
“It Depends”: Viewpoints of Patients, Physicians, and Nurses on Patient-Practitioner Prayer in...
17
“It Depends”: Viewpoints of Patients, Physicians, and Nurses on Patient-Practitioner Prayer in the Setting of Advanced Cancer Michael J. Balboni, PhD, ThM, Amenah Babar, MPH, Jennifer Dillinger, MDiv, Andrea C. Phelps, MD, Emily George, RN, MPH, Susan D. Block, MD, Lisa Kachnic, MD, Jessica Hunt, BA, John Peteet, MD, Holly G. Prigerson, PhD, Tyler J. VanderWeele, PhD, and Tracy A. Balboni, MD, MPH Center for Psycho-Oncology and Palliative Care Research (M.J.B., A.C.P., S.D.B., J.H., J.P., H.G.P., T.A.B.), Departments of Psycho-Oncology and Palliative Care (M.J.B., A.C.P., S.D.B., J.P., H.G.P., T.A.B.), Department of Chaplaincy (J.D.), and Department of Radiation Oncology (TA.B.), Dana-Farber Cancer Institute; Boston University School of Theology (M.J.B.); Department of Society, Human Development and Health (A.B.) and Departments of Epidemiology and Biostatistics (T.J.V.), Harvard School of Public Health; Department of Medical Oncology (E.G.) and Department of Radiation Oncology (L.K.), Boston Medical Center; and Harvard Medical School Center for Palliative Care (S.D.B., J.P., H.G.P., T.A.B.), Boston, Massachusetts, USA Abstract Context—Although prayer potentially serves as an important practice in offering religious/ spiritual support, its role in the clinical setting remains disputed. Few data exist to guide the role of patient-practitioner prayer in the setting of advanced illness. Objectives—To inform the role of prayer in the setting of life-threatening illness, this study used mixed quantitative-qualitative methods to describe the viewpoints expressed by patients with advanced cancer, oncology nurses, and oncology physicians concerning the appropriateness of clinician prayer. Methods—This is a cross-sectional, multisite, mixed-methods study of advanced cancer patients (n = 70), oncology physicians (n = 206), and oncology nurses (n = 115). Semistructured interviews were used to assess respondents’ attitudes toward the appropriate role of prayer in the context of advanced cancer. Theme extraction was performed based on interdisciplinary input using grounded theory. Results—Most advanced cancer patients (71%), nurses (83%), and physicians (65%) reported that patient-initiated patient-practitioner prayer was at least occasionally appropriate. Furthermore, clinician prayer was viewed as at least occasionally appropriate by the majority of patients (64%), nurses (76%), and physicians (59%). Of those patients who could envision themselves asking their physician or nurse for prayer (61%), 86% would find this form of prayer spiritually supportive. Most patients (80%) viewed practitioner-initiated prayer as spiritually supportive. Open-ended responses regarding the appropriateness of patient-practitioner prayer in the advanced cancer setting revealed six themes shaping respondents’ viewpoints: necessary conditions for prayer, © 2011 U.S. Cancer Pain Relief Committee Published by Elsevier Inc. All rights reserved. Address correspondence to: Michael J. Balboni, PhD, ThM, Center for Psycho-Oncology and Palliative Care Research, Dana-Farber Cancer Institute, 44, Binney Street, Boston, MA 02120, USA. [email protected]. Disclosures None of the authors have relationships with any entities having financial interest in this topic. NIH Public Access Author Manuscript J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09. Published in final edited form as: J Pain Symptom Manage. 2011 May ; 41(5): 836–847. doi:10.1016/j.jpainsymman.2010.07.008. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of “It Depends”: Viewpoints of Patients, Physicians, and Nurses on Patient-Practitioner Prayer in...

“It Depends”: Viewpoints of Patients, Physicians, and Nurses onPatient-Practitioner Prayer in the Setting of Advanced Cancer
Michael J. Balboni, PhD, ThM, Amenah Babar, MPH, Jennifer Dillinger, MDiv, Andrea C.Phelps, MD, Emily George, RN, MPH, Susan D. Block, MD, Lisa Kachnic, MD, Jessica Hunt,BA, John Peteet, MD, Holly G. Prigerson, PhD, Tyler J. VanderWeele, PhD, and Tracy A.Balboni, MD, MPHCenter for Psycho-Oncology and Palliative Care Research (M.J.B., A.C.P., S.D.B., J.H., J.P.,H.G.P., T.A.B.), Departments of Psycho-Oncology and Palliative Care (M.J.B., A.C.P., S.D.B.,J.P., H.G.P., T.A.B.), Department of Chaplaincy (J.D.), and Department of Radiation Oncology(TA.B.), Dana-Farber Cancer Institute; Boston University School of Theology (M.J.B.);Department of Society, Human Development and Health (A.B.) and Departments of Epidemiologyand Biostatistics (T.J.V.), Harvard School of Public Health; Department of Medical Oncology(E.G.) and Department of Radiation Oncology (L.K.), Boston Medical Center; and HarvardMedical School Center for Palliative Care (S.D.B., J.P., H.G.P., T.A.B.), Boston, Massachusetts,USA
AbstractContext—Although prayer potentially serves as an important practice in offering religious/spiritual support, its role in the clinical setting remains disputed. Few data exist to guide the role ofpatient-practitioner prayer in the setting of advanced illness.
Objectives—To inform the role of prayer in the setting of life-threatening illness, this study usedmixed quantitative-qualitative methods to describe the viewpoints expressed by patients withadvanced cancer, oncology nurses, and oncology physicians concerning the appropriateness ofclinician prayer.
Methods—This is a cross-sectional, multisite, mixed-methods study of advanced cancer patients(n = 70), oncology physicians (n = 206), and oncology nurses (n = 115). Semistructured interviewswere used to assess respondents’ attitudes toward the appropriate role of prayer in the context ofadvanced cancer. Theme extraction was performed based on interdisciplinary input usinggrounded theory.
Results—Most advanced cancer patients (71%), nurses (83%), and physicians (65%) reportedthat patient-initiated patient-practitioner prayer was at least occasionally appropriate. Furthermore,clinician prayer was viewed as at least occasionally appropriate by the majority of patients (64%),nurses (76%), and physicians (59%). Of those patients who could envision themselves asking theirphysician or nurse for prayer (61%), 86% would find this form of prayer spiritually supportive.Most patients (80%) viewed practitioner-initiated prayer as spiritually supportive. Open-endedresponses regarding the appropriateness of patient-practitioner prayer in the advanced cancersetting revealed six themes shaping respondents’ viewpoints: necessary conditions for prayer,
© 2011 U.S. Cancer Pain Relief Committee Published by Elsevier Inc. All rights reserved.
Address correspondence to: Michael J. Balboni, PhD, ThM, Center for Psycho-Oncology and Palliative Care Research, Dana-FarberCancer Institute, 44, Binney Street, Boston, MA 02120, USA. [email protected].
DisclosuresNone of the authors have relationships with any entities having financial interest in this topic.
NIH Public AccessAuthor ManuscriptJ Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
Published in final edited form as:J Pain Symptom Manage. 2011 May ; 41(5): 836–847. doi:10.1016/j.jpainsymman.2010.07.008.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
potential benefits of prayer, critical attitudes toward prayer, positive attitudes toward prayer,potential negative consequences of prayer, and prayer alternatives.
Conclusion—Most patients and practitioners view patient-practitioner prayer as at leastoccasionally appropriate in the advanced cancer setting, and most patients view prayer asspiritually supportive. However, the appropriateness of patient-practitioner prayer is case specific,requiring consideration of multiple factors.
KeywordsPrayer; spirituality; religion; spiritual care; end-of-life care; palliative care
IntroductionPrayer is the most common spiritual practice among patients facing illness1–3 and is afrequent means by which religion and/or spirituality (R/S) helps patients endure and findmeaning in the context of advanced illness.1 In patient surveys, between 19% and 67%indicate that they would like prayer from their nurse or physician,4–7 with the frequency ofdesiring patient-practitioner prayer increasing with greater illness severity and with the formof prayer offered (silent vs. aloud).5,8 In a national sample of physicians, 83% agreed that itwas appropriate to pray with patients under some conditions.9 Physician openness towardparticipating in prayer depends on illness severity,10,11 form of prayer,11 and initiator(patient vs. caregiver).9,11 Only 19% of physicians report at least “sometimes” praying withpatients under any conditions.12 Among nurses, between 53% and 66% frequently offerprivate prayers,13,14 whereas 8%–30% report directly praying with patients.13,15
Recognition of the importance of spiritual care for patients with advanced illness is reflectedin the incorporation of spiritual care into palliative care guidelines.16,17 Among advancedcancer patients, spiritual support from the medical team has been shown to be associatedwith greater hospice use, decreased futile aggressive care, and improved quality of life neardeath.18 Although prayer potentially serves as an important practice in offering R/Ssupport,1 its role in the clinical setting remains disputed.19,20 Furthermore, little data exist toguide the role of patient-practitioner prayer in the setting of advanced illness. Given theimportant role of spiritual support in end-of-life care,16,17,21 the importance of prayer amongpatients facing advanced illness,1–3 and the frequent desire for patient-practitioner prayeramong patients facing serious illness,5,22 data are needed to inform the appropriate role ofprayer in the setting of advanced illness.
