In our own hands: SWAA-Ghana champions the female condom
39
Population Council Population Council Knowledge Commons Knowledge Commons 2006 In our own hands: SWAA-Ghana champions the female condom In our own hands: SWAA-Ghana champions the female condom Kathleen Cravero Michelle Skaer Population Council Victoria Ebin Martha Brady Population Council Follow this and additional works at: https://knowledgecommons.popcouncil.org/departments_sbsr-pgy Part of the Demography, Population, and Ecology Commons, Family, Life Course, and Society Commons, Gender and Sexuality Commons, International Public Health Commons, Maternal and Child Health Commons, Obstetrics and Gynecology Commons, and the Women's Health Commons How does access to this work benefit you? Let us know! How does access to this work benefit you? Let us know! Recommended Citation Recommended Citation Cravero, Kathleen, Michelle Skaer, Victoria Ebin, and Martha Brady. 2006. "In our own hands: SWAA-Ghana champions the female condom," Quality/Calidad/Qualité no. 17. New York: Population Council. This Case Study is brought to you for free and open access by the Population Council.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of In our own hands: SWAA-Ghana champions the female condom
Population Council Population Council
Knowledge Commons Knowledge Commons
2006
In our own hands: SWAA-Ghana champions the female condom In our own hands: SWAA-Ghana champions the female condom
Kathleen Cravero
Michelle Skaer Population Council
Victoria Ebin
Martha Brady Population Council
Follow this and additional works at: https://knowledgecommons.popcouncil.org/departments_sbsr-pgy
Part of the Demography, Population, and Ecology Commons, Family, Life Course, and Society
Commons, Gender and Sexuality Commons, International Public Health Commons, Maternal and Child
Health Commons, Obstetrics and Gynecology Commons, and the Women's Health Commons
How does access to this work benefit you? Let us know! How does access to this work benefit you? Let us know!
Recommended Citation Recommended Citation Cravero, Kathleen, Michelle Skaer, Victoria Ebin, and Martha Brady. 2006. "In our own hands: SWAA-Ghana champions the female condom," Quality/Calidad/Qualité no. 17. New York: Population Council.
This Case Study is brought to you for free and open access by the Population Council.

In Our Own Hands:SWAA-Ghana Championsthe Female Condom
/Quality/Calidad/Qualité /
In Our Own Hands:
SWAA-Ghana Champions
the Female Condom
/Quality/Calidad/Qualité /

Publication of this edition of Quality/Calidad/Qualité is made possible by support provided by FamilyHealth International; by the Robert H. Ebert Program on Critical Issues in Reproductive Health of thePopulation Council; by the Ford Foundation; and by the Gender, Family, and Development Program ofthe Population Council. Statements made and views expressed in this publication are solely the respon-sibility of the authors and not of any organization providing support for Q/C/Q.
The Population Council is an international, nonprofit, nongovernmental organization that seeks to im-prove the well-being and reproductive health of current and future generations around the world andto help achieve a humane, equitable, and sustainable balance between people and resources. TheCouncil conducts biomedical, social science, and public health research and helps build researchcapacities in developing countries. Established in 1952, the Council is governed by an internationalboard of trustees. Its New York headquarters supports a global network of regional and country offices.
Population Council, One Dag Hammarskjold Plaza, New York, NY 10017 USAtel: (212) 339-0500 fax: (212) 755-6052 e-mail: [email protected]
Quality/Calidad/Qualité, a publication ofthe Population Council, presents case stud-ies of high-quality, innovative programs insexual and reproductive health. Q/C/Qspecifically documents educational andclinic-based programs that are makingstrides in one or more of the followingways: (1) addressing the central importanceof gender dynamics in shaping sexual andreproductive health outcomes; (2) improv-ing the quality of care of clinic-based serv-ices; and (3) reaching disadvantaged andunderserved groups. With rare exceptions,featured programs are operating in develop-ing countries.
Q/C/Q case studies—selected by an ex-pert advisory group—are offered not as
models for replication, but as examples forlearning. They demonstrate a responsive-ness to broader social and economic trans-formations; they highlight inventive and af-fordable ways to respond to clients’ needs;and they reflect the self-critical and flexibleattitude required for learning from programexperiences and research evidence. Al-though they are written as practical tools—in accessible style with carefully selecteddetail—they also serve to inspire programleaders and policymakers to enable clientsto become more effective guardians oftheir sexual and reproductive health, andby doing so contribute fundamentally tothe achievement of such broader aims asthe Millennium Development Goals.
Cover photograph by SWAA-Ghana.
Issue No. 17 ISSN: 1097-8194 Copyright © 2006 The Population Council, Inc.
Any part of this publication may be copied or adapted to meet local needs without permission fromthe Population Council, provided that the parts copied are distributed free or at cost (not for profit) andthat the source is identified. The Population Council would appreciate receiving a copy of any materi-als in which the text is used.
Advisory Committee
Delia BarcelonaGary Barker Carmen BarrosoJudith BruceBatya ElulSusana GaldosFrançoise GirardNicole HaberlandKatherine Kurz
Laura LaskiAnn LeonardAnn McCauleyLiz McGroryManisha MehtaSuellen MillerSaumya RamaraoAnn StarrsCynthia Steele
Production Staff
Editor: Debbie Rogow
Editorial and production coordinator:Michelle Skaer
Copyeditor: Karen Tweedy-Holmes
Designer: Mike Vosika
Translators: Charo Quesada (Spanish) andGenevieve Haines (French)

No. 17 • 1
In 1992, a new product appeared onpharmacy shelves in developed coun-tries—pink packets of female condoms.Doctors and journalists alike trumpetedthe innovation. The method prevents bothunwanted pregnancy and the transmis-sion of sexually transmitted infections(including HIV), has a long shelf life, andallows for insertion for up to eight hoursbefore intercourse. Even more important,its use is initiated by the woman.
Why a need for a method that placescontrol in the hands of the woman? First,women and (especially) girls—of whomnearly 20 million are already living withHIV—account for an increasing propor-tion of new cases of HIV/AIDS around theworld, with rates rising most rapidly inAsia, Eastern Europe, and Latin America.If current trends continue, women andgirls infected with HIV could soon out-number men and boys with the diseaseworldwide. In sub-Saharan Africa, wom-en already account for almost 60 percentof those living with HIV, and three out offour HIV-infected young people are girls.
Moreover, the majority of women andgirls who remain at greatest risk (as well asof those who are already infected) are vul-nerable because of the behaviors of oth-ers, rather than as a result of their ownchoices. Although the traditional “ABC”prevention paradigm of Abstain, BeFaithful, and Use Condoms is a worthygoal, few women have the options theyneed to translate this strategy into reality.A number of social and economic factorscombine to constrain women’s ability todetermine whether, when, and with whomthey have sex. In some settings, girls aremarried off as children or are otherwisecoerced into sexual relationships—usual-ly with older men who are more sexually
experienced. Because the double stan-dard for sexual behavior prevails in manyplaces, women commonly remain mono-gamous, knowing that their husbandshave other sexual partners. Nevertheless,the decision regarding whether to use amale condom rests primarily with men,many of whom resist the idea.
No wonder the arrival of the pinkpackets raised hopes about reducingwomen’s vulnerability to HIV globally.When used correctly and consistently,the female condom reduces risk of HIVtransmission by 97 percent (Trussell et al.1994). Studies conducted in more than40 countries found acceptability ratesranging from 41 percent to 95 percent(FHI 2005). Twelve years after the femalecondoms first entered the market, theUnited Nations calculated that 64 mil-lion female condoms had been distrib-uted in more than 100 countries.
The sad truth is, however, that thisnumber is insignificant in light of the im-mense need for the method.
Why has the female condom so farfailed to be adopted widely? Althoughlimited acceptability is an issue (somewomen find that they or their partnerssimply do not like the method),1 a majorcentral obstacle is set at the policy level—that is, the misguided tendency ofmany donors and program leaders tocompare the method in narrow terms tothe male condom. In such a comparison,the cost of the female condom (US$0.58to $0.72 per unit, compared with $0.03for the male condom) seems prohibitive,especially for many users who live onless than a dollar a day. The contrast inprice, however, is almost meaningless: Asthe following article shows, some menwho refuse to use the male condom are
Introduction
by Kathleen Cravero
1 Some women have found it difficult to insert without extensive practice; others dislike its visible outer ring.

2 • Quality /Calidad /Qualité
willing to have their partner use the fe-male condom. To the degree that this pat-tern holds true, the lower cost of themale condom becomes moot. A moremeaningful comparison is to the cost ofprojected cases of HIV.
Skepticism about the female condomis also based on the lack of continuinginterest within some traditional servicesettings. Unlike the male condom, whichhas been distributed successfully throughtraditional provider systems, the femalecondom requires an education-based ap-proach that seeks to raise women’s aware-ness about their very right to protection.Schemes for female-condom distributionthat do not enable women to assume andexercise this right are of negligible value.
As we accelerate work to make the fe-male condom more available, affordable,and acceptable to both women and men,we must also extend efforts to alter pre-vailing gender norms. Throughout theworld, a growing number of initiativesseeking to lower the barriers women facein accessing health and social services areconfronting head-on such issues as vio-lence, education, employment, and prop-erty and inheritance rights. For example,the UNAIDS-led Global Coalition on Wom-en and AIDS is working with men and boysas well as with women and girls, advocat-ing and supporting a range of strategies tochange traditional beliefs and practices thatreinforce pervasive gender inequality.
Normative change is slow. In the mean-time, we must also provide women andgirls with the information and—to the bestof our ability—the means for preventingthe spread of HIV. Today, the female con-dom remains the best tool for preventionavailable that provides women and girlswith a measure of control over their ownsurvival. Although promising progress isbeing made toward the development of amicrobicide—a gel, cream, sponge, orsuppository that women can use to pro-tect themselves, if necessary without theirpartners’ knowledge or consent—at leastfive to ten years will pass before an effec-
tive microbicide reaches the market, evenbacked by sufficient political will andfinancial investment.
Happily, a growing body of evidencefrom various countries shows that in placeswhere the female condom is being thought-fully promoted and distributed, more andmore women—and men—are saying thatthey want to use it. This news is encourag-ing and bodes well for ongoing efforts.Work is also underway to improve the fe-male condom by making it not only lessexpensive and more accessible but alsomore comfortable and acceptable to malepartners. A new model, which has beenwell received in Mexico, South Africa, andThailand, is currently undergoing clinicaltrials in the United States and could reachthe global market within the next two years.
Hence, a renewed programmatic effortis afoot to promote the female condom.The following article describes an innova-tive initiative in Ghana and includes short-er descriptions of efforts in Brazil, SouthAfrica, and Zimbabwe. The Ghanaianproject brought together a diverse rangeof partners—including the government,UN agencies, NGOs, and the FemaleHealth Company—to enable large num-bers of women to obtain female condomsat an affordable price. The program’s suc-cess is a tribute to the value of an effec-tive multisectoral partnership, to thefemale-empowerment strategy launchedby the Ghanaian branch of the Society ofWomen and AIDS in Africa, and to thethousands of women who recognized thattheir lives were at stake and seized theopportunity to act on their own behalf.
References
Family Health International. 2005. “Female Con-dom Acceptability and Sustained Use.” FHIResearch Briefs on the Female Condom No. 4.<http://www.fhi.org/en/RH/Pubs/Briefs/fcbriefs/acceptability.htm>. Accessed 15 December 2005.
Trussell, James, Kim Sturgen, Jennifer Strickler,and Rosalie Dominik. 1994. “Comparativecontraceptive efficacy of the female condomand other barrier methods.” Family PlanningPerspectives 26(2): 66–72.

