Influence of the proportion of particulate autogenous bone graft/platelet-rich plasma on bone...
7
Influence of the proportion of particulate autogenous bone graft/platelet-rich plasma on bone healing in critical-size defects: An immunohistochemical analysis in rat calvaria Maria Nagata a, ⁎, Michel Messora a , Roberta Okamoto b , Natália Campos a , Natália Pola a , Luis Esper a , Michyele Sbrana a , Stephen Fucini a,c , Valdir Garcia a , Alvaro Bosco a a Division of Periodontics, Department of Surgery and Integrated Clinic, Dental School of Araçatuba, São Paulo State University–UNESP, Brazil b Division of Oral and Maxillofacial Surgery, Department of Surgery and Integrated Clinic, Dental School of Araçatuba, São Paulo State University–UNESP, Brazil c Private Practice, Hanover, NH, USA abstract article info Article history: Received 25 November 2008 Revised 18 April 2009 Accepted 22 April 2009 Available online xxxx Edited by: R. Rizzoli Keywords: Bone regeneration Growth factors Platelets Immunohistochemistry Osteoblasts This immunohistochemical analysis evaluated the influence of the proportion of particulate autogenous bone (AB) graft/platelet-rich plasma (PRP) on bone healing in surgically created critical-size defects (CSD) in rat calvaria. 25 rats were divided into 5 groups: C (control), AB, AB/PRP-50, AB/PRP-100 and AB/PRP-150. A 5 mm diameter critical-size defect was created in the calvarium of each animal. In Group C, defect was filled by blood clot only. In Group AB, defect was filled with AB graft. In Groups AB/PRP-50, AB/PRP-100 and AB/ PRP-150, defects were filled with AB graft combined with 50, 100 and 150 μl of PRP, respectively. Animals were euthanized at 30 days post-operative. Osteocalcin (OC) and osteopontin (OP) immunohistochemical staining were performed. OP-positive and OC-positive cells were quantified. The amount of vital bone (VBA) and remaining bone graft particles (RPA) were calculated as percentage of the total area of the original defect. Data were statistically analyzed (ANOVA, Tukey, p b 0.05). Group AB/PRP-100 presented a significantly higher number of OP-positive cells than groups C, AB/PRP-50 and AB/PRP-150 (p b 0.05) and also a significantly higher number of OC-positive cells than all of the other groups (p b 0.05). The number of OP-positive cells in Group AB/PRP-150 was significantly lower than in Group AB (p b 0.05). Statistically significant differences were not found between groups with regard to either VBA or RPA (p N 0.05). However, clear trends were indicated by an increase in VBA in Group AB/PRP-100 when compared to groups C, AB and AB/PRP-150 and an increase in RPA in Group AB/PRP-150 when compared to groups AB, AB/PRP-50 and AB/PRP-100. The proportion AB graft/PRP seems to influence bone healing in CSD in rat calvaria. The highest expression of osteocalcin and osteopontin, and thus the most developed healing, was found in Group AB/PRP-100 indicating that there may be an optimal proportion beyond which increasing the concentration PRP is deleterious. © 2009 Elsevier Inc. All rights reserved. Introduction Researchers continuously strive to improve bone grafting techni- ques and to provide the means to obtain a faster and denser bony regeneration. Marx et al. [1] have proposed the use of platelet-rich plasma (PRP) to obtain faster maturation of autogenous bone grafts. The main rationale for adding PRP to bone grafts is that high con- centrations of platelets in a bony wound will increase the local con- centration of secreted growth factors and subsequently enhance the initial bone healing response [2]. Later on, the direct influence of PRP will fade away and physiological mechanisms of bone repair will continue to work on an accelerated level [3]. However, while some authors have found significant increases in bone formation and matu- ration rates [1,4–6], others have not observed any improvement [7–10]. Inconsistent results found in various studies may, in part, be due to their use of different ratios of PRP to bone graft [11]. A literature review failed to find a rationale to justify the selection of a specific PRP to bone graft ratio. Marx et al. [1] used approximately 70 ml of PRP combined with autogenous bone graft to treat mandibular defects 50 mm in diameter or larger. Mazor et al. [12] and Robiony et al. [13] used 8 ml of PRP to treat osseous defects with different sizes and shapes. Volumes of 1–1.5 ml, 0.5 ml and 3– 4 ml have been reported in studies conducted in rabbits by Aghaloo et al. [7] and Butterfield et al. [14] and in sheep by Jakse et al. [3]. Even though these clinical and animal studies have reported the volume of PRP, they have not described the volume of autogenous bone graft used. Therefore, the proportion of autogenous bone graft/ PRP cannot be calculated. To date, there is no study that has eval- Bone xxx (2009) xxx–xxx ⁎ Corresponding author. Rua José Bonifácio, 1193, CEP: 16015-050 Araçatuba, SP, Brazil. Fax: +55 3636 3332. E-mail address: [email protected] (M. Nagata). BON-08455; No. of pages: 7; 4C: 8756-3282/$ – see front matter © 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.bone.2009.04.246 Contents lists available at ScienceDirect Bone journal homepage: www.elsevier.com/locate/bone ARTICLE IN PRESS Please cite this article as: Nagata M, et al, Influence of the proportion of particulate autogenous bone graft/platelet- ^ rich plasma on bone healing in critical- ^ size defects ^ : An immunohistochemical analysis in rat calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246
Transcript of Influence of the proportion of particulate autogenous bone graft/platelet-rich plasma on bone...

