INFORMATION TO USERS - AU Digital Research Archive |
82
INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. Each original is also photographed in one exposure and is included in reduced form at the back of the book. Photographs included in the original manuscript have been reproduced xerographically in this copy. Higher quality 6” x 9” black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order. Bell & Howell Information and Learning 300 North Zeeb Road, Ann Arbor, Ml 48106-1346 USA 800-521-0600 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of INFORMATION TO USERS - AU Digital Research Archive |
INFORMATION TO USERS
This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer.
The quality of this reproduction is dependent upon the quality of the copy
submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment
can adversely affect reproduction.
In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion.
Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. Each original is also photographed in one exposure and is included in reduced form at the back of the book.
Photographs included in the original manuscript have been reproduced xerographically in this copy. Higher quality 6” x 9” black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order.
Bell & Howell Information and Learning 300 North Zeeb Road, Ann Arbor, Ml 48106-1346 USA
800-521-0600
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
COGNITIVE DECONSTRUCTION IN SEXUALLY COMPULSIVE PRIESTS
by
Carmen Winterschladen
Submitted to the
Faculty of the College of Arts and Sciences
of American University
in Partial Fulfillment of
the Requirements for the Degree
of Master of Arts
in
Psychology
Chair:
Dean^fthe College
7Date
JamraGray. Pn.D.l y ' . C-_ ( ' t J 'k tp c .
David Haaga. Ph.D.
misa Saffiotti. Ph.D.
impson. Ph/O.
1999
American University
Washington. D.C. 20016
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

UMI Number: 1396143
UMI Microform 1396143 Copyright 1999, by UMI Company. All rights reserved.
This microform edition is protected against unauthorized copying under Title 17, United States Code.
UMI300 North Zeeb Road Ann Arbor, MI 48103
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

COGNITIVE DECONSTRUCTION IN SEXUALLY COMPULSIVE PRIESTS
by
Carmen Winterschladen
ABSTRACT
The focus of this study is self-destructive compulsive sexual behavior in Roman Catholic clergy
and male religious. It is hypothesized that Baumeister’s theory of cognitive deconstruction, the process by
which people attempt to escape painful self awareness, may offer an explanatory framework for
understanding the cognitive processes of long-term sexually compulsive males who report a history of
compulsive sexual behavior beginning in adolescence. Baumeister outlines four consequences of cognitive
deconstruction: disinhibition, passivity, absence o f emotion, irrational thinking. The Rorschach protocols
of 112 Roman Catholic clergy who were referred for psychiatric evaluation were examined for evidence of
the consequences of cognitive deconstruction. The protocols of 39 priests diagnosed with compulsive
sexuality were compared to the protocols of 37 priests diagnosed with an anxiety disorder and 36 priests
who did not receive a psychiatric diagnosis at the time of evaluation. It was hypothesized that the
compulsive sexuality group would have significantly more extreme scores on the 13 variables chosen to
reflect cognitive deconstruction. The results did not support the hypothesis. The compulsive sex group
was not significantly different from both the anxiety group and the control group on any of the selected
Rorschach variables.
ii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
AC K N O W LE D G M EN T S
I would like to thank Dr. James Gray for his service as chair of this thesis committee, and Dr.
David Haaga. Dr. Luisa Saffiotti. and Dr. Gary Thompson for their participation on the thesis committee.
I also wish to thank my colleagues at Saint Luke Institute, especially Michelle Short and Amy
Streiby. for their invaluable help and support, without which this project would never have been
completed.
I am also indebted Joe Thompson, who provided technical support at a critical time. Lastly. I
wish to thank my family and friends for their unw avering moral support and sense of humor.
iii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
TABLE OF CONTENTS
ABSTRACT........................................................................................................................................ ii
ACKNOWLEDGMENTS................................................................................................................ iii
LIST OF TABLES.............................................................................................................................v
Chapter
1. INTRODUCTION.......................................................................................................1
Cognitive Deconstruction Theory
Compulsive Sexuality
Cognitive Deconstruction in Compulsive Sexual Behavior
The Research Question
2. METHOD..................................................................................................................23
3. RESULTS..................................................................................................................44
4. DISCUSSION........................................................................................................... 58
The Rorschach as a Measure of Cognitive Deconstruction
Theoretical Network of Cognitive Deconstruction
Failure of the Experimental Design
Instability of the Cognitive Deconstruction State
5. CONCLUSION.........................................................................................................67
REFERENCES.................................................................................................................. 69
iv
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
LIST OF TABLES
1. Rorschach variables and cognitive deconstruction........................................................................26
2. Correlation coefficients for Rorschach variables....................................................................... 28
3. Mean scores of reference groups.................................................................................................29
4. Disinhibition Rorschach variables..............................................................................................45
5. Coping deficit index variable...................................................................................................... 45
6. Adjusted D variable..................................................................................................................... 46
7. FC:CF+C variable........................................................................................................................47
8. Passivity Rorschach variables..................................................................................................... 47
9. Active to passive ratio variable................................................................................................... 48
10. Movement active to movement passive variable........................................................................ 48
11. Absence of emotion Rorschach variables....................................................................................48
12. Affective ratio variable................................................................................................................ 49
13. Vista variable................................................................................................................................50
14. Egocentricity index variable........................................................................................................50
15. Irrational Thought Rorschach variables......................................................................................50
16. M-variable....................................................................................................................................51
17. Human response variable.............................................................................................................52
18. X-% variable................................................................................................................................52
19. ANOVA X-% variable.................................................................................................................53
20. X+% variable...............................................................................................................................53
21. ANOVA X+% variable................................................................................................................ 54
22. WSUM 6 variable.........................................................................................................................54
23. W:M variable................................................................................................................................ 55
v
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
24. Zd variable.....................................................................................................................................55
25. MCMI test data............................................................................................................................. 56
26. MMPI-2 test data........................................................................................................................... 57
vi
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
CHAPTER 1
INTRODUCTION
Cognitive Deconst ruction Theory
In 1990 Baumeister offered a theory of cognitive deconstruction as one explanation of suicidal
behavior. Cognitive deconstruction theory combines cognitive and motivational components and is an
outgrowth of action identification theory (Vallacher & Wegner. 1985,1987). self-discrepancy theory
(Higgins, 1987), objective self-awareness theory ( Duval and Wicklund. 1972), and control theory (Carver
and Scheier, 1982). The central argument of cognitive deconstruction theory is that nonfatal self
destructive or addictive behaviors (such as binge eating) serve to reduce painful awareness of self. He
asserts that suicide may also be an attempt to escape from painful awareness of certain symbolic
interpretations about the self. Cognitive deconstruction has been used to provide an explanatory
framework for understanding the cognitive processes of sex offenders (Ward. Hudson. Marshall. 1995).
This study investigates whether there is evidence that cognitive deconstruction may also relate to the
cognitive processes of self-destructive sexually compulsive patients.
A number of theories propose a relationship between emotional discomfort and inconsistencies or
conflicts in a person’s beliefs, feelings, and actions (Festinger. 1957; Duval and Wicklund, 1972; Carver
& Scheier, 1982, 1990; Higgins, 1987). Several theories have focused on different types of belief
incompatibilities, for example cognitive dissonance (Festinger, 1957), balance theory (Heider, 1958) and
objective self-awareness theory (Duval & Wicklund, 1972). The emotional consequences of belief
incompatibilities are usually described in general terms, such as conflict, stress, or discomfort. This
section will discuss four theories that are relevant to the development of cognitive deconstruction theory
and that address: 1.) different sources of self-inconsistencies or discrepancies (self -discrepancy theory).
2.) the role of self-awareness in one’s motivation to reduce perceived discrepancies (objective self-
awareness
1
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
2
theory). 3.) the role of emotional discomfort in self- regulation (control theory), and 4.) the hierarchical
organization of identities of actions which lead to different views of an action (action identification
theory). Each theory is an antecedent to cognitive deconstruction theory, and they each contain elements
that are central features of cognitive deconstruction theory'. A discussion of these theories will highlight
how' cognitive deconstruction theory builds on them and differs from them.
I.) Higgins* (1987) self-discrepancy theory distinguishes between two different kinds of
discomfort that people holding incompatible beliefs may experience: dejection-related emotions and
agitation-related emotions. The theory proposes that different clusters of emotional vulnerabilities are
linked to different types of discrepancies that people may possess among their self beliefs. The theory' also
distinguishes three basic domains of the self: a) the actual self, w'hich is one's representation of the
attributes that someone (oneself or another) believes one actually possesses; b) the ideal self which is
one’s representation of the attributes that someone would like one to possess (someone’s hopes,
aspirations, or wishes for one, and c) the ought self which is one's representation of the attributes that
someone believes one should or ought to possess (one’s sense of duty, obligation, or responsibilities).
Higgins goes on to discriminate between two basic standpoints of the self from which one can be judged:
a) one’s own personal standpoint and b) the standpoint of some significant other.
When the discrepancy' is between actual/self or actual/other self state representations (self
concept) and ideal/self or ideal/other standards, the individual will likely suffer more from dejection-
related emotions. When the discrepancy is between self concepts and ought/self or ought/other standards,
individuals are likely to suffer more from agitation-related emotions. The greater the magnitude of the
discrepancy', the more the individual will suffer the kind of discomfort associated with that type of self -
discrepancy.
2.) Duval and Wicklund’s (1972) theory of objective self-awareness addresses the nature of the
conditions that cause consciousness to focus on the self as an object and takes as its central assumption
the notion that the person will evaluate himself as soon as the objective state occurs. This process is
predicated on the existence of a psychological system of standards of correctness possessed by each
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
3
person. When attention is focused on the self, there will be an automatic comparison of the self with
standards of correctness. Objective self-awareness will lead to a negative self-evaluation whenever the
person is aware of a self-contradiction or discrepancy between an ideal and his actual state. The negative
affect experienced will be greater when a substantial discrepancy is salient for the person. Consequently
he or she will either attempt to avoid the situation provoking objective self awareness or else alter his or
her actual state (moving his or her attention away from the self and onto the environment) in an effort to
reduce the discrepancy. Even without a loss of self-esteem from a prior failure, the objective state is
uncomfortable when endured for extended time periods.
Duval and Wicklund (1972) argue that it is the passive, nonspeaking, nonacting person who is
most susceptible to objective self-awareness. Placing the person into an active situation should increase
subjective self-awareness, which is the opposite conscious state. Activity necessitates the person focusing
attention on events external to himself and subjective self-awareness will result. Self-awareness will be
difficult in that the person is aware of self only insofar as he is the source or the subject of forces acting on
the environment. There is an assumption that objective self awareness creates a negative affect, which
implies that the person will seek out methods of moving out of the state. The individual who is passive
may have difficulty in transferring his attention away from himself, but when he is occupied with a task,
no matter how routine and automatic, he can easily shift his attention from himself to the task. The task
provides a ready escape from the undesirable state of critical self-evaluation (Duval and Wicklund. 1972).
3.) Carver and Scheier's (1982) control theory describes a model of self-regulation provided by a
discrepancy-reducing feedback loop. The function of the feedback loop is to negate, or reduce, sensed
deviations from a comparison value. When a discrepancy is perceiv ed between the present state and the
reference value, a behavior is performed, and the goal of the behavior is to reduce the discrepancy. The
impact of the antecedent behavior creates a change in the present condition, leading to a different
perception of the situation which then, in tum, is compared anew with the reference value. This
arrangement constitutes a closed loop of control, the purpose of which is to minimize deviations from the
standard of comparison. The central function of the feedback system is to maintain the perception of a
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
4
specific desired condition, i.e.. consistency between the present state and the reference value, not to create
“behavior."'
Carver and Scheier theorize that the standard of comparison comes from a hierarchically
organized system. The highest level of the system is characterized by the abstract integration of
information. Each subordinate level influences the person's behavior, which is aimed at attaining
congruence between the person’s self-image and his or her actual behavior. Actually producing behavior
entails control of more and more concrete behavioral qualities. All of these qualities of behavior represent
lower and lower levels of control in the hierarchy. The approach accounts for the fact that exceedingly
restricted and concrete behavioral acts (i.e. changes in levels of muscle tensions) are used to create
behavioral events that are often so abstract as to seem completely unrelated to those concrete acts.
According to Carver and Scheier (1982) the engagement of the self-regulatory feedback loops
partially depends on the person’s focus of attention The process of directing attention to the self, when a
behavioral standard has been evoked, results in a tendency to compare one's perceptions of one’s present
state or behavior against the standard, leading (when possible) to a reduction of perceptible discrepancies
between the two through self-regulation. There is evidence that self-focus does result in increased
conformity to salient behavioral standards (Hull, 1981; Duval & Wicklund, 1972;. Carver & Scheier,
1990; Snyder 1987). However. Carver and Scheier (1982) suggest that if the person’s expectancy of being
able to reduce the discrepancy is sufficiently unfavorable the person may act on an impulse to withdraw or
disengage from the attempted discrepancy reduction.
4.) The symbolic representation of action is the basis for Vallacher & Wegner's (1985) theory' of
action identification. This theory makes two assumptions: 1.) a person can always offer an identity for his
or her action (identity availability') and 2.) a person’s working knowledge of an action typically consists of
a single prepotent identity, although an action may have several different identities.
According to Vallacher and Wegner (1985), a person’s general knowledge of an action is
determined by the level of the identity of the action within a hierarchical organization. The prepotent
identity can vary between higher and lower levels and so can entail very different understandings of the
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
action at hand. A person with a high level prepotent identity for an action has an effective understanding
of the action. The person can evaluate whether the course of action is worth pursuing or should be
inhibited because he or she is sensitive to the abstract implications of the behavior. Lower levels of
prepotent identity account for the detail underlying the performance of an action. A person whose
prepotent identity of an action is at too low a level will lose sight of the more comprehensive meaning of
the action, while focusing exclusively on the specific details of the behavior.
Another assumption of the theory states that when an action can be identified at both a higher
and a lower level, there will be a tendency for higher level identity to become prepotent. In other words,
movement towards higher levels of identification is a regular feature of the system.
The process of action identification can influence one’s self-concept which in turn constrains the
identities under which actions are chosen, enacted, and communicated. However, self-understanding in
not an inevitable by-product of action identification. A person who fails to maintain much of what he or
she does at a high level identity may have a weak sense of his or her self-defining qualities. Such a
person can be considered a low-level agent in that this person operates on the world primarily at the level
of detail. The low level agent is likely to think about the self in a relatively impoverished way - as the
author of simple movements. In contrast a high level agent tends to conceptualize most of his or her
actions in more meaningful, high level terms. These terms are not far from the person’s self-conceived
qualities as a person. The high level agent is engaged in action that expresses his conception of self,
whereas the low' level agent is engaged in action that is more divorced from an understanding of self.
Vallacher & Wegner (1985) assessed whether people may differ reliably in their characteristic
level of action identification. They assessed the relationships among level of personal agency (high or low
level agent), self-uncertainty, trait unimportance, and self-evaluation. They found that level of personal
agency signals how well defined a person’s self-concept is. The results of their investigation suggests that
low-level agents are less inclined to think about themselves in terms of broad personality traits than are
their high-level counterparts. It seems that people who are relatively insensitive to the broader meanings
and implications of their everyday actions also fail to have a clearly articulated, trait-like understanding of
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
6
themselves. They found the low-level agents tended to manifest anxiety and a weak sense o f personal
control. These data paint a portrait of persons who fail to understand their actions, in a manner
conducive to either effective maintenance or coherent self-understanding. High-level identification seems
to be essential not only for effective action, but for an integrated sense of well-being.
Self-discrepancy theory', objective self-awareness theory, control theory', and action identification
theory have features which are incorporated into cognitive deconstruction theory. Self-discrepancy theory
identifies how the discrepancy between self and relevant standards can stem from one's personal
standpoint or from how one believes others perceive him or her. Cognitive deconstraction theory
recognizes that emotional discomfort may stem from a failure to live up to one's own personal standards
or a failure to meet the perceived standards of others. Both dejection-related emotions and agitation-
related emotion may be present as a result of discrepancy between self and reference values. Baumeister's
(1990) theory goes one step further in focusing on the cognitive processes one may use to cope with an
aversive emotional state that is the result of awareness of self discrepancy'.
Duval and Wicklund’s theory of objective self-awareness defines two distinct forms of conscious
attention. In the objective self-awareness state attention is directed tow ard an aspect of the self, in
subjective self-awareness attention is directed toward the external environment. Critical self-evaluation
will lead to negative affect, and the degree of discomfort the person experiences as a result o f self
evaluation is directly related to the size of the perceived discrepancy' between the actual self and the ideal
representation. Alternatively, a contradiction between behavior and beliefs can lead to critical self-
evaluation. Physical activity is one way to shift a person’s attention away from painful objective self-
awareness. As the person becomes engaged in a task, no matter how routine the task may be. awareness
shifts from the objective state to the subjective state. Baumeister’s (1990) theory of cognitive
deconstruction builds on objective self-awareness theory in that it states that a person will actively attempt
to escape negative affect but goes one step further by' outlining how- mental activity provides a means of
escape. Cognitive deconstruction postulates that dismantling meaningful thought and narrowing one’s
focus to a more concrete level can enable the person to flee the negative affect that results from critical self
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
7
evaluation. Certainly the person may also engage in physical activities or tasks to shift his attention from
objective state to the subjective self-awareness state, but there is an accompanying cognitive activity which
aids in the escape from negative affect.
Vallacher and Wegner’s (1985) theory of action identification suggests that there is a
hierarchical organisation of action identities and that each identity will convey a different understanding
of the action, depending on where the identity falls in the hierarchy. Vallacher and Wegner maintain
that there is a tendency for a person to move from a lower level of identity to a higher level of identity.
Cognitive deconstruction theory also posits a hierarchy of organization. While the theory allows
for shifting between higher or more abstract levels to lower or concrete levels. Baumeister explores the
complex reasons why people do not inevitably move to a higher level of understanding of their actions.
Vallacher and Wegner state that a person may switch from a high-level prepotent identity to a lower level
identity because the higher level identity may not pertain to the ongoing action. Baumeister argues that a
person may switch to a lower level identity (cognitive deconstruction) because the abstract implications of
the action may be a source of negative affect.
In Carver and Scheier’s (1982) control theory, a hierarchically organized system with abstract
thought at the highest level sets the standard for comparison between self and the reference value. They
show how the most concrete actions are used in the service of maintaining a highly abstract self concept.
In contrast Baumeister’s (1990) theory of cognitive deconstruction postulates that one can avoid
recognizing the abstract meaning of concrete actions by purposefully concentrating on the physical
sensations that are present in concrete behavioral acts. The process of deconstructing abstract thought, and
narrowing one’s focus to the concrete, reverses the hierarchical system posited in control theory.
Both theories suggest that if a person expects to fail at reducing discrepancy he or she may
withdraw or disengage rather than attempt discrepancy reduction. According to Baumeister (1990). such a
person would be vulnerable to engaging in cognitive deconstruction.
There are six main steps in cognitive deconstruction theory (Baumeister. 1990).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
8
1.) Unrealistically high expectations or unexpected problems or setbacks contribute to a
discrepancy between a desired or expected outcome in a situation and what actually occurred, resulting in
the perception in an individual that he or she is falling below standards. For example, a young man may
enter seminary with unrealistically high expectations about his ministry. He may see his ordination as a
transforming experience which will bestow on him the authority and interpersonal skills necessary to
dramatically improve his effectiveness with people. He may also imagine that ordination will resolve any
inner conflicts that may trouble him, especially in the area of sexuality. After ordination he settles into his
first assignment and finds that his life as an ordained priest does not meet his expectations and he
continues to struggle with the same problems as before ordination.
2.) Internal attributions are made whereby the disappointing outcomes are blamed on the self,
creating negative implications about the self. The self is linked to some undesirable traits which are the
cause of the problems or setbacks, and disappointing events are seen as a reflection of the self. In the
case of the young priest, his setbacks are handled without any reference to external attributions. He may
believe that his problems stem from his innate failure as a person rather than his inexperience as a priest.
He does not recognize that the standards to which he holds himself may be unrealistic.
3.) An aversive state of high self-awareness comes from comparing the self with the relevant
standards and from the self blame for recent disappointments. The newly ordained priest may become
extremely self-conscious when performing his pastoral duties and may focus his attention on his perceived
deficiencies. He may imagine that others are critically evaluating, which adds to his discomfort.
4.) Negative affect arises from the unfavorable comparison of self with unmet standards. The
individual becomes acutely aware of self as inadequate, incompetent or guilty. Attention is focused on
any evidence that he is failing to meet his own or others’ standards. At this stage the new priest will feel
acute pain at his perceived failure and may feel particularly bad or guilty because the grace that he was
suppose to receive at ordination has not transformed his life. He may engage in cognitive distortions such
as overgeneralization (formulating a general rule based on a few' isolated incidents and applying the rule
broadly to other situations) or personalization (attributing external events to self in the absence of any
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
9
causal connection) (Beck, 1989; Bums, 1981) regarding his perceived failures until he feels overwhelmed
by his view of himself as a complete and utter failure.
5.) The person wishes to escape from this undesirable emotional state by somehow obliterating
awareness of self. In the attempt to escape meaningful thoughts about self, and thereby escape a highly
aversive emotional state, the person engages in mental narrowing. The shift to less meaningful, less
integrative forms of thought and awareness is what is meant by Cognitive Deconstruction. While in the
deconstructed state, the person's time perspective is constricted to a narrow focus. Action is guided by
immediate, proximal goals rather than distal goals. By ceasing to think in meaningful terms about self and
behavior the person can avoid negative conclusions about self, and the emotional pain that accompanies
such conclusions. Deconstructed awareness means that the person is aware of self and action in concrete
ways and rejects abstract levels of meaning or interpretation.
One result of shifting to a deconstructed state is that self-evaluative processes are suspended.
Sustaining deconstructed awareness may be difficult, and so the person desires increasingly strong means
of terminating the aversive thoughts and feelings. In the example of the young priest he may narrow his
focus away from his identity as a priest and instead focus on his physical self. He may become focused on
immediate sexual gratification, or he may use alcohol to numb his feelings or food to distract himself from
thinking of the implications of his perceived failure. This is not the same as when a person may have an
alcoholic drink at the end of the day to unwind. The person is not seeking to unwind; instead he is seeking
an escape from painful self awareness.
6.) The consequences of this deconstructed state include passivity- and impulsivity, suppression
of emotion, irrational thoughts, and a failure to recognize inconsistencies in one's behavior. Accordingly,
the person in a cognitively deconstructed state may be more willing to engage in self-destructive behavior
or behavior which is a source of inner conflict. In the example of the young priest he may chronically
escape negative affect through cognitive deconstruction, engaging in self-destructive activities that focus
his attention on his physical self rather than using feedback to alter his behavior and improve his
functioning.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
10
The different self-awareness theories have each emphasized the negative comparison of self
against salient standards. When the self is perceived as falling below standards, the individual's self
esteem plummets and he may view himself in exaggerated negative terms. Two sets of standards are
relevant. The status quo is often important and self-blame may occur if the individual falls short of his
own past level of performance. Other people's expectations are also important, and failure to meet these
may result in private feelings that one cannot live up to what others expect. In both cases painful
awareness of one's shortcomings results in an acute negative state that the person wishes to escape from
as quickly as possible. The person may terminate this aversive state by ceasing to feel emotion, by ceasing
to blame the self, or by ceasing to be aware of self.
