KNOWLEDGE AND PRACTICE OF STUDENT GIRLS REGARDING PREMENSTRUAL SYNDROME
56
Introduction and Aim of the Study 1 INTRODUCTION Premenstrual syndrome (PMS) refers to a cluster of physical, psychological and behavioral symptoms that occur during the luteal phase of the menstrual cycle and end with the onset of menstruation. PMS is viewed now as a complex psychoneuroendocrinology disorder known to affect emotional and physical well-being. PMS is no longer considered a single condition but a group of menstrually related disorders and symptoms. Adolescent girls in many cultures worldwide, have many factors which put them at high risk for PMS, that include age, genetic, psychological, cultural and psychosocial factors (Lin &Thompson, 2001). Premenstrual dysphoric disorder (PMDD) is a severe form of PMS that is characterized by mood symptoms such as irritable, tense, tired, sad and hypersensitive feelings associated with high levels of interpersonal conflict and enough to interfere markedly with occupational and social functions (Endicott et al., 2000) . Over 150 symptoms contributing to PMS which categorized into behavioral and emotional symptoms such as poor coordination, loss of concentration, insomnia, irritability, mood swings, depression, hostility, and social
Transcript of KNOWLEDGE AND PRACTICE OF STUDENT GIRLS REGARDING PREMENSTRUAL SYNDROME

Introduction and Aim of the Study
1
INTRODUCTION
Premenstrual syndrome (PMS) refers to a cluster of
physical, psychological and behavioral symptoms that
occur during the luteal phase of the menstrual cycle and
end with the onset of menstruation. PMS is viewed now as
a complex psychoneuroendocrinology disorder known to
affect emotional and physical well-being. PMS is no
longer considered a single condition but a group of
menstrually related disorders and symptoms. Adolescent
girls in many cultures worldwide, have many factors
which put them at high risk for PMS, that include age,
genetic, psychological, cultural and psychosocial factors
(Lin &Thompson, 2001).
Premenstrual dysphoric disorder (PMDD) is a severe
form of PMS that is characterized by mood symptoms
such as irritable, tense, tired, sad and hypersensitive
feelings associated with high levels of interpersonal
conflict and enough to interfere markedly with
occupational and social functions (Endicott et al., 2000).
Over 150 symptoms contributing to PMS which
categorized into behavioral and emotional symptoms such
as poor coordination, loss of concentration, insomnia,
irritability, mood swings, depression, hostility, and social

Introduction and Aim of the Study
2
withdrawal, whereas physical symptoms include bloating,
breast tenderness, pelvic pain, sensation of weight
increase, headache, fatigue, urinary frequency and
constipation (Ling & Duff, 2001).
Approximately 95% of girls are affected with PMS,
about 20% to 40% of these girls have more severe
symptoms that interfere with their work or social life, a
generally stressful life and problematic relationships that
may be related to intensity of symptoms (Ried, 2003).
Some girls report moderate to severe life disruptions
secondary to PMS that negatively affect their interpersonal
relationships. PMS may also be a factor in reduced
productivity, work related accidents and absenteeism (Dell
et al., 2001).
Premenstrual syndrome is of unknown cause.
Theories originally emphasized a combination of
biological, psychological and social factors. These factors
such as hormone imbalance, abnormal prostaglandin
metabolism, vitamin deficiency, changes in endorphin
levels, and external stressors also play a part in the girls'
perception of PMS and its severity (Hudson, 2002).
Nurses play an instructive and supportive role to
help girls coping with PMS and its problems. The nursing
role in PMS involves helping girls and their families to

Introduction and Aim of the Study
3
become more informed about premenstrual symptoms,
causes, and rational for any planned treatment. The most
important part of management is to reassure girls,
understand girls concerns and disruptions which
symptoms are causing to girls life. As PMS can be a long-
term problem there are life style modifications which help
girls to cope with symptoms such as practicing exercise,
relaxation techniques and diet modification (Beausang &
Razor, 2004).
Justification of the problem:
Approximately 75% of adolescent girls experience
some kind of problems associated with menstruation. PMS
affects millions of girls during their reproduction years
(Ziv et al., 2000). According to Ahmed et al. (2002), the
prevalence of PMS among 800 students in Assuit
University was 73.9%. Girls had a lack of general
knowledge related to menstruation and do not understand
much about PMS, or recognize that the problems they
have are related to their menstrual cycle, such as,
absenteeism from school, low self-esteem, stressed
relationships, and limited daily home activities and social
events. They may feel symptoms are not severe enough to
discuss, so assessing of adolescent girls knowledge and
their health practices regarding PMS are the main concern
of this study.

Introduction and Aim of the Study
4
Aim of the Study:
To evaluate knowledge and practice of student girls
regarding premenstrual syndrome this aim was achieved
through:
1- Assessment of student girls knowledge about
PMS.
2- Assessment of student girls practices taken to
relief PMS.
Research Questions:
Is there a knowledge deficit regarding PMS that
affects on practices taken by student girls to relief
symptoms?

Review of Literature
5
PREMENSTRUAL SYNDROME
Definition:
Premenstrual syndrome describes a range of
predictable physical and affective symptoms that occur
cyclically during the luteal phase of the menstrual cycle
and resolve at the onset of menstruation. PMS begins 7 to
10 days before menses and ceases with the onset of
bleeding. PMS can be a long term condition, in some girls,
symptoms flare up before every menstrual period. This
pattern continues until menopause, it's a characteristic for
adolescent girls to experience symptoms at the time of
menses in varying degrees of severity from mild to severe
(Dicarlo et al., 2001).
Premenstrual syndrome means a group of physical,
mood, and behavioral changes that occur in a regular
cyclic relationship to the luteal phase of the menstrual
cycle. The mildest PMS changes are known as molimina
which are referring to those symptoms (breast pain,
bloating, acne and constipation) most girls experience at
or near menstruation (Meaden et al., 2005).
Premenstrual dysphoric disorder (PMDD) is a severe
form of PMS characterized by some combination of
marked mood swings, depressed mood, irritability, and