The Religion and Spirituality in Cancer Care study is a multisite, cross-sectional study ofadvanced, incurable cancer patients, oncology nurses, and oncology physicians using mixedqualitative and quantitative methods to characterize patient and practitioner viewpoints ofthe appropriate role of prayer in the setting of life-threatening illness.
MethodsStudy Sample
Patients and practitioners were enrolled between March 3, 2006 and December 31, 2008.Eligibility criteria for patients included diagnosis of an advanced, incurable cancer; activereceipt of palliative radiotherapy; age ≥21 years; and adequate stamina to undergo a 45-minute interview. Oncology physicians and nurses were eligible if they cared for incurablecancer patients. Excluded patients were those that met criteria for delirium or dementia byneurocognitive examination (Short Portable Mental Status Questionnaire23) and those notspeaking English or Spanish.
Balboni et al. Page 2
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Study ProtocolAll research staff underwent a one-day training session in the study protocol and scriptedinterview. Patients and practitioners were from four Boston, Massachusetts sites: Beth IsraelDeaconess Medical Center, Boston Medical Center, Brigham and Women’s Hospital, andDana-Farber Cancer Institute. Patients were randomly selected from radiotherapy schedules;all eligible patients were approached. To mitigate selection bias, study staff informed allpotential participants, “You do not have to be religious or spiritual to answer thesequestions. We want to hear from people with all types of points of view.” Practitioners wereidentified by collecting e-mail addresses from departmental websites. Participants providedinformed consent according to protocols approved by each site’s human subjects committee(institutional review board-approved “implied informed consent” among practitioners). Of103 patients approached, 75 (response rate [RR] = 73%) participated, with no differences inparticipants vs. nonparticipants in age, gender, or race. The most frequent reasons for non-participation were “not interested” (n = 8, 32%) and “too busy” (n = 7, 28%). Five patientswere too ill to complete the interview, yielding 70 patients (93% of 75). Of 538 physiciansand nurses contacted, 339 responded (RR = 63%). Eight reported not seeing incurablecancer patients, giving 331 respondents (98% of 339, 206 physicians and 115 nurses).
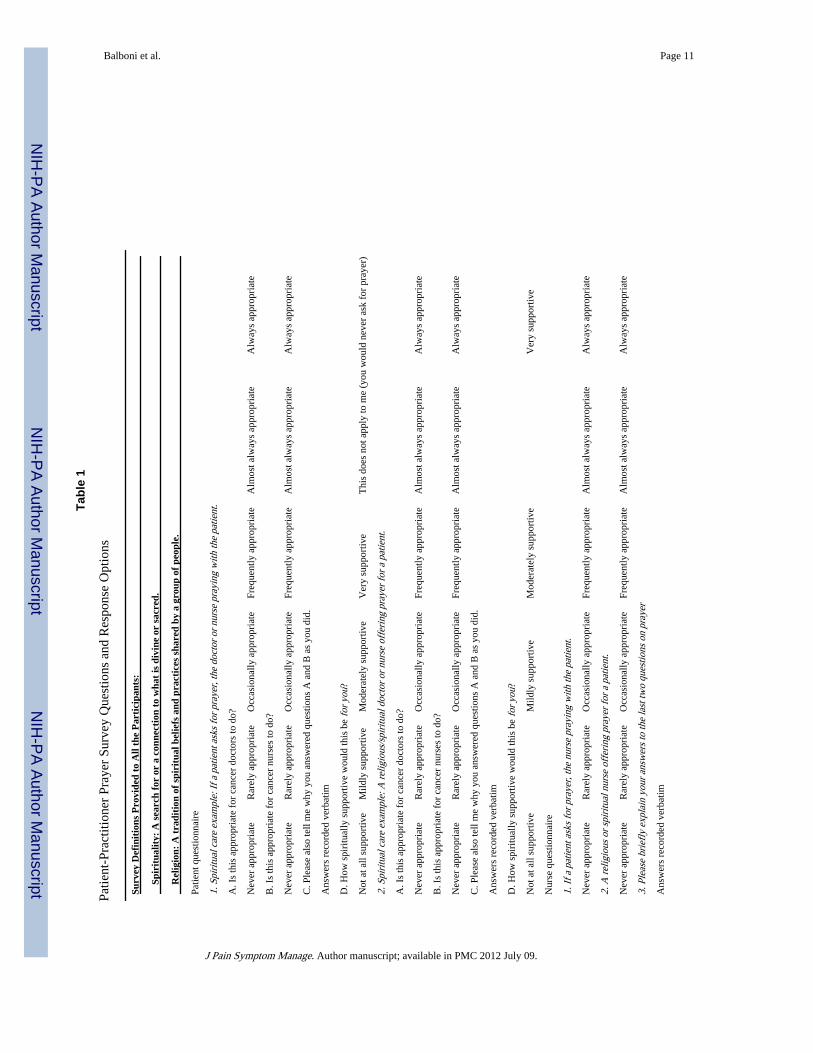
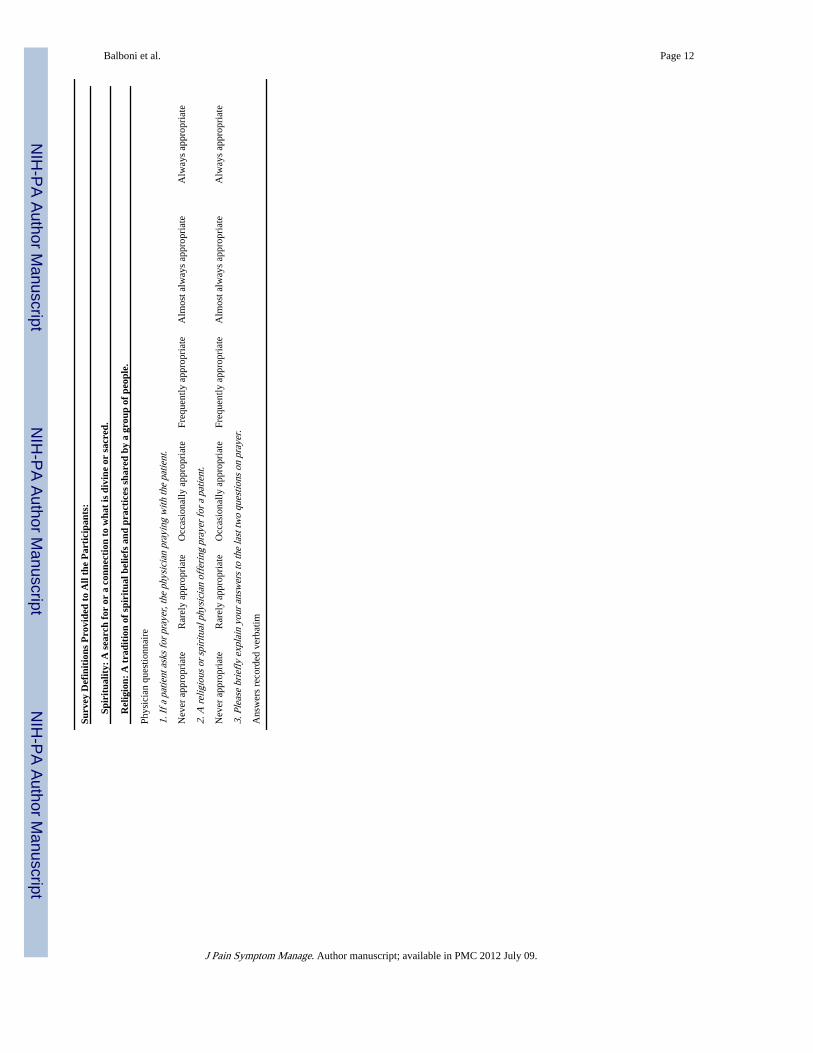
Study MeasuresPerceptions of Patient-Practitioner Prayer—Participants responded to two prayerscenarios—patient-initiated prayer and practitioner-initiated prayer—with items shown inTable 1. Participants rated (6-point scale) their perceptions of the appropriateness of prayerin each setting, and then provided open-ended explanations of their answers (recordedverbatim). Patients then rated how spiritually supportive patient-practitioner prayer would befor them (4-point scale).
Other Measured Variables—Age, gender, race/ethnicity, and years of education werepatient reported. Karnofsky performance status was obtained by physician assessment.Practitioner demographics included age, gender, race, field of oncology (medical, radiation,or surgical oncology), and years of practice.
