Interventions for the prevention and treatment of postpartum psychosis: a systematic review
10
REVIEW ARTICLE Interventions for the prevention and treatment of postpartum psychosis: a systematic review Shelley Doucet & Ian Jones & Nicole Letourneau & Cindy-Lee Dennis & Emma Robertson Blackmore Received: 29 March 2010 / Accepted: 10 November 2010 / Published online: 3 December 2010 # Springer-Verlag 2010 Abstract Postpartum psychosis is a serious disorder that can cause negative consequences for the mother, infant, and entire family. While reports of this condition date back for centuries, little is known about what interventions are most effective for this population. The purpose of this systematic review was to examine the research evidence on interventions for the prevention and treatment of postpartum psychosis. Studies were searched using CINAHL, EMBASE, MEDLINE, PsycINFO, and PubMed databases. All primary research studies published in English since 1970 that explored interventions for the prevention or treatment of postpartum psychosis were included. The search resulted in 26 studies on interventions for postpartum psychosis, with 10 focusing on prevention and 17 focusing on treatment. Studies on the prevention of postpartum psychosis have examined the effects of mood stabilizers, antipsychotics, and hormone therapy, while those examining treatment have included electrocon- vulsive therapy, mood stabilizers, antipsychotics, hormones, and the beta blocker propranolol. Only preliminary evidence suggests which interventions may be effective strategies to prevent (e.g., lithium) and treat (e.g., electroconvulsive therapy) postpartum psychosis. Due to methodological limi- tations in the studies reviewed, extensive evidence-based recommendations for the prevention and treatment of post- partum psychosis cannot be made. The known risk factors and negative consequences of postpartum psychosis point to the importance of preventative and acute treatment measures. Well-designed prospective studies are needed to determine the efficacy of prevention and treatment interventions for women who experience postpartum psychosis. Keywords Postpartum psychosis . Prevention . Treatment . Systematic review Postpartum psychosis (PP) is a psychiatric emergency that requires immediate medical attention. Despite the experience of PP dating back centuries (Brockington 1996), little is known about what interventions are most effective for this vulnerable population. Research on interventions for women who experience PP has been limited due to barriers such as the relative rarity of this disorder and exclusion from drug trials for safety concerns. Affecting one to two per 1,000 deliveries (Kendell et al. 1987), PP can cause several negative consequences, including impaired mother–infant bonding (Hipwell et al. 2000), infant abuse and neglect (Chandra et al. 2006), the risk of recurrent psychiatric illness S. Doucet (*) Department of Nursing and Health Sciences, University of New Brunswick, 100 Tucker Park Road, P.O. Box 5050, Saint John, NB E2L 4L5, Canada e-mail: [email protected] I. Jones MRC Center for Neuropsychiatric Genetics and Genomics, Department of Psychological Medicine and Neurology, Cardiff University, The Henry Wellcome Building for Biomedical Research in Wales, Academic Avenue, Heath Park, Cardiff CF14 4XN, UK N. Letourneau Faculty of Nursing, University of New Brunswick, PO Box 4400, Fredericton, NB E3B 5A3, Canada C.-L. Dennis Faculties of Nursing and Medicine, Department of Psychiatry, University of Toronto, 155 College Street, Rm. 280, Toronto, ON M5T 1P8, Canada E. R. Blackmore Department of Psychiatry, University of Rochester Medical Center, BOX PSYCH 4-9200, 300 Crittenden Boulevard, Rochester, NY 14642-8409, USA Arch Womens Ment Health (2011) 14:89–98 DOI 10.1007/s00737-010-0199-6
Transcript of Interventions for the prevention and treatment of postpartum psychosis: a systematic review

REVIEW ARTICLE
Interventions for the prevention and treatmentof postpartum psychosis: a systematic review
Shelley Doucet & Ian Jones & Nicole Letourneau &
Cindy-Lee Dennis & Emma Robertson Blackmore
Received: 29 March 2010 /Accepted: 10 November 2010 /Published online: 3 December 2010# Springer-Verlag 2010
Abstract Postpartum psychosis is a serious disorder that cancause negative consequences for the mother, infant, and entirefamily. While reports of this condition date back for centuries,little is known about what interventions are most effective forthis population. The purpose of this systematic review was toexamine the research evidence on interventions for theprevention and treatment of postpartum psychosis. Studieswere searched using CINAHL, EMBASE, MEDLINE,PsycINFO, and PubMed databases. All primary researchstudies published in English since 1970 that exploredinterventions for the prevention or treatment of postpartum
psychosis were included. The search resulted in 26 studies oninterventions for postpartum psychosis, with 10 focusing onprevention and 17 focusing on treatment. Studies on theprevention of postpartum psychosis have examined the effectsof mood stabilizers, antipsychotics, and hormone therapy,while those examining treatment have included electrocon-vulsive therapy, mood stabilizers, antipsychotics, hormones,and the beta blocker propranolol. Only preliminary evidencesuggests which interventions may be effective strategies toprevent (e.g., lithium) and treat (e.g., electroconvulsivetherapy) postpartum psychosis. Due to methodological limi-tations in the studies reviewed, extensive evidence-basedrecommendations for the prevention and treatment of post-partum psychosis cannot be made. The known risk factors andnegative consequences of postpartum psychosis point to theimportance of preventative and acute treatment measures.Well-designed prospective studies are needed to determine theefficacy of prevention and treatment interventions for womenwho experience postpartum psychosis.
Keywords Postpartum psychosis . Prevention . Treatment .
Systematic review
Postpartum psychosis (PP) is a psychiatric emergency thatrequires immediate medical attention. Despite the experienceof PP dating back centuries (Brockington 1996), little isknown about what interventions are most effective for thisvulnerable population. Research on interventions for womenwho experience PP has been limited due to barriers such asthe relative rarity of this disorder and exclusion from drugtrials for safety concerns. Affecting one to two per 1,000deliveries (Kendell et al. 1987), PP can cause severalnegative consequences, including impaired mother–infantbonding (Hipwell et al. 2000), infant abuse and neglect(Chandra et al. 2006), the risk of recurrent psychiatric illness
S. Doucet (*)Department of Nursing and Health Sciences,University of New Brunswick,100 Tucker Park Road, P.O. Box 5050, Saint John, NB E2L 4L5,Canadae-mail: [email protected]
I. JonesMRC Center for Neuropsychiatric Genetics and Genomics,Department of Psychological Medicine and Neurology,Cardiff University,The Henry Wellcome Building for Biomedical Research in Wales,Academic Avenue, Heath Park,Cardiff CF14 4XN, UK
N. LetourneauFaculty of Nursing, University of New Brunswick,PO Box 4400, Fredericton, NB E3B 5A3, Canada
C.-L. DennisFaculties of Nursing and Medicine, Department of Psychiatry,University of Toronto,155 College Street, Rm. 280,Toronto, ON M5T 1P8, Canada
E. R. BlackmoreDepartment of Psychiatry,University of Rochester Medical Center,BOX PSYCH 4-9200, 300 Crittenden Boulevard,Rochester, NY 14642-8409, USA
Arch Womens Ment Health (2011) 14:89–98DOI 10.1007/s00737-010-0199-6

(Robertson et al. 2005; Terp et al. 1999), suicide (Appleby etal. 1998), and infanticide (Spinelli 2004). PP is at timesconfused or used interchangeably with postpartum depression.Postpartum depression refers to a non-psychotic depressiveepisode that often requires treatment and affects approximately13% of mothers within 12 weeks of giving birth (O’Hara andSwain 1996). PP is more severe than postpartum depression,often requiring hospitalization, and is characterized bydelusions, hallucinations, bizarre behavior, depression, mania,and mood lability that usually presents within the first 2 weekspostpartum (Heron et al. 2008; Sit et al. 2006).