Review of Literature
6
anxiety, which may be combined with physical symptoms
(Hylan et al., 1999).
Pathophysiology of Premenstrual Syndrome:
1- Normal hormonal changes along the menstrual cycle
Hypothalamic gonadotropin releasing hormone
(GnRH) stimulates the anterior pituitary gland to release
follicle stimulating hormone (FSH) and Luteinising
hormone (LH). FSH stimulates the initial secretion of
estrogen by the follicles and LH further stimulates
follicular development and full secretion of estrogen,
triggers ovulation, promotes formation of the corpus
luteum and stimulates the corpus luteum to produce
estrogen and progesterone. Moderate levels of estrogen
inhibit release of GnRH and secretion of LH and FSH.
High levels of progesterone also inhibit GnRH and LH
secretion. High levels of estrogen during the last part of
the preovulatory phase can actually exert positive
feedback on both the hypothalamus and anterior pituitary
gland resulting in the LH surge that triggers ovulation.
This positive effect of estrogen does not occur if
progesterone is present at the same time (Miner et al.,
2002).
Review of Literature
7
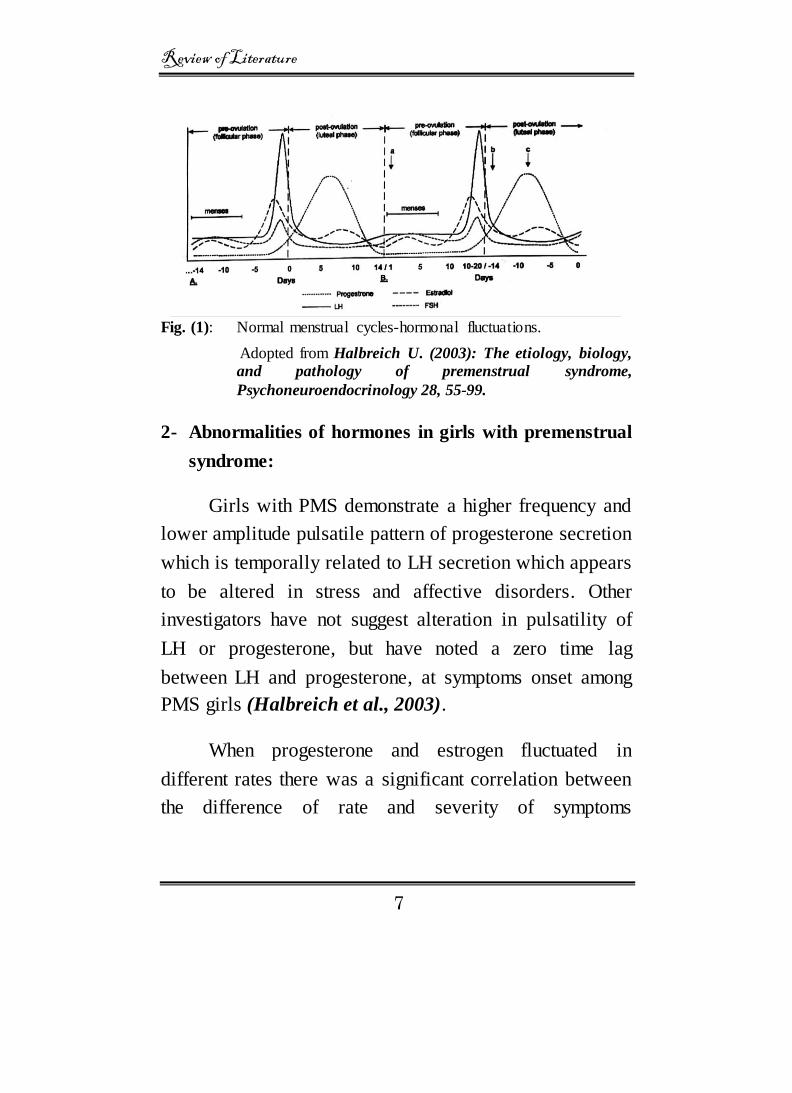
Fig. (1): Normal menstrual cycles-hormonal fluctuations.
Adopted from Halbreich U. (2003): The etiology, biology,
and pathology of premenstrual syndrome,
Psychoneuroendocrinology 28, 55-99.
2- Abnormalities of hormones in girls with premenstrual
syndrome:
Girls with PMS demonstrate a higher frequency and
lower amplitude pulsatile pattern of progesterone secretion
which is temporally related to LH secretion which appears
to be altered in stress and affective disorders. Other
investigators have not suggest alteration in pulsatility of
LH or progesterone, but have noted a zero time lag
between LH and progesterone, at symptoms onset among
PMS girls (Halbreich et al., 2003).
When progesterone and estrogen fluctuated in
different rates there was a significant correlation between
the difference of rate and severity of symptoms

Review of Literature
8
contributing to premenstrual symptoms formation
(Schmidt et al., 1998).
Both estrogen and progesterone interact with the
renin-angiotensin-aldosterone system (RAAS), which
influences electrolytes and fluid imbalance, aldosterone
acts to increase sodium and water retention, estrogen may
stimulate the RAAS by inducing the syntheses of
angiotensinogen in the liver, these estrogen and
progesterone effects have been suggested to underlie
menstrual related symptoms such as bloating and also
contribute to weight gain (Parsey & Pony, 2000).
Estrogen influences some of the major
neurotransmitters involved in regulation of mood,
behavior and cognitive functions including serotonin,
noradrenalin, gamma amino butyric acid (GABA),
dopamine and acetylcholine. Various serotonergic
receptors and systems appear to play different roles in the
modulation of PMS. Whole blood serotonin levels during
luteal phase have been shown to be lower in girls with
PMS as compared with girls with no PMS but also
abnormal serotonergic activity prior to the symptomatic
period is important for symptom formation (Mitwally et
al., 2002).

Review of Literature
9
Endogenous opioids activity is closely related to
hypothalamic pituitary gonadal (HPG) axis activity, the
contributing rate of the significant late luteal phase
decreases in opioids activity, that withdrawal may
contribute to symptoms formation of irritability, decreased
self-control impulsivity, aggression and anxiety (Blumer
et al., 1998).
A gradual but steady drop in serum calcium starting
about 10 days before the menstrual flow takes place. This
calcium drop is a stress condition and the adrenals are
affected in a manner that cause retention of salts and water
in the body resulting headache and depression, when the
menstrual flow occurs, the calcium drops further causing
uterine and muscular cramps, convulsions may result if the
calcium drop is markedly low (Gorman et al., 2001).
Etiology of premenstrual syndrome:
The exact cause of PMS is unknown, theories about
causes of PMS include progesterone deficiency, estrogen
excess, increased activity of aldosterone, vitamin B6
deficiency and serotonin deficiency, current research
suggests that PMS is most likely of multifactorial origin,
with involvement of neurohormones and neurotransmitters
(Stud, 2003).
Review of Literature
10
1- Progesterone and estrogen theory
Recurrence of psychometric symptoms in relation to
the luteal phase led to the theory that, hormonal
production in the corpus luteum causes premenstrual
symptoms that, estrogen and progesterone played a role
in PMS, mainly because of their fluctuating patterns that
occur during the menstrual period (Cohen et al., 2002).
Excess estrogen, deficient progestin, and
inappropriate ratio of the two sex steroids or inadequate
corpus luteal function are associated with PMS. Recent
clinical studies haven't consistently implicated abnormal
estrogen or progesterone levels in PMS, although certain
PMS symptoms can be reproduced through hormonal
manipulation (Pregler & Decherney, 2002).
Estrogen's ability to affect serotonergic neurological
function has led some researchers and clinicians to
postulate that PMS involves problems with serotonin
system (Nelson, 1998).
2- Serotonin theory:
Serotonin is a neurotransmitter that is known to play
an important role in our mood, appetite, and behavior
patterns. Some studies have demonstrated blood serotonin
levels to be significantly lower in the luteal phase of the
Review of Literature
11
menstrual cycle of girls with PMS, reduced serotonergic
neurotransmission has been linked with depressed mood,
irritability, anger, aggression, poor control impulses and
increased craving for carbohydrates (Lewis et al., 2000).
PMS is related to enhanced sensitivity to
progesterone in girls with underlying serotonin deficiency.
This mechanism doesn't explain all cases because some
girls don't respond to treatment with selective serotonin
reuptake inhibitors (Kessel, 2000).
3- Prostaglandin theory:
Prostaglandins are produced in the breast, brain,
gastrointestinal tract, kidney and reproductive tract. These
areas often present with physical symptoms, so
deficiencies in prostaglandins related to inability to
convert linoleic acid to prostaglandin in precursors may be
involved in PMS (Steiner & Born, 2000).
4- Endorphin theory:
There is a relative decrease in the luteal phase
endorphin levels in some girls who suffer from PMS,
because these endogenous opiates are associated with a
sense of well-being, a decline in their production is seen as
a cause of these symptoms (Beckmann et al., 1998).