No. 17 • 3
In Our Own Hands:SWAA-Ghana Champions the Female Condom
by Michelle Skaer and Victoria Ebin
A group of women hotel workers watch-es intently as Rebecca Attipoe, a mem-ber of the Society for Women and AIDSin Africa (SWAA), holds a small, clear,plastic item, which she calls a femalecondom. Using the device does not lookeasy to these women. Talking to theirsexual partners about it seems even moredifficult. Worrying every night aboutAIDS and unwanted pregnancy, howev-er, seems harder still. After Rebeccaanswers their questions, several womenstep forward. With their health and livesat stake, they decide to try it.
These women, like 75 percent of allwomen in Ghana, enjoy a measure ofeconomic autonomy. Working primarilyin farming and informal employment,one out of three are the heads of theirhouseholds (GSS et al. 2004). Despitetheir economic role, however, mostGhanaian women have little power oversexual decisions affecting their healthand lives. Typically, they cannot insistupon fidelity from their husbands, muchless from extramarital sexual partners.Nor can most require their partners touse protection against infection or un-wanted pregnancy; use of contracep-tives, and of male condoms in particu-
lar, remains low.1 Commonly, moreover,women are coerced to have sex. As oneGhanaian reproductive health profes-sional has commented, “Most womenown houses but still need educating inhow to negotiate [sex]” (Akai-Nettey2003).
Around the world, gender inequalityin sexual decisionmaking puts women atparticular risk of health consequences.Of particular concern, of course, isHIV/AIDS. Compared with other Africancountries, the HIV prevalence rate inGhana is relatively low: 3.6 percent ofthe adult population, with a rate of 5.3percent in some regions (NACP 2001).The virus, however, disproportionatelyaffects women and girls. Among 15–24-year-olds, the HIV rate is more than fourtimes higher for females than for males(NACP 2001:17).
Until the late 1990s, the Ghanaiangovernment’s HIV/AIDS programmingwas limited.2 Ghana’s well-establishedfamily planning program continued toemphasize long-acting methods, such asNorplant®‚ rather than barrier methodsthat offer protection against HIV/AIDSand many sexually transmitted infections(STIs). Public awareness about HIV/AIDS
1 The DHS found overall contraceptive use among currently married women to be 25.2 percent, with thepill accounting for 5.5 percent, injectables for 5.4 percent, periodic abstinence for 5.1 percent, and malecondoms for 3.1 percent (GSS and MI 2004).
2 The first education campaign began in 1986; the National AIDS Policy was drafted in 1996; and in 2001the National AIDS Commission was established.

4 • Quality /Calidad /Qualité
and condoms was close to universal;however, local studies found that only 42percent of men perceived themselves tobe at risk of infection. In one survey, only16 percent of adult men and 6 percent ofwomen reported using a condom duringtheir most recent sexual encounter (GSSand MI 2000).
In recent years, several factors haveheightened the sense of urgency aboutthe epidemic. First, the HIV rates inneighboring countries—which are two tothree times higher than those in Ghana—underscore the risk of rapid spread of thevirus. (The discrepancy between the ratein Ghana and the rates across its bordersalso raises concerns about whetherGhana’s reported rates of infection maybe underestimated.) Approximately 200people in Ghana become infected withHIV each day. Moreover, at least three-fourths of female sex workers in Accraand Kumasi, the two major Ghanaiancities, are HIV-positive.
Society for Womenand AIDS in Africa(SWAA)Across the region, an early driving forcefor attention to HIV/AIDS, and in particu-lar, to women’s needs with regard to theepidemic, has been the Society for Wom-en and AIDS in Africa (see box below:SWAA International). In the late 1990s,however, the Ghana branch of SWAA wassmall and relatively inactive. The organi-zation, with no funding or paid staff, hadnot undertaken any large projects. Two ofits leaders, Alice Lamptey and BerniceHeloo, had been involved in their profes-sional lives in small acceptability trials ofthe female condom, but SWAA-Ghanahad not begun to advocate for the method.
Two incidents changed the organiza-tion’s path.
First, Alice Lamptey and Bernice Heloowere invited to represent SWAA in aworking group established specifically to
Around the world, women have re-sponded collectively to the AIDS epi-demic. One of the earliest and best-established of the women’s organiza-tions—with affiliated branches in eightcountries, including Ghana—is theSociety for Women and AIDS in Africa(SWAA). Initially, SWAA focused oncare (including improving access toantiretroviral drugs) for people livingwith HIV as well as support for them,for their children, and for AIDS or-phans. By the late 1990s, the organiza-tion also began to focus on methods ofpreventing transmission of the virus,advocating for access to the femalecondom and for research toward the
development of an effective microbi-cide (SWAA 2004). The eight SWAAbranches range in size from a singlewoman to large groups (composed pri-marily of volunteers with some paidstaff). Some operate without any fund-ing, whereas others have strong donorsupport. Some branches focus on pro-viding direct services and communitycare, and others lead advocacy andeducational campaigns. SWAA Interna-tional, based in Senegal, provides assis-tance to the all of the loosely affiliatedbranch offices through capacity-build-ing and communications support.
For more information, visit <www.swaainternational.org>.
SWAA International

No. 17 • 5
introduce the female condom into Ghana.This working group arose out of the gov-ernment’s AIDS task force, in whichmembers learned from the UNAIDS (theJoint United Nations Programme onHIV/AIDS) and UNFPA (United NationsPopulation Fund) representatives (Cyn-thia Eledu and Moses Mukasa, respec-tively) about the successful experiencewith the method in South Africa. TheAIDS task-force members decided to es-tablish a working group that includedthe government, international organiza-tions (UNAIDS and UNFPA), and se-lected nongovernmental organizations(NGOs), including SWAA.
At about the same time, Alice Lamp-tey attended an international SWAAmeeting in Dakar, where members wereenthusiastically promoting an organiza-tion-wide campaign for the female con-dom. Lamptey knew that SWAA-Ghanahad gained, through the new workinggroup, an important avenue for makingthe female condom a viable option forwomen in her country. She also knewthat in order to take advantage of thatopportunity, the Ghana branch wouldhave to be revitalized.
On her return to Accra, Lamptey set towork. SWAA-Ghana reorganized itsstructure, holding its first general elec-tion; Charity Binka, a well-known jour-nalist and women’s activist, became itsfirst president. An executive committeeappointed four members to manage afemale condom promotion project. Be-yond collaborating with the government’sworking group to introduce the method,SWAA’s project plan called for the orga-nization to operate its own network fordistributing it directly to users. Fundswere secured from the Danish Interna-tional Development Agency (DANIDA)and from UNAIDS. The organizationestablished an office and hired RebeccaAttipoe as the project coordinator.
Nothing inspires like having a mission,and now SWAA-Ghana had found one.
SWAA’s Role in the FemaleCondom Working Group
SWAA-Ghana joined the female con-dom working group along with threeother NGOs: the Ghana Social Market-ing Foundation (GSMF), Planned Parent-hood Association of Ghana (PPAG), andthe Ghana Registered Midwives Associ-ation. For the most part, the group mem-bers were already well acquainted withone another. For example, Lampteywore “two hats” on the working group;she also worked at the Ghana SocialMarketing Foundation. Indeed, the in-volvement of the NGO representativesenlivened the working group and creat-ed a strong sense of partnership.
SWAA mobilized to promote the female condom; with fundssecured from DANIDA, the organization established an of-fice, hired Rebecca Attipoe as project coordinator, and pur-chased a truck.
Phot
o:V
icto
ria
Ebin
6 • Quality /Calidad /Qualité
SWAA played an integral role fromthe outset; Alice Lamptey, together withher colleague Kojo Lokko of GSMF,drafted a strategy proposal for the group.
This document outlined the femalecondom introduction process and identi-fied a number of issues on which thegroup developed an easy consensus. Forexample, drawing on acceptability datafrom more than 40 countries, the groupdecided against investing time and re-sources on another comprehensiveacceptability study. Another key decisionconcerned defining the target user popu-lation. The group wanted to avoid thenegative association with sex workersthat had hindered the female condomcampaigns in other countries. Accord-ingly, they decided to position themethod as a “mainstream” contraceptivebarrier that protects against unwantedpregnancy and HIV infection and tomarket it widely. The target user popula-tion included all sexually active men
and women (both married and unmar-ried), with an emphasis on reaching18–30-year-olds in urban and periurbanareas within the regions of highest HIVprevalence (Glasgow 2001).
The working group easily allocatedresponsibility for distributing the method
through various channels. The governmentand Planned Parenthood agreed to offerthe method in their clinics; the GhanaSocial Marketing Foundation assumedresponsibility for arranging pharmacysales of a more expensive “brand-name”female condom; the Ghana RegisteredMidwives Association agreed to promotethe method among its clients; and theWest Africa Project To Combat AIDS en-listed to reach out to sex workers and toother women through midwives. SWAA’srole was to distribute the female condomthrough its local networks, focusing onthe regions with the highest HIV-infectionrates and the communities not reachedby other programs. Although SWAA hadnever been involved with large-scalecommodity supply, the organization wasprepared to invest in developing the insti-tutional infrastructure and skills to carryout its role in the cooperative plan.
The Fight Over Pricing
The most difficult issue facing the work-ing group was establishing a unit pricefor the female condom, and on this mat-ter, SWAA fought an uphill battle. Toenable programs to provide the methodwith limited outside support over thelong term, some working group mem-bers suggested a unit price of 6,000–8,000 cedis (at the time approximatelyUS$1).3 SWAA balked and a conflict en-sued. Alice Lamptey recalls that she pro-tested, “Men’s condoms cost 100 cedis,and women should pay 8,000? How canwe ask women to pay that? You’re tellingthem to go to hell and get infected. If wefix the price above what women canafford, we will be condemning them toHIV infection.”
To ascertain how much women wouldactually pay, the working group asked
3 The global public-sector price was set in 1996 by UNAIDS and the manufacturer, the Female HealthCompany.
The Ghana Social Marketing
Foundation tested the product at
this price by placing 8,000 female
condoms in 160 pharmacies. The
entire inventory was sold within
a week.

No. 17 • 7
the Ghana Social Marketing Foundationto undertake further in-depth marketresearch. Almost all respondents saidthey would buy the female condom if itcost the same as a male condom (100cedis, or less than $0.02). The averageacceptable price named by respondentswas 450 cedis (GSMF 1999).4
At the next meeting, the workinggroup slashed the proposed price from8,000 to 500 cedis ($1.12 to $0.07), butLamptey argued that the lowered pricestill placed too great a burden on poorwomen at risk of HIV infection and pre-dicted that, at 500 cedis, the methodwould stay on the shelves. SWAA un-derstood that the relatively high unitprice of the female condom strained
donor budgets, but argued that it was agood investment from both a publichealth perspective and as a women’srights issue. Lamptey recalled that “Itwas a matter of equity. . . . We cannotdiscriminate against women.”
SWAA’s efforts to restructure donorpriorities prevailed. At the final meetingbefore the introduction, Moses Mukasaof UNFPA agreed that the agencywould subsidize the extra cost. The fe-male condom would be sold for 300cedis ($0.04). The Ghana Social Mar-keting Foundation tested the product atthis price by placing 8,000 female con-doms in 160 pharmacies.
The entire inventory was sold with-in a week.
The Ghana Social Marketing Foundation undertook market research to determine a price that women couldafford. Alice Lamptey argued that a reasonable price “was a matter of equity. . . . We cannot discriminateagainst women.”
Phot
o:M
elis
sa M
ay
4 The study also attempted to gauge the strength of market demand. Two-thirds of respondents stated thatthey did not consider themselves at risk of acquiring HIV infection. Forty-four percent reported that theyhad taken action within the last three months to avoid becoming pregnant; the greatest proportion (19percent) were relying on the male condom. About 40 percent of respondents had heard of the femalecondom, but only two of 468 respondents had ever used it.

