Jesuit Health Care Handbook
76
Jesuit Health Care Handbook for the Assistancy of Canada and the United States April 2015
-
Upload
khangminh22 -
Category
Documents
-
view
7 -
download
0
Transcript of Jesuit Health Care Handbook

Jesuit Health Care Handbookfor the Assistancy of Canada and the United States
April 2015

ACKNOWLEDGEMENTS (2014)
The 2014 revision of the Jesuit Health Care Handbook forthe United States Assistancy was undertaken by acommittee consisting of Arnie Shafer (CFN and OREprovincial assistant for health care), Paul Cochran, SJ(Superior of the Regis Community in Spokane,WA), TerryKult (Health Care Coordinator for Omaha, NE) and DavidGodleski, SJ (Delegate for Formation and Jesuit Life –Jesuit Conference). The committee would like to thankNancy Gallagher (Director, Manresa Hall, Philadelphia),Harry Geib, SJ (Superior of St. Claude La ColombiereJesuit Community in Baltimore), Margaret MaryMonahan (Executive Director at Murray-Weigel Hall),Richard Twohig, SJ (former Superior of ColombiereCenter in Clarkston, MI) and the other ProvincialAssistants for Health Care (Deirdre Banscher (MAR), AnaCasey (MIS-NOR), Jane Glynn-Nass (CDT-WIS),Catherine Morency (NEN), Jacqueline Perez (NYK)) fortheir time, energy and diligence in their work on therevisions of the different sections of the Handbook. Wealso wish to express our gratitude to Ron Amiot, SJ, andJane Ferdon, OP for their review of the updated drafts ofthe sections.
We are very grateful to Myles Sheehan, SJ, M.D., andJosephTetlow, SJ who contributed the original articleentitled Spirituality and Aging.
The final editing of this Handbook could not have beenaccomplished without the assistance of Becky Sindelarand Doris Yu and we are thankful for the fine service theyprovided.
Should any part of this work be cited in scholarlymaterial, the citation should read as follows: ProvincialAssistants for Health Care of the Jesuit Conference ofCanada and the United States,Washington, DC 20036.
©1997 by the New England Province of the Society ofJesus.Revised 2006.Revised 2014.All rights reserved.
Printed in the United States of America.
No part of this book may be used or reproduced in anymanner whatsoever except for brief citation or review inscholarly material without written permission of the NewEngland Province.
Please contact the Jesuit Conference at 1016 16thStreet, NW, Suite 400,Washington, DC 20036 for allinquiries concerning reproduction of any part of thismaterial.
HOWTO SEARCHTHIS DOCUMENT
PC users:
1. Press CTRL+F (“Control” and “F” keys).2. Type your search term.3. Hit “Enter.”4. Occurrances of your term will be
highlighted in the text throughout thedocument.
To the right of the search field arebuttons to view the previous and nextoccurrances of your search term. Or youmay press CTRL+G to see the nextoccurrance.
To bring up an advanced search function, hitSHIFT+CTRL+F (“Shift,” “Control” and “F”keys).
Macintosh users:
1. Press ⌘+F (“Command” and “F” keys).2. Type your search term.3. Hit “Enter.”4. Occurrances of your term will be
highlighted in the text throughout thedocument.
To the right of the search field arebuttons to view the previous and nextoccurrances of your search term. Or youmay press ⌘+G to see the nextoccurrance.
To bring up an advanced search function, hitSHIFT+⌘+F (“Shift,” “Command” and “F”keys).
To download the latest version of the freeAdobe Acrobat Reader, visithttps://get.adobe.com/reader/

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . .
. . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
. . . . .. . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . .
. . . . . . . . . . . .. . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
JESUIT HEALTH CARE HANDBOOK 3
CONTENTS
FOREWARD
I. CONVERSATION GUIDE FOR SUPERIORS1. What sort of things can be done to encourage good health among the men of a
community?2. As a Jesuit superior, what role should I play in the medical care of the men in my
community?3. What sort of medical records should be kept on each man?4. How do I know if an older man is doing well or not? If he is getting old, shouldn’t
I expect certain changes?5. How do I recognize and care for men who are showing signs of failing?6. Are there ways to structure a community to provide more support for some men
without turning an apostolic community into a nursing home?7. Is it worth confronting older men about smoking and drinking?8. What about odd and eccentric behaviors?9. What should be done about meals?10. What should be done with men who appear to be having memory loss?11. I’m concerned about the ability of some of the older men in the community to
drive safely.What can I do about men who may be having problems driving a car?12. Are there ways to include older men more in community life13. What sort of health planning should I encourage in younger men?14. What are advance directives?15. What sort of things can be done to make a community more comfortable for
older men?16. Are there some practical considerations that can be helpful in providing cura
personalis for older men in a community?17. Are there specific policies a community should have on health care issues?18. When should men be referred to the province health care center?What options
are there other than the health care center?19. How can I help men prepare for transitions and retirement?20. How can I attend to the spiritual needs of the men in my community?21. How can I recognize men who might be depressed in the community?22. Should I involve the families/friends in the care of older Jesuits?
II. ANNUAL CHECKLIST FOR SUPERIORS1. How is the man’s physical health at this time?2. How does the man take care of himself?3. How does the man relate to his community?4. What is the man’s room like?5. Is the man’s health care file up-to-date?6. How is the superior’s relationship to the man?7. Some items for the community and consultors to consider
III. RESOURCES & BIBLIOGRAPHY1. Assessment Programs2. Healthy Celibate Living3. Mental Health Resources4. Online Resources (Mental Health)5. Aging and Spirituality6. AgingTopics7. Online Resources on Aging8. General Resources
5
6
6
78
89
1010101111
12121313
13
1314
1414151515
1616161616171717
181818181919202020

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . .. . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
JESUIT HEALTH CARE HANDBOOK4
CONTENTS
9. Elders and Driving10. Disease-related websites
IV. PRACTICAL GUIDELINES FORTHE HEALTH CARE OF JESUITS4.1 Taking ownership of one’s own health care4.2 Interactions with Health Care Professionals4.3 Specific Steps to take in Emergency Situations4.4 Communicable Diseases4.5 Medical Records4.6 General Principals for Community Record Keeping4.7 Funeral Preparation4.8 Transitions4.9 Personal Belongings4.10 How to Make Older Men Feel Valued in Community4.11 Spirituality and Aging in Community4.12 Loneliness4.13 Ways to Recognize Depression4.14 Utilization of Local Resources4.15 Family & Friends of Jesuits4.16 Overview on Professional Counseling and Psychotherapy4.17 Guidelines for Counseling and Psychotherapy4.18 Guidelines for Long-TermTherapy at a Treatment Center4.19 Overview on Alcoholism4.20 Guidelines to Address Alcohol Issues4.21 Suggestions for a Driving Conversation4.22 Furniture and Furnishing for a Community4.23 Food Preparation Consideration
V. IGNATIAN SPIRITUALITY ANDAGING5.1 Spirituality and Aging by Myles Sheehan, S.J., and JosephTetlow, S.J. (2014)5.2 Ignatian Spirituality and theAging, Sick and Dying Jesuit byWilliamA Barry, S.J. (1993)
VI. GENERAL DIRECTIVES FOR HEALTH CARE INA JESUIT RETIREMENT FACILITY ORNURSING CARE CENTER
VII. APPENDIX7.1 “Challenges to Healthy Jesuit Living” from Community As Mission: Jesuit Life
Now and Into the Future (U.S. Jesuit Conference, 2012)7.2 Jesuits Aging 2006 by Myles Sheehan, S.J.7.3 Sample - Community Health Care Information Form7.4 Sample - Authorization for the Release of Medical Information Form7.5 Sample - Quality Improvement Report (Health Care Facility)7.6 Sample - New Resident Intake Form for Health Care Facility7.7 Sample - Health History Form for Jesuits
2121
222224262727293032353536373738383940404141434546
474750
56
60
60646869707275

This handbook is divided into seven sections:Section One, Conversation Guides for Superiors,contains introductory comments and generaldirectives for superiors in the form of questionsand answers. SectionTwo, An Annual Checklistfor Superiors, is offered as a practical tool forsuperiors to assess the health care needs andareas that may need attention in communities.SectionThree, Resources and Bibliography, offersadditional resources with added hyperlink/webpage topics.Section Four, Practical Guidelines forthe Health Care of Jesuits, provides a wide rangeof advice on quality of life questions andpracticalities affecting community life. SectionFive, Ignatian Spirituality and Aging, offersreflections on situating the aging process withinthe context of Ignatian and Jesuit spirituality.Section Six, General Directives for Health Care ina Jesuit Retirement Facility or Nursing CareCenter. Section Seven, Appendix, whichprovides some samples of common forms aswell as additional material.
It is the sincere hope of the American Provincialsthat the directives and advice contained hereinwill be of help to the superiors of the Assistancyas you endeavor to help the men entrusted toyour care.
JESUIT HEALTH CARE HANDBOOK 5
FOREWARD

I. Conversation Guides For Superiors
The purpose of this section is to assist Jesuitsuperiors with some commonly askedquestions about health care for the men intheir communities.These questions andanswers are an attempt to frame some of thecommon health-related questions that ariseabout the older men in our communities.Section Four, Practical Guidelines for theHealth Care of Jesuits, contains concreterecommendations for superiors about a widevariety of community needs and items thataffect the quality of life of individuals, andthese are to be considered practicalsuggestions, which augment the generalquestions and answers contained in thissection. It should be noted that superiors andall others involved in health care for Jesuitsare strongly urged to consult a professional asappropriate for assistance with any of theitems contained herein.
1.What sort of things can be done toencourage good health among the men of acommunity?
Recognizing the importance of cultivating healthyhabits and encouraging men to take responsibilityfor maintaining their health is an essential part ofthe job of a Jesuit superior. At the same time,there is a limit to what a superior can do.Individual Jesuits need to take charge of theirown health. There are three areas in which asuperior of a community, in conjunction with theminister, can create the conditions in which goodhealth is encouraged. First, encourage men totake care of themselves. This means inquiringinto whether they have a physician andsuggesting a reasonable frequency for thesecheckups. It is recommended that at least everytwo years younger men should see a physician toidentify subtle changes in health.
A difficult task for the superior is to ask menabout behaviors that are potentially self-destructive. Although an individual in thecommunity may be a productive and good Jesuit,it is worth asking him about behaviors thatsuggest something is wrong. This requires thesuperior not to accept as the status quo
behaviors that might be brushed over. Assumethat a middle-aged professor in a universitycommunity has three to four drinks every night atpre-prandials. This is too much. The man shouldbe confronted. He need not be an alcoholic to beusing alcohol in a way that is unhealthy. Therector should ask him: “Why do you have three orfour drinks a night?You become loud andgregarious after those drinks. Is your work goingwell? Is there something bothering you?”Another man may be noted by the superior to berapidly gaining weight and eating large portions atmealtimes: “You have gained a lot of weightlately and seem to be eating heavily; what is thatabout? I am worried about your health with thisweight gain. Could I help you in some way?”
Smoking is a difficult habit to stop and smokersare not pariahs. At the same time, heavysmokers may want to quit and find themselvesunable to do so. There are medications andeffective smoking cessation programs available.Encouraging a man to stop smoking may givehim the push he needs to stop. “I have noticedthat you find it hard to give up smoking; is thereanything I can do to encourage you in this?”Second, create the conditions in the communitywhere men are able to live a healthy lifestyle.Practically speaking, this means doing fourthings. First, provide meals that are nutritious andallow a choice for those who wish to follow alow-fat, low-cholesterol diet. Second, discouragesmoking in common areas. Third, encouragereasonable exercise and opportunities for fitness.This can mean providing access to healthequipment or a gym. Fourth, encourage sharedleisure and opportunities for relaxation. ManyJesuits work too hard, and the potential forloneliness and isolation in our lives is real.Whether it is a special meal, a villa day, or someother opportunity to relax in each other’scompany, encouraging men to come togetherand have some fun is an important part ofcommunity health. Men who consistently refuseopportunities like these may be depressed,angry, anxious, or overly involved in work to thedetriment of their overall well-being. Third, set anexample by your own behavior. All your talk aboutgood health to the community will be ineffectualif you drink too much, smoke like a fiend, eat toexcess, and never take a day off.
JESUIT HEALTH CARE HANDBOOK6
SECTION I Conversation Guides For Superiors

2. As a Jesuit superior, what role should I playin the medical care of the men in mycommunity?
This will be determined by a number of factorsincluding your personality and the personality ofthe man, the size of your community, and thetype of illnesses that come up during your periodof governance. Some specific issues to considerfor all superiors include:
• selecting a physician from a list of providersapproved by your insurance company.
• normally, a Jesuit will choose his doctor likeother Americans, deciding on the basis of arecommendation or a personal acquaintance.
• the choice of physicians used currently by menin your community
• positive interactions with physicians when youhave questions about a man's condition
• dealing with specialty physician choices when aman is hospitalized
Superiors should make certain that the men intheir community have a doctor and a dentist andhave regular checkups. The superior should alsobe aware of the name of health care providers ofhis men, so he can contact them in the event ofan emergency. The PAHC and/or local health carecoordinator can assist in establishing this list.Thechoice of a physician is a highly personal matterand one that will usually be decided by theindividual Jesuit. Today the managed carenetwork of many insurance programs mayalter this individual choice. In somecommunities, most of the men will see a fewphysicians. This has the benefit of dealing withphysicians who are usually aware of the Jesuitcommunity, are willing to help in emergencies,and provide faithful service to our members. Atthe same time, close relations between a Jesuitcommunity and a physician or a group ofphysicians need periodic review. In caring forolder men, the hallmarks of a good physician area willingness to talk to the older man, parsimonywith medications, careful investigation ofproblems rather than assigning them to “old age,”and therapeutic efforts aimed at maintaining orimproving function. Physicians who frequentlyprescribe tranquilizers, sleeping pills andexcessive pain medication to older members ofthe community may not be the best choice.
Likewise, some physicians will show a misplacedrespect for our men and not question orphysically examine Jesuits as thoroughly as theywould a lay person. It is wise for a superior tohave a good relationship with one or twophysicians who can assist in providing secondopinions about men and arranging referrals.Occasionally a Jesuit will have a chronic problemand will benefit from a referral to a specialist.Ordinarily, the man’s physician will arrange for areferral. From time to time, however, a problemmay occur with a Jesuit that the man and/or hissuperior will feel needs further investigation.Particularly useful is obtaining a comprehensivegeriatric assessment for older men who appearto be having difficulties. This type of assessmentaims to look at the man from a number ofperspectives in an effort to develop a care planthat will maintain or improve his functionalabilities, as well as diagnose and treat anyproblems. If the Jesuit’s physician is unable torecommend a referral for a comprehensivegeriatric assessment, consult with the ProvinceHealth Care Assistant. Together you may need tocall to a local university teaching hospital and thedepartment of geriatrics for assistance.Thenormal channel of communication about aJesuit’s health should be between the Jesuit andhis physician, with the Jesuit notifying hissuperior and the designated local health careprovider of any significant change or problem.With some Jesuits, however, either because ofan acute illness or frailty, there is a need for amember of the community, usually either thesuperior or the minister, to discuss theindividual’s condition with his physician. Suchcommunication can be facilitated byaccompanying the Jesuit to his appointment and,with the man’s permission and in his presence,speaking with the physician. Doctors will notroutinely answer questions about the condition oftheir patients to another person without thepermission of the patient. Federal legislation toprotect patient privacy, known as HIPAAregulations (Health Insurance Portability andAccountability Act), can create some newbarriers for Jesuit superiors trying to makesure that they are kept in the loop regardinghealth issues. Practically speaking, the best wayto make sure that a doctor will communicate witha Jesuit superior regarding the health of a Jesuitis to have the Jesuit provide a release to his
JESUIT HEALTH CARE HANDBOOK 7
SECTION I Conversation Guides For Superiors

physician designating the Jesuit superior and hissuccessors as an individual to whom thephysician can speak (a sample Consent forRelease of Health Information form can be foundin the Appendix). Realize that no doctor is goingto speak with a Jesuit superior if the Jesuit tellsthe doctor not to talk to the superior. Realistically,if you are the superior and you are concernedabout a Jesuit under your care and you needhealth related information, and the man is notdemented or unconscious, that Jesuit is going tohave to tell the doctor to talk to you. If the Jesuitis demented, unconscious, or otherwise unableto participate in the decision making process,then the doctor will contact the person the Jesuithas listed on his advance directive (see below fora description of advance directives) or theJesuit’s next of kin. This makes it crucial thatJesuit superiors, probably with the help of theProvincial Assistant for Health Care (PAHC), beactive in developing and keeping on hand a copyof the advance directive for each communitymember.When a Jesuit becomes ill and istransferred to a hospital, decision making may bedifficult. Normally, it is the patient who is toldabout his condition and who consents or refusesto the plans of the physician. This may beproblematic in the case of a frail, elderly Jesuit.First, most physicians will not think to call aJesuit superior, and many doctors will not havethe slightest idea what a Jesuit is, let alone aJesuit superior. Second, with other olderpatients, physicians will routinely discuss thecare of the patient with the patient’s family,provided the patient agrees. Physicians may wellspeak with the relatives of a Jesuit rather thanwith a superior. Third, an older Jesuit may not beinclined to ask questions or disagree with theauthority of a physician. Fourth, if the older Jesuitis too ill to participate in the decision-makingprocess, physicians will look to the next of kin toassist in decisions. They will not think of religioussuperiors or ministers.When a Jesuit is admittedto a hospital, the superior or minister can doseveral things to avoid mishaps and poorcommunication. First, accompany the man to thehospital or emergency room and have thesuperior or minister listed as next of kin onhospital records. Second, if the man has madeout an advance directive (living will, durablepower of attorney for health care, or health careproxy), bring that document to the hospital so
that it is available to the staff. Third, call theJesuit’s family members so they are informed.Make it clear that you are involved in caring fortheir relative and tell them to call if they havequestions. Keeping family in the loop ofinformation lessens the chance of a nastyconflict. Fourth, speak with the nurse and thephysician of the Jesuit. Make it clear that you arethe one to be called in the event of a problem.Show them a copy of the advance directive thatdesignates you as the person to be contacted.Conflict can develop between family membersand Jesuit superiors regarding decisions aboutlife-sustaining care of critically ill Jesuits. Apreviously prepared advance directive is crucial inresponding to this question. If a Jesuit names afamily member rather than another Jesuit as hisproxy, then the Jesuit community has no controlover the decision-making process.
3.What sort of medical records should be kepton each man?
It is unreasonable to expect the superior tobecome a medical librarian. The PAHC has anelectronic health record that provides criticalinformation. In the event that you do not haveregular access to the PAHC, an alternative formmay be needed. The type of information thatshould be readily available in the event of anemergency includes: the name of the man’sphysician, a list of medications that the mantakes, a list of any possible allergies, and thenames and telephone numbers of familymembers who should be contacted. As importantas collecting this information is, it is alsoimportant to provide a means for the informationto be available when the superior’s office islocked up on a night or on a weekend when thesuperior may be away.When the superior isaway, another individual in the community shouldbe responsible for providing emergencyinformation. If your Province does not have aspecific form, a sample is provided in thishandbook in the Appendix or contact your PAHCfor an electronic health record copy.
4. How do I know if an older man is doing wellor not? If he is getting old, shouldn’t I expectcertain changes?
JESUIT HEALTH CARE HANDBOOK8
SECTION I Conversation Guides For Superiors

The most important piece of information for asuperior in a community with older Jesuits is torecognize that changes in older Jesuits shouldnot be chalked up to old age. Although it is truethat with increasing age individuals experiencedecline, these changes are not the direct resultof aging per se but represent illness. Memoryloss, difficulty walking, depression, incontinence,personality changes, falls, and frailty are notnormal. An older man in a community whoseems not to be himself or who, for example,becomes forgetful, needs a medical assessment.Why bother with a medical assessment?Although decline does occur with aging, many ofthe changes that occur can be reversible. Asudden change in the status of an older person isoften a sign that a serious illness is brewing. Forexample, an 80-year-old man who has beenindependent and does well in the communitysuddenly becomes confused over the course of48 hours. He should be taken to an emergencyroom. This presentation of a sudden change inmental status may be the first sign of a drugreaction, a serious infection, a heart attack, astroke, or other condition. It is not part of normalaging. Appropriate assessment and treatmentcan return an older person to his previousbaseline. It is true, however, that many illnessesare chronic and not always curable withadvancing age. Rather than simply assume thatthis is the case with an older individual, however,it makes sense to seek competent medicalattention and establish a diagnosis. It may be thatsome treatment can be provided or interventionssuggested that would improve function andincrease independence.
5. How do I recognize and care for men whoare showing signs of failing?
It is a common occurrence to be living with aman and be told by a visitor to the communitythat Father X seems to be doing poorly. The dailycontact of community life can make it difficult tonotice the changes over time that are readilyapparent to an individual who has not seen theman for some time. Recognizing changes overtime in older men requires paying attention totheir functional ability. Functional ability describeshow well a man is able to negotiate the commondemands of everyday life. Some specific items,
referred to as activities of daily living (ADLs),include his ability to bathe, dress, use the toilet,feed himself, groom, and walk independently.Other items, known as instrumental activities ofdaily living (IADLs), describe a man’s ability toperform the tasks that make it possible to remainindependent and include arranging fortransportation and travel outside of thecommunity, independent management ofmedications, using a phone, managing finances,shopping, and cleaning. Typically, instrumentalactivities of daily living are lost first in olderindividuals as a consequence of illness ordementia. Many will first note a problem with aparent because of a problem in paying the bills orrunning errands. But Jesuits in community, asopposed to lay people, often have many of theinstrumental activities of daily living taken care ofby the community. As a consequence, physicaland mental problems with Jesuits are oftenrelatively hidden until they present themselves atan advanced stage. The two key points forsuperiors who are in charge of a large number ofolder men are a discerning eye and a high degreeof suspicion. Discernment is required in notingchanges among the men in a community. Asuperior would do well to be concerned over amember of the community who, for example,begins to dress poorly or whose hygienedeteriorates. Likewise, problems with memory,continence, weight loss, and falls are signs ofimportant changes. The high degree of suspicionrequires that superiors not shrug aside changesin older men but pay careful attention and have alow threshold to refer to a physician. The superiorshould not be satisfied when he notices afunctional change in one of his men and thephysician brushes the concern off with acomment about the individual’s age. It may wellbe that a competent physician will not find aspecific explanation. He or she should stillacknowledge the problem, discuss what hasbeen done to investigate the problem, and sharehis or her thoughts as to what is the cause andwhether or not further investigation is warranted.If a man continues to deteriorate and the man’sphysician does not seem to do much, then thesuperior may consider having the man seeanother doctor or arranging for a comprehensivegeriatric assessment . Consult the PAHC or localhealth care professional for guidance in thisreferral.
JESUIT HEALTH CARE HANDBOOK 9
SECTION I Conversation Guides For Superiors