Review of Literature
12
Abnormal prostaglandin production in girls with
PMS also may interfere with beta-endorphin synthesis
causing PMS alleviation of symptomatology when
moderate exercise is undertaken, presumably because of
an exercise-associated increase in endorphin production
(Gstrzenski, 2002).
5- Hypoglycemia
Studies have suggested that PMS may be related to
abnormally low blood sugar (hypoglycemia), girls with
PMS seem to have a high intake of salt and refine
carbohydrates resulting in premenstrual hypoglycemic
episodes, sometimes associated without bursts of crying
and violent behavior (Hammond & Riddick, 2000).
6- Vitamin deficiency
Deficiencies in number of vitamins, minerals and
other nutrients may by associated with premenstrual
distress and behavior symptoms. Deficiencies of
magnesium, manganese, B vitamins, vitamin E, calcium
and linoleic acid and its metabolites have been reported in
girls with PMS (Bendich, 2000).
7-Genetic factors
There is a genetic predisposition to PMS, study of
monozygotic twins demonstrated that over 90% exhibited

Review of Literature
13
similar PMS symptoms to their twin. In contrast, about
50% of dizygotic twins and non-twin sibling had similar
PMS symptoms (Kendler et al., 1998).
Fig.(2): The etiology and Pathophysiology of PMS.
Adopted from Halbreich u, (2003): The etiology, biology and
evolving pathology of premenstrual syndrome, Psychoneuro-
endocrinology, 28, 55-99.
Symptoms of premenstrual syndrome:
Symptoms of PMS were not recognized as occurring
specifically during the late luteal phase. They were more
broadly described as being related to the general process
of menstruation and more closely linked to the actual
bleeding of menses, symptoms can begin any time after
ovulation but there must be a symptom-free interval

Review of Literature
14
during the follicular phase of the menstrual cycle
(Pearlstien et al., 2003).
Fig. (3): Several premenstrual symptom patterns .
Adopted from Moline ML& Zendell SM (2000): Evaluating
and managing premenstrual syndrome. Med Gen, 212.
Pattern 1, symptoms begin during the week before
menstruation and remit during menses. Pattern 2 differs in
that symptoms begin around the time of ovulation and
persist through the luteal phase. In pattern 3, a brief of
symptoms occurs around ovulation with the symptoms
returning during the second week of the luteal phase. The
fourth pattern depicts symptoms that begin at ovulation
and continue through menses leaving only a symptom-free
week to 10 days.
Review of Literature
15
Over 150 symptoms have been attributed to PMS,
there is considerable variation in the duration of
symptoms. It varies widely from one girl to another and
from cycle to the next in the same person, great variability
is found in the degree, but few are severely affected (Dog,
2001).
Symptoms may increase during periods in which
girls experience rapid hormonal changes such as puberty,
after pregnancy, discontinuation of oral contraceptives and
after periods of menstrual irregularity (Johnson, 2004).
Some girls reported symptoms that distressing them for
several days around ovulation and then again in the
premenstrual week, other girls may have troubles for only
several days before menses (Pearlstien et al., 2000).
Classification of premenstrual symptoms
Premenstrual symptoms can be classified as
affective, cognitive, autonomic, behavioral, neuro1ogic
and dermatologic symptoms.
I. Affective symptoms include sadness, anxiety, anger,
irritability and mood swings.
II. Cognitive symptoms manifested as decreased
concentration, paranoia, rejection, and suicidal
ideation.

Review of Literature
16
III. Autonomic symptoms include nausea, diarrhea, and
palpitation.
IV. Behavioral symptoms are demonstrated by decreased
motivation, poor impulse control, decrease efficiency
and social isolation.
V. Numbness and tremors are the neuralgic symptoms.
VI. Dermatologic symptoms are dry hair and pain
experience by women with PMS can manifested as
headache, breast tenderness and muscle pain
(Littleton &Engerbretson, 2005).
Major symptoms of PMS, include headache ,fatigue,
lower back pain, painful breast and feeling of abdominal
fullness, general irritability, mood swings, fear of losing
control, and crying spells may also occur (Morse, 1999)
(Table 1).

Review of Literature
17
Table (1): Symptoms of Premenstrual Syndrome (Morse,
1999).
Physical symptoms Headache, dizziness
Abdominal bloating or swelling; swelling of extremities Weight gain
Breast tenderness Hot flashes
Abdominal cramps Generalized muscle and joint pain Fatigue
Appetite changes: binge eating, food craving Sleep changes: excessive or insomnia
Reduced sexual interest
Behavioral symptoms Depression or sadness
Feelings of hopelessness Marked anxiety
Confusion, forgetfulness, poor concentration Accident prone Irritability and anger
Emotional liability: tearfulness or crying easily, loneliness, mood instability
Reduced interest in normal daily activities Social avoidance Lethargic or energetic
Hendrick (2002) classified PMS into both physical
and emotional symptoms and listed common symptoms as,
breast swelling, tenderness, fatigue, bloating, constipation
or diarrhea, headache, food cravings, muscle pain, tension,
irritability, mood swings, depression and trouble
concentrating or remembering.
Review of Literature
18
Researchers' studies of adolescent girls discovered
that the most common manifestation of PMS was negative
affect characterized by mood swings, stress and
nervousness, and physical symptoms as breast tenderness,
abdominal bloating, fatigue and edema (Derman et al.,
2004).
Moline and Zendell (2000), also classified
symptoms of premenstrual syndrome into physical
symptoms, behavioral symptoms and psychological
symptoms (Table 2).
Table (2): Common Symptoms of Premenstrual Syndrome
(Moline & Zendell, 2000).
Behavioral symptoms: Fatigue, insomnia, dizziness, changes
in sexual interest, food cravings or overeating.
Psychological symptoms: Irritability, anger, depressed mood,
crying and tearfulness, anxiety, tension, mood swings, lack of concentration, confusion, forgetfulness, restlessness,
loneliness, decreased self-esteem and tension.
Physical symptoms: Headaches, breast tenderness and
swelling, back pain, abdominal pain and bloating, weight gain, swelling of extremities, water retention, nausea, muscle and
joint pain.

