Implementing bedside handover: strategies for change management: Implementing bedside handover
Upload
independentCategory
view
1download
0
Implementing a national approach to universal child and family health
services in Australia: professionals’ views of the challenges and
opportunities
Virginia Schmied RN RM PhD1, Caroline Homer RM PhD
2, Cathrine Fowler RN PhD3, Kim Psaila RN BA MN (Hons)
1,
Lesley Barclay PhD AO4, Ian Wilson MBBS PhD
5, Lynn Kemp RN BHSc PhD6, Michael Fasher MBBS
7 and
Sue Kruske RN RM PhD8
1School of Nursing and Midwifery, University of Western Sydney, Penrith, New South Wales, Australia, 2Centre for
Midwifery, Child and Family Health, Faculty of Health, University of Technology Sydney, Broadway, New South Wales,
Australia, 3Tresillian Chair in Child and Family Health, Faculty of Health, University of Technology Sydney, Broadway,
New South Wales, Australia, 4University Centre for Rural Health, University of Sydney, Uralba St Lismore, New South
Wales, Australia, 5Learning & Teaching, Graduate School of Medicine, University of Wollongong, Wollongong, New
South Wales, Australia, 6Centre for Health Equity Training Research and Evaluation (CHETRE), UNSW Centre for
Primary Health Care and Equity, Population Health, South Western Sydney Local Health District, Ingham Institute,
Liverpool, New South Wales, Australia, 7Sydney Medical School, University of Sydney and School of Medicine,
University of Western Sydney, Sydney, New South Wales, Australia and 8The School of Nursing and Midwifery,
The University of Queensland, Brisbane, Queensland, Australia
Accepted for publication 30 May 2014
Correspondence
Virginia Schmied
School of Nursing and Midwifery
University of Western Sydney
Building EB Parramatta Campus,
Locked Bag 1797
Penrith South, Penrith,
New South Wales 2751, Australia
E-mail: [email protected]
What is known about this topic
• Children have higher levels of well-being in countries where child health issupported by access to a universalchild health service.
• The Australian system of universalCFH services is inconsistent acrossjurisdictions, fragmented acrossdisciplines and sectors, and does notmeet population needs.
What this paper adds
• This is the first study to synthesise theviews of CFH nurses, midwives, GPsand practice nurses about thechallenges of implementing a nationalapproach to universal CFH services.
• Challenges include data availability,information exchange, communicationbetween disciplines, workforcelimitations, equity in service deliveryand tensions around role boundaries.
• System improvement strategies includelinkage of national data sets, effectivecommunication pathways, co-locationof services and interprofessionallearning.
AbstractAustralia has a well-accepted system of universal child and family health (CFH)services. However, government reports and research indicate that these servicesvary across states and territories, and many children and families do not receivethese services. The aim of this paper was to explore professionals’ perceptions ofthe challenges and opportunities in implementing a national approach touniversal CFH services across Australia. Qualitative data were collected betweenJuly 2010 and April 2011 in the first phase of a three-phase study designed toinvestigate the feasibility of implementing a national approach to CFH servicesin Australia. In total, 161 professionals participated in phase 1 consultationsconducted either as discussion groups, teleconferences or through emailconversation. Participants came from all Australian states and territories andincluded 60 CFH nurses, 45 midwives, 15 general practitioners (GPs), 12 practicenurses, 14 allied health professionals, 7 early childhood education specialists, 6staff from non-government organisations and 2 Australian government policyadvisors. Data were analysed thematically. Participants supported the concept ofa universal CFH service, but identified implementation barriers. Key challengesincluded the absence of a minimum data set and lack of aggregated nationaldata to assist planning and determine outcomes; an inconsistent approach totransfer of information about mothers and newborns from maternity services toCFH nursing services or GPs; poor communication across disciplines andservices; issues of access and equity of service delivery; workforce limitationsand tensions around role boundaries. Directions for change were identified,including improved electronic data collection and communication systems,reporting of service delivery and outcomes between states and territories,professional collaboration, service co-location and interprofessional learning anddevelopment.
Keywords: child and family nursing, child health, family health, generalpractice, midwives, universal child and family health services
© 2014 John Wiley & Sons Ltd 1
Health and Social Care in the Community (2014) doi: 10.1111/hsc.12129
Introduction
Studies demonstrate that events during pregnancyand the early years of life strongly influence healthand development (National Scientific Council on theDeveloping 2007, Robinson et al. 2011). Governmentshave an obligation to devise health and social sup-port systems that ensure effective parenting and pro-mote positive early child development (McCain &Mustard 2002). In countries where child health is sup-ported by such policy, children have higher levels ofwell-being (Kuo et al. 2006). One significant compo-nent of a system of early childhood services is anavailable, accessible universal health service (Kuoet al. 2006, Oberklaid et al. 2013).
Australia has a well-accepted system of universalhealth services for children and families informed byprinciples of primary healthcare, prevention, earlyintervention and utilises a strengths-based approach(Australian Health Ministers Advisory Council 2011,Schmied et al. 2011). Government-funded child andfamily health (CFH) nurses (also known as maternaland child health nurses in some states and territories)provide services for families and children from birth toschool entry, including health and development sur-veillance, immunisation, information about health andparenting issues, and support for families, throughmultiple contact points at the primary level (AustralianHealth Ministers Advisory Council 2011). Contactoccurs at home or in a centre. Midwives provide carethrough pregnancy, birth and up to 6 weeks in thepostnatal period and general practitioners (GPs) pro-vide primary care services for families across the life-span including care for pregnant women and newborns.
Despite these services, a recent analysis of thewell-being of Australia’s children (ARACY 2013) indi-cates that the health of Australian children, particu-larly Indigenous children, does not comparefavourably with the health of children in many othercountries. This could be related to the complex sys-tem of healthcare provision. Australia has eight statesand territories, a federal government and a networkof local government authorities. A significant propor-tion of healthcare is the domain of the states and ter-ritories (known hereafter as jurisdictions). Thisincludes care provided by CFH nurses and midwives.GPs, in contrast, are funded through Medicare, a uni-versally available federal public health insurancemechanism. There is a constant tension between thefederal and state/territory systems. Published litera-ture and government reports indicate that universalCFH services are inconsistent across jurisdictions,fragmented across disciplines and sectors, and do notadequately meet the needs of the population (Brother-
hood of St Laurence 2005, Hirst 2005, Brinkman et al.2012). While jurisdictional policies reflect commoncore principles (Schmied et al. 2011), there are consid-erable differences; for example, the frequency ofscheduled contacts offered to all children and familiesfrom birth to 5 years varies from none to 10(Brinkman et al. 2012). To address the inconsistencyin universal CFH services, the Australian governmentcommissioned a National Framework for Universal Childand Family Health Services (Australian Health Minis-ters Advisory Council 2011), which articulates avision for universal health services for children andfamilies from birth to 8 years of age.