6. Are there ways to structure a community toprovide more support for some men withoutturning an apostolic community into anursing home?
When an older man begins to have somefunctional declines and needs more assistance tolive in the community, there are resourcesavailable to assist the man. The first place tobegin is with the Provincial Assistant for HealthCare (PAHC). Either the PAHC or the local healthcare professional can assist with arranging ahome assessment or explain how to go aboutgetting a referral for an assessment. The purposeof this assessment is to investigate the functionof the man in his own setting, see what hisneeds are, and arrange for further services. Thenurse may recommend a variety of services thatwill come to the community. The nurse,depending on the man’s condition, can monitorhis progress, check vital signs, change dressings,and provide other skilled nursing needs.Examples of other potential services include ahome health aide who can help the man withbathing and grooming and a home physicaltherapist to assist the man in regaining strengthand function and to train the man in the use ofadaptive devices such as canes and walkers.Some services will be provided free of charge ifcovered under Medicare. Other services may becharged. Some communities with a large numberof older men may consider providing moreassistance for these men on a regular basis.Helping men retain their function and ability tolive in community can often be a goodinvestment for two reasons. First, it contributesto the man’s well-being when he knows that helpis available to him in the community and he neednot fear a transfer to a retirement center ornursing home if a problem develops. Second, itcan be less expensive to provide some help for aman in his own community rather than transferhim to another environment. The type ofassistance that a community wants to providewill depend on a number of factors, including itsfinances, size, ability to recruit help, and theapostolate of the community. Some examples ofhelp that should be considered includeassistance with laundry and room housekeepingand hiring an individual to assist with bathing andgrooming. In communities with relatively fewmembers where older men may be isolated
during the day, consideration should be given toobtaining some type of signaling device (e.g.,Lifeline) that can summon help for a man shoulda sudden crisis, such as a fall, occur.
7. Is it worth confronting older men aboutsmoking and drinking?
Older men who smoke and drink to excessshould be confronted with their behavior forthree reasons. First, there are health gainsobtained by stopping drinking and smoking, evenfor old men. Second, the community usually willbe relieved by the change in behavior. Third, it isthe job of the superior to be concerned about thehealth and well-being of his men. Avoiding adiscussion about smoking and drinking simplybecause the man is old is ageist.
8.What about odd and eccentric behaviors?
Many of our communities have men whosepeculiar habits and behavior would not bepossible in any other setting. Some of thesebehaviors represent long-term personalitydisorders that have never been confronted. Otherproblematic behaviors are the result ofdepression, obsessive-compulsive disorders, orchronic anxiety. It is very difficult for a superior toknow how or when to confront individuals. Thosewho have a long-term history of problematicbehavior may not respond favorably. Superiors,however, should try to assist men who are clearlyacting strangely, even if this strange behavior hasbeen ignored for years. Inquiring about the man’shistory among other community members andattempting to ascertain if any professional helphas been given in the past are reasonable firststeps. It is also reasonable to arrange for aconversation with the man and simply mentionthe behavior and ask the man why he does it. Asan example: “Father Jones, I have noticed thatyou will not eat in the dining room with the restof the community!Why is this?” A prudentsuperior would do well to make the attempt toget to know a man a bit first and make it clearthat the man, despite his behavior, is a valuedmember of the community. Some behaviorscreate issues for the health and safety of thecommunity and must be confronted, even if it
JESUIT HEALTH CARE HANDBOOK10
SECTION I Conversation Guides For Superiors

makes everyone very uncomfortable. As anexample, most Jesuits are aware of an older manwho will fill his room with artifacts and debris ofhis Jesuit life, creating a garbage dump.Behaviors like these, that create a problemwhere fire, vermin, and safety are real concerns,cannot be tolerated. In situations like this, contactthe PAHC to develop a planned approach tocarefully evaluate the room or identify if there is amental health issue connected with this behavior.Some of the hoarding behaviors that are seencan be a manifestation of a personality style ordownright disorder. Interventions have thepotential to lead to tremendous disruption for aperson who is at best fragilely balanced. Prior tomaking ad hoc interventions, it may be necessaryto work in conjunction with a psychologist orpsychiatrist to provide assistance to the Jesuitand the superior in interventions like these.
9.What should be done about meals?
Mealtime is an important part of Jesuitcommunity. It provides an opportunity not onlyfor obtaining nourishment but for conversationand relaxation. At the same time, proper nutritionis an essential part of fostering good health.Because meals are so important, and becausemany Jesuits have very strong feelings on whatthey like or what they feel is healthy, superiorsoften have a difficult task in making decisionsabout what will be served in the dining room.
Some suggestions may be of help: First,encourage choice and moderation. Some Jesuitswill prefer meat and potatoes while others willopt for low-caloric, low-salt, and low-fat items. Ifpossible, a choice of two entrees will helpprovide options that will keep the communitywell fed and content. Encourage the cook to cutback on salt, heavy sauces, and high fat items.Second, have the menus planned and reviewedwith the help of a dietician. He or she can, incooperation with the cook, make sure thechoices available provide for a balanced diet. Ifyou contract your food service, check into havingtheir dietician assess the needs and choices ofyour community.Third, be cautious in cutbacksthat involve meals. Many communities are forcedto economize and can no longer afford mealservice three times a day, seven days a week. In
communities with older men, who may neverhave been in a kitchen since they entered theSociety as teenage boys, it is unreasonable toexpect that all will be able to fend forthemselves. A particularly important mealtime forolder men is breakfast. For many older persons,breakfast is the meal where they will consumethe most of their calories for the day. Althoughabolishing meal service at breakfast may provideattractive economies, it may lead to nutritionaldecline among older men.
10.What should be done with men whoappear to be having memory loss?
Although changes in memory are common withadvancing age, they are not a part of normalaging. A gradual memory loss could be a sign ofa number of conditions, including a problem withmedications, misuse or abuse of alcohol, anunderlying medical disorder like thyroidimbalance depression, or a dementing illnesscaused by strokes or Alzheimer’s disease.Evaluation is crucial. Consult with the PAHC orthe local designee to arrange for thisconsultation. There are reversible causes ofmemory loss, such as thyroid imbalance, adversemedication interactions, and some vitamindeficiencies. Second, even if a reversible cause isnot found, establishing a diagnosis provides theopportunity for better planning for the man andhis community. Although an individual may bediagnosed with Alzheimer’s disease, it does notmean that a man is incapable of participating inand making a contribution to community life.When the diagnosis of a dementing illness ismade, the superior should plan for the future,ideally with the help of the older man. First, theman needs emotional support in dealing with thediagnosis. Second, data concerning a living willand the appointment of a proxy decision makershould be reviewed or established while the manis still capable of understanding. Third, safetyissues in the community need to be addressed.Most likely the man should no longer drive. Ifwandering is a concern, an identification braceletshould be obtained.Wandering and otherbehaviors may necessitate a transition plan to asafer Jesuit community. The diagnosis of ademanding illness, however, does not mean thatthe man must be moved. That should be
JESUIT HEALTH CARE HANDBOOK 11
SECTION I Conversation Guides For Superiors

determined on the basis of his ability to continuesafely in the community.
11. I’m concerned about the ability of some ofthe older men in the community to drivesafely.What can I do about men who may behaving problems driving a car?
Because the ability to drive is important forpersonal independence, it can be very tough for asuperior to confront men in the community whomay be having problems. Anyone can have anaccident and older men should not be afraid theywill be barred from driving because they havehad a fender bender. At the same time, a laissez-faire attitude toward dangerous driving is notappropriate because of the risk to others. Lessimportant than the chance that someone couldbe hurt, but not a trivial concern, is the fact thatthe community can be held responsible for theliability incurred by a community member who isat fault in an accident.
Superiors on occasion must order men not todrive. For the older man about whom there areconcerns but real uncertainty, some hospitalsoffer driving testing programs through theoccupational therapy department. Some autoinsurance companies offer defensive drivingcourses and hands-on assessment as part of thepolicy services. Limiting a man’s driving privilegeneed not be an all-or-nothing decision. Based onthe advice of a physician and/or an occupationaltherapy driving evaluation, some compromisesmay be possible. For example, a man may driveto a parish a few miles away for supply work onSundays. He has no problem with this route, butlonger driving, night driving, or highway drivingare all problematic. Limiting the man to drivingwithin the neighborhood of the community maybe possible. Such prudential decisions, however,are difficult and require balancing safety with theneeds of the man to remain independent and notisolated. Men who drive drunk, habitually haveaccidents, or have serious vision problems mustbe ordered to cease driving. Driving guidelinesare already available in many provinces. Additionalconversation guides are available in section 4.21.
12. Are there ways to include older men morein community life?
Many communities find the older members areinvolved and active. In some settings, however,older men may not be fully integrated into thecommunity and seem somewhat aimless anddrift through the day. There are a number ofpossible explanations for this type of behavior,including boredom and a lack of stimulation nowthat an active career of teaching or pastoral workis over. One possible solution is to provide morestructured activities during the day. Many of theolder men will remember a regular order thatprovided a framework for their life. Now,however, the only order may be the times ofmeals. Providing some sort of scheduledactivities may be useful. Suggestions wouldinclude communal liturgical events, daily videos,and occasional outings. Obviously, arranging forthese activities can be difficult in a communitywhere there are only a few older men and therest of the community is working at theapostolate during the day. Part of regular order inthe past included set times for prayer and groupworship. Reviving such customs can provide thetype of structure in life that some older men lack.Regularly scheduled times for visits to theBlessed Sacrament, meditation, and rosary aresome examples. Other devotions, likeBenediction, may well be popular among oldermen and encourage group participation.Community meetings can be another time whenolder and younger members can mingle. It is areasonable idea to have some meetings devotedto outside speakers, media/slide shows of arecent trip of a community member, or othergroup activities that encourage companionship.Although it is important that a community be ableto discuss difficult issues and speak frankly,many older men are very uncomfortable withfaith sharing or open discussion of some issues.Taking care in planning meetings so that there isa balance in the type of formats that can createopportunities for everyone to come together aswell as provide settings where frank discussionscan be held.
JESUIT HEALTH CARE HANDBOOK12
SECTION I Conversation Guides For Superiors

13.What sort of health planning should Iencourage in younger men?
In working with younger men, superiors canencourage the men to take responsibility for theirhealth. Concrete suggestions include regularmedical checkups and dental care, physicalexercise, moderation in work and appropriate useof leisure time, cessation of tobacco use, andmoderation in alcohol use. All men should beencouraged to develop an advance directive forhealth care. In addition, young and middle-agedmen may need to be assisted in considering theirown aging process and think a bit about whatthey would like to do in the future. The PAHCand/or local health professional can be excellentcoaches in promoting healthy lifestyle choices.
14.What are advance directives?
Advance directives refer to a class of documentsand statements whereby individuals attempt todirect the type of medical care they would wantto receive in the event of a serious illness oraccident and the individual is unable to participatein the decision-making process. Different stateshave different legal requirements about advancedirectives. In some states, a living will is allowedwhere specific treatments are mentioned. Inother states, the legal method of establishing anadvance directive is to appoint a health careproxy: a person who will act in the name of thepatient should he be too sick to discuss with thephysician and decide for himself. Some statesallow a combination of living will and theappointment of a proxy decision maker. Otherjurisdictions refer to appointing a durable powerof attorney for health care decisions. This createsa role like that of the health care proxy. Advancedirectives are an important part of arranging foran individual Jesuit’s health care. Given that manyphysicians will turn to the Jesuit’s nearest livingrelative rather than a Jesuit superior, theappointment of a Jesuit as the health care proxyfor another Jesuit provides a mechanism thatensures that the Society will remain involved inserious decision making.
15.What sort of things can be done to make acommunity more comfortable for older men?Some attention to furniture, bathrooms, lighting,and other parts of the physical environment areuseful in making a community an accessible andsafe place for older Jesuits. (See section 4.22)
16. Are there some practical considerationsthat can be helpful in providing curapersonalis for older men in a community?
Visiting a Jesuit in his room is an excellent way toget a better idea of what is going on with thisman. Get a sense of what his living surroundingsare like. Is the room a mess? Is the furniturecomfortable and adapted to the needs of theolder man? Are there hazards that can becorrected like electrical cords and clutter on thefloor? Providing the man with some assistance tofix up the room as well as replace worn-out anduseless furniture is important. Other things tonotice include the types of belongings the oldermen may have. For instance, an older man maylove classical music and have only an old radio.Without being extravagant, a modestly pricedsound system and a few CDs might make theman’s life that much happier. Likewise, see if theman has any hobbies. Provide some extra moneyto encourage him in pursuing these types ofactivities (of course that depends on the hobby!).Clothing and personal hygiene are other areaswhere men may need some help. Many oldermen pay little attention to their personalappearance. Occasionally, some of the clothingchosen by our men comes from their desire tomodel the vow of simplicity or poverty, sinceclothing may be taken from the common’s tableor closet it can make them appear slovenly orsilly. Offer to take an older man shopping and gethim clean, reasonable clothing, e.g., two or threepairs of pants, several shirts, and a week’s supplyof underwear.
Emphasize that it is important to the Society thathe look neat and clean. If men have difficulty inmatching clothing, or prefer not to wear casualclothes, it is reasonable to encourage theindividuals to wear clean clerical clothing andreplace old and threadbare clerics or cassocks.Some men may not be able to do their laundry.Finding a way to help a man out is important to
JESUIT HEALTH CARE HANDBOOK 13
SECTION I Conversation Guides For Superiors

maintaining his dignity and appearance. Visitingthe room of an older Jesuit can also give someearly evidence of a problem that he may be ableto disguise outside the room. The point is not toinvade a man’s privacy or embarrass him; it is toimprove his ability to function and ensure that hisdignity is respected. If there is an odor of urine inthe room or, if there are other problems withhygiene, then this should not be left unattended.Neglecting an older Jesuit’s decline is neitherloving nor an example of personal care.
17. Are there specific policies a communityshould have on health care issues?
Communities need to consider two things. First,the appropriate Province policies can be obtainedand reviewed. Keeping track of advancedirectives and permission to contact the Jesuit’sphysician are very important. Some Provinceshave specialized forms for release of medicalinformation referred to as consent forAUTHORIZATION FOR RELEASE OF HEALTHINFORMATION PURSUANTTO HIPAA. Thisconsent form allows the superior or designatedhealth care professional to participate in medicalcare discussion, discharge planning, andcoordination of the plan of care. An example ofsuch a consent form is included in the Appendix.
Second, the superior and his consulters candiscuss problems that seem particularly commonor distressing in the community, and then,perhaps with the advice of professionals, tailor apolicy to the needs of the community. As anexample, the various provinces have policies ondealing with alcoholism.Within the framework ofthose policies, a community may develop its ownplan for aftercare and a list of resources andphysicians with particular expertise in the care ofmen with alcohol problems.
18.When should men be referred to theProvince health care center?
What options are there other than the health carecenter? An issue that needs to be considered byeach community is the question of criteria forreferral to the Province health care center. Thismust be coordinated with Province policy. At the
same time, communities have varying resourcesto meet the challenges that may be posed by anolder man with health problems and/or severefunctional limitations. Likewise, it may be that acommunity can deal with one or two men with avariety of problems but any additional older menmay overextend the personal or financialresources of the community. Ideally, theProvincial Assistant for Health Care, perhaps inconjunction with the director of the health carecenter, can assist superiors in planning for thecare of older men. The PAHC may be able tosupply the superior with a variety of resources tocare for men outside of the health care center.Types of resources can include lists of physicianswho can provide a second opinion; rehabilitationfacilities; possible short-term nursing home stays;community-based adult day care programs, andprofessionals who will come into the community,like visiting nurses, home health aides, andphysical therapists.
19. How can I help men prepare for transitionsand retirement?
For many older Jesuits, aging is a particularlydifficult time because they find themselves withlittle to do after a lifetime of busy apostolic workand have made no plans for the time when activework as a teacher or in a parish comes to an end.It is wise to begin discussing the transitionprocess prior to the need. The point is not tomake concrete plans for the future but toencourage men to begin considering possibilitiesfor the future. Specific items to discuss includethe use of leisure time, hobbies, and otherministries that may attract the man. As menbecome older, more concrete planning isnecessary. The man should be encouraged todevelop a specific plan or lists of possibilities thathe would like to pursue upon retiring from anapostolate. Too often, men say they look forwardto reading or doing some research but they makeno concrete plans.When retirement comes, theyare lost. Our spirituality has the potential to be atremendous resource in planning for thetransitions that aging will inevitably bring. Prayer,spiritual conversations, and devoting the annualretreat to asking the Lord about our desires,fears, and where the Lord is leading us as we ageare all appropriate.
JESUIT HEALTH CARE HANDBOOK14
SECTION I Conversation Guides For Superiors

20. How can I attend to the spiritual needs ofthe men in my community?Like most questions, this will depend on the menbut some suggestions may be helpful. First, askthe older men what they want or if they feelanything is lacking. Second, review theopportunities available in the community for thespiritual needs of the men: availability ofconfessors, accessibility of the chapel for menwith functional impairments, regular communityEucharist and prayer, and devotional opportunitiesfrom which all can profit but may be particularlyappealing to older men, such as benediction andlitanies. Third, consider an occasional day ofrecollection for the older men of the entirecommunity so that they can come together.Group activities when the entire community canpray together can be an important way to bridgesome of the occasional distance that may be felt.
21. How can I recognize men who might bedepressed in the community?
Depression is a relatively common problemamong people of all ages, not just the elderly. Inolder persons, depression can be neglected, asthe changes due to this illness may be ascribedto aging or simply attributed to a change inpersonality. It should be emphasized thatdepression is a treatable illness. It does notrepresent a failure or weakness on the part of theperson who is suffering. (Refer to section 4.13)
22. Should I involve the families/friends in thecare of older Jesuits?
When a Jesuit becomes frail or ill, it is naturalthat his family/friends want to make certain thathe is receiving good care and is being properlylooked after. On occasion, some communitieshave had difficult problems with family/friendsdemanding certain treatments or being intrusiveinto the life of the community. It also is the case,however, that families/friends have properlyidentified areas of concern where their relativemay not be well cared for and important issuesare neglected. Hopefully, the community alreadywelcomes family/friends in a variety of ways:special dinners during the year, liturgies, and get-togethers. It is much easier to deal with a crisis
when there is a pre-existing relationship betweenthe community, the community superior, and thefamily/friends of an older Jesuit. It is wise to aska close family member from time to time how heor she thinks a relative is doing. This may providea valuable insight into the man’s condition as wellas build a foundation for discussions if futureproblems occur.When there is a problem with anolder Jesuit, the superior should notify the family.This is obviously the case in the event of anemergency hospitalization. In less urgentsituations, however, it is wise to contact family.For example, a man may be having a slow declinein functional ability and generally not appearing tobe doing well. The superior could initiate aconversation with a family member that reviewsseveral points: first, that the changes in the olderJesuit have been noticed and are of concern;second, that the man has been seen by thedoctor and the doctor’s recommendations havebeen followed or another opinion sought; andthird, that there are plans to care for the man inthe future. Occasionally, family members can beextremely difficult. Approaching the family priorto a crisis may prevent some difficult behavior. Insituations where the family appearsunreasonable, the superior would do well todiscuss the situation with his consulters for theirsupport and advice.
In a hospital setting, it is essential that thesuperior do everything possible to be the contactperson regarding issues in the care of Jesuits.Considerable confusion can exist regarding theissue of next of kin, and many nurses andphysicians would look to a brother, sister, niece,or nephew rather than think to call a man’ssuperior. Conflicts between family and religioussuperiors regarding care decisions in the hospitalwhen the patient is unable to participate in thedecision-making process can be very difficult andrequire legal consultation.
JESUIT HEALTH CARE HANDBOOK 15
SECTION I Conversation Guides For Superiors

II. Annual Checklist for Superiors
A Jesuit is part of the one mission of the Societyof Jesus regardless of his age, training, andlocale. An integral part of participating in this onemission is the health (mind, body, and spirit) ofthe individual Jesuit and his community. Thesuperior of the community is tasked withoverseeing how each individual Jesuit lives outhis mission, i.e., that he has the necessary healthand support to labor with Christ in the Lord’svineyard.
It is highly recommended that the superior (or hisdelegate for health care) and PAHC meet yearlywith each man in his community for a shortcolloquy regarding each Jesuit’s health care.Preferably this would be separate from theannual colloquy that superiors conduct in theircommunities. This would allow the opportunityto review health care files as well as to have aconversation on health issues that are specific tothe man but also include the community.
It is highly advisable for the superior and hisconsulters to have a yearly review of how thecommunity enables the individual Jesuit to liveout his mission. Sometimes called a “systemsreview,” this process could help uncoverstrengthens and weakness in the community,e.g., kitchen and meal patterns, common areasof concern, transportation issues, safety in andaround the community, and hospitality andsupport concerns of the vowed religious life.
Some items to consider as part of a healthcare colloquy (and annual colloquy):
1. How is the man’s physical health at thistime?
• Have there been significant changes in health?Hospitalizations?
• Does he have a primary physician? Is there aHIPAA waiver on file?
• Has he had age appropriate exams? Has heshared the results with the superior or healthcare delegate?
• Has there been unexplained weight loss/gainduring the year?
2. How does the man take care of himself?
• Does he follow healthy patterns ofeating/exercise?
• Does he take appropriate time away for rest,relaxation and renewal of his spirit and body?
• Does he have any hobbies or interests outsideof his apostolic work?
• Does he read extensively, watch movies and/orsports or attend opera or symphonies?
• Does he maintain good relations with his familyof origin? Does he have a network of friends tosupport him emotionally/spiritually?
• Are there concerns regarding food/alcoholconsumption? Is he dressing and groominghimself appropriately? Does he wear clean andwell-mended clothes, bathe regularly, etc.?
• Is he safely independent for his daily activitiesof living or does he need significant assistancefrom others?
3. How does the man relate to hiscommunity?
• Does he regularly interact with other communitymembers? Or is he isolated and withdrawn?
• Is he present for community liturgies andmeetings? Does he excuse himself forapostolic or personal reasons?
• Are there signs of memory loss, depression,anxiety or other tensions that affect membersof his community?
• Are there issues of “commandeering” parts ofthe community, cars, TV rooms, etc., for hisexclusive use?
• Does the community value the man and hismission—regardless of his age or type ofassignment? And vice versa?
• Is the man able to live safely and comfortably inthe community, i.e., is the furniture and lightingage appropriate, is healthy and nutritious foodavailable at regular times, etc.?
4.What is the man’s room like?
• Has the superior/health care delegate visitedthe man in his room?
• Is it clean and uncluttered? Appropriatelighting? No tripping hazards, i.e., extensioncords, excess furniture, etc.?
JESUIT HEALTH CARE HANDBOOK16
SECTION II Annual Checklist For Superiors

• Is the room cleaned regularly? Are there smellsthat suggest health problems, e.g., urine orincontinence, rotting foods, etc.?
• Does the man need/want assistance with bedlinens and laundry?
5. Is the man’s health care file up-to-date?
• Is there a current Power of Attorney for him?Advance directives? Current list of medicinesbeing taken and seeing his doctors as needed?
• Is there a list of nearest relatives/friends to benotified in case of a health care crisis?
• Is the health care file immediately available tothe superior/acting superior/health caredelegate when an emergency occurs?
• Has he been in contact with the PAHC?
6. How is the superior’s relationship to theman?
• How well does the superior know the man andhis physical and health care needs? Hisspiritual and emotional needs?
• Is there tension/avoidance on either person’spart? Distrust that leads to breakdown in therelationship?
7. Some items for the community andconsultors to consider:
1. Do members of the community feel safe andcared for?
2. Are community meetings always geared toyounger members or are there a variety oftopics and formats?
3. Do I make sure that older men have the samespiritual care as younger men?
4. What are the opportunities for spiritualdirection, retreats, and access to Confession?
5. Do I encourage older men to attendcommunity liturgies or do I avoid the topic?
6. Are there other devotions or liturgies that thecommunity should have? (e.g., Benediction,communal Rosary?)
7. Do I make it clear I value the prayer life of menwho cannot be physically active in theapostolate?
8. Do I have a plan to help the men considertransitions?
9. Am I a reasonable example of decent healthhabits?
10. Do I discuss with young and middle-agedmembers of the community their health andthe need for them to take reasonable care ofthemselves?
11. Is there a policy about driving that considerswhat to do with men who should not bedriving? Are there alternative transportationoptions in the area?
12. What are our hopes and dreams for thefuture?
JESUIT HEALTH CARE HANDBOOK 17
SECTION II Annual Checklist For Superiors

III. Resources and Bibliography
Assessment Programs
Guest House Institute: Promotes expertise in thefield of addiction to Catholic leadership, dioceses,orders, universities, and seminaries. It has a largeexpert speakers’ bureau compromised of Catholicclergy, recovering lay and ministry professionals,and international academicians.www.guesthouseinstitute.org
National Catholic Council onAddictions (NCCA):The NCCA, an affiliate of the USCCB, is anorganization that promotes hope, healing, andreconciliation to those suffering from the diseaseof addiction; it also addresses the impact ofaddictions on family, society, and church.Spirituality and addiction resources. Servicesinclude educational workshops on SubstanceAddiction Ministries in local parishes.www.nccatoday.org
Saint JohnVianney Center: St John Vianneyspecializes in the treatment of behavioraldisorders and psychiatric illnesses for Catholicclergy, consecrated religious, and clergy of othermajor Christian denominations.www.sjvcenter.org
St. Louis Consultation Center: Comprehensiveassessment and treatment services aim to aid anindividual and his superior in understanding thenature of the individual’s problems. Effectivetreatment begins with an accurate assessmentof the individual’s spiritual, emotional, andpsychological state. It also is important tounderstand the impact of the individual’sdifficulties on the larger community of which heor she is a part.www.Stlconsult.org
Saint Luke Institute: Brings the healing ministryof Christ to clergy and men and women religiousthrough expert consultation,psychological/spiritual healing, and education.www.sli.org
Servants of the Paraclete: Provide holistic,integrated programs devoted to the spiritual andvocational renewal of priests and religious brothers.www.theservants.org
The Southdown Institute: Offers a five-dayresidential assessment program, a 14-weekresidential treatment program for religious andclergy suffering from a range of emotional/mentalhealth concerns, and a two- year Continuing Carefollow-up program and educational lectures,workshops, and consultation sessions.www.southdown.on.ca
Healthy Celibate Living
Manuel, S.J., Gerdenio Sonny. (2012) LivingCelibacy: Healthy Pathways for Priests.Mahwah,NJ: Paulist Press.
Amidst the Church's continuing clergy sexabuse crisis and the suspicions the publicmight have about celibacy and Catholicpriesthood, Living Celibacy hopes to makewhat constitutes healthy celibate living.
Mental Health Resources
American Psychiatric Association. (2013).Diagnostic and Statistical Manual of MentalDisorders (5th ed.). Washington, DC: AmericanPsychiatric Press.
A comprehensive clinical manual on mentalhealth classifications and disorders, includingtreatment protocols and prognosis.
Midden, P. (2012). New Creations: TheTreatmentof Priests. St. Louis, MO:Wittmann Blair.
This book offers ordinaries and religioussuperiors a candid look into dealing with theirproblematic priests and religious. It describestime-tested approaches and strategies thatare straightforward and respectful of theneeds of the man, those around him, and theChurch at large.
Patterson, K., Grenny, J., McMillan, R., Switzler,A. (2002). Crucial Conversations: Tools for TalkingWhen Stakes Are High. McGraw Hill.
Real, Terrence. (2003). I Don’tWant to Talk AboutIt: Overcoming the Secret Legacy of MaleDepression. NewYork, NY. Simon & Schuster.
JESUIT HEALTH CARE HANDBOOK18
SECTION III Resources & Bibliography

