
Re-thinking Thought: Foucault, Deleuze, and the Possibility of ...
Upload
independentCategory
view
2download
0
TITLE PAGE
ORIGINAL ARTICLE
KIDNEY EXCHANGES: AN APPEALING POSSIBILITY
AUTHOR: EMANUELA MADDALENA, MD Nephrology Dialysis and Transplantation Unit Azienda Ospedaliera Città della Salute e della Scienza Torino
KEY WORDS: KIDNEY PAIRED DONATION (KPD); NEAD CHAINS; DOMINO KIDNEY PAIRED DONATION; LIVING NON DIRECT DONATION; SAMARITAN DONATION;
Abstract ‘s word count: 227.
Text’s word count: 2945.
TOTAL COLOR FIGURES: 4 (GRAPHICS).
ADDRESS FOR CORRESPONDENCE: [email protected]
Mobile Phone: 3317277293
Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
Footnotes
Study Design: Emanuela Maddalena
Writing Paper: Emanuela Maddalena
Partecipating in reaserch: Emanuela Maddalena
Analysis of data: Emanuela Maddalena
Figures: Emanuela Maddalena
Conflict of Interest: None
Disclosure: None
Source of Support: None
2

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
ABSTRACT
Renal transplant is now the best option for patients affected by CKD, both for organ survival
and improvement in quality of life.
If a patient affected by chronic kidney disease in dialysis has family members or friends willing
to donate to him one of their kidneys, but there are incompatibilities such as blood group type or
cross-match incompatibility, a kidney exchange can bypass this obstacle in various ways.
Kidney Paired Donation is the most common form of Kidney exchange and consists in
matching an incompatible pair (candidate recipient and prospective donor) with another incompatible
couple, allowing a living donor to donate the organ not directly to his intended recipient but to the
recipient of another couple (non direct donation) in exchange for another kidney: thus two patients
who have an incompatible prospective donor receive a transplant through a kidney exchange. A pair
consists in a kidney transplant candidate and his intended but incompatible living donor (parents,
partners, brothers, close friends).
In the last decade many countries have developed exchange programs, EPs, with different
modalities that we will describe in this paper: we also discuss the ethical and legal questions raised by
this kind of kidney exchange and the cultural assumptions that favor or not the adoption of these
exchanges in Italy.
3

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
ESSENTIAL DATA FOR RENAL TRANSPLANTS: US – ITALY -EUROPE From 2001 to 2013 210.781 kidney transplants were performed in the United States, according to
US Registry (1): of these 80-.208 were from living donors (Graph 1): on 1 August 2014 there are
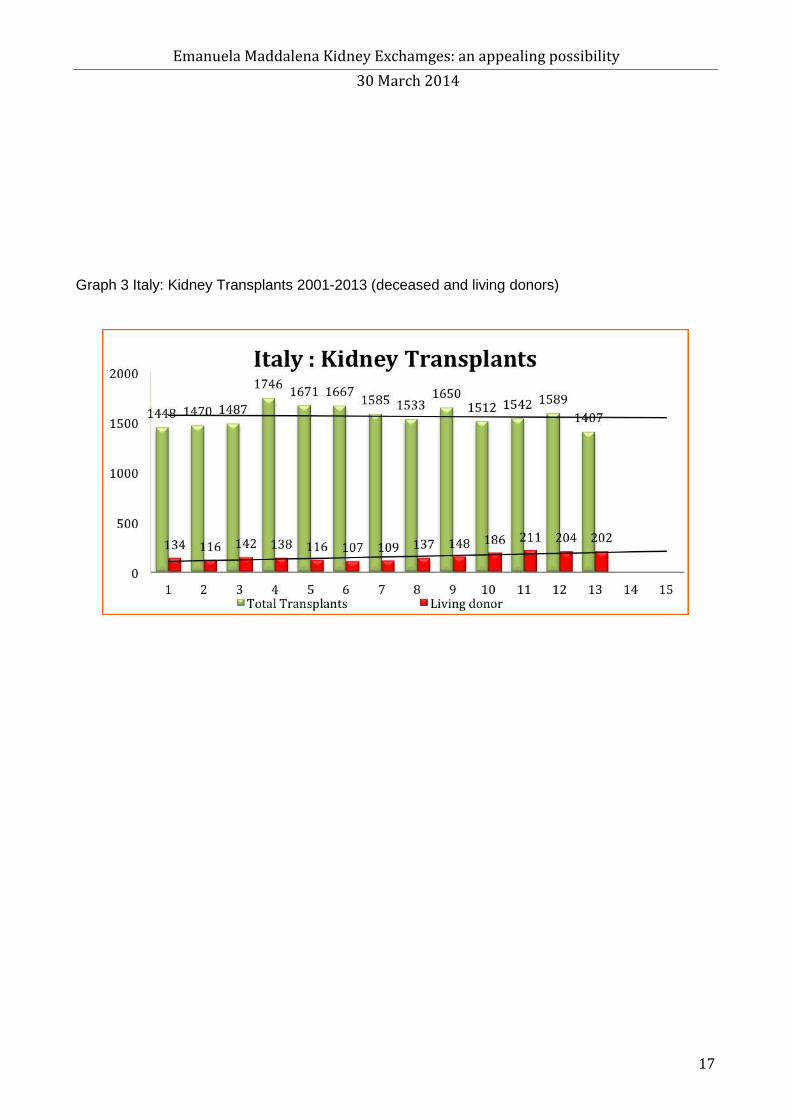
108.667 patients on the waiting lists for cadaver kidneys in the USA. In Italy from 2001 to 2013 20307 kidney transplants were performed (Graph2) of which 2950 from
