Impact of the SIAGA Maternal and Neonatal Communication Campaign on Knowledge of Danger Signs and...
21
JOURNAL OF HEALTH & MASS COMMUNICATION E DITED BY Fiona Chew, Syracuse University E DITORIAL B OARD MEMBERS Linda Aldoory, University of Maryland Julie Andsager, Iowa State University R. Warwick Blood, University of Canberra Owen Carter, Curtin University of Technology Perth Prabu David, Ohio State University Timothy Edgar, Emerson University Soledad Liliana Escobar-Chaves, University of Texas Health Science Center - Houston Brain R. Flay, Oregon State University Thomas H. Feeley, University of Buffalo Vicki S. Freimuth, University of Georgia Daniela B. Friedman, University of South Carolina Patricia Geist-Martin, San Diego State University William D. Grant, Upstate Medical University Edward C. Green, Harvard University Nancy G. Harrington, University of Kentucky Laurie Hoffman-Goetz, University of Waterloo Robert C. Hornik, University of Pennsylvania Gary L. Kreps, George Mason University Marilee Long, Colorado State University Edward Maibach, George Mason University Thomas A. Morton, University of Exeter Kimberly A. Neuendorf, Cleveland State University Richard M. Perloff, Cleveland State University Brian A. Primack, University of Pittsburgh Joey Reagan, Washington State University Rajiv N. Rimal, Johns Hopkins University Donna Rouner, Colorado State University Clifford W. Scherer, Cornell University Barbara F. Sharf, Texas A&M University Nancy Signorielli, University of Delaware Arvind Singhal, University of Texas - El Paso Brian Southwell, University of Minnesota Melanie Wakefield, The Cancer Council Victoria, Australia Kim B. Walsh-Childers, University of Florida Kim Witte, Michigan State University Itzhak Yanovitzky, Rutgers University Marco Yzer, University of Minnesota
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Impact of the SIAGA Maternal and Neonatal Communication Campaign on Knowledge of Danger Signs and...

JOURNAL OF HEALTH & MASS COMMUNICATION
EDITED BY
Fiona Chew, Syracuse University
EDITORIAL BOARD MEM BERS
Linda Aldoory, University of Maryland
Julie Andsager, Iowa State University
R. Warwick Blood, University of Canberra
Owen Carter, Curtin University of Technology Perth
Prabu David, Ohio State University
Timothy Edgar, Emerson University
Soledad Liliana Escobar-Chaves, University of Texas
Health Science Center - Houston
Brain R. Flay, Oregon State University
Thomas H. Feeley, University of Buffalo
Vicki S. Freimuth, University of Georgia
Daniela B. Friedman, University of South Carolina
Patricia Geist-Martin, San Diego State University
William D. Grant, Upstate Medical University
Edward C. Green, Harvard University
Nancy G. Harrington, University of Kentucky
Laurie Hoffman-Goetz, University of Waterloo
Robert C. Hornik, University of Pennsylvania
Gary L. Kreps, George Mason University
Marilee Long, Colorado State University
Edward Maibach, George Mason University
Thomas A. Morton, University of Exeter
Kimberly A. Neuendorf, Cleveland State University
Richard M. Perloff, Cleveland State University
Brian A. Primack, University of Pittsburgh
Joey Reagan, Washington State University
Rajiv N. Rimal, Johns Hopkins University
Donna Rouner, Colorado State University
Clifford W. Scherer, Cornell University
Barbara F. Sharf, Texas A&M University
Nancy Signorielli, University of Delaware
Arvind Singhal, University of Texas - El Paso
Brian Southwell, University of Minnesota
Melanie Wakefield, The Cancer Council Victoria,
Australia
Kim B. Walsh-Childers, University of Florida
Kim Witte, Michigan State University
Itzhak Yanovitzky, Rutgers University
Marco Yzer, University of Minnesota

JOURNAL OF HEALTH & MASS COMMUNICATION
Volume 1, Numbers 1/2 Winter/Spring 2009
INAUGURAL EDITORIAL
5 Fiona Chew, Founding Editor of the JOURNAL OF HEALTH & MASS COMM UNICATION
Build It and (S)he Will Come
ESSAY
8 Brian G. Southwell
Health Communication as Interdisciplinary Intersection Rather than Separate
Field
ARTICLES
11 Paula M. Frew, Wendy Macias, Kayshin Chan, and Ashley C. Harding
In “Step” with HIV Vaccines? A Content Analysis of Local Recruitment
Campaigns for an International HIV Vaccine Study
40 Suruchi Sood, Manisha Sengupta, Corinne L. Shefner-Rogers and Anne Palmer
Impact of the Siaga Maternal and Neonatal Communication Campaign on
Knowledge of Danger Signs and Birth Preparedness in West Java, Indonesia
58 Amanda Hinnant
Getting the Science Right: An Experiment on How Readers Evaluate Medical
News Coverage in Magazine Health Journalism
77 Karyn Ogata Jones and Renee Pelton
Attribute Agenda Setting and Breast Cancer in Newspapers
90 Randy M. Page, Rosemary Thackeray, Brad Neiger and Marissa Black
Analysis of Food and Beverage Brand Websites Targeting Children: Internet
Marketing Strategies, Content, and Features
109 Cynthia-Lou Coleman, L. David Ritchie and Heather Hartley
Assessing Frames and Metaphors in News Coverage of Prescription Drug
Advertising
129 Cory L. Armstrong
Examining the Blame Frame: Portrayals of Women in Newspaper Content
about Dieting

