
Hepatitis Portfolio R&D Day - VIR Bio Overview
91
VIR BIOTECHNOLOGY, INC. Hepatitis Portfolio R&D Day APRIL 27, 2022 1
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Hepatitis Portfolio R&D Day - VIR Bio Overview

V I R B I O T E C H N O L O G Y , I N C .
Hepatitis Portfolio R&D Day
A P R I L 2 7 , 2 0 2 2
1

Forward-Looking Statements
Statements in this presentation that are not statements of historical fact are forward-looking statements. Such forward-looking statements include, without limitation, statements regarding the near-term financial performance (including near-term collaboration revenue related to binding agreements for doses of sotrovimab) of Vir Biotechnology, Inc. (the “Company or “Vir”), the expected success, cost, and timing of the Company’s research and clinical development plans and clinical trials, the Company’s goals with respect to the prophylaxis or treatment of COVID-19, HBV, HDV, influenza A and HIV, the Company’s objectives, strategy, technology platform and clinical trial designs, the potential benefits of the Company’s collaborations, and the Company’s ability to complete certain milestones. Words such as “believe,” “anticipate,” “plan,” “expect,” “intend,” “will,” “may,” “goal,” “potential,” “could,” “aim” and similar expressions are intended to identify forward-looking statements, though not all forward-looking statements necessarily contain these identifying words. These forward-looking statements are based on the beliefs of the management of the Company as well as assumptions made by and information currently available to the Company. Such statements reflect the current views of the Company with respect to future events and are subject to known and unknown risks, including business, regulatory, economic and competitive risks, uncertainties, contingencies and assumptions about the Company, including, without limitation, risks inherent in developing the Company’s products and technologies, future results from the Company’s ongoing and planned clinical trials such as unexpected data or clinical site activation rates or clinical trial enrollment rates that are lower than expected, difficulties arising from the Company’s collaborations, challenges in accessing adequate manufacturing capacity, the Company’s ability to obtain adequate financing to fund its planned clinical trials and other expenses, statements related to regulatory authorizations and approvals, trends in the industry, changes in the competitive landscape, delays or disruptions due to the COVID-19 pandemic, geopolitical changes or other external factors, including supply chain disruptions, the legal and regulatory framework for the industry, unexpected litigation or disputes and future expenditures. In light of these risks and uncertainties, the events or circumstances referred to in the forward-looking statements may not occur. The actual results may vary from the anticipated results and the variations may be material. Other factors that may cause the Company’s actual results to differ from current expectations are discussed in the Company’s filings with the U.S. Securities and Exchange Commission, including the section titled “Risk Factors” contained therein. These forward-looking statements should not be taken as forecasts or promises nor should they be taken as implying any indication, assurance or guarantee that the assumptions on which such forward-looking statements have been made are correct or exhaustive or, in the case of the assumptions, fully stated in this presentation. You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date this presentation is given. Except as required by law, the Company undertakes no obligation to publicly update any forward-looking statements, whether as a result of new information, future events or otherwise. The Company claims the protection of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995 for all forward-looking statements.
This presentation discusses product candidates that are under clinical study, and which have not yet been approved for marketing by the U.S. Food and Drug Administration. No representation is made as to the safety or effectiveness of these product candidates for the use for which such product candidates are being studied.
The trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of such products.
Marketing Authorization/Emergency Use of SotrovimabSotrovimab has received marketing authorization in the European Union, Australia, Great Britain, Japan, and Saudi Arabia, and has been granted temporary authorization in multiple other countries, including Bahrain, Canada, Egypt, Kuwait, Qatar, Singapore, and the United Arab Emirates. In the United States, sotrovimab has not been approved, but has been authorized for emergency use by FDA under an EUA, to treat mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death. Due to the high frequency of the Omicron BA.2 subvariant, sotrovimab is not currently authorized in any U.S. region.
The emergency use of sotrovimab is only authorized for the duration of the declaration that circumstances exist justifying the authorization of the emergency use of drugs and biological products during the COVID-19 pandemic under Section 564(b)(1) of the Act, 21 U.S.C. § 360bbb-3(b)(1), unless the declaration is terminated, or authorization revoked sooner.
L E G A L D I S C L A I M E R
© 2022 Vir Biotechnology, Inc. 2

© 2022 Vir Biotechnology, Inc.
AGENDA
1
2
4
Introduction
George Scangos, Ph.D., Chief Executive Officer
Overview and challenges of treating hepatitis B
Jordan Feld, M.D. M.P.H., R. Phelan Chair in Translational Liver Disease Research, Professor of Medicine, University of Toronto, Research Director, Toronto Centre for Liver Disease, Senior Scientist, Sandra Rotman Centre for Global Health, TGRI, Toronto General Hospital
Review Vir’s hepatitis B development program to date and announce new program directives
Carey Hwang, M.D., Ph.D., SVP, Clinical Research, Head of Chronic Infection
Q&A and closing remarks 5
© 2022 Vir Biotechnology, Inc. 3
3 Vir’s hepatitis portfolio strategy
Phil Pang, M.D., Ph.D., Chief Medical Officer

George Scangos, Ph.DC h i e f E x e c u t i v e O f f i c e r
© 2022 Vir Biotechnology, Inc. 4

Vir is a commercial-stage immunology company
focused on treating and preventing
the world’s most serious infectious diseases
© 2022 Vir Biotechnology, Inc. 095

A pivotal timefor VIR
6
COVID-19: coronavirus disease 2019HIV: human immunodeficiency virus
1
2
3
$917.2 million sotrovimab collaboration revenues in 2021 and $1.1B expected in 1H22. Strong balance sheet. Resources we believe will save lives, build more value
Pursuing a robust and diverse pipeline in large infectious diseases: COVID-19, hepatitis B and D, influenza and HIV, with multiple clinical value drivers in 2022
Validated and new technologies driving innovation behind late-stage programs
© 2022 Vir Biotechnology, Inc.

Disease Area Product Candidate Treatment / Prophylaxis Preclinical Phase 1 Phase 2 Phase 3 Authorized Collaborator
COVID-19 Sotrovimab Treatment (Early-IV) mAb GlaxoSmithKline
Sotrovimab Treatment (Early-IM) GlaxoSmithKline
Sotrovimab Treatment (Hospitalized) GlaxoSmithKline
Sotrovimab Prophylaxis GlaxoSmithKline
VIR-7832 Treatment mAb GlaxoSmithKline
HBV VIR-2218 Treatment siRNA Alnylam
VIR-2218 + PEG-IFN-⍺ Treatment siRNA Alnylam
VIR-3434 Treatment mAb
VIR-2218 + VIR-3434 Treatment siRNA Alnylam
VIR-2218 + BRII-179 Treatment siRNA Alnylam, Brii Biosciences
VIR-2218 + TLR81 + PD-12 Treatment siRNA Alnylam, Gilead
Influenza A VIR-2482 Prophylaxis
HIV VIR-1111* Prophylaxis Bill & Melinda Gates Foundation
C L I N I C A L D E V E L O P M E N T P I P E L I N E
†
*Vaccine designed to establish proof of concept in Phase (Ph) 1 clinical trial to determine whether unique immune response observed in non-human primates can be replicated in humans; ultimately, any candidates we advance as a potential HIV vaccine will require modifications to VIR-1111 before further clinical development.Sotrovimab and VIR-2482 incorporate Xencor’s XtendTM technology. VIR-7832 and VIR-3434 incorporate Xencor’s XtendTM and other Fc technologies.
PEG-IFNα: peginterferon alfa-2a1: GS-9688; 2: nivolumab†sotrovimab for early treatment by IV currently has marketing approval, temporary authorization or emergency use authorization in >40 countries and an application has been submitted to the FDA requesting an amendment to the EUA for sotrovimab to include IM administration.
© 2022 Vir Biotechnology, Inc.
†
Antibody siRNA T cell
7

Jordan Feld, M.D., M.P.H. R . P h e l a n C h a i r i n T r a n s l a t i o n a l L i v e r D i s e a s e R e s e a r c h , P r o f e s s o r o f M e d i c i n e , U n i v e r s i t y o f T o r o n t o
© 2022 Vir Biotechnology, Inc. 8

Hepatitis B: Why we need new
therapy
Jordan J. Feld MD MPH
Interim Director, Toronto Centre for Liver Disease
R. Phelan Chair in Translational Liver Disease Research
Sandra Rotman Centre for Global Health
University of Toronto

Should the big 3 be the big 4?
Thomas NEJM 2019

HBV is the major driver of hepatitis-
related mortality
WHO Global Hepatitis Report, 2017.
De
ath
s (
millio
ns
) in
20
15
Viral hepatitis HIV/AIDS Tuberculosis Malaria0
0.5
1
1.5
1.34
1.06
1.37
0.44
HCV
(30%)
HBV
(66%)
A & E
(4%)
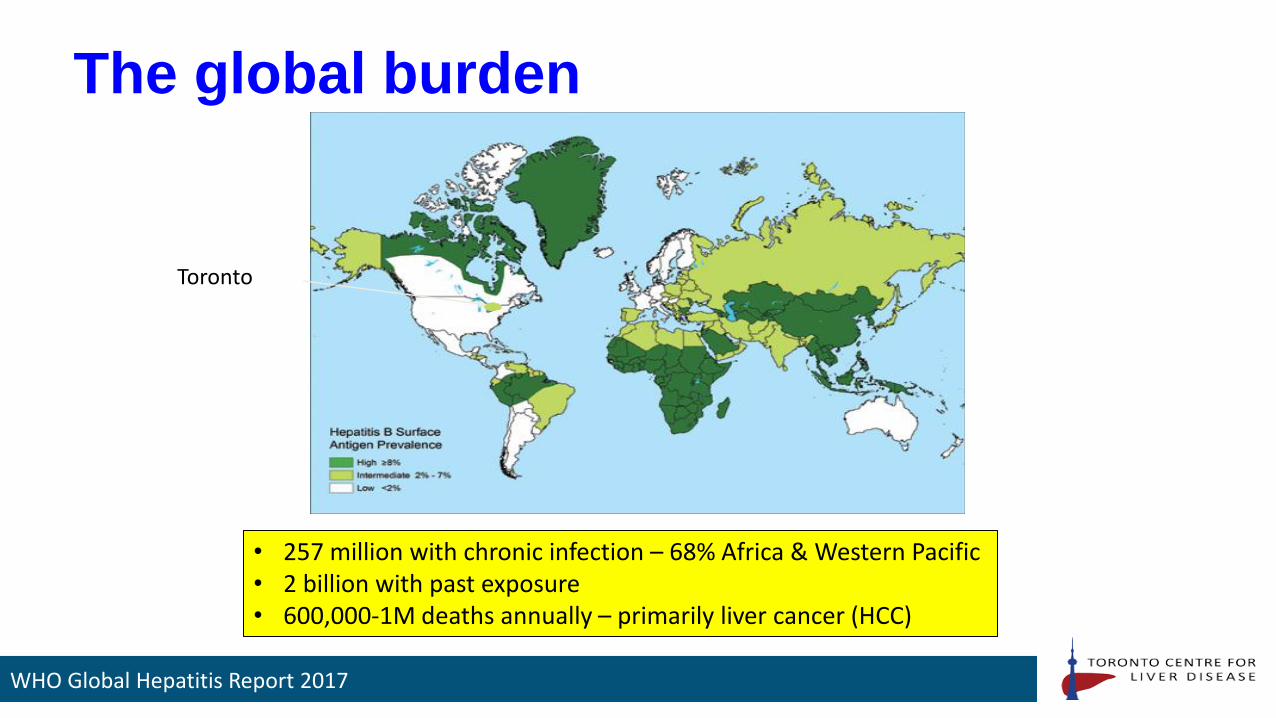
The global burden
Toronto
• 257 million with chronic infection – 68% Africa & Western Pacific• 2 billion with past exposure• 600,000-1M deaths annually – primarily liver cancer (HCC)
WHO Global Hepatitis Report 2017

