
Is nephrogenesis affected by preterm birth? Studies in a non-human primate model
11
doi:10.1152/ajprenal.00163.2009 297:1668-1677, 2009. First published Sep 16, 2009; Am J Physiol Renal Physiol Bertram and M. Jane Black Lina Gubhaju, Megan R. Sutherland, Bradley A. Yoder, Anthony Zulli, John F. You might find this additional information useful... 38 articles, 13 of which you can access free at: This article cites http://ajprenal.physiology.org/cgi/content/full/297/6/F1668#BIBL including high-resolution figures, can be found at: Updated information and services http://ajprenal.physiology.org/cgi/content/full/297/6/F1668 can be found at: AJP - Renal Physiology about Additional material and information http://www.the-aps.org/publications/ajprenal This information is current as of April 20, 2010 . http://www.the-aps.org/. American Physiological Society. ISSN: 0363-6127, ESSN: 1522-1466. Visit our website at (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2005 by the respective cells and vasculature, as well as to the control of body fluid volume and composition. It is published 12 times a year publishes original manuscripts on a broad range of subjects relating to the kidney, urinary tract, and their AJP - Renal Physiology on April 20, 2010 ajprenal.physiology.org Downloaded from
Transcript of Is nephrogenesis affected by preterm birth? Studies in a non-human primate model

doi:10.1152/ajprenal.00163.2009 297:1668-1677, 2009. First published Sep 16, 2009;Am J Physiol Renal Physiol
Bertram and M. Jane Black Lina Gubhaju, Megan R. Sutherland, Bradley A. Yoder, Anthony Zulli, John F.
You might find this additional information useful...
38 articles, 13 of which you can access free at: This article cites http://ajprenal.physiology.org/cgi/content/full/297/6/F1668#BIBL
including high-resolution figures, can be found at: Updated information and services http://ajprenal.physiology.org/cgi/content/full/297/6/F1668
can be found at: AJP - Renal Physiologyabout Additional material and information http://www.the-aps.org/publications/ajprenal
This information is current as of April 20, 2010 .
http://www.the-aps.org/.American Physiological Society. ISSN: 0363-6127, ESSN: 1522-1466. Visit our website at (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2005 by therespective cells and vasculature, as well as to the control of body fluid volume and composition. It is published 12 times a year
publishes original manuscripts on a broad range of subjects relating to the kidney, urinary tract, and theirAJP - Renal Physiology
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

Is nephrogenesis affected by preterm birth? Studies in a non-humanprimate model
Lina Gubhaju,1 Megan R. Sutherland,1 Bradley A. Yoder,2 Anthony Zulli,3 John F. Bertram,1
and M. Jane Black1
1Department of Anatomy and Developmental Biology, Monash University, Clayton; 2Department of Pediatrics, Universityof Utah, Salt Lake City, Utah; and 3Department of Cardiology, University of Melbourne, Austin Health and Northern Health,Heidelberg, Victoria, Australia
Submitted 18 March 2009; accepted in final form 9 September 2009
Gubhaju L, Sutherland MR, Yoder BA, Zulli A, Bertram JF,Black MJ. Is nephrogenesis affected by preterm birth? Studies ina non-human primate model. Am J Physiol Renal Physiol 297:F1668 –F1677, 2009. First published September 16, 2009;doi:10.1152/ajprenal.00163.2009.—Nephrogenesis occurs predomi-nantly in late gestation at a time when preterm infants are alreadydelivered. The aims of this study were to assess the effect of pretermbirth and the effect of antenatal glucocorticoid treatment on nephro-genesis. Preterm baboons, which were delivered at 125 days gestationand ventilated for up to 21 days postnatally, were compared withgestational controls. A cohort of preterm baboons that had beenexposed to antenatal glucocorticoids were compared with unexposedpreterm baboons. The number of glomerular generations was esti-mated using a medullary ray glomerular-counting method, and glo-merular number was estimated using unbiased stereology. CD31 andWT-1 localization was examined using immunohistochemistry andVEGF was localized using in situ hybridization. The number ofglomerular generations was not affected by preterm birth, and totalglomerular numbers were within the normal range. Kidneys weresignificantly enlarged in preterm baboons with a significant decreasein glomerular density (number of glomeruli per gram of kidney) in thepreterm kidney compared with gestational controls. Neonates exposedto antenatal steroids had an increased kidney-to-body weight ratio andalso more developed glomeruli compared with unexposed controls.Abnormal glomeruli, with a cystic Bowman’s space and shrunkenglomerular tuft, were often present in the superficial renal cortex ofboth the steroid-exposed and unexposed preterm kidneys; steroidexposure had no significant effect on the proportion of abnormalglomeruli. The proportion of abnormal glomeruli in the pretermkidneys ranged from 0.2 to 18%. In conclusion, although nephrogen-esis is ongoing in the extrauterine environment, our findings demon-strate that preterm birth, independent of steroid exposure, is associatedwith a high proportion of abnormal glomeruli in some, but not allneonatal kidneys. Whether final nephron endowment is affected inthose kidneys exhibiting a high proportion of abnormal glomeruli isyet to be confirmed.
baboon; kidney; glomerulogenesis
THE INCIDENCE OF PRETERM BIRTH is currently high, with 13% ofall babies born preterm in the United States (17) and 8% inAustralia (25). In addition, the survival of preterm infants,including extremely preterm infants, has improved substan-tially over recent years such that infants born as early as 26 wkof gestation now have a 60–80% chance of survival (28, 34).
In the human kidney, nephrogenesis commences at aroundweek 5 of gestation and is complete by 36 wk of gestation (32).
After this point, no more new nephrons are formed for the lifeof the individual. Nephrogenesis predominantly occurs in lategestation at a time when preterm infants are already delivered(20). It is important to gain an understanding of the effects ofpreterm birth on nephrogenesis since there is accumulatingepidemiological data linking premature birth with an increasedincidence of hypertension (8, 22) and adverse renal function(23) later in life; this may be linked to a reduced nephronendowment after birth (4).
To our knowledge, there has only been one previouslypublished study which has investigated the effects of pretermbirth on nephrogenesis. In the autopsy study, conducted byRodriguez et al. (31), a reduced number of glomerular gener-ations, potentially indicative of a nephron deficit, were reportedin kidneys of infants that were born preterm. It is important tonote, however, that the cohort of preterm infants in the humanautopsy study included a number of infants that were not onlypreterm but also intrauterine growth restricted (IUGR). Since itis well known that IUGR adversely impacts nephrogenesis (19,40), it is difficult to clearly differentiate the effects of pretermbirth and IUGR on nephrogenesis in the previous study. Inaddition, any abnormal effects observed in the human autop-sied kidneys may have been a direct result of a failure of thebaby to thrive after birth rather than preterm birth per se. Hencein this study we have examined the effects of preterm birth, inthe absence of IUGR, in a non-human primate model where theneonates were in relatively good health after birth.
The improved survival of preterm neonates, such as thoseborn as early as 27 wk of gestation, can be largely attributed tothe use of antenatal glucocorticoids. These have been shown toaccelerate lung maturation, thus reducing neonatal morbidityand mortality (11). Previous experimental studies have dem-onstrated a link between glucocorticoid exposure early in uteroand a reduction in nephron endowment (5, 30, 38). There is noevidence to date, however, as to the effects of clinical doses ofantenatal glucocorticoids on nephrogenesis.
