
Journal of Mental Health Education
81
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Journal of Mental Health Education


Journal of Mental Health Education
The Journal of Mental Health Education is the official publication of The
Department of Mental Health Education, NIMHANS. The journal is peer-reviewed,
is published annually, and accepts high-quality work or writings in the broad fields of
mental, neurological and neurosurgical health and promotion. The journal is being
published through funding from the Dr. RN Moorthy Foundation.
With the goal of dissemination of knowledge to increase the wider public awareness of
mental health and to promote research in the field Mental Health Education, the
Department of Mental Health Education publishes the Journal of Mental Health
Education, a peer-reviewed online Journal with Annual print compilation of issues. The
first issue of the journal was published in 2017 under the Editorship of Prof. S.K.
Chaturvedi and Dr. Meena K.S.
Further details about the Department of Mental Health Education and its activities are
available at http://mentalhealtheducationnimhans.org/
Journal Ethics
The Journal is committed to meeting and upholding the standards of ethical behavior at
all stages of the publication process. We follow closely the industry associations, such
as the Committee on Publication Ethics (COPE), International Committee of Medical
Journal Editors (ICMJE) and World Association of Medical Editors (WAME), that set
standards and provide guidelines for the best practices in order to meet these
requirements.
Open Access Publication and Creative Commons Licensing
This is an open access Journal and articles are distributed under the terms of the
Creative Commons Attributions-Non-Commercial-Share Alike 4.0 License, which
allows others to remix, tweak, and build upon the work non-commercially, as long as
appropriate credits is given and the new creations are licensed under the identical terms.
Digital Archiving
The contents of the Journal will be saved on a cloud server in case of a Website
Malfunction. Ahead of Print Policy Articles published online under the Ahead of Print
model are considered published and can be cited and quoted using the DOI as the
reference source.

Areas of Publication
This multidisciplinary Journal focuses publishing high quality, peer-reviewed papers in
the area of mental, neurological and neurosurgical health and promotions, book-reviews
and brief articles. The Journal highlights issues in education, training and developing
a skilled, healthy and committed mental health workforce. The Journal of Mental
Health Education is keen to receive original papers on mental health education and
mental health promotion, methodology, training, research, policy development and
practice- particularly from a nation and international perspective.
It considers for publication original research articles in the following areas:
Mental Health Education
Community Mental Health Education
First Aid for Mental Health
Prevention, Promotion and Intervention in Mental Health
Design, Implementation, Monitoring and Evaluation of Programs in Mental Health
Mental Health Awareness
Mental Health Literacy
Stigma and Discrimination in Mental Health
Digital Mental Health Education
Public Mental Health
Advocacy and policy making
Research Methodologies in Mental Health
Health Education Materials
Mental Health Education and Media
Aids and Methodologies in Mental Health Education
Theories and Evidence Based Research in Mental Health Education
Legal and Ethical Principles in Mental Health Education
In the above mentioned subjects, the Journal invites submission of original research
papers, brief reports, case discussions, debates, commentaries and controversies,
narrative and systematic reviews, essays, letter to editor, correspondence and book
reviews.
Potential readership for this Journal includes but not limited to mental health
professionals (psychiatrists, psychologists, psychiatric social workers, mental health
nurses), health educators, public health professionals, people from the media, non-
government organizations, administrators and policy makers working in the field of
Mental Health.

EDITORIAL BOARD JMHEDU
Concept and Mentor
Dr. Santosh K. Chaturvedi
Former Dean & Senior Professor of Psychiatry,
National Institute of Mental Health &
Neurosciences, Bangalore, India
Chief Editor
Dr. K. S. Meena
Additional Professor
Head of Department of Mental Health Education NIMHANS,
Bangalore, India
Deputy Editor
Dr. Latha K.
Assistant Professor
Department of Mental Health Education NIMHANS,
Bangalore, India
International Editorial Board
Dr Helal Uddin Ahmed
Associate Professor
Dept. of Child Adolescent & Family Psychiatry,
National Institute of Mental Health, Dhaka, Bangladesh
Dr. Afzal Javed
Chairman
Pakistan Psychiatric Research Centre, Fountain House, Lahore, Pakistan

Dr. Mitchell Weiss
Health Social Scientist & Professor
Swiss Tropical and Public Health Institute, University of Basel, Basel,
Switzerland
Dr. Matcheri S Keshavan
Professor of Psychiatry
Harvard Medical School, Boston, MA
Dr. Shinfuku Naotaka
Emeritus Professor
Kobe University School of Medicine, Japan
Dr. Gabriel Ivbijaro
Immediate Past President WFMH
Professor at NOVA University, (Lisbon) Portugal Medical Director,
The Wood Street Medical Centre, UK
Dr. Ali Ahsan Mufti
Assistant Professor
Jinnah Medical College Consultant Psychiatrist Ibadat Hospital, Peshawer
National Editorial Board
Dr. Rajaram Subbian
Psychosocial Consultant
Executive Director of Basic Needs, India
Core Team from NIMHANS, Editorial Board
Dr. Aravinda.B.A.Banavaram
Associate Professor, Department of Epidemiology, NIMHANS, Bangalore, India
Dr. Aruna Rose Mary Kapanee
Associate Professor, Department of Clinical Psychology, NIMHANS, Bangalore,
India
Dr.Arivazhagan
Professor, Department of Neurosurgery, NIMHANS, Bangalore, India
Dr. Poornima Bhola
Professor, Department of Clinical Psychology, NIMHANS, Bangalore, India

Dr. Prabha. S. Chandra
Professor, Department of Psychiatry, NIMHANS, Bangalore, India
Dr. Prabhat Kumar Chand
Professor of Psychiatry, Head of Centre for Addiction Medicine
NIMHANS, Bangalore, India
Dr. Geetha Desai
Professor, Department of Psychiatry, NIMHANS, Bangalore, India
Dr. Sailaxmi Gandhi
Professor and Head, Department of Nursing, NIMHANS, Bangalore, India
Dr. Kavitha Jangam
Associate Professor, Department of Psychiatric Social Work, NIMHANS,
Bangalore, India
Dr. Deepak Jayarajan
Associate Professor, Psychiatric Rehabilitation Services, NIMHANS,
Bangalore, India
Dr. Santosh Loganathan
Professor, Department of Psychiatry, NIMHANS, Bangalore, India
Dr. Reeta Mani
Additional Professor, Department of Neurovirology, NIMHANS, Bangalore,
India
Dr. N Manjunatha
Associate Professor, Department of Psychiatry, NIMHANS, Bangalore, India
Dr. Seema Mehrotra
Professor and Head, Department of Clinical Psychology, NIMHANS,
Bangalore, India
Dr. D. N. Nandakumar
Professor and Head, Department of Neurochemistry, NIMHANS, Bangalore,
India
Dr. Nandeesh. B. N
Associate Professor, Department of Neuropathology, NIMHANS, Bangalore,
India
Dr. Prasanthi Nattala
Additional Professor, Department of Nursing, NIMHANS, Bangalore, India
Dr. G. Radhakrishnan
Associate Professor, Department of Nursing, NIMHANS, Bangalore, India

Dr. Manoj. K. Sharma
Professor, Department of Clinical Psychology, NIMHANS, Bangalore, India
Dr. John Vijay Sagar
Professor & Head, Department of Child and Adolescent Psychiatry, NIMHANS,
Bangalore, India
Dr. Priya Treesa Thomas
Associate Professor, Department of Psychiatric Social Work, NIMHANS,
Bangalore, India
Dr. Mathew Verghese
Senior Professor and Head, Geriatric Psychiatry Unit, Department of Psychiatry,
NIMHANS, Bangalore, India
Dr. Vandana V. P
Additional Professor and Head, Department of Speech Pathology and Audiology,
NIMHANS, Bangalore, India
Dr. B. K. Yamini
Additional Professor, Department of Speech Pathology and Audiology,
NIMHANS, Bangalore, India
Dr. P T Sivakumar
Professor of Psychiatry, Consultant in Geriatric Psychiatry Unit,
Department of Psychiatry, NIMHANS, Bangalore, India
Dr. Vranda M.N.
Additional Professor, Department of Psychiatric Social Work,
NIMHANS, Bangalore, India
Dr. Anish V Cherian
Associate Professor, Department of Psychiatric Social Work NIMHANS,
Bangalore, India
Dr. Debanjan Banerjee
Senior Resident, Department of Psychiatry NIMHANS, Bangalore, India
Dr. Lakshmana G
Assistant Professor, Department of Social Work, School of Social and
Behavioural Sciences, Central University of Karnataka, Kalaburgi, Karnataka

Associate Editors
Deepika Saini
Masters in Psychology, Currently a fellowship student in the Department of Mental
Health Education, NIMHANS, Bangalore, India
Dr. Rajeev Jayaram Paleri
MBBS, Currently a fellowship student in the Department of Mental Health
Education, NIMHANS, Bangalore, India
Student Editor
Manjiri Gokhale
Pursuing BSc PJCs (Psychology, Journalism, Computer Science), currently an
intern at the department of Mental Health Education

CONTENTS
S.NO TITLE PAGE NO.
EDITORIAL
i. What do I do? Predicament of Mental Health Education
during Pandemic
Dr. Santosh K Chaturvedi
1
COMMENTARY
1. A brief commentary on COVID 19: A Disguised Lesson of
Positivity
Shivani Haritay
4
2. Psychosocial impact of COVID 19 on Migrants
Muhammed Noorudheen
7
ORIGINAL ARTICLE
3. Academic Stress among 10th Standard Students during
COVID-19 Lockdown Period
Megha S. Rao
11
4. Awareness generation in the communities: field experience from the
CBOs
N. Janardhana
19
REVIEW ARTICLE
5. Policing During COVID-19 Pandemic and its Impact on
Mental Health
Apurva Kumar Pandya
40

S.NO TITLE PAGE NO.
BRIEF COMMUNICATION
6. Experience of Interning in the field of Mental Health Education
Manjiri Gokhale
58
7. NIMHANS Arogya Jagruti Kendra- A window to Educate
Minds and Empower Communities
Deepika Saini
65

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
What do I do? The predicament of Mental Health Education during
Pandemics and looking forward
Dr. Santosh K Chaturvedi
Address for correspondence: Santosh K Chaturvedi, Former Dean & Senior Professor of
Psychiatry, National Institute of Mental Health & Neurosciences, Bangalore -560029, India
How to cite this article:
Chaturvedi S. What do I do? The predicament of Mental Health
Education during Pandemics and looking forward. Journal of
Mental HealthEducation.2021;3(1):1-3
The role of mental health education
was exemplified during this current
pandemic. On one hand, its role was
in promotion of health in general and
mental health in particular, on the
other hand it had to deal with mental
health issues related to the pandemic.
There were numerous mental health
issues which emerged, some
unimaginable. There were fears and
anxieties related to contracting or
spreading infection, and there were
stigma issues towards frontline
workers and health professionals.
Mental health education professionals
thus needed to focus on the emerging
issues which kept changing by the
days.
1

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
They had to put other general mental health promotion and education issues on the back
burner, those issues were still as relevant as ever. This was similar to the situation of
medical profession; the predicament of doctors who were mired in confusion about what
their duty is and what they should do; save one life at the cost of losing another! Is it their
duty to follow the instructions or orders from their health leaders and systems or listen to
the voice of their conscience? If they follow the directions from their health leaders, they are
consigned to live with the guilt of not doing their duty lifelong.
The features of this ‘what do I do?’ phenomenon is related to healthcare delivery and related
matters, including mental health education. These have been experienced and reported by
many of our colleagues facing this predicament. The dilemma is the compromised autonomy
of the mental health education workers, their inability to do what they think is right and
needed. Mental health education programs on common mental disorders, situations and
conditions were halted, even though these had some links with the pandemic. In the pre
Covid-19 times general public were all advised to do regular physical activity, go for a walk
or a swim, or regular outdoor exercises in order to improve their respiratory and cardiac
functions and attaining well- being. All these were prohibited during the lockdown making
people more vulnerable to deal with the pandemic stress.
Stigma is an important theme in mental health education programs. One of the key objectives
of mental health promotion and education programs is reducing stigma towards mental illness
and those with mental illness. The pandemic has caused so much mental tension, anxieties
and fears that the role of mental health professionals and interventions has seemingly become
as important as the search for cure or treatment of the viral infection. There is also
tremendous stigma towards covid-19, people who turned positive on testing, or were at high
risk, or primary or secondary contacts. On the positive side, the government and public
have become well aware of the mental health issues, fears, anxieties and stress related to
covid-19 and launched extensive and mental health education on this aspect. Mental health
counsellors are being sought after and multiple telephone help-lines have been launched.
The counselling for such mental health issues and stigma could mainly be provided through
remote methods, like, tele-counselling and chats. Numerous health education materials in
the form of pamphlets, videos and use of technology to deal with this stigma have been
launched to counter the effect of stigma, negative impact of rumors, and to provide accurate
and authentic information. Thus, stigma associated with Covid-19 pandemic has reduced
stigma towards mental health and seeking mental health services and counselling. The
rumors and misinformation proved to be more than or as contagious as the virus itself.
This has led to fear in the public. This also led to stigma, not only against the infection, but
2

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
those who were even remotely associated with it. Rumors, like the virus, are infectious.
Fear and anxiety produced by such rumors are transmitted even if social distancing is
maintained. These cause widespread panic. A suitable way to deal with these would be
providing authentic knowledge and information through appropriate health information and
mental health education. These should be in different forms in order to reach the general
population, through mass media and social media.
A task force was set up to address the mental health aspects of the pandemic and make a plan
for action for psychosocial support. The committee suggested certain interventions may be
executed in the post-pandemic period, which included - preparations for addressing long
term reactions, which may evoke varied emotional response from the population, such as
suicide attempts, substance use and alike; support people in adjusting themselves to the ‘new
normal’ state, by providing continued psychosocial support; enhance the resilience, coping,
and adaptation levels in the community by devising specific awareness and interventions
programs and promote healthy lifestyles and habits to prevent future pandemics or the
morbidities associated with pandemics. Specific interventions on psychosocial support for
Covid-19 response included development of sensitization/training material for frontline
workers including health professionals for providing psychosocial support to such people,
sensitization of frontline workers including health professionals, development and
dissemination of messages to address anxiety, stigma and discrimination. For caregivers, it
was suggested to develop and disseminate messages for addressing psychosocial issues of
family caregivers’ burden and trauma including health professionals and other frontline
workers and development and dissemination of messages for addressing psychosocial
issues of people of vulnerable groups among the general population. Other suggestions to
be considered were development of sensitization/training material for frontline workers
including health professionals for providing psychosocial support vulnerable groups of
people; and development and dissemination of messages for addressing social stigma
attached with people in quarantine/isolation and frontline workers. As can be seen in these
suggestions, the role of mental health education in management of the impact of the
pandemic are of paramount significance. The health education and mental health education
sections and departments need more support and resources in order to meet the goals and
objectives of facing the psychosocial consequences of the pandemic. Being in the midst of
multiple strains and waves, it is clear, people have to live with this and similar pandemics
in future. Being prepared to face the uncertainties this time will definitely be of great help
and support.
3

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
A brief commentary on COVID 19: A Disguised Lesson of Positivity
Shivani Haritay Masters of Public Health, KLE JNMC, Belagavi, Karnataka
Address for correspondence: Shivani Haritay, Masters of Public Health, KLE JNMC,
Belagavi, Karnataka.
E-mail: [email protected]
How to cite this article:
Haritay S. A brief commentary on
COVID-19: A Disguised Lesson of
Positivity. Journal of Mental Health
Education. 2021;3(1):4-6
“Having an attitude that looks for
the positive and tries to be
optimistic can help you to filter out
some of the constant barrage of bad
or discouraging news- the figures
of the disease and how it’s
growing,” Wilcox said.
Covid-19 has created havoc all over
the world, leaving traces of death.
Negativity in the form of stress has
been witnessed in every aspect of
our lives. The constant fear of
being tested positive for COVID-
19 has been challenging for every
individual and a sense of being safe
is lost due to rise in the cases.
Major steps to cope up with this
pandemic crisis included restriction
of movement and social distancing,
which led individuals to be isolated
at home, affecting their mental
4