This paper explores health professionals’ percep-tions of the challenges and opportunities related toimplementing a national approach to universal CFHservices across Australia. The data reported here arefrom the first phase of a three-phase mixed-methodsstudy investigating the feasibility of implementing anational approach to CFH services in Australia.
Methods
Qualitative description (Sandelowski 2010) informeddata collection and analysis in phase 1 of this three-phased sequential mixed-methods study. Phase 1 wasconducted between July 2010 and April 2011 and wesought health and other professionals’ perceptions ofthe challenges in implementing a universal CFH ser-vice in Australia. Qualitative description offers astraight description of experiences and is useful whengathering information to inform service improvement(Greenhalgh et al. 2004) as well as informing thesequential phases of a mixed-methods study (Creswell& Clark 2007). In phase 2, we conducted two nationalsurveys of midwives (655 respondents) and CFHnurses (1098 respondents) and held one-to-one inter-views with 71 GPs to determine their perspectives oftheir role in CFH services and the facilitators of andbarriers to the provision of universal services for chil-dren and families. Results on the role of CFH nurses inAustralia (Schmied et al. 2014), issues of continuity ofcare (Psaila et al. 2014a), the extent of collaborationbetween midwives and CFH nurses (Psaila et al. inpress) and the transition of care from maternity to CFHservices (Psaila et al. 2014b) are published elsewhere.In phase 3, we sought illustrations of exemplary ser-vices where innovation had occurred, particularlywhere universal CFH service providers were workingcollaboratively to meet the needs of children and fami-lies. Twenty one services participated in this phase andthe findings are reported elsewhere. A parallel studyof consumers of CFH services (N = 700) has also beenconducted. Consumer representative groups such as
© 2014 John Wiley & Sons Ltd2
V. Schmied et al.

the Australian Breastfeeding Association participatedin phase 1.
The study was approved by the University ofWestern Sydney Human Research Ethics Committee.
Participants and recruitment
We invited representatives from five Australian profes-sional organisations: Australian College of Midwives(ACM); Maternal Child and Family Health Nurses ofAustralia (MCaFHNA); The Royal Australian Collegeof General Practitioners (RACGP); Australian PracticeNurse Association (APNA); and the Australian GeneralPractice Network (AGPN) (now the Australian Medi-care Local Alliance). We requested each organisation tonominate professional leaders as representatives. Wedetermined that professional leaders were individualswho contributed actively to the development oradvancement of their profession and advocated forresources and support to meet the needs of familieswith children. Some participants were on the executivecommittee or subcommittees of their respective profes-sional organisations and they represented their associa-tion at local, state and national levels. Otherparticipants demonstrated their leadership contribu-tion by providing policy advice or acting as changeagents, and some participants contributed regularly tothe professional literature. In some instances, the pro-fessional leaders were service managers or clinicalnurse/midwife consultants. Participants were pro-vided, in advance via email, information about thestudy, with the questions to be asked during the con-sultations, and consent forms.
We also sought the perspective of other profes-sionals who work with children and families, includ-ing allied health professionals, early childhoodeducation specialists and policy advisors. Invitationsto participate were sent via email through organisa-tions involved as study partners.
In total, 161 professionals participated in the con-sultations. This included 60 CFH nurses, 45 midwives,15 GPs, 12 practice nurses, 14 allied health profession-als, 7 early childhood education specialists, 6 staff fromnon-government organisations (NGOs) and 2 Austra-lian government policy advisors (see Box 1). The non-government organisations provided family supportand advocacy or services for consumers of CFH ser-vices such as Aboriginal families, young parents andfamilies from refugee and migrant backgrounds.
Data collection
We held five separate focus groups via teleconferencewith groups representing their professional associations:
one teleconference with eight CFH nurses, one withfive midwives, one with six GPs and two teleconfer-ences with twelve practice nurses (six in each)(see Box 1). In addition, we held 2 consultative dis-cussion groups with 52 CFH nurses (one discussiongroups) and 40 midwives (one discussion group) atnational conferences. To obtain further informationfrom GPs, one researcher facilitated a discussion viaemail (e-conversation) with nine members of the RAC-GP. We also held one videoconference and one tele-conference with allied health professionals (e.g. socialwork, speech and occupational therapy) and two face-to-face consultations, one with representatives from arange of NGOs and the other with early childhoodeducation specialists. In addition, we conducted 2one-to-one interviews with State government policymakers. All jurisdictions were represented.
The discussion groups ranged from 1 to 1½ hours.Two to three members of the research team were inattendance. One researcher led as group facilitator,while the other researcher/s took notes and observedgroup interaction. Questions were tailored to eachprofessional group. Topics included the group’s rolein delivering CFH services; facilitators of and barriersto undertaking their role; changes needed in organi-sational and professional practice; and knowledge ofpractice innovations (see Box 2 with the key promptsasked during the consultations). Each consultation
Box 1 Number of participants from each professional group
MCaFHNA Group 1 – face-to-face discussion
group/workshop
42
Group 2 – teleconference with
state-based representatives
8
Group 3 – face-to-face focus
group
10
RACGP e-conversation 9
AGPN Focus group via teleconference 6
APNA Focus group 1 via teleconference 6
Focus group 2 via teleconference 6
ACM Group 1 – face-to-face discussion
group/workshop
40
Group 2 – teleconference with
state-based representatives
5
Allied health Teleconference 5
Face-to-face focus group including
videoconference
9
NGO Face-to-face focus group 6
Early childhood
education specialists
Face-to-face focus group 7
Policy makers and
key stakeholders
One-to-one interviews 2
ACM, Australian College of Midwives; MCaFHNA, Maternal
Child and Family Health Nurses of Australia; RACGP, Royal
Australian College of General Practitioners; APNA, Australian
Practice Nurse Association; AGPN, Australian General Practice
Network; NGO, non-government organisation.
© 2014 John Wiley & Sons Ltd 3
Implementing a national approach to universal CFH services
was digitally audio-recorded with consent fromparticipants.