Hence, the aims of the current study were first to assess theeffects of preterm birth on nephrogenesis, and second todetermine the effects of prenatal glucocorticoid treatment onnephrogenesis. To address these aims, we have used a baboon(non-human primate) model, where the ontogeny of the kidneyclosely resembles that of the human (18) and the pretermneonates are cared for in a neonatal intensive care unit afterbirth in a similar manner as human infants (6). In our model,the baboons are delivered at 125 days gestation (0.67 of totallength of gestation), a time point at which nephrogenesis is stillongoing in the baboon (18) and is approximately equivalent to27 wk of gestation in the human (27).
Address for reprint requests and other correspondence: M. J. Black, Dept. ofAnatomy and Developmental Biology, STRIP2, Bldg. 76, Monash Univ.,Victoria 3800, Australia (e-mail: [email protected]).
Am J Physiol Renal Physiol 297: F1668–F1677, 2009.First published September 16, 2009; doi:10.1152/ajprenal.00163.2009.
0363-6127/09 $8.00 Copyright © 2009 the American Physiological Society http://www.ajprenal.orgF1668
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

METHODS
Induction of Preterm Delivery and Postnatal Care
All animal experiments were undertaken at the Southwest Foun-dation for Biomedical Research (San Antonio, TX). All animal-handling procedures were approved to conform to the AmericanAssociation for Accreditation of Laboratory Animal Care guidelines.Fetal baboons were delivered prematurely by caesarean section at 125days gestation (term � 185 days). After birth, all preterm neonateswere intubated, administered 100 mg/kg surfactant (Survanta; donatedby Ross Products, Columbus, OH), and ventilated with pressure-limited infant ventilators (InfantStar; donated by Infrasonics, SanDiego, CA). All preterm neonates were also treated with ampicillinand gentamycin for the first 7–10 days of life. Further doses ofantibiotics were only administered in cases of clinically suspectedinfection; two preterm animals were administered additional doses ofvancomycin and a cephalosporin antibiotic, Fortaz (days 10–13 of lifein one preterm neonate and days 10–17 of life in the other pretermneonate).
A detailed description of the postnatal clinical and nutritionalmanagement of the preterm baboons has been previously published(39). Briefly, during the first 24 h of life, all animals receivedheparinized normal saline and 5% dextrose/water and supplementalcalcium infusion. Sufficient fluids were administered to maintainelectrolyte homeostasis, a minimal urine output of 1–2 ml �kg�1 �h�1,and blood pressure within the normal range. Parenteral nutrition wasinitiated at 24 h of life with amino acids, electrolytes, vitamins, andtrace elements. If clinically stable, enteral nutrition was initiated onday 7 of life; 10 ml �kg�1 �day�1 of donated human breast milk wasadministered by intermittent gastric infusion and once 100 ml �kg�1 �day�1
was tolerated, feeds were changed to Primilac (Bio-Serv, Frenchtown,NJ). Serum electrolytes, glucose, and hematocrit were maintainedwithin the normal range for the extremely low birth-weight infant.
None of the animals had, or required, Foley catheters or any otherform of urinary drainage device. There were also no animals that hadidentifiable urinary tract anomalies or obstructions at the time ofnecropsy.
Effect of Preterm Birth on Nephrogenesis in the Context ofAntenatal Steroids
Fetal baboons were delivered prematurely by caesarean section at125 days gestation (term � 185). Neonates were euthanized atdelivery (125 days gestation; n � 4; 2 males and 2 females) ormaintained in intensive care for 6 (n � 2; all males), 14 (n � 2; allmales), or 21 days (preterm�21 days; n � 4; all males) before beingeuthanized. Gestational-age-matched controls for the preterm�21days group were delivered and euthanized at 146 days gestation (n �4; 3 males and 1 female). All animals in the preterm�21 days groupand the 125- and 146-day gestational control groups were exposed toantenatal maternal steroids in utero. In those animals, pregnant ba-boons weighing �15 kg received 6 mg betamethasone (CelestoneSoluspan; Schering Pharmaceuticals, Kenilworth, NJ) by intramuscu-lar injection at 123 and 124 days of gestation (a dose of �0.4ml �kg�1 �day�1) (24, 33). Those same animals were compared withnon-betamethasone-exposed controls in the subsequent study de-scribed below. It is to be noted that only individual data is shown forthe baboons euthanized at 6 and 14 days, and they were only includedin the linear regression analyses; these baboons were not exposed toantenatal steroids. Kidneys from time points late in gestation (175 and185 days; n � 5; 4 males and 1 female) were used for comparisonwhen the number of glomerular generations formed within the kidneywas considered. Previously, we have shown that nephrogenesis in thebaboon is ongoing at 125 days gestation and complete by 175 daysgestation (18), so the kidneys from the 175- and 185-day gestationalcontrol groups were combined.
Effect of Prenatal Maternal Glucocorticoids on Nephrogenesis
The four betamethasone-exposed baboons euthanized at 125 daysgestation (utilized in the study described above) were compared withnon-betamethasone-exposed controls (125 days gestation; n � 6; 3males and 3 females). The four betamethasone-exposed pretermneonates maintained for 21 days postnatally (utilized in the studydescribed above) were compared with preterm controls (not exposedto antenatal betamethasone) at postnatal day 21 (preterm�21 days;n � 4; 2 males and 2 females). At postnatal day 21, the baboons wereeuthanized.
Tissue Processing, Embedding, and Sectioning
Kidneys were immersion-fixed at necropsy, cut into halves, slicedinto 2-mm slices, and sampled using a smooth fractionator approach(29). The sampled slices (8–15 slices/kidney) were embedded inglycolmethacrylate to be used for the estimation of the number ofglomeruli, the number of glomerular generations, kidney volume,mean renal corpuscle volume, and the proportion of abnormal glo-meruli. Complete slices containing both cortex and medulla wererandomly selected from the remaining slices, embedded in paraffin,and sectioned at 5 �m for the immunohistochemical analyses.
Qualitative and Quantitative Assessment of Nephrogenesis
Morphological assessment of nephrogenesis. The presence of un-differentiated metanephric mesenchyme, the branching ureteric bud,and developing glomerular structures in the form of comma- andS-shaped bodies in the outer cortex indicated that nephrogenesis wasongoing. Developed glomeruli exhibited a well-defined glomerulartuft surrounded by a distinct Bowman’s space and capsule.
Measurement of nephrogenic zone thickness. The width of thenephrogenic zone was measured using image-analysis software (Im-age Pro Plus v. 6.0 for Windows, Media Cybernetics; Silver Spring,MD). This method was based on a previous method used to measurenephrogenic zone thickness to assess renal maturity in human neona-tal kidneys (9, 12). From the serially sectioned glycolmethacrylatesections, one complete intact section from each sampled kidney slice(8–15 complete sections/kidney) was used to estimate the width of thenephrogenic zone. Each section was viewed at �200 magnification,and the width of the nephrogenic zone was measured in three separateregions of each kidney section. The nephrogenic zone was defined asthe area in the outer renal cortex exhibiting developing glomerularstructures in the form of comma and S-shaped bodies. An averagenephrogenic zone width was determined for each kidney.
