Long-term outcome and post-treatment effects of psychoanalytic psychotherapy with young adults
17
Copyright © The British Psychological Society Reproduction in any form (including the internet) is prohibited without prior permission from the Society Long-term outcome and post-treatment effects of psychoanalytic psychotherapy with young adults Annika Lindgren 1,2 *, Andrzej Werbart 1,2 and Bjo ¨rn Philips 1,3 1 Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden 2 Institute of Psychotherapy, Stockholm County Council, Sweden 3 Centre for Dependency Disorders, Stockholm County Council, Sweden Objectives. The short- and long-term effects of open-ended, long-term psycho- analytic psychotherapy for young adults were investigated. Possible changes during the year and a half follow-up, as well as predictors of change, were explored. Design. Patients aged 18–25 years who accepted the offered psychoanalytic individual or group psychotherapy were included. Patients filled out questionnaires and were interviewed at intake, termination, and follow-up. Alliance data were collected after the second session of psychotherapy proper. Methods. The primary outcome measures were the Symptom Checklist-90 and the Inventory of Interpersonal Problems. The Helping Alliance Questionnaire-II was used to measure alliance. Mixed model ANOVAs were used to analyse changeover time and prediction of change in relation to gender, treatment format, treatment duration, and in individual psychotherapy, therapist- and patient-rated alliance. Results. All outcome measures changed significantly from intake to follow-up. None changed significantly during the follow-up period, but there was a tendency towards recurring symptoms and an improvement in one of the object relational measures during the follow-up. The latter was the only outcome measure that did not change significantly during treatment. Lower therapist-rated alliance was predictive of greater change in psychiatric symptoms for patients with high levels of symptoms at intake. Conclusions. The long-term effectiveness of psychoanalytic psychotherapy for young adults was supported. Low therapist-rated alliance implies that the therapists have identified problematic interactions, which might have mobilized their effort to solve the problems. Further research on cases reporting no gain or even deterioration is needed. Meta-analyses of psychotherapy outcome demonstrate that psychotherapy in general affects a diverse range of disorders and conditions (Doidge, 1997; Fonagy, Roth, & Higgitt, 2005). Earlier research indicates that different treatment modalities produce equivalent outcome (Lambert, Bergin, & Garfeild, 2004). All psychotherapy models are * Correspondence should be addressed to Annika Lindgren, Karolinska Institutet, Sektionen fo ¨r psykoterapi, Bjo ¨rnga ˚rdsgatan 25, S-118 56 Stockholm, Sweden (e-mail: [email protected]). The British Psychological Society 27 Psychology and Psychotherapy: Theory, Research and Practice (2010), 83, 27–43 q 2010 The British Psychological Society www.bpsjournals.co.uk DOI:10.1348/147608309X464422
Transcript of Long-term outcome and post-treatment effects of psychoanalytic psychotherapy with young adults

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Long-term outcome and post-treatment effects ofpsychoanalytic psychotherapy with young adults
Annika Lindgren1,2*, Andrzej Werbart1,2 and Bjorn Philips1,3
1Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden2Institute of Psychotherapy, Stockholm County Council, Sweden3Centre for Dependency Disorders, Stockholm County Council, Sweden
Objectives. The short- and long-term effects of open-ended, long-term psycho-analytic psychotherapy for young adults were investigated. Possible changes during theyear and a half follow-up, as well as predictors of change, were explored.
Design. Patients aged 18–25 years who accepted the offered psychoanalyticindividual or group psychotherapy were included. Patients filled out questionnaires andwere interviewed at intake, termination, and follow-up. Alliance data were collectedafter the second session of psychotherapy proper.
Methods. The primary outcome measures were the Symptom Checklist-90 and theInventory of Interpersonal Problems. The Helping Alliance Questionnaire-II was usedto measure alliance. Mixed model ANOVAs were used to analyse changeover time andprediction of change in relation to gender, treatment format, treatment duration, and inindividual psychotherapy, therapist- and patient-rated alliance.
Results. All outcome measures changed significantly from intake to follow-up. Nonechanged significantly during the follow-up period, but there was a tendency towardsrecurring symptoms and an improvement in one of the object relational measuresduring the follow-up. The latter was the only outcome measure that did not changesignificantly during treatment. Lower therapist-rated alliance was predictive of greaterchange in psychiatric symptoms for patients with high levels of symptoms at intake.
Conclusions. The long-term effectiveness of psychoanalytic psychotherapy for youngadults was supported. Low therapist-rated alliance implies that the therapists haveidentified problematic interactions, which might have mobilized their effort to solve theproblems. Further research on cases reporting no gain or even deterioration is needed.
Meta-analyses of psychotherapy outcome demonstrate that psychotherapy in general
affects a diverse range of disorders and conditions (Doidge, 1997; Fonagy, Roth, &
Higgitt, 2005). Earlier research indicates that different treatment modalities produce
equivalent outcome (Lambert, Bergin, & Garfeild, 2004). All psychotherapy models are
* Correspondence should be addressed to Annika Lindgren, Karolinska Institutet, Sektionen for psykoterapi, Bjorngardsgatan25, S-118 56 Stockholm, Sweden (e-mail: [email protected]).
TheBritishPsychologicalSociety
27
Psychology and Psychotherapy: Theory, Research and Practice (2010), 83, 27–43
q 2010 The British Psychological Society
www.bpsjournals.co.uk
DOI:10.1348/147608309X464422

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
intended to bring long-lasting effects, and a continued progression after treatment
termination is assumed in psychoanalytic theory (Dreher, 2002, p. 25). The same
desirable outcome should also apply to psychodynamic long-term psychotherapy, as it is
based on psychoanalytic theory. However, the research support for this theoretical
assumption is weak. Published studies of long-term effects of psychotherapy, all
naturalistic and quasi-experimental in design, have reported mixed results. A Swedishstudy of subsidized psychoanalytic treatments and psychoanalytic psychotherapies
reported a positive development from pre-treatment to follow-up with decreased levels
of psychiatric suffering during the post-treatment period (Blomberg, Lazar, & Sandell,
2001; Sandell et al., 2000), especially for patients in psychoanalysis. A German
retrospective study of a similar population found that between 70 and 80% of the
patients reported that their well-being had increased and that the change achieved
during treatment was stable during the post-treatment period (Leuzinger-Bohleber,
Stuhr, Ruger, & Beutel, 2003). A study that followed 62 patients in either long-termbehaviour therapy or long-term psychoanalytic psychotherapy found that both groups
decreased their levels of suffering during treatment and the gains remained over a 7-year
follow-up (Brockmann, Schluter, & Eckert, 2006). Interpersonal problems continued to
decrease during follow-up for patients who had been in psychoanalytic psychotherapy.
A 1-year follow-up of 23 patients in psychoanalytic therapy also revealed stable change
in psychiatric symptoms and a tendency towards improvement of interpersonal
problems over the follow-up period (Leichsenring, Biskup, Kreische, & Staats, 2005).
Also, an effectiveness study of open-ended psychodynamic psychotherapy revealed asignificant change during treatment, but due to attrition rates it was not possible to
analyse data beyond the first year from inclusion (Roseborough, 2006). A meta-analysis
of psychodynamic psychotherapies with duration of at least 1 year of treatment
identified 11 studies that reported follow-up data (Leichsenring & Rabung, 2008). The
meta-analysis found that the treatments produced large effect sizes and that treatment
gains seemed to be stable over the follow-up period. However, no formal tests of post-
treatment changes were conducted.
Only two studies specifically focusing on young adults, the target population of thepresent study, have been found. Positive change in self-rated problems from intake to
one year later was reported from community-based psychodynamic psychotherapy
including both adolescents and young adults (Baruch & Fearon, 2002). However, it is not
clear whether the patients were still in treatment at the 1-year follow-up, or if and when
they had terminated their psychotherapy. A study of adolescents and young adults
participating in an in-patient multi-treatment programme reported that increase of
complexity in object relations or schemas of self and significant others was related to
improvement in expert-rated general clinical functioning during treatment, but noinformation about post-treatment changes was presented (Blatt, Stayner, Auerbach, &
Behrends, 1996).