Bone xxx (2009) xxx–xxx
BON-08455; No. of pages: 7; 4C:
Contents lists available at ScienceDirect
Bone
j ourna l homepage: www.e lsev ie r.com/ locate /bone
ARTICLE IN PRESS
Influence of the proportion of particulate autogenous bone graft/platelet-richplasma on bone healing in critical-size defects: An immunohistochemical analysisin rat calvaria
Maria Nagata a,⁎, Michel Messora a, Roberta Okamoto b, Natália Campos a, Natália Pola a, Luis Esper a,Michyele Sbrana a, Stephen Fucini a,c, Valdir Garcia a, Alvaro Bosco a
a Division of Periodontics, Department of Surgery and Integrated Clinic, Dental School of Araçatuba, São Paulo State University–UNESP, Brazilb Division of Oral and Maxillofacial Surgery, Department of Surgery and Integrated Clinic, Dental School of Araçatuba, São Paulo State University–UNESP, Brazilc Private Practice, Hanover, NH, USA
⁎ Corresponding author. Rua José Bonifácio, 1193, CBrazil. Fax: +55 3636 3332.
E-mail address: [email protected] (M. Nagata)
8756-3282/$ – see front matter © 2009 Elsevier Inc. Adoi:10.1016/j.bone.2009.04.246
Please cite this article as: Nagata M, et al,healing in critical-
^size defects
^: An immuno
a b s t r a c t
a r t i c l e i n f oArticle history:Received 25 November 2008Revised 18 April 2009Accepted 22 April 2009Available online xxxx
Edited by: R. Rizzoli
Keywords:Bone regenerationGrowth factorsPlateletsImmunohistochemistryOsteoblasts
This immunohistochemical analysis evaluated the influence of the proportion of particulate autogenous bone(AB) graft/platelet-rich plasma (PRP) on bone healing in surgically created critical-size defects (CSD) in ratcalvaria. 25 rats were divided into 5 groups: C (control), AB, AB/PRP-50, AB/PRP-100 and AB/PRP-150. A5 mm diameter critical-size defect was created in the calvarium of each animal. In Group C, defect was filledby blood clot only. In Group AB, defect was filled with AB graft. In Groups AB/PRP-50, AB/PRP-100 and AB/PRP-150, defects were filled with AB graft combined with 50, 100 and 150 μl of PRP, respectively. Animalswere euthanized at 30 days post-operative. Osteocalcin (OC) and osteopontin (OP) immunohistochemicalstaining were performed. OP-positive and OC-positive cells were quantified. The amount of vital bone (VBA)and remaining bone graft particles (RPA) were calculated as percentage of the total area of the originaldefect. Data were statistically analyzed (ANOVA, Tukey, pb0.05).Group AB/PRP-100 presented a significantly higher number of OP-positive cells than groups C, AB/PRP-50and AB/PRP-150 (pb0.05) and also a significantly higher number of OC-positive cells than all of the othergroups (pb0.05). The number of OP-positive cells in Group AB/PRP-150 was significantly lower than inGroup AB (pb0.05). Statistically significant differences were not found between groups with regard to eitherVBA or RPA (pN0.05). However, clear trends were indicated by an increase in VBA in Group AB/PRP-100when compared to groups C, AB and AB/PRP-150 and an increase in RPA in Group AB/PRP-150 whencompared to groups AB, AB/PRP-50 and AB/PRP-100.The proportion AB graft/PRP seems to influence bone healing in CSD in rat calvaria. The highest expression ofosteocalcin and osteopontin, and thus themost developed healing, was found in Group AB/PRP-100 indicatingthat there may be an optimal proportion beyond which increasing the concentration PRP is deleterious.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Researchers continuously strive to improve bone grafting techni-ques and to provide the means to obtain a faster and denser bonyregeneration. Marx et al. [1] have proposed the use of platelet-richplasma (PRP) to obtain faster maturation of autogenous bone grafts.The main rationale for adding PRP to bone grafts is that high con-centrations of platelets in a bony wound will increase the local con-centration of secreted growth factors and subsequently enhance theinitial bone healing response [2]. Later on, the direct influence of PRPwill fade away and physiological mechanisms of bone repair willcontinue to work on an accelerated level [3]. However, while some
EP: 16015-050 Araçatuba, SP,
.
ll rights reserved.
Influence of the proportionhistochemical analysis in rat
authors have found significant increases in bone formation and matu-ration rates [1,4–6], others have not observed any improvement[7–10]. Inconsistent results found in various studies may, in part, bedue to their use of different ratios of PRP to bone graft [11].