Estimation of glomerular generation number. One complete intactsection from each glycolmethacrylate block (8–15 blocks/kidney) wasexamined. In each sampled section, five clearly distinguishable med-ullary rays from separate regions were identified. The number ofdeveloped glomeruli (inclusive of normal and abnormal glomeruli)along one side of each medullary ray were counted, and an averagenumber for each kidney was then determined (36).
Estimation of the number of developed glomeruli, kidney volume,and mean renal corpuscle volume. Glycolmethacrylate blocks (8–15/kidney) were serially sectioned at 20 �m with every tenth andeleventh sections collected and stained with hematoxylin and eosin.Kidney volume was then estimated using the Cavalieri principle (29).One pair of complete intact sections from each block was used for theestimation of glomerular number. Using an unbiased physical disec-tor/fractionator technique, renal corpuscle volume and the number ofglomeruli (and thereby nephrons) in the kidneys were stereologicallyestimated (3, 18). In the counting of glomeruli, only developedglomeruli (inclusive of normal and abnormal glomeruli) exhibiting awell-defined Bowman’s space and capsule were included; developingglomerular structures such as comma-shaped and S-shaped bodieswere not counted.
F1669IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

Characterization of Abnormal Glomeruli
Quantitative assessment of abnormal glomeruli. While the stereo-logical estimation of glomerular number was being undertaken, ineach field of view the number of normal and abnormal glomeruli(exhibiting a shrunken glomerular tuft and dilated Bowman’s space)was recorded and the percentage of abnormal glomeruli within thewhole kidney was determined.
Immunohistochemical analysis with the endothelial cell markerCD31 and podocyte marker Wilms tumor suppressor gene-1. Five-micrometer paraffin sections were deparaffinized, rehydrated, andrinsed in water and 10 mM Tris hydrochloride. For Wilms tumorsuppressor gene-1 (WT-1) staining, heat-induced antigen retrieval(3 � 5 min in a microwave) was undertaken in Tris-EDTA buffer (10mM Tris Base, 1 mM EDTA, 0.05% Tween 20, pH 9.0). Endogenousperoxidase activity was blocked by placing slides in an endogenousenzyme block solution (Dako) for 15 min. Sections were then incu-bated with 1% goat serum for 20–30 min. Subsequently, sectionswere incubated with the primary antibody, either a mouse anti-humanCD31 monoclonal antibody (1:15 dilution, JC70A, Dako) or a mouseanti-human WT-1 monoclonal antibody (1:100 dilution, M3561,Dako) overnight. The negative control consisted of a mouse IgGantibody raised against bacterial glucose oxidase (Dako). The sectionswere then incubated for 2 h with the Envision molecule (Dako), and3�3�-diaminobenzidine tetrachloride was used to detect antibody bind-ing. All sections were counterstained with hematoxylin.
In situ hybridization of VEGF mRNA. For the synthesis of ribo-probes, a cDNA fragment of human VEGF121 (gift of Steven Stacker,Ludwig Institute, Melbourne, Australia) was cloned into a BSKSplasmid (Stratagene, La Jolla, CA) and linearized with HindIII. Ananti-sense riboprobe was generated from the template incorporatingDIG-UTP (Roche Applied Science, Mannheim, Germany) into run-off transcripts using T7 RNA polymerase. A sense riboprobe was alsogenerated. In situ hybridization was undertaken in 4-�m paraffinsections as described by Sutherland et al. (36).
Statistical Analysis
Statistical analyses were performed using GraphPad Prism Ver-sion 4.0 for Windows (GraphPad Software, San Diego, CA). Aone-way analysis of variance was utilized to compare data betweenthe 125- and 146-day gestational control groups and the preterm�21 days group. This was followed by a Tukey’s post hocanalysis.
Data between steroid-exposed and unexposed neonates were ana-lyzed using a Student’s t-test. To compare data between steroid-exposed and unexposed neonates from different postconceptional timepoints, a two-way analysis of variance was utilized. Physiological datawere analyzed using a repeated measures two-way analysis of vari-ance followed by Bonferroni’s post hoc analysis.
Linear regression analyses were performed to determine whetherthere were significant correlations between glomerular number andpostconceptional age, birth weight, kidney weight, kidney volume,and renal corpuscle volume. Included in these analyses were data fromsteroid-exposed and unexposed animals and animals from the pre-term�6 days and preterm�14 days groups. An analysis of covariancewas used to determine any differences in the linear regressionsbetween the preterm group and the gestational controls. Statisticalsignificance was accepted as P � 0.05.
RESULTS
Effect of Preterm Birth on Nephrogenesis in the Context ofAntenatal Steroids
Postnatal fetal physiology. Arterial blood gases (pH, PaCO2,
PaO2), fluid intake, urine output, and mean arterial blood pres-
sure of preterm neonates from birth until postnatal day 21 wereall within the accepted clinical range.
Body weights, kidney weights, and kidney volumes. Allfetal baboons had birth weights above the 10% reference
Fig. 1. A: representative photomicrographs of kidney sections from the 125 (top)- and 146 (middle)-day gestational control groups and the preterm�21 daysgroup (bottom), all demonstrating evidence of ongoing nephrogenesis in the outer renal cortex. NZ, nephrogenic zone; C, comma-shaped body; UB, ureteric bud.B: nephrogenic zone thickness of gestational controls (125 and 146 days gestation) compared with the preterm�21 days group. Data were analyzed using a 1-wayanalysis of variance followed by Tukey’s post hoc analysis. Nephrogenic zone thickness in the 125-day gestational controls was significantly greater (*P � 0.05)compared with the 146-day gestational controls and the preterm�21 days group. C: number of glomerular generations in the gestational controls (125, 146, and175/185 days gestation) compared with the preterm�21 days group. Data were analyzed using a 1-way analysis of variance followed by Tukey’s post hoc test.The number of glomerular generations was significantly less in the 125-day gestational controls compared with the 146- and 175/185-day gestational controlsand the preterm�21 days group (*P � 0.0001). D: linear regression analysis of glomerular number vs. postconceptional age in preterm kidneys showing asignificant linear relationship between postconceptional age and glomerular number. E: linear regression analysis of glomerular generations vs. postconceptionalage in preterm kidneys showing a significant linear relationship between postconceptional age and the number of glomerular generations.
