Knowledge on Water, Sanitation and Hygiene Among the mothers of under-5 children
45
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 1 Knowledge on Water, Sanitation and Hygiene Among the mothers of under-5 children Guide Teacher Dr. Md. Mahmudul Haque MBBS, MPH, BCS, WHO Fellow Assistant Professor, NIPSOM Part-time faculty, MPH, ASAUB Submitted by Md. Mamunur Rashid ID No.: 11-3-41-0017 Master’s of Public Health, Batch-3 (Regular) ASA University
Transcript of Knowledge on Water, Sanitation and Hygiene Among the mothers of under-5 children

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 1
Knowledge on Water, Sanitation and Hygiene
Among the mothers of under-5 children
Guide Teacher Dr. Md. Mahmudul Haque
MBBS, MPH, BCS, WHO Fellow Assistant Professor, NIPSOM
Part-time faculty, MPH, ASAUB
Submitted by Md. Mamunur Rashid ID No.: 11-3-41-0017
Master’s of Public Health, Batch-3 (Regular) ASA University
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 2
SUBMISSION SHEET
This dissertation is submitted to the Department of Public Health, ASA University, in partial
fulfilment of the requirement for the degree of Master of Public Health during the academic
session.
_______________________________
Md. Mamunur Rashid
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 3
DECLARATION
I certify that the research work titled “Knowledge on Water, Sanitation and Hygiene Among the
mothers of under-5 children” is my own work. The work has not been presented elsewhere for
assessment. Where material has been used from other sources it has been properly
acknowledged/ referred.
Signature of Student

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 4
ACKNOWLEDGEMENT
“No project is ever a work of only one person and this one is no exception”
To conduct a survey and go through all the stages of data collection, from planning to analysis
and from writing to the printing of final copy was a difficult task that was not possible
without many people. Many thanks are due to these peoples and institutes, without whose help I
would not have completed this dissertation.
First of all, I like to thanks ASA University especially the Chairman of the MPH department
Prof. Dr. Md. Abdul Bari for giving me the chance to conduct this research through this MPH
course. Thank you to all of those who have helped listened and encouraged me throughout this
study. I am indebted to my supervisor Dr. Md. Mahmudul Haque whose guidance, advice and
patience has been immeasurable.
I would also like to express my sincere gratitude to Prof. Dr. ASM Amanullah for his convivial
support towards development of this report. I would also like to thank Dr. Jesmin Akter, the
MPH Course Coordinator; whose dynamism, untiring efforts and dedication made a difficult
dream come true. My sincere thanks to all members of the ASA University, both staff and
students, whose continuous support have made this research possible.
Last but not least, I would like to thank all of the participants in the study for the time and help
given throughout. Without their participation, this research would not have been possible.
Lastly, I wish to acknowledge the forfeits of my family who supported and encouraged me
during the whole MPH course and while preparing this dissertation.

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 5
ACRONYMS AND ABBREVIATIONS
ADP Annual Development Programme
BANBEIS Bangladesh Bureau of Education, Information and Statistics
BBS Bangladesh Bureau of Statistics
BCC Behaviour Change Communication
BRAC Bangladesh Rural Advancement Committee (formerly known as)
CSO Civil Society Organization
DGHS Directorate General of Health Services
DPHE Department of Public Health Engineering
DSK Dustha Shastha Kendra
GDP Gross Domestic Product
GOB Government of Bangladesh
HH Household
ICDDR,B International Centre for Diarrhoeal Disease Research, Bangladesh
IEC Information Education and Communication
KAP Knowledge Attitude and Practice
LGD Local Government Division
LGED Local Government Engineering Department
LGI Local Government Institution
MIS Management Information System
MDG Millennium Development Goal
MOU Memorandum of Understanding
NGO Non Government Organization
PHC Primary Health Care
PPPHW Public-Private Partnership for Hand Washing
TB Tuberculosis
UN United Nations
UNICEF United Nations Children‟s Fund
WASH Water, Sanitation and Hygiene
WATSAN Water and Sanitation
WHO World Health Organization
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 6
TABLE OF CONTENTS
CONTENT PAGE
ABSTRACT................................................................................................................... 1
CHAPTER ONE: INTRODUCTION.......................................................................... 2-4
1.1 Background
1.2 Statement of problem
1.3 Rationale of the study
CHAPTER TWO: LITERATURE REVIEW............................................................ 5-8
2.1 Status of Water Sanitation and Hygiene in Global Scenario
2.2 Status of Water Sanitation and Hygiene in the context of Bangladesh
CHAPTER THREE: RESEARCH METHODOLOGY........................................... 9-12
3.1 Research Objectives
3.1.1 General objectives
3.1.2 Specific objectives
3.2 Research questions
3.3 Study Area and population
3.4 Study Design and Method
3.5 Sampling Unit
3.6 Sample size and Sampling Method
3.7 Data collection tools
3.8 Data collection technique
3.9 Criteria of the study
3.10 Ethical considerations
3.11 Validity and Reliability of the Study
3.12 Limitations of the study
3.13 Data management and analysis
3.14 Data cleaning
3.15 Operational definition
CHAPTER FOUR: FINDINGS OF THE STUDY..................................................... 15-23
4.1 Demographic profile of the respondents
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 7
4.2 Knowledge related to water
4.3 Knowledge related to sanitation
4.4 Knowledge related to hygiene
4.5 Summary Results
CHAPTER FIVE: CONCLUSION AND RECOMMENDATION.......................... 24-25
References...................................................................................................................... 26
Annexure: 1 (Bangla Questionnaire).............................................................................. 27-31
Annexure: 2 (English Questionnaire)............................................................................. 32-37
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 8
LIST OF TABLES
______________________________________________________________________________
Table: 1 Status of drinking pure water p. 16
Table: 2 Status of Latrine use p. 17
Table: 3 Habit of Hand washes before taking food p.18
LIST OF FIGURES
______________________________________________________________________________
Figure: 1 Age Structure p.13
Figure: 2 Mother with number of children p.14
Figure: 3 Marital Status p.14
Figure: 5 Income status p.15
Figure: 6 Types of water in preparing baby‟s food p.16
Figure: 7 Disposal methods of solid and liquid waste p.17
Figure: 8 Understanding on the necessity of sanitary latrine use p.18
Figure: 9 Necessity of hand wash p.19
Figure: 10 Knowledge on Hand washing techniques p.20
Figure: 11 Causes of worm to children p.20
Figure: 12 Causes of diarrhoea p.21
Figure: 13 Decontamination process baby‟s feeding accessories p.22

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 9
ABSTRACT
Water Sanitation and Hygiene (WASH) is still a burning issue in the context of developing
countries like Bangladesh as many diseases related to it are causing the maximum number
of child‟s death. This study focused on evaluating knowledge level of the participants on
WASH among the mother groups of under-5 children in two urban slums located at
Mohammadpur and Adabor Thana in Dhaka.
The research is targeted to mother groups because it has been found that the diarrhoeal diseases
caused due to poor sanitation and hygienic condition as well as impure drinking water is the
leading cause of under-5 mortality and morbidity. One on one interview was conducted with 70
mothers at respected areas through a structured questionnaire. The general objective of this study
is to systematically assess level of the knowledge on water, sanitation and hygiene among the
mother groups of under-5 children.
The design for the study is cross-sectional descriptive study. The data are collected from the
mother groups of under-5 children from the Adabor and Mohammadpur Thana of City
Corporation Area of Dhaka district. All the data has been collected through one on one interview
using a predefined questionnaire.
The findings/results of this research may not be generalized to other Thana, Districts and the
country as a whole, as it done within a limited time with a short sample size in a cluster area.
Among the mothers, 56 of them are married and living with their husband. The mean income
shows as Tk. 6511 only which is in line with the national GDP. Level of education found
significantly poor as 28 respondents said they only can sign their name and 7 respondents are
completely illiterate. The concept of drinking pure water found significantly low among the
mothers; 40 respondents said they use direct tap water in preparing their baby‟s food. In terms of
waste disposal (both liquid and solid), respondents generally through it here and there, this
pollutes the environment significantly. The knowledge on the urgency of sanitary latrine was
also found poor. 60 respondents expressed that they don‟t know the right techniques of hand
washing.

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 10
CHAPTER ONE: INTRODUCTION
1.1 Background
In many countries there exists a high prevalence of water and sanitation related diseases, causing
many people, children in particular, to fall ill or even die. Improved hygiene practices are
essential if transmission routes of water and sanitation related diseases are to be cut. Whereas
appropriate hygiene education can bring about the intention to change hygiene behaviour, for
most hygiene behaviours appropriate water and sanitation facilities are needed to allow people to
transform intention to change into real change.
Access to water and sanitation is a fundamental human right and essential to life, health and
dignity. Timely and adequate provision of clean water and sanitation services to uprooted people
is particularly important, given the vulnerability of their situation. The UN believes that all
refugees, asylum seekers, internally displaced people and returnees should have access to
adequate drinking water whether they stay in camps or in urban areas (ECOSOC, 2002).
The provision of adequate sanitation services is equally important. Proper disposal of all waste as
well as control of the carriers of communicable diseases, including mosquitoes, rats, mice and
flies, is crucial to mitigate health risks and prevent epidemics.
Access to Water, Sanitation and Hygiene (WASH) is a pre-condition for people to acquire good
health, well-being and even benefit from economic development. Without it, the increasing rate
of population and economic growth tend to negatively affect the most vulnerable segments in
society: women, children and marginalized communities.
It is obvious that to reduce infant and child mortality, improve quality of life, and
reduce poverty, greater efforts and investment are needed to increase safe water, affordable
hygienic sanitation and adequate hygiene promotion. Improvement of water, sanitation and
hygiene promotion provides a range of benefits for people‟s well-being, particularly the poor and
marginalized. Improved sanitation and promotion of hygienic behaviour reduce health risks, and
eventually contribute to the socio-economic development of the nation.
The disease burden from unsafe water, sanitation and hygiene (WASH) is estimated at the global
level taking into account various disease outcomes, principally diarrhoeal diseases. The risk
factor defined as including multiple factors, namely the ingestion of unsafe water, lack of water
linked to inadequate hygiene, contact with unsafe water, poor personal and domestic hygiene and
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 11
agricultural practices, and inadequate development and management of water resources or water
systems (Glass Report, 2009).
1.2 Statement of problem
Inadequate and unsafe water, poor sanitation, and unsafe hygiene practices are main causes of
the diarrhoea, which results 50 out of thousand under- 5 child deaths in Bangladesh (DGHS,
2011).
Water, sanitation and hygiene are also linked to many other diseases that kill children or stunt
their development, including helminth infections, trachoma, cholera, fluorosis and arsenicosis.
There is also emerging evidence linking better hand-washing practices with reduced incidence of
acute respiratory infections.
In the context of Bangladesh, sanitation coverage is just 39% (Water Aid, 2008) which results in
widespread diseases the majority of people do not have a latrine and have to defecate in the open.
Water-related diseases are very common in Bangladesh but for the majority of the population the
causes of ill health are shrouded in superstition.
Diarrhoeal morbidity rates are increasing. The only way to sustainably reduce this massive
burden of disease is through the use of safe drinking water, sanitation and improved hygiene
practices, in particular hand washing with soap.
1.3 Rationale of the study
Many people believe that simply providing a fresh, clean water supply will substantially reduce
water-borne illnesses. What most people do not know is that safe hygiene practices and access to
sanitation are crucial for combating the main health threats to children under five, in particular
diarrhoea.
In recent years, sanitation has raised up the international policy agenda. In 2002, sanitation was
included in the Millennium Development Goals (MDGs), and specifically within MDG 7 Target
10 which sets the aim of halving „by 2015‟. The proportion of people without sustainable access
to safe drinking water and basic sanitation yet at national level in most developing countries,
hygiene and sanitation do not yet receive much attention, despite important health implications
(Ahmed, et al., 2002).
Water, Sanitation and Hygiene is linked in many ways to people‟s livelihoods and sustainable
development in general; it is an important input not just for Target 10 of Millennium