living donors, according the italian Registry (2): on 11 August 2014 there are 6590 patients on the
standard waiting lists in Italy. In the US Registry the average time on the waiting lists for a kidney transplant is 1.5 year; 5.2 years
for a highly sensitized patient vs average time of 3.8 years for patients with c-PRA < 10%.: in Italy
the average time on a waiting list for a kidney transplant is 3 years (1,2). From 2004 to 2013 31.809 kidney transplants were performed in the Eurotransplants countries (3),
according to Eurotranplant Registry: of these 11.320 were from living donors (Graph 3): on
February 2014 there were about 10857 patients on the waiting lists for deceased donor in the
Eurotransplant Registry.
BIOLOGICAL BARRIERS TO TRANSPLANTATION The two traditional biological barriers to transplantation are incompatibility of ABO group type or
cross-match incompatibility. These barriers are now surmountable by desensitization protocols that
allow transplants against group or against cross-match: if successful, these protocols allow
transplants in patients who have an intended living donor incompatible because of group type
(transplant against group) or of anti-donor antibodies, DSA (transplant against cross-match). They are now frequently used and with better results, but they are still only an extreme possibility.
Hyper-immune patients (c- PRA >15%) with anti-donor antibodies (DSA) have a high probability
of having a positive cross-match and so usually find it most difficult to find a compatible donor and
remain on the waiting list for a long time (7,8).
Highly hyper-immune patients (c- PRA > 80%) either will find no compatible .donor or will have
to wait for years on waiting lists of cadaver donors.
4
Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
In the world sensitized patients on waiting lists are about 30%: of these 15% are highly hyper-
immune (C-PRA > 80%) and have a very high chance of having a positive cross-match. It is
estimated that in the USA every year less than 15% of highly sensitized patients receive a transplant
(7, 8, 12).
These patients can be treated by desensitization protocols whether they are on waiting lists for a
deceased donor or have an intended incompatible donor: these protocols are meant to reduce the
level of anti-donor antibodies so as to increase the possibility of finding a compatible organ . TYPES OF EXCHANGES
KIDNEY PAIRED DONATION The simplest form of kidney exchange is the two ways Kidney Paired Donation: two incompatible
couples of donor-recipient exchange donors. This simple model (direct exchange) can be described
in this way: an intended donor of group A who has an intended recipient of group B gives the organ
to the recipient of group A (of another incompatible couple) who has a potential donor of group B
and viceversa.