8 • Quality /Calidad /Qualité
SWAA Helps Lead theNational Training
SWAA played an important role in de-signing and implementing the femalecondom working group’s two-day train-ing of trainers (TOT) workshops. Repre-sentatives from the Ministry of Health(MOH) and all participating NGOs (in-cluding ten SWAA members) attendedthe first round of TOT workshops, whichdrew on materials produced by the man-ufacturer (the Female Health Company)5
and included the following topics:
• Clinical aspects and prevalence ofHIV/AIDS
• How gender inequality increaseswomen’s vulnerability to HIV
• Overview of the female condom(with emphasis on dual protectionagainst infection and pregnancy)
• Education and counseling issues (in-cluding negotiating skills)
• Logistics (supply, distribution chan-nels, storage, reporting)
• How to plan a training for direct dis-tributors
The trainers demonstrated proper useof the method using a plastic model.They also encouraged female partici-pants to try inserting the method duringthe night between days one and two ofthe workshop, and later to insert it eighthours in advance of a time they antici-pated having sex. Trainees’ likelihood oftrying the method varied, depending, inpart, on the effectiveness of the trainer.
The Public Launch of the Method
The TOT participants went on to train4,400 direct distributors, from clinicstaff and pharmacists to hairdressersand tailors (Glasgow 2001). UNAIDSdistributed a total of 15,000 femalecondoms for the trainers and directproviders to use during educationaldemonstrations.
SWAA cooperated with the workinggroup in planning a public educationcampaign to introduce the femalecondom formally in Ghana. The offi-cial launch of the introduction processtook place on 25 May 2000 at the Na-tional Theatre in Accra. More than1,500 people attended the high-profileevent. A representative of the FirstLady of Ghana delivered the keynotespeech. Political leaders, representa-tives from international organizations,traditional chiefs, and “queen moth-ers” were all in attendance. The NGOsparticipated, as did women’s associa-tions, market sellers, and hairdressers.The event even included a “mascot” ina female condom costume (UNAIDSand WHO 2000).
Alice Lamptey and Bernice Helooshared with their fellow working groupmembers a sense of excitement andmomentum about ushering in a newstage in HIV prevention. SWAA-Ghana, however, was about to take a different approach in carrying outits promise to help distribute the fe-male condom.
5 The Female Health Company (FHC) was founded on the belief that women have the right to protect them-selves against HIV and other infections and have need for a technology to enable them to exercise thatright. FHC manufactures the female condom, holds exclusive worldwide rights to its design, and cur-rently distributes the method to 80 countries through public-sector procurement and commercially in 17countries. In 1996, FHC formed a foundation to carry out advocacy and education activities promotingwomen’s health and reproductive rights around the world (see www.femalehealth.org).
No. 17 • 9
Recasting CommodityDistribution as anEducation PackageTaking on direct distribution of a tech-nology was a new challenge for SWAA,and the organization charted its owncourse. In terms of institutional capaci-ty, the organization was not fully pre-pared for the task. In terms of its cre-ative vision, however, SWAA was per-haps the ideal organization to introducethe female condom across Ghana.Indeed, the organization’s approachturned traditional commodity distribu-tion on its head: Instead of focusing firston the details of a particular method oron racking up a number of “acceptors”(with counseling as an add on), SWAAfelt that its main job was to convince
women that they had a right to protecttheir own lives and to provide themwith some basic skills in negotiation—and a technology in their hands—toexercise that right. In this case, the tech-nology happens to be the female con-dom; substitute another technology (forexample, a microbicide), and the basicstrategy would remain the same. AsRebecca Attipoe, the project coordina-tor, described this moment, “SWAAbecame involved with the female con-dom because it is woman-controlled.Now that the government and partnershad put a structure in place for thefemale condom, SWAA could reachwomen with an empowering messageabout the method.”
SWAA leaders understood thatwomen need to learn about a method
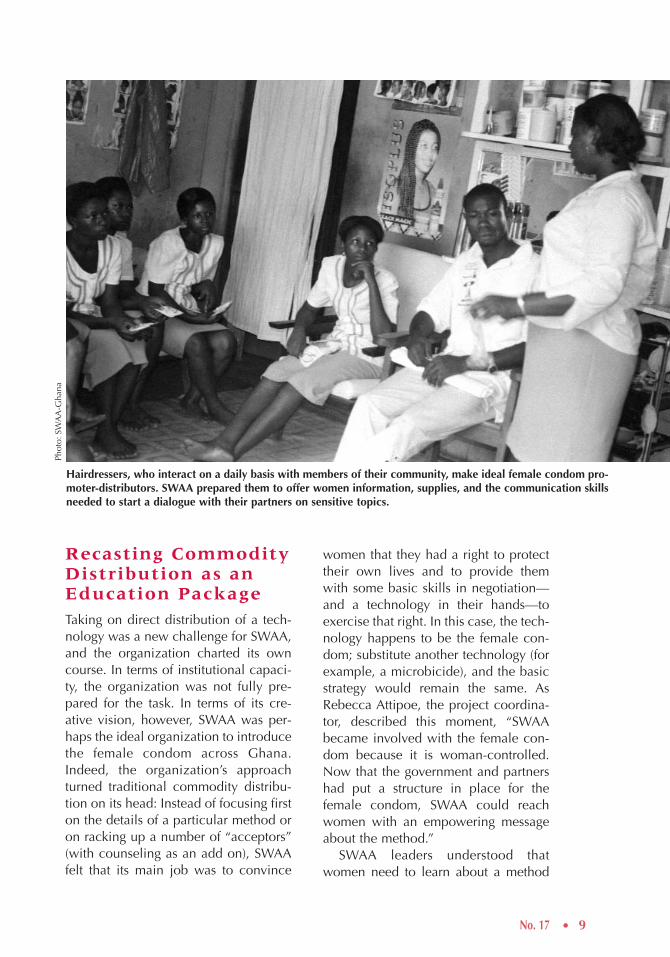
Hairdressers, who interact on a daily basis with members of their community, make ideal female condom pro-moter-distributors. SWAA prepared them to offer women information, supplies, and the communication skillsneeded to start a dialogue with their partners on sensitive topics.
Phot
o:SW
AA
-Gha
na
Recruiting andTraining SWAADistributorsBy the end of 2000, the number ofSWAA trainers had grown from ten to80. Through local associations in urbanand rural areas, these trainers beganoffering one-day workshops to individu-als who wanted to become direct dis-tributor-promoters. The priority was onreaching individuals—for example,hairdressers, market women, and seam-stresses—who interact on a daily basiswith members of their community.6 Inhopes of promoting support among
like the female condom in the context ofa frank discussion—about their sexualrelationships, about the sexual practicesof the men in their lives, and about whatis involved in inserting the method intothe vagina. As one SWAA representativecommented, “It’s crossing a big socialbarrier for women to talk about sex.”SWAA believed that a grassroots effortwas the most effective way to foster suchconversations. Discussions about the fe-male condom were embedded in, andopened, larger conversations about sex-uality, reproduction, and power withinmale–female relationships.
The distribution project was, at itsheart, an empowerment campaign, andSWAA threw itself into the task. Theorganization developed a system forprocuring commodities from the govern-ment and purchased a truck. Staff alsoadapted the existing training and materi-als. For example, they changed the mes-sage on the national promotional posterfrom “Safe, Simple and Reliable” to“Safe and Reliable.” As Rebecca Attipoesays, “It’s not all that simple, and wedon’t want women to lose their confi-dence if they don’t get it right at first.”On the national brochure, they replacedthe image of a middle-class woman in asuit with a woman in traditional dress.“She could be a farmer or marketwoman,” remarks Rebecca. “This is whowe need to reach.”
It is unusual for an advocacy NGO tofield an army of commodity suppliers,but the female condom is not a typicaltechnology. SWAA kept its eye not onwomen’s compliance with a set of in-structions but on their increased sense ofagency. Ultimately, within the Ghanaiancontext, SWAA has proved most capableof promoting the female condom.
10 • Quality /Calidad /Qualité
6 Rebecca Attipoe explained that female apprentices (such as those learning to be seamstresses) are amongthose in greatest need of a method to protect themselves, because they are on their own for the first time,and they often have to depend on men to survive.
By the end of 2000, the 1,000 SWAA dis-tributor-promoters had sold (or had givenaway) about 170,000 female condoms.
7 This number compares with 300 distributor-promoters trained by the Ghana Midwives Association and 55trained by Planned Parenthood Association of Ghana. The MOH and the Ghana Social MarketingFoundation trained nearly 3,000 individuals each, but the distributors reached by these groups were notexpected to organize group meetings, discuss sensitive sexual issues, or teach women sexual negotiationskills. Hence, SWAA positioned itself to reach directly the greatest number of possible users.
No. 17 • 11
men, SWAA also recruited local maleleaders to help distribute the femalecondom.
In Ghana’s Western Region, SWAAmembers Elizabeth Ennuson, MargaretAsantinwa Sackey, and Agatha Aggreyset out to recruit 100 distributor-promoters at a workshop. They con-tacted dozens of associations—youthand women’s organizations, Christianministers and congregations, socialclubs, fishmongers, students, marketwomen, Muslim women’s groups,hairdressers, and associations of thewives of police and of prison officers.They also informed potential partici-pants that transportation costs andlunch would be paid by SWAA. To
their amazement, three hundred peo-ple attended, including students, house-wives, and religious leaders.
SWAA trainers continued to recruitover a period of several months, untilthey had trained about 1,000 people topromote and distribute the female con-dom;7 at least one-third of the traineeswere men.
The training for potential distributor-promoters was a combination of socialanalysis, technical information, andskill-building for talking about sexuali-ty. The SWAA trainers taught partici-pants about HIV and about how wom-en become particularly vulnerable tothe disease. They also explained whatthe female condom is and how to
Phot
o:V
icto
ria
Ebin
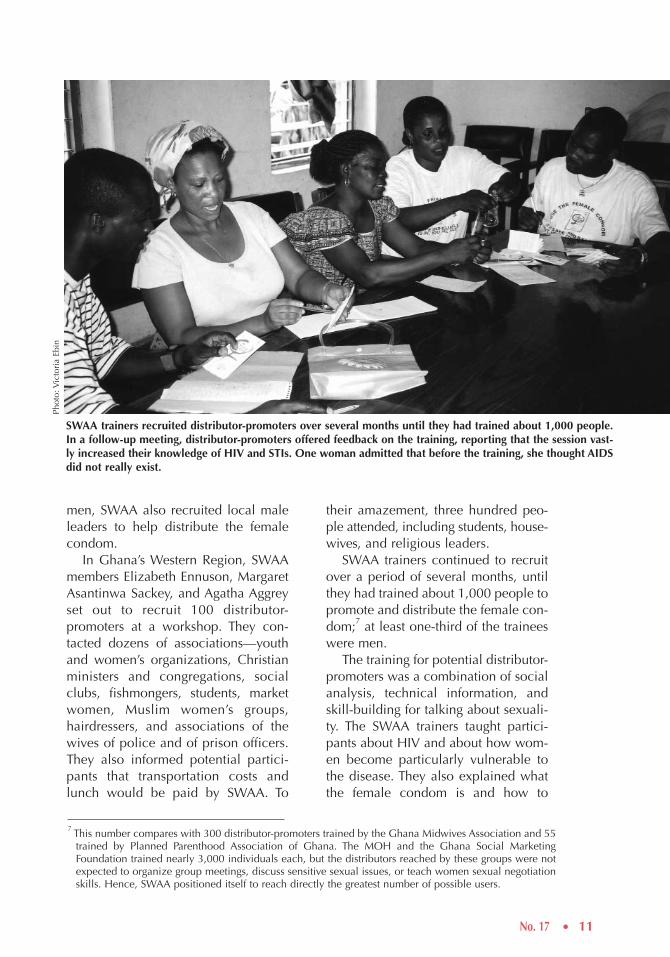
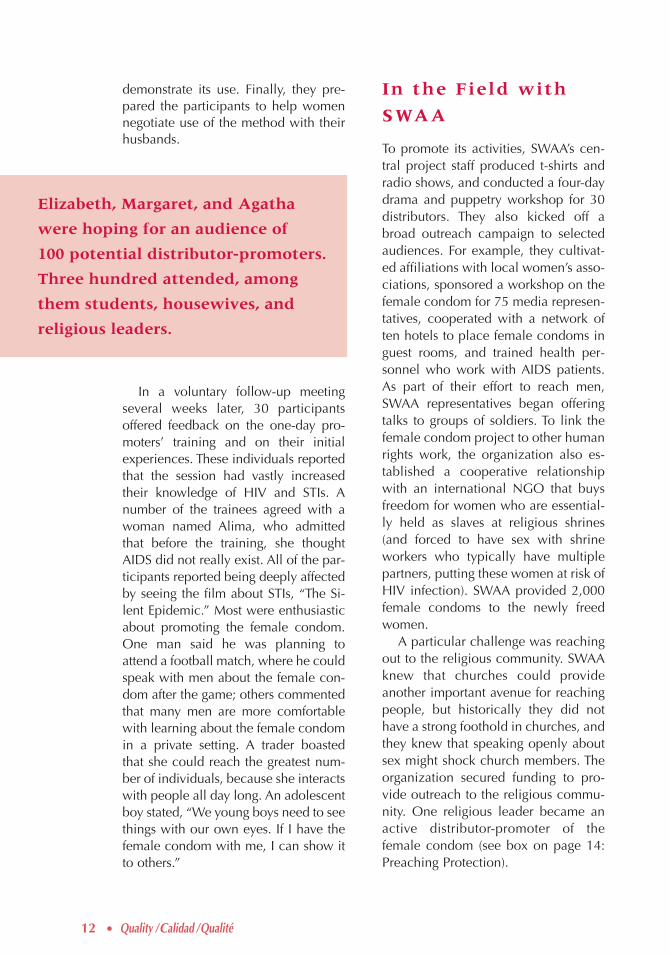
SWAA trainers recruited distributor-promoters over several months until they had trained about 1,000 people.In a follow-up meeting, distributor-promoters offered feedback on the training, reporting that the session vast-ly increased their knowledge of HIV and STIs. One woman admitted that before the training, she thought AIDSdid not really exist.
12 • Quality /Calidad /Qualité
In the Field with
SWAA
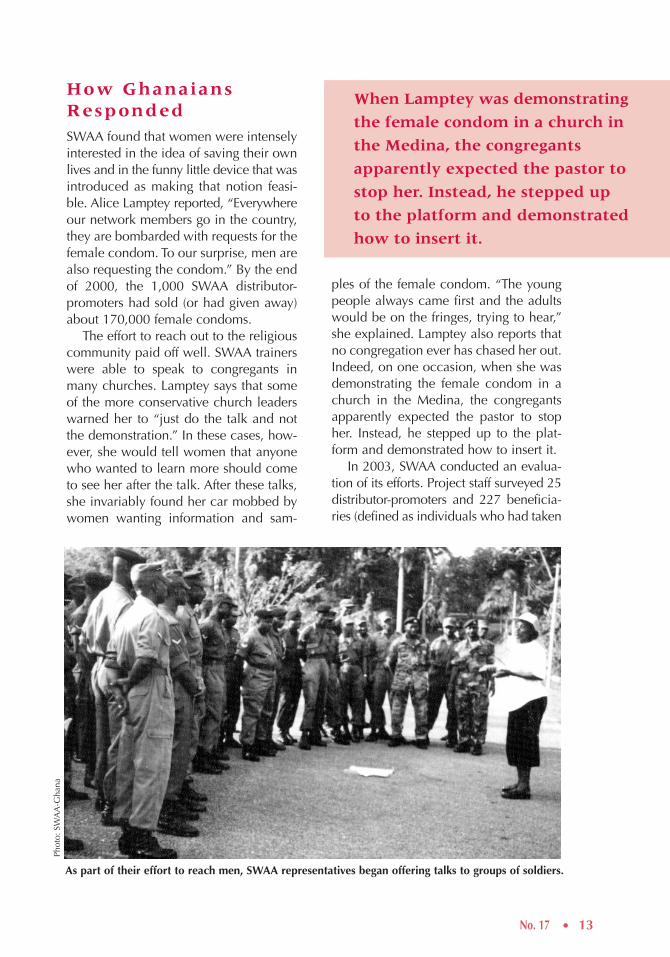
To promote its activities, SWAA’s cen-tral project staff produced t-shirts andradio shows, and conducted a four-daydrama and puppetry workshop for 30distributors. They also kicked off abroad outreach campaign to selectedaudiences. For example, they cultivat-ed affiliations with local women’s asso-ciations, sponsored a workshop on thefemale condom for 75 media represen-tatives, cooperated with a network often hotels to place female condoms inguest rooms, and trained health per-sonnel who work with AIDS patients.As part of their effort to reach men,SWAA representatives began offeringtalks to groups of soldiers. To link thefemale condom project to other humanrights work, the organization also es-tablished a cooperative relationshipwith an international NGO that buysfreedom for women who are essential-ly held as slaves at religious shrines(and forced to have sex with shrineworkers who typically have multiplepartners, putting these women at risk ofHIV infection). SWAA provided 2,000female condoms to the newly freedwomen.
A particular challenge was reachingout to the religious community. SWAAknew that churches could provideanother important avenue for reachingpeople, but historically they did nothave a strong foothold in churches, andthey knew that speaking openly aboutsex might shock church members. Theorganization secured funding to pro-vide outreach to the religious commu-nity. One religious leader became anactive distributor-promoter of thefemale condom (see box on page 14:Preaching Protection).
demonstrate its use. Finally, they pre-pared the participants to help womennegotiate use of the method with theirhusbands.
In a voluntary follow-up meetingseveral weeks later, 30 participantsoffered feedback on the one-day pro-moters’ training and on their initialexperiences. These individuals reportedthat the session had vastly increasedtheir knowledge of HIV and STIs. Anumber of the trainees agreed with awoman named Alima, who admittedthat before the training, she thoughtAIDS did not really exist. All of the par-ticipants reported being deeply affectedby seeing the film about STIs, “The Si-lent Epidemic.” Most were enthusiasticabout promoting the female condom.One man said he was planning toattend a football match, where he couldspeak with men about the female con-dom after the game; others commentedthat many men are more comfortablewith learning about the female condomin a private setting. A trader boastedthat she could reach the greatest num-ber of individuals, because she interactswith people all day long. An adolescentboy stated, “We young boys need to seethings with our own eyes. If I have thefemale condom with me, I can show itto others.”
Elizabeth, Margaret, and Agatha
were hoping for an audience of
100 potential distributor-promoters.
Three hundred attended, among
them students, housewives, and
religious leaders.
No. 17 • 13
How GhanaiansRespondedSWAA found that women were intenselyinterested in the idea of saving their ownlives and in the funny little device that wasintroduced as making that notion feasi-ble. Alice Lamptey reported, “Everywhereour network members go in the country,they are bombarded with requests for thefemale condom. To our surprise, men arealso requesting the condom.” By the endof 2000, the 1,000 SWAA distributor-promoters had sold (or had given away)about 170,000 female condoms.
The effort to reach out to the religiouscommunity paid off well. SWAA trainerswere able to speak to congregants inmany churches. Lamptey says that someof the more conservative church leaderswarned her to “just do the talk and notthe demonstration.” In these cases, how-ever, she would tell women that anyonewho wanted to learn more should cometo see her after the talk. After these talks,she invariably found her car mobbed bywomen wanting information and sam-
ples of the female condom. “The youngpeople always came first and the adultswould be on the fringes, trying to hear,”she explained. Lamptey also reports thatno congregation ever has chased her out.Indeed, on one occasion, when she wasdemonstrating the female condom in achurch in the Medina, the congregantsapparently expected the pastor to stopher. Instead, he stepped up to the plat-form and demonstrated how to insert it.
In 2003, SWAA conducted an evalua-tion of its efforts. Project staff surveyed 25distributor-promoters and 227 beneficia-ries (defined as individuals who had taken
As part of their effort to reach men, SWAA representatives began offering talks to groups of soldiers.
Phot
o:SW
AA
-Gha
na
When Lamptey was demonstrating
the female condom in a church in
the Medina, the congregants
apparently expected the pastor to
stop her. Instead, he stepped up
to the platform and demonstrated
how to insert it.
14 • Quality /Calidad /Qualité
the female condom home). The resultsindicated that 90 percent of distributorsand users had shared information aboutthe female condom with friends or familymembers. Seventy-nine percent had dis-cussed method use with her or his partner;among these couples, 87 percent of part-ners agreed, immediately or eventually, totry the method. Men as well as womenwere purchasing the condoms.
At the time of the survey, not all ofthese couples had tried the method, how-ever: Among the promoters, 87 percenthad ever used the female condom;among the general beneficiaries, 60 per-
cent had tried it. Of the group of ever-users, two-thirds were continuing to usethe female condom. Among this group,47 percent reported using the methodalways or most of the time. (These datawere corroborated by responses to ques-tions about how many times the methodwas used in the previous five sexual en-counters: 34 percent reported using it allfive times, and another 21 percent statedthat they had used it three or four times.)
The evaluation also documentedproblems with management informationsystems, counseling, and outreach inareas that lack radio.
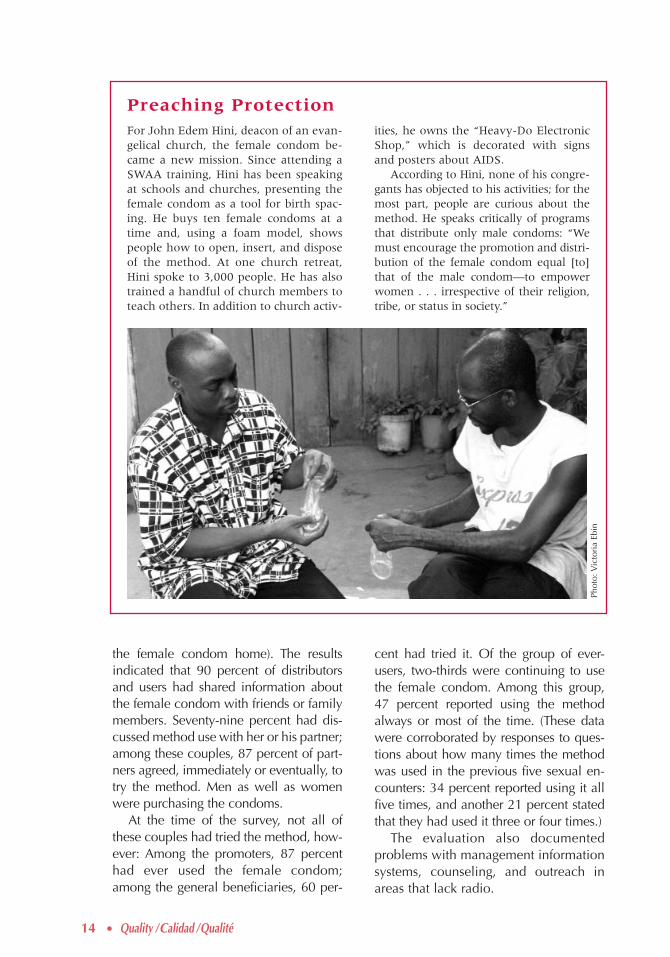
For John Edem Hini, deacon of an evan-gelical church, the female condom be-came a new mission. Since attending aSWAA training, Hini has been speakingat schools and churches, presenting thefemale condom as a tool for birth spac-ing. He buys ten female condoms at atime and, using a foam model, showspeople how to open, insert, and disposeof the method. At one church retreat,Hini spoke to 3,000 people. He has alsotrained a handful of church members toteach others. In addition to church activ-
ities, he owns the “Heavy-Do ElectronicShop,” which is decorated with signsand posters about AIDS.
According to Hini, none of his congre-gants has objected to his activities; for themost part, people are curious about themethod. He speaks critically of programsthat distribute only male condoms: “Wemust encourage the promotion and distri-bution of the female condom equal [to]that of the male condom—to empowerwomen . . . irrespective of their religion,tribe, or status in society.”
Preaching Protection
Phot
o:V
icto
ria
Ebin
No. 17 • 15
Experiences of Usersat SWAA and otherDistribution Sites
Although SWAA has been the mostconsistently active promoter of thefemale condom in Ghana, otherprovider organizations from the work-ing group have also continued distrib-uting the method. In interviews, staffmembers from these organizations andSWAA members shed light on thediversity of users’ perspectives andexperiences. The following discussionsynthesizes reports from the variousprovider groups and their clients.
User Profi les
As the working group had hoped, thefemale condom has appealed to adiverse population in Ghana. One groupof users are women whose partners areunwilling to use the male condom, but
are more comfortable with the femalecondom. The Planned Parenthood clinicin Accra describes the typical user as arelatively educated married woman whowants to delay pregnancy, is unable touse other methods, and whose partner isunwilling to use the male condom. Asone user stated: “My husband will notuse the male condom. [With the femalecondom,] my experiences with unwant-ed pregnancies are over.”
By contrast, other programs havefound that women, particularly young-er women, are using the female con-dom primarily to protect themselvesfrom infection. Some women (and men)use the method only when they have anactive infection, discontinuing use aftertreatment. Another group of users con-sists of women who have multiple part-ners, including some sex workers. Asone sex worker indicated, “In situationswhere no condom was used, I waspricked by my conscience.” In one sur-
Phot
o:V
icto
ria
Ebin
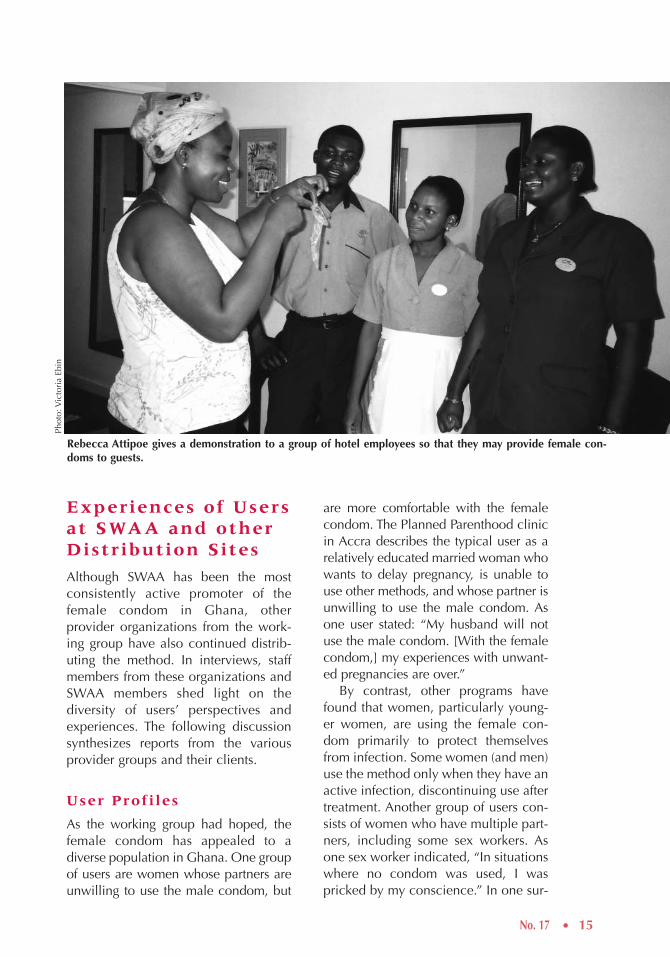
Rebecca Attipoe gives a demonstration to a group of hotel employees so that they may provide female con-doms to guests.

