
Perceptions Of Postnatal Mothers Regarding Perinatal Loss ...
Upload
khangminh22Category
view
0download
0
Bureau of Women’s & Children’s Health Office of Children’s Health
7/1/2019
High Risk Perinatal Program Community Health Nursing Policy & Procedure Manual

2 | P a g e
Table of Contents
1 Introduction ............................................................................................................................... 1
1.1 History of the High Risk Perinatal Program (HRPP) ...................................................................... 1
2 High Risk Perinatal Program (HRPP) .......................................................................................... 2
2.1 Philosophy ....................................................................................................................................... 2
2.2 Mission Statement ........................................................................................................................... 2
2.3 Goals ................................................................................................................................................ 2
2.4 Overview .......................................................................................................................................... 2 A. Transport Services .................................................................................................................................... 2 B. Hospital Services ....................................................................................................................................... 3 C. Community Health Nursing ...................................................................................................................... 4
3 Roles & Responsibilities ............................................................................................................. 6
3.1 Arizona Department of Health Services (ADHS) .............................................................................. 6
3.2 Contractor ........................................................................................................................................ 6
3.3 Nurse Consultant ............................................................................................................................. 7
3.4 Partnerships ..................................................................................................................................... 7
4 Program Overview .................................................................................................................... 8
4.1 Objective .......................................................................................................................................... 8
4.2 Responsibilities ................................................................................................................................ 8
4.2 Requirements .................................................................................................................................. 9
5 Home Visitation Services ......................................................................................................... 10
5.1 Introduction ................................................................................................................................... 10
5.2 Eligibility Requirements ................................................................................................................. 10
5.3 Enrollment ..................................................................................................................................... 10 A. By Hospital ............................................................................................................................................. 10 B. By Community Health Nurse .................................................................................................................. 11
5.4 Program Participation .................................................................................................................... 11 A. Full Participation ..................................................................................................................................... 11 B. Partial Participation ................................................................................................................................ 11 C. Late Enrollment ...................................................................................................................................... 11 D. Adoption and Foster Care ...................................................................................................................... 12
3 | P a g e
6 Visit Guidelines ........................................................................................................................ 13
6.1 Introduction ................................................................................................................................... 13
6.2 Protocols ........................................................................................................................................ 13
6.3 Documentation .............................................................................................................................. 13
6.4 Referrals ......................................................................................................................................... 13
6.5 Case Dismissal Guidelines .............................................................................................................. 13 A. Dismissal Reasons ................................................................................................................................... 13 B. Dismissal Procedures for Eligible, Non-Responsive Families .................................................................. 14 C. Transferring Cases .................................................................................................................................. 14
7 Visit Guidelines for Special Populations .................................................................................. 15
7.1 Children and Youth with Special Health Care Needs (CYSHCN) .................................................... 15 A. Introduction ............................................................................................................................................ 15 B. Eligibility Requirements .......................................................................................................................... 15 C. CYSHCN Enrollment Procedures ............................................................................................................. 15 D. Home Visitation Guidelines .................................................................................................................... 16
7.2 Newborn Screenings ...................................................................................................................... 16 A. Introduction ............................................................................................................................................ 16 B. Eligibility Requirements .......................................................................................................................... 16 C. Enrollment Procedures ........................................................................................................................... 16 D. Home Visitation Guidelines .................................................................................................................... 16
8 Visit Procedures and Tools ...................................................................................................... 18
8.1 Visit Protocols ................................................................................................................................ 18
8.2 Educational Tools ........................................................................................................................... 18
8.3 Community Healthy Nursing (CHN) Visit Form .............................................................................. 18
8.4 Family Service Plans (FSP) .............................................................................................................. 19
8.5 Infant Screening Tools ................................................................................................................... 20 A. Ages and Stages Questionnaire .............................................................................................................. 20 B. Nursing Neonatal and Pediatric Assessment .......................................................................................... 21 C. Children’s Health Survey......................................................................................................................... 21
8.6 Maternal Assessment Tools & Support ......................................................................................... 21 A. Postpartum Mood Disorder.................................................................................................................... 21 B. Edinburgh Postnatal Depression Scale (EPDS) ........................................................................................ 21 C. Maternal Wellness Assessment/Preconception Care ............................................................................ 22
8.7 Environmental Screening Assessment .......................................................................................... 22
8.8 Determining Level of Risk ........................................................................................................... 22
9 Community Collaboration ....................................................................................................... 24

4 | P a g e
10 Personnel & Training ............................................................................................................... 25
10.1 Roles and Qualifications ............................................................................................................. 25 A. Community Health Nurse .................................................................................................................. 25 B. Social Worker .................................................................................................................................... 25 C. Early Interventionist (EI) .................................................................................................................... 25
10.2 Staff Education Requirements ..................................................................................................... 25
10.3 Orientation .................................................................................................................................. 25
10.4 Continuing Education .................................................................................................................. 27
10.5 Education Log .............................................................................................................................. 27
10.6 Tailoring Education ...................................................................................................................... 27
10.7 Supervision .................................................................................................................................. 27
11 Reporting ................................................................................................................................. 28
11.1 Notice of Implementation or Change ......................................................................................... 28
11.2 Monthly Invoice ........................................................................................................................... 28
11.3 Monthly Reports ......................................................................................................................... 28
11.4 Annual Plan .................................................................................................................................. 28
12 Continuous Quality Improvement ........................................................................................... 29
12.1 Introduction ................................................................................................................................. 29
12.3 Indicators ..................................................................................................................................... 29
12.3 Goals and Outcomes .................................................................................................................... 29
12.4 Responsibility ............................................................................................................................... 29
13 Billing Process & Policy ............................................................................................................ 30
13.1 Billing Policy ................................................................................................................................. 30
13.2 Billing Procedures ........................................................................................................................ 30
13.3 Billing Definition .......................................................................................................................... 30 A. Proximity ................................................................................................................................................ 30 B. Type of Visit ............................................................................................................................................ 31
14 Contract Monitoring................................................................................................................ 32
14.1 ADHS Responsibilities .................................................................................................................. 32
14.2 Contractor Responsibilities .......................................................................................................... 32
15 Procedural Safeguards ............................................................................................................ 33

5 | P a g e
15.1 Information Sharing ..................................................................................................................... 33
15.2 Data Usage Statement ................................................................................................................ 33
15.3 Administrative Records ............................................................................................................... 33
15.4 Patient Records............................................................................................................................ 33
16.5 Personnel ..................................................................................................................................... 33
15.6 Customer Service Policy .............................................................................................................. 33
15.7 Consent ........................................................................................................................................ 34
15.8 Review and Inspection of Records............................................................................................... 34
15.9 Confidentiality ............................................................................................................................. 35
15.10 Termination of Contract ............................................................................................................. 35
1 Glossary ................................................................................................................................... 36
2 Forms....................................................................................................................................... 41
3 Forms Matrix ........................................................................................................................... 42
4 Educational Materials ............................................................................................................. 66

6 | P a g e
Contact Information Arizona Department of Health Services Bureau of Women’s and Children’s Health Office of Children’s Health High Risk Perinatal Program (HRPP) 150 North 18th Avenue, Suite 320 Phoenix, Arizona 85007-3242 Laura Bellucci, Office Chief Office of Children’s Health (602) 364-1454
Brenda Nichols Program Director (602) 364-1462 Christina Becerra Home Visiting Program Manager (602) 364-3256 HRPP Coordinator (602) 364-0058
How to Use this Manual The purpose of this manual is to document the program’s policies for management. The manual is to be used as a reference and information resource for community nursing contractors, Arizona Department of Health Services (ADHS) administration and other interested parties in fulfilling the mission of the High Risk Perinatal Program. The policies contained herein are the minimum acceptable requirements to contract with ADHS to provide community nursing services to Arizona’s maternal and neonatal population. This manual will be reviewed at least annually and revised as necessary. Suggestions for changes to the manual to clarify a policy or to update a procedure may be sent in writing or emailed to the HRPP Program Manager at the address at the end of this chapter. The suggestions will be considered during the review process. Please note that the policy and procedure manual is dated and numbered. As revisions occur or new policies and procedures are developed, they will be added to the manual. Old policies or procedures will be deleted from the manual. Revisions to the manual will be distributed to all contractors at least thirty (30) days prior to the effective date of any change. Contractors are required to adhere to the policies and procedures set forth in this manual, and are also responsible for incorporating all policy changes into their operations.

1 | P a g e
1 Introduction
1.1 History of the High Risk Perinatal Program (HRPP) Prior to 1967, Arizona had one of the highest infant mortality rates in the country. In an effort to reduce the high infant morbidity and mortality, Arizona applied for and received a federal demonstration grant. The grant was designed to reduce infant deaths by transporting critically ill newborns born in rural hospitals to intensive care centers. As a result, there was a dramatic decrease in neonatal mortality. In 1972, the State Legislature provided state funding for the program, which eventually became the Newborn Intensive Care Program (NICP). The system provided care to those infants transported to metropolitan hospitals (Level III’s) and expanded to include infants born in Level II or Level III hospitals. Comprehensive and periodic developmental assessments were an additional component of the follow-up services provided in specific areas of the state. In 1975, ADHS received a Robert Wood Johnson Grant to develop regionalized perinatal care with a focus on the maternal transport system. Under this grant, the Maternal Transport Program (MTP), the Arizona Perinatal Program (APP), the Arizona Medical Association (AMA) and the University of Arizona began to develop guidelines for Level I, II, and III perinatal hospital services, a perinatal data system and the system of maternal transport. In 1977, it was demonstrated that babies did very well if transported to hospitals closer to their homes following the acute phase of their illness. Therefore, back transport was added as a component of the NICP. In the late 1980s, the need for home-based community health nursing services for those infants who may not have been critically ill at birth but were diagnosed with problems at a later date was identified. Part C of the Public Law for Individuals with Disabilities Education Act (IDEA), provided incentive for the development of a system of early intervention services which could provide a comprehensive, culturally appropriate, multi-disciplinary, family centered approach to all families. In 1993, ADHS awarded contracts to developmental clinics to determine eligibility for the Arizona Early Intervention Program (AzEIP). In 2002, funding for the developmental clinic component was eliminated. Arizona physicians and therapists then had few options for the evaluation of their developmentally delayed patients. Physicians began working closely with the Arizona legislature to restore funding for this much needed service. In FY 2007 the legislature partially restored funding to allow the HRPP/NICP to provide developmental assessments to program enrollees who do not meet Arizona Early Intervention (AzEIP) eligibility criteria and are uninsured or underinsured. The Community Health Nursing component works with families to improve their infant’s developmental outcomes. Services may be provided through a child’s third birthday. Research has demonstrated that the health of the mother before she becomes pregnant plays a significant role in the wellbeing of the newborn. To address those issues the CHN also incorporates post-partum wellness assessment and guidance about inter-conception wellness into her family centered care. During FY 2009, the state experienced a severe budget downfall. As the result of budget reductions, and in an effort to serve the sickest infants, the Program changed eligibility to infants who have spent at least 5 days in the NICU and restricted back transports to families who live over 30 miles from the NICU. The developmental services component was eliminated at that time also as a result of underutilization.

2 | P a g e
2 High Risk Perinatal Program (HRPP)
2.1 Philosophy HRPP depends on partnerships with families, medical communities, funding sources, and policy makers to provide risk appropriate transport, newborn hospital care, and community health nursing for high risk pregnant women and critically ill newborns. These services should be accessible to all critically ill newborns and their families in Arizona regardless of geographic location and ability to pay; in order to protect families from catastrophic costs.
2.2 Mission Statement The mission of HRPP is to reduce maternal and infant morbidity and mortality through a regionalized statewide system of coordinated care that includes consultation, transportation, hospital care and community health nursing.
2.3 Goals Transport: Medical consultation and transport for high risk mothers and infants to the most appropriate level of medical care. Hospital: Medical treatment, education and developmentally appropriate care for high risk infants. Working with perinatal partners to reduce the impact of catastrophic medical costs on families with high risk infants through reduced fees and financial support. Community Health Nursing: Monitor the health and development of high risk infants through in-home follow-up providing family support, education, and resources.
2.4 Overview The High Risk Perinatal Program consists of main 3 components: A. Transport Services B. Hospital Services C. Community Health Nursing Services
A. Transport Services
Transport Services consist of: a. Medical Consultation and Case Management
The ADHS contracts with neonatology and maternal fetal medicine groups throughout the state to provide free 24/7 medical consultation regarding the treatment, stabilization and, if needed, approval of coordination of inter-facility neonatal and maternal transport.
b. Information and Referral The ADHS provides access to a toll free telephone service that serves as the crucial link between referring health care providers and consulting maternal fetal medicine (MFM) specialists and neonatologists. If, at the time of consult, a transport is deemed necessary, the contracted neonatologist or MFM will make transport arrangements with a contracted transport company. 1-800-552-5252

3 | P a g e
c. Medical Transportation Families benefit from the Transport Services by having a coordinated system in place to ensure appropriate inter-facility transport and admission to high risk perinatal centers. The services are initiated without prior authorization or verification of payment source to prevent delays in service delivery. The ADHS contracts with medical transport companies to provide air and ground transport, as well as team services, for high risk pregnant women and neonates. The HRPP transport providers must obtain prior authorization and direction from a board certified MFM or neonatologist licensed and practicing in Arizona and contracted with the ADHS. The transport providers must be accompanied by a program contracted transport team.
B. Hospital Services
Hospital services consist of: a. Hospital Care
The ADHS contracts with all Level II, Level IIE (Enhanced), Level III, and Level IV perinatal centers (see glossary) that are certified by the Arizona Perinatal Trust (APT) to provide the appropriate level of hospital care to Program babies and their families. Contracts are in place with neonatology groups to provide appropriate medical care to program infants during the newborn intensive, intermediate or continuing care hospitalization.
In addition, the Program contracts with all Level IIE, Level III, and Level IV centers to support the implementation of developmental care practices in their newborn intensive care unit.
b. Financial Assistance to Families As a payor of last resort, HRPP Hospital Services provides limited financial assistance for families who enroll. Financial assistance includes inpatient physician services and forward or back transport (if needed). It is provided to families only after they have applied for all other possible benefits. These benefits may include 3rd party private insurance, AHCCCS, county and other government programs; and these benefits must be billed first. If the newborn is not added, enrolled, and maintained on the family’s insurance, HRPP will deny payment and the family will be solely responsible. Families are not protected from costs with providers who do not contract with ADHS. The program does not pay for any services provided at non-contracted facilities prior to transport to a contracted hospital. Health care costs related to the mother are not included coverages and will be denied. Hospitals, using the ADHS formulas, establish the liability for each family requesting financial assistance. All contracted hospital and physicians agree not to bill the family more than their established family liability Family liability is based on one amount per family rather than per child in the event of a multiple birth delivery. The liability is established once to cover all associated inpatient costs for the infant(s). At any time, HRPP may request documentation demonstrating that a family’s liability has been met. The HRPP Claims Coordinator works with the family and the providers to track the distribution of family liability payments. The family’s liability is the total amount that the family must pay to contracted providers before a bill is considered for payment by HRPP. The family liability is generally applied to hospital and physician bills accordingly: 75% to hospitals and 25% to specialty services. When a hospital does not require the entire 75%, the remaining liability is applied to physicians in the NICU, or

4 | P a g e
transport. Conversely, if the specialty services do not require the 25%, the remainder will be applied to the hospital bill. The family will be responsible for the entire established family liability.
C. Community Health Nursing
Community Health Nursing delivers a statewide, coordinated system of specialized nursing services to infants who are enrolled in the Program. The Community Health Nurse (CHN) provides support to families during the transition of the infant to home; conducts physical, developmental, psychosocial and environmental assessment and screening of the discharged infant. The CHN administers a post-partum depression screening and scoring of the mother and provides education about inter-conception health. The CHN connects mothers and infants to community resources. The CHN collaborates with the mothers on issues related to their own wellbeing in an effort to improve their ability to meet the needs of the enrolled infants and decrease the likelihood of a poor birth outcome with subsequent pregnancies. This program collaborates with the Office for Children with Special Health Care Needs (OCSHCN) to provide services to children who have a chronic medical condition and whose families express a desire for information, support, and/or coordination with multiple service providers and resources. The CHNs also assists with blood spot collections for the Newborn Screening (NBS) program as needed.