This model can be extended to increasing numbers of couples (three-way Kidney Paired Donation,
four-way Kidney Paired Donation)
Initially the couples enrolled in the KPD programs were only incompatible ones; more recently
there have been in these programs compatible couples who join the program for altruistic motives
(to help another patient to find a compatible kidney) or for clinical reasons (to find a better organ,
with better compatibility, or adequate size, or minor age difference). Worldwide the number of KPD exchanges and of non direct donations is increasing. In the USA in 2012 (11,12) KPD transplants were about 10 % of living donor kidney transplants
(graph 4) , although a greater increase was expected after the centralization of programs on a
national basis (programs in many countries are now on a national basis).
A recent American study (14) analyzed data of 34.843 living donor kidney transplants (LDKTs)
performed between 2006 and 2011 in 207 American transplant centers: 2089 (6%) were performed
in KPD modality. However, the percentage increase is lower than expected, probably because few
transplant centers use this modality (KPD) on a large scale. The study shows great differences in
the percentages of the use of this modality, ranging from less than 1% in most centers (1/100 living
donors) to a maximun of 8.8 % in few a great centers, showing that in fact most KPD transplants
are performed in a few big centers. The authors conclude that, if this modality was encouraged in
all transplant centers, the annual increase of LDKTs would be about 1000 transplants / year.
5

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
As an example we include the largest monocentric series. The Transplant Center of Cornell
University of New York published data of its series of 44 couples enrolled in the national program
(KPDPP): 54% of the couples was incompatible for group and 43% had been subjected to
desensitization protocols for the presence of anti-donor antibodies: in total 50 transplants were
performed. Average waiting time for a transplant was 157 days (from the enrollment in the
program), 14 kidneys were allocated to patients on cadaver waiting lists; rejection rate after one
year was 9.1 %, patient and organ survival after 1 year was 98% and 94% respectivelly
Another recent Turkish (16) study (data from three transplant centers) shows the outcomes of 272
KPD transplants compared with the results of 1885 transplants from living direct donor (LD): organ
survival after 1 year is similar (KPD 96.7% vs LD 96.5%) as is the rejection rate (KPD 19.4 % vs
LD19.3 %.).
The algorithm of allocation in KPD pools is fundamental and must be specifically designed for this
type of transplant, because the donors both in KPD and in altruistic or specific donation do not
choose their recipients, but the recipient is assigned by the algorithm: so criteria of allocation must
be carefully and expressly studied (10, 18, 19).
In theory the best algorithm is the one that allows the maximum number of negative cross-matches,
the best HLA matches,. the maximum number of matches for pediatric and hyper-immune patients,
and the minimum age difference between donors and recipients.
The choice of the mathematical model of optimization of the algorithm can increase the chances of
finding a match by 15%. However, even adfopting both strategies of implementation, using the best
algorithm and increasing the size of the pool, 50% of patients of KPD pools is destined to remain
long on the waiting list or not to find a negative cross-match at all (10,18,19).
The USA are the obligatory point of reference because of the quantity of cases ( 9, 13,15,20,21,22,
23 24,25).
DOMINO KIDNEY PAIRED DONATION
Domino exchanges are chains of simultaneous transplants that begin with an altruistic donor
(Living non direct donor) and end with the donation of an organ to a recipient on the list from
cadaver donors. In exchange programs in domino mode the first donor who starts the chain of
transplants is an altruistic (or non direct) donor who donates the kidney to a recipient of an
incompatible couple enrolled in a KPD program: this begins a chain of transplants that ends with
6

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
the allocation of the kidney of the chain’s last donor (Domino Donor) to a recipient on the cadaver
waiting list (25, 26).