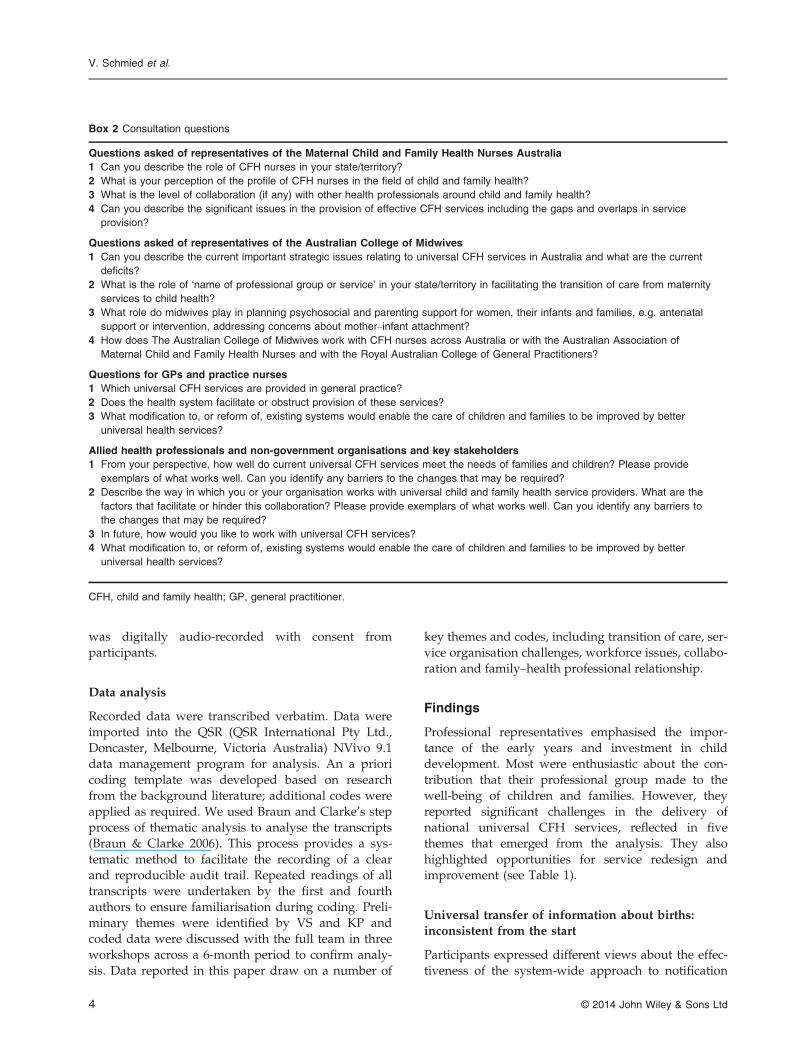
Data analysis
Recorded data were transcribed verbatim. Data wereimported into the QSR (QSR International Pty Ltd.,Doncaster, Melbourne, Victoria Australia) NVivo 9.1data management program for analysis. An a prioricoding template was developed based on researchfrom the background literature; additional codes wereapplied as required. We used Braun and Clarke’s stepprocess of thematic analysis to analyse the transcripts(Braun & Clarke 2006). This process provides a sys-tematic method to facilitate the recording of a clearand reproducible audit trail. Repeated readings of alltranscripts were undertaken by the first and fourthauthors to ensure familiarisation during coding. Preli-minary themes were identified by VS and KP andcoded data were discussed with the full team in threeworkshops across a 6-month period to confirm analy-sis. Data reported in this paper draw on a number of
key themes and codes, including transition of care, ser-vice organisation challenges, workforce issues, collabo-ration and family–health professional relationship.
Findings
Professional representatives emphasised the impor-tance of the early years and investment in childdevelopment. Most were enthusiastic about the con-tribution that their professional group made to thewell-being of children and families. However, theyreported significant challenges in the delivery ofnational universal CFH services, reflected in fivethemes that emerged from the analysis. They alsohighlighted opportunities for service redesign andimprovement (see Table 1).
Universal transfer of information about births:inconsistent from the start
Participants expressed different views about the effec-tiveness of the system-wide approach to notification
Box 2 Consultation questions
Questions asked of representatives of the Maternal Child and Family Health Nurses Australia
1 Can you describe the role of CFH nurses in your state/territory?
2 What is your perception of the profile of CFH nurses in the field of child and family health?
3 What is the level of collaboration (if any) with other health professionals around child and family health?
4 Can you describe the significant issues in the provision of effective CFH services including the gaps and overlaps in service
provision?
Questions asked of representatives of the Australian College of Midwives
1 Can you describe the current important strategic issues relating to universal CFH services in Australia and what are the current
deficits?
2 What is the role of ‘name of professional group or service’ in your state/territory in facilitating the transition of care from maternity
services to child health?
3 What role do midwives play in planning psychosocial and parenting support for women, their infants and families, e.g. antenatal
support or intervention, addressing concerns about mother–infant attachment?
4 How does The Australian College of Midwives work with CFH nurses across Australia or with the Australian Association of
Maternal Child and Family Health Nurses and with the Royal Australian College of General Practitioners?
Questions for GPs and practice nurses
1 Which universal CFH services are provided in general practice?
2 Does the health system facilitate or obstruct provision of these services?
3 What modification to, or reform of, existing systems would enable the care of children and families to be improved by better
universal health services?
Allied health professionals and non-government organisations and key stakeholders
1 From your perspective, how well do current universal CFH services meet the needs of families and children? Please provide
exemplars of what works well. Can you identify any barriers to the changes that may be required?
2 Describe the way in which you or your organisation works with universal child and family health service providers. What are the
factors that facilitate or hinder this collaboration? Please provide exemplars of what works well. Can you identify any barriers to
the changes that may be required?
3 In future, how would you like to work with universal CFH services?
4 What modification to, or reform of, existing systems would enable the care of children and families to be improved by better
universal health services?
CFH, child and family health; GP, general practitioner.