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
health indirectly as recreational activities like travelling, exploring streets and others were
completely stopped for a period of time which added to their frustration and anger. The sense
of anxiety about one’s own health had brought changes in eating and sleeping patterns.2
The present crisis is a transitional phase as the past shows us to value the present that is most
important to us and to look into the future to discover the newness of life. 3 COVID-19 has
been a disguised teacher who taught us the key lessons of life. The transmission of
COVID- 19 has indicated that if one does not take care of himself, he can be at the risk of
getting infected or infecting those around him. The second most important lesson was to
value the smallest steps like maintaining hygiene and sanitation, following the simplest
rules and regulations set by the government. Thirdly, to be aware of one's own action
towards the environment, following the guidelines of wearing a mask and gloves is
absolutely right but discarding them in a proper way is also equally important. Fourth
lesson was learning how to respect time, the questions like how much time did I lose being
sad, angry, or gain a moment being happy? During this phase time played a vital role, it
reconnected one to his own hobbies and cultivated an art of adjustment. Fifth, the share of
responsibilities at home, the gender based roles merged during this time, for family time
played a vital role. Sixth, the greatness of sacrifices by our health care frontline workers, law
and order officials and others proved to be a true inspiration. Lastly COVID-19 through its
nature of virus showcased it mightiness of power over humanity, the greatest take away
from it was together if humans decide to accept change, no power can conquer the will of a
man, today every individual has united together to fight back against the pandemic, with a
hope to end this crisis sooner. Positive emotions, such as comfort, happiness, joy, love, and
gratitude, can help maintain and improve human mental health.3 To conclude being
positive during a challenging time like a pandemic, seems little tough but looking at the
broader aspect and with a choice in change of thought, positivity can help in coping not
only stress but also one’s own routine making it more productive and cheerful. Covid-19
has paved a path in shaping human life in every aspect while battling with the crises.
References
1. Readers Blog by Times of India. India :Archie Mishra April 19 2020, (cited on
September 21, 2020) available at
https://timesofindia.indiatimes.com/readersblog/bubblybarebones/15ways-to-stay-
positive-du ring-covid-19-12287/ (last accessed on September 21, 2020)
2. Centers for Disease Control and Prevention (2020) Coping with Stress available at
5

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress- anxiety.html
(last accessed on September 21, 2020
3. Yamaguchi, K., Takebayashi, Y., Miyamae, M., Komazawa, A., Yokoyama, C., & Ito, M.
Role of focusing on the positive side during COVID-19 outbreak: Mental health perspective
from positive psychology Psychological Trauma: Theory, Research, Practice, and Policy
2020. 12(S1), S49 S50.
6

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Psychosocial impact of COVID-19 on Migrants
Muhammed Noorudheen1, Lekshmi Vimala2, Anish V Cherian3
1MPhil Scholar, Department of Psychiatric Social Work, NIMHANS, Bengaluru
2PhD Scholar, Department of Psychiatric Social Work, NIMHANS, Bengaluru
3Assistant Professor, Department of Psychiatric Social Work, NIMHANS, Bengaluru
*Address for Correspondence: Muhammed Noorudheen, MPhil Scholar, Department of
Psychiatric Social Work, NIMHANS, Bengaluru, India,
E-mail: [email protected]
How to cite this article:
Noorudheen M, Vimala L, Cherian
A V. Psychosocial impact of
COVID- 19 on migrants. Journal of
Mental Health Education.
2021;3(1):7-10
Though the pandemic is not a new
concept to humankind, the current
Covid-19 outbreak is different
from all the previous ones that we
have overcome. The virus in itself
may not be life-threatening, but
most of the population could get
affected due to the absence of
vaccines and ‘herd immunity’ not
being applicable. It puts the health
care system under strain leading to
catastrophic repercussions.1 In the
absence of a vaccine, the only
viable option available to help
flatten the curve, is to follow the
precautionary measures diligently
7

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
lockdowns included. Currently there are restrictions of social interaction in workplace,
schools and other public spheres, except for essential public services such as fire, police,
hospitals.2 However, this measure has seen adverse after effects in the informal sector, with
the worst brunt being borne by the migrant laborers, who are left with no job, money or
shelter3 and asked to stay put till end of the lockdown, as their movement would act as a
risk factors. Migrant workers have been chronicled as highly vulnerable to stress due to
displacement, undernutrition, low immunization coverage rate, and various physical and
mental health conditions.4 They are also often exposed to challenging and unsafe
conditions, occupational hazards, poor living conditions, and the absence of a supportive
family or societal structure. They also do not have access to educational or health
programmers.5 Difficulties in communication due to language barriers, traditional beliefs,
and socio-economic status are significant challenges for migrants.6 There is inadequate data
that connects migration, livelihood strategies, and the economic growth in India, which has
resulted in inaccurate policies and a lack of political commitment to improve the lives of the
migrants.7,12 Though migration has been found to be a leading cause of mental health issues8
and suicide9,the subject is not much explored in India. Women are potentially more
affected by the loss of livelihood, domestic violence, and forced early marriages. In
addition, Prof. Aman pointed out that 133 people died by suicide out of distress about the
COVID infection, loneliness, travel restrictions imposed during the lockdown, and the
hopelessness over their inability to return home.10
Policy changes at the state level have to be brought to ensure proper dissemination of services
to the migrant workers. Though there are policies that exist to protect the migrants (such as
the National Rural Employment Guarantee Act, 2005 and the Minimum Wages Act, 1948),
these are fragmented in nature and do not address the concerns related to physical and mental
health in its entirety.5 Disaster preparedness and risk reduction need to be implemented
from a disaster perspective, such as awareness raising, early warning, emergency
communication and effective recovery. These all have to be application level from the
systematic framework. Sensitization and training of concerned policy makers and health
stakeholders such as government officials, healthcare workers, and private employers are to
be done on a large scale so that adequate information about the necessary health and public
services will help prevent expected psychological distress and promote mental health well-
being among migrants. The existing community and religious organizations can be
developed to mobilize the psychosocial support and resources required.11 Alternative
identity cards can be issued to the migrant workforce (similar to what has been
implemented in Kerala) to provide education and welfare services including health
provisions and child policies.12
8

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
The economic and sociocultural changes experienced that acts as a risk factor for poor
mental health also needs to be addressed.8 Helplines and Crisis interventions need to be
available to the migrant workforce during disaster and times of emergency (such as the
current outbreak) to take care of the specific needs of the migrant population so that events
similar to the ‘long walk’13 that happened recently in New Delhi can be avoided.
References
1. Ackerman. D. Infectious disease experts explain how the coronavirus pandemic is different
from a flu pandemic. Business Insider India. [Internet] [2020, April]. Available from:
https://www.businessinsider.in
2. Sardar T, Nadim SS, Chattopadhyay J. Assessment of 21 days’ lockdown effect in some
states and over all India: a predictive mathematical study on COVID-19 outbreak. arXiv
preprint arXiv:2004.03487. 2020 Apr 7.
3. Slater J, Masih N. In India, the world’s biggest lockdown has forced migrants to walk
hundreds of miles’ home. The Washington Post. Mar. 2020 Mar;28. Available from
https://www.washingtonpost.com
4. Nitika AL, Nongkynrih B, Gupta SK. Migrants to urban India: need for public health action
Indian journal of community medicine: official publication of Indian Association of
Preventive & Social Medicine. 2014 Apr;39(2):73.
5. Borhade A. Health of internal labour migrants in India: some reflections on the current
situation and way forward. Asia Europe Journal. 2011 Apr 1;8(4):457-60.
6. Virupaksha HG, Kumar A, Nirmala BP. Migration and mental health: An interface. Journal
of natural science, biology, and medicine. 2014 Jul;5(2):233.
7. Deshingkar, Priya and Akter, Shaheen. Migration and Human Development in India
Published in: Human Development Research Paper (HDRP) Series. 2009, Dec Vol.13.
8. Firdaus G. Mental well-being of migrants in urban center of India: Analyzing the role of
social environment. Indian journal of psychiatry. 2017 Apr;59(2):164.
9. Anil RA, Nadkarni A. Suicide in India: a systematic review. Shanghai archives of
psychiatry.2014 Apr;26(2):69.
10. Dheeraj Mishra. RTI Shows the Government Did Collect Data on Deaths of Migrant
Workers During Lockdown. The Wire. 2020 Sep 17. Available from
https://thewire.in/rights/centre-indian-railways-lockdown-deaths-migrant-workers-shramik-
special-rti
11. Reitmanova S, Gustafson DL. Mental health needs of visible minority immigrants in a small
9
https://thewire.in/rights/centre-indian-railways-lockdown-deaths-migrant-workers-shramik-special-rti
https://thewire.in/rights/centre-indian-railways-lockdown-deaths-migrant-workers-shramik-special-rti

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
urban center: Recommendations for policy makers and service providers. Journal of
Immigrant and Minority Health. 2009 Feb 1;11(1):46-56.
12. Aggarwal, V, Singh, P. Mitra, R. Low interstate migration is hurting India's growth and
states are to blame. Business Standard. 2019, August 26. Available from
https://www.business-standard.com
13. Nayar PK. The Long Walk. Journal of Extreme Anthropology. 2020 Mar 29;4(1):E1-6.
10

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Academic Stress among 10th Standard Students during COVID-19
Lockdown Period
Megha S Rao1, Sindhu V 2 1Lecturer, Department of Psychology, M.E.S College of Arts, Commerce & Science,
Bangalore
2Former Behaviour Trainer from YourDOST organization, Bangalore.
*Address for Correspondence: Megha S Rao, Lecturer, Department of Psychology,
M.E.S College of Arts, Commerce & Science.
E-mail: [email protected]
How to cite this article:
Rao S, V. S. Academic stress among 10th
standard students during COVID- 19
Lockdown period. Journal of Mental
Health Education. 2021;3(1)11-18
Abstract
Aim: To understand the level
of academic stress among 10th
standard students who were
taking tests on a daily basis
through online mode due to
COVID-19 lockdown.
Method: A total of 60 students
(30 boys and 30 girls) were
selected using a purposive
sampling method. The
Educational Stress Scale for
Adolescents (ESSA, Sun,
Dunne, Hou, & Xu, 2011a)
which is a revised 16 item
scale which includes five
factors – pressure from study,
workload, worry about grades,
11

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
self-expectation and study despondency was used for the study. Along with this scale, a
question on how this lockdown period helped participants to cope with the situation was asked
and the responses were collected using Google forms. Mean, Median, independent samples t-
test, Pearson Product Moment Correlation were the statistics used to analyze the data.
Results: It was found that there is no significant difference in the academic stress level among
boys and girls. However, the mean scores indicated that girls were more stressed compared
to boys. It was also found that there was a significant positive relationship between pressure
from study and worry about grades and study-despondency. Low levels of academic stress
were found among boys and girls. Low level of stress under the factors word-load, self-
expectancy and study-despondency and average level of stress under pressure from study
and worry about grades was reported.
Conclusion: Involving in various activities would help students cope better with the
academic stress.
Key words: Academic stress, 10th standard students, online mode, COVID-19
Background
Coronavirus Disease 2019 (COVID-19) is an infectious disease caused by a newly
discovered Coronavirus.1 Dr. Sameer Malhotra, director and head, Department of Mental
Health and Behavioral Sciences, Max Healthcare says that students who are giving board
exams are concerned about the uncertainty that future holds.2 S. Arumainadhan, the
President of the Tamil Nadu Students’ Parents Welfare Association, Chennai said that “This
situation is stressful for students. There is a lot of stress that the students are burdened with
during board exams and now this COVID-19 will stress them even more.”3
Methodology
The study used survey methods which were exploratory in nature. A purposive sample of 60
students (30 boys and 30 girls), studying in tenth standard were chosen to understand the
level of stress as they were dealing with uncertainty and were taking many subject related
tests. Consent for participation was obtained and responses were collected using Google
forms between 1st and 6th of May 2020. A question “Has this lockdown period helped you
develop or learn anything new? If yes, please mention what new skill you have learnt” was
asked mainly to understand how students were dealing with the lockdown period.
12

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Tools: The revised version of Educational Stress Scale for Adolescents (ESSA, Sun, Dunne,
Hou, & Xu, 2011a) was used to estimate the level of academic stress. It contains 16
statements rated on a 5-point Likert scale ranging from 1 (Strongly disagree) to 5 (Strongly
agree). The total score ranges from 16 to 80: a high score indicating greater stress. This scale
has five factors: ‘Pressure from study’ (four items about the perceived pressure from daily
learning, from parents, peer competition and students’ concern about the future); ‘Workload’
(three items regarding perceived burden of homework, schoolwork and examinations);
‘Worry about grades’ (three items regarding stressful emotions due to dissatisfaction with
academic grades); ‘Self- expectation stress’ (three items about stressful feelings when self-
expectation failed to be met) and ‘Despondency’ (three items about dissatisfaction and lack
of confidence and concentration in academic study). This instrument has satisfactory to good
internal consistency with Cronbach’s α = .82 for the total scale. Test-retest reliability is
satisfactory with .78 for the total scale.
Analysis
SPSS Version 16.0 was used to calculate the mean and median to understand the level of
stress under five factors. Independent samples T-Test was computed to see if there is a
significant gender difference in academic stress and Karl Pearson Product Moment
correlation to understand the relationship between all the five factors.
Results and discussion
Table 1 (Appendix 1), shows Academic stress does not differ significantly among boys and
girls of 10th standard students taking tests on a daily basis during the lockdown period of
COVID-19. However, the mean scores indicate that the academic stress is slightly higher
among girls (mean=49.933, SD=7.49) than boys (mean=49.500, SD=8.754) with a t-value
0.206. This finding indicates girls reporting more academic stress than boys.
Table 2 (Appendix 1), shows a significant relationship between the different areas of
Academic stress across gender by 10th standard students taking tests on a daily basis during
the lockdown period of COVID-19. Pressure from study has a positive correlation with
worry about grades (r=0.434, p<0.01). Pressure from study has a positive correlation with
self- despondency (r=0.472, p<0.01). This indicates that increased pressure from study can
increase worry about grades and self-despondency.
The findings of the study show that participants experience low levels of academic stress
13

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
(35%) compared to average (33.3%) and high (31.7%) levels of Academic stress.
Average level of stress under the factors Pressure from study (low= 33.3%, average=35%,
high=31.7%) and Worry about grades (low=40%, average=41.7%, high=18.3%).
Low level of stress under the factors workload (low= 40%, average=28.3%, high=31.7%),
Self-expectancy (low=32.3%, average=9.4%, high=20.8%) and Study-despondency (low=
30.2%, average=15.6%, high=16.7%).
The level of stress was found to be low among the participants as they had involved themselves
in different activities. Girls were involved in cooking, household chores, drawing, playing
games, chess, learning songs, acting and reading story books. Few had taken the opportunity
to improve their academic progress for board exams and one of the participants was
involved in learning how to ride a bike. Boys were involved in cooking, solving Rubik’s
cube, practicing yoga, exercising, trying to build their body, riding, household chores and a
few of them had taken the opportunity to improve their academic progress for board exams,
and one of the boys had mentioned that he was practicing anger management and being
calm at times.
However, a few boys did mention that they were not happy as they felt depressed staying
alone and not meeting their friends for a long time. Among 60 participants, 17 participants
indicated that they had not been involved in any major activities as such.
Suggestions
From this study we can understand that although there is uncertainty, participants coped with
their stress level by involving themselves in different activities. Stress is caused by thinking
about the future and not being focused completely. To manage the stress level, a certain
strategy to cope with academic stress can help the mover come.
The coping strategies may include learning new skills through practice, using positive self-
talk, taking responsibility for mistakes, forgiving ourselves, focusing on what we can control
and practicing good self-care.
Implications
The result of this study helps parents, students and teachers understand that pressure from
studying can have an impact on study-despondency and their worry about grades. However,
adapting and accommodating coping strategies or focusing on different activities may lower
the level of academic stress.
14