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 12
Development Goal 7 but for all of the Goals. It is a key input for the achievement of universal
primary education and reductions in child mortality (Goals 2 and 4) and is directly linked to the
eradication of poverty and hunger, the empowerment of women, improvements in maternal
health and the reduction of diseases (Goals 1, 3, 5 and 6).
In addition to coverage disparities between regions, there are significant inequities within the
districts: clear rural-urban disparities as well as coverage and service level disparities between
richer and poorer households. The urban poor usually have very low access to water and
sanitation services, and pockets of people - such as indigenous groups-often have even lower
access.
The Alma-Ata conference held in 1978 also had determined an adequate supply of safe
water and basic sanitation as one of the element of primary health care (PHC).The study is
targeted to the mother groups of under-5 years of age children because the diseases associated
with water, sanitation and hygiene are the leading cause of under-5 mortality and morbidity and
the mothers are directly linked with the child‟s health as they are the one who take care of their
children (Gautam, et al., 2010).
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 13
CHAPTER TWO: LITERATURE REVIEW
The study problem is selected after thorough literature search and discussion with the colleagues.
The related information required for the study has been collected from different sources such as
DGHS Year book, Health Bulletin, Library of different institutions i.e. WaterAid Bangladesh,
ICDDR,B, CARITAS Resource Centre, DSK Library, different related journals, publications and
internet search.
The related national and international literatures on water sanitation and hygiene among different
group published by different organizations are reviewed and attempted to present in this section.
The various facts and figures reviewed from different literatures, that are directly or indirectly
relevant to the study topic are presented here as follows:
2.1 Status of Water Sanitation and Hygiene in Global Scenario
A large fraction of the world‟s illness and death is attributable to communicable disease. 62%
and 31% of all deaths in Africa and Southeast Asia, respectively, are caused by infectious
diseases. This trend is especially notable in developing countries where acute respiratory and
intestinal infections are the primary cause of morbidity and mortality among young children.
Inadequate sanitary conditions and poor hygiene practices play major role in the increased
burden of communicable disease within these developing countries. Previous hand hygiene
studies have indicated that children with proper hand washing practices are less likely to report
gastrointestinal and respiratory symptoms. Hand washing with soap has been reported to reduce
diarrheal morbidity by 44% and respiratory infections by 23%. However, globally the rates at
which hands are washed with soap range from only 0-34% of the time (Vivas, et al., 2010).
A study conducted by the Global Public-Private Partnership for Hand Washing (PPPHW) which
included several Sub-Saharan African countries reported that 17% of the participants washed
their hands with soap after using toilet, while 45% used only water.
According to Ricard Gine, 884 million people do not use improved sources of drinking water and
26oo million people do not use improved sanitation. 84% of the world population, without an
improved drinking water source, lives in rural areas in developing regions, 94% of the urban
population uses improved sources. In rural areas, it is only seven out of ten people without
improved sanitation live in rural areas. In developing regions, use of improved sanitation in

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 14
urban areas is 68% but it is only 40% in rural areas (Ricard, 2010). Almost 900 million people
lack access to an improved water supply and 2.6 billion to basic sanitation (Howard, et al.,
2010). Many studies have reported the results of interventions to reduce illness through
improvements in drinking water, sanitation facilities, and hygiene practices in less developed
countries. Diarrhoeal disease is one of the leading causes of morbidity and mortality in less
developed countries, especially among the children aged under -5 years.
Since 1990, over 1 billion people have gained access to improved drinking water and sanitation
services. Nonetheless, 2.6 billion people- over half of the developing world population- do not have
improved sanitation facilities, and 1.1 billion are still using water from unimproved sources. Barely
one third of the population of South Asia uses improved sanitation facilities. (UNICEF, 2006).
According to the survey done by Kashmir Charitable Trust in District Muzaffarabad, Pakistan, in
August 2008, 48% people haven‟t any latrines and go to open fields for defecation and among people
having latrines, only 48% of women use it. 72% of the respondent of the survey reported that muddy
water to be dirty and 6% said that filtering by clean cloth can make water clean. Also 55% of the
survey population use stones to clean themselves after defecation (Kashmir Charitable Trust, 2008).
A Survey done by WE Consult Lda for Unicef Mozambique in 18 districts of Mozambique in
2009, had found only 15% of the households practices some form of household water treatment.
The water quality at the household is significantly lower than at the source, indicating
unhygienic practices during collection, transport and storage. 54% of all households still
practices open defecation. The coverage of improved sanitation facilities is on average only 2%
for the whole survey area. The majority of the households bury the stools of the children or
disposes them in the latrine. Although almost everyone washes the hands, only 1% uses the
proper practice, which is washing with running water and using soap or ashes. The vast majority
washes the hands in a basin or bucket (UNICEF, 2009).
2.2 Status of Water Sanitation and Hygiene in the context of Bangladesh
In Bangladesh, the high incidence of diarrhoeal and other diseases related to faecal
contamination, causes an estimated 110,000 child (under 5) deaths each year (11% of total child
deaths). Over 65 million episodes of diarrhoeal diseases occur annually among children under
five years of age. An average child in Bangladesh suffers 3-4 episodes of diarrhoeal diseases

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 15
every year. Much of this is thought to be preventable with improvements in sanitation, water
quality and hygiene practices (BBS, 2007).
A large number of people in Bangladesh lack access to potable drinking water. Among them,
urban slum dwellers face the greatest challenges. Their water quality is affected by unsafe water
supply, unhygienic sanitation facilities, poor solid waste management, unhygienic practices
particularly with regard to hand washing, insecure land tenure, poor socio-economic backing,
and crowded living conditions (Sobsey, 2003). The people from these high-risk areas often suffer
from diarrhoea and other water borne diseases. Due to lack of education, knowledge and basic
awareness, people often have a poor understanding of the relationship between health, water,
sanitation and hygiene. In some instances, people may still practice unhygienic habits even
though this understanding does exist.
A World Bank report cited Bangladesh‟s urban population as having grown almost nine-fold
from 2.6 million in 1961 to approximately 22 million in 1991 with an annual urbanization rate of
7.5 percent (World Bank, 2000). Over 37% of the city populations live in slums that occupy only
4% of city land (Ahmed, et al.2002). Slums are the most densely populated areas with over 200
times the normal density of Bangladesh at 531,000 persons per square mile. Overcrowding
creates huge increases in communicable diseases like diarrhoea (CUS, 2006).
24 % of urban households are estimated to have no sanitary latrines. In pockets such as slums,
sanitary latrine coverage is even lower than the average of 14% for towns and cities.
Furthermore, over 80% of the low income populations have no legal access to safe water.
Hanging latrines and indiscriminate garbage dumping by Households, industries, clinics etc. are
very common in the urban areas (Gautam, et al. 2010).
Bangladesh faces multiple challenges in its water, sanitation and hygiene sector. According to
the Joint Monitoring Programme of WHO and UNICEF, the latrine coverage in Bangladesh
increased from 33% in 2003 to 36% in 2006, and the safe drinking water supply coverage
increased from 75% in 2003 to 80% in 2006. The Government‟s target for sanitation, 100%
coverage by 2013, goes significantly beyond the Millennium Development Goal (MDG) 7.
Hygiene-related diseases in Bangladesh cost 5 billion taka (US$ 80 million) each year for
treatment alone. Moreover; Bangladesh strives to realize its relatively ambitious targets of
achieving 100% sanitation and water supply coverage for a population of over 144 million by the
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children 16
year 2013. Several critical challenges towards achieving its goals, such as reaching the poorest
people and hard to reach areas, must be overcome (Gautam, et al. 2010).
The battle against the diseases in Bangladesh started in the 70s with the introduction of hand
pumps (popularly known as tube wells) as safe sources of drinking water. By the 90s, over 10
million tube wells dotted the countryside. In contrast, the safe disposal of excreta received little
attention. Moreover, unlike the popular craze for tube wells, people hardly had any demand for
sanitation. Almost everyone defecated in the open (Water Aid, 2008).
In the 80s, DPHE (Department of Public Health Engineering) devised low-cost sanitary latrines
by doing away with the expensive brickwork and concrete. Local materials were used for
building the super-structure. To make latrine components available to the villagers, DPHE set up
many local based production centres. They started to sell the rings and slabs at subsidized price
to the public. Yet the demand was lukewarm, and a key component – social mobilization, was
still missing. However, other important development was taking place in the 80s. The
decentralized latrine production centres of DPHE brought the technology closer to the people.
Many NGOs became interested. They sent their members to receive training from DPHE. Then
the NGOs started to set up their own latrine production centres.
In the 90s, with the low-cost design completed and production centres established, the DPHE
turned its attention to the last lacuna of social mobilization for creating demand. . It started a
national program on social mobilization for sanitation (SOC-MOB). DPHE, with its partners
including UNICEF and various NGOs, mounted a massive campaign for sanitation through
social mobilization. People were encouraged to install pour-flush ring-slab sanitary latrines if
possible.
People who could not afford the low-cost sanitary latrines were encouraged to build home-made
pit latrines. Thus the first attempt at having open-defecation free communities started during this
time.
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
17
CHAPTER THREE: RESEARCH METHODOLOGY
3.1 Research objectives
3.1.1 General objectives
To assess the knowledge on water, sanitation and hygiene among the mother groups
of under-5 children.
3.1.2 Specific objectives
To describe the socio demographic, cultural information of respondents.
To find out the incidence of disease due to unhygienic practices
To identify gaps between knowledge regarding WASH.
3.2 Research questions
For the purpose of the study, three research questions were identified and focused on these
questions, the questionnaire was developed.
What is the knowledge on water sanitation and hygiene (WASH) among mothers
of under-5 children?
What are the incidences of disease due unhygienic hand wash practices?
What are the gaps between the knowledge on WASH among the mother groups of under-
5 children?
3.3 Study Area and population
Mohammadpur and Adabor Thana of Dhaka City Corporation are chosen purposively for the
study. Mother group of under-5 children of the selected areas was interviewed under the study.
3.4 Study design and method
This is a Cross-sectional Descriptive study on the knowledge regarding WASH among the
mother with under 5 children at Urban slam areas of DCC. Due to time and resource limitations,
the study method selected as quantitative with structured questionnaire.
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
18
3.5 Sampling Unit
Individual mothers
3.6 Sample size and Sampling Method
A total of 70 mothers with under-5 child will be interview for this study. The number of mothers
was selected purposively due to time and resource constraint. Considering the limitation, the
sample size was not determined following any recognized sample size determination formula.
Mothers were selected through the snowball sample collection technique.
3.7 Data collection tools
Structured face-to-face interviews with pre-tested questionnaires were used to elicit information
from the respondents. Data are collected by using structured interview questionnaire.
The questionnaire consists of four main parts:
➢ Socio-demographic information of the respondents
➢ Knowledge on water access and use
➢ Knowledge on sanitation
➢ Knowledge related to hygiene
3.8 Data collection technique
Individual one on one interview was held with the mothers.
Data collection
Information was collected at household level by visiting each family.
Age of child was confirmed by further interviewing the family members and scrutinizing
the available records.
After ensuring the confidentiality and building a rapport, interview of mothers of under
five children was undertaken to record the social status of mother covering following
areas:
o Mothers education
o Mother‟s employment
o Mothers role in providing treatment support towards their children
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
19
3.9 Criteria of the study
All mothers having children less than 5 years of age were studied irrespective of social class,
caste, ethnicity etc.
3.10 Ethical considerations
Purpose and the objective of the research were explained before to the respondents.
Written consent of the respondent was taken prior to data collection.
Privacy and confidentiality of the respondents information maintained
3.11 Validity and Reliability of the Study
Bangla language is used during data collection with respondents though the questionnaire
developed both in Bangla and English
Research carried out under assistance of the respective guide teacher.
The researcher directly involved in data collection, cross-checking, data processing and
data analyzing.
Each filled questionnaire was re-checked just after the interview in order to correct any
miss/under response.
Regular review of literature done according to the need.
3.12 Limitations of the study
This is a small-scale study done for the partial fulfilment of the requirement of the
MPH program within short period of time hence covers small study areas.
Limited resources as a student.
Difficult to generalize the result to district and the country.
3.13 Data management and analysis
All filled questionnaire were checked on the spot for its completeness.
All the collected information examined on the basis of the research objectives.
Data entries, editing and coding/recoding done in SPSS (Version 12.0) program. MS
Excel is used for preparing the graphs and tables. MS Word used for the producing the
report.
Findings are presented through texts, tables & figures
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
20
3.14 Data cleaning
As a first step in data cleaning, frequency tables were produced for all variables, showing the
minimum and maximum values entered as well as some basic statistics such as average and
median values.
3.15 Operational Definition
Educational status of the mother :
Illiterate: Cannot read and write
Literate: Can read and write
Primary education: Up to Grade V
Secondary education: Grade IX to X
Higher Secondary: XI to XII1
Occupation of the mother :
Housewife: Work done only at their home
Service: Work done on basis of their salary
Agriculture: Work done in farm for cultivation
Student: Studying in certain level
Labourer: Work done on daily wage basis
Diseases related to Water, Sanitation and Hygiene
Diarrhoea, helminth infections, cholera, dysentery.
Proper hand washing
6 steps of hand washing
Recommended by WHO (Wet, Soap, Scrub, Rinse, Dry and Water off )
Disadvantaged population:
“Groups with diminished capacity to take advantage of opportunities for better
health and who are often denied those opportunities, whether due to internal or
external factors” (UNI-SOL 1999).
Health-seeking behaviour:
Health-seeking behaviour refers to the sequence of remedial actions that
individuals undertake to rectify perceived ill health (Ward, et al. 1996).
1 As per the definition of “Bangladesh Bureau of Education, Information and Statistics (BANBEIS)”