5 | P a g e
Baby born outside of HRPP contracted hospital and needs
risk appropriate NICU care
Baby inborn at HRPP contracted hospital and needs higher level of care than can be provided at birth hospital
MATERNAL TRANSPORT High-risk pregnant women who
need risk appropriate care
1-800 STATE TRANSPORT LINE Link between referring health care providers and consulting maternal fetal
medicine specialists and neonatologists
Mother arrives at hospital End of Maternal Services
End of Program
HOSPITAL STAY >120 hours stay at Arizona Perinatal
Trust (APT) certified Level II, IIE, III, IV HRPP contracted hospitals
BACK OR FORWARD TRANSPORT
Infant can be transported to APT certified hospital
within family’s community
*Back or forward to non-APT certified hospitals with program approval OUT-OF-STATE
NICU Graduate Arizona Resident
HRPP NICU Graduate
Child identified with special healthcare
need after discharge or during home visit
COMMUNITY HEALTH NURSING Home visit(s) for high risk HRPP infants or
OCSHCN infants, toddlers, and children
COMMUNITY SERVICES (DDD, AzEIP, OCSHCN, WIC, AHCCCS, IHS, additional HV programs, Medical Home, etc.)
CONSULTATION & CASE MANAGEMENT Neonatology and maternal fetal medicine groups provide medical
consultation regarding the treatment, stabilization and, if needed, approval and coordination of inter-facility neonatal and maternal transport.
Authorized physician secures appropriate hospital bed, coordinates transport (air or ground) with contracted
transport company and follows up with a return call to sending physician to relay detailed
INFANT TRANSPORT
KEY Consult/Transport Hospital Follow Up Services
ENROLLMENT OPTIONS
HIGH-RISK PERINATAL PROGRAM FLOWCHART

6 | P a g e
3 Roles & Responsibilities
3.1 Arizona Department of Health Services (ADHS) The ADHS is designated as the state agency responsible and accountable for program goals and expenditures. The HRPP is administered by ADHS, Public Health Prevention Services, and the Bureau of Women’s and Children’s Health (BWCH). The HRPP performs a variety of roles in the oversight of the Program: as a regulator, as a partner, monitor, facilitator, technical advisor, educator, and payer. A. ADHS and its contractors share a dynamic role in the development and evolution of the HRPP. B. HRPP collaborates with the APT and AHCCCS for establishing standards of care and participation
within the regionalized system. C. ADHS provides the criteria, policies and requirements for developing and implementing the high
quality, developmentally, risk appropriate transport, and intensive care services state wide for high risk pregnant women and newborns. The philosophy reflects the core requirements of HRPP, while also attempting to promote the family centered approach that is the cornerstone of the program.
D. ADHS contracts with perinatal centers (Levels II, IIE, III, and IV Hospitals) which may recruit and manage a unique group of specialized providers, such as neonatologists, MFM specialists, pediatricians, nurses, paramedics, respiratory therapists, social workers, developmental interventionists, communication specialists and other ancillary personnel.
E. The ADHS Community Health Nursing program contracts with local public and private agencies that may recruit and manage a unique group of specialized providers, community health nurses, social workers, and early interventionists, (speech/language pathologists, physical and occupational therapists).
3.2 Contractor Services are contracted through providers statewide. Coordination among all service programs and rural specialists is essential for an efficient, statewide, family centered program. The contractor is expected to: A. Provide a home based visitation program to:
a. Infants and toddlers meeting program eligibility b. Infants and toddlers and children meeting Children and Youth with Special Health Care Needs (CYSHCN) eligibility c. Mothers and families of HRPP enrolled infants
B. Provide individualized family-centered, developmentally appropriate, and coordinated home visiting services in a setting and at a time which is most appropriate for meeting the needs of the child and family.
C. Provide a program that at a minimum recruits, hires, trains and supervises community health nurses, early interventionists and social workers.
D. Provide orientation for new staff, continuing education and ongoing supervision of staff. E. Provide a physical, developmental, psychosocial and environmental screening and assessment of
the enrolled infant including evidence based education, family support, and early intervention along with referral services to community resources.
F. Provide maternal screenings and support. G. Provide assistance to the ADHS Newborn Screening Program in locating families and facilitating the
collection of newborn blood spot with a previously abnormal test result. H. Designate a CHN to attend the weekly Discharge Planning meetings at Level IIE, III, and IV Newborn
Intensive Care Units or special care nurseries as designated by ADHS. I. Collaborate and coordinate with parents, team members and other community providers in order
to offer a family centered approach to care.
7 | P a g e
J. Establish a linkage with referral sources for children and their families needing services within the Contractor’s community.
K. Establish a linkage to tobacco cessation referral sources. L. Meet data and reporting deadlines as outlined.
Written notification will precede any changes in Contractor responsibilities. Contractors will be given a 30 day notice to implement changes.
3.3 Nurse Consultant The HRPP Nurse Consultant is a contractor who shall provide quality training, education, consultation, and technical assistance to HRPP Community Health Nursing Contractors to support families and medically fragile infants. The Consultant’s coordination of services will result in quality services as expected by the ADHS Program. Coordination of services include, but are not limited to, training, education, activities, evaluation, and quality assurance. A. Provide guidance on developmental assessments, education, referral, anticipatory guidance and
advocacy services to HRPP Community Health Nursing in relation to program implementation; B. Provide ongoing support and training opportunities which empower CHNs to promote a family
centered approach, implementing developmental, and risk appropriate services to women and children with the following anticipated outcomes;
C. Provide consultation, support, and technical assistance to CHNs following HRPP standards, guidelines, policies and procedures;
D. Lead efforts focused on updating current forms, creating standardization of services based on best practices, such as risk assessment and what a typical visit would look like and including the infant’s developmental needs;
E. Collaborate with HRPP staff in discussing strategies, ongoing assessments, and implementation.
3.4 Partnerships HRPP partners with other ADHS programs such as the Office for Children with Special Health Care Needs and Newborn Screening to ensure that infants and children throughout the state are receiving necessary services. Current programs include: A. Home Visiting for Children and Youth with Special Health Care Needs (CYSHCN) B. Newborn Blood Spot Collection

8 | P a g e
4 Program Overview This chapter provides a synopsis of major programmatic functions and responsibilities of the Community Health Nursing Program Contractors. This general summary is not intended to be an all-inclusive description of the Contractor responsibilities. More comprehensive detailed descriptions of these responsibilities are contained throughout this policy manual and in each Contractor’s contracted Scope of Work with ADHS.
4.1 Objective The objective of the HRPP Community Health Nursing program is to assist in the smooth transition of medically fragile infants and their families from a NICU or SCN to home and to provide a coordinated, family centered, culturally responsive, developmentally appropriate, and coordinated home visiting service to these infants and other children/families identified with special health care needs. This care will include collaborating with the mothers on issues related to their own wellbeing in an effort to improve their ability to meet the needs of the enrolled infants and decrease the likelihood of a poor birth outcome with subsequent pregnancies.
4.2 Responsibilities The Contractor shall:
A. Provide a home-based visitation program to: a. Infants and toddlers meeting HRPP program eligibility b. Infants and toddlers and children meeting Children and Youth with Special Health Care Needs
(CYSHCN) eligibility c. Mothers and families of enrolled infants, toddlers and children B. Complete a physical, developmental, psychosocial, special needs and environmental assessment(s) of
the enrolled infant including evidence-based education, family support and early intervention along with referral services to community resources as needed;
C. Provide maternal postpartum wellness screening and interconception assessment, in addition providing support, education, and resources as needed;
D. Contact the Family within one (1) week of receipt of HRPP Enrollment & Discharge Forms; E. Conduct home visits, including but not limited to, first (1st) home visit within two (2) weeks after initial
contact; F. Visit enrolled infants a minimum of four (4) times within a year from the date of discharge and/or
prioritize visitation to ensure the infants are seen as appropriate according to their risk and need; G. Provide assistance to the ADHS Newborn Screening Program in locating families with a previously
abnormal test result and facilitate the collection of newborn blood spot; H. Collaborate and coordinate with other contracted CHN agencies when providing services in the same
area. Service areas are assigned by zip code; I. Coordinate with other providers and make referrals to appropriate services within the community and
prevent duplication of services; J. Designate a CHN to attend the weekly Discharge Rounds at Level IIE, III, and IV NICUs and/or SCNs as
appropriate; K. Provide a home based visitation program, which shall include community health nurses (CHN), and
may include early interventionists and/or a social worker; L. Provide a program that recruits, hires, trains, supervises and encourages ongoing professional
competency of CHNs, early interventionists and social workers that have contact with infants, toddlers and families;
M. Maintain documentation of orientations, continuing education and ongoing supervision for all program staff;
9 | P a g e
N. Participate in the continuous quality improvement process (CQI) based on specific indicators, one of which is to be determined by ADHS;
4.2 Requirements The Contractor shall: A. Employ Arizona licensed Registered Nurses with Basic Life Support Certification, experienced in
pediatrics and/or NICU and a Bachelor of Science Degree. Social Workers shall be a licensed Master Social Worker and/or hold a Master of Social Work degree. Early Interventionists shall have a minimum of a Bachelor’s degree and be licensed in early childhood, early childhood special education or a closely related field, hold a valid Arizona license as a speech-language pathologist, or be certified as an audiologist, physical therapist or occupational therapist.
B. Provide to ADHS upon request: education logs, completed client visit forms, monthly invoices, logs of clients seen, monthly reports, and other program related information and documentation.
C. Maintain all necessary permits and licenses, when applicable, and be licensed to provide service in Arizona.
D. Provide an Annual Plan using designated template. E. Designated nurses and/or support staff will be trained on the HRPP Efforts to Outcome (ETO) data
management system within 60 days of hire. F. Data, including documentation of contact attempts, visits, screening, referrals, and dismissals, must
be entered into HRPP ETO data management system within seven (7) days of the contact or visit date.
G. A minimum of one individual must attend the annual HRPP hosted meetings and conferences. H. CHNs must be trained in ASQ3/ASQ-SE by an approved trainer within 6 months of hire. I. CHNs must ensure that enrolled infants and children receive the initial ASQ within 1 year of program
enrollment. All services, screening tools, and assessments implemented for this Contract shall be performed in accordance with the Community Health Nursing Policy and Procedure Manual.

10 | P a g e
5 Home Visitation Services
5.1 Introduction HRPP CHNs serve a very special purpose in the transition from NICU to home. Home visiting services are based on health, development, environment and relationship risk. Periodic monitoring of the child's medical and developmental needs identifies infants who would benefit from referral to other early intervention programs. The service planning process must be flexible, coordinated and culturally sensitive. Immediate needs and concerns must be explored with the family as well as long term and future goals. Through these home visits, families receive support and education as well as referral to appropriate community resources.
5.2 Eligibility Requirements A. The primary caregiver/parent of the infant must:
a. Reside in Arizona when eligibility is determined and throughout period of service delivery. b. A residential street address. P.O. Box address is not acceptable; AND,
B. The infant(s) must meet one or more of the criteria below in order to be eligible for the program: a. Infants who require 120 hours or more of continuous care in a NICU or SCN beginning within
96 hours of birth. (Example: infant is discharged 24 hours after birth and is readmitted to NICU at 4 days of age with a neonatal condition that was present but not detected at birth);
b. Infants approved for admission or transported to a Pediatric Intensive Care Unit (PICU) of a Level III or IV hospital due to cardiac conditions for which the NICU is not equipped;
c. Infants who required NICU or SCN care and who subsequently expire after medical intervention occurred;
d. Infants with special health needs other than the above may be authorized for enrollment upon the request of a neonatologist and at the discretion of the contracted agency. The neonatologist name and reason for the request must be included.
e. Any infant who was in a NICU in another state whose parents now reside in Arizona qualify for CHN follow-up services.
C. Infants who do not meet the established criteria for HRPP may be eligible for Community Health Nursing services for Children and Youth with Special Health Care Needs (CYSHCN). See Section 8 Visit Guidelines for Special Populations for more information.
5.3 Enrollment A. By Hospital
ADHS contracted hospitals enroll an infant meeting the eligibility criteria. Each contracted hospital shall have designated and trained personnel available to explain the Program to eligible families and assist them with enrollment. HRPP requires that hospital personnel be responsible for completion of all forms required for enrollment. a. Enrollment in the HRPP occurs when the following touchpoints are completed by a hospital in the
Efforts to Outcome (ETO) database: • Enrollment Form- Demographics • Enrollment Form – Signature Page • HRPP Discharge Summary
b. The birth hospital is usually considered the enrolling hospital, provided that the infant spends 120 hours in their NICU or SCN. The enrolling hospital is required to complete and distribute ALL HRPP forms and enter into ETO. I. If the infant is transported within the first 120 hours, the contracted receiving hospital will
be considered the enrolling hospital, and is required to distribute, complete, and enter all
11 | P a g e
forms into ETO. II. If the infant is transported after the first 120 hours, the contracted birth hospital is required
to distribute, complete, and enter into ETO all of the forms.
B. By Community Health Nurse An infant meeting the HRPP eligibility criteria may be enrolled by a CHN only when: a. the family qualified but was not offered the program at the hospital b. the family initially declined services but changed their mind within 30 days of birth c. the infant spent 120 hours in a NICU out of state but resides in Arizona d. a special request was made by a neonatologist or pediatrician e. sibling of eligible infant (twin) f. a child does not meet HRPP eligibility criteria but would qualify under CYSHCN (see below).
Enrollment in the HRPP or CYSHCN occurs when the following data is entered by a CHN in ETO: • Enrollment Form- Demographics • Enrollment Form – Signature Page
5.4 Program Participation When enrolling at the hospital, families will be offered two options to choose from; full or partial. A. Full Participation
a. Full participation provides the family with the opportunity for developmental follow-up visits from a community health nurse, and possible financial support for, hospital inpatient services, and transport to/from another hospital if needed. When full participation is selected, families must enroll their infant on their third party and/or AHCCCS plan, if eligible, within insurance guidelines to cover the infant’s medical bills. Failure to do so may result in HRPP/NICP financial assistance being denied and family will be responsible for all hospital, physician, and transport charges.
B. Partial Participation
a. Partial participation may be requested if the family does not wish to disclose their financial information, they do not have insurance or they are sure their insurance company will pay all hospital inpatient costs for the baby. Partial participation provides the family with community nursing follow-up services only.
b. Families will not receive any financial assistance for transport, back transport, or physician services.
C. Late Enrollment
Enrollment in the program, which occurs beyond 30 days of the infant’s birth, is accepted at the discretion of the CHN contracting agency based on capacity and risk. a. Reasons for a Late Enrollment:
• Enrollment Hospital never offered program • Parent originally declined participation • Child from an out of state NICU • Referred by provider for neonatal follow up as a child or youth with special health care needs • Sibling of eligible infant (twin) • CYSHCN enrollment
b. To complete a late enrollment, use the Enrollment Form c. Notify the HRPP Program Manager of any denied requests by the Contractor to accept a late
enrollment.

