Longitudinal Effects of Medical Students' Communication Skills on Future Performance
7
MILITARY MEDICINE, 180, 4:24, 2015 Longitudinal Effects of Medical Students’ Communication Skills on Future Performance Ting Dong, PhD*; Lt Col (Sel) Jeffrey S. LaRochelle, USAF MC*; Steven J. Durning, MD, PhD*; LTC Aaron Saguil, MC USA†; Kimberly Swygert, PhD‡; CDR Anthony R. Artino Jr., MSC USN* ABSTRACT Background: The Essential Elements of Communication (EEC) were developed from the Kalamazoo consensus statement on physician–patient communication. The Uniformed Services University of the Health Sciences (USU) has adopted a longitudinal curriculum to use the EEC both as a learning tool during standardized patient encounters and as an evaluation tool culminating with the end of preclerkship objective-structured clinical examinations (OSCE). Medical educators have recently emphasized the importance of teaching communication skills, as evidenced by the United States Medical Licensing Examination testing both the integrated clinical encounter (ICE) and commu- nication and interpersonal skills (CIS) within the Step 2 Clinical Skills exam (CS). Purpose: To determine the associa- tions between students’ EEC OSCE performance at the end of the preclerkship period with later communication skills assessment and evaluation outcomes in the context of a longitudinal curriculum spanning both undergraduate medical education and graduate medical education. Methods: Retrospective data from preclerkship (overall OSCE scores and EEC OSCE scores) and clerkship outcomes (internal medicine [IM] clinical points and average clerkship National Board of Medical Examiners [NBME] scores) were collected from 167 USU medical students from the class of 2011 and compared to individual scores on the CIS and ICE components of Step 2 CS, as well as to the communication skills component of the program directors’ evaluation of trainees during their postgraduate year 1 (PGY-1) residency. In addition to bivariate Pearson correlation analysis, we conducted multiple linear regression analysis to examine the predictive power of the EEC score beyond the IM clerkship clinical points and the average NBME Subject Exams score on the outcome measures. Results: The EEC score was a significant predictor of the CIS score and the PGY-1 communication skills score. Beyond the average NBME Subject Exams score and the IM clerkship clinical points, the EEC score explained an additional 13% of the variance in the Step 2 CIS score and an additional 6% of the variance in the PGY-1 communication skills score. In addition, the EEC score was more closely associated with the CIS score than the ICE score. Conclusion: The use of a standardized approach with a communication tool like the EEC can help explain future performance in communication skills independent of other education outcomes. In the context of a longitudinal curriculum, this information may better inform medical educators on learners’ communication capabilities and more accurately direct future remediation efforts. INTRODUCTION The importance of teaching, assessing, and improving the communication skills of physicians-in-training cannot be over- emphasized—physicians must be competent communicators to effectively practice medicine. 1 The Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Medical Specialties (ABMS) have jointly identified communication and interpersonal skills (CIS) as one of the six general competencies for physicians. 2,3 The Institute of Medi- cine also specifies communication skills as one of the six essential curricular domains for effective patient care. 4 Post- graduate accredited training programs are required to demon- strate that they teach and evaluate trainees’ communication skills. The importance of communication skills is also demon- strated in licensing examinations. The U.S. Medical Licensing Examination requires students to take a clinical skills exami- nation with standardized patients as part of Step 2, 5 the Step 2 Clinical Skills (CS) assessment; this has a separate subcom- ponent and passing standard for the evaluation of CIS. The development and administration of CIS assessment tools is challenging and resource intensive. It is difficult to assess communication skills through inauthentic means (such as a written test), as it requires in vivo demonstration. 1 Com- petence in communication skills is not only about the presence of specific behaviors but also about the timing of effective verbal and nonverbal behaviors in the context of interactions with patients. 6 In 1999, leaders and representatives from medical schools, residency programs, continuing medical edu- cation providers, and prominent medical educational organiza- tions in North America gathered in Kalamazoo for the purpose of identifying and specifically articulating ways to facilitate the teaching and evaluation of physician–patient communica- tion. 7 After examining 5 models of physician–patient commu- nication that had been used by the conference attendees, the group reached a consensus on a set of Essential Elements of Communication (EEC). *Department of Medicine, Uniformed Services University of the Health Sciences, 4301 Jones Bridge Road, Bethesda, MD 20814. †Department of Family Medicine, Uniformed Services University of the Health Sciences, 4301 Jones Bridge Road, Bethesda, MD 20814. ‡National Board of Medical Examiners, 3750 Market Street, Philadelphia, PA 19104. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of Defense or the U.S. Government. doi: 10.7205/MILMED-D-14-00565 MILITARY MEDICINE, Vol. 180, April Supplement 2015 24 Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015. Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Longitudinal Effects of Medical Students' Communication Skills on Future Performance

MILITARY MEDICINE, 180, 4:24, 2015
Longitudinal Effects of Medical Students’ Communication Skillson Future Performance
Ting Dong, PhD*; Lt Col (Sel) Jeffrey S. LaRochelle, USAF MC*; Steven J. Durning, MD, PhD*;LTC Aaron Saguil, MC USA†; Kimberly Swygert, PhD‡; CDR Anthony R. Artino Jr., MSC USN*