Table 1. Birth weight, necropsy weight, kidney weight, kidney volume, kidney weight-to-body weight ratio, kidneyvolume-to-kidney weight ratio, glomerular number, and mean renal corpuscle volume of gestational controls at 125 days and146 days gestation and preterm neonates at postnatal day 21
Gestational Controls Preterm
125 Days (n � 4) 146 Days (n � 4) �21 Days (n � 4)
Birth weight, g 35312† (329–375) 59725*(532–654) 41922† (354–460)Necropsy weight, g 35312† (329–375) 59725*(532–654) 40030† (320–466)Kidney weight, g 1.370.16 (1.01–1.77) 1.820.18 (1.31–2.16) 2.730.41*(1.90–3.87)Kidney volume, mm3 903113 (636–1,170) 1,348196 (819–1,768) 1,719270 (1,391–2,523)Kidney weight-to-body weight
ratio, g/kg 3.90.5 (2.7–5.4) 3.10.4 (2.0–3.7) 6.70.5*† (5.9–8.3)Kidney volume-to-body weight
ratio, mm3/g 2.604 (1.7–3.6) 2.30.4 (1.2–3.0) 4.30.4*†(3.5–5.4)Glomerular number 117,2358,766 (101,439–137,765) 270,48633,631*(202,266–352,621) 283,53512,358*(249,772–304,186)Average renal corpuscle volume,
�10�4 mm3 5.870.52 (5.03–7.38) 3.970.35 (2.37–4.29) 3.650.43 (3.14–4.72)
Values are means SE with data range in parentheses; n � No. of animals. All animals were exposed to antenatal glucocorticoids. *P � 0.05 vs. 125 daysgestation, †P � 0.05 vs. 146 days gestation by 1-way analysis of variance followed by Tukey’s post hoc test.
F1670 IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

range for premature baboons delivered at this gestationaltime point. There was no significant difference in birthweights between the 125-day gestational control group andthe preterm�21 days group (Table 1). Necropsy weights ofthe preterm�21 days group were significantly less (P �
0.002) compared with the 146-day gestational age-matchedcontrols. Although all preterm baboons lost weight afterbirth, relative kidney weights and volumes were signifi-cantly increased compared with the 125- and 146-day ges-tational controls.
F1671IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

Assessment of nephrogenesis. In the preterm kidneys atpostnatal day 6, 14, and 21 and in the 125- and 146-daygestational controls, there was morphological evidence of on-going nephrogenesis (Fig. 1A). In the preterm kidneys atpostnatal day 21, nephrogenic zone thickness was significantlyless compared with the 125-day gestational control group butnot significantly different from the 146-day gestational controlgroup (Fig. 1B).
The number of glomerular generations increased signifi-cantly from 125 days gestation to 175/185 days gestation (Fig.1C). The number of glomerular generations in the preterm�21days group was not significantly different from the number ofgenerations in the 146-day gestational age-matched controls,and was significantly higher than the 125-day group.
In accordance with the glomerular generation data, thenumber of developed glomeruli in the preterm�21 days groupwas significantly greater compared with the 125-day gesta-tional controls, but was not significantly different from the146-day gestational age-matched controls (Table 1).
Statistically significant correlations were found betweenglomerular number and postconceptional age (r2 � 0.781, P �0.0001) and between glomerular generations and postconcep-tional age (r2 � 0.613, P � 0.003) when all preterm animalswere combined (Fig. 1, D and E). In the two kidneys from thepreterm�6 days group, there were 184,234 and 202,316 de-veloped glomeruli and in the kidneys from postnatal day 14(n � 2) there were 140,185 and 178,661 developed glomeruli.
Birth weight correlated significantly with glomerular num-ber in both the preterm neonates (r2 � 0.438, P � 0.02) and thegestational controls (r2 � 0.680, P � 0.01). In the pretermneonates, there was no significant correlation between nec-ropsy weight and glomerular number.
Importantly, there was a very strong correlation betweenkidney weight and glomerular number in both the pretermneonates (r2 � 0.703, P � 0.0007) and gestational controls (r2 �0.664, P � 0.01); however, there was a significant differencein the slopes of the regression lines (P � 0.048) such that in thepreterm kidneys there were 83,840 glomeruli/g compared with193,400 glomeruli/g in the gestational controls (Fig. 2).
There was no significant difference in the mean renal cor-puscle volume between the preterm�21 days groups and the146-day gestational age-matched control group (Table 1).There was no significant correlation between renal corpusclevolume and glomerular number.
Effect of Prenatal Maternal Glucocorticoidson Nephrogenesis
Postnatal fetal physiology. Exposure to antenatal maternalglucocorticoids at 123 and 124 days gestation did not signifi-cantly affect arterial blood-gas levels (pH, PaO2
, PaCO2) follow-
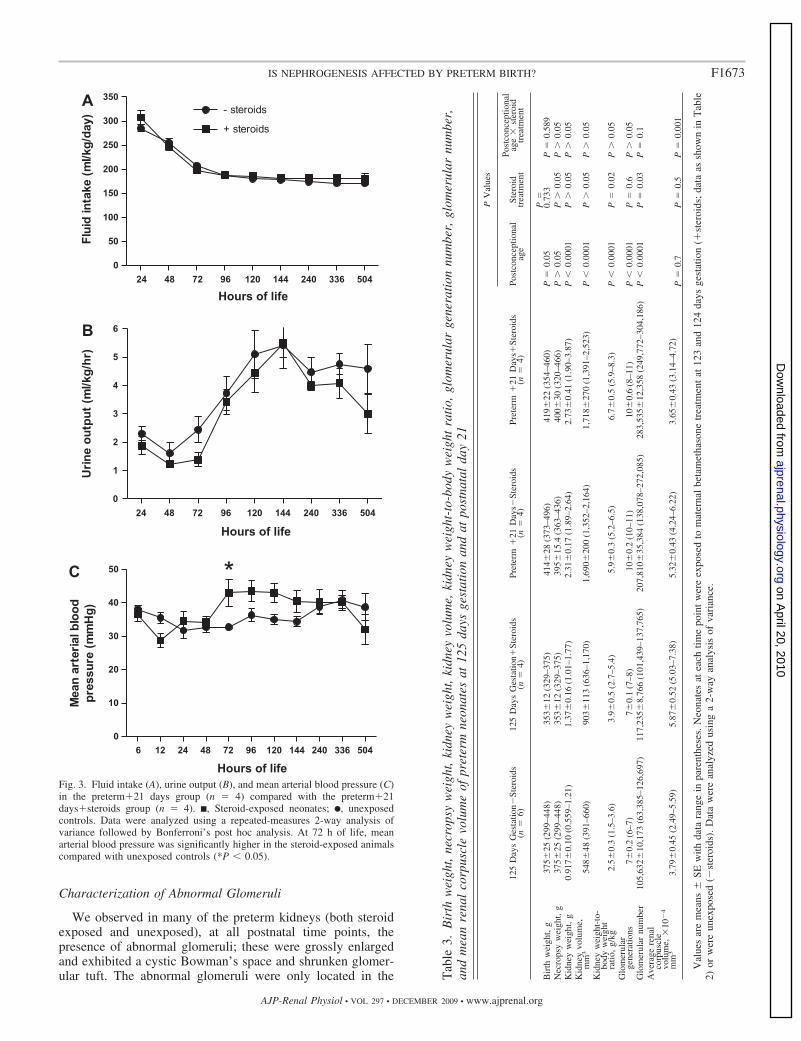
ing preterm delivery at 125 days gestation (Table 2). There wasno significant difference in fluid intake or urine output betweenthe two groups (Fig. 3, A and B). At 72 h of life, however,mean arterial blood pressure was significantly elevated in thesteroid-exposed group (P � 0.05) (Fig. 3C). There was nosignificant difference in mean arterial blood pressure betweenthe two groups at postnatal day 21.