In the present study, we have tried to overcome the most recurrent critique among
psychoanalytic scholars against the common design of outcome studies (e.g. Blatt &
Zuroff, 2005; Kazdin, 2008; Schneider et al., 2002; Westen, Novotny, & Thompson-
Brenner, 2004). To increase the external validity, we have adopted a naturalistic stance.
The psychotherapies have been conducted in accordance with standard descriptions
and procedures of psychoanalytic psychotherapy without use of an explicit treatmentmanual, and the battery of instruments included measures of symptoms as well as
concepts central to psychoanalytic theory. Instead of using psychiatric diagnoses as
inclusion criteria, a developmental approach was adopted. Following the tradition from
28 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
child and adolescent psychotherapy, the present study focuses on psychotherapy for
young adults, ages 18–25. This is understood as a transitional period, when the young
individual leaves adolescence and forms his/her position and identity within adult
society. According to psychoanalytic developmental theory, this is the period when
intellectual and emotional capacities should consolidate in order to be able to meet the
demands of life and society. It is assumed that the encounter with life tasks andexistential questions might stir heightened levels of stress, especially when the
psychological development is interrupted or disturbed for some reason (Emde, 1985;
Escoll, 1987). In addition, young adults report higher levels and prevalence of
psychiatric problems than other groups of adults (Statistics Sweden, 2006).
When experimental restrictions are kept at a minimum, it is warranted to examine
other factors that might influence outcome in addition to the treatment. Some of the
commonly explored predictor variables of outcome in other patient samples, such as
patient– and therapist-rated alliance, gender, treatment duration, and individual versusgroup therapy seem reasonable for evaluating the present patient population. Alliance,
defined as the agreement on goals and tasks, and the emotional bond between the
therapist and the patient (Bordin, 1979), has been established as a robust predictor or
mediator of outcome (Horvath & Symonds, 1991; Martin, Garske, & Davis, 2000) in
psychotherapy for adult patients. Better agreement and quality of collaboration is
predictive of a better outcome. Gender and treatment modality in general have not been
associated with outcome (Burlingame, Fuhriman, & Mosier, 2003; Clarkin & Levy, 2004;
Fuhriman & Burlingame, 1994), that is women and men tend to profit equally frompsychotherapy, and no difference in effectiveness between individual and group
psychotherapy has been found. However, we do not know if this is the case in a
population of young adults. Owing to the disparate results in the literature about the
association between treatment duration and outcome (Feaster, Newman, & Rice, 2003;
Orlinsky, Ronnestad, & Willutzki, 2004), we included duration for evaluation.
The present study had three objectives: (1) to evaluate the short- and long-term effect
of psychoanalytic psychotherapy for young adults, (2) to evaluate maintenance and
further development of therapy gains after termination, and (3) to explore whethergender, treatment duration, treatment format (individual or group psychotherapy), and
patient- and therapist-rated alliance (only in individual psychotherapy) predicts and
moderates changes in psychiatric symptoms and level of interpersonal distress during
treatment and/or during the follow-up period. Two treatment modalities, individual and
group psychoanalytic psychotherapy were included in the present study. Even though
earlier research indicates that the two produce equivalent outcome, this does not mean
that the change processes or interventions leading to change are the same in group and
individual psychotherapy. In order to stay true to the complexity of this naturalisticstudy, we still decided to treat the outcome of both psychotherapy modalities as one
outcome. Psychotherapy modality was included in the analyses of possible predictors of
outcome. In order to facilitate comparisons with other studies on either individual or
group psychotherapy, we will include descriptive data and effect sizes for both
treatments separately on our two main outcome measures.
Method
This study uses data from the Young Adult Psychotherapy Project (YAPP), an ongoing
naturalistic, prospective, and longitudinal study of young adults in psychoanalytic
Long-term outcome for young adults 29

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
psychotherapy. The research project and the participants have been fully described
elsewhere (Philips, Wennberg, Werbart, & Schubert, 2006); we will provide a brief
overview here. All psychotherapies were conducted within the regular work at the
Institute of Psychotherapy, Stockholm County Council. Patients applied for
psychotherapy through a telephone service and were offered consultation with a
psychotherapist when a vacancy was available. A few patients were referred from thecounty council’s psychiatric out-patient clinics.
ParticipantsYAPP comprised 134 young adults, aged 18–25, who applied for psychotherapy. Age,
acceptance of the offered psychoanalytic psychotherapy, and providing informed
consent to participation in the study were the inclusion criteria. No exclusion criterion
was adopted. Seventy-three per cent of the participants were women, and mean age at
inclusion was 22 years (SD ¼ 2:2). There was a great variation in both type and number
of complaints expressed by the patients. Common complaints were depressiveness,
anxiety, interpersonal problems, and low self-esteem. Self-reports of suffering andexpert assessed functioning show that the patients were moderately suffering from
different symptoms at intake, while their capacities to describe themselves and
important others in a modulated way were quite good (see Table 2). Self-reported
personality disorders, in accordance with the DSM-IV and ICD-10 Personality
Questionnaire (DIP-Q; Ottosson et al., 1995, 1998), were found in 41 patients (31%),
which is a lower prevalence than has been reported in a recent study of adult patients in
psychiatric care in Stockholm (Noren et al., 2007).
AttritionDuring the inclusion period, 170 patients applying for psychotherapy fulfilled the age
criterion. Thirty-six patients did not enter the project, as they did not wish toparticipate, failed to appear for the initial sessions, or due to administrative error.
Drop-out was defined as a treatment shorter than 3 months. A time period shorter
than 3 months was chosen as the definition of drop-out since 10 to 12 sessions once a
week is a common length of psychodynamic short-term psychotherapy, and this project
did not include short-term psychotherapy as a treatment option. Sixteen patients
dropped out of psychotherapy, all during the first month of treatment, or did not reach a
treatment contract with their psychotherapists. There are more men than expected
among the drop-outs (37.5%) compared with among completers (26.1%). Neither agenor suffering at intake differed between the groups. Further analyses of predictors of
drop-out will be reported in a separate study (Roos, Wennberg, Philips, & Werbart,
2009).
Owing to the design with open-ended psychotherapies, three patients are still in
treatment at the time of the present study and are thus excluded from the analyses. Of
the remaining 131 patients, 115 came to the research evaluation at termination and 99
patients came to the follow-up 1.5 year post-treatment. Owing to internal missing data,
that is patients not answering all questions on all questionnaires, the N for the differentquestionnaires varies slightly with each measurement point.
Following a design of intention-to-treat, all patients with data at intake (except the
three still in psychotherapy) were included in the analyses. Accordingly, all proportions
were calculated with 131 as the sample population. The analyses of prediction of
30 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
outcome from alliance were based on all available ratings at the second session
following the contract agreement in individual psychotherapy, i.e. 69 patient ratings and
73 therapist ratings.
TreatmentsAll participants were offered either individual (N ¼ 92) or group psychoanalytic
psychotherapy (N ¼ 42). The treatment option depended on what modality was
available at the moment. No formal criterion for recommending either treatment was
formulated. However, if both group and individual therapy was available when a patient
called, a clinical decision on what to offer was made by the therapist receiving the call.
The psychotherapies were not manualized but were intended to be psycho-
analytically informed psychotherapies. The treatments in general aimed at helping the
young adults to overcome developmental arrests and to better handle strains in everydaylife. All therapists met every week in clinical teams, where treatment problems and
clinical experiences were discussed. There is no process data collected that makes it
possible to evaluate the therapists interventions, but it is obvious that both therapists
and patients are describing psychodynamic psychotherapies at the interviews at
termination and follow-up ( Johansson & Werbart, 2009; Lilliengren & Werbart, 2005).