Review of Literature
19
Risk factors of premenstrual syndrome:
1- Age:
Premenstrual syndrome is higher in adolescents, it
affects girls with ovulatory cycles, older adolescents tend
to have more severe symptoms than younger adolescents
whose age at menarche was 12 years. Symptoms of PMS
diminish after age of 35 years and resolve completely at
menopause (Lowdage, 2001).
2- Psychosocial factors:
Regarded the incidence of PMS that increased after
major life events and stressors, these events are associated
with somatic health symptoms. Girls are reporting
significant life stressors which are more likely to rate
premenstrual symptoms, stressors such as premature
parental loss, childhood sexual abuse and interpersonal
difficulties; combination of lack of parental warmth and
lack of social support system (Wood et al., 1999).
3- Psychiatric disorders:
As many as 70% of girls with PMS have a history of
mood disorders including major depression, anxiety
disorders, and personality disorders, although a past
history of mood disorders is very common with PMDD,
Review of Literature
20
the relation between them including high life time rates for
phobia and obsessive-compulsive disorder should not be
neglected that irritability, impulsivity, anger, anxiety,
tension and nervousness are very prevalent premenstrually
(Lemelledo et al., 2000).
4- Hereditary factors:
There are high correlations between premenstrual
tension of mothers and daughters. A similarity of PMS
subtype was noted if the mother had nervous symptoms,
69.8% of daughters had similar symptoms, and 62.5% of
the daughters with symptoms-free mothers were also
symptoms free (Kendler et al., 1998).
5- Life style factors:
Physical activity and dietary patterns have long been
influencing PMS. Alcohol consumption, caffeine intake
have been found to be higher with PMS prevalence among
girls who consumed more as compared with non drinkers,
A significant greater prevalence of PMS in girls who have
not reported exercising on regular basis (Deuster et al.,
1999). Also, life style plays a significant role in PMS,
symptoms appear to be most troubling in girls who smoke,
rarely exercise and who reported environmental stress
(Sternfeld et al., 2002).

Review of Literature
21
6- Other risk factors:
Other risk factors associated with increase risk of
PMS are: low parity because fewer pregnancies mean
more menstrual cycles and greater exposure to cyclic
changes in estrogen and progesterone. A woman who uses
oral contraceptives (OCs) may be less likely to have
premenstrual symptoms suggesting that briefer exposure
to estrogen and progesterone fluctuations protects against
PMS (Johnson, 1998).
Premenstrual symptoms is prevalent regardless of
parity, race culture or socio-economic group, there is no
single cause for PMS, it's a combination of physiological,
psychological and social factors that are involved (Pregler
& Decherney, 2002).
Prevalence of premenstrual symptoms:
Studies on the prevalence of premenstrual symptoms
and syndromes have produced mixed results depending
upon the diagnostic criteria and the method of measuring
symptoms (Spitzer et al., 2000).
Researchers, who undertook broad surveys
questioning girls about general premenstrual symptoms,
found the highest prevalence of premenstrual dysphoric
and have been already reported in adolescent girls aged 14

Review of Literature
22
and over. Approximately 50- 80% of girls experienced at
least a few premenstrual symptoms that may be varied
from mild to severe (Wittchen et al., 2002).
Premenstrual conditions grouped into 3 broad
categories: Severe PMDD that affects about 2% to 9% of
girls, moderate to severe PMS that affects about 20% to
40% of girls, and mild PMS which affects up to 80% of
girls at the reproductive age (Bornstein et al., 2003).
In Egypt, a study conducted by Amasha 1995, to
assess prevalence of premenstrual tension syndrome
among nursing students in Port Said City, the prevalence
rate was 77.2%. Of these girls 39.3% suffered from mild
PMS, 24% from moderate and 13.9% had severe PMS.
Effects of premenstrual syndrome on adolescent girls
Adolescent girls develop an altered body image,
decrease in self esteem, lack of self-confidence and
subsequently affect their relationship with others. On
reaching adulthood, these affects may give rise to broken
engagement, marital distress, difficulty in pursing
education goals or becoming withdrawn and socially
isolated (Hylan et al., 1999).
Adolescent girls with PMS have been reported to
view their bodies in a negative light, with feeling of failure

Review of Literature
23
and shame having been expressed. PMS puts a consistent
strain on family relationships, includes increased family
conflict, disrupted communication and decreased family
cohesion (Baram, 2000). Impaired work productivity in
adolescent girls with PMS was reported perimenstrually
and continued also during the early follicular phase
(Chawla et al., 2002).
There are close link between mood and sexuality
premenstrually. Many girls are less interested in sexual
activity premenstrually due to that they suffer from
symptoms such as tiredness, breast tenderness and mood
changes which lead to tension within relationships
(Ganger & Allanch, 2001).
Premenstrual syndrome affects adolescent girls on
limiting daily home activities, participation in social
events, class concentration, home work tasks, also extends
to sleep deprivation and causes school absenteeism among
adolescent girls (Montero et al., 1999).

Review of Literature
24
Fig. (4): Vicious circles of negative thinking in PMS. Adopted from Ganger E,& Allanch V, (2001): Gynecological
Nursing. Harcourt: London, pp. 109-125.
PMS Symptoms
Guilt Low mood Low mood
" I'm less in control. I
won't perform as well
as I should "
Being out of control is
confirmed as dreadful
Perceives further difficulty.
"I can't do it, so I am
useless, a failure."
Irritable outburst Tries harder
Anxiety, tension
depressed mood
Guilt : " I should be in
control. I should be able to do this "
Resentment: "There are too
many demands on me.
Nobody cares about me or
helps me."

Review of Literature
25
Diagnosis of premenstrual syndrome
There is no consensus for diagnosis of clinically
significant PMS. The essential components include
confirmation of the expected relationship of the symptoms
to the menstrual cycle (First et al., 1997).
Diagnosis of PMS is made only if the following
criteria are met; symptoms occur in the luteal phase and
resolve with in a few days of menses onset, symptoms free
period occur in the follicular phase, the recurrence,
cyclicity, timing of symptoms are documented by daily
symptom reports, symptoms are not explained by another
chronic physical or mood disorder, it causes emotional and
physical distress and suffering or impaired of daily
functions (ACOG, 2000).
Premenstrual symptoms are varied and no specific
diagnostic test exists, a premenstrual disorder may be
unrecognized or misdiagnosed as another condition, a
wide range of medical problems should be ruled out, such
as anemia and endometrioses, dysmenorrhea, thyroid
disorder, diabetes mellitus, psychiatric disorders such as
major depression, dythymia, bipolar disorder, generalized
anxiety and panic disorder (Mortola, 2000).