12 | P a g e
D. Adoption and Foster Care Infants are entitled to the same HRPP services when placed into foster care or adopted. It is the responsibility of the hospital personnel to notify and inform the responsible agency and/or family regarding the array of services available.

13 | P a g e
6 Visit Guidelines
6.1 Introduction The service planning process must be flexible, coordinated and culturally responsive to accommodate changes that occur within the family over time. Long term and future goals must be explored with the family as well as immediate needs or concerns. Home visiting services are based on health, development, environment and relationship risk.
6.2 Protocols A. CHN Contractors are expected to:
a. Contact the family within one week of receiving the enrollment forms. b. Attempt to visit a new family within two (2) weeks of initial contact.
B. CHN Contractors will receive all referrals through ETO. C. If the parent does not wish to participate in the program, the CHN will dismiss the participant from
the program in ETO selecting the appropriate reason for dismissal. A CHN Visit Form should be completed if the decision was made during a visit.
6.3 Documentation A. CHNs are required to complete the following documentation in ETO. Please see the CHN ETO
Procedure Manual for guidance. A chart is provided in appendix with timelines and purpose for each document.
B. If CHN programs maintain paper charts, they may be requested at the time of site visit for review. C. Charts will be reviewed in ETO at minimum one time per year.
6.4 Referrals Referrals must be recorded from each visit in the External Service Referral touchpoint within seven (7) days of the visit date. They are categorized by priority level. Priority level of the referral determines the estimated time period for next follow-up with the client regarding the referral outcome. Follow-up notes should also be recorded in ETO. A. Level 1 – low priority referral for services that do not need follow-up. This would include information
on community resources or educational resources for the client/family but not an immediate health or behavioral health concern/need that requires action. No required follow-up.
B. Level 2 - high priority referral for services that need follow-up verification. This would be immediate health, behavioral health, child developmental needs, and food scarcity, etc. Recommended follow-up at next visit.
C. Level 3- emergency priority referral for services that need follow-up verification. This would be emergency situations where the health, behavioral health and/or safety of the family may be at risk. Immidiate action taken at visit, follow up with family as necessary.
6.5 Case Dismissal Guidelines A. Dismissal Reasons
a. Goals Met/Service Complete – Infants 12 months or greater adjusted age and have no medical or developmental problems
b. Moved Out of State c. Lost to Follow-Up – When several attempts have been made to reach a family, such as a letter,
phone call, or home visit and there is no response. d. Declined Nursing Follow-Up – Prior to home visits being established, the CHN makes contact with
the family and they verbally refuse nurse home visitation.

14 | P a g e
e. Voluntary Withdrawal -Parent declines services after initially receiving services. f. In Other Services – Infant has been enrolled in other services that fulfill similar needs or target-
specific needs (i.e., DDD, AzEIP, Healthy Families, etc.) g. Low Risk h. Child Death i. Transferred j. Transferred to IHS
B. Dismissal Procedures for Eligible, Non-Responsive Families
When a family cannot be contacted, i.e., moved with no forwarding address or ability to be contacted by phone, they are considered “Lost to follow-up”. The following are guidelines for documentation of closure to community nursing services. a. CHN must make at least 2 contact attempts. Initial contact must be by phone, followed up with a
text message. b. CHN will use clinical judgment to determine whether a drop-in home visit needs to be made prior
to closure. c. No response – send letter via mail. d. No response from letter, close in 30 days.
C. Transferring Cases
When a family is moving out of one service area into another HRPP service area the CHN should ask the family if they are interested in continuing services in their new community. If so, the CHN should refer the family to the new CHN contractor through ETO. Upload into ETO all forms and documents to the most recent CHN Visit Form touchpoint.

15 | P a g e
7 Visit Guidelines for Special Populations
7.1 Children and Youth with Special Health Care Needs (CYSHCN) A. Introduction
The Office for Children with Special Health Care Needs (OCSHCN) partners with HRPP by contracting with specially trained community health nurses (CHNs) throughout Arizona to provide a culturally appropriate, multi-disciplinary, family centered approach for children with chronic medical conditions or a demonstrated risk for developmental delay. The community health nurse provides support from hospital to home, conducts physical and developmental assessments, provides anticipatory guidance, and makes referrals to other community resources as appropriate (AzEIP, DDD, WIC, etc.). Children with special health care needs are defined as; “Those with a physical, developmental, behavioral or emotional condition that has lasted or is expected to last 12 months or longer; who require health or related services that children in general do not.” This definition is very broad and goes well beyond developmental conditions, to include any condition requiring specialized care or services that most children do not need or use.
B. Eligibility Requirements Infants and/or children should meet the following eligibility criteria: Eligible individuals shall reside in Arizona, ages birth -19 years old and one of the following:
• Former HRPP clients ages 3-19. • Infants not eligible for HRPP but referred by neonatologist. • Siblings of a HRPP infant and other children living in the home referred by a family member or
provider. • Children age 0 – 19 who are referred by a provider.
The criteria above is defined as:
• Infants previously enrolled in HRPP who also meet the definition of special health care needs, but are no longer eligible for HRPP.
• Infants with special health care needs, who do not meet the criteria of a NICU/SCN stay of 120 hours, may be enrolled upon submission of a request from a pediatrician to a local contracting agency.
• Siblings and/or other children ages birth - 19 years, not enrolled in HRPP and living in the home, who have a special health care need and whose families demonstrate or desire a need for information, support, and/or coordination with multiple service providers and resources OR whose provider expresses a concern related to the child’s health or need for family supports and resources.
• Children ages birth - 19 years not enrolled in HRPP who have a special health care need and whose provider expresses a concern related to the child’s health or need for family supports and resources.
C. CYSHCN Enrollment Procedures Infants and children meeting the above eligibility requirements may be enrolled as a child or a youth with special health care needs (CYSHCN) and be referred for Community Health Nursing. A community health nursing program may enroll an eligible child by completing the following steps: a. The Enrollment Form should be signed and dated by the parent at the initial CHN visit. It is
required to include a brief reason for the enrollment. b. Complete the Enrollment Form touchpoint and upload the Enrollment Form into ETO within seven

16 | P a g e
(7) days of the signature date.
Outside agencies or community organization can inquire about enrollment by contacting the ADHS Program Manager. The provider will complete the Enrollment Form and submit via email, or at minimum complete the Demographics Form. The Program Manager will refer the infant to the appropriate CHN agency via ETO data management system.
D. Home Visitation Guidelines
Infants, toddlers and children may be seen for up to 6 months under the CYSHCN CHN services. Home visits beyond this period require prior approval from OCSHCN via email request to the HRPP Program Manager. The Community Health Nurse should refer families as appropriate. CHN contractors should have a network of providers, programs and services for families. Information within this manual also applies to children enrolled as a CYSHCN client.
7.2 Newborn Screenings A. Introduction
HRPP partners with the Office of Newborn Screening to provide follow up newborn blood spot collections. These visits include the coordination and referral to community services for infants identified as needing repeat bloodspot as needed.
B. Eligibility Requirements Infants and/or children should meet the following eligibility criteria: a. Shall reside in AZ, with an concurrent birth within the state; AND b. Received a previous abnormal or incomplete result for bloodspot
The contractor should collect and verify demographic information on the baby such as DOB, birth hospital and mother’s name and DOB.
C. Enrollment Procedures
a. Infants will be enrolled into the HRPP program in the ETO Data management system. b. The Newborn Blood Spot Collection Touchpoint will be completed to demonstrate that
collection/visit was completed.
D. Home Visitation Guidelines Upon notification from the ADHS Office of Newborn Screening, contractors will provide assistance in locating families and facilitating the collection and submission of another newborn screening test for infants with a previously abnormal test result. The CHN will make a home visit and provide education about Newborn Screening and a follow up blood test. All procedures in the Newborn Screening Guidelines are to be followed. The blood spot collection will be sent to the Arizona State Laboratory to be analyzed. The Arizona Newborn Screening Provider Guidelines details the specifics for ordering collection kits, techniques for specimen collection, shipping and handling practices. There are also best practice recommendations for meeting hearing screening, diagnoses, and early intervention milestones. The guidelines can be located here: https://azdhs.gov/preparedness/state-laboratory/newborn-screening/index.php#healthcare-providers-education The website www.aznewborn.com provides free brochures in English and Spanish for dissemination to families as well as links to other clinical references, including the core panel of disorders screened

17 | P a g e
for in Arizona. Once visit is complete, CHN will provide ADHS Office of Newborn Screening status of case as well as Community Nursing Visit form which outlines areas discussed. CHN may offer CYSHCN enrollment based on the needs of the infant and family.

18 | P a g e
8 Visit Procedures and Tools 8.1 Visit Protocols
The Olds model for home visitation of HRPP infants recommends a frequent schedule of home visits. Once a week for the first six weeks, every other week until 21 months, and once a month from months 21-24. (David Olds, PH.D. Prenatal and Infancy Home Visitation By Nurses, 1998). Budget constraints prevent HRPP from following that model. Contractors are required to evaluate their allocated funding each fiscal year and prioritize visitation to ensure the infants are seen as appropriate according to their risk. HRPP recommends a minimum of four visits the first year, however a visiting schedule needs to be discussed with the family to determine frequency. Some families may choose to opt out after the first visit; some may require support until 3 years of age. Nursing impression and family concerns determine what visits are needed until the child turns 3 years of age. All visits must be documented. Optimal minimum visit schedule for moderate to high risk infants not receiving services from any other provider would be:
• Initial visit • 2 month • 4 month • 6 month • 8 or 9 months • 12 month visit
8.2 Educational Tools A main component to the CHN Visit is providing education to the parent related to infant health and development. Educational Packets are as follows:
• Initial Packet - First Visit • Second Packet - 4-6 months • Third Packet - 8-12 months
List of ADHS approved educational materials are listed in the appendix.
8.3 Community Healthy Nursing (CHN) Visit Form The CHN Visit Form is an ETO touchpoint to be filled out by the home visitor after each visit. This form contains the required information for payment of services and must be completed for all HRPP and CYSHCN visits. It does not need to be completed for a Newborn Blood Spot Collection visit. The CHN shall ensure: A. All home visits must be entered into Efforts to Outcome (ETO) database B. A copy of the CHN Visit Form is filed in the client’s chart according to agency protocols (if applicable) C. Demographics are updated as needed using the following guidelines:
a. First name: The name that the infant is given at birth and is called by the parents. b. Last name and/or Family Name: This should match the infant’s last name as designated by the
parents upon enrollment, if different than the hospital label. c. Alias last name: This should match the name given on the hospital label.

19 | P a g e
Health Status “Good” when infants have normal growth and development parameters:
• Consistent growth, height, weight and head circumference as indicated on the growth charts and the other assessment information collected by the CHNs using WHO standards
• No trips to the ER, OTC medications needed except vitamins, normal physical exam and no family or CHN concerns
“Fair” when infants have normal childhood illnesses such as ear infection or: • A chronic condition exists that does not require frequent trips to the doctor or
hospitalizations. • Feeding problems exist but the child’s growth parameters are still on the growth
chart. • Some equipment, such as apnea monitor and/ prescription medications are taken
such as those for seizures, etc. “Poor” when infants have conditions that may be considered “life threatening” or need
frequent hospitalizations or surgeries.
d. Medical Home Mark “Yes” if the family has a consistent source of medical care such as:
• A physician or practitioner they can call if their child is sick anytime within a 24-hour period of time.
• A place they can take their child for care other than an emergency room, i.e., Doctor’s Office, clinic, community health center, etc.
e. Purpose of CHN Visit This field should be utilized to provide additional detail regarding the purpose of the visit and is particularly important when there is a need for multiple visits within a short period of time. Using as few words as is possible. The home visitor should describe the ongoing situation (i.e., postpartum depression, nutritional follow-up/weight check, resources, and referral, etc.) If following regular visiting schedule, use initial visit for first visit and developmental follow up when using ASQ screening.
8.4 Family Service Plans (FSP) The purpose of the FSP is to identify family resources, priorities, and concerns and is developed by the home visitor in conjunction with the family. The FSP is usually initiated on the first visit with the family and includes assessment planning. The FSP is fluid and used as a guiding tool on subsequent visits. This is not duplicating data collected elsewhere, only data important to the family and outcome goals identified. Infant/child, maternal and family strengths and needs are identified, i.e., “What is the family most proud of with their child and what are they the most concerned about?” “How does mother view her own health in relationship to possible subsequent pregnancies?”
A. A FSP is required to be completed at each home visit B. The FSP can:
• Identify child and family desired outcomes. • Explore the family’s natural helping network, such as extended family members, friends or
neighbors. • Explore child and family health insurance benefits and provide information about services
available in the community.