The obliteration of self awareness can be accomplished by rejecting higher-level abstract
meaning and interpretation of oneself and shrinking self perception to the most concrete terms. By
directing thought to the movements and sensations of direct bodily experience, one can strip away the
many layers of meaning associated with one's personal identity. Since emotion, attribution, and self-
awareness all involve meaning, a shift to a deconstructed state void of meaningful thought could
effectively terminate all three. By focusing attention on oneself as merely a body, blotting out awareness of
self as an identity with enduring attributes, one can avoid interpreting the meaning of one's actions.
Engaging in actions that are unplanned, irresponsible, and lacking in any long-term context are features
of the type of impulsive and uninhibited behavior that persons in a deconstructed state often exhibit.
Concrete thinking that focuses on immediate goals prevents the individual from recognizing the
implications of his or her behavior.
Ideally, the individual copes with disappointing outcomes by constructing new integrative
meanings for the relevant circumstances in his or her life. If a person is unable to reinterpret his or her
circumstances in a positive fashion he or she may remain stuck in the present, struggling to remain in the
deconstructed state in order to avoid the negative affect that is associated with meaningful thought. The
cognitive shift to a deconstructed state may not be enough to stop unpleasant feelings, and the person may
become receptive to stronger means of escape. To help sustain the deconstructed state the individual may
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
11
adopt an attitude of passivity, engaging in deconstructed activity' which is without interpretation, such as
compulsive behavior. The person operating in a deconstructed state is passive with respect to important,
meaningful actions and may engage in seemingly random, aimless, impulsive, or mindless activity.
Baumeister (1990) states that there are four relev ant consequences of Cognitive Deconstruction:
disinhibition, passivity, absence o f emotion, and irrational thought. According to Baumeister (1990)
disinhibition, or the removal of inner restrains, makes the individual willing to engage in actions that
violate normal patterns of behavior. The cognitively deconstructed state removes meaningful constructs
or implications about one’s behavior from the person’s awareness. Since inhibitions are to some degree
dependent on meaningful interpretation about one's behavior, this can effectively remove certain inner
restraints which usually serve to inhibit behavior. The person acting in a deconstructed state may engage
in irrational behavior or behavior that is contrary to the person’s normal standards and values. The lack
of self-awareness that is the by-product of cognitive deconstruction may enable a person to engage in
behavior which may be a source of conflict for the person.
In his work on suicide as an escape from the self. Baumeister (1990) states that impulsive
behavior is a reflection of the disinhibition produced by the deconstructed state and is not necessarily a
stable personality trait. Disinhibition as a result of cognitive deconstruction may account for some of the
self-destructive, risky, and compulsive behaviors in which a person may engage. An example of this is
the priest who becomes narrowly focused on his sexual needs and the excitement he may experience from
sexual cruising. He may spend hours in this activity with no regard for the consequences. He may risk
arrest, violence, and disease, as well as public humiliation, in his pursuit of a sexual experience. The
quest for intense sensations may itself be characteristic of many forms of escape from unpleasant affect
which is purportedly the reason one enters a deconstructed state. The attempt to immerse oneself in
immediate, intense sensations in order to escape broader awareness of events, and their implication, could
be a form of sensation-seeking, and appears to be a central feature in other forms of escape from self-
awareness, including alcohol use (Hull. 1981) and sexual masochism (Baumeister. 1988. 1989).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
12
According to Baumeister (1990). passivity is a second consequence of dcconstruction. A passive
style may serve as further evidence of the general rejection of meaning, in that adopting a passive
approach enables a person to evade responsibility and to avoid implicating or assessing the self. A
proactive approach involves planning, assessing the capacities of the self, considering the meaningful
implication of one's actions, evaluating if one’s behaviors are consistent with one’s goals and values, and
self-regulating accordingly. Passivity, as a consequence of cognitive deconstruction, facilitates
deconstruction and escape from meaningful implications about the self.
The absence o f emotion is another presumed byproduct of cognitive deconstruction, since the
purpose of the process is to escape from the negative affect associated with meaningful, integrative
interpretations. Lack of affect is sometimes used as a sign of deconstructed, low-level thinking
(Pennebaker, 1989), and so successful escape to low levels of awareness should be characterized by lack of
affect. According to Baumeister (1990), the affect is available, but the person is striving to keep it out of
awareness. Persons using cognitive deconstruction to avoid negative affect keep the painful affect at bay
by avoiding meaningful thought. In the deconstructed state neither positive nor negative affect occur
with any regularity or spontaneity. In avoiding intense emotion the person will be somewhat estranged
from his emotion, but may feel generally bored or vaguely unhappy.
A vulnerability to fantasy or irrational thought is another consequence of cognitive
deconstruction. Most people cannot remain permanently in a deconstructed state, but the person seeking
escape may often be reluctant to face the pain that may accompany thinking realistically about his or her
life in meaningful terms. The suspension of normal, critical thinking can leave a mental vacuum which
makes the individual vulnerable to bizarre thoughts and fantasies. The use of fantasy" may be a
compensatory strategy to help the person avoid realistic thought about his situation.
In summary, to escape from the self is to free oneself of the struggle to maintain a certain image.
According to Baumeister (1991), some people have escapist impulses (watching television or playing or
watching sports) because of stress or boredom. The person may actually be content with himself or
herself and may feel no need to forget the self. Escapist activities may be a response to problems, stress.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
13
or oppressive conditions, but this is different than escaping as a response to painful feelings about the self,
where the need to escape is ongoing. The person's feelings of pain about the self drives the impulse to
escape from a meaningful identify, which results in cognitive deconstruction. In this type of escape,
attention is focused intensely on the body and the person becomes absorbed in physical feelings. In other
words, the person can leave behind the burden of his identity and become just a body.
Compulsive Sexuality
The DSM-IV provides the category of Sexual Disorder Not Otherwise Specified for coding a
sexual disturbance that does not meet the criteria for any specific Sexual Disorder and is neither a Sexual
Dysfunction nor a Paraphilia. An example of a sexual disturbance warranting this diagnosis is “Distress
about a pattern of repeated sexual relationships involving a succession of lovers who are experienced by
the individual only as objects to be used” (DSM-IV. 1994. p.538). In this study, the diagnosis of “ Sexual
Disorder NOS: Compulsive Sexuality” (302.9) has been given to individuals who meet the above criteria.
The DSM-IV specifies that sexual behavior, when engaged in excessively, does not warrant a diagnosis of
Obsessive Compulsive Disorder (303.3) as “the person usually derives pleasure from the activity and may
wish to resist only because of its deleterious consequences” (DSM-IV. 1994. p.422).
There is general agreement in the literature that the pattern of sexual behavior that corresponds
to the DSM-IV description exists (Carnes. 1983. 1991; Coleman. 1988. 1992; Earle & Crow, 1990;
Griffin-Shelley, Benjamin. Benjamin. 1995; Goodman. 1993; Kraft-Ebbing. 1886; Laaser. 1991; Money.
1986; Quadland. 1985; Robinson et al., 1993; Robinson etal.. 1994; Taylor. 1996). The two terms that
are commonly used to label the behavior are sexual addiction or sexual compulsivity and many use the
terms interchangeably.
Researchers and clinicians note the development of compulsive sexual behavior is linked to early
childhood trauma and/or abuse and to restrictive attitudes of sexuality and intimacy (Carnes, 1991;
Coleman, 1988; Money. 1986). The sexual experience is used as a coping mechanism for numbing painful
feelings such as inadequacy, isolation, and loneliness. Preoccupation with sexual behavior and fantasies is
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
14
thought to be rooted in a chaotic and abusive childhood in which retreat into an imaginary' world provided
an escape from physical or emotional abuse or neglect. (Laaser. 1991) This is related to Baumeister’s
argument that some sexual behavior (sexual masochism) can be a form of escape from the self by reducing
the self from identity to body. For the sexually compulsive person, sexual behavior can function both to
produce pleasure and provide an escape from internal discomfort. Through compulsive or addictive sexual
behavior, an individual can create a false sense of security, well-being, and intimacy, thereby distracting
him or herself from the painful realities of life.
Carnes (1983) identifies a number of beliefs and behaviors that typify' the sex addict. At his or
her core the person believes that he or she is basically a bad. unworthy person. This belief is consistent
with the second step in Baumeister’s theory of cognitive deconstruction in which the self is linked to
undesirable traits and the fourth step in which the individual becomes acutely aware of the self as
somehow bad. Earle and Crow (1990) have identified another belief that fuels compulsive sexual
behavior: If I have to depend on my social skills to get close to anyone, it will never happen. It is thought
that compulsive sexual behavior both compensates for and reinforces these beliefs. For some, compulsive
sexual behavior is an attempt to connect intimately with others. (Laaser. 1991)
On the basis of his research and clinical experience. Carnes (1991) outlines a number of signs
that indicate the presence of sexual addiction. These signs include, but are not limited to the following:
1.) A pattern of out-of-control behavior. The amount extent and duration of behavior regularly
exceeds what the person intended. 2.) Severe consequences due to sexual behavior including arrest
personal injury, and serious professional and financial difficulties 3.) Inability to stop despite adverse
consequences. 4.) Persistent pursuit of self-destructive or high-risk behavior. 5.) Sexual obsession and
fantasy as a primary coping strategy. Sexual preoccupation becomes an "analgesic fix." Sex becomes a
primary tool to regulate one’s emotional life. Sexual fantasy, including planning, thinking, and looking
for sexual opportunities may absorb hours of the person's daily activity. This feature also coincides with
cognitive deconstruction in which escape from the self is a strategy for avoiding or regulating painful
emotions associated with the self. 6.) Severe mood changes around sexual activity. Often a feeling of
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
15
euphoria will accompany the beginning phase of the pursuit of sexual activity, followed by despair and
shame after the encounter. 7.) Sexual obsession becomes the organizing principle of daily life. The person
may neglect important social, occupational, or recreational activities because of sexual behavior.
Clergy and Sexual Compulsivitv
Sexually compulsive clergy share many of the same attributes as sexually compulsive people in
the general population. They tend to have distorted or unrealistic beliefs about themselves, their behavior,
and other people. Their low self esteem is reinforced by their tendency to focus their attention on their
perceived deficiencies. They' have difficulty coping with stress, and they' wish to escape from or suppress
unpleasant emotions. Frequently they have at least one powerful memory of an intense “high"
experienced at a crucial time in their lives. A major feature is their ability' to deny they have a problem.
The celibate priest faces profound professional consequences if his behavior is exposed, and this can lead
to entrenched fear and denial. (Carnes. 1987; Earle & Crow. 1990; Laaser, 1991) This description is
consistent with Baumeister’s assertion that people seek to escape from the self to avoid thinking bad
thoughts about oneself, usually in the wake of some calamity, or to find temporary' relief from the stressful
burden of maintaining an inflated or unrealistic image of self. (Baumeister. 1991)
All sexual addicts have sought ways to rigidly control their behavior. Frequently, the sexually
compulsive priest will turn to religious formulas which never work. Ordination may be seen as way to
control their sexual desires and behaviors. They expect the role of pastor to bestow on them respect
admiration, and authority. They' often believe that ordination will free them from their compulsion to
sexually act out. Sometimes they' embrace a “magical thinking’' style in which they' believe they have a
special relationship with God and will be protected from all consequences, especially if they' cover their
“bad” sexual behavior with “good” works. (Laaser. 1991)
Priests involved in compulsive sexual activity will, like their counterparts in the secular world,
construct elaborate excuses for their behavior and deny they have a problem which warrants professional
treatment. Most of the priests who engage in compulsive sexual activity are homosexual (Berry, 1992;
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
16
Sipe. 1990. 1994. Taylor, 1996) and are fearful of having theii orientation disclosed. The problem of
denial keeps the sexually compulsive pastor isolated and alone. He leads a double life, appearing in public
in his “priest” role while privately engaging in sexual behaviors which are contradictory to his value
system and jeopardize the life he has built (Schwartz. 1994).
The cycle of sexually compulsive behavior is the same for both priests and the general
population: stress or emotional pain, acting out the impulses, shame and remorse, promise of reform, brief
period of reform, acting out again. (Earle & Crow. 1990: Goodman. 1993) According to Carnes (1983).
shame may be particularly powerful when the authority of the church is inv oked to curtail sexual behavior
in childhood. Sexual pleasure may then be fused with sexual and religious guilt and shame. Self image
and sexual identity' may be further damaged if the child or adolescent discovers he has some homosexual
feelings, and he must carry the M l weight of the church’s moral condemnation of homosexuality.
Carnes and other therapists who have worked with sexually compulsive patients note that clergy
seem particularly vulnerable to sexual addiction. Cames (1987) lists five occupational hazards that are
unique to the clergy and may contribute to their vulnerability in this area.
1.) Traditionally, priests have been idealized as symbols of church life. When the idealization is
personalized, parishioners may develop enhanced expectations of their priests which lead the priest to
withdraw into a secret separate life as a way to escape the burden of such expectations.
2.) The public role of a pastoral leader involves the promotion of moral standards and may
underscore the double life that the sexually compulsive priest leads.
3.) Clergy commonly find themselves in relationships in which others depend on them. The
authority and credibility that comes with the role of priest may serve as a cloak for their behavior, which
again adds to the potential for secrecy and shame.
4.) The spiritual formation of clergy emphasize selfless devotion to the service of others.
Misguided altruism can lead some clergy to emotional impoverishment and over-extension, sometimes
called burnout. As a result clergy may feel angry and resentM, feelings which can fuel rationalization of
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
17
their addictive behaviors. For example, the priest who tells himself that after a grueling week of endless
pastoral duties he deserves to have the fun and excitement his cruising behavior brings.
5.) Lastly, some clergy may chose religious life as a way to avoid or cure problems. The classic
example is the choice of celibacy as a way to cope with ego-dystonic homosexuality or excessive sexual
behaviors. Choosing celibacy for these reasons only exacerbates the pain of obsession for those prone to
sexual addiction.
Clinicians who have worked with sexually compulsive priests note that their clinical
presentations are often complex, and many may have multiple addictions as well as other
psychopathology. (Carnes, 1987: Irons & Laaser. 1994: Taylor. 1996, Robinson et al,1993) This is
consistent with Carnes' (1989) description of sex addicts in the general population in which he reports
that most sex addicts have more than one, and on average, three paraphilias.
Cognitive Deconstruction in Compulsive Sexual Behavior
The DSM-IV category of Sexual Disorder. Not Otherwise Specified is used for coding a sexual
disturbance that does not meet the criteria for any specific Sexual Disorder. Three examples of sexual
disturbance warranting the diagnosis are given: I.) marked feelings of inadequacy" concerning sexual
performance 2.) persistent marked distress about sexual orientation, and 3.) distress about a pattern of
repeated sexual relationships involving a succession of lovers who are experienced by the individual only
as things to be used (DSM-IV. 1994. p. 538). This last example captures the essential feature of
compulsive sexual behavior.
The person involved in compulsive sexual behavior often uses cognitive distortions to justify the
behavior to himself or herself. The person's affective deficits will also facilitate the problem behavior.
Clinicians working with patients with compulsive sexual behavior note the prevalence of cognitive
distortion, minimization, and denial in their perception of their behavior (Abel, Gore, Holland. Camp.
Becker, Rathner, 1989; Abel. Becker. Cuningham-Rathner.1984; Cames. 1983. 1991; Coleman. 1987;
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
18
Earle & Crow. 1990: Goodman, 1993; Henderson. Kalichman. 1990: Kalichman. 199l;Laaser. 1991;
Levin. Stava. 1987; Ward. Hudson. Marshall. 1995).
In my clinical experience, the priests who are referred for evaluation because of sexual behavior
problems exhibit the same cognitive and emotional deficits that characterize the descriptions of secular
patients. However, they are different in that most of the priests who are referred for a psychiatric
evaluation because of sexual behavior problems report feeling conflict or distress about their homosexual
feelings and often believe or fear that homosexual feelings are morally wrong and may disqualify a person
from active ministry. Often, this translates into a general feeling of inadequacy' which results in fragile
self esteem and painful self-awareness. (Carnes, 1987) In the clinical interview, the patients describe in
great detail their struggle to control their sexual behavior. Often patients report that perceived criticism
or failure to live up to their own standards, or the standards of others, precipitates their engaging in high
risk sexually compulsive behavior.
Baumeister’s construct of cognitive deconstruclion may offer a theoretical explanation for a
number of the features in the clinical presentation of sexually compulsive patients, including priests.
Frequently, the sexually compulsive priest displays a distorted pattern of thinking about his life
circumstances and about the long-term consequences of his behavior, focusing instead on immediate
sexual gratification. His perception of the compulsive behavior is often distorted: for example, he may
rationalize to himself that frequenting gay bars where he often picks up sexual partners is an appropriate
pastime, especially if he promises himself that “this time” it will be different and he will avoid sexual
contact with anonymous partners. Many sexually compulsive priests report an absence or blunting of
affect prior to or during the compulsive behavior, as well as a more general tendency to distance from
emotions. The compulsive behavior tends to be impulsive and is contrary to the normal standards and
values of priesthood. During times of even minimal stress the person’s inner restraints seem to melt away
and he numbly seeks out anonymous sexual contacts. Previous experiences of being physically hurt,
robbed, arrested, or blackmailed do not deter him from cruising and other forms of high-risk behavior.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
19
Many of the sexually compulsive priests who arc referred for psychiatric evaluation have been
engaging in compulsive behavior for years. According to Baumeister (1991) and Ward et al. (1995).
people who begin compulsive sexual behavior, or sexual abusive behavior, in adulthood should display a
cognitive style which reflects repeated switching from concrete or deconstructed levels to higher abstract
levels. While some report that the behavior began fairly late in adulthood, it is not unusual for a client to
report engaging in some form of sexually compulsive behavior since adolescence. In using cognitive
deconstruction as an explanation for the cognitive processes typically seen in sex offenders (denial,
minimization, rationalization, lack of empathy, and suppression of negative emotions during the offense
process) Ward et al. (1995) hypothesize that sex offenders who begin offending in adolescence may
engage in a chronic form of cognitive deconstruction which may be a result of their never having
developed an abstract style of self regulation. They argue that poor developmental experiences contribute
to early onset offending and may lead a vulnerable adolescent to rely on cognitive deconstruction as a
chronic coping mechanism.
Consequently, adolescent sex offenders may, as a result of the deficits which may arise from
inappropriate developmental experiences, attempt to resolve problems and escape negative affect by-
engaging in cognitive processing that remains at the concrete or deconstructed level. The constant stress
of their developmental circumstances may have hindered them from developing an abstract style of
problem-solving and self-regulation, which would allow them to evaluate the long-term consequences of
their behavior. Therefore, the incorporation of cognitive deconstruction as a chronic coping strategy- could
differentiate early onset offenders from those sex offenders whose first offense is in adulthood, or who first
begin engaging in compulsive sex in adulthood.
There is evidence from the clinical presentations of priests who began engaging in sexually
compulsive behavior in adolescence that many of the features and consequences of cognitive
deconstruction have been incorporated into their general cognitive and behavioral style. For example,
many sexually compulsive priests who struggle to gain control of their behavior report that they seem to
be most at risk for acting out when they have experienced a disappointment or when they- feel they are
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
20
unable to perform adequately, or they are not sufficiently appreciated by colleagues or religious superiors.
Their passive interpersonal style hinders them from initiating appropriate problem-solving strategies,
which may contribute to feelings of worthlessness, self-blame, and in the person magnifying their
perceived faults and inadequacies. Typically, this results in the person impulsively engaging in sexual
cruising behavior or some other behavior that will likely lead to sexual contact. Often the person says that
he was acting in a numbed state in which he thought only of obtaining his goal of immediate sexual
satisfaction. At the time he is unable to engage in the higher level abstract thinking that enables him to
interpret the meaning of his behavior, engage in self-evaluative processes, or assess the long-term
consequences of his actions. Indeed, the interpretive vacuum left by cognitive deconstruction is likely to
lead the person to reconstruct new beliefs that “solve"’ the issue of his sexual deviancv and support his
behavior. For example, he will often justify his cruising behavior by constructing irrational beliefs that
support his behavior, such as his cruising behavior is really just a form of community outreach.
The cognitive processes and behaviors described by the sexually compulsive priest seem to
contain all the consequences of cognitive deconstruction as outlined by Baumeister (1990). The person's
inner constraints fail to inhibit his behavior, resulting in impulsive behavior that is incompatible with the
person’s values as a priest who has taken a vow of celibacy. His passivity helps him avoid responsibility
for his behavior and assessing the appropriateness of his actions. His quest to obtain sexual gratification
helps push negative affect out of his awareness and distracts his mind from broader, more meaningful
concerns. He will often construct irrational beliefs that support his behavior.
The Research Question
This study focused on Roman Catholic priests and religious (members of religious orders who are
not ordained priests) who were referred for psychiatric evaluation because of compulsive sexual behavior,
and who report beginning sexually compulsive behavior before adulthood (age 2 1). The most frequent
reason for referral is a history of cruising for anonymous partners, but the presenting problem can include
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
21
other forms of nonparaphilic behavior (multiple partners, compulsive fixation on an unattainable
partner, compulsive autoeroticism, compulsive use of pornography).
It was hypothesized that early onset sexually compulsive priests have incorporated cognitive
deconstruction as part of their general behavioral and cognitive style. Their Rorschach protocols were
examined for evidence of the four consequences of cognitive deconstruction (disinihibition, passivity,
absence o f emotion, irrational thinking). The Rorschach variables chosen to reflect the presence of
cognitive deconstruction were: I.) Coping Deficit Index (CDI), 2.) Adjusted D Score. 3.) FC:CF+C
Ratio, 4.) Active to Passive Movement Ratio (a:p ratio). 5.) Human Movement Active to Human
Movement Passive Ratio (Ma:Mp ratio). 6.) Affective Ratio (Afr ratio). 7.) Vista (V). 8.) Egocentricity
Index, 9.) M-. 10.) H: (H) Hd (Hd). 11.) X-%. 12.) X+%, 13.) WSUM6. The definition of each variable,
along with reliability and validity data will be discussed later in the paper.
Two Rorschach variables relating to effort in processing (W:M) and processing efficiency (Zd)
were also examined. These variables are not related to cognitive deconstruction, and it was hypothesized
that there would be no difference among the groups on these variables.
The Rorschach protocols of the early onset sexually compulsive priests were compared with the
Rorschach protocols of two other groups of priests. Priests who were referred for psychological
evaluation because of occupational problems or as part of the candidate assessment process served as a
control group providing data on a nonpsychiatric sample of priests. No Axis I or Axis II diagnosis is a
selection criterion for this group. However, they may have one or more conditions that may be a focus of
clinical attention, such as V62.90 Religious or Spiritual Problem or V62.2 Occupational Problem,
nicotine dependence, or learning disability. It was expected that the Rorschach protocols of this group
would be generally within the normal range and free of any indications of marked psychopathology.
The other comparison group was comprised of priests who were diagnosed at the time of their
evaluation as having an anxiety disorder. The presence of a sexual disorder, eating disorder, or alcohol or
drug dependence would exclude them from this group, as these are other forms of escape from the self
which could indicate the chronic use of cognitive deconstruction as a coping mechanism.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
22
Hypothesis
The Rorschach protocols of the early onset sexually compulsive sample (group 1) will be different from
the anxiety sample (group 2) and the nonpsychiatric sample (group 3) in the following ways:
1.) There will be a significantly higher number of subjects in group 1 obtaining a positive CDI: CDI>3.