A literature review failed to find a rationale to justify theselection of a specific PRP to bone graft ratio. Marx et al. [1] usedapproximately 70 ml of PRP combined with autogenous bone graft totreat mandibular defects 50 mm in diameter or larger. Mazor et al.[12] and Robiony et al. [13] used 8 ml of PRP to treat osseous defectswith different sizes and shapes. Volumes of 1–1.5 ml, 0.5 ml and 3–4 ml have been reported in studies conducted in rabbits by Aghalooet al. [7] and Butterfield et al. [14] and in sheep by Jakse et al. [3].Even though these clinical and animal studies have reported thevolume of PRP, they have not described the volume of autogenousbone graft used. Therefore, the proportion of autogenous bone graft/PRP cannot be calculated. To date, there is no study that has eval-
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246

2 M. Nagata et al. / Bone xxx (2009) xxx–xxx
ARTICLE IN PRESS
uated the influence of the proportion of autogenous bone graft/PRPon bone healing. The purpose of this immunohistochemical ana-lysis was to evaluate the influence of the proportion of particu-late autogenous bone (AB) graft/platelet-rich plasma (PRP) onbone healing in surgically created critical-size defects (CSD) in ratcalvaria.
Material and methods
Experimental model
The experimental protocol was approved by the São Paulo StateUniversity–UNESP, Dental School of Araçatuba Institutional AnimalCare and Use Committee. Twenty five, 5 to 6-month-old, male rats(Rattus norvegicus, albinus, Wistar) weighing 450 to 500 g (UNESP,Dental School of Araçatuba, Animal Care Unit) were used. The ratswere kept in a roomwith a 12 hour light/dark cycle and temperaturebetween 22 and 24 °C. They were randomly assigned to one of 5experimental groups: Group C (control), Group AB, Group AB/PRP-50,Group AB/PRP-100 and Group AB/PRP-150.
Surgical procedure
The rats were anesthetized by an intramuscular injection ofxylazine (6 mg/kg body weight) and ketamine (70 mg/kg bodyweight). After aseptic preparation, a semilunar incision was made inthe scalp in the anterior region of the calvarium, allowing reflection ofa full-thickness flap in a posterior direction. A 5 mm diameter critical-size defect was made with a trephine used in a low-speed handpieceunder continuous sterile saline irrigation. The defect included aportion of the sagittal suture.
One L-shaped mark was made 2 mm anterior and one 2 mmposterior to the margins of the surgical defect using a small taperedcarbide fissure bur and a surgical stent. The long axes of the L-shapedmarks were located on the longitudinal axis bisecting the surgicaldefect. The marks were filled with amalgam. Their purpose was toallow identification of the center line of the original defect duringlaboratory processing and also to be used as references to accuratelylocate the original bone margins of the surgical defect during immu-nohistochemical analysis.
In Group C, the surgical defect was filled with a blood clot only. InGroup AB, the defect was filled with 0.01 ml of particulate autogenousbone graft. In Groups AB/PRP-50, AB/PRP-100 and AB/PRP-150, thedefects were filled with 0.01 ml of particulate autogenous bone graftcombined with 50, 100 and 150 μl of PRP, respectively. Autogenousbone obtained from the calvarium during creation of the surgicaldefect was prepared in a bone mill. The bone was grounded to aparticle size of 172.0 to 210.5 μm. The soft tissues were then repo-sitioned and sutured to achieve primary closure. Each animal receivedan intramuscular injection of 24,000 IU of penicillin G-benzathine(Pentabiótico⁎ Veterinário Pequeno Porte, Fort Dodge® Saúde AnimalLtda., Campinas, SP, Brazil) postsurgically.
PRP preparation
A 3.15 ml volume of autologous blood was drawn from eachanimal, via cardiac puncture, into a syringe containing 0.35 ml of 3.2%sodium citrate to prevent coagulation. The blood sample wascentrifuged at 160 g for 20 min at 22 °C to separate the plasmacontaining the platelets from the red cells. The plasma was drawn offthe top and centrifuged at 22 °C for an additional 15 min at 400 g toseparate the platelets. The platelet-poor plasma was then drawn offthe top, leaving the platelet-rich plasma and buffy coat. Then, thebuffy coat and platelet-rich plasma (0.35 ml) were re-suspended,activated and used within minutes. A 10% solution of calcium chloride(Calcium Chloride 10% Solution, ScienceLab.com Inc., Houston, TX,
Please cite this article as: Nagata M, et al, Influence of the proportionhealing in critical-
^size defects
^: An immunohistochemical analysis in rat
USA) was used to activate PRP samples (0.05 ml of calcium chloridefor each 1 ml of PRP).
Platelet counts
Brecher liquid was used to lyse the erythrocytes and dilute thewhole blood and PRP samples. The platelets in the dilutedwhole bloodand PRP samples were then countedmanually in a Neubauer chamber.In addition, PRP and whole blood smears were stained with “PanóticoRápido LB” (LaborClin, Pinhais, PR, Brazil) in order to assess themorphology of the platelets. The platelet counts and the analysis of theplatelet morphology were performed by a veterinary hematologist.