Online Resources
Carlat Report: Behavioral Health Bulletinwww.carlatbehavioralhealth.com
Monthly topic on mental health therapyoverviews.
Men and Mental Health: Depression, anxiety,bipolar, eating disorders, etc.www.nimh.nih.gov/topics/topic-page-mens-mental-health.shtml
National Institute of Mental Health: Educationoutreach/www.nimh.nih.gov
Aging & Spirituality
Bernardin, J. (1997). The Gift of Peace. Chicago,IL. Loyola Press.
He shares personal reflections and insights tothe struggle to find peace in ministry as onestands on the threshold of eternal life.
Buchanan, Missy. (2008). Living with Purpose in aWorn Out Body: Spiritual Encouragement forOlder Adults. Upper Room Books.
Callanan, M., Kelly, P., (1997). Final Gifts. NewYork: Bantam.
Hospice care and communication used by thedying to talk about their journey.
Chittister, Joan. (2008). The Gift of Years:Growing Older Gracefully. NewYork: Blue Bridge.
In The Gift of Years, Sister Joan Chittisterdescribes the task of growing older gracefullythrough the three stages of being “old”: “old”(age 65-74), “old old” (age 75-84), and “oldestold” (age 85 and over). Each of the 40 shortchapters (averaging about five pages) startswith a quotation by writers ranging fromSeneca to Carl Jung and ends with a briefsummation of burdens and blessings of therelevant element in these later years. Some ofthe 40 topics seem negative, for example fear,ageism, sadness, and loneliness, butChittister is able to draw positive results fromthem.
Griffin, Emilie. (2012). Green Leaves for LateYears. IVP Books.
Kidd, Sue Monk. (1990).When the HeartWaits:Spiritual Direction for Life’s Sacred Questions.NewYork: HarperCollins.
Sue Monk Kidd’s memoirWhen the HeartWaits views challenges in the transitionalperiod commonly known as midlife. However,most of her reflections are relevant to anytransitional period, including retirement.
McKevitt, Gerald. (2012). “The Gifts of Aging:Jesuit Elders in Their OwnWords.” Studies in theSpirituality of Jesuits (43/3) Autumn.http://www.jesuit.org/Assets/Publications/File/Studies_Autumn_2011_43-3.pdf
Moody, Harry R., and David Carroll. (1997). TheFive Stages of the Soul: Charting the SpiritualPassagesThat Shape Our Lives. NewYork:Anchor Books.
According to Harry Moody’s underlyingpremise in The Five Stages of the Soul, not allpeople advance spiritually at the same pace,but spirituality does normally develop withinthe second half of life in the same sequenceof stages: Call, Search, Struggle,Breakthrough, and Return. Moody exemplifieseach stage by its effects on his own life andon the lives of acquaintances and varied publicfigures, past and future. The Calls that initiatethe Search come in a wide variety of forms,for example vague feelings of emptiness,physical disorders, and beauties of art ornature, dreams, sudden spiritual insights, ornear-death experiences.
O’Nan, Stewart. (2011). Emily, Alone. NewYork:Penguin Books.
The title of the novel highlights one keyproblem faced by elders like Emily, the feelingof “aloneness.” Instead of a traditional plot,O’Nan has created a beautifully developedcharacter study of Emily Maxwell, an 80-year-old widow who has settled into relativelypassive old age, accepting dependency onothers, bemoaning the infrequency of visitsfrom her children and grandchildren, relivingscenes from her past, and living a routine lifein the present. That is, until she findsindependence by courageously driving her
JESUIT HEALTH CARE HANDBOOK 19
SECTION III Resources & Bibliography

new car around her Pittsburgh suburb. Latershe drives home to visit her parents’ graves, thefirst time in ten years. Here again O’Nan echoesa gerontological description of one stage ofaging: the Return, with its internal reconciliation,its service, and its sense of peace.
Schacter-Shalomi, Zalman, and Ronald S. Miller.(1995). From Age-ing to Sage-ing: A ProfoundNew Vision of Growing Older. NewYork:WarnerBooks.
Against a rich background of history andpsychology, From Age-ing to Sage-ing tracesattitudes toward old age in the past and thenturns to ways in which modern retirees canfind meaning, purpose, and a sense ofcompletion in their later years. The bookaddresses a mixed audience, primarily eldersand middle age adults planning foruncertainties of retirement, but health careprofessionals, nursing home operators, andfamily caregivers can also learn from it. RabbiZalman asserts that instead of producingdepression and isolation, aging can beaccompanied by positive effects when theaging person accepts the retirement years asa time for contemplatively “harvesting” thepast, enjoying the present, and deepening asense of oneness with the human and naturalworld.
AgingTopics
Sheehan S.J., RP Myles. (2012, September).Aging Gracefully, a production of Catholic TV.http://www.sjnen.org/news-and-events/aging-gracefully-catholictv-series-by-fr-myles-sheehan
Topics include: 1) Spirituality andWellness ofAging, 2) Fear, Health Issues & PsychologicalIssues of Aging, 3) Talking toYour Physician, 4)The Gifts of Aging, 5) Thinking and Preparingfor Death.
Adelson, Rachel. (2013). Staying Power: Age-proof Your Home for Comfort, Safety and Style.Thornhill, Ontario: SageTree Publishing.
Callone, Pat. (2007). Alzheimer’s Disease: TheDignityWithin: A Handbook for Caregivers,Family and Friends. Demos Medical Publishing,LLC.
Morris, Virginia. (2004). How to Care for AgingParents (3rd ed.) NewYork, NY:Workman.
Radin, L., Radin, G. (2007).What If It’s NotAlzheimer’s? Frontotemporal Dementia.Amherst, NewYork: Prometheus Books.
Excellent resource on cognitive declineassociated with executive function tasks andmemory.
Online Resources on Aging
Alzheimer’s Disease and Related Dementias:Learn about signs and symptoms, stages,diagnosis, research progress, treatment and careof Alzheimer’s disease and dementia.www.alz.org
The Family Caregiver Alliance-National Centeron Caregiving. San Francisco.http://www.caregiver.org/Fact-Sheets
Fact sheets on aging, caregiving, etc.
General Resources
CDC. Center for Disease Control andPrevention. Atlanta, GA.Online resource for creditable resources onpublic health topics. Immunizations schedules,foreign travel vaccines, health promotion, andeducation, etc.http://www.cdc.gov/
National Library of Medicine: Medline Plus.8600 Rockville Pike, Bethesda, MD.Online resource for consumer health information,including videos, illustration, and druginformation. Search “Health Topics.”http://www.nlm.nih.gov/medlineplus
NRRO: National Religious RetirementOrganizationMultiple resources on aging from the UnitedStates Conference of Catholic Bishops.http://www.usccb.org/about/national-religious-retirement-office/
JESUIT HEALTH CARE HANDBOOK20
SECTION III Resources & Bibliography
Elders & DrivingWebsites
http://www.seniordrivers.org - AutomobileAssociation of America contains brochures,driving tips for seniors, video clips, and otherhelpful ideas from AAA.
http://www.nhtsa.dot.gov/people/injury/olddrive -National HighwayTraffic SafetyAdministration: Research studies, booklets andmaterials, including Driving Safely while AgingGracefully.
http://www.aarp.org/55alive - AARP 55 AliveMature Driving Site to locate AARP DriverSafety education classes in your area; take theonline Driver Safety course; other information onolder drivers.
http://www.aging-parents-and-elder-care.com/Pages/Checklists/Elderly_Drivers.html -An article on driving by elders, which includes achecklist of telltale signs of decline in drivingabilities; also includes ways for elder drivers toadjust to changing abilities.
http://driving.phhp.ufl.edu/ -Website for theUniversity of Florida National Older DriverResearch andTraining Center.Their focus is onhelping older drivers to maintain their safe drivingability as long as possible.
http://www.beverlyfoundation.org - The BeverlyFoundation’s mission is to foster new ideas andoptions to enhance mobility and transportationfor today's and tomorrow's older population. Thefoundation pursues this mission through aspecialized series of research programs,community demonstrations, and technicalassistance products.
http://www.aota.org/olderdriver - The Older DriverSite of the American Occupational TherapyAssociation includes a link to find a drivingspecialist or program.
http://www.ama-assn.org//ama/pub/news/news/older-driver-safety.page- Website of the American MedicalAssociation on Older Driver Safety.
www.seniordriving.aaa.com - Automobile Club ofAmerica
Disease-relatedWebsites
Adult Immunization Recommendations:http://www.cdc.gov/vaccines
Agency for Healthcare Research and Quality:www.guidelines.gov
Alcoholics Anonymous:www.aa.org
Al-Anon Family Groups:www.al-anon.org
American Cancer Society:www.cancer.org
American Diabetes Association:www.diabetes.org
American Heart Association:www.americanheart.org
American Lung Association:www.lungusa.org
Parkinson’s Disease Association:www.parkinson.org
U.S. Preventive ServicesTask Force:www.uspreventiveservicestaskforce.org
JESUIT HEALTH CARE HANDBOOK 21
SECTION III Resources & Bibliography

IV. Practical Guidelines for the HealthCare of Jesuits
4.1Taking ownership of one’s own health care
Introduction
The Society of Jesus in the United Statessupports the promotion of health in each of itsmembers in accordance with the teachings of St.Ignatius as found in the Exercises and theConstitutions. It is through the maintenance ofoptimum physical, mental, and spiritual healthand well-being that each Jesuit can best becapable of effective apostolic ministry and be inthe position to be missioned.
Each Jesuit has the primary responsibility formaintaining his own health and meets annuallywith the PAHC or the local health carecoordinator. This affords an opportunity for healthpromotion and review of current health status.
General guidelines for taking responsibility forhealth care:
1. Each Jesuit should have a primary physician,dentist, or specialist as required who has accessto his health history and to whom he can go forcomprehensive health needs.
If you are in need of a new primary physician,dentist, or other specialist(s), Jesuits should askeither the superior or PAHC for professionalreferrals while remaining within the network ofapproved providers.
2. Any non-emergency surgery (necessary butnot immediately so) should be discussed withthe local superior or the superior who has thefinancial responsibility for health care needs.
3. Long-term treatments such as physicaltherapy, experimental treatments, extendedpsychiatric treatment, or experimental diagnostictesting should be discussed with your superior.
4. “Second opinions” may be initiated by Jesuitsonly after consultation with the local superior.Physician-requested second opinions may bemade without further consultation with the localsuperior or the health care representative of the
Provincial.
The following preventive healthrecommendations, which are age specific, shouldbe used as guidelines to optimize the health ofthe Jesuit.
In addition, please be aware of the immunizationguide from CDC. Their adult immunizationrecommendations can be found athttp://www.cdc.gov/vaccines
Preventive health recommendations(Ages 19 – 39)
Schedule: Every 1 – 3 years
Leading causes of death and future chronicillness
• Motor vehicle crashes related to alcohol andcell phone use
• Heart Disease• Obesity• Injuries (non-motor vehicle)• Suicide
Screening
• Diet behavior counseling – BMI 18-25, lifestylechoices, and stress management
• Physical activity• Tobacco/alcohol/drug use• Depression screening• Sexual practices• Use a helmet for some physical activities likebiking
Physical exam
• Height and weight• Blood pressure: 120/80 average – lower isbetter
• Complete skin exam• Clinical testicular exam• Family history of heart disease or diabetes:Lipid panel, glucose A1C
Preventive care
• Immunizations• Influenza (Flu) Annual
JESUIT HEALTH CARE HANDBOOK22
SECTION IV Practical Guidelines for the Health Care of Jesuits

• TD/Tdap: GiveTdap vaccine (adult booster)once. Td booster every 10 years.
• Measles, mumps, rubella (MMR): 1 – 2 doses• Meningococcal: 1 or more doses• Hepatitis A: 2 doses strongly recommendeddue to ministry assignments
• Hepatitis B: 2 doses strongly recommendeddue to ministry assignments
• HPV (Gardasil for men): speak with yourphysician
• Dental services every 6 months/yearly• Eye exam• Hearing screening (persons exposed toexcessive noise)
• TB skin screening: risk related to unexpectedexposure at homeless shelters, correctionalinstitutions, nursing homes, substance abusefacilities, and immigrants/refugees centers
Remain alert for:
• Depression symptoms, poor sleep patterns,isolation
• Abnormal bereavement• Sexual integration• Suicide risk• Malignant skin lesions
Counseling: “Healthy Eating and Living”
• Dietary choices: (1) 5 servings of fruit andvegetables a day, more is better; (2) Animalmeat – 4-6 oz. daily; (3) Stay alert to our fastfood society, especially saturated fats andprocessed foods.
• Daily exercise of at least 30-45 minutes a day.Walking is free, no excuses.
• Stress management skills: Yoga, meditation,group support, cognitive therapy for anxiety,days off, annual vacation, and retreat. Buildfriendships and use a spiritual director/guide.
Preventive health recommendations(Ages 40 – 64)
Schedule: Every 1 – 2 years
Leading causes of death and chronic illness
• Heart Disease• Cerebrovascular disease – stroke• Obstructive lung disease
• Cancer: colorectal cancer and lung cancer• Pneumonia/Influenza
Screening
• Diet behavior and weight management: BMIunder 27
• Physical activity: low impact exercise, corestrength, and cardio exercise, 6 hrs./week
• Alcohol/tobacco• Prescription drug abuse• Travel-related illness• Ergonomics of work environment• Sleep apnea• Safety helmets
Physical exam
• Height and weight• Blood pressure: 120/80 or lower• Blood test: comprehensive metabolic profile,lipid panel, TSH, B12, VitD3
• Complete skin exam• PSA: age 50 for white males, 45 for African-Americans (www.guideline.gov)
• Review family history for heart disease,especially if incident prior to age 50.
Preventive care
• Over 45 yrs.: ask MD about daily low dose ofaspirin
• Immunizations: Influenza: yearly seasonalvaccine
• Zoster (Shingles) age 60+ (Especially if youhave already had an incident of shingles)
• Tdap: one booster shot as an adult;recommend aTd-tetatnus/diphterian every 10years
• TB skin screening: related to ministryexposures and travel
• Dental services every 6 months• Eye exam• Hearing screening• Colonoscopy screening: at age 50 and every 10years to age 70
Remain alert for:
• Prescription drugs and driving impairments• Mental health treatment and aftercare needs• Midlife vocational/occupational unrest
JESUIT HEALTH CARE HANDBOOK 23
SECTION IV Practical Guidelines for the Health Care of Jesuits

• Depression/abnormal bereavement
Counseling: “Healthy Eating and Living”
• Diet and exercise: Time to take seriousinventory of health choices and potential risk forfuture conditions that could limit one’savailability for future ministry assignments.Seek assistance from a physician or lifecoach/personal trainer.
• Relaxation and hobbies• Annual vacation and retreat/Spiritual direction
Preventive health recommendations(Ages 65 and older)
Schedule: Every 3 – 6 months depending onmedical history
Leading causes of death and chronic illness
• Heart Disease, cerebrovascular disease –stroke
• Lung cancer, obstructive lung disease• Cancer: Colorectal cancer, bladder cancer• Pneumonia/influenza
Screening
• Diet behavior and weight management: BMIunder 27 (over 30 is a diabetes risk)
• Physical activity: consider a personal trainer orlocal program to guide you in age appropriateactivities, cardio exercise, core strengthening,gait, and balance. Goal: 30–45 minutes/day, 5times a week.
• Alcohol/tobacco: limiting alcohol consumptionand tobacco cessation programs
• Prescription drug overuse: request a completeprescription review annually with primarydoctor.
• Driving assessment per Province guidelines• Cognitive changes: appropriate screening fordepression vs. memory disorders
• Functional status at home/work environment
Physical Exam
• Height and weight• Blood pressure: 135/85 or lower (physicianguidelines)
• Blood test: comprehensive metabolic profile,
lipid panel, TSH, B12, VitD3, PSA• Complete skin exam• Hearing evaluation• Bone density screening• Electrocardiogram• Urology: PSA and prostate care
Preventive Care
• Colonoscopy every 10 years• Immunizations: Pneumonia, Shingles (Zoster),Tetanus/diphtheria, annual flu vaccine
• TB skin screening: related to ministryexposures and travel
• Hearing evaluation and interventions• Dental services every 6 months• Glaucoma testing by an eye specialist
Remain alert for:
• Changes in cognitive function• Medications that increase risk of falls• Signs of depression and personal neglect• Abnormal bereavement• Peripheral arterial disease• Malignant skin lesions• Tooth decay, loose teeth, and gingivitis• Injury prevention: use of safety belts, smokedetectors, heating pads
• Fall prevention related to rugs and extensioncords. Clothing that is oversized and worn outshoes.
Counseling: “Healthy Eating and Living”
• Diet and exercise: Be mindful of caloriebalance, avoid fast food, high sugar dietaryintake. Breakfast is important each day.Adequate water intake – 6 glasses/day. Ageappropriate exercise program. Tai Chi or Yogafor balance and strength.
• Engage in hobbies and relaxation• Annual vacation and retreat. Spiritual directorand Jesuit delegate for Senior Formation.
4.2 Interactions with healthcare professionals
Superiors may find themselves at a loss in theirinteractions with health care professionals. Theproblems can include what sort of doctors tocontact for problems in the community, dealing
JESUIT HEALTH CARE HANDBOOK24
SECTION IV Practical Guidelines for the Health Care of Jesuits

with doctors and nurses in emergency situations,and negotiating a long-term relationship betweenhealth care providers and the community.Together with the assistance of the PAHC, strongliaisons can be developed.
In choosing a doctor for the community orhelping men find an individual physician, onedoes well to choose either a family practitioner ora general internist. That individual can then serveas the gatekeeper for more specialized careshould it be needed. Men should be discouragedfrom seeing a variety of specialists on their own.
Many Jesuits will have an old friend or studentserve as their physician. This is not a goodpractice. Frequently the older Jesuit will not bereceiving the professional care that he requires,but rather using this doctor as an excuse for nothaving comprehensive medical care.We are allfamiliar with the Jesuit who refers to an individualas his physician but it turns out that he only callshim to fill a prescription and not to seek acomprehensive medical evaluation or thepreventive care he needs. Naturally, many Jesuitswill turn to former students, or superiors may askalumni or benefactors to our institutions toprovide medical care for the community. In manycases this works well. There is, however, thepotential for an unhappy relationship on bothsides with the physician reluctant to send a bill, illat ease in confronting unhealthy behaviors, notperforming full examinations out of a misplacedfear of modesty, and in general not getting thegood care that one would from a regularphysician who is not “a friend.” Professionalrelationships work best when they are conductedprofessionally and not on the presumption offriendship or obligation.
How can superiors find good doctors for thecommunity?
One option is to ask the respected members ofthe community from whom they seek for theirmedical care. In other situations, superiors maywish to consult friends and colleagues as to whois good. Some special concerns involveaccessing geriatric or psychiatric care. A goodinternist or family practitioner may well be able tomeet the needs of an aging community. Inchoosing a physician, a superior may wish to ask
if a physician has a certificate of addedqualification in geriatric medicine. Another optionis to review the network of physicians that areapproved by your insurance carrier.In finding psychiatrists, one would do well toseek the advice of an internist or familypractitioner who provides care for Jesuits and askher or him for a candid opinion on who wouldbest meet the needs of Jesuits in yourcommunity. A problem for health careprofessionals in dealing with Jesuits is they donot understand our governance. The Americanhealth care system focuses on the patient, andphysicians are reluctant to speak to other peopleabout the health of a particular patient. Manydoctors would not know what to do with a callfrom Father Superior or Father Minister becausethey do not understand what Jesuits are about.The issue is a delicate one and raises questionsabout a superior’s style within the community.Men should be trusted to have a confidentialrelationship with their physician. It probably isunethical for a physician to speak about a man’shealth with a superior unless the man has givenclear permission for that conversation. HIPAAregulations, discussed previously, can make thiseven more problematic. This can becomeparticularly difficult if a man is ill and confused,and the superior has a real need to know so thatthe man can be helped in the community. Menshould be encouraged to speak to their doctorabout our governance system. Jesuits shoulddiscuss with their physician their advancedirective for health care and make sure that sheor he has a copy on file.
Emergency situations
When a Jesuit is admitted to a hospital,especially in an emergency situation, a superioror his designate must move quickly to make itclear to those providing care for the Jesuit thathe is the one to be contacted for decisions if theman himself cannot participate in the decisions.Obviously the physicians will ask the ill Jesuitwhat he wants, but in many situations the Jesuitmay be too sick to answer. Procedures to follow:1. Make certain that a copy of the man’s advancedirective is placed on the chart and that thenurses and doctors know about it. 2. Make surethat the Jesuit superior is listed as the next of kinon the admitting information. 3. Once the man
JESUIT HEALTH CARE HANDBOOK 25
SECTION IV Practical Guidelines for the Health Care of Jesuits

goes from the emergency room to the hospitalroom, speak with the secretary on the floor andmake sure that the records state that the personto be notified in an emergency is the superior orhis designate. (Also make certain that the phonenumber given to the hospital is one where youcan be reached and not the switchboard thatcloses at 8:00 p.m.) NOTE: Some communitieshave copies of the advance directives and theman’s medical history by the car sign-out sheetsin a community so that this information is readilyavailable when an emergency situation occursand the information is needed.
4.3 Specific steps to take in emergencysituations
1. Planning for emergencies before theyhappen.
Community members should be encouraged toreceive certification in basic life support from theAmerican Red Cross. These classes provideinstruction in basic life support for individualswho are choking, experiencing respiratorydistress, or who have had a cardiac arrest. Theseclasses are either free or have a minimaldonation. One can find out more about theseclasses by calling the local branch of theAmerican Red Cross. Alternately your localhospital probably provides training andcertification in basic life support. Although itmight seem obvious, having members of thecommunity trained in maintaining an airway,restoring breathing, and assisting circulation canhelp an emergency have a positive outcomerather than become a tragedy. Evaluate theavailability or purchase of an AED (AutomaticExternal Defibrillator).
2. Dealing with the emergency.
Some emergencies are obvious and it is clearwhat should be done. In the case of someonewho collapses, a person who is suffering a heartattack, or a person who falls with injuries, theonly prudent course is to call 911 or the localemergency number and have the persontransported to the hospital by paramedics.
3. Recognizing the hidden emergency.
What might be harder is to recognize what trulyare emergency situations but may be hidden inthe general hustle and bustle of community life.Some examples: a sudden change in a man’smental status where he becomes confused,belligerent, or angry. It could be the only sign ofa serious life-threatening illness, such as aserious infection, a stroke, a heart attack, orsome other dire process.
New onset of chest pain requires immediateassessment, as many heart attacks can bepresent with relatively few symptoms. Rapidassessment is essential. The person who isdescribing chest pain or indigestion should betaken by ambulance to an emergency room forassessment. Obviously individuals with a knownmedical history of angina or stomach upset whohave been told by their physician to takemedications should seek medical attentionpromptly if symptoms increase in severity orfrequency. Falls and lack of consciousness arevery serious. Although people do occasionallysimply trip over a rug or lose their balance, oneneeds to have a high index of suspicion that, infact, a person has fallen as a consequence of lossof consciousness. Similarly individuals who faintor pass out may have a serious condition andrequire immediate assessment by a physician. Itis not appropriate after someone has “passedout” or had a serious fall to put them to bed andsee how they are in the morning. They may bedead. Occasionally many older persons willcomplain of difficulty with breathing. The possiblecauses for complaint are multiple, yet requireskilled assessment and should not be subject toself-diagnosis in treatment by our own members.Shortness of breath may be an indication ofasthma, a heart attack, heart failure, a blood clotto the lungs, pneumonia, another infection, or thepresence of other conditions that could have life-threatening consequences. It is impossible toprovide a list of all the potential problems thatcould occur in a community. The key, however, isnot to accept an approach that minimizessymptoms and avoids expert evaluation. Suddenchanges in the health status of individuals requireassessment and are not to be brushed under therug. You are always wise to call 911 first ratherthan wait and regret your procrastination.
JESUIT HEALTH CARE HANDBOOK26
SECTION IV Practical Guidelines for the Health Care of Jesuits

4.4 Communicable diseases
In the event that a community member has hadexposure to a diagnosed communicable disease,the superior will need to contact the PAHC forappropriate suggestions on how to managementthe infectious disease.
A few such diseases are listed below andextensive information can be found on the CDCweb site: www.cdc.gov
1) Tuberculosis2) Hepatitis A3) Hepatitis B4) Hepatitis C5) Influenza6) Norovirus7) Vancomycin resistant enterococcus (VRE)8) Methicillin-resistant Staphylococcus
aureus (MRSA)9) HIV/AIDS
Key recommendations for limited medicalsupplies in each community in dealing withcommunicable diseases should includedisposable gloves, alcohol-based hand rub, andface masks. Washing hands with soap and waterroutinely is always advisable.
Responsibility for routine cleaning anddisinfection of environmental surfaces should beassigned using a bleach disinfectant. Dispose oftrash in leak proof bags/containers.
4.5 Medical records
1. Community Medical Form.
An example of a possible basic medical form foryour community is located in the Appendix(Section 7.3).2. Updating Medical Records. Sincemost Jesuit Communities are not health carefacilities, only basic medical information isnecessary to have on file. Realizing that, what isimportant for a superior to know about individualJesuits residing in the community? Know theman’s main conditions, his allergies, and anyimportant highlights and main conditions in hismedical history, as well as the name of hisprimary physician.
The Provincial Assistants for Health Care (PAHC)have developed a standardized document thatcan be used by all communities. If there is aninfirmary in the community, then the health careprofessional and the appropriate staff shouldkeep up those records on the members of thehouse. If a person is being moved to a non-Jesuithealth care facility, it is strongly encouraged thatthe superior or PAHC facilitate communicationbetween the man’s primary doctor and theadmission coordinator at the health care facility.The superior is strongly encouraged to obtain atyped discharge summary to accompany thehospitalized Jesuit on his way to the nursingfacility.
When a Jesuit is being moved to a Jesuit-managed facility, similar documentation andtransfer information is critical. Please consultwith the PAHC for a checklist of dischargeinformation, diagnostic testing results, labs, andtherapy notes.
Organ Donation: One of the difficulties withJesuits for organ donation is that in much of, ifnot all of the United States, the person’s legalnext of kin, e.g., sister, brother, niece, etc., (notreligious superior) has the authority to grantpermission for donation. Given that many Jesuitshave expressed a preference for organ donation,they need to speak with their family as well astheir superior regarding their preference in theevent that in sudden death it may be difficult for asuperior to really do much to facilitate an organdonation. The double tragedy of a sudden death,especially in a younger person, is the loss ofmultiple organs that could provide life for manypeople, which makes this issue especiallyimportant for younger members of the Society.
Special Burial Requests: Men should be told tobring these to the attention of the superior inorder to avoid difficulties at the time of death.Often men who are suffering from a terminaldisease assemble detailed burial requests. Thisshould be seen as a way of getting some controlover the chaos of illness. As in many cases ofthis nature, pastoral care should dictate anyconversation about this.
Advance Directives: Advance directives aredocuments that provide for the health care of an
JESUIT HEALTH CARE HANDBOOK 27
SECTION IV Practical Guidelines for the Health Care of Jesuits