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Limitations
● Limited scope for generalization of the study’s conclusion due to small sample size.
● Participants only from urban areas were considered.
● Participants were not selected randomly.
Conclusion
The level of stress is low on academics as a whole among 10th standard students, taking tests
on a daily basis during the lockdown period due to COVID-19. Participants have shown low
levels of stress under workload, Self-despondency and Self-expectancy. There is no
significant difference across gender in academic stress. There is a significant relationship
between pressure from study and worry about grades, study-despondency across gender.
References
1. World Health Organization, Health topic, Coronavirus available at
https://www.who.int/health-topics/coronavirus#tab=tab_1
2. Ghosh S, (2020), Express News Service, New Delhi, available at
https://www.newindianexpress.com/lifestyle/health/2020/may/07/anxiety-feeling-of-
uncertainty-mental-health-talks-rise-amid-covid-19-lockdown-2140214.html
3. Deeksha J (20/03/2020), TN students, parents hoping state will go CBSE way, postpone
Class 10 exams, available at https://www.edexlive.com/news/2020/mar/20/tn-students-
parents-hoping-state-will-go-cbse- way-postpone-class-10-exams-10790.htm
15

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
APPENDIX 1
Table 1 shows mean, standard deviation, t-value and significant difference in Academic
stress across gender, by 10th standard students taking tests on a daily basis during lockdown
of COVID-19.
Scale Groups Mean SD p-value t-value
Academic stress Boys 49.5000 7.49
Girls 49.9333 8.784
0.497 0.206
16

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Table 2 shows the significant relationship between different areas of Academic stress
across gender i.e. Pressure from study, workload, and worry about grades, self-expectation
and study- despondency by 10th standard students taking online classes during lockdown
of COVID-19.
Factors of
PFS WL WA G
SE SD
Acade
mic
stress
PFS
1
0.1
76
0.43
4**
0.1
45
0.472*
*
WL 0.176 1 -
0.16
9
0.1
07
0.039
WAG 0.434
**
-
0.1
69
1 0.1
26
0.213
SE 0.145 0.1
07
0.12
6
1 0.154
SD 0.472 **
0.0 39
0.21 3
0.1 54
1
p<0.01
PFS=Pressure from study, WL=Workload, WAG= Worry about
grades, SE=Self-Expectation and SD= Study-Despondency.
17

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
18
Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Awareness generation in the communities: field experience
from the CBOs N. Janardhana1*, DM. Naidu2, Guru Raghevendra3
1Dr, N. Janardhana, MSW, M.Phil, Ph.D, Professor, Department of Psychiatric
Social Work, NIMHANS, Bangalore, Karnataka.
2DM. Naidu (deceased), Programme Manager, Basic Needs India, Bangalore.
3Guru Raghevendra, Programme Manager, Samarthanam Trust, Bangalore.
*Address of correspondence: N. Janardhana, MSW, M.Phil, Ph.D, Professor,
Department of Psychiatric Social Work, NIMHANS, Bangalore, Karnataka.
E-mail: [email protected]
How to cite this article:
Janardhana N, Naidu M D, Raghevendra G.
Awareness generation in the communities: field
experience from the CBOs. Journal of Mental
Health Education. 2021.3(1):19-39.
Abstract
Mental illness attracts less
empathy and more distrust than
any other forms of illness. People
may consciously or
unconsciously isolate themselves
from people with mental illness
and their families. Lot of
misconception govern the faith of
people with mental illness.
Mental illness often generates
misunderstanding, prejudice,
confusion and fear. There is an
urgent need for developing
awareness generation in order to
reduce ill effects of stigma.
researcher have collated various
means of awareness generation
program while working with
19

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
the partners in initiating community based rehabilitation program for people with
mental illness in the community. Researcher have shared various mediums of
awareness generation like, street theatre, puppet shows, wall writings, booklets, rallies,
etc., as means of generating awareness in the community. Intervention programs need
to be designed using locally available community resources. The awareness generation
should involve community members, so that they can sustain the program.
Key words: Stigma, Discrimination, Community Based Rehabilitation,
Introduction
The word Stigma means a mark of shame associated with a particular circumstance,
quality or a person. In the context of mental health issues, stigma is a mark of
degradation associated with person living with mental illness1,2. It is not just that
person who becomes mentally ill gets stigmatised but the entire family has to face the
brunt3,4. This has been the age-old issue, and passed on from generation to generation.5
Such people were called as lunatics, mad, mental, loose, incapable etc. In the East,
people still believe that mental illness is caused due to witchcraft, misdeeds in the
previous lives, curse, etc.6 These sort of perceptions, misconceptions, myths and
apprehensions leads to stigmatise people with mental illness and their family
members.5,7 The stigma is so tremendous that people feel ashamed and deny their
illness. Therefore, the first and foremost element that shrouds the realm of mental
illness is stigma attached to it. It is a huge burden on the family members. The very
thought of someone in the family getting mental illness is a big shock and they do not
want to believe it. Hence, they first go to temples, black magicians, witches and faith
healers and waste whole lot of financial and other resources, before reaching menstal
health care services8. The burden of stigma may exceed the burden of the disease in its
impact on social, emotional, and work functioning, thus negatively affecting the overall
quality of life.9
Janardhana and Naidu in their study have found various forms of stigma faced by
families of people with mental illness10. They have reported harmful treatment,
chaining and locking in the rooms, social boycott for the families, denial of property
rights for persons with mental illness, legal separations due to mental illness, caregivers
20

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
getting ostracized, and also denial of right treatment. In another study with children
with disabilities, Janardhana et al.,4 (2016) have found various ugly forms of
discrimination and stigma seen are social boycott, denial of property rights, physical
restraints, decreased prospectus of marital life due to disabled member in the family,
discriminations from the state policies, and women with disabilities face more brunt of
their disabilities.
Due to stigma associated with mental illness, families become victims of
discrimination and human rights abuse. When poverty, physical neglect and social
marginalization intersect, the impact on the people with mental illness and their
families can be devastating. People with mental illness are kept hidden away at their
home, denied basic rights of mobility, education and employment. They are viewed as
incapable and dependent persons.10 Such discrimination in some cases starts from their
family members and spreads right up to the policy makers and state authorities as the
policies for people with mental illness are not user friendly. 11 As a result of such
discrimination the people with mental illness and their families face chronic health
issues, socio-economic burden and destitution. Sometimes it is so difficult to
define the marginalization — they are outside the margin or within the community
meaning, locked in the rooms, institutionalized, families isolating themselves, enrolling
in special homes, not admitting that they have a person with mental illness in their
families, and etc.12 Social attitudes and stigma play an important role in limiting
the opportunities for people with mental illness for their full participation in social
and economic life, often even within their own families.13
Stigmatizing attitudes towards mental disorders are responsible for substantial distress
among caregivers, and delay in seeking appropriate help for treating their family
member with mental illness14,15 and often find it difficult to rehabilitate them as they do
not have adequate opportunities for employment.15,16 Moreover, stigma is not confined
only to severe mental illness but also to common mental disorders. 17,21
Researchers have proved that stigma has become one of the public health problem and
need to develop strategies and mechanisms to create awareness in the community so
that people with mental illness would get adequate opportunities for living with
dignity.22,25 World Health Organization has called for action amongst its member
nations to develop strategies of creating awareness to reduce stigma26, and several
activities in this area have been implemented by both government and non-
21

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
governmental organization23. The researchers in the current paper have shared their
experiences of using different methods and mediums of awareness generation by
utilizing the local resources available within their reach.
Method
The researchers were working in Basic Needs India, a registered Trust and a resource
group in community mental health and development. The Basic Needs India partnered
with the CBOs and NGOs for including mental health issues in their development
activities in all south Indian states. Basic Needs India, a resource group in community
mental health and development, worked with partner organizations like SACRED in
Ananthpur and Kurnool district, Andhra Psradesh; Samuha in Koppal and Raichur
district, Grameena Abyadaya Seva Samasthe, Dodabalapura, Karnataka; ADD India
and Vidyasagar partners in states of Tamil Nadu and Kerala. The researchers supported
these organizations in building their capacities to include people with mental illness in
their disability programs in their project areas in rural areas. During the process of
capacity building, the field staff/CBR workers would come out with different methods
using materials available within their reach in developing awareness materials.
Researchers have tried to capture some of the methods and materials used for creation
of awareness materials in writing this paper. The aim of this paper is to capture various
methods of awareness generation which can be used in the community for dealing with
the ill effects of stigma. During the review and consultation with the partner
organization, people with mental illness and other disability groups were also evolving
strategies for dealing with stigma and discriminations. The researcher would like to
share community based strategies evolved for dealing with the stigma in the current
paper.
Means of awareness generations with people’s participation and utilizing
community resources
Sl
no
Modes of
awareness
generation
Key features
1 Street theatres Street theatre troops are
made in their locality
involving field staff, and
volunteers in the
22

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
community. Language and
cultural factors are taken in
to consideration while
writing the script for the
street theatres. This would
attract people to participate
and also has scope for
interaction after the street
theatres, and helps in
identifying people with
mental illness, as
community members would
identify and refer them to
the field staff.
2 Posters using
materials in
their reach
Waste materials like used
tyres, cement gunny bags
and other materials are used
to write posters which are
cost effective and also easy
to carry for the field staff to
places where they conduct
awareness programs.
3 Wall writing The awareness material
generated would stay for
long time till they repaint.
Most of the family
members have volunteered
to give space for such
writing, they have taken
responsibility for
safeguarding such writing.
This would address the
sustainability of program.
4 Wall painting It generated community
participation, people in the
community actively
participate in filling paints
for the sketches. It also
makes them own the
painting. This would be
long lasting addressing the
sustainability of the
program.
23

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
5 Press clubs Print media need to actively
participate in capturing the
experiences of people with
mental illness and their
families. People with
mental illness and their
caregivers should be
encouraged to share their
experiences during
observation of world
mental health day and
world disability day, so that
people would get sensitized
about the needs, and their
attitudes can be changed
and create safe environment
for people with mental
illness
6 Books in local
language
Demystifying the technical
information into a simple
booklet for people to
understand the concept of
mental health and mental
illness. These books can be
kept in public transport
vehicle, so that people can
read while traveling.
7 Puppet shows Scripts prepared can be
enacted through puppet
shows, which would attract
children and people in the
community, this also helps
to relate to the problems
and would be able to
identify people with mental
illness in their areas
8 Caregivers
groups and
associations
Encouraging caregivers to
form self-help groups also
help to save money and get
loans for livelihood
activities. These groups
would generate strengths
for the families to evolve
24

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
support for dealing with
their problems.
9 Medicine box
using materials
in their reach
Developed by field staff to
deal with the problems of
medicine adherence, as
people tend to get confused
about which medicine and
when to take.
10 Recorded DVD
(Videos)
The DVDs are used in the
local cable networks, and
during community festivals,
which would create
awareness on mental
illness.
11 Songs Field staff taking interest in
creating songs and tuning is
also an effective method
generating awareness.
12 Rallies Rallies organized as part of
observing world mental
health day and world
disability day is used as a
platform for sensitizing the
district authorities and local
community about the needs
of people with mental
illness in their areas.
13 Observations of
world mental
health and
world disability
day
When people with mental
illness, their alliance
partners, families and local
community take
responsibility for such
events. The panchayats also
would participate and
support such initiatives by
observing cost of such
celebrations.
25

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Awareness Materials
The partner organizations utilised the local resources in developing awareness
materials. Below given are some of how the examples a flex with symptom of mental
illness was prepared. This was displayed in all the awareness program (street theatre,
community group meeting and on camp days). Another partner organization created
awareness materials using used tyres covered with the empty cement gunny bags, and
colours were used to write messages on it. Another partner organization in Bihar
collected empty cement bags from the construction site, with the help of Self Help
Group, got them stitched and used as banner during the camp day.
Caregivers along with people with mental illness, NGO personnel addressing press club
during world mental health day observation. Caregivers and people with mental illness
wanted to sensitize print media and also used print media in presenting their
psychosocial needs so that people in the community do not ostracise people with
mental illness.
26

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Puppet show in Pudukotai
Regular awareness sessions designed around a puppet show were held in the street of a
village that lies within their area of operation. The ‘stage’ was a simple suspended
banner behind which the puppeteers worked. The banner summarized causes,
treatments and symptoms of mental illness, the purpose being to demystify the subject
and to raise the awareness of the public towards mental health issues.
A short puppet show based on the story of a family break-up and the recovery of a
mentally ill person was followed by a play that showed the effects of bi-polar disorder.
The acting was dramatic and held the attention of the audience, which was made up
almost entirely of women and children, around one hundred people altogether. The
performance was around twenty minutes long in total and was followed by a short
address to the audience that reinforced some of the main messages.
Street Theatre in Bangalore urban Slum
Awareness sessions designed around a case study from their experience from the field.
8 field staff enacted different roles in the street theatre staged a woman with mental
illness, portraying how she would become victim of socio cultural practices and
violence acting as precipitator for mental illness. The story also depicted the role of
field staff in identifying people with mental illness, facilitating treatment process in and
then home based intervention, involvement in livelihood opportunities. The ‘stage’ was
27

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
simple and attracted crowd on the busy street of slum. The performance was around
thirty minutes long in total and was followed by a short address to the audience that
reinforced some of the main messages.
Wall writing
Community members were encouraged to take responsibility for owning the awareness
pictures. Public building had been identified with the support of the community
members, an artist was invited to draw an outline for the awareness charts. The
community members were encouraged to take responsibility for filling the colours in
the outline diagram. The community members took responsibility of owning it, and
guarding it from all damages. These become an effective tool in changing their
attitudes towards mental illness and also promote inclusion of people with mental
illness. The messages about mental illness had been written on the walls of the main
road in the village and in the National and state highways, which also added towards
reduction of stigma in the community.
Community Owning Wall Writing
PC: Apsa
28

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Awareness materials in the Public Transport (Auto)
A small Handbook with 25 pages of basic information on mental illness for the lay
individual was developed, and kept in small cotton bags which can be tied to the back
side of the driver seat of the auto-rickshaw. The passengers traveling in the auto could
pick up these books, and read while travelling.
29

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Federation of people with disabilities advocating for the rights of people with mental
illness
People with disabilities were encouraged to include people with mental illness in their
disability groups as mental illness is one of the disability. With the support of other people with
disabilities, rally was organized to sensitize government officials and community members
about their needs. Through these rallies, it was intended to spread awareness and expected
people to recognize people with mental illness, facilitate and create opprtunities for people
with mental illness in their neighbouhoods.
30

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
A field staff in order to deal with the problem of drug adherence was appointed as people were
forgetting about the medicines to be taken in morning, afternoon, and night. The self help
group members and the field staff developed a medicine box using the cardboard which had
3x7 compartments for 7 days. They also made a small bag with three openings of different
colors; red indicating morning; white indicating afternoon and black indicating night.
Medicines were kept in this bag, as it was more convenient for people to take medicines
prescribed for morning, afternoon and night.
Field staff were talented, and wrote songs and tuned them. The same medium was used for
awareness generation. One of the partner from Andhra Pradesh composed a song “manam
marithe ie jagathu mareanu (if we change, society will also change). These songs were sung in
public platforms, caregivers’ meeting and disabled people’s organizations. This acted as a
medium of collecting people and encouraged people’s participation in social cause.
31