Review of Literature
26
Diagnostic criteria are important for distinguishing
between PMS and other disorders. For determining the
effective treatment, diagnosis is determined by results of
diaries, physical examination, laboratory tests (Strine et
al., 2005).
In women with severe dysphoric symptoms research
criteria can be used to establish the diagnosis of PMDD.
(Table 3)
Table (3): Criteria for diagnosis of premenstrual dysphoric
disorder (American Psychiatric Association,
2000)
Symptoms occur 1 week before menses and resolve in the first few days after menses begins
Five or more of the following (one must be among the first four):
Markedly depressed mood with feelings of hopelessness
Marked anxiety or tension
Marked affective liability
Irritability and anger
Decreased interest in usual activities and social withdrawal
Lack of energy
Appetite change (over eating or under eating)
Change in sleep pattern (hypersomnia or insomnia)
Feeling out of control or overwhelmed
Difficulty with concentration
Somatic symptoms such as abdominal bloating, breast tenderness,
headaches, or joint pain
Symptoms are severe enough to interfere with work, school, usual activities, or interpersonal relationships

Review of Literature
27
The patient keeps a
premenstrual daily
symptom diary for two to three months
Are the patient's
symptoms
consistent with PMS
No
Evaluate the patient
for
other physical and
psychiatric disorders.
Yes
Are the patient's
symptoms
restricted to the luteal phase
of the menstrual cycle
No
Yes
Do the patient's
symptoms interfere with
daily functioning?
No Premenstrual
symptoms
Yes
Evaluate the severity of
the patient's symptoms and refer to the
diagnostic criteria for
PMS and PMDD
Fig. (5): Diagnosis of Premenstrual Symptoms, PMS, and PMDD. Adopted from Kessel, B. (2000): Premenstrual syndrome
advanced in diagnosis and treatment. Obstet Gynecol Clinic
North Am; 27: 625-39.

Review of Literature
28
1-Daily Symptom Reports
Daily prospective rating of symptoms, is initially the
most strong method of confirming diagnosis of symptoms
associated with PMS which typically begin during the late
luteal phase and resolve promptly with the onset of
menstruation, and this is helpful to girls having a complete
prospectively daily report about severity of symptoms
throughout their menstrual cycles (Halbreich et al., 2000).
A number of instruments have been used for rating
PMS symptoms, daily symptom reports by girls remain
the most useful diagnostic tool, they must keep a
menstrual calendar for 3 months on which she carefully
records daily symptoms, rating them on a scale of 0 to 4
with (0) used for no symptoms and (4) used for severe and
debilitating symptoms. Common tools included the
Menstrual Distress Questionnaire (MDQ), the
Premenstrual Assessment Form (PAF), and the
Prospective Record of the Impact and Severity of
Menstruation (PRISM) (Angest et al., 2001).

Review of Literature
29
Fig. (6): Premenstrual Daily Symptom Diary.
Adopted from Dickerson et al. (2003): Premenstrual
syndrome. American Family Physician, 76 (8): 1743-1752.
2-Physical examination
History consists of a list of girl premenstrually
related symptoms and how they interfere with her daily

Review of Literature
30
life, the timing of each symptom in relation to menses
should be reviewed carefully, other important aspect was
medical history through review of the symptoms of
conditions that can mimic PMS, history of drugs that can
affect mood or hormone levels including birth control
pills, thyroid medications and tranquilizers, should be
taken (Praschak-Rieder et al., 2001).
Physical and pelvic examination will assist in
diagnosing PMS because it will help to rule out possible
causes of the symptoms such as thyroid disorder, cardiac
abnormality, major depression, alcohol problems, drug
abuse, endometriosis, pelvic mass and allergies. Many
women experience both psychiatric disorder and PMS
simultaneously, that chronic minor depression is the most
common condition, the diagnostic challenge is to sort out
those with PMS only, another diagnosis only, or both
diagnosis concurrently (Pearlstein, 2002).
Family history, particularly that related to the
adolescent mother and female siblings is relevant because
the nature patterns of menstruation have a genetic basis
(Deuster et al., 1999).

Review of Literature
31
3-Laboratory tests
There is no hormone or laboratory tests that indicate
PMS diagnosis, standard hematology and blood chemistry
profiles are conducted to confirm general good heath
thyroid function test that may be obtained to screen out
thyroid (Freeman, 2003).

Review of Literature
32
MANAGEMENT OF
PREMENSTRUAL SYNDROME
Treatment for PMS depends largely on the severity
of the symptoms, and treatment goals should include
building self-esteem and self-control, reduction of stress,
eliminate symptoms, reduce their impact on activities and
interpersonal relationships (Moline & Zendell, 2000).
Non Pharmacological Treatment
Relaxation technique and exercise
Relaxation techniques are helpful tools for coping
with stress and promoting long-term health by slowing
down the body and quieting mind. Techniques generally
entail, refocusing attention, and increasing body awareness
(Lazar, 2000).
When we become stressed our bodies engage in
something called the (fight or flight response) which refers
to changes that occur in the body it prepares to either fight
or run, these changes include increased heart rate, blood
pressure, rate of breathing and 300-400 % increase in the
Review of Literature
33
amount of blood being pumped to the muscles, over time
these reactions raise cholesterol levels, disturb intestinal
activities, depress the immune system and leave us feeling
(stressed out) (Holroyd et al., 2001).
On the other hand, the relaxation response refers to
changes that occur in the body when it is a deep state of
relaxation, changes include decreased blood pressure,
heart rate, muscle tension and rate of breathing, as well as
feelings of being calm and in control, reduce the
perception of pain and reduce symptoms. Massage therapy
has also shown to decrease anxiety, depressed mood and
pain immediately after massage sessions, that include
reduced pain, menstrual distress and fluid retention
(Hernandez-Reif et al., 2000).
Exercises the most frequently (18%) used form of
treatment for PMS among alternative therapies, exercise
infrequently prescribed as integral part of a life-style
modification program, exercise founded to be helpful by
possible increasing endogenous production of endorphins
(Strine et al., 2005).