individual if he is not able to speak for himselfbecause of illness, accident, or some othercatastrophe. Advance directives can take multipleforms ranging from verbal statements to formaldocuments. In most states, however, the bestway for an individual to secure his wishes in theevent of serious illness is accomplished by thecompletion of a relatively simple form.Depending on the state, advance directives willeither consist of a living will format or theappointment of an individual to speak for theperson. This latter option can either be a durablepower of attorney for health care or a health careproxy. In many states, features of a living will anda proxy can be provided in the same document. Itis important not to confuse durable power ofattorney with power of attorney. The formerremains in effect if the person is incapable ofmaking medical decisions. The latter ceases toremain in effect just when you need it! It iscustomary for a Jesuit to designate the superiorto speak for them. If the superior is not chosen,it is imperative for the superior to know who theproxy is so that the individual can be locatedwhen a crisis occurs. It is best to avoid lengthyliving wills or various statements made in writingby the Jesuit, as these are often subject toconsiderable interpretations and confusion due tothe lack of clarity in the language or when theperson’s seemingly clear wish becomeshopelessly muddied. Especially to be avoided arevague documents such as a “Catholic LivingWill” or statements as “I desire to be treated inaccord with the teachings of the CatholicChurch.” Although such statements are laudable,they cause great confusion among physicians ofvery good will who wish to take care of theJesuit but lack training in what those statementsmean. It is also to be noted that themagisterium’s competence does not extend topurely medical decision making in the provisionof therapies in a specific medical condition.Superiors should consult their Province for formsthat are applicable in the state in which thecommunity lives. This will ensure that the rightdocument is being used. In Provinces with manystates, it is important that either different formsare provided for each state or a competentlawyer has drafted a document that will behonored in several jurisdictions. A final issue thatshould be decided on the Provincial level, andusually with legal counsel, is whether Jesuits can
simply designate the superior (rather than anamed individual) or his successor as the proxydecision maker. If that is not the case, amechanism in the community should beoperative to attend to this when the superior ischanged. The real issue with these documents isthat an individual Jesuit and his superior speakhonestly about what the man would want in theevent of a life-threatening illness. Thisconversation should take place in the context ofthe superior’s concern for the individual Jesuitand his desire to make sure that he receivesgood medical care. Also, this conversation is anopportunity to express the superior’s concernabout reasonable stewardship over medicalresources, avoiding unnecessary pain andsuffering, and the witness of Christian faith in theResurrection in a society where many do notbelieve in eternal life. This conversation may bemore crucial than any written form in that itprovides the superior (or some other proxy) withreal knowledge about what the man would wantif he cannot speak for himself. It is not theproxy’s job to make life and death decisions. It isthe proxy’s job to provide what he feels is themost likely response of the sick Jesuit in thissituation so that the doctor can make treatmentdecisions accordingly. Although thecommunication between proxy and Jesuit isessential, it is equally important that the Jesuit letthe physician know his wishes prior to a healthcare crisis. Such communication prior to a crisiscan guide the physician in his or her approach toan illness and provide for much better care thanwould be the case if the physician is uncertain,afraid of legal reprisals, and essentially “doingeverything” out of a misguided feeling that this isnecessary.
Community held medical records
As indicated above, a model form for brief recordkeeping purposes within your community can befound in the Appendix (Section 7.3). You may wishto add certain categories, but this one is probablysufficient for emergency situations.
Another option is to work with the ProvinceAssistant for Health Care. The Assistancy hasinvested in an electronic database containing thehealth care record for Jesuits in the U.S. Thisdatabase is HIPAA compliant and can only be
JESUIT HEALTH CARE HANDBOOK28
SECTION IV Practical Guidelines for the Health Care of Jesuits

accessed by authorized Province healthprofessionals. These records are encrypted andpassword protected. Page one of this form canbe printed for your emergency file use, and ablank copy of this can be found in the Appendix(Section 7.7).
Medical forms such as this should be completedand easily accessible during an emergency. Somecommunities keep a copy of each Jesuit’scompleted form in a sealed envelope in the samebinder as the car check-out sheets. This way the
information is accessible if a superior is notavailable at the time an emergency occurs.Obviously once the forms are returned, they areonce again sealed in a new envelope.
4.6 General principles for community recordkeeping
The following pages provide recommendationsconcerning the record keeping process/protocolfor the health care records on individual Jesuits.
JESUIT HEALTH CARE HANDBOOK 29
SECTION IV Practical Guidelines for the Health Care of Jesuits
Types of records Paper copy Computer Who has access For what purpose? Disposition
Medical (updatedafter medicalchange/ yearlyphysical)
Rector’s/supe-rior's/minister's of-fice (to beforwarded to anynew community forfiling)
If community hasa system for this
SuperiorProvince HealthCare Assistant orcoordinatorHospital/physician
Legal/ReferenceArchival decision atdeath
Advance DirectiveProvince Offices,Local Superior
No
SuperiorProvince HealthCare Assistant orcoordinatorProvince Office
Legal/ReferenceAccession toArchives at Death
Organ Donor/BodyDonor to Science
Local Community Yes
SuperiorProvince HealthCare Assistant orcoordinator
InformationAccession toArchives at Death
Special Burial Re-quests
Province Of-fices/Local Supe-rior (exists inwritten form)
Yes
Province OfficeLocal SuperiorIn certain Statesfamily and closefriends (.e.g,Texas)
InformationAccession toArchives at Death
Will (Original andCopy)
Finance Office ofProvince
No Province Treasurer Legal/Reference
Original must befiled in Office ofClerk of County inwhich Jesuit died.Copy Accession toArchives at Death
Death CertificateFinance Office ofProvince
No Province Treasurer Legal/ReferenceAccession toArchives at Death
It is recommended that all of these records should be retained permanently.
General principles for community record keeping
It is recommended that the following record keeping process be established for the health care recordson individual Jesuits:

4.7 Funeral preparations
Some superiors have reported experiencingdifficulties and discomfort before the tasks ofarranging a fellow Jesuit's funeral and dealingwith other concerns subsequent to his death.This is especially true when that Jesuit'sspecific wishes have not been reliablydetermined. The following generic checklist isoffered as an instrument for local adaptation asa means of addressing these concerns,minimizing ambiguities, and resolving questionsthat may arise after a Jesuit's death. Whatfollows on pp. 62 - 67 is a possible instrumentyou may wish to reproduce within yourcommunity. It is offered as a sampleworksheet; feel free to make your ownmodifications to suit the needs of yourparticular community. You might also checkwith your Province office to see whetheranother instrument is available.
Individual circumstances will, of course,suggest how this instrument, formatted as aquestionnaire, might best be employed: as astructured interview in fraternal dialoguebetween superior and subject, perhaps, and/oras a prayerful exercise in which a Jesuit mightengage in solitary reflection.
Sample Letter to Jesuits about FuneralPreparations
Dear Brothers: Peace to you
Death and disabling incapacity are not topics thatinvite easy reflection or conversation. Prompted,however, by the frequent experience ofambiguities generated by the absence ofdocumentation, my consultors and I are trying toestablish, for those individuals who wish tosupply one, a record of preferences and otherinformation that might otherwise be neglected oroverlooked at the time of your death. Thus, youare invited to review the following checklist,indicating your wishes in regard to these variousmatters.
Funeral preparations
Medical directives
1. Are Health Care Proxy and Durable Power ofAttorney for Health Care documents on filewith the local superior?
a. ☐Yesb. ☐ No
2.What directions, if any, are in place for:a. Organ donation:b. Donation of my body to science:
Memorial card
1. Do you wish the customary photograph ofyourself on the card?
a. If yes, where is there a photo availablefor such use?
b. If no, what would you prefer instead ofyour photo?
2. What text would you like to appear on thecard?
a. ☐ Suscipeb. ☐ Anima Christic. Scripture Passage:d. Other:
3. Other places (besides the usual houses of theProvince) to which I would like cards to be sent(e.g., persons listed in your address book, ifwe can find them):
4. The death notice and obituary will be sent tonewspapers in various cities. Please list thecity/cities to which the death notice andobituary should be sent.
a.b.c.d.
Wake
1. I would prefer the casket to be:☐ Closed☐ Open
JESUIT HEALTH CARE HANDBOOK30
SECTION IV Practical Guidelines for the Health Care of Jesuits

2. Any additional instructions (e.g., Scripturepassages to be used)
Funeral
1. Name of person you’d like to have preside atthe funeral Mass:
2. Name of pallbearers (if any)a.b.c.d.e.f.
3. Names of priests you’d like to haveconcelebrate, if they are available:
a.b.c.
4. Homilist (please indicate two or three choicesin order of preference)
a.b.c.
5. Music preferences – music you would stronglydesire to have or have a strong desire NOT tohave. Please be specific.
a.b.c.d.e.f.
6. Any specifics regarding the GeneralIntercessions?
7. Gift bearers (please indicate their names)?a.b.c.d.
8. Preference for Eucharistic Prayer:
9. Eulogist:
10. Any other issues:
Burial
1.What type of burial would you prefer?a. ☐Traditionalb. ☐ Cremation
2. Burial will, of course, be in one of our usualJesuit plots. I prefer that the burial be
a. ☐ where the death occursb. ☐ Elsewhere – please specify:c. ☐ I am indifferent regarding the place
of burial
Other
Please specify any other matters that need to beaddressed (e.g., flowers, needs of familymembers, etc.)
Matters relating to personal effects
1. Have you made a last will and testament orprepared any similar document that willfacilitate the final disposition of your effects?
a. ☐ Yes. If so, where is this to befound? ___________________ (Itwould be good for your localsuperior to have a copy of thisdocument)
b. ☐ No. Please consider creating such adocument.
2. If you do not care to be that formal, pleasetake the time to identify articles (books,papers, photographs, audio tapes, CDs, DVDs,etc.) which should not be discarded but shouldbe passed along to a specific person. Pleaseidentify that person in writing and alsospecify the exact location of these articles.
3. If there is a bank account (savings, checking,or other) under your name, please provide theinformation necessary to close the account.
i. Name of bank:ii. Name of account holder:iii. Account number:iv. Address of account holder:v. Other persons on this account:
i. Name of bank:ii. Name of account holder:
JESUIT HEALTH CARE HANDBOOK 31
SECTION IV Practical Guidelines for the Health Care of Jesuits

iii. Account number:iv. Address of account holder:v. Other persons on this account:
i. Name of bank:ii. Name of account holder:iii. Account number:iv. Address of account holder:v. Other persons on this account:
4. If you have a safe deposit box(es), pleaseprovide the following:
a. Name of location where the box(es)are held:
b. Where are the keys to the box(es):c. Other persons who have access to thebox(es):
5. If you have other materials in containers (e.g,suitcases, safes) with combination locks,please provide the combinations so that wecan retrieve the materials:
6. Please provide all user names and passwordson any electronic or Internet account (e.g.,Google, online banking, Netflix, Facebook,etc.):
7. Please provide the physical location of all creditcards/debit cards:
8. Please provide the following information foreach credit card or debit card account:
i. Name of bank/credit card company:ii. Name of account holder:iii. Account number:iv. Expiration date on card:v. Address of account holder:vi. Other persons on this account:
4.8Transitions
It is very difficult to give clear-cut criteria fortransition from an independent community to acommunity that provides more assistance, e.g., aProvince health care facility. Normally a move isconsidered when a person needs assistance in theactivities of daily living.These include the following:being able to move around from bed to chairwithout a problem, dressing oneself, using thetoilet, maintaining continence throughout the day,bathing, grooming, and feeding oneself.When a layperson has problems with these activities, he orshe needs either assistance at home or placementin a nursing facility.What about Jesuits? As anexample, an older Jesuit who was formerly doingquite well and then had a stroke now needs helpwith dressing. It makes no sense to send him tothe nursing community when a member of thecommunity can help him button his shirt andfastens his belt without great fuss.This is part ofthe ordinary care, which we owe each other.Another Jesuit, however, may have problems withmaking it to the bathroom, in dressing, showering,and falling frequently. In this case, provided theman has had a thorough evaluation by a physicianand these deficits cannot be remedied, then it isappropriate that he move to a community withassisted living or a nursing home. Issues like theseraise the question of transitions in Jesuitcommunities.There are a number of reasons why itmight be necessary for an aging Jesuit to leave acommunity that has been his home for many years.These transitions are never truly easy, but in manycases there are ways to think and plan that mayhelp both the man and the community during thetransition process.
For temporary assistance while a man is still in anactive community, Medicare Home Health Compare(www.medicare.gov/homehealthcompare/) is agood resource.
How should a superior approach the subjectof transitions?
1. Transition is a part of every Jesuit’s life, and it isnot part of our vocation to become rooted in aplace. In community meetings, superiors mightwish to emphasize this topic and provideopportunities for both younger and older
JESUIT HEALTH CARE HANDBOOK32
SECTION IV Practical Guidelines for the Health Care of Jesuits
Name of account User name Password

members to discuss transitions in their life. Inindividual conversations with older Jesuits thesuperior should ask open-ended questionssuch as: “What do you think the future holdsfor you? Have you thought about what youwant for the future?” Some Jesuits will likelyspontaneously discuss their fears and theirhopes for the future. Others may avoid thetopic or announce their plan to stay in aspecific community until they are carried out.Although there is no way to deal with everypossible problem, the superior should early onmove beyond the superficial and encourage theman to think about what transition will be likeand how when the time comes for thistransition, the superior will be most helpful forthis man. In some ways there will be anelement of preaching to the converted becauseit is likely that the man who thinks seriouslyabout his life and where God is calling him willhave both an easy transition and serve as anexample to the community. The cranky ordifficult Jesuit, or the Jesuit who simplyrefuses to look beyond the surface, willprobably have a difficult transition. There is littlethat the superior can do except provide aconscious effort for planning and providing acontext for transitions.
2. Discussions about transitions should be part ofall Jesuit life as they are something that we allexperience frequently. Men in a communityfor a long period of time should be challengedto consider their next step and urged to think,pray, and discuss with the superior theirhopes, fears, and expectations regarding thismove.
3. Difficulties in transitions can be eased if thosewho remain behind in a community make theeffort to keep in touch with the man who hasbeen moved. (How would you feel if youmoved and none of your friends called, wrote,or visited?)
Options in transitions
Skilled Nursing Care
Why does an older Jesuit have to move onsometimes?The most obvious reason is an
overwhelming illness that requires skilled nursingcare that can be found in some of our health carefacilities. As an example, the transition is veryhard for a Jesuit who has had a stroke, a heartattack, or a major surgery and cannot comehome.When an illness like this occurs suddenly,very little planning can be done. This transitionhappens to many older Americans. The best thatcan be said is that as Jesuits we are relativelyprivileged, for the most part, by having facilitieswhere we will be cared for by Jesuits and thosewho work with us in this health care ministry.
Assisted Living Community
Another more difficult transition is when a Jesuitsimply appears to be increasingly incapable ofindependent living. His capability to remain in thecommunity depends on three factors: (1) Theability of the community to provide safe andresponsible support 24/7; (2) The type of functionlimitations experienced by the older Jesuit; (3)Possible resources available to keep the man incommunity.
1. The ability of a community to provide safeand responsible care.
This is a particularly neuralgic issue becausetransitions will work well in a community wherethe older Jesuits are loved and cared for incontrast to communities that look at the care ofolder people as a potentially difficultresponsibility. In the former community atransition may not be easy, but there is a farbetter chance that it will be done well rather thanin the latter type. Younger Jesuits need toconsider aging apartheid that promotesseparation of Jesuits rather than a cura personalisthat is the tradition of the Society or the livedexperience of many middle-aged Americans thatstruggle to combine career and family as theyprovide care for aging parents. Transitions arebest when there is a place of hope to which aperson can move. Thus, it may be necessary tocreate a community for older members ofanother community because their collectiveinfirmities do truly limit the apostolic availabilityand potential of the few young men who areworking in a specific apostolate. In a case likethis, the new community should be one that
JESUIT HEALTH CARE HANDBOOK 33
SECTION IV Practical Guidelines for the Health Care of Jesuits

combines a physically attractive setting, a warmatmosphere, and an appropriate environment thatwill make it easy for the older man to maintainhis level of functional ability.
The other part in assisting older Jesuits withtransitions is that either health care communitiesor communities designed for older Jesuits shouldbe visited by younger Jesuits and not kept in acordon sanitaire situation.What will make anytransition easier is to make a man know thatthose with whom he has lived care for him andwill demonstrate that care by driving to visit himin his new community.
2. The type of function limitationsexperienced by the older Jesuit.
What indicates the need for a possible transferfor health care support?
1. Difficulties with hygiene that impact negativelyon the man and the community.
2. Irascible behavior that creates an unpleasantenvironment for other community members.
3. A gradual deterioration of function andbehavior that has received adequate medicalevaluation and is not chalked up to functions ofold age.
Probably the key is the individual’s ability to carefor himself in a manner that is safe and dignifiedand does not create an excessive difficulty forother generous community members. The kindsof problems that can happen include greatinstability in walking, frequent falls, bowel andbladder incontinence, inability to dress oneself,and inability to shower or bathe on a very regularbasis and take prescription medication accurately.Many of these problems may be hidden by anindividual out of fear that he will be forced tomove.
What is especially difficult is that earlyrecognition may reveal a treatable medicalproblem that can be reversed throughpreventative medicine. For those individualswhose growing infirmities do, however, clearlylimit the man’s ability to contribute to community
or truly have a negative impact on thecommunity, then the individual or individuals inquestion must be moved. It would be hoped thatthe community would see the man becomingfrail over time and have the good sense andinquire how he is doing, take him to the doctorand tell the doctor what is wrong, and try to gethim better. It is important that the superior not letthis slide. If he does not have the courage to talkabout these changes, then one can guaranteetension within the house and a difficult transition.
3. Possible resources available to keep theman in community.
Another issue in considering transitions is howmuch support should a community provide to aman who is failing. Everybody needs help fromtime to time and communities should be able togive a man some help with dressing, provide forassistance with transportation, and, in a charitablemanner, help with means of hygiene and personalcare. The difficulty facing a community is menwho are clearly holding on in a desperate effort toavoiding moving. A number of men can have anumber of needs that may not be big individuallybut collectively are too much for a community tobear. There is no way to establish a clear calculusfor when an individual is too much or thecommunity is overburdened. People need to behonest and caring, but critical of ageist attitudesand assumptions. At the same time, a communitymust realize that our apostolic communities arenot nursing homes. A superior who finds himselfburdened by these decisions might seek theguidance of either a physician with specialexpertise and qualification in geriatrics or a nursegeriatric practitioner who can come into thecommunity, perhaps share a meal or two in thecommunity setting, and gain a sense of who trulyseems to be failing. Specific assistance that maybe available to communities includeshomemaking and home health aide services thatcan be privately contracted or maybe, in somecases, reimbursed by Medicare. Such servicesinclude assistance with bathing, dressing, helpwith medications, and simple actions likeassistance with laundry and light housekeeping ina man’s room.You can find the services in yourarea by calling the local hospital, asking to speakwith the social work or social service department,
JESUIT HEALTH CARE HANDBOOK34
SECTION IV Practical Guidelines for the Health Care of Jesuits

and asking them to provide a list of home care orhome nursing organizations. Another option is tocall the visiting nurse association listed in yourphone book and ask for a listing of their services.A final note about the transition process, whichagain may prove difficult, but may help easetransitions: One should be critical of those Jesuitswho continually complain about older Jesuits andare too self-absorbed to participate in the care oftheir older brothers. One also needs to confrontan attitude that will occasionally be found in anolder Jesuit that the community is his, and that hehas the license to continually criticize the Church,the apostolate, the community, and other Jesuits,and that he is not accountable to normal Jesuitgovernance. Unfortunately there will be difficultcases in which the main issue is control and afight over power in a man who is unwilling torecognize that he is no longer capable of livingindependently or that his behavior poisons thecommunity. Regrettably, in such situations, thesuperior, perhaps with the help of the Provincial,has to exercise the authority of his office in whatmight seem to be a heavy-handed manner.
N.B. For some communities and Provinces, if theman’s health care needs cannot be met in theProvince-supported facility the transition to a non-Jesuit facility is a reasonable option. Thisconsideration may be due to psychological andphysical needs beyond the scope of care at theProvince health care facility. Consultation withthe PAHC is strongly recommended.
4.9 Personal belongings
Jesuits transitioning and their personalbelongings.
It can be difficult when Jesuits leave acommunity where they have lived for many yearsto go to another community or health care facilityand they must reconcile the need to leave somebelongings behind. Although there is no reasonwhy a Jesuit cannot bring a modest amount ofpersonal items to the health care facility,extensive personal libraries, knick knacks, andother clutter sometimes cannot make the movewith the man. Another problem is that someJesuits are collectors of newspapers andmagazines. Unless these are of some particular
value or unusual magazines, then the man willneed to discard them. On occasion one can bestruck by the starkness of the rooms of some ofour men in our health care facilities. This mayreflect the austerity of their lives, or it may be asign that no one took the trouble to make surethat the man had those few belongings that areimportant in his new setting. When a manmoves to a new community, there should becoordination with the new superior as to whatconstitutes a reasonable amount of personalbelongs in this new setting. Especially importantwould be photographs, picture albums, andperhaps other cherished mementos.
4.10 How to make older men feel valued incommunity
Jesuit superiors face the challenge of making allin their care feel appreciated and valued. This canbe a challenge with some men! As men age theymay have particular vulnerability to feeling thatthey are unimportant, not valued, andapostolically worthless. There is no magic way tocounter this attitude except the ongoing care andconcern of a sympathetic superior who is willingto listen, encourage, and, from time to time, befirm with older Jesuits.
What are some practical suggestions?
If the community is not very large, the superiorshould make a point on occasion of taking anolder man out to lunch or for some outing wherehe can talk and have a pleasant time. This socialencounter may lead to more real exchange ofinformation than would be the case with a formalaccount of conscience where an older Jesuit mayhide his feelings of sadness under the cloak oftraditional religious language. Another thing for asuperior to do is to ask older men about theirhobbies, encourage them in the pursuit of thesehobbies or to take one up, and to provide themen in question with reasonable financialsupport. A third possibility is to visit the manwhere he lives, i.e., in his room. Take a look at thesurroundings or furnishings for their comfort andsafety. See what mementos and pictures theman has and engage him in conversation aboutthese memories. The superior can also ask theentire community to take part in caring for older
JESUIT HEALTH CARE HANDBOOK 35
SECTION IV Practical Guidelines for the Health Care of Jesuits

men. Some of the practical items just suggestedcan be done by any Jesuit with a heart. As anexample, if you notice one of the older men isnot dressing well or looking a bit shabby, suggestto one of the younger men to take him shoppingand give him some money to outfit the older manin an appropriate manner. The particular outingdoes not matter so long as the older Jesuit has asense that someone cares that he is alive. Oldermen should be encouraged to attend communitysocials and especially liturgical functions. All toooften some older men will celebrate a privatemass early in the morning and then feel excusedfrom the community celebration late in theafternoon. Tell him he is a valued member of thecommunity and that in addition to his privatemass, he belongs in prayer with his brotherseven if he does not wish to concelebrate at thattime. Community meetings can often be anawkward time with younger men more facile indiscussing feelings and emotions whereas oldermen can feel embarrassed or simply confused bytopics like intimacy, sexuality and ministry,appropriate relations with lay people, etc. Notevery community meeting need be an exercise inself-revelation. Instead, a meeting might focus ona topic in liturgy or Scripture or history or travelthat does not present obvious possibilities fordivision and could be enjoyed by all. Men whoare eating at meals that minimize their time withthe community are Jesuits who may be feelinglonely and otherwise disturbed. The superiorshould discus with the man the behaviors henotes and ask what is going on. For other Jesuitsloneliness is a persistent feeling, despite theirefforts to throw themselves into work andcommunity. It can be a trial of one’s vocation thata particular Jesuit is lonely because he is awayfrom good friends, family, and other connectionsthat give support to his life. Helping members ofa community through this transition time requiresthat other members of the community reach outand notice that the other person is there andefforts should be made to make him feel wanted.This need not be elaborate, but involves simpleand repeated offers to share a meal, go to amovie, share a walk, etc.With older men as theyretire and physical infirmities multiply, lack ofcontact with the surrounding world and loss ofpeers because of death and illness can create asituation where loneliness is a clear andreasonable response. Again, probably the best
way to help in situations like these is to keepone’s eyes open, notice them, and ask the manhow he is doing, if is he lonely, and what he orother community members can do to help withthis loneliness. Many Jesuits have created abarrier around themselves to privatize their life incommunity. These barriers should gently butfirmly be knocked down so that these mencannot retreat into intractable loneliness anddepression.
4.11 Spirituality and aging in community
Ignatius’ vision of people created to praise,reverence, and serve our Lord is especiallyimportant during the later stages of life in theSociety. Since much of our spiritual life isprivatized, little can be said here beyond a fewpractical suggestions. This presupposes dailyMass and regular structured community spiritualexercises.
1. Ask them what religious practices areimportant to them and try to provide thesepractices. Although benediction may not be theform for most of the community, do realize thatthis may have been an important part of thespirituality of older Jesuits.
2. Try to provide regularized options for theSacrament of Reconciliation, etc.
3. Continue to stock the house library with goodreligious reading material. It may be helpful tosurvey your house as to the desires of yourmen. If biographies of the saints are importantto many in your house, focus on that as anarea of spiritual reading that needsaugmentation.
4. St. Ignatius wished that each house have agarden for the sake of reflection. Try to keepyour garden up to some standard ofpleasantness and provide seating forcommunity members.
5. Encourage annual retreats and provide thetransportation an older man needs to a placeconducive to his annual reflection and renewal.Some older men opt for a “house retreat” soas not to appear a burden to the superior or
JESUIT HEALTH CARE HANDBOOK36
SECTION IV Practical Guidelines for the Health Care of Jesuits

put the community out because of a mobilityproblem.
6. Encourage men to exercise their priestlysacramental life in a parish setting or otherreligious context.
7. Have spirituality as a topic for a communitymeeting, though be careful not to focus on thisas a sharing of emotions, which can confusemany of the elderly not used to communicatingin this way.
8.Organize some lectures on a topic of Jesuithistory, Jesuit spirituality, or theology.
9.Encourage growth in companionship amongcommunity members and use creative meansto evoke a sense of “friends in the Lord.”
10. Call on the elderly to speak to the communityon parts of the heritage of the Society thatcome from the time they entered.
11. Organize times for common prayer for thosewho prefer it.
4.12 Loneliness
This topic cannot be addressed in anycomprehensive form.What can be said issomething about how to notice this internalpsychological state when it surfaces in yourcommunity. Some of this topic has been touchedon in the discussion of transitions, personalbelongings, hobbies, and making older men feelvalued in community. Loneliness often coexistswith depression and one should have a highindex of suspicion that the man who iswithdrawn and lonely is suffering from a majordepressive illness and needs help and perhapsmedication. There are other situations when menrightly or wrongly feel themselves alone; theirJesuit brothers can ameliorate that. Among anyJesuits, individuals who seem reclusive, avoidcommunity gatherings, spend excessive amountsof time in their rooms and develop a style ofeating at meals that minimizes their time with thecommunity are Jesuits who may be feeling lonelyor otherwise disturbed. The superior shoulddiscuss with the man the behaviors he notes andask what is going on. For other Jesuits
loneliness is a persistent feeling, despite theirefforts to throw themselves into work andcommunity. It can be a trial of one’s vocation thata particular Jesuit is lonely because he is awayfrom good friends, family, and other connectionsthat give support to his life. Helping members ofa community through this transition time requiresthat other members of the community reach outand notice that the other person is there andefforts should be made to make him feel wanted.This need not be elaborate, but involves simpleand repeated offers to share a meal, go to amovie, share a walk, etc.
With older men as they retire and physicalinfirmities multiply, lack of contact with thesurrounding world and loss of peers because ofdeath and illness can create a situation whereloneliness is a clear and reasonable response.Again, probably the best way to help in situationslike these is to keep one’s eyes open, noticethem, and ask the man how he is doing, if he islonely, and what can he or other communitymembers do to help them with their loneliness.Many Jesuits have created a barrier aroundthemselves to privatize their life in community.These barriers should gently but firmly beknocked down so that these men cannot retreatinto intractable loneliness and depression.
4.13Ways to recognize depression
Although some individuals may be chronicallydepressed and down in the dumps, truedepression represents an observable change inthe behavior of most people. Recognizing thatmay sometimes be very easy. An individual whohas previously been active, friendly, and a goodcommunity member suddenly becomeswithdrawn and moody and avoids people in thecommunity. He also has difficulties with workand outside friendships. Depression may wellbe the cause. Occasionally depression is moresubtle, and there are a variety of symptoms thatmay be helpful in recognizing depression. Hereis a list of some of the more commonsymptoms:
• A change in sleep patterns, frequentlymanifested by early morning awakening with aninability to fall asleep again;
JESUIT HEALTH CARE HANDBOOK 37
SECTION IV Practical Guidelines for the Health Care of Jesuits