ABSTRACT Background: The Essential Elements of Communication (EEC) were developed from the Kalamazooconsensus statement on physician–patient communication. The Uniformed Services University of the Health Sciences(USU) has adopted a longitudinal curriculum to use the EEC both as a learning tool during standardized patientencounters and as an evaluation tool culminating with the end of preclerkship objective-structured clinical examinations(OSCE). Medical educators have recently emphasized the importance of teaching communication skills, as evidencedby the United States Medical Licensing Examination testing both the integrated clinical encounter (ICE) and commu-nication and interpersonal skills (CIS) within the Step 2 Clinical Skills exam (CS). Purpose: To determine the associa-tions between students’ EEC OSCE performance at the end of the preclerkship period with later communication skillsassessment and evaluation outcomes in the context of a longitudinal curriculum spanning both undergraduate medicaleducation and graduate medical education. Methods: Retrospective data from preclerkship (overall OSCE scores andEEC OSCE scores) and clerkship outcomes (internal medicine [IM] clinical points and average clerkship NationalBoard of Medical Examiners [NBME] scores) were collected from 167 USU medical students from the class of 2011and compared to individual scores on the CIS and ICE components of Step 2 CS, as well as to the communicationskills component of the program directors’ evaluation of trainees during their postgraduate year 1 (PGY-1) residency.In addition to bivariate Pearson correlation analysis, we conducted multiple linear regression analysis to examine thepredictive power of the EEC score beyond the IM clerkship clinical points and the average NBME Subject Exams scoreon the outcome measures. Results: The EEC score was a significant predictor of the CIS score and the PGY-1communication skills score. Beyond the average NBME Subject Exams score and the IM clerkship clinical points, theEEC score explained an additional 13% of the variance in the Step 2 CIS score and an additional 6% of the variance inthe PGY-1 communication skills score. In addition, the EEC score was more closely associated with the CIS score thanthe ICE score. Conclusion: The use of a standardized approach with a communication tool like the EEC can help explainfuture performance in communication skills independent of other education outcomes. In the context of a longitudinalcurriculum, this information may better inform medical educators on learners’ communication capabilities and moreaccurately direct future remediation efforts.
INTRODUCTIONThe importance of teaching, assessing, and improving the
communication skills of physicians-in-training cannot be over-
emphasized—physicians must be competent communicators
to effectively practice medicine.1 The Accreditation Council
for Graduate Medical Education (ACGME) and the American
Board of Medical Specialties (ABMS) have jointly identified
communication and interpersonal skills (CIS) as one of the six
general competencies for physicians.2,3 The Institute of Medi-
cine also specifies communication skills as one of the six
essential curricular domains for effective patient care.4 Post-
graduate accredited training programs are required to demon-
strate that they teach and evaluate trainees’ communication
skills. The importance of communication skills is also demon-
strated in licensing examinations. The U.S. Medical Licensing
Examination requires students to take a clinical skills exami-
nation with standardized patients as part of Step 2,5 the Step 2
Clinical Skills (CS) assessment; this has a separate subcom-
ponent and passing standard for the evaluation of CIS.
The development and administration of CIS assessment
tools is challenging and resource intensive. It is difficult to
assess communication skills through inauthentic means (such
as a written test), as it requires in vivo demonstration.1 Com-
petence in communication skills is not only about the presence
of specific behaviors but also about the timing of effective
verbal and nonverbal behaviors in the context of interactions
with patients.6 In 1999, leaders and representatives from
medical schools, residency programs, continuing medical edu-
cation providers, and prominent medical educational organiza-
tions in North America gathered in Kalamazoo for the purpose
of identifying and specifically articulating ways to facilitate
the teaching and evaluation of physician–patient communica-
tion.7 After examining 5 models of physician–patient commu-
nication that had been used by the conference attendees, the
group reached a consensus on a set of Essential Elements of
Communication (EEC).
*Department of Medicine, Uniformed Services University of the Health
Sciences, 4301 Jones Bridge Road, Bethesda, MD 20814.
†Department of Family Medicine, Uniformed Services University of the
Health Sciences, 4301 Jones Bridge Road, Bethesda, MD 20814.
‡National Board of Medical Examiners, 3750 Market Street, Philadelphia,
PA 19104.
The views expressed in this article are those of the authors and do not
necessarily reflect the official policy or position of the Department of
Defense or the U.S. Government.
doi: 10.7205/MILMED-D-14-00565
MILITARY MEDICINE, Vol. 180, April Supplement 201524
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

From the standpoint of learning communication skills, many
research studies have shown that these skills can be taught.8,9
Yedidia et al9 found that communications curricula signifi-
cantly improved third-year medical students’ “overall commu-
nications competence as well as their skills in relationship
building, organization and time management, patient assess-
ment, and negotiation and shared decision-making.” Aspegren8
also pointed out that those students with the lowest pre-
training scores benefit the most from communication skills
curriculum and that the best time to learn these skills in
medical school is most likely during clinical clerkships.
At the Uniformed Services University of the Health
Sciences (USU), we have adopted a longitudinal curricu-
lum using the EEC (see the Appendix) as both a learning
tool during standardized patient encounters and as an eval-
uation tool culminating with the end of preclerkship objective-
structured clinical examination (OSCE). Students are provided
with a copy of the EEC on their second day of medical school
and immediately begin developing skills related to the first
two domains (opening the discussion and building the rela-
tionship). Students build upon their communication skills
through standardized patient interactions, real patient inter-
views, and small-group discussions, using the domains of
the EEC as a guide. The EEC then becomes the primary
assessment tool for communication skills during standardized
and real patient encounters over the course of the preclerkship
training period.