20 | P a g e
• Identify other agencies or services for which the child may be eligible, facilitate referrals, and enrollment.
• Assist the family in identifying needed services as appropriate. • Identify outcomes to meet infant, child, maternal, and/or familial needs. This can include
potential or actual dates. C. It should be signed by the caregiver at each visit and included in the client’s file. D. The FSP is not a legal document, which means that services identified as needed are not required to
be provided by the CHN program. Efforts shall be taken, however, to facilitate the referral of families to appropriate service providers and encourage enrollment.
E. Guidelines for using the FSP: • Infants and toddlers are uniquely dependent on their families for their survival and
nurturing. This dependence necessitates a family-centered approach to early intervention. • Each family has its own structure, values, roles, beliefs and coping styles. Respect and
acceptance of this diversity is essential to family-centered early intervention. • Early intervention systems and strategies must reflect a respect for racial, ethnic and cultural
diversity of families. • Respect for family, autonomy, independence and decision making means that families must
be able to choose the level and nature of early intervention involvement. • Family/professional collaboration and partnership is the key to family- centered early
intervention and successful implementation of the planning process. • No one agency or discipline can meet the diverse and complex needs of infants and toddlers
with special needs and their families. Therefore, a team approach to planning and implementing the FSP is recommended.
• A family need or concern is only a need if the family perceives it to be relevant. • Any information the family does not want to be on the plan must not be included and must
remain confidential. • The FSP is a “working” document. The process must lead to outcomes that assist the family
in achieving their goals for themselves and their child.
8.5 Infant Screening Tools A. Ages and Stages Questionnaire
The Ages and Stages Questionnaire (ASQ-3) should be used to assess the child’s performance on various age-appropriate tasks. This tool is valuable in screening children for possible problems, confirming suspicions with an objective measure, and in monitoring children at risk for developmental problems, such as those who have experienced perinatal difficulties. It is designed to compare a given child’s performance on a variety of tasks to performance of other children the same age. The ASQ:SE-2 is designed to measure a child’s social and emotional developmental needs. At minimum, a child should receive at least one ASQ screening within the first year of the program. The Ages and Stages Questionnaires include a series of questionnaires designed to identify infants and young children who show potential developmental problems. Each questionnaire features 30 developmental items that are written in simple, straightforward language. The items are divided into five areas: communication, gross motor, fine motor, problem solving, and personal-social. An overall section addresses general parental concerns. Children are identified as needing further testing and possible referral to early intervention services when their ASQ scores fall below designed cutoff points. The ASQ materials consist of reproducible master questionnaires, age- appropriate scoring and data summary sheets, and the User’s Guide which also contains activity sheets for parents that correspond

21 | P a g e
to the ASQ age intervals. A Spanish translation master set of questionnaires is also available.
B. Nursing Neonatal and Pediatric Assessment All “regular” home visits by the Community Health Nurse should include an assessment of the infant/child’s physical, developmental, environmental, and family relationship status. The assessment form should be used to describe any Concerns of the parent or home visitor, to describe the home visitor’s Impressions, and to document the Plan for follow up. The level of risk should also be recorded here.
C. Children’s Health Survey As a collaboration with the Office for Children with Special Health Care Needs, the Children’s Health Survey will be implemented as resource for identifying a child with special health care needs. It can be administered as early as one year of age. The child or infant should be screened:
• After turning 1 year of calendar age • Age greater than 1 at entry into the program • Or a Re-screen can be completed if there is a significant medical consequence
8.6 Maternal Assessment Tools & Support A. Postpartum Mood Disorder
Postpartum Mood Disorders affect millions of women worldwide, regardless of race, age, culture, or socioeconomic status. Symptoms of Postpartum Mood Disorders vary and may include feelings of sadness, anger, frustration and confusion. A mother experiencing a Postpartum Mood Disorder may feel alone and ashamed of her symptoms. Fathers are also impacted by Postpartum Mood Disorders and have their own experience that may be very different from the mother. These differences place an enormous amount of stress on the couple's relationship and it can prove a difficult time for the entire family. Postpartum Support International (PSI) (http://www.postpartum.net/learn-more/pregnancy-postpartum-mental-health/) provides information and resources to mothers and fathers on Postpartum Mood Disorders. The resources there are intended to provide couples, families, and professionals with information and tools to help mothers and families heal from Postpartum Mood Disorders. *Information taken from PSI (http://www.postpartum.net/)
B. Edinburgh Postnatal Depression Scale (EPDS) The EPDS was developed for screening postpartum women in outpatient, home visiting settings, or at the 6 –8 week postpartum examination. It has been utilized among numerous populations including U.S. women and Spanish speaking women in other countries. The EPDS consists of 10 questions. The test can usually be completed in less than 5 minutes. Responses are scored 0,1, 2, or 3 according to increased severity of the symptom. Items marked with an asterisk (*) are reverse scored (i.e., 3, 2, 1, and 0). The total score is determined by adding together the scores for each of the 10 items. Validation studies have utilized various threshold scores in determining which women were positive and in need of referral. Cut-off scores ranged from 9 to 13 points. Therefore, to err on safety’s side, a woman scoring 9 or more points or indicating any suicidal ideation (that is she scores 1 or higher on question #10) should be immediately referred for follow-up. Even if a woman scores less than 9, if the clinician feels the client is suffering from depression, an appropriate referral should be made. The EPDS is only a screening tool. It does not diagnose depression – that is done by appropriately licensed

22 | P a g e
health care personnel. Users may reproduce the scale without permission providing the copyright is respected by quoting the names of the authors, title and the source of the paper in all reproduced copies. *Information taken from the American Academy of Pediatrics (https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/practicing-safety/Documents/Postnatal%20Depression%20Scale.pdf) The EPDS is to be completed at each first home visit of HRPP enrolled children (foster/adoptive excluded). Any score equal to or higher than 9 must be referred for follow up care. A referral may include PPMD support, primary care physician, crisis line, and/or other appropriate referral. The referral must be noted on the FSP and in the External Referral touchpoint in ETO. Once the screening has been completed the CHN will educate the mom on postpartum depression, how to score and together review the results. The screening tool will be left with the mother for future use. Every mother in the program should be provided information on the PSI Helpline. The PSI Helpline can be reached at 1-800-944-4773.
C. Maternal Wellness Assessment/Preconception Care “Preconception care is defined as a set of interventions that aim to identify and modify biomedical, behavioral, and social risks to a woman’s health or pregnancy outcome through prevention and management.” Recommendations to Improve Preconception Health and Health Care-United states, A Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR 2006; 55 (No.RR-6):3-4. The Community Health Nurse, by virtue of following HRPP enrolled infants, is in the unique position of being in the home and working with the mother of a premature infant or infant with a less than optimal birth outcome. The mother who has had a preterm infant is at a statistically higher risk of having another preterm infant. The goal of this aspect of the CHN follow up visit is reduction of risk factors that can lead to preterm delivery in a subsequent pregnancy. To this end, the CHN will use appropriate screening tools to screen and then provide education to the mother of the infant about: reproductive awareness; environmental toxins and teratogens; nutrition and folic acid; genetics; substance use including tobacco and alcohol; medical conditions and medications; infectious diseases and vaccination; and psychosocial conditions. The CHN helps to link her to community services when appropriate. Additional information can be found on the ADHS Women’s Health website (https://www.azdhs.gov/prevention/womens-childrens-health/womens-health/index.php) and Power Me A2Z (https://www.powermea2z.org/power-your-family/).
8.7 Environmental Screening Assessment During the Neonatal & Pediatric Assessment, the CHN will observe the home for safety concerns. The CHN will document concerns observed or reported by caregiver and provide education and/or resources to address the concerns. All families will receive education on home safety during initial and subsequent visits by the CHN.
8.8 Determining Level of Risk All enrolled infants are identified upon discharge from the hospital as “high risk” or “at risk” for developmental delay. Families who have a child that is considered to be in the “high risk”

23 | P a g e
category should be strongly encouraged to receive follow-up services through the Community Nursing Services component of the program. Infants who have an established condition at the time of discharge should be referred, by the discharging hospital, directly to the Arizona Department of Economic Security’s Division of Developmental Disabilities (DDD), or the Arizona Early Intervention Program (AzEIP). The CHN will use the Nursing Neonatal and Pediatric Assessment (NNPA) at each regular visit until one year of age. At this time, the CHN will determine the risk of the infant.
Level of risk on the Neonatal & Pediatric Assessment should be determined as follows: • High Risk: Two or more areas of concern in two or more categories • Moderate Risk: One area of concern in two categories or two areas of concerns in one
category • Low Risk: One area of concern in one category
Nursing judgement and the infant’s medical assessment at the time of discharge from the hospital should be considered during the risk assessment.

24 | P a g e
9 Community Collaboration An essential component of community nursing services is the collaboration with hospitals, primary care providers, and other agencies to assist infants, children and their families in accessing appropriate services. Community Nursing providers are expected to: Learn about the community. Know what resources are available and how to connet families to needed services. Attend hospital discharge planning meetings at Level IIE, III and IV hospitals within the service area. It is encouraged to introduce yourself to parents nearing discharge if the opportunity is available. A. Share information to the home visitor responsible for visiting those families discharged into
their service area B. Meet with hospital personnel to:
a. Develop a collaborative relationship b. Receive discharge information c. Provide feedback to hospital personnel d. Provide training on HRPP and other community resources
C. Attend multi-disciplinary staffing meetings in person or via phone as requested by agencies and/or families. These may include hospital discharge rounds, staffings with the DCS, AzEIP, DES, DDD, or others as appropriate.

25 | P a g e
10 Personnel & Training
10.1 Roles and Qualifications A. Community Health Nurse
Arizona Licensed Registered Nurses with Basic Life Support Certification, experienced in maternal and child health, pediatrics and/or NICU and a BSN Degree.
B. Social Worker Licensed Master-level Social Worker, experience with children and families and have Basic Life Support certification.
C. Early Interventionist (EI) EIs may be used to provide specialized support and guidance. EIs shall meet the professional requirements and rules of professional conduct for that discipline or profession as prescribed by the State of Arizona. EIs shall have a minimum of a Bachelor’s degree in early childhood, early childhood special education, speech therapy, physical therapy, occupational therapy, hearing, nutrition or a closely related field. A CHN may request the accompaniment of an early interventionist. This should be used only when an infant does not qualify for AzEIP or DDD and a family has identified concerned that require additional support. *Social Workers and Early Interventionists should only conduct visits with the CHN and with prior approval from the ADHS Program Manager.
10.2 Staff Education Opportunities and Requirements Maintain records of education completed on the provided HRPP log. HRPP provides educational opportunities for designated HRPP staff. Currently, bi-annual CHN trainings and an Annual HRPP conference are offered. Continuation of these opportunities is based on funding. The educational requirements for designated HRPP staff are as follows: A. Complete program orientation prior to being assigned a case load. B. HRPP requires a minimum of 6 CEUs annually. 1 CEU in PMAD, 1 CEU in NAS, 1 CEU in ACES
and 3 additional in program related education. The required topic are subject to change based on trending topics and needs. Contractors will be notified annually of any changes.
Attendance over and above the CEU requirements is based on the availability of funding.
10.3 Orientation The Orientation is intended to give the CHN an overview of the program requirements and their role and job responsibilities. The orientation program provides basic information on several critical areas of the Community Nursing Program. Through this initial orientation process, community nurses demonstrate that they possess sufficient knowledge about the program, and that they have mastered the necessary skills to begin conducting client contact activities safely and competently.

26 | P a g e
A. Program Introduction and Training HRPP CHN Policy & Procedure Manual*
All CHN must complete a comprehensive review of the Policy and Procudure manual with the supervisor, documenting on the Education log dates of completion. HRPP Training should include the following: 1. Introduction and History of HRPP 2. HRPP Philosophy, Mission and Goals 3. Roles and Responsibilities 4. Program Overview 5. Home Visitation Services 6. Visit Guidelines 7. Visit Guidelines for Special Populations 8. Visit Procedures and Tools
8.1 Visit Protocols 8.2 Educational Tools (Parent Education Packets) 8.3 CHN Visit Form 8.4 Family Service Plan (FSP) 8.5 Infant Screening Tools 8.6 Maternal Assessment Tools & Support 8.7 Environmental Screening Assessment 8.8 Determining Level of Risk
9. Community Collaboration 10. Personal and Training 11. Reporting 12. Continuous Quality Improvement 13. Billing Process and Policy 14. Contract Monitoring 15. Procedural Safeguards
B. Additional Training Requirements
1. Agency HRPP Processes & Communication Flow* 2. Observation of Home Visit* (shadowing, up to 5) 3. Supervised Home Visit* 4. Efforts to Outcome (ETO) Data Management System
*Must be completed before CHNs can be assigned a caseload. Must be completed within 60 days of hire Shadowing visits for a nurse in training shall be billable, up to five visits. The other areas should be completed within six months, but the CHN should have general knowledge before completing visits independently. The information in these areas must, at minimum, address the learning objectives of the orientation training which conforms to ADHS Community Nursing Policy and Procedure Manual. Training must also include relevant information from the Contractor’s specific community to allow community nurses to successfully work within that community.

27 | P a g e
10.4 Continuing Education All continuing education should be designed to strengthen the skills, provide updated information and support the activities of the community health nurse. A continuing education plan should be developed annually for all workers that include the training needs identified through the Education Log. A copy of the continuing education log will be available to the ADHS Site Review Team for review during a formal site visit. HRPP requires a minimum of 6 CEUs annually. 1 CEU in PMAD, 1 CEU in NAS, 1 CEU in ACES and 3 additional in program related education. The required topic are subject to change based on trending topics and needs. Contractors will be notified annually of any changes.
Community Health Nurses are strongly encouraged to attend conferences and workshops for continuing education. Attendance for training is based on availability of funds.
10.5 Education Log The Education Log is found in the appendix. It is required that all contractors use this form to track
the following by all CHNs and other professionals conducting visits as part of HRPP services to be reviewed at annual site visit. A. Orientation B. Continuing Education
10.6 Tailoring Education Orientation experiences shall be designed to meet the needs and experiences of each new CHN, i.e., nurses who have worked in the NICU would be best served by more exposure to the public health nursing role whereas, nurses experienced in the public health role would benefit most from spending time observing care offered to the critically ill infant in the NICU. A new CHN would benefit from spending time observing infant evaluations by a developmental specialist. Specific questions regarding the assessment of the neuromotor development of the infant can be addressed during these opportunities. Encourage new CHNs to attend AzEIP evaluations when possible. A new CHN would also benefit from the mentoring experience of following a very experienced nurse or practitioner making home visits. The amount and duration of the supervised home visits depend on the needs and experience of each CHN.
10.7 Supervision Contracted agencies are required to have standard procedures in place to evaluate the quality of services and skills of home visitors which may include annual employee evaluations, skills assessments, and client satisfaction surveillance.

28 | P a g e
11 Reporting All forms and reports are used by the Community Nursing Program to collect information for program planning, development and evaluation. Information gathered, both at the ADHS and Contractor level is used to evaluate the effectiveness of the Program. In this chapter, data collection forms will be fully explained.
11.1 Notice of Implementation or Change A. The contractor shall notify the ADHS Program Manager of any new professional staff and
changes to existing staff within 30 days of the change. This should be included on your monthly report.
B. ADHS will notify the contractor of reporting changes with 30 days notice of the required change in reporting. This will be done via email.
11.2 Monthly Invoice Contractors are required to submit a monthly invoice by the 21st of the month following the service month. This should be accompanied by: A. Log of service that includes the name of the participant, date of the visit, and type of service B. List of Discharge Planning Rounds attended including the hospital, name of CHN, and date C. Supporting documentation for training days, which includes a list of trainings, CHN name,
dates, and a copy of the certificate If the log or invoice is incomplete or illegible, it will be sent back to the Contractor for completion before payment is authorized.
11.3 Monthly Reports A monthly report must be submitted by the 21st of the month following describing the following: A. Program strengths, priorities and concerns B. Training/education activities, certifications and training needs C. Current program staff
11.4 Annual Plan An annual plan must be developed which a comprehensive description of the agency, program management, and program goals for the year. The plan must be completed on contractor’s letterhead or HRPP template and submitted annually by July 31st. The template will be distributed by the HRPP Program Manager on an annual basis. See the same template in the appendix. The Annual Plan includes information related to the Continuous Quality Improvement indicator identified by ADHS HRPP program team for the year.

29 | P a g e
12 Continuous Quality Improvement
12.1 Introduction The ADHS Bureau of Women's and Children's Health (BWCH) recognizes the need to support the development of effective quality assessment and improvement initiatives into its programs. Contractors must develop a systematic process for continuous monitoring of the quality of patient/client services. This document provides guidelines for the development and/or ongoing implementation of a continuous quality management and improvement program.
Quality management and improvement is an ongoing process to monitor and improve health services. The process is summarized in The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) Ten Step Model (adaptation): A. Assign responsibility for activities. B. Delineate scope of care. C. Identify criteria and indicators for review. D. Establish thresholds for evaluation and implement. E. Data collection. F. Review actions with analysis of data and reports. G. Evaluate care and assess prior interventions. H. Cooperative planning and implementation of change (a new plan) as necessary. I. Assess effectiveness and document improvement. J. Communication-establish a feedback system for communication about trend, interventions
and evaluations.
12.3 Indicators The indicator is what is looked at to determine how well the organization is doing on an aspect of care. It is a measurable variable that relates to the quality of services. Each indicator has its own performance or effectiveness goal and has the potential to impact the health of the patient. In recognition of the fact that both state-wide trends and local concerns must be addressed by the ongoing quality improvement process, the BWCH will identify two indictors per contract year that must be included in CQI activities. Contractors may select additional quality improvement activities.
12.3 Goals and Outcomes Performance or effectiveness goals may be selected. Performance goals identify the organization's target for the result of a process or system. Performance goals measure the compliance of the organization or its providers in relation to its processes or systems. Effectiveness goals, on the other hand, measure a change in health, patient/client performance, or patient/client satisfaction as a result of the performance of the organization or its providers. Performance goals may be drawn from a variety of sources including various regulations and standards governing health care practice, organizational policy and procedures or contractual requirements.
12.4 Responsibility The person identified to be in charge of documenting the plan, collecting the data, reporting results, developing and documenting strategies and results. Results of each contractor’s performance related to quality improvement indicators are to be reported on the quarterly reports and available for scheduled formal site visits.