WHO Elimination Targets
WHO

Prevention is better than cure
Taiwan: A vaccine success story
Ni Gastro 2007, WHO 2017
HB
sAg
Posi
tivi
ty (
%)
1984 No vaccine
1989 Vaccine<5 yo
1994 1999
2004
Age (years)
• Marked reduction in HBsAg prevalence with universal vaccination• Increasing but plateauing global coverage → 79% in 2012 and 82% in 2014 • Only 38% coverage of birth-dose

Limited benefits
375
300
150
75
0
Death
s (
x1000)
210
341
242
112
20101990
HCC ESLD
5.1 5.2 5.8
4.8225
20101990
HCC ESLD
20101990 20101990
10
8
4
2
0
6
Absolute numbers
Age
sta
nd
ard
ized
de
ath
rat
e
(pe
r 1
00
,00
0)
Age Standardized Rates
HBV-related HCC increasing despite vaccine and therapy, partially due to population growth & aging but still concerning
Lozano Lancet 2012, Stanaway Lancet 2016

Bottom line - vaccine
• Highly effective
• Very safe
• Coverage is the problem:
– Good, but far from perfect, uptake → particularly in some high prevalence
regions
– Birth dose even worse (globally 38%)
– Incomplete or absent vaccination has major health consequences…
• Conclusion: Vaccine is necessary but not sufficient to eliminate HBV

The vaccine does not help
those already infected…

Chronic HBV infection – Natural History
Infection
HBeAg+ HBeAg- HBeAb+
months-years
Immune Active
5-30 years
Immune Tolerant
ALT
HBV DNA
months-years
Immune Control
(Inactive Carrier)
HBsAg+ HBsAg- HBsAb+

What happens after eAg loss?
5-30 years months-years
Infection
Immune Tolerant
Immune Active
E Negative Chronic HBV
HBeAg+ HBeAg- HBeAb+
months-years
ALT
E Negative ‘Inactive Carrier’ vs
TreatObserve
HBV DNA
It’s a dynamic disease: Long-term follow-up required

From the patient’s perspective
◼ Patients feel perfectly fine!!!
◼ Almost always entirely asymptomatic…until it’s too late
◼ Even if they have cirrhosis HBsAg

When to treat
5-30 yearsmonths-years
Infection
Immune Tolerant
Immune ActiveHBeAg Negative
Chronic HBV
(Definition?)
HBeAg+ HBeAg- HBeAb+
months-years
ALT
HBV DNA
Treatment
Treatment
Treatment?Immunosuppression
(Chemo/HIV/BMT)
Treatment
Immune Control
(Inactive Carrier)
Treatment

The guidelines
HBeAg + HBeAg - Cirrhosis
HBV DNA ALT HBV DNA ALT HBV DNA ALT
AASLD* >20,000 IU/mL
≥2x ULN or significant
histologic disease (≥A3 or ≥F2)
>2,000 IU/mL
≥2x ULN or significant
histologic disease (≥A3 or ≥F2)
Detectable Any
EASL >2,000 IU/mL> ULN and/or
significant histological disease
>2,000 IU/mL> ULN and/or
significant histological disease
Detectable Any
APASL >20,000 IU/mL
>2x ULN or significant
histologic disease (≥A3 or ≥F2)
>2,000 IU/mL
>2x ULN or significant
histologic disease (≥A3 or ≥F2)
>2,000 IU/mL Any
* ALT ULN of 25 for F and 35 for M
Terrault Hepatology 2018, EASL HBV Guidelines J Hep 2017, Sarin Hepatol Int 2016
Current guidelines are complicated and hard to implement

Under-diagnosis & Under-Treatment: A huge problem
9.9%
18.9%
HBsAg+
Global USA – Insured Population
Yeo & Nguyen APT 2021
Strikingly low diagnosis & treatment rate in high and low/middle income countries
1.6%
Ever treatedDiagnosed
3.5%
32.2%

Therapy only works in people who get it…
WHO
Begs the question…should we treat everyone?
• Some push for treatment of all HBsAg+
• Particularly in LMIC where diagnostics may be more costly than
treatment and f/u is often difficult
• Rationale:
– Likely more cost effective than current guidelines – esp in LMICs
– Drugs are safe, resistance rarely a problem
– Benefits hard to see in a cohort study may be apparent at population level (HCC)
– Transmission benefit
With the right therapy – indication would likely be HBsAg+ (ie like HCV)

What are the goals of therapy?
Learning from natural history
0
100
80
60
40
20
0 5 10 15 20 25
Su
rviv
al p
rob
ab
ilit
y (
%) Inactive CHB
HBeAg-/HBV DNA+
or HBeAg reversion
HBeAg+ persistence
Time (years)
• Very inactive disease and ideally HBsAg loss associated with excellent long-term and cancer-free survival
• A good goal for therapy
Fattocvich Gut 2008, Yang NEJM 2002
sAg + /eAg +
sAg + /eAg -
sAg - /eAg -Cu
mu
lati
ve H
CC
In
cid
ence
(%
)
Survival HCC

Highly effective therapy
• Current therapy taken long-term
– Suppresses HBV DNA
– Normalizes ALT
– Prevents fibrosis progression
– Promotes fibrosis regression – even in cirrhosis
– Prevents and even reverses hepatic decompensation
– Reduces, but does not eliminate, the risk of HCC
Lim Gastro 2014, Papaetheodoridis J Hep 2015, Zoutendijk Gut 2013, MarcelllinLancet 2013, Chang Hepatology 2010

But suppressive therapy is not a cure1378 Korean patients on LAM/ETV vs 1014 inactive CHB
• Treatment reduces but does not eliminate risk of HCC• Spontaneous (immune) control better than suppressing
HBV DNA with treatment
Cho Gut 2014
Complete respondersInactive
CHB
p<0.001 p<0.015
Non-cirrhotic Cirrhotic
Cu
mu
lati
ve in
cid
en
ce o
f H
CC
Cu
mu
lati
ve in
cid
en
ce o
f H
CC
Complete responders
Inactive CHB

HBsAg loss is the goal5409 Korean patients treated with LAM/ETV, 110 lost HBsAg
Kim Gut 2014
HBsAg loss is effectively a cure of CHB
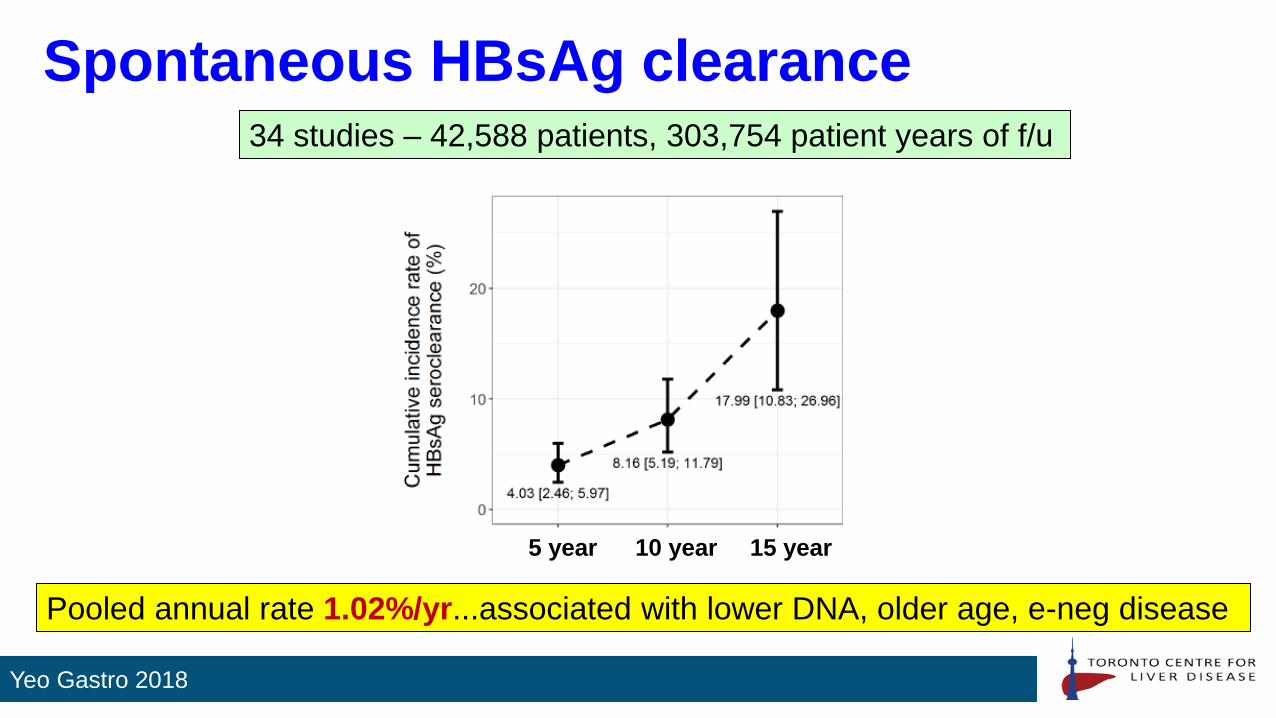
Spontaneous HBsAg clearance
Yeo Gastro 2018
Pooled annual rate 1.02%/yr...associated with lower DNA, older age, e-neg disease
34 studies – 42,588 patients, 303,754 patient years of f/u
5 year 10 year 15 year