© 2014 John Wiley & Sons Ltd4
V. Schmied et al.
that a woman had given birth and was returninghome. CFH nurse representatives from Victoria werethe most positive about the system for universal con-tact with families, reflecting an effective mandatedbirth notification system where maternity services arerequired by law (Department of Education and EarlyChildhood Development 2011) to notify the maternaland child health service of every birth in the localgovernment area:
In Victoria, we have compulsory notification of births,whether it’s hospital-based or a community-based birth. Ithink the statistics bear out that we do 97% of the popula-tion [who] get a home visit. (MCaFHNA group 1)
In other jurisdictions, participants reported adiverse range of systems to transfer information frommaternity services to CFH nursing services or GPs.Some were considered effective:
We [CFH service] have electronic databases that actively‘talk’ to maternity databases. So all births from hospitalsthat participate, and in my area they are automaticallytransferred over. We have a 97% home visit rate too,because of that. (MCaFHNA group 1)
However, a NSW CFH nurse noted:
There’s no birth notification, so we cannot rely on thematernity hospitals referring, or the clients self-referringand you don’t know if anyone is missing. (MCaFHNAgroup 1)
Another participant reported:
In Queensland, it really depends on the hospital. Someseem to have good systems but this is not universal, withthe private sector being particularly bad at informing thelocal CFH Service. (MCaFHNA group 1)
Across Australia, particularly in remote areas,CFH services often relied on informal notification:
In remote Indigenous communities, the women have to flyout to a large regional centre at 34 or 36 weeks. So weknow who’s out of community waiting to give birth [butnot when they come back]. We very much rely on local gos-sip, to say such-and-such had their baby. (MCaFHNAgroup 1)
When systems are not in place, professionalsreported that the onus is placed on women to makecontact with services:
Maternity units inform women of the service and may givea brochure, a fridge magnet [with service contact numbers]or tell women they should contact the service. (MCaFHNAgroup 1)
Many participants were also concerned about thetimeliness and type of information received:
The information we get is often delayed, and we don’t getit . . . in a timely manner. And a lot of times we’ll walkin . . . somewhat blind [i.e. with insufficient information].(MCaFHNA group 3)
Another related challenge in the delivery and eval-uation of universal CFH services is the access toaggregated and comparative data. Data collected onchildren and families in each jurisdiction are not col-lated or reported nationally; one participant stated‘we are desperate for a national minimum data set’(PA1). One nurse argued, ‘ideally we would use thesame tools nationally’ (MCaFHNA group 2).
Communication – the elephant in the room
There was a general view that professionals provid-ing CFH services do not communicate well. A repre-sentative from a NGO stated:
We have these silos, health sits here, education sits here,child protection sits here. It’s almost a mortal sin to talk toone another. (NGO group)
The lack of communication between sectors andservices was highlighted:
For the most part though, we work in silos. As a GP, I willread the personal health record [of the child], which con-tains information from the child health nurses, but haveonly contacted them directly on one occasion that I canremember. (GP e-conversation)
You’ve got all these individual services being offered outthere that keep things to themselves. (APNA group 1)
The limited mechanisms for sharing informationand linking data about children and families acrossprofessions, services and government agenciesemerged strongly as a key barrier to effective com-munication and collaboration. A GP described:
Table 1 Themes identified
Challenges Opportunities
• Universal transfer of
information about births:
inconsistent from the start
• Communication – the
elephant in the room
• Equity and access in
universal CFH services
• Mismatch between policy
expectations and workforce
capacity
• No one knows what I do
• Structures that work
• Building collaboration
• Seizing opportunities
© 2014 John Wiley & Sons Ltd 5
Implementing a national approach to universal CFH services
The whole issue of connectivity between providers, I stillthink that is the elephant in the room. Until we can actuallyhave an efficient, obviously secure system, whereby oneprovider can interact and communicate with another pro-vider, we are still going to be having gaps and potentially,duplication. (AGPN group)
Equity and access in universal CFH services
Concerns about lack of equity and access to serviceswere common across the consultations. GP partici-pants noted:
We are not reaching the hard to reach . . . families who areunable to afford fees, long waiting lists. (GP e-conversation)
In other cases, specialist services have long wait-ing lists for those without private health insurance:
We have very good access to private speech pathologists inan area like this, very good access, but it’s very expensiveeven if you have top [private] medical insurance. To getthat access to the public system, your child will already beat school before that happens. (GP e-conversation)
Services were not always accessible because oftransport or opening hours:
Access is really only for those people who have transport,others can’t get there because the bus doesn’t go there. Theycould get there with two children, but three children on thebus is another issue. (MCaFHNA group 1)
When they [mothers] return to work from being on maternityleave, the hours of operation for a CFH nurse make it increas-ingly difficult, only 9 to 5. (Allied Health group)
Despite increasing emphasis on ‘reaching out’ tothose who do not access CFH services, some participantsbelieved that CFH nursing services continue to primarilysupport families with high levels of personal resources,which really only require scheduled universal services:
In some communities, the CFH nurse caters for the worriedwell and services are not available on the outskirts of townwhere there [are] massive social issues. There is no opportu-nity for someone just to drop in. (NGO group)
NGO representatives also believed that some womenor families felt judged by the universal CFH service:
Young parents and those from disadvantaged backgroundsare the people who least access service for fear of judge-ment. (NGO group)
Mismatch between policy expectationsand workforce capacity
Workforce numbers, capacity and skill were seen asthe major challenge to providing a universal CFH
service to Australian children and families. A short-age of CFH nurses limited the capacity to meet policyexpectations. This shortage stemmed from two issues:the number of funded positions available and thenumber of qualified nurses prepared to work in cer-tain geographical areas. Shortages were consideredparticularly severe in certain locations:
The number of staff prepared to work in remote areas aswell as work in CFH is few and far between. So, althoughwe have developed a programme of universal visitsfor children, it still just doesn’t get done. (MCaFHNAgroup 2)
CFH nurses in some districts reported that theywere not able to meet local policy requirements, par-ticularly for universal home visiting within the firstmonth after birth:
If someone’s deemed to be a low priority, they are actuallynot given a universal first home visit, which doesn’t followour framework [jurisdictional policy]. They are given theoption of coming to a clinic and they may or may not come.(MCaFHNA group 3)
Women don’t hear from the CFH nurses for well over2 weeks. So the women had already done the toughestpatch with their babies . . . and there was nothing inbetween. (ACM group 2)
Even in Victoria, where participants reported anadequate CFH nursing workforce, geographical varia-tion occurred; for example, in one metropolitan areaparticipants stated:
We were finding it extremely difficult to get staff and Ithink that shows the vulnerability of this area, that many ofthe professionals don’t live out here and so it was very hardto get them to work in these areas. (MCaFHNA group 1)
Another common concern was availability of refer-ral services:
What’s the use of identifying a problem when we don’thave any services to actually refer the families to, particu-larly around developmental issues? Thus, GPs may bereluctant to be curious about development and behaviour.(GP e-conversation)
GPs identified their restricted capacity to conductchild developmental assessments and to supportfamilies:
Current funding rebates and incentives primarily focus onchronic care and services for well children and families arenot prioritised. (GP e-conversation)
And as a consequence
. . .many GPs have lost skills with the fragmentation of ser-vices. (GP e-conversation)
© 2014 John Wiley & Sons Ltd6
V. Schmied et al.

‘No one knows what I do!’
It was evident that the professional groups providinguniversal CFH services rarely communicated witheach other, leading to misunderstandings about dis-crete role and function. Some participants suggested:
This can lead to tension between professional groups.(ACM group 1)
One GP acknowledged:
I am not fully aware of who sees the children whom I seeand what value each contact actually could and does bring.(GP e-conversation)
Each professional group expressed concern thattheir contribution to the well-being of children andfamilies was not known or appropriately valued bythe other groups. The phrase ‘they don’t know whatwe do’ reflected the perspective of CFH nurses, GPs,practice nurses and midwives alike (see Box 3).