2.) Significantly more group 1 subjects will obtain an Adjusted D score in the minus range: Adj D<0.
3.) There will be a significantly higher number of group I subjects obtaining a FC.CF+C ratio in which
the CF+C will be greater than the FC by at least 1 point: CF+OFC.
4.) There will be a significantly higher incidence of group 1 subjects obtaining an a:p ratio in which the
value for passive movement exceeds the value for active movement by more than one point: p>a+l.
5.) Significantly more group 1 subjects will obtain a Ma:Mp ratio in which the value for Mp is one point
more than the value for Ma: Mp>Ma.
6.) Significantly more group 1 subjects will have an Affective ratio less than .53: Afr. ratio<53
7.) Significantly more group 1 subjects will have a Vista response: VXD.
8.) Significantly more group 1 subjects will have an egocentricity index (3r+(2)/R) value of .32 or below:
(3r+(2)/R) = or <.32.
9.) Significantly more group 1 subjects will have an M- response: M-X).
10.) Significantly more group 1 subjects will obtain a H: (H) Hd (Hd) ratio in which the stun of pure H
or human responses will be less than 2 and less than the sum of human detail or fictional responses: H<
2 and H<(H) Hd (Hd).
11.) Significantly more group 1 subjects will have a X-% of .20 or greater: X-%= or >.20.
12.) Significantly more group lsubjects will have aX+%less than .60: X+%<60.
13.) Significantly more subjects in group I will have a WSUM6 >9.
14.) There will be no significant difference in the W:M ratio among the 3 groups.
15.) There will be no significant difference in the ZD scores among the 3 groups.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
CHAPTER2
METHOD
Subjects
This study examined the archival psychological testing data of 112 Roman Catholic clergy who
participated in a week-long psychological evaluation at a psychiatric hospital for priests and religious.
All the subjects were diagnosed by a psychological evaluation team at a summary meeting that takes
place on the last day of the evaluation process. Diagnoses are made according to the criteria of the
Diagnostic Statistical Manual of Mental Disorders - Third Edition. Revised (DSM-IH-R. 1987) or the
Diagnostic Statistical Manual of Mental Disorders - Fourth Edition (DSM-IV. 1994). The DSM-IH- R
(1987) definition of Sexual Disorder Not Otherwise Specified is unchanged in the DSM-IV (1994). The
diagnosis of Sexual Disorder Not Otherwise Specified is made on the basis of clinical interviews and the
patient’s self report about his sexual behavior. Projective testing is not used to make a diagnosis of
Sexual Disorder Not Otherwise Specified.
The evaluation team includes a chairperson (either a Ph.D. clinical psychologist or psychiatrist)
who is a senior staff clinician. Four different clinicians served as chairperson for the majority of the
subjects in this study. Their level of experience doing psychological assessments of this population using
the Rorschach varies from five to 12 years. The rest of the evaluation team is comprised of clinical staff
who also provide individual and group therapy for both inpatients and outpatients. The staff, which
includes clinical psychologists, clinical social workers, and pastoral counselors, rotate among the
evaluation teams. A neuropsychologist with 12 years of experience works full-time as a member of each
evaluation team and is present for all the summaries. There are no data available on the diagnostic
reliability among the evaluation teams.
The subjects were homogenous for variables such as sex, marital status, socioeconomic status,
faith affiliation, and occupation.
23
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
24
The subjects were organized into three diagnostic groups: early onset sexual compulsives, anxiety
disorders, and nonpsychiatric control group.
Group 1: Compulsive Sexual Behavior
The 39 subjects in this group did not have an anxiety disorder and all reported early onset (before
age 21) compulsive sexual behavior. At the time of evaluation they' were diagnosed with a Sexual
Disorder according to DSM-IV (1994) criteria. Distress or impairment resulting from a pattern of
repeated sexual relationships involving a succession of lovers who are experienced by the individual only
as things to be used (DSM-IV 1994. p. 538). compulsive cruising for anonymous partners, compulsive
fixation on an unattainable partner, compulsive autoeroticism, compulsive use of pornography.
Group 2: Anxiety Disorders
This group was comprised of 37 subjects diagnosed with any of the following Anxiety Disorders
according to DSM-IV (1994) criteria: Panic Disorder. Specific Phobia. Social Anxiety Disorder.
Obsessive Compulsive Disorder. Acute Stress Disorder. Generalized Anxiety Disorder. Anxiety Disorder
due to a General Medical Condition, Substance-Induced Anxiety Disorder, Anxiety Disorder Not
Otherwise Specified. Subjects in this group did not have a diagnosed sexual disorder.
Group 3: No Psychiatric Diagnosis
The 36 subjects in this group experienced problems serious enough to warrant the same
psychological evaluation process as subjects in the compulsive sexual behavior group and the anxiety
disorder group. However, there may have not been enough information at the time to give them a
diagnosis other than a V code (relational problems, problems related to abuse or neglect or additional
conditions that may be a focus of clinical attention), nicotine dependence, or learning disability.
Measures
The Rorschach Inkblot Test
The Rorschach protocols were administered and scored by staff psychologists using the Exner
Comprehensive System. The tests were administered and scored prior to the evaluation summary; the
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

25
testing psychologist was. therefore, blind to the patient’s diagnoses. The level of experience in
administering and scoring the Rorschach varied among the psychologists. New psychologists on staff
were trained and supervised by the senior clinical psychologist or the neuropsychologist, each with 12
years' experience in the Rorschach. Most of the Rorschach protocols in this study were administered by
staff psychologists with at least five years of Rorschach testing experience. There are no data available on
the inter-rater reliability among the examiners.
The Rorschach Inkblot Test is one of the most frequently used projective techniques worldwide. It
is thought that in the process of structuring an ambiguous stimulus such as an inkblot the subject will
unveil deep, otherwise inaccessible facets of his or her personality makeup. The emphasis in scoring is
on the perceptual elements of the test and the interpretation of a protocol is based on a structural
summary of the responses, which utilizes ratios, indices and combinations of variables, rather than single
scores. The Rorschach. A Comprehensive System (TRACS) (Exner. 1974) integrates elements from
different scoring systems and provides standardized administration, scoring, and interpretive procedures.
All the protocols in this study were scored using the Comprehensive System.
The Rorschach was chosen over the other available psychological tests (MMPI. MCMI. NEO-PI)
because of the availability of clusters of variables that yield information on how a person may approach
affect and emotional stimuli, interpersonal relationships, cognitive ideation and mediation, and impulse
control. These variables are related to the four consequences of cognitive deconstruction (disinhibition,
passivity, absence o f emotion, irrational thinking). The notion that cognitive deconstruction could be
incorporated into a person’s general personality style and used as a chronic coping strategy (albeit an
ineffective one), suggests that the consequences of cognitive deconstruction would be reflected in some of
the enduring traits that are measured by the Rorschach Inkblot Test variables chosen for this study.
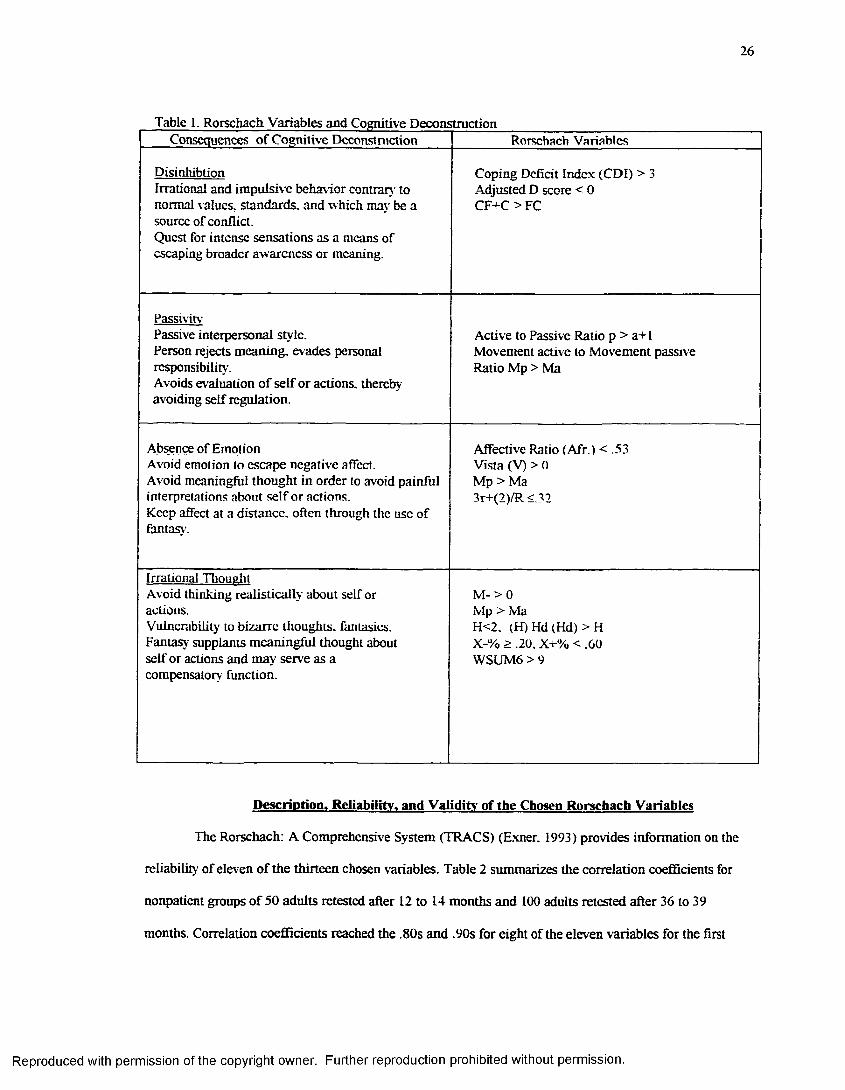
Table 1 outlines the Rorschach variables which are intended to measure the four main
consequences of cognitive deconstruction as outlined by Baumeister (1990).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
26
Table 1. Rorschach Variables and Cognitive DeconstructionConsequences of Cognitive Deconstruction Rorschach Variables
DisinhibtionIrrational and impulsive behavior contrary to normal values, standards, and which may be a source of conflict.Quest for intense sensations as a means of escaping broader awareness or meaning.
Coping Deficit Index (CDI) > 3 Adjusted D score < 0 CF+C > FC
PassivitvPassive interpersonal style.Person rejects meaning, evades personal responsibility.Avoids evaluation of self or actions, thereby avoiding self regulation.
Active to Passive Ratio p > a+I Movement active to Movement passive Ratio Mp > Ma
Absence of EmotionAvoid emotion to escape negative affect.Avoid meaningfttl thought in order to avoid painful interpretations about self or actions.Keep affect at a distance, often through the use of fantasy.
Affective Ratio (Afr.) < .53 Vista (V) > 0 Mp > Ma 3r+(2)/R <32
Irrational ThoualitAvoid thinking realistically about self or actions.Vulnerability to bizarre thoughts, fantasies. Fantasy supplants meaningful thought about self or actions and may serve as a compensatory function.
M- > 0 Mp > MaH<2. (H) Hd (Hd) > H X-% > .20. X+% < .60 WSUM6 > 9
Description. Reliability, and Validity- of the Chosen Rorschach Variables
The Rorschach: A Comprehensive System (TRACS) (Exner. 1993) provides information on the
reliability of eleven of the thirteen chosen variables. Table 2 summarizes the correlation coefficients for
nonpatient groups of 50 adults retested after 12 to 14 months and 100 adults retested after 36 to 39
months. Correlation coefficients reached the .80s and .90s for eight of the eleven variables for the first
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
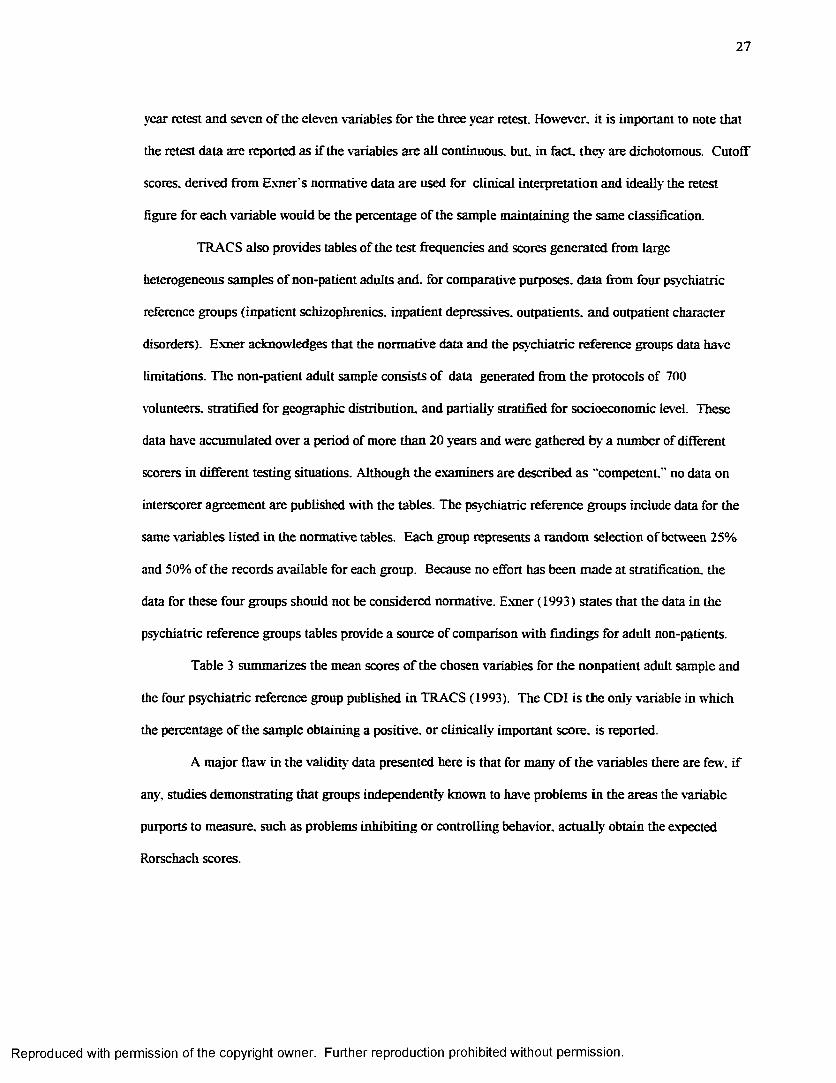
2 7
year retest and seven of the eleven variables for the three year retest. However, it is important to note that
the retest data are reported as if the variables are all continuous, but. in fact, they are dichotomous. Cutoff
scores, derived from Exner's normative data are used for clinical interpretation and ideally the retest
figure for each variable would be the percentage of the sample maintaining the same classification.
TRACS also provides tables of the test frequencies and scores generated from large
heterogeneous samples of non-patient adults and. for comparative purposes, data from four psy chiatric
reference groups (inpatient schizophrenics, inpatient depressives. outpatients, and outpatient character
disorders). Exner acknowledges that the normative data and the psychiatric reference groups data have
limitations. The non-patient adult sample consists of data generated from the protocols of 700
volunteers, stratified for geographic distribution, and partially stratified for socioeconomic level. These
data have accumulated over a period of more than 20 years and were gathered by a number of different
scorers in different testing situations. Although the examiners are described as "competent-” no data on
interscorer agreement are published with the tables. The psychiatric reference groups include data for the
same variables listed in the normative tables. Each group represents a random selection of between 25%
and 50% of the records available for each group. Because no effort has been made at stratification, the
data for these four groups should not be considered normative. Exner (1993) states that the data in the
psychiatric reference groups tables provide a source of comparison with findings for adult non-patients.
Table 3 summarizes the mean scores of the chosen variables for the nonpatient adult sample and
the four psychiatric reference group published in TRACS (1993). The CDI is the only variable in which
the percentage of the sample obtaining a positive, or clinically important score, is reported.
A major flaw in the validity' data presented here is that for many of the variables there are few, if
any, studies demonstrating that groups independently known to have problems in the areas the variable
purports to measure, such as problems inhibiting or controlling behavior, actually obtain the expected
Rorschach scores.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
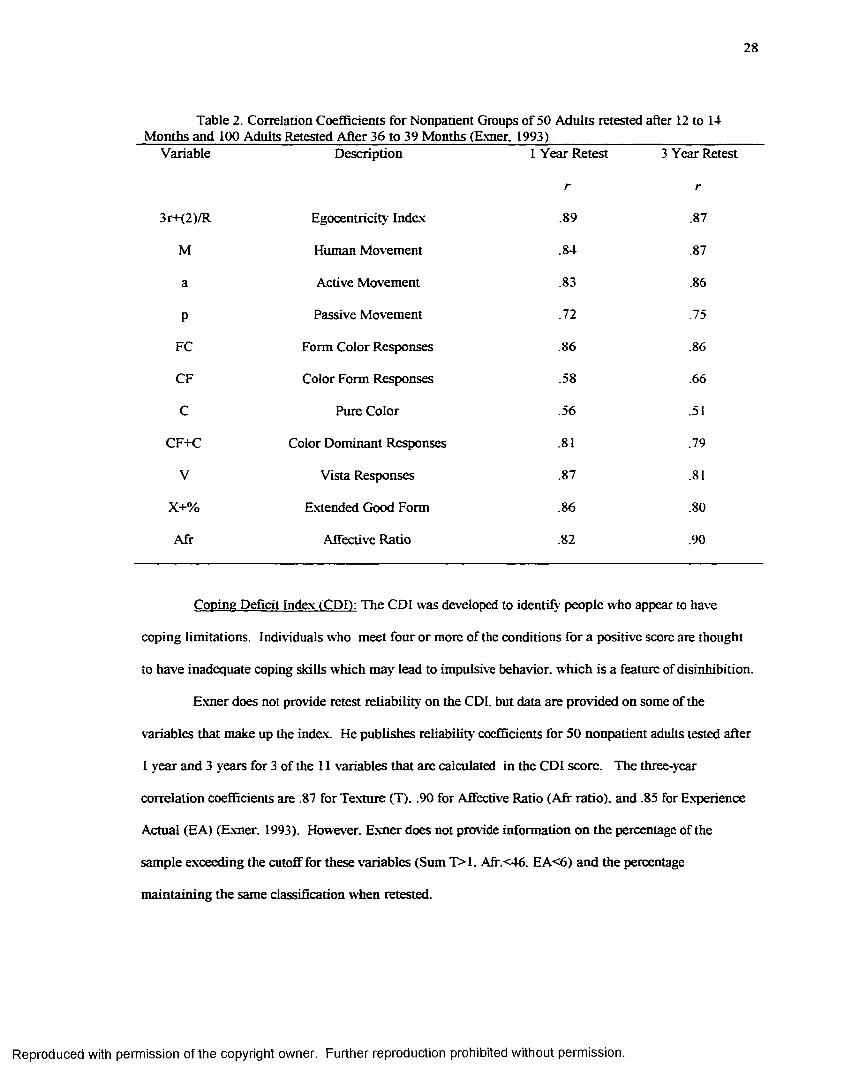
28
Table 2. Correlation Coefficients for Nonpatient Groups of 50 Adults retested after 12 to 14 Months and 100 Adults Retested After 36 to 39 Months (Exner. 1993)_________________________
Variable Description 1 Year Retest 3 Year Retest
r r
3r+(2)/R Egocentricity Index .89 .87
M Human Movement .84 .87
a Active Movement .83 .86
P Passive Movement .72 .75
FC Form Color Responses .86 .86
CF Color Form Responses .58 .66
C Pure Color .56 .51
CF+C Color Dominant Responses .81 .79
V Vista Responses .87 .81
x+% Extended Good Form .86 .80
Afr Affective Ratio .82 .90
Coping Deficit Index (CDD: The CDI was developed to identify people who appear to have
coping limitations. Individuals who meet four or more of the conditions for a positive score are thought
to have inadequate coping skills which may lead to impulsive behavior, which is a feature of disinhibition.
Exner does not provide retest reliability on the CDI. but data are provided on some of the
variables that make up the index. He publishes reliability coefficients for 50 nonpatient adults tested after
1 year and 3 years for 3 of the 11 variables that are calculated in the CDI score. The three-year
correlation coefficients are .87 for Texture (T). .90 for Affective Ratio (Afr ratio), and .85 for Experience
Actual (EA) (Exner. 1993). However. Exner does not provide information on the percentage of the
sample exceeding the cutoff for these variables (Sum T>1. Afr. <46. EA<6) and the percentage
maintaining the same classification when retested.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
29
Table 3. Mean Scores of Reference GroupsVariable Nonpatient
Adult N=700InpatientSchizophrenicN-320
Inpatient Depressive N=315
OutpatientN=440
OutpatientCharacterDisorderN=180
CDI >3 3% 25% 44% 28% 48%
Adj.D. .20 .69 -.57 .38 .19
FC:CF+C 4.09:2.44 1.54:1.66 1.58:2.30 1.23:2.46 .98:1.33
a:p 6.48:2.69 5.51:4.25 4.79:3.66 3.92:3.24 2.82:2.43
Ma:Mp 3.04:1.31 3.38:2.75 1.94:1.67 1.90:1.78 1.39:1.27
Afr ratio .69 .52 .47 .53 .49
Vista .26 .60 1.09 .42 .24
3r+(2)/R .40 .38 .33 .41 .46
M- .03 2.42 .58 .39 .47
X-% .07 .37 .20 .16 .20
X+% .79 .40 .53 .64 .58
WSUM6 3.28 44.69 18.20 9.59 11.31
H: (H) Hd (Hd) 3.40:2.03 3.17:4.25 2.05:3.16 2.10:3.06 1.94:2.62
People who have elevated or positive scores (CDI>3) are likely to have impoverished or
unrewarding social relationships and they may have difficulty contending with the natural demands of a
social world. (Exner. 1993) They may also have histories that are marked by limited interpersonal
effectiveness or success. The coping limitations signified by a positive CDI also raise a more general
question concerning capacity for control. The capacity for control is usually defined in terms of the ability
to form and direct responses: however, even in cases in which that capacity' appears to exist but a marked
kind of social immaturity also exists, there is a potential vulnerability for problems in everyday living.
A positive CDI raises serious questions about the capacity for control and or the tolerance for
stress, even if the values of the Adjusted D Score and EA are within normal limits. Subjects who are
positive on the CDI appear to have more trouble in many coping situations. They tend to feel helpless or
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
30
out of place when confronted with ev eryday social demands and this sense of helplessness can often give
rise to control problems and ineffective behaviors. Thus, even though the Adjusted D Score may be zero
or greater, positive CDI subjects frequently become disorganized and or ineffective when confronted with
social demands. If the value for the CDI is 4 or 5 it suggests that the personality organization of the
subject is somewhat less mature than might be expected, which can create a vulnerability for problems in
coping with the requirements of everyday living. Subjects with a positive CDI may experience problems
controlling their behavior in times of stress.
Exner (1993) reports that data from 440 outpatients support the postulate that the CDI tends to
identify those who have coping limitations or deficiencies which may result in interpersonal problems.
The outpatients were sorted into two groups, and the target group included all subjects who identified
“interpersonal difficulties” as part of their presenting problem. The CDI was calculated for all 440
subjects and 125 were found to have a positive CDI. It was found that 97 of the subjects who had a
positive CDI were in the group who complained of interpersonal problems (n=204). The other 28
subjects with a positive CDI were in the group with no interpersonal complaints (n=236). The finding
that 48% of the target group had an elevated CDI. compared to 12% of the group with no interpersonal
complaints is statistically significant (p<001). Exner notes that the subjects in the target group did not
necessarily have more interpersonal problems than the subjects in the other group, but apparently subjects
who complained about interpersonal difficulties were more aware of those problems. This may have been
because this group had experienced problems in control.