• Lack of interest in normal activities, work,friendships;
• Anger;• Persistent guilty ruminative thoughts, or as maybe the case among Jesuits, severe scruplesand persistent “desolation”;
• Lack of energy, feelings of persistent fatigue,unable to do regular duties because of thisfatigue;
• Changes in concentration, which may manifestas memory loss, mild confusion, and evenamong older men as to be thought of asAlzheimer’s disease or other dementingillnesses;
• Changes in appetite, weight loss or gain maybe seen;
• Abuse or overuse of alcohol to medicate lonelyfeelings;
• The signs of psychomotor slowing are oftenseen with depression and include: listlessappearance and a shuffling gait. (Someindividuals rather than having psychomotorslowing will exhibit psychomotor agitation withpacing, hand wringing, weeping, and otherhigh-energy agitating manifestations.)
Depression may well be the common factorbehind many problems seen in community life.Reclusive behavior, individuals who act strangely,and people who seem angry and bitter all of thetime could well have a depressive component totheir illness. Superiors should have access to agood psychiatrist for consultation (and forthemselves) and advice on community members.Superiors should have a low threshold to contactthe primary care physician when depression issuspected. He or she may institute treatment orrefer the man to a psychiatrist. Always takeseriously any suicidal desires or behaviors ofcommunity members. This does require anemergency assessment through the emergencyroom of your local hospital.
4.14 Utilization of local resources
Each superior is strongly encouraged to haveregular conversations with the PAHC and thelocal health care coordinator. By workingtogether, these groups can discuss and planoptions to meet the specific needs of yourcommunity. A variety of resources may be
accessible depending on the town or city wherethe community lives. One way to start is to ask adoctor or nurse with whom one has a goodrelationship and see if he or she can make areferral to an appropriate agency. Anotherresource, which can be invaluable, is to contactthe local social work department of your localhospital and make an appointment with one ofthe social workers, recognizing that you willprobably need to pay for their time and to ask heror him for advice for referrals for neededresources. A third option is to look in the phonebook and find a council on aging. Many localareas have these councils, which serve as aclearing house for information for resources andactivities for older individuals. A fourth optionwould be to call the local visiting nurseassociation and to ask for advice on these issues.They will likely be able to give you some goodleads. Consider a small high school communitywhere an older man may be going blind and isalone for a significant part of the day. Contactinga social worker can lead to a referral for TalkingBooks, which are provided free of charge for thevisually disabled, as well as applications for otherspecial services that are available in many states.Other problems in living experienced bycommunity members may also have localcommunity resources available to help them. Thekey to finding these resources is the willingnessto spend some time networking and lookingbeneath the surface at what is in many cities andtowns a fairly extensive network of socialservices. Likewise, many of the older men in thecommunity who feel they have nothing to do andlittle work can be valuable resources by agreeingto do volunteer help in a variety of tasks. Look inyour phone book or you can call RSVP (RetiredSenior Volunteer Programs). They will provide alist of volunteer activities that desperately needthe skills and services of many Jesuits. OlderJesuits may also help you to surfaceopportunities and services in your area, thusgiving them a sense of investment andresponsibility in their own care.
4.15 Families and friends of Jesuits
The relationship between a Jesuit’s family oforigin, their friends, and his Jesuit brothers canbe summarized by the following statement:
JESUIT HEALTH CARE HANDBOOK38
SECTION IV Practical Guidelines for the Health Care of Jesuits

It is the conviction that life as a religiouscontinues to have meaning and value to theJesuit. The decision to join the Society of Jesuswas a free choice and is one that has beenconstantly reaffirmed over the years by thedecision to continue living the religious life in theSociety of Jesus. It is expected that choicesmade by a Jesuit and the decisions made by aJesuit’s religious superiors should be honoredand upheld. A third party may be consulted butshould not be looked to for final decisionsregarding a Jesuit. The Society of Jesus takesvery seriously its responsibility for and role inproviding cura personalis for its members.
Jesuits are expected to inform and consult afamily of origin during an illness. But, the Societyof Jesus has final responsibility for decisionsabout a Jesuit’s health, and the hope and desireis that family and friends will honor decisionswithout interference. This desire in no waymanifests a lack of love for family and friends, butit does recognize the desire of a Jesuit to entrustdecisions about his care to the Society of Jesus.It is expected that the usual presumptions foundin civil law that look to the family for decisionsshould be put aside in favor of the wishes of theSociety of Jesus.
How can a Superior communicate well withfriends and family?
The best way to communicate well with a familyis to create an ongoing relationship with families.It may be worthwhile to consider an annualgathering where families are especially welcome.The community should welcome families,recognizing the occasional need to set someboundaries.
How to deal with challenges?
When a superior is confronted by a situation thatappears to be difficult either for the superiorhimself, the Jesuit, or the community, it is wiseto obtain some professional advice. These typesof problems frequently involve long-standingpsychological issues in the family or friends’circle. An excellent resource can be a socialworker skilled in family therapy. The ProvincialAssistant for Health Care can also be an advocatefor you.
4.16 Overview on professional counseling andpsychotherapy
In our life together, we Jesuits provide mutualsupport, encouragement, and love throughcommunity life and friendship, spiritual direction,community prayer, retreats, and efforts towardpersonal and theological renewal. Yet we knowwell that these ordinary means of growth andhealing are sometimes not sufficient to helpsome of our men to continue their developmentas persons and as Jesuits.
When stress, anxiety, or depression begin toburden or incapacitate, a Jesuit should feelinvited, in consultation with his superior, to seekthe aid of trained counselors.While our culturesometimes views such assistance as a sign ofweakness, let us enjoy a quiet confidence basedon the experience of many of our men who havegained useful insight into their own situations andburdens through the help received from a trainedtherapist. Counseling is not a panacea, but it isone more gift from God to us in our journey tohim.
Occasionally a man may not realize that hisbehavior is manifesting extreme tension oranxiety. It is difficult for many of us to admit thatwe need help, not only to increase our apostoliceffectiveness but also to remove the obstaclesblocking our own growth. Knowledgeable andtrustworthy Jesuits with whom we live and workmay help us to gain a realization when we are inthis need. More ordinarily, superiors arerequested to deal with the suggestion from acommunity member that a particular Jesuit mayneed professional counseling help when othermeans have proven ineffective. We thereforehave provided some guidelines in the nextsection to assist in a superior’s deliberationsabout counseling for a member.
When full confidentiality permits it, the processmay involve a community, insofar as we may inour different ways assist a companion in need ofprofessional help. The guidelines do look towardthe role of the local community — superior,consultors, and members — in the process ofaffecting individual members of their community.But in order for all of us to be entirely trusting ofthe full confidentiality we are meant to have from
JESUIT HEALTH CARE HANDBOOK 39
SECTION IV Practical Guidelines for the Health Care of Jesuits

our superiors, these guidelines pertain especiallyto local superiors.
These guidelines do not address preventivemeans, or those ordinary means which theSociety and our wider culture usually provide forour continual personal development in living andserving together. Rather, these statements focuson those already existing situations of distress orunfreedom in our lives that may be provingunresponsive to more customary help.
4.17 Guidelines for counseling andpsychotherapy
1. In a spirit of brotherly love, when a Jesuitlearns in a non-confidential way that a fellowJesuit is in need of professional help and is notreceiving it, he should discuss the matter withthe individual’s superior. Should wise andcareful reflection indicate it would be helpful,the Jesuit should broach the subject, perhapswith the individual himself, and encourage theindividual to take appropriate steps forrecovery.
2. Members of the Jesuit community, butespecially the superior and communityconsultors, should accept it as part ofresponsible community life that we giveappropriate assistance and encouragement toa community member who needs to receive orwho is already receiving counseling or therapy.The two key words here are “responsible” and“appropriate.” Responsible:We are profoundlycovenanted and mutually involved.We are aSociety, a companionship, called tocommunion, to be friends in the Lord.Appropriate: Let realism be a central elementof our love and care and also reverence: a finesense of the feelings, reputation, and privacyof one another.
3. Where serious problems arise the superiorshould be in continuing contact with theappropriate Provincial Assistant and whennecessary with the Provincial. Should anycommunity involvement be appropriate in theprocess, care should be taken by all thatconfidentiality is preserved.
4. The local superior should have a list ofrecommended psychiatrists and psychologistsin his area. Jesuit psychiatrists andpsychologists in the Province are available togive advice when requested by superiors, e.g.,as to when to seek professional help inparticular cases, what kind of help, etc. Localsuperiors should also have adequateinformation about hospitalization facilities andprocedures in their area. Furthermore,communities should see the financial costsinvolved in counseling or therapy as a wise andimportant apostolic investment.
5. Superiors should not feel unduly burdened.Their task is to decide whether professionalevaluation is appropriate or necessary. Thefurther decision as to whether (and what kindof) treatment would be appropriate liesprimarily with the professional. Furthermore,wherever initial evaluation is not done with apsychiatrist, at least a psychologically-mindeddoctor should be part of the evaluation, so thatgeneral medical conditions are evaluated alongwith emotional ones.
6. When a community member leaves the housefor a time, for counseling or therapy purposes,community members, with the approval of thesuperior, should maintain good personalcontact with the individual and actively seekhis return to community and to his formerwork.
7. When someone in the course of counseling ortherapy needs to live, whether briefly or atlength, in a Jesuit community where he hasnot previously been residing, superiors andmembers of the host community shouldwelcome him in a full spirit of brotherly love,generously offering any assistance that mayhelp return him to full health and to his formerwork and/or community.
4.18 Guidelines for longer-term therapy at atreatment center
As we become more knowledgeable aboutsevere mental illness and its ramifications, wehave come to realize that short-term treatmenton an outpatient basis, or, worse, ignoring
JESUIT HEALTH CARE HANDBOOK40
SECTION IV Practical Guidelines for the Health Care of Jesuits

aberrant behavior, serve neither the individualinvolved nor the community in which he resides.Jesuits who could be absorbed in largercommunities in the past and were considered tobe merely eccentric are now understood to sufferfrom mental illness and to be unhappy in theirplight. For the welfare of both individuals andcommunities, these needs must be met in thefuture. In exploring possible structures to addressthis problem, other Jesuit resources have beencontacted, but no combination of such resourcesseems feasible at this time, for example, if aProvince does not have the financial or personnelresources on its own to respond to this need.Hence, it is clear that such a Province must use anon-Jesuit resource as its principal health careagency in this area. It is the practice of the USAJesuits to provide for the medical, spiritual, andfraternal care of the mentally or emotionallyimpaired members in religious housesadministered by competent and experiencedreligious communities. The local superior,together with the Provincial Assistant for HealthCare, will be the principal advisors to theProvincial and his consultors on whether anindividual is in need of a residential program todeal with his mental or emotional problems. Thesuperior will carefully document the individual’sbehavior patterns that appear to be aberrant. It isexpected that the superior will have professionalevaluation reports from qualified medical personsand evidence that all other alternatives andmedical procedures have been tried. Funding willbe determined by the insurance program of theProvince (or where applicable, the localcommunity) and the economic situation of thecommunity in which the man resides.
4.19 Overview on alcoholism
The Society of Jesus in the U.S. recognizes andaccepts alcoholism as a disease. This diseasegenerally manifests itself as a threefold illness ofbody, mind, and spirit. Unless arrested,alcoholism leads to irreparable damage orpremature death.
In fraternal charity and in varying degrees ofcompetence, all Jesuits have an obligation inconscience to help the suffering alcoholic toobtain adequate treatment. This obligation is just
as urgent as that of securing adequate treatmentfor any serious disease.
Clinical experience shows that persons afflictedwith the disease of alcoholism need help andprofessional treatment. They are rarely able tohelp themselves effectively. Finally, because ofthe addictive nature of the disease, they areincapable of a sound and realistic judgment as towhether or not they need treatment.
The provincial assistant for health care should beconsulted about a Jesuit with a drinking problem.He or she can offer information and makerecommendations about the available andnecessary treatment options for the Jesuit.
4.20 Guidelines to address alcohol issues
Introduction
The purpose of these suggestions is to help asuperior bring a problem drinker in his communityto the point where the man is willing to accepthelp in seeking a solution to his problems.
It’s not always easy to see when the man’sdrinking has crossed the line from moderate orsocial use to problem drinking. But if heconsumes alcohol to cope with difficulties or toavoid feeling bad, he is in potentially dangerousterritory.
Alcoholism and alcohol abuse can sneak up onthe man, so it’s important to be aware of thewarning signs and take steps to encourage theman to cut back if you recognize them.Understanding the problem is the first step toaddressing it.
Understanding the Problem
Alcoholism and alcohol abuse are due to manyinterconnected factors. People who have a familyhistory of alcoholism or who associate closelywith heavy drinkers are more likely to developdrinking problems. Finally, those who suffer froma mental health problem such as anxiety,depression, or bipolar disorder are alsoparticularly at risk, because alcohol may be usedto self-medicate.
JESUIT HEALTH CARE HANDBOOK 41
SECTION IV Practical Guidelines for the Health Care of Jesuits

Indicators the man may have a drinking problem.Does he:
• Feel guilty or ashamed about his drinking?• Lie to others or hide his drinking habits?• Have community, friends, or family memberswho are worried about his drinking?
• Need to drink in order to relax or feel better?• “Black out” or forget what he did while he wasdrinking?
• Regularly drink more than he intended to?
The bottom line is how alcohol affects theman. If the man’s drinking is causingproblems in his and the community’s life, thenhe may have a drinking problem.
Alcohol abuse - signs and symptoms
Substance abuse experts make a distinctionbetween alcohol abuse and alcoholism (alsocalled alcohol dependence). Unlike alcoholics,alcohol abusers have some ability to set limits ontheir drinking. However, their alcohol use is stillself-destructive and dangerous to themselves orothers.
Common signs and symptoms of alcohol abuseinclude:
• Repeatedly neglecting his responsibilities incommunity and/or at work because of hisdrinking.
• Using alcohol in situations where it’s physicallydangerous, such as drinking and driving ormixing alcohol with prescription medicationagainst doctor’s orders.
• Experiencing repeated legal problems onaccount of his drinking. For example, gettingticketed for driving under the influence or fordrunk and disorderly conduct.
• Continuing to drink even though his alcohol useis causing problems in his relationships.
• Drinking as a way to relax or de-stress. Manydrinking problems start when people usealcohol to self-soothe and relieve stress.Getting drunk after every stressful day, atsocial, dinner, and/or haustus.
Not all alcohol abusers become full-blownalcoholics, but it is a big risk factor. Sometimesalcoholism develops suddenly in response to a
stressful change, such as new or loss of ministry,retirement, or another loss. Other times, itgradually creeps up on the man as his toleranceto alcohol increases. If he is a binge drinker ordrinks every day, the risk of developingalcoholism is greater. This is a critical moment;early intervention can prevent development offull-blown alcoholism.
Alcoholism (alcohol dependence) – signs andsymptoms
Alcoholism is the most severe form of problemdrinking. Alcoholism involves all the symptoms ofalcohol abuse, but it also involves anotherelement: physical dependence on alcohol. If yourely on alcohol to function or feel physicallycompelled to drink, you’re an alcoholic.
Commons signs of withdrawal symptoms mayinclude:
• Anxiety or jumpiness• Shakiness or trembling• Sweating• Nausea and vomiting• Insomnia• Depression• Irritability• Fatigue• Loss of appetite• Headache
Rationalizations you may hear from the manabout his drinking:
• I can stop drinking anytime I want to.• My drinking is my problem. I’m the one it hurts,so no one has the right to tell me to stop.
• I don’t drink every day, so I can’t be analcoholic. OR I only drink wine or beer, so Ican’t be an alcoholic.
• I’m not an alcoholic because I have a job andI’m doing okay.
• Drinking is not a “real” addiction like drugabuse.
Denial is one of the biggest obstacles togetting help for alcohol abuse and alcoholism.The desire to drink is so strong that the mindfinds many ways to rationalize drinking, evenwhen the consequences are obvious. By
JESUIT HEALTH CARE HANDBOOK42
SECTION IV Practical Guidelines for the Health Care of Jesuits

keeping the man from looking honestly at hisbehavior and its negative effects, denial alsoexacerbates alcohol-related problems withwork and relationships.
Toward a solution*
Intervention by a superior
1. Documentation is important. Gatherinformation, i.e., eyewitnesses, complaints orconcerns from co-workers or communitymembers.
2. Promptly undertake an informed, planned, one-on-one brotherly intervention. The aim is tolead the man to make his own decision toaccept help. The superior can stress to theman that he is following his obligation torespond to this serious health problem and toprovide treatment options. It is important forthe man’s sense of support, hope, and lovethat this be done in a spirit of fraternal love andconcern.
3. If the man agrees to accept help, the superiorshould contact the Provincial Assistant forHealth Care to identify the best treatmentoption for the man. See additional resources inSection 3: Assessment Programs.
4. If the man is resistant, plan for a groupintervention.
Intervention by group
1. Identify key support people, i.e., Provincial, hisAssistant for Health Care, Prefect of Health,minister, personal doctors.
2. Have a clear plan for referral/intervention.Again, documentation is important.
3. Direct Provincial involvement may be needed –communication between superiors andProvincials in the man must be moved.
Provincials/Leadership cannot let addictionsgo untreated.
Follow-through (aftercare)
After the intervention, the problem is notcompletely solved, so the superior cannotdismiss it from his mind when the Jesuit brotheragrees to accept help. That is the best beginning.A superior needs to continue contact with theman while he is in treatment. Moreover, he mustmaintain this close follow-up when the manreturns to the community. The superior isencouraged to provide the necessary supports toenable the man to continue with his recoveryprogram.
1. Support for aftercare.
2. Foster small groups within the community orlocal area, where the man with addictionproblems can share with other Jesuits, as inAA, SA, etc.
The recovery program will engage him for therest of his life.
4.21 Suggestions for a driving conversation
Starting the conversation
This guide provides some suggestions for aconversation about driving. Local superiors areencouraged to seek professional assistance inthose situations when concerns arise about thedriving skills of their community members. YourProvince may already have guidelines in place;please check with the assistant for health care inyour province.
Ten questions for the individual Jesuit driver toask himself about his ability to drive:
1. Have you noticed a change in your drivingskills?
JESUIT HEALTH CARE HANDBOOK 43
SECTION IV Practical Guidelines for the Health Care of Jesuits
* This material was adapted from two sources: (1) Challenges to Healthy Jesuit Living: RECOMMENDATION MATRIX in JesuitConference of the United States Task Force on Challenges to Healthy Jesuit Living and (2) National Clearinghouse for Alcohol &Drug Information.

2. Do others honk or show signs of irritationswhen you drive?
3. Have you lost confidence in your driving ability,leading you to drive less often?
4. Have you ever become lost when you aredriving?
5. Have you ever forgotten where you are going?
6. Do you think at present you are a safe driver?
7. Have you had any car accidents in the pastyear?
8. Have you had any minor fender benders withother cars or objects in parking lots?
9. Have you had any recent traffic tickets?
10. Have others criticized your driving or refusedto ride with you?
If you answeredYES to any of the abovequestions, you may need to have your drivingskills screened. Seek further consultation withyour local superior. A physician order would beneeded for further assessment.
Ten questions your local superior or other Jesuitsmight ask about your driving:
1. Do you feel uncomfortable riding with theindividual Jesuit driver?
2. Have you noticed any abnormal or unsafedriving behavior?
3. Has the driver had any recent crashes?
4. Has the driver had any near misses that can beattributed to mental or physical decline?
5. Has the driver received any recent traffictickets?
6. Are other drivers forced to drive defensively toaccommodate the individual Jesuit driver’serrors in judgment?
7. Have there been times when the individual
Jesuit driver has become lost or confused?
8. Does the individual Jesuit driver require manycues or directions from passengers?
9. Does the individual Jesuit driver need a co-pilotto alert him to potentially dangeroussituations?
10. Have others commented on the individualJesuit driver’s unsafe driving?
If you answeredYES to any of these questionsabout the driving skills of the individual Jesuitdriver, then an assessment and functionalscreening by a physician is appropriate. Amedical order would include a hands-on drivingassessment by an occupational therapist and, ifindicated, a neuropsychological screening (usuallynot covered by medical insurance).
Key points:ConversationClinical EvaluationBehind theWheel EvaluationRehabilitation through on the roadinstructions, adaptive driving equipment,community accessibility options.
The driving conversations: 5 stage talks witholder drivers
To understand the 5 Stages of The DrivingConversation, click on the links to the pagesbelow:
Stage 1. Rethinking the driving conversations- Ideally you begin this conversation before anyissues have presented themselves. Establishyour concern for the future and align yourselfwith being on the same team as your agingcommunity member.
Stage 2. What to do at the first signs ofchange - What to look for as early signs ofchange in driving habits. Self-assessment toolsoffered. Providing support to preserve maximumfreedom.
Stage 3. The warning bells - Learn the signalsthat there are more serious concerns.Whatprofessional medical assessments could be
JESUIT HEALTH CARE HANDBOOK44
SECTION IV Practical Guidelines for the Health Care of Jesuits

suggested? Referrals to Driving RehabilitationSpecialists and adaptive devices for the car arediscussed.
Stage 4. When it’s time to retire from driving -Critical questions to know when it's time to hangup the keys. Methods to ease the transition arediscussed. Alternative approaches if drivingcessation will not be voluntary.
Stage 5. Preserving independence afterdriving - Planning ahead to maintain freedom.What are some creative transportationalternatives to driving?
What NOT to do
The decision to retire from driving is NOT anultimatum. It is not a single conversation. Ideallythis conversation takes place in a way in whichthe individual and superior create a plan. Thesuperior has the final decision concerning driving.Check with your Province office for specificdriving policy.
4.22 Furniture and furnishings for acommunity
When should a superior be concerned about thepersonal belongings of a man?The superiorneeds to be concerned when there is anexcessive amount of clutter that may cause asafety hazard or certain devices that may run therisk of fire, electrical shock, or other hazard.Superiors should know their house and have asense of clutter or hazardous devices thatindividual Jesuits keep in their rooms.
General Principles:
When considering furniture and the furnishingsfor a community, take into account older menand those with physical limitations, eithertemporary or permanent. Furniture needs to besafe, comfortable and easy to use.
Particularly for older men, many of whom havesome problem with leg weakness or arthritis, it isimportant to avoid low chairs that make it almostimpossible for them to get up once seated.
Ideally, furniture should have relatively high seatswith good arm supports, so the man can steadyhimself getting down or getting up. Regrettably,the overstuffed lazy boy type chair favored bymany men is usually too low, quite difficult to getup from, and encourages immobility rather thanfunctional independence.With regard to safety,an excessive amount of furniture is a hazard, asis too many furniture groupings.
The issues of clutter and fire safety may becomeobvious with men who have a propensity for“saving” many items like newspapers, letters,and other materials that may be painful for themto discard.
Lighting:
Loss of visual acuity caused by cataracts andother changes in the eye is common to olderpeople. Good lighting is an important way toavoid accidents. Overhead lighting casts fewershadows and can help increase the safety of theJesuit Community for its older members. Inconsultation with someone skilled in lightingdesign or interior renovations, light fixtures thatare aesthetically pleasing and functional can bechosen.
Hallways:
Hallways pose special challenges because ofcarpeting, lighting, and the need some older menhave for support in navigating down their length.Carpeting should be relatively light and a sharpdistinction should be made between hallwaysand stairways so that men will have visual cluesand not fall down the stairs. Likewise, hallwaysshould be well-lit at all times, and all members ofthe community should be made to realize that itis false economy to shut the lights out for theevening when an older man may wander and fall.Carpeting should be well-maintained and withoutscatter rugs or potential barriers that could leadto falls. Particularly useful for some older menmay be the addition of a hallway railing that couldprovide them with support as they walk down thecorridor.
Bathrooms:
Consider installing ADA height toilets and grab
JESUIT HEALTH CARE HANDBOOK 45
SECTION IV Practical Guidelines for the Health Care of Jesuits

bars. Shower stalls that require a high step for aman to enter should be renovated. Consult acontractor or medical equipment vendor tochange the shower pan to entry-free access.Consider purchasing temperature sensitivefaucets and hand-held shower nozzles.
Flooring:
Consider non-skid flooring material.
4.23 Food preparation considerations
Community meals provide a special challenge forsuperiors who need to juggle four sometimesmutually exclusive goals: 1. Provide adequatenutrition; 2. Discourage food faddism both for theyoung and the old; 3. Maintain peace in thecommunity; 4. Stay within a budget. Despitepassing fads and dire warnings about fat andfiber from various quarters, moderation both inchoice of foods and amounts is reasonable.Although they can be a source of problems wheneaten in excess, a dash of salt, an occasionalegg, a bit of butter, and red meat are notpoisonous. It should not be the case, however,that every meal be laden with fat, salt, gravies,rich sauces, and fatty meats. In seeking help inplanning a menu, a dietician could be consulted.A professional can usually be found through alocal hospital or clinic. Ask your chef to prepare alist of typical menus and, ideally, the superior, thedietician, and cook can meet to formulate ahealthy plan. It is extremely important forsuperiors not to be swayed by well-meaning ifover- zealous members of the community whofeel obliged to impose strict diets that mayrepresent their own idiosyncratic views onnutrition rather than true scientific knowledge. Aspecial problem that many younger Jesuits donot seem to recognize with older men is that theelderly may have diminished appetites andweight loss. Although an overweight older Jesuitwith a history of heart disease needs to bestrongly counseled about his diet, do notoverlook the thin older man who is losing weight.
Special diets and food fads:
Rectors are often faced with communitymembers requesting special diets. Obviously it is
the responsibility of the community to meet theneeds of those with special problems, e.g.,diabetes, hypercholesterolemia, or specificconditions indicated by their doctor as a genuinehealth problem. One needs to considerbudgetary constraints and a reasonable regard forpoverty in dealing with Jesuits who seek diets forunproven or faddish reasons. (If a person is avegetarian, then it is appropriate that thevegetables already planned for the communitymeal are well-prepared. If however, someonesuddenly announced that he felt a need for abrown-rice diet, one could question whether thisis a reasonable request.)
Rules of thumb:
1. Make sure the men’s calorie requirements arebeing meet. Some men can benefit from high-calorie drinks like Ensure or Boost.
2. A daily ingestion of fast foods should beavoided due to the excess intake of salt,sugars, fats, and processed additives. 3. Don’tgive in to fad diets.
4. For men with limited cooking experience whohave to prepare their own meals, provide ahealthier choice such a frozen entrée like“Smart Ones, Healthy Choice.” Therecommended entrée guidelines are at least300 calories per serving with sodium between600-800mg and 10 grams of protein.
JESUIT HEALTH CARE HANDBOOK46
SECTION IV Practical Guidelines for the Health Care of Jesuits