Analytical MethodsQuantitative Methodology—Differences between patient and practitioner quantitativelyassessed perspectives of the appropriateness of patient-practitioner prayer (dichotomized bya median split to “never” and “rarely” vs. “occasionally,” “frequently,” “almost always,”and “always” appropriate) were assessed using Chi-squared statistics. Predictors of viewingpatient-practitioner prayer as at least occasionally appropriate were assessed usingunivariable logistic regression models. Multivariable analyses were then performed andincluded all significant and marginally significant (P ≤ 0.10) univariable predictors.Statistical analyses were performed with SAS version 9.1 (SAS Institute Inc., Cary, NC). Allreported P-values are two-sided and considered significant when less than 0.05.
Qualitative Methodology—The analysis followed standard qualitative methodology24—triangulated analysis, employment of multidisciplinary perspectives (medicine, chaplaincy,theology, sociology), and the use of reflexive narratives—aimed to maximize thetransferability of interview data. Transcriptions were independently coded line by line bytwo researchers (M. J. B. and J. D.), and were then compiled into two preliminary codingschemes. Following principles of grounded theory,25 a final set of themes and subcodesinductively emerged through an iterative process of constant comparison, with input fromM. J. B., J. D., A. C. P., and T. A. B. Transcripts were then recoded by M. J. B. and J. D.each working independently. The interrater reliability score was high (kappa = 0.79).
Balboni et al. Page 3
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
ResultsSample Characteristics
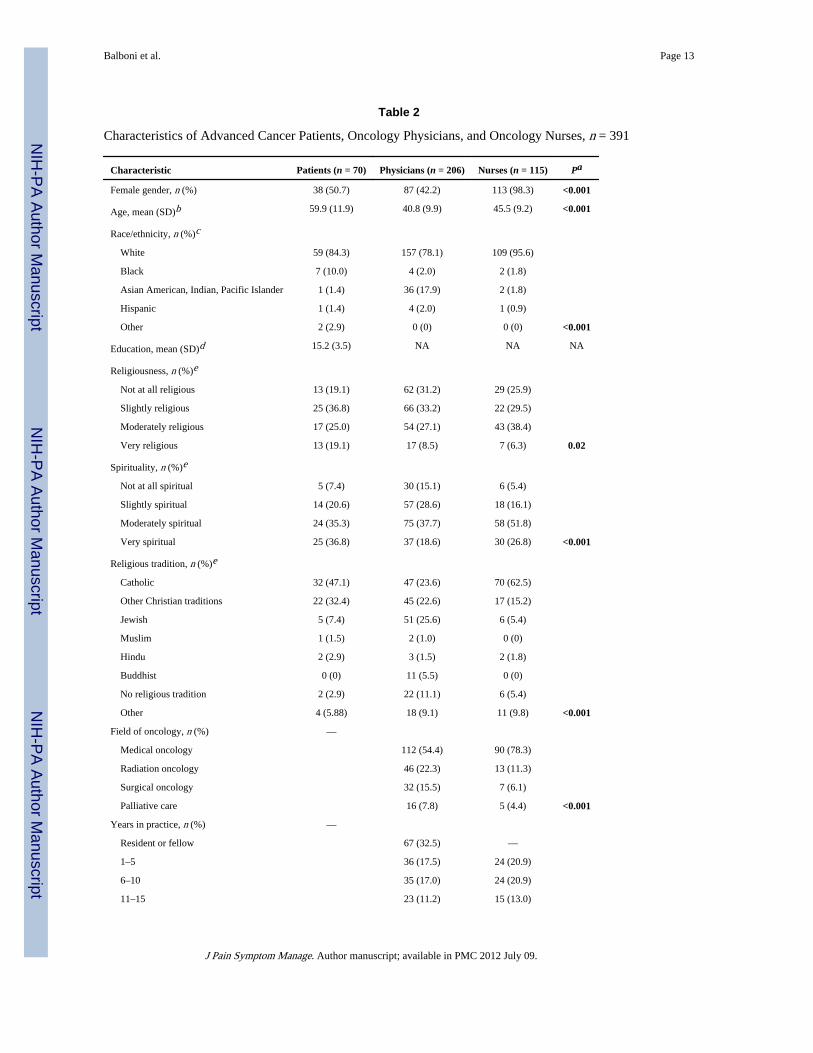
Sample characteristics are shown in Table 2. There were significant differences betweenpatients, physicians, and nurses in regard to age, gender, race, religiousness, spirituality, andreligious identification. The majority of patients (87.5%), physicians (78%), and nurses(77%) were both (slightly, moderately, or very) spiritual and religious.
Quantitative Assessment of Perceptions of Patient-Practitioner PrayerThe majority of respondents indicated that patient-initiated prayer and practitioner-initiatedprayer are at least occasionally appropriate in the cancer setting (Fig. 1). Nurses weresignificantly more likely than physicians to view both forms of patient-practitioner prayer asat least occasionally appropriate. When comparing participants’ views of patient-vs.practitioner-initiated prayer, patients, nurses, and physicians more frequently rated patient-initiated prayer as at least occasionally appropriate (Chi-squared value = 4.34, degrees offreedom [DF] = 1, P = 0.03; Chi-squared value = 35.97, DF = 1, P < 0.001; Chi-squaredvalue = 30.08, DF = 1, P < 0.001, respectively).
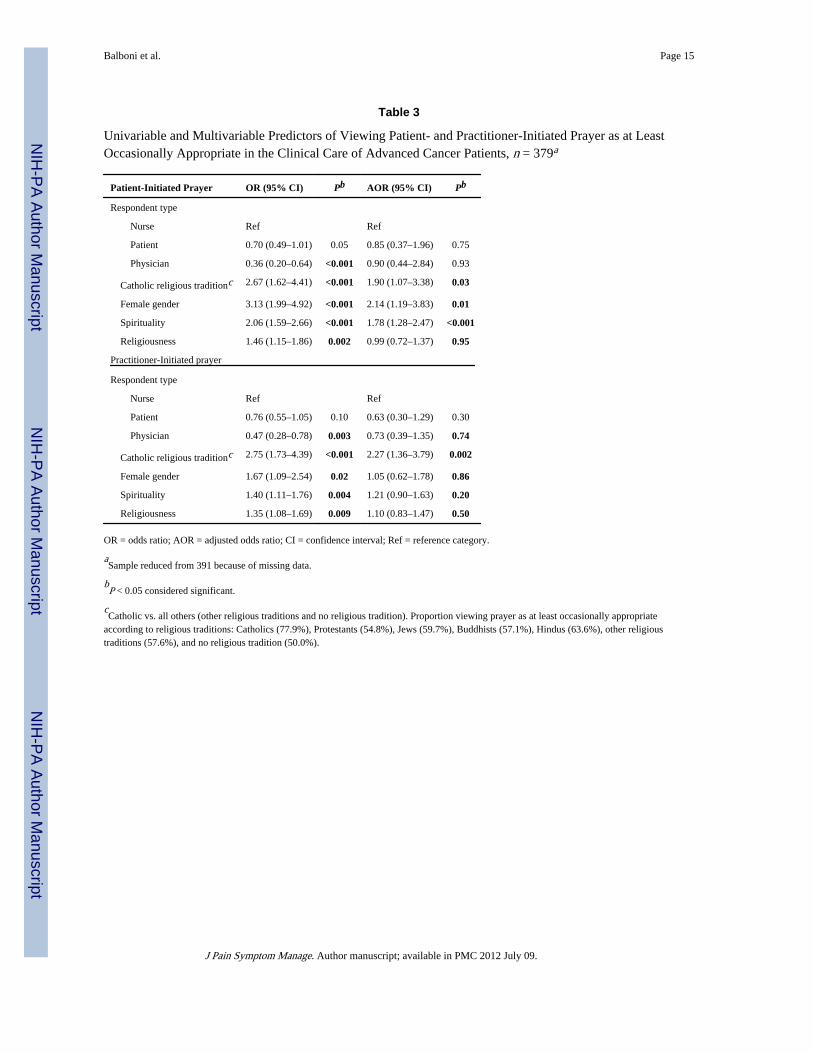
Univariable and multivariable analyses of predictors of perceptions of prayer in theadvanced cancer clinical setting are shown in Table 3. In univariable analyses, respondentswere more likely to view patient-initiated prayer and practitioner-initiated prayer as at leastoccasionally appropriate if they were female, more spiritual, and more religious. Perceptionsof patient-practitioner prayer also were influenced by religious affiliation, with Catholicsbeing the most likely to perceive patient-practitioner prayer as at least occasionallyappropriate. Age, race, years of practice, and field of oncology were not predictive ofperceptions of practitioner-initiated prayer. In multivariable analyses, Catholic religioustradition, female gender, and increasing spirituality were significant predictors of viewingpatient-initiated prayer as at least occasionally appropriate; whereas Catholic religioustradition was the only factor that remained a significant predictor of viewing practitioner-initiated prayer as at least occasionally appropriate. Notably, in multivariable analyses,respondent type (patient, physician, or nurse) no longer predicted perceptions of patient-practitioner prayer.