Another barrier to conducting research related to PP is thatthe nosology of this disorder remains disputed. The evidencesuggests, however, that PP is usually mania or affectivepsychosis linked temporally with childbirth (Brockington1996). The Diagnostic and Statistical Manual of MentalDisorders, Fourth Edition (DSM-IV; American PsychiatricAssociation 2000), and the International Classification ofDiseases, Tenth Revision (ICD-10;World Health Organization1992) do not recognize PP as a distinct condition; rather, PPis diagnosed within various non-postpartum psychiatricdisorders if the onset occurs within 4 and 6 weeks postpar-tum, respectively. The differential diagnosis for PP episodescan include major depression with psychotic features, bipolarI, bipolar II, schizoaffective, unspecified functional psychosis,and brief psychotic disorder. Studies suggest that PP is often amanifestation of a bipolar disorder condition that is triggeredby childbirth (Brockington et al. 1981; Jones and Craddock2001; Kendell et al. 1987). Approximately 25–50% ofwomen who give birth and have a history of bipolar disorderexperience an episode of PP (Brockington 1996; Jones andCraddock 2001), while rates as high as 74% have beenreported with women who also have a family history of PP(Jones and Craddock 2001). Recent epidemiological researchsuggests that in primiparous women, the relative risk forhospital admission with bipolar disorder during the firstmonth postpartum is 23 (Munk-Olsen et al. 2006). Thisfinding is four times higher than the relative risk for hospitaladmission with schizophrenia. Further support for theincreased risk of bipolar disorder recurrence postnatallycomes from research demonstrating high relapse rates amongwomen who discontinue their lithium (Viguera et al. 2000).In a retrospective study, Viguera et al. (2000) found that 70%of women who stopped their lithium treatment duringpregnancy experienced a recurrence of their bipolar disorderin the postpartum period, compared to 24% of non-pregnantmatched women. A personal history of PP also predisposesapproximately 57% of women to experience another episodeafter a subsequent pregnancy (Robertson et al. 2005).
Considering it is well documented that a history ofbipolar disorder or PP are significant risk factors for arelapse postnatally, preventative strategies are warranted.Given the seriousness of PP, gaining a better understanding
of effective treatment interventions is also critical in orderto address the immediate effects and decrease the long-termhealth consequences.
Aim
While there are general guidelines available on the treatmentof bipolar disorder or affective psychosis (e.g., AmericanPsychiatric Association http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx), specific guidelines onthe prevention and treatment of PP for perinatal healthprofessionals are primarily limited to the UK (e.g., NICE,SIGN, and CEMACH). In light of the seriousness of PP, agreater understanding of effective interventions is essential toimprove outcomes for this vulnerable population. Thepurpose of this systematic review was to examine theevidence on interventions for the prevention and treatmentof PP. It is beyond the scope of this review to evaluate theevidence of reproductive safety for medications used inpregnancy or breastfeeding; a review examining this specificarea has already been previously published (Stowe 2007).
Methods
Search methods
Databases systematically searched for this review includedCINAHL (1982–2009), EMBASE (1980–2009), MEDLINE(1950–2009), PsycINFO (1806–2009), and PubMed (1966–2009). Due to the dearth of research on PP, and to ensure thatno studies were missed, all studies including the key searchterms postpartum psychosis, puerperal psychosis, or postnatalpsychosis were reviewed for inclusion. Additional literaturewas located through reviewing the citations of the retrievedstudies and by contacting subject experts.
Inclusion and exclusion criteria
All primary research studies published in English andsince 1970 that explored the effectiveness of interven-tions for the prevention or treatment of PP were includedin this review. For the prevention studies, the interven-tion must have begun prior to the presentation of manicor affective psychotic symptoms either during pregnancyor immediately postpartum. For the treatment studies, theonset of mania or affective psychosis had to haveoccurred within the first year postpartum. As previouslystated, although symptoms generally develop within2 weeks of delivery, research studies can identifysubjects with PP using two different strategies. Someauthors use specific diagnostic criteria ascertained
90 S. Doucet et al.

through medical records while others use temporalcriteria that links symptoms to childbirth. As such, weused the criterion of onset of mania or affectivepsychosis within 1 year of parturition to ensure thatkey studies were not omitted. Studies based solely onbaby blues or postpartum depression were excluded;however, studies that included mixed samples includingboth women who experienced postpartum depression andPP were included to ensure that research on preventionand treatment strategies for PP was thoroughly reviewed.
Quality appraisal, data abstraction, and synthesis
Due to the limited number of studies on interventions forPP, all research designs were included. Studies, caseseries, or case reports of very poor methodological qualitywere excluded when we could not establish the preventionor treatment intervention used. Data were extracted usingan abstraction form and details related to disorderdefinition (i.e., diagnostic/screening criteria used), popu-lation sampled (i.e., participant characteristics, samplesize, recruitment process, inclusion/exclusion criteria),study design (i.e., method and timing of assessment,outcome measures, length of follow-up), intervention,and results were collected. Interventions were categorizedas prevention or treatment, and were subcategorizedaccording to the specific interventional approach used.
Results
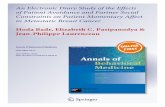
The first author reviewed the titles of approximately 800papers. After scanning the titles for inclusion, approxi-mately 270 abstracts were specifically examined accord-ing to the inclusion criteria. The search resulted in 26intervention studies (one study included both preventionand treatment interventions). Table 1 summarizes theresults of 10 studies that explored the prevention of PP.Table 2 summarizes the results of 17 studies that exploredthe treatment of PP. All studies that met the inclusioncriteria for this review were those that examined biologicalinterventions such as pharmacotherapy and electroconvulsivetherapy.
Prevention of PP
Research on the prevention of PP has focused on the effectsof mood stabilizers, antipsychotics, and hormone therapy.The sample size for the 10 prevention studies ranged from 1to 29, while over half (60%) of the studies had between 17and 29 participants. Half (50%) of the studies were smallclinical trials, while the remainder were primarily casestudies or retrospective reports.
Mood stabilizers Six studies evaluated the effects of moodstabilizers for the prevention of PP. In an open clinical trialconducted in Canada, the Netherlands, and the UK, 21women who met the Research Diagnostic Criteria (RDC)for history of PP were administered lithium at 34 weeksgestation or within 24 h of delivery (Stewart et al. 1991). At6 months postpartum, only two (10%) women hadexperienced an episode of PP. In an earlier case study byStewart (1988) in Canada, four women who had a history ofPP were administered prophylactic lithium immediatelyfollowing delivery and there were no reported relapses of PP.