Current treatment is not much better…
TDF+PegIFN x 24w
TDF+PegIFN x 16w +
TDFx12w
TDFx120wPegIFNx48w
9.1%
Hard to achieve with monotherapy or current combos, not much better
than natural history…upside – lots of room for improvement!
Composite of numerous trials, not head-to-head, Marcellin Gastro 2016
2.8%
0%
7%
1%3%
~1%1.1% 1.7%
0%
10%
20%
30%
Peg
IFN
Lamiv
udine
Adef
ovir
Ente
cavi
r
Tenofo
vir
Pla
cebo
HB
sA
g L
oss

The problem with the current state of affairs
• Massive under-diagnosis
• Complicated treatment guidelines– People who need treatment are often not on treatment
• Once you start, you can’t stop
• Adherence drops off – risk of severe flares
• Despite treatment – people remain HBsAg+– Cancer risk (lower but not gone)
– Cost
– Stigma – a very real issue – patients want curative therapy for everyone –even those with low risk of bad outcomes (eg. inactive carriers)

Goals of Therapy
• Cure the infection
– True cure = all traces of HBV gone from the liver (ie. like HCV)
– This is VERY difficult (if not impossible) → cccDNA + integrated HBV DNA
• Functional cure
– Use the markers of excellent natural history…
1. HBsAg loss (ideally with anti-HBs)
2. Possibly…sustained off treatment inactive disease without HBsAg loss
(HBeAg –ve, DNA undetectable, normal ALT, normal histology) (some
call this ‘partial cure’)

Is there consensus?
Sterilizing cure(cccDNA loss)
Too hard to achieve
Sustained Virological Response(sAg +ve, DNA negative, off therapy)An advance but not enough of one
Functional Cure(sAg loss with undetectable DNA
& Normal ALT)Challenging but achievable goal
88% of attendees at EASL/ASSLD HBV Endpoints conference chose Functional Cure as the preferred goal
for future therapies
EASL/AASLD Endpoints Meeting

HBsAg
• Preferred endpoint…but some issues1. May mean different things with different targets
• Natural clearance = cccDNA loss/silencing…ie what we want
• Targeting transcripts or protein → does this effect cccDNA transcription? Does it lead to immune control?
• Other Antivirals → may depend on mechanism
• Immune target – immune control - probably what we want…but hard to assess and flares are scary!
• False negative → integrated DNA could produce sAg even in people who have cleared/silenced all cccDNA
2. Decline is SLOW! • Need long-term therapy to see an effect – integrated DNA may never go away – major issue to avoid
excluding a good drug
• If surrogate, what decrease in quant HBsAg matters? 0.5 log, 1 log, <100 IU/mL?
3. Similar challenges likely with HBV RNA, HBcrAg etc• Potentially other issues given uncertainty of ‘what they mean’ and whether that differs by MOA of therapy

Considerations for cureHCV
• Ineffective, poorly tolerated
therapy
• Multiple lifecycle targets
• No long-lasting nuclear reservoir
or integration
• Limited involvement of immune
system
HBV
• Well tolerated, very effective therapy –
high bar
• Single viral enzyme
• cccDNA persistent & hard to reach +
DNA integration
• Immune control important …flares (in
healthy people)
Bottom line…it won’t be as easy to cure HBV as it was to cure HCV!

Potential targets in the lifecycle
O-
5’Cap (A)n 3’
Translocation
dAdAdG
new (-) strand DNA synthesis
pgRNA
DNA Synthesis
Encapsidationof pg RNA
Golgi complex
Release
CCC DNA
DNArepair
HBV RNATranscripts
PregenomicRNA
Attachment andPenetration
S Ag
e Ag
HBV Virion
EnvelopeProteins
S, M, L
e Ag
PolymeraseProteinCore
Protein
uncoating
transport to cellnucleus
Block Entry
Target cccDNA- Destruction- Inactivation
Target HBV RNA
Target packaging
Target DNA synthesis
Target Assembly/Export
Stimulation of innate and/or
adaptive immunity

ImmunotherapiesInnate
• Cytokine therapy
– IFN
• TLR agonists
– TLR7, TLR8
• RIG-I agonists
Adaptive
• Therapeutic vaccine
• Checkpoint inhibitors
– PD-1
– PD-L1
Immune restoration through inhibition of viral antigens
Attractive but a little bit stressful…flares can be good, but flares can scary!

Attractive combinations
Nuc
HBV DNASuppression + +
ImmuneTarget
RNAi
Monoclonal Antibodies
Nucleic Acid Polymers
cccDNAi
+/- CAM
+/- RNAi
+/- cccDNAi
TLR agonist
αPD1/PDL1
Therapeutic vaccine
Mix and match…complicated matrix!
Viral ProteinDepletion(s, x, core)

It’s not just choosing the right
target/compound…• Other MAJOR issues
1. Correct population
• Highest need?
• Easiest to show an effect?
• Immune tolerant/e+/e-/inactive/NA suppressed…
2. Correct endpoint
• Is sAg loss the same with an NA as with an siRNA?
• Do we need to look in the liver? Do we need new biomarkers – HBV RNA, HBV crAgothers?
3. Correct combinations
• Lots of possibilities – a huge matrix!!
4. Safety!
• A major concern…especially with immunotherapies

Inarigivir – a novel approach
with dual antiviral activity
RIG-I
RIG-I
TYPE III IFNs
OATP1
DAA EFFECT TARGETING REPLICATION COMPLEX
HBV pgRNA5’ 3’
HBV pgRNA5’ 3’
Dual antiviral effect against HBV
HBV polymerase
Reverse transcription
Viral replication
ε ε
INARIGIVIR
Hepatocyte
RIG-I ACTIVATION AND BINDING TO
HBV PGRNA
• Dose-dependent decline in HBV DNA & HBV RNA > in HBeAg-neg patients and those with low qHBsAg levels• HBV RNA effects persisted after cross-over to tenofovir – ‘new set-point’? Interesting proof-of-concept
HBV DNA HBV RNA
Placebo 25 mg 50 mg 100 mg Placebo 25 mg
Placebo 25 mg 50 mg 100 mg Placebo 25 mg 50 mg 100 mg
P<0.01P<0.01
Log
dec
line
in H
BV
DN
ALo
g d
eclin
e in
HB
V D
NA
HBeAg-negative
HBeAg-positive
50 & 100 mg
6 pts with undetectable HBV RNA at BL
HBV RNAHBV DNA
0
1
-1
-2 -2
-1.5
-1
-0.5
0
0.5
Log
dec
line
in H
BV
RN
A
-6
-4
-2
2
4
0
Log
dec
line
in H
BV
RN
A
-3
-2
-1
1
2
0
Yuen et al, AASLD 2018, Abstract 75, Agarwal HBV Forum 2020
• Looked promising…until it didn’t…• ALT elevations noted but then pancreatitis, lactic acidosis, liver failure• 7 patients admitted → 1 death!• Cholestasis and coagulopathy in 2 with slow resolution• Halt development

HDV▪ Worst form of viral hepatitis
▪ Decreasing global prevalence (HBV vaccination & mortality!)
▪ Population attributable fraction of HBsAg-positive patients suggested HDV accounted for:
‒ 18% of cirrhosis
‒ 20% of HCC
‒ Over-represented among all bad outcomes and high-risk populations
Stockdale. J Hepatol 2020, Kamal JVH 2021
Group
People who inject drugs33 samples (I2 = 86.7%, T
2 = 1.16)
Commercial sex workers5 samples (I2 = 91.5%, T
2 = 1.19)
Men who have sex with men2 samples (I2 = 0.0%, T
2 = 0.0)
Hemodialysis recipients11 samples (I2 = 21.0%, T
2 = 0.49)
HIV, excluding generalized epidemics18 samples (I2 = 74.4%, T
2 = 0.56)
Hepatitis C virus infection17 samples (I2 = 90.7%, T
2 = 1.21)
Cirrhosis29 samples (I2 = 77.2%, T
2 = 0.85)
Hepatocellular carcinoma20 samples (I2 = 38.4%, T
2 =0.26)
Odds Ratio (95% CI)
19.00 (12.26-29.45)
18.70 (6.70-52.17)
16.00 (3.94-64.92)
3.42 (1.38-8.48)
6.57 (4.08-10.59)
10.02 (5.49-18.26)
6.68 (4.37-10.20)
4.80 (3.18-7.26)
Odds RatioGreater odds of anti-HDV relative to control populations

How much HDV is out there?Among HBsAg-positive, estimated prevalence of HDV is 4.5% (95%CI: 3.6-5.7) ~12M
Anti-HDV Prevalence, %
<11.1-2.02.1-5.05.1-10.010.1-30.030.1-50.0>50
Data not availableNot applicable
Stockdale. J Hepatol. 2020
HDV Hot-spots - But data quality questionable – wide range of estimates

HDV Therapy
• No approved therapies
• Very limited data with pegIFN-alpha
– Long-term, high dose
• NA – ineffective (HDV only cares about HBsAg)
The future: Any therapy that reduces/clears HBsAg or blocks HBV entry should work for HDV