V. Ignatian Spirituality and Aging
5.1 Spirituality and aging
In these pages, the Jesuit Health Care Handbookfocuses on Jesuit spirituality and the ageingJesuit. The pages aim to help superiors in theircura personalis and cura apostolica. They alsomean to offer support to those who give ouraging men health or other professional care.
The guiding perspective throughout can only bethat aging is a time of opportunity and newpossibilities. Both Jesuit spirituality andgerontology urge seeing it that way. Although thechallenges are real and not to be disguised byPollyanna like sentiments, aging presents olderJesuits real possibilities for human growth andholiness.
Jesuit spirituality and aging
Our spirituality begins in the Principle andFoundation, the authentic experience of Godcreating and caring for us all our life long. Agingwith this foundation, we continue aware that Godis with us and loves us, providing us grace tomove toward the goal of our existence. Hence,we are free to take each day of our age as a gift.We reject the view that getting old is a negativeexperience, a view frequently bruited in theUnited States today, and that the elderly aresomehow less alive or vital than the young.
Not all Jesuits take age as a gift, as anyone cansee. Some ignore the reality of their aging. Someeffectively deny it by continuing in work – workthat may no longer be especially productive. AJesuit can keep engaging in a plethora of tasksthat keep him from integrating into his later yearshis long experience of everyday life and of grace.
But as a rule, Jesuits not only adapt but find newdepth as we age.We find spiritual consolationeven in our last years. These are proving longerthan most of us expected, an added time to findgetting old challenging. As one asked, notwithout humor, “What do you do when you findyourself in a marathon you didn’t sign up for?”We have been men who said the “Suscipe”anticipating to be put to work.We gave ourselvesto God precisely by giving ourselves all our lives
long to often arduous work for others. From thisactive life, we come to a time when we may wellbe able to give more time to prayer, reflection,and spiritual reading. To prayer in our aging, webring a rich variety of experiences.
Aging Jesuits are generally aware that, as we canbe less active the way we were when younger,we need to experience a greater givenness tocontemplative action.We can experience thiseven in debilitating illness: Fr. General Nicolássaid to a man – paralyzed but clear-minded – whoregretted that he could not pray: “Your bodyprays all day long.” For many, though not for all,this change to a more contemplative life comesto prove satisfying.
Living the Spiritual Exercises
A Jesuit will manage this shift better if he has letthe Spiritual Exercises keep informing hisappreciation of his life and vocation as he ages.We must again and again rediscover that we areloved as we are, even though we have to liveongoing conversions, as flawed as any man andas prone to habits of sin. A man who seemsclinically depressed may actually rather bespiritually desolate, giving himself to serious sinor to blatant spiritual or religious negligence.None of us lives a celibate life for long withouthaving to choose again and again to follow Christand make our own his affections and desires.
We are, however, notably pragmatic men.We areeager to put our imitation of Christ into action.With the onset of age, we confront theunappetizing need – the unaccustomed need –simply to wait. Americans are not good atwaiting, and we are Americans. In old age, ourexperience seems to be inflicted on us and wemust accept much more than in earlier years. Ifwe are open to it, we are graced with a deeperunderstanding Jesus Christ in His Passion.Humanly, He failed, and older Jesuits are readierto empathize with Him in the human failure heaccepted. Looking back over our years, enough ofus are tempted to feel that they have beenempty.We watch this feeling lead some men toliving a closed-in life of practical despair. Butgenerally, Jesuits come to appreciate that Godhas been with us all along, His passionate,infinite love present at every stage of our life
JESUIT HEALTH CARE HANDBOOK 47
SECTION V Ignatian Spirituality and Aging

here, and waiting for us beyond it.
The ages of Jesuit life in the Constitutions
The Constitutions also give a lens to focus theJesuit’s aging and spirituality. In this perspective(as suggested by Fr. Pat Lee, Oregon Provincial(2008-2014)), the succeeding sections of theConstitutions mark out a path from early fervor,to education and training for mission, to decidingthe best way to proceed in work in the Kingdom.Then, in Part VIII, the process of Jesuitdevelopment comes to its fruition with the olderJesuit who now can give to God totally throughprayer. The mission to pray for the Society andthe Church is not a euphemism for being put outto pasture, but a valuable mission entrusted to aman who is now beyond inordinate affectionsand excess self-love, self-will, and self-interestand can truly communicate with God in prayer,lifting up the needs of our Society, the Church,and the world.
Does Pat’s vision match the reality of what weexperience in our encounters with aging Jesuitsor in our own lives as we age in the Society?
The aging Jesuit and humane gerontology
One of the truisms from gerontology is that theolder people get the less alike they are. There istremendous variability from one older Jesuit toanother. And thinking about this man as aperson, it is useful not to have stereotypicalviews of what older Jesuits are supposed to belike, but view aging for each individual holistically.This means considering men from a variety ofperspectives: biological, psychological, social,spiritual, community life, and apostolic life. Thegoal of health for Jesuits is not physical andpsychological perfection but integration to be themost effective apostle possible. Each of theperspectives is interwoven. When we thinkabout the spiritual life of the older Jesuit, thereremains the goal of availability for the apostolatethat is possible, with each of the different partsof the man that make him who he is at thatmoment coming to bear.
• Thus, although aging should not be equatedwith illness, illness is a common part of agingand that affects a man’s spirituality, sometimes
shaking him with deep questions of personalmeaning.
• Likewise, psychological aspects of apersonality, deeply rooted through the years,will be part of how a man approaches prayer,his relationship with God, his interactions withothers, and his ability to cope with thechallenges of aging.
• The social history of a Jesuit includes what hehas done during his life, his friendships,successes, failures, and ability or lack of abilityto adapt to change that inevitably occurs withaging. The man who is clinging on to work,feels that a particular apostolate absolutelydepends on him, views himself asirreplaceable, and who cannot appreciate whohe is separate from what he does or has donemay well have a very challenging time spirituallywhen change is forced either by illness or theorder of a superior.
• Community life is part of Jesuit life, and manymen as they age have had a variety ofexperiences, some very good and some not sogood. For some, aging may be a time ofwithdrawal and, without the stimulus of workand an active ministry, real isolation as there isa lack of experience in relating to other Jesuitsin ways that are personal and based on deepfriendships.
• Again, the spiritual life of an older Jesuit whohas been engaged in community life, open tothe variety of personalities, accustomed tosharing his life and presence with his Jesuitbrothers will have a depth and richness thatmay be lacking in men who have never fullyaccepted Jesuit community as a place for theheart and spirit to reach out and flourish.
The aging Jesuit and illness
Spiritual and physical illnesses can reinforce eachother at any time of life. But with decreasedindependence these interactions become moreobvious and problematic. Illness, with decreasedpersonal freedom, can constitute a real spiritualcrisis for Jesuits as much as for any person. TheJesuit who faces these challenges with a historyof regular prayer, spiritual direction, openness,and a real desire to find God in the midst of theirproblems will discover how God loves them innew ways. But the man who is rooted in his owndesires, who is caught in his own self and
JESUIT HEALTH CARE HANDBOOK48
SECTION V Ignatian Spirituality and Aging
sinfulness, can find illness shattering. For menbring their habits, fears, joys, and ways of relatingto others to their older years. Men who havebeen immersed in Jesuit spirituality and truly findthe meaning and love of their lives in theirrelationship with Jesus may well know hardtimes, but will also likely be more resilient.
It is not infrequent that an older Jesuit is deeplyproblematic and creates chaos around himself,disturbing other Jesuits and presentingchallenges for those who care for them,particular for staff in our health care facilities.Men like this require compassion, because notevery problem of distressing behavior has aspiritual source. Men who have lived deeplyspiritual and wonderful Jesuit lives can developtough behaviors related to dementing illnessesand the like. Some may have to struggle withdepression and can be tough to deal with.
But there are a few older Jesuits who are justplain mean, inappropriate, and difficult. Chancesare they have been this way for most of theirlives and with aging their disturbed personalityhas no outlet other than those around them andthose who care for them. These are tough cases,and pious admonitions will not do too well. Butthe real love and care shown by brother Jesuitsand health care providers can provide theopportunity for grace to be real, immediate, andreceived by men who may well have not hadmuch affection or happiness in their lives.
Summarizing: Jesuit spirituality and aging
One of the dangers in considering aging is tosimply reduce it to managing a collection ofproblems. That would be wrongheaded andignore the reality that God’s grace is as availableto an old Jesuit as it is to a novice on the thirtyday retreat. It is too easy to think that men aresimply set in their ways and avoid encouragingand facilitating real spiritual growth. Probablyeven more important for superiors is helping menin middle age and older to think and prayseriously about what they want and what Godseems to be offering them as they age. Just asmen as they age are encouraged to consider theirdiet, exercise, and appropriate preventive healthcare practices, Jesuit superiors should thinkabout encouraging men to develop a deeper and
more intimate spiritual life and friendship withJesus.
What sort of ways can a superior show care andassistance for the spiritual depth and life ofJesuits as they age? Likely, many superiors havea variety of experiences and ways of proceeding,so what follows is only meant to assist inconsidering the question, and is not any sort ofdefinitive answer.
1. Make sure the yearly fraternal conversationincludes discussion about prayer, attendance atEucharist, spiritual direction, and a yearlyretreat. Markers for concern would be the manwho does not have a director, does his ownretreat, is vague about prayer, and attendsEucharist only when convenient.
2. Spiritual life is not separate from the otherperspectives mentioned above in considering aholistic view of aging. The physical,psychological, social, community, and apostolicelements of a Jesuit life are supposed to be allpart of spiritual life, and likewise, it is hopedthat a Jesuit’s spiritual life will influence theseother elements. Be ready to ask or encouragediscussion about these different elements of aman’s life and how they are finding, or notfinding God.
3. Be ready to challenge men as they age whohold on to positions of influence or who arekeen to view their presence as irreplaceableand essential. In this, also be aware that manyJesuits with age bring a perspective andwisdom that can be very beneficial in anapostolate and this is very different from afailure to appreciate that they are aging andthat the contributions best made are not thesame as when they were younger. Wisdomand grace look different than fear, rigidity, andcontrolling behavior.
4. Use community meetings as an opportunity todiscuss aging, especially by allowing older mento tell their stories and be open to sharing theirhopes and fears. Silence is a great way tomake sure that isolation and the evil spirit canhurt us at any time in our lives. With aging, theenemy of human nature has a number of tricksto encourage us to feel alone, unappreciated,
JESUIT HEALTH CARE HANDBOOK 49
SECTION V Ignatian Spirituality and Aging

and tempted to despair.
5. Make sure that community members visit menwho are in the province health center, or if thatis not geographically convenient, that regularcommunication is encouraged. It can be hardfor an older man spiritually who finds himselfin the health center and whose previouscommunity, where he may have lived most ofhis lifetime, does not visit, call, or provide anyevidence of care and concern.
6. Encourage men who are in their middle ageand early older years to consider a thirty dayretreat that will ask God to reveal how best toface aging and death.
7. Share with older Jesuits who need more carethat giving up some degree of independence,that may be already threatened by illness andfrailty, can be a much needed gift that willallow more freedom for Jesuit caregivers aswell as those who work with us to providecare. Just as an elderly family member whostubbornly clings to a home or refuses help,and thus exhausts their children with addedwork and worry, so an older Jesuit can controla community or be a source of disruption thatdetracts from apostolic and community energy,activity, and life. (This idea suggested by KateMorency, RN)
8. At superiors’ gatherings, ask your peers fortheir best ideas on encouraging spiritual depthand growth with age.
5.2 Ignatian spirituality and the aging, sickand dying Jesuit
William A. Barry, S.J.Nov. 12, 1993
It is a great pleasure to welcome all of you to theNew England Province and to Campion Center.This is the first meeting of its kind, I believe,bringing together men and women from all ourprovinces who have a care and concern forelderly, sick and dying Jesuits. I hope that thisweekend will be very profitable for all of you andfor the continuing work of providing quality carefor our elderly, sick and dying Jesuits.
I have been asked to focus my remarks thisevening on Jesuit spirituality and the aging, sickand dying Jesuit and those who care for him. AsI thought about the topic, I ran through a numberof possible starting points. I recalled howIgnatius cared for his sick companions. Once,when Simon Rodrigues was sick, Ignatius walkedmiles to comfort him, a deed that Simonremembered later in life when he had so badlytreated Ignatius the General. Or I could speak ofhow Ignatius, in spite of his insistence on strictpoverty, wanted everything done for those whowere sick in the house. Indeed, he made surethat the Roman house had a villa house outsideRome so that his men could get away from thepestilential air of Rome where they often gotsick. But finally I came back to the heart ofIgnatian spirituality, the Spiritual Exercises andto the very beginning of them, the “Principle andFoundation.” There we ponder God’s dream increating the world and each one of us. Let me,therefore, begin my presentation here.
Why did God create a universe with people in it?It certainly was not because God was lonely andneeded company. God, we believe, is the perfectcommunity of Father, Word and Holy Spirit whoneeds nothing else to be fulfilled. Then whycreate a universe and us? It is as if the threePersons said to one another, “Our community lifeis so good; why don't we create a world wherethere will be other persons whom we can inviteinto our community life!” In other words, Goddesires our world and us into existence so thatwe might enjoy theTrinitarian life of God. We aremade for God, and, as Augustine says, we shallbe restless and frustrated until we attain unionwith God. In creating us God has implanted in usa deep desire for union with God, a desire thatwe often experience as a welling up of a desirefor “we know not what,” for the “All,” for unionwith the Mystery we call God. When that desirewells up in us, we feel a deep joy and awholeness that is hard to explain or describe.We are, as C. S. Lewis puts it, “Surprised by Joy,”and this “Joy” is the desire for God.
Let me give you a concrete example of thewelling up of such a desire. It comes fromFrederick Buechner’s autobiographical memoirSacred Journey. After his father’s tragic suicide
JESUIT HEALTH CARE HANDBOOK50
SECTION V Ignatian Spirituality and Aging
his mother took him and his brother to Bermuda.Near the end of his stay he was sitting on a wallwatching ferries come and go with a girl whowas also thirteen. Quite innocently, he says,
our bare knees happened to touch for amoment, and in that moment I was filledwith such a sweet panic and anguish for Ihad no idea what that I knew my lifecould never be complete until I found it...It was the upward reaching andfathomlessly hungering, heart breakinglove for the beauty of the world at itsmost beautiful, and, beyond that, for thatbeauty east of the sun and west of themoon which is past the reach of all butour most desperate desiring and is finallythe beauty of Beauty itself, of Being itselfand what lies at the heart of Being.1
Buechner himself acknowledges that there aremany ways of explaining this experience.However, he goes on to say that “looking back atthose distant years I choose not to deny, either,the compelling sense of an unseen giver and aseries of hidden gifts as not only another part oftheir reality, but the deepest part of all.”2
When I have the experience of desiring “I knownot what,” I am experiencing God creating menow in all the particulars of my presentexistence. While I am caught in that experience,I do not worry about my past failures and sins orabout what the future might hold. I feel at onewith the universe and as whole as I couldpossibly be. Moreover the desire I experience isthe deepest desire within me. That desire is intune with God's one intention in creating theuniverse, and that desire can become the rulingpassion of my life, if I let it. When we experiencethis desire, it is God's Holy Spirit drawing us intothe community which is theTrinity. While we arein the power of this desire, everything elsebecomes relative before the absolute Mysterywe desire. Moreover, insofar as this desirereigns in our hearts, we desire to live out ourlives in harmony with this desire and want to do
whatever will more readily bring us to the objectof our desire. Hence, we want to live in harmonywith God's creative purpose in creating us, tochoose what will be more in tune with our desirefor union with God. Ignatius spells out theimplications of the foundational experience ofGod's creative touch in the Principle andFoundation.
Ignatius, too, experienced this “Joy,” this desirefor “he knew not what,” and he reflected on thisexperience a long time. He distilled the results ofhis reflection and his study of theology in the“Principle and Foundation” which, in somewhatdry language, expresses why God made us.Here is the text:
Human beings are created to praise,reverence, and serve God our Lord, andby means of doing this to save theirsouls.
The other things on the face of the earthare created for the human beings, to helpthem in the pursuit of the end for whichthey are created.
From this it follows that we ought to usethese things to the extent that they helpus toward our end, and free ourselvesfrom them to the extent that they hinderus from it.
To attain this it is necessary to makeourselves indifferent to all created things,in regard to everything which is left toour free will and is not forbidden.Consequently, on our own part we oughtnot to seek health rather than sickness,wealth rather than poverty, honor ratherthan dishonor, a long life rather than ashort one, and so on in all other matters.
Rather, we ought to desire and chooseonly that which is more conducive to theend for which we are created. (TheSpiritual Exercises, n. 23)
JESUIT HEALTH CARE HANDBOOK 51
SECTION V Ignatian Spirituality and Aging
1 Frederick Buechner, The Sacred Journey. San Francisco: Harper & Row, 1965, 52.2 Ibid., 56.

Because God is God and because our onlyultimate happiness lies in living in harmony withGod’s intention for the universe and for each oneof us, Ignatius calls upon us to be “indifferent” toall created things. In his recent translation Ganssnotes that the term is a key technical term inIgnatian spirituality. However, “(I)n no way doesit mean unconcerned or unimportant. It impliesinterior freedom from disordered inclinations.”3
Because I am made for union with God and withall other creatures, I want to treat other creaturesin accordance with God’s intentions, and notabuse them for a purpose contrary to or differentfrom what God intends.
I believe that you can now see where I amheading in this talk. If the deepest desire of myheart (and of anyone’s heart) is union with God,then everything else pales to insignificance incomparison with God. Hence, it is a matter of“indifference” whether I am successful in mycareer or not, whether I am rich or poor, whetherI am sick or healthy. Ignatius and those whohave imbibed his spirituality expect to find God inall things, in every circumstance of life, insickness or in health, in a long life or in a shortone, and so forth. Ignatian spirituality draws aperson toward the realization that the “pearl ofgreat price,” namely God, is worth more thananything else that he or she possesses; to buythat pearl one would, indeed, sell all that one has.Thus, we who follow this spirituality beg God tohelp us to the “indifference” Ignatius speaks of.We want to be “indifferent” to sickness orhealth, to a long life or a short one. But only a bitof self knowledge reveals to each of us how farfrom this ideal we are. The mere repetition of thewords of the “Principle and Foundation” will notmake us indifferent, will not make us acceptingof our lot in life when sickness, old age and dyingstare us in the face.
The attainment of the ideal of Ignatianindifference toward sickness or health is a lifelong process. Moreover, it is not attained by theforce of will power alone; in fact, unaided
attempts to attain indifference by will poweralone will only bring us to despair or to ajoylessness that is totally foreign to Ignatianspirituality. The only pathway to the attainment ofIgnatian indifference is a life long commitment toprayer, to the relationship with God which willgradually rub away all our disordered inclinationsthrough a growing love for God above all things.Ignatius himself did not easily attain to thisindifference in the face of illness and death. Letme give you some examples from hisAutobiography which indicate a growing changein his image of God and in his love for God.
After his initial conversion Ignatius went to thesmall town of Manresa where he spent almost ayear in prayer and other spiritual exercises. Priorto going on the journey to Manresa he says ofhimself that he considered entering theCarthusians. However, his ardor to enter cooled,as he says, because “he feared that he would notbe able to give vent to the hatred that he hadconceived against himself.”4 This self hatred tellsus much about his image of God at this time. IfIgnatius hates himself so violently, we canspeculate that he harbors an image of himselfbefore an implacable God. Not long after hisarrival in Manresa he begins to attack his bodyand his former attitudes toward ambition andvainglory by terrible fasts and penances, to thepoint that he did permanent damage to hishealth. Moreover, he began to have great swingsof mood which led him into terrible bouts ofscruples. The agony of his struggle with thesescruples can be seen in this paragraph from theAutobiography.
Once, being very disturbed because ofthem, he set himself to pray and withgreat fervor he cried aloud to God,saying, “Help me, Lord, for I find noremedy among men, nor in any creature.No task would be too irksome for me if Ithought I could get help. Lord, show mewhere I may get it, and even if I have tofollow after a little puppy to get theremedy I need, I will do it.”
JESUIT HEALTH CARE HANDBOOK52
SECTION V Ignatian Spirituality and Aging
3 George E. Ganss, The Spiritual Exercises of Saint Ignatius: ATranslation and Commentary. St. Louis, MO: The Institute of JesuitSources, 1992, 151.4 A Pilgrim's Journey:The Autobiography of Ignatius of Loyola. Introduction, Translation and Commentary by Joseph N.Tylenda. Wilmington, DE: Michael Glazier, 1985, n. 12.