Copyright © 2009. The authors of each of the articles published in this issue own the copyrights to their works.
For permission to reprint, please contact them (see title page for contact information).
Journal of Health & Mass Communication (ISSN 1940-9354 print, 1940-9362 online) is a peer-reviewed
scientific journal that publishes theoretical and empirical papers and essays and book reviews that advance an
understanding of mass media effects or processes with respect to health-related issues or topics. Submissions may
have a psychological, social, historical or cultural orientation but must focus on mass communication and health.
All theoretical and methodological perspectives are welcomed. All manuscripts undergo blind peer review.
JHMC is published online and in hard copy form. The online version is open access, which means it is available
at no charge to the public. Visit www.MarquetteJournals.org to view the contents of this journal and others.
Subscriptions are available for hard copy versions. Visit the MarquetteJournals.org Web site for additional
information.
MANUSCRIPTS SUBMISSION GUIDELINES
Exclusivity: All manuscripts should be original and should
not be under consideration at other journals or other
publications. Peer Review: All manuscripts will undergo
masked peer review. The normal review period is three
months or less. Submissions: The ideal length for submitted
papers is 20-30 double-spaced pages (6,000 to 8,000 words
using 12-point Times Roman or equivalent), including
references, tables and figures. Longer manuscripts will be
considered when space is available. The submission and
review process will be electronic. All manuscripts should be
prepared using Microsoft Word or converted to that format.
One electronic copy should be e-mailed to the appropriate
journal listed below Manuscript Preparation: Manuscripts
for all journals except the Journal of Media Law & Ethics
should be prepared according to the guidelines of the
Publication Manual of the American Psychological
Association (latest edition), with some exceptions provided
below. Submissions to JMLE should be prepared according
to Bluebook. Please double-space all material except tables
and figures. Please do NOT use footnotes. Endnotes are
permitted, but they must be manually inserted (i.e., please do
not use the automatic endnote insertion functions in word
processing systems). Microsoft Word and WordPerfect are
the required software programs for formatting manuscripts.
The title page should include the title of the manuscript;
names and affiliations of all authors, as well as their
addresses, phone numbers and e-mail addresses; and five key
words for referencing the document in electronic database
systems. Only the title page should contain identifying
information. The second page should include the manuscript
title and an abstract of 150 to 250 words. All figures and
tables must be formatted to 5.5 inches in width and no more
than 8.5 inches in height.
Copyright and Production Notes: All works submitted must
be original and must not have been published elsewhere.
Authors of works that are selected for publication shall retain
the copyright to their works. As such, they control the future
distribution and reprinting of their works. However, authors
shall give Marquette Books LLC a nonexclusive right to
publish the work in its journals or in other publications or
books that it may produce at the same time or in the future
(works submitted to the Russian Journal of Communication
also must allow reprinting rights to the Russian
Communication Association). Authors shall be given credit
in such works and will continue to control the copyright to
their works. After a manuscript is accepted for publication,
the author or authors are expected to provide a computer file
of the manuscript and to copyedit the page proofs when they
are completed. Permissions: Authors are responsible for
obtaining permission from copyright owners to use lengthy
quotations (450 words or more) or to reprint or adapt a table
or figure that has been published elsewhere. Authors should
write to the original copyright holder requesting nonexclusive
permission to reproduce the material in this journal and in
future publications generated by Marquette Books. All
requests are for nonexclusive rights. Email an electronic
copy of manuscripts to: Fiona Chew, editor,
Journal of Health & Mass Communication is published by
Marquette Books LLC
5915 S. Regal St., Suite 118B
Spokane, Washington 99223-6970
509-443-7047 voice / 509-448-2191 faxwww.MarquetteJournals.org • [email protected]

Suruchi Sood is an assistant professor in the Department of Health, Behavior and Society at the Johns
Hopkins Bloomberg School of Public Health ([email protected]); Manisha Sengupta is an
independent consultant in the Bloomberg School; Corinne L. Shefner-Rogers is an independent
consultant with the Bloomberg School and adjunct professor in the Department of Family and
Community Medicine, School of Medicine, at the University of New Mexico; and Anne Palmer is
senior program officer at the Center for Communication Program in the Bloomberg School.
40 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
IMPACT OF THE SIAGA MATERNAL AND
NEONATAL COMMUNICATION CAMPAIGN
ON KNOWLEDGE OF DANGER SIGNS
AND BIRTH PREPAREDNESS IN
WEST JAVA, INDONESIA
SURUCHI SOOD, MANISHA SENGUPTA,
CORINNE L. SHEFNER-ROGERS AND ANNE PALMER4
In 2004, an impact assessment of the SIAGA Maternal and Neonatal
Communication Campaign was conducted in West Java, Indonesia. This paper
examines the impact of the SIAGA campaign on knowledge about pregnancy danger
signs and birth preparedness behaviors in women of childbearing age in three study
districts of West Java. A total of 891 women was surveyed about maternal health
knowledge and behaviors. Analyses included logistic regression modeling of the
impact of exposure to the SIAGA campaign on several dependent variables.
Overall, there was evidence of a strong relationship between different levels of
exposure to the SIAGA campaign and increased awareness about severe bleeding
as a danger sign, increased knowledge about community-based life-saving services,
increased birth preparedness and antenatal care behaviors. Education and
residence emerged as significant control variables associated with these outcomes.
Keywords: maternal and neonatal health, mass media campaign, community
mobilization, birth preparedness