HDV Pipeline
Entry InhibitorBLV
Hepatitis Delta Virus
NTCP
ImmunomodulatorspegIFNλpegIFNα
Viral Entry
Hepatocyte
Replication
HDV RNA
S-HDAg
HDV RNA
Transcription and Editing
TranslationNucleus
Farnesyl-transferase
L-HDAg
Prenylation
PrenylatedL-HDAg
Release of New Virions
Inhibitors of HBsAg Release (NAPs)
REP-2139REP-2165
Prenylation Inhibitor
LNF
Loureiro Liver Int 2021
Goal of therapy: HDV RNA decline by 2 log (or negative) + normal ALT

Summary
• Despite an effective vaccine, burden of HBV still enormous
• Current therapy is very safe and effective but not curative → high bar
to improve upon
• Science is complex – cccDNA & integrated DNA are challenging
• HBsAg loss is an imperfect (but still best available) endpoint
• Combination therapy – antivirals +/- immunomodulatory likely
necessary
• Study design – population, MOAs, safety – challenging
• HDV – no effective therapy – HBsAg loss effective here too
• Lots of potential – need to be a bit patient – this is not HCV 2.0!
Phil Pang, M.D., Ph.D.C h i e f M e d i c a l O f f i c e r
© 2022 Vir Biotechnology, Inc. 47

HBV functional cure through cocktails of antivirals and immunomodulators
UNMET NEEDS VIR’S ANSWER
© 2021 Vir Biotechnology, Inc.
In pursuit of a functional cure
The Polaris Observatory Collaborators. Lancet Gastroenterol Hepatol 2018
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8309973/
*Functional cure: undetectable hepatitis B virus surface antigen (HBsAg), defined as less
than 0.05 international units per milliliter, as well as HBV DNA less than the lower limit of
quantification, in the blood six months after the end of therapy
EASL: The European Association for the Study of the Liver
AASLD: The American Association for the Study of Liver Diseases
HBV: Hepatitis B
~300M
<7%
Approximately 300 million people in the world live with chronic Hepatitis B (HBV)
Current therapies either require life-long therapy or have poor tolerability with functional cure* rates less than 7%
Recent presentations at EASL and AASLD demonstrate progress and breadth
© 2022 Vir Biotechnology, Inc. 48
H B V

1. Vir’s goal: be the first company to develop treatments that achieve meaningful HBV functional cure rates, moving from 3% to more than 30%
2. Differentiated HBV cure pipeline: designed to optimize the likelihood of success
• We believe a pure antiviral strategy is not enough
• Need to also remove tolerogens (via our siRNA, VIR-2218, and our mAb, VIR-3434) and
• Add an immunostimulant (our mAb VIR-3434)
• Differentiated in evaluating five complimentary immunostimulant mechanisms: PEG-IFN-⍺, VIR-3434, our collaborations with BRII-179, TLR8 (GS-9688) + PD-1 (nivolumab)
• Evaluating three different patient populations: NRTI-suppressed, viremic, inactive carriers
3. Intend to leverage our existing clinical-stage assets, VIR-3434 and VIR-2218, for a new Hepatitis Delta (HDV) program
• Derisked MOAs: entry inhibition and dual knock-down of HbsAg
• No drug related safety signals identified to date
• Potential for near-term proof of concept (2023)
• Potential for convenient monthly dosing and to be used in the hepatically-impaired
© 2022 Vir Biotechnology, Inc.
49
NRTI: Nucleoside reverse transcriptase inhibitorsMOA: Mechanism of actionHbsAg : Hepatitis B surface antigen
K E Y T A K E A W A Y S

© 2022 Vir Biotechnology, Inc. 50
STOP CLEAR
Antivirals Immunomodulators
Break ToleranceVIR-3434VIR-2218⍺PD-1
Stimulate T-CellsVIR-3434
PEG-IFN-⍺BRII-179
TLR8 (GS-9688)
Block ReplicationVIR-2218
NRTIsPEG-IFN-⍺
Block EntryVIR-3434
Goal to STOP the virus and CLEAR already infected cells:Differentiated Assets and Differentiated Combinations
H B V

Targeting multiple HBV patient populations in clinical trials
Evaluating multiple HBV patient populations to identify most potentially responsive patient populations
• NRTI-suppressed• Viremic• Inactive carriers
New opportunity to evaluate HDV patients with VIR-2218 and VIR-3434
© 2022 Vir Biotechnology, Inc. 51
0 20 40 60
HBeAgAnti-HBe
YEARS
Immune tolerant
Immune clearance HBeAg-positive
chronic hepatitus
Inactive carrier state
Reactivation HBeAg-negative chronic hepatitus
HBV DNA
HBsAg
ALT
HBeAg+ Chronic HBV Infection /
Immune Tolerant (IT)
HBeAg+ Chronic Hepatitis B /
Immune Active (IA)
HBeAg- Chronic HBV Infection /
Inactive Carrier (IC)
HBeAg- Chronic Hepatitis B / Reactivation
VIR: Evaluating multiple patient populations to identify most responsive patient groups
(potential future evaluation) ✓ ✓ ✓
Current SOC: NRTIs and Peg-IFN-alpha are only recommended for chronic hepatitis B patients ✓ ✓
NRTI: Nucleoside/nucleotide reverse transcriptase inhibitors
H B V

New chronic Hepatitis Delta (HDV) treatment program
HDV is the most severe form of viral hepatitis • High rates of cirrhosis and hepatocellular carcinoma (HCC);
significant economic burden
Significant unmet need • No approved therapy in the US
• High potential treatment rate given disease severity
• Opportunity independent of HBV functional cure
Leverages VIR-2218 and VIR-3434 combination • Derisked MOAs: entry inhibition and dual knock-down of HbsAg
• No drug related safety signals identified to date
• Potential for near-term proof of concept (2023)
• Potential for convenient monthly dosing and to be used in the hepatically-impaired
© 2022 Vir Biotechnology, Inc. 52MOA: Mechanism of actionHbsAg : Hepatitis B surface antigen

Carey Hwang, M.D., Ph.D.S V P , C l i n i c a l R e s e a r c h , H e a d O f C h r o n i c I n f e c t i o n
© 2022 Vir Biotechnology, Inc. 53
© 2022 Vir Biotechnology, Inc.
AGENDA
1
2
4
5
54
3
Hepatitis B (HBV) unmet need
Review of preclinical and Vir clinical data to date
Introduction of new Hepatitis Delta (HDV) Program
HDV unmet need
Expected clinical data milestones
© 2022 Vir Biotechnology, Inc.

