Improving pathway compliance and clinician performance by using information technology
6
Improving Pathway Compliance and Clinician Performance by Using Information Technology R Blaser a , M Schnabel b , O Heger a , E Opitz a , R Lenz a , K A Kuhn c a Institute of Medical Informatics, Philipps-University Marburg, Germany b Department of Trauma, Reconstructive and Hand Surgery, Philipps-University Marburg, Germany c Institute of Medical Statistics and Epidemiology, Technical University Munich, Germany Abstract To deliver patient-specific advice at the time and place of a consultation, to improve clinician performance and compliance by using computer-based decision support, and to integrate such IT solutions with the clinical workflow are important strategies for the implementation of clinical pathways. User acceptance plays a critical role: additional effort has to be balanced with enough benefit for the users. Experiences from routine use of an online surgical pathway at Marburg University Medical Center show that it is possible to successfully address this issue by seamlessly integrating patient-specific pathway recommendations with documentation tasks which have to be done anyway and by substantially reusing entered data to accelerate routine tasks (e.g. by automatically generating orders and reports). Keywords: Clinical Pathways; Clinical Decision Support Systems; Systems Integration; User Acceptance 1. Introduction For more than a decade, studies on the incidence and nature of adverse events in medicine have shown that errors in medicine are not rare and may cause severe harm [1-3]. The nature and preventability of adverse events have been studied, and cognitive overload of physicians was found to be among the reasons. Evidence-based clinical guidelines or pathways can reduce variability in practice and improve patient care outcomes [4]. Implementation strategies for guidelines and pathways which deliver patient-specific advice at the time and place of a consultation are most likely to be effective [4, 5]. Computer- based decision support (e.g. reminder systems) can improve clinician performance and guideline compliance [6, 7]. Such a capability depends on the availability of the data to make the appropriate recommendations [8]. Suitable interaction mechanisms for data entry during consultation and for the representation of patient-specific recommendations and warnings are needed. These IT solutions should be integrated with the clinical workflow and give back to the user something of value in order to minimise and to offset the inconvenience of using the system [5, 8]. In 2003 we analysed quality problems with discharge letters at the Department of Trauma, Reconstructive and Hand Surgery at University Medical Center, Marburg, Germany. Based Connecting Medical Informatics and Bio-Informatics R. Engelbrecht et al. (Eds.) ENMI, 2005 199 Section 3: Decision Support and Clinical Guidelines
-
Upload
uni-erlangen -
Category
Documents
-
view
0 -
download
0
Transcript of Improving pathway compliance and clinician performance by using information technology

Improving Pathway Compliance and Clinician Performance by Using
Information Technology
R Blasera, M Schnabelb, O Hegera, E Opitza, R Lenza, K A Kuhnc
aInstitute of Medical Informatics, Philipps-University Marburg, Germany bDepartment of Trauma, Reconstructive and Hand Surgery, Philipps-University Marburg, Germany
cInstitute of Medical Statistics and Epidemiology, Technical University Munich, Germany
Abstract To deliver patient-specific advice at the time and place of a consultation, to improve clinician performance and compliance by using computer-based decision support, and to integrate such IT solutions with the clinical workflow are important strategies for the implementation of clinical pathways. User acceptance plays a critical role: additional effort has to be balanced with enough benefit for the users. Experiences from routine use of an online surgical pathway at Marburg University Medical Center show that it is possible to successfully address this issue by seamlessly integrating patient-specific pathway recommendations with documentation tasks which have to be done anyway and by substantially reusing entered data to accelerate routine tasks (e.g. by automatically generating orders and reports).