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 41
Mass media public health campaigns can be effective in changing knowledge, attitudes,
and behaviors for a variety of health issues including family planning, HIV/AIDS, drug use,
tobacco use, heart disease, and drunk driving (Piotrow et al., 1997; Dearing, 2001; Cappella
et al., 2001; Worden & Flynn, 2002; Flora, 2001; Winsten & DeJong, 2001; Lederman et
al., 2001). Health communication messages may be more effective when linked with
community-level programs, and when they encourage interpersonal dialogue (Rogers &
Storey, 1987; Wallack & Dorfmann, 2001; Papa et al., 2000; Rogers et al., 1999; Sharan &
Valente, 2002; Sood et al., 2004). The germinal work by Farquhar et al, (1977) — the
Stanford Heart Disease Prevention Program — utilized a quasi-experimental design and
compared the effects of media and intensive interpersonal counseling on physiological risk
indicators as well as knowledge and behaviors related to cardiovascular disease, and serves
as a heuristic model for this specific paper.
Very few behavior change interventions have focused on improving maternal and
neonatal health by changing health-seeking behaviors, for example using a skilled healthcare
provider for delivery (Koblinsky, 2004). Since the 1990s, safe motherhood programs have
focused on promoting the use of a skilled attendant for childbirth as a primary means for
preventing maternal death. The presence of a skilled attendant at delivery is the most valid
indicator of the impact of safe motherhood programs (Starrs, 1998). Skilled healthcare
providers can recognize life threatening complications during childbirth and postpartum, and
either treat the complication or refer the woman to a higher level of care as necessary.
Different studies report a wide range of estimates of maternal mortality ratio (MMR)
for Indonesia, but a range of estimates of 300 — 400 maternal deaths per 100,000 live births
has been generally accepted as the prevailing level (UNFPA, 2007). In other South-east
Asian countries, the MMR is lower than Indonesia’s. In Burma, this ratio is 230;
Philippines, 170; Vietnam, 160; Thailand, 44; Malaysia, 39; and Singapore, six (UNICEF,
2004). The issue of high maternal mortality remains at the top of the health care agenda in
Indonesia, in order to meet the Millennium Development Goals (MDGs) # 5 “improve
maternal health,” Indonesia will have to ensure a reduction in maternal mortality to nearly
100 / 100,000 live births by 2015 (UNFPA, 2007)
In Indonesia a woman dies every hour from pregnancy, complications during delivery,
late referral to hospital services and poor emergency obstetric care (UNFPA, 2007). The
majority of deaths result from severe bleeding (World Health Organization, 2004a). In 1991,
the Government of Indonesia trained and deployed 54,000 village midwives (bidan di desa),
one per village, throughout the nation. Despite the presence of these community-based
bidan, pregnant women continued to use traditional providers (dukun) for delivery. Dukun
are preferred because they are older, married women who are long-standing members of the
village community, compared to bidan who were young, unmarried women from another
village. In 2003-2004, 50 percent of all home births were delivered by nurses or bidan, and
32 percent were delivered by dukun (Badan Pusat Statistik, 2003).

Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
42 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
The SIAGA Campaign in West Java, Indonesia combined mass communication
messages with community mobilization activities and had four major components: (1) Suami
SIAGA (Alert husband), (2) Warga SIAGA (Alert citizen), (3) Bidan SIAGA (Alert
midwife), (4) Desa SIAGA (Alert village). The word SIAGA is both a concept and an
acronym. SIAGA translates as “alert” or “ready” in Bahasa Indonesia (the Indonesian
language). The SIAGA concept embodies the Indonesian value of shared responsibility and
community help (gotong royong). The acronym, SIAGA, stands for Siap (ready), Antar (take
or transport), jaGA (stand by or guard). A SIAGA community, husband, or midwife, is one
who protects a pregnant woman and is ready to transport her to a healthcare facility when
needed. See Table 1 for the SIAGA Communication Campaign Components.
The present study was designed to evaluate the impact of the SIAGA campaign.
Specifically, we examined the dose-response relationship between exposure to a
combination of mass media and intensive community mobilization activities, and levels of
awareness, knowledge, and birth preparedness behaviors regarding pregnancy, childbirth,
and postpartum care.
Methods
Sources of Data
In 2004, Johns Hopkins University’s Center for Communication Programs, in
collaboration with the University of Indonesia’s Center for Health Research, conducted an
impact assessment of the SIAGA Communication Campaign. The objective of the
assessment was to determine the impact of the SIAGA campaign on (1) awareness about
severe bleeding as a danger sign during pregnancy, delivery, and postpartum, (2) knowledge
about community life-saving services, (3) birth preparedness, (4) use of antenatal care, (5)
use of a skilled healthcare provider for antenatal care, (6) use of a skilled attendant for
delivery, (7) obtaining postpartum care for the mother, and (8) obtaining postpartum care
for the child.
The research design for the impact assessment was a post-test non equivalent quasi field
experiment with four campaign exposure groups (no exposure, low, medium and high
exposure) to the SIAGA communication campaign. The sample included 865 married
women who had a live birth in the past 15 months. Approximately 10 women per village
were systematically randomly sampled from a total of 96 villages and municipalities drawn
from three study districts in West Java where both mass media and community mobilization
activities were implemented: Kabupaten Kuningan, Kabupaten Cirebon, and Kota Cirebon.
Initially, a stratified cluster sample was used to randomly select 35 villages from the 55
where mass media and intensive community mobilization activities were implemented (high
exposure). Next, 31 out of 62 villages with mass media and general community mobilization

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 43
activities (medium exposure) and finally 30 villages that received only mass media messages
(low exposure) were sampled. Women who were not exposed to any of the messages or
activities conducted by the SIAGA communication campaign were considered as the “no
exposure” group during analysis. Some 26 women who were exposed only to the
TABLE 1DESCRIPTION OF THE SIAGA COMMUNICATION CAMPAIGN COMPONENTS

Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
44 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
mobilization activities were excluded from the analyses leaving a total of 865 women in the
study sample.
Ethical approval for this study was obtained from the Johns Hopkins University
Bloomberg School of Public Health Committee on Human Research.
Measures
The independent measure of exposure to the SIAGA communication campaign, as
described above, was calculated as a four-level variable. These four categories were, to
some extent, a function of the area in which the respondents resided. For example, women
who lived in areas in which community mobilization activities were not conducted were
only eligible to belong to either the “no exposure” or the “low exposure” group.
The dependent variables for this study included several topics pertaining to knowledge
and behaviors. The knowledge level variables included: awareness about severe bleeding
as a danger sign and knowledge about community life-saving services. The specific
behaviors included actions undertaken to prepare for child birth and use of specific services
during pregnancy, childbirth and in postpartum. The knowledge and behavior related
variables were measured as follows:
Awareness of severe bleeding as a danger sign. This variable was measured as a
dichotomous variable (0=not aware, 1=aware). Awareness was assessed separately for the
pregnancy, delivery, and postpartum periods.
Knowledge of community-based life-saving services. Four dichotomous variables were used
to measure knowledge about life-saving services in the community. Respondents were asked
whether they knew about notifying the community, transportation services, blood donation
services, and available funds that could be used in the event of an obstetric emergency.
Birth preparedness. Five variables were used to measure birth preparedness. Questions
included asking respondents whether they had notified others in their community, arranged
for a skilled attendant to be present for delivery, and arranged transportation, funds, and a
blood donor in case of an obstetric emergency. In Indonesia, healthcare facilities may not
have adequate blood supplies in the event of an obstetric emergency. Pregnant women are
encouraged to identify a potential blood donor (with matching blood type) that will
accompany her to the healthcare facility when needed. These birth preparedness items are
central to the concept of birth preparedness, and to preventing delays in receiving treatment
for pregnancy-related complications (Stanton, 2004). Each question yielded a dichotomous
answer (0=no; 1=yes).
Use of antenatal care. Respondents were asked whether they received antenatal care at least
four times during their pregnancy. The World Health Organization guidelines for adequate

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 45
antenatal care (World Health Organization, 2001) calls for a minimum of four antenatal care
visits. This variable was dichotomous (0=no; 1=yes).
Use of a skilled attendant for delivery. The survey questionnaire included a question about
whether a woman used a skilled attendant for delivery. The presence of a skilled healthcare
provider during childbirth contributes to improved maternal health outcomes, and to a
reduction in maternal deaths (Starrs, 1998; World Health Organization, 2004b). Possible
responses included “no” (coded as “0”) or “yes” (coded as “1).
Obtaining postpartum care for the mother. This variable was measured using a dichotomous
question that asked women whether they had received postpartum care within the first four
hours following delivery.
Obtaining postpartum care for the child. Women respondents were asked if their newborn
had received postpartum care (i.e., care in the first four hours following delivery). Postpartum
care contributes to improved neonatal outcomes (Koblinsky, 2004; Starrs, 1998). This
variable was dichotomous (0=no; 1=yes).
The following potential confounding variables were included in the analyses: (1) Age
of the respondent (mean years), (2) residence (urban or rural), (3) education (at least some
primary school or junior high school and above), and (4) socioeconomic status (household
expenditures in the amount of Rupiahs (Rps). 300,000 or less, Rps. 301,000 to 700,000, or
Rps. 700,001 or more; one US Dollar is approximately. 8,000 Indonesian Rupiahs). In
addition to these commonly used control variables, we included “duration at current
residence” (measured as “two years or less,” or “more than two years”) as a potential
confounder. An individual’s familiarity with her community may contribute to her
knowledge and use of community-based resources.
Statistical Analysis
Statistical analysis included descriptive statistics for exposure and the dependent
variables. In addition, a series of multivariate logistic regression analyses were conducted.
A first set of analyses used “no exposure” as a reference category and examined the impact
of mass media (low) exposure. A second set of analyses used the exposure to mass media
alone (low) as the reference category and compared it to medium and high exposure
separately, so as to distinguish between specific groups. All analyses were conducted using
STATA version 9.0. Probability levels were set at p<.05

Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
46 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
RESULTS
Descriptive Analysis
Table 2 shows the descriptive characteristics of the respondents by level of exposure to
the SIAGA Communication Campaign. The mean age of respondents was 28 years. Some
25 percent (N=217) of respondents were not exposed to the SIAGA campaign message. At
least 38 percent (N=331) of women in the study sample were exposed to only mass media
messages, and 23 percent (N=200) were presented with mass media messages and general
community mobilization activities. Fourteen percent (N=117) of respondents were exposed
TABLE 2PERCENTAGE DISTRIBUTION OF RESPONDENTS’
CHARACTERISTICS BY LEVEL OF EXPOSURE