In the Netherlands, the first country with a national program of KPD exchanges used since 2005,
Roodnat (28) published data about the results of the Good Samaritan/ Domino Paired Donation
Program They report (28) a series of 29 domino chains, of which 24 are two ways chains starting
from a domino or an altruistic donor, 4 three ways chains and one four ways chain, with a total of
51 altruistic donors and 35 domino donorsributed fairly among patients on the waiting lists.
CHAINS
This exchange is a chain from extended altruistic donation non simultaneous; it is a variant of a
domino paired donation, in which an altruistic donor is associated to a pool of KPD incompatible
pairs: the difference from the other exchanges is that the last donor of the chain (bridge donor) does
not give the kidney at the same time as the others, but his donation is carried out at a later time, so
as to start another chain. The donor who starts the new chain is called the “bridge donor” (6, 9, 14,
20.22, 26, 29, 30).
In theory chains can continue indefinitely (never ending chains) until the chain is interrupted
(broken chain) because a donor refuses the donation (reneging donor): a NEAD chain is formed of
segments in which each segment is similar to domino kidney paired donation with the exception of
the last donation which is postponed to a later time so as to generate a second chain.
The main differences from domino kidney paired donation are that not all transplants are performed
simultaneously, and that the last donor of a chain does not give the organ to a recipient on a waiting
list. NEAD appears for the first time in an article by Rees (30) published in 2009 in the New
England Journal of Medicine, which describes a chain of 10 transplants performed in 2007 over six
months, beginning with an altruistic donation with the involvement of six US transplant centers in
five different states. The advantage of NEAD chains lies in the fact that by being able to break the
chains, because not all transplants are carried out simultaneously, it is possible to perform longer
chains and so increase the number of transplants generated by a single altruistic donation. One of
the most recent case studies about chains is that by Melcher (14) published on JAMA Surgery in
2013. The study analyzes 77 donor chains started by 77 altruistic donors between February 2008
and December 2012 (46 months): out of the 77 chains 66 ended with the allocation of an organ to a
recipient on a waiting list, 7 were interrupted because of the unexpected unsuitability of the bridge
donor. The average number of grafts per chain was 4.8, no chains broken in 2011. One third of
transplant recipients was group 0. In total. 77 chains had allowed the performance of 373
7

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
transplants with an average of five donations for one altruistic donation (5 transplants for a single
altruistic donation)
From the ethical point of view the critical point of the NEAD chains is the breaking of the chain
because of the bridge donor’s possible withdrawal.
The risk is much greater than in the other types of exchanges because of the time between the organ
donation and the actual transplant of it to a recipient, time for unexpected problems to arise for
various reasons, clinical, rethinking, or economic and family problems (6, 33).
However, the risk of a change of mind by the bridge donor is considered acceptable by the
professionals, because it involves a lower risk than in a KPD exchange, where transplants are
performed strictly conteporaneously (either all or none) precisely to overcome this risk. If one of
the donors in a KPD exchange withdraws after his receiver has received the kidney the second
recipient would suffer a double loss, because he would not receive the organ and lose a potential
living donor.
AUPKE
This is a kind of exchange very recently introduced, in which a compatible couple is associated to a
incompatible pair: this allows an incompatible recipient (and his intended donor) to receive a
transplant. This type of exchange is analogous to KPD, the difference being that one couple donor-
recipient is compatible, the other incompatible pair.
The acronym “AUPKE”, altruistic unbalanced exchange, was coined by Woodle and Ross (32)
bioethicists who were the first to evaluate the ethical acceptability of this new mode of exchange
meant to expand living donors pools.
In AUPKE the compatible donor-recipient pair make an non direct rather than a direct donation: the
reason why a compatible pair makes a non direct donation instead than a direct one can be altruistic
or clinical. Clinical reasons can be the wish to obtain an organ with a better compatibility or a better
size or less age difference.
The exchange is said to be altruistically unbalanced because a different degree of altruism is
required of the compatible pairs (who could make a direct donation) compared to the degree
required of an incompatible pair (who could not make a direct donation).