30 | P a g e
13 Billing Process & Policy
13.1 Billing Policy A. Payments are contingent on availability of funds. The HRPP will notify Contractors when
allocated funds are exhausted. B. Late Enrollment Forms and CHN Visit Forms must be entered into HRPP ETO before any
request for payment is considered. C. Services for infants who are not HRPP must be billed as CYSHCN or NBS as appropriate.
13.2 Billing Procedures A. The Contractor shall electronically submit the monthly invoice for CHN services by the 21st
day of the month following the service using the designated template. The invoice template will be sent to each contractor annually or as needed by the HRPP Program Manager.
B. A visit summary must be submitted with the monthly invoice. C. Documentation for billable trainings and discharge planning attendance (agenda,
certificate, etc.) must be submitted for each attendee with monthly invoices. D. Each Contractor has a unique Contract Number and Purchase Order number. The contract
number must be included on all Contractor invoices and correspondence to ADHS. E. The billing time period and contractor’s name must also be entered in the designated
invoice template. The invoice must contain the signature of the Contractor’s authorized representative and the date of signature.
F. Any revisions to the invoice must be resubmitted to the Program Manager with original signature of the Contractor’s authorized representative and the date of signature.
G. The Program Manager’s signature line in the bottom left hand corner of the page is for payment authorization by ADHS
H. The signed invoice and required documentation should be submitted to: [email protected] or mailed to: Arizona Department of Health Services Bureau of Women’s & Children’s Health ATTN: Community Nursing Services 150 North 18th Avenue, Suite 320 Phoenix, AZ 85007
13.3 Billing Definition Contractors are reimbursed for managing the care of each infant referred for services per the conditions of the contract. Home visitors are required to provide services according to the needs of the infant/toddler and family based on risk assessment. Unit billing rates are reflected in the Provider contract price sheet and are defined as follows: A. Proximity
a. Distance Level 1 – Total miles between two points ranging from one to 30 miles. This includes from office to home visit, from CHN home to first visit, or from visit one to visit two.
b. Distance Level 2 – Total miles between two points ranging from 31 to 60 miles. This includes from office to home visit, from CHN home to first visit, or from visit one to visit two.
c. Distance Level 3 – Total miles between two points greater than or equal to 61 miles. This includes from office to home visit, from CHN home to first visit, or from visit one to visit two.

31 | P a g e
B. Type of Visit
b. Interim – Usually shorter in duration. An interim visit does not require a full assessment of child. Examples of an Interim visit: Weight check, follow-up on feeding issues, environmental assessment, referral to community resources.
c. Regular – Complete a physical, developmental, psychosocial and environmental assessment of infants, provide family support and early intervention along with referral services to community resources as needed and provide interconception support and education to the mother.
d. Discharge Rounds - Family-centered Multidisciplinary visit at the hospital focused on learning about multiple patients and sharing the program. The nurse may meet with families during this time to explain the program.
e. Family Visit- This is a visit that addresses social or emotional concerns of the family. This visit does not include a full assessment of the infant. This would be billed as a single visit regardless of the number of children in the family.
f. Bereavement – Counseling and referral to appropriate community resources (can occur in the hospital or in the home). There are not to be more than two bereavement visits per family. Bill at the family visit rate.
g. Staffing Visit – This visit is usually a Multidisciplinary visit (participation in IFSP,joint visit with another discipline, Foster Care Review Board, DCS staffing, a nurse making a home visit with a health professional when the nurse IS NOT doing a full assessment of the child, etc.). This visit can occur in the office or in the home. Bill at the family visit rate.
h. Pre-Discharge- Visit with the infant/family in the hospital before or after enrollment in the program and before initial discharge. This visit is charged at the “distance 1” “interim” rate. Parent/guardian must be present for visit to occur. If this visit occurs during the same time frame as discharge rounds, you may only bill for discharge rounds.
i. Shadow - ADHS will reimburse the contractor for each newly hired CHN to shadow a home visit with an existing program nurse. The contractor shall be reimbursed up to 50% of the visit rate charged by the agency’s visit rate (not the mileage rate for the person shadowing), and shall not exceed 5 shadow visits per new hire.
j. Newborn Blood Spot Collection - This is an urgent request from the ADHS Newborn Screening program to contact, re-screen, and collect a sample from an infant with a previously abnormal test result.

32 | P a g e
14 Contract Monitoring The purpose of contract monitoring is to establish a mechanism for the evaluation of contracts executed by ADHS to ensure services were delivered pursuant to the terms and conditions of the contract, statues, rules, and other policies applicable or made a part of the contract. During the monitoring process, ADHS shall provide training and technical assistance to the contracted provider, engage in dialog to identify public health concerns, and provide general overview of the ADHS services. The monitoring process provides a structured framework for reviewing and assessing the Community Health Nursing contractor’s progress, program strengths and compliance with Standards. HRPP Program Manager will conduct an annual site visit for each contractor.
14.1 ADHS Responsibilities A. Determine the appropriate contract monitoring method and document the plan. B. Prepare and provide the contractor with a comprehensive Contract Monitoring Guide. C. Schedule the on-site review (as appropriate) with the Contractor a minimum of (5) days in
advance of the review. D. Provide the contractor with a draft agenda, a list of the review team members, a copy of the site
review monitoring guide, and a list of patient charts which should be available for review. E. Conduct interviews with administrators, staff, clients, family members and others as appropriate. F. Review charts. G. Provide feedback on performance to the Contractor during the on-site review exit conference. H. Provide the opportunity for the Contractor to discuss program strengths and identify issues and
concerns. I. Provide the Contractor with a “Draft” of the complete Site Review Monitoring Guide and a Site
Review Summary which covers: Areas of Strengths, Concerns of the Program, Recommendations for Improvement, and Required Corrections.
J. Provide the Contractor with the opportunity to review and respond to the Site Review Summary. The Contractor will be given fourteen (14) days to inform ADHS if there are any corrections that should be made to the content.
The Site Review Guide can be found in the appendix.
14.2 Contractor Responsibilities A. Cooperate with the HRPP in the monitoring process by making information and records available
and by allowing interviews and inspections of the facilities. B. Notify the ADHS Program Manager regarding any desired training or technical assistance that will
be required during the on-site visit. C. Request the attendance of the staff directly responsible for the contract. D. Make space available for the meeting and review of patient records. E. Have the following materials available for review at the site: Personnel Records and Client Charts. F. Identify strengths, concerns, and education/technical assistance needs during the site visit. G. Respond to the Site Review Draft within fourteen (14) days of receipt if corrections need to be
made. H. Prepare and submit to HRPP a written plan of corrective action, if required, within fourteen (14)
days of receipt.

33 | P a g e
15 Procedural Safeguards
15.1 Information Sharing CHNs will, as is appropriate, be part of an infant’s medical team and work collaboratively with all other team members. This will include, at a minimum, sharing any results, findings related to the infant’s health and well-being. Sharing of information may be at a staff meeting, by fax, by phone, or any other forum, once permission to share information has been retrieved from the parent/guardian.
15.2 Data Usage Statement All data collected from HRPP parents and contracted vendors will be used exclusively for enrollment verification, medical claims coordination, and coordinating future care and services for the participant and or family. ADHS will de-identify all data used for statistical analysis.
15.3 Administrative Records The contractor must maintain records of employed personnel, including background, education, registration, license or certification in their respective fields, details of the HRPP Orientation, and any ongoing training received.
15.4 Patient Records Patient records must be retained according to existing legal requirements. The contractor is expected to store and maintain all client records in a safe, secure location. The Office of Women’s and Children’s Health program administration and the ADHS Office of Auditing shall have access to client records in order to conduct necessary evaluations or programmatic review.
16.5 Personnel The contractor must designate a primary contact for the HRPP program. This person is responsible for ongoing communication, updating or collecting missing information, and coordinating contract monitoring visits with the HRPP Program Manager as well as being the official contact for all other contract issues. That name must be submitted to the Program Manager by July 1, annually and as changes occur.
15.6 Customer Service Policy The Contractor must develop and implement a process by which clients may present concerns about the operation and management of the program and services received. When developing a customer service policy, the following must be included: A. Contractors must inform the client of the right to express concerns and must assist the client with
the process. B. Client concerns must be addressed in a timely manner. C. Client problems and issues must be tracked to identify trends. D. Contractors must incorporate findings and feedback into a plan to identify and correct future
problems. E. The Contractor must include in writing the address and the phone number of HRPP Program
Director in the last step in the customer service process.

34 | P a g e
15.7 Consent Consent in this context means permission from the family. It ensures that:
• The family has been fully informed of all information relevant to the activity for which consent is sought, in the family’s native language or mode of communication.
• The family understands and agrees in writing to the activity for which consent is sought. The written, signed agreement describes the activity and a list of records (if any) to be released and to whom.
• The family understands that consent is voluntary and they may revoke it at any time. • The family has the right to determine whether the infant/toddler or any other family
member will accept or decline referrals to other providers or an early intervention service without jeopardizing other early intervention services under IDEA, Part C
A. Parental Consent
Parental Consent shall be obtained in writing before: • Conducting physical, developmental, psychosocial and environmental assessment of
infant • Initiating the provision of referral to other providers or early intervention services • Initiating the provision of interconception support and education to the mother
B. Parental Consent Not given
If parental consent is not given, reasonable effort shall be made to ensure that the family: • Is fully aware of the nature of the CHN visit and assessment or service that would be
available • Understands that the child will not be able to receive the CHN visit , assessment or
services unless consent is given.
15.8 Review and Inspection of Records Parents shall be permitted to examine, inspect and review (without unnecessary delay) any records relating to their child’s evaluations, assessments, FSP, and eligibility determination. Every parent of a child enrolled in the program has the right to examine, inspect and review the records of their child and family related to:
• CHN visit • Assessments and evaluations • Eligibility determinations • Individual complaints dealing with the child
A. Requests for Review of Records
Each provider shall comply with a parent’s request to examine, inspect, and review the records of his/her child and family:
a. Without unnecessary delay b. Before any assessment c. Before any referrals to other providers or early intervention service d. Within 45 days of the request

35 | P a g e
B. Procedures for Record Review When a parent makes a request to examine, inspect, and review the records of his/her child and family the following steps will be taken: a. The contractor shall provide the parent with written instructions on his/ her rights and
how to access the records, and ensure that the parent understands these instructions. b. A date and time, that is convenient to the parent, will be set up to explain the purpose for
which the information in the records shall be used and to provide explanations and interpretations of the records. This may be done:
• At the same time the parent is inspecting and reviewing the records. • Immediately following the parent’s inspection and review of the records, or at a
later date and time.
C. Corrections to Records A parent may request to make corrections to information in his/her child’s records which they believe is inaccurate, misleading, or violates the privacy or other rights of the child or family. Each provider shall decide whether to make the requested corrections to the information in the child’s records within a reasonable amount of time, but no later than 45 days.
15.9 Confidentiality The confidentiality of personally identifiable information at collection, storage, disclosure, and destruction stages shall be protected. Each participating agency shall maintain, for public inspection, a current listing of the names and positions of those employees who may have access to personally identifiable information and those other parties who obtained access to the records.
15.10 Termination of Contract Upon termination of the contract, all administrative documents, data and reports prepared by the Contractor under the Contract shall be maintained for a period of three years beyond termination.

36 | P a g e
Appendix
1 Glossary AAP (American Academy of Pediatrics): AAP is a professional organization for pediatricians and affiliate members involved with the care of children. ADES (Arizona Department of Economic Security): Lead Agency for AZEIP ADHS (Arizona Department of Health Services): ADHS is the Arizona State agency responsible for administering public health services and addressing a variety of community health programs. AHCCCS (Arizona Health Care Cost Containment System): AHCCCS is an Arizona State agency that administers (through its managed care plans) health care benefits and services for people who are eligible for Medicaid or other low-income medical assistance programs. Anticipatory Guidance: Information given by the health care provider to assist parents or guardians in the understanding of the expected growth and development of their children. APIB (Assessment of Preterm Infants’ Behavior): APIB is a comprehensive, systematic assessment method of determining the developmental, neurological and/or behavioral characteristics of a Preterm infant. APT (Arizona Perinatal Trust): A private non-profit agency that administers the voluntary certification of Arizona hospitals for their obstetrical and neonatal care services. The agency also works to establish standards of care. The HRPP only contracts with hospitals that are certified by the APT/APRS, Inc.
ASQ (Ages & Stages Questionnaire): A parent-completed child monitoring system designed to identify infants and young children who show potential developmental problems ASQ:SE (Ages & Stages Questionnaire Social-Emotional): A highly reliable, parent completed tool with a deep, exclusive focus on children’s social and emotional development, pin pointing behaviors of concern. Authorization: The ADHS process for accepting enrollment requests for eligible maternal/neonatal clients. AzEIP (Arizona Early Intervention Program): AzEIP is Arizona’s implementation of a federal law requiring that early intervention services be provided to infants and toddlers who have, or who are at risk for, certain disabling conditions. Back Transport: Any authorized transport of an HRPP infant from one HRPP contracted hospital to an equal or lower level HRPP contracted hospital. BWCH (Bureau of Women’s and Children’s Health): Provides services and facilitates the development of systems to improve the health of women, children, and adolescents. This includes: technical assistance, consultation, system and community development, direct care, and contracts for services and education. Case Management: A process that provides high quality, cost effective health care by decreasing fragmentation, increasing clients□ quality of life and containing health costs. Case management can be provided to groups of clients, in addition to individuals and families.

37 | P a g e
CYSHCN (Children and Youth with Special Health Care Needs): “Those with a physical, developmental, behavioral or emotional condition that has lasted or is expected to last 12 months or longer; and who require health or related services that children in general do not. This definition is very broad and goes well beyond developmental conditions, to include any condition requiring specialized care or services that most children do not need or use.” Client: An enrolled patient who receives eligible neonatal, child or maternal services. CHN (Community Health Nurse): Primary home visitor in the HRPP program who addresses the emotional, social, medical and developmental needs of the infant and parental concerns. Consent: The agreement to and acceptance of a course of action, when: a. the parent or parents have been fully informed of all information relevant to the activity for which
consent is sought, in the parent’s native language or other mode of communication. b. the parent or parents understand and agree in writing to the carrying out of the activity for which
consent is sought, and the consent describes the activity and lists the records (if any) that will be released and to whom.
c. the parent or parents understand that the granting of consent is voluntary on the part of the parent or parents and may be revoked at any time.
Contractor: A public or private organization that has a contract with ADHS to develop, manage and provide HRPP services. CQI (Continuous Quality Improvement): A systematic process of identifying, describing, and analyzing strengths and problems and then testing, implementing, learning from, and revising solutions.
Developmental Care: An approach to providing individualized care to infants based on an individual assessment of the infant’s developmental/behavioral status and capabilities. This care is based on the Synactive Theory of Development. Developmentally Appropriate: Refers to the provision of services and activities that are designed to optimize the developmental status and capabilities of the individual to whom they are targeted. Disabilities: In this context, it refers to a child who presents with special health care needs. Discharge Rounds: A type of visit for the HRPP program. It is a family-centered multi-disciplinary visit at the hospital focused on learning about multiple patients and sharing the program. DDD (Division of Developmental Disabilities): Part of the AZ Department of Economic Security (DES). Assists people with disabilities achieve independence and provides support to family members and care givers. EI (Early Interventionist): The early interventionist is part of the home visiting team at a contracted agency. Eligibility: Pertains to meeting the requirements for enrollment in the High Risk Perinatal/Newborn Intensive Care Program, AzEIP, or any other early intervention agency for services.