UK researchers evaluated the effectiveness of lithiumprophylaxis in a retrospective study including 17 womenwho met the RDC criteria for bipolar disorder or history ofpuerperal affective psychosis (Austin 1992). Within3 months postpartum, only two (22%) of the nine womenwho received prophylactic lithium relapsed in comparisonto six (75%) of the eight women who did not receiveprophylactic lithium. It should be noted that three of thewomen in the treatment group were also included in thestudy of Stewart et al. (1991). In another retrospective studyincluding US women who met the DSM-III-R criteria forbipolar disorder, 14 of the 27 women received variouscombinations of prophylactic mood stabilizers (Cohen et al.1995). All but one woman received lithium alone or incombination with either carbamazepine or an antidepres-sant. Only one (7%) of the 14 in the treatment grouprelapsed, in comparison to eight (62%) of the 13 in the non-treatment group at 3 months postpartum. The relative riskof relapse was 8.6 times greater for women who did notreceive prophylactic mood stabilizers.
Support for the prophylactic effect of lithium also comesfrom a prospective study of 11 women from the Nether-lands who met DSM-III criteria for bipolar disorder (vanGent and Verhoeven 1992). Five of the women werestudied during two pregnancies. Of the 16 pregnancies,eight women received prophylactic lithium, two receivedprophylactic carbamazepine, one received prophylactichaloperidol, while five received no medications. Within3 months postpartum, three (27%) of the 11 women whowere treated with either lithium, carbamazepine, or halo-peridol experienced a manic or psychotic relapse comparedto three (60%) of five women who refused treatment.
The effects of the mood stabilizer divalproex inpreventing postpartum relapse were evaluated in an openclinical trial including 26 US women with a DSM-IVdiagnosis of bipolar disorder (Wisner et al. 2004). Fifteenof the women received divalproex immediately postpartum,while 11 of the women received only symptom monitoring.Participants were assessed weekly for 20 weeks using theStructured Clinical Interview for DSM-IV, the HamiltonRating Scale for Depression, the Bech–Rafaelson ManiaScale, the Mania Rating Scale, the Global Assessment of
Prevention and treatment of postpartum psychosis 91

Tab
le1
Postpartum
psycho
sispreventiv
einterventio
nstud
ies
Study
Design
Participants
Interventio
nsResults
Notes
Austin
1992
Retrospectiv
estudy
17UK
wom
enwho
met
theRDC
criteriaforbipolardisorder
orpuerperaleffectivepsychosis
Liprophylaxis(serum
levelsof
0.4mmol/1
ormore)
during
pregnancy(7/9)or
with
in48
hfollo
wingdeliv
ery(2/9)
2/9(22%
)in
thetreatm
entgrouprelapsed,
comparedto
6/8(75%
)in
thenon-
treatm
entgroupat
3monthspostpartum
Three
inthetreatm
entgroup
werealso
included
inthe
studyby
Stewartet
al.(1991)
Cohen
etal.1995
Retrospectiv
estudy
27USwom
enwho
met
DSM-III-R
criteriaforbipolardisorder
4/27
also
hadahistoryof
PP
Various
prophylactic
moodstabilizers
Li
alone=
9LiandCBZ=2Liandan
antid
epressant=
2CBZ=1
1/14
(7%)of
thetreatm
entgrouprelapsed,
comparedto
8/13
(62%
)in
thenon-
treatm
entgroupat
3monthspostpartum
Doses
werenotspecified
Kum
aret
al.2003
Openclinical
trial
29UK
wom
enwith
aRDCdiagnosis
ofhypomania,mania,or
schizoaffectivedisorder
Prophylactic
transdermal
17ß-estradiolwith
in48
hof
birthin
dosesof
200,
400,
or800μg/day,
reducedover
12days
12/29(41%
)relapsed,of
which,thosewho
received
thedose
of800μg/dayrequired
less
subsequent
psychotropic
medication
andrecoveredsooner
Onset
ofrelapsewas
with
in14
days
postpartum
for10
wom
en,and75
and77
days
for2wom
en
Murray1990
Casestudy
One
UK
wom
anwith
ahistoryof
PP
Duringsecond
pregnancyprophylactic
progesterone
400mg/dwas
administered
andincreasedto
800mg/dafterdeliv
ery.
After
3rd
pregnancy,
thioridazine
prophylaxis50
mgtid
Prophylactic
progesterone
didnotprevent
relapseof
PPthat
occurred
9days
postpartum
.Prophylactic
thioridazine
didpreventrelapseafter3rd
pregnancy
Study
isalso
included
underthe
treatm
entof
PP.
Thiorida-zine
was
takenoffmarketbecause
ofadverseeffects
Sharm
aet
al.2006
Openclinical
trial
25Canadianwom
enwith
ahistory
ofbipolardisorder
Prophylactic
olanzapine
alone(5–1
0mg)
orin
combinatio
nwith
anantid
epressantor
moodstabilizer=
11.Antidepressants,
moodstabilizers,or
nomedication=14
2/11
(18%
)wom
enin
theolanzapine
group
relapsed,in
comparisonto
8/14
(57%
)of
thewom
enin
theno
olanzapine
group
with
in4weekpostpartum
Sichelet
al.1995
Openclinical
trial
11USwom
enwho
met
DSM-III-R
criteriaforhistoryof
PP(n=7)
orPPD
(n=4).Noneexperienced
non-postpartum
affectiveillness
Prophylactic
oral
estrogen
(5mg,
bid)
immediately
afterdeliv
ery(dosereduced
over
4week).2/11
also
received
IVestrogen
toensure
compliancefor2days
1/11
(9%)relapsed
attheone-year
follo
w-up
Onset
ofrelapsewas
1weekpostpartum
All10
who
compliedwith
treatm
entdidnotrelapseNo
indicatio
nof
whether
the
relapsewas
PPD
orPP
Stewart1988
Caseseries
FourCanadianwom
enwith
historyof
PP,
3/4diagnosedwith
bipolardisorder
Prophylactic
Li(900–1
,200
mg/d)
immediately
follo
wingdeliv
ery
Lipreventedrelapsein
all4cases,maintained
at6month
follo
w-up
Stewartet
al.1991
Openclinical
trial
21wom
enfrom
Canada,
theNetherlands,
ortheUK
with
ahistoryof
PP
accordingto
theRDC
Prophylactic
Li(750–1
,200
mg/d)
at34-w
eek
gestation(5/21)
orwith
in24
hafterdeliv
ery
(16/21)
2/21
(10%
)relapsed
with
in8days
postpartum
,both
mild
Nootherrelapseat
6months
One
motherwho
beganLi
before
deliv
erysuffered
astillbirth
vanGentand
Verhoeven
1992
Prospectiv
ethree-center
study
Elevenwom
enfrom
theNetherlands
who
met
DSM-IIIcriteriaforbipolar
disorder,5becamepregnant
twice
Prophylactic
Li(serum
levelsup
to0.7mmol/1)=
8CBZ=2Haloperidol=1Refused
treatm
ent
group=5
3/11
(27%
)of
thetreatm
entgroup
experiencedmanic/psychotic
relapsewith
in3months,
comparedto
3/5(60%
)who
refusedtreatm
ent
The
prophy-lactic
effectsof
Li,
CBZ,andhaloperidolwere
notspecified
Wisneret
al.2004
Openclinical
trial
26USwom
enwith
aDSM-IV
diagnosisof
bipolardisorder
Divalproex(250
mg/bidas
tolerated)