This kind of exchange has the advantages of allowing a transplant from a living donor to a patient
who could not receive it (AB0 incompatibility or positive cross-match), of removing a patient of
group 0 from the waiting list from deceased donor, of being able to be made in one transplant
8

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
center, and of not needing the organizational complexity of the chains involving different transplant
centers.
However this kind of exchange immediately raised serious ethical concern because of the high
potential for coercion of the compatible donor pair, far superior than in other forms of exchanges .
The most critical aspect of this exchange is that the donor may be subject to a double pressure by
the transplant center and by the partner (33).
In fact the authors themselves, Woodle and Ross, propose that in this kind of exchange, then
extended to chains, the center itself provides the donor with the assistance of a third party
independent of both the center and the receiver, the “independent donor advocate: in other words,
it would protect the interests of the donor, against the multiple pressures from the others parts,
including its receiver. One the most extensive case studies of this kind of exchange is that published
by the Transplant Center of Columbia University and Presbiterian Hospital where in 2007 the first
three ways AUPKE exchange (three pairs) was performed, completing six transplant operations at
the same time with six different teams (34)
VOLUNTARY EXCHANGES The experience of Istanbul Transplant Centre (16,17) has recently been reported with the
publication of the data of a year of voluntary living donor kidney exchanges. In the program 22
couples were enrolled and 16 two ways exchanges, 1 three way exchange, 1 four ways exchange
were performed, allowing living transplants to 21 patients who would not have received it without
the program. The authors report an increase of 6.1% of transplants of the center utilizing this
program, and propose it should practised on a large scale .
CONCLUSIONS
There are two aspects in the ethics of kidney exchanges and samaritan donations, in my opinion.
If the objection is that in crossover donation the principle of unavailability and inviolability of the
body, cornerstone of our religious philosophical and legal system, is breached, it seems to me that
this principle can only be challenged in very exceptional cases.
This principle, however, is breached also in direct living kidney donations: therefore the objection
to samaritan donations and kidney exchanges bacause of the inviolability of the body is valid but
should also apply to the direct living donation from related donors.
If the real problem is the fear that, once the possibility of exchanging organs is legalised, forms of
marketing organs become easier, this, although possible, is, in my opinion, a purely theoretical risk:
in reality the complex and multidisciplinary transplant network offers sufficient guarantees that it 9

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
will not happen, at least in our country and in the present organization. Samaritan donation instead
is more problematic.
In Italy actually is only planned as an exceptional method, as currently planned in Italy by CRT
(38)
Although the existence of samaritan or altruistic non direct donors is possible, even if rare, it is easy
to understand that “ ultimate and personal motivations” are difficult to verify (from a legal point of
view they are not)
It is obviously simpler to verify a kinship or other type of proximity than to verify the deep reasons
of a samaritan donation: at the moment the Catholic Church has taken no official position on
crossover, samaritan or altruistic donation, the two new forms of living transplatation. Mons Sgreggia (39) one of the most famous exponents of Catholic bioethics, underlines that the Church’s ethical position on transplants is based on two key principles: the protection of the life of
the donor and the disinterestedness of the donation (solidarity in a social sense and charity in
christian terms). The Church does not think that samaritan donation or exchanges infringe these
principles. He thinks that it is right to emphasise the principle of unavailability of the body, but
believes that in the case of organ donation there is no question about the protection of the donor’s
life, provided his physical, mental, social, and working integrity is safeguarded.
As for Pope John Paul II’s prohibition of organ exchange 40 ) in his speech, to 18 Congress of the
International Society for Organ Transplants (…any procedure which tends to commercialize the organs or to consider it as a unit of exchange is morally unacceptable..) , I think a situation
similar to that of section 301 of NOTA is possible (6), that the Pope meant to forbid the use of the
body as an object and the sale of organs (in 2000 exchanges such as KPD were not a legal medical
option ) . Kidney exchanges between incompatible donors are acceptable provided the donor’s is guaranteed
The possibility of withdrawal from a negotiated agreement must be a calculated risk and the
possibility for the donor to change his must be guaranteed: there must no kind of formal or legal
consequence.