Concern about who was best to provide universalservices to children and families also dominated somediscussions. CFH nurse representatives were particu-larly vocal in this regard, expressing concern about thequalifications and/or the skills and experience of GPs,practice nurses and pharmacy nurses in this field:
Practice nurses often ring me to ask advice on growth anddevelopment because they don’t get the education aroundthat. So we’re not seeing the client, but yet we’re sharingknowledge. (MCaFHNA group 1)
We [CFH nurses] encourage breastfeeding. We find that thewoman goes to the doctor . . . asking for some assistancewith breastfeeding, and a lot of times, doctors . . . becausethey don’t have a lot of experience with breastfeeding, theytend to just say, ‘Go home and feed him with for-mula’ . . . instead of saying, ‘go and see the CFH nurse’.(MCaFHNA group 3)
GPs also noted that increasing fragmentation of ser-vices and the advent of specialist paediatrics ‘haveremoved the assessment and care of well babies fromgeneral practice . . . resulting in deskilling for GPs’.One GP added that employment of practice nurses hasimpacted the relationship that a GP has with a family:
I wonder with the advent of practice nurses doing all ourimmunisation, whether this has fragmented and lessenedthe care we provide at the early age. It used to be a fullconsult psychosocial review, which has now been replacedby a stab from the nurse. (GP e-conversation)
Opportunities and strategies for change
Participants were asked to describe what was work-ing well in the delivery of universal CFH servicesand to identify opportunities for service improvementand strategies for change. One policy advisor pro-posed that a national approach to universal CFH ser-vices was now more feasible:
I think for the first time ever we probably could have anational system because all are on board now . . . becauseeverybody (jurisdictions) has now started talking more andthere’s a lot of sharing, so aligning (jurisdictions) wouldn’tactually be all that difficult and with the electronic healthrecords, there is potential. (PA1)
This participant described the CFH nursing serviceas an ‘extraordinary resource that needed to be usedeffectively to achieve positive outcomes’.
Structures that work
Participants described practice change or innovationsthat had worked or were needed. They provided illus-trations where the current CFH service system workedwell or where local adaptations had enhanced service
Box 3 Data extracts representing the theme: ‘No one knows what I do!’
No one knows what I do!
General practitioners Child and family health nurses
Contribution to health not appreciated, our strengths not seen by
other health professionals . . . (General practice) is often viewed
from a deficit model – that is acute services only see what has
gone wrong – ‘the failures’. (GP e-conversation)
The GPs do not refer back to Child Health Services regularly
enough. They sort of think of us as something that isn’t really
available. They just forget that we’re there sometimes,
depending on where you are. (MCaFHNA group 3)
Practice nurses Midwives
I find our team of doctors are very reluctant to let go of the
responsibility to nurses, with health promotion, especially with the
Medicare system not having lots of financial incentives for
nurses’ time in that area. (PN group 1)
Antenatal care’s all done by our doctors, even when they have a
midwife. (PN group 2)
If I was inventing the perfect system, I would like to see that we
had closer relationships and ties with the community setting.
This is one of the biggest issues, I feel, they really don’t
understand how we operate in the hospital and perhaps we
don’t understand how they operate in the community. (ACM
group 2)
GP, general practitioner; MCaFHNA, Maternal Child and Family Health Nurses of Australia; PN, practice nurse; ACM, Australian
College of Midwives.
© 2014 John Wiley & Sons Ltd 7
Implementing a national approach to universal CFH services

access. For example, CFH nurses from Victoria spokepositively about the long-standing structure locatingCFH nursing services within local government:
. . .one of the really strong things that Victoria offers is thatwe come under the umbrella of the local government, whoreally value our service, because they can see that it actuallysupports the families living within their local governmentarea . . . It actually promotes connection between families,and it promotes the use of other services such as theplaygroups and the kindergartens in the area. (MCaFHNAgroup 2)
Some midwife participants also promoted the ben-efits of managing or integrating CFH nursing serviceswith maternity services:
We are under the same management structure, that helps.(ACM group 1)
However, examples of effective services were rare;most professionals agreed that mechanisms to ‘untan-gle’ the mass of services, reduce the confusion andguide families within the system were needed. Onepolicy advisor also advocated the idea of ‘one entrypoint’ for all sectors (health, early childhood educa-tion, family support).
Building collaboration
Most CFH nurses and midwives spoke positivelyabout regular multidisciplinary meetings recentlyestablished in some jurisdictions to address the psy-chosocial needs of families. Participants emphasisedincreasing opportunities to support collaborationthrough shared learning and discussion, ‘we havebeen sharing in-service [education] and that hasimproved communication’ (MCaFHNA group 1). Par-ticipants also offered several examples of local serviceinnovation that could inform service-level change, forexample, joint antenatal visiting with midwives andCFH nurses to assist families with complex needs
(MCaFHNA group 1). Exemplars of service innova-tion – one from a rural/remote area; another from ametropolitan service for young parents – are pre-sented in Box 4.
CFH nurse and GP participants were enthusiasticabout a new model of service collaboration in NSWdesigned to integrate GP services with state govern-ment-funded community health:
[This model] is basically about the communication and col-laboration among all of the services; community health,GPs and hospitals. A CFH nurse (employed as a liaison)provides the linkage, and communication among thesegroups. (MCaFHN group 3)
Co-location of services was identified by nurses,midwives and NGO staff as one way to improvecommunication and collaboration:
We do our antenatal visits at the CFH clinics, so the womenbecome familiar with that environment. We introduce themto some of the CFH nurses while they’re in that environ-ment so when they have got a baby, they know exactlywhere to go. (ACM 2)
Seizing opportunities
Other participants described initiatives that werefacilitated by specific funding opportunities such asthe National Perinatal Depression Initiative (PerinatalMental Health Consortium 2008). One jurisdictionestablished nurse liaison roles to ensure that womenwith perinatal depression were linked into appropri-ate services. This included negotiating with generalpractice for CFH liaison nurses to refer women need-ing psychological services directly rather than themhaving to also see the GP.
Although still in the planning stage at the time ofdata collection, GP participants considered that Medi-care Locals offered a significant opportunity for thefuture delivery of CFH services:
Box 4 Exemplars of practice innovation
Exemplar 1: Remote setting in Queensland
In those small towns, they have employed a community midwife. Traditionally, the CFH nurses have been providing generalist
community health and CFH and school health, so the community midwife now joins that team. The women are seen by the
community midwives antenatally and they may provide clinical care or they may also be providing a lot of transport assistance to
get them to and from appointments and linking them into other services where they’re getting care as well. Then there’s a transition
period where the CFH nurse comes to a late pregnancy visit. Then they both visit hospital and then the midwife does the handover
in the home to the child health nurse, so they’re actually employed by the service. (ACM group 2)
Exemplar 2: Young mothers group in metropolitan New South Wales
We run a young mums group and we have a postnatal group that the CFH nurse comes and facilitates that group. So we run it in the
same setting and the groups overlap, so they start to see that there’s a group for them to join into. So in terms of a group model like
the antenatal care’s in groups, the postnatal care’s in groups, the CFH nurse is there, it’s a familiar space. (ACM group 2)
CFH, child and family health; ACM, Australian College of Midwives.