16 • Quality /Calidad /Qualité
vey of 132 SWAA users, fear of infectionwas the single most important motive foruse, although more than 40 percent ofthe respondents cited protection from in-fection and from unwanted pregnancy asfactors (Boraas and Asante 2003).
One user group—regardless of wheth-er their concern is about pregnancy orinfection—is women whose partnersobject to using the male condom for avariety of reasons. The female condomhas a niche where otherwise there wouldbe no protection, which recasts the poli-cy debate about the method. As BerniceHeloo commented, “Issues of pricing andaccessibility are important. But the fe-male condom gives many women theirsole protection over their health. From apolicy and program perspective, it can-not be compared with the male condom.”
Method Acceptabil ity
Many users are skeptical when they firstsee a female condom, but they developcomfort with it over time. As one userexplained, “The female condom looksbig, but it fits very well and does not feelany different from the male condom.”According to several midwife-distribu-tors, women say that men do not objectto the female condom because “they areonly interested in having sex. They do noteven notice that it is there.” Experiencewith other methods also shapes opinions;one man in Akim Oda reported, “I thinkI will use the female condom forever be-cause, so far, it has not burst, as has hap-pened with the male condom.”
Some users report increased comfortor pleasure during intercourse. For exam-ple, the Ghana Registered Midwives As-sociation reported that some olderwomen use the method because thelubrication makes intercourse easier. Astudent commented, “I get more sensa-tion when I use the female condom.” A(male) truck driver commented, “Thefemale condom is more pleasant . . .
because it does not feel as tight as themale [condom].”
Of course, not all users were satisfiedwith the method. Those who had discon-tinued use did so because either they ortheir partner found the method unpleas-ant (noisy or difficult to use). Some menand women reported reduced sensationduring intercourse. Others found it cum-bersome and noisy, or “too big andthick.” Some women have nicknamedthe method “polytank,” a reference tothe large plastic water containers usedthroughout the country. One PlannedParenthood nurse explained that somewomen find that the outer ring of thecondom can get in the way. Some usersbelieved that the female condom is dan-gerous and could get stuck in the repro-ductive tract. Another concern was thatthe method could encourage promiscuity.
Some promoters have found challeng-ing their attempts to help potential userssort through sensitive issues that affectacceptability. Even among SWAA’s ownmember-promoters, few adopted thefemale condom as their own method.These women cited the same “difficultywith their husbands” that many otherwomen reported.
Tension CharacterizingSexual Relationships
The intrinsic characteristics of the meth-od are not the only, or perhaps even theprincipal, determinant of acceptability.Rather, the social context in which sex istaking place affects method use, andmany women are having sex in a contextof unease or mistrust. For example, onemidwife who distributes the method ex-plained that to negotiate barrier-methoduse, most couples need guidance in howto initiate discussions about the intimateaspects of sex. A Planned Parenthoodnurse encourages married women to“start negotiating before getting to thebedroom.” Victoria Tutu, a midwife at