In a study of the Rorschachs of 98 children and adolescents who had been severely burned.
Holaday and Whittenberg (1994) reported that their sample of bum victims appeared similar to the index
group of helpless individuals with coping deficits, leading them to predict that the CDI would be positive
on many of the protocols. They found significant differences between their sample and Exner’s normative
data (1993, p.302). They found that 49% of the patients met the criteria for a positive score (4) on the
CDI and 68% met 3 or more conditions. They conclude that their study supports Exner’s (1990)
assertion that the CDI is a measure of learned helplessness. It is thought that learned helplessness is
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
31
related to reactive depression that follows an uncontrollable precipitating event which is viewed by the
individual as the source o f present and future distress (Brehn & Smith. 1986). In this sample the
experience of being severely burned is identified as the trigger for learned helplessness.
In summary, the CDI yields useful information about the adequacy of an individual's coping
skills and how likely he may be to have control problems secondary' to experiencing stressful situations.
According to Exner and Ritzier (personal communication. June 29. 1997). an elevation of the CDI
suggests that in times of stress, the person may have difficulty inhibiting his or her behavior, one of the
consequences of cognitive deconstruction.
Adjusted D: According to Exner (1993). this score offers information regarding the more typical
or usual capacity to formulate and control behaviors. It is the best single index of the ability to maintain
control under demand or stress situations and it provides information regarding the usual capacity for
control, whereas the D score offers information about that capacity as it is at the time of testing. The
score is independent of how adaptive the person's behavior is. Exner (1993) does not provide any
information on retest reliability for this variable.
The Adjusted D score is obtained by using the formula Experience Actual (EA) -Adj es. Exner
(1993) reports that EA (Sum M +WSUMC) is thought to provide information about the extent to which
resources are organized in a manner that makes them accessible. Exner cites the following study as
supporting the theory that EA relates to internal resources. He reports that 30 patients and 30 nonpatients
were retested after an 18 month interval. The mean EA for the nonpatients was 6.25 at the first test and
6.75 at the second test. The patient group was subdivided into two groups on the basis of independent
ratings of improvement provided by both (a) professional and (b) relatives. The mean EA for the
unimproved patient group was 3.50 at pretreatment and 4.25 at the second test. The mean EA for the
patient group rated as improved was 3.75 at pretreatment and 7.25 at the second test.
Subjects with D or Adjusted D scores in the minus range have fewer available resources than are
required in light of the frequency and or intensity of demands made on them. They are overloaded, they
are experiencing more demands for response formulation than they are able to prepare and implement at
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
32
the moment. The overload predisposes them to inefficient or ineffective functioning. At times, they may
not process information adequately, may not form decisions carefully or thoroughly, or may not
implement decisions fully or effectively. They are vulnerable to impulsiveness in both thinking and
behavior. If only the D score is in the minus range, the overload can be expected to be transient, but if the
Adjusted D score is in the minus range, the condition is more chronic (Exner. 1991.1993).
According to Exner (1993). people who have scores in the minus range may be in an almost
continuous state of overload and function best in routine and predictable environments. New or complex
situations often cause them to become distracted or inefficient and their behaviors may not be adaptive.
The result is that many of their behaviors are inadequate or even inappropriate, and when new demands
occur, their lives usually become disorganized in some ways. People with Adjusted D scores of less than
minus 1 usually have histories that include numerous events marked by faulty judgment, emotional
disruption, and or behavioral ineffectiveness. They are chronically vulnerable to ideational and or
affective impulsiveness and typically function adequately for extended periods only in environments that
are highly structured and routine and over which they have some sense of control (Exner. 1991. 1993).
Whereas a D score in the minus range may be the result of some situational stress, the overload
condition reflected in the minus Adjusted D score can be the result of a perpetuated developmental
failure. This occurs in cases of more immature people whose lives seem to be marked by one chaotic
event after another, or whose general pattern of activity will be marked by an excessive frequency of
ineffective and or maladaptive behaviors. The minus Adjusted D score may not just reflect immaturity, it
can also reflect pathology (Exner. 1991. 1993).
The FC:CF+C Ratio: This ratio provides an index of the extent to which emotional discharges
are modulated (Exner, 1991, 1993; Groth- Mamat, 1990). The data of the ratio are most meaningful
when studied in relation to the D scores. If either or both of the D scores fall into the minus range, the
capacity for control will be much more limited, and the capacities for modulation of affect will be more
vulnerable to interference by even modest but unexpected stressful experiences (Exner. 1991. 1993).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
33
Exner (1993) provides correlation coefficients at 1 year and 3 years for each individual variable.
For FC he reports r to be .86 after 1 year and 3 years. For CF he reports r to be .58 after 1 year and .66
after 3 years. For C he reports r to be .56 after 1 year and .51 after 3 years.
According to Exner (1993), less cognitive effort is required to identify colors than forms. Color
responses can involve a more passive process, but when specific form demands are injected into the
translation of color stimuli, it suggests that more cognitive control has been inserted into the process. For
this reason. FC responses point more to affective experiences that have been controlled and or directed by
cognitive elements. On the other hand. CF and C responses suggest instances in which the subject has
been more prone to give way to the affective stimulus, and inject less cognitive modulation into the
translation of the stimulus field.
If a record has a value for CF+C that is equal to or as much as two points greater than the value
for FC. and the value for Pure C is greater than 1. it indicates some potentially serious modulation
problems. People who score this way are often overly intense in their emotional displays and frequently
convey impressions of impulsiveness. This problem could be the product of control difficulties; it could
equally reflect a less mature psychological organization in which the modulation of affect is not regarded
by the subject as being very important.
Exner. Armbruster, and Viglione (1978) report that the directionality of the ratio is stable over
time. In their study of 100 nonpatient adults retested after 3 years it was found that if the value in one
side of the ratio exceeded the other by at least 1 point in the first test, the same directionality existed in the
second test. Weiner and Exner (1991) and Exner and Sanglade (1992) found the stability of the
directionality of the ratio also exists among outpatients up to a least one year of treatment.
There is some evidence that suggests that a higher frequency of CF+C responses may correlate
with impulsive or aggressive behaviors. Sommer and Sommer (1958) assessed the relationship between
assaultive behavior and two types of color responses, aggressive and nonaggressive. They predicted that
subjects giving aggressive color responses would show more assaultive behavior than non aggressive
color subjects. An inspection of subjects' case histories found that, for physical assaultiveness, the
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
34
aggressive color subjects significantly exceeded the nonaggressive color subjects. They also found that
the aggressive color subjects contained more pure C responses than the nonaggressive color group. The
nonaggressive color group had more FC responses than the aggressive color group.
The FC: CF+C ratio appears to yield information about a subject's ability to modulate affect and
emotional discharges. If color dominates, it suggests that the subject may tend to be overwhelmed by
affective impulses, which would contribute to a tendency to engage in impulsive behavior, one of the
consequences of cognitive deconstruction.
a:p ratio: This relationship concerns flexibility in ideation and attitudes. If the value for passive
movement exceeds the value for active movement by more than one point (p>a+l). it indicates the
subject will tend to assume a more passive role in interpersonal relations. Subjects with this score
usually prefer to avoid responsibility for decision making and are less prone to search out new solutions
to problems or initiate new patterns of behavior.
Exner (1993) reports reliability correlation coefficients for active movement to be .83 after 1 year
and .86 after 3 years. For passive movement he reports r to be .72 after 1 year and .75 after 3 years . High
frequency- of active movement responses does not equate with an unusual frequency- of active behaviors, or
with any special class of behaviors.
Exner devised an index of behavioral passivity using 20 items in the Katz Adjustment Scale
which was completed for 279 outpatients by a significant other of the patient 9 months after treatment
had been initiated. All subjects were volunteers in a long term treatment effects study which required
psychological testing and behavioral evaluations at 9 month intervals for at least 3 years. Examination of
the Rorschach data collected at the 9 month interval revealed that 83 of the 279 patients had a:p ratios in
which p exceeded a by more than 1 point. These subjects had a mean score for the passivity index of 11.6
(SD=4.2). A comparison group of 83 patients was randomly drawn from the other 196 subjects. This
group obtained a mean score on the passivity index of 5.3 (SD=3.3), yielding a significant difference
between the groups (p<.001). (Exner. 1978)
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
35
Exner (1974) found active movement responses occurred significantly more in the records of
acute schizophrenics, subjects with a history of assaultiveness (regardless of diagnosis), and a group of
individuals with character disorders. He found that passive movement answers occurred more frequently
in the records o f long-term inpatient schizophrenics, depressive individuals, and outpatient neurotics. He
also found that a proportional difference score, comparing the frequencies of active and passive movement
answers differentiated patients from nonpatients.
Blatt et al. (1976) analyzed and compared the Rorschachs of normal adolescents and young
adults with the Rorschachs of a sample of adolescent and young adult psychiatric inpatients and found
that patients gave a greater number of responses that were inert or passive as well as poor form quality.
The Ma:Mp Ratio: This variable concerns some characteristics of thinking. It includes only
human movement responses with total Active entered on the left and total Passive entered on the right.
Exner (1993) lias suggested that when Mp is greater than Ma, it indicates fantasy may be a prominent
feature of the subject’s ideation, which he calls a “Snow White” feature. Subjects with this type of score
are more likely to take flight into passive forms of fantasy as a defensive maneuver, and are less likely to
initiate decisions or behaviors if there is a likely alternative that others will do so.
If the value for Ma is greater than one and the value for Mp is one point more than the value for
Ma. it indicates that the subject has a stylistic tendency to use fantasy excessively. People with this type of
score are prone to defensively substitute fantasy for reality in stressful situations much more often than
most people. This form of avoidance/denial provides some tempo ran' relief from stress by replacing, in
the imagination, an unpleasant situation with one that is easily managed. It also tends to breed
dependency on others because of the implicit assumption that if one avoids facing a problem situation
eventually external forces will bring some resolution. If the value for Mp is two or more points greater
than the value for Ma. it indicates the presence of a marked style in which flight into fantasy has become a
routine tactic for dealing with unpleasant situations. In this case, the person can be said to have a Snow
White syndrome, which is characterized mainly by the avoidance of responsibility or decision-making.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
36
The Affective Ratio (Afr): provides information about an individual's responsiveness to
emotional stimulation. If the value of the Afr is less than average but no more than one standard
deviation below the average range, it suggests that the subject is less interested in or less willing to process
emotional stimuli. If the value for Afr is less than average and more than one standard deviation below the
average range, it indicates a marked tendency to avoid emotional stimuli. Such a person may be quite
uncomfortable around emotion and. as a result, often become much more socially constrained or even
isolated.
Exner reports the retest reliability for Afr ratio after 3 years to be .90 for 50 nonpatient adults.
Vista Variable: This variable seems to be related to negative emotional experience that is
generated by self-focusing behavior. The presence of a Vista in a protocol is thought to indicate that the
subject is experiencing discomfort, or even pain, as a result of ruminative self-inspection which is focused
on perceived negative features of the self.
Exner (1993) reports the correlation coefficient for this variable to be .87 after 1 year and .81
after 3 years in nonpatient groups of 50 adults. He does not report correlation coefficients for patient
groups.
Exner (1993) reports that a Vista response may indicate the subject is trying to distance from
painful feelings of inferiority or depression, which may be the source of some anxiety for the subject. The
Vista variable may indicate the person is self critical, attempts to avoid unpleasant stimuli, and may find
introspection painful. Meltzer (1944) studied the Rorschachs of 50 stuttering children and 50 non
stuttering children matched for sex. age, grade, school, and intelligence. He reports that the stuttering
group produced significantly more Vista responses than the nonstuttering group.
Exner and Wylie (1977) found that an elevation in Vista responses is significantly correlated
with effected suicides that occur within 60 days after being tested. Exner (1993). reports that he has cross
validated this finding by examining the Rorschach protocols of 101 subjects who effected their own death
within 60 days of being tested. Fiske and Baughman (1958) and Exner (1993) report that Vista responses
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
37
also tend to increase in the records of patients who have been in uncovering forms of psychotherapy for at
least 6 months as contrasted with pretreatment records.
Egocentricitv Index (3r+(2)/R): According to Exner (1993). the Egocentricity Index is a crude
measure of self-focusing or self-attending behavior and may possibly provide information about the
subject’s self esteem. If the value is above the average range, greater than .45. it suggests that the person
tends to be much more involved with himself or herself than others. If the value is below' average, less
than .32. it suggests that the person’s estimate of personal worth tends to be quite negative. Exner (1993)
suggests that such individuals regard themselves less favorably when compared with others.
The two determinants which make up this index are pairs (2) and reflections (Fr.rF). Exner
(1993) reports that the hypothesis that reflection and pair answers might be related to overinvolvement
with the self was tested by administering a sentence completion blank to 750 nonpatient adults. Most of
the 30 stems contained the personal pronouns I, me, or my. Responses were scored for whether the answer
focused on the self (S) (example: “I worry about my future’*) or focused on others (O) (example: "I worry
about the homeless”). Eighty subjects. 40 with the highest number of S responses, and 40 with the highest
number of O responses, were administered the Rorschach by 14 examiners. Reflection responses appeared
in the records of 37 of the 40 high S subjects as contrasted with only 2 records of the high O responses.
The blank, entitled the Self Focus Sentence Completion (SFSC) was then standardized on a population of
2500 subjects. The 30 subjects from each extreme were administered the Rorschach. Reflection and pair
responses appeared more than twice as often among the 30 high S subjects as among the records of the
high O group.
Human Movement Response (M): This score is used for responses involving the kinesthetic
activity of a human, or of an animal or fictional character in human-like activity.
Exner (1993) reports the correlation coefficients for a nonpatient group of 50 adults retested after
1 year to be .84. He reports a correlation coefficient of .87 for a nonpatient group of 50 adults retested
after 3 years. He does not report retest correlation coefficients for patient groups.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
38
According to Piotrowski (1960) and Exner (1974). subjects who give more cooperative M's are
generally oriented toward more socially effective behaviors. Subjects who give significantly large
numbers of passive M are more prone to avoid decision responsibility and prefer to be more dependent on
others for direction. Exner (1993) reports M is positively correlated with abstract thinking and requires
some delaying operations.
Rorschach suggested that when the form quality of a Movement response is poor (M-), the
likelihood of psychopatholgy appears to be greater (Exner. 1993). Exner and Weiner (1982) have
suggested that M- response is probably related to deficient social skills and poor interpersonal
relationships and included M- as one of the critical criteria for the differentiation of schizophrenia. The
presence of good quality M’s has been regarded as a positive prognostic indicator, especially for seriously
disturbed subjects. Because the frequency of M is usually low. ranging from 3 to 9 for the nonpatient
adult sample, most are expected to include an appropriate use of form. M responses appear to reflect the
deliberate directing of thinking and the more they deviate from the realities of the stimulus field, the more
likely the thinking activity will be marked by deviation. According to Exner (1993), M's may also include
projections that, in some ways, represent some of the inner qualities of the subject. The presence of one
M- response is sufficient to raise concern about peculiarity in ideation. If the frequency is greater than 1.
the likelihood of a marked thinking problem is increased considerably. Two or more M- responses is an
unusual finding, and may indicate the presence of disoriented thinking or psychosis. If most or all of the
M- responses are passive, it increases the probability that characteristics are present from w hich
delusional operations evolve.
Greenwald (1990) reports that, in a sample of students at a large urban university, the M-
variable yielded a significant negative correlation with the Barron Ego Strength Scale. Blatt et al. (1976)
report that a hospitalized sample of adolescents and adults had significantly more minus form quality
human movement responses (M-) than a sample of normal adolescents and young adults.
Interpersonal interest variables: H is the code for a Whole Human response and involves the
percept of a whole human form. (H) is the code for a Whole Human. Fictional or Mythological response
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
39
and involves the percept of a whole human form that is fictional or mythological, such as clowns, fairies,
giants, witches, fairy tale characters, angels, dwarfs, devils, ghosts, science fiction creatures that arc
humanoid, human-like monsters, and silhouettes of human figures. Hd is the code for Human Detail and
involves the percept of an incomplete human form, such as an arm, leg, fingers, feet the lower part of a
person, a person without a head. etc. (Hd) is the code for Human Detail, Fictional or Mythological and
involves the percept of an incomplete human form that is fictional or mythological such as, the head of the
devil, the arm of a witch, the eyes of an angel, parts of science fiction creatures that are humanoid, a jack-
o-lantem. and all masks.
H: (H) Hd (Hd): This entry provides information about interest in people. The entry includes
both primary and secondary contents. The sum of Pure H responses is entered on the left and the sum of
the other human contents is entered on the right and may provide some information about the extent to
which conceptions of others may be based more on imagination than real experience. Exner does not
provide any information on the retest reliability' of this variable.
The evaluation of human content has several uses. The absolute frequency of all human content
provides some information about interest in people. A breakdown of human contents into those that are
Pure H (versus those that are Hd or parenthesized human figures) seems to indicate whether the subject’s
conceptions of people, including the self, are based on actual experience or are derived more from
imaginary conceptions. The actual substance of human content answers often provides useful projected
information about how people, and the self, are conceptualized. The most critical human content datum
related to self image is the relation between Pure H and other human contents, expressed in the ratio H:
(H)+Hd+(Hd). According to Exner (1993), all nonpatient adults give more Pure H responses than
combination of others, and more Pure H responses than other forms of human content relate to a more
realistic estimate of self image.
When interpreting the H: (H)+Hd+(Hd) ratio with regard to self image, a value on the left side
that is at least equal to. or greater than, the right side is desirable. If the majority of the human contents
include whole figures scored H, it suggests that self image and self value are probably based more on
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
40
experience than on imagination. In other words, interactions, rather than fantasies, have contributed
significantly to formulations regarding the self. If the majority of human contents are scored Hd or have
parenthesized human contents, it suggests that self image and or self value tend to be based largely on
imaginary rather than on real experience. If the proportion of parenthesized human content is larger than
the number of pure H responses it may indicate a detachment from the real world, and probably signal an
investment in fantasy. Subjects with a score such as this are often less mature and frequently have very
distorted notions of themselves. This more limited self awareness will sometimes serve negatively in
decision making and problem solving activity and creates a potential for difficulties in relating to others.
There is evidence that the appearance of the human response varies directly with cognitive
development and social maturity, is consistent over time for the same subject and occurs frequently in the
records of well-adjusted normal adults. (Barry, Blyth. & Albrecht 1952; Blatt et al. 1976). Blatt and
Ritzier (1974) found that distorted human responses, particularly human-inanimate blends, increase in
frequency across patients as severity of pathology increases. Blatt et al. (1976) found that a sample of
psychiatric inpatients consistently gave a significantly greater number of minus human responses than
did normals.
X- % and X+%: These variables are part of the basic data concerning cognitive mediation and
provide information about the perceptual accuracy and conventionality of the responses as well as the
psychological functioning of the subject. The X-% concerns the proportion of the perceptual distortion
that has occurred in the record and is calculated by dividing the number of Form Quality responses that
are designated minus by R. the total number of responses in the protocol. The X+% concerns the extent to
which the form used in responses is conventional and perceptually accurate. The score is determined by
dividing the sum of all of the Form Quality responses that are designated superior or ordinary by the total
number of responses in the protocol.
Exner does not provide any retest reliability data for the X-%. only for the X+% variable, which
is an indication of the extent to which the form used in responses is conventional and perceptually
accurate. The data published in The Rorschach. A Comprehensive System (TRACS) (Exner. 1993)
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
41
suggest that the X+% score is stable among nonpatient adults over long periods. The X+% reliability
coefficient for a group of 50 adults retested after one year was .86. The X+% reliability coefficient for a
group of 100 adults retested after three years was .80.
Other researchers have found a relationship between X+%. X-% and cognitive distortion. In a
stuch' of personality characteristics of incarcerated individuals who had committed at least one sexual
homicide, researchers compared their Rorschach scores to the scores of a sample of incarcerated non-
sexually offending violent psychopaths. The X-% scores for both samples were elevated in comparison to
scores published in TRACS for nonpatient adults. (Meloy. Gracono. Kenney. 1994)
Wald et al. (1990) compared the X+% and X-% scores of mothers of incest victims with a control
group of mothers matched for socioeconomic status, age. education, and marital status. The experimental
group mean scores of .55 for X+% and .23 for X-% appear consistent with the researchers' prediction that
mothers of incest victims would exhibit deficits in reality testing as evidenced by their X+% score and
considerable distortion in perceptual accuracy (poor form quality), as evidenced by their X-% score. The
control group scores were in line with the nonpatient scores published by TRACS, the X+% was .76 and
the X-% was .07.
WSUM6: The WSUM6 variable is the weighted sum of six special scores that are used to mark
the presence of an unusual characteristics in thinking in the response. The six scores are used when the
answer contains some form of Unusual Verbalization (UV). which is thought to reflect some form of
cognitive slippage. (Exner, 1993; Adair, Wagner, 1992; Meloy, Gacono. Kenney, 1994: Weiner. 1995)
When some form of cognitive disarray occurs, either momentarily or for longer periods of time, it will
often manifest verbally. Four of the six special scores are designated level 1. for those answers in which a
mild or modest instance of illogical, fluid, peculiar, or circumstantial thinking is present; or level 2, for
answers in which a moderate or severe instance of dissociated, illogical, fluid, or circumstantial thinking
is present. The scores, together with their designated level, are know as The Critical Special Scores and
can be conceptualized as a crude continuum identifying the presence of cognitive mismanagement or
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
42
dysfunction. The Critical Special Scores are thought to identify' mild cognitive slippage, serious instances
of faulty thinking, and severe cognitive dysfunction (Exner, 1993).
According to Exner (1993), responses which warrant a Critical Special Score are not necessarily
cause for serious concern, provided that they occur with low frequencies. Exner reports that nearly 81%
of the subjects in the adult nonpatient reference group (n=700) gave at least one response which warranted
a Special Score, and the mean of the mean score for the WSUM6 variable for the non-patient group was
3.28. It is suggested in TRACS that when the WSUM6 score exceeds one standard deviation above the
mean (WSUM6 score >9) the data are too compelling to avoid concluding that some disturbance in
thinking exists.
When Meloy et al. (1994) compared the Rorschach protocols of men imprisoned for sexual
homicide with those of a sample of incarcerated, non-sexually offending violent psychopaths they found
the sexual homicide group had a mean WSUM6 score of 23.17 whereas the comparison group had a mean
score of 14.22.
Netter and Viglione (1994) compared the Rorschach scores of a sample of chronic schizophrenic
inpatients to a control group and a malingering (experimental) group. The schizophrenic group obtained a
WSUM6 score within the range expected if the variable is a valid index of thought disorder, the mean
score was 42.73.
Processing Variables
W:M Ratio: This ratio concerns the processing motivation or effort. The W (whole) response is
related to the degree to which a person can interact in an efficient, active manner with his or her
environment (Groth-Mamat. 1990). As noted earlier, the M variable is the number of Human Movement
responses. Elevated frequencies for W signal the investment of more effort than might be necessary for
the task. The frequency' of M responses can be regarded as a crude index of some of the functional
capabilities that are necessary for achievement-oriented activities (Exner, 1993). According to Exner
(1993). if frequency of W answers is substantially greater than the number of M responses it probably
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
43
indicates that the subject is striving to accomplish more than is reasonable in light of current functional
capacities.