A sizable minority of patients (38.6%) indicated they would never ask their nurse orphysician for prayer. Of those who would potentially request prayer, most (86.0%) ratedreceiving prayer in that setting as at least mildly supportive (62.8% moderately to verysupportive). Most patients (80.0%) rated a practitioner offering prayer as at least mildlyspiritually supportive (55.7% moderately to very supportive).
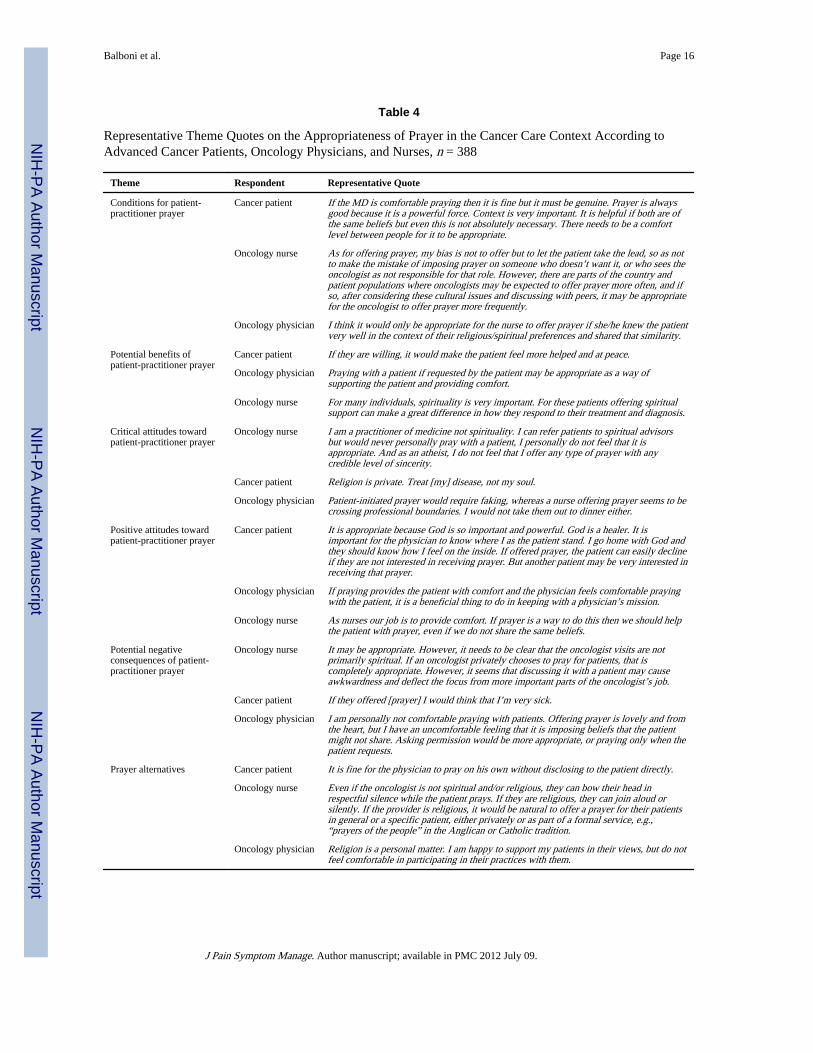
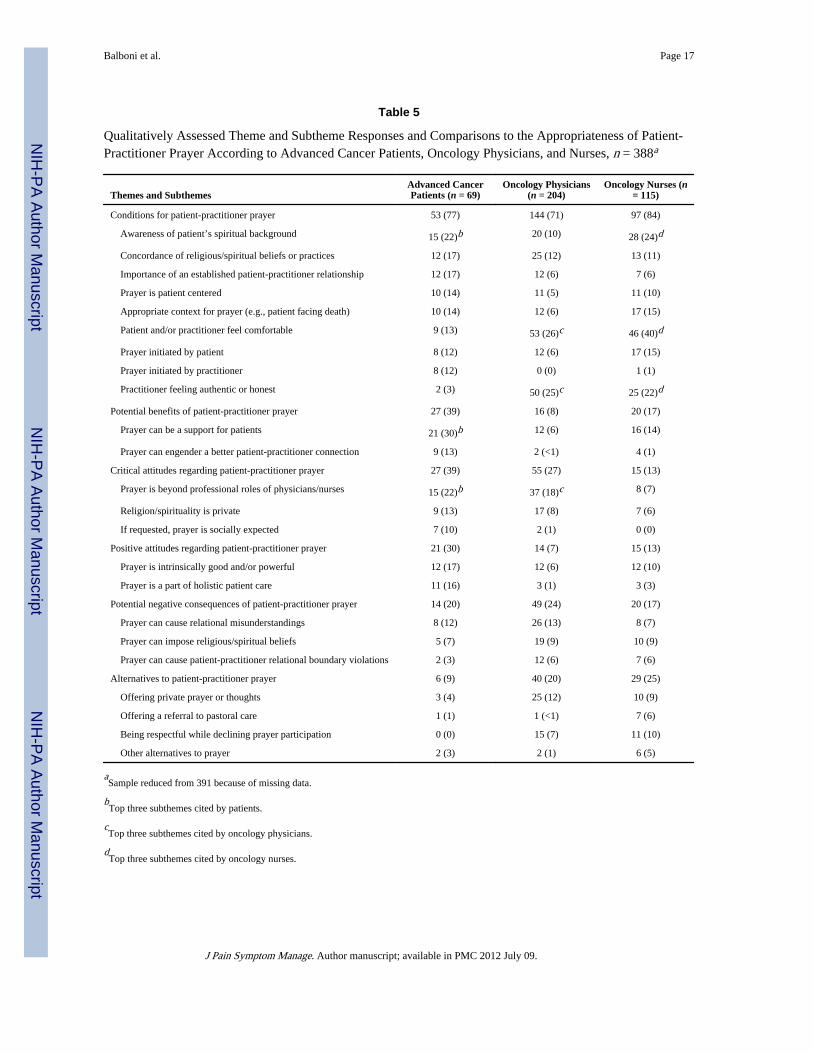
Qualitative Assessment of Perceptions of Patient-Practitioner PrayerThe six primary themes extracted from participants’ open-ended descriptions of theappropriate role of patient-practitioner prayer in the cancer setting are shown in Table 4 withillustrative quotes. Qualitative theme and subtheme frequencies are provided in Table 5.
The “conditions for patient-practitioner prayer” theme was defined as the conditionsrequired for prayer to be appropriate in the clinical setting. One physician exemplified thistheme by stating, “It depends on the spirituality of the patient, the relationship between thepatient and physician, and the comfort level of the physician.” Among patients, the mostcited conditions were the practitioner knowing the patient’s spiritual background, thepresence of a prior established patient-physician relationship, and concordance of patientand practitioner R/S beliefs. For example, one patient expressed feeling uncomfortablereceiving prayer from a practitioner with potentially differing beliefs by emphatically stating
Balboni et al. Page 4
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

“I don’t know who the person is praying to.” For physicians and nurses, the most frequentlycited condition was the practitioner and/or patient feeling comfortable, a theme exemplifiedby a nurse: “I think it depends on the spirituality of the nurse and her comfort bringing thisinto care.”
The “potential benefits of patient-practitioner prayer” theme was defined as potentialpositive outcomes of patient-practitioner prayer. The most frequently raised subtheme wasthe potential for prayer to be a source of support for cancer patients, as illustrated by onepatient: “Because I think prayer is as important a part of the treatment as conventionalmedicine itself. It is another way for doctors and nurses to hold out a hand.” Another viewnoted prayer can foster a better patient-practitioner relationship. One patient stated,“Because [prayer] would make me feel that they care for me to take time to pray. It showsthat they are feeling people.” Similarly, one physician explained, “[Prayer] can’t hurt and itfosters closeness between doctor and patient.”
The “critical attitudes regarding patient-practitioner prayer” theme was defined as criticalpresuppositions underlying participants’ perceptions of patient-practitioner prayer. The mostcommon subtheme for all groups was the view that prayer may violate professionalboundaries. One patient explained, “The patient expects objectivity from the physician. Tochange that role would not be offensive but it would be a challenge to get used to. I have animage of a doctor I knew who would remove his stethoscope when talking to patients on aspiritual level.” One physician said, “Ideally there should be a division of labor between thephysician and spiritual guide. The two strike me as separate roles and disciplines.” The nextmost common subtheme for all groups was that R/S are private matters. One nurse stated,“[I] want to keep my religious beliefs and practices private.”
The “positive attitudes regarding patient-practitioner prayer” theme was defined as positivepresuppositions underlying respondents’ views of patient-practitioner prayer. The mostcommon subtheme was that prayer is intrinsically good and/or powerful, as illustrated byone nurse who said, “To me a prayer is not about religion. It is a group of words which canbring about hope, meaning and peace to a person.” A second subtheme was the view thatprayer is part of a holistic approach to patient care, illustrated by one patient who inexplaining the appropriateness of patient-practitioner prayer stated, “Doctors and nursesneed to touch the patient where the patient is. This is important to healing.” Similarly, aphysician stated, “While prayer is personal, it may be appropriate in the context of holistichealing.”