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Caregivers Association at Erumalainayakanpatti
The work of caregivers’ associations came up on frequent occasions during the review and it
appeared to be one of the most effective features of the work of Basic Needs India. Through
ADD India and St Joseph Development Trust, organized all the caregivers in the project area
of Theni District and registered a Caregivers Association to discuss issues of the caregivers and
their mentally ill family members in the Association meeting held monthly once. The
Association made plans for observing world mental health day, world disability day and
caregivers’ day. With the support of the partner organizations, rallies were organized, giving
representations and advocating with the district authorities of availing health and welfare
needs.
Kittur Rani Chennamma Self-help Group
Self-help groups are a platform for creating awareness programmes. The self-help group of
women in Marasandra in Y N Hoskota was clearly working hard to be strong in the face of
personal tragedy and unrelenting poverty. Comprising twelve members, they explained that
their main purpose is to promote savings of Rs.100 per month per person so that individuals
can accumulate enough to buy a buffalo/cow. This would then be a source of regular income;
the milk being sold to a cooperative at a guaranteed rate per litre. One of the women had lost
her husband to snakebite and so the group was rallying around to support her and her three
children. The link with mental illness comes through the treasurer, Krishnaveni, who had been
accepted into the group for her literacy skills and was in remission after taking treatment for
her schizophrenia. The point here is that her illness was not seen by people because she had
skills to offer.
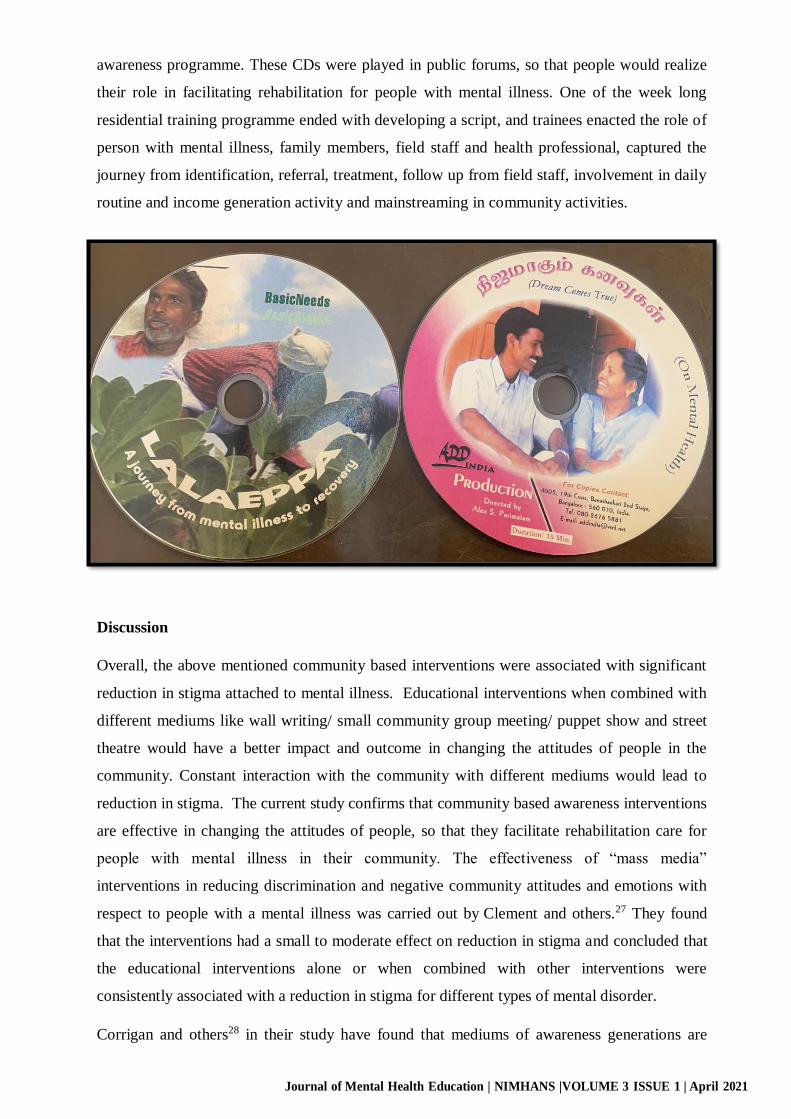
Videos capturing the journey of a person (Lalaeppa) with mental illness were recorded in their
place of residence by a trained cinematographer and these CDs were used for creating
32
Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
awareness programme. These CDs were played in public forums, so that people would realize
their role in facilitating rehabilitation for people with mental illness. One of the week long
residential training programme ended with developing a script, and trainees enacted the role of
person with mental illness, family members, field staff and health professional, captured the
journey from identification, referral, treatment, follow up from field staff, involvement in daily
routine and income generation activity and mainstreaming in community activities.
Discussion
Overall, the above mentioned community based interventions were associated with significant
reduction in stigma attached to mental illness. Educational interventions when combined with
different mediums like wall writing/ small community group meeting/ puppet show and street
theatre would have a better impact and outcome in changing the attitudes of people in the
community. Constant interaction with the community with different mediums would lead to
reduction in stigma. The current study confirms that community based awareness interventions
are effective in changing the attitudes of people, so that they facilitate rehabilitation care for
people with mental illness in their community. The effectiveness of “mass media”
interventions in reducing discrimination and negative community attitudes and emotions with
respect to people with a mental illness was carried out by Clement and others.27 They found
that the interventions had a small to moderate effect on reduction in stigma and concluded that
the educational interventions alone or when combined with other interventions were
consistently associated with a reduction in stigma for different types of mental disorder.
Corrigan and others28 in their study have found that mediums of awareness generations are
33

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
effective in stigma reduction. They also have found that the quantitative evidence that stigma
interventions are effective for specific categories of mental disorder, including depression and
psychosis/schizophrenia. They concluded that there is clear need to undertake further research
to evaluate the effectiveness of stigma reduction interventions for these conditions need to be
the focus of future researches.
The current study does confirm that educational components and those with a consumer
contact components are effective in reducing stigma. Further investigation of the effectiveness
of standalone educational interventions for the specific clinical conditions may be required.
There is a clear need for further research investigating the effect of consumer contact, whether
there is a difference in the effectiveness of contact, education and education combined with
contact. There is some evidence to suggest that population level interventions using mass
media campaigns and social marketing can be effective29.
Although researchers have found evidence that different mediums of awareness generation do
have impact in stigma reduction 18, 19, our findings suggest that different mediums presented in
this article have been integrated in to the activities of the integrated community development.
However, employing parallel measures of awareness generation along with scope for live
interaction with the community members would have better impact, similar finding has been
reported by Stauart30. Community based interventions delivered via community participation
was found to be effective. Many community based interventions programs are delivered face-
to-face with scope for interaction from the community and also scope for reflecting on some of
the messages made these mediums more effective. Similar views have been shared by others
employing the awareness programmes 31 -34.
Griffiths et al.,35 have reported that there is paucity of studies that had investigated the effects
of stigma interventions for different types of mental disorder and for different intervention
types, particularly in the case of consumer contact. It is clear that different mediums of high-
quality awareness generation is required and need of the day in order to facilitate community
care for people with mental illness.
The different methods of awareness generation given in this paper is different from the
psychoeducation models used in the institutional care. The psychoeducation models use one to
one interaction with the family members, concentrate more on medicine adherence and relapse
prevention. Whereas, the different modes of awareness generation given in the paper
concentrate more on dealing with myths and misconception directly dealing with the attitudes
of people in the community, which would help in reintegrating people into the community life
and also experiencing dignified living for people with mental illness. The reintegration can be
achieved only when people provide opportunities for livelihood, interactions, inclusion in
34

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
community activities for people with mental illness.
Future Research
However, future researches should concentrate in testing out the effective modes of awareness
generation with scientific methodologies in different cultural settings so that these mediums
can be up-scaled with community participation to reach the unreached. Future research is
needed to systematically compare the efficacy of single-level vs. multi-level stigma
interventions in order to determine the conditions under which multi-level stigma interventions
may be preferable to single-level interventions. Future research is also needed to evaluate how
changes at one level of stigma (e.g., intrapersonal) would impact on other levels of stigma
(e.g., community). Research should also focus on identifying mechanisms of change in multi-
level stigma interventions, and to explore the barriers and facilitators to the dissemination of
multi-level stigma interventions across diverse cultures. Finally, there is a need to improve the
quality of studies in this area, particularly with respect to reducing stigma and facilitating care
and rehabilitation of people with mental illness in their own community.
Limitations:
The paper addressed a clinically important topic that has rarely been explored. The current
study has some limitations. The current paper analysed various modes of awareness
generations used by Community based organizations for generating awareness about mental
illness. However the authors have not made any efforts in terms of testing out the efficacies of
different strategies, which is a main limitation of this paper. Efforts of such Community based
organizations need to be appreciated, recognized, applauded, emphasized not acknowledged in
the literature. There is a need for developing measures to assess the impact of different modes
of awareness generation. There may be many more modes and strategies of awareness
generations which are not covered in this paper is one of the limitations of this paper. The
awareness generations done by different people and in different places can have different
outcome, authors were not able to capture what worked well and what did not workout. The
field workers do not have any formal training in mental health, with the support of the
psychiatric social worker they were able to generate materials for awareness, more professional
inputs would have strengthened the materials, which acted as one of the limitations of this
paper. Data also would have been collected with people attending such awareness programme
so that we would have found out the impact of awareness generations on attitudes related to
mental illness.
35

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Conclusion:
Stigma is inherently a multi-sectoral and cross cutting phenomenon and thus affects all spheres
of life for people with mental illness and their families. Myths and misconceptions prevailing
towards mental illness leads to stigmatised behaviours reducing opportunities for participation
and inclusion for people with mental illness in the communities. Changing attitudes of people
only can create opportunities for people with mental illness to lead and experience their life
with dignity. Need to develop strategies using local resources in order to create an awareness
programmes. The authors have shared their experiences of different modes of awareness used
in their mental health and development programme. It becomes necessary for mental health
sector to invest on developing various means of awareness generation, concentrating various
community groups in the community.
These efforts would sustain in the community and also help in overcoming the ill effects of
stigma. There is a need for convergence between different sectors, need to invest their time and
resources to help such initiatives and also observe them in their regular programmes. Such
modes of awareness efforts would be sustained in the community, in order to deal with stigma,
so that lives of people with mental illness and their families would be eased and experience
dignified life. More attention is required from the learned and scientific group in reaching out
to people, and their scientific skills clubbed with field staff efforts would go a long way in
developing scientific means of awareness generation. There is an urgent need for partnership
from scientific communities, policy makers, authorities in-charge for implementation of
programmes at the district and state levels, and other stakeholder, so that the experiences can
be captured with strong methodologies, replicated and propagated for its implementation
throughout the country. Despite progress over the past decade in the development of multi-
level stigma interventions, much work remains to strengthen and broaden with scientific
research in not only testing the efficacy but also being innovative in fully utilizing the
technology in the new digital India.
Acknowledgement: would like to acknowledge the field staff of GASS in Dodabalapura,
Narendra Foundation in Pavagad, Samuha in Koppal, Raichur and Karwara districts of
Karnataka, Field staff of the partners of ADD India and Vidya sagar in Tamil Nadu and Kerala,
field staff of SACRED in Ananthpur and Kurnool districts of Andhra Pradesh. Would like to
thank people with mental illness and their caregivers, people with disabilities, and field staff
who have permitted the authors to take photographs and use the same for publication in
developing the sector.
36

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Reference:
1. Janardhana, Maria, and Naidu (2004) ‘Mental health and development: Basic Needs India
experience’ – Disability News, Action Aid International India, Vol 14, 46-49, November.
2. Janardhana and Naidu (2006) ‘Community mental health and development model evolved
through consulting people with mental illness; Mental health by the people, edited by R.
Srinivas Murthy.
3. Janardhana N, Naidu DM. Inclusion of people with mental illness in Community Based
Rehabilitation: need of the day. International Journal of Psychosocial Rehabilitation. 2011 Jul
1;16(1).
4. Janardhana N, Muralidhar D, Naidu DM, Raghevendra G. Discrimination against differently
abled children among rural communities in India: Need for action. Journal of natural science,
biology, and medicine. 2015 Jan;6(1):7.
5. World health organization. Future trends and challenges in rehabilitation, Geneva Switzerland
World Health Organization 2001a.
6. Srinivasa Murthy R. Mental health by the people. Peoples Action For Mental Health,
Bangalore. 2006.
7. World Health organization Report. Mental Health: New Understanding, New Hope, Geneva
Switzerland, WHO 2001 b
8. Navaneetham JN, Raghunandan S, Naidu DM, Hampanna H. Availability and accessibility of
treatment for persons with mental illness through a community mental health programme.
Disability, CBR & Inclusive Development. 2011 Oct 15;22(2):124-33.
9. Sirey JA, Bruce ML, Alexopoulos GS, Perlick DA, Friedman SJ, Meyers BS. Stigma as a
barrier to recovery: perceived stigma and patient-rated severity of illness as predictors of
antidepressant drug adherence. Psychiatry Serv. 2001;52:1615–20.
10. Janardhana N, Naidu DM. Stigma and Discrimination experiences by families of
mentally ill-Victims of mental illness. Contemp Soc Work J 2011;3:83-8.4.
11. Addlakha R. Mainstreaming disability into the child rights agenda. InfoChange News &
Features. June; 2007.3.
12. Parish SL, Rose RA, Dababnah S, Yoo J, Cassiman SA. State-level income inequality
and family burden of U.S. families raising children with special health care needs. Soc
Sci Med 2012;74:399-407.5.
13. Augustine JS. The Indian family in transition. New Delhi: Vikas; 1982.
14. Barney LJ, Griffiths KM, Jorm AF, et al. Stigma about depression and its impact on help-
seeking intentions.Aust N Z J Psychiatry. 2006;40:51–4.
37

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
15. Corrigan PW, Edwards AB, Green A, et al. Prejudice, social distance, and familiarity with
mental illness.Schizophr Bull. 2001;27:219–25.
16. Link BG, Struening EL, Rahav M, et al. On stigma and its consequences: evidence from a
longitudinal study of men with dual diagnoses of mental illness and substance abuse. J Health
Soc Behav. 1997;38:177–90.
17. Gerlinger G, Hauser M, De Hert M, et al. Personal stigma in schizophrenia spectrum disorders:
a systematic review of prevalence rates, correlates, impact and interventions. World
Psychiatry. 2013;12:155–64.
18. Griffiths KM, Christensen H, Jorm AF. Predictors of depression stigma. BMC
Psychiatry. 2008;8:25.]
19. Griffiths KM, Batterham PJ, Barney L, et al. The Generalised Anxiety Stigma Scale (GASS):
psychometric properties in a community sample. BMC Psychiatry. 2011;11:184.
20. Mond JM, Robertson-Smith G, Vetere A. Stigma and eating disorders: is there evidence of
negative attitudes towards anorexia nervosa among women in the community? J Ment
Health. 2006;15:519–32.
21. Griffiths KM, Nakane Y, Christensen H, et al. Stigma in response to mental disorders: a
comparison of Australia and Japan. BMC Psychiatry. 2006;6:21.
22. Commonwealth of Australia. Fourth National Mental Health Plan: an agenda for collaborative
government action in mental health 2009 - 2014. Canberra: Commonwealth of Australia, 2009.
23. Minister of Health. Te Tahuhu – improving mental health 2005-2015. The second New
Zealand Mental Health and Addiction Plan. Wellington: Ministry of Health, 2005.
24. The Scottish Government. Mental Health Strategy for Scotland: 2012-1015. Edinburgh:
Scottish Government, 2012.
25. World Health Organization. Geneva: World Health Organization; 2013. Mental Health Action
Plan: 2013-2020.
26. Sartorius N, Schulze H. Reducing the stigma of mental illness: a report from a Global
Programme of the World Psychiatric Association. Cambridge: Cambridge University Press;
2005.
27. Clement S, Lassman F, Barley E, et al. Mass media interventions for reducing mental health-
related stigma. Cochrane Database Syst Rev. 2013;7:
28. Corrigan PW, Morris SB, Michaels PJ, et al. Challenging the public stigma of mental illness: a
meta-analysis of outcome studies. Psychiatr Serv. 2012;63:963–73.
29. NICE (2007). NICE public health guidance 06: Behaviour change at population, community
and individual levels. NICE: London.
30. Stuart H. Reducing the stigma of mental illness. Global Mental Health. 2016;3.
31. Calear AL, Griffiths KM, Christensen H. Personal and perceived depression stigma in
Australian adolescents: magnitude and predictors. J Affect Disord. 2011;129:104–8. ]
38