When the frequency of W responses is disproportionately low in relation to the M frequency, it
suggests that the subject is very cautious and possibly over conservative in defining objectives for
achievement (Exner. 1991. 1993).
ZD Variable: This variable relates to processing efficiency and the score for this variable
differentiates between underincorporators, with ZD score less than -3.0. and overincorporators, with ZD
score greater than +3.0. An underincorporative style suggests that the subject scans the stimulus field
hastily and haphazardly and often may neglect critical cues in the environment. An overincorporative
style suggests that the subject invests more effort and energy into scanning activities, which indicates a
cautious, thorough approach to ensure all stimulus cues are included in the input (Exner. 1993).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
CHAPTER 3
RESULTS
Data Analysis
Hypotheses were tested using chi-square analyses of the data for each Rorschach variable.
Additionally, one way analysis of variance (ANOVA) techniques were used to analyze the X+% and X-%
variables, the only variables that meet the assumptions for parametric tests.
Results
The study hypothesized that extreme scores on thirteen Rorschach variables reflect the
consequences of Cognitive Deconstruction (disinhibition, passivity, absence o f emotion, and irrational
thinking). It was expected that subjects in the compulsive sex group would obtain significantly more
extreme scores than subjects in the anxiety and control groups, which would offer some support for the
hypothesis that cognitive deconstruction theory may provide a framework for understanding the cognitive
processes of earlv-onset sexually compulsive patients. The results do not support the hypothesis. The
compulsive sex group was not significantly different from both the anxiety and the control groups on any
of the variables, although the compulsive sex subjects had significantly more positive CDI scores than
subjects in the anxiety group. However, there was no significant difference in the number of subjects
obtaining positive CDI scores between the compulsive sex and the control groups. Four other variables
(Ma:Mp, W:M, Vista, M-) yielded significant differences among the groups, but not in the direction
expected.
Tables 4, 8. 11, and 15 summarize the frequency data and chi-square values for the cluster of
variables that measure each of the four consequences of cognitive deconstruction (disinhibition, passivity,
absence o f emotion, irrational thought). Tables 5-7, 9-10, 12-14, 16-18, 20, and 22 list each variable, the
44
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
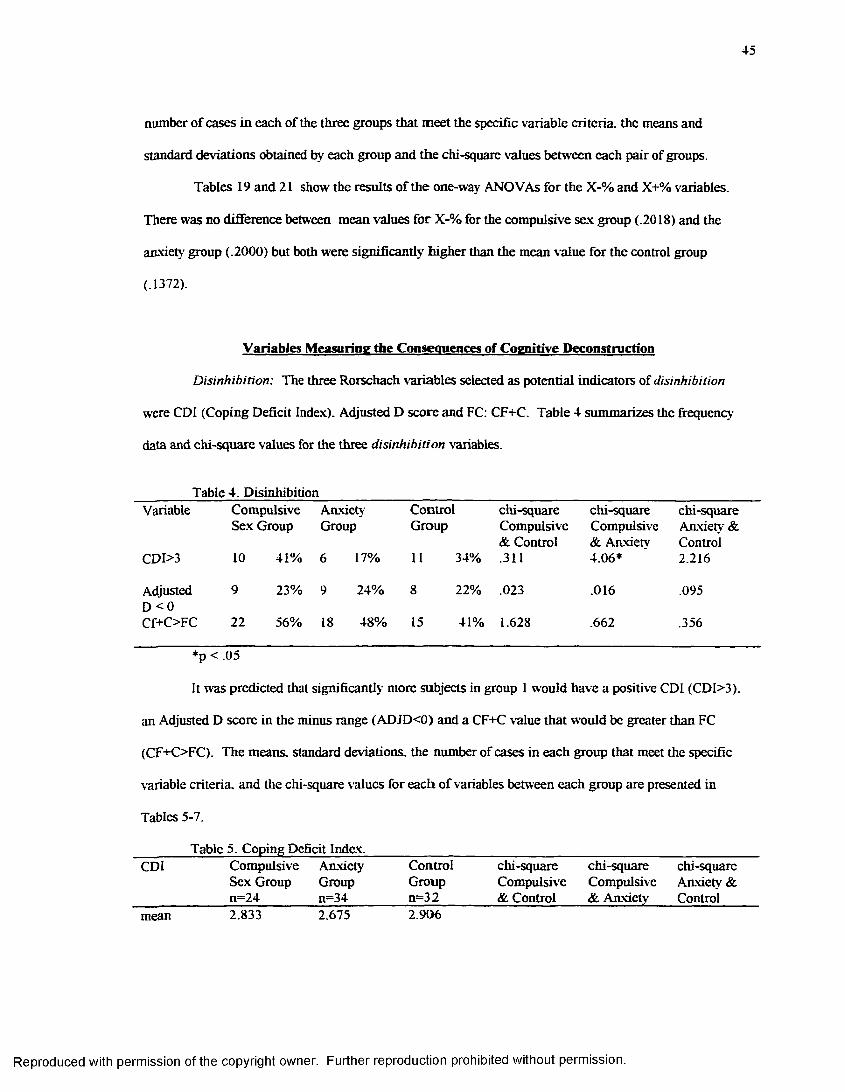
45
number of cases in each of the three groups that meet the specific variable criteria, the means and
standard deviations obtained by each group and the chi-square values between each pair of groups.
Tables 19 and 21 show the results of the one-way ANOVAs for the X-% and X+% variables.
There was no difference between mean values for X-% for the compulsive sex group (.2018) and the
anxiety group (.2000) but both were significantly higher than the mean value for the control group
(.1372).
Variables Measuring the Consequences of Cognitive D econstruction
Disinhibition: The three Rorschach variables selected as potential indicators of disinhibition
were CDI (Coping Deficit Index). Adjusted D score and FC: CF+C. Table 4 summarizes the frequency
data and chi-square values for the three disinhibition variables.
Table 4. DisinhibitionVariable Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety && Control & Anxiety Control
CDI>3 10 41% 6 17% 11 34% .311 4.06* 2.216
Adjusted 9 23% 9 24% 8 22% .023 .016 .095D <0Cf+C>FC 22 56% 18 48% 15 41% 1.628 .662 .356
*p < .05
It was predicted that significantly more subjects in group 1 would have a positive CDI (CDI>3).
an Adjusted D score in the minus range (ADJD<0) and a CF+C value that would be greater than FC
(CF+C>FC). The means, standard deviations, the number of cases in each group that meet the specific
variable criteria, and the chi-square values for each of variables between each group are presented in
Tables 5-7.
Table 5. Coping Deficit Index.______________________________________________________CDI Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety & _________ ii=24________ n=34_________n=32________ & Control & Anxiety Controlmean 2.833 2.675 2.906
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
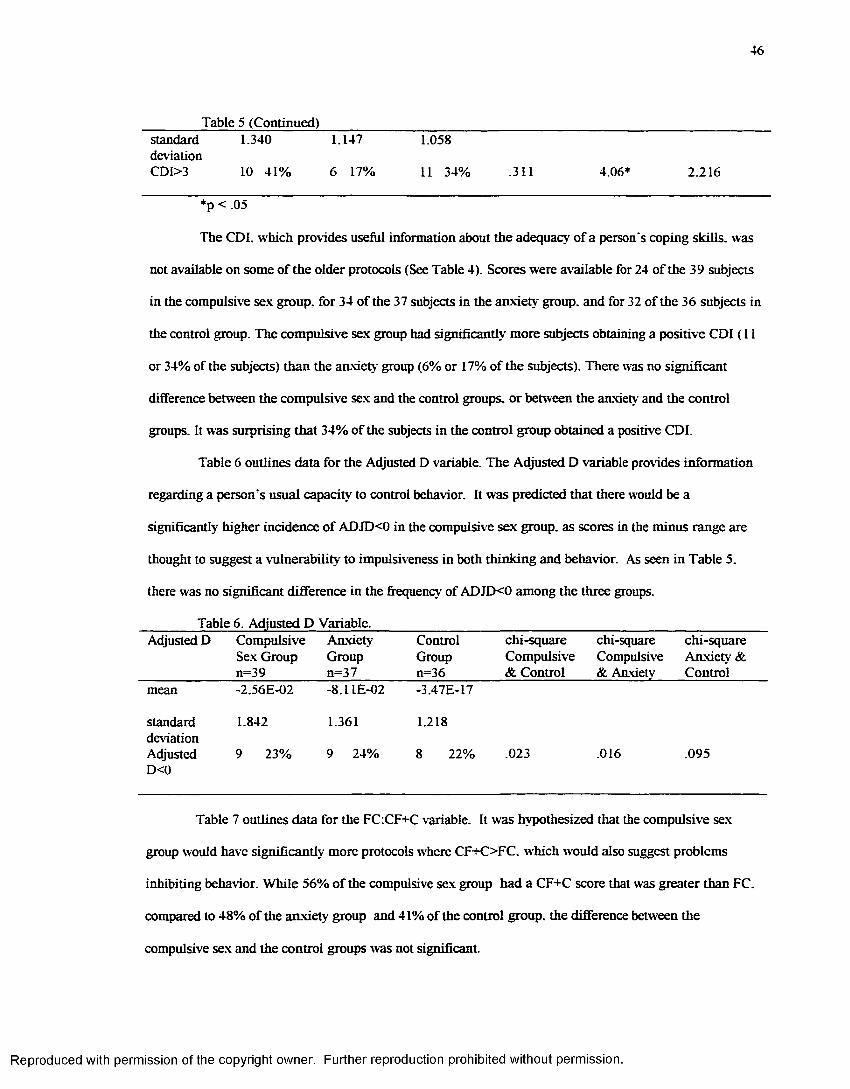
46
________ Table 5 (Continued)_______________________________________________________________standard 1.340 1.147 1.058deviationCDI>3 10 41% 6 17% 11 34% .311 4.06* 2.216
*p < .05
The CDI. which provides useful information about the adequacy of a person's coping skills, was
not available on some of the older protocols (See Table 4). Scores were available for 24 of the 39 subjects
in the compulsive sex group, for 34 of the 37 subjects in the anxiety group, and for 32 of the 36 subjects in
the control group. The compulsive sex group had significantly more subjects obtaining a positive CDI (11
or 34% of the subjects) than the anxiety group (6% or 17% of the subjects). There was no significant
difference between the compulsive sex and the control groups, or between the anxiety and the control
groups. It was surprising that 34% of the subjects in the control group obtained a positive CDI.
Table 6 outlines data for the Adjusted D variable. The Adjusted D variable provides information
regarding a person’s usual capacity to control behavior. It was predicted that there would be a
significantly higher incidence of ADJD<0 in the compulsive sex group, as scores in the minus range are
thought to suggest a vulnerability to impulsiveness in both thinking and behavior. As seen in Table 5.
there was no significant difference in the frequency of ADJD<0 among the three groups.
_______ Table 6. Adjusted D Variable.________________________________________________________Adjusted D Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &_____________ n=39 n=37 n=36 & Control & Anxiety Controlmean -2.56E-02
standard 1.842deviationAdjusted 9 23%D<0
Table 7 outlines data for the FC:CF+C variable. It was hypothesized that the compulsive sex
group would have significantly more protocols where CF+C>FC. which would also suggest problems
inhibiting behavior. While 56% of the compulsive sex group had a CF+C score that was greater than FC.
compared to 48% of the anxiety group and 41% of the control group, the difference between the
compulsive sex and the control groups was not significant.
-8.UE-02 -3.47E-17
1.361 1.218
9 24% 8 22% .023 .016 .095
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
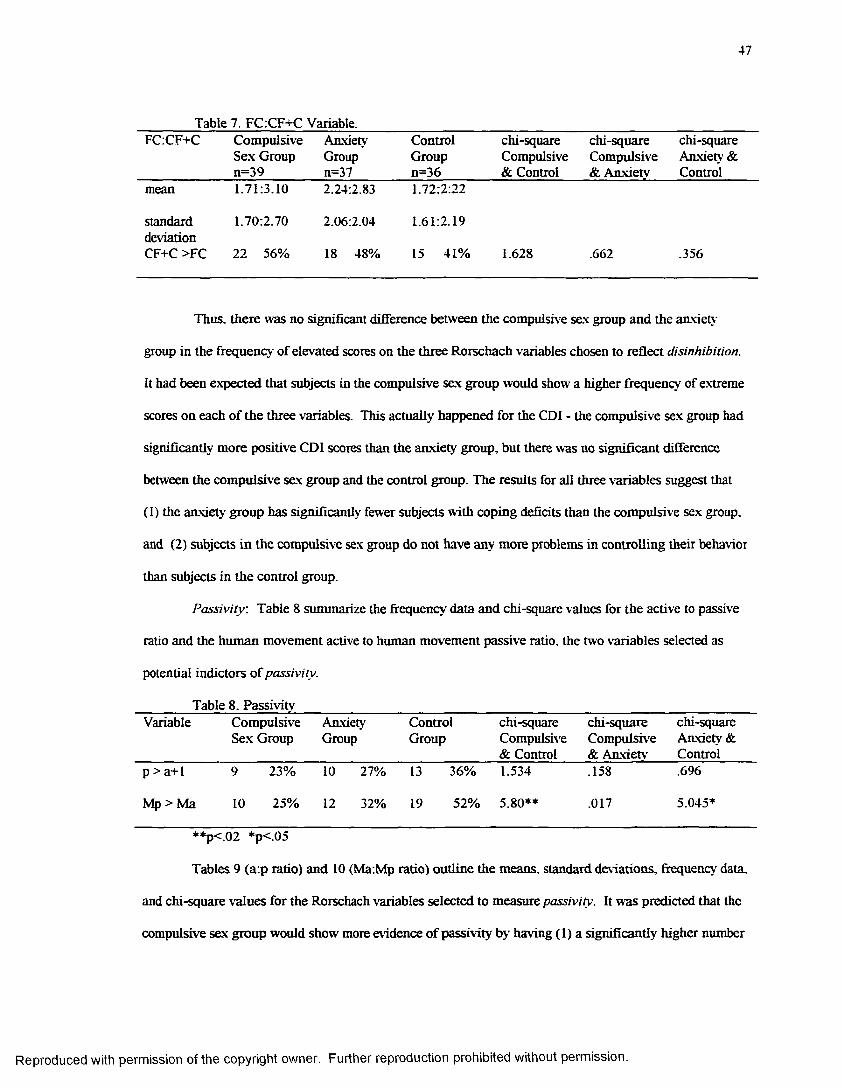
47
_______ Table 7. FC.CF+C Variable.______________________________________________________FCCF+C Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &_____________n=39_______ n=37________ n=36________ & Control & Anxiety Controlmean 1.71:3.10 2.24:2.83 1.72:2:22
standard 1.70:2.70 2.06:2.04 1.61:2.19deviationCF+C >FC 22 56% 18 48% 15 41% 1.628 .662 .356
Thus, there was no significant difference between the compulsive sex group and the anxiety
group in the frequency of elevated scores on the three Rorschach variables chosen to reflect disinhibition.
It had been expected that subjects in the compulsive sex group would show a higher frequency of extreme
scores on each of the three variables. This actually happened for the CDI - the compulsive sex group had
significantly more positive CDI scores than the anxiety group, but there was no significant difference
between the compulsive sex group and the control group. The results for all three variables suggest that
(1) the anxiety group has significantly fewer subjects with coping deficits than the compulsive sex group,
and (2) subjects in the compulsive sex group do not have any more problems in controlling their behavior
than subjects in the control group.
Passivity : Table 8 summarize the frequency data and chi-square values for the active to passive
ratio and the human movement active to human movement passive ratio, the two variables selected as
potential indictors of passivity.
Table 8. PassivityVariable Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety && Control & Anxiety Control
p > a+1 9 23% 10 27% 13 36% 1.534 .158 .696
Mp > Ma 10 25% 12 32% 19 52% 5.80** .017 5.045*
**p<02 *p<05
Tables 9 (a:p ratio) and 10 (Ma:Mp ratio) outline the means, standard deviations, frequency data,
and chi-square values for the Rorschach variables selected to measure passivity. It was predicted that the
compulsive sex group would show more evidence of passivity by having (1) a significantly higher number
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
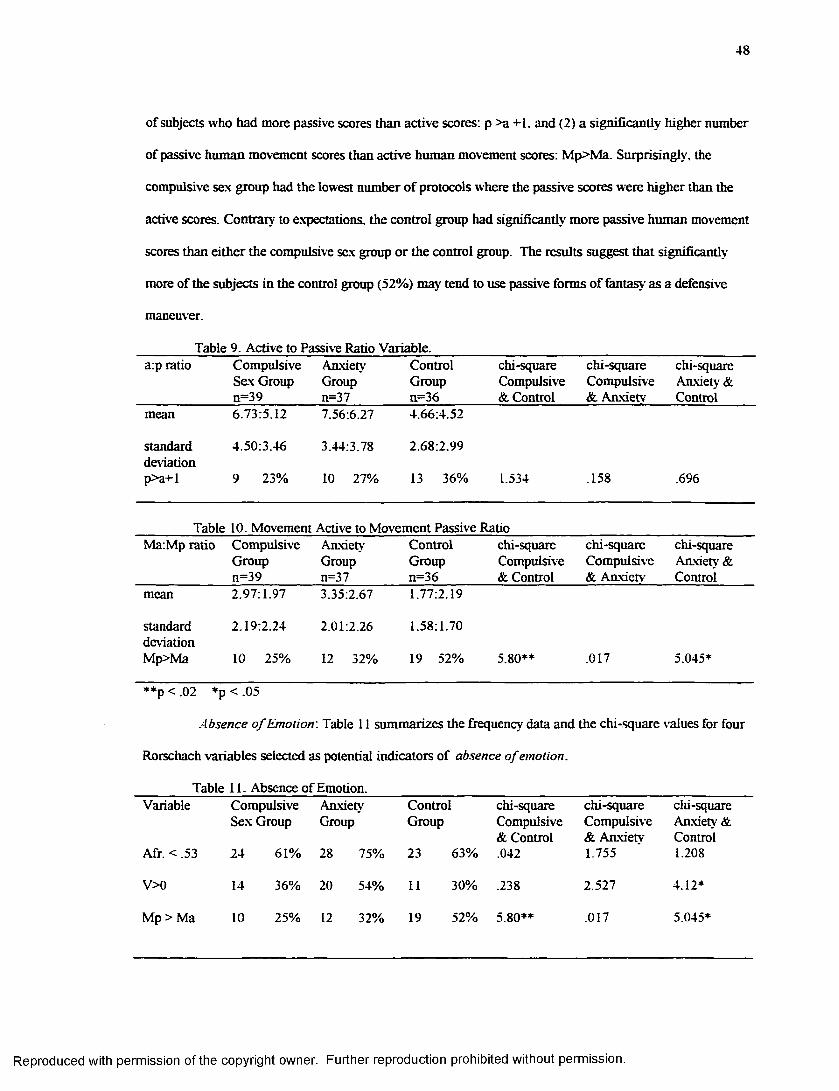
48
of subjects who had more passive scores than active scores: p >a +1, and (2) a significantly higher number
of passive human movement scores than active human movement scores: Mp>Ma. Surprisingly, the
compulsive sex group had the lowest number of protocols where the passive scores were higher than the
active scores. Contrary to expectations, the control group had significandy more passive human movement
scores than either the compulsive sex group or the control group. The results suggest that significandy
more of the subjects in the control group (52%) may tend to use passive forms of fantasy as a defensive
maneuver.
Table 9. Active to Passive Rado Variable.a:p rado Compulsive
Sex Groupn=39
AnxietyGroupn=37
ControlGroupn=36
chi-square Compulsive & Control
chi-square Compulsive & Anxietv
chi-square Anxiety & Control
mean 6.73:5.12 7.56:6.27 4.66:4.52
standarddeviationp>a+l
4.50:3.46
9 23%
3.44:3.78
10 27%
2.68:2.99
13 36% 1.534 .158 .696
Table 10. Movement Active to Movement Passive RatioMa:Mp ratio Compulsive
Groupn=39
AnxietyGroupn=37
ControlGroupn=36
chi-square Compulsive & Control
chi-square Compulsive & Anxietv
chi-square Anxiety & Control
mean 2.97:1.97 3.35:2.67 1.77:2.19
standarddeviationMp>Ma
2.19:2.24
10 25%
2.01:2.26
12 32%
1.58:1.70
19 52% 5.80** .017 5.045*
**p < .02 *p <.05
Absence o f Emotion: Table 11 summarizes the frequency data and the chi-square values for four
Rorschach variables selected as potential indicators of absence o f emotion.
Table 11. Absence of Emotion.Variable
Afr. < .53
Compulsive Sex Group
24 61%
AnxietyGroup
28 75%
ControlGroup
23 63%
chi-square Compulsive & Control .042
chi-square Compulsive & Anxiety 1.755
chi-square Anxiety & Control 1.208
V>0 14 36% 20 54% 11 30% .238 2.527 4.12*
Mp > Ma 10 25% 12 32% 19 52% 5.80** .017 5.045*
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
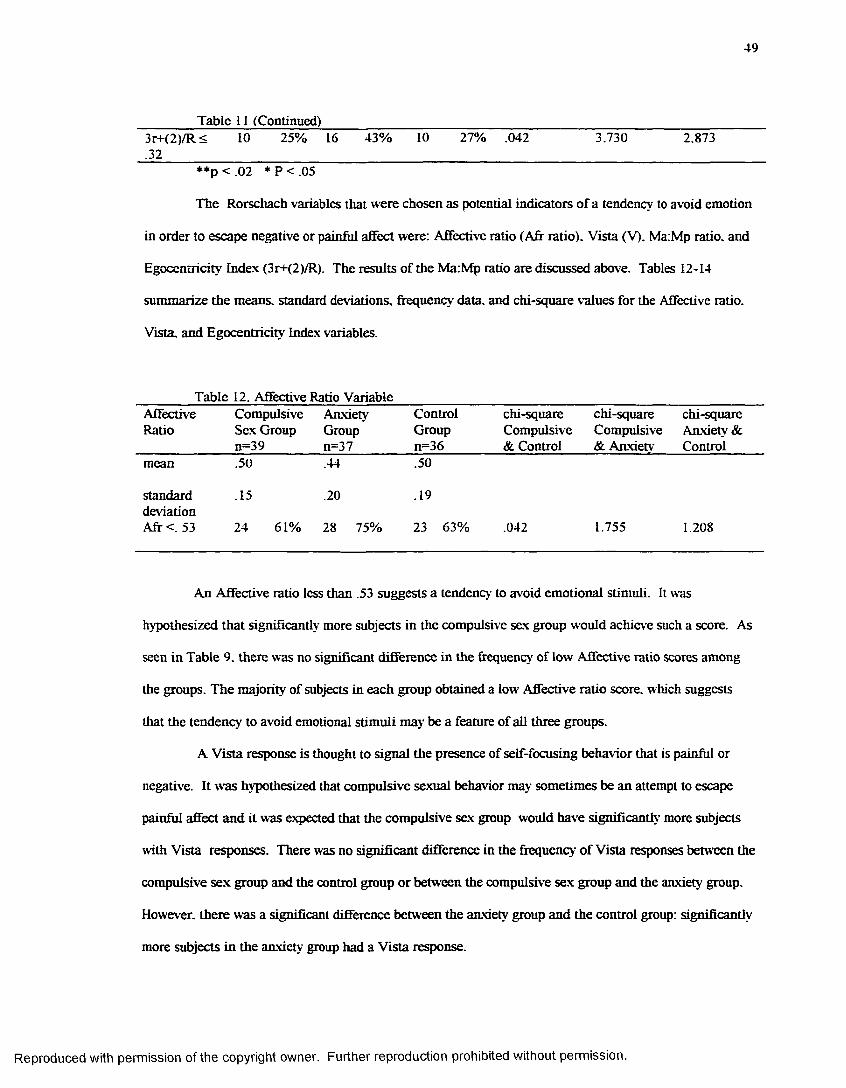
49
Table 11 (Continued)3r+<2)/R<.32
10 25% 16 43% 10 27% .042 3.730 2.873
**p < .02 * P < .05
The Rorschach variables that were chosen as potential indicators of a tendency to avoid emotion
in order to escape negative or painful affect were: Affective ratio (Afr ratio). Vista (V). Ma:Mp ratio, and
Egoccntricity Index (3r+(2)/R). The results of the Ma:Mp ratio are discussed above. Tables 12-14
summarize the means, standard deviations, frequency data, and chi-square values for the Affective ratio.