The “potential negative consequences of patient-practitioner prayer” theme was defined aspossible deleterious outcomes of patient-practitioner prayer. Subthemes included thepotential for patient-practitioner prayer to cause relational misunderstandings. Thissubtheme was illustrated by one physician who explained, “The physician might be seen asgiving up on the medical/scientific approach.” Also raised were concerns regarding prayercausing an imposition of religious beliefs, as illustrated by one patient who stated, “Youdon’t want the patient to feel pressured by the doctor’s religiosity.” A third subtheme wasthe potential for prayer to cause boundary violations in the patient-practitioner relationship.One physician shared, “[Patient-practitioner prayer] depends on the oncologist’s comfort,beliefs and relationship with the patient. In some cases there is a boundary, in others there isnot.”
The “prayer alternatives” theme was defined as alternatives to prayer considered potentiallymore appropriate than patient-practitioner prayer. Alternatives included showing respectwithout active participation in prayer, described by one nurse who shared, “I have stoodrespectfully in the room when prayers were offered of other faiths. If of my faith and the
Balboni et al. Page 5
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
patient asked me to stay, I have said blessings of recovery.” Another alternative was privatepractitioner prayer. One physician described, “Private prayer is appropriate as a way todemonstrate caring for a patient. Sometimes I might pray for a patient without theirknowledge just as a human being, which I think is always or almost always appropriate, butI am wary as an oncologist of taking a more formal, spiritual role.”
DiscussionOur findings indicate that the majority of patients, nurses, and physicians view patient-practitioner prayer as at least occasionally appropriate in the advanced cancer setting, andthat most patients would find this practice spiritually supportive. Although viewed as lessfrequently appropriate than patient-initiated prayer, the majority of respondents viewedpractitioner-initiated prayer as at least occasionally appropriate, a finding that stands incontrast to assertions that prayer should always be patient initiated.20,26 These findings areconsistent with prior reports indicating that patient-practitioner prayer is more frequentlyconsidered appropriate in the setting of life-threatening illnesses when compared with othersettings.5,11 Our study indicates that engagement of patient-practitioner prayer is best done,however, after considering key factors influencing the appropriateness of prayer in theclinical setting, indicated by six qualitatively derived themes.
First, optimal conditions for prayer should be appreciated, such as knowing the patients’spiritual background, sharing concordance of beliefs, and weighing personal comfort andability to be authentic. The noted conditions highlight the central role of taking a spiritualhistory,27 which provides cues to guide all subsequent spiritual care, including theappropriateness of prayer in the clinical setting. Factors found to quantitatively predictperceptions of the role of prayer in the clinical setting (e.g., Catholic religious tradition,increasing spirituality, gender) can also aid in informing the optimal context for patient-practitioner prayer.
Next, although practitioners should acknowledge that prayer is spiritually supportive formost patients, they also should weigh potential negative consequences, such as creatingdiscomfort or distance with a patient who may not share the same belief system, may beuncomfortable with prayer in the medical setting, or may feel the clinician is imposing his orher R/S beliefs. Strategies to mitigate negative outcomes can be considered, such as ensuringconcordance in R/S beliefs or offering prayer in a manner that provides comfortable ways todecline (e.g., simultaneously offering chaplaincy referrals).28 Beyond considering potentialconsequences, engagement in patient-practitioner prayer requires reflection by clinicians ontheir own and their patients’ underlying attitudes. For example, if practitioners feel thatprayer is beyond their personal beliefs or professional roles, they should feel no obligation toparticipate in prayer. However, practitioners should weigh this view with the potential forprayer and other forms of spiritual care to benefit the patient and foster holistic care.Bringing these contrasting influences together, practitioners can offer spiritual careconsistent with their own beliefs and professional commitments, such as calling onchaplaincy or remaining respectfully silent during patient prayer.29 Likewise, a practitionerwho holds that patient-practitioner prayer is a part of holistic care must weigh this attitudeagainst potential negative consequences. Beyond reflecting on underlying attitudes,clinicians also should be aware of the potential for countertransference and non–patient-centered motivations in the practice of patient-provider prayer,30 such as a clinician offeringprayer in response to a personal emotion or agenda (e.g., to ease guilt over diseaseprogression). The ability to prudentially consider potential consequences, underlyingattitudes, personal emotions, and motivations regarding patient-practitioner prayer hinges onpractitioners incorporating spiritual assessments as part of initial and ongoing care and being
Balboni et al. Page 6
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

constructively aware of personal viewpoints, emotional responses to patients, and biasesregarding R/S in the medical setting.
Finally, caregivers should consider prayer alternatives, such as offering private prayer orrelying on other members of the health care team such as chaplains,31 while communicatingrespectful acknowledgment of patients’ R/S beliefs and practices even if decliningparticipation.29 Patient-practitioner prayer involves some degree of shared experience of R/Sand a shared willingness to invite that experience into the patient-practitioner relationship.Whether personal irreligiousness, deeply held R/S beliefs, or conviction that prayer isoutside the practitioner’s role, a number of factors circumscribe the appropriateness ofpatient-practitioner prayer. The frequent differences between patients and practitioners inregard to R/S characteristics, as noted in our sample and in others,32 only further highlightthe importance of spiritual care approaches that sidestep potential conflicts associated withdivergent beliefs and practices. Examples of such conflicts not only include a religiouspractitioner imposing R/S beliefs on a patient, but also can include an irreligious practitionerfailing to acknowledge a patient’s R/S beliefs or issues, potentially disregarding existentialneeds1 and medically relevant information.33 Awareness and facility with other forms ofspiritual care (e.g., taking a spiritual history) equips practitioners to navigate R/S on a case-by-case basis, recognizing that although the role of prayer should always remain voluntary,practitioners hold a central role as facilitators of spiritual care in the setting of advancedillness.21,27,31,34
Study limitations include the fact that respondents were surveyed from a single U.S. region.Given that this region has lower than national averages of religiosity, spirituality, and dailydependence on prayer,35 our study may underestimate the perceived appropriateness ofpatient-practitioner prayer and overestimate negative perceptions, although suchcharacteristics may aid in conservatively informing the role of prayer in the medical setting.Last, the generalizability of these findings to other diseases or illness severities is unknown;further studies are required to define the role of patient-practitioner prayer in other settings.
In conclusion, this study demonstrates that the majority of patients, physicians, and nursesview patient-practitioner prayer as at least occasionally appropriate in the setting ofadvanced cancer. Furthermore, most patients view patient-practitioner prayer as spirituallysupportive. Perceptions of prayer are shaped by key factors that inform its appropriatenesson a case-by-case basis. These factors highlight the essential role of regular spiritualassessments by clinicians21,27 and the importance of a multidisciplinary approach in theprovision of patient-centered spiritual care.
AcknowledgmentsThis research was supported in part by an American Society of Clinical Oncology Young Investigator Award to Dr.Tracy Balboni.