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
21
CHAPTER FOUR: FINDINGS OF THE STUDY
4.1 Demographic Profile of the Respondents
Age Structure
To understand the demographic profile of the respondents, age structure considered as a vital
indicator. According to this study, 85% respondent‟s age are within 30 years. More specifically,
33% respondents age are 20 or below. 29% respondent‟s age are within the range of 21-25 and
23%‟s age between 26-30 years. Only 6% respondents are belongs to the age group of 36 and
above. The mean ages of the respondents are 25 where 18 minimum and 45 is the maximum age.
Status of mother with number of children
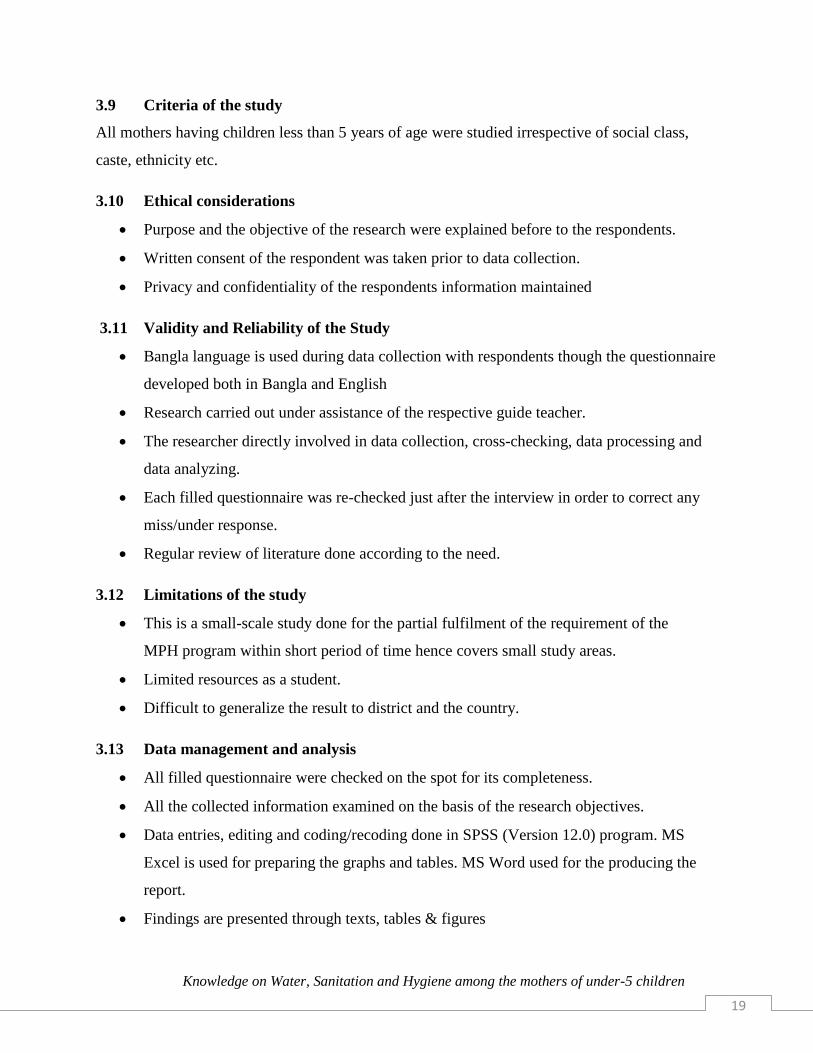
Most of the respondents have two children in an average. It is also observed that, respondent
having two or less children belongs to the age group of below 25. 11 respondents said that they
have 5 children or more.
Figure 2: Mother with number of children
Figure 1: Age Structure
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
22
Most of the respondents have two children in an average. It is also observed that, respondent
having two or less children belongs to the age group of below 25. 11 respondents said that they
have 5 children or more.
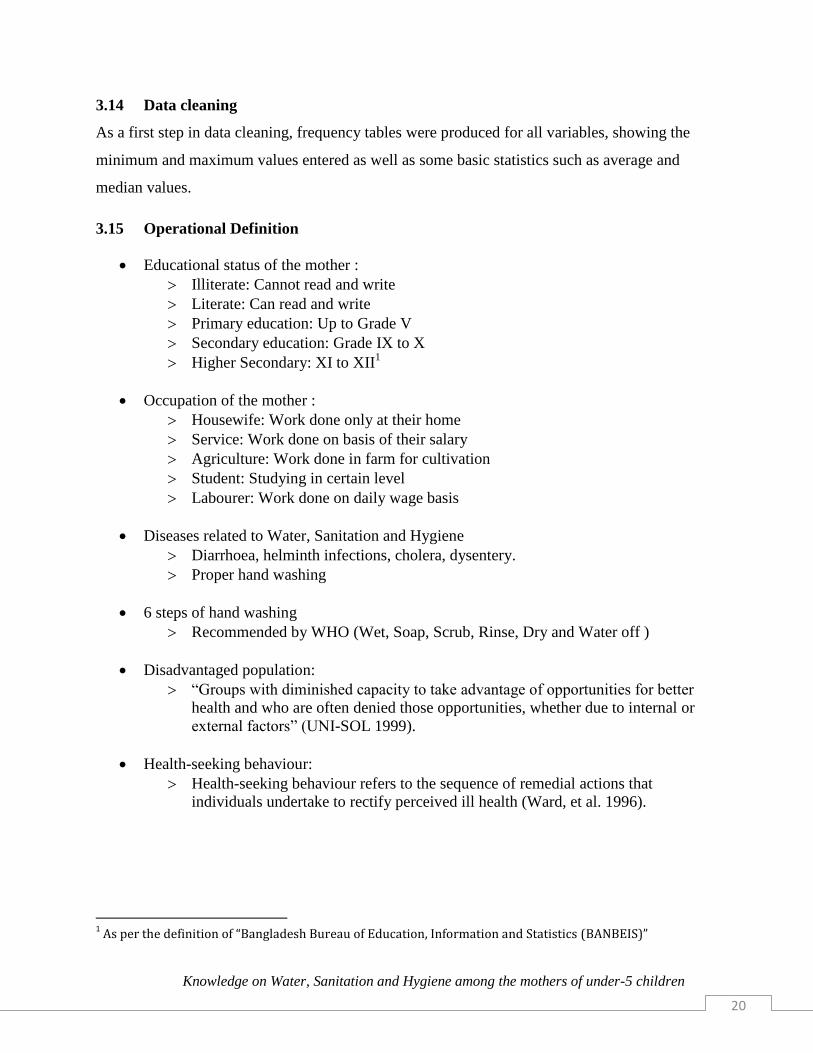
Marital Status
Significant level of respondents (96%) are found married. Rest 4% exists with divorced and
widowed.
0
5
10
15
20
25
30
1 Children 2 children 3 children 4 children 5 children > 5 children
Figure 3: Marital Status
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
23
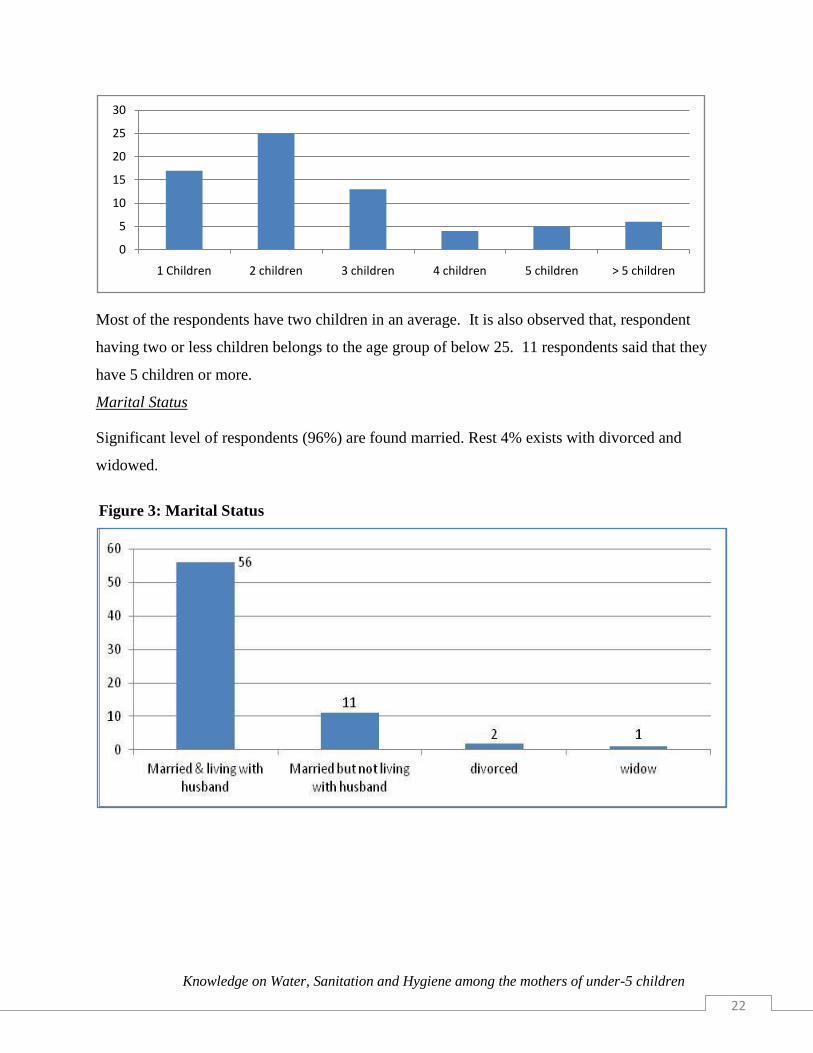
Income Status
It is noteworthy that, within the same community, earning levels vary significantly. In exploring
the income status, the researcher tried to find out the gross income of the respondent‟s family.
The lowest income found as Tk. 1800 where as the highest is Tk. 14000. The mean income of
the respondents is Tk. 6511.
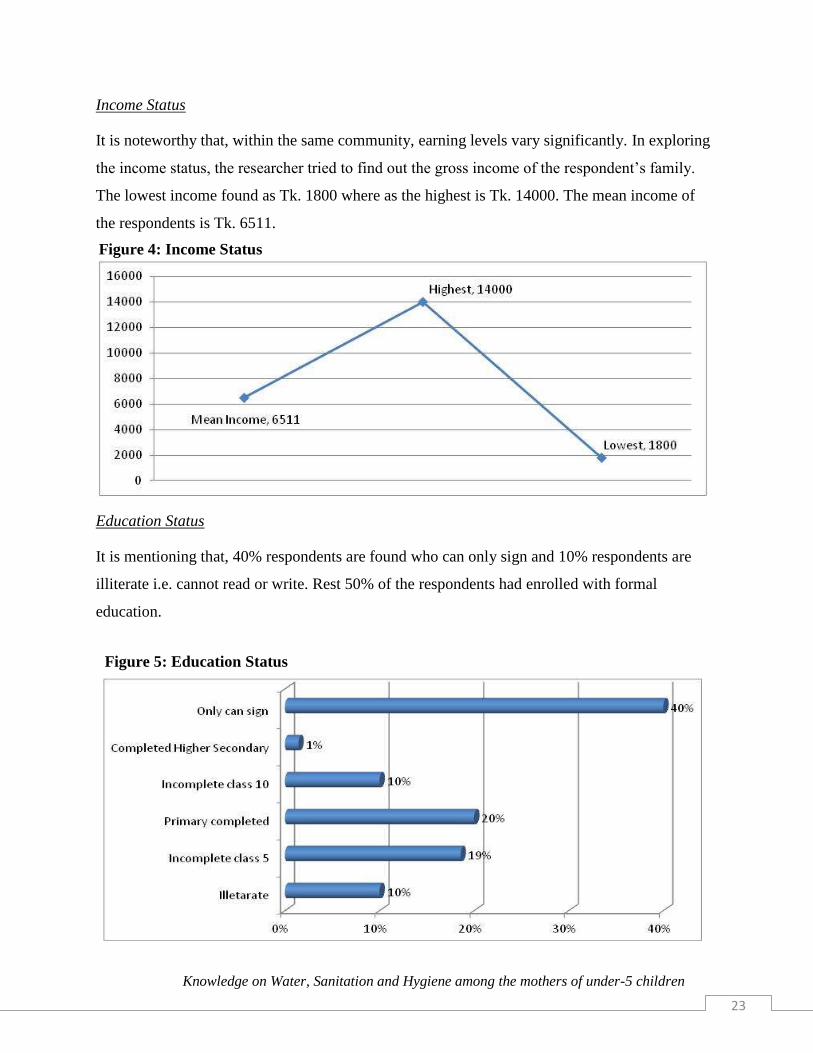
Education Status
It is mentioning that, 40% respondents are found who can only sign and 10% respondents are
illiterate i.e. cannot read or write. Rest 50% of the respondents had enrolled with formal
education.
Figure 5: Education Status
Figure 4: Income Status