Treatment duration was adapted to the needs of the individual patient and was
formalized in a written renegotiable contract between therapist and patient. Five
psychotherapy groups were conducted within the project. One of the groups was semi-open and open-ended, while the others were closed with a time frame of 1 or 1.5 years.
The patients stayed in treatment for an average of 19 months (SD ¼ 13:8,range ¼ 1–55).
PsychotherapistsThirty-seven different therapists were involved in this study, all with a psychoanalytic
orientation (26 female and 11 male). They represented various professionalbackgrounds: physicians (6), psychologists (14), social workers (15), or other (2).
Fifteen were psychoanalysts and licensed psychotherapists, 19 were licensed
psychotherapists, and 3 had basic training in psychodynamic psychotherapy. As to
their experience in psychotherapeutic work, the mean time from license for the 34
licensed psychotherapists was 10.3 years (median 12.5 years; range 1–15 years).
Individual therapy was conducted by 34 therapists (between 1 and 7 patients each) and
group therapy by 6 therapists. Most of the therapists had been working within a clinical
project aiming at developing and providing psychoanalytic psychotherapy for youngadults.
InstrumentsThree instruments were used to measure different aspects of symptoms and health:
Symptom Checklist-90 (SCL-90; Derogatis, 1994), a self-report questionnaire was
used to assess psychiatric symptoms experienced over the last 7 days. Items are rated on
five-point Likert-scales ranging from zero (‘not at all’) to four (‘very much’). The GlobalSeverity Index (GSI) was used for the analyses in this study. The SCL-90 demonstrates
adequate reliability (Derogatis, Rickels, & Rock, 1976) and for the Swedish translation a
Cronbach’s alpha of .97 has been reported (Fridell, Zvonomir, Johansson, & Malling
Thorsen, 2002).
Long-term outcome for young adults 31
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Self-rated health (SRH; Bjorner et al., 1996) is a single-item measure where the
respondent rates his/her present subjective mental and somatic health. The item is rated
on a seven-point Likert-scale ranging from one (‘very bad’) to seven (‘very good’). SRH
has been shown to be a good predictor of mortality and health problems (Heidrich,
Liese, Lowel, & Kiel, 2002; Larsson, Hemmingsson, Allebeck, & Lundberg, 2002; Mossey
& Shapiro, 1982; Shadbolt, Barresi, & Craft, 2002), and the item has shown good test–retest reliability in a previous study (r ¼ :92; Lorig et al., 1996).
Global Assessment of Functioning Scale (GAF; American Psychiatric Association,
1994) was used for measuring symptomatic and social functioning. The ratings were
based on interviews at intake, except for one-third of the group. Their ratings were
based on case presentations by the therapists. A group of trained raters did all
assessments, and consensus ratings were used in order to increase reliability of
assessments. An independent rater later rated 40 cases (approximately 10% of all cases
over the three time-points) and the intra-class correlation was ¼ .74.Three instruments were used to measure aspects of personality:
The Inventory of Interpersonal Problems (IIP; Horowitz, Rosenberg, Baer, Ureno, &
Villasenor, 1988) was used to measure the degree of interpersonal suffering. The 64
items circumplex version of IIP was used (Alden, Wiggins, & Pincus, 1990). Each item
was rated on five-point Likert-scales ranging from zero (‘not at all’) to four (‘very much’).
A later translation than the presently used has shown adequate psychometric properties
in a Swedish sample (Weinryb et al., 1996). The internal consistency (Cronbach’s alpha)
of the eight clusters in the present Swedish translation of IIP has been reported as .78to .91 (Rosander & Stiwne, 1997). The average of all items was calculated as a measure
of interpersonal distress.
The structural analysis of social behaviour intrex questionnaire (SASB; Benjamin,
1974, 1983) was used to assess levels of positive and negative self-concepts. The
instrument comprises 36 items about oneself rated on 11-point Likert-scales ranging
from 0 (‘not true’) to 100 (‘true’). The reported internal consistency of the Swedish
version of the questionnaire is . 0:90 for all of the subscales (Armelius, 2001).
Following Adamson and Lyxell (1996), means of clusters two through four and clusterssix through eight were used as indicators of positive and negative self-concepts.
The Differentiation-Relatedness of Self and Object Representations Scale (DRS;
Blatt & Auerbach, 2001; Diamond, Blatt, Steyner, & Kaslow, 1995) was used to evaluate
the degree of complexity and differentiation in cognitive-affective schemas of concepts
of self and others. The ratings were based on information obtained through the Object
Relation Inventory (Blatt, Wein, Chevron, & Quinlan, 1979; Diamond et al., 1995; Gruen
& Blatt, 1990). Each patient received independent ratings of representations of mother,
father, and him/herself. A group of trained raters made all assessments. A reliability studybased on part of the present material reported the inter-rater agreement as an intra-class
correlation of .71 (Hjalmdahl, Claesson, Werbart, & Levander, 2001). Consensus ratings
were used in order to increase reliability of assessments.
Finally, the Helping Alliance Questionnaire (HAq-II; Luborsky et al., 1996) was used
to measure both patient- and therapist-rated alliance in individual psychotherapy. The
instrument comprises 19 items rated on six-point Likert-scales ranging from one
(‘I strongly feel it is not true’) to six (‘I strongly feel it is true’). The HAq-II demonstrates
excellent reliability and good convergent validity with other alliance measures(Luborsky et al., 1996). The questionnaire was translated to Swedish by the principal
investigator of the present study and has been used in several studies, although no
psychometric data have been previously published. The internal consistency
32 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
(Cronbach’s alpha) of the Swedish version was .91 for the patient questionnaire and .88
for the therapist questionnaire in this sample.
ProceduresThe psychotherapists were free to accept or reject a patient based on assessment of the
patient’s motivation for treatment and a general idea about suitability for the specific
treatment modality. Only one patient was rejected. Every second patient who was
assigned to individual therapy (N ¼ 47 of 92) and all patients assigned to group therapy(N ¼ 42) underwent a research interview pre-therapy. All patients were interviewed at
termination and at follow-up 1.5 years after termination. All patients completed
background and personality questionnaires pre- and post-treatment as well as at the
follow-up. Alliance was measured every third month starting from the second
psychotherapy session. The information from patient questionnaires and research
interviews was not disclosed to the psychotherapists during the treatment.
Data analysisInspection of descriptive statistics of all measures at all time-points revealed a positively
skewed distribution pattern in GSI at termination and follow-up, and a negatively
skewed distribution in DRS at all three time-points. DRS was thus reflected and bothmeasures were then log-transformed before any analyses of outcome were performed.
To analyse outcome, a series of mixed model ANOVAs with one within fixed-factor
(time) was performed. GSI and IIP were chosen as the two primary outcome measures,
whereas the other measures were seen as secondary outcome measures. The variance
structure for analyses of all outcome measures was set to compound symmetry
heterogeneous based on Akaike’s information criterion and an inspection of estimated
variance components. Bonferroni correction of the alpha level was performed for the
repeated comparisons between time-points and across outcome variables. In order tokeep the familywise error at 5%, the alpha level was set to .003 for each separate
significance test.
Effect sizes of change were calculated for each measure and each time period (intake
to termination, termination to follow-up, and intake to follow-up) based on estimated
marginal means and standard deviation at intake obtained through the mixed model
analyses. Z-scores representing standardized values within each measure over the three
time-points were used to illustrate the amount of change in all measures.
In order to evaluate the obtained change, we compared the effect sizes with resultsfrom earlier published studies. Research on long-term psychodynamic psychotherapy is
scarce (Crits-Christoph & Barber, 2000). Only six studies with a mean treatment
duration exceeding 18 months were identified in a recently published meta-analysis of
long-term psychodynamic psychotherapy (Leichsenring & Rabung, 2008). For this
reason, the comparison was based on data from two meta-analyses on short-term
psychodynamic psychotherapy. Leichsenring, Rabung, and Leibing (2004) reported that
adult patients treated for a diverse range of psychiatric disorders achieved a within-
group effect size in the range of 0.80–0.95 for general psychiatric symptoms and socialfunctioning. The lower 95% confidence limits for these measures ranged from 0.56
to 0.65. Thus, we decided that effect sizes below 0.56 were small or modest, effect
sizes in the interval 0.56 to 0.95 were of medium size, whereas effect sizes above 0.95
where large.