References1. Alcorn SA, Balboni MJ, Prigerson HG, et al. “If God wanted me yesterday, I wouldn’t be here
today”: religious and spiritual themes in patients’ experiences of advanced cancer. J Palliat Med.2010; 13:581–588. [PubMed: 20408763]
2. Balboni TA, Vanderwerker LC, Block SD, et al. Religiousness and spiritual support amongadvanced cancer patients and associations with end-of-life treatment preferences and quality of life.J Clin Oncol. 2007; 25:555–560. [PubMed: 17290065]
3. Koenig HG. Religious attitudes and practices of hospitalized medically ill older adults. Int J GeriatrPsychiatry. 1998; 13:213–224. [PubMed: 9646148]
Balboni et al. Page 7
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
4. King DE, Bushwick B. Beliefs and attitudes of hospital inpatients about faith healing and prayer. JFam Pract. 1994; 39:349–352. [PubMed: 7931113]
5. MacLean CD, Susi B, Phifer N, et al. Patient preference for physician discussion and practice ofspirituality. J Gen Intern Med. 2003; 18:38–43. [PubMed: 12534762]
6. Oyama O, Koenig HG. Religious beliefs and practices in family medicine. Arch Fam Med. 1998;7:431–435. [PubMed: 9755735]
7. Taylor EJ, Mamier I. Spiritual care nursing: what cancer patients and family caregivers want. J AdvNurs. 2005; 49:260–267. [PubMed: 15660550]
8. McCord G, Gilchrist VJ, Grossman SD, et al. Discussing spirituality with patients: a rational andethical approach. Ann Fam Med. 2004; 2:356–361. [PubMed: 15335136]
9. Curlin FA, Lawrence RE, Odell S, et al. Religion, spirituality, and medicine: psychiatrists’ and otherphysicians’ differing observations, interpretations, and clinical approaches. Am J Psychiatry. 2007;164:1825–1831. [PubMed: 18056237]
10. Luckhaupt SE, Yi MS, Mueller CV, et al. Beliefs of primary care residents regarding spiritualityand religion in clinical encounters with patients: a study at a midwestern U.S. teaching institution.Acad Med. 2005; 80:560–570. [PubMed: 15917361]
11. Monroe MH, Bynum D, Susi B, et al. Primary care physician preferences regarding spiritualbehavior in medical practice. Arch Intern Med. 2003; 163:2751–2756. [PubMed: 14662629]
12. Curlin FA, Chin MH, Sellergren SA, Roach CJ, Lantos JD. The association of physicians’religious characteristics with their attitudes and self-reported behaviors regarding religion andspirituality in the clinical encounter. Med Care. 2006; 44:446–453. [PubMed: 16641663]
13. Taylor EJ, Amenta M, Highfield M. Spiritual care practices of oncology nurses. Oncol NursForum. 1995; 22:31–39. [PubMed: 7708523]
14. Taylor EJ, Outlaw FH. Use of prayer among persons with cancer. Holist Nurs Pract. 2002; 16:46–60. [PubMed: 11913227]
15. King MO, Pettigrew AC, Reed FC. Complementary, alternative, integrative: have nurses kept pacewith their clients? Medsurg Nurs. 1999; 8:249–256. [PubMed: 10661161]
16. National Consensus Project for Quality Palliative Care. [Accessed March 1, 2010] Clinical practiceguidelines for quality palliative care. 2009. Available fromhttp://www.nationalconsensusproject.org/Guidelines_Download.asp
17. World Health Organization. [Accessed May 15, 2009] Integrated Management of Adolescent andAdult Illness (IMAI) modules: palliative care: symptom management and end-of-life care. 2004.Available fromhttp://www.who.int/3by5/publications/documents/en/genericpalliativecare082004.pdf
18. Balboni TA, Paulk ME, Balboni MJ, et al. Provision of spiritual care to patients with advancedcancer: associations with medical care and quality of life near death. J Clin Oncol. 2010; 28:445–452. [PubMed: 20008625]
19. Sloan RP, Bagiella E, VandeCreek L, et al. Should physicians prescribe religious activities? NEngl J Med. 2000; 342:1913–1916. [PubMed: 10861331]
20. Post SG, Puchalski CM, Larson DB. Physicians and patient spirituality: professional boundaries,competency, and ethics. Ann Intern Med. 2000; 132:578–583. [PubMed: 10744595]
21. Puchalski C, Ferrell B, Virani R, et al. Improving the quality of spiritual care as a dimension ofpalliative care: the report of the Consensus Conference. J Palliat Med. 2009; 12:885–904.[PubMed: 19807235]
22. Ehman JW, Ott BB, Short TH, Ciampa RC, Hansen-Flaschen J. Do patients want physicians toinquire about their spiritual or religious beliefs if they become gravely ill? Arch Intern Med. 1999;159:1803–1806. [PubMed: 10448785]
23. Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficitin elderly patients. J Am Geriatr Soc. 1975; 23:433–441. [PubMed: 1159263]
24. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001; 358:483–488. [PubMed: 11513933]
25. Corbin, JM.; Strauss, AL. Basics of qualitative research: Techniques and procedures fordeveloping grounded theory. 3. Los Angeles, CA: Sage Publications; 2008.
Balboni et al. Page 8
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
26. Pembroke NF. Appropriate spiritual care by physicians: a theological perspective. J Relig Health.2008; 47:549–559. [PubMed: 19093681]
27. Puchalski CM. Spirituality and end-of-life care: a time for listening and caring. J Palliat Med.2002; 5:289–294. [PubMed: 12006231]
28. Koenig, HG. Spirituality in patient care: Why, how, when, and what. 2. Philadelphia, PA:Templeton Foundation Press; 2007.
29. Lo B, Kates LW, Ruston D, et al. Responding to requests regarding prayer and religiousceremonies by patients near the end of life and their families. J Palliat Med. 2003; 6:409–415.[PubMed: 14509486]
30. Josephson, AM.; Peteet, JR. Handbook of spirituality and worldview in clinical practice. 1.Washington, DC: American Psychiatric Publishing, Inc; 2004.
31. Handzo G, Koenig HG. Spiritual care: whose job is it anyway? South Med J. 2004; 97:1242–1244.[PubMed: 15646763]
32. Curlin FA, Lantos JD, Roach CJ, Sellergren SA, Chin MH. Religious characteristics of U.S.physicians: a national survey. J Gen Intern Med. 2005; 20:629–634. [PubMed: 16050858]
33. Phelps AC, Maciejewski PK, Nilsson M, et al. Religious coping and use of intensive life-prolonging care near death in patients with advanced cancer. JAMA. 2009; 301:1140–1147.[PubMed: 19293414]
34. Sulmasy DP. Spirituality, religion, and clinical care. Chest. 2009; 135:1634–1642. [PubMed:19497898]
35. The Pew Forum on Religion & Public Life. [Accessed March 1, 2010] US religious landscapesurvey. Available from http://religions.pewforum.org/maps
Balboni et al. Page 9
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
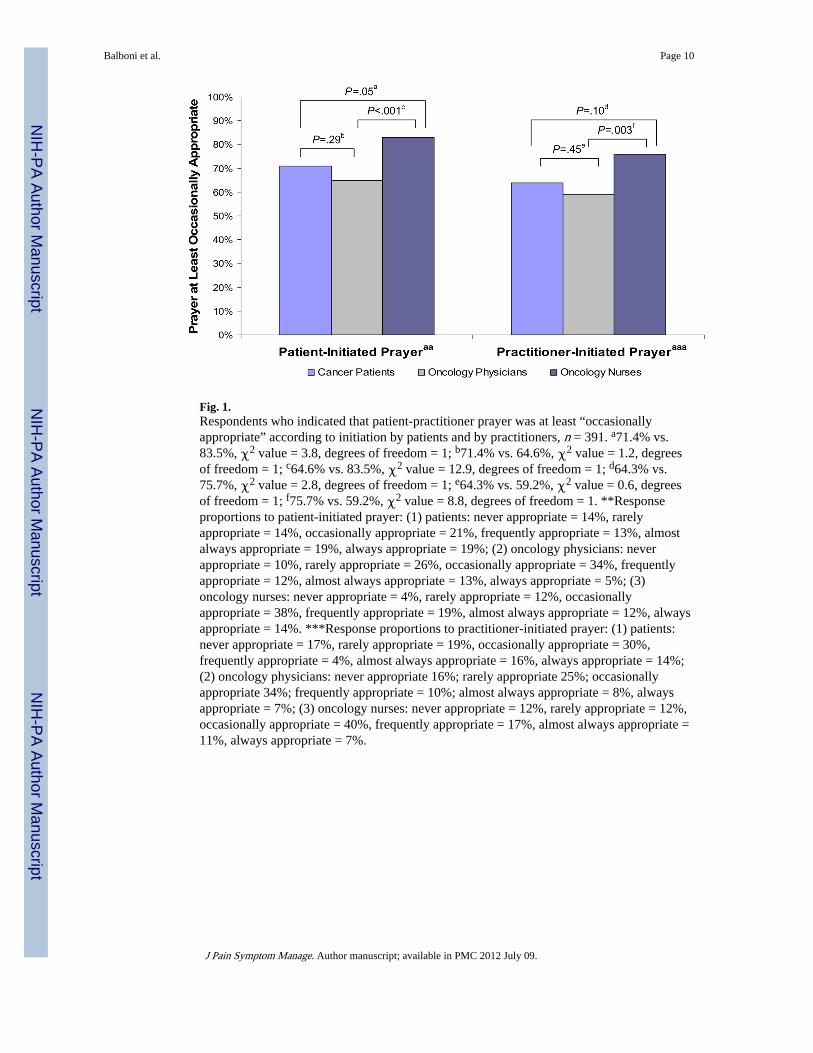
Fig. 1.Respondents who indicated that patient-practitioner prayer was at least “occasionallyappropriate” according to initiation by patients and by practitioners, n = 391. a71.4% vs.83.5%, χ2 value = 3.8, degrees of freedom = 1; b71.4% vs. 64.6%, χ2 value = 1.2, degreesof freedom = 1; c64.6% vs. 83.5%, χ2 value = 12.9, degrees of freedom = 1; d64.3% vs.75.7%, χ2 value = 2.8, degrees of freedom = 1; e64.3% vs. 59.2%, χ2 value = 0.6, degreesof freedom = 1; f75.7% vs. 59.2%, χ2 value = 8.8, degrees of freedom = 1. **Responseproportions to patient-initiated prayer: (1) patients: never appropriate = 14%, rarelyappropriate = 14%, occasionally appropriate = 21%, frequently appropriate = 13%, almostalways appropriate = 19%, always appropriate = 19%; (2) oncology physicians: neverappropriate = 10%, rarely appropriate = 26%, occasionally appropriate = 34%, frequentlyappropriate = 12%, almost always appropriate = 13%, always appropriate = 5%; (3)oncology nurses: never appropriate = 4%, rarely appropriate = 12%, occasionallyappropriate = 38%, frequently appropriate = 19%, almost always appropriate = 12%, alwaysappropriate = 14%. ***Response proportions to practitioner-initiated prayer: (1) patients:never appropriate = 17%, rarely appropriate = 19%, occasionally appropriate = 30%,frequently appropriate = 4%, almost always appropriate = 16%, always appropriate = 14%;(2) oncology physicians: never appropriate 16%; rarely appropriate 25%; occasionallyappropriate 34%; frequently appropriate = 10%; almost always appropriate = 8%, alwaysappropriate = 7%; (3) oncology nurses: never appropriate = 12%, rarely appropriate = 12%,occasionally appropriate = 40%, frequently appropriate = 17%, almost always appropriate =11%, always appropriate = 7%.