© 2014 John Wiley & Sons Ltd8
V. Schmied et al.
The linking of all child health services under one fundingarrangement as is proposed in Medicare Locals could iden-tify gaps in local services and set priorities for integratedcare. (GP e-conversation)
In Australia, Medicare Locals have been estab-lished to plan health services within local communi-ties and ensure that decisions about health servicesare made by local communities in line with localneeds. Another group said:
The concept of Medicare Local is an approach to bring thatabout. So what we’re doing is we are going to identifywhat services are available and bring all the players to thetable and have a database of the services. (AGPN focusgroup)
However, CFH nurses appeared concerned aboutMedicare Locals encroaching on their role:
I want nurses on all the boards of Medicare Locals [tospeak for CFH nurses], ‘don’t try and take over our turf,just know that we’re here, and refer to the service, of childand family health’. (MCaFHNA group 2)
Discussion
The findings illustrate the different perspectives pro-fessionals hold about the challenges and opportuni-ties in delivering a universal CFH service inAustralia. Participants came from all jurisdictionsand represented a range of disciplines. They identi-fied challenges in data availability, informationexchange, communication between disciplines, work-force limitations, and access and equity in servicedelivery. All professional groups suggested thatothers, including consumers, were unaware of theservices provided by each professional group, resultingin service gaps, overlaps and tensions around roleboundaries. While some of these concerns have beenreported previously (Brotherhood of St Laurence2005, Hirst 2005, Brinkman et al. 2012), this is thefirst national study to include perspectives from allprofessional groups involved in delivering universalCFH services.
In earlier studies, Kuo et al. (2006) found littleco-ordination among services for well children whenexamining services across five resource-rich countries.Others have identified the transition of care frommaternity services to CFH nursing services, GPs andother relevant agencies as problematic (Homer et al.2009). Nationally, there is a call for timely, relevantand structured clinical handover to support safepatient care (ACSQHC 2012), and the NationalMaternity Services Plan (Australian Health MinistersConference 2010) argues for mechanisms to facilitatethe sharing of standardised information.
There is limited research on the transition of care.Homer et al. (2009) identified a variety of models inNSW. Some were structured, but many had evolvedin an ad hoc way depending on local context. Simi-larly, in the Northern Territory, Bar-Zeev et al. (2012)reported an inconsistent approach to transition ofcare for women living in remote Australian commu-nities. The need for referral mechanisms and collabo-ration between birthing facilities and communityservices such as child health and GPs has been em-phasised, particularly the need to extend the serviceto women who birth in private care (Brodribb et al.2012, Jenkinson et al. in press). These problems arenot confined to Australia. In Sweden, midwives andchild health nurses described the need for joint actionto facilitate continuity of care across fragmented ser-vices in pregnancy, birth and the postnatal period(Barimani & Hylander 2012).
Study participants were concerned that with cur-rent limitations on funded positions or qualified pro-fessionals, they were not able to provide acomprehensive universal CFH service. In Australia,there has been a steady increase in the annual num-ber of births since 2003, yet at the same time, thenumber of CFH nurses has decreased (Cowley et al.2012). Furthermore, the role of CFH service providershas expanded with renewed focus on psychosocialscreening and support as well as other health promo-tion activities to promote social and emotional func-tioning in families (Australian Health MinistersAdvisory Council 2011). Similarly, in the UK, Cowleyet al. (2007) report workforce constraints have meantthat in some areas, health visitors offer restrictiverather than comprehensive services. They argue thata restricted service is reactive, largely focused onchild protection and vulnerable families, with littletime for such proactive public health activities(Cowley et al. 2007).
Apart from workforce issues, participantsappeared particularly concerned that the contributionthat their group made to universal CFH services wasnot understood by others, including consumers. Sev-eral consultations highlighted tension around profes-sional boundaries. Lane (2006) reporting oncollaboration in maternity services and Bar-Zeev et al.(2012) reporting on CFH services in the Northern Ter-ritory both note that guarding professional bound-aries was a barrier to effective collaboration. Studiesof health visitors in Norway and Scotland found thatthey experienced ‘collaborative strain’, jurisdictionalthreats and team conflicts as they believed that oth-ers, such as GPs, were not clear about role definitionand responsibility in ‘grey’ work areas (Ellefsen 2002).Concern about professional boundaries is perhaps most
© 2014 John Wiley & Sons Ltd 9
Implementing a national approach to universal CFH services

evident in a climate of change, but, unless addressed,is a significant barrier to effective collaboration.Axelsson and Axelsson (2006) stress the importanceof seeing beyond one’s own interests; too often, theneeds of the family are forgotten in the quest forprofessional priorities.
Opportunity for change
The most effective system for identifying and sup-porting all families was reported by Victorian repre-sentatives where there is a mandatory system oftransfer of information to CFH services followingbirth. Recent data from Western Australia also indi-cate that mandatory notification has resulted in asimilarly high proportion of women and infants beingfollowed up within 2 weeks of birth (Western Austra-lian Auditor General 2010). Greater considerationshould therefore be given nationally to implementingsimilar legislation.
Participants also offered their perspectives onstrategies for improvement, including the co-locationof services and introduction of interprofessionallearning. Integrated service delivery achieved throughpartnerships and inter-professional collaboration areconsidered essential to providing a comprehensiveuniversal service for pregnant women, children andfamilies, particularly for those vulnerable to poor out-comes (Rodr�ıguez & des Rivi�eres-Pigeon 2007). GPsin this study believed that Medicare Locals, a recentAustralian government initiative, offered an opportu-nity to improve primary healthcare service deliveryto children and families. Medicare Local policy em-phasises planning services on the basis of local needsand finding solutions based on local knowledge (Aus-tralian Government 2013, Gardner et al. 2013).