The purpose of this study was to determine the associa-
tions between students’ EEC OSCE performance during the
preclerkship period with later communication skills assess-
ment and evaluation outcomes in the context of a longitudinal
curriculum spanning both undergraduate medical education
(UME) and graduate medical education (GME). The out-
comes were the CIS and integrated clinical encounter (ICE)
scores of Step 2 CS, as well as the communication skills
component of the program directors (PDs) evaluation of
trainees’ during their postgraduate year 1 (PGY-1) residency.
If poor performance can be diagnosed as early as the end of
the preclerkship period by EEC assessment, this would better
inform medical educators on learner ability, and more accu-
rately direct remediation efforts. The research hypotheses
were (1) students’ EEC score would explain a significant
amount of variance in the Step 2 CS CIS score and the PGY-1
communication skills score, beyond the variance explained by
other established clerkship performance measures, and (2) the
associations between EEC score and Step 2 CS ICE score
would be weaker compared with those between EEC score
and CIS score since both EEC and CIS scores are measures
of students’ communication skills.
METHODS
Study Context and Participants
This investigation was part of the larger Long-Term Career
Outcome Study conducted at the F. Edward Hebert School of
Medicine, USU. As the United States’ only federal medical
school, USU matriculates approximately 170 medical students
annually and, at the time of this study, offered a traditional
4-year curriculum: 2 years of basic science courses followed
by 2 years of clinical rotations (clerkships). The participants
of the present study were students graduating in 2011 (N =167; 58 were female [34.7%] and 109 were male [65.3%]).
Measures
EEC Score
The EEC score on the OSCE consists of seven domains (open
the discussion, build the relationship, gather information,
understand the patient perspective, share information, reach
agreement, and provide closure), in addition to an overall
global rating. Each domain has a 5-point Likert-type scale
associated with behavioral anchors. Standardized patients are
trained on how to use the EEC assessment tool and complete
their evaluations after each encounter with a student. The
overall score on each OSCE station is converted into a per-
centage of available points, and the average across all OSCE
stations is recorded as the final EEC score on the OSCE.
According to a previously conducted but unpublished
generalizability study at the USU, the second-year OSCE
stations demonstrated a moderate generalizability coefficient
(r = 0.52), with 18.1% and 3.7% of the overall variance
explained by the OSCE station and rater, respectively. Over-
all, 40.8% of the total variance was explained by student
ability. These generalizability values are slightly lower than
the published reliabilities for the Step 2 CS components of
CIS, data gathering, and patient note, but are in line with
other school-level OSCE reliabilities.10 The EEC reliability
estimate is higher, as a study by Joyce et al found the internal
reliability coefficient (Cronbach’s a) of standardized patient
EEC scores to be 0.90.11
Average NBME Subject Exams Score
The third-year curriculum consisted of the school’s core clerk-
ship rotations: family medicine, internal medicine (IM), general
surgery, psychiatry, pediatrics, and obstetrics and gynecology.
All core clerkship rotations use the relevant NBME Subject
Exam, which is given near the end of the core rotation. The
average NBME Subject Exam score was the un-weighted mean
of the scores across the clerkships. Nationally, the mean scores
(2009–2010) ranged from 73.1 (SD = 8.9) in general surgery
through 78.2 (SD = 8.8) in psychiatry.
IM Clerkship Clinical Points
During the student’s IM clerkship, teachers recommended
grades for each student, and reported the number of clinics
spent with each student. Teacher-recommended grades were
weighted according to the number of clinics the teacher spent
with the students and summarized into a measure called
clinical points.
MILITARY MEDICINE, Vol. 180, April Supplement 2015 25
Effects of Medical Students’ Communication Skills on Future Performance
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
CIS and ICE Scores of Step 2 CS
We accessed the students’ CIS and ICE scores of Step 2
through a collaboration with the NBME. The ICE subcompo-
nent is a composite score of data gathering and data interpre-
tation skills via both spoken and written communication.
Performance on the ICE subcomponent is rated by the stan-
dardized patients for the history taking and physical exami-
nation portion (via checklist), and by trained physician raters
for the patient note (via a 1–9 scale). The final ICE score is on
the standardized score scale, scaled to have a mean of zero
and SD of 1. The CIS subcomponent includes assessment of
the patient-centered communication skills of fostering the
relationship, gathering information, providing information,
helping the patient make a decision, and supporting emo-
tions. Examinees’ performance of the CIS subcomponent is
evaluated by the standardized patients. This component is
scored as a combination of three 1 to 9 scales, with final CIS
scores ranging from 3 to 27.12
PGY-1 Communication Skills Score
We collect PGY-1 data annually from PDs. The items in our
most recent survey were designed to parallel the six ACGME
competencies. Each spring we identify the programs where
our interns and residents are trained, and we mail the evalua-
tion forms for each trainee to the respective GME PDs. The
psychometric properties of this evaluation form were recently
investigated, and the results indicated reasonable validity and
reliability.13 The structure of the form suggested five factors
or subscales—Medical Expertise, Military-unique Practice,
Professionalism, System-based Practice, and Communication
and Interpersonal Skills. We used the CIS subscale score,
which was calculated as the average of the four items in this
subscale, as an outcome in the present study (hereafter
referred to as the “PGY-1 communication skills score”).
Statistical Analyses
First, we examined the descriptive statistics and the bivariate
correlations of all the measures included. Next, we conducted
multiple linear regression analyses to examine the predictive
power of the EEC score beyond the IM clerkship clinical
points and the average NBME Subject Exams score on the
outcome measures. The USU’s Institutional Review Board
provided ethical approval for the present study.