This is the primary aim to be pursued if one decides to go down the way of kidney exchanges like
kidney paired donation: it is an attractive and promising way, but it inevitably raises complex
ethical problems not easily solved.
10
Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
REFERENCES
1. UNITED NETWORK FOR ORGAN SHARING WEB SITE: HTTP://OPTN.TRANSPLANT.HRSA.GOV (7 AGOSTO 2013 ).
2. SIT.SISTEMAINFORMATIVOTRAPIANTI,HTTP://WWW.TRAPIANTI.SANITA.IT/STATISTICHE/HOM
E.ASP ( 9 AGOSTO 2013).
3. EUROTRANSPLANT:STATISTICS.EUROTRANSPLANT.ORG:HTTP://STATISTICS.EUROTRANSPLA NT.ORG ( 6/3/2013).
4. RAPAPORT F.T. “ THE CASE FOR A LIVING EMOTIONALLY RELATED INTERNATIONAL KIDNEY
DONOR EXCHANGE”. TRANSPLANT PROCEEDINGS 1986: 18 (SUPPL 2): 5-9.
5. BARSOTTI D.“ IL TRAPIANTO DA DONATORE VIVENTE: LA MODALITÀ CROSS-OVER”, G ITAL NEFROL, 2009, 26 (4): 488-98.
6. KIERAN H. AND KIMBERLY D.K “ CUSTOMS CONTRACTS AND KIDNEY EXCHANGES”, DUKE
LAW JOURNAL, 62: 645-670, 2012. 7. MARFO K, LU A, LING M ”DESENSITIZATION PROTOCOLS AND THEIR OUTCOME”, CLIN J AM
SOC NEPHROL, 6: 922-936, 2011.
8. LOBASHEVSKY AL, HIGGINS NG, ROSNER KM “ANALYSIS OF ANTI - HLA ANTIBODIES IN
SENSITIZED KIDNEY TRANSPLANT CANDIDATES SUBJECT TO DESENSITIZATION WITH INTRAVENOUS IMMUNOGLOBULIN AND RITUXIMAB”, TRANSPLANT 2013, GIUGNO 2013: 182-
90.
9. MONTGOMERY RA “LIVING DONOR EXCHANGE PROGRAMS: THEORY AND PRACTICE”, BRIT MED BULL, 2011, 98: 21-30.
10. DE KLERK M, KAL-VAN GESTEL JA, HAASE KROMWIJK BJ, CLAAS FH “ LIVING DONOR
KIDNEY EXCHANGE PROGRAM”. CLIN TRANSPL.2011: 287-90.
11. YABU JM, PANDO MJ, BUSQUE S, MELCHER ML “ DESENSITIZATION COMBINED WITH
PAIRED EXCHANGE LEADS TO SUCCESSFUL TRANSPLANTATION IN HIGLY SENSITIZED KIDNEY
RECIPIENTS: STRATEGY AND REPORT OF FIVE CASES”, TRANSPLANT. PROC: 45 (1): 82-87
12. FERRARI P, HUGHUES PD, COHNEY SJ “ ABO-INCOMPATIBLE MATCHING SIGNIFICANTLY
ENHANCES TRANSPLANTS RATES IN KIDNEY PAIRED DONATION”: TRANSPLANTATION, LUGLIO 2013 .
13. MASSIE A.B, GENTRY SE, MONTGOMERY R.A “CENTRAL- LEVEL UTILIZATION OF KIDNEY
PAIRED DONATION”, AM J TRANSPLANT, 13: 1317-1322, 2013.
11

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
14. MELCHER M.L, VEALE JL, JAVAID B “KIDNEY TRANSPLANT CHAINS AMPLIFY BENEFIT OF
NON DIRECT DONOR”, JAMA SURG, 2013: 148 (2): 165-69.