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
32. Coppens E, Van Audenhove C, Scheerder G, Arensman E, Coffey C, Costa S, Koburger N,
Gottlebe K, Gusmão R, O’Connor R, Postuvan V. Public attitudes toward depression and help-
seeking in four European countries baseline survey prior to the OSPI-Europe intervention.
Journal of affective disorders. 2013 Sep 5;150(2):320-9..]
33. Barney LJ, Griffiths KM, Christensen H, et al. Exploring the nature of stigmatising beliefs
about depression and help-seeking: implications for reducing stigma. BMC Public
Health. 2009;9:61.
34. Rao D, Elshafei A, Nguyen M, Hatzenbuehler ML, Frey S, Go VF. A systematic review of
multi-level stigma interventions: state of the science and future directions. BMC medicine.
2019 Dec;17(1):41.
35. Griffiths KM, Carron‐Arthur B, Parsons A, Reid R. Effectiveness of programs for reducing the
stigma associated with mental disorders. A meta‐analysis of randomized controlled trials.
World psychiatry. 2014 Jun;13(2):161-75.
39

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Policing During COVID-19 Pandemic and its Impact on Mental
Health
Dr. Apurva Kumar Pandya1*, Dr. Somen Saha2
1Economic Evaluation, Specialist, Indian Institute of Public Health, Gandhinagar
2Associate Professor, Indian Institute of Public Health, Gandhinagar
*Address for correspondence: Dr. Apurva Kumar Pandya, Indian Institute of Public
Health Gandhinagar, Opp. Air Force Headquarter, Near Lekawada Bus Stand, Lekawada,
Gandhinagar-382042
E-mail: [email protected]
Introduction
How to cite this article:
Pandya A K, Saha S. Policing During
COVID-19 Pandemic and its Impact on
Mental Health. Journal of Mental Health
Education. 2021;3(1)40-57
The coronavirus disease 2019
(COVID-19) pandemic has put
the world on a standstill.
Governments are forced to take
immediate measures to control
such a pandemic which include
lock- down, forced isolation
of infected patients, quarantine
affected people and social
distance. Therefore, viral
outbreaks are often paralleled
with symptoms of fear, anxiety,
and depression (Banerjee, 2020;
Brooks et all 2020; Ho et al,
2020; Roy et all, 2020; Yao et
al, 2020; Zhang et al, 2020).
Review Article
40

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Police personnel have been a part of “essential workers” who are the first responders
taking on active roles in the fields to prevent the infections and maintain law and order
(van Dijk, & Crofts, 2017). The World Health Organization and other international
agencies have recognized police personnel as first responders who are most vulnerable to
mental health problems (Inter-Agency Standing Committee 2020; International
Federation of Red Cross and Red Crescent Societies, 2020;WHO 2020).
The State Police Force (SPF) is a state-level agency which is in charge of maintaining law
& order. The primary role of SPF is to uphold and enforce laws, control and prevent crimes.
The Central Armed Police Forces (CAPF) refers to a group of seven security forces such as
Central Reserve Police Force, Central Industrial Security Force, Border Security Force, Indo
Tibetan Border Police, Assam Rifles, Sashastra Seema Bal, and National Security Guard
under the authority of Ministry of Home Affairs in India. They protect the borders of the
nation from external aggression and infiltration and aid the state governments in internal
security, including insurgency, anti-nasalism and counter terrorism. The SPF has been the
forefront of the COVID-19 pandemic in India. Personnel from CAPF (particularly Central
Reserve Police Force & Border Security Force) were also engaged in the pandemic
management, especially during lock-down phase. Police personnel had coordinated local
shutdowns, enforced stay-at-home mandates and at present they are encouraging use of
masks and social distancing in addition to their other usual responsibilities. The study
conducted in 2019 revealed that the police force is understaffed and overburdened. The
COVID-19 pandemic might have exerted tremendous stress and mental pressure on already
strained police personnel. Public health and policing experts acknowledge COVID-19
pandemic as a significant stressor for police personnel which compounds the stress
associated with their professional roles. They are not only vulnerable to infection but are also
at high risk to develop mental health problems. However, their mental health and
psychosocial support care remain neglected. We have reviewed existing literature on
COVID-19 pandemic and its impact on police personnel with an objective to map studies
conducted on police personnel mental health in the context of COVID-19, identify policing
practices, strategies and recommendations to protect police personnel from stress and risk of
infection of COVID-19.
Methods
Rapid scoping review was conducted using Arksey and O’Malley’s scoping review
framework (Arksey & O’Malley, 2005). The empirical studies and grey literature on
Policing and COVID- 19was reviewed. Electronic databases namely PubMed, PsychINFO,
41

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
and Google Scholar were accessed. The following keywords “police,” “policing” “COVID-
19 pandemic,” “risk of infection,” “prevention,” “protection of COVID-19 transmission,”
“mental health” were used. These key words were combined with Boolean operators to
narrow down the search results. Subsequently, manual searches were executed to identify
additional articles based on the references mentioned in the articles selected for full-text
review.
Initial search yielded articles (PubMed 305; PsychINFO 13; Google Scholar 13000) of
which 13013 were excluded based on title and abstract review. Later 223 articles were
rejected based on abstract review. Finally, 82 full texts were selected for review, of which
total 18 records met the inclusion criteria. The PRISMA chart is presented in Figure 1. Full
text of selected articles was critically appraised and data was synthesized using a meta
ethnography approach (Britten et al, 2002; Hoon, 2003).
Outcome measure
Prevalence of mental morbidity was considered as an outcome measure.
Inclusion criteria
Records were included when they met following criteria:
● Studies carried out on state police or law enforcement or para-military force in the
context of COVID-19.
● Studies focused on mental well-being, occupational stress or mental health problems.
● Studies documented policing practices, strategies or recommendations on policing
during health emergencies.
● Grey literature such as reports, and guidelines.
Exclusion criteria
Records were excluded when studies conducted with defense personnel or military personnel
and those studies published in other than English language.
Data extraction
The literature search was done by one researcher. The results were matched by repeating
search exercises using key words and removing duplicating and unqualified records based
on the exclusion criteria by another reviewer. Initial data extracted from the selected studies
and data synthesis was done by AKP and was reviewed by SS. Full text of selected articles
was critically appraised.
42

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Results
Out of total studies reviewed, only one study was conducted on police personnel during
COVID- 19 pandemic as of 30th September 2020. Most studies were conducted in developed
countries such as the USA, and UK indicating lack of research priority on this topic among
researchers and practitioners.
COVID-19 presents a serious risk of infection and harm to police personnel (Alcadipani,
Cabral, Fernandes, & Lotta, 2020). Various incidents during lockdown were noted where
people attacked police personnel. For example, police personnel, beaten up by a group of
people in Punjab, reported one police officer’s hand was chopped off and two were injured
(Ghazali, & Sanyal, 2020). Similar incidents of beating up of police personnel were recorded
in Maharashtra (Deccan Herald, 2020). The risks to physical health of police personnel from
COVID-19 are clear as they continue to work in the COVID-19 environment. As of 21st
September 2020, 99602 police personnel including CRPF personnel were tested positive and
574 personnel succumbed to death (Police Foundation of India, 2020). Furthermore,
incidents of police suicide deaths were also recorded (Times of India, April, 27, 2020).
COVID-19 poses a significant risk of harm to self, which represents one of the most significant
factors linked to poor mental health outcomes following critical incidents, traumas, and
disasters. Fear of COVID-19 infection is widespread among police personnel.
Recent study conducted in Maharashtra, 50 percent of police personnel are mentally
disturbed due to fear of COVID-19 and faces challenges at the workplace (Kokane,
Maurya, & Muhammad, 2020). The current situation of COVID-19 necessitates police
personnel to work under trauma inducing conditions for longer than usual emergency
situations, which may impact their physical and mental health. Thus, tracking the longer-
term psychological outcomes of police personnel is particularly important. Police personnel
who are infected by the virus and/ or who lost someone, or suffer from chronic physical
health or psychiatric conditions should be taken care and protected from adverse effects of
COVID-19.
Impact on Family Members of Police Personnel
Whilst the sustained stress experienced by police personnel themselves may be harmful, the
pandemic has significant implications for police families as well. Studies have not
documented the impact of COVID-19 on families of police personnel; however, few
studies have reported impact of traumatic conditions and emergencies on the families of
police personnel. In the aftermath of Hurricane Katrina, many police had to cope with the
43

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
impact of the hurricane on themselves and their families (West et al, 2008). Faust and
Vander Ven (2014) described Hurricane Katrina as a worst-case scenario, as police were
both victims and first-line responders. Of relevance to this discussion, research undertaken
by Behere, Basnet and Campbell (2017) found that one family member's threat to life
predicts mental health of family and particularly impacts children’s mental health. Further,
in the context of COVID-19, police personnel are fearful of bringing home the virus to
their families. In turn, it is likely that family members also, at the same time, worry about
their family member who is offering services to the police (Drew & Martin, 2020). Unlike
other public health emergencies, the job of police personnel in the era of COVID- 19 is
directly affecting the mental health of family members. However, research on the
prevalence of mental health problems among family members of police personnel is
lacking. It is assumed that usual levels of stress caused by the “routine” threat of policing
among family members will be significantly increased in the COVID-19 context (Stogner,
2020; Drew & Martin, 2020).
Impact of COVID-19 on Mental Well-being
COVID-19 pandemic presents challenges for police leadership in supporting personnel in an
environment that has both physical and mental health impacts (Kirby, 2020; Reicher, & Stott,
2020; Shirzad, Abbasi Farajzadeh, Hosseini Zijoud, & Farnoosh, 2020). A recent study
conducted with police personnel in Maharashtra reported that half of the police personnel
had mental disturbance due to fear of COVID-19 virus and one-third police were facing
mental stress due to other reasons related to their occupation (Kokane, Maurya, Muhammad,
2020). This is nearly double than the psychological disturbance indicated among the general
population (28%) in the systematic review conducted (Rajkumar, 2020). The COVID-19
pandemic has affected police personnel as well as their families across the globe (Sriwijitalai,
& Wiwanitkit, 2020; Laufs, & Waseem, 2020)
Knowledge of COVID-19 and Precautionary Measures Used by Police Personnel
Inadequate knowledge and occupational exposure both are attributed as risk factors for
infection among healthcare workers (Jiang, et al, 2020) which is relevant to police personnel
as well. A qualitative research conducted in Maharashtra demonstrated that 50 percent of
police personnel received information about the virus from social media such as WhatsApp
and Facebook (Kokane, Maurya, Muhammad, 2020). Huge gaps in adhering to precautions
were observed in the study. The same study reported that one-third of the total police
professionals were using masks, sanitizer, and gloves in working hours to protect
themselves; about 10 percent of police personnel were taking care of their personal health,
and about half of them (51%) washed their clothes while returning home from the duty. This
44

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
indicates a need for creating awareness on precautions among police personnel and their
families.
Effectiveness of Mental Health Interventions for Police Personnel
Police leaders must consider what programs and initiatives are needed to support the
psychological outcomes of COVID-19. Literature indicates mixed outcomes of mental health
interventions for police personnel. Among the most recognized interventions in policing is
the Critical Incident Stress Management (CISM), providing an “emotional first aid” to
stabilize and restore pre-crisis functioning (Mitchell, 2003); Critical Incident Stress
Debriefing (CISD), a specific technique designed to assist others in dealing with the
physical or psychological symptoms associated with trauma exposure (Malcolm et al,
2005); Mental Health First Aid (MHFA) training (Intveld, 2016),peer intervention
programs (Aronie, & Lopez, 2017), trauma resilience training (Arnetz, Nevedal,Lumley,
Backman, & Lublin, 2009) and psychological first aid programs, such as Recognize,
Evaluate, Advocate, Coordinate, and Track (REACT) (Marks et al., 2017). While
reviewing these interventions for police personnel deployed during emergencies,
Castellano and Plionis(2006) concluded that interventions lack consistent outcomes and
more rigorous program evaluations are needed. The evidence on effective mental health
programs in COVID-19 context is not definitive, hence, locally suitable short-term and
long-term programs should be implemented in Indian context and effectiveness of such
interventions should be documented.
Addressing Mental Health of Police Personnel: Learning from Previous Emergencies
The prevalence of post-traumatic stress disorder (PTSD) in police and first responders is
associated with critical incidents and disasters. Different types of traumatic experiences
produce different mental health problems. Based on a systematic review of the literature,
prevalence of post- traumatic stress disorder was noted between 8 and 12 percent during
and after 9/11 World Trade Center attacks in USA (Lowell et al., 2018; Laufs, & Waseem,
2020) whereas shortly after Hurricane Katrina, 19 percent of police personnel reported
PTSD symptoms whereas 26% reported symptoms of Major Depressive Disorder (West et
al., 2008). Long-term impacts of emergencies on police personnel mental health have also
been documented. A study on prevalence of PTSD of police involved in 9/11 found that
PTSD rates increased over time (Bowler et al., 2012). PTSD, depression or anxiety can
develop up to six years following disastrous events (Wang et al, 2010). For example, a
study conducted 20 months’ post-earthquake in Nepal revealed prevalence of mental
morbidities among the general population (Kvestad et al, 2019). These indicate long-term
impact of traumatic events on police personnel and highlight the need to address short-term
45

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
and long-term interventions to address mental health issues of police personnel.
Best Practices on Policing: Positive Policing during the Pandemic in India
Positive policing perhaps one of the most important aspects of law enforcement, but often
neglected as being secondary to the important role of enforcing the law. Positive policing is
potential to transform police organizations by changing negative police subculture, and
negative public perception.
During the pandemic, positive policing can be practiced that can create a lasting impact on
the lives of people and change the image of the police as follow:
● Collaboration between police and public health engagement. There may be a need to
share resources and strengths between the police and health department. For example, the
police had a resource for contact tracing of at-risk people (potential contact with the affected
patient), and helped people in need of urgent healthcare in rural areas where there were no
health facilities. Cyber police helped take actions to "fake and misleading" messages on
social media.
● Becoming an example by actions and positive messaging. Police can play a crucial role
in spreading a message of positivity, community and strength. Many police personnel have
adopted innovative ways to appeal to people to educate and stay home. For example, Tamil
Nadu traffic police devised “corona helmet” to educate people and urge to remain home,
Maharashtra police efforts in creating mass awareness.
Assisting people in need is vital in this crucial time. For example, in the National Capital,
police had helped the elderly in arranging grocery; Meerut police distributed food to the
needy while Bareilly police fed the hungry and poor. Documenting best-practices among
police personnel across the country can be inspiring and motivating not only for peers but
also help spreading positive messages about policing to the public and in turn, can create a
positive image of the police. In this direction, Police Foundation of India has recently
documented best-practices across police forces in the times of COVID-19 which is
appreciable. Disseminating these practices to police personnel across police organizations
would be a welcome step.
46