No. 17 • 17
Adabraka, is more pragmatic, remindingwomen that they can insert the condomup to eight hours before having sex, sothat “If you don’t trust men, you can stillprotect yourself.”
Tutu’s comment touches only lightlyon the deep tensions that often character-ize Ghanaian women’s sexual encoun-ters. For example, many clients need acontraceptive (and ideally, a microbicide)that they can use not only independentlybut surreptitiously.8 Moreover, many arehesitant to mention the method to theirhusbands because it brings to the surfacethe reality of sexual infidelity and canmake either partner the object of suspi-cion. As one woman explained, “If thewife comes home and shows him afemale condom, he’s going to think, ‘I’mfaithful to her, and she gives me this?’”
Although the threat of conflict andviolence may impede some women’sability to use the female condom, othersturn to the method precisely because ofthe difficult circumstances that they arefacing. For example, sex workers mustmanage thorny relationships with theirclients; one nurse who provides servicesto sex workers reports, “If a woman seesthat a man is diabolical, she will some-times use the female condom. Thefemale condom is good for womenbecause sometimes men are trickish.”
Providers also report that women atrisk of experiencing coerced sex are usingthe method. One nurse commented onthe challenge of facing the double threatsof forced sex and a resulting disease orpregnancy. She cited the example of wom-en firefighters who go off with male co-workers to the bush: “They go to the fieldwith men and they know men are goingto push them for sex . . . or even attackthem. They say they’re going to urinateand then they put in the female condom.”
Stumbling BlocksWith most new temporary methods, ini-tial interest is high as people experimentwith the technology, and then settles ata much lower level that reflects ongoinguse among those who find the methodacceptable. The use levels in Ghana fol-lowed this trajectory. The biggest obsta-cle to positioning the female condom asa viable option in Ghana, however, hasnot been low acceptability. Rather,SWAA found its efforts mired in logisti-cal obstacles to access—problems withsupply and pricing at the national level.
Securing Supplies
From the outset, uneven supplies under-mined the method’s introduction. In asense, the pitfalls of the introductionwere symptoms of its own success:Enthusiasm among women—and rela-tive disinterest in the donor world—threw the supply system off balance.
The problems began even before theofficial launch of the method, when dif-ficulty securing donor support resultedin an initial procurement that was small-er than that which the national femalecondom working group had anticipated.Moreover, many of the people whowere being trained as distributors (by allof the participating organizations) hadbegun offering the method in the weeksbefore the national launch date; by thatday, therefore, early demand had alreadypartially depleted supplies. To avoid los-ing momentum when the working groupwas unable to find donors willing tosupport subsequent purchases, MosesMukasa used UNFPA country programmoney to arrange for airlifting an addi-tional but limited supply of the methodto Ghana. He also met with World Bankrepresentative Peter Harrold, who facili-
8 In Northern Ghana, for example, where fewer women have access to education and where socioeconomiclevels are lower than in other regions of the country, many women are reluctant to give up injectables forthis reason.

18 • Quality /Calidad /Qualité
tated the purchase of one million femalecondoms for the Ghana Ministry ofHealth.9 Mukasa explained, “The per-sonality of characters was important inthis collaborative effort. The World Bankrepresentative cared about AIDS.”
Unfortunately, the shipment arrangedby the World Bank did not arrive formore than a year. The samples intendedfor use as community-demonstrationsupplies quickly disappeared. The dis-tributor-promoters found many womenwilling to use the female condom, butthese women were frustrated when theycould not be resupplied. In manyplaces, women visited distribution cen-ters to request the method, only to beturned away.
By the time new supplies arrived, thedistribution system was destabilized,and many women had given up trying toobtain the method. This setback madepredicting demand difficult and resultedin fewer requests leading to procure-ment of the next order. This lack of sta-bility further suppressed both providers’and users’ interest and threatened tospin the entire female condom deliverysystem into a downward spiral.
A year after the official launch of thefemale condom, interest in the methodwas beginning to wane.10 The GhanaSocial Marketing Foundation, frustratedby the lack of steady supplies, aban-doned its plans to add a “high-end”brand for the private sector. PlannedParenthood of Ghana provides the
method but has observed that its clientsoften do not return; staff were unclearabout the number of their clients whoare restocking the method at pharma-cies nearer to their homes and howmany have discontinued use. At theMOH clinics, demand for the methodhad never been as high as in other sec-tors; counseling in the resource-poorpublic clinics may not have been ade-quate to teach women enough aboutthe female condom so that they couldimagine being able to use it successful-ly. The West Africa Project to CombatAIDS and STIs (WAPCAS) reported hav-ing reasonable success in promoting themethod among the sex workers who areregular clients at the Adabraka Clinic.
Presently, the female condom ac-counts for only a small fraction of allcontraceptive use in Ghana.11
Ensuring steady supplies is essential ifthe female condom is to develop a nichein a country. The stakeholders in pro-moting access to the female condom—among which SWAA is now in a leadingrole—must take several steps back andtry to overcome the sense that the pro-ject “has slipped from sight.” Oneimportant requirement is that of gradual-ly building back demand in a mannerthat will allow distribution agencies topredict supply needs. National advocacyand publicity campaigns, together with arenewed investment in social marketing,are necessary for the female condom toreach its potential.
9 The money for this purchase came from a fund supplied by the World Bank, the (UK) Department forInternational Development, the Danish International Development Agency, the European Union, and thegovernment of the Netherlands.
10 Although SWAA has no quarterly records documenting commodity flow, MOH and the Ghana SocialMarketing Foundation records show that consumption at the public clinics and pharmacies began to leveloff after the first year.
11 Although the majority of users still rely on hormonal methods, a very small number of Ghanaian womenhas adopted the female condom as their contraceptive method. Official figures for contraceptive use,however, presumably underestimate overall use of the method, because they exclude those individualswho use the method specifically, even if only briefly, for disease protection (MOH/GHS 2001).
“You need money to buy it, and somewomen just don’t see money on a dailybasis.” Kathlyn Ababio, a midwife andpresident of the Ghana Registered Mid-wives Association, gives free samples towomen who she feels are at elevated riskof an infection. She explains, “Infection iseasier to prevent than to cure.”
SWAA’s InstitutionalChallenges
In addition to these structural problems,SWAA faces its own organizational chal-lenges. Currently, SWAA carries out pro-curement, distribution, and follow-upwith minimal documentation. As a result,the organization is uncertain about thenumber of distributors who have beentrained or how they are carrying out their
No. 17 • 19
Regulating Pricing
Pharmacies continue to sell the method,and many women who first hear aboutthe female condom at a clinic find itmore convenient to restock at a localpharmacy. Because the Ghana SocialMarketing Foundation is not involvedwith supplying the method, no mecha-nism exists to regulate and enforce pricecontrols, however.
SWAA currently sells the female con-dom for 300 cedis ($0.04), a price com-parable to that of the male condom,which is sold by most providers in a set ofthree condoms for 900 cedis.12 SWAA isconcerned, however, about the afford-ability of the method if the price increas-es. One SWAA promoter expressed con-cern that even the current nominal costrepresents a barrier for many women:
12 SWAA is able to purchase female condoms for $0.02 with subsidies from the Ghanaian government andUNFPA.
Despite the challenges, SWAA-Ghana’s staff members maintain their commitment to promoting the femalecondom, stating that the cost is a small price to pay for reducing HIV-infection rates and empowering women.
Phot
o:V
icto
ria
Ebin
20 • Quality /Calidad /Qualité
work. Bernice Heloo (the current presi-dent of SWAA-Ghana) explains thatSWAA does not know who is buying thefemale condom, why they are buying it,or whether and how they are using it. Theorganization’s leaders are hoping todevelop a management information sys-tem to track and analyze commodity flowand monitor project activities at all levels.
Another goal is to strengthen thecounseling skills of SWAA’s promoters.SWAA’s evaluation indicated that distrib-utors often lack the capacity to fosterwomen’s negotiation and communica-tion skills and to address such sensitiveissues as infidelity and trust in marriage.To this end, SWAA is hoping to offeranother training of trainers workshop toenable promoters to position the female
condom not as stand-alone technology,but as a tool within an educational pack-age. The refresher training will alsoaddress questions about reusing thefemale condom (see the Afterword).
The most immediate concern facingSWAA, however, is that the DANIDAfunding for the female condom project($200,000 per year) has ended. Current-ly, UNAIDS funds are enabling SWAA
to continue its promotion of the femalecondom.13 Because the organization iscommitted to making the method avail-able to poor women using an intensiveeducational approach, distribution andsales can never provide significant rev-enues. To expand its coverage to theentire country, Rebecca Attipoe esti-mates that SWAA would require rev-enues of $500,000 per year.
Some critics of SWAA’s effort mayexpress concern that such budgetary re-quirements are excessive. SWAA’s posi-tion is that this cost is a small price topay for reducing HIV-infection rates andempowering women.
Looking AheadDespite daunting obstacles to securingsteady and affordable supplies, theGhanaian experience, and SWAA’s ex-perience in particular, can well serveother countries’ governments, providers,and organizations hoping to empowerwomen by incorporating the female con-dom into HIV-prevention efforts. Ghanais one of the few countries that has intro-duced the female condom nationallythrough a wide range of channels. Theworking group members attribute theirachievements to their successful collab-oration. As Alice Lamptey reflected, “Theright sort of partnership has been key toour success. None of us could have doneit alone.” Each partner brought itsstrength to the undertaking. UNAIDSfacilitated the process and broughteveryone together. UNFPA provided re-sources to ensure affordability. UNAIDSnegotiated a reduced price from the Fe-male Health Company. The governmentof Ghana made a commitment to offer-ing women a method they could control,
The female condom campaign
offered SWAA a vehicle for
revitalizing itself as an organiza-
tion. The project was providing
a relatively weak organization
with a mobilizing focus and an
opportunity to enhance its own
credibility nationally and locally.
13 Another grant was awarded in 2003 by the Open Society Institute that enabled SWAA International toinclude SWAA-Ghana in a project to test strategies, strengthen collaborative networks, and generatelessons for female condom work in several countries.