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 47
to mass media message and intensive community mobilization activities. The majority of
respondents lived at their current residence for more than two years.
The levels of education, socioeconomic status, and residences differed significantly
among the four exposure groups. Respondents that were not exposed to the SIAGA
campaign were least likely to live in urban areas (13.8%) and most likely to have a primary
school education (82%). The majority (62%) of women in the “no exposure” category were
also most likely to have monthly household expenditures of Rps. 300,001-700,000. We were
able to make valid comparisons across the four exposure groups by controlling for these
potential confounders using multiple logistic regression analyses.
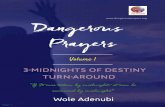
Table 3 presents the dependent variables by level of exposure. These data suggest a
strong dose-response effect of exposure to the SIAGA campaign on awareness of bleeding
as a danger sign during pregnancy, delivery, and postpartum, and on knowledge of
community-based life-saving services. Birth preparedness activities were highest for
respondents that were exposed to both the mass media messages and intensive community
mobilization activities. The results for antenatal care visits and use of a skilled provider for
delivery indicated that these behaviors increased with exposure to a combination of mass
media and community mobilization activities. The majority of women in the study sample
received postpartum care for themselves and for their child regardless of exposure status.
Awareness about Bleeding
Awareness of severe bleeding as a danger sign during pregnancy, childbirth, and the
postpartum period varied significantly among the women with no exposure (reference
category) and those exposed to the mass media campaign (Table 4). The second set of
multivariate analyses revealed that awareness of severe bleeding did not vary significantly
among women with low exposure (mass media only) when compared to the medium
exposure category (mass media and general community mobilization) and the high exposure
category (mass media and intensive community mobilization. The only exception was that
women with a high level of exposure (i.e., exposure to both the mass media component and
the intensive community mobilization activities) were two times more likely (AOR=2.04;
CI= 1.28,3.26; p<.05) to recognize severe bleeding during childbirth as a danger sign than
women with low exposure to the SIAGA campaign (Table 4). Among the control variables,
age and education were associated with significantly higher awareness levels of bleeding
as a danger sign during pregnancy, childbirth, and postpartum.
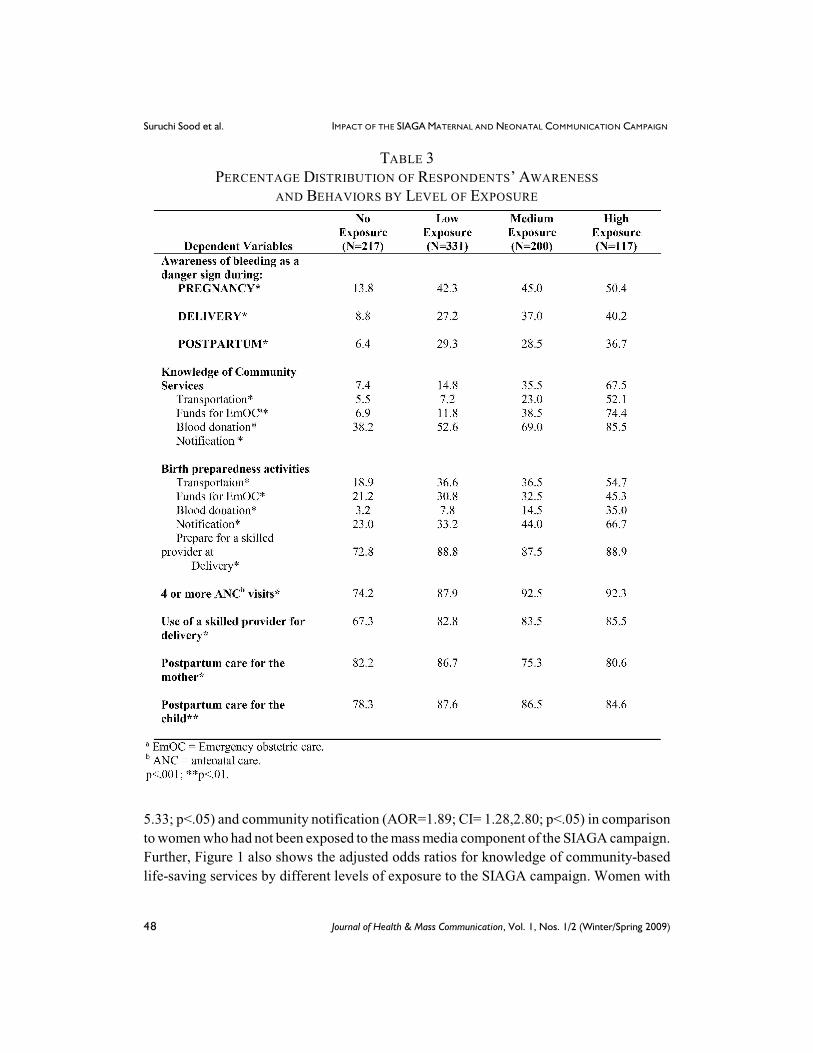
Knowledge about Life-Saving Services
The findings presented in Figure 1 indicate that women in the low exposure category
were significantly more likely to be aware of transportation schemes (AOR=2.77; CI= 1.45,
Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
48 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
5.33; p<.05) and community notification (AOR=1.89; CI= 1.28,2.80; p<.05) in comparison
to women who had not been exposed to the mass media component of the SIAGA campaign.
Further, Figure 1 also shows the adjusted odds ratios for knowledge of community-based
life-saving services by different levels of exposure to the SIAGA campaign. Women with
TABLE 3PERCENTAGE DISTRIBUTION OF RESPONDENTS’ AWARENESS
AND BEHAVIORS BY LEVEL OF EXPOSURE

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 49
both medium and high levels of exposure were significantly more likely to know about the
various community bases life saving services in comparison to women who were only
exposed to the mass media campaign. A strong dose response relationship was also
suggested.
Residence in a rural area was associated with significantly higher awareness of
community-based life-saving services.
TABLE 4RELATIONSHIP BETWEEN LEVELS OF EXPOSURE TO THE SIAGA COMMUNICATION
CAMPAIGN AND AWARENESS OF SEVERE BLEEDING AS A DANGER SIGN
Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
50 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
Birth Preparedness
The results pertaining to birth preparedness activities indicate that women exposed to
the mass media campaign were significantly more likely to report arranging for
transportation (AOR=1.87; CI=1.19,2.93; p<.01), community notification (AOR=1.73;
CI=1.12,2.66; p<.01) and preparing to use a skilled provider (AOR=1.99; CI=1.22, 3.25;
p<.01) in comparison to their counterparts with no exposure to the SIAGA campaign.
Comparisons among women with low exposure (mass media only) and those who were
exposed to the mass media and general community mobilization activities revealed few
significant differences. The only exception was with regards to making arrangements for
blood donation. Women exposed to both mass media and general community mobilization
activities were significantly more likely to report arranging for blood donation (AOR=2.01;
CI=1.12,3.59; p<.01). However, as the results from Table 5 indicate women who were
exposed to both mass media messages and intensive community mobilization activities were
FIGURE 1RELATIONSHIP BETWEEN LEVEL OF EXPOSURE TO THE SIAGA
COMMUNICATION CAMPAIGN AND KNOWLEDGE ABOUT COMMUNITY SCHEMES