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Discussion
Police organizations play a critical role during public health emergencies (Sharma &
Hossain, 2019; van Dijk, & Crofts, 2017). Recent efforts by police organizations to protect
the country from COVID-19 pandemic must be acknowledged. During enforcement of
lockdown, police personnel went through high risk situations coupled with long hours of duty,
multiple shifts and inadequate personal protective equipment.
Various organizations put forth guidelines for police personnel. However, recommendations
for coping in the longer term are limited. All guidelines lack information about the fact that,
while they may not experience immediate distress, delayed psychological effects can be
expected and they should monitor their psychological health over time and seek support even
following the pandemic.
State Police Force (SPF) and Its Role in Managing Pandemic
The SPF played a central role in responding to COVID-19 pandemic. It is common to
observe negative police-citizen interactions that are characterized by low-levels of trust
with several instances of the police brutality and poor accountability structures (Common
Cause & Lokniti, 2018). Negative public perception of police force severely affects
people’s satisfaction with the rule of law and results in a trust deficit. At the same time
police personnel experience the occupational stress and limited resources (Common Cause
& Lokniti, 2018; Singh & Kar, 2015). These challenging working conditions make police
work even more taxing and it is likely that the COVID-19 pandemic might have
exacerbated their stress. Despite miniscule resources, SPF has taken up the challenge of
enforcing the lockdown and promoting public health. They are playing the role of not only
maintaining public order but also aiding public health officials in ensuring compliance with
state or local public health orders. Even after lockdown is lifted, they are expected to work
closely with the Health department and ensure compliance with state or district or local
corporation’s COVID-19 related public orders. Such additional duties for a longer duration
exert extreme stress. While shortage of personal protective equipment has made the fight
tougher, considering their nature of duty, increasing physical and mental health demands
are more taxing. Despite they are at the risk of contracting COVID-19 and other physical
and mental health ailments, their healthcare needs particularly during pandemic are not
addressed.
This pandemic has perhaps gathered attention from researchers and public health experts on
attending healthcare needs of police personnel to prepare them for the long haul.
47

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Recommendations for Police Leadership Team
Based on the findings of this review and the key insights drawn, a call to action is urgently
needed to support police personnel as they continue to experience the stresses of an active
COVID-19 environment. At the same time, it is equally important to strategically plan
interventions for post- pandemic situations. Evidence-based guideline on addressing mental
health concerns during and after COVID-19 pandemic for police leadership team is required.
● Police organization leaders should clearly establish how police personnel are to interact
with the community and enforce the rules. The role of police personnel should be focused
on informing the public about the current restrictions and encouraging individuals to
comply with the state and local emergency health declarations.
● It is also critical that police organizations develop a contingency plan for potential staffing
shortages as a result of the spread of COVID-19. It is important to cross-train personnel for
temporary duty reassignment to assure proper coverage of essential duties.
● Police organizations need to develop a methodology for identifying specific groups of
police personnel that may require additional support—those that are at higher risk due to
greater trauma exposure (occupational duties, crisis in the family, sickness, death in the
family), previous medical and psychiatric history. Such at-risk police personnel should be
offered less stressful duties along with mental health intervention.
● Police agencies need to educate their police personnel on the delayed impact of COVID-
19 for themselves and their families, ensuring understanding that mental health concerns are
not necessarily immediate.
● Given the unique nature of COVID-19 compared with other types of trauma experienced by
police, continuing health monitoring of the police personnel is warranted.
● Adequate psychosocial support intervention should be available to assist personnel in
managing their mental health during the active COVID-19 period and provide continued
access to support in the longer term.
● Psychosocial support intervention should recognize psychological issues such as depression
and anxiety and timely link with specialized mental health care services. Such intervention
should also include police families, considering both are impacted.
● Conduct concurrent monitoring and evaluation of interventions and support services,
ensuring that programs and initiatives are evidence-based and serve to maximally impact on
improving police mental health.
● Integrate interventions with the system for sustainability and long-term. There is a need for a
48

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
holistic support and recovery system for the police personnel so that efficiency of police
force can be utilized effectively in future for such type of public health crisis.
Recommendations for Psychosocial Support Intervention
Strengthening psychosocial support for improving mental health of police personnel have
the potential to play a major role in overall wellbeing. Psychosocial support helpline along
with the low-cost primary prevention model such as “peer counseling” program has potential
to improve the mental health conditions. Further, use of technology such as mobile based
training applications for educating police personnel on coping strategies can be explored.
Self-management Strategies Reported in the Literature
Various national and international organizations have published guidelines and training
manuals for police personnel (CDC, 2020; Inter-Agency Standing Committee 2020; PHFI,
2020; WHO, 2020). We have synthesized key points as follow:
Precautions for protecting from COVID 19 infection during the field duty
● Maintain a physical distance of at least 6 feet.
● Use Personal Protective Equipment.
● Wear a mask.
● Practice cough hygiene (While coughing or sneezing, cover the mouth with a handkerchief
or cough or sneeze into the upper sleeve, not your hands.)
● Practice proper hand hygiene. Wash hands with soap and water for at least 20 seconds or
sanitizer. Wash hands after touching surfaces like car handles, door handles or elevator doors
etc. Avoid touching your face, nose or eyes with unwashed hands.
● Disinfect vehicle. All surfaces that may have come in contact with the patient or materials
contaminated during interacting with people (e.g., touching floors, walls and work surfaces)
as well as patrol car equipment, steering wheel, gear shift, a dispatch radio module, door
handles and edges should be thoroughly cleaned and disinfected using soap/detergent and
water or 1% Sodium Hypochlorite solution. Vehicles can be cleaned after every shift.
● Clean essential items/gears. COVID-19-infected droplets may be able to live on nearly any
surface. Clean and disinfect duty belt and other equipment like a gun or stick prior
to reuse. Consider sanitizing items that are frequently touched during a shift such as a phone,
laptop, clipboard, etc.
● Seek help. Seek medical care early if a fever, cough and difficulty breathing are experienced.
49

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Precautions during the duty in the camp
Personnel can protect themselves from infection when they are in the camps by following
steps.
● Maintain physical distancing
● Practice proper hand hygiene.
● Practice cough hygiene.
● When you cough or sneeze, cover your mouth with a handkerchief or cough or sneeze into
your upper sleeve, not your hands.
● If you have symptoms like fever, cough, sore throat, or shortness of breath, seek immediate
medical care and inform the supervisor.
Protecting partners, families and friends after shift
Police duties can potentially expose themselves to COVID-19. Before coming back into
direct contact with their family, police personnel should maintain physical distancing
measures. Based on COVID 19 pandemic guidelines for law enforcement published by the
International Criminal Police Organization, follow steps given in the box while returning
home.
Precautions to protect families from infection
● Clean or decontaminate your work equipment, including shoes, avoiding the spread of
particles/dust;
● Take off duty clothes and wash them with laundry soap as soon as feasible. Handle them and
wash them in a way that limits exposure to skin, eyes, environment and other clean clothes
(avoid shaking clothes);
● Take a shower or wash exposed skin with soap and water;
● Self-monitor for signs of illness as well those of family members.
Precautions while enforcing crowd control
Larger gatherings offer more opportunities for person-to-person contact and therefore pose
a greater risk of COVID-19 transmission. Some steps towards positive policing are presented
below.
● Meet with community elders/ religious leaders at the event venue: Explain to them
50

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
respectfully, try to convince them, be respectful, develop a contingency plan that addresses
various scenarios described below which you may encounter during a COVID-19outbreak.
● Establish relationships with key community partners and stakeholders: When forming
key relationships with local stakeholder for any events, include relevant partners such as the
local public health department, community leaders, faith-based organizations, vendors,
suppliers, hospitals, hotels, airlines, transportation companies, and law enforcement.
Collaborate and coordinate with them on broader planning efforts. Clearly identify each
partner’s role, responsibilities, and decision-making authority. Participate in community-
wide emergency preparedness activities.
● Stay away from uncooperative individuals. When dealing with uncooperative individuals,
limit contact and practice hand hygiene.
● Avoid or limit direct contact with documents. Avoid touching documents and if
documents are touched, wash hands immediately with soap and water or use sanitizer.
● Stay away from uncooperative individuals. When dealing with uncooperative individuals,
limit contact and practice hand hygiene.
● Avoid or limit direct contact with documents. Avoid touching documents and
documents are touched, wash hands immediately with soap and water or use sanitizer.
Stress-management strategies during COVID 19 pandemic
Police personnel engaged in an emergency, and those deployed in the field duties are
facing tremendous stress.
● Avoid information overload and rumours: Limit news consumptions of news from TV or
social media. It creates fear, panic, and anger. Access latest information from the website of
the Ministry of Health and Family Welfare, Government of India, helpline numbers, or from
the WHO.
● Improve eating habits. Eat sufficient, healthy, nutritious food. Eat fruits and keep yourself
and keep yourself hydrated.
● Stay positive. Focus on positive aspects. Talk about the positive incident with colleagues.
● Deep breathing. Sit, close your eyes and take deep breaths. Whenever you are stressed,
angry or affected by overthinking, take a pause, drink water if needed and take a deep
breath for 1 to 5 minutes or more.
● Engage in physical activity. Move around, basic stretching exercises may help. Physical
activities help reduce fear, anxiety and improves mood.
● Stay connected with family. Stay in contact with family and friends through phone or video
calls or email.
51

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
● Avoid drugs. Avoid using tobacco, alcohol or other drugs. In the long term, these can
worsen mental and physical well-being.
● Develop an attitude of gratitude. Studies show gratitude to improve well-being. Maintain
a gratitude diary. One can write a gratitude journal. Appreciate and thank the Universe by
writing at-least 1 positive thing that happened in a day.
● Follow spiritual or a religious ritual. Studies indicate that it can improve wellbeing, help
in coping with stress and reduce symptoms of mental illness. Based on a person's preferred
spiritual path or religion, engage in prayers, namaaz, yoga, meditation, chanting, mantra
recitation, worship, and so.
● Provide social support to your colleagues. Talk with colleagues, stay connected and
extend personal help if any colleague needs support.
● Talk to the supervisor. Talk with a supervisor if you are directly impacted or have a family
member impacted by a stressful event in the family. And prepare a flexible duty schedule.
● Seek mental health help. If you are not able to manage symptoms of stress, sleeplessness,
irritability, fear, seek help. Talk with a medical officer in the camp or use a helpline number
for assistance. For psychosocial support, use psychosocial support helpline.
Precautions and strategies for Supervisors and Administrators
Supervisors and administrators play a vital role in protecting the health (including mental
health) of their subordinates.
● Educate police personnel of hand and cough hygiene.
● Avoid public duty, if police personnel are not well.
● Roll call briefing. Physical distance should be maintained while police attendance in the
evening.
● Flexible schedule for vulnerable staff. If personnel are not well, provide immediate medical
care. If personnel are having a family crisis, provide an alternate schedule that is less
stressful.
● Providing Medical Checks for police personnel. Police personnel should be provided with
guidance on protection from COVID 19 and regular health check-ups. Screening booths
should be set up at police quarters.
Implication for Future Research
Future study can map existing studies (completed and on-going studies) on mental health as
52

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
well as mental health programs for police personnel in India. This will help assess
effectiveness and scale-up best programs. Prospective research can focus on assessing
prevalence of mental morbidities, resilience and coping mechanisms used by police
personnel of different cadres in the context of COVID-19 pandemic and in general.
Implementation research to create evidence is commanded. It may be perhaps more
pertinent to undertake a clinical and cost effectiveness analysis to see how investing in
mental health can improve health outcomes of the police, their performance and the
policing.
Conclusion
The COVID-19 pandemic has exacerbated stress among both police personnel and their
families. Protecting police personnel during the pandemic such as COVID-19 is essential. In
the absence of mental health service provision within the police force, intervention to prevent
mental health problems and treat mental health conditions among police personnel is
inescapable. In this crucial time, implementation of sustainable mental health interventions
and generating evidence on its effectiveness are needed without delay.
References
1. Alcadipani, R., Cabral, S., Fernandes, A., & Lotta, G. (2020). Street-level bureaucrats under
COVID-19: Police officers’ responses in constrained settings. Administrative Theory &
Praxis,1-10.
2. Arksey, H., & O'Malley, L. (2005). Scoping studies: towards a methodological
framework. International Journal of Social Research Methodology, 8(1), 19-32.
3. Aronie, J., & Lopez, C. E. (2017). Keeping each other safe: An assessment of the use of peer
intervention programs to prevent police officer mistakes and misconduct, using New Orleans’
EPIC program as a potential national model. Police Quarterly, 20(3), 295–321.
4. Arnetz, B. B., Nevedal, D. C., Lumley, M. A., Backman, L., & Lublin, A. (2009). Trauma
resilience training for police: Psychophysiological and performance effects. Journal of
Police and Criminal Psychology, 24(1), 1–9.
5. Brooks R., Lopez C. 2020. Policing in a Time of Pandemic: Recommendations for Law
Enforcement. Retrieved from https://ethics.harvard.edu/files/center-
ethics/files/whitepaper7a .pdf
6. Behere, A. P., Basnet, P., & Campbell, P. (2017). Effects of Family Structure on Mental
Health of Children: A Preliminary Study. Indian journal of psychological medicine, 39(4),
457–463. https://doi.org/10.4103/0253-7176.211767
7. Banerjee D. (2020). The COVID-19 outbreak: crucial role the psychiatrists can play. Asian
53

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Journal of Psychiatry, 102(14).
8. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ.
(2020). The psychological impact of quarantine and how to reduce it: a rapid review of
the evidence. The Lancet.
9. Britten, N., Campbell, R., Pope, C., Donovan, J., Morgan, M., & Pill,R. (2002). Using
meta ethnography to synthesize qualitative research: a worked example. Journal of
health services research &policy, 7(4), 209-215.
10. Bowler, R. M., Harris, M., Li, J., Gocheva, V., Stellman, S. D., Wilson, K., ... & Cone, J.
E. (2012). Longitudinal mental health impact among police responders to the 9/11
terrorist attack. American Journal of Industrial Medicine, 55(4), 297-312.
11. Castellano, C., & Plionis, E. (2006). Comparative analysis of three crisis intervention
models applied to law enforcement first responders during 9/11 and hurricane Katrina.
Brief Treatment and Crisis Intervention, 6(4), 326.
12. Common Cause and Lokniti. (2018). Status of policing in India report 2018—A study of
performance and perceptions. New Delhi: Common Cause & Lokniti - Centre for the
Study Developing Societies (CSDS).
13. Common Cause & Lokniti-CSDS. (2019). Status of policing in India report 2019—A
study of police adequacy and working conditions. New Delhi: Common Cause & Lokniti
- Centre for the Study Developing Societies (CSDS). Retrieved from
https://www.commoncause.in/uploadimage/page/Status_of_Policing_in_India_Report_2
019 _by_ Common_Cause_and_CSDS.pdf
14. Deccan Herald. (May 2, 2020). Videos of attacks on cops enforcing lockdown emerge
in Maharashtra; minister assures action. Retrieved from
https://www.deccanherald.com/national/west/coronavirus-videos-of-attacks-on-cops-
enforcing-lockdown-emerge-in-maharashtra-minister-assures-action- 832647.html
15. Drew, J. M., & Martin, S. (2020). Mental health and well-being of police in a health
pandemic: Critical issues for police leaders in a post-COVID-19 environment. Journal of
Community Safety and Well-Being, 5(2), 31-36.
16. Faust, K. L., & Ven, T. V. (2014). Policing Disaster: An Analytical Review of the
Literature on Policing, Disaster, and Post‐Traumatic Stress Disorder. Sociology Compass,
8(6), 614-626.
17. Ghazali, M., & Sanyal, A. (April 12, 2020). Punjab Cop's Hand Chopped, 2 Injured In
Attack By Group Defying Lockdown. ND TV. Retrieved from
https://www.ndtv.com/india- news/punjab-policemans-hand-chopped-two-others-
injured-in-attack-by-group-defying- coronavirus-lockdown-2210329
54