Review of Literature
34
Aerobic exercise, even just taking 30 minutes walk
every day, is beneficial in lowering the intensity and
number of premenstrual symptoms, although an aerobic
exercise, yoga releases muscle tension, regulates breathing
and reduces stress, some evidence indicates that exercise
can also reduce fluid retention, negative affect, bloating
and improve problems of concentration, pain, fear and
guilt (Kaur et al., 2004).
Herbal Therapy
1- Evening primrose oil
The most publicized and popular choice treatment of
PMS, is herbal product contains gamma linoleic acid. This
essential omega-6 fatty acid is a prostaglandin precursor.
Some researchers believed that girls in the premenstrual
phase of their cycle had deficiency in gamma linoleic acid,
leading to symptoms that attribute to abnormal
prostaglandin synthesis. Evening primrose oil 3 to 6g daily
has been used to treat breast tenderness, other putative
uses are for irritability, ankle swelling and depressive
symptoms (Bosarge, 2003).
Review of Literature
35
2- Chaste berry (Vitex angus-castes)
The fruit of chaste tree, was used for variety of
gynecologic conditions such as premenstrual syndrome,
cyclical breast discomfort, menstrual cycle abnormalities
and dysfunctional uterine bleeding. Chaste berry
therapeutic effects are attributed to its direct effects on
various hormones especially prolactin and progesterone
(Czygan & Mayer, 2005).
Chaste berry reduced some symptoms, especially
breast tenderness, edema, constipation, irritability,
depressed mood, anger and headache. Over the past 50
years, European trials of chaste berry have reported
improvement of premenstrual and menstruation related
disorders (Schellenberg, 2001).
There is no drug interaction with chaste berry, it is
usually well tolerated with only minor adverse effects
reported. Side effects generally include mild
gastrointestinal complaints, dizziness, headache, tiredness,
and dry mouth (Loch et al., 2000).The dosages of chaste
berry used is 20-40mg/day of the fruit extract, fluid extract
Review of Literature
36
40 drops/ daily and tincture 35-45 drops 3 times daily, also
have been used (Mills & Bone, 2000).
Pharmacological Therapy
1- Diet therapy
A- Vitamin B6:
Vitamin B6 is a cofactor in neurotransmitter
synthesis, this vitamin has been suggested as a treatment
for PMS on the basis of its role in carbohydrate and
gonadal steroid metabolism, daily doses of 50-100 mg
may reduce severity of premenstrual depressive and
physical symptoms, no more than 100 mg daily because of
the risk of peripheral neuropathy (Hudson, 1999).
B- Calcium:
Calcium supplementation effect against pre-
menstrual symptoms of moderate severity, 1200 mg of
calcium administered daily result in a clinically significant
reduction in cluster of physical and emotional symptoms,
it relieve symptoms of water retention, negative affect
food cravings and pain (Thys-Jacob et al., 1998).

Review of Literature
37
C- Vitamin E:
Vitamin E exerts its effect through prostaglandin
synthesis or regulation of central neurotransmitters, it may
relieve some mood and physical symptoms, including
anxiety and breast tenderness with dose 400 Iu daily
(Stevinson & Ernest, 2001).
D- Magnesium:
Girls with PMS have lower levels of magnesium in
erythrocytes and leukocytes despite normal plasma
magnesium levels. Magnesium helps to stabilize blood
sugar levels, acting as a mild laxative, replacing
magnesium in dose 200-400mg, once daily reduced fluid
retention, can reduce constipation that exacerbates
menstrual pain and bloating with adverse reaction mild
somatic diarrhea (Golberg, 2001).
2- Non Steroidal Anti Inflammatory Drugs (NSAIDs)
Non steroidal anti inflammatory drugs effectively
treat the pain component of PMS, administered 3 to 4 days
premenstrual reduce breast tenderness, only naproxen
sodium and mefenamic acid have been evaluated for PMS

Review of Literature
38
therapy. The most frequent adverse reactions to NSAIDs
are gastrointestinal with dyspepsia, gastric erosion, peptic
ulcerations and gastrointestinal hemorrhage are much less
common. With dose of 500 mg three times daily, pain-
related symptoms begin in the luteal phase and persist
until menstruation. NSAIDs therapy should be initiated
just prior to the onset of pain and continued until
menstruation ceases if dysmenorrhea is also a problem
(Rickels & Freeman, 2000).
3- Hormones:
A) Progesterone:
Progesterone is the most controversial treatment
regimen of premenstrual syndrome and this is based on the
theory that women who suffer from PMS are deficient of
progesterone in the luteal phase (Freeman et al., 2001).
Recent meta analysis found that progesterone and
other progestogens were no more effective, progesterone
described to be effective, delivered either as a vaginal or
rectal suppository or oral microrized progesterone, that
dosage should be 200-400mg twice daily, given for at least

Review of Literature
39
5 days before the expected onset of symptoms (Wyatt et
al., 2001).
B) Estrogens:
Administration of estrogens late in the luteal phase
(to minimize decline in the hormone) relieves pre-
menstrual migraine, for over all management, estrogen
must be given continuously to suppress ovarian activity.
Dose of estradiol 50mg or 75mg with 100mg of
testosterone are inserted (Kessel, 2000).
C) Oral contraceptive pills:
The primary mechanism used for PMS therapy
through its capacity to suppress ovulation, it provides
significant relief for menstrual pain and breast tenderness,
psychological symptoms don't significantly improve, in
addition oral contraceptive may lead to depression in some
girls. Dose with ethinyl estradiol 30 mg plus drospirenone
3 mg (yasmin) alleviated bloating, breast tenderness and
swelling, the drospirenone component has anti androgenic
properties and may also reduce acne (Brown et al., 2002).
Review of Literature
40
D) Gonadotropin releasing hormone agonists (GnRH):
A synthetic analog of naturally GnRH which
suppresses ovulation by inhibiting the release of pituitary
gonadotropin, GnRH agonists have been shown to be
more effective in treating behavioral and physical
symptoms of PMS. Some improvements of premenstrual
depression and irritability have been demonstrated for
lower dosages of GnRH (Sundstrom et al., 1999).
Lower dosage 100 mg of GnRH in a form of
intramuscular, subcutaneously and intranasally, can lead to
atrophic vaginities, urinary tract symptoms, decrease of
skin collagen content and chemical menopause. Use of
GnRH more than six months increases risk of
osteoporosis, that needs to add-black therapy with
estrogen and progesterone to minimize long term adverse
effects (Rapport et al., 2002).
E) Danazol
It is an androgenic agent that inhibits gonadotropin
release, by improving mastaligia and not for other
symptoms. Continues danazol thereby also relieves other
Review of Literature
41
PMS symptoms, 200 mg twice a day for three months
given during the luteal phase of menstrual cycle is the
recommended dose (O'Brien & Abukhalil, 1999).
4- Anxiolytics
There is evidence that alpazolam taken during luteal
phase may have efficacy in treatment of PMDD in dose of
0.25mg up to 0.5 mg. It increases food craving and caloric
intake in some girls coupled with its mild cognitive,
memory impairing and withdrawal (Landen et al., 2001).
5- Diuretics
Abdominal bloating, edema and weight gain are
most common premenstrual symptoms that initially are
treated by sodium restriction. Diuretics are to be considered,
if dietary alterations are unsuccessful in reducing fluid
retention, and not effective for the treatment of all
symptoms (psychological and somatic) but they provide
some relieve from premenstrual weight gain and bloating,
diuretics may cause intravascular depletion, electrolyte
disturbance, fatigue, headache and irregular bleeding
(Dickerson et al., 2003).