Tissue processing
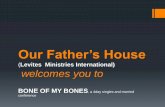
All animals were euthanized at 30 days post-operative. The areaof the original surgical defect and the surrounding tissues wereremoved en bloc. The blocks were fixed in 10% neutral formalin, rinsedwith water and then decalcified in 18% ethylenediaminotetraaceticacid (EDTA) solution. After initial decalcification, each specimen wasdivided longitudinally into two blocks exactly along the center line ofthe original surgical defect using the long axis of both L marks asreferences. Transverse cuts were then made using the short axis ofeach L mark as references. Each specimen then measured 9 mm inlength along the longitudinal axis running through the center of thedefect, allowing for precise identification of the original surgical defectmargins during image analysis procedure (Fig. 1). Following addi-tional decalcification, they were processed and embedded in paraffin.Serial sections 6 μm thick were cut in a longitudinal direction startingat the center of the original surgical defect and then subjected toimmunohistochemical reactions using the immunoperoxidase detec-tion method. In addition, bone samples were recovered from anuntreated area of the frontal skull. These samples were also subjectedto immunohistochemical reactions to determine the basal expressionof the evaluated markers in the original bone (OB) of the calvariumwithout surgery.
Osteocalcin (OC) and osteopontin (OP) immunohistochemicalstaining were performed in all specimens. OP and OC are extracelullarmatrix proteins synthesized and secreted during the process of osteo-blast differentiation and mineralization [15]. While OP is an early andeffective marker of bone formation, OC indicates the later phase ofbone formation [15].
The following primary antibodies were used: anti-OC and anti-OPproduced in goats (Santa Cruz Biotechnology, Santa Cruz, CA, USA).Titling of primary antibodies was standardized before the ex-periments. The primary antibodies with 1:100 titling showed thebest immunolabeling. The biotynilated rabbit anti-goat (Pierce Bio-technology, Rockeford, IL, USA) were used as secondary antibodies atthe titling of 1:200. The StreptABComplex/HRP (Dako, Carpinteria, CA,USA) was then used to amplify the signal of the reaction developedwith Diaminobenzidine (Dako, Carpinteria, CA, USA) as the chromo-gen. The procedure was completed by nuclear counterstaining usinghematoxylin. All samples were accompanied by a negative control.
Image analysis procedure
The most central histological section of each surgical defectwas selected. The image analysis was performed by a calibratedexaminer blinded with respect to the treatment rendered. Theimages of the histologic sections were captured by a digital cameraconnected to a light microscope with an original magnification of×160. The digital images were saved on a computer. A compositedigital image was then created by combining 8 smaller imagesbecause it was not possible to capture the entire defect in one imageat the level of magnification that was used. The composite image wascreated based on anatomic reference structures (e.g. blood vessels
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246
Fig. 1. (A) Longitudinal cut along the center line (Y) of critical-size defect; (B) transverse cuts (X); (C) dimensions of specimen to be embedded in paraffin.
3M. Nagata et al. / Bone xxx (2009) xxx–xxx
ARTICLE IN PRESS
and bone trabeculae) within each of the histologic sections. The“ImageLab 2000” software (Diracon Bio Informática Ltda., VargemGrande do Sul, SP, Brazil) was used for the image analysis.
The following criteria, based on thework of Messora et al. [6], wereused to standardize the analyses of the digital images:
1) The total area (TA) to be analyzed corresponded to the entirearea of the original surgical defect. This area was determined byfirst identifying the external and internal surfaces of the originalcalvarium at the right and left margins of the surgical defect,and then connecting them with lines drawn following their res-pective curvatures. Considering the total length of the histologic
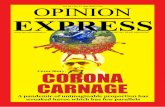
Fig. 2. Group AB/PRP-100—expressions of osteopontin (A) and osteocalcin (B); Group C—exporiginal magnification ×400). Osteopontin=arrow head; Osteocacin=arrow. DAB=diami
Please cite this article as: Nagata M, et al, Influence of the proportionhealing in critical-
^size defects
^: An immunohistochemical analysis in rat
specimen, 2 mm were measured from the right and left edges ofthe specimen towards the center in order to determine themargins of the original surgical defect.
2) OP-positive and OC-positive cells (bone lining cells and osteo-cytes) were quantified within the confines of the TA. Thespecificity of the immunocytochemical localization was verifiedby the absence of staining in all negative control preparations.
3) The vital bone area (VBA) and the remaining bone graft particlesarea (RPA) were delineated within the confines of the TA. TA wasmeasured in mm2 and was considered 100% of the area to beanalyzed. The VBA and RPA were also measured in mm2 andcalculated as a percentage of TA.
ressions of osteopontin (C) and osteocalcin (D) (DABwith hematoxylin counterstaining;nobenzidine.
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246

Fig. 3. Expressions of osteopotin in Group AB (A), Group AB/PRP-50 (B) and Group AB/PRP-150 (C). Expressions of osteocalcin in Group AB (D), Group AB/PRP-50 (E) and GroupAB/PRP-150 (F) (DAB with hematoxylin counterstaining; original magnification ×400). Osteopontin=arrow head; Osteocalcin=arrow. DAB=diaminobenzidine.