No. 17 • 21
managing licensing and procurement,and providing the method in publicfamily planning clinics. The NGO sec-tor, with the capacity to provide appro-priate education and counseling, tookthe lead in providing the method be-yond clinic settings. Although this part-nership was eased by the fact that manymembers of the group had previouslyestablished professional relationships,their shared commitment to enablingwomen to save their own lives was whatgave the working group its vitality.
Over the long haul, however, SWAA-Ghana carried the project into villagesacross the country. In doing so, the orga-nization approached its work not ascommodity distribution but as an edu-cation and empowerment campaign.Despite the remaining challenges, theirefforts to date have reconfigured thework of preventing HIV transmissionacross the country and have providedlessons for the field about how to viewdistribution of technologies related tosexuality and gender.
Moreover, the female condom cam-paign offered SWAA-Ghana a vehiclefor revitalizing itself as an organization.The project was providing a relativelyweak organization with a mobilizingfocus and an opportunity to enhance itsown credibility nationally and locally. Itenabled the organization to build itsgrassroots base, to strengthen its affilia-tion with religious groups, and to culti-vate a relationship with the media. Thecampaign provided a vehicle for exten-sive institutional development, becauseSWAA was forced to reckon with itsown internal strengths and weaknessesin order to develop its capacity in train-ing, in developing materials, in man-agement information systems, and inmonitoring program activity. Finally,through its collaboration with SWAAInternational on the Women’s Protec-tion Initiative, SWAA-Ghana raised its
profile and helped to generate networksand lessons across the region.
Sorting out problems of commoditylogistics—including pricing and sup-ply—is not easy. It will demand evengreater commitment and creativity toimplement programs that—reflectingemerging policy mandates—seek tochange power relations between malesand females in family life, schooling,employment, policymaking, and otherdimensions of daily life that shape sexu-al decisionmaking. Echoing some of themost far-reaching community health-promotion drives, SWAA-Ghana’s expe-rience illustrates how an NGO musthelp create women’s social capacity touse the very technology it is distributing.
The organization’s leaders hope tosecure enough funding to enable SWAA-Ghana to scale up nationally, working inpartnership with the government tosecure supplies. As Alice Lamptey says:“I’m sold on NGOs and what they cando. I believe in NGOs. [With more] sup-port . . . we could do more.”
As SWAA-Ghana carries the female condom projectforward, they continue to emphasize the importance ofengaging men.
Phot
o:V
icto
ria
Ebin
22 • Quality /Calidad /Qualité
As a result of the strong influence ofthe Brazilian feminist movement, theMinistry of Health approached thefemale condom already sensitized tothe way in which gender issues affectcontraceptive use and HIV-preven-tion efforts. For years, feminist organi-zations have provided input to statecommissions on issues of quality ofcare and women’s rights. Indeed,both the National AIDS Program andthe National Women’s Health Pro-gram within the Ministry have femi-nist leadership. When the femalecondom became available, the MOHquickly responded with a large-scaleacceptability trial (conducted by theUniversity of Campinas and involving2,400 participants) to determine ifthe female condom would help to fillthe gap in HIV-protection mecha-nisms for women in Brazil.
Acceptability rates exceeded ex-pectations: 93 percent of the womentried the female condom and 76 per-cent of them continued to use it,yielding a 70 percent acceptabilityrate. Study participants reported
using some form of protection duringintercourse 65 percent of the time,compared with 31 percent beforethey entered the study. These resultsencouraged the government to pro-ceed with a national distributioncampaign. The campaign began inOctober 1999, and the Ministry allo-cated $1.28 million for the programper year. They expected to providetwo million female condoms for25,000 women.
Because the introduction researchalso found that acceptability rateswere elevated when users were con-tacted through community-baseddistribution, the MOH developedstrong partnerships with NGOs thatcould provide necessary communityoutreach. To reach high-risk groups,some of the NGOs were selected fortheir particular ability to reach sexworkers and HIV-positive womenand their partners.
The Ministry of Health selected340 programs (health services andeducational and advocacy groups) todistribute the female condom. Train-
The experience in Ghana is unusualboth because of the level of multisec-toral collaboration and because a wom-en’s NGO became the leading local dis-tributor of a new technology. In an effortto deliver the female condom to womenas quickly as possible, the Ghanaianteam had decided to compromise onthe degree of research and documenta-tion associated elsewhere with the intro-duction. In other countries, the pro-
cess—involving different models—hasbeen more closely studied, and theseexperiences have generated their ownlessons for the field. Brief summariesbelow describe the process of introduc-ing the female condom in three coun-tries (Brazil, South Africa, and Zim-babwe) in which the government main-tained a more ongoing active role thanin Ghana in making the female condomavailable to its citizens.
Brazil: Feminist Perspectives Penetrate the State Apparatus
Experiences from Other Countries

No. 17 • 23
ing was provided for three profession-als from each program. Topics cov-ered in training included sexuality,gender roles, myths, taboos, sexualpractices, dual-method protection,and self-esteem. The two-day trainingsessions were followed by an obser-vation period. The MOH also de-signed educational awareness sessionsfor female users.
Thanks to well-developed projec-tions of demand, strong ideologicalcommitment within the public sector,and (relative to African countries) ade-quate resources, Brazil’s MOH hasbeen able to ensure that female con-doms are consistently available at nocost in many locations throughout thecountry. From 2000 to 2002, theMOH ordered more than eight million
female condoms for free distribution.As distribution has increased, thenumber of participating NGOs hasalso increased each year to reachmore users. In addition to the govern-ment’s free distribution, female con-doms are sold through DKT do Brazil,a social marketing organization thathad launched a female condom dis-semination campaign for World AIDSDay as early as 1997.
By 2002, the female condom wasavailable at 417 locations across Bra-zil.14 The government and its partnerNGOs continue to study female con-dom use in an attempt to overcomebarriers and to reach women who areat risk and who lack the power orskills to insist that their partners usethe male condom.
Brazil purchases more female condoms than any country in the world. Underlyingthe method’s success are: a strong feminist influence in the Ministry of Health, anational HIV-prevention campaign based on frank societal dialogue about sexual-ity, a research community with expertise in contraceptive introduction, andNGOs able to collaborate in distribution.
Phot
o:Eu
gene
Zhu
kovs
ky
14 Currently, taxes and embargoes in Brazil threaten the security of female condom supplies.
24 • Quality /Calidad /Qualité
In South Africa, the governmentintroduced the female condom intandem with another new technolo-gy: emergency contraception. Thisinitiative responded to a 1994 assess-ment of existing reproductive healthservices, which found that womenhad severely limited contraceptivechoice. In 1998, with the goals ofimproving quality of care and in-creasing the options available to pre-vent transmission of HIV and otherSTIs and to prevent unwanted preg-nancies, the National Department ofHealth launched the National Intro-duction of the Female Condom andEmergency Contraception.
In deciding how to position thefemale condom, the NationalDepartment of Health, working withthe Reproductive Health ResearchUnit (RHRU) of the University ofWitwatersrand, involved providerswho served different populationsthroughout the country. The plancalled for free distribution of femalecondoms to clients in 31 pilot clinics(both government and PlannedParenthood sites) and to sex workers,and for subsidized distributionthrough the private sector. HealthDepartment provincial coordinators(seven nurses and one public healthofficer) were selected to monitor staffat clinic distribution sites, providethem with support, and collect data.
A series of three-day trainingsfocused on counseling and logisticsrelated both to the female condomand to emergency contraception.
Although clinic staff were the mainparticipants, providers to the sex-worker community, the provincialcoordinators, and several additionaltrainers also attended the workshops.
Each clinic received an initial sup-ply of 3,000 female condoms andwas required to file reports on theirdistribution in order to receive more.In the first 18 months of the program,9,406 government clinic clients and1,381 Planned Parenthood clientstook female condoms home to try.These clients were predominantlywomen aged 20–29 who continuedto use hormonal contraceptives.Nearly 14 percent of these womenreturned for additional supplies. Thisproportion is considered an underes-timate of actual continuation, how-ever. Some sites experienced short-ages of forms and, therefore, failed toreport on distribution fully. Moreover,Planned Parenthood staff reportedthat some women found restockingmore convenient at local pharmaciesor gas stations participating in thepilot study.
For distribution to sex workers,the government worked through theSex Worker Advocacy Task Force(SWEAT). SWEAT serves 4,500 sexworkers on the streets and in mas-sage parlors and those affiliated withescort services. In the first 18 months,SWEAT distributed 11,698 female con-doms, despite a three-month gap dur-ing which time the supply dried up.
To establish private-sector distrib-ution, the Health Department pur-
South Africa: A Joint Introduction of theFemale Condom and EmergencyContraception
chased 150,000 female condomsand donated them to the Society forFamily Health (SFH) to be sold inpackages of two under the brandname care at pharmacies, gas sta-tions, and spaza shops (conveniencestores). SFH sold care for R4.25($0.32 in 2000), half the recom-mended retail price (Bank of Canada2005). In the first year, more than20,000 female condoms were sold at
590 locations. Two provinces (Gua-teng and Kwazulu-Natal) accountedfor most of these sales, however careremained virtually unavailable infour rural provinces.
The RHRU, working in collabora-tion with Family Health International(FHI), provided technical assistance,particularly in monitoring the prog-ress of the introduction. For the per-formance evaluation, the RHRU in-terviewed 39 public-sector providersand 198 women who had receivedthe female condom at least once. Ofthe 177 who had ever used it for sex-ual intercourse, 32 percent had usedit three or fewer times, 33 percent
had used it four to ten times, and 35percent reported using it more thanten times. Some women used femaleand male condoms interchangeably,resulting in greater overall methoduse. Of the 86 women who had usedthe female condom in the monthprior to their interview, 38 had alsoused the male condom. Eighty-eightpercent reported that, overall, theyused protection more often than theyhad before the female condom wasavailable to them, and 93 percentsaid they might purchase the femalecondom if it were not available forfree. Almost all women (96 percent)recalled that a provider had giventhem instructions and a demonstra-tion when they first received themethod.
Distribution varied considerablyamong clinics. Low distribution rateswere associated with staff turnover,specifically with the departure ofproviders who had attended thetraining. The RHRU recommendedformalizing the transfer of informa-tion to other staff and fostering effortsto reach men to increase methodacceptability.
Based on the success of the pilot,the government increased the num-ber of distribution sites, to a total of204 sites by late 2005, including pri-mary health-care services, hospitals,services for sex workers, truck-stops,workplaces, NGOs, and youth cen-ters. The gradual introduction of themethod has fostered steady increasesin use, and South Africa has becomethe one of the largest consumers offemale condoms in the world. Plansare evolving for continued expan-sion of the method’s availability.
Based on the success of
the pilot, the government
increased the number of
distribution sites to
include primary health-
care services, hospitals,
services for sex workers,
truck-stops, workplaces,
NGOs, and youth centers.
No. 17 • 25