38 | P a g e
EPDS (Edinburgh Postnatal Depression Scale): A tool used to identify mothers at risk for perinatal/postpartum depression. Enrollment: A process of voluntarily requesting to receive High Risk Perinatal Program (HRPP) by the parent or legal guardian for his or her eligible infant or by the transported mother. Family-Centered: Recognition that the family is the constant in a child’s life and that service systems and personnel must support, respect, encourage and enhance the strength and competence of the family. Family Liability: A term used to describe the total amount of money a family will be required to pay for services provided for their HRPP enrolled infant during the infant’s hospital stay in an HRPP contracted hospital(s). The services covered are inpatient and transport related only. The time period covered is from the infant’s initial transport/enrollment until his or her final discharge to home or to a non- contract facility. This may cover more than one admission if there was a back or forward transport, but does not cover readmissions of enrolled infants after a discharge to home or to a non-contracted facility. FSP (Family Service Plan): Resources, concerns, priorities and outcome tool; this form is used with the family to plan goals for case management and education. Family Visit: A visit that addresses the social or emotional concerns of the family. This visit does not include a full assessment of the infant. HRPP Program Manager: The Program Manager is an ADHS employee who is responsible for the agency’s implementation and oversight of a specific program component of the HRPP. The Program Manager provides consultation and technical assistance, coordinates activities among contractors and among HRPP team members, receives and reconciles invoices, manages the Program budget, and answers questions that arise. The Program Manager is also responsible for writing and negotiating contracts, writing and updating the CHN Policy and Procedure Manual continuous quality improvement and monitoring contractor compliance. IFSP (Individualized Family Service Plan): This acronym is used by AzEIP and DDD for children from birth to 3 years of age. This plan is used for special services for children with developmental delays. It is a written plan for providing early intervention services to an eligible child and the child’s family. IFSP Team: A team of professionals including, the parents, who through consensus, collaboration and coordination, support the family in meeting the needs of their child. Hospital Visit: A visit with the infant/family in the hospital after enrollment in the program and after initial discharge. Interconception Care: The care provided to mothers between pregnancies to improve health outcomes for women and newborns. Included interventions that modify risk factors in order to promote healthy outcomes of subsequent pregnancies. Level I: A hospital certified by the APT to provide basic obstetrical and/or newborn care. Level II: A hospital certified through the APT to provide basic and intermediate obstetrical and newborn care.

39 | P a g e
Level II EQ (Enhanced Qualifications): A hospital certified by the APT to provide all services provided by Level II hospitals plus management of pregnancy labor and delivery at 28 weeks gestational age or greater. Level III: A hospital certified by the APT to provide basic and intensive obstetrical and/or newborn care.
Maternal Transports: Maternal transports by contracted providers are paid by HRPP/NICP after all other third-party payments. The HRPP Request for Maternal Transport Form must be completed and signed by the patient or responsible party and must include the name of the authorizing contracted maternal fetal medicine specialist and name of Level II EQ or III perinatal center to which the patient is transported.
Multi-disciplinary: Refers to a service or activity carried out collaboratively between at least two separate disciplines. Each discipline involved carries out its own part, but the resulting product includes the input presented in an integrated fashion. Natural Environments: To the maximum extent appropriate for the needs of the child, early intervention services must be provided in settings that are natural or normal for the child’s age for peers who have no disability, including home and community settings. Neonatal & Pediatric Nursing Assessment: A gathering of information using medical information (hospital discharge summary), observation, and parental interview to assess the physical, developmental, psychosocial, and environmental health of the infant and family.
Neonatal Back Transports: Neonatal back transports by contracted providers are paid by the HRPP/NICP after all other third-party reimbursements if the a contracted neonatologist authorizes the transport and where the distance from the family home to the hospital is over 30 miles and the family is enrolled as full participants. Payment for transport to a non-contracted hospitals provided only with a prior authorization from the Transport Services Program Director.
Neonatal Transports: Neonatal transports completed by contracted providers are paid once the HRPP enrollment is complete and after all other third-party reimbursements. Families must enroll their infant in third party insurance or apply for AHCCCS within the required timeframes and maintain insurance. Failure to do so will result in HRPP financial assistance being denied and the family being liable for the cost of the transport. The HRPP Request for Neonatal Transport Form must be completed and signed by the patient or responsible party and must include the name of the authorizing contracted neonatologist and name of Level II, II E or III perinatal center to which the patient is transported. NICU (Neonatal Intensive Care Unit): The NICU is an area of the hospital that offers specialized care to medically compromised infants that are often born premature.
NIDCAP (Neonatal Individualized Developmental Care and Assessment Plan): A formal and standardized assessment of an infant’s developmental and behavioral status presented along with a suggested care plan to enhance the developmental status of the infant. Non-contracted Ground Transports: Non-contracted ground transport providers may participate in the Transport Program and may be reimbursed as payer of last resort. However, if they choose to participate, they must abide by the Transport Services Policy and Procedure Manual.

40 | P a g e
Nurse Consultant: The HRPP Nurse Consultant is a contractor who shall provide quality training, education, consultation, and technical assistance to HRPP Community Health Nursing Contractors to support families and medically fragile infants. OCSHCN (Office for Children with Special Health Care Needs): ADHS Office dedicated to serving children and youth with special health care needs.
Referral: Linking infants and/or families to resources and services to support their physical, developmental, psychosocial and economic needs. Risk Appropriate: Determining the need for frequency of services in an environment that most closely meets the needs of the individual. Risk Criteria: A set of conditions or circumstances that indicate areas of risk (high, intermediate, low), based on nursing assessment and judgement The level of risk aids in the prioritization of visiting families. SCN (Special Care Nursery): A nursery with specialists who care for premature infants but the infants are typically healthier and stronger than those in the NICU. Service Coordination: Activities carried out to assist and enable a child eligible under Part C and the child’s family to receive the rights, procedural safeguards and services that are authorized to be provided under the State’s early intervention program. Staffing: Multi-disciplinary staffing is a term used for the purpose of reimbursement for services provided by the Contractor such as CPS (Child Protective Services) or DDD (Division of Developmental Disabilities) staffing, hospital discharge staffing, IFSP, etc. The family is usually present as are other disciplines as appropriate. SW (Social Worker): The social worker is a member of the home visiting team at the contracted agency.

41 | P a g e
2 Forms The following visit forms are provided within this document:
a. Visit Forms • Enrollment Form – Demographics Page • Enrollment Form – Signature Page • HRPP Discharge Summary • Contact Form • CHN Visit Form • Family Service Plan (FSP) • Nursing Neonatal & Pediatric Assessment (NNPA) • Edinburgh Postnatal Depression Scale (EDPS) • Children’s Health Survey
b. Reporting
• Annual Plan • Monthly Report • Educational Log
c. Site Visit
• Site Visit Review Guide • Chart Audit Guide

3 Forms Matrix All Programs Form Purpose Where By When Enrollment Form - Demographics
Tool for contractor use to collect demographic information to input an infant and parent/guardian(s) into the ETO database
Paper version is provided as a tool. Information must be entered into ETO.
Must be entered into ETO within 30 days of birth OR within 7 days of discharge whichever comes first Can also be used as needed to update contact information.
Enrollment Form – Signature Page
Authorization form for participation in HRPP. Must choose level of participation. Collect financial information to determine a family’s liability and potential assistance. This is also completed for late enrollment and CYSHCN services.
The form must be completed and signed. The Enrollment Form touchpoint must also be completed for enrollment into the program with the form uploaded. Financial information must be entered if Full Participation is being selected.
Parents must sign the form within 30 days of birth. Must be entered into ETO within 30 days of birth OR within 7 days of discharge whichever comes first
Parent/Guardian Profile Collect demographic and contact information for the participant’s parent/guardian(s)
This is a touchpoint located in ETO. Information is collected on the Enrollment Form - Demographics at the time of enrollment.
At the time of enrollment.

43 | P a g e
Community Health Nursing Visit Forms Form Purpose Where By When Contact Form Collect contact attempts to reach a
family during outreach. Paper version is provided as a tool. Contact attempts prior to home visitation services are required to be entered. The contracting agency may continue to use the touchpoint to track client contract as desired.
Entered into ETO within seven days (1 week) of the contact attempt.
CHN Visit Form Collects pertinent information from the home visit. This identifies how visits are invoiced in the ETO system.
This is a touchpoint located in ETO. Information is collected from the paper Family Service Plan (FSP) and is identified by the areas highlighted in gray.
Entered into ETO within seven days (1 week) of the visit.
Family Service Plan (FSP)
Collects pertinent information from the home visit.
This remains in the client chart at the contractor agency. It can be uploaded to ETO as part of the CHN Visit Form if desired.
It should be completed at each regular home visit with an infant where an assessment is done.
Nursing Neonatal & Pediatric Assessment (NNPA)
Assesses the physical, developmental, and social health of the infant. Conducts an environmental assessment.
This is placed in the client’s file at the contracting agency.
It should be completed at each regular home visit with an infant where an assessment is done.
Edinburgh Postnatal Depression Scale (EPDS)
To screen mothers for postpartum depression.
This is a touchpoint located in ETO, collecting the score, referrals, and whether the client declined.
Entered into ETO within 7 days (1 week) of the visit. To be completed at the initial visit and at subsequent visits on an as needed basis.

44 | P a g e
ASQ-3 Ages & Stages Questionnaire
Assess the child’s performance on various age appropriate tasks and monitors children at risk for developmental problems.
This is a touchpoint located in ETO. A copy should be placed in the client’s file at the contracting agency if applicable.
Entered into ETO within 7 days (1 week) of the visit.
ASQ:SE-2 Ages & Stages Questionnaire Social-Emotional
Designed to measure a child’s social and emotional developmental needs.
This is a touchpoint located in ETO. A copy should be placed in the client’s file at the contracting agency if applicable.
Entered into ETO within 7 days (1 week) of the visit.
Children’s Health Survey
Identifies children and youth with special health care needs. To be completed at 1 year of age for all participants.
This is a touchpoint located in ETO. A copy should be placed in the client’s file at the contracting agency if applicable.
Entered into ETO within 7 days (1 week) of the visit. To be completed at 1 year of age for all participants or at the time of enrollment if over 1 year of age.
External Service Referral Guide
Categorizes referrals by level. Paper version is provided as a tool. Information regarding referrals and follow-up is documented in ETO.
Entered into ETO within 7days (1 week) of the visit.
Newborn Blood Spot Collection
Records the completion of a newborn blood spot collection.
This is a touchpoint located in ETO.
Entered into ETO within 7 days (1 week) of the visit. Please see the Arizona Newborn Screening Program Guidelines for more information.

45 | P a g e
Reporting Forms Form Purpose Where By When Monthly Invoice Invoice template to bill for
monthly services. This is a form provided by ADHS at the beginning of a contract year. It is updated as needed. Contractors are required to use the template provided.
Due to ADHS via email at [email protected] by the 21st day of the month following service.
Monthly Report Collects information about the current status of the program, program statistics, and continuous quality improvement measurements.
This is a form provided by ADHS at the beginning of a contract year. It is updated as needed. Contractors are required to use the template provided.
Due to ADHS via email at [email protected] by the 21st day of the month following service.
Annual Plan Plan from contracting agency for their program in the upcoming contract year.
This is a form provided by ADHS at the beginning of a contract year. It is updated as needed. Contractors are required to use the template provided.
Due to ADHS via email at [email protected] by July 31st of each contract year.
Education Log For contracted agencies to demonstrate completion of an initial orientation to HRPP and log continuing education.
Contractors are required to use the template provided. It must be maintained for each home visitor in their personnel file.
Ongoing

46 | P a g e
Transport Form Purpose Where By When Maternal Transport Enrollment Form
Collect mother’s demographics, emergency contact, information and transport information.
Paper version is provided as a tool. Information must be entered into ETO.
Must be entered into ETO within 14 days.
Neonatal Transport Enrollment Form
Collect infant’s demographics, emergency contact, information and transport information.
Paper version is provided as a tool. Information must be entered into ETO.
Must be entered into ETO within 14 days.
Hospital Form Purpose Where By When HRPP Discharge Summary
Medical discharge information from the hospital. Provides diagnoses and referral information. Encourages continuum of care from hospital to community health nursing program.
Paper version is provided as a tool. Information must be entered into ETO. Additional information from the hospital can be attached to the HRPP Discharge Summary touchpoint in ETO
Must be entered into ETO within 7 days (1 week) of discharge.
Decline Participation Records a family’s decline to participate the HRPP program.
This remains in the client chart at the contracted hospital.
Hospitals are required to offer the program within 30 days of birth.