4 M. Nagata et al. / Bone xxx (2009) xxx–xxx
ARTICLE IN PRESS
Statistical analysis
The data normality and homogeneity of variances were verified.Each parameter (whole blood platelet count, PRP platelet count,number of OP-positive cells, number of OC-positive cells, VBA andRPA) was evaluated separately. The significance of differences bet-ween groups was determined by an analysis of variance (ANOVA),followed by a post hoc Tukey's test when the ANOVA suggested asignificant difference between groups (pb0.05).
Results
All animals tolerated the surgical procedures well and werehealthy during the entire experimental period.
Platelet count study
The platelets exhibited normal morphology. Platelet counts con-firmed that the PRP preparation technique used in this study producedsamples of highly concentrated platelets. The PRP smears showed
Fig. 4.Mean number of platelets per microliter (μl) and standard deviations in the samples ofstatistically significant at pb0.05. AB=autogenous bone; PRP=platelet-rich plasma.
Please cite this article as: Nagata M, et al, Influence of the proportionhealing in critical-
^size defects
^: An immunohistochemical analysis in rat
higher concentrations of platelets than the whole blood smears. Theaverage whole blood platelet count was 465.803±93.46×103 plate-lets/μl while the average PRP platelet countwas 2611.80±313.34×103
platelets/μl. Thus, the concentration of the platelets in the PRP wasmore than 5 times greater than that of the whole blood.
Qualitative immunohistochemical analysis
All groups presented positive immunolabels for OP and OC (Figs. 2and 3). Except for Group C, all the other groups showed an increase inthe expression of OP and OC when compared to the original bone(OB). Positive immunolabels for OP and OC were observed in the bonegraft particles, newly formed bone and connective tissue. The highestexpression of both proteins occurred in Group AB/PRP-100 (Figs. 2Aand B) while the lowest expression was observed in Group C (Figs. 2Cand D). Groups AB and AB/PRP-50 (Figs. 3A, B, D and E) demonstratedsimilar expressions of these proteins which were greater than thatseen in Group AB/PRP-150 (Figs. 3C and F). Most bone graft particlesthroughout the surgical defect were not surrounded by bone liningcells positive for OP and OC in Group AB/PRP-150.
PRP of groups AB/PRP-50, AB/PRP-100 and AB/PRP-150. Analysis of variance. Nonewas
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246

Table 1Mean (±SD) of OP-positive and OC-positive cells within the surgically created defect and in the original calvaria bone with comparison among groups.
Protein OB C AB AB/PRP-50 AB/PRP-100 AB/PRP-150
OP 76±60.8 16.4±14.4a 350.6±82.1b 320.3±53.4 642.5±234.1c 124±73.07OC 101.5±43.1 24.40±11.0 278±100.1 294±129.2d 735.3±224.4e 164.8±131.8
Comparisons for OP: acompared to AB/PRP-50 and AB/PRP-100 (pb0.05); bcompared to OB and AB/PRP-150 (pb0.05); ccompared to OB, C, AB-PRP-50 and AB/PRP-150 (pb0.05).Comparisons for OC: dcompared to C (pb0.05); ecompared to OB, C, AB, AB/PRP-50 and AB/PRP-150 (pb0.05).OP=osteopontin; OC=osteocalcin; OB=original bone; C=control; AB=autogenous bone; PRP=platelet-rich plasma; SD=standard deviations.
5M. Nagata et al. / Bone xxx (2009) xxx–xxx
ARTICLE IN PRESS
Statistical analysis
No significant differences (pN0.05) were observed in either thewhole blood or PRP platelet count among groups AB/PRP-50, AB/PRP-100 and AB/PRP-150 (Fig. 4).
A detailed description of the immunohistochemical data is given inTable 1. In summary, the results can be described as follows:
OP-positive cells. Groups AB and AB/PRP-100 presented asignificant increase in the number of OP-positive cells whencompared to OB (pb0.05). Group AB/PRP-100 also presented asignificantly higher number of OP-positive cells than groups C, AB/PRP-50 and AB/PRP-150 (pb0.05). The number of OP-positive cellsin Group AB/PRP-150 was significantly lower than in Group AB(pb0.05) (Table 1).OC-positive cells. Group AB/PRP-100 presented a significantincrease in the number of OC-positive cells when compared toOB (pb0.05). Group AB/PRP-100 also presented a significantlyhigher number of OC-positive cells than groups C, AB, AB/PRP-50and AB/PRP-150 (pb0.05) (Table 1).
Means and standard deviations of VBA and RPA for all groups aredocumented in Fig. 5. Statistically significant differences were notfound between groups with regard to either VBA or RPA (pN0.05).
Discussion
Although the biological rationale for the use of PRP to enhancebone formation is theoretically sound, the precise methodology thatwill result in the optimal benefit from this therapy has yet to beelucidated [16]. The present immunohistochemical analysis evaluatedthe influence of the proportion of particulate autogenous bone graft/PRP in the expression of bone matrix proteins.