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
24
4.2 Knowledge Related to Water
Status of drinking purified water
Only 19% respondents are using purified water for drinking. Out of them, 69% of them use boil
water and 15% filtering the water before drinking.
% of respondent using purified water Methods of Purification
19%
Boil 69%
Filter 15%
Others 15%
Source of water in preparing baby’s food
57% respondents said they use direct tap water for preparing their baby‟s food. Only 24%
respondents boil and 4% filter the water before preparing the baby foods. Rest of the respondents
mentioned other ways of purification.
4.3 Knowledge Related to Sanitation
For the purposes of this study, safe sanitation for low-income areas includes the safe disposal of
faeces to avoid the spread of diseases, and facilities adequate for privacy and dignity that are also
within easy reach (with no queuing). Improved sanitation therefore should mean the number of
Figure 6: Types of water in preparing baby’s food
Table 1: Status of drinking pure water
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
25
sanitary facilities that are better than the most basic safe sanitary measure, rather than in
comparison with non-availability.
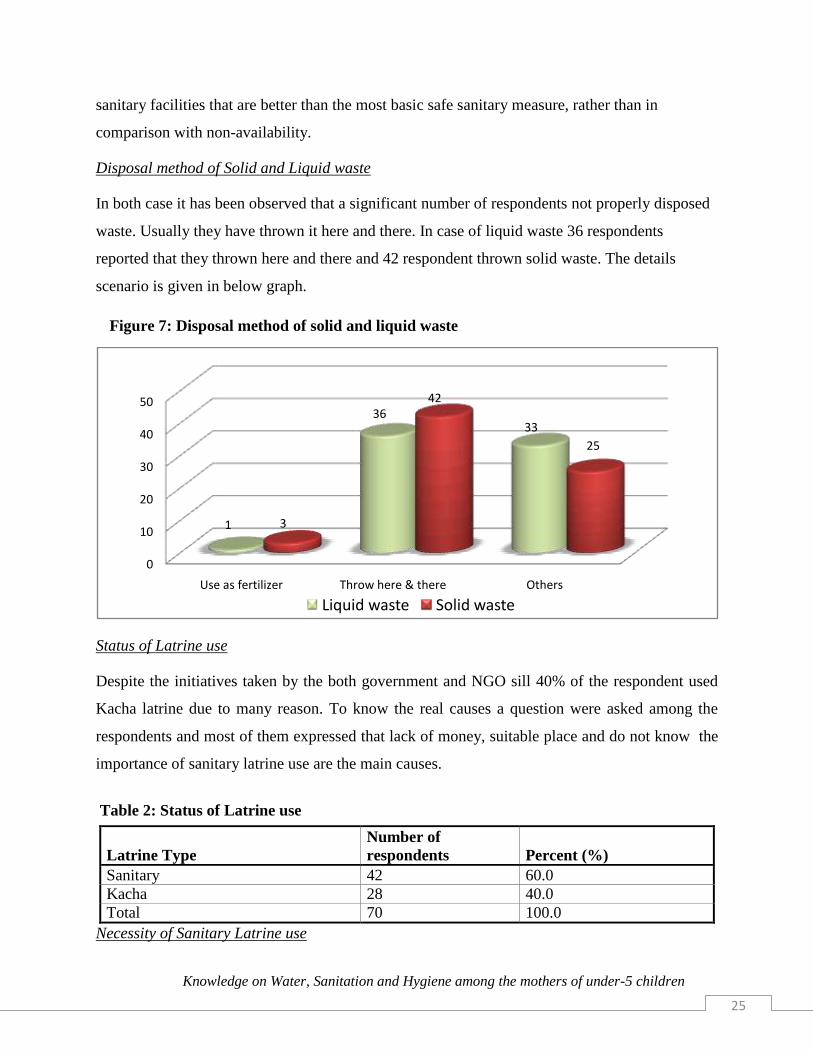
Disposal method of Solid and Liquid waste
In both case it has been observed that a significant number of respondents not properly disposed
waste. Usually they have thrown it here and there. In case of liquid waste 36 respondents
reported that they thrown here and there and 42 respondent thrown solid waste. The details
scenario is given in below graph.
Status of Latrine use
Despite the initiatives taken by the both government and NGO sill 40% of the respondent used
Kacha latrine due to many reason. To know the real causes a question were asked among the
respondents and most of them expressed that lack of money, suitable place and do not know the
importance of sanitary latrine use are the main causes.
Latrine Type
Number of
respondents Percent (%)
Sanitary 42 60.0
Kacha 28 40.0
Total 70 100.0
Necessity of Sanitary Latrine use
0
10
20
30
40
50
Use as fertilizer Throw here & there Others
1
3633
3
42
25
Liquid waste Solid waste
Table 2: Status of Latrine use
Figure 7: Disposal method of solid and liquid waste
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
26
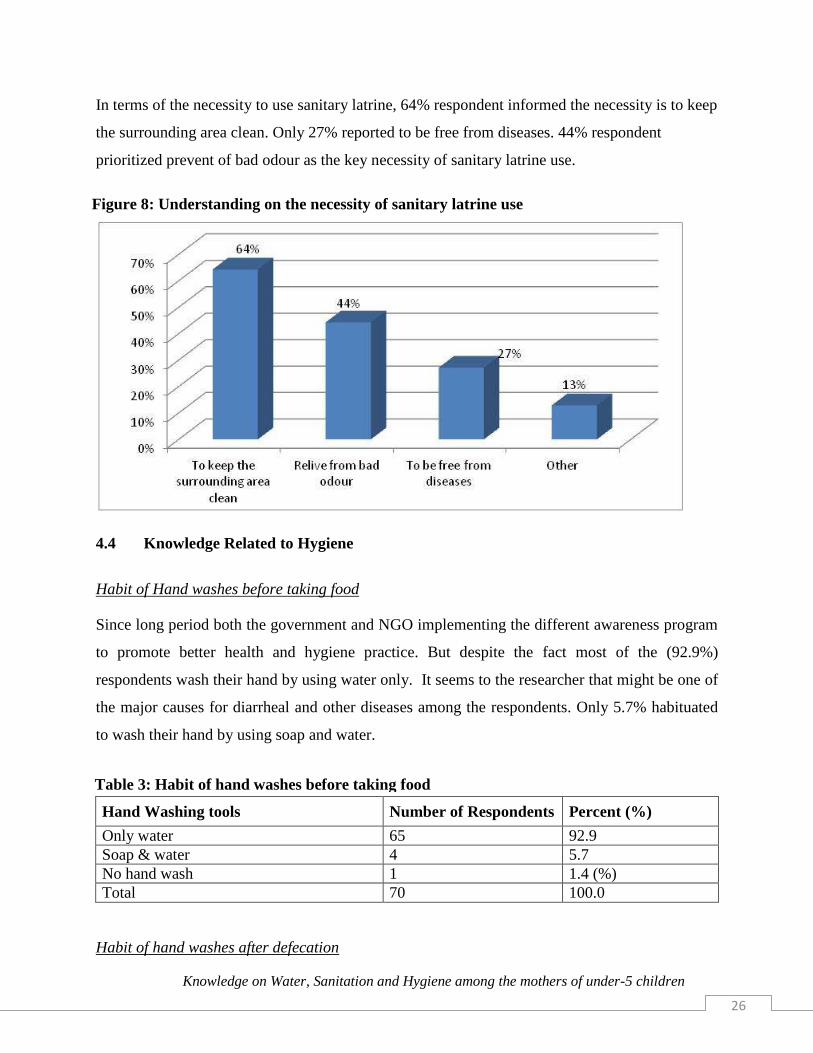
In terms of the necessity to use sanitary latrine, 64% respondent informed the necessity is to keep
the surrounding area clean. Only 27% reported to be free from diseases. 44% respondent
prioritized prevent of bad odour as the key necessity of sanitary latrine use.
4.4 Knowledge Related to Hygiene
Habit of Hand washes before taking food
Since long period both the government and NGO implementing the different awareness program
to promote better health and hygiene practice. But despite the fact most of the (92.9%)
respondents wash their hand by using water only. It seems to the researcher that might be one of
the major causes for diarrheal and other diseases among the respondents. Only 5.7% habituated
to wash their hand by using soap and water.
Hand Washing tools Number of Respondents Percent (%)
Only water 65 92.9
Soap & water 4 5.7
No hand wash 1 1.4 (%)
Total 70 100.0
Habit of hand washes after defecation
Figure 8: Understanding on the necessity of sanitary latrine use
Table 3: Habit of hand washes before taking food