Body weights, kidney weights, and kidney volumes. Antena-tal exposure to steroids (123 and 124 days gestation) did notaffect fetal birth weight at 125 days gestation, necropsy weightat postnatal day 21, or absolute kidney weights or kidneyvolumes (Table 3). Kidney weight-to-body weight ratio, how-ever, was significantly greater in the animals exposed toantenatal steroids (P � 0.02).
Assessment of nephrogenesis. There were no apparent mor-phological differences in kidney structure between the steroid-exposed and unexposed preterm groups at postnatal day 21.Kidneys from both the preterm�21 days group and the pre-term�21 days�steroids group exhibited a clearly visible neph-rogenic zone, and there was no significant difference in thewidth of the nephrogenic zones (94.2 6.5 vs. 100.5 10.6�m, respectively).
There was no difference in the number of glomerular gen-erations formed within the kidney between the steroid-exposedand unexposed groups (Table 3).
There was a significant increase in the number of developedglomeruli in the steroid-exposed kidneys (Table 3). The num-ber of developed glomeruli was 9% higher in the steroid-exposed kidneys compared with unexposed controls at 125days gestation and 27% higher at postnatal day 21.
The response of renal corpuscle volume in relation to ma-ternal steroid treatment was different in kidneys at 125 daysgestation compared with preterm kidneys at postnatal day 21(Table 3). At 125 days gestation, there was a significantincrease in renal corpuscle volume whereas on postnatal day 21there was a significant decrease.
Fig. 2. Linear regression analyses of glomerular number vs. kidney weight inpreterm neonates (F) and gestational controls (Œ). There was a significant linearrelationship between kidney weight and glomerular number in both the pretermneonates and gestational controls (P � 0.05). An analysis of covariancedemonstrated a significant difference in the slopes of the two regression lines(P � 0.048).
Table 2. Arterial blood gases (pH, PaCO2, PaO2
) of thepreterm�21 days group compared with the preterm�21days�steroids group at postnatal day 21
Preterm �21 Days(n � 4)
Preterm �21 Days�Steroids(n � 4)
pH 7.320.03 7.290.03PaCO2, mmHg 47.74.5 53.21.9PaO2, mmHg 79.70.3 67.06.4
Values are means SE. Data were analyzed using Student’s t-test.
F1672 IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from
Characterization of Abnormal Glomeruli
We observed in many of the preterm kidneys (both steroidexposed and unexposed), at all postnatal time points, thepresence of abnormal glomeruli; these were grossly enlargedand exhibited a cystic Bowman’s space and shrunken glomer-ular tuft. The abnormal glomeruli were only located in the
Fig. 3. Fluid intake (A), urine output (B), and mean arterial blood pressure (C)in the preterm�21 days group (n � 4) compared with the preterm�21days�steroids group (n � 4). ■, Steroid-exposed neonates; F, unexposedcontrols. Data were analyzed using a repeated-measures 2-way analysis ofvariance followed by Bonferroni’s post hoc analysis. At 72 h of life, meanarterial blood pressure was significantly higher in the steroid-exposed animalscompared with unexposed controls (*P � 0.05).
Tab
le3.
Bir
thw
eigh
t,ne
crop
syw
eigh
t,ki
dney
wei
ght,
kidn
eyvo
lum
e,ki
dney
wei
ght-
to-b
ody
wei
ght
rati
o,gl
omer
ular
gene
rati
onnu
mbe
r,gl
omer
ular
num
ber,
and
mea
nre
nal
corp
uscl
evo
lum
eof
pret
erm
neon
ates
at12
5da
ysge
stat
ion
and
atpo
stna
tal
day
21
PV
alue
s
125
Day
sG
esta
tion�
Ster
oids
(n�
6)12
5D
ays
Ges
tatio
n�St
eroi
ds(n
�4)
Pret
erm
�21
Day
s�St
eroi
ds(n
�4)
Pret
erm
�21
Day
s�St
eroi
ds(n
�4)
Post
conc
eptio
nal
age
Ster
oid
trea
tmen
t
Post
conc
eptio
nal
age
�st
eroi
dtr
eatm
ent
Bir
thw
eigh
t,g
375
25(2
99–4
48)
353
12(3
29–3
75)
414
28(3
73–4
96)
419
22(3
54–4
60)
P�
0.05
P�
0.73
3P
�0.
589
Nec
rops
yw
eigh
t,g
375
25(2
99–4
48)
353
12(3
29–3
75)
395
15.4
(363
–436
)40
030
(320
–466
)P
0.
05P
0.
05P
0.
05K
idne
yw
eigh
t,g
0.91
70.
10(0
.559
–1.2
1)1.
37
0.16
(1.0
1–1.
77)
2.31
0.
17(1
.89–
2.64
)2.
73
0.41
(1.9
0–3.
87)
P�
0.00
01P
0.
05P
0.
05K
idne
yvo
lum
e,m
m3
548
48(3
91–6
60)
903
113
(636
–1,1
70)
1,69
020
0(1
,352
–2,1
64)
1,71
827
0(1
,391
–2,5
23)
P�
0.00
01P
0.
05P
0.
05K
idne
yw
eigh
t-to
-bo
dyw
eigh
tra
tio,
g/kg
2.5
0.3
(1.5
–3.6
)3.
90.
5(2
.7–5
.4)
5.9
0.3
(5.2
–6.5
)6.
70.
5(5
.9–8
.3)
P�
0.00
01P
�0.
02P
0.
05G
lom
erul
arge
nera
tions
70.
2(6
–7)
70.
1(7
–8)
10
0.2
(10–
11)
10
0.6
(8–1
1)P
�0.
0001
P�
0.6
P
0.05
Glo
mer
ular
num
ber
105,
632
10,1
73(6
3,38
5–12
6,69
7)11
7,23
58,
766
(101
,439
–137
,765
)20
7,81
035
,384
(138
,078
–272
,085
)28
3,53
512
,358
(249
,772
–304
,186
)P
�0.
0001
P�
0.03
P�
0.1
Ave
rage
rena
lco
rpus
cle
volu
me,
�10
�4
mm
33.
79
0.45
(2.4
9–5.
59)
5.87
0.
52(5
.03–
7.38
)5.
32
0.43
(4.2
4–6.
22)
3.65
0.
43(3
.14–
4.72
)P
�0.
7P
�0.
5P
�0.
001
Val
ues
are
mea
ns
SEw
ithda
tara
nge
inpa
rent
hese
s.N
eona
tes
atea
chtim
epo
int
wer
eex
pose
dto
mat
erna
lbe
tam
etha
sone
trea
tmen
tat
123
and
124
days
gest
atio
n(�
ster
oids
;da
taas
show
nin
Tab
le2)
orw
ere
unex
pose
d(�
ster
oids
).D
ata
wer
ean
alyz
edus
ing
a2-
way
anal
ysis
ofva
rian
ce.
F1673IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

outer renal cortex and exhibited an immature morphology; theclearly recognizable glomerular anlage was surrounded by acup-shaped layer of epithelial cells.