Taken up with these thoughts he wasmany times vehemently tempted tothrow himself into a deep hole in hisroom which was near the place where heused to pray.5
The self hatred has taken a very violent turn,indeed, to the point where he was tempted tosuicide. What kind of image of God lies behindsuch scruples? It has to be a God who isrelentless in his pursuit of every last detail of thesinner's faults, indeed, a God who will never besatisfied with any examination of conscience thesinner has so far done. God must be a terriblejudge ready to pounce on every sin or sinfultendency. Unless this image of God changes,suicide is the only out. As you care for usJesuits, be aware that some, hopefully very few,still live as though this were the real image ofGod.
Fortunately, Ignatius kept on praying to God fordeliverance. After a couple of days free fromscruples, they returned. Ignatius says:
But on the third day, which was aTuesday, the remembrance of his sinsreturned to him while he was at prayer,and as one thing leads to another, hethought of sin after sin from his past lifeand felt obliged to confess them again.After these thoughts, there came uponhim a loathing for the life he was thenliving and he had a strong temptation togive it up. In this manner the Lord choseto awaken him as from a dream.6
Ignatius, we can speculate, has realized that theimage of God with which he has operated thusfar in Manresa was a product of the demon andnot an image of the true God. He goes on to say:
Now that he had some experience withthe different spirits through the lessonsthat God had given him he began tothink about the way that that spirit hadcome to him. Thus, he decided, and with
great clarity of mind, never to confess hispast sins again and from that day forwardhe was free of his scruples, and he heldit for certain that our Lord had desired toset him free because of His mercy.7
God is not implacable, but merciful, and Ignatiuscan count on this God. Thus he need notcontinually grub around in his mind for possibleunconfessed sins.
What I want to emphasize is that this change inIgnatius’ image of God did not come aboutthrough theological argument or throughpreaching, but through experience and reflectionon experience. Ignatius experienced differentmoods and thoughts; he reflected on thesedifferences; finally he came to the point wherehe realized that some thoughts and emotionscame from God and some did not come fromGod. The encounter with God in prayer and in lifechanged his image of God. Gradually theexperience of God transformed his image of Godand his image of himself in relation with God.Such a transformation is, Ignatius believed, opento anyone who gives God a chance, to anyonewho pays attention to his or her experience,reflects on it and discerns what is of God fromwhat is not of God in his or her experience.Ignatius believed that at every moment of ourlives we are in the presence of God, we areencountering God, and that, if we pay attentionto our experience with the expectation ofknowing God, we can gradually be weaned fromour false images of God, from our inordinateattachments that keep us from recognizing the“pearl of great price,” and from our fears ofsickness, old age and death. If we are faithful tosuch attention to our experience, Ignatiusbelieved, we would quite literally find God in allthings, in good times and in bad, in sickness andin health, in success and in failure. Through hisown faithfulness to the practice of suchdiscernment of spirits Ignatius was brought tosuch a state of indifference that he could, hesays, come to peace in fifteen minutes if theSociety of Jesus were to be dissolved. In
JESUIT HEALTH CARE HANDBOOK 53
SECTION V Ignatian Spirituality and Aging
5 Ibid., 23 24.6 Ibid., 25.7 Ibid., 25.

addition, people who describe him in his lateryears as General of the Society speak of hissense of humor and his ease with others, a farcry from the man tortured by scruples inManresa.
In his Autobiography Ignatius describes threeinstances when he was threatened with death.The differences in his reactions to the thought ofimminent death tell us a great deal about how alifetime of paying attention to God changed hisimage of God and his attitude toward death. Thefirst occurred at Manresa when a fever broughthim to death's door. He was convinced that hewas about to die. He says:
At that instant the thought came into hismind that he was numbered among therighteous, but this brought him so muchdistress that he tried everything todismiss it and to dwell on his sins. Hehad more difficulty with that thoughtthan with the fever, but no matter howhe toiled to overcome it, he was unabledo so. When the fever lessened and hewas no longer in danger of death, heloudly cried out to certain ladies who hadcome to visit him that the next time theysaw him at death's door they were, forthe love of God, to shout aloud that hewas a sinner and that he should be evermindful of the sins he had committedagainst God.8
Some of the Jesuits who are in your charge maystill be in this stage of fear of God. Pastoral careof them would include help to experience God asmerciful and kind to all.
Contrast this last experience, where Ignatius isstill caught up in terror of God, with the next onehe describes. He was on ship from Spain to Italy,and in a storm everyone on board was convincedthat death was inevitable.
Thus, making use of his time, he made acareful examination of conscience andprepared himself for death, but he felt no
fear because of his sins nor was he afraidof being condemned, but he wasespecially disturbed and sorry, knowingthat he had not put to good use all thegifts and graces that God our Lord hadgranted him.9
Notice that Ignatius knows that he is a sinner andthat this knowledge saddens him. But it doesnot frighten him as it did before. Because of hisfurther experiences of God he now trusts in themercy of God. He seems now to believe that heis a sinner loved and forgiven by an all mercifulGod. This experience reminds us of thedescription of the Jesuit from GC 32: “What is itto be Jesuit? It is to know that one is a sinner,yet called to be a companion of Jesus as Ignatiuswas.” It is to be hoped that most of the sick andelderly Jesuits we care for have reached this levelof intimate knowledge of God.
Finally Ignatius describes a time in the year 1550,just six years before his actual death, when heand everyone else were convinced that he wasabout to die of a fever.
Thinking of death at the time, heexperienced such joy and so muchspiritual consolation in the thought ofhaving to die that he burst into tears.This came to be of such frequentoccurrence that many times he stoppedthinking of death just so as not to haveso much consolation.10
Now Ignatius seems to be so in love with Godthat the thought of death and complete unionwith God overjoyed him. Thoughts of his sins donot seem to arise. The self God image seems tobe that of beloved to lover. God has taughtIgnatius the ultimate lesson of who God really isfor Ignatius, and for all of us, Lover parexcellence. Fidelity to the relationship with Godhas changed Ignatius’ image of God as well ashis image of himself.
Ignatius urges the one who directs the SpiritualExercises to “allow the Creator to deal
JESUIT HEALTH CARE HANDBOOK54
SECTION V Ignatian Spirituality and Aging
8 Ibid., 32.9 Ibid., 33.10 Ibid., 33.

immediately with the creature and the creaturewith its Creator and Lord” (n. 15). In thatencounter with God each of us can be freed ofthose attachments that make us inordinatelyafraid of sickness, old age and death. In our carefor our elderly and sick brothers in Christ we cancontinue this Ignatian direction with the surehope that God can be found in all things, even insickness and diminishment. Death itself is, webelieve, only the door that reveals fully what Goddesires for all of us, namely union with God andwith one another forever.
So as we ponder the central principles of Ignatianspirituality with regard to the care of sick, elderlyand dying Jesuits, we can well remember thatIgnatius would have us take good care of ourelderly and sick brothers; but even more we needto remember that even these days ofdiminishment and sickness and dying are timesfor encountering the living God, are, indeed,times for helping our brothers to say again in anew and deeper way the prayer of Ignatius:
“Take, Lord, and receive all my liberty,my memory, my understanding, and allmy will, all that I have and possess. You,Lord, have given all that to me. I nowgive it back to you, O Lord. All of it isyours. Dispose of it according to yourwill. Give me love of yourself along withyour grace, for that is enough for me.”(n. 234)
JESUIT HEALTH CARE HANDBOOK 55
SECTION V Ignatian Spirituality and Aging

VI. General Directives for Health Carein a Jesuit Retirement Facility orNursing Care Center
While it is important to retain the unique quality,traditions, and Province identity that exist in eachProvince’s retirement or nursing care centers,certain standards should be consistently upheldthroughout the Assistancy. This section outlinesthose best practices and expected policies thatshould be implemented, if necessary, and upheldif already in place. Those centers that are state-licensed may have additional requirements.
Each health care center or Province should have awritten plan for ongoing QA (Quality Assurance)and QI (Quality Improvement). Ideally thereshould be regular reviews conducted by anoutside party or team; inter-Province cooperationmay be employed in this regard.
Further, it is recommended that a plan beestablished to see that these areas areaddressed in a timely fashion. Finally, thereshould be a Province strategy for the regularimprovement of these areas. This may be bestachieved by the formation of a quality assurancecommittee that meets regularly to discuss qualitymeasures. These measures may include reviewof falls and other incidents, medication errors, in-house wound development, etc. In the Appendixcan be found a sample tool that may be of usefor tracking and trending quality measures in ahealth care facility.
I. Mission statement
A mission statement should be drafted for eachfacility. It should be specific to the level of careprovided (independent, assisted living, and/orinfirmary or skilled level of care) and placedwithin the context of Ignatian spirituality and aJesuit vision of mission.
II. Retirement/Nursing care centers policy
A.Transition process
1. There should be anticipatory discussions withthe Jesuit before the move, with his immediate
superior and the Assistant for Health Care tothe Provincial, about the demonstrated changein his health care needs that require a move toa facility that can better meet his needs. Duringthe discussions every effort should be made tohelp the Jesuit understand the decision andfeel that he is a partner in the decision.
2. The determination of the center/facility that theJesuit will move to will be determined by themedical, functional, and/or cognitive needs ofthe Jesuit (a tool should be developed by eachunique venue to make this assessmentuniform and as objective as possible). Eachcare facility should have written criteria on thelevels of care provided and available services.
3. If at all possible, the Jesuit should receive avisit from the care facility to which he will bemoving. During this visit a medical, functional,and cognitive assessment should be done (atool should be developed by each uniquevenue to make this assessment uniform andobjective as possible).This time can also beused to address any concerns the Jesuit mighthave and also allow for discussion on thespace limitations of the facility (if there are any)as well as the daily routines of thecenter/facility.
4. The superior of the Jesuit’s current communityshould inform the man’s family and, whenappropriate, his friends about the changes inthe Jesuit’s condition that necessitate theneed for a move to a higher level of care.
5. Medical records should be requested and sentto the receiving facility before the Jesuitmoves to the new facility.
6. A medical history, a list of medications, andother pertinent medical information should betransmitted to the receiving facility. Eachprovince should develop a tool to facilitateseamless transitions. (A sample copy of a newresident intake form is included in theAppendix in Section 7.6.) A copy of theJesuit’s Advance Directive should be sent tothe receiving community so they can preparefor the man’s admission.
7. When possible a celebratory party/dinnershould be held for the Jesuit before leaving his
JESUIT HEALTH CARE HANDBOOK56
SECTION VIGeneral Directives for Health Care in a JesuitRetirement Facility or Nursing Care Center

current community and the receivingcommunity should provide a clear welcome.
8. On admission to the new facility, a completenursing assessment is done and a plan of careis initiated. Regular assessments and follow-upare done according to the facility’s protocols.
B.Assessment
In each care facility, a formal system to establisha thorough profile of each arriving Jesuit shouldbe in place. In most cases a portion is done bythe PA for health care or charge nurse of thefacility while the other section is done by thesuperior of the community. It should include, butnot be limited to, the following:
• Acuity levels/ROM• Interests and Hobbies• Family/Friends• A discussion with the new resident of theassets of the place
• A two-month plan for incorporation into the newresidence (special attention during this time)
• Staff introductions and interaction as to howthe staff may be helpful
• A comprehensive functional assessment of aperson’s needs and exactly what he can andcannot do; activities of daily living
• Complete medical physical• Activities the man did and did not do in the past• Work history• Fears, anxieties, hopes, wishes• Spiritual needs• Development of a nursing care plan• Required activity care plan• Spiritual care plan (sacrament of the sick,confession, breviary, etc.)
• Medical care plan from the physician• Make sure documents exist on advancedirectives, living wills, etc.
• Plan for records transfer• Mental status exam• Physical assessment• Immunization screening• A problems list for all of the above• A primary care physician and dentist should beobtained
• Often an initial screening by a psychiatrist ishelpful
• Facilities that have a dietician should also havethe new resident screened
• Each facility should establish its own plan forperiodic re-evaluation of the person.
• The Provincial, the local superior, and thesuperiors of the Province should share a clearunderstanding as to a facility’s areas ofcompetence.
• A system should be established whereby anongoing evaluation of each Jesuit iscommunicated to the Jesuit superior of the facility.
• A system should exist that informs a Jesuit’sprevious community of his state.
• The man’s family should receive regularevaluation updates.
C. Safety
1. Environment
A disaster plan (for earthquakes, tornadoes, etc.)should be in effect. The plan should be tested atregular intervals.
Many facilities have created Safety Committeesthat meet at regular intervals to discuss issuesregarding safety.
2. Environmental Integrity
The following areas should conform to safety forJesuits and staff. An outsider should mandate anassessment of each care facility. If any area isfound to be in need of repair, updating, orreplacing, then a schedule should be developedto address the need(s) based on high-to-lowpriority.
• Electrical• Tub, bathroom, shower• Night lighting• Carpet edges• Floor coverings• Step edges• Call bells• Side rails when needed• Furniture should be adequate• Cleanliness; a policy needs to be in place forhygiene standards
• Policy on regular evaluation for the environment• Scheduled maintenance
JESUIT HEALTH CARE HANDBOOK 57
SECTION VIGeneral Directives for Health Care in a JesuitRetirement Facility or Nursing Care Center

• Good functioning equipment• Variety in diet, especially for those followingspecial diets
• House transportation should be accessible toresidents
• Is the house accessible for those who residethere?
• Safe food handling standards, includingtemperature of foods, should be monitoredregularly
3. Infection Control
Policy should exist based on Standard UniversalPrecautions. Good medical policy should bedeveloped for the following:
• Contaminated waste disposal• Laundry sanitation• Health care standards for employees (TBtesting, etc.)
• Needle/Stick Protocol for Staff• MRSA/CDIFF (Nursing Home)• A procedure for Quality Assessment and RiskManagement
• A system for incident reporting and systematicreporting of errors
• A plan for total quality control should beestablished to address problems and how tosolve them, i.e., falls, medical errors, employeeinjury, misdiagnosis, etc.
• A policy on the use of restraints (who and why)and a policy on review
• A policy on medical restraints (who and why) andreview to assess the need for this over time
• Protocol for Patient Abuse (a policy on how tohandle this and training to understand when itis happening)
• Policy that coincides with state law on protocolfor reporting incidents
D. Staffing
Professional (licensed) and certified care (C.N.A.,M.A., caregivers, etc.) must be administered in acaring, supportive environment that helps createa family, community atmosphere, whilemaintaining as much independence as possible.Generally, an RN needs to be on the staff or at aminimum an RN must be available and clinicalresponsibilities delegated according to the nurse
practice acts of the states in which the facilitiesare located. Additional regulations may apply ifthe facility is licensed.
The following items should be made clear:
• Job descriptions• A clear Personnel Policy Manual• Levels of pay should conform to the area of thecountry in which the facility is located.
• Generally, an activity director is needed; againflexible based on the level, people, etc.
• Personnel files should be maintained for eachemployee, which includes annual reviews,disciplinary concerns, and, when appropriate,copies of verified licensure.
• Background checks where appropriate/required
Site specific, general principles for staffingminimums should be established for all levels ofcare.
Retired:
Assisted:
Full Nursing:
E. Jesuits and care givers:
A clear understanding should exist between theJesuit superior and the facility’s healthcoordinator and/or clinical director. Maintaining agood working relationship will beneficially impactthe Jesuits and the community as a whole.
The superior should not make decisionsindependently of the health care coordinator orclinical director; rather, he should enter intoregular conversations with the health carecoordinator and/or clinical director about the menand the facility. The superior should make everyeffort to ensure that the above mentionedguidelines are incorporated. Regular face-to-facemeetings are beneficial.
A new superior should begin his work byrespecting the continuity that exists in a placeand the good program the coordinator hasestablished. The coordinator needs to have theflexibility required to work with a variety of
JESUIT HEALTH CARE HANDBOOK58
SECTION VIGeneral Directives for Health Care in a JesuitRetirement Facility or Nursing Care Center

superiors. The ideal situation is one in which ateam approach is taken.
Each facility should have a written chain ofcommand and policies in place regardingsupervision of staff, as well as general guidelinesfor communicating with the men about their careneeds. Specific areas to keep in mind includeresponsibility for hiring and firing of staff;informing men of a need to stop driving;transitioning to a different level of care; non-compliance; refusal of care; and acceptingneeded assistance with hygiene, etc.
F. Medications
Each facility should have written policies andprocedures regarding:
• Medication orders• Administration control• Error reporting• Refusal of medications
JESUIT HEALTH CARE HANDBOOK 59
SECTION VIGeneral Directives for Health Care in a JesuitRetirement Facility or Nursing Care Center

VII. Appendix
7.1 “Challenges to Healthy Jesuit Living” fromCommunity As Mission: Jesuit Life Nowand Into the Future (US JesuitConference, 2012)
Challenges to Healthy Jesuit Living
Recommendation Matrix
One of GC35’s most striking statements is foundin Decree 3, #41: “Thus, Jesuit community is notjust for mission: it is itself mission.” Communityas mission implies a transformation of Jesuitculture with a new grace, and members of theSociety being transformed by this grace as well.
The key framework of such a transformation isMutual Relationship, and understanding of ourlives in common as built on mutuality and bestexpressed in “covenant” terms: the Society (inits unity, as the province, represented by theprovincial), a local community, and its individualJesuits have a commitment to one another tosupport and develop the mission of Jesuitcommunity. Covenant, rather than “policies,”“programs,” or “tools,” stresses mutualresponsibility and accountability to others: The
Society, a community and an individual Jesuit allhave specific contributions or investments tomake, and all are answerable to one another forthe fulfillment of community as mission.
This covenanted interplay touches our deepestdesires for wholeness and holiness, evokingpossibilities of hope, healing and love in theexperience of Jesuit life. TheTask Force wasconvinced that the desire for such a change ortransformation in community culture alreadyexists among brother Jesuits, and needs only tobe awakened and structurally encouraged.
How do we make this happen?The matrix whichfollows looks at the roles of leadership (at boththe province and local level) and individualmembers in making such a transformation takeplace. The matrix presumes a less institutional,more covenantal way of looking at Jesuitcommunity, especially in dealing with some of itsparticular challenges. The matrix seeks toincorporate the reality of difficulties into thedeeper expression of community life. Rather thanexclude and isolate “difficult people,” this is anopportunity to incorporate healthier models ofJesuit life across all dimensions and developways of supporting and engaging those withdifficulties as members of the community’smission.
JESUIT HEALTH CARE HANDBOOK60
SECTION VII Appendix

JESUIT HEALTH CARE HANDBOOK 61
SECTION VII Appendix
Issue/Value Leadership Best Practices Individual Best Practices
Health Care • Provide community resources to sup- porthealthy diet and exercise (e.g., gym incommunity or access to gym; personaltrainers, as appropriate)
• Use health care coordinators well (e.g.,consulting on medications)
• Be clear about role of prefect of health inlocal communities.
• Medical record of medications andconditions on back of the door to anindividual’s room for ready access inemergency situations
Nutrition consultation for kitchens, pro-viding cooks who take proper responsibilityfor the nutritional needs of the community• Regular health updates (e.g., newsletter)• Attractive alternatives to alcohol-basedsocial hour
• Attention to strategic investment in healthcare across the spectrum from proactiveto crisis
• Who gives attention to the physical andemotional health of a provincial and hissocius?
• Personal attention to diet and exercise• Regular medical attention: check-ups forPSA, blood pressure, cholesterol levels, etc.
• Self-monitoring of cholesterol, salt andsugar intake, blood pressure, weight,factors within one’s control.
• Awareness of alcohol and food intake• Be compliant with medicine and seebenefit of medicine
• Individuals become more aware of andtake responsibility for health costs andproviders.
• Individuals understand insurance coveragethat is provided by the province
Toxic Behaviors:
(narcissistic;grossly insensitive;self-protective; avoidresponsibility;isolated; source ofdisharmony andfragmentation ofcommunity)
The man who“doesn’t need help”.
• Acknowledge that we have people withthese behaviors
• Listen to and understand the concerns ofthe community
• Identify and document problematicbehavior
• Develop incremental interventions,beginning with common norms of thegospel and religious life.
• Confront and set boundaries (not adaptingto the individual, giving him too muchinformal power)
• Need a plan to deal with the individual thatis supported at all levels of governance;consider group intervention at times(rather than one-on-one)
• Provincial needs to take directresponsibility at appropriate moment
• The individual must be made aware thatcontinued disruptive behavior will haveserious consequences. Theseconsequencesmust be clear andmade clear.
• Communication between superiors andprovincial in cases where an individualmust be moved
• Realize that some men cannot live life incommunity
• Develop criteria and accountability for menliving outside community
• The community is ready to take part ininterventions for the man’s sake and theirown.
• The man must gain awareness and under-standing of his personal anger andresentment.
• He must be shown the documented ac-count of his destructive behavior.
• He ultimately needs to be given a plan forwhich he is responsible.
• He must acknowledge the consequencesif he does not change his behavior(“Toxic” members may not become an-gels, but may become more responsible ifconfronted with the truth in love.)
Challenges to Healthy Jesuit Living - Recommendation Matrix

JESUIT HEALTH CARE HANDBOOK62
SECTION VII Appendix
Issue/Value Leadership Best Practices Individual Best Practices
Difficult Transitions • Identify, acknowledge and help normalize stressfultransitions
• Encourage men in transition to share experience with oneanother and with superiors
• Provide workshops for cohort group transitions (e.g. newlyordained)
• Life-coaching in 50's; promoting re-training; how to livewith leisure.
• Facilitate transitions to new province structures,encouraging: “Open Houses” across “borders”; visitingand getting acquainted with other regions and personnel;erasing caricatures and old images; one Society
• Handle transitions to health care facilities with“intentionality” and care.
• Engage in early identification and dialogue.• Superiors encourage move to health care when appropriateand not just wait until a crisis. (cf. Wisconsin Provincepolicy)
• Health care facilities provide intellectual stimulus; goodbooks; connection to current events and people; “ElderHostel” type experiences.
• Develop contact with the outside world in health carefacilities: readers for the sightless; companions outdoorsfor the immobile – balancing need with reasonable“boundary” measures.
• Do “dying” better; (e.g., talk; missioning letter; vigil withdying; men intentionally reflect on reality of death; book-let/journal on one’s Jesuit life)
• Potentially stressfultransitions
- Post-ordination- Loss ofparents/siblings- Change in assignment- Loss of Jesuit friends(death/departures)- Job loss and failure &loss of satisfaction- Mid-life issues- Diminishment
• Older Jesuits in places havebegun to form groups toreflect on the end of lifeand/or the end of life asthey have known it. Aspirituality for aging.
• One doesn’t let his mind orinterests dry up with aging.
• In health care facility TVdoes not replace books,while one still has sight.Options for the sightless.
• The man in transition doesnot lose initiative.
Spiritual • Consistent use of the spiritual resources of the Society ofJesus
- Spiritual direction- Annual retreat- Continuing formation- Prayer/liturgy- Manifestation of conscience in which provincials andsuperiors build a trusting relationship that is not one-sided or “institutional”, and allows for the oneaccepting the manifestation to share his own innerlife and experience as a brother; a form oftransformative experience that leadership can provideto elicit trust.
• Promote education and development of competent spiritualdirectors
• Promote open conversation to bridge and respect diver-gent ecclesiologies or politics that can perpetuate splits.
• Adaptive use of spiritual resources in times of crisis (e.g.,hospitalization, collective “crisis”)
• Foster creative, culturally responsive spiritual expressioncommunally and individually.
• Attention to people who feel marginalized by the Church• Recognize that the men themselves have desires forchange; ride their energy; sharing of dreams.
• Consistent use of thespiritual re- sources of theSociety of Jesus
- Spiritual direction- Annual retreat- Continuing formation- Prayer/liturgy- Open manifestation ofcon- science
• A spirit open to culturalchange in its many aspects;a spirituality of “desires”
• Able to deal with feelings ofshame and humiliation,collectively and personally,and move on.
• Identification with “sinners”vs. dissociation from them.
• Proactive hospitality towardother Jesuits, and towardcolleagues and friends, menand women; expanding thenotion of Jesuit community.

JESUIT HEALTH CARE HANDBOOK 63
SECTION VII Appendix
Issue/Value Leadership Best Practices Individual Best Practices
Crisis Management • National referral directory of therapists,treatment programs, etc.
• Mandate integrated approach especially inregard to faith
• Seen as part of a proactive incrementalprocess – programs, etc., are steps afterother alternatives have been explored
• Leadership develops crisis managementteams to support superiors
• Companionship for man in crisis
• Community awareness of the "signs" ofphysical and psychological crises (e.g.,suicidal tendencies, conduct in ministry) --and call attention, ask for help.
• Community discretion and confidentiality;respects privacy.
Environmental • Build structures that promote social inter-action
• Public spaces that promote appropriatefamily and colleaguehospitality/interaction.
• Private spaces for community interactions.• Demonstrated commitment to environ-mental sustainability (clean air; recycling;energy conservation)
• Separation of living and working situations• Create incentives for sustainability (e.g.paying public transportation costs)
• Attentiveness to one's own living space• Personal responsibility for environmentalsustainability
• Investment in design and care ofcommunal space.
• Concern for creation on all levels;conservation
• Uses public transportation; shares rides,etc.

7.2 Jesuits Aging 2006 – A Presentation byMyles Sheehan, S.J., M.D.
Over the next ten years or so, the Society ofJesus in the United States will decrease in size,and then, if current predictions are accurate, beconstant at about 1000 members.
Diminishment is not something that is easy toview with excitement and consider anopportunity. But I do. I believe that the currenttime in our Church gives American Jesuits anopportunity similar to that of Ignatius and his firstcompanions. It is a time of turmoil and changewhere we can labor along with Christ. That mayseem like pious delusional thinking. And it wouldbe delusional if I thought that we wouldrecognize new opportunities without changes,choices, uprooting, and opposition. Realizingsome of our future opportunities requires us tobe much more creative about aging in the Societyin the United States. Creativity about aging forAmerican Jesuits has several components. Thefirst is to re-consider what we mean by health inthe Society of Jesus.With a better understandingof health in the context of our charisma andmission, then I believe we will have the chanceto look with optimism and excitement at some ofthe challenges we face. Reconsidering what wemean by health as Jesuits requires thinking abouthealth from more than a medical perspective.Health in the Society of Jesus is not an end initself: our health is part of our ability to fulfill ourmission. In my 21 years in the Society, I havebeen struck that we talk a lot about the problemsassociated with poor health and the infirmitiesthat old age can bring. Part of this is acommendable desire to make sure that our menreceive excellent care and are treatedappropriately. Indeed, in the past two decades Ihave been gratified by improved standards ofcare, better staffing and facilities, and, in general,a much improved approach to some of themedical problems of aging. But being a healthyJesuit is not defined by infirmity or illness, oreven the absence of medical problems. Healthhas a variety of components. Those in health caremay well be familiar with the model of GeorgeEngels that looks at health as having biological,psychological, and social components. It remindsphysicians and other providers that the people forwhom we care are not just diseases or bodies,
but they are people whose health includes avariety of psychological and social factors.
When we think about health for Jesuits, then Ibelieve we need to add some other dimensionsto Engel’s bio psychosocial model. Let mesuggest six, acknowledging that none aremutually exclusive and there is a fair amount ofoverlap: Apostolic, biologic, psychological, social,community, and spiritual. In what follows, I amgiving some rough outlines, not attemptingdefinitions that are perfect. What is the apostolicdimension of Jesuit health?
The basic question is whether or not a man isready for mission and has the necessary qualitiesand skills to work and be with people, sufficientprudence to deal with work related issues, andthe freedom to be available for the missions thatthe Society proposes as part of a discernmentprocess.What about the biological dimension ofhealth?
I would emphasize the prevention of disease,care for existing conditions, and a habitual patternof living that avoids fads and extremes butattempts to minimize risks to health andemphasizes reasonable exercise and a prudentdiet. The psychological dimension of health for aJesuit is clearly related to all the others?
It would certainly include the balance andpsychological health to live the life of the vowswithout anguish, to reflect on experience andponder the best course, and the maturity to avoidboth an obsessive need to placate authority or animmature failure to deal with unresolvedauthority issues. Psychic health for a Jesuitincludes responding to the challenges ofcommunity living, having the ability to maintaingood relations while not being afraid of honestdiscussion and fair disagreement. The socialdimension of health includes both the person’splace in the larger society and the network ofrelationships in which a person lives and works?
Social health for a Jesuit would certainly includethe ability to engage and work with others in anapostolate. But in our current society, it alsoincludes the ability to function to interact withindividuals where there is a loss of previousrespect and regard for Jesuits and priests, and
JESUIT HEALTH CARE HANDBOOK64
SECTION VII Appendix