HIGH RISK PERINATAL PROGRAM (HRPP) The State of Arizona established a High Risk Perinatal Program to provide a system of Transportation, Hospital, Medical, and Follow-up for high risk newborns whose parents reside in Arizona.
HRPP DISCHARGE SUMMARY
Date of Death: / /
Discharge Date:* / /
Infant’s First Name: Middle Initial:
Infant’s Last Name: Infant’s Alias Name:
DOB: / /
Birth Weight:
Gestational Age: Weeks APGAR: @ 1____5_____10____
Respiratory Diagnosis/Complications ☐Air Leak Syndrome ☐Apnea - ☐Ongoing ☐Resolved ☐BPD (or Chronic Lung Disease ☐Pneumothorax ☐Meconium RDS ☐Pleural Effusion ☐Pneumonia ☐PPHN (pulmonary hypertension) ☐Respiratory Distress ☐Respiratory Insufficiency ☐Subglottic Stenosis/Tracheomalacia ☐ TTN ☐Other_________________________________
Primary Care Physician:
NICU/SCN Admit Date:* / /
Birth Length (cm):
Fetal Growth: ☐AGA ☐SGA ☐LGA
To:*
Birth OFC (HC) (cm):
Discharge Weight (grams): Discharge Length (cm): Discharge OFC (cm):
Respiratory Treatment (RT) ☐CPAP Only ☐NC ☐ECMO ☐Nitric Oxide ☐IPPV/NIPPV ☐Surfactant ☐Jet Ventilation ☐Tracheostomy ☐Oscillator ☐Vapotherm/HFNC ☐Other__________________________________ Cardiovascular Diagnosis/Complication ☐Cardiac Anomaly_________________________ ☐Cardiac Dysrhythmias ☐Congenital Heart Disease ☐Shock Hypotension w/ Pressor Support ☐Systemic Hypertension ☐Other__________________________________ Cardiovascular Treatment ☐PDA – Medication ☐PDA - Surgical ☐Other__________________________________
Neurological Diagnosis ☐Abnormal Neurological Exam ☐PVL ☐Acquired Hydrocephalus ☐Reservoir ☐Congenital Hydrocephalus ☐Seizures ☐Cooling Therapy ☐Shunt ☐Hypoxic Encephalopathy ☐IVH-Grade I / II ☐IVH - Grade III / I ☐Meningitis ☐ Microcephaly ☐Mylomeningocele ☐Other___________________________________
Dysmorphology ☐Anomaly Requiring Surgery_________________ ☐Chromosomal Anomaly ☐Cleft Lip ☐Dysmorphic Infant ☐Cleft Palate ☐Type of Syndrome ________________________ ☐Other _____________________________
Other Diagnoses ☐Congenital Viral Infections ☐IUGR ☐Multiple Birth (# of Births__________) ☐NAS ☐Positive Drug Screen For: ☐Amphetamines ☐Benzodiazepines ☐Buprenorphine ☐Cocaine ☐Fentanyl ☐Heroin ☐Methadone ☐Opiates ☐SSRIs ☐Suboxone ☐THC ☐ROP/Vision Screen- ☐Pass/WNL ☐Refer/Abnormal Time Frame for Vision Screen Follow-up _________________ ☐SGA-Symmetrical ☐Suspected/Proven Sepsis ☐Symptomatic Hypoglycemia (BG <40) ☐Other___________________________________
Discharge Information / Adaptations ☐Apnea Monitor ☐Oxygen ☐Car Bed ☐Pulse Oximeter ☐CPR ☐Special Feeding ☐Feeding Pump ☐Special Therapy ☐Medication ☐Suction Machine ☐Ostomy Supplies ☐Ventilator ☐Other___________________________________
Gastrointestinal/Genitourinary ☐GE Reflux ☐GI Anomaly ☐GU Anomaly ☐Proven NEC ☐Renal Failure ☐Surgery__________________________________ ☐Other ___________________________________
Developmental ☐Kangaroo Care ☐NIDCAP (# completed ______) ☐OT Evaluation ☐PT Evaluation ☐Speech Evaluation ☐Other___________________________________
Newborn Screening ☐Bloodspot Screen - ☐1st ☐2nd ☐3rd ☐Car Seat Study - ☐Pass ☐Fail ☐CCHD Screen - ☐Pass ☐Fail ☐Hearing Screen - ☐Pass ☐Refer
Referral to ☐HRPP Community Home Nursing ☐ASDB ☐AzEIP ☐CRS ☐DCS ☐DDD ☐Developmental Follow-up Clinic ☐Health Start ☐Healthy Families ☐Home Health Agency ☐SSI ☐Smooth Way Home ☐WIC Other____________________________________
Immunizations ☐DTaP ☐HepB ☐HIB ☐Pediatrix ☐Pneumoccoccal ☐Polio ☐Synagis (date __________) ☐Refused ☐Other__________________________________
Social Concerns ☐Adoption ☐Domestic Violence/Child Abuse History ☐Edinburgh Postnatal Score _________________ ☐Family Conflict/Anger ☐Father of Baby Not Involved ☐History of Parental Substance Abuse ☐Housing Inadequate or Homeless ☐Infant Placed in Foster Care ☐Language Barrier________________________ ☐No Family/Community Support System ☐No Transportation/Limited Transportation ☐Parent has Chronic Illness ☐Parent has Cognitive Limitation ☐Parent has Developmental Disability ☐Parent(s) incarcerated ☐Parent has Mental Illness ☐Parental Unemployment ☐Siblings have Chronic Illness or Dev. Disability ☐Problems Buying Food & Other Necessities ☐Single Parent ☐Teen Parent ☐Other__________________________________
Notes:
Hematological ☐Anemia ☐Polycythermia ☐Thrombocytopenia ☐Twin to Twin Tranfusion Syndrome ☐Other __________________________________

48 | P a g e
Infant’s First Name* Infants Last Name* Alias Last Name (same as hospital label) DOB*
☐PARTIAL/LATE PARTICIPATION: (No financial assistance)
I request participation in the HRPP community home nursing. I reside in the State of Arizona and my infant meets the HRPP criteria. Reason for partial/late enrollment: ☐Sibling of eligible infant ☐Enrollment Hospital never offered program ☐Parent originally declined participation ☐Out of state NICU ☐Children and Youth with Special Health Care Needs*
I request participation in the ADHS OCSHCN Community Health Nursing Program and authorize the one-time release of any necessary medical, social or other relevant information held by any institution or individual that provides services to my child to the ADHS and to their contracted providers for provider quality management purposes.
*The Office for Children with Special Health Care Needs (OCSHCN) in collaboration with the office of Women’s and Children’s Health, High Risk Perinatal Program, Community Health Nursing with in the Arizona Department of Health Services (ADHS) supports eligible infants and children with special health care needs through referrals and linking families to series for which the infant or child may be eligible.
Source of Referral___________________________________________________________________________________
Reason for Referral__________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
/ /
HIGH RISK PERINATAL PROGRAM (HRPP) ENROLLMENT FORM – Signature Page
ENROLLMENT SELECTION

49 | P a g e

50 | P a g e

51 | P a g e

52 | P a g e

53 | P a g e
Edinburgh Postnatal Depression Scale (EPDS) Name Baby’s DOB As you are pregnant or have recently had a baby, we would like to know how you are feeling. Please check the answer that comes closest to how you have felt IN THE PAST 7 DAYS, not just how you feel today. Here is an example, already completed:
I have felt happy Yes, all the time Yes, most of the time No, not very often No, not at all
This would mean: “I have felt happy most of the time” during the past week. Please complete the other questions in the same way
In the past 7 days: 1. I have been able to laugh and see the funny side
of things As much as I always could Not quite so much now Definitely not so much now Not at all
2. I have looked forward with enjoyment to things
As much as I ever did Rather less than I used to Definitely less than I used to Hardly at all
*3. I have blamed myself unnecessarily when things
went wrong Yes, most of the time Yes, some of the time Not very often No, never
4. I have been anxious or worried for no good
reason No, not at all Hardly ever Yes, sometimes Yes, very often
*5. I have felt scared or panicky for no good reason
Yes, quite a lot Yes, sometimes No, not much No, not at all
*6. Things have been getting on top of me Yes, most of the time I haven’t been able to cope at all Yes, sometimes I haven’t been coping as well as usual No, most of the time I have coped quite well No, I have been coping as well as ever
*7. I have been so unhappy that I have had difficulty
sleeping Yes, most of the time Yes, sometimes Not very often No, not at all
*8. I have felt sad or miserable
Yes, most of the time Yes, quite often Not very often No, not at all
*9. I have been so unhappy that I have been crying
Yes, most of the time Yes, quite often Only occasionally No, never
*10. The thought of harming myself has occurred to
me Yes, quite often Sometimes Hardly ever Never

54 | P a g e
HIGH RISK PERINATAL PROGRAM (HRPP)
Children’s Health Survey
1. Does your child currently need or use medicine prescribed by a doctor (other than vitamins)? ☐Yes - Go to Question 1a ☐No - Go to Question 2 1a. Is this because of ANY medical, behavioral, or other health conditions? ☐ Yes - Go to Question 1b ☐ No - Go to Question 2 1b. Is this a condition that has lasted or is expected to last for at least 12months? ☐ Yes - Go to Question 2 ☐ No - Go to Question 2
2. Does your child need or use more medical care, mental health, or educational services than is usual for most childre same age? ☐ Yes - Go to Question 2a ☐ No - Go to Question 3 2a. Is this because of ANY medical, behavioral, or other health conditions? ☐ Yes - Go to Question 2b ☐ No - Go to Question 3 2b. Is this a condition that has lasted or is expected to last for at least 12 months? ☐ Yes - Go to Question 3 ☐ No - Go to Question 3
3. Is your child limited or prevented in any way in his or her ability to do the things most children of the same age can d ☐ Yes - Go to Question 3a ☐ No - Go to Question 4 3a. Is this because of ANY medical, behavioral, or other health conditions? ☐ Yes - Go to Question 3b ☐ No - Go to Question 4 3b. Is this a condition that has lasted or is expected to last for at least 12 months? ☐ Yes - Go to Question 4 ☐ No - Go to Question 4
4. Does your child need or get special therapy, such as physical, occupational, or speech therapy? ☐ Yes - Go to Question 4a ☐ No - Go to Question 5 4a. Is this because of ANY medical, behavioral, or other health conditions? ☐ Yes - Go to Question 4b
☐ No - Go to Question 5 4b. Is this a condition that has lasted or is expected to last for at least 12 months? ☐ Yes - Go to Question 5 ☐ No - Go to Question 5
5. Does your child have any kind of emotional, developmental, or behavioral problems for which he or she needs to get or counseling? ☐ Yes - Go to Question 5a ☐ No 5a. Is this because of ANY medical, behavioral, or other health conditions? ☐ Yes - Go to Question 5b ☐ No 5b. Is this a condition that has lasted or is expected to last for at least 12 months? ☐ Yes ☐ No
Infant’s Name: Date of Visit: / / HRPP #:

55 | P a g e
High Risk Perinatal Program (HRPP) Community Health Nursing Monthly Report (Due on the 21st of each month along with CER)
PROGRAM NAME: Agency name here SUBMITTED BY: Your name here PHONE: 555-555-5555
MONTH: July YEAR: 2019-2020 SUBMITTED: 8/21/2019
Current Program Staff: List names of CHN and support staff. Update monthly as needed. (Highlight changes).
Program Statistics: # # # of referrals provided # of newly hired CHNs this month # of families contacted w/in 7 days of receiving referral # of CHNs trained in ASQ w/in 6 months of hire Average # of days between receiving referral and 1st visit # of CHNs training to become IBCLC certified # of referral NOT received w/in 7 days of discharge # of CHNs trained on the effects of second hand smoke # of initial ASQ w/in four months of referral # of babies diagnosed as NAS # of babies receiving a CYSHCN screening # of babies considered SEN
Explain program statistics from ETO Supervisor’s Report that fall outside of the normal limits.
Continuous Quality Improvement:
1. STAFF TRAINIING: A minimum of six (6) hours of training are required annually. One hour of training needs to be completed in each of the following: Adverse Childhood Experiences (ACEs), Neonatal Abstinence Syndrome (NAS), and Perinatal Mood and Anxiety Disorders.
2. SCREENING AND SUPPORT FOR PERINATAL MOOD AND ANXIETY DISORDERS (PMAD): • Mother is screened for depression using the Edinburgh Postnatal Depression Scale (EPDS) at the initial visit • AND, if positive, mother receives appropriate referral, follow-up and/or enrollment in services
Programmatic Expectations: Mother is screened using the Edinburgh Postnatal Depression Scale (EPDS) at the initial visit. A positive result is a score equal or greater to 9 OR "yes" on question #10. If positive, the mother should be referred to the appropriate level of care. # of initial visits # screened with EPDS at initial visit # screened with EPDS after the initial visit # positive on EPDS (scoring greater or equal to 9) # provided appropriate follow up referrals/services # declining participation/did not take the EPDS
56 | P a g e
High Risk Perinatal Program (HRPP) Community Health Nursing Monthly Report (Due on the 21st of each month along with CER)
Accomplishments/Unique Events/Special Projects: Concerns & Barriers: Identify program concerns and barriers. How are you addressing them?

57 | P a g e
High Risk Perinatal Program (HRPP) Community Health Nursing
Annual Plan
1
Objective: Community Health Nursing assists in the smooth transition of medically fragile High Risk Perinatal Program (HRPP) enrolled infants and their families from a NICU or special care nursery to home and to provide family centered, culturally responsive, developmentally appropriate, and evidence-informed coordinated home visiting services to these infants and other children/families identified with special health care needs. This care will include collaborating with the mothers on issues related to their own wellbeing in an effort to improve their ability to meet the needs of the enrolled infants and decrease the likelihood of a poor birth outcome with subsequent pregnancies.
Program Priorities Identify two priorities to be accomplished by the end of the fiscal year. Use SMART goals to describe the priority. Specific, Measurable, Achievable, Realistic, and Time-bound are characteristics of SMART goals. Ensure that priorities align with HRPP Community Health Nursing Objective. Click here to enter text.
Planning and Implementation Describe your agency’s implementation plan. This may include identifying all steps for planning, quality improvement, and implementation. Include information related to staff oversight of service implementation and/or quality improvement. Click here to enter text. How will you determine the effectiveness of your program? Click here to enter text. How will you evaluate the quality of service provided by your staff? Click here to enter text. What mechanism will you use to provide feedback to your team? Click here to enter text. What barriers to do you anticipate during the implementation period? How will you address them? Click here to enter text.
Responsibility Identify the individual(s) that will have responsibility for overseeing the program. Describe the roles and responsibilities of each individual. Click here to enter text.

58 | P a g e
High Risk Perinatal Program (HRPP)
Community Health Nursing Education and Training Log
Name: __________________________________________ Start Date:___________________
Job Title: ______________________________________________________________________
Staff Education Requirements
A. Orientation and Additional Training Requirements B. Continuing Education
ORIENTATION Program Introduction and Training Date Completed Initials 1. Introduction and History of HRPP 2. HRPP Philosophy, Mission and Goals 3. Roles and Responsibilities 4. Program Overview 5. Home Visitation Services 6. Visit Guidelines 7. Visit Guidelines for Special Populations 8. Visit Procedures and Tools
(review each tool and document date completed) 8.1 Visit Protocols 8.2 Educational Tools (Parent Education Packets) 8.3 CHN Visit Form 8.4 Family Service Plan (FSP) 8.5 Infant Screening Tools (Nursing Neonatal & Pediatric Assessment , Ages & Stages Questionnaire (ASQ), ASQ-3 and ASQ-SE:2 formalized training, Edinburgh Postnatal Depression Scale (EPDS))
8.6 Maternal Assessment Tools & Support 8.7 Environmental Screening Assessment 8.8 Determining Level of Risk
9. Community Collaboration 10. Personal and Training 11. Reporting 12. Continuous Quality Improvement 13. Billing Process and Policy 14. Contract Monitoring 15. Procedural Safeguards

59 | P a g e
Additional Training Requirements Date Completed Initials 1. Agency HRPP Processes & Communication Flow* 2. Observation of Home Visit (shadowing, up to 5) * 3. Supervised Home Visit* 4. Efforts to Outcome (ETO) Data Management System 5. ASQ-3 Training^
*Must be completed (at minimum) before a CHN can be assigned a caseload. Must be completed within 60 days of hire ^Must be completed within 6 months of hire
Trainings, Conferences & Meetings Continuing Education Log HRPP requires a minimum of 6 CEUs annually. 1 CEU in PMAD, 1 CEU in NAS, 1 CEU in ACES and 3 additional in program related education. The required topic are subject to change based on trending topics and needs. Contractors will be notified annually of any changes. Training Title Date Completed Initials
High Risk Perinatal Program (HRPP) Community Health Nursing
Education and Training Log Continued