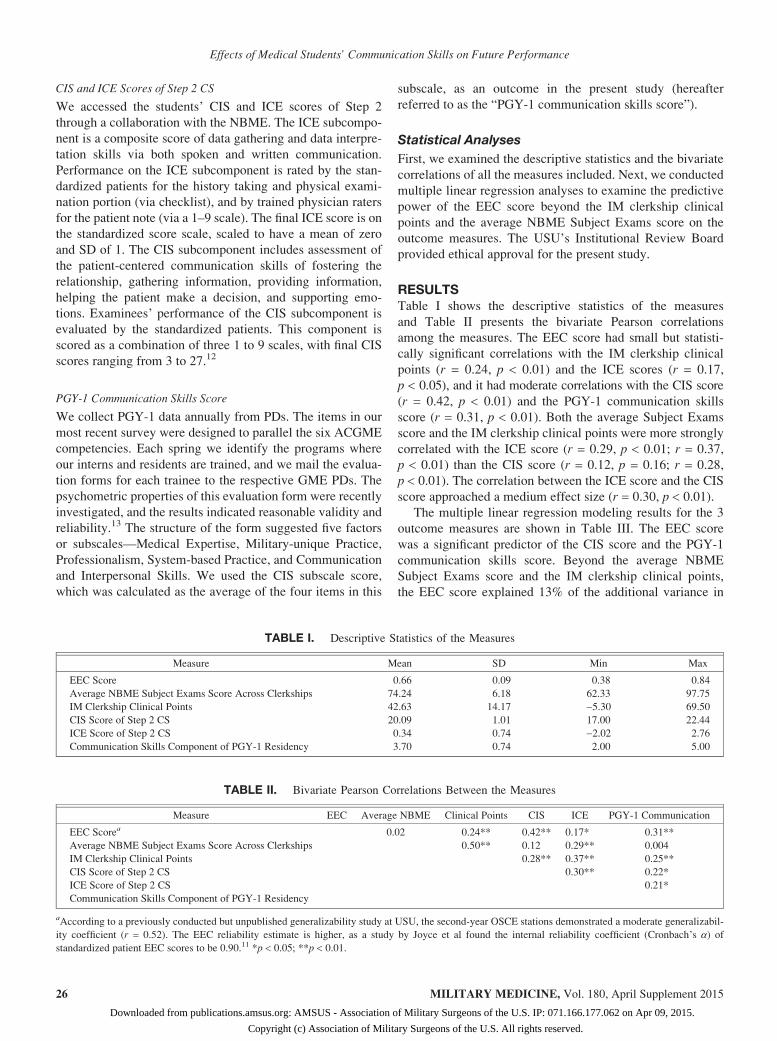
RESULTSTable I shows the descriptive statistics of the measures
and Table II presents the bivariate Pearson correlations
among the measures. The EEC score had small but statisti-
cally significant correlations with the IM clerkship clinical
points (r = 0.24, p < 0.01) and the ICE scores (r = 0.17,
p < 0.05), and it had moderate correlations with the CIS score
(r = 0.42, p < 0.01) and the PGY-1 communication skills
score (r = 0.31, p < 0.01). Both the average Subject Exams
score and the IM clerkship clinical points were more strongly
correlated with the ICE score (r = 0.29, p < 0.01; r = 0.37,
p < 0.01) than the CIS score (r = 0.12, p = 0.16; r = 0.28,
p < 0.01). The correlation between the ICE score and the CIS
score approached a medium effect size (r = 0.30, p < 0.01).
The multiple linear regression modeling results for the 3
outcome measures are shown in Table III. The EEC score
was a significant predictor of the CIS score and the PGY-1
communication skills score. Beyond the average NBME
Subject Exams score and the IM clerkship clinical points,
the EEC score explained 13% of the additional variance in
TABLE I. Descriptive Statistics of the Measures
Measure Mean SD Min Max
EEC Score 0.66 0.09 0.38 0.84
Average NBME Subject Exams Score Across Clerkships 74.24 6.18 62.33 97.75
IM Clerkship Clinical Points 42.63 14.17 −5.30 69.50
CIS Score of Step 2 CS 20.09 1.01 17.00 22.44
ICE Score of Step 2 CS 0.34 0.74 −2.02 2.76
Communication Skills Component of PGY-1 Residency 3.70 0.74 2.00 5.00
TABLE II. Bivariate Pearson Correlations Between the Measures
Measure EEC Average NBME Clinical Points CIS ICE PGY-1 Communication
EEC Scorea 0.02 0.24** 0.42** 0.17* 0.31**
Average NBME Subject Exams Score Across Clerkships 0.50** 0.12 0.29** 0.004
IM Clerkship Clinical Points 0.28** 0.37** 0.25**
CIS Score of Step 2 CS 0.30** 0.22*
ICE Score of Step 2 CS 0.21*
Communication Skills Component of PGY-1 Residency
aAccording to a previously conducted but unpublished generalizability study at USU, the second-year OSCE stations demonstrated a moderate generalizabil-
ity coefficient (r = 0.52). The EEC reliability estimate is higher, as a study by Joyce et al found the internal reliability coefficient (Cronbach’s a) ofstandardized patient EEC scores to be 0.90.11 *p < 0.05; **p < 0.01.
MILITARY MEDICINE, Vol. 180, April Supplement 201526
Effects of Medical Students’ Communication Skills on Future Performance
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

the CIS score and 6% additional variance in the PGY-1 com-
munication skills score. For the ICE score, 16% of the vari-
ance was accounted for by the average NBME Subject Exams
score and the IM clerkship clinical points, while the EEC
score explained only a modicum of additional variance (R2
change = 0.01). However, if we remove the EEC component
score from the overall OSCE score, the remainder of the
OSCE accounts for an additional 7% of the variance in the
ICE score.