Keywords: Clinical Pathways; Clinical Decision Support Systems; Systems Integration; User Acceptance
1. Introduction
For more than a decade, studies on the incidence and nature of adverse events in medicine have shown that errors in medicine are not rare and may cause severe harm [1-3]. The nature and preventability of adverse events have been studied, and cognitive overload of physicians was found to be among the reasons. Evidence-based clinical guidelines or pathways can reduce variability in practice and improve patient care outcomes [4]. Implementation strategies for guidelines and pathways which deliver patient-specific advice at the time and place of a consultation are most likely to be effective [4, 5]. Computer-based decision support (e.g. reminder systems) can improve clinician performance and guideline compliance [6, 7]. Such a capability depends on the availability of the data to make the appropriate recommendations [8]. Suitable interaction mechanisms for data entry during consultation and for the representation of patient-specific recommendations and warnings are needed. These IT solutions should be integrated with the clinical workflow and give back to the user something of value in order to minimise and to offset the inconvenience of using the system [5, 8]. In 2003 we analysed quality problems with discharge letters at the Department of Trauma,
Reconstructive and Hand Surgery at University Medical Center, Marburg, Germany. Based
Connecting Medical Informatics and Bio-InformaticsR. Engelbrecht et al. (Eds.)ENMI, 2005
199
Section 3: Decision Support and Clinical Guidelines

on this analysis we systematically elaborated easy to implement IT solutions which have the potential to prevent treatment errors and to improve the documentation quality by using structured data entry and reminders [9]. We used these interaction mechanisms not only to increase the quality of our discharge letters by implementing a kind of a “mini-pathway” for the letter writing process, but also to support the online implementation of major parts of clinical pathways by integrating the routine documentation process with patient-specific advice in the context of the clinical pathway. In this paper we describe our computer-based implementation of a surgical pathway at the
Department of Trauma, Reconstructive and Hand Surgery at Marburg University Medical Center, and we report on first experiences from routine use.
2. Background
Setting
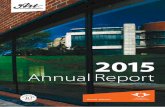
In 2001/2002 the care process for patients with proximal femoral fracture at the Department of Trauma, Reconstructive and Hand Surgery was analysed and weak points were identified (e.g. delays in timing the operation, clarification of osteoporosis) by a prospective study on 169 patients with a one year follow up (96.6% survivors). Based on the process analysis, a formal barrier analysis, and a literature and guideline research a target pathway was defined. The pathway was finalised through a multi-tiered consensus process and adopted by the board of directors. Figure 1 shows a simplified diagram of the pathway. For each step in the pathway there exists a detailed description with recommendations, e.g. for indicated X-ray examinations or appropriate medication. In order to train the clinicians and to integrate the clinical pathway into daily routine,
academic detailing and pathway controlling are used as implementation strategies. The integration of an online model of core parts of the pathway into the Marburg Health Information System was aimed at to get active decision support at the time and place of a consultation and to receive additional benefits for the clinicians from data reuse.
IT infrastructure
Marburg University Medical Center has established a responsive IT infrastructure and a holistic Health Information System (HIS) on the basis of a commercially available product, which is in widespread use in Germany, Austria, and Switzerland: the Orbis®/OpenMed-system. The Marburg HIS represents one of the most advanced installations of this system, and significant impulses for improving the system have resulted from the Marburg project [10, 11]. The system offers functionality for business/financial purposes and patient data management, as well as basic clinical functionality (e.g. ICD/ICPM and reports), and comprises an integrated CASE1 tool for rapid implementation of integrated clinical modules (“generator tool”). This generator tool is part of a vendor-specific application framework which allows to incrementally add new application modules or to adapt generic applications to specific requirements, and thereby provides the fundamentals for a responsive IT-infrastructure and demand driven software development. A detailed description of the implementation of the generator tool can be found in [11]. We have also developed an adapted software engineering process which is primarily intended to achieve an IT-alignment to healthcare process requirements [10, 12].
1 CASE: Computer Aided Software Engineering
Connecting Medical Informatics and Bio-InformaticsR. Engelbrecht et al. (Eds.)ENMI, 2005
200
Section 3: Decision Support and Clinical Guidelines

Prehospital phaseAdmission
Anamnesis andclinical examination
Clinical suspicion ofproximal femoral fracture?
Therapy depending ondiagnosis/symptom
Imaging diagnostics
Proximal femoral fracture& operation indicated?