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
18. Ho, C. S., Chee, C. Y., & Ho, R. C. (2020). Mental health strategies to combat the
psychological impact of covid-19 beyond paranoia and panic. Annals of the Academy
of Medicine. 49(1),1-3.
19. Hoon, C. (2013). Meta-synthesis of qualitative case studies: An approach to theory
building. Organizational Research Methods, 16(4), 522-556.
20. Intveld, R. (2016) Expanding the role of EAP through peer support. The Journal of
Employee Assistance, 46: 20-24
21. India Today. (2020). Cops of Corona. Available at:
https://www.youtube.com/watch?v=159bbNuPfRs
22. International Federation of Red Cross and Red Crescent Societies (2020). Mental Health
and Psychosocial Support for Staff, Volunteers and Communities in an Outbreak of
Novel Coronavirus. IFRC: Hong Kong.
23. Inter-Agency Standing Committee (2020): Interim briefing note: Addressing mental
health and Psychosocial aspects of COVID-19 outbreak. Retrieved from
https://interagencystandingcommittee.org/system/files/2020-03/IASC%20Interim%20
Briefing%20Note%20on%20COVID-
19%20Outbreak%20Readiness%20and%2Response %20Operations %20-
%20MHPSS_0.pdf
24. International Criminal Police Organization. (2020). COVID 19 pandemic guideline
for law enforcement Retrieved from https://www.interpol.int/en/News-and-
Events/News/2020/INTERPOL-issues-international-guidelines-to-support-law-
enforcement- response-to-COVID-19 Jiang, L., Ng, I. H. L., Li, D., Tan, L. W. L., Ho,
H. J. A., Mark, I., & Chen, C. (2018). Infectious disease transmission: survey of contacts
between hospital-based healthcare workers and working adults from the general
population. Journal of Hospital Infection, 98(4), 404-411.
25. Kirby, T. (2020). Spotlight patient perspectives UK senior police officer with COVID-
19. Lancet Respire [Internet]. 2600(20):30164. Available from:
http://dx.doi.org/10.1016/S2213-2600(20)30164-8
26. Kokane, P., Maurya, P., Muhammad, T. (2020). Understanding the Incidence of Covid-
19 among the police force in Maharashtra through a mixed approach. doi:
https://doi.org/10.1101/2020.06.11.20125104
27. Kvestad, I., Ranjitkar, S., Ulak, M., Chandyo, R. K., Shrestha, M., Shrestha, L., ... &
Hysing, M.(2019). Earthquake exposure and post-traumatic stress among Nepalese
mothers after the 2015 earthquakes. Frontiers in Psychology, 10, 734.
28. Laufs, J., & Waseem, Z. (2020). Policing in pandemics: A systematic review and best
55

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
practices for police response to COVID-19. International Journal of Disaster Risk
Reduction,51, 101812.https://doi.org/10.1016/j.ijdrr.2020.101812
29. Lowell, A., Suarez-Jimenez, B., Helpman, L., Zhu, X., Durosky, A., Hilburn, A., ... &
Neria, Y. (2018). 9/11-related PTSD among highly exposed populations: a systematic
review 15 years after the attack. Psychological Medicine, 48(4), 537-553.
30. Malcolm, A. S., Seaton, J., Perera, A., Sheehan, D. C., & Van Hasselt, V. B. (2005).
Critical incident stress debriefing and law enforcement: An evaluative review. Brief
Treatment and Crisis Intervention, 5(3), 261
31. Marks, M. R., Bowers, C., DePesa, N. S., Trachik, B., Deavers, F. E., & James, N. T.
(2017). REACT: A paraprofessional training program for first responders—A pilot
study. Bulletin of the Menninger Clinic, 81(2), 150-166.
32. Mitchell, J. T. (2003). Crisis intervention & CISM: A research summary. Retrieved
fromhttps://www.uflac.org/images/shared/Peer%20Support/Crisis-Intervention-and-
CISM- A- Research-Summary.pdf.
33. Ministry of Health and Family Welfare (13 April, 2020). COVID status. Government of
India. Retrieved from https://www.mohfw.gov.in/
34. National Centre for Disease Control. (14 April 2020). Advisories on COVID 19
pandemic in India. Ministry of Health & Family Welfare, Government of India.
35. Retrieved from https://ncdc.gov.in/index4.php?lang=1&level=0&linkid=127&lid=432.
36. PHFI (2020). Health and safety measures for police personnel on COVID-19. Training
Manual for Biju Patnaik State Police Academy, Odisha, Bhubaneswar. Training Division,
Public Health Foundation of India (PHFI), India.
37. Police Foundation of India. (2020). COVID-19 resources. Retrieved from
https://www.policefoundationindia.org/covid-19-resources.
38. Rajkumar, R. P. (2020). COVID-19 and mental health: A review of the existing
literature. Asian Journal of Psychiatry, 52; 102066
39. Reicher, S., & Stott, C. (2020). Policing the coronavirus outbreak: Processes and
prospects for Collective Disorder. Policing: A Journal of Policy and Practice.
40. Roy D., Tripathy S, Kar, S. K, Sharma, N., Verma, S K, & Kaushal, V. (2020). Study of
knowledge, attitude, anxiety & perceived mental healthcare need in Indian population
duringCOVID-19 pandemic. Asian Journal of Psychiatry, 51, 102083.
https://doi.org/10.1016/j.ajp.2020.102083
41. Sharma, R., & Hossain, M. M. (2019). Strengthening public health partnerships in India:
Envisioning the role of law enforcement during public health emergencies. Indian Journal
of Community Medicine, 44(3), 188.
56

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
42. Shirzad, H., Abbasi Farajzadeh, M., Hosseini Zijoud, S. R., & Farnoosh, G. (2020). The
role of military and police forces in crisis management due to the COVID-19 outbreak
in Iran and the world. Journal of Police Medicine, 9(2), 63–70.
43. Singh, S., & Kar, S. K. (2015). Sources of occupational stress in the police personnel of
North India: An exploratory study. Indian Journal of Occupational and Environmental
Medicine, 19(1),56
44. Sriwijitalai, W., & Wiwanitkit, V. (2020). Incidence of COVID-19 among immigration
police: Observation from Thailand. Medical Journal of Armed Forces India.
45. Stogner, J., Miller, B. L., & McLean, K. (2020). Police stress, mental health, and resiliency
during the COVID-19 pandemic. American Journal of Criminal Justice, 45(4),718-730.
46. van Dijk, A., & Crofts, N. (2017). Law enforcement and public health as an emerging field.
Policing and Society, 27(3), 261-275.
47. Wang, Z., Inslicht, S. S., Metzler, T. J., Henn-Haase, C., McCaslin, S. E., Tong, H., Neylan,
T. C., & Marmar, C. R. (2010). A prospective study of predictors of depressive symptoms
in police. Psychiatry Research, 175, 211–216.
48. West, C., Bernard, B., Mueller, C., Kitt, M., Driscoll, R., & Tak, S. (2008). Mental health
outcomes in police personnel after Hurricane Katrina. Journal of Occupational and
Environmental Medicine,50(6), 689-695.
49. World Health Organization. (2020). Coronavirus situation report. Retrieve from
https://www.who.int/docs/default-source/corona viruse/situation- reports/20200316- sitrep-
56- COVID- 19.pdf?sfvrsn=9fda7db2_2
50. Yao H, Chen JH, Xu YF. (2020). Patients with mental health disorders in the COVID-
19epidemic. The Lancet Psychiatry.7(4), e -21.
51. Zhang, J., Wu, W., Zhao, X., & Zhang, W. (2020). Recommended psychological crisis
intervention response to the 2019 novel coronavirus pneumonia outbreak in China: a model
of West China Hospital. Precision Clinical Medicine, 3(1),3-8.
57

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Experience of Interning in the field of Mental Health Education Manjiri Gokhale
Student intern, Department of Mental Health Education, NIMHANS, Bangalore
*Address of Correspondence: Manjiri Gokhale, Jyoti Nivas College Autonomous,
Bengaluru, India
E-mail: [email protected]
How to cite this article:
Gokhale M. Experience of Interning
in the field of Mental Health
Education. Journal of Mental Health
Education. 2021;3(1):58-64.
Abstract
Most of the mental health disorders
(due to their invisibility to the
human eye) have an underlying
stigma and discrimination. This is
largely due to lack of awareness
and sensitivity. Owing to our
cultural boundaries and prejudicial
perspectives, we often blindside our
mental health. Therefore, it is a
need of the house to promote mental
health and raise awareness among
the public. Mental Health
Education and promotion, thus
becomes a critical factor in a
country’s development. This helps
debunk myths, counter the stigma
and promote a healthy environment
for the welfare of the people. It
further helps reduce the socio-
58

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
economic burden. In a developing country like India, education plays a key role in
converting an individual from a liability to an asset. The purpose of an internship is to
prepare students with realistic expectations of their future careers and to provide them with
opportunities to polish career skills and to gain on-the- job experience. Therefore, internship
opportunities not only serve as a tool to educate and promote community welfare but also
aids to shape an individual to create a better future.
Keywords: Mental Health, Mental Health Education, Internship, Internship Experience
Background
According to a research study conducted by the World Health Organization (WHO), it was
found that an estimated 450 million people globally suffer from mental disorders.
Approximately 80% of the people with mental disorders live in low-middle income countries
(LMICs), where four out of five people with serious mental health problems living in LMICs
do not receive the needed mental health care services. Mental illness accounts for 14% of all
disability adjusted life years (DALYs) lost worldwide, and is one of the major contributors
to the global burden of disease. [1] Mental health is the foundation for well-being and
effective functioning of an individual and for a community. It is more than the absence of
mental illness, it is a state of well-being in which the individual realizes his or her own
abilities, can cope with the normal stresses of life, can work productively and fruitfully, and
is able to make a contribution to his or her community.[2] Despite these known facts, most
of the mental health disorders (due to their invisibility to the human eye) like anxiety,
depression, suicide have an underlying stigma and discrimination which hinder the process
of treatment seeking among patients. This is largely due to lack of awareness and sensitivity.
Owing to our cultural boundaries and prejudicial perspectives, we often blindside our mental
health paying less or no attention and care to it. Therefore, it is a need of the hour to promote
mental health and raise awareness among the public.
The Department of Mental Health Education, NIMHANS- is an integral part of the Institute
and actively involved in teaching, research and training activities in the field of health
education. Its focus is to prepare students, health care professionals, caregivers, and the
community at large to promote health in individual and group settings, and among diverse
populations using culturally appropriate health education methodologies. Its goal is to
facilitate voluntary health-related behavioral and social change through the application
59

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
of principles of behavioral and social sciences. [4]
Internships involve students working with and for an organization/institute in a fashion that
will make them more acquainted with the real time field work and have a context to apply
the knowledge gained from their classwork to real life situations. Internship in the field of
mental health education is crucial because an individual’s holistic wellbeing is what sets
them apart as assets rather than a liability.
Experience as an Intern
The field of psychology and related studies is vast, but its growth is slow in a country like
India where the societal constructs have a powerful influence over the ever widening
treatment gap. If not dealt with at a grass root level, this field will have no strong base to
develop on. Knowing this, I wished to work in the field of Mental Health Education. The
National Institute of Mental Health and Neurosciences (NIMHANS), is one of the only
institutes in India that has a dedicated department for this cause. The Department of Mental
Health Education is an exclusive department that aims at promoting and educating
individuals and communities to raise awareness, tackle stigma and help bridge the treatment
gap that will add in the exponential growth of this much needed field. When I first applied
to the Department of Mental Health Education, my expectations were to gain an insight to a
mental health setting and also learn more about this field both theoretically and practically.
During my internship course, the department offered the interns with a perfect blend of
theoretical and practical knowledge, where the interns had an opportunity to expand their
network, interact with academicians and also provided a hands-on experience of curating
IEC (Information, Communication and Education) material.
Observing the trend of media and mental health, the Department of Mental Health Education
aimed at adopting the process of developing IEC materials to help reach out to a wider
spectrum of the public to raise awareness about mental health, neurological and
neurosurgical disorders. IEC materials are a combination of brochures, booklets, videos,
posters etc. that consist of health information about various mental and neurological
disorders and mental wellbeing portrayed in an innovative, simplistic and understandable
manner that can be accessed by patients, caregivers and the general public who avail the
services at the Outpatient Department, NIMHANS. To create IEC material, one must
understand that beyond just gathering the “right” information, it requires creativity to make
it appealing to the readers, the material must be well drafted and edited. These factors play
60

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
a crucial role in dissemination of information. During the internship, I had an opportunity
to enhance content creation and public relations skills. It provided me with an opportunity
to visit specialized clinics and departments to know more about the severe mental health
disorder I wished to curate the content on.
In any field, research work serves as a key to establish facts and reach new conclusions, it is
the reason we investigate limitations and propose new ideas for a progressive growth. The
department of Mental Health Education, has its own journal that provides a platform for
professionals and students working in the broad fields of mental, neurological and
neurosurgical health and promotion to submit their quality work/research/findings in the
journal. [13].
I had an exclusive opportunity to work closely with the faculty members and the editorial
team and work on the journal. This helped me stay connected with the latest findings,
initiatives and progress of this field. It helped me know and understand the current status of
the field so that as a future psychologist I can contribute more to this field. But beyond just
content creation and learning opportunities, the internship program helped me improve my
interpersonal relationship skills, it enhanced my communications skills and boosted my
confidence while I learnt to work in a time bound goal-oriented manner.
Implications / Significance
Mental Health and physical health both play an integral role in a person’s existence. Despite
this, mental health is still portrayed by some as a luxury. [2] Noting the above misconception,
Mental Health Education and promotion becomes a critical factor in a country’s
development. This helps debunk myths, counter the stigma and promote a healthy
environment for the welfare of the people. On the background of oversupply of graduates,
more and more professional-degree postgraduates need to prove their working ability
through internships beyond their degree. [8] An internship courses with the Department of
Mental Health Education, NIMHANS (National Institute of Mental Health and
Neurosciences) has provided me with an exclusive opportunity to bridge the gap between
literacy and education. It helps apply theoretical knowledge to real world problems and gain
the real taste of the field. Working under the Department of Mental Health Education gave
interns a chance to expand their network, interact with academicians and learn from them.
It also helped them get access to many IEC (Information Education and Communication)
materials that served as a key in this learning process.
61

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
Strengths/Limitations
The internship period at NIMHANS- under the department of Mental Health Education
helped us flourish in two major aspects:
1. Personal Aspect: Working closely with the department made me realize my potential and
inclination towards psychology and mental health education. Understanding the magnitude
of difference between healthy and unhealthy lifestyles, the internship program aided and
helped me learn how to make “better choices’. Highlighting the role of caregivers, it helped
me know the rising need of caregivers and the need to recognize and value mental health.
Engaging in departmental activities boosted my confidence as I got an opportunity to
showcase my skills and enhance my event management skills. It helped me know and value
“teamwork” more and personally it shaped us to be a better fit in the real working world.
All in all, it holistically enhanced the personal growth and development.
2. Professional Aspect: Working with the Department of Mental Health education provided me
with an enriching opportunity to expand our practical knowledge. It further encouraged us
to improve on our interpersonal communication skills and tap into our creative side- helping
us understand the relation between media, creativity and mental health.
More importantly, working on the development of IEC Material on severe mental health
disorder gave us an in-depth insight to the subject that helped us improve academically and
the intensive training helped in converting this theoretical knowledge to application-based
methods that helped promote mental health. The Department of Mental health education
provided me with an opportunity to work closely with the department’s journal: “Journal of
Mental Health Education” to help understand the research and review process. Along with
this, it aided me to understand the importance of deadlines and gave me an insight about
how it feels to be working in a mental health setting in real life.
Conclusion
There is no health without mental health.
The focus of the Department of Mental Health Education is to prepare students, health care
professionals, caregivers and the community at large to promote health in individual and
group settings, and among diverse populations using culturally appropriate mental health
education methodologies. Internships are very useful in acquiring (practical) knowledge,
especially in bridging the theoretical and practical knowledge. Through internship, they can
authentically feel the process of combining two kinds of knowledge, and get to know the
62