DISCUSSIONThe aim of this study was to investigate the strength of the
association between students’ EEC OSCE performance at the
end of the preclerkship period and later communication skills
assessment and evaluation outcomes at both the UME and
GME level. The results demonstrate that the EEC score is a
strong predictor of the CIS score on Step 2 CS and a good
predictor of the PGY-1 communication skills score. These
findings provide fairly robust validity evidence for USU’s
EEC evaluation method. The use of a standardized approach
with a communication tool such as the EEC can help inform
future performance in communication skills independent of
other education outcomes. In the context of a longitudinal
curriculum, this information may better inform medical edu-
cators on learners’ communication capabilities and more
accurately direct future remediation efforts (there was approxi-
mately one year between EEC assessment and Step 2 CS
Exam and another 18 months to PGY-1 PDs evaluation).
As our results suggest, for the ICE score, the EEC was a
poor predictor. However, the average NBME Subject Exams
score, the IM clerkship clinical points, and the overall OSCE
score without the EEC component score were significantly
associated with this component. This finding indicates that
clinical knowledge as measured by the Subject Exams and
preceptor observations are better predictors of the ICE per-
formance. To some extent, what EEC tested was different
from the rest of the OSCE and this provides another piece of
construct validity evidence for our EEC assessment.
There are several important limitations of the present, single-
institution study. In particular, since the reliabilities of the EEC,
OSCE, IM clinical points, and PGY-1 factors do not reach the
levels adequate for high-stakes decisions, the correlations
between measures may have been weakened, thereby impacting
our ability to accurately calculate the adjusted correlation coef-
ficients. A larger sample size consisting of multiple classes of
students would also increase the generalizability of the findings.
In conclusion, our EEC assessment appears to be a good
predictor of students’ later performance on communication
skills evaluation of Step 2 CS and the first year of residency.
As such, this tool could be used as a sign of poor performance
of communication skills as early as the start of the third-year
clerkship where specific interventions can be effectively
applied and tested before graduation from medical school.
Future studies should focus on the longitudinal development
within individual domains on the EEC, and the impact this
may have future performance.
TABLE III. Multiple Linear Regression Models of the Outcomes
Explanatory Variables
Unstandardized Regression Coefficient Standardized Regression Coefficient R2 Change
CIS ICE PGY-1 CIS ICE PGY-1 CIS ICE PGY-1
Average NBME Subject Exams Score 0.004 0.02 −0.02 0.02 0.16 −0.14 0.08 0.16 0.08
IM Clerkship Clinical Points 0.01* 0.01** 0.01* 0.18 0.27 0.25
EEC score 3.87** 0.65 1.85** 0.37 0.09 0.25 0.13 0.01 0.06
*p < 0.05; **p < 0.01.
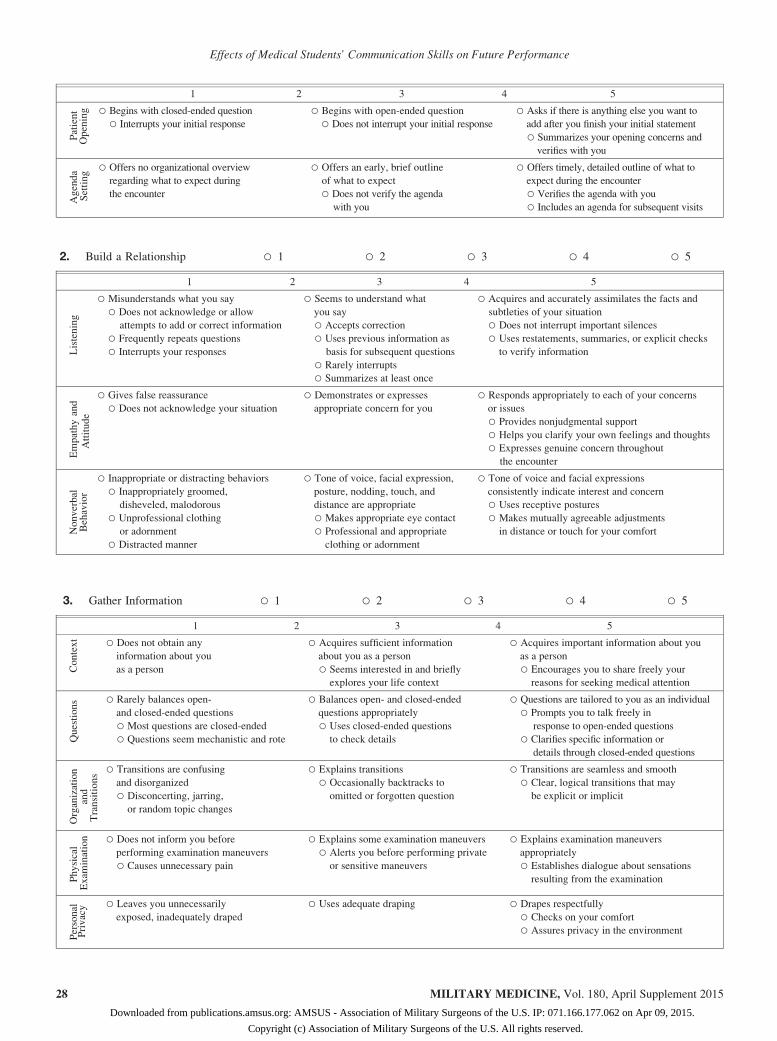
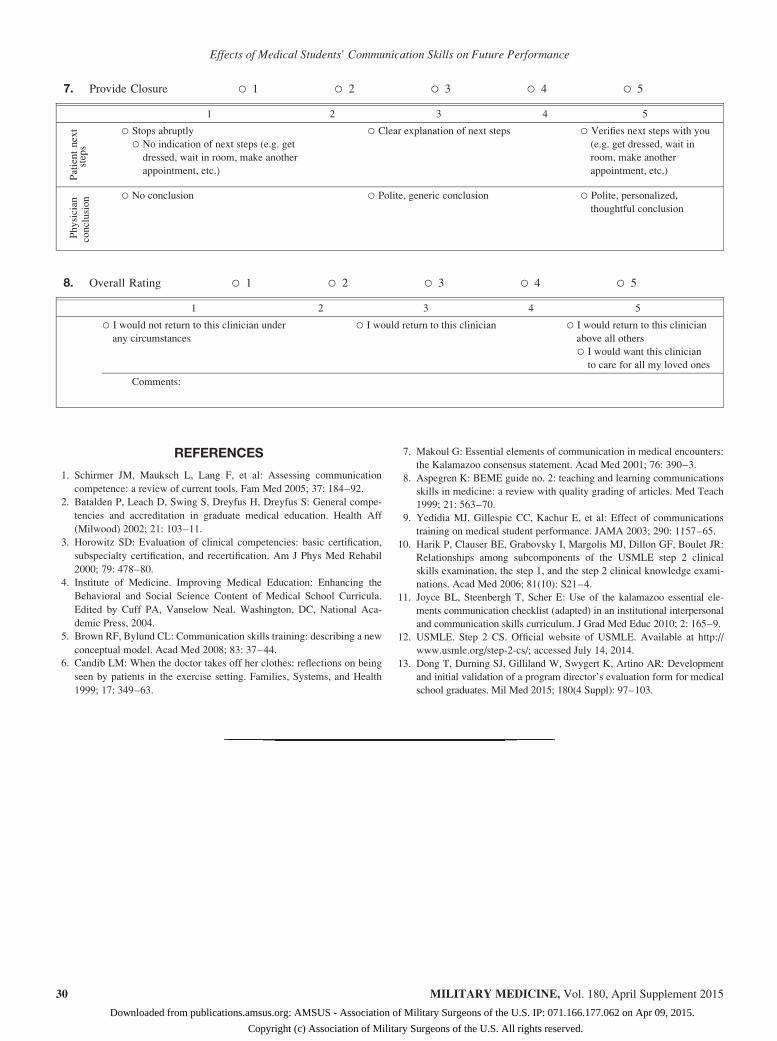
APPENDIX