where sometimes one can run into overt hostility.The community dimension of health for Jesuits isoften critical and frequently overlooked.
The community aspect of health would includebeing able to live with others in a way that allowsinteraction, maintains reasonable hygiene inpersonal quarters, and engages with othercommunity members at meals, recreation,worship, and meetings. A Jesuit who isdisruptive in community, absent, or otherwiseweird is not a healthy Jesuit. Spiritual healthshould be central to our understanding of what itmeans to be a healthy Jesuit.
The characteristics of spiritual health wouldinclude the ability to pray, a regular prayer life,regular conversation and direction about one’sspiritual life, and the use of prayer as a strengthand guide for behavior and interactions in theapostolate and in the community. In other words,a healthy spiritual life will be made manifest by itsfruits in community and in apostolic work.Appropriately, superiors and others have beenincreasingly insistent that Jesuits see physiciansand that attention be paid to their medical care. Itis not my impression that superiors are as directabout requiring individuals to have a spiritualdirector and to take a yearly retreat. You mighthave a Jesuit with great blood pressure, fantasticlab results, and a colon as clean as a whistle oncolonoscopy; but without a spiritual life you havean unhealthy Jesuit. Looking at health for a Jesuitfrom a perspective that is bigger than justmedical diagnoses and idiosyncratic behaviors,suggests that health for Jesuits depends on theindividual but it also depends on the health ofcommunities, the nurturing and maintenance of aspiritual life, and committed superiors who knowtheir men well and are willing to have sometimesdifficult conversations. Perhaps a more sensitiveindicator of health in the Society is not the list ofdiagnoses of the individual Jesuits, but the“mission ability” of the men. Part of thedifficulties with mission may be a failure to lookholistically at Jesuits as individuals who aremeant to be on mission. A Jesuit is not reallyhealthy unless he is engaged in a mission. Howdoes a more expansive definition of healthdirected at mission allow us to face thechallenges of the next few years? I believe itallows us to face an incontrovertible fact with
flexibility and a recognition that God is presentingus with an opportunity. The fact is that as theAssistancy drops from a bit under four thousandcurrently to around 1000 men in ten to fifteenyears, we cannot continue financially to maintainour current structure of health centers andinfirmaries. There are too many beds for thefuture needs of Jesuits, although the next fewyears will be busy ones as we reach the crest ofthe aging wave of American Jesuits. Healthyaging for older Jesuits can include a variety offutures that will allow mission directedinvolvement. Mission directed life is not aboutsitting around until one is sent to the provinceinfirmary. Non-Jesuit American men as they agemove in a variety of ways to a variety of differentfutures. They move geographically, they have aset of other interests, some develop second orthird careers, and, in what may be calledretirement settings, they have new friendshipsand live in new communities. I worry that incomparison far too many Jesuits stay put at anapostolate for decades. Some of them truly arewisdom figures who continue to provideenormous service. But let us be honest. Thereare other men who have no idea where else togo and who do not have the support andencouragement, or even the challenge, to moveto a new kind of future. At any given time, thismay only be a handful of men. But over theyears, this wasted potential becomes substantial.Our Jesuit rhetoric about not retiring is nothelpful. It creates an incentive to hang on in asetting when there are other good opportunitiesbeyond the confines of where one has spentmost of one’s adult life. Quite frankly, there aremen who are too frightened to move out of theircommunities. Some hide behind a feeling thatthey are irreplaceable or that the Catholic andJesuit character of an institution is somehowdependent on their ongoing presence. Thus theyputter about in their community, generouslytrying to do the best they can but, perhaps,missing the much greater apostolic fruit thatcould be available in a new apostolate.Recognizing a new stage in life with differentpossibilities is part of what healthy aging is about.So what’s the opportunity?
The opportunity is to develop a plan for aging inthe Society that shows the same kind ofawareness of God’s Providence that Ignatius
JESUIT HEALTH CARE HANDBOOK 65
SECTION VII Appendix

showed in the Constitutions. It means less focuson institutions and more on individuals comingtogether on mission. And it is directed atmaintaining and directing zeal for souls ratherthan allowing the enemy of human nature havingus settle for hanging around a recreation roomwhen there is so much need. Let me outline foursuggestions before finishing on changingdemographics and the meaning of health in theSociety. First, the cornerstone of newopportunities for Jesuits is always theirexperience of prayer and the Spiritual Exercisesinterwoven with their experience of life. AlthoughTertianship is the definitive close to Jesuitformation, it should not be the end of Jesuitspiritual growth and change. I would suggest thatthe Assistancy create opportunities for men intheir late middle age to spend serious time withGod, and with each other, praying about whereGod is leading them as they grow in years. Thiswould mean developing retreats as well as get-togethers similar to what is now done for men information.
At a recent meeting of our health carecoordinators, this idea received much attentionand support. No doubt there would be someresistance in the beginning. That will change ifthe programs are done well, with care, and withobvious respect for the needs and hopes of themen involved. It also is an immediate response tothe feelings of neglect that some older men maybe having in the midst of planning for the future.Some of the current Assistancy planning canleave older Jesuits thinking that their time is past.Many of the health care coordinators expressedconcerns that older men felt left out. Change ininstitutional commitments, communities, andpatterns of living may create a sense that thecontributions of the past are not valued.Attending to the more holistic health needs ofolder men now, rather than simply waiting untilthey become sick or infirm, is a way to combineboth cura personalis with attention to apostolicneeds.
Second, Jesuits who are aging and want to moveon in ministry should not find themselves “alldressed up and nowhere to go.”We can createfrustration by having nothing availableapostolically as men look to their future. I wouldsuggest that the Assistancy look to a set of
ministries that are appropriate for older men andboth meets real needs as well as provides goodcommunity life in a setting that is congenial tomen who may face some physical challenges.We need to avoid isolated locales or stickingJesuits alone as they age in rural parishes orother sites where there will only be a disaster ifthey become frail. We need to be much morecreative about mission. Although Provinces haveattempted to look at new career positions, thiswould be an ideal place to look beyond Provincesand across the Assistancy. Third, thinking aboutmission concretely means to dream about thekind of opportunities that might be available forolder Jesuits. In considering the future of ourcurrent health facilities we must recognize theirtremendous apostolic potential. It may be thatthe facilities, some of which have substantialsurrounding land, could be converted into amixed retirement community, a place that wouldallow older persons from a variety ofbackgrounds to come together. Using some ofthis resource to provide housing for people oflow income is a way to combine our desire forjustice with our recognition of the needs of olderpersons. Ministry for older Jesuits in such asetting could include work in direction, retreats,pastoral care, and other possibilities. Imaginedeveloping a community for older persons thatincludes Jesuits, alumni from our institutions, andhousing for low and middle income elderly in asetting that allows recreation, conversation, andfriendships. Not only would the Jesuits have anumber of pastoral opportunities, it could well bethat there would be work that the other olderpersons could do that might benefit a school, orprovide assistance to others in need, etc. Indeed,one can think of partnership with a Jesuituniversity and the creation of some type ofcourses, activities, and immersions that couldallow the wisdom of older Jesuits, and older laypeople, to come forth in new ways.We also needto realize the tremendous potential of a group ofJesuits who would live in an adult community notowned or operated by the Society. (I hesitate touse the word retirement community because ofthe baggage associated with the word in Jesuitcircles.) The lay people in this setting might thinkof themselves as retired. Jesuits, however, wouldbe involved in the lives of other people and thuswould find themselves busy and active. There willbe the need to create an appropriate community
JESUIT HEALTH CARE HANDBOOK66
SECTION VII Appendix

structure for the Jesuits and think a bit abouthow to work issues of governance. But thepotential outweighs the problems. The fastestgrowing segment of the American population arethose 85 years of age and older. Those are a lotof souls that need care, and conversion, and thegrace of Christ. And we have Jesuits who aretheir contemporaries and who could provideextraordinary apostolic service. I would suggestthe signs of the times point in an obviousdirection. Something less obvious to consider aswell. If older Jesuits are working withgrandparents, they may well find themselvesserving as advisors and trusted mentors to thegrandchildren! Again, Ignatius found himselfoverwhelmed by opportunities in a time filledwith change and confusion. Are we holding on sotightly to past models that we are missing God’scall? A fourth, and fairly obvious consideration, isthat there are many other possible models forministry as Jesuits get older. Frankly, thepotential is only limited by our fear of doingsomething different and by the logistic needs tohave organization and care given to developingthese new apostolates. This speaks to a need forthe possibility of someone at the Assistancy tohelp coordinate these ventures across provinces.This individual would be available to helpprovincials and superiors think about theapostolic uses of older men rather than simplydeal with problem cases. He (or she) would lookto organizing retreats and other gatherings forJesuits in their late middle age and older. Andshe (or he) would have responsibility forconsidering how best to work with superiors inconsidering the apostolic potential of older men.In other words, this individual would be helpingus consider the future and the resources ofhealthy Jesuits, men who want to be on amission, rather than our current somewhatobsessive focus on the personal care of menwho are sick or our sometimes seeming oversolicitude for maintaining institutions. I havementioned challenges of caring for our older menas we face a period of change. There arechallenges in considering a more holisticunderstanding of health for Jesuits, andchallenges in developing new opportunities formen in the Society in the United States as theyage. The fundamental challenge is to take God’saction across the lifespan seriously and, both asindividual Jesuits and as friends in the Lord
united in mission, to make sure that as we agewe are led by the Spirit, deepening ourrelationship with Jesus and further progressing inour love of the Father. Ignatius’ ideal of the manwith Final Vows remains an ideal that we areblessed to see instantiated in many fine Jesuits.For the rest of us, however, time and otherconcerns can take us away from prayer, regularspiritual reading, and a habit of encouraginghealthy relationships with superiors who reallyknow us well. Human nature is such that formany Jesuits the period after Tertianship can be atime when they may not make progresspersonally and spiritually. This can be especiallythe case given that many people will live for fouror five decades after Final Vows. And for somethese four or five decades will be living in amanner that is privatized, isolated, and not fullyengaged with the community.What a waste ofthe graces that we have received! Ignatius wasalmost obsessive in his detailed prescriptions forthose in formation. Perhaps part of his reticenceabout the life of those after Final Vows was thatin the sixteenth century there were not thatmany years left for most men after they finishedformation. Men usually died in their forties,fifties, and sixties. Happily, that is not the casetoday. Don’t you think Ignatius would have beenexcited by the opportunity for many more yearsof fruitful ministry for himself and hiscompanions?Why should we be so dull as not totake advantage of this gift?We are being forcedfor a variety of reasons to think about our presentand our future. There is so much that is excitingand filled with opportunity. The prospect of ahealthier Society of Jesus, with health definedbroadly and directed toward mission, issomething that fills me with hope. The dark spiritmakes me worry that people will not have thecourage to change, that we are so stuck innurturing institutions rather than individualJesuits it may be too late, and all our rhetoric cantie us up in knots rather than set us free. Butthat’s the dark Spirit. Not the Spirit of God. And Itruly believe that the Spirit is speaking somethingvery important for us to attend to at this time.
JESUIT HEALTH CARE HANDBOOK 67
SECTION VII Appendix

7.3 Sample of community health careinformation form
Community Medical Information Form
JESUIT HEALTH CARE HANDBOOK68
SECTION VII Appendix
Community Medical Information Form
The following information is requested in case of an emergency. Please feel free to provide allor as much information as you think would be helpful in case you are not able to speak foryourself. Please return to my box as soon as possible.
Date completed:_____________________________Name:______________________________________Hospital of Choice:___________________________Name of your Current Physician:________________________________________________________Name of the Office/Clinic:___________________________________________________________________Do you have any pre-existing conditions an emergency room should be aware of?Yes____ No ____List medical diagnoses:__________________________________________________________________________________________________________________________________________________________________________Allergies (e.g., medications, latex, or foods):__________________________________________________________________________________________________________________________________________________________________________Are you taking any regular medications? Yes____ No ____Please list your medications below, including dosage information:____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Person to be notified in case of emergency (include telephone #):_____________________________________________________________________________________Have you granted durable power of attorney?Yes____ No ____If yes, where is that document located?_____________________________________________________________________________________Are you an organ donor? Yes____ No ____If yes, where do you keep the document indicating this?_____________________________________________________________________________________
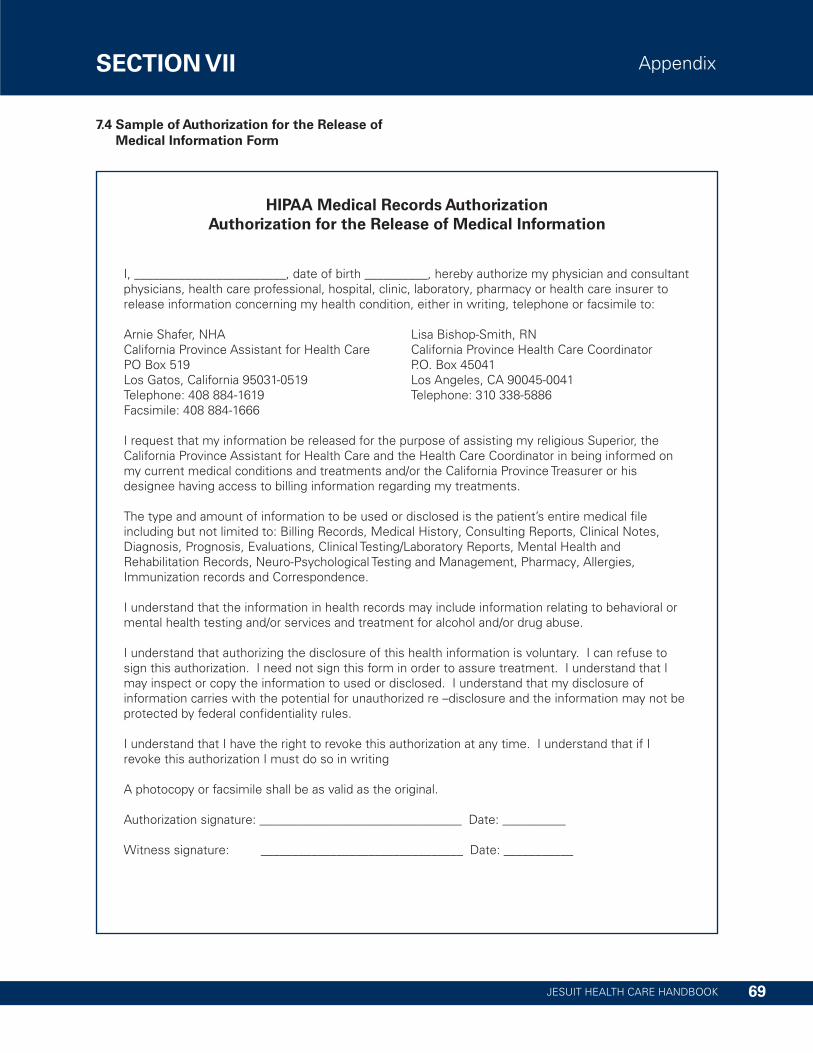
7.4 Sample of Authorization for the Release ofMedical Information Form
JESUIT HEALTH CARE HANDBOOK 69
SECTION VII Appendix
HIPAA Medical Records AuthorizationAuthorization for the Release of Medical Information
I, ________________________, date of birth __________, hereby authorize my physician and consultantphysicians, health care professional, hospital, clinic, laboratory, pharmacy or health care insurer torelease information concerning my health condition, either in writing, telephone or facsimile to:
Arnie Shafer, NHA Lisa Bishop-Smith, RNCalifornia Province Assistant for Health Care California Province Health Care CoordinatorPO Box 519 P.O. Box 45041Los Gatos, California 95031-0519 Los Angeles, CA 90045-0041Telephone: 408 884-1619 Telephone: 310 338-5886Facsimile: 408 884-1666
I request that my information be released for the purpose of assisting my religious Superior, theCalifornia Province Assistant for Health Care and the Health Care Coordinator in being informed onmy current medical conditions and treatments and/or the California ProvinceTreasurer or hisdesignee having access to billing information regarding my treatments.
The type and amount of information to be used or disclosed is the patient’s entire medical fileincluding but not limited to: Billing Records, Medical History, Consulting Reports, Clinical Notes,Diagnosis, Prognosis, Evaluations, Clinical Testing/Laboratory Reports, Mental Health andRehabilitation Records, Neuro-Psychological Testing and Management, Pharmacy, Allergies,Immunization records and Correspondence.
I understand that the information in health records may include information relating to behavioral ormental health testing and/or services and treatment for alcohol and/or drug abuse.
I understand that authorizing the disclosure of this health information is voluntary. I can refuse tosign this authorization. I need not sign this form in order to assure treatment. I understand that Imay inspect or copy the information to used or disclosed. I understand that my disclosure ofinformation carries with the potential for unauthorized re –disclosure and the information may not beprotected by federal confidentiality rules.
I understand that I have the right to revoke this authorization at any time. I understand that if Irevoke this authorization I must do so in writing
A photocopy or facsimile shall be as valid as the original.
Authorization signature: ________________________________ Date: __________
Witness signature: ________________________________ Date: ___________

7.5 Sample Quality Improvement Report
JESUIT HEALTH CARE HANDBOOK70
SECTION VII Appendix
Data Source Acceptable Outside AcceptableParameters
If outside acceptable parameters, note action(s)taken
1. InternalTracking ofQuality Measuresincluding:FallsWeight LossPainManagementHypnotic UsePressure Ulcers
X • Falls with Major Injury:• Residents who have moderate to severe pain:• Prevalence of hypnotic use more than two times in lastweek: Residents with pressure ulcers:
2. QualityDashboard
X • Hand hygiene:• Mortality Nursing Facility:• Presence of Advanced Directives:
3. ResidentCouncil MeetingMinutes
X • No issues identified at this time.
4. Safety andEnvironmental
X
5. DietaryServices
X • Temperatures at the point of service are monitoredmonthly. They continue to be satisfactory.
• Diet order audits are conducted on a quarterly basis toensure the accuracy of diets being served.
• Monitoring of 5% or more weight loss continues on1st and 2nd floors.
6. PharmacyReport
7. InfectionControl Reports
8. MMDS
9. Rehabilitation
10. ReportableAccident Data
X • There were (#) SNF resident incidents/accidents,which is a decrease from last quarter.
• There were (#) ALF resident incidents/accidents, whichis a decrease from last quarter. One of these incidentsresulted in a DPH reportable.
• Number of reportable incidents.
Jesuit Health Center Name (Quarterly or Monthly)Quality Improvement ReportDate__/__/__

JESUIT HEALTH CARE HANDBOOK 71
SECTION VII Appendix
Data Source Acceptable Outside AcceptableParameters
If outside acceptable parameters, note action(s)taken
11. EmployeeIncidents/Accidents
X • There were (#) employee incidents/accidents thisquarter.
12. Policy andProcedureChanges
X
13. StaffDevelopment/Turnover
X •The turnover rate (%)• Alzheimer’s and Dementia training• Blood Borne Pathogens training• Fire Safety and Disaster training• MSDS training• Employee Handbook/Policies
CURRENT QUALITY IMPROVEMENT PROJECTS:• 2nd floor main shower rooms• Updating the Infection Prevention Policy and Procedure Manual• Maintenance/Housekeeping checklist audit for vacant rooms• 2013 Action Plan• Organize and review the medical record filing system• Audit of HIPAA Privacy and Security
COMPLETED QUALITY IMPROVEMENT PROJECTS:• Implemented the MOLST/POLST for all Jesuits• All Health Center employees completed the Alzheimer’s Habilitation Training• Empty Room Audit for Maintenance and Housekeeping• 2013-2015 Strategic Plan• Implementation of Consistent Assignments (3 months and Jesuits did not like it)• Employee Satisfaction Survey
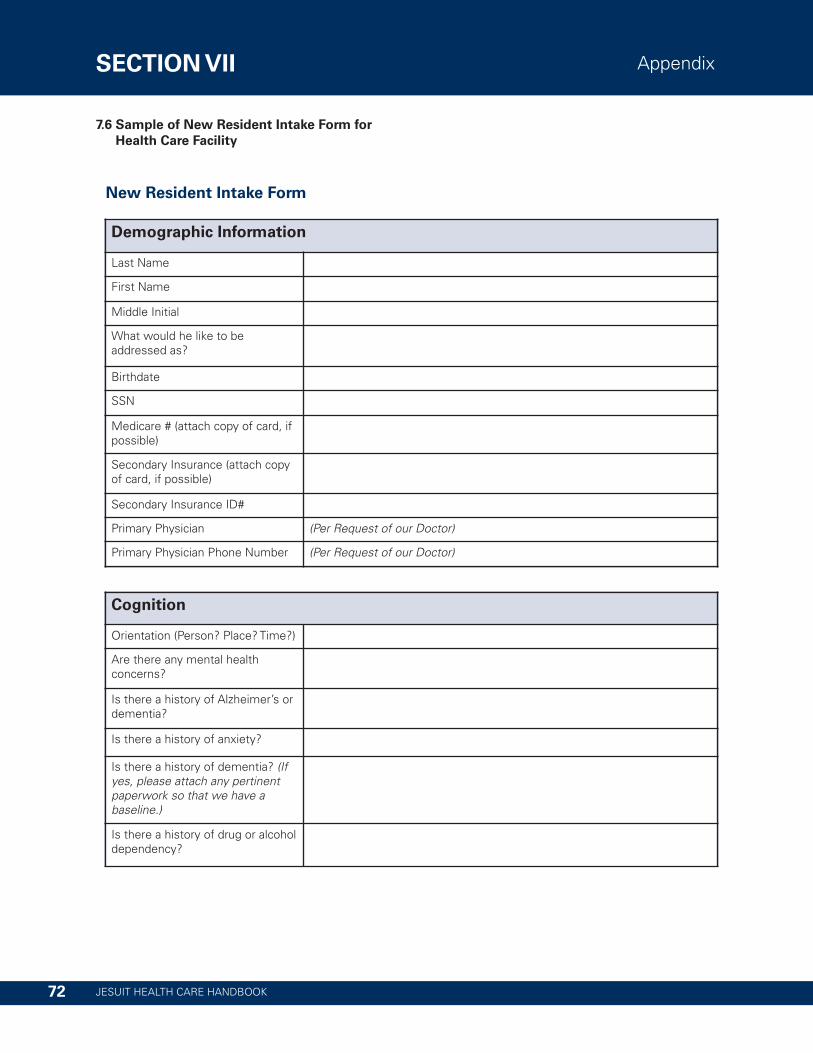
7.6 Sample of New Resident Intake Form forHealth Care Facility
JESUIT HEALTH CARE HANDBOOK72
SECTION VII Appendix
Demographic Information
Last Name
First Name
Middle Initial
What would he like to beaddressed as?
Birthdate
SSN
Medicare # (attach copy of card, ifpossible)
Secondary Insurance (attach copyof card, if possible)
Secondary Insurance ID#
Primary Physician (Per Request of our Doctor)
Primary Physician Phone Number (Per Request of our Doctor)
New Resident Intake Form
Cognition
Orientation (Person? Place?Time?)
Are there any mental healthconcerns?
Is there a history of Alzheimer’s ordementia?
Is there a history of anxiety?
Is there a history of dementia? (Ifyes, please attach any pertinentpaperwork so that we have abaseline.)
Is there a history of drug or alcoholdependency?

JESUIT HEALTH CARE HANDBOOK 73
SECTION VII Appendix
Current Medical Information
Medication List – Please attachcopy
I am attaching the most current medication list & the patient will be sentwith a 2-3 week supply of medicationsORI do not have a current medication list. I will inform the Jesuit to bring all oftheir medications to St. Camillus, in addition to a 2-3 week supply ofmedications
Medication Administered by:(please circle one)
Self-Administered MedicationsORStaff Administers MedicationsORRN sets up in Mediset and Patient administers to self
Medicinal Allergies
Food Allergies
Current Height &Weight _______ Inches & _________lbs.
Driving Able to safely drive & has a current driving license OrDoes not currently drive
Medical History – Please attachcopy
Please send with paper copies of Jesuit’s medical history for our doctor toreview
Surgical History – Please attachcopy
Please send with paper copies of Jesuit’s medical history for our doctor toreview
Special Diet?
Does he have an AdvanceDirective? If so, please attach copy
Yes & it will be sent with the JesuitORThere is no Current AD on File
Is he a DNR? If so, please attachcopy
Yes, he is a DNR and a copy will be sent with himORNo, he does not have a DNR order on file

JESUIT HEALTH CARE HANDBOOK74
SECTION VII Appendix
Personal Care/Mobility Information
Bathing & Frequency Is able to bathe self ORRequires some assistance with bathing ORRequires total assistance with bathing
Oral Care Independent ORRequires some assistance with oral care ORRequires total assistance with oral care
Shaving Independent ORRequires some assistance with shaving ORRequires total assistance with shaving
Toe Nail Care Independent ORRequires some assistance with nail care ORSee’s podiatrist on a regular basis
Dressing Independent ORRequires some assistance with dressing ORRequires total assistance with dressing
Mobility/Transfers Independent Or Stand by assist for transfersAssist of one with transfers Or Max assist of two with transfersOther:__________________________
Assistive Equipment Needed Hospital bed Single Point CaneWheelchair Quad CaneWalker Side Rails on BedReacher CommodeShower chair Toilet Seat RiserShower Bench No equipment neededCall Light (necklace to call for assistance) Other: ___________________
Elimination Status Continent of Bowel & Bladder ORContinent of Bowel, Incontinent of Bladder ORIncontinent of Bowel & BladderOther:_______________________
Dentures No Dentures OR Partial Dentures (upper or lower) OR Full Dentures
Hearing Status No Hearing Impairment ORHard of Hearing – will need a Hearing Aid EvaluationOR Currently has Hearing Aids (R or L)
Vision No visual Impairments ORWears Glasses ORWears Contacts AND/ORHistory of Glaucoma? AND/OR History of Cataracts?And/OrWill need to establish care with Ophthalmologist upon arrival
Respiratory Equipment Currently does not use any respiratory equipmentOR Currently using oxygen (please attach orders and company used)OR Currently uses Nebulizer (please bring all equipment and contactinformation from the rental company)OR Currently uses a CPAP/BiPap (please bring all equipment and contactinformation from the rental company)

SECTION VII Appendix
7.7 Sample of Health History Form for Jesuits
JESUIT HEALTH CARE HANDBOOK 75
Society of Jesus Health History Form
Preferred Hosp. _________________________________Primary Doctor _________________________________
Phone _________________________________Office _________________________________
Last Physical ____________Last Dental Exam____________Last Eye Exam ____________Record Updated ____________Blood Pressure _____ / _____BloodType ____________Height, inches ____________Weight, pounds ____________
Medicare Qualified Programs Effective DateMedicare A _______________ _______________Medicare B _______________ _______________Medicare C _______________ _______________
State Medicaid _______________________________Prov. Medical Plan _______________________________Other Medical Plan _______________________________
Current Presciption Meds
Current Non-Presciption Meds
Birth Date _____________ Age ____________
Emergency Contacts: Name / Phone / Relationship
1. ______________________________________________
2. ______________________________________________
Allergies and Reactions
Major Diagnoses
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
� Childhood
� Cholera
� Flu
� Hepatitus A (1) (2)
� Hepatitus B (1) (2) (3)
� Meningococcal
� Pneumo Vac
� Shingles
� TB
� Tdap
� Tetanus-Diptheria Booster
� Typhoid
� Other
Immunizations Date

Jesuits.org