Long-term outcome for young adults 33

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
To determine whether results at follow-up were equivalent to termination, we
used data from a meta-analysis of placebo or waiting list controls in randomized,
controlled studies of short-term psychodynamic psychotherapy (Leichsenring &
Rabung, 2006). An average effect size of 0.12 with a 95% confidence interval ranging
from 20.05 to 0.28 has been reported for these control groups. Effect sizes below
20.05 were interpreted as an indication of deterioration, whereas effect sizes greaterthan 0.28 were seen as indications of a tendency to improve. In addition, percentage
of improved patients was calculated based on the reliable change index (RCI;
Jacobson, Roberts, Berns, & McGlinchey, 1999; Jacobson & Truax, 1991) on GSI and
IIP. The RCI was chosen rather than the cut-off level of two standard deviations above
the mean of the norm group as a measure of clinically significant change, since
approximately 75% of the included patients in this study reported levels below this
cut-off at intake. Thus, they had no room to become clinically significantly changed.
The RCI was based on Cronbach’s alpha following recommendations from Evans,Margison, and Barkham (1998). A value above 1.96 was interpreted as a reliable
improvement, while a value below 21.96 was interpreted as a reliable deterioration.
The internal consistencies reported in the Swedish SCL-90 manual (Fridell et al.,
2002) and the Swedish IIP manual (Psykologiforlaget, 2002) were used to calculate
the RCI of GSI and IIP.
Finally, in order to further explore the outcome, analyses of the association between
change in the two primary outcome measures (GSI and IIP) and possible predictors of
change were performed. The mixed model analyses were rerun with one predictorvariable included at a time. The interaction between predictors and time was analysed
through a piecewise model that divided time into two periods, during treatment and
during follow-up (Schwartz, 1993), since the analyses of outcome indicated a difference
in rate of change during and after psychotherapy. The predictor variables were gender,
duration of treatment, treatment modality (individual or group psychotherapy), patient-
rated alliance, and therapist-rated alliance in individual psychotherapy. The analyses
were rerun with intake level of the dependent variable added as a covariate to the
analyses whenever a significant predictor was found. This was done in order to checkwhether intake level explained the significant results. No correction of alpha-level was
adapted to these exploratory analyses.
Results
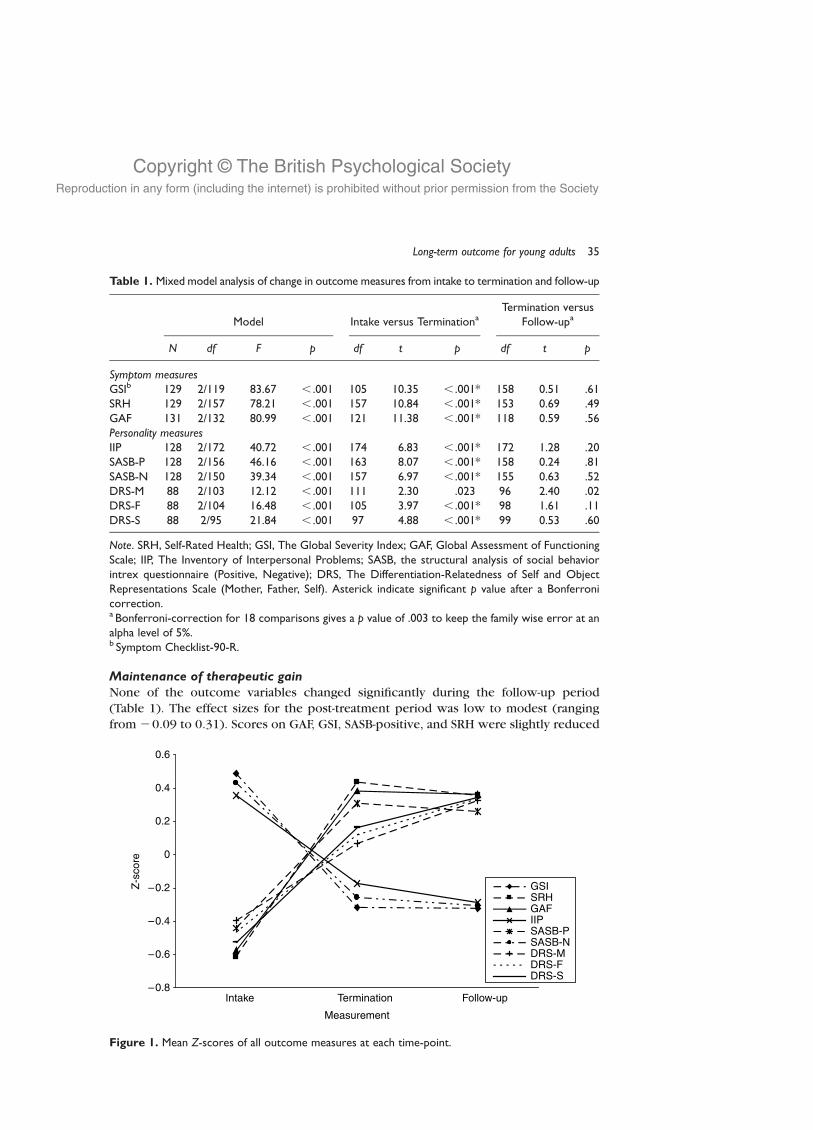
Short- and long-term outcomeThe mixed model analyses showed that eight of nine outcome measures were
significantly changed at termination, and by follow-up all nine outcome variables were
significantly changed (Table 1 and Figure 1). Effect sizes of change during treatment
were modest to high, whereas the effect sizes of change from intake to follow-up were
medium to high (Tables 2 and 3).
Based on the RCI cut-off scores, 66 patients (50.4%) showed significant improvement
from intake to follow-up, whereas five patients (3.8%) showed impairment in severity on
the GSI. Concerning interpersonal problems (IIP), 46 patients (35.1%) showedimprovement and 6 patients (4.6%) deteriorated by follow-up. The corresponding
numbers for change between intake to termination were 58 patients (44.3%) improved
and 8 patients (6.1%) deteriorated on the GSI, and 41 patients (31.3%) improved and
4 patients (3.1%) deteriorated on the IIP.
34 Annika Lindgren et al.
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Maintenance of therapeutic gainNone of the outcome variables changed significantly during the follow-up period
(Table 1). The effect sizes for the post-treatment period was low to modest (ranging
from 20.09 to 0.31). Scores on GAF, GSI, SASB-positive, and SRH were slightly reduced
Table 1. Mixed model analysis of change in outcome measures from intake to termination and follow-up
Model Intake versus TerminationaTermination versus
Follow-upa
N df F p df t p df t p
Symptom measuresGSIb 129 2/119 83.67 , .001 105 10.35 , .001* 158 0.51 .61SRH 129 2/157 78.21 , .001 157 10.84 , .001* 153 0.69 .49GAF 131 2/132 80.99 , .001 121 11.38 , .001* 118 0.59 .56Personality measuresIIP 128 2/172 40.72 , .001 174 6.83 , .001* 172 1.28 .20SASB-P 128 2/156 46.16 , .001 163 8.07 , .001* 158 0.24 .81SASB-N 128 2/150 39.34 , .001 157 6.97 , .001* 155 0.63 .52DRS-M 88 2/103 12.12 , .001 111 2.30 .023 96 2.40 .02DRS-F 88 2/104 16.48 , .001 105 3.97 , .001* 98 1.61 .11DRS-S 88 2/95 21.84 , .001 97 4.88 , .001* 99 0.53 .60
Note. SRH, Self-Rated Health; GSI, The Global Severity Index; GAF, Global Assessment of FunctioningScale; IIP, The Inventory of Interpersonal Problems; SASB, the structural analysis of social behaviorintrex questionnaire (Positive, Negative); DRS, The Differentiation-Relatedness of Self and ObjectRepresentations Scale (Mother, Father, Self). Asterick indicate significant p value after a Bonferronicorrection.a Bonferroni-correction for 18 comparisons gives a p value of .003 to keep the family wise error at analpha level of 5%.b Symptom Checklist-90-R.