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
27
A significant number of respondents reported that they use only water to wash hands after
defecation. The data also represent poor knowledge on hygiene. Only 27 respondents use soap,
ash or other elements with water to wash their hands after defecation.
Hand Washing tools Number of Respondents Percent (%)
Only water 43 61.4
Soap & water 22 31.4
Ash & water 4 5.7
Others 1 1.4
Total 70 100.0
Necessity of Hand Wash
The main purpose of washing hands is to cleanse the hands of pathogens (including bacteria
or viruses) and chemicals which can cause personal harm or disease. This is especially important
for people who handle food or work in the medical field, but it is also an important practice for
the general public.
From the above table, the data indicates most of the respondents consider that, hand wash is
necessary to be clean and get rid of the diseases. Only 16 respondents reported hand wash
necessary to be healthy.
There‟s a standard technique (six steps technique) for hand wash defined by World Health
Organization (WHO). Only 14% respondents mentioned that they know the techniques of Hand
wash properly.
Table 4: Habit of hand washes after defecation
Figure 9: Necessity of hand wash
Figure 10: Knowledge on hand washing techniques
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
28
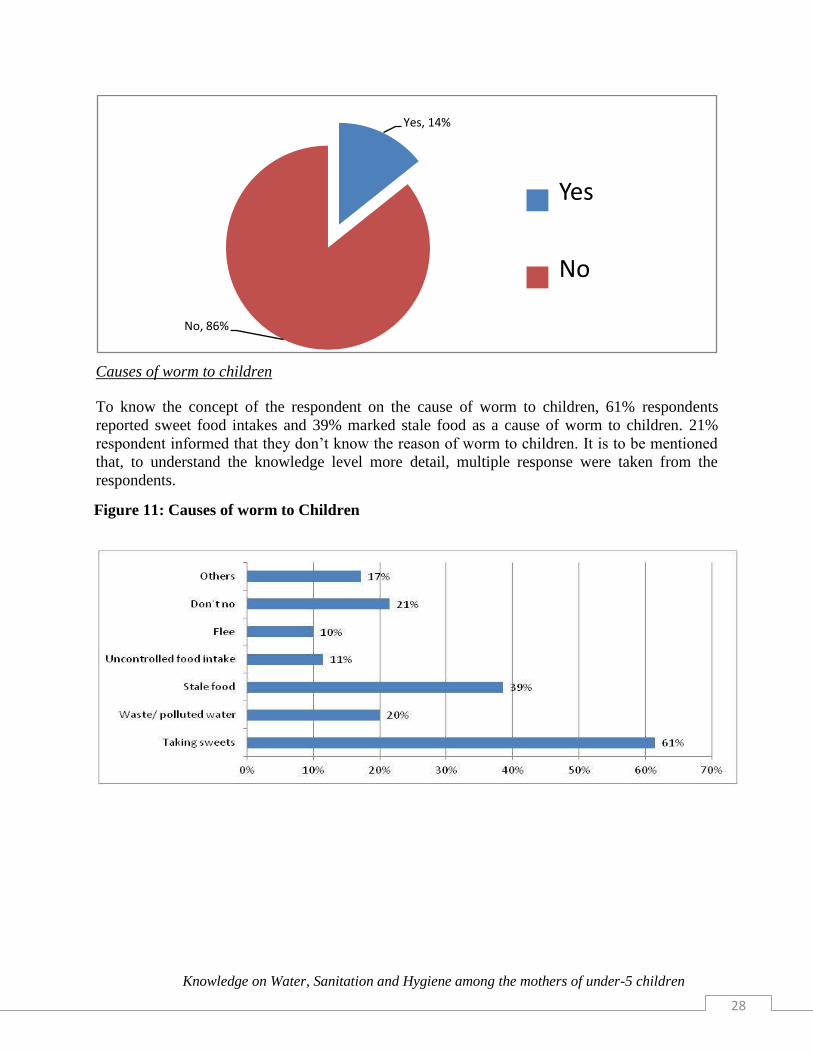
Causes of worm to children
To know the concept of the respondent on the cause of worm to children, 61% respondents
reported sweet food intakes and 39% marked stale food as a cause of worm to children. 21%
respondent informed that they don‟t know the reason of worm to children. It is to be mentioned
that, to understand the knowledge level more detail, multiple response were taken from the
respondents.
Yes, 14%
No, 86%
Yes
No
Figure 11: Causes of worm to Children

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
29
Causes of Diarrhoea
Only 17 respondents reported unsafe drinking water as a cause of diarrhoea. 28 respondents also
noticed dirty environment as a cause. 17 respondents indicate that they don‟t know the reasons of
diarrhoea. The details of the respondents responses are mentioned in the below table.
*Multiple responses
Moreover, half of the respondents reported that they experienced Diarrhoea among their family
members in last six months and they mostly used packet saline as a measure to overcome from
diarrhoea. Only 6 of them discussed the matter with the health workers and 5 respondents
reported that they don‟t take any measure to overcome the situation. In term of the knowledge
regarding sugar salt solution, 53 respondents said they know about it.
Baby depends on only breast feeding
11 respondents reported that their babies are dependent only on breast feeding where as 59
reported they feed baby other foods as well along with breast feeding. Other than breast feed, 44
respondents reported the use of naked hands to prepare their baby‟s food.
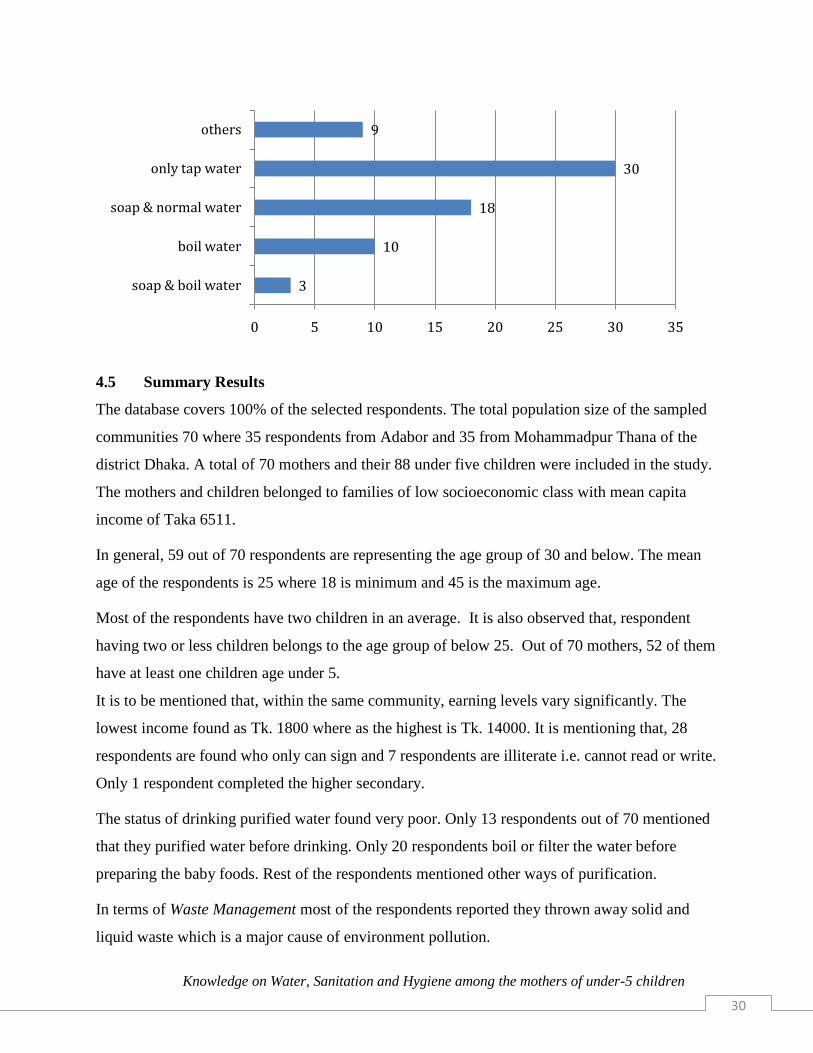
For the decontamination purpose, 30 respondents reported that they use only tap water. Only
three respondents mentioned that they use soap and boil water for decontamination. The
following graph indicates clearly the decontamination status of the mother groups.
28
10
26
9
17
1
0 5 10 15 20 25 30
Dirtyenvironment
Pathogens from stools
Use of unhygienic food
Use of unsafe drinking water
Don't no
Others
Figure 12: Causes of Diarrhoea (respondent’s perception)
Figure 13: Decontamination process of baby’s feeding accessories
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
30
4.5 Summary Results
The database covers 100% of the selected respondents. The total population size of the sampled
communities 70 where 35 respondents from Adabor and 35 from Mohammadpur Thana of the
district Dhaka. A total of 70 mothers and their 88 under five children were included in the study.
The mothers and children belonged to families of low socioeconomic class with mean capita
income of Taka 6511.
In general, 59 out of 70 respondents are representing the age group of 30 and below. The mean
age of the respondents is 25 where 18 is minimum and 45 is the maximum age.
Most of the respondents have two children in an average. It is also observed that, respondent
having two or less children belongs to the age group of below 25. Out of 70 mothers, 52 of them
have at least one children age under 5.
It is to be mentioned that, within the same community, earning levels vary significantly. The
lowest income found as Tk. 1800 where as the highest is Tk. 14000. It is mentioning that, 28
respondents are found who only can sign and 7 respondents are illiterate i.e. cannot read or write.
Only 1 respondent completed the higher secondary.
The status of drinking purified water found very poor. Only 13 respondents out of 70 mentioned
that they purified water before drinking. Only 20 respondents boil or filter the water before
preparing the baby foods. Rest of the respondents mentioned other ways of purification.
In terms of Waste Management most of the respondents reported they thrown away solid and
liquid waste which is a major cause of environment pollution.
3
10
18
30
9
0 5 10 15 20 25 30 35
soap & boil water
boil water
soap & normal water
only tap water
others