Matrix proteins define the specific properties of mineralizedtissues and are expressed in a tightly controlled fashion. Theirsequential expression depends on the location and differentiation
Fig. 5. Means of VBA and RPA (% of total defect area) and standard deviations for
Please cite this article as: Nagata M, et al, Influence of the proportionhealing in critical-
^size defects
^: An immunohistochemical analysis in rat
stage of the producing cells [17]. In vitro and in vivo studies havedemonstrated that PRP may modulate the expression of some bonematrix proteins depending on the concentration of platelets used[16–18]. This study demonstrated that PRP samples with similarplatelet concentrations (platelets per μl) may produce differentpatterns of OP and OC expression. These results may possibly beattributed to two factors. The first factor is the variations in the levelsof growth factors (GFs). This hypothesis is based on the results ofother studies that have shown differences in the levels of GFs in PRPsamples with similar platelet concentrations [19–21]. The secondfactor is the variation in the volume of PRP used in the differentexperimental groups in the present study. When a small amount ofbone graft is mixed with a large volume of PRP the bone cells in boththe autograft and adjacent tissue are exposed to high concentrationsof PRP. In an in vitro study, Choi et al. [11] showed that the viabilityand proliferation of alveolar bone cells are stimulated by low butsuppressed by high concentrations of PRP. According to these authors,dilution of the PRP concentration to a level suitable for cellproliferation may be necessary to enhance bone cell growth withinthe treated bone graft. In the present study, the number of OP-positive cells in Group AB/PRP-150 was significantly lower than inGroup AB. Therefore, since OP is related to osteoblast function [16,22],this seems to indicate that the larger volume of PRP used in GroupAB/PRP-150 had a cytotoxic effect on the healing of autogenous bonegraft. This result corroborates the findings of Choi et al. [11]. It isimportant to emphasize that a decrease in VBA and an increase in RPAin Group AB/PRP-150 when compared to groups AB, AB/PRP-50 andAB/PRP-100 indicates a clear trend, although the differences were notstatistically significant. These findings suggest an impaired bonehealing in Group AB/PRP-150.
Another aspect that should be taken into consideration to explainthe results observed in the present study is the possibility that thedifferent volumes of PRP may have influenced the bioavailability ofGFs. The efficiency of GFs in enhancing bone regeneration is likely tobe dependent on their dosage, spatial distribution and temporalrelease [23]. In this study, a smaller volume (Group AB/PRP-50) may
all groups. VBA=vital bone area; RPA=remaining bone graft particles area.
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246

6 M. Nagata et al. / Bone xxx (2009) xxx–xxx
ARTICLE IN PRESS
have presented an insufficient amount of GFs during bone healing. Arecent in vivo study [24] supports, in part, this hypothesis. Histologicanalyses were conducted to determine whether the healing of full-thickness skin wounds in rabbits can be accelerated by differentvolumes of PRP [24]. When a small volume was used, the PRP seemedto have no effect onwound healing. One possible explanation given bythe authors was the inability of this volume to cover the woundcompletely. In addition, a smaller volume would contain less GFs.
In the present study, Group AB/PRP-100 presented a significantincrease in the number of OC-positive cells when compared to AB. Thisresult corroborates the findings of Thowarth et al. [15]. These authorsdemonstrated that autogenous bone grafts with PRP presented highervalues of OC than the grafts without PRP at 2 and 4 weeks post-operative. The higher number of OC-positive cells in Group AB/PRP-100 suggests an earlier calcification of the newly formed bone in thisgroup, since OC indicates the mineralization process in boneformation implemented by the calcification of the osteocytes in thecollagen layer [15]. With regard to the number of OP-positive cells,significant differences were not observed between groups AB/PRP-100 and AB. A possible explanation for this result may be related to theperiod of observation selected in the present study (30 days post-operative), since OP is an early marker of bone formation. In the studyconducted by Thorwarth et al. [15], the effects of PRP on theexpression of bone matrix proteins were identified particularly inthe early phase (2 weeks post-operative). It is important to considerthat complete detection of OP may have been hampered because itsproduction is almost undetectable in osteoblasts actively expressingOC [17,25].
In the present study, Group AB/PRP-100 showed a significantlyhigher number of OP-positive cells and OC-positive cells than theportions of untreated bone of same origin (OB) at 30 days pos-operative. Thorwarth et al. [15] also demonstrated higher values ofboth proteins in autogenous bone graft combined with PRP than inuntreated bone at 4 weeks post-operative. They observed that theexpressions of OC and OP were similar to that of untreated bone at 12and 26 weeks post-operative.
The pattern of OP and OC expressions and the values of VBA andRPA observed in Group AB/PRP-100 suggest that this group had themost developed healing process. Some studies have demonstratedthat PRP may increase the proliferation of the endothelial cells [26],pre-osteoblasts [27], osteoblasts [11,28] and osteoclasts [29] in thesurgical site. It could be speculated that these PRP effects might havecontributed to the improved healing observed in Group AB/PRP-100.
One limitation in the methodology of the present study is that theimmunohistochemical staining can only indicate the presence orabsence of proteins in the bone matrix. Therefore, it is impossible todistinguish between proteins expressed before surgery and thoseexpressed after surgery [17]. Nevertheless, the data from this study arean important source of information since they reveal the processes ofbone formation on a qualitative level.