Figure 1. Mean Z-scores of all outcome measures at each time-point.
Long-term outcome for young adults 35
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
during follow-up. The change was greater than an effect size of 2 .05 for GAF, GSI,
and SRH, which indicated a tendency towards deterioration. The change in positive
direction for DRS-mother was large enough to support a conclusion that the results
at termination and follow-up were not equivalent, even though the difference was
not significant.
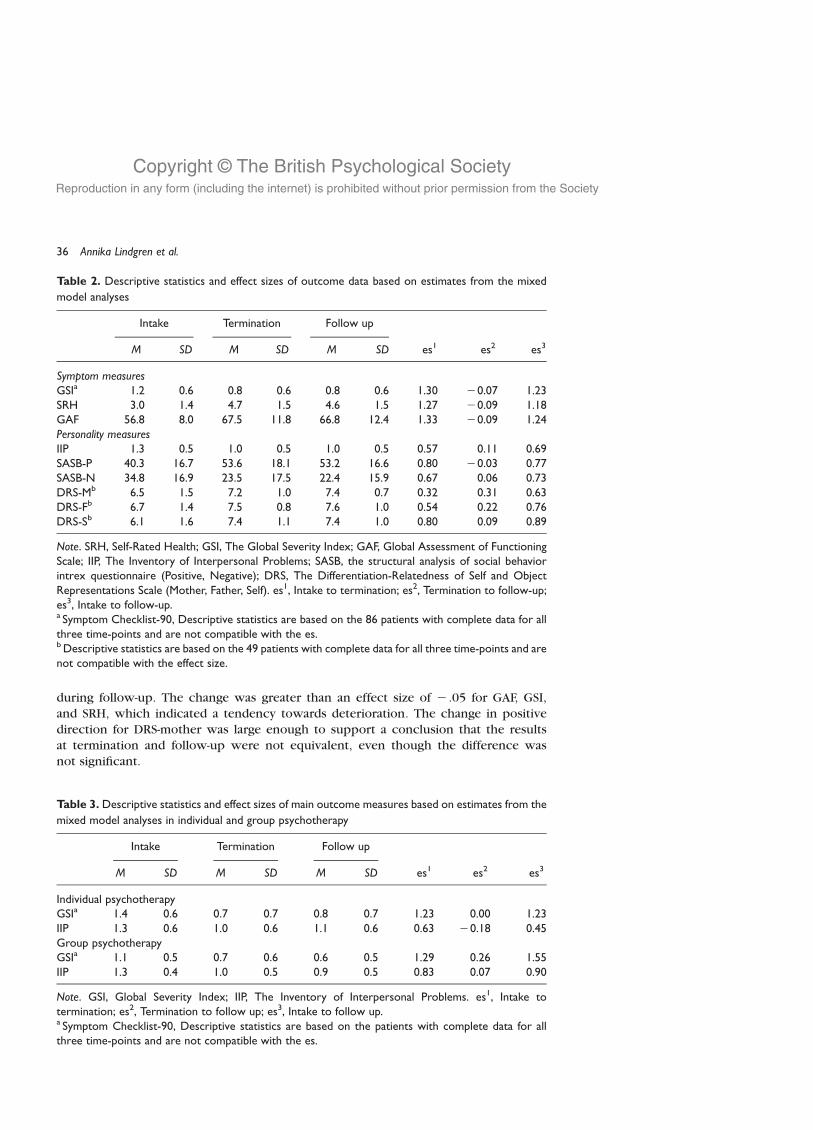
Table 2. Descriptive statistics and effect sizes of outcome data based on estimates from the mixed
model analyses
Intake Termination Follow up
M SD M SD M SD es1 es2 es3
Symptom measuresGSIa 1.2 0.6 0.8 0.6 0.8 0.6 1.30 20.07 1.23SRH 3.0 1.4 4.7 1.5 4.6 1.5 1.27 20.09 1.18GAF 56.8 8.0 67.5 11.8 66.8 12.4 1.33 20.09 1.24Personality measuresIIP 1.3 0.5 1.0 0.5 1.0 0.5 0.57 0.11 0.69SASB-P 40.3 16.7 53.6 18.1 53.2 16.6 0.80 20.03 0.77SASB-N 34.8 16.9 23.5 17.5 22.4 15.9 0.67 0.06 0.73DRS-Mb 6.5 1.5 7.2 1.0 7.4 0.7 0.32 0.31 0.63DRS-Fb 6.7 1.4 7.5 0.8 7.6 1.0 0.54 0.22 0.76DRS-Sb 6.1 1.6 7.4 1.1 7.4 1.0 0.80 0.09 0.89
Note. SRH, Self-Rated Health; GSI, The Global Severity Index; GAF, Global Assessment of FunctioningScale; IIP, The Inventory of Interpersonal Problems; SASB, the structural analysis of social behaviorintrex questionnaire (Positive, Negative); DRS, The Differentiation-Relatedness of Self and ObjectRepresentations Scale (Mother, Father, Self). es1, Intake to termination; es2, Termination to follow-up;es3, Intake to follow-up.a Symptom Checklist-90, Descriptive statistics are based on the 86 patients with complete data for allthree time-points and are not compatible with the es.b Descriptive statistics are based on the 49 patients with complete data for all three time-points and arenot compatible with the effect size.
Table 3. Descriptive statistics and effect sizes of main outcome measures based on estimates from the
mixed model analyses in individual and group psychotherapy
Intake Termination Follow up
M SD M SD M SD es1 es2 es3
Individual psychotherapyGSIa 1.4 0.6 0.7 0.7 0.8 0.7 1.23 0.00 1.23IIP 1.3 0.6 1.0 0.6 1.1 0.6 0.63 20.18 0.45Group psychotherapyGSIa 1.1 0.5 0.7 0.6 0.6 0.5 1.29 0.26 1.55IIP 1.3 0.4 1.0 0.5 0.9 0.5 0.83 0.07 0.90
Note. GSI, Global Severity Index; IIP, The Inventory of Interpersonal Problems. es1, Intake totermination; es2, Termination to follow up; es3, Intake to follow up.a Symptom Checklist-90, Descriptive statistics are based on the patients with complete data for allthree time-points and are not compatible with the es.
36 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Eighty-six patients completed the GSI and IIP at all three time-points. Thirty-nine
(29.8% of 131 included patients) reported a significant improvement in GSI scores at
both termination and follow-up, whereas 9 patients (6.9%) had lost their significant
improvement from termination to follow-up, and 16 patients (12.2%) had values above
the critical value of RCI 1.96 at follow-up but not at termination. The corresponding
numbers for IIP were 28 patients (21.4%) with stable improvement, 4 patients (3.1%)had lost their significant improvement, and 11 (8.4%) had reached a significant
improvement at follow-up.