Quantitative assessment of abnormal glomeruli. There waswide variation in the proportion of abnormal glomeruli withinthe preterm kidneys (Tables 4 and 5); steroid exposure did notaffect the proportion of abnormal glomeruli in the kidney. Theproportion of abnormal glomeruli in the preterm kidneysranged from 0.2 to 18.3%. Of the 12 preterm kidneys analyzed(inclusive of steroid exposed and unexposed), 50% had morethan 4% of their glomeruli appearing abnormal. In threepreterm kidneys, the proportion of abnormal glomeruli was10%. In one of the preterm baboons, the morphology of thekidney was grossly abnormal, with 18% of the glomeruliabnormal. The proportion of abnormal glomeruli in the kidneysof the gestational controls was considered negligible (Table 4).
Immunohistochemical localization of endothelial cellmarker CD31. In kidney sections at 146 days gestation, thewell-developed glomeruli adjacent to the nephrogenic zonedemonstrated profuse positive staining for CD31 (Fig. 4A). Inthe preterm kidneys, the abnormal glomeruli exhibited littleCD31 immunostaining compared with well-developed glomer-uli observed in the same section.
Immunohistochemical localization of podocyte marker WT-1.Profuse WT-1 staining was observed in the glomerular tuft ofwell-developed, normal glomeruli from preterm kidneys (Fig.4B). In the abnormal glomeruli from the preterm kidneys,however, WT-1-positive immunostaining was localized to thelayer of epithelial cells surrounding the spherical mass of cellsof the glomerular tuft. Positive immunostaining was also lo-calized to the epithelial cells of Bowman’s capsule in theabnormal glomeruli.
In situ localization of VEGF mRNA. VEGF mRNA waslocalized to the glomerular podocytes in both the pretermkidneys and gestational controls including the abnormal glo-meruli (Fig. 4C).
DISCUSSION
The findings of this study clearly demonstrate that nephro-genesis continues after preterm birth in the steroid-exposed andunexposed primate kidney. There was an increase in thenumber of glomerular generations and total glomeruli in theextrauterine environment, with no differences found betweenthe preterm kidneys and their gestational age-matched controls,in the context of antenatal steroids. Interestingly, exposure toantenatal glucocorticoids before preterm birth led to renalhypertrophy and an increase in the number of developedglomeruli in the kidney compared with unexposed kidneys.
Many of the glomeruli located in the outer renal cortex of thepreterm kidney, in both the steroid-exposed and unexposedbaboon neonates, often appeared abnormal. Immunohisto-chemical analyses of these abnormal glomeruli showed thatthey were in a relatively immature state of development, poorlyvascularized, and are therefore likely to be nonfunctional.
Although all preterm baboons lost weight after birth, thereappeared to be substantial postnatal kidney growth, with therelative kidney weights and kidney volumes significantlyhigher in the preterm animals compared with the gestationalcontrols. Similar findings have been previously reported inpreterm babies (21). The renal hypertrophy observed in thepreterm kidneys did not appear to be attributed to differencesin the thickness of the nephrogenic zone or in the size ofglomeruli, thus implying tubular hypertrophy.
Our results demonstrate that nephrogenesis unequivocallyoccurs postnatally in both steroid-exposed and unexposedpreterm neonates; morphologically, there was evidence of anephrogenic zone and, when assessed quantitatively, the num-ber of glomerular generations and the total number of devel-oped glomeruli increased with postnatal age. The averagenumber of developed glomeruli in the preterm kidneys (inclu-sive of steroid-exposed and unexposed preterm kidneys) was�245,673, ranging from 138,078 to 304,186, which appears tobe within the normal range for term baboon kidneys, albeit atthe lower end (18). Total glomerular number is also expectedto increase further since nephrogenesis, although nearing com-pletion, was not finished by postnatal day 21.
In the context of antenatal steroids, there was no significantdifference in the number of glomerular generations formed inthe kidney between the preterm�21 days kidneys and their146-day gestational age-matched controls. These findings arenot consistent with those of Rodriguez et al. (31), who reportedfewer glomerular generations within the kidneys of autopsiedpreterm infants. However, the discrepancy in findings is likelyexplained by a number of the preterm human neonates beingintrauterine growth restricted in the study by Rodriguez et al.,which is known to influence nephron endowment (19, 40).
We have previously reported a very strong correlation be-tween renal size and glomerular number (18), and this associ-ation appears to be maintained after premature delivery sincekidney weight significantly correlated with glomerular numberin the preterm baboons. However, in the present study ourlinear regression analyses indicate that glomerular density (thenumber of glomeruli per gram of kidney) is substantially lessin the preterm kidneys (83,840 glomeruli/g) compared withgestational controls (193,400 glomeruli/g); this is likely to bedue to the relative increase in kidney size after preterm birth
Table 4. Proportion of abnormal glomeruli in kidneys of gestational controls and preterm baboon neonates
Gestational Controls Preterm
125 Days 146 Days 175/185 Days �6 Days �14 Days �21 Days
Proportion of abnormal glomeruli, % 1.3 0.2 0.0 4.3 10.7 18.31.2 0.0 0.0 6.5 6.1 1.40.3 0.0 0.0 2.02.4 0.0 0.0 2.6
0.0Average, % 1.30.4 0.050.05 0.00.0 5.41.1 8.42.3 6.14.1
Values are means SE. Animals from the 125 days gestation, 146 days gestation, and preterm�21 days groups were all exposed to antenatal glucocorticoids.
F1674 IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

and not a change in the absolute number of glomeruli formed.Further studies would be necessary to investigate whether thisdifference in glomerular density reflects a change in renaltubular mass.
Our findings have demonstrated that antenatal exposure toglucocorticoids before preterm birth increases the number ofdeveloped glomeruli within the preterm baboon kidney. Cer-tainly, this indicates that glucocorticoid administration has
Table 5. Proportion of abnormal glomeruli in steroid-exposed baboons (data as shown in Table 5) compared with unexposed controls
125 Days Gestation�Steroids 125 Days Gestation�Steroids Preterm�21 Days� Steroids Preterm�21 Days�Steroids
Proportion of abnormal glomeruli, % 0.2 1.3 0.2 18.32.9 1.2 12.8 1.40.6 0.3 0.2 2.00.2 2.4 4.7 2.60.50.0
Average, % 0.70.4 1.30.4 4.53.0 6.14.1
Values are means SE.
Fig. 4. Representative photomicrographs ofkidney sections from the 146-day gestationalcontrol group and the preterm�21 daysgroup immunostained with an endothelialcell marker (CD31; A), the Wilm’s tumorsuppressor gene-1 (WT-1; B), and in situhybridization for vascular endothelial growthfactor (VEGF; C). The glomeruli from the146-day gestational control group show pro-fuse positive brown staining for CD31 (A).The abnormal glomeruli in the preterm�21days group are poorly vascularized, asshown by the scant positive brown stainingfor CD31 (A). WT-1-positive staining is local-ized to podocytes within the glomerular tuft ofdeveloped, normal glomeruli (B). In abnormalglomeruli, WT-1 staining is localized to podo-cytes surrounding the immature glomerular an-lage (B). WT-1-positive immunostaining canalso be observed in the parietal epithelial cellsof Bowman’s capsule (arrows). VEGF-positiveimmunostaining (dark purple staining) was lo-calized to the podocytes in the glomerular tuft(arrows, C). In an abnormal glomerulus from apreterm kidney, VEGF-positive podocytesstained dark purple were also observed (ar-rows, C).