Essential Elements of Communication Checklist—Adaption From the University of New Mexico Medical School,Communication Skills Competency Committee, November 2005
Evaluator ________________ Room ______ Time _________ Student Code ____________
Patient Name _____________________ Date _______
Essential Elements of Communication – Global Rating Scale 2005 (EEC – GRS)
1. Open the Discussion ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Introduction
○ No greeting
○ Does not call you by name
○ Initiates use of inappropriate variation
of your name
○ Inappropriate familiarity or informality
○ Does not identify self by name or title
○ Polite greeting
○ Calls you by or establishes your
appropriate name
○ Appropriate formality
○ Accurately introduces self with
full name and title
○ Personal greeting shows genuine interest
○ Displays welcoming nonverbal behavior
MILITARY MEDICINE, Vol. 180, April Supplement 2015 27
Effects of Medical Students’ Communication Skills on Future Performance
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
1 2 3 4 5
Patient
Opening ○ Begins with closed-ended question
○ Interrupts your initial response
○ Begins with open-ended question
○ Does not interrupt your initial response
○ Asks if there is anything else you want to
add after you finish your initial statement
○ Summarizes your opening concerns and
verifies with you
Agenda
Setting
○ Offers no organizational overview
regarding what to expect during
the encounter
○ Offers an early, brief outline
of what to expect
○ Does not verify the agenda
with you
○ Offers timely, detailed outline of what to
expect during the encounter
○ Verifies the agenda with you
○ Includes an agenda for subsequent visits
2. Build a Relationship ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Listening
○ Misunderstands what you say
○ Does not acknowledge or allow
attempts to add or correct information
○ Frequently repeats questions
○ Interrupts your responses
○ Seems to understand what
you say
○ Accepts correction
○ Uses previous information as
basis for subsequent questions
○ Rarely interrupts
○ Summarizes at least once
○ Acquires and accurately assimilates the facts and
subtleties of your situation
○ Does not interrupt important silences
○ Uses restatements, summaries, or explicit checks
to verify information
Empathyand
Attitude
○ Gives false reassurance
○ Does not acknowledge your situation
○ Demonstrates or expresses
appropriate concern for you
○ Responds appropriately to each of your concerns
or issues
○ Provides nonjudgmental support
○ Helps you clarify your own feelings and thoughts
○ Expresses genuine concern throughout
the encounter
Nonverbal
Behavior
○ Inappropriate or distracting behaviors
○ Inappropriately groomed,
disheveled, malodorous
○ Unprofessional clothing
or adornment
○ Distracted manner
○ Tone of voice, facial expression,
posture, nodding, touch, and
distance are appropriate
○ Makes appropriate eye contact
○ Professional and appropriate
clothing or adornment
○ Tone of voice and facial expressions
consistently indicate interest and concern
○ Uses receptive postures
○ Makes mutually agreeable adjustments
in distance or touch for your comfort
3. Gather Information ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Context ○ Does not obtain any
information about you