Balboni et al. Page 10
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 11
Tabl
e 1
Patie
nt-P
ract
ition
er P
raye
r Su
rvey
Que
stio
ns a
nd R
espo
nse
Opt
ions
Surv
ey D
efin
itio
ns P
rovi
ded
to A
ll th
e P
arti
cipa
nts:
Sp
irit
ualit
y: A
sea
rch
for
or a
con
nect
ion
to w
hat
is d
ivin
e or
sac
red.
R
elig
ion:
A t
radi
tion
of
spir
itua
l bel
iefs
and
pra
ctic
es s
hare
d by
a g
roup
of
peop
le.
Patie
nt q
uest
ionn
aire
1. S
piri
tual
car
e ex
ampl
e: If
a p
atie
nt a
sks
for p
raye
r, th
e do
ctor
or n
urse
pra
ying
with
the
patie
nt.
A. I
s th
is a
ppro
pria
te f
or c
ance
r do
ctor
s to
do?
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
B. I
s th
is a
ppro
pria
te f
or c
ance
r nu
rses
to d
o?
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
C. P
leas
e al
so te
ll m
e w
hy y
ou a
nsw
ered
que
stio
ns A
and
B a
s yo
u di
d.
Ans
wer
s re
cord
ed v
erba
tim
D. H
ow s
piri
tual
ly s
uppo
rtiv
e w
ould
this
be
for y
ou?
Not
at a
ll su
ppor
tive
Mild
ly s
uppo
rtiv
eM
oder
atel
y su
ppor
tive
Ver
y su
ppor
tive
Thi
s do
es n
ot a
pply
to m
e (y
ou w
ould
nev
er a
sk f
or p
raye
r)
2. S
piri
tual
car
e ex
ampl
e: A
relig
ious
/spi
ritu
al d
octo
r or n
urse
off
erin
g pr
ayer
for a
pat
ient
.
A. I
s th
is a
ppro
pria
te f
or c
ance
r do
ctor
s to
do?
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
B. I
s th
is a
ppro
pria
te f
or c
ance
r nu
rses
to d
o?
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
C. P
leas
e al
so te
ll m
e w
hy y
ou a
nsw
ered
que
stio
ns A
and
B a
s yo
u di
d.
Ans
wer
s re
cord
ed v
erba
tim
D. H
ow s
piri
tual
ly s
uppo
rtiv
e w
ould
this
be
for y
ou?
Not
at a
ll su
ppor
tive
Mild
ly s
uppo
rtiv
eM
oder
atel
y su
ppor
tive
Ver
y su
ppor
tive
Nur
se q
uest
ionn
aire
1. If
a p
atie
nt a
sks
for p
raye
r, th
e nu
rse
pray
ing
with
the
patie
nt.
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
2. A
relig
ious
or s
piri
tual
nur
se o
ffer
ing
pray
er fo
r a p
atie
nt.
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
3. P
leas
e br
iefl
y ex
plai
n yo
ur a
nsw
ers
to th
e la
st tw
o qu
estio
ns o
n pr
ayer
Ans
wer
s re
cord
ed v
erba
tim
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 12
Surv
ey D
efin
itio
ns P
rovi
ded
to A
ll th
e P
arti
cipa
nts:
Sp
irit
ualit
y: A
sea
rch
for
or a
con
nect
ion
to w
hat
is d
ivin
e or
sac
red.
R
elig
ion:
A t
radi
tion
of
spir
itua
l bel
iefs
and
pra
ctic
es s
hare
d by
a g
roup
of
peop
le.
Phys
icia
n qu
estio
nnai
re
1. If
a p
atie
nt a
sks
for p
raye
r, th
e ph
ysic
ian
pray
ing
with
the
patie
nt.
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
2. A
relig
ious
or s
piri
tual
phy
sici
an o
ffer
ing
pray
er fo
r a p
atie
nt.
Nev
er a
ppro
pria
teR
arel
y ap
prop
riat
eO
ccas
iona
lly a
ppro
pria
teFr
eque
ntly
app
ropr
iate
Alm
ost a
lway
s ap
prop
riat
eA
lway
s ap
prop
riat
e
3. P
leas
e br
iefl
y ex
plai
n yo
ur a
nsw
ers
to th
e la
st tw
o qu
estio
ns o
n pr
ayer
.
Ans
wer
s re
cord
ed v
erba
tim
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 13
Table 2
Characteristics of Advanced Cancer Patients, Oncology Physicians, and Oncology Nurses, n = 391
Characteristic Patients (n = 70) Physicians (n = 206) Nurses (n = 115) Pa
Female gender, n (%) 38 (50.7) 87 (42.2) 113 (98.3) <0.001
Age, mean (SD)b 59.9 (11.9) 40.8 (9.9) 45.5 (9.2) <0.001
Race/ethnicity, n (%)c
White 59 (84.3) 157 (78.1) 109 (95.6)
Black 7 (10.0) 4 (2.0) 2 (1.8)
Asian American, Indian, Pacific Islander 1 (1.4) 36 (17.9) 2 (1.8)
Hispanic 1 (1.4) 4 (2.0) 1 (0.9)
Other 2 (2.9) 0 (0) 0 (0) <0.001
Education, mean (SD)d 15.2 (3.5) NA NA NA
Religiousness, n (%)e
Not at all religious 13 (19.1) 62 (31.2) 29 (25.9)
Slightly religious 25 (36.8) 66 (33.2) 22 (29.5)
Moderately religious 17 (25.0) 54 (27.1) 43 (38.4)
Very religious 13 (19.1) 17 (8.5) 7 (6.3) 0.02
Spirituality, n (%)e
Not at all spiritual 5 (7.4) 30 (15.1) 6 (5.4)
Slightly spiritual 14 (20.6) 57 (28.6) 18 (16.1)
Moderately spiritual 24 (35.3) 75 (37.7) 58 (51.8)
Very spiritual 25 (36.8) 37 (18.6) 30 (26.8) <0.001
Religious tradition, n (%)e
Catholic 32 (47.1) 47 (23.6) 70 (62.5)
Other Christian traditions 22 (32.4) 45 (22.6) 17 (15.2)
Jewish 5 (7.4) 51 (25.6) 6 (5.4)
Muslim 1 (1.5) 2 (1.0) 0 (0)
Hindu 2 (2.9) 3 (1.5) 2 (1.8)
Buddhist 0 (0) 11 (5.5) 0 (0)
No religious tradition 2 (2.9) 22 (11.1) 6 (5.4)
Other 4 (5.88) 18 (9.1) 11 (9.8) <0.001
Field of oncology, n (%) —
Medical oncology 112 (54.4) 90 (78.3)
Radiation oncology 46 (22.3) 13 (11.3)
Surgical oncology 32 (15.5) 7 (6.1)
Palliative care 16 (7.8) 5 (4.4) <0.001
Years in practice, n (%) —
Resident or fellow 67 (32.5) —
1–5 36 (17.5) 24 (20.9)
6–10 35 (17.0) 24 (20.9)
11–15 23 (11.2) 15 (13.0)
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 14
Characteristic Patients (n = 70) Physicians (n = 206) Nurses (n = 115) Pa
16–20 20 (9.7) 11 (9.6)
21+ 25 (12.1) 41 (35.7) <0.001f
SD = standard deviation; NA = not assessed.
aP-values based on χ2 tests for categorical variables and analysis of variance for continuous variables; P < 0.05 considered significant.
bAge missing for 25 physicians and 8 nurses.
cRace/ethnicity missing in five physicians and one nurse.
dEducational status of physicians and nurses not assessed, but given the training requirements of these professions, can be assumed to be at least a
postgraduate education.
eReligiousness, spirituality, and religious tradition missing in seven physicians and three nurses.
fResident or fellow category combined with practice one to five years to create single category of less than five years of practice.