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
31
In terms of latrine use, despite the initiatives taken by the both government and NGOs it is still
40% of the respondent used Kacha latrine due to many reasons. To know the real causes a
question were asked among the respondents and most of them expressed that lack of money,
suitable place and do not know the importance of sanitary latrine use are the main causes.
In the knowledge of hygiene, only 5.7% respondents are habituated to wash their hand by using
soap and water. Moreover, a significant number of respondents reported that they use only water
to wash hands after defecation. The data also represent poor knowledge on hygiene.
In terms of hand wash, only 16 respondents reported hand wash necessary to be healthy and
only 10 respondents know how to wash hands properly.
Respondents have a very limited knowledge on the causes of Worm and Diarrhoea. They mostly
identified intake of sweet product as a cause of worm to children and 17 respondents‟ said that
they don‟t know the causes of diarrhoea though most of them know how to prepare sugar salt
solution.
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
32
CHAPTER FIVE: CONCLUSION AND RECOMMENDATION
CONCLUSION
During 2008, in the countries shown, over 350,000 children died before their fifth birthday due
to diarrhoea caused by poor sanitation and unsafe water (Black, et al. 2010). Many more fell
seriously ill, compromising their future potential and overburdening health services. At current
rates of progress, the
As per the Bangladesh Demographic and Health Survey (BDHS) 2011, the under-5 child
mortality rate in the country has dropped to 53 per 1,000 in 2011 from 65 in 2007. This is a
factor that will help the country achieve the Millennium Development Goal-4 targeting to cut
this rate to 48 per cent by 2015. But still the rate is significantly high compare to neighbouring
countries.
According to different study and observation, the child mortality considerably depends on the
water, sanitation and hygiene practice of the mother‟s group. Thus the study designed to assess
the knowledge of mothers with under children on Water, Sanitation and Hygiene.
As per the study, still 40% of the respondent used Kacha latrine due to many reason. To know
the real causes a question were asked among the respondents and most of them expressed that
lack of money, suitable place and do not know the importance of sanitary latrine use are the
main causes.
To know the concept of the respondent on the cause of worm to children, 61% respondents
reported sweet food intakes and 39% marked stale food as a cause of worm to children. 21%
respondent informed that they don‟t know the reason of worm to children. These findings
indicate the low level of knowledge on causes of worm to children.
If we look at the educational status most of the respondents are illiterate (10%) and only can
sign (40%), besides the mean income of the respondents are Tk. 6511 only. This low profile of
education and income status creates barriers in accessing proper knowledge on wash and also
practicing good hygiene in the family.
Experience shows that hygiene, especially behavioural change, receives limited attention in
traditional interventions. The success of any hygiene promotion effort involves changing habitual
practices. Hand washing with soap or ash after defecation, before eating, after cleaning
children‟s bottoms, before feeding children, and before serving food has a great impact on

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
33
people‟s health. For many years, people were unaware of the necessity of washing hands with
soap or ash. They did not know about the relation between hand washing and related diseases.
This situation has improved and the number of people who are washing their hands with
soap/ash is increasing. Hand washing has become important hygiene behaviour.
There has been considerable improvement since the 1990, but there remain many critical areas
which require urgent attention in order to free the citizens from undignified, inhumane and
unhygienic living conditions. Following points can be considered to overcome this scenario:
Ensure effective targeting of new investments to poor and un-served populations.
Improve water, sanitation and hygiene behaviour among the under privileged group
Develop effective means of hygiene promotion
Ensure sustainable promotion of safe drinking water (at least a single method)
Create awareness through providing knowledge on the benefits of using sanitary latrine
Aware the community people about the environmental effects of unhygienic practices
Develop strong strategy to promote proper hand wash
Public awareness on water and sanitation linkages should be included and emphasized in
all development initiatives, for maximum public health benefits within urban poor
communities.
The adoption of sanitation technologies within low-income communities requires
appropriate designs and applications.
Further research is needed on the design of messages and campaigns on hygiene
awareness for urban poor communities.
REFERENCES
A.P. Vivas, B. Gelaye, N. Aboset, A. Kumie, Y. Berhane, M.A. Wiliams. 2012, Knowledge,
Attitude and Practices (KAP) of Hygiene among School Children in Angolela,
Ethiopia. Washington: Bizu Gelaye; [updated 2010; cited 2012 Sept 20].
Ricard Gine, 2010, Key Challenges for the Rural WASH Sector (Water, Sanitation and Hygiene) in
Developing Countries. Science against Poverty Conference; 8-9 April 2010; La Granja.

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
34
Guy Howard, Katrina Charles, Kathy Pond, Anca Brookshaw, Rifat Hossain and Jamie Bartram.
2010, Securing 2020 Vision for 2030: Climate Change and Ensuring Resilience in
Water and Sanitation Services.
Kashmir Charitable Trust, 2012, PRE KAP Report on Sanitation and Hygiene. Muzaffarabad District.
UNICEF Mozambique, 2009,Water, Sanitation and Hygiene. Maputo, Mozambique: [updated
2009 Jan; cited 2012 Sept 19].
Bangladesh Bureau of Statistics, 2007
S.A. Ahmed, 2012, Water & Sanitation Program, personal communication April 2002, based on
“Health Care Expenditures in Bangladesh” in “Health Situation and Health Care
Expenditures in Bangladesh, Evidences from Nationally Representative Surveys”.
DGHS, 2011, Health Bulletin.
Gautam, O.; Adhikari,B.; Rajbhandari,K.; Jones,O., 2010, Stages of Hygiene Monitoring: An
Operational Experience from Bangladesh. South Asia Hygiene Practitioners' Workshop.
Annette Prüss-Üstün, David Kay, Lorna Fewtrell and Jamie Bartram., 2007, Unsafe water,
Sanitation and Hygiene. In: Comparative Quantification of Health Risks. P. 321-48.
UNICEF, 2006, Water, Sanitation and Hygiene Strategies for 2006-2015. CHAPTERed Nations
Children‟s Fund.
Water Aid Bangladesh, 2011, Water, Sanitation and Hygiene: ; [cited 2011 Apr 17].
UNICEF Mozambique , 2011,Water, Sanitation and Hygiene. Maputo, Mozambiqu,
[updated2009 Jan; cited 2011 Apr 18].
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
35
Annexure: 1
m¤§wZ cÎ
wb¤œ 5 eQ‡ii wkï Av‡Q Ggb gv‡q‡`i cvwb, ¯v¯’ weavb I cwi®‥vi cwi”QbœZv m¤úw©KZ Ávb I avibv
welqK cÖkœcÎ, 2012
AvB wW Rwic GjvKv t
Avmmvjvgy-AvjvBKzg| Avgvi bvg †gv: gvgybyi iwk`| wb¤œ 5 eQ‡ii wkï Av‡Q Ggb gv‡q‡`i cvwb, cqtwb®‥vkb I cwi®‥vi
cwi”QbœZv m¤úw©KZ Ávb I avibv wb‡q Avwg GKwU M‡elbv KiwQ| GB M‡elbvwU Avgvi Avkv wek¦we`¨vj‡q wkÿv Kvh©µ‡gi
GKwU Ask| Gwel‡q wKQ~ Rvbvi Rb¨ Avcbvi mv‡_ K_v ej‡Z PvB| G e¨cv‡i Avcbv‡K wKQy e¨w³MZ cÖkœ wRÁvmv Kiv
cÖ‡qvRb| Avcwb Avgv‡K hv ej‡eb Zv K‡Vvifv‡e †Mvcb ivLv n‡e| Avcwb PvB‡j GB mv¶vrKv‡i AskMÖnb †_‡K weiZ
_vK‡Z cv‡ib| mv¶vrKvi ce©wU m‡ev©”P 20 wgwbU ¯’vqx n‡Z cv‡i| mv¶vrKvi ïiæi ci Avcwb †h †Kvb mg‡q mv¶vrKvi
cÖ`vb eÜ K‡i w`‡Z cvi‡eb| Avcwb hw` mv¶vrKvi w`‡Z ivRx _v‡Kb, Zv n‡j m¤ú~Y© mZ¨ K_v ejv AZ¨šÍ ¸iæZ¡c~b©|
Avcwb Avgv‡K GB M‡elbv m¤ú©wKZ †h ‡Kvb cÖkœ Ki‡Z cv‡ib; Avwg Avgvi mxwgZ mv‡a¨ Zvi DËi †`qvi †Póv Ki‡ev|
Avwg wK Zvn‡j Avcbvi mv¶vrKvi ïiæ Ki‡Z cvwi ?
n¨uv bv
Avwg GB m¤§wZ cÎwU m¤ú~b© c‡owQ/Avgv‡K eywS‡q ejv n‡q‡Q| GB mvÿvZKv‡i AskMÖn‡b Avgvi †Kvb AvcwË †bB|
DËi cÖ`vbKvixi ¯vÿi/wUc mB t .................................................................
cÖkœKZ©vi ¯vÿi t .................................................................