as a person
○ Acquires sufficient information
about you as a person
○ Seems interested in and briefly
explores your life context
○ Acquires important information about you
as a person
○ Encourages you to share freely your
reasons for seeking medical attention
Questions ○ Rarely balances open-
and closed-ended questions
○ Most questions are closed-ended
○ Questions seem mechanistic and rote
○ Balances open- and closed-ended
questions appropriately
○ Uses closed-ended questions
to check details
○ Questions are tailored to you as an individual
○ Prompts you to talk freely in
response to open-ended questions
○ Clarifies specific information or
details through closed-ended questions
Organization
and
Transitions
○ Transitions are confusing
and disorganized
○ Disconcerting, jarring,
or random topic changes
○ Explains transitions
○ Occasionally backtracks to
omitted or forgotten question
○ Transitions are seamless and smooth
○ Clear, logical transitions that may
be explicit or implicit
Physical
Exam
ination ○ Does not inform you before
performing examination maneuvers
○ Causes unnecessary pain
○ Explains some examination maneuvers
○ Alerts you before performing private
or sensitive maneuvers
○ Explains examination maneuvers
appropriately
○ Establishes dialogue about sensations
resulting from the examination
Personal
Privacy ○ Leaves you unnecessarily
exposed, inadequately draped
○ Uses adequate draping ○ Drapes respectfully
○ Checks on your comfort
○ Assures privacy in the environment
MILITARY MEDICINE, Vol. 180, April Supplement 201528
Effects of Medical Students’ Communication Skills on Future Performance
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
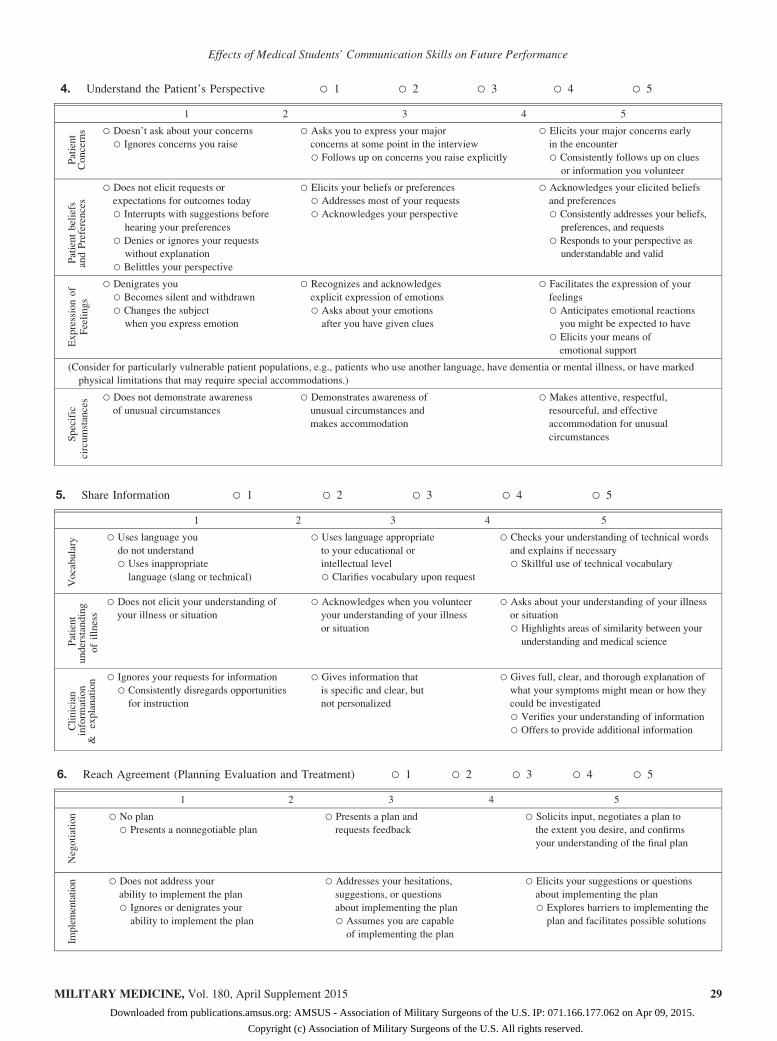
4. Understand the Patient’s Perspective ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Patient
Concerns ○ Doesn’t ask about your concerns
○ Ignores concerns you raise
○ Asks you to express your major
concerns at some point in the interview
○ Follows up on concerns you raise explicitly
○ Elicits your major concerns early
in the encounter
○ Consistently follows up on clues
or information you volunteer
Patientbeliefs
andPreferences
○ Does not elicit requests or
expectations for outcomes today
○ Interrupts with suggestions before
hearing your preferences
○ Denies or ignores your requests
without explanation
○ Belittles your perspective
○ Elicits your beliefs or preferences
○ Addresses most of your requests
○ Acknowledges your perspective
○ Acknowledges your elicited beliefs
and preferences
○ Consistently addresses your beliefs,
preferences, and requests
○ Responds to your perspective as
understandable and valid
Expressionof
Feelings
○ Denigrates you
○ Becomes silent and withdrawn
○ Changes the subject
when you express emotion
○ Recognizes and acknowledges
explicit expression of emotions
○ Asks about your emotions
after you have given clues
○ Facilitates the expression of your
feelings
○ Anticipates emotional reactions
you might be expected to have
○ Elicits your means of
emotional support
(Consider for particularly vulnerable patient populations, e.g., patients who use another language, have dementia or mental illness, or have marked
physical limitations that may require special accommodations.)