Vista, and Egocentricity Index variables.
Table 12. Affective Ratio VariableAffectiveRatio
Compulsive Anxiety Sex Group Group n=39 n=37
ControlGroupn=36
chi-square Compulsive & Control
chi-square Compulsive & Anxietv
chi-square Anxiety & Control
mean .50 .44 .50
standard deviation Afr < 53
.15 .20
24 61% 28 75%
.19
23 63% .042 1.755 1.208
An Affective ratio less than .53 suggests a tendency to avoid emotional stimuli. It was
hypothesized that significantly more subjects in the compulsive sex group would achieve such a score. As
seen in Table 9. there was no significant difference in the frequency of low Affective ratio scores among
the groups. The majority of subjects in each group obtained a low Affective ratio score, which suggests
that the tendency to avoid emotional stimuli may be a feature of all three groups.
A Vista response is thought to signal the presence of self-focusing behavior that is painful or
negative. It was hypothesized that compulsive sexual behavior may sometimes be an attempt to escape
painful affect and it was expected that the compulsive sex group would have significantly more subjects
with Vista responses. There was no significant difference in the frequency of Vista responses between the
compulsive sex group and the control group or between the compulsive sex group and the anxiety group.
However, there was a significant difference between the anxiety group and the control group: significantly
more subjects in the anxiety group had a Vista response.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
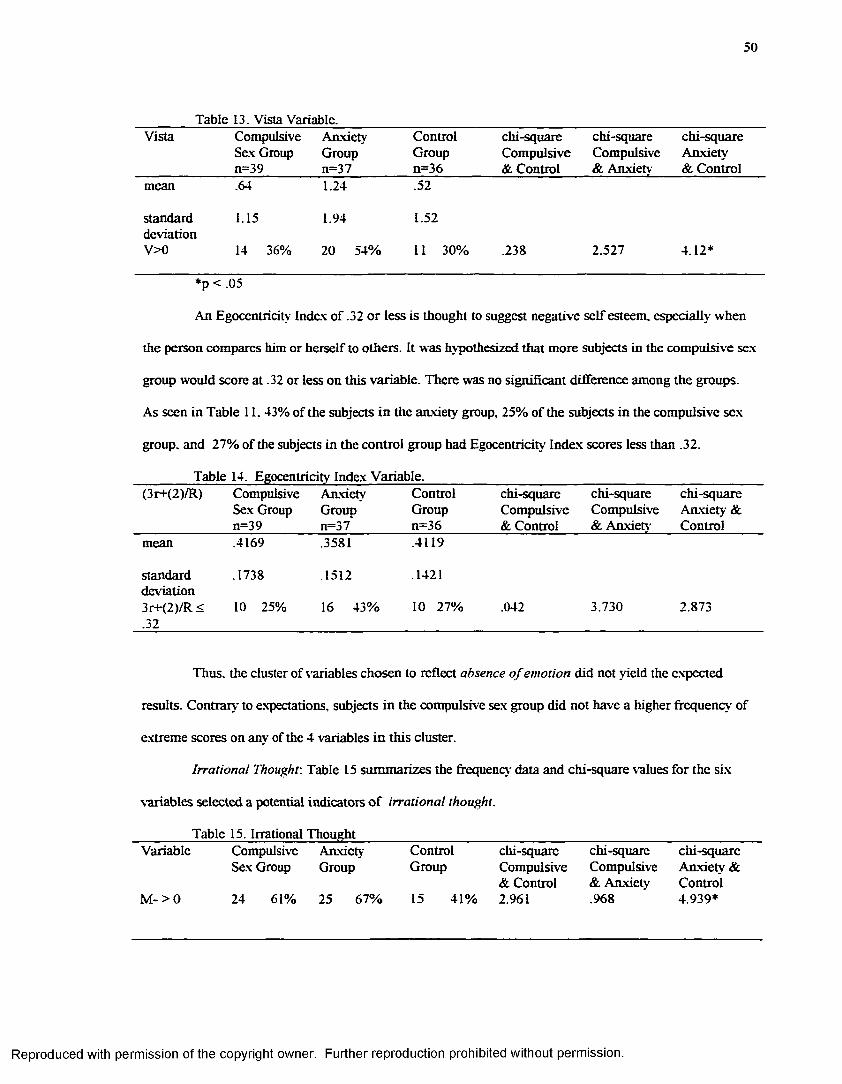
50
Table 13. Vista Variable.__________________________________________________________Vista Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety_____________ n=39_______ n=37_________n=36________& Control & Anxiety & Controlmean .64 1.24 .52
standard 1.15 1.94 1.52deviationV>0 14 36% 20 54% 11 30% .238 2.527 4.12*
*p < .05
An Egocentricity Index of .32 or less is thought to suggest negative self esteem, especially when
the person compares him or herself to others. It was hypothesized that more subjects in the compulsive sex
group would score at .32 or less on this variable. There was no significant difference among the groups.
As seen in Table 11, 43% of the subjects in the anxiety group, 25% of the subjects in the compulsive sex
group, and 27% of the subjects in the control group had Egocentricity Index scores less than .32.
_______ Table 14. Egocentricity Index Variable._______________________________________________(3r+(2)/R) Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &_____________ n=39________n=37________ n=36________ & Control & Anxiety Controlmean .4169 .3581 .4119
standard .1738 .1512 .1421deviation3r+(2)/R< 10 25% 16 43% 10 27% .042 3.730 2.873.32
Thus, the cluster of variables chosen to reflect absence o f emotion did not yield the expected
results. Contrary' to expectations, subjects in the compulsive sex group did not have a higher frequency of
extreme scores on any of the 4 variables in this cluster.
Irrational Thought: Table 15 summarizes the frequency' data and chi-square values for the six
variables selected a potential indicators o f irrational thought.
_______ Table 15. Irrational Thought________________________________________________________Variable Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety && Control & Anxiety Control
M- > 0 24 61% 25 67% 15 41% 2.961 .968 4.939*
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
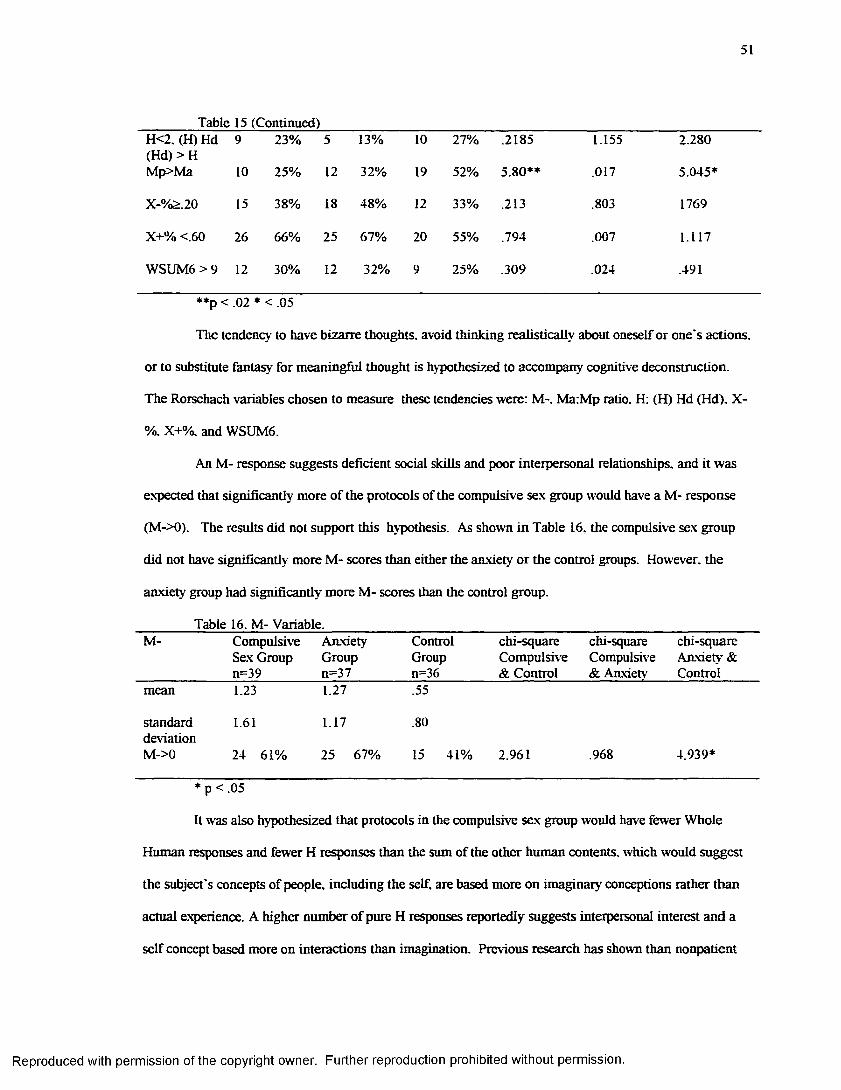
51
Table 15 (Continued)H<2. (H) Hd (Hd) > H
9 23% 5 13% 10 27% .2185 1.155 2.280
Mp>Ma 10 25% 12 32% 19 52% 5.80** .017 5.045*
X-%>.20 15 38% 18 48% 12 33% .213 .803 1769
X+% <.60 26 66% 25 67% 20 55% .794 .007 1.117
WSUM6 > 9 12 30% 12 32% 9 25% .309 .024 .491
**p < .02 * < .05
The tendency to have bizarre thoughts, avoid thinking realisticaUv about oneself or one’s actions,
or to substitute fantasy for meaningful thought is hypothesized to accompany cognitive deconstruction.
The Rorschach variables chosen to measure these tendencies were: M-. Ma:Mp ratio. H: (H) Hd (Hd). X-
%, X+%. and WSUM6.
An M- response suggests deficient social skills and poor interpersonal relationships, and it was
expected that significantly more of the protocols of the compulsive sex group would have a M- response
(M->0). The results did not support this hypothesis. As shown in Table 16. the compulsive sex group
did not have significantly more M- scores than either the anxiety or the control groups. However, the
anxiety group had significantly more M- scores than the control group.
_______ Table 16. M- Variable._____________________________________________________________M- Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &_____________n=39________n=37________ n=36________ & Control & Anxiety Controlmean 1.23 1.27 .55
standard 1.61 1.17 .80deviationM->0 24 61% 25 67% 15 41% 2.961 .968 4.939*
_____
It was also hypothesized that protocols in the compulsive sex group would have fewer Whole
Human responses and fewer H responses than the sum of the other human contents, which would suggest
the subject’s concepts of people, including the self, are based more on imaginary conceptions rather than
actual experience. A higher number of pure H responses reportedly suggests interpersonal interest and a
self concept based more on interactions than imagination. Previous research has shown than nonpatient
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
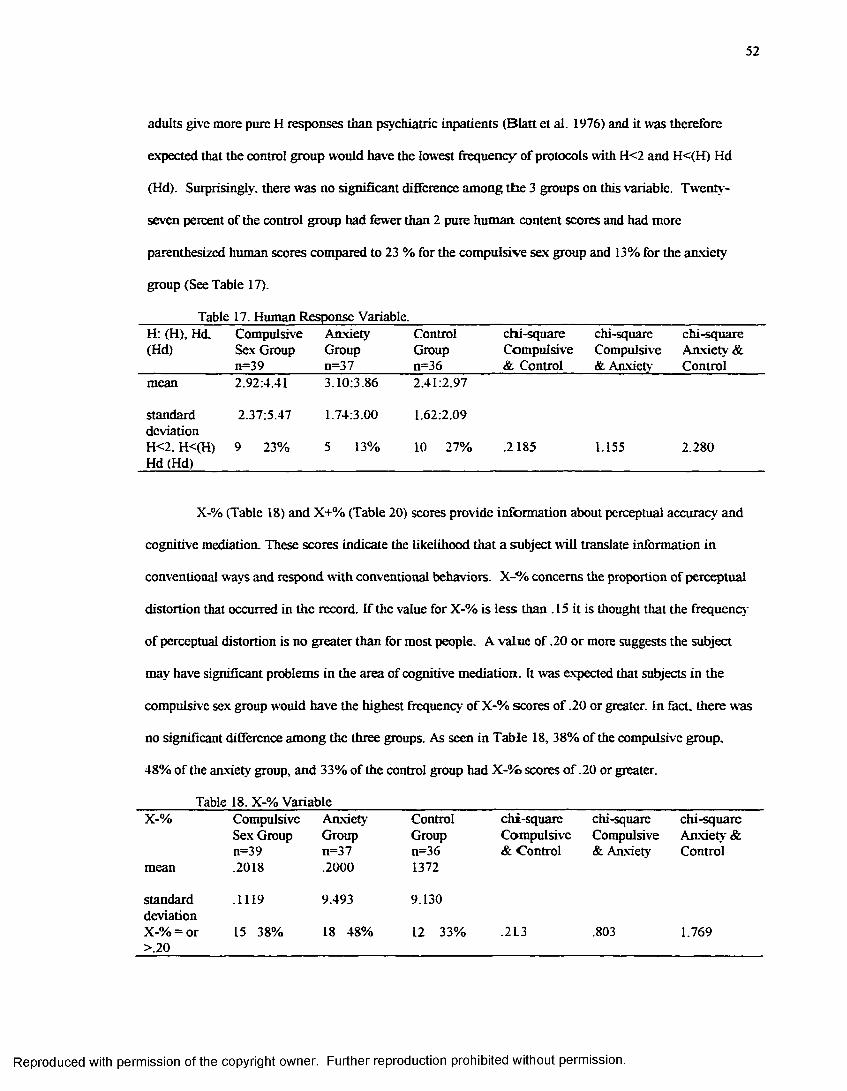
52
adults give more pure H responses than psychiatric inpatients (Blatt et al. 1976) and it was therefore
expected that the control group would have the lowest frequency of protocols with H<2 and H<(H) Hd
(Hd). Surprisingly, there was no significant difference among the 3 groups on this variable. Twenty-
seven percent of the control group had fewer than 2 pure human, content scores and had more
parenthesized human scores compared to 23 % for the compulsive sex group and 13% for the anxiety
group (See Table 17).
_______ Table 17. Human Response Variable.________________________________________________H: (H), Hd. Compulsive Anxiety Control chi-square chi-square chi-square(Hd) Sex Group Group Group Compulsive Compulsive Anxiety &_____________n=39________n=37________ n=36_________& Control & Anxiety Controlmean 2.92:4.41 3.10:3.86 2.41:2.97
standard 2.37:5.47 1.74:3.00 1.62:2.09deviationH<2. H<(H) 9 23% 5 13% 10 27% .2185 1.155 2.280Hd (Hd)_______________________________________________________________________________
X-% (Table 18) and X+% (Table 20) scores provide information about perceptual accuracy and
cognitive mediation. These scores indicate the likelihood that a subject will translate information in
conventional ways and respond with conventional behaviors. X-% concerns the proportion of perceptual
distortion that occurred in the record. If the value for X-% is less than . 15 it is thought that the frequency
of perceptual distortion is no greater than for most people. A value of .20 or more suggests the subject
may have significant problems in the area of cognitive mediation. It was expected that subjects in the
compulsive sex group would have the highest frequency of X-% scores of .20 or greater. In fact, there was
no significant difference among the three groups. As seen in Table 18, 38% of the compulsive group.
48% of the anxiety group, and 33% of the control group had X-%> scores of .20 or greater.
Table 18. X-% VariableX-% Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &n=39 n=37 n=36 & Control & Anxiety Control
mean .2018 .2000 1372
standard .1119 9.493 9.130deviationX-% = or 15 38% 18 48% 12 33% .2L3 .803 1.769>.20
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
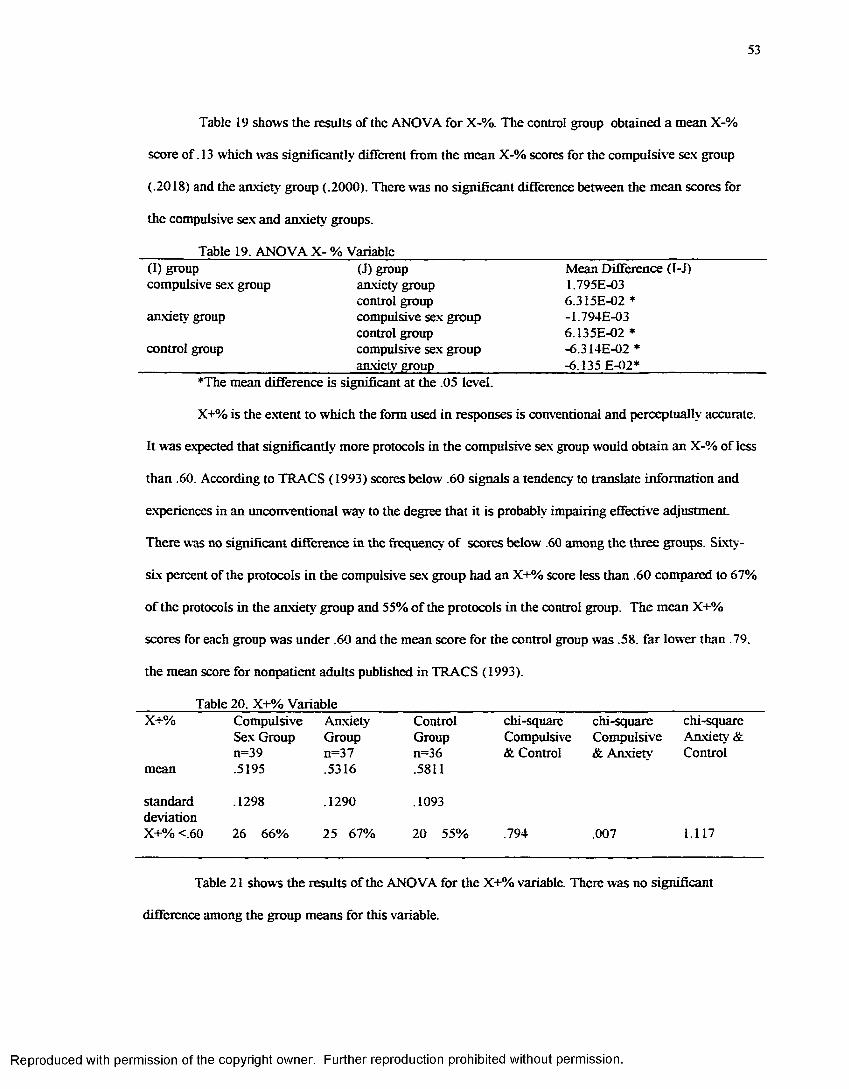
53
Tabic 19 shows the results of the ANOVA for X-%. The control group obtained a mean X-%
score of .13 which was significantly different from the mean X-% scores for the compulsive sex group
(.2018) and the anxiety group (.2000). There was no significant difference between the mean scores for
the compulsive sex and anxiety groups.
_______ Table 19. ANOVA X- % Variable____________________________________________________(I) group (J) group Mean Difference (I-J)compulsive sex group anxiety group 1.795E-03
control group 6.315E-02 *anxiety group compulsive sex group -1.794E-03
control group 6.135E-02 *control group compulsive sex group -6.314E-02*
______________________________ anxiety group__________________ -6.135 E-02*_________________♦The mean difference is significant at the .05 level.
X+% is the extent to which the form used in responses is conventional and perceptually accurate.
It was expected that significantly more protocols in the compulsive sex group would obtain an X-% of less
than .60. According to TRACS (1993) scores below .60 signals a tendency to translate information and
experiences in an unconventional way to the degree that it is probably impairing effective adjustment.
There was no significant difference in the frequency of scores below .60 among the three groups. Sixty-
six percent of the protocols in the compulsive sex group had an X+% score less than .60 compared to 67%
of the protocols in the anxiety group and 55% of the protocols in the control group. The mean X+%
scores for each group was under .60 and the mean score for the control group was .58. far lower than .79.
the mean score for nonpatient adults published in TRACS (1993).
Table 20. X+% VariableX+% Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &n=39 n=37 n=36 & Control & Anxiety Control
mean .5195 .5316 .5811
standard .1298 .1290 .1093deviationX+% <.60 26 66% 25 67% 20 55% .794 .007 1.117
Table 21 show's the results of the ANOVA for the X+% variable. There was no significant
difference among the group means for this variable.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
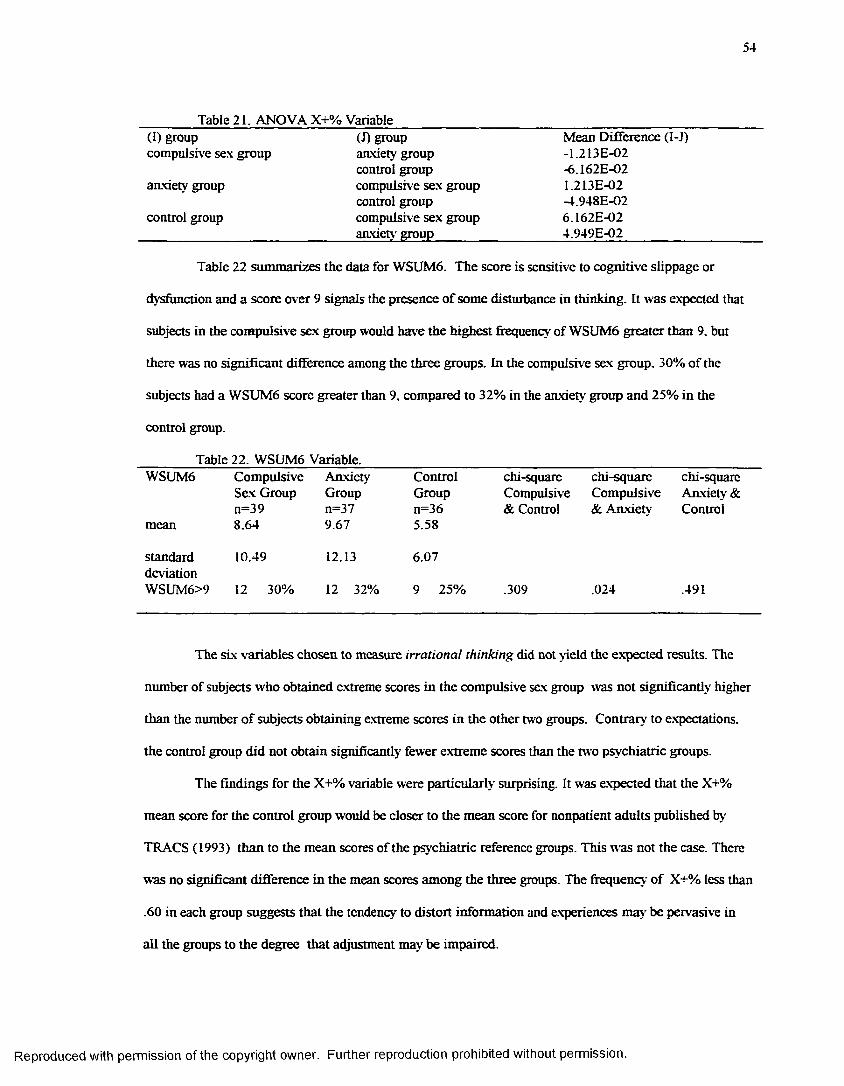
54
_______ Table 21. ANOVA X+% Variable__________________________________________________(I) group (J) group Mean Difference (I-J)compulsive sex group anxiety group -1.213E-02
control group -6.162E-02anxiety group compulsive sex group 1.213E-02
control group -4.948E-02control group compulsive sex group 6 .162E-02______________________________ anxiety group_________________ 4.949E-02__________________
Table 22 summarizes the data for WSUM6. The score is sensitive to cognitive slippage or
dysfunction and a score over 9 signals the presence of some disturbance in thinking. It was expected that
subjects in the compulsive sex group would have the highest frequency of WSUM6 greater than 9. but
there was no significant difference among the three groups. In the compulsive sex group. 30% of the
subjects had a WSUM6 score greater than 9. compared to 32% in the anxiety group and 25% in the
control group.