HBV Global Prevalence Estimate: ~300 M1
≤1.0% 1.1-2.5% 2.6-5.0% 5.1-10.0% >10.0%HBsAg prevalence:
HBV: A significant global health threat
55
1. The Polaris Observatory Collaborators. Lancet Gastroenterol Hepatol 2018. 2. World Health Organization
~900K deaths per year from complications of
chronic HBV2
H B V U N M E T N E E D
New Infections Each Year Estimate: ~1.5M2
© 2022 Vir Biotechnology, Inc.
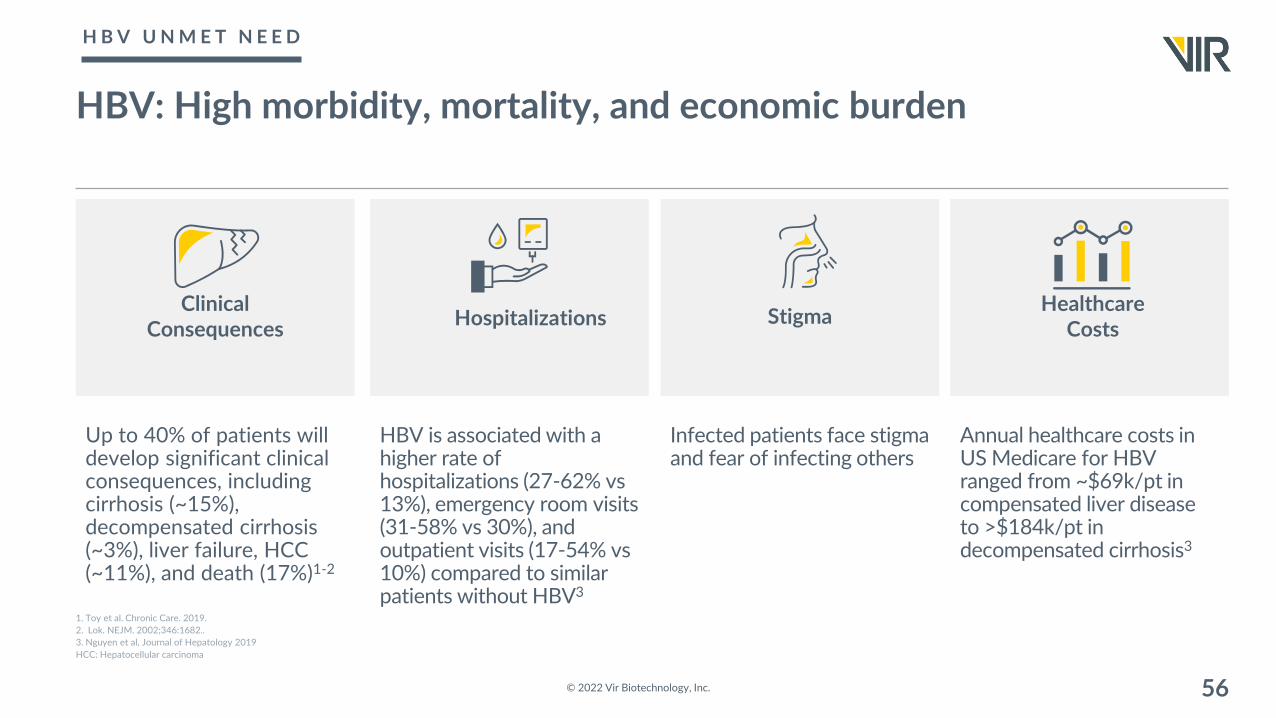
HBV: High morbidity, mortality, and economic burden
Up to 40% of patients will develop significant clinical consequences, including cirrhosis (~15%), decompensated cirrhosis (~3%), liver failure, HCC (~11%), and death (17%)1-2
© 2022 Vir Biotechnology, Inc. 56
1. Toy et al. Chronic Care. 2019. 2. Lok. NEJM. 2002;346:1682.. 3. Nguyen et al, Journal of Hepatology 2019HCC: Hepatocellular carcinoma
Clinical Consequences Hospitalizations Stigma
Healthcare Costs
HBV is associated with a higher rate of hospitalizations (27-62% vs 13%), emergency room visits (31-58% vs 30%), and outpatient visits (17-54% vs 10%) compared to similar patients without HBV3
Infected patients face stigma and fear of infecting others
Annual healthcare costs in US Medicare for HBV ranged from ~$69k/pt in compensated liver disease to >$184k/pt in decompensated cirrhosis3
H B V U N M E T N E E D
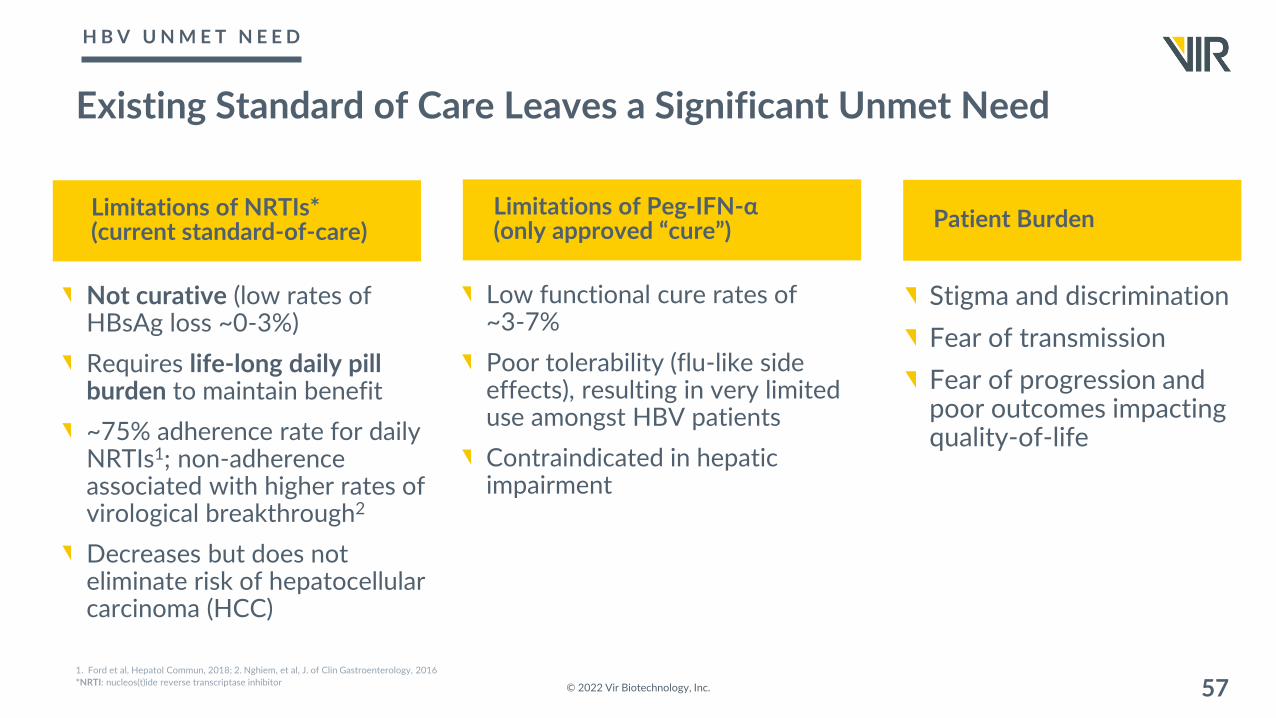
Existing Standard of Care Leaves a Significant Unmet Need
© 2022 Vir Biotechnology, Inc. 571. Ford et al, Hepatol Commun, 2018; 2. Nghiem, et al, J. of Clin Gastroenterology, 2016*NRTI: nucleos(t)ide reverse transcriptase inhibitor
Not curative (low rates of HBsAg loss ~0-3%)
Requires life-long daily pill burden to maintain benefit
~75% adherence rate for daily NRTIs1; non-adherence associated with higher rates of virological breakthrough2
Decreases but does not eliminate risk of hepatocellularcarcinoma (HCC)
Low functional cure rates of ~3-7%
Poor tolerability (flu-like side effects), resulting in very limited use amongst HBV patients
Contraindicated in hepatic impairment
Limitations of NRTIs* (current standard-of-care)
Limitations of Peg-IFN-α (only approved “cure”)
Stigma and discrimination
Fear of transmission
Fear of progression and poor outcomes impacting quality-of-life
Patient Burden
H B V U N M E T N E E D

HBV: Significant unmet need and patient opportunity for functional cure regimen
© 2022 Vir Biotechnology, Inc. 581.WHO Fact Sheet - https://www.who.int/news-room/fact-sheets/detail/hepatitis-b, 2. Harris et al, Am J of Man Care 2020 3).Vir internal assumptions; MOA: mechanism of action
CURRENT GLOBAL PATIENT FLOW
Prevalence~300M WW1
Diagnosed~30M1 (~10%)
NRTI Treated today~7M1 Globally (~2%)
(~120k US,~220k EU)2-3
(limited to immune active patients)
FUTURE STATE
• Vir HBV functional cure through combination of antivirals and immunomodulators
• Distinct MOA (e.g. VIR-3434)• Evaluating five different
immunomodulators • Evaluating three patient
populations
H B V U N M E T N E E D

Chronic HBV: Our approach to achieving functional cure
Chronic HBV (CHB) is a viral disease resulting in immune dysfunction
Immune dysfunction is a result of the expression of a large amount of HBV antigens, which act to suppress the immune system
Believe a functional cure for CHB results from regaining immunologic control
© 2022 Vir Biotechnology, Inc. 59
We hypothesize that knocking down HBV antigens will remove the block on the immune system, and in the setting of an immune modulator, result in immune control
P R E C L I N I C A L

Chronic HBV: Reversal of functional cure via immunosuppression
© 2022 Vir Biotechnology, Inc. 60
functionally cured patient
(HbsAg < LLOQ)
rituximab-containing
chemotherapy+ =
Seto W, et al. J Clin Oncol 2014; 32(33): 3736-43
P R E C L I N I C A L

© 2022 Vir Biotechnology, Inc. 61
Mueller SN, Ahmed R. PNAS 2009; Oxenius A, et al. Eur J Immunol 2012; Schietinger A, Greenberg PD. Trends Immunol.2014; Tay SS, et al. PNAS 2014; Wherry EJ. Nat Immunol 2011.
High Hepatic Antigen Levels
Dysfunctional Immune Response
Low Hepatic Antigen Levels
Functional Immune Response
1
T cell activation in liver
2
Functional effector
Naïve CD8 T cell
Functional effector
T cell activation in lymph nodes
Antigen clearancein liver
Functional effectorLiverLiver
1
T cell activation in liverNonfunctional
T cell
T celldeletion
2
3
Functional effector
Naïve CD8 T cell
ExhaustedT cell
T cell activation in lymph nodes
Antigen persistence in liver
High antigen load can drive T cell dysfunction
P R E C L I N I C A L

Reduction of HBsAg improves responses to therapeutic vaccination in mouse HBV models
© 2022 Vir Biotechnology, Inc. 62
AAV, adeno-associated virus; Ctrl, control; HBs, hepatitis B surface antibody; TherVacB, therapeutic hepatitis B vaccine.Adapted from Michler T, et al. EASL 2018.
Functional cure associated with generation of HBV-specific CD8+ T cells
- - - + + +
Ctrl HBV1 HBV2 Ctrl HBV1 HBV20
5
10
15
20
25
0.841 3
0.334 8
0.014 4
0.017 8
siRNA
TherVacB - - - + + +
Ctrl HBV1 HBV2 Ctrl HBV1 HBV20
2
4
6
8
10
0.980 1
0.499 9
0.007 5
0.239 6
Rea
ctiv
e C
D8
T C
ells
, %
IF
Nγ+
of C
D8+
Functional cure achieved in all 12 mice treated with HBV siRNA + TherVacB
4 5-12 -8
AAV-HBV1.2 WT mice
Weeks
-4 0
HBsAg siRNATherVacB
2
P R E C L I N I C A L

VIR-2218 Phase 2 DataPotential Best-In-Class siRNA
Ongoing Clinical Trials
Vir’s broad HBV functional cure portfolio
© 2022 Vir Biotechnology, Inc. 63
Substantial, Durable, and Dose Dependent Reduction of HBsAg through 48 weeks1
Currently in
Phase 2 PEG-IFN-⍺
Currently in
Phase 2
VIR-3434
mAb
Currently inPhase 2
GS-9688TLR-8 agonist
nivolumabPD-1 antagonist
Currently in
Phase 2
BRII-179T cell vaccine
Mea
n C
hang
e in
Log
10H
BsA
g (IU
/mL)
Placebo 20 mg 50 mg 100 mg 200 mg
Week
Note: current and planned trials are/will be conducted in patients with chronic HBV on nucleotide/nucleoside reverse transcriptase inhibitors (NRTIs), which are standard of care treatmentPEG-IFN: pegylated interferon alpha.1. Gane E, et al. Oral presentation at: The International Liver Congress – EASL; June 25, 2021; Virtual.