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
defects and scarcity in their own theory study. Beyond just theoretical knowledge, working
closely with the Department of Mental Health Education - NIMHANS, aided in personal and
professional growth- providing me with an array of tasks that helped us enhance our
management skills, communication skills and interpersonal relations and also shaped us to
be a better fit in the real working world.
References
1. Bhumika t Venkatesh. Journal of family medicine and primary care. [Online]. Available
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4535113/ [Accessed 30 March
2021].
2. World Health Organization. Promoting Mental Health. [Online]. Available from:
https://www.who.int/mental_health/evidence/en/promoting_mhh.pdf [Accessed 25
March2021].
3. Department of mental health education. National Institute of Mental Health and
Neurosciences (NIMHANS). [Online]. Available from: https://nimhans.ac.in/mental-health-
education/ [Accessed 30 March 2021].
4. Pola, B.G.U.P.T.A, David J Burns, Jaime S Schiferl. An exploration of student satisfaction
with internship experiences in marketing. Business education and accreditation.2010;2(1).
5. World health organization. World Health Organization. [Online]. Available from:
https://www.who.int/india/health-topics/mental-health [Accessed 30 March 2021].
6. World health organization. World Health Organization. [Online]. Available from:
https://www.who.int/mental_health/evidence/atlas/profiles/ind_mh_profile.pdf
[Accessed30 March 2021].
7. Mengyuan chen. The significance of internship to the cultivation of professional-degree
postgraduate: from student subject perspective. [Online]. Available from:
https://cies2020.org/wp-content/uploads/334359-MengyuanChen-Peking University.pdf
[Accessed 25 March 2021].
8. Ssrn. An Exploration of Student Satisfaction with Internship Experiences in Marketing.
[Online]. Available from: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1871152
[Accessed 25 March 2021].
9. World journal of education. The Mode of Theoretical Knowledge and Practical Knowledge
Combination: The Significance of Internship. [Online]. Available from:
https://files.eric.ed.gov/fulltext/EJ1158954.pdf [Accessed 25 March 2021].
10. Nimhans. Mental Health Education. [Online]. Available from:
63

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
http://mentalhealtheducationnimhans.org/ [Accessed 25 March 2021].
11. World health organization. Promoting Mental Health. [Online]. Available from:
https://www.who.int/westernpacific/activities/promoting-mental-health [Accessed 25
March 2021].
12. Journal of mental health education. Department of Mental Health Education - NIMHANS.
[Online]. Available from: jmhedu.org [Accessed 30 March 2021].
13. Martin, P.R.I.N.C.E, Vikram Patel, Shekhar Saxena, Mario Maj, Joanna Maselko. No health
without mental health. The Lancet Psychiatry. [Online] 2007 ;370(--):. Available from:
https://www.thelancet.com/ [Accessed 31-March-2021].
64

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
NIMHANS Arogya Jagruti Kendra- A window to Educate Minds and
Empower Communities
Deepika Saini1, Dr. Rajeev Jayaram Paleri1*, Dr. Meena K. S2, Dr. Latha K.3
1 Fellowship Student, Department of Mental Health Education, NIMHANS, Bangalore
2Additional Professor and Head, Department of Mental Health Education, NIMHANS,
Bangalore
3Associate Professor, Department of Mental Health Education, NIMHANS, Bangalore
*Address of Correspondence: Dr. Rajeev Jayaram Paleri, Department of Mental Health
Education, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru,
India
E-mail: [email protected]
How to cite this article:
Saini D, Paleri R J, K. S M, K L.
NIMHANS Arogya Jagruti Kendra- A
window to Educate Minds and Empower
Communities. Journal of Mental Health
Education. 2021;3(1):65-71.
Abstract
The purpose of this brief
communication is to examine
innovative ideas as a way
forward in creating Mental
Health Awareness. NIMHANS
Arogya Jagruti Kendra (NAJK),
an initiative by Department of
Mental Health Education,
NIMHANS was put forth to
create awareness on the mental
health & neurological disorders
with the help of brochures short
videos and direct interaction of
mental health professionals with
65

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
patients and caregivers. IEC materials include a range of products like: infographics, flyers,
leaflets, brochures, short videos and direct interaction of mental health professionals with
patients and caregivers. The initiative will foresee different ways to disseminate information
about mental health and illness to the patients and caregivers attending Outpatient
departments at the institute and to the public. The NAJK is a Learning Resource Centre
where patients and caregivers can access various resources related to various disorders and
health related information. Though it has its own strengths and challenges, the center looks
forward to increasing the flow of patients and caregivers seeking access to information
thereby meeting the objective of service deliverables.
Keywords: Mental Health Education, learning resource center, innovative ideas,
mental illness, mental disorder, caregivers.
Background
Mental health as defined by WHO is “a state of well-being in which the individual realizes
his or her own abilities, can cope with the normal stresses of life, can work productively
and fruitfully, and is able to make a contribution to his or her community. By this definition
one realizes the importance of having a healthy mind and the ability to cope with daily life
stressors. Globally the burden of Mental illness is 13.2%. (WHO, 2000) a. Health
promotion is an approach in improving public health that requires active participation by
the stakeholders. It may be understood as actions and advocacy to address the full range of
potentially modifiable determinants of health, including actions that allow people to adopt
and maintain healthy lives and those that create living conditions and environments that support
health (WHO, 1998a) 1. In India, many initiatives have been taken since the last decade to
improve knowledge and increase awareness relating to mental illness. From traditional
methods of print media to newer mobile technology based and Non-Specialist Mental Health
Programs, each state has come up with newer initiatives to reach the target population. In the
year 2014, the state of Gujarat, trained non-specialist community mental health workers for
screening, tracking and providing mental health care in remote regions of Gujarat.2 They
taught the people to use mobile phones and answer the self-report questionnaire developed
by WHO. They customized and added questions for epilepsy and alcohol abuse to make it
culturally appropriate and target the problem occurring in that area.
Information Education Communication (IEC) is the process of learning that empowers
people to make decisions, modify behaviours and change social conditions.3 IEC materials
include a range of products like: infographics, flyers, brochure, social media posts,
television advertisements, audio spots for radio, posters, billboards or murals. The primary
66

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
goal of the IEC program is to inspire and educate people about prevention, care and/or
treatment of various health issues and for a better understanding of the same in a more
comprehensive way.
The Ministry of Health & Family Welfare, Himachal Pradesh, developed 30 second audio
spots to disseminate information regarding general health issues, mental health and
substance use by broadcasting it on Radio channels. The spots were short, catchy and
informative. The Department of Mental Health Education, NIMHANS started an innovative
initiative in its OPD block which is called the NIMHANS Arogya Jagruti Kendra (NAJK).
This learning resource center in the OPD allows the patients and caregivers to access
varied health information related to mental health, neurological and neurosurgical disorders.
It is a walk-in space and has different kinds of brochures, manuals and a digital display
displaying educational videos for the visitors. The patients & caregivers can also interact
with the students at NAJK who are trained by experts from a multidisciplinary team
including Mental Health Education, Psychiatry, Clinical Psychology, Psychiatric Social
Work, Neurology, Neurosurgery, Nursing and allied fields. This innovative initiative aims
at strengthening the knowledge related to mental health & neurological conditions by
integrating it into the OPD setting, and also disseminates information regarding specific
disorders and well-being through a wide range of resources.
Observation and Experience
The department, in its academic pursuits, receives students from various backgrounds and
trains them in the field of Mental Health Education during their tenure. One of the
objectives of their training includes guiding patients and caregivers to access the resources at
NAJK and to develop the same. In addition, they also learn to disseminate knowledge on
various psychiatric, neurological and neurosurgical disorders among the people who visit
the center. The concept of NAJK is innovative and exciting to explore as many hospitals that
specialize in psychiatric illnesses do not have such spaces where visitors could gain
information about disorders.
For decades, it has been observed that the mentally ill have been treated very badly. It was
believed that mental illness was caused by demonic possession, witchcraft, or an angry God
(Szasz, 1960). For example, in medieval times, abnormal behaviors were viewed as a sign that
a person was possessed by demons.4
On this background, we understand that there lies a strong connection between socio- cultural
beliefs and mental health which plays a major role in the way mental health is perceived
67

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
by people which further affect the treatment of Mental Health Disorders. Culture is an
abstraction, reflecting the total way of life of a society. It is a precipitate of the group’s history
and an expression of its adaptation to the physical environment. Culture is constantly in the
process of change and it is transmitted from one generation to the next. All societies have it
though their styles vary from one group to another.5 Over the years, there has been an
initiative by the government and private organizations to spread awareness, information and
facts related to Mental illnesses and health to bridge the gap between the orthodoxical
perspective and scientific treatment.
The department of Mental Health Education tries to bridge this gap by creating simple, easily
understandable content in the areas of psychiatric, neurological and neurosurgical disorders.
With various IEC Materials out for display at the entrance of the NAJK, the public is drawn
to have a look at the materials for more information about the disorder they would like to
know about or even about ways to maintain a good mental well-being. Posters and short
videos are displayed on digital signage at the entrance of the OPD block and waiting areas to
educate and expand the visitors’ knowledge regarding disorders and healthy lifestyle. The
department has taken various steps including distributing flyers to other Outpatient
Departments, for the doctors to guide their patients or caregivers to the NAJK for further
information about mental health topics.
The turnout of patients and caregivers in NAJK over the last 3 months has been tremendous.
Ona day to day basis, the fellows interact with patients and caregivers who visit to NAJK
and it was disheartening to realize people have no or very little information regarding the
problems they are going through and it draws our attention towards the bridging the gap
between trying to create awareness using IEC material and how many people actually receive
it. This has been supported in a study by Thakur et al that lack of information is the major
barrier to the effective access to services. Adding to the lack of information is the
inappropriate usage of funds provided by the Government. The funds are underutilized or
used for conventional information material such as print advertisements. A majority of the
IEC materials available at the district level is not relevant as per the local needs and
requirements. The focus should be to develop local context-specific IEC materials. IEC
materials need to be adapted at the state and district levels, and reproduced considering the
sociocultural context and need, and then be disseminated in the community, especially
hard- to-reach areas.6 The curiosity of the visitors often draws them to the NAJK to interact,
know more about their problems and pick up brochures. Patients and caregivers provide
feedback where they suggest improvements in the NAJK and request for other relevant topics
on which IEC material can be created. A lot of patients through the feedback form have
68

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
expressed a need for starting discussion groups for family and Self-help groups for
patients, as they feel that talking to others who can understand what it is like to deal with a
mental illness and caring for them would prove to be of great help. Self-help groups for
mental health problems are the most prevalent form of self-help. There are several thousand
groups in Australia, the U.K., the U.S. However, in India where there are less trained
mental health professionals, SHGs prove to be essential and beneficial for both rural and
urban populations. Under the “Manam Inidhu” an initiative by Tamil Nadu Corporation for
Development of Women, Schizophrenia Research Foundation (SCARF) and the Institute of
Mental Health, members of self-help groups (SHGs) across Tamil Nadu will be trained as
mental health counsellors.7 NAJK as an initiative, helps to reach out to more audience,
understand the nuances of how mental illness is perceived by the population, the treatment
gap that persists, the need to fill in through educating the masses, and normalizing
discussing and talking about Mental illness.
Implications/ Significance
There has been a very slow progress in understanding mental health and its importance
when compared to physical health. With the arrival of the Pandemic, COVID- 19, people
have begun to understand the importance of Mental Health and seeking treatment for all
mental disorders. The NAJK is crucial in drawing people into the world of knowledge and
thereby spreading awareness among the people about Mental Health which is further
crucial in obtaining the right treatment at the right time, thereby helping to reduce stigma
related to mental health disorders and treatment gap, which are the two main causes of
global burden of mental health disorders. This is achieved through effective dissemination
of booklets and brochures. It also helps the people in identifying mental health disorders,
seeking necessary treatment, self- help and improving mental well-being. The NAJK also
invites emails from people to seek out information from various other authentic sources.
Strengths and Limitations
The location of the NAJK near the entrance proves to be of very crucial strength as it draws
in the attention of a majority of people who enter the OPD as they are passing by to their
respective departments. The availability of various IEC materials and its display on standees
calls in people to read and collect the IEC Materials to improve their knowledge on Mental
Health and its well-being. The NAJK also conducts theme based programs by initiating
exhibitions, public awareness programs, development of IEC materials and undertaking
unique campaigns to generate awareness.
Despite all the strengths, the NAJK has got scope for improvement. Most of the patients
and caregivers come from different part of India and from neighboring countries. The waiting
69

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
time for consultation deprives the caregivers of visiting the center for accessing the
resources. This can be addressed by the trainees and volunteers reaching out to them in the
waiting halls and making help accessible. Development of newer IEC materials in multiple
languages according to needs can be enforced with interaction with patients and caregivers.
Implementing these in the coming months can strengthen the services of NAJK and
educate and empower the persons seeking services at the hospital.
Conclusion
The NIMHANS Arogya Jagruti Kendra, a learning resource center to disseminate awareness
about mental health, its disorders and well-being, is an innovative strategy brought into
action for patients and caregivers coming to the OPD. The NAJK can be further
strengthened by being provided with space in key locations within the specific Out Patient
Departments, thereby improving dissemination of awareness on mental health and
neurological disorders. The NAJK plays a key role in answering the queries of its visitors and
thus, improving mental health literacy and reducing mental health stigma. The innovative
approach of NAJK started by NIMHANS, not only makes mental health services more
accessible and affordable but also empowering in nature by encouraging patients and
caregivers in early detection, prevention of mental health illness, appropriate treatment
referral to existing primary healthcare services.
References
1. Merging Evidence. Promoting Mental Health [Internet]. Who.int. [cited 2021 Mar1].
Available from: https://www.who.int/mental_health /evidence/en/promoting_mhh.pdf
2. Appasani RK. mh2: Mobile Health for Mental Health [Internet]. 217.112.]. Available from:
http://146.189.217.112/globalassets/office-of-undergraduate-medical-education- media/i me
ghp/appasani_ghpposter.pdf [cited 2021 Mar 31]
3. Pratheepa, M., & Nithya, M. (2014). Relevance of HIV IEC Materials-A study among
PLHIVs. IOSR Journal of Humanities and Social Science (IOSR-JHSS, 19(3), 53–58.
http://www.iosrjournals.org/iosr-jhss/papers/Vol19 issue3/Version- 4/K019345358.pdf
4. Lumen Learning. Mental health treatment: Past and present
[Internet]. Lumen learning.com. [cited 2021 Mar 31]. Available
from:https://courses.lumenlearning.com/intropsychmaster/chapter/mental-health- treatment-
past- and-present/
5. Gautam S, Jain N. Indian culture and psychiatry. Indian Journal of
Psychiatry.2010;52(7):309.
70
https://courses.lumenlearning.com/intropsychmaster/chapter/mental-health-treatment-past-and-present/
https://courses.lumenlearning.com/intropsychmaster/chapter/mental-health-treatment-past-and-present/

Journal of Mental Health Education | NIMHANS |VOLUME 3 ISSUE 1 | April 2021
6. Thakur J, Jaswal N, Grover A. Is focus on prevention missing in national health programs?
A situation analysis of IEC/BCC/Health promotion activities in a district setting of Punjab
and Haryana. Indian Journal of Community Medicine. 2017;42(1):30.
7. SHG members to be trained as mental health counsellors in TN [Internet]. The Hindu.2021
[cited 3 April 2021].
Available from: https://www.thehindu.com/news/national/tamil-nadu/shg- members-to-be-
trained-as- mental-health-counsellors-in-tn/article29863696.ece
71




