Table 22. WSUM6 Variable.WSUM6 Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &n=39 n=37 n=36 & Control & Anxiety Control
mean 8.64 9.67 5.58
standard 10.49 12.13 6.07deviationWSUM6>9 12 30% 12 32% 9 25% .309 .024 .491
The six variables chosen to measure irrational thinking did not yield the expected results. The
number of subjects who obtained extreme scores in the compulsive sex group was not significantly higher
than the number of subjects obtaining extreme scores in the other two groups. Contrary to expectations,
the control group did not obtain significantly fewer extreme scores than the two psychiatric groups.
The findings for the X+% variable were particularly surprising. It was expected that the X+%
mean score for the control group would be closer to the mean score for nonpatient adults published by
TRACS (1993) than to the mean scores of the psychiatric reference groups. This was not the case. There
was no significant difference in the mean scores among the three groups. The frequency of X+% less than
.60 in each group suggests that the tendency to distort information and experiences may be pervasive in
all the groups to the degree that adjustment may be impaired.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
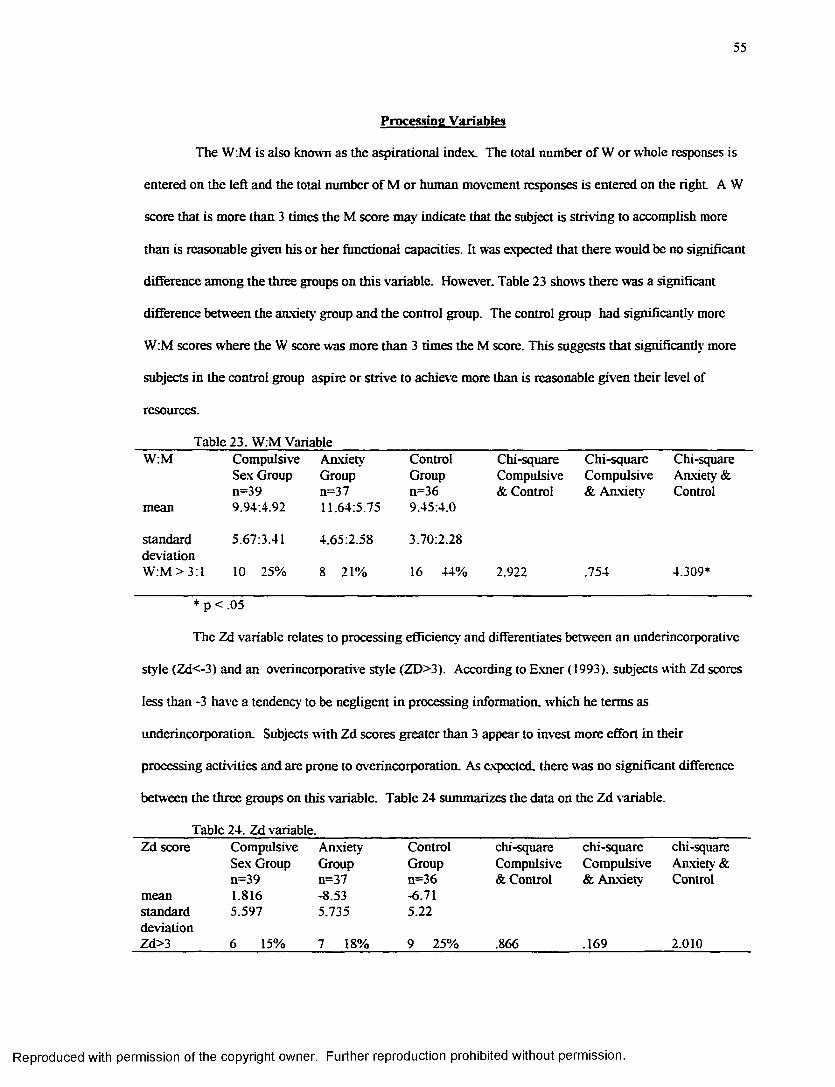
55
Processing Variables
The W:M is also known as the aspirational index. The total number of W or whole responses is
entered on the left and the total number of M or human movement responses is entered on the right. A W
score that is more than 3 times the M score may indicate that the subject is striving to accomplish more
than is reasonable given his or her functional capacities. It was expected that there would be no significant
difference among the three groups on this variable. However. Table 23 shows there was a significant
difference between the anxiety group and the control group. The control group had significantly more
W:M scores where the W score was more than 3 times the M score. This suggests that significantly more
subjects in the control group aspire or strive to achieve more than is reasonable given their level of
resources.
Table 23. W:M VariableW:M Compulsive Anxiety Control Chi-square Chi-square Chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &n=39 n=37 n=36 & Control & Anxiety Control
mean 9.94:4.92 11.64:5.75 9.45:4.0
standard 5.67:3.41 4.65:2.58 3.70:2.28deviationW:M > 3:1 10 25% 8 21% 16 44% 2.922 .754 4.309*
* p < .05
The Zd variable relates to processing efficiency and differentiates between an underincorporative
style (Zd<-3) and an overincorporative style (ZD>3). According to Exner (1993). subjects with Zd scores
less than -3 have a tendency to be negligent in processing information, which he terms as
underincorporation. Subjects with Zd scores greater than 3 appear to invest more effort in their
processing activities and are prone to overincorporation. As expected, there was no significant difference
between the three groups on this variable. Table 24 summarizes the data on the Zd variable.
Table 24. Zd variable.Zd score Compulsive Anxiety Control chi-square chi-square chi-square
Sex Group Group Group Compulsive Compulsive Anxiety &n=39 n=37 n=36 & Control & Anxiety Control
mean 1.816 -8.53 -6.71standard 5.597 5.735 5.22deviationZd>3 6 15% 7 18% 9 25% .866 .169 2.010
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
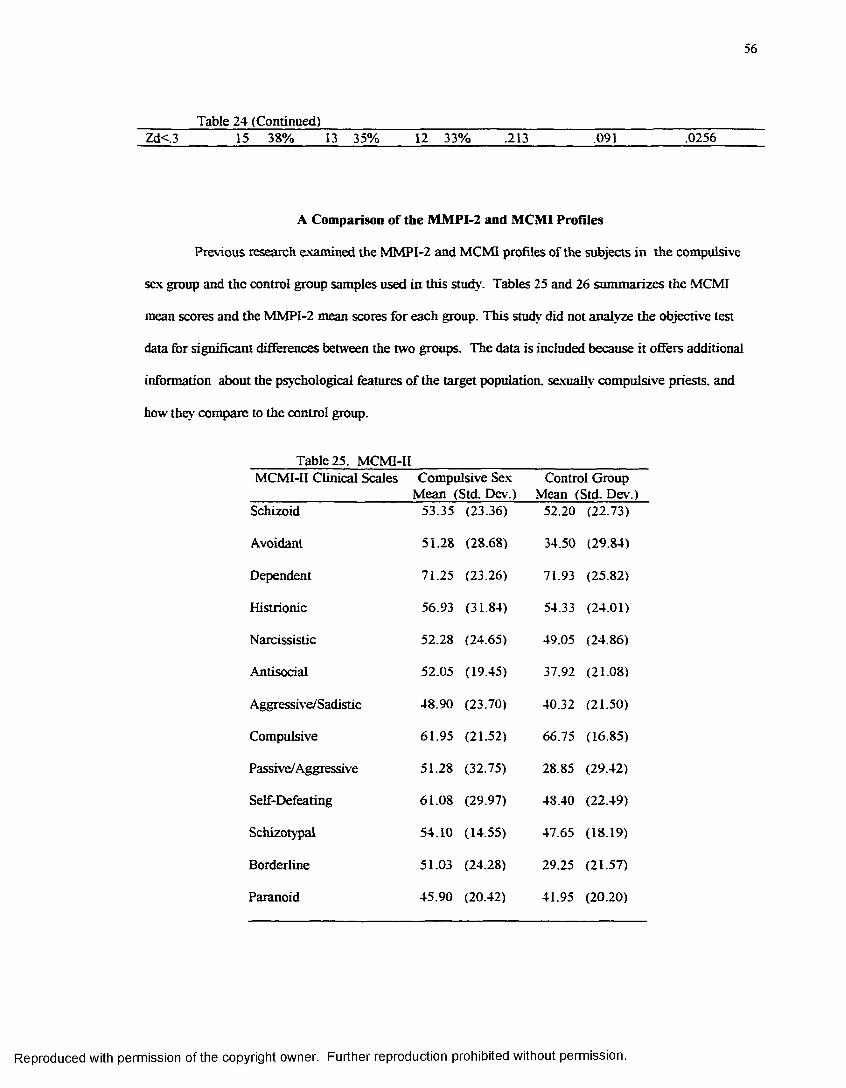
56
_______ Table 24 (Continued)_________________________________________________________Zd< 3 15 38% 13 35% 12 33% .213 .091 .0256
A Comparison of the MMPI-2 and MCMI Profiles
Previous research examined the MMPI-2 and MCMI profiles of the subjects in the compulsive
sex group and the control group samples used in this study. Tables 25 and 26 summarizes the MCMI
mean scores and the MMPI-2 mean scores for each group. This study did not analyze the objective test
data for significan t differences between the two groups. The data is included because it offers additional
information about the psychological features of the target population, sexually compulsive priests, and
how they compare to the control group.
Table 25. MCMI-IIMCMI-II Clinical Scales Compulsive Sex Control Group ______________________ Mean (Std. Dev.) Mean (Std. Dev.)Schizoid 53.35 (23.36) 52.20 (22.73)
Avoidant 51.28 (28.68) 34.50 (29.84)
Dependent 71.25 (23.26) 71.93 (25.82)
Histrionic 56.93 (31.84) 54.33 (24.01)
Narcissistic 52.28 (24.65) 49.05 (24.86)
Antisocial 52.05 (19.45) 37.92 (21.08)
Aggressive/Sadistic 48.90 (23.70) 40.32 (21.50)
Compulsive 61.95 (21.52) 66.75 (16.85)
Passive/Aggressive 51.28 (32.75) 28.85 (29.42)
Self-Defeating 61.08 (29.97) 48.40 (22.49)
Schizotypal 54.10 (14.55) 47.65 (18.19)
Borderline 51.03 (24.28) 29.25 (21.57)
Paranoid 45.90 (20.42) 41.95 (20.20)
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
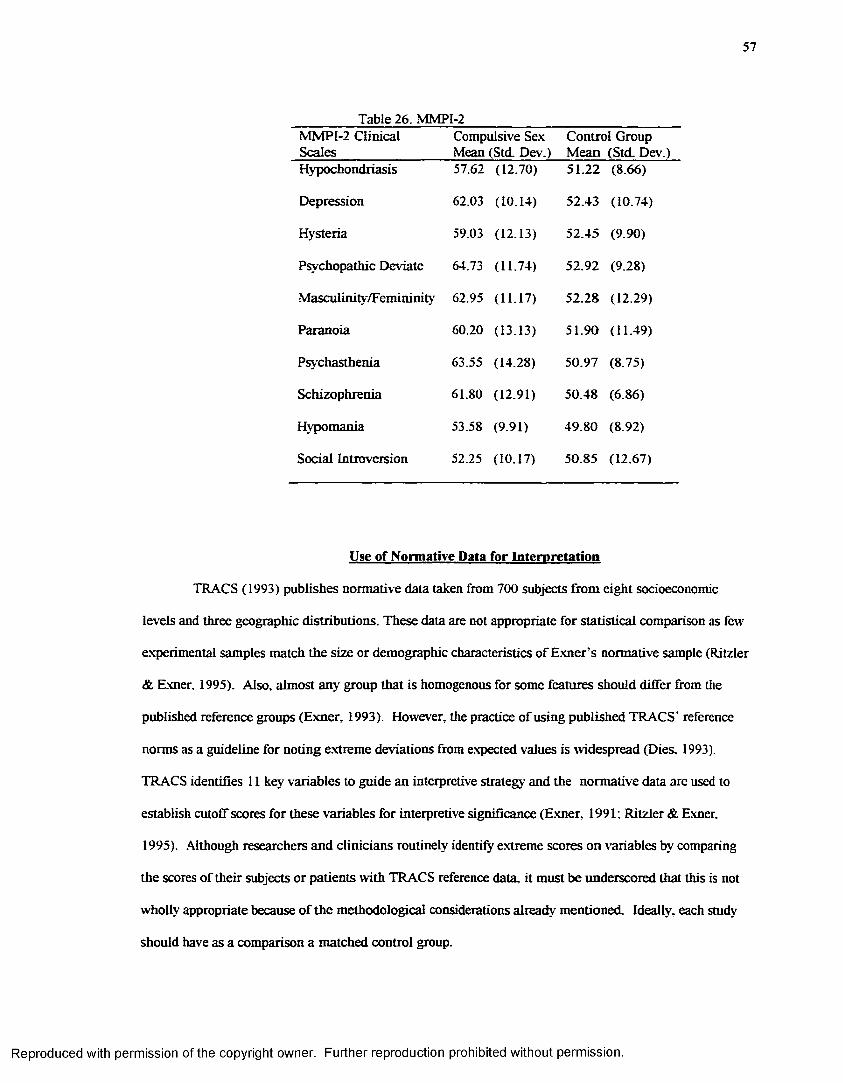
57
Table 26. MMPI-2MMPI-2 Clinical Scales
Compulsive Sex Mean (Std. Dev.)
Control Group Mean (Std. Dev.)
Hypochondriasis 57.62 (12.70) 51.22 (8.66)
Depression 62.03 (10.14) 52.43 (10.74)
Hysteria 59.03 (12.13) 52.45 (9.90)
Psychopathic Deviate 64.73 (11.74) 52.92 (9.28)
Masculinity/Femininity 62.95 (11.17) 52.28 (12.29)
Paranoia 60.20 (13.13) 51.90 (11.49)
Psychasthenia 63.55 (14.28) 50.97 (8.75)
Schizophrenia 61.80 (12.91) 50.48 (6.86)
Hypomania 53.58 (9-91) 49.80 (8.92)
Social Introversion 52.25 (10.17) 50.85 (12.67)
Use of Normative Data for Interpretation
TRACS (1993) publishes normative data taken from 700 subjects from eight socioeconomic
levels and three geographic distributions. These data are not appropriate for statistical comparison as few
experimental samples match the size or demographic characteristics of Exner’s normative sample (Ritzier
& Exner. 1995). Also, almost any group that is homogenous for some features should differ from the
published reference groups (Exner, 1993). However, the practice of using published TRACS’ reference
norms as a guideline for noting extreme deviations from expected values is widespread (Dies, 1993).
TRACS identifies 11 key variables to guide an interpretive strategy and the normative data are used to
establish cutoff scores for these variables for interpretive significance (Exner. 1991: Ritzier & Exner.
1995). Although researchers and clinicians routinely identify extreme scores on variables by comparing
the scores of their subjects or patients with TRACS reference data, it must be underscored that this is not
wholly appropriate because of the methodological considerations already mentioned. Ideally, each study
should have as a comparison a matched control group.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
CHAPTER4
DISCUSSION
Cognitive deconstruction theory states that a person may try to escape from negative affect caused
by internal attributions of failure by rejecting and avoiding meaningful thought. The person rejects the
broader ideas that are associated with higher level thinking, focusing on concrete movements and sensations
in the present, thereby escaping the emotional discomfort that may accompany painful self-awareness. The
theory has been offered as a possible model for understanding the cognitive processes that may underlie the
initiation, maintenance, and justification of self-destructive sexually compulsive behaviors. Baumeister
(1990) lists four consequences of cognitive deconstruction: disinhibition, passivity, absence o f emotion,
irrational thinking. The features and consequences of cognitive deconstruction theory seemed to be
particularly relevant to the features noted in the clinical presentations of many sexually compulsive priests.
This study was the first attempt to investigate whether the consequences of cognitive
dcconstruction (disinhibition, passivity, absence o f emotion, irrational thinking) could be found in the
Rorschach protocols of a population hypothesized to engage in deconstruction. Extreme scores on thirteen
Rorschach variables were chosen to indicate the presence of the four consequences of cognitive
deconstruction. It was hypothesized that the sample of sexually compulsive priests would yield
significantly more protocols with extreme scores on the chosen variables than two comparison groups: a
group of priests diagnosed with an anxiety disorder and a control group of priests who underwent
psychological evaluation.
While there were some significant differences among the groups, the results did not support the
hypothesis that a sample of priests with sexually compulsive behavior would have significantly more
scores on the Rorschach that signaled the four consequences of cognitive deconstruction (disinhibition,
passivity, absence o f emotion, irrational thinking). There could be a number of explanations for the
results.
58
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
59
Methodological issues related to alpha and beta error sources need to be taken into account when
interpreting the results. It may be that the statistically significant differences among the groups may not be
a reflection of any real differences, instead, they may be the result of alpha or Type I error. Archer and
Krishnamurthy (1993) point out that when a large number of significance tests are computed within a
single study, an inflation of p values occurs and an increasing number of the obtained differences that
achieve statistical significance may occur due to chance. Alternatively, beta or Type II error reflects the
sensitivity of the statistical test in detecting true differences. The probability of rejecting the null
hypothesis when it is false is referred to as the power for a test: analyses that yield low power elevate the
probability of failing to reject a “false” null hypothesis. The probability of a Type I error and the
probability of a Type II error are inversely related (Agresti & Finlay, 1986). The vulnerability of this study
to Type I error does not alter the overall conclusions, since the significant differences were not in the
direction expected: the compulsive sex group was not significantly different from either the anxiety or the
control groups on any variable.
A major limitation of this study is the lack of available data on Rorschach scorer reliability.
Weiner (1991) offers the following guidelines to establish interrater reliability: at least 20 protocols in a
study should be scored by two or more examiners. There should be at least 80% agreement on variables
central to the particular study. Categories examined should include location, determinants, form level,
and content. Moreover, there are no available data on the reliability of the different evaluation teams in
formulating psychiatric diagnoses.
According to Cronbach and Meehl (1955). when an investigator's prediction and data are
discordant the results can be interpreted in three ways: the test does not measure the construct variable,
the theoretical network which generated the hypothesis is incorrect or the experimental design failed to
test the hypothesis properly.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
60
The Rorschach as a Measure of Cognitive Deconst ruction
Data to support the validity of the chosen Rorschach variables as measures of psychological
attributes related to a person’s resources, capacity for control, openness to emotional stimulation,
interpersonal style, self-esteem, and cognitive mediation have been presented earlier in the text. The
Rorschach is interpreted as an indirect measure of various psychological attributes, providing information
about underlying propensities to certain kinds of psychological responses (Meyer. 1996). It was not
purported that these variables are a direct measure of the construct of cognitive deconstruction.
Consideration of what scores in a Rorschach protocol actually mean is a matter of construct validity: do
the test scores actually reflect the presence of the psychological attribute they are intended to measure? In
this study, the Rorschach variables were used to infer the presence of the psychological qualities that are
purported to be the consequences of cognitive deconstruction. For some of the chosen variables there was
a direct connection between the psychological construct and a consequence of cognitive deconstruction.
For example, an a:p ratio of p>a+l indicates passivity and directly relates to passivity as a consequence of
cognitive deconstruction. The interpretation of passive scores on the Rorschach, and passivity as a
consequence of cognitive deconstruction both refer to a passive interpersonal style and a tendency to
avoid personal responsibility.
For other variables, the connection was more indirect. For example, the Vista response, one of
the variables used to assess absence o f emotion, is thought to be related to negative or painful emotional
experience that is generated by self-focusing behavior. However, while the presence of negative emotion is
considered to be a causal factor in the need to avoid emotion in cognitive deconstruction, not everyone
who experiences emotional pain uses avoidance as a means of coping. While a Vista response may signal
the presence of painful affect related to self evaluation, it does not necessarily mean the person is
suppressing the painful affect, or is estranged from his or her emotions.
It was expected that evidence of the consequences of cognitive deconstruction would be present in
the Rorschach protocols of a population that exhibits behavior hypothesized to be used by some people to
escape negative emotions. One explanation for the discordance between the predictions and the results is
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
that the Rorschach is not a good measure of the consequences of cognitive deconstruction. It may be that
this population of priests does in fact use the process of cognitive deconstruction as a means of escaping
negative emotions, and that they turn to compulsive sexual behavior as a way of m ainta in ing the
deconstructed state. The negative findings may instead be pointing to a weak link between the theory and
the test measurement used.
A more direct measure of the presence of cognitive deconstruction may yield different results.
Any conclusions about the presence of cognitive deconstruction in sexually compulsive priests should be
deferred until more valid measures of the construct are available. Even if this study had yielded positive
results, follow-up studies using a measure that is more directly related to cognitive deconstruction would
be necessary to support the hypothesis that sexually compulsive priests engage in cognitive deconstruction.
Theoretical Network of Cognitive Deconstruction
The second possible interpretation of the results is that the theoretical network which generated
the hypothesis is flawed. According to Cronbach and Meehl (1955). if a construct is too loosely defined, it
will not yield verifiable inferences. Baumeister (1990) developed the theory of cognitive deconstruction as
an explanation o f the processes that may be involved in a person’s flight from negative and painful
implications about the self, and posits that this flight from higher level cognitive activity produces several
consequences. He argues that addictions and similar compulsive behaviors typically involve an escape
from an aversive state as much as a pursuit of pleasure. It may be difficult to use the presence of the
consequences o f cognitive deconstruction to assess the presence of the construct because some of these
attributes may be the nonspecific consequences of psychopathology in general, rather than specific
consequences of cognitive deconstruction. Therefore, the presence of these attributes may be due to a
number of factors other than cognitive deconstruction. Even had group 1 obtained significantly more
protocols with extreme scores on the 13 variables indicating the presence of the consequences of cognitive
deconstruction. the results would not be sufficient to establish the actual presence of construct.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
62
Disinhibition, passivity, absence o f emotion, and irrational thinking could be the result of other aspects of
psychopathology.