Predictors and moderators of changeTherapist-rated alliance measured after session 2 was significantly related to change in
SCL-90 GSI during treatment (F½1; 122� ¼ 4:76, p ¼ :03), whereas a tendency towards asignificant association was found for patient-rated alliance in relation to the same
measure (F½1; 114� ¼ 3:67, p ¼ :06). The association between therapist-rated alliance
and change in SCL-90 GSI was negative, that is, lower levels of therapist-rated alliance
were related to greater change. The association between patient-rated alliance and
change in SCL-90 GSI showed a reversed pattern, that is, higher level of patient-rated
alliance was related to greater change in SCL-90 GSI. The tendency towards significant
association between patient-rated alliance and change in SCL-90 GSI was lost when the
intake level of SCL-90 GSI was added as a covariate to the analyses (F½1; 127� ¼ 0:968,p ¼ :33). When the same was done with therapist-rated alliance as a moderator, a three-
way interaction was found in relation to change in SCL-90 GSI during treatment
(F½1; 144� ¼ 4:274, p ¼ :04). A median split based on intake level of SCL-90 GSI showed
that the negative association between therapist-rated alliance and change in psychiatric
symptoms was significant for patients with higher ratings on SCL-90 GSI at intake
(r ¼ 2:36), but no association was found in the group of patients with lower ratings
(r ¼ :01). A significant negative main effect was found for treatment duration in relation
to IIP (F½1; 172� ¼ 4:12, p ¼ :04), meaning that patients with lower average levels ofinterpersonal distress over all three time-points stayed longer in treatment, but
treatment duration was not related to change in interpersonal distress. Neither gender,
treatment duration, nor treatment format (individual or group psychotherapy)
predicted changes on GSI and IIP up to termination or follow-up.
Discussion
The long-term effectiveness of psychoanalytic psychotherapy for young adults was
supported in the present study. There was a significant positive change in all nine
outcome variables from intake to follow-up. All outcome measures except one changed
significantly during treatment, and none of the measures changed significantly from
termination to follow-up. The rating of differentiation-relatedness in object
representation of mother changed significantly from intake to follow-up, but not
during the treatment or follow-up period separately. Effect sizes of change in alloutcome measures during treatment were moderate to high, and modest or negligible
for change during the follow-up period. An indication of recurring psychiatric symptoms
and health problems during the follow-up period was found, as well as an indication for
continued progression for one of the object relation measures. Reliable improvement of
psychiatric symptoms at follow-up was achieved by approximately 50% of the patients
Long-term outcome for young adults 37

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
while on a measure of interpersonal problems, 35% of patients showed reliable
improvement.
Lower levels of therapist-rated alliance predicted greater change in psychiatric
symptoms for patients with high levels of psychiatric symptoms at intake. A tendency
towards an association between higher patient-rated alliance and change in psychiatric
symptoms was found. None of the other possible predictors were associated withchanges in psychiatric symptoms or interpersonal distress.
The major limitation of this study is also its main asset, i.e. its naturalistic design. This
approach facilitates optimization of external validity, but the lack of a comparison group
makes it impossible to rule out the time effect. The treatment model in this study
conceptualized the patients’ problems as arrests in development, and all gains could be
true effects of maturation rather than treatment effects. However, effect sizes were
comparable to within-group effect sizes usually reported in randomized controlled
studies of short-term treatments (Leichsenring et al., 2004) and they exceed the upperlimit of the confidence interval for change occurring in psychiatric patients participating
in control groups not receiving specific treatment. This supports the conclusion that the
results presently reported are true treatment effects. In addition, the broken line of
development in almost all outcome measures illustrates a difference in amount
of change during and after treatment, which indicates that the psychotherapies have had
an effect on outcome. However, the results need to be replicated.
The theoretical assumption of continued development and improvement after
treatment termination could not be supported. In accordance with findings on short-term psychodynamic psychotherapy (Leichsenring et al., 2004), the therapeutic gains
were maintained during the follow-up. However, while lacking statistical significance,
not all variables were equivalent at termination and follow-up. Effect sizes indicated that
symptom variables displayed the most change during treatment, and a slight recurrence
of problems was in evidence. Object relational variables changed least during treatment
but continued to develop slightly, whereas measures of self-image and interpersonal
problems remained stable during the follow-up period. These results agree with
psychological theory in that symptoms are generally understood to be reactive andcontextually dependent, whereas character or personality can be understood as a
quality of functioning or ability (see e.g. Kopta, Howard, Lowery, & Beutler, 1994). Once
achieved it is either stable or continues to develop.
The present study replicated earlier results indicating that alliance moderates
outcome, whereas it has been hard to identify other consistently significant predictors
of outcome. Gender and treatment format were not associated with change in either
psychiatric symptoms or interpersonal distress, which is in accordance with earlier
findings (Clarkin & Levy, 2004). Treatment duration has sometimes been associated withoutcome and sometimes not (Orlinsky et al., 2004); however, in the current study it was
not predictive of change in either psychiatric symptoms or interpersonal distress.
A shortcoming of the present study is the lack of outcome data during treatment. The
collection of such data would have made it possible for us to evaluate the pattern of
change during the treatment, and it would have given us a possibility to evaluate if it had
been sufficient with shorter treatments than the ones given. An additional limitation of
the present study is the lack of adherence data that would have assured treatment
fidelity.Patients with lower levels of interpersonal distress stayed longer than others in
psychotherapy. Perhaps, patients with less problematic interpersonal experiences
endure the interaction with their psychotherapists better, regardless of treatment
38 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
outcome. An earlier study has reported that the presence of any personality disorder on
the one hand, and higher adaptive defensive style on the other hand, predicted longer
treatments (Perry, Bond, & Roy, 2007).
The tendency towards significant association between patient-rated alliance and
change in psychiatric symptoms during treatment went in the expected direction
(Martin et al., 2000), which supports the validity of the present translation of the HAq-II.The association was lost, however, when we controlled for the patients’ intake level of
psychiatric symptoms. Due to lack of data it was not possible to check whether early
symptom change from intake until the second session predicted the early patient-rated
alliance, which has been observed by others (Barber, Connolly, Crits-Christoph, Gladis,
& Siqueland, 2000; DeRubeis & Feeley, 1990; Feeley, DeRubeis, & Gelfand, 1999). More
studies investigating this pattern of alliance and symptom change are needed, not least
in adolescents and young adults.
Lower therapist-rated alliance predicted greater change in psychiatric suffering forpatients reporting more psychiatric symptoms at intake, which is a paradox. We do not
have other process data that could help us explain the finding, but one plausible
explanation is related to the theory of alliance rupture (eg. Safran, Muran, Samstag, &
Stevens, 2002). Therapeutic alliance has been one of the top issues within the research
community as well as within the clinical society during the last two decades. Low alliance
ratings means that the therapists have identified problematic interactions, which might
havemobilized their effort to solve theproblems. If thiswas the case, itwould also be easier
for the therapists to identify problematic interactions with patients that suffered more.To summarize, we found significant changes in all outcome measures from intake to
follow-up. Changing the perspective from variables to individuals, we found that the
majority of patients reported reduced levels of psychiatric symptoms and interpersonal
problems, and between 35 and 50% displayed statistically significant improvement at
either termination and/or follow-up. This supports the effectiveness of long-term
psychoanalytic psychotherapy for young adults both in the short and the long
perspective. However, a small group of patients got worse from intake to follow-up,
which should not be ignored. Further research on cases reporting no gain or evendeterioration is needed if we as clinicians are to be able to recommend treatment for a
specific patient.
Acknowledgements
The project was supported by grants from the Bank of Sweden, Tercentenary Foundation and the
Research and Development Secretariat at Stockholm County Council. The project has been
approved by the Regional Research Ethics Committee at the Karolinska Institutet, and all
participants have given their informed consent.
References
Adamson, L., & Lyxell, B. (1996). Self-concept and questions of life: Identity development during
late adolescence. Journal of Adolescence, 19, 569–582.
Alden, L. E., Wiggins, J. S., & Pincus, A. L. (1990). Construction of circumplex scales for the
inventory of interpersonal problems. Journal of Personality Assessment, 55, 521–536.
American Psychiatric Association (1994). Diagnostical and statistical manual of mental
disorders (4th ed.). Washington, DC: Author.
Long-term outcome for young adults 39
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Armelius, K. (2001). Reliabilitet och validitet for den svenska versionen av SASB –
sjalvbildstestet (Reliability and validity for the Swedish version of SASB – the self image
test). Unpublished manuscript.