Review of Literature
42
Spironolacton is the agent of choice because of its
potassium sparing diuretics at dosage of 10 mg daily,
shown to effectively relieve Premenstrual symptoms such
as breast tenderness, fluid retention, it is administrated
only during the luteal phase (Arias, 2002).
6- Antidepressant
Anti depressants are widely used in treating the
mood disturbances related to PMS, It appears to work by
increasing brain chemical (opioids, serotonin) levels,
which are affected by ovarian hormones, its importance is
in the control of mood and emotion (Dimmock et al.,
2000).
Selective serotonin-reuptake inhibitors are the first-
line agents of treating PMS, SSRI has a significant impact
on the treatment of depression and effective disorders, it
works by increasing serotonin levels in the brain by
inhibiting reuptake of serotonin (Pearlstein et al., 2000).
Fluoxetine is the first SSRI at dose of 20 mg or 60
mg daily reducing premenstrual emotional and physical
symptoms, sertraline also at dose 50-150mg daily with
Review of Literature
43
side effects usually transient and minor such as dizziness,
headaches, nausea and insomnia (Tana & Gradyweliky,
2003).
7- Surgery
Surgical treatment, principally hysterectomy plus
bilateral oophorectomy, this would remove all ovarian
functions by removing uterus at the same time, A
hysterectomy and bilateral oophorectomy results in the
relief of all genuine PMS cyclical symptoms.
Hysterectomy plus bilateral oophorectomy is controversial
because it's irreversible and associated with significant
risks. Surgery may be considered in severely affected
cases who fail to respond to other therapies and also have
significant gynecologic problems for which surgery would
be appropriate (Wyatt et al., 2000).

Review of Literature
44
Fig (7): Treatment strategies for premenstrual syndrome.
Adopted from Lewis SM, Heitkemper MM, Dirksen SR,
(2000): Medical surgical nursing. Boston: Mosby, pp. 1521-
1523.
Education and counseling
Knowledge of possible
causes and treatment
Daily diary
Family understanding
Support groups
Diet
Well balanced
Avoid caffeine,
alcohol
Reduce refined
Carbohydrates
Adequate intake of
vitamin B6
Stress management
Relaxation
techniques
Abdominal
breathing
Mental imagery
Progressive muscle
relaxation
Exercise
Aerobics
Walking
Swimming
Selective serotonin
Reuptake Inhibitors (SSRI)
Antidepressants
Good relief for mood symptoms
Prostaglandin Inhibitors
Administration 2-4 times
Daily at onset of symptoms
Combination oral
Contraceptives
Used for women with no
contraindications
Diuretics
Administration 2-4 during
luteal phase
Other Agents
Tranquilizers and sedatives
Gonadotropin inhibitors
(Danazol)
Evening Primrose Oil ("natural therapy")
NO NPHARMACO LO GIC STRATEGIES
PHARMACO LO GIC STRATEGIES
Review of Literature
45
NURSING MANAGEMENT
OF PREMENSTRUAL SYNDROME
Nursing management of premenstrual syndrome
starts with understanding, and caring approach, that
acknowledges the reality of what is happening to the girl
who is suffering, and provides knowledge about the
menstrual cycle, the symptoms and their effects. It also
provides reassurance by various support groups for
seeking more information, helpful literature, building self-
esteem, self-control, stress relief, eliminating symptoms,
and facilitating the body's natural healthy process to
increase feelings of well being, and helping girls to feel in
control for PMS (Endicott, 2000).
Nurses must begin any management of PMS or
PMDD with an expression of empathy and support towards
girls so as to acknowledge not only the symptoms she is
experiencing but also the possible cultural stigma that she
may be bearing or trying to avoid (Varney et al., 2004).
Nurse as Educator
1- Health education about premenstrual syndrome:
Nurses are in a prime position to help girls who
needed guidance and support. It is important to begin with

Review of Literature
46
the process of building therapeutic communication to
establish trust between nurse and girls. Most girls feel
uncomfortable talking about their body habits and
functions, this trust will alleviate girls anxiety, reservation
and embarrassment in discussing menstrual problems.
Nurses should be aware of culture as well as family values
and previous life experiences of girls (Alderman, 2000).
All adolescent girls need reassurance that
menstruation is a normal function. When nurses are asked
for advice regarding menstrual problems, they have
available opportunity to engage in health teaching
concerning menstrual physiology and hygiene, as well as
the importance of a well balanced diet, exercise, general
health maintenance. Health teaching can dispel any myths
in relation to menstruation and feminity (Wong et al.,
2006).
Nurses are expected to be knowledgeable about
PMS providing girls a name and reason for the feeling that
may be causing her out of control. Providing discussions
of family and friends participation in PMS support group
enables them to develop ways of coping and establish
channels of communication with close family members for
understanding and help during PMS days (Marvan &
Escobedo, 1999).

Review of Literature
47
Nursing activities are directed to provide an
atmosphere of acceptance and subsequent empowerment
by increasing personal awareness and sensitivity to
individual needs. Nurses should provide actual
information concerning PMS and the current theories on
its etiology and treatment. Explanations help girls with
PMS understand the complexity and ways they can regain
a better sense of control. Girls need to be assured that their
symptoms are real, PMS exists and they are not "crazy".
Providing support to the girls in making life style changes
reduces PMS (Young Kin & Davis, 1998).
Nurses can provide girls information regarding
sexuality and that the promotion of healthy attitudes
towards sexuality will help to empower adolescent girls to
make healthy decisions about sexual behavior. Nurses also
can initiate a dialogue with girls through inquiring them
about pubertal changes, including menstrual patterns and
then gradually guiding the interview toward sexuality.
Mothers are the major source of information on topics of
sex and menstruation for their daughters and therefore it's
helpful to involve mothers in general discussions about
sexual health (Beausang & Razer, 2004).

Review of Literature
48
2- Health education about diet
Nutritional counseling through general dietary
modification is an area where nurses can be especially
helpful in assisting girls to develop a holistic symptom
management program over time. Nurses should encourage
girls to eat fresh foods rather than processed ones,
maintain balanced nutritional intake, regular eating times,
also eating fresh fruits, and vegetables which contain
vitamins and minerals, foods rich in vitamin B6 such as
liver, egg, and milk. Magnesium has been also successful
in relieving premenstrual mood fluctuations, it presents in
whole grain, sea food, also milk, yoghurt, and cheese are
good sources of calcium, and eating frequent and small
portions of foods high in complex carbohydrates improves
mood symptoms by raising level of tryptophan, (Young,
2002).
On the other hand, nurses should advice girls to
restrict foods containing chocolate and coffee which are
associated with increase in severity of premenstrual
symptoms, particularly anxiety, tension depression and
irritability. As well, sodium restriction has been proposed
to minimize bloating, fluid retention, breast tenderness and
swelling (Wyatt et al., 2000).