Future research to validate or support the theory- may need to look for more direct evidence of the
steps leading to cognitive deconstruction (disappointment followed by internal attributions of failure,
leading to negative affect from which the person wishes to escape).
Failure of the Experimental Design
The negative findings may also be due to the failure of the experimental design to test the
hypotheses properly. This study compared the Rorschach protocols of three groups of Roman Catholic
clergy, all referred to a psychiatric hospital for evaluation. It was hypothesized that a significantly higher
number of the protocols of the group diagnosed with compulsive sexuality would have scores that
indicated the presence of the consequences of cognitive deconstruction (disinhibition, passivity, absence o f
emotion, irrational thinking). However, as noted earlier, the variables that were chosen to measure these
attributes also relate to more general problems in functioning, such as inadequate coping skills (CDI).
ability to modulate emotional discharges (FC:CF+C). responsiveness to emotional stimulation (Afr ratio),
and perceptual accuracy (X-% and X+%).
It is possible that all priests referred for evaluation share some common psychological features,
making it more likely for the comparison groups to have similar scores on the variables in question. On
most of the 13 Rorschach variables, there was no difference among the three samples. While the
compulsive sex group did obtain significantly more positive CDI scores than the anxiety group, suggesting
they maybe have inadequate coping skills, there was no difference between the compulsive sex and the
control groups on this variable. The significant differences that were observed among the groups suggest
that: (1) more subjects in the control group may be interpersonally passive compared to the subjects in the
other two groups (Mp>Ma), (2) more subjects in the control group are likely to strive to accomplish more
than is reasonable given their resources (W:M>3:1) compared to subjects in the anxiety group, and (3)
more subjects in the anxiety group may experience painful self-focusing behavior (VX)). interpersonal
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
63
problems, and poorer social skills (M-) than subjects in the control group. As three of the variables which
yielded significant results relate to aspects of interpersonal functioning (CDL Ma:Mp. M-) it would appear
that all three subject groups have some problems in this area.
An examination of the objective personality tests used in the evaluation process yields additional
information about the psychological features of some of the priests referred for evaluation. It is important
to note that there is no evidence that MCMI results are related to Rorschach results, and the
interrelationship between MMPI results and Rorschach results is weak at best. In 1996. Taylor examined
the Millon Clinical Multiaxial Inventory (MCMI) and the Minnesota Muitiphasic Personality Inventory'
(MMPI) profiles of the compulsive sex and the control samples used in this study. Tables summarizing
these data were presented in the results section (tables 24 and 25). The two samples had very' similar
profiles on the MCMI, which seems to support the notion that many, if not all. priests referred for
evaluation share some common features. Although neither sample obtained elevated group mean scores
(BR>74) on the personality and severe pathology scales, both groups obtained their highest scores on the
Dependent and Compulsive scales. The compulsive sex group had sub-clinical elevations on Dependent,
Compulsive, Self-defeating, and Histrionic scales while the control group had sub-clinical elevations on
Dependent Compulsive, Histrionic, and Schizoid scales. The compulsive sex group scored significantly
higher than the control group on the antisocial, passive-aggressive, and borderline scales.
The MMPI-2 group mean scores for the control group were all within normal limits. However,
the mean scores for the compulsive sex group were moderately elevated on eight of the ten clinical scales.
As noted earlier, the interrelationship between the MMPI and Rorschach is weak. Archer and
Krishnamurthy (1993) examined 37 studies that have reported interrelationships between MMPI and
Rorschach variables in adult populations. They report that 73% of the studies revealed either no
statistically significant relationships or minimal associations between MMPI scales and Rorschach
variables. The authors conclude that the Rorschach and the MMPI may be measuring different aspects of
personality functioning.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
64
The results of the MMPI may appear to challenge the notion that the psychological features of the
control group and the compulsive sex group are too similar yield any differences in psychological test
scores. However, there is evidence that some people who look healthy on standard mental health scales,
such as the MMPI. may in fact be maintaining an “illusion of mental health” based on defensive denial of
distress (Shelder, et. al.. 1993). This is a possible explanation for why a control group comprised of
individuals referred for a week-long residential psychological evaluation looks healthy on the MMPI. but
not on the projective testing. Shedler (1993) suggests that people in this group, known as defensive
deniers. need to see themselves as well-adjusted. Shedler (1993) argues that they preserve belief in their
“adjustment” by disavowing much of their emotional life, and consequently, they have little awareness of
their needs, wishes, and feelings. Such people may have scores that fall with in normal limits but. for this
group, the scales appear to measure defensive denial rather than mental health.
Keddy et al. (1990) studied the psychological profiles of a group of Catholic clergy and religious
who were referred for residential treatment for a variety of presenting problems including interpersonal
problems, depression, sexual identity problems, alcoholism, and vocational issues. The Rorschach
protocols of the participants indicated a tendency toward rigidity, losing control in emotionally charged
situations and having unmodulated outbursts of emotion, and an idiosyncratic world view. The data from
Rorschach protocols pointed to a consistent constellation of problems including an overemphasis on
intellectual abilities, difficulty modulating emotional discharges, a tendency' to avoid emotional
complexity, difficulty in engaging in productive introspection, and an idiosyncratic world view. These
findings corresponded to the reasons for referral, such as angry outbursts or sexual acting out.
Kennedy et al. (1977) obtained a randomly selected national sample of 271 priests and. on the
basis of a clinical interview, grouped them into four categories along a continuum of development.
Sixty-five percent were labeled as either maldeveloped or underdeveloped. 29% were considered
developing, and only 6% were seen as maturely developed. The maldeveloped had long histories of
serious psychological problems, including underlying hostile feelings, poor self-esteem, and disruptive
sexual conflicts. The underdeveloped were described as over-identifying with their role as priest and
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
65
failing to develop a personal sense of themselves. Their lives were shaped by the expectations of others,
they had few experiences of intimacy, and tended to handle their feelings through repression and
inteliectualization. The developing priests were judged to have begun to grow as persons after a delay at
an earlier level. They were characterized by high motivation and vitality. The maturely dev eloped priests
were the reference points for maturity and normality in this population. They achieved a mature level of
personal integration and were characterized as independent and self-sufficient. They tended to be
responsible and aggressive in their work and achieved warm, close relationships with others, including
women.
A major limitation of this study is the lack of a normal (non priest) random sample comparison
group. It is unclear what percentage of a normal group would fall into the different categories, and
without this reference it is uncertain whether the emotional development of the priest population is any
different than the development of the general public.
These two studies suggest that there may be a homogeneity in the psychological makeup and
functioning of Roman Catholic clergy that that transcends diagnostic labels. Their symptoms and
behavioral problems may differ, but at their core many of the priests are likely to share similar attributes.
This may account for the similarity in the Rorschach protocols of the three groups of priests in this study.
It would have been preferable to compare the Rorschach protocols of the target group of sexually
compulsive priests to the protocols of a randomly selected group of priests who were not referred for
psychological evaluation. This would help determine what are typical scores for this population and
thereby establish cutoff scores for clinical interpretation.
Instability of Cognitive Deconstruction State
According to Baumeister (1991) and Ward et al. (1995) people who begin engaging in
compulsive sexual behavior, or sexually abusive behavior, in adulthood should display a cognitive style
which reflects repeated switching from deconstructed levels to higher abstract levels. The natural
tendency of the mind is to drift toward broader meanings; staying at a lower level of awareness may
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
66
require exertion or distraction. This repeated switching between higher/abstract and lower/concrete levels
is consistent with the notion of a hierarchical system for identifying and executing behavior that is a
feature of action identification theory (Vallacher & Wegner, 1985. 1987). control theory (1982. 1990).
and objective self awareness theory (Duval & Wicklund. 1972).
It may be that early-onset sexually compulsive priests are in a deconstructed state only while they
are acting out sexually, at other times they may shift to a more abstract level of thinking The Rorschach
protocols may reflect the state of the subject at the time of testing, when they may be in a more abstract
level of awareness. Typically, the intervention or catastrophe that precipitates the priest’s referral for
evaluation also forces him to confront his problems in a meaningful way. resulting in a broader and more
abstract level of thinking. The week-long evaluation includes at least two comprehensive clinical
interviews and a spiritual assessment that includes spiritual exercises. Thus, it may be that the evaluation
process shifts the priest to a more abstract level of awareness, therefore providing little evidence of the
more narrow states that characterize cognitive deconstruction.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
CHAPTER 5
CONCLUSIONS
This study did not support the hypothesis that early-onset sexually compulsive priests have
incorporated cognitive deconstruction into their general cognitive and behavioral style, as evidenced by a
high number of extreme scores on Rorschach variables that measure the consequences of cognitive
deconstruction. Although there was not evidence that this population was significantly different from the
two comparison groups, the results do not rule out the possibility that sexually compulsive priests may
shift into a cognitively deconstructed state while actually engaging in sexually compulsive behavior.
A number of explanations for the negative results of this study have been discussed. The
construct needs to be more tightly defined so that construct validation does not rely on the presence of
consequences of the construct but targets actual features of cognitive deconstruction. Other factors that
account for the results are the homogeneity of the population used in this study and the measure used to
detea the presence of cognitive deconstruction.
Researchers and clinicians have noted the similarity in the psychological profiles of Roman
Catholic clergy. Some of the most frequent descriptions of priests (non-patient and patient) include:
passive, socially inept, distanced from emotion, displaying poorly modulated emotional discharges, rigid,
intellectually defended, and idiosyncratic in their views. These descriptions are consistent with the
Rorschach protocols obtained by the three groups, and with the results of study of a national, randomly
seleaed. representative sample of priests (Kennedy et al.. 1977). As noted earlier, the Roman Catholic
priesthood seems to attraa persons who share a number of psychological traits.
Among the various psychological test data available for the target population, the Rorschach was
determined to be the most likely to yield information on psychological attributes that were related to the
consequences of cognitive deconstruaion. While the Rorschach variables chosen did relate to the
consequences of cognitive deconstruction, the variables did not relate to the different steps involved in the
67
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

68
process of cognitive deconstruction. Also, the variables relate to more general pathology, m aking it
difficult to establish a causal link between extreme scores on the chosen variables and cognitive
deconstruction.
Future research using more direct measures of cognitive deconstruction by focusing on the actual
steps involved in the process, rather than the consequences, may yield different results. Also, it is
noteworthy that the control group consisted of priests experiencing a high enough level of dysfunction to
warrant referral for residential psychological evaluation rather than outpatient consultation. A control
group of priests who were higher functioning (and thus not referred for residential psychological
evaluation) may look significantly different on the psychological testing when compared to the
experimental group.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
69
REFERENCES
Abel. G.G.. Becker. J.G., Cunningham-Rathner. J. (1984). Complication, consent and cognitions in sex between children and adults. International Journal of Law and Psychiatry. 7. 89-103.
Abel. G.G.. Gore. D.K.. Holland. C.L.. Camp. N. Becker. J.V.. Rathner. J. (1989). The measurement of the cognitive distortions of child molesters. Annals of Sex Research. 137-152.
Archer. R_. Krishnamurthy. R. (1993). A review of MMP1 and Rorschach interrelationships in adult samples. Journal of Personality Assessment. 61(2). 277-293.
Adair, H., Wagner, E. (1992). Stability of unusual verbalizations on the Rorschach for outpatients with schizophrenia. Journal of Clinical Psychology. 48(2). 250-256.
Agresti, A., Finlay. B. (1986). Statistical methods for the social sciences. San Francisco: Dellen Publishing Company.
American Psy chiatric Association (1987). Diagnositic and Statistical Manual of Mental Disorder. Third Edition. Revised. Washington. D.C.: American Psychiatric Association Press.
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorder, Fourth Edition. Washington. D.C.: American Psychiatric Association Press.
Bam'. J.. Blyth. D.. Albrecht. R. (1952). Relationships between Rorschach scores and adjustment level. Journal of Consulting Psychology. 16. 30-36.
Baumeister. R. (1991). Escaping the self. New York: Basic Books.
Baumeister. R. (1990). Suicide as escape from the self. Psychological Review. 97. (1). 90-113.
Baumeister. R. (1988). Masochism as escape from the self. Journal of Sex Research. 25. 28-58.
Baumeister. R. (1989). Masochism and the self. Hillsdale. NJ.: Earlbaum.
Beck, A. & Weishaar, M. (1989). Cognitive Therapy. In A. Freeman. K. Simon. L. Beutler (Eds.) Comprehensive Handbook of Cognitive Therapy. New York: Plenum Press.
Berry, J. (1992). Lead us not into temptation: Catholic priests and the sexual abuse of children: New York: Doubleday.
Blatt, S., Brenneis, C., Schimek, J.. Glick, M. (1976). Normal development and psychopathological impairment of the concept of the object on the Rorschach. Journal of Abnormal Psy chology. 85. (4), 364-373.
Blatt. S.. Ritzier, B. (1974). Thought disorder and boundary disturbance in psychosis. Journal of Consulting and Clinical Psychology. 42. 370-381.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
70
Brehin. S. & Smith, T. (1986). Social psychological approaches to psychological and behavior change. In SL. Garfield & A.E. Bergin (Eds.), Handbook of psychotherapy and behavior change. 69-117. New York: Wiley.
Burns. D. (1981). Feeling good. New York: Penguin Books.
Carnes. P. (1983). Out of the Shadows: Understanding sexual addition. Minneapolis: Compcare.
Carnes, P. (1987). Sexual Addiction: Implications for spiritual formation. Studies in Formative Spirituality. 8 (2). 165-174.
Carnes. P. (1989). Contrary to love. Minneapolis: Compcare.
Carnes. P. (1991). Don’t call it love: Recovering from sexual addiction. New York: Bantam.
Carnes. P. (1996). Addiction or compulsion: politics or illness: Sexual Addiction &Compulsivitv. 3. (2). 127-150.
Carver. C. & Scheier. M. (1982). Control theory: A useful conceptual framework for personality- social, clinical, and health psychology'. Psychological Bulletin. 92. 111-135.
Carver. C. & Scheier. M. (1990). Origins and functions of positive and negative affect: A control-process view. Psychological Review. 97. (1), 19-35.
Choca. J.. Shanley. L.. Van Denburg, E. (1992). Interpretative guide to the Millon Clinical Multiaxial Inventory. Washington DC: American Psychological Association.
Coleman. E. (1988). Sexual Compulsivity: Definition, etiology, and treatment considerations. In E. Coleman (E d.) Chemical Dependency and Intimacy Dvsfuncion. New York: The Haworth Press.
Coleman. E.. (1992). Is your patient suffering from Compulsive Sexual Behavior? Psychiatric Annals. June. 22 (6), 320-325.
Cronbach. L.J. & Meehl. P.E. (1955). Construct validity in psychological tests. Psychological Bulletin. 52. 281-302.
Dies. R. (1995). Subject variables in Rorschach research. In John E. Exner (Ed.), Issues and methods in Rorschach research. 99-121.Mahwah, New Jersey: Lawrence Erlbaum Associates.
Duval. Shelly. & Wicklund, Robert. (1987). A theory of objective self awareness. New York: Academic Press.
Earle. R. & Crow, G. (1990). Sexual Addiction: Understanding and treating the phenomenon. Contemporary Family Therapy. 12 (2). 89-104.
Exner. J.J. (1974). The Rorschach: A comprehensive system. Volume 1. New York: Wiley'.
Exner. J. J. (1991). The Rorschach: A comprehensive svstem. Volume 2: Interpretation (2nd edition). New York: Wiley.
Exner. J. J. (1993). The Rorschach: A comprehensive svstem. Volume 1: Basic foundations (3rd edition). New York: Wiley.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
71
Exner. J., Armbruster. G.. Viglione. D. (1978). The temporal stability of some Rorschach features. Journal of Personality Assessment 42. 474-482.
Exner, J. & Murillo. L. (1975).Early prediction of post hospitalization relapse. Journal of Psychiatric Research. 12. 231-237.
Exner. J. & Sanglade. A. (992). Rorschach changes following brief and short term therapy. Journal of Personality Assessment 59. 59-71.
Exner. J. & Weiner. I. (1982). The Rorschach: A comprehensive system, volume 3. assessment of children and adolescents. New York: Wiley.
Exner, J. & Wylie. J. (1977). Some Rorschach data concerning suicide. Journal of Personality Assessment 41. 339-348.
Festinger, L. (1957). A theory of cognitive dissonance. Evanston. II: Row Peterson.
Fisk, D. & Baughman, E. (1958). The relationship between Rorschach scoring categories and the total number of responses. Journal of Abnormal and Social Psychology. 48. 25-30.
Green. R. (1991). The MMPI-2/MMPI an interpretive manual. Needham Heights: Allvn andBacon.
Greenwald, D. (1990). An external construct validity study of Rorschach personality variables. Journal of Personality Assessment 55. (3&4). 768-780.
Griffin-Shelly. E.. Benjamin, L.. Benjamin. R. (1995). Sex addiction and dissociation. Sexual Addiction & Compulsivitv. 2. (4). 295-306.
Groth-Mamet G. (1990). Handbook of psychological assessment. New York: Wiley.
Goodman. A. (1993). Diagnosis and treatment of sexual addiction. Journal of Sex & Marital Therapy. 19 (3). 225-251.
Holaday. M. & Wittenberg, T. (1994). Rorschach responding in children and adolescents who have been severely burned. Journal of Personality Assessment 62. (2). 269-279.
Heider. F. (1958). The psvcholoev of interpersonal relations. New York: Wiley.
Henderson. M.C.. Kalichman, S.C. (1990). Sexually deviant behavior and schizotypv: a theoretical perspective with supportive data. Psychiatric Quarterly. 61. (4). 273-284.
Higgins, E.T. (1987). Self-discrepancy: A theory relating self and affect. Psychological Review. 94,319-340.
Hull, J.G. (1981). A self-awareness model of the causes and effects of alcohol consumption. Journal of Abnormal Psychology. 90. (6). 586-600.
Irons, R. & Laaser, M. (1994). The abduction of fidelity: Sexual exploitation by clergy - Experience with inpatient assessment. Sexual Addiction & Compulsivitv. l.(2). 119-129.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
72
Irons. R. & Schneider. J. (1994). Sexual addiction: Significant factor in sexual exploitation by health care professionals. Sexual Addiction & Compulsivitv L 3. 198-214.
Kaclichman, S.C. (1991). Psychopathology and personality characteristics of criminal sexual offenders as a function of victim age. Archives of Sexual Behavior. 20. (2). 187-197.
Keddy. P.. Erdberg, P., Sammon, S. (1990). The psychological assessment of Catholic clergy and religious referred for residential treatment. Pastoral Psychology. 38 (3). 147- 159.
Kennedy. E., Heckler. V.. Kobler, F., Walker R. (1977). Clinical assessment of a profession: Roman Catholic clergymen. Journal of Clinical Psychology. 33 (1). 120-128.
Kraft-Ebbing. R. Psvchonathia sexualis (F.J. Rebman translation). New York, Paperback Library. 1965 (first edition. 1886).
Laaser. M. (1991). Sexual addiction by clergy. Pastoral Psychology. 39. 213-235.
Levin. S.M.. Stava. L. (1987). Personality characteristics of sex offenders: a review. Archives of Sexual Behavior. 16. (1). 54-67.
Levine. M. Meltzoff. J. (1956). Cognitive inhibition and Rorschach movement responses. Journal of Consulting Psychology. 20. (2). 119-122.
Meltzer, H. (1944). Personality differences between stuttering and non-stuttering children as indicated by the Rorschach Test. The Journal of Psychology. 17. 49-59.
Meloy, J.R., Gracono, C.B., Kenny. L. (1994). A Rorschach investigation of sexual homicide. Journal of Personality Assessment 62. fl). 58-67.
Meyer. G.J. (1996). Construct validation of scales derived from the Rorschach Method: A review of issues and introduction to the Rorschach Rating Scale. Journal of Personality' Assessment 67 (3). 598- 628.
Money. J. (1986). Love mans: Clinical concepts of sexual/erotic health and pathology. Paraphilia, and gender transportation in childhood, adolescence, and maturity. New York: Irvington Press.
Netter, B„ Viglione, D.(1994) An empirical stud)’ of malingering schizophrenia on the Rorschach. Journal of Personality Assessment 62(1). 45-57.
Pennebaker, J.W. (1989). Stream of consciousness and stress: Levels of thinking. In J.S. Uleman & J.A Bargh (Eds.), The direction of thought: Limits of awareness, intention, and control. 327-350.
PiotrowskL Z. (I960). The movement score. In M. Rickers-Ovsiankina (Ed.) Rorschach Psychology. New' York: Wiley.
Quadland, M. (1985). Compulsive sexual behavior: Definition of a problem and an approach to treatment. Journal of Sex & Marital Therapy. 11 (2). 121-132.
Ritzier, B., Exner. J. (1995). Special issues in subject selection and design. In John J. Exner (Ed.) Issues and methods in Rorschach research. Mahway, New Jersey:Lawrence Erlbaum Associates. 123-143.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
73
Robinson . E. Montana. S.. Thompson. G. (1993). A descriptive study of sexually troubled clergy. PaDer Dresented at 13th annual ASTA Conference: Boston. 1993.
Robinson. E.. Greer, J., Estadt B.. Thompson. G. (1994). Shadows of the lantern bearers: a studv of sexually troubled clergy. Ann Arbour. MI: UMI Dissertation Sendees.
Robinson, T. & Valcour, F. (1995). The use of depo-provera in the treatment of child molesters and sexually compulsive males. Sexual addiction & Compulsivitv. 2. (4). 227-234.
Schwartz. M. (1995). Victim to Victimizer. Sexual Addiction & Compulsivitv. 2. (2). 81-88.
Shedler, J., Mayman. M.. Manins. M„ (1993). The illusion of mental health. American Psychologist 48 (11). 1117-1131.
Sipe. A.W. R. (1990). A secret world: Sexuality and the search for celibacy. New York: Brunner/ Mazel. Inc.
Sipe, A.W. R. (1994). The problem of sexual trauma and addiction in the catholic church. Sexual Addiction & Compulsivitv. 1. 2. 130-137.
Sommer, R. & Sommer. D. (1958). Assaultiveness and two types of Rorschach color responses. Journal of Consulting Psychology, 22. 57-62.
Syder, M. (1987). Public appearances private realities. New York: W.H. Freeman Company.
Taylor, G. (1996). An empirical comparison of intermittent and compulsive sexually exploitative clergy. Unpublished Doctoral Dissertation. Loyola College.
Vallacher, R. & Wegner, D. (1985). A theory of action identification. Hillsdale. NJ: Erlbaum.
Vallacher. R. & Wegner, D.(1987). What do people think they’re doing: Action identification and human behavior. Psychological Review. 94. 3-15.
Wald, B., Archer, R.. Winstead, B. (1990). Rorschach characteristics of mothers of incest victims. Journal o f Personalitlv Assessment 55. (3&4), 417-424.
Ward, T., Hudson. S.M., Marshall, W.L. (1995). Cognitive distortions and affective deficits in sex offenders: a cognitive deconstructionist interpretation. Sexual Abuse: A Journal of Research and Treatment 7. (1). 67-83.
Weiner, I. & Exner. J. (1991). Rorschach changes in long-term and short-term psychotherapy. Journal of Personality Assessment 56. 453-465.
Weiner. I. (1995). Methodological considerations in Rorschach research. Psychological Assessment 7(3). 330-337.
Weiner, I. (1991). Editor’s note: interscorer agreement in Rorschach research. Journal of Personality Assessment 56. 1.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.