VIR-2218 + PEG-IFN-α
© 2022 Vir Biotechnology, Inc. 64

Trial Design of VIR-2218 with an immunommodulator (PEG-IFNα)
All participants are virally suppressed
Preliminary data from Cohorts 1-4 through Week 24 are presented herein
© 2022 Vir Biotechnology, Inc. 65
HBsAg assay LLOQ and LLOD are < 0.05 IU/mL.LLOD, lower limit of detection; LLOQ, lower limit of quantitation; q4w, every 4 weeks; qw, every week; mg, microgram; PEG-IFN⍺, peginterferon alfa-2a, SC, subcutaneous.VIR-2218 Dose 200 mg SC | PEG-IFNα 180 µg SC
WEEK 484036322824201612080400 44
Participants discontinue PEG-IFNα if they have HBsAg < LLOQ at 2 consecutive visits
VIR-2218 Q4W x 6
Cohort 1
VIR-2218 Q4W x 6
PEG-IFN⍺ QW x 24
Cohort 3
VIR-2218 Q4W x 6PEG-IFN⍺ QW x 12
Cohort 2
VIR-2218 Q4W x 6
PEG-IFN⍺ QW x 48
Cohort 4
VIR-2218 Q4W x ≤ 13
PEG-IFN⍺ QW x ≤ 44
Cohort 5
V I R - 2 2 1 8

Concurrent initiation of VIR-2218 and PEG-IFNα combination achieved greatest reductions in HBsAg through week 24
© 2022 Vir Biotechnology, Inc. 66
*Participant achieved HBsAg < LLOQ (0.05 IU/mL).HBeAg-negative, hepatitis B e antigen; PEG-IFN⍺, peginterferon alfa-2a.Yuen et al., AASLD 2021
HBsAg change from baseline at Week 24 (log10 IU/mL)
** *HBeAg-negativeHBeAg-positive
HBeAg-negativeHBeAg-positive
HBeAg-negativeHBeAg-positive
HBeAg-negativeHBeAg-positive
Cohort 1 Cohort 2 Cohort 3 Cohort 4
VIR-2218 only VIR-2218 lead-in +PEG-IFN⍺ (12 wk)
VIR-2218 + PEG-IFN⍺ (24 wk)
VIR-2218 + PEG-IFN⍺ (≤ 48 wk)
Week 4, n 15 15 17 13
Mean Change in HBsAg (log10 IU/mL) -0.51 -0.51 -0.92 -1.01
Week 12, n 14 15 16 11
Mean Change in HBsAg (log10 IU/mL) -1.39 -1.42 -1.98 -2.05
At Week 24, n 15 15 13 9
Mean Change in HBsAg (log10 IU/mL) -1.89 -2.03 -2.55 -2.30
V I R - 2 2 1 8

Three participants achieved HBsAg < LLOQ by week 24
© 2022 Vir Biotechnology, Inc. 67
HBsAg,: hepatitis B surface antigen; HBeAg, hepatitis B e antigen; anti-HBs, hepatitis B surface antibody; PEG-IFN⍺, peginterferon alfa-2a.1.HBeAg at baseline was very low (0.16 IU/mL); the participant achieved HBeAg loss by Week 4. HBsAg assay LLOQ and LLOD are < 0.05 IU/mL; anti-HBs considered positive at > 10 mIU/mL.Yuen et al., AASLD 2021
Week
HB
sAg
(IU/m
L)
Participant A
100
10
1
0.1LOQ
150
125
100
75
50
25
00 4 8 12 16 20 24
HBsAg ALT
Participant B
100
10
1
0.1LOQ
150
125
100
75
50
25
00 4 8 12 16 20 24
Week
HBsAg ALT
Participant C
100
10
1
0.1LOQ
150
125
100
75
50
25
00 4 8 12 16 20 24
HBsAg ALT
Week
ALT (U
/L)
Participant A B C
Cohort 2 3 4
Age (years) 36 56 39
Gender Male Male Male
Baseline HBeAg status Negative Positive1 Negative
Baseline HBsAg (IU/mL) 134 151 156
Anti-HBs at Week 24 Positive (130.6 mIU/mL) Negative Positive (84 mIU/mL)
V I R - 2 2 1 8

Proof of principle and next steps
VIR-2218 with PEG-IFNα has demonstrated clinically meaningful HBsAg reductions with no clinically significant safety signalsConcurrent initiation of VIR-2218 and PEG-IFNα resulted in greatest HBsAg reductions with most patients having achieved HBsAg <100 IU/mL and 55% achieved <10 IU/mL at Week 24These results suggest that treatment with an siRNA could unlock the potential of immunomodulatorsTrial expanded to explore if response rates differ between 24 and 48 weeks of therapy
68© 2022 Vir Biotechnology, Inc.
V I R - 2 2 1 8

VIR-2218 + VIR-3434
© 2022 Vir Biotechnology, Inc. 69
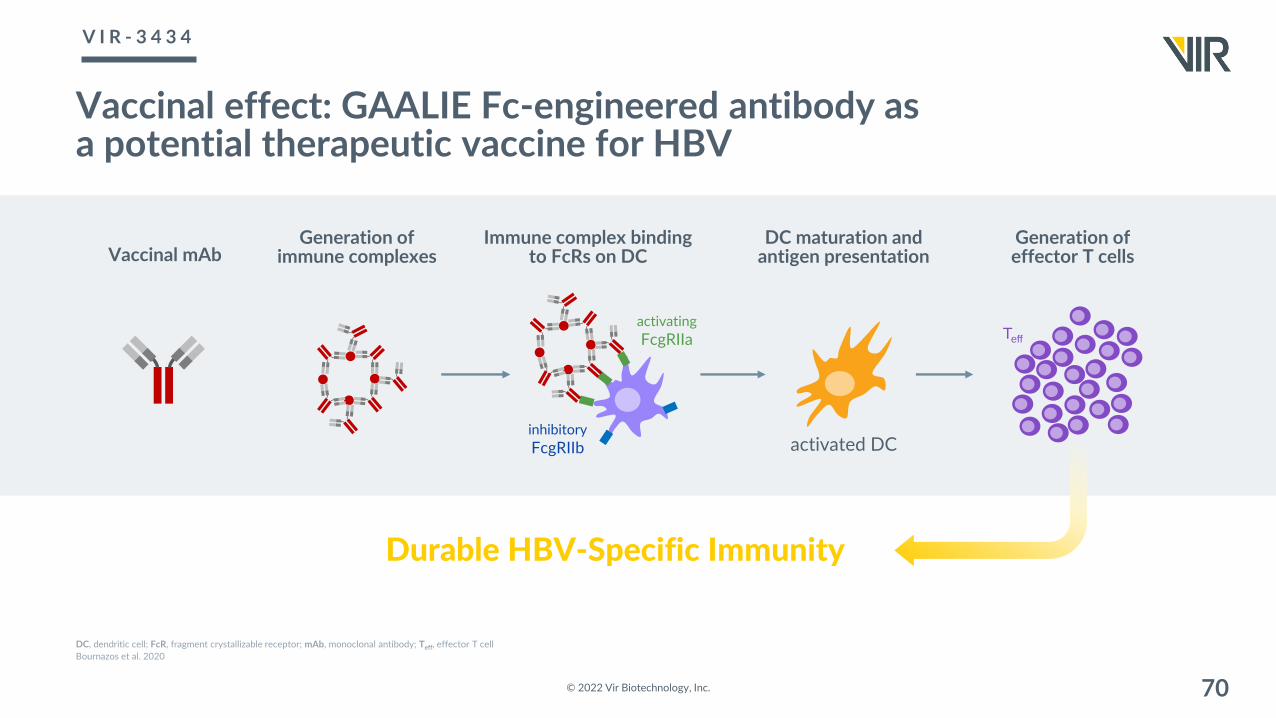
Vaccinal effect: GAALIE Fc-engineered antibody as a potential therapeutic vaccine for HBV
© 2022 Vir Biotechnology, Inc. 70
DC, dendritic cell; FcR, fragment crystallizable receptor; mAb, monoclonal antibody; Teff, effector T cell Bournazos et al. 2020
Generation ofimmune complexes
Immune complex binding to FcRs on DC
Generation of effector T cells
Durable HBV-Specific Immunity
activated DC
DC maturation and antigen presentation
activatingFcgRIIa
inhibitoryFcgRIIb
Teff
Vaccinal mAb
V I R - 3 4 3 4

7E3-GAALIE (anti-sLeA carbohydrate) reduced lung metastatic foci of B16 tumor cells compared to 7E3-WT
FY1-GAALIE (anti-HA stem mAb) induced a CD8+ T cell-mediated protection from infection with influenza virus
Turning antibodies into T-cell vaccines via Fc GAALIE mutation in preclinical studies
© 2022 Vir Biotechnology, Inc. 71
Isotype
wild type-Fc
GAALIE-Fc
Wei
ght (
%)
Time (days)0 7 14
80
90
100
PBS
WT
GA
GAALIEIsotype
Isotype
Isotype
Isotype
Anti-CD8
Anti-CD8
Anti-CD8
Anti-CD8
mAb WT, GA, or GAALIE
Infection InfectionCD8+ depletion Isotype or
anti-CD8 mAb
Monitor survival/ weight loss
Day 0-4 h Day 3
Weizenfeld, P, et al. JClinInvest. 2019; 129(9):3952–3962.Bournazos, S, et al. Nature. 2020; 588,485–490.
GAALIE cancer antibody: superior protection from metastasis
GAALIE flu antibody: superior protection from infection
V A C C I N A L E F F E C T

VIR-3434 SAD trial design
Part A SADHealthy Volunteers
Part B SAD Virally SuppressedHBsAg < 3,000 IU/mL1
Part C SAD Virally SuppressedHBsAg ≥ 3,000 IU/mL2
Part D SADViremic (HBV DNA ≥ 1,000 IU/mL)Any HBsAg
72
IV, intravenous; SAD, single ascending dose; SC, subcutaneous1. Cohort 1b (6 mg SC) enrolled participants with screening HBsAg < 1,000 IU/mL. 2 Cohort 1c (18 mg SC) enrolled participants with any screening HBsAg
300 mg SCn=8
18 mg SCn=8
75 mg SCn=8
900 mg SCn=8
90 mg SCn=8
300 mg SCn=8
6 mg SC1
n=8
3,000 mg IVn=8
900 mg IVn=8
75 mg SCn=8
300 mg SCn=8
18 mg SC2
n=8
300 mg SCn=8
75 mg SCn=8
OngoingComplete Planned
In each cohort, 8 participants are randomized 6:2 to receive a single dose of VIR-3434 or placebo by SC injection
© 2022 Vir Biotechnology, Inc.
V I R - 3 4 3 4

Increasing doses of VIR-3434 correlate with maximum decline in HBsAg
The largest (> 2 log10 IU/mL) and most sustained reductions in HBsAg were observed in the 75 mg cohort
Mean reduction at 75 mg was 1.96 log10 IU/mL at nadir and 1.5 log10 IU/mL at Day 29
73
1. Free VIR-3434 was undetectable in all available samples. 2. Free VIR-3434 concentrations were lower than anticipated in all available samples.HBsAg measured with Abbott ARCHITECT®.Agarwal et al., AASLD 2021Maximum decline does get lower with each dose
V I R - 3 4 3 4
© 2022 Vir Biotechnology, Inc.