and
symptom
monito
ring
immediately
postpartum
=15
Postpartum
symptom
monito
ring
alone=
11
10/15(67%
)of
thewom
enwho
received
divalproex
and8/11
(73%
)of
thewom
enwho
wereunmedicated
relapsed
with
in20
weekpostpartum
.Nosignificantdifferencesbetweengroups
RDC
ResearchDiagn
ostic
Criteria,
DSM
Diagn
ostic
andStatistical
Manualof
MentalDisorders,PPpo
stpartum
psycho
sis,PPD
postpartum
depression
,Lilithium
,CBZcarbam
azepine
92 S. Doucet et al.
Tab
le2
Postpartum
psycho
sistreatm
entinterventio
nstud
ies
Study
Design
Participants
Interventio
nsResults
Notes
Ahokasand
Aito
1999
Caseseries
Twowom
enfrom
Finland
with
onsetof
PP
1–4weeks
postpartum
Bothcasestreatedwith
sublingual
17ß-estradiol
(4–6
mg/day)
1case
was
first
treatedwith
CPZ200mg/dfor2weeks
CPZhadlittle
effect
Psychotic
symptom
sdecreased
with
in1weekon
estradiolas
measuredby
theBPRS,
andboth
madeacompleterecovery.Bothwom
anstoppedtreatm
entandrelapsed
with
in2weeks
Ahokaset
al.2000a
Open-labeltrial
Tenwom
enfrom
Finland
meetin
gtheICD-10
criteriaforpsychosiswith
postpartum
onset,
(meanonset=12.3
days,SD=8.3)
All11
received
sublingual
17ß-estradiol
(3–6
mg/d)
2wom
enfirsttreatedwith
CPZ300–
400mg/dforup
to3week.
Twowom
enfirsttreated
with
haloperidol8–20
mg/dforup
to17
days
CPZandhaloperidolhadlittle
effect
Psychotic
symptom
sdecreasedwith
in1weekon
estradiolas
measuredby
theBPRS.1wom
anwho
stoppedtreatm
entrelapsed
with
in1week
Twowom
enalso
received
psycho-therapy
before
estradiolwith
little
effect
Ahokaset
al.2000b
Caseseries
Twowom
enfrom
Finland
with
onset
ofPP1–2weeks
postpartum
Bothcasestreatedwith
sublingual
17ß-estradiol
(3–4
mg/d)
1case
was
firsttreatedwith
haloperidol
upto
20mg/dfor17
days
Haloperidol
hadlittle
effect
Psychotic
symptom
sdecreasedwith
in10
days
onestradiolas
measured
byBPRS1wom
anwho
stoppedtreatm
entrelapsed
with
in1week
Atkinsonand
Atkinson1983
Casestudy
One
UK
wom
anwith
onsetof
PP
with
in7weeks
postpartum
Progesterone(injectio
nsandsupposito
ries)
Hallucinatio
nsanddelusionsdecreasedwith
in1month,
afternotresponding
toatranquilizer
Writtenby
affected
mother
andhusbandDosenot
specified
Forrayand
Ostroff2007
Caseseries
FiveUSwom
enwith
severe
treatm
ent
refractory
PPandPPD
Onset
3weeks—11
monthspostpartum
ECT3tim
esaweek
All5wom
enim
proved
with
in3–6sessions
whenprior
pharmacotherapy
was
unsuccessful
Huang
etal.2008
Casestudy
One
wom
anfrom
Taiwan
with
ahistoryof
mania
Onset
ofPP
1month
postpartum
Lialoneor
variouslycombinedwith
CBZ,valproic
acid,andhaloperidol.HRTwith
conjugated
estrogen
0.625mg/dandmedroxy-progesterone2.5mg/day
Poortreatm
entresponse
with
alltreatm
ents,except
forHRT,
which
was
effectivewith
in2weeks
Iruela
etal.1992
Casestudy
One
wom
anfrom
Spain
with
onsetof
psychosis3days
postpartum
Antidepressantsandanxiolytics.Haloperidol
(4mg/day)
andmethotrim
eprazine
(75mg/day).
Pim
ozide(8
mg/day)
Pim
ozidewas
effectivewith
in4days
andremained
asym
ptom
atic
at3year.Allothertreatm
entswere
ineffective
Antide-pressant
andanx-
iolytic
drugsnotspecified
Kornhuber
and
Weller1991
Casestudy
One
wom
enfrom
Germanywith
onset
ofpsychosis1weekpostpartum
Zuclopenthixoldecanoate600mgClozapine
200mg
Zuclopenthixoldecanoatecaused
severe
extrapyram
idal
side
effects.Clozapine
was
substituted
andwas
effectivewith
in1week
Lichtenberg
etal.1988
Casestudy
One
wom
anfrom
Israel
with
onsetof
psychosis3days
postpartum
Liup
to1,200mg/day
Responded
tolithium
with
in10
days
ofinitiating
treatm
entandrecoveredwith
inamonth
Alsohadahistoryof
GM2
Ganglio-sidosis
MarshallandNursing
care
study1981
Casestudy
One
UK
wom
anwith
onsetof
psychosis8days
postpartum
CPZtablets(25mg,
bid)
andlorazepam
tablets
(2.5
mg,
bid)
Changed
toCPZtablets(50mg,
bid)
andim
ipraminetablets(25mg,
tid)
CPZandlorazepam
was
noteffective.
Increaseddose
ofCPZcombinedwith
imipraminedecreased
symptom
swith
in1weekandremainedsymptom
free
at12
week
Murray1990
Casestudy
One
UK
wom
anwith
onsetof
psychosis5days
postpartum
after1s
t
pregnancyand9days
postpartum
after2n
d
CPZ50
mg,
tidSym
ptom
sim
proved
rapidlywith
CPZafterboth
pregnancies
Study
isalso
included
under
thepreven-tionof
PP
O’Reagan1981
Casestudy
One
Canadianwom
anwith
onsetof
psychosis11
days
postpartum
Antipsychotics,ECT,
antid
epressants,andLi
Propranolol
(adrenergicblocking
agent)up
to450mg/day
ECTprovided
good
results,temporarily
Antipsychotics,
antid
epressants,andLihadno
effect
Propranolol
“cured”patient’spsychosis
Antipsy-chotic
and
antid
e-pressantdrugs
notspecified
Reedet
al.1999
Retro-spective
case-notestudy
114wom
enfrom
theUK
PPwith
in3months=
58Non-postpartum
psychosis=
56Postpartum
group=3–6ECTsessions
Non-
postpartum
group=1–23
ECTsessions
Wom
enwho
experiencedPPhadsignificantly
greater
clinical
improvem
entfollo
wingECTcomparedto
thenon-postpartum
psychosisgroup
Silb
ermann
etal.1975
Prospectiv
estudy
Com
pari-son
group
was
retro-spectiv
e
19wom
enfrom
theNetherlands
experiencing
postpartum
delirium
Treatmentgroup(13/19)=
combinatio
nof
Li
(upto
1,200mg/d)
andperfenazine(upto
30mg/d)
Com
parisongroup(6/19)=oneor
moreantip
sychotics
The
treatm
entgroupwas
symptom
free
with
in7–15
days,
less
likelyto
relapse,
andhadsignificantly
faster
recovery
times
(mean12
weekcomparedto
20week)
Onset
timenotspecified
Stanw
orth
1982
Casestudy
1wom
anfrom
theUK
with
onsetof
psychosis
1weekpostpartum
CPZ(upto
250mg/day)
2ECTtreatm
ents
Little
improvem
entwith
CPZalone.