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 15
Table 3
Univariable and Multivariable Predictors of Viewing Patient- and Practitioner-Initiated Prayer as at LeastOccasionally Appropriate in the Clinical Care of Advanced Cancer Patients, n = 379a
Patient-Initiated Prayer OR (95% CI) Pb AOR (95% CI) Pb
Respondent type
Nurse Ref Ref
Patient 0.70 (0.49–1.01) 0.05 0.85 (0.37–1.96) 0.75
Physician 0.36 (0.20–0.64) <0.001 0.90 (0.44–2.84) 0.93
Catholic religious traditionc 2.67 (1.62–4.41) <0.001 1.90 (1.07–3.38) 0.03
Female gender 3.13 (1.99–4.92) <0.001 2.14 (1.19–3.83) 0.01
Spirituality 2.06 (1.59–2.66) <0.001 1.78 (1.28–2.47) <0.001
Religiousness 1.46 (1.15–1.86) 0.002 0.99 (0.72–1.37) 0.95
Practitioner-Initiated prayer
Respondent type
Nurse Ref Ref
Patient 0.76 (0.55–1.05) 0.10 0.63 (0.30–1.29) 0.30
Physician 0.47 (0.28–0.78) 0.003 0.73 (0.39–1.35) 0.74
Catholic religious traditionc 2.75 (1.73–4.39) <0.001 2.27 (1.36–3.79) 0.002
Female gender 1.67 (1.09–2.54) 0.02 1.05 (0.62–1.78) 0.86
Spirituality 1.40 (1.11–1.76) 0.004 1.21 (0.90–1.63) 0.20
Religiousness 1.35 (1.08–1.69) 0.009 1.10 (0.83–1.47) 0.50
OR = odds ratio; AOR = adjusted odds ratio; CI = confidence interval; Ref = reference category.
aSample reduced from 391 because of missing data.
bP < 0.05 considered significant.
cCatholic vs. all others (other religious traditions and no religious tradition). Proportion viewing prayer as at least occasionally appropriate
according to religious traditions: Catholics (77.9%), Protestants (54.8%), Jews (59.7%), Buddhists (57.1%), Hindus (63.6%), other religioustraditions (57.6%), and no religious tradition (50.0%).
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 16
Table 4
Representative Theme Quotes on the Appropriateness of Prayer in the Cancer Care Context According toAdvanced Cancer Patients, Oncology Physicians, and Nurses, n = 388
Theme Respondent Representative Quote
Conditions for patient-practitioner prayer
Cancer patient If the MD is comfortable praying then it is fine but it must be genuine. Prayer is alwaysgood because it is a powerful force. Context is very important. It is helpful if both are ofthe same beliefs but even this is not absolutely necessary. There needs to be a comfortlevel between people for it to be appropriate.
Oncology nurse As for offering prayer, my bias is not to offer but to let the patient take the lead, so as notto make the mistake of imposing prayer on someone who doesn’t want it, or who sees theoncologist as not responsible for that role. However, there are parts of the country andpatient populations where oncologists may be expected to offer prayer more often, and ifso, after considering these cultural issues and discussing with peers, it may be appropriatefor the oncologist to offer prayer more frequently.
Oncology physician I think it would only be appropriate for the nurse to offer prayer if she/he knew the patientvery well in the context of their religious/spiritual preferences and shared that similarity.
Potential benefits ofpatient-practitioner prayer
Cancer patient If they are willing, it would make the patient feel more helped and at peace.
Oncology physician Praying with a patient if requested by the patient may be appropriate as a way ofsupporting the patient and providing comfort.
Oncology nurse For many individuals, spirituality is very important. For these patients offering spiritualsupport can make a great difference in how they respond to their treatment and diagnosis.
Critical attitudes towardpatient-practitioner prayer
Oncology nurse I am a practitioner of medicine not spirituality. I can refer patients to spiritual advisorsbut would never personally pray with a patient, I personally do not feel that it isappropriate. And as an atheist, I do not feel that I offer any type of prayer with anycredible level of sincerity.
Cancer patient Religion is private. Treat [my] disease, not my soul.
Oncology physician Patient-initiated prayer would require faking, whereas a nurse offering prayer seems to becrossing professional boundaries. I would not take them out to dinner either.
Positive attitudes towardpatient-practitioner prayer
Cancer patient It is appropriate because God is so important and powerful. God is a healer. It isimportant for the physician to know where I as the patient stand. I go home with God andthey should know how I feel on the inside. If offered prayer, the patient can easily declineif they are not interested in receiving prayer. But another patient may be very interested inreceiving that prayer.
Oncology physician If praying provides the patient with comfort and the physician feels comfortable prayingwith the patient, it is a beneficial thing to do in keeping with a physician’s mission.
Oncology nurse As nurses our job is to provide comfort. If prayer is a way to do this then we should helpthe patient with prayer, even if we do not share the same beliefs.
Potential negativeconsequences of patient-practitioner prayer
Oncology nurse It may be appropriate. However, it needs to be clear that the oncologist visits are notprimarily spiritual. If an oncologist privately chooses to pray for patients, that iscompletely appropriate. However, it seems that discussing it with a patient may causeawkwardness and deflect the focus from more important parts of the oncologist’s job.
Cancer patient If they offered [prayer] I would think that I’m very sick.
Oncology physician I am personally not comfortable praying with patients. Offering prayer is lovely and fromthe heart, but I have an uncomfortable feeling that it is imposing beliefs that the patientmight not share. Asking permission would be more appropriate, or praying only when thepatient requests.
Prayer alternatives Cancer patient It is fine for the physician to pray on his own without disclosing to the patient directly.
Oncology nurse Even if the oncologist is not spiritual and/or religious, they can bow their head inrespectful silence while the patient prays. If they are religious, they can join aloud orsilently. If the provider is religious, it would be natural to offer a prayer for their patientsin general or a specific patient, either privately or as part of a formal service, e.g.,“prayers of the people” in the Anglican or Catholic tradition.
Oncology physician Religion is a personal matter. I am happy to support my patients in their views, but do notfeel comfortable in participating in their practices with them.
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Balboni et al. Page 17
Table 5
Qualitatively Assessed Theme and Subtheme Responses and Comparisons to the Appropriateness of Patient-Practitioner Prayer According to Advanced Cancer Patients, Oncology Physicians, and Nurses, n = 388a
Themes and SubthemesAdvanced CancerPatients (n = 69)
Oncology Physicians(n = 204)
Oncology Nurses (n= 115)
Conditions for patient-practitioner prayer 53 (77) 144 (71) 97 (84)
Awareness of patient’s spiritual background 15 (22)b 20 (10) 28 (24)d
Concordance of religious/spiritual beliefs or practices 12 (17) 25 (12) 13 (11)
Importance of an established patient-practitioner relationship 12 (17) 12 (6) 7 (6)
Prayer is patient centered 10 (14) 11 (5) 11 (10)
Appropriate context for prayer (e.g., patient facing death) 10 (14) 12 (6) 17 (15)
Patient and/or practitioner feel comfortable 9 (13) 53 (26)c 46 (40)d
Prayer initiated by patient 8 (12) 12 (6) 17 (15)
Prayer initiated by practitioner 8 (12) 0 (0) 1 (1)
Practitioner feeling authentic or honest 2 (3) 50 (25)c 25 (22)d
Potential benefits of patient-practitioner prayer 27 (39) 16 (8) 20 (17)
Prayer can be a support for patients 21 (30)b 12 (6) 16 (14)
Prayer can engender a better patient-practitioner connection 9 (13) 2 (<1) 4 (1)
Critical attitudes regarding patient-practitioner prayer 27 (39) 55 (27) 15 (13)
Prayer is beyond professional roles of physicians/nurses 15 (22)b 37 (18)c 8 (7)
Religion/spirituality is private 9 (13) 17 (8) 7 (6)
If requested, prayer is socially expected 7 (10) 2 (1) 0 (0)
Positive attitudes regarding patient-practitioner prayer 21 (30) 14 (7) 15 (13)
Prayer is intrinsically good and/or powerful 12 (17) 12 (6) 12 (10)
Prayer is a part of holistic patient care 11 (16) 3 (1) 3 (3)
Potential negative consequences of patient-practitioner prayer 14 (20) 49 (24) 20 (17)
Prayer can cause relational misunderstandings 8 (12) 26 (13) 8 (7)
Prayer can impose religious/spiritual beliefs 5 (7) 19 (9) 10 (9)
Prayer can cause patient-practitioner relational boundary violations 2 (3) 12 (6) 7 (6)
Alternatives to patient-practitioner prayer 6 (9) 40 (20) 29 (25)
Offering private prayer or thoughts 3 (4) 25 (12) 10 (9)
Offering a referral to pastoral care 1 (1) 1 (<1) 7 (6)
Being respectful while declining prayer participation 0 (0) 15 (7) 11 (10)
Other alternatives to prayer 2 (3) 2 (1) 6 (5)
aSample reduced from 391 because of missing data.
bTop three subthemes cited by patients.
cTop three subthemes cited by oncology physicians.
dTop three subthemes cited by oncology nurses.
J Pain Symptom Manage. Author manuscript; available in PMC 2012 July 09.




