Summary
In virally suppressed participants with HBsAg < 3,000 IU/mL, a single dose of 6 mg to 75 mg of VIR-3434 resulted in rapid HBsAg reductions of > 1 log10 IU/mL in most participants
Single doses of VIR-3434 showed no clinically significant safety signals; all adverse events (AEs) were Grade 1 or 2
These data support the potential for VIR-3434 to have a meaningful role in the functional cure of chronic HBV infection
74© 2022 Vir Biotechnology, Inc.
V I R - 3 4 3 4

VIR-2218 Q4W
VIR-3434 Q4W
Regimen 3
VIR-2218 Q4WVIR-3434 Q4W
VIR-2218 Q4WVIR-3434 Q4WPEG-IFNα QW
VIR-2218 Q4WVIR-3434 QW
VIR-2218 Q4WVIR-3434 QW
Regimen 4
Regimen 5
Regimen 1
Regimen 2
Initial data expected 2H2022
© 2022 Vir Biotechnology, Inc.
WEEK 484036322824201612080400 44 484036322824201612080400 44
Part A: short treatment courses designed to rapidly evaluate safety, PK, and HBsAg suppression, when VIR-3434 is given weekly
Part B*: additional cohorts to determine dose, length of treatment, and evaluate triple cocktails, when VIR-3434 is given every 4 weeks
WEEK
Evaluating functional cure potential from combinations
Each regimen will enroll up to 30 participants with chronic HBV infection who are virally suppressed on NRTI therapy
Participants will be followed for at least 48 weeks post-treatment and be assessed for safety and efficacy
75
VIR-3434 18-75mg dosing in Part A, dosing TBD for Part B; VIR-2218 200mg dose in Part B; PEG-IFNα 180mcg dose in Regimen 5MARCH: Monoclonal Antibody siRNA Combination against Hepatitis B; QW: weekly; Q4W, every 4 weeks; NRTI: nucleos(t)ide reverse transcriptase inhibitor*Not exhaustive - additional cohorts may be added; PK: Pharmacokinetics
M A R C H T R I A L ( V I R - 2 2 1 8 + V I R - 3 4 3 4 )

Available data from Part A suggest no clinically significant safety signals and evidence of additivity between VIR-2218 and VIR-3434
Part A*• Available data suggests no clinically significant safety signals with combination therapy• Available data suggests evidence of additivity between VIR-2218 and VIR-3434 in HbsAg
reductions • Full data set delayed by war in Ukraine
o Scientific presentation of data now anticipated in 2H2022
Part B of MARCH Trial • Trial initiation anticipated in 2Q2022• Will evaluate additional cohorts to determine dose, length of treatment, and the value of triple
cocktails, when VIR-3434 is given every 4 weeks • 24 vs 48 weeks of VIR-2218 with and without VIR-3434 and PEG-IFN-⍺
© 2022 Vir Biotechnology, Inc. 76* As some of our clinical trial sites for the MARCH trial are in Ukraine and Moldova, we will continue to monitor the war to determine potential delay in expected timetables.
M A R C H T R I A L U P D A T E

Initial on-treatment data from MARCH Part A
© 2022 Vir Biotechnology, Inc. 77
Data on file
No discontinuations or clinically significant safety signals were observed.
M A R C H T R I A L U P D A T E

VIR-2218 + Other Immunomodulators
© 2022 Vir Biotechnology, Inc. 78

RATIONALE AND TRIAL DESIGN
Both trials evaluate the hypothesis of reducing toleragens and adding an immunomodulator to enhance immune responses
Rationale for combining VIR-2218, GS-9688 (TLR8 agonist) and nivolumab (anti-PD-1)
• VIR-2218 reduces tolerogens (e.g. HBsAg)
• GS-9688 stimulates antiviral and T-cell supporting cytokines
• Nivolumab reverses T-cell exhaustion to improve HBV-specific T and B cell responses
79
GS-9688 (TLR8 agonist) and nivolumab (anti-PD-1) : in collaboration with GileadBRII-179: in collaboration with BriiMOA: mechanism of action
Rationale for combining VIR-2218 and BRII-179
• VIR-2218 reduces tolerogens • BRII-179 induces sustained HBV-
specific host immune responses– Reducing tolerogens improved
responses to therapeutic vaccines in mouse HBV models
© 2022 Vir Biotechnology, Inc.
G I L E A D & B R I I T R I A L S
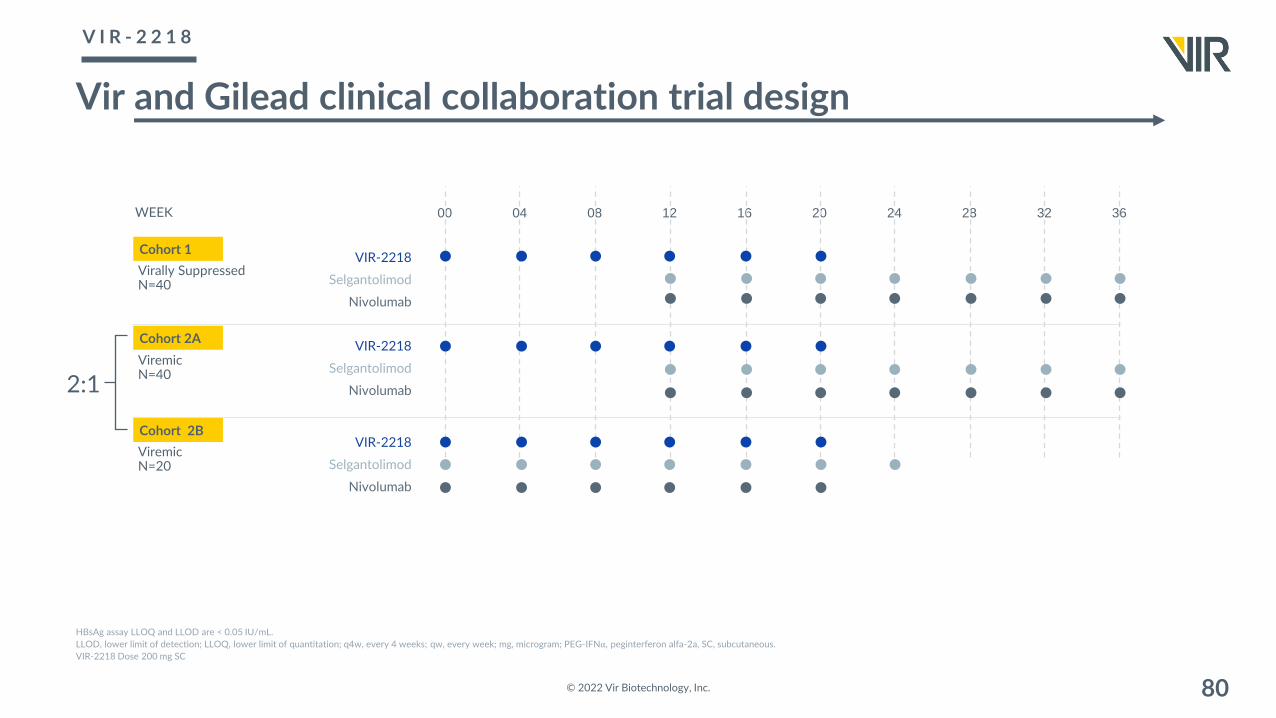
Vir and Gilead clinical collaboration trial design
© 2022 Vir Biotechnology, Inc. 80
HBsAg assay LLOQ and LLOD are < 0.05 IU/mL.LLOD, lower limit of detection; LLOQ, lower limit of quantitation; q4w, every 4 weeks; qw, every week; mg, microgram; PEG-IFN⍺, peginterferon alfa-2a, SC, subcutaneous.VIR-2218 Dose 200 mg SC
WEEK 36322824201612080400
Virally SuppressedN=40
Cohort 1
Cohort 2B
Cohort 2A
VIR-2218
Selgantolimod
Nivolumab
ViremicN=40
ViremicN=20
VIR-2218
Selgantolimod
Nivolumab
VIR-2218
Selgantolimod
Nivolumab
2:1
V I R - 2 2 1 8

Vir and Brii clinical collaboration trial designBRII-835 (VIR-2218) reduces HBsAg followed by administration of therapeutic vaccine to boost immune response
© 2022 Vir Biotechnology, Inc. 81
Nrtl=nucleos(t)ide reverse transcriptase inhibition; Rand=Randomization#Nrtl Discontinuation Monitoring: Participants who meets the Nrtl Discontinuation Criteria at Week 44 may be eligible to discontinue from Nrtl therapy and enter into the Nrtl Discontinuation Monitoring Period on the first day of Week 48.¶Participants that have NOT achieved Nrtl discontinuation criteria by Week 44 will be discharged from the study completion of all follow-up visits by Week 72. *Floater Participants: Up to 60 participants may be added to any existing cohort(s) as expansions of the existing cohorts(s) if further data is required. The allocation of floater participants is not required to be distributed evenly.
STUDY WEEK 484036322824201612080400 44 52 56 60 64 68 72 76 80 84 88 82 92 96
STUDY DAY 33628025222419616814011284562801 308 364 392 420 448 476 504 532 560 588 616 616 644 672-42
BRII-835 100mg
Cohort A
BRII-835 100mg
Cohort C*
BRII-835 100mg
BRII-179 40μg, IFN-⍺
Cohort B*
BRII-179 40μg
NRTI Treatment
FOLLOW-UP
48-week NRTI Discontinuation Monitoring*
NRTI Treatment 48-week NRTI Discontinuation Monitoring*
NRTI Treatment 48-week NRTI Discontinuation Monitoring*
FOLLOW-UP
FOLLOW-UP
V I R - 2 2 1 8