Proportionate universalismIn a climate of constraint and workforce limitations,governments could be tempted to offer services onlyto those considered most in need. There is strong evi-dence, however, that providing services primarily tothe disadvantaged will not eliminate populationhealth burdens (Hertzman & Power 2004, Brinkmanet al. 2012). Children from all social and economicbackgrounds may experience poor health and devel-opment, even though the most disadvantaged experi-ence this at a disproportionate rate. Commentatorstherefore argue that services be provided from a uni-versal platform with an increasing scale and intensityproportionate to the level of disadvantage, anapproach now termed ‘progressive’ or ‘proportionateuniversalism’ (Australian Health Ministers AdvisoryCouncil 2011, Oberklaid et al. 2013).
It is important to emphasise that the role ofsupporting child health and development and effec-tive parenting should be shared across professions,services and communities. Oberklaid et al. (2013)describe the core components of proportionate univer-salism for children and families as health and educa-tion services and family support for all families, withmore intensive interventions directed to those mostlikely to benefit. This approach facilitates engagementof all parents, avoids the risk of stigmatisation andallows for identification of problems and subsequentaccess to assessment and care when parents or profes-sionals have particular concerns about a child. Theargument for proportionate universalism is compel-ling and is advocated by Australian governments(Australian Health Ministers Advisory Council 2011).However, as conceptualisation of proportionate uni-versalism is not fully developed, it may have givenrise to the notion that the universal CFH service isprimarily concerned with case-finding and enablingthose who need it to access appropriate help andsupport, rather than being focused on proactive,universal prevention (Cowley et al. 2012). In this study,a number of groups believed that their workload wasdriven by performance indicators such as the propor-tion of families to receive a first home visit by CFHnursing services within 2 weeks after birth. In the con-text of workforce shortages, in some jurisdictions, therole of the CFH nurse appears to be restricted to pro-viding a home visit to new parents with limited provi-sion of ongoing services (Grant 2012). In this context,CFH nurses report high levels of job dissatisfaction.
Strengths and limitationsThis study has a number of limitations. Participantswere leaders in their respective professional groupsand active members of professional associations andtheir views may not represent all within that profes-sion, particularly those who provide ‘front-line’ ser-vices on a day-to-day basis. We experienced somedifficulty recruiting GPs and participant numbers aresmall in comparison with the midwife and CFHnurse participants. However, the perspectives offeredby all professional groups around the identifiedthemes were generally congruent. We were some-what surprised that participants did not canvass theopportunities for the use of SMART phone technol-ogy in the delivery of services. This may be a limita-tion of the questions that guided the groupdiscussions. Further studies should explore theseopportunities. This study is unique in canvassing theviews of maternity and CFH service providers at anational level and to include CFH nurses, midwivesand GPs and practice nurses.
© 2014 John Wiley & Sons Ltd10
V. Schmied et al.

Conclusion
This study examined the perspectives of diverse profes-sionals towards implementing a national approach touniversal CFH services in Australia. A number of con-cerns expressed by the participants have been reportedin government and commissioned reviews, but theperspectives of midwives, CFH nurses, GPs and practicenurses have never been synthesised. The findings of thisstudy demonstrate that strategies are needed to increasecommunication and collaboration between professionalsand across services through improved electronic datacollection and communication systems, service innova-tion such as co-location of services and opportunitiesfor interprofessional learning and development.
Acknowledgements
This study was funded by the Australian ResearchCouncil as a linkage grant. Our research partnerswere the Western Australian Department of Health;The Northern Territory Department of Health andFamilies; the Queensland Department of Health; Vic-torian Department of Education and Early ChildhoodDevelopment; the New South Wales Department ofFamily and Community Services; the Maternal Childand Family Health Nurses of Australia; the Austra-lian College of Midwives; The Royal Australian Col-lege of General Practitioners; Australian PracticeNurse Association and the Australian General Prac-tice Network (AGPN) (now the Australian MedicareLocal Alliance). We thank Chris Rossiter for finalediting and proofreading of this paper.
Conflicts of interest
All authors declare that they have no conflicts ofinterest. The only supporting source is the researchfunding outlined in the Acknowledgements.
Author contributions
VS, SK, CH, CF, LB, IW, LK and MF conceived thestudy, participated in its design and the submission ofapplication for competitive funding. VS, KP, SK, CFand CH undertook data collection. VS and KP con-ducted the preliminary analysis. All authors contrib-uted to the discussion of preliminary themes, the finalanalysis, and drafting and approval of this manuscript.
References
ACSQHC (2012) National safety and quality health service stan-dards. Commonwealth of Australia. Available at: http://
www.safetyandquality.gov.au/our-work/accreditation/nsqhss/ (accessed on 13/10/2013).
ARACY (2013) Report card: the wellbeing of young Australians.Australian Research Alliance for Children and Youth.Available at: http://www.aracy.org.au/documents/item/126 (accessed on 15/9/2013).
Australian Government (2013) Medicare Locals. Common-wealth of Australia. Available at: http://www.medicarelocals.gov.au/internet/medicarelocals/publishing.nsf (accessedon 15/12/2013).
Australian Health Ministers Advisory Council (2011)National Framework for Universal Child and Family HealthServices. Canberra: Australian Government Department ofHealth and Ageing. Available at: http://www.health.gov.au/internet/main/publishing.nsf/Content/AFF3C1C460BA5300CA257BF0001A8D86/$File/NFUCFHS.PDF (accessedon 13/11/2013).
Australian Health Ministers Conference (2010) NationalMaternity Services Plan. Commonwealth of Australia.Available at: http://www.health.gov.au/internet/publications/publishing.nsf/Content/BFE6AE67A9BC1BF1CA257A1B001B4B2D/$File/maternity%20plan.pdf (accessedon 13/11/2013).
Axelsson R. & Axelsson S.B. (2006) Integration and collabo-ration in public health – a conceptual framework. Interna-tional Journal of Health Planning and Management 21 (1),75–88.
Barimani M. & Hylander I. (2012) Joint action betweenchild health care nurses and midwives leads to continu-ity of care for expectant and new mothers. InternationalJournal of Qualitative Studies on Health and Well-being 7,1–11.
Bar-Zeev S.J., Barclay L., Farrington C. & Kildea S. (2012)From hospital to home: the quality and safety of a post-natal discharge system used for remote dwelling Aborigi-nal mothers and infants in the top end of Australia.Midwifery 28 (3), 366–373.
Braun V. & Clarke V. (2006) Using thematic analysis inpsychology. Qualitative Research in Psychology 3 (2), 77–101.
Brinkman S.A., Gialamas A., Rahman A. et al. (2012) Juris-dictional, socioeconomic and gender inequalities in childhealth and development: analysis of a national census of5-year-olds in Australia. BMJ Open 2 (5), e001075.
Brodribb W., Zadaroznyi M., Dane A. & Price T. (2012)Evaluating the Implementation of the Universal PostnatalContact Services in Queensland: The Experiences of HealthCare Providers and Mothers. St Lucia, Brisbane: Queens-land Centre for Mothers & Babies, The University ofQueensland. Available at: http://espace.library.uq.edu.au/eserv/UQ:286473/Fulltext.pdf (accessed on 1/12/2013).