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
36
†mKkvb-1 RbwgwZK Z_¨
101 Avcbvi bvg ejyb ÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑ
102 Avcbvi eqm ÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑ
103 Avcbvi evox †Kvb †Rjvq ÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑÑ
cÖkœ bs cÖkœ ‡Kv‡Wi aib wb‡ ©k
104 Avcbvi mšÍvb KqRb? 1
2
3
4
5
5 Gi AwaK
1
2
3
4
5
6
105 Avcbvi mšÍvb‡`i KqR‡bi eqm 5 eQi ev
Zvi wb‡P?
1
2
2 Gi AwaK
1
2
3
106 Avcwb †Kvb K¬vm ch©šÍ cov‡jLv K‡i‡Qb? wbi¶i (co‡Z Ges wjL‡Z cv‡i bv )
Amgvß cÖv_wgK (cÂg †kªYx ch©šÍ)
cÖv_wgK mgvß
Amgvß gva¨wgK (`kg †kªYx ch©šÍ)
gva¨wgK mgvß
Amgvß D”P gva¨wgK
D”P gva¨wgK mgvß
Amgvß mœvZK
mœvZK mgvß
Amgvß mœvZ‡KvËi
mœvZ‡KvËi mgvß
ïay ¯^v¶i w`‡Z cv‡i
1
2
3
4
5
6
7
8
9
10
11
12
107 ‡ckvMZ Z_¨ - Avcwb eZ©gv‡b ‡Kvb †ckvq
wb‡qvwRZ?
M„wnbx
QvÎx
K…wlKvR
PvKzixRxwe
w`bgRyi
Ab¨vb¨
1
2
3
4
5
6
108 Avcbvi ‣eevwnK Ae¯’v weevwnZ Ges ¯vgxi mv‡_&
weevwnZ wKš‘ ^vgx mv‡_ _v‡K bv
ZvjvKcÖvßv&
weaev
Ab¨vb¨ (D‡jøL Kiæb) ----------------
1
2
3
4
5
109 Avcwb †Kvb ag© Abymvix Bmjvg
wn›`y
‡e․×
wLªóvb
Ab¨vb¨
1
2
3
4
5

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
37
110 Avcbvi msmv‡i gvwmK Mo Avq K‡Zv?
(MZ 6 gv‡mi Mo )
----------- UvKv
msmv‡ii mKj
DcvR©‡bi Mo
†mKkvb-2 (cvwb e¨envi m¤©úwKZ cÖkœ)
201 Avcbvi my‡cq cvwbi cÖavb Drm wK? b`xi cvwb
cyKz‡ii cvwb
PvcKj
‡U‡ci cvwb
Ab¨vb¨
1
2
3
4
5
202 my‡cq cvwbi Drm ch©šÍ †h‡Z Avcbvi KZ
mgq jv‡M?
5wgwbU A_ev Zvi Kg mgq
6 †_‡K 10 wgwbU
11 †_‡K 20 wgwbU
21 †_‡K 30 wgwbU
30 wgwb‡Ui AwaK
1
2
3
4
5
203 cvwb LvIqvi Av‡M Avcwb wK cvwb
weï×Kib K‡i _v‡Kb?
nu¨v
bv
1
2
204 hw` DËi n uv nq, Zvn‡j cvwb weï×Kib
Kivi Rb¨ mvavibZt †Kvb c×wZ e¨envi
K‡i _v‡Kb?
cvwb wm× K‡i
wdëvi ev QvuKbxi gva¨‡g
‡K¬vwib/cvwb weï×Ki †Ue‡jU
Ab¨vb¨
1
2
3
4
203 hw` bv nq
Z‡e 204 DËi
w`‡Z n‡e bv
205 Avcbvi wkïi Lvevi •Zix‡Z Avcwb †Kvb
ai‡bi cvwb e¨envi K‡ib?
wm× cvwb
QvuKbxi gva¨‡g cwi‡kvwaZ wKš‘ wm× bq
QvuKbxi gva¨‡g cwi‡kvwaZ Ges wm×
mivmwi ‡U‡ci cvwb
Ab¨vb¨
1
2
3
4
5
†mKkvb-3 (cqtwb®‹vkb m¤©úwKZ cÖkœ)
301 Avcbvi evmvi Zij eR©¨ mg~n Avcwb wK
K‡ib?
evMv‡b e¨envi Kwi
Mevw` cïi Lv`¨
Gw`K-Iw`K †d‡j †`B
Ab¨vb¨
1
2
3
4
302 Avcbvi evmvi KwVb eR©¨ mg~n Avcwb wK
K‡ib?
cywo‡q †dwj
gvwU Pvucv †`B
Gw`K-Iw`K †d‡j †`B
‣Re mvi •Zix‡Z e¨envi Kwi
Ab¨vb¨
1
2
3
4
5
303 gjZ¨v‡Mi Rb¨ Avcwb †Kvb ai‡bi cvqLvbv
e¨envi K‡ib?
‡mwbUvix cvqLvbv
KuvPv cvqLvbv
1
2
304 Avcwb †Kb GKwU †mwbUvix cvqLvbv •Zix
Ki‡Qb bv? (hw` Avcwb KvuPv cvqLvbv
e¨envi K‡i _v‡Kb)
cÖ‡qvRbxqZv †eva Kwi bv
ch©vß UvKv bvB
chv©ß RvqMvi Afve
wKfv‡e Ki‡Z nq Zv Rvwb bv
Ab¨vb¨
1
2
3
4
5
303 Gi DËi
hw` 1 nq Z‡e
304 cÖ‡hvR¨ n‡e
bv
305 Avcbvi 5 eQ‡ii bx‡P wkïi gj †Kv_vq
‡d‡jb?
bvjvi cvwb‡Z
‡Lvjv RvqMvq
Wv÷we‡b/KwVb e‡R© I mv‡_
M‡Z© cy‡Z †d‡j
1
2
3
4
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
38
cvqLvbvq
Ab¨vb¨
5
6
306 †mwbUvix cvqLvbv e¨envi Riæix †Kb? Avk-cvk cwi®‥vi ivLvi Rb¨
`yM©Ü †_‡K ~‡i _vKvi Rb¨
‡ivM-evjvB †_‡K wbivc` _vKvi
Ab¨vb¨
1
2
3
4
GKvwaK DËi
n‡Z cv‡i|
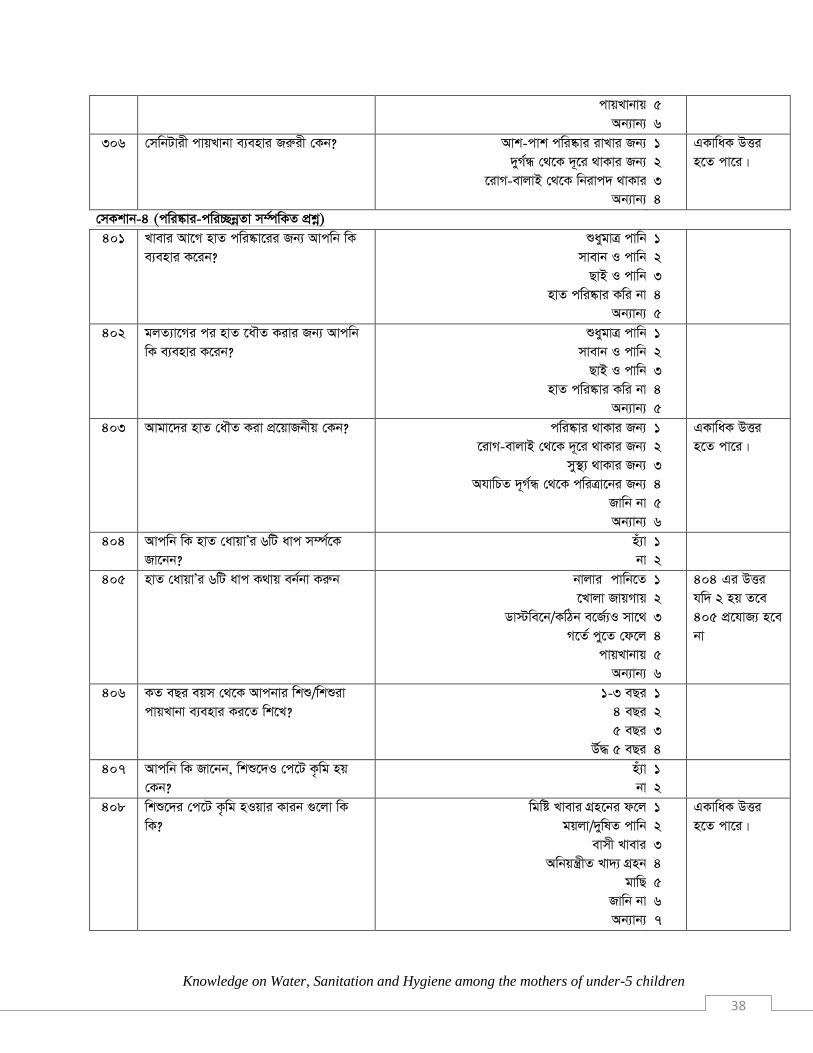
†mKkvb-4 (cwi®‹vi-cwi”QbœZv m¤©úwKZ cÖkœ)
401 Lvevi Av‡M nvZ cwi®‥v‡ii Rb¨ Avcwb wK
e¨envi K‡ib?
ïaygvÎ cvwb
mvevb I cvwb
QvB I cvwb
nvZ cwi®‥vi Kwi bv
Ab¨vb¨
1
2
3
4
5
402 gjZ¨v‡Mi ci nvZ ‡a․Z Kivi Rb¨ Avcwb
wK e¨envi K‡ib?
ïaygvÎ cvwb
mvevb I cvwb
QvB I cvwb
nvZ cwi®‥vi Kwi bv
Ab¨vb¨
1
2
3
4
5
403 Avgv‡`i nvZ †a․Z Kiv cÖ‡qvRbxq †Kb? cwi®‥vi _vKvi Rb¨
‡ivM-evjvB †_‡K ~‡i _vKvi Rb¨
my¯’¨ _vKvi Rb¨
AhvwPZ ~M©Ü †_‡K cwiÎv‡bi Rb¨
Rvwb bv
Ab¨vb¨
1
2
3
4
5
6
GKvwaK DËi
n‡Z cv‡i|
404 Avcwb wK nvZ †avqvÕi 6wU avc m¤ú©‡K
Rv‡bb?
nu¨v
bv
1
2
405 nvZ †avqvÕi 6wU avc K_vq eb©bv Kiæb bvjvi cvwb‡Z
‡Lvjv RvqMvq
Wv÷we‡b/KwVb e‡R© I mv‡_
M‡Z© cy‡Z †d‡j
cvqLvbvq
Ab¨vb¨
1
2
3
4
5
6
404 Gi DËi
hw` 2 nq Z‡e
405 cÖ‡hvR¨ n‡e
bv
406 KZ eQi eqm †_‡K Avcbvi wkï/wkïiv
cvqLvbv e¨envi Ki‡Z wk‡L?
1-3 eQi
4 eQi
5 eQi
D©× 5 eQi
1
2
3
4
407 Avcwb wK Rv‡bb, wkï‡`I †c‡U K…wg nq
†Kb?
nu¨v
bv
1
2
408 wkï‡`i †c‡U K…wg nIqvi Kvib ¸‡jv wK
wK?
wgwó Lvevi MÖn‡bi d‡j
gqjv/ ywlZ cvwb
evmx Lvevi
Awbqš¿xZ Lv`¨ MÖnb
gvwQ
Rvwb bv
Ab¨vb¨
1
2
3
4
5
6
7
GKvwaK DËi
n‡Z cv‡i|
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
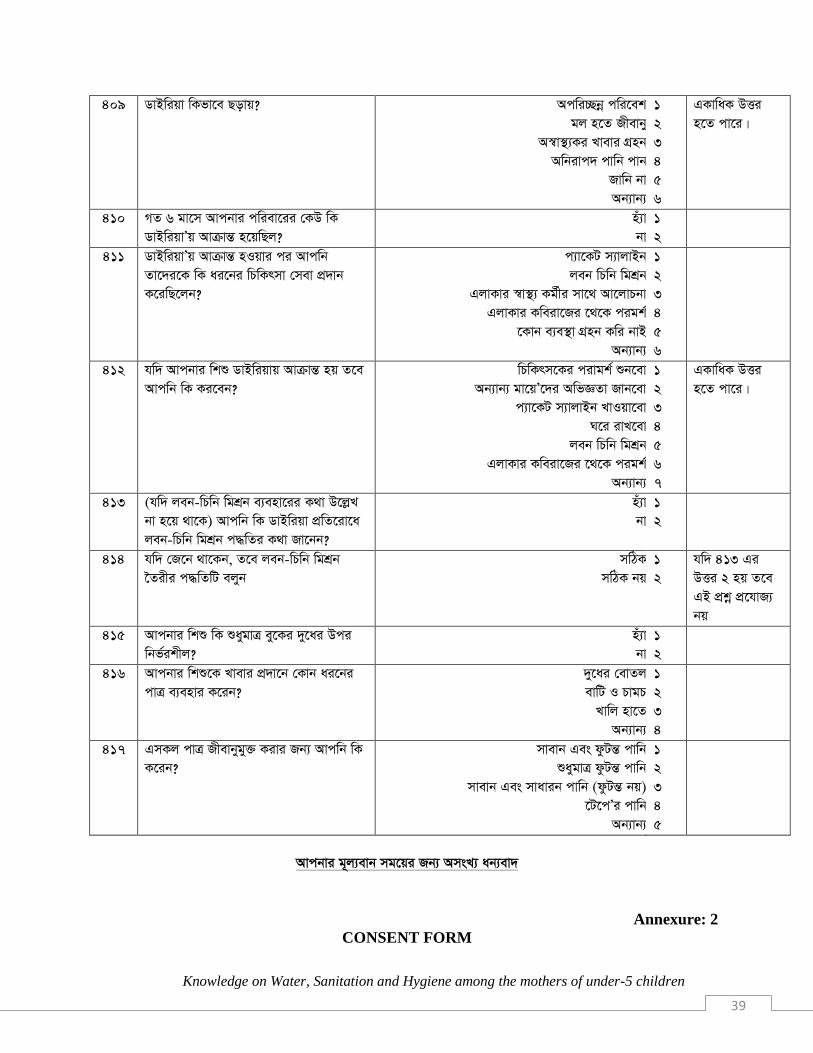
39
409 WvBwiqv wKfv‡e Qovq? Acwi”Qbœ cwi‡ek
gj n‡Z Rxevby
A¯v¯’¨Ki Lvevi MÖnb
Awbivc` cvwb cvb
Rvwb bv
Ab¨vb¨
1
2
3
4
5
6
GKvwaK DËi
n‡Z cv‡i|
410 MZ 6 gv‡m Avcbvi cwiev‡ii †KD wK
WvBwiqvÕq AvµvšÍ n‡qwQj?
nu¨v
bv
1
2
411 WvBwiqvÕq AvµvšÍ nIqvi ci Avcwb
Zv‡`i‡K wK ai‡bi wPwKrmv †mev cÖ`vb
K‡iwQ‡jb?
c¨v‡KU m¨vjvBb
jeb wPwb wgkÖb
GjvKvi ¯v¯’¨ Kg©xi mv‡_ Av‡jvPbv
GjvKvi Kweiv‡Ri ‡_‡K cigk©
‡Kvb e¨e¯’v MÖnb Kwi bvB
Ab¨vb¨
1
2
3
4
5
6
412 hw` Avcbvi wkï WvBwiqvq AvµvšÍ nq Z‡e
Avcwb wK Ki‡eb?
wPwKrm‡Ki civgk© ïb‡ev
Ab¨vb¨ gv‡qÕ‡`i AwfÁZv Rvb‡ev
c¨v‡KU m¨vjvBb LvIqv‡ev
N‡i ivL‡ev
jeb wPwb wgkÖb
GjvKvi Kweiv‡Ri ‡_‡K cigk©
Ab¨vb¨
1
2
3
4
5
6
7
GKvwaK DËi
n‡Z cv‡i|
413 (hw` jeb-wPwb wgkÖb e¨env‡ii K_v D‡jøL
bv n‡q _v‡K) Avcwb wK WvBwiqv cÖwZ‡iv‡a
jeb-wPwb wgkÖb c×wZi K_v Rv‡bb?
nu¨v
bv
1
2
414 hw` †R‡b _v‡Kb, Z‡e jeb-wPwb wgkÖb
‣Zixi c×wZwU ejyb
mwVK
mwVK bq
1
2
hw` 413 Gi
DËi 2 nq Z‡e
GB cÖkœ cÖ‡hvR¨
bq
415 Avcbvi wkï wK ïaygvÎ ey‡Ki `y‡ai Dci
wbf©ikxj?
nu¨v
bv
1
2
416 Avcbvi wkï‡K Lvevi cÖ`v‡b †Kvb ai‡bi
cvÎ e¨envi K‡ib?
`y‡ai †evZj
evwU I PvgP
Lvwj nv‡Z
Ab¨vb¨
1
2
3
4
417 GmKj cvÎ Rxevbygy³ Kivi Rb¨ Avcwb wK
K‡ib?
mvevb Ges dzUšÍ cvwb
ïaygvÎ dzUšÍ cvwb
mvevb Ges mvavib cvwb (dzUšÍ bq)
‡U‡cÕi cvwb
Ab¨vb¨
1
2
3
4
5
Avcbvi g~j¨evb mg‡qi Rb¨ AmsL¨ ab¨ev`
Annexure: 2
CONSENT FORM