15. BINGAMAN AVV, WRIGHT FH, KAPTURCZAK M. “SINGLE CENTRE KIDNEY PAIRED DONATION:
THE METHODIST SAN ANTONIO EXPERIENCE”, AM J TRANSPLANT: 12 (8): 2125-32, 2012 16. YUCETIN L, TIFF S, KECECIOGLU N “PAIRED EXCHANGE KIDNEY TRANSPLANTATION
EXPERIENCE OF TURKEY”, TRANSPLANT PROC, APRIL: 45 ( 3) : 860-3, 2013. 17. HACAR SH, EROGLU A, TILIF S “A NOVEL EXPERIENCE IN LIVING DONOR
TRANSPLANTATION”, TRANSPL. PROCEED, GIUGNO 2013.
18. BOHMIG GA, FIDLER S, CHRISTIANSEN FT “TRANSNATIONAL VALIDATION OF THE AUSTRALIAN ALGORITHM FOR VIRTUAL CROSSMATCH ALLOCATION IN KIDNEY PAIRED DONATION”, HUMAN IMMUNOL; 74 (5): 500-505.
19. DE KLERK M, VITVILIET MD, HAASSE- KROMIJK JJM “HURDLES, BARRIERS, AND SUCCESS
OF A NATIONAL LIVING DONOR KIDNEY EXCHANGE PROGRAM”, TRANSPLANTATION; 86
1749-53, 2008.
20. MONTGOMERY RA “LIVING DONOR EXCHANGE PROGRAMS: THEORY AND PRACTICE”, BRIT
MED BULL, 2011, 98: 21-30.
21. SEGEV D.L, KURCIKA LM, GENTRY SE “UTILIZATION AND OUTCOME OF KIDNEY PAIRED
DONATION IN THE UNITED STATES”, TRANSPLANTATION, 86 (4): 502-510, 2008. 22. AKKINA S.K, MUSTER H, STEFENS E. “DONOR EXCHANGES PROGRAMS IN KIDNEY
TRANSPLANTATION: RATIONALE AND OPERATIONAL DETAILS FROM THE NORTH CENTRAL DONOR EXCHANGE COOPERATIVE”, AM J KIDNEY DIS 2011, JAN 57 (1): 152-168.
23. CHKOTUA A.“PAIRED KIDNEY DONATION: OUTCOMES, LIMITATIONS, AND FUTURE
PERSPECTIVES” TRANSPLANTATION PROCEEDINGS, 2012, 44: 1790-92.
24. LEESER DB, AULL MJ, AFANEH C “LIVING DONOR KIDNEY PAIRED DONATION TRANSPLANTATION: EXPERIENCE AS A FOUNDING MEMBER OF THE NATIONAL KIDNEY
REGISTRY”, CLIN TRANSPLANT 2012 MAGGIO- GIUGNO; 25 (3): E 213-22 25. MONTGOMERY RA, GENTRY SA, MARKS WH “DOMINO PAIRED KIDNEY DONATION: A
STRATEGY TO MAKE BEST USE OF LIVE NON DIRECT DONATION”, LANCET, 268 : 419-21 , 2006.
26. GENTRY S.E, MONTGOMERY SA, SWIHART BJ “THE ROLES OF DOMINOS NON-
SIMOULTANEOUS CHAINS IN KIDNEY PAIRED DONATION”, AM JOURNAL TRANSPLANT
2009: 9 (6): 1330-1336.
27. LEE J, LEE SU, CHUNG SY “CLINICAL OUTCOMES OF MULTICENTER DOMINO KIDNEY PAIRED
DONATION”. AM J TRASNPLANT, 9: 2424- 2438, 2009.
28. ROODNAT J.I “ ALTRUISTIC DONOR TRIGGERED DOMINO PAIRED KIDNEY DONATION FOR
UNSUCCESFUL COUPLES FROM KIDNEY EXCHANGES PROGRAM”, AM J TRANSPLAN, 2010: 821-27.