60 | P a g e
ARIZONA DEPARTMENT OF HEALTH SERVICES COMMUNITY HEALTH NURSING
SITE REVIEW GUIDE Contractor: Date: Attendees: ADHS Reviewer:
CODE: H=Have R=Requested O=Observation C=Compliant P=Partially Compliant N=Non-Compliant
STANDARD
C O D E
SOURCE COMMENTS
PROGRAM ADMINISTRATION
Provide a home-based visitation program to infants and toddlers meeting program eligibility including those with special health care needs, and all families of enrolled infants. (5.2, Contract)
Home Visit #, Client Files & Data
Maintain all necessary permits and licenses, when applicable, and be licensed to provide service in Arizona (5.3, Contract)
There is a primary contact designated for the program who is responsible for ongoing communication, updating or collecting missing information, and coordinating contract monitoring visits
Annual Plan & Monthly Report
Provide an Annual Plan using designated template Annual Plan
Submit monthly report within 21 days of the end of the quarter using the template provided. (12.3)
Monthly Report & Tracking Log
Submit invoices by the 21st day of the month with supporting documentation as applicable (14.2)
Tracking Log
The contractor maintains Administrative Records of employed personnel in a safe, secure location. (16.3)
Site Visit
The contractor maintains Patient Records in a safe, secure location according to the agency’s existing legal requirements. (16.4)
Site Visit
Provide a copy of the program’s customer service policy. (16.6) Site Visit
STAFF RECRUITMENT/CREDENTIALING
Provide a program that recruits, hires, trains, supervises and encourages ongoing professional competency of CHNs, early interventionists and social workers that have contact with infants, toddlers and families. (5.2, Contract)
Personnel Files
Staff should maintain the required credentials: Licensed Registered Nurses, Basic Life Support Certification, ASQ

61 | P a g e
STANDARD
C O D E
SOURCE COMMENTS
STAFF EDUCATION
Provide orientation for new staff, continuing education and ongoing supervision of staff. (4.2, Contract)
Personnel Files & Education Log
Provide Education Logs demonstrating compliance with HRPP Orientation and annual Staff Education Requirements (5.3, Contract, 11.2, 11.3)
Personnel Files & Education Log
A minimum of one individual must attend the annual HRPP hosted meetings and conferences (5.3, Contract)
Personnel Files & Education Log
Designated nurses and/or support staff will be trained on the HRPP Efforts to Outcome (ETO) data management system within 60 days of hire (5.3, Contract)
Personnel Files & Education Log
CHNs must be trained in ASQ3/ASQ-SE by an approved trainer within 6 months of hire
Personnel Files & Education Log
DOCUMENTATION
Data, including documentation of contact attempts, visits, screening, referrals, and dismissals, must be entered into HRPP ETO data management system within seven (7) days of the contact or visit date (4.2, 5.3, Contract)
Data
HOME VISITING STANDARDS OF CARE Provide individualized family-centered, developmentally appropriate, and coordinated home visiting services in a setting and at a time which is most appropriate for meeting the needs of the child and family. (4.2, Contract)
Home Visit #, Client Files & Data
Complete a physical, developmental, psychosocial, special needs and environmental assessment(s) of the enrolled infant including evidence-based education, family support and early intervention along with referral services to community resources as needed. (5.2, Contract)
Client Files & Site Visit
Provide maternal postpartum wellness screening and interconception assessment, in addition providing support, education, and resources as needed (5.2, Contract)
Client Files & Site Visit
Provide assistance to the ADHS Newborn Screening Program in locating families with a previously abnormal test result and facilitate the collection of newborn blood spot. (5.2, Contract)
Site Visit
CHNs must ensure that enrolled infants and children receive the initial ASQ within 1 year of program enrollment (5.3, Contract)
Client Files & Data
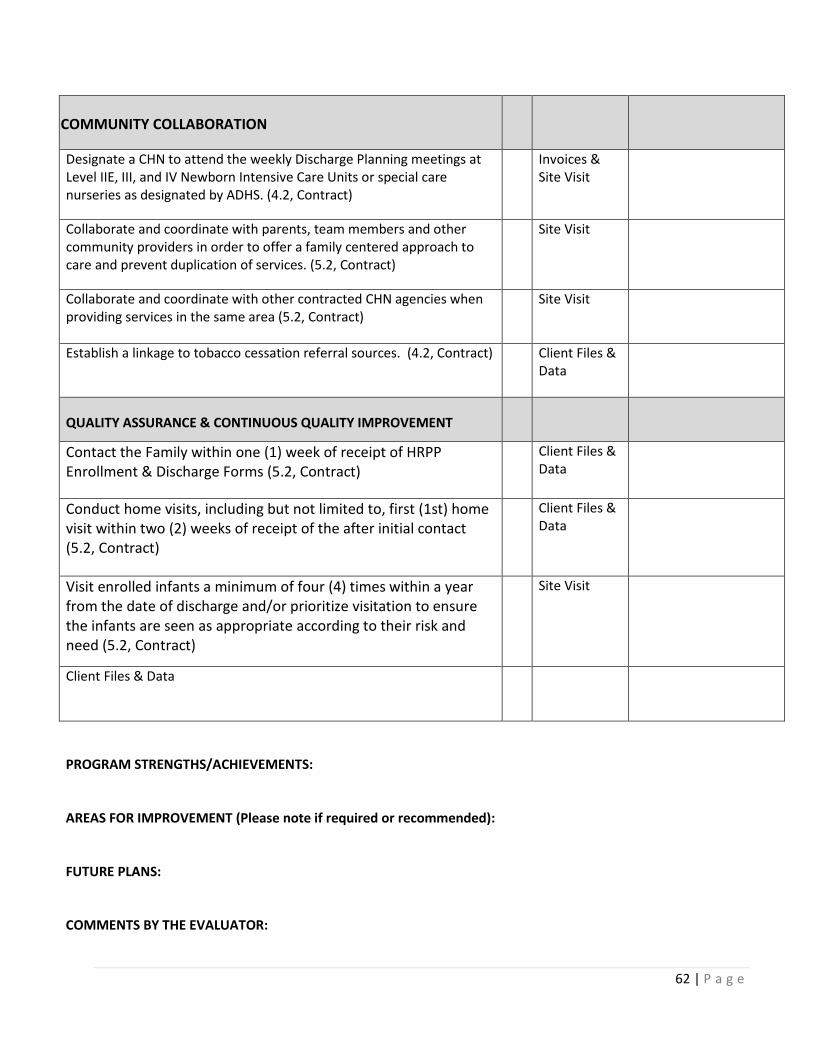
62 | P a g e
PROGRAM STRENGTHS/ACHIEVEMENTS: AREAS FOR IMPROVEMENT (Please note if required or recommended): FUTURE PLANS: COMMENTS BY THE EVALUATOR:
COMMUNITY COLLABORATION
Designate a CHN to attend the weekly Discharge Planning meetings at Level IIE, III, and IV Newborn Intensive Care Units or special care nurseries as designated by ADHS. (4.2, Contract)
Invoices & Site Visit
Collaborate and coordinate with parents, team members and other community providers in order to offer a family centered approach to care and prevent duplication of services. (5.2, Contract)
Site Visit
Collaborate and coordinate with other contracted CHN agencies when providing services in the same area (5.2, Contract)
Site Visit
Establish a linkage to tobacco cessation referral sources. (4.2, Contract) Client Files & Data
QUALITY ASSURANCE & CONTINUOUS QUALITY IMPROVEMENT
Contact the Family within one (1) week of receipt of HRPP Enrollment & Discharge Forms (5.2, Contract)
Client Files & Data
Conduct home visits, including but not limited to, first (1st) home visit within two (2) weeks of receipt of the after initial contact (5.2, Contract)
Client Files & Data
Visit enrolled infants a minimum of four (4) times within a year from the date of discharge and/or prioritize visitation to ensure the infants are seen as appropriate according to their risk and need (5.2, Contract)
Site Visit
Client Files & Data

63 | P a g e
HRPP Chart Audit Review Agency: Date: Reviewer:
Last Name First Name DOB Visit Date(s)
1 2 3 4 5 6 7 8 9
10 11 12

64 | P a g e
External Referrals Level 1 – Low Priority referral for services that do not need follow-up. This would include information on community resources or educational resources for the client/family but not an immediate health or behavioral health concern/need that requires action. Level 2 - High Priority referral for services that need follow-up verification. This would be immediate health, behavioral health, child developmental needs, and food scarcity Level 3- Emergency Priority referral for services that need follow-up verification. This would be emergency situations where the health, behavioral health and/or safety of the family may be at risk.
This is not an extensive list. Add referrals as needed.
Level 1 Service Providers AHCCCS - general information
Adult Education - GED/Technical/Community College
Adoption Services
Alcohol/ Substance Use/Abuse Counseling/Treatment
Asthma - American Lung Association
AZEIP (Arizona Early Intervention Program)
Birth to 5 Hotline (877-705-5437)
Breastfeeding (and Pregnancy) Hotline (800-833-4642)
Breastfeedinginc.ca
Childbirth Education Classes
Child Care Providers/Services
Community Health Centers
Division of Developmental Disabilities (DDD)
Dental/Oral Health Care Services
Disease Self-Management Programs
Domestic Violence/Sexual Violence Counseling
Drug Use - Marijuana/Heroin/Opiates/Meth/Other Drugs
Counseling/Treatment Services
Education Services - Children/Family
Employment Services/Opportunities
Early Headstart/Headstart
Faith Based Services - Church
Family Planning Services
Feedingmatters.org
Hearing/Vision Testing
Home/Health Safety Hazards
Home Visiting Program (Healthy Families, Health Start,
Housing/Landlord Tennant/Pests
Immunizations (Child/Children)
Immunizations (Family)
Kids Care
KidsHealth.org
Lead Exposure/Blood Lead Testing
Midwives/Birthing Centers
Mother to Baby Exposures mothertobaby.org
Parents as Teachers, Family Spirit, Other)
Parenting classes
Prenatal Care Providers – OB/GYN
Primary Care Providers
Poison Prevention/Control (800-222-1222)
Postpartum Support International - PMAD Warm line
PowerMeA2Z.org
Pregnancy and Breastfeeding Hotline (800-833-4642)
Salvation Army/Goodwill
Safekids.org General Safety; Car Seat Safety Check
Safe Sleep/Crib/Car Seat Safety
Seatcheck.org (Car Seat Information)
Social Security Administration (SSA)
Supplemental Security Income (SSI)
Tobacco Smoke/Tobacco Cessation Services
Transportation Services
Unemployment Assistance
Utility Assistance
WIC (Women, Infants and Children)
Womenshealth.gov
ZerotoThree.org

65 | P a g e
Level 2 Services Providers ADHS - (OCSHCN)
Adoption Services
AHCCCS - Health care coverage Enrollment/Eligibility
Alcohol/ Substance Use/Abuse (800-662-4357)
Arizona Long Term Care Services (ALTCS) Cranial Tech
Asthma - American Lung Association
AZEIP (Arizona Early Intervention Program)
Behavioral Health Counseling
Bereavement Counseling
Breastfeeding Counselor/IBCLC
Child Care Providers/Services
Community Health Centers
CRS (Children’s Rehabilitation Services) Dental/Oral
Health Care Services
Department of Child Safety (DCS)
DES Family Assistance: Job service /SNAP/TANF
Division of Developmental Disabilities (DDD)
Domestic Violence/Sexual Violence Counseling
Domestic Violence Advocate
Domestic Violence Shelter
Drug Use - Marijuana/Heroin/Opiates/Meth/Other Drug
Counseling/Treatment Services
Family Planning Services
FeedingMatters.org
Food Bank/ Food Box
Hanger Clinic Services
Hearing/Vision Testing
Home/Health Safety Hazards
Housing/Landlord Tennant/Pests
Housing Hazards - Bed Bugs/Lead/Other environmental
Immunizations - Child (Children)
Immunizations - Family
Lead Exposure/Blood Lead Testing
Midwives/Birthing Centers
Newborn Screening
OB/GYN Provider
Postpartum Support International - PMAD Warm line
Pregnancy Options Counseling
Prenatal Care Provider
Postpartum Care appointments
Primary Care Provider Safe Sleep – Pack n Plays/Cribs for Kids
Sliding Fee Health care clinics
Specialty Care Provider
Substance Use/Abuse Counseling/Treatment Services
Transportation Services – Urgent/Emergency
Tobacco Cessation Services – ASHLINE/Arizona Lung
Well Child Care appointments
Well Woman Care appointments
(WIC) Women Infants and Children
Level 3 Services Providers 911
Behavioral Health Counseling
Bereavement Counseling
Department of Child Safety (DCS) Neglect/Abuse
Domestic Violence/Sexual Violence Counseling
Domestic Violence Advocate
Domestic Violence Shelter
Emergency Care/Urgent Care
Food Bank/Food Box
Housing
Police
Poison Control
Primary Care Provider
OB/GYN Provider
Specialty Care Provider
Substance Use/Abuse Counseling/Treatment Services
Transportation Services – Emergency

66 | P a g e
4 Educational Materials More information to be provided by July 1, 2019.
Parent Education Packets
Initial Packet Time/Ages: First Visit Handout Name Where to Locate Tummy Time: Activities to Strengthen Baby (Pathways.org)
Available in English, Spanish, Portuguese, and French Canadian. Can be printed or ordered at https://pathways.org/print/
Assure the Best: Baby’s Physical Development (Pathways.org)
Available in English, Spanish, and a variety of 13 other languages. Can be printed or ordered at https://pathways.org/print/
What does a safe sleep environment look like?
Available to print or order. https://safetosleep.nichd.nih.gov/resources/caregivers English: https://www.nichd.nih.gov/sites/default/files/2019-02/Safe_Sleep_Environ_update.pdf Spanish: https://www.nichd.nih.gov/sites/default/files/2019-02/Safe_Sleep_Environ_Span_update.pdf
Shaken Baby Door Hanger order from Beth Eggers-Sedlet 603-708-0484 or [email protected] Walker/Saucer Flyer Attached Recommended Child and Adolescent Immunization Schedule
https://www.cdc.gov/vaccines/schedules/downloads/child/0-18yrs-child-combined-schedule.pdf Can also be ordered at: https://wwwn.cdc.gov/pubs/CDCInfoOnDemand.aspx?ProgramID=84
TDAP Print Out Interconception Care http://www.azdhs.gov/documents/prevention/womens-childrens-
health/reports-fact-sheets/preconception-health/HighRiskPregnancy.pdf
Power Me A2Z booklet from ADHS
https://www.powermea2z.org/health-resource-order-form/
Edinburgh Postnatal Depression Scale (EPDS)
Available in 13 additional languages (including Spanish). http://www.perinatalservicesbc.ca/Documents/Resources/HealthPromotion/EPDS/EPDSQuestionnaireApril2013.pdf Scoring guide http://www.perinatalservicesbc.ca/Documents/Resources/HealthPromotion/EPDS/EPDSScoringGuide_March2015.pdf
PMAD Flyer
RSV Vision flyer

67 | P a g e
Second Packet Time/Ages: 4-6 month visit Handout Name Where to Locate Tooth Decay ADHS Oral Health Flyer
copy attached limited brochures available at ADHS oral health
Safety Booklet print out http://www.safehomesafebaby.com/downloads/safety_guide.pdf
TV Time hand out
Early Literacy Attached
Developmental Feeding Attached in English and Spanish
Third Packet Time/Ages: 8-12 month visit Handout Name Where to Locate Lead Poisoning Flyer from ADHS
also available at azhealth.gov/lead or call 602-364-3118
Oral Care/Tooth Decay Flyer 1-3 Years
Gun Safety Handout Positive Discipline Flyer Child Safety Checklist Car Seat Safety Handout Age Appropriate Toys Handout
Copyright © 2022 FDOKUMEN




















