pathology and anaplastic Wilms' tumour Comparison of 1.800 laparoscopic andofWilms' tumour (nephroblastcrna): the (SlOP 93-01 trial): a randomised open partial nephrectomies for single renal
controlled trial. Lancet 364(9441).International Society of Paediatric1229-1235 (2004).
rumors.}. Urol. 178(1).41-46 (2007).Oncology approach. Am.}. Surg. Patbol.(2009).
Expert Rw. Anticancer Th~T_1·' (7), (2010
Supplied by The British Library - "The world's knowledge"

Management of adults with Wilms' tumor: recommendations based on international consensus
Author list & affiliationsHeidi Segers'Deprartrnenr of Oncology/Hematology, Erasmus MC-SophiaChildren's Hospital. Dr Molewaterplein, 603015 GJ, Rotterdam,The Netherlands
Marry M van den Heuvel-Eibrink"Deptarrrncnt of Oncology/Hematology, Erasrnus MC-SophiaChildren's Hospital, Dr Molewaterplein, 603015 GJ, Rotterdam,The NetherlandsTel.: +31 104636691Fax: +31 [email protected]
MaxJ CoppesCcnter for Cancer and Blood Disorders, Children's National MedicalCenter, Washington, DC, USA
Michael AitchisonDepartment of Urology, NHS Greater Glasgow & Clyde, GartnavelGeneral Hospital/Western Infirmary, Glasgow, Scotland, UK
Christophe BergeronCentre Leon Berard/Insritut d'Hernato-Oncologie Pediarrique,Lyon, France. '.
Beatriz de CamargoPcdiatric Hematology Oncology Program, Research Cenrcr, InstitutoNacional do Cancer, Rio de Janeiro, Brazil
Jeffrey S DomeDepartments ofPediarrics and Oncology, University of Alberta,Edmonton, AB, Canada
Paul GrundyCenrer for Cancer and Blood Disorders, Children's National MedicalCenrcr, Washington, DC, USA
Gemma GatraEvaluative Epidemiolgy Unit, Fondazione IRCCS Istituto Nazionaledei Tumori, Milano, Italy
Norbert GrafDepartment ofPediatric Hematology and Oncology, UniversityHospital for children, Homburg/Saar, Germany
Paul GrundyDepartments of Pcdiarrics and Oncology, University of Alberta,Edmonton, AB, Canada
John A KalapurakalDepartment of Radiation Oncology, Robert H Lurie Cancer Center,Northwestern University, Chicago, IL, USA
Jan de KrakerDepartment ofPediatric Oncology, Emma Children's Hospital,
'AMC, Amsterdam, The Netherlands
•. Elizabeth J Perlman'. Department of Pathology and Laboratory Medicine, Children's
Memorial Medical Cenrer, Chicago, IL, USA
Harald ReinhardAsklepios Hospital, Pediatric Haematology and Oncology, D-53757Sankt Augustin, Germariy
Filippo SpreaficoPediatric Unit, Fondazione IRCCS Istituto Nazionale dei Tumori,Milano, !raly
Gordan VujanicDepartment of Histopathology, School of Medicine CardiffUniversity, Heathl'ark, Cardiff, UK
Anne B WarwickDivision ofPediatric Hematology/Oncology, Department ofPediatrics, Medical College of Wisconsin, Milwaukee,WJ,USA
Kathy Prirchard-jonesUCL Institute of Child Health & Great Ormond Street Hospital,London, UK
'These authors equally contributed to the production of thismanuscript.
WWw.experc-revicws.com 1113
Supplied by The British Library - "The world's knowledge"