Initial treatment(emergency area) and
operation planning
Ward/ICU andoperative treatment
Clarification ofosteoporosis
Discharge, documentation
Poststationary treatment
IT support in routine use
yes
nono yes
Figure 1: Clinical pathway for proximal femoral fracture (simplified
3. Materials and methods
Our intention was to utilise the potential of our responsive IT-infrastructure and our adapted software engineering process to develop an IT-supported pathway that is aligned to the clinical work process. Based on the results from pathway controlling, those core parts of the clinical pathway were identified for which computer-based decision support could be used effectively or necessary data should be entered. The clinical pathway model and other results from the pathway development process (e.g. quality affecting factors from the formal barrier analysis) as well as the experiences from pathway controlling and from our previous work described in [9] flowed into the specification of user-defined forms for structured data entry and of rules for recommendations and warnings. According to our adapted software engineering process the users were intensively
involved in the development of the application aligned to their requirements and integrated with the clinical workflow. The generator tool was used to rapidly develop and iteratively refine prototypes of the application directly based on the common database of the Marburg HIS. Feasibility and usability analyses were performed to test the interaction design and different mechanisms for the representation of rules.
Connecting Medical Informatics and Bio-InformaticsR. Engelbrecht et al. (Eds.)ENMI, 2005
201
Section 3: Decision Support and Clinical Guidelines

After the application was intensively tested and approved by the key users, it was activated in the routine system at the end of August 2004. IT-support for further parts of the pathway (clarification of osteoporosis and generation of discharge letters) followed in April 2005. Feedback from the clinicians is used to continuously improve the application resulting in two minor updates since begin of routine use.
4. Results
Figure 1 shows the parts of the clinical pathway which are supported by IT. The application consists of 10 forms for structured data entry and decision support:
Structured entry of data from admission, anamnesis and clinical examination; Selection of procedures for imaging diagnostics with rule-based recommendations
derived from previously entered data; online orders of the selected procedures to the radiology department can be placed (previously entered patient data is reused);
Documentation of the principle diagnosis and other diagnoses (ICD codes and additional medical description);
Selection of procedures and medication for the initial treatment in the emergency area, and operation planning (e.g. selection of appropriate implant) with rule-based recommendations and warnings derived from previously entered data;
Structured entry of instructions for the ward; Structured data entry for clarification of osteoporosis.
A report for further treatment on the ward can be generated from previously entered data, and these data also can be reused for other routine documentation (e.g. discharge letters). As an example, figure 2 shows the form for initial treatment. Patient-specific pathway
information is given by preselected medication and procedures. Those selections which correspond with an existing pathway recommendation are marked with a superscript “p”. Deviation from the pathway is possible but needs to be documented (variance documentation). The user can navigate through the forms in the predefined order (“previous” or ”next”) or he can jump directly to the desired form. So far, the application contains about 20 rules e.g. for medication, for X-ray
recommendations based on the age of the patient and documented diagnoses, and for warnings, e.g. if a documented allergy contraindicates the use of the selected implant. These rules are represented by using catalogues (e.g. for diagnoses and for X-ray examinations) and correlations between the catalogue entries. During eight months of routine use, the online pathway was successfully used for 84% of
the patients with proximal femoral fracture (n = 123). User feedback was very positive and additional effort for data entry was accepted as enough benefit from data reuse was given back to the users (e.g. generation of online orders and reports).
5. Discussion and Conclusion
More detailed studies on user satisfaction by means of standardised questionnaires and on pathway compliance are about to follow, but user feedback already shows that this clinical module is acceptable and usable in the daily routine.