Goodim
provem
ent
with
CPZandECT
Steiner
etal.1973
Openclinical
trial,
con-secutiv
eassignmentto
1of
2treatm
entgroups
10wom
enfrom
Israel
with
psychosisassociated
with
child
bearingMeanonsettim
eforthe
propranololgroupwas
14days
and35
days
fortheCPZgroup
Propranolol
(upto
3,200mg/d)
=5/10
CPZ
(upto
800mg/d)
=5/10
Bothtreatm
entseffective;
however,wom
entreatedwith
propranololweredischarged
sooner,hadgreater
symptom
improvem
ent,andsymptom
sim
proved
morerapidlyas
measuredby
theBRPSandtheCGI
Usedmeanonsettim
e;howeverrangenotspecified
Targum
etal.1979
Caseseries
TwoUSwom
enwith
ahistoryof
bipolardisorder
with
onsetof
PP
with
in2weeks
postpartum
(after
with
draw
alfrom
Liduring
pregnancy)
Case1:
treatedwith
thioridazine
for1weekandrestarted
onLiCase2:
treatedwith
CPZandrestartedon
Li
Bothcasesrecoveredwith
in17
days
BPRSBrief
Psychiatric
RatingScale,ICD
InternationalClassificationof
Diseases,CGIcogn
itive
glob
alim
pression
,PPpo
stpartum
psycho
sis,PPD
postpartum
depression
,CPZchlorpromazine,
ECTelectrocon
vulsivetherapy,
Lilithium
,CBZcarbam
azepine,
HRTho
rmon
ereplacem
enttherapy
Prevention and treatment of postpartum psychosis 93

Function, and the Asberg Side Effects Scale. Within20 weeks postpartum, 10 (67%) of the 15 women whoreceived divalproex relapsed, compared to eight (73%) ofthe 11 unmedicated women. There were no significantdifferences between the two groups. While divalproex wasnot effective, none of the women who relapsed experienceda severe episode that required admission, which may beassociated with the close clinical supervision of theparticipants.
Overall, prophylactic lithium was supported in fivestudies (Austin 1992; Cohen et al. 1995; Stewart 1988;Stewart et al. 1991; van Gent and Verhoeven 1992). Theprophylactic effects of carbamazepine were demonstrated intwo studies (Cohen et al. 1995, van Gent and Verhoeven1992), while prophylactic divalproex was not supported inone study (Wisner et al. 2004).
Antipsychotics Only one study to date has explored theeffects of antipsychotics for the prevention of PP. An opentrial exploring the effects of prophylactic olanzapine wasconducted in Canada including 25 women with a history ofbipolar disorder, of which 11 received olanzapine alone orin combination with an antidepressant or mood stabilizer,while 14 received either antidepressants, mood stabilizers,or no medication (Sharma et al. 2006). The treatmenteffects were assessed using the Schedule for AffectiveDisorders and Schizophrenia—Lifetime Version, the HamiltonRating Scale for Depression—31 items, the Young ManiaRating Scale, and the Personal Mood Diary. At 4 weekspostpartum, only two (18%) of the 11 women who receivedolanzapine experienced an affective relapse according to theDSM-IV criteria, in comparison to eight (57%) of the 14 whodid not receive olanzapine.
Hormone therapy Three studies reported the effects ofhormone therapy for the prevention of psychosis postpar-tum. To determine the effects of prophylactic oral estrogen,an open clinical trial was conducted with 11 US womenwho had a history of either PP or postpartum depression(Sichel et al. 1995). None of the 10 women who compliedwith the estrogen treatment relapsed. The preventive effectsof estrogen were less promising in an open clinical trialwith 29 pregnant women from the UK who met the RDCfor hypomania, mania, or schizoaffective disorder (Kumaret al. 2003). The Schedule for Affective Disorders andSchizophrenia–Lifetime Version was used to assess thetreatment effects of prophylactic transdermal estrogen thatwas administered 48 h after birth in doses of 200, 400, or800 μg/day. Estrogen was not effective in reducing the rateof relapse; however, of the 12 out of 29 who relapsed, thosewho received a dose of 800 μg/day required less subse-quent psychotropic medication and recovered sooner. In acase study with a woman from the UK, prophylactic
progesterone administered during pregnancy and postpar-tum was not effective in preventing a relapse of PP (Murray1990). In summary, there are mixed findings for thepreventative effects of estrogen and there is no evidenceto support the prophylactic use of progesterone.
Treatment of PP
Research on the treatment of PP has examined the effects ofelectroconvulsive therapy (ECT), antipsychotics, moodstabilizers, hormones, and the beta-blocker propranolol.The sample size for the 17 treatment studies and casereports ranged from 1 to 114, with 15 (88%) studiesincluding 10 or fewer participants; over half (53%) of thestudies had only one participant. Not surprising, themajority (76%) of treatment studies were case reports.
Electroconvulsive therapy Three studies have explored theeffects of ECT in the treatment of PP. In a retrospectivestudy with 114 women, UK researchers compared theclinical response to ECT in women with postpartum andnon-postpartum psychosis (Reed et al. 1999). According toblind ratings, the postpartum group was found to havegreater clinical improvement following ECT compared tothe non-postpartum group. In a case study of a woman fromthe UK, treatment with chlorpromazine alone resulted inlittle clinical improvement, while the addition of ECTresulted in positive outcomes (Stanworth 1982). Anothercase study described five US women who had severe andtreatment refractory PP or depression with onset between3 weeks and 11 months postpartum (Forray and Ostroff2007). All women were treated with ECT and improvedwithin three to six sessions. Overall, these studies providebeginning support for the beneficial effects of ECT in thetreatment of PP.