Review of Literature
49
Nurses can encourage girls limit consumption of
refined sugar, salt, red meat, alcohol and caffeinated
beverages. Girls can be encouraged to include whole
grains, legumes, seeds, nuts, vegetables fruits, and
vegetable oils in their diets (Lowdermilk et al., 1999).
3- Health education about exercise & relaxation
technique
Girls complaining from PMS might play a role of
student, sister, mother and care giver, all these social roles
experienced by girls lead to considerable emotional strain.
Nurses must provide girls an opportunity to discuss
stressors in their life that could be exacerbating their
symptoms, also can be learned strategies for managing
time across the menstrual cycle and how to redefine their
roles of mothers, friends, or coworkers that can ultimately
reduce stress (Taylor, 2000).
The nurse should inform girls about stress
management such as relaxation technique and aerobic
exercise, telling her benefits of a regular exercise program
that may help decrease fluid retention, this include
reading, watching television and aerobic activity like
fitness. Walking or gagging exercise also has been found
to increase blood levels of beta-endorphin. Exercise also
reduces stress by providing a time away from home by

Review of Literature
50
providing a useful outlet for any anger and aggression,
promoting relaxation and helping to sleep at night (Steege
& Blumenthal, 2004).
The nurse has to encourage girls to using such
techniques which are recommended to treat symptoms of
PMS, such as massage, reflexology, Reiki and yoga, with
an explanation of these therapies how to be performed and
possible complications (Long et al., 2000).
Nursing role as a care giver
An empathic relationship with a health care
professional to whom the girl feels free to voice concerns
is highly beneficial. The nurse can encourage girls to keep
a journal to help them identify life events associated with
PMS. Stress reduction education, self-care groups, and
self-care literature can also help girls gain control over
their bodies (Olds et al., 2004).
Nurses first step in assessing PMS is to obtain
history regarding symptoms, history is essential for
arriving at correct diagnosis. Menstrual history includes
age of menarche, regularity and duration of periods, and
number of pads or tampons used. Other areas that may
provide important information helping nurses to assess the
PMS problem accurately, include family history of
menstrual problems particularly related to adolescent

Review of Literature
51
mothers and female siblings. These are relevant because
the nature and patterns of menstruation have a genetic
basis, past medical history, medication and substance use,
sexual behavioral and other related issues such as weight
changes, nutrition, exercise and sports (Littleton &
Engerbretson, 2005).
One of the most difficult experiences facing the
adolescent girl is the gynecologic examination. She has
often feels of apprehension, and needs continuity of
support in the form of anticipatory guidance. Routine
check up such as cervical screening, physical and pelvic
examinations provide an opportunity for the nurse to
enquire about the girl' menstrual cycle and problems she is
experiencing. The nurse should rule out other possible
causes for the symptoms that the girl is experiencing such
as thyroid disorder, cardiac abnormality and pelvic mass
that could be source of symptoms thought to be related to
PMS and could be discovered on examination (Nelson,
1998).
Nurses in schools and clinics must teach girls how to
use daily symptom diary which is a useful educational
tool, in addition to its diagnostic value. The diary provides
the girl a visual record of the symptomatic intervals with
their onset and resolution each month, which can be
helpful to the girl and her family. The pictorial validation
Review of Literature
52
of the girl' cycle may stimulate her to schedule activities
so as to minimize stress and negative influences that might
exacerbate her symptoms as well as to be helpful to gain a
sense of mastery over the disorder (Moline & Zendell,
2000).
Improving detection of PMS is a vital role to the
nurse who can encourage girls to report premenstrual
symptoms and keep a prospective symptom diary. For
girls with irregular menstrual cycle or difficulties to keep a
calendar of symptoms, the nurse can recommend daily
measurements of basal body temperature throughout the
cycle, the time of ovulation can be pin pointed using this
method, allowing girls determine their symptoms
occurring during the luteal phase (Yonkers, 1999).
Symptoms management, stress reduction, and health
promoting approaches that include behavioral and
cognitive strategies present additional intervention options
for PMS. Specific nursing activities include simple
relaxation therapy, breathing exercise, stretching exercise,
progressive muscle relaxation and autogenic training.
The nurse should encourage girls to practice exercise,
medication imagery and creative activities to reduce stress
(Smeltzer & Bare, 2004).

Review of Literature
53
The nurse helping girls to take medications as
prescribed, by providing instructions about the desired
effects of medication, and by enrolling in a PMS group
that meets to discuss problems which may help girl learn
that others recognize and understand what she is
experiencing. Nurses must help the girl to make concrete
arrangements, and to obtain relief when she feels that she
may harm herself. A neighbor friend or family member
should be identified to provide immediate relief, without
question or explanations (McKinney et al., 2005).
Nurses should advice girls who are taking herbs
about the characteristics of these herbs, she should
emphasize that the herb should be pure, safe, effective,
and labeled with the following information: name of the
herb, the part of plant used, expiration date, name and
address of manufacturer. The nurse should inform her also
about important precautions during herbal treatment, these
precautions include: cautions in taking herbs during
pregnancy and lactation, avoiding regular use of large
variety of herbs together, possible stopping of herbal
therapies at least 2 weeks before elective surgery,
reporting adverse side effects to doctor, and learning as
much as possible about used herbs (Eliason & Kruger,
2000).

Review of Literature
54
Nursing efforts towards empowerment of adolescent
girls are likely to be more effective than efforts toward
compliance, that the nurse should identify the girl
appropriate levels of self-care, whereas the latter implies
the need for girls to simply follow instructions without
acknowledging the adolescent's level of maturity and
ability to take responsibility, and take care of their own
bodies can provide a sense of independence and
fulfillment (Coupey, 2000).
Frye and Silverman (2000) mentioned that, the
nurse must tell girls that although PMS is complex but is
as well highly treatable, and improvement is virtually
certain with combination of several interventions. In
addition, by reassuring girls that PMS affects millions of
girls and helping to alleviate feelings of isolation caused
by symptoms, nurses can take active role that helps girls to
take proper medication as prescribed and provide
instructions about desired effects of medications.
Many girls with PMS have sleep difficulties either
insomnia or excessive sleepiness, the nurse should
encourage these girls to adopt consistent bed times and
wake times not only at least during the luteal phase of the
cycle, but also preferably all month long. Consistent bed
times tend to decrease sleep latency, and an important part
of good sleep hygiene includes keeping a regular schedule,

Review of Literature
55
limiting caffeine and alcohol consumption after noon and
limiting the use of sedative-hypnotics (Bendich, 2000).
The nurse should encourage sedentary woman about
daily short walk at her own place that will be far more
likely to bring results than starting her a more rigorous
regimen that requires warm-up, wind-down and
calculations of pulse rate. Even basic stretching exercises
can be useful in promoting a general feeling of well being
and reducing stress due to PMS (Blake et al., 2002).