26 • Quality /Calidad /Qualité
In Zimbabwe, various governmentalbodies have been actively involved inlicensing, pricing, distribution, anddirect provision of the female condom.The government’s involvement beganin 1994, when representatives from theNational AIDS Coordination Pro-gramme and Zimbabwe National Fam-ily Planning Council (ZNFPC) met withresearchers from the University ofZimbabwe to discuss the results of aWHO-funded acceptability study ofthe female condom. The study wasconducted with diverse populations,and participants were divided into fourgroups: rural, urban, and two groups ofsex workers. At least 66 percent ofrespondents from each group preferredthe female to the male condom. In therural and urban groups, 82 percentwere married women, many of whomwere at risk of acquiring HIV infectionfrom their husbands but were unable toconvince them to use a male condom.
Several steps had to be taken beforedistribution could begin. First, the gov-ernment’s Medical Control Councilhad to approve the device, whichrequired that a plan be developed formaking the method available towomen at an affordable price. Severalmore years passed in dialogue to estab-lish this plan; this process engaged thegovernment agencies, UNAIDS, andthe Women and AIDS Support Network(WASN), a Zimbabwean NGO to whichthe original university researchers alsobelonged.
WASN simultaneously carried out amedia campaign and community-mobilization effort that culminated ina petition carrying 30,000 signaturespresented to the government on WorldAIDS Day in December 1996. The Min-ister of Health agreed to offer his sup-
port, and by September 1996, theMedical Control Council had approvedthe female condom for use.
Once the method was approved, thegovernment undertook the marketingcampaign, in collaboration with Popu-lation Services International (PSI). Thiscampaign folded the introduction of thefemale condom into a male condompromotion campaign supported byBritish and US aid programs.
To enable married women to negoti-ate method use without raising sensitivequestions about disease and infidelity,the introduction emphasized the femalecondom’s contraceptive function. Tofurther differentiate between the maleand female condoms, the method wasrenamed as a “contraceptive sheath”under the brand name care.
Key decisions had to be made re-garding pricing. Funds were secured tofurther subsidize the UNAIDS-negotiat-ed price ($0.63), allowing for a userprice of $0.15 per condom.
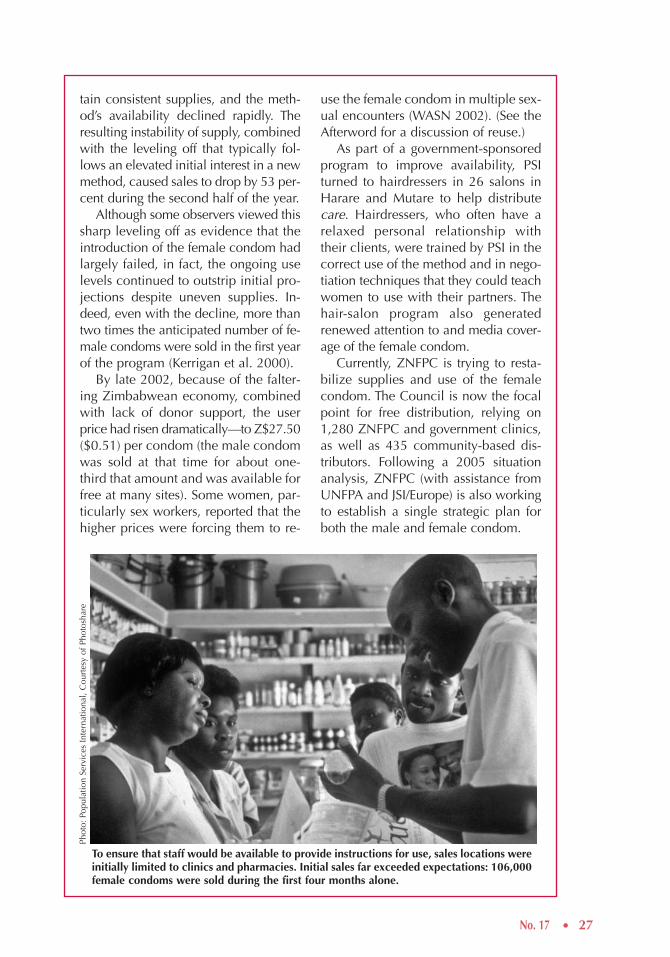
To ensure that staff would be avail-able to provide instructions for care’suse, sales locations were initially limitedto clinics and pharmacies. PSI sent train-ers to visit the pharmacies, public clin-ics, and pharmaceutical wholesalers toprovide them with educational materi-als. Over time, supermarkets, hair sa-lons, and other locations were allowedto carry the female condom. The gov-ernment and PSI forecasted that a real-istic goal was to sell 80,000 condomsduring their first year on the market.
In response to the marketing cam-paign and to women’s desperate needfor protection against HIV, initial salesfar exceeded expectations: 106,000 fe-male condoms were sold during the firstfour months alone. Unfortunately, do-nor support was not adequate to main-
Zimbabwe: After a Meteoric Jump and EarlyFalloff, Use Continues to Outstrip Projections
No. 17 • 27
tain consistent supplies, and the meth-od’s availability declined rapidly. Theresulting instability of supply, combinedwith the leveling off that typically fol-lows an elevated initial interest in a newmethod, caused sales to drop by 53 per-cent during the second half of the year.
Although some observers viewed thissharp leveling off as evidence that theintroduction of the female condom hadlargely failed, in fact, the ongoing uselevels continued to outstrip initial pro-jections despite uneven supplies. In-deed, even with the decline, more thantwo times the anticipated number of fe-male condoms were sold in the first yearof the program (Kerrigan et al. 2000).
By late 2002, because of the falter-ing Zimbabwean economy, combinedwith lack of donor support, the userprice had risen dramatically—to Z$27.50($0.51) per condom (the male condomwas sold at that time for about one-third that amount and was available forfree at many sites). Some women, par-ticularly sex workers, reported that thehigher prices were forcing them to re-
use the female condom in multiple sex-ual encounters (WASN 2002). (See theAfterword for a discussion of reuse.)
As part of a government-sponsoredprogram to improve availability, PSIturned to hairdressers in 26 salons inHarare and Mutare to help distributecare. Hairdressers, who often have arelaxed personal relationship withtheir clients, were trained by PSI in thecorrect use of the method and in nego-tiation techniques that they could teachwomen to use with their partners. Thehair-salon program also generatedrenewed attention to and media cover-age of the female condom.
Currently, ZNFPC is trying to resta-bilize supplies and use of the femalecondom. The Council is now the focalpoint for free distribution, relying on1,280 ZNFPC and government clinics,as well as 435 community-based dis-tributors. Following a 2005 situationanalysis, ZNFPC (with assistance fromUNFPA and JSI/Europe) is also workingto establish a single strategic plan forboth the male and female condom.
To ensure that staff would be available to provide instructions for use, sales locations wereinitially limited to clinics and pharmacies. Initial sales far exceeded expectations: 106,000female condoms were sold during the first four months alone.
Phot
o:Po
pula
tion
Serv
ices
Inte
rnat
iona
l, C
ourt
esy
of P
hoto
shar
e

28 • Quality /Calidad /Qualité
Lessons LearnedAcross the globe, efforts to enable women to protect themselves against infection and un-wanted pregnancy have generated similar lessons. Some of the most important lessonslearned from female condom programs in Brazil, Ghana, South Africa, and Zimbabwe are:
• The female condom has a real—and fairly heterogeneous—potential user popula-tion. To reach this target audience, however, the method may have to be positionedinitially as a contraceptive with additional benefits of protection against diseaserather than being targeted to sex workers as the primary users.
• Distribution of a method such as the female condom depends on a structure for pro-viding education and counseling about sexuality, power in intimate relationships,and fears of HIV infection. From a planning perspective, the technology is almost sec-ondary to facilitating this interpersonal exchange.
• Government, social marketing agencies, and NGOs all have roles to play in intro-ducing the female condom. NGOs, and women’s groups in particular, may be bestsuited to organize and foster the discussions that surround initial distribution and pro-motion of the female condom. Pharmacies, however, are often the most convenientsite for some women to obtain resupplies of the method, although wide-scale distri-bution through pharmacies will depend on continuing subsidies.
• The comparison with male condoms —which women cannot use and which menoften will not use—is a spurious one, financially as well as programmatically. Ifwomen who are learning that they have the right to protect their own lives are goingto be able to secure the means to do so, international donors and, where feasible gov-ernments, must invest in large enough procurements to lower the method’s unit costand to avert crises in supply and demand.
References
Akai-Nettey, Regina. 2003. Personal communication.
Boraas, Christy and Lydia Asante. 2003. Evaluation of the SWAA-Ghana Female Condom PromotionProject. Accra: Prolink.
Ghana Social Marketing Foundation (GSMF). 1999. Pricing Study on the Female Condom Report.Report submitted to the Ministry of Health on behalf of the Female Condom Working Group.
Ghana Statistical Service (GSS) and Macro International (MI). 2000. Ghana Demographic and HealthSurvey 1998. Calverton, MD: GSS and MI.
Ghana Statistical Service (GSS), Noguchi Memorial Institute for Medical Research (NMIMR), andORC Macro. 2004. Ghana Demographic and Health Survey 2003. Calverton, MD: GSS, NMIMR,and ORC Macro.
Glasgow, Muriel. 2001. “Promotion of the female condom: Where we came from; where we are;where we’re going.” UNAIDS Case Study. Geneva: UNAIDS.
Kerrigan, Deanna, Steve Mobley, Naomi Rutenberg, Andrew Fisher, and Ellen Weiss. 2000. TheFemale Condom: Dynamics of Use in Urban Zimbabwe. Washington, DC: Population Council.
Ministry of Health (MOH) and Ghana Health Service (GHS). 2001 Annual Report. Accra: MOH/GHSReproductive and Child Health Unit, Public Health Division.
National AIDS/STI Control Programme (NACP). 2001. HIV/AIDS in Ghana: Background, Projections,Impacts, Interventions, and Policy. Third edition. Accra: Disease Control Unit, Ministry of Health.
UNAIDS and WHO. 2000. The Female Condom: A Guide for Planning and Programming. Geneva:UNAIDS and WHO.
World Resources Institute (WRI). 2003. “Food and Agriculture: Ghana” Earthtrends Country Profiles.Washington, DC: WRI. <http://earthtrends.wri.org/pdf_library/country_profiles/agr_cou_288.pdf>.Accessed 15 December 2005.
pandemic, women need an expandedarray of and easier access to such prod-ucts. Program designers must recognizethe diversity of potential users of thefemale condom and incorporate that un-derstanding into their marketing, prod-uct positioning, and distribution chan-nels and mechanisms. Moreover, wemust seize the opportunity that thefemale condom presents to build a plat-form for the introduction of future HIV-prevention products.
As we enter the third decade of theHIV/AIDS pandemic, the female con-dom is the only means by which wom-en can take protection against STIs,HIV, and unwanted pregnancy intotheir own hands. The preceding casestudy documents the importance ofgovernment–NGO alliances that canbring the method to women at thegrassroots level and enable them to pro-tect themselves and their partners. If,however, we are to stem the tide of the
No. 17 • 29
Afterwordby Martha Brady
The female condom is the only means by which women can take protection against STIs, HIV, and unwant-ed pregnancy into their own hands.
Phot
o:V
icto
ria
Ebin