Besides the biological effects of PRP on the healing of autogenousbone grafts, it is also important to take into consideration that twofactors may directly influence the incorporation of bone grafts. Thefirst is the type of bone graft used. The bone grafts used in the presentstudy were mainly cortical bone. This type of bone revascularizesmore slowly than cancellous bone [30]. Consequently, the incorpora-tion of cortical bone grafts is slower than that of cancellous bonegrafts. Over time, cancellous grafts are completely replaced bycreeping substitution, whereas cortical grafts remain an admixtureof necrotic and viable bone for prolonged periods of time [31]. Thesecond is the size of the bone graft particles used. In a study conductedin rabbits, the early stages of bone regeneration were influenced bythe particle size of autogenous bone grafts [32]. The total volume ofnewly formed bone in defects with small particles was larger andmore mature compared to defects with large particles after 2 and4weeks [33]. However, it is important to point out that there are limits
Please cite this article as: Nagata M, et al, Influence of the proportionhealing in critical-
^size defects
^: An immunohistochemical analysis in rat
to the reduction of graft particle size. A study conducted in monkeysshowed that the size of the bone particles should exceed 125 μm toprevent removal by macrophages [34]. The size of the graft particlesused in the present study was between 172 and 210 μm.
One of drawbacks of the present study was that the small samplesize, coupled with the relatively high covariance, led to statisticaloutcomes that might not have been sensitive enough to detect thedifferences between the experimental treatments in all instances.Additional studies with larger sample sizes should be conducted toimprove statistical sensitivity and to investigate possible relationshipsbetween two of the variables (VBA and RPA) and the numbers of OC-and OP-positive cells for each group.
Within the limits of this study, it can be concluded that theproportion autogenous bone graft/PRP seems to influence bonehealing in CSD in rat calvaria. The highest expression of osteocalcinand osteopontin, and thus the most developed healing, was found inGroup AB/PRP-100 indicating that there may be an optimal propor-tion beyond which increasing the concentration PRP is deleterious.
Acknowledgments
Natália de Campos received a scholarship from São Paulo StateFoundation for Research (FAPESP: 06/58094-7).
References
[1] Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR.Platelet-rich plasma: growth factor enhancement for bone grafts. Oral Surg OralMed Oral Pathol Oral Radiol 1998;85:638–46.
[2] Plachokova AS, Nikolidakis D, Mulder J, Jansen JA, Creugers NH. Effect of platelet-rich plasma on bone regeneration in dentistry: a systematic review. Clin OralImplants Res 2008;19:539–45.
[3] Jakse N, Tangl S, Gilli R, Berghold A, Lorenzoni M, Eskici A, et al. Influence of PRP onautogenous sinus grafts. An experimental study on sheep. Clin Oral Implants Res2003;14:578–83.
[4] Fennis JP, Stoeling PJ, Jansen JA. Mandibular reconstruction: a histological andhistomorphometric study on the use of autogenous scaffolds, particulate cortico-cancellous bone grafts and platelet rich plasma in goats. Int J Oral Maxillofac Surg2004;33:48–55.
[5] Simon Z, Friedlich J. The use of autogenous bone grafting with platelet-rich plasmafor alveolar ridge reconstruction: a clinical report. J Calif Dent Assoc 2006;34:895–9.
[6] Messora MR, Nagata MJ, Mariano RC, Dornelles RC, Bomfim SR, Fucini SE,et al. Bone healing in critical-size defects treated with platelet-rich plasma: ahistologic and histometric study in rat calvaria. J Periodontol Res 2008;43:217–23.
[7] Aghaloo TL, Moy PK, Freymiller EG. Investigation of platelet rich plasma in rabbitcranial defects: a pilot study. J Oral Maxillofac Surg 2002;60:1176–81.
[8] Froum SJ, Wallace SS, Tarnow DP, Cho SC. Effect of platelet-rich plasma on bonegrowth and osseointegration in human maxillary sinus grafts: three bilateral casereports. Int J Periodontics Restorative Dent 2002;22:45–53.
[9] Choi BH, Im CJ, Huh JY, Suh JJ, Lee SH. Effect of platelet-rich plasma on boneregeneration in autogenous bone graft. Int J Oral Maxillofac Surg 2004;33:56–9.
[10] Gerard D, Carlson ER, Gotcher JE, Jacobs M. Effects of platelet-rich plasma on thehealing of autologous bone grafted mandibular defects in dogs. J Oral MaxillofacSurg 2006;64:443–51.
[11] Choi BH, Zhu SJ, Kim BY, Huh JY, Lee SH, Jung JH. Effect of platelet-rich plasma(PRP) concentration on the viability and proliferation alveolar bone cells: an invitro study. Int J Oral Maxillofac Surg 2005;34:420–4.
[12] Mazor Z, Peleg M, Garg AK, Luboshitz J. Platelet-rich plasma for bone graftenhancement in sinus floor augmentation with simultaneous implant placement:patient series study. Implant Dent 2004;13:65–72.
[13] Robiony M, Polini F, Costa F, Politi M. Osteogenesis distraction and platelet-richplasma for bone restoration of the severely atrophicmandible: preliminary results.J Oral Maxillofac Surg 2002;60:630–5.