12

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
29. ROTH AE. “UTILIZING LIST EXCHANGE AND NON DIRECT DONATION THROUGH “ CHAIN” KIDNEY
PAIRED DONATIONS”, AM J TRANSPLANT, 6 (11): 2694-2705.
30. REES M.A, KOPKE JE, PELLETIER RP.“A NON-SIMOULTANEOUS, EXTENDED, ALTRUISTIC –
DONOR CHAIN” N ENGL J MED, 360 (11): 1096-101, 2009.
31. ROSS L.F, WOODLE E.S “ETHICAL ISSUES IN INCREASING LIVING KIDNEY DONATIONS BY
EXPANDING KIDNEY PAIRED PROGRAMS”, TRANSPLANT 2000, 69 (8): 1539- 43.
32. ROSS L.F, WOODLE E.S “THE ALTRUISTIC UNBALANCED PAIRED KIDNEY EXCHANGE: PROOF OF CONCEPT AND SURVEY OF POTENTIAL DONOR AND RECIPIENT ATTITUDE” TRANSPLANTATION; 89 (1): 15-22, 2010.
33. FORTIN M.C. “IS IT ETHICAL TO INVITE COMPATIBLE PAIRS TO PARTICIPATE IN EXCHANGES
PROGRAMS?” J MED ETHICS , JANUARY 24, 2013
34. RATNER LE, RATNER EL, KELLY J “ALTRUISTIC UNBALANCED PAIRED KIDNEY EXCHANGE AT
COLUMBIA UNIVERSITY/ NEW YORK PRESBYTERIAN HOSPITAL: RATIONALE AND PRATICAL
CONSIDERATIONS”, CLIN TRANSPLANT 2008: 107-12. LEGGE 26 GIUGNO 1967 N.458
“TRAPIANTO DI RENE TRA PERSONE VIVENTI”.
35. LEGGE 26 GIUGNO 1967 N.458 “TRAPIANTO DI RENE TRA PERSONE VIVENTI”.
36. COMITATO NAZIONALE DI BIOETICA, 23 APRILE 2010 : “LA DONAZIONE DA VIVO DEL RENE A
PERSONE SCONOSCIUTE, PRESIDENZA DEL CONSIGLIO DEI MINISTRI.
37. CFR. KANT I., “LEZIONI DI ETICA”, LATERZA, ROMA 1991.
38. PETRINI VENETTONI NANNI COSTA “IL TRAPIANTO CROSS- OVER: ASPETTI GENERALI E DI
ETICA” UNITÀ DI BIOETICA - CENTRO NAZIONALE TRAPIANTI, 2010.
39. SGRECCIA E. “ INTERVISTA RADIO VATICANA “LA DONAZIONE DA VIVO A PERSONE
SCONOSCIUTE”, FONDAZIONE “UT VITAM HABEANT”, WWW.ILDONODELLAVITA.IT, MARZO
2010.
40. GIOVANNI PAOLO II. DISCORSO AI PARTECIPANTI A UN CONVEGNO SUL TRAPIANTO DI ORGANI,
2000.
ACKNOWLEDGMENTS: to Dott.ssa Caterina Maddalena (correction of translation) 13
Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
ORIGINAL ARTICLE
KIDNEY EXCHANGES: AN APPEALING POSSIBILITY
AUTHOR: EMANUELA MADDALENA, MD
GRAPHICS( FIGURES)
Email address: [email protected]
14

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
GRAPHICS
Graph 1 US Kidney Transplants 2001-13 (deceased and living donors)
15

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
Graph 2: Eurotransplants: Kidney Transplants 2004-13 (deceased and living donors) 16
Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014 Graph 3 Italy: Kidney Transplants 2001-2013 (deceased and living donors)
17

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
Graph 4 US: Kidney Paired Donation 2001-12
18

Emanuela Maddalena Kidney Exchamges: an appealing possibility
30 March 2014
19
Copyright © 2022 FDOKUMEN




