Barber, J. P., Connolly, M. B., Crits-Christoph, P., Gladis, L., & Siqueland, L. (2000). Alliance predicts
patients’ outcome beyond in-treatment change in symptoms. Journal of Consulting and
Clinical Psychology, 68, 1027–1032.
Baruch, G., & Fearon, P. (2002). The evaluation of mental health outcome at a community-based
psychodynamic psychotherapy service for young people: A 12-month follow-up based on self-
report data. Psychology and Psychotherapy: Theory, Research and Practice, 75, 261–278.
Benjamin, L. S. (1974). Structural analysis of social behavior. Psychological Review, 81, 392–425.
Benjamin, L. S. (1983). The Intrex user the ’s manual, part I and II. Madison, WI: Intrex
Interpersonal Institute, (Computer program manual).
Bjorner, J. B., Sondergaard Kristensen, T., Orth-Gomer, K., Tibblin, G., Sullivan, M., & Westerholm,
P. (1996). Self-rated health: A useful concept in research, prevention and clinical medicine.
No. 96:9. Stockholm: Swedish Council for Planning and Coordination of Research (FRN).
Blatt, S. J., & Auerbach, J. S. (2001). Mental representation, severe psychopathology, and the
therapeutic process. Journal of the American Psychoanalytic Association, 49, 113–159.
Blatt, S. J., Stayner, D. A., Auerbach, J. S., & Behrends, R. S. (1996). Change in object and self-
representations in long-term, intensive, inpatient treatment of seriously disturbed adolescents
and young adults. Psychiatry: Interpersonal and Biological Processes, 59, 82–107.
Blatt, S. J., Wein, S. J., Chevron, E., & Quinlan, D. M. (1979). Parental representations and
depression in normal young adults. Journal of Abnormal Psychology, 88, 388–397.
Blatt, S. J., & Zuroff, D. C. (2005). Empirical evaluation of the assumptions in identifying evidence
based treatments in mental health. Clinical Psychology Review, 25, 459–486.
Blomberg, J., Lazar, A., & Sandell, R. (2001). Long-term outcome of long-term psychoanalytically
oriented therapies: First findings of the Stockholm outcome of psychotherapy and
psychoanalysis study. Psychotherapy Research, 11, 361–382.
Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working alliance.
Psychotherapy: Theory, Research and Practice, 16, 252–260.
Brockmann, J., Schluter, T., & Eckert, J. (2006). Langzeitwirkungen psychoanalytischer und
verhaltenstherapeutischer langzeitpsychotherapien: Eine vergleichende studie aus der praxis
niedergelassener psychotherapeuten [Long-term effects of long-term psychoanalytic and long-
term behavior therapy. A comparative study from the general practices of psychotherapists].
Psychotherapeut, 51, 15–25.
Burlingame, G. M., Fuhriman, A., & Mosier, J. (2003). The differential effectiveness of group
psychotherapy: A meta-analytic perspective. Group Dynamics: Theory, Research, and
Practice, 7, 3–12.
Clarkin, J. F., & Levy, K. N. (2004). The influence of client variables on psychotherapy. In M. J.
Lambert (Ed.), Bergin and Garfield’s handbook of psychoterapy and behavior change
(pp. 194–226). New York: Wiley.
Crits-Christoph, P., & Barber, J. P. (2000). Long-term psychotherapy. In C. R. Snyder & R. E. Ingram
(Eds.), Handbook of psychological change: Psychotherapy processes and practices for the
21st century (pp. 455–473). New York: Wiley.
Derogatis, L. R. (1994). Symptom-Checklist-90-R: Administration, scoring and procedures
manual (3rd ed., revised). Minneapolis: National Computer Systems.
Derogatis, L. R., Rickels, K., & Rock, A. F. (1976). The SCL-90 and the MMPI: A step in the validation
of a new self-report scale. British Journal of Psychiatry, 128, 280–289.
DeRubeis, R. J., & Feeley, M. (1990). Determinants of change in cognitive therapy for depression.
Cognitive Therapy and Research, 14, 469–482.
Diamond, D., Blatt, S. J., Steyner, D., & Kaslow, N. (1995). Differentiation-relatedness of self and
object representations. Revised scale. Unpublished research manual, New Haven, CT.
Doidge, N. (1997). Empirical evidence for the efficacy of psychoanalytic psychotherapies and
psychoanalysis: An overview. Psychoanalytic Inquiry, 17(Suppl.), 102–150.
40 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Dreher, U. (2002). What are the aims of psychoanalysis? In M. Leuzinger-Bohleber & M. Target
(Eds.), Outcomes of psychoanalytic treatment: Perspectives for therapists and researchers
(pp. 17–29). London: Whurr Publishers.
Emde, R. N. (1985). From adolescence to midlife: Remodelling the structure of adult development.
Journal of the American Psychoanalytic Association, 33, 59–112.
Escoll, P. J. (1987). Psychoanalysis of young adults: An overview. Psychoanalytic Inquiry, 7, 5–30.
Evans, C., Margison, F., & Barkham, M. (1998). The contribution of reliable and clinically
significant change methods to evidence-based mental health. Evidence-Based Mental Health,
1, 70–72.
Feaster, D. J., Newman, F. L., & Rice, C. (2003). Longitudinal analysis when the experimenter does
not determine when treatment ends: What is dose–response? Clinical Psychology and
Psychotherapy, 10, 352–360.
Feeley, M., DeRubeis, R. J., & Gelfand, L. A. (1999). The temporal relation of adherence and
alliance to symptom change in cognitive therapy for depression. Journal of Consulting and
Clinical Psychology, 67, 578–582.
Fonagy, P., Roth, A., & Higgitt, A. (2005). Psychodynamic psychotherapies: Evidence-based
practice and clinical wisdom. Bulletin of the Menninger Clinic, 69, 1–58.
Fridell, M., Zvonomir, C., Johansson, M., & Malling Thorsen, S. (2002). SCL-90. Svensk normering,
standardisering och validering av symtomskalan. (Swedish standardization and
validation of SCL-90). Stockholm: Statens Institutionsstyrelse.
Fuhriman, A., & Burlingame, G. M. (1994). Group psychotherapy: Research and practice. In
A. Fuhriman & G. M. Burlingame (Eds.), Handbook of group psychotherapy: An emprical and
clinical synthesis (pp. 3–40). New York: Wiley.
Gruen, R. J., & Blatt, S. J. (1990). Change in self- and object representation during long-term
dynamically oriented treatment. Psychoanalytic Psychology, 7, 399–422.
Heidrich, J., Liese, A. D., Lowel, H., & Kiel, U. (2002). Self-rated health and it’s relation to all-cause
and cardiovascular mortality in southern Germany. Annual Epidemiology, 12, 338–345.
Hjalmdahl, Y., Claesson, M., Werbart, A., & Levander, S. (2001). Bedomning av differentiering-
relaterande i sjalv-och objektrepresentationer I: En validitetsstudie. [Differentiation-
relatedness of self and object relations I: Validity of the Swedish version]. No. 20. Stockholm:
Institute of Psychotherapy and Psychotherapy Section at Karolinska Institutet.
Horowitz, L. M., Rosenberg, S. E., Baer, B. A., Ureno, G., & Villasenor, V. S. (1988). Inventory of
interpersonal problems: Psychometric properties and clinical applications. Journal of
Consulting and Clinical Psychology, 56, 885–892.
Horvath, A. O., & Symonds, B. (1991). Relation between working alliance and outcome in
psychotherapy: A meta-analysis. Journal of Counseling Psychology, 38, 139–149.
Jacobson, N. S., Roberts, L. J., Berns, S. B., & McGlinchey, J. B. (1999). Methods for defining and
determining the clinical significance of treatment effects: Description, application, and
alternatives. Journal of Consulting and Clinical Psychology, 67, 300–307.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining
meaningful change in psychotherapy research. Journal of Consulting and Clinical
Psychology, 59, 12–19.