30 • Quality /Calidad /Qualité
Technology MattersOne avenue for moving forward is inthe arena of technology. For example,ongoing debates about reuse of thefemale condom will affect the afford-ability and accessibility of the meth-od.15 Refinements to existing infection-prevention products and accelerationof new products (for example, newfemale condoms, cervical barriers,and microbicides) are also promising.For example, the Female HealthCompany intends to launch a second-generation female condom; the “FC2”is expected to reduce the “noise”effect often cited as a drawback of thecurrent product. Moreover, new man-ufacturing processes and a change inmanufacturing locale are expected,ultimately, to drive down the price ofthe FC2.
Other investments in user-con-trolled technologies also are under-way: Modified female condoms of dif-ferent materials produced by means ofnew manufacturing processes arebeing designed and tested. The diap-hragm’s effectiveness against HIV in-fection is also being studied. We know,however, that no single technologywill provide an answer for all women.Currently, the female condom remainsthe only female-initiated device thatprovides effective simultaneous pro-tection against STIs, HIV, and unwant-ed pregnancy.
But the Major Need is for a NewProgrammatic Wave
While scientific development contin-ues, the promotion of currently avail-able technologies must advance with arenewed sense of urgency and with abolder approach to programming. Inmany settings, the approach to offeringthe female condom has fallen intostand-alone “take it or leave it” inter-ventions that have resulted in lower-than-anticipated levels of acceptabilityand uptake. As the previous case stud-ies demonstrate, rather than imple-ment this narrow vision, we must iden-tify ways to create synergies amongprograms through experimentationwith innovative and integrated servicemodels, venues, providers, and mes-sages. Such initiatives can also pavethe way for the introduction of futureprevention technologies.
Female condom introduction mustmove beyond “projects” to large-scaleprograms. In this regard, the methodmust be incorporated into overallcountry programs and bilateral andmultilateral (for example, UNFPA)plans. Due attention must also begiven to the female condom in the Re-productive Health Commodity Secur-ity assessments underway in manycountries. Success will require a com-mitment to overcoming political, eco-nomic, and social barriers.
15WHO convened a consultative process to consider the advantages and risks associated with washingand reusing the female condom. As of December 2005, WHO recommends, “the use of a new maleor female condom for every act of sexual intercourse where there is risk of unplanned pregnancy orof acquiring a sexually transmitted infection (STI), such as HIV. Recognizing the urgent need for risk-reduction strategies for women who cannot or do not access new condoms, the consultation devel-oped a draft protocol for safe handling and preparation of female condoms intended for reuse.” Formore information, see <http://www.who.int/reproductive-health/stis/reuse.en.html>.
No. 17 • 31
The female condom must be madeavailable by means of a range of healthand nonhealth systems, both public andprivate. Such a diverse strategy has bothpractical and political appeal. Someparticularly promising ideas are de-scribed below:
The female condom could be effec-tively positioned as an integral part of HIVprevention, care, and treatment strategies.Some approaches to be tested include:
• The provision of female condoms aspart of counseling within antiretrovi-ral treatment (ART) programs, partic-ularly in countries where such pro-grams are being scaled up.
• The provision of the female condomto women in serodiscordant couplesidentified through voluntary counsel-ing and testing programs and throughmother-to-child transmission-preven-tion programs.
• The positioning of female condoms as a“care” product for HIV-positive women.
Because in some settings, marriagemay increase young women’s risk ofacquiring STIs, including HIV, intensi-
fied efforts are needed to destigmatizecondom use and disease protectionwithin marriage. Field efforts can gener-ate important lessons about reshapingthe image of condoms to representrespect for health and future fertilityrather than distrust or infidelity, andabout reorienting antenatal care serv-ices to include protection messages andfemale condom distribution as needed.
The female condom can be presentedas a product intended to safeguard futurefertility and improve vaginal health, es-pecially where the social significance ofinfertility is profound. Provision of themethod should be an integral part ofSTI-prevention efforts.
Finally, addressing deep-seated gen-der inequalities is central to any seriousprotection strategy. Indeed, efforts to in-troduce the female condom and otherinfection-prevention methods must becarried out in tandem with initiatives toreconfigure the power dynamics be-tween partners and the communicationbetween men and women. Undoubted-ly, such broad social initiatives mustreach men as well as women.
Addressing deep-seated gender inequalities is central to any serious protection strategy. Effortsmust be carried out in tandem with initiatives to reconfigure the power dynamics between part-ners and the communication between men and women.
Phot
o:V
icto
ria
Ebin
32 • Quality /Calidad /Qualité
A diario, mujeres y niñas contraen VIHporque no pueden lograr que los com-pañeros con los que mantienen rela-ciones sexuales utilicen condones. Elcondón femenino es el único medio deprotección cuyo uso es iniciativa de laspropias mujeres. Hasta la fecha, muypocos países cuentan con experienciaamplia en la promoción del condón fem-enino, por lo tanto esos esfuerzos apor-tan lecciones valiosas para las estrategiasde protección de VIH.
Este artículo describe los esfuerzos dela filial en Ghana de SWAA (siglas eninglés de la Sociedad para las Mujeres ySIDA en África). SWAA-Ghana fue invi-tada a participar en un comité multisec-torial cuyo fin era ayudar a introducir elcondón femenino en dicho país. SWAAinsistió para que el comité redujera drás-ticamente el precio a las usuarias, liderólos talleres para capacitadores-de-capac-itadores y, más adelante, y se convirtieróen el distribuidor principal de condonesfemeninos en Ghana.
El enfoque de SWAA para la introduc-ción del producto dió un vuelco total ala distribución tradicional de productos:en lugar de centrarse en los detalles delmétodo, el objetivo de SWAA fue con-vencer a las mujeres sobre su derecho aproteger sus propias vidas y facilitarleslos conocimientos necesarios para la ne-gociación del ejercicio de esos derechos,con una tecnología a su disposición. Consu dedicación a este objetivo, la organi-zación, que carecía de experiencia endistribución de productos y hasta en-tonces había funcionado sin personalremunerado o proyectos de importancia,hizo llegar el condón femenino a lasmujeres en todo Ghana.
Más de 80 socias de SWAA reclutarony capacitaron a mil personas para la dis-tribución del condón femenino en suspropias comunidades. En el contexto deconversaciones francas sobre sexuali-
dad, reproducción y poder en las rela-ciones hombre-mujer, los distribuidoresencontraron con un enorme interéssobre el método. Aunque el énfasis en lafunción anticonceptiva del método eraimportante para su imagen, la mayoríade las mujeres lo utilizaban, al menos enparte, como protección contra infec-ciones. Algunas mujeres informaron quesus parejas se habían negado a utilizarcondones masculinos pero estaban dis-puestos a utilizar el condón femenino.
La introducción del condón femeninoha tenido sus problemas. La dificultadmayor ha sido mantener su abastec-imiento continuo. Los donantes vac-ilaron a la hora de hacer pedidos y facil-itar un producto relativamente caro.Cuando el abastecimiento se hizo pocofiable, muchas usuarias que se habíanmostrado satisfechas se vieron frustradasy dejaron de utilizar el método, a conse-cuencia de lo cual la operación perdió elimpulso inicial. SWAA reconstruye ahorala demanda de forma gradual al tiempoque garantiza un abastecimiento másconfiable.
Lecciones incluyen lo siguiente: 1) Lapoblación usuaria potencial del condónfemenino es heterogénea pero, para evi-tar el estigma conectado a VIH, podríaser importante presentar el método comoun anticonceptivo; 2) Las ONG serían lasmás adecuadas para ofrecer la educación(sobre sexualidad, problemas de género,y temor a VIH) clave para la distribuciónde este método; y 3) Los donantes debeninvertir en adquisiciones más volumi-nosas del producto si se desea que lasmujeres tengan acceso a esta tecnologíatan importante.
La próxima edición de programaciónpodría considerar estrategias tan innova-doras como presentar este método comoun producto para salvaguardar la fertili-dad futura, y intentar borrar el estigma dela protección dentro del matrimonio.
Resumen en Español
No. 17 • 33
Chaque jour, des femmes et des jeunesfilles contractent le VIH, impuissantesqu’elles sont à imposer le préservatif àleur partenaire sexuel. La seule méthodede protection dont l’usage peut être con-trôlé par les femmes elles-mêmes est lepréservatif féminin. Peu de pays dis-posent à ce jour d’une vaste expériencede la promotion du préservatif féminin.Les leçons tirées de leurs initiatives ensont d’autant plus précieuses à l’élabora-tion de stratégies de prévention utiles à lalutte contre le VIH.
Cet article décrit les efforts de labranche ghanéenne de l’organisationSWAA (Society for Women and AIDS inAfrica/Association pour les FemmesAfricaines contre le SIDA). Invitée à sejoindre à un groupe multisectorielchargé de l’introduction du préservatifféminin dans le pays, SWAA-Ghana ainsisté sur une réduction considérable ducoût de la méthode aux utilisateurs etpris la tête des ateliers nationaux de «formation des formateurs », devenantbientôt le principal organisme de distrib-ution du préservatif féminin au Ghana.
L’approche adoptée pour l’introduc-tion de la méthode a révolutionné lemode de distribution traditionnel : plutôtque de se concentrer sur les détails de laméthode, SWAA a cherché à convaincreles femmes de leur droit de protéger leurpropre vie et à les initier, technique enmain, aux principes élémentaires de lanégociation, pour les rendre aptes àexercer ce droit. Vouée à ce nouvel ob-jectif, l’organisation, qui n’avait alorsaucune expérience de la distribution deproduits et avait jusque-là opéré sanseffectifs salariés ni projets de vaste enver-gure, a apporté le préservatif féminin auxfemmes du Ghana.
Plus de 80 membres de l’organisationont recruté et formé 1 000 personneschargés de distribuer la méthode dansleurs propres communautés. Dans lecontexte de la discussion franche desquestions de sexualité, de procréation, et
de pouvoir au sein des relations entre leshommes et les femmes, ces agents de dis-tribution ont découvert un profondintérêt pour la méthode. La fonction con-traceptive du préservatif a, certes, étésoulignée pour son image, mais lamajorité des utilisatrices ont adopté laméthode, en partie du moins, pour seprotéger contre le risque d’infection. Cer-taines ont même déclaré que leur parte-naire, bien qu’ayant refusé le préservatifmasculin, s’était montré disposé à enaccepter la version féminine.
L’introduction du préservatif fémininne s’est toutefois pas déroulée sans diffi-cultés. Le plus gros problème aura étél’assurance d’approvisionnements conti-nus. Les donateurs se sont montrés hési-tants à commander et entretenir desstocks d’un produit relativement onéreux.Face à l’approvisionnement peu fiable,beaucoup d’utilisateurs sinon satisfaitesont fini par abandonner la méthode et lacampagne a perdu son élan. SWAA s’ef-force aujourd’hui de rétablir progressive-ment la demande, tout en cherchant àassurer une réserve plus stable.
Leçons tirées : 1) Le préservatif fémi-nin peut intéresser une population utilisa-teur potentielle hétérogène mais, pouréviter la connotation négative associéeau VIH, il peut être important de présen-ter la méthode parmi les contraceptifs ;2) les ONG pourraient bien être lesmieux placées pour assurer l’éducation(sur la sexualité, les questions de genre etla peur du VIH) essentielle à la distribu-tion de la méthode ; et 3) les donateursdoivent investir dans de plus vastessources d’approvisionnement si l’on veutassurer l’accès des femmes à cette impor-tante technique.
Il pourra être utile aussi, lors de laprochaine vague de programmation,d’envisager les stratégies innovatrices depositionnement de la méthode en tantque produit apte à préserver la féconditéà venir et de banalisation de la protectionau sein du mariage.
Résumé en Français

34 • Quality /Calidad /Qualité
About the Authors
Martha Brady (Afterword) is a Program Asso-ciate with the Gender, Family, and Develop-ment Program of the Population Council.
Kathleen Cravero (Introduction) is Chair, Lea-dership Council of the Global Coalition onWomen and AIDS, established by UNAIDS in2004.
Victoria Ebin (Coauthor) is an anthropologistand consultant who works with the media inAfrica and the Caribbean on improving cover-age of reproductive health.
Michelle Skaer (Coauthor) is a Staff Assistantwith the Gender, Family, and DevelopmentProgram of the Population Council.
Acknowledgments
In acknowledgement of their valuable input,the authors wish to thank the following indi-viduals (listed in alphabetical order): Henri-ette Ahrens, Rebecca Attipoe, Mags Bek-sinksa, Cira Endsley, Suzanne Fischer, TheresaHatzell Hoke, Bernice Heloo, Alice Lamptey,Mary Ann Leeper, Simone Martins, Maria Joséde Oliveira Araújo, Beth Robinson, MitchellWarren, and Ellen Weiss, as well as represen-tatives of the Planned Parenthood Associationof Ghana, the United Nations PopulationFund Ghana office, the Ghanaian Ministry ofHealth, the Ghana Registered Midwives Asso-ciation, the UNAIDS Ghana office, and theGhana Social Marketing Foundation.
We invite your comments on Quality/Calidad/Qualité. If you would like to be included on ourmailing list, please send an e-mail to: [email protected]. Most past editions are available on-line at <www.popcouncil.org/publications/qcq/default.htm>. Single or multiple print copies ofpast editions may be ordered by e-mail.
No. 1 Celebrating Mother and Child on the Fortieth Day: The Sfax Tunisia Postpartum Program, 1989. (E)
No. 2 Man/Hombre/Homme: Meeting Male Reproductive Health Care Needs in Latin America, 1990. (E,S)
No. 3 The Bangladesh Women’s Health Coalition, 1991. (E)
No. 4 By and For Women: Involving Women in the Development of Reproductive Health Care Materials,1992. (E,S)
No. 5 Gente Joven/Young People: A Dialogue on Sexuality with Adolescents in Mexico, 1993. (E,S)
No. 6 The Coletivo: A Feminist Sexuality and Health Collective in Brazil, 1995. (E,P,S)
No. 7 Doing More with Less: The Marie Stopes Clinics of Sierra Leone, 1995. (E)
No. 8 Introducing Sexuality within Family Planning: Three Positive Experiences from Latin Americaand the Caribbean, 1997. (E,S)
No. 9 Using COPE to Improve Quality of Care: The Experience of the Family Planning Association ofKenya, 1998. (E,S)
No. 10 Alone You Are Nobody, Together We Float: The Manuela Ramos Movement, 2000. (E,S)
No. 11 From Patna to Paris: Providing Safe and Humane Abortion, 2001. (E)
No. 12 Universal Sexuality Education in Mongolia: Educating Today to Protect Tomorrow, 2002. (E)
No. 13 What about Us? Bringing Infertility into Reproductive Health Care, 2002. (E)
No. 14 “My Father Didn’t Think This Way”: Nigerian Boys Contemplate Gender Equality, 2003. (E,F)
No. 15 Linking Reproductive Health to Social Power: Community Health Workers in Belize and Pakistan,2004. (E)
No. 16 Healing Wounds, Instilling Hope: The Tanzanian Partnership Against Obstetric Fistula, 2004.(E,F,Sw)
(E) = English; (F) = French; (P) = Portuguese;(S) = Spanish; (Sw) = Swahili

Q/C/Q No. 17
/Quality/Calidad/Qualité /