[14] Butterfield KJ, Bennett J, Gronowicz G, Adams D. Effect of platelet-rich plasmawithautogenous bone graft for maxillary sinus augmentation in a rabbit model. J OralMaxillofac Surg 2005;63:370–6.
[15] Thorwarth M, Rupprecht S, Falk S, Felszeghy E, Wiltfang J, Schlegel KA. Expressionof bone matrix proteins during de novo bone formation using a bovine collagenand platelet-rich plasma (prp)—an immunohistochemical analysis. Biomaterials2005;26:2575–84.
[16] Graziani F, Ivanovski S, Cei S, Ducci F, Tonetti M, Gabriele M. The in vitro effect ofdifferent PRP concentrations on osteoblasts and fibroblasts. Clin Oral Implants Res2006;17:212–9.
[17] Thorwarth M, Wehrhan F, Schultze-Mosgau S, Wiltfang J, Schlegel KA. PRP
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246

7M. Nagata et al. / Bone xxx (2009) xxx–xxx
ARTICLE IN PRESS
modulates expression of bonematrix proteins in vivowithout long-term effects onbone formation. Bone 2006;38:30–40.
[18] Wiltfang J, Kloss FR, Kessler P, Nkenke E, Schultze-Mosgau S, Zimmermann R, et al.Effects of platelet-rich plasma on bone healing in combination with autogenousbone and bone substitutes in critical-size defects. An animal experiment. Clin OralImplants Res 2004;15:187–93.
[19] Weibrich G, Kleis WK, Hafner G, Hitzler WE. Growth factor levels in platelet-richplasma and correlations with donor age, sex, and platelet count. J CraniomaxillofacSurg 2002;30:97–102.
[20] Lacoste E, Martineau I, Gagnon G. Platelet concentrates: effects of calcium andthrombin on endothelial cell proliferation and growth factor release. J Periodontol2003;74:1498–507.
[21] Martineau I, Lacoste E, Gagnon G. Effects of calcium and thrombin on growth factorrelease from platelet concentrates: kinetics and regulation of endothelial cellproliferation. Biomaterials 2004;25:4489–502.
[22] LiuW, Toyosawa S, Furuichi T, Kanatani N, Yoshida C, Liu Y, et al. Overexpression ofCbfa1 in osteoblasts inhibits osteoblast maturation and causes osteopenia withmultiple fractures. J Cell Biol 2001;155:157–66.
[23] Tsay RC, Vo J, Burke A, Eisig SB, Lu HH, Landesberg R. Differential growth factorretention by platelet-rich plasma composites. J Oral Maxillofac Surg 2005;63:521–8.
[24] Lee HW, Reddy MS, Geurs N, Palcanis KG, Lemons JE, Rahemtulla FG, et al.Efficacy of platelet-rich plasma on wound healing in rabbits. J Periodontol2008;79:691–6.
[25] Stein GS, Lian JB. Molecular mechanisms mediating proliferation/differentiation
Please cite this article as: Nagata M, et al, Influence of the proportionhealing in critical-
^size defects
^: An immunohistochemical analysis in rat
interrelationships during progressive development of the osteoblast phenotype.Endocr Rev 1993;14:424–42.
[26] Fréchette JP, Martineau I, Gagnon G. Platelet-rich plasmas: growth factor contentand roles in wound healing. J Dent Res 2005;84:434–9.
[27] Gruber R, Kandler B, Fischer MB, Watzek G. Osteogenic differentiation induced bybone morphogenetic proteins can be suppressed by platelet-released supernatantin vitro. Clin Oral Implants Res 2006;17:188–1893.
[28] Ogino Y, Ayukawa Y, Kukita T, Koyano K. The contribution of platelet-derivedgrowth factor, transforming growth factor-beta1, and insulin-like growth factor-Iin platelet-rich plasma to the proliferation of osteoblast-like cells. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2006;101:724–9.
[29] Gruber R, Karreth F, Fischer MB, Watzek G. Platelet-released supernatants stimu-late formation of osteoclast-like cells through a prostaglandin/RANKL-dependentmechanism. Bone 2002;30:726–32.
[30] Albrektsson T. Repair of bone grafts. A vital microscopic and histological inves-tigation in the rabbit. Scand J Plast Reconstr Surg 1980;14:1–12.
[31] Goldberg VM, Stevenson S. The biology of bone grafts. Semin Arthroplasty 1993;4:58–63.
[32] Pallesen L, Schou S, Aaboe M, Hjørting-Hansen E, Nattestad A, Melsen F. Influenceof particle size of autogenous bone grafts on the early stages of bone regeneration:a histologic and stereologic study in rabbit calvarium. Int J Oral MaxillofacImplants 2002;17:498–506.
[33] Shapoff CA, Bowers GM, Levy B, Mellonig JT, Yukna RA. The effect of particle size onthe osteogenic activity of composite grafts of allogeneic freeze-dried bone andautogenous marrow. J Periodontol 1980;51:625–30.
of particulate autogenous bone graft/platelet-^rich plasma on bone
calvaria, Bone (2009), doi:10.1016/j.bone.2009.04.246