Johansson, L., & Werbart, A. (2009). Patients’ view of therapeutic action in psychoanalytic group
psychotherapy. Group Analysis, 42, 120–142.
Kazdin, A. E. (2008). Evidence-based treatment and practice: New opportunities to bridge clinical
research and practice, enhance the knowledge base, and improve patient care. American
Psychologist, 63, 146–159.
Kopta, S. W., Howard, K. I., Lowry, J. L., & Beutler, L. E. (1994). Patterns of symptomatic recovery
in psychotherapy. Journal of Consulting and Clinical Psychology, 62, 1009–1016.
Lambert, M. J., Bergin, A. E., & Garfeild, S. L. (2004). Introduction and historical overview.
In M. J. Lambert (Ed.), Bergin and Garfeild’s handbook of psychotherapy and behavior
change (pp. 3–15). New York: Wiley.
Long-term outcome for young adults 41
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Larsson, D., Hemmingsson, T., Allebeck, P., & Lundberg, I. (2002). Self-rated health and mortality
among young men: What is the relation and how may it be explained? Scandinavian Journal
of Public Health, 30, 259–266.
Leichsenring, F., Biskup, J., Kreische, R., & Staats, H. (2005). The Gottingen study of
psychoanalytic therapy: First results. International Journal of Psychoanalysis, 86, 433–455.
Leichsenring, F., & Rabung, S. (2006). Change norms: A complementary approach to the issue of
control groups in psychotherapy outcome research. Psychotherapy Research, 16, 594–605.
Leichsenring, F., & Rabung, S. (2008). Effectiveness of long-term psychodynamic psychotherapy:
A meta-analysis. JAMA, 300, 1551–1565.
Leichsenring, F., Rabung, S., & Leibing, E. (2004). The efficacy of short-term psychodynamic
psychotherapy in specific psychiatric disorders: A meta-analysis. Archives of General
Psychiatry, 61, 1208–1216.
Leuzinger-Bohleber, M., Stuhr, U., Ruger, B., & Beutel, M. (2003). How to study the ‘quality of
psychoanalytic treatments’ and their long-term effects on patients’ well-being: A
representative, multi-perspective follow-up study. International Journal of Psychoanalysis,
84, 263–290.
Lilliengren, P., & Werbart, A. (2005). A model of therapeutic action grounded in patients’ view of
curative and hindering factors in psychoanalytic psychotherapy. Psychotherapy: Theory,
Research, Practice, Training, 42, 324–339.
Lorig, K., Stewart, A., Ritter, P., Gonzalez, V., Laurent, D., & Lynch, J. (1996). Outcome measures
for health education and other health care interventions. Thousand Oaks, CA: Sage
Publications.
Luborsky, L., Barber, J. P., Siqueland, L., Johnson, S., Najavits, L. M., Frank, A., et al. (1996). The
revised helping alliance questionnaire (Haq-II). Journal of Psychotherapy Practice and
Research, 5, 260–270.
Martin, D. J., Garske, J. P., & Davis, M. (2000). Relation of the therapeutic alliance with outcome
and other variables: A meta-analytic review. Journal of Consulting and Clinical Psychology,
68, 438–450.
Mossey, J. M., & Shapiro, E. (1982). Self-rated health: A predictor of mortality among the elderly.
American Journal of Public Health, 72, 800–808.
Noren, K., Lindgren, A., Hallstrom, T., Thormahlen, B., Vinnars, B., Wennberg, P., et al. (2007).
Psychological distress and functional impairment in patients with personality disorders.
Nordic Journal of Psychiatry, 61, 260–270.
Orlinsky, D. E., Ronnestad, M. H., & Willutzki, U. (2004). Fifty years of psychotherapy process-
outcome research: Continuity and change. In M. J. Lambert (Ed.), Bergin and Garfield’s
handbook of psychotherapy and behavior change (pp. 307–389). New York: Wiley.
Ottosson, H., Bodlund, O., Ekselius, L., Grann, M., von Knorring, L., Kullgren, G., et al. (1998).
DSM-IV and ICD-10 personality disorders: A comparison of a self-report questionnaire (DIP-Q)
with a structured interview. European Psychiatry, 13, 246–253.
Ottosson, H., Bodlund, O., Ekselius, L., von Knorring, L., Kullgren, G., Lindstrom, E., et al. (1995).
The DSM-IV and ICD-10 personality questionnaire (DIP-Q): Construction and preliminary
validation. Nordic Journal of Psychiatry, 49, 285–291.
Perry, J. C., Bond, M., & Roy, C. (2007). Predictors of treatment duration and retention in a study of
long-term dynamic psychotherapy: Childhood adversity, adult personality and diagnosis.
Journal of Psychiatric Practice, 13, 221–232.
Philips, B., Wennberg, P., Werbart, A., & Schubert, J. (2006). Young adults in psychoanalytic
psychotherapy: Patient characteristics and therapy outcome. Psychology and Psychotherapy:
Theory, Research and Practice, 79, 89–106.
Psykologiforlaget (2002). Inventory of interpersonal problems: IIP. Swedish manual. Stockholm:
Psykologiforlaget AB.
Roos, J., Wennberg, P., Philips, B., & Werbart, A. (2009). Young adults who drop-out from long-
term psychoanalytic psychotherapy; results from a prospective longitudinal study.
Manuscript submitted for publication.
42 Annika Lindgren et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Rosander, M., & Stiwne, D. (1997). Inventory of interpersonal problems, IIP: Konstruktion och
normering av svensk kortversion. [Inventory of interpersonal problems, IIP: Construction
and norms of a Swedish short version]. Unpublished manuscript, Linkopings universitet,
Sweden.
Roseborough, D. J. (2006). Psychodynamic psychotherapy: An effectiveness study. Research on
Social Work Practice, 16, 166–175.
Safran, J. D., Muran, J. C., Samstag, L. W., & Stevens, C. (2002). Repairing alliance ruptures. In J. C.
Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and
responsiveness to patients (pp. 235–254). New York: Oxford University Press.
Sandell, R., Blomberg, J., Lazar, A., Carlsson, J., Broberg, J., & Schubert, J. (2000). Varieties of long-
term outcome among patients in psychoanalysis and long-term psychotherapy: A review of
findings in the Stockholm outcome of psychoanalysis and psychotherapy project (STOPP).
International Journal of Psychoanalysis, 81, 921–942.
Schneider, W., Buchheim, P., Cierpka, M., Dahlbender, R. W., Freyberger, H. J., Grande, T, et al.
(2002). Operationalized psychodynamic diagnostics: A new approach in psychodynamic
psychotherapy. In L. E. Beutler & M. L. Malik (Eds.), Rethinking the DSM: A psychological
perspective. Decade of behavior (pp. 177–200). Washington, DC: American Psychological
Association.
Schwartz, J. C. (1993). The mixed-model anova: The truth the computer packages, the books. The
American Statistician, 47, 48–59.
Shadbolt, B., Barresi, J., & Craft, P. (2002). Self-rated health as a predictor of survival among
patients with advanced cancer. Journal of Clinical Oncology, 20, 2514–2519.
Statistics Sweden (2006). Health and medical care 1980–2005 (No. 113).
Weinryb, R. M., Gustavsson, J. P., Hellstrom, C., Andersson, E., Broberg, A., & Rylander, G. (1996).
Interpersonal problems and personality characteristics: Psychometric studies of the Swedish
version of the IIP. Personality and Individual Differences, 20, 13–23.
Westen, D., Novotny, C. M., & Thompson-Brenner, H. (2004). The empirical status of empirically
supported psychotherapies: Assumptions, findings and reporting in controlled clinical trials.
Psychological Bulletin, 130, 631–663.
Received 24 January 2008; revised version received 15 May 2009
Long-term outcome for young adults 43