Mood stabilizers Three studies have examined the effectsof lithium in the treatment of PP. A case study of an Israeliwoman revealed a positive response to lithium within10 days of initiating treatment and patient recovery within amonth (Lichtenberg et al. 1988). The woman also had ahistory of GM2 Gangliosidosis, wherein approximately onethird who have this disorder also experience psychosis. Aprospective study of 19 women from the Netherlandscompared the treatment effects of a group who receivedlithium combined with perfenazine to a group who receivedone or more antipsychotic treatments (Silbermann et al.1975). The lithium treatment group was symptom freewithin 7–15 days, was less likely to relapse, and hadsignificantly faster recovery times, with a mean of 12 weekscompared to 20 weeks. In a case study, two US womenwith a history of bipolar disorder experienced PP within
94 S. Doucet et al.

2 weeks postpartum (Targum et al. 1979). One woman wastreated with lithium and thioridazine and the other womanwith lithium and chlorpromazine. Both women recoveredwithin 17 days. In summary, there have been very fewstudies examining the effect of lithium. This treatmentoption was found to be effective in one case study where itwas used as monotherapy (Lichtenberg et al. 1988) and intwo studies where it was used as adjunct therapy (Silbermannet al. 1975; Targum et al. 1979).
Antipsychotics The effects of antipsychotics in the treat-ment of PP have been examined in four studies. Onestudy described a UK woman who experienced PP aftertwo separate pregnancies and reported that treatment withchlorpromazine was successful during both episodes(Murray 1990). In another case study with a UK womanexperiencing PP, chlorpromazine combined with loraze-pam was ineffective (Marshall and Nursing Care Study1981). However, when chlorpromazine was increased andcombined with imipramine, the woman’s psychotic symp-toms decreased within 1 week and she remained symptomfree at 12 weeks.
In a case study of a woman from Germany with PP,treatment with clozapine was effective within a week(Kornhuber and Weller 1991). In another case study, aSpanish woman was refractory to treatment with variousdrugs, including antidepressants, anxiolytics, and the anti-psychotics haloperidol and methotrimeprazine (Iruela et al.1992). Another antipsychotic, pimozide, was administeredand was effective within 4 days. Overall, very few studieshave explored the effects of antipsychotics in the treatmentof PP. There are reports of successful treatment withchlorpromazine, clozapine, and pimozide.
Hormone therapy Five studies have examined the effects ofhormonal treatment among women diagnosed with PP.Three studies conducted in Finland examined the treatmenteffects of sublingual estrogen in women who had estrogendeficiency and PP (Ahokas and Aito 1999; Ahokas et al.2000a; Ahokas et al. 2000b). A total of 14 women weredescribed in the three reports. Using the Brief PsychiatricRating Scale (BPRS), psychiatric symptoms were reportedto have decreased within 2 weeks of estrogen treatment.Four women discontinued their estrogen treatment andexperienced a relapse within 2 weeks. The case study of awoman from the UK reported a positive outcome for theeffects of progesterone in the treatment of PP after thewoman did not respond to an unspecified tranquilizer(Atkinson and Atkinson 1983). In a recent case study, aTaiwanese woman with a history of mania was treated forPP with hormone replacement therapy, which consists ofestrogen and progesterone (Huang et al. 2008). Thistreatment was reported to be effective within 2 weeks after
the woman was refractory to antipsychotics and moodstabilizers. With only a few individual case reports, it is notpossible at present to conclude that any evidence exists forthe hormonal treatment of PP.
Propranolol This drug is a beta-adrenergic blocker that isprimarily used to treat hypertension (Prichard and Gillam1996). Propranolol was first used to treat PP in 1973(Steiner et al. 1973), although the mechanism in whichpropranolol works on treating psychiatric conditions is notwell understood. To compare the effects of propranolol andchlorpromazine, an open clinical trial was conducted with10 Israeli women experiencing PP (Steiner et al. 1973).Both treatments were effective in reducing the severity ofpsychotic symptoms as measured by the BPRS and theCognitive Global Impression (CGI) instruments; however,women treated with propranolol were discharged sooner(61 days compared to 104 days), symptoms improved morerapidly (3 days compared to 55 days), and demonstratedgreater mean improvement on the BPRS and the CGI. Theuse of propranolol was also supported in a case study of aCanadian woman who was unresponsive to antipsychotics,antidepressants, lithium, and ECT (O’Reagan 1981). Pro-pranolol was said to have “cured” the patient’s psychosis.Overall, only two studies to date have supported the effectsof propranolol in the treatment of PP (O’Reagan 1981;Steiner et al. 1973).
Discussion
The aim for this systematic review was to examine theeffectiveness of interventions for the prevention andtreatment of PP. A total of 26 studies were reviewed, with10 examining preventative interventions and 17 examiningtreatment interventions (one study included both preventionand treatment interventions). Studies were conducted innine countries, with the majority conducted in the UK(33%), followed by the US (19%). The years of publicationfor the included studies ranged from 1973 to 2008, whileapproximately two thirds (65%) of the studies werepublished more than 10 years ago. The methodologicalquality of the studies differed significantly, resulting in alimited evidence base to guide current practice and decisionmaking. In particular, the study sample sizes were generallysmall, reports were often retrospective, and the designswere primarily case reports. While the evidence providedfrom this research is limited, it does highlight promisingareas for additional research and may provide clinicianswith some suggestions to guide management. In addition,for some treatment approaches with a considerable evi-dence base in non-postpartum samples—mood stabilizers
Prevention and treatment of postpartum psychosis 95

and antipsychotics for example—further evidence in post-partum cases may be reassuring. For novel treatmentoptions such as hormonal manipulation, however, the lackof data is far more concerning reflecting the need foradditional research before conclusions about efficacy canbe drawn. Overall, further research is warranted usingrigorous methodology to evaluate current preventative andtreatment options.
The studies included in this review used a variety ofdiagnostic criteria to determine participant study inclu-sion and intervention efficacy. The standardized diagnos-tic criteria used for inclusion in the preventative studiesincluded the DSM III (van Gent and Verhoeven 1992),DSM III-R (Cohen et al. 1995; Sichel et al. 1995), DSM-IV (Sharma et al. 2006; Wisner et al. 2004), and the RDC(Austin 1992; Kumar et al. 2003; Stewart et al. 1991).Five prevention studies used standardized questionnairesto determine the relapse of postpartum psychosis, includ-ing the Schedule for Affective Disorders and Schizophre-nia—Lifetime Version (Kumar et al. 2003; Sharma et al.2006), the Mania Rating Scale (Wisner et al. 2004), theYoung Mania Rating Scale (Sharma et al. 2006), theBech–Rafaelson Mania Scale (Wisner et al. 2004), theHamilton Rating Scale for Depression (Sharma et al. 2006;Wisner et al. 2004), the Global Assessment of Function(Wisner et al. 2004), the Asberg Side Effects Scale(Wisner et al. 2004), the Personal Mood Diary (Sharmaet al. 2006), the DSM III-R checklist (Sichel et al. 1995),the Structured Clinical Interview for DSM-IV (Wisner etal. 2004), and a “standard data form” (Stewart et al. 1991).Only one treatment study (Ahokas et al. 2000a) reportedusing standardized diagnostic criteria to diagnose postpar-tum psychosis, namely the ICD-10. Questionnaires wereused to assess the treatment effects in seven studies;specifically the BPRS (Ahokas and Aito 1999; Ahokas etal. 2000b; Steiner et al. 1973), the CGI (Steiner et al.1973), and various unstandardized scales (Forray andOstroff 2007; Reed et al. 1999; Silbermann et al. 1975).Overall, eight of the prevention studies and only seven ofthe treatment studies used some form of a standarddiagnostic assessment. The diagnostic measures werediverse, making comparisons between studies difficult tointerpret. Moreover, the studies included in this reviewrepresent a variety of prevention and treatment approachesin various combinations, further precluding any clearcomparisons between studies. For these reasons, resultsfrom this review should be interpreted with caution.