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 51
significantly more likely to undertake birth preparedness activities, such as prepare
transportation, notify their community about their pregnancy, prepare emergency funds and
TABLE 5RELATIONSHIP BETWEEN LEVEL OF EXPOSURE TO THE
SIAGA COMMUNICATION CAMPAIGN AND BIRTH PREPAREDNESS ACTIVITIES

Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
52 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
prepare for emergency blood donation than women who were only exposed to the mass
media campaign.
Among those exposed to the SIAGA campaign, regardless of the level of exposure,
urban residence was associated with significantly lower likelihood of making preparations
in case of an obstetric emergency and notifying the community about a woman’s pregnancy.
However, urban residence was also associated with significantly greater levels of
preparation to deliver with a skilled provider across of levels of exposure. At the same time,
regardless of the level of exposure to the SIAGA campaign, education was associated with
higher levels of birth preparedness activities, specifically preparing transportation, prepare
money for emergency obstetric care and prepare to use a skilled provider for delivery.
Use of Antenatal Care
Women who were exposed to the mass media component of the SIAGA campaign were
significantly more likely than those not exposed to the SIAGA campaign to report having
received four or more antenatal care visits (AOR=1.89; CI=1.15, 3.08; p<.001). However,
there were no significant differences among the antenatal care visits with increasing levels
of exposure to the SIAGA campaign.
Skilled Attendance at Delivery
There was no significant difference among those not exposed to the SIAGA
communication campaign and those exposed to the mass media component, with regards to
the use of a skilled provider for delivery. Use of a skilled attendant for delivery did not vary
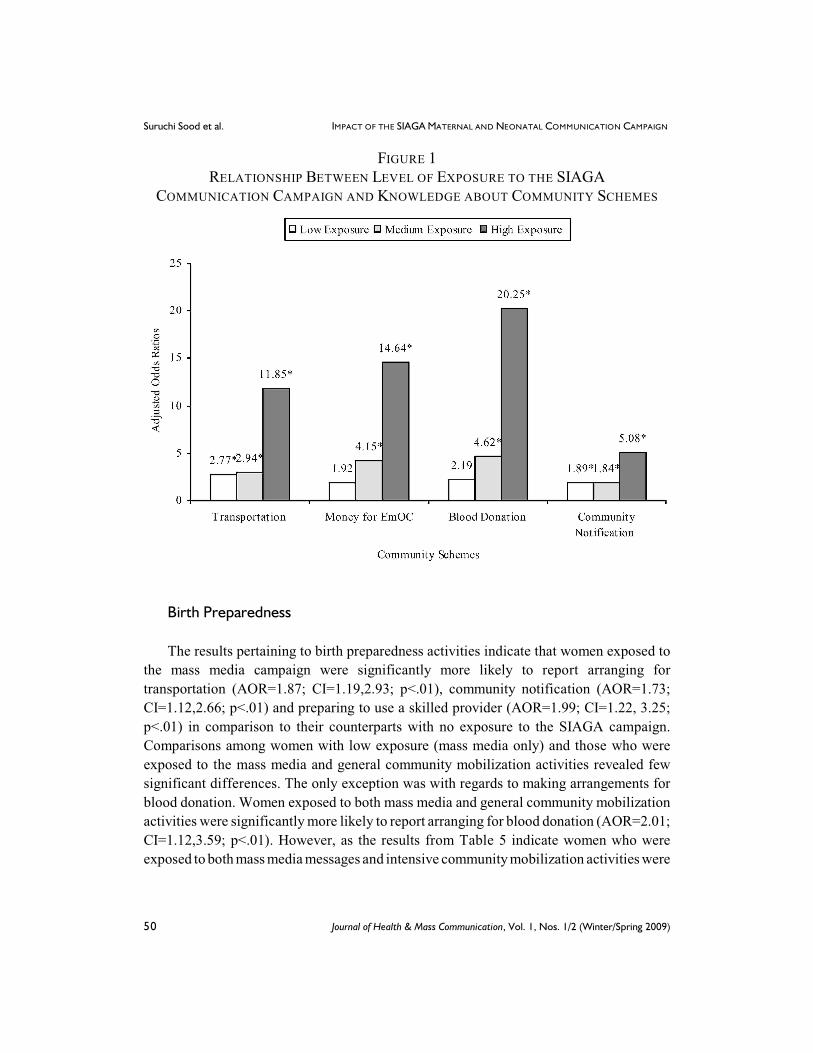
significantly with increasing levels of exposure to the SIAGA campaign (Table 6).
Postpartum care for the mother or the newborn did not vary significantly with increasing
levels of exposure to the SIAGA campaign. Interestingly, women who were exposed to the
mass media and general community mobilization activities were significantly less likely to
report having received post partum care for themselves, than women who were exposed only
to the mass media campaign (AOR=0.49; CI=0.30, 0.80; p<.01) (Table 6).
DISCUSSION
The SIAGA campaign in West Java, Indonesia was designed to increase awareness,
knowledge, and behaviors associated with positive maternal health outcomes. The aim of
the present study was to assess the influences of exposure to SIAGA campaign messages
and activities promoting maternal health knowledge and behaviors. The results of the
present study showed that exposure to the mass media component of the SIAGA campaign
IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 53
TABLE 6. RELATIONSHIP BETWEEN LEVEL OF EXPOSURE TO THE
SIAGA COMMUNICATION CAMPAIGN AND ANTENATAL CARE, USE OF SKILLED ATTENDANT AND POSTPARTUM CARE

Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
54 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
was associated with increased awareness about severe bleeding as a danger sign. Exposure
to the mass media in combination with intensive community mobilization activities was
associated with increased birth preparedness. A strong dose-response effect of exposure to
the campaign on knowledge of community based life saving schemes was observed.
The consistency of the findings related to the impact of high levels of exposure to the
campaign underscores the effectiveness of using intensive community mobilization activities
to encourage behavior change. Program planners, however, must weigh the costs (i.e.,
human and material resources) of implementing such time and cost intensive activities.
We failed to find significant associations between level of exposure to the SIAGA
campaign and (1) use of a skilled attendant for delivery, or (2) use of postpartum care for
the mother and newborns. These results are especially important since skilled attendance at
delivery is considered a key indicator for maternal mortality reduction. Despite these non-
significant results, it would be premature to conclude that the SIAGA campaign itself was
unsuccessful in increasing the use of skilled healthcare providers for childbirth, given that
actual use of skilled attendants for delivery was relatively high for the study sample
regardless of their exposure status. The SIAGA messages and activities may have focused
more directly on preparing for obstetric emergencies than on the importance of using a
skilled provider for delivery, or on the value of postpartum care. Also, time from campaign
end to evaluation and the fact that births are a rare event may have affected these findings.
A number of socio-demographic characteristics were considered to control for the
differences among the respondents not exposed to the SIAGA campaign in comparison to
those with low exposure (mass media only), as well as, comparisons between those exposed
to the mass media component only and those who were exposed to medium (mass media
plus general community mobilization), and high (mass media plus intensive community
mobilization) levels of the SIAGA campaign that may help to explain certain birth
preparedness and delivery behaviors. Urban residents were (1) significantly less likely to
know about community-based life-saving services, (2) significantly less likely to prepare
funds for the birth of their child or notify the community about the pending birth, and (3)
significantly more likely to prepare for a skilled provider for delivery and (4) significantly
more likely to use a skilled provider at delivery. It may be that the establishment of
community-based life-saving services was weaker in urban areas than in rural areas. Urban
residents may not have the same sense of community as rural dwellers, thus urban residents
may not be as knowledgeable about community activities, and may be less inclined to notify
their community members about a pregnancy. Residents in urban areas may also have better
access to various levels of medical care and therefore do not feel the need to prepare for the
birth of a child in the same way as residents in rural areas.
Not surprisingly, education was significantly correlated with a number of outcome
indicators. Women who were better educated were more likely (1) to be aware of severe
bleeding as a danger sign during the pregnancy, delivery, and postpartum periods

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 55
(specifically those exposed to the mass media campaign (low exposure) and those exposed
to the mass media campaign and intensive community activities (high exposure), (2) to
prepare money, transportation, and a skilled healthcare provider in case of an obstetric
emergency regardless of the level of exposure, and (3) to have four or more antenatal care
visits using a skilled antenatal care provider (specifically those exposed to the mass media
campaign (low exposure) and use a skilled provider at delivery, regardless of the level of
exposure to the SIAGA campaign. Finnegan and Viswanath (1999) suggested that unlike the
mass media, community mobilization activities span educational boundaries and reduce the
“knowledge gap” that might exist in a given community. Our findings showed that the
SIAGA campaign reached more women with higher education levels via mass media and
general community mobilization activities than with intensive community mobilization
activities. Prior research indicates that maternal mortality is higher among poor women with
lower levels of education (Abou-Zahr & Royston, 1991; Thaddeus & Maine, 1994). It is
critical to make specific efforts to reach a wider cross-section of women, especially low-
literate and illiterate women, with maternal mortality reduction messages and activities
through community and social mobilization activities.
This study had several limitations that need to be addressed in future research. The study
only included women with a live birth. It is possible that the selection of women with a live
birth was correlated to the presence of a skilled attendant independent of campaign
exposure. Future research could include statistics pertaining to both live and non-live births.
The use of cross-sectional data limited our ability to identify causal relationships between
exposure to the intervention and maternal health awareness and behaviors. Another
limitation was that we were unable to examine the impact of community mobilization
activities independently of mass media exposure. A fourth limitation of this study was that
we were unable to conduct a cost-effectiveness analysis to determine the relative impact of
community mobilization activities. Cost effectiveness is an important factor providing
accountability for campaign spending and might serve as a focus for further analysis. One
of the research challenges in the field of public health communication is the lack of adequate
scholarly investigation of the impact of behavior change communication strategies that
integrate mass media campaigns with community-based health promotion activities. A future
research agenda could include the collection of longitudinal data that would allow for
estimating time trends, and the availability of cost estimates for cost-benefit analysis.
Despite these limitations, the overall findings were encouraging, showing strong effects
of exposure on indicators associated with positive maternal outcomes. A key implication
from these findings is the importance of integrating mass media and intensive community
mobilization activities to improve preparation for obstetric emergencies, thus contributing
to reducing maternal mortality.