Brotherhood of St Laurence (2005) Breaking cycles, buildingfutures. Promoting inclusion of vulnerable families inantenatal and universal early childhood services I. Avail-able at: https://www.eduweb.vic.gov.au/edulibrary/public/beststart/ecs_breaking_cycles_best_start.pdf (accessedon 12/10/2013).
Cowley S., Caan W., Dowling S. & Weir H. (2007) What dohealth visitors do? A national survey of activities and ser-vice organisation. Public Health 121 (11), 869–879.
Cowley S., Kemp L., Day C. & Appleton J. (2012) Researchand the organisation of complex provision: conceptualis-ing health visiting services and early years programmes.Journal of Research in Nursing 17 (2), 108–124.
© 2014 John Wiley & Sons Ltd 11
Implementing a national approach to universal CFH services

Creswell J.W. & Clark V.L.P. (2007) Designing and Conduct-ing Mixed Methods Research. Sage Publications, ThousandOaks, CA.
Department of Education and Early Childhood Development(2011) Maternal and child health service guidelines, Maternaland Child Health. State Government of Victoria. Availableat: https://www.eduweb.vic.gov.au/edulibrary/public/earlychildhood/mch/mchsguidelines.pdf (accessed on 13/11/2013).
Ellefsen B. (2002) The experience of collaboration: a compar-ison of health visiting in Scotland and Norway. Interna-tional Nursing Review 49 (3), 144–153.
Gardner K., Yen L., Banfield M., Gillespie J., McRae I. &Wells R. (2013) From coordinated care trials to medi-care locals: what difference does changing the policydriver from efficiency to quality make for coordinatingcare? International Journal for Quality in Health Care 25(1), 50–57.
Grant J. (2012) Between a rock and a hard place: managingprofessional practice alongside organisational directives inchild and family health nursing. Australian Journal of Childand Family Health Nursing 9 (2), 9–15.
Greenhalgh T., Glenn R., Macfarlane F., Bate P. & Kyriaki-dou O. (2004) Diffusion of innovations in service organi-zations: systematic review and recommendations. TheMilbank Quarterly 82 (4), 581–629.
Hertzman C. & Power C. (2004) Child development as adeterminant of health across the life course. Current Paedi-atrics 14 (5), 438–443.
Hirst C. (2005) Re-birthing: report of the review of maternityservices in Queensland. Queensland Health, QueenslandGovernment. Available at: http://www.qcmb.org.au/media/pdf/Rebirthing%20report.pdf (accessed on 13/11/2013).
Homer C., Henry K., Schmied V., Kemp L., Leap N. & Brig-gs C. (2009) ‘It looks good on paper’: transitions of carebetween midwives and child and family health nurses.Women and Birth 22 (2), 64–72.
Jenkinson B., Young K.B. & Kruske S. (2014) Maternity ser-vices and the discharge process: a review of practice inQueensland. Women and birth 27 (2), 114–120.
Kuo A.A., Inkelas M., Lotstein D.S., Samson K.M., SchorE.L. & Halfon N. (2006) Rethinking well-child care in theUnited States: an international comparison. Pediatrics 118(4), 1692–1702.
Lane K. (2006) The plasticity of professional boundaries: acase study of collaborative care in maternity services.Health Sociology Review 15, 341–352.
McCain M.N. & Mustard J.F. (2002) The Early Years StudyThree Years Later. From Early Child Development to HumanDevelopment: Enabling Communities. Toronto: The Founders’Network of the Canadian Institute for Advanced Research.Available at: http://www.aicafmha.net.au/enews/info/MustardAugust2002.pdf (accessed on 13/11/2013).
National Scientific Council on the Developing (2007) The sci-ence of early childhood development. Centre on the Develop-ing Child, Harvard University. Available at: http://developingchild.net/pubs/persp/pdf/Science_Early_Childhood_Development.pdf (accessed on 13/10/2013).
Oberklaid F., Baird G., Blair M., Melhuish E. & Hall D.(2013) Children’s health and development: approaches toearly identification and intervention. Archives on Disease inChildhood 98 (12), 1008–1011.
Perinatal Mental Health Consortium (2008) Perinatal MentalHealth: National Action Plan: 2008-2010. Canberra: Beyond-blue. Available at: http://www.beyondblue.org.au/docs/default-source/8.-perinatal-documents/bw0125-report-beyondblues-perinatal-mental-health-(nap)-full-report.pdf?sfvrsn=2 (accessed on 13/11/2013).
Psaila K., Schmied V., Fowler C. & Kruske S. (2014a) Dis-continuities between maternity and child and familyhealth services: health professional’s perceptions. BMCHealth Services Research 14 (4), 1–12.
Psaila K., Kruske S., Fowler C., Homer C. & Schmied V.(2014b) Smoothing out the transition of care betweenmaternity and child and family health services: perspec-tives of child and family health nurses and midwives.BMC Pregnancy and Birth 14 (151), 1–13.
Psaila K., Schmied V., Fowler C. & Kruske S. (2014) Inter-professional collaboration at transition of care: perspec-tives of child and family health nurses and midwives.Journal of Clinical Nursing doi: 10.1111/jocn.12635.
Robinson M., Mattes E., Oddy W.H. et al. (2011) Prenatalstress and risk of behavioral morbidity from age 2 to14 years: the influence of the number, type, and timing ofstressful life events. Development and Psychopathology 23(2), 507–520.
Rodr�ıguez C. & des Rivi�eres-Pigeon C. (2007) A literaturereview on integrated perinatal care. International Journal ofIntegrated Care 7, e28.
Sandelowski M. (2010) What’s in a name? Qualitativedescription revisited. Research in Nursing and Health 33 (1),77–84.
Schmied V., Donovan J., Kruske S., Kemp L., Homer C. &Fowler C. (2011) Commonalities and challenges: a reviewof Australian state and territory maternity and childhealth policies. Contemporary Nurse 40 (1), 106–117.
Schmied V., Fowler C., Rossiter C., Homer C. & Kruske S.(2014) Nature and frequency of services provided by childand family health nurses in Australia: results of a nationalsurvey. Australian Health Review 38 (7), 177–185.
Western Australian Auditor General (2010) PerformanceAudit – Universal Child Health Checks. Perth: Governmentof Western Australia. Available at: https://audit.wa.gov.au/wp-content/uploads/2013/05/report2010_11.pdf (accessedon 13/11/2013).
© 2014 John Wiley & Sons Ltd12
V. Schmied et al.
Copyright © 2022 FDOKUMEN