Prevention
Research on the prevention of PP has focused on the effectsof mood stabilizers, antipsychotics, and hormone therapy.Lithium was the most commonly studied prevention
approach with research suggesting it may decrease the rateof relapse from approximately 50% to less than 22%(Austin 1992; Cohen et al. 1995; Stewart 1988; Stewart etal. 1991). Further support for the use of lithium comes fromstudies demonstrating high relapse rates among womenwho discontinue their lithium during pregnancy (Targum etal. 1979; Viguera et al. 2000). There is insufficient evidenceto suggest whether lithium is equally effective whenadministered prophylactically through pregnancy or startedimmediately in the postpartum period.
Only one study has focused on the effects ofantipsychotics in the prevention of PP and positiveresults have been found in a small trial of olanzapine(Sharma et al. 2006). Additional research is clearlyrequired, but the dearth of evidence for prophylacticantipsychotic medication in the postpartum context mustbe considered in light of the more robust evidence base forthese medications in non-postpartum samples. In the caseof hormonal prophylaxis, however, the evidence base ispoor and without the studies demonstrating efficacy inmood disorders more generally there is insufficientevidence to support their use at present. What is veryclear is that women with a history of PP or bipolardisorder who do not receive prophylactic treatment are atan increased risk for relapse of affective symptoms (Austin1992; Cohen et al. 1995). Larger naturalistic and possiblyrandomized controlled trials are required to examine theeffects of prophylactic interventions.
Treatment
Research on the treatment of PP has examined the effects ofECT, mood stabilizers, antipsychotics, hormones, andpropranolol. The limited evidence supports the use ofECT in the treatment of PP when administered alone(Forray and Ostroff 2007; Reed et al. 1999), as well aswhen combined with the antipsychotic chlorpromazine(Stanworth 1982). Overall, the use of antipsychotics in thetreatment of PP requires further investigation before anyconclusions can be drawn about their effectiveness postna-tally. Their use at this time, however, must be considered inlight of the large body of evidence of efficacy in non-postpartum episodes.
Lithium is commonly used in the treatment of PP;however, the evidence to support this treatment option isscarce. In the few studies conducted to date (Lichtenberg etal. 1988; Silbermann et al. 1975; Targum et al. 1979),lithium treatment for PP is generally supported. Theeffectiveness of lithium in the treatment of bipolar disorderis well documented and it has been suggested that lithium isequally effective with postpartum women as it is with non-postpartum women (Abou-Saleh and Coppen 1983). Fur-ther comparative investigations are needed that examine
96 S. Doucet et al.

whether the effects of lithium are equally effective intreating episodes of PP.
Three studies conducted by the same group (Ahokas andAito 1999; Ahokas et al. 2000a, b) have found beneficialeffects of estrogen. The potential beneficial use of proges-terone (Atkinson and Atkinson 1983) and hormone replace-ment therapy (Huang et al. 2008) were described throughcase studies. There is insufficient research to recommendhormone treatment; however, preliminary results wouldsuggest that further studies are indicated—particularly asthe involvement of hormonal factors in etiology come to bebetter understood.
There is an array of differences reported across studieson the effect of interventions for PP. Health professionalsshould therefore gain knowledge on what methods havebeen effective for women in the past and if any adverseeffects were experienced (Sharma 2003). Although we havefocused in this review on biological approaches, treatmentshould also go beyond the medical symptoms and includepsychosocial and psychological therapy given the complexand multiple needs of women diagnosed with PP.
Safety of medication during pregnancy and breastfeeding
An important consideration is the reproductive safety ofmedication in pregnancy and breastfeeding. While beyondthe scope of this review, there is clearly a need to conduct arisk benefit analysis with each individual woman. Althoughsome medications are associated with particular problems,there are no universal recommendations that can be madeabout whether to continue or stop and the decision mustultimately lie with the woman and her family. Moreover,women with bipolar disorder need to be informed early intheir illness about the risks in childbirth and the reproductivesafety of medication and family planning should be discussedwhen drugs are prescribed.
Limitations
The review only included studies published in English.Although most cases of PP occur within the first 2 weeksafter giving birth (Heron et al. 2007), we included onsetwithin 1 year postpartum. In 10 (38%) of the studiesincluded in this review, women had onset times beyond2 weeks postpartum. This may preclude any clear inferencesto be made about the participants who exceeded 2 weeks inonset, as they may be cases that are coincidentally psychoticin the postpartum period, and not truly cases of PP.
Implications for future research
There are numerous gaps in the research on strategies toprevent and treat PP. Agreement is needed on the diagnosis
and classification of the disorder that is not dealt with in aparticularly helpful way in current DSM-IV and ICD-10criteria. While acquiring large representative samples andconducting randomized controlled trials is problematic,collaborative multicenter naturalistic studies are possibleand would provide very helpful data.
Future research could also focus on gaining a betterunderstanding of the causes of PP, as this will act as a guidefor research on prevention and treatment. Given the equivocalevidence on hormone therapy in both the prevention andtreatment of PP, research on the etiology of PP could furtherexamine the role of hormonal factors to guide management.
Conclusion
Firm recommendations on effective interventions arelimited until further research is conducted on all forms ofprevention and treatment for PP. PP represents a psychiatricemergency, thus the timely recognition of symptoms andearly treatment is critical to the well-being of the affectedwoman and her family. The well-established risk factors(e.g., bipolar disorder) and potentially severe consequences(e.g., suicide and infanticide) of PP point to the importanceof preventive measures. Multicenter prospective studies aredesperately needed to provide guidance on prevention andtreatment interventions.