Specific
circumstances ○ Does not demonstrate awareness
of unusual circumstances
○ Demonstrates awareness of
unusual circumstances and
makes accommodation
○ Makes attentive, respectful,
resourceful, and effective
accommodation for unusual
circumstances
5. Share Information ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Vocabulary
○ Uses language you
do not understand
○ Uses inappropriate
language (slang or technical)
○ Uses language appropriate
to your educational or
intellectual level
○ Clarifies vocabulary upon request
○ Checks your understanding of technical words
and explains if necessary
○ Skillful use of technical vocabulary
Patient
understanding
ofillness
○ Does not elicit your understanding of
your illness or situation
○ Acknowledges when you volunteer
your understanding of your illness
or situation
○ Asks about your understanding of your illness
or situation
○ Highlights areas of similarity between your
understanding and medical science
Clinician
inform
ation
&explanation ○ Ignores your requests for information
○ Consistently disregards opportunities
for instruction
○ Gives information that
is specific and clear, but
not personalized
○ Gives full, clear, and thorough explanation of
what your symptoms might mean or how they
could be investigated
○ Verifies your understanding of information
○ Offers to provide additional information
6. Reach Agreement (Planning Evaluation and Treatment) ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Negotiation ○ No plan
○ Presents a nonnegotiable plan
○ Presents a plan and
requests feedback
○ Solicits input, negotiates a plan to
the extent you desire, and confirms
your understanding of the final plan
Implementation ○ Does not address your
ability to implement the plan
○ Ignores or denigrates your
ability to implement the plan
○ Addresses your hesitations,
suggestions, or questions
about implementing the plan
○ Assumes you are capable
of implementing the plan
○ Elicits your suggestions or questions
about implementing the plan
○ Explores barriers to implementing the
plan and facilitates possible solutions
MILITARY MEDICINE, Vol. 180, April Supplement 2015 29
Effects of Medical Students’ Communication Skills on Future Performance
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
REFERENCES
1. Schirmer JM, Mauksch L, Lang F, et al: Assessing communication
competence: a review of current tools. Fam Med 2005; 37: 184–92.
2. Batalden P, Leach D, Swing S, Dreyfus H, Dreyfus S: General compe-
tencies and accreditation in graduate medical education. Health Aff
(Milwood) 2002; 21: 103–11.
3. Horowitz SD: Evaluation of clinical competencies: basic certification,
subspecialty certification, and recertification. Am J Phys Med Rehabil
2000; 79: 478–80.
4. Institute of Medicine. Improving Medical Education: Enhancing the
Behavioral and Social Science Content of Medical School Curricula.
Edited by Cuff PA, Vanselow Neal. Washington, DC, National Aca-
demic Press, 2004.
5. Brown RF, Bylund CL: Communication skills training: describing a new
conceptual model. Acad Med 2008; 83: 37–44.
6. Candib LM: When the doctor takes off her clothes: reflections on being
seen by patients in the exercise setting. Families, Systems, and Health
1999; 17: 349–63.
7. Makoul G: Essential elements of communication in medical encounters:
the Kalamazoo consensus statement. Acad Med 2001; 76: 390–3.
8. Aspegren K: BEME guide no. 2: teaching and learning communications
skills in medicine: a review with quality grading of articles. Med Teach
1999; 21: 563–70.
9. Yedidia MJ, Gillespie CC, Kachur E, et al: Effect of communications
training on medical student performance. JAMA 2003; 290: 1157–65.
10. Harik P, Clauser BE, Grabovsky I, Margolis MJ, Dillon GF, Boulet JR:
Relationships among subcomponents of the USMLE step 2 clinical
skills examination, the step 1, and the step 2 clinical knowledge exami-
nations. Acad Med 2006; 81(10): S21–4.
11. Joyce BL, Steenbergh T, Scher E: Use of the kalamazoo essential ele-
ments communication checklist (adapted) in an institutional interpersonal
and communication skills curriculum. J Grad Med Educ 2010; 2: 165–9.
12. USMLE. Step 2 CS. Official website of USMLE. Available at http://
www.usmle.org/step-2-cs/; accessed July 14, 2014.
13. Dong T, Durning SJ, Gilliland W, Swygert K, Artino AR: Development
and initial validation of a program director’s evaluation form for medical
school graduates. Mil Med 2015; 180(4 Suppl): 97–103.
7. Provide Closure ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
Patientnext
steps
○ Stops abruptly
○ No indication of next steps (e.g. get
dressed, wait in room, make another
appointment, etc.)
○ Clear explanation of next steps ○ Verifies next steps with you
(e.g. get dressed, wait in
room, make another
appointment, etc.)
Physician
conclusion ○ No conclusion ○ Polite, generic conclusion ○ Polite, personalized,
thoughtful conclusion
8. Overall Rating ○ 1 ○ 2 ○ 3 ○ 4 ○ 5
1 2 3 4 5
○ I would not return to this clinician under
any circumstances
○ I would return to this clinician ○ I would return to this clinician
above all others
○ I would want this clinician
to care for all my loved ones
Comments:
MILITARY MEDICINE, Vol. 180, April Supplement 201530
Effects of Medical Students’ Communication Skills on Future Performance
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 071.166.177.062 on Apr 09, 2015.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.