F1675IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

accelerated glomerular maturation, which is in accordance withprevious studies demonstrating that glucocorticoids induceorgan maturation (13). Our findings also support the improve-ment in renal function demonstrated to occur in preterm infantsexposed to steroids (1). Exposure to steroids also resulted in agreater increase in kidney weight-to-body weight ratio, sug-gesting that glucocorticoid treatment may be leading to renalhypertrophy. Previous studies in the preterm lamb, baboon, andhuman neonate have shown that glucocorticoid treatment in-creases mean arterial pressure, renal blood flow, and glomer-ular filtration rate, implicative of renal functional maturation,(1, 10, 35) which may be contributing to the renal hypertrophyobserved in the current study. Indeed, mean arterial bloodpressure was observed to be significantly elevated at 72 h oflife in the preterm baboons exposed to antenatal steroids.Similar findings have also been reported in human infants, inwhich the effects of prenatal glucocorticoids appear to belimited to the early postnatal period (1, 37).
In accordance with previous studies (31, 36), abnormalglomeruli exhibiting a dilated Bowman’s space surrounding anunderdeveloped glomerular tuft were observed in the outerrenal cortex of both steroid-exposed and unexposed pretermkidneys, suggesting glomeruli formed in the extrauterine envi-ronment are “at risk”; developed glomeruli deep in the cortexwere not affected. The glomerular abnormalities appear to be adirect consequence of premature birth and/or treatments in thepostnatal care of the preterm neonate, since the number ofabnormal glomeruli in the gestational control kidneys wasnegligible. Immunostaining with the endothelial cell markerCD31 showed that the abnormal glomeruli in the pretermkidneys were poorly vascularized, even though VEGF wasexpressed. The abnormal glomeruli appeared to be in a rela-tively immature state of development with a layer of WT-1-positive epithelial cells (indicative of podocytes) surrounding aspherical mass of relatively undifferentiated cells. PositiveWT-1 immunostaining was also localized to the epithelial cellsof Bowman’s capsule (parietal podocytes), which has beendemonstrated previously in the human kidney (2). Interest-ingly, Bariety et al. (2) noted that capsules without a glomer-ular tuft, or a retracted tuft, contained a greater number ofparietal podocytes compared with normal glomeruli lining theentirety of Bowman’s capsule. Furthermore, Gibson et al. (14)have also shown that in atubular cystic glomeruli in humankidneys, Bowman’s capsule is always lined by parietal podo-cytes. It is therefore conceivable that the cystic abnormalglomeruli observed in the preterm kidneys may be atubular,and as such would never be functional.
Not all kidneys from the premature baboons contained thesame proportion of abnormal glomeruli, ranging from 0.2% toas high as 18%. Hence preterm birth may not always adverselyimpact kidney development, or alternatively there may be adifference in the rates of resorption of dysfunctional glomeruli(26). Another likely explanation is that factors in the postnatalcare of the neonate (which varies between neonates) adverselyimpact nephrogenesis. In particular, pharmacological agentsadministered to the neonate in the postnatal period, such asaminoglycoside antibiotics, are known to be nephrotoxic (7,15, 16). In the present study, since all preterm neonates wereexposed to antibiotics after birth, it is possible that the glomer-ular abnormalities in the kidneys have been caused by exposureto nephrotoxic antibiotics. However, if this is the case, it is
difficult to explain why there was such variation in the pro-portion of abnormal glomeruli within the preterm kidneys,given that all neonates received the same regime of antibiotics,except for two animals that were administered additional dos-es; these animals were not the neonates with the high propor-tion of abnormal glomeruli. Further studies are required toelucidate whether exposure to antibiotics is nephrotoxic to thepreterm infant and/or whether other medications, or factors inthe postnatal care of the preterm infants, lead to the adverserenal effects that we observe. If definitive associations arefound, this may lead to potential interventions to improve therenal health of preterm babies.
In conclusion, using a non-human primate model the currentstudy has clearly demonstrated ongoing nephrogenesis afterpreterm birth. The rate of glomerular formation remains similarfollowing preterm birth; however, glomerular density (numberof glomeruli per gram of kidney) was significantly reduced inthe preterm kidney, suggesting that the non-glomerular com-partments are growing at a faster rate. Of concern, manypreterm neonates exhibited abnormal glomeruli in the outerrenal cortex, suggesting that extrauterine nephrogenesis leadsto an increased risk of abnormal glomerular development.Whether this will impact final nephron endowment is yet to bedetermined, since nephrogenesis was still ongoing.
ACKNOWLEDGMENTS
We thank the Southwest Foundation for Biomedical Research (San Anto-nio, TX) for provision of the baboon kidneys, in particular Jacqueline Coalsonand Vicki Winter from the University of Texas Health Science Center forassistance in obtaining the kidneys. The authors also thank Alison Cox andAssociate Professor Darren Kelly from the Department of Medicine at theUniversity of Melbourne for assistance with the VEGF in situ hybridization.
GRANTS
This work was supported by National Institutes of Health BPD ResourceCenter Grant HL52636, P51RR13986 for facility support, and the NationalHealth and Medical Research Council of Australia.
L. Gubhaju and M. R. Sutherland were recipients of an Australian Post-graduate Award while undertaking this work.
DISCLOSURES
No conflicts of interest are declared by the authors.
REFERENCES
1. al-Dahan J, Stimmler L, Chantler C, Haycock GB. The effect ofantenatal dexamethasone administration on glomerular filtration rate andrenal sodium excretion in premature infants. Pediatr Nephrol 1: 131–135,1987.
2. Bariety J, Mandet C, Hill G, Bruneval P. Parietal podocytes in normalhuman glomeruli. J Am Soc Nephrol 17: 2770–2780, 2006.
3. Bertram J. Analysing renal glomeruli with the new stereology. Int RevCytol 161: 111–172, 1995.
4. Brenner B, Garcia D, Anderson S. Glomeruli and blood pressure. Lessof one, more the other? Am J Hypertens 1: 335–347, 1988.
5. Celsi G, Kistner A, Aizman R, Eklof AC, Ceccatelli S, de Santiago A,Jacobson SH. Prenatal dexamethasone causes oligonephronia, sodiumretention, and higher blood pressure in offspring. Pediatr Res 44: 317–322, 1998.
6. Coalson J, Winter V, Siler-Khodr T, Yoder B. Neonatal chronic lungdisease in extremely immature baboons. Am J Respir Crit Care Med 160:1333–1346, 1999.
7. Cullen L, Young R, Bertram J. Studies on the effects of gentamicin onrat metanephric development in vitro. Nephrology 5: 115–123, 2000.
8. Dalziel S, Parag V, Rodgers A, Harding J. Cardiovascular risk factorsat age 30 following pre-term birth. Int J Epidemiol 36: 907–915, 2007.
9. dos Santos AM, Fonseca Ferraz ML, Pinto Rodriguez ML, Dos ReisMA, Miranda Correa RR, de Paula Antunes Teixeira V, da Cunha
F1676 IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from

Castro EC. Assessment of renal maturity by assisted morphometry inautopsied fetuses. Early Hum Dev 82: 709–713, 2006.
10. Ervin MG, Seidner SR, Leland MM, Ikegami M, Jobe AH. Direct fetalglucocorticoid treatment alters postnatal adaptation in premature newbornbaboons. Am J Physiol Regul Integr Comp Physiol 274: R1169–R1176,1998.