Connecting Medical Informatics and Bio-InformaticsR. Engelbrecht et al. (Eds.)ENMI, 2005
202
Section 3: Decision Support and Clinical Guidelines

To deliver patient-specific advice at the time and place of a consultation, to improve clinician performance and compliance by using computer-based decision support, and to integrate such IT solutions with the clinical workflow are important strategies for the implementation of guidelines and clinical pathways [5-8]. Our solution can reach this goal by seamlessly integrating patient-specific pathway information into the routine documentation. Data is made available through structured data entry during consultation, and rule-based recommendations are given to the users in an unobtrusive way by means of preselected medication or procedures. The integrated generator tool and our software engineering process [10-12] make it possible to integrate the IT solution with the clinical workflow and to rapidly adapt it to the users needs. These approaches also can cause negative effects which have to be considered. Interaction
mechanisms for recommendations have to be designed carefully to avoid biases or errors, and it is important to intensively involve the physicians [13]. User acceptance plays a critical role and is one of the major obstacles on the way to online guidelines and pathways [5,8]. Additional effort (e.g. from data entry) has to be balanced with enough benefit for the users. We address this issue by integrating parts of the online pathway with documentation tasks which have to be done anyway and by substantially reusing entered data to accelerate routine tasks (e.g. by automatically generating orders and reports). It is important to concentrate on core parts of the pathway and to keep the online implementation as simple as possible. So far, comparatively simple methods for the representation of rules and for workflow support sufficed for our implementation. In order to be able to implement more
Figure 2: Form for initial treatment with preselected medication and procedures according to the recommendations in the clinical pathway as well as variance documentation.
Connecting Medical Informatics and Bio-InformaticsR. Engelbrecht et al. (Eds.)ENMI, 2005
203
Section 3: Decision Support and Clinical Guidelines

complex rules and workflows, if needed, we are testing the ARDEN engine and the workflow engine which are incorporated into the generator tool. The effectiveness of our approach is continuously being evaluated and improved.
Presently adaptations of the interaction mechanisms are being discussed to further increase user benefit and user acceptance.
6. References
[1] Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, Hebert L, Newhouse JP, Weiler PC, Hiatt H. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med 1991; 324(6):377-384.
[2] Thomas EJ, Studdert DM, Burstin HR, Orav EJ, Zeena T, Williams EJ, Howard KM, Weiler PC, Brennan TA. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care 2000; 38(3):261-271.
[3] Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The Quality in Australian Health Care Study. Med J Aust 1995; 163(9):458-471.
[4] Grimshaw JM, Russell IT. Effect of clinical guidelines on medical practice: a systematic review of rigorous evaluations. Lancet 1993;342:1317-22.
[5] Shiffman RN, Liaw Y, Brandt CA, Corb GJ. Computer-based guideline implementation systems: a systematic review of functionality and effectiveness. J Am Med Inform Assoc 1999; 6(2):104-114.
[6] Johnston ME, Langton KB, Haynes RB, Mathieu A. Effects of computer-based clinical decision support systems on clinician performance and patient outcome. A critical appraisal of research. Ann Intern Med 1994; 120(2):135-142.
[7] Elson RB, Connelly DP. Computerized decision support systems in primary care. Prim Care 1995; 22(2):365-384.
[8] Zielstorff RD. Online practice guidelines: issues, obstacles, and future prospects. J Am Med Inform Assoc 1998; 5(3):227-236.
[9] Blaser R, Schnabel M, Mann D, Jancke P, Kuhn KA, Lenz R. Potential Prevention of Medical Errors in Casualty Surgery by Using Information Technology. In: Haddad HM, Papadopoulos GA, Omicini A, Wainwright RL, Liebrock LM, Palakal MJ, Andreou A, Pattichis C, eds. Proceedings of the 19th ACM Symposium on Applied Computing (SAC 2004). New York: ACM, 2004; pp. 285-290.
[10] Kuhn KA, Lenz R, Elstner T, Siegele H, Moll R. Experiences with a generator tool for building clinical application modules. Methods Inf Med 2003; 42(1):37-44.
[11] Lenz R, Elstner T, Siegele H, Kuhn KA. A practical approach to process support in health information systems. J Am Med Inform Assoc 2002; 9(6):571-585.
[12] Lenz R, Kuhn KA. Towards a Continuous Evolution and Adaptation of Information Systems in Healthcare. Int J Med Inf 2004; 73(1):75-89.
[13] Anderson JG. Clearing the way for physicians' use of clinical information systems. Communications of the ACM 1997; 40(8):83-90.
Address for Correspondence
Rainer Blaser Institut für Medizinische Informatik Klinikum der Philipps-Universität Marburg D-35033 Marburg GERMANY e-mail: [email protected]
Connecting Medical Informatics and Bio-InformaticsR. Engelbrecht et al. (Eds.)ENMI, 2005
204
Section 3: Decision Support and Clinical Guidelines