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
40
Good morning/afternoon. My name is Md. Mamunur Rashid; I am conducting a study about
Knowledge on Water, Sanitation and Hygiene Among mother groups of under-5 children that
has been approved by ASA University.
Taking part in this study is voluntary. If you agree to participate, I will ask you some questions
about you and your family. The interview will take about 20 minutes. There are no anticipated
problems but in case some questions make you feel uncomfortable, you are free to express your
discomfort or decide not to respond. You can choose not to participate or withdraw from the
interview at any point and that will not affected you in any way.
I will do my best to ensure that your personal information is kept private. Your record will not be
accessed by any other persons except the university concern individuals. It will be kept in a
secure place and only used for purposes of the study.
At this time, do you want to ask me anything about the study? If you have any questions at any
time even after the interview, please feel free to ask.
_____________________________________________________________________________
This consent form has been read and explained to me and I have understood, and my questions
have been addressed. I therefore willingly agree to take part in the study.
Signature/Thumb print of the participant and date_________________________, ____________
Names of Interviewer, Signature and date____________________, ___________,____________

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
41
RESEARCH QUESTIONNAIRE
Date: …..........………….. Respondent No.:
…………
Section A (Socio-demographic Information)
1. Name of respondent : ……………………………...................................
2. Age of respondent : ………………..............
3. District of Origin : ...................................................................
4. Thana (Please ) : Mohammadpur Adabor
5. Education :
Illiterate Primary level Jr. Secon. Level Secondary level
Above
6. Occupation: (Please on the right answer)
House wife Agriculture Service Student Labour Others…….....
7. Religion: (Please on the right answer)
Hindu Buddhist Christian Muslim Other……...
8. Marital Status....................................................................
9. Average Monthly income:..........................................................
Section B (Questions related to water)
1. What is the main source of your drinking water?
a) River
b) Well
c) Standpipe/tap
d) Stagnant pool or dam
e) Other …………
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
42
2. What time does it take to reach the source of water?
a) 5 or less than 5 minutes
b) 5-15 minutes
c) 15-30 minutes
d) 30 minutes or more
3. Do you purify drinking water before use?
a) Yes
b) No
4. If yes, which method do you use for purification of water? a) Boil
b) Filter
c) Chlorinate/Tablet
d) Other………….
5. What kind of water do you use to dilute or mix in the baby’s food? a) Boiled water
b) Un boiled but filtered
c) Boiled and Filtered water
d) Direct Tap water
e) Other…………..
Section C (Questions related to sanitation)
1. How do you manage Liquid Wastes coming from household activities?
a) Use in kitchen Gardening
b) Feed to cattle
c) Throw haphazardly
d) Other……….
2. How do you dispose Solid Waste that comes out of your house?
a) Burn
b) Bury
c) Throw haphazardly
d) Prepare compost
e) Other………
3. What type of latrine you use for defecation?
a) Sanitary Latrine (well built, structured)
b) Non-sanitary Latrine
4. If there’s no sanitary latrine, why you are not initiating to build a sanitary
latrine?
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
43
a) Not necessary
b) No money
c) No place
d) Didn‟t know
e) Other………
5. Where do you dispose of stools of children younger than 3 years?
a) Put/rinsed in drain or ditch
b) Left in the open
c) Throw in into garbage/ with solid waste
d) Buried
e) Used toilet or rinsed in toilet
f) Other...............................
6. Why is it important to have latrines? (Multiple choices)
a) To keep surroundings clean
b) Free from odour
c) Safe from disease
d) Other…………….
Section D (Questions related to hygiene)
1. What do you use to wash your hands before having meal? a) Only water
b) Soap and water
c) Ash and water
d) Don‟t wash hands
e) Other………...
2. What do you use to wash your hands after defecation? a) Only water
b) Soap and water
c) Ash and water
d) Don‟t wash hands
e) Other………...
3. Why should we wash our hands? (Multiple choices)
a) To be clean
b) To get rid of diseases
c) To be healthy
d) To reduce foul odour
e) Don‟t know
f) Other……….
4. Do you know the 6 steps of hand washing?

Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
44
a) Yes
b) No
5. (If yes) please describe
a) Correct
b) Incorrect
6. Age of your children they begin using latrine. a) About 1
b) About 2
c) About 3
d) About 4
e) About 5
f) Children do not use latrines
7. Do you know what causes worms to children? (Multiple choices)
a) Eating sweet things
b) Dirty water
c) Stale food
d) Unbalanced diet
e) Flies
f) Don‟t know
g) Other……………
8. How diarrhoea spreads? (Multiple choices) a) Dirty environment
b) Pathogens from stools
c) Use of unhygienic food
d) Drinking unsafe water
e) Don‟t know
f) Other……………..
9. In previous 6 months, had any one suffered from any diarrhoeal disease?
a) Yes
b) No
10. How do you treat yourself or family members after getting diarrhoea?
a) Use Packet Saline
b) Use homely made sugar-salt solution
c) Take to HPs
d) Take to Traditional Healers
e) Do nothing
f) Other………..
11. What you do in case child gets attack of diarrhoea?
Knowledge on Water, Sanitation and Hygiene among the mothers of under-5 children
45
a) Consult medical personnel
b) Consult Peer
c) Use ORS
d) Keep Home
e) Do nothing
f) Other………….
12. (If sugar-salt solution is not used) have you heard about sugar-salt solutions
for treating diarrhoea?
a) Yes
b) No
13. Do you know the process of preparing Sugar-Salt Solutions? a) Yes
b) No
14. If yes, how do you prepare? Please describe.
a) Correct
b) Incorrect
15. Are your babies exclusively breastfed? a) Yes
b) No
16. On what you fed your baby/babies? a) Bottle
b) Plate and spoon
c) Naked hand
c) Other……..
17. How is baby bottle or cup cleaned?
a) Soap, boiled water
b) Boiled water only
c) Soap, un-boiled water
d) Tap water
e) Other…….
Thank you for your time.