References
Abou-Saleh MT, Coppen A (1983) Puerperal affective disorders andresponse to lithium. Br J Psychiatry 142:539
Ahokas A, Aito M (1999) Role of estradiol in puerperal psychosis.Psychopharmacology 147:108–110
Ahokas A, AitoM, RimonR (2000a) Positive treatment effect of estradiolin postpartum psychosis: a pilot study. J Clin Psychiatry 61:166–169
Ahokas A, Aito M, Turtiainen S (2000b) Association between oestradioland puerperal psychosis. Acta Psychiatr Scand 101:167–170
American Psychiatric Association (2000) Diagnostic and statisticalmanual of mental disorders, 4th edn. American PsychiatricAssociation, Washington, text revision
Appleby L, Mortensen PB, Faragher EB (1998) Suicide and othercauses of mortality after post-partum psychiatric admission. Br JPsychiatry 173:209–211
Atkinson S, Atkinson T (1983) Puerperal psychosis: a personalexperience. Health Visit 56:17–19
Austin MV (1992) Puerperal affective psychosis: is there a case forlithium prophylaxis? Br J Psychiatry 161:692–694
Brockington IF (1996) Motherhood and mental health. OxfordUniversity Press, Oxford
Brockington IF, Cernik KF, Schofield EM, Downing AR, Francis AF,Keelan C (1981) Puerperal psychosis: phenomena and diagnosis.Arch Gen Psychiatry 38:829–833
Chandra PS, Bhargavaraman RP, Raghunandan VNGP, Shaligram D(2006) Delusions related to infant and their association withmother–infant interactions in postpartum psychotic disorders.Arch Womens Ment Health 9:285–288
Prevention and treatment of postpartum psychosis 97

Cohen LS, Sichel DA, Robertson LM, Heckscher E, Rosenbaum JF(1995) Postpartum prophylaxis for women with bipolar disorder.Am J Psychiatry 152:1641–1645
Forray A, Ostroff RB (2007) The use of electroconvulsive therapy inpostpartum affective disorders. J ECT 23:188–193
Heron J, Robertson-Blackmore E, McGuinness M, Craddock N, JonesI (2007) No latent period in bipolar affective puerperal psychosis.Arch Womens Ment Health 10:79–81
Heron J, McGuinness M, Robertson Blackmore E, Craddock N, JonesI (2008) Early postpartum symptoms in puerperal psychosis. Br JObstet Gynaecol 115:348–353
Hipwell AE, Goossens FA, Melhuish EC, Kumar R (2000) Severematernal psychopathology and infant–mother attachment. DevPsychopathol 12:157–175
Huang MC, Wang YB, Chan CH (2008) Estrogen-progesteronecombination for treatment-refractory post-partum mania. PsychiatryClin Neurosci 62:126
Iruela LM, Ibañez-Rojo V, Gilaberte I, Oliveros SC (1992) Newpossible indications of pimozide. J Clin Psychiatry 53:172–173
Jones I, Craddock N (2001) Familiarity of the puerperal trigger inbipolar disorder: results of a family study. Am J Psychiatry158:913–917
Kendell R, Chalmers J, Platz C (1987) Epidemiology of puerperalpsychoses. Br J Psychiatry 150:662–673
Kornhuber J, Weller M (1991) Postpartum psychosis and mastitis: anew indication for clozapine? Am J Psychiatry 148:1751–1752
Kumar C, McIvor RJ, Davies T (2003) Estrogen administration doesnot reduce the rate of recurrence of affective psychosis afterchildbirth. J Clin Psychiatry 64:112–118
Lichtenberg P, Navon R, Wertman E, Dasberg H, Lerer B (1988) Post-partum psychosis in adult GM2 Gangliosidosis: a case report. BrJ Psychiatry 153:387–389
Marshall S, Nursing care study (1981) Puerperal psychosis: with a lotof help from her friends. Nurs Mirror 152:46–47
Munk-Olsen T, Laursen TM, Pedersen CB, Mors O, Mortensen PB(2006) New parents and mental disorders: a population-basedregister study. JAMA 296:2582–2589
Murray D (1990) Recurrence of puerperal psychosis not prevented byprophylactic progesterone administration. J Nerv Ment Dis178:537–538
O’Hara MW, Swain AM (1996) Rates and risk of postpartumdepression: a meta-analysis. Int Rev Psychiatry 8:37–54
O’Reagan JB (1981) Treatment of acute postpartum psychosis. CanMed Assoc J 125:1083
Prichard BNC, Gillam PMS (1996) Treatment of hypertension withpropranolol. Br Med J 1:7–16
Reed P, Sermin N, Appleby L, Faragher B (1999) A comparison ofclinical response to electroconvulsive therapy in puerperal andnon-puerperal psychoses. J Affect Disord 54:255–260
Robertson E, Jones I, Haque S, Holder R, Craddock N (2005) Risk ofpuerperal and non-puerperal recurrence of illness followingbipolar affective puerperal (post-partum) psychosis. Br J Psychiatry186:258–259
Sharma V (2003) Pharmacotherapy of postpartum psychosis. ExpertOpin Pharmacother 4:1651–1658
Sharma V, Smith A, Mazmanian D (2006) Olanzapine in theprevention of postpartum psychosis and mood episodes in bipolardisorder. Bipolar Disord 8:400–404
Sichel DA, Cohen LS, Robertson LM, Ruttenberg A, Rosenbaum JF(1995) Prophylactic estrogen in recurrent postpartum affectivedisorder. Biol Psychiatry 38:814–818
Silbermann RM, Beenen F, de Jong H (1975) Clinical treatment ofpost partum delirium with perfenazine and lithium carbonate.Psychiatr Clin 8:314–326
Sit D, Rothschild AJ, Wisner KL (2006) A review of postpartumpsychosis. J Womens Health 15:352–368
Spinelli MG (2004) Maternal infanticide associated with mentalillness: prevention and promise of saved lives. Am J Psychiatry161:1548–1557
Stanworth HM (1982) After-care of puerperal psychosis in thecommunity. Nurs Times 78:922–925
Steiner M, Latz A, Blum I, Atsmon A, Wijsenbeek H (1973) Propranololversus chlorpromazine in the treatment of psychoses associated withchildbearing. Psychiatr Neurol Neurochir 76:421–426
Stewart DE (1988) Prophylactic lithium in postpartum affectivepsychosis. J Nerv Ment Dis 176:485–489
Stewart DE, Klompenhouwer JL, Kendall RE, Van Hulst AM (1991)Prophylactic lithium in puerperal psychosis: the experience ofthree centres. Br J Psychiatry 158:393–397
Stowe ZN (2007) The use of mood stabilizers during breastfeeding. JClin Psychiatry 68(Suppl 9):22–28
Targum S, Davenport Y, Webster M (1979) Postpartum mania inbipolar manic-depressive patients withdrawn from lithium carbonate.J Nerv Ment Disord 167:572–574
Terp IM, Engholm G, Moller H, Mortenson PB (1999) A follow-upstudy of postpartum psychoses: prognosis and risk factors forreadmission. Acta Psychiatr Scand 100:40–46
van Gent EM, Verhoeven WM (1992) Bipolar illness, lithiumprophylaxis, and pregnancy. Pharmacopsychiatry 25:187–191
Viguera AC, Nonacs R, Cohen LS, Tondo L, Murray A, BaldessariniRJ (2000) Risk of recurrence of bipolar disorder in pregnant andnonpregnant women after discontinuing lithium maintenance.Am J Psychiatry 157:179–184
Wisner KL, Hanusa BH, Peindl KS, Perel JM (2004) Prevention ofpostpartum episodes in women with bipolar disorder. BiolPsychiatry 56:592–596
World Health Organization (1992) The ICD-10 Classification of Mentaland Behavioral Disorders. World Health Organization, Geneva
98 S. Doucet et al.









![“Ekomo’s Interventions” [María Nsue Angüe]](https://static.fdokumen.com/doc/165x107/632104d980403fa2920c8b06/ekomos-interventions-maria-nsue-anguee.jpg)