New Opportunities in Hepatitis
A D D I T I O N A L H B V P O P U L A T I O N S A N D H E P A T I T I S D
© 2022 Vir Biotechnology, Inc. 82
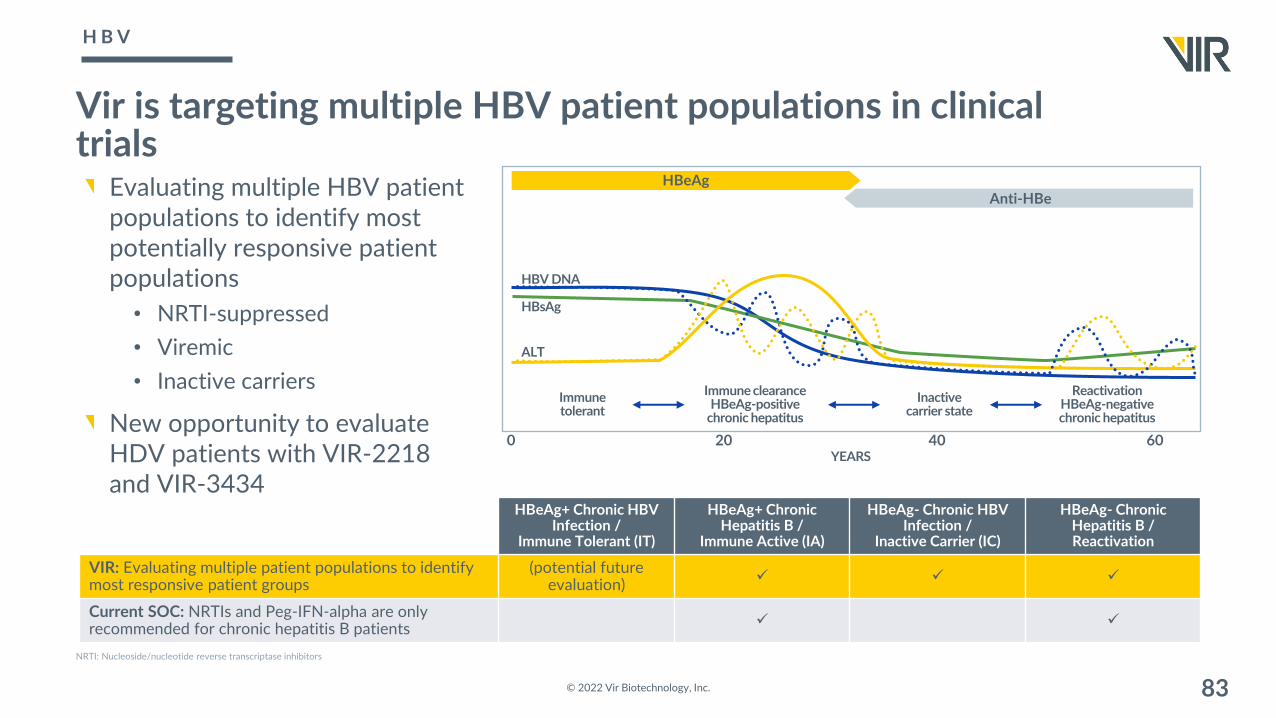
Vir is targeting multiple HBV patient populations in clinical trials
Evaluating multiple HBV patient populations to identify most potentially responsive patient populations
• NRTI-suppressed• Viremic• Inactive carriers
New opportunity to evaluate HDV patients with VIR-2218 and VIR-3434
© 2022 Vir Biotechnology, Inc. 83
0 20 40 60
HBeAgAnti-HBe
YEARS
Immune tolerant
Immune clearance HBeAg-positive
chronic hepatitus
Inactive carrier state
Reactivation HBeAg-negative chronic hepatitus
HBV DNA
HBsAg
ALT
HBeAg+ Chronic HBV Infection /
Immune Tolerant (IT)
HBeAg+ Chronic Hepatitis B /
Immune Active (IA)
HBeAg- Chronic HBV Infection /
Inactive Carrier (IC)
HBeAg- Chronic Hepatitis B / Reactivation
VIR: Evaluating multiple patient populations to identify most responsive patient groups
(potential future evaluation) ✓ ✓ ✓
Current SOC: NRTIs and Peg-IFN-alpha are only recommended for chronic hepatitis B patients ✓ ✓
NRTI: Nucleoside/nucleotide reverse transcriptase inhibitors
H B V

• Combination leveraging existing Vir assets for HDV chronic therapy; derisked MOAs: entry inhibition and dual knock-down of HbsAg
• Differentiated with the potential for: convenient monthly dosing, broader patient populations (hepatically-impaired), no drug related safety signals identified to date
• Independent of already significant potential HBV opportunity
UNMET NEEDS VIR’S ANSWERNew opportunity in HDV: VIR-2218 & VIR-3434
Stockdale et al. J Hepatol. 2020;73(3):523-532
Koh et al. Gastroenterology 2019;156:461–476
Miao et al J Infect Dis. 2020 Apr 27;221(10):1677-1687
MOA: Mechanism of action
HbsAg : Hepatitis B surface antigen
3.9x• HDV increases risk of poor outcomes
compared to HBV alone (3.9x greater risk for HCC, 2x greater risk for HCC, and death)
• High unmet need for treatment to reduce burden
© 2022 Vir Biotechnology, Inc. 84
• Estimated ~12 million people HDV infected (~100k in U.S. and ~100-200k in Europe)
• Represents ~5% of HBV positive people • No approved therapy in US
~12M
H D V

Associated with rapid progression to cirrhosis and high rates of decompensated liver disease, HCC, and liver-related events
Early treatment is critical to slowing progression of diseaseSignificant annual healthcare utilization costs associated with HDV infection
HDV is the most aggressive form of viral hepatitis and is associated with poor prognosis; unmet need is significant
© 2022 Vir Biotechnology, Inc. 85
~41% Mean of ~5 YRS to progress to cirrhosis
~6% Mean of ~10 YRS to progress to HCC
~17% CIRRHOSIS HCC DEATH
Prevalence of Liver Diseases in HDV patients
Miao Z, Zhang S, Ou X, et al. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of Hepatitis Delta Virus Infection. J Infect Dis. 2020;221(10):1677-1687.
H D V U N M E T N E E D

Significant unmet need in HDV with current therapies
No approved therapy in US
Pegylated interferon-alpha (PEG-IFN-alpha) efficacy is limited, resulting in low utilization
• Contraindicated in hepatic impairment
Nucleos(t)ide analogues have little or no effect on HDV replication
Hepcludex (bulevirtide) conditional approval in EU requiring daily SC injections
86Gastroenterology & Hepatology Volume 14, Issue 6 June 2018 SC: subcutaneous injection
© 2022 Vir Biotechnology, Inc.
LIMITATIONS OF CURRENT TREATMENTS
H D V U N M E T N E E D

HDV Significant Unmet Need and Patient Opportunity
© 2022 Vir Biotechnology, Inc. 871. Vir internal analysis of CDC NHANES data and 2019 US Census, 2. Eurostat 2021; 3. Stockdale et al. J Hepatol 2020; 4. Safaie, et al. Virus Res 2018; 5. Kushner et al. J Hepatol 2015;
HDV PATIENT FLOWHDV Prevalence
~5% of HBV 12M WW
~200-300K US+EU1-3
Diagnosed
~5-10% today4-5
Treated
Significant unmet need
High disease severity resulting in urgency to diagnose and treat
VIR-2218 and VIR-3434 combination differentiated with the potential for convenient monthly dosing and broader patient population (hepatically-impaired) with no drug related safety signals identified to date
H D V U N M E T N E E D

VIR-2218 + VIR-3434 combination for chronic HDV therapy
Combination treatment leveraging independent and potentially synergistic MOAs to suppress HDV viremia
Potential to be more convenient and more tolerable than other pipeline agents
Potential to be used in hepatically-impaired patients
No drug related safety signals identified to date
Potential POC (viral suppression) 2023
© 2022 Vir Biotechnology, Inc. 88MOA: mechanism of actionPOC: proof of concept
Silence Viral RNA2
Inhibition of viral entry1
VIR-3434
VIR-2218
Immunomodulation: HBsAg Tolerogen Reduction
Antiviral Activity
Clearance of HBsAg3
VIR-3434
HBV HDV
HBV Virions SVPs HDV Virons
HDV RNPcccDNAintDNA
Viral RNA
ProteinsHBV DNA
NRTIs

VIR-3434 monotherapy Phase 1 1H2022
VIR-2218 monotherapy Phase 2 1H2022
PEG-IFN-⍺ Phase 2 2H2022
VIR-3434 (MARCH Part A)*mAb Phase 2 2H2022
VIR-3434 (MARCH Part B)mAb Phase 2 2H2023
VIR-3434 + VIR-2218 (STRIVE/THRIVE) Phase 2 2H2023
BRII-179T cell vaccine Phase 2 2H2022
GS-9688TLR-8 agonist
Phase 2 1H2023nivolumabPD-1 antagonist
VIR-2218 + VIR-3434 Phase 2 2023
© 2022 Vir Biotechnology, Inc. 89
E X P E C T E D C L I N I C A L D A T A M I L E S T O N E SNext Clinical Data
VIR-2218 +
HBV
HDV
* As some of our clinical trial sites for the MARCH trial are in Ukraine and Moldova, we will continue to monitor the war to determine potential delay in expected timetables.

1. Vir’s goal: be the first company to develop treatments to achieve meaningful HBV functional cure rates, moving from 3% to more than 30%
2. Differentiated HBV cure pipeline: designed to optimize the likelihood of success
• We believe a pure antiviral strategy is not enough• Need to also remove tolerogens (via our siRNA, VIR-2218, and our mAb, VIR-3434) and
• Add an immunostimulant (our mAb VIR-3434)
• Differentiated in evaluating five complimentary immunostimulant mechanisms: PEG-IFN-⍺, VIR-3434, our collaborations with BRII-179, TLR8 (GS-9688) + PD-1 (nivolumab)
• Evaluating three different patient populations: NRTI-suppressed, viremic, inactive carriers
3. Intend to leverage our existing clinical-stage assets, VIR-3434 and VIR-2218, for a new Hepatitis Delta (HDV) program• Derisked MOAs: entry inhibition and dual knock-down of HbsAg• No drug related safety signals identified to date• Potential for near-term proof of concept (2023)• Potential for convenient monthly dosing and to be used in the hepatically-impaired
© 2022 Vir Biotechnology, Inc. 90
NRTI: Nucleoside reverse transcriptase inhibitorsMOA: Mechanism of actionHbsAg : Hepatitis B surface antigen
K E Y T A K E A W A Y S

ClosingQ & A a n d F i n a l R e m a r k s
© 2022 Vir Biotechnology, Inc. 91




