11. Feldman D, Carbone J, Belden L, Borgida A, Herson V. Betametha-sone vs dexamethasone for the prevention of morbidity in very-low-birthweight neonates. Am J Obstet Gynecol 197: 284e281–284, 2007.
12. Ferraz FML, Dos Santos AM, Cavellani CL, Rossi RC, Correa RR,Dos Reis MA, de Paula Antunes Teixeira V, da Cunha Castro EC.Histochemical and immunohistochemical study of the glomerular devel-opment in human fetuses. Pediatr Nephrol 23: 257–262, 2008.
13. Fowden A, Szemere J, Hughes P, Gilmour R, Forheard A. The effectsof cortisol on the growth rate of the sheep fetus during late gestation. JEndocrinol 151: 97–105, 1996.
14. Gibson I, Downie T, More I, Lindop G. Atubular glomeruli andglomerular cysts—a possible pathway for nephron loss in the humankidney? J Pathol 179: 421–426, 1996.
15. Gilbert T, Gaonach S, Moreau E, Merlet-Benichou C. Defect ofnephrogenesis induced by gentamicin in rat metanephric organ culture.Lab Invest 70: 656–666, 1994.
16. Gilbert T, Lelievre-Pegorier M, Merlet-Benichou C. Immediate andlong-term renal effects of fetal exposure to gentamicin. Pediatr Nephrol 4:445–450, 1990.
17. Goldenberg R, Culhane J, Iams J, Romero R. Epidemiology and causesof preterm birth. Lancet 371: 75–84, 2008.
18. Gubhaju L, Black MJ. The baboon as a good model for studies of humankidney development. Pediatr Res 58: 505–508, 2005.
19. Hinchliffe SA, Lynch MR, Sargent PH, Howard CV, Van Velzen D.The effect of intrauterine growth retardation on the development of renalnephrons. Br J Obstet Gynaecol 99: 296–301, 1992.
20. Hinchliffe SA, Sargent PH, Howard CV, Chan YF, van Velzen D.Human intrauterine renal growth expressed in absolute number of glomer-uli assessed by the disector method and Cavalieri principle. Lab Invest 64:777–784, 1991.
21. Huang HP, Tsai IJ, Lai YC, Cheng CH, Tsau YK. Early postnatal renalgrowth in premature infants. Nephrology 12: 572–575, 2007.
22. Johansson S, Iliadou A, Bergvall N, Tuvemo T, Norman M, Cnattin-gius S. Risk of high blood pressure among young men increases with thedegree of immaturity at birth. Circulation 112: 3430–3436, 2005.
23. Keijzer-Veen M, Schrevel M, Finken M, Dekker F, Nauta J, Hille E,Frolich M, van der Heijden B. Microalbuminuria and lower glomerularfiltration rate at young adult age in subjects born very premature and afterintrauterine growth retardation. J Am Soc Nephrol 16: 2762–2768, 2005.
24. Koenen SV, Mecenas CA, Smith GS, Jenkins S, Nathanielsz PW.Effects of maternal betamethasone administration on fetal and maternalblood pressure and heart rate in the baboon at 0.7 of gestation. Am J ObstetGynecol 186: 812–817, 2002.
25. Laws P, Abeywardana S, Walker J, Sullivan E. Australia’s Mothersand Babies 2007. Sydney, Australia: AIHW National Perinatal StatisticsUnit, 2007.
26. Ma J, Rossini M, Yang H, Zuo Y, Fogo A, Ichikawa I. Effects ofpodocyte injury on glomerular development. Pediatr Res 62: 417–421,2007.
27. McCurnin DC, Pierce RA, Chang LY, Gibson LL, Osborne-LawrenceS, Yoder BA, Kerecman JD, Albertine KH, Winter VT, Coalson JJ,Crapo JD, Grubb PH, Shaul PW. Inhaled NO improves early pulmonaryfunction and modifies lung growth and elastin deposition in a baboonmodel of neonatal chronic lung disease. Am J Physiol Lung Cell MolPhysiol 288: L450–L459, 2005.
28. Noble L. Developments in neonatal technology continue to improve infantoutcomes. Pediatr Ann 32: 595–603, 2003.
29. Nyengaard J. Stereologic methods and their application in kidney re-search. J Am Soc Nephrol 10: 1100–1123, 1999.
30. Ortiz LA, Quan A, Zarzar F, Weinberg A, Baum M. Prenatal dexa-methasone programs hypertension and renal injury in the rat. Hypertension41: 328–334, 2003.
31. Rodriguez MM, Gomez AH, Abitbol CL, Chandar JJ, Duara S,Zilleruelo GE. Histomorphometric analysis of postnatal glomerulogenesisin extremely preterm infants. Pediatr Dev Pathol 7: 17–25, 2004.
32. Saxen L. Organogenesis of the Kidney. Cambridge, UK: CambridgeUniversity Press, 1987, p. 173.
33. Schlabritz-Loutsevitch NE, Lopez-Alvarenga JC, Comuzzie AG,Miller MM, Ford SP, Li C, Hubbard GB, Ferry RJ Jr, NathanielszPW. The prolonged effect of repeated maternal glucocorticoid exposureon the maternal and fetal leptin/insulin-like growth factor axis in Papiospecies. Reprod Sci 16: 308–319, 2009.
34. Slattery M, Morrison J. Preterm delivery. Lancet 360: 1489–1497, 2002.35. Stonestreet BS, Hansen NB, Laptook AR, Oh W. Glucocorticoid
accelerates renal functional maturation in fetal lambs. Early Hum Dev 8:331–341, 1983.
36. Sutherland MR, Gubhaju L, Yoder BA, Stahlman MT, Black MJ. Theeffects of postnatal retinoic acid administration on nephron endowment inthe preterm baboon kidney. Pediatr Res 65: 397–402, 2008.
37. van den Anker J, Hop W, de Groot R, van der Heijden B, Broerse H,Lindemans JS, Sauer PJ. Effects of prenatal exposure to betamethasoneand indomethacin on the glomerular filtration rate in the preterm infant.Pediatr Res 36: 578–581, 1994.
38. Wintour EM, Moritz KM, Johnson K, Ricardo S, Samuel CS, DodicM. Reduced nephron number in adult sheep, hypertensive as a result ofprenatal glucocorticoid treatment. J Physiol 549: 929–935, 2003.
39. Yoder B, Siler-Khodr T, Winter V, Coalson J. High-frequency oscil-latory ventilation. Am J Respir Crit Care Med 162: 1867–1876, 2000.
40. Zimanyi MA, Denton KM, Forbes JM, Thallas-Bonke V, ThomasMC, Poon F, Black MJ. A developmental nephron deficit in rats isassociated with increased susceptibility to a secondary renal injury due toadvanced glycation end-products. Diabetologia 49: 801–810, 2006.
F1677IS NEPHROGENESIS AFFECTED BY PRETERM BIRTH?
AJP-Renal Physiol • VOL 297 • DECEMBER 2009 • www.ajprenal.org
on April 20, 2010
ajprenal.physiology.orgD
ownloaded from




