Suruchi Sood et al. IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN
56 Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009)
ACKNOWLEDGMENTS
We gratefully acknowledge the women participants in West Java, Indonesia who completed the survey
questionnaires. We sincerely thank the Maternal and Neonatal Health Program managed by JHPIEGO
Corporation. Funding for this research was provided by the United States Agency for International
Development (Cooperative Agreement HRN-A-00-98-0043-00). Some of the results shown here were
presented at the 55 International Communication Association Conference, New York, May 26-30,th
2005.
REFERENCES
Abou-Zahr C. & Royston E. (1991). Maternal mortality: A global fact book. Geneva: World Health
Organization.
Badan Pusat Statistik-Statistics Indonesia (BPS) and ORC Macro. (2003). Indonesia Demographic
and Health Survey 2002-2003. Calverton, Maryland, USA: BPS and ORC Macro.
Cappella, J.N., Fishbein, M., Hornik, R., Ahern, R.K. & Sayeed, S. (2001). Using theory to select
messages in antidrug media campaigns: Reasoned action and media priming. In Rice R.E., &
Atkin C.K. (Eds.), Public communication campaigns, Third Edition (pp. 214-230). Thousand
Oaks, CA: Sage.
Dearing, J. (2001). The cumulative community response to AIDS in San Francisco. In Rice R.E., &
Atkin C.K. (Eds.), Public communication campaigns, Third Edition (pp. 305-308). Thousand
Oaks, CA: Sage.
Farquhar, John W., Maccoby, N., Wond, P.D., Alexander J.K., Breitrose, H., Brown, B.W. Jr.,
Haskell, W.L., McAlister, A.L., Meyer, A.J., Nash, N.D., and Stern, M.P. (1977). “Community
Education for Cardiovascular Health,” Lancet, 1-8023: 1192-5.
Finnegan, J.R. &Viswanath, K. (1999). Mass media and health promotion: Lessons learned, with
implications for public health campaigns. In Bracht N. (Ed.), Health promotion at the community
level: New advances (pp. 119-126). Thousand Oaks, CA: Sage.
Flora J. (2001). The Stanford community studies: Campaigns to reduce cardiovascular disease. In Rice
R.E., & Atkin C.K. (Eds.), Public Communication Campaigns, Third Edition (pp. 193-213).
Thousand Oaks, CA: Sage.
Koblinsky M. (2004). Behavior change and maternal and early newborn health: Dilemmas for safe
motherhood. Aberdeen, Scotland: IMMPACT Project Digald Baird Center for Research on
Women’s Health, Department of Obstetrics and Gynecology, University of Aberdeen.
Lederman, L.C., Stewart, L.P., Barr, S.L., Powell, R.L., Laitman, L., & Goodhart, F.W. (2001). RU
SURE? Using communication theory to reduce dangerous drinking on a college campus. In Rice
R.E., & Atkin C.K. (Eds.), Public Communication Campaigns, Third Edition (pp. 295-304).
Thousand Oaks, CA: Sage.
Papa, M.J., Singhal, A., Law, S., Pant, S., Sood, S., Rogers, E.M., & Shefner-Rogers, C.L. (2000).
Entertainment-education and social change: An analysis of parasocial interaction, social learning,
collective efficacy, and paradoxical communication. Journal of Communication, 50,31-55.

IMPACT OF THE SIAGA MATERNAL AND NEONATAL COMMUNICATION CAMPAIGN Suruchi Sood et al.
Journal of Health & Mass Communication, Vol. 1, Nos. 1/2 (Winter/Spring 2009) 57
Piotrow, P.T., Kincaid, D.L., Rimon II, J.G., & Rinehart, W. (1997). Health communication: Lessons
from family planning and reproductive health.Westport. CT: Praeger.
Rogers, E.M., & Storey J.D. (1987). Communication campaigns. In Berger C. R., & Chaffee, S. H.
(Eds.), Handbook of communication science (pp. 817-846). Newbury Park, CA.
Rogers, E.M., Vaughan, P., Swalehe, R.M.A., Rao, N., Svenkerud, P., & Sood, S. ( 1 9 9 9 ) .
Effects of an entertainment-education radio soap opera on family planning and HIV/AIDS
prevention behavior in Tanzania. Studies in Family Planning, 50, 17-36.
Sharan M., & Valente TW. (2002). Spousal communication and family planning adoption: Effects of
a radio drama in Nepal. International Family Planning Perspectives, 28(1), 16-25.
Sood, S., Sengupta, M., Mishra, P.R., & Jacoby, C. (2004). Come gather around together: An
examination of radio listening groups in Fulbari, Nepal. Gazette, 66(1), 63-86.
Stanton C. (2004). Methodological issues in the measurement of birth preparedness in support of safe
motherhood. Evaluation Review, 28(3), 179-200.
Starrs, A. (1998). The safe motherhood agenda: Priorities for the next decade. New York: Safe
Motherhood Interagency Group.
Thaddeus, S, & Maine, D. (1994). Too far too walk: Maternal mortality in context. Social Science and
Medicine, 38(8), 91-111.
UNFPA (2007). Reproductive and Maternal Health. Retrieved October 31 , 2007 fromst
http://indonesia.unfpa.org/mmr.htm
UNICEF (2004). At a glance: Indonesia. Retrieved April 27, 2006 from http://www. unicef.org/
infobycountry/indonesia_statistics.html.
Wallack, L., & Dorfmann, L. (2001). Putting policy in health communication. In Rice, R.E., & Atkin,
C.K. (Eds.), Public Communication Campaigns, Third Edition (pp. 295-304). Thousand Oaks,
CA: Sage.
Winsten, J.A., & DeJong, W. (2001). The designated driver campaign. In Rice, R.E., & Atkin, C.K.
(Eds.), Public Communication Campaigns, Third Edition (pp. 290-294). Thousand Oaks, CA:
Sage.
Worden, J.K., & Flynn, B.S. (2002). Using mass media to prevent cigarette smoking. In Hornik RC
(Ed.), Public health communication: Evidence for behavior change (pp. 23-34). Mahwah, NJ:
Lawrence Erlbaum.
World Health Organization (2001). WHO Antenatal care randomized trial: Manual for the
implementation of the new model. Geneva: WHO.
World Health Organization (2004a). Beyond the numbers: Reviewing maternal deaths and
complications to make pregnancy safer. Geneva: WHO.
World Health Organization (2004b). Making pregnancy safer. WHO Fact Sheet. Geneva: WHO.